use of three-dimensional catheter guidance and trans-esophageal echocardiography to eliminate...
TRANSCRIPT

Use of Three-Dimensional Catheter Guidance andTrans-Esophageal Echocardiography to EliminateFluoroscopy in Catheter Ablation of Left-SidedAccessory PathwaysJOHN CLARK, M.D., J.R. BOCKOVEN, M.D., JOHN LANE, M.D., C.R. PATEL, M.B.B.S.,and GRACE SMITH, M.D.From The Heart Center, Akron Children’s Hospital, Akron, Ohio
Background: Newer technologies such as three-dimensional mapping and echocardiography can de-crease x-ray exposure during catheter ablation. Many right-sided tachycardias can now be ablated with-out fluoroscopy. Left-sided tachycardias, however, have not yet been ablated using a zero fluoroscopyapproach.
Objective: This study sought to examine the utility of trans-esophageal echocardiography (TEE) inproviding adequate imaging as an alternative to fluoroscopy for transseptal puncture. When combinedwith NavX guidance (St. Jude Medical, St. Paul, MN, USA), fluoroscopy may not be necessary.
Methods: Ten pediatric patients with supraventricular tachycardia (SVT) had accessory pathwaysmapped to the left side. Right atrial and coronary sinus geometries were created using NavX. Once aleft-sided pathway was confirmed, a transseptal puncture was performed. A guide wire was placed in theSVC and confirmed by TEE. A transseptal sheath and dilator were advanced over the wire and positionedwith TEE guidance so that the tip of the dilator was tenting the fossa ovalis. A transseptal needle wasadvanced across the fossa. Left atrial location of the needle tip was confirmed on TEE by saline contrastinjection. The sheath and dilator were advanced over the needle with continuous pressure monitoring andTEE. Once the sheath was appropriately positioned, the ablation was completed using NavX guidance.
Results: All patients had acutely successful ablations and none required the use of fluoroscopy. Numberof cryo lesions ranged from five to 19, with a mean of 9. Mean procedure time was 4.4 hours, with a rangeof 3.2 hours to 7.2 hours. There were no complications. One patient had recurrence.
Conclusions: Three-dimensional mapping combined with TEE shows potential for eliminating fluo-roscopy use during catheter ablation. (PACE 2008; 31:283–289)
ablation, cryoablation, NavX, pediatric, three-dimensional mapping, trans-esophagealechocardiography, transseptal puncture
IntroductionCatheter ablation of accessory pathway me-
diated tachycardia is the treatment of choicefor many patients with clinical supraventriculartachycardia (SVT). The success rate for this pro-cedure is greater than 90% for most substrates.1Newer technologies allow for minimal fluoroscopyuse during catheter ablation. Several authors havereported experience with ablation of tachycar-dia substrates on the right side of the heart us-ing no fluoroscopy.2–5 Left-sided tachycardias aremore challenging to ablate without radiation ex-posure. We report 10 patients with left-sided ac-cessory pathways who underwent catheter abla-tion by transseptal approach without the use of
No conflicts of interest for any author.
Address for reprints: John Clark, M.D., Akron Children’s Hospi-tal, One Perkins Square, Akron, OH 44308. Fax: 330-543-8208;e-mail: [email protected]
Received September 12, 2007; revised November 7, 2007;accepted November 30, 2007.
fluoroscopy. NavX (St. Jude Medical, St. Paul,MN, USA) geometry and transesophageal echocar-diography (TEE) were used to guide sheaths andcatheters.
MethodsThe study group consisted of 10 patients who
underwent electrophysiology study for treatmentof SVT due to a left-sided accessory pathway. Theonly inclusion criteria were a documented left-sided accessory pathway and a structurally normalheart. Prior to procedure, consent was obtained forparticipation in the study. When appropriate, as-sent was also obtained. Patient age ranged fromnine years to 17 years (mean = 14.4 years). Therewere two females and eight males (Table I). Threepatients had manifest pre-excitation. All patientshad structurally normal hearts. Two patients hadpreviously undergone ablation attempts withoutthe use of NavX guidance.
All procedures were done under general anes-thesia. A two-pole catheter was placed on the
C©2008, The Authors. Journal compilation C©2008, Blackwell Publishing, Inc.
PACE, Vol. 31 March 2008 283
CLARK, ET AL.Ta
ble
I.
Stu
dyG
roup
Pat
ien
t1
Pat
ien
t2
Pat
ien
t3
Pat
ien
t4
Pat
ien
t5
Pat
ien
t6
Pat
ien
t7
Pat
ien
t8
Pat
ien
t9
Pat
ien
t10
Age
(yea
rs)
1515
1615
1716
99
1116
Gen
der
Mal
eM
ale
Mal
eM
ale
Mal
eM
ale
Fem
ale
Fem
ale
Mal
eM
ale
Wei
ght(
kg)
102.
265
82.1
5753
.670
.636
.829
.162
64.3
Pat
hway
loca
tion
PL
PL
PP
SP
PS
PL
PS
#1-R
A.#
2-L
#1-R
PP
S.#
2-P
PS
PP
SP
LP
roce
dure
time
(min
utes
)25
120
726
529
618
943
033
324
725
119
4F
luor
otim
e(m
inut
es)
00
00
00
00
00
Cat
hete
rtip
size
(mm
)6
46
66
4an
d6
4an
d6
44
6C
ryom
aptim
e(s
econ
ds)
205
4119
976
8387
074
230
010
953
Num
ber
ofle
sion
s5
85
66
1319
119
7To
tall
esio
ntim
e(m
inut
es)
2032
2024
25.4
5276
4437
.828
Acu
tesu
cces
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sR
ecur
renc
eN
oN
oN
oN
oYe
sN
oN
oN
oN
oN
o
L=
left
late
ral;
PL
=le
ftpo
ster
o-la
tera
l;P
PS
=le
ftpo
ster
ior
para
sept
al;R
A=
right
ante
rior;
RP
PS
=rig
htpo
ster
ior
para
sept
al.
patient’s back and the electrodes were secured inplace using an electrocautery-grounding pad. Thiscatheter served as the reference catheter. A sin-gle multi-pole catheter was placed from the rightfemoral vein. Using NavX guidance, the catheterwas advanced up the inferior vena cava (IVC) untilatrial signals were obtained. A right atrial geome-try was then created, including superior vena cava(SVC), IVC, right atrium, and tricuspid valve. Oncethe right atrial and tricuspid valve geometries werecomplete, the tricuspid annulus served as a land-mark to position the coronary sinus (CS) catheter.Using the geometry in the same manner that a flu-oroscopic image would be used, the catheter waspositioned in the right atrium and given a down-ward deflection to position the tip across the tri-cuspid valve into the right ventricle. The catheterwas then pulled downward to contact the inferiormargin of the tricuspid valve. Clockwise rotationof the catheter then would bring the tip back acrossthe tricuspid valve and into contact with the loweratrial septum. Further clockwise rotation engagedthe tip of the catheter into the mouth of the CS.Release of the flexion on the catheter then allowedthe catheter to extend into the CS. A CS geometrywas then drawn. The resulting geometry is shownin Figure 1.
Standard atrial and ventricular protocols werethen performed. For patients with manifest path-ways, pathway location was mapped by localizingshortest atrioventricular (A-V) intervals in sinusrhythm. For patients with concealed pathways, lo-cation was mapped by the earliest retrograde ac-tivation during SVT. In these patients, a secondmapping catheter was inserted via the right or leftfemoral vein and positioned in the right ventricu-lar apex for mapping during ventricular pacing. Toplace this catheter, it was first positioned to recorda His electrogram and then given a downward de-flection. The catheter was then advanced so thatthe curve of the catheter contacted the right ven-tricular outflow tract and deflected the tip towardthe right ventricular apex. The flexion was thenreleased to allow the catheter tip to contact themyocardium.
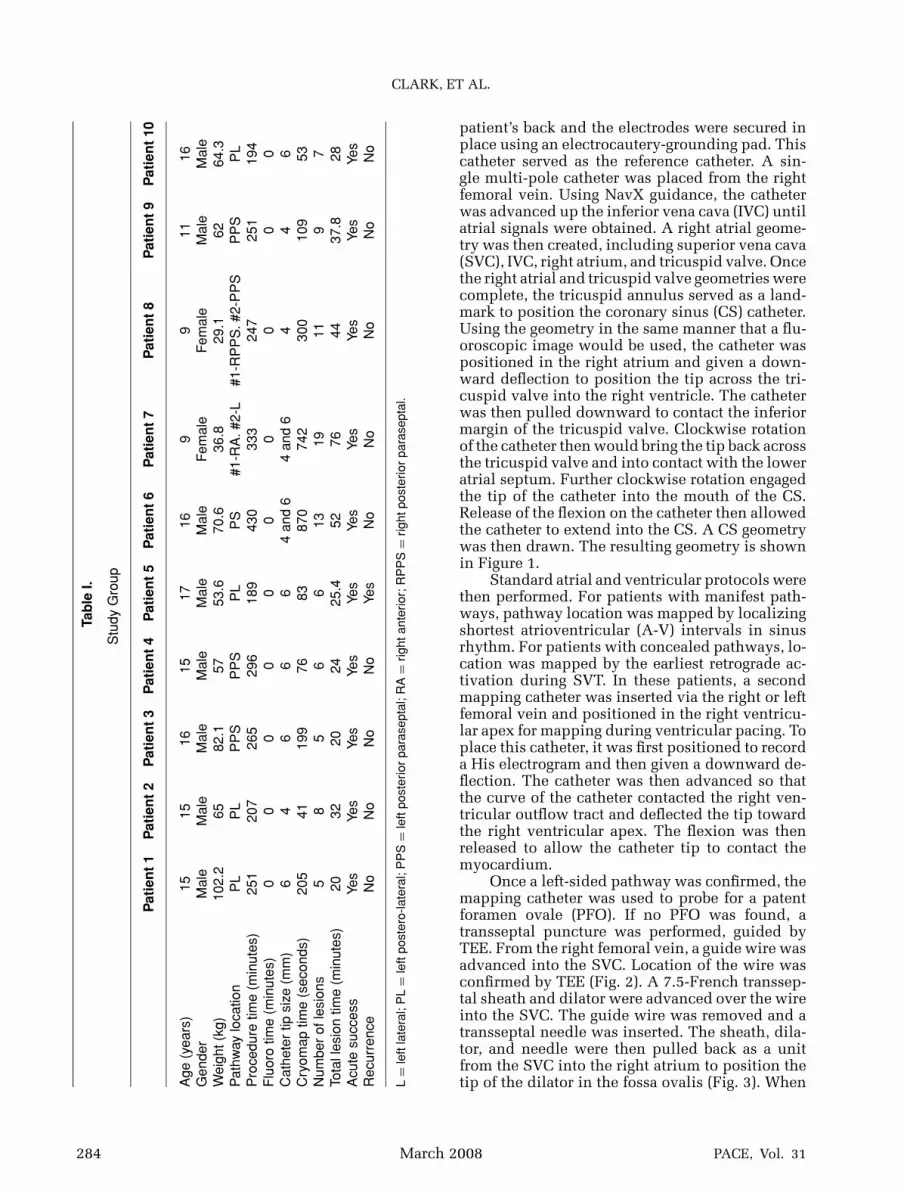
Once a left-sided pathway was confirmed, themapping catheter was used to probe for a patentforamen ovale (PFO). If no PFO was found, atransseptal puncture was performed, guided byTEE. From the right femoral vein, a guide wire wasadvanced into the SVC. Location of the wire wasconfirmed by TEE (Fig. 2). A 7.5-French transsep-tal sheath and dilator were advanced over the wireinto the SVC. The guide wire was removed and atransseptal needle was inserted. The sheath, dila-tor, and needle were then pulled back as a unitfrom the SVC into the right atrium to position thetip of the dilator in the fossa ovalis (Fig. 3). When
284 March 2008 PACE, Vol. 31

TRANSSEPTAL PUNCTURE WITHOUT FLUOROSCOPY
Figure 1. Standard AP (left) and lateral views as drawn in NavX for patient 7. Right atrial geometryis drawn in purple. Coronary sinus geometry is drawn in gold. Blue spheres represent lesionsplaced for her right anterior manifest accessory pathway. Red spheres represent lesions on herleft lateral concealed pathway. The cryocath is shown in orange with the distal tip marked ingreen.
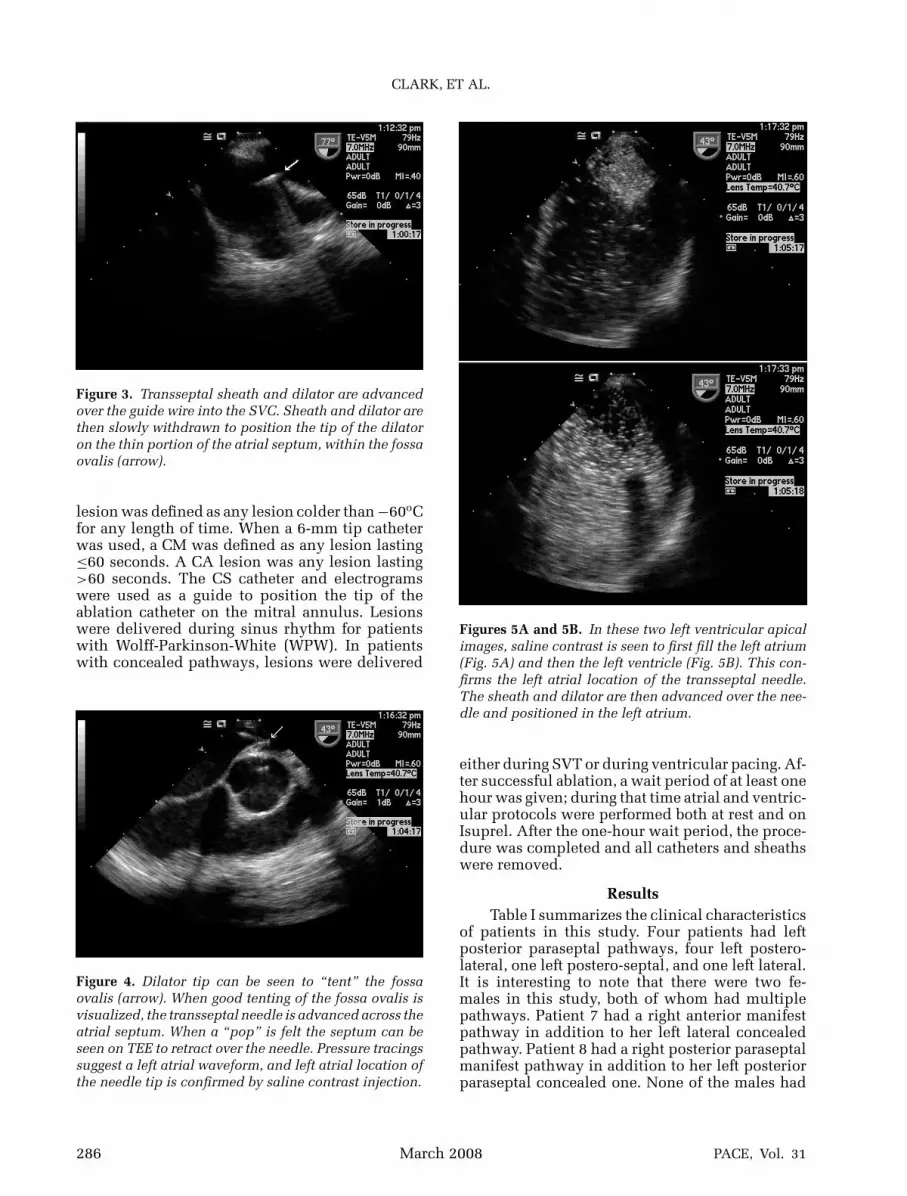
adequate position was seen on the bicaval view,other views were obtained to optimize location ofthe dilator tip. Particular attention was paid to theaortic short-axis view. From this view, the tip couldbe well seen to indent the fossa, and the anterior-posterior orientation could be established (Fig. 4).When the dilator tip could be seen tenting the fossaand aiming posterior to the aortic valve, then thetransseptal needle was advanced out of the dila-tor. The needle could be seen to perforate the fossaand come to rest within the left atrium. A left atrialpressure tracing could then be seen. At this point,the needle was held in position and the TEE viewchanged to an apical left ventricle (LV) view. Salinecontrast was injected which showed left atrial fill-ing, confirming the left atrial location of the needletip (Figs. 5A and 5B).
After establishing good needle position, thedilator and sheath were carefully advanced overthe needle with continuous pressure monitoringand TEE imaging. Once the sheath was in good po-sition, the needle and dilator were carefully with-drawn. The sheath was evacuated of any air andflushed with heparinized saline. Final position ofthe sheath in the left atrium was confirmed onTEE by both direct visualization (Fig. 6) as wellas saline contrast injection. The patient was thengiven IV heparin to maintain activated clottingtimes of around 250 seconds.
A cryoablation (CA) catheter (CryoCath Inc.,Kirkland, Canada) was advanced through thesheath into the left atrium. From this point on, theprocedure was completed using standard ablationprotocols. In three patients, a 4-mm tip catheterwas used. In five patients, a 6-mm tip was used;and in two patients, both a 4-mm and a 6-mm tipwere used. When a 4-mm tip catheter was used,a cryomap (CM) was defined as any lesion be-tween −30oC to −59oC for ≤60 seconds. A CA
Figure 2. A guide wire (arrow) is advanced into the SVC.
PACE, Vol. 31 March 2008 285
CLARK, ET AL.
Figure 3. Transseptal sheath and dilator are advancedover the guide wire into the SVC. Sheath and dilator arethen slowly withdrawn to position the tip of the dilatoron the thin portion of the atrial septum, within the fossaovalis (arrow).
lesion was defined as any lesion colder than −60oCfor any length of time. When a 6-mm tip catheterwas used, a CM was defined as any lesion lasting≤60 seconds. A CA lesion was any lesion lasting>60 seconds. The CS catheter and electrogramswere used as a guide to position the tip of theablation catheter on the mitral annulus. Lesionswere delivered during sinus rhythm for patientswith Wolff-Parkinson-White (WPW). In patientswith concealed pathways, lesions were delivered
Figure 4. Dilator tip can be seen to “tent” the fossaovalis (arrow). When good tenting of the fossa ovalis isvisualized, the transseptal needle is advanced across theatrial septum. When a “pop” is felt the septum can beseen on TEE to retract over the needle. Pressure tracingssuggest a left atrial waveform, and left atrial location ofthe needle tip is confirmed by saline contrast injection.
Figures 5A and 5B. In these two left ventricular apicalimages, saline contrast is seen to first fill the left atrium(Fig. 5A) and then the left ventricle (Fig. 5B). This con-firms the left atrial location of the transseptal needle.The sheath and dilator are then advanced over the nee-dle and positioned in the left atrium.
either during SVT or during ventricular pacing. Af-ter successful ablation, a wait period of at least onehour was given; during that time atrial and ventric-ular protocols were performed both at rest and onIsuprel. After the one-hour wait period, the proce-dure was completed and all catheters and sheathswere removed.
ResultsTable I summarizes the clinical characteristics
of patients in this study. Four patients had leftposterior paraseptal pathways, four left postero-lateral, one left postero-septal, and one left lateral.It is interesting to note that there were two fe-males in this study, both of whom had multiplepathways. Patient 7 had a right anterior manifestpathway in addition to her left lateral concealedpathway. Patient 8 had a right posterior paraseptalmanifest pathway in addition to her left posteriorparaseptal concealed one. None of the males had
286 March 2008 PACE, Vol. 31

TRANSSEPTAL PUNCTURE WITHOUT FLUOROSCOPY
Figure 6. When the transseptal procedure is complete,the sheath can be seen (arrow) adjacent to the anteriorleaflet of the mitral valve.
multiple pathways. All patients had an acutelysuccessful CA and none required the use of flu-oroscopy. There were no complications. Radiofre-quency energy was not used in this study.
Procedure time ranged from 189 minutes to430 minutes, with a mean of 266 minutes. Patient6 had the longest procedure time. This patient hadpreviously undergone radiofrequency ablation of aleft postero-septal pathway with subsequent recur-rence. He was brought back to the catheterizationlaboratory for attempted CA and was enrolled inthe study. Initial lesions were placed just insidethe CS using a 4-mm tip catheter. This was tran-siently successful but the pathway recurred duringthe one-hour wait period. He subsequently had at-tempts from a left atrial approach with the samecatheter. He again had transient success. He finallyhad attempts with a 6-mm tip catheter and hadsuccessful elimination of his pathway with no re-currence to date.
The CM time ranged from 41 seconds to 870seconds, with a mean of 268 seconds. The numberof CA lesions ranged from 5 to 19, with a mean of9. The mean CA time was 36 minutes. There wereno complications.
At 6-month follow-up, there was one recur-rence. Patient 3 had a left posterior parasep-tal WPW pathway. He had CA with a 6-mmtip catheter. Although his pathway conductionwas eliminated quickly into the first lesion andhe showed no evidence of recurrence in thecatheterization laboratory, he showed manifestpre-excitation one-week post procedure and sub-sequently had recurrence of SVT.
DiscussionCatheter ablation is a well-established ther-
apy for treatment of SVT in children. In most in-
stances, the procedure is curative. One of the risksof catheter ablation is radiation exposure.6–9 Thisrisk is cumulative and lifelong. It therefore posesa greater concern in the pediatric population. TheAmerican College of Cardiology recommends thatall catheterization laboratories adopt the princi-ples of “ALARA” (radiation doses “as low as rea-sonably achievable”).10 These guidelines are in-tended for the protection of both the patient andthe staff. There is increasing interest in methodsto minimize radiation exposure during catheterprocedures, and various authors have publishedmethods to lower the total dose.11–14 In addi-tion, newer technologies have evolved, which of-fer opportunities to lower radiation exposure. Onesuch technology is three-dimensional navigationsystems.15–18
In 2002, Drago et al. first reported catheterablation of SVT without fluoroscopy.2 In that se-ries, the CARTO system was used (Cordis Web-ster, Marlton, NJ, USA). Subsequently, severalauthors have reported using NavX.3–5 There aresome advantages to NavX for this purpose. First,NavX allows visualization of any electrophysiol-ogy catheter, not just the ablation catheter. Sec-ond, NavX allows for the use of either radiofre-quency or CA. Availability of CA is importantto increase the safety of procedures on or nearthe atrial septum. In our own laboratory, we havebeen using three-dimensional NavX guidance toreplace fluoroscopy since 2005.4 By this means,we were able to eliminate fluoroscopy use forall right-sided tachycardia mechanisms, includ-ing A-V nodal reentry, accessory pathways, ectopictachycardias, junctional tachycardias, and ventric-ular tachycardias. The only remaining indicationfor fluoroscopy was to perform a transseptal punc-ture.
Transseptal sheaths and dilators cannot be vi-sualized on NavX. Verma et al. have reported vi-sualization of the tip of the transseptal needle onNavX.19 However, the needle tip cannot be seenuntil it is advanced out of the dilator. This ap-proach, therefore, does not assist in positioningthe transseptal dilator and sheath against the fossaovalis, and is of limited clinical use. Echocardio-graphy is commonly used as an adjunct to fluo-roscopy in the performance of transseptal punc-ture. Daoud has suggested that echo guidanceshould be standard of care for all transseptal pro-cedures.20 Intracardiac localization of the sheath,dilator, and needle tip are better assessed by echothan by fluoroscopy. However, what has not beenpreviously evaluated is the use of echo to supplantfluoroscopy, rather than as an adjunct to it. Thepresent study demonstrates the initial feasibilityfor TEE to replace fluoroscopy in the performanceof transseptal puncture.
PACE, Vol. 31 March 2008 287

CLARK, ET AL.
An alternative approach would be to use in-tracardiac echocardiography (ICE). TEE offers sev-eral benefits in the pediatric population. First, TEEdoes not require venous access and can be per-formed on almost all patients who would be under-going catheter ablation. ICE catheters are of signif-icant size and require extra venous access, whichis a major hurdle in pediatric procedures. Second,TEE gives a greater variety of views of the heart,which allows for more ability to confirm the loca-tion of the sheath, dilator, and needle before andafter it is advanced across the septum. Finally, TEEis easy to position without fluoroscopy. Maneuver-ing an ICE catheter from the left femoral vein tothe right atrium, and then manipulating it to ob-tain the necessary images without the use of x-ray,could prove to be challenging.
This study suggests that when TEE is com-bined with NavX guidance, there appears to be po-tential for complete elimination of fluoroscopy forall electrophysiologic procedures. This has ben-efits for both the patient and the staff. The mostobvious benefit is the elimination of the risks as-sociated with x-ray exposure, but there are other,less obvious ones as well. One is the ability to per-form a catheter ablation on a patient during preg-nancy without risking radiation exposure to thefetus. Fortunately, this is an uncommon scenario,but when needed, it would be a welcome tool.Another benefit is staff comfort. In our laboratory,lead aprons are no longer worn and this makes fora much more comfortable working environment.Fluoroscopy is always immediately available. Inthe rare instance that it would be needed, apronscan be donned for that portion of the procedureand then removed. Another benefit that we havewitnessed is the ability to permit a staff member tocontinue working in the catheterization laboratorywhile pregnant, since no x-ray is being used.
Procedure time for these 10 patients was rel-atively long. On average, it took about one hourlonger than our procedures using fluoroscopy. Al-though the sample size is too small for statisti-cal analysis, the average procedure time for our10 most recent procedures with fluoroscopy was181 minutes, compared to 266 minutes without.This was not unexpected. We were most interestedin learning the procedure and in determining themost useful TEE views to complete the procedure
safely and successfully. As experience is gained,procedure times will decrease. Sheaths and dila-tors with electrode markers that can be seen onNavX would shorten the time further. However,after an adequate learning curve, if the use of TEEstill proves to add significant time to the proce-dure, this would negatively influence its useful-ness. Longer procedure times could pose a greateranesthetic risk and this must be balanced againstany potential benefit.
The primary drawback of TEE is that it re-quires general anesthesia. This is not an issuefor many pediatric institutions because the pro-cedures are often done under general anesthesiaalready. However, most adult institutions do notutilize general anesthesia for a routine ablation.Therefore, in the adult population, the use of ICEmay offer advantages over TEE. Other limitationsof the study include the small size of the studypopulation, and the need for an additional physi-cian for performance of the TEE. Lastly, the costeffectiveness of TEE versus ICE versus fluoroscopyalone was not systematically studied. Cost analysismust consider the use of fluoroscopy alone becausein most pediatric institutions transseptal punctureis performed with only fluoroscopic guidance. Itmust also factor in risk benefit.
CA was used for all patients in this study.Acute success was achieved in 100% with a 10%recurrence. Although the study size is too smallfor statistical analysis, the results are comparableto those reported in the pediatric registry using ra-dio frequency.1
LimitationsThis study is not a randomized trial and the
population size is small. It therefore does not havethe statistical power to conclude safety or efficacyof this new approach.
ConclusionUsing TEE imaging, the intraprocedural func-
tions of fluoroscopy were adequately performedby echocardiography. Combined with NavX guid-ance, none of the patients required fluoroscopy.These data provide a basis for exploring the use ofTEE and NavX to achieve a zero x-ray approach tocatheter ablation. Larger studies will be needed toprove the usefulness of these technologies.
References1. Kugler JD, Danford DA, Houston KA, Felix G. Pediatric radiofre-
quency catheter ablation registry success, fluoroscopy time, andcomplication rate for supraventricular tachycardia: Comparison ofearly and recent eras. J Cardiovasc Electrophysiol 2002; 13:336–341.
2. Drago F, Silvetti MS, Di Pino A, Grutter G, Bevilacqua M, LeibovichS. Exclusion of fluoroscopy during ablation treatment of right acces-
sory pathway in children. J Cardiovasc Electrophysiol 2002; 13:778–782.
3. Grubb NR, Petzer E, Lang C, Colthart A, Elhag O. A zero fluoroscopyapproach for electrophysiologic studies and catheter ablation forcommon supraventricular tachycardias. Heart Rhythm 2006; 3:S123.(Abstract)
288 March 2008 PACE, Vol. 31

TRANSSEPTAL PUNCTURE WITHOUT FLUOROSCOPY
4. Smith G, Clark J. Elimination of fluoroscopy use in a pediatric elec-trophysiology laboratory utilizing three-dimensional mapping. Pac-ing Clin Electrophysiol 2007; 30:510–518.
5. Tuzcu V. A nonfluoroscopic approach for electrophysiology andcatheter ablation procedures using a three-dimensional navigationsystem. Pacing Clin Electrophysiol 2007; 30:519–525.
6. Park T, Eichling J, Schechtman K, Bromberg B, Smith J, Lind-say B. Risk of radiation induced skin injuries from arrhyth-mia ablation procedures. Pacing Clin Electrophysiol 1996; 19:1363–1369.
7. Rosenthal L, Beck T, Williams J, Mahesh M, Herman MG, DinermanJL, Calkins H, et al. Acute radiation dermatitis following radiofre-quency catheter ablation of atrioventricular nodal reentrant tachy-cardia. Pacing Clin Electrophysiol 1997; 20:1834–1839.
8. Lindsay B, Eichling J, Ambos H, Cain M. Radiation exposure to pa-tients and medical personnel during radiofrequency catheter abla-tion for supraventricular tachycardia. Am J Cardiol 1992; 70:218–223.
9. McFadden SL, Mooney RB, Shepherd PH. X-ray dose and associatedrisks from radiofrequency catheter ablation procedures. Br J Radiol2002; 75:253–265.
10. Limacher M, Douglas P, Germano G, Laskey WK, Lindsay BD,McKetty MH, Moore ME, et al. Radiation safety in practice of cardi-ology. J Am Coll Cardiol 1998; 31:892–913.
11. Davies AG, Cowen AR, Kengyelics SM, Moore J, Pepper C, CowanC, Sivanathan MU. X-ray dose reduction in fluoroscopically guidedelectrophysiology procedures. Pacing Clin Electrophysiol 2006;29:262–271.
12. Kotre CJ, Charlton S, Robson KJ, Birch IP, Willis SP, Thornley M.Application of low dose rate pulsed fluoroscopy in cardiac pacingand electrophysiology: Patient dose and image quality implications.Br J Radiol 2004; 77:597–599.
13. Den Boer A, de Feyter PJ, Hummel WA, Keane D, Roelandt JR. Re-duction of radiation exposure while maintaining high-quality flu-oroscopic images during interventional cardiology using novel x-ray tube technology with extra beam filtering. Circulation 1994;89:2710–2714.
14. Fenner JW, Morrison GD, Kerry J, West N. A practical demonstrationof improved technique factors in paediatric fluoroscopy. Br J Radiol2002; 75:596–602.
15. Krum D, Goel A, Hauck J, Schweitzer J, Hare J, Attari M, Dhala A,et al. Catheter location, tracking, cardiac chamber geometry creation,and ablation using cutaneous patches. J Interv Card Electrophysiol2005; 12:17–22.
16. Papagiannis J, Tsoutsinos A, Kirvassilis G, Sofianidou I, Koussi T,Laskari C, Kiaffas M, et al. Nonfluoroscopic catheter navigation forradiofrequency catheter ablation of supraventricular tachycardia inchildren. Pacing Clin Electrophysiol 2006; 29:971–978.
17. Ventura R, Rostock T, Klemm HU, Lutomsky B, Demir C, WeissC, Meinertz T, et al. Catheter ablation of common-type atrial flut-ter guided by three-dimensional right atrial geometry reconstruc-tion and catheter tracking using cutaneous patches: A random-ized prospective study. J Cardiovasc Electrophysiol 2004; 15:1157–1161.
18. Rotter M, Takahashi Y, Sanders P, Haissaguerre M, Jais P, Hsu LF,Sacher F, et al. Reduction of fluoroscopy exposure and procedureduration during ablation of atrial fibrillation using a novel anatom-ical navigation system. Eur Heart J 2005; 26:1415–1421.
19. Verma S, Borganelli M. Real-time, three-dimensional localization ofa Brockenbrough needle during transseptal catheterization using anonfluoroscopic mapping system. J Invasive Cardiol 2006; 18:324–327.
20. Daoud EG. Transseptal catheterization. Heart Rhythm 2005; 2:212–214.
PACE, Vol. 31 March 2008 289