Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 1
PT for Hypermobility Spectrum Disorders
A Zebra Among Us: Recognition & Management of
Hypermobility Spectrum Disorders Combined Sections Meeting 2018
New Orleans, LA, February 21-24, 2018 LeslieNRussek,PT,DPT,PhD,OCS
ClarksonUniversity,Canton-PotsdamHospital,Potsdam,NYStephanieSaboPT,MPT
Cincinna:Children’sHospitalMedicalCenter,Cincinna:,OHJaneSimmondsDProf,MCSP,MACP,SFHEA
GreatOrmondIns:tuteofChildHealth,UniversityCollegeLondon,London,UKHeatherPurdin,MS,PT,CMPT
GoodHealthPhysicalTherapy&Wellness,Portland,OR
1
Disclosures The speakers have no financial or other conflicts of interest.
PT for Hypermobility Spectrum Disorders 2
Affiliations [email protected] [email protected] [email protected] [email protected]
PT for Hypermobility Spectrum Disorders 3
Learning Objectives Attheendofthiscourse,parDcipantswillbeableto:
1. Describetypicalclinicalpresenta:onofpa:entswithhypermobilityspectrumdisorder(HSD)throughthelifespan,includingpediatric,adolescent,andadultpa:entswithinthecontextoftheICFmodel.
2. Applythe2017Interna:onalClassifica:ontoiden:fyHypermobilitySpectrumDisordersandhEDS.
3. Proposeevidence-basedapproachesforphysicaltherapymanagementforindividualswithhypermobilityspectrumdisorders.
4. Recognizecommonchallengesandpi]allsworkingwiththesecomplexpa:ents.
PT for Hypermobility Spectrum Disorders 4
Outline • 25min:Introduc:ontoEDS,hEDS,HSD(LRussek)• 25min:Pediatriccase(StephanieSabo,presentedbyL.Russek)
– Exam,evalua:on,motordelays,motorcontrolissues,bracing• 25min:Adolescentcase(JaneSimmonds)
– Exam,evalua:on,stra:fiedmanagement,POTS,fa:gue,GIproblems,psychosocialissues
• 25min:Adultcase(HeatherPurdin)– Exam,evalua:on,chronicpain,MCAD,
• 20min:QA(panel)
PT for Hypermobility Spectrum Disorders 5
Many Types of EDS • Hypermobile (III): Loose joints, joint pain. Most common. • Classical (I & II): Velvety, stretchy, fragile skin. Common. • Vascular (IV): Possible arterial/organ rupture. Most serious. • Kyphoscoliosis: Joint laxity, muscle hypotonia,
developmental delay. Severe functional loss over time. • Arthrochalasia (VII): Congenital hip dislocation, lax joints. • Dermatosparaxis (VII): Severe skin fragility & bruising.
• Malfait, 2017
PT for Hypermobility Spectrum Disorders 6

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 2
Vascular Ehlers-Danlos Syndrome
PT for Hypermobility Spectrum Disorders www.ehlersdanlosnetwork.org/vascular.html
7
Classical Ehlers-Danlos Syndrome
PT for Hypermobility Spectrum Disorders 8
Many Names of Hypermobility • Generalizedjointhypermobility/laxity(GJH)
– Mightormightnothavepainorsymptoms• Jointhypermobilitysyndrome(JHS)&hypermobilitysyndrome
(HMS):termsodenusedbyrheumatologists• Ehlers-DanlosSyndrome–hypermobilitytype(EDS–HTortypeIII)
terminologyusedbygene:cists• NewlyproposedterminologyhypermobileEhlers-DanlosSyndrome
(hEDS)andHypermobilitySpectrumDisorder(HSD)• Wewillrefertoitas‘hypermobility’or‘HSD’
PT for Hypermobility Spectrum Disorders 9
Hypermobility Spectrum Disorder
Individual
JointLaxity
GJH
EDS
hEDS
Asymptomatic Mild Symptoms Severe Symptoms
GJH = (asymptomatic) joint hypermobility; EDS = Ehlers-Danlos Syndrome; hEDS = hypermobile EDS Castori, 2017
Localized-HSD Generalized-HSD Peripheral-HSD Historical-HSD
PT for Hypermobility Spectrum Disorders 10
Prevalence of EDS • HSDisthemostcommonsystemicinheritedconnec:ve:ssue
disorderinhumans(Tinkle,2017)– intheUKprevalenceofHSDassociatedwithchronicwidespreadpain
orseverelydisablingpain(Mulvey,2013)isalmostashighasfibromyalgia(Fayaz,2016)and100:meshigherthanrheumatoidarthri:s.(Humphreys,2013)
• Affects~10millionpeopleintheU.S.(Tinkle,2017)– 30xnumberofTHA/yr;60xnumberofACLreconstruc:ons/yr
• HSDinmusculoskeletalhealthcare:30-55%
• InOmaniwomen,probablynotthishighintheUS.(Clark,2011)• 80-90%ofallEDSishEDS(Tinkle,2017)
PT for Hypermobility Spectrum Disorders 11
Pathophysiology • Autosomaldominantconnec:ve:ssuedisorder• Thereisnogene:cmarkerknownforhEDS
– IncontrasttomostoftheotherformsofEDS• Heterogeneouspathophysiology
– TenascinXabnormality?– TypeIIIcollagenabnormality?– Exactconnec:ve:ssueabnormalityisunknown– (Tinkle,2017;Malfait,2017)
PT for Hypermobility Spectrum Disorders 12
Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 3
Common Signs & Symptoms • Musculoskeletal: joint hypermobility, subluxations/dislocations, sprains,
muscle spasm, TMD, flat feet, finger deformities, arthralgia, myalgia, fractures, pain, proprioceptive deficits, kinesiophobia
• Integumentary: stretchy skin, easy bruising, atrophic scarring, poor wound healing, frequent hernias
• Cardiovascular: dysautonomia, postural orthostatic tachycardia syndrome Other: gastritis, IBS, incontinence, developmental delay, poor coordination, anxiety, mast cell activation, organ prolapse
• Disability due to pain, fatigue, anxiety, depression (Castori, 2011; Colombi, 2015; Scheper, 2016; Tinkle, 2017)
PT for Hypermobility Spectrum Disorders 13
Major Comorbidities • Chronic pain: fibromyalgia, myofascial pain, OA, TMD
– Hyperalgesia (Scheper, 2017)
• Developmental delay in children • Dysautonomia: POTS, thermoregulation, gut, sexual
dysfunction • Mast Cell Activation Disorder: systemic inflammation • Gastrointestinal disorders: GERD, IBS, malabsorption
syndrome (Tinkle, 2017)
• Tethered cord syndrome (Henderson, 2017)
PT for Hypermobility Spectrum Disorders 14
HSD Through the Life Span 1. Hypermobile phase
– Hypermobile joints – Clumsiness/motor delay – Constipation/diarrhea – Abdominal hernias
2. Pain phase – Chronic musculoskeletal pain – Strains, sprains, dislocations – Unrefreshing sleep – Chronic fatigue – Memory/cognitive problems – Gastric reflux, abdominal pain – Paresthesias – Tachycardia – Incontinence/UTI
3. Stiffness phase – Widespread pain – Fatigue – Tendinosis/tendon rupture – Chronic gastritis – Stiffness
– (Castori, 2011; Tinkle, 2017)
PT for Hypermobility Spectrum Disorders 15
Evolving Diagnostic Criteria • Un:l2017:
– BeightonScale(Beighton,1973)mostodenusedforGJH• Carter-Wilkinson(Carter,1964)• Rotés/HospitaldelMar(Bulbena,1992)
– VillafrancheClassificaDonusedmostlybygene:cistsforchildren:EDS-HT(Beighton,1998)
– BrightonCriteriausedmostlybyrheumatologistsforadults:JHS(Grahame,1998)
• NewcriteriaforhEDS:“The 2017 international classification of the Ehlers-Danlos syndromes.”(Malfait,2017)
• NoclearguidelinesregardingHSD;Mustexcludeotherpoten:aldiagnoses
PT for Hypermobility Spectrum Disorders 16
2017 hEDS Diagnostic Criteria Mustmeetall3criteria:
1. Generalizedjointhypermobility
2. Featuresofheritableconnec:ve:ssuedisorder• Mustmeet≥2of3categories,A-C
3. Absenceofexclusioncriteria• (Malfait,2017)
PT for Hypermobility Spectrum Disorders 17
BeightonScore≥5/9
• 2:Bend5thfingerback>90°• 2:Touchthumbtoforearm• 2:Elbowhyperextension>10°• 2:Kneehyperextension>10°• 1:Palmstofloor,kneesstraight
• Prepubescent≥6/9• Pubescent-50years≥5/9• Over50years≥4/9
Pts with limited ROM for cause, add 1 point if ≥2/5 on the 5-Item Questionnaire: 1. Can you now (or could you ever) place your hands flat on the floor without
bending your knees? 2. Can you now (or could you ever) bend your thumb to touch your forearm? 3. As a child, did you amuse your friends by contorting your body into strange
shapes or could you do the splits? 4. As a child or teenager, did your shoulder or kneecap dislocate on more than
one occasion? 5. Do you consider yourself “double-jointed”?
(Malfait, 2017; diagram from Juul-Kristensen)
1: Generalized Joint Hypermobility
PT for Hypermobility Spectrum Disorders 18

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 4
2: Features of Heritable Connective Tissue Disorder
• Musthave≥2ofthefollowing3categories:A. Systemicmanifesta:ons
• ≥5of12op:onsB. FamilyhistoryC. Musculoskeletalcomplica:ons
• ≥1of3op:ons
PT for Hypermobility Spectrum Disorders 19
2A: Systemic Manifestations i. Unusuallysod/velvetyskinii. Mildskinhyperextensibility(forearm)iii. Unexplainedstraiae/stretchmarksiv. Bilateralpapulesofheelv. Recurrent/mul:pleabdominalherniasvi. Atrophicscarringin≥2sitesvii. Pelvicfloor,rectal,uterineprolapseviii. Dentalcrowdingorhigh,narrowpalateix. ArachnodactylybilateralSteinbergorWalkersignx. Armspan/height≥1.05xi. Mitralvalveprolapsemildorgreaterxii. Aor:crootdila:onMeetsSystemicManifestaDonsifYESto≥5items
PT for Hypermobility Spectrum Disorders 20
2A: Systemic Manifestations i. Unusuallysodorvelvetyskinii. Mildskinhyperextensibility(>1.5cmonvolar,non-
dominantforearm)iii. Unexplainedstraiae/stretchmarksinany�or
prepubertal�w/osignificantweightchange
PT for Hypermobility Spectrum Disorders 21
2A: Systemic Manifestations iv. Bilateralpiezogenicpapulesofheel*v. Recurrentormul:pleabdominalhernias(umbilical,
inguinal,crural;nothiatalhernia)*Piezogenic papules are sub-cutaneous fat herniations through the fascia; they may appear as white nodules only with weight bearing Malfait, 2017
PT for Hypermobility Spectrum Disorders 22
vi. Atrophicscarringinvolvingatleast2sites(notlikeclassicalEDS)
Malfait, 2017 Hypermobile EDS, Castori, 2015
PT for Hypermobility Spectrum Disorders 23
Hypermobile EDS Classical EDS 2A: Systemic Manifestations 2A: Systemic Manifestations
vii. Pelvicfloor,rectal,and/oruterineprolapseinchildren,�,nulliparous�w/omorbidobesity
viii. Dentalcrowdingandhighornarrowpalateix. Bilateralarachnodactyly
– Bilateral Steinberg OR bilateral Walker sign
PT for Hypermobility Spectrum Disorders 24

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 5
2A: Systemic Manifestations x. Armspan/height*≥1.05xi. Mitralvalveprolapsemildorgreaterxii. Aor:crootdila:on,z-score>+2
*Arm span is from tip of middle finger to tip of middle finger
PT for Hypermobility Spectrum Disorders 25
2B: Family History • 1stdegreerela:veindependentlymeetsdiagnos:ccriteriaforhEDS
PT for Hypermobility Spectrum Disorders 26
2C: Musculoskeletal Complications 1. Pain≥2limbs,recurringdailyforatleast3months2. Chronicwidespreadpainfor≥3months3. Recurrentjointdisloca:onsorfrankjointinstabilityin
absenceoftrauma(aorb)a. 3+atrauma:cdisloca:onsofsamejointOR2+disloca:onsof2
differentjointsatdifferent:mesb. Medicalconfirma:onofjointinstabilityat2+jointsnotrelatedto
trauma
• Ifyesto≥1item(andnotduetootherconnecDveDssuedisorder,e.g.
lupus,RA),thenposiDveformusculoskeletalcomplicaDons
PT for Hypermobility Spectrum Disorders 27
2: Features of Heritable Connective Tissue Disorder
• Insummary,tomeetthecriterion:FeaturesofheritableconnecDveDssuedisorder
• Musthave≥2ofthefollowing3categories:
A. Systemicmanifesta:onsB. FamilyhistoryC. Musculoskeletalcomplica:ons(notexplainedbyanother
connec:ve:ssuedisorder)
PT for Hypermobility Spectrum Disorders 28
3: Absence of Exclusion Criteria TomeetthisCriterion,all3ofthefollowingmustbeABSENT:
1. Unusualskinfragility(shouldpromptconsidera:onofothertypesofEDS)
2. Otherheritableoracquiredconnec:ve:ssuedisorder(e.g,lupusorRA)
3. Neuromusculardisordersthatmaycausejointhypermobilitybymeansofhypotoniaorconnec:ve:ssuelaxity(e.g.,Marfan,otherEDS,OI,etc.)
PT for Hypermobility Spectrum Disorders 29
Patient Examination • Useabiopsychosocialapproach
• Lookforcontribu:ngfactorsaswellassigns,symptoms,&involved:ssues
PT for Hypermobility Spectrum Disorders 30

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 6
International Classification of Functioning Disability and Health
PT for Hypermobility Spectrum Disorders 31
Engelbert , 2017; Pacey, 2014 PhD thesis
PT for Hypermobility Spectrum Disorders 32
Gastrointestinal
Dysautonomia
Fatigue
Psychological
Pain
Urogenital
Cardiovascular Neuromusculoskeletal
Symptom Profile Ninis, 2015
PT for Hypermobility Spectrum Disorders 33
Where To Start? Focus on patient’s primary activity & participation restrictions Engelbert, 2017
• Startatthebiggestcomplaint&worktowardsmallerissues• Lookforthekeystructures/problemsthatarecausingthe
pa:ent’sdeficits
PT for Hypermobility Spectrum Disorders 34
Principles of the Subjective Exam • Thorough,biopsychosocialinterview• Qualityoflifeassessment• Psychosocialassessmenttoolsasindicated(e.g.,depression,anxiety,etc.)
• Iden:fyhabitsandlifestylechoicesthatcontributetoprimarycomplaints– E.g.,sleephygiene,postures,ac:vi:es
• Whathashelped/harmedinthepast– Avoidiatrogenicinjuries(Bovet,2012)
PT for Hypermobility Spectrum Disorders 35
Outcome Measures • BristolImpactofHypermobility– Theonlycondi:on-specific– 55ques:ons– ~10mintocomplete– Validated– Reliability,MCIDnotyetdetermined
– (Palmer,2017)
PT for Hypermobility Spectrum Disorders 36

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 7
What is Different in HSD? • TissuesinHSDaremorefragile(Tinkle,2017)• Maybedamagedbymoresubtlestressesorcontribu:ngfactors
(“theprincessandthepea”)– Areslowertoheal(Tinkle,2017)
• Gravitycanhaveabigimpact• Abnormalpainprocessing/hyperalgesia(Chopra,2017;Scheper,2017)• Mul:plecomorbidi:escancompoundproblems
– E.g.,Poorcoordina:on�microtrauma– Fa:gueorpain�decondi:oning– POTS:anxiety�muscletriggerpoints– MCAD�excessiveinflammatoryresponse
PT for Hypermobility Spectrum Disorders 37
Principles of the Physical Exam • Iden:fy:ssuescausingsymptoms• Iden:fystressorsaffec:ngthose:ssues
1. Isthereanimbalancebetweenlaxjointsand:ghtmuscles?2. Doespoorposture,alignmentorgravitystressjoints/muscles?3. Arebodymechanicsstretchingorstressingjoints/muscles?4. Ispoorpropriocep:onormotorcontrolleadingtoinstability?5. Whatiscausingmuscletriggerpoints?
• POTStest,ifappropriate
PT for Hypermobility Spectrum Disorders 38
Interventions • PaDenteducaDon!!!• Exercise(appropriate)• Painmanagement,focusingonself-care• Assis:veandortho:cdevices?• Manualtherapy?
(Engelbert,2017;ClinicalGuidelines;Chopra,2017)
PT for Hypermobility Spectrum Disorders 39
Patient Education EducateandempowerthepaDent/family
• Paineduca:on&self-management• Bodymechanics/ergonomics
• Ortho:cs,braces,&splintsif/whenneeded• Appropriateexercise/ac:vity• Sleephygiene&fa:guemanagement• POTSself-management• Psychological&socialwellness,relaxa:onstrategies• Dietandfluidmanagement• Otherissues:GIdysfunc:on,MCAD,incon:nence,etc.Refertootherprofessionalsasappropriate(Engelbert,2017;Chopra,2017)
PT for Hypermobility Spectrum Disorders 40
Exercise Prescription • Propriocep:on,stabiliza:on,motorcontrol&coordina:on
• Strengthening• Appropriatestretching,stabilizingasneeded• Cardiovascularcondi:oning
– “GradedExerciseTherapy”• (POTS-specificexercise)(Engelbert,2017;Palmer,2014)
PT for Hypermobility Spectrum Disorders 41
Pain Management (in Clinic) • Physiologicalquie:ng• Biofeedback• TENS(trialforhomedevice)• Manualtherapy• Dryneedling(iflegalinyourstate)• Shi<topa=entself-management
– Avoidextensiveuseofmodali=esintheclinic(Chopra,2017;Engelbert,2017)
PT for Hypermobility Spectrum Disorders 42

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 8
Medications • Li|ledefini:veresearchevidenceformedica:ons• NSAIDsfortrueinflamma:on
– NSAIDsmayslow:ssuehealing,aggravateGIsymptoms• Tricyclics,an:-seizure,SNRImedsforneuropathicpain• Topicalanalgesicsandan:-inflammatorymedica:ons• Acetaminophen• Cau:ons:
– Opiatesforshorttermuseonly– Musclerelaxersmayaggravateinstability
PT for Hypermobility Spectrum Disorders 43
Chopra, 2017 Tinkle, 2017
Barriers To Treatment • Nega:vepastexperienceswithPT(Bovet,2016)• Iatrogenicinjuries(Bovet,2016)• Barrierstodoingexercise:(Simmonds,2017)
– Fear– Pain– Fa:gue
PT for Hypermobility Spectrum Disorders 44
Applying Evidence-Based Practice
• Althoughmoreresearchisavailablenow,manyques:onsaboutop:maltreatmentremainunanswered
• Wethereforerelyontheprinciplesofevidence-basedprac:ce
PT for Hypermobility Spectrum Disorders 45
Review • Hypermobility-relatedcomplaintsarecommon
– Hypermobilityaffectsmostbodysystems• The2017diagnos:ccriteriaforhEDSarerestric:ve
– ConsiderHypermobilitySpectrumDisorders• PTexamina:onshouldbebiopsychosocial(ICFmodel)
– Accountfor:ssuefragility– Lookforcontribu:ngfactors
• PTmanagementshouldaddresscontribu:ngfactorsPT for Hypermobility Spectrum Disorders 46
Case Examples • Theremainderofthissessionwillbethroughcaseexamples– Pediatriccase:StephanieSabo,presentedbyL.Russek
• Addressesassessment,motordelays,motorcontrolissues,bracing– Adolescentcase:JaneSimmonds
• Addressesassessment,stra:fiedmanagement,POTS,fa:gue,GIproblems,psychosocialissues
– Adultcase:HeatherPurdin• Addressesassessment,chronicpain,MCAD
PT for Hypermobility Spectrum Disorders 47
Managing Pediatric Patients with HSD
Case and slides provided by Stephanie Sabo, PT, MPT
PT for Hypermobility Spectrum Disorders 48

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 9
Common Presentation in Children
• Difficultywithprolongedwalkingorstanding• Legpainworseineveningoratnightandwith/aderac:vity• Legpainsymptomsrelievedbyrubbingorheat• Historyof“growingpains”• Difficultysi~nginchairatschool,figi:ng• Trips,falls,beinglabeled“clumsy”(Bernie,2011;Adib,2005)• Grossmotordelays(Tirosh1991,Davidovitch1994,Bernie2011)• Coordina:ondifficul:es(Kirby2007)
PT for Hypermobility Spectrum Disorders 49
Developmental Condition vs. Hypermobility in Young Children?
• Standardizedmotorcompetencytestsarenotadequate– Donotcapturethefullimpactofjointhypermobilityonmotorfunc:onandqualityoflife
– Qualityofmovementandcompensa:onsshouldbethefocusoftheassessment
– Childrencanodenachieveindividualmotoritems,butnotefficientlyorrepe::vely
– (Remvig,2011)PT for Hypermobility Spectrum Disorders 50
Prevalence
• 34-35%inschoolagechildren• (Arroyo,1988;Remvig,2011;Junge,2013)
• NOgenderdifferencefoundat10y/o
• (Remvig,2011)
• Postpubertalgenderdifferences• (Quatman,2008)
PT for Hypermobility Spectrum Disorders 51
Additional Hx: Prior Therapies • Itisimportanttoaskaboutwhetherthechildhashadpriortherapyand
whetheriswasperceivedashelpful– Some:mespriortherapyreportedtobeofli|lebenefitandworsenedsymptoms– Askifhypermobilitybeingtargetedinpriortherapies;ifhypermobilitywasnot
recognized,lesslikelythattherapywassuccessful• Authorssuggestthefollowingpoten:alreasonsforpreviouslyfailed
therapies:– Techniquesbeingtooaggressive– Dura:ontoshort– Frequencytohigh– Failingtoappreciatefullscopeofinterven:onsrequired
(Keer, 2003; Hakim 2003)
PT for Hypermobility Spectrum Disorders 52
Referral Sources • Pediatrics• Rheumatology• Gene:cs• DevelopmentalPediatrics• Orthopedics• PainManagement
PT for Hypermobility Spectrum Disorders 53
Referral Sources • TheEDS/hypermobilitypopula:ondoesn’tfitanyspecialtyarea
perfectly• Jointhypermobilityand/oritsimpactonfunc:onmaybeiden:fied
duringtreatmentofanothercondi:on,soitishelpfultoscreen• Children:
– Mayormaynotcomewiththisdiagnosisonthereferral– Mayhaveseenmanyphysiciansorservicesmul:ple:meslookingfor
answers• Pa:entandfamilyodenexpressfrustra:onswithdelayindiagnosis
orlackofexplana:onforsymptoms.
PT for Hypermobility Spectrum Disorders 54

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 10
• MotherwithhEDS• Over2-hourdrivefromtherapy• Parentsseparated• Limitedinvolvementofbiologicalfather
IMPAIRMENTS PARTICIPATION
PERSONAL FACTORS ENVIRONMENT
• Paininankles&knees,7/10-10/10– Worsewithac:vity&atnight
• Headaches• Poorposture• Poorbalance• Abnormalgait• Jointhypermobility• Muscle:ghtness:HS,heelcords• Poormotorcontrol&motorskills
• Difficultywalking>20minutes• Difficultysi~nginchairatschool
• Troubleatschool• Troublewithsocialfunc:on,playingwithfriends
Tommy,age4
• Anxious• A|en:ondeficit/hyperac:vitydisorder
• Self-imageas“clumsy”anduncoordinated
I want to play just like all the
other kids
ACTIVITY
PT for Hypermobility Spectrum Disorders 55
Tommy: Initial Presentation • 4yearoldmalereferredtoPTbyPediatricRheumatologist
– Onsetofsymptoms~1yearago,withincreasedcomplaintsinthelast6months
– Motherwithbehavioranda|en:onconcerns:“doesn’teversits:ll”
– SenttoRheumatologybyprimarycarephysician– 6monthslaterseenbyGene:cs(perRheumatologyReferral)
• Motherwithhypermobility/EDS
Insert subject
PT for Hypermobility Spectrum Disorders 56
Tommy: Initial Presentation • Paininanklesandknees2-3x/week
– 7/10onNumericRa:ngScale(NRS)– increaseswithphysicalac:vity– increasesinevening/night
• Upto10/10onNRS;motherhastakenhimtoemergencydepartmentforpain
• Bilateralhipandkneexrays-normal• Usesrubbingandmedica:onforrelief(e.g.,overthecounter
TylenolorMotrin)• Pa:entalsohascomplaintsofheadaches
Insert subject
PT for Hypermobility Spectrum Disorders 57
Tommy: Findings • Posture:
– Shouldersforward/rounded,increasedlordosis/anteriorpelvic:lt,genurecurvatum,calcanealvalgusandpesplanus,genuvalgum,externalrota:onatfeet
• Gait:– Decreasedkneeflexion,overprona:onofrearfoot-midfoot,audiblefootslap,
ERatfeet• ROM:
– HipER85o,HipIR70o,KneeExtension+8o,AnkleDorsiflexion30o,Ankleinversion60o
• Flexibility:– Hamstrings-40o;heelcords20o
PT for Hypermobility Spectrum Disorders 58
Measuring Flexibility • Assessmuscleflexibility
– Differen:atemuscleflexibilityandjointmobility
• Isolatemusclelengthvs.jointlaxity– Reinforceneedtostrengthenmusclesaroundloosejoints
• Muscularimbalances– Commonlyseelimita:onsinhamstringsandgastrocnemiusmusclegroups
PT for Hypermobility Spectrum Disorders 59
Tommy: Findings • Singlelimbstance:right:4-5seconds;led:4-5seconds
– Notedunsteadiness,withlateraltrunklean,trunkflexion,increasedanklestrategies,andadduc:onofoppositeLE
• Bridgeinhooklyingfor3secondsx3reps– Notedunsteadinessanddecreasedeccentriccontroluponlowering
• Miniwallsqua~ngfor10secondsx3reps– Noteddifficultywithmiddlerangecontrol:pushingkneeintogenu
recurvatumandpelvisforwardintoAPTwithoutcueing• Modifiedheelraises:singleUEsupportfor3secondsx3reps
– Notedtoini:allycompletethroughfullankleplantarflexionbutlockingoutankles;whencompletedinmiddlerange,demonstratedunsteadinessandsteppingstrategies
PT for Hypermobility Spectrum Disorders 60
Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 11
Measuring Strength • Assesscorestrength
– Qualityofmovementisveryimportant:focusonac:va:onofkeymusclegroupsthroughhips,coreandpelvis• Forexample:bridgingmayini:atethroughtrunkextensionandlackcoreac:va:on
– Under-u:liza:onofkeyposturalmusclesiscommon-Transverseabdominus,mul:fidus,gluteals,serratusanterior
– Co-contrac:onisodenlacking/decreased– (Falkerslev,2013;Jensen,2013;Grahame,2009)
PT for Hypermobility Spectrum Disorders 61
Common Strength Deficits
• Pts have difficulty maintaining stable, neutral postures and effectively controlling movement
• Efficient use of proper positions to accomplish tasks is not natural
• Pts often initially demonstrate a full crab walk position when asked to perform a bridge
• Even athletic patients can have difficulty sustaining a neutral core with simple bridging
PT for Hypermobility Spectrum Disorders 62
Strength
• Assessextremitystrengthusingfunc:onalstrengthtes:ng(nomanualmuscletes:ng):– Alltes:ngshouldbedoneinneutraljointposi:ons,where
strengthandenduranceareodendecreased– Avoidposi:onsatendofjointrange
• lockedjointsareassociatedwithligamentousdependency– Assessthequalityofmuscleco-contrac:on– Lookformuscleimbalances
• Oden,keyposturalmusclesareveryweakandnotproperlyu:lized
PT for Hypermobility Spectrum Disorders 63
Tommy: Ankle Strength
• With heel raises, Tommy positions ankles in end range to help stabilize
• He is unable to maintain a static position
PT for Hypermobility Spectrum Disorders 64
Tommy: Leg Strength Wall sits: • Note wide base of support with genu
valgum and increased pronation/ calcaneal valgum and knee flexion
• He has muscle endurance limitations and genu recurvatum with knee extension
• He has overall poor quality of movement and poor mid range control
PT for Hypermobility Spectrum Disorders 65
Balance and Proprioception • AssessbalanceandpropriocepDon
– Observecompensatorypa|ernsofmovement– Assessforalteredawarenessofbodyposi:oninspace(common)
• Mul:plestudiesconfirmpropriocep:vedeficits:– Lowerlimbpropriocep:onisdecreasedinBenignJointHypermobilitySyndrome
– Decreasedpropriocep:oninUEjoints(fingers)(Smith,2013;Rombaut,2010;Fatoye,2009;Sahin2008;Schubert-Hjalmarsson,2012)
PT for Hypermobility Spectrum Disorders 66

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 12
Balance and Proprioception
Single leg stand: • Observe duration of
single limb stance AND the quality of the movement
PT for Hypermobility Spectrum Disorders 67
Balance and Proprioception
Devia:onstolookfor• Lateral trunk lean (gluteus medius weakness) • Unsteadiness • Trendelenburg (hip drop) • Trunk flexion • Adduction of opposite leg using other limb for stability • Increased ankle strategies • Pronation through midfoot • Locking out knee • Internal rotation of stance limb
PT for Hypermobility Spectrum Disorders 68
Tommy: Intervention/Treatment Plan • FrequencyforPTservices:recommendedfollowupvisit
~4-6weeksaderevalua:on;however,pa:entwaslosttofollowupfor6monthsduetofamilyhavingsocialconcerns
• EducaDon:jointprotec:on,ac:vitymodifica:on,sodjoints• OrthoDcs:fi|edwithortho:csatevalua:on• HEP:bridging,resistedhipabduc:on,squats,passive
hamstringstretch• Treatments:completedHEP4x/weekfromevalua:onun:l
6monthfollowupvisit
PT for Hypermobility Spectrum Disorders 69
Basic Principles of Intervention • Beginlowlevelforbaseline
– Odenneedtobeginingravityeliminatedposi:onsand/oruseisometrics
• Progressatslowrate• Considerthewholeperson
– Notjustonejointata:me– Nonmusculoskeletalmanifesta:ons
• Customizetreatmentbasedonindividualneedsandgoals (Celletti, 2013)
PT for Hypermobility Spectrum Disorders 70
Joint Protection • Posturalre-educa:onandawareness
– Reducesstressonmusclesandjoints– Reducepainandfa:gueover:me
• Focusonawarenessofneutraljointposi:ons.Avoid:– Kneeandelbowhyperextension– Anteriorpelvic:lt/hiphanging(forwardand
laterally)– Wsi~ng– Roundedshoulderandforwardhead (Rombaut, 2012)
PT for Hypermobility Spectrum Disorders 71
Joint Protection
• Pa:entsshouldbeinstructedhowtoavoidoverstretchingjointsandtoreducemechanicalstressonjoints– Forexample:individualscanprac:cefindingandmaintaininga“sodknee”
posi:on,withkneesneutralorveryslightlyflexed
• Lackofposturalmuscleac:va:onreinforcesposturaldeficits• Avoidexcessivejointmovement,whichcouldleadtotears
andruptureofthesod:ssuessurroundingthejoint• (Rombaut,2012)
PT for Hypermobility Spectrum Disorders 72

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 13
Controlled Stretching • Paya%en(ontotechnique:
– Stabilizesurroundingjointstostretchspecific:ghtmuscleswithoutstressingotherstructures
• Contrastpa:ent’sini:alposi:onforstandinghamstringstretch(top)withperformanceAFTERinstruc:oninproperform(bo|om)
PT for Hypermobility Spectrum Disorders 73
Orthoses: Summary of Evidence • Thereislimited,inconclusiveevidence,evenasitrelatestothegeneral
“flatfeet”diagnosisinthepediatricpopula:on• Systema:creviewsfindthatstudiesusedifferentpa:entpopula:onsand
widelyvaryingtypeoforthoses (Evans,2011)• Noinforma:ontoconsistentlysupportusingortho:csornot• Planusfootinearlylifeisassociatedwithadultdegenera:vejointdisease
andinterven:onisindicated (Gross,2011)• Anecdotalexperiencewithuseofortho:csinthehypermobilepopula:on
isveryposi:ve (LocalCCHconsensus,2016)
PT for Hypermobility Spectrum Disorders 74
Minimal Control Orthotics
• Providesomesupporttopronated(flat)feet
• Canreducestressonalllowerextremityjoints
• Customizable
Cascade DAFO Fast Fit http://cascadedafo.com
Vasyli orthotics www.vasylimedical.com
PT for Hypermobility Spectrum Disorders 75
Models of Therapy • ConsultaDve:Emphasisisonhomeexerciseprogramsthatareperiodicallyupdatedbythetherapist
• Intermediate:1-3x/wk• Intensive:Frequentsessionsoverashortperiodof:me
PT for Hypermobility Spectrum Disorders 76
Consultative Model • Emphasisonhomeprogrammingandselfmanagement(odenusedinini:alstages)– Homeexerciseprogramestablishedatini:alsession– Educa:onwithchildandcaregivers:posture,jointprotec:on…– Ortho:cs,ifindicated
• Followupplanestablished– Individualized,emphasizingselfmanagement– Frequencyoftherapyisdeterminedattheevalua:on– Follow-upoden4to6weekslater
PT for Hypermobility Spectrum Disorders 77
Intensive Treatment Model • Mul:disciplinaryprogram,including
OT,PT,MD,Psychology,ChildLife– Seekstoprovideknowledge,aswellas
aphysicalboost– Providestoolsforselfmanagement– ProvidessocialInterac:ons– Par:cipantsbecometheirownexperts– Facilitateshomeadherenceand
lifelongmanagement– IncreasesindependencewithHEP (Bathen, 2013; Birt, 2013)
PT for Hypermobility Spectrum Disorders 78

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 14
Example Intensive Model • 2-weekprogram• Par:cipantsgroupedbygenderandage• AllwithEDSand/orjointhypermobilitycondi:ons• Benefits:
– IntensiveexposuretoPTempowersparentsandchildren– Par:cipantsgainknowledge,skillsandconfidencetoadaptexercisesandself-
managesymptoms
• Adolescentsfacedthemostdifficul:eswithfinding:me,privacyandmo:va:ontodotheexerciseprogramathome
PT for Hypermobility Spectrum Disorders 79
Intensive Model (2 week program) • Programstarted2011
• Outcomemeasurespreandpost:– PedsQL,COPM,TampaScaleKinesiophobia
• Psychologyusescogni:vebehavioraltherapyandgroupsessions
• MusicincorporatedinexercisesessionsandwithChildLife
• ChildLifehelpspa:entswritele|ersofencouragementtothenextgroupcomingintotheprogram
• HEPbooksareconstructedwithpicturesofthepa:entdoingtheexercises
• (Celle~,2013;Castori,2012)
PT
MD
Child Life
Aqua-tics PSY
OT
PT for Hypermobility Spectrum Disorders 80
PT for Hypermobility Spectrum Disorders 81
Outcome Measures • CanadianOccupa:onalPerformanceMeasure(COPM)
• PediatricQualityofLifeMeasure(PedsQL)• TampaScaleforKinesiophobia(TSK)
PT for Hypermobility Spectrum Disorders 82
Tommy: Outcome At 6 months: • Leg pain decreased from
daily to 1-2x/month • Improved quality of
movements • Improved ability to sustain
hold counts • Decreased postural
compensations
PT for Hypermobility Spectrum Disorders 83
Summary of Pediatric Case • Hypermobilepa:entsareinmostpediatriccaseloads• Func:onalimpactofjointhypermobilitypainandfa:gueissignificant
andisodenunder-appreciated• Standardtherapyfrequentlyfailsthesepa:ents• Specific,targetedjointstabiliza:on,neuromusculartrainingand
educa:onareneeded• Lowintensityandslowprogressionofinterven:onisindicated• Livescanbechanged!
PT for Hypermobility Spectrum Disorders 84

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 15
Thanks To: Stephanie Sabo PT, MPT
Physical Therapist II [email protected]
• Cincinnati Children's Hospital Medical Center Joint Hypermobility Team 2014. “Identification and Management of Pediatric Joint Hypermobility” CCHMC EBDM Website Guideline 43 pages 1-22.
Available at https://www.cincinnatichildrens.org
PT for Hypermobility Spectrum Disorders 85
Managing Adolescents with HSD and HEDS Jane Simmonds DProf, MCSP, MACP, SFHEA
Outline of Adolescent Case
• Consider issues which arise in adolescence
• Stratified approach to management Hypermobility Spectrum Disorders and Hypermobile Ehlers Danlos Syndrome
• Case study
• Plans for research
PT for Hypermobility Spectrum Disorders 87
Reflect on the key physiological and psychological changes during adolescence 1. Hormonal changes
2. Growth – Peak Height Velocity
3. Developing independence Seminal study (Kirk,1967) described three quarters of patients developed symptoms prior to age 15 years Hypermobile adolescents 2 times more likely to develop musculoskeletal problems than non hypermobile counterpart. Risk increases 12 fold if overweight (Tobias, 2013)
PT for Hypermobility Spectrum Disorders 88
DS
Joint Laxity
hEDS
Asymptomatic Mild Signs Significant Signs & Symptoms & Symptoms
GJH = (asymptomatic) joint hypermobility; hEDS = hypermobile EDS EDS = Ehlers-Danlos Syndrome
GJH
(Castori, 2017)
PT for Hypermobility Spectrum Disorders 89
SPECTRUM
SIMPLE/ACUTE INTERMEDIATE COMPLEX/CHRONIC
PT for Hypermobility Spectrum Disorders 90

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 16
STRATIFIED MANAGEMENT
SIMPLE/ EARLY
Episode of acute musculoskeletal injury, sprains, dislocation, subluxations
enthesopathies
(Pacey 2010; Smith 2005)
PT for Hypermobility Spectrum Disorders 91
STRATIFIED MANAGEMENT
SIMPLE/ EARLY
Episode of acute musculoskeletal injury, sprains, dislocation, subluxations
enthesopathies
(Pacey, 2010; Smith, 2005)
PT for Hypermobility Spectrum Disorders 92
STRATIFIED MANAGEMENT
SIMPLE/ EARLY
Episode of acute musculoskeletal injury, sprains, dislocation, subluxations
enthesopathies
SIMPLE/ EARLY Ice, electrotherapy, tape, support, exercise,
screen, education – rehabilitate and prevent
PT for Hypermobility Spectrum Disorders 93 PT for Hypermobility Spectrum Disorders 94
STRATIFIED MANAGEMENT
SIMPLE/ EARLY
Episode of acute musculoskeletal injury, sprains, dislocation, subluxations
enthesopathies
SIMPLE/ EARLY Ice, electrotherapy, tape, support, exercise,
screen, education – rehabilitate and prevent
INTERMEDIATE Recurrent episodes, series of episodes at
different sites, deconditioning, some central/ peripheral sensitization, mild
systemic conditions
PT for Hypermobility Spectrum Disorders 95
STRATIFIED MANAGEMENT
SIMPLE/ EARLY
Episode of acute musculoskeletal injury, sprains, dislocation, subluxations
enthesopathies
SIMPLE/ EARLY Ice, electrotherapy, tape, support, exercise,
screen, education – rehabilitate and prevent
INTERMEDIATE Recurrent episodes, series of episodes at
different sites, deconditioning, some central/ peripheral sensitization, mild
systemic conditions
INTERMEDIATE Physiotherapy modalities have temporary
effect, no effect or exacerbate Modified / adapted approach
Functional Restoration
(Engelbert 2017; Scheper 2017)
PT for Hypermobility Spectrum Disorders 96

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 17
Subjective Assessment
Listen and develop the therapeutic
alliance
Listen to the history carefully……. Explore expectations with young person and parent Identify problems – prioritize – Pain – local/ general/ acute/ chronic (sensitization) – Joint instability – subluxations, dislocations, clicking – Fatigue – sleep, fluid, diet – Anxiety - Low mood/ depression – Gastrointestinal dysmotility – Dysautonomia – Postural Tachycardia Syndrome (POTS) – Gynaecology and bladder problems – Allergies
Explore impact – Physical activity/ Sport/ Hobbies Physical Education – Social, School, General health – Family history and thorough developmental history **
PT for Hypermobility Spectrum Disorders 97
Subjective Assessment
Identify barriers to
rehabilitation
Listen to the history carefully……. Explore expectations with young person and parent Identify problems – prioritize – Pain – local/ general/ acute/ chronic (sensitization) – Joint instability – subluxations, dislocations, clicking – Fatigue – sleep, fluid, diet – Anxiety - Low mood/ depression – Gastrointestinal dysmotility – Dysautonomia – Postural Tachycardia Syndrome (POTS) – Gynaecology and bladder problems – Allergies
Explore impact – Physical activity/ Sport/ Hobbies Physical Education – Social, School, General health – Family history and thorough developmental history **
PT for Hypermobility Spectrum Disorders 98
Subjective Assessment
Identify personal strengths and
interests to drive rehabilitation
Listen to the history carefully……. Explore expectations with young person and parent Identify problems – prioritize – Pain – local/ general/ acute/ chronic (sensitization) – Joint instability – subluxations, dislocations, clicking – Fatigue – sleep, fluid, diet – Anxiety - Low mood/ depression – Gastrointestinal dysmotility – Dysautonomia – Postural Tachycardia Syndrome (POTS) – Gynaecology and bladder problems – Allergies
Explore impact – Physical activity/ Sport/ Hobbies Physical Education – Social, School, General health – Family history and thorough developmental history **
PT for Hypermobility Spectrum Disorders 99
Objective Assessment Careful active and passive joint range and muscle length Functional assessment * Posture and gait – compensatory patterns Sit to stand/ squat – gluteal, quadriceps Single leg dip Heel raise – tibialis posterior Balance – Single leg / Y Balance Test / Hop/ Jump Repositioning tests – proprioception/ kinaesthetic Strength/ activation (careful testing* - through range) Test for POTS (standing test…refer on)
Observe Carefully
PT for Hypermobility Spectrum Disorders 100
Dysautonomia/ Postural Tachycardia Syndrome (POTS)
Near syncope on standing Venous pooling with colour changes Tachycardia –standing and changing position Can result in massive anxiety Excessive heart rate on exercise Hyperventilation Heat intolerance Nausea Mathias (2011); Kizilbash (2014)
PT for Hypermobility Spectrum Disorders 101
Dysautonomia/ Postural Tachycardia Syndrome (POTS)
Near syncope on standing Venous pooling with colour changes Tachycardia –standing and changing position Can result in massive anxiety Excessive heart rate on exercise Hyperventilation Heat intolerance Nausea
Mechanisms Illness
Hormonal Deconditioning Hypermobility Mathias (2011); Kizilbash (2014)
PT for Hypermobility Spectrum Disorders 102

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 18
Chair
Walking
Chair
Artefact corrected heart rate
PT for Hypermobility Spectrum Disorders 103
Autonomic Testing Typical response POTS patient
Tilt Test Rise of ≥30 BPM adults Rise of ≥ 40 BPM in adolescents
Time Time Mathias (2011); Raj (2013); Kizilbash (2014)
PT for Hypermobility Spectrum Disorders 104
Autonomic Testing Typical response POTS patient
Time 10 Minute Standing Test – Alternative to Tilt Test
Time
Tilt Test Rise of ≥30 BPM adults Rise of ≥ 40 BPM in adolescents
Mathias (2011); Raj (2013); Kizilbash (2014)
PT for Hypermobility Spectrum Disorders 105
IMPAIRMENTS ACTIVITY PARTICIPATION
PERSONAL FACTORS ENVIRONMENT
Meet Helen 15 years
• Abletowalkfor15-20mins• Strugglingwithwri:ng• Strugglingtocarryschoolbag• Strugglingonpublictransport–duetosyncope
• Missingschool• Struggleswithdancing,notswimmingorplayingnetball
• Reducedsocialac:vitywithfriends(mainlyonline)
• Motherwithfibromyalgia• Youngerbrother–hEDS• Lovelyfriends
• Female• Highachiever–Astudent• Lowconfidence
• Widespreadhypermobility++• Recurrentshoulder,kneefingersubluxa:ons
• Persistentpainandfa:gue• Decondi:oned+• Anxiousandlowmood• Presyncopeandfastheartratewhenstanding(POTS)
• Dysmenorrhea• Bloa:ngandearlysa:ety
PMHx: Hypermobility detected in early life. Enjoyed being active. Recurrent injuries, subluxations. Physiotherapists treated single areas. PC: Never got on top of problem, injury after injury….now not coping ….
I want to do my exams…play sport,
dance …..go shopping
PT for Hypermobility Spectrum Disorders 106
Gastrointestinal
Dysautonomia
Fatigue
Psychological
Pain
Urogenital
Cardiovascular
Neuromusculoskeletal
Symptom Profile Ninis (2015)
PT for Hypermobility Spectrum Disorders 107
IMPAIRMENTS ACTIVITY PARTICIPATION
PERSONAL FACTORS ENVIRONMENT
Meet Helen 15 years
• Pa:entSpecificFunc:onalScale(PSFS)
• GoalA|ainmentScale
• PedsQL• (Physicalfunc:on,social,emo:onalandschool)
• SelfEfficacyScale(VAS)• CopingScale(VAS)
• PainVisualAnalogueScale(VAS)
• PedsQLMul:dimensionalFa:gueScale
• SingleLegDip• ModifiedStarExcursionBalanceTest(YBalance)
• TiltTest/StandTest• PedsQLGastroIntes:nalSymptomsandWorryScales
PMHx: Hypermobility detected in early life. Enjoyed being active. Recurrent injuries, subluxations. Physiotherapists treated single areas. PC: Never got on top of problem, injury after injury….now not coping ….
Relevant Outcome Measures
PT for Hypermobility Spectrum Disorders 108
Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 19
PT for Hypermobility Spectrum Disorders 109
Management
• Prioritize problems • Motivate and empower – partnership • Educate young person and family on all aspects of the condition • Agree goals (short and longer term) • Pain and fatigue management – including sleep routine • Movement correction • Exercise - recondition
(Engelbert, 2017)
PT for Hypermobility Spectrum Disorders 110
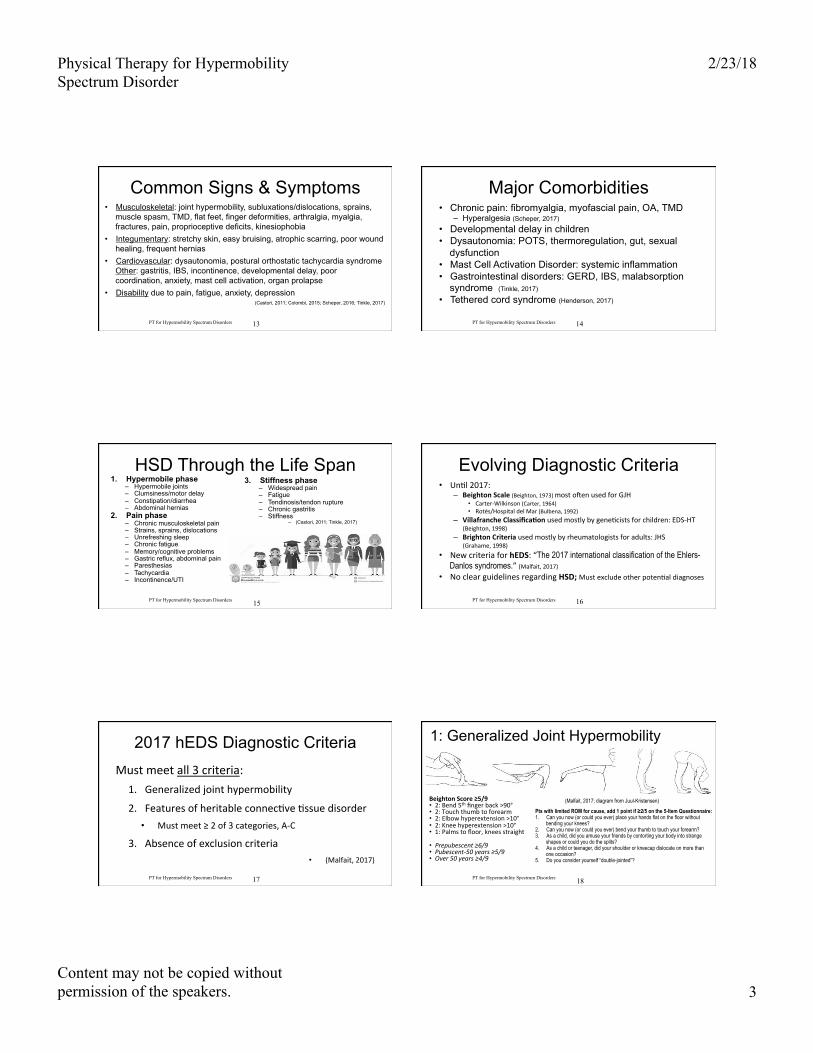
(Simmonds,2017)
Surveyof946paDentsUK
ExperiencesofPhysiotherapy
PT for Hypermobility Spectrum Disorders 111
Liaise with school teachers Dance teacher Coaches
PT for Hypermobility Spectrum Disorders 112
Dislocation and
Subluxation
Panic = muscle spasm Position the joint Analgesic Heat - Breath – Relax - Distract Give it time Do your usual thing… Ice, analgesia Support for a few days…carry on
PT for Hypermobility Spectrum Disorders 113
Limited evidence: wrist/hand neoprene splint not effective for hand pain or writing speed (small sample) (Frohlich, 2011)
Expertopinion-Judicioususe**Canbeveryhelpfulforwhenreturningfrominjuryandforfunc:on
Splinting and Tape
PT for Hypermobility Spectrum Disorders 114

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 20
Orthotics and Footwear
Cochrane Review Recommends supportive footwear and orthotics for flexible flat feet (Evans, 2011)
Improved gait efficiency in young people with Developmental Coordination Disorder and Hypermobility Syndrome (Morrison, 2013)
Expert opinion - Judicious use of orthotics or supportive footwear/ heal cup/ high tops
PT for Hypermobility Spectrum Disorders 115
Management of POTS • Advice – fluids, electrolytes/salt, compression tights
– Positioning, anti syncope manoeuvres • Medications prescribed (Midodrine, Fludrocortizone, Beta blockade)
• Respiratory physiotherapy – hyperventilation • Anxiety management – psychological support • Small meals, low carbohydrate diet and FODMAP • Graded cardiovascular exercise and resistance training – focus on lower limbs
– Morning exercise • Incorporating exercise to manage joint instability • Recumbent to upright exercise
(Mathias, 2011; Fu, 2011; George, 2013; Kizilbash, 2014)
PT for Hypermobility Spectrum Disorders 116
PREMISE FOR EXERCISE: Long term benefits of improved physical fitness and lower limb strength counteract orthostatic intolerance"• Increase blood volume"• Increase cardiac output"• Enhance vascular compression due to increased muscle mass and tone"• Improve endothelilial function"• Improve baro reflex function "
"
PT for Hypermobility Spectrum Disorders 117
PREMISE FOR EXERCISE: Long term benefits of improved physical fitness and lower limb strength counteract orthostatic intolerance"• Increase blood volume"• Increase cardiac output"• Enhance vascular compression due to increased muscle mass and tone"• Improve endothelilial function"• Improve baro reflex function "
"During exercise, people with POTS have a low stroke volume response to exercise – leads to light headedness, dizziness, dyspnoea and weakness!
PT for Hypermobility Spectrum Disorders 118
Application of Exercise • Individualise treatment based on needs and goals • Begin at a low level for baseline
– Weak and poor proprioception (Ferrell 2004; Engelbert 2017)
– Fear and pain (Simmonds, 2017)
• Progress slowly – exercise through range (Pacey 2013) • Considermotorcontrol(Roussel,2009)andengagethought(Boudreau2010)• Consider the whole person – kinetic chain
– Not just one joint at a time – Non musculoskeletal manifestations
• Hands on to teach (Simmonds, 2017)
• Make it relevant and fun and include the family (Birt, 2015)
PT for Hypermobility Spectrum Disorders 119
For Helen
PT for Hypermobility Spectrum Disorders 120

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 21
Pilates ….. Dance
(Simmonds, 2017)
For Helen
PT for Hypermobility Spectrum Disorders 121
For Helen
PT for Hypermobility Spectrum Disorders 122
PT for Hypermobility Spectrum Disorders 123 PT for Hypermobility Spectrum Disorders 124
STRATIFIED MANAGEMENT
SIMPLE/ EARLY Episode of acute musculoskeletal injury,
sprains, dislocation, subluxations enthesopathies
SIMPLE/ EARLY Ice, electrotherapy, tape, support, exercise,
screen, education – rehabilitate and prevent
INTERMEDIATE Recurrent episodes, series of episodes at
different sites, deconditioning, some central/ peripheral sensitization, mild
systemic conditions
INTERMEDIATE Physiotherapy modalities have temporary
effect, no effect or exacerbate Modified / adapted approach
Functional Restoration
COMPLEX LONG TERM Chronic, longstanding, severe, unremitting
pain with profound deconditioning/ comorbidities, disability
PT for Hypermobility Spectrum Disorders 125
STRATIFIED MANAGEMENT
SIMPLE/ EARLY Episode of acute musculoskeletal injury,
sprains, dislocation, subluxations enthesopathies
SIMPLE/ EARLY Ice, electrotherapy, tape, support, exercise,
screen, education – rehabilitate and prevent
INTERMEDIATE Recurrent episodes, series of episodes at
different sites, deconditioning, some central/ peripheral sensitization, mild
systemic conditions
INTERMEDIATE Physiotherapy modalities have temporary
effect, no effect or exacerbate Modified / adapted approach
Functional Restoration
COMPLEX LONG TERM Chronic, longstanding, severe, unremitting
pain with profound deconditioning/ comorbidities, disability
COMPLEX/ LONG TERM Multi disciplinary management programme using functional andcognitive behavioural
approaches (Bathen 2014)
PT for Hypermobility Spectrum Disorders 126

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 22
Summary for Functional Rehabilitation Time to listen reassurance, educate, empower (young person and family)
Condition specific education, advice and support
Give HOPE, agree GOALS, and be CREATIVE
Treat the treatable – prioritise
Pain and fatigue management (young person and parent)
Improve movement – use your hands
Strengthen weak muscle groups
Improve cardiovascular fitness
PT for Hypermobility Spectrum Disorders 127
Future Research and Education
• Understand the factors which influence development of symptoms • Validate and agree outcome measures • Understand what works best for young people • Intervention trials • Education patients and professionals
PT for Hypermobility Spectrum Disorders 128
Acknowledgments Patients and families Professor Rodney Grahame Rosemary Keer Dr Nelly Ninis Dr Hanadi Kazkaz Dr Alan Hakim Professor Christopher Mathias Colleagues in the Hypermobility Unit
PT for Hypermobility Spectrum Disorders 129
PT for Hypermobility Spectrum Disorders 130
Adults with HSD
ByHeatherPurdin,MS,PT,[email protected]
Guido Daniele http://www.guidodaniele.com
PARTICIPATION
PERSONAL FACTORS
ENVIRONMENT
• Widespreadhypermobility• AllogradHSandAchillesusedtostabilizeRshoulderanditsdisloca:ngagain
• PastHxlumbardiscectomy• Weightgain40#sincestoppingpainmedslastyear
• UterineProlapse• Dizzinessandtachycardia• TMJandribsubluxa:ons• Widespreadhives&swelling
• Strugglingtocareforfamilyandhome
• ⬇︎Churchinvolvement
• Female• Driven• Frustratedbymedicalcare• KidswithhEDSneedsupport
• Suppor:vehusband• Sickkids/neardeathexperience
• Recentlyrelocated• StresslevelhighduetonewChurchassignment
I need to look after my
family
ACTIVITY • Limitedarmfunc:onduetoshoulderinstability
• Limitedmobility• PainlimitsADLandIADL
BODY STRUCTURE/FUNCTION
132
MeetMindy,37y/ohomemaker
PT for Hypermobility Spectrum Disorders

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 23
Gravity affects EDS/HSD Pre-operaDveshoulder
subluxaDonNormalshoulderx-ray
PT for Hypermobility Spectrum Disorders 133
Gravity is a problem InferioranteriorsubluxaDon Deltoid,uppertrap,rotatorcuffset
PT for Hypermobility Spectrum Disorders 134
Subluxed Shoulder Causes Neck/Jaw Malalignment
Downsloped R shoulder pulls lower neck to R and head corrects to L
Set shoulder brings head back to neutral
PT for Hypermobility Spectrum Disorders 135
Types of Pain • Iden:fythetype(s)ofpain
– Nocicep:ve:mechanical,inflammatory– Neuropathic:peripheral,(central)– Centralsensi:za:on:neuroplas:city
• Differentpainistreateddifferently
136 PT for Hypermobility Spectrum Disorders
Pain Source
Quality Medications/Referral
Exercise Other Intervention
Mechanical Localized, occurs with certain motions. Sensitized by inflammation
NSAIDs? Primary MD
Strength/Mobility Balance throughout kinetic chain Proprioception
Bracing, taping, Ergonomics training, Muscle setting
Inflammatory Burning in broad area not dermatomal, bruisy
NSAIDs, Allergy meds, MCAD Primary MD, Allergy
Pool Proprioceptive input Mindful movement
Modalities, Tool assisted scraping, Dietary guidance
Nerve Burning in a peripheral nerve or dermatomal pattern, searing
Gabapentin, Lyrica, SNRI’s, LDN, Triptylines Primary MD, Neuro, Nutrition?
Nerve flossing Mindful movement Cardio External focus
Posture training to address entrapped nerves, positions of slack
Central Sensitization
Whole body pain, difficult to localize, wind-up, allodynia
SNRI’s, triptylines, LDN Primary MD, Psych
Cardio Mindful movement External focus
Meditation Breathing Biofeedback 137
PT for Hypermobility Spectrum Disorders
(Chopra, 2017; Castori, 2012)
What is MCAD?
PT for Hypermobility Spectrum Disorders 138 https://ehlers-danlos.com/pdf/Maitland-EDNF-Vegas-Mast-Cell-Activation-Disorders-S.pdf.
Slide from Anne Maitland’s presentation at 2017 EDS Global Learning Conference

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 24
MCAD Presentation
PT for Hypermobility Spectrum Disorders 139
Slide from A. Maiteland, EDS Global Learning Conference, 2017 https://ehlers-danlos.com/pdf/Maitland-EDNF-Vegas-Mast-Cell-Activation-Disorders-S.pdf.
Mindy’s Symptoms - Hives,redrash- Brainfog- Diges:veissues- Bladderirritability- Swellinginlimbs,supraclavicular
- Elevatedurinehistamines
PT for Hypermobility Spectrum Disorders 140
PT for Hypermobility Spectrum Disorders 141 Slide from A. Maiteland, EDS Global Learning Conference, 2017 https://ehlers-danlos.com/pdf/Maitland-EDNF-Vegas-Mast-Cell-Activation-Disorders-S.pdf.
Manage Mast Cell Activation • Iden:fytriggers:
– Alcohol,heat,medica:ons(NSAIDs,an:bio:cs,narco:cs),allergens– Foodsensi:vi:es– Excessiveexercise
• Managephysicalandemo:onalstress• Exerciseregularly,inspiteoffa:gue• Advocateforpa:entge~ngonMastCellStabilizersandmeds
thatblockchemicalmediatorslikean:-histamines– sendpa:enttoMDwithresearchar:cles
– (Akin, 2010; Moulderings, 2011; Seniviratne, 2017; Theoharides 2015)
142 PT for Hypermobility Spectrum Disorders
Dietary Advice • 37%ofpeoplewithIBShavehEDS• FODMAPdietmaybehelpful(expertopinion)
– Fructose,Oligosaccharides,Disaccharides,Monoamines,andPolyols– BacteriathriveonFODMAPfoods/dysbiosiscausesMCAD– MonashUniversity,MelborneAustrialia(Fikree,2017)
• Otherrecommenda:onsarespecula:ve– HeidiCollins,MDdiet–avoidchemicals,gluten,takesupplementstoimprove
nutri:on,reducehistamines– Lowhistaminediet(especiallywithMCAD)– Avoidhardfoodsandexcessivejawmovements(ice,gums,etc.)toavoidTMD– Avoidbladderirritantfoods(e.g.,coffee,citrusproducts)– Avoidlargemeals(especiallyofrefinedcarbohydrates)
143 PT for Hypermobility Spectrum Disorders
Sources of Pain • Don’tjustlookforsymptoma:c:ssue–findthecauseof:ssuesymptoms– E.g.:UTTrPmaybecausingHA,butpoorpropriocep=onandDNFmotorcontrolcauseUTTrP
• Chronicpain-consider– Psychosocialfactors– Stress– Childhoodtrauma
144 PT for Hypermobility Spectrum Disorders

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 25
HSD Through the Life Span 1. Hypermobile phase
– Hypermobile joints – Clumsiness/motor delay – Constipation/diarrhea – Abdominal hernias
2. Pain phase – Chronic musculoskeletal pain – Strains, sprains, dislocations – Unrefreshing sleep – Chronic fatigue – Memory/cognitive problems – Gastric reflux, abdominal pain – Paresthesias – Tachycardia – Incontinence/UTI
3. Stiffness phase – Widespread pain – Fatigue – Tendinosis/tendon rupture – Chronic gastritis – Stiffness
– (Castori, 2011; Tinkle, 2017)
PT for Hypermobility Spectrum Disorders 145
Adverse Childhood Experience • Specificadversechildhoodexperiences(ACEs)increaseriskofchronicpain– Verbalorsexualabuse,parentalpsychopathy,Earlyparentaldeath
– Adults(Sachs-Erickson,2017)– Childrenandadolescents(Nelson,2017)
• MechanismmaybeviaalteredHPAaxisandautonomicdysfunc:on(Elbers,2017)
PT for Hypermobility Spectrum Disorders 146
Set Realistic Goals • Pa:entavoidsdisability/reversesdisability• Fewer“bad”days• Selftreatmentstrategiesreduceneedformedicalinterven:on
• Increasedself-efficacy
PT for Hypermobility Spectrum Disorders 147
Mindy’s Goals • Goodshoulderalignmentwithoutshouldersubluxa:on:60%met• Cantalkunlimitedbyjawpain/locking:Met• ImprovedstabilityBhipstoallow1hourofpainfreewalkingwith
restbreaks:Metwithpain,nopainflarewith30minutesofwalking• IndependentwithprogressiveHEPwithself-reliefforpain:Metfor
basicprogramforshoulders,neck,ribs,hips,core• Improvedbiomechanicsandstabilityofribcageforfull,painfree
ven:la:on:Mostlymet,selftreatsribmalalignment• Improvedmobilityandreducedpaininheadandneck:Partlymet,
needscuestostabilizeneckduringarmuse
PT for Hypermobility Spectrum Disorders 148
Pain Self-Management • Techniquestodecreasepain:
– Painneuroscienceeduca:on(e.g.,“ExplainPain”)– Cogni:vebehavioraltherapy– Relaxa:on– Self-carewithheat,ice,TENS
• Techniquestodecreaseinjury– Jointprotec:onstrategies– Bracing/splin:ng,etc.
149 PT for Hypermobility Spectrum Disorders
Body Mechanics • Postureandergonomicsatschool/work/home• Sleepingposture,surface,support– Engagingmusclesbeforemoving– Assis:vedevices(e.g.,pens,tools,etc.)
150 PT for Hypermobility Spectrum Disorders

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 26
Biomechanical Differences • Shoulderse~ng
– Cueupinsteadofdown– Ballbackinsocket,notjustscapulae–cueupsidedown“G”
• Bicepslongheadsubluxa:on– ReduceERandabduc:onposi:ons
• Hipposteriorsea:ng– Nohipflexorusewithoutglutuseor– Alterposi:onofexercisetoassiststability/posteriorsea:ng
suchasinlongsi~ng
151 PT for Hypermobility Spectrum Disorders
Biomechanical Differences • Ankleprotec:on
– Bedsheetscansubluxtalusanteriorly– Si~ngonankles
• Patellofemoralinstability– TypicalissuesOsgoodSchla|er’s,trackingissues
• Elbow–ulnarnervesubluxa:onusuallyat90+degrees
• Wrist–carpalsubluxa:ons,rota:ons
152 PT for Hypermobility Spectrum Disorders
Biomechanical Differences • Craniocervicalinstability
– Odenjustlongholdintomobiliza:ondirec:onisenoughtonormalize
• SpineInstabili:es– Spondylolisthesis– Retrolisthesis
• Ribse~ng– ½inhalebeforeliding– Ifdepressedribs,inhalewithac:vity– Ifelevatedribs,exhalewithac:vity
153 PT for Hypermobility Spectrum Disorders
Exercise: Do No Harm! • Researchshowsthatmanypa:entswithhEDShavenega:vepastphysicaltherapyexperiencesdueto:
– Iatrogenicjointinjuries
– Unmetrehabilita:onneeds» (Bovet,2016)
154 PT for Hypermobility Spectrum Disorders
Exercise: Do No Harm! Avoidmechanicalpain
• Stabiliza:on&motorcontrolarecri:calThinkbeforemoving
• Tensilestrengthof:ssuesvarieswithac:vity,menses,inflammatorystate,ageetc.
• Slowprogressiontoallowhistologicalchanges
155 PT for Hypermobility Spectrum Disorders
Exercise: Do No Harm!
Cau:onwithoveruse:nerveentrapment,triggerpointsCau:onwithchangingforces
e.g.,exercisebandsincreaseresistance
Allow:ssuerecoverybetweenexercisebouts
2-hourrule:discomfortshouldreturntobaselinewithin2hours
156 PT for Hypermobility Spectrum Disorders

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 27
Exercise Progression • Rememberbasicprinciplesofexerciseprogression
157 PT for Hypermobility Spectrum Disorders
Proprioceptive Exercise • Propriocep:onsignificantlyworseinkneeswithBJHS(Sahin,2008)
– Propriocep:onexercisesimprovepainandfunc:on(Sahin,2008)• Propriocep:veexforkneesreducespainandimprovesqualityof
life(Ferrell,2004)– ClosedChainLEex–bridges,squats,sidelungetos:mulatejoint
receptors• Neckandspinepain-Propriocep:veexmaybelessrelevantthan
behavioralandeduca:onalRx,metaanalysis(McCaskey,2014)
• Backpainreduc:on,muscleenduranceandposturalstabilityimprovementswithlumbarspinalstabexercise(ToprakCelenay,2017)
PT for Hypermobility Spectrum Disorders 158
Exercise: Proprioception • Externalfocusexercises–putalaser
onitanddrawonthewall,thinkBAPS(SenMoCorSystem™)
• Biofeedback(e.g.,Stabilizer™)• Alterna:ngisometrics,dynamic
stabiliza:on• Ballexercises,balance&
propriocep:on• Emphasizegoodmotorcontrol
159 PT for Hypermobility Spectrum Disorders
Exercise Progression Easier
• Morepropriocep:vefeedback– Tac:le,visual,verbal– Externalfocus,e.g.lasers
• Moresupport– Exercisemachines– Againstwall
Harder
• Lessexternalpropriocep:vefeedback
• Lesssupport– Morechallenge,e.g.,unstable
surfaces– Freeweightsorbands
160 PT for Hypermobility Spectrum Disorders
Exercise Progressions Gravityassistedstabiliza:on,maximumtac:lefeedback
Addinggravitytostabilizerswithoutchallengingsubluxa:on
PT for Hypermobility Spectrum Disorders 161
Exercise Progressions Notowelunderthearm,set
upandback,controlresistanceReducingtac:le
feedback/useofwall
PT for Hypermobility Spectrum Disorders 162

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 28
Exercise Progression Easier
• Focusonjointstability– Isolatelegorarmwithout
spinemovement– Isolateshoulderstabilizers– Isolatecore
• Visualiza:on/mind-body– E.g.,jointcompression,
Qigong
Harder
• Focusonintegra:on– Coordinatecoreandlimb
movement– Addexternalchallenge– Complexmovements,e.g.,TaiChi
• Adddistrac:on/mul:tasking
163 PT for Hypermobility Spectrum Disorders
Exercise Progressions Speed/alterna:ngisometrics Againstgravityismoreadvanced
PT for Hypermobility Spectrum Disorders 164
Stabilization Exercises
• Shoulderse~ngwithfeedback
PT for Hypermobility Spectrum Disorders 165
Exercise Progression – Central Sensitization
Easier
• ChronicPain–unstablepla]orm,flowingmo:on,alternateagonist/antagonistorcontract/relaxandstretch
• Externalfocusexercise–laserpointerontarget/visualiza:on
Harder
• ChronicPain-longerholds,isometrics,longersets,stretchlaterinsession
• Focusonbodyposi:on
166 PT for Hypermobility Spectrum Disorders
Craniocervical Flexion vs Proprioception Ex
• Group1exercisingwithStabilizer/longuscolinods• Group2exercisingwithlaseronheadandeyeandheadmovementstotargets(externalfocus)
• BothGroupshadreduc:oninpainandneckdisabilityindex
• Propriocep:ongroup>CCflexionimprovedtolerancetotriggerpointpalpa:on
(Galllego-Izquierdo,2016)
PT for Hypermobility Spectrum Disorders 167
Exercise Progression Easier
• Midrange• Shortdura:on• Slow• Lowimpact• Symmetrical/bilateral • RPEstartat4/10
Harder
• FullRange• Longerdura:on• Fast• Addimpact• Unilateral/asymmetrical• RPE7.5/10ul:mategoal
168 PT for Hypermobility Spectrum Disorders

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 29
Exercise: Strengthening • Strengthenstabiliza:onmmbeforeglobalmm
– SpinestabilityexwithBJHSreducedpain,improvedendurance,improvedposturalstability(ToprakCelenay,2016)
• Possibilityofincreasedjoints:ffnesswithincreasedstrength– Cheerleadersincreasedshoulders:ffness,decreasedant.capsulelaxity(Laudner,2013)– Increasedpatellartendons:ffnessinpa:entswithcEDS(Moller,2014)– Mechanicalstraininhibitscollagenbreakdown(Flynn,2010)
• Needpropriocep:on&motorcontrol(Scheper,2016)• Beawareofstresseson‘incidental’joints,e.g.
– HandsgrippingweightsorTheraband– Wristextensioninquadruped– Spinestabiliza:onforextremityexercise
169 PT for Hypermobility Spectrum Disorders
Cardiovascular Exercise • Chronicpainleadstodecondi:oning• Exercise-inducedanalgesiacanreducepain• Startcardioaderini:alcorestabiliza:ontrainingorusemachinesthatprovidestability(e.g.,recumbentbike)
• Makeitfunsopa:entss:ckwithit170 PT for Hypermobility Spectrum Disorders
Exercise: Stretching • PeoplewithEDScanhave:ghtstructures• Isolatestretchtoproperstructure
– Keepjointsinproperalignmentwhenstretchingmuscles
• Stretchesmayneedtobegentle– Onlydo80%stretchandhold3-5secinpa:entswithperipheralsensi:za:on
– Thiscanminimizeflaresinsensi:zedpa:ents
171 PT for Hypermobility Spectrum Disorders
Bracing and Taping • Mul:direc:onalinstabilitycommon• Hips,Shoulders,SI,Knees,Ribs,
Fingers,Feet…• Benefitmaybefrompropriocep:ve
feedback• Givepa:entresourcestoselfmanage
painfulareasastheyarise• Teachpa:enttousemusclestobrace
fortheac:vity
172 PT for Hypermobility Spectrum Disorders
Picture of Mindy’s Modified Brace
PT for Hypermobility Spectrum Disorders 173
Manual Therapy • Relievemmspasm,TrP,&fascialadhesions• Decreasepain&autonomictone• Realignjointscarefully
– MWM,MET,nervemobs,gradesI-IV– Stabilizenearbystructures
• DONOHARM!– Donotover-mobilize
174 PT for Hypermobility Spectrum Disorders

Physical Therapy for Hypermobility Spectrum Disorder
2/23/18
Content may not be copied without permission of the speakers. 30
Precautions and Red Flags • Spinalfluidincreasedpressure,leaks,syrinxesandheadaches–
– Mindyhaddocumentedleakfromnoseapprox.1cupofspinalfluidaderhusbandpushedonherupperneckwithmassagewhichalleviatedher“worstheadacheinherlife”
• Craniocervicalinstability–isdizzinessfromPOTSorCCI,stress,BPPV?• ChiariMalforma:on–maycauseincreasedspinalfluidpressure,ataxia
especiallyifmalallignedinuppercervical• Tetheredcord–avoidexcessivenervetension/flossingonly
– Saddleanesthesia,difficultywalking,bowel/bladderissues,tension• Precau:onsaswithapregnantpa:entforlaxity
PT for Hypermobility Spectrum Disorders 175
Mindy’s outcomes • 22%increaseinfunc:ononCareConnec:onsform• 4.5/7globalra:ngofchangeonscaleof-7to+7• Worstpainreducedfrom9/10to4-5/10,LBP0/10• Areastreated:Neck,jaw,ribs,shoulder,hips,LB• 21visitsover6months
PT for Hypermobility Spectrum Disorders 176
Summary of Adult Case • Needcomprehensiveevalua:on• Challengetoovercomegravity• Motorcontrolisessen:al• Subtlechangescanbeimportant• Startlow,goslow!
PT for Hypermobility Spectrum Disorders 177
Overall Summary • Hypermobilityspectrumdisordersarecommon• HSDinvolvesmanybodysystems,notjustjoints• Physicaltherapyiskeytomanagement• Programmustbecustomizedtothepa:ent• Lookforzebras!
178 PT for Hypermobility Spectrum Disorders
PT for Hypermobility Spectrum Disorders 179 PT for Hypermobility Spectrum Disorders 180

Physical Therapy for Hypermobility Spectrum Disorders References
The whole issue of Am J Med Genet C Semin Med Genet. 2017;175(1) is devoted to EDS, including hEDS and HSD. These articles, including many cited below, are available at https://www.ehlers-danlos.com/2017-eds-international-classification/.
• Adib N, Davies K, Grahame R, Woo P, Murray KJ. Joint hypermobility syndrome in childhood. A not so benign multisystem disorder?
Rheumatology (Oxford). 2005;44(6):744-750. • Akin C, Valent P, Metcalfe DD. Mast cell activation syndrome: Proposed diagnostic criteria. J Allergy Clin Immunol. 2010;126(6):1099-
1104.e1094. • Arroyo IL, Brewer EJ, Giannini EH. Arthritis/arthralgia and hypermobility of the joints in schoolchildren. J Rheumatol. 1988;15(6):978-980. • Bathen T, Hangmann AB, Hoff M, Andersen LO, Rand-Hendriksen S. Multidisciplinary treatment of disability in ehlers-danlos syndrome
hypermobility type/hypermobility syndrome: A pilot study using a combination of physical and cognitive-behavioral therapy on 12 women. Am J Med Genet A. 2013;161A(12):3005-3011.
• Beighton P, De Paepe A, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Ehlers-Danlos National Foundation (USA) and Ehlers-Danlos Support Group (UK). Am J Med Genet. 1998;77(1):31-37.
• Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis. 1973;32(5):413-418. • Bernie C, Maillard SM. The frequency of parent-reported motor coordination difficulties in children diagnosed with benign joint hypermobility
syndrome. Ped Rheumatol. 2011; 9(Suppl 1):035. • Birt L, Pfeil M, Macgregor A, Armon K, Poland F. Adherence to home physiotherapy treatment in children and young people with joint
hypermobility: a qualitative report of family perspectives on acceptability and efficacy. Musculoskeletal Care. 2014;12(1):56-61. • Boudreau SA, Farina D, Falla D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain
disorders. Man Ther. 2010;15(5):410-414. • Bovet C, Carlson M, Taylor M. Quality of life, unmet needs, and iatrogenic injuries in rehabilitation of patients with Ehlers-Danlos Syndrome
hypermobility type/Joint Hypermobility Syndrome. Am J Med Genet A. 2016;170(8):2044-2051. • Bulbena A, Duro JC, Porta M, Faus S, Vallescar R, Martin-Santos R. Clinical assessment of hypermobility of joints: assembling criteria. J
Rheumatol. 1992;19(1):115-122. • Carter C, Wilkinson J. Persistent Joint Laxity and Congenital Dislocation of the Hip. J Bone Joint Surg Br. 1964;46:40-45. • Castori M. Ehlers-danlos syndrome, hypermobility type: an underdiagnosed hereditary connective tissue disorder with mucocutaneous,
articular, and systemic manifestations. ISRN Dermatol. 2012;2012:751768. • Castori M, Morlino S, Celletti C, et al. Management of pain and fatigue in the joint hypermobility syndrome (a.k.a. Ehlers-Danlos syndrome,
hypermobility type): principles and proposal for a multidisciplinary approach. Am J Med Genet A. 2012;158A(8):2055-2070. • Castori M, Sperduti I, Celletti C, Camerota F, Grammatico P. Symptom and joint mobility progression in the joint hypermobility syndrome
(Ehlers-Danlos syndrome, hypermobility type). Clin Exp Rheumatol. 2011;29(6):998-1005. • Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A. A framework for the classification of joint hypermobility and related conditions. Am
J Med Genet C Semin Med Genet. 2017;175(1):148-157. • Celletti C, Castori M, La Torre G, Camerota F. Evaluation of kinesiophobia and its correlations with pain and fatigue in joint hypermobility
syndrome/Ehlers-Danlos syndrome hypermobility type. Biomed Res Int. 2013;2013:580460. • Chopra P, Tinkle B, Hamonet C, et al. Pain management in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet.
2017;175(1):212-219. • Clark CJ, Simmonds JV. An exploration of the prevalence of hypermobility and joint hypermobility syndrome in Omani women attending a
hospital physiotherapy service. Musculoskeletal Care. 2011;9(1):1-10. • Colombi M, Dordoni C, Chiarelli N, Ritelli M. Differential diagnosis and diagnostic flow chart of joint hypermobility syndrome/ehlers-danlos
syndrome hypermobility type compared to other heritable connective tissue disorders. American Journal of Medical Genetics Part C: Seminars in Medical Genetics. 2015;169(1):6-22.
• Dansie EJ, Turk DC. Assessment of patients with chronic pain. Br J Anaesth. 2013;111(1):19-25. • Davidovitch M, Tirosh E, Tal Y. The relationship between joint hypermobility and neurodevelopmental attributes in elementary school children. J
Child Neurol. 1994;9(4):417-419. • Elbers J, Rovnaghi CR, Golianu B, Anand KJS. Clinical Profile Associated with Adverse Childhood Experiences: The Advent of Nervous System
Dysregulation. Children (Basel). 2017;4(11). • Engelbert RHH, Juul-Kristensen B, Pacey V, et al. The Evidence-based rationale for physical therapy treatment of children, adolescents and
adults diagnosed with joint hypermobility syndrome/hypermobile Ehlers Danlos Syndrome. Am J Med Genet C Semin Med Genet. 2017;175(1):158-167.
• Evans AM, Rome K. A Cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur J Phys Rehabil Med. 2011;47(1):69-89.
• Falkerslev S, Baago C, Alkjaer T, et al. Dynamic balance during gait in children and adults with Generalized Joint Hypermobility. Clin Biomech (Bristol, Avon). 2013;28(3):318-324.
• Fatoye F, Palmer S, Macmillan F, Rowe P, van der Linden M. Proprioception and muscle torque deficits in children with hypermobility syndrome. Rheumatology (Oxford). 2009;48(2):152-157.
• Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364.

• Ferrell WR, Tennant N, Sturrock RD, et al. Amelioration of symptoms by enhancement of proprioception in patients with joint hypermobility syndrome. Arthritis Rheum. 2004;50(10):3323-3328.
• Fikree A, Chelimsky G, Collins H, Kovacic K, Aziz Q. Gastrointestinal involvement in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):181-187.
• Flynn BP, Bhole AP, Saeidi N, Liles M, Dimarzio CA, Ruberti JW. Mechanical strain stabilizes reconstituted collagen fibrils against enzymatic degradation by mammalian collagenase matrix metalloproteinase 8 (MMP-8). PLoS One. 2010;5(8):e12337.
• Frohlich L, Wesley A, Wallen M, Bundy A. Effects of neoprene wrist/hand splints on handwriting for students with joint hypermobility syndrome: a single system design study. Phys Occup Ther Pediatr. 2012;32(3):243-255.
• Fu Q, Vangundy TB, Shibata S, Auchus RJ, Williams GH, Levine BD. Exercise training versus propranolol in the treatment of the postural orthostatic tachycardia syndrome. Hypertension. 2011;58(2):167-175.
• Gallego Izquierdo T, Pecos-Martin D, Lluch Girbes E, et al. Comparison of cranio-cervical flexion training versus cervical proprioception training in patients with chronic neck pain: A randomized controlled clinical trial. J Rehabil Med. 2016;48(1):48-55.
• George SA, Bivens TB, Howden EJ, et al. The international POTS registry: Evaluating the efficacy of an exercise training intervention in a community setting. Heart Rhythm. 2016;13(4):943-950.
• Grahame R. Joint hypermobility syndrome pain. Curr Pain Headache Rep. 2009;13(6):427-433. • Grahame R, Bird HA, Child A. The revised (Brighton 1998) criteria for the diagnosis of benign joint hypermobility syndrome (BJHS). J
Rheumatol. 2000;27(7):1777-1779. • Hakim A, Grahame R. Joint hypermobility. Best Pract Res Clin Rheumatol. 2003;17(6):989-1004. • Henderson FC, Sr., Austin C, Benzel E, et al. Neurological and spinal manifestations of the Ehlers-Danlos syndromes. Am J Med Genet C
Semin Med Genet. 2017;175(1):195-211. • Humphreys JH, Verstappen SM, Hyrich KL, Chipping JR, Marshall T, Symmons DP. The incidence of rheumatoid arthritis in the UK:
comparisons using the 2010 ACR/EULAR classification criteria and the 1987 ACR classification criteria. Results from the Norfolk Arthritis Register. Ann Rheum Dis. 2013;72(8):1315-1320.
• Jensen BR, Olesen AT, Pedersen MT, et al. Effect of generalized joint hypermobility on knee function and muscle activation in children and adults. Muscle Nerve. 2013;48(5):762-769.
• Junge T, Jespersen E, Wedderkopp N, Juul-Kristensen B. Inter-tester reproducibility and inter-method agreement of two variations of the Beighton test for determining Generalised Joint Hypermobility in primary school children. BMC Pediatr. 2013;13:21
• Keer R, Grahame R. Hypermobility syndrome - recognition and management for physiotherapists. London: Butterworth-Heinemann; 2003. • Kirby A, Davies R. Developmental Coordination Disorder and Joint Hypermobility Syndrome--overlapping disorders? Implications for research
and clinical practice. Child Care Health Dev. 2007;33(5):513-519. • Kizilbash SJ, Ahrens SP, Bruce BK, et al. Adolescent fatigue, POTS, and recovery: a guide for clinicians. Curr Probl Pediatr Adolesc Health
Care. 2014;44(5):108-133. • Laudner KG, Williams JG. The relationship between latissimus dorsi stiffness and altered scapular kinematics among asymptomatic collegiate
swimmers. Phys Ther Sport. 2013;14(1):50-53. • Maitland, A, “Mast Cell Activation Disorders.” Presentation at EDS Global Learning Conference, Sept, 2017, Las Vegas, NV. Available on-line at
https://ehlers-danlos.com/pdf/Maitland-EDNF-Vegas-Mast-Cell-Activation-Disorders-S.pdf. Accessed 12/12/17. • Malfait F, Francomano C, Byers P, et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med
Genet. 2017;175(1):8-26. • Mathias CJ, Low DA, Iodice V, Owens AP, Kirbis M, Grahame R. Postural tachycardia syndrome--current experience and concepts. Nat Rev
Neurol. 2011;8(1):22-34. • McCaskey MA, Schuster-Amft C, Wirth B, Suica Z, de Bruin ED. Effects of proprioceptive exercises on pain and function in chronic neck- and
low back pain rehabilitation: a systematic literature review. BMC Musculoskelet Disord. 2014;15:382. • Molderings GJ, Brettner S, Homann J, Afrin LB. Mast cell activation disease: a concise practical guide for diagnostic workup and therapeutic
options. J Hematol Oncol. 2011;4:10. • Moller MB, Kjaer M, Svensson RB, Andersen JL, Magnusson SP, Nielsen RH. Functional adaptation of tendon and skeletal muscle to
resistance training in three patients with genetically verified classic Ehlers Danlos Syndrome. Muscles Ligaments Tendons J. 2014;4(3):315-323.
• Morrison SC, Ferrari J, Smillie S. Assessment of gait characteristics and orthotic management in children with Developmental Coordination Disorder: preliminary findings to inform multidisciplinary care. Res Dev Disabil. 2013;34(10):3197-3201.
• Mulvey MR, Macfarlane GJ, Beasley M, et al. Modest association of joint hypermobility with disabling and limiting musculoskeletal pain: results from a large-scale general population-based survey. Arthritis Care Res (Hoboken). 2013;65(8):1325-1333.
• Nelson SM, Cunningham NR, Kashikar-Zuck S. A Conceptual Framework for Understanding the Role of Adverse Childhood Experiences in Pediatric Chronic Pain. Clin J Pain. 2017;33(3):264-270.
• Ninis N, De Wandelle I, Simmonds JV. Symptom Severity Scale: A descriptor for complex patients with hypermobility spectrum disorders and hypermobile EDS. 2015.
• Pacey V. Joint Hypermobility Syndrome in Children. Sydney, Australia, University of Sydney; 2014. • Pacey V, Nicholson LL, Adams RD, Munn J, Munns CF. Generalized joint hypermobility and risk of lower limb joint injury during sport: a
systematic review with meta-analysis. Am J Sports Med. 2010;38(7):1487-1497. • Pacey V, Tofts L, Adams RD, Munns CF, Nicholson LL. Exercise in children with joint hypermobility syndrome and knee pain: a randomised
controlled trial comparing exercise into hypermobile versus neutral knee extension. Pediatr Rheumatol Online J. 2013;11(1):30.

• Palmer S, Bailey S, Barker L, Barney L, Elliott A. The effectiveness of therapeutic exercise for joint hypermobility syndrome: a systematic review. Physiotherapy. 2014;100(3):220-227.
• Palmer S, Cramp F, Lewis R, Gould G, Clark EM. Development and initial validation of the Bristol Impact of Hypermobility questionnaire. Physiotherapy. 2017;103(2):186-192.
• Palmer S, Manns S, Cramp F, Lewis R, Clark EM. Test-retest reliability and smallest detectable change of the Bristol Impact of Hypermobility (BIoH) questionnaire. Musculoskelet Sci Pract. 2017;32:64-69.
• Quatman CE, Ford KR, Myer GD, Paterno MV, Hewett TE. The effects of gender and pubertal status on generalized joint laxity in young athletes. J Sci Med Sport. 2008;11(3):257-263.
• Raj SR. Postural tachycardia syndrome (POTS). Circulation. 2013;127(23):2336-2342. • Remvig L, Engelbert RH, Berglund B, et al. Need for a consensus on the methods by which to measure joint mobility and the definition of norms
for hypermobility that reflect age, gender and ethnic-dependent variation: is revision of criteria for joint hypermobility syndrome and Ehlers-Danlos syndrome hypermobility type indicated? Rheumatology (Oxford). 2011;50(6):1169-1171.
• Rombaut L, De Paepe A, Malfait F, Cools A, Calders P. Joint position sense and vibratory perception sense in patients with Ehlers-Danlos syndrome type III (hypermobility type). Clin Rheumatol. 2010;29(3):289-295.
• Rombaut L, Malfait F, De Wandele I, et al. Muscle tendon tissue properties in the hypermobility type of Ehlers-Danlos syndrome. Arthritis Care Res (Hoboken). 2012.
• Roussel NA, Nijs J, Mottram S, Van Moorsel A, Truijen S, Stassijns G. Altered lumbopelvic movement control but not generalized joint hypermobility is associated with increased injury in dancers. A prospective study. Man Ther. 2009;14(6):630-635.
• Sachs-Ericsson NJ, Sheffler JL, Stanley IH, Piazza JR, Preacher KJ. When Emotional Pain Becomes Physical: Adverse Childhood Experiences, Pain, and the Role of Mood and Anxiety Disorders. J Clin Psychol. 2017;73(10):1403-1428.
• Sahin N, Baskent A, Cakmak A, Salli A, Ugurlu H, Berker E. Evaluation of knee proprioception and effects of proprioception exercise in patients with benign joint hypermobility syndrome. Rheumatol Int. 2008;28(10):995-1000.
• Scheper MC, Juul-Kristensen B, Rombaut L, Rameckers EA, Verbunt J, Engelbert RH. Disability in Adolescents and Adults Diagnosed With Hypermobility-Related Disorders: A Meta-Analysis. Arch Phys Med Rehabil. 2016;97(12):2174-2187.
• Scheper MC, Pacey V, Rombaut L, et al. Generalized Hyperalgesia in Children and Adults Diagnosed With Hypermobility Syndrome and Ehlers-Danlos Syndrome Hypermobility Type: A Discriminative Analysis. Arthritis Care Res (Hoboken). 2017;69(3):421-429.
• Schubert-Hjalmarsson E, Ohman A, Kyllerman M, Beckung E. Pain, balance, activity, and participation in children with hypermobility syndrome. Pediatr Phys Ther. 2012;24(4):339-344.
• Seneviratne SL, Maitland A, Afrin L. Mast cell disorders in Ehlers-Danlos syndrome. Am J Med Genet C Semin Med Genet. 2017;175(1):226-236.
• Simmonds JV, Herbland A, Hakim A, et al. Exercise beliefs and behaviours of individuals with Joint Hypermobility syndrome/Ehlers-Danlos syndrome - hypermobility type. Disabil Rehabil. 2017:1-11.
• Smith R, Damodaran AK, Swaminathan S, Campbell R, Barnsley L. Hypermobility and sports injuries in junior netball players. Br J Sports Med. 2005;39(9):628-631.
• Smith TO, Jerman E, Easton V, et al. Do people with benign joint hypermobility syndrome (BJHS) have reduced joint proprioception? A systematic review and meta-analysis. Rheumatol Int. 2013;33(11):2709-2716.
• Theoharides TC, Valent P, Akin C. Mast Cells, Mastocytosis, and Related Disorders. N Engl J Med. 2015;373(19):1885-1886. • Tirosh E, Jaffe M, Marmur R, Taub Y, Rosenberg Z. Prognosis of motor development and joint hypermobility. Arch Dis Child. 1991;66(8):931-
933. • Tobias JH, Deere K, Palmer S, Clark EM, Clinch J. Joint hypermobility is a risk factor for musculoskeletal pain during adolescence: findings of a
prospective cohort study. Arthritis Rheum. 2013;65(4):1107-1115. • Toprak Celenay S, Ozer Kaya D. Effects of spinal stabilization exercises in women with benign joint hypermobility syndrome: a randomized
controlled trial. Rheumatol Int. 2017.







