
May 31, 2014
340B UNIVERSITY™
Las Vegas Edition

SESSION 1:THE TOP 5:
340B BASICS FOR HOSPITALS
Mike Benedict

Objectives
1. Define the intent of the 340B Program2. Describe the major 340B stakeholders 3. Explain how to participate in 340B4. Identify how the Prime Vendor Program
supports 340B stakeholders5. List the program rules and explain how to
follow them

Takeaways
1. The intent of 340B: to support entities that serve vulnerable patients so the entities stay in business
2. Major 340B stakeholders: federal government, certain drug manufacturers, certain covered entities, 340B Prime Vendor Program, managed by Apexus
3. Covered entities must register on the HRSA Database; once a year they must recertify accuracy of HRSA 340B database information

Takeaways
4. The 340B Prime Vendor Program provides:
– Truth (call center)
– Teamwork (contracting with distributors and suppliers)
– Teaching (340B University)
5. Covered entities must maintain auditable records:
– Only patients of the covered entity receive 340B drugs
– A Medicaid rebate is not paid on a 340B drug
– All eligibility criteria are met

1. 340B PROGRAM INTENT AND OVERVIEW

340B Intent
To permit covered entities “to stretch scarce Federal resources as far as possible, reaching more eligible patients and providing more comprehensive services.”
H.R. Rep. No. 102-384(II), at 12 (1992)

Which examples below describe 340B program savings used in alignment with 340B program intent? Discuss at your table.A. Supporting an indigent care clinicB. Starting a patient assistance medication programC. Subsidizing medications for patients unable to payD. Adding pharmacy staff
Share

340B Statute
• Resulted from a 1992 federal statute• Manufacturers participating in Medicaid Drug
Rebate Program must sign a PharmaceuticalPricing Agreement (PPA) with the Secretary ofHealth and Human Services– The manufacturer agrees to charge a price for
covered outpatient drugs that does not exceed the340B price

340B Price
• Calculated quarterly– 340B ceiling price =
Average Manufacturer Price (AMP) – Medicaid Unit Rebate Amount (URA)
• Manufacturer submits data to CMS

Relative Pricing
100%
79%
66% 64%58%
53% 51% 49%
0%10%20%30%40%50%60%70%80%90%
100%
42%
Private Sector Pricing
Adapted from a slide by Safety Net Hospitals for Pharmaceutical AccessSource: Data derived from Prices for Brand-Name Drugs Under Selected Federal Programs, Congressional Budget Office (June 2005)

340B Covered Outpatient Drugs*
http://www.ssa.gov/OP_Home/ssact/title19/1927.htm
Drug not directly reimbursed
FDA doesn’t require NDC
Vaccines
Inpatient drugs
Outpatient Prescription Drugs
Over-the-counter drugs (with a prescription)
Clinic administered drugs
Biologics
Insulin

Program Evolution
1992 2014
AccessSub-Regulatory
IntegrityRegulatory

Have you been here?

340B Program Integrity
OPA Program Integrity Page:http://www.hrsa.gov/opa/programintegrity/index.html
Manufacturer Entity• Calculate and charge a
correct 340B price
• Subject to HRSA audits
• Comply with 340B statute and guidelines
• Subject to HRSA and manufacturer audits

Concerns from Peers
• “I’m afraid I’ll have an audit and not be awareof a particular aspect of the program, eventhough I’ve tried to stay on top of everything.”
• “I worry about how to apply certain policies; itseems that there are different interpretations ofthe right thing to do.”

Share
Please share your primary 340B program integrity concern with the person sitting next to you.

Review
Which of the following is a 340B covered outpatient drug?
a) Vaccine
b) Inpatient drugs
c) Over the counter drug not prescribed in writing by an authorized provider
d) None of the above are covered outpatient drugs

Entities Take Action
1. Describe how your entity’s use of the 340B program supports the intent of the 340B program.
2. Identify how your entity can document the use of 340B savings to align with the intent of the 340B program.
3. Incorporate these elements into your 340B related standard operating procedures.
4. Rely on trusted resources identified by OPA as the source of truth for 340B issues: OPA and Apexus.

2. MAJOR 340B STAKEHOLDERS

Major 340B Stakeholders
Manufacturer Calculate and offer 340B price
Entity Provide 340B access
OPA Administer 340B program 340B Drug
to Patient

HRSA Office of Pharmacy Affairs (OPA)
• Health Resources and Services Administration (HRSA)– Oversees 340B program administration (enrollment,
recertification, compliance) – Establishes mechanism to prevent duplicate discounts– OPA support
• The 340B Prime Vendor Program, managed by Apexus– Apexus is not the same thing as HRSA; Apexus communicates
HRSA policy

HRSA-Endorsed Resources
• HRSA• Apexus

340B Eligible Entities*
Federal Grantees/Designees Certain Hospitals• Federally Qualified Health Center• Federally Qualified Health Center Look-Alikes• Title X Family Planning Grantees• State Aids Drugs Assistance Programs• Ryan White Care Act Grantees (A,B,C,D,F)• Black Lung Clinics• Hemophilia Treatment Centers• Native Hawaiian Health Centers• Urban Indian Organizations• Sexually Transmitted Disease Grantees• Tuberculosis Grantees
• Disproportionate Share Hospitals• Children’s Hospitals• Critical Access Hospitals• Free Standing Cancer Hospitals• Rural Referral Centers• Sole Community Hospitals

340B Hospital Eligibility
Entity TypeNon-profit/
Govt. Contract
DSH% GPO Prohibition* Orphan Drug* Applies?
Disproportionate Share Hospital (DSH) Yes >11.75% Yes No
Children’s Hospital (PED) Yes >11.75% Yes No
Free-standing Cancer Hospital (CAN) Yes >11.75% Yes Yes

340B Hospital Eligibility
Entity TypeNon-profit/
Govt. Contract
DSH% GPO Prohibition* Orphan Drug* Applies?
Critical Access Hospital (CAH) Yes N/A No Yes
Rural Referral Center (RRC) Yes > 8% No Yes
Sole Community Hospital (SCH) Yes > 8% No Yes

3. PARTICIPATION IN 340B

1. Ensure it has the capability to follow (and maintain auditable records documenting compliance with) program rules
2. Register on the HRSA 340B database3. Recertify with HRSA annually
To Participate in 340B, an Entity must…

HRSA 340B Database*
• The HRSA 340B Database is the official source of 340B information– Entities*– Contract Pharmacies*– Manufacturers– Medicaid Exclusion File*

340B Database: Statistics
• 340B database:http://opanet.hrsa.gov/opa/default.aspx
• APR 2014– 25,196 registered sites: 11,718 are hospital sites– 14, 485 unique contract pharmacies– >$7.5B/year in 340B drug purchases– ~82% of 340B participants enrolled with Apexus

340B Database: Statistics, continued
• APR 2014– 18% of covered entity sites utilize contract
pharmacies– 89% of covered entity sites use only in-house or in-
house and one contract pharmacy– Of sites using contract pharmacy, 73% have five
or fewer contract pharmacy arrangements

• Entities DO NOT need to log into the 340B database
• All links referenced on the homepage are accessible without a username & password
Working with the HRSA 340B Database

Working with the HRSA 340B Database
• When searching for your covered entity’s profile - LESS IS MORE
• The 340B ID is the most reliable search criteria

Working with the HRSA 340B Database
• Covered entity data is divided between tabs on the 340B profile
• The information about your facility can be found under the applicable tabs

HRSA 340B Database: Medicaid

• Important Notifications & What’s Newo Great resource for important notifications about:
Registration Recertification Change requests Database changes
Working with the HRSA 340B Database

Registration Process*
• New entities, entity sites, contract pharmacies,Medicaid information– 2 week registration periods, quarterly updates
made to OPA Database
• Change requests: changes to existing information,rolling basis
Update Official October 1 January 1 April 1 July 1
Registration Period July 1 – 15 October 1 -15 January 1 – 15 April 1 - 15

Apexus Answers
What types of documentation must a
hospital supply to HRSA to register?

Hospital Cost Report
340B Eligible clinics should be reimbursable ( on lines 50-118)340B Eligible clinics should be reimbursable ( on lines 50-118)
340B Eligibility if line 33 shows DSH% >11.75 or ≥8%, depending upon hospital type340B Eligibility if line 33 shows DSH% >11.75 or ≥8%, depending upon hospital type
Hospital ownership /control on line 21 Hospital ownership /control on line 21
Date and Time of eligibility-signature blockDate and Time of eligibility-signature block
Shows outpatient chargesShows outpatient charges
A
EPart A
S2
S
C
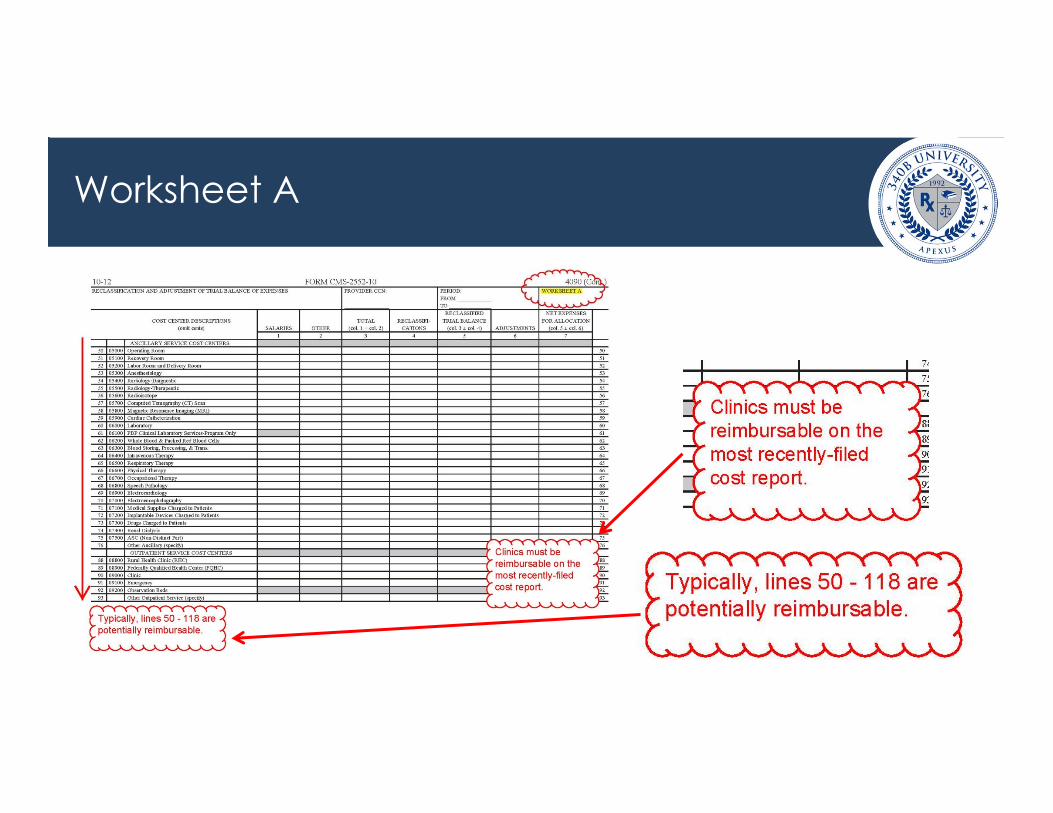
Worksheet A

Worksheet E, Part A

Worksheet S2

Worksheet S

Worksheet C

Outpatient Clinics
• Use 340B only in clinics that:– Appear as reimbursable on the most recently
filed Medicare Cost Report– Are integral parts of the hospital– Use 340B for patients that meet the 340B patient
definition

Apexus Answers
Which outpatient facilities are hospitals required to
register on the 340B database?
Recertification*:
• Entities are required to recertify informationin the HRSA 340B database annually
• HRSA sends a notification email toAuthorizing Official and Primary Contact
• The Authorizing Official performs therecertification online

Recertification Statements*:
• Database entry is complete, accurate, correct
• Entity meets 340B eligibility requirements
• Compliance with 340B requirements/restrictions
• Maintenance of auditable records
• Systems in place to ensure compliance
• Contract pharmacy compliance, entity obtains sufficient information
• Entity contacts OPA for any breach of the above
• Entity acknowledges possibility of payment to manufacturers for failure to notify OPA in timely fashion

Review
Updates sent to OPA during its registration period of October 1-October 15 will be reflected on the OPA database and active as of:
a) January 1
b) October 1
c) April 1
d) July 1

Review
In order to be 340B eligible, outpatient clinics of hospitals must:
a) Be listed as reimbursable on the most recently filed cost report
b) Must be an integral part of the hospitalc) Adhere to all 340B guidelines (i.e. patient
definition, etc.) d) All of the above

Entities Take Action
1. If you have never seen your entity’s record on the OPA database, visit the site, review the record and ensure it is accurate.
2. Identify all potentially eligible 340B areas of your entity; determine if your entity has implemented 340B in all areas that are eligible.
3. For hospitals only: talk to your CFO about the cost report worksheets discussed in this session, and ensure the CFO understands that changes to information on these forms may impact 340B eligibility.

4. THE PRIME VENDOR PROGRAM

Apexus Focus
TEAM
WORK Contract
Services
TEAC
HING 340B University
& 340B OnDemand
TRUTH Apexus
Answers Call

Teamwork: Contracted Supplier Agreements (by year)
17
26
3845
5156
6165
100
0
20
40
60
80
100
120
2005 2006 2007 2008 2009 2010 2011 2012 2013
Con t r ac t s

Teaching: 340B University
• National experts share leading practices at this one ortwo day live educational program
• Aligned with HRSA policy, compliance-focused• Only HRSA-endorsed compliance training• CE for pharmacists and technicians offered• Interactive, opportunities to network, leave with tools to
equip your entity• 10+ Sessions in 2014• Online, on-demand modules under development

Truth: Apexus Answers
• National 340B source of truth, communicates HRSA policy
• Staff in constant communication with HRSA to ensure messaging is consistent
• FAQs available here: https://www.340bpvp.com/resource-center/faqs/
• Average monthly interactions ~2,000
• Tiered levels of response: can handle from basic to complex

5. 340B PROGRAM RULES

Forces Impacting OPA
OPA340B
Stakeholders*
340B Participants(Entities and
Manufacturers)Advocacy
Government (OIG, GAO, CMS, etc.)

Why 340B is like an onion…

340B Policy Options*
Policy Releases
Guideline
Regulation
Statute

Do you see a musician or a woman’s face?

340B Policies*
Guidelines Regulations (proposed**)• Patient Definition*• Contract Pharmacy*• Audits*• Dispute Resolution*• Outpatient Facilities• Duplicate Discounts*
• Manufacturer CivilMonetary Penalties**
• Administrative DisputeResolution**
• Orphan Drugs*


Major 340B Compliance Areas
1. Duplicate Discount Prohibition*2. No Diversion (Patient Definition)*3. Certain Hospitals Only
– Group Purchasing Organization (GPO) Prohibition*– Orphan Drug Exclusion

Duplicate Discount Prohibition
340B Price Medicaid Rebate

Preventing Duplicate Discounts

Patient Definition*
• Records of individual’s care
• Health care services, health care professional
– Employed by, under contractual or other arrangements (referral)
• Entity has responsibility for care
• Service received is consistent with funding or designation status (hospitals exempt)
• Services must be more than dispensing
• Aids Drug Assistance Program (ADAP) exception

GPO Prohibition*
• Applies to:
– Disproportionate Share
– Children’s Hospitals
– Free Standing Cancer Hospitals
• Such hospitals:
“...will not participate in a group purchasing organization or group purchasing arrangement for covered outpatient drugs as of the date of this listing on the OPA website.” OPA GPO Certification Form

• Final Rule
– Published July 23, 2013, effective October 1, 2013
• Free-standing cancer hospitals, Rural Referral Centers, Sole Community Hospitals, and Critical Access Hospitals
• Excluded from 340B: drugs used for the indication for which they received an orphan designation but not when the drug is used for indications independent of that designation
• Both HRSA and manufacturers may audit this exclusion
• OPA published the orphan drug list here in 9/2013: http://www.hrsa.gov/opa/programrequirements/orphandrugexclusion/index.html
• Lawsuit filed from PhRMA 9/27/13
Orphan Drug Exclusion
Entities Take Action
1. Apply the brief tool 340B Compliance Self-Assessment Policy to your entity type
2. Review FAQs on specific policy topics for more information
3. Contact Apexus Answers to help you resolve any questions or concerns

Takeaways
1. The intent of 340B: to support entities that servevulnerable patients so the entities stay in business
2. Major 340B stakeholders: federal government,certain drug manufacturers, certain coveredentities, 340B Prime Vendor Program, managed byApexus
3. Covered entities must register on the HRSADatabase; once a year they must recertifyaccuracy of HRSA 340B database information

Takeaways
4. The 340B Prime Vendor Program provides:– Truth (call center)– Teamwork (contracting with distributors and suppliers)– Teaching (340B University)
5. Covered entities must maintain auditable records:– Only patients of the covered entity receive 340B drugs– A Medicaid rebate is not paid on a 340B drug– All eligibility criteria are met

• Remind leadership they are not required to log in to the HRSA 340B database for change forms or to view profiles
• Check your 340B standard operating procedures to make sure they reflect your entity’s operations
• If a new location/contract pharmacy are added to the HRSA database, remember the quarterly deadlines
• Keep the contact number for Apexus Answers handy
Tips for Pharmacy Technicians

Questions

SESSION 1:THE TOP 5: 340B BASICS FOR
NON-HOSPITALS
Debra Demers

Objectives
1. Define the intent of the 340B program2. Describe the major 340B stakeholders3. Explain how to participate in 340B4. Identify how the 340B Prime Vendor Program
supports 340B stakeholders5. List the program rules and explain how to
follow them

Takeaways
1. The intent of 340B: to support entities that serve vulnerable patients so the entities stay in business
2. Major 340B stakeholders: federal government, certain drug manufacturers, certain covered entities, 340B Prime Vendor, managed by Apexus
3. Covered entities must register on the HRSA Database; once a year they must recertify accuracy of HRSA 340B database information

Takeaways
4. The 340B Prime Vendor Program provides:– Truth (call center)– Teamwork (contracting with distributors and suppliers)– Teaching (340B University)
5. Covered entities must maintain auditable records:– Only patients of the covered entity receive 340B drugs
– A Medicaid rebate is not paid on a 340B drug
– All eligibility criteria are met

1. 340B PROGRAM INTENT AND OVERVIEW

340B Intent
To permit covered entities “to stretch scarce Federal resources as far as possible, reaching more eligible patients and providing more comprehensive services.”
H.R. Rep. No. 102-384(II), at 12 (1992)

Which examples below describe 340B program savings used in alignment with 340B program intent? Discuss at your table.a) Supporting an indigent care clinicb) Starting a patient assistance medication programc) Subsidizing medications for patients unable to payd) Adding pharmacy staff
Share

340B Statute
• Resulted from a 1992 federal statute• Manufacturers participating in Medicaid Drug
Rebate Program must sign a Pharmaceutical Pricing Agreement (PPA) with the Secretary of Health and Human Services– The manufacturer agrees to charge a price for
covered outpatient drugs that does not exceed the 340B price

340B Price
• Calculated quarterly– 340B ceiling price =
Average Manufacturer Price (AMP) – Medicaid Unit Rebate Amount (URA)
• Manufacturer submits data to CMS

Relative Pricing
100%
79%
66% 64%58%
53% 51% 49%
0%10%20%30%40%50%60%70%80%90%
100%
42%
Private Sector Pricing
Adapted from a slide by Safety Net Hospitals for Pharmaceutical AccessSource: Data derived from Prices for Brand-Name Drugs Under Selected Federal Programs, Congressional Budget Office (June 2005)

340B Covered Outpatient Drugs*
http://www.ssa.gov/OP_Home/ssact/title19/1927.htm
Drug not directly reimbursed
FDA doesn’t require NDC
Vaccines
Inpatient drugs
Outpatient Prescription Drugs
Over-the-counter drugs (with a prescription)
Clinic administered drugs
Biologics
Insulin

Program Evolution
1992 2014
AccessSub-Regulatory
IntegrityRegulatory

Have you been here?

340B Program Integrity
OPA Program Integrity Page:http://www.hrsa.gov/opa/programintegrity/index.html
Manufacturer Entity• Calculate and charge a
correct 340B price
• Subject to HRSA audits
• Comply with 340B statuteand guidelines
• Subject to HRSA andmanufacturer audits

Concerns from Peers
• “I’m afraid I’ll have an audit and not be awareof a particular aspect of the program, eventhough I’ve tried to stay on top of everything.”
• “I worry about how to apply certain policies; itseems that there are different interpretations ofthe right thing to do.”

Share
Please share your primary 340B program integrity concern with the person sitting next to you.

Review
Which of the following is a 340B covered outpatient drug?
a) Vaccine
b) Inpatient drugs
c) Over the counter drug not prescribed in writing by an authorized provider
d) None of the above are covered outpatient drugs

Entities Take Action
1. Describe how your entity’s use of the 340Bprogram supports the intent of the 340B program.
2. Identify how your entity can document the use of340B savings to align with the intent of the 340Bprogram.
3. Incorporate these elements into your 340B relatedstandard operating procedures.
4. Rely on trusted resources identified by OPA as thesource of truth for 340B issues: OPA and Apexus.

2. MAJOR 340B STAKEHOLDERS

Major 340B Stakeholders
Manufacturer Calculate and offer 340B price
Entity Provide 340B access
OPA Administer 340B program 340B Drug
to Patient

HRSA Office of Pharmacy Affairs (OPA)
• Health Resources and Services Administration (HRSA)– Oversees 340B Program administration (enrollment,
recertification, compliance) – Establishes mechanism to prevent duplicate discounts– OPA support
• The 340B Prime Vendor Program, managed by Apexus– Apexus is not the same thing as HRSA; Apexus communicates
HRSA policy

HRSA-Endorsed Resources
• HRSA• Apexus

340B Eligible Entities*
Federal Grantees/Designees Certain Hospitals• Federally Qualified Health Center• Federally Qualified Health Center Look-Alikes• Title X Family Planning Grantees• State Aids Drugs Assistance Programs• Ryan White Care Act Grantees (A,B,C,D,F)• Black Lung Clinics• Hemophilia Treatment Centers• Native Hawaiian Health Centers• Urban Indian Organizations• Sexually Transmitted Disease Grantees• Tuberculosis Grantees
• Disproportionate Share Hospitals• Children’s Hospitals• Critical Access Hospitals• Free Standing Cancer Hospitals• Rural Referral Centers• Sole Community Hospitals

3. PARTICIPATION IN 340B

1. Ensure it has the capability to follow (andmaintain auditable records documentingcompliance with) program rules
2. Register on the HRSA 340B Database3. Recertify with HRSA annually
To Participate in 340B, an Entity must…

HRSA 340B Database*
• The HRSA 340B Database is the official source of 340B information– Entities*– Contract Pharmacies*– Manufacturers– Medicaid Exclusion File*

340B Database: 340B Statistics
• 340B database:http://opanet.hrsa.gov/opa/default.aspx
• APR 2014– 25,196 registered sites: 11,718 are hospital sites– 14, 485 unique contract pharmacies– >$7.5B/year in 340B drug purchases– ~82% of 340B participants enrolled with Apexus

340B Database: 340B Statistics, continued
• APR 2014– 18% of covered entity sites utilize contract
pharmacies– 89% of covered entity sites use only in-house or in-
house and one contract pharmacy– Of sites using contract pharmacy, 73% have five
or fewer contract pharmacy arrangements

• Entities DO NOT need to log into the 340B database
• All links referenced on the homepage are accessible without a username & password
Working with the HRSA 340B Database

Working with the HRSA 340B Database
• When searching for your covered entity’s profile - LESS IS MORE
• The 340B ID is the most reliable search criteria

Working with the HRSA 340B Database
• Covered entity data is divided between tabs on the 340B profile
• The information about your facility can be found under the applicable tabs

HRSA 340B Database: Medicaid

• Important Notifications & What’s Newo Great resource for important notifications about:
Registration Recertification Change requests Database changes
Working with the HRSA 340B Database

Registration Process*
• New entities, entity sites, contract pharmacies,Medicaid information– 2 week registration periods, quarterly updates
made to OPA Database
• Change requests: changes to existing information,rolling basis
Update Official October 1 January 1 April 1 July 1
Registration Period July 1 – 15 October 1 -15 January 1 – 15 April 1 - 15

Electronic Handbook
• HRSA/OPA uses it for validation of site information• EHB data incorporated as part of recertification in
FEB 2014• Importance of EHB changes and timing, especially
changes of scope• Possibility of chargeback denial and/or wholesaler
delivery issues if EHB doesn’t match HRSA and entity’s wholesaler information

Apexus Answers
A CHC uses employed healthcare professionals to provide elderly
care services at a non-entity owned clinic. The CHC owns the
records of care. Should the CHC register this
location on the 340B database? Is 340B use permissible?

Recertification*:
• Entities are required to recertify informationin the HRSA 340B database annually
• HRSA sends a notification email toAuthorizing Official and Primary Contact
• The Authorizing Official performs therecertification online

Recertification Statements*:
• Database entry is complete, accurate, correct
• Entity meets 340B eligibility requirements
• Compliance with 340B requirements/restrictions
• Maintenance of auditable records
• Systems in place to ensure compliance
• Contract pharmacy compliance, entity obtains sufficient information
• Entity contacts OPA for any breach of the above
• Entity acknowledges possibility of payment to manufacturers for failure to notify OPA in timely fashion

Review
Updates sent to OPA during its registration period of October 1-October 15 will be reflected on the OPA database and active as of:
a) January 1
b) October 1
c) April 1
d) July 1

Entities Take Action
1. If you have never seen your entity’s record on the OPA database, visit the site, review the record and ensure it is accurate
2. Identify all potentially eligible 340B areas of your entity; determine if your entity has implemented 340B in all areas that are eligible

4. THE PRIME VENDOR PROGRAM

Apexus Focus
TEAM
WORK Contract
Services
TEAC
HING 340B University
& 340B OnDemand
TRUTH Apexus
Answers Call

Teamwork: Contracted Supplier Agreements (by year)
17
26
3845
5156
6165
100
0
20
40
60
80
100
120
2005 2006 2007 2008 2009 2010 2011 2012 2013
Con t r ac t s

• National experts share leading practices at this one or two day live educational program
• Aligned with HRSA policy, compliance-focused• Only HRSA-endorsed compliance training• CE for pharmacists and technicians offered• Interactive, opportunities to network, leave with tools to
equip your entity• 10+ Sessions in 2014• Online, on-demand modules under development
Teaching: 340B University

Truth: Apexus Answers
• National 340B source of truth, communicates HRSA policy
• Staff in constant communication with HRSA to ensure messaging is consistent
• FAQs available here: https://www.340bpvp.com/resource-center/faqs/
• Average monthly interactions ~2,000
• Tiered levels of response: can handle from basic to complex

5. 340B PROGRAM RULES

Forces Impacting OPA
OPA340B
Stakeholders*
340B Participants(Entities and
Manufacturers)Advocacy
Government (OIG, GAO, CMS, etc.)

Why 340B is like an onion…

340B Policy Options*
Policy Releases
Guideline
Regulation
Statute

Do you see a musician or a woman’s face?

340B Policies*
Guidelines Regulations (proposed**)• Patient Definition*• Contract Pharmacy*• Audits*• Dispute Resolution*• Outpatient Facilities• Duplicate Discounts*
• Manufacturer Civil Monetary Penalties**
• Administrative Dispute Resolution**
• Orphan Drugs*


Major 340B Compliance Areas
1. Duplicate Discount Prohibition*2. No Diversion (Patient Definition)*3. Certain Hospitals Only
– Group Purchasing Organization (GPO) Prohibition*– Orphan Drug Exclusion

Duplicate Discount Prohibition
340B Price Medicaid Rebate

Preventing Duplicate Discounts

Patient Definition*
• Records of individual’s care
• Health care services, health care professional
– Employed by, under contractual or other arrangements (referral)
• Entity has responsibility for care
• Service received is consistent with funding or designation status (hospitals exempt)
• Services must be more than dispensing
• Aids Drug Assistance Program (ADAP) exception

Entities Take Action
1. Apply the brief tool 340B Compliance Self-Assessment Policy to your entity type
2. Review FAQs on specific policy topics for moreinformation
3. Contact Apexus Answers to help you resolve anyquestions or concerns

Takeaways
1. The intent of 340B: to support entities that serve vulnerable patients so the entities stay in business
2. Major 340B stakeholders: federal government, certain drug manufacturers, certain covered entities, 340B Prime Vendor, managed by Apexus
3. Covered entities must register on the HRSA Database; once a year they must recertify accuracy of HRSA 340B database information

Takeaways
4. The 340B Prime Vendor Program provides: – Truth (call center)– Teamwork (contracting with distributors and suppliers)– Teaching (340B University)
5. Covered entities must maintain auditable records:– Only patients of the covered entity receive 340B drugs– A Medicaid rebate is not paid on a 340B drug– All eligibility criteria are met

• Remind leadership they are not required to log in to theHRSA 340B database for change forms or to view profiles
• Check your 340B standard operating procedures tomake sure they reflect your entity’s operations
• If a new location/contract pharmacy are added to theHRSA database, remember the quarterly deadlines
• Keep the contact number for Apexus Answers handy
Tips for Pharmacy Technicians

Questions

Chris HatwigChris Shain
George Kenny
SESSION 2:340B PRICING

Objectives
• Identify the activities of the manufacturer and wholesaler in 340B pricing
• Explain 340B price calculation for covered outpatient drugs
• Discuss the manufacturer and wholesaler perspectives on policy issues

Takeaways
• Manufacturers and wholesalers have important roles in supporting program integrity
• Manufacturers have 340B compliance responsibilities
• The 340B price file is one of the most complex• Actions entities take can impact a
manufacturer’s calculations and ultimately impact the manufacturer’s compliance

Panel Question
What are the 340B-related roles and responsibilities for you and your organization?

Manufacturer: Role/Responsibilities
• Uphold responsibilities in the Pharmaceutical Pricing Agreement– Calculate and charge a correct PHS Price– Ensure that you charge the price to valid 340B
entities• Validate customers on indirect sales (chargebacks) to
the OPA database (eligibility)

Pharmaceutical Pricing Agreement
HRSA Responsibilities Manufacturer Responsibilities• Public list of 340B entities, including
Medicaid information• Require entities to maintain
purchasing/dispensing records for covered outpatient drugs and Medicaid reimbursement for these drugs for not less than 3 years
• Charge 340B entities a price that does not exceed the 340B ceiling price
• Retain necessary records for not less than 3 years from date of creation
• Afford Secretary (or designee) reasonable access to records relevant to compliance
• Permit CMS to share AMP and URA with Secretary in order to carry out agreement
• Participate with HRSA 340B Prime Vendor Program (voluntary)

Wholesaler: Role/Responsibilities
• Open accounts with only eligible entities• Deliver correct price to 340B entities• Process chargebacks with manufacturer
correctly

Manufacturer Question
How is the 340B price calculated?

Manufacturer: 340B Calculation
• Weighted average price (net of discounts) to retail community pharmacies
AMP: Average Manufacturer Price
• Lowest price to US customers, certain federal pricing, such as 340B, excluded
BP: Best Price
• Brand: Greater of [(AMP * 231%) or (AMP – BP)] plus inflation penalty
• Generic/OTC: 13% of AMP
URA: Unit Rebate Amount
• 340B Price based on quarterly Medicaid metrics which are based on commercial contracting practices

Manufacturer: 340B Calculation
WAC
AMP
BP
URAminus 340B Unit Priceequals
Units per Package
340B Ceiling Price
times
equals
• 340B Ceiling Price

Manufacturer: 340B Implementation
• Quarterly Pricing– 340B prices change quarterly
– Manufacturers upload to authorized wholesalers 15-30 days prior to beginning of a quarter
– 340B pricing lags behind Medicaid by 2 quarters
Sales transactions occur
Q1 AMP and BP calculated, submitted to CMS;
340B ceiling price calculated, submitted to wholesalers
340B ceiling price becomes effective
(based on Q1 transactions)
Q1 Q2 Q3

Apexus Answers
Why is my 340B price “different” from another 340B
entity’s price?

Panel Question
How do you implement a chargeback?

1. 340B price is established2. Wholesaler purchases at WAC ($10)3. Covered entity places 340B order with wholesaler4. Wholesaler reviews OPA database, then sells to covered
entity at 340B price ($6)5. Wholesaler sends manufacturer a 340B chargeback ($4)6. Manufacturer verifies 340B eligibility of covered entity
(reviews OPA database)7. Manufacturer pays wholesaler the chargeback
Manufacturer: Chargeback Process
Potentially significant Medicaid implications if a manufacturer provides the 340B price to a non-participating entity

Manufacturer: Chargeback Comments
• Manufacturer MUST validate entity on the chargeback to confirm 340B eligibility
• Manufacturer will deny the chargeback if they can not validate eligibility– “Bill-to” address on the chargeback identifies
eligibility– Correct information is critical

Wholesaler: Chargeback Comments
1. 340B Pricing changes quarterly: Unique and Challenging – 340B is the most challenging price file to administer in the
pharmaceutical industry
2. No “verified” central file of all 340B pricingWholesale distributors receive more than 100 different notices from manufacturers, 4 times per year– PVP does provide a comparative price file to Participants which
shows the Big 3 and one regional wholesaler’s 340B pricing for comparison

3. Contract Pharmacy and Entity Identification:– HIN, DEA, 340B ID
4. Returns:– The correct invoice must be chosen when returning a product
Wholesaler: Chargeback Comments

Manufacturer Question
What types of adjustments do manufacturers make to prices?

Manufacturer: Pricing Adjustments
• Standard procedures– Routine Medicaid restatements– Standard Best Price true-ups
• Medicaid restatements resulting from audits/investigations
• Reclassification/banking

Apexus Answers
What steps does an entity take to resolve what it believes to be
an incorrect 340B price?

Apexus Answers
What is the procedure used by manufacturers that wish to
refund payment to covered entities who are overcharged
for 340B?

Panel Question
What are special situations or challenges for you specific to 340B?

Manufacturer: Special Situations
• Penny pricing• Sub-Ceiling prices (voluntary)
– Through 340B Prime Vendor Program (non-FAMP exempt)– Not through 340B Prime Vendor Program (include in non-FAMP)
• Inpatient pricing• Product allocation systems
– 340B customers can be subject to product allocation systems just like commercial customers
• Non-discrimination guidance– Timing issues– Concern about hoarding

Apexus Answers
If a drug is only available through a specialty
pharmacy, how would a 340B patient access that drug?

Wholesaler: Contract Pharmacy Challenges
• Complex 340B contract pharmacy relationships present additional challenges• Manufacturer requirements are not consistent regarding 340B sales reporting
for 340B contract pharmacy• Process:
1. Confirm accurate “bill-to” 340B covered entity and “ship-to” (contract pharmacy)information specific to the relationship on the OPA website
2. Request HIN (5-7 business days)3. Account Set Up (Multi-Ship To Form/Customer Application)4. Set ordering/delivery options5. Covered Entity Authorization6. Complete Credit Application if new customer7. Verify licenses, CSMP setup8. Set up EDI specific to 340B vendor

Entities Take Action
• Keep OPA database information accurate/current to avoid chargeback issues
• Check the OPA website for manufacturer updates

Takeaways
• Manufacturers and wholesalers have important roles in supporting program integrity
• Manufacturers have 340B compliance responsibilities
• The 340B price file is one of the most complex• Actions entities take can impact a
manufacturer’s calculations and ultimately impact the manufacturer’s compliance

• Remember: you have resources to check pricing!Log in to the Apexus 340BPVP.com website to verifypricing, run customized reporting, and keep up-to-date with new contracts
• Communicate pricing changes to leadership;significant price changes may impact purchasingdecisions
Tips for Pharmacy Technicians

Questions

SESSION 3:340B IMPLEMENTATION
Todd Karpinski

Objectives
• Describe 340B delivery models:– Contract Pharmacy– In-House Pharmacy– Mixed-Use Areas
• Discuss implementation strategies ofcompliant programs

340B Pharmacy Options

Pharmacy Options
yContractPhcy
Single Contract
Multiple Contract
Supplement with Contract
Clinic Administered Drugs
Central Fill, Telepharmacy or
Specialty Pharmacy
Pharmacy Services
Mixed-Use
Contract Pharmacy
In-house Pharmacy
Other

Share
1. Your current model for getting 340B drugs to patients
2. One thing you are interested in expanding or changing about your current 340B model

CONTRACT PHARMACY

• 550 bed academic medical center
• 24,000 annual admissions
• >140,000 patient days
• Disproportionate share hospital– 17.25% (FY2011)
• Affiliated with Medical College of Wisconsin
• Only Level I trauma center in Southeastern Wisconsin
• Major referral center: 40 specialties and subspecialties
• >220 Pharmacy FTE’s
• Administration, Pharmacists, Technicians, EPIC® team
Froedtert Hospital

• Froedtert Hospital is the major teaching affiliate of the Medical College of Wisconsin (the “Medical College”)
– A majority of Froedtert Hospital’s medical staff is comprised of Medical College faculty members (816 faculty)
– 330 full-time equivalent residents at Froedtert Hospital– 413 medical students
• Close working affiliation between the two organizations
– Froedtert Hospital and the Medical College jointly operate and own a network of clinical sites for primary care and outpatient clinical initiatives
Affiliation with the Medical College of Wisconsin

• Inpatient– 3,700 orders per day; 12,000 total doses dispensed daily; 4.3 million doses
yearly– 2,000 admission histories per month– Discharge reconciliation and education
• Hospital Outpatient Departments (HOD)– 70,000 doses dispensed yearly– 60,000 injection/IV dispenses yearly– Over 30 Ambulatory Clinics
• Outpatient Pharmacies– 170,000 prescriptions/year
Froedtert Pharmacy Fun Facts

• Froedtert Hospital’s community benefit framework is to improve the quality oflife in the communities we serve through health care programs and servicesthat are measureable, accessible and culturally appropriate; recognizing thegreatest impact is in Milwaukee’s underserved, urban population.
• The Setting:– US 2010 Census: Milwaukee is #4 in poverty among nation’s cities– In Milwaukee County, 30% are on Medicaid and 15% are uninsured
• Our Investments in 2011:– $34 million uncompensated care– $41 million in government shortfalls– Over 10,000 patient accounts adjusted for charity care– $400,000 annual support to FQHC’s and a $2 million pledge for capital support– Over $58 million in health professions education, including college and high school
scholarships/internships for underrepresented students
How do we support the intent of the 340B program?

• Charity Care • Medication Management Home Delivery• Diabetes Smart Start Program• Medication Collection Program• Sharps Collection Program• Medication Repository• Discharge Program (implemented 9/2011)• Ambulatory Care pharmacists • Blood pressure cuffs (Newly Transplanted Patients)
Community Benefit from Pharmacy

AUDIT
Froedtert Hospital 340B Timeline

Takeaways
• Do not outsource your 340B complianceresponsibilities to another party
• Entities can negotiate the terms of theircontract pharmacy agreements
• The intent of 340B is to stretch scarce federalresources as far as possible to help entitiesand their patients

340B Contract Pharmacy - Overview
• HRSA guidance permits entities to partner with outside pharmacies to provide eligible patients with 340B medications– Identification via shared patient and provider data
– Inventory via "Bill To - Ship To” wholesale arrangements
• Entity-Contract Pharmacy relationship types– Direct Contracting with Pharmacy
– Contracting through 340B vendor with Pharmacy

What is a 340B Vendor?
A company providing 340B contract pharmacy programimplementation and management• Not a HRSA requirement• Minimizes impact on retail pharmacy workflow• Collects data from retail pharmacy at the switch• Provides the interface to identify eligible claims (matches
entity data and pharmacy data)• Manages inventory replenishment• Establishes contracts with pharmacies• Provides reports and transparency for auditing

340B Contract Pharmacy
1. Contract Pharmacy dispenses drug (non-340B inventory) to 340B entity’s eligible patient
2. When a full package size of the Rx is reached, the pharmacy or vendor orders a 340B drug to replace it
3. Replacement 340B drugs are “billed to” the entity and “shipped to” the contract pharmacy
4. Entity pays contract pharmacy for its services

1. Eligibility data feeds sent2. Patient presents Rx to pharmacy (or entity sends
electronically to pharmacy)3. Pharmacy submits claim via switch4. Switch communicates with PBM
5. Claim payer eligibility sent6. Periodic 340B eligibility determination7. Periodic 340B replenishment order placed8. 340B replenishment order shipped
1
2
4 5
3
6
8
7
340B Contract Pharmacy - Data

1. Patient receives Rx, pays co-copay2. PBM pays pharmacy (3rd party)3. Pharmacy keeps dispensing fee, pays vendor entity’s 3rd party collections4. Vendor pays entity 3rd party collections, less vendor administrative fees5. 340B replenishment order paid
1 2
3
4
5
340B Contract Pharmacy - Financial

Reality of the Complexity

Apply It: Patient/Prescriber Data Updates
Scenario 1:Pharmacy will update the patient and prescriber data once monthly, per data receipt from entity• Is this frequency of updating appropriate?• What kinds of data files could the entity use as
sources for eligible prescribers/patients?

Apply It: Prescriber Eligibility
Scenario 2:Prescriber eligibility is determined by a match to a prescriber “eligibility” list• Is this enough? What additional information could
be used?

Apply It: Fees
Scenario 3:Self-Pay: Pharmacy shall collect and receive a $15 dispensing fee and a $1 administrative fee from patientInsured: Pharmacy shall collect and retain 30% of the contracted rate + a $19 dispensing feeDispensing Fee: rates will increase according to the consumer price index yearly
• Is this a reasonable fee structure? Does this align with 340B program intent?

Apply It: MCO Medicaid
Scenario 4
The contract will include patients with Private Insurance. Contract Definitions of Private Insurance Private Insurance includes Managed Care Medicaid Plans.1. How can you find out if your state collects Medicaid
rebates on MCO drugs?
2. If your state collects rebates on MCO drugs, is this language appropriate to include in the contract?

Contract Pharmacy Reimbursement
• Cash Pay/Sliding Fee– Reduced pricing at contract pharmacy
• Private Insurance• Medicaid - Managed Care Medicaid Plans
– Check with your state– Entity risk

C-Suite Myths
• “This program runs it self!”– 340B program coordinator / manager essential
• “The first company that approach us is the best/ only one out there!”– Have the conversation first
• “We have to jump on every opportunity!”– Be vigilant when considering any opportunity

HOW DO WE STAY COMPLIANT?

340B Program Coordinator
• Responsible for day to day programmaintenance– Preforming compliance audits– Maintaining provider list– Coordinating data sharing– Reporting metrics– Assisting in staff training

Contract Pharmacy Compliance
• Audit 1: Patient Eligibility – From the vendor’s report, choose 20 patients to audit. Select patients
who are filling the prescription for the first time. Select patients that have multiple first fills prescriptions written by different prescribers. Verify each patient in EPIC to ensure visit was completed by an eligible provider.
– Completed daily
• Audit 2: Hardcopy Prescription Request– Request 20 prescription hardcopies from vendor. Verify patient and
provider eligibility. Verify that dispenses were accumulated appropriately.
– Completed monthly

Contract Pharmacy Compliance – cont’d
• Audit 3: Vendor Prescriber Audit– Evaluate each provider used to dispense 340B eligible
prescriptions for inclusion on eligible provider list. Eligibility isbased on NPI number.
– Updated provider eligibility list is sent each month– Completed monthly

Lessons Learned
• Understand– Work with national organizations– Network with other covered entities– Utilize internal resources
• Be proactive– Review and understand Polices & Procedures– Review audit process with key stakeholders
• Stay engaged– Continue to measure and test compliance
• Entity pays flat fee per claim• Stop-loss function (prevents 3rd party
transmission if loss to entity)• Entity does not pay fees on claim
reversals (net paid claims)• Entity pays lowest of U&C, MAC, and
340B• Entity has access to ALL data
(including prescriptions presented vs. filled with 340B)
• High complexity data management systems
– HL7 interface
• Entity pays fees based on % of revenue or drug cost
• Entity does not keep 3rd party reimbursement
• Vendor recruits patients to its mail order pharmacy
• Early cancellation fees• Entity not permitted to select
wholesaler• Entity may end up purchasing partial
bottles at high rates due to non-replenishment
• Entity not permitted to contract with other 340b vendors
Contract Negotiation, Summary

Entities Take Action
Takeaways
• Do not outsource your 340B compliance responsibilities to another party
• Entities can negotiate the terms of their contract pharmacy agreements
• The intent of 340B is to stretch scarce federal resources as far as possible to help entities and their patients

Questions
Take a deep breath, take a good look, and take
responsibility.

MIXED-USE: GPO
Mike BenedictFern Paul-Aviles
Rob Nahoopii

• Disproportionate Share Hospital• 874-bed Level I Trauma Center
in Charlotte, NC• 2 infusion centers:
– 1 cancer, 1 non-cancer• Behavioral Health Center• Five outpatient retail
pharmacies located in clinicbuildings that provide primarycare and behavioral healthcare
Carolinas Medical Center

• Resources within Pharmacy for 340B compliance– Dedicated
• Enterprise audit tech (former buyer) – shared among 7 facilities• Enterprise 340B Director
– Facility Directors of Pharmacy– Materials management department– Inventory management software, automated dispensing
machines, split-billing software and HIS system– Wholesaler account representative and other wholesaler
experts
Carolinas Medical Center

• Describe what data you feed into your split-billing software and the source for that data
Panel Question

Use of 340B Savings
Offer meds on a sliding scale to indigent patients and numerous
patient assistance programs
Ambulatory clinical pharmacy services in anticog, HIV, asthma,
diabetes (appropriate care)
Built a primary care clinic within Behavioral Health Center using
Family Medicine fellow
Multidisciplinary care teams (RN, CM, PharmD, Health Advocate)
to prevent readmissions
Carolinas Medical Center340B Savings

Use of 340B Savings
• 340B Charity Care Voucher Program– Diabetes Clinic– Family Practice Clinic
• Synagis (palivizumab) Clinic• Pertussis Cocooning Clinic• Discharge Medication Support (Cath Pts)

Takeaways
1. Carefully consider which options you elect if using split billing software
2. Take steps to minimize your WAC spend3. Load correct contracts, including Apexus sub-
WAC pricing4. Define: inpatient, outpatient5. Interpret: covered outpatient drug6. Account: for waste and lost charges

Overview: Mixed-Use
• Mixed-Use Setting in a Nutshell– In a mixed-use area, the entity
dispenses/administers medications to bothinpatients and outpatients from the samelocation (pharmacy)
– Examples• Cardiac Cath Lab, One-day surgery, Emergency
Department, Endoscopy

GPO Prohibition*
• Applies to:– Disproportionate Share
– Children’s Hospitals
– Free Standing Cancer Hospitals
• Such hospitals:“...will not participate in a group purchasing organization or group purchasing arrangement for covered outpatient drugs as of the date of this listing on the OPA website.” OPA GPO Certification Form

Entities Must Ensure
• 340B is limited to OUTPATIENTS• Patients meet patient definition
– Patient status = outpatient (at time of service)– Prescriber = eligible prescriber– Location of service = reimbursable on cost report, registered
on 340B database (if req.)
• No GPO use for covered outpatient drugs for DSH/PEDs/CAN
• No duplicate discounts on Medicaid transactions

Split-Billing Software to the Rescue
• There is one physical drug inventory servingboth inpatients and outpatients
• This software merges data from patient visits(date/time of service, patient status,prescriber, location/clinic, Medicaid status)to help split orders into the right buckets

Accumulators and Eligibility
Accumulator: GPO
Inpatients
Accumulator: 340B
340B eligible outpatients
Accumulator/Default: Non-GPO/WAC
340B ineligible outpatients
Medicaid carve-outLost charges
Clinics within 4-walls but not 340B eligibleIn-house pharmacy
open to public

InpatientGPO
• GPO Contract• DSH Inpatient GPO
Contracts (DSH only)• GPO or Wholesaler Generic
Source Program• Individual Hospital
Agreement
Outpatient(340B eligible)
340B• PHS/340B• PVP Sub-340B (if enrolled in PVP)
• Apexus Generic Portfolio(AGP) (if enrolled in PVP)
• Individual HospitalAgreement (single entity only)
Outpatient(not 340B eligible)Non-GPO/WAC
• WAC Pricing• PVP Sub-WAC (if enrolled in PVP)
• Apexus Generic Portfolio(AGP) (if enrolled in PVP)
• Individual HospitalAgreement (single entity only)
Wholesaler Account Setup-DSH/PED/CAN with GPO Prohibition

Update: Account Load Options

Contracting: Avoid These Pitfalls
• The following situations are not GPO-compliantcontracting practices:- An individual DSH accessing contracts executed by a network
(i.e. IDN, ACO, etc.) in which it is a member
- A wholesaler’s generic source program (unless offered as a subcontracted solution to the Apexus Generics Source portfolio)
- A manufacturer extending a discounted price to a group of covered entities (subject to the GPO prohibition) through a wholesaler, other third party or group purchasing arrangement, that is not supported by an individual contract between the 340B covered entity and the manufacturer. Such agreements should be reproducible for review during an audit of compliant 340B

GPO: Special Situations
• GPO private label products• IVIG• Drug shortages

2 Key Questions HRSA Will Ask:
• What outpatient accounts do you have? • How do you purchase drugs for ineligible
outpatients?

• What is the biggest challenge for youregarding record-keeping/inventorymanagement?
Panel Question

• Steps to take• Pitfalls to avoid• Example
Mixed-use Inventory/Record Keeping Challenges

Minimizing WAC Exposure Tool

• Please share a few strategies to minimizeWAC exposure
Panel Question

Strategy #1: Covered Outpatient Drug
Q: Can a hospital subject to the GPO Prohibition use a GPO fordrugs that are part of/incident to another service and payment is not made as direct reimbursement of the drug (“bundled drugs”)?
A: If the entity interprets the definition of covered outpatient drugreferenced in the 340B Statute (Social Security Act 1927 (k)) and decides that bundled drugs do not meet this definition, a GPO may be used for drugs that are not covered outpatient drugs. The decision the entity makes should be defensible, consistently applied in all areas of the entity, documented in policy/procedures, and auditable.

Strategy #2: GPO “Only” Clinics
In certain off-site outpatient hospital facilities that meet all of thefollowing criteria: 1. Are located at a different physical address than the parent;
2. Are not registered on the OPA 340B database as participating in the 340B Program;
3. Purchase drugs through a separate pharmacy wholesaler account than the 340B participating parent; and
4. The hospital maintains records demonstrating that any covered outpatient drugs purchased through the GPO at these sites are not utilized or otherwise transferred to the parent hospital or any outpatient facilities registered on the OPA 340B database.

Strategy #3: Waste/Lost Charges
• Expired/returns-return company policy, entity policy• Waste/lost charges
– Multi-dose vials, insulin
– Mixed product, but patient doesn’t get dose

Strategy #4: Charge Code to NDC
• Charge code to the correct NDC• Charge quantity to the package size
– Procrit, e.g.• Billing unit: 1000 units• Vial size: 20,000 units/1 mL vial• Package size: 4 vials per box• How many billing units per package?
– 1000
– 20
– 80

Takeaways
1. Carefully consider which options you elect if usingsplit billing software
2. Take steps to minimize your WAC spend3. Load correct contracts, including Apexus sub-
WAC pricing4. Define: inpatient, outpatient5. Interpret: covered outpatient drug6. Account: for waste and lost charges

• Stay up to date with Apexus sub-WAC pricechanges; sign up for Contract News brief
• Educate your colleagues and identify waysto capture lost charges and expired drugs,to avoid unnecessary WAC exposure
• Ensure the CDM to NDC crosswalk staysupdated
Tips for Pharmacy Technicians

Questions

IN-HOUSE PHARMACY
Jenny Clark

Health Partners of Western Ohio
“To eliminate gaps in health outcomes for all members of our community by providing access to quality, affordable, preventive and primary health care.”

Entity Background Slide
• FQHC with 5+ sites • 18,000+ patients • NCQA Level 3 Patient Centered Medical Home• In house, owned and operated, 340B pharmacies• Approximately 18 Pharmacy staff members• Each pharmacy fills 75-250+ RX per day

Use of 340B Savings
INTENT- The 340B Program enables covered entities to stretch scarce Federal resources as far as possible, reaching more eligible patients and providing more comprehensive services.
HPWO Patient Rx Savings in 2013 = $1.58M

340B Savings
Funds:• Integrated Clinical Pharmacy Services• Medication Therapy Management (MTM) clinic and
Med Box Program• Uninsured and underinsured patient services and
prescriptions• Free Delivery Program• Continual Service Expansion

Takeaways
1. The entity is responsible for compliance. 2. Understand your state’s Medicaid billing policy
(ambulatory, physician administered).3. Identify the key Policies and Procedures that are
needed to support your 340B program.4. Continually review 340B program and conduct
self-audits to maintain program compliance.

Pharmacy Model Benefits
In-House Owned Pharmacy Contract Pharmacy Generally lower average operating costs (average $10-15 per prescription) after start up costs are covered.
Less staffing resources needed; Needpharmacy point person and for monthly reporting and compliance.
Pharmacy staff can contribute as part of patient care team, improving patient outcomes and meeting organizational goals.
Less risk for low volume clinics or those with very high rate of uninsured patients.
Achieve higher capture rates for pharmacy; Patients can be very loyal.
Low start up costs: No need for infrastructure development or licensing.
Able to keep uninsured costs very low. No building space requirements.
Pharmacy can be community resource; Retail business can increase business of pharmacy and clinic.
Use negotiated contracts of pharmacy partner; do not need to negotiate your own.

Pharmacy Model Challenges
In-House Owned Pharmacy Contract Pharmacy Higher start up costs ($75-200K start up not including inventory).
Higher ongoing operational costs ($17-25+ per prescription) and potential need for 3rd party administrator too.
Requires space within or immediately proximate to entity site.
Added cost for quarterly drug reconciliation costs.
Greater administrative resources required; Need to develop space, get licensed and hire staff.
Less opportunity for clinical integration of pharmacy services and improved patient outcomes.
Note: Pros and Cons are offered as generalizations and are not mutually exclusive. Entities can have Owned and Contracted Pharmacy programs.

• What are the entity goals of creating a pharmacy program?
• Would your volume and payer mix support an In-house Pharmacy?
• Consider types of clinical services offered or special populations served by entity.
• Would your community benefit from a retail pharmacy?
In-House Pharmacy Considerations

In-House Pharmacy Operation
• 340B Account• Retail Account
Wholesaler
• 340B Inventory• Retail Inventory
In House Pharmacy
• 340B Patient• Retail Patient
Patient
• 340B Provider• Retail Provider
Provider• 340B Billing• Retail Billing
Billing

Planning, Design,
Construction
Licensing and Accreditation
Inventory Model
ChoicesWholesaler
Negotiations
Insurance Contracting
Carve-In vs. Carve-Out
Pharmacy Operating
System
Pharmacy Staffing Plan and Training
Policies and Procedures
Start Up Steps

Detail strategies to
achieve growth rate
Educating patients and prescribers to use pharmacy
Sales and Marketing
Added value services for
clients
Tracking and reporting on
progress
Strategies for Growth –12 month Start-Up Plan

Staffing Considerations
Manage Accounts Receivable
Maximize Technology & Workflow
Regulatory Compliance Plan
Optimize SavingsControl Costs
In-House Pharmacy Keys to Success

Investments to increase pharmacy efficiency and improve 340B compliance• Pharmacy operating system• Robotic dispensing devices• Bar code scanning through dispensing and
check out processes• Interactive voice / text response• Tele-pharmacy
Maximize Technology & Work Flow

Perpetual Inventory System with Par LevelsPerpetual Inventory System with Par LevelsMonthly unused drug
reportQuarterly drug level
checkLabor as a percent of
sales
Cost of GoodsCost of GoodsCost of goods reviewed
at every orderQuarterly price
changes Prime Vendor Program
Control Costs

Eligibility and Registration– A grantee has a new clinic that opens March 15th
– It must be added to the EHB prior to registration in the OPA database.
What steps have to be taken before the clinic can begin using 340B?
Compliance Considerations

Referral Prescriptions– If we refer a patient to an outside clinic, can we
fill their prescriptions from our 340B clinic?
Compliance Considerations

Demonstrating “responsibility for care”– Some examples of auditable records for a 340B
prescription resulting from a referral prescription?
Compliance Considerations
Some methods to help demonstrate responsibility for careOutgoing referral from covered entity
Incoming notes from outside provider
Shared EMR access with outside provider
Referring returning patient for follow up encounter to review outside care

CE maintains a list of providers
who could prescribe at non-
entity location.
CE maintains a list of providers
who could prescribe at non-
entity location.
Pharmacy should have means to verify entity address of floaters•Use provider address
check •Without means to verify
floaters address - NO 340B should be used340B drugs.
Pharmacy should have means to verify entity address of floaters•Use provider address
check •Without means to verify
floaters address - NO 340B should be used340B drugs.
Compliance Considerations
Eligible providers who are “floaters”

• Real time access to patient andprovider eligibility information
Eligibility verification at filling
• Right inventory to right personRetail
inventory
• Do you have responsibility for care?Hospital
prescriptions
• Documentation of Outgoing referraland incoming
Specialist prescriptions
Compliance Considerations

Patient and provider eligibility
Duplicate discounts
Billing for all prescription
Inventory to match
dispensations
Matching return-to-stock
to correct account
Compliance and Business Reporting
End of Month Reporting:• Weekly• Monthly• Quarterly

Case Discussions
Thank You !

In-House Case #1: Patient
• A patient came to our pharmacy withprescriptions from a local hospital discharge.Can we fill these prescriptions with 340B drugs?
1. Is the person an active patient of the health center?
2. Is your health center provider medically responsible forthe care related to these prescriptions?
3. Does your health center have a contract withprescriber ?

In-House Case #2: Provider
• We have a cardiologist that sees health centerpatients once a month because we have nospecialists in the area. Can the health centeruse 340B to fill these prescriptions?
1. Does the health center contract with the specialistto provide services to the patients?
2. Is the health center medically responsible for thecare provided by the specialist to the patients?

In-House Case #3: Referral Patients
• The local mental health providers send uninsured patients to our pharmacy if they can’t afford prescriptions. Under what circumstances can we fill them?
1. Is the person a patient of the health center?2. Can you verify documentation of a referral from
the health center to the specialist and report back from the specialist?

In-House Case #4: Medicaid Billing
• Can we use 340B for the Medicaid managed care patients and bill regular rates (U&C)?
What information do you need to know to make this decision?

In-House Case #5: Multiple provider types
• Our health center provides dental and primarycare. A patient presents to the pharmacy with twoprescriptions, (Rx #1) is from a health center dentistfor an antibiotic and (RX#2) is for birth control froma non-health center OBGYN provider.
1. Can 340b inventory be used for the antibiotic?2. Is the health center medically responsible for the
care provided by the OBGYN to the patient?

• Ensure your entity’s policy for referrals is reflected in the 340B Standard Operating Procedure
• Know your state’s Medicaid 340B billing policy and support it in your operations
• Prior to dispensing prescriptions, verify prescriber and clinic/location 340B eligibility
Tips for Pharmacy Technicians

Takeaways
1. The entity is responsible for compliance.2. Understand your state’s Medicaid billing policy
(ambulatory, physician administered).3. Identify the key Policies and Procedures that are
needed to support your 340B program.4. Continually review 340B program and conduct
self-audits to maintain program compliance.

Questions

Debra DemersFern Paul-AvilesJennifer Hagen
Jenny Clark
SESSION 5:340B & MEDICAID BILLING

Objectives
• Recognize information required to avoidcreation of a duplicate discount
• Review appropriate approaches toMedicaid billing and understand scenariosthat could lead to duplicate discounts

Takeaways
1. Duplicate discounts are prohibited by 340BStatute
2. The entity’s 340B information on the 340BDatabase should reflect practice
3. Contract pharmacies should carve-outMedicaid, absent an arrangement toprevent duplicate discounts

Medicaid
1. Requirement: Prevent duplicate discounts – Medicaid Exclusion File
2. Entity decision: Use 340B for Medicaid (or not)– Some states have requirements for using 340B for
Medicaid
– Some states have very specific Medicaid billing requirements (ex. certain codes or procedures when using 340B drugs)

Medicaid Billing
• How much do you know?– Review 4 question quiz at your table– Discuss options among colleagues at your table
and select choice you think most accurate

Duplicate Discounts
• What is the state’s general policy on Medicaid rebates on340B drugs (for example, does the Medicaid Agency use theOPA Exclusion File?)
• If our entity uses 340B for Medicaid, what procedure should weuse to notify the state Medicaid agency that a 340B drug wasunavailable?
• Does the State Medicaid Agency seek a Medicaid Rebate onclaims from patients:1. That are “Dual Eligible” (Medicaid/Medicare)2. That received physician administered Drugs3. That are billed from Medicaid Managed Care4. In any other circumstance?

Medicaid Message
State 340B policies that incentivize entities to use 340B by offering fair reimbursement will save states money and support entities

State Medicaid Engagement : 19 states
DiscussionsActive Engagements

Medicaid
• 340B University for Medicaid Agencies planned for summer2014
• Apexus engagement:– Providing education and connecting entities with the state during
state policy development– Providing analytics support to State and covered entities
• Challenges & Opportunities:– Shrinking state budgets (+/-)– Managed care policy issues, contract pharmacies– Coordinating policy development and billing systems to enable
entities to use 340B

Apexus Answers
If an entity intends to have some clinics use 340B drugs for
Medicaid and other clinics carve-out, then should each clinic get its own Medicaid
number to distinguish them?

Apexus Answers
My contract pharmacy said I can use 340B for Medicaid
patients. Is this OK?

Apexus Answers
We bill Medicaid in more than one state. Is it OK to have
different billing policies for the different state?
How do we reflect this in the database?

Takeaways
1. Duplicate discounts are prohibited by 340B Statute
2. The entity’s 340B information on the HRSA 340B Database should reflect practice
3. Contract pharmacies should carve-out Medicaid, absent an arrangement to prevent duplicate discounts

• Check your HRSA 340B database listing to ensure your Medicaid information reflects practice
• Ensure Medicaid patients with retroactive eligibility are accounted for in your 340B software/operations and treated consistently with your standard operating procedures)
Tips for Pharmacy Technicians

Questions

Debra DemersFern Paul-AvilesJennifer Hagen
Jennifer ClarkJustin Simon
SESSION 6:340B HOT TOPICS

Objectives
• Apply tools available to assist entities indeveloping and assessing programcompliance
• Discuss 340B compliant approaches used byleading practices to common hot topics

Takeaways
• Stakeholders are not all going to interpret policy the same way
• Defend your decision and document it in your policies and procedures
• Use free tools and resources to support your decisions: FAQs, Apexus Answers

340B “Mega-Reg”
• Comprehensive HRSA regulation (to replaceprogram guidance)
• Expected to be a proposed rule, withcomment period
• Expected in draft form by Summer 2014

Contract Pharmacy OIG Report
• Contract Pharmacy Arrangements in the 340B Program (OEI-05-13-00431) released Feb. 5, 2014– Contract pharmacy arrangements create complications in
preventing diversion and duplicate discounts, and covered entities addressed the complications in different ways.
– Some covered entities in the study offer the 340B discount to uninsured patients at the contract pharmacy and others do not.
– Most covered entities in the study do not conduct all of the HRSA-recommended oversight activities.

Entities Take Action


Patient Definition
• Does the entity:– Have a relationship with the individual and maintain records
of the individual’s health care?– Provide health care services from a health care professional
• Employed by entity• Under contractual or other arrangements (e.g. referral for
consultation) with entity?
– Maintain responsibility for the patient’s health care services?– Provide services consistent with funding or designation status
(hospitals exempt)

Apexus Answers
Are employees of a covered entity eligible to receive
340B drugs?

Apexus Answers
If we refer a patient to an outside clinic, can we use
340B for their prescriptions?

Apexus Answers
In our outpatient pharmacy, we provide services to patients who receive
prescriptions from physicians that do not have
a relationship with our hospital.
Is this compliant?

Inventory/Records
• Does the entity:– Maintain separate, auditable records for all 340B
purchasing and dispensing?– Regularly evaluate 340B utilization reports to
catch and correct problems?

Apexus Answers
If I dispense a manufacturer’s generic product to a 340B
eligible patient, can I restock my inventory with a generic
equivalent from another manufacturer?

Apexus Answers
Can our parent entity transfer 340B drugs to a child site?
Can a hospital under our umbrella organization transfer 340B drugs to
another 340B hospital?What about in an emergency?

Apexus Answers
Does the prescription have to have a fill date that matches
the date of service?

Registration
• Does the entity:– Have all information completely and accurately
reflected in the Office of Pharmacy Affairs (OPA) and PVP (Prime Vendor Program) databases?

Apexus Answers
How do I know which types of 340B Database information are changeable on a rolling
basis vs. only at the quarterly interval?

Changes to 340B Database
• Opt-in vs. opt-out decision• Medicaid carve-in vs. carve out• Add new clinics or contract pharmacies
Registration: Quarterly
Recertification: Annually
• Changes to existing information in 340Bdatabase (e.g., addresses)
• Add/remove Medicaid Provider # or NPI
OnlineChange
Form
Rolling/as required

Apexus Answers
If my contract pharmacy has a change of information
(name change, etc.) how should I notify OPA?

Apexus Answers
Will HRSA make an exception to their registration rules? For example:
– My CEO deleted an email from HRSA that was critical, and HRSA removed our entity
– We made a mistake and forgot to register a site
– We forgot to submit the supporting documentation on the same day we submitted our registration request

Takeaways
• Stakeholders are not all going to interpretpolicy the same way
• Defend your decision and document it inyour policies and procedures
• Use free tools and resources to support yourdecisions: FAQs, Apexus Answers

• Consider making a 340B eligibility checklist to keep at your workstation, if your software doesn’t help you manage this—don’t forget to address referral prescriptions
• Understand the policy for transferring 340B inventory from your entity to a child site, and ensure this is documented in your 340B Standard Operating Procedures
Tips for Pharmacy Technicians

Questions

Rose BabbittFern Paul-Aviles
Robert NahoopiiGeorge KennyMarcy Imada
SESSION 7:AUDIT & DISPUTE PANEL
DISCUSSION

Objectives
• Explain the key points of the audit processes• Describe current events in HRSA and
manufacturer audits• Discuss tools available to self-assess in
preparation for an audit

Takeaways
• HRSA and manufacturers may both audit entities
• There are lessons to be learned from prior audits
• There are specific choices that place an entity at a higher risk of being audited

HRSA AUDITS
Rose Babbitt

Audits
HRSA Audits• Diversion, Orphan Drugs• Duplicate Discounts• Eligibility
• GPO Prohibition• Auditable records
Manufacturer Audits• Diversion, Orphan Drugs• Duplicate Discounts
What are the main areas of focus for a HRSA audit of an entity? How does that differ from a manufacturer audit of an entity?
“Entity shall permit manufacturer/government to audit records that directly pertain to entity compliance”

HRSA Risk-Based/Target Audits
WHO performs the audits, and WHAT is examined?
– HRSA Staff– All covered entities considered for risk
based auditsAudit Focus Areas:
• Entity’s oversight of Contract Pharmacycompliance
• Operations and Internal Controls
• Records of distribution and dispensing

HRSA Audit Steps
What steps are involved in a HRSA audit of an entity?1. Pre-Audit
– Engagement letter from HRSA2. Onsite Audit
– Auditors obtain, review, examine data– Exit interview, preliminary issues
3. Post-Audit– Auditors provide preliminary issues to OPA– OPA reviews issues found during audit, documents,
and addresses concerns– Entity presents corrective action plan to HRSA– Results are preliminary until reviewed by OPA– OPA finalizes report, posts summary on website

HRSA Audit: Next Steps
1 HRSA Notice and Hearing; entity has 30 days to disagree with preliminary report
2 Final report; 60 days to submit corrective action plan*; entity has 30 days to disagree with final report
3 Audit Summary and corrective action on HRSA website
4 Results support education of covered entities*If no corrective action plan within 60 days of final report, entity terminated

What have we learned from the HRSA audits?• FY 2012
– 51 covered entities encompassing over 410 outpatient facilities/sub-grantees and 860contract pharmacy locations
– All 51 audits finalized and posted on website• FY 2013
– 94 audits covering 718 outpatient facilities/sub-grantees and 1,937 contract pharmacylocations
– In process of finalizing audits• FY 2014 - As of March 12, 2014
– 40 on-site audits completed– 2 in process– 42 covered entity audits include 796 outpatient facilities and 2,544 contract pharmacies
HRSA Audits: Lessons Learned

Diversion
340B drugs dispensed at ineligible sites
Not spot checking inventory to check for diversions and correcting them
(variance)
340B drugs dispensed at
ineligible site and by an ineligible
provider
340B drugs dispensed to non-
patient at contract pharmacy
Example HRSA Audit Findings

Example HRSA Audit Findings
Duplicate Discount
Billing Medicaid contrary to
HRSA Medicaid Exclusion File
listing
340B drugs used for Medicaid patients at contract
pharmacy, with no
arrangement to prevent duplicate discounts
Medicaid claims
incorrectly coded when
provided to the state
Incorrect Medicaid or NPI
in HRSA Medicaid
Exclusion File
Outpatient sites incorrectly listed
on HRSA Medicaid
Exclusion File

Example HRSA Audit Findings
Eligibility, Auditable Records
Incorrect Authorizing
Official
Primary location and
contact information
incorrect
Closed child sites remained registered;
incorrect name listed for a child
site
Incorrect address for facility,
incorrect ship-to address,
pharmacy listed as entity with
340B ID
No written contract in place
for contract pharmacies

Audits – Manufacturer Conducted
• Authority– Reasonable cause– Independent auditor
• OPA encourages manufacturers to submit plans and we will workclosely with them throughout the process
• Statistics:– 9 received– 7 approved to move forward– 6 audit reports finalized
• Encourage manufacturers to share lessons learned

• Authority– 340B statute, guidelines
• Requirements– Reasonable cause– Workplan to HRSA– Independent auditor– Limited to Diversion/Duplicate Discounts
• HRSA has received 8 work plans• OPA works with them throughout the process
Audits – Manufacturer Conducted
*Encourage manufacturers to share lessons learned

ENTITY EXPERIENCE (SELF-AUDIT)
Fern Paul-Aviles

Carolinas Healthcare System
• Audit-readiness review– Summary of locations and 340B usage types (100% 340B-
eligible, hospital mixed-use, hospital-based retail)– Deviations from DSH practices– Table with answers to audit questions
• Data examined– Retail prescription dispensing– Inpatient and outpatient types– Policies and procedures – must describe what you do

• Lessons learned– Audit yourself as rigorously as you expect HRSA to
• Policies and procedures• Data extracts for split-billing software
– Inpatient vs. outpatient– When does patient status change? Know!– Bill on dispense/bill on administration
• Duplicate discount avoidance – How Medicaid gets 340B info
• Self-audit
Carolinas Healthcare System

Self-Audit: Eligibility
• Frequency– Monthly – split-billing non-matched items report – more optimization than
compliance– Quarterly – prior to “open enrollment”– Annually – part of Corporate Compliance Workplan
• Sample of prescriptions in mixed-use retail– High-dollar drugs (cancer, transplant, fertility)– Old-way – doctor list; New-way: ICD-9 match or 100% doctor list
• Examine– Patient eligibility– Prescriber eligibility
• Specialists (referral and follow up)
– Drug on formulary

Self-Audit: Inventory/Compliance
• Regular ad hoc reports from vendor– Prior authorizations for specialists– Reviewed by internal entity staff
• Contract with an outside group to audit– NDC vs. replenishment– Inventory management– Any “true-ups”
• Reversed claims• Payment of inventory value

Self-Audit: 340B Database
• Developed a policy to:– Assign responsibility for monitoring/updating– Direct routine review or PRN changes– Address recertification annually

Takeaway
• Compliance is the entity’s responsibility; do not rely on a vendor’s records alone

ENTITY EXPERIENCE
Rob Nahoopii

Lessons Learned-HRSA Audits
Flying by the seat of your pants precedescrashing by the seat of your pants. – Bill Walsh
• Have a solid compliance plan.• Implement monthly auditing of both contract
pharmacy and administered drugs.• Resource staff time for compliance and program
oversight.

Self-Reports
• Use Apexus resource, “Self-Reporting 340B Non-Compliance.” Found at:https://www.340bpvp.com/resource-center/other-resources/other-tools/
• Notify HRSA, then each manufacturer impacted individually.
• There are multiple ways to correct non-compliance, and working with each manufacturer on its ideal mechanism works best.

Lessons Learned-Manufacturer Audits
• Avoid the costly (time and money) impact of amanufacturer audit by working together for anequitable and transparent resolution.
• Share data to help with transparency.
• As a DOP, I had four manufacturer letters. In allcases we engaged in open and honestconversation and they all ended well.

To achieve great things, two things are needed; a plan and not quite enough time.
– Leonard Bernstein
A Wise Person Once Said…

A Compliance Action PlanIs Complicated
Is Do-AbleIs Updated Regularly
Is AuditableIs the Covered Entity’s Responsibility
Remember…

Apexus Self-Audit Tool

MANUFACTURER AUDITS
George Kenny

Apexus Answers
As a manufacturer, what are potential compliance issues
that I might observe?

Manufacturer Audit Issues
• Diversion
– Non-eligible entity or entity service (inpatient)– Non-eligible patient– Reselling of product– Non-Compliance with Orphan Drug Final Rule
(for RRC, SCH, CAH and Freestanding Cancer Hospitals)
• Medicaid Duplicate Discounts
– 340B discount and Medicaid rebate on same unit of utilization– Covered entity responsible for avoiding duplicate discounts– State Medicaid should issue rules for compliance
• Example: UD Modifier for Physician Administered– Managed Medicaid

Other Issues:
• GPO Prohibition• Definition of patient• Maintenance of auditable records• Correct information on OPA database• Multiple ship-to sites• Split billing software and credit /re-bill activity• Healthcare reform impact (ACOs, integration)• Some other issues (ex. GPO Prohibition) are not auditable by
manufacturers,but manufacturers can inform OPA of these issues and OPA will follow-up with covered entities

Manufacturer Audits of Entities: Overview
• If informal negotiations fail, a manufacturer may seek OPA permissionto conduct an audit– Demonstrate reasonable cause
• Evidence of Duplicate Discount and/or Diversion• Unsatisfactory attempt at informal dispute resolution
– Submit proposed audit workplan• OPA response to request (within 15 days)
– Approval– Denial– Request for revision/additional information
• Manufacturer provides Covered Entity with notice of Audit– minimum 15-day period to prepare for audit

Manufacturer Audits of Entities: Overview
• Manufacturer notifies covered entity of audit– Identifies issue(s) & third party auditing firm
• Audit Pre-Work– Document requests (policies, SOPs, etc.)– Data request (inventory, billings, etc.)– Identification of key individuals to be interviewed
• On-Site Audit– Minimal time necessary to complete work (2-5 days)
• Conclusion of Audit– Resolve any outstanding issues– Covered entity comment on findings– Final Audit report provided to OPA and HHS OIG– Recoupment of 340B discount (discount = WAC – 340B)

Covered Entity Self-Disclosure of Non-Compliance
• Covered Entity– Identifies Issue(s)– Corrects Issue(s)– Self-Discloses issue and proposed corrective action plan
(CAP) to OPA– Self Discloses to manufacturer – works in good faith to
implement CAP• Manufacturer
– Identifies impact to manufacturer’s products– Works with covered entity to resolve issue

Corrective Action Plans
• Covered entity must:– Prospectively correct issue
• Conduct root cause analysis of underlying issue• Implement Plan to correct issue moving forward
– Retrospectively correct issue• Identify products (and units) affected• Determine inappropriate discounts
– Repayment challenges• Refund vs. Offset• Work with manufacturers to determine best course

HRSA Audits of Manufacturers
• Manufacturer perspective– Calculation of 340B Ceiling price
• AMP – URA
– Transmission of 340B Ceiling price to distributors– Resolution of inquiries regarding appropriate
prices

AUDITOR’S EXPERIENCES
Marcy Imada

Audit Approval
• Manufacturer seeks OPA permission to conduct an audit– Demonstrate reasonable cause– Submit proposed audit work plan
• OPA response to request (within 15 days)– Approval– Denial– Request for revision/additional information
• Manufacturer must provide covered entity with notice– Minimum 15-day period to prepare for audit

Audit Steps and Scope
• Manufacturer notifies covered entity of audit– Identifies issue(s)– Identifies third party auditing firm– Sets audit timeline (at least 15 day advance notice)
• Audit Pre-Work may include:– Background Questionnaire– Document requests (policies, SOPs, etc.)– Data request (inventory, billings, etc.)– Identification of key individuals to be interviewed
• Scope– Entire period of non-compliance

Audit Steps and Scope – cont’d
• On-Site Audit– Third party auditors (implementing GAGAS standards)
– Minimal time necessary to complete work• Pre-work can shorten on-site requirement• ~2-3 days
• Conclusion of Audit– Resolve any outstanding issues– Draft Audit report– Covered entity comment on findings– Final Audit report provided to OPA and HHS OIG

• Examples of what works well and what to avoid
• Most common findings
Tips From the Auditor

Takeaways
• HRSA and manufacturers may both auditentities
• There are lessons to be learned from prioraudits
• There are specific choices that place anentity at a higher risk of being audited

• Report inventory discrepancies or softwaremalfunctions to leadership; document the issue inwriting and keep records of how the situation wascorrected
• Know your 340B policies and procedures forverifying patient, prescriber, and location eligibility
• Spot check that these procedures are beingfollowed and report issues to leadership
Tips for Pharmacy Technicians

Questions

340B UNIVERSITY WRAP-UP

Take Action
Apexus Answers 340BPVP.com• Register for access to
secure section for contract maximization
Apexus | 340B Prime Vendor Program | 290 E John Carpenter Frwy | Irving, TX 75062

THANK YOU FOR ATTENDING340B UNIVERSITY!







