
EVAR vs. OAR: One Community Hospital’s Experience
Westley Smith

Background
Abdominal Aortic Aneurysm (AAA)
http://www.zenithstentgraft.com/patients/US/aaa/what/index.html

Methods
OAR1.Large mid-line incision
2.Aneurysm dissected
3.Graft stitched into place
4.Aorta and Iliac Sutured
Pictures taken from: http://www.guidant.com/webapp/emarketing/compass/comp.jsp?lev1=proc&lev2=aaa

Methods
EVAR1. Small Infrainguinal
Incision
2. Catheter Insertion
3. Portable C-Arm (radiography)
4. Deployment
http://www.guidant.com/webapp/emarketing/compass/comp.jsp?lev1=proc&lev2=aaa
http://www.llnl.gov/str/pdfs/05_00.3.pdf
http://www.ziehm.com/ZiehmVision.htm
Blood F
low

Candidacy
1. Arteriosclerosis
2. Tortuosity
3. Infrarenal neck length/diameter
4. Iliac diameter
5. Patient preference

Comorbidity and Demographics OAR vs. EVAR Comorbidities
0
10
20
30
40
50
60
70
80
90
CoronaryDisease
CongestiveHeart Failure
Irregular HeartRhythm
Hypertension PeripheralVascularDisease
PulmonaryDisease
Diabetes History ofSmoking
Fre
qu
ency
of
Pat
ien
ts
OAR (n = 28) EVAR (n= 72)
Note. *Between groups Pulmonary Disease measured significantly different X2= 13.688, p= .001
*
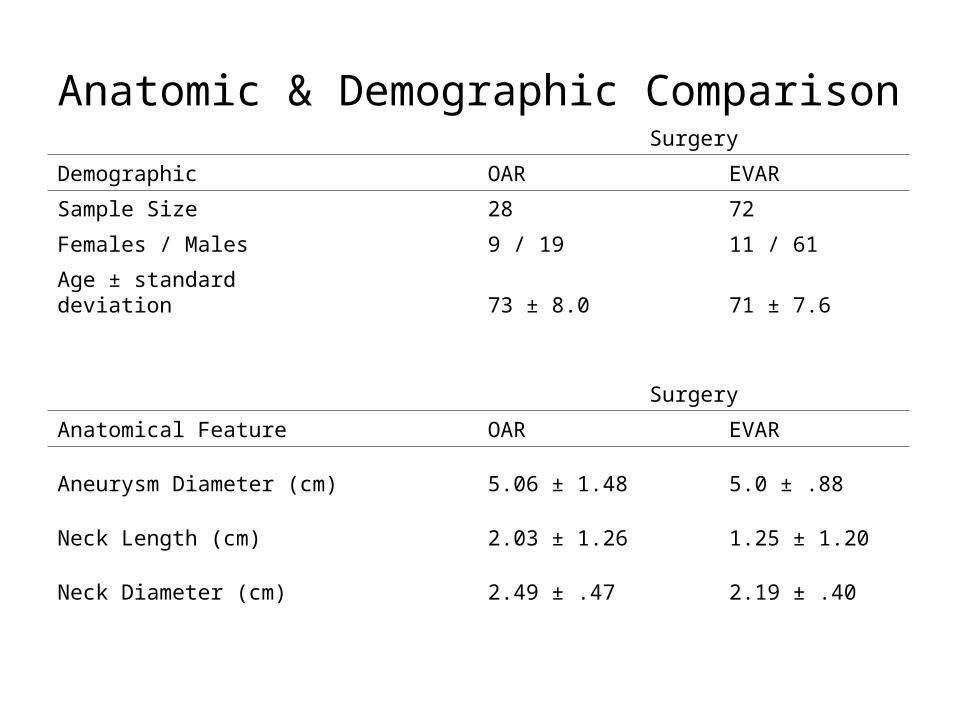
Anatomic & Demographic ComparisonSurgery
Demographic OAR EVAR
Sample Size 28 72
Females / Males 9 / 19 11 / 61
Age ± standard deviation 73 ± 8.0 71 ± 7.6
Surgery
Anatomical Feature OAR EVAR
Aneurysm Diameter (cm) 5.06 ± 1.48 5.0 ± .88
Neck Length (cm) 2.03 ± 1.26 1.25 ± 1.20
Neck Diameter (cm) 2.49 ± .47 2.19 ± .40

The Results
Surgery
Perioperative Variable OAR EVAR Significance
Operative Time (min) 98 ± 41 126 ± 57 No Significance
Anesthetic Time (min) 240 ± 75 203 ± 67 No Significance
Estimated Blood Loss (cc) 1482 ± 1275 353 ± 285 p < .001
Oral Intake (days) 3.87 ± 2.07 .875 ± .95 p < .001
Ambulation (days) 4.46 ± 4.83 2.33 ± 2.00 p = .018

Postoperative Results
Surgery
Postoperative Variable OAR EVAR Significance
Morbidity 17.90% 3.20% χ2 = 16.5, p < .001
Mortality 3.57% 2.80% χ2 = 10.7, p = .005

Conclusions
Candidates for EVAR have tolerated a less invasive procedure without sacrificing postoperative results. The current study is indicative support for the surgeon’s continuation with EVAR – given amendable anatomical characteristics, and pending the long-term results of larger trial facilities.

ReferencesChuter TA, Reilly LM, Faruqui RM, Kerlan RB, Sawhney R, Canto CJ, et al. Endovascular
aneurysm repair in high risk patients. J Vas Surg; 31:122-33, 2000
Marek, J: Endoluminal graft repair of AAA by vascular surgeons at a nonclinical trial center. Presented at the Peripheral Vascular Surgery Society, 11th annual winter meeting, Snowmass, Colorado, January 11-14, 2002.
Moore WS: Two-year follow-up of patients with the EVT/Guidant (Ancure) bifurcated graft for endovascular AAA repair: Advantages and disadvantages of this device. Presented at the 27th Global Veith Meeting, New York City, New York, November 2000.
Abraham CZ, Chuter TA, Reilly LM, Okuhn SP, Pethan LK, Kerlan RB, Sawhney R, Buck DG, Gordon RL, Messina LM, et al: Abdominal aortic aneurysm repair with the Zenith stent graft: Short to midterm results. J Vas Surg; 36:217-225, 2002.
Zarins CK, White RA, Schwarten D, et al: AneuRx stent graft versus open surgical repair of abdominal aortic aneurysms: Multicenter prospective clinical trial. J Vas Surg; 29:292-308, 1999.
Hill BB, Yehuda WG, Lee WA, Arko FR, Cornelius O, Schubart PJ, Dalman RL, Harris JE, Fogarty TJ, Zarins CK, et al: Open versus endovascular AAA repair in patients who are morphological candidates for endovascular treatment. J Endovasc Ther; 9:255-261, 2002.

Special Thanks to:
The Biology Department
&Dr. Daniel McGraw and his Office Staff
Questions





![Best power point evar! [autosaved]](https://cdn.vdocuments.mx/doc/165x107/548bdd07b479592b788b460b/best-power-point-evar-autosaved.jpg)

