Managing falls and fractures in care homes for older people
Falls Prevention and ManagementResource Pack
Falls Prevention ServiceWilson HospitalCranmer Road, MitchamCR4 4TP
Tel: 020 8254 8247Fax: 020 3458 5528
2
ContentsIntroduction 3
Tools for Staff
1. Care home resident falls and fracture risk/intervention tool 4
2. Resident environment and orientation check 5
Tools for Managers
1. Care homes falls questionnaire 6
2. Care homes multifactorial falls risk assessment and management tool 7
3. Care homes falls prevention monitoring form 14
4. Care homes generic falls environmental risk assessment form 16
5. Care homes monthly falls overview form 20
6. Care homes post fall/incident report form 21
Additional information
Annex A – Care homes post fall pathway 25
Annex B – Care homes had a fall poster 26
Annex C – Medicines associated with falls 27
3
IntroductionWhat is this resource pack about?This resource pack provides the answers to many of the questions care home managers have in relation to the prevention and management of falls and fractures and can act as an excellent educational tool for new or existing care home staff.
“Managing falls and fractures in care homes for older people” provides the direction, advice and support that staff in a care home need to make a difference in this area of care. The resource which is research-based not only gives the guidance required, but offers tools which can be used in a care home to help improve or change practice.
Why should I use it?Falls are an inevitable part of ageing. In many cases, taking the right steps at the right time can prevent falls and enable an older person to continue a physically active life. Care home staff have a key role to play in falls prevention, but they need to have knowledge and understanding.
Older people living in care homes are three times more likely to fall than older people living in their own homes, with the result of a fall often being much more serious; there are ten times more hip fractures in care homes than in other environments. Many factors can contribute to this heightened risk, such as physical frailty, the presence of long term conditions, physical inactivity, taking multiple medications and the unfamiliarity of new surroundings. For this reason, it is important that all care homes for older people implement a person centred process to manage and reduce falls and fractures. This will help to improve the overall quality of care for an individual and will have a huge impact on a person’s independence and participation in life.
How should I use it?The resources are split into groups to make them easier to navigate.
There is a section for all staff to use to ensure the home environment and people living in it are safe and risk is minimised and managed where falls are inevitable.
There is a section for managers to monitor falls in the home and develop more proactive management plans for reducing the incidence of falls.
This resource pack has been adapted from the ‘Managing falls and fractures’ Resource Pack as developed by, and with kind permission of, the Care Inspectorate. The full resource can be downloaded at: www.careinspectorate.com
4
Inst
ruct
ions
fo
r us
e: re
fer
to e
ach
area
of r
isk
in tu
rn. C
onsi
der
the
sugg
este
d ac
tions
to h
elp
writ
e a
pers
onal
ised
act
ion
plan
for
a re
side
nt.
Ada
pted
from
a to
ol d
evel
oped
by
Lynn
Fla
nnig
an, N
HS
Lan
arks
hire
Mo
bili
ty/
Bal
ance
Co
nfus
ion/
cog
nitiv
eim
pai
rmen
tF
alls
hi
sto
ryM
edic
atio
nC
ont
inen
ceFo
othe
alth
an
d
foot
wea
r
Diz
zine
ss/
bla
cko
uts
Vis
ion/
hear
ing
Is th
e re
side
nt
unst
eady
or
have
mob
il-ity
pro
b-le
ms?
Doe
s th
e re
side
nt
they
hav
e a
fear
of
fallin
g?
Is th
e re
side
nt
cogn
itive
ly
impa
ired?
Is th
e re
side
nt
mor
e co
nfus
ed
than
nor
mal
?
Co
nsid
er?
• M
ovin
g &
ha
ndlin
g as
sess
-m
ent.
• S
uper
visi
on p
lan.
•
Enc
oura
ging
saf
e ac
tivity
with
use
of
app
rop.
wal
king
ai
ds.
• R
efer
ral t
o ph
ysio
.•
Ass
essm
ent f
or
hip
prot
ecto
rs.
• M
onito
ring
alco
hol i
ntak
e.
Co
nsid
er?
• C
urre
nt h
ealth
eg
pain
, de
hydr
atio
n,
cons
tipat
ion.
• R
ulin
g ou
t in
fect
ion/
delir
ium
.•
See
king
adv
ice
from
GP
/CP
N.
•
Opt
imis
ing
envi
ronm
enta
l sa
fety
.•
Tel
ehea
lthca
re•
Pro
mot
ing
safe
ex
erci
se a
nd a
ctiv
-ity
.•
Ass
essm
ent f
or
hip
prot
ecto
rs.
Co
nsid
er?
• P
re-a
dmis
sion
st
rate
gies
.•
Sup
ervi
sion
pla
n,
usin
g •
Wal
king
aid
s w
here
requ
ired.
•
Enc
oura
ging
saf
e ac
tivity
.•
Ref
erra
l for
fur-
ther
ass
essm
ent e
g ph
ysio
, GP
or
falls
se
rvic
e, if
hig
h ris
k,
unex
plai
ned
falls
or
seve
ral r
ecen
t fal
ls.
• A
sses
sing
for
hip
prot
ecto
rs.
Co
nsid
er?
• A
skin
g ab
out
and
obse
rvin
g fo
r sy
mpt
oms
of
dizz
ines
s/
drow
sine
ss.
• C
heck
ing
BP
(ly
ing/
stan
ding
).•
Med
icat
ion
revi
ew b
y G
P.•
CP
N re
view
.
Co
nsid
er?
• C
heck
ing
for
infe
ctio
n.
• T
oile
ting
regi
me.
•
Pos
ition
ing
near
to
ilet.
• R
efer
ral t
oD
N o
r co
ntin
ence
se
rvic
e.•
App
ropr
iate
cl
othi
ng.
• A
com
mod
e or
ur
inal
.•
Usi
ng n
ight
lig
hts.
Co
nsid
er?
• D
iscu
ssin
g w
ith
resi
dent
and
fam
ily
suita
ble
foot
wea
r. •
Intr
oduc
ing
a fo
otca
re re
gim
e.
• R
efer
ral t
o po
diat
ry.
Co
nsid
er?
• G
P re
view
, in
clud
ing
med
icat
ion
revi
ew.
• C
heck
ing
lyin
g/st
andi
ng B
P.•
Ref
erra
l to
Falls
C
linic
.
Co
nsid
er?
• E
nsur
ing
glas
ses
and
hear
ing
aids
in
plac
e an
d in
goo
d st
ate
of re
pair.
• E
nsur
ing
good
lig
htin
g.•
Che
ck fo
rea
r w
ax.
• R
efer
ral t
o op
ticia
n/au
diol
ogy.
Hav
e th
ere
been
pr
evio
us
falls
? If
so,
how
man
y;
wha
t wer
e th
e ca
uses
&
con
se-
quen
ces?
Is th
e re
side
nt
taki
ng
beno
dia-
zepi
nes,
ps
ycho
trop
ics
4 or
mor
e m
eds;
or
any
othe
r hi
gh
risk
drug
s?
Are
ther
e an
y co
ntin
ence
is
sues
: in
cont
i-ne
nce,
fre
quen
cy o
r ur
genc
y?
Is
foot
wea
r su
itabl
e?
Are
ther
e fo
ot h
ealth
pr
oble
ms?
Doe
s th
ere
side
nt
appe
ar
dizz
y or
hav
e fa
intin
g at
tack
s?
Doe
s th
ere
side
nt
have
im
paire
d he
arin
g or
sig
ht?
Env
ironm
ent
Po
or
nutr
itio
nB
one
he
alth
Co
nsid
er?
• O
rient
atin
g re
side
nt to
en
viro
nmen
t.•
Usi
ng th
e‘E
nviro
nmen
t A
sses
smen
t too
l’.
• A
ids,
app
lianc
es
and/
or s
igna
ge.
Co
nsid
er?
• R
efer
ral t
o G
P o
r di
etic
ian.
• S
tart
ing
a fo
od
reco
rd c
hart
(as
advi
sed
by G
P o
r di
etic
ian)
.•
Foo
d su
pple
men
ts.
(as
advi
sed
by G
P
or d
ietic
ian)
.•
Enc
oura
ging
go
od fl
uid
inta
ke.
Co
nsid
er?
• T
akin
g os
teop
o-ro
sis
med
icat
ions
an
d/or
cal
cium
and
vi
tam
in D
as
pres
crib
ed.
• D
iscu
ssin
g bo
ne
heal
th w
ith G
P.•
Life
styl
e ad
vice
eg
cal
cium
ric
h di
et, s
afe
sunl
ight
ex
posu
re, s
ensi
ble
alco
hol i
ntak
e,
smok
ing
cess
atio
n,
wei
ght-
bear
ing
activ
ity.
Is th
ere
side
nt
unde
rwei
ght
or h
ave
poor
food
in
take
?
Doe
s th
e re
side
nt
have
os
teop
oros
is
or a
re th
ere
oste
opor
osis
ris
k fa
ctor
s?
Is th
een
viro
nmen
t sa
fe a
ndsu
itabl
e?
If s
till a
pro
ble
m -
co
nsid
er r
efer
ral t
o f
alls
clin
ic
Ris
k fa
cto
rs id
entifi
edD
ate
and
initi
als
Act
ion
pla
nD
ate
and
initi
als
Car
e ho
me
resi
dent
falls
and
frac
ture
ris
k/in
terv
entio
n to
ol
Als
o kn
own
as T
ool 6
: Car
e ho
me
resi
dent
falls
and
frac
ture
risk
/inte
rven
tion
tool
Uni
que
iden
tific
atio
n no
: NR
527a
Ver
sion
no:
1
Janu
ary
2015
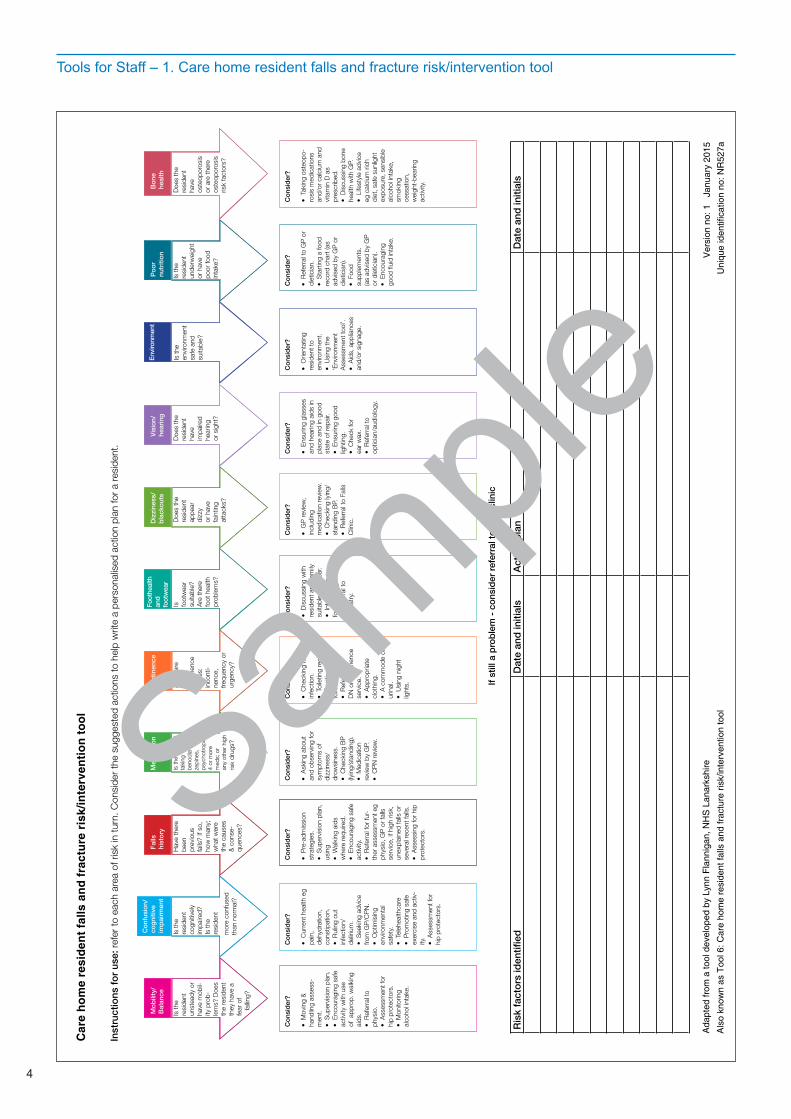
Tools for Staff – 1. Care home resident falls and fracture risk/intervention tool
Sample
5
Fo
otw
ear/
clo
thin
g
Wal
king
A
id/
whe
elch
air
Flo
ori
ngLi
ght
ing
Bat
hro
om
Sur
roun
ding
area
Fur
nitu
reB
ed
Is fo
otw
ear
light
wei
ght
and
non-
slip
? A
re
clot
hes
non-
slip
an
d co
rrec
t le
ngth
?
Do
they
re
quire
a
wal
king
ai
d? Is
thei
r w
alki
ng a
id/
whe
elch
air
clea
n an
d in
a
good
sta
te o
f
re
pair?
Co
nsid
er?
• L
iais
ing
with
ne
xt o
f kin
and
di
scus
sing
with
re
side
nt th
e im
port
ance
of
suita
ble
foot
wea
r an
d cl
othi
ng.
• C
heck
ing
foot
wea
r m
onth
ly.•
Pro
visi
on o
f eq
uipm
ent e
g lo
ng
hand
led
shoe
horn
, he
lpin
g ha
nd if
re
quire
d.
Co
nsid
er?
• R
efer
ral t
o lo
cal
phys
io
depa
rtm
ent.
•
Che
ckin
g co
nditi
on o
f w
alki
ng a
id,
repl
ace
ferr
ules
if
requ
ired.
• C
heck
ing
cond
ition
of
whe
elch
air,
arra
nge
whe
elch
air
repa
ir if
requ
ired.
• If
lap
belts
are
be
ing
used
ap
prop
riate
ly.
Co
nsid
er?
• R
epor
ting
and
reco
rdin
g an
y pr
oble
ms.
• R
earr
angi
ng
furn
iture
if
requ
ired.
•
Enc
oura
ging
go
od
hous
ekee
ping
.
Co
nsid
er?
• N
ight
ligh
t.•
Bed
side
ligh
t.•
Acc
essi
bilit
y to
re
side
nt.
• A
dditi
onal
lig
htin
g if
requ
ired.
• T
imer
ligh
ting
if re
quire
d.
Co
nsid
er?
• P
ositi
on o
f bu
zzer
. •
Pos
ition
of
soap
/han
d to
wel
s.
• U
sing
a r
aise
d to
ilet s
eat/
toile
t fra
me.
•
Is th
ere
spac
e fo
r w
alki
ng a
id/
mov
ing
and
hand
ling
equi
pmen
t?
• S
igna
ge.
• G
rabr
ails
.•
Lig
htw
eigh
t do
or.
• C
ontr
astin
g co
lour
s.•
Pos
ition
of b
ed.
Co
nsid
er?
• A
dditi
onal
lig
htin
g.•
Add
ition
al
sign
age.
• F
loor
s di
ffere
nt
colo
ur fr
om w
alls
. •
Ade
quat
e ha
ndra
ils.
• C
lutt
er fr
ee.
• R
epor
ting
and
reco
rdin
g an
y is
sues
.
Co
nsid
er?
• R
earr
angi
ngfu
rnitu
re.
• R
emov
ing
unne
cess
ary
furn
iture
. •
Are
foot
stoo
ls
able
to b
e m
oved
an
d st
ored
saf
ely?
• A
cces
sibi
lity
to:
–
buz
zer
–
ele
ctric
al
equ
ipm
ent
–
war
drob
es
a
nd d
raw
ers.
Co
nsid
er?
• H
eigh
t.•
Mat
tres
s su
itabi
lity.
• P
ositi
on in
ro
om.
• A
cces
sibi
lity
and
abilit
y to
use
bu
zzer
.•
Gra
b ra
ils.
• N
eed
for
bed
rails
.
Is th
e flo
or-
ing
in g
ood
cond
ition
and
no
n-sl
ip?
Are
al
l thr
esho
lds
flush
? Is
th
ere
ade
quat
e sp
ace,
fr
ee fr
om
c
lutt
er?
Is th
e lig
htin
g su
itabl
e fo
r th
e re
side
nt’s
ne
eds?
Is th
e ba
thro
om
suita
ble
for
the
resi
dent
/st
aff n
eeds
? C
an th
e re
side
nt fi
nd
it ea
sily
?
Are
the
hallw
ays
wel
l lit
and
wel
l sig
n-
post
ed fo
r re
side
nt?
Is
ther
e ea
sy
acce
ss?
Is th
ere
adeq
uate
sp
ace
for
wal
king
aid
/m
ovin
g an
d ha
ndlin
g eq
uipm
ent?
Is th
e be
d su
itabl
e fo
r re
side
nt’s
ne
eds?
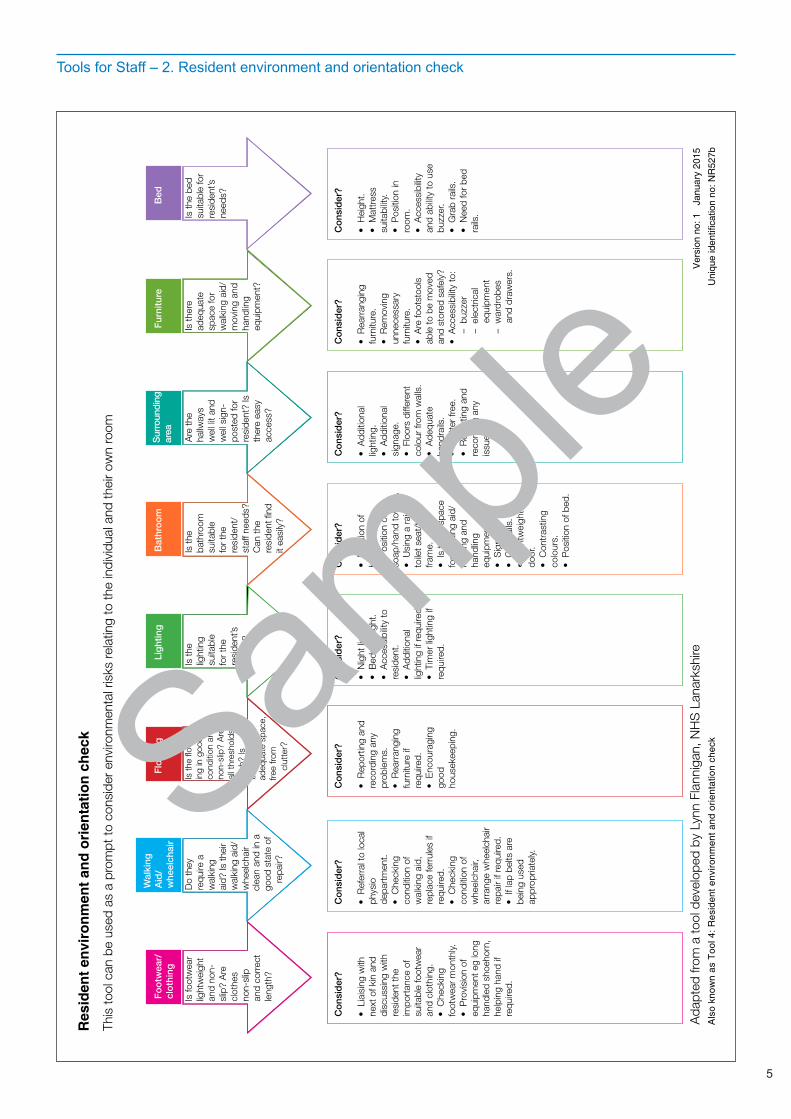
This
tool
can
be
used
as
a pr
ompt
to c
onsi
der
envi
ronm
enta
l ris
ks re
latin
g to
the
indi
vidu
al a
nd th
eir
own
room
Ada
pted
from
a to
ol d
evel
oped
by
Lynn
Fla
nnig
an, N
HS
Lan
arks
hire
Res
iden
t env
iron
men
t and
ori
enta
tion
chec
k
Als
o kn
own
as T
ool 4
: Res
iden
t env
ironm
ent a
nd o
rient
atio
n ch
eck
Ver
sion
no:
1
Janu
ary
2015
Uni
que
iden
tific
atio
n no
: NR
527b
Tools for Staff – 2. Resident environment and orientation check
Sample
6
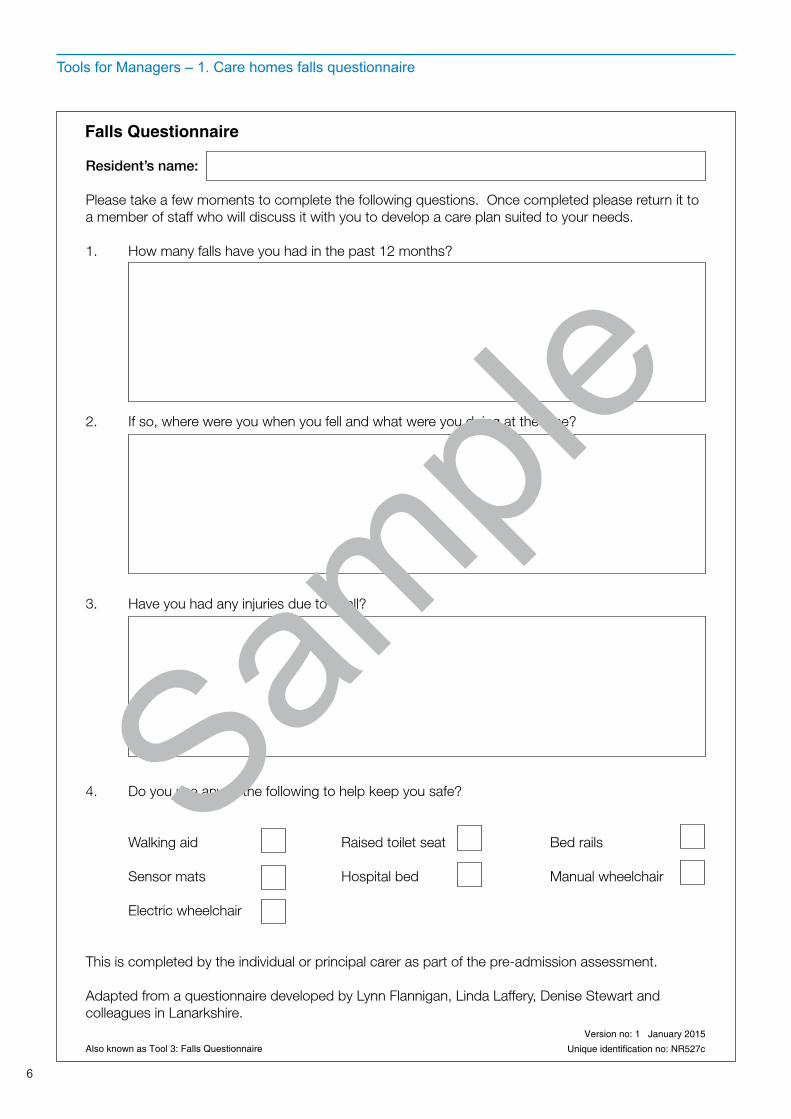
Tools for Managers – 1. Care homes falls questionnaire
Resident’s name:
Please take a few moments to complete the following questions. Once completed please return it to a member of staff who will discuss it with you to develop a care plan suited to your needs.
1. How many falls have you had in the past 12 months?
2. If so, where were you when you fell and what were you doing at the time?
3. Have you had any injuries due to a fall?
4. Do you use any of the following to help keep you safe?
Walking aid Raised toilet seat Bed rails
Sensor mats Hospital bed Manual wheelchair
Electric wheelchair
This is completed by the individual or principal carer as part of the pre-admission assessment.
Adapted from a questionnaire developed by Lynn Flannigan, Linda Laffery, Denise Stewart and colleagues in Lanarkshire.
Falls Questionnaire
Also known as Tool 3: Falls Questionnaire
Version no: 1 January 2015
Unique identification no: NR527c
Sample
7
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
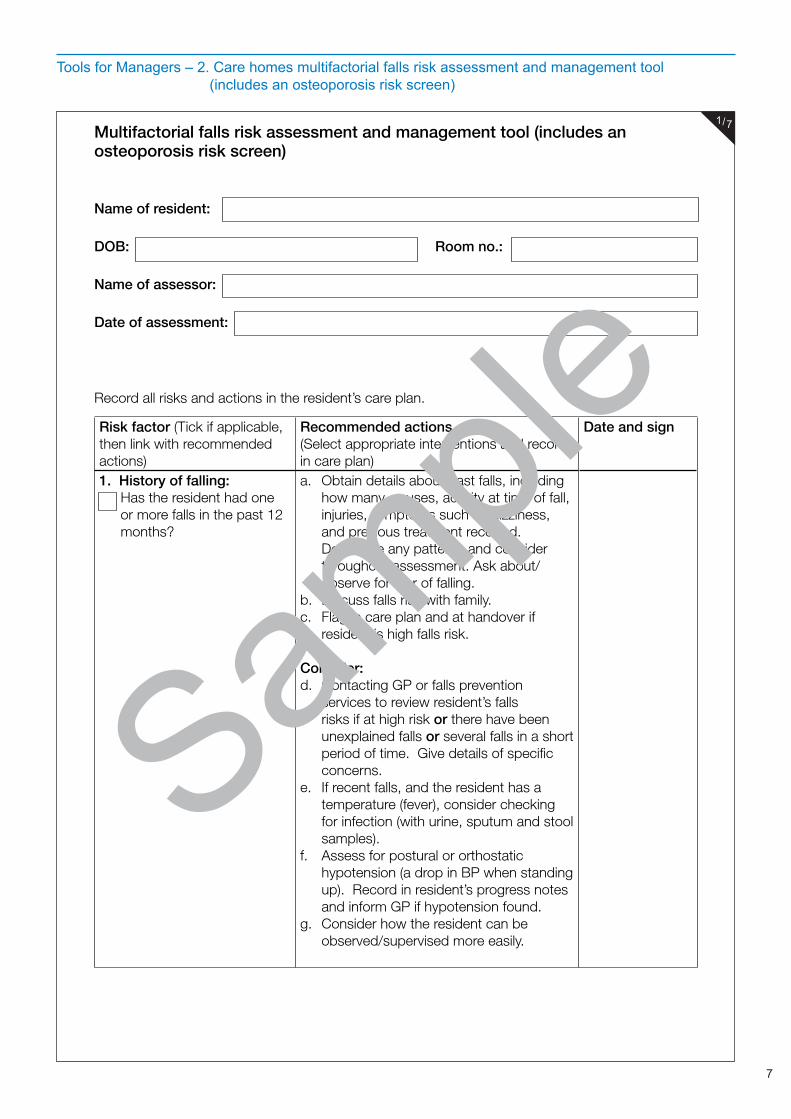
Multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
Name of resident:
DOB: Room no.:
Name of assessor:
Date of assessment:
Record all risks and actions in the resident’s care plan.
Risk factor (Tick if applicable, then link with recommended actions)
Recommended actions (Select appropriate interventions and record in care plan)
Date and sign
1. History of falling:Has the resident had one or more falls in the past 12 months?
a. Obtain details about past falls, including how many, causes, activity at time of fall, injuries, symptoms such as dizziness, and previous treatment received. Determine any patterns and consider throughout assessment. Ask about/observe for fear of falling.
b. Discuss falls risk with family.c. Flag in care plan and at handover if
resident is high falls risk.
Consider:d. Contacting GP or falls prevention
services to review resident’s falls risks if at high risk or there have been unexplained falls or several falls in a short period of time. Give details of specific concerns.
e. If recent falls, and the resident has a temperature (fever), consider checking for infection (with urine, sputum and stool samples).
f. Assess for postural or orthostatic hypotension (a drop in BP when standing up). Record in resident’s progress notes and inform GP if hypotension found.
g. Consider how the resident can be observed/supervised more easily.
1/7
Sample
8
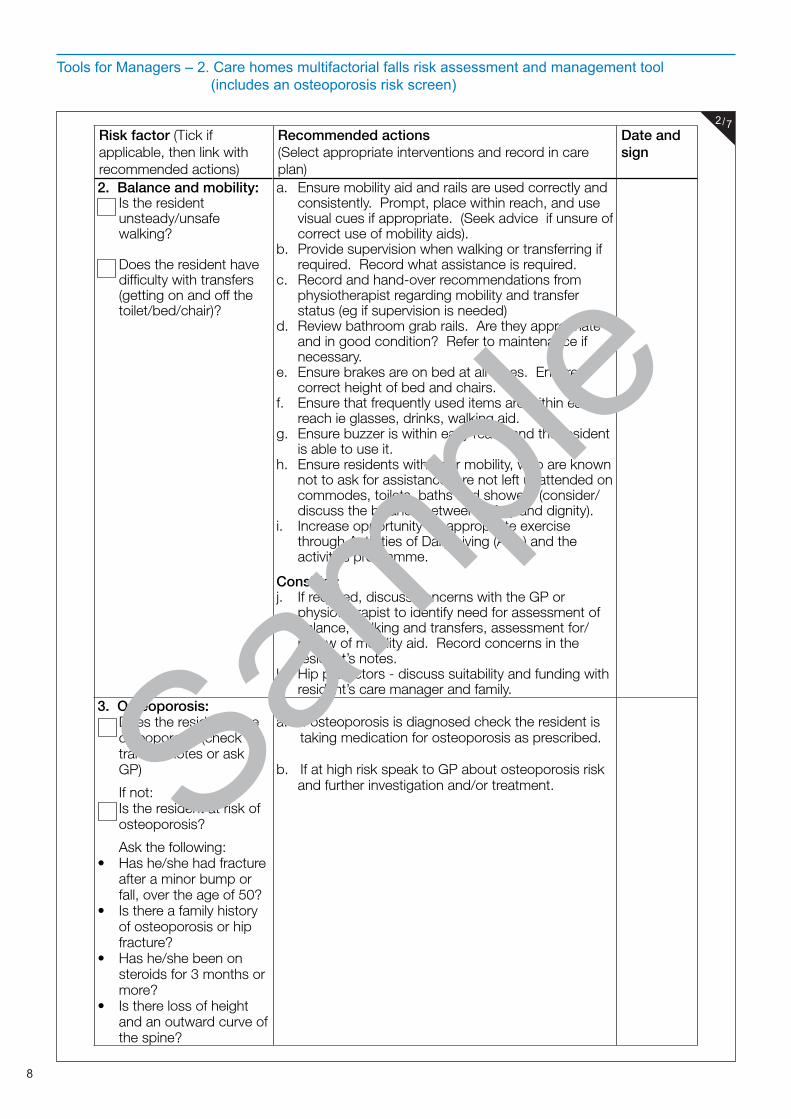
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
Risk factor (Tick if applicable, then link with recommended actions)
Recommended actions (Select appropriate interventions and record in care plan)
Date and sign
2. Balance and mobility:Is the resident unsteady/unsafe walking?
Does the resident have difficulty with transfers (getting on and off the toilet/bed/chair)?
a. Ensure mobility aid and rails are used correctly and consistently. Prompt, place within reach, and use visual cues if appropriate. (Seek advice if unsure of correct use of mobility aids).
b. Provide supervision when walking or transferring if required. Record what assistance is required.
c. Record and hand-over recommendations from physiotherapist regarding mobility and transfer status (eg if supervision is needed)
d. Review bathroom grab rails. Are they appropriate and in good condition? Refer to maintenance if necessary.
e. Ensure brakes are on bed at all times. Ensure correct height of bed and chairs.
f. Ensure that frequently used items are within easy reach ie glasses, drinks, walking aid.
g. Ensure buzzer is within easy reach and the resident is able to use it.
h. Ensure residents with poor mobility, who are known not to ask for assistance, are not left unattended on commodes, toilets, baths and showers (consider/discuss the balance between safety and dignity).
i. Increase opportunity for appropriate exercise through Activities of Daily Living (ADL) and the activities programme.
Consider:j. If required, discuss concerns with the GP or
physiotherapist to identify need for assessment of balance, walking and transfers, assessment for/review of mobility aid. Record concerns in the resident’s notes.
k. Hip protectors - discuss suitability and funding with resident’s care manager and family.
3. Osteoporosis:Does the resident have osteoporosis (check transfer notes or ask GP)
If not:Is the resident at risk of osteoporosis?
Ask the following: • Has he/she had fracture
after a minor bump or fall, over the age of 50?
• Is there a family history of osteoporosis or hip fracture?
• Has he/she been on steroids for 3 months or more?
• Is there loss of height and an outward curve of the spine?
a. If osteoporosis is diagnosed check the resident is taking medication for osteoporosis as prescribed.
b. If at high risk speak to GP about osteoporosis risk and further investigation and/or treatment.
2/7
Sample
9
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
Risk factor (Tick if applicable, then link with recommended actions)
Recommended actions (Select appropriate interventions and record in care plan)
Date and sign
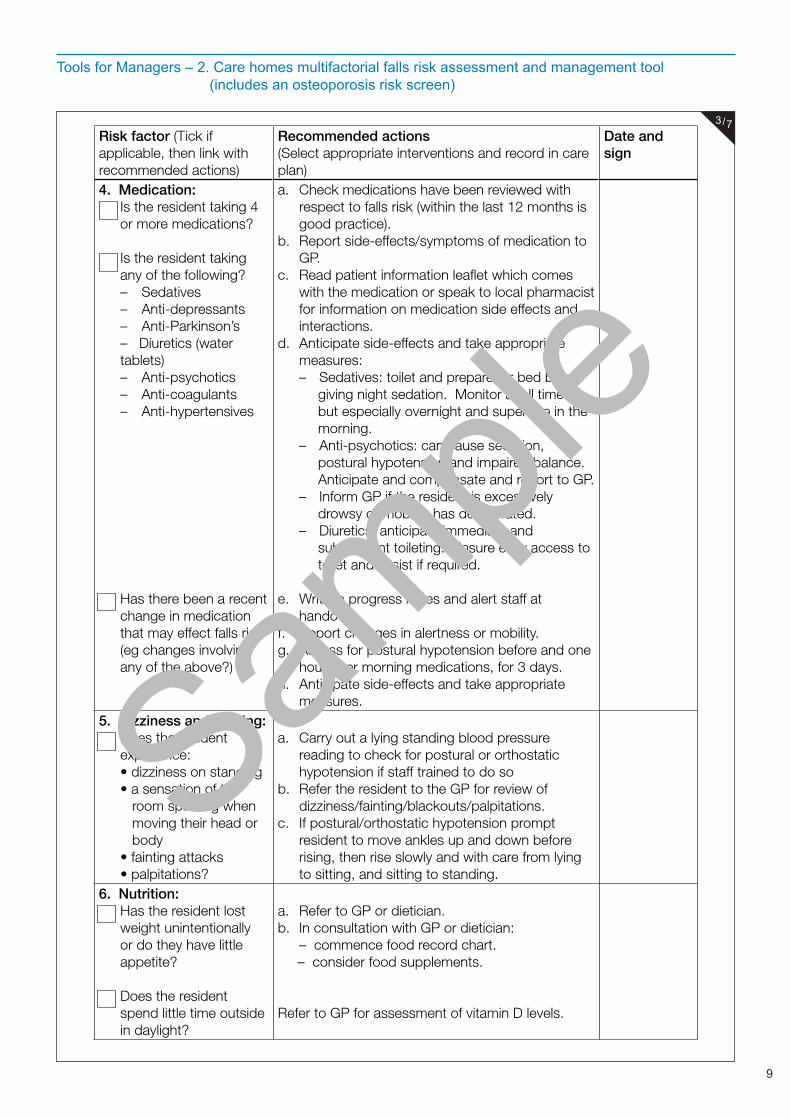
4. Medication:Is the resident taking 4 or more medications?
Is the resident taking any of the following?– Sedatives– Anti-depressants– Anti-Parkinson’s – Diuretics (water tablets)– Anti-psychotics– Anti-coagulants– Anti-hypertensives
Has there been a recent change in medication that may effect falls risk (eg changes involving any of the above?)
a. Check medications have been reviewed with respect to falls risk (within the last 12 months is good practice).
b. Report side-effects/symptoms of medication to GP.
c. Read patient information leaflet which comes with the medication or speak to local pharmacist for information on medication side effects and interactions.
d. Anticipate side-effects and take appropriate measures:– Sedatives: toilet and prepare for bed before
giving night sedation. Monitor at all times, but especially overnight and supervise in the morning.
– Anti-psychotics: can cause sedation, postural hypotension and impaired balance. Anticipate and compensate and report to GP.
– Inform GP if the resident is excessively drowsy or mobility has deteriorated.
– Diuretics: anticipate immediate and subsequent toileting. Ensure easy access to toilet and assist if required.
e. Write in progress notes and alert staff at handover.
f. Report changes in alertness or mobility.g. Assess for postural hypotension before and one
hour after morning medications, for 3 days.h. Anticipate side-effects and take appropriate
measures.5. Dizziness and fainting:
Does the resident experience:• dizziness on standing• a sensation of the room spinning when moving their head or body • fainting attacks• palpitations?
a. Carry out a lying standing blood pressure reading to check for postural or orthostatic hypotension if staff trained to do so
b. Refer the resident to the GP for review of dizziness/fainting/blackouts/palpitations.
c. If postural/orthostatic hypotension prompt resident to move ankles up and down before rising, then rise slowly and with care from lying to sitting, and sitting to standing.
6. Nutrition:Has the resident lost weight unintentionally or do they have little appetite?
Does the resident spend little time outside in daylight?
a. Refer to GP or dietician.b. In consultation with GP or dietician: – commence food record chart. – consider food supplements.
Refer to GP for assessment of vitamin D levels.
3/7
Sample
10
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
Risk factor (Tick if applicable, then link with recommended actions)
Recommended actions (Select appropriate interventions and record in care plan)
Date and sign
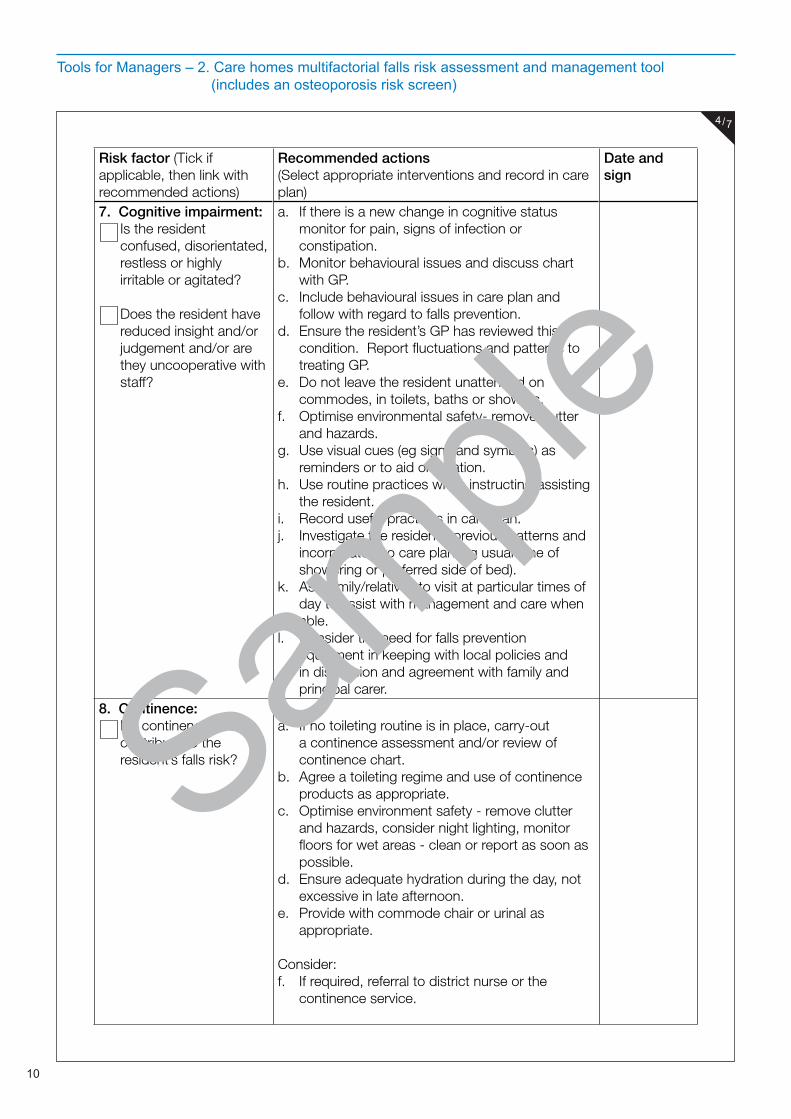
7. Cognitive impairment:Is the resident confused, disorientated, restless or highly irritable or agitated?
Does the resident have reduced insight and/or judgement and/or are they uncooperative with staff?
a. If there is a new change in cognitive status monitor for pain, signs of infection or constipation.
b. Monitor behavioural issues and discuss chart with GP.
c. Include behavioural issues in care plan and follow with regard to falls prevention.
d. Ensure the resident’s GP has reviewed this condition. Report fluctuations and patterns to treating GP.
e. Do not leave the resident unattended on commodes, in toilets, baths or showers.
f. Optimise environmental safety- remove clutter and hazards.
g. Use visual cues (eg signs and symbols) as reminders or to aid orientation.
h. Use routine practices when instructing/assisting the resident.
i. Record useful practices in care plan.j. Investigate the resident’s previous patterns and
incorporate into care plan (eg usual time of showering or preferred side of bed).
k. Ask family/relatives to visit at particular times of day to assist with management and care when able.
l. Consider the need for falls prevention equipment in keeping with local policies and in discussion and agreement with family and principal carer.
8. Continence:Do continence issues contribute to the resident’s falls risk?
a. If no toileting routine is in place, carry-out a continence assessment and/or review of continence chart.
b. Agree a toileting regime and use of continence products as appropriate.
c. Optimise environment safety - remove clutter and hazards, consider night lighting, monitor floors for wet areas - clean or report as soon as possible.
d. Ensure adequate hydration during the day, not excessive in late afternoon.
e. Provide with commode chair or urinal as appropriate.
Consider:f. If required, referral to district nurse or the
continence service.
4/7
Sample
11
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
Risk factor (Tick if applicable, then link with recommended actions)
Recommended actions (Select appropriate interventions and record in care plan)
Date and sign
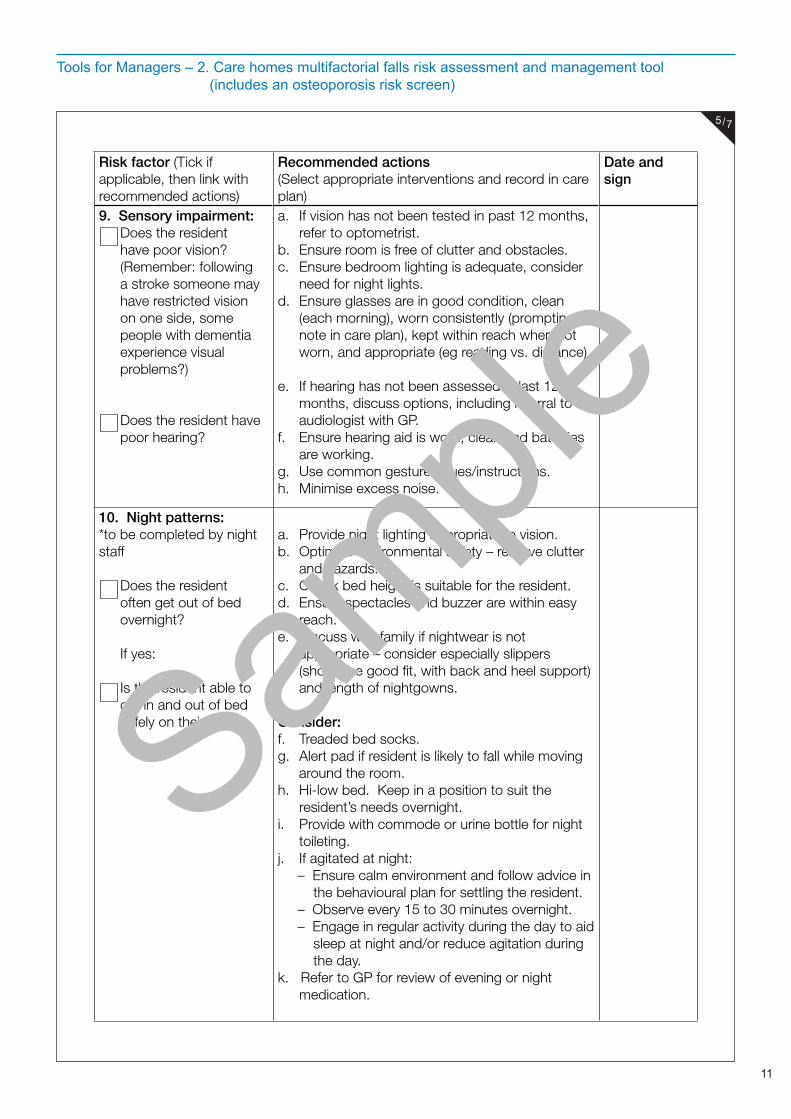
9. Sensory impairment:Does the resident have poor vision? (Remember: following a stroke someone may have restricted vision on one side, some people with dementia experience visual problems?)
Does the resident have poor hearing?
a. If vision has not been tested in past 12 months, refer to optometrist.
b. Ensure room is free of clutter and obstacles.c. Ensure bedroom lighting is adequate, consider
need for night lights.d. Ensure glasses are in good condition, clean
(each morning), worn consistently (prompting, note in care plan), kept within reach when not worn, and appropriate (eg reading vs. distance)
e. If hearing has not been assessed in last 12 months, discuss options, including referral to audiologist with GP.
f. Ensure hearing aid is worn, clean and batteries are working.
g. Use common gestures/cues/instructions.h. Minimise excess noise.
10. Night patterns:*to be completed by night staff
Does the resident often get out of bed overnight?
If yes:
Is the resident able to get in and out of bed safely on their own?
a. Provide night lighting appropriate to vision.b. Optimise environmental safety – remove clutter
and hazards.c. Check bed height is suitable for the resident.d. Ensure spectacles and buzzer are within easy
reach.e. Discuss with family if nightwear is not
appropriate – consider especially slippers (should be good fit, with back and heel support) and length of nightgowns.
Consider:f. Treaded bed socks.g. Alert pad if resident is likely to fall while moving
around the room.h. Hi-low bed. Keep in a position to suit the
resident’s needs overnight.i. Provide with commode or urine bottle for night
toileting.j. If agitated at night: – Ensure calm environment and follow advice in the behavioural plan for settling the resident. – Observe every 15 to 30 minutes overnight. – Engage in regular activity during the day to aid sleep at night and/or reduce agitation during the day. k. Refer to GP for review of evening or night
medication.
5/7
Sample
12
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
Risk factor (Tick if applicable, then link with recommended actions)
Recommended actions (Select appropriate interventions and record in care plan)
Date and sign
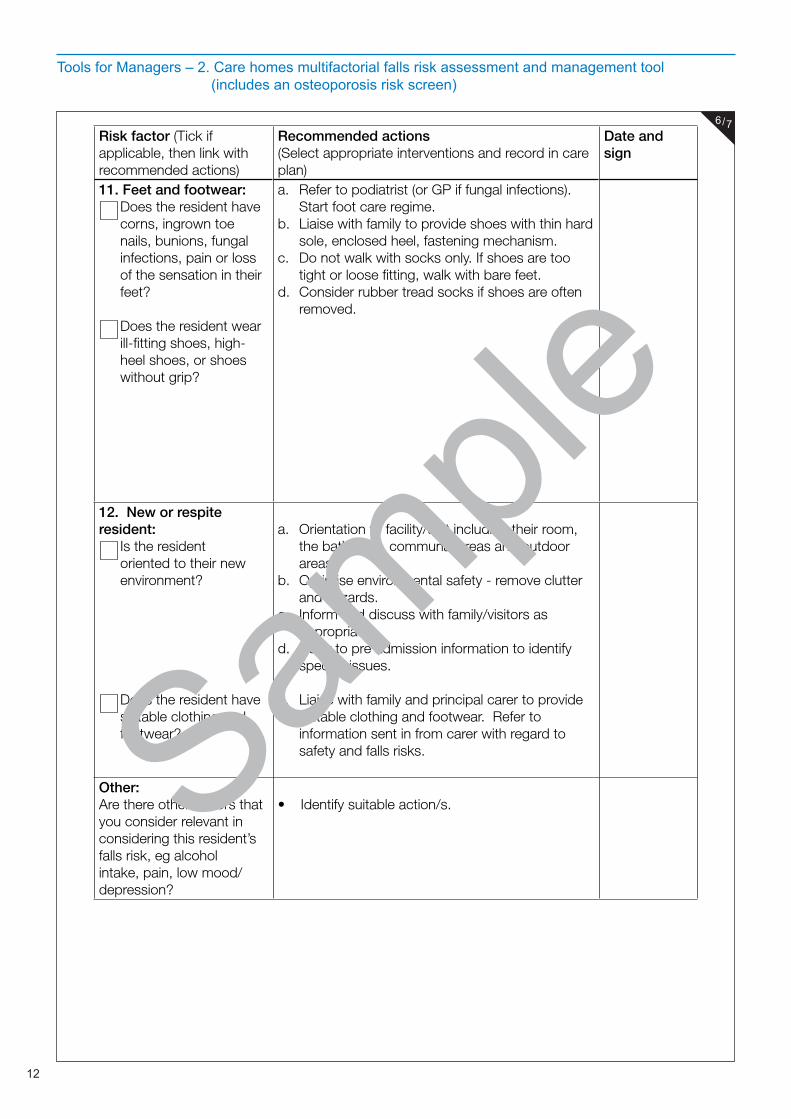
11. Feet and footwear:Does the resident have corns, ingrown toe nails, bunions, fungal infections, pain or loss of the sensation in their feet?
Does the resident wear ill-fitting shoes, high-heel shoes, or shoes without grip?
a. Refer to podiatrist (or GP if fungal infections). Start foot care regime.
b. Liaise with family to provide shoes with thin hard sole, enclosed heel, fastening mechanism.
c. Do not walk with socks only. If shoes are too tight or loose fitting, walk with bare feet.
d. Consider rubber tread socks if shoes are often removed.
12. New or respite resident:
Is the resident oriented to their new environment?
Does the resident have suitable clothing and footwear?
a. Orientation to facility/unit including their room, the bathroom, communal areas and outdoor areas.
b. Optimise environmental safety - remove clutter and hazards.
c. Inform and discuss with family/visitors as appropriate.
d. Refer to pre admission information to identify specific issues.
e. Liaise with family and principal carer to provide suitable clothing and footwear. Refer to information sent in from carer with regard to safety and falls risks.
Other:Are there other factors that you consider relevant in considering this resident’s falls risk, eg alcohol intake, pain, low mood/depression?
• Identify suitable action/s.
6/7
Sample
13
Tools for Managers – 2. Care homes multifactorial falls risk assessment and management tool (includes an osteoporosis risk screen)
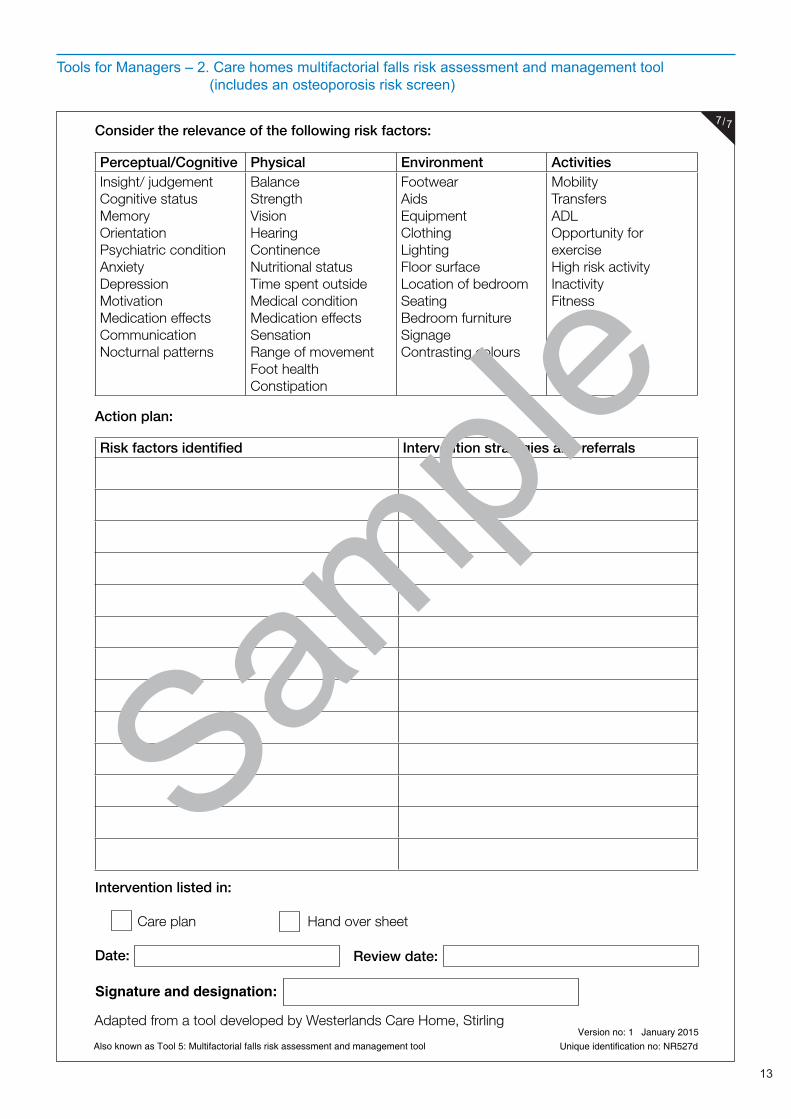
Consider the relevance of the following risk factors:
Perceptual/Cognitive Physical Environment ActivitiesInsight/ judgementCognitive statusMemoryOrientationPsychiatric conditionAnxietyDepressionMotivationMedication effectsCommunicationNocturnal patterns
BalanceStrengthVisionHearingContinenceNutritional statusTime spent outsideMedical conditionMedication effectsSensationRange of movementFoot healthConstipation
FootwearAidsEquipmentClothingLightingFloor surfaceLocation of bedroomSeatingBedroom furnitureSignageContrasting colours
MobilityTransfersADLOpportunity for exercise High risk activityInactivityFitness
Action plan:
Risk factors identified Intervention strategies and referrals
Intervention listed in:
Care plan Hand over sheet
Date:
Signature and designation:
Review date:
Adapted from a tool developed by Westerlands Care Home, Stirling
Also known as Tool 5: Multifactorial falls risk assessment and management toolVersion no: 1 January 2015
Unique identification no: NR527d
7/7
Sample
14
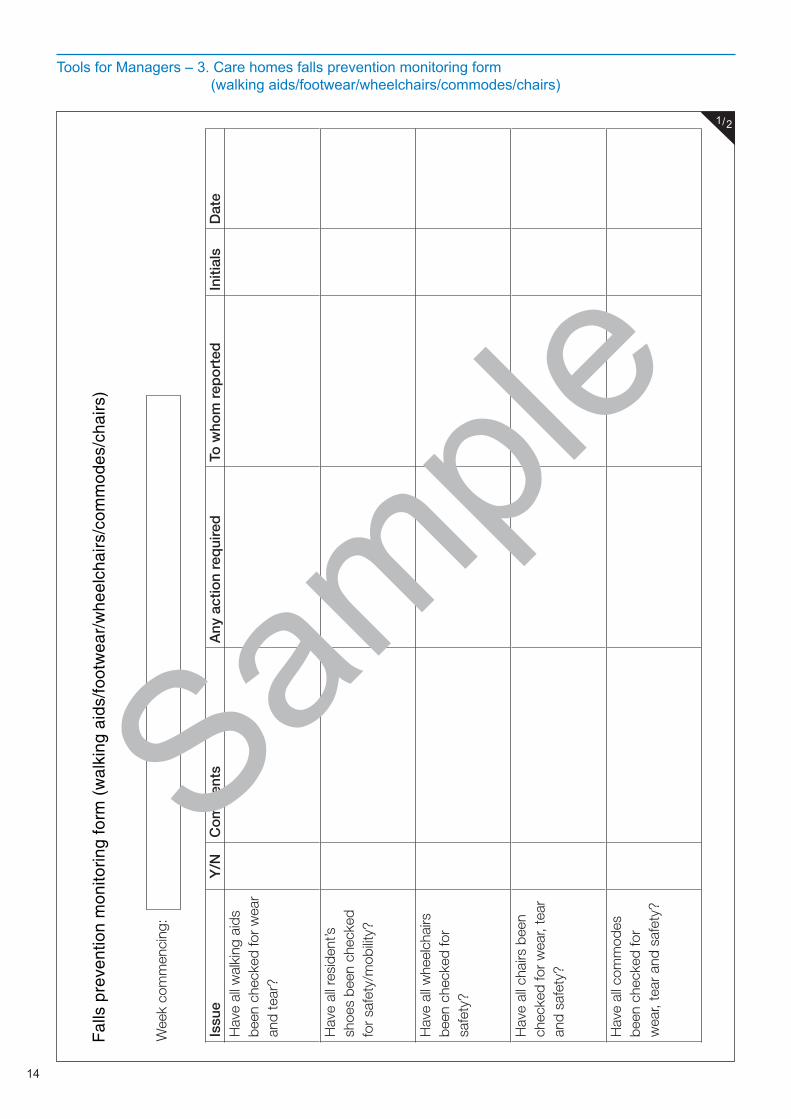
Tools for Managers – 3. Care homes falls prevention monitoring form (walking aids/footwear/wheelchairs/commodes/chairs)
Wee
k co
mm
enci
ng:
Issu
eY
/NC
om
men
tsA
ny a
ctio
n re
qui
red
To w
hom
rep
ort
edIn
itial
sD
ate
Hav
e al
l wal
king
aid
s be
en c
heck
ed fo
r w
ear
and
tear
?
Hav
e al
l res
iden
t’s
shoe
s be
en c
heck
ed
for
safe
ty/m
obilit
y?
Hav
e al
l whe
elch
airs
be
en c
heck
ed fo
r sa
fety
?
Hav
e al
l cha
irs b
een
chec
ked
for
wea
r, te
ar
and
safe
ty?
Hav
e al
l com
mod
es
been
che
cked
for
wea
r, te
ar a
nd s
afet
y?
Fal
ls p
reve
ntio
n m
onito
ring
form
(w
alki
ng a
ids/
foot
wea
r/w
heel
chai
rs/c
omm
odes
/cha
irs)
1/2
Sample

15
Tools for Managers – 3. Care homes falls prevention monitoring form (walking aids/footwear/wheelchairs/commodes/chairs)
Act
ion
take
nD
ate
Nam
e/in
itial
s
Ada
pted
from
tool
dev
elop
ed b
y Ly
nn F
lann
igan
, NH
S L
anar
kshi
reA
lso
know
n as
Too
l 16:
Fal
ls p
reve
ntio
n m
onito
ring
form
(w
alki
ng a
ids/
foot
wea
r/w
heel
chai
rs/c
omm
odes
/cha
irs)
Ver
sion
no:
1
Janu
ary
2015
Uni
que
iden
tific
atio
n no
: NR
527e
2/2
Sample
16
Tools for Managers – 4. Care homes generic falls environmental risk assessment
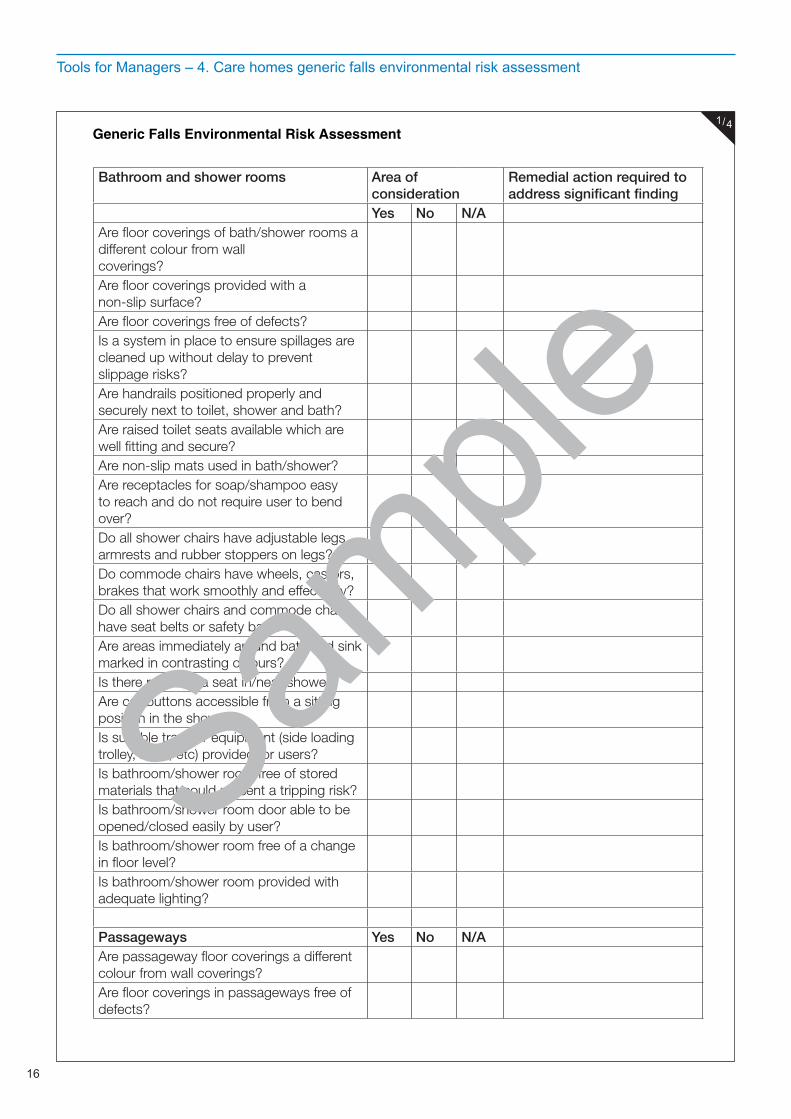
Bathroom and shower rooms Area of consideration
Remedial action required to address significant finding
Yes No N/AAre floor coverings of bath/shower rooms a different colour from wall coverings?Are floor coverings provided with a non-slip surface?Are floor coverings free of defects?Is a system in place to ensure spillages are cleaned up without delay to prevent slippage risks?Are handrails positioned properly and securely next to toilet, shower and bath?Are raised toilet seats available which are well fitting and secure?Are non-slip mats used in bath/shower?Are receptacles for soap/shampoo easy to reach and do not require user to bend over?Do all shower chairs have adjustable legs, armrests and rubber stoppers on legs? Do commode chairs have wheels, castors, brakes that work smoothly and effectively?Do all shower chairs and commode chairs have seat belts or safety bars?Are areas immediately around bath and sink marked in contrasting colours?Is there room for a seat in/near shower?Are call buttons accessible from a sitting position in the shower?Is suitable transfer equipment (side loading trolley, hoist, etc) provided for users?Is bathroom/shower room free of stored materials that could present a tripping risk?Is bathroom/shower room door able to be opened/closed easily by user?Is bathroom/shower room free of a change in floor level?Is bathroom/shower room provided with adequate lighting?
Passageways Yes No N/AAre passageway floor coverings a different colour from wall coverings?Are floor coverings in passageways free of defects?
Generic Falls Environmental Risk Assessment1/4
Sample
17
Tools for Managers – 4. Care homes generic falls environmental risk assessment
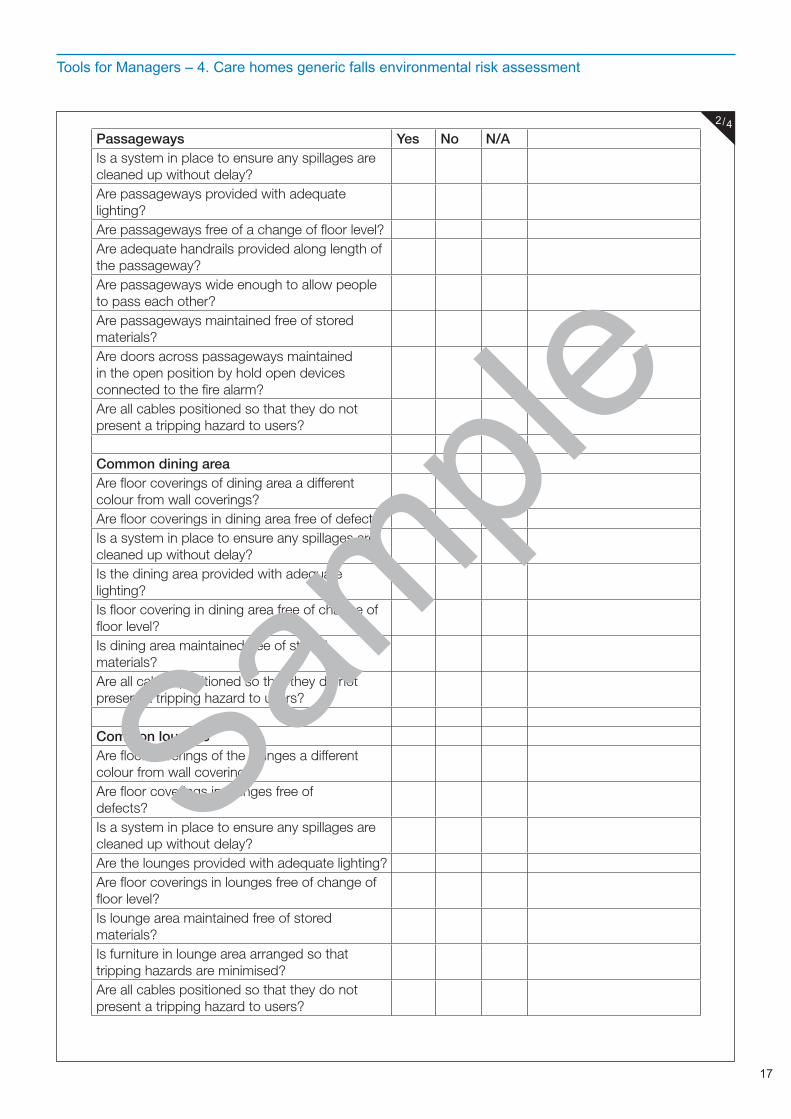
Passageways Yes No N/AIs a system in place to ensure any spillages are cleaned up without delay?Are passageways provided with adequate lighting?Are passageways free of a change of floor level?Are adequate handrails provided along length of the passageway?Are passageways wide enough to allow people to pass each other?Are passageways maintained free of stored materials?Are doors across passageways maintained in the open position by hold open devices connected to the fire alarm?Are all cables positioned so that they do not present a tripping hazard to users?
Common dining areaAre floor coverings of dining area a different colour from wall coverings?Are floor coverings in dining area free of defects?Is a system in place to ensure any spillages are cleaned up without delay?Is the dining area provided with adequate lighting?Is floor covering in dining area free of change of floor level?Is dining area maintained free of stored materials?Are all cables positioned so that they do not present a tripping hazard to users?
Common loungesAre floor coverings of the lounges a different colour from wall coverings?Are floor coverings in lounges free of defects?Is a system in place to ensure any spillages are cleaned up without delay?Are the lounges provided with adequate lighting?Are floor coverings in lounges free of change of floor level?Is lounge area maintained free of stored materials?Is furniture in lounge area arranged so that tripping hazards are minimised?Are all cables positioned so that they do not present a tripping hazard to users?
2/4
Sample
18
Tools for Managers – 4. Care homes generic falls environmental risk assessment
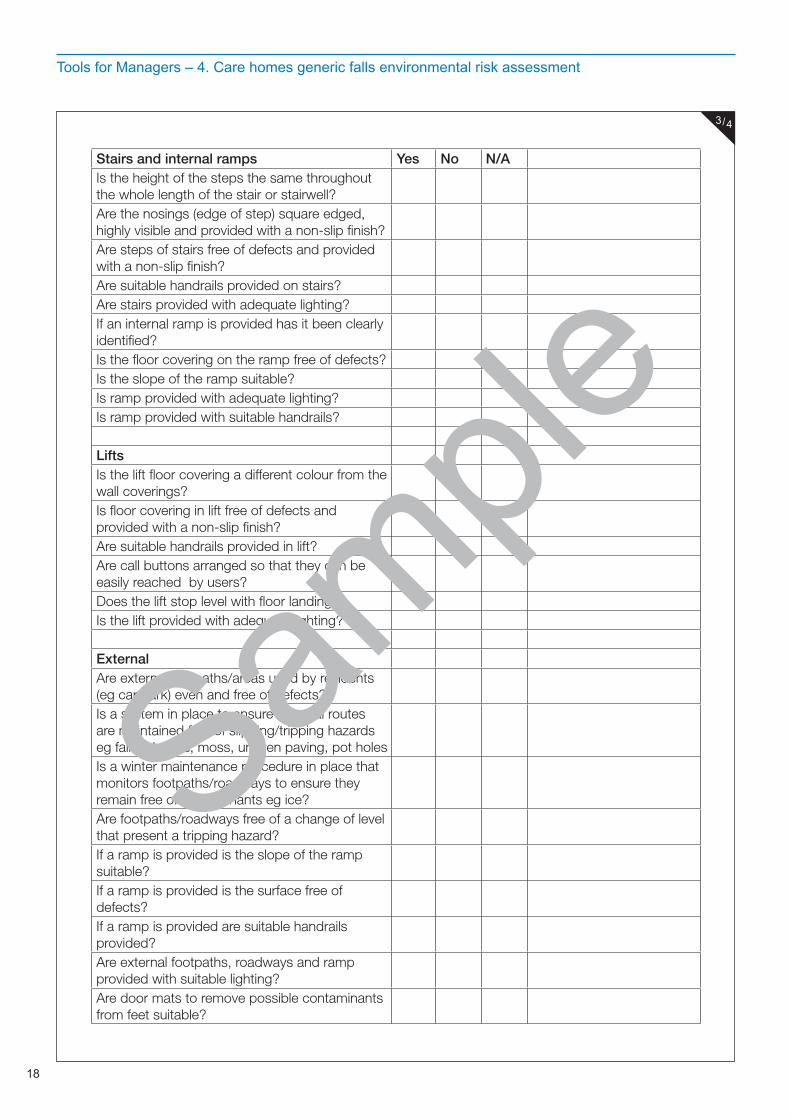
Stairs and internal ramps Yes No N/AIs the height of the steps the same throughout the whole length of the stair or stairwell?Are the nosings (edge of step) square edged, highly visible and provided with a non-slip finish?Are steps of stairs free of defects and provided with a non-slip finish?Are suitable handrails provided on stairs?Are stairs provided with adequate lighting?If an internal ramp is provided has it been clearly identified?Is the floor covering on the ramp free of defects?Is the slope of the ramp suitable?Is ramp provided with adequate lighting?Is ramp provided with suitable handrails?
LiftsIs the lift floor covering a different colour from the wall coverings?Is floor covering in lift free of defects and provided with a non-slip finish?Are suitable handrails provided in lift?Are call buttons arranged so that they can be easily reached by users?Does the lift stop level with floor landing?Is the lift provided with adequate lighting?
ExternalAre external footpaths/areas used by residents (eg car park) even and free of defects?Is a system in place to ensure external routes are maintained free of slipping/tripping hazards eg falling leaves, moss, uneven paving, pot holesIs a winter maintenance procedure in place that monitors footpaths/roadways to ensure they remain free of contaminants eg ice?Are footpaths/roadways free of a change of level that present a tripping hazard?If a ramp is provided is the slope of the ramp suitable?If a ramp is provided is the surface free of defects?If a ramp is provided are suitable handrails provided?Are external footpaths, roadways and ramp provided with suitable lighting?Are door mats to remove possible contaminants from feet suitable?
3/4
Sample
19
Tools for Managers – 4. Care homes generic falls environmental risk assessment
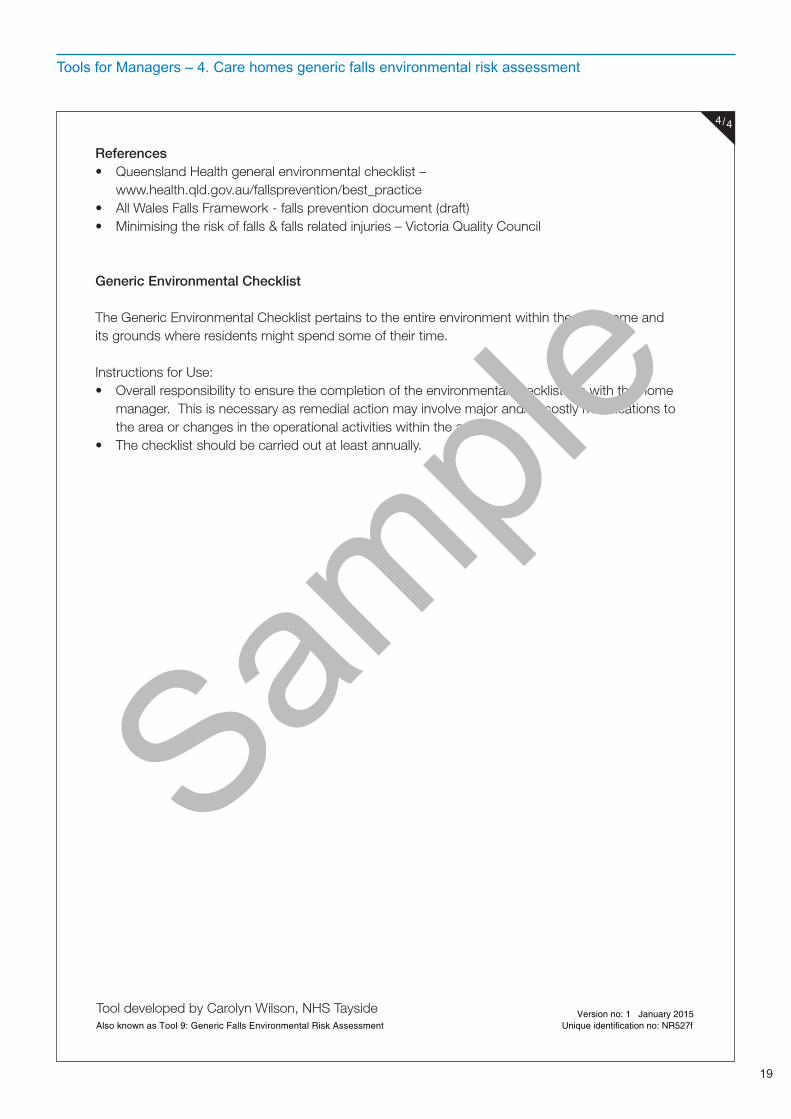
References• Queensland Health general environmental checklist – www.health.qld.gov.au/fallsprevention/best_practice• All Wales Falls Framework - falls prevention document (draft)• Minimising the risk of falls & falls related injuries – Victoria Quality Council
Generic Environmental Checklist
The Generic Environmental Checklist pertains to the entire environment within the care home and its grounds where residents might spend some of their time.
Instructions for Use:• Overall responsibility to ensure the completion of the environmental checklist lies with the home
manager. This is necessary as remedial action may involve major and/or costly modifications to the area or changes in the operational activities within the area.
• The checklist should be carried out at least annually.
Tool developed by Carolyn Wilson, NHS TaysideAlso known as Tool 9: Generic Falls Environmental Risk Assessment
Version no: 1 January 2015Unique identification no: NR527f
4/4
Sample
20
Tools for Managers – 5. Care homes monthly falls overview form
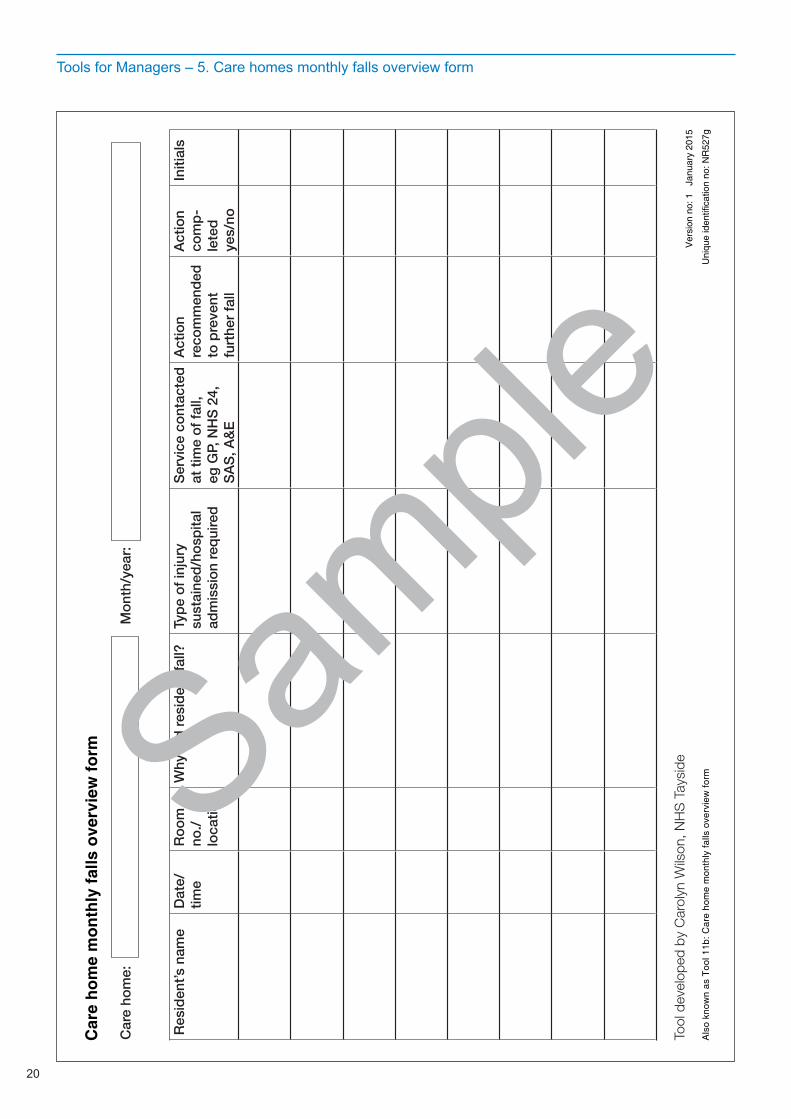
Car
e ho
me:
M
ont
h/ye
ar:
Res
iden
t’s n
ame
Dat
e/tim
eR
oo
m
no./
loca
tion
Why
did
res
iden
t fa
ll?Ty
pe
of
inju
ry
sust
aine
d/h
osp
ital
adm
issi
on
req
uire
d
Ser
vice
co
ntac
ted
at
tim
e o
f fa
ll,
eg G
P, N
HS
24,
S
AS
, A&
E
Act
ion
reco
mm
end
ed
to p
reve
nt
furt
her
fall
Act
ion
com
p-
lete
d
yes/
no
Initi
als
Tool
dev
elop
ed b
y C
arol
yn W
ilson
, NH
S T
aysi
de
Car
e ho
me
mon
thly
falls
ove
rvie
w fo
rm
Als
o kn
own
as T
ool 1
1b: C
are
hom
e m
onth
ly fa
lls o
verv
iew
form
Ver
sion
no:
1
Janu
ary
2015
Uni
que
iden
tific
atio
n no
: NR
527g
Sample
21
Tools for Managers – 6. Care homes post fall/incident report form
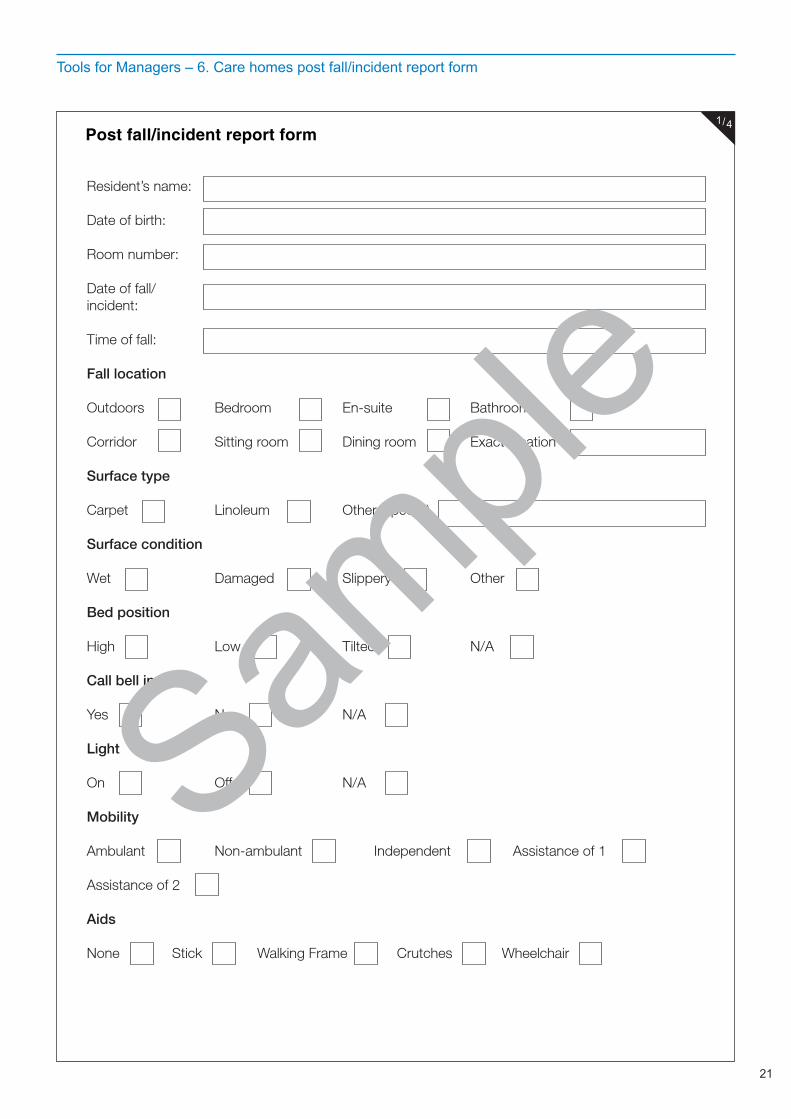
Resident’s name: Date of birth: Room number:
Date of fall/incident: Time of fall:
Fall location
Outdoors Bedroom En-suite Bathroom Corridor Sitting room Dining room Exact location
Surface type
Carpet Linoleum Other (specify)
Surface condition
Wet Damaged Slippery Other
Bed position
High Low Tilted N/A
Call bell in reach
Yes No N/A
Light
On Off N/A
Mobility
Ambulant Non-ambulant Independent Assistance of 1
Assistance of 2
Aids
None Stick Walking Frame Crutches Wheelchair
Post fall/incident report form1/4
Sample
22
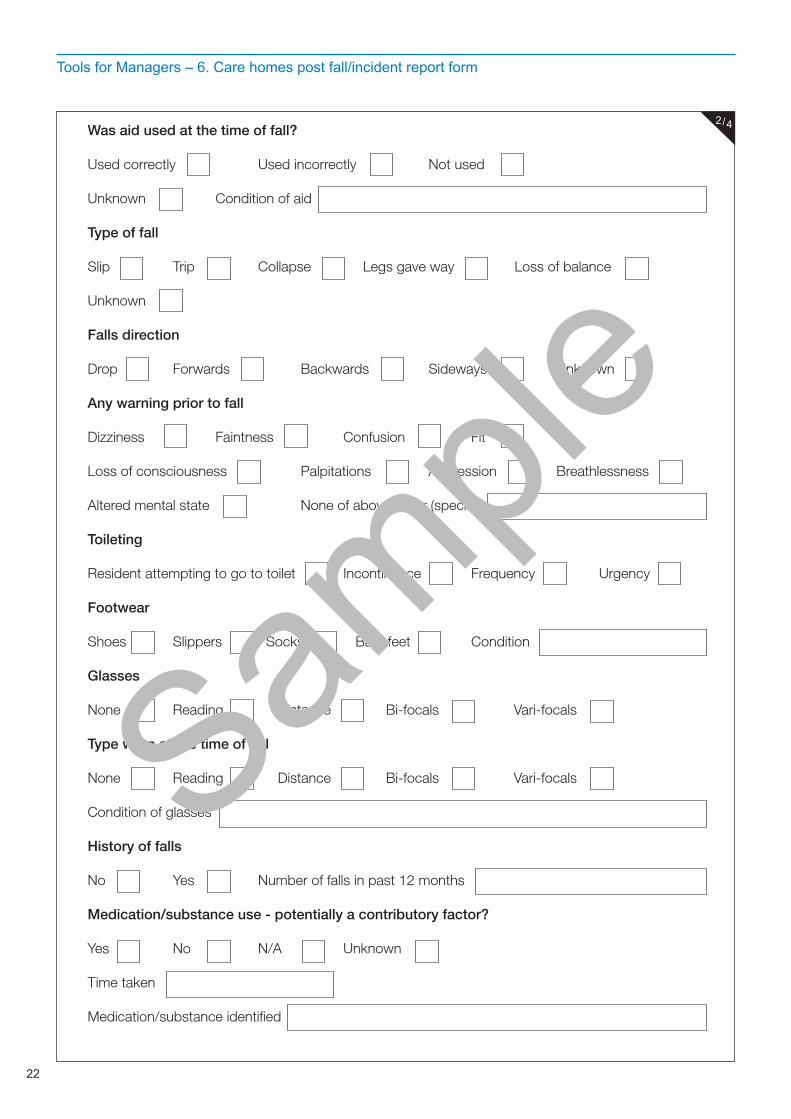
Tools for Managers – 6. Care homes post fall/incident report form
Was aid used at the time of fall?
Used correctly Used incorrectly Not used
Unknown Condition of aid
Type of fall
Slip Trip Collapse Legs gave way Loss of balance Unknown
Falls direction
Drop Forwards Backwards Sideways Unknown
Any warning prior to fall
Dizziness Faintness Confusion Fit
Loss of consciousness Palpitations Aggression Breathlessness Altered mental state None of above/other (specify)
Toileting
Resident attempting to go to toilet Incontinence Frequency Urgency
Footwear
Shoes Slippers Socks Bare feet Condition
Glasses
None Reading Distance Bi-focals Vari-focals
Type worn at the time of fall
None Reading Distance Bi-focals Vari-focals
Condition of glasses
History of falls
No Yes Number of falls in past 12 months
Medication/substance use - potentially a contributory factor?
Yes No N/A Unknown
Time taken
Medication/substance identified
2/4
Sample
23
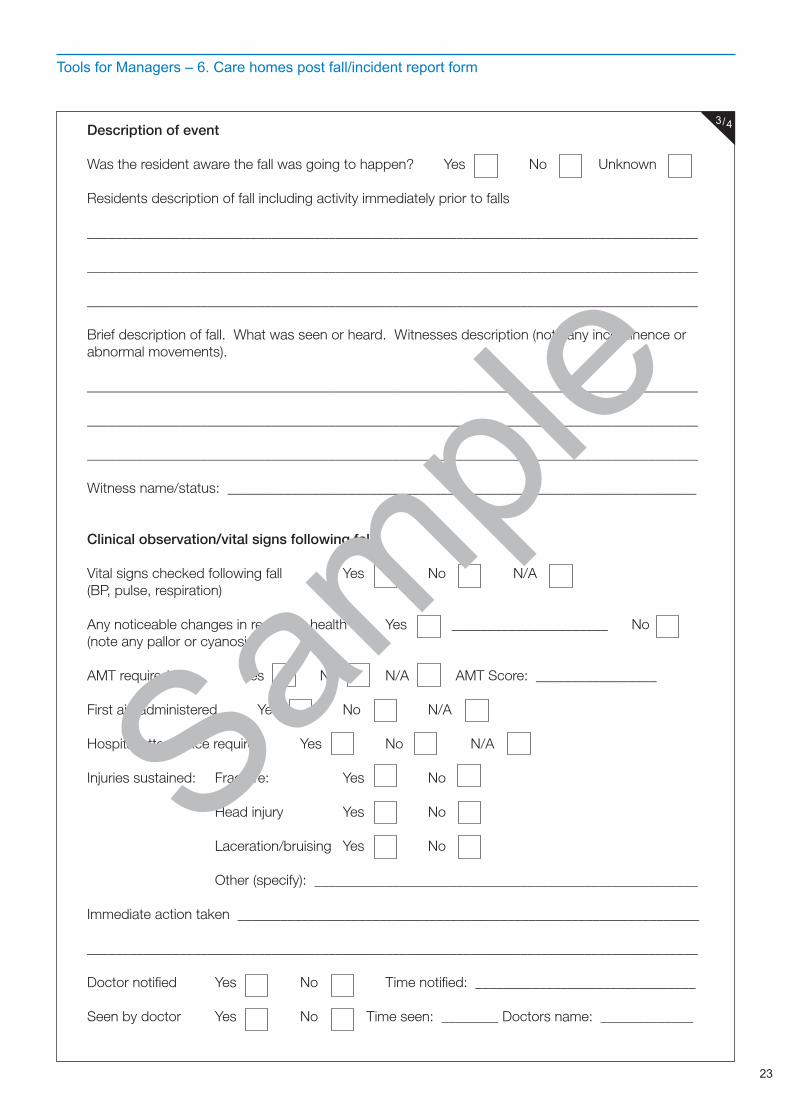
Tools for Managers – 6. Care homes post fall/incident report form
Description of event
Was the resident aware the fall was going to happen? Yes No Unknown
Residents description of fall including activity immediately prior to falls
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
Brief description of fall. What was seen or heard. Witnesses description (note any incontinence or abnormal movements).
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
Witness name/status: __________________________________________________________________
Clinical observation/vital signs following fall
Vital signs checked following fall Yes No N/A(BP, pulse, respiration)
Any noticeable changes in residents health Yes ______________________ No(note any pallor or cyanosis)
AMT required Yes No N/A AMT Score: _________________
First aid administered Yes No N/A
Hospital attendance required Yes No N/A
Injuries sustained: Fracture: Yes No Head injury Yes No
Laceration/bruising Yes No
Other (specify): ______________________________________________________
Immediate action taken _________________________________________________________________
______________________________________________________________________________________
Doctor notified Yes No Time notified: _______________________________
Seen by doctor Yes No Time seen: ________ Doctors name: _____________
3/4
Sample
24
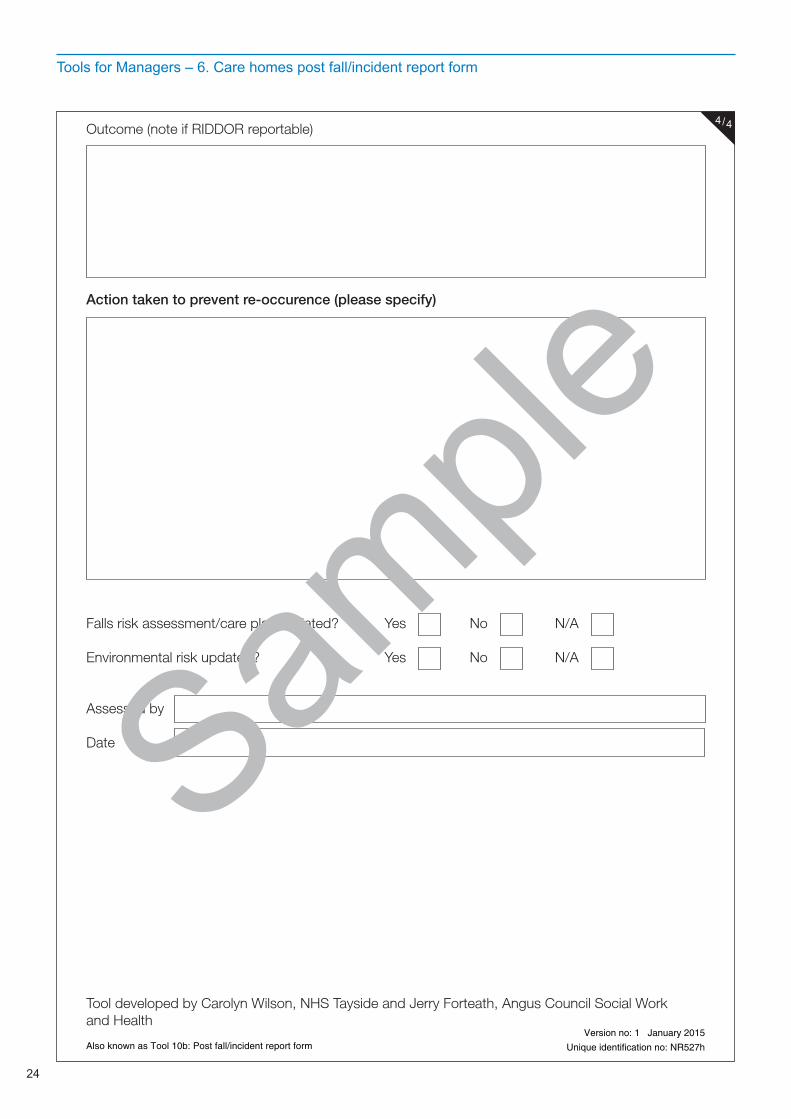
Tools for Managers – 6. Care homes post fall/incident report form
Outcome (note if RIDDOR reportable)
Action taken to prevent re-occurence (please specify)
Falls risk assessment/care plan updated? Yes No N/A
Environmental risk updated? Yes No N/A
Assessed by
Date
Tool developed by Carolyn Wilson, NHS Tayside and Jerry Forteath, Angus Council Social Work and Health
Also known as Tool 10b: Post fall/incident report formVersion no: 1 January 2015
Unique identification no: NR527h
4/4
Sample
25
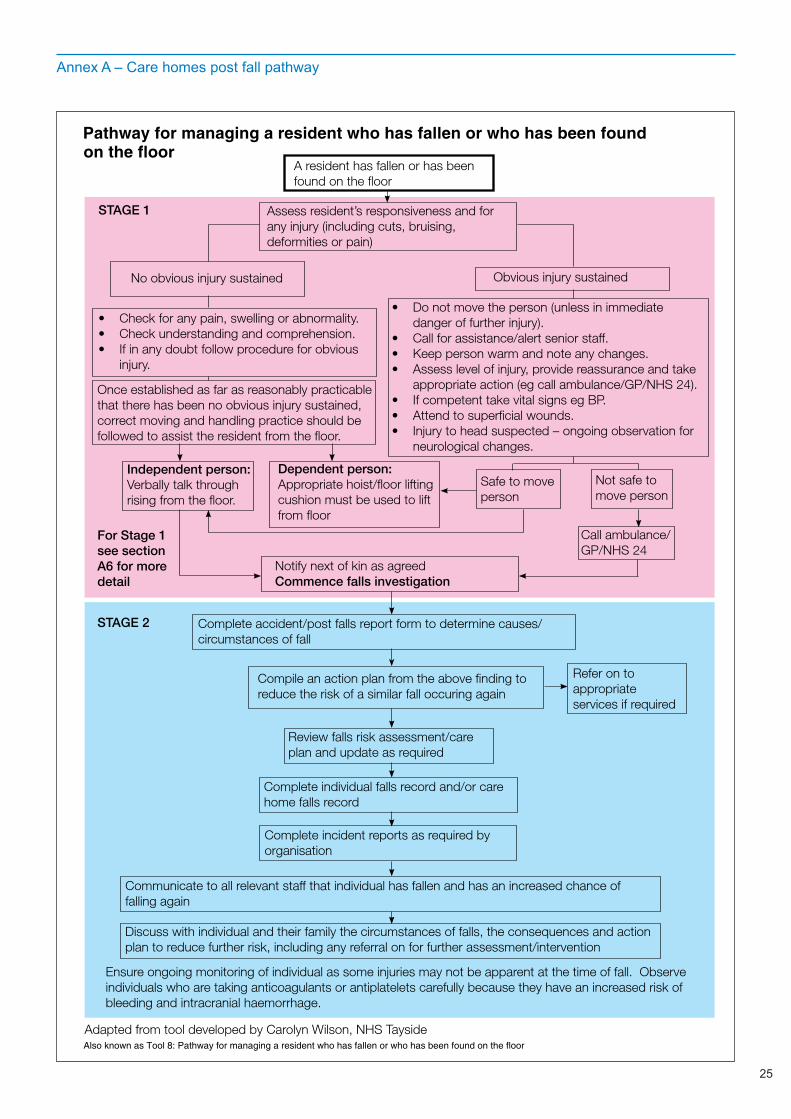
Annex A – Care homes post fall pathway
A resident has fallen or has been found on the floor
Assess resident’s responsiveness and for any injury (including cuts, bruising, deformities or pain)
No obvious injury sustained Obvious injury sustained
• Check for any pain, swelling or abnormality.• Check understanding and comprehension.• If in any doubt follow procedure for obvious
injury.
Once established as far as reasonably practicablethat there has been no obvious injury sustained, correct moving and handling practice should be followed to assist the resident from the floor.
Independent person:Verbally talk throughrising from the floor.
Dependent person:Appropriate hoist/floor lifting cushion must be used to lift from floor
Safe to move person
Not safe to move person
Call ambulance/GP/NHS 24
• Do not move the person (unless in immediate danger of further injury).• Call for assistance/alert senior staff.• Keep person warm and note any changes.• Assess level of injury, provide reassurance and take
appropriate action (eg call ambulance/GP/NHS 24).• If competent take vital signs eg BP.• Attend to superficial wounds.• Injury to head suspected – ongoing observation for
neurological changes.
Notify next of kin as agreedCommence falls investigation
Complete accident/post falls report form to determine causes/circumstances of fall
Compile an action plan from the above finding to reduce the risk of a similar fall occuring again
Refer on to appropriate services if required
Review falls risk assessment/care plan and update as required
Complete individual falls record and/or care home falls record
Complete incident reports as required by organisation
Communicate to all relevant staff that individual has fallen and has an increased chance of falling again
Discuss with individual and their family the circumstances of falls, the consequences and action plan to reduce further risk, including any referral on for further assessment/intervention
STAGE 2
STAGE 1
For Stage 1see sectionA6 for moredetail
Adapted from tool developed by Carolyn Wilson, NHS Tayside
Ensure ongoing monitoring of individual as some injuries may not be apparent at the time of fall. Observe individuals who are taking anticoagulants or antiplatelets carefully because they have an increased risk of bleeding and intracranial haemorrhage.
Pathway for managing a resident who has fallen or who has been foundon the floor
Also known as Tool 8: Pathway for managing a resident who has fallen or who has been found on the floor
26
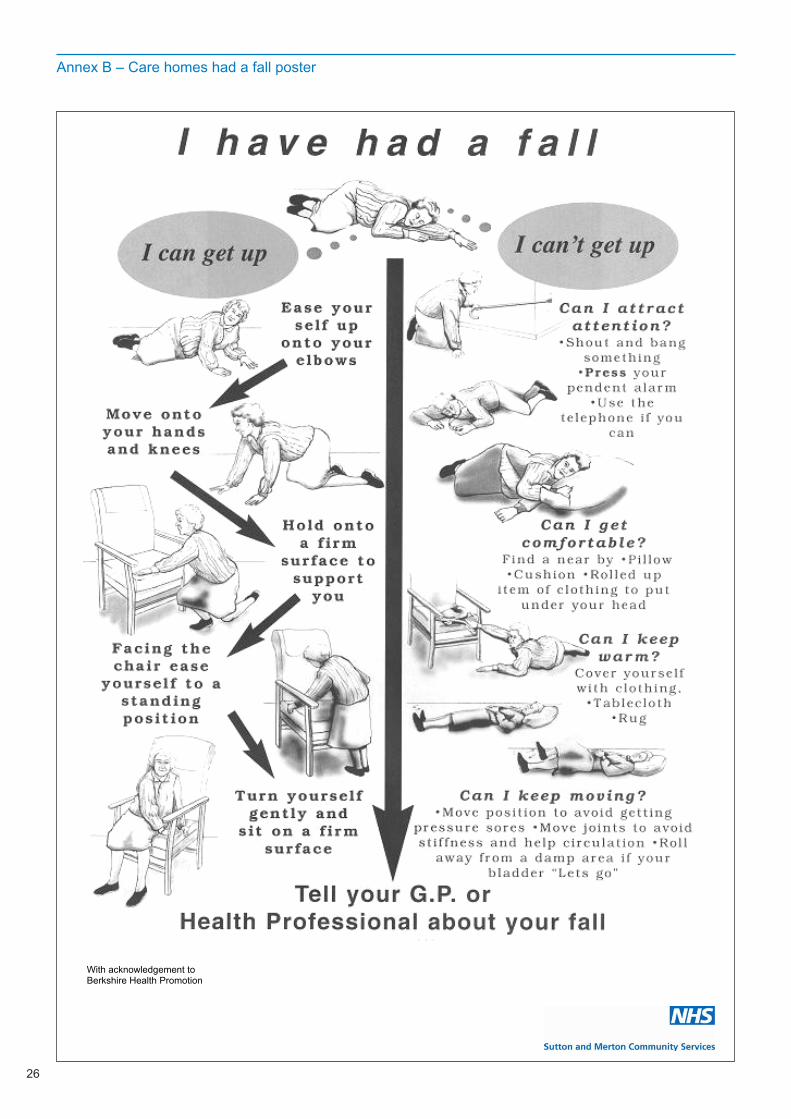
Annex B – Care homes had a fall poster
With acknowledgement to Berkshire Health Promotion
27
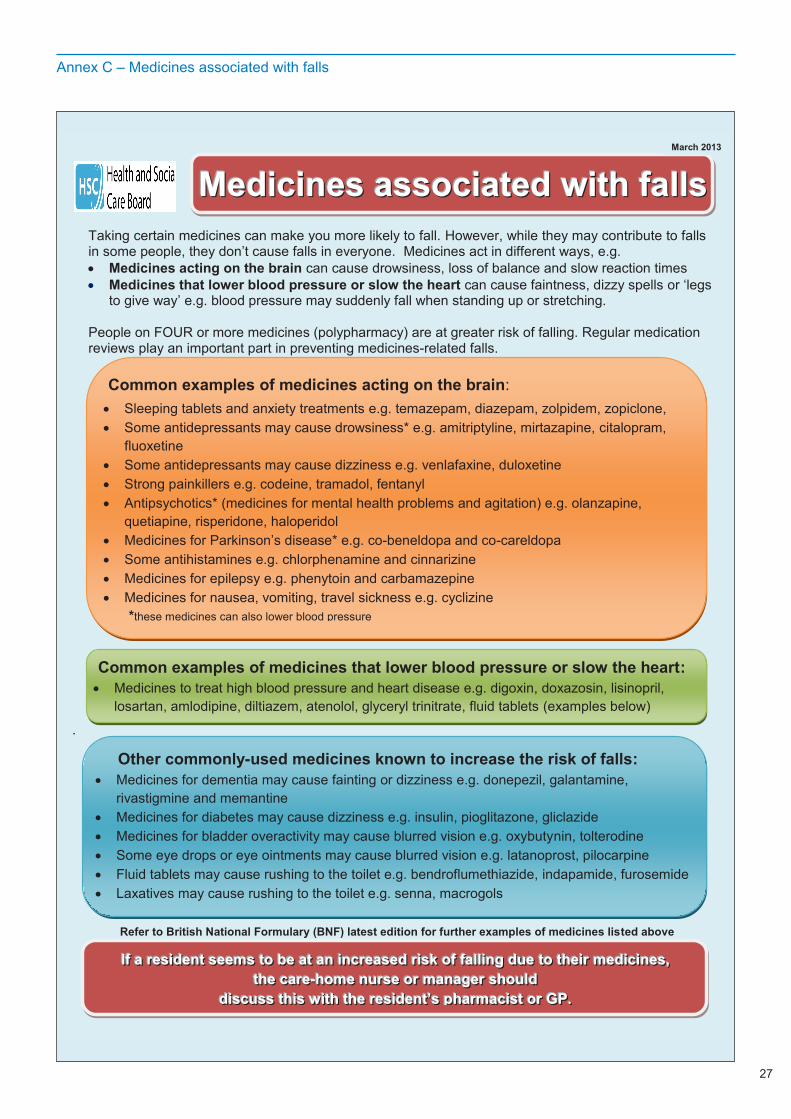
Annex C – Medicines associated with falls
Taking certain medicines can make you more likely to fall. However, while they may contribute to falls in some people, they don’t cause falls in everyone. Medicines act in different ways, e.g. Medicines acting on the brain can cause drowsiness, loss of balance and slow reaction times Medicines that lower blood pressure or slow the heart can cause faintness, dizzy spells or ‘legs
to give way’ e.g. blood pressure may suddenly fall when standing up or stretching.
People on FOUR or more medicines (polypharmacy) are at greater risk of falling. Regular medication reviews play an important part in preventing medicines-related falls.
.
Refer to British National Formulary (BNF) latest edition for further examples of medicines listed above
Common examples of medicines acting on the brain:
Sleeping tablets and anxiety treatments e.g. temazepam, diazepam, zolpidem, zopiclone, Some antidepressants may cause drowsiness* e.g. amitriptyline, mirtazapine, citalopram,
fluoxetine Some antidepressants may cause dizziness e.g. venlafaxine, duloxetine Strong painkillers e.g. codeine, tramadol, fentanyl Antipsychotics* (medicines for mental health problems and agitation) e.g. olanzapine,
quetiapine, risperidone, haloperidol Medicines for Parkinson’s disease* e.g. co-beneldopa and co-careldopa Some antihistamines e.g. chlorphenamine and cinnarizine Medicines for epilepsy e.g. phenytoin and carbamazepine Medicines for nausea, vomiting, travel sickness e.g. cyclizine
*these medicines can also lower blood pressure
Common examples of medicines that lower blood pressure or slow the heart: Medicines to treat high blood pressure and heart disease e.g. digoxin, doxazosin, lisinopril,
losartan, amlodipine, diltiazem, atenolol, glyceryl trinitrate, fluid tablets (examples below)
MMMeeedddiiiccciiinnneeesss aaassssssoooccciiiaaattteeeddd wwwiiittthhh fffaaallllllsss
Other commonly-used medicines known to increase the risk of falls: Medicines for dementia may cause fainting or dizziness e.g. donepezil, galantamine,
rivastigmine and memantine Medicines for diabetes may cause dizziness e.g. insulin, pioglitazone, gliclazide Medicines for bladder overactivity may cause blurred vision e.g. oxybutynin, tolterodine Some eye drops or eye ointments may cause blurred vision e.g. latanoprost, pilocarpine Fluid tablets may cause rushing to the toilet e.g. bendroflumethiazide, indapamide, furosemide Laxatives may cause rushing to the toilet e.g. senna, macrogols
IIIfff aaa rrreeesssiiidddeeennnttt ssseeeeeemmmsss tttooo bbbeee aaattt aaannn iiinnncccrrreeeaaassseeeddd rrriiissskkk ooofff fffaaalllllliiinnnggg ddduuueee tttooo ttthhheeeiiirrr mmmeeedddiiiccciiinnneeesss,,, ttthhheee cccaaarrreee---hhhooommmeee nnnuuurrrssseee ooorrr mmmaaannnaaagggeeerrr ssshhhooouuulllddd
dddiiissscccuuussssss ttthhhiiisss wwwiiittthhh ttthhheee rrreeesssiiidddeeennnttt’’’sss ppphhhaaarrrmmmaaaccciiisssttt ooorrr GGGPPP...
March 2013
28
Copyright © 2015 Care Inspectorate
All rights reserved
Printed January 2015Planned review January 2016
Sutton and Merton Community Services120 The BroadwayLondon, SW19 1RH
www.smcs.nhs.uk
The Care Inspectorate and NHS allow all or part of the text of this document to be reproduced, free of charge, in any format or medium provided it is not for commercial gain. The text may not be changed and must be acknowledged as Care Inspectorate and NHS copyright with the document’s date and title specificed.
This booklet is evidence based wherever the appropriate evidence is available, and represents an accumulation of expert opinion and professional interpretation.
This resource pack has been adapted from the ‘Managing falls and fractures’ Resource Pack as developed by, and with kind permission of, the Care Inspectorate. The full resource can be downloaded at: www.careinspectorate.com
Details of the references used in writing this booklet are available on request from: The Royal Marsden Help CentreFreephone: 0800 783 7176Email: [email protected]
No conflicts of interest were declared in the production of this booklet. The information in this booklet is correct at the time of going to print.
NR527 Version 1, January 2015







