
“Effectiveness of Educational Package on Level of Knowledge and
Attitude Regarding Mission Indradhanush Among Mothers of Under
Five Children In Selected Urban Slum Area, Bengaluru”.
By
Mrs. Jyotima Borgohain Handique
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka
In partial fulf illment
of the requirement for the degree of
Master of Science
in
Community Health Nursing
Under the guidance of
Mrs. Kala. Suneetha
Associate Professor and H.O.D
Department of Community Health Nursing
Padmashree Institute of Nursing
Bengaluru-60
2018

ii

iii

iv

v

vi
ACKNOWLEDGEMENT
I owe my gratitude to my Almighty God, Gurudev who makes everything
possible in our life, for His faithfulness and countless blessing during the entire course
of the study and completion of this work.
I extend my heartfelt thanks to Chairman, Managing Trustee and Directors
of Padmashree Institute of Nursing for their constant support.
I extend my sincere gratitude to Dr. Bhima Uma Maheswari Ph.D (N),
Principal, Padmashree Institute of Nursing, for her valuable guidance, constant
encouragement and support throughout the course of the study.
Words are not enough to express gratitude to my guide Mrs. Kala. Suneetha
Associate Professor cum HOD, Community Health Nursing, Padmashree
Institute of Nursing, she is such aninspiration, her expert guidance, suggestions and
constant support throughout the study is of great value.
I also owe my gratitude to Mrs. Divyasri D.S , Associate Professor,
Community Health Nursing, Padmashree Institute of Nursingfor her guidance and
valuable suggestions throughout my study.
I am extending my sincere thanks to Prof. R. Chinnadurai, Biostatistician,
for his valuable guidance and support in statistical analysis and presentation of data.
I take this opportunity to thank the entire Teaching Faculty, Padmashree
Institute of Nursing for their contribution throughout the course.
I am thankful to all the experts who had spent their valuable time in
validating the research tool and who contributed with their valuable suggestions in
making suitable tool for my study.
I express my sincere thanks to the Medical Officer, Kengeri Upanagar
Primary Health Centre, and Gandhi Gram Urban Health Centre, Bengaluru for
granting me permission to conduct the study.
I am grateful to the Nursing staff and ASHA workers of UHC and PHC for
their help during data collection.

vii
viii
LIST OF ABBREVIATIONS USED
1. AV : Audio-visual
2. BCG : Bacille Calmette Guerin
3. Df : Degree of Freedom
4. et. Al : All others
5. F : Frequency
6. H : Hypothesis
7. H0 : Null hypothesis
8. JE : Japanese Encephalitis
9. n : Total number of sample
10. NS : Non significant
11. P : Probability
12. r : Correlation Co-efficient
13. S : Significant
14. SD : Standard Deviation
15. UIP : Universal Immunization Programme
16. VPD : Vaccine Preventable Diseases
17. WHO : World Health Organisation
18. χ2 : Chi Square
19. ≥ : Greater than or equal
20. < : Less than
21. % : Percentage

ix
LIST OF TABLES
Sl.
No Tables
Pages
1.1 Frequency and percentage distribution of demographic variable of
mothers of under five children according to age, religion, educational
status and occupation.
38
1.2 Frequency and percentage distribution of demographic variable
mothers of under five children according to family income per month,
type of family, number of children, immunization status of the mothers,
previous information about Mission Indradhanush and sources of
information.
40
2.1 Frequency and percentage distribution of pre-test level of knowledge
regarding Mission Indradhanush mothers of under five children.
47
2.2 Range, Mean, SD and Mean percentage of pre-test level of knowledge
regarding Mission Indradhanush among mothers of under five children.
47
2.3 Frequency and percentage distributionof pre-test level of attitude
regarding Mission Indradhanush among. Mothers of under five
children.
48
2.4 Range, Mean, SD and Mean percentage of pre-test level of attitude
regarding Mission Indradhanush among mothers of under five children.
48
3.1 Frequency and percentage distribution of post-test level of knowledge
regarding Mission Indradhanush among mothers of under five children.
49
3.2 Range,Mean, SD, and Mean percentage of post-test level of knowledge
regarding Mission Indradhanush among mothers of under five children.
49
3.3 Frequency and percentage distribution of post-test level of attitude
regarding Mission Indradhanush among mothers of under five children.
50
3.4 Range, Mean, SD, and Mean percentage of the post-test level of
attitude regarding Mission Indradhanush among mothers of under five
children.
50
4.1 Frequency and percentage distribution of mothers according to pre
andpost- test level of knowledge regarding Mission Indradhanush.
51
4.2 Range, mean, SD, and Mean percentage of pre and post- test level of
knowledge regarding Mission Indradhanush among mothers of under
53
x
Sl.
No Tables
Pages
five children.
4.3 Frequency and percentage distribution of mothers according to the pre
and post- test level of attitude regarding Mission Indradhanush.
53
4.4 Range, Mean, SD, and Mean percentage of pre and post- test level of
attitude regarding Mission Indradhanush among mothers of under five
children.
54
5.1 Paired t-test analysis for the significance of pre and post- test knowledge
and attitude regarding Mission Indradhanush among mothers of under
five children.
55
6.1 Correlation between the pre- test knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
56
7.1. Association between pre-test level of knowledge regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables such as age, religion and educational status.
58
7.2 Association between pre-test level of knowledge regarding Mission
Indradhanush among mothers with their selected demographic
variables such as occupation, family income, type of family, number of
children, immunization status of the children, previous information
about Mission Indradhanush and sources of information.
59
7.3 Association between pre-test level of attitude regarding Mission
Indradhanush among moters with their selected demographic variables
such as age, religion and educational status.
61
7.4 Association between pre- test level of attitude regarding Mission
Indradhanush among mothers with their selected demographic variables
such as occupation, family income, type of family, numer of children,
immunization status of the children. previous information about
Mission Indradhanush and sources of information,
62

xi
LIST OF FIGURES
Sl. No Figures Pages
1 Modified conceptual framework based on Pender’s Health
Promotion Model.
16
2 Schematic representation of Research plan of the study. 28

xii
LIST OF GRAPHS
Sl.No. Graphs Pages
1. Percentage distribution of mothers of under five children according
to age.
42
2. Percentage distribution of mothers of under five children according
to religion.
42
3. Percentage distribution of mothers of under five children according
to educational status.
43
4. Percentage distribution of mothers of under five children according
to occupation.
43
5. Percentage distribution of mothers of under five children according
to family income per month.
44
6. Percentage distribution of mothers of under five children according
to type of family.
44
7. Percentage distribution of mothers of under five children according
to number of children.
45
8. Percentage distribution of mothers of under five children according
to immunizatipn status of the children.
45
9. Percentage distribution of mothers of under five children according
to previous information about Mission Indradhanush.
46
10. Percentage distribution of mothers of under five children according
to sources of information.
46
11. Percentage distribution of mothers of under five children according
to pre and post- test level of knowledge regardingMission
Indradhanush.
52
12. Percentage distribution of mothers of under five children according
to pre andpost-test level of attitude regarding Mission Indradhanush.
54
13. Correlation between knowledge and attitude regarding among
Mission Indradhanush mothers of under five children.
57

xiii
LIST OF ANNEXURES
Annexure No.
Content Page No.
I. Letter seeking and granting permission for conducting the
research study.
112-113
II. a. Lesson plan (English)
b. Lesson plan (Kannada)
114-126
127-144
III. Criteria rating scale for content validation of thetool. 145-148
IV. Letter seeking experts’ opinion and suggestions for content
validity of tool.
149
V. List of experts who validated the tool. 150
VI. Content validity certificate. 151-159
VII. a. Certificate of English editing.
b. Certificate of Kannada editing.
160
161
VIII. A.V. Aids - Flash cards, pamphlet and leaflet (English and
Kannada)
162-180

xv
STRUCTURED ABSTRACT
Title
A quasi experimental study to assess the effectiveness of educational package
on level of knowledge and attitude regarding Mission Indradhanush among mothers
of under five children in selected urban slum area, Bengaluru.
Background
Immunization is one of the most important public health interventions to
reduce child mortality associated with infectious diseases. Mission Indradhanush
waslaunched in December 2014 and aimed to fully immunize more than 90% of
newborns and pregnant mothers by 2020 through innovative and planned approached
to reach all children.
Objectives
1. To assess the existing level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children. 2. To assess theeffectiveness of
educational package on Mission Indradhanush among mothers of under five children.
Methods
A quasi experimental study was conducted by using one group pre-test post-
test research design. Simple random sampling technique was adopted to select 60
mothers of under five children.
Results
The overall pre-test mean knowledge score was found to be 10.17 with SD of
4.49 and overall pre-test mean attitude score was found to be 30.58 with SD of 2.39.
The overall post-test mean knowledge score was found to be 17.00 with SD of 3.36
and overall post-test mean attitude score was found to be 37.21 with SD of 2.50.
Paired t-test shows that there was statistical significance at p<0.001 level. It showed,
there was an establishing impact of educational package on knowledge and attitude
regarding Mission Indradhanush among mothers of under five children and there was
significant linear correlation (r=0.486) between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children at p<0.05 level.
xvi
Interpretation and Conclusion
The study concluded that the educational package was effective in improving
the level of knowledge and attitude regardingMission Indradhanushamong mothers of
under five children.
Key words
Knowledge; attitude; mothers; educational package; immunization;Mission
Indradhanush.

1
“A quasi experiental study to assess the effectiveness of educational package on level
of knowledge and attitude regarding Mission Indradhanush among mothers of under
five children in selected urban slum area, Bengaluru”
INTRODUCTION
Background of the study
Today’s healthy children are the future healthy citizen of the country.
According to 2011 census children population of 0 to 6 yrs is 158.8 million which
represents 13.12% of the total population.1
Health care of children below 5 years
should give greater importance because these age groups are vulnerable to various
health problems due to weaker immune system as compared to adults. The child needs
to be protectedfrom six infectious and vaccine preventable diseases, it includes
tuberculosis, tetanus, diphtheria, whooping cough, measles and poliomyelitis. More
than one million children and pregnant mothers can be saved from death by
immunizing them at the right age and right time and by completing the full course of
immunization.2
Immunization is a procedure in which immunobiological substances are
administered to strengthen the defense (immune) mechanism as to protect the
individual against the disease.3
Immunization remains one of the most important
public health intervention and cost effective strategies to reduce child mortality
associated with infectious diseases. It has been seen that five million children are
dying in each year and another five million were disabled by six childhood diseases in
some developing countries like India. Protecting the health and development of
children is a long term contribution to the growth and development of the country as a
whole.4
Vaccines are the antigenic substance which when administered in an
individual, stimulate the production of specific antibodies and protect the individual
against the particular diseases.5
Vaccines are among the most effective tools available
for preventing infectious diseases and their complications. Immunization is vital;
almost one third of deaths under five are prevented by vaccine. Every child has the
right to benefit from the appropriate traditional and new life saving vaccinations.

2
However, the success of an immunization programme depends on high rates of
acceptance and coverage.6
` The health of a child is basically in the hands of their mothers as children
nourish under the care of their mothers. Rearing is determined to a greater extend by
the knowledge and attitude of mothers. To meet the health needs of children, it is
impossible without mother’sinvolvement as they play a primary role in child’s life.
Most mothers know the basics of keeping their child healthy like offering them
healthy foods, making sure that they get enough sleep and ensuring safety, but it is
also very important for the mother to know the importance of immunization to
prevent from six killer diseases and its complication.
Based on the Health problems of underfive children and pregnant mothers, the
Government of India has launched many NationalHealthProgrammes to meet the
health needs of the country, such as-
• Maternal and Child Health Programme ( MCH )
• Integrated Child Development Service Scheme ( ICDS )
• Child Survival and Safe Motherhood Programme ( CSSM )
• Integrated Management of Neonatal and Childhood Illness ( IMNCI )
• National Programme on immunization
• Diarrheal disease control programme
• Vitamin A deficiency control programme
• National Rural Health Mission ( NRHM )7
Withtheongoing health programme, it is resulted in the considerable
improvement of the country’s health in general, as the children form the central part
and development and the wealth of the country depends largely on them. The
Government aims to strengthen and improve the health of children.7
Committed to improving immunization coverage and addressing the eqality agenda,
the Ministry of Health and Family Welfare, Government of India, has implemented
various intensification strategies including its flagship programme “Mission
Indradhanush” launched in December 2014, and delivery system strengthening
exercises through improved micro-plans.8

3
Mission Indradhanushin is a special drive to vaccinate all unvaccinated and
partially vaccinated children under Universal Immunization Programme. The mission
focuses on intervention to improve full immunization coverage in India from 65% in
2014 to at least 90% children in the next fiveyears.9
Mission Indradhanush aimed to
fully immunize more than 90% of newborns by 2020 through innovative and planned
approaches to reach all children. It not only aimed to rapidly increase the
immunization coverage through special drives during specified months but also
focused towards strengthening health system for addressing equality issues in access
to immunization. This initiative will eventually close immunity gap and strengthen
immunization coverage.9
In the first phase, 9.66,495 sessions were conducted and around 7.6 million
children were immunized out of which 1-9 million children were fully immunized.10
Second phase of Mission Indradhanush continued in January 2016 in 352 districts.
Phase III was implemented from April to July in 216 districts of the country. During
all the three phases, as on 1st August 2016, 2.08 crore children have been vaccinated
of which 54.5 lakh children have been fully immunized. In addition, 55.4 lakh
pregnant women were vaccinated against tetanus toxoid. According to Integrated
Child health and immunization Survey 2016, full immunization coverage has
increased by about 5-7% after the launch of Mission Indradhanush.11
This is done through special “catch-up” drives, - the aim to cover all the
children who have been left out or missed out for immunization. It is supported by
WHO,UNICEF, Rotary International and other donor partners. Medical Officer in
Charge for the Block/ Urban Planning has conducted detailed planning for additional
sessions in the planning unit. In urban areas, urban health posts, post-partum centers,
family welfare centers or local leader’s premises in urban slums are used as
immunization sites. For other areas, primary school, anganwadi centers, private
dispensaries, Non Governmental Organization sites or any other location that are
easily accessible and acceptable to community are used as immunization sites.9
There are four rounds of vaccination between April and July, with each round
having seven consecutive working days beginning of 7th
of the month. In addition to
health staff available from the same or neighboring community health center / Block
PHC, NGOs (LIONS, Rotary etc.), it is necessary to utilize retired health workers.

4
The activity are conducted from 9am to 4pm. Sessions are planned based on
availability of the targeted population to maximize the benefits achieved.9
The Government of India, in partnership with the World Health Organization,
UNICEF and other agencies, is leaving no stone unturned to ensure that there are no
children who remain unvaccinated, or partially vaccinated against these seven
preventable diseases. The World Health Organization is assisting with risk - analysis
– identifying children in underserved areas who havenot been fully immunized and
the underlying reasons, to strengthen our efforts. The WHO is also providing us
valuable technical support in micro – planning, training and monitoring the work on
the ground.12
Seeing its wider coverage, Mission Inrdadhanush has been a success till now
in order to improve the immunization coverage particularly in the under-privileged
and underserved communities and reduce mortality rate due to vaccine preventable
diseases.9
Need for the study
Each year 27 million children are born in India. Around 10 per cent of them do
not survive 5 years of age. India contributes to 25 per cent of the over 6.9 million
under five death occurring worldwide over years.13
Globally under five mortality rate
has been decreased by 53% from an estimated rate of 91 death per 1000 live births in
1990 to 43 deaths per 1000 live births in 2015. The average annual rate of reduction
of under five mortality has accelerated from 15% in a year over the period 1990 to
2000 to3.9% for 2000 to 2015; but remain insufficient to reach Millennium
Development Goal-4. About 19,000 fewer children died every day in 2015 than in
1990.14
The proposal is for all countries aiming reduce under five mortality to at least
as low as 25 per 1000 live births. The Government of India is committed to reducing
child mortality and morbidity in the country by improving full immunization coverage
through Universal Immunization programme (UIP) and introducing new and
efficacious vaccines for vaccine preventable diseases.9 India’s UIP has contributed
significantly to ensure equality to children accessing the public health system through
a variety of supply and demand side interventions,though there still remain challenges

5
of inequility. The stedy fall of infant mortality from 80 per 1000 live birth in 1991 to
37 per 1000 live birth in 2015 (SRS) does in part reflect the Govt. of India’s dedicated
efforts under UIP to reduce child mortality and morbidity.8
Attention was given to immunization programme in India after successful
eradication of smallpox in mid 1970s. India has launched Expanded Programme on
Immunization (EPI) for immunizing children against diphtheria, whooping cough and
typhoid in 1978 mainly for urban areas. Oral Polio Vaccine against polio, BCG
against tuberculosis and vaccination against measles were included in 1979-80, 1981-
82 and1985-86 respectively.15
The programme was revised in 1985 and renamed as Universal Immunization
Programme (UIP), is one of the largest health programmes of its kind in the World
catering to a birth cohort of 2.7 crore children annually. The program provides
vaccination against seven lifethreatening diseases (Diphtheria, Whooping cough,
Tetanus, Poliomyelitis, Tuberculosis, Measles and Hepatitis B) in the entire country.
In addition, vaccination against Haemophilus Influenzae type B (Hib) and Japanese
Encephalitis (JE) is provided in selected districts and states of the country.9
In spite of all positive changes, there are ongoing challenges for UIP. Despite
being operational for the past more than 30 years, only 65% children (RSOC 2013-
2014) in India receive all vaccines during their first year of life. It is estimated that
annually more than 89 lakh children majorly in hard to reach and underserved
population do not receive all vaccines that are available under Universal
Immunization programme – the highest number compared with any other country in
the World.8
Evidence shows that unimmunized and partially immunized children are most
susceptible to childhood disabilities and run a 3-6 times higher risk of death as
compared with fully immunized children. There are wide variation in the proportion
of partially immunized and unimmunized children within states and districts. Recent
evaluation have indicated that the reason for inability to reach all vaccines to children
in the country are lack of awareness among parents about the benefits of vaccination,
fear of adverse events following immunization and operational reasons such as non
availability of vaccines or vaccinators during vaccination sessions.9

6
Under Mission Indradhanush all the vaccines provided under UIP are
administered to children and pregnant women. UIP of India prevents mortality and
morbidity in children and pregnant women against 12 vaccine preventable diseases.
The Government has identified 201 high focus districts across the country that have
50% of all unvaccinated or partially vaccinated children in the country. A total of 528
districts covered during the various phases of Mission Indradhanush and more than
2.47 crore children and 67 lakh pregnant women have been vaccinated. With the
launch of Mission Indradhanush, the Government aims at
• Generally high demand for immunization services by addressing
communication challenges.
• Enhancing political, administrative and financial commitment through
advocacy with key stakeholders and
• Ensuring that the partially immunized and unimmunized children are fully
immunized as per National Immunization schedule.9
The Union Health Ministry plans to achieve full immunization coverage under
its “Mission Indradhanush” by 2018. States conduct Mission Indradhanush drives for
seven working days from 7th
of every month, for four consecutive months, excluding
Sundays, holidays and routine immunization days.8
Mission Indradhanush contributed to an increase in Full Immunization
Coverage by 6.7%, as evidenced by Integrated Child Health and Immunization
Survey (INCHIS). This increase would not be sufficient to achieve Full Immunization
Coverage of more than 90% of new-borns by 2020 as aimed under Mission
Indradhanush.Further, Full Immunization Coverage in selected disticts/cities that have
shown slow progress in spite of repeated phases of Mission Indradhanush.8
There are several reasons why India has so many unlimited and party
immunised children–vast pools of illiteracy, lack of awareness about the benefits of
immunization and lack of access to healthcare facilities. Reaching every child who
missed out on immunization is not an easy task. The vulnerable are not just in the
rural hinterland. Many live on the margins of urban India.It is children of migrant
workers often miss out on routine and supplementary immunization.Others at equal
risk include those belonging to populations that are nomadic, living around brick
kilns, urban slums, fishermens’ villages, living in riverine areas with shifting

7
populations and other traditionally underserved and hard- to- reach groups like tribal
communities and those living in forested areas.Those at risk also include populations
which have a health facility exists but lack health workers.12
With the aim to accelerating the full immunization coverage and provide
greater focus on urban areas and other pockets of low immunization coverage, the
Ministry of Health and Family Welfare has drawn up an aggressive action plan to
achieve the target by 2018 and it was launched on 8th
October,2017 as Intensifies
Mission Indradhanush.8
Hon’ble Prime Minister emphasized the need of a supplemental aggressive
action plan to cover all left outs and drop outs in selected districts and urban cities
with low routine immunization coverage in a specific time frame(December 2018).
These districts should focus on improving immunization coverage through need based
interventions in Intensified Mission Indradhanush drives, based on a comprehensive
gap analysis, with strengthened involvement of relevent non- health departments and
enhanced accountability frameworks.8
Inter-ministerial and inter- departmental coordination, action- based review
mechanism and intensified monitoring and accountability framework are the key for
effective implementation of targeted rapid interventions to improve the routine
immunization coverage which will ensure that life saving vaccines reach every child.8
Under the intensified drive, due attention must be given to:
• Urban slum areas and districts where there is maximum scope of
improvement in immunization
• Due- listing of beneficiaries on the basis of robust head- count surveys which
will be validated by supervisors; and
• Improving mobilization of beneficiaries.8
This Intensified Mission will hence be steered based on the information
received from gap assessment, concurrent monitoring by partners, and end- line
surveys. States and districts need to device coverage improvement plans based on gap
self assessment,which will be reviewed at all levels for adherence to achieving goal of
reaching 90% evaluated coverage/ concurrent monitoing by December 2018.8

8
Over half (54%) of the world’s population lived in urban areas and by 2050
this population is expected to increase 66 per cent, adding approximately 2.5 billion
new urban dwellers. Around 90% of the projected increase will occur in Asia and
Africa, which currently have the lowest level of urban dwelling population (48% and
40% respectively). This increasing trends towards urbanization is closely linked
withincreasing population living in slum environment, particularly in low and middle
income countries in Asia and Africa.16
Significant disparities in health outcomes exist in urban areas, with the urban
poor most affected. These disparities are driven by demographic, geographic and
socio- economic factors. The coverage of basic health services, including vaccination,
is usually lower among urban poor communities, increasing their vulnerability to
vaccine preventable diseases. Factors associating with immunization uptake in urban
slums are
• Socio-economic characteristics
The socio-economic circumstances are having low level of income and
education; poor provision ofpublic infrastructure such as water and sanitation;
insecure legal status resulting in exclusion from public health systems; and reduced
or absent provision of basic health services.
• Information, beliefs and behavior
Health services are not acceptable due to lack of information and distrust in
the government. Some parents are unaware of the need of vaccines; either the mother
or both parents being too busy to take their child to be vaccinated; parents travelled to
village or place of origin; parents or caretakers unaware of the location or timing of
the vaccine clinic.
• Health services
The provision of health services are different when compared to the rest of an
urban area, which may have an effect on immunization coverage and lead to
inequalities in coverage among the urban poor in slums. The quality of the services
provided also plays a role: higher patient satisfaction and provision of accurate
information leads to increased attendance for repeat vaccine doses.

9
• Migration status
An Indian slum cited the following reasons for under-immunization for
migrant population: mother or both parents being too busy; parents returned to home
village; parents unaware of place or time of immunization; and lack of awareness for
the need for immunization.16
A study conducted among 731 Saudi parents of 0-12 years old children during
April 2013 in Taif, Saudi Arabia shows that parents had good knowledge on general
role of vaccination in prevention of some infectious diseases 672 (91.9%), timing of
the first dose in vaccination schedule 635 (86.8%). Parents had poor knowledge on
importance of administration of multiple doses of same vaccine 304(41.6%).Parents
attitudes towards immunization was positive except in some aspects related to
vaccination side effects 316 (34.2%) and the probability of occurrence of diseases
against which the child was vaccinated 288 (39.4%). It indicates that although parents
had good knowledge and positive attitudes on some aspects related childhood
immunization, gaps in both studied domains were identified. Educational
interventions are needed to upgrade parents’ knowledge with special emphasis on less
educated and residents of rural areas.17
A study conducted among 500 families having children between 0-5 years in
rural areas of Punjab, India from March 2014-march 2015 revealed that maximum
coverage to BCG vaccination (77.2%) and minimum for measles vaccine (56.2%) was
observed. 55% of children were completely immunized, 28.8% were partially
immunized and 16.2 were not immunized. It is concluded that the main reason for
partial/non immunization was lack of knowledge of families about vaccination.
Considering incomplete knowledge and inappropriate practices the policy makers and
medical profession require to put in much more efforts to sensitive families about
importance regarding immunization in preventing diseases and their consequent
morbidity and mortality.18
A survey study conducted among 60 migrant mothers of under five children in
selected construction sites at Bangalore Urban showed that 55.0% were between 20-
23 years of age, 38.3% had only 1 child, 45% of the children belonged to the ages
below 1 year, 91.7% had no formal education, 68.3% of migrant mothers speak
Kannada, 71.7% of them had inadequate knowledge, whereas 28.3% of them had

10
moderate knowledge while 0% of them had adequate knowledge. The post-test score
showed that (38)63.3% had adequate knowledge and (22)36.6% had moderate
knowledge while none had inadequate knowledge. There is no association between
knowledge scores and demographic variables.19
A study conducted in the urban slums of Bijapur, Karnataka in 2012among
155 mothers/ responsible guardian of children in the age group of 12 to 23 months
revealed that 54 out of 155 respondents (34.84%) where fully immunized, 97
(62.58%) were partially immunized and 4 (2.58%) were unimmunized. It indicates
that the immunization coverage in the urban slum of Bijapur is still way short of the
85% coverage mark due to a lack of information and motivation among the parents.20
A community based cross-sectional study conducted among 150 parents in
slums of Mangalore taluk during August –November 2015shows that 88(57.7%) of
under five children were fully immunized, 62(41.3%) were partially immunized. It
indicates that the immunization coverage was found to be very bad. There is an urgent
need to ensure that regular health education sessions are conducted. Slum areas
should be the target of RCH programme with special focus on immunization related
activities e.g. ensuring that all households with children should have immunization
cards.21
A study conducted among 143 mothers from socioeconomically backward part
of Bangalore, Karnataka. in a teaching hospital in South India shows that even though
most of the mothers had satisfactory knowledge, attitude and practice, almost 25%
children were identified as un-immunized or partially immunized. The study indicated
that there is an urgent need to increase the coverage of Universal Immunization
programme vaccines and there is a direct need to arrange for health education
program sessions for all the parents regarding the importance of complete adherence
of vaccination among children. TV, newspaper and other media can be also promoted
as most important sousces which can be used for spreading educational messages
regarding vaccination.22
From the above studies it shows that the magnitude of unimmunization and
incomplete immunization is huge among under five children specially in urban slum
area. It is important to to create awareness among parents about immunization and its

11
benefits. Mothers are the primary care giver and the decision makers in upbringing of
their children. So, the investigator assumes that the mothers should have depth
knowledge and attitude regarding immunization and Mission Indradhanush. The
investigator choose the mothers of urban slum as her sample to create awareness
about Mission Indradhanush to ensure that they are adequately informed about the
programme and it would help to cover all the children who have been left out or
missed out for immunization.

12
OBJECTIVES
Statement of the problem
A quasi experimental study to assess the effectiveness of educational package
on level of knowledge and attitude regarding Mission Indradhanush among mothers
of under five children in selected urban slum area, Bengaluru.
Objectives of the study
1.To assess the existing level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children.
2. To assess the posttest level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children.
3. To assess the effectiveness of educational package on knowledge and attitude
regarding Mission Indradhanush among mothers of under five children.
4. To determine the correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
5. To associate the pretest level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables.
Operational definitions
1. Effectivenes
It refers to the extent to which the educational package will improve
the knowledge and attitude regarding Mission Indradhanush among mothers
of under five children.
2. Educational package
It refers to the systematically developed educational strategy to teach
the mothers of under five children regarding importance of Mission
Indradhanush, who are all beneficiaries, about the seven life threatening
diseases, Universal immunization schedule by using A.V. aids such as flash
cards, pamphlets and leaflets for a duration of 45 minutes to 1 hour.
13
3. Knowledge
It refers to the level of understanding regarding Mission Indradhanush
among mothers of underfive children which is assessed by structured
questionnaire.
4. Attitude
It refers to belief and opinion regarding Mission Indradhanush among
mothers of under five childrenwhich is elicited by Likert scale.
5. Mission Indradhanush
It is a health programme launched by the Union Government to ensure
immunization of children and pregnant women. This is a focused and
systematic drive to be implemented through a “catch up” campaign mode. The
aim of the “catch up” mode is to cover all the children who have been left out
for immunization.
6. Mothers of under five children
It refers to the mothers who are having children below five years of
age and are residing in selected urban slum.
Assumptions
1. Mothers of under five children may have low knowledge regarding Mission
Indradhanush.
2. Mothers of under five children may have poor attitude towards Mission
Indradhanush.
3. Educational package may improve the knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
4. Knowledge and attitude of mothers of under five children may vary with
their selected demographic variables.
Research Hypotheses
H1- There is a significant difference between the mean pre-test and post-test score of
knowledge and attitude regarding Mission Indradhanush among mothers of under
fivechildren.

14
H2- There is a significant correlation between pre-test knowledge and attitude
regarding Mission Indradhanush among mothers of under five children.
H3- There is a significant association between pre-test level of knowledge and attitude
regarding Mission Indradhanush among mothers of under five childrenwith
theirselected demographic variables.
Delimitations
1. The study was delimited to mothers having children below five years.
2. The data collection was dilimited to 4 weeks
Conceptual framework
Concepts are basically vehicles of thought that involve images. Concepts are
words that describe objects, properties or eventsthatare basic componentsof theory. It
is an idea of an object, property or events which can be empirical or concrete,
inferential or abstract, that is derived from individual perceptual experience. Concept
is defined as a complex mental formulation of an object, property or an event that is
derived from the individual’s perception and experience.23
Conceptualization is the process of forming ideas, which are utilized and
forms the conceptual framework for development of research design. It helps the
researcher to know that data need to be collected and gives direction to an entire
research process.Theories and conceptual models are the primary means of providing
a conceptual context for a study.24
The present study is intended to assess the effectiveness of educational
package regarding Mission Indradhanush among mothers of under five children.
The conceptual model selected for this study is based on “Pender’s Health
Promotion Model” (1996). The Health Promotion Model proposed by Nola Pender
and was designed to be a complementary counterpart to model of health protection.
Health promotion is directed at increasing the well level of wellbeing and human
Health potential.
The model focused on following three areas
1. Individual characteristics and experiences
2. Behavior specific cognition and affect
15
3. Behavioral outcomes.
Individual characteristics
In this study, individual characteristics refers to the demographic variables of
mothers of under five children consisting of age, religion, educational status,
occupation,family income per month,type of family, number of
children,immunization status of the children, previous knowledge and sources of
information.
Behavior specific cognition and affect
Here, it refers to the existing knowledge and attitude regarding Mission
Indradhanush among mothers of under five children. The investigator targeted that the
administration of educational package will improve the level of knowledge and
attitude of mothers of under five children regarding Mission Indradhanush .Structured
interview schedule was developed to assess the knowledge and three point Likert
scale was developed to assess the attitude regarding Mission Indradhanush among the
mothers of under five children.
Perceived barrier to actions such as lack of awareness and lack of the sources
of information were identified. Effort was taken to overcome the perceived barriers
and effective working environment was created in order to fulfill the expectation of
the mothers to achieve the targeted goals.
Educational package regarding Mission Indradhanush was administered to all
the selected mothers of under five children with the help of flash cards, pamphlets and
leaflets for a duration of 45 minutes.
Behavioral outcome
It is the end result of behavior and helps to identify and assess short term and
long term outcomes. In the present study, behavioral outcome refers to the
comparison of pre -test and post-test level of knowledge and attitude scores of
mothers of under five children regarding Mission Indradhanush. Assessment of
improvement in knowledge and attitude of parents was done by statistical
computation. The targeted outcome was met through the administration of educational
package on Mission Indradhanush among mothers of under five children.

16

17
REVIEW OF LITERATURE
Literature review is defined as a broad, comprehensive, in depth, systematic
and critical review of scholarly publication, unpublished printed or audio visual
materials and personal communications. Before starting any research whether it is
single study or an extended project, a literature review of previous study and
experience related to the purpose investigation should be done. One of the most
satisfying purposeof the literature review is the contribution to make the new
knowledge insight and general scholarship of the research. A researcher analyses
existing knowledge before dwelling into a new area of the study, while conducting a
study, when interpreting the results of the study and when making the judgement
about application of new knowledge in nursing practice.
The received related literature has been organized under the following headings:
1. Literature related to knowledge regarding immunization.
2. Literature related to knowledge and attitude regarding immunization.
3. Literature related to effectiveness of educational programme on immunization.
4. Literature related to immunization programme.
Literature related to knowledge regarding immunization
A non-experimental survey was conducted to assess the level of knowledge
regarding immunization among mothers of under five children and associate the
findings with the selected demographic variables in selected area of Pune city. 200
mothers who were having under five children were selected by non-probability
convenient sampling technique. The study results shows that majority of mothers was
having average knowledge 140 (70%), poor 50 (20%) and good 10 (5%). There is also
association between education of mothers and knowledge regarding immunization at
p <0.05 level. The chi square test result indicates that as the standard of education is
higher, the knowledge of immunization was more. The study concluded that mothers
knows the importance of immunization, but they have knowledge deficiency about
some vaccine like BCG,DPT, doses of hepatitis B and vitamin A vaccination.25
A community based cross sectional survey study was done to assess the
immunization status and knowledge regarding newer vaccines among mothers in a
rural area of Rangareddy District, Telangana, India. Fifty children and their mothers

18
were selected for the study by convenient sampling technique. A pre designed, pre
tested questionnaire was used by adapting interview technique. The study result
shows that about three fourth (74%) children were completely immunized and 26%
were partially immunized. About one third of mothers were aware about pentavalent
vaccination, one fourth were aware about IPV and extreme low level of awareness
(2%) was seen regarding Rota virus vaccine. The study concluded that one fourth of
the children were partially immunized with majority missing the booster doses and a
very low level of awareness was seen among mothers regarding various newer
vaccines.26
A hospital based cross-sectional descriptive study was conducted to assess the
maternal knowledge about immunization, vaccines used, vaccination centres and
advantages at tertiary care centre in Maharastra. The study was conducted among the
mothers at pediatric OPD of Government Medical College and hospital, Akola. The
results show that majority of mothers had poor knowledge of vaccine used in
Universal Immunization programme. BCG and OPV were comparatively known to
many. Also the most of the mothers were not aware of advantages of immunization.27
A non experimental researchexploratory study was conducted to assess the
knowledge among mothers of under five children regarding immunization in selected
villages of Moga, Punjab. 100 mothers of under five children were selected from
anganwadis by using simple random sampling method. The finding of the study
revealed that 12% of mothers had good knowledge, 40% of mothers had average
knowledge and 48% of mothers had below average knowledge regarding
immunization. The total mean percentage of mothers knowledge regarding
immunization is (69.12%). There was statistically significant effect of age,
qualification, occupation of mother, family income in rupees, religion, number of
children and source of information on knowledge regarding immunization. So the
study concluded that the level of knowledge vary according to different demographic
variables.28
A non experimental study was conducted to assess the knowledge regarding
immunization among mothers of under five children and prepare health education
programme regarding immunization at Kunderki U.P. India. The mothers of under
five children were selected as sample by using convenient sampling technique. The

19
sample size was 30. The result shows that good knowledge score is 10%, average
knowledge score is 23.34% and poor knowledge score is 66.66%. The study
concluded that the mothers of under five having poor knowledge of immunization.29
A descriptive and non experimental study was conducted to assess the
knowledge regarding immunization among mothers of under five children admitted in
pediatric ward of Prabhakar Kore Hospital, Belagavi, Belgaum with the aim to
develop educational pamphlet. The study was conducted on 50 mothers of under five
children and they were selected by convenient sampling technique. The results
showed that majority of 34 (68%) of mothers of under five children had an average
knowledge regarding immunization, 9 (18%) of mothers had good knowledge and
minimal 7(14%) had poor knowledge. The study concluded that mothers knowledge
regarding immunization is essential for timely utilization of immunization services as
it isthe most cost effective measure to prevent vaccine preventable diseases.30
A non-experimental exploratory study was conducted to assess the knowledge
of mothers of under five children on immunization with a view to develop a
information booklet. The sample comprised of 30 mothers of under five children, who
visited Yenepoya hospital, Mangalore. The study result shows that 30% of mothers
had poor knowledge, 43.4% of mothers had average knowledge, 23.4% of mothers
had good knowledge and 3.33% mothers had excellent knowledge. There is no
significant association between knowledge score and selected demographic variables.
There was a significant association between knowledge and exposure to mass media
in relation to immunization among mothers of under five children.31
Literature related to knowledge and attitude regarding immunization
A survey study was conducted to assess the knowledge and attitude of mothers
towards childhood immunization in Bauchi Local Government, Nizeria.Data was
collected from 322 mothers by in-depth interview schedule. The finding of the study
revealed that the level of mothers’ education relates to their knowledge and tend to
encourage childhood immunization. The study recommends that Government should
employ more health officials, such as nurses to meet the WHO health staff ratio of
one nurse for four patients. There is need to remove all cultural impediments that
prevent women from immunization by empowering them with decision making at

20
home. The study believed that there is the need to encourage women or girl child
education as well as to educating husbands, parents and community leaders on the
dangers associated with lack of immunization especially of the mentioned five killer
diseases.32
A qualitative study was conducted to assess the knowledge, attitude and
perception about routine childhood vaccination among Jewish Ultra-Orthodox
mothers residing in communities with low vaccination coverage in the Jerusalem
district. The study was conducted among mothers and sampling technique used was
focus groups and semi-structured interview. The sample size was 87. The study result
shows that vaccination delay was very common and timeliness was considered
insignificant. Overall there was a sense of self-responsibility accompanied by inability
to influence others. The study concluded that investigating maternal knowledge and
attitudes on childhood immunization provides insights that may insist in planning
tailored intervention programs aimed to increase both vaccination coverage and
timeliness. 33
An institutional based cross sectional study was conducted from March 1st to
April 1st, 2013 to assess knowledge, attitude, and practice of mothers towards
immunization of infants and their associated factors in immunization clinic in health
centers at Addis Ababa, Ethiopia. The study results revealed that only 55.0%, 53.8%
and 84% of respondents had good knowledge, positive attitude and good practice
towards immunization of infants. Good immunization practice was significantly
associated with mothers who heard information about vaccination, mothers who know
the time of starting and completion of immunization, know the number of sessions
needed and place of delivery. The study concluded that knowledge and attitude of
mothers’ about infant vaccination was not adequate. Despite of inadequate knowledge
and attitude of mothers towards infant immunization, 84.0%of mothers found to have
good practice of immunization.34
A cross-sectional survey study was conducted to assess the knowledge,
attitude and practice of mothers’ towards children obligatory vaccination at Damietta
Governorate, Egypt. The sample size was 1050 mothers (210 from 5 districts) and
they were selected randomly according to availability of household list. Four
structured interviewing sheets were used to assess the data. The results revealed that

21
there was a statistically significant correlation between knowledge and practice of the
studied mothers. The study concluded that less than half of the studied mothers had
poor knowledge score while less than one third had good score, more than two thirds
of the studied mothers had good attitude score while the minority had poor attitude
score and more than one third of mothers had good practice while one quarter had
poor practice.35
A study was conducted to assess the knowledge, attitude and practice of
mothers as regards immunization and the influence of socio demographic
characteristics on immunizable children in Jos North, Nigeria. The study was
conducted among 232mothers with children born between 26th
September 2011 and
26th
September 2012 .The study showed only 2.6% had excellent knowledge on
vaccine preventable diseases, 89.6% had an overall good knowledge while5.2% each
had fair and poor knowledge. The education of mother, marital status, religion,
geographical zone and her and/ of the father of the child been immunized as children
significantly influenced their knowledge (p<0.05). The study concluded that proper
health education and health promotion intervention has to be taken as measures to
improve knowledge, attitude and practice of mothers towards immunization.36
A mixed method study was conducted to evaluate the correlation between
parental knowledge-practices and children’s immunization completeness in Mosul,
Iraq. A retrospective cohort study and a prospective cross sectional study was used.
528 children born between 1 January 2003 and 31June 2008 were randomly selected
from public health clinic. Immunization history of each child was collected
retrospectively from their immunization record/card. The results of study indicate that
about half of studied 286 (56.3%) were immunized with all vaccination doses; these
children were considered as having had complete immunization. 66.1% of the parents
was found to have adequate knowledge and practice scores. A significant association
of immunization completeness with total knowledge and practice groups (p<0.05) was
found. The study concluded that future efforts are required to improve immunization
rate and parents’ knowledge and practice.37
A study was conducted to determine the knowledge, attitude and practice of
mothers regarding their understanding of immunization in rural areas in and around
Pondicherry. The study was conducted among 501 mothers of children from 0-5 years

22
of age. The results shows that majority of children (62.6%) included in the study were
born at Aarupadai Veedu Medical College and Hospital and 100% immunization
coverage upto 18 months were recorded for all those children. The knowledge and
awareness of antenatal vaccination is approximately 70-80% of the mothers, 30% of
mothers are not aware that immunization can be done during minor ailments and after
minor adverse reactions. The study concluded that health professional play a major
role in creating both immunization awareness and administration in prescribed date to
mothers.38
A descriptive cross sectional study was conducted to assess the knowledge and
practice of mothers regarding childhood immunization compliant with immunization
completeness in Aurangabad, Maharashtra, India. The study was conducted among
364 mothers attending immunization OPD in Government Medical College during
September to December2015. The results shows that 78.5% children were completely
immunized as per date. 57.97% of the study population was found to have adequate
knowledge-practice scores. A significant association of immunization completeness
with knowledge-practice scores of mothers (p<0.05) was found. It is concluded that
future efforts are required to improve immunization rate and parents’knowledge and
practice.39
A cross-sectional study was conducted to assess the knowledge, attitude and
practice of mothers of under five children regarding immunization in a selected
community, Rishikesh, Uttarakhand. Total 50 subjects were assessed by using semi
structured questionnaire. The result revealed majority 40 (80%) of the under five
children are partially immunized. Majority 25(50%) had moderately adequate
knowledge and 45(90%) have favorable attitude towards immunization. Majority
44(88%) had poor practice whereas 6(12%) demonstrated good practice. There was
significant association between subjectslevel’ of knowledge and attitude while no
association was found between knowledge and practice of mothers of under five
children. The study concluded that it is very clear that the partial vaccination among
under five children in Uttarakhant, India warrant special attention.40
A cross-sectional survey study was conducted to survey mothers’ knowledge
and attitude towards childhood immunization and then determine if these variables
correlate with the timely vaccination coverage of their children in Rural Uganda from

23
September to December 2013. The sample size was 302 women having one child
between 1 month and 5 years from rural Sheema district. The study finding shows that
88% of the children received age-appropriate on time immunization, 93.5%of the
women were able to state that childhood immunizations protect children from
diseases. The study concluded that the factors influencing caregivers’ demand for
childhood immunization vary widely between, and also within, developing
countries.41
A prospective cross-sectional study was carried out for assessment of parents’
knowledge, attitude and practice about child vaccination in Rural areas of Bangalore.
110 parents of under five children were selected and data was collected by using
structured questionnaire. The results shows that a majority of them (72.7%) had good,
(21.8%) had average and (5.4%) had poor knowledge whereas 85.4% of the
respondent were found to have good attitude towards child immunization. 68.1%
children were completely immunized, 7.2% receive incomplete immunization and
remaining 24.5% was uncertain. A very significant correlation was seen between the
parental knowledge and attitude score with p<_0.0001. The study concluded that the
parental knowledge, attitude and practice about child vaccination are important
determinants of the immunization status of their child.42
A descriptive study was conducted to assess the knowledge and attitude on
immunization among the mothers of under five children, Halaga village, Belgaum,
Karnataka. 50 mothers of under five children were selected by convenient and
purposive sampling. The result reveals that mean knowledge value on immunization
of mothers of under five children was 58.1 and attitude score was 41.4. The
correlation between knowledge on immunization and attitude of mothers showed that
there is a positive correlation between knowledge on immunization and attitude
(r=0.483). The study concluded that the mothers of under five children of rural
community area had moderately adequate knowledge on immunization and moderate
positive attitude towards immunization. These findings reveal that the community
health nurses should make little efforts in educating the mothers so as to achieve
100% immunization.43
A cross-sectional survey was conducted to determine the knowledge,
attitude and practice of parents regarding childhood immunization in immunization

24
clinic at Vanivilas hospital, attached to Bangalore Medical College and Research
Institute and a private pediatric clinic in Bengaluru. Data were collected from 200
parents/ guardians (100 from each set up) using structured questionnaire. The result
showed that 172(86%) children were fully immunized. Knowledge (p<0.004) and
practice (p<0.001) of parents opting for optional vaccines were significantly higher in
private setting compared to the government setting. The study concluded that
although childhood immunization practices and attitudes are satisfactory, majority
donot have specific knowledge on vaccines and the duration of protection they offer.
Socio-demographic factors had a significant influence on the immunization status.44
A cross sectional descriptive study was carried out to assess the knowledge,
attitude and perception of mothers with children under five years of age about
vaccination in Mangalore, India. 200 mothers of under five children were selected
from Urban Health centre (74) and a peripheral Health Centre in Bengre (126) and a
semi structured pre validated questionnaire was used to collect data. The results
revealed that around 8 (10.8%) from urban area and 78 (61.9%) from rural area were
illiterate. On a net analysis, 64(86.5%) mothers in the urban area and only 64(50.8%)
mothers in the rural area are found to have favorable knowledge, attitudes,
perceptions and practices towards vaccination. The study concluded that a significant
number of mothers in rural areas were unaware about the vaccination and its
implications and even in the urban areas, there was lacunae in the knowledge, attitude
and perception of mothers towards childhood vaccination.45
Literature related to effectiveness of educational progrommeon immunization
A cross-sectional study was conducted to assess parents’ knowledge and to
evaluate the effect of a short educational intervention on improving parents’
knowledge of childhood immunization. 73 Malaysian parents were enrolled in this
study and changes in total knowledge score before and after the intervention were
measured using a validated questionnaire. The result shows that the majority were
mothers (n=64, 8.7%).Parents’ knowledge about childhood immunization increased
significantly after the intervention compared to the baseline results (p<0.001). There
were significant differences between parents’ knowledge and their educational level
and monthly income (p<0.001 and p=0.005), respectively. The study concluded that a

25
short educational intervention desiagned for parents’ had a positive effect on their
knowledge about immunization.46
A quasi experimental study was conducted to assess the effectiveness of health
teaching programme on knowledge regarding immunization among mothers of under
five children in selected communitysetting, Aurangabad. 40 mothers of under five
children were selected by purposive sampling technique. The study result shows that
the overall pre-test mean knowledge score was found to be14.675 and SD as 4.226.
And the overall post-test mean knowledge score was found to be 21.800 and SD as
4.207. Paired t-test shows statistical significance at 5 per cent level (p<0.05)
establishing the impact of planned teaching on knowledge regarding immunization
among mothers of under five children. The study concluded that post-test mean
knowledge score of mothers indicated significant difference which is a net benefit to
the mothers due to the effectiveness of health teaching program.47
Literature related to immunization programme.
A study was carried out to assess the awareness of mothers about the new
vaccines introduced in the childhood vaccination programme in Delhi State. Total
samples of 388 mothers were interviewed in the immunization clinic of a tertiary care
hospital. The result shows that only 18.3% of the participants were aware that newer
vaccines have been introduced into the programme. 48. 2% of the respondents were
unaware about the same, while 33.5% claimed to have heard about it but were not
sure whether newer vaccines had been introduced. It was observed that as the
education status of mothers improved, their awareness regarding newer vaccines in
the programme also increased. The study concluded that there is a requirement of
focused publicity campaign to increase the awareness and thereby uptake of the new
vaccine among caregiver.48
An one year prospective cross sectional study was carried out to study the
knowledge regarding immunization schedule among parents and the source of
information regarding vaccination. Data were collected from parents of 240 children
admitted in Pediatric ward of Kamla Nehru hospital, Gandhi Medical College,
Bhopal. The study results shows that the highest incidence was of TB 47.92%
followed by tetanus, measles, diphtheria and neotetanus. The incidences of vaccine
preventable diseases were higher among unvaccinated child as compared to

26
vaccinated child except tuberculosis where vaccination rate was higher (52.17). All
vaccine preventable diseases were much common in illiterate fathers and mothers.
The study concluded that there is need to increase awareness and knowledge about the
benefits and importance of vaccination, as well as the harmful consequences of non
complete immunization.49
A descriptive studywas conducted to assess the knowledge and attitude
regarding national vaccine programme among mothers of under five in selected
hospital Mangalore. The sample size consists of 300 mothers. The study result shows
that 289 (96.33%) mothers knew that BCG vaccine prevents Tuberculosis .Only
26(8.66%) mothers were knowledgeable about the measures that can be done if the
child has not given DPT. 11 (3.66%) mothers knew that chicken pox can be prevented
by varicella vaccine. The study concluded that even though the mothers had good
attitude regarding vaccines but they were unaware of Hib vaccine and rotavirus
vaccine and awareness should be created among mothers.50

27
METHODOLOGY
Research methodology is a systematic way to solve the research problems. It
is of vital importance which consists of the various steps that are generally adopted by
a researcher in studying the problem along with the logic behind them. The
methodology of the researcher indicates the general pattern of organizing the
procedure for gathering valid and reliable data for the purpose of the study.
This chapter deals with research approach, research designs, variables, setting
of study, population, sample, criteria for sample selection, sampling technique,
sampling criteria, tool for data collection, validity and reliability, pilot study, method
of data analysis, interpretation and ethical consideration.
Research approach
Research approachindicates the basic procedure for conductingthe research.
Quantitative research approach was used to assess the effectiveness of educational
package on level of knowledge and attitude regarding Mission Indradhanush among
mothers of under five children .
Research design
Quasi experimental one group pre- test and post- test design.23
Pre- test (O1) Intervention (X) Post- test (O2)
Assess pre-test level of
knowledge and attitude
regarding Mission
Indradhanush among
mothers of under five
children through
structured interview
schedule and Likert scale.
Educational package
regardingMission
Indradhanush among
mothers of under five
children by using flash
cards, pamphlets and
leaflets for duration of 45
minutes.
Assess post-test level of
knowledge and attitude
regarding Mission
Indradhanush among
mothers of under five
children through
structured interview
schedule and Likert scale.

28
Figure No. 2: Schematic representation of research plan.
Research design: Quasi experimental one group pre- test post- test design.
Study setting: Kengeri Upanagar urban slum area, Bengaluru.
Population: All the mothers having under five years children in Kengeri Upanagar urban slum area.
Sample size: 60 mothers.
Sampling technique: Simple Random Sampling technique.
Independent variables:
Educational package regarding
Mission Indradhanush
Dependent variables Knowledge
and attitude regarding Mission
Indradhanush
Tool for data collection:
Structured interview schedule and Likert scale
Method of data collection:
1.Informed consent 2. Pre test 3. Educational package 4. Post- test
Data analysis: Descriptive and Inferential statistics
Findings and conclusion
Statement of the problem: A quasi experimental study to assess the effectiveness of
educational package on level of knowledge and attitude regarding Mission Indradhanush
among mothers of under five children in selected urban slum area, Bengaluru.

29
Research variables
Variables are an attributes of a person that varies and takes on different values.
Independent variables
Educational Package on level of knowledge and attitude regarding Mission
Indradhanush.
Dependent variables
Knowledge and attitude regarding Mission Indradhanush among mothers of
under five children.
Demographic variables
Baseline information of motherssuch as age,religion, educational status, occupation,
family income per month, type of family, number of children, immunization status
of children, previous knowledge regarding Mission Indradhanushand sources of
information.
Setting
The study was conducted in Kengeri Upanagar urban slum area, Bengaluru
and the setting was selected according to geographic proximity, feasibility and
availability of the sample.
Population
In this study, population comprised of all the mothers of under five children in
Kengeri Upanagar urban slum area, Bengaluru.
Sample
Mothers of under five children who fulfilled the inclusion criteria were the
samples and the sample size was 60.
Criteria for sample collection
Inclusion criteria
The study includes
1. Mothers having children below five years.
2. Mothers of under five children who can understand Kannada or English.
3. Mothers who are residing in Kengeri Upanagar urban slum area, Bengaluru.

30
Exclusion criteria
The study excludes
1. Mothers of under five children who are not available at the time of data
collection.
2. Mothers of under five children who are not willing to participate in the study.
Sampling technique
The sampling technique adopted for the study was Simple Random Sampling
technique.
Development and description of tool
The tools were prepared on the basis of objectives of the study, by taking
suggestion from the guide, by consulting 6 nursing experts, one biostatistician and one
medical officer. Under the guidance of the guide, final tools were prepared. The tools
consist of 3 sections, Section A consists of structured interview schedule regarding
demographic variables, Section B cons ists of structured interview schedule to assess
the knowledge regarding Mission Indradhanush and Section C consists of 3 points
Likert attitude scale to assess the attitude of mothers regarding Mission Indradhanush.
The following steps were carried out while preparing the tool
1. Review of literature
2. Based on experts opinion
3. Researcher’s personal opinion.
Tools for data collection
The tool consists of the following sections:
Section A
It includes demographic variables which give base line information of mothers
such as age, religion, educational status, occupation, family income per month, type
of family, number of children, immunization status of children, previous
informatiomregarding Mission Indradhanush and sources of information.

31
Section B
Structured interview schedule was used to assess the level of knowledge
regarding Mission Indradhanush among mothers of under five children.
Scoring interpretation
Scoring key was prepared for section B, score ‘1’ was awarded to correct
response and ‘0’ for wrong response in all items. Thus a score of 22 were allotted to
interpret the level of knowledge among mothers of under five children, the scores
were categorized as
1. Inadequate knowledge -<50%
2. Moderate knowledge-50-75%
3. Adequate knowledge- > 75%
Section C
3 points Likert attitude scale was used to assess the attitude of mothers of
under five children regarding Mission Indradhanush.
In section C, for positive questions, score of 3 for agree, score of 2 for
uncertain and score of 1 for disagree, for negative questions, score of 3 for disagree,
score of 2 for uncertain and score of 1 for agree. Thus a total score of 42 were allotted
to interpret the level of attitude among mothers of under five children, the scores were
categorized as
1. Unfavorable attitude -<50%
2. Neutral attitude -50-75%
3. Favorable attitude- >%75%
Development of educational package
The first draft of educational package was developed on the basis of
information obtained during extensive literature review and objectives in the blue
print. The entire content was prepared as a lesson plan. The content was given to 8
experts and modifications were made according to their suggestions and the content
was finalized.

32
Preparation of final draft of educational package
Preparation of final draft was done after incorporating the expert’s opinion and
suggestions. The content was prepared in English and Kannada in the form of lesson
plan and A.V aids. The average time taken to teach on Mission Indradhanush among
mothers of under five children by using A.V aids was 45 minutes duration.
Content validity
The first draft of educational package was based on the objective of the study
and was given to 6 nursing expert in the field of community health nursing, 1 expert
in the field of community medicine and 1 expert in the field of Statistics. The experts
were requested to give their opinion and suggestions regarding the relevance of the
tool for medications to improve the clarity and contents of the items. The tool
consisted of 22 items on knowledge and 14 statements on attitude, comprehension and
application domain, in all items were agreed upon with the suggestions. The final tool
was incorporated with the expert suggestions and opinion.
Reliability
In order to establish reliability of the tool, the test split half method was used.
The calculated “r” value was 0.87 for knowledge and 0.95 for the attitude and the
developed tool was found to be reliable.
Formula
r =� �� ∑���������
∑�� ���∑�� ���
r1
= 2r/1-r
Pilot study
Pilot study is a small version or trial run done in preparation for major study.
The pilot study was conducted in the month of January,2018 for 1 week in Gandhi
gram urban slum area Bengaluru. An administrative approval was obtained from the
Medical Officer of Health and Family Welfare,Gandhi Gram urban health centre,
BMP, Bengaluruto conduct the study. On the first day, the existing level of
knowledge and attitude regarding Mission Indradhanush was assessed with the help of
structured interview schedule and Likert scale respectively. On the same day the
educational package was administered by using flash cards, pamphlets and leaflets for

33
45 minutes. After a period of 7 days of educational package, post-test knowledge and
attitude was assessed by using same structured Interview schedule and Likert scale.
The purpose of the pilot study was to find out the feasibility of conducting the study.
There was significant improvement in the post-test knowledge and attitude
regarding Mission Indradhanush among mothers of under five children. The subjects
expressed their desire to learn and the pilot study revealed that tool was feasible and
appropriate to conduct the main study.
Procedure for data collection
After obtaining the official permission from Medical Officer of Kengeri
Upanagar urban health centre, and written consent obtained from the samples, the
investigator conducted the main study among 60 mothers of under five children who
were selected by simple random sampling technique method and the data was
collected in the month of February 2018 for 4 weeks. The investigator personally
collected the data in the following phase.
Phase I
On the first day, the existing knowledge and attitude regarding Mission
Indradhanush among mothers of under five children was assessed with the help of
structured interview schedule and 3 point Likert scale.
Phase II
On the same day, educational package was given to mothers of under five
children regarding Mission Indradhanush by using flash cards, pamphlets and leaflets
for 45minutes.
Phase III
After a period of 7 days of educational package, post- test level of knowledge
and attitude regarding Mission Indradhanush was assessed by using the same
structured interview schedule and 3 point Likert scale.
Data Analysis
The data was collected and analysed by using descriptive and inferential statistics:

34
Descriptive statistics
1. Frequency and Percentage distribution are used to assess the demographic
variables.
2. Range, Mean and Standard deviation were used to describe pre- test and post-
test level of knowledge and attitude regarding Mission Indradhanush among
mothres of under five children.
3. Correlation co-efficient was used to correlate the correlation between
knowledge and attitude regarding Mission Indradhanush.
Inferential statistics
1. Paired t-test was used to compare pre and post -test knowledge and attitude
regarding Mission Indradhanush amongmothres of under five children.
2. Chi-square test was used to determine the association between the pre- test
level of knowledge and attitude regarding Mission Indradhanush with their
selected demographic variables.
Ethical consideration
1. Formal permission was obtained from the Medical Officer Kengeri Upanagar
Urban Health Centre, Bengaluru.
2. Written consent was obtained from the study samples.
3. The subjects were informed that confidentiality of the data will be maintained
4. The subjects were informed that their participation was on voluntary basis
and can withdraw from the study anytime
5. No ethical issues arose during the study.

35
RESULTS
Organization of study findings
Analysis is the process of evaluating data using analytical and logical
reasoning to examine each component of the data provided.51
This chapter provides
the analysis and interpretation of data collected from the mothers of under five
children in Kengeri Upanagar Urban Slum area, Bengaluru. The data was analysed by
using descriptive and inferential statistics.
The substantive summary of the analysis was under the following sections
Section 1: Description of demographic variables of mothers of under five
children.
Table1.1: Frequency and percentage distribution of demographic variables of the
mothers of under five children according to age, religion, educational
status and occupation.
Table 1.2: Frequency and percentage distribution of demographic variables of the
mothers of under five children according to family income per month in
rupees, type of family, number of children, immunization status of children,
previous information regarding Misssion Indradhanush and the sources of
information.
Section 2: Assessment of pre -test level of knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
Table 2.1: Frequency and percentage distribution of pre-test level of knowledge
regarding Mission Indradhanush among mothers of under five children.
Table 2.2: Range, Mean, Standard deviation and Mean percentage of pre-test level of
knowledge regarding Mission Indradhanush among mothers of under five
children.
Table 2.3: Frequency and percentage distribution of pre-test level of attitude regarding
Mission Indradhanush among mothers of under five children.
Table 2.4: Range, Mean, Standard deviation and Mean percentage of pre-test level
of attitude regarding Mission Indradhanush among mothers of under five
children.

36
Section 3: Assessment of post- test level of knowledge and attitude regarding
Mission Indradhanush amongmothers of under five children.
Table 3.1: Frequency and percentage distribution of post- test level of knowledge
regarding Mission Indradhanush among mothers of under five children.
Table 3.2: Range, Mean, Standard Deviation and Mean percentage of post- test level
of knowledge regarding Mission Indradhanush among mothers of under
five children.
Table 3.3: Frequency and percentage distribution of post- test level of attitude
regarding Mission Indradhanush among mothers of under five children.
Table 3.4: Range, Mean, Standard deviation and Mean percentage of post-test level of
attitude regarding Mission Indradhanush among mothers of under five
children.
Section 4: Assessment of pre and post-test knowledge and attitude regarding
Mission Indradhanush amongmothers of under five children.
Table 4.1: Frequency and percentage distribution of mothers according to pre and
post- test knowledge regarding Mission Indradhanush.
Table 4.2: Range, Mean, Standard deviation and Mean percentage of pre and post-test
knowledge regarding Mission Indradhanush among mothers of under five
children.
Table 4.3: Frequency and percentage distribution of mothers according to pre and
post-test attitude regarding Mission Indradhanush.
Table 4.4: Range, Mean, Standard Deviation and Mean percentage of pre and post-
test attitude regarding Mission Indradhanush among mothers of under five
children.
Section 5: Effectiveness of educational package on level of knowledge and
attitude regarding Mission Indradhanush among mothers of under
five children.

37
Table 5.1: Paired t-test analysis for the significance of pre and post-test knowledge
and attituderegarding Mission Indradhanush among mothers of under five
children.
Section 6: Assessment of correlation between the pre-test level of knowledge and
attitude regarding Mission Indradhanush among mothers of under
five children.
Table 6.1: Correlation between the pre-test knowledge and attitude regarding Mission
Indradhanush among mothers of under five children.
Section 7: Association between pre- test level of knowledge and attitude
regarding Mission Indradhanush with selected demographic
variables.
Table 7.1: Association between pre- test level of knowledge regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables such as age in years, religion and educational status.
Table 7.2: Association between pre- test level of knowledge regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables such as occupation, family income per month, type
of family, number of children, immunization status of children, previous
information regarding Mission Indradhanush and sources of information.
Table 7.3: Association between pre-test level of attitude regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables such as age in years, religion and educational
status.
Table 7.4: Association between pre-test level of attitude regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables such as family income per month, type of family,
number of children, immunization status of children, previous
information regarding Mission Indradhanush and sources of information.

38
Section 1: Description of demographic variables of mothers of under five
children
Table1.1: Frequency and percentage distribution of demographic variables of
mothers according to age, religion, educational status and
occupation.
n=60
SL.NO DemographicVariables Frequency Percentage
1 Age in years
a. 20 years and below 6 10.0
b.21-25 years 28 46.7
c. 26-30 years 18 30.0
d. 31years and above 8 13.3
2 Religion
a.Hindu 42 70.0
b. Christian 3 5.0
c.Muslim 12 20.0
d.Others 3 5.0
3 Educational status
a. No formal education 2 3.3
b. Primary education 15 25.0
c. Secondary education 11 18.3
d. Higher secondary education 21 35.0
e. Graduation and above 11 18.3
4
Occupation
a.Home maker 23 38.3
b.Daily wager 17 28.3
c.Self employed 11 18.3
d.Government employee 2 3.3
e.Private employee 6 10.0
f.Others 1 1.7
Table 1.1 shows the frequency and percentage distribution of selected
demographic variables of mothers of under five children as age in years, religion,
educational status and occupation.
With regards to age, 10.0% (6) mothers were 20 years and below, 46.7% (28)
were 21 -25 years, 30.0% (18) were 26-30 years and 13.3% (8) were 31 years and
above. With respect to religion, 70.0% (42) mothers belong to Hindu religion, 5.0%

39
(3) mothers belong to Christian religion, 20.0% (12) belong to Muslim religion and
5.0% (3) belong to other religion. With regards to educational status of mothers, 3.3%
(2) had no formal education, 25.0% (15) had primary education, 18.3% (11) had
secondary education, 35.0% (21) had higher secondary education and 18.3% (11) had
graduation and above level of education. With regards to occupation of mothers,
38.3% (23) were homemaker, 28.3% (17) were daily wager, 18.3% (11) were self-
employed, 3.3% (2) were government employee, 10% (6) were private employee and
1.7% (1) was other occupations.

40
Table1.2: Frequency and percentage distribution of demographic variables of
the mothers according to occupation, family income per month in
rupees, type of family, number of children, immunization status of the
children, previous information about Mission Indradhanush and the
sources of information.
n=60
Sl. No DemographicVariables Frequency Percentage
5 Family income (rupees/month)
a.≤10,000 37 61.7
b.10,001-15,000 16 26.7
c.15001 and above 7 11.7
6 Type of family
a. Nuclear family 17 28.3
b. Joint family 38 63.3
c. Extended family 5 8.3
7 Number of children
a. 1 27 45.0
b. 2 22 36.7
c. 3 or more 11 18.3
8 Immunization status of children
a. Fully immunized 42 70.0
b. Partially immunized 15 25.0
c. Drop out 3 5.0
9 Have you heard about Mission Indradhanush?
a. Yes 24 40.0
b. No 36 60.0
If yes, specify the sources of information (n=24)
a. Health personal 13 54.2
b. Family member 5 20.8
c. Friends - -
d. Mass media 6 25.0
The above table shows the frequency and percentage distribution of selected
demographic variables of mothers of under five children according to family income
per month in rupees, type of family, number of children, immunization status of
children, knowledge about Mission Indradhanush and sources of information.
With regards to family income per month in rupees, 61.7.% (37) had an
income of ≤ 10,000 per month, 26.7% (16) had an income of 10,001-15,000 per
month, and 11.7 % (7) had an income of 15,001 and above per month .With regards

41
to type of family, 28.3% (17) belongs to nuclear family, 63.3% (38) belongs to joint
family and 8.3% (5) belongs to extended family.With regards to number of children
45% (27) had one child, 36.7% (22) had two children and 18.3% (11) had three or
more children. With regards to immunization status of the children 70.0% (42) were
fully immunized, 25.0% (15) were partially immunized and 5.0% (3) were drop out.
With regards to previous knowledge about Mission Indradhanush 40.0% (24) have
heard about Mission Indradhanush and 60.0% (36) have not heard about Mission
Indradhanush. With regards to source of information, 54.2% (13) heard about Mission
Indradhanush through health personnel, 20.8% (5) heard from family members and
25% (6) heard through mass media.

42
Graph 1: Percentage distribution of mothers of under five children according to
age
Graph 2: Percentage distribution of mothers of under five children according to
religion.
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Below 20
years
21-25 years 26-30 years 31 and
above
10.0%
46.7%
30.0%
13.3%
Per
cen
tage
Age in years
0%
10%
20%
30%
40%
50%
60%
70%
80%
Hindu Christian Muslim Others
70.0%
5.0%
20.0%
5.0%
Per
cen
tage
Religion

43
Graph 3: Percentage distribution of mothers of under five children according to
educational status.
Graph 4: Percentage distribution of mothers of under five children according to
occupation
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
No formal
Education
Primary
Education
Secondary
Education
Higher
Secondary Education
Graduation
and Above
3.3%
25.0%
18.3%
35.0%
18.3%
Per
cen
tage
Educational status
0%5%
10%15%20%25%30%35%40%
38.3%
28.3%
18.3%
3.3%
10.0%
1.7%
Per
cen
tage
Occupation

44
Graph 5: Percentage distribution of mothers of under five children according to
family income per month in rupees.
Graph 6: Percentage distribution of mothers of under five children according to
type of family.
0%
10%
20%
30%
40%
50%
60%
70%
61.7%
26.7%
11.7%
Per
cen
tage
Family income per month
0%
10%
20%
30%
40%
50%
60%
70%
Nuclear Joint Extended
28.3%
63.3%
8.3%Per
cen
tage
Type of family

45
Graph 7: Percentage distribution of mothers of under five children according to
number of children.
Graph 8: Percentage distribution of mothers of under five children according to
immunization status of children.
0%
10%
20%
30%
40%
50%
1 2 3 or above
45.0%
36.7%
18.3%
Per
cen
tage
Number of children
0%
10%
20%
30%
40%
50%
60%
70%
80%
Fully
Immunized
Partially
immunized
Drop out
70.0%
25.0%
5.0%
Per
cen
tage
Immunization status of children

46
Graph 9: Percentage distribution of mothers of under five children according to
previous information about Mission Indradhanush.
Graph 10: Percentage distribution of mothers of under five children according to
sources of information.
40.0%
60.0%
Have you heard about Mission Indradhanush?
Yes
No
0%
10%
20%
30%
40%
50%
60%
Health
personnel
Family
members
Friends Mass media
54.2%
20.8%
0%
25.0%
Per
cen
tage
Sources of information

47
Section 2: Assessment of pre- test level of knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
Table 2.1: Frequency and percentage distribution of pre-test level of knowledge
regarding Mission Indradhanush among mothers of under five
children.
n=60
SI. No
Pre-test level of knowledge Frequency Percentage
1. Inadequate knowledge (<50%) 45 75.0
2. Moderate knowledge (50-75%) 11 18.3
3. Adequate knowledge (>75%) 4 6.7
Total 60 100
The above table shows that in the pre- test, 75.0% (45) of mothers had
inadequate knowledge, 18.3% (11) had moderate knowledge and 6.7% (4) had
adequate knowledge.
Table 2.2: Range, Mean, Standard Deviation and Mean Percentage of pre- test
level of knowledge regarding Mission Indradhanush among mothers
of under five children.
n=60
Pre-test
knowledge Max. Score Range Mean SD Mean%
Over all 22 3-19 10.17 4.49 46.2%
The above table shows that in the pre-test, the range was 3- 19, mean was
10.17, SD was 4.49 and mean percentage was 46.2.

48
Table 2.3: Frequency and percentage distribution of pre-test level of attitude
regarding Mission Indradhanush among mothers of under five
children.
n=60
SI. No Post-test level of knowledge Frequency Percentage
1. Unfavorable attitude (<50%) - -
2. Neutral attitude (50-75%) 40 66.7
3. Favorable attitude (>75%) 20 33.3
Total 60 100
The above table shows that in the pre-test, 66.7% (40) of mothers had neutral
attitude and 33.3% (20) had favorable attitude.
Table 2.4: Range, Mean, Standard Deviation and Mean Percentage of pre-test
level of attitude regarding Mission Indradhanush among mothers of under five
children.
n=60
Pre-test
knowledge Max. Score Range Mean SD Mean%
Over all 42 27-36 30.58 2.39 72.8%
The above table shows that in the pre-test range was 27-36, mean was 30.58,
SD was 2.39 and mean percentage was 72.8%.

49
Section 3: Assessment of post- test level of knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
Table 3.1: Frequency and percentage distribution of the post-test level of
knowledge regarding Mission Indradhanush among mothers of
under five children.
n=60
SI. No Post-test level of knowledge F %
1. Inadequate knowledge (<50%) - -
2. Moderate knowledge (50-75%) 26 43.3
3. Adequate knowledge (>75%) 34 56.7
Total 60 100
The above table shows that in the post- test, 43.3% (26) of mothers had
developed moderate knowledge and 56.7% (34) of mothers developed adequate
knowledge.
Table 3.2: Range, Mean, Standard deviation and Mean percentage of the post-
test level of knowledge regarding Mission Indradhanush among
mothers of under five children.
n=60
Post-test
knowledge Max. Score Range Mean SD Mean%
Over all 22 11-22 17.00 3.36 77.3%
The above table shows that in the post- test, the range was 11-22, mean was
17.00, SD was 3.36 and mean percentage was 77.3%.
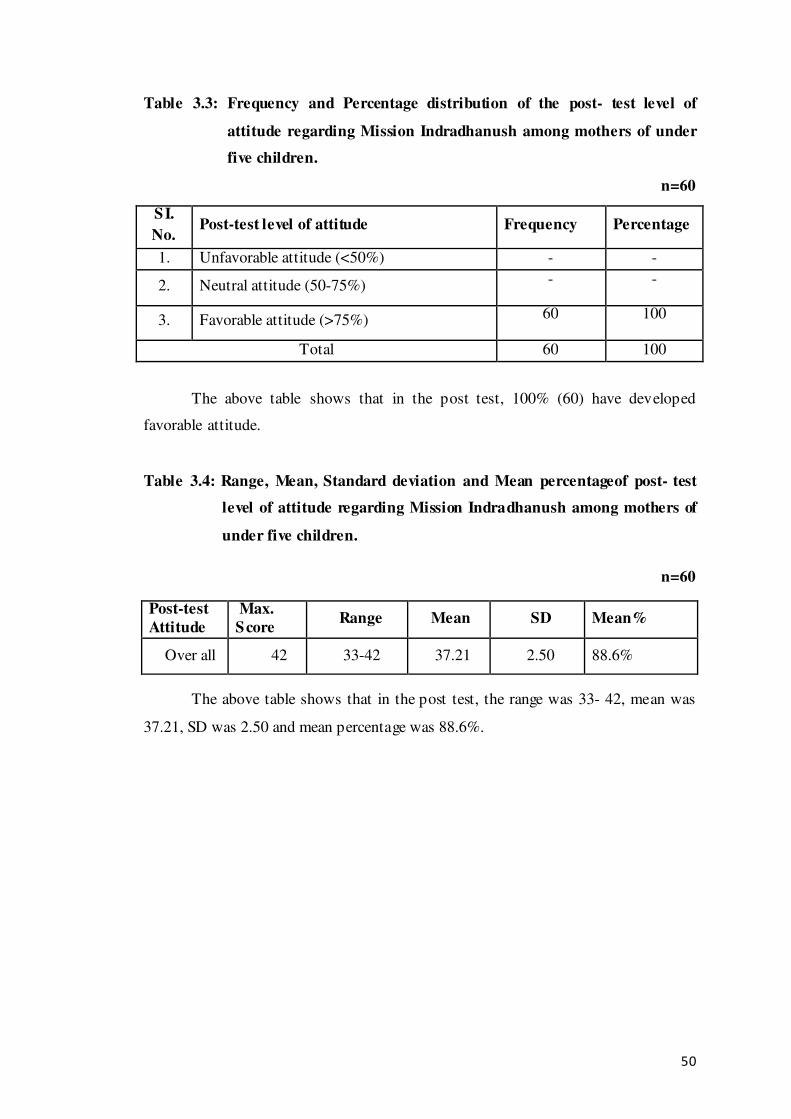
50
Table 3.3: Frequency and Percentage distribution of the post- test level of
attitude regarding Mission Indradhanush among mothers of under
five children.
n=60
SI.
No. Post-test level of attitude Frequency Percentage
1. Unfavorable attitude (<50%) - -
2. Neutral attitude (50-75%) - -
3. Favorable attitude (>75%) 60 100
Total 60 100
The above table shows that in the post test, 100% (60) have developed
favorable attitude.
Table 3.4: Range, Mean, Standard deviation and Mean percentageof post- test
level of attitude regarding Mission Indradhanush among mothers of
under five children.
n=60
Post-test
Attitude
Max.
Score Range Mean SD Mean%
Over all 42 33-42 37.21 2.50 88.6%
The above table shows that in the post test, the range was 33- 42, mean was
37.21, SD was 2.50 and mean percentage was 88.6%.

51
Section 4: Assessment of pre and post-test knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
Table 4.1: Frequency and Percentage distribution of mothers according to pre
and post- test level of knowledge regarding Mission Indradhanush.
n=60
SI.
No. Level of knowledge Pre-test Post-test
F % F %
1. Inadequate knowledge (<50%) 45 75.0 - -
2. Moderate knowledge (50-75%) 11 18.3 26 43.3
3. Adequate knowledge (>75%) 4 6.7 34 56.7
Total 60 100 60 100
The above table 4.1 presents the frequency and percentage distribution of
mothers according to level of knowledge before and after the educational package.
Majority of 75.0% (45) of the mothers had inadequate knowledge, 18.3% (11) had
moderate knowledge and 6.7% (4) had adequate knowledge before the educational
package but after educational package was administered, majority of 56.7% (34) of
mothers had developed adequate knowledge and 43.3% (26) developed moderate
knowledge.
Mothers of under five children according to level of knowledge before educational
package were within inadequate, moderate and adequate but after the educational
package, majority of them had developed adequate knowledge.
It evidenced that the educational package had shown the effect on improving
the level of knowledge regarding Mission Indradhanush among mothers of under five
children.

52
Graph 11: Percentage distribution of Mothers of under five children according
to pre and post-test level of knowledge regarding Mission
Indradhanush.
0.0%
20.0%
40.0%
60.0%
80.0%
Inadequate
knowledge
Moderate
knowledge
Adequate
knowledge
75.0%
18.3%
6.7%0%
43.3%
56.7%P
erce
nta
ge
Level of knowledge
Before
educational
package
After
awareness
package

53
Table 4.2: Range, Mean, SD and Mean percentage of pre and post -test level of
knowledge regarding Mission Indradhanush among mothers of under
five children n=60
SI.
No. Knowledge Max. Score Range Mean SD
Mean%
1. Pre test 22 3-19 10.17 4.49 46.2
2. Post test 22 11-22 17.00 3.36 77.3
The above table shows that in the pre- test range was 3-19, mean was 10.17,
SD was 4.49 and mean percentage was 46.2%. In the post- test, range was 11-22,
mean was 17.00, SD was 3.36 and mean percentage was 77.3%.
Table 4.3: Frequency and Percentage distribution of mothers of under five
children according to the pre and post-test level of attitude regarding
Mission Indradhanush.
n=60
SI. No.
Level of attitude Pre-test Post-test
F % F %
1. Unfavorable attitude (<50%) - - - -
2. Neutral attitude (50-75%) 40 66.7 - -
3. Favorable attitude (>75%) 20 33.3 60 100
Total 60 100 60 100
The above table presents the frequency and percentage distribution of mothers of
under five children according to level of attitude before and after the educational
package. 66.7% (40) of mothers had neutral attitude and 33.3% (20) had favorable
attitude before the educational package, but after the educational package, 100% (60)
of them had developed favorable attitude.
Mothers of under five children according to level of attitude before educational
package were within neutral attitude but after the educational package 100% of have
developed favorable attitude.
It evidenced that the educational package had shown the effect on improving
the level of attitude among mothers of under five children.

54
Graph 12: Percentage distribution of mothers of under five children according to
pre and post-test level of attitude regarding Mission Indradhanush.
Table 4.4: Range, Mean, SD and Mean percentage of pre and post -test level of
attitude regarding Mission Indradhanush among mothers of under
five children.
n=60
SI. No Attitude Max.
Score Range Mean SD Mean%
1. Pre-test 42 27-36 30.58 2.39 72.8%
2. Post-test 42 33-42 37.21 2.50 88.6%
The above table shows that in the pre- test, range was 27-36, mean was 30.58,
SD was 2.39 and mean percentage was 72.8%. In the post test, range was 33-42, mean
was 37.21, SD was 2.50 and mean percentage was 88.6%.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Unfavourable
attitude
Moderate
attitude
Favourable
attitude
0.0%
66.7%
33.3%
0% .0%
100%
Per
cen
tage
Level of attitude
Before
educational
package
After
educational
package

55
Section 5: Effectiveness of educational package on level of knowledge and
attitude regarding Mission Indradhanush among mothers of under
five children.
Table 5.1: Paired t-test analysis for the significance of pre and post- test
knowledge and attitude regarding Mission Indradhanush among
mothers of under five children.
n=60
Sl.
no.
Variables
Max
score
Pre and post knowledge
difference Paired
t-value P-value
Mean
difference
SD of
difference
% of
increase
1. Knowledge 22 6.83 1.13 31.0 14.45* p<0.001
2. Attitude 42 6.63 0.11 15.7 11.16* p<0.001
Note: *- denotes significant ( p<0.001) for df = 59.
The above table depicts the outcome of paired t-test analysis carried over to
assess the significance of pre and post-test mean score of knowledge and attitude
regarding Mission Indradhanush among mothers of under five children. The paired t-
test was found to be significant to overall knowledge and attitude regarding Mission
Indradhanush.
It evidenced that there is a significant difference in knowledge and attitude
after the intervention of educational package.
Testing of hypothesis
H1-: There is a significant difference between the mean pre- test and post- test score
of knowledge and attitude regarding Mission Indradhanush among mothers of
under five children.
H01: There is no significant difference between the mean pre -test and post- test score
of knowledge and attitude regarding Mission Indradhanush among mothers of
under five children.
The table 5.1 represents the mean pre-test and post-test knowledge and attitude
regarding Mission Indradhanush among mothers of under five children respectively.
The paired t- test was carried out and it was found out significant at P<0.001 level,
hence reseaech hypothesis (H1) was accepted and the null hypothesis (H0) was
rejected. It provides evidence that the educational package was significantly effective
in improving the knowledge and attitude regarding Mission Indradhanush among
mothers of under five children.

56
Section 6: Assessment of correlation between pre-test knowledge and attitude
regarding Mission Indradhanush among mothers of under five
children.
Table 6.1: Correlation between the pre-test knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
n=60
Variables Mean SD r p-value
Knowledge 10.17 4.49 0.486*
p<0.05
Attitude 30.58 2.39
Note: *- Significant at 5% level (i.e., p<0.05)/NS-not significant at 5% level
(i.e,>0.05)
The above table 6.1 presents the correlation between knowledge and attitude
regarding Mission Indradhanush among mothers of under five children. The Karl
Pearson’s correlation was found to be (r=0.486) and it was found to be statistically
significant at p<0.05. It was evidenced that there was significant linear correlation
between knowledge and attitude ie., increase in knowledge bears the further increase
in attitude regarding Mission Indradhanush among mothers of under five children.
There was significant trend in increase of attitude with the increase in knowledge
through the regression model (Attitude = 27.29 +0.34 x Knowledge ). The R-square
was 0.24, which implied that chance of increase in attitude was by the influence of
24.0% increase of knowledge and remaining influence was due to other factors.
Testing of Hypothesis
In order to evaluate the correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children, the following
hypothesis were tested.
H2: There is a significant correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children
H02: There is no significant correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children

57
The above table 6.1 indicates that there positive correlation between
knowledge and attitude regarding Mission Indradhanush among mothers of under five
children at p<0.05 level hence, research hypothesis was accepted and null
hypothesis was rejected.
Graph 13: Assessment of correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.

58
Section 7: Association between pre-test level of knowledge and attitude with their
selected demographic variables.
Table 7.1: Association between pre- test level of knowledge regarding Mission
Indradhanush among mothers of under five children with their
selected demographic variables such as age in years, religion and
educational status
n=60
Sl.
No
Demographic
variables
Sample
(n=60)
Level of knowledge Chi-
square
value
p-value ≤ Median >Median
F % F % F %
1 Age in years
a. 20 years and below 6 10.0 5 14.3 1 4.0
8.759,
df=3,
S
p<0.05 b. 21-25 years 28 46.7 19 54.3 9 36.0
c. 26-30 years 18 30.0 9 25.7 9 36.0
d. 31 and above 8 13.3 2 5.7 6 24.0
2 Religion
a. Hindu 42 70.0 19 54.3 23 92.0
10.676,
df=3,
S
p<0.05 b. Christian 3 5.0 3 8.6 0 0
c. Muslim 12 20.0 11 31.4 1 4.0
d. Others 3 5.0 2 5.7 1 4.0
3 Educational status
a.Noformal education 2 3.3 2 5.7 0 0
18.801,
df=4, S p<0.05
b. Primary education 15 25.0 13 37.1 2 8.0
c.Secondary.education 11 18.3 8 22.9 3 12.0
d.Higher Secondary
education 21 35.0 11 31.4 10 40.0
e.Graduation
and above 11 18.3 1 2.9 10 40.0
Note: S-significant (p<0.05); NS-Not significant (p>0.05).
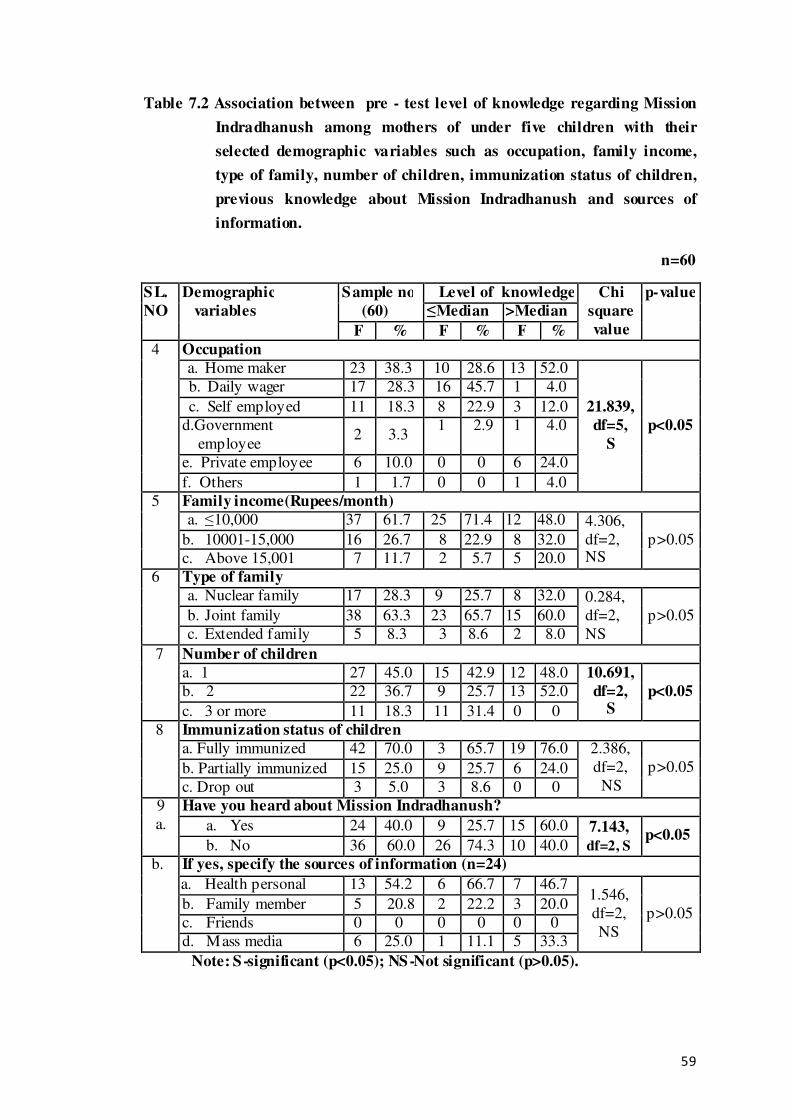
59
Table 7.2 Association between pre - test level of knowledge regarding Mission
Indradhanush among mothers of under five children with their
selected demographic variables such as occupation, family income,
type of family, number of children, immunization status of children,
previous knowledge about Mission Indradhanush and sources of
information.
n=60
SL.
NO
Demographic
variables
Sample no
(60)
Level of knowledge Chi
square
value
p-value
≤Median >Median
F % F % F %
4 Occupation
a. Home maker 23 38.3 10 28.6 13 52.0
21.839,
df=5,
S
p<0.05
b. Daily wager 17 28.3 16 45.7 1 4.0
c. Self employed 11 18.3 8 22.9 3 12.0
d.Government
employee 2 3.3
1 2.9 1 4.0
e. Private employee 6 10.0 0 0 6 24.0
f. Others 1 1.7 0 0 1 4.0
5 Family income(Rupees/month)
a. ≤10,000 37 61.7 25 71.4 12 48.0 4.306,
df=2, NS
p>0.05 b. 10001-15,000 16 26.7 8 22.9 8 32.0
c. Above 15,001 7 11.7 2 5.7 5 20.0
6 Type of family
a. Nuclear family 17 28.3 9 25.7 8 32.0 0.284,
df=2,
NS
p>0.05 b. Joint family 38 63.3 23 65.7 15 60.0
c. Extended family 5 8.3 3 8.6 2 8.0
7 Number of children
a. 1 27 45.0 15 42.9 12 48.0 10.691,
df=2, S
p<0.05 b. 2 22 36.7 9 25.7 13 52.0
c. 3 or more 11 18.3 11 31.4 0 0
8 Immunization status of children
a. Fully immunized 42 70.0 3 65.7 19 76.0 2.386,
df=2,
NS
p>0.05 b. Partially immunized 15 25.0 9 25.7 6 24.0
c. Drop out 3 5.0 3 8.6 0 0
9
a.
Have you heard about Mission Indradhanush?
a. Yes 24 40.0 9 25.7 15 60.0 7.143,
df=2, S p<0.05
b. No 36 60.0 26 74.3 10 40.0
b. If yes, specify the sources of information (n=24)
a. Health personal 13 54.2 6 66.7 7 46.7 1.546,
df=2,
NS
p>0.05 b. Family member 5 20.8 2 22.2 3 20.0
c. Friends 0 0 0 0 0 0
d. Mass media 6 25.0 1 11.1 5 33.3
Note: S-significant (p<0.05); NS-Not significant (p>0.05).

60
The table 7.1 and 7.2 envisages the outcome of chi square analysis being
carried out to bring out the association between the pre-test level of knowledge
regarding Mission Indradhanush among mothers of under five children with their
demographic variables. The categories such as age, religion, educational status,
occupation, family income, number of children, immunization status of the children,
previous information about Mission Indradhanush and the sources of information
were accounted for determining the association with knowledge. Out of which, age,
religion, education and occupation of mothers, family income, number of children and
previous information of the demographic variables of the mothers of under five
children were found significant with level of knowledge regarding Mission
Indradhanush.
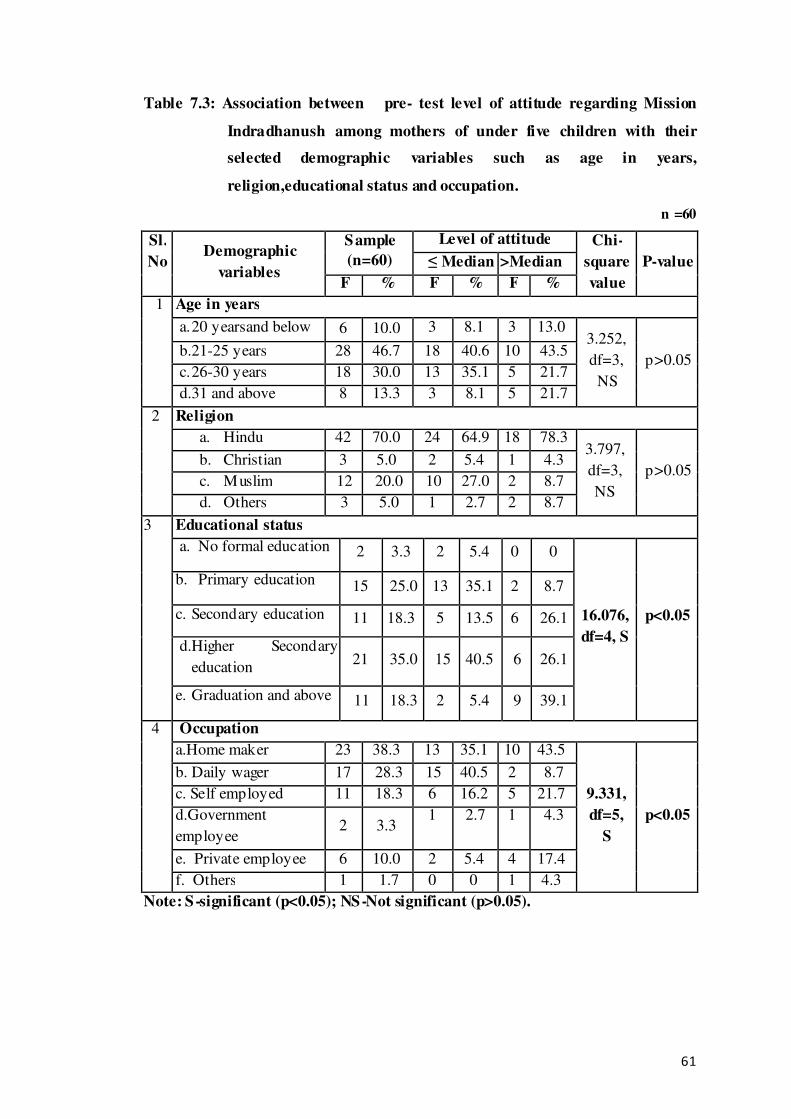
61
Table 7.3: Association between pre- test level of attitude regarding Mission
Indradhanush among mothers of under five children with their
selected demographic variables such as age in years,
religion,educational status and occupation.
n =60
Sl.
No
Demographic
variables
Sample
(n=60)
Level of attitude Chi-
square
value
P-value ≤ Median >Median
F % F % F %
1 Age in years
a. 20 yearsand below 6 10.0 3 8.1 3 13.0 3.252,
df=3,
NS
p>0.05 b.21-25 years 28 46.7 18 40.6 10 43.5
c. 26-30 years 18 30.0 13 35.1 5 21.7
d.31 and above 8 13.3 3 8.1 5 21.7
2 Religion
a. Hindu 42 70.0 24 64.9 18 78.3 3.797,
df=3,
NS
p>0.05 b. Christian 3 5.0 2 5.4 1 4.3
c. Muslim 12 20.0 10 27.0 2 8.7
d. Others 3 5.0 1 2.7 2 8.7
3 Educational status
a. No formal education 2 3.3 2 5.4 0 0
16.076,
df=4, S
p<0.05
b. Primary education 15 25.0 13 35.1 2 8.7
c. Secondary education 11 18.3 5 13.5 6 26.1
d.Higher Secondary
education 21 35.0 15 40.5 6 26.1
e. Graduation and above 11 18.3 2 5.4 9 39.1
4 Occupation
a.Home maker 23 38.3 13 35.1 10 43.5
9.331,
df=5,
S
p<0.05
b. Daily wager 17 28.3 15 40.5 2 8.7
c. Self employed 11 18.3 6 16.2 5 21.7
d.Government
employee 2 3.3
1 2.7 1 4.3
e. Private employee 6 10.0 2 5.4 4 17.4
f. Others 1 1.7 0 0 1 4.3
Note: S-significant (p<0.05); NS-Not significant (p>0.05).

62
Table 7.4: Association between pre- test level of attitude regarding Mission
Indradhanusamong mothers of under five children with their
selected demographic variables such as family income, type of
family, number of children, immunization status, previous
information regarding Mission Indradhanush and sources of
information.
n=60
Note: S-significant (p<0.05); NS-Not significant (p>0.05).
The table 7.3 and 7.4 envisages the outcome of chi square analysis being
carried out to bring out the association between the pre- test level of attitude regarding
Mission Indradhanush among mothers of under five children with their demographic
SL.
NO
Demographic
variables
Sample no
(60)
Level of knowledge Chi
square
value
p-value ≤Median >Median
F % F % F %
5 Family income(Rupees/month)
a. ≤10,000 37 61.7 25 67.6 12 52.2 1.791,
df=2,
NS
p>0.05 b.10001-15,000 16 26.7 9 24.3 7 30.4
c. Above 15,001 7 11.7 3 8.1 4 17.4
6 Type of family
a. Nuclear family 17 28.3 11 29.7 6 26.1 1.696,
df=2,
NS
p>0.05 b. Joint family 38 63.3 24 64.9 14 60.9
c. Extended family 5 8.3 2 5.4 3 13.0
7 Number of children
a. 1 27 45.0 14 37.8 13 56.5 8.410,
df=2,
S
p<0.05 b. 2 22 36.7 12 32.4 10 43.5
c. 3 or more 11 18.3 11 29.7 0 0
8 Immunization status of children
a. Fully immunized 42 70.0 25 67.6 17 73.9 0.272,
df=2,
NS
p>0.05 b.Partially immunized 15 25.0 10 27.0 5 21.7
c. Drop out 3 5.0 2 5.4 1 4.3
9
a.
Have you heard about Mission Indradhanush?
a.Yes 24 40.0
13 35.1 11 47.8 0.952,
df=2,
NS
p>0.05
b.No 36 60.0 24 64.9 12 52.2
b. If yes, specify the sources of information (n=24)
a.Health personal 13 54.2 6 46.2 7 63.6 6.616,
df=2,
S
p<0.05 b. Family member 5 20.8 5 38.5 0 0
c.Friends 0 0 0 0 0 0
d.Mass media 6 25.0 2 15.4 4 36.4

63
variables. The categories such as age, religion, educational status, occupation, family
income, type of family, number of children, immunization status of children, previous
information about Mission Indradhanush and the sources of information were
accounted for determining the association with attitude. Out of which, education,
occupation, number of children and source of information of the demographic
variables of the mothers of under five children were found significant with level of
attitude regarding Mission Indradhanush.
Testing of hypothesis
H3: There is a significant association between the pre- test level of knowledge and
attitude regarding Mission Indradhanush among mothers of under five children
with their selected demographic variables.
H03: There is no significant association between the pre- test level of knowledge and
attitude regarding Mission Indradhanush among mothers of under five children
with their selected demographic variables.
The table 7.1 and 7.2, shows the chi-square value at the level of p<0.05 for
knowledge and prove that there was association between the pre-test level of
knowledge regarding Mission Indradhanush among mothers of under five children
with their selected demographic variables such as age, religion, education,
occupation, number of children and previous information. Hence,research hypothesis
(H3) was accepted and null hypothesis (H03) was rejected.
The table 7.3 and 7.4shows the chi-square value at the level of p<0.05 for
attitude and prove that there was association between the pre-test level of attitude
regarding Mission Indradhanush among mothers of under five children with their
selected demographic variables such as education, number of children and source of
information. Hence null hypothesis (H03) was rejected and research hypothesis (H3)
was accepted.

64
DISCUSSION
This chapter deals with discussion part according to the result obtained from
the statistical analysis based on the data of the study, review of literature and
hypothesis which was formulated to this study. The present study was conducted to
assess the effectiveness of educational package on level of knowledge and
attituderegarding Mission Indradhanush among mothers of under five children in
Kengeri Upanagar urban slum area, Bengaluru.
In order to achieve the objective of the study, a quasi experimental one group
pre-test post-test design was adopted. The samples were selected by random sampling
technique. The data was collected from 60 respondents before and after providing the
educational package regarding Mission Indradhanush. The findings of the study has
been discussed with reference to the objectives, hypothesis and with the findings of
the other studies.
Demographic variables of the subjects
Regarding the frequency and percentage distribution on demographic variables
of mothers of under five children according to the age, religion, educational status,
occupation, family income per month in rupees, type of family, number of children,
immunization status of children, previous information about Mission Indradhanush
and the sources of information.
With regards to age, majority of the mothers of under five children 46.7% (28)
belongs 21-25 years, 30.0% (18) mothers belongs to below 26-30 years, 13.3% (8)
belong to 31 years and above and 10.0% (6) belongs to 20 years and below .
With regards to religion, majority of the mothers 70.0% (42) belongs to Hindu
religion 20.0% (12) belongs to Muslim religion, 5.0% (3) belongs to Christian and
5.0% (3) belongs to other religion.
With regards to educational status of mothers majority of them 35.0% (21) had
secondary education, 25.0% (15) had primary education, 18.3% (11) had graduation
and above, 18.3% (11) had secondary education, and 3.3 % (2) had no formal
education.

65
With regards to occupation of mothers, majority of mothers 38.3% (23) were
home maker, 28.3% (17) were daily wager, 18.3% (11) were self employed, 10.0%
(6) were private employee, 3.3% (2) were government employee and 1.7% (1) were
from others occupation,
With regards to family income per month in rupees, majority of mothers
61.7% (37) had an income of 10,000 and below, 26.7% (16) had an income of
10,001-15.000 and 11.7 % (7) had an income of 15.001 and above.
With regards to type of family, majority of mothers 63.3% (38) belongs to
joint family, 28.3% (17) belongs to nuclear family and 8.3% (5) belongs to extended
family.
With regards to number of children, majority of mothers 45.0% (27) had one
child, 36.7% (22) had two children and 18.3% (11) had three or more children.
With regards to immunization status of the children, majority of children
70.0% (42) were fully immunized, 25.0% (15) were partially immunized and 5.0% (3)
were drop out.
With regards to previous knowledge about Mission Indradhanush, majority
of mothers 60.0% (36) had not heard about Mission Indradhanush and 40.0% (24) had
heard about Mission Indradhanush.
With regards to sources of information, majority of mothers 54.2% (13) had
heard about Mission Indradhanush from health personnel, 25.0% (6) had heard from
mass media, 20.8% (5) had heard from family members and no mothers had heard
from friends.
The first objective was to assess the existing level of knowledge and attitude
regarding Mission Indradhanush among mothers of under five children.
With regards to the pre- test level of knowledge regarding Mission
Indradhanush among mothers of under five children from table 2.1 and 2.2 it is
evident that 75.0% ( 45) of mothers had inadequate knowledge ,18.3% (11) had
moderate knowledge and 6.7% (4) had adequate knowledge from table 2.2. All the

66
pre-test knowledge scores were ranging within 3- 19, mean was 10.17, SD was 4.49
and mean percentage was 46.2%
With regards to the pre- test level of attitude regarding Mission Indradhanush
among mothers of under five children from table 2.3 and 2.4, it is evident that 66.7%
(40) of mothers had neutral attitude and 33.3% (20) had favorable attitude. The
attitude scores were ranging between 27-36, mean 30.58, SD was 2.39 and mean
percentage 72.8%.
The findings of the study was supported by a non experimental study which
was conducted to assess the knowledge regarding immunization among mothers of
under five children and prepare health education programme regarding immunization
at Kunderki U.P. India. The mothers of under five children were selected as sample
by using convenient sampling technique. The sample size was 30. The finding of the
study shows that good knowledge score is 10%, average knowledge score is 23.34%
and poor knowledge score is 66.66%. The study concluded that the mothers of under
five having poor knowledge of immunization.
A descriptive study was conducted to assess the knowledge and attitude
regarding national vaccine programme among mothers of under five in selected
hospital Mangalore. The sample size consists of 300 mothers. The study result shows
that 289 (96.33%) mothers knew that BCG vaccine prevents Tuberculosis .Only
26(8.66%) mothers were knowledgeable about the measures that can be done if the
child has not given DPT. 11 (3.66%) mothers knew that chicken pox can be prevented
by varicella vaccine. The study concluded that even though the mothers had good
attitude regarding vaccines but they were unaware of Hib vaccine and rotavirus
vaccine and awareness shoul d be created among mothers.50
The second objective was to assess post-test level of knowledge and attitude
regarding Mission Indradhanush among among mothers of under five children.
With regards to the post- test level of knowledge and attitude regarding
Mission Indradhanush among mothers of under five children, from table 3.1 and 3.2,
it is evident that 43.3% (26) had moderate knowledge and 56.7%(34) had adequate
knowledge and post- test knowledge scores were ranging between 11-22 with a mean
17.00 and mean percentage 77.3 where SD was 3.36.

67
With regards to post- test level of attitude, all 100% (60) had developed
favorable attitude regarding Mission Indradhanush and all the post- test attitude scores
were ranging between 33-42 with a mean 37.21 and mean percentage 88.6 where SD
was 2.50.
The third objective was to assess the effectiveness of educational package on level
of knowledge and attitude regarding Mission Indradhanush among mothers of
under five children.
With regards to the pre -test and post- test level of knowledge and attitude
regarding Mission Indradhanush among mothers of under five children, from the table
5.1, the ‘t’ value were found to be 14.45 for knowledge and 11.16 for attitude which
was statistically significant at p< 0.001 level.
The findings of the study was supported by a quasi experimental study
conducted to assess the effectiveness of health teaching programme on knowledge
regarding immunization among mothers of under five children in selected community
setting, Aurangabad. 40 mothers of under five children were selected by purposive
sampling technique. The study result shows that the overall pre-test mean knowledge
score was found to be14.675 and SD as 4.226. And the overall post-test mean
knowledge score was found to be 21.800 and SD as 4.207. Paired t-test shows
statistical significance at 5 per cent level (p<0.05) establishing the impact of planned
teaching on knowledge regarding immunization among mothers of under five
children. The study concluded that post-test mean knowledge score of mothers
indicated significant difference which is a net benefit to the mothers due to the
effectiveness of health teaching program.47
The fourth objective was to correlate the pre-test level of knowledge and attitude
regarding Mission Indradhanush among mothers of under five children.
The table 6.1 revealed that there was significant linear correlation (r=0.486)
between knowledge and attitude regarding Mission Indradhanush among mothers of
under five children which is significant at p<0.05 level.
The findings of the study was supported by a descriptive study which was
conducted to assess the knowledge and attitude on immunization among the mothers
of under five children, Halaga village, Belgaum, Karnataka. 50 mothers of under five

68
children were selected by convenient and purposive sampling. The result reveals that
mean knowledge value on immunization of mothers of under five children was 58.1
and attitude score was 41.4. The correlation between knowledge on immunization and
attitude of mothers showed that there is a positive correlation between knowledge on
immunization and attitude (r=0.483). The study concluded that the mothers of under
five children of rural community area had moderately adequate knowledge on
immunization and moderate positive attitude towards immunization.44
A survey study was conducted to assess the knowledge and attitude of mothers
towards childhood immunization in Bauchi Local Government, Bauchi State- Nizeria.
The total sample size was 322 mothers and data was collected by in-depth interview
schedule. The finding of the study revealed that the level of mothers’ education relates
to their knowledge and tend to encourage childhood immunization. The study also
believed that there is the need to encourage women or girl child education as well as
to educating husbands, parents and community leaders on the dangers associated with
lack of immunization especially of the mentioned five killer diseases.32
The fifth objective was to associate between the pre- test level of knowledge and
attitude regarding Mission Indradhanush among mothers of under five children
with their selected demographic variables.
The table 7.1 and 7.2 shows that there was a significant association between
the pre-test level of knowledge regarding Mission Indradhanush among mothers of
under five children with their selected demographic variables such as age, religion,
education and occupation of mothers, number of children and information regarding
Mission Indradhanush.
The table 7.3 and 7.4 shows that there was a significant association between
the pre-test level of attitude regarding Mission Indradhanush among mothers of under
five children with their selected demographic variables such as educational status
of mothers, number of children and sources of information.
The findings is supported by a non-experimental survey was conducted to
assess the level of knowledge regarding immunization among mothers of under five
children and associate the findings with the selected demographic variables in
selected area of Pune city. 200 mothers who were having under five children were

69
selected from selected area by non-probability convenient sampling technique. The
study results shows that majority of mothers was having average knowledge 140
(70%), poor 50 (20%) and good 10 (5%). There is also association between education
of mothers and knowledge regarding immunization at p <0.05 level. The chi square
test result indicates that as the standard of education is higher, the knowledge of
immunization was more. The study concluded that mothers knows the importance of
immunization, but they have knowledge deficiency about some vaccine like
BCG,DPT, doses of hepatitis B and vitamin A vaccination.25
A non experimental research exploratory study was conducted to assess the
knowledge among mothers of under five children regarding immunization in selected
villages of Moga, Punjab. 100 mothers of under five children were selected from
anganwadis by using simple random sampling method. The finding of the study
revealed that 12% of mothers had good knowledge, 40% of mothers had average
knowledge and 48% of mothers had below average knowledge regarding
immunization. The total mean percentage of mothers knowledge regarding
immunization is (69.12%). There was statistically significant effect of age,
qualification, occupation of mother, family income in rupees, religion, numbersof
children and source of information on knowledge regarding immunization. So the
study concluded that the level of knowledge vary according to different demographic
variables.28

70
CONCLUSION
This chapter presents a brief summary of the study with limitation, nursing
implications and recommendations for future research and conclusion
The present study assessed the effectiveness of educational package on level
of knowledge and attitude regarding Mission Indradhanush among mothers of under
five children in Kengeri Upanagara Urban slum area, Bengaluru.
In the pre- test level of knowledge, 45 (75.0%) of mothers had inadequate
knowledge, 11 (18.3%) had moderate knowledge and 4 (6.7%) had adequate
knowledge whereas in post-test, 26(43.3%) of mothers had moderate knowledge and
34 (56.7%) of them had developed adequate knowledge. On the assessment of level of
attitude in pre-test, 40 (66.7%) had neutral attitude and 20 (33.3%) had favorable
attitude and none of them had unfavorable attitude whereas in the post-test, 60 (100%)
had developed favorable attitude. The paired t-test was carried out and it was found to
be significant at p<0.05 level. Hence, research hypothesis was accepted and null
hypothesis was rejected.
The study concluded that educational package is significantly effective in
improving the level of knowledge and attitude regarding Mission Indradhanush
among mothers of under five children.
Nursing Implications
The investigator has drawn the following implications from the studies which
are of vital concern to the field of nursing practice, nursing administration, nursing
education and nursing research.
Nursing Practice
1. Educational package can be effective in improving the knowledge and attitude of
mothers regarding Mission Indradhanush.
2. The community health nurse should identify the various factors which affects the
immunization of children and pregnant mothers, create awareness about
importance of immunization.

71
3. Regular health education programme can be conducted by the nursing personnel
in community setting which helps the mothers to be aware about the ongoing
immunization Programme for children and pregnant mothers, the optional
vaccines, benefits of immunization and about the killer or vaccine preventable
diseases.
4. The study carries an implication that community health nurse plays an important
role in imparting knowledge and helping the mothers regarding Mission
Indradhanush and help the Government to achieve the goals and objectives.
Nursing Education
1. Nurse should equip themselves by reading more books, recent advances and
current health related issues to keep themselves updated.
2. The nursing curriculum should include more on the recent National Health
Programme for effective utilization of the ongoing health programme
including immunization programme so that the public can benefit from various
Health schemes.
Nursing Administration
1. Nurse administrator should collaborate and co-ordinate with the community
leaders in creating awareness in the community for effective utilization of
Universal Immunization Programme including Mission Indradhanush.
2. Nurse administrator should arrange in-service education, training and staff
development programme to nursing personnel regarding latest and ongoing
National health programme including Universal Immunization Programme
and Mission Indradhanush.
3. Nurse administrator should arrange special training to School Teachers,
Anganwadi workers and social workers about Mission Indradhanush and
Universal Immunization Programme, its importance and about vaccine
preventable diseases or killer diseases.

72
Nursing Research
1. The study should be generalized and conducted in a larger population so it can
be used for Evidenced Based Studies .
2. The study should be disseminated through research journals and scientific
papers.
3. The study should be utilized for future studies and references.
Recommendations
1. The study may be replicated using larger population.
2. A similar kind of study can be undertaken in different settings (eg. Tribal and
hilly areas, construction sites etc.)
3. Educational programme may be designed for mothers, Anganwadi workers,
health workers, school teachers, Panchayat members and social workers to
disseminate knowledge regarding Mission Indradhanush.
Limitations
• The study was limited to mothers who were having children below five
years in Kengeri Upanagara urban slum area, Bengaluru .
• The sample size of the study was limited to 60 mothers of under five
children.

73
SUMMARY
The Ministry of Health and Family Welfare, Government of India launched
Mission Indradhanushin December 2014 as a special drive to vaccinate all
unvaccinated and partially vaccinated children under Universal Immunization
Programme. Mission Indradhanush aims to fully immunize more than 90% of
newborns by 2020 through innovative and planned approaches to reach all children as
well as pregnant women, against twelve vaccine preventable diseases. It not only
aimed to rapidly increase the immunization coverage through special drives during
specified months but also focused towards strengthening health systems for
addressing equity issues in access to immunization.
With the aim to accelerating the full immunization coverage and provide
greater focus on urban areas and other pockets of low immunization coverage, the
Ministry of Health and Family Welfare has drawn up an aggressive action plan to
achieve the target by 2018 and it was launched on 8th
October,2017 as Intensified
Mission Indradhanush.
The investigator conducted the present study to assess the effectiveness of
educational package on level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children. This study reveals that there is
substantial increase in knowledge and attitude of mothers after administration of
educational package on Mission Indradhanush.
The above study suggested that the immunization and health of the child is
impossible withoutmothers involvement as they play a primary role in child’s life.
Objectives of the study were
1. To assess the existing level of knowledge and attitude regardingMission
Indradhanush among mothers of under five children.
2. To assess the post-test level of knowledge and attitude regardingMission
Indradhanush among mothers of under five children.
3. To assess the effectiveness of educational package on knowledge and attitude
regardingMission Indradhanush among mothers of under five children.

74
4. To correlate the pre-test knowledge and attitude regardingMission
Indradhanush among mothers of under five children.
5. To associate between the pre-test level of knowledge and attitude regarding
Mission Indradhanush among mothers of under five children with their
selected demographic variables.
The Assumptions of the study were
1. Mothers of under five children may have low knowledge regarding Mission
Indradhanush.
2. Mothers of under five children may have poor attitude towards Mission
Indradhanush.
3. Educational package may improve the knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
4. Knowledge and attitude of mothers of under five children may vary with
their selected demographic variables.
The research hypotheses were stated as follows:
H1- There is a significant difference between the mean pre-test and post-test score
of knowledge and attitude regardingMission Indradhanush among mothers of
under five children.
H2- There is a significant correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
H3- There is a significant association between pre-test level of knowledge and
attitude regardingMission Indradhanush among mothers of under five
children.with their selected demographic variables.
The conceptual framework of this study was based on Pender’s health
promotion model (1996).
An extensive review of literature was done which enabled the investigator to
study the selected problem in depth, to develop conceptual framework, to construct
the tool, analyze and interpret the data.
75
The investigator selected quasi-experimental one group pre-test and post-test
design to assess the effectiveness of educational package on level of knowledge and
attitude regarding Mission Indradhanush among mothers of under five children. 60
mothers were selected through simple random sampling technique.
A structured interview schedule was developed by the investigator which
comprised of three sections: Section A consist of demographic data which gives
baseline information of mothers of under five children such as age, religion,
educational status, occupation, family income, type of family, number of children,
immunization status of the children, previous information about Mission
Indradhanush and sources of information, Section B on Structured interview schedule
to assess the level of knowledge of mothers of under five children regarding
Mission Indradhanush and Section C on 3 point Likert scale to assess the level of
attitude of mothers regarding Mission Indradhanush.
The content validity was obtained from experts and reliability was obtained by
split half method using Spearmen Brown’s prophecy formula method. Feasibility of
the study was confirmed by pilot study. The level of knowledge was assessed under
three categories: adequate knowledge, moderate knowledge and inadequate
knowledge. The level of attitude was assessed under three categories favorable
attitude, neutral attitude and unfavorable attitude.
The data obtained was analyzed and interpreted in terms of the objectives and the
hypotheses of the study. Descriptive and inferential statistics were used for data
analysis.
Major findings of the study
• With regards to age, majority of the mothers of under five children 46.7% (28)
belongs 21-25 years, 30.0% (18) mothers belongs to below 26-30 years,
13.3% (8) belongs to 31 years and above and 10.0% (6) belongs to 20 years
and below .
• With respect to religion, majority of the mothers 70.0% (42) belongs to Hindu
religion 20.0% (12) belongs to Muslim religion, 5.0% (3) belongs to Christian
and 5.0% (3) belongs to other religion.

76
• With regards to educational status of mothers, majority of them 35.0% (21)
had secondary education, 25.0% (15) had primary education, 18.3% (11) had
graduation and above, 18.3% (11) had secondary education, and 3.3 % (2) had
no formal education.
• With regards to occupation of mothers, majority of mothers 38.3% (23) were
home maker, 28.3% (17) were daily wager, 18.3% (11) were self employed,
10.0% (6) were private employee, 3.3% (2) were government employee and
1.7% (1) were from others occupation.
• With regards to family income per month in rupees, majority of mothers
61.7% (37) had an income of 10,000 and below, 26.7% (16) had an income of
10.001-15,000 and 11.7 % (7) had an income of 15,001 and above.
• With regards to type of family, majority of mothers 63.3% (38) belongs to
joint family, 28.3% (17) belongs to nuclear family and 8.3% (5) belongs to
extended family.
• With regards to number of children, majority of mothers 45.0% (27) had one
child, 36.7% (22) had two children and 18.3% (11) had three or more children.
• With regards to immunization status of the children, majority of children
70.0% (42) were fully immunized, 25.0% (15) were partially immunized and
5.0% (3) were drop out.
• With regards to previous knowledge about Mission Indradhanush, majority of
mothers 60.0% (36) had not heard about Mission Indradhanush and 40.0%
(24) had heard about Mission Indradhanush.
• With reference to sources of information, majority of mothers 54.2% (13) had
heard about Mission Indradhanush from health personnel, 25.0% (6) had heard
from mass media, 20.8% (5) had heard from family members and no mothers
had heard from friends.
• In the pre-test, majority75.0% (45) of mothers had inadequate
knowledge,18.3% (11) had moderately adequate knowledge and 6.7% (4) had

77
adequate knowledge and 66.7% (40) of mothers had neutral attitude and
33.3% (20) had favorable attitude.
• After administration of educational package (post-test) majority of mothers
56.7 (34) had adequate knowledge, 43.3% had moderate knowledge and pre-
test Mean (10.17) was lower than the post-test mean (17.00), pre-test Mean
percentage ( 46.2%) was lower than the post- test mean percentage 77.3%) and
pre-test SD (4.49) was higher than the post-test SD (3.36). In the post-test
level of attitude, all 60 (100%) had developed favorable attitude and pre-test
mean (30.58 ) was lower than the post-test mean (37.21), pre-test mean
percentage (72.8%) was lower than the post-test mean percentage (88.6%) and
pre-test SD was (2.39) SD was lower than the post-test SD ( 2.50).
• The paired t-test was carried out and it was found to be significant at p<0.001
level. Hence, research hypothesis (H1) was accepted and null hypothesis (H01)
was rejected. It was evident that the educational package was significantly
effective in improving the level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children.
• There was significant linear correlation (r=0.486) between knowledge and
attitude regarding Mission Indradhanush among mothers of under five
children which is significant at p<0.05 level. Hence, research hypothesis (H2)
was accepted and null hypothesis (H02) was rejected. It was evident that there
is positive linear correlation between knowledge and attitude regarding
Mission Indradhanush among mothers of under five children.
• Chi square analysis being carried out to bring out the association between the
pre-test level of knowledge regarding Mission Indradhanush among mothers
of under five children with their demographic variables. The result of the
study indicated that age, religion, education and occupation of mothers,
number of children and previous information of the demographic variables of
the mothers of under five children had significant association with level of
knowledge regarding Mission Indradhanush, where as education, number of
children and source of information of the demographic variables of the
mothers of under five children had significant association with level of

78
attitude regarding Mission Indradhanush. Hence, research hypothesis (H3) was
accepted and null hypothesis (H03) was rejected. It was evident that there is
association of pre- test level of knowledge and attitude regarding Mission
Indradhanush among mothers of under five children with their selected
demographic variables.

79
REFERENCES
1. Census of India: Provisional Population Totals: India: Census 2011. Available
from: http://www.censusindia.gov.in/2011-prov-results/prov_results_ paper1_
india.html
2. Swarnakar’s. Community Health Nursing. 3rd
Edition. Indoor: N.R. Brothers
Publisher’s Nursing; 2016:468
3. K.K. Gulani. Community Health Nursing. 2nd
edition. Delhi: Kumar Publication
House; 2013: 395
4. A H Suryakantha. Community medicine with recent advances. 4th
edition. New
Delhi. Jaypee Brother’s medical publisher P (Ltd)
5. BT Basavanthapa. Community Health Nursing. 2nd
Edition. New Delhi: Jaypee
Brother Medical Publisher (P) Ltd: 2008: 547
6. UNICEF- Immunization. Available from http://www.unicef.org/immunization/
7. National Health Programmes Related To Child Health. Available from http:
//www. m.authorstream.com
8. Intensified Mission Indradhanush Operation Guidelines. Available from http:
//kamleshvaland. files.wordpress.com/2017/imi-operational-guidelines.pdf
9. Mission Indradhanush Operation Guidelines. Available from
http://www.tripuranrhn.gov.in/guidelines/0701201701.pdf
10. Mission Indradhanush phase 1: Final coverage report. Accessed from
http://www.missionindradhanush.in/about
11. Press Information Bureau. Government of India. Ministry of Health and Family
Welfare. Initiatives and Achievements of Ministry of Health and Family Welfare:
A Year End Review, 2016. Accessed from http://www.pib.nic.in>
newsite>PrintRelease
12. World Health Organization, Mission Indradhanush: Leveraging lessons from polio
success story. Accessed from http://www.searo.who.int/mediacentre/events/polio-
story/en/.

80
13. K. Park. Textbook of preventive and social medicine. 23rd
edition. Jabalpur: M/S
Banarsides Bhanot Publishers;2015:575
14. Under five mortality Available from http://www.who.int/gho/child_health/
mortality/mortality_under_five_text_en/
15. Suresh Sharma. Immunization coverage in India. Working Paper Series No.
E/283/2007, Institute of Economic Growth. Delhi, India.
16. Tim Crocker-Buque, Godwin Mindra and Richard Duncan. Immunization,
Urbanization And Slum: A Review Of Evidence. Available from
http://wwwiunicef.org/health/files/immunization_urbanization_and_slums_workin
g_paper_12122016.docx.
17. Yousif MA, Ahmed Abdulrahman Albarraq, Mustafa Awad A Abdullah and
Abubaker Ibrahim Elbur. Parents’ Knowledge and Attitude on Childhood
Immunization, Taif, Saudi Arabia. Journal of Vaccines & Vaccination. 2013
December.
18. Mandeep Singh Khurana, Supriya Malik, Sunita Arora. Cross sectional study to
assess immunization knowledge and practice among families of children between
0-5 years in rural areas of Punjab, India. International Journal of Contemporary
Pediatrics. 2017; Vol 4, No 5.
19. Juliet Thrani, Deepa S. Nair and Karthika, S..A study to assess the effectiveness of
Planned Teaching Program on the knowledge of immunization among migrant
mothers of under five children in selected construction sites at Bangalore Urban.
Internationl Journal of Current Research. 2017 July; Vol. 9, Issue, 07.
20. M.M. Angadi, Arun Pulikkottil Jose, Rekha Udgiri, K.a. Masali and Vijaya
Sorganvi. A Study Of Knowledge, Attitude And Practices On Immunization Of
Children In Urban Slum Of Bijapur city, Karnataka, India. Journal of clinical and
diagnostic research. 2013 December; Vol 7(12): 2803-2806.
21. Saurabh Kumar, Sudhir Prabhu, Arun P. Jose, SowmyaBhat, Oliver D. Souza,
Narayana V. Assessment of under-five immunization coverageamong the
population of slum areas in Mangalore taluk, India. International Jounnal of
Community Medicine and Public Health. 2017Mar; 4(3):781 -786.

81
22. Aleena Sunny, Sambhu Ramesh and Binal K Shankar. A Study to Assess and
Correlate the Knowledge, Attitude and Practices of Vaccination among Mothers
with Educational Status in a Teaching Hospital in South India. Primary Health
Care: Open Access. 2018; Volume 8, Issue1.
23. Denise F.Polit, Cheryl Tatano Beck, Bernadette P.Hungler. Essentials of Nursing
research, Methods, Appraisal and Utilization. 5th
edition. New York: Lippincott,
175-178.
24. Suresh K. Sharma. Nursing Research and Statistics.First Edition. Haryana India:
Elsevier 2016; 213.
25. N Sujita Devi, Irish, Smitta, Pragati and Vishvendra. A study to assess the
knowledge regarding immunization among mother of under five children of Pune
city. International Journal of Applied Research. 2017; 3(6): 112-1114.
26. Vijoy Kumar M., Anjaneyulu G., Venkata Navya Sree, Gautham Sai W. M..
Immunization status and knowledge regarding newer vaccines among mothers in a
rural area of Rangareddy District, Telangana, India. International Jounnal of
Community Medicine and Public Health. 2016 Nov; 3(11):3157-3160.
27. Nilesh Dayama, Vinet Wartha, Paradhi Garg, Ashutosh Padliwal, Sunit Aggarwal.
Study of Maternal Knowledge Regarding Immunization at Tertiary Care Center in
Mahareshtra. Indian Journal of Applied Research. 2015; Volume 5(12).
28. Varinder Pal Kaur. A Study to Assess the Knowledge among Mothers of Under
Five Children Regarding Immunization in Selected Villages of Punjab.
ResearchGate. 2015 January; 7(2): 119.
29. Farha Azmi, Dr. Ratna Prakash. Assessment of Knowledge towards Immunization
among Mothers of Under Five of UP India: A Quantitative Approach.
International Journal Of Science And Research. 2013; Volume 4.
30. Virupakshappa Savadi, Sumitra l.a, Mahaling hulgibali. A Study To Assess The
Knowledge Regarding Immunization Among Mothers of Under Five Children
Admitted In Pediatric Ward Of Prabhakar Kore Hospital, Belagavi With The Aim
To Develpo Educational Pamphlet. IOSR Journal of Nursing and Health Sciences.
2017 Nov.-Dec.; Vol 6, Issue 6: PP 68-73.

82
31. Jisy Josh, Melba Roshni Lobo, K. Nisha, S. G. Shilpa, J. Umarani. Awareness on
Immunization among Mothers of Under Five Children. International Journal of
Innovative Research and Development 2013 June; Vol 2: Issue 6.
32. Kabir Bello & Abarshi Dauda Danial. Knowledge and Attitude of Mothers
towards Childhood Immunization in Bauchi Local Government, Bauchi State-
Nigeria. International Journal of Innovative Research in Social Sciences &
Strategic Management Techniques. 2017 September; Vol 4, No 2.
33. Stein Zamir C, Israeli A. Knowledge Attitude and Perception about Routine
Childhood Vaccination Among Jewish Ultra-Orthodox Mothers Residing In
Communities With Low Vaccination Coverage In The Jerusalem District.
Maternal chilh health journal. 2017- jan-16; Doi: 10.1007/s10995-017-2272-5.
34. Shieferaw Birhanu, Aderaw Antenah, Yezabnesh Kibie, Ayalew Jejaw.
Knowledge, Attitude and Practice of Mothers Towards Immunization of Infants in
Health Centres at Addis Ababa, Ethiopia. American Journal of Health Research.
2016 January; Volume 4, Issue: Pages 6-17.
35. Heba Adel Ramadan, Sahar Mohamed Soliman, Rabab Gad Abd El-kader.
Knowledge, Attitude and Practice of Mothers towards Children’s Obligatory
Vaccination. IOSR Journal of Nursing and Health Science. 2016 Jul-Aug; Volume
5, Issue 4: pp 22-28.
36. Chris Otubor, G.O., Dangiwa D.A., Ior, L.D, Anukam, N.C. Assessment Of
Knowledge Attitude And Practices Of Mothers In Jos North Regarding
Immunization. IOSR Journal of pharmacy. 2015 June; Volume 5,Issue 6: 34-45.
37. Omer Qutaiba B Al-lela, Mohd Baidi Bahari, Harith Khalid Al-Qazaz, Muhannad
RM Salih, Shzia Q Jamshed and Ramadan M Elkalmi. Are parents’ knowledge
and practice regarding immunization related to pediatrics’ immunization
compliance? A mixed method study. BioMed Central Pediatrics. 2014 January;
14: 20.
38. Dharmalingam A., N.S. Raghupathy, M. Sowmiya, D.Amudharaj, H. M. Jehangir.
Immunization Knowledge, Attitude and Practice among mothers of children from
0-5 years. International Journal of Contemporary Pediatrics.2017; Vol 4, No 3.

83
39. Nafeha Sameen Siddiqui, Arvind K. Gaikwad, Bina M. Kuril, Rajendra T.
Ankushe, Mohan K. Doibale, Sandeep B. Pund, et.al. Is mothers’ knowledge and
practice regarding childhood immunization complient with immunization
completeness? International Journal of Community Medicine and Public Health.
2017 Mar; 4(3): 775-780.
40. Vasantha Kalyani C and Xavier Belsiyal C. Knowledge, Attitude and Practice of
Mothers of Under Five Children Regarding Immunization in a Selected
Community, Rishikesh, Uttarakhand. International Journal of Recent Scientific
Research. 2016 May; Vol. 7, Issue 5: pp. 11301-11305.
41. Bryan J. Vonasek, Francis Bajunirwe, Laura E. Jacobson, Leonidas Twesigye,
James Dahm, Monica J. Grant, et. Al. Do Maternal Knowledge and Attitudes
towards Chidhood Immunizations in Rural Uganda Correlate with Complete
Childhood Vaccination? PLOS| ONE A Peer-Reviewed, open Access
Journal.2016; 11(2).
42. Patel Trushitkumar B, Riju Pathak, Rajindar Singh, Varun Alves, Mahesh N M,
Chaluvaraj TS et. Al.. Assessment of Parents’ Knowledge, Attitude and Practice
about Child Vaccination in Rural areas. Journal of Pharmaceutical Research. 2017
Jul-Sept; Volume 16, Issue 3.
43. Mr Hazaratali Panari, Mrs Anuchithra. Study on Immunization among the Mother
Of Under Five Children, Halag Village, Balgaum, Karnataka. Asian journal of
nursing education and research. 2016; vol 6, issue 2.
44. Jolsna Joseph, Vijayalakshmi Devarashetty, S. Narayana Reddy, M. Sushma.
Parents’ knowledge, attitude and practice on childhood immunization.
International Journal of Basic & Clinical Pharmacology. 2015; Vol 4, No 6.
45. Soundarya Mahalingam, Abhijna Soori, Pradhum Ram, Basavaprabhu Achappa,
Mukta Chowta. Knowledge, Attitude and Perception of mothers with children
under five years of age about vaccination in Mangalore, India. Asian Journal of
Medical Science. 2014 May; Vol 5, No 4.
46. Ammar Ihsan Awadh, Mohamed Azmi Hassali, Omer Qutaiba Al-lela, Siti
Halimah Bux, Ramadan M Elkalmi, and Hazrina Hadi. Does an educational

84
intervention improve parents’ knowledge about immunization? Experience from
Malasia. BioMed Central Pediatrics. 2014 Oct; 14: 254.
47. Sheetal Udaykar, Joanna John K. Assess the Effectiveness of Health Teaching
Programme on Knowledge Regarding Immunization among Mothers of Fewer
than Five Children. International Journal of Science and Research. 2016 June;
Volume 5, Issue 6.
48. Reema Mukherjee, Manisha Arora, Atul Kotwal, Poonam Hooda. Awareness and
attitude of mothers towards new vaccines in the childhood vaccination programme
in Delhi state: a cross sectional study. International Journal of Community
Medicine and Public Health.2017; Vol 4, No 10.
49. Agrawal A, Hanspal R. To study the knowledge regarding immunization schedule
among parents and the source of information regarding vaccination. Pediatric
Review: International Journal of Pediatric Research. 2016; Vol 3, No 12.
50. Ms.Meena, Mrs Sujatha. R. A study on Knowledge and Attitudes Regarding
Vaccines among Mothers of Under Five Children attending Pediatric OPD in a
Selected Hospital at Mangalore. IOSR Journal of Nursing and Health Sciences.
2014(Sep-Oct); Volume3: Issue 5,39-46.
51. P.S.S. Sundar Rao, J. Richard. An Introduction to Biostatistics. A manual for
students in health sciences.3rd
edition. New Delhi: Prentice-Hall of India private
limited 2004.

85
CONSENT FORM
LETTER SEEKING CONSENT FROM THE SUBJECTS FOR
PARTICIPATION IN STUDY
Dear participant,
I am a post graduate nursing student at the Padmashree Institute of Nursing,
Bangalore, and conducting “A study to assess the effective of educational package on
level of knowledge and attitude regarding Mission Indradhanush among mothers of
under five children in selected urban slum area, Bengaluru. Hope you will co-operate
with me for the same.
I request you to answer the given interview questionnaire with the most
appropriate responses. Kindly do not leave any question unattended. The information
given by you will be kept confidential and used only for the study purpose. Kindly
sign the consent form given below.
Thanking You.
Yours faithfully,
Mrs Jyotima Borgohain Handique

86
CzsÀåAiÀÄ£ÀzÀ°è ¥Á¯ÉÆμÀÄîªÀÅzÀPÁÌV «µÀAiÀÄUÀ½AzÀ M¦àUÉ ¥ÀqÉAiÀÄ®Ä ¥ÀvÀæ
DwäÃAiÀÄ ¥Á ÉÆμÀÄîªÀªÀgÉÃ, £Á£ÀÄ ¥ÀzÀä²æà E£ïìnlÆåmï D¥sï £À¹ðAUï, ¨ÉAUÀ¼ÀÆgÀÄ ¸ÁßvÀPÉÆÃvÀÛgÀ £À¹ðAUï «zÁåyð¤AiÀiÁVzÉÝÃ£É ªÀÄvÀÄÛ ¨ÉAUÀ¼ÀÆj£À DAiÀÄÝ £ÀUÀgÀ PÉƼÀZÉ ¥ÀæzÉñÀzÀ°è “LzÀÄ ªÀµÀðQÌAvÀ aPÀÌ ªÀÄPÀ̼À vÁAiÀÄA¢gÀ°è «Ä±À£ï EAzÀæzsÀ£ÀĵïUÉ ÀA§A¢ü¹zÀAvÉ w¼ÀĪÀ½PÉ ªÀÄvÀÄÛ ªÀÄ£ÉÆèsÁªÀzÀ ªÀÄlÖzÀ §UÉÎ ±ÉÊPÀëtÂPÀ ¥ÁåPÉÃeï£À ¥ÀjuÁªÀĪÀ£ÀÄß ¤zsÁðgÀuÉ ªÀiÁqÀ®Ä CzsÀåAiÀÄ£À”-ªÀ£ÀÄß PÉÊUÉÆArzÉÝãÉ. EzÀPÁÌV ¤ÃªÀÅ £À£ÀUÉ ¸ÀºÀPÁgÀ ¤ÃqÀÄ«gÉAzÀÄ §AiÀĹzÉÝãÉ.
¤ªÀÄUÉ PÉÆlÖ ¸ÀAzÀ±Àð£À ±ÉqÀÆå ïUÉ CvÀåAvÀ ¸ÀÆPÀÛ ¸ÀàAzÀ£ÉAiÉÆA¢UÉ GvÀÛj¸À ÉÃPÉAzÀÄ £Á£ÀÄ ¤ªÀÄä°è «£ÀAw¸ÀÄvÉÛãÉ. zÀAiÀÄ«lÄÖ AiÀiÁªÀÅzÉà ¥Àæ±ÉßAiÀÄ£ÀÄß GvÀÛj¸ÀzÉà ©qÀ ÉÃr.¤ÃªÀÅ PÉÆlÖ ªÀiÁ»wAiÀÄ£ÀÄß UÀÄ¥ÀÛªÁV EqÀ ÁUÀĪÀÅzÀÄ ªÀÄvÀÄÛ F CzsÀåAiÀÄ£ÀzÀ GzÉÝñÀPÁÌV ªÀiÁvÀæ G¥ÀAiÉÆÃV¸À ÁUÀĪÀÅzÀÄ.zÀAiÀÄ«lÄÖ F PɼÀUÉ PÉÆlÖ M¦àUÉ ¥ÀvÀæPÉ Ì ¸À»ªÀiÁrj.
zsÀ£ÀåªÁzÀUÀ¼ÉÆA¢UÉ,
¤ªÀÄä «±Áé¹
²æêÀÄw eÉÆåÃwªÀiÁ ¨ÉÆÃUÉÆÃðºÉÃ£ï ºÁåArPï

87
CONSENT FORM
I here with consent for the above said study knowing
that all the information provided by me will be treated with utmost confidentiality by
the investigator which will be helpful to update knowledge and attitude regarding
Mission Indradhanush among mothers of under five chidren.
Date: Name and Signature of the participant
Place: Address:

88
M¦àUÉ ¥ÀvÀæ
£Á£ÀÄ ____________________________________ F ªÉÄïÁÌt¹zÀ CzsÀåAiÀÄ£ÀPÁÌV £À£Àß
M¦àUÉAiÀÄ£ÀÄß F ªÀÄÆ®PÀ ÀÆa ÀÄvÉÛãÉ. £Á£ÀÄ MzÀV¹zÀ ªÀiÁ»wAiÀÄ£ÀÄß vÀ¤SÉzÁgÀgÀÄ CvÀåAvÀ
«±Áé ÁºÀðªÁV ¥ÀjUÀt ÀÄvÁÛgÉ ºÁUÀÆ CzÀÄ LzÀÄ ªÀµÀðQÌAvÀ aPÀÌ ªÀÄPÀ̼À vÁAiÀÄA¢gÀ°è «Ä±À£ï
EAzÀæzsÀ£ÀĵïUÉ ÀA§A¢ü¹zÀAvÉ w¼ÀĪÀ½PÉ ªÀÄvÀÄÛ ªÀÄ£ÉÆèsÁªÀzÀ ªÀÄlÖªÀ£ÀÄß ºÉaÑ ÀĪÀ°è £ÉgÀªÁUÀÄvÀÛzÉ
JAzÀÄ £Á£ÀÄ ¨sÁ«¹zÉÝãÉ.
¢£ÁAPÀ:¨sÁUÀªÀ» ÀĪÀªÀgÀ ºÉ ÀgÀÄ ªÀÄvÀÄÛ À»
ÀܼÀ:«¼Á À:

89
ETHICAL COMMITTEE CLEARANCE CERTIFICATE

90
PROFORMA RORMAT
BLUEPRINT OF KNOWLEDGE AND ATTITUDE
STRUCTURED INTERVIEW SCHEDULE
Section A: Demographic Variables of Mothers of under five childrens
SN TYPE OF QUESTION QUESTION NO.
1 MCQ (Multiple Choice Questions) 1,2,3,4,5,6,7,8,9A,9B,1
Total 11
Section B:Structured Interview Schedule
S
N
TYPE
OF
QUEST
ION
QUESTION NO. MARKS WEIT
AGE
1 MCQ
(Multipl
e Choice
Questio
ns)
1,2,3,4,5,6,7,8,9,10,11,12,13,
14,15,16,17,18,19,20,21,22
1+1+1+1+1+1+1+1+1+1+1+
1+1+1+1+1+1+1+1+1
+1+1=22
Every question consists of:
• 4 options
• Each answer being
scored as 1
100%
Total 22 22 100%
Section C: 3 point Likert Scale
SN TYP
E OF
QUE
STI
ON
QUESTION NO. MARKS WEIT
AGE
1 3
point
Liker
t
Scale
1,2,3,4,5,6,7,8,9,10,11,12,13,14 3+3+3+3+3+3+3+3+3+3+3
+3+3+3 =42
Every question consists of:
• 3 options
• Each answer being
scored on a scale
value of 1-3
100%
Total 14 42 100%

91
SECTION A
DEMOGRAPHIC VARIABLES OF MOTHERS OF UNDER FIVE
CHILDREN
Instruction:
(Please read each statement carefully and give appropriate response)
Please answer the entire question.
1. Age in years
a) 20 years and below
b) 21-25years
c) 26 -30 years
d) 31years and above
2. Religion
a) Hindu
b) Christian
c) Muslim
d) Others
3. Educational status of Mother
a) No formal education
b) Primary education
c) Secondary education
d) Higher secondary education
e) Graduation and above
4. Occupation of Mother
a) Home maker
b) Daily wager
c) Self employed
d) Government employee
e) Private employee
f) Others
92
5. Family income per month
a) Rs. 10,000 and below
b) Rs. 10,001-15,000
c) Above Rs.15,001
6. Type of family
a) Nuclear family
b) Joint family
c) Extended family
7. Number of Children
a) 1
b) 2
c) More than 3
8. Immunization status of children
a) Fully Immunized
b) Partially Immunized
c) Drop out
9. Have you heard about Mission Indradhanush?
a) Yes
b) No
If yes, specify the source of information
i. Health personnel
ii. Family members
iii. Friends
iv. Mass media

93
SECTION B
Structured interview schedule to assess the knowledge of mothers of under five
children regarding Mission Indradhanush
1. What is meant by Mission Indradhanush?
a) Health promotion programme.
b) Health screening and early intervention programme
c) Re-habilitation programme
d) Immunization programme
2. Which Ministry launched Mission Indradhanush?
a) Ministry of Education
b) Ministry of Social Welfare
c) Ministry of Health and Family Welfare
d) NRHM
3. What is the main objective of Mission Indradhanush?
a) To cover all non immunized children
b) To cover all partially immunized children
c) To cover all pregnant mothers
d) To cover all drop out children and pregnant mothers
4. Where are the Mission Indradhanush services available?
a) Areas with high routine immunization coverage
b) Areas with low routine immunization coverage
c) All the government hospitals
d) All the private hospital
5. How to identify the beneficiaries for Mission Indradhanush services ?
a) By survey
b) By screening
c) By blood testing
d) By checking height and weight
6. Which age group of children are beneficiaries of this programme?
a) 0 – 1 year, pregnant mothers
b) 0 – 6 years, pregnant mothers
c) 0 – 5 years, pregnant mothers

94
d) 0 – 10 years, pregnant mothers
7. Mission Indradhanush is mainly for which group of children?
a) Fully immunized
b) Malnourished
c) Partially immunized
d) Sick
8. What may be the reasons for partial immunization?
a) Lack of awareness about benefits of vaccination
b) Fear of adverse effects following immunization
c) Non availability of health services
d) All of the above
9. Who conducts survey for Mission Indradhanush?
a) Health personnels
b) Panchayat members
c) Political leaders
d) NGO
10. Which of the following health personnels are involved in conducting survey
for Mission Indradhanush?
a) Doctors
b) ANMs
c) Laboratory technicians
d) Physiotherapists
11. How many rounds of immunization are conducted under this programme?
a) 2 rounds
b) 3 rounds
c) 4 rounds
d) 5 rounds
12. What is the duration of each round?
a) 3 days
b) 7 days
c) 5 days
d) 6 days

95
13. How many vaccine preventable diseases are covered by Mission
Indradhanush?
a) Seven
b) Six
c) Eight
d) Five
14. What is the working time for Mission Indradhanush?
a) 9 am – 6 pm
b) 9 am– 12 noon
c) 9 am– 4 pm
d) 9 am– 2 pm
15. What are the areas forvaccination under Mission Indradhanush ?
a) Primary School, Post partum centre
b) Anganwadi Centre, NGO sites
c) PHC, local leader’s premises
d) All of the above
16. Which card is given to the beneficiaries under Mission Indradhanush?
a) Adhaar card
b) Vaccination card
c) Ration card
d) Voter ID card
17. What are all the vaccines provided by Mission Indradhanush?
a) Pentavalent,BCG
b) Measles, OPV
c) TT, Hepatitis -B
d) All of the above
18. Which type of vaccine is given to pregnant mothers?
a) DPT
b) TT
c) MMR
d) OPV

96
19. In Karnataka, which day of the week is immunization clinic conducted?
a) Thursday
b) Wednesday
c) Tuesday
d) Monday
20. How the information about Mission Indradhanush is conveyed to the public?
a) Health personnel
b) Mass media
c) Members of panchayat
d) All of the above
21. Which of the following activity will be helpful for awareness for Mission
Indradhanush?
a) Mothers meeting
b) Home visit
c) Community meeting
d) All of the above
22. Which of the following indicates the success of Mission Indradhanush ?
a) Decreased number of partially immunized children and pregnant mothers
b) Increased number of partially immunized children and pregnant mothers
c) Decreased number of sick children
d) Increased number of sick children

97
SECTION C
LIKERT SCALE TO ASSESS THE ATTITUDE OF MOTHERS OF UNDER
FIVE CHILDREN REGARDING MISSION INDRADHANUSH
(3 POINT LIKERT SCALE)
KEYS
A- Agree
B- Undecided
C- Disagree
SL
NO
ITEMS
RESPONSE
Score A U D
1. Mission Indradhanush is helpful programme
for children and pregnant mothers.
2. Mission Indradhanush can help to reduce the
children disease and death rate.
3. It is difficult to receive the services of Mission
Indradhanush
4. Mission Indradhanush will help to cover 100%
full immunization.
5. Mission Indradhanush is beneficial for fully
immunized children.
6. Unimmunized and partially immunized
children are susceptible to childhood diseases
and disability.
7. Unawareness of parents on benefits of
immunization cause partial immunization.
8. All the vaccinations are not necessary for

98
SL
NO
ITEMS
RESPONSE
Score A U D
children.
9. There are fix and mobile sessions of
vaccination.
10. Mission Indradhanush services are provided
free of cost.
11. Mission Indradhanush covers only the less
immunization coverage area.
12. Mission Indradhanush services cover whole
Karnataka.
13. Services of Mission Indradhanush are available
for only few selected months.
14. Mass media has no role in Mission
Indradhanush.

99
PÀæªÀħzÀÞ ¥Àæ±ÁߪÀ½
« sÁUÀ J 5 ªÀµÀðQÌAvÀ QjAiÀÄ ªÀÄPÀ̼À vÁAiÀÄA¢gÀ d£À ÀASÁå zÀvÁÛA±À
ದಯ�ಟು� ಪ�ಂದು ೕ��ಗಳನು� ಎಚ����ಂದ ಓ� ಮತು� ಸ�!ಾದ ಪ#$ %ೕ&.
¸ÁåA¥À¯ï £ÀA. (1) ªÀAiÀÄ ÀÄì
(J) 20 ªÀµÀðUÀ¼ÀÄ ªÀÄvÀÄÛ PÀrªÉÄ (©) 21-25 ªÀµÀðUÀ¼ÀÄ (¹) 26-30 ªÀµÀðUÀ¼ÀÄ (r) 31 ªÀµÀð ªÉÄîàlÄÖ
( ) ( ) ( ) ( )
(2) zsÀªÀÄð (J) »AzÀÆ (©) Qæ²ÑAiÀÄ£ï (¹) ªÀÄĹèA (r) EvÀgÀgÀÄ
( ) ( ) ( ) ( )
(3) vÁ¬ÄAiÀÄ ²PÀët ªÀÄlÖ (J) N¥ÀZÁjPÀ ²PÀët«®è (©)¥ÁæxÀ«ÄPÀ ²PÀët (¹)ªÀiÁzsÀå«ÄPÀ ²PÀët (r) ¥ËæqsÀ±Á¯Á ²PÀët (E) ¥ÀzÀ« ªÀÄvÀÄÛ ªÉÄîàlÄÖ
( ) ( ) ( ) ( ) ( )
(4) vÁ¬ÄAiÀÄ GzÉÆåÃUÀ (J) UÀȺÀ¤ªÀðºÀuÉ (©) ¢£ÀUÀÆ° (¹) ¸ÀéAAiÀÄA GzÉÆåÃV (r) ¸ÀPÁðj GzÉÆåÃV (E) SÁ¸ÀV GzÉÆåÃV (J¥sï) SÁ¸ÀV GzÉÆåÃV
( ) ( ) ( ) ( ) ( ) ( )
(5) PÀÄlÄA§zÀ DzÁAiÀÄ (J) gÀÆ. 10,000 QÌAvÀ PÀrªÉÄ (©) gÀÆ. 10,001 - gÀÆ. 15,000 (¹) gÀÆ.15000 ªÀÄvÀÄÛ ªÉÄîàlÄÖÖ
( ) ( ) ( )
(6) PÀÄlÄA§zÀ «zsÀ (J) ªÀÄÆ® PÀÄlÄA§ (©) dAn PÀÄlÄA§ (¹) KPÀ¥Á®PÀ PÀÄlÄA§
( ) ( ) ( ) (7) ªÀÄPÀ̼À ÀASÉå
(J) 1 (©) 2 (¹) 3 QÌAvÀ ºÉZÀÄÑ
( ) ( ) ( )

100
(8) ªÀÄPÀ̼À ¥ÀæwgÀPÀët ¹Üw (J) ¸ÀA¥ÀÆtð ¥ÀÛwgÀQëvÀ (©) ¨sÁUÀ±ÀB ¥ÀæwgÀQëvÀ (¹) ºÉÆgÀUÀĽ¢ªÉ
( ) ( ) ( ) (9) ¤ÃªÀÅ «Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ PÉý¢ÝÃgÁ?
(J) ºËzÀÄ (©) E®è
ºËzÀÄ JAzÁgÉ- ªÀiÁ»wAiÀÄ ªÀÄÆ®ªÀ£ÀÄß w½¹j. (J) DgÉÆÃUÀ å C¢üPÁj (©) PÀÄlÄA§ ¸ÀzÀ ÀågÀÄ (¹) ¸ÉßûvÀgÀÄ (r) ¸ÀªÀÄƺÀ ªÀiÁzsÀåªÀÄ
( ) ( )

101
« sÁUÀ-©
«Ä±À£ï EAzÀæzsÀ£ÀĵïUÉ ÀA§A¢ü¹zÀAvÉ 5 ªÀµÀðQÌAvÀ QjAiÀÄ ªÀÄPÀ̼À vÁAiÀÄA¢gÀ eÁÕ£ÀªÀ£ÀÄß ¤zsÁðgÀuÉ ªÀiÁqÀ®Ä PÀæªÀħzÀÞ ÀAzÀ±Àð£À C£ÀħAzsÀ
(1) «Ä±À£ï EAzÀæzsÀ£Àĵï JAzÀgÉãÀÄ?
(J) DgÉÆÃUÀ å ¥ÀæZÁgÀ PÁAiÀÄðPÀæªÀÄ (©) DgÉÆÃUÀ å vÀ¥Á¸ÀuÉ ªÀÄvÀÄÛ ¥ÀƪÀð ªÀÄzsÀå¹ÜPÉ PÁAiÀÄðPÀæªÀÄ (¹) ¥ÀÄ£ÀgÀÄfÓêÀ£À PÁAiÀÄðPÀæªÀÄ (r) ¥ÀæwvÀPÀët PÁAiÀÄðPÀæªÀÄ
( ) ( ) ( ) ( )
(2) AiÀiÁªÀ ¸ÀaªÁ®AiÀĪÀÅ «Ä±À£ï EAzÀæzsÀ£ÀĵïDgÀA©ü¹vÀÄ?
(J) ²PÀët ¸ÀaªÁ®AiÀÄ (©) ¸ÀªÀiÁd PÀ Áåt ¸ÀaªÁ®AiÀÄ (¹) DgÉÆÃUÀå ªÀÄvÀÄÛ PÀÄlÄA§ PÀ Áåt ¸ÀaªÁ®AiÀÄ
(r)NRHM
( ) ( ) ( ) ( )
(3) «Ä±À£ï EAzÀæzsÀ£ÀĵïªÀÄÄRå UÀÄjAiÉÄãÀÄ? (J) ¥ÀæwgÀQë À®àqÀzÀ J®è ªÀÄPÀ̼À£ÀÄß M¼ÀUÉƼÀÄîªÀÅzÀÄ (©) ¨sÁUÀ±ÀB ¥ÀæwgÀQë À®àlÖ J®è ªÀÄPÀ̼À£ÀÄß M¼ÀUÉƼÀÄîªÀÅzÀÄ (¹) J®è UÀ©üðt ªÀÄ»¼ÉAiÀÄgÀ£ÀÄß M¼ÀUÉƼÀÄîªÀÅzÀÄ (r) ºÉÆgÀUÀĽzÀ J®è ªÀÄPÀ̼ÀÄ ªÀÄvÀÄÛ UÀ©üðt vÁAiÀÄA¢gÀ£ÀÄß M¼ÀUÉƼÀÄîªÀÅzÀÄ.
( ) ( ) ( ) ( )
(4) «Ä±À£ï EAzÀæzsÀ£Àĵï¸ÉêÉUÀ¼ÀÄ J°è zÉÆgÀPÀÄvÀÛªÉ? (J) C¢üPÀ ¤gÀAvÀgÀ ¥ÀæwgÀPÀët ªÁå¦ÛAiÀÄ ¥ÀæzÉñÀUÀ¼ÀÄ (©) PÀrªÉÄ ¤gÀAvÀgÀ ¥ÀæwgÀPÀët ªÁå¦ÛAiÀÄ ¥ÀæzÉñÀUÀ¼ÀÄ (¹) J®è ¸ÀPÁðj D¸ÀàvÉæUÀ¼ÀÄ (r) J®è SÁ¸ÀV D¸ÀàvÉæUÀ¼ÀÄ
( ) ( ) ( ) ( ) (5) «Ä±À£ï EAzÀæzsÀ£Àĵï¥sÀ¯Á£ÀÄ sÀ«UÀ¼À£ÀÄß J°è UÀÄwð¸ÀÄwÛÃj?
(J) ¸À«ÄÃPÉë¬ÄAzÀ (©) ¹ÌçäAUï¤AzÀ (¹) gÀPÀÛ¥ÀjÃPÉë¬ÄAzÀ (r) JvÀÛgÀ ªÀÄvÀÄÛ vÀÆPÀ vÀ¥Á¸ÀuɬÄAzÀ
( ) ( ) ( ) ( )
(6) AiÀiÁªÀ ªÀAiÀĹì£À ªÀÄPÀ̼ÀÄ F PÁAiÀÄðPÀæªÀÄzÀ¥sÀ¯Á£ÀÄ sÀ«UÀ¼ÁUÀĪÀgÀÄ? (J) 0-01 ªÀµÀð, UÀ©üðt vÁAiÀÄA¢gÀÄ (©) 0-6 ªÀµÀðUÀ¼ÀÄ, UÀ©üðt vÁAiÀÄA¢gÀÄ (¹) 0-5 ªÀµÀðUÀ¼ÀÄ, UÀ©üðt vÁAiÀÄA¢gÀÄ (r) 0-10 ªÀµÀð, UÀ©üðt vÁAiÀÄA¢gÀÄ
( ) ( ) ( ) ( )

102
(7) AiÀiÁªÀ ªÀAiÀĹì£À ªÀÄPÀ̽UÉ «Ä±À£ï EAzÀæzsÀ£Àĵï EgÀÄvÀÛzÉ? (J) ¸ÀA¥ÀÆtðªÁV ¥ÀæwgÀQë¹zÀ ªÀÄPÀ̼ÀÄ (©) C¥Ë¶ÖPÀvɬÄAzÀ PÀÆrzÀ ªÀÄPÀ̼ÀÄ (¹) ¨sÁUÀ±À B ¥ÀæwgÀQë¹zÀ ªÀÄPÀ̼ÀÄ (r) PÁ¬Ä¯ÉAiÀÄ ªÀÄPÀ̼ÀÄ
( ) ( ) ( ) ( ) (8) sÁUÀ±ÀB ¥ÀæwgÀPÀëuÉUÉ PÁgÀtUÀ¼ÁªÀªÀÅ?
(J) ZÀÄZÀÄѪÀĢݣÀ ¥ÀæAiÉÆÃd£ÀUÀ¼À §UÉÎ Cj«£À PÉÆgÀvÉ (©) ¥ÀæwgÀPÀ ëuÉAiÀÄ £ÀAvÀgÀ zÀĵÀàjuÁªÀÄUÀ¼ÁUÀĪÀ §UÉÎ ¨sÀAiÀÄ (¹) DgÉÆÃUÀå ¸ÉêÉUÀ¼À C®¨sÀåvÉ (r) ªÉÄð£À J®èªÀÇ
( ) ( ) ( ) ( )
(9) «Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ ¸À«ÄÃPÉë AiÀiÁgÀÄ ªÀiÁqÀÄvÁÛgÉ? (J) DgÉÆÃUÀ å C¢üPÁjUÀ¼ÀÄ (©) ¥ÀAZÁAiÀÄvÀ ¸ÀzÀ ÀågÀÄ (¹) gÁdQÃAiÀÄ ªÀÄÄRAqÀgÀÄ (r) ¸ÀPÁðgÉÃvÀgÀ ¸ÀA¸ÉÜUÀ¼ÀÄ
( ) ( ) ( ) ( )
(10) «Ä±À£ï EAzÀæzsÀ£ÀÄµï ¸À«ÄÃPÉëAiÀÄ°è AiÀiÁªÀ DgÉÆÃUÀå C¢üPÁjUÀ¼ÀÄ M¼ÀUÉƼÀÄîvÁÛgÉÉ? (J) ªÉÊzÀågÀÄ
(©) ANM
(¹) ¥ÀæAiÉÆÃUÁ®AiÀÄ vÀAvÀædÕgÀÄ (r) ªÀÄ£À±Á ÀÛçdÕgÀÄ
( ) ( ) ( ) ( )
(11) F PÁAiÀÄðPÀæªÀÄzÀ CrAiÀÄ°è ¥ÀæwgÀPÀëtªÀ£ÀÄß JµÀÄÖ ¸ÀÄvÀÄÛUÀ¼À°è PÉÊUÉƼÀî ÁUÀÄvÀÛzÉ? (J) 2 gËAqïUÀ¼ÀÄ (©) 3 gËAqïUÀ¼ÀÄ (¹) 4 gËAqïUÀ¼ÀÄ (¹) 5 gËAqïUÀ¼ÀÄ
( ) ( ) ( ) ( ) (12) ¥Àæw gËAqïUÉ JµÀÄÖ CªÀ¢ü?
(J) 3 ¢£ÀUÀ¼ÀÄ (©) 7 ¢£ÀUÀ¼ÀÄ (¹) 5 ¢£ÀUÀ¼ÀÄ (r) 6 ¢£ÀUÀ¼ÀÄ
( ) ( ) ( ) ( ) (13) «Ä±À£ï EAzÀæzsÀ£Àĵï¢AzÀ JµÀÄÖ ZÀÄZÀÄѪÀÄzÀÄÝ ¤gÉÆÃzsÀPÀ gÉÆÃUÀUÀ¼ÀÄ M¼ÀUÉƼÀÄîvÀÛªÉ?
(J) K¼ÀÄ (©) DgÀÄ (¹) JAlÄ (r) LzÀÄ
( ) ( ) ( ) ( )

103
(14) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ PÁAiÀiÁðªÀ¢ü JµÀÄÖ? (J) ¨É½UÉÎ 9 jAzÀ ¸ÁAiÀÄAPÁ® 6 UÀAmÉ (©) ¨É½UÉÎ 9 jAzÀ ªÀÄzsÁåºÀß 12 UÀAmÉ (¹) ¨É½UÉÎ 9 jAzÀ ªÀÄzsÁåºÀß 4 UÀAmÉ (r) ¨É½UÉÎ 9 jAzÀ ªÀÄzsÁåºÀß 2 UÀAmÉ
( ) ( ) ( ) ( )
(15) «Ä±À£ï EAzÀæzsÀ£Àĵï ZÀÄZÀÄѪÀÄ¢ÝUÁV ¸ÀܼÀUÀ¼ÁªÀªÀÅ? (J) ¥ÁæxÀ«ÄPÀ ±Á¯É, ¥ÉÆøïÖ ¥ÁmïðªÀiï ¸ÉAlgï (©) CAUÀ£ÀªÁr PÉÃAzÀæUÀ¼ÀÄ, NGO
(¹)PHC, ÀܽÃAiÀÄ ªÀÄÄRAqÀgÀ PÀlÖqÀUÀ¼ÀÄ (r) ªÉÄð£À J®èªÀÇ
( ) ( ) ( ) ( )
(16) «Ä±À£ï EAzÀæzsÀ£Àĵï CrAiÀÄ°è ¥sÀ¯Á£ÀÄ sÀ«UÀ½UÉ AiÀiÁªÀ PÁqïð PÉÆqÀ¯ÁUÀÄvÀÛzÉ? (J) DzsÁgï PÁqïð (©) ZÀÄZÀÄѪÀÄzÀÄÝ PÁqïð
(¹)gÉñÀ£ï PÁqïð (r) ªÀÄvÀzÁ£À UÀÄgÀÄw£À PÁqïð
( ) ( ) ( ) ( ) (17) «Ä±À£ï EAzÀæzsÀ£Àĵï¤AzÀ MzÀV À¯ÁUÀĪÀ ZÀÄZÀÄѪÀÄzÀÄÝUÀ¼ÀÄ AiÀiÁªÀªÀÅ?
(J) Pentavalent, BCG
(©)Measles, OPV
(¹)TT, Hepatitis-B
(r) ªÉÄð£À J®èªÀÇ
( ) ( ) ( ) ( )
(18) «Ä±À£ï EAzÀæzsÀ£Àĵï¤AzÀ UÀ©üðt vÁAiÀÄA¢jUÉ AiÀiÁªÀ ZÀÄZÀÄѪÀÄzÀÄÝ PÉÆqÀ¯ÁUÀÄvÀÛzÉ?
(J) DPT
(©)TT (¹)MMR
(r) OPV
( ) ( ) ( ) ( )
(19) PÀ£ÁðlPÀzÀ°è ªÁgÀzÀ AiÀiÁªÀ ¢£À ¥ÀæwgÀPÀët D ÀàvÉæAiÀÄ£ÀÄß £ÀqÉ À¯ÁUÀÄvÀÛzÉ? (J) UÀÄgÀĪÁgÀ (©) §ÄzsÀªÁgÀ (¹) ªÀÄAUÀ¼ÀªÁgÀ (r) ªÀÄAUÀ¼ÀªÁgÀ
( ) ( ) ( ) ( )
(20) «Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ ªÀiÁ»wAiÀÄ£ÀÄß ¸ÁªÀðd¤PÀjUÉ ºÉÃUÉ vÀ®Ä¦¸À¯ÁUÀÄvÀÛzÉ? (J) DgÉÆÃUÀ å C¢üPÁj (©) ¸ÀªÀÄƺÀ ªÀiÁzsÀåªÀÄ (¹) ¥ÀAZÁAiÀÄvÀ ¸ÀzÀ ÀågÀÄ (r) ªÉÄð£À J®èªÀÇ
( ) ( ) ( ) ( )

104
(21) «Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ eÁUÀÈwUÁV F PɼÀV£À AiÀiÁªÀ ZÀlĪÀnPÉAiÀÄÄ ¸ÀºÀPÁjAiÀiÁVzÉ? (J) vÁAiÀÄA¢gÀ ¨sÉÃn (©) ªÀÄ£É ¨sÉÃn (¹) ¸ÀªÀÄÄzÁAiÀÄ ¨sÉÃn (r) ªÉÄð£À J®èªÀÇ
( ) ( ) ( ) ( )
(22) F PɼÀV£À AiÀiÁªÀÅzÀÄ «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ AiÀıÀ¹ì£À §UÉÎ w½¸ÀÄvÀÛzÉ? (J) ¨sÁUÀ±ÀB ¥ÀæwgÀQëvÀ ªÀÄPÀ̼ÀÄ ªÀÄvÀÄÛ UÀ©üðt vÁAiÀÄA¢gÀ ¸ÀASÉåAiÀÄ°è E½PÉ (©) ¨sÁUÀ±ÀB ¥ÀæwgÀQëvÀ ªÀÄPÀ̼ÀÄ ªÀÄvÀÄÛ UÀ©üðt vÁAiÀÄA¢gÀ ¸ÀASÉåAiÀÄ°è KjPÉ (¹) PÁ¬Ä¯ÉAiÀiÁzÀ ªÀÄPÀ̼À ¸ÀASÉåAiÀÄ°è£À E½PÉ (r) PÁ¬Ä¯ÉAiÀiÁzÀ ªÀÄPÀ̼À ¸ÀASÉ åAiÀÄ°è£À KjPÉ
( ) ( ) ( ) ( )

105
« sÁUÀ-¹
«Ä±À£ï EAzÀæzsÀ£ÀĵïUÉ ÀA§A¢ü¹zÀAvÉ 5 ªÀµÀðQÌAvÀ QjAiÀÄ ªÀÄPÀ̼À vÁAiÀÄA¢gÀ
ªÀÄ£ÉÆà sÁªÀ ¤zsÁðgÀuÉUÁV °PÀmïð£ÀÀ ªÀiÁ£ÀzÀAqÀ(3 CA±ÀUÀ¼À °PÀmïð ªÀiÁ£ÀzÀAqÀ)
zÀAiÀÄ«lÄÖ F PɼÀUÉ PÉÆlÖ GvÀÛgÀUÀ¼À£ÀÄß N¢j ªÀÄvÀÄÛ ¤ªÀÄUÉ ÀÆPÀ۪ɤ¸ÀĪÀ DAiÉÄÌAiÀÄ ªÀÄÄAzÉ�
UÀÄvÀð£ÀÄß ªÀiÁr ¤ªÀÄä M¦àUÉAiÀÄ£ÀÄß ÀÆa¹j. ¤ÃªÀÅ MzÀV¹zÀ ªÀiÁ»wAiÀÄ£ÀÄß
UÀÄ¥ÀÛªÁVqÀ ÁUÀĪÀÅzÀÄ.zÀAiÀÄ«lÄÖ-‘M¦ààUɬÄzÉ’(A), ‘C¤¢ðµÀÖ’ (U) , ‘M¦àUÉ¬Ä®è’ (D) JA§ÄzÀ£ÀÄß
ªÀåPÀÛ¥Àr¹j.
\PÀæ. ÀA.
«µÀAiÀÄUÀ¼ÀÄ
¥ÀæwQæAiÉÄUÀ¼ÀÄ ÉÆÌÃgÀÄ A U D
(1) «Ä±À£ï EAzÀæzsÀ£ÀÄµï ªÀÄPÀ̼ÀÄ ªÀÄvÀÄÛ UÀ©üðt vÁAiÀÄA¢jUÉ G¥ÀAiÀÄÄPÀÛªÁzÀ PÁAiÀÄðPÀäªÁVzÉ
(2) «Ä±À£ï EAzÀæzsÀ£Àĵï PÁAiÀÄðPÀæªÀĪÀÅ ªÀÄPÀ̼À gÉÆÃUÀÀ ªÀÄvÀÄÛ ªÀÄgÀtzÀ ¥ÀæªÀiÁtªÀ£ÀÄß PÀrªÉĪÀiÁqÀ®Ä ÀºÀPÁjAiÀiÁVzÉ.
(3) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ ÉêÉUÀ¼À£ÀÄß ¥ÀqÉAiÀÄĪÀÅzÀÄ vÉÆAzÀgÉzÁAiÀÄPÀªÁVzÉ.
(4) «Ä±À£ï EAzÀæzsÀ£Àĵï 100% gÀµÀÄÖ ¥ÀÆtð ¥ÀæwgÀPÀët M¼ÀUÉƼÀî®Ä ¸ÀºÀPÁjAiÀiÁVzÉ.
(5) «Ä±À£ï EAzÀæzsÀ£Àĵï ÀA¥ÀÆtð ¥ÀæwgÀQëv À ªÀÄPÀ̽UÉ G¥ÀAiÀÄÄPÀÛªÁVzÉ.
(6) ¥ÀæwgÀQë ÀzÀ ºÁUÀÆ sÁUÀ±ÀB ¥ÀæwgÀQëv À ªÀÄPÀ̼ÀĪÀÄPÀ̼ÀÄ ¨Á®åzÀ gÉÆÃUÀUÀ½UÉ ªÀÄvÀÄÛ «PÀ®vÉUÉ UÀÄjAiÀiÁUÀÄvÁÛgÉ
(7) ¥ÀæwgÀPÀëuÉAiÀÄ ¥ÀæAiÉÆÃd£ÀUÀ¼À §UÉÎ ¥Á®PÀjUÉ Cj«®è¢gÀĪÀÅzÀÄ ¨sÁUÀ±ÀB ¥ÀæwgÀPÀëuÉUÉ PÁgÀtªÁVzÉ.
(8) ªÀÄPÀ̽UÉ J¯Áè ZÀÄZÀÄѪÀÄzÀÄÝUÀ¼ÀÆ CUÀvÀ å«®è. (9) ZÀÄZÀÄѪÀĢݣÀ ¤UÀ¢vÀ ºÁUÀÆ ¸ÀAZÁj
C¢üªÉñÀ£ÀUÀ¼ÀÄ EgÀÄvÀÛªÉ.
(10) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ ÉêÉUÀ¼À£ÀÄß GavÀªÁV MzÀV¸À ÁUÀÄvÀÛzÉ.
(11) «Ä±À£ï EAzÀæzsÀ£Àĵï PÀrªÉÄ ¥ÀæwgÀPÀët ¥ÀæzÉñÀUÀ¼À£ÀÄß ªÀiÁvÀæ M¼ÀUÉƼÀÄîvÀÛzÉ.
(12) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ ¸ÉêÉUÀ¼ÀÄ Erà PÀ£ÁðlPÀªÀ£ÀÄß M¼ÀUÉƼÀÄîvÀÛªÉ.
(13) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ ÉêÉUÀ¼ÀÄ PÀ ɪÉà DAiÀÄÝ wAUÀ¼ÀÄ ªÀiÁvÀæ ®¨sÀå«gÀÄvÀÛªÉ.
(14) «Ä±À£ï EAzÀæzsÀ£ÀĵïPÁÌV ¸ÀªÀÄƺÀªÀiÁzsÀåªÀĪÀÅ AiÀiÁªÀÅzÉà ¥ÁvÀæ ºÉÆA¢®è.

106
SCORING FOR STRUCTURED KNOWLEDGE QUESTIONNAIRE
Item no. Correct response score
1 d 1
2 c 1
3 d 1
4 b 1
5 a 1
6 b 1
7 c 1
8 d 1
9 a 1
10 b 1
11 c 1
12 b 1
13 a 1
14 c 1
15 d 1
16 b 1
17 d 1
18 b 1
19 a 1
20 d 1
21 d 1
22 a 1

107
SCORING FOR 3 POINT LIKERT SCALE
ITEM
NO
DIRECTION
OF
SCORING
AGREE UNDECIDED DISAGREE
1 + 3 2 1
2 + 3 2 1
3 - 1 2 3
4 - 1 2 3
5 - 1 2 3
6 + 3 2 1
7 + 3 2 1
8 - 1 2 3
9 + 3 2 1
10 + 3 2 1
11 + 3 2 1
12 - 1 2 3
13 + 3 2 1
14 - 1 2 3
Maximum score=42
SCORING
1. Unfavorable attitude:< 50%
2. Neutral attitude :50-75%
3. Favorable attitude:>75%

108
MASTER CHART
Sl.
No
Demographic variables of mothers of under 5 children Pre test Post test
1 2 3 4 5 6 7 8 9 A 9B Knowledge
Total
Attitude
Total
Knowledge
Total
Attitude
Total
1. c A d a a b a a b
11 30 17 38
2. c A c a a b b a b
10 32 15 37
3. c a b e b a a a a b 10 29 14 33
4. c a b b a a c a b
7 30 12 32
5. c a d a b a b b a b 10 30 18 36
6. b a b a a a b b b
10 30 14 34
7. c a d b a b b a a b 9 28 18 37
8. b a a b a c a a a a 4 30 12 34
9. d a d a a a b a a a 10 29 18 37
10. b a e d b b a a a a 14 32 19 37
11. d a b a a a a a b
7 31 13 33
12. b a d a b a a b b
12 35 18 38
13. b a e a c b a a b
12 34 19 39
14. b a e a b b a a b
8 33 18 35
15. a a d a a a a a b
8 28 17 35
16. b a d a b b a a b
8 28 17 35
17. c a e c a a a b b
12 32 20 37
18. b a c a c c a b a d 8 27 16 36
19. b c d a a b b a b
5 30 18 38
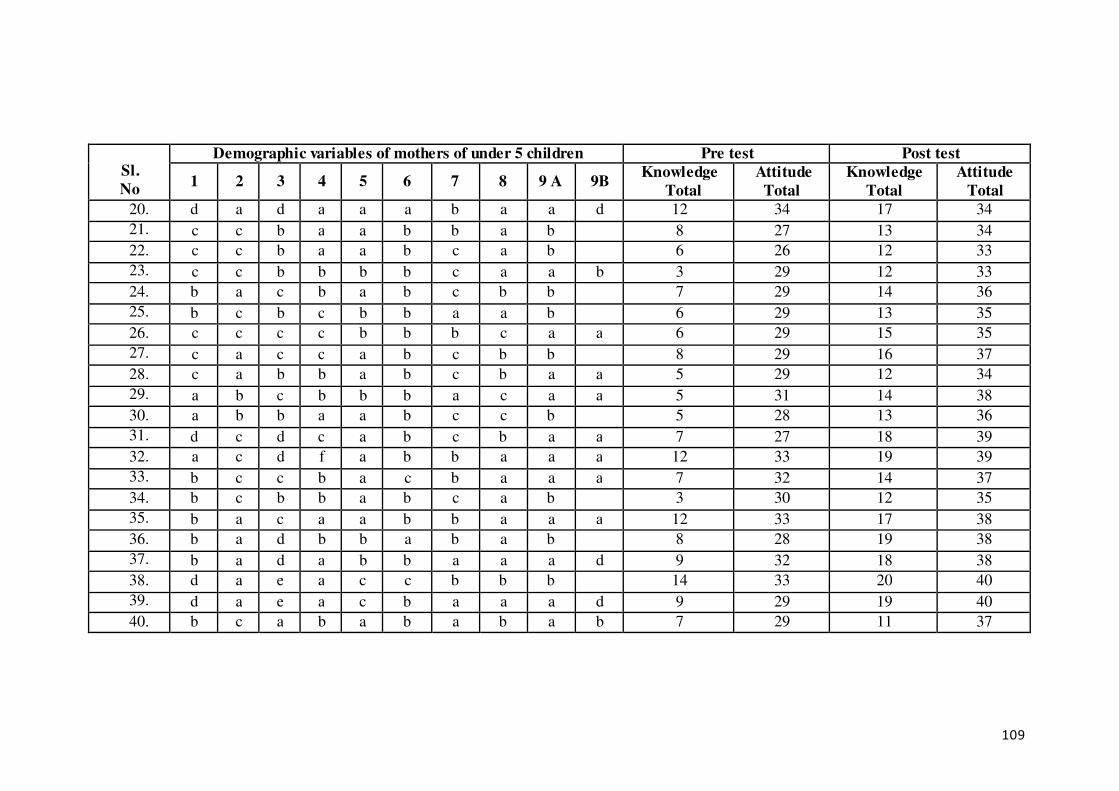
109
Sl.
No
Demographic variables of mothers of under 5 children Pre test Post test
1 2 3 4 5 6 7 8 9 A 9B Knowledge
Total
Attitude
Total
Knowledge
Total
Attitude
Total
20. d a d a a a b a a d 12 34 17 34
21. c c b a a b b a b
8 27 13 34
22. c c b a a b c a b
6 26 12 33
23. c c b b b b c a a b 3 29 12 33
24. b a c b a b c b b
7 29 14 36
25. b c b c b b a a b
6 29 13 35
26. c c c c b b b c a a 6 29 15 35
27. c a c c a b c b b
8 29 16 37
28. c a b b a b c b a a 5 29 12 34
29. a b c b b b a c a a 5 31 14 38
30. a b b a a b c c b
5 28 13 36
31. d c d c a b c b a a 7 27 18 39
32. a c d f a b b a a a 12 33 19 39
33. b c c b a c b a a a 7 32 14 37
34. b c b b a b c a b
3 30 12 35
35. b a c a a b b a a a 12 33 17 38
36. b a d b b a b a b
8 28 19 38
37. b a d a b b a a a d 9 32 18 38
38. d a e a c c b b b
14 33 20 40
39. d a e a c b a a a d 9 29 19 40
40. b c a b a b a b a b 7 29 11 37

110
Sl.
No
Demographic variables of mothers of under 5 children Pre test Post test
1 2 3 4 5 6 7 8 9 A 9B Knowledge
Total
Attitude
Total
Knowledge
Total
Attitude
Total
41. c a d a b b b b b
12 35 20 39
42. c a e e a b a a a a 19 32 22 42
43. c a d e a b b a a a 17 32 22 38
44. d a e e a b b a a d 15 34 22 40
45. b a e e b b a a a a 17 28 20 41
46. d a e e c c a a a d 17 36 21 40
47. b a c c b b a a b
9 34 15 38
48. b a b b a a a a b
6 26 13 36
49. c a b b a a c a b
7 24 13 35
50. c a d b a a b a b
7 29 18 42
51. b a d b a b c b b
6 30 18 40
52. a a b c a a a b b
6 32 14 38
53. b a d c b b b a b
5 28 18 38
54. b d d c a b b a b
4 29 18 40
55. b b c b a a b a b
7 29 16 36
56. b c b b a b a a b
3 29 14 36
57. b d c c a b a a b
5 35 17 40
58. b d e c c a b a b
10 31 22 42
59. a a d a a b a b b
7 26 18 38
60. b a d d c b a a b
5 30 17 38

111

112
ANNEXURE I
LETTER SEEKING AND GRANTING PERMISSION FOR COUNDUCTING
RESEARCH STUDY

113

114
ANNEXURE II (a)
EDUCATIONAL PLAN ON MISSION INDRADHANUSH
Name of the researcher : Mrs. Jyotima Borgohain Handique
Name of the topic : Mission Indradhanush
Group : Mothers of under five children
Method of teaching : Lecture and group discussion
Date and time :--/--/2018
Place : Kengeri Upanagar
Duration : 45 minutes -1 hour
Medium of instruction : Kannada
AV aids : Flash cards, pamphlets and leaflets

115
OBJECTIVES
General objective: At the end of the educational package session, the mothers ofunder five children will gain knowledge regarding Mission
Indradhanush.
Specific objectives: At the end of the educational package, the learner will be able to
1. introduce the concept of Mission Indradhanush
2. enumerate the objectives of Mission Indradhanush
3. explain the strategy of Mission Indradhanush
4. describe about the operational planning Mission Indradhanush
5. explain about the life threatening diseases of children
6. describe about Universal immunization schedule
7. discuss the success of Mission Indradhanush

116
Time Specific
O bjectives Content
Researcher activities
Learning activities
A.V Aids
Evaluation
5 min To
introducethe
concept of
Mission
Indradhanush
Introduction and concept of Mission Indradhanush
� Mission Indradhanush was launched by the
Government of India under Ministry of Health and
Family Welfare, on 25th December 2014.
� Immunization forms the major focus of child survival programme throughout the world.
� It depicts the seven colour of rainbow, target seven
killer diseases such as diphtheria, pertusis or
whooping cough, tetanus, poliomyelitis,
tuberculosis, measles and hepatitis B. Also vaccine to guard against Japanese encephalitis and
haemophilus influenza type B are provided in
selected districts.
� The mission focuses on interventions to improve
full immunization coverage in India from 65% in 2014 to at least 90% children in the next five
years. This is done through special catch-up
drives.
� Under Mission Indradhanush, the government has
identified 201 high focus districts across the country that have nearly 50% of all unvaccinated
or partially vaccinated children in the country.
Researcher
introduce the
concept of
Mission
Indradhanush
Learners
listen
attentively
Flash card What is the
concept of
Mission
Indradhanush?
5 min To enumerate
the objectives
of Mission
Objectives of Mission Indradhanush
General objective
Researcher
enumerate the
Learners
listen
Flash card What are the
objectives of
Mission

117
Indradhanush
The objective is to ensure high coverage of children and pregnant women with all available vaccines
throughout the country, with emphasis on the identified
201 high focus districts.
Specific objectives
With the launch of Mission Indradhanush, the
Government aims at
1. Generating high demand for immunization
services by addressing communication challenges.
2. Enhancing political, administrative and financial commitment through advocacy with key
stakeholders;
3. Ensuring that partially immunized and
unimmunized children are fully immunized as per
National Immunization schedule.
objectives of Mission
Indradhanush
carefully Indradhanush?
3 min To explain
strategy of Mission
Indradhanush
Strategy of Mission Indradhanush
The Government has planned to conduct four special vaccination campaigns between January and June 2015.
All vaccines are already available free of cost under
Universal Immunization programme in India. Under this
mission, Government plans to intensify its efforts and thus
increase accessibility of these vaccines to all the children of India.
Researcher
explains the strategy of
Mission
Indradhanush
Learner
listen carefully
Flash
card
Whatis the
strategy of Mission
Indradhanush?

118
9 min To describe
about the operational
planning of
Mission
Indradhanush
Describe about the operational planning of Mission
Indradhanush The following two operational mechanisms will be
utilized to reach out to the unreached or poorly reached
beneficiaries:
a) Fixed and outreach sessions
Sites for vaccination
In urban areas, urban health posts, post-partum
(PP) centers, family welfare centres or local
leader’s premises in urban slums can also be used
immunization sites. For other areas, primary
schools, anganwadi centers, private dispensaries, non-governmental organization (NGO) sites or any
other locations that are easily accessible and
acceptable to community can be used as
immunization sites.
Availability of human resources
In addition to health staff available from the same
or neighboring community health center
(CHC)/Block PHC, NGOs (LIONS, Rotary etc.), it
is necessary to utilize retired health workers, and
staff available from other government agencies such as Employee’s State Insurance Corporation,
Ventral Government Health Scheme, armed forces,
Researcher
describes about the
operational
planning of
Mission
Indradhanus
Learners
listen attentively
Pamphlets What arethe
operational planning of
Mission
Indradhanush?

119
railways, District Urban Development Agency (DUDA)/State Urban Development agency
(SUDA) and community based organizations to
reach large number of children.
Timing:The activity will be conducted from 9 am to 4 pm. However, sessions should be planned
based on availability of the targeted population to
maximize the benefits achieved.
Team: A team will comprise one vaccinator and
up to two mobilizers (at least one should be from local mohallas/locality). An additional vaccinator
will be included in the team if the estimated
injection load is more than 60-70.
b) Mobile sessions
Mobile sessions should be planned at places where routine immunization coverage is weak and the
small number of beneficiaries does not warrant an
independent session. These areas include peri-
urban areas, scattered slums, brick kilns and
construction sites.
10min To explain
about the life
threatening diseases of
children
Explain about the life threatening diseases of children
The seven vaccine preventable diseases are diphtheria,
whooping cough, tetanus, polio, TB, measles and Hepatitis B.
These seven diseases are common in children and they
can be prevented by immunization. Immunizations are
given to young children starting at birth.
Researcher
explain about
the life threatening
diseases of
children
Learner
listen
carefully
Flash card Explain about
the life
threatening diseases of
children.

120
Children who are not immunized at all or not fully immunized they get these diseases, are often very sick and
many of them die. A number of them remain with
permanent damage (handicap) from the disease.
Tuberculosis - It is spread to other through the air. Sign and symptoms are chronic cough and loss of weight; if the
disease is not treated the child becomes very sick and dies.
But children who have been immunized will not get
tuberculosis.
Whooping cough - It causes cough which occurs continuously and ends with a whoop. The child also has
fever and a running nose. At the end of each whoop the
child may vomit. If the disease is not treated early the
child may die, and those who survive many develop
malnutrition. If the child receives 3 doses of vaccination he is protected against whooping cough.
Diphtheria- Children with diphtheria have fever, and a
membrane which covers the throat causing difficulty in
breathing. This membrane may suffocate the child to
death. It is prevented by 3 doses of immunization.
Tetanus- The germ enter the body through cuts or bruises.
They may enter through a thorn prick or umbilical cord of
new born child. Who have tetanus cannot open their
mouth and they are rigid. And often die if they receive
treatment. Immunization against tetanus is given starting from 6 weeks of age, and to pregnant mothers.

121
Measles- This is a common infection in children and can attack many children at once. It spread from one person to
another through the air during coughing, sneezing or
talking.
The child become very sick with fever skin rash, sticky red eyes and coughing. The cough is like the
barking of a dog. Some develop dehydration due to
diarrhea and vomiting. Some recover but many dies.
There is no medicine to cure measles and it can be
prevented by immunization.
Polio -It is a dangerous disease that causes paralysis of the
body. The germ is passed in faces and many spread from
one person to another by mean of unwashed hands, flues,
contaminated food. If the child does not die from polio, he
remains with permanent paralysis. There is no treatment for polio.
Hepatitis B- It is the inflammation of liver due to the
Hepatitis B virus. People with chronic hepatitis may have
no symptom, but gradual liver damage may be occurring.
They may have symptom of acute hepatitis like loss of appetite, fatigue, low grade fever, muscle & joint ache,
nausea & vomiting, yellow skin &dark urine due to
jaundice

122
5 min To describe about
Universal
immunization
schedule
Describe about Universal immunization schedule
Researcher Describe
about
Universal
immunization schedule
Learner listen
carefully
Leaflet Describe about
Universal
immunization
schedule

123
4 min To discuss the success of
Mission
Discuss the success of Mission Indradhanush
Government of India partnering with WHO, UNICEF and
other partners to leverage the knowledge and
Researcher discuss the
success of
Mission
Learner listen
carefully
Flash card Discuss about the success of
Mission

124
Indradhanush infrastructure built during the polio campaign to step this mission around 2000 doctors and field monitors who were
working with the WHO on the Polio eradication
programme are now part of this nationwide initiative of
vaccinate all unvaccinated and partially vaccinated children.
Under the mission, the Government has indentified 201
high focus districts across the country. These districts
have been identified based on a composite indicator,
considering full immunization coverage, number of partially vaccinated. And unvaccinated children and
whether the district is an identified High Priority Districts
(HPD). Nearly 50% of all unvaccinated or partially
vaccinated children in India are in these 201 districts.
A total in the first phase 9, 66495 sessions were held and around 7.6 million children were immunized .The second
phase 352 districts were selected including 279 mid
priority districts.
But this increase would not be sufficient to achieve
Full Immunization Coverage in selected districts/cities that have been shown slow progress in spite of repeated
phages of Mission Indradhanush, so Government has
modified the mission to Intensified Mission Indradhanush
for low coverage areas.
Seeing its wider coverage mission Indradhanush has been a success till now in order to improve the immunization
coverage particularly in the underprivileged and
Indradhanush Indradhanush

125
underserved communities and reduce childhood mortality due to vaccine preventable disease.
4 min To summarize
and conclude
the topic
Summary and Conclusion
Mission Indradhanush depicting 7 colours of rainbow
provides vaccination to 7 vaccine preventable disease
which includes diphtheria, whooping cough, tetanus,
polio, TB, measles, hepatitis-B. The new vaccines
rotavirus, measles rubella, inactivated polio vaccine, Japanese encephalitis for adults are also included.
With these now 11 vaccines have been covered under this
programme. In one year time 1.62 crores children have
been additionally brought under ambit of immunization an
about 45 lacks have been totally immunized additionally. Mission Indradhanush aims at covering all children by
2020 who are either unvaccinated or are partially
vaccinated against these vaccine preventable diseases.
Researcher summarize
the topic.
Learner listen
carefully

126
Bibliography
1. Mission Indradhanush. Operational Guidelines. Available from http://www.tripuranrhn.gov.in/guidelines/0701201701.pdf
2. Mission Indradhanush phase 1: Final coverage report. Accessed fromhttp://www.missionindradhanush.in/about
3. Md Abu Bashar, Success story of Mission Indradhanush: A road to achieve universal immunization, National Journal of Community
medicine, May 2016; Issue - 5 Volume - 7,
4. Mission Indradhanush Immunization Program, Accessed from http://www.civilsdaily.com/story/mission-indradhanush-immunization-program/
5. Akhilesh Kumar Singh, Research scholar, Department of Economics, Lucknow University, Lucknow, Mission Indradhanush: The Art of
Health and Healing, Indian Streams Research Journal, April 2016; Issue – 3 volume – 6
6. Mission Indradhanush to get a new name as four new vaccines have been added into it accessed from http://www.newsbharati.com/Encyc/2016/5/31/Mission-/indradhanush-programme-vaccination
7. CHAPTER 8. The Six Immunisable Diseases accessed from http://www.nzdl.org/gsdlmod?e=d-00000-00---off-0cdl--00-0----0-10-0---0-
--0direct-10---4-------0-1l--11-en-50---20-about---00-0-1-00-0--4----0-0-11-10-0utfZz-8-
00&cl=CL1.68&d=HASH01221928a8ae1bc2f8253cba.13>=1

127
ANNEXURE II (b)
«Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ ¥ÁoÀ AiÉÆÃd£É
¹zÀÞ¥Àr¹zÀªÀgÀÄ
eÉÆåÃwªÀiÁ ¨ÉÆUÉÆÃðºÉÃ£ï ºÁåArPï
¥ÀzÀä²æà E£Àì¹ÖlÆåmï D¥sï £À¹ðAUï

128
ÉAUÀ¼ÀÆgÀÄ
«Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ ¥ÁoÀ AiÉÆÃd£É
ÀA±ÉÆÃzsÀPÀgÀ ºÉ ÀgÀÄ : ²æêÀÄw eÉÆåÃwªÀiÁ ÉÆUÉÆÃðºÉÃ£ï ºÁåArPï
«µÀAiÀÄzÀ ºÉ ÀgÀÄ : «Ä±À£ï EAzÀæzsÀ£Àĵï
ÀªÀÄƺÀ : 5 ªÀµÀðQÌAvÀ PÀrªÉÄ ªÀAiÀĹì£À ªÀÄPÀ̼À vÁAiÀÄA¢gÀÄ
PÀ°PÁ «zsÁ£À : G¥À£Áå À ªÀÄvÀÄÛ ¸ÀªÀÄƺÀ ZÀZÉð
¢£ÁAPÀ ªÀÄvÀÄÛ ÀªÀÄAiÀÄ : ___/___/________
ÀܼÀ :
CªÀ¢ü : 45 ¤«ÄµÀ¢AzÀ 1 UÀAmÉ
¨ÉÆÃzsÀ£Á ªÀiÁzsÀåªÀÄ : PÀ£ÀßqÀ
±ÀæªÀt-zÀȱÀå À®PÀgÀuÉUÀ¼ÀÄ : ¥sÁè±ï PÁqïðUÀ¼ÀÄ, eÁ»ÃgÀÄUÀ¼ÀÄ ªÀÄvÀÄÛ °Ã¥sï¯ÉmïUÀ¼ÀÄ

129
«Ä±À£ï EAzÀæzsÀ£ÀÄµï §UÉÎ ¥ÁoÀ AiÉÆÃd£É
GzÉÝñÀUÀ¼ÀÄ:
¸ÁªÀiÁ£Àå GzÉÝñÀUÀ¼ÀÄ: F ±ÉÊPÀ ëtÂPÀ ¥ÁåPÉÃeï C¢üªÉñÀ£ÀzÀ £ÀAvÀgÀ, 5 ªÀµÀðQÌAvÀ QjAiÀÄ ªÀÄPÀ̼À vÁ¬ÄAiÀÄÄ «Ä±À£ï EAzÀæzs À£ÀĵïUÉ ¸ÀA§A¢ü¹zÀ eÁÕ£ÀªÀ£ÀÄß ¥ÀqÉAiÀÄĪÀ¼ÀÄ.
«±ÉõÀ GzÉÝñÀUÀ¼ÀÄ:F ±ÉÊPÀëtÂPÀ ¥ÁåPÉÃeï£ÀAvÀgÀ, PÀ°PÉzÁgÀ£ÀÄ F PɼÀV£ÀªÀÅUÀ½UÉ ¸ÀªÀÄxÀð£ÁUÀĪÀ£ÀÄ.:
1) «Ä±À£ï EAzÀæzsÀ£Àĵï£À ¥ÀjPÀ®à£ÉAiÀÄ£ÀÄß ¥ÀjZÀ¬Ä¸ÀĪÀÅzÀÄ..
2) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ GzÉÝñÀUÀ¼ÀÄ £ÀªÀÄÆ¢¸ÀĪÀÅzÀÄ.
3) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ PÁAiÀÄð¤ÃwAiÀÄ£ÀÄß «ªÀj¸ÀĪÀÅzÀÄ.
4) «Ä±À£ï EAzÀæzsÀ£ÀĵïzÀ PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£ÉAiÀÄ §UÉÎ «ªÀj¸ÀĪÀÅzÀÄ.
5) ªÀÄPÀ̼À ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À §UÉÎ «ªÀj¸ÀĪÀÅzÀÄ.
6) ¸ÁªÀðwæPÀ ¥À æwgÀPÀët ±ÉqÀÆå ï §UÉÎ «ªÀj¸ÀĪÀÅzÀÄ.
7) «Ä±À£ï EAzÀæzsÀ£Àĵï AiÀıÀ¹ì£À §UÉÎ ZÀað¸ÀĪÀÅzÀÄ.
130
¸ÀªÀÄAiÀÄ «±ÉõÀ
GzÉÝñÀUÀ¼ÀÄ
«µÀAiÀÄ
¸ÀA±ÉÆÃzsÀPÀgÀ ZÀlĪÀnPÉ
PÀ°PÉzÁgÀgÀ ZÀlĪÀnPÉ
zÀȱÀå-±ÀæªÀt ¸ÁªÀÄVæ
ªÀiË®åªÀiÁ¥À£À
5 ¤«ÄµÀ
«Ä±À£ï EAzÀæzsÀ£ÀÄµï ¥ÀjPÀ®à£É ¥ÀjZÀ¬Ä ÀĪÀÅzÀÄ.
¦ÃpPÉ: ªÀÄvÀÄÛ «Ä±À£ï EAzÀæzsÀ£ÀÄµï ¥ÀjPÀ®à£É:
� sÁgÀvÀ ÀPÁðgÀªÀÅ DgÉÆÃUÀå ªÀÄvÀÄÛ PÀÄlÄA§ PÀ Á åt ÀaªÁ®AiÀÄzÀ CrAiÀÄ°è «Ä±À£ï EAzÀæzsÀ£Àĵï
AiÉÆÃd£ÉAiÀÄ£ÀÄß 25 £É r ÉA§gï 2014 gÀAzÀÄ DgÀA©ü¹vÀÄ.
� ¥ÀæwgÀPÀëuÉAiÀÄÄ «±ÀézÁ åAvÀ ªÀÄPÀ̼À ÀAgÀPÀëuÁ PÁAiÀÄðPÀæªÀÄzÀ ¥ÀæªÀÄÄR «µÀAiÀĪÁVzÉ.
� CzÀÄ PÁªÀÄ£À©°è£À K¼ÀÄ §tÚUÀ¼À£ÀÄß ÀÆa ÀÄwÛzÀÄÝ, D ªÀÄÆ®PÀ K¼ÀÄ ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À£ÀÄß GzÉÝò ÀÄvÀÛzÉ. CªÀÅUÀ¼ÉAzÀgÉ-UÀAl®Ä ªÀiÁj, £Á¬ÄPɪÀÄÄä CxÀªÁ G§â À PɪÀÄÄä, zsÀ£ÀĪÁðAiÀÄÄ, ªÀÄPÀ̼À ¥Á±ÀéðªÁAiÀÄÄ, PÀëAiÀÄgÉÆÃUÀ, zÀqsÁgÀ ªÀÄvÀÄ Û ºÉ¦mÉÊn¸ïB C®èzÉ d¥Á¤ ªÀĹ۵ÉÆÌÃzÀæPÀ ªÀÄvÀÄÛ ºÉªÉÆæü°¸ï E£ï¥sÀÄèAiÀÄ£ïì PÁ¬Ä ÉUÀ¼À «gÀÄzÀÞ ZÀÄZÀÄѪÀÄzÀÝ£ÀÄß ªÀAiÀÄ ÀÌjUÁV DAiÀÄÝ f ÉèUÀ¼À°è MzÀV À ÁUÀÄvÀÛzÉ.
� sÁgÀvÀzÀ°è 2014 gÀ°è£À 65% jAzÀ 90% gÀµÀÄ Ö ªÀÄPÀ̽UÉ ªÀÄÄA¢£À LzÀÄ ªÀµÀðUÀ¼À°è ÀA¥ÀÆtð
ÀA±ÉÆÃzsÀPÀgÀÄ «Ä±À£ï EAzÀæzsÀ£ÀÄµï ¥ÀjPÀ®à£É ¥ÀjZÀ¬ÄvÁÛgÉ.
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
¥sÁè±ï PÁqïð
«Ä±À£ï EAzÀæzsÀ£ÀÄµï ¥ÀjPÀ®à£É JAzÀgÉãÀÄ?

131
¥ÀæwgÀPÀët ªÁå¦ÛAiÀÄ£ÀÄß ÀÄzsÁj À®Ä EgÀĪÀ ªÀÄzsÀå¹ ÜPÉUÀ¼À ªÉÄÃ É F «Ä±À£ï ɼÀPÀÄ ZÉ®ÄèvÀÛzÉ. EzÀ£ÀÄß «±ÉõÀ PÁAiÀiÁðZÀgÀuÉUÀ¼À ªÀÄÆ®P À ªÀiÁqÀ ÁUÀÄvÀÛzÉ.
� «Ä±À£ï EAzÀæzsÀ£Àĵï CrAiÀÄ°è, ÀPÁðgÀªÀÅ sÁgÀvÀzÁzÀ åAvÀ 201 C¢üPÀ MvÀÄÛ ¤ÃqÀĪÀ f ÉèUÀ¼À£ÀÄß
UÀÄgÀÄw¹zÀÄÝ, CzÀgÀ°è ÀĪÀiÁgÀÄ 50% gÀµÀÄ Ö ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃqÀzÀ CxÀªÁ sÁUÀ±À: ZÀÄZÀÄѪÀÄzÀÄ Ý ¤ÃqÀzÀ ªÀÄPÀ̼ÀÄ M¼ÀUÉƼÀÄîvÁÛgÉ.
� «Ä±À£ï EAzÀæzsÀ£Àĵï ÉêÉUÀ¼ÀÄ PÀ£ÁðlPÀzÀ 6 f ÉèUÀ¼À°è ® sÀå«gÀÄvÀÛªÉ.
5 ¤«ÄµÀ
«Ä±À£ï EAzÀæzsÀ£Àĵï GzÉÝñÀUÀ¼À£ÀÄß «ªÀj ÀĪÀÅzÀÄ.
«Ä±À£ï EAzÀæzsÀ£Àĵï£À GzÉÝñÀUÀ¼ÀÄ:
¸ÁªÀiÁ£Àå GzÉÝñÀUÀ¼ÀÄ: ® sÀå«gÀĪÀ J®è
ZÀÄZÀÄѪÀÄzÀÄÝUÀ½AzÀ gÁµÀÖçzÀ°è£À J®è ªÀÄPÀ̽UÉ ªÀÄvÀÄ Û UÀ©üðt ªÀÄ»¼ÉAiÀÄjUÉ ÀA¥ÀÆtð ¥ÀæwgÀPÀëuÉ MzV ÀĪÀÅzÀÄ. C®èzÉ UÀÄgÀÄw¹zÀ 201 C¢üPÀ GvÀÄÛ¤ÃqÀĪÀ f ÉèUÀ¼À §UÉÎ MvÀÄÛ ¤ÃqÀĪÀÅzÀÄ.
«±ÉõÀ GzÉÝñÀUÀ¼ÀÄ:«Ä±À£ï EAzÀæ¥Àæ¸ïÜ DgÀA©ü¹zÀ
ÀA±ÉÆÃzsÀPÀgÀÄ «Ä±À£ï EAzÀæzsÀ£Àĵï GzÉÝñÀUÀ¼À£ÀÄß «ªÀj ÀÄvÁÛgÉ.
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
¥sÁè±ï PÁqïð
«Ä±À£ï EAzÀæzsÀ£Àĵï GzÉÝñÀUÀ¼ÀÄ AiÀiÁªÀªÀÅ?

132
£ÀAvÀgÀ ÀPÁðgÀªÀÅ »ÃUÉ GzÉÝò ÀÄvÀÛzÉ:
1) ÀªÀÄÄzÁAiÀÄzÀ ÀªÁ®ÄUÀ¼À£ÀÄß JzÀÄj ÀĪÀÅzÀjAzÀ ¥ÀæwgÀPÀët ÉêÉUÀ½UÁV C¢üPÀ ÉÃrPÉAiÀÄ£ÀÄß GAlĪÀiÁqÀĪÀÅzÀÄ.
2) ¥ÀæªÀÄÄR ªÀÄzs Àå ÀÜUÁgÀgÀ ÀºÀ sÁVvÀézÀ ªÀÄÆ®P À gÁdQÃAiÀÄ, DqÀ½vÁvÀäPÀ ºÁUÀÆ ºÀtPÁ¹£À §zÀÞvÉAiÀÄ£ÀÄß ªÀ¢üð ÀĪÀÅzÀÄ.
3) gÁ¶ÖçÃAiÀÄ ¥ÀæwgÀPÀët PÁAiÀiÁðªÀ¢üAiÀÄ£ÀéAiÀÄ sÁUÀ±ÀB ¥ÀæwgÀQëvÀªÁzÀ ºÁUÀÆ ¥ÀæwgÀQëvÀªÁU À¢gÀĪÀ ªÀÄPÀ̽U É ÀA¥ÀÆtðªÁV ¥ÀæwgÀPÀëuÉ ªÀiÁqÀ ÁVzÀ JJA§ÄzÀ£ÀÄß
RavÀ¥Àr ÀĪÀÅzÀÄ.
3 ¤«ÄµÀ
«Ä±À£ï EAzÀæzsÀ£Àĵï CrAiÀÄ°è MvÀÄÛ¤ÃqÀĪÀ PÉëÃvÀæUÀ¼À£ÀÄß ¥ÀnÖªÀiÁrj.
MvÀÄÛ ¤ÃqÀĪÀ PÉëÃvÀæUÀ¼ÀÄ
F «Ä±À£ï ªÀÄÆ®PÀ vÀ®Ä¦zÀ ªÀÄÄRå PÉëÃvÀæUÀ¼ÀÄ »ÃVªÉ:
1) SÁ°¬ÄgÀĪÀ G¥À-PÉÃAzÀæUÀ¼À PÉëÃvÀæUÀ¼ÀÄ: 3 wAUÀ½VAvÀ ºÉZÀÄÑ CªÀ¢üAiÀÄ ªÀgÉUÉ AiÀiÁªÀÅzÉà ÀºÁAiÀÄPÀ £À¸ïð
«ÄqÀªÉ Ê¥sïUÀ¼À£ÀÄß (ANM)¤AiÉÆÃf¹®è.
2) ªÀÄÆgÀÄ CxÀªÁ ºÉZÀÄÑ PÀæªÀiÁ£ÀÄUÀvÀ vÀ¦àzÀ ¤gÀAvÀgÀ
ÀA±ÉÆÃzsÀPÀgÀīıÀ£ï EAzÀæzsÀ£Àĵï CrAiÀÄ°è MvÀÄÛ¤ÃqÀĪÀ PÉëÃvÀæUÀ¼À£ÀÄß ¥ÀnÖªÀiÁqÀÄvÁÛgÉ
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
°Ã¥sï Émï & ¥sÁè±ï PÁqïð
«Ä±À£ï EAzÀæzsÀ£Àĵï CrAiÀÄ°è MvÀÄÛ¤ÃqÀĪÀ ªÀÄÄRå PÉëÃvÀæUÀ¼À£ÀÄß ºÉ Àj¹j.

133
¥ÀæwgÀPÀët (RI)C¢üªÉñÀ£ÀUÀ¼ÀÄ:¢üÃWÀðPÁ®zÀ gÀeÉ CxÀªÁ EvÀgÀ EAvÀºÀzÉà PÁgÀtUÀ¼À ªÉÄðgÀĪÀ ANM.
3) ¥ÉÆðAiÉÆà ¤ªÀÄÆð®£Á PÁAiÀÄðPÀæªÀÄ¢AzÀ UÀÄvÀð¹zÀ C¢üPÀ C¥ÁAiÀÄ PÉëÃvÀæUÀ¼ÀÄ (HRAS). EªÀÅUÀ¼ÀÄ F PɼÀPÀAqÀ ¥ÀæzÉñÀUÀ¼À°è ªÁ¹ ÀĪÀ d£À ÀASÉåAiÀÄ£ÀÄß M¼ÀUÉÆüÀîvÀÛªÉ
• ªÀ® ɬÄAzÀ PÀÆrzÀ £ÀUÀgÀ PÉƼÀZÉ¥ÀæzÉñÀUÀ¼ÀÄ.
• C ɪÀiÁj vÁtUÀ¼ÀÄ.
• EnÖUÉ UÀÆqÀÄUÀ¼ÀÄ.
• ¤ªÀiÁðt vÁtUÀ¼ÀÄ.
• EvÀgÀ ªÀ® É vÁtUÀ¼ÀÄ d£À ÀASÉåAiÀÄ£ÀÄß ÀܼÁAvÀj¹zÀ «ÄãÀÄUÁgÀ- UÁæªÀÄUÀ¼ÀÄ, £À¢
¥ÀæzÉñÀUÀ¼ÀÄ
• PÁ¬ÄÝj À ÁgÀzÀÄ ªÀÄvÀÄÛ vÀ®Ä¥À®Ä PÀptªÁzÀ d£À ÀASÉå (PÁqÀÄ ªÀÄvÀÄÛ §ÄqÀPÀlÄÖ d£À ÀASÉåUÀ¼ ÀÄ, UÀÄqÀØUÁqÀÄ ¥ÀæzÉñÀUÀ¼ÀÄ EvÁå¢UÀ¼ÀÄ)
4) JgÀqÀÄ ªÀµÀðUÀ¼À°è zÀqÁgÀ, UÀAl®ªÀiÁj ºÁUÀÆ ¤AiÉÆãÁl¯ï nmÁ£À ï- ¥ÀæPÀgÀtUÀ½AzÀ
UÀÄwð À®àlÖ PÀrªÉÄ RI ªÁå¦ÛAiÀÄ ¥ÀæzÉñÀUÀ¼ÀÄ 5) ÀtÚ UÁæªÀÄUÀ¼ÀÄ, PÉÆ¥Àà®ÄUÀ¼ÀÄ, zsÀ¤¸ï, ¥ÀÄgï §¸ï,

134
§¸Á¸ï (¥ÀæzÉñÀ UÀÆr À®ÄUÀ¼ÀÄ) EvÁå¢UÀ¼À£ÀÄß RI
C¢üªÉñÀ£ÀUÀ½UÁV EvÀgÀ UÁæªÀÄUÀ¼ÉÆA¢UÉ ÀAAiÉÆÃf À Á¬ÄvÀÄ
9 ¤«ÄµÀ
«Ä±À£ï EAzÀæzsÀ£Àĵï PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£ÉAiÀÄ §UÉÎ «ªÀj ÀĪÀÅzÀÄ.
«Ä±À£ï EAzÀæzsÀ£Àĵï£À PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£É
E£ÀÄß vÀ®Ä¥À¢gÀĪÀ CxÀªÁ ¸ÁzsÁgÀtªÁV vÀ®Ä¦zÀ ¥sÀ®£ÀÄ sÀ«UÀ¼À£ÀÄß vÀ®Ä¥ÀĪÀÅzÀPÁÌV F PɼÀV£À JgÀqÀÄ PÁAiÀiÁðZÀgÀuÉ ªÀåªÀ ÉÜUÀ¼À£ÀÄß G¥ÀAiÉÆÃV À ÁVzÉ;
a) ¤¢ðµÀÖ ªÀÄvÀÄÛ vÉÆqÀV¹PÉÆAqÀ C¢üªÉñÀ£ÀUÀ¼ÀÄ:
ZÀÄZÀÄѪÀÄ¢ÝUÁV vÁtUÀ¼ÀÄ £ÀUÀgÀ ¥ÀæzÉñÀUÀ¼À°è, £ÀUÀgÀ DgÉÆÃUÀå PÉÃAzÀæUÀ¼ÀÄ, ¥ÉÆøïÖ-¥ÁlðªÀiï ÉAlgï UÀ¼ÀÄ, PÀÄlÄA§ PÀ Áåt PÉÃAzÀæUÀ¼ÀÄ CxÀªÁ £ÀUÀgÀ PÉƼÀZÉ ¥ÀæzÉñÀUÀ¼À°è£À ªÀÄÄRAqÀg À PÀlÖqÀUÀ¼À£ÀÄß ÀºÀ ¥ÀæwgÀPÀët vÁtUÀ¼ÀAvÉ G¥ÀAiÉÆÃV À§ºÀÄzÀÄ. JvÀgÀ ÀܼÀUÀ¼ÉAzÀgÉ- ¥ÀæxÀ«ÄP À ±Á ÉUÀ¼ÀÄ, CAUÀ£ÀªÁr PÉÃAzÀæUÀ¼ÀÄ, SÁ ÀV D ÀàvÉæUÀ¼ÀÄ, ÀPÁðgÉÃvÀgÀ ÀA ÉÜUÀ¼À (NGO)vÁtUÀ¼ÀÄ CxÀªÁ ÀªÀÄÄzÁAiÀÄPÉÌ ÀÄ®§ªÁV vÀ®Ä¥À§ºÀÄzÁzÀ
EvÀgÀAiÀiÁªÀÅzÉà vÁtUÀ¼À£ÀÄß ¥ÀæwgÀPÀët vÁtUÀ¼ÁV G¥ÀAiÉÆÃV À§ºÀÄzÀÄ.
ÀA±ÉÆÃzsÀPÀgÀīıÀ£ï EAzÀæzsÀ£Àĵï PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£ÉAiÀÄ §UÉÎ «ªÀj ÀÄ vÁÛgÉ
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
PÀgÀ¥ÀvÀæUÀ¼ÀÄ
«Ä±À£ï EAzÀæzsÀ£Àĵï PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£É AiÀiÁªÀÅzÀÄ?

135
ªÀiÁ£ÀªÀ ÀA¥À£ÀÆä®UÀ¼À ®¨sÀåvÉ CzÉà CxÀªÁ ¥ÀPÀÌzÀ ÀªÀÄÄzÁAiÀÄ DgÉÆÃUÀå PÉÃAzÀæ
(CHC)/¨ÁèPï PHC, NCOUÀ¼À°è(LIONS, ROTARYEvÁÛ¢) ® sÀå«gÀĪÀ DgÉÆÃUÀå ¹§âA¢AiÀÄ eÉÆvÉUÉ, ¤ªÀÈvÀÛ DgÉÆÃUÀå PÁAiÀÄðPÀvÀðgÀÄ, ªÀÄvÀÄÛ £ËPÀgÀgÀ gÁdå «ªÀiÁ PÁ¥ÉÆÃðgɱÀ£ï , PÉÃAzÀæ ÀPÁðgÀzÀ DgÉÆÃUÀå AiÉÆÃd£É, Éå£Àå ¥ÀqÉ, gÉà Ééà f¯Áè £ÀUÀgÀ C©üªÀÈ¢Ý Keɤì
(DUDA)/gÁdå £ÀUÀgÀ C©üªÀÈ¢Ý Keɤì (SUDA)ªÀÄvÀÄ Û ÀªÀÄÄzÁAiÀÄ DzsÁjvÀ ÀA ÉÜ EvÁå¢ ÀPÁj KeɤìU À¼À°è
® sÀå«gÀĪÀ ¹§âA¢AiÀÄ£ÀÄß §¼À ÀĪÀ CUÀvÀå«zÀÄÝ, CzÀjAzÁV ºÉaÑ£À ÀASÉåAiÀÄ°è ªÀÄPÀ̼À£ÀÄß vÀ®Ä¥À§ºÀÄzÀÄzÁVzÉ. ÀªÀÄAiÀÄ: F ZÀlĪÀnPÉAiÀÄ ¨É½îUÉ 9 UÀAmÉ ¬ÄAzÀ
4UÀAmÉAiÀĪÀgÉUÉ PÉÊUÉÆüÀî ÁUÀÄvÀÛzÉ. DzÀgÀÆ CzÀg À ¥ÀæAiÉÆÃd£ÀUÀ¼À£ÀÄß ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è MzÀV À®Ä GzÉݲv À d£À ÀASÉåUÉ CÀ£ÀÄUÀÄtªÁV C¢üªÉñÀ£ÀUÀ¼À£ÀÄß AiÉÆÃd À ÁUÀÄvÀÛzÉ. vÀAqÀ: F vÀAqÀzÀ°è M§âg ÀÄ ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃqÀÄÀªÀªÀgÀÄ
ªÀÄvÀÄÛ E§âgÀÄ d£À ÀAUÀæºÀPÁgÀgÀÄ (PÀ¤µÀÖ M§âgÀÄ ÀܽÃaiÀÄgÀÄ EgÀ ÉÃPÀÄ) CazÁf¹zÀ EaeɵÀ£ï
¥ÀæªÀiÁtªÀÅ 60-70 QÌAvÀ ºÉZÁÑzÁUÀ, ºÉÉZÀÄѪÀj ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃqÀĪÀªÀgÀ£ÀÄß ¤AiÉÆÃf À ÁUÀÄvÀÛzÉ.

136
b) ÀAZÁj C¢üªÉñÀ£ÀUÀ¼ÀÄ: ¤gÀAvÀgÀ ¥ÀæwgÀµÀt ªÁå¦ÛAiÀÄÄ ¸ÁzÁgÀtªÁVgÀĪÀ ÀܼÀUÀ¼À°è ÀAZÁj C¢üªÉñÀ£ÀUÀ¼À£ÀÄß AiÉÆÃd À ÁUÀÄvÀÛzÉ. ÀtÚ ÀASÉ åAiÀÄ ¥sÀ Á£ÀÄ sÀ«UÀ½zÁÝUÀ ¥ÀævÉåÃPÀªÁzÀ C¢üªÉñÀ£ÀUÀ¼ÀÄ, ZÀzÀÄjzÀ PÉƼÀZÉ¥ÀæzÉñÀUÀ¼À°è EnÖUÉ §nÖUÀ¼ÀÄ ªÀÄvÀÄÛ PÀlÖqÀ ¤ªÀiÁðt vÁtUÀ¼ÀÄ M¼ÀUÉƼÀÄîîvÀÛªÉ.
10 ¤«ÄµÀ
ªÀÄPÀ̼À ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À §UÉÎ «ªÀj ÀĪÀÅzÀÄ.
ªÀÄPÀ̼ÀÄ ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À£ÀÄß «ªÀj¹j ZÀÄZÀÄѪÀÄzÀÄÝ ¤Ãr vÀqÉUÀlÖ§ºÀÄzÁzÀ K¼ÀÄ gÉÆÃUÀUÀ¼ÉAzÀgÉ- UÀAl®ÄªÀiÁj, £Á¬ÄPɪÀÄÄä, zsÀ£ÀĪÁðAiÀÄÄ, ¥ÉÆðAiÉÆ,PÀëAiÀÄgÉÆÃUÀ ÀqÁgÀ ªÀÄvÀÄ Û ºÉ¦mÉÊn¸ï ©. F K¼ÀÄ gÉÆÃUÀUÀ¼ÀÄ ªÀÄPÀ̼À°è ¸ÁªÀiÁ£À åªÁVzÉ ªÀÄPÀ̼À ¥ÀævÀgÀPÀëuÉAiÀÄ£ÀÄß ºÉaÑ ÀĪÀÅzÀjAzÀ CªÀÅUÀ¼À£ÀÄß vÀqÉUÀlÖ§ºÀÄzÀÄ d£À£ÀzÀ DgÀA sÀ¢AzÀ DgÀA©ü¹ aPÀÌ ªÀÄPÀ̽UÀÄ F ¥ÀæwgÀPÀëUÀ¼À£ÀÄß PÉÆqÀ ÁUÀÄvÀÛzÉ F ¥ÀæwgÀPÀëtUÀ¼À£ÀÄß ¥ÀqÉAiÀÄzÀ CxÀªÁ ¥ÀÆtðªÁV ¥ÀqÉzÀgÀzÀ ªÀÄPÀ̽UÉ F PÁ¬Ä ÉUÀ¼ÀÄ §gÀÄvÀÛªÉ. CªÀgÀÄ DUÁUÀ PÁ¬Ä É ©Ã¼ÀÄvÀÛgÉ; PÉ® ªÀÄPÀ̼ÀÄ F PÁ¬Ä ɬÄAzÀ ªÀÄgÀtºÉÆÃAzÀÄvÀÛªÉ. CªÀgÀ°è ºÀ®ªÁgÀÄ ªÀÄPÀ̼ÀÄ FgÉÆÃUÀUÀ½AzÀ ±Á±ÀévÀ CªÀÄUÀ«PÀ®vÉ ºÉÆÃAzÀĪÀgÀÄ.
PÀëAiÀÄgÉÆÃUÀ(TB)F gÉÆÃUÀªÀÅ UÀƽAzÀ ªÀÄvÉÆÛçâjUÉ ºÀgÀqÀÄvÀÛzÉ ¢ÃWÀðPÁ®zÀ PɪÀÄÄä ªÀÄvÀÄÛ zÉúÀzÀ sÁgÀ E½P É
ÀA±ÉÆÃzsÀPÀgÀÄ ªÀÄPÀ̼À ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À §UÉÎ «ªÀj ÀÄvÁÛgÉ
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
¥sÁè±ï PÁqïð
ªÀÄPÀ̼À ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À §UÉÎ «ªÀj¹j.

137
EªÀÅ FgÉÆÃUÀzÀ ®PàëtUÀ¼ÀÄ FPÁ¬Ä ÉUÉ aQvÉì ¤ÃqÀ¢zÀÝg É ªÀÄUÀĪÀÅ wêÀæ PÁ¬Ä É ©Ã¼ÀÄvÀÛzÉ CxÀªÁ ªÀÄgÀt
ºÉÆÃzÀÄvÀÛzÉ DzÀgÉ ¥ÀæwgÀPÀëtUÀ¼À£ÀÄß ¥ÀqÉzÀÄ ªÀÄPÀ̽UÉ TB
§gÀĪÀÅ¢®è.
UÀÆgÀ®Ä PɪÀÄÄä (Whooping cough) EzÀÄ PÉ«ÄäUÉ PÁgÀtªÁV, ¤gÀAvÀgÀªÁV GAmÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ UÀÆgÀ®Ä ÀºÀ DgÀA sÀªÁUÀÄvÀÛzÉ. D ªÀÄUÀÄ«UÉ dégÀ EgÀ§ºÀÄzÀÄ
CxÀªÁ ªÀÄÆUÀÄ ÉÆÃgÀÄwÛgÀ§ºÀÄzÀÄ. ¥ÀæwUÀÆgÀ°£À PÉÆ£ÉU É ªÀÄUÀÄ ªÁAw ¥ÁrPÉƼÀÀÄzÀÄ F PÁ¬Ä ÉU É ªÀÄÄAavÀªÁV aQvÉì ¤ÃqÀ¢zÀÝgÉ ªÀÄUÀÄ ¸ÁAiÀħºÀÄzÀÄ CPÀ Áävï D ªÀÄUÀÄ §zÀÄPÀĽzÀgÉ CªÀÅUÀ¼À°è C¥Ë¶ÖPÀv É É¼ÉAiÀÄÄvÀÛzÉ ªÀÄUÀÄ«UÉ 3 qÉÆøï ZÀÄZÀÄÑ ªÀÄzÀÄÝ ¤ÃrzÀg É
CzÀ£ÀÄß UÀÆgÀ®Ä PÉ«Ää¤AzÀ gÀQë À§ºÀÄzÀÄ
UÀAl® ªÀiÁj (Diphtheria) ;UÀAl®Ä ªÀiÁj GamÁzÀ
ªÀÄPÀ̽UÉ dégÀ«gÀÄvÀÛzÉ ªÀÄvÀÄÛ UÀAl®Ä ÀÄvÀÛ°£À M¼ÀZÀªÀÄðPÉÌ vÉÆÃAzÀvÉ GAmÁUÉ G¹gÁlzÀ°è vÉÆÃAzÀgÉAiÀiÁUÀÄvÀÛzÉ EzÀjAzÀ ªÀÄUÀÄ«UÉ ¸ÁªÀÅ ÀA sÀ«¸À§ºÀÄzÀÄ ¥ÀæwgÀPÀëtzÀ 3 qÉÆøï UÀ¼À£ÀÄß ¤ÃqÀĪÀÅzÀjAzÀ F PÁ¬Ä ÉAiÀÄ£ÀÄß vÀqÉUÀlÖ§ºÀÄzÀÄ. zsÀ£ÀÄÀªÁðAiÀÄÄ (Tetanus):F PÁ¬Ä ÉAiÀÄ ÀÆPÁëöätÄfëAiÀÄÄ UÁAiÀÄUÀ¼À ªÀÄÆ®PÀ ªÀÄUÀÄ«£À

138
zÉúÀªÀ£ÀÄß ¥ÀæªÉò ÀÄvÀÛzÉ CªÀÅ C©üeÁvÀ ²±ÀÄ«£À xÀ£Àð ¦æPï CxÀªÁ CA©°PÀ ï PÁqÀð ªÀÄÆ®PÀ ÀºÀ CzÀg À zÉúÀPÉÌ ¥ÀæªÉò À§ºÀÄzÀÄ F zsÀ£ÀĪÀÄðAiÀÄÄ ¦ÃrvÀªÁzÀ ªÀÄUÀÄ vÀ£Àß ¨Á¬Ä vÉUÉAiÀÄĪÀÅ¢®è ªÀÄvÀÄÛ CªÀÅ UÀqÀÀ ÁVgÀÄvÀÛªÉ CAvÀºÀ ªÀÄUÀÄ«UÉ ÀPÁ®zÀ°è aQv Éì ¤ÃqÀ¢zÀÝgÉ CªÀÅ ªÀÄgÀtºÉÆÃzÀÄvÀÛzÉ F zsÀ£ÀĪÀÄðAiÀÄÄ «gÀÄzÀÞ ¥ÀævÀgÀPÀëuÉAiÀÄ£ÀÄß ªÀÄUÀÄ d¤¹zÀ 6 ªÁgÀUÀ½ªÀÄzÀ CzÀPÉÌ PÉÆÃqÀ ÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ UÀ©üðt ¹ÛçAiÀÄjUÀÆ PÉÆqÀ§ºÀÄzÀÄ.
zÀqÁgÀ(Measles); CªÀÅ ªÀÄPÀ̼À°è ¸ÁªÀiÁ£ÀåªÁVgÀĪÀ gÉÆÃUÀªÁVzÉ EzÀÄ ºÀ®ªÁgÀÄ ªÀÄPÀ̽UÉ KPÀPÁ®zÀ°è DPÀæ«Ä À§ºÀÄzÀÄ PÉ«ÄäzÁUÀ. ¹Ã¤zÁUÀ CxÀªÁ ªÀiÁvÀ£ÁrzÁUÀ CzÀgÀ ªÉ ÊgÁtÄ UÁ½AiÀÄ ªÀÄÆ®PÀ M§âjAzÉƧâjUÉ ºÀgÀqÀÄvÀÛzÉ F PÁ¬Ä ÉAiÀiÁzÁUÀ ªÀÄUÀÄ wêÀæ PÁ¬Ä É ©Ã¼ÀÄvÀÛzÉ, dégÀ«gÀÄvÀÛzÉ PÀtÄÚ PÉA¥ÀUÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ EgÀÄvÀÛzÉ D PɪÀÄÄä £Á¬ÄAiÀÄ ÉÆUÀ¼ÀÄ«PÉAiÀÄAvÉ EgÀÄvÀÛzÉ PÉ®ªÀÅ ªÀÄPÀ̽U É Éâü ªÀÄvÀÄÛ ªÁAwAiÀiÁV CªÀgÀ°è ¤dð°ÃPÀgÀt
GAmÁUÀÄvÀÛzÉ PÉ®ªÀÅ ªÀÄPÀ̼ÀÄ UÀÄtªÀÄÄRªÁUÀ§ºÀÄzÀÄ ªÀÄvÀÄÛ PÉ®ªÀÅ ¸ÁAiÀħºÀÄzÀÄ zÀqÁgÀ PÁ¬Ä É UÀÄA¥Àr À É AiÀiÁªÀÅzÉ OµÀ¢üUÀ½®è ¥ÀæwgÀPÀët ZÀÄZÀÄÑ ªÀÄzÀÝ£ÀÄß ¤ÃqÀĪÀÅzÀjAzÀ zÀqÁgÀªÀ£ÀÄß §gÀzÀAvÉ vÀqÉUÀlÖ§ºÀÄzÀÄ.

139
¥ÉÆ°AiÉÆÃ: CªÀÅ C¥ÁAiÀÄPÁj PÁ¬Ä ÉAiÀiÁVzÀÄÝ, ªÀÄUÀÄ«£À zÉúÀPÉÌ ¥Á±ÀÑðªÁAiÀÄÄ GAlĪÀiÁqÀÄvÀÛzÉ EzÀg À ªÉÊgÁtÄ ªÀÄÄRUÀ¼À°è ¸ÁUÀÄvÀÛzÉ ªÀÄvÀÄÛ CªÀÅUÀ¼À°è PÉ®ªÀÅ vÉÆüÉaiÀÄzÀ PÉÊUÀ¼ÀÄ, dégÀUÀ¼ÀÄ, PÀ®ä±ÀAiÀÄÄPÀÛ DºÁgÀUÀ½AzÀ M§âjAzÉÆçâjUÉ ºÀgÀqÀ§ºÀÄzÀÄ ¥ÉÆðAiÉÆà PÁ¬Ä ɬÄAzÀ ªÀÄUÀÄ ¸ÁaiÀÄzÀzÀÝgÉ CzÀÄ fêÀ£À ¥ÀAiÀÄðAvÀ ±Á±ÀévÀ ¥Á±ÀéðªÁAiÀÄĪÀŤªÀÄzÀ §¼À®ÄvÀÛzÉ ¥ÉÆðAiÉÆà PÁ¬Ä ÉUÉ AiÀiÁªÀÅzÉ aQvÉì¬Ä®è.
ºÉ¥ÀmÉÊn¸ï ©. (Hepatitis B.): CzÀÄ °ªÀgï£À GjAiÀÄÆvÀªÁVzÉ CzÀÄ ºÉ¥ÀmÉÊn¸ï © JA§ ªÉÊgÁtÄ«¤ªÀÄzÀ §gÀÄvÀÛzÉ ¢ÃWÀðPÁ®¢ªÀÄzÀ ºÉ¥ÀmÉÊn¸ï EzÀÝ d£ÀgÀ®zÀ° AiÀiÁªÀÅzÉ gÉÆÃUÀ®ët PÁt ÀĪÀÅ¢AzÀ DzÀgÉ ¤zsÁ£ÀªÁV °ªÀgï ºÁ¼ÁUÀĪÀÅzÀÄ GamÁºÀ§ºÀÄzÀÄ ºÀ¹ªÀÅ E®è¢gÀĪÀÅzÀÄ, DAiÀiÁ¸À,C®à ¥ÀæªÀiÁtzÀ dégÀ, ¸ÁßAiÀÄÄ ªÀÄvÀÄÛ QÃ®Ä £ÉÆêÀÅ ªÁPÀjP É ªÀÄvÀÄÛ ªÁAw, ºÀ¼À¢ZÀªÀiï, PÀ¥ÀÄà ªÀÄÆvÀæ EvÁå¢UÀ¼ÀÄ ®WÀÄ ºÉ¥ÀmÉÊn¸ï £À gÉÆÃUÀ ®PàëtUÀ¼ÁVªÉ .
5 ¤«ÄµÀ
¸ÁªÀðwæPÀ ¥ÀæwgÀPÀëuÉAiÀÄ ±ÉqÀÆå ï §UÉÎ «ªÀj ÀĪÀÅzÀÄ.
¸ÁªÀðwæPÀ ¥ÀæwgÀPÀëuÉAiÀÄ ±ÉqÀÆå¯ï
ÀA±ÉÆÃzsÀPÀgÀÄ ¸ÁªÀðwæPÀ ¥ÀæwgÀPÀëuÉAiÀÄ ±ÉqÀÆå ï §UÉÎ
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
°Ã¥sï Émï &
¥sÁè±ïPÁqïð
¸ÁªÀðwæPÀ ¥ÀæwgÀPÀëuÉAiÀÄ ±ÉqÀÆå ï §UÉÎ «ªÀj¹j.

140
«ªÀj ÀÄvÁÛgÉ

141
4 ¤«ÄµÀ
«Ä±À£ï EAzÀæzsÀ£Àĵï AiÀıÀ¹ì£À §UÉÎ
«Ä±À£ï EAzÀæ zsÀ£ÀĵïzÀ AiÀıÀ¹ì£À §UÉÎ ZÀað ÀĪÀÅzÀÄ
ÀA±ÉÆÃzsÀPÀgÀÄ «Ä±À£ï EAzÀæzsÀ£Àĵï
PÀ°PÉzÁgÀgÀÄ D ÀQÛ¬ÄAzÀ PÉüÀÄvÁÛgÉ
¥sÁè±ïPÁqïð
EAzÀæzsÀ£Àĵï AiÀıÀ¹ì£À §UÉÎ ZÀað¹j.

142
ZÀað ÀĪÀÅzÀÄ.
¥ÉÆðAiÉÆà ¤ªÀÄÆð®£É PÁAiÀÄðPÀæªÀÄzÀ §UÉÎ WHO zÉÆA¢UÉ PÁAiÀÄð¤ªÀðºÉ ÀÄwÛgÀĪÀ 2000 ªÉ ÊzÀ ågÀÄ ªÀÄvÀÄ Û PÉëÃvÀæ ¤jÃPÀëPÀgÀÄ F «Ä±À£ï PÁAiÀÄðUÀvÀUÉÆý À®Ä ¥ÉÆðAiÉÆà C©üAiÀiÁ£ÀzÀ CªÀ¢üAiÀÄ°è eÁУÀªÀ£ÀÄß ªÀÄvÀÛAiÀÄ ªÀÄÆ®¸ÁPÀAiÀÄ£ÀªÀ£ÀÄß ¸Á¢ü À®Ä WHO,UNICEFªÀÄvÀÄÛ EvÀgÀ ¥Á®ÄzÁgÀjUÀg À
ÀA§A¢üzÀAvÉ sÁgÀvÀ ÀPÁðgÀ –EªÀgÉ°ègÀÆ ZÀÄZÀÄѪÀÄzÀÄ Ý ¤ÃrgÀzÀ ªÀÄvÀÄÛ sÁUÀ±ÀB ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃrgÀĪÀ ªÀÄPÀ̽U É ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃqÀĪÀ F gÁµÀÖç ªÁå¦ C©üAiÀiÁ£ÀzÀ°è ¥Á®ÄzÁgÀgÁVzÁÝgÉ. F «Ä±À£ï CrAiÀÄ°è ÀPÁðJªÀÅ gÁµÀÖç ªÁå¦ 201 C¢üP À MvÀÄÛ ¤ÃqÀ ÉÃPÁzÀ f ÉèU À¼À£ÀÄß UÀÄwð¹zÉ F f¯ÉèUÀ¼À£ÀÄß ÀAAiÀÄÄPÀÛ ÀÆZÀPÀUÀ¼ÀÄ, ¥ÀÆtð ¥ÀæwPÀët ªÁå¦Û, sÁUÀ±ÀB
ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃrzÀ ªÀÄvÀÄÛ ¤ÃrgÀzÀ ªÀÄPÀ̼ÀÄ EªÀÅUÀ¼À£ÀÄß DzsÀj¹ UÀÄwð À¯ÁVzÉ D f ÉèUÀ¼À£ÀÄß C¢üPÀ ¥Àæ±À¹ Û f ÉèUÀ¼ÉAzÀÄ UÀÄwð¹gÀ° CxÀªÁ E®è¢gÀ°, CzÀ£ÀÄß ¥ÀjUÀt ÀzÉ D f Éè UÀ¼À£ÀÄß UÀÄwð À ÁVzÉ ¤ÃrgÀzÀ CxÀªÁ sÁUÀ±ÀB ZÀÄZÀÄÑ ªÀÄzÀÄÝ ¤ÃrzÀ ªÀÄPÀ̼ÀÄ M¼ÀUÉÆüÀîvÁÛgÉ ªÉÆzÀ®£Éà ºÀAvÀzÀ°è 9,66495 C¢üªÉñÀ£ÀUÀ¼À£ÀÄß £ÀqÉ À ÁVzÉ ªÀÄvÀÄÛ ÀĪÀiÁgÀÄ 7.6 zÀ±À®PÀë ªÀÄPÀ̽U É ¥ÀæwgÀPÀëuÉ ¤ÃqÀ ÁVzÉ.JgÀqÀ£Éà ºÀAvÀzÀ°è 279 ªÀÄzsÀå
AiÀıÀ¹ì£À §UÉÎ «ªÀj ÀÄvÁÛgÉ

143
¥Áæ±À ÀÛöå f ÉèUÀ¼À£ÀÄß M¼ÀUÉÆÃAqÀ 352 f É èUÀ¼À£ÀÄß DAiÉÄÌ ªÀiÁqÀ Á¬ÄvÀÄ. «Ä±À£ï EAzÀæzsÀ£Àĵï£À ¥ÀÄ£ÀgÁªÀwðvÀ ºÀAvÀUÀ¼À £ÀAvÀgÀªÀÇ ¤zsÁ£ÀUÀwAiÀÄ ¥ÀæUÀwAiÀÄ£ÀÄß vÉÆÃj ÀĪÀ DAiÀÄÝ f Éè/£ÀUÀgÀUÀ¼À°è ÀA¥ÀÆtð ¥ÀæwgÀPÀët ªÁå¦ÛAiÀÄ£ÀÄß ¸Á¢ü À®Ä F ºÉZÀѼÀªÀÅ ÀªÀÄ¥ÀðPÀªÁV®è. DzÀÝjAzÀ ÀPÁðgÀªÀÅ PÀrªÉÄ ªÁå¦ÛAiÀÄ ¥ÀæzÉñÀUÀ¼À°è F «Ä±À£ï£ÀÄß
wêÀæUÉƽ¹zÀ «Ä±À£ï EAzÀæzs À£ÀÄµï £ÀAvÉ ªÀiÁ¥Àðr¹zÉ.
«Ä±À£ï EAzÀæ zsÀ£Àĵï AiÉÆÃd£ÉAiÀÄ «¸ÁÛgÀªÁzÀ ªÁå¦ÛAiÀÄ£ÀÄß £ÉÆÃrzÁUÀ, C£ÀÄPÀÆ®vÉ MzÀV ÀzÀ ªÀÄvÀÄ Û ÉêÉMzÀV ÀzÀ ÀªÀÄÄzÁAiÀÄUÀ½UÉ ¥ÀæwgÀPÀëuÉAiÀÄ£ÀÄß
ªÁå¥ÀûvÉAiÀÄ£ÀÄß ÀÄzsÁj ÀĪÀÅzÀPÁÌV AiÀıÀ¹éAiÀiÁVzÉ CzÀjAzÁV ZÀÄZÀÄѪÀĢݤAzÀ vÀqÉAiÀħºÀÄzÁzÀ gÉÆÃUÀUÀ½AzÀ ªÀÄPÀ̼À ªÀÄgÀtªÀ£ÀÄß PÀrªÉĪÀiÁqÀ ÁVzÉ
4 ¤«ÄµÀ
«µÀAiÀĪÀ£ÀÄß ¸ÁgÁA±ÀUÉƽ ÀĪÀÅzÀÄ ªÀÄvÀÄÛ G¥À ÀAºÁgÀ UÉƽ ÀĪÀÅzÀÄ
¸ÁgÁA±À ªÀÄvÀÄÛ G¥À ÀAºÁgÀ CzÀÄ PÁªÀÄ£À©°è£À K¼ÀÄ §tÚUÀ¼À£ÀÄß ÀÆa ÀÄwÛzÀÄÝ, D ªÀÄÆ®PÀ K¼ÀÄ ªÀiÁgÀPÀ gÉÆÃUÀUÀ¼À£ÀÄß GzÉÝò ÀÄvÀÛzÉ. CªÀÅUÀ¼ÉAzÀgÉ-UÀAl®Ä ªÀiÁj, £Á¬ÄPɪÀÄÄä CxÀªÁ G§â À PɪÀÄÄä, zsÀ£ÀĪÁðAiÀÄÄ, ªÀÄPÀ̼À ¥Á±ÀéðªÁAiÀÄÄ, PÀëAiÀÄgÉÆÃUÀ,
zÀqsÁgÀ ªÀÄvÀÄÛ ºÉ¦mÉ Ên¸ïB C®èzÉ d¥Á¤ ªÀĹ۵ÉÆÌÃzÀæPÀ ªÀÄvÀÄÛ ºÉªÉÆæü°¸ï E£ï¥sÀÄèAiÀÄ£ïì PÁ¬Ä ÉUÀ¼À «gÀÄzÀÞ
¥sÁè±ïPÁqïð

144
ZÀÄZÀÄѪÀÄzÀÝ£ÀÄß ªÀAiÀÄ ÀÌjUÁV DAiÀÄÝ f ÉèU À¼À°è MzÀV À ÁUÀÄvÀÛzÉ. EzÀgÉÆA¢UÉ FUÀ 11 ZÀÄZÀÄѪÀÄzÀÄÝUÀ¼ÀÄ EzÀgÀrAiÀÄ°è M¼ÀUÉƼÀÄîvÀÛªÉ MAzÀÄ ªÀµÀðzÀ CªÀ¢üAiÀÄ°è ÀĪÀiÁgÀÄ 1.62 PÉÆÃn ªÀÄPÀ̼À£ÀÄß F AiÉÆÃd£ÉAiÀÄ ªÁå¦ÛU É vÀgÀ ÁVzÀÄÝ, ÀĪÀiÁgÀÄ 45 ®PÀë ªÀÄPÀ̽UÉ ÀA¥ÀÆtðªÁV ¥ÀæwgÀPÀëuÉ MzÀV À ÁVzÉ ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃrgÀzÀ CxÀªÁ sÁUÀ±ÀB ¤ÃrzÀ J®è ªÀÄPÀ̽UÀÆ F ZÀÄZÀÄÑ ªÀÄzÀÄÝ ¤Ãr
vÀqÉUÀlÖ§ºÀÄzÀÄ gÉÆÃUÀUÀ¼À «gÀÄzÀÞ ¥ÀæwgÀPÀëuÉ UÁV M¼ÀUÉƼÀî®Ä GzÉÝò À ÁVzÉ

145
ANNEXURE III
CRITERIA RATING SCALE FOR VALIDATION OF THE TOOL
EVALUTION CRITERIA CHECKLIST
Dear Sir/ Madam
Kindly go through the evaluation criteria checklist for the validation of tool.
There are two columns given for your responses and a column for remarks. Kindly
place a tick in the appropriate column your remarks.
SL.NO CONTENT YES NO REMARKS
1. Demographic variables:
All characteristics necessary for the study are
included.
2.
Structured interview
schedule :
• Language is
simple and easy to follow.
• Covers adequate
content.
• All items necessary to
achieve the
objective of the
study are included.
3. Likert scale:
All the items necessary to
achieve the objective of the
study are included.

146
Dear Sir/Madam,
Kindly go through the content and place right mark against the questionnaire in the
following columns ranging from relevant to not relevant, when found to be needs modification, kindly give your opinion in the remark column.
Section A
Demographic variables
Sl .No Items Relevant Needs
modification Not relevant Remarks
1.
2.
3.
4.
5.
6.
7.
8.
9. A
9. B

147
SECTION B
STRUCTURED INTERVIEW QUESTIONNAIRE
Sl.No Items Relevant Needs
modification Not relevant Remarks
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Maximum score = 22

148
SECTION C
3 POINT LIKERT SCALE TO ASSESS THE ATTITUDE REGARDING
MISSION INDRADHANUSH
Sl .No Items Relevant Needs
modification Not relevant Remarks
1.
2.
3.
4.
5.
6.
7.
8.
10.
11.
12.
13.
14.
Suggestion if any:
1.
2.
Date: Signature and seal of the expert
Place: Name and designation

149
ANNEXURE IV
LETTER SEEKING EXPERT’S OPINION AND SUGGESTIONS FOR
CONTENT VALIDITY OF TOOL
From,
Mrs. Jyotima Borgohain Handique
II Year M.Sc. nursing Student.
Padmashree Institute of Nursing
To,
Forwarded Through
Principal
Padmashree Institute of Nursing
Sub: Seeking permission for content validation of the research tool
Respected Sir/Madam,
I, Mrs. Jyotima Borgohain Handique, IInd
year M.Sc. Nursing (community
health nursing) student of Padmashree institute of nursing, request your good self, if
you would kindly accept to validate my research tool on “A study to assess the
effectiveness of educational package on level of knowledge and attitude
regarding Mission Indradhanush among mothers of under five children in
selected urban slum area, Bengaluru” I would be obliged if you would kindly
affirm your acceptance to the undersigned with your valuable suggestion on the topic.
I have attached the details of my study along with the research tool.
Thanking you in anticipation
Yours sincerely,
Mrs. Jyotima Borgohain Handique
Enclosures:
Problem statement and objectives of the study
Structured interview questionnaire andAttitude scale.
Validity certificate

150
ANNEXURE V
LIST OF EXPERTS
1. Dr. B.T Basavanthappa
Principal, Raja Rajeshwari College of Nursing
Bengaluru.
2. Dr. Lukima Saikia
Lecturer,Community Health Nursing
Regional College of Nursing,
Guwahati,Assam.
3. Dr. Lakshmi A.
Principal, HOD,Community Health Nursing
Sarvodaya College of Nursing, Bangalore.
4. Kathyayini N.B.
Associate Professor, Community Health Nursing
Kempegowda College of Nursing, Bangalore.
5. Prof. Prasanna Kuar
HOD, Department of Community Health Nursing
Government College of Nursing
Bangalore.
6. Dr. G. Nagarathana
Professor, Department of Community Health Nursing
Government College of Nursing
Bangalore.
7. Dr. Himashree Bhattacharya
AssistantProfessor, Department of Community Medicine
NEIGRIHMS,Shillong, Meghalaya.
8. Prof . R. Chinnadurai
M.sc,M.Phil.PGDCA
Biostatitician, Padmashree Group Of Institution
Bangalore.

151
ANNEXURE VI
CERTIFICATE OF CONTENT VALIDITY
I hereby certify that I have validated the tool of Mrs. Jyotima Borgohain
Handique, M.Sc. Nursing Student who is undertaking, “A study to assess the
effectiveness of educational package on level of knowledge and attitude
regarding Mission Indradhanush among mothers of under five children in
selected urban slum area, Bengaluru.”
Place: Signature and seal of expert
Date: Name and Designation

152

153

154

155

156

157

158
159

160
ANNEXURE VII (a)
CERTIFICATE OF ENGLISH EDITING

161
ANNEXURE VII (b)
CERTIFICATE OF KANNADA EDITING

162
ANNEXURE VIII
EDUCATIONAL PACKAGE
ON
MISSION INDRADHANSH

163
FLASH CARDS (ENGLISH)
MISSION INDRADHANUSH
INTRODUCTION
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60

164
GOALS AND OBJECTIVES
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
STRATEGY
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60

165
LIFE THREATENING DISEASES OF CHILDREN
BCG VACCINE WHOOPING COUGH
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
BCG VACCINE WHOOPING COUGH
DIPHTHERIA MEASLES
TETANUS
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60

166
POLIOMYELITIS HEPATITIS-B
HEPATITIS-B
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60

167
SUCCESS OF MISSION INDRADHANUSH
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
SUMMARY AND CONCLUSION
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60

168
FLASH CARDS (KANNADA)
«Ä±À£ï EAzÀæzsÀ£Àĵï
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
� EzÀ£ÀÄßPÉÃAzÀæDgÉÆÃUÀå ¸ÀaªÀ ²æà eÉ, ¦, £ÀqÁ Ø 25£Éà r¸ÉA§gï 2014gÀAzÀÄ DgÀA©ü¹zÀgÀÄ. � EzÀÄ 2 ªÀµÀðzÉƼÀV£À ªÀÄPÀ̽UÉ, J®èUÀ©üðt ¹ÛçÃAiÀÄjUÉ K¼ÀÄ ZÀÄZÀÄ ÑªÀÄzÀÄ Ý ¤gÉÆÃzsÀPÀ gÉÆÃUÀUÀ¼À «gÀÄzÀÝ ¥ÀæwgÀPÀëuÉ ¤ÃqÀ®Ä
GzÉÝò¹zÉ.
«Ä±À£ïEAzÀæzsÀ£Àĵï sÁgÀvÀ ÀPÁðgÀzÀDgÉÆÃUÀå «ÄñÀ£ïDVzÉ
GzÉÝò¹zÀ gÉÆÃUÀUÀ¼ÀÄ »ÃVªÉ:
UÀAl®ÄªÀiÁj, £Á¬ÄPɪÀÄÄä, zsÀ£ÀĪÁðAiÀÄÄ, ªÀÄPÀ̼À ¥Á±ÀéðªÁAiÀÄÄ, PÀëAiÀÄgÉÆÃUÀ, zÀqsÁgÀ ªÀÄvÀÄ Û ºÉ¦mÉÊn¸ïB
PÉÃAzÀæDgÉÆÃUÀå ªÀÄvÀÄÛ PÀÄlÄA§ PÀ¯Áåt ÀaªÀgÀÄ
«Ä±À£ïEAzÀæzsÀ£Àĵï DgÀA©ü¹zÀgÀÄ.
gÁµÀÖçzÀ 65% jAzÀ 90% gÀµÀÄÖ ªÀÄPÀ̽UÉ ÀA¥ÀÆtð ¥ÀæwgÀPÀ ët ªÁå¦ÛAiÀÄ£ÀÄß
« ÀÛj ÀĪÀÅzÀÄ
eÁUÀwPÀ ¥ÀæwgÀPÀëtPÁAiÀÄðPÀæªÀÄzÀCrAiÀÄ°èJ®è ZÀÄZÀÄѪÀÄzÀÄÝUÀ¼ÀÄ sÁgÀvÀzÀ°èGavÀªÁVzÉÆgÉAiÀÄÄvÀÛªÉ

169
UÀÄjUÀ¼ÀÄ ªÀÄvÀÄÛGzÉÝñÀUÀ¼ÀÄ
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
�ಾಯ'%ೕ
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
«Ä±À£ï EAzÀæzsÀ£Àĵï-UÀÄjUÀ¼ÀÄ ªÀÄvÀÄÛvÀvÀé
• 2 ªÀµÀðzÉƼÀV£À J®è ªÀÄPÀ̽U É ªÀÄvÀÄÛUÀ©üðt ªÀÄ»¼ÉAiÀÄjUÉ ® sÀå«gÀĪÀJ®è ZÀÄZÀÄѪÀÄzÀÄÝUÀ½AzÀ ÀA¥ÀÆtð ¥ÀæwgÀPÀëuÉMzÀV À¯ÁUÀÄvÀÛzÉ «Ä±À£ïEAzÀæzsÀ£ÀĵïRavÀ¥Àr ÀÄvÀÛzÉ.
• «Ä±À£ïEAzÀæzsÀ£ÀĵïzÀ ¢ÃWÁðªÀ¢ ü UÀÄjUÀ¼ÀÄ: »ÃVªÉ:
- PÉÃAzÀæ ºÁUÀÆgÁdå ÀPÁðgÀUÀ¼ÀÄ ºÁUÀÆ C©üªÀÈ¢Þ ¥Á®ÄzÁgÀg À ÀºÀAiÉÆÃUÀzÀ°èDgÉÆÃUÀå
ªÀåªÀ É ÜAiÀÄ£ÀÄß §®¥Àr ÀĪÀÅzÀÄ,
-
«Ä±À£ïEAzÀæzsÀ£Àĵï ÀÄvÀÄÛUÀ¼ÀÄ
gËAqï 1 –J¦æ¯ï15
gËAqï 1 – ªÉÄà 15
gËAqï 1 –dÆ£ï 15
gËAqï 1 – dÄ ÉÊ 15
«Ä±À£ïEAzÀæzsÀ£Àĵï

170
ಮಕ)ಳ *ಾರಕ ,ೂೕಗಗಳ.
/ಯ ,ೂೕಗ
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
©.¹.f. ZÀÄZÀÄѪÀÄzÀÄÝ UÀÆgÀ®ÄPɪÀÄÄä
UÀAl®ªÀiÁj zÀqsÁgÀ
zsÀ£ÀĪÁðAiÀÄÄ

171
0ೕ1�ೕ
ಪ2ೖ45
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
¤ªÀÄä ªÀÄUÀÄ«UÉ ÀA¥ÀÆtðªÁVZÀÄZÀÄѪÀÄzÀÄÝ ºÁQ¹jCªÀgÀ£ÀÄß ªÀiÁgÀPÀ gÉÆÃUÀUÀ½AzÀ gÀQë¹j

172
«Ä±À£ïEAzÀæzsÀ£ÀĵïAiÀıÀ ÀÄì
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
PADMASHREE INSTITUTE OF NURSING, BANGALORE-60
ªÀiÁ£Àå ¥ÀæzsÁ£ÀªÀÄAwæ ²æà £ÀgÉÃAzÀæ ªÉÆâAiÀĪÀgÀÄ ÀªÀÄUÀæ «Ä±À£ïEAzÀæzsÀÀ£Àĵï 8£Éà CPÉÆÖçgï, 2017gÀAzÀÄ DgÀA©ü¹zÀgÀÄ.PÉêÀ® 2 wAUÀ¼À°è 30.46 ®PÀë ªÀÄPÀ̼ÀÄ ºÁUÀÆ 6.46 ®PÀëUÀ©üðt ªÀÄ»¼ÉAiÀÄgÀÄ ¥ÀæwgÀPÀët ¥ÀqÉzÀgÀÄ.
¸ÁgÁ±À: • ÀA¥ÀÆtð ¥ÀæwgÀPÀ ëtªÀÅ ®PÁëAvÀgÀ ªÀÄPÀ̼À£ÀÄß ««zsÀ ªÀiÁgÀ P À
PÁ¬Ä ÉUÀ½AzÀ gÀQë À§®èzÀÄ. CzÀÄ ¸ÁªÀiÁfPÀC©üªÀÈ¢ ÞUÉCUÀvÀåªÁVzÉ.
• sÁgÀvÀªÀÅ 3 ºÉÆ À ZÀÄZÀÄѪÀÄzÀÄ ÝUÀ¼À£ÀÄß ¥ÀjZÀ¬Ä ÀĪÀÅzÀjAzÀvÀ£Àß ¥ÀæwgÀPÀëtPÁAiÀÄðPÀæªÀĪÀ£ÀÄß « ÀÛj¹zÉ.
• gÁµÀÖçzÀ° è ¥ÀæwgÀPÀët ªÁå¦ÛAiÀÄ£ÀÄß C£ÀĵÁ×£ÀUÉƽ À®Ä
¥ÀæAiÀÄvÀßUÀ¼À£ÀÄß ÀªÀÄVæÃPÀj À®Ä sÁgÀv À ÀPÁðgÀzÀG¥ÀPÀæªÀĪÀÅeÁjAiÀÄ°èzÉ.
¥Àæw ªÀÄUÀÄ«UÉ gÉÆÃUÀªÀÄÄPÀÛ, DgÉÆÃUÀ å¥ÀÆtð ¨Á®åªÀ£ÀÄß ¥ÀqÉAiÀÄĪÀ ºÀQÌzÉ.
¥Àæw ªÀÄUÀÄ«UÉ ÀA¥ÀÆtð ¥ÀæwgÀPÀëtPÁÌV ¥ÀtvÉÆrj

173
OPERATIONS L PLANNING OF
MISS ION INDRADHANUSH
Prepared by:
Jyotima Borgohain Handique
2nd year M.Sc. Nursing
Community Health Nursing
PION
PAMPHLET (ENGLIS H)

174
OPERATIONAL PLANNING O F MISSION
INDRADHANUSH:
The two operat ional mechanisms are ut ilized
to reach out to the unreached or poorly reached
beneficiaries:
a) Fixed and outreach sessions
b) Mobile sessions
a) Fixed and outreach sessions
SITES FOR VACCINAT ION
In urban areas,
• Urban health posts
• Post-partum centers
• Family welfare centers
• Local leader’s premises in urban slums
Other areas,
• Primary schools
• Anganwadi centers
• Private dispensaries
• Non- Government organizat ion
• Any other locat ion that are easily
accessible and acceptable to the
community
AVAILABILIT Y OF HUMAN RESOURCES
• All the health staff from the same or
neighboring community health centre/
• Block PHC,
• NGOs (LIONS, Rotary etc)
• Retired health workers
• Staff available from other Government
• Agencies such as
� Employee’s State Insurance
Corporat ion,
� Central Government Health
Scheme,
� Armed forces
� Railways
� District Urban Development
Agency (DUDA)/
� State Urban Development
Agency (SUDA)
� Community based organizat ions
TIMING:
The activit ies are conducted from 9am to
4pm. However, sessions are planned based on
availability of the targeted populat ion to
maximize the benefits achieved.
TEAM:
A team comprises one vaccinator and up to
two mobilizers (at least one should be from local
mohallas/locality). An additional vaccinator is
included in the team if the est imated injection
load is more than 60-70.
b) Mobile sessions
Mobile sessions are planned at places where
routine immunizat ion coverage is weak and the
small number of beneficiaries does not warrant
an independent session. These areas include
• Peri –urban areas
• Scattered slums
• Brick kilns and
• Construct ion sites.

175
\
«Ä±À£ï EAzÀæzsÀ£Àĵï£À PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£ÉAiÀÄ §UÉÎ
«ªÀj¹j
ತ!ಾ�7ದವರು:.
²æêÀÄw eÉÆåÃwªÀiÁ ¨ÉÆÃUÉÆÃðºÉÃ£ï ºÁåArPï
2;ೕ ವಷ'ದ ಎಂ,ಎ7= .ನ7'ಂ>
ಸಮು?ಾಯ ಆ,ೂೕಗA ನ7'ಂ>
ಪದBCೕ ಇ%=4ಟೂAE ಆF ನ7'ಂ>
GಂಗಳHರು -೬೦

176
«Ä±À£ï EAzÀæzsÀ£ÀÄµï £À PÁAiÀiÁðZÀgÀuÉ AiÉÆÃd£ÉAiÀÄ §UÉÎ «ªÀj¹j E£ÀÄß vÀ®Ä¥À¢gÀĪÀ CxÀªÁ ¸ÁzsÁgÀtªÁV vÀ®Ä¦zÀ ¥sÀ®£ÀĨsÀ«UÀ¼À£ÀÄß vÀ®Ä¥ÀĪÀÅzÀPÁÌV F PɼÀV£À JgÀqÀÄ PÁAiÀiÁðZÀgÀuÉ ªÀåªÀ ÉÜUÀ¼À£ÀÄß G¥ÀAiÉÆÃV À ÁVzÉ; c) ¤¢ðµÀÖ ªÀÄvÀÄÛ vÉÆqÀV¹PÉÆAq À
C¢üªÉñÀ£ÀUÀ¼ÀÄ
• £ÀUÀgÀ ¥ÀæzÉñÀUÀ¼À°è, £ÀUÀgÀ DgÉÆÃUÀå PÉÃAzÀæUÀ¼ÀÄ
• ¥ÉÆà ïÖ-¥ÁlðªÀiï ÉAlgï UÀ¼ÀÄ • PÀÄlÄA§ PÀ Áåt PÉÃAzÀæUÀ¼ÀÄ • £ÀUÀgÀ PÉƼÀZÉ ¥ÀæzÉñÀUÀ¼À°è£ À
ªÀÄÄRAqÀgÀ PÀlÖqÀUÀ¼À£ÀÄß ÀºÀ ¥ÀæwgÀPÀët vÁtUÀ¼ÀAvÉ G¥ÀAiÉÆÃV À§ºÀÄzÀÄ.
CxÀªÁ • ¥ÀæxÀ«ÄPÀ ±Á ÉUÀ¼ÀÄ,
• CAUÀ£ÀªÁr PÉÃAzÀæUÀ¼ÀÄ,
• SÁ ÀV D¸ÀàvÉæUÀ¼ÀÄ,
• ¸ÀPÁðgÉÃvÀgÀ ÀA¸ÉÜUÀ¼À (NGO)
vÁtUÀ¼ÀÄ CxÀªÁ ÀªÀÄÄzÁAiÀÄPÉÌ ¸ÀÄ®§ªÁV vÀ®Ä¥À§ºÀÄzÁzÀ EvÀgÀ AiÀiÁªÀÅzÉà vÁtUÀ¼À£ÀÄß ¥ÀæwgÀPÀët vÁtUÀ¼ÁV G¥ÀAiÉÆÃV¸À§ºÀÄzÀÄ.
ªÀiÁ£ÀªÀ ÀA¥À£ÀÆä®UÀ¼À ® sÀåvÉ • CzÉà CxÀªÁ ¥ÀPÀÌzÀ ¸ÀªÀÄÄzÁAiÀÄ DgÉÆÃU Àå
PÉÃAzÀæ (CHC)/
• ¨ÁèPï PHC • NGO UÀ¼À°è (LIONS, ROTARY
EvÁÛ¢)® sÀ å«gÀĪÀ DgÉÆÃUÀå ¹§âA¢AiÀÄ eÉÆvÉUÉ
• ¤ªÀÈvÀÛ DgÉÆÃUÀå PÁAiÀÄðPÀvÀðgÀÄ • ¸ÀªÀÄÄzÁAiÀÄ DzsÁjvÀ ¸ÀA¸ÉÜ EvÁå¢ ¸ÀPÁj
KeɤìUÀ¼À°è ®¨sÀå«gÀĪÀ ¹§âA¢ • gÁdå «ªÀiÁ PÁ¥ÉÆÃðgɱÀ£ï
• PÉÃAzÀæ ¸ÀPÁðgÀzÀ DgÉÆÃUÀå AiÉÆÃd£É,
• ¸Éå£Àå ¥ÀqÉ, • gÉà ÉéÃ
• f¯Áè £ÀUÀgÀ C©üªÀÈ¢Ý Keɤì (DUDA)/
• gÁdå £ÀUÀgÀ C©üªÀÈ¢Ý Keɤì (SUDA)
• ¸ÀªÀÄÄzÁAiÀÄ DzsÁjvÀ ¸ÀA ÉÜ
• ÀªÀÄAiÀÄ:F ZÀlĪÀnPÉAiÀÄ ¨É½îUÉ 9 UÀAmÉ ¬ÄAzÀ
4UÀAmÉAiÀĪÀgÉUÉ PÉ ÊUÉÆüÀî ÁUÀÄvÀÛzÉ. DzÀgÀÆ CzÀg À ¥ÀæAiÉÆÃd£ÀUÀ¼À£ÀÄß ºÉaÑ£À ¥ÀæªÀiÁtzÀ°è MzÀV À®Ä GzÉݲvÀ d£À ÀASÉåUÉ CÀ£ÀÄUÀÄtªÁV C¢üªÉñÀ£ÀUÀ¼À£ÀÄß AiÉÆÃd À ÁUÀÄvÀÛzÉ.
vÀAqÀ: F vÀAqÀzÀ°è M§âgÀÄ ZÀÄZÀÄѪÀÄzÀÄ Ý ¤ÃqÀÄÀªÀªÀgÀÄ ªÀÄvÀÄÛ E§âgÀÄ d£À ÀAUÀæºÀPÁgÀgÀÄ (PÀ¤µÀÖ M§âgÀÄ ÀܽÃaiÀÄgÀÄ EgÀ ÉÃPÀÄ) CazÁf¹zÀ EaeɵÀ£ï ¥ÀæªÀiÁtªÀ Å 60-70 QÌAvÀ ºÉZÁÑzÁUÀ, ºÉÉZÀÄѪÀj ZÀÄZÀÄѪÀÄzÀÄÝ ¤ÃqÀĪÀªÀgÀ£ÀÄß ¤AiÉÆÃf À ÁUÀÄvÀÛzÉ. b) ÀAZÁj C¢üªÉñÀ£ÀUÀ¼ÀÄ : ¤gÀAvÀgÀ ¥ÀæwgÀµÀt ªÁå¦ÛAiÀÄÄ ¸ÁzÁgÀtªÁVgÀĪÀ ÀܼÀUÀ¼À°è
• ÀAZÁj C¢üªÉñÀ£ÀUÀ¼À£ÀÄß AiÉÆÃd¸À ÁUÀÄvÀÛzÉ.
• ÀtÚ ÀASÉåAiÀÄ ¥sÀ Á£ÀÄ sÀ«UÀ½zÁÝU À ¥ÀævÉåÃPÀªÁzÀ C¢üªÉñÀ£ ÀUÀ¼ÀÄ,
• ZÀzÀÄjzÀ PÉƼÀZÉ¥ÀæzÉñÀUÀ¼À°è EnÖU É §nÖUÀ¼ÀÄ
• ªÀÄvÀÄÛ PÀlÖqÀ ¤ªÀiÁðt vÁtUÀ¼ÀÄ M¼ÀUÉÆüÀîvÀÛªÉ

177
LEAFLET (ENGLIS H)
NATIONAL I MMUNI ZATION SEHEDULE
Prepared by:
Jyotima Borgohain Handique
2nd
year M.Sc. Nursing
Community Health Nursing
PION

178
NATIONAL IMMUNI ZATION SEHEDULE

179
LEAFLET (KANNADA)
c

180







