Download - 2. Update Who Aria 2008, Suprihati

ALLERGIC RHINITIS AND ITS IMPACT ALLERGIC RHINITIS AND ITS IMPACT
ON ASTHMA (ARIA) UPDATE 2008ON ASTHMA (ARIA) UPDATE 2008
Suprihati ENT Depart. Fac of Medicine Diponegoro Univ-Kariadi
Hospital, Semarang

INTRODUCTION
Allergic rhinitis : a symptomatic disorder of the nose induced after
allergen exposure by IgE-mediated inflammation of the membranes lining the nose
3 cardinal symptoms : Sneezing Nasal obstruction Mucous discharge
Important achievement of ARIA WHO workshop (1999) :
A new classification for Allergic rhinitis : * Intermittent allergic rhinitis (IAR) and * Persistent allergic rhinitis (PAR)
The severity of AR : classical symptoms + impairments in how patients function in day-to day life : * mild * moderate to severe
The ARIA WHO workshop

Allergic rhinitis ARIA-WHO classification
Intermittent
Symptom:• < 4 days/ week• or < 4 weeks
Persistent
Symptom
* > 4 days/ week
* and > 4 weeks
Moderate-severe• abnormal sleep • abnormal daily activities• work and school problems• disturbing symptoms
Mild• normal sleep • normal daily activity, sport, recreation • normal work & school • no disturbing symptom
Gloria 2001

Rational for updated of the ARIA recommendations
• some aspects of treatment (complementary & alternative medicines ) • links between upper & lower airways in developing
countries• sport & rhinitis in athletes • rhinitis & links with asthma in pre school children

1. Complementary & alternative medicines are extensively used in the treatment of AR difficult to propose ( not randomized, not controlled, no quantitative measurement)
2. Links between upper & lower airways in developing countries
• Rhinitis is an independent risk factor of asthma• In developing countries rhinitis may be independent • The prevalence generally low than in developed country may be because : under diagnosis lack of awareness limited access to helth care

3. Sport & rhinitis in athletes
Recommendation for athletes address the issue of adapting dx and management to criteria set by International Olympic Committee (IOC) and regulations by the World Anti- Doping Agency ( WADA)
Ex : Oral glucocorticosteroids - prohibited by IOC and WADA Oral B2-agonist prohibited Immunotherapy prohibited Topical steroid - need notification pseudoephedrine - prohibited in competition

4. Rhinitis & links with asthma in pre school children
• The nasal & bronchial mucosa : present similarities• Most important concepts : nose & lung interaction is functional complementarity• Most patients with asthma have rhinitis concept of “ one air one disease”
• In infant & very young children lower respiratory tract symptoms often developed before nasal symptoms

• Chief complain :1. Itching nose2. Sneezing : morning >>3. Serous nose secretion 4. Nasal obstruction at night
• History of other allergic manifestation of patients and other allergic familial manifestations
DIAGNOSIS OF ALLERGIC RHINITISBased on the combination of a typical history of AR symptoms and diagnostic tests

Physical examination
• Nasal passageways• Nasal mucosa• Turbinate• Secretions• Septum• Polyps ?• Sinusitis ?
Including :

IgE examination
Skin Prick Test (in vivo)• Simple• Rapid performance• Low cost• High sensitivity/ specificity
Total serum IgE (in vitro)• Neither very sensitive nor very specific • 35 – 50 % AR Normal IgE levels• Poor correlation with symptom & skin testing result

Watery anterior and sneezing
yes
Nasal obstruction
Symptoms occur at the same time every year
No
Post nasal drip
Colored discharge and/or
facial pain
The patient may be allergic
The patient is likely to be allergic
The patient is unlikely to be allergic
Suspect chronic rhinosinusitis
Confirm diagnosisfor allergic rhinitis
Confirm diagnosisfor rhinosinusitis
Algorithm DX

Symptoms suggestive of Allergic Rhinitis
skin prick test
(+)
eosinophil on nasal cytology
(+) (-)
non allergic rhinitis
NARES
(-)
Allergic rhinitis
Classify andassess severity

MANAGEMENT OF AR
Objectives : • relieving symptoms for improving QOL• to avoid trigger factors • to change the natural history • to avoid / to treat complication
Pharmacologic treatment should take the following factors into account:• Efficacy• Cost-effectiveness of medications• Patient’s preference• Objective of the treatment• Likely adherence to the treatment• Severity and control of the disease• The presence of co-morbidities
Relieving symptoms of AR

1. ANTIHISTAMINE
Consider new antihistamine since : - long acting more practical - no sedating normal daily activity - no / less cardiac effect - broad spectrum effects
except : - patient doesn’t mind sedation effect - is not available - can not be afforded
classic antihistamine can be considered
The first line of pharmacological treatment

2. NASAL DECONGESTANT
• Indicated in patient with prominent nasal
obstruction complaint • As addition / combination with antihistamineLong-term treatment • Systemic nasal decongestant, be careful in hypertension cases & glaucoma.• Topical : rebound effect

3. INTRANASAL CORTICOSTEROID
• long-term treatment safer than systemic • effective to control AR symptomsnotes : * patients should be well informed how to use * symptom relieve is not directly achieved * in some places it is unavailable

EDUCATION
• Explain what is AR / allergic reaction • Explain the meaning of pos. SPT • Confirm whether there is correlation between allergen contact & rhinitis attack• Explain how to do allergen avoidance• Encourage to avoid the allergens
To avoid trigger factors

SPECIFIC IMMUNOTHERAPY ( SIT )
SIT: effective for treating AR
Recommended in patients with :• severe symptoms• fail by pharmacological treatment• positive correlation SPT& history• agree & well informed about duration, schedule of injection & expected results
To change the natural history
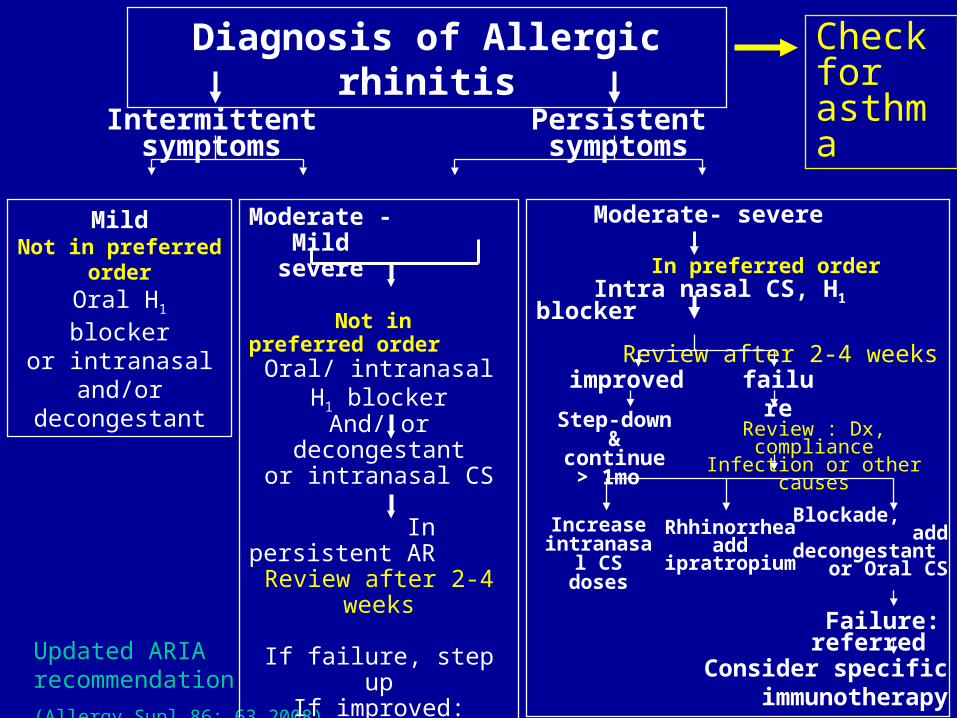
Updated ARIA recommendation
(Allergy Supl 86: 63 2008)
Intermittent symptoms Persistent symptoms
MildNot in preferred orderOral H1 blocker
or intranasaland/or
decongestant
Moderate - Mild severe
Not in preferred orderOral/ intranasal H1
blockerAnd/ or decongestant
or intranasal CS In persistent ARReview after 2-4 weeks
If failure, step upIf improved: continue for
1 mo
Moderate- severe
In preferred order Intra nasal CS, H1 blocker Review after 2-4 weeks
improved failure
Step-down& continue
> 1mo Review : Dx, complianceInfection or other causes
Increase intranasal CS doses
Rhhinorrheaadd
ipratropium
Blockade, add
decongestant or Oral CS
Failure: referred
Consider specific immunotherapy
Diagnosis of Allergic rhinitis Check for asthma
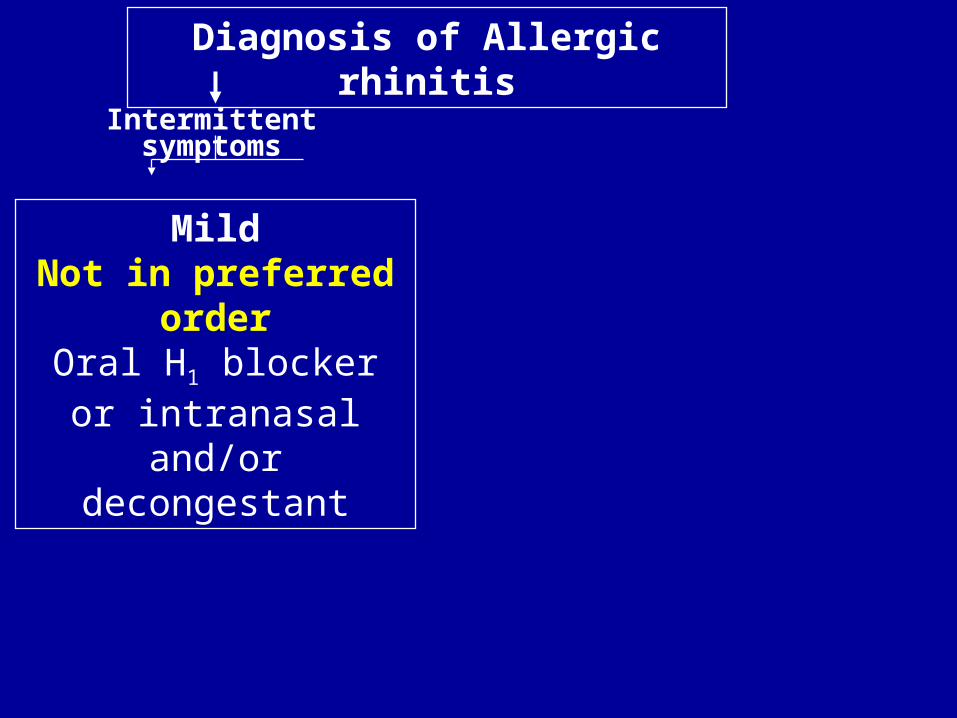
Intermittent symptoms
MildNot in preferred order
Oral H1 blockeror intranasal
and/or decongestant
Diagnosis of Allergic rhinitis
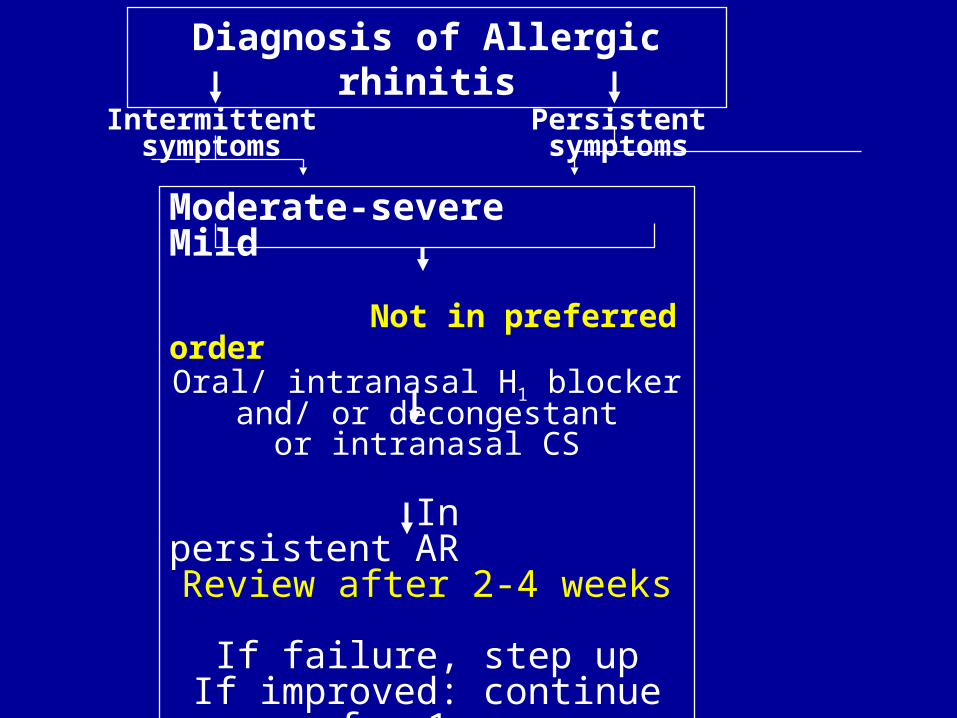
Intermittent symptoms Persistent symptoms
Moderate-severe Mild Not in preferred order
Oral/ intranasal H1 blockerand/ or decongestant
or intranasal CS In persistent AR
Review after 2-4 weeks
If failure, step upIf improved: continue for 1 mo
Diagnosis of Allergic rhinitis

Persistent symptoms
Moderate- severe
improved failure
Step-down & continue > 1mo Review : Dx, complianceInfection or other causes
Increase intranasal CS doses
Rhinorrheaadd ipratropium
Blockade, add decongestant/ Oral CS
Failure: referred to specialist
Consider specific immunotherapy
Diagnosis of Allergic rhinitis
In preferred orderIntranasal CS, H1 blocker
Review after 2-4 weeks


Shekelle guide for level of evidence ( BMJ 1999;318: 593-96)
Level of evidence • Ia : Meta-analysis of RCT• Ib : at least one RCT• IIa : at least one controlled study without randomization• IIb : at least one other type of study• III : Nonexperimental descriptive study• IV : Expert committee reports / opinions

Strength of recommendation
A : category I evidence
B : Category II evidence or extrapolated from
category I
C : Category III evidence
D : category IV evidence







