
“Curiouser and Curiouser”
What Alice, Edward Bear,
Dorothy and Dr. Seuss
Can Tell Us about Health Care Reform
Bob Doherty, SVP, Governmental Affairs and Public Policy, New Mexico Chapter, ACP, November 7, 2014

2
“Curiouser and Curiouser”
Health care reform has become like Alice’s Adventures in Wonderland:
a “curiouser and curiouser” journey to somewhere(but is it where we ought to go?)

3
“Curiouser and Curiouser”
“Would you tell me, please, which way I ought to go from here?"That depends a good deal on where you want to get to," said the Cat.I don't much care where – said Alice.Then it doesn't matter which way you go," said the Cat.– so long as I get somewhere," Alice added as an explanation.“Oh, you're sure to do that," said the Cat, "if you only walk long enough."

4
“Curiouser and Curiouser”—which way ought we go from here?
1. On health care spending?2. On the ACA?3. On GME?4. On physician payment reform?5. On EHRs and health care administration/
paperwork?
(Plus, an update on the 2014 elections! And ACP and Ebola!)

5
“Curiouser and Curiouser”--Slowdown in healthcare spending
Dramatic (but temporary?) slowdown in Medicare spending, due at least in part to ACA changes (provider cuts, re-admissions, delivery system reforms).
Solvency extended to 2030. Eases short-term pressure for more cuts.



8
But even with the slowdown, we still spend more than anyone else

9
What’s next on healthcare spending?
Over the longer term, Medicare financing is still not sustainable
With the GOP Senate take-over, entitlement reform will be on the 114TH Congress’ agenda• “Legacy” issue for President Obama’s remaining two
years?

10
“Curiouser and Curiouser”– the Affordable Care Act
10
What happened in January 2014: Premium tax credits and cost-sharing subsidies available. Beginning of Medicaid expansion. The bulk of the remaining insurance regulations went
into effect, including essential health benefit package, guaranteed issue, premium regulations, etc.
Most people required to have health insurance. The Health Insurance Marketplaces opened in October
2013and closed March 31, 2014.

11
How Did the Marketplaces Do?
11
From 10/1/13 through 9/22/14, estimated 9.4 million individuals selected a QHP through a Health Insurance Marketplace; 8.16 million of them paid 1st premium• Currently enrolled/paid: 7.3 million
57% of Marketplace individual market enrollees were uninsured prior to enrollment.
Percentage uninsured has dropped but less so in states that did not expand Medicaid.
http://acasignups.net/

12
Medicaid Expansion Status
12
The latest:CMS has approve PA plan to expand Medicaid; at least 5 more states expected to join them

13
Percentage of Adults 18 to 64 Years of Age withoutHealth Insurance, January 2012 through June 2014
Health Reform and Changes in Health Insurance Coverage in 2014 Sommers et al, NEJM,July 23,2014
10..3million
gained coverage
19http://www.nejm.org/doi/full/10.1056/NEJMsr1406753#results#t=references

http://www.nytimes.com/interactive/2014/10/29/upshot/obamacare-who-was-helped-most.html?_r=0&abt=0002&abg=0

Whether a state chose to expandMedicaid is the single biggest factor in determining how many people gained health insurance coverage.

16
Patients in non-expansion states remain uninsured
16
• In the states that refuse to expand Medicaid:• People with incomes below the FPL fall into the
“coverage gap” (ineligible for Medicaid, ineligible for ACA premium subsidies)
• Nationwide, 7.6 million people were excluded from Medicaid, including 4.8 million in the coverage gap (79% of whom are in Southeastern U.S.); this number will drop now that HHS has approved expansion waiver proposal in PA (is Utah next)?

Blacks and Hispanics hadsubstantially larger gains in coverage.
Young adults had the biggest reduction in being uninsured of any age group.

More people gained coverage in Republican-leaning areas than in Democratic-leaning ones.

19
What has been the impact in NM?
By mid-April 2014, 32,062 people had finalized their enrollment in the New Mexico exchange, and HHS reported that 78 percent of them received subsidies to lower their premiums.
As of early 2014, it was estimated that nearly 48 percent of the uninsured population in New Mexico would be eligible for expanded Medicaid or CHIP. As of mid-April, 30,147 people had enrolled in Medicaid through the New Mexico exchange. Enrollment in Medicaid continues year-round, so that number is continuing to increase, further lowering the uninsured rate in New Mexico.
http://www.healthinsurance.org/new-mexico/

20
What has been the impact in NM?

21
What has been the ACA’s impact on premiums, availability of employer-sponsored HI?
“The 2014 survey found considerable stability among employer-sponsored plans. Similar percentages of employers offered benefits to at least some employees and a similar percentage of workers at those firms were covered by benefits compared to last year. Family premiums increased at a modest rate [3 percent] and single premiums are not statistically different than those reported last year. On average, covered workers contribute the same percentage of the premium for single and family coverage as they did last year.”Source: 2014 Employer Health Benefits Survey, Kaiser Family Foundation, http://kff.org/report-section/ehbs-2014-summary-of-findings/

Initial filings suggest that in many communities, average 2015 benchmark premiums will be lower than in 2014
http://kff.org/health-reform/press-release/premiums-set-to-decline-slightly-for-benchmark-aca-marketplace-insurance-plans-in-2015/

23
ACP Enrollment Resources Updated
23
Help patients enroll in health coverage:• Updated State-specific guides to the ACA
coverage section• Updated one-pagers for patients• Extensive FAQs on what physicians and patients
need to know about ACA coverage.
http://www.acponline.org/advocacy/state_health_policy/aca_enrollment/
24
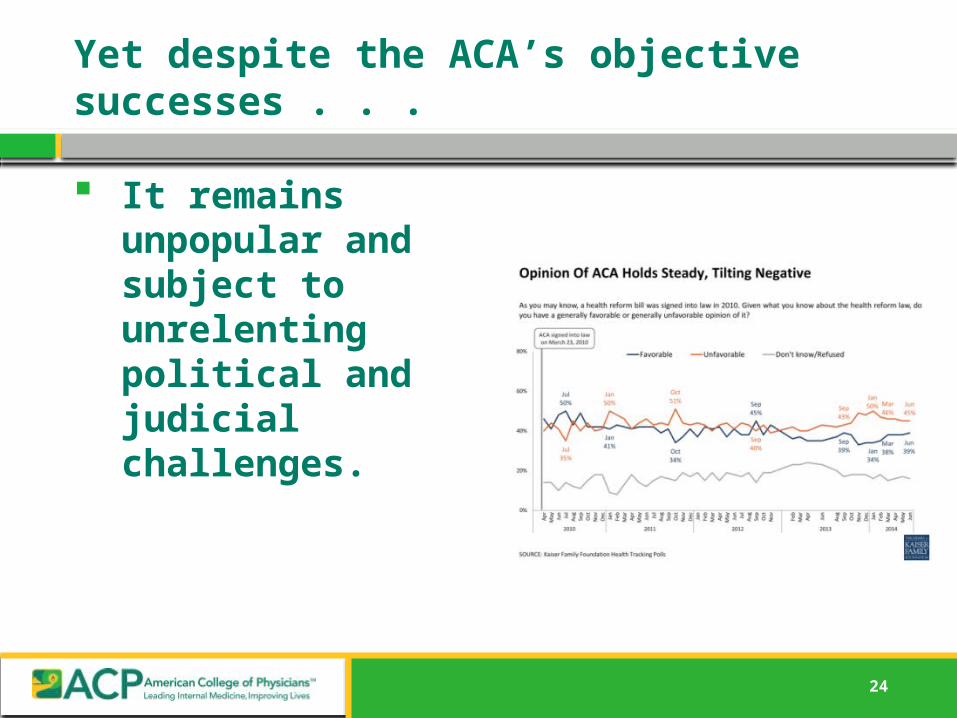
Yet despite the ACA’s objective successes . . .
It remains unpopular and subject to unrelenting political and judicial challenges.

25
Court challenges: Hobby Lobby
25
Supreme Court ruled that the Religious Freedom Restoration Act of 1993 applies to “closely held” companies
Requiring coverage of certain types of contraceptives imposed an unacceptably high burden on owners’ religious beliefs

SOURCE: Kaiser Family Foundation.
Legal Analysis of the Supreme Court Ruling on Hobby Lobby
Is the for-profit employer a “person” capable of religious
belief?
Does the requirement to provide health
insurance for contraceptives
substantially burden the employer?
Does the government have a compelling interest to provide health insurance
coverage for preventive care
including contraceptives?
Is the government meeting the
compelling interest in the least restrictive
way?
Does not violate RFRA Violates RFRA
YES
No RulingYESYES
NO NONO
NO
Burden on Employer Burden on Government
1. 4. 3. 2.

27
ACP’s views on the Hobby Lobby decision
29
We recognize that issues involving religious freedom are controversial and complex, and may divide ACP membership.
Yet our response is focused solely on the potential health impact—we do not claim to have expertise on the legal questions on whether for-profit companies fall under the Religious Freedom Restoration Act of 1993.

28
ACP’s views on Hobby Lobby decision
39
From June 30 statement from ACP PresidentDavid Fleming, MD, FACP:
“The American College of Physicians Is deeply concerned about the adverse impact on healthcare that may result from today’s Supreme Court ruling that allows ‘closely held’ for-profit employers to opt-out of evidence-based contraceptive coverage requirements. We believe that this decision will make it more difficult for women to access affordable contraceptives . . Although we certainly hope that the Supreme Court’s decision does not result in for-profit employers obtaining exemptions for vaccinations and other evidence-based benefits, the ruling clearly does not preclude for-profit employers from challenging such mandates, or the courts from granting further coverage exemptions.”

29
Court challenges: ACA subsidies
29
Statute refers to subsidies being available in“exchanges established by the states.”• IRS ruled that Congress’ intent was for the subsides to
apply in exchanges run by the federal government. One appeals court and one district court ruled
that the subsidies are illegal (Halbig), another appeals court upheld them—in the meantime, the subsidies remain in effect
If subsidies are overruled, it would make premiums unaffordable in majority of states.

PotentialImpact of HalbigDecision on health insurance premiums, by state

31
ACP advocacy to improve the ACA
1. Improve network adequacy standards.2. Require greater transparency in network
adequacy criteria and drug formularies.3. Improve appeals rights for physicians excluded
from a network and for RXs left off of formularies.4. Provide patients with access to out-of-network
physicians at no higher cost if service is unavailable in-network.

32
ACA advocacy to improve the ACA
5. Provide “real-time” access to accurate network directories at time of health plan selection/enrollment.
6. Monitor formularies for potential discriminatory impact on high cost patients.
7. Inform physicians when patient enters 90-day grace period for non-payment of premiums.

33
“Curiouser and Curiouser”—GME financing and workforce
Consensus that the current federal GME financing system is broken because it is not providing enough return on investment:
“At a time when all federal programs are under close scrutiny and the return on the public’s investment in GME is poorly understood, the committee cannot support maintaining Medicare GME funding at the current level without establishing a path toward realignment of the program’s incentives and a plan for documentation of outcomes. The continuation and appropriate level of funding should be reassessed after the implementation of these reforms.”
• IOM (Institute of Medicine). 2014. Graduate medical education that meets the nation’s health needs. Washington, DC: The National Academies Press, http://www.iom.edu/~/media/Files/Report%20Files/2014/GME/GME-RB.pdf

34
“Curiouser and Curiouser”—GME financing and workforce
Consensus that U.S. is facing a shortage of physicians, including primary care, is unraveling:
“Concerns that the nation faces a looming physician shortage, particularly in primary care specialties, are common. The committee did not find credible evidence to support such claims. Too many projections of physician shortages build on questionable provider–patient ratios, fail to consider the marked geographic differences in physician supply, and ignore recent evidence of the impacts of more effective organization, new technology, and deployment of health personnel other than physicians.”
• IOM (Institute of Medicine). 2014. Graduate medical education that meets the nation’s health needs. Washington, DC: The National Academies Press, http://www.iom.edu/~/media/Files/Report%20Files/2014/GME/GME-RB.pdf

35
“Curiouser and Curiouser”—GME financing and workforce
Yet the case for putting billions more into GME is predicated on its projections of physician workforce shortages:
“The IOM recommendations to cut doctor training and funding for care of the sickest patients at teaching hospitals could not come at a worse time. The nation faces an estimated shortage of 130,000 physicians by 2025, split nearly evenly between primary and many other specialties that care for older adults and children with special needs.”
AAMC, IOM’s Vision of GME Will Not Meet Real-world Patient Needs, July 29, 2014, https://www.aamc.org/newsroom/newsreleases/381882/07292014.html

36
“Curiouser and Curiouser”—GME financing and workforce
AAFP proposes to:1. Limit payments for direct graduate medical education and indirect graduate medical education to training for first-certificate residency programs. [Eliminates federal GME funding for IM subspecialty training]
2. Establish primary care thresholds and maintenance-of-effort requirements for all sponsoring institutions and teaching hospitals.
3. Require all sponsoring institutions and teaching hospitals seeking new Medicare- and Medicaid-financed GME positions to meet primary care training thresholds as a condition of residency program expansion.
4. Align financial resources with population health care needs through a reduction in IME payments and allocation of those resources to support innovation in GME.
5. Fund the National Health Care Workforce Commission.
37
“Curiouser and Curiouser”—GME financing and workforce
Yet for all of the attention being paid to GME reform, the status quo has prevailed• Congress hasn’t given hospitals, residency programs and
specialties the billions more that they want, but neither has it cut funding
• GME/IME has been on the budget chopping block for years, yet (so far) has escaped unscathed
• IOM argues for “flat funding” with redistribution of money within a budget neutral pool
• Most GME innovation is being done on a relatively small scale, pilot basis (e.g. teaching health centers)
• But GME reform is coming—its just a matter of when

38
Believing in the impossible
"Alice laughed: "There's no use trying," she said; "one can't believe impossible things.""I daresay you haven't had much practice," said the Queen. "When I was younger, I always did it for half an hour a day. Why, sometimes I've believed as many as six impossible things before breakfast.”
It would be a mistake for us believe in the impossible:
That GME will be immune from the push for accountability/value
That Congress, at time of fiscal restraint, is just going to add hundreds of billions to GME and lift all specialties’ caps
That Congress will just accept our word that there is a physician shortage

39
“Curiouser and Curiouser”—physician payment/delivery system reform
We know that cognitive care is undervalued, yet even the current programs to create incentives for primary care are at risk of going away:• Medicaid primary care pay parity (expires 1/1/15)• Medicare primary care 10% bonus on E/M codes
(expires 1/1/16)

Medicaid pay parity
40
Current law: Medicaid must pay no less than the Medicare for designated primary care and vaccine services provided by internists, pediatricians, and family physicians—and IM and PED subspecialties (funded by federal government).
Physicians in the three eligible specialties must self- attest that they are:• Board certified in IM, FP, PED or• [if not board certified], that 60% of their billable codes
are for the designated primary care and vaccine services

Medicaid pay parity
41
The program expires on 1/1/15 unless Congress extends it.
If the program is allowed to expire, internists in most states would experience Medicaid pay cuts. Average cut of 15% to NM primary care physicians and
IM subspecialists. In April 2014, ACP conducted a survey of a
representative sample of its members: 46 percent of the respondents indicated they had enrolled in the Medicaid Pay Parity program and would accept fewer Medicaid patients in 2015 (40 percent) or drop out of Medicaid entirely in 2015 (6 percent) if the were allowed to expire.

Medicaid pay parity
42
• Senators Patty Murray (D-WA) and Sherrod Brown (D-OH)Introduced a bill (S. 2694) to:
• Prevent an across-the-board Medicaid primary care cut on January 1, 2015 (in most states) by extending the current-law Medicaid Pay Parity program through 2016 to IM, FP, PEDs (and IM and pediatric subspecialties)
• Add ob-gyn physicians as an eligible specialty if 60% if their billing are for designated primary care and vaccine codes (maternity care not included)
• Include NPs as authorized by state law—they would be paid for designated primary care at 100% of the Medicare payment rate that is applicable to NPs ( which is 85% of the physician rate)

43
Current advocacy efforts:
At ACP’s Board of Governors meeting, we asked our chapters to send letters to their congressional delegations to urge extension of the Medicaid pay parity program• Along with release of reports (drafted by ACP staff)
on the impact on each state if it is not continued• Along with a press release to all local media
ACP issued a national report and press release on impact if pay parity is not reauthorized

Medicare SGR and delivery system reform
Congress knows what to do about theMedicare SGR.
But remains unwilling to take the steps needed to overcome partisan differences over how to pay for it.
44

Medicare SGR and Delivery System Reform
45
ACP helped create a bipartisan and bicameral solution to replace the SGR with a payment system that supports value rather than volume.
But the latest SGR “patch” is a big setback to enactment of a permanent solution in the 113th Congress.
But payment and delivery system reform is coming—even without SGR repeal.

46
Why do we need to reform physician payments?
“Here is Edward Bear, coming downstairs now, bump, bump, bump, on the back of his head, behind Christopher Robin. It is, as far as he knows, the only way of coming downstairs, but sometimes he feels that there really is another way, if only he could stop bumping for a moment and think of it.”
A.A. Milne, 1920illustration by E. M. Shepard

47
“There really is another way”
Risk-adjusted monthly per-patient payments (global primary care capitation).
Bundled payments by diagnosis, episodes of care. “Hybrid” models that preserve some elements of
FFS, plus risk-adjusted payments, shared savings (Comprehensive Primary Care Initiative).
FFS—but with dollars at risk based on performance metrics.
Direct (cash) payment? “Retainer” practices? Patient-Centered Medical Homes/PCMH Neighbors

“There really is another way”
NYT: A survey of Blue Cross and Blue Shield plans,showed that the plans collectively have invested$65 billion in new “value-based” models—including PCMHs—involving “215,000 physicians affecting more than 24 million members, including some inMedicare Advantage plans.”
• “The experiments include paying for care delivered in a medical home . . . In its program, Horizon Blue Cross Blue Shield of New Jersey pays a primary care doctor roughly $5 per patient a month to manage a patient’s care. The doctor can earn an additional $11 a month per patient by meeting certain quality and efficiency goals. A practice with 1,000 patients could make an extra $60,000 to $192,000 a year.”
http://www.nytimes.com/2014/07/10/business/health-insurers-are-trying-new-payment-models-study- 64shows.html

“There really is another way”
KHN: “Beginning in 2011 CareFirst increased reimbursement [to] most of its primary care doctors in Maryland, the District and Virginia. . . Doctors who scored well have gotten raises of more than $40,000 on top of round-the-clock nursing assistance for their sickest and riskiest patients http://www.kaiserhealthnews.org/Stories/2014/July/10/CareFirst- primary-care-costs-specialists-hospitals.aspx]
Healthcare Payer News: “In the first year of the medical home contract, Aetna’s 5,650 members being treated by WESTMED [group practice] physicians saw a 35 percent reduction in hospital admissions and had relatively fewer ER visits and hospital readmissions. WESTMED doctors also met almost all of the 10 goals targeting cancer screenings and proactive management of diabetes and heart disease. According to Aetna, those results earned WESTMED some $300,000 in incentive payments.” http://www.healthcarefinancenews.com/news/pcmh- paying-aetna-and-doctors.
65

A Patient CenteredMedical
Or in other words . . .

51
“Curiouser and Curiouser”: health care administration and paperwork
More and more administrative tasks and paperwork are being imposed on physicians, without any assessment of need, value or impact.
Major contributor to dissatisfaction with practice, disincentive to enter or remain in primary care, and less time with patients.

52
Dr. Seuss:
“When at last we are sure you’ve been properly pilled,then a few paper forms must be properly filled, so that you and your heirs may be properly billed.”
From “You Only Get Old Once” by Dr. Seuss, sharedcourtesy of Shari Erickson

Practice Enjoyment
Addressing Administrative Complexities
Practice Redesign
Decreasing Professional Isolation
Addressing Administrative Complexities is one piece of the practice enjoyment puzzle

ACP’s initiative to reduce administrative complexities
Patients Before Paperwork: Reinvigorating the Patient-Physician Relationship,By Challenging Unnecessary Practice Burdens
Goals:1. Educate members,
policymakers, public on what makes up administrative challenges and why they are not all equal
2. Identify which are the highest priorities and why
3. Implement most effective strategies to mitigate or eliminate top priority challenges and help members address those that can’t be eliminated

Addressing Administrative Complexities
Focused Advocacy Efforts
Tools/Services & Practice Support
Relationships &Collaborations
Research
Actions to build this understanding into a key piece of the overall campaign…

56
“Curiouser and Curiouser”—EHRs
EHRs are not living up to their promises, and are a major contributor to physician burn-out.
And we now have data to show the impact on physician time.
57
EHRs—the problem:
Congress dictated a timeline for HITECH that forced CMS and ONC to rush through the initial requirements for EHRs.
• ACP, AMA, and many other societies raised strong opposition to the initial requirements.
• We were concerned that the way certification was set up, it would require specific functions that might or might not be useful, but it made no attempt to ensure that the systems were usable and safe.
• Also, while we argued that true interoperability would be a fundamental requirement for success, ONC was unwilling to push for the base-level technologies and standards that are needed.
• Since then, we have taken every opportunity, both in writing and in person to argue that usability and interoperability were being sacrificed by the Meaningful Use process.

ACP study:
Mean Loss for attending physicians was
48 minutes per clinic day,
4 hours per five day clinic week
JAMA Internal Medicine, September 8, 2014, http://archinte.jamanetwork.com/article.aspx?articleid=1901114

59
EHRs—the solution:
Beginning in the fall of 2013, ACP and AMA staff and members began a cooperative initiative with the major EHR vendors to see if we could find ways outside of the regulatory process to improve usability of EHRs
• The primary causes of poor usability in EHRs are the overwhelming documentation requirements of payers and others, as well as the impossible time pressures placed on EHR vendors by the MU timeline.
• We are working with the vendors to try to address the timeline problem with ONC and CMS, and we have been working on a position paper that addresses the problems caused by documentation requirements. We expect to see this paper published in the next few months.

60
2014 elections and health care reform
Big Republican gains in Senate, House, and statehouses will alter, but not reverse, the course of health care reform
Continued gridlock may be the most likely outcome

Source: National Journal Research; CNN Election Center; Associated Press; NBC News.
Republicans Dominate Competitive Races to Win Senate
Analysis•Republicans won most of 2014’s competitive Senate races, taking seats in Colorado, Arkansas, Georgia, Iowa, and—unexpectedly—North Carolina•Republicans also won special elections this year in Oklahoma and South Carolina•Louisiana will hold a December 6, 2014 runoff election , and Alaska could take until November 18, 2014 to count all remaining ballots, but Republicans have already secured enough seats to control the Senate regardless of these outcomes
OH
WV VA
PA
NY
ME
NC
SC
GA
TN
KY
IN
MIWI
MN
IL
LATX
OK
ID
NV
OR
WA
CA
AZNM
CO
WY
MT ND
SD
IA
UT
FL
AR
MO
MS AL
NE
KS
VT
NHMA
RICT
NJ
DEMD
AK
HI
Senate Seats Gained/Held in the 2014 Midterm Elections
AK
May take until November 18 to count all votes
Democratic Gain
Democratic Hold
Republican Gain
Republican Hold
Independent Gain
Undecided/Runoff
No Election
Democrats: 44Republicans: 52Independents: 2Undecided: 2
Runoff election will be held on December 6,
2014

Source: National Journal Research; CNN Election Center; Associated Press; NBC News.
Republicans Extend Gubernatorial Advantage
Analysis•While Republicans already controlled most governors’ mansions prior to 2014 elections, gains in Arkansas, Illinois, Maryland, Massachusetts, and Connecticut added to the GOP’s sizeable majority of governorships•Legislative activity at the state level has taken on increased importance in recent years due to gridlock at the federal level; as such, increased GOP control of governorships nationwide could give Republicans additional leverage to achieve policy goals at the state level
OH
WV VA
PA
NY
ME
NC
SC
GA
TN
KY
IN
MIWI
MN
IL
LATX
OK
ID
NV
OR
WA
CA
AZNM
CO
WY
MT ND
SD
IA
UT
FL
AR
MO
MS AL
NE
KS
VT
NHMA
RICT
NJ
DEMD
AK
HI
Map of State Governors by Party
AK Democrats: 15Republicans: 31Independents: 0Undecided: 3
Dem Governor
GOP Governor
Undecided*
*Race not called as of 6 AM 11/5

Source: National Journal Research; CNN Election Center; The New York Times.
Republicans Make Significant Gains in House
AnalysisRepublicans were expected to keep control of the House, but strong performances in tossup districts and a handful of wins in states that were expected to lean Democratic mean that the new GOP majority is even
larger than expected
House Seats Gained/Held in the 2014 Midterm Elections
AK Democrats: 175Republicans: 243Independents: 0Undecided: 17
Democratic Gain
Democratic Hold
Republican Gain
Republican Hold
Undecided*
* Races not called as of 6am 11/5/2014; includes runoff elections to be held in LA-5 and LA-6

64
So what does all of this mean for Obamacare?
1. The election was not a referendum on the Affordable Care Act.
• Exit polls show that only 25 percent of voters named Obamacare as the top issue for them compared to 45 percent who named the economy.
• 47 percent of those who cast ballots in the mid-term elections said that Obamacare went too far, but another 48 percent said that the law was just about right or did not go far enough.

65
So what does all of this mean for Obamacare?
2. Although Republicans will have sizeable majorities in both chambers of Congress, they will not be able to repeal Obamacare, because they don’t have the 60 votes required to overcome a Democratic filibuster, and if they were somehow able to get a repeal bill to the president, they don’t have the two-thirds super-majority in both chambers needed to override a veto.

66
So what does all of this mean for Obamacare?
3. The Republican-controlled Congress may be able to advance legislation to alter parts of Obamacare that are peripheral, but not essential, to getting people covered, like the taxes on medical devices and insurance companies, and repeal of the Independent Advisory Board.
4. Republicans will use their control of Congress to exercise more oversight over the administration’s implementation of the ACA.

67
So what does all of this mean for Obamacare?
5. Two programs important to ACP and primary care physicians may face tough sledding in the new Congress, because they were created by the ACA and cost money to continue.
• Medicaid primary care pay parity, which is set to expire at the end of this year, unless Congress authorizes an extension of it during the upcoming “lame duck” session.
• Medicare 10 percent primary care bonus program, which sunsets at the end of 2015.

68
So what does this all mean for Obamacare?
6. With more states having Republican governors and legislatures, continued progress in expanding Medicaid may be slowed, leaving millions of poor Americans in the “coverage gap” (ineligible for Medicaid, ineligible for Obamacare’s premium subsidies).

69
ACP post-election advocacy
We will identify issues where we have opportunities to make progress in the new Congress, such as medical liability safe harbors, regulatory relief.
We will advocate to preserve the elements of the ACA that are most essential to coverage.
We will refine our messages to achieve the most bipartisan support—such as on Medicaid pay parity and Medicare 10% primary care bonus.

70
ACP and Ebola
Updated resources for clinicians:• CDC• Smart Medicine• Checklist
Statement of concern about mandatory quarantines of clinicians
“The College maintains that mandatory quarantines for asymptomatic physicians, nurses and other clinicians, who have been involved in the treatment of Ebola patients, whether in the United States or abroad, are not supported by accepted evidence on the most effective means to control spread of this infectious disease. Instead, such mandatory quarantines may do more harm than good by creating additional barriers to effective treatment of patients with Ebola and impede global efforts to contain and ultimately prevent further spread of the disease.”


72
To recap, imagine that
“Alice” represents your members,patients, public, asking you which way health care ought to go,
And the Cheshire Cat is ACP and the NM Chapter, pointing them in direction to which way health care ought to go

73
“Would you tell me, please, which way I ought to go from here?"
To guaranteed coverage of evidence-based essential services for everyone, without regard to income, where they work, or health status
Despite the opposition, the ACA is taking us to a place where most Americans will have affordable coverage.
• But court challenges, restrictive formularies, state opposition to Medicaid expansion remain barriers
Which way we ought to go: Where we are today:

74
“Would you tell me, please, which way I ought to go from here?"
To sustainable GME financing reforms to ensure accountability and transparency and allocate sufficient resources based on assessment of workforce needs
IOM report offers a thoughtful framework for reform, much (but not all) of which is in accord with ACP policies
Congress is unlikely to make changes in short-term, but over longer-term, GME reform is inevitable and welcome
Long-held consensus that there is a physician workforce shortage is under challenge
Which way we ought to go: Where we are today:

75
“Would you tell me, please, which way I ought to go from here?"
To a payment and delivery system that recognizes and values the role of internal medicine specialists and others who provide primary and comprehensive care
Current Medicaid pay parity program set to expire on 1/1/15, so we need your help in persuading Congress to extend it
“There really is another way” : PCMHs/PCMH-N, ACOs, bundled payments, risk-adjusted capitation
Which way we ought to go: Where we are today:

76
“Would you tell me, please, which way I ought to go from here?"
To a system that minimizes paperwork, regulatory and reporting requirements, and dysfunctional information systems that detract from patient care and the joy of practice
Poorly designed EHRs and federal MU regulations are adding hours to workload and contributing to physician-burnout
• ACP is working with the industry on solutions and leading an effort to advocate for changes in federal standards and rules
Too much paperwork and too many administrative processes!
• ACP’s “Patients Before Paperwork” Initiative will propose solutions
Which way we ought to go: Where we are today:

77
“Would you tell me, please, which way I ought to go from here?"
Through ACP advocacy, we can help lead the United States to• A health care system that covers everyone, costs
less, recognizes the value of internists’ services, ensures stable and transparent GME financing aligned with workforce priorities, puts patients before paperwork, and uses information technology to improve, rather than detract, from patient care.
if only we are willing to walk long enough.







