
BIOS222
Pathology and Clinical Science 2
www.endeavour.edu.au
Session 1
Disorders Of Ears, Nose,
Throat
Bioscience Department

© Endeavour College of Natural Health www.endeavour.edu.au 2
SESSION LEARNING
OUTCOMESAt the end of this session, you should be able to
o Revise and review anatomy and physiology of Ear Nose and Throat.
o Define and identify the common conditions affecting the ears, upper respiratory tract and trachea.
o Analyse and identify the probable causes of these conditions, their clinical manifestations, pathophysiology and complications.
o Make a probable differential diagnosis on the basis of symptomatology and investigations.
o Plan the management of the case with the conditions affecting Ears, Nose and Throat considering prevention, active and supportive treatment of the patient.

© Endeavour College of Natural Health www.endeavour.edu.au 3
SESSION PLAN
o Review Anatomy of the human ear and URT
o Diseases affecting Ears: • Otitis media, Meniere’s disease.
o Diseases affecting the nose and throat: • Acute Coryza, Allergic Rhinitis
• Acute and chronic laryngitis
• Acute epiglottitis
• Acute bronchitis and tracheitis
• Tracheal obstruction
o Acute infection of respiratory system: Influenza

© Endeavour College of Natural Health www.endeavour.edu.au 4
SESSION PLAN
o Review Anatomy of the human ear and URT
o Diseases affecting Ears: • Otitis media, Meniere’s disease.
o Diseases affecting the nose and throat: • Acute Coryza, Allergic Rhinitis
• Acute and chronic laryngitis
• Acute epiglottitis
• Acute bronchitis and tracheitis
• Tracheal obstruction
o Acute infection of respiratory system: Influenza

© Endeavour College of Natural Health www.endeavour.edu.au 5
ANATOMY OF THE HUMAN EAR

© Endeavour College of Natural Health www.endeavour.edu.au 6
ANATOMY OF THE HUMAN EAR
o External ear
• Auricle
• External auditory canal
• Ear drum/Tympanic membrane
Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology, 14th edn, John Wiley &
Sons, Hoboken, NJ

© Endeavour College of Natural Health www.endeavour.edu.au 7
ANATOMY OF THE HUMAN EAR
o Middle ear
• Eustachian
tube
opening
• Auditory
ossicles
• Muscles and
Ligaments
Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology, 14th edn, John Wiley &
Sons, Hoboken, NJ

© Endeavour College of Natural Health www.endeavour.edu.au 8
ANATOMY OF THE HUMAN EAR
o Internal ear
• Bony labyrinth
– The semicircular
canals
– Cochlea
– Vestibule
• Membranous
labyrinth
• Vestibulocochlear
nerve Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology, 14th edn, John Wiley &
Sons, Hoboken, NJ
© Endeavour College of Natural Health www.endeavour.edu.au 9
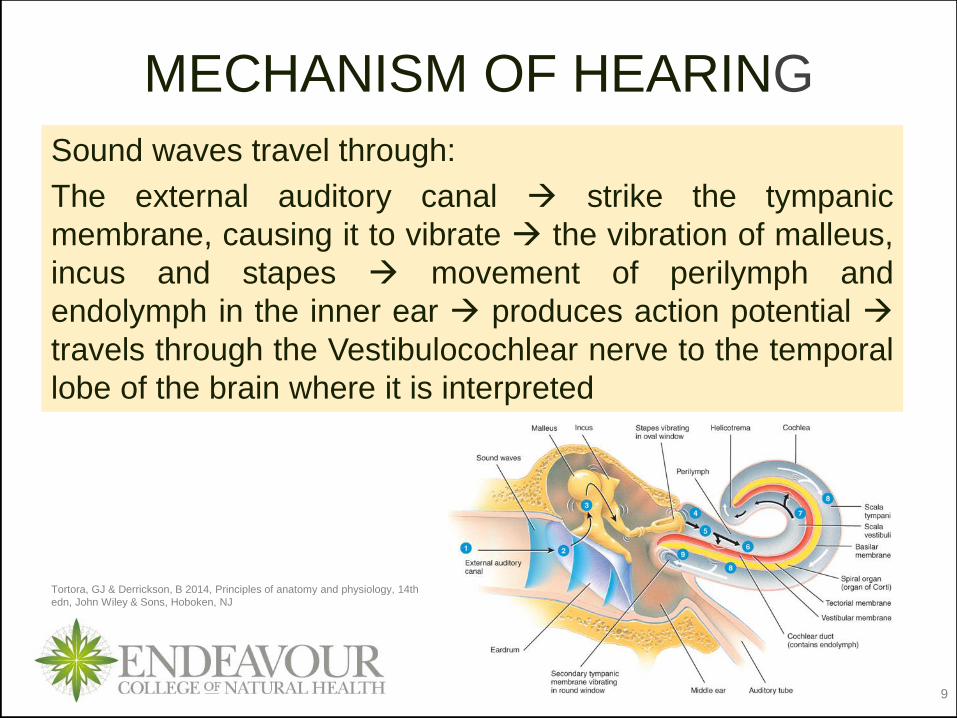
MECHANISM OF HEARING
Sound waves travel through:
The external auditory canal strike the tympanic
membrane, causing it to vibrate the vibration of malleus,
incus and stapes movement of perilymph and
endolymph in the inner ear produces action potential
travels through the Vestibulocochlear nerve to the temporal
lobe of the brain where it is interpreted
Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology, 14th
edn, John Wiley & Sons, Hoboken, NJ

© Endeavour College of Natural Health www.endeavour.edu.au 10
DISEASES AFFECTING EARS

© Endeavour College of Natural Health www.endeavour.edu.au 11
COMMON SYMPTOMS IN DISEASES
AFFECTING THE EARSSigns/Symptoms Common causes/conditions
Tinnitus Over exposure to loud noise, wax on ear drum,
tumours , Meniere’s disease, Osteosclerotic change in
ear ossicles, head injury, metabolic diseases such as
hyperthyroidism,
Hearing loss Congenital, conductive deafness, sensorineural
deafness
Earache Otitis externa or otitis media, Upper respiratory tract
infection, TMJ disease, Cervical spondylosis,
Trigeminal neuralgia, Tonsillitis, Bell’s palsy, Dental
problems, Cancer
Ear discharge Otitis Media, Head injury, Infection,
Vertigo Vestibular neuralgia, Benign Paroxysmal Vertigo,
Meniere’s disease

© Endeavour College of Natural Health www.endeavour.edu.au 12
OTITIS MEDIA
Definition: Inflammation of the middle ear
o Types
• Acute otitis media
• Serous otitis media (otitis media with effusion-OME)
• Chronic suppurative otitis media
o Aetiology:
• Sequel to common cold and other Upper
respiratory infections
• Bacteria: Streptococcus pneumoniae &
Haemophilus influenzae
• Viruses: herpes, varicella, influenza, rhinovirus

© Endeavour College of Natural Health www.endeavour.edu.au 13
OTITIS MEDIA
Upper respiratory
tract infection
Causative
pathogens:
• Bacteria
• Viruses
Triggers inflammation
• Release of
chemical mediators
• Activation of
cellular mediators
• Vasodilation
• Increase capillary
permeability
• Phagocytosis
• Increased blood
flow
• Collection of
fluid and
proteins
• Action of WBCs
• Swelling
• Redness
• Heat (fever)
• Pain
• Impaired hearing
• Fullness in ears
• Exudation
(ottorrhoea)
Pathophysiology : Inflammation usually due to infection.
© Endeavour College of Natural Health www.endeavour.edu.au 14
OTITIS MEDIAo Clinical features of Acute Otitis Media:
• Acute onset of otalgia (or pulling of the ears in an infant)
• Fever (>39°C)
• Hearing loss
• Evidence of middle ear inflammation
• Middle ear effusion (MEE)
o Diagnosis:
• Otoscopic examination of Tympanic membrane
• Tympanometry
• Acoustic reflectometry
• Microbiologic studies

© Endeavour College of Natural Health www.endeavour.edu.au 15
OTITIS MEDIA
Normal ear drum (blood
vessels only at the margins,
i.e. not injected)
Otitis media (injected blood
vessels)
Tympanic membrane appearance on otoscopic examination:
Hawke, M. 2004, Otitis media, Hawke Library, accessed 26 June 2015,
http://otitismedia.hawkelibrary.com/albums/normal/1_G.sized.jpg
© Endeavour College of Natural Health www.endeavour.edu.au 16
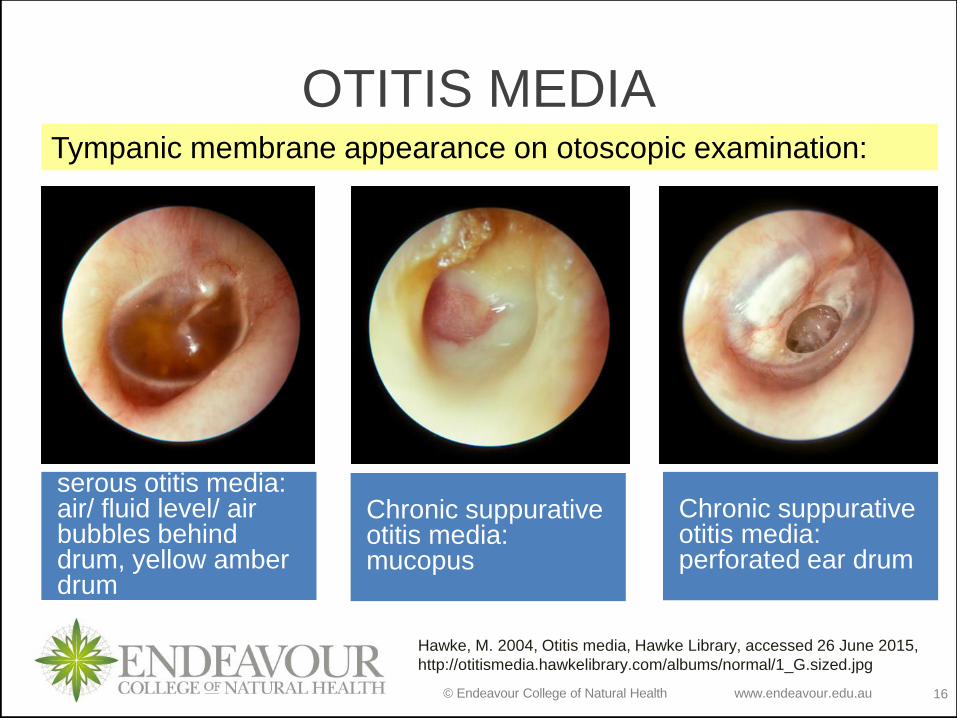
OTITIS MEDIA
serous otitis media: air/ fluid level/ air bubbles behind drum, yellow amber drum
Chronic suppurative otitis media: perforated ear drum
Chronic suppurative otitis media: mucopus
Tympanic membrane appearance on otoscopic examination:
Hawke, M. 2004, Otitis media, Hawke Library, accessed 26 June 2015,
http://otitismedia.hawkelibrary.com/albums/normal/1_G.sized.jpg

© Endeavour College of Natural Health www.endeavour.edu.au 17
OTITIS MEDIA
o Complications:
• Perforation of the
tympanic membrane
• Hearing loss
• Cholesteatoma
• Mastoiditis
• Otologic meningitis
o Management : Control
symptom and underlying
pathologic process
• Pain killers
• Myringotomy
• Antibiotics
• Surgical treatment:
– Tympanostomy tubes (Grommets)
– Adenoidectomy

© Endeavour College of Natural Health www.endeavour.edu.au 18
OTITIS MEDIA
A tympanostomy tube (Grommet) in place in an ear
drum
Images from: http://www.kidshealth.org.nz/grommets-tympanostomy-or-ventilation-
tubes

© Endeavour College of Natural Health www.endeavour.edu.au 19
Otitis media: Middle (Media) Ear (Ot) Inflammation (itis)
Common cold/ other upper respiratory infections: Bacterial: Haemophilus influenzae, Streptococcus pneumonia.
Viral: Herpes, Influenza, Varicella, Rhino
Triggers inflammatory response
Release of inflammatory mediators
Vasodilation of tympanic
membrane blood vessels
Increase pressure in middle ear
WBC activation and
phagocytosis
Collection of inflammatory fluid
(effusion) behind tympanic
membrane
Otoscopic examination of Tympanic
membrane:
• Red injected: AOM
• Yellow, amber (or occasionally blue)
discoloration: OME
• Muco-pus: Chronic OM
• Opacification other than scarring: Chronic
OM
• Decreased or absent motility: Chronic OM
• Perforated drum: Chronic OM with
perforation
Tympanometry & Acoustic reflectometry
detects effusion
Fever
Redness and swelling of respiratory
mucosa and Eustachian tube
leading to adenoid enlargement
Ear pain and bulging of Tympanic
membrane
Pus behind Tympanic membrane
Fullness in ears
Impaired hearing
Ottorrhoea: mucopurulent/serous
Management:
Pain killers
Myringotomy
Antibiotics
Tympanostomy tubes
(Grommets)
Adenoidectomy
Complications:
Perforation of the
tympanic membrane
Hearing loss
Cholesteatoma
Mastoiditis
Otologic meningitis

© Endeavour College of Natural Health www.endeavour.edu.au 20
MENIERE’S DISEASE
o Aetiology:
• Idiopathic
• Trauma
• Infection
• Specific drugs (such as antibiotics)
• Toxins
• Autoimmune reaction
o Definition
• A disorder of the inner ear due to distention of the
endolymphatic compartment of the inner ear.

© Endeavour College of Natural Health www.endeavour.edu.au 21
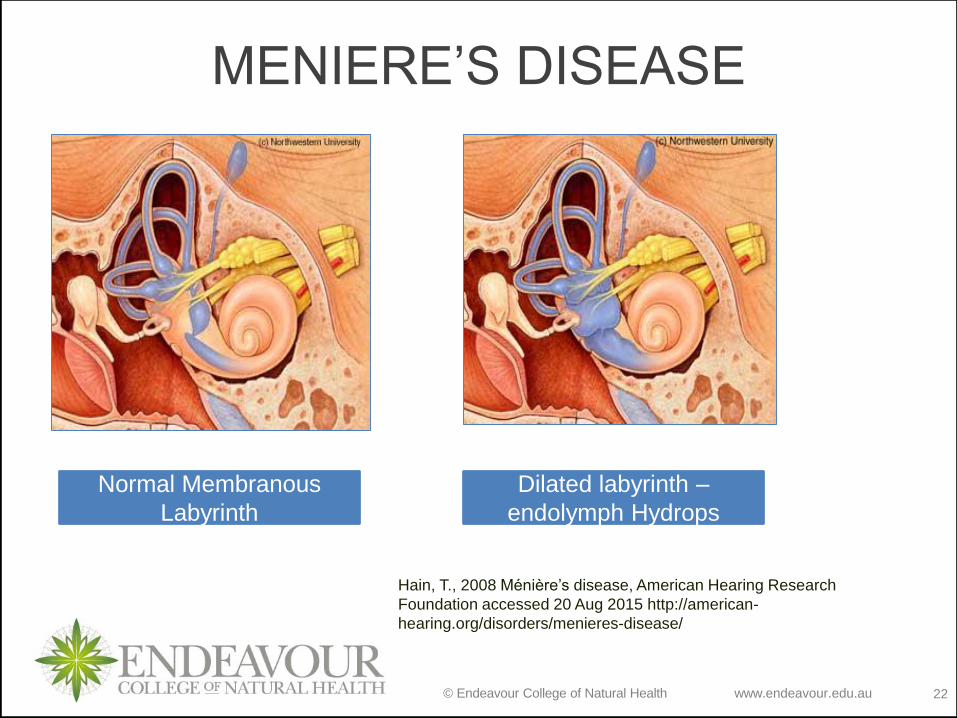
MENIERE’S DISEASEo Pathophysiology:
• An increase in volume and pressure of the endolymph of
the inner ear- endolymphatic hydrops
• Dilation of membranous labyrinth
• Altered function of hair cells in cochlea and vestibular
apparatus
o Clinical features:
• The classic triad: hearing loss, vertigo, and tinnitus.
• A sensation of fullness or pressure in one or both ears
• Pallor, sweating, nausea, and vomiting.
• Nystagmus
© Endeavour College of Natural Health www.endeavour.edu.au 22
MENIERE’S DISEASE
Normal Membranous
Labyrinth
Dilated labyrinth –
endolymph Hydrops
Hain, T., 2008 Ménière’s disease, American Hearing Research
Foundation accessed 20 Aug 2015 http://american-
hearing.org/disorders/menieres-disease/
© Endeavour College of Natural Health www.endeavour.edu.au 23
MENIERE’S DISEASE
o Diagnosis:
• Otoneurological assessment
• MRI to rule out other causes of vertigo
o Differential diagnosis
• Vestibular neuronitis
• Tumour of vestibulocochlear nerve
• Benign paroxysmal positional vertigo

© Endeavour College of Natural Health www.endeavour.edu.au 24
MENIERE’S DISEASE
Management: aimed to reduce the distention of the
endolymphatic space
o Pharmacologic management:
• Suppressant drugs
• Diuretics
• The steroid hormone, prednisone
• A low-sodium diet
o Surgical management:
• Endolymphatic sac surgery
• Vestibular nerve section
© Endeavour College of Natural Health www.endeavour.edu.au 25
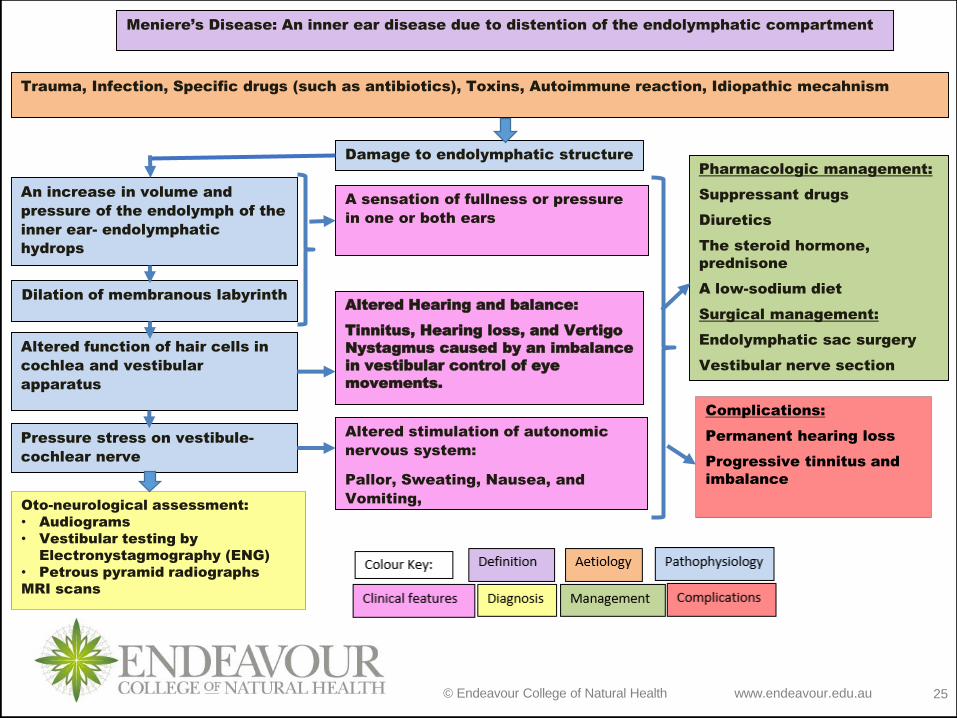
Meniere’s Disease: An inner ear disease due to distention of the endolymphatic compartment
Trauma, Infection, Specific drugs (such as antibiotics), Toxins, Autoimmune reaction, Idiopathic mecahnism
Damage to endolymphatic structure
An increase in volume and
pressure of the endolymph of the
inner ear- endolymphatic
hydrops
Dilation of membranous labyrinth
Altered function of hair cells in
cochlea and vestibular
apparatus
Oto-neurological assessment:
• Audiograms
• Vestibular testing by
Electronystagmography (ENG)
• Petrous pyramid radiographs
MRI scans
A sensation of fullness or pressure
in one or both ears
Altered stimulation of autonomic
nervous system:
Pallor, Sweating, Nausea, and
Vomiting,
Altered Hearing and balance:
Tinnitus, Hearing loss, and Vertigo
Nystagmus caused by an imbalance
in vestibular control of eye
movements.
Pharmacologic management:
Suppressant drugs
Diuretics
The steroid hormone,
prednisone
A low-sodium diet
Surgical management:
Endolymphatic sac surgery
Vestibular nerve section
Complications:
Permanent hearing loss
Progressive tinnitus and
imbalance
Pressure stress on vestibule-
cochlear nerve
© Endeavour College of Natural Health www.endeavour.edu.au 26
DISEASES AFFECTING THE
NOSE AND THROAT

© Endeavour College of Natural Health www.endeavour.edu.au 27
ANATOMY OF NOSE AND THROAT
o Nose
• Conchae
• External nares
• Internal nares
o Throat
• Pharynx
• Epiglottis
• Tonsils
• Larynx
Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology, 14th edn, John Wiley &
Sons, Hoboken, NJ

© Endeavour College of Natural Health www.endeavour.edu.au 28
COMMON SYMPTOMS IN DISEASES
AFFECTING NOSE AND THROAT
o Sneezing
o Nasal discharge/ runny nose
o Headache
o Acute Cough- usually dry
o Change of voice – hoarseness
o Sore throat

© Endeavour College of Natural Health www.endeavour.edu.au 29
ACUTE CORYZAo Definition
• Common cold is a contagious infection of the upper
respiratory tract, involving the nasal mucosa.
o Aetiology
• Viral and Bacterial infections. Mainly rhinoviruses
o Clinical Features:
• Sudden onset, rapid progress
• Burning and tickling sensation in nose
• Sneezing
• Sore throat
• Blocked nose with watery discharge

© Endeavour College of Natural Health www.endeavour.edu.au 30
ACUTE CORYZA
Exposure to
Infectious agents
like rhinoviruses,
bacteria
Triggers inflammation of
nasal and pharyngeal
mucosa
• Release of chemical
mediators
• Activation of cellular
mediators
• Vasodilation
• Increase
capillary
permeability
• Phagocytosis
• Increased blood
flow
• Collection of fluid
and proteins
• Action of WBCs
• Swelling
• Redness
• Heat (fever)
• Pain
• Sneezing
• Fever
• Fullness and
heaviness of head
due to sinusitis
• Nasal discharge
• Sore throat
o Pathophysiology:
© Endeavour College of Natural Health www.endeavour.edu.au 31
ACUTE CORYZA
o Complications
• Sinusitis
• Lower respiratory tract infection
• Otitis media
• Impaired hearing
o Management
• Acute and self-limiting illness
• symptomatic treatment: Rest and antipyretics
• Nasal decongestants
• Antibiotics are ineffective against viral infections and are not recommended

© Endeavour College of Natural Health www.endeavour.edu.au 32
ALLERGIC RHINITISo Definition
• Inflammation of the lining of the nose, caused by
allergens.
o Aetiology
• Seasonal allergic rhinitis:
– Grass, flowers, weed and tree pollens
• Perennial allergic rhinitis:
– House dust (‘dust mite allergen’)
– Fungal spores
– Animal dander (hair and skin flakes)
– Physical or chemical irritants

© Endeavour College of Natural Health www.endeavour.edu.au 33
ALLERGIC RHINITIS
o Pathophysiology: Type 1 hypersensitivity reaction in the
nasal mucosa

© Endeavour College of Natural Health www.endeavour.edu.au 34
ALLERGIC RHINITIS
o Clinical Features
• Sneezing, with profuse watery nasal discharge and
nasal obstruction
• Smarting and watering of the eyes and conjunctival
irritation
• In perennial rhinitis, the symptoms are more
continuous and usually less severe
• Skin hypersensitivity tests with the relevant antigen are
usually positive in seasonal allergic rhinitis, but are
less useful in perennial rhinitis.

© Endeavour College of Natural Health www.endeavour.edu.au 35
ALLERGIC RHINITIS
o Complications
• Sinusitis
• Lower respiratory
tract infection
• Otitis media
• Impaired hearing
o Management
• Antihistaminic drugs
• Nasal spray
• Systemic
corticosteroids in
severe cases
o Prevention
• Avoid contact with allergens

© Endeavour College of Natural Health www.endeavour.edu.au 36
ACUTE LARYNGITIS
o Definition:
• Acute inflammation of the vocal cord often a
complication of acute coryza
o Clinical features:
• Dry sore throat, hoarseness of voice, loss of voice
• Pain on speaking
• Painful, unproductive cough
• Stridor in children
o Aetiology: exposure to noxious agents, or infectious
agents leading to upper respiratory tract infections

© Endeavour College of Natural Health www.endeavour.edu.au 37
ACUTE LARYNGITIS
o Complications:• Chronic laryngitis
• Tracheitis
• Bronchitis
• Pneumonia
o Management:
o Rest of voice
o Steam inhalation
o Paracetamol
o Antibiotics
The image shows thick mucous on the
vocal folds and generalized mucosal
inflammation involving all regions of the
larynx.
http://www.drrahmatorlummc.com/infectiveconditions.htm

© Endeavour College of Natural Health www.endeavour.edu.au 38
CHRONIC LARYNGITIS
o Aetiology:
• Repeated attacks of acute laryngitis
• Excessive use of the voice, especially in dusty
atmospheres
• Heavy tobacco smoking
• Mouth-breathing from nasal obstruction
• Chronic infection of nasal sinuses
o Clinical features:
• Hoarseness or loss of voice
• Irritation of the throat
• Spasmodic cough

© Endeavour College of Natural Health www.endeavour.edu.au 39
CHRONIC LARYNGITIS
o Differential diagnosis
• Bronchial Carcinoma
• Pulmonary TB
• Laryngeal paralysis or tumour
o Management
• Rest the voice
• Inhalation of medicated steam
• Avoid smoking around the patient
http://www.ghorayeb.com/LaryngitisChronic.html
This patient smoked 80 cigarettes daily. The
vocal cords are swollen and covered with
plaques of whitish keratinized mucosa
(leukoplakia). Leukoplakia is related to
smoking and is precancerous.

© Endeavour College of Natural Health www.endeavour.edu.au 40
ACUTE EPIGLOTTITIS
o Aetiology:
• Bacterial infection, mostly H. influenzae type b (Hib)
o Clinical features:
• Fever and sore throat rapidly leading to stridor
• Stridor and cough without hoarseness of voice
o Definition:
• Inflammation of epiglottis, the cartilage that covers the trachea

© Endeavour College of Natural Health www.endeavour.edu.au 41
ACUTE EPIGLOTTITIS
o Complications
• Death from asphyxia due to spasm (hence a medical emergency)
o Management
• Intravenous antibiotic therapy
• Avoid using spatula or tongue depressor while examining the throat (avoids the spasm and thus the asphyxia)
Laryngoscopic view of oedematous and red
epiglottis, with generalised oedema of supraglottic.
http://www.enetmd.com/content/epiglottitis

© Endeavour College of Natural Health www.endeavour.edu.au 42
ACUTE BRONCHITIS AND
TRACHEITIS
o Aetiology:
• Infection usually bacterial or viral
o Clinical features:
• Follows acute coryza
• Chest tightness, wheezing, breathlessness
• Coughing & sputum
o Definition:
• Acute inflammation of the trachea and the bronchial tree

© Endeavour College of Natural Health www.endeavour.edu.au 43
ACUTE BRONCHITIS AND
TRACHEITIS
o Complications
• Bronchopneumonia
• Respiratory failure
• Bronchial asthma
o Management
• Antibiotics
• Endotracheal
intubation
• Analgesics and
paracetamol
o Diagnosis:
• X ray throat and chest for trachea and lungs
• Tracheal / nasopharyngeal swab culture
• Blood oxygen levels
• Blood test to determine the cause of infection
© Endeavour College of Natural Health www.endeavour.edu.au 44
TRACHEAL OBSTRUCTION
o Aetiology:
• Allergic reactions
• Foreign bodies
• Throat cancers
• External tumours pressing on trachea
• Inflammation of trachea or bronchial tree
o Clinical feature
• Stridor
o Complications
• Asphyxia
o Management
• Systematic and
depending upon the
cause

© Endeavour College of Natural Health www.endeavour.edu.au 45
INFLUENZA

© Endeavour College of Natural Health www.endeavour.edu.au 46
INFLUENZA
o Aetiology
• Orthomyxoviridae
family: Mainly Influenza
types A, B, and C
o Definition
• An acute systemic viral
infection that primarily
affects the respiratory
tract and carries a
significant mortality.
Influenza A virus Image from: Bauman, RW, 2010, Microbiology
with Diseases by Taxonomy, 3rd edn, Pearson Higher Ed, USA .
Neuraminidase and hemagglutinin are proteins found on the
envelope, or coat, of the virus that help the virus to lock on to and
invade its target cells.

© Endeavour College of Natural Health www.endeavour.edu.au 47
INFLUENZAo Pathophysiology:
• The virus first targets and kills mucous-secreting, ciliated,
and other epithelial cells of upper respiratory airway,
leaving gaping holes between the underlying basal cells
and allowing extracellular fluid to escape. This leads to the
“runny nose” .
• Viral proteins are released into the blood leading to
release of various cytokines and chemical mediators -
Inflammatory response (fever, headache, fatigue etc).
• Spread of infection to lower respiratory tract may cause
severe shedding of bronchial and alveolar cells down to a
single-cell–thick basal layer
• Pneumonia may result from a viral or a secondary
bacterial infection.

© Endeavour College of Natural Health www.endeavour.edu.au 48
INFLUENZAo Clinical features
• Incubation period: About one day; remain infective for
up to 8 hours on objects outside the body.
• Sudden fever between 39°C and 41°C (102–106°F)
• Pharyngitis, congestion, dry cough
• Malaise, headache, and myalgia
• Most people recover in one to two weeks.
• Associated symptoms:– Body aches, Nausea, Vomiting
– Loss of appetite
– Sweating, Chills, Dizziness, Flushed face
– Worsening of underlying illness, such as asthma or heart failure

© Endeavour College of Natural Health www.endeavour.edu.au 49
INFLUENZAo Complications:
• Viral or bacterial Pneumonia
• Bronchitis
• Sinusitis
• Otitis media
• Myositis
• Myocarditis
• Pericarditis
• Reye syndrome (fatty liver with encephalitis)

© Endeavour College of Natural Health www.endeavour.edu.au 50
INFLUENZAo Management
• Most people recover without needing medical care.
• Rest and medicines to relieve symptoms
• Drink plenty of liquids
• Avoid aspirin (especially teens and children)
• Avoid alcohol and tobacco
• Avoid antibiotics (unless necessary for another
illness)
• Antiviral drugs to treat people who become very sick
with the flu or who are at high risk for flu
complications.

© Endeavour College of Natural Health www.endeavour.edu.au 51
Influenza: An acute systemic viral infection that primarily affects the respiratory tract and
carries a significant mortality.
Orthomyxoviridae family: Influenza types A, B, and C
mucous-secreting, ciliated, and
other epithelial of upper
respiratory airway cells are
attacked.
Gaping holes between the
underlying basal cells and
allowing extracellular fluid to
escape.
Viral proteins are released into
the blood leading to release of
various cytokines and chemical
mediators - Inflammatory
response
Runny nose
Sudden high-grade fever
Pharyngitis, congestion, dry cough
Malaise, headache, and myalgia
Body aches, Nausea, Vomiting
Loss of appetite
Sweating, Chills, Dizziness, Flushed
face
Management:
No medical care required.
Rest and medicines to relieve
symptoms
Drink plenty of liquids
Avoid aspirin
Avoid alcohol and tobacco
Avoid antibiotics
Antiviral drugs
Complications:
Viral or bacterial Pneumonia
Bronchitis
Sinusitis
Otitis media
Myositis
Myocarditis
Pericarditis
Reye syndrome
Spread of infection to lower
respiratory tract, sinuses, middle
ear, heart, liver, muscles
© Endeavour College of Natural Health www.endeavour.edu.au 52
Reading and Resourceso Crowley LV, 2012, An Introduction to Human Diseases – Pathology and
Pathophysiology Correlations, 9th edn, Jones and Bartlett Learning
o Grossman SC & Porth CM 2014, Porth’s Pathophysiology- Concepts of
Altered Health States, 9th edn. Wolters Kluwer Health - Lippincott, Williams
& Wilkins
o Hinson, J, Raven, P & Chew, S 2010, The endocrine system: basic science
and clinical conditions, 2nd edn, Churchill Livingstone Elsevier, Edinburgh
o Jamison, JR 2006, Differential diagnosis for primary care: a handbook for
health care practitioners, 2nd edn, Churchill Livingstone Elsevier,
Edinburgh.
o Jarvis, C, 2012 Physical Examination & Health Assessment, 6th ed.,
Elsevier Saunders, Philadelphia.
o Kumar, P & Clark, M 2012, Kumar and Clark’s clinical medicine, 8th edn,
Saunders Elsevier, Edinburgh.
o Kumar, V, Abbas, AK & Aster, JC 2015, Robbins & Cotran pathologic basis
of disease, 9th edn, Elsevier Saunders, Philadelphia.
© Endeavour College of Natural Health www.endeavour.edu.au 53
Reading and Resourceso Lee, G & Bishop, P 2009, Microbiology and infection control for health
professionals, 4th edn, Pearson Education, Frenchs Forest, NSW.
o McCance, KL, Heuther, SE, & Brashers, VL 2014, Pathophysiology: the
biologic basis for disease in adults and children, 7th edn, Elsevier.
o Michael-Titus, A, Revest, P & Shortland, P 2010, The nervous system: basic
science and clinical conditions, 2nd edn, Churchill Livingstone Elsevier,
Edinburgh
o Mosby’s dictionary of medicine, nursing and health professions 2013, 9th
edn, Elsevier, St. Louis, MO.
o Tortora, GJ & Derrickson, B 2014, Principles of anatomy and physiology,
14th edn, John Wiley & Sons, Hoboken, NJ.
o VanMeter, KC & Hubert, RJ 2014, Gould's pathophysiology for the health
professions, 5th edn, Elsevier, St Louis, MO.
o Walker, BR, Colledge, NR, Ralston, SH, & Penman, ID (eds) 2014,
Davidson’s principles and practice of medicine, 22nd edn, Churchill
Livingstone Elsevier, Edinburgh.

© Endeavour College of Natural Health www.endeavour.edu.au 54
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and
communicated to you by or on behalf of
the Endeavour College of Natural Health pursuant to
Part VB of the Copyright Act 1968 (the Act).
The material in this communication may
be subject to copyright under the Act.
Any further reproduction or
communication of this material by you
may be the subject of copyright
protection under the Act.
Do not remove this notice.







