A1. MODUL – Asepsis and Antisepsis A2. MODUL – Surgical DeontologyA3. MODUL – Surgical interventions A4. MODUL - Bleedings A5. MODUL – Wounds
sterile bandage replacement,suture removal,open wound management,bandaging.
A6. MODUL - Shock
Institute of Surgical Research
„A” Module - Surgical Technics
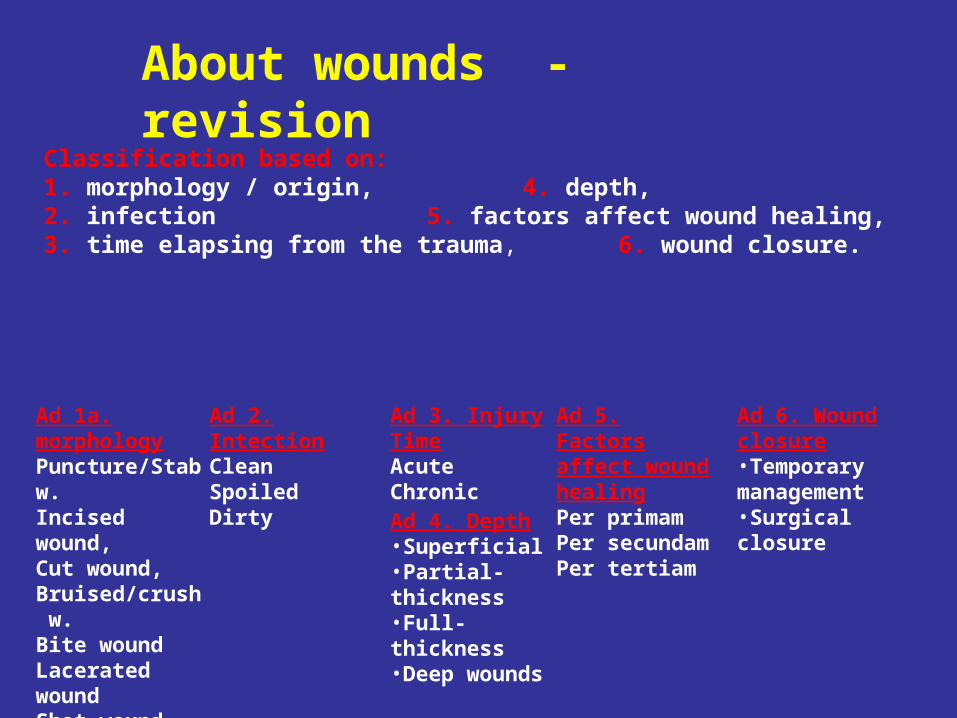
Classification based on:1. morphology / origin, 4. depth,2. infection 5. factors affect wound healing,3. time elapsing from the trauma, 6. wound closure.
About wounds - revision
Ad 1a. morphologyPuncture/Stab w.Incised wound,Cut wound,Bruised/crush w.Bite woundLacerated wound Shot wound
Ad 2. IntectionCleanSpoiledDirty
Ad 3. Injury TimeAcuteChronic
Ad 4. Depth•Superficial•Partial-thickness•Full-thickness•Deep wounds
Ad 5. Factors affect wound healingPer primamPer secundamPer tertiam
Ad 6. Wound closure•Temporary management•Surgical closure
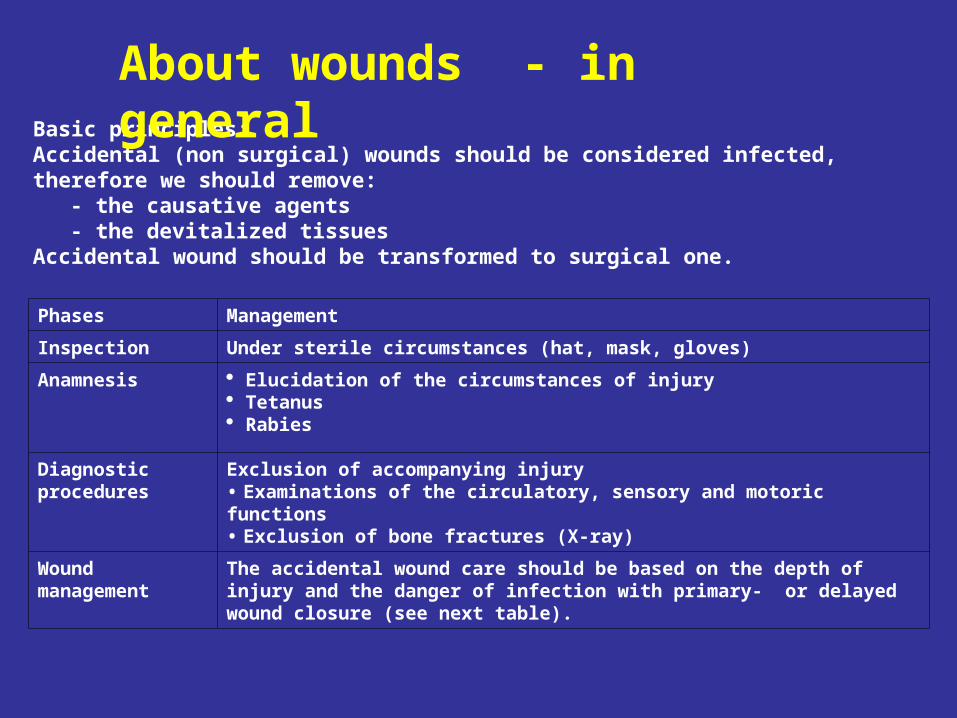
Basic principles: Accidental (non surgical) wounds should be considered infected,therefore we should remove:
- the causative agents - the devitalized tissues
Accidental wound should be transformed to surgical one.
Phases Management
Inspection Under sterile circumstances (hat, mask, gloves)
Anamnesis Elucidation of the circumstances of injury Tetanus Rabies
Diagnostic procedures
Exclusion of accompanying injury• Examinations of the circulatory, sensory and motoric functions• Exclusion of bone fractures (X-ray)
Wound management
The accidental wound care should be based on the depth of injury and the danger of infection with primary- or delayed wound closure (see next table).
About wounds - in general

Types of wound closure
Definite primary wound management (within 12 hrs)
Immediate wound closureAlways perform primary wound closure: penetrating injury of the abdomen chest dura mater
- Primary delayed suture (3-8 days)- Early secondary wound closure (> 14 days )- Late secondary wound closure (4 - 6 weeks )
When primary wound closure is contradicted: infectious signs severely spoiled foreign body pouched, greatly bruised wounds special injury forms of some professions (e.g. surgeons, butcher, veterinarian, pathologist, bacteriologist) bite, shot, deep incised wound hostility wound
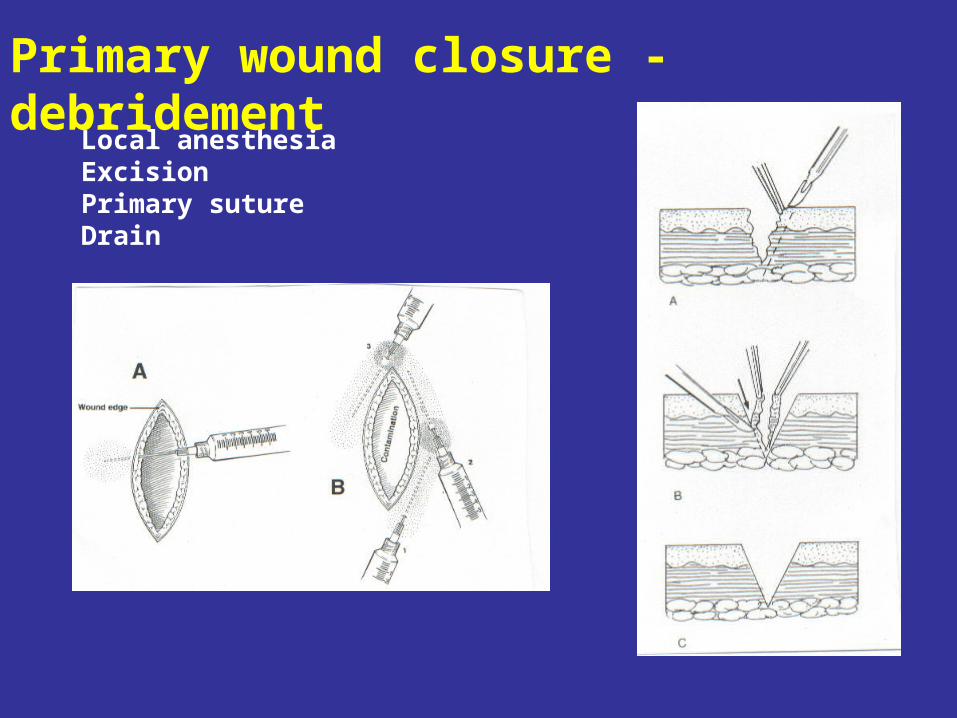
Local anesthesiaExcisionPrimary sutureDrain
Primary wound closure - debridement
Ad 1a. morphologyPuncture/Stab w.Incised wound,Cut wound,Bruised/crush w.Bite woundLacerated wound Shot wound
Ad 2. IntectionCleanSpoiledDirty
Ad 3. Injury TimeAcuteChronic
Ad 4. Depth•Superficial•Partial-thickness•Full-thickness•Deep wounds
Ad 5. Factors affect wound healingPer primamPer secundamPer tertiam
Ad 6. Wound closure• primary wound closure• primary delayed wound suture• early secondary wound closure • late secondary wound closure
Ad 1a. morphologyPuncture/Stab w.Incised wound,Cut wound,Bruised/crush w.Bite woundLacerated wound Shot wound
Ad 2. IntectionCleanSpoiledDirty
Ad 3. Injury TimeAcuteChronic
Ad 4. Depth•Superficial•Partial-thickness•Full-thickness•Deep wounds
Ad 5. Factors affect wound healingPer primamPer secundamPer tertiam
Ad 6. Wound closure• primary wound closure• primary delayed wound suture• early secondary wound closure • late secondary wound closure
Ad 1a. morphologyPuncture/Stab w.Incised wound,Cut wound,Bruised/crush w.Bite woundLacerated wound Shot wound
Ad 2. IntectionCleanSpoiledDirty
Ad 3. Injury TimeAcuteChronic
Ad 4. Depth•Superficial•Partial-thickness•Full-thickness•Deep wounds
Ad 5. Factors affect wound healingPer primamPer secundamPer tertiam
Ad 6. Wound closure• primary wound closure• primary delayed wound suture• early secondary wound closure • late secondary wound closure

Depending on the function:- adherent/taped bandages: (to fix covering bandages or for the approximation of edges of small wounds)
- covering bandages: (to protect the wound and absorb secretion. Prevention from secondary infection and mechanical trauma)
- pressing bandages: (for temporary handling of capillary and venous bleedings under 40-60 mmHg.)
- wedging bandage (used for temporary handling of capillary arterial and venous bleedings until surgical management. Should be relieved in every 2 hrs)
- compressing bandages: (to prevent postoperative bleeding on the limbs, and for the prophylaxis of thrombosis and for the reduction of chronic lymph-edema. Always placed from distal to proximal
- fixing/retention bandage (to immobilize the injured body part or to fix the reposition).
TYPES OF BANDAGES

1. Layer in direct contact with the wound (sterile, hypoallergenic, not irritating, non-sticking)- simple sheet (e.g. Mull sheet: good fluid absorbent, but easily sticks to the wound)- impregnated sheet (vazeline, paraffin: ie. “Jelonet”, non-sticking) (with saline which melts when gets into contact with body fluids i.e. Mesalt.)
2. Absorbent layer (to absorb and store blood and excretions)3. Fixing layer to secure the bandage (adherent tapes i.e. Centerplast,
Leukoplast or Mefix, Mepore; the latter two for bigger surfaces).
Layers of bandages
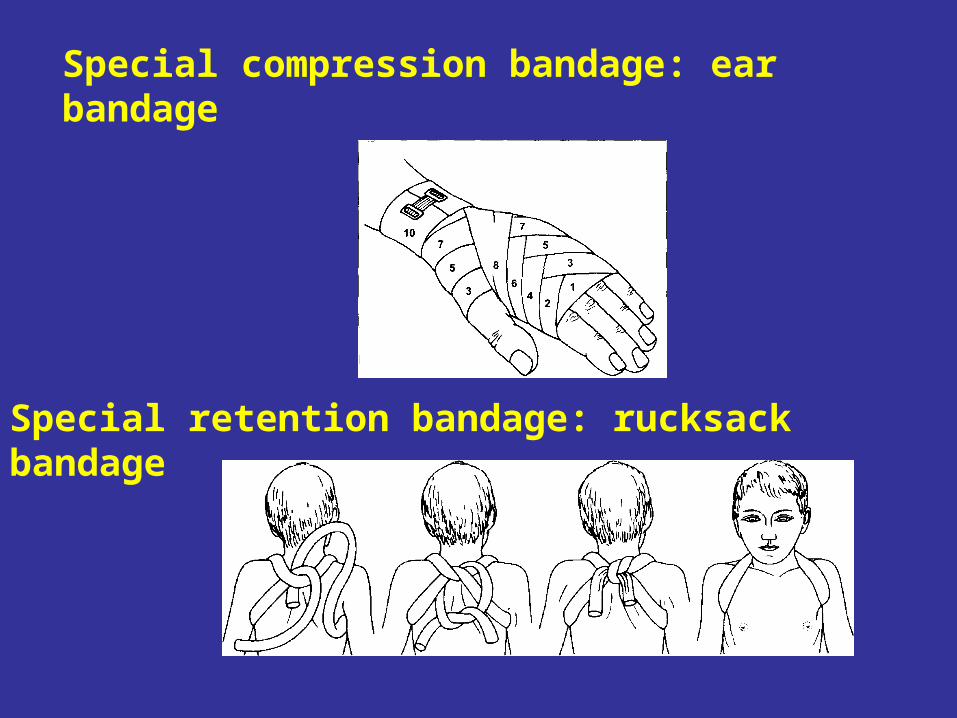
Special compression bandage: ear bandage
Special retention bandage: rucksack bandage

Special retention bandages:
Desault-bandage Charnley-loop

TASKS
OPERATING THEATRE
1. Sterile bandage removalfrom surgical woundRemoval of sutures
2. Sterile bandage removal open wound management
COMPUTER ROOM
1. Steam bandage
2. Compression bandage: ear bandage
3. Retention bandages

1. Surgical wounds – sterile bandage replacement, removal of sutures
NON-STERILEASSISTANT1. Removal of the former bandage
(pouring fluid on the sponge)
6. Fixing
STERILE EQUIPMENTSURGEON
2. Sterile gloving 3. Desinfection (Betadine solution)4. Removal of sutures5. Sterile covering (sterile gauze)
2. Spoiled wounds – open wound management
STERILE EQUIPMENTSURGEON
2. Sterile gloving 3. Wound cleansing (H2O2)4. Rinsing with saline 5. Desinfection (Betadine solution)6. Sterile covering (sterile gauze)
NON-STERILEASSISTANT1. Removal of the former bandage
(pouring fluid on the wound)(pouring fluid on the wound)(pouring fluid on the sponge)
7. Cover, fixing
OPERATING THEATRE: WOUND MANAGEMENT
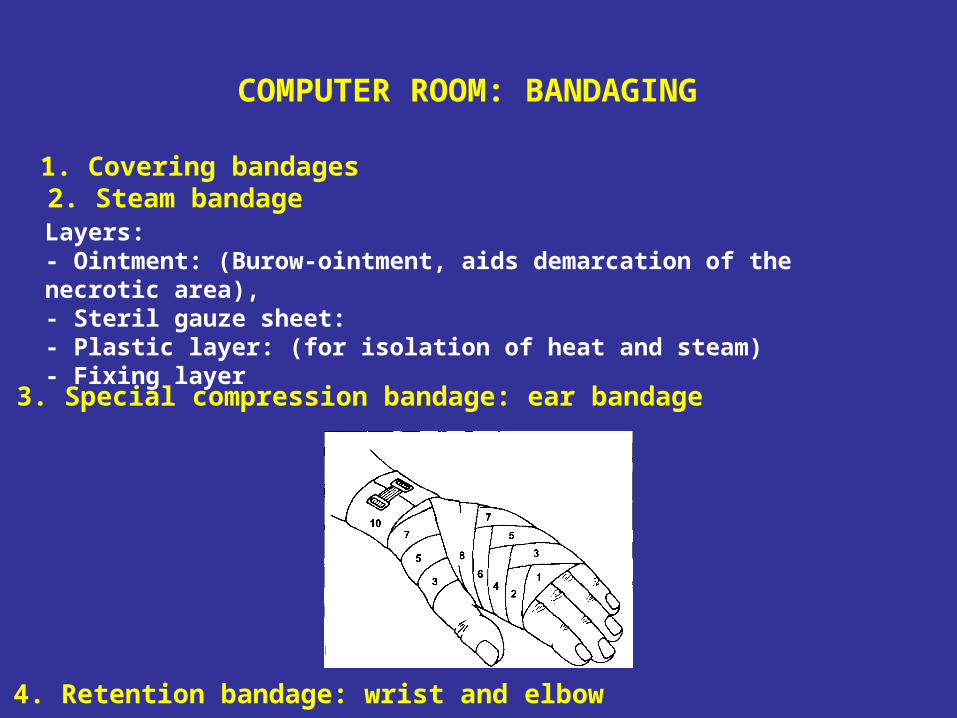
3. Special compression bandage: ear bandage
4. Retention bandage: wrist and elbow
Layers:- Ointment: (Burow-ointment, aids demarcation of the necrotic area), - Steril gauze sheet: - Plastic layer: (for isolation of heat and steam)- Fixing layer
2. Steam bandage
COMPUTER ROOM: BANDAGING
1. Covering bandages
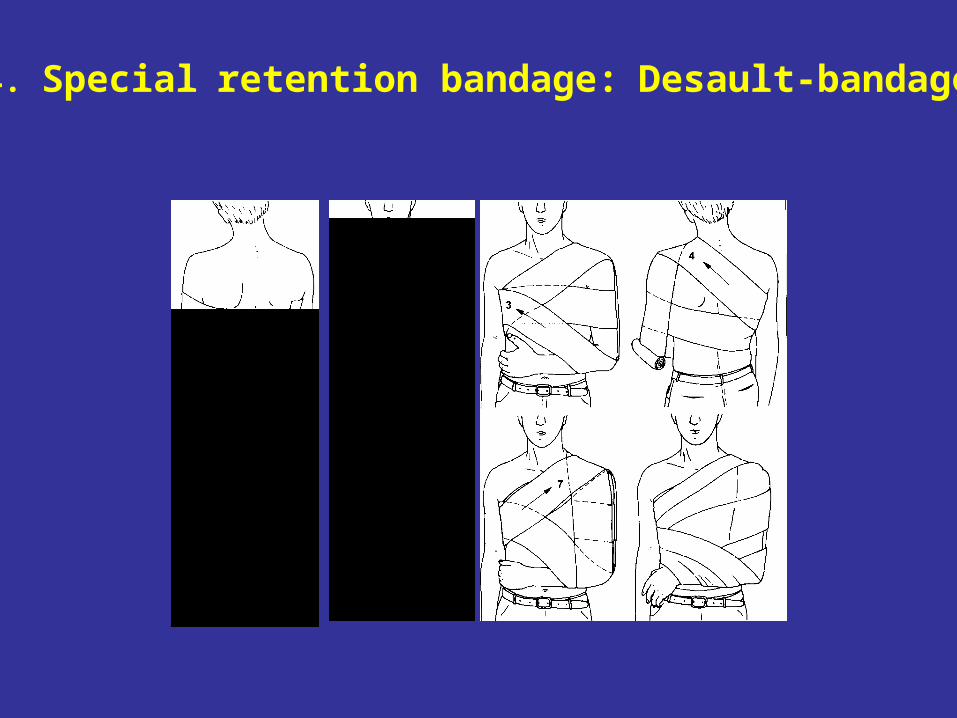
4. Special retention bandage: Desault-bandage







