
Computer-Supported Personal Interventions for Elderly
People with Cognitive Impairment and Dementia
Thesis submitted in partial fulfillment
of the requirements for the degree of
“DOCTOR OF PHILOSOPHY”
by
Vardit Sarne-Fleischmann
Submitted to the Senate of Ben-Gurion University
of the Negev
Approved by the advisors
Approved by the Dean of the Kreitman School of Advanced Graduate Studies
September 2013
Beer-Sheva

2
This work was performed under the supervision of Prof. Noam Tractinsky and
Prof.Tzvi Dwolatzky.
In the Department: Industrial Engineering and Management
Faculty: Engineering

3
Research-Student's Affidavit when Submitting the Doctoral Thesis for
Judgment
I, VarditSarne-Fleischmann, whose signature appears below, hereby declare that
(Please mark the appropriate statements):
× I have written this Thesis by myself, except for the help and guidance offered by my
Thesis Advisors.
___ The scientific materials included in this Thesis are products of my own research,
culled from the period during which I was a research student.
___ This Thesis incorporates research materials produced in cooperation with others,
excluding the technical help commonly received during experimental work. Therefore, I
am attaching another affidavit stating the contributions made by myself and the other
participants in this research, which has been approved by them and submitted with their
approval.
Date: _________________ Student's name: ________________
Signature:______________

4
Acknowledgements
This dissertation could not have been initiated, conducted and completed without the
invaluable guidance, inspiration, and support of my wonderful advisors, Prof. Noam
Tractinsky and Prof. Tzvi Dwolatzky.
Prof. Noam Tractinsky has accompanied me from my first step as a researcher. I was
privileged to work with him, and to gain from his vast knowledge in the area of Human-
Computer Interaction and from his intelligent way of thinking. I deeply appreciate his
willingness to engage in this research, which combines the fields of computing as well
as the needs of older people with dementia. Incessantly, Noam was a role model for me
of a highly reliable, creative and systematic researcher, and most importantly, he was
extremely patient, supportive, and empathic for my needs in this highly demanding and
meaningful period of my life.
Prof. Tzvi Dwolatzky has introduced me to the fascinating world of clinical research,
and gerontology. Throughout our joint way I was deeply impressed by his professional
knowledge and skills as a physician as well as a researcher, and for most by his
humanistic approach towards his patients and colleagues. I appreciate his extremely
motivated and hopeful desire to help patients combat their illness.
I would also like to thank Prof. Arnold Rosin for his engagement in this study. I was
privileged to meet a wonderful person, who inspired me with his rich experience,
enthusiasm and his warm approach and kindness.
Many thanks to Inbal Rief and Studio 97, for developing the reminiscence system. I
would also like to thank Yehudith and Elimelech Lange who developed the Savion
software and provided new versions for this study.
There are many people who helped me conducting this study. I would like to thank
Moran Korem, Terry Hendin, Irit Levy, and the staff of the Memory Clinic in Beer-
Sheeva (Iris Weider, YuliaLipkin, Elad Robin, and Diana Sokolov), who helped in
conducting the evaluations of patients and family members. I would also like to thank
Yafit Fisher, Nelly Fein, Ariel Rosin and the many volunteers who devotedly worked

5
with the patients (Wendy Bocarsky , Sharon Finkel, Michael Kuttner, Mary Jo Elman,
Linda, Esther Puld, and Reuven Gruber).
My grateful thanks are also extended to Prof. Jonathan Rabinowitz for his valuable
guidance in the data analysis.
I would like to express my very great appreciation to the management and staff of the
day care centers where the study was performed, among them are: Moti Zelikowitz,
Marsha Donshik, Marta Milsztein, Ayelet Fisher, Heni Sher, Suzi Martziano, Yelena
Babayev, Klaudia Konson, Hadas Helbershtat, Dafna Green, Ifah Arbel and Shulamit.
My gratitude to Mandy Haner and Sergey Korotchenko who provided outstanding
technical support, to Itamar Doniger from Neurotrax for his help and advice, to Shimon
Amit (Neurotrax) for Mindstreams' technical support, and to Hadas Tractinsky for her
help in the long process of data entry.
I would also like to thank the patients who participated in this study and their family
members.
Lastly and most importantly, I wish to thank my wonderful family who has been my
source of strength and encouragement throughout my life: my parents Haya and
Yishayahu, my brothers David and Oz, my husband Moshe, and my daughters Noga
and Naama.
This study was supported (in part) by grant no.3-00000-9334from the Chief
Scientist Office of the Ministry of Health, Israel, and by the Israeli Ministry of Science
and Technology. I would also like to thank Mr. David (Dede) Goldschmidt from Valley
Venture Capital, for his generous donation in support of this research.

6
Dedication
I would like to dedicate this dissertation to my dearest family for their endless love,
support, and encouragement.

7
Abstract
Dementia is formally described as "a clinical syndrome of cognitive decline that is
sufficiently severe to interfere with social or occupational functioning" (Chertkow,
Feldman, Jacova & Massoud, 2013, p.2). In addition to the cognitive consequences of
dementia, people with dementia frequently experience a wide range of neuropsychiatric
symptoms.
Alzheimer's disease (AD) is the most common cause of dementia, representing
approximately two-thirds of those suffering from this syndrome. Currently there is no
cure for AD or for most of the diseases causing the dementia syndrome.
Pharmacological interventions have limited efficacy and are, at best, symptomatic.
Important for the management of patients with dementia are psychosocial and lifestyle
interventions, which aim primarily to relieve cognitive and behavioral symptoms, to
promote well-being and to provide caregiver support.
Two forms of non-pharmacological therapeutic intervention currently offered to patients
with dementia are reminiscence therapy and cognitive training. Studies have evaluated
the effects of these therapies and have suggested that they may improve cognitive
function in patients with dementia and in adults at risk of developing dementia.
However, due to methodological limitations, few controlled studies and the lack of
sensitive assessment tools, there is still no clear evidence for significant benefits of
these interventions.
Increasingly, computerized systems are being designed for the treatment of patients with
dementia, including web sites for providing information, computerized tools for
monitoring, assistive technology and computer systems offering emotion-oriented
treatments in dementia care.
The study that we performed evaluated two computer-supported interventions for
patients with dementia, namely personalized computerized reminiscence therapy and
computerized cognitive training. The personalized reminiscence system was developed
specifically for the purpose of this study to enable independent use and administration
for both patients and caregivers. The cognitive training system involved the use of a
commercial software for memory enhancement for people with Alzheimer's disease,
dementia and other causes of cognitive decline. In both interventions subjects with
dementia were compared to a control group. The comparison utilized Mindstreams

8
(NeuroTrax Corp., NJ),an innovative computerized neuropsychological tool for
assessing patients' cognitive function. In addition, the effects of the interventions on
family members were evaluated.
A total of 167older subjects with cognitive impairment or dementia, residing in the
community, were recruited for the study. All underwent a preliminary assessment to
determine their cognitive status. Following initial screening 95 suitable subjects were
randomly assigned to one of the following 3 groups: (1) Personal computer-based
reminiscence therapy; (2) Computer-based cognitive training; and (3) Control group.
Both those participants receiving reminiscence therapy as well as those using the
cognitive training program participated in 2 sessions a week, each of 30-minutes
duration, supervised by a mediator, for a period of 3 months. Assessments were
performed at baseline, at one month and at 3 months, and included an evaluation of
cognitive function using the Mindstreams computerized testing battery (NeuroTrax
Corp., NJ), the subject’s psychological and behavioral well-being (using QoL-AD,
WTL and NPI questionnaires), and caregiver burden (using the short version of Zarit
Caregiver Burden Interview).
Data analysis, including both parametric and non-parametric methods, was performed
ona total of 85 participants who, in addition to a baseline evaluation completed at least
one follow-up evaluation at 1 month (T1) and at 3 months (T3). No differences between
groups were found regarding demographic variables of the participants at baseline.
When comparing the reminiscence group vs. the control group, group effects were
found using the parametric analysis at both T1 and T3 for the following variables:
global cognitive score, QoL-AD-patient and WTL. These effects were also
demonstrated using the non-parametric analysis at T3. An improvement in the Go-
NoGo reaction time level 1 (RT L1) measure was demonstrated only at T1 using the
parametric method, while improvements in the Zarit Caregiver's Burden and the NPI
were demonstrated only at T3 using the non-parametric method. Overall, a higher
accordance of the two analysis methods was shown at T3 compared to T1.
When comparing the cognitive training and the control groups, an adverse tendency was
noted, since group effects were found only at T1. These were more modest and related
mostly to the following measures: orientation, verbal and Go-NoGo RT L1. The results
of the two methods of analysis corresponded only for the orientation measure.

9
Although this study has found some positive results for both computer-based
reminiscence and cognitive training interventions compared to a control group, due to
the limited sample size available for final analysis the effects demonstrated were not
adequate to draw firm conclusions. It is suggested that more randomized controlled
trials with a greater sample size and longer periods of evaluations should be conducted
to further test the efficacy of those intervention methods as well as to elucidate the
relative contribution of each intervention and the interesting differences between them.
Keywords: Dementia, Alzheimer's disease, reminiscence, cognitive training, HCI, psychosocial
interventions, assistive technology, emotion-oriented interventions, cognitive function.

10
Table of content
1. INTRODUCTION ...................................................................................................................................... 14
2. LITERATURE REVIEW……......................................................................................................................... 16
2.1 DEMENTIA…………... .................................................................................................................................. 16
2.1.1 Caregiver burden……………………………………………….………………. ........................................................... 17
2.2 PSYCHOSOCIAL INTERVENTIONS IN DEMENTIA CARE…………… ............................................................................. 18
2.2.1 Reminiscence Therapy……………………………………………………….............................................................. 19
2.2.2 Cognitive Training…………………………………………………………………. ........................................................ 21
2.3 COMPUTER-BASED SYSTEMS DESIGNED FOR PEOPLE WITH DEMENTIA…………. ....................................................... 23
2.4 STUDY OBJECTIVES.… ................................................................................................................................. 25
3. THE COMPUTER-BASED SYSTEMS….….. ................................................................................................. 27
3.1 THE REMINISCENCE SYSTEM…… .................................................................................................................... 27
3.1.1 Usability Testing………………………………………………….…………….. ........................................................... 28
3.1.2 Results and modifications of the system……………….……………. ........................................................... 29
3.1.3 Additional findings…………………………………………………………….............................................................. 32
3.2 THE COGNITIVE TRAINING SYSTEM……. .......................................................................................................... 33
3.2.1 Modifications of the Savion software…………………………………. ........................................................... 33
4. STUDY PREPARATION…………… .............................................................................................................. 37
4.1 ETHICS COMMITTEE APPROVALS…………. ........................................................................................................ 37
4.2 CONTACTING SUITABLE ADULT DAYCARE CENTERS……….. ................................................................................... 37
4.3 INTRODUCING THE STUDY TO THE STAFF……. ................................................................................................... 38
4.4 PRESENTING THE STUDY TO POTENTIAL SUBJECTS AND THEIR FAMILY MEMBERS.….. ................................................ 38
4.5 INSTALLATION……….. ................................................................................................................................. 39
4.6 THE ADDITION OF PERSONAL CONTENTS TO THE REMINISCENCE SYSTEM………........................................................ 39
5. METHODS…….… ...................................................................................................................................... 40
5.1 PATIENT SAMPLE…………. ............................................................................................................................ 40
5.2 DESIGN…………………… .............................................................................................................................. 42
5.3 PROCEDURE………………. ............................................................................................................................. 43
5.3.1 The reminiscence therapy session…………………….………………… ........................................................... 43
5.3.2 The cognitive training session……………………………………….……. ........................................................... 44
5.4 MEASUREMENTS…………. ............................................................................................................................ 44
5.4.1 Cognitive function assessment……………………………………….….. ........................................................... 44
5.4.2 Patients’ psychological/ behavioral well-being……………….….. ........................................................... 45
5.4.3 Caregiver burden…………………………………………………………….…. ........................................................... 46

11
6. ANALYSIS AND RESULTS………….. ........................................................................................................... 47
6.1 STATISTICAL ANALYSIS…… ............................................................................................................................ 47
6.2 BASELINE ANALYSIS……….. .......................................................................................................................... 49
6.3 OUTCOME MEASURES DATA…… .................................................................................................................... 51
6.4 ANALYSIS OF RESULTS…… ............................................................................................................................ 52
6.5 AN ALTERNATIVE STATISTICAL ANALYSIS……..................................................................................................... 61
6.6 SUMMARY OF FINDINGS….. .......................................................................................................................... 71
6.7 RESULTS SEGMENTED BY MMSE SCORES….. ................................................................................................... 73
6.7.1 Parametric evaluation………………………….……………………………............................................................. 73
6.7.2 Non-parametric evaluation……………………………………………….. ............................................................ 74
6.7.3 Summary of results according to grouped MMSE scores……………………………………………………………...74
7. DISCUSSION………… ................................................................................................................................. 75
7.1 THE REMINISCENCE THERAPY………… ............................................................................................................. 75
7.2 THE COGNITIVE TRAINING….. ........................................................................................................................ 77
7.3 LIMITATIONS AND FUTURE WORK…….. ........................................................................................................... 79
8. IMPRESSIONS AND CHALLENGES……. .................................................................................................... 81
8.1 IMPRESSIONS OF THE STUDY….. .................................................................................................................... 81
8.1.1 Reminiscence…………………………………………………………………….. ............................................................ 81
8.1.2 Cognitive training……………………………………………………………… ............................................................ 82
8.2 CHALLENGES………… .................................................................................................................................. 84
9. CONCLUSION……… .................................................................................................................................. 86
REFERENCES ................................................................................................................................................ 87
APPENDICES ................................................................................................................................................ 95

12
List of Figures
Figure 1: Navigating between the three levels of the reminiscence system -------------- 28
Figure 2. Old vs. new location of information icon; Old vs. new format of thumbnails
view icon. ------------------------------------------------------------------------------------------ 30
Figure 3. Old vs. new Info layer location and background --------------------------------- 31
Figure 4. Old vs. new audio default sign ------------------------------------------------------ 32
Figure 5. Randomization of participants in each day care center -------------------------- 43
Figure 6. Consort diagram of the study. ------------------------------------------------------- 48
Figure 7. Mean Global scores for study groups in T0, T1 and T3. ------------------------ 54
Figure 8. Mean differences in cognitive measures between T1&To, and T3&T0. ------ 55
List of Tables
Table 1: Psychosocial treatments (APA, 1997) .............................................................. 19
Table 2: The Savion usability evaluation - findings and recommendations ................... 34
Table 3: Inclusion and exclusion criteria ........................................................................ 40
Table 4: Baseline characteristics of the participants, according to study group............. 49
Table 5: Sample mean scores for outcome measures of each of the study groups ......... 52
Table 6: Comparing T1-T0 scores difference between reminiscence & control groups,
and between cognitive training & control groups - ANCOVA results........................... 58
Table 7: Comparing T3-T0 scores difference between reminiscence & control groups,
and between cognitive training & control groups - ANCOVA results........................... 60
Table 8: Changes in outcome measures for reminiscence group between T0 & T1, and
T0 & T3 – Wilcoxon signed-rank test. ........................................................................... 62
Table 9: Changes in outcome measures for cognitive training group between To & T1,
and T0 & T3 – Wilcoxon signed rank test...................................................................... 64
Table 10: Changes in outcome measures for control group between To & T1, and T0 &
T3 – Wilcoxon signed rank test. ..................................................................................... 65
Table 11: Comparing 1 month differences between Reminiscence and control groups
(Mann Whitney test) ....................................................................................................... 66

13
Table 12: Comparing 3 months differences between Reminiscence and Control groups
(Mann Whitney test) ....................................................................................................... 67
Table 13: Comparing 1 month differences between Cognitive training and Control
groups (Mann Whitney test) ........................................................................................... 68
Table 14: Comparing 3 months differences between Cognitive training and Control
groups (Mann Whitney test) ........................................................................................... 70
Table 15: Level of significance and effect size for effects found in the reminiscence
group compared to control group, according to the method of analysis. ....................... 71
Table 16: Level of significance and effect size for effects found in the cognitive
training group compared to control group, according to the method of analysis. .......... 72
Table 17: Comparing scores differences (T1-T0, T3-T0) between reminiscence &
control groups, and between cognitive training & control groups - ANCOVA results for
participants with high MMSE score ............................................................................. 101
Table 18: Comparing scores differences (T1-T0, T3-T0) between reminiscence &
control groups, and between cognitive training & control groups - ANCOVA results for
participants with low MMSE score. ............................................................................. 102
Table 19: Comparing 1 month differences between Reminiscence and control groups -
Mann Whitney test for participants with high MMSE score. ....................................... 103
Table 20: Comparing 3 months differences between Reminiscence and control groups -
Mann Whitney test for participants with high MMSE score. ....................................... 103
Table 21: Comparing 1 month differences between cognitive training and control
groups - Mann Whitney test for participants with high MMSE score.......................... 104
Table 22: Comparing 3 months differences between cognitive training and control
groups - Mann Whitney test for participants with high MMSE score.......................... 104
Table 23: Comparing 1 month differences between Reminiscence and control groups -
Mann Whitney test for participants with low MMSE score ......................................... 105
Table 24: Comparing 3 months differences between Reminiscence and control groups -
Mann Whitney test for participants with low MMSE score. ........................................ 105
Table 25: Comparing 1 month differences between cognitive training and control
groups - Mann Whitney test for participants with low MMSE score. .......................... 106
Table 26: Comparing 3 months differences between cognitive training and control
groups - Mann Whitney test for participants with high MMSE score.......................... 106

14
1. Introduction
According to the Alzheimer’s Association, dementia is "an overall term that describes a
wide range of symptoms associated with a decline in memory or other thinking skills
severe enough to reduce a person's ability to perform everyday activities"
(http://www.alz.org/what-is-dementia.asp).
Dementia typically appears in later life (in most cases after the age of 65 years), but
may rarely occur in individuals in the fourth or fifth decade of life. Patients with this
condition may experience a decline in many cognitive areas, including memory,
attention, language, communication, problem solving and reasoning.
Dementia not only affects the patient, but as the condition progresses and patients
become increasingly dependent on others, the primary burden of support falls on
caregivers. Compared to caregivers of older adults with normal cognition, caregivers of
people suffering from dementia are required to provide a greater degree of care for
longer periods of time (Thies & Bleiler, 2013).
Alzheimer's disease (AD) is the most common cause of dementia, representing
approximately two-thirds of those suffering from this syndrome (Plassman et al., 2007).
Currently there is no cure for AD or for most of the diseases causing the dementia
syndrome. Important for the management of patients with dementia are psychosocial
and lifestyle interventions, aiming primarily to relieve cognitive and behavioral
symptoms and to provide caregiver support.
Two forms of non-pharmacological therapeutic intervention currently offered to patients
with dementia are reminiscence therapy and cognitive training. Reminiscence therapy
stimulates the person's long-term memory (a capability that is generally more preserved
than short-term memory in patients with dementia) and encourages interactions by
means of a variety of familiar stimulations. Reminiscence therapy has been found to
decrease depressive symptoms, facilitate social involvement and encourage participants
to introspect on their lives and achievements (Gibson, 1994; Scogin & McElreath,
1994). To date, there is no clear evidence regarding the effect of reminiscence therapy
on cognitive function, and there is thus a need for additional studies in order to further
evaluate the positive trends that have been reported (Woods, Spector, Jones, Orrell &
Davies, 2005). Conducting reminiscence therapy, however, requires major efforts in
organizing the stimulating material and presenting it to the patient.

15
Cognitive training is another intervention that may be of benefit in maintaining
cognitive function, both in healthy aging as well as in those with mild cognitive
impairment and possibly even dementia. However, the benefits of cognitive training in
patients with early dementia are modest. Systematic reviews (Bahar-Fuchs, Clare &
Woods, 2013; Clare, Woods, Moniz-Cook, Orrell, & Spector, 2003) recommend that
further studies be performed in order to provide more definite evidence.
Increasingly, computerized systems are being designed for the treatment of patients with
dementia. Project CIRCA (Computer Interactive Reminiscence and Conversation Aid)
that was designed in Scotland as a multimedia conversation aid system had great
success in prompting conversations, in promoting a more natural and relaxed
atmosphere, and in allowing the patients to interact with the system. The material
included in project CIRCA was mainly from the UK, with an emphasis on local material
from Dundee, Scotland, the area of residence of the patients. Whereas in project CIRCA
all the patients shared the same background and hence the same reminiscence-evoking
stimuli, we suggest that the effectiveness of such a system may be enhanced
significantly by individually adapting its content to the patient's particular background
and preferences, thus providing personal material for each patient. We previously
developed a prototypical reminiscence therapy system and conducted a preliminary
evaluation of its acceptability by five patients with AD and their caregivers in Israel
(Sarne-Fleischmann &Tractinsky, 2008). The results of our evaluation indicated high
levels of user-satisfaction with the system and a strong tendency for repeated use. We
also found a clear preference for the use of personal rather than general material when
both were available.
The purpose of the study described in this manuscript was to evaluate two computer
supported interventions for patients with dementia, namely personalized computerized
reminiscence therapy and computerized cognitive training. A personalized
reminiscence system was developed specifically for the purpose of the study, and
subjects using either intervention for a period of up to 3 months were compared to a
control group.

16
2. Literature Review
The literature review is structured as follows: Initially I will describe dementia and the
effect of this syndrome on both patients and caregivers. Therapeutic interventions are
then presented, concentrating particularly on reminiscence therapy and cognitive
training. Subsequently, existing computerized systems designed for people with
dementia will be described. Based on the review, the rationale and objectives of the
study will be presented.
2.1 Dementia
A formal definition of dementia describes "a clinical syndrome of cognitive decline that
is sufficiently severe to interfere with social or occupational functioning" (Chertkow et
al., 2013, p.2).
Alzheimer's Disease is the most common cause of dementia, accounting for 60-80
percent of all dementia cases over the age of 65 (Thies & Bleiler, 2013). Other causes of
dementia include vascular dementia (VaD), diffuse Lewy body disease (DLBD), fronto
temporal dementia (FTD), Parkinson's disease dementia (PDD), and Creutzfeldt-Jakob
disease (CJD), mixed dementia (associated vascular and neurodegenerative disease),
among others (Thies & Bleiler, 2013).
While average life expectancy from the onset of symptoms in AD is approximately 8-10
years, it is postulated that the disease process begins long before the appearance of
symptoms.
The number of people suffering from dementia is increasing worldwide. In 2005, a
panel of 12 international experts was assigned by Alzheimer's Disease International to
provide a consensus estimate for the prevalence of dementia worldwide (Ferri et al.,
2005). Based on published studies of dementia, the experts estimated that there were
24.3 million people with dementia in 2001, predicting an additional 4.6 million new
cases annually. The number of people affected was expected to double every 20 years
and to reach 81.1 million by the year 2040. In 2012, the panel's coordinating group
reappraised the global prevalence of dementia, estimating some 35.6 million people
living with dementia in 2010 worldwide, and predicting this to reach 90.3 million by
2040, being approximately 10% higher than the previous report (Prince et al., 2013).

17
Currently there is no cure for AD or for most of the diseases causing the dementia
syndrome. Pharmacological interventions have limited efficacy and are, at best,
symptomatic (Thies & Bleiler, 2013; O'Brien & Burns, 2011; Birks, 2006; Courtney et
al., 2004).Important for the management of patients with dementia are psychosocial and
lifestyle interventions, aiming primarily to relieve cognitive and behavioral symptoms
and to provide caregiver support. Behavioral and Psychological Symptoms of Dementia
In addition to the cognitive consequences of dementia, people with dementia frequently
experience a wide range of neuropsychiatric symptoms, termed the Behavioral and
Psychological Symptoms of Dementia (BPSD) by a workgroup of the International
Psychogeriatric Association (Finkel, Costa E Silva, Cohen, Miller & Sartorius, 1997).
BPSD is defined as "Symptoms of disturbed perception, thought content, mood or
behavior that frequently occur in patients with dementia" (Finkel & Burns, 1999).
Symptoms include apathy, depression, irritability, agitation and anxiety (the most
common symptoms in dementia patients), aggression, wandering, delusions, and sleep
disturbances. Less commonly patients may experience euphoria, hallucinations, and
disinhibition (Cerejeira, Lagarto & Mukaetova-Ladinska, 2012).
BPSD affects the quality of life both of patients and of caregivers and is often
associated with a high level of distress.
2.1.1 Caregiver burden
Dementia does not only affect the patient, but as the condition progresses patients
become increasingly dependent on others, with the primary burden of support falling on
the caregiver. Compared to caregivers of older adults with normal cognition, caregivers
of people suffering from dementia are required to provide a greater degree of care for
longer periods of time (Thies & Bleiler, 2013).
Caring for a person with dementia is very stressful and has negative implications on
caregivers. Brodaty and Donkin (2009) describe four elements of caregiver burden,
namely psychological morbidity (general distress and depression), physical morbidity
(poor physical health), social isolation (due to the role of caregiving) and financial
burden (due to the costs of dementia care and the loss of earnings).
Baumgarten et al (1992) argue that the stressfulness of caring for a demented person
"stems from its novelty, unpredictability, long duration and ambiguity" (Baumgarten et
al, 1992, p.61).

18
In addition to affecting the caregiver's health, the burden of caregiving was also found
to be associated with early placement of relatives with dementia in a nursing home
(Etters, Goodall, & Harrison, 2008).
Both caregiver and patient factors influence the level of burden (Schӧlzel-Dorenbos,
2009, as cited in: Beinart , Weinman, Wade & Brady, 2012). According to these
authors, caregiver characteristics influencing the level of burden include: age (older age
predicts higher burden), duration of caregiving, workload, gender (male caregivers are
inclined to physical illness, whereas female caregivers are more inclined to suffer from
psychological symptoms), educational background, income (lower socioeconomic status
predicts higher burden), psychological state, and relationship with patient, among
others. Patient attributes include the duration and severity of disease, disease symptoms
(behavioral, psychiatric and cognitive), functional abilities, poor quality of life and
educational background.
2.2 Psychosocial interventions in dementia care
The goals of psychosocial (also called non-pharmacological) interventions in dementia
care are to improve quality of life and to manage the behavioral and psychological
symptoms associated with dementia. The effectiveness of this form of treatment has
been increasingly studied and its potential for reducing behavioral and psychological
symptoms, as well as relieving caregiver burden, has been described (Brodaty &
Arasaratnam, 2012; Vernooij-Dassen, Vasse, Zuidema, Cohen-Mansfield & Moyle,
2010; Vasse et al. 2012; Gitlin, Kales & Lyketsos, 2012).
The American Psychiatric Association (APA, 1997) has classified four categories of
psychosocial treatments for people with dementia, namely Emotion-oriented, Behavior-
oriented, Cognition-oriented and Stimulation-oriented (see Lawrence, Fossey, Ballard,
Moniz-Cook & Murray (2012) conducted a systematic review and meta-synthesis of
qualitative studies presenting the use and effectiveness of psychosocial interventions for
people with dementia in nursing homes. Their aim was to identify the beneficial
elements comprising a successful intervention from the perspective of both patients and
staff. Based on their findings, successful psychosocial interventions were perceived by
those
with dementia as enabling them to connect with others, provide the feeling that they
were making a meaningful contribution, and allowing them an opportunity to reminisce.

19
Table 1).
Lawrence, Fossey, Ballard, Moniz-Cook & Murray (2012) conducted a systematic
review and meta-synthesis of qualitative studies presenting the use and effectiveness of
psychosocial interventions for people with dementia in nursing homes. Their aim was to
identify the beneficial elements comprising a successful intervention from the
perspective of both patients and staff. Based on their findings, successful psychosocial
interventions were perceived by those
with dementia as enabling them to connect with others, provide the feeling that they
were making a meaningful contribution, and allowing them an opportunity to reminisce.
Table 1: Psychosocial treatments (APA, 1997)
EMOTION-
ORIENTED
APPROACHES
BEHAVIOR-
ORIENTED
APPROACHES
COGNITION-
ORIENTED
APPROACHES
STIMULATION-
ORIENTED
APPROACHES
Supportive
psychotherapy
Behavior therapy Reality orientation
Skills training
Activity therapy
Recreation therapy
Validation therapy Art therapy
Sensory integration
Simulated presence
therapy
Reminiscence Therapy
The authors argue that adjusting the psychosocial interventions to individual patients
will enhance the clinical benefits. With regard to staff, successful psychosocial
interventions improved their awareness of the person and his family (beyond the
dementia), broadened the concept of their role in caregiving, and better reflected their
approach to influencing the patient.
2.2.1 Reminiscence Therapy
Reminiscence therapy is one of the psychosocial interventions most often included in
European dementia guidelines (Vasse et al., 2012). This form of therapy stimulates the
person's long-term memory (a capability that is generally more preserved than short-

20
term memory in patients with dementia) and encourages interactions by means of a
variety of familiar stimulations. Reminiscence therapy can ameliorate depressive
symptoms, facilitate social involvement and encourage participants to evaluate their
lives and achievements (Gibson, 1994; Scogin & McElreath, 1994). Reminiscence
therapy can be conducted in groups or on an individual basis.
A Cochrane review of reminiscence therapy for people with dementia and their
caregivers (Woods, Spector, Jones, Orrell & Davies, 2005) found the intervention to
have promise, but concluded that more high quality studies were needed to reach
conclusive evidence. The inconclusive evidence may be due to methodological
limitations, the limited number of controlled studies and the lack of sensitive assessment
tools.
A recent systematic review conducted by Ponnusamy and Woods (2012) identified five
randomized control trials (RCT's) evaluating individualized reminiscence therapy for
people suffering from dementia. Sample sizes ranged from 17 to 101 and the total
number of treatment sessions from 6 to 12. The authors found potential for psychosocial
benefit in three trials that included a personalized approach, whereas in the two studies
that employed a general form of reminiscing no benefit was found. None of the five
RCT studies evaluated the impact of the interventions on family members or staff
caregivers.
To date, there is no clear evidence regarding the effect of reminiscence therapy on
cognitive function. Some studies did not demonstrate a significant improvement in
cognition (Jackson, 1991; Nomura, 2002), possibly related to methodological issues.
For example, Goldwasser, Auerbach& Harkins (1987) – included inWoods et al's
(2005) review mentioned previously-studied the cognitive, affective and behavioral
effects of reminiscence group therapy on demented elderly patients, and found a slight
but insignificant improvement in cognitive status. They concluded that rather than using
the Mini-Mental Status Examination (MMSE), which was the cognitive outcome
measure in their study, a more sensitive assessment tool is required for evaluating short
term changes in cognitive status . Similarly, Thorgrimsen, Schweitzer & Orrel (2002) –
also included in the Woods et al's review - conducted a pilot study which included 11
subjects, to evaluate the effects of reminiscence in people with dementia. They found
the MMSE score of people attending the reminiscence group to be stable following 20
weeks of therapy, while the control group decreased by almost 4 points during this

21
period. However, this difference did not reach statistical significance. They conclude
that as significant results are more difficult to obtain with a limited number of
participants, a multicentered randomized controlled trial is required to further evaluate
the positive trend reported.
On a more positive note, some studies have reported a significant improvement in
cognitive function due to reminiscence therapy. Baines, Saxby & Ehler (1987) –
included in Woods et al's review - compared reminiscence and reality orientation (RO)
therapies and found an improvement in cognitive function only for the group of
participants who had received RO therapy prior to receiving reminiscence therapy.
Haight, Gibson and Michel (2006) – included in Ponnusamy and Woods' review -
evaluated the effect of life review (a more structured type of reminiscence therapy)
among people with mild to moderate dementia. The study found that compared to a
control group, patients receiving life review treatment had better cognitive measures as
evaluated by MMSE. Similarly, Morgan and Woods (2010) –included in Ponnusamy
and Woods' review- found a significant improvement in autobiographical memory
comparing to the control group. Haslam et al. (2010) - included in Ponnusamy and
Woods' review- compared group reminiscence to individual reminiscing using a control
group playing a social game. They have also found an improvement in cognitive
function, as measured by the Addenbrooke’s Cognitive Examination Revised tool
(Mioshi, Dawson, Mitchell, Arnold, & Hodges, 2006), only for participants who were
included in the group reminiscence sessions, and not in the individual sessions.
2.2.2 Cognitive Training
According to Bahar-Fuchs et al., (2013) cognitive training is defined as an intervention
which "typically involves guided practice on a set of standardised tasks designed to
reflect particular cognitive functions such as memory, attention or problem-solving"
under the assumption that "any effects of practice will generalise beyond the immediate
training context" (p.7). Similar to reminiscence therapy, cognitive training may be
administered either in groups or individually.
Cognitive training may be of benefit in maintaining cognitive function, both for healthy
older people as well as for those with mild cognitive impairment and possibly even
dementia. A systematic review of ten cognitive and memory training trials in adults

22
with mild cognitive impairment, found a moderate effect on memory performance in
seven of the trials (Gates, Perminder, Fiatarone Singh and Valenzuela, 2011). However,
the benefits of cognitive training in patients with early dementia are modest. A pilot
study involving 22 patients with mild to moderate AD showed an initial improvement in
functional status following cognitive training, and patients tended to regress to the pre-
training level after three months (Farina et al., 2002). However, the cognitive benefit of
the training procedure was minimal in this study. A randomized study evaluating a 6-
week memory training program for 34 patients with mild AD showed a modest
improvement in learning and memory (Cahn-Weiner, Malloy, Rebok & Ott, 2003). A
subsequent systematic review to evaluate the impact of cognitive training, cognitive
stimulation and cognitive rehabilitation for people in the early stages of Alzheimer's
disease or vascular dementia did not find strong support for the use of these
interventions in patients with these conditions (Clare, Woods, Moniz-Cook, Orrell &
Spector,2003). This conclusion was based on the fact that there are methodological
limitations, and that a very limited number of randomized controlled studies are
available. The authors recommended that further studies be performed in order to
provide more definite evidence. A recent update of this review by Bahar-Fuchs et al.
(2013) included 11 randomized controlled trials of cognitive training. Again, no strong
indication for the effectiveness of this intervention was found, and the authors conclude
that more high level RCT's are required, using more sensitive tools as outcome
measures in order to identify changes that may have been missed in previous trials.
In conclusion, both types of interventions (namely reminiscence therapy and the
cognitive training) currently share a set of limitations that prevent researchers from
reaching clear conclusions about their efficacy for people with dementia. These include
methodological limitations, a limited number of controlled studies and a lack of
sensitive uniform assessment tools. Therefore, additional methodologically sound large
RCTs employing more sensitive evaluation tools are needed to determine the value of
these interventions on various aspects of cognitive function of the patients, and to
elucidate the potential benefits for family caregivers.

23
2.3 Computer-based systems designed for people with dementia
Increasingly, computerized systems are being designed for the use of people with
dementia. Lauriks et al. (2007) present four areas of needs for computerized services for
this target users' group: (1)providing general and personalized information regarding the
disease; for both patients and informal carers; (2)supporting the patient with regard to
dementia symptoms; (3) determining social needs; (4) monitoring health and safety.
Addressing these needs, there is a growing trend towards the design of Web sites
catering specifically for the needs ofpeople with dementia (The Alzheimer’s Forum;
Freeman et al., 2005; Holsapple, Pakath & Sasidharan, 2005), the design of
computerized tools for monitoring (Kinney, Kart, Murdoch & Conley, 2004; Taylor,
2005; Lauriks et al. 2007), and the development of assistive technology (LoPresti,
Mihailidis & Kirsch, 2004; Carswell et al., 2009, Lauriks et al., 2007).
A growing trend towards the design of computer systems for the purpose of emotion-
oriented treatments in dementia care is also noticeable (Topo et al., 2004; The Story
Table). An important landmark in the efforts to provide computerized support for such
forms of treatment of dementia is project CIRCA (Computer Interactive Reminiscence
and Conversation Aid). The project was designed in Scotland as a multimedia
conversation aid system, which addresses the challenge of supporting reminiscence
therapy by using contemporary technologies to provide a computer-based, user-friendly
alternative to the traditional methods employed. The project had success in prompting
conversations, in promoting a more natural and relaxed atmosphere, and in allowing
patients to interact with the system (Alm et al., 2004). The material included in project
CIRCA was mainly from the UK, with an emphasis on local material from Dundee,
Scotland, the area of residence of the participating patients. Whereas in project CIRCA
the same material was used by all patients, a similar project focusing rather on
personalized multimedia systems (with a limitation of the supported technology) was
initiated in Baycrest Center, Toronto, Canada (Cohene, Baecker, Marziali & Mindy,
2006).
The importance of a personalized system is especially salient in immigrant or in highly
mobile societies, due to the heterogeneous background of the patients. This is reflected
by the variety of locations, events and languages that can promote reminiscing in
patients in these societies. Moreover, patient-adapted external aids in dementia care are
considered more effective, because they better meet the patients’ capabilities and needs
24
(Woods, 1994; McPherson et al., 2001; Topo et al., 2004) and increase their motivation
(Hofmann, Hock, Kühler& Müller-Spahn, 1996).
Another prototypical personalized reminiscence system was developed and evaluated
for its acceptability by patients and caregivers in Israel (Sarne-Fleischmann
&Tractinsky, 2008). The system improved upon existing systems in several ways.
Unlike the study at Baycrest, the main focus was on open-ended, extensive personal
content rather than on predefined life stories. In addition, the system was web-based
with a more flexible and intuitive user interface including a touch screen as the input
device – rather than a remote control. The technology used in the design of the system
was similar in structure to that used in the CIRCA project. However, whereas CIRCA
included only general content, the personalized system included personal content
relevant to the patient's background and preferences. The system was evaluated by five
patients suffering from AD treated at the Psychogeriatric Institute at the Tel-Aviv
Sourasky Medical Center. Each patient completed2 sessions interacting with the system
with the support of a caregiver. The participants’ behavior during the sessions was
observed and videotaped, and interviews were conducted with both patients and
caregivers. Content analysis was undertaken in order to investigate the effects of the
system on the patients, its usability, patient satisfaction with the system, and the
identification of additional benefits of the system on both patients and caregivers. The
results of the study indicated high levels of user-satisfaction from the experience of
using the system, with a strong tendency for repeated use. The system was found to be
effective in prompting conversations and in evoking personal memories; it was also
helpful in facilitating patient–caregiver interaction. The results also showed a clear
preference for personal rather than general material when both were available. Patients
and caregivers alike recognized the advantage of using the system rather than traditional
reminiscence methods, since various objects are included in one easily accessible
system, and there was a positive effect on the patient's self-esteem as a consequence of
being able to use a computer.
This study was included in a review by Subramaniam and Woods (2010) which
presented11 studies using information and communication technology in reminiscence
work (personal and general forms) for people with dementia, most of them in a
preliminary level. Sample sizes of the studies ranged from one to 23.The authors
concluded that feasibility of these systems was established, and suggest that they should

25
"make it easier for carers to converse and develop and maintain relationships with the
person with dementia, rather than simply keeping the person entertained."
(Subramaniam &Woods, 2010, p.121).
The use of computerized cognitive training systems may also be of value in providing a
more standardized approach to this form of intervention (Hofmann et al., 1996;
Schreiber, Lutz, Schweizer, Kalveram & Jäncke,1998). A prospective study involving
19 residents of a home for the elderly (mean age 83.5 years) who participated in a 14-
week computer-assisted cognitive training program found significant improvements in
working memory, with the positive effect on learning maintained even at follow-up
after 5 months (Günter, Schafer, Holzner & Kemmler, 2003). A more recent
randomized controlled study conducted by the Memory Clinic at the Beersheva Mental
Health Center found a clear benefit on memory and global cognitive function in patients
with dementia who participated in a bi-weekly computerized cognitive training program
for the duration of one month (Dwolatzky, Zilbershlag, Friger & Grinshpun, 2009).
2.4 Study Objectives
In the literature review we indicated the potential benefits of using computerized and
personalized interventions in dementia care, alongside their high availability and their
ease to use, especially when designed to address patients' specific needs and
capabilities. However, there is no empirical evidence for these hypothesized benefits
due to insufficient studies in this area and due to methodological limitations of existing
studies (Bahar-Fuchs et al., 2013; Ponnusamy and Woods, 2012).
Thus, the objectives of this study is to conduct a methodologically sound study to
evaluate the efficacy of the computer-based personalized reminiscence and cognitive
training interventions on the cognitive function and well-being of patients with
dementia, as well as the effects on family caregiver burden, as compared to controls.
We hypothesized that the use of the personalized reminiscence system would result in
improved psychological and behavioral measures (including a relief in caregiver
burden), whereas the cognitive training system would result in improved cognitive
measures.

26
With this purpose in mind, a personalized reminiscence system was developed, which
enabled independent use and administration for both patients and caregivers. The next
section describe these systems in detail.

27
3. The Computer-Based Systems1
The research project involved the use of three computerized systems: A reminiscence
therapy system, a cognitive training system, and a computerized neuropsychological
tool for assessing cognitive function. The reminiscence therapy system was developed
specifically for the purpose of this study and was based on a preliminary pilot study
involving five patients with AD (Sarne-Fleischmann & Tractinsky, 2008). The cognitive
training system involved the use of Savion (Melabev, Jerusalem), a commercial
software for memory enhancement for people with Alzheimer's disease, dementia and
other causes of cognitive decline (Dwolatzky et al, 2009). The neuropsychological
assessment tool was Mindstreams (NeuroTrax Corp., NJ) a computerized testing battery
validated for age-related cognitive decline and dementia (Dwolatzky et al., 2003;
Dwolatzky, Dimant, Simon & Doniger., 2010).
3.1 The reminiscence system
Based on our findings in the pilot study (Sarne-Fleischmann & Tractinsky, 2008), a new
Flash web-based application was developed to enable independent use and
administration for both patients and caregivers by including two main components in
the structure. The front-end component supports the patient’s interaction with the
system during the therapeutic sessions. The back-end component facilitates the addition,
update, and management of content. This component was designed for the use of
caregivers and family. The application was developed by an experienced subcontractor
according to a detailed design and the specifications provided.
Great emphasis was placed on the system’s design and on simplicity of use, given the
specific characteristics and limitations of the target users. Features included a very
simple interface (offering the user a limited number of options in order to avoid
cognitive overload); minimizing visual distractions on the display; avoiding the use of
animations or competing stimuli at any given time; using subtle graphics through
calming color schemes; and using a touch screen for all required interactions to support
______________________________
1Portions of this chapter, were published in: Sarne-Fleischmann, V., Tractinsky, N. Dwolatzky, T. and
Rief, I. Personalized reminiscence therapy for patients with Alzheimer's disease using a computerized
system. In: Proceedings of PETRA. 2011, 48-48.

28
the most natural interaction style.
The new system's hierarchy included only three levels to support simple and intuitive
flow:
1. Login – Entering the system by identifying the patient.
2. Select Album – Selecting the required album from up to six albums presented.
3. Album View – Watching the media files associated with the selected album.
The navigation between the three levels isdone hierarchically and is bi-directional (See
Figure 1).
Figure 1: Navigating between the three levels of the reminiscence system
The reminiscence system has two different interfaces: Hebrew and English. The two
interfaces are separated (each is accessible via a different link) so there is no option of
switching to a different language while interacting with the system.
3.1.1 Usability Testing
In order to evaluate the ease-of-use of the new system, and its appropriateness for the
target audience, a usability evaluation was conducted prior to the commencement of the
evaluation study. Three Alzheimer's patients (one woman and two men) from the
memory clinic in Beer-Sheva were separately asked to test the system. Each evaluation
session lasted up to 45 minutes, and consisted of three parts: Introduction, Using the
system and Summary. The Introduction part began with an explanation regarding the
purpose of the meeting, followed by a general description of the system. The patients
were then asked a few questions regarding their personal preferences (e.g Do you like to
watch photo albums? What kind of photos do you like to watch? Do you like to listen to
Login Select Album
Album View

29
music? What kind of music do you like?). In the second part (Using the System) the
patient was given the opportunity to use the system by selecting an album and watching
its media files. At each step the patients were asked two questions: 1) What would they
like to do now? 2) How do they intend to accomplish this? In the case of the patient
mentioning an activity that was not supported by the system, he/she would be directed
to the existing functions available in each case. This had two purposes: 1) Evaluating
the intuitiveness of the system's user interface, and 2) Establishing the users' mental
model of how to interact with the system. The Summary part of the usability evaluation
included general questions regarding the system and its user interface (e.g Did you like
the system? Would you use it again? What did you like about it? Were there things you
didn't like? What additional functionality would you like the system to include?)
3.1.2 Results and modifications of the system
Based on the usability evaluation's results, several modifications were made to improve
the system.
1. Information – The information icon (c), originally located next to the media
presented, was moved to be aligned with the bottom of the media presented (see Figure
2). This change provided better isolation for the icon from the navigation arrow icon,
thus preventing potential confusion between these icons. In addition, the layer
presenting the information text (d), which originally partially overlapped the media
object, was moved to the side of the object, in order to keep the object visible while
reading the text. In addition, the transparency of the text layer was cancelled to
maximize the visibility of the text (using an opaque background) and to reduce any
distractions (see Figure 3).
2. Thumbnails view icon – The thumbnails view icon (a), originally located at the top
left hand of the screen, caused distractions at times, despite being relatively in low
contrast to the screen’s background. To remedy this problem the icon was moved to the
bottom of the screen, and its colors were made even more subtle (see Figure 2). These
changes moderated the presence of the icon on the screen, leaving it mainly for the use
of the caregiver.

30
Figure 2.Old vs. new location of information icon; Old vs. new format of thumbnails view icon
(Upper and lower figures respectively).
3. Audio default sign – The audio default sign (which is presented when an audio file is
played) confused the participants – perhaps because it was too complex due to the
a
b c
a
b
c

31
inclusion of variety of different note shapes. Consequently, it was changed from a
winding set of musical notes to a much simpler sign (seeFigure 4).
Figure 3. Old vs. new Info layer location and background (Upper and lower figures respectively)
d
d e

32
4. Navigation arrow icons - Although the "clickable" surface of the navigation arrow
icons (b) was larger than the graphics itself (enabling an easier activation), the
participants still experienced slight difficulty with the bounded icons. To overcome this
problem, the arrow icons and their “clickable” boundarieswere enlarged, to facilitate the
press action (seeFigure 2).
Figure 4. Old vs. new audio default sign (left and right figures respectively)
3.1.3 Additional findings
During the evaluation, additional questions regarding the design of the system were
raised. Following a thorough discussion, it was decided to disengage selected findings
in order to sustain a most comfortable screen view with minimal distractions.
One of these findings presented a dilemma, whether to add text labels to icons that were
not intuitively understood by the participants (i.e switch to thumbnails view (a),
information (c) and add to favorite (e) icons). The conclusion was that since these icons
were designed mainly for the use of the caregiver, the lack of accompanying texts will
not influence the patient's capability of using the system, while the texts addition might
have a major effect on the user interface.
We considered whether to include all six albums on the same screen view, and thus
avoid the current navigation between two album screens. Here too, it was decided not to
implement this change, which requires a substantial reduction in the size of the albums
icons.

33
3.2 The Cognitive Training System
The Savion software provides training in four cognitive functions, namely language
skills, calculation, non-verbal memory and visual-spatial skills. It is used either with the
support of a therapist or alone (depending on the user's capabilities). The level of the
training can be easily adjusted to accommodate the user's level of competence.
Although the interface is designed for standard input devices (i.e keyboard and mouse),
in this study the Savion was operated using a touch screen (in those areas supported by
this feature) in order to enable an intuitive operation, and to reduce the user's workload.
It is important to note that the use of the touch screen is not supported by all of the areas
of training provided by the Savion software, since they require the insertion of numbers
using the standard keyboard (the calculation and the non-verbal memory training areas).
Savion has two major versions – English and Hebrew. Both interfaces are installed
jointly, and can be accessed via the same interaction (the interface language can be
switched during the session), as opposed to the reminiscence system.
A new Russian version was developed prior to the commencement of the study. This
version required a separate installation and did not support the switching between the
other two interface languages (Hebrew or English).The Savion main screens are
presented in Appendix A.
3.2.1 Modifications of the Savion software
For the purpose of the study the Savion software was modified to include an improved
user interface, and a tool for tracing the interactions. In addition, the new Russian
version of the Savion was evaluated.
3.2.1.1 Modifications of the UI
Savion is a commercial software which has been used by older people at their homes
and at adult day-care centers, for more than 15 years. The software was developed in
collaboration with an experienced occupational therapist from Melabev, and was
designed for use by patients with significant cognitive impairment.
For the purpose of the study, the usability of the Savion software was evaluated from
the viewpoint and according to the mental model of a novice user, and based on key-

34
principals for designing for the elderly. Each of the available functions was evaluated,
and a number of issues that needed to be revised were found. Table 2 presents the major
findings and the recommendations that were made to the Savion developers to enhance
the usability of the software.
Table 2: The Savion usability evaluation - findings and recommendations
Finding Recommendation
1 Use of colors – In all screens there
seemed to be an intensive use of colors.
The overload was salient in the number
of colors used (more than the maximum
five which is recommended), in the
colors palette (strong colors), and in the
colors combinations, which influenced
the contrast and the visibility of the text.
Due to the loss of visual acuity in
elderly people, combination of colors
should be carefully considered
(especially combinations of yellow,
blue and green, which might be difficult
for elderly people to distinguish). Also,
the use of multiple colors should be
reduced, and subtle hues should be
used.
2 Text – In some of the screens there was
an excessive use of text (usually for
detailed instructions).
Long strings of text used for
instructions should not be presented on
main screens but located in "help"
screens that will be displayed upon
user's request.
General instructions should be
simplified.
3 Critical functions - Command buttons
with critical functionality had the same
appearance as less pivotal buttons. As a
result, critical functions (e.g. exiting the
screen) could be performed
unintentionally.
Critical command buttons should be
distinguished from others by using
different colors and a distant location
on the screen.
4 Inconsistency -With regard to font type To provide a consistent conceptual

35
Finding Recommendation
and size, screens layout, and command
button's size.
structure of screens and functionality,
to enhance familiarity across
all screens.
5 Font - Use of serif typeface font, which
made reading the screen difficult.
Using sans- serif typeface, which is
recommended for elderly users. The
sans-serif typeface does not include the
small lines at the ends of the characters,
and therefore enhances legibility.
6 Setup - A redundant update of setup
features at the beginning of each session
of the specific training areas.
Similar setup features (such as
determining interface language,
defining sounds, or setting general
thresholds) should be grouped into one
setup screen, which will be presented
upon the user's request.
7 Mouse interface – Some of the
functions were supported only by the
keyboard interface and could not be
operated through the mouse interface.
Functionality should be fully operable
through a mouse interface in addition to
a keyboard interface. This will maintain
interface consistency and support the
operation using a touch screen.
The Savion software was modified by its developers, though not all of the
recommendations were implemented. For example, the multiplicity of colors was seen
as enhancing the users' enjoyment of the interaction and awareness of the current
training area (by using different background colors). Another example was the use of
complementary input devices (keyboard in addition to mouse instead of maintaining a
complete input set supported by the mouse only), which was seen by the developers as a
means of enhancing cognitive training.

36
3.2.1.2 Adding a tracing tool
In order to follow each of the sessions conducted with Savion, a new tracing tool was
added by the developers, which recorded the time spent in each of the four training
areas for each session. The tool required the insertion of the participant's number at the
beginning of the session, and generated the date and time while entering and exiting
each of the training areas. The data of all participants who used Savion on the same PC
was saved in a text file. A limitation of the tracing tool was the fact that it did not record
the time that was actually spent on active training (for example: it could not report
whether the user was responding to the exercises, setting up the characteristics of
training, or even having a short break during the session).
3.2.1.3 Preparation of the Russian language user interface
For the purpose of the study, a Russian language user interface was also required to
support a group of Russian speaking participants. The development of a new Russian
version of Savion was completed by the commencement of the study but it was not
scientifically validated. The new version was evaluated by a native Russian-speaker in
order to assure the quality of the translation, and to inquire about the appropriateness of
the selected words in the 'language skills' training area. The evaluation resulted in a few
corrections to the list of words.

37
4. Study Preparation
4.1 Ethics committee approvals
In order to conduct the research in the different geographical locations – three proposals
for clinical trials in human subjects were submitted to the relevant institutional review
boards (IRBs). Proposals were submitted to the Soroka Medical Center Helsinki
committee, the Shaare Zedek Medical Center Helsinki committee, and the Ben-Gurion
University of the Negev Human Subjects Research committee.
The proposals were revised according to each committee's suggestions and requirements
and were subsequently approved.
4.2 Contacting suitable adult daycare centers
The study was designed to be conducted either in adult daycare centers or in assisted
living residences. This decision stemmed from the need to use wide touch screens for
the reminiscence treatments, and since these were not easily portable it was preferred to
situate them in a permanent place at these sites for the duration of the study.
Nine adult daycare centers and one assisted living residence for Alzheimer's patients
were approached in order to determine their willingness to participate in the study. The
institutions' suitability for the study was also evaluated, in terms of the characteristics of
the population attending the centers (demented, high or low functioning elderly), the
number of people visiting the center each day, and the available resources (quiet room
and network connection for conducting the interventions). Seven of the daycare centers
were found to be suitable sites for participation in the study. This included three in
Beer-Sheva, two in Jerusalem, one in Ramat-Gan and one in Bnei-Brak. One assisted
living residence was found suitable for participation, but after several meetings with the
director in order to plan the project, a decision was made by the management to
withdraw from partaking in the study based on procedural considerations.

38
4.3 Introducing the study to the staff
After obtaining the approval of the directors, meetings were held with key members of
the staff in each of the adult daycare centers. The aim of these meetings was to present
the study to the staff and to discuss practical details regarding the performance of the
study. This was an opportunity for both sides to raise questions, discuss potential
difficulties, make detailed plans and find solutions at the local level. Among the issues
that were raised were the best way to approach the subjects and their family members,
the level of qualifications required for those assisting the subjects in performing the
interventions, the availability of the computer room where the treatments would take
place, and who should accompany the subjects to the computer room (for the low
functioning subjects in particular), among others.
In addition, meetings were held with each of the assessors who were responsible for the
evaluation of the subjects. In these meetings, the assessors were introduced to the
study's plan. The questionnaires were presented and discussed, with emphasis on their
major elements based on formal instructions and guidelines. The appropriate way of
approaching both subjects and family members was also discussed. The group of
assessors included: a neuropsychologist, a social worker, a nurse, a physician, and an
assessor with a background in the field of education. The researcher also took part in the
evaluations, particularly that were conducted prior to commencement of treatment (at
T0).
4.4 Presenting the study to potential subjects and their family members
In order to contact potential subjects and their family members before enrollment,
different approaches were adopted at the various sites. In four of the daycare centers, a
lecture explaining the purpose and possible benefits of the study was given in the
evening, to which all members of the daycare center and their families were invited. In
one of the centers the project was presented to family members at a routine family
evening activity, with the older participants subsequently receiving a lecture describing
the study as one of their morning activities.
The next step was to approach potential subjects individually. Three of the daycare
centers preferred to approach the potential subjects and their family members directly.

39
For that purpose, a list of subjects who met the inclusion criteria (see 5.1) based on the
opinion of staff members who knew them well was prepared, and family members were
contacted personally by phone in order to provide a more detailed description of the
study and to answer questions that emerged. Those subjects and their families who
expressed an interest and willingness to participate in the project were invited to a
meeting with the researchers to sign informed consent for participation in the study (see
Methods section).
4.5 Installation
At each of the adult daycare centers a PC with a touch screen was installed and
connected to the available internet resource (LAN or WIFI). Savion and Mindstreams
were installed on the PC's. In two centers where participants were native Russian
speakers, the Savion Russian version was installed instead of the Hebrew/English
version, and the operating system was set to support Russian. Links to the reminiscence
software were also added.
4.6 The addition of personal contents to the reminiscence system
For those participants randomly assigned to the reminiscence study group (see 5.2),
family members of participants were approached to provide personal materials for use
in the reminiscence sessions, as well as accompanying information for each item (i.e a
title and a short description of the item). The material was sent directly to the daycare
center or submitted electronically by mail in the few cases where digital files were
available. The contents were scanned and edited in order to enhance their visibility and
quality. In some cases additional information regarding the background of the
participant and his/her areas of interest was requested, and other relevant material was
found using an internet search engine. In addition, extra material was added as
necessary by relatives during the study. In some cases, participants provided their own
materials.

40
5. Methods
5.1 Patient sample
The participants of this study were older subjects with cognitive impairment or
dementia who resided in the community and regularly attended an adult daycare center
at least twice a week.
The inclusion and exclusion criteria are described in Table 3.
Table 3: Inclusion and exclusion criteria
Inclusion criteria Exclusion criteria
(1) Age – above sixty years old (5) Psychiatric disease
(2) Cognitive impairment – mild cognitive
impairment (MCI) or dementia (MMSE
score of 14-26)not associated with a
known medical condition (such as stroke,
vitamin deficiencies, impaired thyroid
function, among others)
(6) Significant visual or auditory
impairments or any other impairment
which may prevent the participant from
using either of the two computerized
interventions
(3) English / Hebrew / Russian speakers (7) Inability to understand the questions
presented in the Savion software program,
or inability to communicate coherently as
required for the performance of
reminiscence therapy.
(4) Have close relatives who could act as
informants
Due to the diverse symptoms of MCI and dementia, and in order to maintain a certain
level of homogeneity, the age criterion (1) was determined in order to exclude cases of
early onset dementia. In order to encourage the inclusion of subjects with an organic
etiology for their cognitive impairment, participants with psychiatric disease (5) were
excluded from the study. The language criterion (3) was based on the availability of
these interfaces in the two computer systems (see 3.1and3.2). Due to the requirements
of the screening tools (as will be described below) – crucial information regarding the

41
functional capabilities of the participants were to be obtained from a family informant
(4). Moreover, the periodic evaluations (to be described in5.4) included the impressions
of family members who serve as the participants' main caregivers.
Each competent participant, as confirmed by an independent geriatrician, was asked to
provide written informed consent prior to participation in the study. For those patients
who were not competent, the legal guardian was required to provide informed consent.
Subjects without a legal guardian who were determined not to be competent were not
enrolled in the study.
After providing informed consent, the participants' medical files were reviewed in order
to ensure that they conform with inclusion and exclusion criteria, and that their
cognitive impairment was not the result of an associated medical condition (such as
stroke, vitamin deficiencies, impaired thyroid function, among others). In addition, the
participants underwent a preliminary assessment in order to determine the stage of their
illness. The assessment included cognitive and functional evaluations using the
following instruments (see Appendix F):
Mini-Mental State Examination for cognitive screening (Folstein et al., 1975).
Clock Drawing test (Freedman et al., 1994) and CogSym questionnaire for
cognitive screening (Memory Clinic, Mental Health Center, Beersheva). The
latter is a numerical scale based on 10 questions used for elucidating cognitive
symptoms, and is completed both by subjects and by informants.
Lawton and Brody’s Instrumental Activities of Daily Living (IADL) for
assessing functional capabilities (Lawton et al., 1969). This questionnaire is
directed at the participants' informant.
Clinical Dementia Rating (CDR) scale as a global measure rating the severity of
dementia (Morris, 1993). This questionnaire includes two parts: the first is
directed at the informant and the second at the participant, comparing the latter's
response to that of the informant.
Short version (15 questions) of the Geriatric Depression Scale (GDS) as a
screening instrument for depression (Yesavage et al., 1983).
All questionnaires directed to informants were administered by face-to-face or
telephone interviews with first-degree relatives of the participants. All other scales were

42
administered by face-to-face interviews with the participants during morning hours at
the adult daycare centers.
At the end of the screening process, the results of all evaluations were reviewed by a
physician specializing in the treatment of cognitive syndromes, and the cognitive
diagnosis was determined to be either MCI or dementia based on accepted criteria.
5.2 Design
At the completion of screening, subjects were assigned randomly to one of three groups:
1. Personal reminiscence therapy intervention (using the computerized
reminiscence system with personal contents for each participant).
2. Cognitive training intervention (using the Savion computerized cognitive
training system).
3. Control group which continued usual activities in the adult daycare center. This
group did not receive any computerized intervention involving interaction with
one of the research staff. The reason for not offering the control group an
alternative intervention was based on the need to create a 'neutral' group with no
elements of intervention similar to those of computerized reminiscence therapy
or cognitive training.
The usual activities of all participants at the daycare centers and at their homes were not
controlled. The purpose of randomization was to assure as much as possible that
baseline characteristics of the participants of the three groups were similar.
Randomization was stratified according to the daycare center, and to the severity of
cognitive impairment (with CDR scores of 0.5 and 1 representing a milder degree of
cognitive impairment, and CDR scores of 2 and 3 representing more severe
impairment), see Figure 5.

43
Figure 5.Randomization of participants in each daycare center
5.3 Procedure
Both those participants receiving reminiscence therapy as well as those using the
cognitive training program participated in two sessions a week, each of 30-minutes
duration, over a period of three months. The treatments were conducted in a quiet room
at the adult daycare centers in the morning hours, and supervised by a trained mediator.
At the end of each session, the mediator provided a short description of the interaction,
relating to the course of the session and to special occurrences.
5.3.1 The reminiscence therapy session
At the beginning of the session the subject was presented with the albums (the themes)
and was asked to select one and to commence viewing its objects. In those instances
where the subject could not decide as to which album to begin with – the mediator
encouraged him/her to make a selection. While the subject was encouraged to talk about
the presented object, no limitation was placed on the content of the conversation. In
fact, the subject could talk about any topic that the object brought to mind, with no
obligation to provide information about the object itself. When relating to the various
objects the mediators were cautious not to let the subjects feel that their memory was
being tested, but rather to explore the object together (for example, instead of asking
"Do you remember this place?" they would refer to the object as follows: "What a nice
place. What do you think it could be?").
Day care center
CDR 0.5-1
Reminiscence Cognitive Training
Control
CDR 2-3
Reminiscence Cognitive Training
Control

44
The mediators encouraged the subjects to operate the system themselves, by selecting
the required albums, navigating through the objects, and controlling the session and the
discussion as they wished.
5.3.2 The cognitive training session
At the beginning of the session the intervention mediators asked the subjects to choose
their preferred cognitive area for commencing their training session. In the case where
the subject expressed no preference – the mediator would offer him/her one of the four
topics. The mediators were advised to include all four topics in each session, although
this was not mandatory. In those instances where the subject refused to work on one of
the topics – the mediator made an effort to encourage the subject to work on that area in
the next session.
At the end of each session the level that the subject achieved on each topic was
documented, and in addition a short description of the session was noted, as mentioned
previously. This ensured continuity and allowed for intellectual stimulation.
5.4 Measurements
The following describes the measurements that were employed in the study. All
assessments were performed at baseline (T0), at one month (T1) and at 3 months (T3).
Responses from subjects' relatives were obtained by face-to-face or telephone
interviews. The name of the subject's relatives was provided by the staff of the adult
day-care centers.
5.4.1 Cognitive function assessment
In order to evaluate the efficacy of each of the interventions as compared to controls
with regard to cognitive function, the subjects’ cognitive function was measured by the
Mindstreams computerized assessment battery (Dwolatzky et al., 2003; Dwolatzky et
al., 2010). The Moderate-Severe Impairment Battery was administered. This tool takes
about 20 minutes to administer and tests the following cognitive domains:
1. Orientation to time and place
2. Language skills
3. Memory

45
a. Nonverbal memory
b. Delayed nonverbal memory
4. Executive function
a. Similarities and judgment
b. Reality testing
c. Go-NoGo basic test
5. Spatial orientation
At the end of the test, data is uploaded to a server, scores are provided forall of the
individual test components, andin addition a global score indexis calculated for the
test.A summary score for each domain (including the global score) reflects the level of
accuracy, ranging between 0-100 (with 100 being the highest level of accuracy).
Using a computerized tool for assessing cognitive function has several advantages over
using traditional assessment instruments. The computerized evaluation enhances the
sensitivity of test, is able to minimize ceiling or floor effects, is much easier to
administer (in terms of time and cost) and is widely available since it is internet-based.
(Dwolatzky et al., 2003).
The Mindstreams batteries for mild and moderate impairment were validated by
Dwolatzky el al. (2003, 2010) and were found to be effective in providing a clear and
detailed cognitive status of the patients.
Samples of the Mindstreams screens and reports are presented in Appendix B.
5.4.2 Patients’ psychological/ behavioral well-being
Behavioral outcomes were assessed using the NPI - Neuropsychiatric Inventory
(Cummings et al., 1994), which was completed by the subject's first-degree relative.
This tool includes 12 areas, each relating to the presence of a particular behavior, its
frequency, severity and the level of caregiver distress. A total score is calculated
according to the frequency and severity, and ranges between 0-144 (a higher score
reflecting a higher level of symptomatology). Psychological well-being was assessed
using the QoL-AD instrument (Logsdon et al., 1999), and a general question from the
Will to Live questionnaire was administered (Carmel, 2011). The QoL-AD instrument
obtains responses regarding the subject's quality of life both from the subject and the

46
relative, and includes 13 items rated on a four-point scale. Total score of the instrument
ranges between 13-52 (a higher score reflecting better quality of life). The Will to Live
questionnaire was rated by the subject, and ranges between 0-5 (a higher score
reflecting a greater will to live). The questionnaires are presented in Appendix F.
5.4.3 Caregiver burden
For the assessment of caregiver burden and psychological morbidity, the short version
of the Zarit Caregiver Burden Interview (Bedard et al., 2001) was used. This
questionnaire was administered to the subjects' first-degree relatives, and ranges
between 0-48 (a higher score reflecting a higher level of burden). The questionnaire is
shown in Appendix F.

47
6. Analysis and Results
Of the 95 subjects who entered the study, 32 were assigned to the reminiscence therapy
intervention, 32 to the cognitive training intervention, and 31 to the control group.
Attrition in the reminiscence group was the highest (9 participants), though this was
mainly prior to commencing the intervention. Six participants did not receive the
intervention: 3 were excluded due to lack of cooperation of family members (who did
not provide the required personal materials), 1 left the day care center and 2 declined (or
family member declined) to participate in the study. All the participants who were
assigned to the cognitive training group commenced the intervention. One participant
from the control group withdrew due to ill health before T0 evaluation.
Of the remaining 88 participants who underwent T0 evaluation, 11 did not complete T3
evaluation due to the following reasons: Illness (4), death (1), withdrew (2), left the day
care center (1) and excluded due to prolonged absence (3).
Figure 6 presents the number of participants who were enrolled, were assigned to each
study group and completed T1 and T3 evaluations. Since family members'
responsiveness was lower, samples of family evaluations were usually smaller and
therefore are reported separately for each of the statistical tests. Reported analysis
relates to a total of N=85 participants who, in addition to T0 evaluation completed at
least one of T1and T3 evaluations.
6.1 Statistical analysis
SPSS v.20 was used for data entry and statistical analysis. The analysis included the
evaluation of baseline demographic and clinical variables for the three study groups,
followed by an analysis of outcome measures, at T1 and T3compared to T0. All tests
were designed as two tailed.
All effects reported in this chapter relate to improvements in the intervention groups
compared to the control group, unless stated otherwise.

48
Figure 6.Consort diagram of the study(Excluded from study: due to lack of cooperation of participants/family members, or absence)
167 subjects were assessed for eligibility
95 entered study and underwent randomization
32 were assigned to Reminiscence group
23 completed T1 follow up 3 remained in the study but
were lost to follow up
23 completed T3 follow up
1 withdrew
2 were excluded
2 withdrew
1 left day care center 3 were excluded
32 were assigned to Cognitive Training group
28 completed T1 follow up 2 remained in the study but
were lost to follow up
27 completed T3 follow up
1 withdrew 1 left day care center
1 withdrew due to ill health
1 was excluded 1 withdrew due to ill health
31 were assigned to Control group
27 completed T1 follow up
2 remained in the study but were lost to follow up
27 completed T3 follow up
1 died 1 withdrew due to ill
health
2 withdrew due to ill health
72 were excluded: 46 did not meet inclusion criteria
16 declined to participate 6 did not receive family approval 4 were absent when screening
tests took place

49
6.2 Baseline analysis
The mean age of participants was 83.9 years (Standard Deviation [SD] 5.6), ranging
from 71 to 98. MMSE minimum and maximum scores were 14 and 26 respectively with
a mean of 21.40 (SD2.9). Most of them were diagnosed as having a CDR score of 1
(60%), with only one subject having a CDR score of 3. The majority of participants
were female (77.6%).Most were widowed (61.1%). The participants' mean number of
children was 3.4 (SD1.9).
Most were born in West Europe/America/Australia (36.5%) or Africa/Asia (24.7%).
The mean total years of education was 10.55 (SD4.6). Mean scores for clinical tests
were: 7 (SD3.4) for Clock drawing test, 3.8 (SD3.3) for GDS, 21.8 (SD7.8) for IADL,
and 5.5 (SD1.9) for CogSym. Almost half of the participants used medications to treat
dementia (44.7%).A cognitive diagnosis of dementia was the most common and
accounted for almost half of the participants (47.1%).
Demographic and clinical variables were compared between study groups. The Kruskal-
Wallis test was used to compare interval and ordinal variables, and Chi square test was
used for comparing categorical variables. No significant differences between groups
were found for any of the variables (Table 4).
Table 4: Baseline characteristics of the participants, according to study group
Number of participants N=85
Reminiscence Cognitive
Training
Control Kruskal-Wallis
test
Characteristics n=26 (%) n=30 (%) n=29 (%) Statistic Sig.
Age (Mean+SD) 84.35 (5.585) 84.13 (6.202) 83.21 (5.130) 1.468 0.480
Gender (n) 0.766a 0.682
Male 6 (23.1) 8 (26.7) 5 (17.2)
Female 20 (76.9) 22 (73.3) 24 (82.8)
Years of education
(Mean+SD)
10.38 (3.920) 10.73 (4.856) 10.52 (5.054) 0.042 0.979

50
Number of participants N=85
Reminiscence Cognitive
Training
Control Kruskal-Wallis
test
Characteristics n=26 (%) n=30 (%) n=29 (%) Statistic Sig.
Place of birth (n) 3.893a 0.867
Israel 1 (3.8) 4 (13.3) 2 (6.9)
West Europe,
America,
Australia
8 (30.8) 13 (43.3) 10 (34.5)
East Europe 5 (19.2) 4 (13.3) 5 (17.2)
Former Soviet
Union
4 (15.4) 4 (13.3) 4 (13.8)
Africa, Asia 8 (30.8) 5 (16.7) 8 (27.6)
Marital status (n) 1.438a 0.838
Married 10 (38.5) 12 (40) 9 (31)
Widowed 16 (61.5) 17 (56.7) 19 (65.5)
Divorce 0 (0) 1 (3.3) 1 (3.4)
Number of children
(Mean+SD)
3.08 (1.262) 3.10 (1.520) 3.86 (2.489) 1.808 0.405
Missing data 0 1 0
Background diseases
(n)
HTN 15 (57.7) 20 (69) 20 (74.1) 1.682a 0.431
IHD 14 (53.8) 7 (24.1) 11 (40.7) 5.135a 0.077
CVA 6 (23.1) 7 (24.1) 5 (18.5) 0.286a 0.867
NIDDM 6 (23.1) 7 (24.1) 6 (22.2) 0.029a 0.986
Psychiatric 1 (3.8) 0 (0) 0 (0) 2.296a 0.317
Missing Data 0 1 2
Medicine (n) 4.787a 0.571
Rivastigmine 2 (8.7) 3 (11.1) 6 (24)
Donepezil 4 (17.4) 4 (14.8) 5 (20)
Memantine 2 (8.7) 2 (7.4) 0 (0)
None 15 (65.2) 18 (66.7) 14 (56)
Missing data 3 3 4
MMSE (Mean+SD) 20.81 (3.163) 21.77 (2.812) 21.55 (2.640) 1.696 0.428
Clock drawing test
(Mean+SD)
5.96 (3.092) 7.10 (3.498) 7.79 (3.331) 4.140 0.126

51
Number of participants N=85
Reminiscence Cognitive
Training
Control Kruskal-Wallis
test
Characteristics n=26 (%) n=30 (%) n=29 (%) Statistic Sig.
Missing data 0 1 0
CDR (n) 2.663a 0.85
0.5 8 (30.8) 11 (36.7) 9 (31)
1 17 (65.4) 16 (53.3) 18 (62.1)
2 1 (3.8) 2 (6.7) 2 (6.9)
3 0 (0) 1 (3.3) 0 (0)
GDS (Mean+SD) 3.38 (3.395) 3.90 (3.044) 3.97 (3.530) 0.783 0.676
IADL (Mean+SD) 21.92 (6.958) 22.38 (8.330) 21.21 (8.095) 0.132 0.936
Missing data 1 1 0
CogSym (Mean+SD) 5.50 (1.241) 5.87 (2.145) 5.24 (2.132) 2.133 0.344
Cognitive diagnosis (n) 2.339a 0.674
MCI 8 (30.8) 10 (33.3) 5 (17.2)
AD 7 (26.9) 7 (23.3) 8 (27.6)
Other dementia 11 (42.3) 13 (43.3) 16 (55.2)
a χ
2 test
6.3 Outcome measures data
Data for analysis included results of the cognitive measurements yielded from the
Mindstreams computerized testing battery (primary outcome measures) and results of
behavioral and psychological measurements derived from the questionnaires (secondary
outcome measures).
The Mindstreams data comprised,in addition to the global score and its five
components, two variables from the raw data. These variables were derived from the
executive function domain but were not included in its summary score. Both variables
reflected reaction time for the Go-NoGo task. The first variable (Go-NoGo RT L1)
measures the average response time at level 1, i.e. the appearance of a green square. The
second variable (Go-NoGo RT L2) measures the average response time at level 2, i.e.
the appearance of a white squarein the inhibition stage.Missing data were reported
where insufficient data were recorded for either of these two variables. A higher rate of

52
missing data wasascribed for the Go-NoGo RT L2, as reported in the analysis
tables(Tables 6-14).
Missing data for the behavioral and psychological variables were due to the following
reasons: low responsiveness of family members, partial completion of questionnaires,
and irrelevant questions on scales (e.gthe Qol-AD includes a rank for marriage, which is
not relevant for widowed participants). In order to create an equal basis of comparison,
imputation of incomplete questionnaire items (for a maximum of 40% missing data),
was conducted according to the following rule: imputed total score was calculated as the
completed items' average multiplied by the total number of items.
This was conducted for the QoL-Ad scale (with 5 maximum missing itemsout of a total
of 13), and the short version of the Zarit Caregiver's Burden scale (with 2 maximum
missing itemsof a total of 12).
For the NPI– an average of the total sum of frequency × severity (for completed items)
was calculated (with 5 maximum missing 'frequency × severity' itemsout of a total of
12). Due to the missing data rate, a new variable was created to record the number of
disturbing behaviors, which was reported more often.
For the purpose of comparison between groups, two new variables were created for each
of the outcome measures. The new variables measure the differences between T1and T0
and between T3 and T0. The value of these variables was calculated as pre intervention
scores (T0) subtracted from post intervention scores (T1 and T3 respectively).
6.4 Analysis of results
Mean scores for outcome variables for each of the study groups are described in Table
5. Examination of the mean Global Score over time (see Figure 7) indicates a
progressive increase in both intervention groups, with no dose-response relationship in
the control group (although differences in both cognitive training and control groups
were very slight).
Table 5: Sample mean scores for outcome measures of each of the study groups
Means (SD)
Measure Group T0 T1 T3
Global Rem 71.22 (14.54) 75.86 (12.36) 77.63 (13.22)
CT 77.16 (16.25) 77.62 (17.18) 80.20 (18.19)
Control 77.40 (10.84) 76.10 (13) 79.53 (10.36)

53
Means (SD)
Measure Group T0 T1 T3
Orientation
Rem
65.96 (28.13)
64.43 (29.51)
68.78 (29.57)
CT 66.03 (33.80) 67.29 (32.89) 69.70 (31.11)
Control 74.72 (23.44) 66.67 (30.35) 72.85 (25.45)
Verbal Function Rem 79.23 (15.71) 85.22 (13.14) 84.26 (16.84)
CT 80.77 (19.70) 84.79 (16.69) 86.04 (19.91)
Control 83.07 (10.16) 83.52 (10.32) 84.74 (11.61)
Memory Rem 64.06 (24.18) 75.72 (18.63) 76.21 (23.69)
CT 79.85 (20.17) 81.94 (21.12) 82.54 (23.33)
Control 76.70 (17.81) 78.08 (19.36) 83.80 (15.65)
Executive function Rem 77.48 (13.86) 80.43 (11.97) 81.94 (11.12)
CT 78.22 (15.55) 80.15 (18.81) 82.15 (18.87)
Control 78.98 (12.96) 77.33 (14.38) 81.42 (10.35)
Visual Spatial Rem 70.73 (20.15) 66.17 (20.14) 72.22 (20.01)
CT 74.70 (20.98) 62.54 (19.66) 73.41 (22.56)
Control 72.13 (19.95) 69.48 (19.78) 64.56 (21.22)
Go-NoGo RT L1 Rem 759.62 (391.13) 676.09 (307.57) 861.04 (496.26)
CT 924.83 (447.47) 854.25 (437.10) 788.81 (389.91)
Control 769.61 (330.31) 923.96 (444.23) 828.52 (364.88)
Go-NoGo RT L2 Rem 610.77 (226.25) 672.45 (304.67) 684.33 (400.95)
CT 694.88 (370.09) 699 (341.10) 624.87 (278.98)
Control 630.13 (201.26) 668.25 (271.08) 644.61 (278.47)
QoL-AD
participant
Rem 33.03 (5.93) 36.88 (4.76) 35.13 (6.61)
CT 33.36 (5.95) 34.63 (6.27) 33.08 (7.01)
Control 32.93 (7.17) 33.45 (6.47) 32.74 (7.54)
WTL Rem 3.56 (1.42) 4.22 (1.17) 4.22 (1.17)
CT 3.97 (1.07) 4.17 (0.81) 4.08 (1.16)
Control 3.66 (1.17) 3.74 (1.20) 3.48 (1.45)
QoL-AD caregiver Rem 31.53 (7.51) 32.77 (6.24) 31.05 (6.84)
CT 29.46 (5.68) 29.12 (6.39) 30.22 (6.71)
Control 29.13 (5.95) 28.26 (6.35) 30.15 (7.29)
Zarit Caregiver
Burden
Rem 16.86 (8.64) 15.53 (8.94) 13.53 (8.45)
CT 14.47 (9.49) 16.28 (9.83) 11.04 (7.03)
Control 13.91 (7.90) 14.95 (9.34) 12.85 (9.44)

54
Means (SD)
Measure Group T0 T1 T3
NPI-Average Rem 0.68 (0.77) 0.40 (0.63) 0.80 (1.15)
CT 0.86 (0.95) 0.53 (0.77) 0.84 (1.64)
Control 0.78 (0.74) 0.78 (0.94) 1.06 (1.60)
NPI-Number of
behavioral
disturbances
Rem 3.32 (3.00) 2.16 (1.74) 2.40 (2.66)
CT 3.62 (3.17) 2.52 (2.31) 2.96 (2.58)
Control 3 (2.84) 2.65 (2.21) 2.55 (2.65)
Rem=Reminiscence, CT=Cognitive training.
Figure 7.Mean Global scores for study groups in T0, T1 and T3.
Differences from baseline at T1 and T3, for each of the remaining cognitive measures
(except for the Go-NoGo RT L2variable whose sample size was lower due to missing
data)are presented in Figure 8.
The mean scores for orientation in both reminiscence and control groups were lower
than baseline (with a lower decrease in the reminiscence group), whereas the cognitive
training group demonstrated an improvement on this scale.An increase in verbal score

55
Figure 8.Mean differences in cognitive measures between T1&To, and T3&T0 (Error bars show
95% confidence interval).
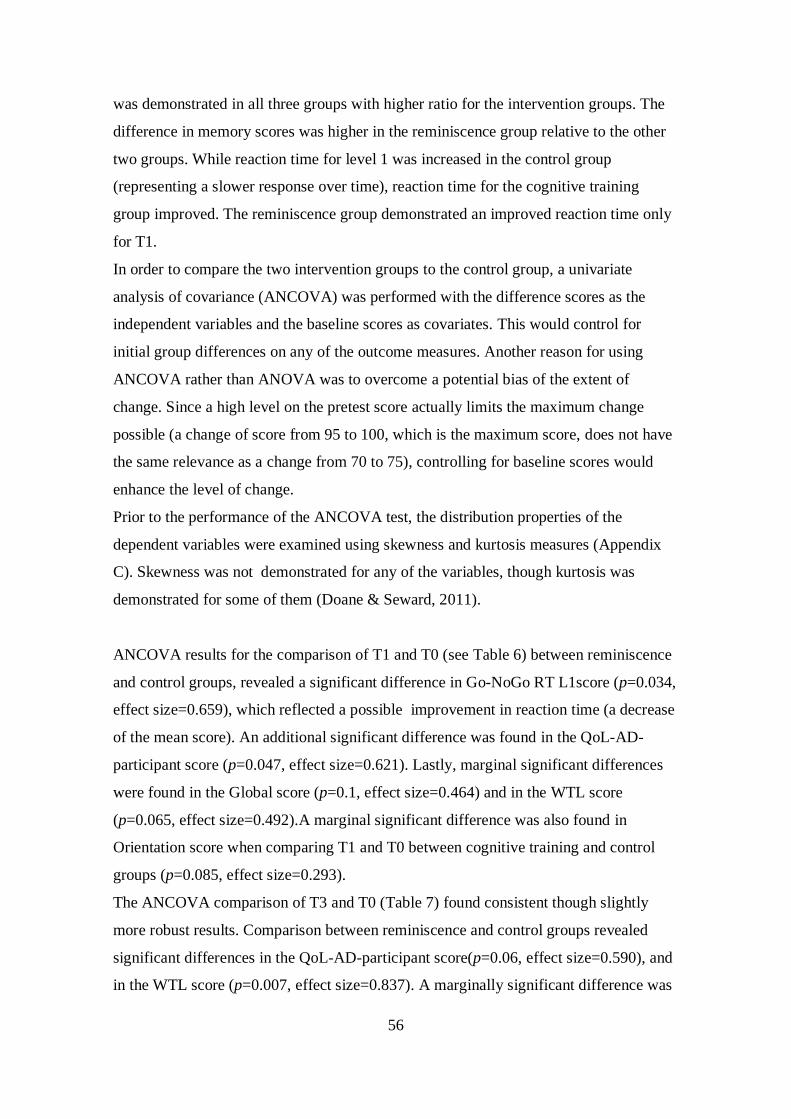
56
was demonstrated in all three groups with higher ratio for the intervention groups. The
difference in memory scores was higher in the reminiscence group relative to the other
two groups. While reaction time for level 1 was increased in the control group
(representing a slower response over time), reaction time for the cognitive training
group improved. The reminiscence group demonstrated an improved reaction time only
for T1.
In order to compare the two intervention groups to the control group, a univariate
analysis of covariance (ANCOVA) was performed with the difference scores as the
independent variables and the baseline scores as covariates. This would control for
initial group differences on any of the outcome measures. Another reason for using
ANCOVA rather than ANOVA was to overcome a potential bias of the extent of
change. Since a high level on the pretest score actually limits the maximum change
possible (a change of score from 95 to 100, which is the maximum score, does not have
the same relevance as a change from 70 to 75), controlling for baseline scores would
enhance the level of change.
Prior to the performance of the ANCOVA test, the distribution properties of the
dependent variables were examined using skewness and kurtosis measures (Appendix
C). Skewness was not demonstrated for any of the variables, though kurtosis was
demonstrated for some of them (Doane & Seward, 2011).
ANCOVA results for the comparison of T1 and T0 (see Table 6) between reminiscence
and control groups, revealed a significant difference in Go-NoGo RT L1score (p=0.034,
effect size=0.659), which reflected a possible improvement in reaction time (a decrease
of the mean score). An additional significant difference was found in the QoL-AD-
participant score (p=0.047, effect size=0.621). Lastly, marginal significant differences
were found in the Global score (p=0.1, effect size=0.464) and in the WTL score
(p=0.065, effect size=0.492).A marginal significant difference was also found in
Orientation score when comparing T1 and T0 between cognitive training and control
groups (p=0.085, effect size=0.293).
The ANCOVA comparison of T3 and T0 (Table 7) found consistent though slightly
more robust results. Comparison between reminiscence and control groups revealed
significant differences in the QoL-AD-participant score(p=0.06, effect size=0.590), and
in the WTL score (p=0.007, effect size=0.837). A marginally significant difference was

57
found in the Global score (p=0.096, effect size=0.381). Comparison of T3 and T0
between cognitive training and control groups found no significant differences.
The results described above should be interpreted with caution. First, these are
exploratory results. The multiplicity of statistical tests might require the adjustment of
p-value to a lower value, which may significantly decrease the power of the findings.
Secondly, it is important to bear in mind the possible bias in these results due to those
methodological limitations described in chapter 7.

58
Table 6: Comparing T1-T0 scores difference between reminiscence & control groups, and between
cognitive training & control groups - ANCOVA results.
Measure p-Value Effect size a p-Value Effect size
a
Reminiscence (n=23) vs.
Control (n=27)
Cognitive Training (n=28) vs.
Control (n=27)
Global 0.1 0.464 0.287
Orientation 0.614 0.085 0.293
Verbal Function 0.301 0.145
Memory 0.268 0.531
Executive function 0.24 0.274
Visual Spatial 0.654 0.126
Reminiscence (n= 23) vs.
Control (n= 24)
Cognitive Training (n= 28) vs.
Control (n=24)
Go-NoGo RT L1 0.034*b
0.659 0.137
Reminiscence (n= 20) vs.
Control (n= 19)
Cognitive Training (n= 20) vs.
Control (n=19)
Go-NoGo RT L2 0.636 0.344
Reminiscence (n=23) vs.
Control (n=27)
Cognitive Training (n=29) vs.
Control (n=27)
QoL-AD participant 0.047* 0.621 0.534
WTL 0.065 0.492 0.234
Reminiscence (n=15) vs.
Control (n=21)
Cognitive Training (n=24) vs.
Control (n=21)
QoL-AD caregiver 0.157 0.661
Reminiscence (n=15) vs.
Control (n=19)
Cognitive Training (n=24) vs.
Control (n=19)
Zarit Caregiver
Burden
0.474 0.789

59
Measure p-Value Effect size a p-Value Effect size
a
Reminiscence (n=11) vs.
Control (n=15)
Cognitive Training (N=17) vs.
Control (N=15)
NPI-Average 0.417 0.398
Reminiscence (n=15) vs.
Control (n=21)
Cognitive Training (n=24)
vs.Control (n=21)
NPI-Number of
behavioral
disturbances
0.215 0.28
Go-NoGo RT L1=Go-NoGo Response Time Level 1.
Go-NoGo RT L2=Go-NoGo Response Time Level 2.
a Cohen's d effect size was calculated only for significant and marginally significant
effects. b A Negative difference (T1<T0).

60
Table 7: Comparing T3-T0 scores difference between reminiscence & control groups, and between
cognitive training & control groups - ANCOVA results.
Measure p-Value Effect size a p-Value Effect size
a
Reminiscence (n=23) vs.
Control (n=27)
Cognitive Training (n=27) vs.
Control (n=27)
Global 0.096 0.381 0.51
Orientation 0.595 0.523
Verbal Function 0.316 0.155
Memory 0.819 0.476b
Executive function 0.321 0.392
Visual Spatial 0.117 0.148
Go-NoGo RT L1 0.708 0.257
Reminiscence (n=17) vs.
Control (n=21)
Cognitive Training (n=20) vs.
Control (n=21)
Go-NoGo RT L2 0.955 0.377
Reminiscence (n=22) vs.
Control (n=27)
Cognitive Training (n=26) vs.
Control (n=27)
QoL-AD participant 0.06 0.590 0.802
WTL 0.007**
0.837 0.153
Reminiscence (n=18) vs.
Control (n=17)
Cognitive Training (n=22) vs.
Control (n=17)
QoL-AD caregiver 0.787 0.9
Zarit Caregiver
Burden
0.277 0.122
Reminiscence (n=10) vs.
Control (n=13)
Cognitive Training (N=16) vs.
Control (N=13)
NPI-Average 0.382 0.605

61
Measure p-Value Effect size a p-Value Effect size
a
Reminiscence (n=19) vs.
Control (n=17)
Cognitive training (n=22)
vs.Control (n=17)
NPI-Number of
behavioral
disturbances
0.717 0.861
Go-NoGo RT L1=Go-NoGo Response Time Level 1.
Go-NoGo RT L2=Go-NoGo Response Time Level 2.
aCohen's d effect size was calculated only for significant and marginally significant
effects. b A Negative difference (T3<T0).
6.5 An alternative statistical analysis
In light of the questionable normal distribution of the dependent variables (the
difference scores) used for the ANCOVA test, an alternative analysis using non-
parametric tests is proposed. The non-parametric analysis also addresses the limited
sample size in each of the study groups.
As in the case of the parametric analysis, the results described in this chapter should be
interpreted with caution, despite their presented statistical power.
First, Wilcoxon signed rank tests were performed for each of the study groups to
compare their outcome variables scores between T1&T0 andT3&T0. In the
reminiscence group (Table 8) significant differences were observed between T1&T0for
the following variables: memory (p=0.012, effect size= 0.522), executive function
(p=0.048, effect size= 0.412) ,QoL-AD-participant (p=0.016, effect size= 0.504), and
WTL (p=0.007, effect size= 0.558). A significant difference was also found in the NPI-
Num-of-Behav (p=0.030, effect size= 0.560), which reflects an improvement in the
number of disturbing behaviors over time (a decrease of the mean score). In addition,
marginal differences were observed for the global score variable (p=0.057, effect
size=0.396) and for the verbal variable (p=0.080, effect size=0.365).

62
When comparing the reminiscence group at T3 to T1(Table 8), significant effects were
observed for the following variables: global score (p=0.003, effect size=0.623), verbal
(p=0.011, effect size= 0.529), memory (p=0.004, effect size= 0.596), QoL-AD-
participant (p=0.039, effect size=0.440 ), and WTL (p=0.001, effect size=0.685 ). A
significant difference was also found in the Zarit caregiver's burden score (p=0.010,
effect size= 0.607), which reflects a possible decreased burden. Only a marginal
significant difference was observed in the NPI-Num-of-Behav variable (p=0.1, effect
size=0.377), which again reflects a possible improvement in the number of disturbing
behaviors over time (a decrease of the mean score).
Table 8: Changes in outcome measures for reminiscence group between T0 & T1, and T0 & T3 –
Wilcoxon signed-rank test.
Reminiscence
Measure Change between T0 & T1 Change between T0 & T3
n p-Value Effect sizea n p-Value Effect size
a
Global 23 0.057 0.396 23 0.003**
0.623
Orientation 23 0.281 23 0.673
Verbal 23 0.080 0.365 23 0.011* 0.529
Memory 23 0.012* 0.522 23 0.004
** 0.596
Executive 23 0.048* 0.412 23 0.131
Visual
Spatial
23 0.638 23 0.808
Go-NoGo
RT L1
23 0.420 23 0.144
Go-NoGo
RT L2
20 0.852 17 0.796
QoL patient 23 0.016* 0.504 22 0.039
* 0.440
WTL 23 0.007**
0.558 22 0.001* 0.685
QoL
caregiver
15 0.432 18 0.862
Zarit 15 0.789 18 0.010*b 0.6067
NPI 11 0.185 10 0.400
NPI-Num
Behaviors
15 0.030*b 0.560 19 0.100
b 0.377
a Effect size was calculated only for significant and marginally significant effects.
bNegative effect.

63
In the cognitive training group (Table 9), significant differences were observed between
T1&T0 for the following variables: verbal (p=0.009, effect size= 0.491), NPI (p=0.026,
effect size=0.541), and NPI-Num-of-Behav (p=0.021, effect size=0.469 ). For the two
NPI variables a negative difference was observed, which reflected a possible
improvement in behavior (a decrease in scores). However, a significant negative
difference was observed for the visual-spatial variable (p=0.007, effect size= 0.507),
which reflects a possible decreased functionality over time.
When comparing the cognitive training group at T3 to T0 (Table 9), significant
differences were observed for the following variables: verbal (p=0.007, effect
size=0.520), executive function (p=0.036 , effect size=0.405 ), and Zarit caregiver's
burden (p=0.042 , effect size=0.433), which had a negative difference reflecting a
possible decrease in burden.

64
Table 9: Changes in outcome measures for cognitive training group between To & T1, and T0 &
T3 – Wilcoxon signed rank test.
Cognitive Training
Measure Change between T0 & T1 Change between T0 & T3
n p-Value Effect sizea n p-Value Effect size
a
Global 28 0.387 27 0.136
Orientation 28 0.344 27 0.260
Verbal 28 0.009**
0.491 27 0.007**
0.520
Memory 28 0.249 27 0.360
Executive 28 0.172 27 0.036* 0.405
Visual
Spatial
28 0.007**b
0.507 27 0.573
Go-NoGo
RT L1
28 0.333 27 0.186
Go-NoGo
RT L2
20 0.243 20 0.911
QoL patient 29 0.186 26 0.416
WTL 29 0.249 26 0.463
QoL
caregiver
24 0.875 22 0.626
Zarit 24 0.177 22 0.042*b
0.433
NPI 17 0.026*b
0.541 16 0.142
NPI-Num
Behaviors
24 0.021*b
0.469 23 0.280
a Effect size was calculated only for significant and marginally significant effects.
bNegative effect.
In the control group (Table 10), a significant difference was observed between T3&T0
memory score (p=0.028, effect size= 0.423). In addition, two negative direction
differences (reflecting a decrease in measure scores) were observed: A significant
differencebetween T3&T1was found in the visual-spatial variable (p=0.036, effect size=
0.403), and a marginal significant difference between T1&T0 was observed in the
orientation variable (p=0.06, effect size= 0.362).
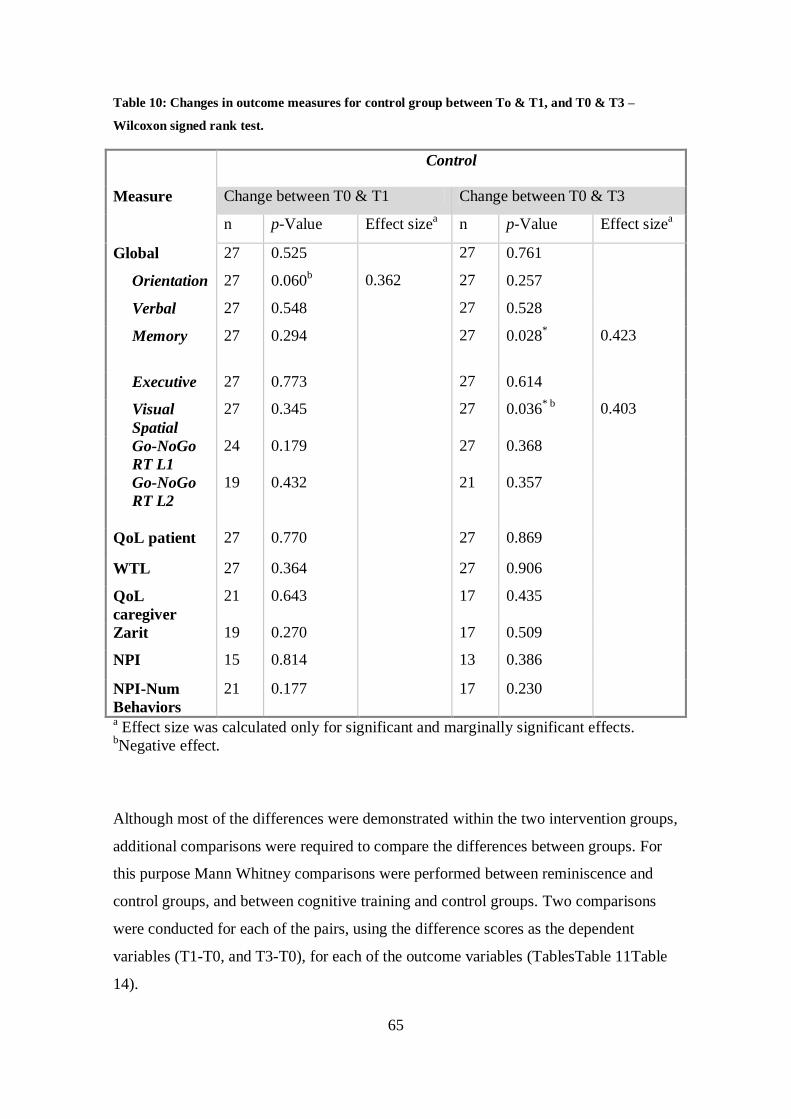
65
Table 10: Changes in outcome measures for control group between To & T1, and T0 & T3 –
Wilcoxon signed rank test.
Control
Measure Change between T0 & T1 Change between T0 & T3
n p-Value Effect sizea n p-Value Effect size
a
Global 27 0.525 27 0.761
Orientation 27 0.060b 0.362 27 0.257
Verbal 27 0.548 27 0.528
Memory 27 0.294 27 0.028* 0.423
Executive 27 0.773 27 0.614
Visual
Spatial
27 0.345 27 0.036* b
0.403
Go-NoGo
RT L1
24 0.179 27 0.368
Go-NoGo
RT L2
19 0.432 21 0.357
QoL patient 27 0.770 27 0.869
WTL 27 0.364 27 0.906
QoL
caregiver
21 0.643 17 0.435
Zarit 19 0.270 17 0.509
NPI 15 0.814 13 0.386
NPI-Num
Behaviors
21 0.177 17 0.230
a Effect size was calculated only for significant and marginally significant effects.
bNegative effect.
Although most of the differences were demonstrated within the two intervention groups,
additional comparisons were required to compare the differences between groups. For
this purpose Mann Whitney comparisons were performed between reminiscence and
control groups, and between cognitive training and control groups. Two comparisons
were conducted for each of the pairs, using the difference scores as the dependent
variables (T1-T0, and T3-T0), for each of the outcome variables (TablesTable 11Table
14).

66
When comparing the reminiscence and control groups, significant group effects were
found only for T3-T0 (Table 12). These were found for global score (p=0.037, effect
size= 0.295), and for WTL (p=0.007, effect size= 0.385).Also, marginal significant
effects of group for T3-T0 were observed for QoL-participant (p=0.089, effect size=
0.243), and for Zarit caregiver's burden (p=0.069, effect size= 0.308). For the latter, a
lower mean rank was observed in the reminiscence group, which possibly reflects lower
levels of burden for the reminiscence group in relation to the control group. Lastly, a
marginal significant effect for T3-T0 was found for NPI (p=0.084, effect size= 0.361),
with higher mean rank in the reminiscence group, possibly reflecting lower levels of
disturbing behavior for the control group in relation to the reminiscence group.
Table 11: Comparing 1 month differences between Reminiscence and control groups (Mann
Whitney test)
Measure Mean Rank Statistics
Reminiscence Control U Z p- value Effect
sizea
n=23
n=27
Global 28.80 22.69 234.5 -1.479 0.139
Orientation 26.41 24.72 289.5 -.437 0.662
Verbal 27.74 23.59 259 -1.027 0.304
Memory 28.59 22.87 239.5 -1.384 0.166
Executive 28.54 22.91 240.5 -1.363 0.173
Visual Spatial 24.70 26.19 292 -.361 0.718
n=23 n=24
Go-NoGo RT
L1
20.74 27.13 201 -1.596 0.110
n=20 n=19
Go-NoGo RT
L2
19.35 20.68 177 -0.365 0.715
n=23 n=27
QoL patient 28.89 22.61 232.5 -1.519 0.129
WTL 28.52 22.93 241 -1.448 0.148
n=15 n=21
QoL caregiver 20.07 17.38 134 -0.756 0.449

67
Measure Mean Rank Statistics
Reminiscence Control U Z p- value Effect
sizea
n=15 n=19
Zarit 15.2 19.32 108 -1.210 0.226
n=11 n=15
NPI 12.14 14.50 67.5 -0.787 0.431
n=15 n=21
NPI-Num
Behaviors
16.97 19.60 134.5 -0.758 0.449
a Effect size was calculated only for significant and marginal significant effects.
Table 12: Comparing 3 months differences between Reminiscence and Control groups (Mann
Whitney test)
Measure Mean Rank Statistics
Reminiscence Control U Z p- value Effect
sizea
n=23
n=27
Global 30.15 21.54 203.5 -2.083 0.037* 0.295
Orientation 26.78 24.41 281 -0.605 0.545
Verbal 28.00 23.37 253 -1.144 0.253
Memory 27.65 23.67 261 -0.966 0.334
Executive 27.48 23.81 265 -0.886 0.376
Visual Spatial 28.76 22.72 235.5 -1.463 0.143
n=23 n=27
Go-NoGo RT
L1
27.02 24.20 275.5 -0.681 0.496
n=17 n=21
Go-NoGo RT
L2
18.50 20.31 161.5 -0.499 0.618
n=22 n=27
QoL patient 28.84 21.87 212.5 -1.700 0.089 0.243
WTL 30.82 20.26 169 -2.697 0.007**
0.385

68
n=18 n=17
QoL caregiver 16.94 19.12 134 -0.628 0.53
Zarit 14.94 21.24 98 -1.820 0.069 0.308
n=10 n=13
NPI 14.75 9.88 37.5 -1.730 0.084 0.361
n=19 n=17
NPI-Num
Behaviors
18.03 19.03 152.5 -0.292 0.771
aEffect size was calculated only for significant and marginal significant effects.
When comparing the cognitive training and control groups, no significant group effects
were found. However, marginally significant group effects (Table 13) were found for
T1-T0 for orientation (p=0.052, effect size= 0.263), for verbal (p=0.097, effect size=
0.224, and for Go-NoGo-RT-L1 (p=0.086, effect size= 0.238).
Table 13: Comparing 1 month differences between Cognitive training and Control groups (Mann
Whitney test)
Mean Rank Statistics
Measure Cognitive
training
Control U Z p-value Effect
sizea
n=28
n=27
Global 30 25.93 322 -0.943 0.346
Orientation 31.95 23.91 267.5 -1.947 0.052 0.263
Verbal 31.39 24.48 283 -1.661 0.097 0.224
Memory 28.64 27.33 360 -0.304 0.761
Executive 30.45 25.46 309.5 -1.153 0.249
Visual Spatial 25.52 30.57 308.5 -1.173 0.241
n=28 n=24
Go-NoGo RT
L1
23.16 30.40 242.5 -1.716 0.086 0.238

69
n=20 n=19
Go-NoGo RT
L2
20.93 19.03 171.5 -0.520 0.603
n=29 n=27
QoL patient 29.83 27.07 353 -0.632 0.528
WTL 28.21 28.81 383 -0.154 0.878
n=24 n=21
QoL caregiver 23.69 22.21 235.5 -0.377 0.707
n=24 n=19
Zarit 21.96 22.05 227 -0.025 0.980
n=17 n=15
NPI 14.91 18.30 100.5 -1.034 0.301
n=24 n=21
NPI-
Num Behaviors
21.25 25 210 -0.979 0.328
a Effect size was calculated only for significant and marginal significant effects.

70
Table 14: Comparing 3 months differences between Cognitive training and Control groups (Mann
Whitney test)
Mean Rank Statistics
Measure Cognitive
training
Control U Z p- value Effect
sizea
n=27
n=27
Global 29.69 25.31 305.5 -1.021 0.307
Orientation 29.91 25.09 299.5 -1.166 0.244
Verbal 30.89 24.11 273 -1.613 0.107
Memory 25.24 29.76 303.5 -1.059 0.290
Executive 30.59 24.41 281 -1.445 0.148
Visual Spatial 29.65 25.35 306.5 -1.010 0.313
n=27 n=27
Go-NoGo RT
L1
24.15 30.85 274 -1.566 0.117
n=20 n=21
Go-NoGo RT
L2
20.10 21.86 192 -0.470 0.639
n=26 n=27
QoL patient 27.94 26.09 326.5 -0.436 0.663
WTL 28.19 25.85 320 -0.579 0.562
n=22 n=17
QoL caregiver 19.82 20.24 183 -0.113 0.910
Zarit 18.18 22.35 147 -1.138 0.255
n=16 n=13
NPI 15.25 14.69 100 -0.177 0.859
n=22 n=17
NPI-Num
Behaviors
20.18 19.76 183 -0.118 0.906
a Effect size was calculated only for significant and marginal significant effects.

71
6.6 Summary of findings
Table 15 and Table 16 summarize the significant and marginally significant effects that
were found in the between group analyses. Effect size was determined according to
Cohen's criteria (Cohen, 1988).All effects described in the tables represent possible
improvements in the intervention group (reminiscence or cognitive training) compared
to control group.
Table 15: Level of significance and effect size for effects found in the reminiscence group compared
to control group, according to the method of analysis.
T1-T0 T3-T0
Measure ANCOVA Mann Whitney ANCOVA Mann Whitney
Global MS
(ES=Medium)
--- MS
(ES=Small-
Medium)
S
(ES=Medium)
Go-NoGo RT
L1
S
(ES=Medium)
--- --- ---
QoL-AD
patient
S
(ES=Medium)
--- MS
(ES=Medium)
MS
(ES=Small-
Medium)
WTL MS
(ES=Medium)
--- S
(ES=Large)
S
(ES=Medium)
Zarit --- --- --- MS
(ES=Medium)
NPI --- --- --- MS
(ES=Medium)
MS=Marginally significant
S=Significant
ES=Effect Size
--- = No effect found

72
Table 16: Level of significance and effect size for effects found in the cognitive training group
compared to control group, according to the method of analysis.
T1-T0 T3-T0
Measure ANCOVA Mann Whitney ANCOVA Mann Whitney
Orientation MS
(ES=Small)
MS
(ES=Small-
Medium)
--- ---
Verbal --- MS
(ES=Small-
Medium)
--- ---
Go-NoGo RT
L1
--- MS
(ES=Small-
Medium)
--- ---
MS=Marginally significant
S=Significant
ES=Effect Size
--- = No effect found
The summary of results shows some consistency over time for the effects that were
found in the reminiscence group (Table 15) for the following measures: global score,
QoL-AD-patient and WTL. Although these effects were not demonstrated using the
non-parametric analysis in the T1-T0 comparison, they are salient in all other three
analyses. Improvements in the Go-NoGo RT L1 measure was demonstrated only in T1-
T0 analysis when using the parametric method, while improvements in the Zarit
Caregiver's Burden and the NPI were demonstrated only in T3-T0 analysis when using
the non-parametric method.
Overall, a higher accordance of the two analysis methods was shown in the T3-T0
analysis compared to the T1-T0 analysis.
When comparing the cognitive training and the control groups (Table 16), an adverse
tendency was noticed. Here, effects were found only in T1-T0 analysis. These were
more modest (in terms of significance level and effect size), and related mostly to the

73
following measures: orientation, verbal and Go-NoGo RT L1. Accordance of the two
analysis methods was found only for the orientation measure.
6.7 Results segmented by MMSE scores
In order to gain a wider insight regarding the potential effect of both treatments on the
participants' cognitive function, a further analysis of the primary outcome measures was
conducted. The analysis was based on the separation of participants into different
groups according to their MMSE scores: a high MMSE score group (where scores
ranged from 22 to 26), and a low MMSE score group (where scores ranged from 14 to
21). Both parametric and non- parametric evaluations were conducted for each of the
MMSE score groups (see appendices D and E respectively).
6.7.1 Parametric evaluation
ANCOVA results of the comparison between reminiscence and control groups in the
high MMSE group, revealed only marginally significant differences in the following
variables when comparing T3 and T0: global score (p=0.051, effect size=0.736) and
verbal function (p=0.088, effect size=0.59). No differences were demonstrated for the
T1 to T0 comparison (Table 17). In the low MMSE group, no differences were found in
any of the T1-T0 or T3-T0 comparisons (Table 18).
The ANCOVA comparison between cognitive training and control groups in the high
MMSE group, revealed a decrease of the visual-spatial score in the cognitive training
group at T1 compared to T0, which was marginally significant (p=0.094, effect
size=0.928). No effects were found for the T3 to T0 comparison (Table 17). However, a
positive effect was observed in the low MMSE group (Table 18): T3- T0 yielded a
significant difference in the visual-spatial score (p=0.047, effect size=0.82), reflecting
an improvement in the cognitive training group over time. In addition, the comparison
of T1 to T0 revealed a marginally significant difference in the global score (p=0.071,
effect size=0.84).

74
6.7.2 Non-parametric evaluation
Analysis of primary outcome measures using Mann Whitney evaluation showed similar
results. When comparing the reminiscence and control groups, a group effect was found
only in the high MMSE group. The effect was revealed in the global score for T3-T0
comparison (Table 12), and was marginally significant (p=0.053, effect size=0.369).
When comparing the cognitive training and control groups, the high MMSE group
showed a significant group effect for T1-T0 (Table 21), which was observed in the
visual-spatial score (p=0.005, effect size=0.497), with a lower mean rank for the
cognitive training group, which again, reflects a decrease over time. No effects were
found for T3-T0 comparison in this group (Table 22). However, differences were found
in the low MMSE group: For T1-T0 comparison (Table 25), significant effects were
found for global score (p=0.031, effect size=0.442) and orientation (p=0.042, effect
size= 0.448). Also, marginally significant effect was observed in the verbal function
score (p=0.084, effect size=0.367). Lastly, a marginally significant difference was found
also in T3-T0 comparison (Table 26), for the visual-spatial score (p=0.067, effect size=
0.387).
6.7.3 Summary of results according to grouped MMSE scores
Table 17 presents the summary of the results, and includes the main findings that were
observed in both methods (parametric and non-parametric).
Table 17: Summary of results segmented by MMSE scores – main findings
High MMSE Low MMSE
Group T1-T0 T3-T0 T1-T0 T3-T0
Reminiscence --- Global score --- ---
Cognitive
Training
Visual Spatial(b)
--- Global score
Orientation
Verbal
Visual Spatial
--- = No effect found
b=Negative effect

75
7. Discussion
Based on the current research of using individual reminiscence therapy and cognitive
training interventions in dementia care, this study's objective was to evaluate the
benefits of two such computer-based interventions, while addressing the calls for more
rigorous studies. This was done by taking the following steps mentioned by
Subramanian and Woods (2012) and Bahar-Fuchs et al. (2013).
1) Selecting a wide range of outcome measures, in order to assess impact on both
subjects and family members. Outcome variables included aspects of cognitive
function, behavior, quality of life (from both subject and caregiver's points of view) and
caregiver burden.
2) Including subjects with a wide range of cognitive impairment (MMSE score of 14-
26) to address 'ceiling' or 'floor' effects
3) Including subjects from seven different day care centers in order to mitigate the effect
of 'institution's settings'.
4) Controlling for baseline differences between treatment and control groups by
stratifying the allocation to groups according to the severity of pre-treatment cognitive
impairment in each daycare center.
5) Ensuring the quality of the implementation of the interventions (reminiscence therapy
and cognitive training) in order to create a clear format for each intervention,
minimizing the effect of other elements as much as possible.
Based on the study’s results, both the computer-based reminiscence and cognitive
training interventions demonstrated possible differences over time for several outcome
measures. The results showed different trends in the effects of each of the interventions.
However, most of these results are of low statistical power and need to be cautiously
interpreted since they may be due to methodological limitations.
7.1 The reminiscence therapy
A between- subjects analysis comparing the reminiscence and control groups showed
some improvement in the intervention group in three measures: global cognitive score,
QoL-AD-patient and WTL. Although this improvement was not significant in most

76
instances, it was consistent at both the one month and the three months follow-up
evaluations, representing a medium effect size.
Since no effects were found for any of the individual measures constituting the global
score (orientation, verbal function, memory, executive function and visual-spatial), the
subtle change found in the global score may be ascribed to the accumulation of small
but consistent improvements in some or all of its five components.
Both quality of life and the will to live (as reported by the participants) showed a subtle
change over time in the reminiscence group compared to the control group. Since the
WTL measure was found in previous study to be influenced by the perceived quality of
life (Carmel, 2001), the change in both measures strengthen the findings that the
computer-based reminiscence intervention might had a positive effect on the
psychological well-being of the participants. This effect was not seen in the cognitive
training group, and therefore might be explained by the therapeutic nature of the
reminiscence intervention, which is classified as a combination of cognitive and
emotion-focused approaches (Ponnusamy and Woods ,2012).
It is interesting to note that although quality of life, as perceived by the participants,
seemed to have improved in the reminiscence group –this finding was not corroborated
by family members (no effect was found in the QoL-AD-family measure). This could
stem from the fact that the QoL-AD tool evaluates subjective impressions. Both
participants and family members are asked to rate each of the 13 aspects of life
according to their own beliefs. Some of these aspects do not necessarily reflect mood
(for example: physical health, living situation, friends, money, etc).While the participant
might feel an improvement in QoL and thus rate life aspects higher, the family member
may not alter impressions of his relative’s quality of life (apart from energy, memory
and mood that may have changed due to the intervention).Also, most of the participants
did not live with their family informants, and therefore subtle changes in the patients'
QoL could have been missed by the caregivers.
Marginally significant effects of the reminiscence intervention were found in the NPI
and Zarit caregiver's burden's measures, but only at three months of treatment.
However, these effects were demonstrated only when using the non-parametric analysis
method, and did not reach a level of significance. Together with the fact that the sample
size of the analyzed data of both measures was low (due to a high rate of missing data),
only tentative conclusions can be reached based on this finding.

77
Regarding the Zarit caregiver's burden measure: lower levels of burden reported by
family members could be the result of a methodological bias, reflecting their awareness
that their relative was being engaged in a treatment that might be beneficial (family
members of participants in the reminiscence group were not blinded to the assignment
to groups, since they had to provide the personal materials that was used in the
intervention). This is also supported by the fact that no effect was found in the quality of
life of patients as perceived by family members.
The possible improvement that was observed in the NPI measure concur with the
conclusions of Brodaty and Arasaratnam's meta-analysis (2012) that psychosocial
interventions may be effective in reducing behavioral symptoms. However, as has been
argued, this finding should be regarded with caution due to the particular high rate of
missing data associated with the NPI tool in our study.
In the reminiscence group, we found a reduced reaction time in the Go-NoGo task,
which is included in the executive function index, as determined by the ANCOVA in
T1. This effect was not demonstrated either by using the non-parametric analysis or at
the T3 evaluations. Although this effect was found to be significant at T1, the relevance
of this finding is limited, since the use of ANCOVA assumes normal distribution of the
data.
7.2 The cognitive training
When comparing the cognitive training intervention group to controls, only marginally
significant effects were found after one month of treatment. However, no effects were
observed at three months. At T1, a possible improvement in orientation was found in
both methods of analysis, with a small to medium effect size. When referring to the four
cognitive areas of training of the program (language skills, calculation, non-verbal
memory and visual-spatial skills), this finding seems surprising since there was no
specific orientation training administered. In contrast, other areas that are included in
the Savion training software (such as verbal and memory skills) did not demonstrate any
change. If this finding may be ascribed to the routine of treatments (the conduction of
frequent training sessions over a period of time, it should have been also observed in the
reminiscence group. However, whereas the reminiscence group demonstrated a subtle
general change in the global cognitive score, the cognitive training group demonstrated

78
a specific change in the orientation skill, which might be the result of general reinforced
senses achieved by the constant practice of this training.
Additional effects were observed in verbal function and in the reaction time of the Go-
NoGo task, though these findings were not confirmed when using the parametric
analysis method.
These findings may imply that there might be a positive effect of the computer-based
cognitive training intervention on some of the cognitive function measures. This is in
line with Bahar-Fuchs et al.'s (2013) systematic review on RCTs of cognitive training
interventions, which found no clear indication of benefit for cognitive training but
concluded that more sensitive tools are needed for evaluation. The current study used
the Mindstreams tool which enables a more sensitive and detailed evaluation of aspects
of cognitive function, and subtle changes following one month of treatment were
noticed. However, the significant results of a previous study (Dwolatzky, 2009), which
included a similar intervention (a one month bi-weekly treatments with the Savion
system), were not replicated in this study. Whereas Dwolatzky found clear evidence for
the effectiveness of cognitive training after one month in global score and memory in
subjects with mild dementia, these effects were not demonstrated in the current study.
This could be due to a greater range of pre-intervention cognitive impairment of the
participants in our study, since we included participants with cognitive impairment
ranging from mild cognitive impairment (MCI) to mild and moderate dementia.
Nevertheless it should be noted that the analysis of results segmented by MMSE scores
for the cognitive outcome measures showed that whereas the high MMSE group
(MMSE score of 22-26) demonstrated only a decrease in the visual-spatial measure in
the cognitive training group compared to control (at one month), more significant
changes with a larger effect size were found in fact in the low MMSE group. These
included effects in global score and orientation at T1 evaluation, and effect in visual-
spatial measure at T3 evaluation.
Conversely, the low MMSE group demonstrated no effects in the reminiscence group
compared to control, while the high MMSE showed marginally significant effects with
medium effect size in global score and verbal function. Despite the limited samples size
which decrease the statistical power of the results, the difference in trends between the
two types of interventions might be ascribed to the nature of each intervention: whereas

79
cognitive training demands lower cognitive capabilities and can be applied using a very
low level of exercise (the Savion software supports the adjustment of difficulty level),
reminiscence therapy requires a reasonable ability for conversing and speaking
coherently in order to benefit from the intervention.
7.3 Limitations and future work
Despite addressing the limitations in previous studies, which were noted by
Subramanian and Woods (2012) and Bahar-Fuchs et al. (2013), this study is not free of
its own limitations. First, allocation to the groups was not blinded, and therefore
subjects' self report could have been influenced by their knowledge
of group assignment. Family members of subjects who were assigned to the
reminiscence group were also aware of the allocation, since they had to provide the
personal materials, and were therefore at the same risk for bias.
Second, the assessors were not blinded to the subjects’ condition, thus having a
potential bias on the evaluation. Of note though is that in the case of administering the
cognitive function evaluation using the Mindstreams tool, the evaluation process is
structured and is minimally dependent on the administrator's input, and therefore the
potential for bias in assessing the participants’ cognitive functioning is limited, although
still exist.
Third, the control group was not offered an alternative intervention in order to create a
"neutral" or "sham therapy" group. The fact that the control group was not engaged in a
one-on-one intervention could also serve as a bias factor, since it can be argued that the
personal contact between the subject and the person administering the intervention may
have a beneficial effect on the participants. However, since different effects were found
for each of the intervention groups in this study, it can be concluded that the personal
contact with the mediator was not the main factor for the improvements that were
found, but rather the intervention itself. Moreover, a previous study by Haslam et al.
(2010) which compared group intervention of reminiscence, individual reminiscence
and group participation in a social activity, found enhanced memory performance and
enhanced well being in the group-based interventions rather than in the individual
reminiscence group. This finding mitigates the effect of the one-on-one interaction.

80
Fourth, we could not reach the desired sample size of the study. This study was initially
planned to include 159 subjects for a treatment duration of six months. Due to various
challenges in the recruitment process (See Section 8.2 for more details), a final sample
size of only 95 participants out of 167 recruited patients actually entered the study and
underwent randomization (see chapter 6). Due to a high rate of withdrawal during the
study, only 81% of participants completed all three evaluations. In addition, missing
data further decreased the sample size. The limited sample size available for analysis
significantly weakened the statistical power of the data analysis. The duration of
treatment was also shortened to three months instead of the planned six months, as a
result of the various challenges we encountered. However, the treatment's duration and
frequency of this study is still more extensive than most of the RCT studies that
evaluated individualized reminiscence therapy for people suffering from dementia
(Ponnusamy and Woods ,2012).
Fifth, since this was an exploratory study, multiple statistical tests were conducted to
inquire possible effects. According to the recommendations for the analysis of these
types of studies, corrections to the p-value which was used were not done, since this
could decrease the power of finding and as a result major findings might be missed
(Bender & Lange, 2001; Perneger, 1998; Rothman, 1990) .As a result, the likelihood of
type I error was high, and thus interpretation of the results should be made cautiously.
Sixth, strict adherence to protocol was sometimes difficult to maintain, due to external
factors that were beyond our control. For example: evaluations that were postponed or
missed due to participants' absence, a change in the schedule of the day care center or a
family member who could not be reached for an interview. Also, missing treatments due
to similar reasons resulted in postponing or even cancelling scheduled evaluations.
Rocket attacks in the southern district of Israel during November 2012 led to 3 of the
adult day care centers located in Beer-Sheva being closed for 8 days. This had
implications on the study in terms of breaking the continuity of treatments, postponing
evaluations and placing more stress on participants.
Lastly, another limitation stemmed from the fact that the adult day care centers' staff
proposed a list of potential participants who they believed would meet the inclusion
criteria, and these participants were approached to participate in the study. Although all
the participants underwent screening to evaluate their suitability, other suitable
candidates may have been overlooked.

81
8. Impressions and Challenges
In addition to the statistical analyses, I collected data and personal observations, both
my own and those of the other research staff who administered the interventions to the
study participants. The main impressions from those observations are presented in this
chapter.
8.1 Impressions of the study
Although the participants’ initial responses to the computerized systems varied, a
common trend was noticed following the first few sessions. When first introduced to
either system most of the participants expressed concern over their lack of experience in
working with computers and that they may not succeed in working with the software.
After the second session most subjects were used to the software, knew what to expect
at any point and could operate the software themselves. The ease of use of the
reminiscence system by the subjects was also demonstrated in our previous study
(Sarne-Fleischmann & Tractinsky, 2008).
In general, most of the participants liked the interventions, many looked forward to their
bi-weekly treatments and a number even came to look for the research assistant
administering the intervention, or would wait for outside the computer room for their
turn. This was true particularly for the higher functioning subjects whose schedule was
more free, and who used to select their own activities at the day care center.
The following sections describe impressions of each group's intervention.
8.1.1 Reminiscence
A range of behaviors was observed in the reminiscence group. Some subjects were more
verbal and tended to converse fluently with the person administering the session. These
participants were satisfied with only a few objects during a session, and usually used
them as a trigger for additional associative memories. However, more introverted
participants tended to observe more objects during a session and were rather "bounded"
to the presented object. Consequently, the "optimal" number of objects for each
participant was, to some extent, dependent on the level of the participant's cognitive
function. Participants who suffered from significant memory impairment would relate to

82
the same objects every session, repeating the same stories, whereas participants with
higher cognitive function would feel bored when watching the same objects. Still, for
the participants who repeated the same stories, eventually new details that had not been
mentioned previously would emerge, triggered by the same objects.
Photos of deceased family members or friends usually provoked distressful feelings,
although some participants nevertheless wished to relate to them in their discussions.
It usually took more time for the participants in the reminiscence group to trust the
research staff member and to speak more freely about their memories (compared to the
participants in the cognitive training group). This was to be expected since the
reminiscence intervention involved more personal content, and therefore a basic level of
familiarity was required in order to establish a meaningful conversation. This may also
support the statistical finding of stronger effects in the reminiscence group after three
months of treatments than after one month of working with the system.
Adjusting the contents to the participant seemed to be one of the key factors for the
success of the computer-based system. The personal contents must include materials
that the participant would like to talk about and this should be constantly reappraised.
Family members, who in most cases served as the agents who provided the personal
materials, were not always aware of their relative's areas of interest. Therefore,
materials obtained from family members should be used as baseline objects, but there is
also a constant need for renewing the repository of personal contents, according to the
impressions gained in the course of treatments. Such monitoring and updating is likely
to increase the benefit of personalized reminiscence therapy.
Lastly, the computer-based reminiscence sessions must be handled carefully by an
appropriate and qualified administrator, who is sensitive enough to the participant's
needs, and is able to navigate the conversation according to the feedback received
during each session.
8.1.2 Cognitive training
Most of the subjects in the cognitive training group were able to use the system and
worked the computer themselves, with only a little assistance from supervisors. Some
also used the keyboard themselves when needed (in the case of typing numbers).

83
However, subjects usually preferred to use the touch screen interface, for all features
that were supported by the program.
Participants who expressed their satisfaction from using the system also seemed to
become more alert during the 3 months duration of the treatment sessions. One of the
participants defined the contribution of treatment as helping her to become more
attentive to questions she is being asked, and solving problems more easily in daily life.
Another subject's daughter has reported an improvement in her mother's behavior, as
she remembered to take her daily medicines.
Subjects usually became more confident and positive through working on the computer.
A few subjects refused to participate initially, but usually became more enthusiastic
later on.
Most of the participants had 1-2 areas of cognitive training that they liked most, and
one area they felt to be more challenging. Some of the participants preferred to work
more with the areas they felt they were more competent with, while some preferred to
work on those areas presenting a greater challenge.
It was sometimes difficult to keep participants focused at the training session, since as
the supervisors and the subject got to know each other better, the subjects would prefer
to talk about other matters. In such instances, time was allotted for discussion at the end
of the session.

84
8.2 Challenges
The study posed many administrative challenges due to the special characteristics of the
study population and the influence of many external factors.
The study demanded a long period of preparation, mainly because of the need to
coordinate with different centers and personnel that were not part of the research team,
and usually had their own busy timetable. For example: asking for informed consent of
participants required coordination between the signing researcher, the independent
specialist (who confirmed the competence of candidates), the staff of the day care
center, and the candidate’s availability (due to different days of attending the day care
center).
Also, the process of attaining approvals from the management of the day care center
was longer than expected in some, due to formal administrative requirements or
managerial decisions. For example, the manager of a large day care center canceled its
participation in the study just before the study was about to commence.
In addition, major efforts were made in approaching the candidates' family relatives and
introducing them to the study's goals and procedure, in order to obtain their approval for
participation. Presenting the study to groups of relatives at the day care centers as well
as individual telephonic approaches yielded a very modest response, and resulted in a
prolonged recruitment process.
Cooperation of family relatives remained a challenge throughout the study. This was
reflected many times in the need for recurrent requests to complete interviews for the
purpose of screening and periodic evaluations (T0, T1 and T3), which sometimes led to
missing evaluations where responses were delayed. Furthermore, numerous instances of
lack of cooperation were found in the reminiscence group, when subjects' relatives were
asked to provide personal contents for the intervention sessions. Lack of responsiveness
of the relatives after several attempts usually led to the exclusion of the subject from the
study (in cases where the subject could not provide the personal contents himself).
One of the study’s major challenges was to maintain the continuity of treatments,
adhering to the protocol requirements of two treatments per a week for each subject, for
a duration of three months. The difficulties stemmed from a range of reasons: First,
subjects' absence due to illness, medical tests, personal events and external carers'
unavailability (in the case where escort to the day care center was required). Secondly, a
changing schedule of activities at the day care centers (due to: trips, special lectures,

85
parties, etc) also affected the planned schedule of treatments, in addition to holiday
vacations when the centers were closed. Although we tried as much as possible to
address these changes and to reschedule treatment sessions , this was not always
possible due to the different days each subject attended the day care center, or to
unavailability of the computer rooms that in some centers were used for other purposes
on different days and hours.
All of these issues and challenges strained the study’s resources and required constant
monitoring and adjustments in study administration, prolonged its duration and
decreased the number of participants in the study and of data points (i.e., evaluations at
T1 and T3) of those who did participate in the study.
Lastly, the multiplicity of centers and their dispersed locations, the long duration of
treatments, and the large number of screening and evaluation tests needed for both
subjects and family caregivers, required considerable financial support. Unfortunately,
the support for this study was limited, only partially addressing its actual needs.
Working within these limited resources required occasionally creative solutions to
overcome the difficulties and to preserve the continuity of the study.

86
9. Conclusion
Reminiscence therapy and cognitive training are two different non-pharmacological
treatments that are used in dementia care. Due to methodological limitations, few
controlled studies and lack of sensitive assessment tools, there is still no clear evidence
as to whether these interventions provide significant benefits in patients with cognitive
impairment.
Increasingly, computerized systems are being designed for the treatment of patients with
dementia, while some of them are used to support existing treatment interventions.
The goal of this dissertation was to conduct a methodologically sound study to evaluate
the contribution of computer-based personalized reminiscence and cognitive training
interventions on the cognitive function and well-being of patients with dementia, as well
as the effects on family caregiver burden.
This study found some positive results for both computer-based reminiscence and
cognitive training interventions over an intervention period of three months compared to
a control group. These included improvements in some aspects of cognitive function in
the two intervention groups, and improvements in quality of life and the will to live
among the reminiscence group's participants. However, due to the limited sample size
available for final analysis these effects were insufficient to draw firm conclusions.
An interesting finding was the difference in the outcomes of each intervention, which
supports the benefits of the interventions themselves rather than the possible effect of
personal contact with a supervisor.
In light of our findings, we believe that these two computer-supported interventions
have potential as therapeutic modalities for elderly people with cognitive impairment
and dementia. Since computer-based systems improve the availability of these
interventions, patients may benefit from using them in their own homes with the support
of family members or personal caregivers. In addition, this would allow for ongoing
exposure to the programs and increase the possible clinical and research prospects of
these non-pharmacological interventions.

87
References
[1] Alm, N., Astell, A., Ellis, M., Dye, R., Gowans, G., & Campbell, J. (2004). A
cognitive prosthesis and communication support for people with dementia. Journal
of Neuropsychological Rehabilitation 14 (1&2), 117-134.
[2] Bahar-Fuchs, A., Clare, L. & Woods, B. (2013). Cognitive training and cognitive
rehabilitation for mild to moderate Alzheimer’s disease and vascular dementia.
Cochrane Database of Systematic Reviews, Issue 6.
[3] Baines, S., Saxby, P. & Ehlert, K. (1987). Reality orientation and reminiscence
therapy. A controlled cross-over study of elderly confused people. The British
Journal of Psychiatry 151, 222-231.
[4] Baumgarten, M., Battista, R., Infante-Rivard, C., Hanley, J., Becker, R. & Gauthier,
S. (1992). The psychological and physical health of family members caring for an
elderly person with dementia. Journal of Clinical Epidemiology, 45, 61–70.
[5] Bédard, M., Molloy, D. W., Squire, L., Dubois, S., Lever, J. A. & O'Donnell, M.
(2001). The Zarit Burden Interview: A New Short Version and Screening Version.
Gerontologist, 41, 652-657.
[6] Beinart, N., Weinman, J., Wade, D. & Brady, R. (2012). Caregiver burden and
psycho educational interventions in Alzheimer's disease: a review. Dementia and
Geriatric Cognitive Disorders Extra, 2(1), 638-48.
[7] Bender, R. & Lange, S. (2001). Adjusting for multiple testing-when and how?
Journal of Clinical Epidemiology, 54, 343–349.
[8] Birks, J. (2006). Cholinesterase inhibitors for Alzheimer's disease (2006). Cochrane
Database Systematic Reviews, 25 (1).
[9] Brodaty, H. & Arasaratnam, C. (2012). Meta-analysis of non pharmacological
interventions for neuropsychiatric symptoms of dementia. American Journal of
Psychiatry, 169, 946–953.
[10] Brodaty, H. & Donkin, M. (2009). Family caregivers of people with
dementia. Dialogues in Clinical Neuroscience, 11,217–228.

88
[11] Cahn-Weiner, D. A, Malloy, P. F., Rebok, G. W. & Ott, B. R. (2003). Results of
a randomized placebo-controlled study of memory training for mildly impaired
Alzheimer's disease patients. Applied Neuropsychology, 10(4), 215-223.
[12] Carmel, S. (2001). The will to live: gender differences among elderly persons.
Social Science and Medicine , 52, 949-958.
[13] Carmel, S. (2011). The will to live as an indicator of well-being and a predictor
of survival in old age. In: Poon, L. & Cohen-Mansfield, J. (Eds.), Understanding
well-being in the oldest-old (pp. 281-289). Cambridge: Cambridge University Press.
[14] Carswell, W. , McCullagh, P. J., Augusto, J. C, Martin, S., Mulvenna, M.
D., Zheng, H. et al. (2009). A review of the role of assistive technology for people
with dementia in the hours of darkness. Technology and health care 17(4), 281-304.
[15] Cerejeira, J., Lagarto, L. & Mukaetova-Ladinska, E. B. (2012). Behavioral and
psychological symptoms of dementia. Frontiers in Neurology 3, 73.
[16] Chertkow, H., Feldman, H. H., Jacova, C. & Massoud, F. (2013). Definitions of
dementia and predementia states in Alzheimer's disease and vascular cognitive
impairment: consensus from the Canadian conference on diagnosis of dementia.
Alzheimer's Research and Therapy, S(Suppl 1):S2; 1-8.
[17] Clare, L. & Woods, B. (2008). Cognitive rehabilitation and cognitive training
for early-stage Alzheimer’s disease and vascular dementia. The Cochrane Library;
Issue 4.
[18] Clare, L., Woods, R.T., Moniz-Cook E.D., Orrell, M. & Spector, A. (2003).
Cognitive rehabilitation and cognitive training for early stage Alzheimer’s disease
and vascular dementia. Cochrane Database of Systematic Reviews, Issue 4.
[19] Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).
Hillsdale, NJ: Lawrence Erlbaum Associates.
[20] Cohene, T., Baecker, R. M., Marziali, E., & Mindy, S. (2006). Memories of a
life: A design case study for Alzheimer’s disease. In J. Lazar (Ed.), Universal
Usability (pp. 357–487). Chichester: John Wiley and Sons.
[21] Courtney, C., Farrell, D., Gray, R., Hills, R., Lynch, L., Sellwood, E., et al.
(2004). Long-term donepezil treatment in 565 patients with Alzheimer's disease
(AD2000): randomized double-blind trial. Lancet 363, 2105-2115.

89
[22] Cummings, J.L., Mega, M., Gray, K., Rosenberg-Thompson, S., Carusi, D.A. &
Gornbein, J. (1994). The Neuropsychiatric Inventory: comprehensive assessment of
psychopathology in dementia. Neurology 44, 2308-2014.
[23] Doane, D.P. & Seward, L.E. (2011). Measuring Skewness: A Forgotten
Statistic? Journal of Statistics Education, 19(2),1-18.
[24] Dwolatzky, T., Dimant, L., Simon, E. S & Doniger G. M. (2010). Validity of a
short computerized assessment battery for moderate cognitive impairment and
dementia. International Psychogeriatrics, 22(5), 795-803.
[25] Dwolatzky, T., Whitehead, V., Doniger, G.M., Simon, E.S., Schweiger, A.,
Jaffe, D. et al. (2003). Validity of a novel computerized cognitive battery for mild
cognitive impairment. BMC Geriatrics 3, 4-16.
[26] Dwolatzky, T., Zilbershlag, Y., Friger, M. & Grinshpun, Y. Computerized
cognitive training in patients with mild dementia. (2009, July). Presented at: The
19th International Association of Gerontology and Geriatrics World Congress of
Gerontology and Geriatrics, Paris, France.
[27] Etters, L., Goodall, D. & Harrison, B.E. (2008). Caregiver burden among
dementia patient caregivers: a review of the literature. Journal of the American
Academy of Nurse Practitioners, 20(8), 423–428.
[28] Farina, E., Fioravanti, R., Chiavari, L., Imbornone, E., Alberoni, M., Pomati, S.
et al. (2002). Comparing two programs of cognitive training in Alzheimer's disease:
a pilot study. Acta Neurologica Scandinavica, 105, 365-371.
[29] Ferri, C. P., Prince, M., Brayne, C., Brodaty, H., Fratiglioni, L., Ganguli, M. et
al. (2005). Global prevalence of dementia: A Delphi consensus study. Lancet
366:2112–2117.
[30] Finkel, S. I, Costa E Silva, J., Cohen, G., Miller, S. & Sartorius, N. (1997)
Behavioural and psychological signs and symptoms of dementia: a consensus
statement on current knowledge and implications for research and treatment.
International Journal of Geriatric Psychiatry 12 (Issue 11), 1060-1061.
[31] Folstein, M. F., Folstein, S. E., McHugh, P. R. (1975). "Mini-Mental State": a
practical method for grading cognitive states of patients for the clinician. Journal of
Psychiatric Research 12, 189-98.

90
[32] Freedman, M., Leach, L., Kaplan, E., Delis, D., Shulman, K. & Winocur, G.
(1994). Clock drawing: a Neuropsychological Analysis. New York: Oxford
university press.
[33] Freeman, E., Clare, L., Savitch, N., Royan, L., Litherland, R., & Lindsay, M.
(2005). Improving website accessibility for people with early-stage dementia: A
preliminary investigation. Aging & Mental Health 9(5), 442-448.
[34] Gates, N., Sachdev, P., Fiatarone-Singh, M. & Valenzuela, M. (2011). Cognitive
and memory training in adults at risk of dementia: A Systematic Review. BMC
Geriatrics 11(1), 55-69.
[35] Gibson, F. What can reminiscence contribute to people with dementia? (1994).
In J. Bornat (Ed), Reminiscence reviewed: Evaluation, Achievements, Perspectives
(pp.46-60). Buckingham: Open University Press.
[36] Gitlin, L. N., Kales, H. C. & Lyketsos, C. G. (2012). Nonpharmacologic
management of behavioral symptoms in dementia. The Journal of the American
Medical Association, 308, 2020–2029.
[37] Goldwasser, A.N., Auerbach, S.M. & Harkins, S.W. (1987). Cognitive, affective
and behavioral effects of reminiscence group therapy on demented elderly.
International Journal of Aging and Human Development 25(3), 209-222.
[38] Günter, V. K., Schafer, P., Holzner, B. J., Kemmler, G. W. (2003). Long-term
improvements in cognitive performance through computer-assisted cognitive
training: a pilot study in a residential home for older people. Aging Mental Health,
7(3), 200-206.
[39] Haight, B. K., Gibson, F., Michel, Y. (2006) The Northern Ireland life
review/life storybook project for people with dementia, Alzheimer's & Dementia 2,
56-58.
[40] Haslam, C., Haslam, S. A., Jetten, J., Bevins, A., Ravenscroft, S. & Tonks, J.
(2010). The social treatment: the benefits of group interventions in residential care
settings. Psychology and Aging, 25, 157–167.
[41] Hofmann, M., Hock, C., Kühler, A., & Müller-Spahn, F. (1996). Interactive
computer-based cognitive training in patients with Alzheimer’s disease. Journal of
Psychiatric Research 30(6), 493-501.

91
[42] Holsapple, C. W., Pakath, R. & Sasidharan, S. (2005). A website interface
design framework for the cognitively impaired: A study in the context of
Alzheimer’s disease. Journal of Electronic Commerce Research 6(4), 291-303.
[43] http://www.alz.org/what-is-dementia.asp. Last accessed: September 2013.
[44] Jackson, A. (1991). To reminisce or not to reminisce. Irish Journal of
Psychological Medicine, 8(2), 147-148.
[45] Kinney, J. M., Kart, C. S., Murdoch, L. D., & Conley, C. J. (2004). Striving to
provide safety assistance for families of elders: The SAFE house project. Dementia,
3, 351-370.
[46] Lauriks, S., Reinersmann, A., Van der Roest, H. G., Meiland, F. J., Davies, R.
J., Moelaert, F., et al. (2007). Review of ICT-based services for identified unmet
needs in people with dementia. Ageing Research Reviews, 6(3), 223–46.
[47] Lawrence, V., Fossey, J., Ballard, C., Moniz-Cook, E. & Murray, J. (2012).
Improving quality of life for people with dementia in care homes: making
psychosocial interventions work. British Journal of Psychiatry, 201(5), 344-51.
[48] Lawton, M.P. & Brody, E.M. (1969). Assessment of older people: self-
maintaining and instrumental activities of daily living. Gerontologist, 9(3), 179-186.
[49] Logsdon, R. G., Gibbons, L. E., McCurry, S. M. & Teri, L. (1999). Quality of
life in Alzheimer's disease: patient and caregiver reports. Journal of mental health
and aging, 5, 21-32.
[50] LoPresti, E.F., Mihailidis, A., & Kirsch, N. (2004). Assistive technology for
cognitive rehabilitation: state of the art. Neuropsychological Rehabilitation, 14, 5-
39.
[51] McPherson, A., Furniss, F.G., Sdogati, C., Cesaroni, F., Tartaglini, B., &
Lindesay, J. (2001). Effects of individualized memory aids on the conversation of
persons with severe dementia: a pilot study. Aging & Mental Health 5(3), 289-294.
[52] Mioshi, E., Dawson, K., Mitchell, J., Arnold, R., & Hodges, J. R. (2006). The
Addenbrooke’s Cognitive Examination Revised (ACE-R): A brief cognitive test
battery for dementia screening. International Journal of Geriatric Psychiatry, 21,
1078–1085.

92
[53] Morgan, S. & Woods, R.T. (2010). Life review with people with dementia in
care homes: a preliminary randomized controlled trial. Non-pharmacological
Therapies in Dementia,1, 43–59.
[54] Morris, J. (1993). The CDR: current version and scoring rules. Neurology, 43,
2412-2413.
[55] Nomura, T. (2002). Evaluative research on reminiscence groups for people with
dementia. In: Webster, J. D. & Haight, B. K. (Eds) Critical advances in
reminiscence work: From theory to application (pp. 289-299). New York, NY, US:
Springer Publishing Co.
[56] O'Brien, J. T. & Burns, A. (2011). Clinical practice with anti-dementia drugs: a
revised (second) consensus statement from the British Association for
Psychopharmacology. J Psychopharmacology, 25(8), 997-1019.
[57] Perneger, T. V. (1998). What's wrong with Bonferroni adjustments, British
Medical Journal, 31, 1236-1238.
[58] Plassman, B. L., Langa, K. M., Fisher, G. G, Heeringa, S. G., Weir, D. R.,
Ofstedal, M. B., et al. (2007). Prevalence of dementia in the United States: The
aging, demographics, and memory study. Neuroepidemiology, 29(1–2), 125–32.
[59] Prince, M., Bryce, R., Albanese, E., Wimo, A., Ribeiro, W. & Ferri, C. P.
(2013). The global prevalence of dementia: A systematic review and meta analysis.
Alzheimer's & Dementia 9(1), 63-75. e2.
[60] Rothman, K. J. (1990). No adjustments are needed for multiple comparisons.
Epidemiology ,1(1), 43-6.
[61] Sarne-Fleischmann, V. & Tractinsky, N. (2008). Development and evaluation
of a personalized multimedia system for reminiscence therapy in Alzheimer’s
patients. Int. J. Social and Humanistic Computing, 1(1), 81–96.
[62] Schreiber, M., Lutz, K., Schweizer, A., Kalveram, K.Th. & Jäncke, L. (1998).
Development and Evaluation of an Interactive Computer-Based Training as a
Rehabilitation Tool for Dementia. Psychologische Beitraege, 40(1), 85-102.
[63] Schӧlzel-Dorenbos, C. J., Draskovic, I., Vernooij-Dassen, M. J. & OldeRikkert,
M. G. (2009). Quality of life and burden of spouses of Alzheimer disease patients.
Alzheimer Disease and Associated Disorders, 23, 171–177.

93
[64] Scogin, F. & McElreath, L. (1994). Efficacy of psychosocial treatments for
geriatric depression: a quantitative review. Journal of Consulting and Clinical
Psychology, 62, 69-74.
[65] Subramaniam, P. & Woods, B. (2010) Towards the therapeutic use of
information and communication technology in reminiscence work for people with
dementia: a systematic review, International Journal of Computers in Healthcare
1(2), 106 – 125.
[66] Subramaniam, P. & Woods B. (2012). The impact of individual reminiscence
therapy for people with dementia: systematic review. Expert Review of
Neurotherapeutics, 12(5), 545-555.
[67] Taylor, F. (2005). Care managers’ views on assistive technology. Journal of
Dementia Care, 13, 32-36.
[68] The Alzheimer’s Forum .http://www.alzforum.org. Last accessed: September
2013.
[69] The Story Table. http://www.storytable.com/html/home.html. Last accessed:
September 2013.
[70] Thies, W. & Bleiler, L.(2013). Alzheimer’s disease facts and figures.
Alzheimer's & Dementia 9, 208-245.
[71] Thorgrimsen, L., Schweitzer, P. & Orrell, M. (2002). Evaluating reminiscence
for people with dementia: a pilot study. The Arts in Psychotherapy, 29, 93–97.
[72] Topo, P., Mäki, O., Saarikalle, K., Clarke, N., Begley, E., Cahill, S., et al. (2004)
Assessment of a music-based multimedia program for people with dementia.
Dementia 3(3), 331-350.
[73] Vasse E., Vernooij-Dassen, M., Cantegreil, I., Franco, M., Dorenlot, P., Woods,
B. et al. (2012). Guidelines for psychosocial interventions in dementia care: a
European survey and comparison. Int. Journal of Geriatric Psychiatry, 27(1),40-48.
[74] Vernooij-Dassen, M., Vasse, E., Zuidema, S., Cohen-Mansfield, J. & Moyle, W.
(2010). Psychosocial interventions for dementia patients in long-term care.
International Psychogeriatrics, 22(7),1121-1128.
[75] Woods, B. (1994). Management of memory impairment in older people with
dementia. International Review of Psychiatry 6, 153–161.

94
[76] Woods, B., Spector, A. E, Jones, C. A, Orrell, M. & Davies, S. P. (2005).
Reminiscence therapy for dementia. Cochrane Database of Systematic Reviews,
Issue 2.
[77] Yesavage, J.A., Brink, T.L., Rose, T.L., Lum, O., Huang, V., Adey, M.B et al.
(1983). Development and validation of a geriatric depression screening scale: A
preliminary report. Journal of Psychiatric Research, 17, 37-49.

95
Appendices
Appendix A: Savion screens
Language - Synonyms
Math

96
Memory
Shapes

97
Appendix B: Mindstreams sample report and screens
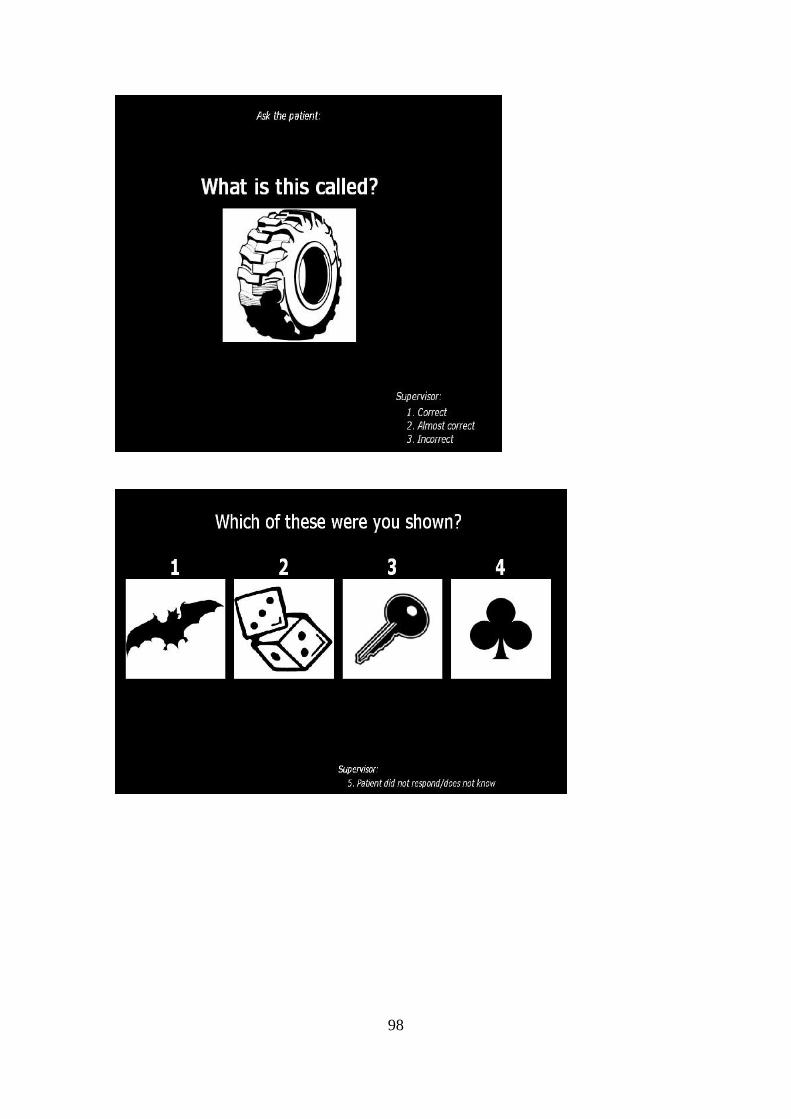
98

99

100
Appendix C: Normality test for dependent variables - results of skewness and Kurtois
measures for primary outcome measures
N Skewness Kurtosis
Statistic Statistic Std. Error Statistic Std. Error
Global_T1T0 78 .099 .272 -.130 .538
Orientation_T1T0 78 -.110 .272 -.144 .538
Verbal_T1T0 78 .770 .272 1.044 .538
Memory_T1T0 78 -.001 .272 .828 .538
Executive_T1T0 78 -.627 .272 1.707 .538
VisualSpatial_T1T0 78 .512 .272 .449 .538
Go-NoGo RT L1_T1T0 75 .595 .277 2.512 .548
Go-NoGo RT L2_T1T0 59 .654 .311 2.619 .613
Global_T3T0 77 .201 .274 1.301 .541
Orientation_T3T0 77 .217 .274 .852 .541
Verbal_T3T0 77 -.070 .274 .127 .541
Memory_T3T0 77 -.301 .274 1.779 .541
Executive_T3T0 77 .301 .274 1.576 .541
VisualSpatial_T3T0 77 .421 .274 .615 .541
Go-NoGo RT L1_T3T0 77 -.308 .274 .604 .541
Go-NoGo RT L2_T3T0 58 -.588 .314 3.137 .618
Valid N (listwise) 49
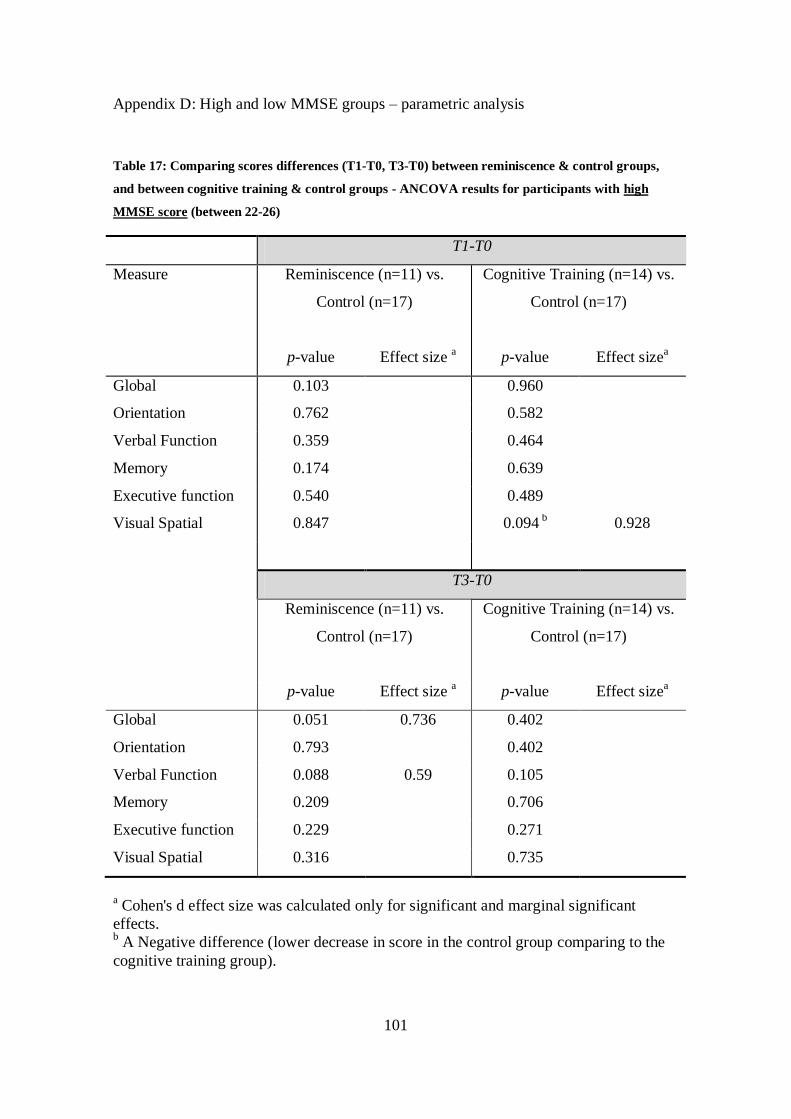
101
Appendix D: High and low MMSE groups – parametric analysis
Table 17: Comparing scores differences (T1-T0, T3-T0) between reminiscence & control groups,
and between cognitive training & control groups - ANCOVA results for participants with high
MMSE score (between 22-26)
T1-T0
Measure Reminiscence (n=11) vs.
Control (n=17)
Cognitive Training (n=14) vs.
Control (n=17)
p-value Effect size a p-value Effect size
a
Global 0.103 0.960
Orientation 0.762 0.582
Verbal Function 0.359 0.464
Memory 0.174 0.639
Executive function 0.540 0.489
Visual Spatial 0.847 0.094 b 0.928
T3-T0
Reminiscence (n=11) vs.
Control (n=17)
Cognitive Training (n=14) vs.
Control (n=17)
p-value Effect size a p-value Effect size
a
Global 0.051 0.736 0.402
Orientation 0.793 0.402
Verbal Function 0.088 0.59 0.105
Memory 0.209 0.706
Executive function 0.229 0.271
Visual Spatial 0.316 0.735
a Cohen's d effect size was calculated only for significant and marginal significant
effects. b A Negative difference (lower decrease in score in the control group comparing to the
cognitive training group).

102
Table 18: Comparing scores differences (T1-T0, T3-T0) between reminiscence & control groups,
and between cognitive training & control groups - ANCOVA results for participants with low
MMSE score(between 14-21).
T1-T0
Measure Reminiscence (n=12) vs.
Control (n=10)
Cognitive Training (n=14) vs.
Control (n=10)
p-value Effect size a p-value Effect size
a
Global 0.351 0.071 0.84
Orientation 0.429 0.042
Verbal Function 0.454 0.134
Memory 0.705 0.409
Executive function 0.386 0.331
Visual Spatial 0.977 0.898
T3-T0
Reminiscence (n=12) vs.
Control (n=10)
Cognitive Training (n=13) vs.
Control (n=10)
p-value Effect size a p-value Effect size
a
Global 0.685 0.447
Orientation 0.739 0.974
Verbal Function 0.741 0.276
Memory 0.351 0.316
Executive function 0.787 0.664
Visual Spatial 0.167 0.047* 0.82
a Cohen's d effect size was calculated only for significant and marginal significant
effects.

103
Appendix E: High and low MMSE groups – non parametric analysis
Table 19: Comparing 1 month differences between Reminiscence and control groups - Mann
Whitney test for participants with high MMSE score (between 22-26).
Measure Mean Rank Statistics
Reminiscence
(n=11)
Control
(n=17)
U Z Exact
p-value
Effect
sizea
Global 17.18 12.76 64 -1.388 0.175
Orientation 14.09 14.76 89 -0.230 0.853
Verbal 16.05 13.50 76.5 -0.820 0.430
Memory 13.50 12.53 60 -1.579 0.122
Executive 16.55 13.18 71 -1.059 0.306
Visual Spatial 14.09 14.76 89 -0.212 0.853
a Effect size was calculated only for significant and marginal significant effects.
Table 20: Comparing 3 months differences between Reminiscence and control groups - Mann
Whitney test for participants with high MMSE score(between 22-26).
Measure Mean Rank Statistics
Reminiscence
(n=11)
Control
(n=17)
U Z Exact
p-value
Effect
sizea
Global 18.27 12.06 52 -1.952 0.053 0.369
Orientation 14.73 14.35 91 -0.123 0.926
Verbal 16.73 13.06 69 -1.180 0.264
Memory 17.41 12.62 61.5 -1.510 0.134
Executive 17.18 12.76 64 -1.390 0.175
Visual Spatial 15.91 13.59 78 -0.730 0.487
a Effect size was calculated only for significant and marginal significant effects.

104
Table 21: Comparing 1 month differences between cognitive training and control groups - Mann
Whitney test for participants with high MMSE score (between 22-26).
Measure Mean Rank Statistics
CT
(n=14)
Control
(n=17)
U Z Exact
p-value
Effect
sizea
Global 14.64 17.12 100 -0.754 0.468
Orientation 16.68 15.44 109.5 -0.390 0. 710
Verbal 16.36 15.71 114 -0.210 0.860
Memory 14.93 16.88 104 -0.599 0.570
Executive 17.39 14.85 99.5 -0.774 0.444
Visual Spatial 11.04 20.09 49.5 -2.768 0.005**b
0.497
CT=Cognitive Training a Effect size was calculated only for significant and marginal significant effects. bNegative effect (lower decrease in score in the control group comparing to the cognitive training group)
Table 22: Comparing 3 months differences between cognitive training and control groups - Mann
Whitney test for participants with high MMSE score(between 22-26).
Measure Mean Rank Statistics
CT
(n=14)
Control
(n=17)
U Z Exact
p-value
Effect
sizea
Global 16.00 16.00 119 0 1.0
Orientation 17.25 14.97 101.5 -0.723 0.493
Verbal 17.89 14.44 92.5 -1.098 0.297
Memory 15.25 16.62 108.5 -0.419 0.681
Executive 17.39 14.85 99.5 -0.774 0.444
Visual Spatial 15.07 16.76 106 -0.518 0.625
CT=Cognitive Training a Effect size was calculated only for significant and marginal significant effects.

105
Table 23: Comparing 1 month differences between Reminiscence and control groups - Mann
Whitney test for participants with low MMSE score (between 14-21).
Measure Mean Rank Statistics
Reminiscence
(n=12)
Control
(n=10)
U Z Exact
p-value
Effect
sizea
Global 12.71 10.05 45.5 -0.956 0.346
Orientation 12.46 10.35 48.5 -0.799 0.456
Verbal 12.42 10.40 49 -0.743 0.497
Memory 12.21 10.65 51.5 -0.561 0.582
Executive 12.75 10.00 45 -0.990 0.346
Visual Spatial 12.00 10.90 54 -0.397 0.722
a Effect size was calculated only for significant and marginal significant effects.
Table 24: Comparing 3 months differences between Reminiscence and control groups - Mann
Whitney test for participants with low MMSE score (between 14-21).
Measure Mean Rank Statistics
Reminiscence
(n=12)
Control
(n=10)
U Z Exact
p-value
Effect
sizea
Global 12.75 10.00 45 -0.989 0.346
Orientation 12.21 10.65 51.5 -0.602 0.582
Verbal 12.04 10.85 53.5 -0.437 0.674
Memory 11.21 11.85 56.5 -0.232 0.821
Executive 11.58 11.40 59 -0.066 0.974
Visual Spatial 13.25 9.40 39 -1.390 0.180
a Effect size was calculated only for significant and marginal significant effects.

106
Table 25: Comparing 1 month differences between cognitive training and control groups - Mann
Whitney test for participants with low MMSE score (between 14-21).
Measure Mean Rank Statistics
CT
(n=14)
Control
(n=10)
U Z Exact
p-value
Effect
sizea
Global 15.14 8.80 33 -2.167 0.031 0.442
Orientation 15.00 9.00 35 -2.193 0.042 0.448
Verbal 14.64 9.50 40 -1.799 0.084 0.367
Memory 13.96 10.45 49.5 -1.203 0.235
Executive 13.43 11.20 57 -0.761 0.472
Visual Spatial 14.32 9.95 44.5 -1.498 0.138
CT=Cognitive Training a Effect size was calculated only for significant and marginal significant effects.
Table 26: Comparing 3 months differences between cognitive training and control groups - Mann
Whitney test for participants with low MMSE score(between 14-21).
Measure Mean Rank Statistics
CT
(n=13)
Control
(n=10)
U Z Exact
p-value
Effect
sizea
Global 13.88 9.55 40.5 -1.520 0.131
Orientation 12.77 11.00 55 -0.641 0.563
Verbal 13.23 10.40 49 -0.997 0.343
Memory 10.46 14.00 45 -1.245 0.232
Executive 13.62 9.90 44 -1.303 0.208
Visual Spatial 14.27 9.05 35.5 -1.857 0.067 0.387
CT=Cognitive Training a Effect size was calculated only for significant and marginal significant effects.

107
Appendix F: Screening and evaluation tools
GDS
Choose the best answer for how you have felt over the past week:
Score 1 0
No Yes 1. Are you basically satisfied with your life?
Yes No 2. Have you dropped many of your activities and interests?
Yes No 3. Do you feel that your life is empty?
Yes No 4. Do you often get bored?
No Yes 5. Are you in good spirits most of the time?
Yes No 6. Are you afraid that something bad is going to happen to you?
No Yes 7. Do you feel happy most of the time?
Yes No 8. Do you often feel helpless?
Yes No 9. Do you prefer to stay at home, rather than going out and
doing new things?
Yes No 10. Do you feel you have more problems with memory than
most?
No Yes 11. Do you think it is wonderful to be alive now?
Yes No 12. Do you feel pretty worthless the way you are now?
No Yes 13. Do you feel full of energy?
Yes No 14. Do you feel that your situation is hopeless?
Yes No 15. Do you think that most people are better off than you are?

2
התערבויות אישיות מבוססות מחשב עבור זקנים עם ירידה קוגניטיבית ודמנציה
"דוקטור לפילוסופיה"מחקר לשם מילוי חלקי של הדרישות לקבלת תואר
מאת
פליישמן-סרנה ורדית
הוגש לסינאט אוניברסיטת בן גוריון בנגב
3102ספטמבר ד"תשרי תשע
באר שבע

3
התערבויות אישיות מבוססות מחשב עבור זקנים עם ירידה קוגניטיבית ודמנציה
"דוקטור לפילוסופיה"מחקר לשם מילוי חלקי של הדרישות לקבלת תואר
מאת
פליישמן-סרנה ורדית
הוגש לסינאט אוניברסיטת בן גוריון בנגב
________________________________________יםאישור המנח
________________________________________
______________ש קרייטמן"אישור דיקן בית הספר ללימודי מחקר מתקדמים ע
3102 ספטמבר ד"תשרי תשע
באר שבע

4
:העבודה נעשתה בהדרכת
נעם טרקטינסקי' פרופ
ר צבי דוולצקי"ד
הנדסת תעשייה וניהול: במחלקה
הנדסה: בפקולטה

5
הצהרת תלמיד המחקר עם הגשת עבודת הדוקטור לשיפוט
(:אנא סמן: )בזאתה /אני החתום מטה מצהיר
להוציא עזרת ההדרכה שקיבלתי מאת , חיברתי את חיבורי בעצמי___
.ים/מנחה
___ החומר המדעי הנכלל בעבודה זו הינו פרי מחקרי מתקופת היותי
תלמיד/ת מחקר.
למעט עזרה , בעבודה נכלל חומר מחקרי שהוא פרי שיתוף עם אחרים___
לפי כך מצורפת בזאת הצהרה על .טכנית הנהוגה בעבודה ניסיונית
.שאושרה על ידם ומוגשת בהסכמתם, תרומתי ותרומת שותפי למחקר
_________________ה /שם התלמיד________ תאריך
__________חתימה

6
תקציר
דמנציה מוגדרת באופן רשמי כתסמונת רפואית של ירידה קוגניטיבית חמורה מספיק בכדי להפריע
בנוסף להשלכות הקוגניטיביות של (. 3' עמ, 3102, ועמיתיו Chertkow)לתפקוד חברתי או תעסוקתי
.םפסיכיאטריי-אנשים עם דמנציה חווים מגוון רחב של תסמינים נוירו, דמנציה
שלישים ממספר הלוקים ואחראית לכשני, מחלת האלצהיימר היא הגורם הנפוץ ביותר של דמנציה
כיום אין עדיין תרופה למחלת האלצהיימר או לרוב המחלות הגורמות לתסמונת . בתסמונת זו
ובמקרה הטוב הן יכולות לתת מענה , להתערבויות תרופתיות ישנה יעילות מוגבלת. הדמנציה
מינים יכולות להקל על תס, התערבויות פסיכו סוציאליות והקפדה על סגנון חיים. לתסמינים
.קוגניטיביים והתנהגותיים ולתת תמיכה למטפלים
מחקרים שבדקו . שתי התערבויות שאינו תרופתיות הינן טיפול בהעלאת זיכרונות ואימון קוגניטיבי
את ההשפעות של טיפולים אלו סברו כי בכוחן לשפר את התפקוד הקוגניטיבי באנשים עם דמנציה
מספר מועט של , בשל מגבלות מתודולוגיות, עם זאתיחד . ובמבוגרים עם סיכון לפתח דמנציה
אין עדיין עדות ברורה לתועלות משמעותיות , מחקרים מבוקרים וחוסר בכלי הערכה רגישים דיים
.של התערבויות אלו
נעשה תכנון של מערכות ממוחשבות לטיפול באנשים עם דמנציה הכולל אתרי , באופן גובר והולך
טכנולוגיה מסייעת ומערכות מחשב למטרות , ממוחשבים לניטור כלים, אינטרנט המספקים מידע
.טיפולים על בסיס רגשי בטיפול בדמנציה
מערכת ממוחשבת לטיפול : מחקר זה בדק שתי התערבויות מבוססות מחשב עבור חולי דמנציה
שתי ההתערבויות הושוו לקבוצת . ומערכת ממוחשבת לאימון קוגניטיבי, אישי בהעלאת זיכרונות
ההשוואה נעשתה באמצעות כלי נוירו פסיכולוגי ממוחשב המיועד להערכת התפקוד . ביקורת
.בנוסף נבדקו ההשפעות של ההתערבויות על בני משפחות החולים. הקוגניטיבי של החולים
גויסו למחקר ועברו , המתגוררים בקהילה, נבדקים מבוגרים עם ירידה קוגניטיבית או דמנציה 061
נבדקים שובצו באופן אקראי לאחת 59מתוכם . על מנת לקבוע את חומרת המחלההערכה ראשונית
אימון קוגניטיבי מבוסס ( 3); העלאת זיכרונות אישית מבוססת מחשב( 0: )משלוש הקבוצות הבאות
הנבדקים שקיבלו טיפול בהעלאת זיכרונות או אימון קוגניטיבי השתתפו . קבוצת ביקורת( 2); מחשב
. חודשים 2למשך תקופה של , י מטפל"שהועברו ע, דקות כל אחד 21בני , ועבשני טיפולים בשב
: וכללו, חודשי טיפולים 2ולאחר , לאחר חודש של טיפולים, ההערכות בוצעו לפני תחילת הטיפולים
, (NeuroTraxשל חברת , י שימוש במבחן המיינדסטרימס הממוחשב"ע)הערכת תפקוד קוגניטיבי
, AD-Qolי שימוש בשאלוני איכות חיים "ע)ות התנהגותיות אצל החולים רווחה פסיכולוגית והפרע
י שימוש בגרסה "ע)ועומס בקרב המטפל , (NPIוהפרעות התנהגותיות , WTLהרצון לחיות
(.Zarit Caregiver Burden Interviewהמקוצרת של שאלון עומס מטפל
משתתפים אשר בנוסף 59ונים לגבי וכלל נת, פרמטריות-ניתוח הנתונים נעשב בשיטות פרמטריות וא
לא נמצאו הבדלים בין . חודשים 2השלימו לפחות אחת מהערכות חודש או , לביצוע הערכות הבסיס
.הקבוצות מבחינת המשתנים הדמוגרפיים בתחילת המחקר
השפעות של הקבוצה נמצאו בניתוח , בהשוואה בין קבוצת העלאת הזיכרונות לקבוצת הביקורת
, נבדק-איכות חיים, global score: חודשים עבור המשתנים הבאים 2חודש ובזמן הפרמטרי בזמן

7
שיפור במדד זמן התגובה . חודשים 2פרמטרי בזמן -שיפורים אלו נמצאו גם בניתוח א. והרצון לחיות
Go-NoGo RT L1 בעוד ששיפור בעומס המטפל , נמצא רק בהערכת חודש בשיטה הפרמטרית
(enZarit Caregiver's Burd ) ובהפרעות ההתנהגותיות(NPI ) חודשים 2נמצאו רק בהערכות
2הייתה תאימות גבוהה יותר בין שתי שיטות הניתוח בהערכת , באופן כללי. פרמטרית-בשיטה א
.חודשים יחסית להערכת חודש
היות וההשפעה , נצפתה מגמה הפוכה, בהשוואת קבוצת האימון הקוגניטיבי מול קבוצת הביקורת
השפעה זו הייתה מועטה והתייחסה בעיקר למדדים . ה נמצאה רק בהערכת חודששל הקבוצ
תאימות בין שתי שיטות הניתוח . NoGo RT L1-Goזמן תגובה -ו orientation ,verbal: הבאים
.orientation-נמצאה רק עבור מדד ה
עבור שתי ההתערבויות מבוססות המחשב בהשוואה חיוביותלמרות שהמחקר מצא תוצאות
ההשפעות שנמצאו , בשל גודלו המצומצם של המדגם עליו בוצע הניתוח הסופי, לקבוצת הביקורת
נדרשים מחקרים מבוקרים אקראית נוספים , לפיכך. אינן מספיקות להסקת מסקנות חד משמעיות
ים שנמצאו בין שני סוגי ההתערבויות ראוי כי ההבדלים המעניינ, בנוסף. בעלי מדגם רחב יותר
.ייחקרו לעומק יותר
-אינטראקצית אדם, אימון קוגניטיבי, העלאת זיכרונות, מחלת אלצהיימר, דמנציה: מילות מפתח
תפקוד , התערבויות מוכוונות רגש, טכנולוגיה מסייעת, התערבויות פסיכו סוציאליות, מחשב
.קוגניטיבי







