
i
Abstract of dissertation entitled
“Evidence-based guideline of postnatal telephone lactation support
on duration of breastfeeding”
Submitted by
Wong Ho Yan
for the Degree of Master of Nursing
at The University of Hong Kong
in July 2016
In the recent decades, the benefits of breastfeeding to both the mothers and the infants have
gained increasing significance among the public. The breastfeeding rate on hospital discharge
showed remarkable increase from19% in 1992 to 85.8% in 2012. Despite the effort made by the
government as well as the NGOs, such as the Baby Friendly Hospital Initiative Hong Kong
Association, the current percentage of breastfeeding in 6 months after delivery in Hong Kong still
lags behind the recommendations of the World Health Organization (WHO).
Considering the traditional Chinese cultural belief, the Chinese mothers are usually expected
to stay at home in the first month of postnatal period. In order to provide continuous postnatal
breastfeeding support for them, telephone support intervention would be considered as a feasible
method in this situation. Even those mothers remain at home in the early postnatal period, they are
still able to access professional breastfeeding support with the use of telephone which is an easy
communication medium nowadays.
For the evidence-based guidelines, it is developed from five selected studies which indicated
that telephone breastfeeding support is effective in prolonging breastfeeding duration. To consider
the implementation potential of the innovation, the implementation plan and its evaluation would be
thoroughly discussed in the later part of this project.

ii
Evidence-based guideline
of postnatal telephone lactation support
on duration of breastfeeding
by
WONG HO YAN
School of Nursing
The University of Hong Kong
A thesis submitted in fulfillment of the requirements for
the Degree of Master of Nursing
at The University of Hong Kong.
July 2016

iii
Declaration
I declare that this dissertation represents my own work, except where due acknowledgment
is made. It has not been previously included in a thesis, dissertation, or report submitted to this
university or to any other institution for a degree, diploma, or other qualifications.
Signed……………………………………………………………………
WONG HO YAN
iv
Acknowledgements
I would like to express my sincere gratitude to my supervisor, Professor Elizabeth Hui, who
provides vulnerable advice, guidance as well as psychological support to me throughout my
dissertation. She did promote interactive atmosphere in the tutorials which facilitated us to
exchange our ideas. And she always provided constructive feedback for my dissertation work. Her
passion and enthusiasm deeply impresses me and drives me to pursuing evidence-based guidelines
related to breastfeeding.
In addition, I would like to give thanks to my supportive classmates. We did enjoy our
learning time in this programme. Not only did I gain knowledge, but also friendship.
Finally, I would like to show my appreciation to my beloved family, including my parents,
my husband and my upcoming new family member who always show understanding and
encouragement throughout my two-year master study.

v
Table of Contents
Abstract ……………………………………………………………………..……………………………………i
Cover page……………………………………………………………………..……………………………… ii
Declaration……………………………………………………………………………………..………………iii
Acknowledgements …………………………………………………………………………………………… iv
Table of contents ……………………………………………………………………………………………… v
Lists of appendices ……………………………………………………………………………………………vi
Chapter 1 - Statement of the Problem……………………………………………………………. 1
Background………………………………………………………………………………….………….1
Affirming the need……………………………………….…………………………………………..2-4
Objective and Research Question……………………..…………………………………….….………4
Significance of clinical issue…………………………………………………………………….……..4
Chapter 2 – Critical Appraisal .....……..………………..………………………………..………6
Search and appraisal strategy……………………………………………………….…………….….6
Table of evidence…………………………………………...…………………………………………7
Quality assessment………………………………………………………………………………….…9
Summary and Synthesis……………………………………………………………………………….12
Chapter 3 - Implementation Potential ………………………………………………………….. 18
Transferability of the findings …………………………………………………………………18-20
Feasibility of the innovation ………………………………………………………………………. 20
Cost-benefit ratio of the innovation ………………………………………………………..……….23
Conclusion ………………………… ………………………………………………………...........25
Chapter 4 – Implementation plan ………………………………..………………………………26
Communication plan …………………………………………………………………………...…..26
Pilot study plan ……………………………………………………………………………………..28
Evaluation plan ……………………………………………………………………………………..29
Outcomes measurement …………………………………………………………………………….31
Basis for effectiveness ……………………………………………………………………...………32
Conclusion …………………………………………………………………………………….32-33
References ……………………………………………………………………………………...34-36

vi
List of appendices
Appendix A: PRISMA diagram …………………………………………………………………….37
Appendix B: Table of Evidence ………………………..……………………………....……………38
Appendix C: Quality assessment using SIGN methodology checklists for RCTs ………..….…39-40
Appendix D: Timeframe for the innovation …………………………………………..……………41
Appendix E: Material and non-material costs of implementing the innovation …………………...42
Appendix F: Material costs of not implementing the innovation …………………………………..42
Appendix G Calculation of cost-benefit ratio: …………………………………………………..…42
Appendix H: Grades of Recommendations ……………………………………………..…….… 43
Appendix I: Levels of Evidence ……………………….…..………………...…………..…….… 43
Appendix J: Breastfeeding data collection form ……………………………..………………...…44
Appendix K: Telephone support checklist …………….…………………………...……..…….… 45
Appendix L: Questionnaire for the level of satisfaction among nurses …………………..…….… 46
Appendix M: Evidence-Based Practice Guideline …………………………………...…………47-48
1
Chapter 1 - Statement of the Problem
Background
Breastfeeding is not only beneficial to infants but also to the mothers and the society. For
infants, breast milk is the best gift to nourish their growth. Its benefits are well recognized by the
public throughout the years. The components of breast milk uniquely satisfies the health needs of
infants in different stages of development and it provides the most ideal nutrients to promote the
growth and development of infants (World Health Organization [WHO], 2003). Unlike the artificial
milk, the constituents of breast milk vary in order to satisfy the health needs in different
developmental stages among the infants. Colostrum is produced during the first few days of
postpartum and it contains plenty of immune protective matters to provide the newborns with a
natural barrier against the pathological agents. Therefore, breastfeeding infants are less prone to
various infant illnesses, such as gastroenteritis, pneumonia, otitis media, eczema, asthma and
Sudden infant death syndrome (SIDS) (Kramer et al., 2001). Breastfeeding is proven to have dose
dependent protective effect on the health outcomes of infants. Evidence showed that there is a direct
cause-and-effect relationship between breastfeeding intervention and positive infant health
outcomes while reducing infant morbidity (Kramer et al., 2001). For the maternal benefits of
breastfeeding, oxytocin released during breastfeeding minimizes the risk of postpartum hemorrhage
by stimulating uterine contraction. There is also lower incidence of ovarian cancer and Type 2
diabetes among lactating mothers (Danforth et al., 2007; Jordan et al., 2010). It is worth promoting
breastfeeding to the public through breastfeeding support intervention.
Regarding to the local situation in Hong Kong, there was a continuous increasing trend of
breastfeeding initiation rate over the past decades. One of the reasons to explain this phenomenon is
that more women become more aware of the health benefits of breastfeeding and they tend to
choose breastfeeding for their infants. According to the latest statistics retrieved from Baby Friendly
Hospital Initiative Hong Kong Association (BFHIHKA), the breastfeeding initiation rate in 2014

2
and 2015 had slightly increased from 84.2% to 86.3% (BFHIHKA, 2015). However, the
breastfeeding rate substantially declines in the few months of postpartum. It implies that local
mothers may acknowledge the benefits of breastfeeding and the majority of mothers choose
breastfeeding for their infants.
In Hong Kong, there are both governmental and non-governmental organizations to promote
breastfeeding, such as Hospital Authority, Maternal Child Health Centres (MCHCs), BFHIHKA and
the La Leche League Hong Kong, via hotline services, educational talk and support groups to
support lactating mothers in breastfeeding concerns. They have greatly contributed in promoting the
duration and rate of breastfeeding. The breastfeeding rate on discharge showed remarkable growth
from 19% in 1992 to 85.8% in 2012 (BFHIHKA, 2015). Despite the efforts made by these
organizations, most mothers decide to stop breastfeeding especially after 1 month of postpartum and
only 32.7% mothers breastfed until 6 months postpartum (CHP, 2014).
Therefore, an evidence-based breastfeeding support intervention for mothers during
postnatal period is vital to provide effective breastfeeding intervention in prolonging duration of
breastfeeding.
Affirming the needs
According to the recommendation by the World Health Organization (WHO), exclusive
breastfeeding is recommended for infants up to 6 months of age, and it can be continued until two
years of age or beyond, accompanied with the introduction of complementary food (WHO, 2003).
Exclusive breastfeeding is defined as the practice of solely giving an infant breast milk for the first
6 months of life without any type of food or drink (WHO, 2003). In the regular survey conducted by
Family Health Service of the Department of Health in 2013, the exclusive breastfeeding rate even
drop from 22.1% at 1 month to 2.3% at 6 months which is far below the WHO recommendation
(CHP, 2014). In addition, the ever breastfeeding rate substantially drop after first month of
postpartum. It indicates that there is room for improvement on current breastfeeding support
3
intervention.
The majority of mothers would attend MCHCs after discharged from hospital for a wide
range of child care services and postnatal support services, such as child immunization programme
and breastfeeding coaching service. MCHCs have implemented a new breastfeeding policy,
incorporating the 'Ten Steps to Successful Breastfeeding' and the International Code of Marketing
of Breastmilk Substitutes since 2000 in order to protect and promote breastfeeding (Leung, 2009).
Breastfeeding promotion has become a major component of current MCHCs services, targeting
from pregnant women to postnatal women through breastfeeding support group, breastfeeding
coaching service and education talk. Since MCHCs provides health promotion services to eligible
persons without any charges, it attracts many local women to utilize the services. Therefore,
MCHCs is an feasible place to implement the innovation of this study. For breastfeeding coaching
services, it is conducted by nurses who have completed professional breastfeeding training and they
are competent to provide hands-on demonstration and individual coaching for those lactating
mothers with breastfeeding concerns. Throughout the coaching service, mothers would learn about
the proper breastfeeding techniques, such as latching on and attachment, and it help minimize the
risk of breastfeeding complications. Although the coaching services are comprehensive, it requires
mothers to take their initiatives to seek for professional help at the first step. For the Chinese
culture, women during postnatal period should stay at home at the first month of postpartum to
promote their recovery. This is a major challenge for them to assess coaching services. Furthermore,
they are usually reluctant to seek help for their breastfeeding problems since they perceive it should
be managed by them. In view of providing effective breastfeeding support intervention among
Chinese mothers, telephone breastfeeding support would be considered as a feasible approach to
provide continuous support for lactating mothers even after discharge. For those lactating mothers
during the period of “sitting month”, they can be easily reached via telephone support. Unlike the
traditional hotline services that mothers take active role to make calls, telephone support is operated
4
in a proactive approach which nurses take initiatives to contact the mothers. Telephone is chosen as
an ideal communication medium since it would not be influenced by geographical limitations and it
is a convenient, economical way compared to other kinds of breastfeeding support intervention,
such as home visit (Tahir & Al-Sadat, 2012).
For those researches including telephone breastfeeding support, the findings are
inconclusive. According to the research conducted by Pugh et al. (2010), the intervention group
received combined intervention (hospital visits provided by a breastfeeding support team, home
visits and telephone support) and their results indicated no increase in duration of breastfeeding.
This do not mean telephone breastfeeding support alone would not be effective to prolong duration
of breastfeeding. Therefore, an evidence-based protocol of telephone lactation support to prolong
duration of breastfeeding is required to provide standardized way to prolong duration of
breastfeeding.
Objective and Research Question
The objective of the dissertation is to prolong the duration of breastfeeding through
telephone support intervention during postnatal period. The proposed research question is
“Among breastfeeding mothers in the postnatal period, does telephone breastfeeding support
intervention prolong breastfeeding duration, compared to usual care?”
Significance of clinical issue
According to World Health Organization (WHO) and United Nations Children's Fund
(UNICEF), exclusive breastfeeding (EBF) is recommended for infants up to the first 6 months of
life and continued breastfeeding with appropriate complementary food can be provided up to 2
years of age or beyond (WHO, 2003). There are extensive evidences shown that the benefits of
breastfeeding is dose dependent, infants receiving longer duration of breastfeeding experience better
health outcomes (Kramer & Kakuma, 2004). Early cessation of breastfeeding not only increases the
risk of childhood obesity, gastroenteritis, necrotizing enterocolitis, lower respiratory infections,

5
Type 1 and 2 diabetes and sudden infant death syndrome (Kramer et al., 2001). It also associates
with adverse health impacts among mothers, such as breast and ovarian cancers, Type 2 diabetes
and postpartum depression (Kramer et al., 2001). In addition, breastfeeding is beneficial to our
society and the health care system. Nowadays, people become more aware of sustainable
development and environmental conservation. Compared to formula feeding, breastfeeding is more
environmental-friendly since mothers just directly feed their infants without extra preparation,
thereby reducing the environmental burden from disposal of artificial cans. For the health care
system, breastfeeding infants are less prone to common childhood illnesses, such as diarrhea and
pneumonia which are the primary causes of child mortality worldwide. Therefore, it reduces
hospital admission and duration of hospitalization, in which directly relieves financial burden on
health care system. In addition, telephone is a well-accepted medium of communication as it works
independent of neither geographical limitation nor physical barriers. And it is particularly beneficial
among Chinese mothers since most of them would “sit month” in the first month of postpartum
which is a delicate period of adaptation in both physiological and psychological way.
6
Chapter 2 – Critical Appraisal
Although telephone lactation support is suggested as an effective intervention to prolong the
duration of breastfeeding, there are still lack of relevant guidelines that standardize nursing practice
among local institutions. Therefore, systematic review allows people to critically appraise the
quality of selected articles. The role of systematic review is to provide health care professionals
with updated and evidence-based clinical information which helps maintain quality of care. It also
assists in standardizing current nursing practice. In this study, our objective is to prolong
breastfeeding duration via professional telephone lactation support. To perform critical appraisal,
the first step is to select relevant articles by keyword searching. After the articles are filtered, the
table of evidence (TOE) would be used as a tool to appraise the articles and facilitate the
comparison among the selected articles in terms of intervention, effect size and so forth.
Search and appraisal strategy
Eligible criteria of study participants
To be eligible for study selection, participants have to meet the criteria shown as follows: (1)
Hong Kong Chinese women aged 18 or above; (2) without significant obstetric complications
during pregnancy, such as pre-clampsia or postpartum hemorrhage; (3) intended to breastfeed; (4)
no history of major medical or psychiatric diseases that may interfere breastfeeding; (5) term
delivery at 37 gestational weeks or beyond; (6) no physical anomalies of mothers and babies that
may contradict with breastfeeding.
For exclusion criteria, mothers who are multiple pregnancy would be excluded in this study
as it is regarded as high risk obstetric case. When their infants who are transferred to Special Care
Baby Unit (SCBU) or Neonatal Intensive Care Unit (NICU) during the study would also be
excluded.
The study search was conducted on 9 and 12 July 2015. Two electrical databases, PubMed
and CINAHL Plus were selected for searching articles. There was no filter used at the beginning of
7
article searching. Keywords used in the searching process include “breastfeed”, “breastfeeding”,
“telephone support”, “telephone breastfeeding support”, “telephone lactation support”, “telephone
support intervention”, “telephone intervention” , “telephone counseling”, “duration of
breastfeeding”, “breastfeeding duration”. After the searching result generated, additional filters
were applied to limit the results, including randomized control trial, English for article language.
There is no limitation of published year of the articles.
The flow diagram of articles searching is presented in PRISMA diagram (Refer to Appendix
A). A total of 587 articles were retrieved from these databases; 487 articles were retrieved from
PubMed and 100 articles from CINAHL. After removing the duplicated articles from the above
databases, there were remaining 494 articles. By screening the title and abstract, 478 articles were
excluded. There were 16 articles which were further screened for their eligibility. Finally, 5 relevant
articles were selected for critical appraisal. There was also 1 article retrieved by manual searching
through the above eligible studies. However, it was excluded after screening through the titles and
abstract since the intervention group received combined intervention support during postnatal
period, including home visit and telephone support (Pugh et al., 2010). Therefore, the effectiveness
of telephone support alone could not be evaluated.
Table of Evidence
Table of evidence provides quick reference of each selected article by clearly presenting data
in different columns. Table of evidence is used to present the summary of the 5 selected studies,
including citation, study design, level of evidence, sample characteristics, treatment received from
intervention and control group, outcome(s) measured and effect size.
Study design & Level of Evidence
All of the five selected studies are randomized controlled trials (RCT). According to the
grading system of Scottish Intercollegiate Guidelines Network (SIGN) in 2011 on the levels of
evidence, four out of these studies were 1+ (Carlsen et al., 2013; Dennis et al., 2002; Simonetti et
8
al., 2012; Tahir & Al-Sadat, 2013) while one study was categorized as 1++ (Fu et al., 2014). The
number of sample size from the above studies ranged from 114 to 1948. For the study with largest
sample size, it was 3 arms study, including 2 intervention groups and 1 control group.
Characteristics of study participants
Participants were recruited from Hong Kong, Malaysia, Denmark, Canada and Italy (Carlsen
et al., 2013; Dennis et al., 2002; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat, 2013).
Two studies focused on primiparous women in postnatal period (Fu et al., 2014; Dennis et al., 2002)
while Carlsen et al. (2013) targeted on whether telephone support prolongs the duration of
breastfeeding among the obese women as it was found that obese women are easier to have
breastfeeding difficulties. Among all of the selected studies, participants are intended to breastfeed
and without significant maternal illnesses. For their infants, all of them are term delivery, without
physical anomalies.
Intervention group
Four of the selected studies had telephone lactation support conducted by lactation
counselors (Carlsen et al., 2013; Tahir & Al-Sadat, 2013), nurses (Fu et al., 2014), midwives
(Simonetti et al., 2012). In Dennis's study (2002), telephone support was provided by peer
counselors. One of the studies was 3 arms studies which consisted of 2 intervention groups and 1
control group (Fu et al., 2014). In the study of Fu et al. (2014), the 2 intervention groups included
breastfeeding support session and weekly telephone support. For the qualification of health
professions, those lactation counselors had completed lactation management and counseling course
based on WHO module in the study (Tahir & Al-Sadat, 2013). In the study by Fu et al. (2014), the
intervention was delivered by nurses, who were either experienced midwives or certified lactation
consultants, with the completion of relevant program and extensive experience on lactation support.
For the peer counselors in those studies by Dennis et al. (2012), they had breastfeeding experience
for at least 6 months duration with completion of orientation session to ensure standardization of
intervention.
9
Control Group
In the control group, participants received standard of care or conventional postnatal care
without telephone breastfeeding support service in all of the above studies (Carlsen et al., 2013;
Dennis et al., 2002; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat, 2013).
Outcomes measured
The primary outcome in the above studies was to assess the rate of breastfeeding in both
exclusive and any method (exclusive breastfeeding and partial breastfeeding) in different intervals,
such as 1, 3 and 6 months of postpartum. In the study conducted by Dennis et al. (2002), its
secondary outcome was maternal satisfaction of infant feeding.
Effect size
The detailed results of the above studies were shown in relative risk (RR) and odd ratio
(OR) (Refer to Appendix B). The effect size in 1 month ranges from 1.627 to 1.89 in terms of odd
ratio and from 1.1 to 1.8 in terms of relative ratio. For the effect size in 3 month, the range is wider
than 1 month, ranging from 1.2 to 2.45 (odd ratio) and from 1.21 to 1.9 (relative ratio).
Quality assessment
To assess the quality of each selected article, SIGN methodology checklist is chosen as the
appraisal tool. SIGN was established in 1993 and it aims at improving the quality of health care
system by standardizing the existing practice and thus maximizes health benefits among patients. It
is divided into 2 sections in the methodology checklist, including internal validity and the overall
assessment of the study. The details of each study are presented in the table of Quality Assessment
(Refer to Appendix C).
Appropriate and clearly focused questions
All of the above studies had clear and appropriate research question which contained all
elements of “patient-intervention-comparison-outcome” (PICO) format which covered the effectiveness
of telephone lactation support on rate of breastfeeding during postnatal period.

10
Randomization
Four studies used randomization for random assignment by different methods, such as random
allocation program, online randomization program (Carlsen et al., 2013; Dennis et al., 2002; Fu et al.,
2014; Tahir & Al-Sadat, 2013). In the study by Simonetti et al. (2012), randomization was
mentioned for study participants but the method was not specified.
Concealment
Only 2 studies achieved the criteria of allocation concealment (Fu et al., 2014; Tahir & Al-Sadat,
2013). In Fu's study (2014), the research nurses and study sites were informed of treatment allocation 48
hours prior to recruitment of study participants. Tahir and Al-Sadat (2013) used a list of random codes to
ensure adequate concealment. In the other 3 studies, no concealment method was mentioned (Carlsen et
al., 2013; Dennis et al., 2002; Simonetti et al., 2012).
Blinding
Since the intervention was conducted by either nurses or peer counselors, it was impossible to
blind either participants or those delivering the intervention. Nevertheless, it is possible to blind the
researcher enumerators who were responsible for data collection and analysis. Four studies succeeded in
blinding the researchers (Carlsen et al., 2013; Dennis et al., 2002; Fu et al., 2014; Tahir & Al-Sadat,
2013). In only one study, the presence of blinding was not clear since it did not mention whether the
researchers were blinded of treatment allocation (Simonetti et al., 2012).
Comparable group
For the baseline characteristics of both intervention and control group, there was no statistical
significance at the beginning of the study. Therefore, study participants in all five studies were
comparable (Carlsen et al., 2013; Dennis et al., 2002; Fu et al., 2014; Simonetti et al., 2012; Tahir &
Al-Sadat, 2013).
Difference between groups is the treatment under investigation
In all five studies, there was no key difference between the treatment groups and control groups
and the intervention was the only difference between two groups (Carlsen et al., 2013; Dennis et al.,

11
2002; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat, 2013).
Valid and reliable outcome measures
All studies clearly mentioned their outcomes which were measured in a valid and reliable way
(Carlsen et al., 2013; Dennis et al., 2002; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat,
2013).
Percentage of dropouts
In all five studies, the dropout rate did not exceed 20%, which was favorable. The detailed
figures of dropout rate in each group are shown in the table of quality Assessment (Refer to Appendix
C).
Intention–to-treat analysis
Only two studies adopted Intention-to-treat analysis (Fu et al., 2014; Tahir & Al-Sadat, 2013).
In the data analysis, they used the original number of participants in each group even though some
participants dropped out. In the remaining three studies, participants who dropped out were not
included throughout the study after randomization (Carlsen et al., 2013; Dennis et al., 2002;
Simonetti et al., 2012).
Results are comparable for all sites
Only 1 study involved multi-centre approach and the results were comparable among all sites
(Fu et al. 2014). For the remaining four studies, their study conducted in a single site only (Carlsen et
al., 2013; Dennis et al., 2002; Simonetti et al., 2012; Tahir & Al-Sadat, 2013).
Ratings of the studies
Two studies were categorized as high quality (++) as they showed adequate randomization
and allocation concealment (Fu et al., 2014; Tahir & Al-Sadat, 2013). In the other 2 studies, they
had randomization but no allocation concealment; therefore, their ratings were classified as
acceptable (+) (Carlsen et al., 2013; Dennis et al., 2002). In the pilot study conducted by Simonetti
et al. (2012), the randomization method was not clear and it did not have allocation concealment. It
was classified as low quality (-).
12
Summary and Synthesis
Summary of study result
All of the five reviewed studies investigated the effect of postnatal telephone lactation
support on breastfeeding outcomes: the rate of exclusive and any breastfeeding at different intervals
in postnatal period.
Diversity of conclusions
In general, all studies showed that telephone lactation support provided by health
professionals was effective to increase the rate of both exclusive and any breastfeeding at various
postnatal periods. According to the result of each study, the intervention was statistically significant
at specific interval. In the study by Tahir & Al-Sadat (2013), it showed that telephone lactation
support was effective in increasing the exclusive breastfeeding rate at the first month postpartum,
but not effective at the fourth and sixth month of postpartum. Fu et al. (2014) showed similar
findings in their study. Professional telephone breastfeeding support significantly increased the rate
of exclusive and any breastfeeding in the early postnatal period: the first month of postpartum.
Carlsen et al. (2013) showed that telephone intervention by lactation consultant prolongs the
duration of both exclusive and any breastfeeding among obese women across the first 6 month of
postpartum. In the study by Dennis et al. (2002), it indicated that telephone support by peer
counselors was statistically effective in maintaining breastfeeding up to 3 months postpartum. In the
pilot study by Simonetti et al. (2012), structured telephone support was shown effective in prolong
duration of breastfeeding during the first 5 months postpartum.
Characteristics of participants
In all of the five studies, the target participants were assessed for their intention to breastfeed
during the recruitment process, only mothers intended to breastfeed would be eligible for the studies
(Carlsen et al., 2013; Dennis et al., 2002; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat,
2013). Four studies reported that their study participants were of good past health without

13
significant obstetric and medical illness that may impair their ability to breastfeed (Carlsen et al.,
2013; Dennis et al., 2002; Fu et al., 2014; Tahir & Al-Sadat, 2013).
Qualifications of researchers who delivered intervention
In the four out of five studies, the telephone support was conducted by health professionals
who were certified lactation consultants, nurses or registered midwives (Carlsen et al., 2013; Fu et
al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat, 2013). Only one study reported that the
intervention was delivered by peer counselors (Dennis et al., 2002). To ensure the competency of
both health professions and peer counselors, lactation counselors (LC) had completed the lactation
management and counseling course prior to the study (Tahir & Al-Sadat, 2013). Counseling
guidelines and standard operation procedure booklet were issued to each lactation counselor (Tahir
& Al-Sadat, 2013). The research nurses were either experienced midwives or certified LC and they
possessed extensive experience in breastfeeding support and counseling skills (Fu et al., 2014).
They were provided additional training on study protocol before the study, in order to ensure the
evidence-based quality of study intervention (Fu et al., 2014).For the qualification of peer
counselors, they were provided with handbook and orientation session which aimed at developing
their skills in telephone support and referrals to increase standardization of the intervention (Dennis
et al., 2002). In the two studies, the intervention was performed by certified LCs (Carlsen et al.,
2013) and WHO-UNICEF licensed midwife (Simonetti et al., 2012) but it was not clear that
whether there was relevant training equipped for them prior to the study.
Duration & frequency of intervention
In the five studies, the duration of intervention varied from 3 to 6 month of postpartum.
Tahir & Al-Sadat (2013) reported that telephone support were delivered by LCs twice monthly until
6 month of postpartum, so participants in intervention group received 12 telephone calls at the end
of the study. Whilst Fu et al. (2014) reported that telephone support would be provided on weekly
basis up to 4 weeks postpartum or whenever mothers stopped breastfeeding. In Carlsen et al. (2013)
14
study, telephone support were provided for 3 times during the first month of postpartum, then
participants would be contacted every second week until 2 months postpartum, and monthly call
until 6 months of postpartum or whenever mothers stopped breastfeeding. Dennis et al. (2002)
reported that there was no standardized frequency of telephone contacts and it was provided based
on individual participant's need. In the pilot study by Simonetti et al. (2012), telephone support was
provided in the structured format. The timing of telephone calls were mutually agreed by both
mothers and midwives and the frequency of intervention was at least once per week.
Time of initial call
Three studies mentioned the timing of first call (Carlsen et al., 2013; Dennis et al., 2002; Fu
et al., 2014). The initial telephone call was made within 2 days after discharged from hospital
(Dennis et al., 2002); within 3 days after discharged from hospital (Fu et al., 2014) and within the
first 7 days (Carlsen et al., 2013).
Format of intervention (structured / patient-initiated)
Four studies provided their intervention based on their proposed frequency and it was
usually conducted on weekly basis (Carlsen et al., 2013; Fu et al., 2014; Simonetti et al., 2012;
Tahir & Al-Sadat, 2013). Dennis et al. (2002) reported that the intervention were participant-
initiated which participants determined the frequency of telephone call according to their individual
needs.
Content of telephone support intervention
Three studies described the content of telephone support intervention (Carlsen et al., 2013;
Fu et al., 2014; Simonetti et al., 2012). During each telephone support, participants were assessed
their breastfeeding knowledge and the well-being of mothers and infants, breastfeeding advice
would be provided accordingly (Carlsen et al., 2013). In Fu et al. study, its content focused on their
breastfeeding knowledge and emotional well-being. Guidelines on managing breastfeeding
problems, such as poor latching, would be provided on individual basis (Fu et al. 2014). Simonetti
15
et al. reported that relevant information and support on breastfeeding would be given in each
telephone call.
Synthesis
In accordance with the diversity of results among the five reviewed studies, the study design
and content of intervention would be compared and possible reasons would be provided to explain
the diversity.
Qualifications of health professions and peer counselors
In the five reviewed study, the intervention was mainly conducted by healthcare professions
(Carlsen et al., 2013; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat, 2013) and it was
performed by peer counselors in one study (Dennis et al., 2002). Since both healthcare professions
and peer counselors received different type of training courses prior to the study, their competency
and qualification were not standardized, in which may impair the accuracy of study results.
Intention-to-treat analysis
Only two out of five reviewed studies adopted intention-to-treat analysis. In Carlsen et
al.(2013) study, the dropout rate was 13.6% in the control group and 2.78% in the intervention
group respectively. When the dropout rate is relatively high in this study, the accuracy of study
result would be impaired especially without intention-to-treat analysis.
Duration & frequency of intervention
Four studies provided telephone support on weekly basis throughout the studies and the
study results showed that the duration of intervention was positively correlated to duration of
breastfeeding (Carlsen et al., 2013; Fu et al., 2014; Simonetti et al., 2012; Tahir & Al-Sadat, 2013).
Time of initial call
In order to provide continuous breastfeeding support after hospital discharge, the initial call
should be made within 2 days after hospital discharge. Breastfeeding mothers, especially the
primiparous mothers, may encounter breastfeeding problems, such as breast engorgement which is

16
commonly seen after day 3 of postpartum and it does require timely advice and management.
Content delivered via telephone support intervention
In the five reviewed studies, the content of telephone breastfeeding support mainly provided
mothers with breastfeeding knowledge, assessment of well-being of both mothers and infants and
advice of managing breastfeeding difficulties. In the early phase, lactating mothers may be
inexperienced and lack adequate breastfeeding knowledge. During this period, correct concepts and
basic principles of breastfeeding should be delivered, such as importance of correct attachment and
latching on. In addition, it is important to assess the psychological concerns of mothers during the
early postpartum period. In the later phase, some mothers need to return to work after maternity
leave. Therefore, storage of breast milk and use of milk pump can be taught.
Implications for innovation
In general, telephone breastfeeding support is shown effective to prolong the duration of
exclusive and any breastfeeding based on the result of five reviewed studies. And it should be
promoted among Chinese women due to cultural concerns. Most Chinese women sit month during
the first month of postpartum and they are often pressured by their relatives, such as mother-in-law,
to start formula feeding (Fu et al., 2014). Therefore, continuous breastfeeding support should be
provided via telephone intervention to ensure accessibility of these mothers as well as provide
timely breastfeeding advice. For the duration of intervention, it should be provided for at least 1
month since the first 1 month of postpartum is the critical period for mothers to adapt physically
and psychologically. The optimal timing of initial call would be 2 days after hospital discharge to
address mothers' concern and emotional needs timely. Prior to the innovation, the nurses who
deliver the intervention should complete certified refresher course organized by well-recognized
breastfeeding organization to ensure their competency and quality of intervention. For the content
of telephone intervention, it should be individualized as lactating mothers may have different
breastfeeding concerns. In addition, the content may be divided into several phases in the

17
postpartum period in order to best suit the needs of lactating mothers. Telephone breastfeeding
support should be provided for at least 1 month of postpartum since lactating mothers are the most
in need during the early period of postpartum.
18
Chapter 3 – Implementation Potential
Target setting and audience
The proposed setting of implementing the innovation would be the designated private
hospital. The target population is the local Chinese women who have no significant obstetric
complications throughout pregnancy, deliver term babies, intend to breastfeed and are willing to
participate postnatal lactation telephone counseling.
Transferability of the findings
Similarity of the settings and target population
The settings of the reviewed studies are local public hospitals with maternity service and our
proposed setting in the innovation is private hospital with maternity service as well. The nature of
maternity service in public or private hospitals in Hong Kong is generally similar and they
recognized the clinical significance of breastfeeding among both mothers and their infants.
Therefore, it is expected the innovation would be feasible in the proposed setting.
Compared to the target population of the reviewed studies and the innovation, the
characteristics of participants in these two groups are also similar and comparable. The target
population in the selected studies and the innovation are the local mothers who had term deliveries,
intended to breastfeed, no significant obstetric history during pregnancy.
Philosophy of Care of the designated private hospital
The designated private hospital is one of the local private hospitals with religious background.
Its mission is to ensure the physical, emotional and spiritual well-being of individuals for the Glory
of God by providing holistic healthcare. Care is its core business and value.
Philosophy of care underlying the innovation
To achieve holistic care, the maternity department of the private hospital advocates
breastfeeding which is regarded as the ideal nutrition for the newborn according to the World Health
Organization. The goal of the innovation is to prolong the duration of breastfeeding through
19
postnatal lactation telephone counseling as the mean of continuous postnatal support even after
hospital discharge. Current research evidences support that prolonging the duration of breastfeeding
would lead to positive health outcomes by reducing the risk of common infant illnesses, such as
gastroenteritis and pneumonia (Kramer et al., 2001).
The philosophy of care underlying the innovation is consistent with the private hospital, which
is to provide holistic care via continuous postnatal lactation support for those lactating women for
the sake of promoting their physical, emotional and spiritual well-being as well as health benefits
among newborns.
Expected number of clients benefited from the innovation.
There are average 2,500 deliveries per annual in the designated private hospital. By
excluding those complicating pregnancies and foreign pregnant mothers which do not satisfy the
inclusion criteria of the innovation, there are approximately 1,500 mother-infant pairs per year (125
mother-infant pairs per month). According to the hospital statistics, nearly 90% mothers intended to
breastfeed. It is supposed that all of the mothers who meet the inclusion criteria would participate
the innovation. By calculation, it is estimated that there are around 110 mother-infant pairs fulfill
the inclusion criteria and would be benefited from the innovation per month.
Projected timeframe for implementing and evaluating the innovation
The total duration of this innovation is 12 months. Prior to the implementation of innovation, it
will take 6 months to establish the protocol of the innovation, implement the pilot test as well as
obtain approval from the stakeholders of the hospital. It includes the arrangement of nurses’
manpower for telephone counseling, preparation of orientation and refresher programme for all
participated nurses and required equipment to implement the innovation. It takes 3 months to
implement the innovation. There are several stages, including recruiting participants,
implementation of the innovation (postnatal lactation breastfeeding counseling performed by
qualified nurses) and data collection. The final part would be data analysis and evaluation based on

20
the collected data (Refer to Appendix D).
Feasibility of the innovation
For those participated nurses, they are provided with orientation and refresher programme
prior to the innovation, for the sake of ensuring their competency of telephone counseling skills and
consolidating their breastfeeding knowledge. They have freedom to implement the innovation based
on their clinical judgment as long as it would not violate the protocol of the innovation or cause
harm to the participated mothers. Under the circumstance that the nurses consider as undesirable,
they possess their choice to terminate the innovation.
In order to avoid excessive workload for the participated nurses during implementing the
innovation, extra manpower would be provided to share their routine workload. During the
implementation of innovation, there would be additional 3 relieving nurses from the nursery service
in every work shift. Therefore, the current staff function and workload would not be significantly
interfered during the innovation.
The administration had started advocating the importance and benefits of breastfeeding for
both mothers and their newborns for years since the existing clinical evidence showed that
breastfeeding babies would have less risk of common infant illnesses, such as pneumonia (Kramer
et al, 2001). The purpose of innovation perfectly matches with the direction of present clinical
practice since our aim is to prolong the duration of breastfeeding via postnatal lactation telephone
support, in order to promote positive health outcomes for the infants. The organizational climate is
conducive to research utilization. As a result, the implementation of the innovation would be highly
supported by the administrators and stakeholders of the hospital.
Consensus between the administrators and the staff
Since the administrators has advocated for the benefits of breastfeeding for both lactating
mothers and their infants via a series of baby-friendly activities. For example, those mothers who
prefer breastfeeding would be provided with early skin to skin contact with their newborns soon

21
after delivery. In addition, nurses also conduct breastfeeding education for those lactating mothers
so as to equip them with correct techniques and minimize risk of undesirable outcomes of
ineffective breastfeeding. Thus, the staff had well understood the significance and advantages of
breastfeeding and the majority of them have positive attitude towards the innovation. As the
implementation of this innovation would lead to change in their current workflow, it is anticipated
that the minority of staff may be reluctant to change. The most common reason is that they perceive
they do not possess sufficient knowledge to handle the cases and they feel incompetent to perform
telephone counseling. Some of them are worried about the unknown situation and dare stick on the
existing practice. To resolve these possible resistances, the orientation and refresher programme
would be provided prior to the implementation, to ensure that they have good understanding of the
innovation and facilitate their cooperation and support. These interventions are expected to
minimize the staff’s concern and rectify their attitudes.
Under the circumstance that the telephone counseling work impairs the daily routine operation
in the clinical setting, it may cause friction within the organization. To minimize the risk of possible
disturbance to the daily operation, there would be maximum 15 telephone call limits for each
participated nurse in every shift. For the sources of extra manpower support, there are additional 3
registered nurses designated from the nursery department which is within the nursing department.
According to the expected number of eligible mother-infant pairs, there are approximately 110
breastfeeding mother-infant pairs per month. To calculate the nurses’ workload, they have to handle
about 30 cases per week. Ideally, assuming that all the eligible mothers participate the innovation
and the dropout rate is zero, the accumulating cases would increase by 30 cases per week. The
maximum duration of each telephone call would be allowed for 20 minutes and special
consideration for time allocation is available if additional referral or support is required for those
mothers when necessary.
22
Skills required for participated staff
For all participated staff, they are required to complete the orientation and refresher
programme prior to the implementation of innovation. The programme would be delivered in 2
sessions and each session last for 3 hours. Working hour compensation would be provided for all
attending staff. The first session would be the orientation session and introduce our aims and
purposes of innovation to the staff. And the second session would mainly cover breastfeeding
knowledge and basic skills of telephone counseling by inviting guest speakers and experts. After the
completion of this programme, certificates will be given to each participated staff to qualify their
clinical competency on breastfeeding skills and fundamental counseling techniques.
Hardware required during implementation
Besides of preparation for participated staff, there is also essential equipment to run the
innovation, including sufficient number of telephone for use of breastfeeding counseling, logbook
and learning materials distributed to nurses during orientation and refresher programme. Extra five
telephones are required for this innovation. The relevant expenditure would obtain financial support
from the department and stakeholders of the hospital.
Special arrangement for participated staff
To minimize the possibility of disturbance to daily operation in the clinical setting, the
orientation and refresher programme will be arranged after the staffs are off their duty. Therefore,
the number of staff in each work shift would not be affected, ensuring the quality of care and
service.
Evaluation tool for measuring the outcomes
A tailor-made breastfeeding evaluation form would be used to collect the data which is
reported by postnatal mothers via telephone counseling at scheduled frequency during the
implementation of innovation.

23
Potential benefits and risks for participated mothers during the implementation
Our innovation relies on telephone as communication tool to deliver breastfeeding message
and psychological support to those participated mothers during implementation. The major
advantage of this innovation is to provide continuous support to those breastfeeding mothers even
after discharged from hospital. Since there is not sufficient time for mothers to learn breastfeeding
techniques within short period of hospitalization after delivery, they may not be competent to
manage breastfeeding problems themselves at home. Through telephone breastfeeding support,
mothers are allowed to raise their concern about breastfeeding and they can obtain correct
breastfeeding knowledge from nurses sooner. Existing research evidence has already shown that
prolonging breastfeeding duration reduce risk of common infant illness and shorten the duration of
hospitalization in which help reduce medical expenditure for the community and the Government
(Kramer et al., 2001). There is no side effect or potential hazard that mothers would be exposed.
Risks of maintaining current practice
In the Chinese cultural practice, postnatal women are expected to stay at home during the
first month of postpartum to promote enough rest and recovery. Without telephone breastfeeding
counseling, those breastfeeding mothers may be reluctant to seek for professional support due to
their cultural concern. In addition, their relatives may advise them to start formula feeding when
they have breastfeeding problems, such as insufficient breast milk supply, thus increasing the
likelihood of terminating breastfeed.
Material costs of implementing the innovation
These include expenditure for fixed assets, including extra telephones; learning materials used
in the orientation and refresher programme and logbooks for nurses to record mothers’ concern and
breastfeeding problems during telephone counseling (Refer to Appendix E).
Material costs of not implementing the innovation
If there is without telephone breastfeeding counseling for those mothers, they are prone to
24
encounter breastfeeding problems after discharged from hospital and early cessation of
breastfeeding would likely occur. For those infants without breastfeeding, they are exposed higher
risk of common infant illnesses, such as pneumonia and gastroenteritis (Ball, Thomas & Anne,
1999). It would directly increase the financial burden of healthcare expenditure. On the other hand,
purchasing formula milk would also contribute to additional expenditure of infant care compared to
breastfeeding which is more economical and eco-friendly (Refer to Appendix F).
Potential non-material costs of implementing the innovation
Since the innovation implies change in existing practice, it is expected that few number of
staffs who are opposed to the innovation even after the orientation and refresher programme, it may
impair staff morale. Participated staffs are also required to attend the programme after their work;
therefore it may reduce their leisure time and cause physical fatigue after attending the programme.
Potential non-material benefits of implementing the innovation
Prolonging the duration of breastfeeding is beneficial to both infants and lactating mothers.
For those infants, Pokhrel et al. (2014) showed that supporting mothers to continue breast feeding
until 4 months are expected to reduce the incidence of common infant infectious diseases and thus
saving at least £11 million annually. Besides of substantial health outcomes of infants resulting from
prolonging the duration of breastfeeding, lactating mothers also benefit from this innovation. Since
oxytocin would be released during breastfeeding, it helps promote uterine involution and reduce
risk of postpartum hemorrhage. Studies also showed that lactating mothers are less prone to breast
and ovarian cancer later in life (Danforth et al., 2007; Jordon et al., 2010). For nurses, they can
enjoy higher job satisfaction by helping mothers in prolonging duration of breastfeeding.
The cost-benefit ratio is 14.2% and the detailed calculation is shown in Appendix G. It is
calculated by cost of innovation minus actual cost (without innovation), the result is divided by
actual cost. Although the result is a positive number, the potential benefits of implementing the
innovation are not taken into account in the calculation. Both the lactating mothers and the infants

25
have positive health outcomes when prolonging the duration of breastfeeding. Therefore, the
innovation is worth implementing in the hospital.
Conclusion
In conclusion, this innovation is transferable and feasible to implement. Apart from
improving health outcomes of both mothers and infants, the innovation also help reduce medical
expenditure by shortening duration of hospitalization. Breastfeeding is more economical and eco-
friendly than formula feeding without the concern of formula powder can disposal.
26
Chapter 4 - Implementation plan
The implementation plan is composed of several parts, including communication plan, pilot
study plan, evaluation plan as well as the basis for implementation.
Communication plan
The major function of the communication plan is to get the stakeholders involved, and to
provide communication channel among them to ensure that they can obtain the latest information
simultaneously. In addition, the detailed process of establishing communication plan would be
described.
Identifying the stakeholders
“Stakeholder” in the communication plan refers to a person who has interest or concern to
the innovation. Stakeholders can have influence on the implementation’s outcomes. In this study,
the stakeholders include hospital administrators, the Department of Manager (DOM), Nurse
Officers (NOs), as well as frontline nurses who participate in the innovation.
Establishment of the communication team
Followed by identifying the stakeholders, a communication team would be established in
order to facilitate sharing of updated information among the stakeholders, which helps the
implementation of the communication plan. One of the functions of the communication team is to
educate the frontline staffs through emails, circulars or information seminars, which equip them
with knowledge about the potential clinical advantages of the innovation and the required skills for
implementation. The communication team consists of a total of six team members, including one
lactation consultant (LC), two nurse officers (NOs), the innovation author and two frontline nurses.
There would be one link person in each work position. It ensures that comprehensive feedback from
different levels of staff would be collected. And the frontline nurses would be responsible to
implement the innovation.

27
Detailed process of communication plan
The initial step of communication plan is to prepare the details of innovation and send the
proposal to the responsible hospital administrators via email 4 weeks prior to the formal meeting, in
order to obtain their approval and support for the innovation. The details of innovation would be
presented in PowerPoint format and it includes the objectives, proposed workflow of the program,
implementation potential in terms of transferability and feasibility, potential clinical benefits and
risks, as well as estimated material and non-material costs. The background information for
supporting the innovation is the five selected studies and they will be attached as appendix in the
proposal. During the formal meeting with the hospital administrators, a brief presentation about the
general workflow of the innovation would be presented by the innovation author. After that, they
are welcome to raise their concerns and inquiries in the Question & Answer session. Their feedback
would be also collected for modifying the details of innovation if necessary.
A meeting with the LC and the NOs will be arranged 2 weeks after obtaining approval from
hospital administrators, to allow sufficient time for the innovation author to modify the innovation
based on the feedback obtained from hospital administrators. This meeting aims at discussing
allocation of manpower and resources during the implementation. Since the innovation requires
additional nurses’ manpower to perform telephone counseling during the implementation stage,
comprehensive workflow of innovation and staff allocation must be mutually agreed to maintain
quality of care of existing nursing service. It also ensures the workload of frontline nurses is
acceptable during implementation.
Prior to the implementation of innovation, it is necessary to ensure all participating staff are
familiarized with the program details and possess sufficient clinical competency to implement the
innovation. All participating nurses need to attend two orientation sessions conducted by guest
speakers in the hospital prior to the implementation. During the orientation session, all of the details
28
of the innovation including the objectives, workflow of the program, potential clinical benefits and
manpower allocation would be clearly stated in order to obtain understanding and support from all
participating staff. It is expected that some nurses will be reluctant to change their current practice
and that is why a clear explanation and manpower support is crucial to ease their concern. In
addition, all participating staff are also encouraged to raise their opinions at the end of the
orientation session and supportive measures would be provided accordingly if possible. Regular
meetings will also be provided in order to facilitate their real-time feedback during the
implementation. Besides, they are also encouraged to provide their feedback via email.
Pilot Study Plan
Pilot study is defined as a small-scale research study conducted before the intended study.
Its purpose is to test the feasibility of the innovation in the reality and therefore it is also named as
“feasibility study”. Although the pilot study cannot eliminate all systematic errors, it can help
reduce the likelihood of type I & type II errors which would result in wastage of manpower and
resources. It also provides a way to identify potential problems of the innovation and allow the
innovation author to look for solutions before implementation. In terms of cost effectiveness,
conducting a pilot study provides a preliminary result about the efficacy of research protocol with
minimal resources input (Hilla, Christa & Gisela, 2006). It can also identify implementation
strategy and relevant facilitators to the innovation.
Timeline of pilot study
The duration of the pilot study is 4 weeks. It is divided into 4 parts: subject recruitment,
implementation, data collection and data evaluation. Subject recruitment will be performed in the
first week. Implementation will follow in the 2 weeks thereafter. Data collection and data evaluation
will be performed in the last week after the implementation. The pilot study aims to recruit 20
postnatal women who delivered their babies within one week and fulfilled our recruitment criteria

29
as stated in the actual innovation. It provides a reasonable number of subjects for frontline nurses to
practice their telephone support skills while not causing excessive workload to them. Verbal
consent is obtained from each eligible participant after recruitment.
All the frontline nurses have to complete the orientation session prior to the implementation of
pilot study to ensure their competency fulfilling our clinical standard. During the orientation session,
they will be equipped with fundamental telephone counseling skills and breastfeeding knowledge
which promotes those postnatal women to successfully breastfeed even after discharge from
hospital. A telephone support checklist (Refer to Appendix K) would be provided for nurses as
simple tips to deliver common telephone support methods to the clients.
After the implementation of the pilot study, the communication team is responsible for data
collection and evaluation, which can tell the feasibility of the innovation. For the part of data
collection, we will collect data including types of intervention delivered by nurses, average time of
each telephone counseling and duration of breastfeeding reported by mothers. Besides, regular
meeting with frontline staff would be conducted to collect their feedback about the pilot study
which helps to modify the innovation if necessary. Expected feedbacks from them include issues
like whether they encounter any difficulties during implementation or whether the telephone
counseling checklist is suitable or adequate for them to carry out their counseling.
Throughout the evaluation, the communication team would examine the overall workflow of
the pilot study, identify any risk factors that may impair the implementation or outcomes and
suggest possible solutions accordingly. The workload of frontline nurses would be assessed to
ensure adequate support to them and maintain good staff morale. After the completion of pilot study,
the results and suggested amendment, if any, of the innovation would be reported to the hospital
administrators in form of a written report.
Evaluation Plan
The evaluation plan is used to assess the effectiveness of the innovation by evaluating the
30
identified outcomes. In the innovation, the primary outcome is the breastfeeding rate in all forms,
including exclusive breastfeeding and partially breastfeeding in different intervals (1 month and 2
months after delivery) in postnatal period. And the secondary outcome is the level of satisfaction
among frontline nurses.
Primary outcome
The breastfeeding rate in all forms, including exclusive breastfeeding and partially
breastfeeding at 1 month and 2 months after delivery in postnatal period would be the primary
outcome (client outcome) of the innovation. Nurses would use standardized breastfeeding form and
telephone support tips card to collect breastfeeding data which is verbally reported by eligible
participants in each telephone call. To determine the effectiveness of the innovation, these collected
breastfeeding data would be compared with other clients who do not participate in the innovation in
the hospital.
Secondary outcome
For the outcome of health care professionals, the satisfaction level among the frontline
nurses would be considered. They are provided with regular meeting during the innovation to
express their feedback and concerns with regard to the innovation. In addition, a tailor-made
questionnaire form (Refer to Appendix L) would be used to assess their satisfaction level about the
innovation.
Characteristics of clients
During the recruitment process, only those local mothers who choose to breastfeed at the
first registration would be invited for the innovation. For their eligibility, they are required to have
good past health without significant obstetric history during pregnancy which may impair their
capability to breastfeed.
Sample size calculation
The sample size calculation of the innovation is performed by the Piface Application version
31
1.76 (Lenth, 2011). To determine whether the breastfeeding rate is improved after the
implementation of the innovation, two-tailed z-test statistical method is used for testing one
proportion. Taking the level of significance at 5% and the power at 80%, the calculated sample size
is 194 when setting null value as 0.4 and actual value as 0.5. According to one of the selected
studies (Fu et al., 2014), the dropout rate is set as 5%, the required sample size is 204.2 (rounding
up to 205). It is estimated that there are 55-65 eligible participants recruited each week. As a result,
the recruitment period lasts for 4 weeks to acquire sufficient number of sample size in the
innovation.
Outcomes measurement
Primary outcome (Breastfeeding rate)
A standardized breastfeeding data collection form (Refer to Appendix J) would be used to
assess clients’ feeding method in each telephone counseling. Nurses would assess the infant’s age
and their feeding method as verbally reported by the clients. Whenever a client claims that she
would stop breastfeeding, telephone counseling will no longer be provided. The total duration of
breastfeeding would be calculated from the day of starting breastfeeding to the day that the client
stops breastfeeding.
Secondary outcome (Level of satisfaction among nurses)
It is worth considering the level of satisfaction among nurses since the participating nurses
are required to handle additional workload during the innovation. Nurses may provide precious
feedback towards the innovation. A tailor-made questionnaire (Refer to Appendix L) would be used
to assess their level of satisfaction. It would be distributed to all participating nurses after the
completion of the innovation. The questionnaire adopts 10-point Likert scale (1= totally disagreed,
10= totally agreed) which allows nurses to rate each statement according to their perception.
Data analysis
The aim of outcomes measurement is to determine if the breastfeeding rate is improved after

32
the innovation by comparing to those mothers who do not participate the innovation in the hospital.
The two-tailed z-test statistical method is used for testing one proportion in this innovation. For the
analysis of the level of satisfaction among the frontline staff, the two-tailed paired t-test would be
used to compare with the results before implementing the innovation.
Basis for effectiveness
There are some criteria to determine if the innovation is effective to improve the
breastfeeding rate and the level of satisfaction among nurses.
Primary outcome (Breastfeeding rate)
In accordance with the local breastfeeding statistics conducted by Department of Health in
2012 (Ching, 2014), the breastfeeding rate in all forms (including exclusive breastfeeding & partial
breastfeeding) at 1 month after delivery is 68.6%. The innovation is therefore considered effective if
the breastfeeding rate in all forms in 1 month is higher than the above percentage.
Secondary outcome (Level of satisfaction among nurses)
A successful innovation is not only supported by statistically significant figures, but also
welcomed by frontline nurses’ recognition. Nurses’ feedback can be reflected via the questionnaire
that assesses their level of satisfaction. The overall expected percentage is 70% of nurses would rate
at least 7/10 for more than 5 statements in the questionnaire.
Conclusion
In the past several decades, the public has become more aware of the benefits of
breastfeeding to both mothers and infants. Despite of the effort of the Government and the local
organizations, the overall breastfeeding rate in Hong Kong (including exclusive breastfeeding and
partial breastfeeding) still lags behind WHO recommendations. Therefore, it is proposed telephone
support to those breastfeeding mothers after hospital discharge would help them maintain longer
duration of breastfeeding and thus improve breastfeeding rate in 1 month.
There are various ranges of supportive measures for mothers to maintain breastfeeding, such
33
as postnatal breastfeeding peer support group, breastfeeding talk and breastfeeding coaching. With
consideration to Chinese traditional culture, postnatal mothers tend to “sit month” for 1 month after
delivery. Nevertheless, the first month after delivery is the most crucial period for them since they
need professional assistance to overcome the difficulties of breastfeeding, such as management of
breast engorgement, and desired breastfeeding position for those mothers with post-operative
wound pain. All of the results in the selected studies showed that telephone support had positive
outcomes on breastfeeding duration. Telephone support is therefore chosen as an ideal
communication tool to provide continuous breastfeeding support in the early postnatal period. After
the implementation of pilot study and its evaluation, postnatal telephone support with evidence-
based guidelines is recommended to prolong duration of breastfeeding in Hong Kong.

34
References
American Academy of Pediatrics. Policy statement: breastfeeding and the use of human milk.
Pediatrics 2012;129:e827–41.
Ball, Thomas M., and Anne L. Wright. "Health care costs of formula-feeding in the first year of
life." Pediatrics 103.Supplement 1 (1999): 870-876.
BFHIHKA (2015). Reports on annual survey. Retrieved from
http://unicef.org.hk:8080/download/WBWReport2015_E.pdf
Carlsen, E. M., Kyhnaeb, A., Renault, K. M., Cortes, D., Michaelsen, K. F., & Pryds, O. (2013).
Telephone-based support prolongs breastfeeding duration in obese women: a randomized
trial. The American journal of clinical nutrition,98(5), 1226-1232.
Centre for Health Protection (February 2014), Non-communicable diseases watch. Retrieved from
www.chp.gov.hk/files/pdf/ncd_watch_feb2014.pdf (Centre for Health Protection [CHP],
2014)
Centre for Health Protection. (2014). Non-communicable diseases watch. Optimising breastfeeding
practices: A link to life long health. Centre for Health Protection of the Department of
Health. (Centre for Health Protection [CHP], 2014)
Ching, R. (2014, February). Optimising Breastfeeding Practices: A Link to Life Long
Health. Retrieved April, 2016, from
http://www.chp.gov.hk/files/pdf/ncd_watch_feb2014.pdf
Danforth, K. N., Tworoger, S. S., Hecht, J. L., Rosner, B. A., Colditz, G. A., & Hankinson, S. E.
(2007). Breastfeeding and risk of ovarian cancer in two prospective cohorts. Cancer causes
& control, 18(5), 517-523.
Dennis, C. L., Hodnett, E., Gallop, R., & Chalmers, B. (2002). The effect of peer support on breast-
feeding duration among primiparous women: a randomized controlled trial. Canadian
Medical Association Journal, 166(1), 21-28.

35
Fu, I. C. Y., Fong, D. Y. T., Heys, M., Lee, I. L. Y., Sham, A., & Tarrant, M. (2014). Professional
breastfeeding support for first‐ time mothers: a multicentre cluster randomised controlled
trial. BJOG: An International Journal of Obstetrics & Gynaecology, 121(13), 1673-1683.
Hannula L, Kaunonen M, Tarkka M-T. A systematic review of professional support interventions
for breastfeeding. J Clin Nurs 2008;17:1132–43.
Hilla, B., Christa, V. W., & Gisela, V. R. (2006). Fundamentals of Research
Methodology for Health Care Professionals. (2nd ed). Lansdowne: Juta & Co. Ltd.
Jordan, S. J., Siskind, V., Green, A. C., Whiteman, D. C., & Webb, P. M. (2010). Breastfeeding and
risk of epithelial ovarian cancer. Cancer Causes & Control, 21(1), 109-116.
Kramer, M. S., Chalmers, B., Hodnett, E. D., Sevkovskaya, Z., Dzikovich, I., Shapiro, S., ... &
PROBIT Study Group. (2001). Promotion of Breastfeeding Intervention Trial (PROBIT): a
randomized trial in the Republic of Belarus.Jama, 285(4), 413-420.
Kramer, M. S., & Kakuma, R. (2004). The optimal duration of exclusive breastfeeding.
In Protecting Infants through Human Milk (pp. 63-77). Springer US.
Kramer MS, Kakuma R. The optimal duration of exclusive breastfeeding: a systematic review. Adv
Exp Med Biol 2004;554:63– 77
Leung, J. (2009). Current role of maternal and child health service. Medical Bulletin, 14(3), 16-19.
Lenth, R. V. (2006-9). Java Applets for Power and Sample Size [Computer
software]. Retrieved 10th May, 2016, from http://www.stat.uiowa.edu/~rlenth/Power.
Pokhrel, S., Quigley, M. A., Fox-Rushby, J., McCormick, F., Williams, A., Trueman, P., ... &
Renfrew, M. J. (2014). Potential economic impacts from improving breastfeeding rates in
the UK. Archives of disease in childhood, archdischild-2014.
Pugh, L. C., Serwint, J. R., Frick, K. D., Nanda, J. P., Sharps, P. W., Spatz, D. L., & Milligan, R. A.
(2010). A randomized controlled community-based trial to improve breastfeeding rates
among urban low-income mothers. Academic pediatrics, 10(1), 14-20.

36
SIGN 50: A guideline developer’s handbook. Scottish Intercollegiate Guidelines Network, 2008.
Simonetti, V., Palma, E., Giglio, A., Mohn, A., & Cicolini, G. (2012). A structured telephonic
counselling to promote the exclusive breastfeeding of healthy babies aged zero to six
months: a pilot study. International journal of nursing practice, 18(3), 289-294.
Tahir, N. M., & Al-Sadat, N. (2013). Does telephone lactation counselling improve breastfeeding
practices?: A randomised controlled trial. International journal of nursing studies, 50(1), 16-
25.
World Health Organization. (2003). Beyond survival: 2nd edition, Integrated delivery care practices
for long-term maternal and infant nutrition, health and development
World Health Organization. (2003). Global Strategy for Infant and Young Child
Feeding. Geneva: World Health Organization. (World Health Organization [WHO], 2003)

37
Appendices
Appendix A: PRISMA diagram
Records identified through
PubMed searching
(n=487)
Additional records identified
through CINAHL
(n=100)
Records of duplicates removed
(n=93)
Records screened
(n=494) Records excluded
(n=478)
Full-text articles
assessed for eligibility
(n= 16 )
Full-text articles excluded
with reasons (n=11)
Reasons of excluded:
(1) combined intervention,
containing telephone
support and other
intervention; (2) outcome
measured not match with
our study
Number of reviewed
articles included (n=5)

38
Appendix B: Table of Evidence
Sample characteristics Intervention Control Outcomes Effect size
1
2
3
4
5
Citation/ Design/
Origin of country/
Level of Evidence
Tahir, N. M., &
Al-Sadat, N.
(2013) / RCT,
Malaysia (1+)
(1) 88.2% Malay women ;
(2) uncomplicated
pregnancy: singleton & term
delivery; (3) intended to
breastfeed; (n=357)
Telephone lactation counseling
given by lactation counselors
via telephone twice monthly
(n=179)
Received standard care, such as
breastfeeding talks and
breastfeeding advice
(n=178)
Rate of exclusive breastfeeding at
1,4 & 6 month after delivery
1 month: OR 1.627
4 month: OR:1.173
6 month: OR: N/A
Fu, I. C. Y.et al.
(2014) / RCT,
Hong Kong (1+
+)
(1) Hong Kong Chinese
primiparas;
(2) intended to breastfeed;
(3) without major obstetric
or medical complications;
(4) term pregnancy
(n=722)
2 intervention arms:
(1) In-hospital group: 30mins BF
support sessions for 3 times
(n= 191);
(2) Telephone group: weekly
telephone support for up to 4
weeks postpartum or until
breastfeeding had been completely
stopped
(n=268)
Received standard postnatal care
such as routine group postnatal
lactation education & post-
discharge followup
(n=263)
Rate of any and exclusive
breastfeeding at 1, 2, and 3
months.
Telephone VS Control (any
BF)
1 month: OR 1.63 P=0.01
2 month: OR 1.48 P=0.03
3 month: OR 1.37 P=0.08
Telephone VS Control
(exclusive BF)
1 month: OR 1.89 P=0.003
2 month: OR 1.43 P=0.12
3 month: OR 1.20 P=0.45
Carlsen, E. M. et
al. (2013)/ RCT,
Danmark (1+)
(1) women who participated
in the Treatment of Obese
Pregnant study;
(2) intended to breastfeed;
(3) without history of breast
surgery
(n=226)
(1) received telephone support, by
lactation consultant during first 6
months
(n=108)
(1) provided standard
breastfeeding support during
hospitalization;
(2) received routine follow up
(n=118)
Rate of any and exclusive
breastfeeding at 3 & 6 months of
postpartum.
Exclusive BF
3 month: OR 2.45 P=0.003
Partial BF
6 month: OR 2.25 P=0.008
Dennis, C. L. et
al. (2002)/ RCT,
Canada (1+)
(1) aged 25-34 women
intended to breastfeed;
(2) Acquired college or
undergraduate university
education level;
(3) without significant
maternal illness that may
impair breastfeeding
(n=359)
(1) Telephone support conducted
by peer volunteer, no standard
frequency of telephone contact as
mother requested
(n=132)
Received conventional in-hospital
care & community postpartum
support services
(n=126)
Primary outcome: rate of
breastfeeding;
Secondary outcome: maternal
satisfaction of infant feeding
1 month: RR 1.10 P= 0.03
3 month: RR 1.21 P=0.01
Simonetti et al,
(2012)/ RCT,
Italy (1-) Pilot
study
(1) Italian healthy
primiparous mothers;
(2) term delivery;
(3) Intended to
BF (n= 114)
Received structured telephone
support by licensed midvives;
timing of phone calls are agreed by
participants and midvives.
(n=55)
Provided conventional counselling
program consisting of periodical
visits with the physician
(n=59)
Rate of exclusive breastfeeding at
1,3 & 5 month after delivery
1 month: RR 1.8
3 month: RR 1.9
5 month: RR 2.1
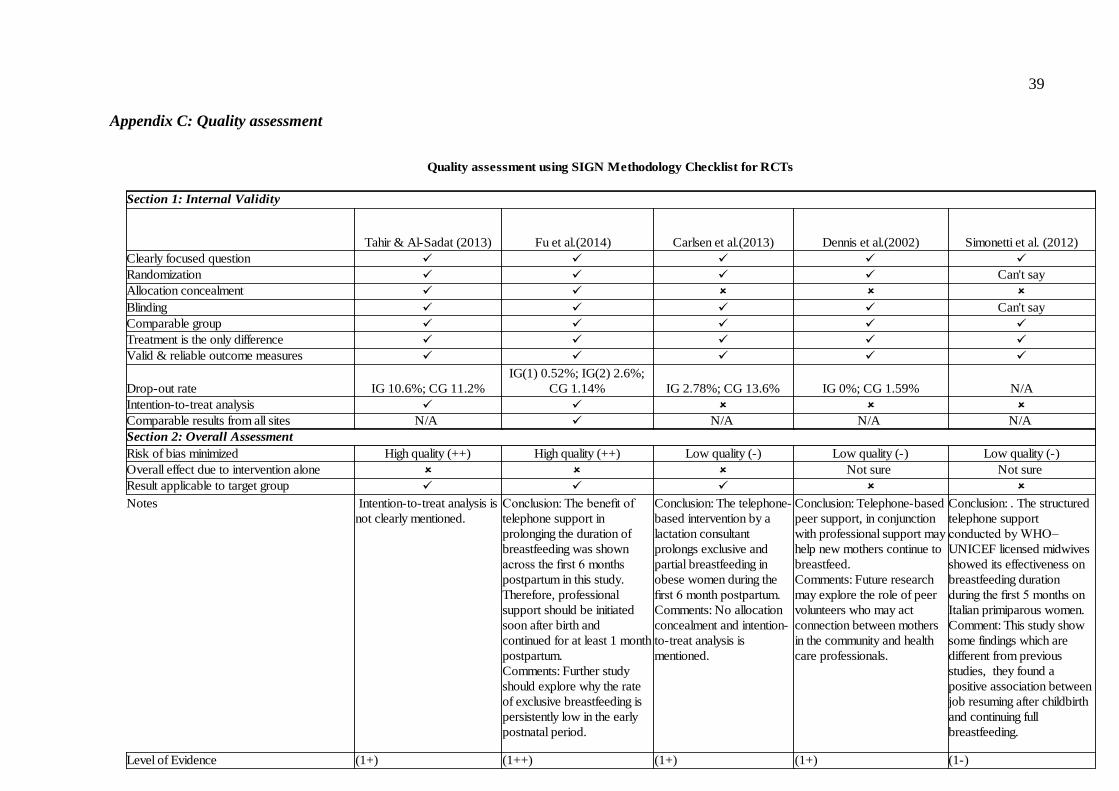
39
Appendix C: Quality assessment
Quality assessment using SIGN Methodology Checklist for RCTs
Section 1: Internal Validity
Tahir & Al-Sadat (2013) Carlsen et al.(2013) Dennis et al.(2002) Simonetti et al. (2012)
Clearly focused question
Randomization Can't say
Allocation concealment
Blinding Can't say
Comparable group
Treatment is the only difference
Valid & reliable outcome measures
Drop-out rate IG 10.6%; CG 11.2% IG 2.78%; CG 13.6% IG 0%; CG 1.59% N/A
Intention-to-treat analysis
Comparable results from all sites N/A N/A N/A N/A
Section 2: Overall Assessment
Risk of bias minimized High quality (++) High quality (++) Low quality (-) Low quality (-) Low quality (-)
Overall effect due to intervention alone Not sure Not sure
Result applicable to target group
Notes
Level of Evidence (1+) (1++) (1+) (1+) (1-)
Fu et al.(2014)_
IG(1) 0.52%; IG(2) 2.6%;
CG 1.14%
Intention-to-treat analysis is
not clearly mentioned.
Conclusion: The benefit of
telephone support in
prolonging the duration of
breastfeeding was shown
across the first 6 months
postpartum in this study.
Therefore, professional
support should be initiated
soon after birth and
continued for at least 1 month
postpartum.
Comments: Further study
should explore why the rate
of exclusive breastfeeding is
persistently low in the early
postnatal period.
Conclusion: The telephone-
based intervention by a
lactation consultant
prolongs exclusive and
partial breastfeeding in
obese women during the
first 6 month postpartum.
Comments: No allocation
concealment and intention-
to-treat analysis is
mentioned.
Conclusion: Telephone-based
peer support, in conjunction
with professional support may
help new mothers continue to
breastfeed.
Comments: Future research
may explore the role of peer
volunteers who may act
connection between mothers
in the community and health
care professionals.
Conclusion: . The structured
telephone support
conducted by WHO–
UNICEF licensed midwives
showed its effectiveness on
breastfeeding duration
during the first 5 months on
Italian primiparous women.
Comment: This study show
some findings which are
different from previous
studies, they found a
positive association between
job resuming after childbirth
and continuing full
breastfeeding.

40
Footnotes:
: Yes
: No
IG: Intervention group
CG: Control group
N/A: Not applicable
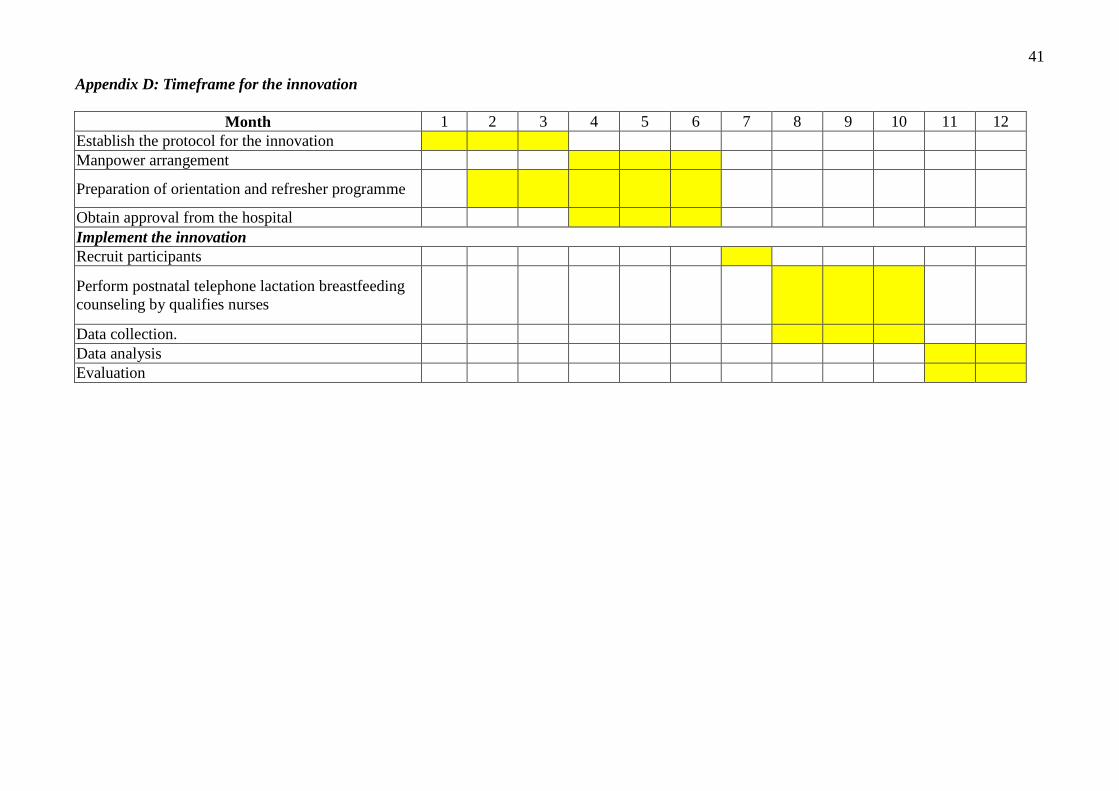
41
Appendix D: Timeframe for the innovation
Month 1 2 3 4 5 6 7 8 9 10 11 12
Establish the protocol for the innovation
Manpower arrangement
Preparation of orientation and refresher programme
Obtain approval from the hospital
Implement the innovation
Recruit participants
Perform postnatal telephone lactation breastfeeding
counseling by qualifies nurses
Data collection.
Data analysis
Evaluation
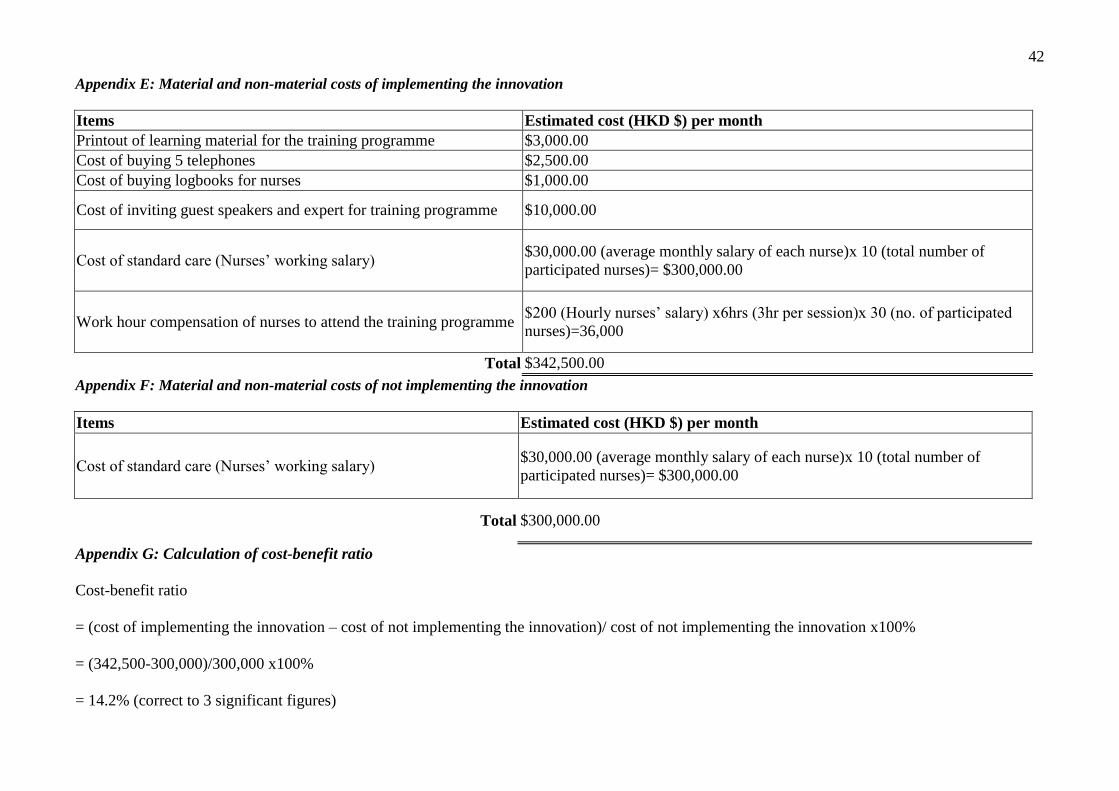
42
Appendix E: Material and non-material costs of implementing the innovation
Items Estimated cost (HKD $) per month
Printout of learning material for the training programme $3,000.00
Cost of buying 5 telephones $2,500.00
Cost of buying logbooks for nurses $1,000.00
Cost of inviting guest speakers and expert for training programme $10,000.00
Cost of standard care (Nurses’ working salary) $30,000.00 (average monthly salary of each nurse)x 10 (total number of
participated nurses)= $300,000.00
Work hour compensation of nurses to attend the training programme $200 (Hourly nurses’ salary) x6hrs (3hr per session)x 30 (no. of participated
nurses)=36,000
Total $342,500.00
Appendix F: Material and non-material costs of not implementing the innovation
Items Estimated cost (HKD $) per month
Cost of standard care (Nurses’ working salary) $30,000.00 (average monthly salary of each nurse)x 10 (total number of
participated nurses)= $300,000.00
Total $300,000.00
Appendix G: Calculation of cost-benefit ratio
Cost-benefit ratio
= (cost of implementing the innovation – cost of not implementing the innovation)/ cost of not implementing the innovation x100%
= (342,500-300,000)/300,000 x100%
= 14.2% (correct to 3 significant figures)

43
Appendix H: Grades of Recommendations (SIGN, 2004)
Grades Statements
A
At least one meta-analysis, systematic review, or RCT rated as 1++, and directly applicable to the target population; or A body
of evidence consisting principally of studies rated as 1+, directly applicable to the target population, and demonstrating overall
consistency of results
B A body of evidence including studies rated as 2++, directly applicable to the target population, and demonstrating overall
consistency of results; or Extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to the target population and demonstrating overall
consistency of results; or Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or Extrapolated evidence from studies rated as 2+
Appendix I: Levels of Evidence (SIGN, 2004)
Level of evidence Evidence statements
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies. High quality case control or cohort studies with a very
low risk of confounding or bias and a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a moderate probability that the
relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not
causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
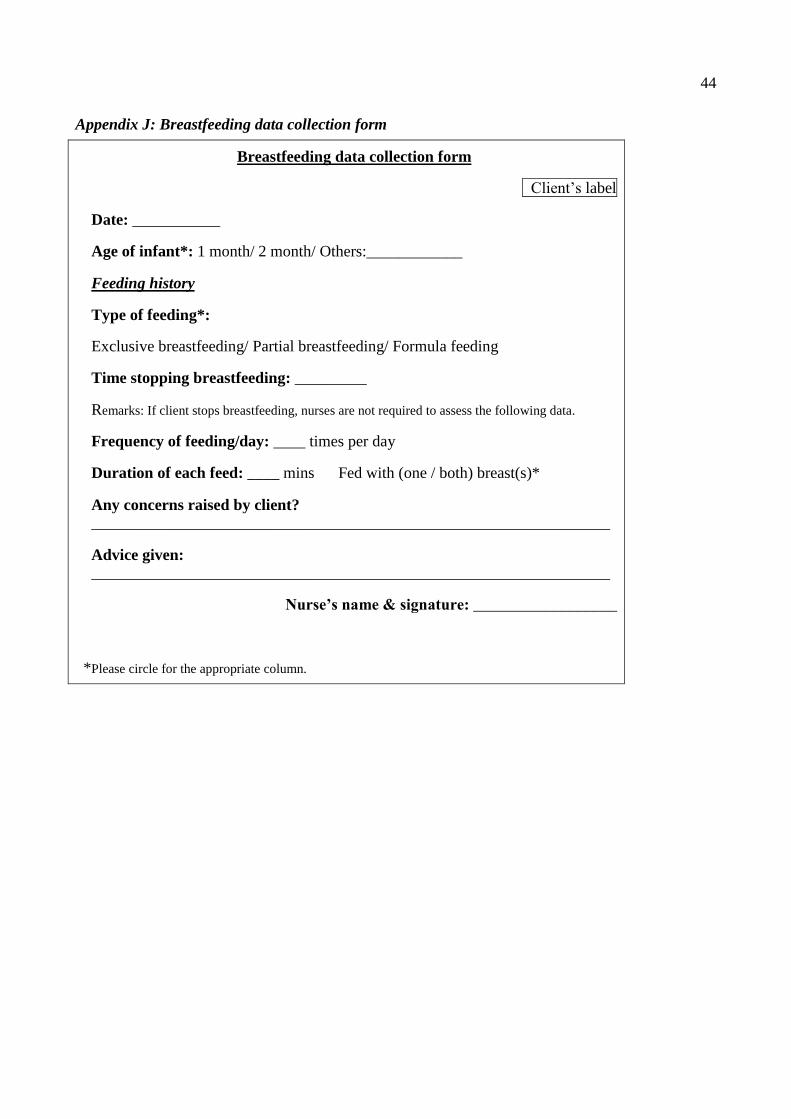
44
Appendix J: Breastfeeding data collection form
Breastfeeding data collection form
Client’s label
Date: ___________
Age of infant*: 1 month/ 2 month/ Others:____________
Feeding history
Type of feeding*:
Exclusive breastfeeding/ Partial breastfeeding/ Formula feeding
Time stopping breastfeeding: _________
Remarks: If client stops breastfeeding, nurses are not required to assess the following data.
Frequency of feeding/day: ____ times per day
Duration of each feed: ____ mins Fed with (one / both) breast(s)*
Any concerns raised by client?
_________________________________________________________________
Advice given: _________________________________________________________________
Nurse’s name & signature: __________________
*Please circle for the appropriate column.
45
Appendix K: Telephone support checklist
Telephone support tips card
Tips: Nurses can implement the following telephone support tips to the clients according to their
individual needs.
1. Actively listen to the client’s concern(s) and identify their needs on
breastfeeding.
2. Provide fundamental breastfeeding knowledge, such as common types of
positioning, signs of correct latch on.
3. Identify any barrier(s) of breastfeeding and provide appropriate management
accordingly, such as management of breast engorgement.
4. Assess client’s emotional status. Whether their family members support
breastfeeding.

46
Appendix L: Questionnaire for the level of satisfaction among nurses
Please circle the number which indicates your feelings about the innovation the most.
Strongly disagree ----------------------> Strongly agree
Preparation stage
1. The duration of orientation program is
appropriate to me. 1 2 3 4 5 6 7 8 9 10
2. The content of orientation program is
appropriate to the innovation. 1 2 3 4 5 6 7 8 9 10
Implementation stage
3. The content of breastfeeding form facilitates
me to record the data efficiently. 1 2 3 4 5 6 7 8 9 10
4. The manpower arrangement is acceptable and
reasonable. 1 2 3 4 5 6 7 8 9 10
5. I am competent to handle telephone support
and deliver breastfeeding knowledge to clients
accordingly.
1 2 3 4 5 6 7 8 9 10
6. The communication team is helpful and
supportive. 1 2 3 4 5 6 7 8 9 10
Evaluation stage
7. I am overall satified with the innovation. 1 2 3 4 5 6 7 8 9 10
8. I think the innovation is helpful in supporting
breastfeeding among mothers. 1 2 3 4 5 6 7 8 9 10
47
Appendix M: Evidence-Based Practice Guideline
Evidence-Based Practice Guideline
Title of the guidelines
Telephone breastfeeding counseling for lactating mothers after discharged from hospital.
Objectives of the guidelines
The objectives of this Protocol are to:
- Provide continuous psychological support for those mothers via telephone counseling;
- Deliver breastfeeding knowledge and skills to those mothers based on the existing evidence,
- Prolong the duration of breastfeeding among those lactating mothers after discharged from
hospital.
Target group of the guidelines
The target population is those mothers who had no significant obstetric history during
pregnancy and had term delivery, intend to breastfeed, are willing to participate telephone
breastfeeding counseling after hospital discharge.
Evidence-based recommendations
There are some recommendations developed from the 5 selected articles. The grading of
recommendations is based on the SIGN guidelines in Appendix D.
1. Participated nurses are required to complete the relevant breastfeeding training
programme prior to conducting telephone breastfeeding counseling (Grade B)
Available evidence: In order to maintain uniformity and quality of care, the participated nurses
should be qualified by relevant training or refresher courses on breastfeeding management and
counseling skills (1+ Tahir & Al-Sadat, 2013).
2. The willingness of breastfeed must be assessed during the selection process. Only
those mothers who meet the inclusion criteria and declare to intend for breastfeeding would be
eligible for the innovation. (Grade A)
48
Available evidence: The intention to breastfeed is assessed and only those mothers who plan to
breastfeed will be recruited (1+ Fu et al., 2014).
3. The timing of telephone support should be mutually agreed by both nurses and
mothers. (Grade B)
Available evidence: Timing of telephone calls are commonly agreed by nurses and mothers to
minimize the possible interruption of their daily family routines (1+ Fu et al., 2014; 1-
Simonetti, 2012).
4. The content in telephone counseling should focus on delivering breastfeeding
knowledge, assessing their breastfeeding concerns and emotional health. In addition, cultural
issues should be also addressed. (Grade A)
Available evidence: The telephone counseling with well-organized content can help mothers to
resolve their breastfeeding concerns and psychological needs (1+ Fu et al., 2014). Chinese
mothers may need to deal with family pressure to stop breastfeeding since they worry
breastfeeding is unable to satisfy infants’ needs.







