Introduction toIntroduction toPacemakersPacemakers
• March 3, 2009
• David Stultz, MD
• Southwest Cardiology, Inc.
(c) 2000-2009 David Stultz, MD
Topics to be coveredTopics to be covered
IndicationsIndications
Pacemaker nomenclaturePacemaker nomenclature
Insertion TechniqueInsertion Technique
ComplicationsComplications
Orientation toOrientation to ““the boxthe box”” (Pacemaker)(Pacemaker)
TroubleshootingTroubleshooting
Questions?Questions?
(c) 2000-2009 David Stultz, MD
General indications for a temporaryGeneral indications for a temporarypacemakerpacemaker
Heart rate is slow, causingHeart rate is slow, causing hemodynamichemodynamic compromisecompromise Sick sinus syndromeSick sinus syndrome
SinusSinus bradycardiabradycardia or atrial fibrillation with slow heart rateor atrial fibrillation with slow heart rateresponse (generally <40response (generally <40 bpmbpm))
Heart blockHeart block 33rdrd degreedegree 22ndnd degree type 2 (degree type 2 (MobitzMobitz))
Malignant Tachyarrhythmia caused byMalignant Tachyarrhythmia caused by bradycardiabradycardia TorsadesTorsades de Pointesde Pointes
(c) 2000-2009 David Stultz, MD
Clinical settings for temporaryClinical settings for temporarypacemakerpacemaker
SyncopeSyncope
Myocardial infarctionMyocardial infarction
Especially inferiorEspecially inferior
Shock due toShock due to bradycardiabradycardia
MyocarditisMyocarditis
LymeLyme diseasedisease
(c) 2000-2009 David Stultz, MD
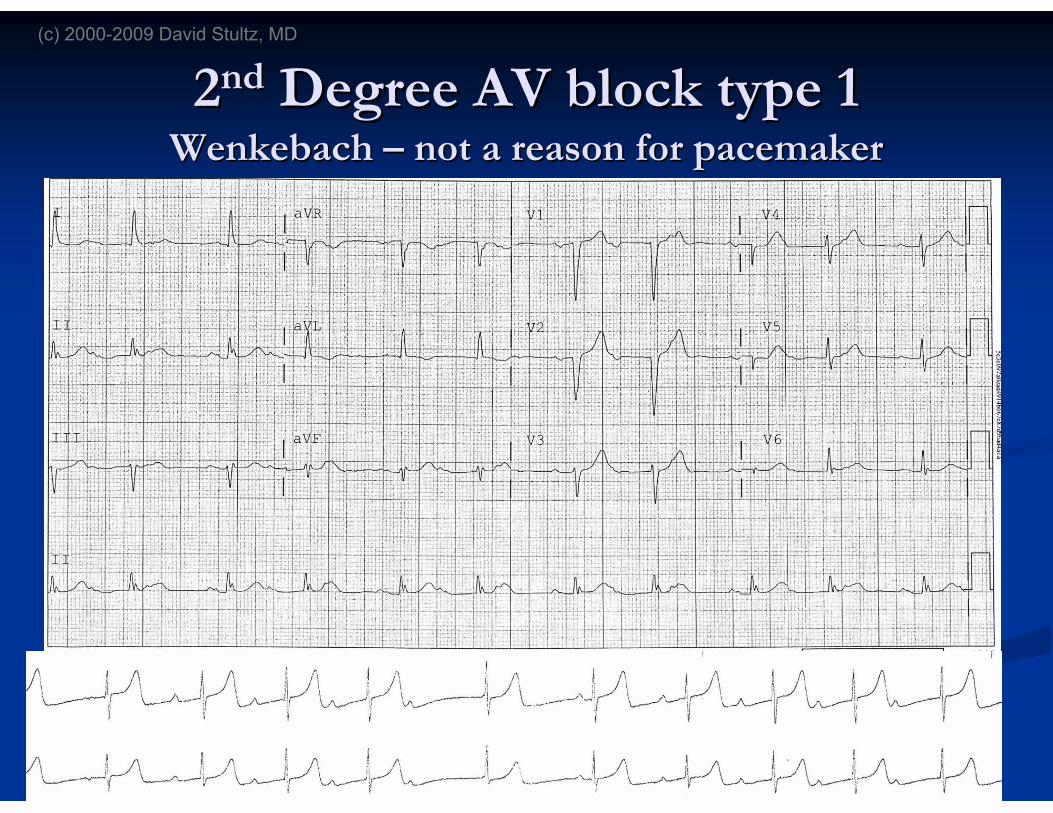
22ndnd Degree AV block type 1Degree AV block type 1WenkebachWenkebach –– not a reason for pacemakernot a reason for pacemaker
(c) 2000-2009 David Stultz, MD
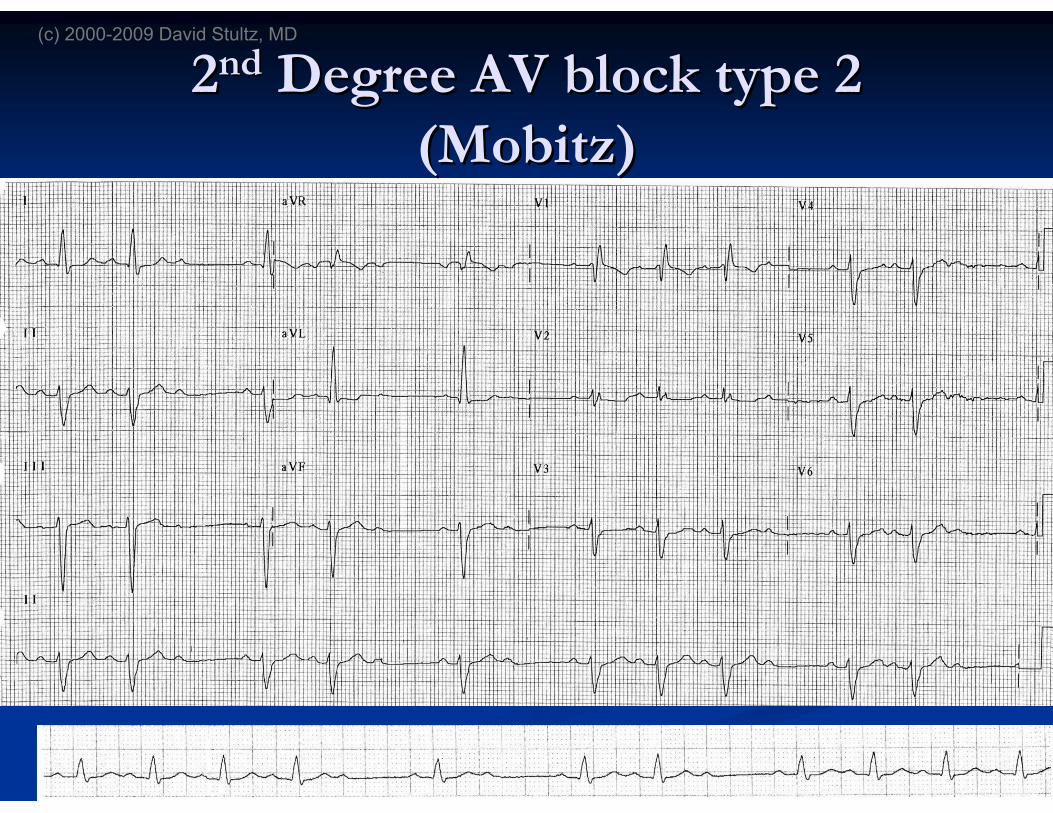
22ndnd Degree AV block type 2Degree AV block type 2((MobitzMobitz))
(c) 2000-2009 David Stultz, MD
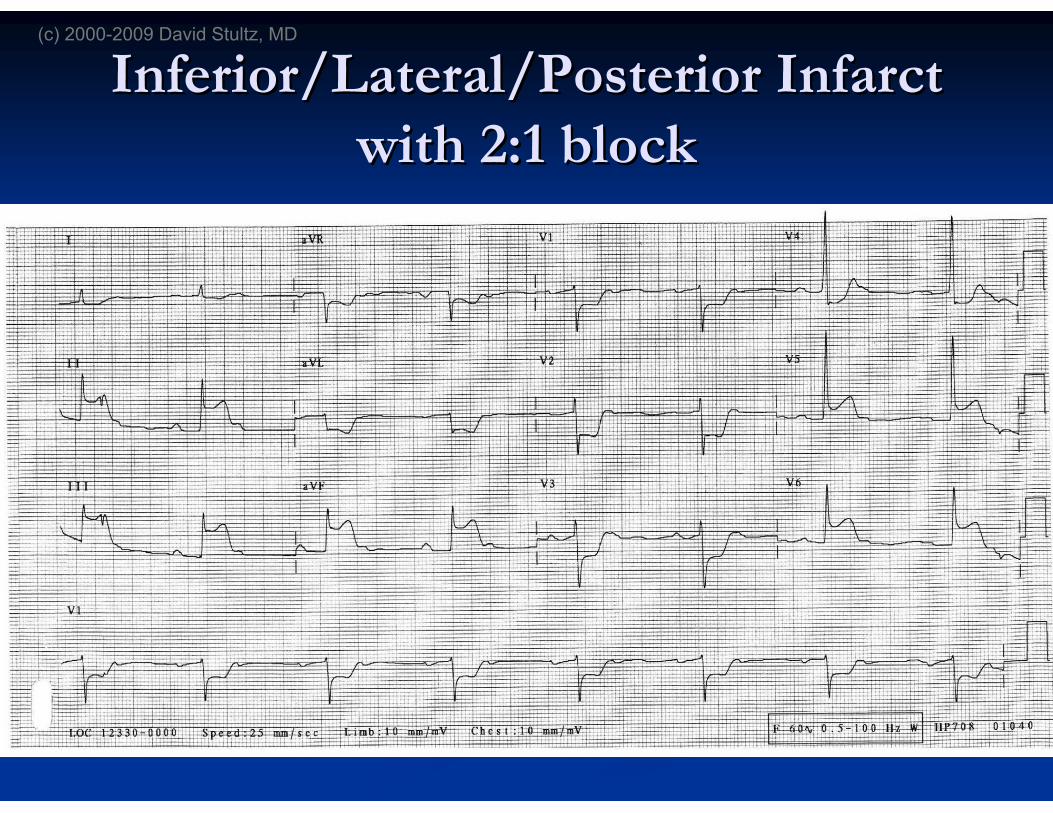
Inferior/Lateral/Posterior InfarctInferior/Lateral/Posterior Infarctwith 2:1 blockwith 2:1 block
(c) 2000-2009 David Stultz, MD
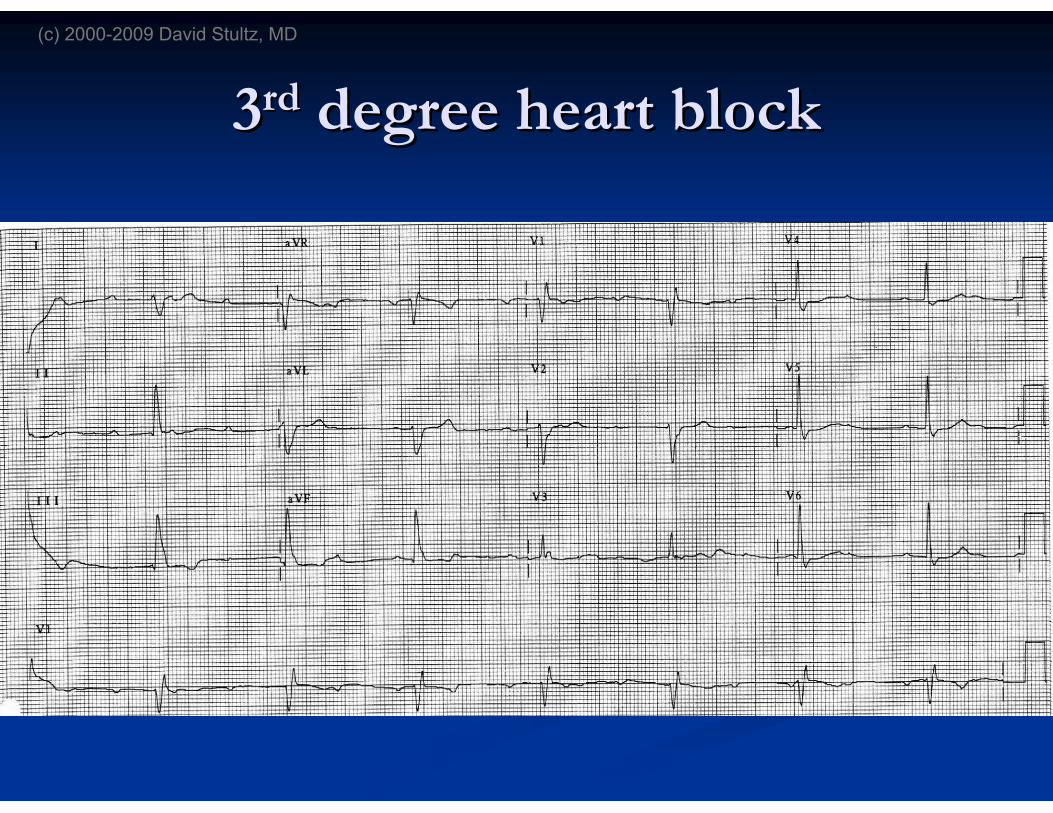
33rdrd degree heart blockdegree heart block
(c) 2000-2009 David Stultz, MD
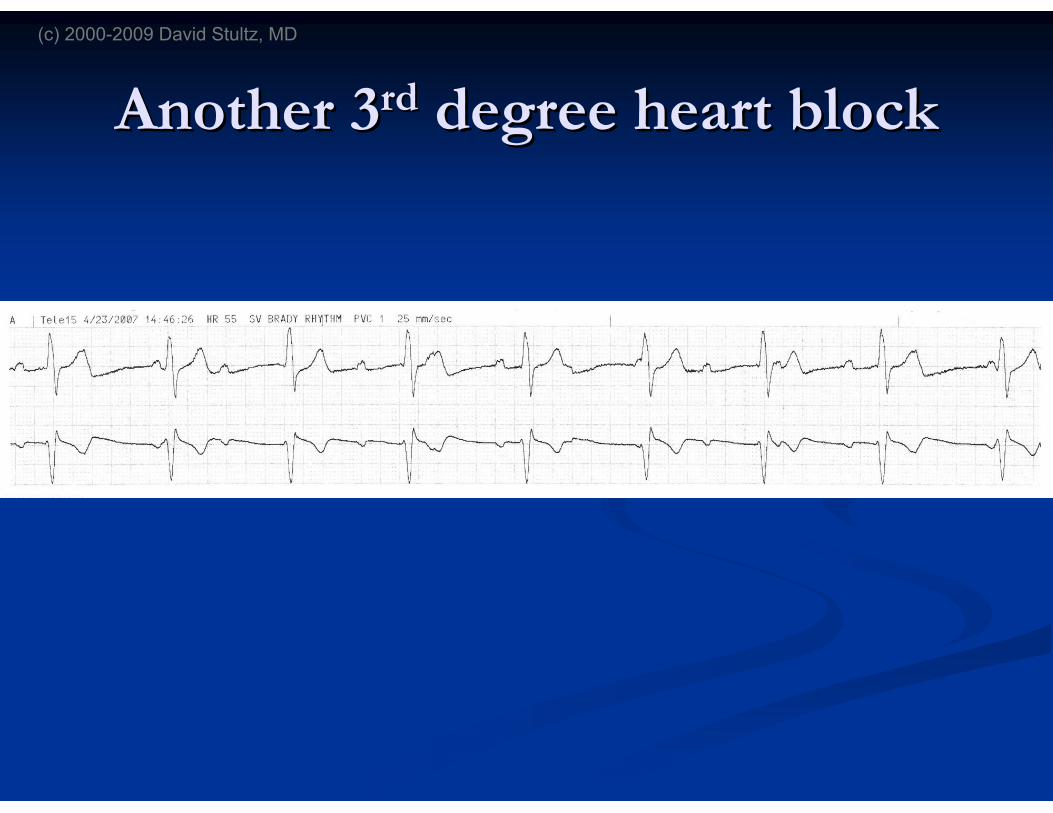
Another 3Another 3rdrd degree heart blockdegree heart block
(c) 2000-2009 David Stultz, MD
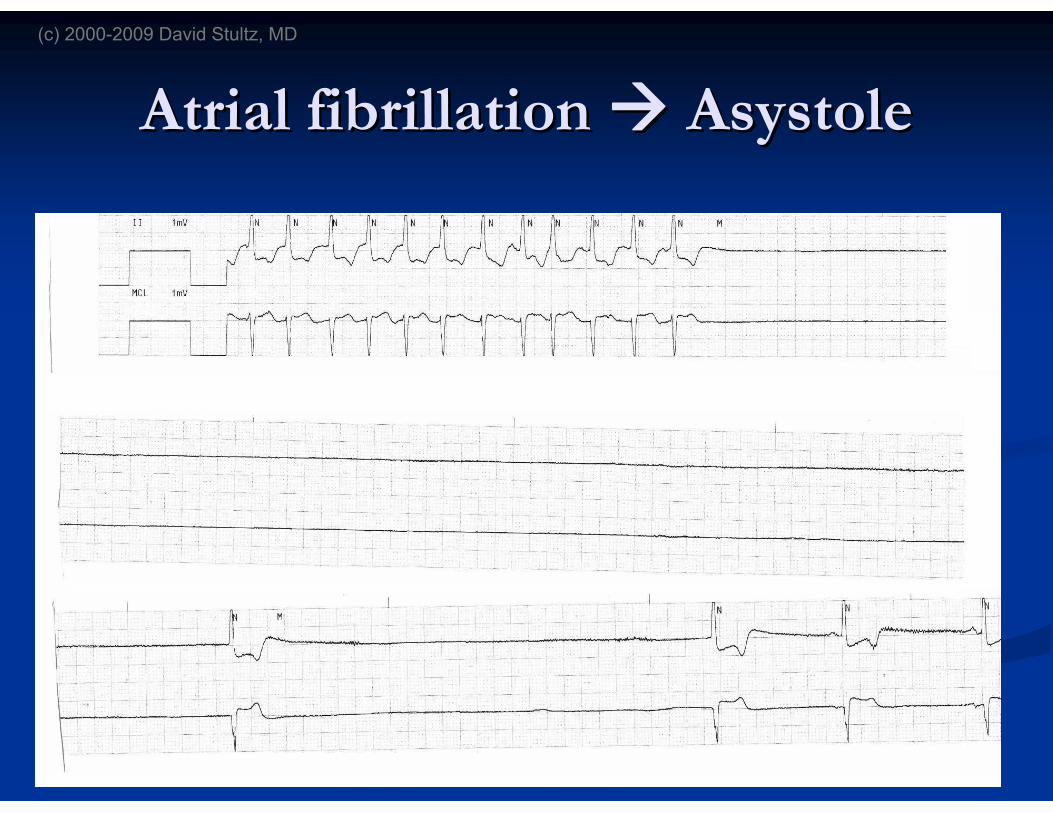
Atrial fibrillationAtrial fibrillation AsystoleAsystole
(c) 2000-2009 David Stultz, MD
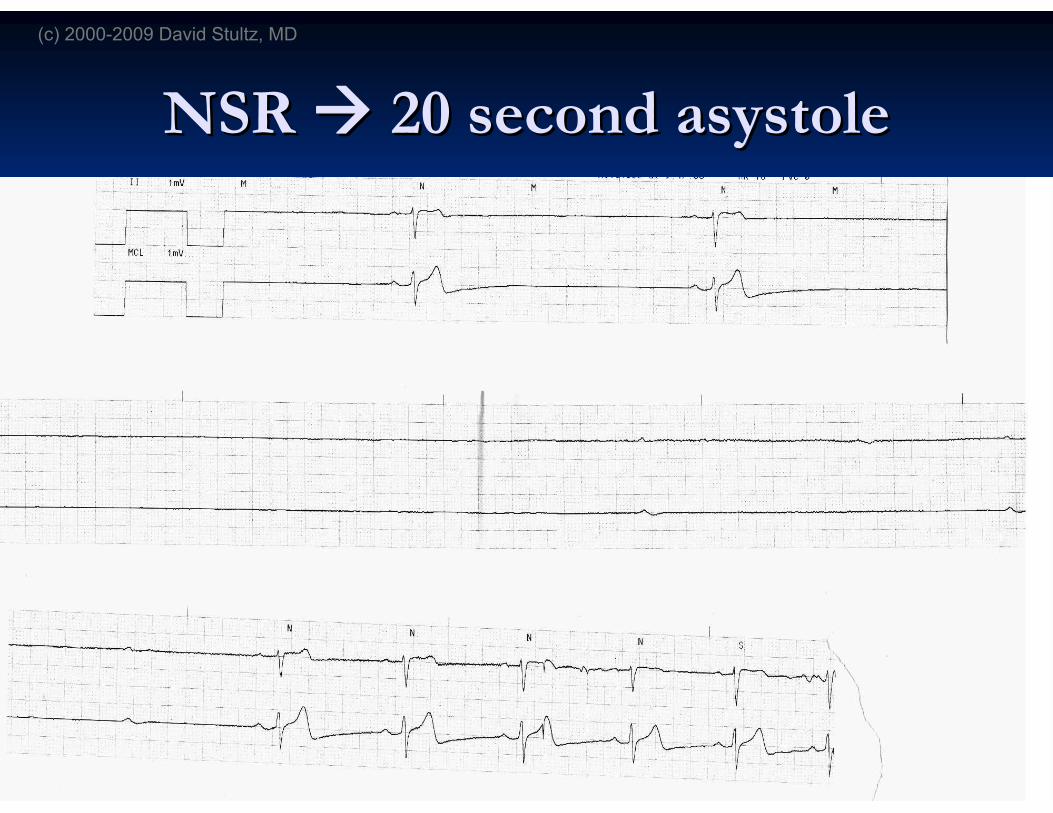
NSRNSR 20 second20 second asystoleasystole
(c) 2000-2009 David Stultz, MD
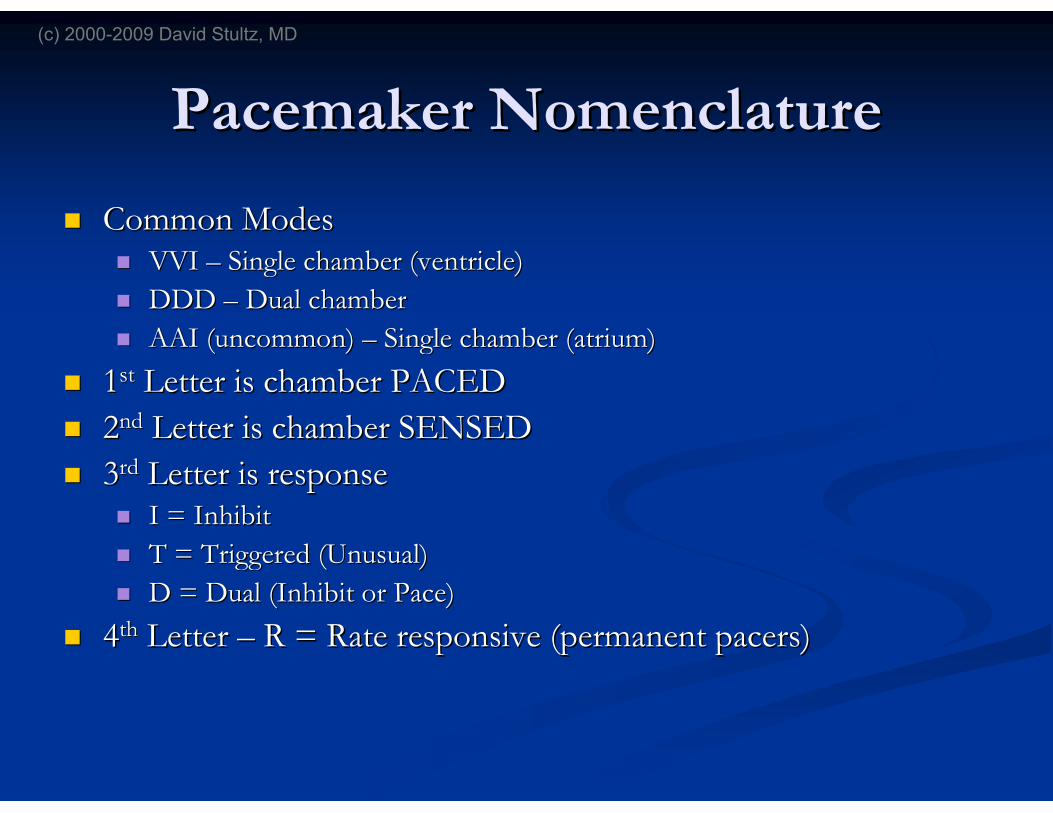
Pacemaker NomenclaturePacemaker Nomenclature
Common ModesCommon Modes VVIVVI –– Single chamber (ventricle)Single chamber (ventricle)
DDDDDD –– Dual chamberDual chamber
AAI (uncommon)AAI (uncommon) –– Single chamber (atrium)Single chamber (atrium)
11stst Letter is chamber PACEDLetter is chamber PACED
22ndnd Letter is chamber SENSEDLetter is chamber SENSED
33rdrd Letter is responseLetter is response I = InhibitI = Inhibit
T = Triggered (Unusual)T = Triggered (Unusual)
D = Dual (Inhibit or Pace)D = Dual (Inhibit or Pace)
44thth LetterLetter –– R = Rate responsive (permanent pacers)R = Rate responsive (permanent pacers)
(c) 2000-2009 David Stultz, MD
Components of a pacemaker systemComponents of a pacemaker system
LeadLead
Wire connects to heartWire connects to heart
PercutaneousPercutaneous
Ventricular wire sits in RV apexVentricular wire sits in RV apex
EpicardialEpicardial (post surgery)(post surgery)
http://www.oscor.com/images/lead%20pics/RU-STR-Polaris%20lead2%20copy.jpg
(c) 2000-2009 David Stultz, MD

The CanThe CanAKAAKA ““Pulse Generator,Pulse Generator,”” ““BatteryBattery””
http://upload.wikimedia.org/wikipedia/commons/thumb/b/b1/Pacemaker_GuidantMeridianSR.jpg/549px-Pacemaker_GuidantMeridianSR.jpg
http://www.staff.vu.edu.au/CriticalCare/Critical%20Care/Images%20_l1/spacer.gif
http://intensivecare.hsnet.nsw.gov.au/five/images/generator.jpg
Single chamber Dual chamberPermanent single chamber
Temporary
(c) 2000-2009 David Stultz, MD
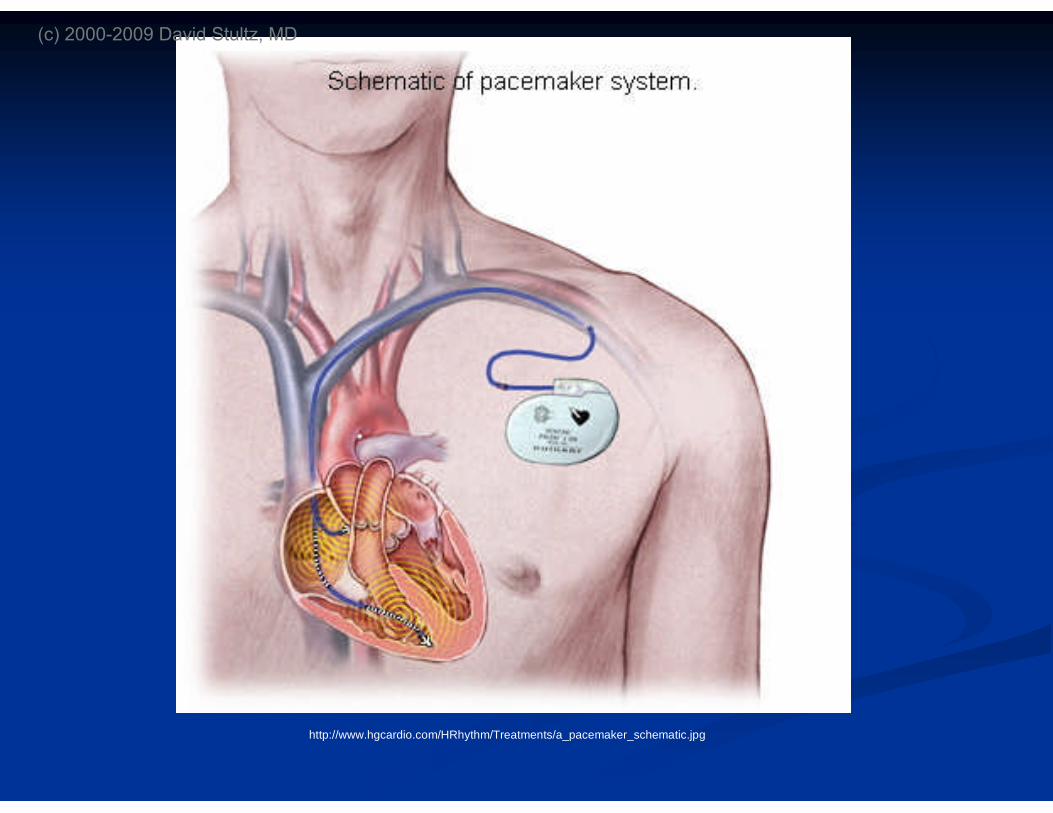
http://www.hgcardio.com/HRhythm/Treatments/a_pacemaker_schematic.jpg
(c) 2000-2009 David Stultz, MD
Sites of insertion for a temporarySites of insertion for a temporarypacemakerpacemaker
Right internal jugularRight internal jugular
LeftLeft subclaviansubclavian veinvein
RightRight subclaviansubclavian veinvein
Either femoral vein (Fluoroscopy required)Either femoral vein (Fluoroscopy required)
Left IJ is possible but very difficultLeft IJ is possible but very difficult
(c) 2000-2009 David Stultz, MD
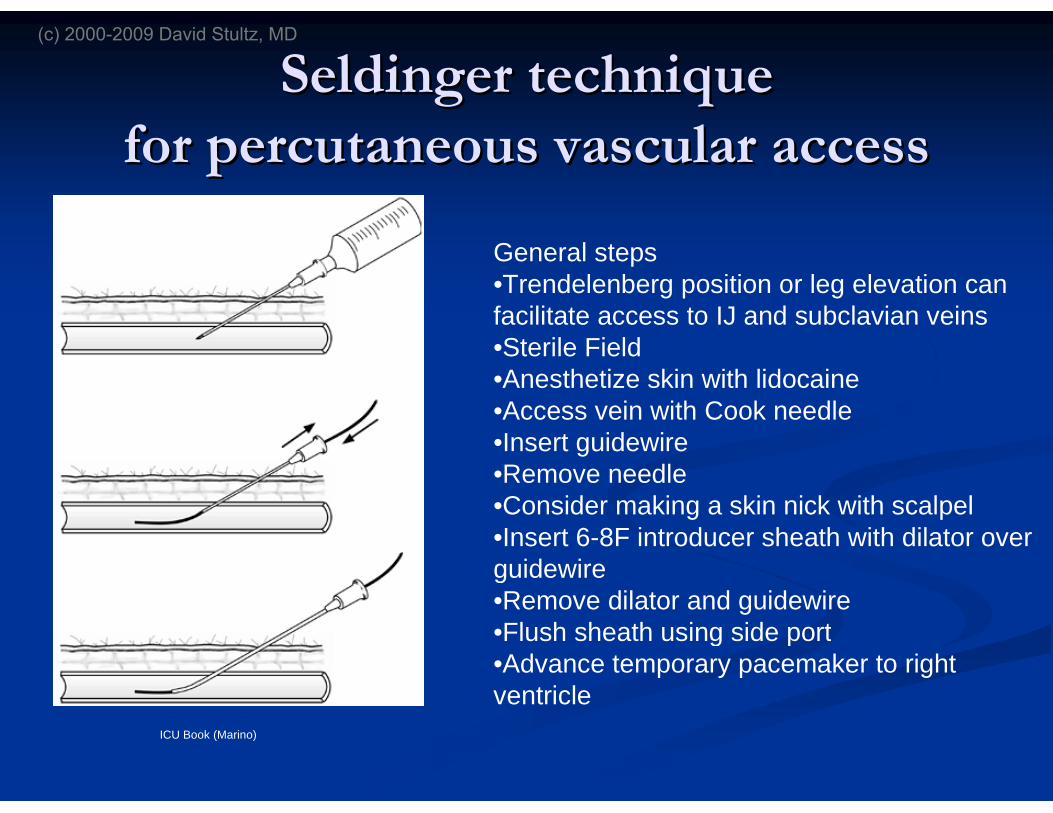
SeldingerSeldinger techniquetechniqueforfor percutaneouspercutaneous vascular accessvascular access
ICU Book (Marino)
General steps•Trendelenberg position or leg elevation canfacilitate access to IJ and subclavian veins•Sterile Field•Anesthetize skin with lidocaine•Access vein with Cook needle•Insert guidewire•Remove needle•Consider making a skin nick with scalpel•Insert 6-8F introducer sheath with dilator overguidewire•Remove dilator and guidewire•Flush sheath using side port•Advance temporary pacemaker to rightventricle
(c) 2000-2009 David Stultz, MD
Complications of temporaryComplications of temporarypacemaker insertionpacemaker insertion
Blood loss/Blood loss/hematomahematoma
InfectionInfection
Arrhythmia (especially during insertion)Arrhythmia (especially during insertion) PVCPVC’’s are commons are common
Heart blockHeart block Especially in patients with underlying LBBBEspecially in patients with underlying LBBB
Bundle branch blockBundle branch block
PneumothoraxPneumothorax (about 1+% when(about 1+% when subclaviansubclavian accessaccessused)used)
Cardiac perforationCardiac perforation TamponadeTamponade
(c) 2000-2009 David Stultz, MD
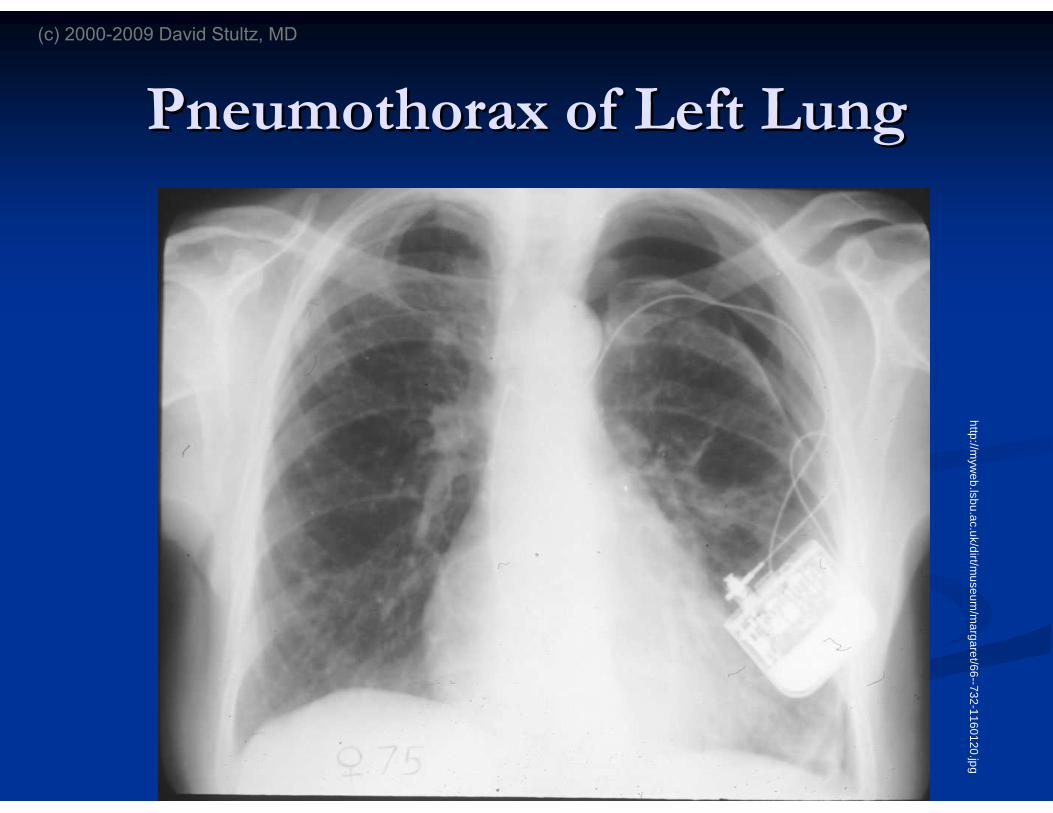
PneumothoraxPneumothorax of Left Lungof Left Lungh
ttp://m
ywe
b.ls
bu
.ac.u
k/d
irt/mu
se
um
/ma
rga
ret/6
6--7
32
-11
60
12
0.jp
g
(c) 2000-2009 David Stultz, MD
Functions of a pacemakerFunctions of a pacemaker
SensingSensing
The deviceThe device ‘‘seessees’’ a native heart beata native heart beat
PacingPacing
The device delivers a shock to stimulate a heart beatThe device delivers a shock to stimulate a heart beat
(c) 2000-2009 David Stultz, MD

VVI ExplainedVVI Explained
A VVI pacemakerA VVI pacemaker
Paces the ventriclePaces the ventricle
Senses the ventricleSenses the ventricle
In response to a sensed event it INHIBITS theIn response to a sensed event it INHIBITS thepacing responsepacing response
So if it doesnSo if it doesn’’t SENSE a native heart beat in a specifiedt SENSE a native heart beat in a specifiedperiod, it will deliver a pace.period, it will deliver a pace.
(c) 2000-2009 David Stultz, MD
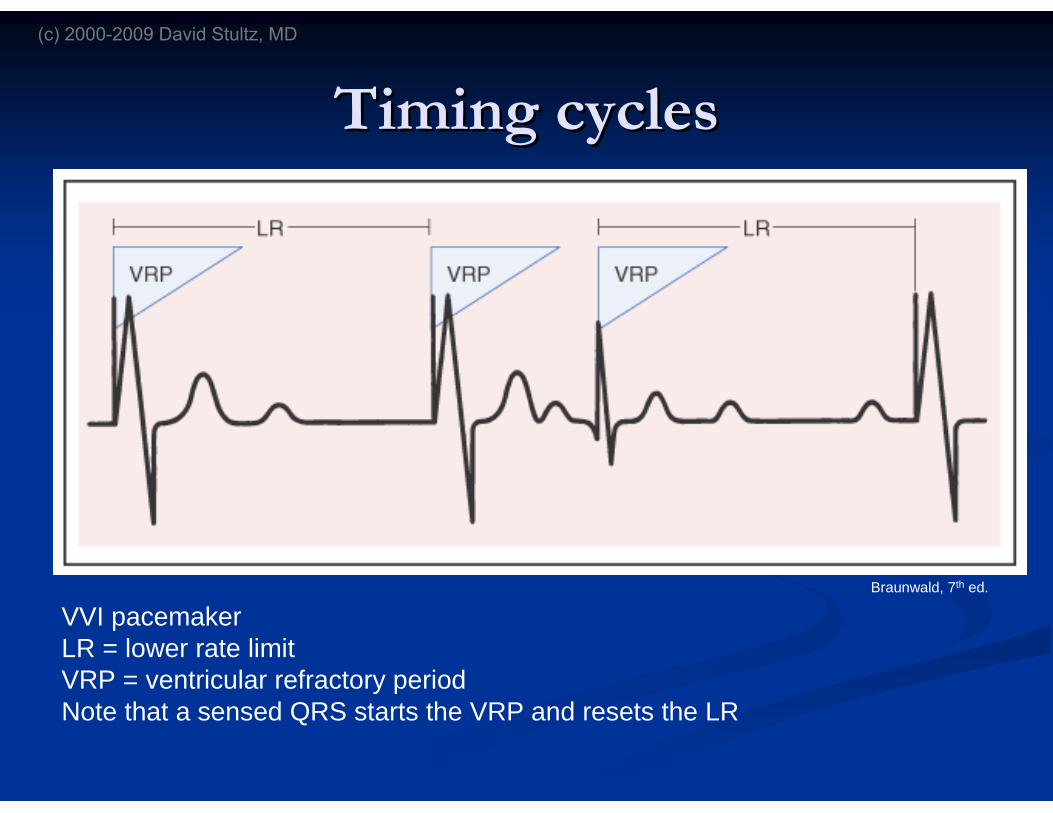
Timing cyclesTiming cycles
VVI pacemakerLR = lower rate limitVRP = ventricular refractory periodNote that a sensed QRS starts the VRP and resets the LR
Braunwald, 7th ed.
(c) 2000-2009 David Stultz, MD
The dials on the TemporaryThe dials on the Temporarypacemakerpacemaker
RateRate
Determines the lower rate limit of the deviceDetermines the lower rate limit of the device
Heart rate should not go lower than the set rateHeart rate should not go lower than the set rate
OutputOutput
In milliamps, the amount ofIn milliamps, the amount of ‘‘juicejuice’’ the devicethe deviceoutputs with each pacer spikeoutputs with each pacer spike
(c) 2000-2009 David Stultz, MD
SensitivitySensitivity
SensitivitySensitivity asynchronousasynchronous InIn millivoltsmillivolts, the amount of energy that has to be, the amount of energy that has to be
detected in order for the device todetected in order for the device to ‘‘sensesense’’ a beata beat
HigherHigher millivoltsmillivolts = less sensitive= less sensitive More likely for the pacemaker to pace at the lower rateMore likely for the pacemaker to pace at the lower rate
regardless of what the heart does on its ownregardless of what the heart does on its own
LowerLower millivoltsmillivolts = more sensitive= more sensitive More likely to pick up noise, andMore likely to pick up noise, and ‘‘sensesense’’ a ventricular beata ventricular beat
even though nothing actually happenedeven though nothing actually happened
(c) 2000-2009 David Stultz, MD
SensitivitySensitivity
http://www.univie.ac.at/cga/courses/BE513/EKG/qrs.gif
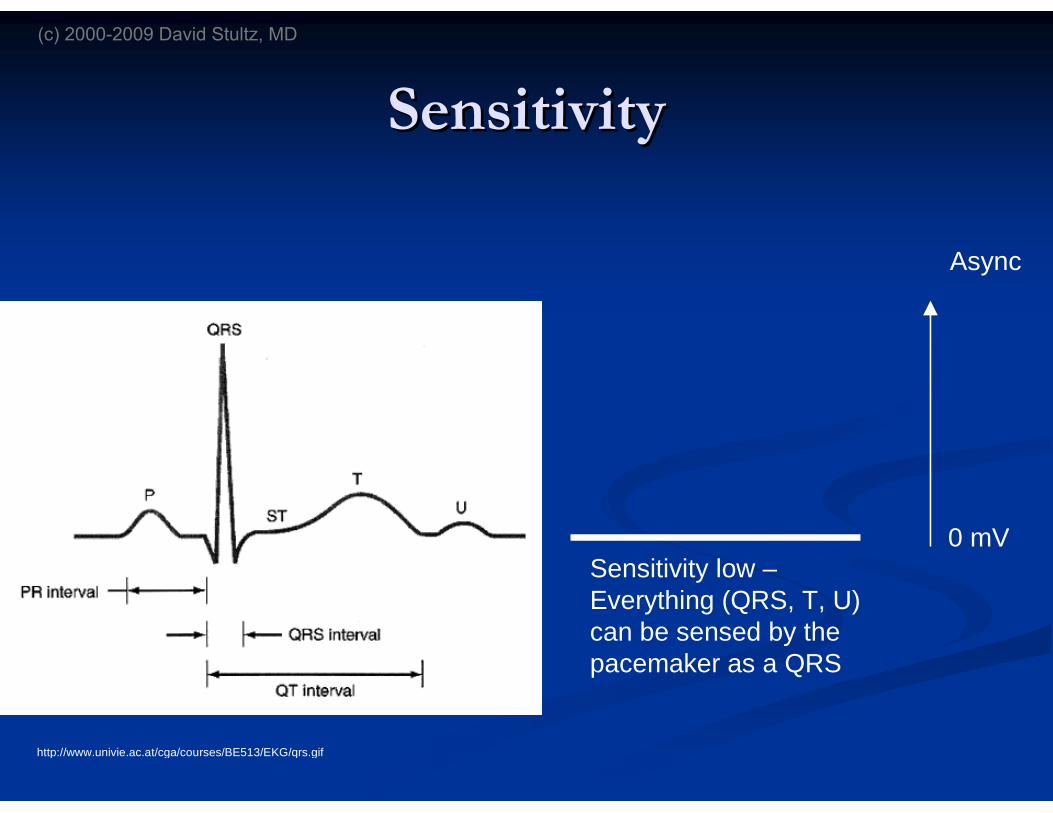
0 mV
Async
Sensitivity low –Everything (QRS, T, U)can be sensed by thepacemaker as a QRS
(c) 2000-2009 David Stultz, MD
SensitivitySensitivity
http://www.univie.ac.at/cga/courses/BE513/EKG/qrs.gif
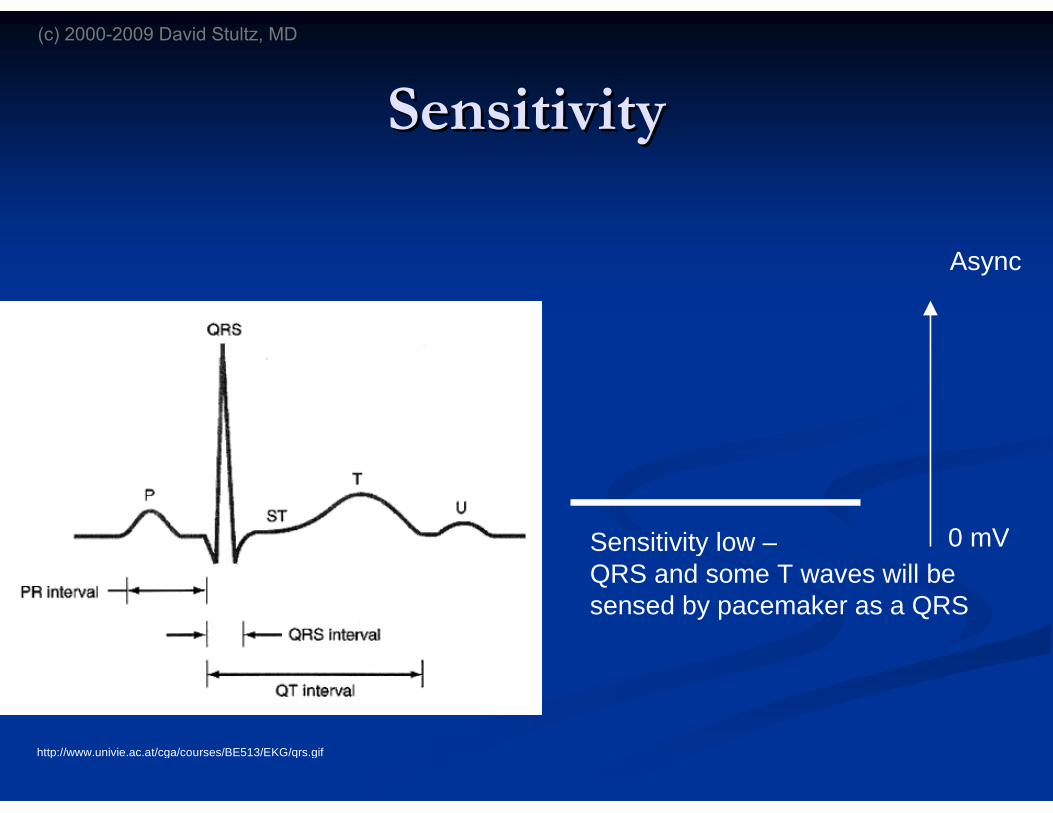
0 mV
Async
Sensitivity low –QRS and some T waves will besensed by pacemaker as a QRS
(c) 2000-2009 David Stultz, MD

SensitivitySensitivity
http://www.univie.ac.at/cga/courses/BE513/EKG/qrs.gif
0 mV
Async
Sensitivity just rightQRS will be sensed,T waves will not
(c) 2000-2009 David Stultz, MD

SensitivitySensitivity
http://www.univie.ac.at/cga/courses/BE513/EKG/qrs.gif
0 mV
Async
Sensitivity too highNothing will be sensed
(c) 2000-2009 David Stultz, MD

Testing thresholdsTesting thresholds
Output ThresholdOutput Threshold Set Sensitivity toSet Sensitivity to ‘‘asynchronousasynchronous’’
Set Rate just above the native heart rateSet Rate just above the native heart rate 6060--8080 bpmbpm
Start output at 5Start output at 5--1010 mAmA, and gradually turn down, and gradually turn downuntil ventricular capture is lostuntil ventricular capture is lost
The last point before losing capture is the thresholdThe last point before losing capture is the threshold
Pacemaker output should be set at 2Pacemaker output should be set at 2--3x the3x thethresholdthreshold
(c) 2000-2009 David Stultz, MD
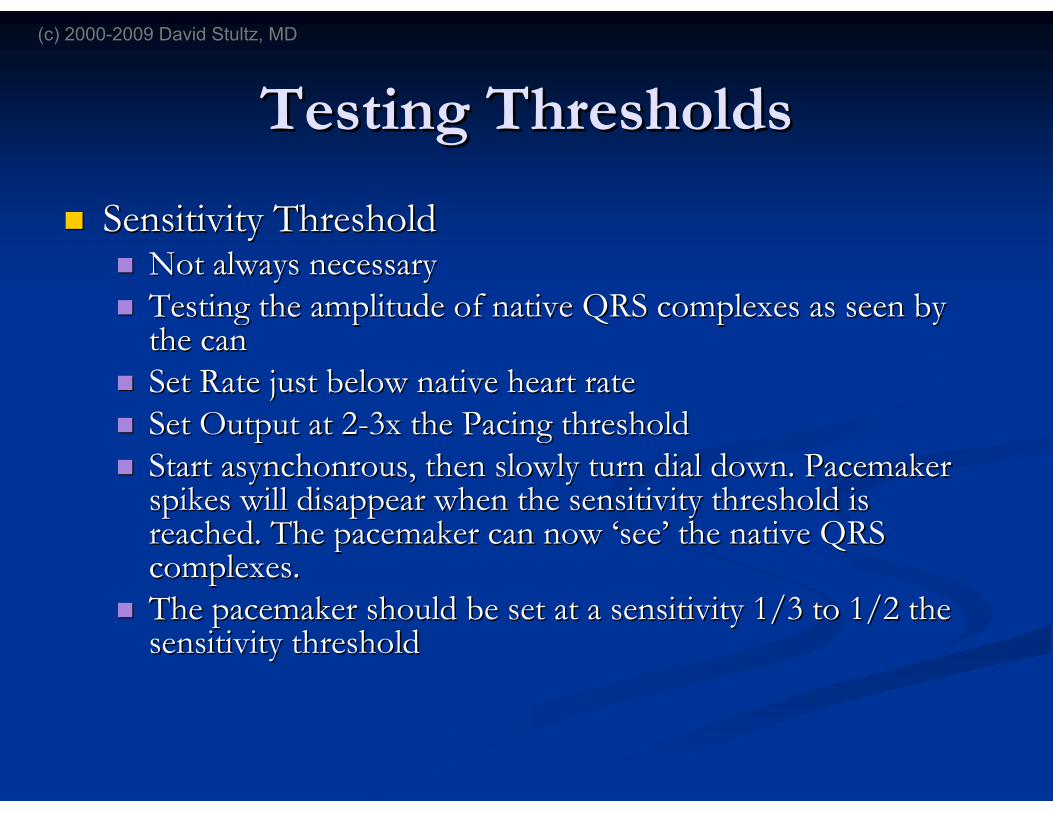
Testing ThresholdsTesting Thresholds
Sensitivity ThresholdSensitivity Threshold Not always necessaryNot always necessary Testing the amplitude of native QRS complexes as seen byTesting the amplitude of native QRS complexes as seen by
the canthe can Set Rate just below native heart rateSet Rate just below native heart rate Set Output at 2Set Output at 2--3x the Pacing threshold3x the Pacing threshold StartStart asynchonrousasynchonrous, then slowly turn dial down. Pacemaker, then slowly turn dial down. Pacemaker
spikes will disappear when the sensitivity threshold isspikes will disappear when the sensitivity threshold isreached. The pacemaker can nowreached. The pacemaker can now ‘‘seesee’’ the native QRSthe native QRScomplexes.complexes.
The pacemaker should be set at a sensitivity 1/3 to 1/2 theThe pacemaker should be set at a sensitivity 1/3 to 1/2 thesensitivity thresholdsensitivity threshold
(c) 2000-2009 David Stultz, MD
Troubleshooting PacemakersTroubleshooting Pacemakers
Normal behavior that looks strangeNormal behavior that looks strange
Failure to CaptureFailure to Capture
UndersensingUndersensing
OversensingOversensing
Cross Talk (Dual Chamber only)Cross Talk (Dual Chamber only)
(c) 2000-2009 David Stultz, MD
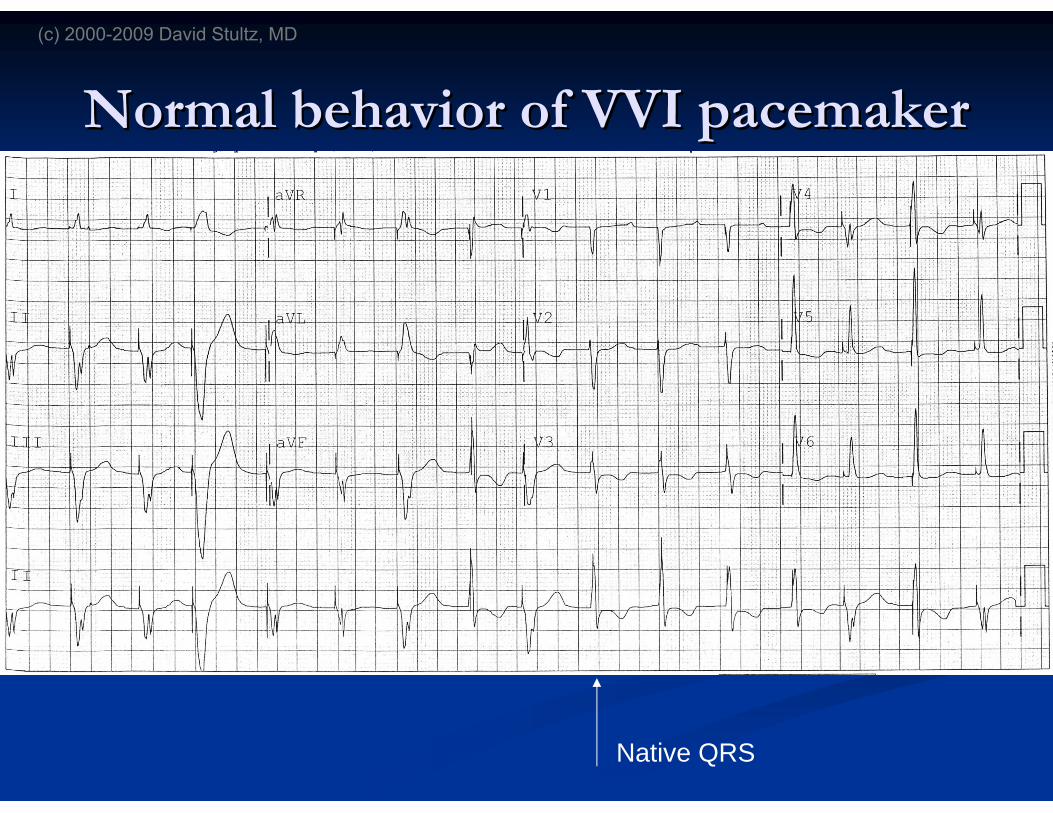
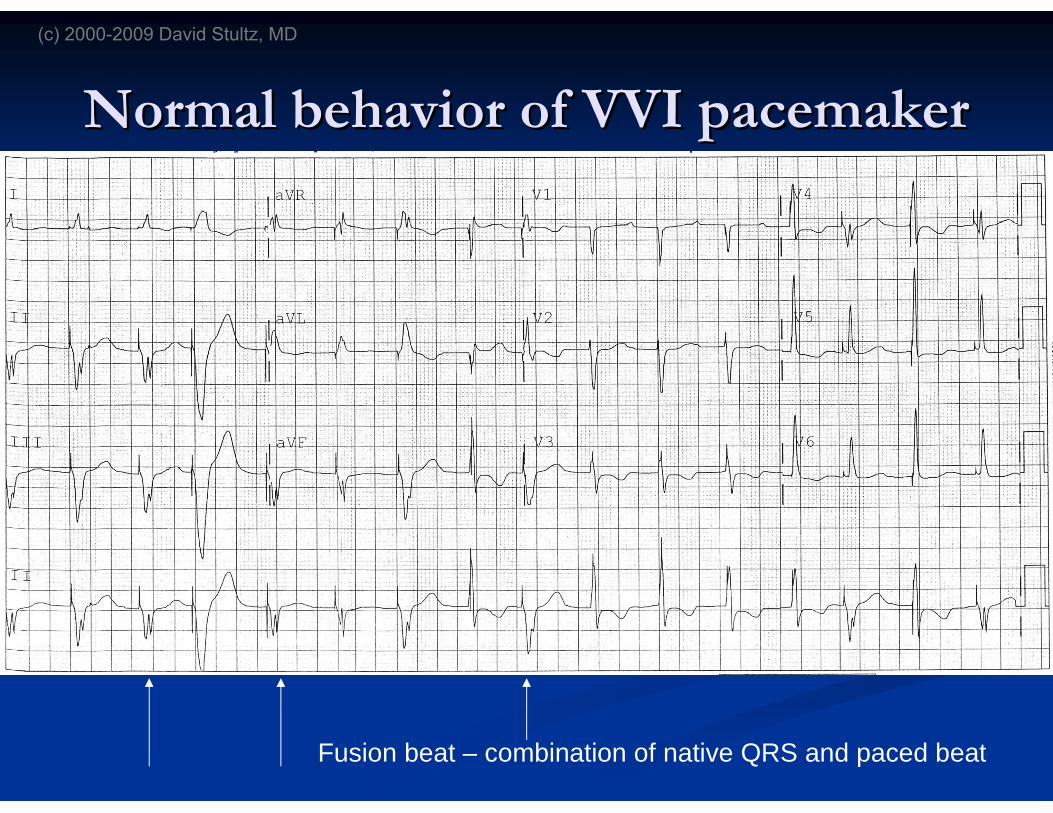
Normal behavior of VVI pacemakerNormal behavior of VVI pacemaker
Native QRS
(c) 2000-2009 David Stultz, MD
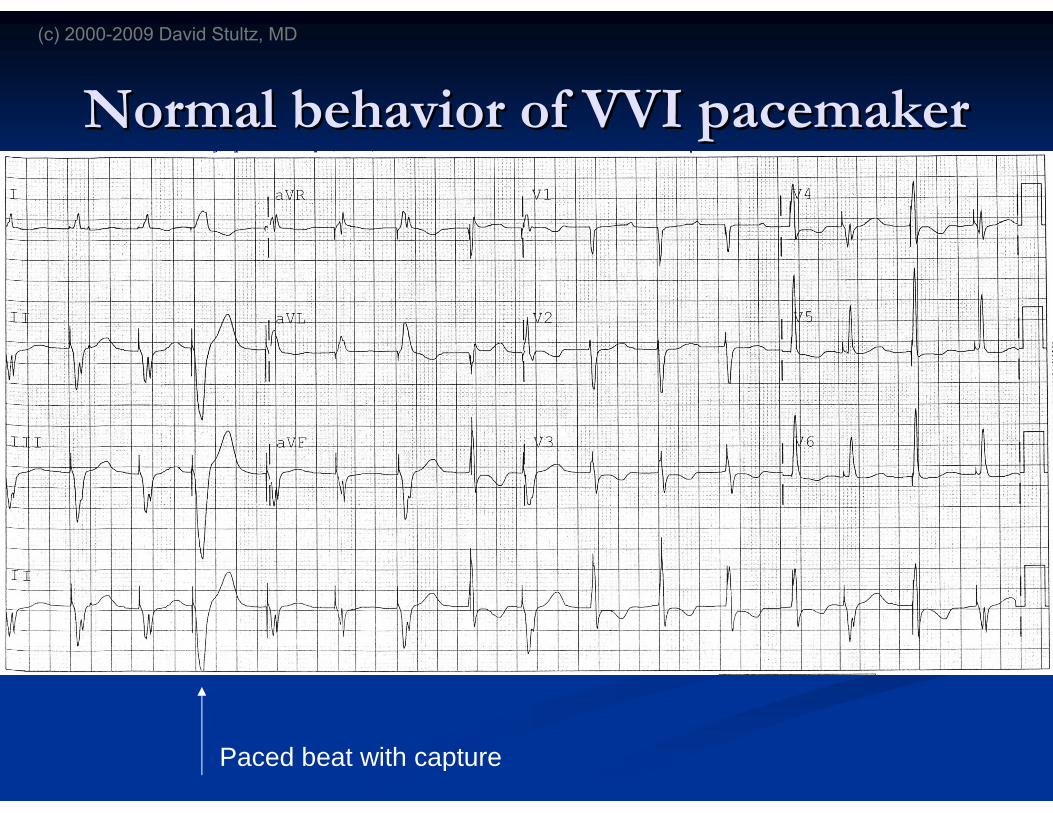
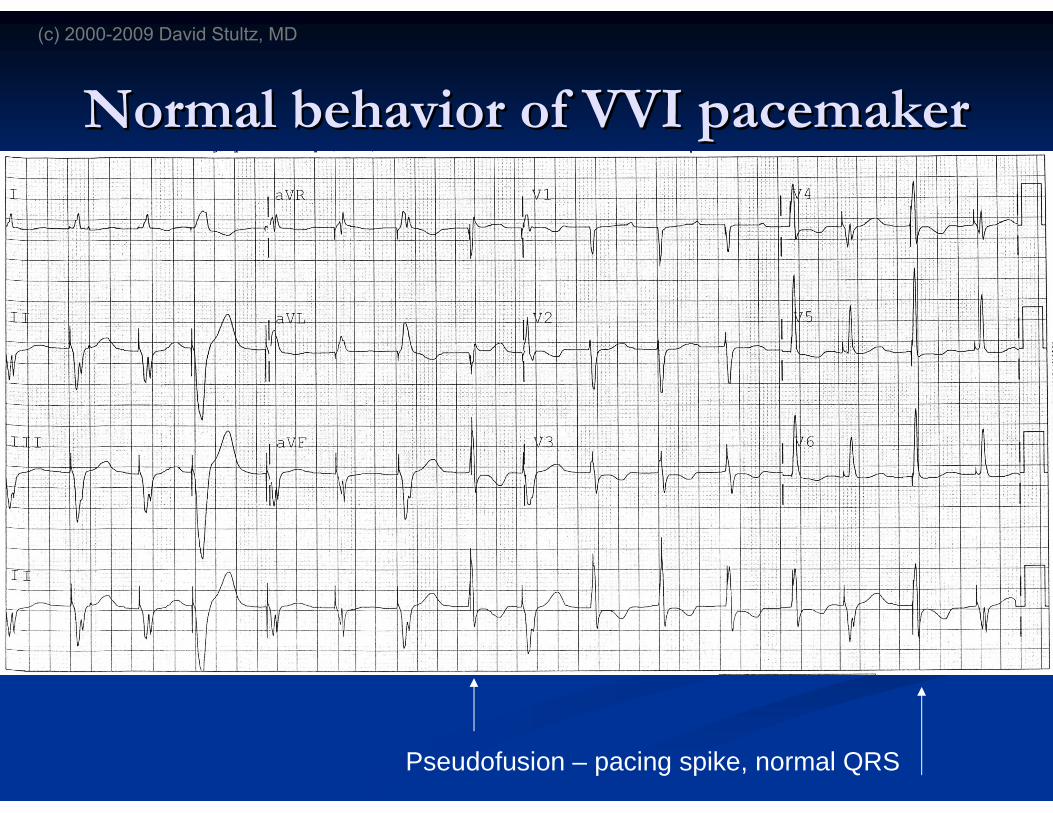
Normal behavior of VVI pacemakerNormal behavior of VVI pacemaker
Paced beat with capture
(c) 2000-2009 David Stultz, MD
Normal behavior of VVI pacemakerNormal behavior of VVI pacemaker
Fusion beat – combination of native QRS and paced beat
(c) 2000-2009 David Stultz, MD
Normal behavior of VVI pacemakerNormal behavior of VVI pacemaker
Pseudofusion – pacing spike, normal QRS
(c) 2000-2009 David Stultz, MD
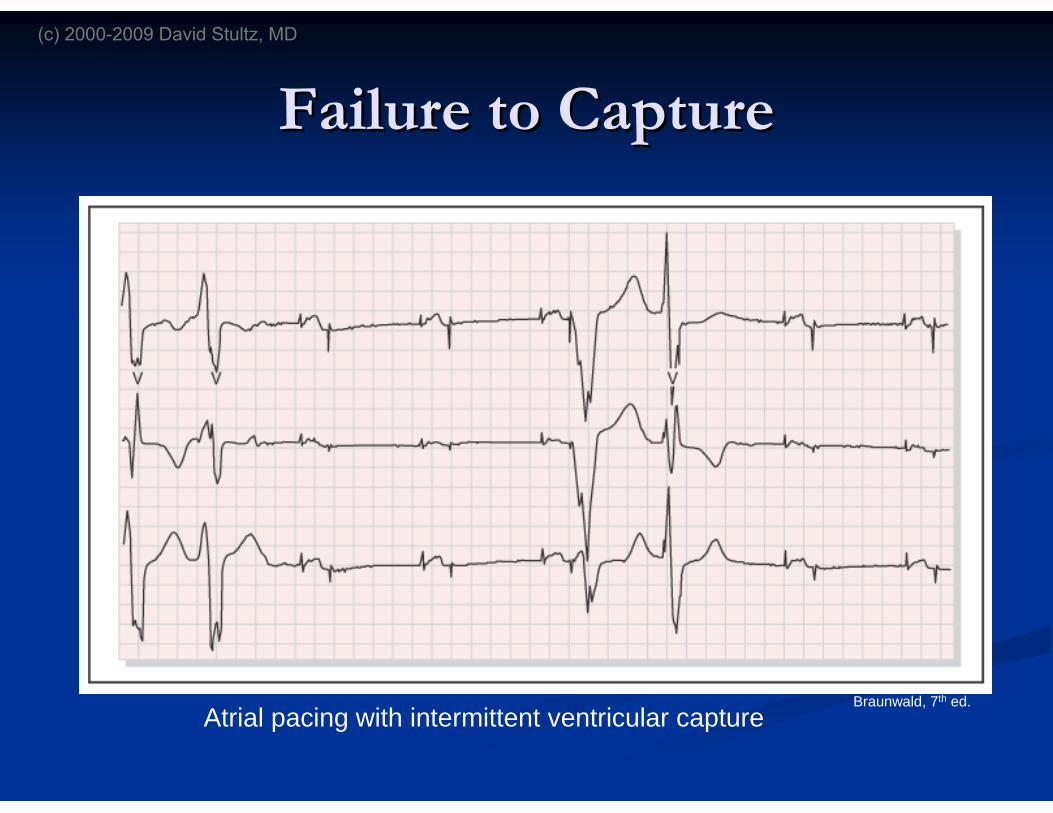
Failure to CaptureFailure to Capture
Atrial pacing with intermittent ventricular captureBraunwald, 7th ed.
(c) 2000-2009 David Stultz, MD
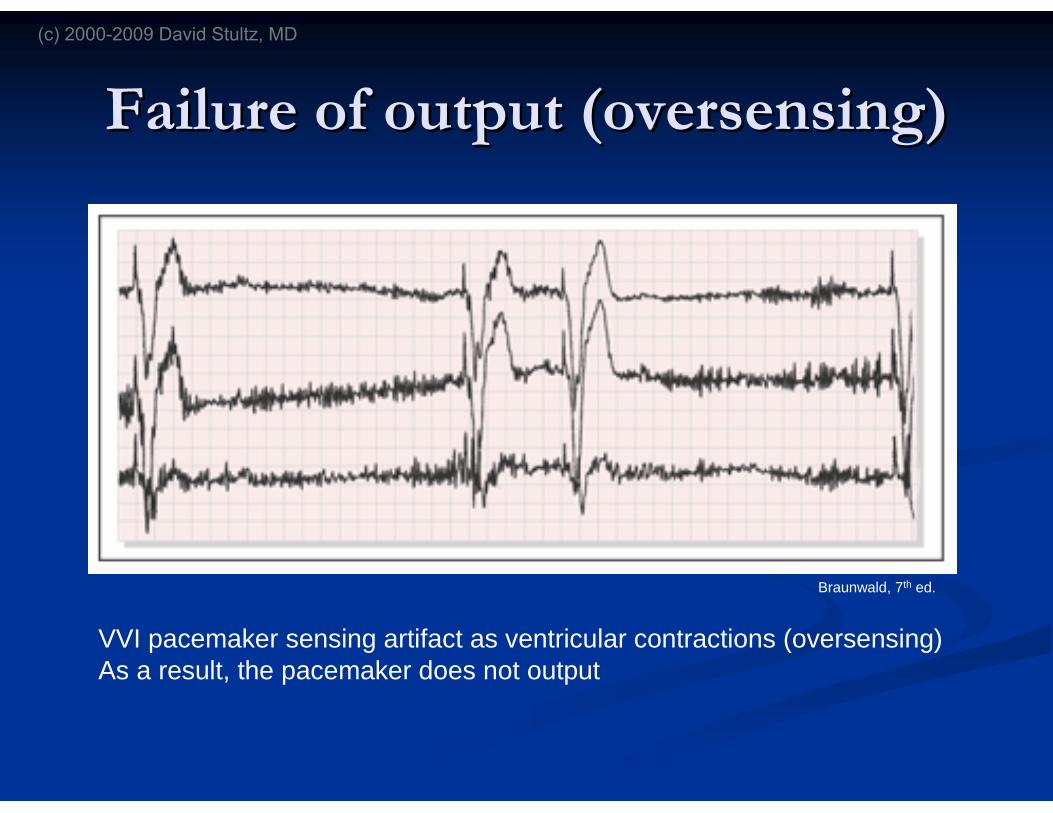
Failure of output (Failure of output (oversensingoversensing))
VVI pacemaker sensing artifact as ventricular contractions (oversensing)As a result, the pacemaker does not output
Braunwald, 7th ed.
(c) 2000-2009 David Stultz, MD
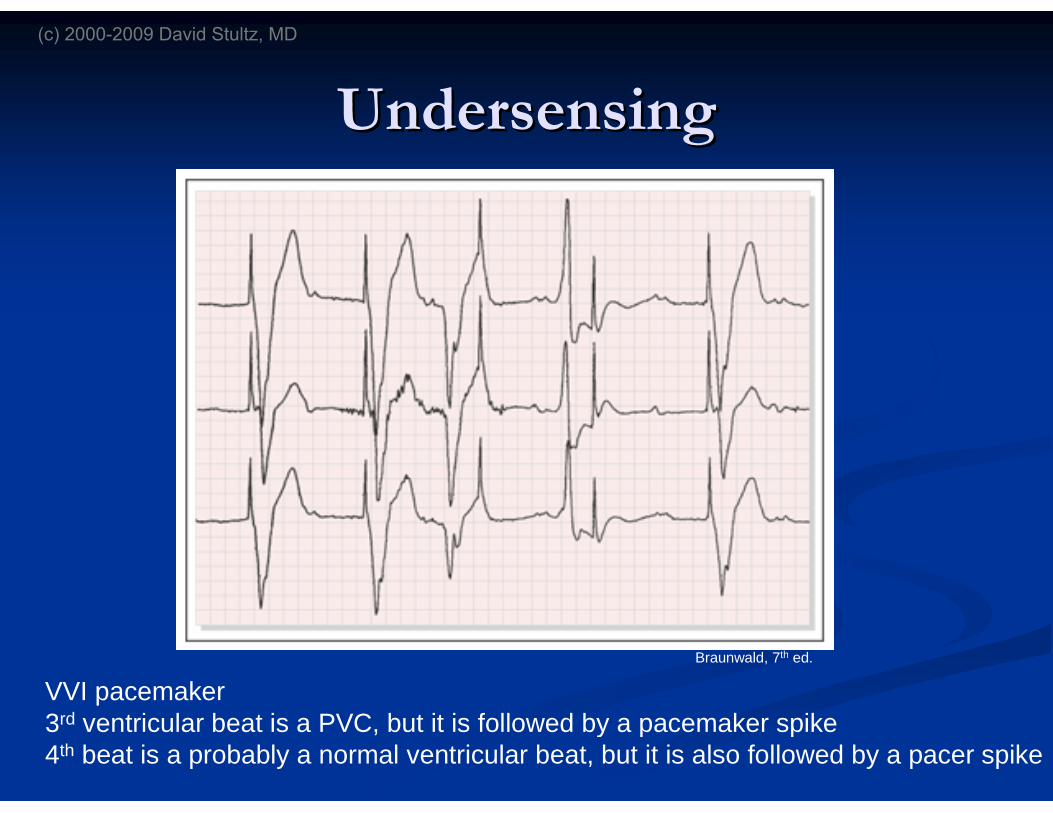
UndersensingUndersensing
VVI pacemaker3rd ventricular beat is a PVC, but it is followed by a pacemaker spike4th beat is a probably a normal ventricular beat, but it is also followed by a pacer spike
Braunwald, 7th ed.
(c) 2000-2009 David Stultz, MD
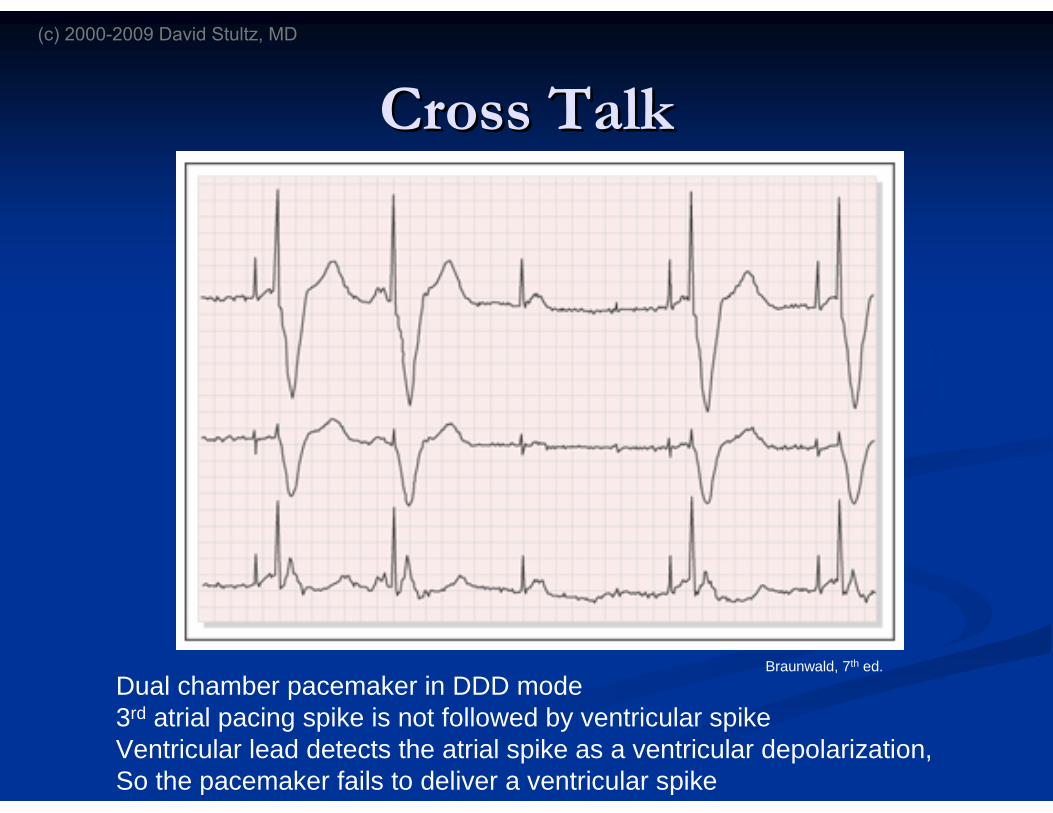
Cross TalkCross Talk
Dual chamber pacemaker in DDD mode3rd atrial pacing spike is not followed by ventricular spikeVentricular lead detects the atrial spike as a ventricular depolarization,So the pacemaker fails to deliver a ventricular spike
Braunwald, 7th ed.
(c) 2000-2009 David Stultz, MD
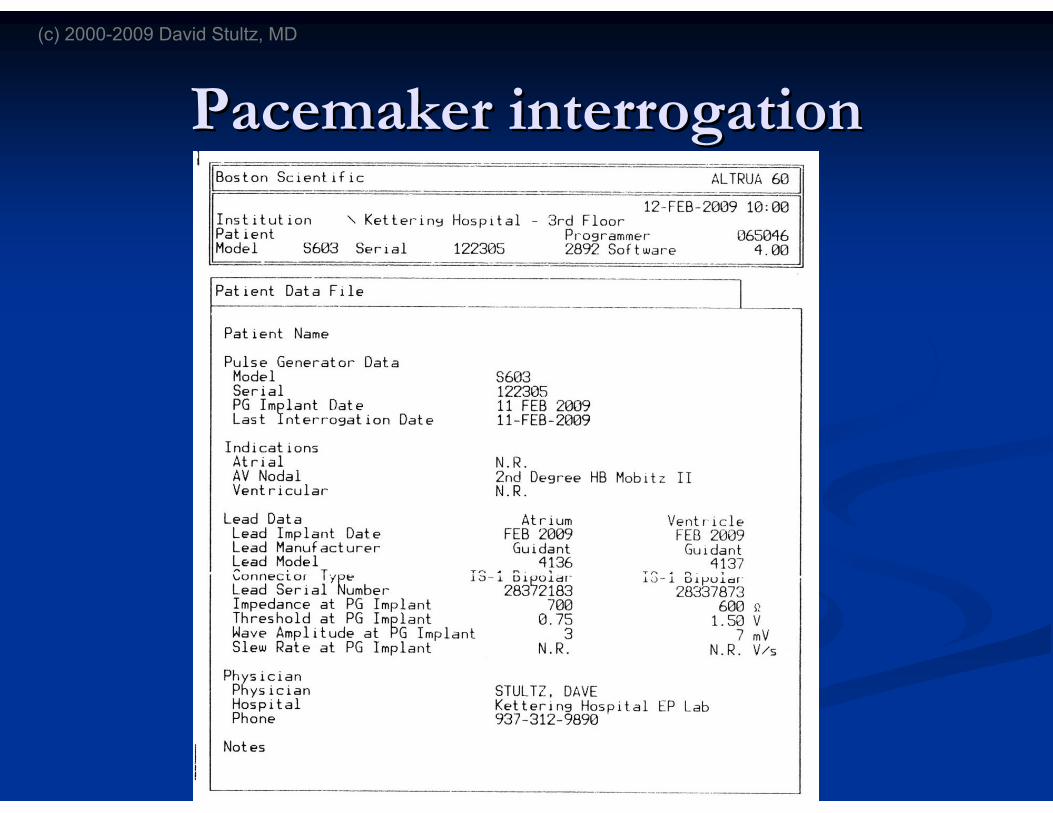
Pacemaker interrogationPacemaker interrogation
(c) 2000-2009 David Stultz, MD
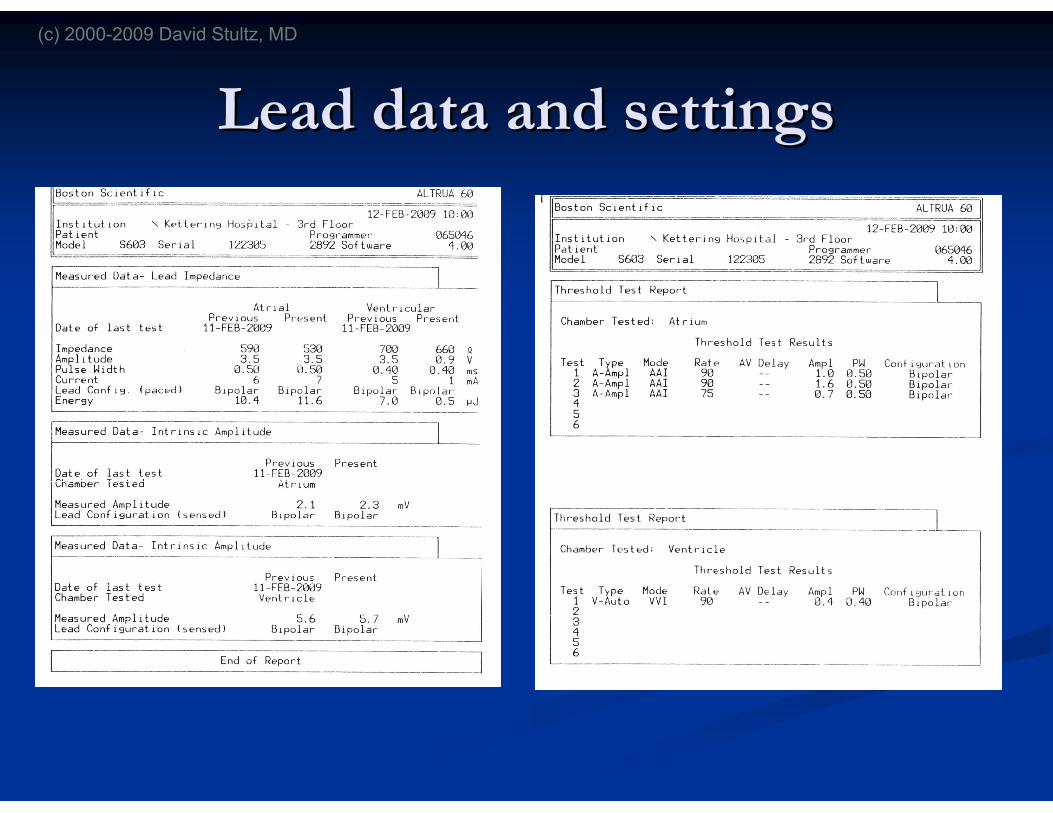
Lead data and settingsLead data and settings
(c) 2000-2009 David Stultz, MD
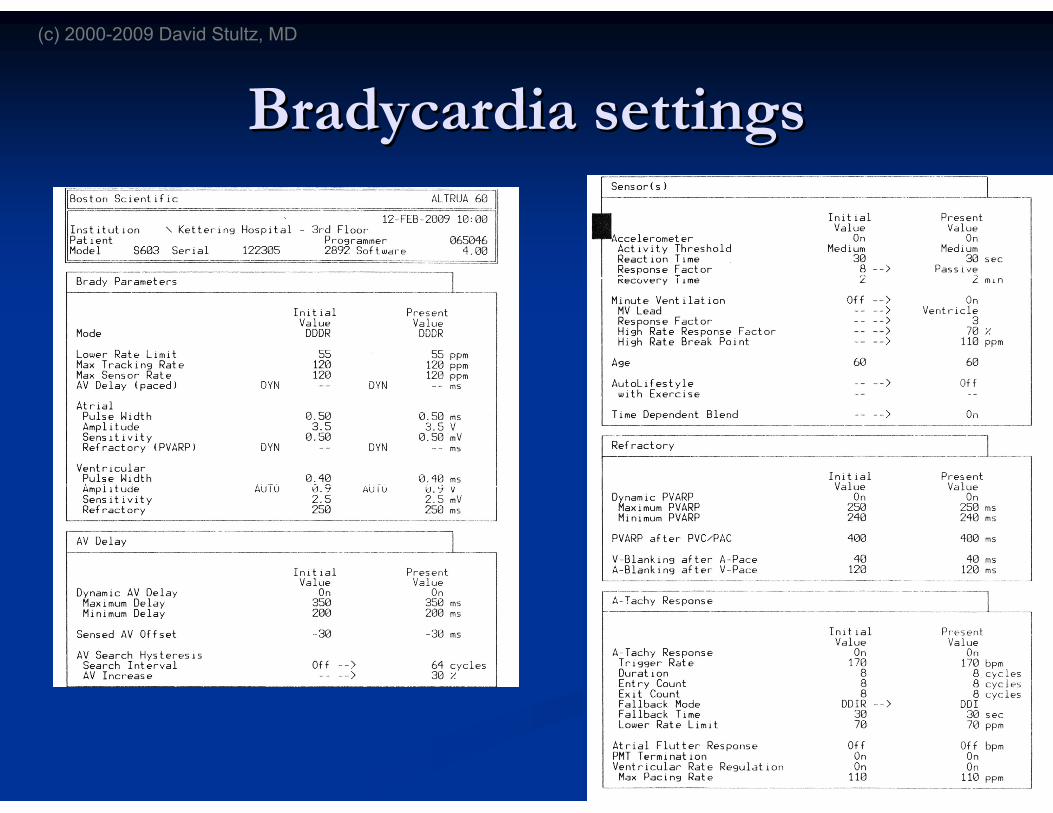
BradycardiaBradycardia settingssettings
(c) 2000-2009 David Stultz, MD
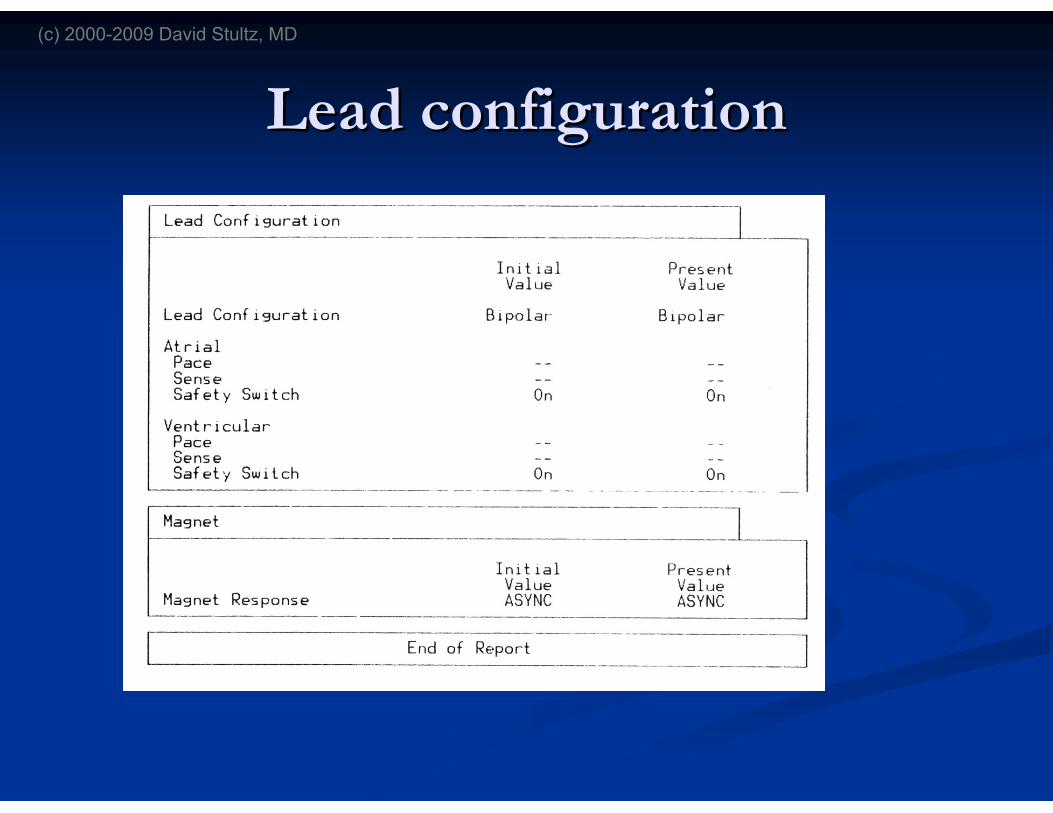
Lead configurationLead configuration
(c) 2000-2009 David Stultz, MD







