Download - Anil - Thorax
Anatomy of the ThoraxLSS Year 1
Anil Chopra
ContentsThorax 1 – Anatomy of the Chest Wall......................................................................1Thorax 2 – Lungs, Pleura and Diaphragm................................................................7Thorax 3 – Superior Mediastinum and Great Vessels............................................14Thorax 4 – Organisation of Nerves in the Thorax – Mon 26th Feb 2007...............23Thorax 5 – Lymphatic System, Breasts and Breast Cancer...................................33Thorax 6 – The Posterior Mediastinum...................................................................37
Thorax 1 – Anatomy of the Chest WallAnil Chopra
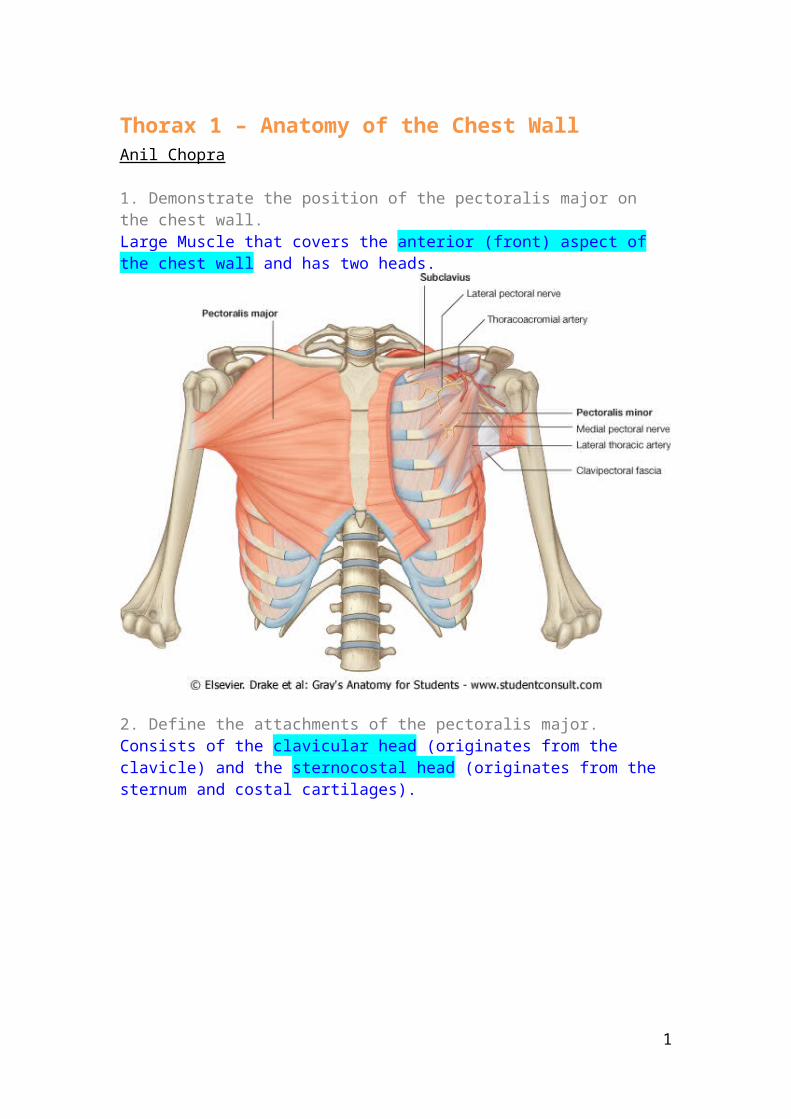
1. Demonstrate the position of the pectoralis major on the chest wall.Large Muscle that covers the anterior (front) aspect of the chest wall and has two heads.
2. Define the attachments of the pectoralis major.Consists of the clavicular head (originates from the clavicle) and the sternocostal head (originates from the sternum and costal cartilages).
3. Outline the actions of the pectoralis major.
1

Contracts when pushing.
4. Name the space between adjacent ribsIntercostal Spaces
5. Name and summarise the functions of the muscles which are found between ribsIntercostal muscles. There are 3: External intercostal muscles – articulates downward and laterally Internal intercostal muscles – articulates perpendicular to external intercostals. Innermost intercostal muscles – fairly trivial.
Their job is to move the ribs as well as stiffen the chest wall improving efficiency of breathing movements.
Just below each rib in the Costal groove, starting from the top, there is the intercostal vein, artery and then the nerve (VAN).
2
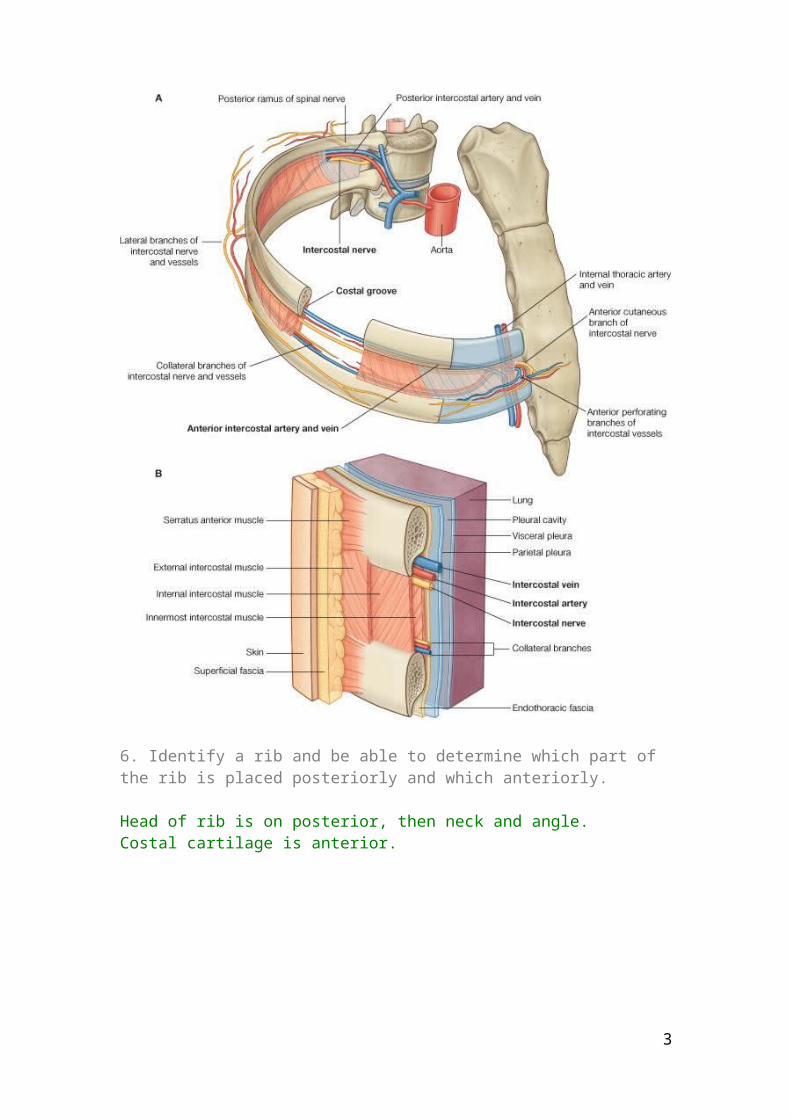
6. Identify a rib and be able to determine which part of the rib is placed posteriorly and which anteriorly.
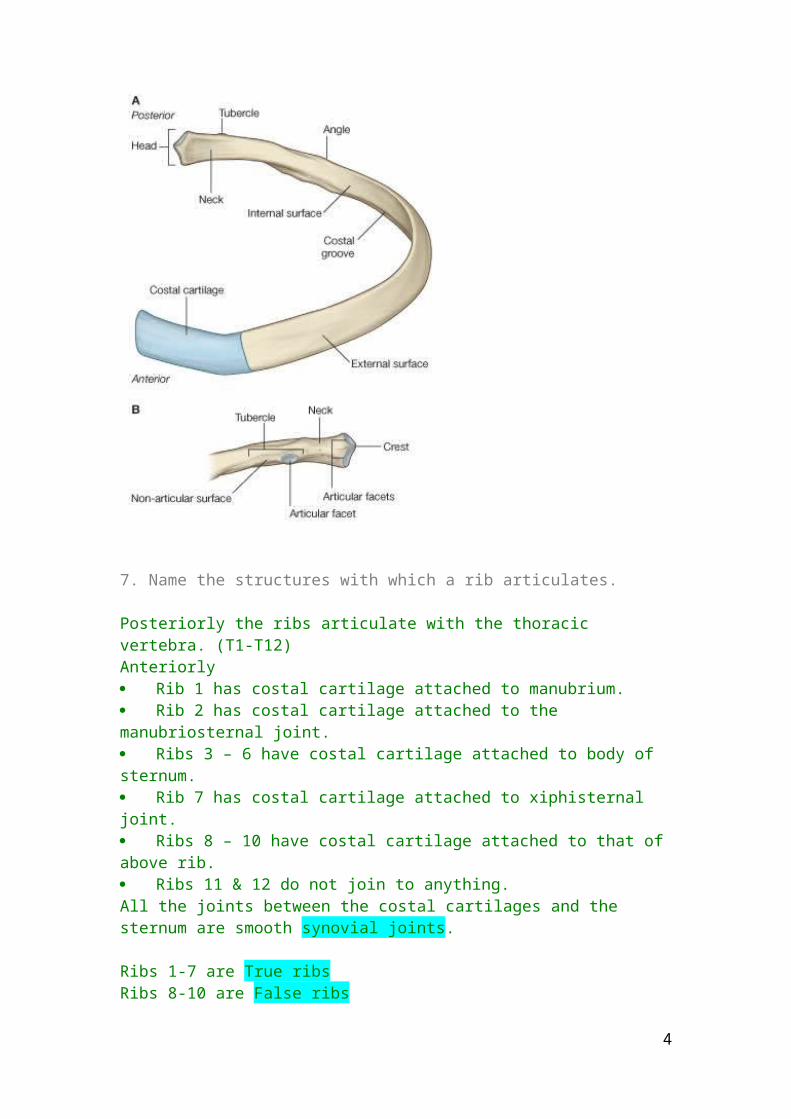
Head of rib is on posterior, then neck and angle.Costal cartilage is anterior.
7. Name the structures with which a rib articulates.
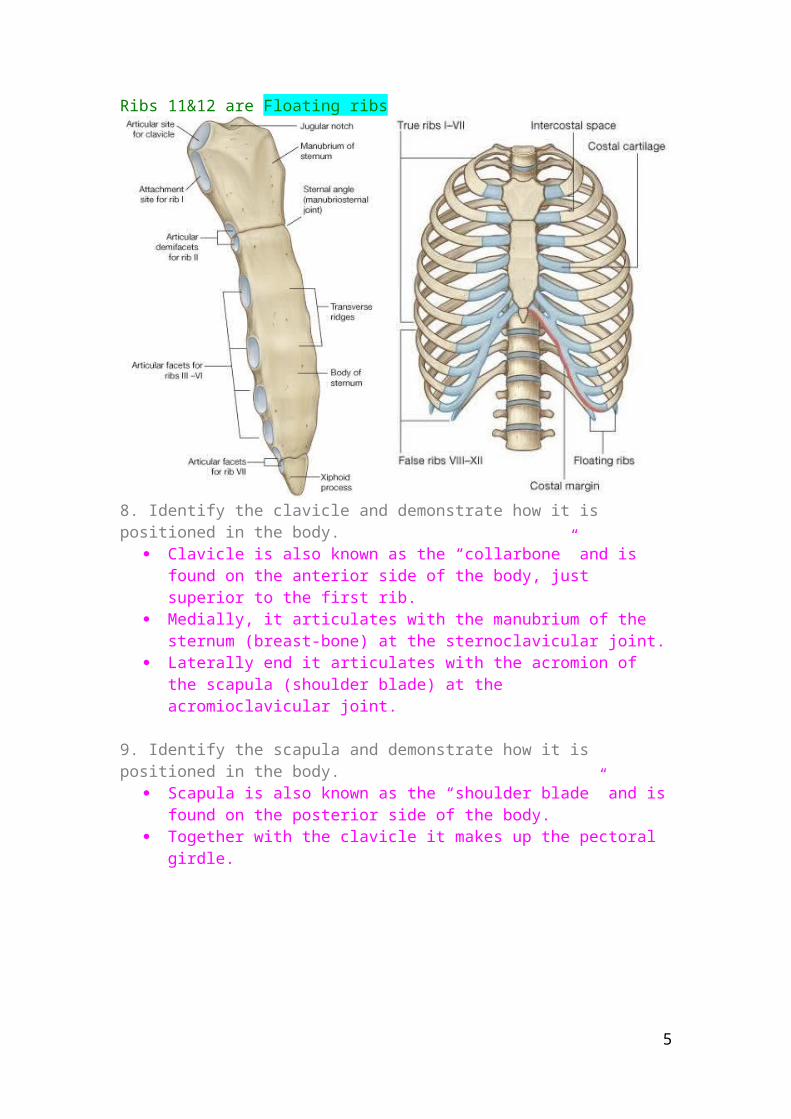
Posteriorly the ribs articulate with the thoracic vertebra. (T1-T12)Anteriorly Rib 1 has costal cartilage attached to manubrium. Rib 2 has costal cartilage attached to the manubriosternal joint. Ribs 3 – 6 have costal cartilage attached to body of sternum. Rib 7 has costal cartilage attached to xiphisternal joint. Ribs 8 – 10 have costal cartilage attached to that of above rib. Ribs 11 & 12 do not join to anything.All the joints between the costal cartilages and the sternum are smooth synovial joints.
Ribs 1-7 are True ribsRibs 8-10 are False ribsRibs 11&12 are Floating ribs
3
8. Identify the clavicle and demonstrate how it is positioned in the body. Clavicle is also known as the “collarbone” and is found on the anterior side of
the body, just superior to the first rib. Medially, it articulates with the manubrium of the sternum (breast-bone) at the
sternoclavicular joint. Laterally end it articulates with the acromion of the scapula (shoulder blade) at
the acromioclavicular joint.
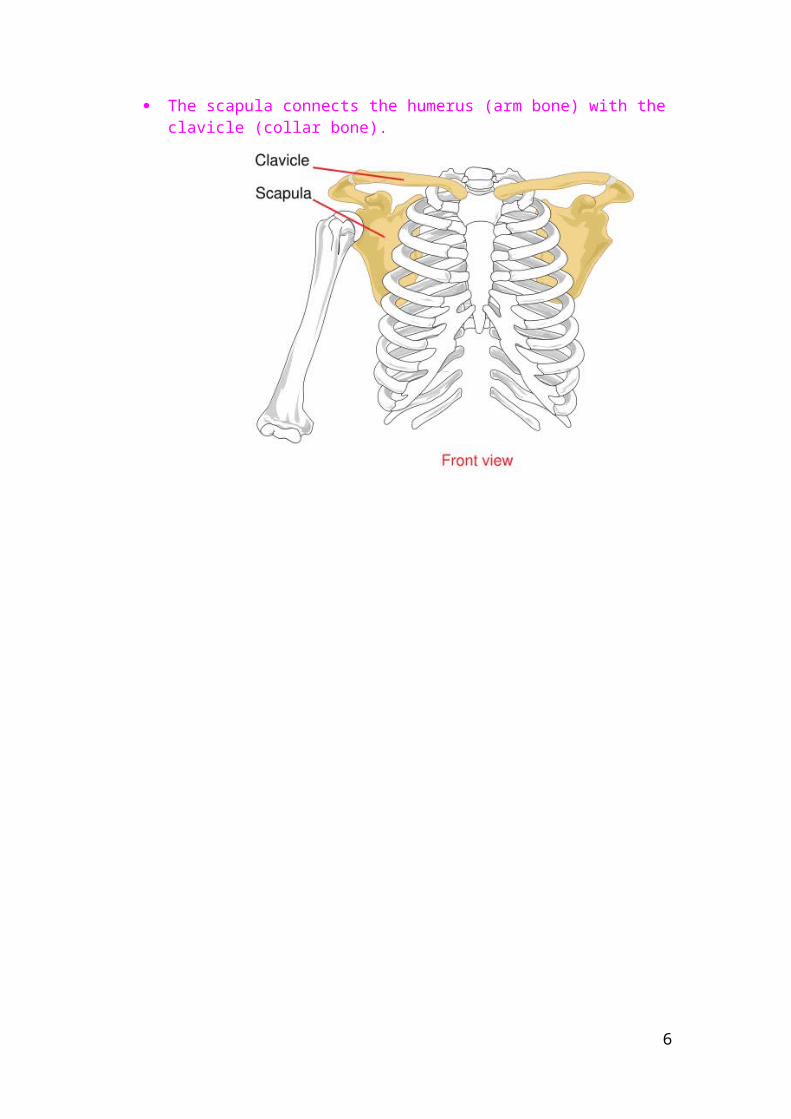
9. Identify the scapula and demonstrate how it is positioned in the body. Scapula is also known as the “shoulder blade” and is found on the posterior
side of the body. Together with the clavicle it makes up the pectoral girdle. The scapula connects the humerus (arm bone) with the clavicle (collar bone).
4
10. Identify a thoracic vertebra. There are 12 thoracic vertebrae T1- T12. Each corresponds to a rib.
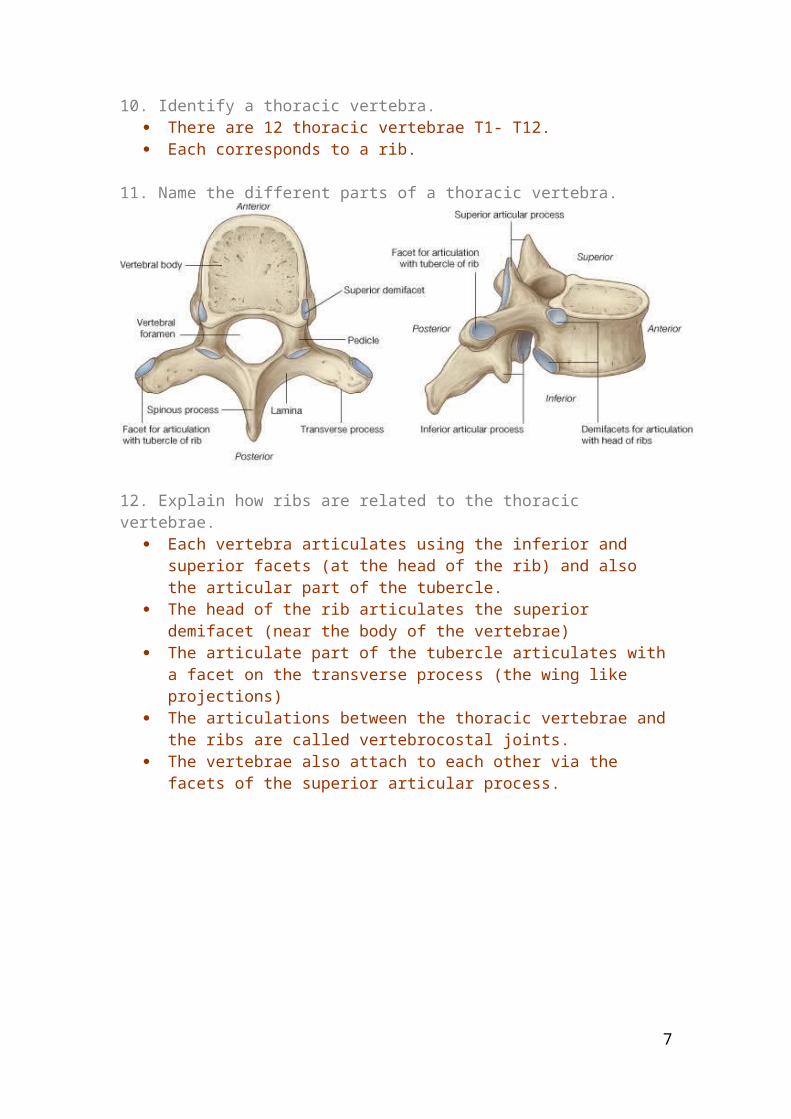
11. Name the different parts of a thoracic vertebra.
12. Explain how ribs are related to the thoracic vertebrae. Each vertebra articulates using the inferior and superior facets (at the head of
the rib) and also the articular part of the tubercle. The head of the rib articulates the superior demifacet (near the body of the
vertebrae) The articulate part of the tubercle articulates with a facet on the transverse
process (the wing like projections) The articulations between the thoracic vertebrae and the ribs are called
vertebrocostal joints. The vertebrae also attach to each other via the facets of the superior articular
process.
5
13. Explain how vertebrae articulate with each other and how they support loads and absorb jolts.
Vertebrae articulate with each other by thin intervertebral discs between them (which also limits movement)
The disk is made of cartilage. It is therefore a synovial joint. Each disc has an outer fibrous ring consisting of fibrocatilage called annulus
fibrosus and an inner soft, pulpy, highly elastic substance called the nucleus pulposus.
The discs form strong joints, permit various movements of the vertebral column and absorb vertical shock. Under compression, they flatten, broaden and bulge from their intervertebral spaces.
6
Thorax 2 – Lungs, Pleura and DiaphragmAnil Chopra
1. Name the contents of an intercostal space.
Intercostal space contains: External intercostal muscles Internal intercostal muscles Innermost intercostal muscles Intercostal Vein (in costal groove) Intercostal Artery (in costal groove) Intercostal Nerve (in costal groove) Collateral branches
2. Define the pleura.
The pleura is a layer of flattened cells supported by connective tissue that lines each pleural cavity and covers the exterior of the lungs.
7

3. Name the layers of the pleura.
Pleura consist of 2 layers:Visceral Pleura: this covers the surface of the lungs and is the innermost layer.
Parietal Pleura: this lines the innermost surface of the chest wall and is in contact with the ribs and intercostal muscles. It is the outermost layer.
These 2 layers are separated by the pleural cavity which contains serous fluid produced by the cells in the pleura. This helps the lungs glide as they expand and collapse.
4. Define the extent of the lungs.The lungs are conical in shape:
The apex (top) of the lungs reach as high as 3-4 cm above the first costal cartilage, in the base of the neck.
The base (bottom) of the lungs is concave and rests on the diaphragm.5. Define the extent of the pleura
.The parietal pleura consists of 4 parts:
the part relating to the intercostal spaces is the costal part the part relating to the diaphragm is the diaphragmatic part the part covering the mediastinum is the mediastinal part the part lining the cervical extension of the cavity is the cervical pleura
In the mediastinal part, there is a space which is made for the root or hilum of the lung.
8

The visceral pleura is continuous with the parietal pleura all the way around the lungs attached to the outside of them, including running into both opposed surfaces of the fissures.
Superiorly the pleural cavity projects 3-4cm above the first costal cartilage. Anteriorly the pleural cavities approach one another in the upper part of the
sternum. In the lower part the right side is closer to the midline than the left side because of the space made by the pericardium etc.
Inferiorly the pleura reflects onto the diaphragm. o On the left side the diaphragm separates the left lobe of the liver, the
spleen and the stomach. o On the right side the diaphragm separates the right lobe of the liver.
During quiet breathing…o The inferior margin of the lungs comes down to as far as about rib VI in the
midclavicular line (middle of clavicle) rib VIII in the midaxillary line (runs down side of body) and reaches the vertebral column at TX.
o The inferior margin of the pleural cavity comes down as far as rib VIII on the midclavicular line, rib X on the midaxillary line, and reaches the vertebral column at TXII.
o The space between the two margins is the costodiaphragmatic recess.
6. State how the right and left lungs are normally distinguishable.The right lung:
o Has 3 lobes, the inferior lobe, the superior lobe and the middle lobe. o Has 2 fissures, the oblique fissure, separating the inferior lobe from the
superior and middle lobes; and the horizontal fissure separating the superior lobe from the middle lobe.
o On its mediastinal surface in contact with the heart, inferior vena cava, superior vena cava, azygos vein oesophagus.
o Is larger than the left lung.The left lung:
o Has only 2 lobes, the inferior lobe and the superior lobe.o Has 1 fissure, the oblique fissure, that separates the superior and inferior
lobes. o On its mediastinal surface is in contact with the heart, aortic arch, thoracic
aorta, and oesophagus. It contains a notch where the heart projects into the pleural cavity from the middle mediastinum.
9

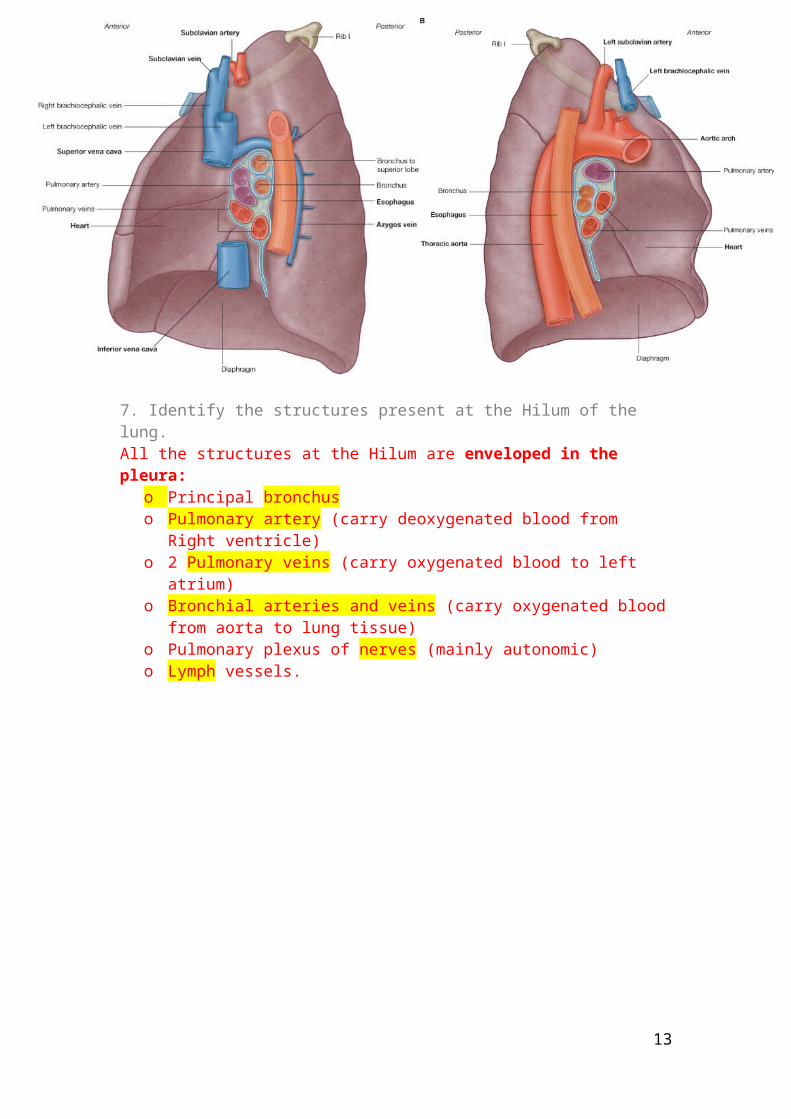
7. Identify the structures present at the Hilum of the lung.All the structures at the Hilum are enveloped in the pleura:
o Principal bronchuso Pulmonary artery (carry deoxygenated blood from Right ventricle)o 2 Pulmonary veins (carry oxygenated blood to left atrium)o Bronchial arteries and veins (carry oxygenated blood from aorta to lung tissue)o Pulmonary plexus of nerves (mainly autonomic)o Lymph vessels.
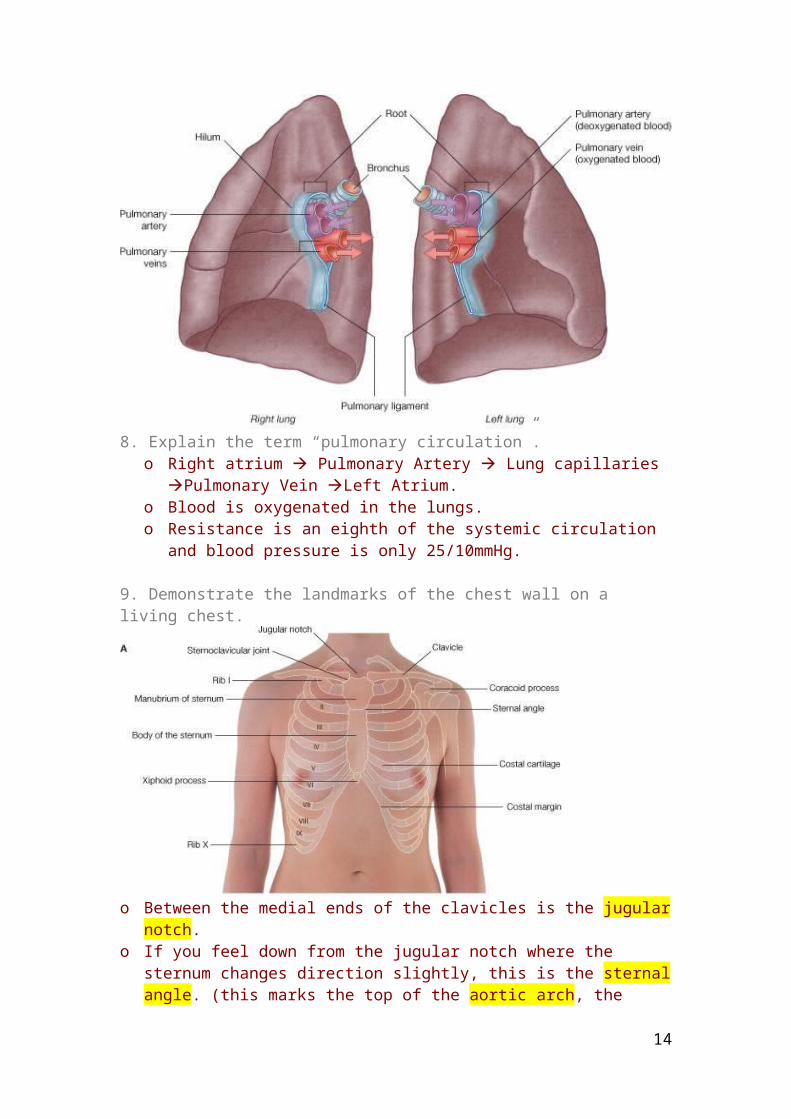
8. Explain the term “pulmonary circulation”.o Right atrium Pulmonary Artery Lung capillaries Pulmonary Vein
Left Atrium.o Blood is oxygenated in the lungs.o Resistance is an eighth of the systemic circulation and blood pressure is only
25/10mmHg.
10
9. Demonstrate the landmarks of the chest wall on a living chest.
o Between the medial ends of the clavicles is the jugular notch.o If you feel down from the jugular notch where the sternum changes direction
slightly, this is the sternal angle. (this marks the top of the aortic arch, the tracheal bifurcation and the level of the 2nd costal cartilage.
o In men the nipple lies in the 4th intercostal space (between 4th and 5th ribs)o In women, beneath the breast is the 6th rib.
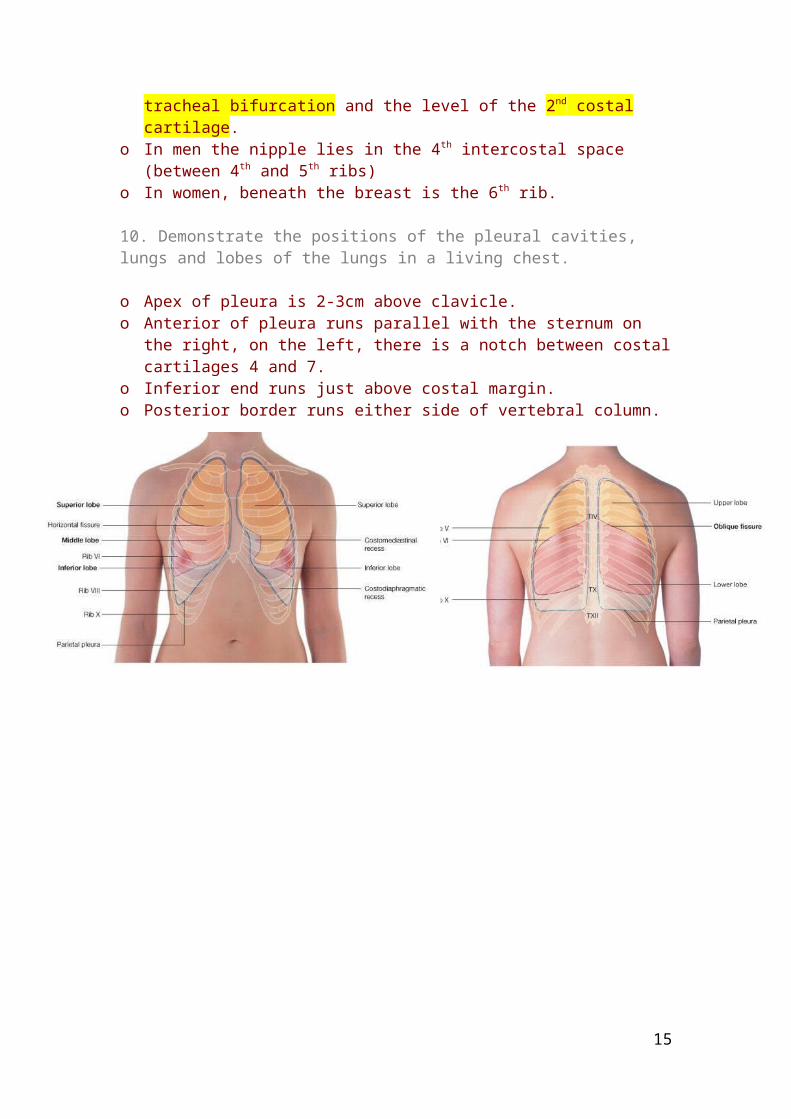
10. Demonstrate the positions of the pleural cavities, lungs and lobes of the lungs in a living chest.
o Apex of pleura is 2-3cm above clavicle.o Anterior of pleura runs parallel with the sternum on the right, on the left, there is a
notch between costal cartilages 4 and 7. o Inferior end runs just above costal margin.o Posterior border runs either side of vertebral column.
11

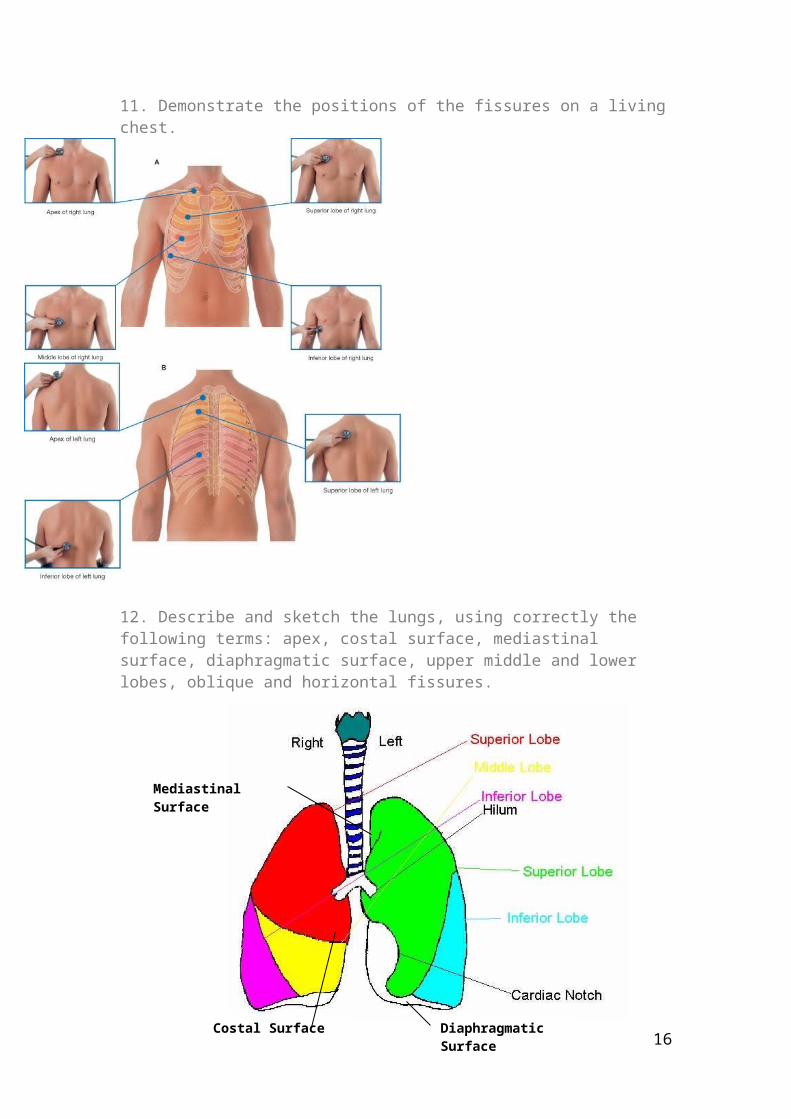
11. Demonstrate the positions of the fissures on a living chest.
12. Describe and sketch the lungs, using correctly the following terms: apex, costal surface, mediastinal surface, diaphragmatic surface, upper middle and lower lobes, oblique and horizontal fissures.
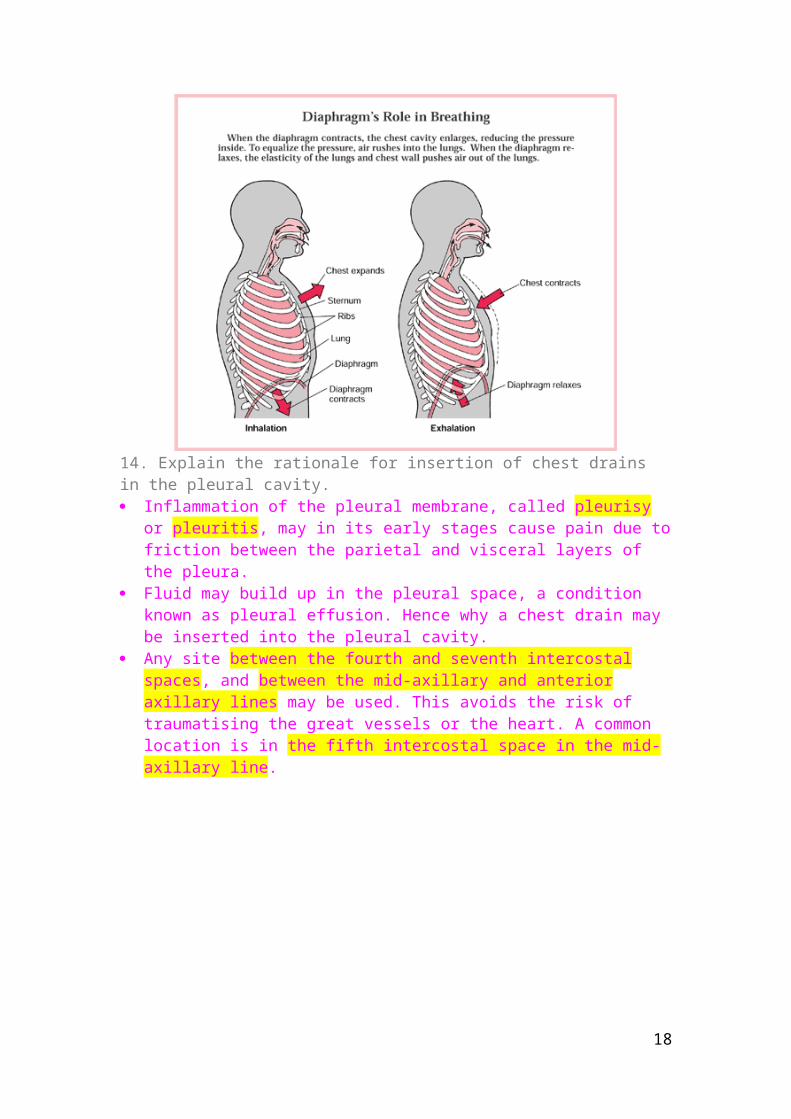
13. Explain the structural basis for breathing, including the differences between light, deep and forced breathing.
Breathing is controlled by the nervous system and produced by the skeletal muscle.
Lungs ventilate the air sacs – the site of gas exchange. Movements of both the diaphragm and the ribs cause an increase of the
thoracic cavity capacityo The muscles in the wall cause expansion of the pleural cavity.o The elastic lungs expand with the pleural cavity.o Air is sucked down the trachea and bronchi into the lungs.
12
Diaphragmatic Surface
Costal Surface
Mediastinal Surface
The Ribs move up forward and upward with a bucket-handle like action. This increases the anteroposterior, as well as the transverse dimensions of the thoracic cavity.
The Diaphragm is the main inspiratory muscle. When it contracts the vertical dimension of the thoracic cavity is greatly increased. This also pushes the contents of the abdominal cavity down and out.
Inspiration is caused by the increase in thoracic cavity capacity which results in a reduction in the intrapleural pressure. This causes expansion of the lung and therefore entry of the air through the respiratory passages.
Quiet inspiration uses only the diaphragm. Forced inspiration uses both the diaphragm and intercostal muscles.
Expiration is caused by the elastic recoil in the tissue around the lungs and rib cage. Quiet expiration uses only the diaphragm. Forced expiration uses both the diaphragm and abdominal muscles.
14. Explain the rationale for insertion of chest drains in the pleural cavity. Inflammation of the pleural membrane, called pleurisy or pleuritis, may in its
early stages cause pain due to friction between the parietal and visceral layers of the pleura.
Fluid may build up in the pleural space, a condition known as pleural effusion. Hence why a chest drain may be inserted into the pleural cavity.
Any site between the fourth and seventh intercostal spaces, and between the mid-axillary and anterior axillary lines may be used. This avoids the risk of traumatising the great vessels or the heart. A common location is in the fifth intercostal space in the mid-axillary line.
13
Thorax 3 – Superior Mediastinum and Great VesselsAnil Chopra
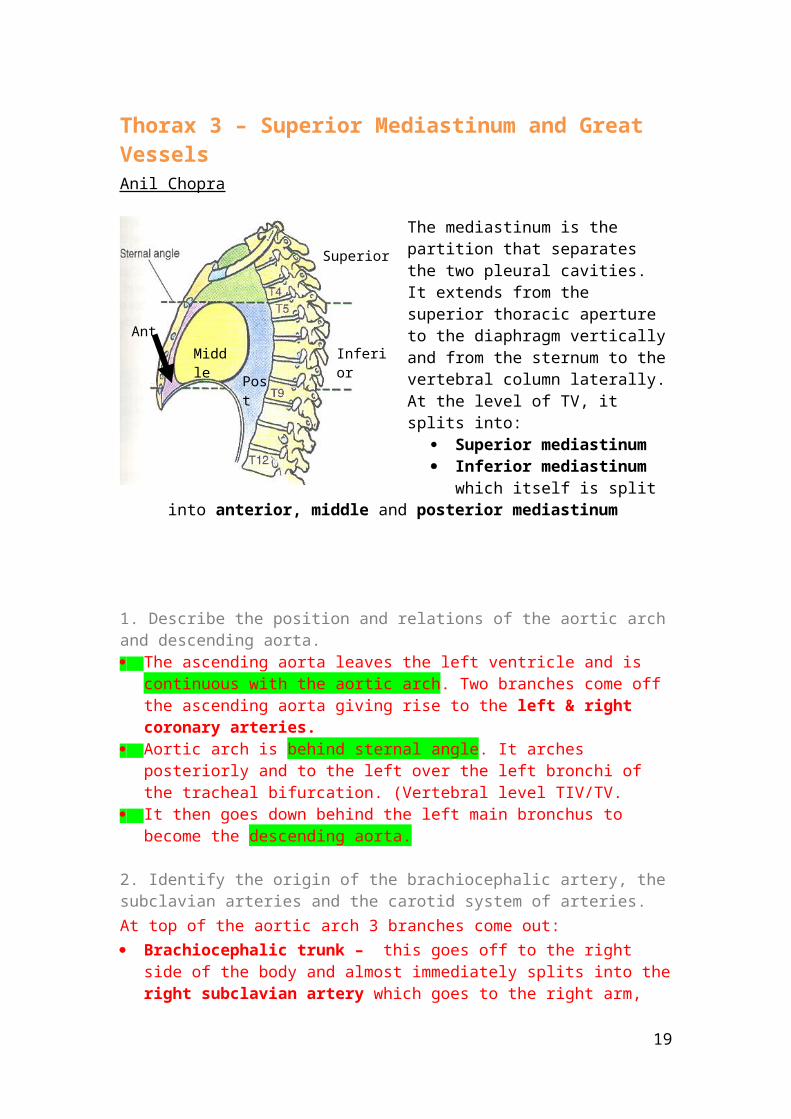
The mediastinum is the partition that separates the two pleural cavities. It extends from the superior thoracic aperture to the diaphragm vertically and from the sternum to the vertebral column laterally. At the level of TV, it splits into:
Superior mediastinum Inferior mediastinum which
itself is split into anterior, middle and posterior mediastinum
1. Describe the position and relations of the aortic arch and descending aorta. The ascending aorta leaves the left ventricle and is continuous with the aortic arch.
Two branches come off the ascending aorta giving rise to the left & right coronary arteries.
Aortic arch is behind sternal angle. It arches posteriorly and to the left over the left bronchi of the tracheal bifurcation. (Vertebral level TIV/TV.
It then goes down behind the left main bronchus to become the descending aorta.
2. Identify the origin of the brachiocephalic artery, the subclavian arteries and the carotid system of arteries.At top of the aortic arch 3 branches come out: Brachiocephalic trunk – this goes off to the right side of the body and almost
immediately splits into the right subclavian artery which goes to the right arm, and the right common carotid artery which goes up to the head.
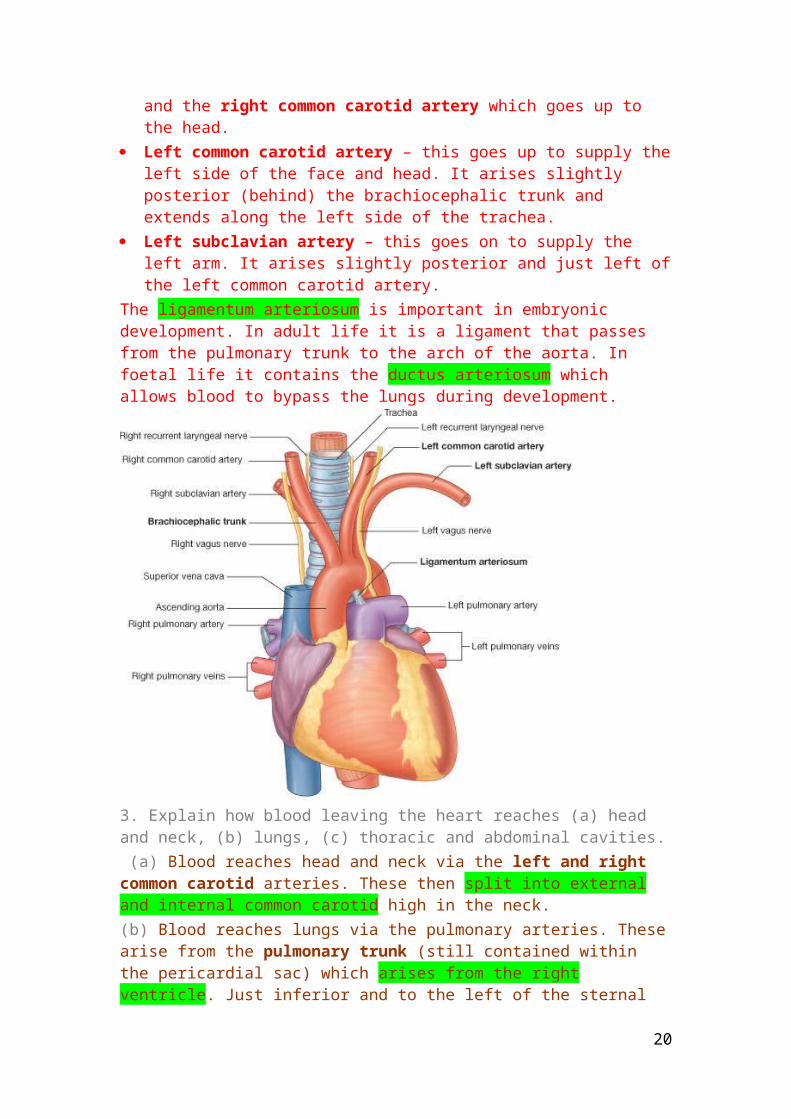
Left common carotid artery – this goes up to supply the left side of the face and head. It arises slightly posterior (behind) the brachiocephalic trunk and extends along the left side of the trachea.
Left subclavian artery – this goes on to supply the left arm. It arises slightly posterior and just left of the left common carotid artery.
The ligamentum arteriosum is important in embryonic development. In adult life it is a ligament that passes from the pulmonary trunk to the arch of the aorta. In foetal life it contains the ductus arteriosum which allows blood to bypass the lungs during development.
14
MiddleAnt
Post
Inferior
Superior
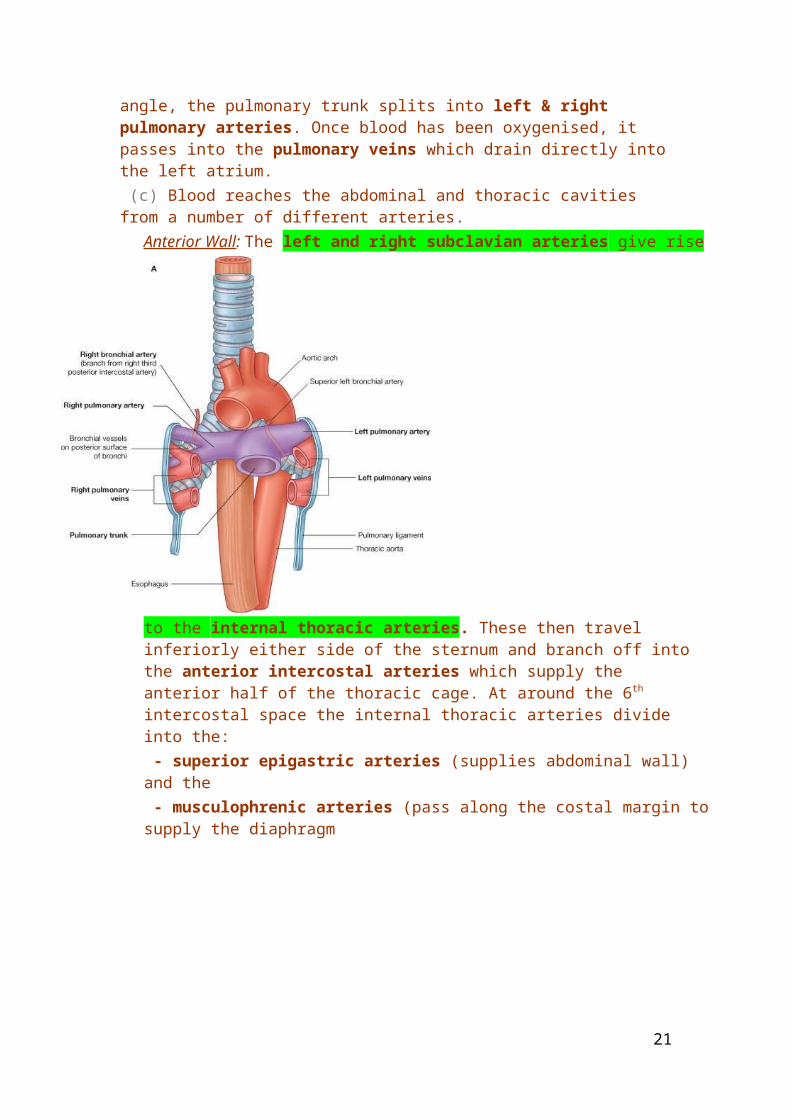
3. Explain how blood leaving the heart reaches (a) head and neck, (b) lungs, (c) thoracic and abdominal cavities. (a) Blood reaches head and neck via the left and right common carotid arteries. These then split into external and internal common carotid high in the neck.(b) Blood reaches lungs via the pulmonary arteries. These arise from the pulmonary trunk (still contained within the pericardial sac) which arises from the right ventricle. Just inferior and to the left of the sternal angle, the pulmonary trunk splits into left & right pulmonary arteries. Once blood has been oxygenised, it passes into the pulmonary veins which drain directly into the left atrium. (c) Blood reaches the abdominal and thoracic cavities from a number of different arteries.
15
Anterior Wall: The left and right subclavian arteries give rise to the internal thoracic arteries. These then travel inferiorly either side of the sternum and branch off into the anterior intercostal arteries which supply the anterior half of the thoracic cage. At around the 6th intercostal space the internal thoracic arteries divide into the: - superior epigastric arteries (supplies abdominal wall) and the - musculophrenic arteries (pass along the costal margin to supply the diaphragm
16

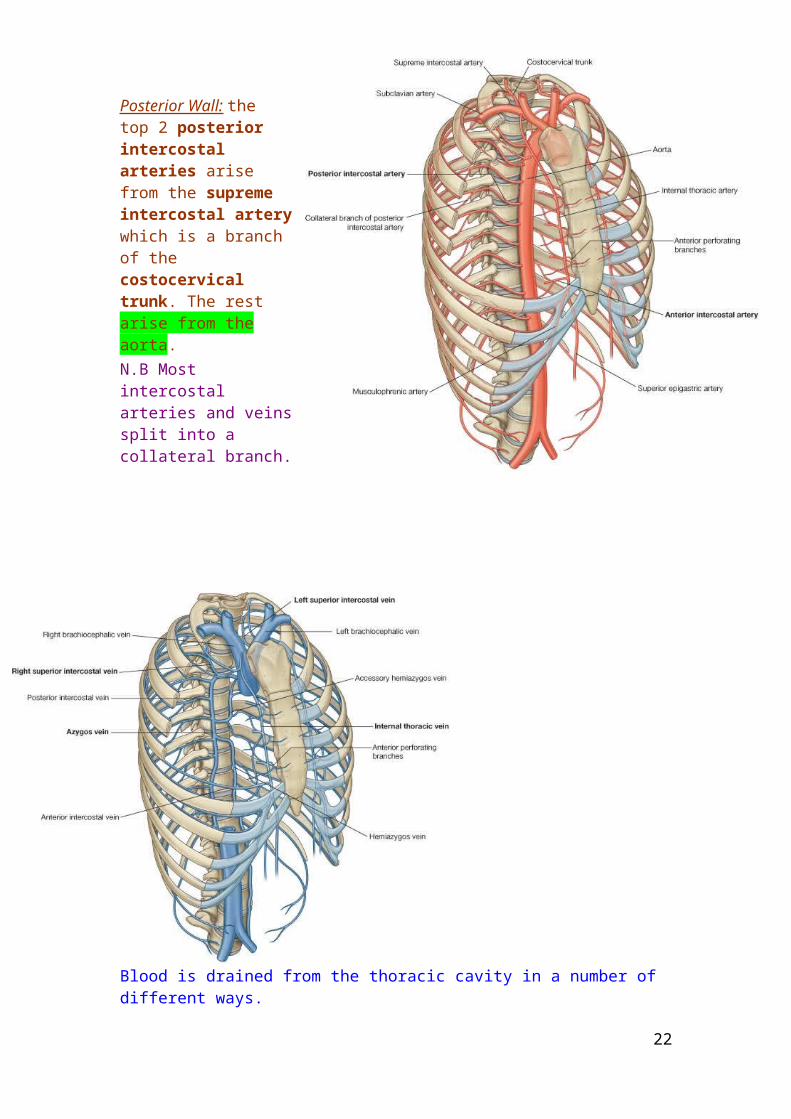
Posterior Wall: the top 2 posterior intercostal arteries arise from the supreme intercostal artery which is a branch of the costocervical trunk. The rest arise from the aorta.N.B Most intercostal arteries and veins split into a collateral branch.
Blood is drained from the thoracic cavity in a number of different ways.Anterior Wall: The anterior intercostal veins drain into the internal thoracic veins which themselves drain into the brachiocephalic vein.Posterior Wall: The superior part of the posterior wall is drained by the left and right upper posterior intercostal veins which drain into the azygous vein. The rest of the posterior wall is drained by the intercostal veins draining into the azygous vein on the right side and the hemiazygous and accessory hemiazygous veins on the left side. The hemiazygous and accessory hemiazygous drain into the azygous which drains directly into the inferior vena cava.
17
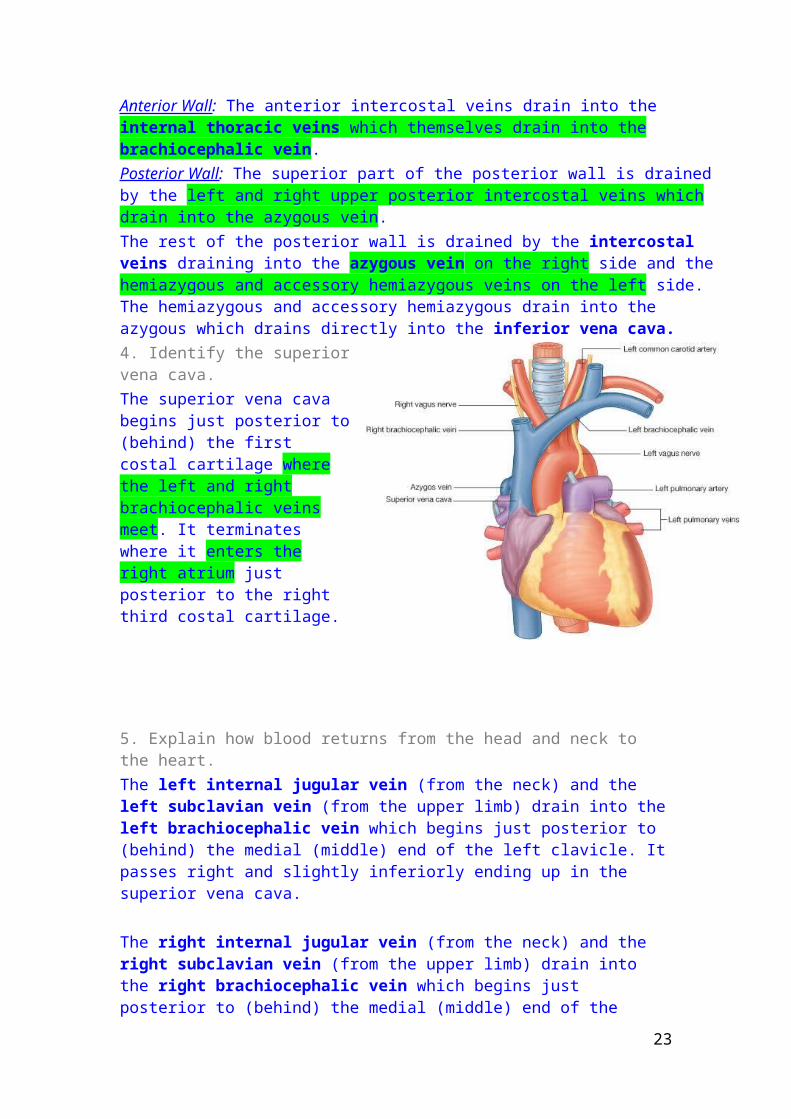
4. Identify the superior vena cava.The superior vena cava begins just posterior to (behind) the first costal cartilage where the left and right brachiocephalic veins meet. It terminates where it enters the right atrium just posterior to the right third costal cartilage.
5. Explain how blood returns from the head and neck to the heart.The left internal jugular vein (from the neck) and the left subclavian vein (from the upper limb) drain into the left brachiocephalic vein which begins just posterior to (behind) the medial (middle) end of the left clavicle. It passes right and slightly inferiorly ending up in the superior vena cava.
The right internal jugular vein (from the neck) and the right subclavian vein (from the upper limb) drain into the right brachiocephalic vein which begins just posterior to (behind) the medial (middle) end of the right clavicle. It passes vertically downward ending up in the superior vena cava.
6. Outline the principles and main applications of conventional X-ray and CT imaging. X-Ray:
o Radiation in the form of X-rays are passed posterior to anterior. o High density e.g. bone/flowing blood stops all x-ray (blood has heavy
metal ions in it therefore absorb the x-rays) and shows up white; low density e.g. lung fields are trans-radiant and show up black. (heavy atomic nuclei are needed to stop X-rays)
o Image is “backwards” i.e. always refer to things from patients point of view (left and right)
CT imaging: o Shows an image as if looking through the feet at a sectiono X-ray beam traces a section at multiple angles around the body –
visualises soft tissue in much more detail than conventional X-ray.
18
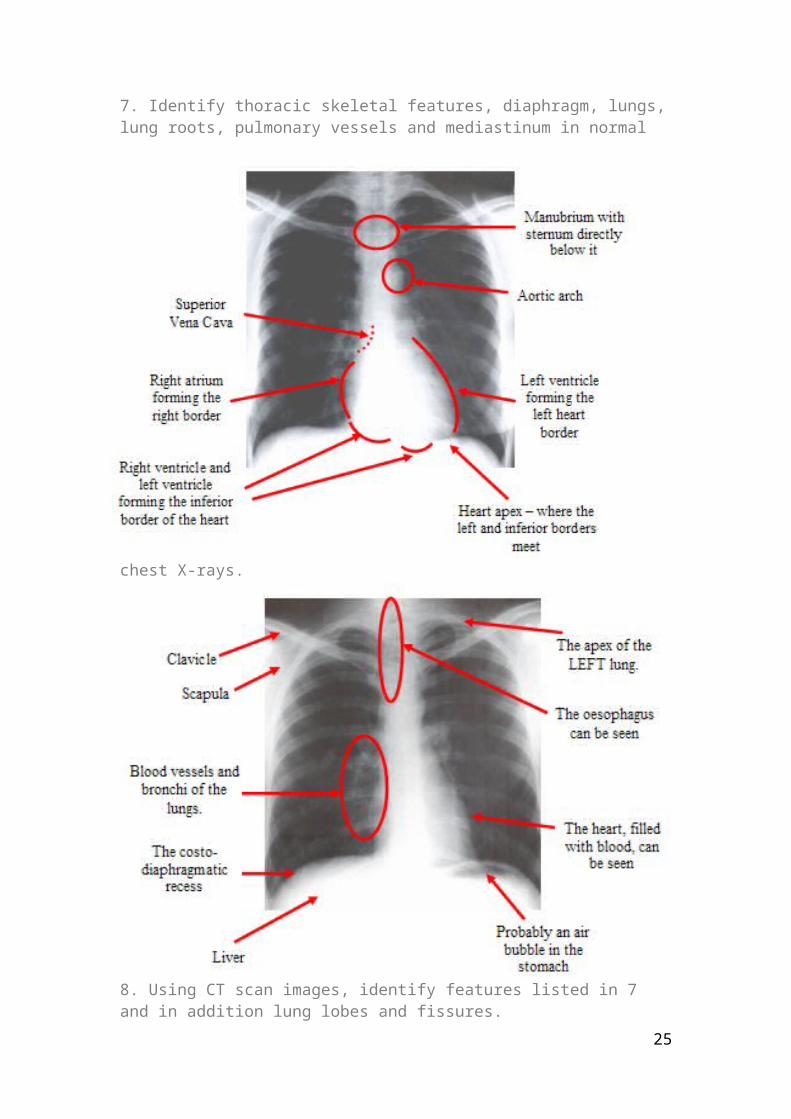
7. Identify thoracic skeletal features, diaphragm, lungs, lung roots, pulmonary vessels and mediastinum in normal chest X-rays.
8. Using CT scan images, identify features listed in 7 and in addition lung lobes and fissures.
19
& 9.Relate appearances seen in CT sections of the chest to those in the living or dissected body; recognise the approximate vertebral level of any chest CT image.
1) Right Clavicle 2) Sternum 3) Pectoralis Major Muscle 4) Pectoralis Minor Muscle 5) Axillary Vein 6) Rib 7) Subclavian Vein 8) Trachea 9) Left Brachiocephalic Vein 10) Left Common Carotid Artery 11) Left Subclavian Artery 12) Vertebral Body 13) Scapula 14) Level of Slice
20
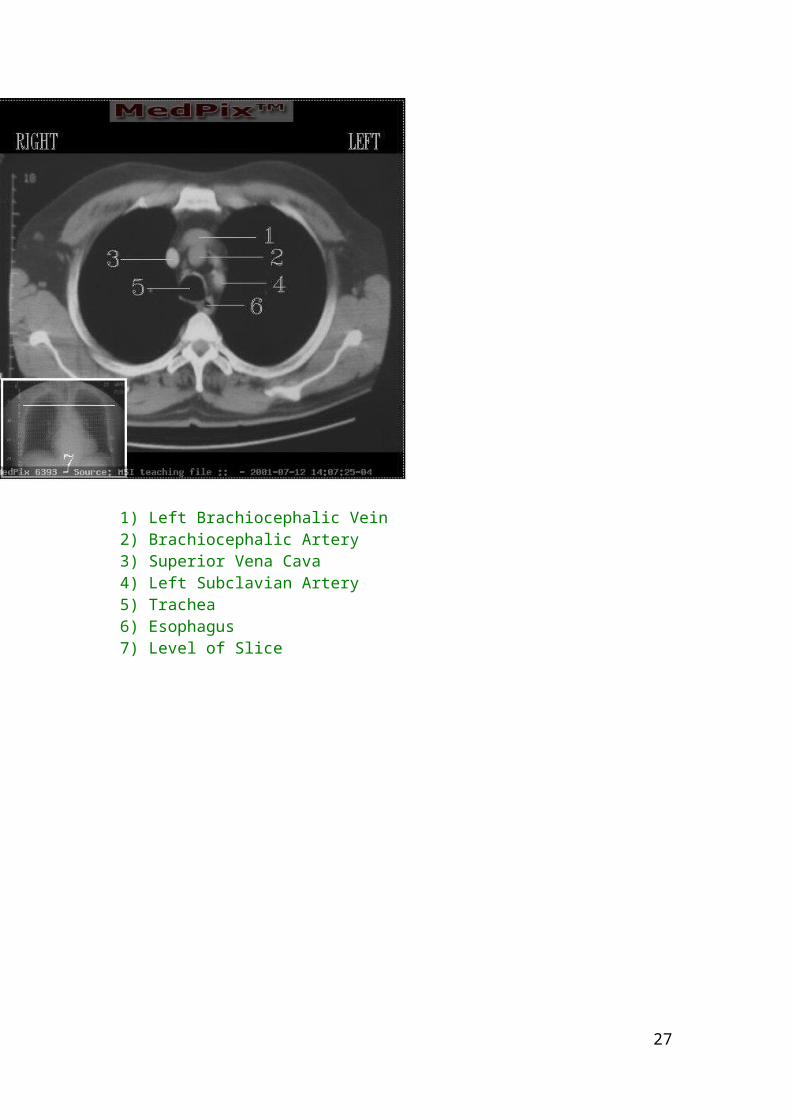
1) Left Brachiocephalic Vein 2) Brachiocephalic Artery 3) Superior Vena Cava 4) Left Subclavian Artery 5) Trachea 6) Esophagus 7) Level of Slice
21
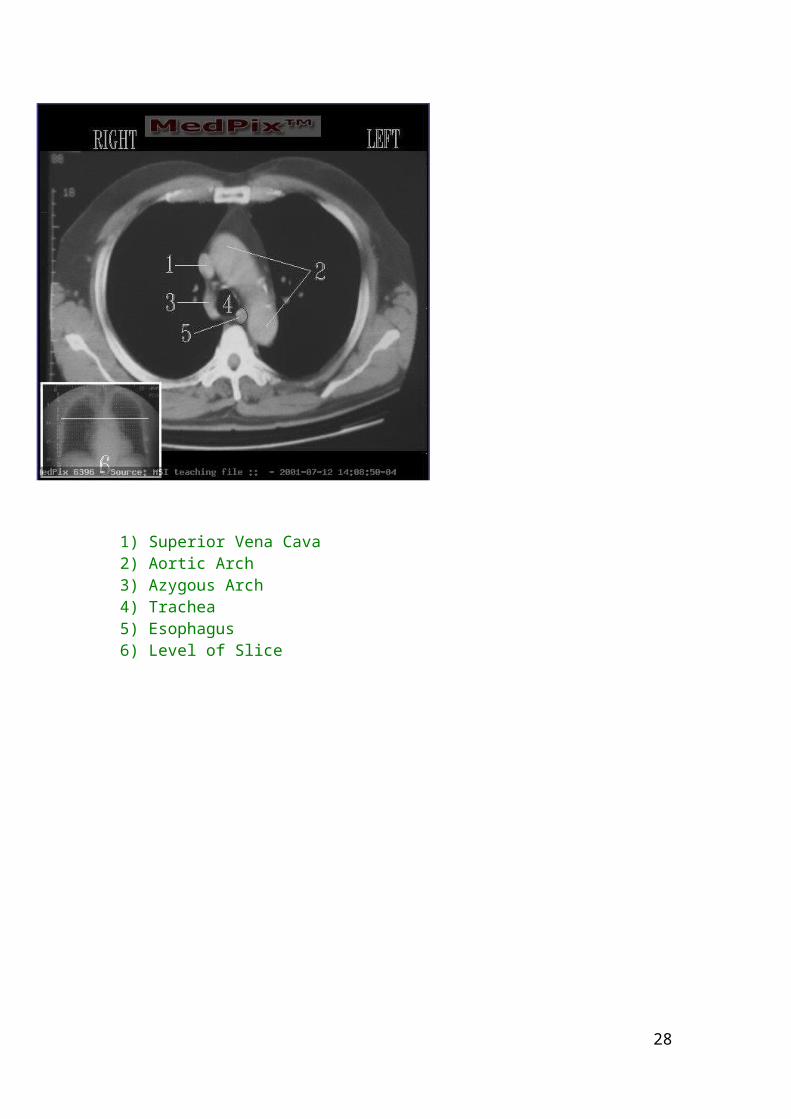
1) Superior Vena Cava 2) Aortic Arch 3) Azygous Arch 4) Trachea 5) Esophagus 6) Level of Slice
22
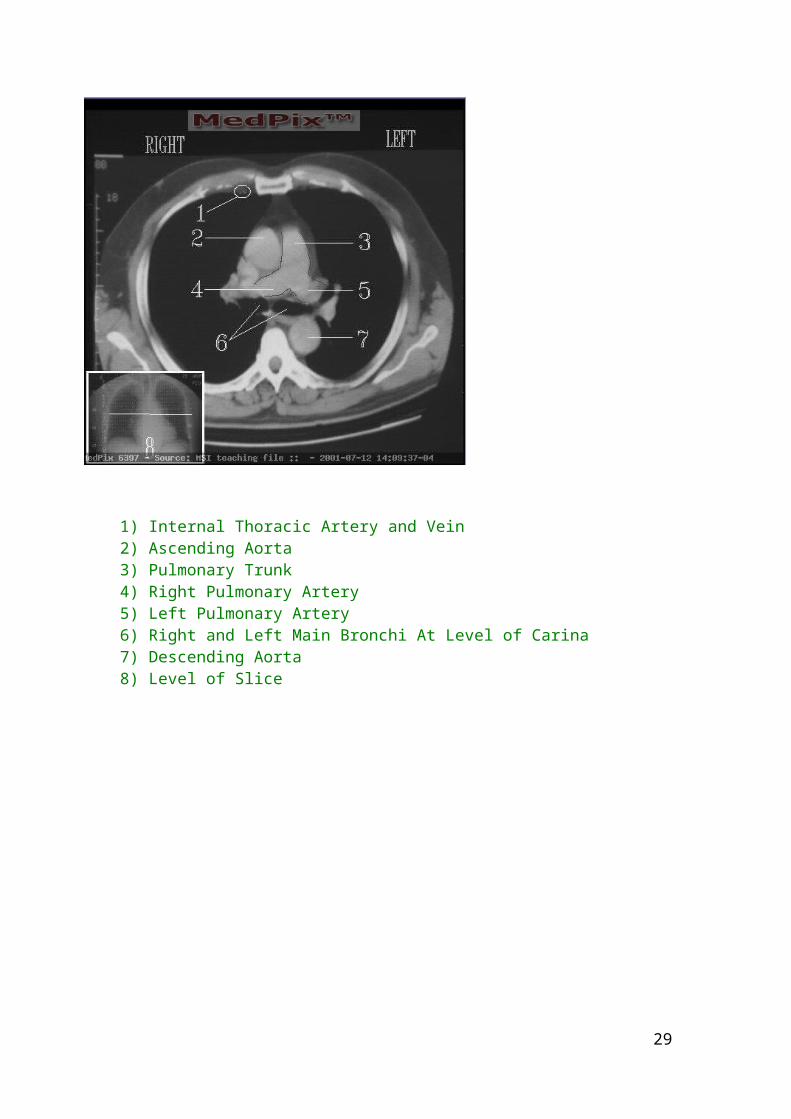
1) Internal Thoracic Artery and Vein 2) Ascending Aorta 3) Pulmonary Trunk 4) Right Pulmonary Artery 5) Left Pulmonary Artery 6) Right and Left Main Bronchi At Level of Carina 7) Descending Aorta 8) Level of Slice
23
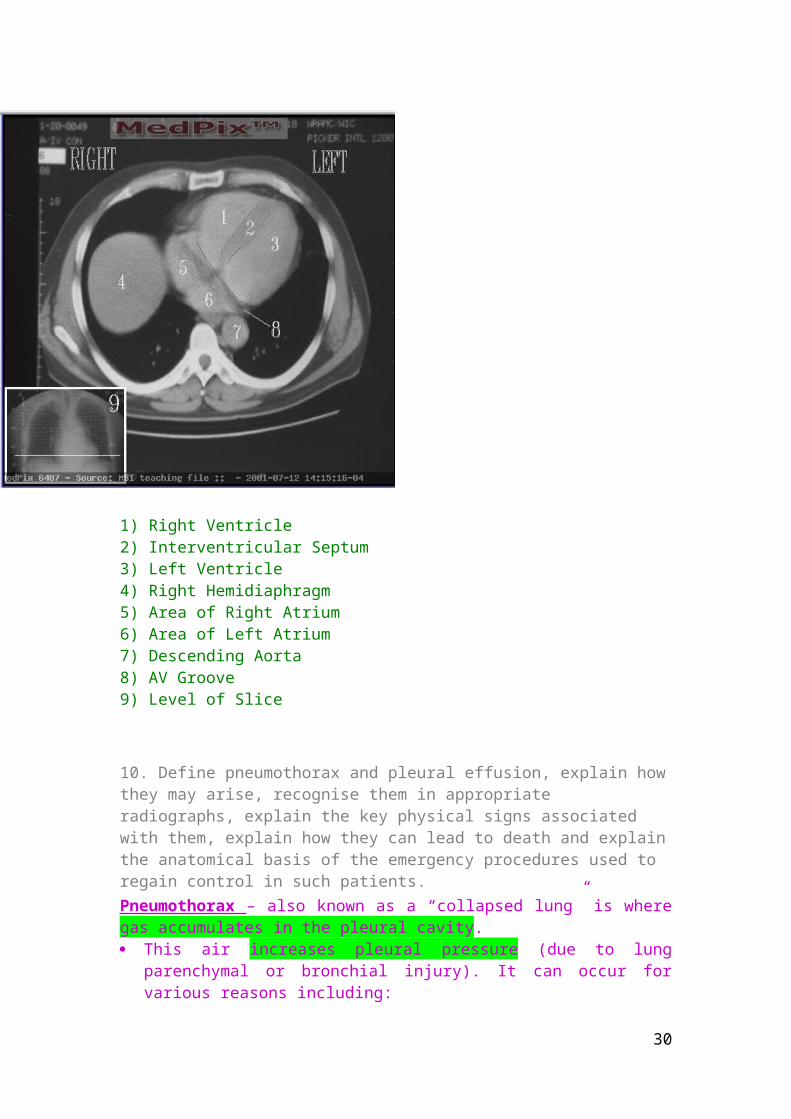
1) Right Ventricle 2) Interventricular Septum 3) Left Ventricle 4) Right Hemidiaphragm 5) Area of Right Atrium 6) Area of Left Atrium 7) Descending Aorta 8) AV Groove 9) Level of Slice
10. Define pneumothorax and pleural effusion, explain how they may arise, recognise them in appropriate radiographs, explain the key physical signs associated with them, explain how they can lead to death and explain the anatomical basis of the emergency procedures used to regain control in such patients.Pneumothorax – also known as a “collapsed lung” is where gas accumulates in the pleural cavity. This air increases pleural pressure (due to lung parenchymal or bronchial injury).
It can occur for various reasons including: A penetrating chest wound Barotrauma to the lungs Spontaneously (most commonly in tall slim young males and in Marfan
syndrome) Chronic and acute lung pathologies including emphysema, asthma,
tuberculosis Cancer
24
Catamenial pneumothorax -due to endometriosis in the chest cavity (i.e. where the endometrium incorrectly grows in parts of the body other than the uterus)
This causes the chest wall to spring out, and the lung to collapse. As pressure in the pleura increases, the mediastinal structures are pushed to the opposite side and compresses the opposite lung.
This can lead to hypoxia, and venous return decreases due to the pressure on the vena cava and the right atrium. This causes a decrease in cardiac output and hypotension. If left untreated, death.
This shows up on radiographs as transparent lung fields; Physical signs are:
tachypnoea (hyperventilation) tachycardia (increased heart rate) cyanosis (bluish coloration of the skin due to the presence of deoxygenated
haemoglobin in blood vessels) dyspnoea (laboured breathing) chest pain
Emergency procedure is the needle thoracostomy – puncture usually 2nd intercostal space, along the mid-clavicular line.
Pleural effusion –
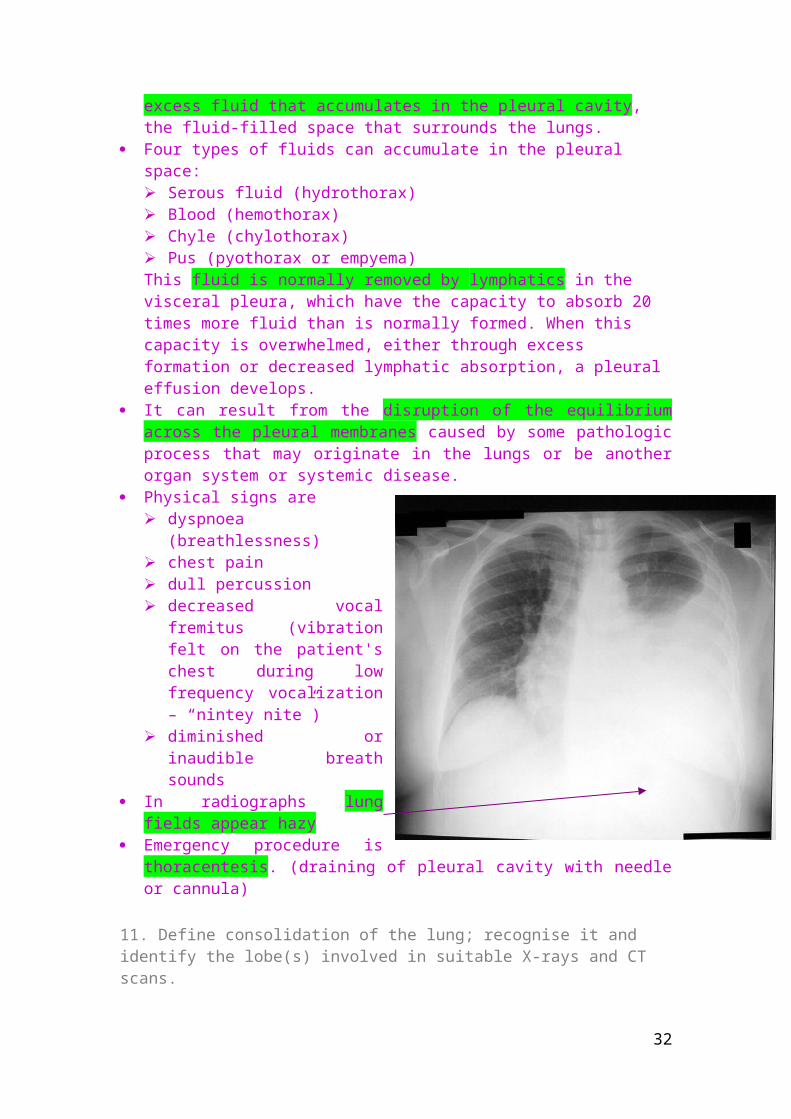
excess fluid that accumulates in the pleural cavity, the fluid-filled space that surrounds the lungs.
Four types of fluids can accumulate in the pleural space: Serous fluid (hydrothorax) Blood (hemothorax) Chyle (chylothorax) Pus (pyothorax or empyema) This fluid is normally removed by lymphatics in the visceral pleura, which have the capacity to absorb 20 times more fluid than is normally formed. When this capacity is overwhelmed, either through excess formation or decreased lymphatic absorption, a pleural effusion develops.
It can result from the disruption of the equilibrium across the pleural membranes caused by some pathologic process that may originate in the lungs or be another organ system or systemic disease.
25
Pneumothorax has occurred on the left hand side (characterised by transparent lung field)
The diaphragm is much lower due to pressure from the pleural cavity
Heart is on the wrong side of the body, due to the pressure from the left pleural cavity
The trachea is displaced to the right side

Physical signs are dyspnoea (breathlessness) chest pain dull percussion decreased vocal fremitus
(vibration felt on the patient's chest during low frequency vocalization – “nintey nite”)
diminished or inaudible breath sounds
In radiographs lung fields appear hazy
Emergency procedure is thoracentesis. (draining of pleural cavity with needle or cannula)
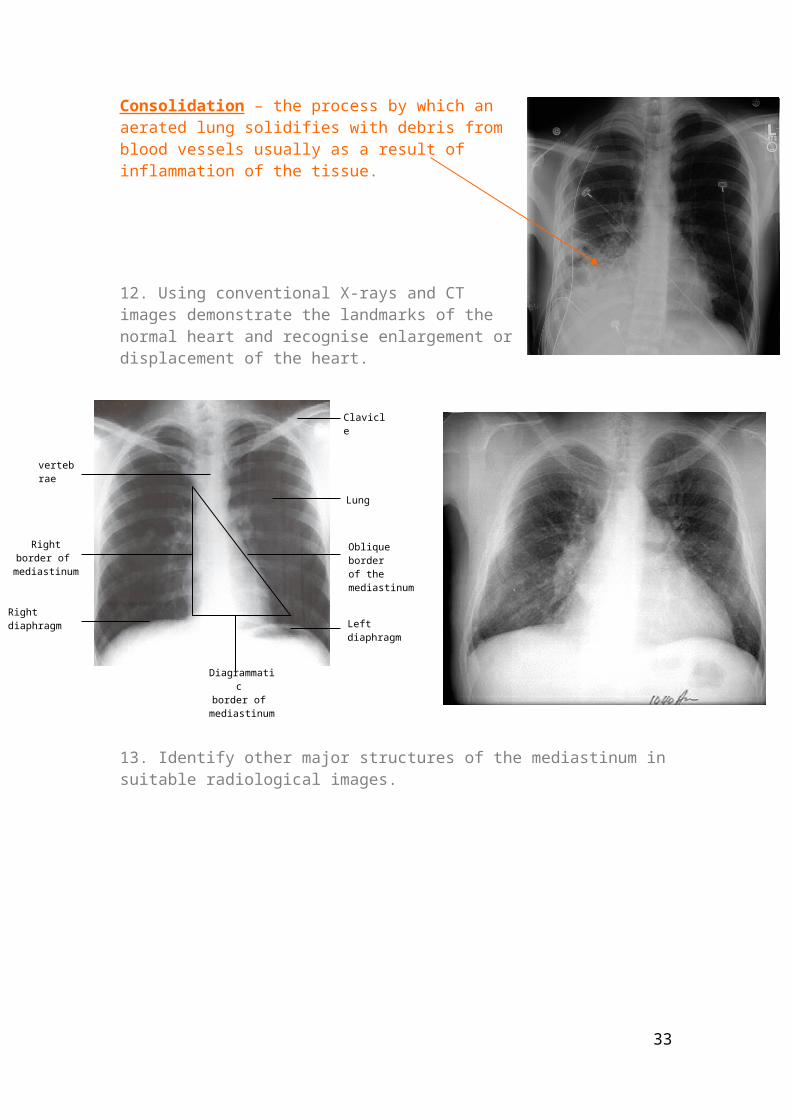
11. Define consolidation of the lung; recognise it and identify the lobe(s) involved in suitable X-rays and CT scans. Consolidation – the process by which an aerated lung solidifies with debris from blood vessels usually as a result of inflammation of the tissue.
12. Using conventional X-rays and CT images demonstrate the landmarks of the normal heart and recognise enlargement or displacement of the heart.
26
Clavicle
Lung
Left diaphragm
Diagrammatic border of
mediastinum
vertebrae
Right border of mediastinum
Right diaphragm
Oblique border of the mediastinum
13. Identify other major structures of the mediastinum in suitable radiological images.
Brochogram (airways) Angiogram (blood vessels)
27
Thorax 4 – Organisation of Nerves in the Thorax – Mon 26th Feb 2007Anil Chopra
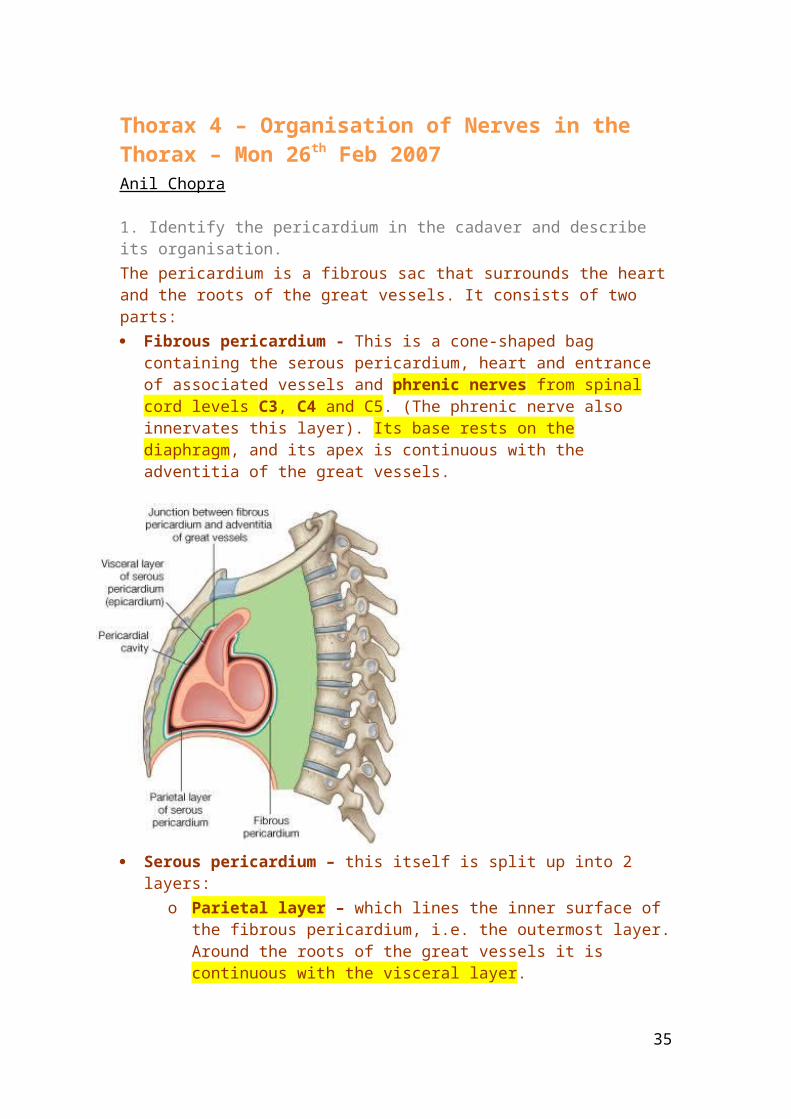
1. Identify the pericardium in the cadaver and describe its organisation.The pericardium is a fibrous sac that surrounds the heart and the roots of the great vessels. It consists of two parts: Fibrous pericardium - This is a cone-shaped bag containing the serous
pericardium, heart and entrance of associated vessels and phrenic nerves from spinal cord levels C3, C4 and C5. (The phrenic nerve also innervates this layer). Its base rests on the diaphragm, and its apex is continuous with the adventitia of the great vessels.
Serous pericardium – this itself is split up into 2 layers:
o Parietal layer – which lines the inner surface of the fibrous pericardium, i.e. the outermost layer. Around the roots of the great vessels it is continuous with the visceral layer.
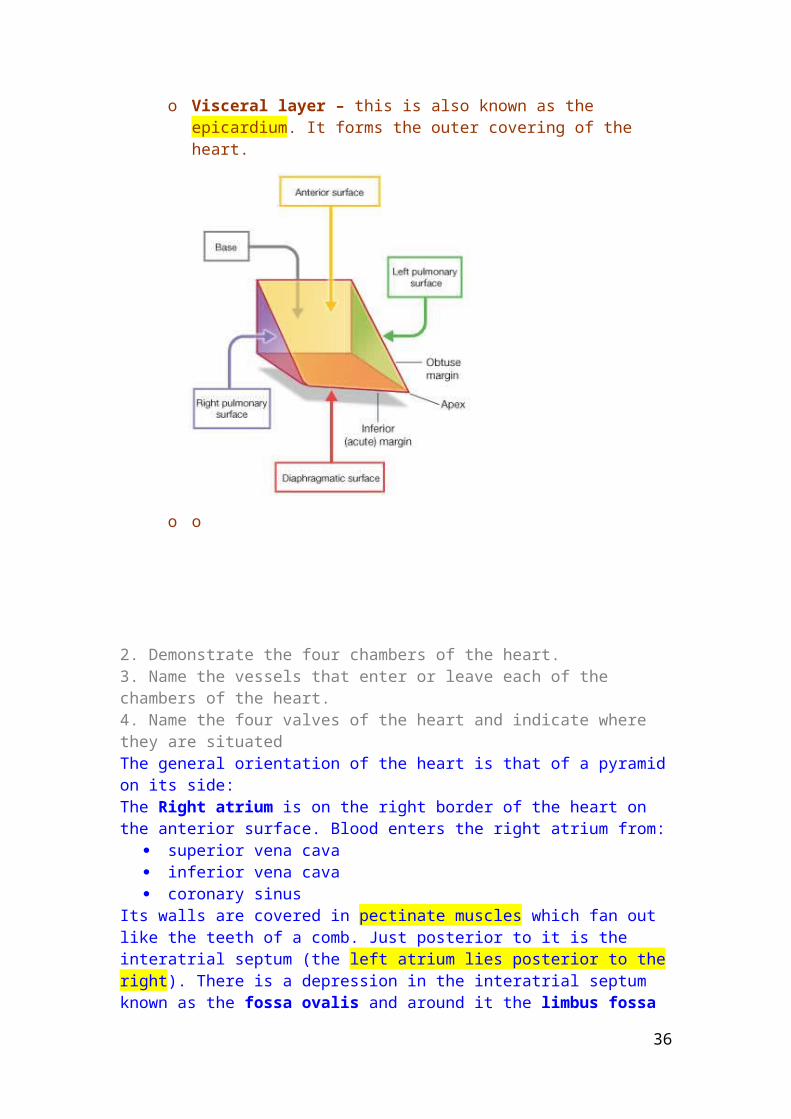
o Visceral layer – this is also known as the epicardium. It forms the outer covering of the heart.
28
o o
2. Demonstrate the four chambers of the heart.3. Name the vessels that enter or leave each of the chambers of the heart.4. Name the four valves of the heart and indicate where they are situatedThe general orientation of the heart is that of a pyramid on its side:The Right atrium is on the right border of the heart on the anterior surface. Blood enters the right atrium from:
superior vena cava inferior vena cava coronary sinus
Its walls are covered in pectinate muscles which fan out like the teeth of a comb. Just posterior to it is the interatrial septum (the left atrium lies posterior to the right). There is a depression in the interatrial septum known as the fossa ovalis and around it the limbus fossa ovalis. This is very important during foetal life as it was the foramen ovale, a hole between the left and right atria so blood can bypass the non-functioning lungs before birth.
29
The right ventricle is on the diaphragmatic border of the heart and also faces anteriorly, blood moving from right atrium to right ventricle therefore moves in a horizontal direction. Its outflow is the pulmonary trunk. There are 3 papillary muscles in the right ventricle:
Anterior papillary muscle is the largest. Posterior papillary muscle arises from posterior wall Septal papillary muscle which arises from the septum.
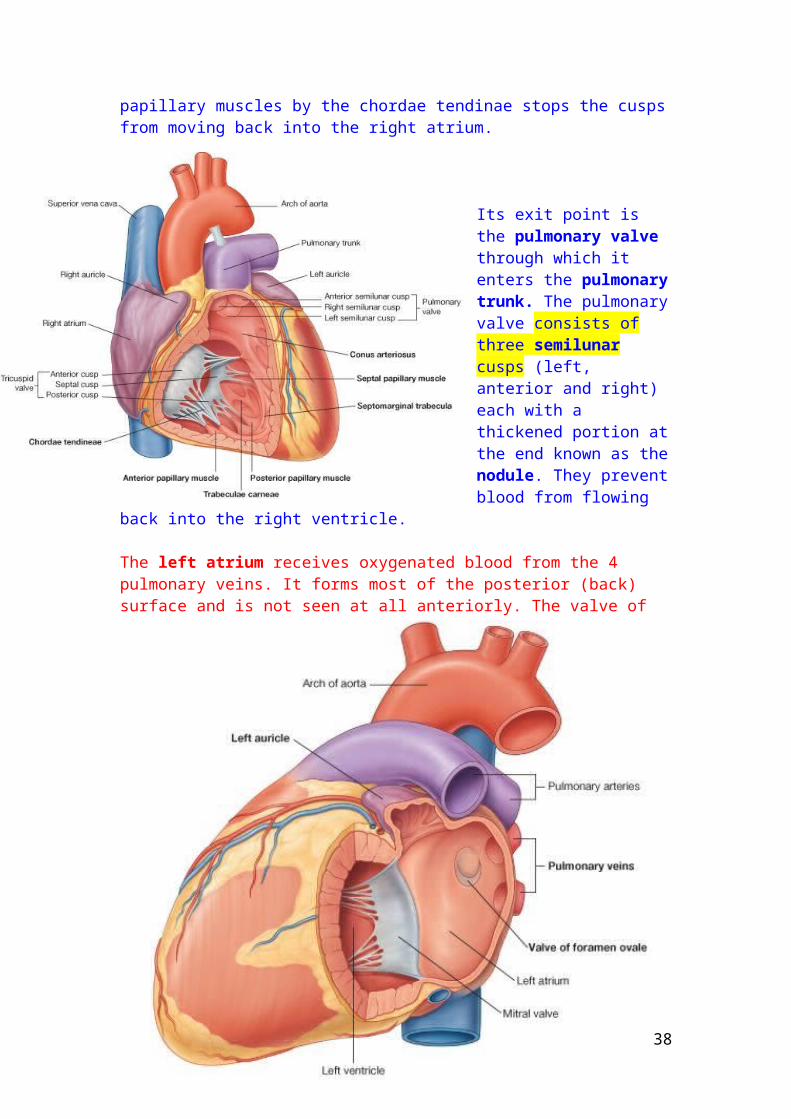
Its entry point is the tricuspid valve. This is the right atrioventricular valve consisting of 3 cusps; anterior, posterior and septal. The attachment of the cusps to the papillary muscles by the chordae tendinae stops the cusps from moving back into the right atrium.
Its exit point is the pulmonary valve through which it enters the pulmonary trunk. The pulmonary valve consists of three semilunar cusps (left, anterior and right) each with a thickened portion at the end known as the nodule. They prevent blood from flowing back into the right ventricle.
30

The left atrium receives oxygenated blood from the 4 pulmonary veins. It forms most of the posterior (back) surface and is not seen at all anteriorly. The valve of the foramen ovale is also seen in the interatrial septum. Its exit point is the mitral valve.
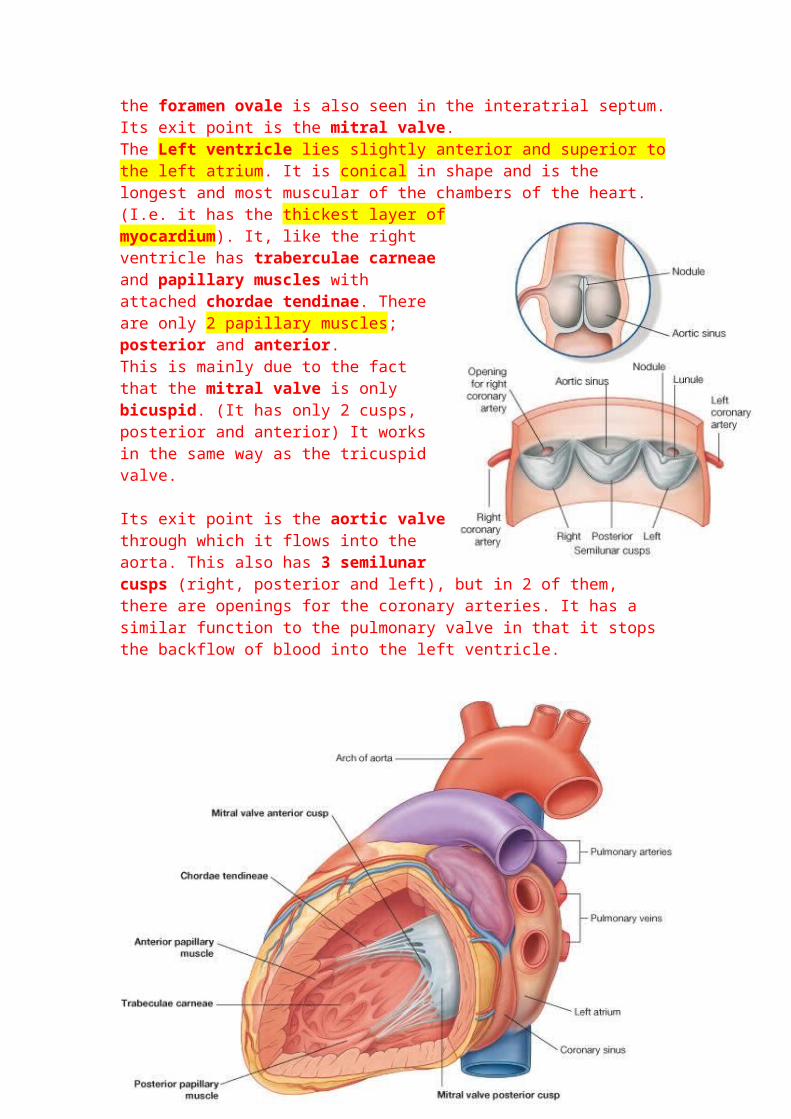
The Left ventricle lies slightly anterior and superior to the left atrium. It is conical in shape and is the longest and most muscular of the chambers of the heart. (I.e. it has the thickest layer of myocardium). It, like the right ventricle has traberculae
31
carneae and papillary muscles with attached chordae tendinae. There are only 2 papillary muscles; posterior and anterior.This is mainly due to the fact that the mitral valve is only bicuspid. (It has only 2 cusps, posterior and anterior) It works in the same way as the tricuspid valve.
Its exit point is the aortic valve through which it flows into the aorta. This also has 3 semilunar cusps (right, posterior and left), but in 2 of them, there are openings for the coronary arteries. It has a similar function to the pulmonary valve in that it stops the backflow of blood into the left ventricle.
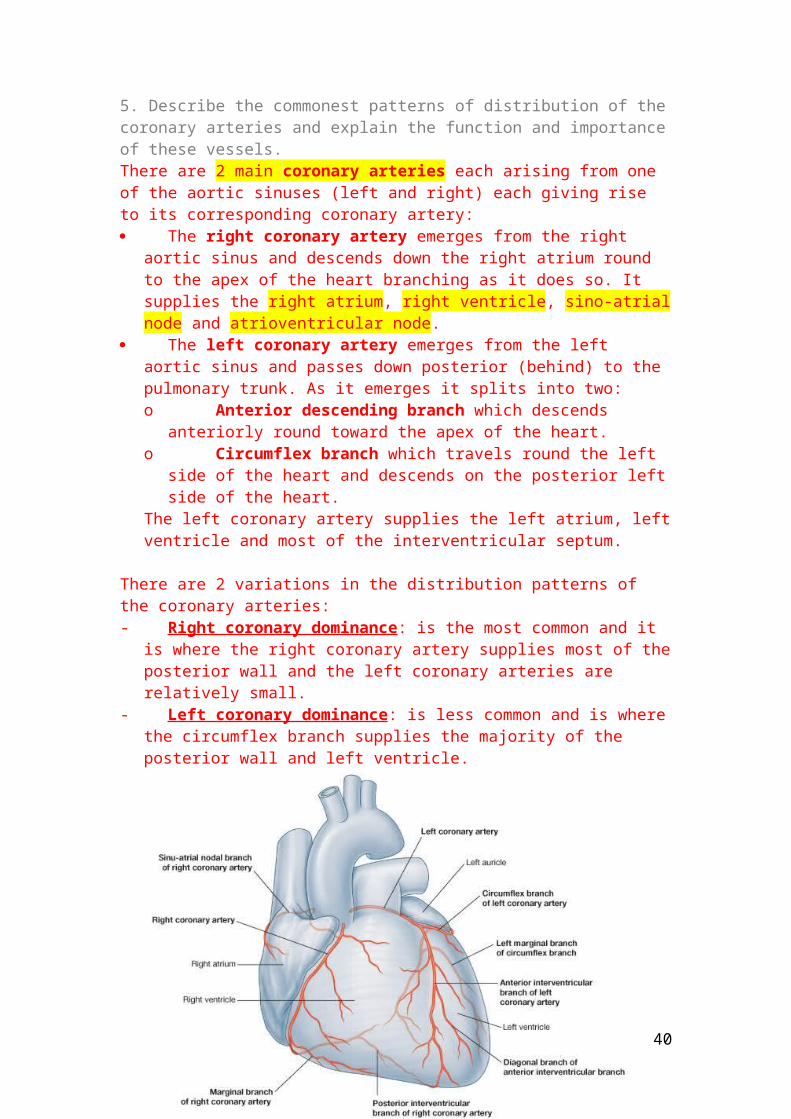
5. Describe the commonest patterns of distribution of the coronary arteries and explain the function and importance of these vessels.There are 2 main coronary arteries each arising from one of the aortic sinuses (left and right) each giving rise to its corresponding coronary artery: The right coronary artery emerges from the right aortic sinus and descends
down the right atrium round to the apex of the heart branching as it does so. It supplies the right atrium, right ventricle, sino-atrial node and atrioventricular node.
The left coronary artery emerges from the left aortic sinus and passes down posterior (behind) to the pulmonary trunk. As it emerges it splits into two:o Anterior descending branch which descends anteriorly round toward
the apex of the heart.o Circumflex branch which travels round the left side of the heart and
descends on the posterior left side of the heart.The left coronary artery supplies the left atrium, left ventricle and most of the interventricular septum.
There are 2 variations in the distribution patterns of the coronary arteries:- Right coronary dominance : is the most common and it is where the right
coronary artery supplies most of the posterior wall and the left coronary arteries are relatively small.
- Left coronary dominance : is less common and is where the circumflex branch supplies the majority of the posterior wall and left ventricle.
32
33

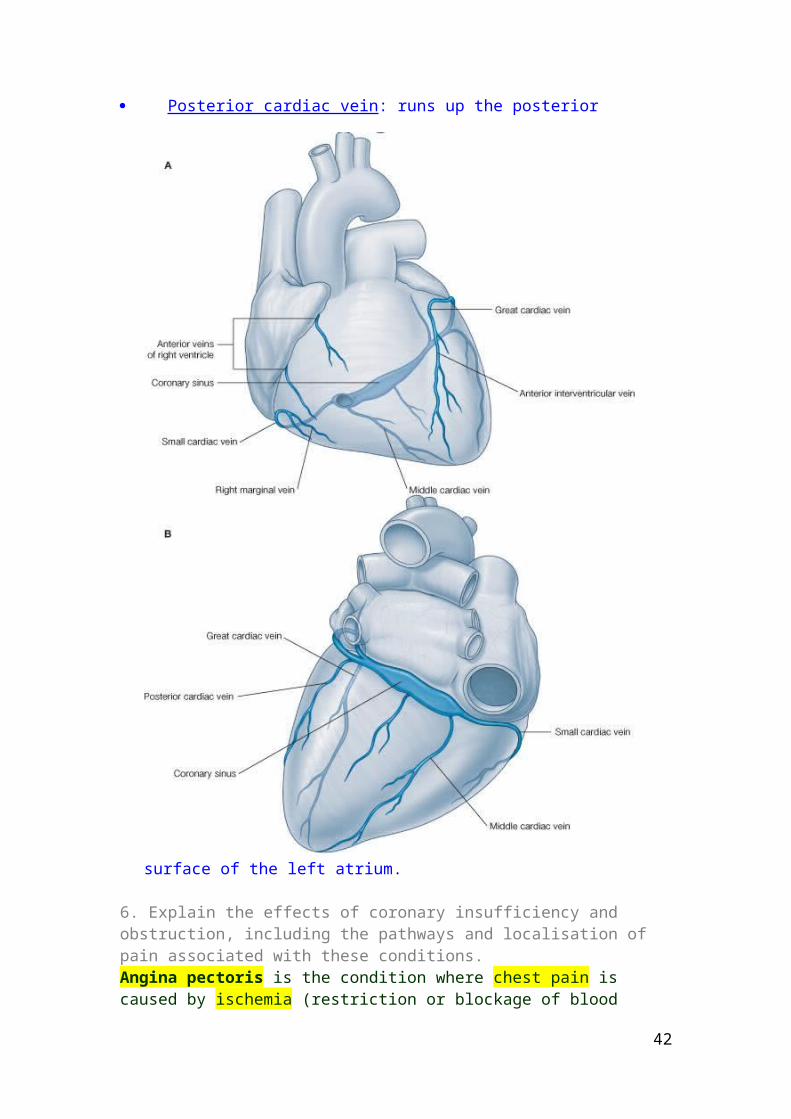
There are 4 main cardiac veins that drain into the coronary sinus which itself drains into the right atrium. Great cardiac vein : begins at the apex of the heart and runs up the anterior
(front) wall along the atrioventricular sulcus, when it reaches the top it goes round the end following the path of the circumflex artery and enlarges at the posterior end to form coronary sinus.
Middle cardiac vein : also begins at the apex but runs up the posterior side in the atrioventricular sulcus.
Small cardiac vein : begins in the lower anterior (front) sector of the anterior sulcus. It travels round the back of the right atrium where it finishes in the coronary sinus.
Posterior cardiac vein : runs up the posterior surface of the left atrium.
34
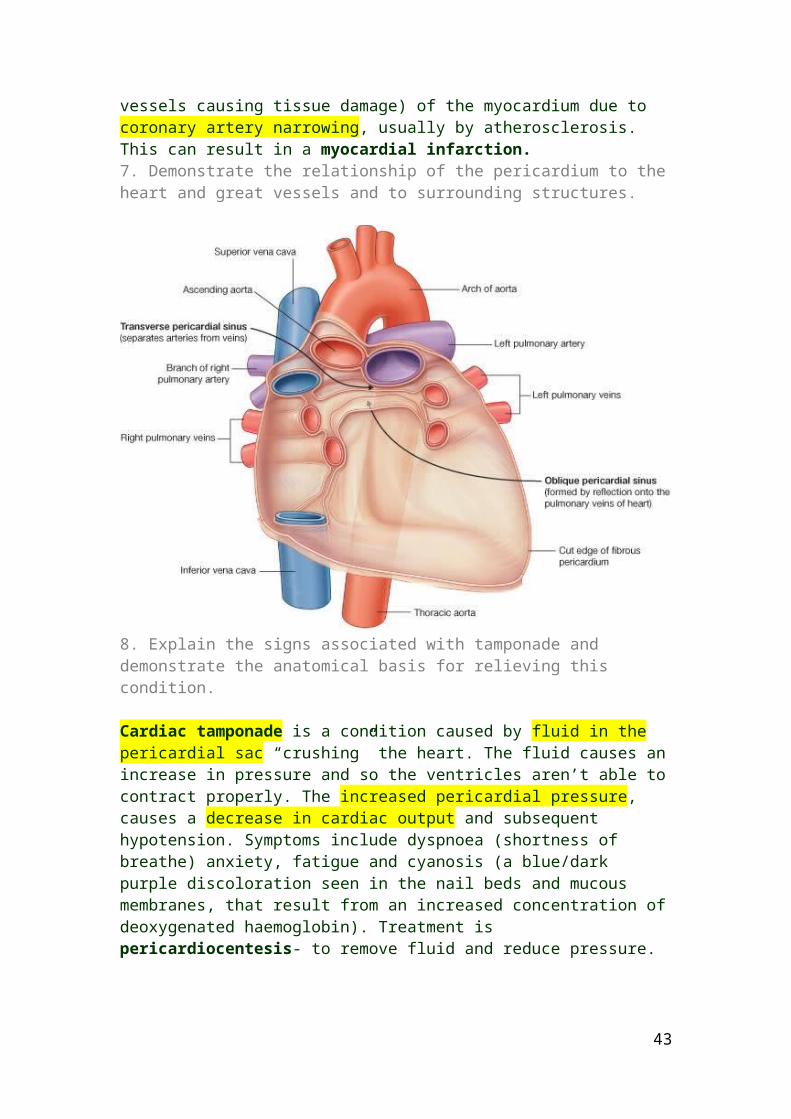
6. Explain the effects of coronary insufficiency and obstruction, including the pathways and localisation of pain associated with these conditions.Angina pectoris is the condition where chest pain is caused by ischemia (restriction or blockage of blood vessels causing tissue damage) of the myocardium due to coronary artery narrowing, usually by atherosclerosis. This can result in a myocardial infarction.7. Demonstrate the relationship of the pericardium to the heart and great vessels and to surrounding structures.
8. Explain the signs associated with tamponade and demonstrate the anatomical basis for relieving this condition.
Cardiac tamponade is a condition caused by fluid in the pericardial sac “crushing” the heart. The fluid causes an increase in pressure and so the ventricles aren’t able to contract properly. The increased pericardial pressure, causes a decrease in cardiac output and subsequent hypotension. Symptoms include dyspnoea (shortness of breathe) anxiety, fatigue and cyanosis (a blue/dark purple discoloration seen in the nail beds and mucous membranes, that result from an increased concentration of deoxygenated haemoglobin). Treatment is pericardiocentesis- to remove fluid and reduce pressure.
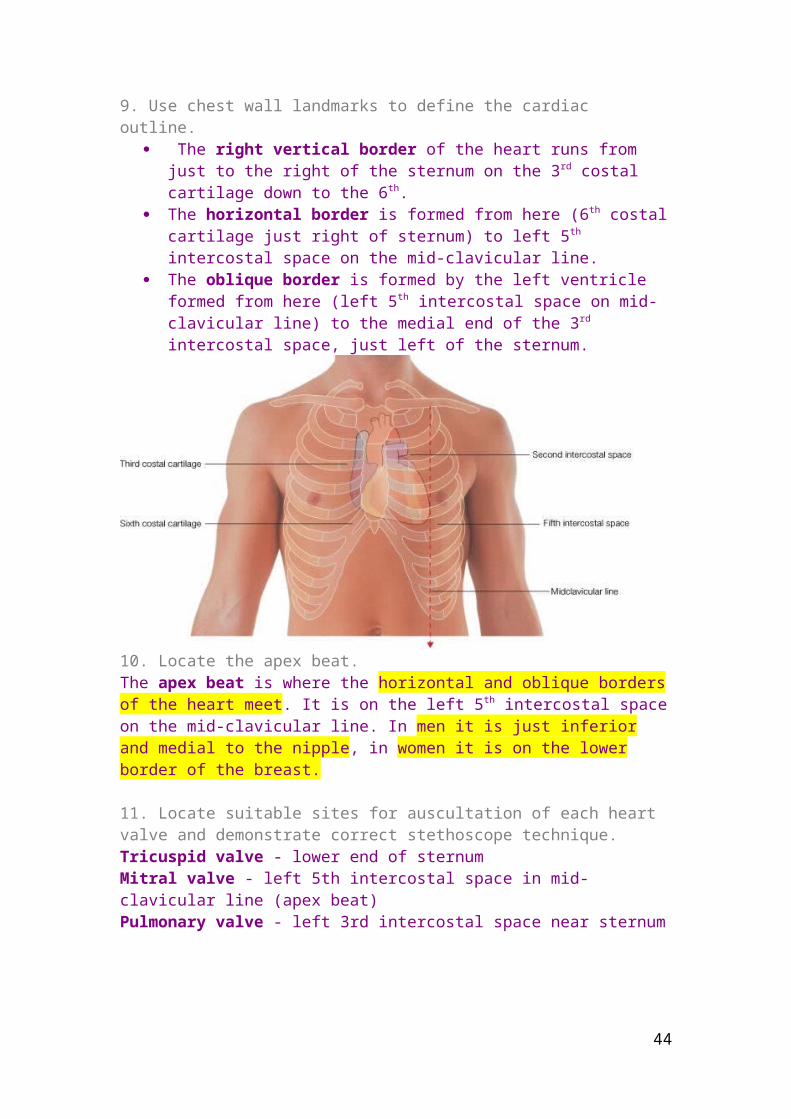
9. Use chest wall landmarks to define the cardiac outline. The right vertical border of the heart runs from just to the right of the
sternum on the 3rd costal cartilage down to the 6th. The horizontal border is formed from here (6th costal cartilage just right of
sternum) to left 5th intercostal space on the mid-clavicular line.
35
The oblique border is formed by the left ventricle formed from here (left 5th intercostal space on mid-clavicular line) to the medial end of the 3rd intercostal space, just left of the sternum.
10. Locate the apex beat.The apex beat is where the horizontal and oblique borders of the heart meet. It is on the left 5th intercostal space on the mid-clavicular line. In men it is just inferior and medial to the nipple, in women it is on the lower border of the breast.
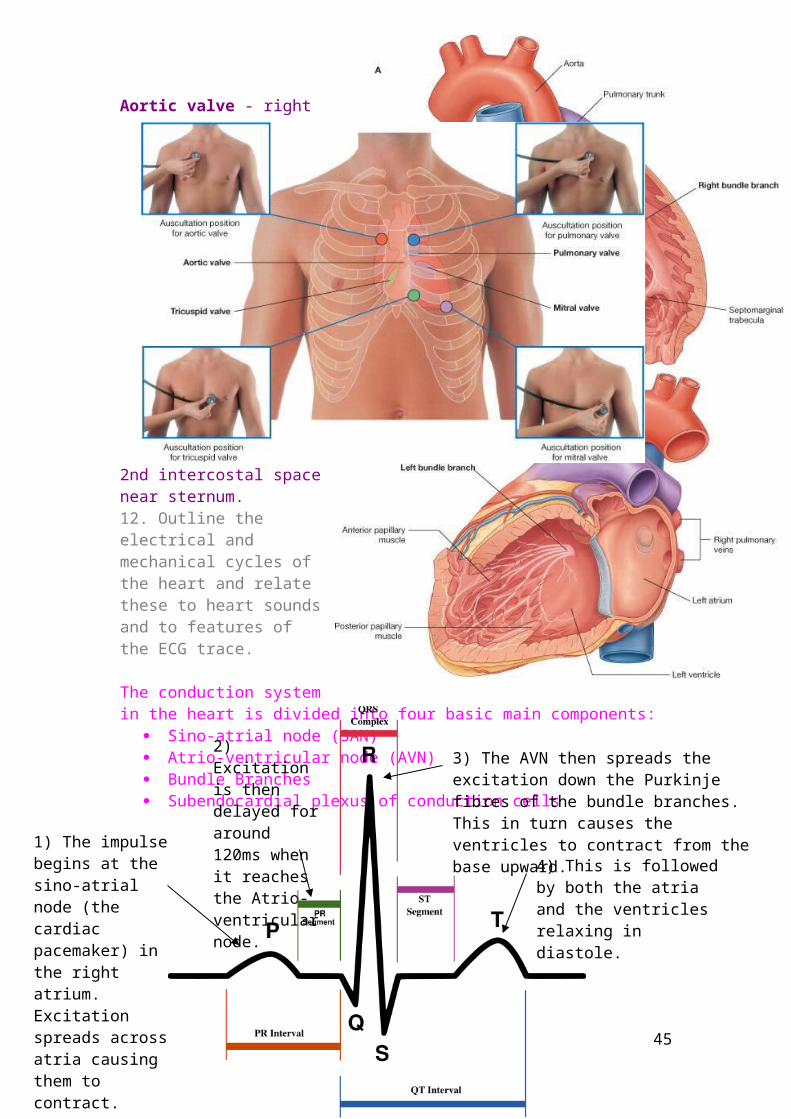
11. Locate suitable sites for auscultation of each heart valve and demonstrate correct stethoscope technique.Tricuspid valve - lower end of sternum Mitral valve - left 5th intercostal space in mid-clavicular line (apex beat) Pulmonary valve - left 3rd intercostal space near sternum Aortic valve - right 2nd intercostal space near sternum.
36

12. Outline the electrical and mechanical cycles of the heart and relate these to heart sounds and to features of the ECG trace.
The conduction system in the heart is divided into four basic main components:
Sino-atrial node (SAN) Atrio-ventricular node
(AVN) Bundle Branches Subendocardial plexus
of conduction cells
37
1) The impulse begins at the sino-atrial node (the cardiac pacemaker) in the right atrium. Excitation spreads across atria causing them to contract.
2) Excitation is then delayed for around 120ms when it reaches the Atrio-ventricular node.
3) The AVN then spreads the excitation down the Purkinje fibres of the bundle branches. This in turn causes the ventricles to contract from the base upward.
4) This is followed by both the atria and the ventricles relaxing in diastole.
13. Explain the pathways by which the heart, lungs and the chest wall receive their motor and sensory nerve supplies.VagusThe vagus nerve is the 10th cranial nerve (Cranial nerve
X).- Arises from the medulla and - Splits into the left (runs anterior to
aortic arch but posterior to left ling root) and right (runs posterior to right lung root).
- Has parasympathetic pathways to the heart, glands, and lungs.
- Also has sensory content from enteroceptors in gut and lungs.
- Both left and right vagus nerves form a plexus round the oesophagus.
- Splits into the recurrent laryngeal nerve that runs back up to supply skeletal muscles in the larynx
Sympathetic Trunk- All sympathetic nerves run from spinal levels T1 to L2.- Supply all parts of the body.- Two chains of sympathetic ganglia run either side of the spinal cord.- Give stimulatory effect to the heart and lungs.
Recurrent Laryngeal- A branch of the vagus nerve that supplies the skeletal muscles in the larynx.
Thoracic Somatic- These usually arise from the main
branches of thoracic spinal nerves 1- 11.- Each segment supplies a
dermatome and group of muscles.- The spinal root emerging splits
into a dorsal and ventral root. The dorsal root contains sensory fibres and the ventral root contains motor fibres.
- Each then splits into 2 rami one of which supplies posterior muscles and one of which supplies its particular dermatome
Enteric Nervous System- Intrinsic nerves of the
oesophagus.- This plexus of ganglia and
axons is located in the oesophageal wall where it co-ordinates the activity of the oesophagus.
38
- The parasympathetic supply stimulates it, sympathetic supply inhibits it.
39
Thorax 5 – Lymphatic System, Breasts and Breast Cancer Anil Chopra
1. Summarise the main functions and anatomical organisation of the lymphatic system.
Lymphatic drain tissue fluid from thorax viscera that has not returned to the venous end of the blood in capillaries.
Uncompensated fluid would result in the build up of fluid in tissues (oedema) and loss of blood volume.
Various forces act across capillary walls affecting the fluid content of the blood.
Lymph contains fluid from tissues, particulate matter, fat, few cells and few proteins.
The lymph then flows into the blind ended lymph vessels.
They are thin-walled and lined by endothelial cells.
At various points they pass through lymph nodes. At these lymph nodes they pass fixed reticular macrophages that remove
bacteria. (it cannot however remove cancerous cells) The lymph system is split into deep and superficial lymphatics. Lymph from lower limbs drains into cisterna chyli and then into the thoracic
duct which itself drains into the brachiocephalic vein. Lymph from the lower limbs drains into the cervical lymph nodes in the
neck. Lymph from the upper limbs drains into the
axillary lymph nodes.
40
2. Describe the lymphatic drainage of the chest viscera (particularly the lungs and bronchi) and outline the implications of this pattern for the spread of lung cancer.
Lymphatic drainage from the lungs, bronchi and mediastinum drain into the left and right bronchomediastinal trunks.
The parasternal nodes run up anteriorly either side of the sternum draining the front of the thorax, intercostal nodes run up posteriorly either side of the spinal cord and the tracheobronchial nodes run around the trachea and bronchi.
These all drain into the left brachiocephalic vein. Cancer cells may travel in the blood or lymph and establish new tumours
where they lodge .When metastasis occurs via lymphatic vessels, secondary tumour sites can be predicted according to the direction of lymph flow, from the primary tumour site. Cancerous lymph nodes feel enlarged, firm, non-tender, and fixed to underlying structures. By contrast, most lymph nodes that are enlarged due to an infection, are not firm, are moveable and are very tender.
3. Define the roles of breast examination and imaging within the epidemiological context of breast cancer incidence.
Breast cancer affects one woman in eight. It usually develops from the ducts of the epithelium. Not all lumps are cancers. They are somewhat dependent on oestrogen.
41
Tumours may put tension on suspensory ligaments. This may cause skin puckering (indentations) or inverted nipples.
They may attach to muscles and are very prone to spreading in the lymph or venous drainage of the breast.
4. Describe the lymphatic and venous drainage of the breast and relate these to the pathways of metastasis of breast cancer.
Breasts develop in both genders, in males however they are rudimentary and consist of small ducts, composed of cords of cells which do not extend beyond the areola.
They overlie the anterior muscles of the chest wall and lie between ribs 2 and 6.
They have an axillary tail/process leading to the axilla. This must always be checked on examination for lumps.
They are raised structures in the thoracic wall that contain mammary glands. Each breast contains around 12-16 lobes which contain structures known as
alveoli. Each has a small duct which opens out into the nipple surrounded by pigmented skin – the areola.
Underneath the areola are the lactiferous sinuses which are milk-filled spaces that the baby sucks on.
Breasts contain internal suspensory ligaments which are used in supporting the breast. Tensing the pectoral muscles (push down on hips) causes suspensory ligaments to lift breast.
The bulk of it is adipose tissue but when pregnant, this turns to glandular tissue.
Lymph drainage of breast parallels arterial supply. Arterial supply to lymph nodes mainly from the thoracic arteries and axillary artery.
Cancers can travel in the internal thoracic (parasternal) and axillary lymph nodes.
42
Cancers can also block lymph drainage and therefore increase pressure cause lymph to take alternative routes.
5. List the imaging techniques used in the diagnosis of breast cancer and outline their
value and limitations. Mammogram – this is a breast x-ray. CT scans – computerised tomography. Bone scan – this uses radioactive isotopes. Self examination – is increasingly popular making sure women check their
breasts and the axillary process. Ultrasound – is also used.
43
Thorax 6 – The Posterior Mediastinum Anil Chopra
1. Define the posterior mediastinumEverything in the thorax that is below the plain of the sternal angle and posterior to (behind) the pericardium is the posterior mediastinum.
2. Describe the relative positions of the descending aorta, the oesophagus, the vagus nerves and the thoracic duct as they descend through the posterior mediastinum.Descending aorta: this begins at vertebral level T IV (4) and it is continuous wit the arch of the aorta. It continues anteriorly down to T XII (12) there it passes through the aortic hiatus of the diaphragm.
Oesophagus: this is a muscular tube running down from the pharynx in the neck to the stomach in the abdomen. Throughout the top part of the thorax it is situated to the right of the aorta until around vertebral level T VII (7) where it bends slightly anterior and left. It then proceeds inferiorly (down) anterior to (in front of) the aorta.
Vagus nerves: cranial nerve X (10) passes posterior to the lung roots and forms the oesophageal plexus. They run down the length of the oesophagus to the stomach where they eventually become the posterior and anterior vagal trunks.
Thoracic Duct: is a lymph duct that returns lymph from the lower limbs, abdomen and pelvis to the blood. It begins below the diaphragm at the cisterna chyli, comes up between the oesophagus and the aorta and then crosses behind the oesophagus at around vertebral level T VI (6).
44
Phrenic Nerves: pass from cervical vertebra C III, IV and V to the diaphragm anterior to the lung roots.
3. Describe the nerve supply, arterial supply, venous drainage and lymphatic drainage of the oesophagusNerve Supply: the oesophagus is supplied by the enteric nervous system. There are oesophageal branches arising from the vagus nerve and the sympathetic chain. The smooth muscle fibres surrounding the oesophagus are stimulated by the parasympathetic branches of the autonomic nervous system. The left and right vagus nerves form the oesophageal plexus. This network of nerves runs down the oesophagus until it eventually becomes the anterior and posterior vagal trunks which
Arterial Supply: the oesophagus is mainly supplied by branches of the descending (or thoracic) aorta.
Venous Drainage: the oesophagus is drained entirely by the azygous system of veins. On the left side of the body, the inferior and superior (accessory) hemiazygous veins drain into the large azygous vein running down the
Lymph Drainage: lymph from cells in the oesophagus is drained by the thoracic duct.
45

4 .Explain how and at which vertebral levels the inferior vena cava, the oesophagus and the descending aorta pass through the diaphragm.
46
Vessel Crosses Diaphragm at
Vertebral Level
Inferior Vena Cava:
vena caval foramen
T VIII (T8)
Oesophagus: oesophageal hiatus
T X (T10)
Descending Aorta:
Aortic hiatus T XII (T12)







