
PD ExpertBriefings: A Closer Look at Anxiety and Depression
in Parkinson’s Disease Led By: Laura Marsh, M.D.
To hear the session live on:
Tuesday, March 6, 2012 at 1:00 PM ET.
DIAL: 1 (888) 272-8710 and enter the passcode 6323567#.
To learn more, please visit:
http://www.pdf.org/parkinson_briefing_anxiety
If you have any questions, please contact [email protected] or at (212) 923-4700
PD ExpertBriefings: A Closer Look at Anxiety and
Depression in Parkinson’s Disease
Presented By: Laura Marsh, M.D.
Michael E. DeBakey Veterans Affairs Medical Center and Baylor College of Medicine
Tuesday, March 6, 2012 at 1:00 PM ET

Welcoming Remarks
Robin Elliott Executive Director
Parkinson’s Disease Foundation

Disclosures Research Support National Institutes of Health: R01-MH 069666, Dystonia
Foundation American Psychiatric Association > 2 years: NIH: P50 NS 58377, Boehringer Ingelheim GmbH, Forest Research Institute, Eli Lilly, Michael J. Fox Foundation
Consultancies : All > last 2 Years Acadia Pharmaceutical, Boehringer Ingelheim GmbH, Merck Serono, Ovation
Royalties Taylor & Francis/Informa
Approved/Unapproved Uses This presentation may discuss use of medications that do not have FDA approval for treatment of psychiatric aspects of PD

Depression , PD, or Both?

Learning Objectives
1. Recognize and distinguish depressive and anxiety symptoms over the course of PD
2. Describe methods for evaluating depression and anxiety in PD patients.
3. Discuss treatments for depression and anxiety in PD

0
20
40
60
80
100
Range of Psychiatric Diagnoses in PD (MOOD-PD Study, n=250)
Lifetime Prevalence Current Prevalence
!"#$$%&'(")*&*$
Impulse Control Disorder
Delirium Psychosis Anxiety Disorder
Mood Disorder
Substance Use
Disorder
%
Depressive Disorders in PD • ~40 percent prevalence (range 3% - 90%) • Several Types
– Major Depression – Minor Depression – Dysthymia – Bipolar Disorder, Depressive Episode – Adjustment Disorder with Depressed Mood – Depressive Disorder, Not otherwise specified
• Clinically significant depressive symptoms 35 percent • Anxiety disorders are a common co-occurrence • Rates of recurrence or treatment resistance unclear
Reijnders 2008; Mayeux, 1981; Starkstein, 1992; Meara, 1999; Global PD Survey, 2002; Weintraub 2004

Anxiety Disorders in PD
Kummer et al., 2008; Maricle et al., 1995, Witjas et al., 2002, Arabia 2007
• ~25-45 percent prevalence • Several Types
• Episodic (Panic Disorder) • Situational (Phobias) • Continuous (Generalized Anxiety) • PD-Specific (Wearing-off anxiety/panic)
• Depressive disorders commonly co-occur • Not understandable reactions to motor symptoms
• Non-motor fluctuations • Onset of Anxiety may precede PD

Co-occurrence of Depressive and Anxiety Disorders Increases the Complexity of Psychiatric Aspects of PD
% of total sample (n=250) with diagnosis Marsh et al., Unpublished
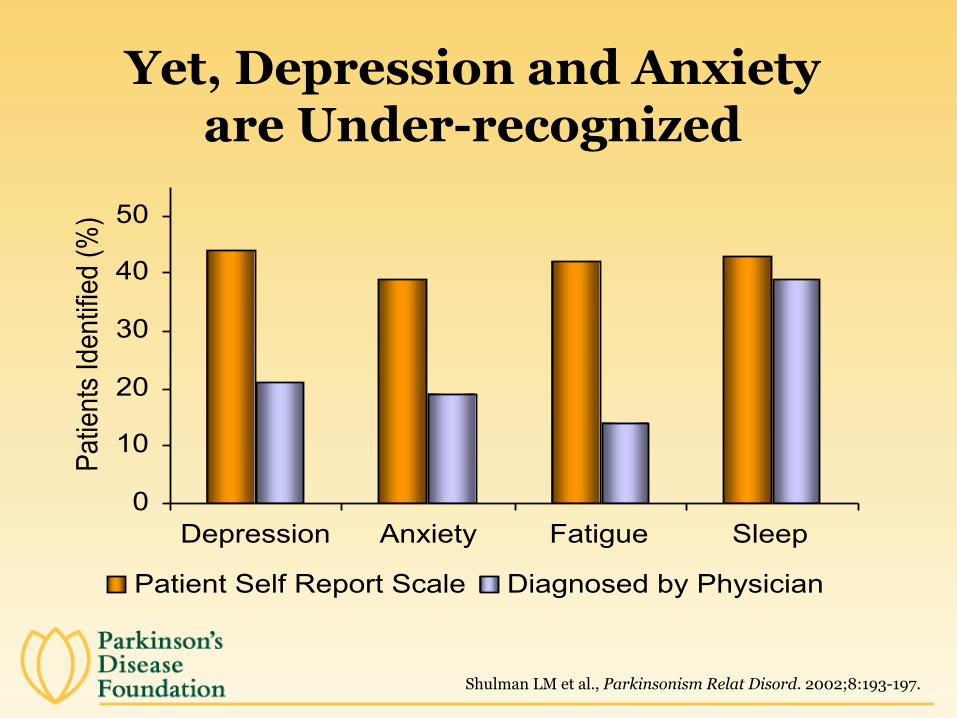
Yet, Depression and Anxiety are Under-recognized
0
10
20
30
40
50
Depression Anxiety Fatigue Sleep
Patie
nts
Iden
tifie
d (%
)
Patient Self Report Scale Diagnosed by Physician
Shulman LM et al., Parkinsonism Relat Disord. 2002;8:193-197.

Barriers to Recognition and Treatment of PD-Depression and Anxiety
• Motor symptoms • Define the disease • Primary focus of care/interest • Mask psychiatric changes/Symptom overlap
• Mood and anxiety symptoms • Regarded as ‘understandable’ reactions • Occur with other mood disorders
• Social barriers • Require extra time to assess and initiate treatment • Don’t ask, don’t tell • Interfere with clinician-patient relationship • Stigma

Overlap of Depression and Anxiety with Features of
Parkinson’s Disease at its Different Stages

• 86 yo WWF, PD since age 72, died of cancer • Champion Senior Division in Table Tennis • Onset Major Depressive Episode age 69
– Recurrent episodes of depression • Diagnosed with PD age 72 with dragging foot x 3
years, left hand tremor x 6 months • Onset Generalized Anxiety Disorder age 80 • Cognitive changes age 80, decline age 82 • Intermittent Visual Hallucinations age 81 • Imbalance age 83
A Typical Case History

Before Parkinson’s Disease

• Classic Motor Triad – Tremor – Rigidity – Bradykinesia/Akinesia (slowness)
• Gait and Postural Disturbances
• Absence of Parkinson-Plus Features
• Motor signs ≠ Disability ≠ Psychological distress
Schrag et al., 2001
Essential Motor Features of PD

However, Initial PD Symptoms Can Overlap with Mood Disorder Symptoms
1st PD Symptom (n=183) # Tremor 129 (70 percent) Gait disturbance 21 Stiffness 18 Slowness 18 Muscle pain, cramps, aching 15 Loss of dexterity 14 Handwriting disturbance 9 Depression, nervousness 8 Speech disturbance 7 General fatigue, muscle weakness 5 Drooling 3 Loss of arm swing 3 Facial masking 3
Yahr, 1967

• Ishihara and Brayne 2006 (review) – On average, affective diagnoses precede PD by 4 to 6 years – RR 3.13 (1.95-5.01) Schuurman et al., 2002 – RR 2.4 (1.72-2.93) Nilsson et al., 2001 – RR 2.40 (2.10-2.70) Leentjens et al., 2003
0 2
4 6
8 10
12
14
16
Fr
eque
ncy
-70 -60 -50 -40 -30 -20 -10 0 10 20 30 Duration between Earliest Major Depression Episode Onset and PD Diagnosis (years)
(MOOD-PD Study, Unpublished Data)
n % Major Depression Before PD Dx 51 46 Major Depression at or after PD Dx 60 54
Onset of depressive disorder is not related to disease stage or disability

0 2
4 6
8 10
12
14
16
Fr
eque
ncy
-70 -60 -50 -40 -30 -20 -10 0 10 20 30 Duration between Anxiety Disorder Onset and PD Diagnosis (years)
n % Anxiety Dx Before PD Dx 76 66 Anxiety Dx at or after PD Dx 39 34
Anxiety disorders can occur long before or after onset of PD motor symptoms
(MOOD-PD Study, Marsh et al.)

n=413 early untreated PD followed over 15 months, diagnosed with + Depression if Geriatric Depression Scale-15>5
– 28 percent + Depression screen at least once – 40 percent + Depression cases left untreated
– Depressive symptoms predicted – Increased need to start symptomatic PD meds (HR=1.86; 95 percent CI 1.29-2.68) – Increased physical disability (ADLS) (p<0.0002)
Ravina et al., 2007
Depressive Symptoms Influence Onset of Motor Treatment in Early PD
NET-PD Study/Neuroprotective Treatment Trials

– If depressive symptoms occur in early PD, they mostly remain mild – 47 percent of depressed patients remitted within 6 months
– However, mild depressive symptoms also predicted – Development of more severe mood symptoms (RR=6.16 [95 percent CI 2.14.17.73]) – Greater PD severity, older age, longer PD duration, failure to remit (HR0.83-0.92)
Ravina et al., 2009
Over Time, Depression Improves or Worsens
NET-PD Study/NeuroprotectiveTreatment Trials

Sydney Multi-center Study – 15-year Follow-up – n=149, 52 surviving (71 + 8; 55-86 years) – Most disabling long term symptoms
– Cognitive decline - 84 percent – Dementia - 48 percent, MCI - 36 percent – Hallucinations – 50 percent – Depression – 39 percent
Hely et al., 2005
Neuropsychiatric Features are Disabling over Disease Course

Non-psychiatric Impact of Depression and Anxiety on PD
Depression • Motor deficits • Cognitive impairment • Disability • Quality of Life Deficits • Caregiver burden • Economic Strain • Concurrent psychiatric
conditions
Reijnders 2008; Mayeux, 1981; Starkstein, 1992; Meara, 1999; Global PD Survey, 2002; Weintraub 2004; Siemers 1993; Dissanayaka 2010;Vazques 1993; Lauterbach 2003; L 2011; Henderson 1992; Pontone 2009;, 2011
Anxiety Increased PD motor symptoms • Motor Deficits • Motor complications
• Freezing • On-Off Fluctuations • Dyskinesias
• Gait difficulties • Quality of life/ self-perceived health status
Antiparkinsonian Treatments Can Have Adverse Neuropsychiatric Effects
• Levodopa/Carbidopa
• Dopamine agonists – Bromocriptine – Pergolide – Pramipexole – Ropinirole – Rotigotine
• MAO-B inhibitors – Rasagiline – Selegiline
• Other – Anticholinergics – Amantadine – Benztropine – Trihexyphenidyl
• Nonpharmacologic – Exercise/PT – Acupuncture – Deep Brain Stimulation – Pallidotomy – Other

Adverse Neuropsychiatric Medication Effects
- Mood Changes - Psychosis - Confusion/delirium - Disinhibition - Impulse Control Disorders
- gambling, hypersexuality, pathological eating and spending

Antiparkinsonian Medications are Associated with Fluctuating Mood
Effects
• Motor - Loss of efficacy - End of dose deterioration/On-off
phenomena - Dose-limiting side effects
- Hyperkinesia/Dyskinesias - Dystonias - Concomitant fluctuating psychiatric
and cognitive symptoms

Nonmotor Fluctuations • Dysautonomic
– Drenching sweats, hot sensation, flushing, dry mouth, dyspnea, dysphagia, constipation, distal cold sensations, excessive salivation, urinary urgency, visual complaints, palpitations, bloating, chest pain
• Cognitive/Psychiatric – Slowed thinking, mental hyperactivity, impaired
memory, mental emptiness – Off-Anxiety (81 percent), Off-depression (63 percent),
On-hypomania (24 percent), irritability, psychosis
• Sensory/Vegetative – Fatigue, akathisia, tightening sensations, tingling, pain
Witjas et al, Neurology 2002; 59: 408-413; Racette et al., J Neuropsychiatry Clin Neurosci 2002; 14: 438-442.

6am 7am 8am 9am 10am 11am Noon 1p 2pm 3pm 4p 5p 6p
Off
On
Dyskinetic Happy
Neutral
Anxious/ Sad
levodopa
Motor state
Motor Mood
Mood/Cognitive state
Fluctuating Mood States Motor and “Non-motor” Fluctuations

Improving Recognition of Depressive and Anxiety
Disorders in PD

Depression/Anxiety
Depressive/ Anxiety Disorders

Symptom Overlap of Depressive and Anxiety Disorders in PD Depressive Disorder Anxiety Disorder
Parkinsonism Decreased facial expression Psychomotor changes – Slowness, motor restlessness
On-off fluctuations Restlessness Insomnia
Somatic Pain, Muscle tension Fatigue, energy loss Insomnia, Decreased appetite Weight Loss
Muscle tension, Fatigue Autonomic Symptoms Insomnia
Cognitive Impairment
Executive dysfunction Decreased memory & Concentration
Executive dysfunction Decreased concentration
Other Psychiatric Sx
Anxiety, ICDS, Apathy, Psychosis Depression, ICDs, Psychosis

Depression
• An emotion characterized by sad and unhappy feelings
• An understandable psychological reaction, especially to loss
• A loosely used term – Frustration, anger, disgust, anxiety, overwhelmed,
apathetic, tired

Depressive Disorder
• A psychiatric (medical) condition
• An abnormal, ‘un-understandable’, and persistent mental state
• Accompanied by physical and mental changes
• Affects function and causes significant distress

DSM Criteria helpful, but Depressive Disorders have Distinct
Emotional Features • A pervasive change in Mood
• Persistent sadness • Decreased interest and enjoyment, anhedonia • Pessimism, hopelessness • Negative ruminations • Inappropriate guilt • Negative view of sense of self • Morbid and/or suicidal thoughts • Feeling overwhelmed, anxious, unable to cope • Irritability

Psychological Features of Anxiety
Excessive • Apprehension • Worry • Anticipation • Overly-detailed • Emotional Reactivity • Fearfulness/Avoidance • Somatic concerns • Ruminative
Unlike Depressive Disorders, no pervasive
• Guilt • Sadness • Decreased self-worth • Lack of interest • Morbid thoughts

Prevalence of Specific Anxiety Disorders
Category / % Prior studies
Pontone 2011
Dissanayaka 2010
Leentjens (2011)
PopulationNEMESIS/ NCS
Panic disorder 13 – 30 5 8 4 1.5/1
Specific Phobia 16 - - 5.5/5.5
Generalized Anxiety Disorder
0 - 40 4 3 21 0.8/1.6
Social phobia 15 7 13 10 3.7/4.5
Agoraphobia - 1.6 - 16 -/2.3
Post-traumatic stress disorder
- 0 - - -
Anxiety Dis NOS
- 22%* - 11%** -
*DSM-IV-TR; **Based on NPI anxiety subscale cut-off >3

Apathy
• Prevalence - ~ 30 percent as a feature of a depressive disorder - ~ 10 percent as an independent disorder
• Clinical features
– Loss of motivation – Emotional indifference – Reduced goal-directed activities – People with primary apathy do NOT complain

Emotionalism/ Pathological Crying
• Prevalence in PD – 40-50 percent – Associated with Depressive Disorders,
Delirium, Benzodiazapines
• Clinical Features – Heightened, excessive sentimentality/tear – Inappropriate, unmotivated, involuntary – Precipitated by a variety of emotions – Social embarrassment/Phobic avoidance
Depression and Anxiety Rating Scales
• Large and growing range of measurement tools
• Use in PD has increased attention to mood disturbances as a feature of the PD
• May be useful for screening and tracking mood symptoms

Symptoms Assessed in Different Rating Scales
Instrument Ham-D BDI-I CESDR PHQ9 GDS
Dysphoria x x x x x
Anhedonia x x x x x
Weight/Appetite Changes
x x x x
Sleep Disturbance x x x x
Psychomotor Retardation
x x x
Fatigue x x x x
Worthlessness/Guilt
x x x x x
Bradyphrenia ? x x x
Suicide/Death x x x x
# DSM Criteria 7 7 9 9 5
# Somatic Sx 3 3 4 4 1
DSM Depressive Criteria: Sad mood, Anhedonia/Interest, Appetite, Sleep, Agitation/Retardation, Energy, Self-attitude/guilt, Cognitive, Suicidality

Treatment of Depression and Anxiety

Psychiatric Treatment
• Targeted and individualized approach • Adjust/Optimize anti-parkinsonian regimen • Treat medical conditions/delirium • Specific treatments for depression/anxiety
– Psychiatric medications • Anti-depressants • Sleep medicines • Anti-anxiety medicines • Anti-psychotics
– Non-pharmacological Interventions

Anxiety Treatments
No evidence-based reports of behavioral or pharmacological treatment trials
for PD-anxiety

Pharmacological Treatments

Are Dopamine Agonists Antidepressants?
• Dopamine agonists – Moller et al., 2005; Reichman et al., 2004
• Open-label pramipexole ↓ PD Depressive symptoms – Barone et al., 2006, n=67
• 12 wk RCT pramipexole (1.5-4.5 mg/d) vs sertraline (50 mg/day)
• More pts in remission on pramipexole (61% vs 27%) – Barone et al., 2010, n=287
• 12 wk RCT pramipexole (0.125-1 mg tid) vs Placebo • Decreased Depressive and Motor Symptoms in Pramipexole
group • Improved depression independent of motor function

Somatic Antidepressant Treatments Med Class Reuptake Inhibition SNRIs Serotonin-Norepinephrine
Tricyclic Antidepressants, Venlafaxine, Duloxetine
NDRIs Norepinephrine-Dopamine Buproprion
SSRIs Serotonin Fluoxetine, sertraline, paroxetine, fluvoxamine, es/citalopram
SARIs Serotonin Antagonist Trazodone, nefazodone
NASAs Norepinephrine/ Serotonin Antagonists Mirtazipine
Other Treatments Electroconvulsive Therapy (ECT) Transcranial Magnetic Stimulation (TMS)

Recent Placebo-Controlled Antidepressant Trials in PD
– Devos et al., 2008, n=48 • 14 days: Desipramine 75 mg > Citalopram 20 mg, Placebo • 30 days: Desipramine = Citalopram > Placebo
– Menza et al., 2009, Dobkin et al., 2010, n=52 • 8 weeks: Nortriptyline (64 mg) >paroxetine 32 mg, placebo • Residual mood symptoms may persist despite + response
– Richard et al., (in press) (SAD-PD Study), n=115, 17 sites • 12 weeks: Paroxetine (24 mg), venlafaxine XR (121mg)>
Placebo • 44% Placebo-treated subjects ‘responded’ and 32% remitted
Menza et al., Neurology 2009; Dobkin et al., AGJP 2010
Important Medication Interactions and Side Effects
• Potential for hypertensive Crisis or Serotonin Syndrome – Selegeline, Rasagaline plus MAO’s
• Orthostasis • GI Upset • Sedation • Anticholinergic side effects • Benzodiazepine side effects • Increased parkinsonism
– Antidepressants (+) – Lithium – Sodium Valproate – Amoxapine – Neuroleptics

Non-pharmacologic Interventions • Education
– Psychiatric aspects of PD – Coping strategies – Caregiver issues
• Psychotherapy – Counseling/problem-solving – Supportive, directive, insight-oriented, grief counseling,
Cognitive-behavioral therapy – Caregiver support
• Rehabilitative therapies – Occupational, Physical, Speech Therapies – Exercise/Exercise classes/Personal trainers – Relaxation training
• Social Supports – Socialization, Support groups, Home care

Evaluate Your Coping Strategies
Best if 1) Flexible
• Use Active and Passive Approaches • If problem can be changed, use Active Strategy
(e.g., Do something). If it cannot be changed, use passive approach (e.g., acceptance)
2) Dynamic • What worked in 2000 may not work in 2012
3) Individualized
Frazier and Marsh, 2005

Cognitive Behavior Treatment (CBT) Trials for Mood Dos in PD
n Dx Sessions Outcome RCT? Dobkin 2006 3 Major Depr 12-14 Min Δ Anxiety Case Series
Dobkin 2007 15 Major Depr 10-14 Trend ↓ anxiety
Pilot study
Dobkin 2011 56 Major Depr 10-14 ↓ Depression Yes
Dreisig 1999 79 Depression 6 Impr Anx 1 month
Feeney 2005 4 Depr/Anxiety 8 group No Δ Anxiety Pilot
Macht 2007 3 Depr, Social anxiety, freezing
12-18 months ↓ anxiety Case series
Veazey 2009 14 Anxiety/Depression
9 (8 on phone) ↓ anxiety (BAI)
Yes-CBT vs Support grp
Armento M, In review

Components of CBT in People with Parkinson’s
Basic CBT components Automatic thoughts, Triggers, PD specific adaptations
Problem Solving Cognitive Restructuring Breathing strategies Written strategies Exposure Social Skills Training Activity Scheduling Health Promotion Stress management Self Monitoring Behavior Modification Sleep Hygiene Relaxation Caregiver Strategies to reinforce therapy for patient Symptom (depression/anxiety) management
Armento M, In review

Additional Caveats

Understand what symptoms and signs of the disturbance are expected to
improve with treatment What was the person’s baseline before onset of mood changes and
before onset of PD?
Caregivers-put your oxygen mask on first! • How does depression or anxiety in the caregiver influence
the patient’s presentation?
Define relationship of depressive or anxiety disturbance to: • Motor fluctuations, dyskinesias, other motor symptoms • PD meds and other medications • Cognitive, medical other psychiatric comorbidities
Determine if life or daily events influence the mood or anxiety presentation?
• Keep 24-hour diary to chart moods, motor state, and meds

Conclusions • Depressive and Anxiety Disorders
– Features overlap with motor and other PD symptoms – Have a negative impact on multiple aspects of PD – Are under-recognized and under-treated in clinical
settings – Are treatable with a variety of modalities – Treatment response needs to be monitored – Scales may be helpful adjuncts to care
• Treating depressive and anxiety disorders effectively, and to remission, reduces excess disability

Questions and Answers







