4/30/19
1
Jeremy Horst
DDS,PhD
UCSF+UW
Medical Models of Caries
for the Modern Dental Practice
• At the conclusion of the session, the participant will be able to:
• 1. Explain the history, clinical evidence, safety, indications, and protocol for using SDF to treat dental caries.
• 2. Explain the indications, benefits, and risks for SDF, SMART, and Hall crowns to patients.
• 3. Guide patients through deciding whether to start with surgical versus topical caries management.
• 4. Demonstrate the technique for applying high viscosity glass ionomer cement as a sealant.
• 5. Propose to patients simple and effective strategies beyond brushing and flossing to prevent caries.
THANK YOU
Peter Milgrom
Joe DeRisi
Jong Seto
John Frachella
Steve Duffin
Douglas Young
Jeanette MacLean
Jason Hirsch
Martin MacInytre
Thuan Le
Pam DenBesten
Ling Zhan
John Featherstone
Eleni Ellenikiotis
Helen Yuan
Alex Yamana
4/30/19
2
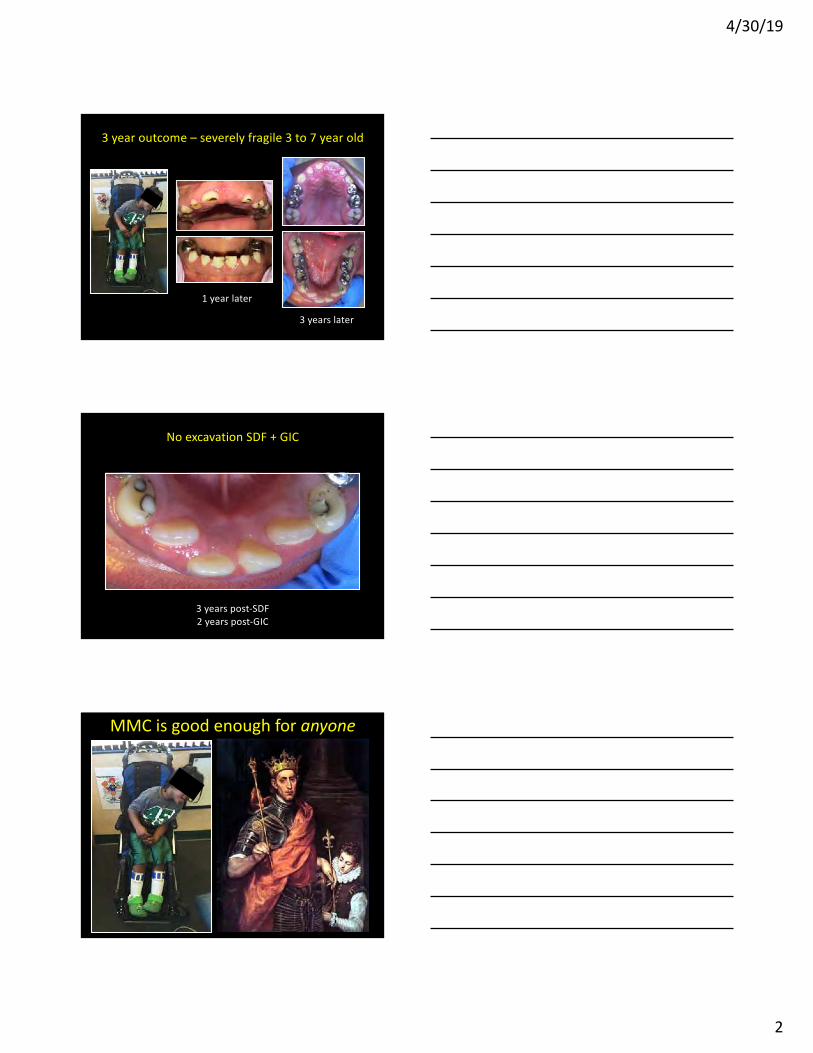
3 year outcome – severely fragile 3 to 7 year old
1 year later
3 years later
No excavation SDF + GIC
3 years post-SDF
2 years post-GIC
MMC is good enough for anyone

4/30/19
3
SDF Outline _
1. SDF – status & basics
2. SDF clinical evidence & use
3. SDF mechanisms
4. Glass ionomer
5. Hall crowns
SDF - what is it?
Colorless liquid
25% silver: antimicrobial
8% ammonia: solvent
5% fluoride: remineralization
SDF vs SN + FV
SDF
25% silver
8% ammonia
5% fluoride
> effect data
SN + FV
16% silver
9% nitrate
2.5% fluoride
> safety data
BOTH are safe & effective.

4/30/19
4
SDF - what does it do?
- Arrests dental caries
- Prevents dental caries
• directly & indirectly
- Decreases dentin hypersensitivity
Accessible
cavity.
1. Isolate with cotton.
2. Air dry.
3. Apply with microbrush.
Arrested cavities
after 1 year
How do you use it?

4/30/19
5
US acceptance
FDA clearance
UCSF protocol & guidelines
FDA “breakthrough status”
Advantage, Willamette protocols
Medicaid funding
IHS protocol & recommendation
ADA resolution
AAPD policy & guidelines
CDA Journal 2018 Jan & Feb
~20% of dentists, ~all pedodontists.
FDA/NIDCR/UMich/NYU/UIowa pivitol trialADA recommendation
October 2018, the ADA
“Clinicians are encouraged to prioritize use of
[nonrestorative treatments] based on
effectiveness, safety, and feasibility." - JDR
"38% silver diamine fluoride solution applied
biannually [is] effective for arresting advanced
cavitated carious lesions on any coronal surface
(moderate to high certainty).” - JADA
Dr. Jason Hirsch
Esthetics? SSC or SDF

4/30/19
6
Dr. John Frachella
Esthetics? Handled.
SMART
Dr. Jason Hirsch

4/30/19
7
Issues à prompts
• What are your goals for your oral health?
• Which matters more to you:
looks or comfort?
• Do you prefer:
multiple easy visits, or
fewer visits that are more intense?
Patient Name:
Date of Birth:
Medical Record Number: !
!
San!Francisco!Department!of!Public!Health!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
Dental!Services!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!INFORMED!CONSENT!FOR!SILVER!DIAMINE!FLUORIDE!
!Facts!for!consideration:!
• Silver!diamine!fluoride!(SDF)!is!a!liquid!that!helps!stop!tooth!
decay.!SDF!is!applied!every!3,!6!or!12!months.!
• A!small!amount!of!SDF!is!applied!to!the!decayed!tooth!area.!
• After!SDF!application!no!eating!or!drinking!for!60!minutes!
and!no!tooth!brushing!until!the!following!morning.!
• The!decayed!area!will!stain!black!permanently.!Healthy!
tooth!structure!will!not!stain.!!
• I!should!not!be!treated!with!SDF!if:!1)!I!am!allergic!to!silver.!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
2)!There!are!painful!sores!or!raw!areas!on!my!gums!or!anywhere!in!my!mouth.!
!!!
Benefits!of!receiving!SDF:!
• Helps!stop!tooth!decay.!
• Fast.!
• Do!not!need!to!numb!teeth.!
• Does!not!hurt.!
!
Risks!of!receiving!SDF:!
• The!affected!area!will!stain!black!permanently.!This!means!SDF!is!working.!
• ToothJcolored!fillings!and!crowns!may!discolor!if!SDF!is!applied!to!them.!!
• After SDF treatment, a filling or crown might still be needed.!
• If!accidentally!applied!to!the!skin!or!gums,!a!brown!or!white!stain!may!appear!that!causes!no!
harm,!cannot!be!washed!off!and!will!disappear!in!one!to!three!weeks.!
• Permanent dark spots if spilled on clothing.!
• Allergic reaction.!
• Risk!that!the!procedure!will!not!stop!the!decay.!
• Not every cavity can be treated with SDF!
!
Alternatives!to!SDF,!not!limited!to!the!following:!
• No!treatment,!which!may!lead!to!continued!break!down!of!the!tooth.!Symptoms!may!get!worse.!
• Placement!of!fillings!or!crowns,!extractions!or!referral!to!a!specialist.!
!
I have read this form. I understand the treatment and have had the chance to ask questions. I have seen the photo
of how teeth may look after SDF discolors the cavities. I understand that I may refuse treatment with SDF. I
understand that I can decide to have no treatment or I can have fillings, crowns, or extractions done at this or
another dental office.
I consent and authorize SFDPH Dental Services to use Silver Diamine Fluoride to help stop tooth decay.
Signature!of!patient/parent/guardian!!______________________________________________________!Date____________!
!
!
Signature!of!witness____________________________________________________________________________Date!____________!!
Consent = Conversation
This is a consent document.
Risks?
Benefits?
Alternatives?
Simple language.
Show pictures!
sites.google.com/site/jeremyahorst/SDFconsents
Tesoriero & Lee 2016
4/30/19
8
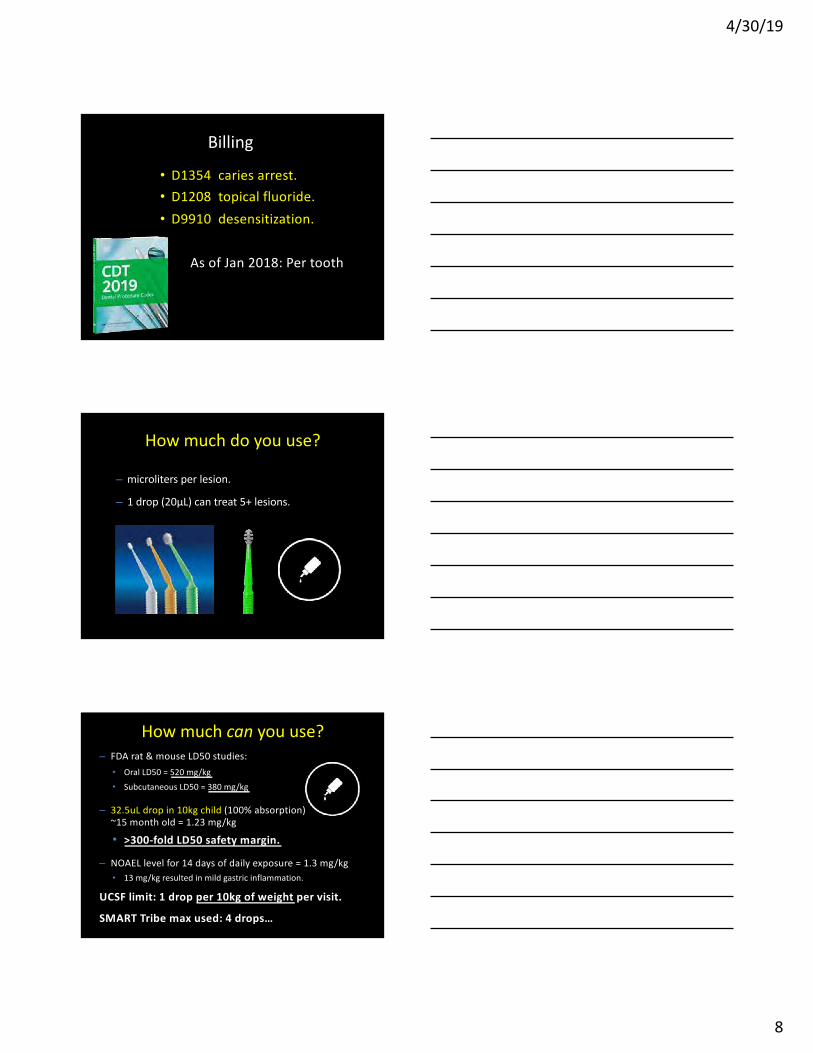
Billing
• D1354 caries arrest.
• D1208 topical fluoride.
• D9910 desensitization.
As of Jan 2018: Per tooth
How much do you use?
– microliters per lesion.
– 1 drop (20μL) can treat 5+ lesions.
How much can you use?
– FDA rat & mouse LD50 studies:
• Oral LD50 = 520 mg/kg
• Subcutaneous LD50 = 380 mg/kg
– 32.5uL drop in 10kg child (100% absorption)
~15 month old = 1.23 mg/kg
• >300-fold LD50 safety margin.
– NOAEL level for 14 days of daily exposure = 1.3 mg/kg
• 13 mg/kg resulted in mild gastric inflammation.
UCSF limit: 1 drop per 10kg of weight per visit.
SMART Tribe max used: 4 drops…

4/30/19
9
=
32.5 µL
50,000 ppm F
2.3 L
0.7 ppm FHow much Fluoride?
6 1=
SDF, how safe is it?
• No adverse reports in >80 years of use in Japan.
• Contraindication
– Silver allergy.
• Relative contraindication:
– Significant desquamative processes
e.g. ulcerative gingivitis, stomatitis
→ Protect by petroleum jelly
• Side effects:
– Small, white mucosal lesions
• disappear in 48 hours.
– It will stain the lesion black.
– 14 days: mild gastric inflammation.
n arrested (SD) 95% CI adverse events
SDF 30 .72 (.38) .55 to .85flu, nausea,
redness, spot
placebo 36 .05 (.18) .00 to .16
diarrhea x 2,
tummy ache,
toothache + diarrhea
Stopping Cavities Trial
purpose: Safety & Arrest Effectiveness

4/30/19
10
The US safety study in
Person and Clinic Protection
Permanent staining of clinic surfaces & clothes.
– Does not come out after setting.
– Clean immediately with copious water,
ethanol, or high pH solvents such as ammonia.
Temporary staining of skin
– Rinse.
–Will go away in days.
– No harm.
SDF staining
time 0 1 day 1 week
Castillo et al, J Dent Res 2011
Duffin, J Cal Dent Assoc 2012
4/30/19
11
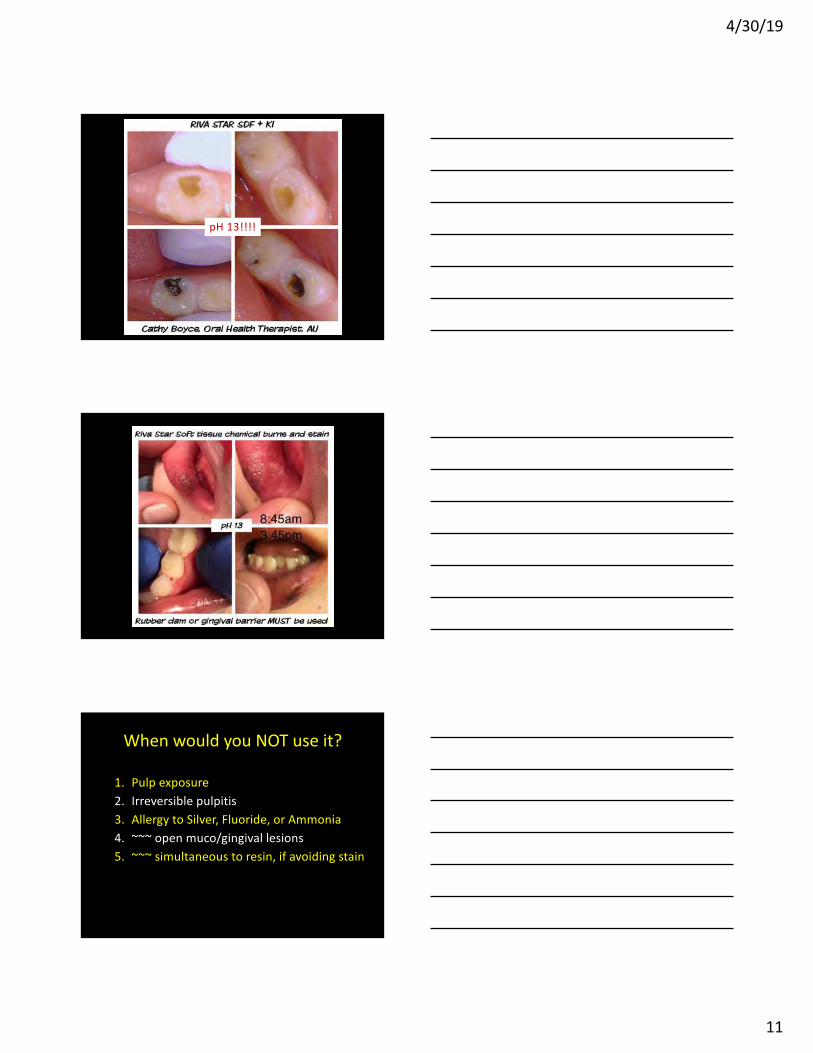
pH 13!!!!
When would you NOT use it?
1. Pulp exposure
2. Irreversible pulpitis
3. Allergy to Silver, Fluoride, or Ammonia
4. ~~~ open muco/gingival lesions
5. ~~~ simultaneous to resin, if avoiding stain

4/30/19
12
SDF Outline _
1. SDF – status & basics
2. SDF clinical evidence & use
3. SDF mechanisms
4. Glass ionomer
5. Hall crowns
Ca
rie
s A
rre
stin
kid
s
Horst, Adv Dent Res 2018
9%
9%
4/30/19
13
Ca
rie
s A
rre
st
in k
ids
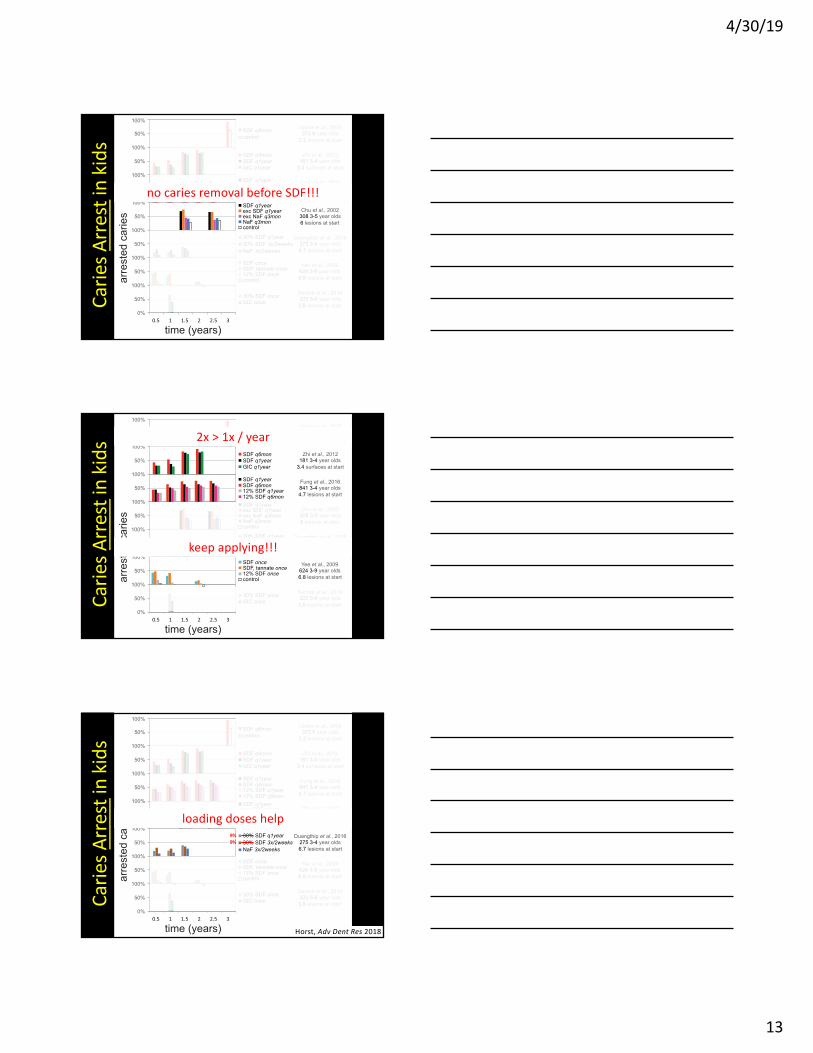
no caries removal before SDF!!!
Ca
rie
s A
rre
stin
kid
s 2x > 1x / year
keep applying!!!
Ca
rie
s A
rre
stin
kid
s
Horst, Adv Dent Res 2018
9%
9%
loading doses help

4/30/19
14
Ca
rie
s A
rre
st
in k
ids
similar effect vs ART
Suggested frequency protocol
• For mild caries:
q6mo
baseline
2-6 wk
3 mo
6 mo
12 mo
18 mo
• For moderate caries:
q6mo + 2-6 week loading dose
• For severe caries:
q6mo + two 2-6 week loading doses + 3mo
0%#
50%#
100%#
0.5# 1# 1.5# 2# 2.5# 3#
SDF#q1year#
+#OHI#q6mon#
control##
Zhang et al., 2013 227 60-89 year olds
0.91 lesions at start
0%#
50%#
100%#
SDF#q1year#
SDF,#KI#q1year#
control##
Li et al., 2016 67 72 year olds
1.9 lesions at start
0%#
50%#
100%#
SDF#q1year#
NaF#q3mon#
Chlorhex#q3mon#
0%#
50%#
100%#
0.5# 1# 1.5# 2# 2.5# 3#
SDF#q1year#
+#OHI#q6mon#
Tan et al., 2010 203 79 year olds
control: 2.5 new lesions
Zhang et al., 2013 227 60-89 year olds
control: 1.3 new lesions
Arr
est
Older adults
Pre
ve
ntio
n
time (years)

4/30/19
15
Kanellis. CDAJ, 2018
SN+FV trial
@Amish U.Iowa
TABLE 2
Major and Minor Failures at 24 Months*
Silver Nitrate Group Conventional Group
Major Failure Minor Failure Major Failure Minor Failure
17 / 237 5 / 237 3 / 93 0 / 93
7.2% 2.1% 3.2% 0%
*Reported at the tooth level.
Baseline
6 months
12 months
18 months
24 months
Ca
rie
s P
reve
nti
on
in k
ids
pre
vente
d fra
ction o
f caries lesio
ns
0%
0.5 1 1.5 2 2.5 3
time (years)
50%
100%
50%
100%
50%
100%
50%
100%
50%
100%
50%
100%
50%
100%
50%
100%
SDF q1year
Resin Sealant
NaF q6mos
Liu et al., 2012
482 9.1 year olds
control: 4.6 new lesions
SDF q1year
exc SDF q1year
exc NaF q3mos
NaF q3mos
Chu et al., 2002
308 3-5 year olds
control: 1.6 new lesions
SDF once
GIC Sealant
Monse et al., 2012
708 6-8 year olds
control: 0.44 new lesions
40% AgF once
849 5-8 year olds
control: 11.7 new lesions
background: 10% SnF2
Green, 1989
50%
100%
SDF q1year
SDF q6mos
Nguyen et al., 2017
295 2-3 year olds
control: 9.0 new lesions
SDF 3x/1week
25 6-8 year olds
control: 0.88 new lesions
Sato & Saito, 1970
SDF q6mos
Llodra et al., 2005
373 6 year olds
control: 2.5 new lesions
50%
100%
SDF q3mosTsutsumi et al., 1981
58 5-7 year olds
mean (61%)
weighted average
SDF q3mos
Yoshida et al., 1976
26 1-2 year olds
control: 2.2 new lesions
Horst & Heima, Compendium 2019
4/30/19
16
0%#
50%#
100%#
0.5# 1# 1.5# 2# 2.5# 3#
SDF#q1year#
+#OHI#q6mon#
control##
Zhang et al., 2013 227 60-89 year olds
0.91 lesions at start
0%#
50%#
100%#
SDF#q1year#
SDF,#KI#q1year#
control##
Li et al., 2016 67 72 year olds
1.9 lesions at start
0%#
50%#
100%#
SDF#q1year#
NaF#q3mon#
Chlorhex#q3mon#
0%#
50%#
100%#
0.5# 1# 1.5# 2# 2.5# 3#
SDF#q1year#
+#OHI#q6mon#
Tan et al., 2010 203 79 year olds
control: 2.5 new lesions
Zhang et al., 2013 227 60-89 year olds
control: 1.3 new lesions
Arr
est
Older adults P
reve
ntio
n
time (years)
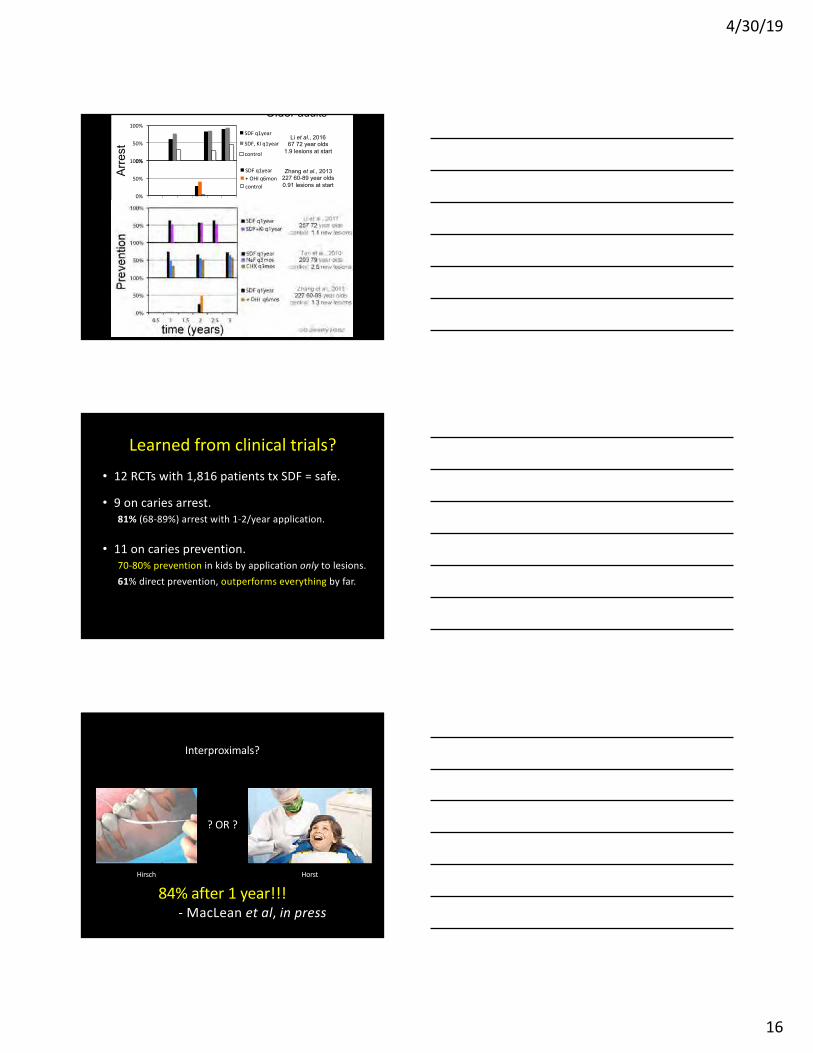
Learned from clinical trials?
• 12 RCTs with 1,816 patients tx SDF = safe.
• 9 on caries arrest.
81% (68-89%) arrest with 1-2/year application.
• 11 on caries prevention.
70-80% prevention in kids by application only to lesions.
61% direct prevention, outperforms everything by far.
? OR ?
Interproximals?
Hirsch Horst
84% after 1 year!!!
- MacLean et al, in press
4/30/19
17
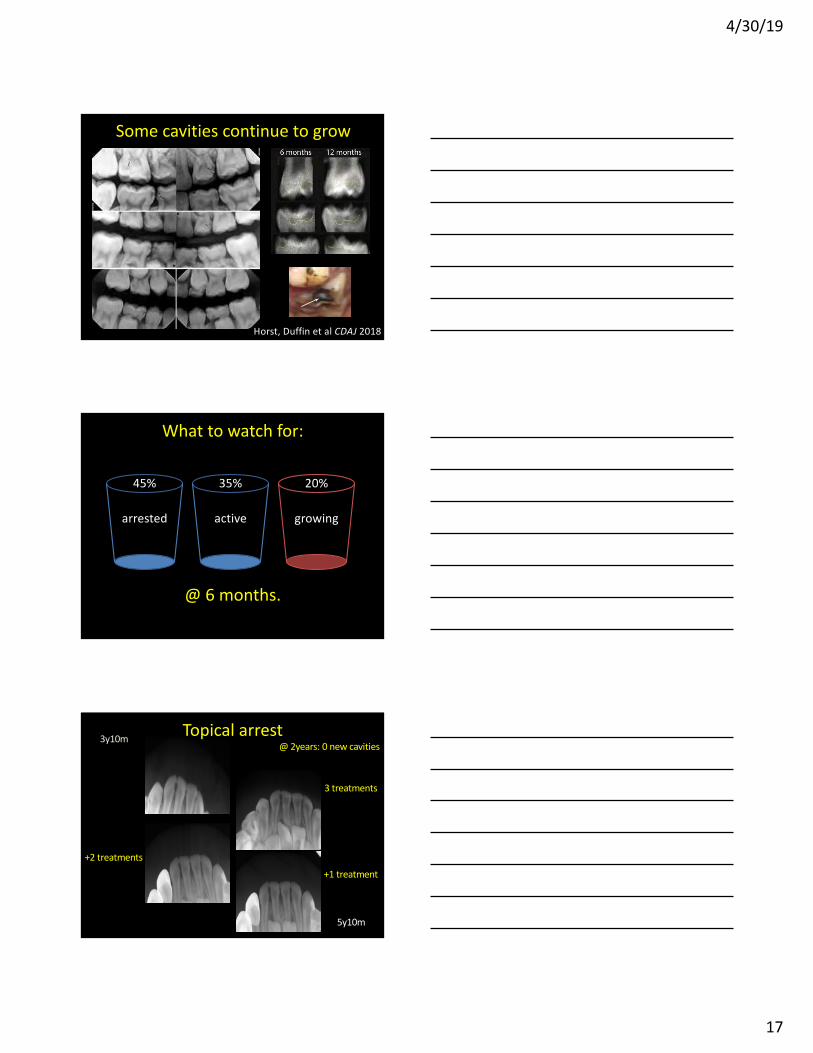
Horst, Duffin et al CDAJ 2018
Some cavities continue to grow
arrested
What to watch for:
active growing
@ 6 months.
45% 35% 20%
3y10m
3 treatments
+9 months
+2 treatments
+6 months+1 treatment
+6 months
5y10m
Topical arrest@ 2years: 0 new cavities

4/30/19
18
3y10m
3 treatments
+9 months
+2 treatments
+6 months+1 treatment
+6 months
5y10m
Topical arrest@ 2years: 0 new cavities
3 treatments
+9 months
@ 2years: 0 new cavities
Topical arrest
3y10m
5y10m
3y10m
3 treatments
+9 months
Topical arrest
5y10m
@ 2years: 0 new cavities

4/30/19
19
arrested
What to watch for:
active growing
@ 6 months.
45% 35% 20%
Ca
rie
s A
rre
st
in k
ids
6mo 18mo
SDF Outline _
1. SDF – status & basics
2. SDF clinical evidence & use
3. SDF mechanisms
4. Glass ionomer
5. Hall crowns

4/30/19
20
Hamama, Aust Dent J 2015
SDF chases bugs
down into tubules
SDF: sustained antimicrobial effects
– Treated dentin resists plaque formation.
– demineralized dentin resists more.
– Zombie Effect: Silver-killed bugs kill active bugs.
• Ideal substantivity.
0
1
2
−2 −1 0 1 2
log2(groupB
groupA)
−lo
g1
0(p
.va
lue
)
FDR<0.05
|logFC|>2
both
Caries legions after treatment
resistance genes
No changes
metagenomic
NextGen Sequencing
Milgrom + Horst et al. J Dent, 2018
●
●
●
●
●●
●
● ●●
●●
●●
● ●
●●●
●● ●● ● ●●●●● ●●
●●●● ●●●● ●● ●●● ●● ●
●●●● ● ●●● ● ●● ●● ●●
●●
● ●●
●●
●●
●
●
●
●
●● ●
●
●●●
●
●
●
●●
●●● ● ●●●●
●
●●
●●
● ●●
●
●●
●● ●
●
●● ●● ● ●● ●● ●●● ●●● ● ●● ●●●●●● ●● ●●● ●●●●● ●●●●●●● ●●● ●●●●● ●● ●● ●●●● ●●●● ●●● ● ●●● ●●● ●●●●●● ●● ●●●●●●●●● ●●● ●●●● ●●● ● ●● ●●● ●●● ●●● ●●●● ●●● ●●● ●●●●● ●●●●●●●● ●●●● ●●● ●●●● ●●● ●●●●●●●●●●●●●●●●●●●●●
● ●●●●●●●●●●●●● ●●
●●●●●
●●●●●●●●●
●●●●●●● ●●●●●●●●●●●●●●●●●●
−15 −10 −5 0 5 10 15
02
46
log2FoldChange
−lo
g1
0(p
va
lue
)
●
●
●
●
●
●
●
●●
●
●
●●
●●
●
●●
●●●
●
●●
●●
●●● ●●
●●● ●●●●
●
●
●Lactobacillus reuteri
Acidithiobacillus caldus
Sulfuriferula sp. AH1
●
●
●
FDR<0.01
|LogFC|>2
both
Lactobacillus
reuteri
Sulfuriferula sp. AH1
Acidithiobacillus caldus
failure
-1 0 1 2 3
log2FoldChange
PropionibacteriumStreptococcus mutans
FDR<0.05
|LogFC|>1
3
Streptococcus
mutans
microbes

4/30/19
21
SDF microstructures
SDF casts silver rebar millimeters into dentin,
reinforcing the lesion and sustaining kill.
Seto, Horst, Frachella, Duffin, MacLean
Silver wires in
dentinal tubules
Seto, Horst,
Frachella, Duffin
SDF penetration testing
Seto, Horst

4/30/19
22
Before10 minutes1 hour
kinetics of SDF penetration
Seto, Horst, Frachella, Duffin
Kitchen SMARTs
with Drs. Steve Duffin & John Frachella
Horst, Seto, Frachella, Duffin

4/30/19
23
SDF Outline _
1. SDF – history & status
2. SDF clinical evidence
3. SDF mechanisms
SDF pro tips
1. 3x in 2 weeks.- Dr. Steve Duffin
2. Cover immediately with varnish.- Dr. Steve Duffin
3. Superfloss to soak posterior interproximals.- Dr. Jason Hirsch
4. Vaseline on lips & skin, toothpaste on tongue,
scented lip balm under nose.
- Dr. Jeanette MacLean
5. Cover it with GIC
- Drs. John Frachella & Cate Quas
SDF take-homes
1. Arrests 81% of lesions when used 1+/year.
2. Prevents 62% of new lesions.
3. Dry before use.
4. Safe.
5. Stains the crap out of everything.
4/30/19
24
When would you use it?
UCSF Indications:
1. Extreme caries risk (Xerostomia, S-ECC)
2. Behavior or Medical management
challenges.
3. More lesions than treatable at 1 visit.
4. Difficult to treat lesions.
5. Patients without access to care.
SDF Outline _
1. SDF – status & basics
2. SDF clinical evidence & use
3. SDF mechanisms
4. Glass ionomer
5. Hall crowns
Locker...Kay, Br Dent J 195:375
What about Sealants?
71% prevention on treated surfaces
4/30/19
25
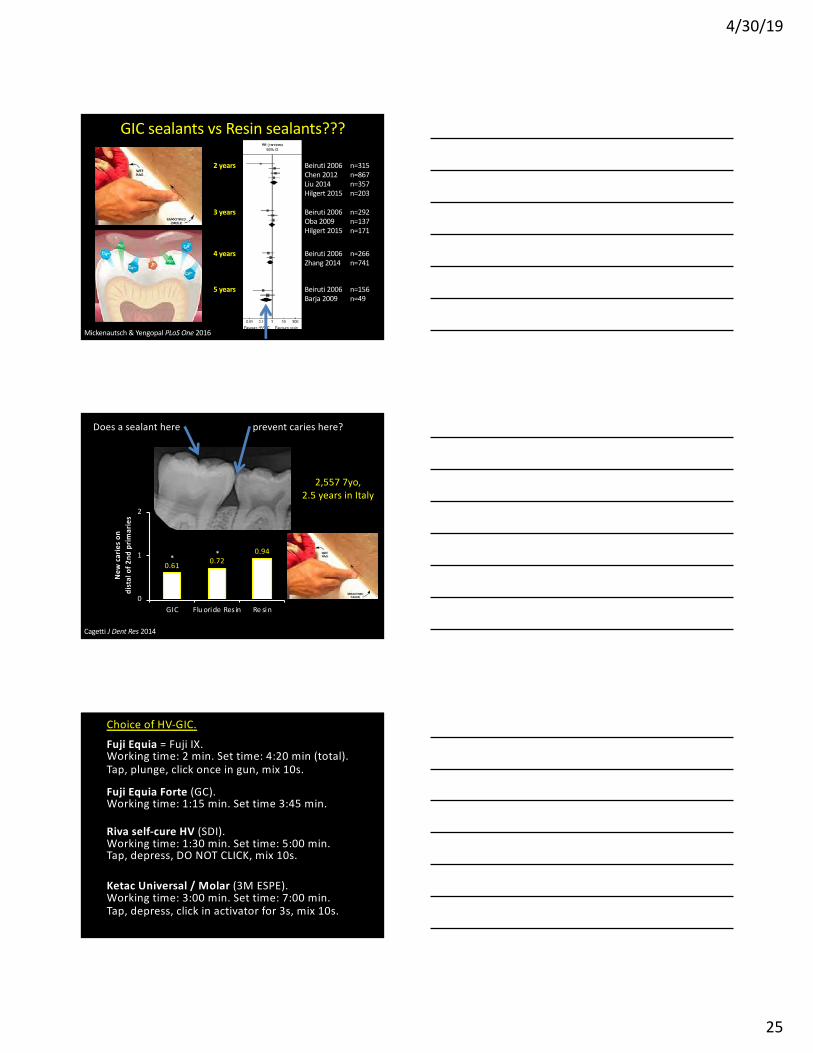
Mickenautsch & Yengopal PLoS One 2016
2 years
3 years
4 years
5 years
Beiruti 2006 n=315
Chen 2012 n=867
Liu 2014 n=357
Hilgert 2015 n=203
Beiruti 2006 n=292
Oba 2009 n=137
Hilgert 2015 n=171
Beiruti 2006 n=266
Zhang 2014 n=741
Beiruti 2006 n=156
Barja 2009 n=49
GIC sealants vs Resin sealants???
Does a sealant here prevent caries here?
2,557 7yo,
2.5 years in Italy
Cagetti J Dent Res 2014
0.610.72
0.94
0
1
2
GIC Flu oride Res in Re sin
Ne
w c
ari
es
on
dis
tal
of
2n
d p
rim
ari
es
**
Choice of HV-GIC.
Fuji Equia = Fuji IX. Working time: 2 min. Set time: 4:20 min (total).
Tap, plunge, click once in gun, mix 10s.
Fuji Equia Forte (GC). Working time: 1:15 min. Set time 3:45 min.
Riva self-cure HV (SDI). Working time: 1:30 min. Set time: 5:00 min. Tap, depress, DO NOT CLICK, mix 10s.
Ketac Universal / Molar (3M ESPE). Working time: 3:00 min. Set time: 7:00 min.
Tap, depress, click in activator for 3s, mix 10s.

4/30/19
26
Choice of HV-GIC.
NO!!!
You’ve got 45s to stop messing with it.
Control the moisture.
Then after the SETTING time, drill with
copious water IFF necessary.
Where’s the margin?
Courtesy of Rella Christensen

4/30/19
27
Amalgam
Original Magnification 300x
[Powerpoint and projectors affect magnification]
Courtesy of Brian Novy
Results
composite
Original Magnification 300x
[Powerpoint and projectors affect magnification]
Courtesy of Brian Novy
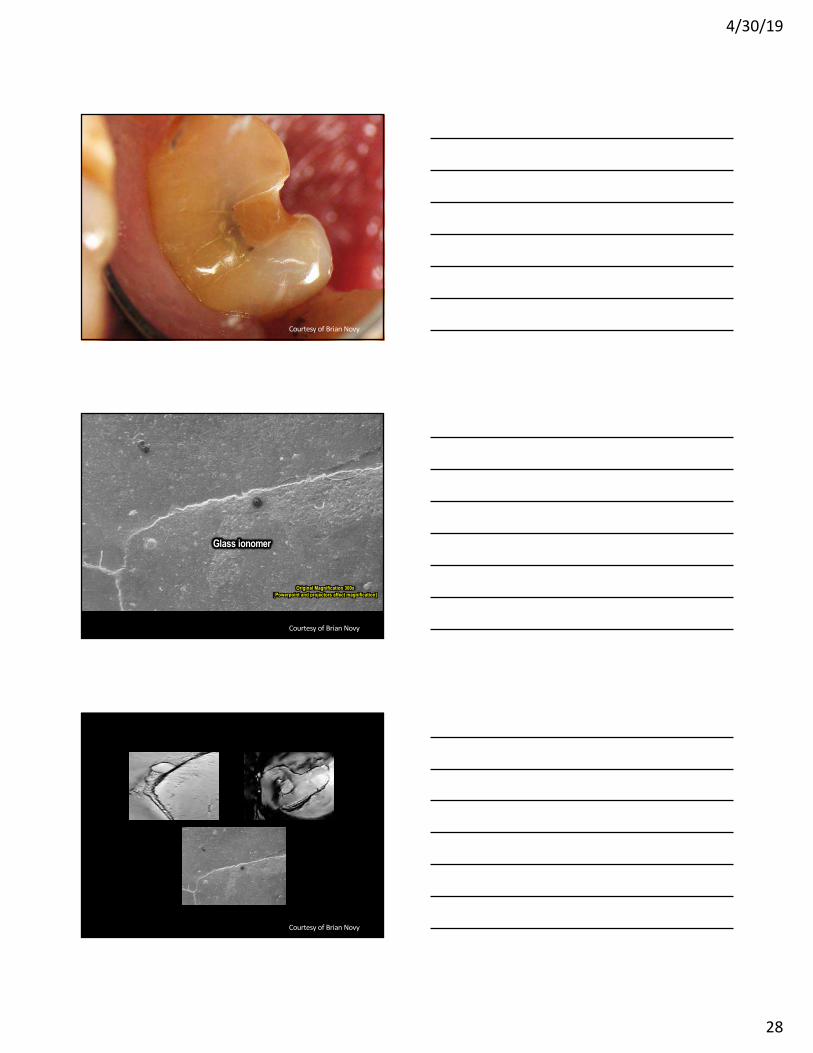
Glass ionomer
Original Magnification 300x
[Powerpoint and projectors affect magnification]
Courtesy of Brian Novy
4/30/19
28
Courtesy of Brian Novy
Glass ionomer
Original Magnification 300x
[Powerpoint and projectors affect magnification]
Courtesy of Brian Novy
Courtesy of Brian Novy
4/30/19
29
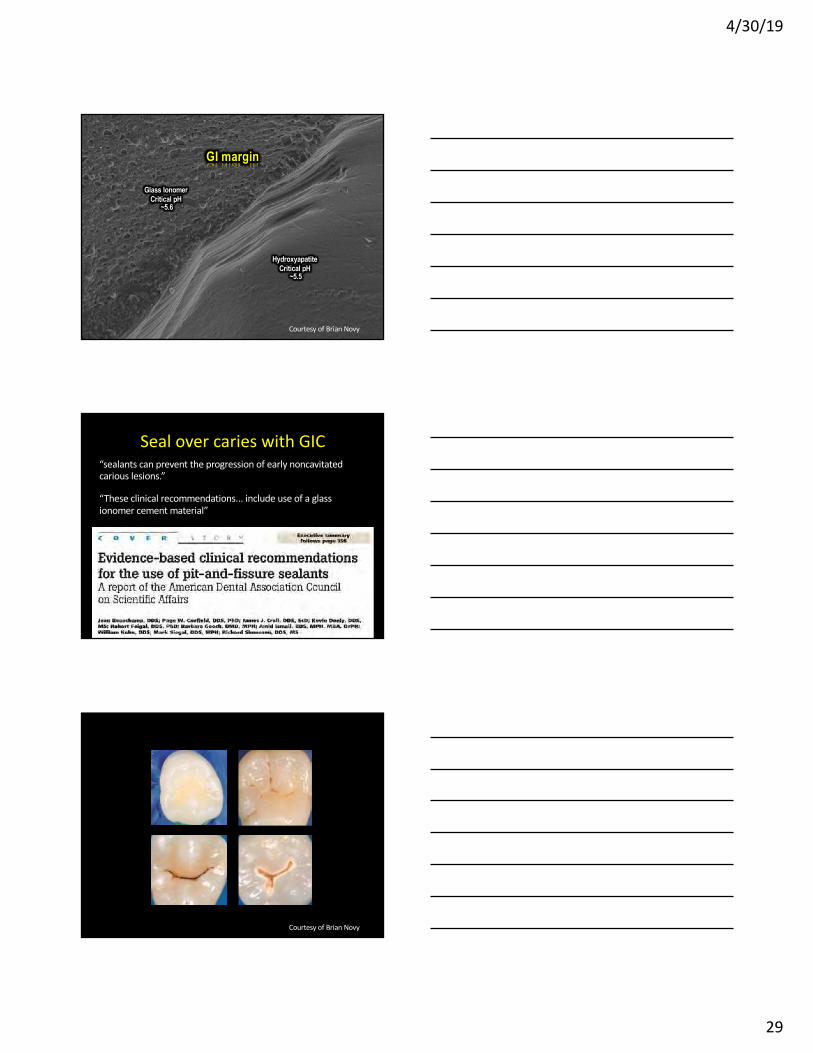
GI margin
Glass Ionomer Critical pH
~5.6
Hydroxyapatite Critical pH
~5.5
Courtesy of Brian Novy
Seal over caries with GIC
“sealants can prevent the progression of early noncavitated
carious lesions.”
“These clinical recommendations... include use of a glass
ionomer cement material”
Courtesy of Brian Novy
4/30/19
30
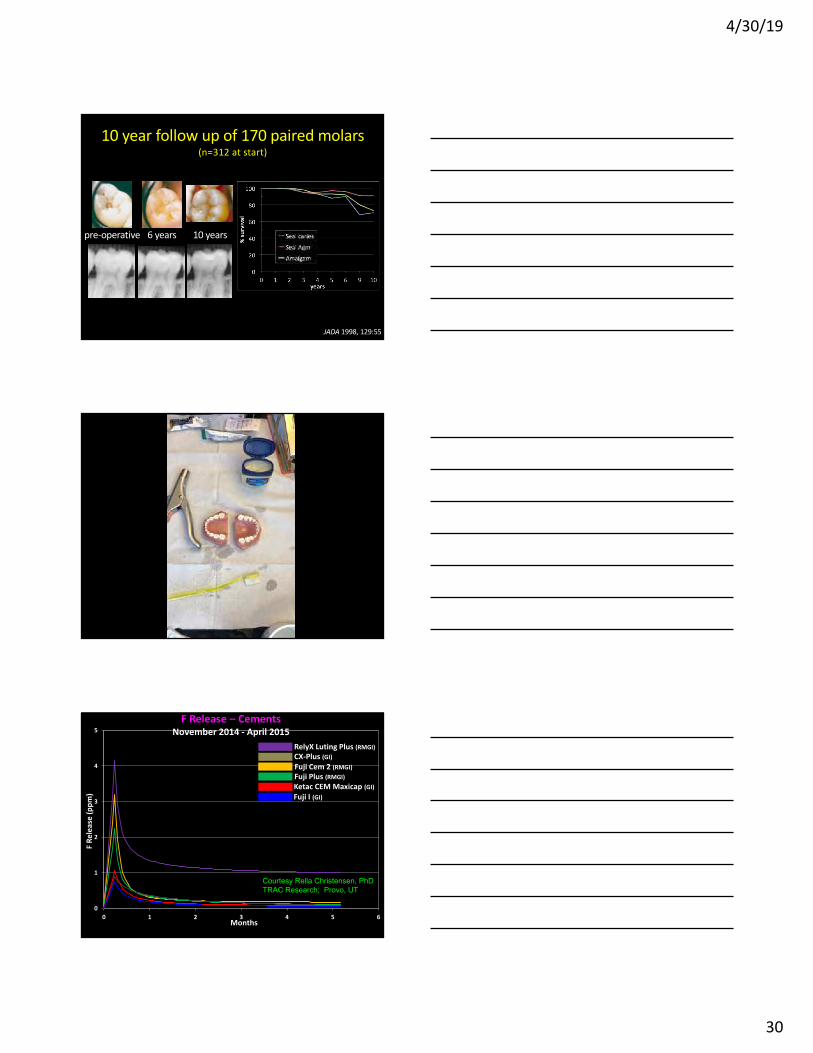
pre-operative 6 years 10 years
JADA 1998, 129:55
10 year follow up of 170 paired molars(n=312 at start)
0
1
2
3
4
5
0 1 2 3 4 5 6
F R
ele
ase
(p
pm
)
Months
RelyX Luting Plus (RMGI)
Fuji Cem 2 (RMGI)
CX-Plus (GI)
Fuji Plus (RMGI)
Ketac CEM Maxicap (GI)
Fuji I (GI)
F Release – Cements November 2014 - April 2015
Courtesy Rella Christensen, PhD
TRAC Research; Provo, UT

4/30/19
31
0
1
2
3
4
5
0 1 2 3 4 5 6
F R
ele
ase
(p
pm
)
Months
RelyX Luting Plus (RMGI)
Fuji Cem 2 (RMGI)
CX-Plus (GI)
Fuji Plus (RMGI)
Ketac CEM Maxicap (GI)
Fuji I (GI)
F Release – Cements November 2014 - April 2015
Courtesy Rella Christensen, PhD
TRAC Research; Provo, UT
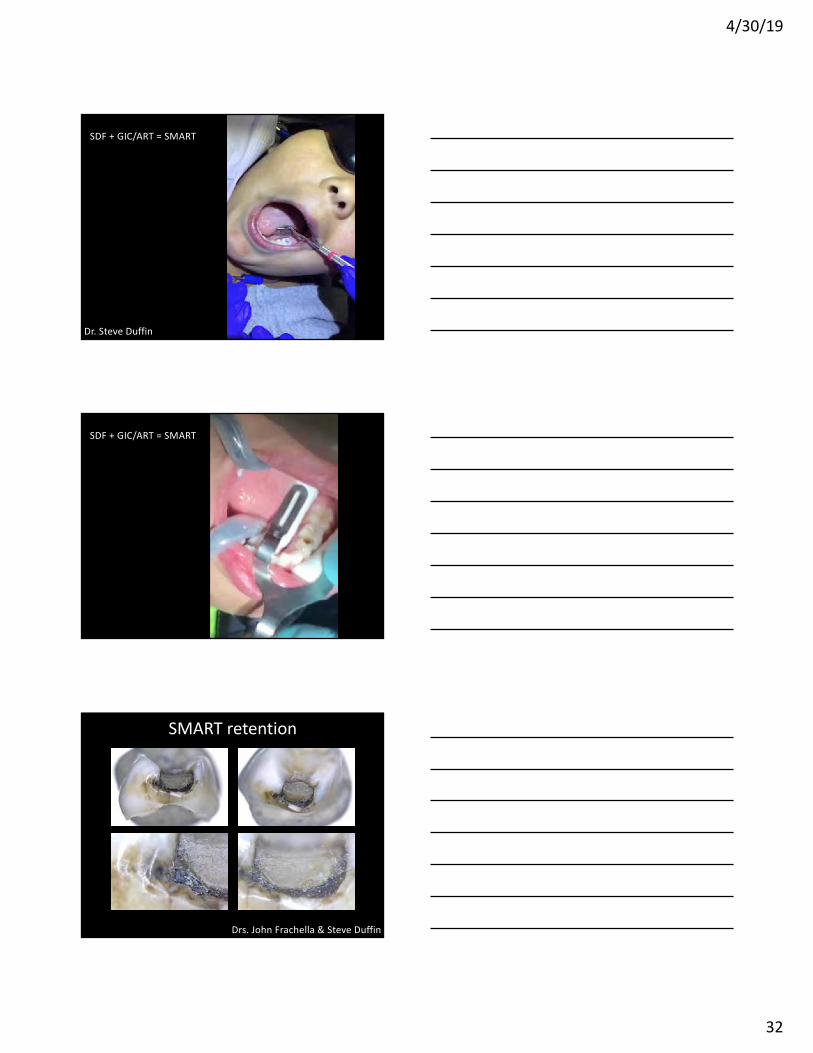
SDF + GIC: silver modified ART
SMART
• Glass Ionomer Cements (GICs) add the benefit of
sustained fluoride release and a seal!
• Protocol: SDF, then standard GIC protocol.
Drs. John Frachella & Cate Quas
(they darken over time)
SMART armamentarium
4/30/19
32
SDF + GIC/ART = SMART
Dr. Steve Duffin
SDF + GIC/ART = SMART
SMART retention
Drs. John Frachella & Steve Duffin
4/30/19
33
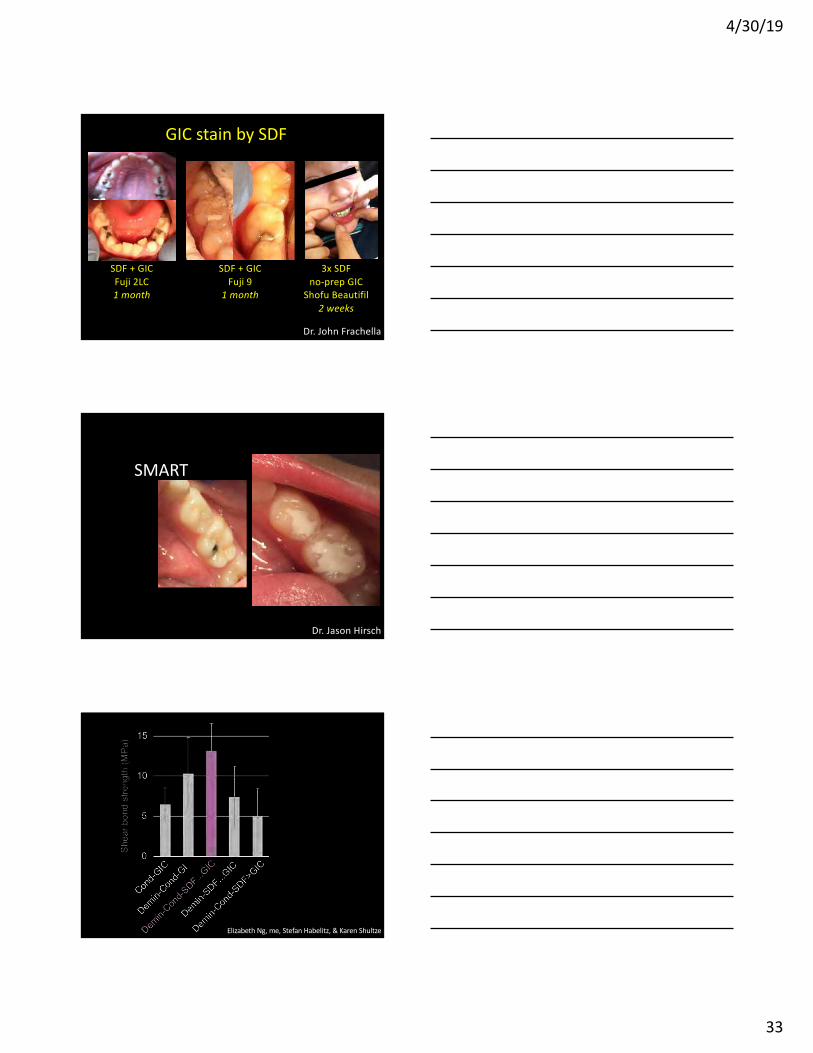
GIC stain by SDF
SDF + GIC
Fuji 2LC
1 month
SDF + GIC
Fuji 9
1 month
3x SDF
no-prep GIC
Shofu Beautifil
2 weeks
Dr. John Frachella
SMART
Dr. Jason Hirsch
Elizabeth Ng, me, Stefan Habelitz, & Karen Shultze
4/30/19
34
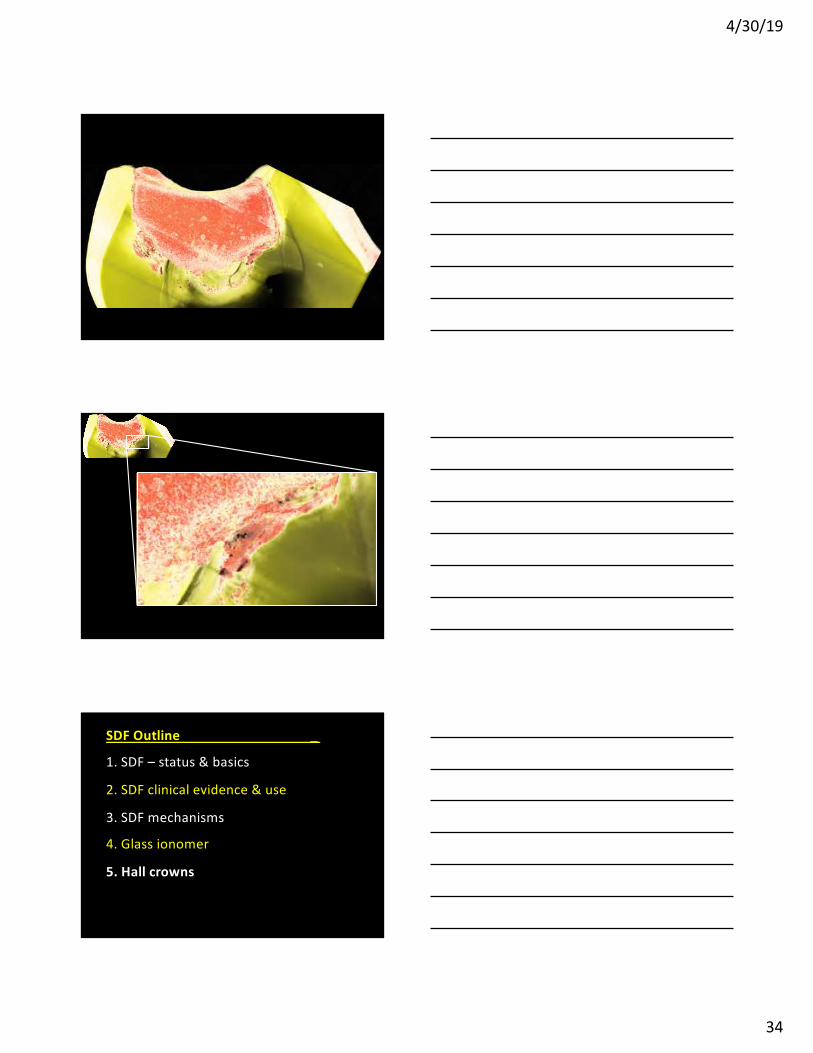
SDF Outline _
1. SDF – status & basics
2. SDF clinical evidence & use
3. SDF mechanisms
4. Glass ionomer
5. Hall crowns
4/30/19
35
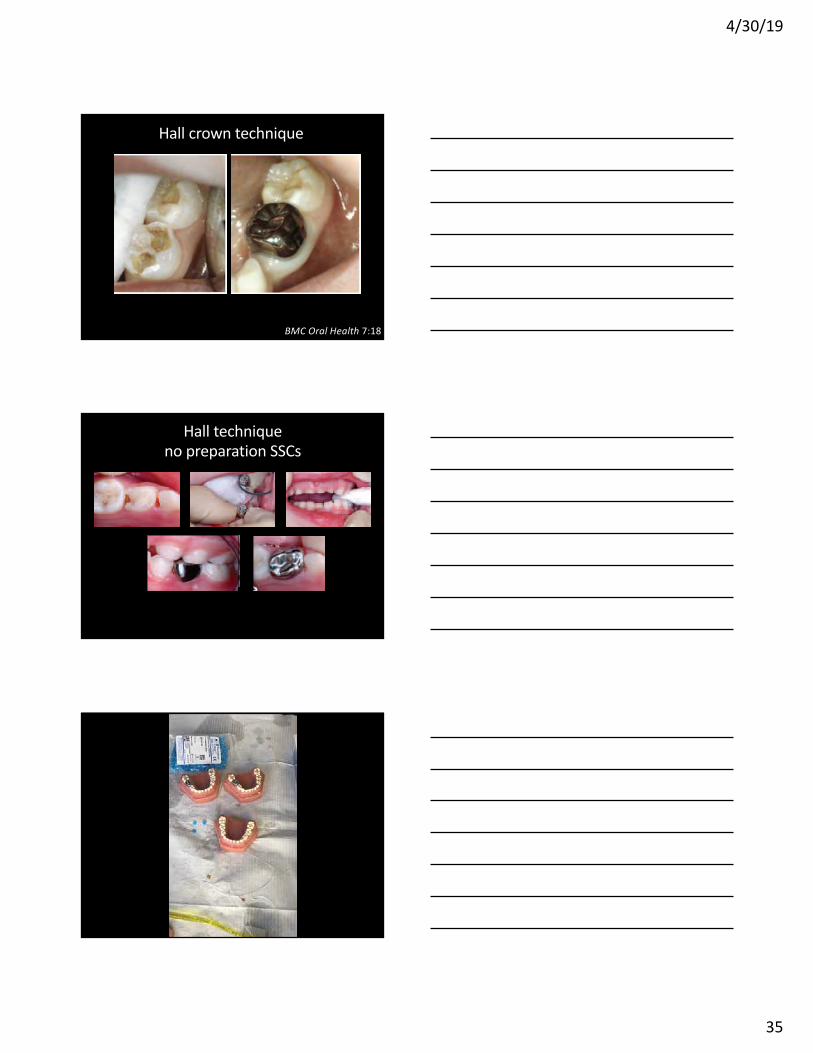
Hall crown technique
BMC Oral Health 7:18
Hall technique
no preparation SSCs
4/30/19
36
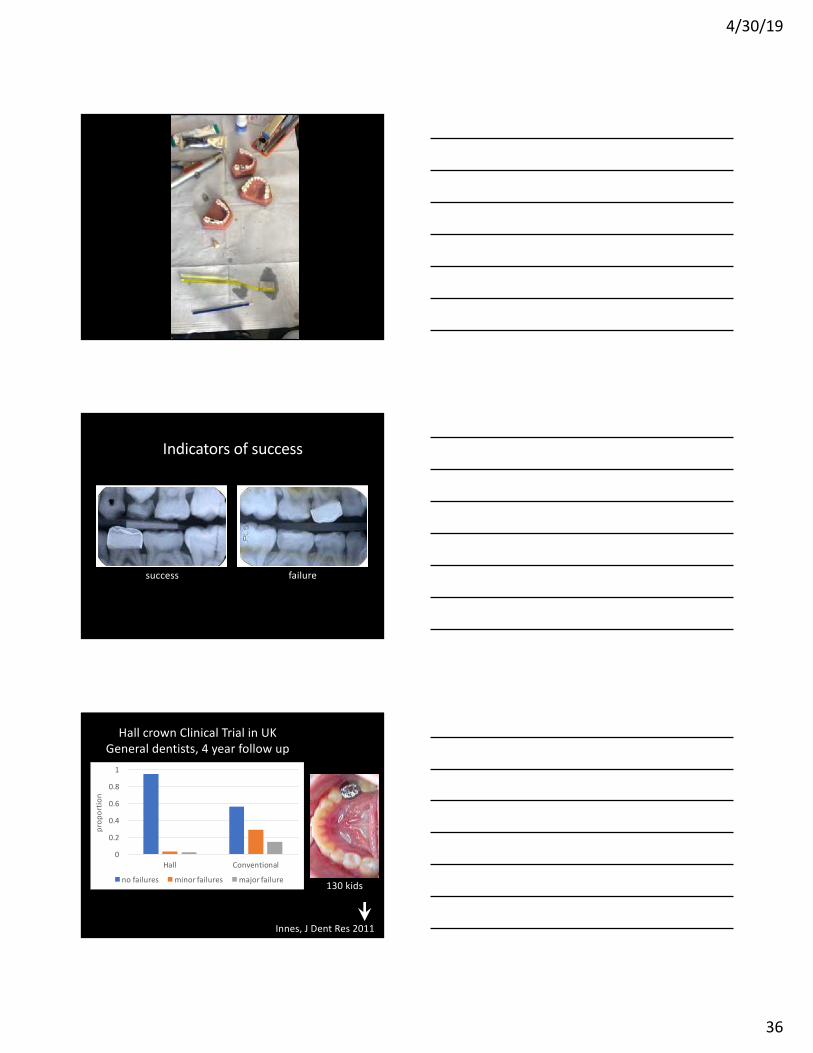
success
Indicators of success
failure
Innes, J Dent Res 2011
Hall crown Clinical Trial in UK
General dentists, 4 year follow up
0
0.2
0.4
0.6
0.8
1
Hall Conventional
proportion
nofailures minorfailures majorfailure130 kids

4/30/19
37
Hall crown Clinical Trial in Germany
treatment by Pediatric dentists, 2.5 year f/u
Santamaria et al., 2017
148 kids
Craig & Powell, 2013
NRCT
Non-restorative
caries therapy
0%
20%
40%
60%
80%
100 %
Hall NR CT Co nvent ion al
pro
po
rtio
n (
%)
no fai lur es minor failures major failu re
1.00
0.98
0.96
0.94
0.92
0.90
0.88
0.86
0.84
0.82
0.80
0
1
2
2 4
117 98
1167
SU
RV
IVA
L P
RO
BA
BIL
ITY
Years
JADA 2014
Halls in the USA
6 Hall crowns
vanderZee & vanAmerongen 2010
0
0.5
1
1.5
2
2.5
3
-1 7 15 23
canineoverlap(mm)
dayspost-treatment
48 kids
The high bite self-adjusts

4/30/19
38
preference
Innes, J Dent Res 2011
The Hall Technique A minimal intervention, child centred approach to managing the carious primary molar
A Users Manual Version 4
Text copyright Nicola Innes, Dafydd Evans, Matthew Stewart, Alex Keightley
wikipedia.org/wiki/Hall_Technique
4/30/19
39
SDF Outline _
1. SDF – status & basics
2. SDF clinical evidence & use
3. SDF mechanisms
4. Glass ionomer
5. Hall crowns
THANK YOU
You can get these slides and more at:
http:// bit.ly / DrJeremy
Watch the SDF video any time:
youtube.com/watch?v=zUAJkqcItco
My email:
jahorst @ gmail.com
4/30/19
40
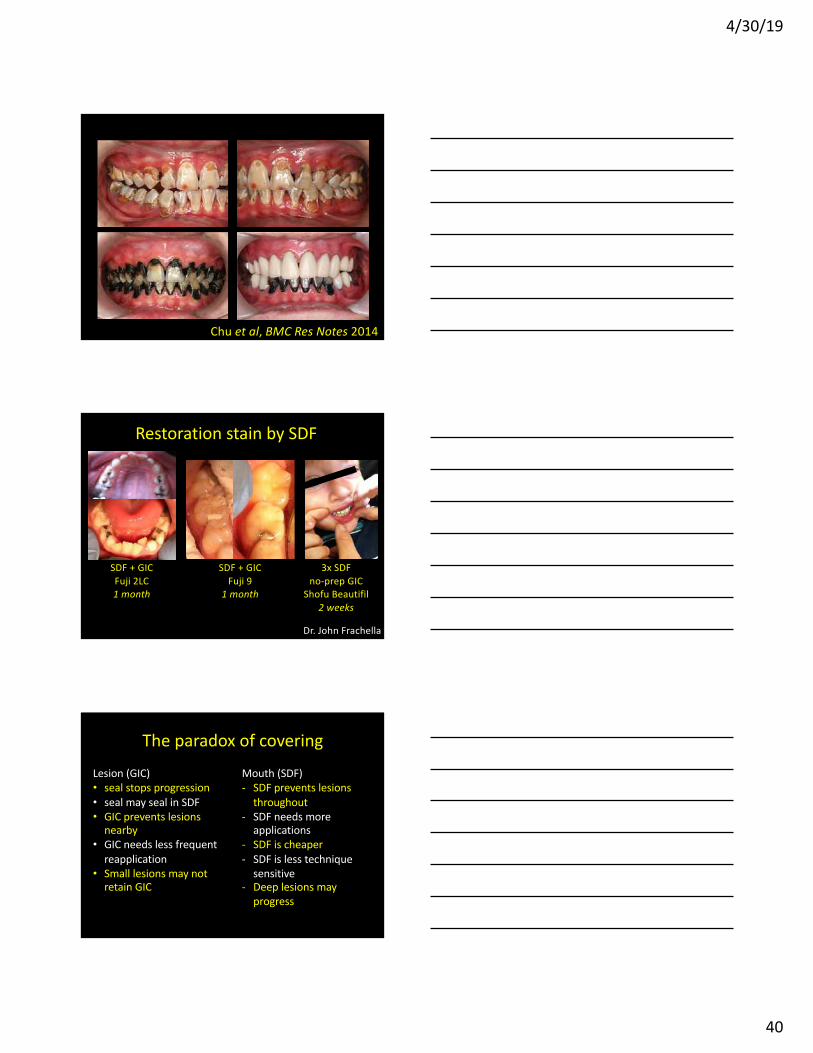
Chu et al, BMC Res Notes 2014
Restoration stain by SDF
SDF + GIC
Fuji 2LC
1 month
SDF + GIC
Fuji 9
1 month
3x SDF
no-prep GIC
Shofu Beautifil
2 weeks
Dr. John Frachella
The paradox of covering
Lesion (GIC)
• seal stops progression
• seal may seal in SDF
• GIC prevents lesions
nearby
• GIC needs less frequent
reapplication
• Small lesions may not
retain GIC
Mouth (SDF)
- SDF prevents lesions
throughout
- SDF needs more
applications
- SDF is cheaper
- SDF is less technique
sensitive
- Deep lesions may
progress
4/30/19
41
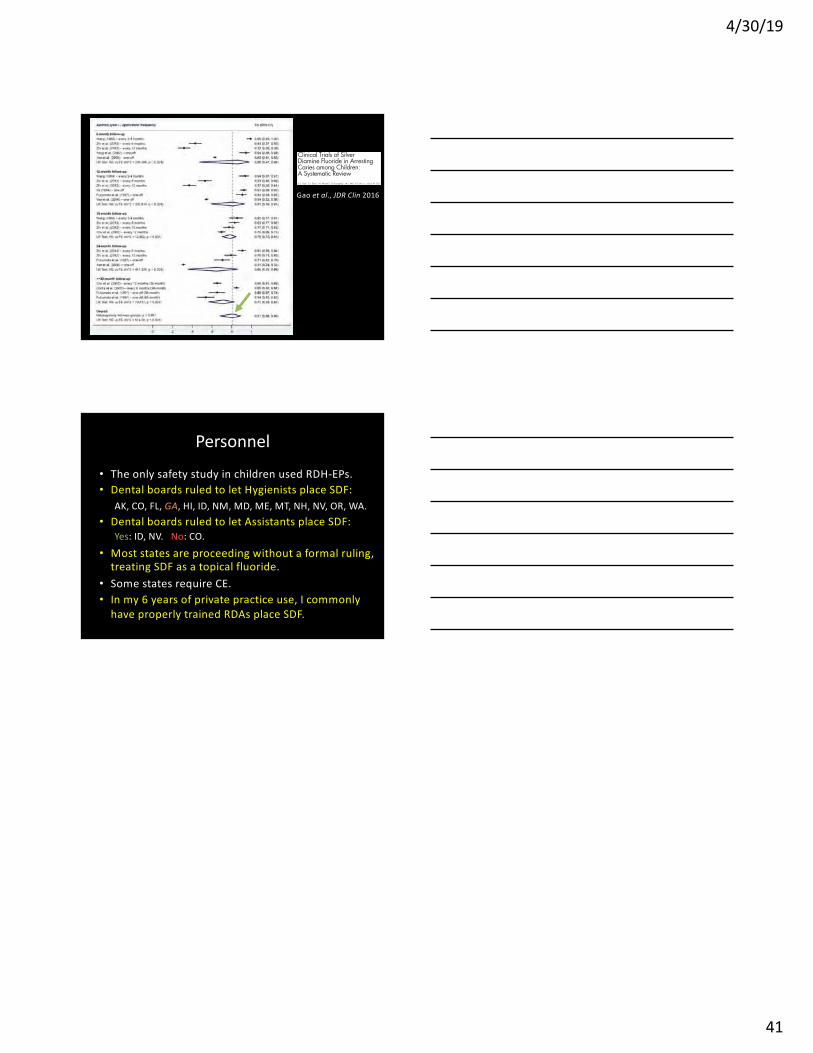
1 1 2 1 1, E.C.M. Lo1 1
Gao et al., JDR Clin 2016
Personnel
• The only safety study in children used RDH-EPs.
• Dental boards ruled to let Hygienists place SDF:
AK, CO, FL, GA, HI, ID, NM, MD, ME, MT, NH, NV, OR, WA.
• Dental boards ruled to let Assistants place SDF:
Yes: ID, NV. No: CO.
• Most states are proceeding without a formal ruling,
treating SDF as a topical fluoride.
• Some states require CE.
• In my 6 years of private practice use, I commonly
have properly trained RDAs place SDF.







