
Diabetic Ketoacidosis
Case Study By:
Tiffany Peters
2/25/16

2
Introduction
L.D. is a 66 year old African-American male who was admitted to St. Francis Hospital on
February 19, 2016. Upon examination in the Emergency Room, he was found to have altered
mental status and hyperglycemia. He was transferred the ICU for critical care management of
diabetic ketoacidosis, hyperkalemia, and acute kidney injury. He currently weighs 113.4 kg and
is 69 inches tall with a BMI of 36.8. His ideal body weight for height is 72.7 kg. Due to a BMI >30
and 156% IBW, his body weight has been adjusted to 83 kg which will be used to calculate his
calorie and protein needs. This patient was chosen for a case study review due to his
complicated medical condition, disease process, and critical care state. This study begins at
admission on February 19, 2016 and concludes on February 25, 2016. The focus of this study is
diabetes disease process and complications from poorly controlled blood sugars requiring
critical care management.
Social History
L.D. is a single man who has never been married and has no children. He lives with his
brother and mother in a small home. He is his mother’s primary care-taker along with his
brother. Mr. D stated that he spends most of his time helping his mother and has let his own
health become his last priority. He was a former lab technician, but has been on disability for a
few years. His current health insurance helps to pay for his doctor visits and diabetes
medication. L.D. has a Catholic background and relies on prayer to encourage him through this
time.
Normal Anatomy and Physiology of Organs Affected by Diabetes

3
Diabetes mellitus is a condition in which the body either has an absence of insulin or
insulin is used inefficiently.1 Without the effects of insulin, the body cannot regulate blood
glucose levels effectively. Normally, the pancreas controls glucose in the bloodstream by
producing the hormones insulin and glucagon. Insulin signals cells to take in glucose to be used
as energy. With type 2 diabetes, the cells either resist insulin or the pancreas does not produce
enough insulin to reduce blood glucose. This causes hyperglycemia which creates multiple
complications such as neuropathy, decreased wound healing, and increased risk for
cardiovascular and kidney disease. Diabetic ketoacidosis is a result of the lack of glucose as an
energy source. The body turns to breaking down adipose tissue to use fat for energy.2 These
free fatty acids are turned into ketones. Ketones are very acidic and eventually lead to osmotic
diuresis which causes metabolic acidosis.
Past Medical History
L.D. has a past medical history of type 2 diabetes mellitus, hypertension, and
hypercholesterolemia. His surgical history includes hip replacement. He denies any history of
heart disease or any other significant medical history related to diabetes. There is no other
record of previous visits or documentation of past medical history for this patient as this is his
first admission to St. Francis Hospital.
Present Medical Status and Treatment
Diabetic ketoacidosis (DKA) is diagnosed when blood glucose levels are above 250
mg/dL along with a decreased blood pH, decreased sodium bicarbonate, and elevated serum
ketones.2 The higher the blood glucose and ketone levels, the more osmotic diuresis occurs
resulting in electrolyte imbalances and possible dehydration.1 Metabolic stability and resolving

4
fluid and electrolyte imbalance is the first priority for treating DKA. Without immediate
attention, a diabetic coma or death may occur.1
Upon admission, L.D. complained of dizziness, lightheadedness, and unsteady balance.
He was assessed and reported to have altered mental status with severe hyperglycemia. He was
also noted to have hyperkalemia and probable acute kidney injury. This is a likely occurrence in
patients with diabetic ketoacidosis. Due to hyperglycemia, lack of insulin and L.D.’s elevated
serum sodium level, it is suspected he was having some impairment of the Na-K pump causing
rhabdomyolysis. This is the most common cause of acute renal failure in these cases.3 The
patient was immediately admitted to the medical intensive care unit for management of these
conditions. He was started on vigorous IV fluids to treat hypovolemia after he was found to
have erythrocytosis. Insulin infusion was also started right away to correct blood glucose levels.
The intensivist chose to give the patient Kayexalate plus insulin, glucose, and sodium
bicarbonate to treat hyperkalemia instead of treating the potassium directly because the
elevated level was most likely due to the acidosis. During metabolic acidosis, the buildup of
hydrogen ions cause a decrease in pH which elevates serum potassium levels. Once the acidosis
is corrected, potassium levels will return to normal.1
Within 24 hours, Mr. D’s condition had stabilized. The hyperkalemia and acute kidney
injury was resolved and blood glucose levels had dropped. Aggressive IV fluid was continued
given his initial volume depletion. The intensivist transitioned him to a subcutaneous insulin
regimen due to the patient having never been on insulin therapy and his extreme uncontrolled
diabetes. It is just as effective as intravenous insulin, and is beneficial because L.D. will need to
continue this regimen as part of his diabetes control.2 However, once starting an oral diet, he

5
had a recurrence of severe hyperglycemia and insulin therapy was adjusted again.
Readjustments are sometimes needed until the right dosing has been reached. It was also
noted that L.D. had developed thrombocytopenia of unclear etiology. He continued to be
monitored for this condition.
On February 22, L.D. was moved out of ICU to a regular hospital room. At this time, the
patient felt very weak; however, the acidosis had resolved. He was consulted to an
Endocrinologist and was seen by the diabetes educator and dietitian intern for diabetes
education and assessment. Thrombocytopenia remained an issue, but the patient was clearly
not septic nor had he been given any heparin medication to cause this issue. Blood pressure
was being monitored and addressed with Diovan and Norvasc.
Due to thrombocytopenia, the patient was not receiving any blood thinner medication.
He was encouraged to ambulate for deep vein thrombosis prophylaxis. He had several bouts of
nausea and emesis on day four of his hospital stay. This was most likely due to the
hyperosmolar state brought on by severe hyperglycemia. By the next day, L.D. was feeling
much better with no complaints of gastrointestinal distress. He continued on Levemir and
Novolog to control his diabetes. He was educated by a certified diabetes educator on how to
give himself insulin injections. By this time, the thrombocytopenia was improving, but he was
monitored for signs and symptoms of bleeding for the next 24 hours. He continued to improve
and all medical conditions were resolved. The patient was discharged on February 25, 2016.
Labs
Upon presentation to the ER, Mr. D. had a serum glucose of 1033 mg/dL and serum
potassium of 7.3 mg/dL. Before moving him to the floor, the patient was given insulin to

6
address his elevated blood sugars. His admission and final lab results are listed in the table
below.
Admission lab values 2/19/16
Final lab values 2/25/16
Normal lab values
Sodium 146 140 136-144
Potassium 4.7 3.8 3.6-5.1
Chloride 112 107 101-111
TCO2 23 29 22-32
Glucose 304 153 70-100
BUN 46 13 6-25
Creatinine 1.8 1.0 0.6-1.2
Calcium 9.4 8.7 8.5-10.5
Hemoglobin 15.3 12.8 12-18
Hematocrit 51.4 38.8 35-51
Anion gap 26 10-20
Total Protein 5.1 6.5-8.1
Total Bili 0.8 0.3-1.2
ALT/SGPT 15 10-42
AST/SGOT 15 10-40
Albumin 2.9 3.6-5.3
Alk Phos 22 42-121
Hemoglobin A1C
14.3 4.0-6.0
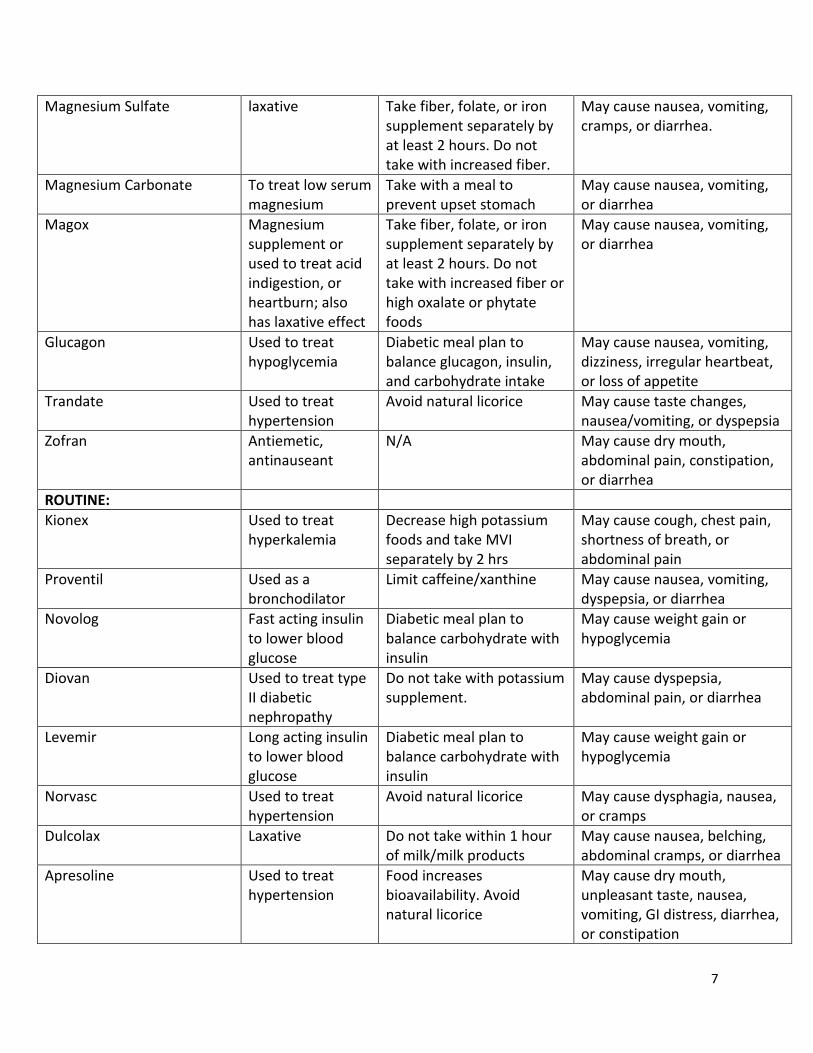
Medications
Medication Purpose Drug/Nutrient Interaction Possible Side Effects
PRN:
Normal Saline Flush To clear medications from the port to make sure the drug was delivered fully.
May alter how other medications work
Possible allergic reaction. Symptoms include rash, itching/swelling, severe dizziness, and trouble breathing.
Potassium Chloride to prevent or to treat low blood levels of K+ (hypokalemia)
Not to be taken while using salt substitutes.
May cause GI irritation, nausea, vomiting, abdominal pain, diarrhea, or flatulence.
Dextrose (50%) Used for dehydration and/or to control blood sugars
May lower serum sodium and increase serum potassium
Hyperglycemia, edema
7
Magnesium Sulfate laxative Take fiber, folate, or iron supplement separately by at least 2 hours. Do not take with increased fiber.
May cause nausea, vomiting, cramps, or diarrhea.
Magnesium Carbonate To treat low serum magnesium
Take with a meal to prevent upset stomach
May cause nausea, vomiting, or diarrhea
Magox Magnesium supplement or used to treat acid indigestion, or heartburn; also has laxative effect
Take fiber, folate, or iron supplement separately by at least 2 hours. Do not take with increased fiber or high oxalate or phytate foods
May cause nausea, vomiting, or diarrhea
Glucagon Used to treat hypoglycemia
Diabetic meal plan to balance glucagon, insulin, and carbohydrate intake
May cause nausea, vomiting, dizziness, irregular heartbeat, or loss of appetite
Trandate Used to treat hypertension
Avoid natural licorice May cause taste changes, nausea/vomiting, or dyspepsia
Zofran Antiemetic, antinauseant
N/A May cause dry mouth, abdominal pain, constipation, or diarrhea
ROUTINE:
Kionex Used to treat hyperkalemia
Decrease high potassium foods and take MVI separately by 2 hrs
May cause cough, chest pain, shortness of breath, or abdominal pain
Proventil Used as a bronchodilator
Limit caffeine/xanthine May cause nausea, vomiting, dyspepsia, or diarrhea
Novolog Fast acting insulin to lower blood glucose
Diabetic meal plan to balance carbohydrate with insulin
May cause weight gain or hypoglycemia
Diovan Used to treat type II diabetic nephropathy
Do not take with potassium supplement.
May cause dyspepsia, abdominal pain, or diarrhea
Levemir Long acting insulin to lower blood glucose
Diabetic meal plan to balance carbohydrate with insulin
May cause weight gain or hypoglycemia
Norvasc Used to treat hypertension
Avoid natural licorice May cause dysphagia, nausea, or cramps
Dulcolax Laxative Do not take within 1 hour of milk/milk products
May cause nausea, belching, abdominal cramps, or diarrhea
Apresoline Used to treat hypertension
Food increases bioavailability. Avoid natural licorice
May cause dry mouth, unpleasant taste, nausea, vomiting, GI distress, diarrhea, or constipation

8
Treatment
The initial treatment for diabetic ketoacidosis is IV fluids and insulin. It is imperative to
also correct electrolyte balance. IV fluids of 0.9% normal saline was started right away for L.D.
and continued vigorously until volume depletion was stabilized. There have been several
studies discussing the use of Plasma-Lyte as an alternative to 0.9% normal saline in volume
repletion for patients with diabetic ketoacidosis. According to Stowe,4 patients recover faster
when using Plasma-Lyte and also tend to have lower serum chloride and higher bicarbonate
levels. This is because it contains organic acid buffers that are very similar to plasma. It contains
a lower concentration of chloride, which when compared to normal saline, is less likely to lead
to hyperchloremia. Plasma-Lyte was also found to improve mean arterial pressure and urine
output more rapidly. Normal saline has been proven to be safe; however, Plasma-Lyte seems to
be an extremely effective alternative. More evidence is needed to determine safety for regular
use in the intensive care unit.4 To treat L.D.’s extreme hyperglycemia, he was started on insulin
therapy. Normally, a patient would be put on an IV insulin. However, the intensivist felt it would
be more beneficial to use subcutaneous insulin to correct his glucose levels. Mr. D. will need to
use insulin for an extended amount of time to get his diabetes under control, therefore, starting
him on injections would help get the correct dosing figured out for long term use. According to
Westerburg,2 using subcutaneous insulin was just as effective on clinical outcomes as using
intravenous insulin. A rapid acting insulin such as Novolog or Humulin is administered at 0.3
units per kg every one to two hours. Adjustments can be made as needed. L.D. was also placed
on Levemir which is a long acting insulin. This is used as a “background” insulin which helps

9
reduce extreme peaks and valleys of glucose levels. He will continue on this regimen to control
his diabetes.
Medical Nutrition Therapy
L.D. stated his diet is varied and irregular. Taking care of his mom is his top priority and
her schedule often dictates his eating patterns. In the morning, he is busy getting his mother
ready and fixing her meals. He mentioned he skips lunch often. L.D mostly eats at home, but
will occasionally eat out. He cooks and prepares most of the meals for his family. He enjoys
afternoon snacks, however, they consist of mostly desserts and sweets. An analysis of foods he
would normally eat is listed in the table below.
Breakfast Carbs (g) Protein (g) Fat (g) Sodium (mg) Calories
1 cup cereal 33 3 2 240 158
½ cup fat free milk 6 4 0 51 42
16 oz glass orange juice 57 3 1 10 244
1 slice toast 13 2 1 177 69
2 Tbs jam 28 0 0 15 109
Lunch
Turkey sandwich with mayo, lettuce, and cheese
37 23 17 1319 399
8 oz ice tea 13 0 0 7 47
Snack
1 Donut 32 4 12 248 255
12 oz Coke 35 0 0 15 136
Dinner
1 grilled chicken breast (5 oz) 0 30 3 388 161
½ cup summer squash 6 1 0 1 27
¾ cup mashed potatoes 3 27 4 400 159
Bedtime snack
6 peanut butter sandwich crackers 25 5 10 302 207
Once L.D. was stabilized and transferred out of the intensive care unit to a regular
hospital room, he was placed on a 2000 calorie diabetic diet. He eats 90-100% of his meals

10
which would provide approximately 1800-2000 calories and 72-96 grams of protein per day. At
22-25 kcal/kg and 0.8-1.0 g/kg protein using his adjusted body weight for weight maintenance,
L.D.’s needs are 1826-2075 kcal and 66-83 grams protein. This diet is designed to control
carbohydrate intake for patients who have diabetes. Each meal is served on a strict schedule to
maintain consistent intake. It is very important for patients to eat every 4-5 hours to regulate
their blood glucose levels and for proper dosing of medications and insulin. On this diet, Mr. D.
was given 5 carbohydrate servings every meal which is equivalent to 75 grams per meal. This
also gives a daily total of 225 grams carbohydrate and is equal to 45% of daily caloric intake.
The patient was compliant with his diet and stated he enjoyed the food. He remained on the
ADA diet throughout his stay at the hospital. Along with medication, the controlled
carbohydrates brought down his blood glucose levels from 304 to 153 mg/dL. This is a
significant improvement considering his hemoglobin A1C of 14.3.
The major nutrition related problem for this patient is maintaining a scheduled eating
pattern at home. From his diet history, it is very obvious that he does not eat consistently and
skips many meals. He has poor self-monitoring skills which is why changing his eating habits will
play a major role in overall control of his disease. Clinical studies have confirmed that following
the recommendations for the nutrition therapy of diabetes can decrease A1C levels in 3-6
months.5 In Mr. D’s case, there is no need for alternative feeding methods. If his intake
becomes compromised, Glucerna Shakes may be added to his diet in order to supplement
calories and protein. In order for success upon discharge, L.D. should be referred by his doctor
to see an outpatient diabetes educator for additional education and careful monitoring of
medications, diet, and glucose control. Before discharge, L.D. was very motivated to start taking

11
better care of his disease. He was encouraged by the information which empowers him to make
better choices concerning his diet.
Prognosis
L.D.’s current prognosis is very good. His diabetic ketoacidosis has resolved and he was
feeling much better at time of discharge. For this patient, the biggest challenge is ahead of him.
Because of his poor self-monitoring skills and compliance with diabetes control, L.D. will need
to make some considerable changes to his normal daily routine. In order to decrease his
hemoglobin A1C and prevent more complications, it is imperative for him to check his blood
glucose levels every day, take his medications and insulin, and be consistent and compliant with
the American Diabetes Association diet. His success with this will be greatly strengthened by
seeing an outpatient diabetes educator. His main goal is to manage his disease at home to
prevent diabetic ketoacidosis and any other complications from happening in the future.
Summary & Conclusion
During this study, I was able to see the full blown effects of uncontrolled diabetes. This
patient had the highest blood glucose levels I have ever seen in a patient. Researching diabetic
ketoacidosis opened my eyes to how the body reacts to insulin and hyperglycemia. It gave me a
greater appreciation for the body’s natural way of compensating for the lack of human
responsibility. As always, I enjoyed interacting with this patient and asking deeper questions to
truly get an overall picture of his life outside of the hospital. This allowed me to pinpoint
specific areas in his diet that needed work. I felt very satisfied after educating this patient
because I felt he really wants to make a change, and I made a difference in helping him achieve
it.
12
References
1. Nelms, M. Sucher, K., Lacey, K., and Roth, S.L. Nutrition Therapy & Pathophysiology. 2nd ed. Brooks/Cole Cengage Learning, Belmont, CA; 2011
2. Westerberg, D. P. (2013). Diabetic ketoacidosis: evaluation and treatment. American family physician, 87(5).
3. Deng, D., Xia, L., Chen, M., Xu, M., Wang, Y., & Wang, C. (2015). A case of fulminant type 1 diabetes associated with acute renal failure. Neuro endocrinology letters, 36(2), 115-118.
4. Stowe, M. (2012) Plasma-Lyte vs. Normal Saline: Preventing Hyperchloremic Acidosis in Fluid Resuscitation for Diabetic Ketoacidosis. School of Physician Assistant Studies. 296
5. American Diabetes Association. (2012). Standards of medical care in diabetes--2012. Diabetes care, 35, S11.







