
COPP MODULE
COMMON OFFICE PRACTICE PEDIATRIC PROBLEMS[A MODULE OF IAP TAMILNADU STATE CHAPTER 2017]
1

TEAM• Scientific advisors Dr P Ramachandran, Dr S Balasubramanian• Conveners Dr S Thirumalai Kolundu, Dr Sunil Srinivasan• Scientific Coordinator Dr A Somasundaram • Academic coordinators Dr S Narmada, Dr R.V Dhakshayani • Academic committee [MODERATORS]
• Dr NC Gowrishankar,• Dr T N Manohar,• Dr K Nedunchelian,• Dr Rema Chandramohan,• Dr R Somasekar,• Dr S Thangavelu,• Dr V V Varadarajan
2

CONTRIBUTORSDr RV Dhakshayani Dr A SomasundaramDr Giridhar Dr Somu SivabalanDr Hemchand K Prasad Dr S SrinivasDr E Mahendar Dr P SudhakarDr S Mangalabharathi Dr Sudharshana skanda Dr Manikandan Dr B SumathiDr Manikumar Dr Suresh Dr S Narmada Dr VenkateshwaranDr Palaniraman Dr C VijayabhaskarDr R Selvan

Dr. Manigandan Chandrasekaran, MBBS,DCH, MRCPCH, CCT,FRCPCH, MD (Research)
• Consultant Neonatologist, Cloudnine Hospitals, • Finished his Specialist training in Neonatology in London• Has done Management Course in London Emperial College
NHS Trust• Faculty in
– NEST – Neonatal Emergency Simulation Team training course – Neonatal Resuscitation, India advanced provider course for doctors
and nurses– Cranial Ultrasound course– Neonatal Neurology examination and investigations course– MRCPCH clinical examination training course – Smart course
• He has 17 publications in Peer reviewed journals, authored in chapters in 2 textbooks and has 7 presentations to his credit
4

Incessant Cry in Neonates and Infants
Dr C ManigandanModerator
Dr. Rema Chandramohan
5

Overview
• Normal cry and sleep
• Definition
• Etiology
• Management

• Physiological behaviour • 6 - 8 weeks – average
2 – 3h/24h • Worse in late afternoon or
evening• Disappears by 3 - 4 months
0
1
2
3
4
0 2 4 6 8 10 12
Age (Weeks)
Tim
e (H
ours
)
Brazelton TB. Crying in infancy. Pediatrics. 1962;29:579-588.
Crying – Normal pattern

Average Sleep
• Birth: 16 - 18 h
• 3 months: 14 -15h
• 6 week - tired after awake for 1.5 hours
• 3 month - tired after 2 hours

Definition – No consensus
• Persistent cry, excessive cry and problem crying• Excessive Crying – “Rule of 3”
>3 hours/day >3 days/week
>3 week• Paroxysmal, qualitatively different from normal cry,
associated with hypertonia and inconsolability• Incidence - 1.5% to 11.9%
Wessel MA, et al Paroxysmal fussing in infancy, sometimes called colic. Pediatrics. 1954;14(5):421-435

Etiology
10

Common Causes of Crying
• Hunger/Thirst• Soiled or wet diapers• Too hot or too cold• Flatus• Loneliness• A sudden or startling
movement• Excessive tiredness• Wanting to be held

System-wise Causes Common and Important
• Corneal abrasion
• Foreign body
• Acute otitis media
• Nasal congestion
• Oral thrush
• Bronchiolitis 12

System-wise Causes
Common and Important
• Intussusception
• GERD
• Colic
• Milk-protein allergy
• UTI
• Genital tourniquet 13

Common and Important
• Early CP
• Meningitis
• Hypoglycemia
• Dehydration
System-wise Causes
14

Common and Important
• Digital tourniquet
• Fractures
• Septic arthritis
• Insect bites
• Diaper dermatitis
• Post - immunisation
System-wise Causes
15

Approach to Diagnosisand Management
16

Key aspects of Management
• Careful assessment to identify infants with a serious illness
• Treatment of benign causes
• Parental guidance and counseling

Diagnosis
• History
• Physical examination
• Lab investigations
Key to diagnosis

Observation FATT & DRIP
FREQUENCYFrom one to infinity
DURATIONElapsed time
AGE of the childNumber of days, weeks, months, or years since birth
RHYTHMFrom waltz to hiphop
TIME of dayM o r n i n g , a f t e r n o o n , evening, or night
INTENSITYRelaxed to vigorous
TONEFrom whimper to wail
PITCHLow (purr) to high (screech)
19
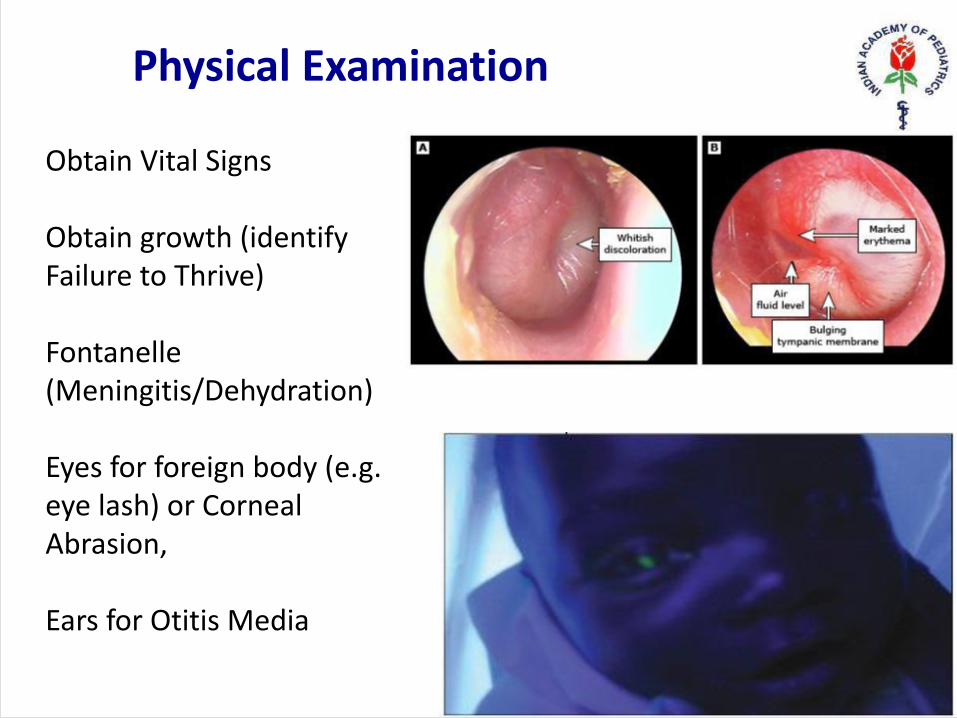
Obtain Vital Signs
Obtain growth (identify Failure to Thrive)
Fontanelle (Meningitis/Dehydration)
Eyes for foreign body (e.g. eye lash) or Corneal Abrasion,
Ears for Otitis Media
Physical Examination

• Nose - obstruction• Mouth for Stomatitis, Thrush or
frenulum tear• Lung Exam for respiratory
disease• Cardiovascular exam for
perfusion and pulses (consider Heart Failure), Evaluate for SVT
• Abdominal exam for acute abdominal signs
• Examine for abdominal mass (e.g. Intussusception)
• Examine for blood in the stool (e.g. Anal Fissure)
Physical Examination

• Genitourinary exam - Incarcerated Hernia, Testicular Torsion
• Neurologic Exam (early CP)• Joint exam for Septic Arthritis,
Osteomyelitis• General exam for signs of
Trauma or Fracture • Decreased extremity use• Skin Exam, Bruising or rashes• Evaluate for Hair Tourniquet
Physical Examination

Lab investigations
• Limited value• X-ray chest – Pneumonia / Bronchiolitis/fractures• US Abdomen – Intussusception • Urine analysis – UTI • Rest – according to clinical findings

Symptoms suggestive of organic causes
• Extreme, prolonged and high-pitched cry• Lack of a diurnal rhythm in crying• Presence of abnormal symptoms • Positive physical examination• Persistence of crying past 4 months of age

Sudden onset – Consider
• Urinary tract infection• Otitis media• Raised intracranial pressure• Hair tourniquet of fingers / toes• Corneal foreign body / abrasion• Incarcerated inguinal hernia

Crying as a presenting symptom
• Supraventricular tachycardia• Foreign body in airway• Diaper rash• Cow’s milk allergy• Sickle cell crisis• DPT immunization• Insect bites

Painful Surgical conditions
• Strangulated Hernia
• Torsion testes
• Intussusception
• Malrotation
• Mid-gut Volvulus
Painful medical conditions
• Insect bite
• Hair tourniquet
• Corneal abrasion
• Otitis media
• Diaper dermatitis

• Viral illness• UTI• AOM • Meningitis• Septic arthritis• Cellulitis• Sepsis• Gasteroenteritis
Febrile conditions

Look for clues
• Corneal abrasion / ocular foreign body• Megalocornea – glaucoma• Retinal hemorrhage / detachment• Bulging tympanic membrane• Incarcerated hernia• Anal fissure• Hair tourniquet• Rib fractures• Open diaper pin injury

• High-grade fever• Refusal to feed / difficulty in feeding • Lethargy• Paroxysms of abnormal activity• Unexplained bruising• Sustained tachycardia > 180/min• Bilious vomiting• Bloody stools • Paradoxical irritability / full fontanel• Not moving an extremity
Red Flags

Treatment
31

Medications – Commonly prescribed
Little role
• Pain relief – Paracetamol, ibuprofen• Antipyretics – Paracetamol • Saline nasal drops • Antibiotics – according to the infection• Anti-reflux medications

Medications – No strong evidence• Dicyclomine – contraindicated (<6months) -
risk of serious adverse events• Simethicone (Infacol Drops / Colic aid Drops)
has no beneficial effect over placebo• Fennel oil/Dill oil – no proven benefit• Enzymes (neopeptine drops ) – no evidence • Hypoallergenic formula – some benefit (2 SRs)
– only after evidence
• Lactobacillus reuteri• Meta-analysis of 6 RCTs
–Significant reduction in crying duration in BF infants in 3 week treatment
• Not available in India
Probiotics

Home remedies ?
• Gripe water – could cause problems if sodium or sugar or alcohol present
• Vasambu, Omam, Uramarundu herb mixture, Asafetida in warm water, Garlic – Avoid (aspiration, infection, dangerous in surgical conditions)
• Calming procedures – Prone positioning, warm compresses and abdominal massages – may be beneficial
• Dietary modification - may benefit

Parental Counseling
36

Explain Normal Patterns
• Explain the infant's cry / sleep / feeding patterns • Encourage parents to recognize signs of tiredness• Avoid excessive stimulation - noise, light, handling• Aim to settle the baby for all sleep in a predictable way• Darken the bedroom for daytime sleeps• Respond before baby is too worked up

Soothing strategies
• Swing• Blankets• Music• Teddy bears • Holding • Swaddling• Infant massage• Singing (to)


Coping strategies
• Identify the cry • Try the obvious • Speak softly, bring the pitch and volume down• Hold his arms and body to avoid startles • Swaddle him • Pick him up to cuddle • Try massaging his back and limbs gently • Sing to him and Walk with him • Use white noise or motion

REST intervention
REST for mothers
• Reassurance• Empathy • Support• Time out for the parents
REST for infants
• Regulation • Entrainment• Structure • Touch
Conclusion
• Commonly benign • Can be the only presentation of a serious illness• Key - detailed history and physical exam (head to toe)• Identify ‘Red flags’• Parental reassurance• Avoid unnecessary investigations and medications

THANK YOU
43







