
Cannabinoids and Epilepsy
Gregory D. Cascino, MD, FAAN Whitney MacMillan, Jr. Professor of
Neuroscience Mayo Clinic
Rochester, MN

Disclosure
• American Academy of Neurology Board of Directors
• Neurology journal Associate Editor
• Mayo Foundation Mayo Medical Ventures
• Human Epilepsy Project The Epilepsy Study Consortium

Research Support
• GW Pharmaceuticals, London, UK Randomized, double-blind, placebo-controlled trial of CBD in Lennox-Gastaut syndrome

EPILEPSY Patient population
• March 30, 2012 (iom.edu) • Consensus report • 1 in 26 people have epilepsy Recurrent, unprovoked events One seizure with biomarkers for
recurrence Prevalence: 1-4% Incidence: 180,000 per year

EPILEPSY goals of therapy
• No seizures • No side effects of treatment • No life-style limitations • QOL related to seizure-free outcome

EPILEPSY adverse effects
• 25,000-50,000 die of seizures or related causes each year
• Cognitive disorder • Depression and Anxiety disorders • SUDEP (sudden unexplained death in
epilepsy) • Risk of sudden death is 24 times controls

EPILEPSY efficacy of treatment
• Neurology 2003;60(Suppl 4):S2-12 • About 30-40% will have a difficult to
control seizure disorder • The 1st and 2nd AEDs are highly predictive
of medical outcome

EPILEPSY efficacy of treatment
• 2.2 million people with epilepsy • Drug-resistant: two AEDs are
ineffective • 750,000 patients with drug-resistant
epilepsy
INTRACTABLE EPILEPSY efficacy of treatment • Epilepsia 2007;62:375-381
• PENN Epilepsy Center • Refractory epilepsy • Randomized add-on trials • Seizure-free rates: 0-7%

INTRACTABLE EPILEPSY treatment strategies
• Curative surgical therapy • focal cortical resection, reoperation
• Palliative surgery • VNS, corpus callosotomy
• Antiepileptic drug medication • Ketogenic or Atkins diet • Investigational studies
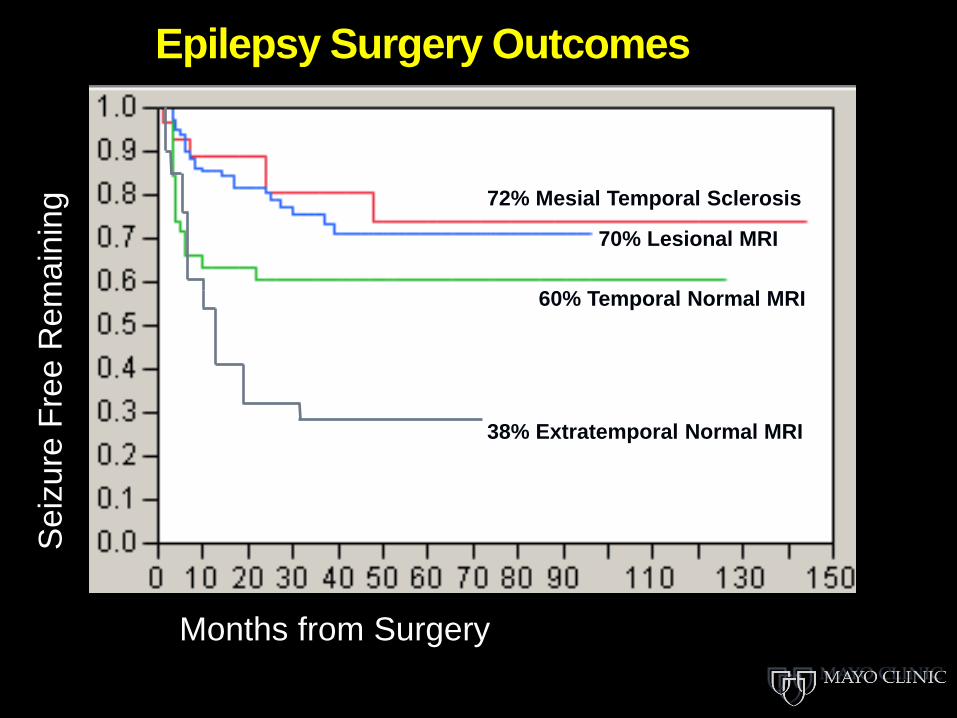
38% Extratemporal Normal MRI
60% Temporal Normal MRI
70% Lesional MRI
72% Mesial Temporal Sclerosis
Mayo Epilepsy Surgery Outcomes
Months from Surgery
Sei
zure
Fre
e R
emai
ning

TRENDS IN EPILEPSY SURGERY 1990-2008
• Englot et al. (UCSF) • Nationwide Inpatient Sample • 6,653 resective surgeries • No increase in epilepsy surgery
during this period despite Grade A evidence
• Neurology 2012;78:1200

HISTORY • In the 19th century, marijuana was used to
treat epilepsy. Gowers reported, Cannabis indica (marijuana), which was first recommended in epilepsy by Dr. Reynolds, is sometimes, though not very frequently, useful. It is of small value as an adjunct to the bromide, but is sometimes of considerable service given separately … I have administered [it] in many cases, and with the effect of delaying the paroxysms and mitigating their severity in some individuals

BACKGROUND • Cannibas sativa – ~8,000 BC in China • 2700 BC – cannibas (ma) for
menstruation, gout, rheumatism, malaria, constipation, and absentmindedness (Abel, 1980)
• 1st Century AD in China > 100 ailments • Medicinal use in ancient Egypt, India,
Africa, Greece, Rome and Arab world
BACKGROUND • Cannabis sativa • Unique compounds are called cannabinoids • Main active ingredient is the cannabinoid 9-tetrahydrocannabinol (THC): psychoactive • Cannabinol and cannabidiol are other cannabinoids

• Cannabis indica – reference in Ancient
Vedas text in India, ~ 1700 BC • Indica strains have more sedative
properties
BACKGROUND

Exogenous Cannabinoids
Cannabidiol (CBD) Non-psychoactive Very slight CB1/CB2 indirect antagonist; opposes some CNS effects of THC Antagonist at GPR55 receptor, ? CBD receptor
Δ9 Tetrahydrocannabinol (THC) Psychoactive CB1 agonist

MARIJUANA NIH: Drug Facts
• Marijuana refers to the dried leaves, flowers, stems, and seeds from the hemp plant, Cannabis sativa.
• The plant contains the mind-altering chemical delta-9 tetrahydrocannabinol (THC) and other related compounds.
• People use marijuana by smoking, eating, drinking, and inhaling it.
SCHEDULE 1 DRUGS U.S. Controlled Substance Act
• The drug or other substance has a high potential for abuse.
• The drug or other substance has no currently accepted medical use in treatment in the United States.
• There is a lack of accepted safety for use of the drug or other substance under medical supervision.

SCHEDULE 1 DRUGS U.S. Controlled Substance Act
• Except as specifically authorized, it is illegal for any person: to manufacture, distribute, or dispense, or possess with intent to manufacture, distribute, or dispense, a controlled substance; or to create, distribute, or dispense, or possess with intent to distribute or dispense, a counterfeit substance.

HISTORY Anecdotal evidence for many illnesses: nausea related to chemotherapy anorexia and wasting from AIDS glaucoma muscle spasticity Tourette syndrome multiple sclerosis epilepsy

Charlotte’s Web • Dr. Gupta highlighted a little girl named
Charlotte with Dravet Syndrome • She was given an oil that is low in THC
and high in CBD • Company now calls the oil Charlotte’s
Web • She had a remarkable reduction in
seizures • Charlotte continues to do well, but is
NOT seizure-free
DRAVET SYNDROME • Drug-resistant seizures beginning
in the first 12 months of life • Incidence: 1/30,000 • Episodes of status epilepticus • Myoclonic seizures occur around
the age 18 months of age • Seizures associated with fever,
vaccinations, hot baths, or warm temperatures

DRAVET SYNDROME • 80% SCNIA gene mutation • Genetic and developmental
epilepsy syndrome • Severe myoclonic epilepsy of
infancy (SMEI) • Development initially may be
normal; may evolve with language and cognitive deficits

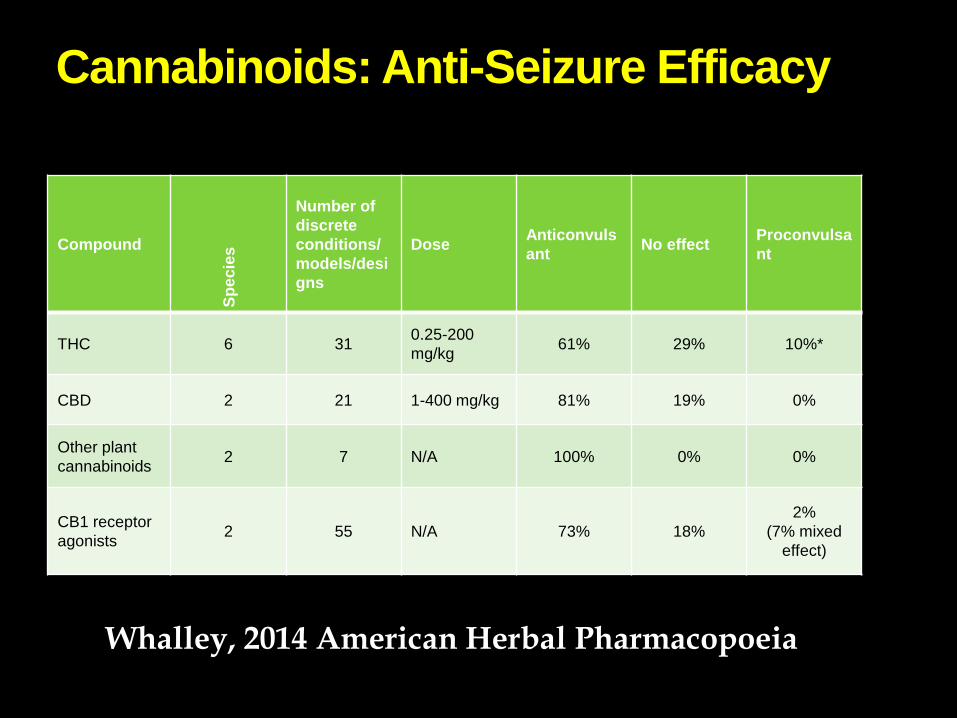
Cannabinoids: Anti-Seizure Efficacy
Compound Sp
ecie
s Number of discrete conditions/models/designs
Dose Anticonvulsant No effect Proconvulsa
nt
THC 6 31 0.25-200 mg/kg 61% 29% 10%*
CBD 2 21 1-400 mg/kg 81% 19% 0%
Other plant cannabinoids 2 7 N/A 100% 0% 0%
CB1 receptor agonists 2 55 N/A 73% 18%
2% (7% mixed
effect)
Whalley, 2014 American Herbal Pharmacopoeia


MINNESOTA MEDICAL CONDITIONS Amyotrophic Lateral Sclerosis Cancer/cachexia Crohn's disease Glaucoma HIV/AIDS Seizures Severe and persistent muscle
spasms Terminal illness Tourette's Syndrome

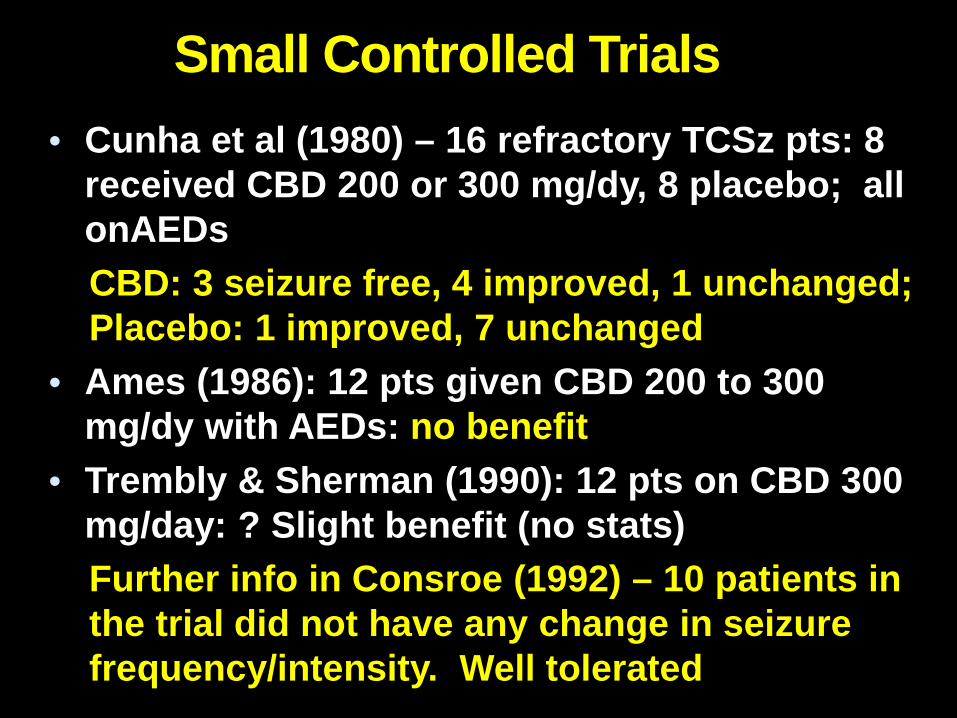
Small Controlled Trials • Cunha et al (1980) – 16 refractory TCSz pts: 8
received CBD 200 or 300 mg/dy, 8 placebo; all onAEDs CBD: 3 seizure free, 4 improved, 1 unchanged; Placebo: 1 improved, 7 unchanged
• Ames (1986): 12 pts given CBD 200 to 300 mg/dy with AEDs: no benefit
• Trembly & Sherman (1990): 12 pts on CBD 300 mg/day: ? Slight benefit (no stats) Further info in Consroe (1992) – 10 patients in the trial did not have any change in seizure frequency/intensity. Well tolerated

Survey of 19 Pediatric Epilepsy Patients on CBD>THC
• 19 children (2-16 years) used a CBD-enriched medical marijuana
• 16 (84%) reduction in seizure frequency
• 2 were seizure free • 8 (42%) >80% reduction in seizures • 6 had a 25-60% reduction in seizures. (Porter & Jacobson, Epilepsy & Behavior, 2013)

Survey of 19 Pediatric Epilepsy Patients on CBD-enriched Cannabis
• Benefits included improved alertness, mood, and sleep.
• Side effects: drowsiness and fatigue. • Diagnoses: Dravet syndrome (13),
Doose syndrome (4), Lennox Gastaut syndrome (1), and idiopathic epilepsy (1). (Porter & Jacobson, Epilepsy & Behavior, 2013)
American Academy of Neurology American Academy of Neurology Guideline – Summary (2014) “Oral cannabinoids are of unknown efficacy in nonchorea-related symptoms of HD, Tourette syndrome, cervical dystonia, and epilepsy.”

American Academy of Neurology
• Not sufficient evidence to make any definitive conclusions regarding the effectiveness of marijuana-based products
• Most currently available marijuana-based products are not regulated by any agency and may not contain the products mentioned by labeling

American Academy of Neurology • Supports all efforts to conduct rigorous research to evaluate the long-term safety and effectiveness of marijuana-based products • For research purposes, requests the reclassification of marijuana-based products from their current Schedule 1 status

Epidiolex (98% CBD) Studies
NYU enrolled 25 children and young adults with TRE – Dravet, LGS, Focal epilepsy, CDKL4, etc 5 other site are enrolling or will soon
enroll 25 children/site (UCSF, Lurie Children’s, MGH, CHOP, Great Ormond St) Orphan drug indication approved by
FDA for Dravet and LGS – plans for RCT

EFFICACY AND SAFETY OF EPIDIOLEX (CANNABIDIOL) IN CHILDREN AND YOUNG
ADULTS WITH TREATMENT-RESISTANT EPILEPSY: INITIAL DATA FROM AN
EXPANDED ACCESS PROGRAM
American Epilepsy Society, 2014


Efficacy results for the 23 patients • After 3 months of therapy, 39% of patients
had a >50% reduction in seizures; there was a 32% median reduction in seizures. Seizure-freedom at 3 months occurred in 3/9 Dravet patients and 1/14 other patients. One patient with Dravet had marked seizure worsening; the only serious adverse event.
• 18 (78%) had adverse effects; most commonly fatigue, somnolence and decreased appetite

CBD FOR MEDICAL USE • JAMA 2015;313:2456-73 • Systematic review and Meta-analysis • 79 trials, 6462 participants
• Moderate evidence for chronic pain and spasticity
• Low evidence for nausea with chemotherapy, Tourette, sleep disorder, weight gain with HIV
• Increased adverse effects

CBD: Anti-seizure effect
From Whalley with permission
• CBD has anticonvulsant effects in > 6 seizure models in rats and mice; independently of CNS CB1 receptors (Jones et al, Seizure 2012; Hill et al, Endocannabinoids 2013:164-204; Hill et al, Brit J of Pharm 2013; Karler & Turkanis, J Clin Pharm 2013)
• CBD reduces epileptiform activity in vitro (Jones et al. 2010, J Pharm Exp Ther)
• CBD reduces mortality in pentylenetetrazol (PTZ) induced seizures (Jones et al. 2010, J Pharm Exp Ther)

CBD: Mechanisms of Action
• Full mechanism of action is unknown • Based on animal studies:
• NMDA receptor antagonist • Potential calcium channel modulation • Possible serotonin properties • Possible positive effects on memory and
learning • Decrease inhibition of aberrant inhibitory cells
(GABA)
CBD: Mechanisms of Action
• G-protein-coupled receptor GPR55 antagonist: presynaptic Ca++ release (Sylantyev et al, PNAS 2013)
• Inhibit the degradation (FAAH) and reuptake of anandamide, ECs (Bisogno. 2001, Brit J Pharm)
• Equilibrative nucleoside transporter • 5-HT1a receptor • Neuroprotective and anti-inflammatory effects • Alters Ca2+ flux (De Petrocellis et al. 2011, Brit J
of Pharm; Bisogno et al. 2001, Brit J of Pharm, Qin et al 2008, J Neurosci)

DRUG INTERACTIONS
• Epilepsia 2015; Jun 26. doi: 10.1111/epi.13060. [Epub ahead of print]
• Clobazam (CLB) and CBD are metabolized in the P450 (CYP) pathway
• 13 patients: increased CLB and CBD levels
• 10 of 13 patients had side effects (improved by CLB dose reduction)
• 9 of 13 had >50% seizure reduction

Current Opinion • Data from methodologically limited
clinical trials of CBD, parental reports of CBD-enriched medical marijuana and animal studies suggest that CBD may have valuable anti-seizure properties and the benefit: risk ratio may be favorable
• Randomized, placebo-controlled clinical trials are warranted

LENNOX-GASTAUT STUDY Mayo Clinic, Rochester, MN
TITLE: A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of cannabidiol (GWP42003-P; CBD) as adjunctive treatment for seizures associated with Lennox-Gastaut syndrome in children and adults.
LENNOX-GASTAUT STUDY • Age: 2-55 years old • Phase 3 study • PI: Dr. Elaine Wirrell (Mayo) • CBD in LGS • 1:1:1 randomized trial: two dose levels of
CBD and placebo • Assess efficacy: reduction in drop
seizures and non-drop seizures • Assess adverse effects
Dr. Elson So: CBD in epilepsy • Rigorous scientific data are lacking • Anecdotal reports and case studies are not
equivalent to a clinical trial • About one-third of patients have >50% reduction
in seizures during short-term follow-up • “Dramatic” responses (seizure-free) are
uncommon <10% • Dravet syndrome may be the most responsive • Long-term adverse effects, drug interactions
and pregnancy exposure needs to be more fully studied

Who should not receive CBD • First seizure or new-onset epilepsy • When less than two antiepileptic medications
have failed • Patients who are seizure-free on existing
medications • When the diagnosis of epilepsy is unclear • As a single agent • In patients with poor compliance with
established therapies • As an alternative to epilepsy surgery or
evaluation
EPILEPSIA’S SURVEY • Epilepsia 2015;56:1-6 • 776 completed survey • Recommend CBD for severe
epilepsy: • 96% of patients and public • 83% of general physicians, nurses,
AHP • 48% of epileptologists and
neurologists
SUMMARY • CBD is not a natural substance but is a
drug • THC is psychoactive and is not the same
substance as CBD • Studies need to be completed evaluating
the efficacy and safety; including seizure-types- age of patients- co-medications
• The laws regarding CBD in U.S. are state specific and confusing to patients and physicians







