
9/21/15
1
Congestive Heart Failure 2015
JP Mehegan/ Mercy Cardiology
Definition
n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms)
n When the heart is unable to pump sufficiently and at the appropriate pressure to meet the bodies needs
n Symptoms; dyspnea, edema, fatigue; activity intolerance
n STARTING POINT
Types of Heart Failure
n Systolic ; heart failure with abnormal LV function; ejection fraction < 40%
n Diastolic; heart failure with normal LV systolic function and abnormal cardiac relaxation (diastolic function); 50%
n Other; valvular, ischemia, MI, constriction/pericardial disease
The Problem (USA)• 5,000,000 patients• 6,500,000 hospital days / year• 300,000 deaths / year• More than half of those diagnosed will be
dead in 5 years• 6% of health care budget (38 billion)• Incidence doubling in last ten years
Heart Failure Costs
60% Inpatient care $23.1 billion
39% Outpatient care
$14.7 billion
1% Transplants $270 million Total = $38.1 billion
(5.4% of total healthcare costs)
O’Connell JB et al. J Heart Lung Transplant. 1994;13:S107-S112
Stages in the evolutionof Heart Failure
n A. HF risk factors; no documented heart disease or symptoms
n B. Heart disease; no symptoms. Asymptomatic LV dysfunction
n C. Prior or current symptomatic CHFn D. Refractory HF symptoms
AHA / ACC HF guidelines 2005

9/21/15
2
Stages in Prevention and Treatment of Heart Failure
n A. Treat risk factors, avoid toxins. ACE-In B. ACE-I, Beta blockersn C. ACE-I, Beta blockers, dig, diuretics,
aldosterone antagonists, ARB, resynchronization (Bi-V pacing), new therapies
n D. Ultrafiltration, inotrope therapy, VADs and transplant
Classification of Functional Status; NYHA
n 1. No physical limitationsn 2. Symptoms with moderate activity,
exercise.n 3. Symptoms with mild activity; activities
of daily livingn 4. Symptoms at rest
Initial / Ongoing Evaluation
n H&Pn Assess functional capacity (NYHA, 6 min
walk)n Assess volume status: (edema, rales, jugular,
hepatomegaly, body weight)n Lab assessment: routine: electrolytes, renal
function, ECHO, X ray ,TSH, EKGn BNP
Causes of Cardiomyopathy/ CHF
n 135 Causes of cardiomyopathyn CAD; prior MI, diffuse ischemia (70%)n Hypertensionn Endocrine; diabetes, thyroidn Drugs/ Toxins; ETOH, cocaine, chemon Afib/ flutter; rate relatedn Infection, familial, nutritional, idiopathic
B type natriuretic peptide!BNP
n Role in the emergency room70 yo with PND, orthopnea, edema and vascular congestion on CXR70 yo with COPD, wheezing, rales and edema, clear CXR
n Role in the clinic
Treatment Objectives
n Increase Survivaln Improve LV functionn Improve symptoms/ Quality of Lifen Improve exercise capacityn Block neurohormonal changes and
prevent progressive HFn CHF Trials App ($2.99)

9/21/15
3
Beta blocker
Mineralocorticoid receptor
antagonist
Drugs That Reduce Mortality in Heart Failure With Reduced Ejection Fraction
ACE inhibitor
Angiotensin receptor blocker
Drugs that inhibit the renin-angiotensin system have modest effects on
survival
Based on results of SOLVD-Treatment, CHARM-Alternative, COPERNICUS, MERIT-HF, CIBIS II, RALES and EMPHASIS-HF
10%
20%
30%
40%
0%
% D
ecre
ase
in M
orta
lity
TreatmentPharmacologic Therapy
n ACE inhibitors/ARBs/Vasodilators
n Beta Blockersn Diureticsn Digitalisn Spironolactone/ Eplerenome
ACE-I. Clinical Effects
n Improve symptomsn Reduce remodeling / progressionn Reduce hospitalizationn Improve survival
ACE-i Practical Usen Start with low dosen Increase dose as toleratedn Renal function & serum K+ after 1-2
weeksn Dose NOT determined by symptoms n Target randomized trial doses n Reduce diuretics if possible
Mortality Reduction with ACE-i
Study ACE-i Clinical SettingCONSENSUS (1987) Enalapril CHFSOLVD treatment Enalapril CHFAIRE Ramipril CHFVheft-II Enalapril CHFTRACE Trandolapril CHF SAVE Captopril LVD/MISMILE Zofenopril High risk HOPE (2000) Ramipril High risk
ACE-i Dose (mg)
Initial MaximumCaptopril 6.25 / 8h 50 / 8hEnalapril 2.5 / 12 h 10 to 20 / 12hFosinopril 5 to 10 / day 40 / dayLisinopril 2.5 to 5.0 / day 20 to 40 / dayQuinapril 10 / 12 h 40 / 12 hRamipril 1.25 to 2.5 / day 10 / day
AHA / ACC HF guidelines 2005

9/21/15
4
ACE-i Adverse Effects
n Hypotensionn Worsening renal functionn Hyperkalemian Cough 5-10%(iron pill may prevent)n Angioedema (1/1000)n Rash, ageusia, neutropenia (1-2%)n ACE intolerant use ARB
Angiotensin Receptor Blockers!ARBs
n As added therapyn As alternative therapy (ACEi intolerant)n FDA approved; Valsartan 40 mg BID
start, 160 mg BID targetn Candesartan; 4 mg QD start, 32 mg QD
targetn Most commonly used ( not approved and
underdosed), Losartan, target 150 mg QD
Val-HeFT5010 patients ���
≥18 years; EF <40%; NYHA II-IV; LVIDd >2.9 cm/m2
ACE inhibitors, diuretics,���digoxin, β-blockers
Valsartan���40 mg bid titrated to���
160 mg bid
Randomized to
Receiving background therapy
Placebo
Cohn JN et al. Eur J Heart Fail. 2000;2:439-446.
Effect of Valsartan on Combined Morbidity/Mortality Endpoint*
Months3 6 9 12 15 18 21 24 270
6570758085909510
0
Probability of Event-
Free Survival���
0
*All-cause mortality, sudden death with resuscitation, hospitalization for worsening heart failure, or therapy with IV inotropes or vasodilators. Cohn JN et al. N Engl J Med. 2001;345:1667-1675.
30
ValsartanPlacebo
P = 0.00913.2% Risk Reduction
Reduction in Combined Morbidity/Mortality Endpoint* with Valsartan (No ACE-I Subgroup)
Hazard ratio (Cox model) : 0.560*First morbid event, including death or hospitalization
Time Since Randomization (months)
4050
6070
8090
100
0 3 6 9 12 15 18 21 24 27 30
P < 0.00144.0% Risk reduction
Valsartan, n=185
Placebo, n=181
Probability of Event-
Free probability���
Maggioni et al. J Am Coll Cardiol 2002;40:1414-21
CHARM
7,601 patients with heart failure 3 Individual component randomized trials with the ARB candesartan (4
or 8 mg/day, titrated to target dose of 32 mg) or placebo
CHARM Added § Patients with LVEF
<40% and treated with an ACE-inhibitor
CHARM Alternative
§ Patients with LVEF <40% and
ACE-inhibitor intolerant
CHARM Preserved § Patients with LVEF >40%
with or without ACE-inhibitor
Endpoints (follow-up minimum 2 years): ! Primary – Component trials: cardiovascular mortality or HF hospitalization
! Primary – Overall trial results: All-cause mortality

9/21/15
5
SS-25
At risk, n Placebo 1272 1017 852 736 338 Candesartan 1276 1074 914 793 395
Primary Outcome !CV Death or CHF Hospitalization !
CHARM Added
1 2 3 Time, yr
0
10
20
30
40
50 Placebo
Candesartan %
3.5
HR 0.85 (95% CI: 0.75, 0.96), p = 0.011 Adjusted HR = 0.85, p = 0.010
483 (37.9%) 538 (42.3%)
15% risk reduction
0
NNT = 23
ß-Adrenergic Blockers Mechanism of action
n Increase Density of ß1 receptorsn Inhibit cardiotoxicity of catecholaminesn Block Neurohormonal activationn HRn Antiischemicn Antihypertensive• Antiarrhythmic• Antioxidant, Antiproliferative
ß-Adrenergic Blockers Clinical Effects
n Improve symptoms (only long term)n Reduce remodeling / progressionn Improve LV systolic functionn Reduce hospitalizationn Reduce sudden deathn Improve survival
ß-Adrenergic Blockers When to start
n Patient stablen Not volume overloadedn No need for i.v. inotropic drugsn Stable dose of ACEi /Diuretic/ Dig
ß-Adrenergic Blockers Contraindications
n Asthma (not COPD)n AV blockn Symptomatic hypotension /
Bradycardia n PVD and Diabetes are NOT
contraindications
ß-Adrenergic Blocker Adverse Effects
n Hypotensionn Fluid retention / worsening heart failuren Fatiguen Bradycardia / heart block
n Reduce dosen Consider cardiac pacingn DON’T GIVE UP

9/21/15
6
ß-Adrenergic Blockers Dose (mg)
Initial TargetBisoprolol 1.25 / 24h 10 / 24hCarvedilol 3.125 / 12h 25 / 12h
Carvedilol XL 10/ 24h 80/24hMetoprolol succinnate 12.5-25 / 24h 200 / 24h
Start Low, Increase SlowlyIncrease the dose every 2 - 4 weeks
35% ReductionIn death
Carvedilol Effect on Survival
What is Target Dose?
What is Target Dose
Which Agent Should We Use?n Substantial differences in Beta–Blocking Agents
n Beta-1 Selectivityn Alpha-1 blockaden Ancillary Properties
n Antioxidant n Endothelin regulation
COMET!Carvedilol vs Metoprolol Tartrate
n 5.7%mortalityn reduction

9/21/15
7
Digitalis. Clinical Effects
n Improve symptoms and measured exercise
n Reduction in hospitalization for CHFn Does not improve survival
DIG trial
N=6800
NYHA II-III
N Engl J Med 1997;336:525
Digitalis. Indications
In combination with ACE-i + diuretics if persisting symptoms
AF, to slow AV conduction
Dose 0.125 to 0.250 mg / day
AHA / ACC Guidelines 2005
Diuretics. Indications
1.Symptomatic HF, with fluid retention• Edema• Dyspnea• Lung Rales• Jugular distension• Hepatomegaly• Pulmonary edema (Xray)
Loop Diuretics / Thiazides. Practical Use
n Start with low dose. Titrate to achieve dry weight
n Monitor serum K+ / renal function at “frequent intervals”
n Reduce dose when fluid retention is controlled
n Teach the patient when, how to change dosen Combine to overcome “resistance”n Do not use alone
Loop diuretics. Dose (mg)
Initial Maximum
Bumetanide 0.5 to 1.0 / 12-24h 10 / day
Furosemide 20 to 40 / 12-24h 400 / day
Torsemide 10 to 20 / 12-24h 200 / day
9/21/15
8
Thiazides, Loop Diuretics. Adverse Effects
• K+, Mg+ wasting (sudden death???)• Na+
• Stimulation of neurohormonal activity• Hyperuricemia (15 - 40%)• Hypotension. Ototoxicity. Metabolic Alkalosis.
Diuretic Resistancen Neurohormonal activationn Hypertrophy of distal nephronn Reduced tubular secretion (renal failure,
NSAIDs)n Decreased renal perfusion (low output)n Altered absortion of diureticn Noncompliance with drugs/ Dennys
biscuits and gravy
Managing Resistance to Diuretics
• Restrict Na+/H2O intake (Monitor Sodium)• Increase dose (individual dose, frequency, i.v.)
• Combine: furosemide + thiazide / spiro / metolazone
• Reduce dose of ACE-I Stop NSAIDS• Dopamine (increase cardiac output)
Aldosterone in Heart Failure
n Levels up 20X from normaln Produces adverse effects
n Cardiac remodelingn Na++ retentionn Up SNSn Down arterial compliance
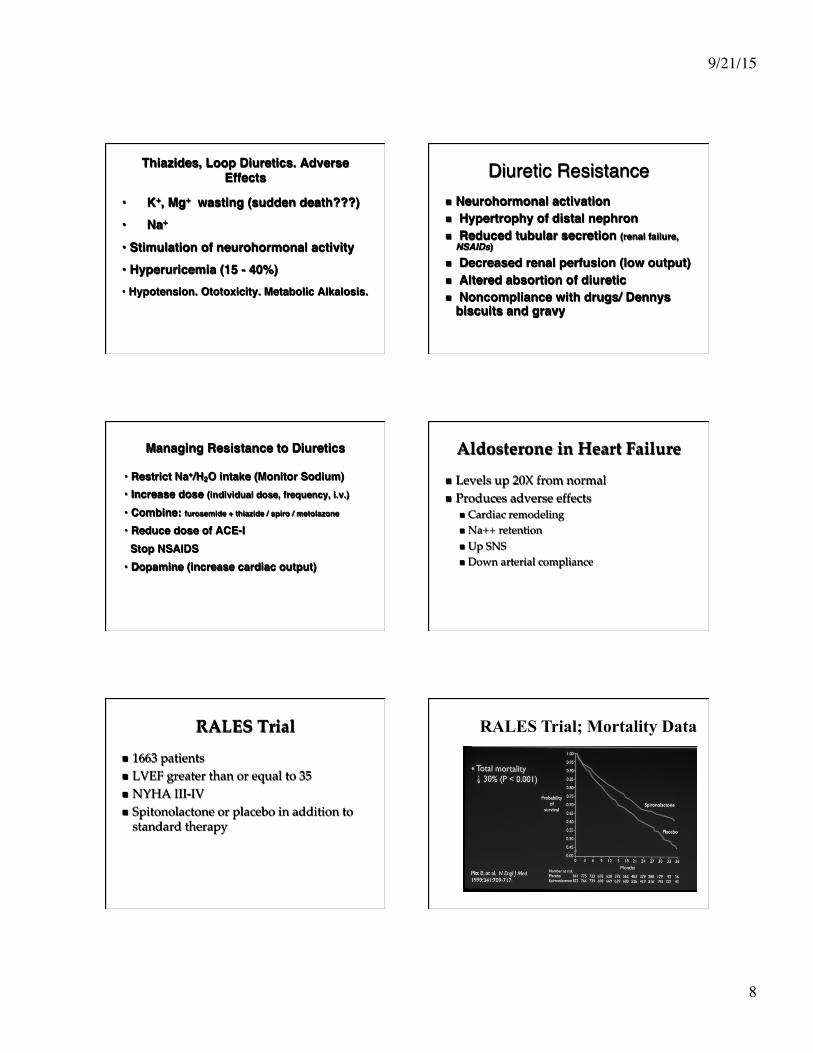
RALES Trial
n 1663 patientsn LVEF greater than or equal to 35n NYHA III-IVn Spitonolactone or placebo in addition to
standard therapy
RALES Trial; Mortality Data

9/21/15
9
Adverse Effects of Spironolactone
RALES Clinical
Hyperkalemia NA 34%
Mild NA 34%
Severe 2% 11%
Azotemia NA 12%
EMPHASIS-‐HF: Major results
EMPHASIS-HF
Outcome Eplerenone (%)
Placebo (%) Adjusted hazard ratio (95% CI)
p
Cardiovascular death/heart-failure hospitalization
18.3 25.9 0.63 (0.54–0.74) <0.001
Cardiovascular death 10.8 13.5 0.76 (0.61–0.94) 0.01 Heart-failure hospitalization 12.0 18.4 0.58 (0.47–0.70) <0.001 Hospitalization for hyperkalemia
0.3 0.2 1.15 (0.25–5.31) 0.85
NYHA Class II HF (N=2737) LV EF < 30% Eplerenone 25-‐50mg QD vs. Placebo
Aldosterone Antagonist Recomendations
n Add to standard treatment if:n Advanced symptomsn No contraindications
n Increased K +n Azotemia
n Follow K+ and BUN/Cr
Aldosterone Antagonist Recomendations
n Decrease KCL by 50%n Lab Follow-up
n Low riskn K+ and BUN/Cr level at week 1& 4
n High Riskn K+ and BUN/Cr level at day 3 and at week 1 & 4
PARADIGM-HF
n Entresto formerly LCZ696n Approved July 2015n ARB-Neprilysin inhibition vs enalapril 10
mg BIDn Valsartan-Sacubitriln Starting dose 49/51 mg BID, target 97/103
BID
Neprilysin Inhibition Potentiates Actions of Endogenous Vasoactive Peptides That Counter
Maladaptive Mechanisms in Heart Failure
Inactive metabolites
Neurohormonal activation
Vascular tone Cardiac fibrosis,
hypertrophy Sodium retention
Neprilysin Neprilysin inhibition

9/21/15
10
0
16
32
40
24
8
Enalapril (n=4212)
360 720 1080 0 180 540 900 1260
Days After Randomization 4187 4212
3922 3883
3663 3579
3018 2922
2257 2123
1544 1488
896 853
249 236
LCZ696 Enalapril
Patients at Risk
1117
Kap
lan-
Mei
er
Estim
ate
of C
umul
ativ
e R
ates
(%
)
914
LCZ696 (n=4187)
HR = 0.80 (0.73-0.87) P = 0.0000002
Number needed to treat = 21
PARADIGM-HF: Cardiovascular Death or Heart Failure Hospitalization (Primary Endpoint)
LCZ696 (n=4187)
Enalapril (n=4212)
P Value
Prospectively identified adverse events Symptomatic hypotension 588 388 < 0.001 Serum potassium > 6.0 mmol/l 181 236 0.007 Serum creatinine ≥ 2.5 mg/dl 139 188 0.007 Cough 474 601 < 0.001
Discontinuation for adverse event 449 516 0.02 Discontinuation for hypotension 36 29 NS Discontinuation for hyperkalemia 11 15 NS Discontinuation for renal impairment 29 59 0.001
Angioedema (adjudicated) Medications, no hospitalization 16 9 NS Hospitalized; no airway compromise 3 1 NS Airway compromise 0 0 ----
PARADIGM-HF: Adverse Events
10%
Angiotensin Neprilysin Inhibition With LCZ696 Doubles Effect on Cardiovascular Death of Current
Inhibitors of the Renin-Angiotensin System
20%
30%
40%
ACE inhibitor
Angiotensin receptor blocker
0%
% D
ecre
ase
in M
orta
lity
18%
20%
Effect of ARB vs placebo derived from CHARM-Alternative trial Effect of ACE inhibitor vs placebo derived from SOLVD-Treatment trial
Effect of LCZ696 vs ACE inhibitor derived from PARADIGM-HF trial
Angiotensin neprilysin inhibition
15%
ENTRESTO
n Entresto $400/month, $4800/yearn Enalapril $4/ month $48/ year
Biventricular pacing

9/21/15
11
Cardiac resynchronization







