International Epidemiologic Databases to Evaluate AIDS
Abstract-MOAB0202 XVIII International AIDS Conference, July 2010, Vienna, Austria
18-month mortality and loss to follow-up in ART-treated children in Asia and Africa
The pediatric IeDEA multiregional collaborationLeroy, V.1, Malateste K. 1, Rabie H. 2, Pagakrong L.3, Ayaya S. 4, Dicko, F. 5,
Davies MA. 6, Kariminia A. 7, Wools-Kaloustian K. 8, Aka, A. 9,, Aurpibul, L 10, Yiannoutsos, C. 8, Signaté-Sy, H, 11, Dabis, F. 1
for the International IeDEA pediatric Working Group.
1. Inserm U897, Bordeaux 2 University, Bordeaux, France. 2. Tygerberg Children's Hosp., Stellenbosch Univ., Cape Town, South Africa.3. Khon Kaen Univ., Thailand.4. Moi Teaching and Referral Hosp., Eldoret Kenya. 5. Hop Gabriel Touré, Bamako, Mali. 6. Center for Infectious Diseases Epidemiology and Research, School of Public Health and
Family Med., Univ. of Cape Town, South Africa.7. National Centre in HIV Epidemiology and Clinical Research, Sydney, Australia. 8. Indiana Univ. School of Medicine, Indianapolis, USA. 9. Centre de Prise en Charge, de Recherche et de Formation, CePReF, Abidjan, Côte d’Ivoire. 10. Chiang Mai University, Thaïland. 11. Hopital Albert Royer, Dakar, Sénégal.

18-month pediatric mortality and loss to follow-up in IeDEA
• Background:– Updated information on mortality and loss to follow-up
(LTFU) on ART are needed– Hypotheses: 1) high mortality among children LTFU and
2) higher LTFU with rapid ART scale-up • Requires large data sets, well-suited for multi-regional analysis
• Objective: To study 18-month mortality and LTFU rates after ART initiation, and baseline patient and programmatic determinants in a multiregional analysis

• IeDEA is a global collaboration of HIV treatment cohorts• Eligible study sites: IeDEA pediatric clinical centres
– Africa (4), Asia-Pacific (1), Central/South America (1) – Standardized data collection
• Inclusion criteria: – Positive PCR <18 mo or EIA ≥18 mo– Age: 0 to 15 years at HAART initiation – ARV-naive
• Except for exposure to perinatal PMTCT prophylaxis
– Starting HAART (≥3 ARV drugs)
Methods (1)

• Baseline: date of HAART initiation• Outcomes
– Mortality – LTFU: >6 months since the last visit
• Statistical analysis – 6-, 12-, and 18-month Kaplan-Meier probabilities – Cox model analysis of baseline determinants stratified
by region • Programmatic and patient variables
Methods (2)

Sites characteristics by region
Region Site (n) N
Public, Academic
(%)
Free access to lab tests
(%)
Free access to OI
prophylaxis(%)
Home visits & phone tracing
(%)
Asia 11 1,454 85.0 86.0 77.2 81.4
East Africa 23 3,114 99.8 100.0 100.0 91.5
Southern Africa 10 6,162 90.0 96.1 96.1 64.4
West Africa 10 2,881 77.1 86.0 41.0 29.9
TOTAL 54 13,611 89.0* 93.8* 83.3* 65.1*
*between-region heterogeneity p <0.01

Baseline characteristics at HAART initiation by region
Region NMedian
age, years (IQR)
Median CD4
percent (IQR)
HAART initiation
<2005 (%)
Initial HAART regimen (%)
2NRTI + 1 NNRTI
2 NRTI + 1 PI Other
Asia 1,454 7 (4-10) 7 (2-14) 40.0 93.4 0.9 5.7
East Africa 3,114 6 (3-9) 12 (7-16) 6.4 97.0 0.9 2.1
Southern Africa 6,162 4 (2-8) 14 (9-21) 21.6 66.4 30.1 3.5
West Africa 2,881 5 (2-9) 13 (7-19) 31.6 69.3 29.3 1.4
TOTAL 13,611 5 (2-9)* 12 (6-18)* 22.2* 76.9* 20.1 3.0*between-region heterogeneity p <0.01

Mortality and LTFU at 18 months by region
Region NMedian
follow-up (mo)
Deaths(%)
LTFU*(%)
Transferred out (%)
Asia 1,454 34 5.4 4.1 8.0
East Africa 3,114 15 4.3 14.0 0.4
Southern Africa 6,162 17 5.7 9.0 16.4
West Africa 2,881 21 7.4 21.8 1.1
TOTAL** 13,611 18 5.7 12.3 8.6
*>6 months since last visit**between-region heterogeneity p <0.01
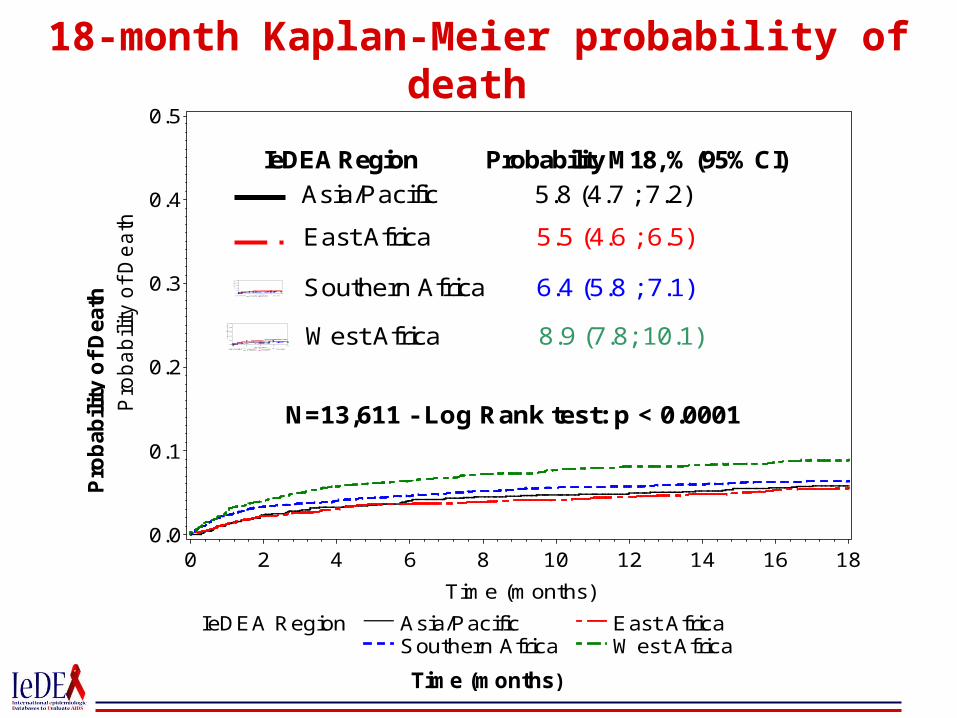
18-month Kaplan-Meier probability of death
P
rob
ab
ility
of
De
ath
Time (months)
IeDEA Region Asia/Pacific East AfricaSouthern Africa W est Africa
Pro
ba
bili
ty o
f D
ea
th
0.0
0.1
0.2
0.3
0.4
0.5
Time (months)
0 2 4 6 8 10 12 14 16 18
N=13,611 - Log Rank test: p < 0.0001
Asia/Pacific 5.8 (4.7 ; 7.2)
IeDEA Region Probability M18, % (95% CI)
Age at Baseline <12 months [1-3[ years [3-5[ years[5-10[ years +10 years
Pro
ba
bilit
y o
f D
ea
th
0.0
0.1
0.2
0.3
0.4
0.5
Time (months)
0 3 6 9 12
West Africa 8.9 (7.8; 10.1)
Age at Baseline <12 months [1-3[ years [3-5[ years[5-10[ years +10 years
Pro
ba
bility
o
f D
ea
th
0.0
0.1
0.2
0.3
0.4
0.5
Time (months)
0 3 6 9 12 Southern Africa 6.4 (5.8 ; 7.1)
East Africa 5.5 (4.6 ; 6.5)

Correlates of 18-month mortality, adjusted analysisVariables at HAART initiation Death at M18
% (n=777) aRR CI (95%) p
Age
10-15 years 5.5 Ref. - -
5-10 years 4.3 0.8 (0.7-1.0) 0.14
3-5 years 4.0 0.9 (0.6-1.1) 0.29
1-3 years 5.7 1.2 (0.9-1.5) 0.18
<12 months 12.8 2.8 (2.2-3.6) <0.01
Clinical stage
A,B or I,II,III 4.1 Ref. - -
AIDS or IV 10.1 2.0 (1.7-2.4) <0.01
Unknown 5.4 1.2 (0.9-1.5) 0.13
%CD4
≥ 20% 4.2 Ref. - -
10%-20% 4.3 1.2 (0.8-1.6) 0.34
<10% 9.9 2.9 (2.2-3.8) <0.01
Missing 5.0 1.5 (1.2-2.1) <0.01
Severe anemia (hgb <7 g/dl)
No 6.6 Ref. - -
Yes 20.4 2.8 (2.1-3.6) <0.01
Unknown 4.2 1.0 (0.9-1.3) 0.58

18-month Kaplan-Meier probability of LTFU
Pro
ba
bil
ity
of
los
s to
fo
llo
w-u
p
Time (months)
IeDEA Region Asia/Pacific East AfricaSouthern Africa W est Africa
Pro
ba
bili
ty o
f lo
ss t
o f
ollo
w-u
p
0.0
0.1
0.2
0.3
0.4
0.5
Time (months)
0 2 4 6 8 10 12 14 16 18
N=13,611 - Log Rank test: p < 0.0001
Asia/Pacific 4.5 (3.5 ; 5.8)
IeDEA Region Probability M18, % (95% CI)
Age at Baseline <12 months [1-3[ years [3-5[ years[5-10[ years +10 years
Pro
ba
bility o
f D
ea
th
0.0
0.1
0.2
0.3
0.4
0.5
Time (months)
0 3 6 9 12West Africa 24.7 (23.0; 26.4)
Age at Baseline <12 months [1-3[ years [3-5[ years[5-10[ years +10 years
Pro
ba
bility o
f D
ea
th
0.0
0.1
0.2
0.3
0.4
0.5
Time (months)
0 3 6 9 12 Southern Africa 11.5 (10.6 ; 12.5)
East Africa 17.0 (15.6 ; 18.6)

Correlates of 18-month LTFU, adjusted analysisLTFU M18 % (n=1680) aRR CI (95%) p
Age (Ref. 10-15 years)
6-10 years 10.3 1.0 (0.8-1.2) 0.99
3-5 years 10.4 0.9 (0.8-1.1) 0.51
1-2 years 15.4 1.2 (1.0-1.5) 0.01
<12 months 18.5 1.8 (1.5-2.2) <0.01
HAART regimen (Ref. 2NRTI+1NNRTI)
2NRTI+1PI 14.5 1.5 (1.3-1.7) <0.01
Other 19.3 1.6 (1.3-2.1) <0.01
Clinical stage (Ref. A,B or I,II,III)
AIDS or IV 14.0 1.3 (1.2-1.5) <0.01
Unknown 14.5 1.9 (1.6-2.2) <0.01
%CD4 (Ref. ≥20%)
10-20% 10.3 0.8 (0.7-1.0) 0.03
<10% 10.6 1.0 (0.8-1.2) 0.90
Missing 13.9 1.1 (0.9-1.3) 0.27
Severe anemia (Ref. None)
Yes 19.7 1.4 (1.0-1.8) 0.02
Unknown 10.6 1.0 (0.9-1.2) 0.48
Year of HAART initiation (Ref. <2005)
2005-2007 13.8 2.5 (2.1-2.9) <0.01
≥2007 14.2 3.6 (3.0-4.3) <0.01

Programmatic correlates of 18-month LTFU, adjusted analysis
LTFU at M18 % (n=1680)
aRR CI (95%) P
Type of facility
Public 13.3 Ref. - -
Private 4.7 0.2 (0.1-0.2) <0.01
Unknown 5.5 0.1 (0.07-0.2) <0.01
Non-urban vs urban 12.6 2.1 (1.7-2.5) <0.01
Cohort size
<250 10.7 Ref. - -
250-500 14.9 1.0 (0.8-1.3) 0.77
500-800 16.7 2.6 (2.1-3.3) <0.01
≥ 800 7.4 1.4 (1.1-1.8) <0.01
Pay for lab tests, unknown vs free 28.9 2.1 (1.5-3.1) <0.01
Pay for HAART, unknown vs free 28.6 6.2 (3.9-9.7) <0.01
LTFU tracing
Home visit and phone call 11.2 Ref. - -
Only phone call 6.8 0.4 (0.3-0.5) <0.01
Only home visit 11.7 1.1 (0.7-1.8) 0.58
No phone call and no home visit 27.8 1.0 (0.3-1.0) <0.01

Methodologic challenges
• Multiple sources of heterogeneity• Operational definition of LTFU• Variability by site in patient tracking system and access
to free services
• Informative censoring– Missing data was not uncommon for the outcomes and
predictors• The impact varied by outcome • Demonstrates need to ascertain outcomes of those LTFU

Conclusions
• The 18-month risks of death and LTFU differed substantially across regions – Reflects impact of delayed HAART and importance of retention– Recent initiation of HAART and increased cohort size were
associated with higher LTFU• Overload of health facilities
– Requiring patients to pay for care is associated with LTFU• Need to advocate for free access to all HIV services for children
• Innovative and feasible approaches to retain children in ART programs are urgently required

Acknowledgments • All the patients followed up in the IeDEA pediatric centers • IeDEA West Africa principal investigators
– François Dabis– Emmanuel Bissagnéné
• Bordeaux and Abidjan IeDEA West Africa Regional Center staff:– Charlotte Lewden, Elodie Rabourdin, Valériane Leroy, Didier K.
Ekouévi, Karen Malateste, Rodolphe Thiebaut– Gérard Allou, JC Azani, Patrick Coffie, Hughes Djétouan, Bertin
Kouadio
• All the investigators and pediatric coordinators from the Pediatric IeDEA Regions contributing to the project: Asia (Annette Sohn), East Africa (Kara Wools-Kaloustian), Southern Africa (Mary-Ann Davies), Western Africa (A. Azondekon)
• The IeDEA Pediatric Working Group: Mary-Ann Davies (Chair), Melanie Bacon, Andrea Ciaranello, Rosemary McKaig, Lynne Mofenson, Robin Huebner, Lori Schwarze
• Funders: NIAID, NICHD, NCI







