11/8/12
1
Hostility, Anger, and Aggression Meaning and Interventions
Michael Brunner, Ph.D., LP Clinical Director
November 8, 2012
1
Learning Objectives • Identify two categories of aggression and the purposes served by
hostility, anger, and aggression. • List three factors, diagnoses, and other causes of hostility, anger,
and aggression. • Understand and describe the mutually destructive relationship
between hostility, anger, and aggression and chemical use. • Describe four targets for treatment of hostility, anger, and
aggression and the timing of interventions to address the issue. • Describe and be able to employ five treatment interventions for
hostility, anger, and aggression.
November 8, 2012
2
Pre-test Question # 1 Impulsive aggression is associated with: a. High levels of emotional arousal b. Low levels of emotional arousal c. Anger or fear d. Both a & c e. Both b & c
November 8, 2012
3

11/8/12
2
What Distinguishes Hostility, Anger, and Aggression • Hostility is an Attitude (way of thinking) ▫ Suggesting strong anger or opposition towards
another person • Anger is an Emotion ▫ Along with fear, sadness, and happiness is
considered one of the primary emotions • Aggression is a Behavior ▫ The physical display of both hostility and anger
November 8, 2012
4
Premeditated Aggression
• Planned behavior not typically associated with frustration or response to immediate threat
• Might not be associated with emotional arousal • Clear goals in mind • Also referred to as: ▫ Predatory ▫ Instrumental ▫ Proactive
November 8, 2012
5
Siever, L. J. American Journal of Psychiatry 2008; 165 (4), 429-42
Impulsive Aggression • Characterized by high levels of emotional
arousal • Provoked by someone or something • Anger or fear are associated with it • Usually in response to a threat • Also referred to as: ▫ Reactive ▫ Affective ▫ Hostile
November 8, 2012
6
Siever, L. J. American Journal of Psychiatry 2008; 165 (4), 429-42
11/8/12
3
Hostility, Anger, and Impulsive Aggression • They travel together – they typically occur at the
same time. • Awareness of one can signal the emergence of
another - for example, hostility can signal impending aggression.
• The root cause of these experiences – hostility, anger, and impulsive aggression - is typically similar.
November 8, 2012
7
Post-test Question # 1
Impulsive aggression is associated with: a. High levels of emotional arousal b. Low levels of emotional arousal c. Anger or fear d. Both a & c e. Both b & c
November 8, 2012
8
The Role and Purpose of Hostility, Anger, and Aggression
November 8, 2012
9

11/8/12
4
Pre-test Question # 2 Preparing the body to respond to stress in the
environment is the responsibility of which of the following?
a. The sympathetic nervous system b. The parasympathetic nervous system c. The autonomic nervous system d. All of the above
November 8, 2012
10
What Purpose does Hostility, Anger, and Aggression Serve?
Hostility, anger, and aggression has meaning: 1. It is a signal to others. It is COMMUNICATION.
November 8, 2012
11
So, if the purpose of Anger, Hostility, and Aggression is communication, what exactly is being communicated?
November 8, 2012
12
11/8/12
5
November 8, 2012
13
You don’t want to be near me right now . . . Really.
I’m feeling
backed into a
corner.
I don’t feel safe.
November 8, 2012
14
But, hostility, anger, and aggression are not just a means of communication.
They’re also adaptive – they serve an important purpose for the person.
Hostility, Anger, and Aggression are Primitive Survival Tools To the person expressing it, the message to oneself is
clear:
TAKE ACTION When functional, the goal is to: ▫ Get Something ▫ Protect Something
November 8, 2012
15

11/8/12
6
• Stress is the perception of a physical or psychological threat and the perception that one’s responses are not adequate to deal with it.
• Within the body, there is a cascade of physiological events that prepares the person to respond to the stress.
• The stress response has also been referred to as the fight or flight response.
The Body’s Response to Stress: Anger in Action
November 8, 2012
16
The Brain and the Body Responding to Stress
1. The cerebral cortex perceives the threat. 2. A signal is sent to the amygdala – the brain center
that activates the fight or flight response / the stress response system.
3. The brain prepares the body for response to the threat via central (brain-related) and peripheral (body-related) responses.
4. Once the threat is dealt with, the stress-response system is turned off.
November 8, 2012
17
Peripheral Nervous System
Consists of: • Sensory neurons running from stimulus receptors
that inform the CNS of the stimuli. • Motor neurons running from the CNS to the muscles
and glands - called effectors - that take action.
November 8, 2012
18
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/PNS.html

11/8/12
7
The Stress Response: The Autonomic Nervous System
November 8, 2012
19
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/PNS.html
November 8, 2012
20
If the fight or flight response is an adaptive response to stress
and hostility, anger, and aggression are revealed in
this response, then
these experiences can be regarded as adaptive – sometimes.
So, when is it that hostility, anger, and/or aggression pathological, unhealthy, or
maladaptive?
When is Premeditated Aggression Pathological? • Almost always . . . ▫ There is a “manipulative” quality to it ▫ Sometimes pleasure is derived from this type of
aggression ▫ There may be little to no arousal in the regions of
the brain that would signal an emotional reaction to the aggression.
November 8, 2012
21
11/8/12
8
When is Impulsive Aggression, Anger, or Hostility Pathological? • When it is exaggerated in relation to the
emotional provocation. • When it is the predominant response to stress. • It feels or is beyond one’s control. • It causes problems or dissatisfaction in one’s life.
November 8, 2012
22
Section 1 Summary - Hostility, Anger, and Aggression: 1. Carries meaning. 2. Is communication. To others it says, “Pay attention!” 3. Is a message to oneself. It announces, “Take action!” 4. Serves to propel the person to either get something or
protect something. 5. Is integrally related to the adaptive stress / fight or
flight response. 6. Though adaptive, it can cause significant problems in
people’s lives when gone awry.
November 8, 2012
23
Post-test Question # 2 Preparing the body to respond to stress in the
environment is the responsibility of which of the following?
a. The sympathetic nervous system b. The parasympathetic nervous system c. The autonomic nervous system d. All of the above
November 8, 2012
24

11/8/12
9
Hostility, Anger, and Aggression in Chemical Dependence treatment Data from residents at Fountain Centers’
programs in Albert Lea, Rochester, Mankato, Faribault, Owatonna, Fairmont, Waseca, and Jackson, MN
November 8, 2012
25
Fountain Centers
November 8, 2012
26
Questions Used to Assess Hostility, Anger, and Aggression
• Global Appraisal of Individual Needs Short Screener (GAIN-SS) ▫ Four Questions used to assess hostility, anger, and aggression:
1. When was the last time that you did the following things two or more times?
a) Were a bully or threatened other people? b) Started physical fights with other people?
2. When was the last time that you… a) Had a disagreement in which you pushed, grabbed, or shoved someone? b) Purposely damaged or destroyed property that did not belong to you?
▫ Answered: 3 = Past month; 2 = 2 to 12 months ago; 1 = 1+ years ago; 0 = Never
November 8, 2012
27

11/8/12
10
Fountain Centers Clients
• Purposely damaged or destroyed property that did not belong to you?
November 8, 2012
28
Men Women Adolescent Males
Adolescent Females
N 144 81 29 12
Past month or 2-12 months
15% 13% 47% 33%
1+ Year Ago 30% 19% 17% 33%
Never 55% 68% 37% 33%
Fountain Centers Clients
• Purposely damaged or destroyed property that did not belong to you?
November 8, 2012
29
Men Women Adolescent Males
Adolescent Females
N 144 8 81 28 29 12
Past month or 2-12 months
15% 0% 13% 0% 47% 33%
1+ Year Ago 30% 38% 19% 21% 17% 33%
Never 55% 62% 68% 79% 37% 33%
Fountain Centers Clients • Have you bullied or threatened other people?
November 8, 2012
30
Men Women Adolescent Males
Adolescent Females
N 147 90 29 12
Past month or 2-12 months
13% 27% 30% 50%
1+ Year Ago 26% 21% 27% 8%
Never 61% 52% 43% 42%
National average for bullying for adolescents in one study estimated to be 13% (Nansel et al JAMA (2001) 285 (19), 2094-2100).

11/8/12
11
Fountain Centers Clients • Have you bullied or threatened other people?
November 8, 2012
31
Men Women Adolescent Males
Adolescent Females
N 147 8 90 28 29 12
Past month or 2-12 months
13% 0% 27% 0% 30% 50%
1+ Year Ago 26% 25% 21% 32% 27% 8%
Never 61% 75% 52% 68% 43% 42%
Fountain Centers Clients • Started physical fights with other people?
November 8, 2012
32
Men Women Adolescent Males
Adolescent Females
N 146 82 30 12
Past month or 2-12 months
12% 17% 50% 50%
1+ Year Ago 25% 24% 27% 17%
Never 64% 59% 23% 33%
One study found that 40.7% of adolescent males and 24.4% adolescent females were in a physical fight in the last year. (MMWR (2012) 61(4) 7).
The rate of simple assault as measured by the BJS for those age 12 and older in 2011 was 1.5% (Bureau of Justice Statistics, National Crime Victimization Survey, 2002, 2010, and 2011; http://www.bjs.gov/content/pub/pdf/cv11.pdf).
Fountain Centers Clients • Started physical fights with other people?
November 8, 2012
33
Men Women Adolescent Males
Adolescent Females
N 146 8 82 28 30 12
Past month or 2-12 months
12% 0% 17% 0% 50% 50%
1+ Year Ago 25% 13% 24% 11% 27% 17%
Never 64% 87% 59% 89% 23% 33%

11/8/12
12
Fountain Centers Clients
• Had a disagreement in which you pushed shoved, or grabbed someone?
November 8, 2012
34
Men Women Adolescent Males
Adolescent Females
N 145 78 29 12
Past month or 2-12 months
23% 35% 77% 83%
1+ Year Ago 42% 24% 10% 8%
Never 35% 41% 13% 8%
Fountain Centers Clients
• Had a disagreement in which you pushed shoved, or grabbed someone?
November 8, 2012
35
Men Women Adolescent Males
Adolescent Females
N 145 8 78 28 29 12
Past month or 2-12 months
23% 0% 35% 7% 77% 83%
1+ Year Ago 42% 38% 24% 43% 10% 8%
Never 35% 62% 41% 50% 13% 8%
Factors, Diagnoses, and Other Common Issues Associated with Hostility, Anger, and Aggression
November 8, 2012
36
11/8/12
13
Pre-test Question # 3 In the study by Caspi et al (2002) which of the
following was found to confer the greatest risk to future aggression and violence?
a. Childhood abuse b. Genes c. The interaction between genes
and the environment d. Having a “hostile”
temperament as a child
November 8, 2012
37
November 8, 2012
38
Predictors of Aggression/Violence • Static – Unalterable Factors ▫ Previous history of violence ▫ Male ▫ Young adult ▫ Lower intelligence ▫ History of head injury ▫ History of military service ▫ Weapons training ▫ Past diagnosis of major mental
illness
• Dynamic – Can be changed to improve outcome ▫ Substance use ▫ Current symptoms of major
mental illness � Persecutory delusions � Command hallucinations � Depression
� Hopelessness � Suicidality
▫ Treatment Nonadherence ▫ Impulsivity ▫ Access to weapons
November 8, 2012
39
Anderson, Western Innovations in Clinical Neuroscience (2011) 8(3): 34-9; Bobes et al., Acta Psychiatry Scananavia (2009) 119, 218-25; Fazel et al., Journal of Clinical Psychiatry (2009) 70(3), 362-9; Swanson et al. Hospital Community Psychiatry (1990) 41(7), 761-70. (Slide and references: 2012 NEI Congress)
11/8/12
14
Other Factors that Influence Anger and Aggression • Low self-esteem* • Under-socialized ▫ Lacking skills to negotiate situations that may provoke
conflict • Situational Factors ▫ Pain and discomfort ▫ Frustration – being blocked from achieving a goal
• Problems with or disordered sleep
November 8, 2012
40
*Donenllan, Psychological Science (2005) 16(4), 328-35.
Genes and Propensity to Aggression • In recent years, certain genes have been found to be
associated with a propensity to aggression and violence in certain situations.
• For example, a variant of the MAO gene, one that controls the breakdown of neurotransmitters, is associated with increased aggression and violence. * This gene was dubbed “the warrior gene.”
• Multiple genes in interaction with other genes, not single genes, are being found to create a heightened risk for complex behaviors such as aggression.
November 8, 2012
41
*Brunner et al Science (1993) 262, 578.
Environmental Influences on Aggression • It has long been known that childhood maltreatment is a
universal risk factor for antisocial behavior. • Boys exposed to erratic, coercive, and punitive parenting
are at risk for conduct disorder, antisocial personality symptoms, and becoming violent offenders.
• The earlier the maltreatment occurs, the greater the risk for these later problems.
• However, there are large differences between children who are exposed to maltreatment – not all go on to become delinquents or adult criminals.
November 8, 2012
42
Widom, Science (1989) 244, 160; Rutter et al, Antisocial Behavior by Young People (1998), Cambridge U. Press; Kelley et al, Dev. Psychopathology (2001) 13, 891.

11/8/12
15
Genes and Environment and Aggression • Genes interact with the environment. ▫ For example, in 2002 a study found that men with a copy of
“the warrior gene” only exhibited violence if they experienced maltreatment as children. ▫ Being raised in a caring environment neutralized the
negative effect of the gene on later aggression and violence. • This gene-environment interaction has been found in
other studies as well involving this gene since 2002.
November 8, 2012
43
Caspi et al., Science, (2002) 297: 851-4.
What May Happen to At-Risk Genes Over Time in a Stressful Environment
Time 1 Time 2 Time 3 (etc) Outcome
November 8, 2012
44
Mild Stress
Moderate to High Stress
I cause trouble.
Chronic Stress is the Culprit
• Individuals who experience chronic “stress” are at greatest risk for problems later in life.
• Experiencing this stress as a child creates even greater risks as it results in structural and functional changes to the developing brain.
• If, on top of this, you are born with compromised genes you are at greatest risk for impairment, both as a child and as an adult.
November 8, 2012
45
11/8/12
16
What May Happen to At-Risk Genes Over Time in a Nurturing Environment
Time 1 Time 2 Time 3 (etc) Outcome
November 8, 2012
46
Do those in Fountain Centers with More Recent Aggression have More Adverse Childhood Experiences* (ACEs)?
• ACEs are a series of 10 questions assessing the number of negative experiences in childhood that an individual reports.
• An individual can achieve a score from 0 to 10, with lower scores representing fewer ACEs.
• Each “Yes” answer earns a score of 1. • Higher scores are associated with a host of adverse
outcomes in adulthood including physical and mental health and social problems.
November 8, 2012
47
*Felitti et al, Am J Prev Med (1998). 14(4), 245-58.
The prevalence of ACE Scores in the ACE study population is as follows: 0 = 33%, 1 = 26%, 2 = 16%, 3 = 10%, >4 = 15%.
ACEs Questions November 8, 2012
48
While you were growing up, during your first 18 years of life: 1. Did a parent or other adult in the household often or very often… Swear at you, insult you, put you down, or humiliate you? or Act in a way that made you afraid that you might be physically hurt? 2. Did a parent or other adult in the household often or very often… Push, grab, slap, or throw something at you? or Ever hit you so hard that you had marks or were injured? 3. Did an adult or person at least 5 years older than you ever… Touch or fondle you or have you touch their body in a sexual way? or Attempt or actually have oral, anal, or vaginal intercourse with you? 4. Did you often or very often feel that … No one in your family loved you or thought you were important or special? or Your family didn’t look out for each other, feel close to each other, or support each other?

11/8/12
17
ACEs Questions (cont’d)
November 8, 2012
49
5. Did you often or very often feel that … You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? or Your parents were too drunk or high to take care of you or take you to the doctor if you needed it? 6. Were your parents ever separated or divorced? 7. Was your mother or stepmother: Often or very often pushed, grabbed, slapped, or had something thrown at her? or Sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard? or Ever repeatedly hit at least a few minutes or threatened with a gun or knife? 8. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
9. Was a household member depressed or mentally ill, or did a household member attempt suicide? 10. Did a household member go to prison?
Do females who report more recent aggression* also report more adverse childhood experiences (ACEs)?
• Were a bully or threatened other people • Purposely damaged or destroyed property that did not belong
to you
November 8, 2012
50
Bully or Threatened
Others
Destroyed Property
Past month or 2-12 months
5.7 (n = 29) 5.9 (n = 14)
1+ Year Ago or Never
3.2 (n = 62) 3.6 (n = 75)
* Selected the GAIN-SS questions with the highest correlation to the ACEs score.
t Correlations in this range are generally regarded as moderate to strong.
The prevalence of ACE Scores in the ACE study population is as follows: 0 = 33%, 1 = 26%, 2 = 16%, 3 = 10%, >4 = 15%.
r = .43t
r=.34t
Do males who report more recent aggression* also report more adverse childhood experiences (ACEs)? • Were a bully or threatened other people r = .36
• Purposely damaged or destroyed property that did not belong to you r = .36
November 8, 2012
51
Bully or Threatened
Others
Destroyed Property
Past month or 2-12 months
4.3 (n = 27) 3.7 (n = 32)
1+ Year Ago or Never
2.0 (n = 144) 2.1 (n = 136)
* Selected the GAIN-SS questions with the highest correlation to the ACEs score.
The prevalence of ACE Scores in the ACE study population is as follows: 0 = 33%, 1 = 26%, 2 = 16%, 3 = 10%, >4 = 15%.
t Again, correlations in this range are generally regarded as moderate to strong.

11/8/12
18
Diagnostic and Statistical Manual – Fourth Edition – Text Revision
(DSM-IV-TR)
Possible causes of aggression, anger, and
hostility
November 8, 2012
52
Cluster B Personality Disorders # 1 Antisocial - A pervasive pattern of disregard for, and violation of, the rights of others that begins in childhood or early adolescence (often diagnosed as conduct disorder) and continues into adulthood Tend to be callous and unconcerned for the feelings of others. Tend to have a very low tolerance for frustration and a low threshold for discharge of aggression. Often maintain persistent irritability.
November 8, 2012
53
Cluster B Personality Disorders # 2 Borderline - also known as emotionally unstable personality disorder, is a psychological condition marked by a prolonged disturbance of personality function, characterized by depth and variability of moods. Tend to think in black-and-white terms, often manifests itself in idealization and devaluation episodes and chaotic and unstable interpersonal relationships, self-image, identity, and behavior, as well as a disturbance in the one's sense of self. React with anger when experiencing perceived rejection, being alone, or perceived failure. Rapid swings from anger to anxiety to depression. Anger is inappropriate. Has difficulty controlling anger.
November 8, 2012
54

11/8/12
19
Narcissistic - a personality disorder in which the individual is described as being excessively preoccupied with issues of personal adequacy, power, prestige, and vanity. Tend to be controlling, blaming, self- absorbed, intolerant of others’ views, unaware of others' needs, and of the effects of their behavior on others. React with anger and rage when experiencing criticism, real or imagined, and when they feel their sense of self is threatened.
Cluster B Personality Disorders # 3
November 8, 2012
55
Impulse Control Disorders
Intermittent Explosive Disorder is a behavioral disorder characterized by extreme expressions of anger, often to the point of violence, that are disproportionate to the situation at hand. Impulsive aggression is unpremeditated and is defined by a disproportionate reaction to any provocation, real or perceived.
November 8, 2012
56
Other Causes of Hostility, Anger, and Aggression # 1
• Brain Injury
• Cognitive Deficits
• Social Skills Deficits
• Thought Disorders ▫ Especially delusions
November 8, 2012
57

11/8/12
20
Other Causes of Hostility, Anger, and Aggression # 2 • Medical Conditions ▫ Any disease condition that taxes the physical
status of the individual
• Alcohol or other drug use or withdrawal ▫ Chronic use of drugs of abuse can permanently
alter the structure and function of the brain, including predisposing a person to precipitous anger.
November 8, 2012
58
Susceptibility to Aggression and Psychiatric Diagnosis
Co-Occurring Problem
Type of Aggression
Psychosis and cognitive impairment
Deviant Behaviors
Anxiety and trauma
Reactive and impulsive; with trauma – triggered by cues associated with trauma
Emotional sensitivity and dysregulation
Impulsive or reactive; e.g., borderline PD
Psychopathy Premeditated; e.g., Antisocial PD
November 8, 2012
59
Susceptibility to Aggression
Siever, L. J. American Journal of Psychiatry 2008; 165 (4), 429-42
Section 2 Summary • Static factors, such as age and gender, and dynamic
factors, such as mental illness and substance use, can increase the prediction of hostility, anger and aggression.
• There are several common factors associated with hostility, anger, and aggression: 1. Genes and the interaction between genes and the
environment. 2. Personality disorders, particularly Cluster B. 3. Impulse control disorders – those with no known cause. 4. Brain injuries, cognitive and social skills deficits, thought
disorders, medical conditions, and drug use and withdrawal.
November 8, 2012
60

11/8/12
21
Post-test Question # 3 In the study by Caspi et al (2002) which of the
following was found to confer the greatest risk to future aggression and violence?
a. Childhood abuse b. Genes c. The interaction between genes
and the environment d. Having a “hostile”
temperament as a child
November 8, 2012
61
The Association Between Chemical Use and Hostility, Anger, and Aggression
November 8, 2012
62
Pre-test Question # 4
What would be the best treatment intervention for someone whose anger is associated with anxiety?
a. Seeking Safety / milieu-based program emphasizing predictability
b. Relaxation strategies such as meditation
c. Skills training such as DBT d. Exercise and sleep hygiene
November 8, 2012
63
11/8/12
22
The Association with Chemical Use
November 8, 2012
64
Chemical Use Hostility, Anger, & Aggression
May increase or decrease
with substance use
Intoxication, Aggression, and Substance Use
November 8, 2012
65
Hostility, Anger, and Aggression Hypotheses Outcome as substances clear
the body
Chemical use or withdrawal is the cause
A co-occurring disorder is the cause
Use substances to control
Co-occurring Disorders as “Medicating” Problems
• Clearly, many drug users consume alcohol and other drugs to make unpleasant emotions, such as anger, and life more tolerable.
• This “solution” is at best a short-term attempt to cope and not getting at the underlying problems.
• More typically, chemical use worsens the very problems the user is trying to sooth with chemicals by: ▫ Preventing the development of adaptive coping strategies. ▫ Making the person more vulnerable to adverse consequences, thus
increasing anger, despair, and feelings of lack of control in one’s life. ▫ Damaging brain circuits required for management of anger and
impulses.
November 8, 2012
66
11/8/12
23
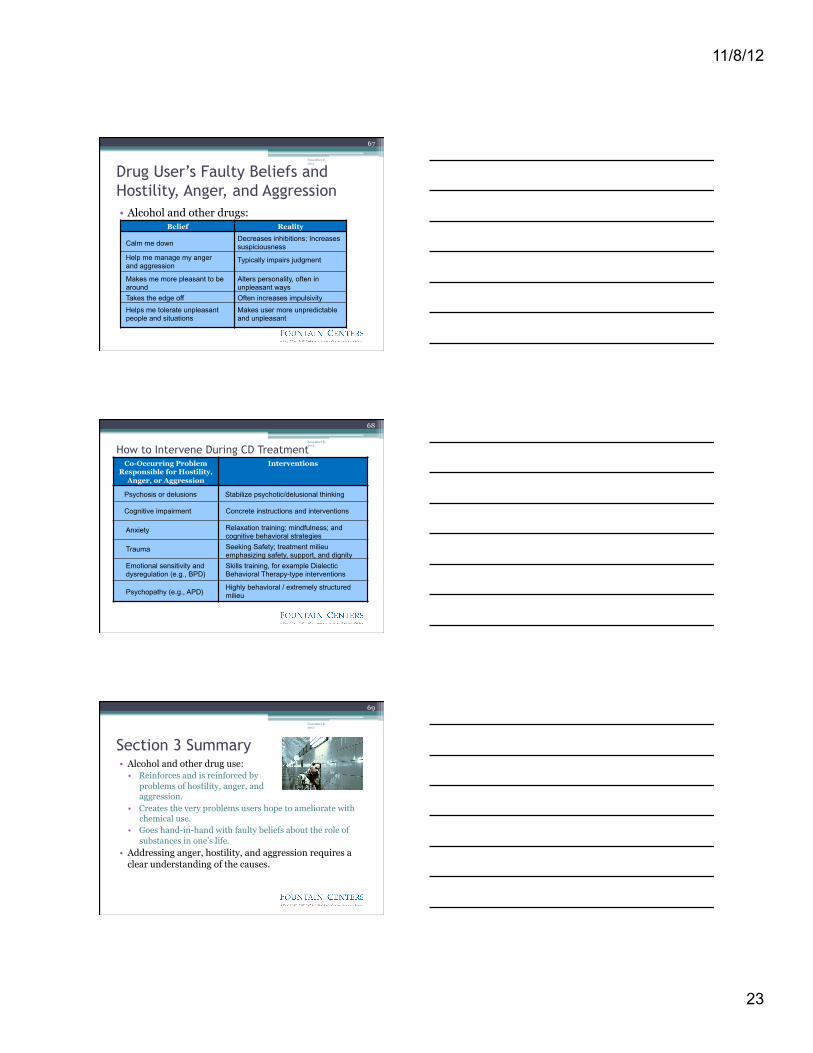
Drug User’s Faulty Beliefs and Hostility, Anger, and Aggression • Alcohol and other drugs:
November 8, 2012
67
Belief Reality
Calm me down Decreases inhibitions; Increases suspiciousness
Help me manage my anger and aggression
Typically impairs judgment
Makes me more pleasant to be around
Alters personality, often in unpleasant ways
Takes the edge off Often increases impulsivity
Helps me tolerate unpleasant people and situations
Makes user more unpredictable and unpleasant
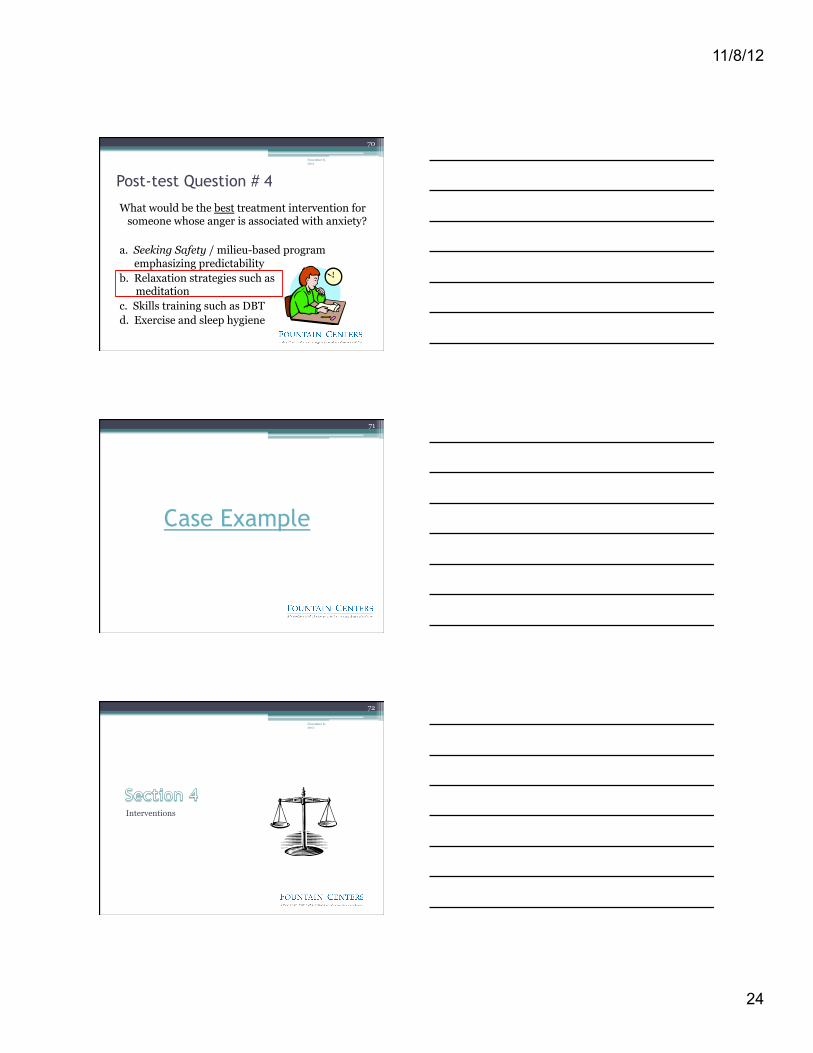
How to Intervene During CD Treatment November 8, 2012
68
Co-Occurring Problem Responsible for Hostility,
Anger, or Aggression
Interventions
Psychosis or delusions Stabilize psychotic/delusional thinking
Cognitive impairment Concrete instructions and interventions
Anxiety Relaxation training; mindfulness; and cognitive behavioral strategies
Trauma Seeking Safety; treatment milieu emphasizing safety, support, and dignity
Emotional sensitivity and dysregulation (e.g., BPD)
Skills training, for example Dialectic Behavioral Therapy-type interventions
Psychopathy (e.g., APD) Highly behavioral / extremely structured milieu
Section 3 Summary
November 8, 2012
69
• Alcohol and other drug use: • Reinforces and is reinforced by
problems of hostility, anger, and aggression.
• Creates the very problems users hope to ameliorate with chemical use.
• Goes hand-in-hand with faulty beliefs about the role of substances in one’s life.
• Addressing anger, hostility, and aggression requires a clear understanding of the causes.
11/8/12
24
Post-test Question # 4
What would be the best treatment intervention for someone whose anger is associated with anxiety?
a. Seeking Safety / milieu-based program emphasizing predictability
b. Relaxation strategies such as meditation
c. Skills training such as DBT d. Exercise and sleep hygiene
November 8, 2012
70
71
Case Example
Interventions
November 8, 2012
72

11/8/12
25
Pre-test Question # 5
For someone who is acutely agitated, the type of intervention that is most likely to be successful will focus on:
a. “Top-down”, prefrontal processing b. “Bottom-up”, amygdala-directed
strategies c. Interventions with specific, clear,
concise directions d. Removing triggers from the situation
November 8, 2012
73
“Top-Down” Regulation of Brain Functioning During Calm Times
November 8, 2012
74
PFC – Prefrontal Cortex DLPFC – Dorsolateral PFC DMPFC – Dorsomedial PFC rIPFC – Right Inferior PFC VMPFC – Ventromedial PFC NA – Norepinephrine DA - Dopamine
The Prefrontal Cortex regulates thought and action. The PFC is often referred to as “the brakes,” slowing down impulse-driven actions.
Arnsten, A. F. T. (2009) Nature Reviews Neuroscience
Notice the many direct and indirect connections to other brain regions.
“Bottom-Up” Regulation of Brain Functioning During Stressful Times
November 8, 2012
75
Arnsten, A. F. T. (2009) Nature Reviews Neuroscience
The Amygdala regulates fear and reward processing and emotion. “Drives,” impulses, and instinctual responding is regarded as originating here.
When the amygdala fires up, prefrontal processing shuts down.

11/8/12
26
Therapeutic Interventions
• Different targets: ▫ The person ▫ The person’s emotions ▫ The symptoms ▫ Self-awareness
November 8, 2012
76
Person Emotions
Symptoms Self-
Awareness
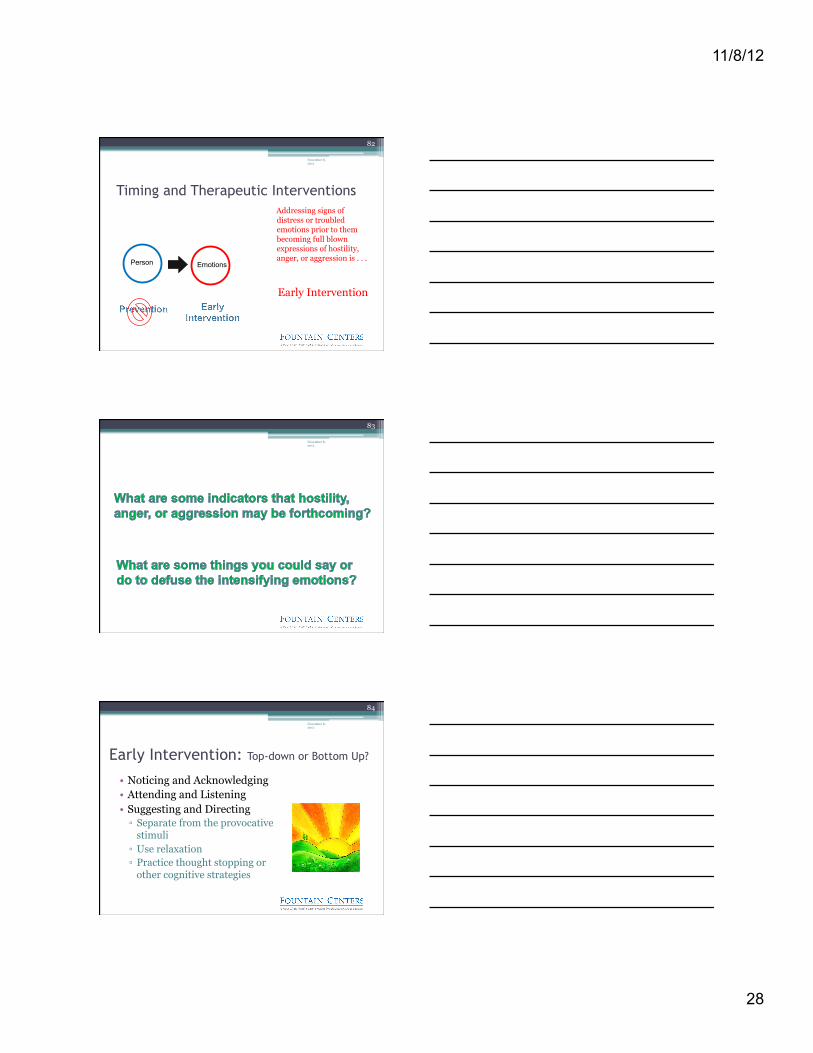
Timing and Therapeutic Interventions
Intervening with a person who is at risk for hostility, anger expression, and aggression prior to their display of the associated behavior and emotions is . . .
PREVENTION.
November 8, 2012
77
Person
November 8, 2012
78
11/8/12
27
Prevention # 1
• Know your client ▫ Be aware of the factors associated with the anger.
� The causes and diagnoses provide a guide for treatment interventions.
▫ Inoculation ▫ Address anger as an issue from the outset.
� “How is this issue likely to play out in treatment?” � “How has this caused you problems in the past?” � “When I/we see this issue in your treatment, what would be
the most helpful way to address it with you?”
November 8, 2012
79
Prevention # 2: Top-down or Bottom Up?
• Focus on the Relationship ▫ Genuineness ▫ Empathy and understanding
• Show Interest ▫ Listening ▫ Inquiring
• Demonstrate Positive Regard
November 8, 2012
80
Prevention # 3: Top-down or Bottom Up?
• Include strategies for management of hostility, anger, and aggression in the treatment plan.
• Give the client homework assignments to practice anger management strategies.
• Treatment Interventions: ▫ Relaxation training / meditative practices ▫ Cognitive behavioral strategies, especially focused on thinking
errors and relapse prevention ▫ Skills training, especially role playing around issues involving
intense emotional exchanges, communication, and assertiveness ▫ Involvement in a healing community, e.g., AA/NA, faith group
November 8, 2012
81
11/8/12
28
Timing and Therapeutic Interventions Addressing signs of distress or troubled emotions prior to them becoming full blown expressions of hostility, anger, or aggression is . . .
Early Intervention
November 8, 2012
82
Person Emotions
November 8, 2012
83
Early Intervention: Top-down or Bottom Up?
• Noticing and Acknowledging • Attending and Listening • Suggesting and Directing ▫ Separate from the provocative
stimuli ▫ Use relaxation ▫ Practice thought stopping or
other cognitive strategies
November 8, 2012
84
11/8/12
29
Timing and Therapeutic Interventions
November 8, 2012
85
Person Emotions Symptoms
Timing and Therapeutic Interventions
November 8, 2012
86
Symptoms
Intervening with a client after hostility, anger, or aggression has been displayed is . . .
De-escalation
When Anger or Aggression are Being Expressed, Remember . . . • Rational, top-down, prefrontal processing of
information is absent. Therefore, talking rationally is not an option.
• Emotional, bottom-up, amygdala-driven reacting predominates. Therefore, interventions aimed at calming the person are most likely to be successful.
November 8, 2012
87

11/8/12
30
De-escalation: Top-down or Bottom Up?
• Containing ▫ Separate from others and
potential hazards. • Redirecting ▫ Clear, concise messages about what you need
the individual to do. ▫ Repeat the message.
• Calming ▫ Help the individual employ self-calming
strategies.
November 8, 2012
88
Timing and Therapeutic Interventions
November 8, 2012
89
Person Emotions Symptoms Self-
Awareness
Timing and Therapeutic Interventions
November 8, 2012
90
Self-Awareness
After de-escalating, the opportunity exists for new learning or . . .
Consolidation

11/8/12
31
November 8, 2012
91
Consolidation: Top-down or Bottom Up? • Process and learn from the experience • Identify triggers for anger • Develop new strategies for anger management • Practice new skills • Rinse, wash, repeat
November 8, 2012
92
Anger
Section 4 Summary
• Interventions to address hostility, anger, and aggression vary depending on one’s target and timing.
November 8, 2012
93
Target Stage
Person Prevention
Emotion Early Intervention
Symptom De-escalation
Self-Awareness Consolidation
11/8/12
32
Post-test Question # 5
For someone who is acutely agitated, the type of intervention that is most likely to be successful will focus on:
a. “Top-down”, prefrontal processing b. “Bottom-up”, amygdala-directed
strategies c. Interventions with specific, clear,
concise directions d. Removing triggers from the situation
November 8, 2012
94
Summary – Anger, Hostility, and Aggression • It has meaning. It is useful to understand what a
person’s anger is communicating. • There are multiple causes of anger and factors
associated with it. Knowing the causes is like having the early stages of trip mapped out.
• Chemical use worsens problems of anger. • Interventions can be matched to the stage at
which anger is observed to be at issue.
November 8, 2012
95
November 8, 2012
96







