Download - Critical illness polyneuropathy
DR. SACHIN ADUKIA
Critical illness polyneuropathyand myopathy

Definitions
Critical illness polyneuropathy (CIP) refers to ICU-acquired weakness with
electrophysiological evidence of an axonal polyneuropathy.
Critical illness myopathy (CIM) refers to ICU-acquired weakness with myopathy
that is documented electrophysiologically or histologically.
Critical illness neuromyopathy (CINMP) refers to electrophysiological or
histologic findings of both critical illness polyneuropathy and critical illness
myopathy.

History
Osler described neuromuscular dysfunction in patients with sepsis
Olsen reported peripheral neuropathy complicating protracted coma.
In 1977, myopathy was described in a patient with status asthmaticus
who received high doses of hydrocortisone and simultaneous
neuromuscular blockade.

Introduction
Neuromuscular weakness develops in ≥25 percent of patients who are ICU and ventilated for atleast 7 days
may result in a lifelong loss of function CIP first described by Bolton and colleagues in 1984
causes severe limb weakness prolonged weaning, increases stay in ICU compromises rehabilitation

Muscles involved in CIP/CIM
affects the limbs (particularly LL) in a symmetric pattern.
proximal predominant (shoulders and hip girdle)
involvement of respiratory muscles can impede weaning from
mechanical ventilation.
Facial and ocular muscles are rarely involved.
Autonomic features are not seen
Pathology in CIM
Also known as acute quadriplegic myopathy and thick filament myopathy
There is loss of thick filament myosin and Type II fiber atrophy, mainly with
proximal weakness
Pathologically classified into five subtypes:
(1) thick filament myopathy
(2) acute myopathy with scattered necrosis
(3) acute myopathy with diffuse necrosis
(4) disuse cachectic myopathy
(5) rhabdomyolysis
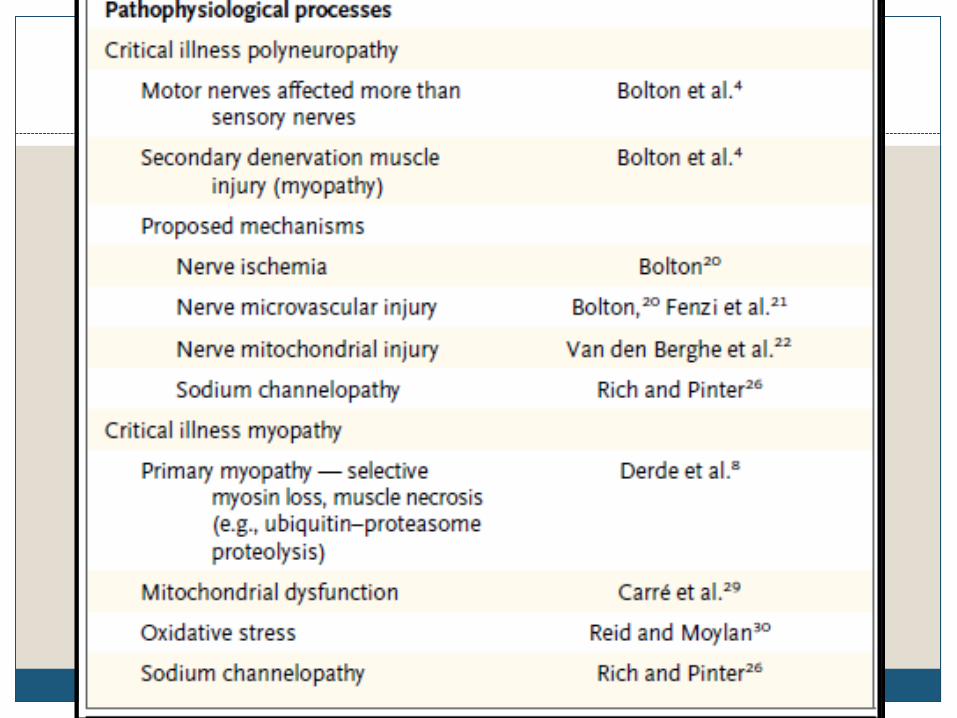
Postulated pathophysiology- CIM
Reduced muscle membrane excitability reduced uptake and release of calcium by the sarcoplasmic reticulum producing a
decrease in muscle contractility. Decreased contractile protein function and muscle fibre force generation. Mitochondrial dysfunction and bioenergetic failure with consequent reduction in
oxygen utilization and ATP production. Muscle denervation either pharmacological (neuromuscular block) or structural (CIP)
mechanisms produces an increased expression of corticosteroid receptors within myocytes, sensitizing them to the deleterious effects of corticosteroids.
Muscle atrophy during critical illness occurs - 3–4% decrease in muscle cross-sectional area per day. Is due to increased proteolysis, decreased protein synthesis, and increased apoptosis.
Pathology and Pathophysiology for CIP
dysfunctional microcirculation leads to neuronal injury and axonal
degeneration.
E-selectin expression in peripheral-nerve vascular endothelium, suggesting endothelial-
cell activation with microvascular leak and alterations in microvascular environment.
Hyperglycemia exacerbates this by inducing neural mitochondrial dysfunction
presents as morphological signs of axonal degeneration in both type 1 and type 2
fibers, resulting in extensive denervation atrophy of muscles
Clinical features
Muscle wasting is variable and frequently disguised by oedema.
flaccid and usually symmetrical weakness
Usually noted as lack of movement after regaining consciousness, loss of deep tendon
reflexes that had been present earlier
earliest sign may be facial grimacing without limb movement to pain
EOM involvement – warrants investigation for different aetiology
Facial muscles - relatively spared
CIP may show a distal loss of sensitivity to pain, temperature, and vibration
But difficult to assess sensory system in Critically ill patient
Autonomic function is not affected.
Difficulty in Weaning
Weaning problems - involvement of the phrenic nerves and the
diaphragm, and intercostal and other accessory respiratory muscles
Neuromuscular weakness typically becomes apparent during
attempted weaning

Full ventilatory support can trigger muscle atrophy within 72 hours
in adults Evidence of oxidative stress and protein breakdown in the muscles
Levine et al. noted atrophy in diaphragm myofibers within 18
hours of complete diaphragmatic inactivity
Jaber et al. reported a loss of diaphragmatic strength within hours
after initiating mechanical ventilation
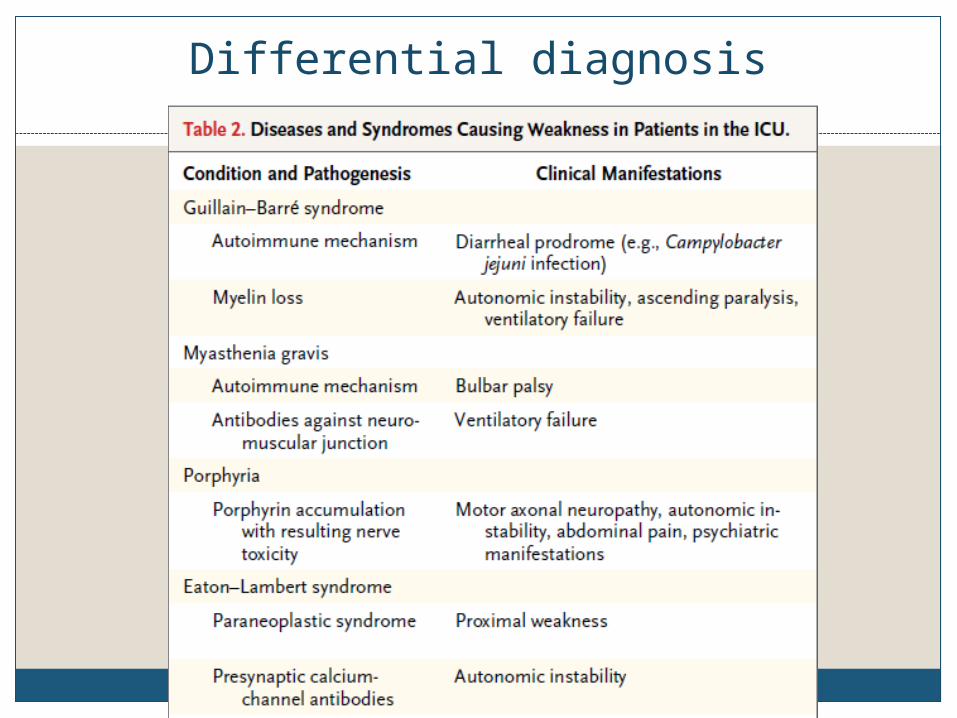
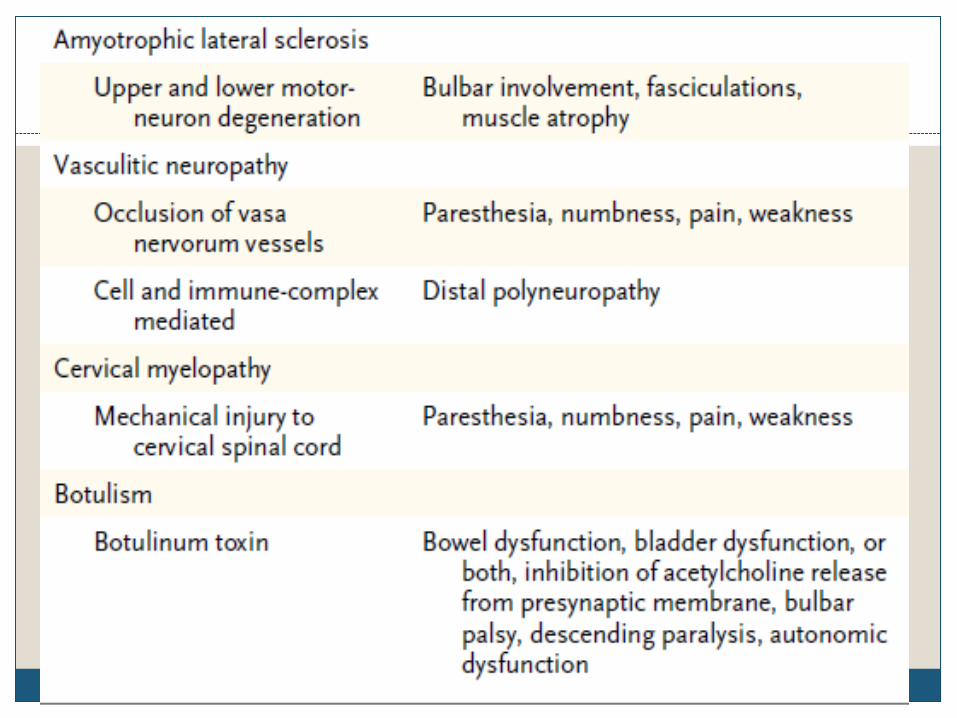
Differential diagnosis
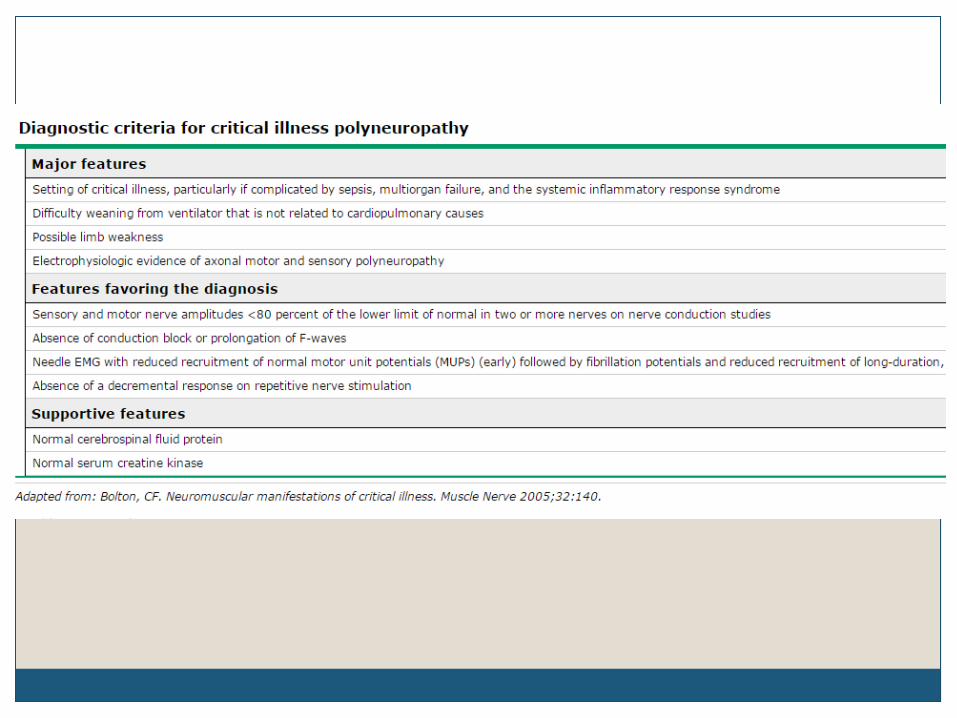
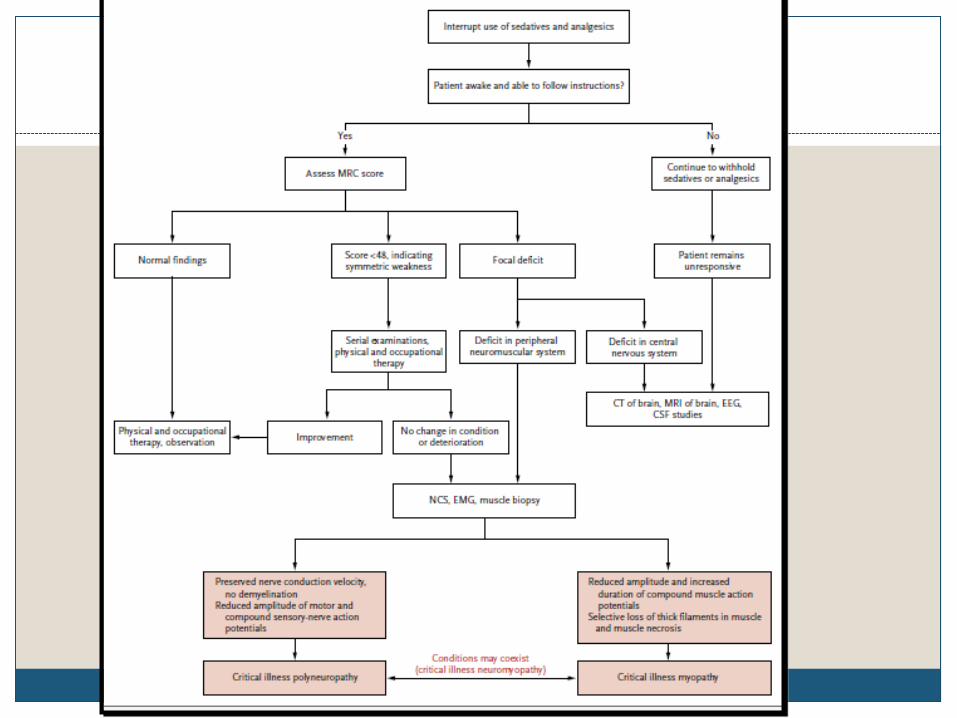
Diagnosis
Serum CK -not helpful since they are normal if muscle necrosis is absent or
scattered ,which is usually the case
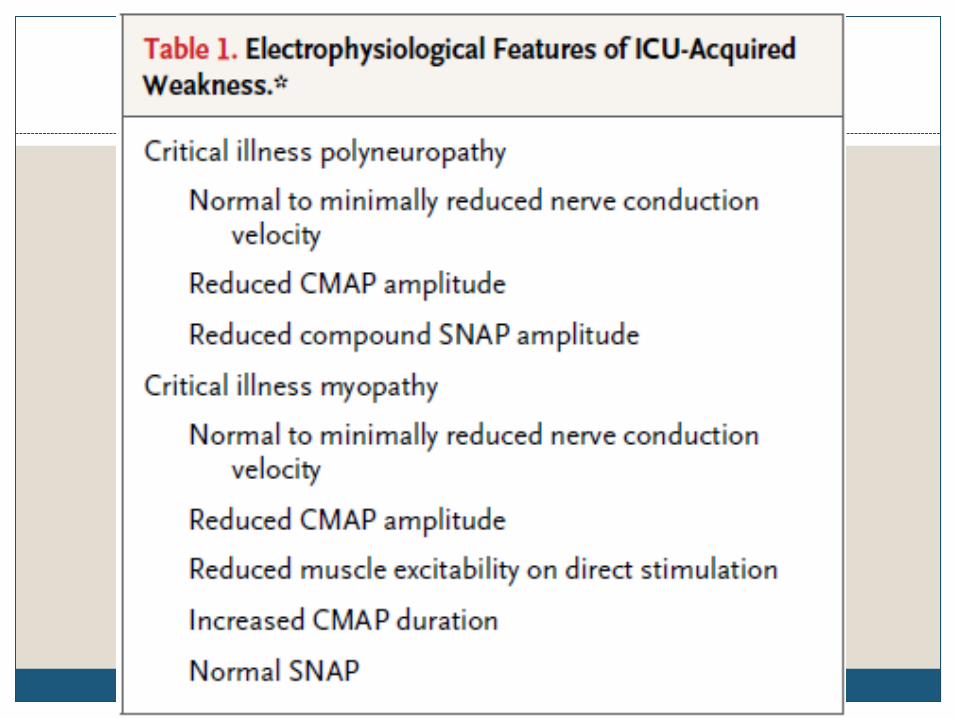
Routine electrophysiological examination often times cannot discriminate
between CIP and CIM in critically ill, sedated, uncooperative or extremely
weak patients
Local oedema can interfere with optimal sensory nerve stimulation and
recording
To differentiate between CIP and CIM – patient co operation is needed for
voluntary motor unit potential recruitment
Muscle biopsy

CRIMYNE study
CRIMYNE for critical illness to monitor for CIM and/or CIP)
showed that serial electrodiagnostic studies are helpful in predicting
development of CIM and/or CIP
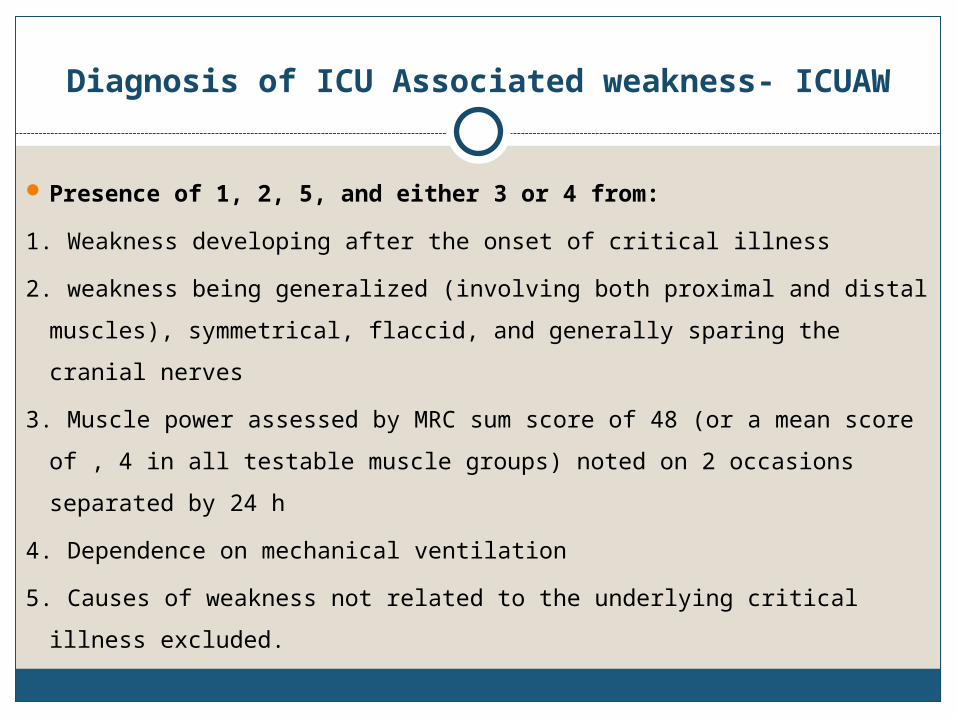
Diagnosis of ICU Associated weakness- ICUAW
Presence of 1, 2, 5, and either 3 or 4 from:
1. Weakness developing after the onset of critical illness
2. weakness being generalized (involving both proximal and distal muscles),
symmetrical, flaccid, and generally sparing the cranial nerves
3. Muscle power assessed by MRC sum score of 48 (or a mean score of , 4 in all
testable muscle groups) noted on 2 occasions separated by 24 h
4. Dependence on mechanical ventilation
5. Causes of weakness not related to the underlying critical illness excluded.
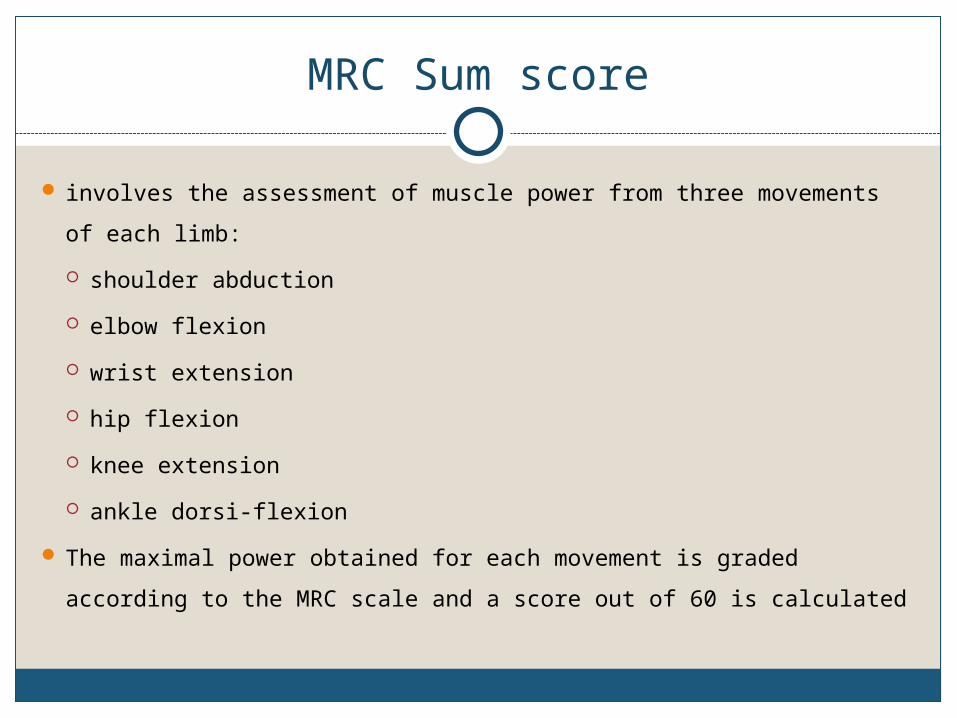
MRC Sum score
involves the assessment of muscle power from three movements of each limb:
shoulder abduction
elbow flexion
wrist extension
hip flexion
knee extension
ankle dorsi-flexion
The maximal power obtained for each movement is graded according to the
MRC scale and a score out of 60 is calculated

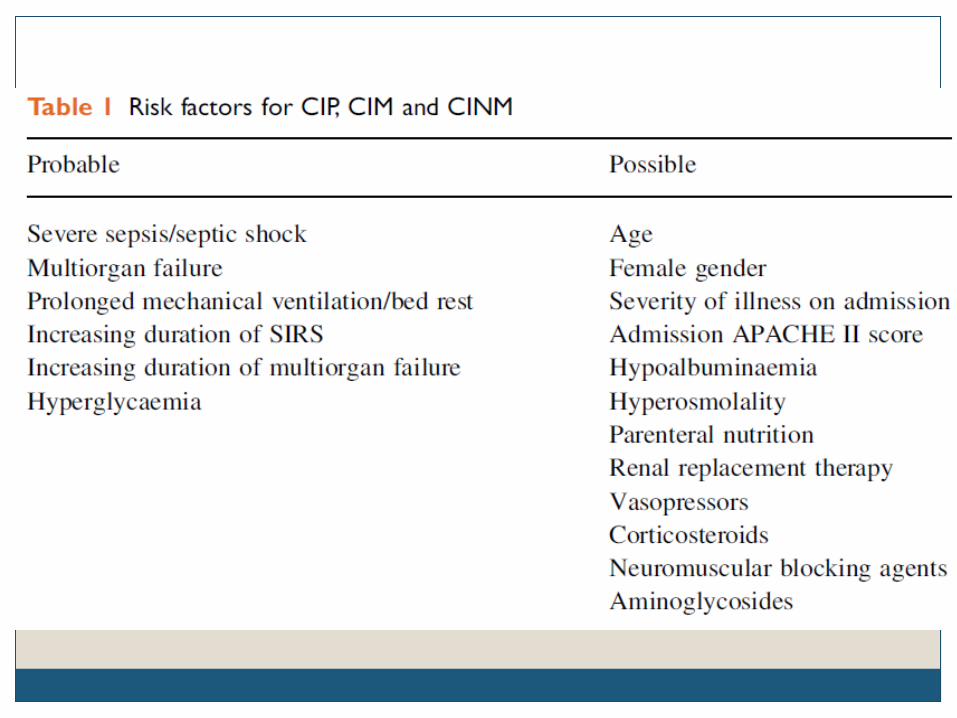
Prevention and therapy
Aggressive treatment of sepsis
Corticosteriods and Neuro-muscular blockade agents, if indicated, to use at minimal dose for shortest period
Rehabilitation programs
Avoiding additional pressure neuropathies by careful positioning
Several specific therapies have been mentioned – nutrition supplements, antioxidant therapy, testosterone derivatives, growth hormones immunoglobulins
NONE EFFECTIVE

Insulin therapy
Intensive insulin therapy- Insulin itself has some potential beneficial
effects
anti-inflammatory effects
endothelial protection,
improvement of dyslipemia, and
neuroprotective effects in animals
an anabolic hormone2 unpublished studies report that intensive insulin therapy (target blood
glucose 80 to 110 mg/dL) may lower the incidence of CIM and CIP
Physiotherapy and training
Applying an early activity protocol ICU environment may contribute unnecessarily to
immobilizationSedation substantially reduce the likelihood of ambulation

Electrical muscle stimulation
An RCT including 24 patients with COPD receiving MV showed that EMS
sessions of 30 minutes in 28 days significantly improves muscle strength
and decreases no. of days needed before mobilization to chair
results in a shorter duration MV and shorter ICU stay
does not require patient cooperation and can be applied to any muscle group
Recovery from CIP/ CIM
Patients who survive ARDS or sepsis or both have these problems with the greatest
frequency and intensity.
patients requiring prolonged mechanical ventilation, neuromuscular recovery is
typically prolonged and incomplete.
Up to 65% of such patients have functional limitations after discharge
Neuromuscular abnormalities may last for many years in some
A 1 year follow-up of 13 survivors from the CRIMYNE study showed
a mixture of tetraplegia, partial recovery, and full recovery in combined CIM/CIP
complete recovery in three to six months for CIM alone
minority of patients with CIP has persistent weakness.

Prognosis
CIPNM significantly increases the length of MV and the
lengths of ICU and hospital stay
Mortality increases from 19-56.5% to 48-84%
Recovery CIM > CIP > CINM

Conclusion
Critical illness myopathy and/or critical illness neuropathy are frequent and serious
complications to intensive care that:
– delay weaning from mechanical ventilation
– increase the stay in ICU
– compromise rehabilitation
- may result in a lifelong loss of function and in a reduction in quality of life.
Ensure maximal functional status for survivors of ICU stays using multimodal
therapeutic approach including:
– screening and early diagnosis is possible
– intensive insulin therapy
– minimal sedation
– early physiotherapy
– electrical muscle stimulation
References
Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. New England Journal of
Medicine. 2014 Apr 24;370(17):1626-35.
Appleton R, Kinsella J. Intensive care unit-acquired weakness. Continuing Education in Anaesthesia,
Critical Care & Pain. 2012 Apr 1;12(2):62-6.
Ydemann M, Eddelien HS, Lauritsen A. Treatment of critical illness polyneuropathy and/or myopathy
a systematic review. Dan Med J. 2012 Oct 1;59(10):A4511.
Zhou C, Wu L, Ni F, Ji W, Wu J, Zhang H. Critical illness polyneuropathy and myopathy: a
systematic review. Neural regeneration research. 2014 Jan 1;9(1):101.
Bolton CF. Neuromuscular manifestations of critical illness. Muscle Nerve 2005; 32:140.
Hermans G, Wilmer A, Meersseman W, et al. Impact of intensive insulin therapy on neuromuscular
complications and ventilator dependency in the medical intensive care unit. Am J Respir Crit Care
Med 2007; 175:480
Thank You







