Download - Cerebellar cyst a case on mri

Cerebellar cyst: A case on MRI
Dr Rekha khare
MD. Radiology

Case presentation
• A young asian man about 22year came for MRI
• Clinical presentation was in favor of
Cerebellar dysfunction :
Ataxia/ incordination/ gait disturbance
Headache

Investigations
• His routine lab investigations Blood & Urine were with in normal limit
• MRI findings in different sequences:
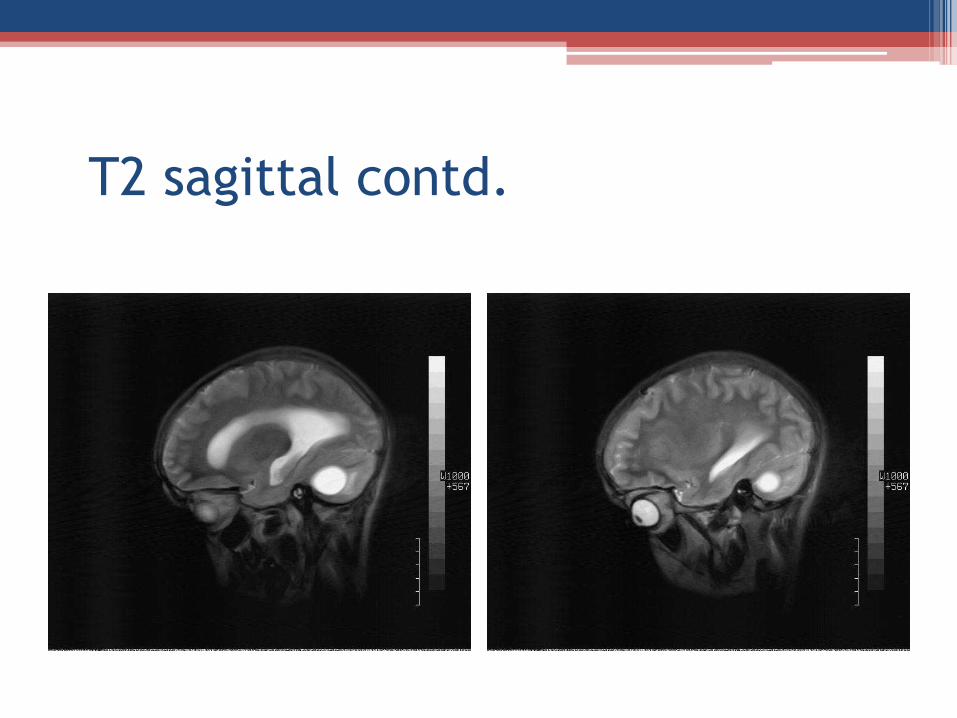
A large left cerebellar cystic mass with non enhanced wall. Cyst is with a small mural nodule vividly enhanced and with flow voids. Cyst is crossing midline and compressing IV ventricle so causing dilatation of 3rd and lateral ventricleImpression: left cerebellar cyst crossing midline
and causing hydrocephalus
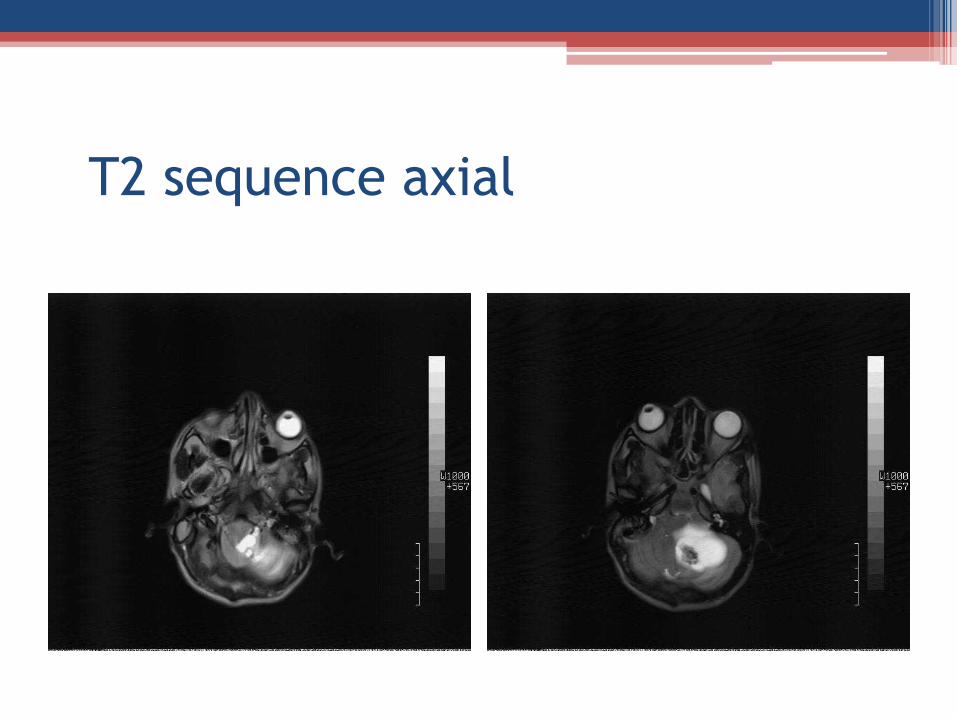
T2 sequence axial

T2 axial contd.

T2 axial contd.
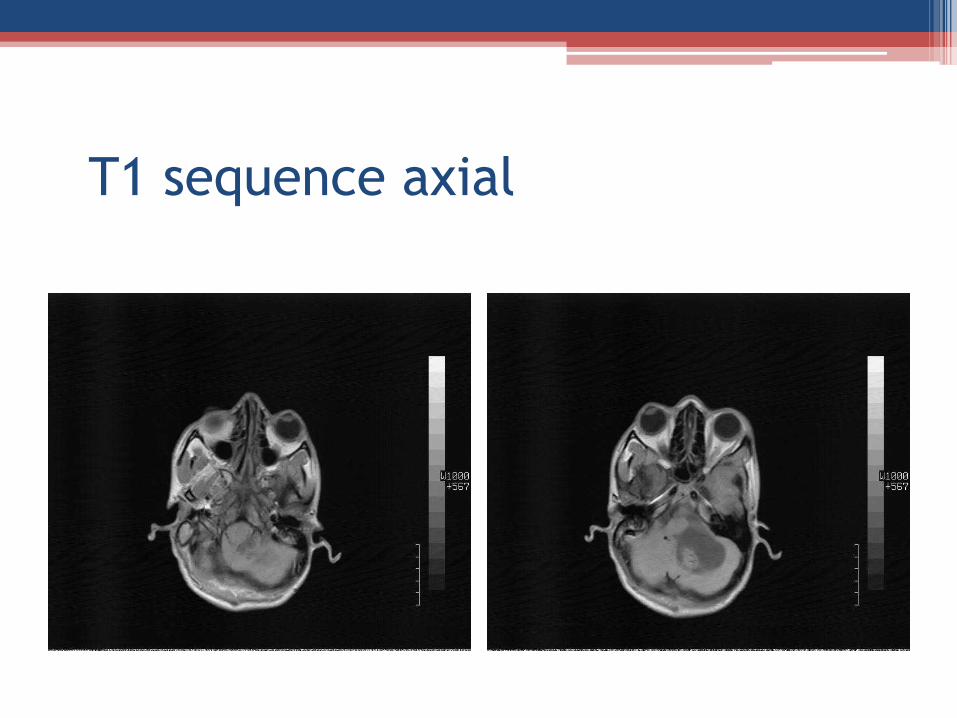
T1 sequence axial

T1 axial contd.

T1 axial contd.

Flair sequence

Flair contd.

Flair contd.

GRE sequence
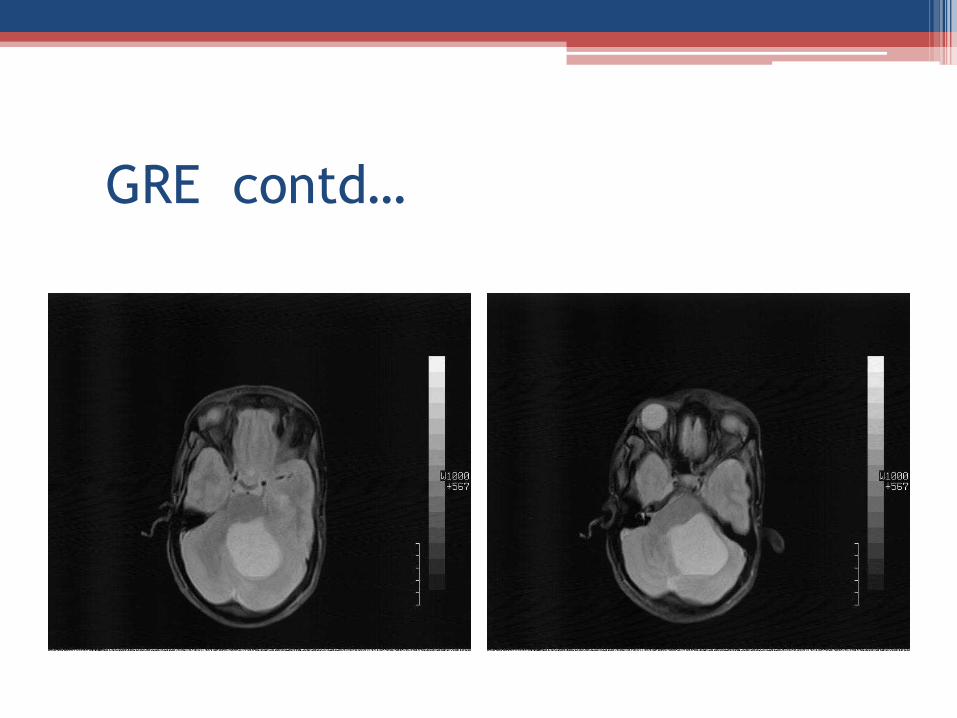
GRE contd…

GRE contd.

T2 sequence sagittal

T2 sagittal contd.

T2 sagittal contd.
T2 sagittal contd.

T1 sequence with contrast

T1 with contrast contd.

T1 with contrast contd.
D/D Cerebellar cyst
• Haemangioblastoma
• Astrocytoma
• Sub acute infarction
• Vascular lesion
• Adult Meduloblastoma – rare much more solid
• Metastasis –usually old with primary

Haemangioblastoma
Cushing and Bailey introduced the term Haemangioblastoma in 1928
Clinical symptoms:Headache-70%Hydrocephalus /ICH- 50%Cerebellar dysfunction- 50-60%altered mental state-10%
Polycythemia due to erythropoietin production occurs in 5-40%
SYMPTOMS DEPENDS ON ANATOMIC LOCALIZATION

Haemangioblastoma
• It accounts for 1% of all intracranial tumor, in isolation in 80% but is linked with
Von Hippel Lindau syndrome
• Most common in cerebellum
• In adult between 30-65% earlier withVHL
• Male : Female :: 1.3- 2.6

Site Haemangioblastoma
• Intracranial – 87-97%
95%------ posterior fossa85% ----- cerebellar hemisphere10% -----cerebellar vermis5% -------medulla5% -------supratentorial
Rarely up to CP angle
• Spinal – 3-13%

Histo-pathology Haemangioblastoma
• Mural nodule with cyst wall not demonstrating tumor involvement in most cases
• Fluid of cyst often xanthochromatic
• Micro-vascular tumor composed of thin walled vessels with surrounding stroma of connective tissue

Haemangioblastoma on CT
• Cyst with nonenhancing wall
• Vividly enhanced mural nodule often has prominent serpentine flow voids
• Calcification is not a feature
• Relatively mild edema and mass effect
** Mistaken for a low density glioma or gliomatous cyst unless the mural nodule is identified in post enhanced scan

Haemangioblastoma on MRI
• T1- Fluid filled cyst
Hypo intense to isointense mural nodule vividly enhancing
• T2- Fluid filled cyst like CSF
Hyper intense mural nodule , flow voids due to enlarged vessels at the periphery to cyst

Haemangioblastoma on angiography
• Enlarged feeding arteries often dilated draining veins are demonstrated with dense tumor blush centrally

Von-Hippel Lindau disease
• It is autosomal dominant hereditary syndrome first described in 1926 by
Arvid Vilhelm Lindau
• Patient may present with--1. cerebellar dysfunction- ataxia and in
coordination with or without hydrocephalus2. Long H/O minor neurological problem or
sudden exacerbation

VHL contd…..
• VHL includes retinal angiomatosis, CNS haemangioblastoma and various visceral tumors most commonly involving the kidneys and adrenal gland
• This syndrome is classified as PHAKOMATOSIS although it does not include any cutaneous manifestation.
• It’s dominating mode of transmission compels performing alerts screening of family members of patient diagnosed with VHL

Diagnostic work up VHL
• Family history
• Detailed funduscopy
• Haematocrit & RBC count
• MRI with contrast
• Arteriography with DSA
• Spinal Angiography if spinal lesion on MRI
• Urine for Metanephrine- if +ve then 24 hrs VMA
• Abdominal CT scan esp. for pancreas, renal and suprarenal

Vascular lesion
• Arterio -venous malformation
• Cavernoma
Both with or without bleed, confirmed on Angiography

Astrocytoma
• Pilocytic astrocytoma- in children
• GBM - in adults
• Ependymoma

Pilocytic astrocytoma on MRI
Iso-Hypointense solid component compared to adjacent brain on T1 and significantly Hyper intense solid component on T2

Ependymoma on MRI
• Typically heterogenous mass in all modalities
Area of necrosis, calcification, cystic changes and hemorrhage frequently seen

Diagnosis of our case
• On the basis of MRI imaging and clinicalpicture most suggestive diagnosis of our case isHaemangioblastoma
• Patient has been referred to specialist

Brain Tumor: Systemic approach
For analysis of potential brain tumor Questions that need to be answered
1. Age of the patient2. Localization- intra versus extra axial
Which anatomical compartmentMid line crossing
3. CT or MRI- calcification, fat, cystic4. Contrast enhancement5. Effect on surrounding structure- mass effect, edema6. Solitary or multiple7. Pseudotumour

References
• Haemangioblastoma-Central nervous system
Dr Bruno Di Muzio and Dr Frank Gaillard et al
radiopaedia.org/article/
• Haemangioblastoma: Medscape Reference
emedicine.medscape.com/article
• Haemangioblastoma: wikipedia.org/wiki/haemangioblastoma
• Brain tumor: systemic approach Robin Smithnis and Walter Montanera Radiology Assistant

References contd…..
• Haemangioblastoma: Neuroradiology
neuroradiology.ws/haemangioblastoma.htm
• Cerebellar haemangioblastoma: An unusual cause of syncope eradiology.bidmc.harvard.edu/learning lab/mohamed.pdf
• Tumors of uncertain histogenesis-haemangioblastoma Text book of Radiology and Imaging vol 2 David Sutton

Have a good time







