
Intracranial Fetus-in-Fetu: CT Diagnosis
Su-Tso Yang 1•2 and Siaw-Wong Leow 1
Summary: The authors present a case of fetus-in-fetu in which
the CT findings are compatible with an earlier description by
Nocera et al., i.e., a "round or tubular collection of very low
density fat surrounding a central bony structure (probably one
of the legs)." Additionally, sonography showed a heterogeneous
mass with limb-like structures in the left lateral ventricle. Plain
films can confirm the presence of a vertebral column and identify
specific bony structures, but CT is a valuable aid in cases where
plain films were not obtained or are inconclusive.
Index terms: Fetus, abnormalities and anomalies; Fetus, com
puted tomography
Fetus-in-fetu is a rare pathologic condition that involves the incomplete twinning of monozygotic twins at the primitive stage when axial development begins (1-3). It is mostly situated in the upper retroperitoneum (4, 5); however, in the case reported here, it was intracranial in location. The preoperative diagnosis of intracranial fetusin-fetu is usually not established accurately (1, 6), due to its extremely low incidence and confusion with teratoma. We report a case in which the retrospective CT findings are compatible with Nocera et al's suggestion for preoperative CT diagnosis (7) .
Case Report
A 2-month-old Taiwanese girl was admitted to our hospital with the chief complaint of progressive enlargement of the head size over a 1-month period . There had been a normal pregnancy and delivery (Cesarean section) ; however, the head size was large at birth.
On admission, the patient 's growth and development were compatible with her age. The head girth was 49 em, which is outside the 97 percentile on the head size/age curve. Physical examination revealed a bulging anterior fontanelle and sunset eyes. Laboratory data including the measurement of alpha-fetoprotein (AFP) level (28.71 IU/
ml, normal range for 2-month-old infants: <45 IU/ mL) were all within normal limits. The sonographic findings were noncommunicating hydrocephalus and a heterogeneous mass with limb-like structures in the left lateral ventricle (Fig. 1 ).
Computed tomography (CT) of the brain without contrast enhancement demonstrated an oval heterogeneous mass with mixed densities of soft tissues, calcification, and fat ; the mass was about 4 X 5 em and arose from the pineal region (Fig. 2A), extended into the occipital horn of the left lateral ventricle , and was surrounded by a wellformed capsule. Compression of the cerebra l aqueduct resulted in severe obstructive hydrocephalus. The preoperative diagnosis was teratoma of the pineal gland.
A left transoccipital surgical approach was used, and a
Fig. 1. Sonography shows a heterogeneous mass with limblike structures in the left lateral ventricle.
Received September 6, 1991 ; accepted and revision requested October 22; revision received January 23, 1992. 1 Department of Radiology, China Medical College Hospital, Taiwan, Republic of China. 2 Address reprint requests to Su-Tso Yang, Department of Radiology , China Medical College Hospita l, 75 Yute Road , Taichung, Ta iwan, Republic of
China.
AJNR 13:1326-1329, Sep/ Oct 1992 0 195-6108/ 92/ 1305-1 326 © American Society of Neuroradiology
1326
AJNR: 13, September /October 1992
A 8
6
I I ·If !:11
3 4
FETUS-IN-FETU 1327
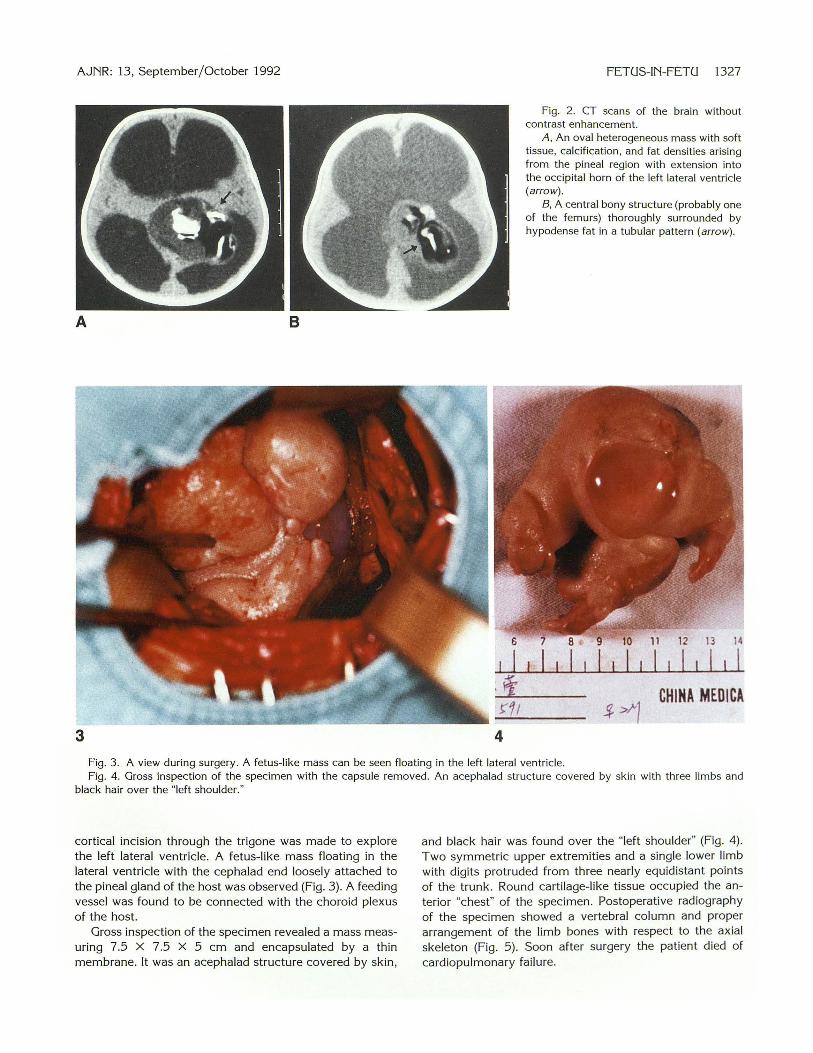
Fig. 2. CT scans of the brain without contrast enhancement.
A, An oval heterogeneous mass with soft tissue, calcification , and fat densities arising from the pineal region with extension into the occipital horn of the left lateral ventricle (arrow).
8, A central bony structure (probably one of the femurs) thoroughly surrounded by hypodense fat in a tubular pattern (arrow).
13 14
I I $>1 CHINA MEDICA
Fig. 3 . . A view during surgery. A fetus-like mass can be seen floating in the left lateral ventricle. Fig . 4. Gross inspection of the specimen with the capsule removed. An acephalad structure covered by skin with three limbs and
black hair over the "left shoulder."
cortical incision through the trigone was made to explore the left lateral ventricle . A fetus-like. mass floating in the lateral ventricle with the cephalad end loosely attached to the pineal gland of the host was observed (Fig. 3) . A feeding vessel was found to be connected with the choroid plexus of the host.
Gross inspection of the specimen revealed a mass measuring 7.5 X 7.5 X 5 em and encapsulated by a thin membrane. It was an acephalad structure covered by skin,
and black hair was found over the "left shoulder" (Fig. 4). Two symmetric upper extremities and a single lower limb with digits protruded from three nearly equidistant points of the trunk. Round cartilage-like tissue occupied the anterior "chest" of the specimen. Postoperative radiography of the specimen showed a vertebral column and proper arrangement of the limb bones with respect to the axial skeleton (Fig. 5). Soon after surgery the patient died of cardiopulmonary failure.

1328 YANG
Discussion
Intracranial fetus-in-fetu is usually not diagnosed preoperatively ( 1, 6) . One reason for misdiagnosis is its extremely low incidence as compared with intracranial teratoma (8, 9). Less than 1 00 cases of fetus-in-fetu have been reported in the literature, and only two of them were intracranial in location (1, 6). Another reason related to the differential features between fetus-in-fetu and teratoma. Because fetus-in-fetu develops through the stage of primitive streak and somite ( 1, 1 0) , the presence of a vertebral column is an essential criterion (11) . Other supportive diagnostic features are the formations of limbs and internal organs. Fetus-in-fetu increases in sizes, which may cause local mass effect and hemorrhage (12) . On the contrary, teratoma is a true tumor, which does not have vertebral development and formations of limbs and internal organs. Because it has potential for malignant transformation , the clinical manifestations are diverse.
A third reason for misdiagnosis is that no laboratory test is available to clearly differentiate teratoma from fetus-in-fetu . Although AFP elevation has been shown to be extremely high in malignant teratomas, elevated values were seen in about half of immature teratomas and less than 6 % of mature teratomas (13 , 14). Reviewing the
Fig. 5. Postoperative radiograph of the specimen. A vertebral column (arrow) and proper arrangement of limb bones with respect to the axial skeleton.
AJNR: 13, September / October 1992
literature of fetus-in-fetu, only one case specified the measurement of AFP, and its result was within normal limits (4). The AFP level in our case was also within normal range. Thus, while the detection of elevated serum AFP level is diagnostic of malignant teratomas (15), its negativity is not specific for fetus-in-fetu because of other possibilities such as mature and immature teratomas.
According to Knox and Webb, the plain radiograph is valuable in making the definitive diagnosis (16) because a vertebral column and/or specific bony structures can be identified; however, their statement was made without the benefit of CT. In cases where plain films are omitted or do not outline the presence of a vertebral column and/or specific bony structures, CT can be a valuable aid. Because the vertebral column may not be clearly demonstrated in the usual 8-mm thick section, Nocera et a!' s feature of "a round or tubular collection of very low density fat surrounding a central bony structure (probably one of the legs)" (7) would be a Valuable preoperative sign. Retrospective study of our CT scans supports his opinion. In our case, the "central bony structure" is probably one of the femurs . It is thoroughly surrounded by hypodense fat in a tubular pattern (Fig. 2B).
Therefore, the preoperative CT diagnosis depends mainly on limb formation, while on plain films one searches for the presence of a vertebral column and specific bony structures.
References 1. Afahar F, King TT, Berry CL. Intraventricular fetus-in-fetu . J Neuro
surg 1982;56:845-849 2. Martinez-Urrutia MJ, Pereira PL, Lassaletta L , Gracia R, Utrilla J.
Abdominal mass: "Fetus in fetu." Acta Paediatr Scand 1990;79:121 -122
3. George V, Meera K . Tripta D. Fetus in fetu. J Pediatr Surg
1983; 18:288-289 4. Eng HL, Chuang JH, Lee TV, Chen WJ. Fetus in fetu : a case report
and rev iew of the literature. J Pediatr Surg 1989;24:296-299 5. Sutthiwan P, Sutthiwan I, Tree-trakan T. Fetus in fetu. J Pediatr Surg
1983; 18:290- 292 6. Kimmel DL, Moyer EK, Peale AR , et al. A cerebral tumor containing
five human fetuses: a case of fetus in fetu. Anat Rec 1950;106:141-158
7. Nocera RM, Davis M, Hayden CK, Schwartz M, Swischuk LE. Fetus
in-fetu. AJR 1982; 138:762-764 8. Ventureyra ECG, Herder S. Neonatal intracranial teratoma . J Neuro
surg 1983;59:879-883 9. Lipman SP, Pretorius DH, Rumack CM , Manco-Johnson ML. Fetal
intracranial teratoma: US diagnosis of three cases and a review of the
literature. Radiology 1985;157:491-494 10. Will is RA. The borderland of embryology and pathology. London:
Butterworth , 1958:1 47

AJNR: 13, September / October 1992
11 . Tada S, Yasukochi H, Ohtaki C, Fukuta A , Takanashi R. Fetus in
fetu. Br J Radio/1 974;47: 146-148
12. Lamabadusuriya SP, Soysa PE, Walpita PR. A case of fetus in fetu.
Arch Dis Child 1972;47:305
13. Tsuchida Y, Hasegawa H. The diagnostic value of alpha-fetoprotein
in infants and children with teratomas: a questionnaire survey in
Japan. J Pediatr Surg 1983; 18:153-155
FETUS-IN-FETU 1329
14. Bi llmire DF, Grosfeld JL. Teratomas in childhood: analysis of 142
cases. J Pediatr Surg 1986;2 1 :548-551
15. Takeuchi J , Handa H, Oda Y, Uchida Y. A lpha-fetoprotein in intracra
nial malignant teratoma. Surg Neuro/1 979; 12:400-403
16. Knox AJS, Webb AJ. The clinical featu res and trea tment of fetus in
fetu: two case reports and a review of the literature. J Pediatr Surg
1975; 10:483-489







