
Clinical Radiology (1990) 42, 244-249
Chest Radiographs After Permanent Pacing. Are They Really Necessary? D. GRIER, P. G. COOK and G. G. H A R T N E L L
Department of Radiodiagnosis, Bristol Royal Infirmary, Bristol
The chest radiographs of 600 consecutive patients undergoing insertion of a permanent cardiac pacemaker were reviewed to determine the incidence and nature of abnormalities present.
Abnormalities were detected on the chest radiographs of 131 patients (21.8%). Unsatisfac- tory electrode tip position and other features related to the electrode wire were commonest (14.4%). Complications related to the lungs and pleura were present in 5.5%, and those related to the generator and pouch least frequent (1.9%).
Complications occurred more frequently following installation of a replacement system (48.3%) compared to new systems (17.2%). Important complications not initially detected included pneumothorax (8/15) and poor electrode loop (26/27).
Chest radiographs following permanent cardiac pacing frequently demonstrate significant abnormalities whose detection is improved by awareness of their incidence and nature. Grier, D., Cook, P.G. & Hartnell, G.G. (1990). ClinicalRadiology 42, 244 249. Chest Radiographs After Permanent Pacing. Are They Really Necessary?
Permanent cardiac pacemaker insertion is a common procedure (9000 systems installed annually in the United Kingdom) and over 300 new systems are implanted annually at the Bristol Royal Infirmary. Many complica- tions may occur, related either to the procedure of insertion or the presence of foreign material in the body (Steiner and Tegtmeyer; 1983).
It is common practice to obtain one or more chest radiographs following insertion of the pacemaker to show satisfactory electrode position, and to demonstrate com- plications such as a pneumothorax. However, there is little published data relating specifically to the value of chest radiographs, in terms of the number and type of abnormalities demonstrated, and it is sometimes felt that these are often unnecessary.
As all investigations involving ionizing radiation need to be justified, both medically and financially, we reviewed the incidence and nature of pacing complica- tions identified on the chest radiograph and their poten- tial importance for patient management.
MATERIALS AND M E T H O D S
The chest radiographs of 600 consecutive patients undergoing permanent cardiac pacemaker insertion at Bristol Royal Infirmary were retrospectively reviewed. All pacemakers were inserted by percutaneous puncture of the subclavian vein, and fashioning of a superficial pouch for the generator in the sub-cutaneous tissues of the upper chest wall. PA and lateral chest radiographs were routinely obtained after insertion and further radio- graphs performed at the discretion of the clinician.
The radiographs were read by two of us (D. G. and P. C.). Note was made of Whether the pacemaker was the first system or a replacement system and on which side it was installed. Abnormalities related to the pacing wire or its insertion were recorded.
Correspondence to: Dr D. Grier, Department of Radiodiagnosis, Bristol Royal Infirmary, Marlborough Street, Bristol BS2 8HW.
Electrode tip position was considered satisfactory when directed antero-inferiorly at the apex of the right ventricle, and unsatisfactory if the tip was in the right atrium, superior or inferior vena cavae, pulmonary artery, or in a sub-optimal position in the right ventricle (i.e. directed posteriorly or superiorly).
A good pacing wire loop was present when the wire crossed the right atrium, with a gentle curve whose apex was directed inferiorly and to the right, and without kinks or subsidiary loops. If the electrode passed through the atrium into the right ventricle with a large radius of curvature it was considered taut, and if excess wire caused 'prolapse' or subsidiary loops or kinks occurred it was considered redundant.
The contemporary clinical notes and radiological reports relating to these patients were reviewed to determine the number of complications detected at the time the radiograph was taken and their significance for patient management.
RESULTS
The majority of first systems were installed on the left side, but replacement systems were more evenly divided between left and right (Table 1).
Abnormalities were detected on the radiographs oft 31 patients (21.8%) (Table 2). Complications were seen on the radiographs of 88 of 512 (17.2%) of patients undergo" ing installation of a first system, and in 43 of 89 (48.3%) patients in whom a replacement system was inserted.
Table 1 - Site and nature of pacemaker system inserted J
Left (%) Right (%) Total (%)
First system 468 (78.0) 43 (7.2) 511 (85.2) Replacement 44 (7.3) 45 (7.5) 89 (I4.8~ system Total 512 (85.3) 88 (14.7) 600 (100.0)
RADIOGRAPHY OF PACING 245
Table 2 - Complications detected on chest radiographs
Complication Number (%) f
pulmonary and pleural t~eurnothorax 15 (2.6) pleurat effusion 8 (1.3) Atelectasis 6 (1.0) Mediastinal emphysema 2 (0.3) Subcutaneous emphysema 2 (0.3)
Sub-total 33 (5.5)
pacing wire Unsatisfactory position 33 (5.5) Multiple wires 17 (2.7) Redundant loop 15 (2.6) Taut loop 12 (2.0) Fractured wire 8 (1.3) Myocardial perforation 2 (0.3)
Sub-total 87 (14.4)
Generator and pouch Air-fluid level Box twiddler
Sub-total
Total
6 (1.0) 5 (0.9)
11 (1.9)
131 (21.8)
Pneumothorax was the commonest pulmonary or pleural abnormality (15 cases; 2.6%), accompanied by mediastinal and sub-cutaneous emphysema in two cases, and shift of the mediastinum in one case.
Pacing wire abnormalities were the most numerous complication detected. Electrode tip mal-position occurred in 33 patients (5.5%), with inappropriate sites including the superior and inferior vena cavae, right atrium and lying free in the right ventricle or the pulmonary artery. Loop abnormalities (taut and redun- dant loops) were found in 27 patients, fractured elec- trodes in eight patients and myocardial perforation in two patients.
Six patients had an air-fluid level in the generator pouch. In a further five patients a subsequent radiograph showed that the pacemaker generator had rotated con- siderably within its pouch when compared to the film taken immediately afterinsertion.
Review of the clinical notes and radiological reports was possible in 102/131 (77.9%) of the patients with complications. An abnormality was commented on in 39 (38.2%) of patients, either in the radiological report (34 cases; 33.3%) or in the clinical notes (21 cases; 20.6%). Several major complications were not detected (Table 3).
Three patients in whom we identified a loop abnor- mality re-presented within, 3 weeks of pacemaker inser- tion with failure to pace. Fluoroscopy demonstrated electrode tip displacement which required repositioning. All patients with an air-fluid level in the generator pouch required treatment for infection at this site (although none required removal of the pacemaker system). Only one of the 15 patients in whom a pneumothorax was
detected needed intercostal drainage because of a large symptomatic pneumothorax with mediastinal shift.
In one patient the electrode passed from the left subclavian vein via a persistent left sided superior vena cava through the coronary sinus before entering the right atrium and ventricle. Though not a complication as such, this unusual course may be mistaken for an abnormality if not recognized.
DISCUSSION
A wide range of complications may occur following insertion of permanent cardiac pacemakers. Many of these are welt known and have been previously described
(a)
Table 3 - Major complications not detected
COmplication Not detected (%)
~neurnothorax 8/15 (53.3) Oor loop 26/27 (96.3)
Air-fluid level 6/6 (100.0) t~°x twiddler 5/5 (100.0)
(b)
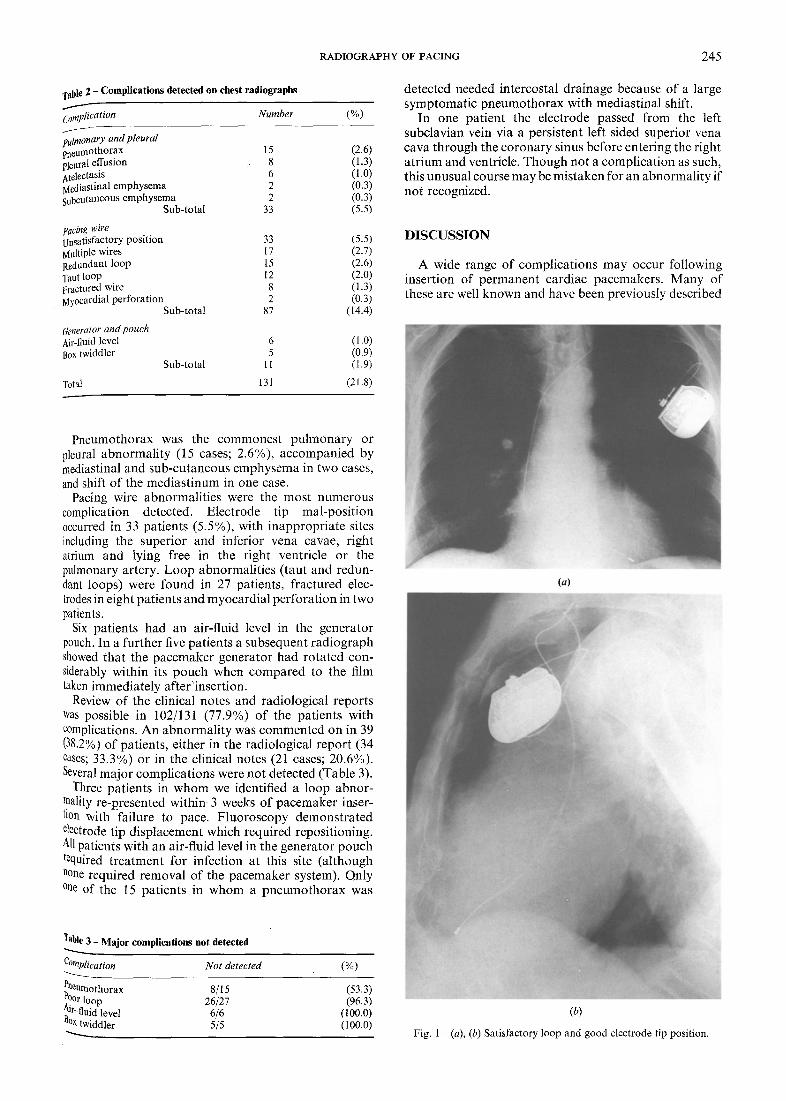
Fig. 1 - (a), (b) Satisfactory loop and good electrode tip position.
246 CLINICAL RADIOLOGY
(a) (a)
OA
[
(b)
DB
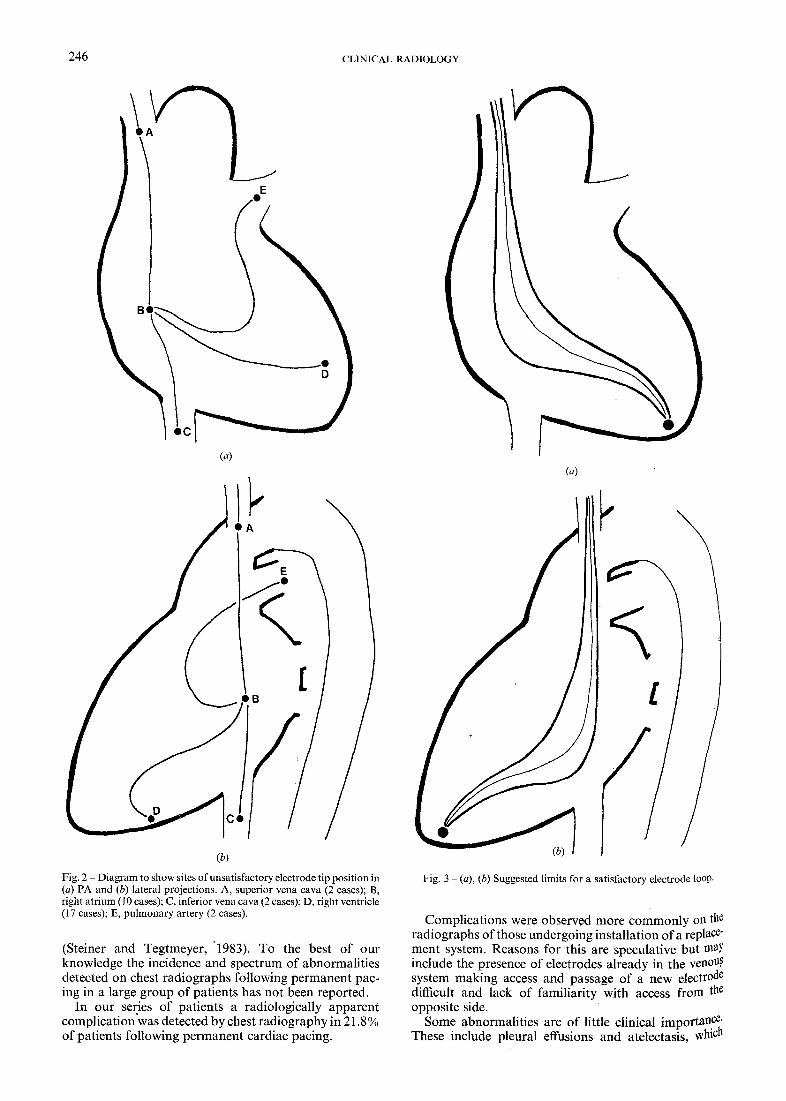
Fig. 2 - Diagram to show sites of unsatisfactory electrode tip position in (a) PA and (b) lateral projections. A, superior vena cava (2 cases); B, right atrium (10 cases); C, inferior vena cava (2 cases); D, right ventricle (17 cases); E, pulmonary artery (2 cases).
(Steiner and Tegtmeyer, ~1983). To the best of our knowledge the incidence and spectrum of abnormalities detected on chest radiographs following permanent pac- ing in a large group of patients has not been reported.
In our series of patients a radiologically apparent complication'was detected by chest radiography in 21.8 % of patients following permanent cardiac pacing.
(b)
Fig. 3 - (a), (b) Suggested limits for a satisfactory electrode loop.
Complications were observed more commonly on the radiographs of those undergoing installation of a replace" ment system. Reasons for this are speculative but may include the presence of electrodes already in the venoU.S system making access and passage of a new electrode difficult and lack of familiarity with access from the opposite side.
Some abnormalities are of little clinical importance. These include pleural effusions and atelectasis, which
RADIOGRAPHY OF PACING 247
require no specific therapy, and probably reflect pleural trauma at the time of insertion or local hypoventilation secondary to discomfort on breathing.
The incidence ofpneumothorax (2.6%) compares with tl0 to 6% in other reported series for central venous cannulation (Mitchell and Clark, 1979), and is the commonest single complication of the procedure of pacemaker insertion. Pneumothoraces in our series were not initially detected for two main reasons. In two patients the pneumothorax was on the opposite side to the pacemaker system; review of the notes revealed an unsuccessful attempt on this side. The common practice 0frequesting a penetrated radiograph to ensure adequate visualization of the electrode tip frequently obliterates lung markings making a pneumothorax more difficult, or impossible to detect. Sub-cutaneous or mediastinal emphysema should alert one to the possibility of a pneumothorax, and ensure that the lungs are adequately demonstrated. However, as only one pneumothorax (under tension) required intercostal drainage, detection of clinically asymptomatic pneumothoraces may be of little importance.
The presence of considerable subcutaneous emphy- sema may interrupt the circuit of a unipolar system leading to an abnormally high pacing threshold or failure to pace (Hearne and Maloney, 1982; Smith et al., 1985).
Ideally the electrode tip should be wedged between the trabeculae at the apex of the right ventricle. Here it is less likely to become displaced and maximal endocardial contact occurs allowing a good pacing threshold (Hall and Rosenbaum, 1971). In this position the tip is directed anteriorly and inferiorly on the lateral radiograph and to the left on the PA radiograph (Dunbar, 1984) (Fig. la, b). All other sites should be considered poor though it is appreciated that in some patients this optimal position
(a)
(b)
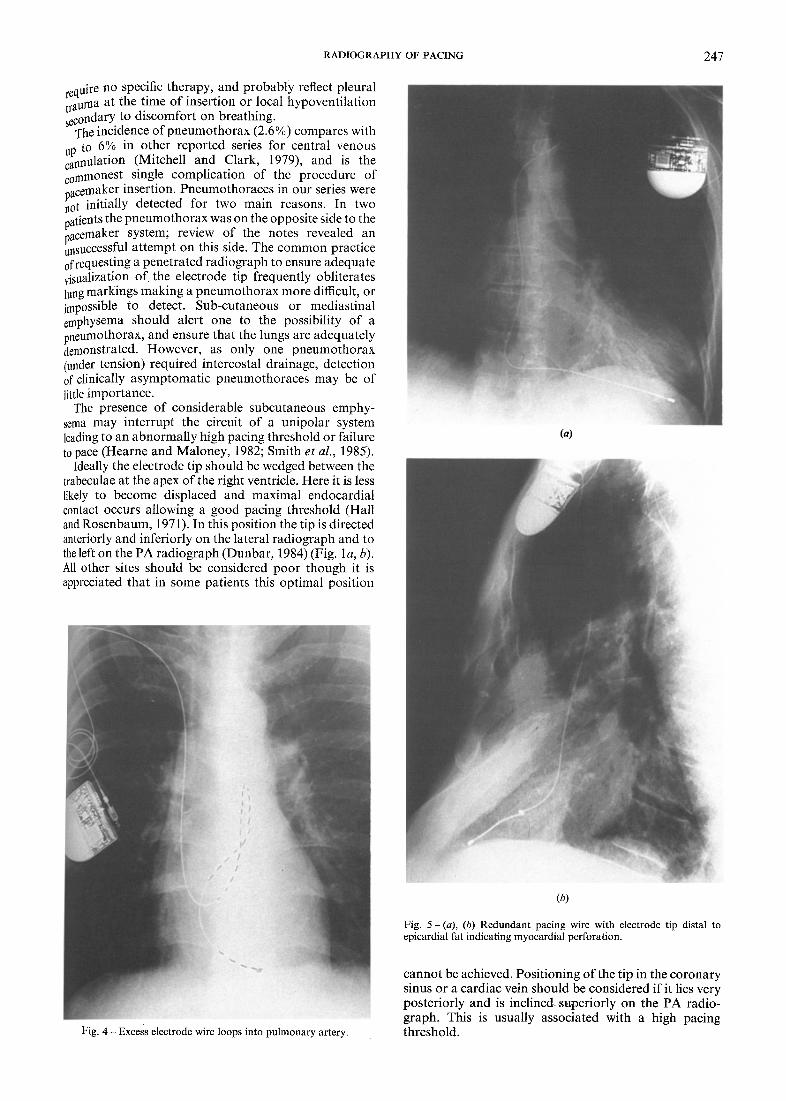
Fig. 5 - (a), (b) Redundant pacing wire with electrode tip distal to epicardial fat indicating myocardial perforation.
Fig. 4 = Excess electrode wire loops into pulmonary artery.
cannot be achieved. Positioning of the tip in the coronary sinus or a cardiac vein should be considered if it lies very posteriorly and is inclined~superiorly on the PA radio- graph. This is usually associated with a high pacing threshold.
248 CLINICAL RADIOLOGY
Unsatisfactory electrode tip position was detected in our series in 5.5% of cases (Fig. 2a, b). Another study reported an incidence of 7.7% for poor electrode position (Kaul et al., 1980). However, these figures do not distinguish between those which become displaced fol- lowing insertion but before the radiograph is obtained, and those initially poorly placed. In addition to early displacement a high pacing threshold may result.
A 'poor loop' appears to be under-recognized by radiologists and clinicians alike, but is important because of the potential complications that may ensue (Steiner and Morse, 1978; Steiner & Tegtmeyer, 1983). The electrode should curve smoothly to the left through the right atrium and continue inferiorly and leftwards in the right ventricle. There should be no kinks or secondary loops, or 'prolapse' of the electrode inferiorly or to the right in the right atrium (Fig. 3a, b).
Insufficient electrode length within the great veins and right heart produces a 'taut' loop with the possibility of early tip displacement following implantation (11.1% of all poor loops in this series). Redundant electrode (Fig. 4)
may predispose to tip displacement and exert undue pressure on the endocardium leading tO myocardial penetration and perforation (0.3 % in our ~eries). If the tip of the electrode lies within 3 mm of the epicardial fat myocardial penetration has occurred and if it lies within or beyond the epicardial fat perforation has occurred (Steiner & Tegtmeyer, 1983) (Fig. 5). A poor loop may also lead to functional and mechanical tricuspid valve abnormalities (Gibson et aI., 1980).
Despite the use of newer alloys, electrode fracture is still a significant cause of early system failure, and may be detected on the chest radiograph provided that the two ends are separated (Fig. 6). Detection may be difficult however, if the ends remain opposed (Varrriale et al.,
(a)
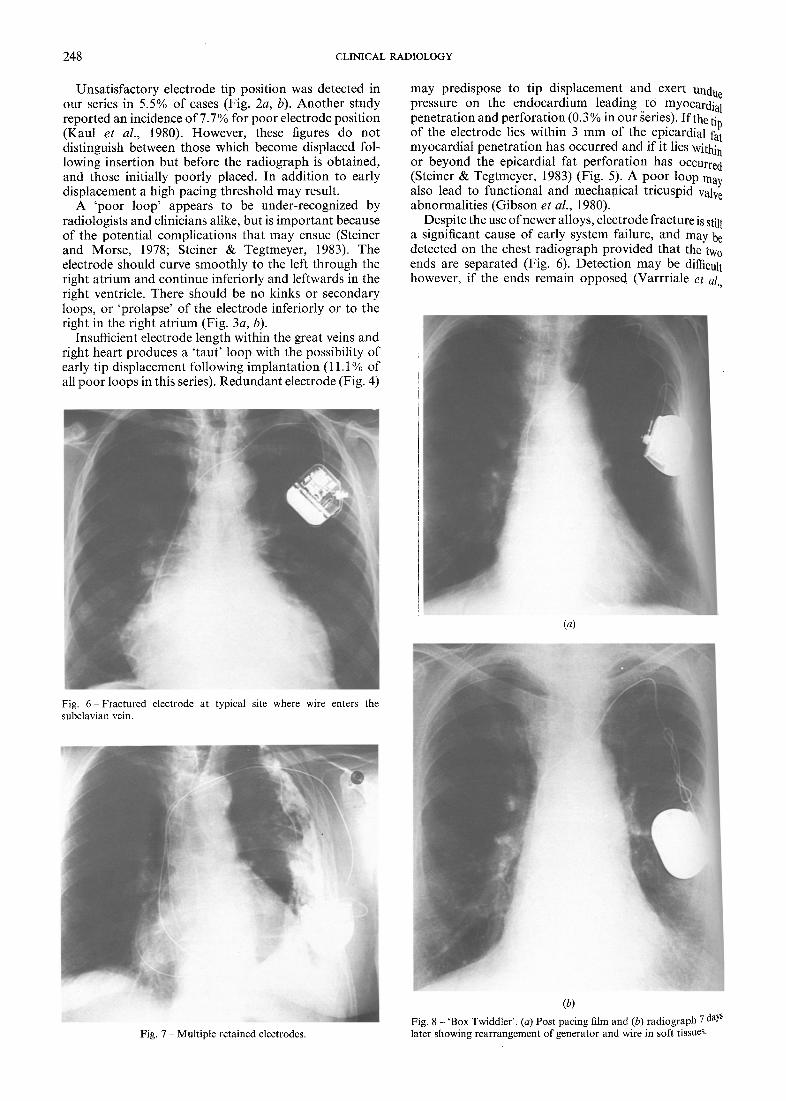
Fig. 6 Fractured electrode at typical site where wire enters the subclavian vein.
Fig. 7 Multiple retained electrodes.
(b) Fig. 8 - 'Box Twiddler'. (a) Post pacing film and (b) radiograph 7 dayS later showing rearrangement of generator and wire in soft tissues-

RADIOGRAPHY OF PACING 249
1982). ECG leads and clips may also obscure a fractured wire.
Multiple retained wires are a common finding, often indicating previous infection or rising thresholds; four was the maximum number detected in one patient in our series (Fig. 7). It is generally considered unnecessary to remove these surgically unless infected (Rettig et al., 1979), but multiple leads may increase the risk of thrombo-embolic disease (Kinney et al., 1979; Gundersen et al., 1982).
The presence of an air-fluid level in the pacemaker pouch (1.0%) was associated with infection in all cases. Other series have reported infection rates of between 0.13% and 12.6% (Anonymous, 1986), but the associ- ation with an air fluid level has not been described.
The pacemaker box 'twiddler' manipulates the genera- tor within its pouch (either consciously or not) and may be recognized on serial radiographs by a change in orientation of the generator and electrode in the chest wall (Fig. 8) (Weiss and Lorber, 1987). It is important to detect as reeling in or out of the electrode may occur leading to tip displacement or myocardial penetration, and in extreme cases a knot may be tied in the electrode leading to fracture and failure to pace.
Our study indicates that chest radiographs following permanent cardiac pacemaker insertion are justified as they demonstrate a significant number of important abnormalities, though many of these are not noted at the time. Awareness of these complications amongst clini- cians and radiologists is poor and needs improvement to allow their more frequent detection and to permit appropriate management.
Following insertion of a permanent cardiac pace- maker, PA and lateral radiographs which are not over- exposed should be obtained. If the tip of the wire is not clearly visible a penetrated PA film is also required.
REFERENCES
Anonymous (1986) Editorial. Preventing pacemaker infection. Lancet, 537 538.
Dunbar, RD (1984). Radiologic appearance of compromised thoracic catheters, tubes and wires. Radiologic Clinics of North America, 22, 699-722.
Gibson, TC, Davidson, RC & DeSilvey, DL (1980). Presumptive tricuspid valve malfunction induced by a pacemaker lead; A case report and review of the literature. PACE, 3, 88 95.
Gundersen, T, Abrahamsen, AM & Jorgensen, I (1982). Thrombosis of superior vena cava as a complication of transvenous pacemaker treatment. Acta Mediea Scandinavia, 212, 85-88.
Hall, WM & Rosenbaum, HD (1971). The radiology of cardiac pacemakers. Radiologic Clinics of North America, 9, 343 353.
Hearne, SF & Maloney, JD (1982). Pacemaker system failure secondary to air entrapment within the pulse generator pocket. Chest, 82, 651 654.
Kaul, TK, Macfarlane, PW, Thomson, RM & Bain, WH (1980). An analysis of electrocardiographic, radiographic, and vectorcardio- graphic findings in patients with implanted cardiac pacemakers. American Heart Journal, 99, 686 693.
Kinney, EL, Allen, RP, Weidner, WA, Pierce, S, Leaman, DM & Zellis, RF (1979). Recurrent pulmonary emboli secondary to right atrial thrombus around a permanent pacing catheter; A case report and review of the literature. PACE, 2, 196 202.
Mitchell, SE & Clark, RA (1979). Complications of central venous catheterization. American Journal of Roentgenology, 133, 467-476.
Rettig, G, Doenecke, P, Sen, S, Volkmer, I & Bette, L (1979). Complications with retained transvenous pacemaker electrodes. American Heart Journal, 98, 587 593.
Smith, SA, Weissberg, PL & Tan, L (1985). Permanent pacemaker failure due to surgical emphysema. British Heart Journal, 54, 220- 221.
Steiner, RM & Morse, D (1978). The radiology of cardiac pacemakers. Journal of the American Medical Association, 240, 2574-2576.
Steiner, RM & Tegtmeyer, CJ (1983). The radiology of cardiac pacemakers. Cardiovascular Clinics, 14, 63 95.
Varriale, P, Kwa, RP & Vyas, P (1982). The 'Lead Tug' sign for the diagnosis of early and inapparent lead fracture. Chest, 82, 787-788.
Weiss, D & Lorber, A (1987). Pacemaker twiddler's syndrome. International Journal of Cardiology, 15, 357 360.
![Large Scale Automated Reading of Frontal and Lateral Chest ... · classification of thoracic diseases in chest radiographs. arXiv preprint arXiv:1711.08760, 2017. [4] Ivo M Baltruschat,](https://cdn.vdocuments.mx/doc/165x107/5f9b65946fb17324741f211a/large-scale-automated-reading-of-frontal-and-lateral-chest-classification-of.jpg)


![A chest radiograph scoring system in ... - BMC Medical Imagingdata collected in epidemiological studies of acute respira-tory infections [7]. For example, chest radiographs are a component](https://cdn.vdocuments.mx/doc/165x107/611d2ab1b132b339a353139f/a-chest-radiograph-scoring-system-in-bmc-medical-imaging-data-collected-in.jpg)



