
Carlos L. Arteaga, M.D.Departments of Medicine and Cancer Biology
Breast Cancer Research ProgramVanderbilt Ingram Comprehensive Cancer Center
Vanderbilt University School of Medicine
Are We About To Cure HER2-Are We About To Cure HER2-Positive Breast Cancer?Positive Breast Cancer?

Slamon et al. Science 237:177, 1987
Median Survival
HER2 overexpression 3 yrsHER2 normal 6-7 yrs
HER2/Neu (ErbB2) oncogene is associatedwith poor prognosis in breast cancer
HER2 protein overexpression (IHC)
HER2 geneamplification (Southern)

HER2 (ErbB2) is Oncogenic
HER2Control
HER2
Soft Agar

ErbB4HER4
EGFR/ErbB1HER1
ErbB2HER2
ErbB3HER3
Lig
ands
EC
IC
Ligands and Receptors of the HER (ErbB) family
100
100
100
44
82
33
36
59
24
48
79
28
EGFTGF
AmphiregulinHB-EGF
BetacellulinEpiregulin
? Heregulin(Neuregulin)
HeregulinHB-EGF
BetacellulinEpiregulin
Ligand binding
Tyr-Kinase
C-terminus
Some facts about the HER2 receptor network and HER2+
breast cancer
• HER2 is the most potent kinase and HER2-HER3 the most potent signaling dimer of this receptor network
• The main survival program activated by the HER (ErbB) network is the PI-3 kinase/Akt pathway
• The antibody trastuzumab and the tyrosine kinase inhibitor lapatinib are approved by the FDA for the treatment of HER2+ breast cancer

EGF30001: Phase III trial of paclitaxel ± lapatinibin first line or metastatic breast cancer

No benefit from lapatinib when analyzing the whole cohort

Benefit from the addition of lapatinib to paclitaxelwas significant in patients with HER2+ cancers

Adjuvant trastuzumab prolongs survival ofpatients with HER2+ breast cancer
Romond, Perez, Bryant, et al. NEJM 2005
07442776612171672Trastuzumab05937468911621679Control0133801145523793351No. at risk
0
% S
urv
ivin
g d
isease-f
ree
1 2 3 4 50
50
60
70
80
90
100
Years after randomization
Trastuzumab(133 events)
p<0.0001HR=0.48
Control(261 events)
87.1%85.3%
67.1%
75.4%

70
10
20
30
40
50
60
70
80
90
0
100
* Censors 4 patients who died due to causes other than breast cancer
10
20
30
40
50
60
0
Time (weeks)
CapecitabineLapatinib +
Capecitabine
0.00016P-value (log-rank, 1-sided)
69 (43%)45 (28%)Progressed or died*19.736.9Median TTP, wks
161160No. of pts
0.51 (0.35, 0.74)
Hazard ratio (95% CI)
% p
ati
en
ts f
ree f
rom
pro
gre
ssio
n*
Lapatinib prolongs progression-free survivalafter trastuzumab (Geyer et al. NEJM 2006)

Processing of trastuzumab-DM1 conjugate
Derivative ofMaytansine
Trastuzumab
Linker: MCC
• Normal-tissue target expression
• Fc-mediated uptake
• Non-specific uptake
HER2
Target-dependent cytotoxic activity

Trastuzumab-DM1 but not trastuzumab induces apoptosisand cell lysis and works in trastuzumab-resistant tumors
Lewis Phillips et al. Cancer Res. 68:9280, 2008

Krop et al. SABCS 2009 (late breaking abstract 710)

• HER2+ disease by FISH or 3+ IHC by local lab• Measurable disease by CT scan as per RECIST• Prior anthracycline, trastuzumab, taxane,
capecitabine and lapatinib therapy in any setting• Prior treatment with two HER2-directed regimens in the
metastatic setting• Documented progression on their most recent treatment
regimen• No history of significant cardiac disease; left ventricular
ejection fraction (LVEF) ≥50%• No history of Grade ≥3 hypersensitivity to trastuzumab or
toxicity requiring discontinuation • No Grade ≥3 peripheral neuropathy• No untreated or symptomatic brain metastases, or any
treatment for brain metastases within 3 months of first dose
• HER2+ disease by FISH or 3+ IHC by local lab• Measurable disease by CT scan as per RECIST• Prior anthracycline, trastuzumab, taxane,
capecitabine and lapatinib therapy in any setting• Prior treatment with two HER2-directed regimens in the
metastatic setting• Documented progression on their most recent treatment
regimen• No history of significant cardiac disease; left ventricular
ejection fraction (LVEF) ≥50%• No history of Grade ≥3 hypersensitivity to trastuzumab or
toxicity requiring discontinuation • No Grade ≥3 peripheral neuropathy• No untreated or symptomatic brain metastases, or any
treatment for brain metastases within 3 months of first dose
Key eligibility criteria

Clinical activity of trastuzumab-DM1 (n=110)
Krop I et al. SABCS 2009 (late breaking abstract 710)
Tumour response IRF(n=110)
Investigator(n=110)
Objective response rate, %(95% CI)
32.7(24.1–42.1)
30.0(22.0–39.4)
CR 0 1.8
PR 32.7 28.2
SD* 46.4 52.7
PD 18.2 13.6
UE 1.8 0.9
Missing 0.9 2.7
Clinical benefit rate, %(95% CI)
44.5(35.1–54.3)
40.0(31.1–49.3)
IRF, independent review facilityObjective response – CR or PR determined by two consecutive tumour assessments at least 28 days apartClinical benefit – objective response or SD maintained for at least 6 months
IRF, independent review facilityObjective response – CR or PR determined by two consecutive tumour assessments at least 28 days apartClinical benefit – objective response or SD maintained for at least 6 months

Implications• Even in advanced stages, HER2+ tumors
remain HER2-dependent
• Single agent anti-HER2 therapies do not inhibit the HER2 network completely
• Combinations of HER2-targeted drugs early in the treatment of HER2+ breast cancers is the rational way to go
• The optimal combination(s) of anti-HER2 agents up front may abrogate acquired resistance, shorten the duration of therapy, and dispense the need of chemotherapy

BT474 HR5
25016010575
P-Tyr
HER3
p85
lapatinib
+ +
p85 i.p.
+ lapatinib
P-HER3
HER3
P-Akt
Akt
In order to induce an antitumor effect, anti-HER2therapies should inhibit the PI3K/Akt pathway
Akt

Yakes et al. Cancer Res. 62:4132, 2002; Junttila et al. Cancer Cell 15:429, 2009
Trastuzumab disrupts ligand-independent HER2/HER3/PI3K complexes

Contributed by Jenny Chang (Baylor), SABCS 2008

HER3 pre HER3 post
His
tosc
ore
0
50
100
150
200
250
300
Pre
-the
rapy
Pos
t-th
erap
y (2
wks
)
Inhibition of the HER2 with lapatinib is followed byupregulation of HER3 in primary HER2+ tumors
In collaboration with Jenny Chang (Baylor)
p=0.01
P-HER3 was also upregulated upon txNo change in S473 P-AktInhibition of P-HER2 was incompleteUnder review

lapatinib
BT474 SKBR3
HER3
SUM225
β-actin
0 1 4 13 24 48 h0 1 4 13 24 48 0 1 4 13 24 48
lapatinib: 0 1 4 13 24 48 h0 1 4 13 24 48
BT474
P-HER3 (Y1289) short
P-HER3 (Y1289) long
P-HER3 (Y1197)
P-HER3 (Y1222)
P-HER2 (Y1248)
HER2
EGFR
HER3
SKBR3
P-EGFR (Y1068)
Akt
S6
P-S6
P-Akt (S473)
P-Akt (T308)
P-Erk
Erk
β-actin
Upon inhibition of the HER2 kinase, HER2+ cells upregulate total and activated HER3
Garrett J, Arteaga CL. Unpublished

Met
PPI3K p110
p85
Akt
PI3K p110
p85
Akt
IGF-IR
IRS-1PPP
P
lapatinib
Activation of Compensatory Pathways
Is compensatory upregulation of HER3a possible mechanism of drug resistance?
P
EGFR
P
HER2 ErbB3
P
Tyrosine kinases that can activate HER3: MET, EGFR, FGFR2,
Src, IGF-IR (?), BRK (?)
Implication: Upregulation of HER3 provides a mechanismfor maintenance of PI3K and escape from drug action

HER3
P-HER3 (Y1289)
β-actin
0 1 4 13 24 48 0 1 4 13 24 48 hBEZ235
SKBR3BT474
Inhibition of either HER2 or PI3K/Akt results in upregulation
of HER3 RNA and protein and P-HER3

Active Akt mutant limits lapatinib-inducedupregulation of HER3 mRNA and protein

FOXO3a TO-PRO-3 Merge
2°
Ab
alo
ne
DM
SO
4 h
la
p1
h l
ap
C N C N C N
DMSO 13 h lap 24 h lap
FOXO3a
Upregulation of HER3 upon inhibition of HER2 blockadeis dependent on PI3 kinase and FoxO3a

HER3
β-actin
ctrl HER3 ctrl HER3 siRNA
BT474 SKBR3
DMSO 0.33 µM lap 1.0 µM lap
siC
TR
Lsi
HE
R3
dmso Lap 0.33 Lap 1.0
mea
n ar
ea o
f aci
ni (
% o
f con
trol
)
0.0
0.2
0.4
0.6
1.0
1.2
ctrl siRNAHER3 siRNA
*
**
p<0.05*
RNAi of HER3 enhances lapatinib action against HER2+ br ca cells

100
300
500
700
900
1100
1300
7 9 13 16 20 23 27 30 34 37
tum
or v
olu
me
(mm
3)
ctrl, n=9
lap, n=8
AMG-888, n=8
lap+AMG-888, n=9
*
#
**
#
**
##
**
##
**
* **
Neutralizing HER3 monoclonal antibody sensitizesBT-474 xenografts to lapatinib
days * p<0.05, ** p<0.01 versus control # p<0.05, ## p<0.01 versus lapatinib
Tx

p=.006
p=.00005
p=.034
p=.000007
p=.029
cont
rol
Pre-tx 2 weeksla
patin
ibla
p +
AMG
-888
Combination of lapatinib and AMG-888 inhibits FDG-PET

HE
R3
*
Fox
O3a
*
lap lap+AMG-888ctrl
P-A
kt
*
Biomarkers of combined HER2 and HER3 inhibition

Trastuzumab inhibits recovery of P-HER3 after lapatinib
P-HER3
lapatinib lap + trast
β-actin
0 1 4 13 24 48 1 4 13 24 48 h
BT
474
0 1 4 13 24 48 1 4 13 24 48 h
SK
BR
3 P-HER3
β-actin
Garret J, …….., Arteaga CL, Unpublished
Src, MET, FGFR2, IGF-IR,EGFR inhibitors and pertuzumabDid not block recovery of P-HER3

31
Phase III study to test if total HER2 blockade improves clinical outcome
RANDOMIZATION
Lapatinib 1000 mg/day PO Trastuzumab 4 2 mg/kg IV qw N=148
Lapatinib 1500 mg/day PO N=148
Stratification Factors
• Visceral Disease
• Hormone Receptor
Key Inclusion
• HER2+(FISH+/ IHC3+) MBC
• Progression on• Anthracycline
• Taxane
• Trastuzumab
• Progression on most recent trastuzumab regimen
Crossover if PD after 4wk therapy (N=73)
Study conducted and funded by GlaxoSmithKline

Lapatinib + trastuzumab improves OS compared to lapatinib in patients progressing on or after
trastuzumab
Blackwell KL, et al. J Clin Oncol 2010; 28;1124–1130

Neoadjuvant lapatinib randomized Phase III trial
neo-ALTTO (adjuvant lapatinib ± trastuzumab
treatment optimization) trial (n=450)

Summary• Current therapeutic inhibitors of HER2 do
not inhibit output to HER3 and PI3K/Akt completely
• Compensatory upregulation of HER3 function occurs by transcriptional and post-translational mechanisms
• To completely inhibit the HER2 network (and the PI3K pathway), compensatory upregulation of HER3 should be eliminated
• The best therapeutic strategy to eliminate HER3 function remains to be determined

Anti-HER3 (ErbB3) strategies in clinical development
• Human antibody (IgG1) AMG-888 (AMGEN-U3)
• Human antibody (IgG2) MM-121 (Merrimack-Sanofi)
• HER3 antisense EZN-3920 (Enzon Pharmaceuticals)

PI3K/AKT pathway inhibitors in clinical development
Hsp70Hip, etc
IP
Hsp90
IP
Hsp90
Release of the mature/refolded
protein
ATP
ATP
Protein
p23
p23
Protein
Protein
IP
17AAG
Ubiquination/degradation
p23
Hsp90
17-AAGProtein
Protein
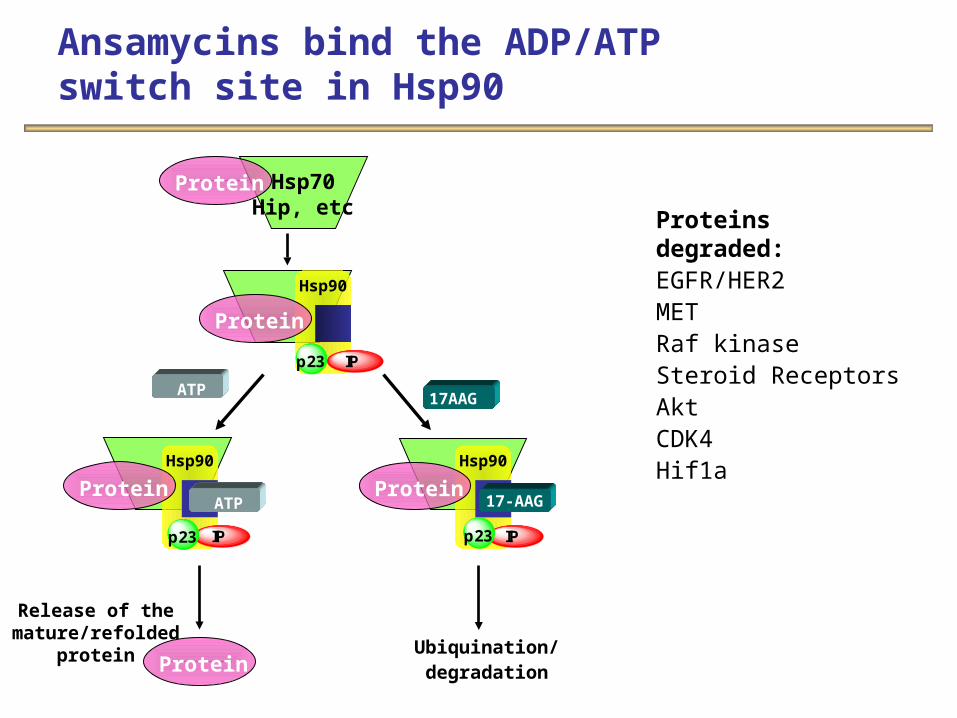
Proteins degraded:EGFR/HER2METRaf kinaseSteroid ReceptorsAktCDK4Hif1a
Ansamycins bind the ADP/ATP switch site in Hsp90
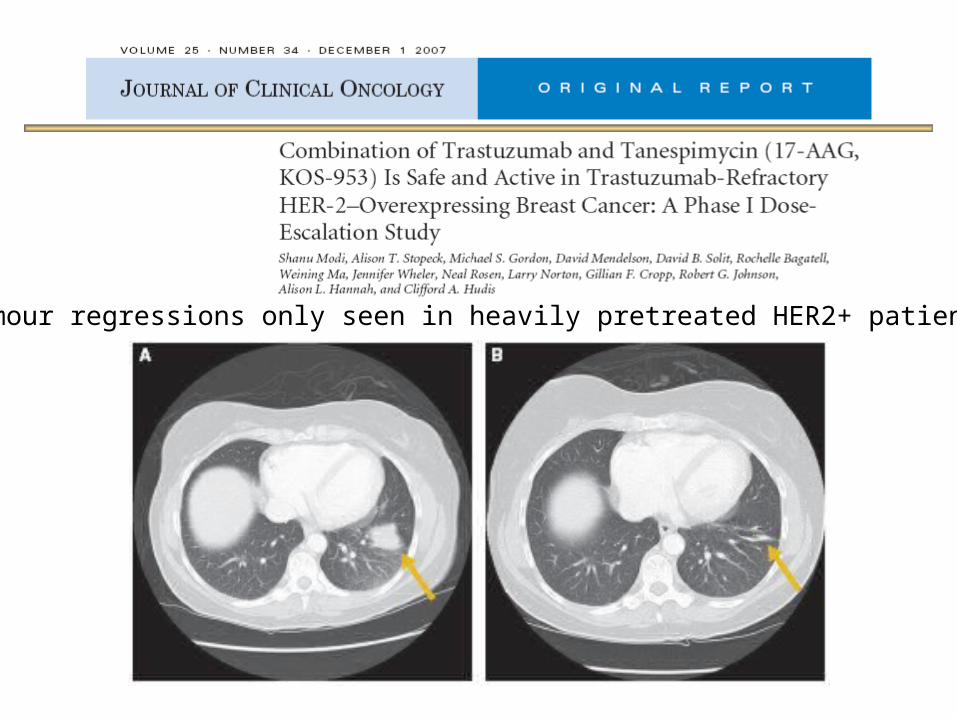
Tumour regressions only seen in heavily pretreated HER2+ patients

Best response and target lesion change (n=25)*
* One additional patient had complete regression of a single target lesion but overall response of progressive disease based on non-target lesions. One patient withdrawn for clinical progression without radiological assessment

Response rates for novel HER2-targeting agents after progression on trastuzumab
17-AAG Pertuzumab Neratinib
0
10
20
30
40
50
60
70
80
90
P<0.0001
Resp
onse
ra
tes
(%)
T-DM1
N=31 N=66N=45 N=112
Modi S et al, ASCO 2008; Gelmon KA et al, ASCO 2008; Swaby R et al, ASCO 2009; Burris HA et al, ESMO 2009

We have a good problem (many drugs) in HER2+ breast cancer – we are just learning how to combine them now
• Pertuzumab (anti-HER2 antibody)
• Irreversible HER2 kinase inhibitors (neratinib)
• HER3 antibodies (AMG-888, MM-121)
• PI3K inhibitors (GDC-0941, XL-147, BKM120)
• Akt inhibitors (MK-2206)
• IGF-IR inhibitors (R1507, MK-0646, OSI-906)
• HSP90 inhibitors
• Trastuzumab-DM1 (fusion toxin)
• Bevacizumab and other angiogenesis inhibitors
• MET, Src, and TGF inhibitors

Implications• There are several 2-drug combinations that can
aim at completely inhibiting the HER2 network and its output to PI3K– Lapatinib + trastuzumab– Trastuzumab + AMG-888– Trastuzumab + pertuzumab– Trastuzumab (or lapatinib) + a PI3K or a AKT inhibitor– Trastuzumb-DM1 + a PI3K or a AKT inhibitor
• Neoadjuvant therapy provides a space where these can be compared (using path CR as an endpoint)
• Some molecular phenotypes may be more sensitive to some specific combinations (i.e., tumors with PI3K pathway mutations)
• Although efficacy may be equivalent, toxicity and cost will be major differentiating factors

Acknowledgements
Vanderbilt Charles ManningWilliam Pao
Baylor (Houston) Jenny ChangBhuvanesh Dave
Stanford Anne Brunet
AMGEN-U3 Dan FreemanRobert RadinskyThore Hetmann
Novartis Carlos Garcia-Echeverria







