Download - 10.tobacco cessation programme

1
TOBACCO CESSATION PROGRAMME
CHAITANYA.PII MDSDept of Public Health Dentistry

PREVIOUS QUESTIONS
• Tobacco cessation Counselling. Apr2012, Oct 2013.
2

CONTENTS:• Introduction to Tobacco.• Tobacco production in India.• Tobacco cessation clinics in India.• Global adult Tobacco survey(GATS).• Behavioural counselling for cessation.• Fagerstrome scale for smokers and non -smokers.• Prochaska diclemente model.• Nicotine replacement therapy • Pharmacotherapy• Studies related to success of tobacco cessation.• References.
3

TOBACCO• Plant: Nicotiana• Family: Solanaceae.• Geographical origin: North America• Ingredients: Nicotine.• Species: N. tabacum
4

5

6http://www.mapsofworld.com/world-top-ten/tobacco-producing-countries.html Last accessed on 28/03/2016.
2012

7
LIST OF COUNTRIES BY CIGARETTE CONSUMPTION PER CAPITA
https://en.wikipedia.org/wiki/List_of_countries_by_cigarette_consumption_per_capita Last accessed on 28/03/2016.

The Global Adult Tobacco Survey (GATS) is a nationally representative household survey that was launched in February 2007
16 low- and middle-income countries where more than half of the world’s smokers live and that bear the highest burden of tobacco use
TOPICS FOCUSED:Tobacco use prevalence Second-hand tobacco smoke exposure and policies CessationKnowledge, attitudes and perceptionsExposure to mediaEconomics
Bangladesh, Brazil, China, Egypt, India, Indonesia, Mexico, Pakistan, Philippines, Poland, Russian Federation, Thailand, Turkey, Ukraine, Uruguay and Viet Nam. 8

• Global Adult Tobacco Survey (GATS) in 2010revealed that 47.9% of males 20.3%of females, 34.6% of the adult used tobacco in one or the other form in India
9

10

Source:- Global adult survey report 2010, Union Ministry of Human Health and Family Welfare INDIA 11

How people develop dependence to tobacco?
12

13
On Oral cavity

14
Oral Lesions and Conditions Related to Tobacco Use

15
Potential Negative Impact on Periodontal Tissues from Smoked Tobacco
• Change in vasculature – reducing immune response.
• Suppression of hemorrhagic responsiveness(bleeding).
• Reduction of oxygen in the periodontal pocket – affecting composition of
subgingival flora.
• Interference with cytokine production – inhibiting the immune response.
• Increase in proteolytic enzymes – leading to periodontal destruction.
• Compromised PDL attachment to root surface – poor healing following
periodontal therapy.
• Decrease in lymphocyte production.

16http://www.theguardian.com/news/datablog/2012/mar/23/tobacco-industry-atlas-smokingLast accessed on 28/3/2016

TOBACCO CESSATION CLINICS
2002
5 centers are established.Later it reached to 18 centers.
17

18

• Concept and operational plan was prepared by technical experts from three premier institutions.
19
Institute of Human Behaviour and Allied sciences, Delhi
Postgraduate institute of Medical Education and Research, Chandigarh
National Institute of Mental health and Neurosciences, Bangalore

In the first 5 yrs of tobacco cessation clinic establishment.
34741 cases were registered.
69% - behavioral strategies employed.
31%- pharmacotherapy+
Behavioral counseling.
20
Murthy P, Saddichha S; Tobacco cessation services in India: Recent developments and the need for expansion Indian Journal of Cancer, 2010, Volume 47,Suppl 1 .

21
Three Components for Tobacco Cessation

ARRANGE5 A’S
22

• Ask - Identify and document tobacco use status for every patient at every visit.
(You may wish to develop your own vital signs sticker, based on the sample
below).
• Advise - In a clear, strong, and personalized manner, urge every tobacco user to
quit.
• Assess - Is the tobacco user willing to make a quit attempt at this time?
• Assist - For the patient willing to make a quit attempt, use counseling and
pharmacotherapy to help him or her quit
• Arrange - Schedule follow up contact, in person or by telephone, preferably
within the first week after the quit date.
23

PATIENTS WHO ARE UNWILLING TO QUIT
TOBACCO
5 R’S
24

FAGERSTROME SCALE
25

Fagerstrom scale for nicotine dependence - smoking
26
MAX SCORE = 10 27
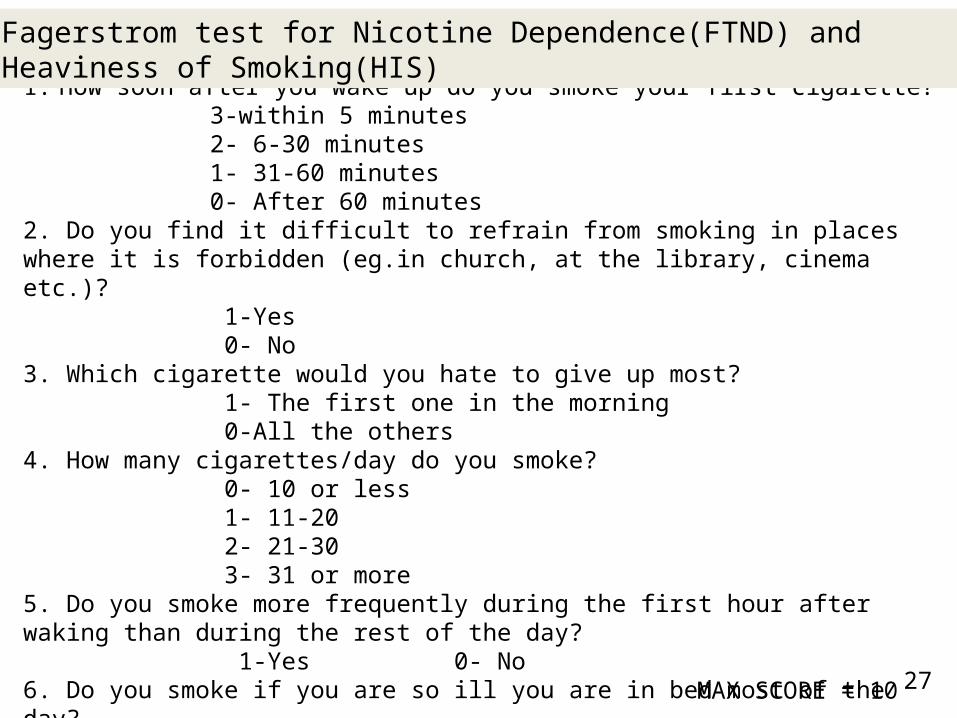
1. How soon after you wake up do you smoke your first cigarette? 3-within 5 minutes 2- 6-30 minutes 1- 31-60 minutes 0- After 60 minutes2. Do you find it difficult to refrain from smoking in places where it is forbidden (eg.in church, at the library, cinema etc.)? 1-Yes 0- No3. Which cigarette would you hate to give up most? 1- The first one in the morning 0-All the others4. How many cigarettes/day do you smoke? 0- 10 or less 1- 11-20 2- 21-30 3- 31 or more5. Do you smoke more frequently during the first hour after waking than during the rest of the day? 1-Yes 0- No6. Do you smoke if you are so ill you are in bed most of the day? 1- Yes 0-No
Fagerstrom test for Nicotine Dependence(FTND) and Heaviness of Smoking(HIS)

Scores on Fagerstrom test
Level of Dependence First line of Treatment
Second Line of Treatment
0 to 2 Very low Dependence Psychological or Behavioral Intervention
3 to 5 Medium Dependence Psychological or Behavioral Intervention
NRT(2mg) (Nutritional supplement)
6 to 7 High Dependence NRT(2mg) along with Psychological or Behavioral Intervention
NRT(4mg)
Above 8 Very High Dependence NRT(4mg) along with Psychological or Behavioral Intervention
Pharmacological intervention
28

29
MAX SCORE = 10 30
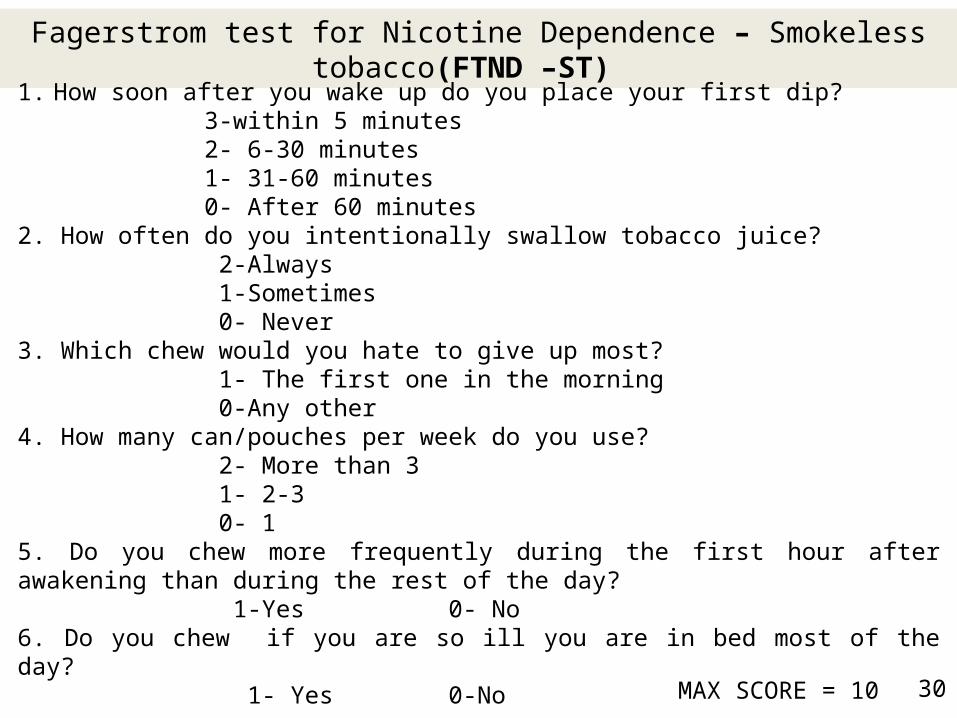
Fagerstrom test for Nicotine Dependence – Smokeless tobacco(FTND –ST)
1. How soon after you wake up do you place your first dip? 3-within 5 minutes 2- 6-30 minutes 1- 31-60 minutes 0- After 60 minutes2. How often do you intentionally swallow tobacco juice? 2-Always 1-Sometimes 0- Never3. Which chew would you hate to give up most? 1- The first one in the morning 0-Any other4. How many can/pouches per week do you use? 2- More than 3 1- 2-3 0- 1 5. Do you chew more frequently during the first hour after awakening than during the rest of the day? 1-Yes 0- No6. Do you chew if you are so ill you are in bed most of the day? 1- Yes 0-No

31
Scores on Fagerstrom test
Level of Dependence First line of Treatment
Second Line of Treatment
0 to 4 Very low Dependence Psychological or Behavioral Intervention
5 to 8 Medium Dependence Psychological or Behavioral Intervention
NRT(2mg) (Nutritional supplement)
9 to 10 High Dependence NRT(2mg) along with Psychological or Behavioral Intervention
NRT(4mg)
Above 10 Very High Dependence NRT(4mg) along with Psychological or Behavioral Intervention
Pharmacological intervention

Prochaska and Diclemente
The Transtheoretical Model (TTM)(1983)
32

33
http://www.prochange.com/transtheoretical-model-of-behavior-change last accessed on 28/3/2016

34
Stage of Readiness Patient Response to: “What are your thoughts and feelings about Quitting smoking?”
Goal of intervention
Typical Physician Intervention
Precontemplation “I like to smoke” Introduce ambivalence
“Your emphysema will improve after you quit smoking”
Contemplation “I like to smoke, but I know I need to quit”
Resolve ambivalence
“How will your life be better after you’ve quit smoking?”
Preparation “I’m ready to quit” Identify successful strategies
“Choose a ‘quit day’ and let’s make plans for it”
Action “I’m not smoking, but I still think about smoking from time to time”
Provide solutions to specific relapse triggers
“How can you deal with your desire to smoke in those situations?”
Maintenance “I used to smoke” Solidify patient’s commitment to a smoke free life
“This would be a good time to share your experience with other people”
Summary of physician counselling based on the stages of change

NICOTINE REPLACEMENT THERAPY
35

NICOTINE REPLACEMENT THERAPY(NRT)
36

37

2 mg (< 25 cigarettes/day) 4 mg (≥ 25 cigarettes/day)
User controls dose• Oral substitute for cigarettes• Available without prescription
Disadvantages:Difficult for denture wearers to use
side effects:•Mouth irritation•Stomach ache• Sore jaw• Nausea• Hiccups 38

urge to smoke Within 30 min after wake up
Urge to smoke no sooner than 30 min
9–20 lozenges/day during first 6 weeks, thendecrease dose gradually until treatment isstopped
Advantages:•Easy to use• Oral substitute for cigarettes• Available without prescription
Adverse effects:•Insomnia• Nausea• Hiccups• Coughing
39

•Easy to use• Unobtrusive• Available without prescription.
Disadvantages:•User cannot adjust dose if craving occurs• Nicotine released more slowly than in other products
Adverse effects:•Skin irritation• Insomnia
40

•User controls dose• Hand-to-mouth substitute forcigarettes
Disadvantages;•Frequent puffing needed• Device visible when used
Adverse effects:•Mouth and throat irritation• Cough• Rhinitis
41

dosage:1–2 doses/hr(1 mg total; 0.5 mg in each nostril)(maximum, 40 mg/day)
•User controls dose• Offers most rapid delivery of nicotine and highest nicotine levels of all nicotine replacement products.
Adverse effects:•Nasal irritation• Sneezing• Cough• Tearing
42

Pharmacotherapeutic approach
43

44
Bupropion SR 1-2 wks before quit date
150mg/d for 3days, then 150mg bid for 7-12wks
May continue use for 6mon after quit date

45
Varenicline 1wk before quit date
0.5mg/d for 3d; then 0.5mg bid for 4d; then 1.0mg bid for 3mon
May continue use for 6

Recommended:-75–100 mg/dayTreatment should be started 10–28 days before the quit date at a dose of 25 mg/day; the dose should be increased as tolerated.
Side effects:•Dry mouth• Sedation• Dizziness• Tremor
Nortriptyline is a tricyclic anti depressant .It has a sedative effect which ‐helps to improve sleep
46

Studies – success of tobacco cessation
47

• A real-life study of the effectiveness of different pharmacological approaches to the treatment of smoking cessation: re-discussing the predictors of success
• Study place: University of Sao PauloMedical School, brazil. 836 – smokers. 25 cigarettes/day
Fagerstrome Score - 6.6.Result: tobacco cessation teaching in hospital has higher
success rates. Nortriptyline + NRT Higher success rates(46.4%).
48
Gustavo Faibischew Prado, Elisa Maria Siqueira Lombardi, Marco Anto nio Bussacos,Frederico Leon Arrabal-Fernandes, Ma´rio Terra-Filho, Ubiratan de Paula Santos; A real-life study of the effectiveness of different pharmacological approaches to the treatment of smoking cessation: re-discussing the predictors of success; CLINICS 2011;66(1):65-71

Settings and Design: This is a community based tobacco cessation program of one year duration conducted among women in a low socioeconomic area of Mumbai, India. Subjects and Methods: It involved three interventions conducted at three months interval, comprised of health education, games and counseling sessions and a post intervention follow up.
49
• Tobacco use among family members and in the
community was primary reasons for initiation
and addiction to tobacco was an important
factor for continuation, whereas health
education and counseling seemed to be largely
responsible for quitting. The quit rate at the end
of the programme was 33.5%.
GA Mishra, SV Kulkani, Majumdar PV, SD Gupta, SS Shastri; Community-based
tobacco cessation program among women in Mumbai, Indian Journal of Cancer, Dec
2014, Volume 51, supplement 1

• AIMS:• To assess the tobacco quit rates among employees, through self report history, and validate it with
rapid urine cotinine test; compare post-intervention KAP regarding tobacco consumption with the pre-intervention responses and assess the tobacco consumption pattern among contract employees and provide assistance to encourage quitting.
• SETTINGS AND DESIGN:• This is a cohort study implemented in a chemical industry in rural Maharashtra, India.• MATERIALS AND METHODS:• All employees (104) were interviewed and screened for oral neoplasia. Active intervention in the form
of awareness lectures, focus group discussions and if needed, pharmacotherapy was offered. Medical staff from the industrial medical unit and from a local referral hospital was trained. Awareness programs were arranged for the family members and contract employees.
• RESULTS:• Forty eight per cent employees consumed tobacco. The tobacco quit rates increased with each follow-
up intervention session and reached 40% at the end of one year. There was 96% agreement between self report tobacco history and results of rapid urine cotinine test. The post-intervention KAP showed considerable improvement over the pre-intervention KAP. 56% of contract employees used tobacco and 55% among them had oral pre-cancerous lesions.
• CONCLUSIONS:• A positive atmosphere towards tobacco quitting and positive peer pressure assisting each other
in tobacco cessation was remarkably noted on the entire industrial campus. A comprehensive model workplace tobacco cessation program has been established, which can be replicated elsewhere.
50
GA Mishra, SV Kulkani, Majumdar PV, SD Gupta, SS Shastri; Workplace tobacco cessation program in India: A success story. Indian Journal of Occupational and Environmental Medicine; December 2009, Volume 13, Issue 3.

World No Tobacco Day 2016: Get ready for plain packaging
packaging of tobacco products is an important demand reduction
measure. It reduces the attractiveness of tobacco products, restricts
use of tobacco packaging as a form of advertising, limits misleading
packaging and labelling, and increases the effectiveness of health
warnings.
For World No Tobacco Day, 31 May 2016, WHO and the Secretariat
of the WHO Framework Convention on Tobacco Control are calling
on countries to get ready for plain (standardized) packaging of
tobacco products.
http://www.who.int/campaigns/no-tobacco-day/2016/en/. Last accessed on 28/03/2016. 51

Barriers of tobacco cessation
• The lack of training and sensitization of health
professionals limits the assessment and
intervention of tobacco use.
52

Lack of trained health professionals to provide quitting support
53

Lack of knowledge of ill effects of tobacco.
54

55

References
1. Daly & bachelor,Richard Watt – Essential Dental Public Health.
2. Esther v Wilkins – clinical practice for dental hygienist.
3. Prochaska JO, DiClemente CC. Toward a comprehensive model of change.
In: Miller WR, Heather N, eds. Treating addictive behaviors: processes of
change. New York: Plenum, 1986:3–27.
4. Clinical practice. Treatment of tobacco use and dependence. N Engl J Med
2002;346:506-512.
5. Murthy P, Saddichha S; Tobacco cessation services in India: Recent
developments and the need for expansion;Indian Journal of Cancer,
2010;Volume 47 ;Suppl 1
6. WHO – GLOBAL ADULT TOBACCO SURVEY (GATS)-2007.
56

7. GA Mishra, SV Kulkani, Majumdar PV, SD Gupta, SS Shastri; Community-
based tobacco cessation program among women in Mumbai, Indian Journal of
Cancer, Dec 2014, Volume 51, supplement 1
8. GA Mishra, SV Kulkani, Majumdar PV, SD Gupta, SS Shastri;
Workplace tobacco cessation program in India: A success story. Indian Journal of
Occupational and Environmental Medicine; December 2009, Volume 13, Issue 3.
9. Cherian Varghesea ; Initiating tobacco cessation services in India: challenges
and opportunities;WHO South-East Asia Journal of Public Health
2012;1(2):159-168 .
10. Krishna M. Palipudi, Prakash C. Gupta, Dhirendra N. Sinha, Linda J. Andes,
Samira Asma, Tim McAfee, on behalf of the GATS Collaborative Group; Social
Determinants of Health and Tobacco Use in Thirteen Low and Middle Income
Countries: Evidence from Global Adult Tobacco Survey; Plos one; March 2012,
Volume 7, Issue 3,e33466 57

11. http://www.who.int/campaigns/no-tobacco-day/2016/en/. Last accessed on
28/03/2016.
12. Brian A King, Sara A Mirza, Stephen D Babb, and for the GATS
Collaborating Group; A cross-country comparison of second hand smoke
exposure among adults: findings from the Global Adult Tobacco Survey
(GATS); Tob Control. 2013 July ; 22(4): e5.
13. Gustavo Faibischew Prado, Elisa Maria Siqueira Lombardi, Marco Anto
nio Bussacos,Frederico Leon Arrabal-Fernandes, Ma´rio Terra-Filho, Ubiratan
de Paula Santos; A real-life study of the effectiveness of different
pharmacological approaches to the treatment of smoking cessation: re-
discussing the predictors of success; CLINICS 2011;66(1):65-71.
58
59
14.http://www.mapsofworld.com/world-top-ten/tobacco-producing countrieshtml.
Last accessed on 28/03/2016.
15.https://en.wikipedia.org/wiki/List_of_countries_by_cigarette_consumption_
per_capita Last accessed on 28/03/2016.
16. Norman O. Harris; Primary Preventive Dentistry, 7th Edition, 2009, Julie Levin
Alexander publishers.17. http://www.theguardian.com/news/datablog/2012/mar/23/tobacco-industry-atlas-smoking Last accessed on 28/3/2016

60







