
NAMAF - 2017 ANNUAL REPORT
2017 ANNUAL REPORT
NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS2
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS2
Taki
ng
Namibia’s HealthcareNamibia’s HealthcareNamibia’s HealthcareHands inHands inHands in

Namibia’s HealthcareNamibia’s HealthcareHands inHands in

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS4
1. General Information 8
1.1 Mission and Vision 101.2 Core Mandate 111.3 Key Partners and their Roles 141.4 Medical Aid Funds and their Relationship to Namaf 20
2. Leadership and Corporate Governance 24
2.1 Management Committee 262.2 Secretariat 322.3 Chairperson’s Report 342.4 Chief Executive Offi cer’s Report 38
3. Operations 48
3.1 Registration and Renewal of Practice Numbers 503.2 Coding Structure 513.3 Marketing and Awareness Interventions 543.4 Stakeholder Relations 553.5 Development of the Strategic Plan 56
4. Litigation: Namaf vs NaCC 58
4.1 Background 604.2 The Appeal in Supreme Court 61
CONTENTS

5NAMAF - 2017 ANNUAL REPORT
7. Annual Financial Statements 76
6. Medical Aid Industry 66 6.1 Demographics 686.2 Healthcare Benefi ts 706.3 Utilisation of Healthcare Services 736.4 Accessibility and Affordability 75
5. The Way Forward 62
CONTENTS

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS6
A� Com A� ordability Committee
FIM Bill Financial Institutions Market Bill
HCPs Healthcare providers
HPCNA Health Professions Councils of Namibia
MAFs Medical Aid Funds
MC Management Committee
MoHSS Ministry of Health and Social Services
MoF Ministry of Finance
MoU Memorandum of Understanding
Namaf Namibian Association of Medical Aid Funds
NAMFISA Namibia Financial Institutions Supervisory Authority
NAMFISA Act Namibia Financial Institutions Supervisory
Authority Act, 2001 (Act No. 3 of 2001)
NMRC Namibia Medicines Regulatory Council
PN Practice number
PNS Practice numbering system
PSEMAS Public Service Employees Medical
Aid Scheme
ACRONYMS

7NAMAF - 2017 ANNUAL REPORT
777777NAMAF - 2017 ANNUAL REPORT

8NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS
8NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS
GENERAL INFORMATION

9NAMAF - 2017 ANNUAL REPORTNAMAF - 2017 ANNUAL REPORT
GENERAL INFORMATION
NAMAF - 2017 ANNUAL REPORT999999

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS10
*value = cost/quality, where quality is a combination of
(1) structure (access); (2) processes; and (3) outcomes.
VISION
MISSION
To be a recognised leader in the provision of a conducive
environment for a sustainable private healthcare funding
industry. To enable the optimum functionality of the Namibian private healthcare industry to maximise value* for benefi ciaries of medical aid funds.
1.1 Vision and Mission

11NAMAF - 2017 ANNUAL REPORT
1.2 Core Mandate
The Namibian Association of Medical Aid Funds (Namaf) is a juristic body, established in terms of the Medical Aid Funds Act, 1995 (Act No. 23 of 1995) (herea� er referred to as the Medical Aid Funds Act). Namaf is responsible for market conduct regulation and supervision. This is done, in part, to protect members of medical aid funds (MAFs) against abuse from both medical aid funds and providers of healthcare services. In terms of the constituting Act, all medical aid funds are obliged to a� liate to Namaf.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS12
The object of Namaf, in terms of section 10(3) of the
Medical Aid Funds Act, is to promote, coordinate,
control and encourage the establishment,
development and functioning of the medical aid funds
in the country. To this end, Namaf issues practice
numbers, which are legally required for any medical
service provider who wishes to claim directly from
medical aid funds. Namaf also publishes procedure
codes and billing guidelines which serve as the
common mode of communication between medical
aid funds and medical service providers when it comes
to the submission of claims and the processing and
assessment of those claims.

13NAMAF - 2017 ANNUAL REPORT
Training and education of both internal and external stakeholders is central to promoting the establishment, functioning and development of medical aid funds in Namibia. Internal education and training of MAFs and healthcare providers (HCPs) creates understanding of rules and regulations, policies and procedures, as well as the roles and responsibilities of the di� erent industry players. This awareness enables compliance, as well as good clinical and corporate governance and optimal functioning in the claims management system and tari� benchmarking process. Engaging and communicating with medical aid members and the general public about the basic functioning of MAFs and Namaf’s role to protect consumer interests encourages the responsible use of medical aid funds’ resources and reduces the risk of fraud, waste and abuse.
Therefore, internal and external training creates stability and sustainability within the industry for the benefi t of all stakeholders.
Namaf acts as a stakeholder coordinator by connecting and facilitating communication between MAFs, HCPs and other key industry stakeholders.
This industrywide stakeholder engagement creates awareness and understanding of the issues facing the industry, allows stakeholders to interact with each other, and to give input into decision-making processes that inform policy, and contributes to an e� ective system.
Through its role as a functional coordinator of the industry, Namaf ensures that there is no overlap or duplication between the roles and functions of di� erent stakeholders. In future, functional coordination will include the management of a central database of claims data and medical cost structures data.
i. Promote: iii. Control:
ii. Coordinate: iv. Encourage:
Setting standards, providing guidelines on industry best practice, and publishing and enforcing regulations is central to e� ectively controlling the industry as a whole and defi ning the environment within which MAFs and HCPs operate.
This framework must complement other legislative instruments within the industry in order to ensure an e� ective overall system. As part of the control function, Namaf is responsible for policy formulation and industry compliance in terms of Section 18 of the Medical Aid Funds Act, which underpins the market conduct regulation identity of Namaf.
Namaf encourages compliance through engaging stakeholders in the process of formulating rules, regulations, policies and procedures. This increases stakeholder buy-in, support and participation and thus ensures a stable industry with a clear sense of direction.
Through its role in the industry, Namaf also plays a vital part in amending national laws and guiding government policies. Although Namaf is not involved in the day-to-day operations or the benefi t structures of MAFs, it encourages optimal and coordinated functioning of MAFs, which includes streamlined and standardised processes and procedures, centralised data analyses, and maintenance of tari� and procedure codes.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS14
1.3.1 Regulatory Bodies
i. Namibia Financial Institutions Supervisory Authority (NAMFISA)
NAMFISA is an independent institution established through the Namibia Financial Institutions Supervisory Authority Act, 2001 (Act No. 3 of 2001) (herea� er referred to as the NAMFISA Act) to regulate and supervise fi nancial institutions, including MAFs, in the fi nancial services industry with the aim of protecting the public. The Authority is the Registrar of non-banking fi nancial institutions and thus all private medical aid funds must be registered with NAMFISA. As the Registrar, NAMFISA can instruct MAFs, which are deemed to be fi nancially unsound, to take steps to rectify the situation, amend its rules, and ultimately to dissolve any MAF that fails to comply.
In terms of the Medical Aid Funds Act, Namaf is responsible for market conduct regulation, while NAMFISA, in addition to being the Registrar
1.3 Key Partners and their Roles

15NAMAF - 2017 ANNUAL REPORT
and fi nancial supervisor, is responsible for the governance structures of MAFs through the approval of rules of the respective funds as formulated by the respective Boards of Trustees. Thus, collaboration between Namaf and NAMFISA is essential for the protection of the consumer and the fi nancial sustainability and stability of the private healthcare funding industry.
ii. Health Professions Councils of Namibia (HPCNA)
The HPCNA is the regulator of health professionals in Namibia. All healthcare
providers must register with the Council in order to practise in the medical fi eld in Namibia. In addition, the Council defi nes and determines the scope of service of HCPs.
The HPCNA is made up of the following fi ve councils, which are administered by one secretariat:
• Medical and Dental Council • Nursing Council • Pharmacy Council• Social Work and Psychology Council• Allied Health Professions Council
The registration of an HCP with the respective council involves a strictly regulated evaluation process to determine the knowledge, skills and competencies of the HCP. Upon registration, the Council issues a practitioner number.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS16
Although Namaf has no jurisdiction over healthcare providers in Namibia, it does issue practice numbers, which are necessary if an HCP’s claims are to be recognised by MAFs. These numbers can only be provided if an HCP has a certifi cate of registration from the HPCNA. As such, the Council is one of the main pillars to help Namaf determine if an HCP is qualifi ed and thus eligible for a practice number.
Consumer complaints about an HCP’s billing or treatment must be directed to the HPCNA. Namaf plays a support role in such instances by helping the Council to better understand the basis of a complaint by evaluating the procedure codes, which clearly defi ne the separate interventions displayed in the disputed bill. This will show whether the billing approach adopted by an HCP follows the billing guidelines published by Namaf.
iii. Namibia Medicines Regulatory Council (NMRC)
The NMRC is a statutory body established in terms of the Medicines and Related Substances Control Act, 2003 (Act No. 13 of 2003) to regulate the use of medicines and scheduled substances in Namibia. The registration of medicines is the focal point of its regulatory framework.
At present, the pharmaceutical industry in Namibia is not regulated. Most of the HCPs in the industry make use of MediKredit SA’s NAPPI (National Pharmaceutical Product Index) codes to identify medicines. However, these codes are not standardised across the country, and most HCPs make changes according to their needs, which leads to a lack of NAPPI code consistency in Namibia.
Since medicines make up a large portion of the total claims paid by MAFs, a need to create a standardised coding structure, which will enable proper regulation of the industry to the benefi t and for the protection of the consumer, has been identifi ed.
Namibia Medicines Regulatory Council

17NAMAF - 2017 ANNUAL REPORT
iv) Namibian Competition Commission (NaCC)
The NaCC was established in terms of the Competition Act, 2003 (Act No. 2 of 2003) to regulate competition issues across all sectors of the Namibian economy. In terms of the Act, the Commission is the principal institution to promote and safeguard fair competition in Namibia by promoting the e� ciency, adaptability and development of the Namibian economy.
The NaCC and Namaf are both regulators mandated to protect the interests of consumers. As such, there is an overlap in functions, which necessitates close collaboration and clearly defi ned roles in order to prevent duplication of e� orts, confl icts or collusion.
1.3.2. Government Ministries
i) Ministry of Health and Social Services (MoHSS)
The Ministry of Health and Social Services is mandated to oversee and regulate public, private, and non-government sectors in the provision of quality health and social services, ensuring equity, accessibility, a� ordability and sustainability.
The Medical Aid Funds Act, created under the auspices of the Minister of Health and Social Services, provides the legal framework within which Namaf and MAFs operate. As needs or circumstances within the industry change, the Minister can amend the Act. Therefore, the Minister is a critical partner determining Namaf’s existence, continuity and sustainability.
As per the Medical Aid Funds Act, Namaf reports to the Minister of Health and Social Services and provides him/her with industry data and information, which informs and infl uences future policy decisions.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS18
ii) Ministry of Finance
The core mandate of the Ministry of Finance includes oversight over fi nancial regulations, public fi nancial institutions and the fi nancial sector.
Since 2016, Namaf has been formally reporting to the Minister of Finance in matters relating to fi nancial aspects of the entity. The change came about when NAMFISA, as Registrar, detected a lack of market conduct regulation at industry level at the time, and thus felt it prudent to engage in market conduct regulation to fi ll the gap created by Namaf inaction, thus making NAMFISA the only regulator. Since NAMFISA reports to the Minister of Finance, the entity succeeded in aligning the line oversight in respect of the Medical Aid Funds Act with the Ministry of Finance.
iii) Ministry of Home A� airs and Immigration
One of the primary objectives of the Ministry of Home A� airs and Immigration is to facilitate lawful migration into and out of Namibia. As part of this role, it is responsible for issuing the necessary visas and permits for foreign healthcare providers wishing to practise in Namibia. Government and private hospitals o� en recruit foreign doctors to fi ll positions in hospitals in rural areas.
To ensure that permits issued by the Ministry of Home A� airs and Immigration do not contradict the provisions and ethical rules of the Health Professions Councils of Namibia, collaboration and coordination between Namaf and the Ministry is essential.
iv) Ministry of Industrialisation, Trade and SME Development The Ministry of Industrialisation, Trade and SME Development is mandated
to develop and manage Namibia’s economic regulatory framework, promote economic growth and development through the formulation and implementation of appropriate policies with the view to attract investment, increase trade, and develop and expand the country’s industrial base.
The Ministry also provides permits to foreign medical professionals who seek to bring in direct investment and create employment for Namibians. In order to ensure that foreign medical professionals satisfy all the requirements of the Health Professions Councils of Namibia, it is essential for the Ministry to consider health-related policies before issuing permits. This is important, because HCPs can only receive a practice number from Namaf once the HPCNA has issued the relevant documentation. Similarly, the Ministry must consider the requirements that a foreign HCP’s practice or surgery must satisfy in terms of the criteria of the Ministry of Health and Social Services.

19NAMAF - 2017 ANNUAL REPORT
Due to the nature and complexity of the healthcare industry and in the interest of protecting the consumer, collaboration and cooperation between several stakeholders is needed in the process of issuing approval for foreign investments in the medical fi eld.
1.3.3 Associations of Health Professionals
Medical professionals under the Medical and Dental Council, the Nursing Council, the Pharmacy Council, the Social Work and Psychology Council and the Allied Health Professions Council form various associations under their councils to serve their respective interests.
Namaf engages theses associations on industry issues that pertain to their scopes of practice as and when necessary. For example, the advancement of medical technology and treatments gives rise to new practices and the need for new procedure codes to capture these practices. In such cases, associations prepare submissions to Namaf, which are subsequently approved or denied by the Namaf Management Committee (MC).
Due to the nature and complexity of the healthcare industry and in the interest of
protecting the consumer, collaboration and cooperation between several stakeholders is needed
in the process of issuing approval for foreign investments in the medical fi eld.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS20
1.4 Medical Aid Funds and their Relationship to Namaf Medical aid funds are Namaf’s principal stakeholders. Their existence is
closely linked to the establishment of Namaf through the Medical Aid Funds Act.
1.4.1 Background and Rationale
In most countries, the responsibilities associated with the provision of healthcare services lie with the government as part of its social contract with the populace. However, the extent and quality of the healthcare provided by the state can vary signifi cantly. In market economies, this creates the opportunity for private sector healthcare professionals to o� er their services and for individual citizens to procure healthcare services in accordance with their fi nancial means.

21NAMAF - 2017 ANNUAL REPORT
The economic or commercial rationale for establishing a Medical Aid Fund is built on the law of averages and statistical probabilities combined with the natural human inclination towards risk aversion. These three forces evidence themselves in the context of human health by the general recognition that while an individual may be healthy at present, there is a risk that he/she may fall into ill health that requires minor treatment or may be the victim of a major health event which requires treatment that may be una� ordable to the individual.
However, when considering a group of persons, the odds are much smaller that all of these said persons will become ill or experience a major health event. This represents a phenomenon called risk pooling, whereby the risk of contracting a potentially impoverishing healthcare event is shared among groups of individuals as opposed to single persons. Through this pooling of the individual health risks across multiple persons, a lower overall risk profi le for the group is achievable. Thus, the concept of an MAF is similar to many other forms of collective or collaborative structures or societies where a greater return is achieved by the collective grouping than could be achieved by all of the members as individuals.
The monthly contributions that members of MAFs make then provide a pool of funds which can be used for the purpose of the MAF, which is to give fi nancial or other assistance for medical costs incurred by members in the event that members or their dependents fall ill or experience a major health event.
1.4.2 The Adoption of Legislation
In Namibia, legislation was adopted in 1995 to formally regulate the type of collective activity dealing with health risks. A medical aid fund is a legal entity established under the Medical Aid Funds Act, which defi nes a fund as “any business carried on under a scheme established with the object of providing fi nancial or other assistance to members of the Fund and their dependents in defraying expenditure incurred by them in connection with rendering of any medical service.”
Viewed as a whole, the Medical Aid Funds Act is in essence a protective social legislation, requiring registration of funds with the Registrar, who is the Chief Executive O� cer of NAMFISA. Namaf is the market conduct regulator and
The economic or commercial rationale for establishing a Medical Aid Fund is built on the law of averages
and statistical probabilities combined with the natural human inclination towards risk aversion.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS22
supervises and controls the operations of MAFs. For the purpose of achieving its objective, Section 12 of the Medical Aid Funds Act empowers Namaf to “consider any matter a� ecting medical aid funds or the members of such funds and make representations or take such actions in connection therewith as the Association may deem advisable and that Namaf may generally do anything that is conducive to the achievement of its object and the exercise of its powers, whether or not it relates to any matter expressly mentioned in this section.”
It is out of these considerations that Namaf enhanced the processes through which the practice numbers, which are legally required, are issued to healthcare providers as a means of identifying providers and enabling Namaf and its a� liated funds to better manage their claims. In addition, Namaf publishes procedure codes and billing rules and guidelines, which, if correctly interpreted, inform benchmark tari� s.
1.4.3 Medical Aid Funds A� liated to Namaf
In terms of Section 11 of the Medical Aid Funds Act, all private MAFs must be a� liated to Namaf, which supervises and controls the operations of MAFs.
i) Renaissance Health ii) Napotel iii) Nammed iv) Road Contractors Company (RCC) Medical Aid Scheme v) Namibia Health Plan (NHP) vi) Namibia Medical Care (NMC) vii) BankMed Namibia viii) Heritage Health Namibia ix) Namdeb Medical Scheme

23NAMAF - 2017 ANNUAL REPORT

24NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS
24NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS
LEADERSHIP ANDCORPORATE GOVERNANCE

25NAMAF - 2017 ANNUAL REPORTNAMAF - 2017 ANNUAL REPORT
LEADERSHIP ANDCORPORATE GOVERNANCE
NAMAF - 2017 ANNUAL REPORT252525252525

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS26
2.1 Management Commitee
In terms of Section 13(1) of the Medical Aid Funds Act, the management of
Namaf vests in the Management Committee (MC), which is expected
to execute Namaf’s mandate. The MC is also mandated to appoint the
CEO and sta� members of the Namaf secretariat.
Benny AmuenjeChairperson
Lea Namoloh Vice-Chairperson
Gabriel Tjombe Treasurer
Pieter Theron Co-opted Member
Ella Mbahijona Member

27NAMAF - 2017 ANNUAL REPORT
The MC is elected by the authorised
representatives nominated by all the
registered medical aid funds. MAFs with
more than 2,000 members nominate
a maximum of two people for election,
while MAFs with less than 2,000
members nominate one authorised
representative.
These representatives elect from
among themselves seven (7) members
to constitute the Management
Committee of Namaf. In keeping with
the provision of Section 11 of the Medical
Aid Funds Act that the Association will
consist of registered funds in Namibia,
the Management Committee resolved
to co-opt authorised representatives
from the a� liated funds that did not
manage to secure a place through the
electoral process, as non-voting MC
members.
Glynis Labuschagne Member
Dolly Nashandi Member
Desley SomsebMember
Alison Begley Co-opted Member
Ella Mbahijona Member
Stephen TjiuoroCEO (Ex-O� cio)

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS28
2.1.1 Management Committee Membership
The members of the MC hold o� ce for three years, where a� er they are eligible for re-election. During June of the reporting period, a new Management Committee was elected.
2014 – 11 June 2017
Benny Amuenje – Chairperson Alison Begley – Vice-Chairperson Gabriel Tjombe – Treasurer Glynis Labuschagne – Member Dolly Nashandi – Member Gert Grobler – Member
(contract ended 12 June 2017) Suzie Chamberlain – Member
(contract ended 12 June 2017) Lea Namoloh – Co-opted Member Ella Mbahijona – Co-opted Member Desley Somseb – Co-opted Member Anton Rostee – Co-opted Member
From 12 June 2017 to present
Benny Amuenje – Chairperson Lea Namoloh – Vice-Chairperson Gabriel Tjombe – Treasurer Glynis Labuschagne – Member Dolly Nashandi – Member Ella Mbahijona – Member Desley Somseb – Member Alison Begley – Co-opted Member Pieter Theron – Co-opted Member Anton Rostee – Co-opted Member (resigned 29 June 2017) Asser Uiseb – Co-opted Member
(resigned 8 October 2017) 2.1.2 Meetings
According to the Medical Aid Funds Act, the MC must meet at least four times per year with intervals of no more than 3 months in between. The MC exceeded this requirement, holding fi ve (5) ordinary and four (4) extra ordinary meetings during the period under review.
1.4.1 Background and Rationale
1.3.2. Government Ministries

29NAMAF - 2017 ANNUAL REPORT
1.4.1 Background and Rationale
1.3.2. Government Ministries
2.1.3 Sub-Committees of the Management Committee
i) A� ordability Committee
The A� ordability Committee (A� Com) is an advisory committee to the MC o� ering guidance on a� ordability issues (e.g. recommendations about adjustments to benchmark tari� s) and clinical issues (e.g. modifi cation, deletion and/or introduction of new procedure codes). The A� Com does not have decision-making powers. It is comprised of representatives of the MAF administrators and one MC member, who acts as the chairperson of the A� Com. Each Namaf-a� liated MAF nominates one representative to the A� Com.
During the reporting period, the A� Com membership changed.
1 January – 30 June 2017
Gert Grobler – Chairperson Alison Begley – Member Callie Schafer – Member (joined May 2017) Sonja Malan – Member Gertrud Baisako – Member Ella Mbahijona – Member Mike Baartman – Member Karl Weyhe – Member Roni Skolnic – Member Joern Wiedow – Member Beth Clayton – Member Elize Fahl – Member Celeen Jacobs – Member (resigned April 2017)
1 July – 31 December 2017
Alison Begley – Chairperson Gert Grobler – Member Callie Schafer – Member Sonja Malan – Member Gertrud Baisako – Member Ella Mbahijona – Member Mike Baartman – Member Karl Weyhe – Member Roni Skolnic – Member Joern Wiedow – Member Beth Clayton – Member Elize Fahl – Member
The A� Com held fi ve (5) meetings during the year under review.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS30
ii) Statutory and Legal Committee
The Statutory and Legal Committee was established during the period of uncertainty resulting from the NaCC court case and the publication of the FIM Bill. The committee was tasked with devising responsive strategies to determine the existence of Namaf in the event that the FIM Bill, which was set to repeal the Medical Aid Funds Act, had been passed and the courts had ruled in favour of the NaCC.
In 2017, the Statutory and Legal Committee comprised of Alison Begley (Chairperson), Callie Schafer, Sonja Malan, Roni Skolnic and Joern Wiedow. It held two (2) meetings during the reporting period.
2.1.4 Stakeholder Forums
In the second quarter of 2013, three stakeholder forums were established with the aim of improving communication and strengthening the relationship between Namaf and its key stakeholders. The forums have no decision-making powers. Issues discussed at the forums are brought to the A� Com, which can make recommendations to the MC based on forum discussions, if deemed necessary.
i) Medical Aid Fund Administrators Forum
The Medical Aid Fund Administrators Forum is a stakeholder engagement forum established to discuss industry-wide issues of an administrative nature. Representatives from each of the medical scheme administrators in Namibia and Namaf secretariat representatives attend the forum. During the reporting period, the Medical Aid Fund Administrators Forum met three (3) times.
ii) Private Hospital Forum
The Private Hospital Forum was established as a joint forum for the medical aid funds industry and private hospitals to discuss issues of mutual concern. It is not a negotiation forum and thus does not discuss matters relating to tari� s or fees. Representatives of the MAFs, the private hospital industry and Namaf attend the forum. During the reporting period, the Private Hospital Forum met three (3) times.

31NAMAF - 2017 ANNUAL REPORT
iii) Peer Review Forum
The Peer Review Forum provides the medical funding industry and private medical practitioners a platform to discuss issues of mutual concern. It can make recommendations on amendments to Namaf rules and guidelines, but since it is not a negotiation forum, matters relating to tari� s or fees are not within its purview. The forum consists of representatives of private MAFs, private medical practitioners in good standing with Namaf, and members of the Namaf secretariat. During the reporting period, the Peer Review Forum met three (3) times.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS32
Justina NeluluStephen Tjiuoro Maggie da Silva Mota
2.2 Secretariat

33NAMAF - 2017 ANNUAL REPORT
Ramona Mathupi Tina Riruako
PNS ADMINISTRATIONOFFICER OFFICE ASSISTANT
PERSONAL ASSISTANT TO THE CEOPERSONAL ASSISTANT TO THE CEO
PNS ADMINISTRATIONOFFICER OFFICE ASSISTANT
NAMAFCHIEF EXECUTIVE OFFICER
Stephen Tjiuoro
Rehetta Isaak ACCOUNTANTJustina Nelulu
FORENSIC & FINANCIALANALYST
FORENSIC & FINANCIALANALYST
HEAD: BENEFIT AND RISKMaggie da Silva Mota
Charlene du Preez Ramona Mathupi Tina Riruako
Charlene Du Preez
Rehetta Isaak
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS34
CHAIRPERSON’S REPORT
On behalf of the Management Committee, it is indeed a great pleasure to
present the Annual Report of the Namibian Association of Medical Aid Funds for the
period 1 January 2017 to 31 December 2017. Namaf’s
fi rst-ever annual report is a considerable milestone
and o� ers a concise account of the Association’s
performance, governance and outlook, as well as an
overview of the medical aid industry in 2017.
The reporting period saw a number of signifi cant developments in terms of leadership, management and strategy. Naturally, the year was not without its challenges, foremost among them the uncertainty created by the proposed Financial Institutions Market Bill and the legal battle between the Namibian Competition Commission and Namaf.
I am pleased to say that we weathered the storm and that thanks to the unwavering commitment of the MC and the secretariat, we are better poised than ever to carry out our mandate as per the Medical Aid Funds Act, 1995 (Act No. 23 of 1995) to promote, coordinate, control and encourage the establishment, development and functioning of medical aid funds in Namibia.
Leadership and Corporate Governance
During the Annual General Meeting in June 2017, the representatives of all nine medical aid funds a� liated to Namaf elected a new Management Committee (MC).
As per Section 13 of the Medical Aid Funds Act, the Boards of Trustees of MAFs with more than 2,000 members nominated two authorised representatives, while MAFs with fewer than 2,000 members nominated one authorised representative. These representatives constituted the electoral college and elected from among themselves seven members to constitute the Management Committee of Namaf. In keeping with the provision of Section 11 that the Association must consist of registered funds in Namibia, the Management Committee resolved to co-opt authorised representatives from the a� liated funds, which did not manage to secure a place through the electoral process, as non-voting MC members.
To prepare MC members for the tasks ahead, they participated in an orientation facilitated by an external consultant. The orientation, a fi rst in Namaf’s history, proved invaluable in creating clarity on Namaf’s governance structure and a deeper understanding of the Association’s pivotal role within the industry.

35NAMAF - 2017 ANNUAL REPORT
I want to thank the outgoing MC members for the strategic insight and valuable experience they brought to the MC during their tenure.
During the reporting period, the MC appointed Stephen Tjiuoro as CEO. Upon taking up o� ce on 1 April 2017, he was presented with a combination of pertinent operational as well as strategic issues, chief among which was the absence of a strategic plan to guide Namaf’s operations and a� airs. He has since demonstrated a clear ability to identify the challenges that Namaf faces and to lead the necessary responses.
Key Highlights
One of my major concerns has long been that Namaf has been operating without a strategic plan since its inception in 1997. Unfortunately, the strategic plan intended for the period of 2012 to 2016 was never implemented. Therefore, one of the key objectives for 2017 was the development of a strategic plan.
In order to guide the formulation of a clear strategy, we tasked Fisher Consulting to conduct a climate survey in order to assess stakeholder perceptions. The results of the survey were presented to the MC in September 2017 and gave meaningful insights into the perceptions and expectations that key stakeholders have of Namaf.
The survey also made it clear that there was a need to intensify engagement with our key stakeholders in order to clarify Namaf’s crucial role within the industry. Thus the CEO was tasked with devising a stakeholder engagement strategy. The strategy was successfully implemented and led to productive engagements, which will undoubtedly enhance collaboration and communication within the industry going forward.
The fi ndings of the climate survey formed the foundation for our strategic objectives and culminated in the development of the Strategic Plan 2018 – 2020. For the fi rst time in the history of the Association, we have a yardstick that charts the way into the future and measures how we conduct business. I am confi dent that the Strategic Plan will enable us to steer the ship in the right direction and am looking forward to the fundamental changes it will introduce upon implementation in 2018.
Namaf v NaCC
A key triumph during the reporting period was the outcome of the appeal in the Supreme Court in the case Namaf v NaCC. The Supreme Court ruled in favour of Namaf, stating that the NaCC does not have jurisdiction over the Association and that the setting of benchmark tari� s by Namaf does not constitute anti-competitive behaviour. The ruling rea� rmed the identity of Namaf and its role as market conduct regulator in the private medical aid industry, allowing Namaf to take charge of and protect the interests of the members of medical aid funds. It was a seminal and landmark judgment, distinguishing the Namibian judicial landscape from the regional powerhouse, South Africa, and defi ning how the competition law is applied in Namibia.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS36
Challenges
Amidst the failure of Namaf to fully exercise its market conduct regulation role in 2016, NAMFISA, as Registrar, changed Namaf’s reporting line from the Ministry of Health and Social Services to the Ministry of Finance. This was problematic, since Namaf regulates the conduct of medical aid funds, which relates to health and not fi nance, and created role confusion between NAMFISA as Registrar and fi nancial regulator and Namaf as market conduct regulator. During the reporting period, we began engaging our political principles in order to restore Namaf’s reporting line to the Ministry of Health and Social Services. In addition, the possibility of closer collaboration between the entities was discussed, and a Memorandum of Understanding was dra� ed to begin the demarcation process between NAMFISA and Namaf.
Into the Future
Under the guidance of the MC, the implementation of the Strategic Plan in 2018 will undoubtedly start the year on a positive note. Activities will centre around meeting stakeholder expectations across several key areas; enabling processes within Namaf through data collection, cleansing, analysis and interpretation; optimising the utilisation of human, physical and digital resources; and improving fi nancial sustainability by optimising income, e� ciently using resources, and developing a contingency reserve and robust corporate governance.
In order to enhance the speed and depth of strategy implementation, an annual plan will be devised for 2018. It will guide Namaf’s operations for the year and enable us to measure performance and progress. In addition, ongoing information sharing and feedback from the secretariat on achievements and challenges will be vital to the successful implementation of the strategy. Our CEO and his sta� are ready to tackle the tasks and challenges ahead with vigour and determination.
During the MC orientation, it became clear that the chairmanship of sub-committees must lie with an MC representative in order to ensure an e� cient reporting and recommendation process to the MC. Therefore, the decision was taken to restructure the governance of sub-committees, giving impetus to two new sub-committees to be established in 2018, namely the Clinical Coding Committee and the Statutory and Forensic Committee, and to restructuring the membership and responsibilities of the A� ordability Committee.

37NAMAF - 2017 ANNUAL REPORT
Appreciation
I would like to sincerely thank Honourable Dr. Bernard Haufi ku, Minister of Health and Social Services, and Honourable Calle Schlettwein, Minister of Finance, for their unwavering support and for shaping the legislative environment that enabled Namaf to make great strides in 2017.
My gratitude also goes to our CEO and his team for their dedication in continuing to shape Namaf into a major industry player. We look forward to ongoing cooperation and collaboration as they assist Namaf to deliver e� ectively on its mandate.
In closing, I wish to thank my fellow Management Committee members for their commitment and expertise in delivering on their fi duciary responsibilities and ensuring good governance. I am confi dent that they will continue to navigate Namaf into an increasingly bright future.
Benny Amuenje Chairperson of the Namaf Management Committee

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS38
CEO’S REPORTAs the executive leader of the Namibian Association
of Medical Aid Funds, allow me to begin by expressing
my gratitude to the Management Committee,
the Chairman, my team in the secretariat and our
stakeholders, especially the Ministry of Health
and Social Services, the Ministry of Home A� airs
and Immigration, the CEO of the Health Professions
Councils of Namibia, the CEO of NAMFISA and his sta� ,
the legal team at ENSafrica law fi rm, and our a� liated
medical aid funds, as well as their Principal O� cers and
Administrators.
Their phenomenal support and commitment during the 2017 fi nancial year enabled Namaf to overcome numerous challenges and to achieve several key strategic and operational milestones. It was truly a year characterised by cooperation and collaborative success.
In my report, I will present an overview of the context within which Namaf operated for several years, followed by an outline of the Association’s operations and fi nances during the reporting period.
Background: An Environment of Challenges
For years, Namaf operated within an environment characterised by a lack of understanding of the Association’s role within the private health insurance industry. The prevalent perception was that Namaf served merely as a lobby group without any legal powers. Naturally, this had a signifi cant impact on the Association’s operations and performance, as well as its ability to deliver on its mandate.
This perception stood in stark contrast to Namaf’s actual role, as described in the Medical Aid Funds Act, as a regulator with the legal power to control, promote, encourage and co-ordinate the establishment, development and functioning of all medical aid funds in Namibia. Within these main functions, Namaf acts as:
• Coordinator of the development and maintenance of clinical coding structures
• Manager of compliance to legal requirements applicable to healthcare providers dealing directly with medical aid funds by managing the registration and maintenance of the practice numbering system
• Provider of guidance on clinical and fi nancial risk management principles
• Infl uencer of healthcare policy developments

39NAMAF - 2017 ANNUAL REPORT
These functions and roles are carried out with the ultimate objective of ensuring access, a� ordability and sustainability within the private medical aid industry.
When I took up o� ce in April 2017, the Namaf secretariat was understa� ed and doing its utmost to regulate a market worth N$3.5 billion on a budget of N$10 million, which is about 0.28% of industry turnover. A rudimentary assessment of the operational environment showed a lack of coherent and well-established business processes.
The o� ce was unable to run e� ciently for several reasons, including the absence of an operational strategy, the lack of a meaningful compliance framework due to the minimal number of internal policies, a shortage of proper regulations necessary for overseeing the industry, the nonexistence of guidelines for the registration of practice numbers (PN), and misuse of the practice numbering system by service providers. In addition, the ongoing legal confl ict between Namaf and the Namibian Competition Commission created considerable uncertainty in terms of Namaf’s future as a regulator within the country.
Far from being deterred, the o� ce of the CEO resolved to tackle these challenges head on.
Addressing the challenges
One of my fi rst undertakings was to compile a short-term strategy outlining the most pertinent strategic and operational issues facing Namaf and the interventions to address them. The o� ce of the CEO committed to undertaking the following activities during the three-month period leading up to August 2017:
• Cleaning up the practice numbering system and fi les of healthcare providers registered with Namaf;
• Developing the rules contemplated in Section 18(1) of the Medical Aid Funds Act specifying the acts and omissions in respect of which the Management
Affordability
Access
Control
Encourage
Promote
Coordinate
Development
Establishment
Functioning Sustainability
Affordability
Function Goals ObjectivesFunction Goals Objectives

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS40
Committee (MC) may take disciplinary steps against any registered fund;• Arranging and facilitating a targeted trustee and MC member training
session as a precursor to the review of the Namaf strategy• Reviewing and activating the strategy, which was originally developed
in 2010/2011 but never rolled out, and incorporating new dynamics in the objectives previously identifi ed; and
• Carrying out the planned activities geared towards stakeholder management, including the Namaf Annual Conference, and consultations with the HPCN, MoHSS, MoF, NaCC, Ministry of Industrialisation, Trade and SME Development, Ministry of Home A� airs and Immigration, BIPA (registrar of companies) and NAMFISA.
I am pleased to say that thanks to the hard work of the secretariat, the unwavering support of the Chairman and MC, and the cooperation of key stakeholders, we were able to achieve all of these objectives. Looking back at the circumstances under which Namaf was functioning early in 2017, it is truly remarkable that we accomplished what we did during the reporting period.

41NAMAF - 2017 ANNUAL REPORT
Review of Operations
Renewal and registration of practice numbers
In order for Namaf to fulfi l its mandate of creating order and structure in the private health insurance industry, it deploys the provision of Section 5(1) of the regulations made in terms of the Medical Aid Funds Act, which requires any medical service provider who wishes to claim directly from medical aid funds to obtain a practice number from Namaf. In essence, these numbers are a tool for mitigating the risk of fraud, misuse and waste. However, despite their importance, the PNs and the information they contain are not widely understood in the industry.
Administering the practice number system is part of the core business of Namaf. In January of every year, mandatory PN renewals and registration of new service providers takes place. However, when I assumed o� ce in April 2017, the PN renewal and registration process had not begun. In addition, the fi les of many of the registered service providers were found to be incomplete, yet the absence of clear guidelines and standards made the task of cleaning up the practice numbering system di� cult.
Thus, a high operational priority was the development of guidelines for the PN registration and renewal process. These would defi ne the minimum requirements to be met before issuance of a practice number and enable Namaf to ensure compliance with set standards.
The decision was taken to allow service providers to renew and register in 2017 as they had in previous years, while Namaf was in the process of developing the necessary guidelines. Upon completion, the guidelines were immediately communicated to service providers, e� ectively enabling them to update their fi les long before the renewal process in January 2018. The guidelines brought major changes, meaning that most service providers had to adjust the internal systems they had in place.
In order for the PN registration and renewal guidelines to take legal e� ect in 2018, they will have to be converted into regulations through the formal government gazetting process. However, we already saw overwhelming compliance in 2017, although the guidelines had not yet become law.
This came as a result of PSEMAS, the State owned and operated medical benefi t scheme for public servants, adopting Namaf’s guidelines and requiring all their contracted service providers to comply during their 2017 renewal and registration process.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS42
Stakeholder engagement
In order to assess the needs, perceptions and expectations of key stakeholders in the private health insurance industry and to understand the value they add to Namaf business, we contracted Fisher Consulting to conduct a climate survey during the reporting period. The goal of this industry analysis was to gather insights that would guide the envisaged strategy formulation process. Among other things, the survey results published in September 2017 identifi ed the key partnerships required for Namaf to successfully carry out its mandate, as well as a general lack of understanding of Namaf’s role among those stakeholders.
In response to these fi ndings, a robust stakeholder engagement strategy was deployed. One of the initiatives under this strategy was a two-day workshop with the HPCN, NAMFISA, the Ministry of Health and Social Services, the Ministry of Finance, the Namibian Competition Commission, the Ministry of Industrialisation, Trade and SME Development, and the Ministry of Home A� airs and Immigration. Initial deliberations centred around each entity’s current activities in relation to medical service providers and how each entity’s actions and decisions impact the other role players. The second day of the workshop focused on enhancing participants’ understanding of Namaf’s governance structure and mandate.
The workshop was a valuable networking exercise, laying the foundation for enhanced communication and collaboration, and creating appreciation for each participating stakeholder’s valuable contribution to the overall healthy functioning of the industry.

43NAMAF - 2017 ANNUAL REPORT
Towards strategy development
In order for any organisation to function e� ectively, it requires a strategic plan that provides a sense of direction and outlines measurable goals. Strategic planning is a useful tool for guiding day-to-day decisions, evaluating progress and changing approaches when moving forward.
It follows that the absence of a strategic plan has prevented Namaf from functioning and operating optimally since its establishment in 1997. Thus, a primary task before the o� ce of the CEO during the reporting period was the development of a strategic plan.
As a precursor to the envisaged strategic planning, it was necessary for MC members to become empowered and develop a clear understanding of Namaf’s governance structure and reporting lines, as well as the basic tenets of their responsibilities as MC members and representatives of medical aid funds, including their fi duciary and fi nancial oversight responsibilities and legal obligations. Thus, a training session for trustees and MC members took place before undertaking strategic planning sessions.
The increased awareness and understanding resulting from the training session, together with the fi ndings of the climate survey, laid a vital foundation for e� ective strategic planning. The strategy development process, which took place from 4 to 6 October 2017, was facilitated by an expert consultant and attended by selected industry stakeholders, MC members, executive management and key sta� .
The process was informed by the Business Model Canvas developed by Alex Osterwalder and Yves Pigneur, and included an industry analysis and SWOT analysis. The fi ndings of the climate survey were also used as an input to the strategy review and development process.
The resultant Strategic Plan for 2018 – 2020 is a transformation strategy. It outlines Namaf’s strategic framework, together with its accompanying strategic goals, a business plan, and specifi c strategic initiatives and targets, and describes the infrastructure that needs to be put in place in order for Namaf to fully execute its mandate as per the Medical Aid Funds Act. This infrastructure includes e� ective business processes, advanced computer systems and qualifi ed human resources.
Human resources
During the reporting period, two key positions were fi lled in order to start building the secretariat’s ability to e� ectively carry out operations and fulfi ll Namaf’s mandate. Maggie da Silva Mota was appointed as the Head of Benefi t and Risk Management in June. This is an executive management position responsible for the management and control of all operational functions with regards to issuing of practice numbers, publishing of benchmark tari� s and ensuring the availability of relevant and e� ective procedure codes.
Responsibilities also include complete customer care, resolving escalated customer queries and analysing and identifying risk mitigating interventions to ensure clinical health governance in order to support Namaf in its core mandate and facilitate the

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS44
In order for Namaf to e� ectively respond to the legal mandate as
stipulated in the Medical Aid Funds Act, it is essential to have a clear
governance structure and reporting lines. These form the bedrock upon
which risk management and a compliance framework are built.
prevention of fraud, waste and abuse in order to contribute to a sustainable medical aid fund industry in Namibia.
In July, Charlene Du Preez was recruited as Forensic and Financial Analyst. One of the primary functions of the position is the identifi cation of service providers guilty of fraudulent practices through the analysis and investigation of their claims.
Clarifi cation of the roles of Namaf and NAMFISA
In order for Namaf to e� ectively respond to the legal mandate as stipulated in the Medical Aid Funds Act, it is essential to have a clear governance structure and reporting lines. These form the bedrock upon which risk management and a compliance framework are built.
As per the Medical Aid Funds Act, Namaf is the market conduct regulator of medical aid funds in Namibia and NAMFISA is the fi nancial supervisor and Registrar. There is a lack of clarity in terms of the roles and responsibilities of each entity, and an overlap of their legal mandates, compounded by the change of the reporting line from the Ministry of Health and Social Services to the Ministry of Finance in 2016. This situation needed to be urgently addressed to enable Namaf to start developing the rules specifying the acts or omissions in respect of which management may take disciplinary steps against any registered medical aid fund, as envisaged in Section 18 of the Medical Aid Funds Act.
In order to gain role clarity and initiate the demarcation process, a delegation from Namaf and NAMFISA undertook a visit to the Council of Medical Schemes in South Africa, which houses the functions of market conduct regulation as well as fi nancial supervision. Valuable lessons were drawn from the exercise, which led to the formulation of a dra� Memorandum of Understanding by December of the reporting period. Although not a legally binding document, I am confi dent that the MoU will bring about improved collaboration between Namaf and NAMFISA and pave the way for the development of legislation that clearly defi nes the regulatory roles of each entity.
45NAMAF - 2017 ANNUAL REPORT
Performance Review
Income
Namaf’s income is mainly derived from the a� liation fees paid by medical aid funds and from the registration and renewal of practice numbers. The two components make up 92% of the Association’s total income. During the reporting period, the total income increased by 17%. This increase is primarily attributed to the annual infl ationary adjustment of 6.85%, the recorded growth in principal membership of 5%, and an increase of 119% in respect of new practice number registrations.
Expenses
The year’s operating expenses increased by 17% in comparison to the previous year. This is attributable to:
• Conference expenses: There was an increase of N$105,720 in conference expenses during the year under review, which is 147% more than during the previous year. This was brought about by an increase in the number of trips taken in 2017 compared to the previous year. Trips included attendance of conferences held by the Board of Healthcare Funders of South Africa and the Association of Healthcare Funders of Zimbabwe, as well the visit to the Council of Medical Schemes in South Africa by four MC members and two sta� members.
• Consulting fees: An increase of 91% (amounting to N$174,405) in this expense line was brought about by the fees paid to the facilitators of the climate survey and the strategy development.
• Meeting fees: A 37.5% increase (amounting to N$135,267) in meeting fees was brought about by the fees paid to the MC members for attending the three-day Namaf strategic development session, as well as the two-day meeting with the Council of Medical Schemes in South Africa.
Financial information at a glance
5% Principal membership
growth
17%Income
119% New practice number
registrations
17% Expenses
303%
Defi cit
2.3% Total
assests
17%
Investments
146% Current
liabilitites
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS46
• Rental cost: In May 2017, Namaf relocated to new o� ce premises, which lead to an increase of 56% (amounting to N$197,189) in rental cost. Previously, the monthly rental cost stood at N$28,973, whereas the rent for the new o� ce is N$50,000 per month.
• Security expense: In December 2016, Namaf contracted 24-hour security services, leading to an additional expense of N$164,404 over the duration of the reporting year.
• Salaries & wages: There was a reduction of 16.5% (amounting to N$658,090) in terms of salary expenses in comparison to 2016, when the former CEO’s termination pay-out was made.
Overall defi cit
Namaf recorded a defi cit of N$202,934 in the year under review, which is an increase of 303.5% compared to the previous year’s defi cit. Namaf’s annual budget for 2017 provided for an expected surplus of N$49,917. However, due to operational and strategic exigencies, Namaf under the new management incurred expenses totalling N$691,000, which were not included in the initial budget. Approval in respect of these expenses was sought from and granted by the MC.
Investments
Namaf’s investment decreased by N$550,895 in the year under review. The decrease is ascribed to the withdrawals made to fi nance the extra expenditures.
Total assets
The increase of 2.4% in total assets is ascribed to the acquisition of boardroom furniture, four additional o� ce laptops and an amount of N$280,880 (included under Trade & Other Receivables) owed by the Namibian Competition Commission (NaCC) in respect of the legal proceedings between Namaf and the NaCC.
Current liabilities
The increase of 146% in the current liabilities is ascribed to the prepaid income of N$164,489 for the registration of practice numbers, which were yet to be registered as at 31 December 2017. It is also ascribed to unpaid creditors invoices amounting to N$192,629.
Outlook for 2018
The implementation of the Strategic Plan in 2018 assures me of a positive outlook going forward. The strategic framework built around meeting stakeholder expectations, enabling processes, optimal resource utilisation and prudent fi nancial management will lend impetus, structure and focus to the activities of the o� ce of the CEO during the next reporting period and beyond.

47NAMAF - 2017 ANNUAL REPORT
In order to meet these objectives, we will invest in human capital. The provision for the formulation of rules made in Section 18 of the Medical Aid Funds Act has been identifi ed as one of the key tools for regulating the conduct of medical aid funds. Yet we cannot aspire to publish regulations without the necessary human resource capacity. Therefore, we will recruit a legal expert to steer legislative and policy issues. In addition, as understanding of Namaf’s role among industry stakeholders is vital for e� ective functioning, key marketing sta� will be recruited to devise a marketing strategy and build on the awareness creation and training e� orts undertaken in 2017.
Another key highlight will be the full automation of the PN registration and renewal process. Not only will this greatly simplify and streamline registration and renewal for service providers and Namaf alike, but will also allow the secretariat to focus on the essential function of risk mitigation and investigation of potential cases of fraud, waste and abuse, instead of the cumbersome administration of a paper-based management, fi ling and record system.
In order for the PN guidelines to take legal e� ect, they will be submitted to the Minister of Health and Social Services for approval and subsequent publishing in the Gazette, as required by the Medical Aid Funds Act. This will mark an important milestone enabling Namaf to exercise its regulatory and disciplinary responsibilities over the business of medical aid funds.
In conclusion, good health matters greatly at both the individual and organisational level of existence. Therefore, going forward we commit to promoting a healthy medical aid industry that adheres to good governance and sound fi nancial management, and o� ers value to its benefi ciaries in terms of access to quality healthcare services.
We look forward to the continued and unmatched support of the Chairman, the entire Management Committee and our stakeholders, and face 2018 armed with the commitment to achieve our strategic goals and objectives.
Stephen TjiuoroChief Executive O� cer of the Namibian Association of Medical Aid Funds
Going forward we commit to promoting a healthy medical aid industry that adheres to good
governance and sound fi nancial management, and o� ers value to its benefi ciaries in terms of access to
quality healthcare services.

4848
OPERATIONS

49NAMAF - 2017 ANNUAL REPORTNAMAF - 2017 ANNUAL REPORT
494949494949
OPERATIONS

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSNAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS
3.1 Registration and Renewal of Practice Numbers
Practice numbers are a means of identifying healthcare providers and are linked to a scope of practice, which in turn links to procedure codes specifi c to the scope. Essentially, this information defi nes the procedures that an HCP performs and is allowed to bill patients for. Thus, the practice numbers, which are a requirement for claiming from MAFs, enable Namaf and its a� liated funds to manage claims. The claims data received from MAFs allows Namaf to identify irregularities and link these to the HCPs through the practice number. As such, practice numbers are part of the risk mitigating process aimed at consumer protection.
During the reporting period, Namaf issued 474 new registrations, renewed 1,598 practice numbers, and revoked or suspended 69 practice numbers. In addition, 35 practice numbers were deactivated on request of healthcare practitioners. Since the administration of practice numbers is a manual process, and thus very time-consuming, it dominated the work of the Namaf secretariat during 2017. The absence of a proper fi ling system made the process even more cumbersome. Thus, four temporary sta� were recruited to expedite the process.
It is a legal requirement under Section 5 of the regulations made under the Medical Aid Funds Act that practice numbers must be issued in compliance with the regulations and criteria as stipulated by Namaf. Due to the current absence of such regulations and criteria, the practice number registration process is not yet streamlined or standardised. A signifi cant milestone during the reporting period was the adoption of dra� guidelines to inform the procedures that HCPs must follow during practice number registration and renewal. Although the new procedures were not used during the 2017 registration, they were already distributed to HCPs during the reporting period in preparation for the next PN registration in January 2018.
Plans to fully automate the registration and renewal process within the next reporting period are underway. This will enable HCPs to register, renew and pay fees online, thereby making the process much faster and easier for HCPs, as well as the Namaf secretariat.
Namaf is responsible for
issuing practice numbers (PNs)
to healthcare providers. This
includes new registrations as
well as annual renewals of
practice numbers.
50NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS

51NAMAF - 2017 ANNUAL REPORT
Namaf’s coding structure consists of practice numbers, a descriptor of the intervention or treatment to be provided, a relative value expressed in units which is, among others, a measure of the skill level and complexities inherent in the execution of such an intervention, and the conversion factor, which if multiplied by the units under relative values, will provide the benchmark tari� for a particular procedure. Figure 1 provides a summary of the coding structure.
Therefore, the procedure codes contain the intelligence needed for the processing of claims by MAFs and for identifying possible instances of fraud, waste and abuse. As new treatment procedures are developed, or new technology is deployed in the medical industry, Namaf adds to or amends the coding structure to accommodate these developments.
The procedure codes and billing guidelines published by Namaf inform benchmark tari� s.
Figure 1: Coding structure components
ClinicalEvidence
ResponsibilityValue
ProffesionalResponsibility
PracticeCosts
Scope ofPractice
Time
Code Terminology Relative ValueConversion
Factor
Costing
X -
CodingStructure
ReferencePrice
3.2 Coding Structure

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS52
3.2.1 Procedure Codes
Procedure codes translate medical treatments and procedures into numbers. In Namibia, the internationally accepted CPT® (Current Procedural Terminology) code structure, originally developed by the American Medical Association (AMA), is referenced during the development and maintenance processes that apply to the procedure coding systems used by Namaf. CPT® codes are numbers assigned to every task and service a medical practitioner may provide to a patient including medical, surgical and diagnostic services.
Associated with the CPT® code structure is the ICD-10 coding structure (International Classifi cation of Diseases and Related Health Problems, 10th revision), developed by the World Health Organization (WHO). It translates the written description of medical and health information into standard codes, e.g. J03.9 is an ICD-10 code for acute tonsillitis (unspecifi ed), and G40.9 denotes epilepsy (unspecifi ed). The ICD-10 code structure is a framework to facilitate and organise the communication of a diagnosis of a patient’s condition. Namibia is yet to implement the ICD coding structure.
These two coding structures are fundamental to the design of MAF benefi ts, because they provide a framework within which to describe health events and the associated treatment.
It is important to note that procedure codes represent compulsory industry standards, meaning that all HCPs are legally required to make use of them when interacting with medical aid funds. These codes can be described as a ‘common language’ that is applied by all parties in order to ensure common understanding.
3.2.2 Billing Guidelines
Namaf is responsible for publishing billing guidelines. The billing guidelines are linked to the procedure codes, as they place a value or cost on the treatments of the health events enshrined in the procedure codes. The billing guidelines assign a relative value to these medical procedures, based on factors like the skill needed to perform the procedure and the complexity of the procedure. This value is expressed in units, which are used to calculate the benchmark tari� s.
Similar to the procedure codes, the billing guidelines represent mandatory industry standards that HCPs must adhere to when interacting with medical aid funds. Like the procedure codes, the billing guidelines form the basis for common understanding within the industry.

53NAMAF - 2017 ANNUAL REPORT
3.2.3 Benchmark Tari� s
On an annual basis, Namaf consults with the various associations representing di� erent healthcare professions on the monetary value or cost linked to the procedure codes. Based on those consultations, and by looking at procedure coding and billing guidelines, the benchmark tari� s are set. These are an agreed guideline for the cost of specifi c treatments and procedures and represent a specifi c threshold according to which an MAF is willing to reimburse for healthcare treatment and services rendered to a member.
Namaf-a� liated MAFs may accept these tari� s but are not bound to adhere to them and may use a completely di� erent set of tari� s to cost their benefi t packages in order to di� erentiate their benefi t options from other MAFs. In other words, the benchmark tari� s, unlike the procedure codes and billing guidelines, are not mandatory or prescriptive.
Similarly, it is vital to understand that benchmark tari� s in no way prescribe what a healthcare provider can or should charge a patient for a specifi c treatment or service. The healthcare provider can charge more or less than the benchmark tari� , subject to his/her preference. When a healthcare provider charges more than the relevant MAF’s benefi t tari� for a treatment or service, which is very o� en the case, then the MAF will only pay the benefi t tari� amount and the patient is usually responsible for paying the di� erence.
The coding structure is well established in Namibia and functions e� ectively within the medical aid industry.
It becomes clear that the coding structure is the language informing communication in the industry. It is the tool for controlling expenses and safeguarding against fraud, abuse and misuse from HCPs and MAFs. Therefore, it is essential for key role players in the industry, such as MAFs, their administrators, and healthcare providers, to fully understand the coding structure, so that the consumer is protected.
However, Namibia has not adopted formal coding structure training for stakeholders, and the majority of industry players has not attended the training o� ered by AfriCode. The resultant lack of understanding of the coding structure and how to interpret the data enshrined within it is problematic, because it leaves the consumer vulnerable to being overcharged by HCPs, and MAFs not detecting problems or discrepancies with claims.
On an annual basis, Namaf consults with the various associations representing di� erent
healthcare professions on the monetary value or cost linked to the procedure codes.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS54
3.3 Marketing and Awareness Interventions
During the reporting period, Namaf contracted Fisher Consulting to conduct a climate survey to guide Namaf’s strategy formulation, and to enable Namaf to meet the needs and expectations of key stakeholders/customers in order to build trust, loyalty and a spirit of teamwork. The objectives of the survey were to evaluate stakeholder perception of the Namaf brand and the level of stakeholder satisfaction, to ascertain stakeholder opinion about the communication and relationship with Namaf, and to identify the needs, challenges and expectations of stakeholders.
From June to August, focus groups for (i) MAF Administrators, (ii) MAF Providers (open and closed funds), (iii) enabler linkages stakeholders (HPCNA, NAMFISA, NMRC, MoF, MoHSS), and (iv) Service Provider Associations (individual service provider associations and healthcare facility associations) were conducted to collect qualitative data. One of the key fi ndings of the survey was that there is a widespread lack of understanding of Namaf’s role within the industry. Thus, increased stakeholder engagement and education is of vital importance.
The members of the MC and several NAMFISA sta� undertook an educational visit to the South African Council of Medical Schemes (CMS). The CMS houses both the market conduct regulatory and the fi nancial supervisory roles, while in Namibia, Namaf is the market conduct regulator and NAMFISA is the fi nancial supervisor and Registrar.
The NAMFISA Act, which was promulgated a� er the Medical Aid Funds Act, added to the roles of the Registrar as described in the Medical Aid Funds Act. This created signifi cant overlap between the functions of Namaf and NAMFISA, which was not anticipated when the Medical Aid Funds Act was promulgated. This overlap presents a signifi cant operational challenge. Thus, the aim of the visit was to learn how the CMS splits its roles within the organisation in order to understand where and how to demarcate Namaf and NAMFISA’s roles.
Towards the end of the reporting period, the entities were working towards the fi nalisation of the dra� Memorandum of Understanding, which will balance and clarify the roles of Namaf and NAMFISA.

55NAMAF - 2017 ANNUAL REPORT
As part of its marketing e� orts during the reporting period, Namaf also refurbished its website, adding a substantial amount of information and making it more user-friendly. As at the end of the reporting period, Namaf did not have a marketing department or marketing manager, making the website the only marketing tool at present.
Since marketing is a major component of the ‘promote’ function of Namaf, there is a need for a marketing department to be established in the near future.
Based on the fi ndings of the climate survey (see 3.3), Namaf conducted two signifi cant stakeholder relation interventions.
From June to September, Namaf held meet-and-greet sessions with all the associations representing di� erent healthcare professions. The purpose of the meetings was to understand the associations’ expectations of Namaf and to clarify Namaf’s regulatory role within the industry. One of the major points that was clarifi ed was that MAFs and HCPs are Namaf’s customers, as they pay for a service that Namaf renders (provision of practice numbers, and management and development of clinical coding structures), and that the other entities and institutions that Namaf deals with are stakeholders.
In addition, Namaf conducted a two-day industry workshop in Windhoek on 21 and 22 June 2017 with the HPCNA, NMRC, Ministry of Health and Social Services, Ministry of Home A� airs and Immigration, and Ministry of Industrialisation, Trade and SME Development. This was a major milestone as the di� erent stakeholders had not previously had a platform to discuss matters pertaining to regulating and administering the medical aid industry. The purpose of the workshop was to clarify the roles of Namaf and the other stakeholders. In addition, the demarcation between the market conduct regulatory and fi nancial supervisory roles was discussed, thereby marking the initial stages of the demarcation process between Namaf and NAMFISA.
3.4 Stakeholder Relations

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS56
Since its inception in 1997, Namaf has been operating without a strategic plan. Although a strategic plan, intended for the period of 2012 to 2016, was developed in 2010/2011, it was never rolled out. Thus, a major milestone during the reporting period was the development of the Namaf Strategic Plan 2018 – 2020.
The strategy development process was informed by two inter-related activities: (i) the climate survey to gather intelligence to inform the strategy development process, and (ii) a three-day workshop in October 2017 with executive management, key sta� and an expert consultant to analyse current operations and the results of the climate survey in order to devise feasible strategic alternatives.
The process culminated in the development of strategic goals centered around (i) meeting stakeholder expectations, (ii) enabling processes (starting with data collection, analysis and interpretation to drive e� ective communication, investigation, and wider regulatory actions), (iii) the optimal use of resources, and (iv) prudent fi nancial management.
The Namaf Strategic Plan will be published and rolled out during the next reporting period.
3.5 Development of the Strategic Plan

57NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS58
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS58
LITIGATION

59NAMAF - 2017 ANNUAL REPORTNAMAF - 2017 ANNUAL REPORT
LITIGATION
NAMAF - 2017 ANNUAL REPORT595959595959

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS60
In response, Namaf and the MAFs instituted proceedings in High Court, seeking an order that Namaf and its members are not undertakings as defi ned in the Competition Act, because Namaf and the members do not carry on business for gain or reward, and thus are not subject to the jurisdiction of the Competition Commission or the Competition Act.
In addition, we maintained that Namaf and its members were precluded by the Medical Aid Funds Act from distributing profi ts to fund members, or anyone else, and that the setting of benchmark tari� s was designed to achieve a non-commercial socio-economic objective, thus excluding that activity from the Act. Namaf further argued that the issue of benchmark tari� s was authorised by the Medical Aid Funds Act and as a result excluded from the jurisdiction of the NaCC.
In March 2016, the High Court dismissed the application and ruled in favour of the NaCC, stating that Namaf is not exempt from the application and force of the Competition Act. The court referred to the defi nition of a medical aid fund in the Medical Aid Funds Act, which states that a fund is a business, and found that a fund operates for gain or reward, even if its profi ts are not distributed. In addition, the court stated that the issuing and publication of benchmark tari� s in respect of medical services was unlawful as it was in contravention of the anti-competition provisions of the Competition Act, and that benchmark tari� s in respect of medical services were not an activity designed to achieve a socio-economic objective. Consequently, Namaf members were asked to cease the practice of setting benchmark tari� s.
In 2015, the Namibian Competition Commission conducted an investigation under the Competition Act, 2003 (Act No. 2 of 2003) and notifi ed Namaf and its
a� liated medical aid funds that the process for the determination and annual review of benchmark tari� s amounted to a contravention of Section 23 of the Competition Act, which proscribes concerted practices between undertakings
which directly or indirectly fi x purchase or setting prices.
4.1 Background

61NAMAF - 2017 ANNUAL REPORT
The judgement of the High Court threatened the very existence, purpose and functioning of Namaf. Therefore, Namaf and its nine a� liated MAFs appealed the judgement in the Supreme Court. As with the High Court case, the Supreme Court case hinged on the question of whether medical aid funds, and by extension Namaf, were included under the Competition Act’s defi nition of undertakings.
In July of the reporting period, the Supreme Court overturned the decision of the High Court, ruling that while medical aid funds are businesses in the form of enterprises and are statutorily enjoined to apply sound business principles in their operations, this is to protect their members’ interests by ensuring the solvency of funds.
In other words, medical aid funds are not undertakings within the meaning of the Competition Act, because they do not carry out their business for the purpose of achieving a gain or reward.
As the MAFs are not undertakings as per the defi nition of the Competition Act, it also followed that Namaf does not fall within that defi nition. The court ruled that funds are non-profi t concerns, because the Medical Aid Funds Act prohibits funds from distributing a surplus. Instead, any surplus is retained for the future benefi t of a fund’s members.
The Supreme Court’s ruling was a seminal and landmark judgment, distinguishing the Namibian judicial landscape from the regional powerhouse, South Africa, and defi ning how the competition law is applied in Namibia. It clearly established that the NaCC has no jurisdiction over Namaf or its a� liated medical aid funds.
4.2 The Appeal in Supreme Court

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS62
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS62
THE WAY FORWARD

63NAMAF - 2017 ANNUAL REPORTNAMAF - 2017 ANNUAL REPORT
THE WAY FORWARD
NAMAF - 2017 ANNUAL REPORT636363636363

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS64
In addition, Namaf operates many areas of its business in the absence of approved internal policies, thus rendering it di� cult to apply a meaningful compliance framework. Consequently, there is a need to develop rules and regulations to guide the medical aid industry, as well as internal policies aligned to the strategic directions enshrined in the Strategic Plan 2018 – 2020.
In order to address the operational challenge of the overlap between the functions of Namaf and NAMFISA, the fi nalisation of the MoU between NAMFISA and Namaf will take place in 2018. Although not a legally binding document, the MoU will outline the terms and details of an understanding, including each party’s requirements and responsibilities. It is hoped that it will be the fi rst step towards changing legislation to require Namaf to report to the MoHSS instead of the MoF.
The lack of understanding of the coding structure among stakeholders was identifi ed as hampering the optimal functioning of the MAF industry. Thus, plans are underway to hold training on the coding structure for key stakeholders during April 2018. The training will be conducted by AfriCode.
During the next reporting period, two additional sub-committees will be established:
(i) The Clinical Coding Committee, comprised of medical experts, will be responsible for advising the MC on the introduction of new procedure codes and the deletion of redundant ones based on technological and medical advancements and developments. This function previously fell under the mandate of the A� ordability Committee.
(ii) The Statutory and Risk Committee will take over the functions of the Statutory and Legal Committee but have a wider mandate. It will be responsible for all legal issues, including regulations and risk management.
One of the major operational challenges facing Namaf is the lack of Namaf rules and regulations. Without rules and regulations, Namaf cannot prescribe
and enforce behaviours expected of MAFs and members of medical aid funds, meaning that it cannot fully exercise its regulatory role.

65NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS66
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS66
MEDICAL AID INDUSTRY

67NAMAF - 2017 ANNUAL REPORTNAMAF - 2017 ANNUAL REPORT
MEDICAL AID INDUSTRYAID INDUSTRY
NAMAF - 2017 ANNUAL REPORT676767676767

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS68
200
195
190
185
180
175
170
165
1602014 2015 2016 2017
173,526 180,240 187,797 196,276
Thou
sand
s
Benefi ciaries
173,53
190.28
187.80
196.28
Figure 2: Number of lives covered by Namaf a� liated MAFs 2014 – 2017
Benefi ciaries
6.1 Demographics
The number of lives/benefi ciaries covered by the medical aid funds a� liated to Namaf has been growing steadily over the four years leading up to 2017, when 196,276 lives were covered (see Figure 2).

69NAMAF - 2017 ANNUAL REPORT
Figure 3 shows the distribution between the genders in each of the respective years, noting that the number of female benefi ciaries has been growing at a faster rate than the number of male benefi ciaries.
105.00
100.00
95.00
90.00
85.00
80.00
75.00
2014 2015 2016 2017
84,815.50 88,282.50 92,438.17 97,259.92
88,710.33 92,001.00 95,358.33 99,016.17
Thou
sand
s
Male
Female
Figure 3: Gender distribution of benefi ciaries 2014 – 2017
Female Male
29.70
29.65
29.60
29.55
29.50
29.45
29.40
29.352014 2015 2016 2017
29.46 29.53 29.59 29.65Benefi ciaries
29.46
29.53
29.59
29.65
Figure 4: Age distribution of benefi ciaries 2014 – 2017
Average Age
Figure 4 shows that the average age of the covered benefi ciaries has remained almost constant over the four years up to 2017.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS70
25,000
20,000
15,000
10,000
5,000
0-5
5-10
10-15
15-2
020
-25
25-3
030
-35
35-4
040
-45
45-5
050
-55
55-6
060
-65
>65
Figure 5: Age categories 2017
% Benefi ciariesNo. of Benefi ciaries
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
4.00
3.50
3.00
2.50
2.00
1.50
1.00
0.50
-2014 2015 2016 2017
2,325,819,403 2,410,741,350 2,825,938,482 3,137,572,791
2,688,639,049 2,778,831,998 3,260,274,257 3,638,890,390
Billio
ns
Benefi t Amount
Claimed Amount
Figure 6: Total value of claims received and benefi ts paid 2014 – 2017
2.692.78
3.26
3.64
2.332.41
2.83
3.14
The total value of claims received increased from N$2.69 billion in 2014 to N$3.64 billion in 2017. The total value of the claims paid by MAFs increased from N$2.33 billion in 2014 to N$3.14 billion in 2017.
The numbers of benefi ciaries in each of the age bands for the 2017 benefi t year are shown in Figure 5. It is worth noting that less than 4% of the benefi ciaries of MAFs are older than 65 years of age.
6.2 Healthcare Benefi ts

71NAMAF - 2017 ANNUAL REPORT
1.80
1.60
1.40
1.20
1.00
0.80
0.60
0.40
0.20
-2014 2015 2016 2017
1,291.18 1,284.47 1,446.72 1,544.97
1,116.94 1,114.33 1,253.99 1,332.13
Thou
sand
s
Average Claims/MonthAverageBenefi ts/Month
Figure 7: Average value of claims and benefi ts per life per month 2014 – 2017
Figure 7 provides the same fi gures as Figure 6 on a per life per month basis, which o� ers a perspective that is net of any membership growths or shrinkages during the period analysed.
As indicated in Figure 7, the average claims received per covered life per month increased from N$1,291 in 2014 to N$1,544 in 2017. The average benefi t amounts paid increased from N$1,116 to N$1,332 over the same period.
The di� erence between the claims received and the benefi ts paid increased from N$174.24 per average benefi ciary per month to N$212.84 per average benefi ciary per month.
Figure 8: Claims split 2017
Medical Specialists12%
Radiology5%
Medicines17%
Dentistry5%
Other11% Gen Practitioner
10%
Pathology6%
Hospitals34%
Of the benefi ts paid in 2017, hospitals account for 34% of the benefi ts paid, medicines for 17%, medical specialists for 12% and general practitioners for 10% (see Figure 8).

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS72
1.2
1.0
0.8
0.6
0.4
0.2
02014 2015 2016 2017
Billio
ns
Figure 9: Hospital claims received and benefi ts paid 2014 – 2017
Claimed AmountBenefi t Amount
Hospitals
0.78 0.79
0.951.080.81 0.81
0.97
1.11
Figure 10: Pharmacy claims received and benefi ts paid 2014 – 2017 Figure 10: Pharmacy claims received and benefi ts paid 2014 – 2017
Billio
ns
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
02014 2015 2016 2017
Claimed AmountBenefi t Amount
Pharmacies
0.42
0.530.57
0.67
0.72
0.44
0.510.54
Figure 9 shows that the value of claims received from hospital and related facilities increased from N$0.81 billion in 2014 to N$1.11 billion in 2017. The value of the claims paid increased from N$0.78 billion to N$1.08 billion over the same period.
As shown in Figure 10, the value of claims received from pharmacies increased from N$0.53 billion in 2014 to N$0.72 billion in 2017. The value of the claims paid increased from N$0.42 billion to N$0.54 billion over the same period.
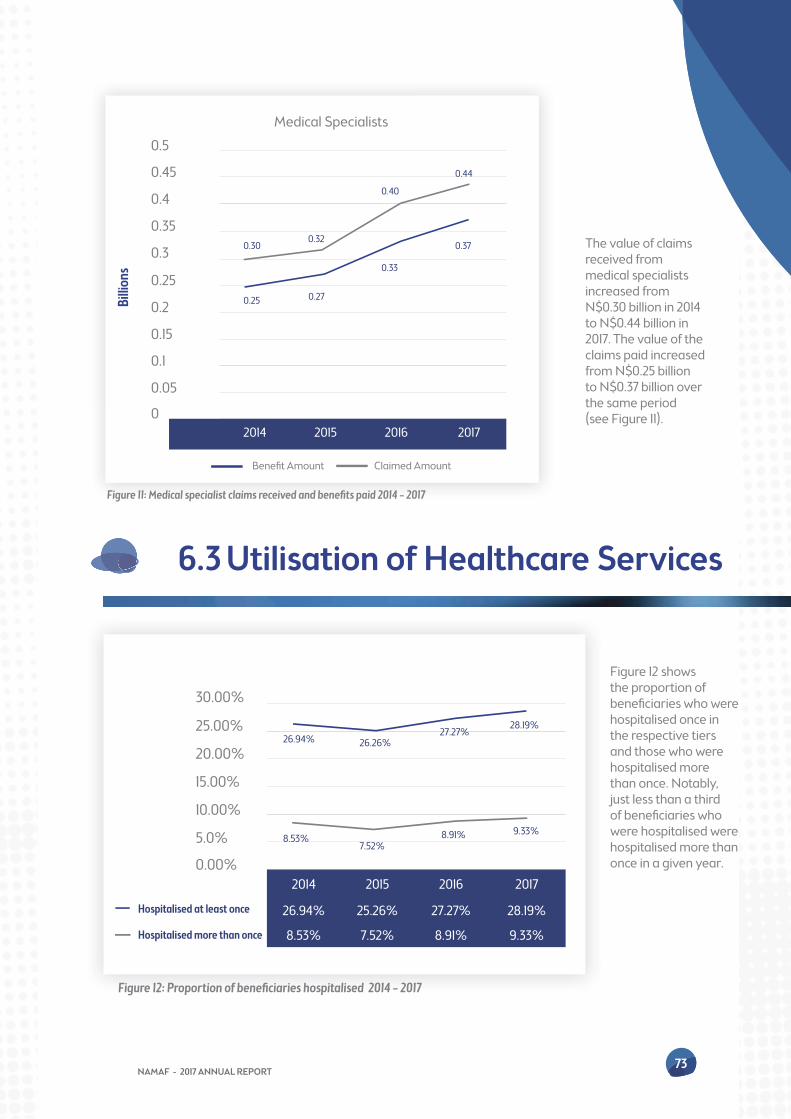
73NAMAF - 2017 ANNUAL REPORT
The value of claims received from medical specialists increased from N$0.30 billion in 2014 to N$0.44 billion in 2017. The value of the claims paid increased from N$0.25 billion to N$0.37 billion over the same period (see Figure 11).
0.5
0.45
0.4
0.35
0.3
0.25
0.2
0.15
0.1
0.05
02014 2015 2016 2017
Billio
ns
Figure 11: Medical specialist claims received and benefi ts paid 2014 – 2017
Claimed AmountBenefi t Amount
Medical Specialists
0.25
0.30
0.27
0.32
0.33
0.40
0.37
0.44
30.00%
25.00%
20.00%
15.00%
10.00%
5.0%
0.00%2014 2015 2016 2017
26.94% 25.26% 27.27% 28.19%
8.53% 7.52% 8.91% 9.33%
Hospitalised at least once
Hospitalised more than once
Figure 12: Proportion of benefi ciaries hospitalised 2014 – 2017
8.53%7.52%
8.91% 9.33%
26.94% 26.26%27.27%
28.19%
6.3 Utilisation of Healthcare Services
Figure 12 shows the proportion of benefi ciaries who were hospitalised once in the respective tiers and those who were hospitalised more than once. Notably, just less than a third of benefi ciaries who were hospitalised were hospitalised more than once in a given year.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS74
24.00%
23.50%
23.00%
22.50%
22.00%
21.50%
21.00%
20.50%2014 2015 2016 2017
22.25% 21.56% 22.83% 23.52%Specialist Claims
Figure 13: Utilisation trends for medical specialist services 2014 – 2017
78.00%
77.80%
77.60%
77.40%
77.20%
77.00%
76.80%
76.60%
76.40%
76.20%
76.00%
75.80%2014 2015 2016 2017
77.65% 77.03% 76.50% 77.71%GP Services
Figure 14: Utilisation trends for GP services 2014 – 2017
Figure 13 indicates the utilisation trends for medical specialist services. The proportion of benefi ciaries of medical aid funds utilising specialist services has steadily increased since 2015.
Figure 14 shows that more than 75% of the covered benefi ciaries have accessed GP services during the respective benefi t years.

75NAMAF - 2017 ANNUAL REPORT
94.00%
93.50%
93.00%
92.50%
92.00%
91.50%2014 2015 2016 2017
92.21% 93.61% 93.39% 93.07%Pharmacy Services
Figure 15: Utilisation trends for pharmacy services 2014 – 2017
The high-level statistics and trends illustrated in this section show that:
• The average age of benefi ciaries covered has remained more or less constant over time;
• Benefi ciaries aged 65 years and older (pensioners) represent a small proportion of the total benefi ciaries covered;
• The claims incurred and benefi ts paid per average benefi ciary per month have increased by just under 5% per annum;
• The largest proportion of expenditure is represented by hospital, medicine and medical specialist costs;
• High proportions of benefi ciaries covered have claimed from their medical aid funds; and
• The gap between the claimed and paid amounts has increased by N$38.60 per average benefi ciary per month or 22.15% over the four years to December 2017.
The impact of the high annual increases in contributions coupled with the high increases in out-of-pocket expenditure will have a negative e� ect on the access to and the a� ordability of healthcare going forward. Therefore, addressing this will be one of Namaf’s main focus areas.
6.4 Accesibility and A� ordability
More than 90% of covered benefi ciaries have accessed pharmacy services in the respective benefi t years, as shown in Figure 15.

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS76
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS76
ANNUAL FINANCIAL STATEMENTS

77NAMAF - 2017 ANNUAL REPORT
ANNUAL FINANCIAL STATEMENTS
NAMAF - 2017 ANNUAL REPORT77777777777777

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS78
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
ANNUAL FINANCIAL STATEMENTS FOR THE YEAR ENDED 31 DECEMBER 2017
REGISTERED OFFICE 8 Newton Street
NMC House
Windhoek
Namibia
POSTAL ADDRESS P.O. Box 11974
Klein Windhoek
Namibia
AUDITORS PricewaterhouseCoopers
Namibia
BANKERS Nedbank Namibia Limited
First National Bank
CONTENTS PAGE
Statement of Management Committee’s responsibilities 79
Independent auditor’s report 80-82
Report of the Management Committee 83
Statement of fi nancial position 84
Statement of comprehensive income 85
Statement of changes in equity 86
Cash fl ow statement 87
Notes to the fi nancial statements 88-94
Detailed statement of comprehensive income 95

79NAMAF - 2017 ANNUAL REPORT
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
STATEMENT OF MANAGEMENT COMMITTEE’S RESPONSIBILITIESFOR THE YEAR ENDED 31 DECEMBER 2017
1. The Management Committee is responsible to maintain adequate accounting records and the content and integrity of the annual
fi nancial statements and related fi nancial information included in this report. It is their responsibility to ensure that the annual fi nan-
cial statements fairly present the state of a� airs of the Association as at the end of the fi nancial year and the results of its operations
and cash fl ows for the year then ended, in conformity with the accounting policies of the association. The external auditors are
engaged to express an independent opinion on the annual fi nancial statements.
2. The annual fi nancial statements are prepared in accordance with the accounting policies of the Association which are consistently
applied and supported by reasonable and prudent judgements and estimates.
3. The Management Committee acknowledges that it is ultimately responsible for the system of internal fi nancial control established
by the Association and places considerable importance on maintaining a strong control environment. To enable the Management
Committee to meet these responsibilities, it sets standards for internal control aimed at reducing the risk of error or loss in a cost
e� ective manner. The standards include the proper delegation of responsibilities within a clearly defi ned framework, e� ective ac-
counting procedures and adequate segregation of duties to ensure an acceptable level of risk.
These controls are monitored throughout the Association and all employees are required to maintain the highest ethical standards
in ensuring the Association’s business is conducted in a manner that in all reasonable circumstances is above reproach. The focus
of risk management in the association is on identifying, assessing, managing and monitoring all known forms of risk across the
Association. While operating risk cannot be fully eliminated, the association endeavours to minimise it by ensuring that appropriate
infrastructure, controls, systems and ethical behaviour are applied and managed within predetermined procedures and constraints.
4. The external auditors are responsible for independently reviewing and reporting on the Association’s annual fi nancial statements.
The annual fi nancial statements have been audited by the Association’s external auditors and their report is presented on pages 80
to 82.
5. The a� airs of the Association shall be controlled by the management of the Association, which shall exercise and perform the pow-
ers, duties and functions of the Association with due regard to the provisions of the Medical Aid Funds Act.
The annual fi nancial statements set out on pages 83 to 96, which have been prepared on the going concern basis, were approved and
authorised for issue by the Management Committee and were signed on its behalf by:
Chairman
Date:
CEO

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS80
INDEPENDENT AUDITOR’S REPORT TO THE MEMBERS OF THE MANAGEMENT COMMITTEE OF NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS (NAMAF)FOR THE YEAR ENDED 31 DECEMBER 2017
Our opinion
In our opinion, the fi nancial statements of Namibian Association of Medical Aid Funds (the Association) for the year ended 31 December
2017 are prepared, in all material respects, in accordance with the basis of accounting described in note 1 to the fi nancial statements.
What we have audited
Namibian Association of Medical Aid Funds (NAMAF)’s fi nancial statements set out on pages 83 to 96 comprise:
• the report of the Management Committee for the year ended 31 December 2017;
• the statement of fi nancial position as at 31 December 2017;
• the statement of comprehensive income for the year then ended;
• the statement of changes in equity for the year then ended;
• the statement of cash fl ows for the year then ended; and
• the notes to the fi nancial statements, which include a summary of signifi cant accounting policies.
Basis for opinion
We conducted our audit in accordance with International Standards on Auditing (ISAs). Our responsibilities under those standards are
further described in the Auditor’s responsibilities for the audit of the fi nancial statements section of our report.
We believe that the audit evidence we have obtained is su� cient and appropriate to provide a basis for our opinion.
Independence
We are independent of the Association in accordance with the International Ethics Standards Board for Accountants Code of Ethics for
Professional Accountants (Parts A & B) and other independence requirements applicable to performing audits of fi nancial statements
in Namibia. We have fulfi lled our other ethical responsibilities in accordance with this and in accordance with other ethical requirements
applicable to performing audits in Namibia
Basis of accounting
We draw attention to note 1 to the fi nancial statements, which describes the basis of accounting. The fi nancial statements are prepared in
accordance with the Association’s own accounting policies to satisfy the fi nancial information needs of the Association’s members. As a
result, the fi nancial statements may not be suitable for another purpose. Our opinion is not modifi ed in respect of this matter.
Other information
The Association’s Management Committee is responsible for the other information. The other information comprises the Association
information, the statements of responsibility of the Management Committee and the detailed income statement describe additional
content of other information, but does not include the fi nancial statements and our auditor’s report thereon.

81
INDEPENDENT AUDITOR’S REPORT TO THE MEMBERS OF THE MANAGEMENT COMMITTEE OF NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS (NAMAF) (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
Other information (continued)
Our opinion on the fi nancial statements does not cover the other information and we do not and will not express an audit opinion or any
form of assurance conclusion thereon.
In connection with our audit of the fi nancial statements, our responsibility is to read the other information identifi ed above and, in doing
so, consider whether the other information is materially inconsistent with the fi nancial statements or our knowledge obtained in the
audit, or otherwise appears to be materially misstated.
If, based on the work we have performed, we conclude that there is a material misstatement of this other information, we are required
to report that fact. We have nothing to report in this regard.
Responsibilities of the Management Committee for the fi nancial statements
The Management Committee is responsible for the preparation and fair presentation of the fi nancial statements in accordance with the
accounting policies of the Association, and for such internal control as the Management Committee determine is necessary to enable the
preparation of fi nancial statements that are free from material misstatement, whether due to fraud or error.
In preparing the fi nancial statements, the Management Committee is responsible for assessing the Association’s ability to continue as
a going concern, disclosing, as applicable, matters related to going concern and using the going concern basis of accounting unless the
Management Committee either intend to liquidate the Association or to cease operations, or have no realistic alternative but to do so.
Auditor’s responsibilities for the audit of the fi nancial statements
Our objectives are to obtain reasonable assurance about whether the fi nancial statements as a whole are free from material misstate-
ment, whether due to fraud or error, and to issue an auditor’s report that includes our opinion. Reasonable assurance is a high level of
assurance, but is not a guarantee that an audit conducted in accordance with ISAs will always detect a material misstatement when it
exists. Misstatements can arise from fraud or error and are considered material if, individually or in the aggregate, they could reasonably
be expected to infl uence the economic decisions of users taken on the basis of these fi nancial statements.
As part of an audit in accordance with ISAs, we exercise professional judgement and maintain professional scepticism throughout the
audit. We also:
• Identify and assess the risks of material misstatement of the fi nancial statements, whether due to fraud or error, design and per-
form audit procedures responsive to those risks, and obtain audit evidence that is su� cient and appropriate to provide a basis for
our opinion. The risk of not detecting a material misstatement resulting from fraud is higher than for one resulting from error, as
fraud may involve collusion, forgery, intentional omissions, misrepresentations, or the override of internal control.
• Obtain an understanding of internal control relevant to the audit in order to design audit procedures that are appropriate in the
circumstances, but not for the purpose of expressing an opinion on the e� ectiveness of the Association’s internal control.
NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS82
INDEPENDENT AUDITOR’S REPORT TO THE MEMBERS OF THE MANAGEMENT COMMITTEE OF NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS (NAMAF) (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
Auditor’s responsibilities for the audit of the fi nancial statements (continued)
• Evaluate the appropriateness of accounting policies used and the reasonableness of accounting estimates and related disclosures
made by the Management Committee.
• Conclude on the appropriateness of the Management Committee’ use of the going concern basis of accounting and, based on the
audit evidence obtained, whether a material uncertainty exists related to events or conditions that may cast signifi cant doubt on
the Association’s ability to continue as a going concern. If we conclude that a material uncertainty exists, we are required to draw
attention in our auditor’s report to the related disclosures in the fi nancial statements or, if such disclosures are inadequate, to modify
our opinion. Our conclusions are based on the audit evidence obtained up to the date of our auditor’s report. However, future events
or conditions may cause the Association to cease to continue as a going concern.
We communicate with the Management Committee regarding, among other matters, the planned scope and timing of the audit and
signifi cant audit fi ndings, including any signifi cant defi ciencies in internal control that we identify during our audit.
PricewaterhouseCoopers
Registered Accountants and Auditors
Chartered Accountants and Auditors
Per: Louis van der Riet
Partner
Windhoek
Date:
82

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
REPORT OF THE MANAGEMENT COMMITTEEFOR THE YEAR ENDED 31 DECEMBER 2017
1. The Management Committee presents its annual report, which forms part of the audited fi nancial statements of the Association for
the fi nancial year ended 31 December 2017.
General review
2. The Association is incorporated under the Medical Aid Funds Act and it serves as a controlling body in respect of the medical aid fund
industry.
Events subsequent to statement of fi nancial position date
3. There have been no facts or circumstances of a material nature that have occurred between the accounting date and the date of
this report.
Financial results
4. Full details of the fi nancial results of the Association are disclosed in the statement of comprehensive income and the notes thereto.
Management Committee
5. The management of the Association during the fi nancial year and up to the date of this report is as follows:
Name
B Amuenje (Chairperson)
LA Namoloh (Vice Chairperson)
G Tjombe (Treasurer)
DH Somseb (Member)
E Mbahijona (Member)
GD Labuschagne (Member)
LD Nashandi (Member)
A Begley (Co-opted Member)
P Theron (Co-opted Member)
AR Roostee (Co-opted Member)
A Uiseb (Co-opted Member)
K Mbaukua (Co-opted Member)
S Charmberlain (Member)
G Grobler (Member)
Date appointed
12 June 2017
12 June 2017
12 June 2017
12 June 2017
12 June 2017
12 June 2017
12 June 2017
14 July 2017
14 July 2017
24 February 2016
18 July 2017
26 January 2018
08 April 2015
02 June 2014
Date resigned
-
-
-
-
-
-
-
-
-
29 June 2017
04 October 2017
21 May 2018
12 June 2017
12 June 2017
83NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS84
Notes 2017N$
2016N$
ASSETS
Non-current assetsProperty, plant and equipment 2 166 488 89 999
Current assets 3 319 432 3 313 519
Investments 4 2 586 775 3 137 670
Trade and other receivables 5 359 233 70 280
Cash and cash equivalents 6 373 424 105 569
Total assets 3 485 920 3 403 518
EQUITY AND LIABILITIES
Capital and reservesRetained surplus 3 005 347 3 208 281
Current liabilitiesTrade and other payables 7 480 573 195 237
Total equity and liabilities 3 485 920 3 403 518
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
STATEMENT OF FINANCIAL POSITIONFOR THE YEAR ENDED 31 DECEMBER 2017
84

Notes 2017N$
2016N$
Revenue 9 592 890 8 190 507
Administrative expenses (10 049 945) (8 580 724)
Operating defi cit for the year ( 457 055) ( 390 217)
Interest received 3 254 121 339 924
Defi cit for the year ( 202 934) ( 50 293)
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
STATEMENT OF COMPREHENSIVE INCOMEFOR THE YEAR ENDED 31 DECEMBER 2017
85NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS86
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
STATEMENT OF CHANGES IN EQUITYFOR THE YEAR ENDED 31 DECEMBER 2017
Notes 2017N$
2016N$
Retained surplus
At the beginning of the year 3 208 281 3 258 574
Defi cit for the year (202 934) (50 293)
At the end of the year 3 005 347 3 208 281
86

Notes 2017N$
2016N$
Cash fl ow from operating activities
Cash outfl ows from operations 8 (432 241) (1 311 844)
Interest received 3 254 121 339 924
Net cash used in operating activities ( 178 120) ( 971 920)
Cash fl ows from investing activities
Property, plant and equipment acquired 2 ( 104 920) ( 62 900)
Investments 4 550 895 1 035 981
Net cash generated from investing activities 445 975 973 081
Net change in cash and cash equivalents 267 855 1 161
at the beginning of the year 105 569 104 408
at the end of the year 6 373 424 105 569
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSA STATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUND, ACT 23 1995
CASH FLOW STATEMENTFOR THE YEAR ENDED 31 DECEMBER 2017
87NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS88
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTSFOR THE YEAR ENDED 31 DECEMBER 2017
1. Accounting policies
1.1 Basis of accountingThe fi nancial statements are prepared in accordance with the accounting policies of the Association. The basis of accounting
and the presentation and disclosures contained in the fi nancial statements are not intended to, and do not, comply with all of
the requirements of International Financial Reporting Standards.
1.2 Property, plant and equipmentProperty, plant and equipment is stated at historical cost less accumulated depreciation.
Depreciation is calculated on the straight-line method to write o� the cost of each asset over its estimated useful life as follows:
Furniture & fi ttings 10 years
O� ce equipment 3 years
Computer equipment 3 years
The carrying values of equipment are reviewed for impairment when events or changes in circumstances indicate the carrying
value may not be recoverable. If any such indication exists and where the carrying values exceed the estimated recoverable
amount, the assets or cash-generating units are written down to their recoverable amount.
Gains and losses on disposal of equipment are determined by reference to their carrying amount and are taken into account in
determining operating profi t. On disposal of revalued assets, amounts in revaluation and other reserves relating to that asset
are transferred to retained earnings.
1.3 Financial assetsThe Association classifi es its fi nancial assets in the following categories: at fair value through profi t or loss and loans and re-
ceivables. The classifi cation depends on the purpose for which the fi nancial assets were acquired. Management committee de-
termines the classifi cation of its fi nancial assets at initial recognition and re-evaluates this designation at every reporting date.
1.4 LeasesLeases where a signifi cant portion of the risks and rewards of ownership are retained by the lessor are classifi ed as operating
leases. Payments made under operating leases (net of any incentives received from the lessor) are charged to the statement
of comprehensive income on a cash-fl ow basis over the period of the lease.
Leases of assets under which all the risks and benefi ts of ownership are e� ectively retained by the lessor are classifi ed as op-
erating leases. Payments made under operating leases are charged to the statement of comprehensive income on a straight-
line basis over the period of the lease.
When an operating lease is terminated before the lease period has expired, any payment required to be made to the lessor by
way of penalty is recognised as an expense in the period in which termination takes place.
88

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTS (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
1.5 Trade receivablesTrade receivables are carried at original invoice amount less provision made for impairment of these receivables. Such pro-
vision for impairment of trade receivables is established if there is objective evidence that the Association will not be able to
collect all amounts due according to the original terms of receivables.
1.6 Cash and cash equivalentsCash and cash equivalents are carried in the statement of fi nancial position at cost. For the purposes of the cash fl ow state-
ment, cash and cash equivalents comprise cash on hand, deposits held at call with banks, other short-term highly liquid in-
vestments with original maturities of three months or less, and bank overdra� s. In the statement of fi nancial position, bank
overdra� s are included in borrowings in current liabilities.
1.7 Trade payablesTrade payables are carried at the fair value of the consideration to be paid in future for services that have been received or
supplied and invoiced or formally agreed with the supplier.
1.8 ProvisionsProvisions are recognised when the Association has a present legal or constructive obligation as a result of past events, when
it is probable that an outfl ow of resources embodying economic benefi ts will be required to settle the obligation, and when a
reliable estimate of the amount of the obligation can be made.
1.9 Revenue recognitionActuarial, sub-committee, consultancy and a� liation feesThese revenue streams comprise income from all medical aid funds. The fees are payable every month based on the previous
month’s member numbers of the relevant medical aid funds.
Annual renewal fees and practice number registration feesThese revenue streams comprise of income from registered health care professionals. Annual renewal fees are payable on an
annual basis. Registration fees are payable as and when registration takes place.
When the outcome of a transaction involving the rendering of services can be estimated reliably, revenue associated with the
transaction is recognised by reference to the stage of completion of the transaction at the end of the reporting period. The
outcome of a transaction can be estimated reliably when all the following conditions are satisfi ed:
• the amount of revenue can be measured reliably;
• it is probable that the economic benefi ts associated with the transaction will fl ow to the company;
• the stage of completion of the transaction at the end of the reporting period can be measured reliably; and
• the costs incurred for the transaction and the costs to complete the transaction can be measured reliably.
When the outcome of the transaction involving the rendering of services cannot be estimated reliably, revenue shall be recog-
nised only to the extent of the expenses recognised that are recoverable.
89NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS90
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTS (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
1.9 Revenue recognition (continued)
Service revenue is recognised by reference to the stage of completion of the transaction at the end of the reporting period.
Stage of completion is determined by the proportion of costs incurred to date bear to the total estimated costs of the trans-
action.
Revenue is measured at the fair value of the consideration received or receivable and represents the amounts receivable for
goods and services provided in the normal course of business, net of trade discounts and volume rebates, and value added tax.
Other income includes interest income, which is accounted for as it accrues to the Association.
Interest income from fi nancial instruments measured at fair value through profi t or loss, is recognised in the statement of
comprehensive income using the e� ective interest rate method.
2. Property, Plant & Equipment
2.1 31 December 2017
Opening net carrying amount 60 534 29 465 89 999
Additions 69 972 34 948 104 920
Depreciation charge ( 9 686) ( 18 745) ( 28 431)
Closing net carrying amount 120 821 45 668 166 488
Cost 357 074 223 778 580 852
Accumulated depreciation (236 254) (178 110) (414 364)
Net carrying amount 120 821 45 668 166 488
Furniture & fi ttings
N$
O� ce & computerequipment
N$ N$
Total
90

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTS (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
2.2 31 December 2016
Opening net carrying amount 27 652 45 032 72 684
Additions 62 900 - - 62 900
Depreciation charge ( 30 018) ( 15 567) ( 45 585)
Closing net carrying amount 60 534 29 465 89 999
Cost 287 102 188 830 475 932
Accumulated depreciation ( 226 568) ( 159 365) ( 385 933)
Net carrying amount 60 534 29 465 89 999
Furniture & fi ttings
N$
O� ce & computerequipment
N$ N$
Total
2017N$
2016N$
3. Interest received
Interest received on current account 5 016 3 425
Interest received on investment 249 105 336 499
254 121 3 208 281
91NAMAF - 2017 ANNUAL REPORT
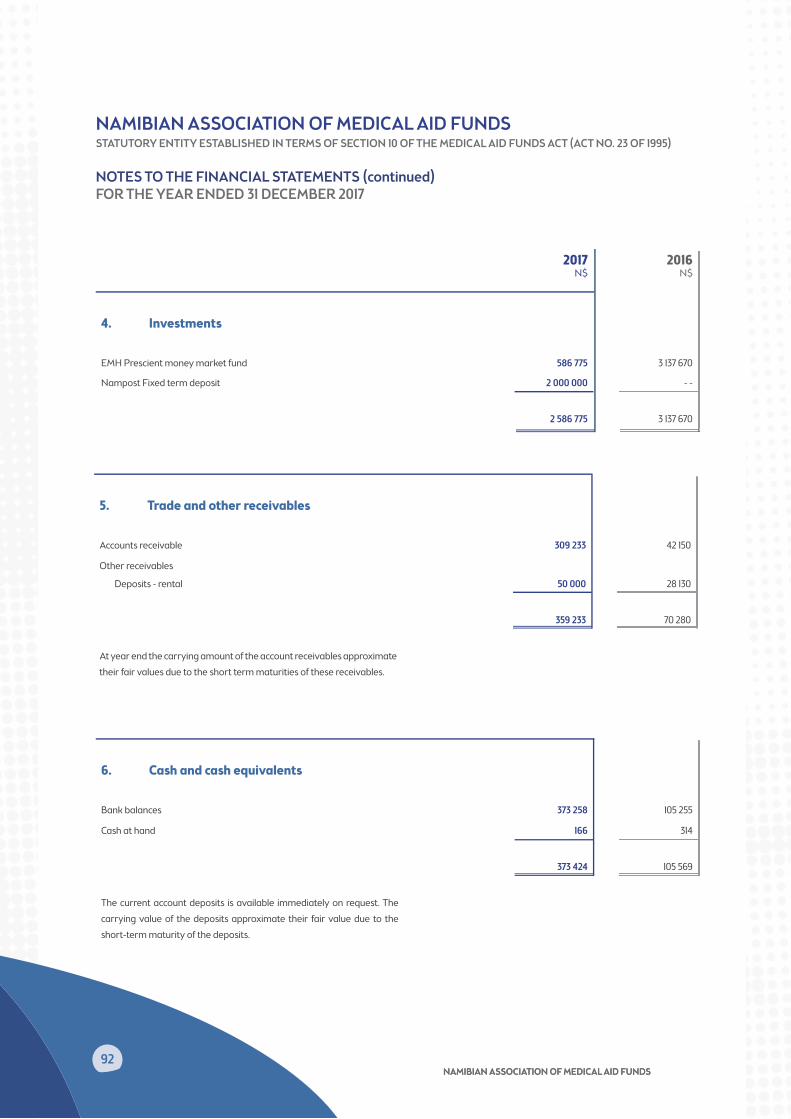
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS92
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTS (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
2017N$
2016N$
4. Investments
EMH Prescient money market fund 586 775 3 137 670
Nampost Fixed term deposit 2 000 000 - -
2 586 775 3 137 670
5. Trade and other receivables
Accounts receivable 309 233 42 150
Other receivables
Deposits - rental 50 000 28 130
359 233 70 280
At year end the carrying amount of the account receivables approximate their fair values due to the short term maturities of these receivables.
6. Cash and cash equivalents
Bank balances 373 258 105 255
Cash at hand 166 314
373 424 105 569
The current account deposits is available immediately on request. The carrying value of the deposits approximate their fair value due to the short-term maturity of the deposits.
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS9292

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTS (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
2017N$
2016N$
7. Trade and other payables
Accruals 69 357 16 599
Trade payables 192 629 165 188
Prepaid renewal and registration income 164 489 - -
Leave pay accrual 54 098 13 450
480 573 195 237
At year end the carrying amount of the payables approximate their fair values due to the short-term maturities of these payables.
8. Cash generated from operations
Reconciliation of surplus for the year to cash generated from operations:
Defi cit for the year
Adjusted for:
(202 934) (50 293)
Depreciation 28 431 45 585
Interest income (254 121) (339 924)
Leave pay 40 648 (209 010)
Severance pay - - (182 393)
Bad debts written o� /(bad debts reversed) 72 450 98 372
Changes in working capital:
Trade and other receivables (361 404) (90 776)
Trade and other payables 244 689 (583 405)
Cash fl ows generated from operations (432 241) (1 311 844)
93NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS94
2017N$
2016N$
9. Bad debts written o� /(bad debts recovered)
Renewal fee receivable 72 450 78 813
Sundry debtors - - 19 559
72 450 98 372
10. Investment in Namibian Health Funders Consortium Trust
Trust capital 100 100
Less Accumulated impairment ( 100) 100
- - - -
The Trust is a related party and was created to administer the Medicines Formulary for the benefi t of medical aid funds, but became dormant due to resistance from the Namibian medicine market.
11. Contingent assets
Contingent assets represent items that, at 31 December 2017, are not recognised in the statement of fi nancial position because there is signifi cant uncertainty at date as to the necessity for the Association to receive payments in respect of the legal fee refund.
In respect of the legal fee refund from the Namibian Competition Commission, additional consideration of N$ $474 212 will be received from the Namibian Competition Commission. No gain has been recognised during the fi nancial year, as the receipt of the additional consideration is not virtually certain as it is dependent on the approval of the high court.
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
NOTES TO THE FINANCIAL STATEMENTS (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
94

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
DETAILED STATEMENT OF COMPREHENSIVE INCOMEFOR THE YEAR ENDED 31 DECEMBER 2017
2017N$
2016N$
Income 9 592 890 8 190 507
A� liation fees 7 232 749 6 450 223
Practice number registration/renewal fees 1 625 964 1 304 106
Coding Structures Fees 198 000 195 000
Trustee Training Income 155 295 --
Other Receipts 380 881 231 700
Rent recovery from sub tenant -- 8 053
Sundry income -- 1 426
Less: Administrative expenses 10 049 945 8 580 724
Accounting fees 92 783 - -
Actuarial fee expenses 1 620 077 1 313 499
Advertising 77 234 94 308
Auditors' remuneration 47 156 47 350
Bad debts written o� /(debts reversed) 72 450 98 372
Bank charges 25 892 14 284
Conference expenses 177 552 71 832
Cleaning 14 390 4 840
Consulting expenses 366 405 192 000
IT services 167 561 150 774
Depreciation 28 431 45 585
Directors & o� cers liability cover 10 762 9 302
Entertainment 16 391 20 128
Insurance 14 633 12 219
Leave pay expense 40 648 (209 010)
Legal and professional fees 1 426 183 1 309 606
Mediscor (NRPF) 24 000 24 000
Meeting attendance 494 879 359 612
Municipal charges 64 677 45 243
O� ce expenses 64 992 34 761
Postage and courier 12 898 10 685
Printing and stationery 77 209 43 193
Provider Practice Number - fees to BHF 477 776 373 532
Rent paid - o� ce 544 866 347 677
Repairs and maintenance 29 196 19 701
Salaries and wages 3 323 808 3 981 898
Security expenses 186 147 20 743
Severance pay expense -- (182 393)
95NAMAF - 2017 ANNUAL REPORT

NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS96
2017N$
2016N$
Sponsorship 23 927 30 419
Sta� development 5 250 7 500
Sta� recruitment 154 782 - -
Sub-committee meetings 98 717 103 938
Telephone and fax 99 746 103 691
Travel and accommodation 21 268 22 535
Trustee training and workshop costs 100 802 - -
ICD10 Training expense - - 53 607
VET Levy expense 24 243 - -
Workshops (strategic project) 22 216 5 295
Operating (defi cit) for the year (457 055) (390 217)
Interest received 3 254 121 339 924
Defi cit for the year (202 934) (50 293)
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDSSTATUTORY ENTITY ESTABLISHED IN TERMS OF SECTION 10 OF THE MEDICAL AID FUNDS ACT (ACT NO. 23 OF 1995)
DETAILED STATEMENT OF COMPREHENSIVE INCOME (continued)FOR THE YEAR ENDED 31 DECEMBER 2017
This statement is unaudited and does not form part of the fi nancial statements. It has been included for the members' purposes only.
969696
Notes
NAMAF - 2017 ANNUAL REPORT

9898
Notes
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS


NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS100
Windhoek O� ceAddress: No. 8 Newton Street, NMC HouseTel: +264-61-257211 or 257212Fax; +264-61-257213Email; [email protected]://www.namaf.org.na
NAMIBIAN ASSOCIATION OF MEDICAL AID FUNDS100100
Windhoek O� ceAddress: No. 8 Newton Street, NMC HouseTel: +264-61-257211 or 257212Fax; +264-61-257213Email; [email protected]; [email protected]://www.namaf.org.nahttp://www.namaf.org.na
NMC HouseNo. 8 Newton StreetWindhoekTel: +264 61 257 211 / 257 212Fax: +264 61 [email protected]://www.namaf.org.na







