
International SymposiumInternational SymposiumCentenary of Chagas Disease 1909 Centenary of Chagas Disease 1909 .. 2009 2009
Use of Polymerase Chain Reaction Use of Polymerase Chain Reaction (PCR) to Establish Drug Efficacy(PCR) to Establish Drug Efficacy
- Value and Limitations- Value and Limitations
Constança BrittoConstança Britto [email protected]@ioc.fiocruz.br
Oswaldo Cruz Foundation, FIOCRUZOswaldo Cruz Foundation, FIOCRUZ
July, 2009 – Rio de JaneiroJuly, 2009 – Rio de Janeiro

Chemotherapy during the acute stage of Chagas disease leads to parasitological cure in up to 80% of the cases, but its effectiveness in the long-lasting chronic phase remains unclear.
I- Etiological Treatment should focus I- Etiological Treatment should focus on Parasite Clearanceon Parasite Clearance
Conventional Serology may remain positive for several years despite repeated negative parasite detection methods. Rather poor sensitivity of Xenodiagnosis and Hemocultive
The main limitations are:
(i) long-term follow-up (persistence of specific antibodies);
(ii) continuing administration of toxic nitroimidazole derivatives;
(iii) differences in drug susceptibility among distinct T. cruzi strains;
(iv) lack of reliable tests to ensure parasite elimination.

II- PCR contributions for the II- PCR contributions for the diagnosis of Chagas diseasediagnosis of Chagas disease
The use of PCR to detect minimal amounts of T. cruzi DNA in the blood of chagasic patients opened new possibilities for the diagnosis of chronic infections and evaluation of chemotherapeutic treatment (Moser et al. 1989; Sturm et al. 1989; Avila et al. 1991; 1993; Britto et al. 1993; Wincker et al, 1994; Britto et al, 1995).
HIGHER SENSITIVITY (Multiple genome targets)
SPECIFICITY IMPROVEMENT(DNA sequences with the ability to distinguish between organisms)
Target DNA sequence
Chromosome
DNA in vitro amplification
PCR to assess therapy in Chagas disease

III- Is PCR a valid technique to III- Is PCR a valid technique to address cure?address cure?
PCR performance for the analysis of clinical specimens has revealed discordant results concerning sensitivity, depending on:
(i) epidemiological characteristics of the studied populations (geographic areas, high genetic heterogeneity of T. cruzi strains, etc);
(ii) volume of blood collected (intermittent presence and quantity of circulating parasites at the time of blood collection);
(iii) method used to isolate DNA;
(iv) selection of parasite target-sequences, reagents used, as well as thermo-cycling conditions.
Several therapeutic studies confirm the usefulness of PCR to evaluate treatment outcome in Chagas disease, as a complement to
serological tests.

IV- The value of PCR to establish IV- The value of PCR to establish drug efficacydrug efficacy
PCR appears remarkably useful for the early detection of treatment failure, in cases of resistance or reactivation of T. cruzi infection.
If the persistence of positive PCR is considered therapeutic failure, assessment of parasite load by quantitative real-time PCR could be correlated with the impact of trypanocidal treatment on the disease evolution. Clearance of parasitaemia and disappearance of antibodies are taken as cure criteria.
There is no guarantee that a single “flash” of negative PCR means parasitological cure.
The value of PCR tests lies mainly in the positive results they yield.
330 bpfragment
Detection of a single parasite in 20mL of blood
lysate

V- Treatment of congenital infectionsV- Treatment of congenital infections
Schijman et al (2003) evaluated treatment outcome (Nf and Bz) in 40 infected infants monitored for 2-3 years by PCR (satellite DNA) and conventional methods. Two mL of blood were collected for PCR.
Cure achieved by negativation of PCR + serology in 100% of infants with <3 months, in 66.7% between 7 months-2 years old and in 12.5% with >3 years old.In those infants who started therapy in their first months of life (<3 months), cure was achieved early after treatment.
Parasite search by microhematocrit, hemoculture and PCR-based on satellite nuclear DNA (100 µL plasma)
PCR (during treatment & at the end of follow-up) confirmed 100% of Bz treatment efficacy in association with conventional serology negativation (Russomando et al, 1998).
Parasite clearance more rapidly assessed by PCR [15 days after treatment] than serology [3-8 months] during a 4 years follow-up (Russomando et al, 1998).

VI- Treatment in early lifeVI- Treatment in early life
Galvão et al, 2003: J Clin Microbiol 41: 5066-70.
Cohort of T.cruzi seropositive schoolchildren from an endemic Brazilian area;
Blood samples (5 mL) were taken at baseline and 36 months after treatment with Bz (n=58) or placebo (n=53); Bz group: 39.6% positive PCR (for kDNA)
Placebo: 64.2% positive PCR (P=0.01)
Untreated patients had 1.6-fold-higher chance of remaining PCR positive than the Bz group (P<0.05);
Adequate correlation between high proportion of negative PCR and decrease in antibody titers in the Bz group; PCR positivity occurred in patients without reductions in antibody titers;
PCR is a useful tool for revealing therapeutic failure on a short-term basis.
Infants infected during the early years of life represent those patients amenable to specific treatment with great possibility of cure
(Andrade et al. 1996; Sosa Estani et al. 1998).

VII- Treatment of chronic infectionsVII- Treatment of chronic infections
The efficacy of available drugs is limited for chronic patients (Urbina, 2002). The drugs are able to reduce the parasite population in blood and the risk for disease progression (Viotti et al, 1994; 2006). Up to 80% of chronic treated patients do not achieve parasitological cure as assessed by the persistence of positive serology (very slow decrease in antibody titers), now confirmed using PCR-based methods.
(Britto C et al, 1995) Polymerase chain reaction detection of Trypanosoma cruzi in human blood samples as a tool for diagnosis and treatment evaluation. Parasitology 110: 241-247.
32 Bz-treated seropositive chronic patients attending the Hospital of Infectious Diseases (Fiocruz).
Positive PCR (kDNA) observed in only 9 out of 32 treated patients who remained reactive with conventional serology
(5 years post-treatment).

Selection of patients (1979) Department of Tropical Medicine, University of Brasilia
100 Xeno+ patientsasymptomatic
85 – treated (Nf or Bz)(37 in the acute phase & 48 in
the chronic phase)
15 – control group
BA
GO
Vector transmission has been interrupted for more than 20 years

Therapy evaluation in a 20 years follow-up
PCR was more sensitive than Xenodiagnosis in
determining therapeutic failure, 20 years after
chemotherapy
XENO (pre & post-treatment)
PCR (post-treatment)
PCR +
10 (27%)
17 (35%)
8 (53%)
Total
N=37
N=15
N=48
Acute
Chronic
Placebo
XENO +
5 (13.5%)
8 (16.7%)
4 (26.7%)
PCR -
27 (73%)
31 (65%)
7 (47%)
XENO -
32 (86.5%)
40 (83.3%)
11 (73.3%)

TotalPCR + PCR -N=37
N=15
N=48 17 (35%)17 (35%)
10 (27%)10 (27%)
8 (53%)8 (53%)
27 (73%)
31 (65%)
7 (47%)
Sero ?Sero + Sero -
5 (18%)
0 (0%)
12 (38%)16 (52%)
15 (56%)
7 (100%)
7 (26%)
3 (10%)
0 (0%)
PCR -
Acute Phase
Chronic Phase
Placebo Group
Acute Phase
Chronic Phase
Placebo Group
The agreement of negative results between serology The agreement of negative results between serology and PCR is probably indicative of cureand PCR is probably indicative of cure
Herein, as only one point in time was analyzed by PCR, a negative result could not be assumed as definitive cure.

Treatment of patients with Chronic Chagas Treatment of patients with Chronic Chagas Cardiomyopathy (CCC)Cardiomyopathy (CCC)
Multicenter, randomized, placebo controlled clinical trial of 3,000 patients with
CCC (excludes severe disease). Full-scale trial follow-up will be 5 years
(ending in 2011).
BENEFIT includes a pilot study (600 patients) to evaluate whether 60 days of Benznidazole therapy will reduce parasite activity determined by PCR negativation
and parasite load measure.
PCR performed at randomization, at the end of therapy (60 days) and after 2 years of follow-up.
Participation of 8 countries and 60 centers, conducted by the Canadian Institute of Health Research and WHO/TDR, with the Latin American coordinating center at Dante Pazzanese Institute (SP, Brazil).
PCR Core Lab in Brazil (Oswaldo Cruz Institute/FIOCRUZ, RJ) = responsible for PCR analyses from 16 Brazilian centers.
This is the largest trial yet conducted in Chagas disease. The study will clarify the role of trypanocidal therapy in preventing cardiac disease progression and death.
Am Heart J 2008; 156: 37-43

I- Rapid quantification of T. cruzi in host tissue by real-time PCR (Cummings & Tarleton, 2003)
Accurate quantification of tissue parasite burden in experimental infected mice using SYBR green with two distinct primer sets: satellite nuclear DNA and kDNA.
II- Development of a real-time PCR assay for T. cruzi detection in blood samples (Piron et al, 2007)
TaqMan probe directed to satellite DNA for parasite detection in blood of chronic individuals and acute congenital infection = qualitative assay (90% concordance with Nested PCR for the same parasite target).
The system was used to quantify T. cruzi epimastigotes DNA in reconstituted blood samples, reaching a detection limit of 10 parasites/mL.
A useful tool for monitoring parasite burden in hosts under treatment
nu
clea
rkDN
A
VIII- Real-time PCR for evaluating therapyVIII- Real-time PCR for evaluating therapy

III. Accurate real-time PCR strategy for monitoring bloodstream parasitic loads in Chagas disease patients (Duffy et al, 2009)
Dynamic range of T. cruzi satellite DNA based Q-PCR in
reconstituted blood
Melting curve analysis of satellite amplicons from reference stocks
melting temperatures > 85ºC
SybrGreen targeted to T. cruzi repetitive satellite sequence. To estimate parasite load in pediatric patients (n=43) and for the follow-up of those receiving treatment with Bz (n=38); aging 15 days to18 years old. To monitor Chagas disease reactivation in heart-transplanted patients (n=3) who received immunosuppressive therapy.

IV. PIDC – Chagas Disease Integrated Program (FIOCRUZ)
2008 Meeting: Thematic area of Diagnosis Development and validation of reagents and calibrators for Real Time PCR (TaqMan qPCR) – Oswaldo Cruz Institute (RJ), Carlos Chagas Institute (PR), BioManguinhos
DNA extraction standardization by an automated platform Generating a recombinant plasmid (internal calibrator)
A question to be addressed: Which target should be considered??
• Both assays yielded the same detection limit • kDNA was more effective if one considers the lower Ct values inferred from each point of the curve (higher number of sequence targets)• Satellite DNA gave more reproducible results inter-assays
Dynamic range of T. cruzi kDNA based Real-Time PCR [n = 6]. Serial dilutions of epimastigote DNA
representative of T. cruzi populations.
Standard curve generated from Dm28c (TcI)epimastigotes DNA in blood (10-fold dilutions)
26,62
19,49
28,8232,81
36,3638,57
31,9828,80
25,8722,10
y = - 3,1455x + 42,07R2 = 0,9898
y = - 3,1675x + 35,148R2 = 0,9977
05
10152025303540
0.01 0.1 1 10 100Parasite equivalents/mL blood
Cyc
le N
um
ber
(C
t)
kDNA
satellite DNA
Cl Brener(TCIIe)
Dm28c(TCI)
Y(TCIIb)
INPA 4167(Z3)
Cl Brener(TCIIe)
Dm28c(TCI)
Y(TCIIb)
INPA 4167(Z3)
Cl Brener(TcIIe)
Dm28c(TcI)
Y(TcIIb)
INPA 4167(Z3)
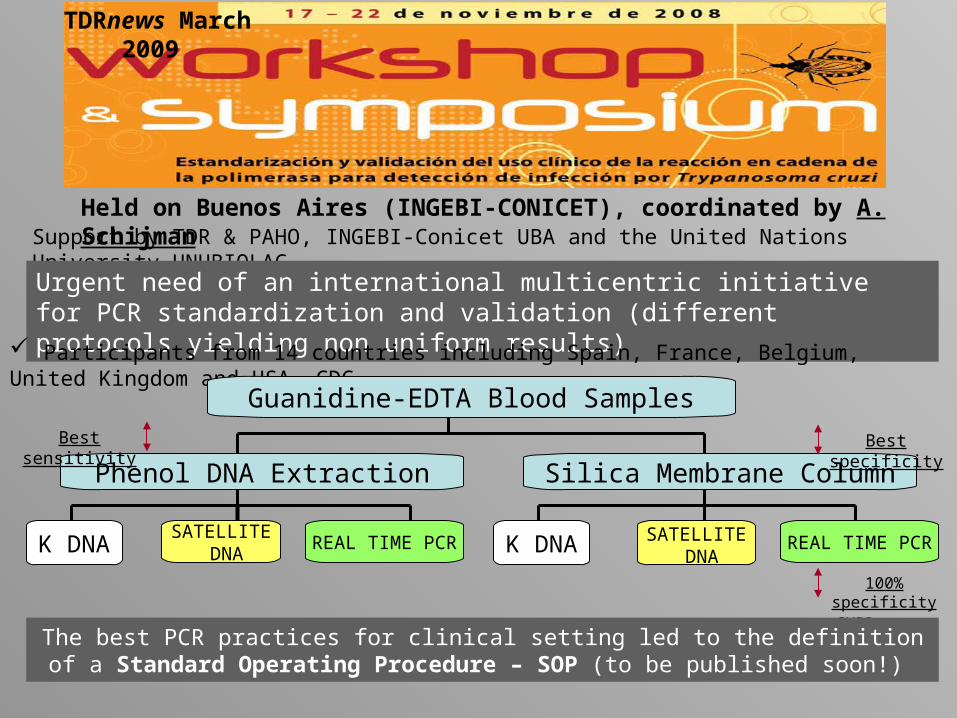
Held on Buenos Aires (INGEBI-CONICET), coordinated by A. Schijman Support by TDR & PAHO, INGEBI-Conicet UBA and the United Nations University UNUBIOLAC
Urgent need of an international multicentric initiative for PCR standardization and validation (different protocols yielding non uniform results)
Participants from 14 countries including Spain, France, Belgium, United Kingdom and USA -CDC
Guanidine-EDTA Blood Samples
Phenol DNA Extraction Silica Membrane Column
K DNASATELLITE
DNAREAL TIME PCR K DNA SATELLITE
DNAREAL TIME PCR
Best specificity
100% specificitySYBR green
Best sensitivity
TDRnews March 2009
The best PCR practices for clinical setting led to the definition of a Standard Operating Procedure – SOP (to be published soon!)

THANK YOU ...THANK YOU ...
AND ENJOY RIO !!!!AND ENJOY RIO !!!!







