
Intermittent Exotropia - A Case Of Pseudo divergence Excess
Krishna Banjade Consultant optometrist in pediatrics and strabismus

ABBREVIATIONS
X’ - Exophoria XT - Exotropia X(T) - Intermittent Exotropia CT – Cover Test PD – Prism Dioptre IOP – Intra Ocular Pressure PACD – Peripheral Anterior Chamber Depth RAPD – Relative Afferent Pupillary Defect Sx – Surgery RTC – Return To the Clinic

PATIENTS DETAIL
Age : 10 Years/ Male
Profession - Student
Address- Lucknow, Uttar Pradesh, India
First visit - 05/07/2014

VISIT 1Visit 1
CHIEF COMPLAINTS
(OU) Gradual progressive painless blurring of vision for near and distance since 5 years
Occasional outward deviation of eyeballs noticed by parents since 4 years
Photophobia since 1 year
HISTORY
Recent ophthalmic consultation locally - diagnosed Alternate exotropia - referred to our hospital for further management
No h/o using glasses/contact lens/patching
No h/o head and ocular injury
No h/o seizures, Asthma and CAD
Normal pre, peri and postnatal birth history with normal physical , emotional and cognitive development
CONTD…
Family history- mother myopic
Not aware of any allergy
No h/o systemic diseases
No h/o past lasers, surgeries and medications
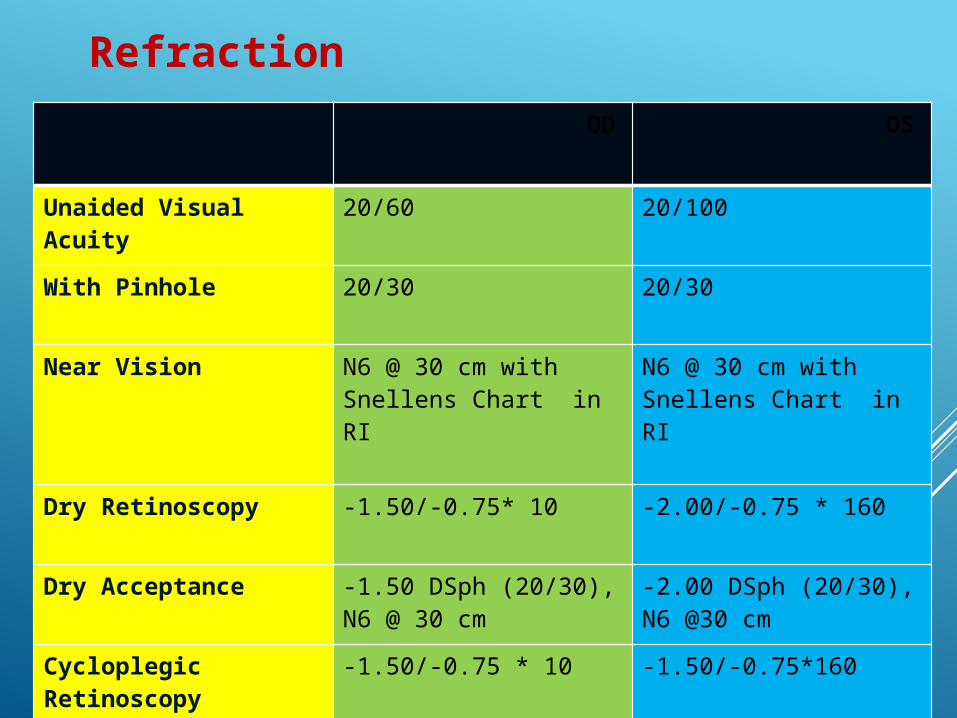
OD OS
Unaided Visual Acuity
20/60 20/100
With Pinhole 20/30 20/30
Near Vision N6 @ 30 cm with Snellens Chart in RI
N6 @ 30 cm with Snellens Chart in RI
Dry Retinoscopy -1.50/-0.75* 10 -2.00/-0.75 * 160
Dry Acceptance -1.50 DSph (20/30), N6 @ 30 cm
-2.00 DSph (20/30), N6 @30 cm
Cycloplegic Retinoscopy(cyclopentolate)
-1.50/-0.75 * 10 -1.50/-0.75*160
Refraction

Facial Asymmetry nil
Abnormal head posture nil
Nystagmus nil
EOM Movement Full, Free and Painless
Hirschberg's Test LXT 10 Degree
Cover Test 25-30 PD X(T) ( Distance) 12 PD X(T (Near)
Stereo Acuity using Random Dot Stereogram Test
80 sec of arc
External Examination

OD OS
Lids Flat Flat
Conjunctiva Quiet Quiet
Cornea Clear Clear
AC PACD > 1/2 CT, Quiet PACD > 1/2 CT, Quiet
Pupil R/R/R, No RAPD R/R/R
Iris Normal color and pattern
Normal color and pattern
Lens Clear Clear
IOP With GAT 13 mm of Hg @ 11:10am
14 mm of Hg @ 11:10am
Slit Lamp Examination

OD OS
Media Clear Clear
Retina On On
Macula Healthy Healthy
C/D 0.2 0.2
Fundus examination
DIAGNOSIS ?

DIAGNOSIS
(OU) Compound Myopic Astigmatism Intermittent Exotropia
PLAN OF RX
Glasses
Reassure
EOM Sx If Required
Patch Test next visit
RTC 3/12

INTERMITTENT EXOTROPIA
Obstracles to development or maintenance of BSV
Defective action of MR Muscles
Defective fusional convergence (1)
New born infants with transient exodeviation (2)
Refractive Errors, Anisomyopia and Anisoastigmatism (3)
Differs from Exophoria1. Worth C. Squint, its causes, pathology and treatment ed. 6. London 1929, Bailliere, Tyndall and Cox 2. 2. Archer SM, Helveston EM: Strabismus and Eye Movement Disorders. In Isenberg SJ (ed) The eye in Infancy
1994 Mosby, pg 255.3. Jampolsky A, Flom BC, Weymouth FS, Moster LE. Unequal corrected visual acuity as related to anisometropia Arch Ophthalmol. 1955;54:893

Tropia Phase of Intermittent exotropia observed when :
In Child - Tired, sick or day dreaming In Adults - Also after imbibing alcoholic beverages or taking
sedatives
PREVALENCE
Comprises 50-90% of cases of Exotropia
Affects 1 % of general population (1,2)
Nearer a country is to the equator the higher the prevalence of exodeviations (3)
1.Govindan M, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood exotropia: a population based study. Ophthalmology. 2005 Jan;112(1):104-8.
2. Noorden GK von. Exodeviations. In: Binocular Vision and Ocular Motility 5 th ed., 1996 Mosby, pg 343
3. Jenkins R. Demograhics: geographic variations in the prevalence and management of exotropia. Am. Orthopt. J. 1992,42:82.
NATURAL HISTORY
Remains obscure
Some cases
First at distance and then at near
Not all the cases are progressive, may be constant or even improve
ExophoriaIntermitte
nt exotropia
constant
Noorden GK von. Exodeviations. In: Binocular Vision and Ocular Motility 5 th ed., 1996 Mosby, pg 343

FACTORS TO BE RECORDED FOR PROGRESSION
Amount of Loss of fusional control with increasing strabismus
Development of a secondary convergence insufficiency
Increase in size of basic deviation
Development of Suppression

SYMPTOMS OF INT. XT
Transient Diplopia
Asthenopic symptoms
Photophobia (1)
Micropsia (2)
1. Manley DR. Classification of the exodeviations. In: Manley D ed.: Symposium on horizontal ocular deviations. St. Louis. 1971. Mosby-Year Book Inc. p128
2. Noorden GK von. Exodeviations. In: Binocular Vision and Ocular Motility 5 th ed., 1996 Mosby, pg 361

PATCH TEST
Noorden GK von: Atlas of Strabismus, ed 4. St Louis, Mosby–Year Book, 1983

Visit 2nd
1ST FOLLOW UP 10/09/2014
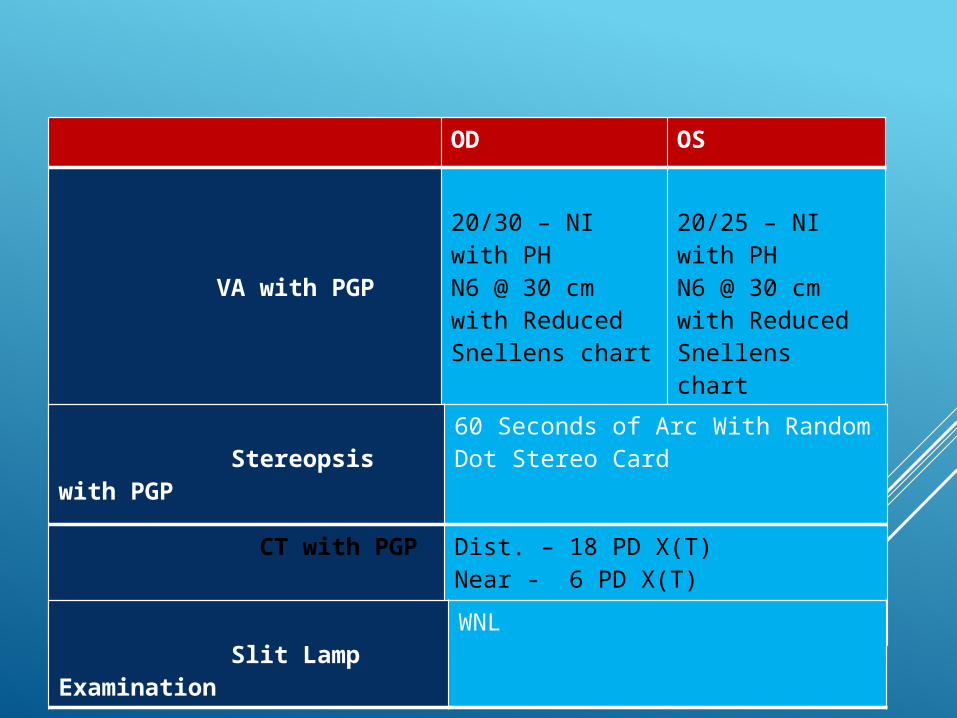
OD OS
VA with PGP
20/30 – NI with PHN6 @ 30 cm with Reduced Snellens chart
20/25 – NI with PHN6 @ 30 cm with Reduced Snellens chart
Stereopsis with PGP
60 Seconds of Arc With Random Dot Stereo Card
CT with PGP Dist. – 18 PD X(T)Near - 6 PD X(T)
Slit Lamp Examination
WNL
PROVISIONAL DIAGNOSIS
Basic Intermittent Exotropia
Divergence Excess
Convergence Insufficiency
Simulated or Pseudo-divergence Excess

Basic Intermittent Exotropia - Deviation for distance and near within 10∆
- Normal Accommodative, Fusional and
Proximal convergence
• Divergence Excess - Deviation for distance > 10∆ than near even after patch test
- High AC/A Ratio
Convergence Insufficiency - Near deviation > 10∆ than distance deviation
Simulated / Pseudo divergence Excess - Larger exotropia for distance than near but
near deviation increases within 10 PD
of distance deviation after Patch Test
Burian HM: Exodeviations: Their classification, diagnosis, and treatment. Am J Ophthalmol 62:1161, 1966

COVER TEST AFTER 1 HOUR PATCHING( WITH PGP)
Distance = 20-25 PD X(T)
Near = 20-25 PD X(T)

FINAL DIAGNOSIS
(OU) Compound Myopic Astigmatism
Intermittent Exotropia
(Pseudo divergence Type)
PLAN OF RX
Continue same glass
RTC 6-8 months

• Patch Test is the main criterion for differentiating true and pseudo divergence exotropia
• Nevertheless, not all intermittent exotropia are progressive nor do they need surgical interventions
• Proper clinical history with relation to classical symptoms plays vital role for the diagnosis

Thank you…







