
ДВС синдром = Судсанд цус түгээмлээр бүлэгнэх хам шинж
буюу
Disseminated Intravascular Coagulation
Syndrome- DICS
2011.12.05

What is DICSyndrome?
DIC is a clinicopathologic syndrome characterized by widespread
intravascular fibrin formation in response to excessive blood protease activity that overcomes the natural
anticoagulant mechanisms..,

“DIC is an acquired syndrome characterized by the intravascular
activation of coagulation with loss of localization arising from different
causes. It can originate from and cause damage to the microvasculature, which if sufficiently severe, can
produce organ dysfunction”
Why???

Common Clinical Causes of Disseminated Intravascular Coagulation
SepsisTrauma and tissue injuryVascular disordersCancerImmunological (complement activation, release of tissue factor)
Obstetric complicationsDrugsLiver diseasesEnvenomationMiscellaneous etc..,

Conditions Associated With DIC
• Malignancy– Leukemia–Metastatic disease
• Cardiovascular– Post cardiac arrest– Acute MI– Prosthetic devices
• Hypothermia/Hyperthermia
• Pulmonary– ARDS/RDS– Pulmonary embolism
• Severe acidosis• Severe anoxia• Collagen vascular
disease• Anaphylaxis

The pathophysiology of DIC is complex. The mechanisms that activate or “trigger” DIC act on processes that are involved in, the processe normal hemostasis—namelys of platelet adhesion and aggregation and contact-activated (intrinsic) and tissue factor–activated (extrinsic) pathways of coagulation.

The release of several proinflammatory cytokines such as interleukin 6 \IL-6\ and tumor necrosis factor \TNF\ play central roles in mediating the coagulation defects in DIC and symptoms associated with systemic inflammatory response syndrome.

Uncontrolled trombin generation
Fibrin deposits in microcirculation Consumption of platelets & coagulation factors
Red blood cell damage & hemolysis
Ischemic tissue
damage
Failure multiple organs
Secondary fibrinolysis
Diffusing bleeding
Vessel patency FDP d-dimer
The pathophysiology of disseminated intravascular coagulation (DIC). Interactions between coagulation and fibrinolytic pathways result in bleeding and thrombosis in the microcirculation in patients with DIC.

Thrombin- and stasis-induced release of tissue plasminogen activator
Fibrinolytic activity in patients with DIC
Abr
upt o
nset
of D
IC
Plasminogen Plasmin
Fibrin Fibrin degradation products
Plasminogenactivator
inhibitor-1
2-Plasmin inhibitor
During DIC FXII FXIIa PrekallikreinKallikrein
PC APC inhibits PAI-1

• Bacteria• Virus• Parasitis• Mycotic• Endotoxin
Sepsis, snake toxin, Drug
Mechanism..,

• Extensive burns• Brain injury \gunshot\• Fat embolism• Rhabdomyolisis
Trauma & Tissue injury
Mechanism..,

• Blood • Other organs cancer• Carcinoma \pancreas, prostate, breast, lung etc..,\
Neoplasm = cancer
Mechanism..,

• Abruptio placentae• septic abortion & chorioamnionitis• Amniotic fluid embolism• Intrauterine fetal death
Obstetric complications
Mechanism..,
• Fulminant hepatic failure• Cirrhosis• Fatty liver of pregnancy
Liver diseases
Mechanism..,

• Shock• Respiratory distress syndrome• Massive transfussion• Acute iron toxicity• Anaphylaxis etc..,
Miscellaneous
Mechanism..,

• Complement activate• Kallikrein-Kinin
Hyperfibrinolysis
Mechanism..,

Clinical course..,
Acute & ChronicStages:
I-stage hypercoagulationII-stage III-stage hypocoagulationIV-stage terminal stage
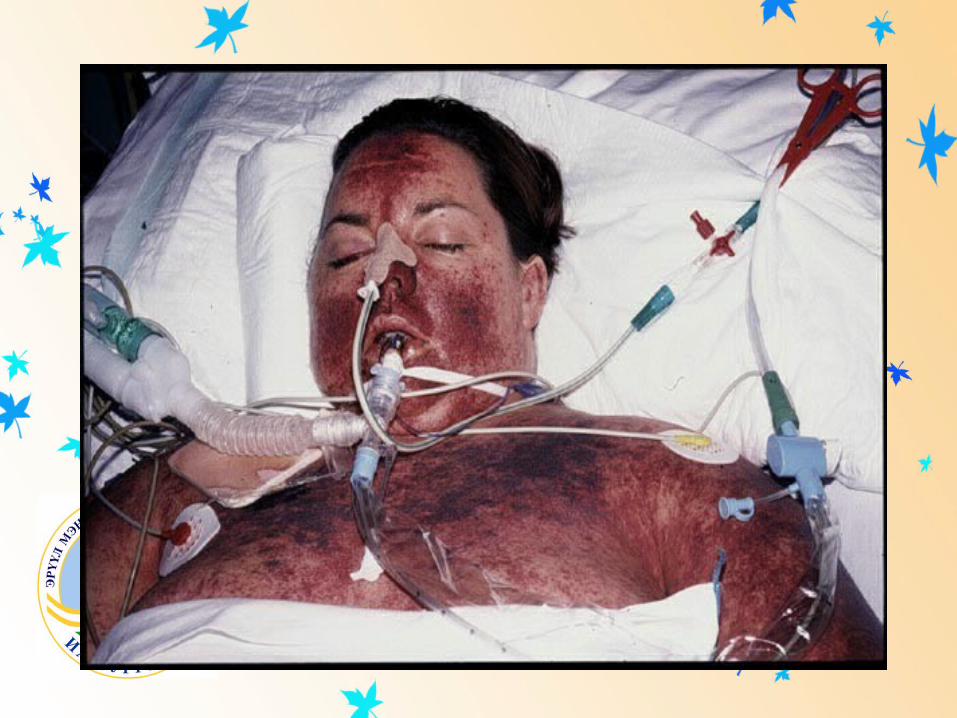
Clinical course..,Clinical manifestations of DIC syndrome
are related to the magnitude of the imbalance of hemostasis, to the underlying disease, or to both. The most common findings are bleeding ranging from oozing from venipuncture sites, petechiae, and ecchymoses to severe hemorrhage from the gastrointestinal tract or lung or into the central nervous system.
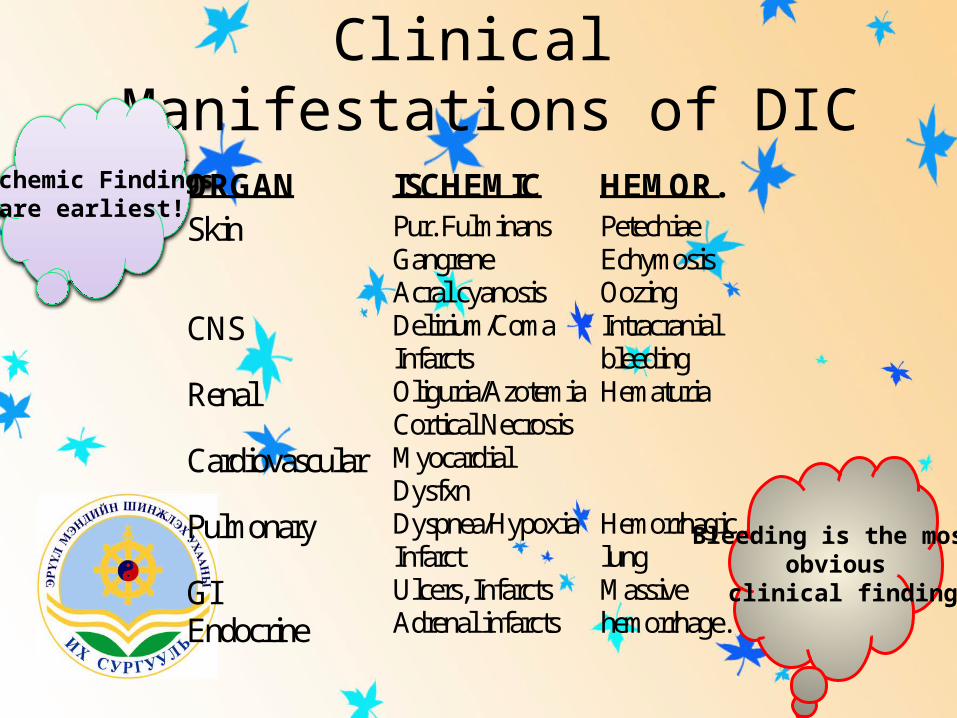
Clinical Manifestations of DIC
ORGAN ISCHEMIC HEMOR.Skin Pur. Fulminans
GangreneAcral cyanosis
PetechiaeEchymosisOozing
CNS Delirium/ComaInfarcts
Intracranialbleeding
Renal Oliguria/AzotemiaCortical Necrosis
Hematuria
Cardiovascular MyocardialDysfxn
Pulmonary Dyspnea/HypoxiaInfarct
Hemorrhagiclung
GIEndocrine
Ulcers, InfarctsAdrenal infarcts
Massivehemorrhage.
Ischemic Findingsare earliest!
Bleeding is the most obvious
clinical finding
Clinical course.., acute DICsyndrome
Hemocoagulation & shockThrombosis & HemorragicHypovolemia & AnemiaOther organs dysthropy, dysfunctional symphtomeMetabolytic syndrome..,
Hemodynamic complications and shock are common among patients with acute DIC.

Clinical course.., chronic DICsyndrome
In chronic DIC the bleeding symptoms are discreet and restricted to skin or mucosal surfaces. The hypercoagulability of DIC manifests as the occlusion of vessels in the microcirculation and resulting organ failure. Thrombosis of large vessels and cerebral embolism can also occur.

Clinical Manifestations of DIC

Diagnosis..,
The diagnosis of clinically significant DIC is based on the presence of clinical and/or laboratory abnormalities of coagulation or thrombocytopenia. The laboratory diagnosis of DIC should prompt a search for the underlying disease if it is not already apparent.
Diagnosis..,
The laboratory investigation should include coagulation tests [aPTT, PT, thrombin time (TT)] and markers of fibrin degradation products (FDP), in addition to platelet and red cell count and analysis of the blood smear.
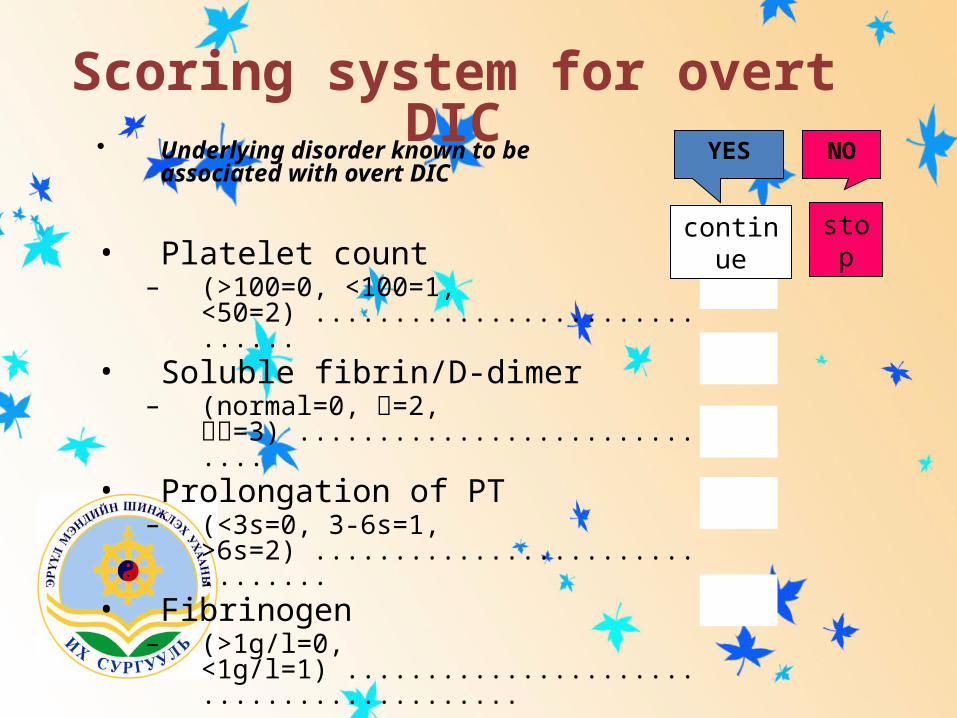
Scoring system for overt DIC
• Platelet count– (>100=0, <100=1, <50=2) ..............................
• Soluble fibrin/D-dimer– (normal=0, =2, =3) .............................
• Prolongation of PT– (<3s=0, 3-6s=1, >6s=2) ................................
• Fibrinogen– (>1g/l=0, <1g/l=1) ..........................................
• Calculate sum ........................................
YES NO
stopcontinue
• Underlying disorder known to be associated with overt DIC

Scoring system for overt DIC
• Platelet count– (>100=0, <100=1,
<50=2) ................... ...........• Soluble fibrin/D-dimer
– (normal=0, =2, =3) .............................• Prolongation of PT
– (<3s=0, 3-6s=1, >6s=2) ................................
• Fibrinogen– (>1g/l=0,
<1g/l=1) ..........................................
• Calculate sum ........................................
YES NO
stopcontinue
• Underlying disorder known to be associated with overt DIC
Polytrauma
85 1
8 3
+3 1
2,2 0
5
- Example -
Scoring system for overt DIC
• If the calculated score is– 5: compatible with overt DIC
repeat scoring daily– <5: suggestive (not affirmative)
for non-overt DIC repeat next 1-2 days.

Scoring system for non-overt DIC• Presence of underlying disorder
– (no=0, yes=2) ..........................................................
• Platelet count + changes– (100=0, <100=1) + (=-1, stable=0, =1) .......
• Sol.fibrin/D-dimer + changes– (normal=0, =1) + (=-1, stable=0, =1) ........
• Prolongation of PT + changes– (3s=0, >3s=1) + (=-1, stable=0, =1) ...........
• Antithrombin– (normal=-1,
low=1) .................................................• Protein C
– (normal=-1, low=1) .................................................
• Calculate sum ...............................................

Diagnosis.., acute DICsyndrome Prolongation of PT and/or aPTTPlatelet counts <100,000/mm3
Elevated levels of FDPRapid decline in platelet numbersLow levels of coagulation inhibitors
AT III, protein CLow levels of coagulation factors
Factors V,VIII,X,XIIIThe presence of schistocytes (fragmented red cells) in the blood smear
\in approximately 50% of cases\The most sensitive test for DIC is the FDP level
The D-dimer test is more specific for detection of fibrin (but not fibrinogen) degradation products and indicates that the cross-linked fibrin has been digested by plasmin. D-dimer values >2,000 ng/ml have been reported to be consistent with DIC
High-grade DIC is also associated with levels of antithrombin III or plasminogen activity <60% of normal.

Chronic DIC has been described in many patients with intrauterine fetal death or giant hemangiomas (Kasabach-Merritt syndrome) and in many cases of adenocarcinoma
Other etiologic factors that may produce chronic DIC include various forms of vasculitis, acute leukemia, aneurysms, hemangiomatous transformation of the spleen, and renal allograft rejection
Diagnosis.., chronic DICsyndrome
Diagnosis.., chronic DICsyndromePlasma levels of FDP or D-dimers are elevated. aPTT, PT, and fibrinogen values are within the normal range or high.Mild thrombocytopenia or normal platelet counts are also common findingsRed cell fragmentation is often detected but at a lower degree than in acute DIC.
Differential diagnosis• Liver diseases– Patients with severe liver disease are at risk for bleeding
and manifest laboratory features including thrombocytopenia (due to platelet sequestration, portal hypertension, or hypersplenism), decreased synthesis of coagulation factors and natural anticoagulants, and elevated levels of FDP due to reduced hepatic clearance. However, in contrast to DIC, these laboratory parameters in liver disease do not change rapidly.
• Hypofibrinogenemia• Hemolytic-uremic syndrome• Vitamin K deficiency

Therapy..,
• DIC always is the end result of a serious underlying disorder.
• Anticoagulants• Antifibrinolytic therapy• Replacement Therapy with Platelets and
Coagulation Factors• Physiologic coagulation inhibitors

Therapy..,
• Anticoagulant
Antithrombin IIIProtein C concentrateTissue Factor Pathway Inhibitor (TFPI)Heparin

Therapy..,
• Antifibrinolytic
– Tranexamic acid– ∊-aminocaproic acid- EACA

Therapy..,
• Plasma therapy• Indications
– Active bleeding– Patient requiring invasive procedures– Patient at high risk for bleeding complications
• Fresh frozen plasma(FFP):– provides clotting factors, fibrinogen, inhibitors, and
platelets in balanced amounts.– Usual dose is 10-15 ml/kg

Therapy..,
• Blood• Replaced as needed to
maintain adequate oxygen delivery.
Blood loss due to bleedingRBC destruction (hemolysis)

Баярлалаа
Амжилт
Хүсье

Пресентаци авбал аваарай..,







