
RANDOLPH S. MARSHALL
I N T E R P R E T A T I O N IN D O C T O R - P A T I E N T
I N T E R V I E W S : A S O C I O L I N G U I S T I C A N A L Y S I S
ABSTRACT. This paper discusses interpretation in doctor-patient interviews from a sociolinguistic perspective. A meaning-centered orientation to clinical practice calls for practitioners to create a clinical picture of the illness that is compatible with the patient's experience. This requires that appropriate interpretation of symptoms take place. Using transcripts of doctor-patient interviews, this paper demonstrates that another interpretive process, necessary to understanding illness, occurs at the level of conversation. Contrasting examples illustrate that without an adequate degree of "conversational cooperation," inter- pretation cannot take place. The results of poor conversational interpretation are the creation of an inaccurate clinical picture and the loss of clinically relevant information. The anthropological and sociolinguistic paradigms are linked by showing how differing perspec- tives on the illness affect conversational interpretation.
INTRODUCTION
Anthropologists have demonstrated the importance of understanding the patient's perception of illness in the delivery of successful medical care. Work by Kleinman (1978), Good and Good (1980), and others have shown that illness can be understood in different ways by the participants in the medical encounter, especially when the doctor and patient come from different cultures. The reality of the illness may be constructed by the patient according to culturally bound beliefs. The patient's perception of the illness - - including its etiology, its classification, and its prognosis - - may be at odds with the doctor 's perception which has been built largely from academic training and clinical experience. In cross-cultural case studies presented in the literature, it has been shown that when doctor and patient are unable to reach a common understanding of the illness, there are detrimental consequences to the patient's health status (Kleinman 1978, Katon and Kleinman 1980, Weaver and Sklar 1980). Management of the illness may be more difficult, and both patient and practitioner may become frustrated and discouraged.
Differing perceptions of illness are not limited to cross-cultural encoun- ters. Anthropologists have elicited a variety of explanatory models from patients within a single culture (Helman 1978, Pfifferling 1980, Stoeckle and Barsky 1980, Gillick 1985). One might argue that restricting investi- gations of health beliefs to cross-cultural data obscures the idiosyncratic perceptions of individuals. Symptoms may be grounded in cultural beliefs, but their meaning is modified by individual experience, regardless of the
Culture, Medicine and Psychiatry 12 (1988) 201--218. © 1988 by Kluwer Academic Publishers.

202 R A N D O L P H S. M A R S H A L L
cultural group to which the individual belongs. Since the health care visit in this country is largely a one-on-one encounter, it is important to try to understand the perceptions of illness operating in individual practitioner- patient interactions.
Good and Good (1980) address this issue and recommend a reorienta- tion of clinical practice. They argue that human illness is fundamentally semantic or meaningful to the individual. They argue further that clinical practice is inherently interpretive or hermeneutic, as is represented by the physician's task of deducing an underlying biological disease from sub- jective and objective manifestations. The clinician's imperative, they say, is to use an interpretive approach to explore the patient's illness meanings and "decode the patient's semantic network of the illness" in order to arrive at appropriate therapeutic responses. I will argue in this paper that the interpretation called for by the Goods does not happen without interpretation occurring simultaneously at the level of conversation.
The objectives of this paper are threefold: (1) to illustrate the conversa- tional processes necessary for conversational interpretation to occur; (2) to demonstrate that conflicting perceptions of the illness can interfere with conversational interpretation; and (3) to consider how understanding the conversational mechanisms involved in the interaction might help doctors to communicate better. I will pursue these objectives using a sociolinguistic method of analysis.
The study of doctor-patient communication has been approached from several perspectives. A brief review of the literature follows. For a more comprehensive review of doctor-patient communication, see Inui and Carter (1985) and Pendleton (1983).
Researchers most closely allied to the traditional goals of medical interviews have assessed doctor-patient communication by using patient satisfaction and compliance as outcome measures (Davis 1968, Korsch and Negrete 1972, Zola 1980). Studies of this type have been criticized for their inconsistency (West 1984) and their use of uncontrollable variables (Pendleton 1983). Other researchers have applied coding schemes to textual data in order to categorize interactional styles (Byrne and Long 1976, Korsch and Negrete 1972, Stone 1979). Critics of these methods point out that no degree of detail in coding can approach the sensitivity gained by examining textual data as an unabstracted document (Inui and Carter 1985).
Anthropologists and sociologists have elicited perceptions of the health care encounter using ethnographic methods (Kleinman 1980, Good and Good 1980, Helman 1978, Pfifferling 1980, Stoeckle and Barsky 1980). Within the anthropological/interpretive paradigm, the doctor-patient en-

D O C T O R - P A T I E N T IN T E RV IE W S 203
counter is viewed as the meeting of conflicting world views. Mishler (1984) has augmented the anthropological paradigm by offering textual evidence that doctor and patient "speak" with discordant voices -- the "Voice of Medicine" and the "Voice of the Lifeworld," respectively. His contention that successful doctor-patient encounters include a doctor's attentiveness to the Voice of the Lifeworld is corroborated by the data in this paper.
Of the studies that employ direct analysis of doctor-patient transcripts in the tradition of conversational analysis (as pioneered by Sacks, Schegloff and Jefferson 1974), some have concerned themselves primarily with the structure of conversation in the interview (Shuy 1983, Frankel 1985). Others demonstrate the creation and perpetuation of interactional assyme- try (West 1984, Fisher 1983, Todd 1983). Detailed analyses of transcripts have also begun to address broader interactional issues, such as the influence of beliefs and expectations (Cicourel 1982), role shifts (Tannen and Wallat 1983), and bureaucratic constraints (Freeman 1986) on com- munication in the health encounter.
The approach to studying doctor-patient communication used in this paper builds on structural analyses of doctor-patient interviews and draws on the interpretive approach to conversational analysis developed by Gumperz (1982b). An attempt will be made to link the interpretive paradigm of anthropology with the interactional paradigm of conversa- tional analysis.
Sociolinguistics can expand our knowledge of perceptions of illness by examining the verbal and non-verbal cues that participants use to achieve understanding within the interaction. Doctors and patients enter an inter- action with incomplete, though overlapping knowledge and expectations of the health encounter. The patient's knowledge of the illness comes from personal knowledge of his or her own health, as well as from second hand sources such as friends and relatives' experiences, medical articles, and the popular press. In addition to such popular forms of knowledge, the doctor's perspective includes "expert" knowledge drawn predominantly from academic training, clinical experience, and information about the patient's medical history. Given the incompleteness of the participants' knowledge as they enter the encounter, a central conversational task of the participants in the interview is to fill in each other's gaps in knowledge, continuously restructuring information gathered with the implicit goal of reaching a shared understanding (Gumperz 1982b). The analysis used in this paper is based upon principles of conversation outlined here.

204 R A N D O L P H S. M A R S H A L L
C O N V E R S A T I O N A L T H E O R Y
When we talk to one another, a process of mental monitoring runs beneath the conversation. It allows us to understand what is being said and formulate appropriate responses. Although we may not be able to follow a part of the conversation or get a particular point across, we are not necessarily aware of whether our interpretation of what is going on matches that of the other participants in the conversation. The verbal manipulations with which we attempt to gain understanding seem to happen without our having to be aware of how we are trying to orient ourselves or even, perhaps, that appropriate orientation is our goal.
Several factors influence understanding in a conversation. As compe- tent speakers, we have a working knowledge of conversational rules. Some of these rules are universal principles of human interaction. By these rules we know that a response is supposed to follow a greeting and that an answer should follow a question. Other rules are culturally bound. Being able to use them appropriately requires experience interacting with mem- bers of that particular cultural group. Examples of culturally bound rules include knowing what topics are appropriate for a given setting, knowing how to open or close a conversation, knowing what a pause might mean, and recognizing an appropriate moment for an interjection.
In addition to knowledge of conversational rules, participants bring beliefs and expectations to an interaction. These expectations may be modified through verbal and non-verbal aspects of the interaction itself. Cicourel (1982), for example, has shown how a patient's beliefs about her illness and expectations for her medical encounters affected the way she interacted with the doctor. Conflicting test results and prior experience with medical bureaucracy made this patient suspicious about the validity of the information that a doctor offered and resulted in her challenging the doctor's competency.
Finally, doctor-patient interviews are constrained by interactional fac- tors that are unique to a medical encounter. These include bureaucratic constraints such as time pressure, institutional protocol, and third party payor requirements (Freeman 1986), role shifts (Tannen and Wallat 1983), and the cognitive strategies that are followed in the process of medical diagnosis (Harvey et al. 1984: 1--39; Kassirer & Gorry 1978).
In the midst of this complex interactional environment, conversation proceeds in the following way: Hearing an utterance, we do not simply process what is said in literal terms. Using our cultural knowledge and our current understanding of the situation, we go beyond the surface meaning of the words, using what Grice (1975) calls "implicature" to infer meaning

DOCTOR-PATIENT INTERVIEWS 205
from the utterance. Consider an example offered by Grice (1975): A college professor responds to a request to evaluate a student with the statement: "He has good handwriting." The words in his utterance have a literal meaning. The professor, however, is relying upon the listener's knowledge of the usual criteria for evaluating college students for his utterance to be interpreted as a poor evaluation of the student. If the listener's interpretation is correct -- that is, shared by the person who spoke -- the conversation moves on. If the interpretation is incorrect -- does not match that of the speaker -- the conversation is disrupted in some way. Evidence of disruption appears in the text of the interaction. Thus, conversation can be seen as a continuous interpretive process. It requires a dynamic involvement of both participants in framing and refraining a perception of the situation.
The sociolinguistic method used in this paper can demonstrate how closely the participants' perceptions of the situation match. The analysis proceeds by identifying indicators of "conversational cooperation" within the transcript. Such indicators include adequate contextualization of utterances (Gumperz 1982b), as well as smooth transitions in speaking turns, even rhythm or pacing, cooperative sentence building, 'duetting' (making similar statements simultaneously), and receiving confirmatory utterances to summarizing statements (Tannen 1984: 54--94). Non-coop- eration in a conversation may be identified not only by an absence of the cooperative indicators, but by breaks in rhythm, abrupt changes in topic that the other participant does not follow, and overlapping utterances that disrupt the flow of talk.
Examples of indicators of conversational cooperation and non-coop- eration will be demonstrated in the analysis of the transcripts in this paper. Conversational cooperation will be shown to facilitate interpretation at a conversational level. Conversational non-cooperation will be shown to result in confusion, inaccuracy and loss of information.
ANALYSIS OF INTERVIEWS
The three transcripts analyzed here are drawn from a collection of 215 doctor-patient interviews videotaped for purposes of analyzing diagnosis and treatment of chronic lung disease (Gerbert & Hargreave, in press). The participants knew they were being videotaped, but studies showed that the presence of the camera and operator made tittle difference to the interview (Gerbert et al. 1982). Doctor and patient are both Anglo, with English as their first language. This makes communication problems arising in the interview more likely to be attributable to the doctor-patient

2 0 6 R A N D O L P H S. M A R S H A L L
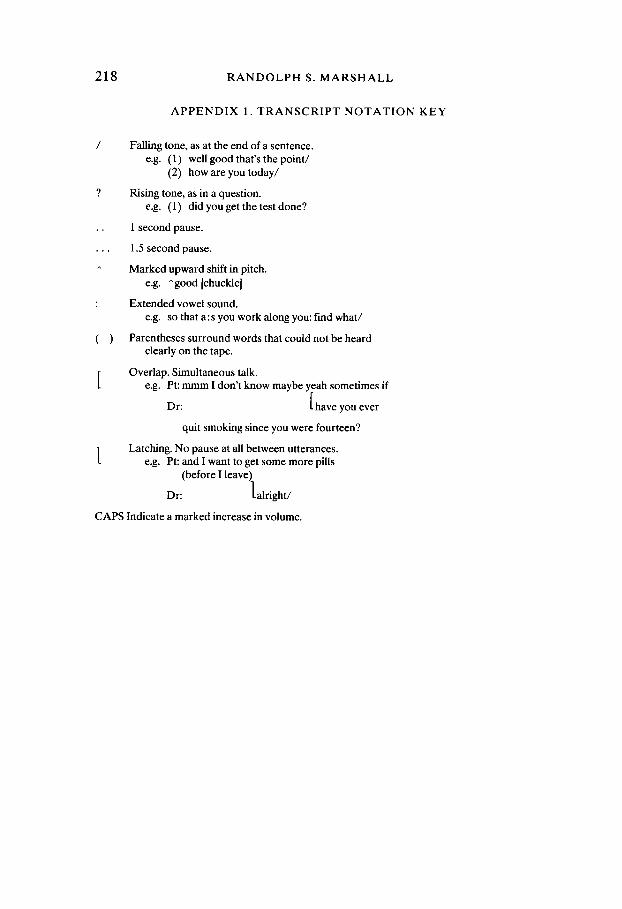
interaction per se, rather than to an additional language barrier. The doctor in all three interviews is a general practitioner who has seen the patient at least once before. (See Appendix 1 for Transcript Notation Key.)
Figure 1. Interview ¢~ 1
161 Dr: [4 sec 1 let's get back to the- the- cough business u: h
162 it's all gone now but over the last few months have you
163 had a- you know a persisting cough?
164 Pt: oh it was horrible yeah I had to prop myself up I
165 Dr: [u :m
166 Pt: couldn't lay down fiat at all 1
167 Dr: [ uh-huh does- does the not
168 being able to lie down fiat was because what /what
169 happened 1
170 Pt: [as soon as I'd lay down I'd start coughing/
171 and even sittin' in the chair it got to the point uh
172 the husband'd get mad and say WHAT ARE YOU HACKING like
173 that for I s' can't help it/
174 Dr: okay do you actually get to sleep- wake up out of a
175 sound sleep in the middle of the night coughing? or is
176 it a matter of you just can't lie fiat/
177 Pt: o h / n - for a long time I couldn't hardly get to sleep/
178 I just- the cough would just keep me awake I'd- doze
179 off and sit up and doze off and slide up more on a
180 pillow/
181 Dr: so did you find yourself actually waking out
182 of a sound sleep F
183 Pt: [oh yeah uh-huh 1
184 Dr: [ u h - h u h / u h and did what you just sort
185 of sat up /
186 Pt: I'd sit- sit up 1
187 Dr: [was there any other symptom at that
188 point/

D O C T O R - P A T I E N T INTERVIEWS 207
189 Pt:
190 Dr:
191 Pt:
192 Dr:
193 Pt:
194 Dr:
195
196 Pt:
197 Dr:
198
199 Pt:
200 Dr:
201
202
203 Pt:
204 Dr:
205 Pt:
206
207 Dr:
208
209 Pt:
210 Dr:
211
212 Pt:
no:?
you were just coughing
lyeah
you didn't have pain?
no just-just the breathing it just seemed like I-
was there
any sense of pressure anywhere?
yeah up in here/[indicates chest with her hand]
alright/so you- you sort of had a uh- a pressure
anything else that you noticed/or do you remember/
I can't remember now
[and the last time that you did that
was when/that you woke up out of a sound sleep with
pressure and trouble breathing/
oh I'd say about two and a half weeks ago/since the
right
cough left I haven't had that real heavy heavy
pressure/
was that a night time every- every night kind
of thing?for was it every so often/
[r oh yeah every night/
and now that has gone away miraculously as the cough
disappeared
urn yeah/
In the in te rv iew segment shown in F igure 1, the d o c t o r is t rying to elicit
the s y m p t o m s of conges t ive hea r t fai lure. A classic s y m p t o m , k n o w n as
p a r o x y s m a l noc tu rna l dyspnea , is de f ined as waking up s u d d e n l y in the
midd l e of the night unab le to ca tch one ' s b rea th . T h e r e m a y b e an
a s soc ia t ed s y m p t o m of ches t p ressure . T h e d o c t o r ' s po in t e d ques t ion ing
fi l ters out all the i n fo rma t ion o f fe r red by the pa t i en t excep t s t a t ements that
might conf i rm a cl inical p i c tu re o f hea r t fai lure. W i t h the excep t ion of he r
initial s t a t emen t a b o u t no t be ing able to lie fiat, the pa t i en t p r o d u c e s the
sought af ter s y m p t o m s only af ter pe r s i s t en t and res t r ic t ive ques t ion ing by
the doc to r . By look ing at the i n fo rma t ion that the pa t i en t offers on he r

208 RANDOLPH S. MARSHALL
own and the line of questioning pursued by the doctor, we can identify conflicting perceptions of the illness operating simultaneously in the interview.
For the patient, the cough meant that she could not lie flat. It made her husband mad at her, kept her awake, was associated with trouble breathing and heavy chest pressure, and it has not been a problem since she recovered two and a half weeks ago.
For the doctor, the cough led him to the fact that the patient couldn't lie fiat, that she woke up out of a sound sleep with chest pressure and trouble breathing, and that this constellation of symptoms could mean that the patient has chronic heart failure. (A persistent cough, by the way, does not fit the classic presentation of heart failure.) The doctor separates the cough from the rest of the symptoms by noting that "that" (the symptoms of heart failure) has gone away "as" the cough did (line 210).
Figure 2 illustrates the two perceptions of illness in schematic form. To indicate the difference in the way the models emerge in the interview, I have represented the doctor's model as a linear progession and the patient's model as a list.
Figure 2. Conflicting perceptions of the illness.
Patient's Perception
cough: -- couldn't lie flat - - made her husband mad
at her - - kept her awake -- assoc, with trouble
breathing and pressure - - was over 2 1/2 weeks ago
Doctor's Perception
cough - couldn't lie flat
woke up out of sound sleep
pain?
pressure? 1
woke up out of sound sleep with pressure and
trouble breathing
What are the consequences of maintaining disjunct perceptions of the situation? The immediate consequence in this case is that the doctor has created an inaccurate clinical picture of the patient's illness. The physi- cian's question near the end of the segment - - When did you last wake up out of a sound sleep with pressure and trouble breathing? - - disagrees with the patient's perception that prior to two and a half weeks ago, she had had a cough that prevented her from lying flat, annoyed her husband, and kept her awake. The doctor alters the picture of the illness she

DOCTOR-PATIENT INTERVIEWS 209
presents even further when he returns to the topic a few minutes later and asks:
line 236 Dr: yeah [12 sec] okay is there any other time you get this pressure business in the chest you were saying had been wak- had been waking you up?
The patient never stated -- in response to the doctor or on her own -- that chest pressure woke her up.
In addition to inaccuracy, there is also loss of information. By not responding to some of the information the patient offers, the doctor will not be able to use it in planning a treatment regimen. As the research on explanatory models has shown, this can produce frustration and unsuc- cessful management of the illness. Follow-up data on this interview are not available to assess the health status of the patient. However, in a debriefing session the doctor and the patient were asked individually: "For each of the following symptoms, please tell me if you/the patient did or did not have that symptom today" (Gerbert & Hargreave, in press). Responding to this question, the doctor and patient disagreed on two symptoms: "cough" and "general worsening of lung condition." It is likely that disagreements on the presence of these symptoms will be manifested in differences in opinion about what treatment will be useful.
This segment is not an isolated occurrence. Later in this interview, the doctor and patient run through a similar pattern, the doctor this time probing for symptoms of a heart attack (transient chest, jaw and arm pain) and the patient offerring incidents of pain in different parts of her body that she associates with other events in her life -- chest pain following a breast exam, jaw pain following a trip to the dentist (which, incidentally, resulted in her husband getting mad at her for taking pain medication). The doctor eventually abandons the line of questioning after altering the patient's statements and losing information as in the earlier segment.
This example shows that a doctor and patient can proceed through an interview working with conflicting perceptions of the illness. Let us now consider the conversational mechanisms that allow the conflicting percep- tions to occur.
Two lines of evidence suggest conversational interpretation is failing. The first concerns turn-taking. Following the response to his initial question, the doctor inserts a request for a speaking turn ("u:m" in line 165) before the patient has completed her answer. This attempt is not successful, which is fortunate for him because the symptom he is inter- ested in follows his attempted interjection. In other instances, however, the doctor cuts off the patient's answers before they are completed (lines

210 R A N D O L P H S. M A R S H A L L
186--187, 189--190, and 193--194). In two of these instances (186--187 and 193--194), the interruptions changed the topic.
Another sign of conversational non-cooperation in this segment is the difference in discourse structure. The patient uses a narrative strategy to offer information about her illness, as in her story about her husband getting mad at her (lines 170--173) and her description of dozing off and sliding up on the pillow (lines 177--180). In contrast, the doctor pursues restrictive questions that request "either/or" or "yes/no" responses (lines 174--175, 181--182). As a consequence of mismatched discourse strate- gies, each participant is unable to use the cues that the other produces which indicate what is being attempted in the conversation. The patient receives no feedback from the doctor that can tell her whether or not the information she is offerring is being heard or understood. From the doctor's perspective, he must repeat himself and ignore some responses to his questions in order to elicit the answers he is looking for.
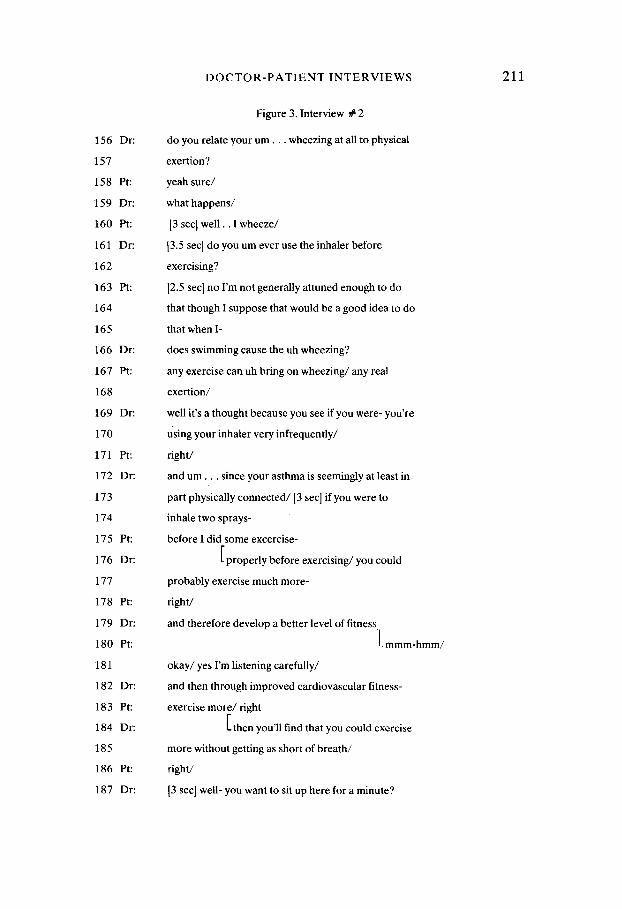
For purposes of comparison, I will now turn to an interview in which a high degree of conversational cooperation occurs. The segment opens with the doctor inquiring about the relationship between the patient's wheezing and his exercising, a topic which the patient initiated early in the interview (38 Pt: I've lost my wind and that's what really bothers me/). (See Figure 3.)
In this segment, the rhythm or pacing is even. The participants cooper- ate in building sentences. They display "duetting." They repeatedly receive confirmatory utterances in response to assessments. With regard to the principles of conversation discussed previously, each participant is able to use the other's utterances to build on what has come before and in so doing maintain an orientation to the ideas that are being developed. As a consequence, the proposal that the inhaler be used before exercise is offered by the doctor and is received and worked with by the patient without the inaccuracies and information loss that plagued the other interview. Furthermore, the doctor uses the patient's perspective of the illness -- that losing his 'wind' is the most important aspect of his asthma - - in proposing a treatment plan. Thus, he is able to interpret the meaning of the patient's illness and suggest a therapeutic regimen that is both appropriate medically and meets the needs that the patient has presented. Mishler (1984) reaches similar conclusions about a successful doctor- patient interaction in his discussion of attentiveness to the "Voice of the Lifeworld."
The final interview segment, shown in Figure 4, further highlights conversational processes that may disrupt interpretation.
The first problematic process is the doctor's use of unassigned pro-
D O C T O R - P A T I E N T I N T E R V I E W S 2 1 1
156 Dr:
157
158 Pt:
159 Dr:
160 Pt:
161 Dr:
162
163 Pt:
164
165
166 Dr:
167 Pt:
168
169 Dr:
170
171 Pt:
172 Dr:
173
174
175 Pt:
176 Dr:
177
178 Pt:
179 Dr:
180 Pt:
181
182 Dr:
183 Pt:
184 Dr:
185
186 Pt:
187 Dr:
Figure 3. Interview # 2
do you relate your u m . . . wheezing at all to physical
exertion?
yeah sure/
what happens/
I3 sec I well . . I wheeze/
[3.5 sec] do you um ever use the inhaler before
exercising?
[2.5 sec] no I'm not generally attuned enough to do
that though I suppose that would be a good idea to do
that when I-
does swimming cause the uh wheezing?
any exercise can uh bring on wheezing/any real
exertion/
well it's a thought because you see if you were- you're
Using your inhaler very infrequently/
right/
and u r n . . , since your asthma is seemingly at least in
part physically connected/[3 sec] if you were to
inhale two sprays-
before I did some excercise-
properly before exercising/you could
probably exercise much more-
right/
and therefore develop a better level of fitness
~- mmm-hmm/
okay/yes I'm listening carefully/
and then through improved cardiovascular fitness-
exercise more/f ight
then you'll find that you could exercise
more without getting as short of breath/
right/
[3 sec I well- you want to sit up here for a minute?

212
1. Pt:
2 Dr:
3
4 PI:
5 Dr:
6 Pt:
7 Dr:
8
9
10
11
12
13 Pt:
14 Dr:
15 Pt:
16 Dr:
17
18 Pt:
19 Dr:
20
21
22
23
24
25 Pt:
R A N D O L P H S. M A R S H A L L
Figure 4 -- Interview # 3
my potassium's low huh/
yeah it was uh and we can do that to- today too/you- I
put you on Moduretic before did 1 not?
mmm-hmm/
okay and you're taking one a day on- on the
mmm-hmm
(Moduretic)/uh your potassium is still 3.3 and I would
imagine that that's still low because of before and
let's put- I'll plan on supplementing you with
potassium for about another two weeks and then we'll
and then we'll drop it off/do you have any of the Slo-
K left?
yeah/
good/how many do you have?
I don't know/I've got- I've got refills on it/
okay/okay/let me just check your blood pressure
today/[5 sec]
so should I take Slo-K (once a day?)
u:h yeah/yeah/I think the 3.3 is a little bit low u:h
with 3.5 and 5 is about the- is about the normal level
3.3 will never bother you but you might feel a little
bit better you might have some uh I would imagine that
it would go up slowly over the next uh uh . . . six months
or so with your being on the Moduretic/
mmm-hmm/
nouns. The pat ient opens by asking whe the r her po tass ium level is low.
T h e d o c t o r answers the li teral mean ing of the quest ion, then goes on to
offer a plan to do "that" today, too. T h e pat ient may or may not k n o w
what "that" refers to; no e luc ida t ion of the word takes p lace and no fur ther
re fe rence is m a d e to a p r o c e d u r e involving po tass ium levels. Later , the
d o c t o r repeats this, leaving "before" of line 8 un re fe r enced in the text. O n e
may offer an a l ternat ive explana t ion that the doc to r and pat ient are so
famil iar with the si tuation that expl ica t ion is unnecessary; however , this

D O C T O R - P A T I E N T I N T E R V I E W S 213
would be in marked contrast to the text of other interviews in which either pronouns are referenced or there is evidence that both participants are using unassigned words to mean the same thing. Leaving words ambig- uously referenced increases the potential for confusion. The fact that no attempt at clarification is made suggests that the participants are unaware of the ambiguity or that they are unable to develop the cooperation necessary to rectify it.
A second problem arises when the doctor makes an assumption about the intent of the patient's first question. By answering with a plan to do "that" today, he can be said to be answering an unstated intent of the patient's question (e.g. Can you do something for my low potassium today?) A little further on, the doctor mentions the potassium level again (line 7), this time offering an explanation of why the potassium is low (line 8). Finally, near the end of this segment the doctor reintroduces the topic once more (lines 19--24), this time wandering through several aborted attempts to give significance to the patient's potassium level, though no request for such an explanation has been explicitly requested. Answering the intent of a question requires confirmation from the first speaker as to whether the question's intent was interpreted correctly. In these exchanges, no confirmations are sought or offered. The doctor is thus forced to carry the burden of interpretation alone.
A third disrupter of conversational interpretation is the doctor's use of medical logic. His monologue of lines 7--12, followed by his question about the remaining SIo-K makes sense if one knows Moduretic's pharma- cologic action on potassium (K +) excretion in the kidneys. The patient, however, reveals her lack of understanding by reopening the topic after a 5 second pause (line 18). This exchange suggests that for the patient, the doctor's statements do not contain sufficient contextualization for informa- tion to be transferred clearly. Cicourel (1975) has shown the problem of insufficient contextualization to arise commonly in doctor-patient interviews. He suggests that inadequate contextualization may be the result of the cognitive strategy of the doctor who, while pursuing a decision- making tree that makes sense medically, leaves the patient uninformed as to the significance of the questions being asked.
I am referring again to a cognitive process that is mediated by con- versational mechanisms. Because the doctor and patient do not provide each other with cues that indicate whether understanding is taking place, they are unable to mediate what may look to the patient as a cryptic questioning strategy. The patient reveals her lack of understanding by reopening a topic that the doctor has closed.
The rest of the interview maintains a similar level of non-cooperation.

214 R A N D O L P H S. M A R S H A L L
Much time is wasted in trying to obtain and convey information under non-cooperative conditions.
D I S C U S S I O N
The interviews presented in this paper demonstrate the importance of conversational cooperation in a doctor-patient interview. Although most of the interviews reviewed for this study fell between the extremes presented here, the same principles appeared in all the interviews. In order for the Goods' clinical imperative to be realized -- interpreting symptoms and reacting with appropriate therapeutic responses -- a physician must not only be capable of understanding different ways of perceiving the illness; he or she must also be capable of engaging conversational coop- eration to facilitate interpretation (Grice's implicature) at the level of conversation. The use of non-cooperative turn-taking, discordant discourse structures, unassigned pronouns, and unconfirmed assumptions was shown to interfere with conversational interpretation. On a cognitive level, con- flicting perceptions of the illness and the doctor's tendency to follow an isolated path of clinical reasoning were shown to inhibit the establishment of the conversational cooperation needed for clear and accurate transfer of information to take place.
The analysis of transcripts as demonstrated here suggests that any lapse in conversational cooperation has the potential for resulting in communi- cation difficulties. Teaching medical students and practitioners to analyze their own and others' interviews may sensitize them to the ways in which conversational cooperation can influence the outcome of an interview. Understanding the mechanisms of conversational interpretation may pro- vide information about real problems of the interactional process.
Understanding conversational interpretation, however, does not alter the structure and operation of the sociocultural environment in which the interaction takes place. An assumption was made for the purposes of analysis in this paper that the doctor and patient wished to communicate as best they could and were striving to converse effectively. Success or failure in reaching a shared understanding in an interview was therefore dependent upon the degree to which participants were "able" to cooperate conversationally, rather than on how willing they were to do so.
Pursuing the notion that participants in a doctor-patient encounter do not exist independent of the social structure that allows the interaction, sociologists examining language in doctor-patient encounters have pro- posed that doctors perpetuate a power differential in the interview by the maintenance of a particular structure (Mishler 1984) and content

D O C T O R - P A T I E N T I N T E R V I E W S 215
(Waitzkin 1979, Waitzkin and Stoekle 1972) of their verbal interaction. The effect of the power inequity may be the delivery of unsatisfactory health care. In sociolinguistic terms, a power inequity may influence conversational cooperation directly, and consequently disrupt information transfer, accurate and efficient diagnosis, and the interpretation of the patient's illness meanings.
Conclusions about power, however, depend upon definition. Some conversational analysts suggest that power may be measured in terms of interactional assymetry, which they define by the greater number of interruptions the doctor produces relative to the number the patient produces and by the doctor's control of topic initiation (West 1984, Fisher 1983, Todd 1983). Defining power inequity simply in terms of assymetry may preclude adequate examination of the interaction. The second inter- view segment (Figure 3) illustrates that an extremely assymetrical inter- action -- in which topic changes are controlled exclusively by the doctor - - can produce cooperative and efficient transfer of information. The influence of power on conversational processes and health outcome is an important line of research which lies beyond the scope of this paper.
The data analyzed here are limited to doctors and patients who share a communicative background. Cross-cultural communication difficulties in non-medical institutional settings have been analyzed with sociolinguistic methods (Gumperz 1982a). There is a need for additional sociolinguistic research in intercultural medical settings to expand the knowledge base of physicians and physician educators.
UC Berkeley/UCSF Joint Medical Program, San Francisco 66 Overlook Terrace New York, N.Y. 10040
N O T E
This paper is the result of two years of seminar and tutorial work with John Gumperz. He has provided invaluable guidance and support. The tenets of conversational theory discussed in this paper were drawn from ideas developed in his book, Discourse Strategies (1982b). Sarah Freeman was extremely helpful in introducing me to the practical and theoretical aspects of studying doctor-patient communication. I would also like to thank Barbara Gerbert for her advice and the use of her videotapes.
Funding for this project was provided by a Smithkline Beckman Medical Perspec- tives Fellowship.
R E F E R E N C E S
Byrne, P. S. and B. E. L. Long 1976 Doctors Talking to Patients. London: HMSO.

216 R A N D O L P H S. M A R S H A L L
Cicourel, A. V. 1975 Discourse and Text: Cognitive and linguistic processes in studies of social struc-
ture. Versus: Quaderni di Studi Semotici 12:33--84. Cicourel, A. V.
1982 Language and Belief in a Medical Setting. In Georgetown University Round Table on Language and Linguistics 1982. Heidi Byrnes, ed. Washington, D.C.: Georgetown University Press.
Fisher, Sue 1983 Doctor/Patient Talk: How treatment decisions are negotiated in doctor-patient
communication. In The Social Organization of Doctor-Patient Communication. S. Fisher and A. Todd, eds. Washington, D.C.: CAL Press.
Frankel, R. M. 1985 From Sentence to Sequence: Understanding the Medical Encounter Through
Microinteractional Analysis. Discourse Processes 7: 35--170. Freeman, Sarah
1986 Organizational constraints as communicative variables in medical settings: the case of referral requests. Paper presented at the 84th Annual Meetings of the American Anthropological Society, Washington, D.C.
Gerbert, Barbara, and W. A. Hargreave In press Measurement of Adequacy of Physician Performance: A comparison of four
methods. Medical Care. Gerbert, B., R. B. Countiss, M. Kemeny, and D. S. Gullion
1982 Utilization of Videotaped Observations to Assess Physician Care: A Method- ology for Evaluating Treatment. Research in Medical Education. Proceedings of the 21 st Annual Conference.
GiUick, Muriel R. 1985 Common-Sense Models of Health and Disease. NEJM 313: 700--703.
Good, Byron J., and Mary Jo DelVecchio Good 1980 The Meaning of Symptoms: A Cultural Hermeneutic Model for Clinical Practice.
In The Relevance of Social Science for Medicine. Chapter 8. L. Eisenberg and A. Kleinman, eds. Dordrecht: Holland/Boston: USA: D. Reidel Publishing Company.
Gumperz, J. J. (ed.) 1982a Language and Social Identity. Cambridge: Cambridge University Press.
Gumperz J. J. 1982b Discourse Strategies. Cambridge: Cambridge University Press.
Harvey, A. Mcgehee 1984 The Principles and Practice of Medicine, 21st ed. Norwalk, CT: Appleton-
Century-Crofts. Helman, Cecil
1978 Feed a Cold, Starve a Fever. Culture, Medicine and Psychiatry 2: 107--137. Inui, Thomas S. and William B. Carter
1985 Problems and Prospects for Health Services Research on Provider-Patient Com- munication. Medical Care 23:521--538.
Katon, Wayne and Arthur Kleiman 1980 Doctor-Patient Negotiatin and Other Social Science Strategies In Patient Care.
In The Relevance of Social Science for Medicine. L. Eisenberg and A. Kleinman, eds. Dordrecht: Holland/Boston: USA: D. Reidel Publishing Co..
Kassirer, Jerome P. and G. Anthony Gorry 1978 Chnical Problem Solving: A Behavioral Analysis. Ann Int Med 89:245--255.
Kleinman, Arthur, Leon Eisenberg, and Byron Good 1978 Culture, Illness, and Care; Clinical Lessons from Anthropologic and Cross-
Cultural Research. Ann Int Med 88:251--258.
D O C T O R - P A T I E N T I N T E R V I E W S 217
Mishler, Elliot G. 1984 The Discourse of Medicine: Dialectics of Medical Interviews. Norwood, NJ:
Ablex Publishing Corp. Pendleton, David
1983 Doctor-Patient Communication: A Review. In Doctor-Patient Communication, Chapter One, Pendleton D. and John Hasler, eds. London: Academic Press.
Pfifferling, John-Henry 1980 A Cultural Prescription for Medicocentrism. In The Relevance of Social Science
for Medicine. L. Eisenberg and A. Kleinman, eds. Dordrecht: Holland/Boston: USA: D. Reidel Publishing Co..
Sacks, H., E. A. Schegloff and G. Jefferson 1974 A Simplest Systematics for the Organisation of Turn-taking in Conversation.
Language 50: 696--735. Stoeckle, John D. and Arthur J. Barsky
1980 Attributions: Uses of Social Science Knowledge in the Doctoring of Primary Care. In The Relevance of Social Science for Medicine. L. Eisenberg and A. Kleinman, eds. Dordrecht: Holland/Boston: USA: D. Reidel Publishing Co..
Stone, George C. 1979 Objectives and Evaluation Criteria in Teaching Communication Skills. Presented
in Symposium on Teaching and evaluating interpersonal skills in health profes- sions. Am Psych Assoc. New York.
Shuy, R. W. 1983 Three Types of Interference to an Effective Exchange of Information in the
Medical Interview. In The Social Organization of Doctor-Patient Communica- tion. Fisher, S. and A. Todd, eds. Washington, D.C.: CAL Press.
Tannen, Deborah and Cynthia Wallat 1983 Doctor/Mother/Child Communication: Lingustic Analysis of a Pediatric Interac-
tion. In The Social Organization of Doctor-Patient Communication. Fisher, S. and A. Todd, eds. Washington, D.C.: CAL Press.
Tannen, Deborah 1984 Conversational Style: Analyzing Talk Among Friends. Norwood, NJ: Ablex.
Todd, Alexandra Dundas 1983 A diagnosis of doctor-patient discourse in the perscription of contraception. In
The Social Organization of Doctor-Patient Communication. S. Fisher and A. Todd, eds. Wash, DC: CAL Press.
Waitzkin, Howard 1979 Medicine, Superstructure and Micropolitics. SocSciandMed 13A:601--609.
Waitzkin, Howard and John D. Stoeckle 1972 Communication of Information About Illness. Advances in Psychosomatic
Medicine 8: 180--215. Weaver, Charlotte and David Sklar
1980 Diagnostic Dilemmas and Cultural Diversity in Emergency Rooms. Western Journal of Medicine 133: 356--366.
West, Candace 1984 Routine Complications: Troubles With Talk Between Doctors and Patients.
Bloomington: Indiana University Press. Zola, Irving
1980 Structural Constraints in the Doctor-Patient Relationship. In The Relevance of Social Science for Medicine. L. Eisenberg and A. Kleinman, eds. Dordrecht: Holland/Boston: USA: D. Reidel Publishing Co.
218 R A N D O L P H S. M A R S H A L L
A P P E N D I X 1. T R A N S C R I P T N O T A T I O N K E Y
/ Falling tone, as at the end of a sentence. e.g. (1) well good that 's the poin t /
(2) how are you today/
9 Rising tone, as in a question. e.g. (1) did you get the test done?
1 second pause.
•. 1.5 second pause.
^ Marked upward shift in pitch. e.g. ^good [chuckle]
: Extended vowel sound• e.g. so that a :s you work along you: find what /
( ) Parentheses surround words that could not be heard clearly on the tape.
Overlap• Simultaneous talk. e.g. Pt: m m m I don' t know maybe yeah sometimes if
f
Dr: [ have you ever
quit smoking since you were fourteen?
Latching. No pause at all between utterances• [ e.g. Pt: and I want to get some more pills
(before I leave)
Dr: [ a l r igh t /
CAPS Indicate a marked increase in volume.







