
1
What does the Bush Administration’s Medicaid Reform Proposal Mean for
Home and Community-Based Services?
Joan AlkerSenior Researcher
Institute for Health Care Research and PolicyGeorgetown [email protected]

2
Medicaid serves as a critical health care safety net for specific groups of low-income people
Provides health care coverage to 47 million low-income people in the United States
Serves over 8 million people with disabilities Covers more than 1 in 5 children and pays for 40% of all births in the
United States Largest source of financing for long-term care and covers nearly 70% of
nursing home residents Largest source of coverage for HIV/AIDS care Largest funder for state and local spending on mental health services

3
Medicaid is a federal/state matching program
Federal government matches state spending on an open-ended basis Formula for reimbursement depends on states per capita income Matching rates vary from 50 percent in high per capita income states to 77
percent in low per capita income states like Mississippi

4
Medicaid Fills Medicare’s GapsOver One-Third of Medicaid Benefit Spending -- $68 billion – is
for Services for Medicare BeneficiariesThis Grows Over Time with the Baby Boomers’ Retirement
Spending onMedicare
Beneficiaries35%
Spending onAll Other
Beneficiaries65%
Source: Secretary’s Advisory Committee on Regulatory Reforms, June 2002. Data for 1999.

5
Medicaid Long Term Care Spending (1998)
Other3%
ICF/MR15%
Nursing Facility
53%
Mental Health5%
Home Care24%
Source: Urban Institute estimates, based on HCFA-2082 and HCFA-64 reports.
Total = $58.7 billion

6
“Mandatory" Groups “Optional” Groups
• Children under age 6 ≤ 133% FPL
• Children age 6 - 18 ≤ 100% FPL
• Children in foster care
• Pregnant women ≤ 133% FPL
• Parents with incomes below state-
established minimums (median = 60% FPL)
• People with disabilities and the elderly
receiving SSI (incomes ≤ 74% FPL)
• Low-income Medicare beneficiaries
• Children and parents above minimum
requirements
• Pregnant women 133% FPL
• People with disabilities and the elderly 74%
FPL, including those in nursing homes
• Disabled and elderly people served under
Home and Community Based waivers
• Women with breast and cervical cancer
• Certain disabled people who are employed
and buy into coverage
Medicaid has both mandatory and optional eligibility groups

7
Care for Older People and People with Disabilities is the Most Costly
(Medicaid Expenditures Per Enrollee, 2001)
$1,447$2,283
$11,238
$12,322
$0
$3,000
$6,000
$9,000
$12,000
$15,000
Children Parents Disabled Elderly
Source: CBO January 2002 Baseline.
8
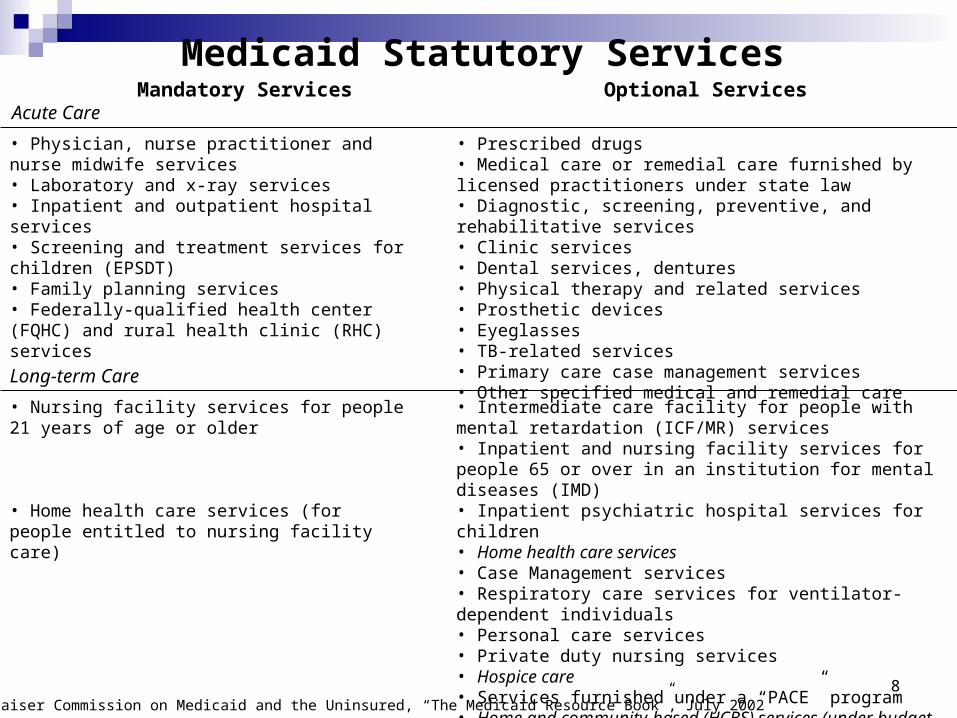
Mandatory Services Optional Services
• Physician, nurse practitioner and nurse midwife services• Laboratory and x-ray services• Inpatient and outpatient hospital services• Screening and treatment services for children (EPSDT)• Family planning services• Federally-qualified health center (FQHC) and rural health clinic (RHC) services
• Prescribed drugs• Medical care or remedial care furnished by licensed practitioners under state law• Diagnostic, screening, preventive, and rehabilitative services• Clinic services• Dental services, dentures• Physical therapy and related services• Prosthetic devices• Eyeglasses• TB-related services• Primary care case management services• Other specified medical and remedial care
Source: Kaiser Commission on Medicaid and the Uninsured, “The Medicaid Resource Book”, July 2002
Medicaid Statutory Services
Acute Care
Long-term Care
• Nursing facility services for people 21 years of age or older
• Home health care services (for people entitled to nursing facility care)
• Intermediate care facility for people with mental retardation (ICF/MR) services• Inpatient and nursing facility services for people 65 or over in an institution for mental diseases (IMD)• Inpatient psychiatric hospital services for children• Home health care services• Case Management services• Respiratory care services for ventilator-dependent individuals• Personal care services• Private duty nursing services• Hospice care• Services furnished under a “PACE” program• Home and community-based (HCBS) services (under budget neutrality waiver)

9
Medicaid plays a major role in the health care system and is a major contributor to state economic activity
Program is projected to be larger than Medicare in 2003 $155 billion in federal dollars, $116 billion in state dollars in 2003 Accounts for nearly 17% of the nation’s health care expenditures
Single largest source of federal financing to states (43%) Provides key financial support to safety net health centers, hospitals and other
providers Economic engine in many communities

10
Medicaid is a significant source of national health spending
17% 17%
11%
17%
48%
Total PersonalHealth Care
Hospital Care ProfessionalServices
Nursing HomeCare
PrescriptionDrugs
SOURCE: Heffler, S. et al., 2002. Based on National Health Care Expenditure Data, Centers for Medicare and Medicaid Services, Office of the Actuary.
Total National
Spending(billions)
$1,130 $412 $422 $92 $122
Medicaid as a share of national
spending (2000):

11
States are experiencing severe fiscal challenges
12
State budget problems are leading to Medicaid cuts
49 states and the District of Columbia will cut Medicaid spending in the current fiscal year
32 states have had to cut Medicaid spending twice during the year States are:
Freezing or cutting payments to providers Controlling prescription drug costs Reducing Medicaid benefits Restricting Medicaid eligibility Increasing beneficiary co-payments
13
Looking to the future, statesare worried
Many states say they cannot continue to afford Medicaid if costs rise as projected
Medicaid pays for costs that should be covered by Medicare—35% of Medicaid spending is for services for “dual eligibles”, persons who receive both Medicaid and Medicare
Prescription drug costs are increasingly rapidly The need for long-term services and supports will increase significantly

14
States need immediate help
States need short-term funding so that they can maintain their commitment to Medicaid and avoid further cutting services and eligibility – Congress has been debating a temporary increase in the “FMAP”
Current recession means that since more people are out of work, more people count on Medicaid for health care coverage
After fixing short-term problems, there are long-term challenges to be addressed

15
Bush Administration’s response
The Administration has consistently opposed a temporary increase in the FMAP
The President’s FY2004 budget includes a radical restructuring of the way Medicaid is paid for and run

16
The President’s Medicaid proposal
At least 2/3 of the spending (and possibly all) will be “block granted”. States choose to participate – if they don’t however, they get no fiscal relief. States that choose to participate receive capped federal payments that they
have to pay back in later years. The proposal is “budget neutral” – offering $12.7billion over 7 years that is paid back in years-8-10.
Eliminates the SCHIP program as we know it. No required state matching payments/ a “maintenance of effort” system instead “Carte blanche” flexibility

17
How does block grant proposal work? States would receive 2 annual, capped
allotments from federal govt; one for acute care and one for LTC
States could move some portion of the funds between 2 accounts (10%?)
Up to 15% of each allotment for DSH and admin

18
Key features of the President’s proposal
Capped federal payments to states
Payments front loaded to provide fiscal relief, but reductions in later years - $12.7 billion over 7 years; “budget neutral” over 10 years.
In comparison 80 Senators voted for a Sense of the Senate in March which would provide states with at least $15billion in increased FMAP over 1 year.

19
Capped Federal Payments
Based on 2002 spending, adjusted forward using 10-year growth projections
Funding no longer based on actual changes in enrollment Funding no longer based on actual changes in health care costs,
utilization, new technology

20
Bush plan would allow for “complete” flexibility for “optional” beneficiaries
What does this mean?:
Optional services could be provided for some groups of people but not others Some services could be covered in some parts of the state but not others States could adopt closed formularies for drugs: high cost drugs could be
excluded even if needed Federal standards on cost sharing could be relaxed or eliminated Current “mandatory” services, such as mental health care or hospital care, could
be cut out of the benefits package for “optional” people States might not have to meet nursing home quality standards
Impact on mandatory beneficiaries is unclear

21
Risk #1:Difficult to predict spending changes in Medicaid over time

22
105
115
125
135
145
1999 2000 2001 2002
Actual 2002
CBO 2002
CBO 2001
CBO 2000
CBO 1999
CBO 1998
CBO 1997
CBO Federal Medicaid Spending Projections, 1999-2002
Variance in actual 2002 expenditures vs. projections is $17 billion or 12% of all 2002 federal payments.
Source: Congressional Budget Office historical budget tables, previous editions of its Economic and Budget Outlook.
(billions of dollars)

23
Medicaid Long Term Care Average Annual Expenditure Growth Rates 1990-1998
9.1%
18.2%
8.2%
3.4%
4.7%
0%
5%
10%
15%
20%
All LTC Home Care Nursing Home ICF/MR Mental Health
Source: Urban Institute estimates, based on HCFA-2082 and HCFA-64 reports.

24
Risk #2: Capped Funding Inevitably Results In Winners and Losers Among States
Base year differences Differences in growth rates States do not have to take the block grant option
But states may not be able to predict if they will be a winner or a loser No fiscal relief if state does not opt in
25
Risk #3: States likely to withdraw a significant portion of their funding

26
Under Current Law When A State Cuts State Spending, It Loses Federal Funds
Amount of federal dollars lost if a state reduces state Medicaid spending by $125 million, at different match rates
FederalDollars
Lost(millions)
$125
$232
$375
Match Rate
StateFundsSaved
(millions)
50%
65%
75%
$125
$125
$125
Under The Proposal, A State Could Cut State Spending Without Losing Federal Funds (as
long as it meets the MOE requirement)
FederalDollars
Lost(millions)
$0
State Funds Saved
(millions)
$125
Amount of federal dollars lost if a state reduces state Medicaid spending by $125 million
Bush plan could lead to lost state support for Medicaid

27
Under Current Law When a State Invests State Funds to Expand Coverage, Federal
Funds Grow
Amount of federal dollars gained if a state expands state Medicaid spending, at different match rates
Match Rate
New StateInvestment(millions)
50%
65%
75%
$125
$125
$125
Additional Federal Funds
(millions)
$125
$232
$375
Under The Proposal, If A State Invests State Funds To Expand Coverage, Federal Payments
Do Not Grow (assuming the state is receiving its full federal allotment)
Additional Federal Funds
(millions)
New State Investment(millions)
$125 $0
Amount of federal dollars gained if a state expands state Medicaid spending
Bush plan would diminish state incentives to invest in Medicaid

28
What Spending Would be Under the Cap?

29
Most Spending in Medicaid is “Optional” (1998)
Mandatory Expenditures For Mandatory Groups
35%
Optional Services forMandatory
Groups21%
All Services forOptional Groups
44%
Optional Expenditures
65%
Source: Urban Institute estimate, based on data from federal fiscal year 1998 HCFA2082 and HCFA-64 reports, 2001
Note: Expenditures do not include disproportionate share hospital (DSH) payments, administrative costs, or accounting adjustments.

30
Most “Optional” Spending is for the Elderly and Disabled
(Optional Spending by Eligibility Group, 1998)
Source: Urban Institute estimate, based on data from federal fiscal year 1998 HCFA2082 and HCFA-64 reports, 2001
Disabled45.0%
Parents9.0%
Children8.0%
Elderly38.0%
Optional Spending = $100 billion
Note: Expenditures do not include disproportionate share hospital (DSH) payments, administrative costs, or accounting adjustments.

31
ElderlyDisabled
Mandatory Services for Mandatory Groups
Optional Services for Mandatory Groups
All Services for Optional Groups
Children Parents
Distribution of Medicaid Spending by Eligibility Group and Type of
Service, 1998
15%
20%
65%
41%
14%
45%34% 34%
32%73%
17%
10%
Note: Expenditures do not include disproportionate share hospital (DSH) payments, administrative costs, or accounting adjustments.
Source: Urban Institute estimates, based on data from federal fiscal year 1998 HCFA 2082 and HCFA-64 reports, 2001

32
Optional Spending for Long Term Care (1998)
Home and Community-
Based Waivers
16%
Mental Health5%
Nursing Facility
51%
Other Home Care10%
ICF-MR17%
Home Health Care1%
Source: Urban Institute estimate, based on data from federal fiscal year 1998 HCFA2082 and HCFA-64 reports, 2001
Note: Expenditures do not include disproportionate share hospital (DSH) payments, administrative costs, or accounting adjustments.
Total = $58.7 billion

33
Other solutions?
Increasing the Medicaid “FMAP” Medicare prescription drug benefit Increasing the Medicaid Drug Rebate Other controls on prescription drug costs Federalizing “duals”/federalizing LTC







