dose response in prostate cancer
TRANSCRIPT
The evidence for dose The evidence for dose escalation in prostate escalation in prostate
cancercancer
A. Choudhury
SpR, Clinical Oncology
OutlineOutline
• Radiobiology
• Evidence for dose escalation
• The CHHiP trial
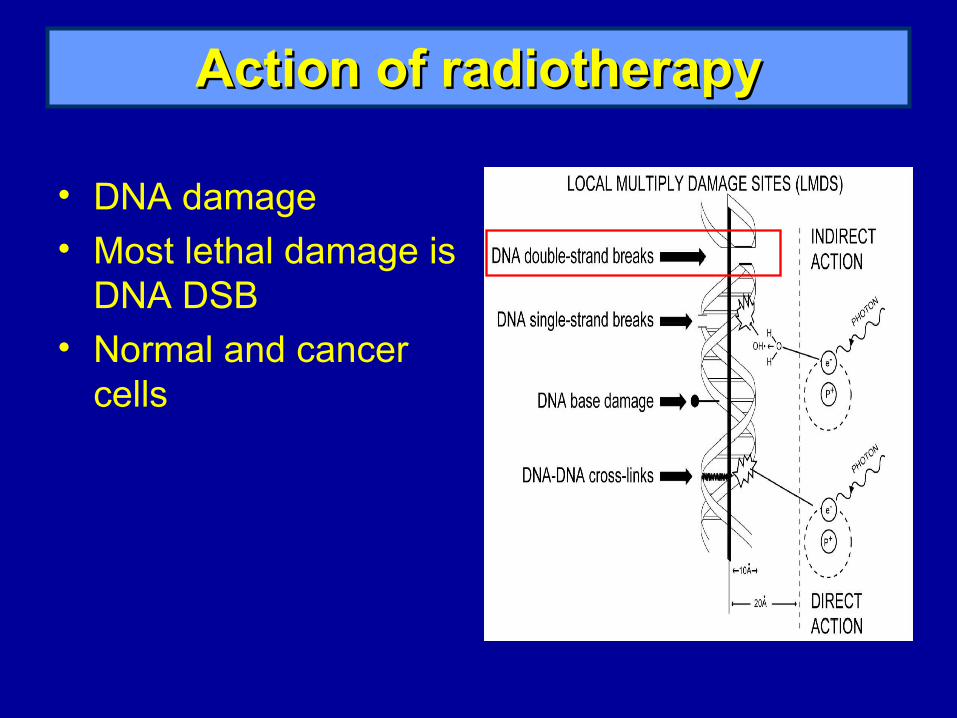
Action of radiotherapyAction of radiotherapy
• DNA damage• Most lethal damage is
DNA DSB• Normal and cancer
cells
Factors affecting radiosensitivityFactors affecting radiosensitivity
Intrinsic Factors
• DNA repair
• Repopulation
• Redistribution
Extrinsic Factors
• Micro-environment
• Blood supply
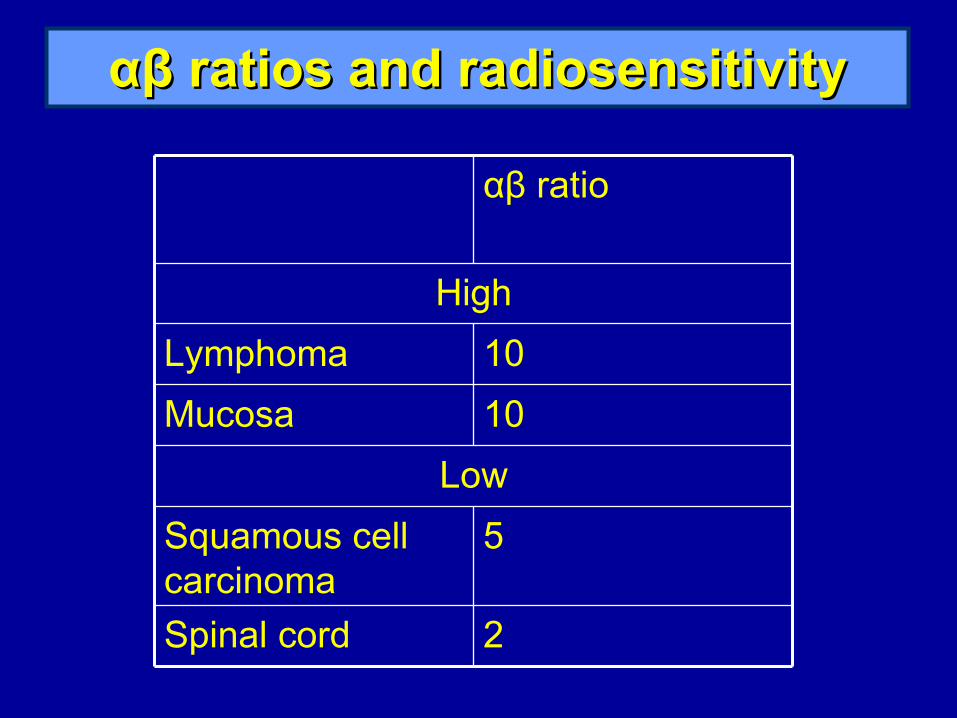
αβαβ ratios and radiosensitivity ratios and radiosensitivity
2Spinal cord
5Squamous cell carcinoma
Low
10Mucosa
10Lymphoma
High
αβ ratio

Effe
ct
Tumour Dose
Tumour control
The therapeutic ratioThe therapeutic ratio
normal tissue damage
Maximum tumour kill with minimum normal tissue toxicity

Normal tissue constraintsNormal tissue constraints
• Rectum:
30% <70Gy and mean dose <50 Gy
• Bladder:
50% <70Gy
• Femoral heads:
50% <50Gy
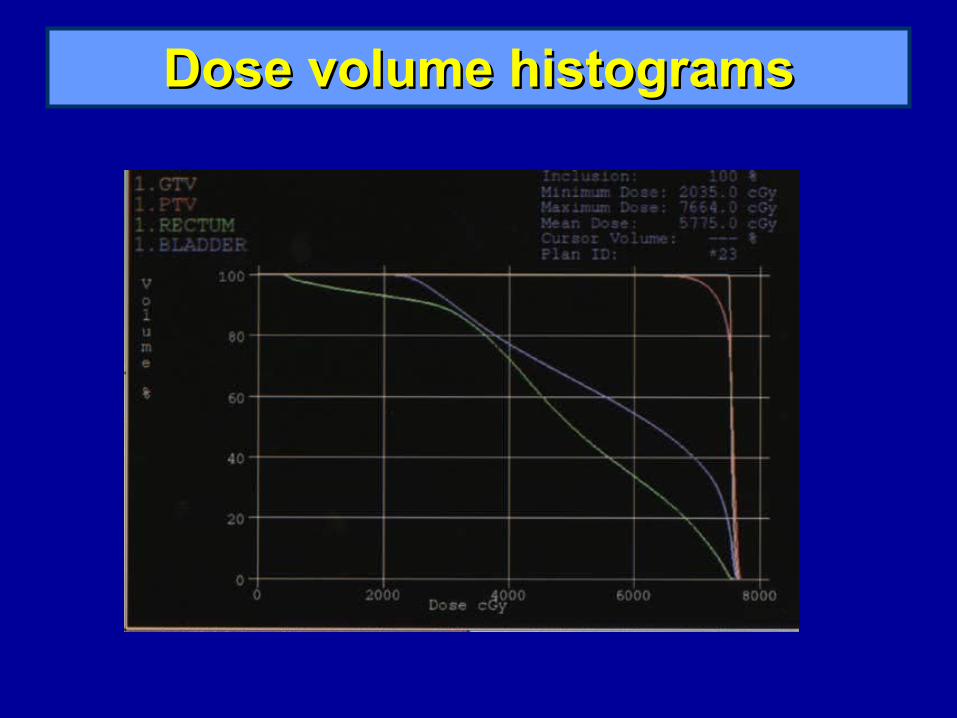
Dose volume histogramsDose volume histograms
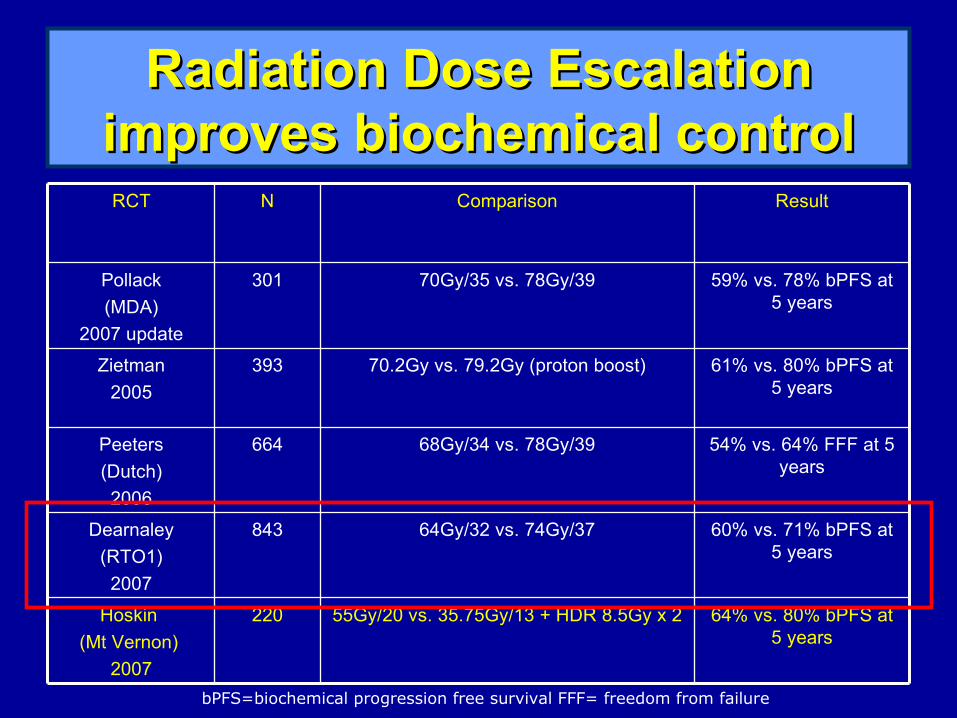
Radiation Dose Escalation Radiation Dose Escalation improves biochemical controlimproves biochemical control
64% vs. 80% bPFS at 5 years
55Gy/20 vs. 35.75Gy/13 + HDR 8.5Gy x 2220Hoskin
(Mt Vernon)
2007
60% vs. 71% bPFS at 5 years
64Gy/32 vs. 74Gy/37843Dearnaley
(RTO1)
2007
54% vs. 64% FFF at 5 years
68Gy/34 vs. 78Gy/39664Peeters
(Dutch)
2006
61% vs. 80% bPFS at 5 years
70.2Gy vs. 79.2Gy (proton boost)393Zietman
2005
59% vs. 78% bPFS at 5 years
70Gy/35 vs. 78Gy/39301Pollack
(MDA)
2007 update
ResultComparisonNRCT
bPFS=biochemical progression free survival FFF= freedom from failure

RT01 trialRT01 trial
• UK-based trial – largest phase III study• Compared 64Gy/32# v 74Gy/37#• Significant improvement in biochemical
progression-free survival• Significantly greater late bowel toxicity
HR=1·47 (95%CI: 1·12–1·92) (RTOG ≥2.0 ie >4-6 bowel opening,
moderate cramping) • No significant increase in bladder toxicity.

Conformal CT planned Conformal CT planned radiotherapyradiotherapy
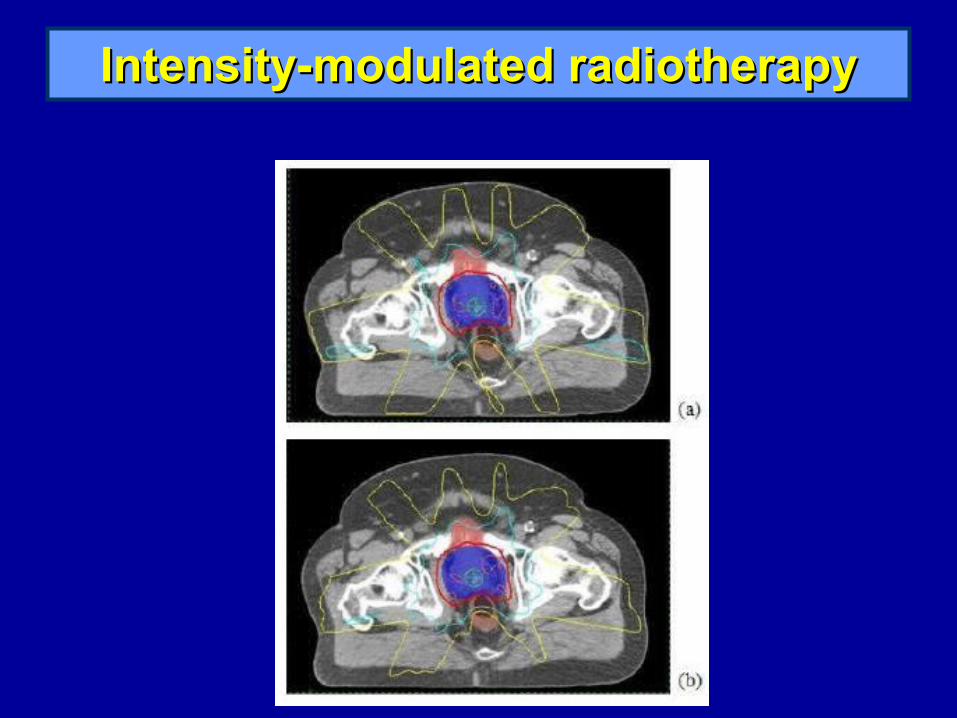
Intensity-modulated radiotherapyIntensity-modulated radiotherapy

Radiation Dose Escalation Radiation Dose Escalation improves biochemical controlimproves biochemical control
64% vs. 80% bPFS at 5 years
55Gy/20 vs. 35.75Gy/13 + HDR 8.5Gy x 2220Hoskin
(Mt Vernon)
2007
60% vs. 71% bPFS at 5 years
64Gy/32 vs. 74Gy/37843Dearnaley
(RTO1)
2007
54% vs. 64% FFF at 5 years
68Gy/34 vs. 78Gy/39664Peeters
(Dutch)
2006
61% vs. 80% bPFS at 5 years
70.2Gy vs. 79.2Gy (proton boost)393Zietman
2005
59% vs. 78% bPFS at 5 years
70Gy/35 vs. 78Gy/39301Pollack
(MDA)
2007 update
ResultComparisonNRCT
bPFS=biochemical progression free survival FFF= freedom from failure
Mount Vernon trialMount Vernon trial
• Phase III RCT – 220 patients
55Gy/20# v 35.75Gy/13# + 17Gy/2# HDR
• Significantly improved biochemical progression-free survival (p=0.03) with HDR
• No increase in toxicity

HDR brachytherapyHDR brachytherapy
• 12-15 metal catheters inserted peripherally to about 1 cm beyond gland
• Template sutured and needles fixed in position
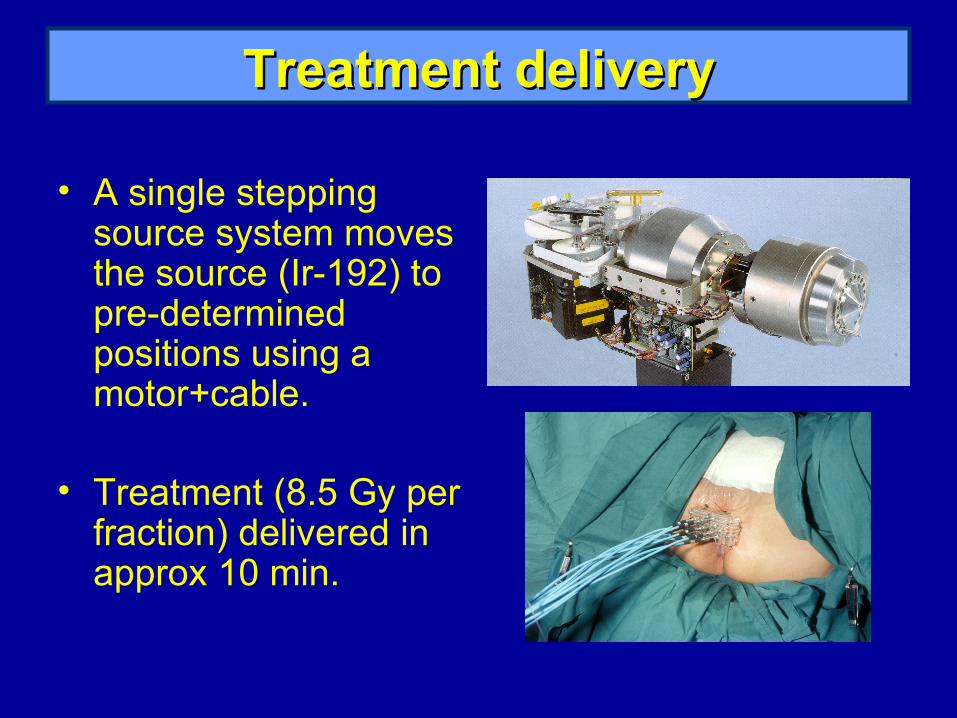
Treatment deliveryTreatment delivery
• A single stepping source system moves the source (Ir-192) to pre-determined positions using a motor+cable.
• Treatment (8.5 Gy per fraction) delivered in approx 10 min.

Equivalent dosesEquivalent doses
αβ ratio
77.0122.0214.535.75Gy/13# +17Gy/2#
External beam + HDR boost
70.198.2155.855Gy/20#
87.7113.1165.274Gy/37#
External beam
103.51.5
Hoskin et al, 2007
CHHiP TrialCHHiP Trial
• Conventional or Hypofractionated High Dose Intensity Modulated Radiotherapy for Prostate Cancer
• Hypothesis: hypofractionated radiotherapy schedules for localised prostate cancer will improve the therapeutic ratio by either:
a) Improving tumour control
b) Reducing normal tissue side effects

Eligibility criteriaEligibility criteria
• Histologically proven carcinoma of the prostate • Clinical disease stage T1b – T3a, N0, M0 (1997
TNM System) • PSA ≤ 30ng/ml • Estimated risk of seminal vesicle involvement
under ≤30% • WHO performance status 0 or 1 • No previous androgen deprivation • Life expectancy likely to be in excess of 10 years
(5 years for poorly differentiated cancers)
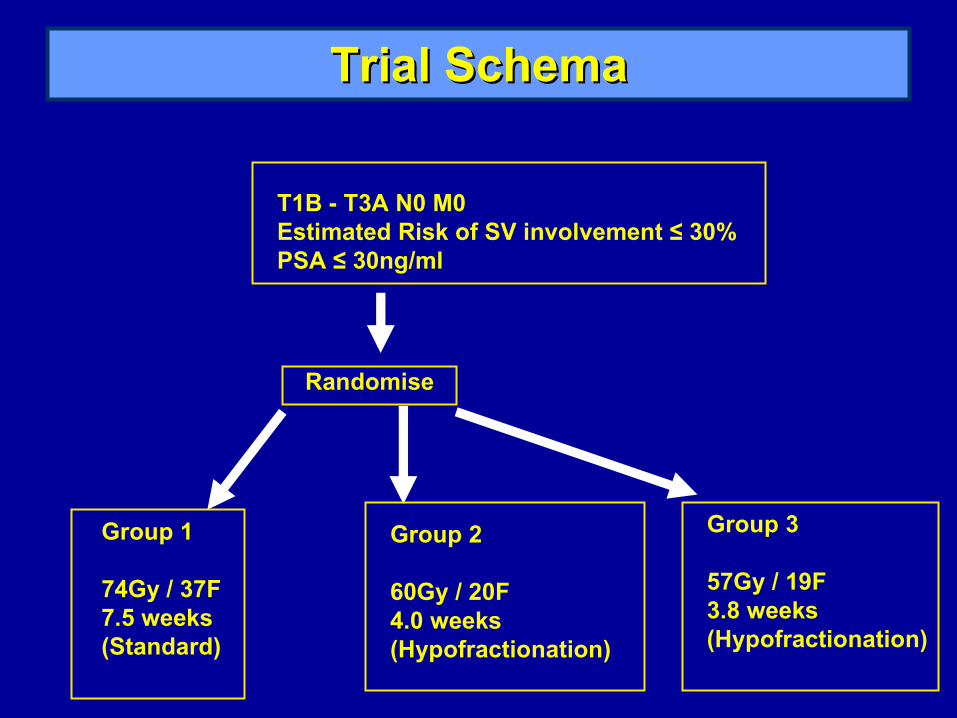
Trial SchemaTrial Schema
T1B - T3A N0 M0 Estimated Risk of SV involvement ≤ 30% PSA ≤ 30ng/ml
Randomise
Group 1
74Gy / 37F 7.5 weeks (Standard)
Group 2
60Gy / 20F 4.0 weeks (Hypofractionation)
Group 3
57Gy / 19F 3.8 weeks (Hypofractionation)
Normal tissue constraints (CHHiP)Normal tissue constraints (CHHiP)
• Rectum:
30% ≤ 65Gy
• Bladder:
50% ≤ 50Gy
• Femoral heads:
50% ≤ 50Gy
The FutureThe Future
• Proton therapy
• Radiosensitisers- chemotherapy: weekly docetaxel- novel agents
• Predictive factors for radiotherapy response