use of lhrh analogue to obtain reversible castration in a patient with benign metastasizing...
TRANSCRIPT

British Journal of Obstetrics and Gynaecology M a y 1986, Vol. 93, pp. 455-460
Use of LHRH analogue to obtain reversible castration in a patient with benign metastasizing leiomyoma
W. M. HAGUE Research Fellow, N. A. ABDULWAHID Research Fellow, H. S. JACOBS Professor of Reproductive Endocrinology, Cobbold Laboratories, Middlesex Hospital, London W l & I. CRAFT Director of Gynaecology, Cromwell Hospital, London SW5
Summary. The use of superactive LHRH analogue to provide a reversi- ble form of castration is discussed in the context of the management of a patient with benign metastasizing leiomyoma. The aetiology and prog- nosis of this rare disease are briefly considered.
Castration has been used as a therapeutic man- oeuvre in several malignant conditions whose sex-hormonal dependence is believed to be important (Lipsett & Lippman 1981). But there are pathologies whose hormonal dependence is in doubt, and both doctor and patient may be reluctant to embark on ablative surgery with no guarantee of response. Treatment with superac- tive analogues of luteinizing hormone releasing hormone (LHRH) has been shown to cause pituitary desensitization to endogenous LHRH, producing effective and reversible gonadal sup- pression (Sandow 1983). We present here a patient with a rare condition of uncertain endocrine dependence, benign metastasizing leiomyoma, in whom use of the superactive LHRH analogue, buserelin (HOE 766), pro- vided a medical castration, with suppression of the disease, and therefore a clear indicator for irreversible castration by ovariectomy. Follow- ing surgery, the disease regressed still further, thus confirming the initial hypothesis.
Patient and methods
The patient, a Portuguese engineer born in 1950, initially presented in 1979 with chest pain. Chest X-ray revealed discrete nodules in the lungs which, after thoracotomy, were found to have the pathological features of leiomyomata. A few months earlier, she had undergone termination of her fourth pregnancy and, in 1973, had had a myomectomy after the spontaneous abortion at 20 weeks gestation of a twin pregnancy. Follow- ing referral to us in April 1979, she underwent
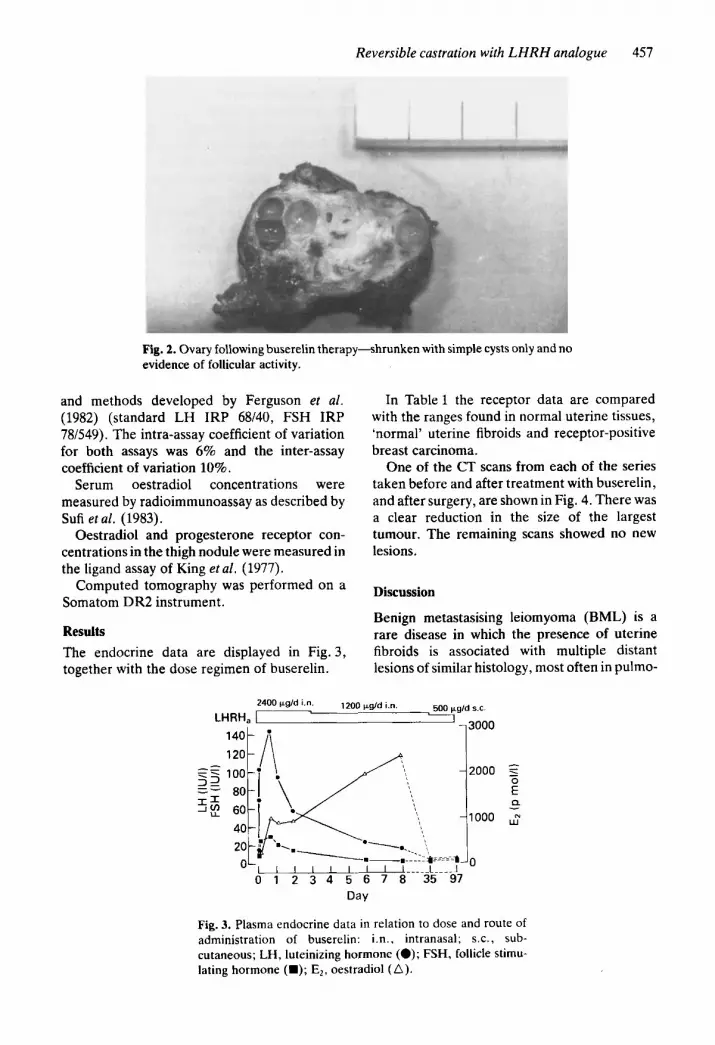
hysterectomy and unilateral oophorectomy, the latter for an incidental benign cyst. The histo- logy of the uterus showed entirely benign leiomyomata, both within the myometrial tissue and also within, but not breaching the walls of, blood-vessels (Figs l a and lb). Chest X-ray at that time was clear, but CT scan of the chest showed some small opacities. In 1982 and 1984, nodules were excised from her right leg, both histologically similar to the uterine lesions (Fig. lc); the second was shown to contain both oestradiol and progesterone receptors. Shortly after the second excision, she had further chest pain and the residual lesions in her chest were shown on CT scan to have enlarged. As she was reluctant to have further surgery, medical cas- tration was attempted using a superactive analo- gue of LHRH (buserelin), administered initially by intranasal spray and subsequently by sub- cutaneous injection. Flushing developed after 6 days of therapy, and she noticed superficial dys- pareunia in the second week. After 3 months of therapy, repeat CT scan confirmed a reduction in the size of the chest lesions. Surgical oophorectomy was therefore performed with the removal of a small, shrunken ovary that showed simple cysts but no evidence of follicular activity (Fig. 2). She thereafter remained well on treatment with medroxyprogesterone (40 mg/ day). Six months after surgery, a fourth CT scan showed further diminution in the chest opacities. Methods Serum gonadotrophin concentrations were measured by radioimmunoassay using reagents
455

456 W, M . Hagueetal.
Fig. 1. Histology of (a) intrauterine leiomyoma X350, (b) intravascular intra- uterine leiomyoma X88 and (c) thigh nodule X88: (all haematoxylin and eosin).
Reversible castration with LHRH analogue 457
Fig. 2. Ovary following buserelin therapy-shrunken with simple cysts only and no evidence of follicular activity.
and methods developed by Ferguson et al. (1982) (standard LH IRP 68/40, FSH IRP 7W.549). The intra-assay coefficient of variation for both assays was 6% and the inter-assay coefficient of variation 10%.
Serum oestradiol concentrations were measured by radioimmunoassay as described by Sufi et al. (1983).
Oestradiol and progesterone receptor con- centrations in the thigh nodule were measured in the ligand assay of King et al . (1977).
Computed tomography was performed on a Somatom DR2 instrument.
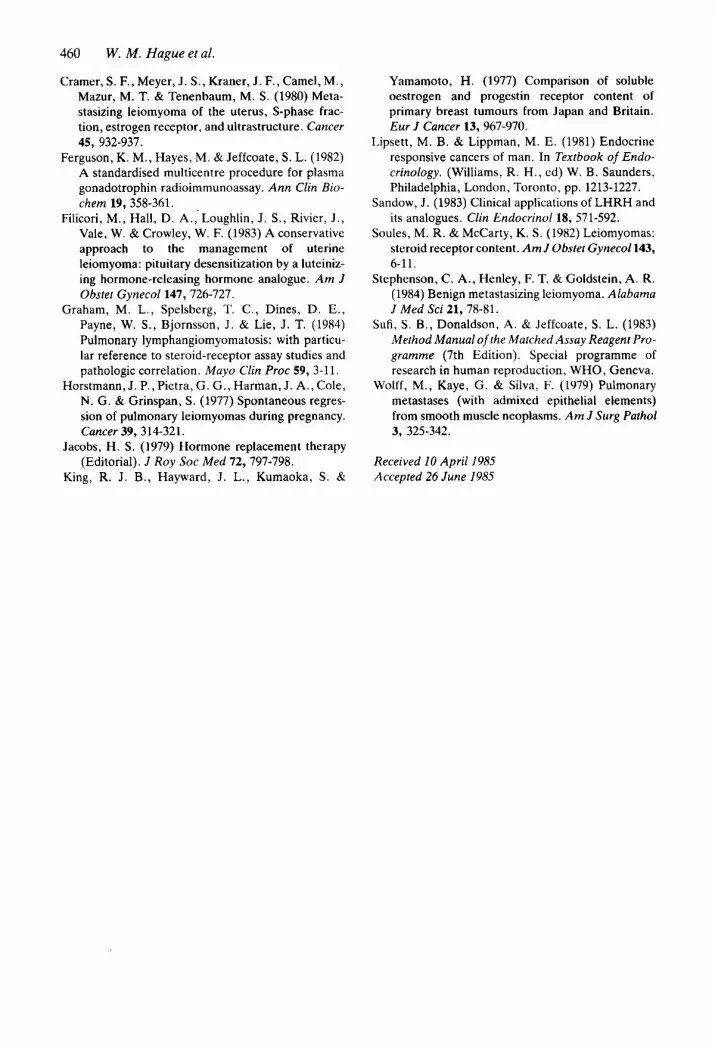
Results The endocrine data are displayed in Fig. 3, together with the dose regimen of buserelin.
In Table 1 the receptor data are compared with the ranges found in normal uterine tissues, 'normal' uterine fibroids and receptor-positive breast carcinoma.
One of the CT scans from each of the series taken before and after treatment with buserelin, and after surgery, are shown in Fig. 4. There was a clear reduction in the size of the largest tumour. The remaining scans showed no new lesions.
Discussion
Benign metastasising leiomyoma (BML) is a rare disease in which the presence of uterine fibroids is associated with multiple distant lesions of similar histology, most often in pulmo-
80 2000
Q
1000 ;
=-=a .I I 0 97
Dav
Fig. 3. Plasma endocrine data in relation to dose and route of administration of buserelin: i.n., intranasal; s .c . , sub- cutaneous; LH, luteinizing hormone (0); FSH, follicle stimu- lating hormone (m); E,, oestradiol (A).

458
Table 1. Receptor studies
W. M. Hague et al.
Oestradiol Progesterone receptor receptor
Tissue (fmol/mg) ( f m o h g )
‘Metastasis’ 14 16 Myometrium 40- 50 120-250 Fibroid 40- 80 120-400 Endometrium
Proliferative 70-200 15C-500 Secretory 25- 70 50-200
Breast carcinoma 15- 20 15- 20
nary tissue (Stephenson et al. 1984). The ambi- guity of the nomenclature reflects the almost completely benign nature of the histology, with low mitotic indices, lack of nuclear pleomor- phism and no evidence of invasiveness, despite the multiple distant lesions-‘metastases’.
BML appears to be identical to the condition of multiple leiomyomatous hamartomas
(Horstmann et al. 1977). They both form part of a spectrum which includes intravenous leiomyomatosis, leiomyomatosis peritonalis dis- seminata, and lymphangioleiomyomatosis. All of these conditions have the common feature of benign leiomyomata which are found respec- tively within blood vessels, the peritoneal cavity or lymphatics. Our case has features of both BML and intravenous leiomyomatosis.
The aetiology is a matter of debate which resolves around the possibilities of true meta- stases, low grade sarcomatous change, or meta- plastic transformation of smooth muscle elements (Wolff etal . 1979). We note the curious similarity of BML to endometriosis, with its dis- tant deposits of benign endometrial tissue, and the various aetiological theories of trans- coelomic spread, blood-borne spread or meta- plastic transformation, together with its favourable response to endocrine ablation.
In general BML is a disease of women of childbearing years, although a few cases have
Fig. 4. CT scans through the thorax from the series done in (a) March 1984, (b) July 1984, (c) January 1985. (d) Indicates the position in 4a, of liver (A), some of left diaphragm (B) posterior mediastinum (C) and ‘metastases’ (M), the latter having shrunk or disappeared in 4b and 4c.

Reversible castration with LHRH analogue 459
indeed, began to notice flushing attacks even while the oestradiol level was still rising.
The significance of these observations is uncertain, but further experience with the drug will provide a dose regimen that will minimize any oestrogen flare and thus any possible stimu- lation of tumour growth as might occur in patients with breast carcinoma.
A further modification to future treatment regimens might be to add progestagen, such as we gave following surgery. Such high dose pro- gestagen therapy has been shown to abolish the vasomotor symptoms of oestrogen deprival (Albrecht et al . 1981), and has the further advan- tage of inhibiting the production of further oestrogen receptor (Jacobs 1979). Progestagen therapy has also been used in the management of the possibly related condition pulmonary lymphangiomyomatosis (Graham et al. 1984).
We believe that our data confirm the need for oophorectomy in patients with benign meta- stasizing leiomyomyomatosis. For the uncertain case, we suggest that the use of buserelin or a similar LHRH analogue, in combination with receptor studies, may provide the optimal way of selecting those who will respond to castration, with all its distressing side-effects, both in this and in other conditions with uncertain endocrine dependence.
been described after the menopause. It has also been described in pregnancy. Presentation may be with pulmonary or abdominal symptoms, or it may be diagnosed on investigation of an asymp- tomatic pelvic mass.
There is evidence of hormonal dependence both from receptor studies (Cramer et al. 1980) and from results of treatment by oophorectomy (Banner et al. 1981). The prognosis of the disease can be shown to relate to the oestrogen status of the patient as well as to the surgical removal of the uterine tumours. Combining the data from the literature on all the patients with BML or multiple leiomyomatous hamartomas whose follow-up has been documented, all three of those who had had no pelvic surgery pro- gressed, and all but one of the 21 who had had uterine surgery alone (either myomectomy, total or sub-total hysterectomy) either pro- gressed (52%) or remained static (46%). The one patient of the group treated by hysterectomy who regressed had received progesterone therapy. In contrast, of the patients who under- went castration, 6 out of 11 (54%) regressed.
Therapy with a superactive analogue of LHRH has also been used to shrink straightfor- ward uterine fibroids as a means of avoiding uterine surgery in young women (Filicori et al. 1983), a treatment consistent with the presence of oestrogen receptors in these tumours (Soules & McCarty 1982).
As shown in Table 1, the receptor data in the thigh nodule was comparable with that found in receptor-positive breast carcinoma, but much lower than that found in ‘normal’ fibroids. These results might support the thesis that the tumours are indeed not true metastases, but rather meta- plastic in nature.
The dose of buserelin used initially was mas- sive, with the intention of achieving pituitary desensitization and thus ovarian suppression as quickly as possible. Because there was no uterus present, we were unable to time the onset of therapy with menstruation and low endogenous levels of gonadotrophin. Our endocrine results (Fig. 3) show that we in fact caused initial stimu- lation of both luteinizing hormone and follicle stimulating hormone output to very high levels, with an associated rise of plasma oestradiol comparable to that seen in multiple ovulation. However, it is noteworthy that the patient did not complain of any exacerbation of her chest pain during the initial phase of treatment, and
Acknowledgments
W. M. H. is a Frances and Augustus Newman Foundation Research Fellow. We are grateful to Dr P. Magill of Hoechst for supplies of bus- erelin, to Dr R. J. B. King, Imperial Cancer Research Fund for the receptor assays, to the Endocrine Laboratories, Chelsea Hospital for women for the oestradiol assay, to the Histo- pathology Department, Royal Free Hospital for the photomicrographs, and to Dr G. Farrar- Brown for the photograph of the excised ovary.
References
Albrecht, B. H., Schiff, I., Tulchinsky, D. & Ryan, K. J. (1981) Objective evidence that placebo and oral medroxyprogesterone acetate therapy diminish menopausal vasomotor flushes. Am J Obstel Gynecol 139, 631-635.
Banner, A. S., Carrington, C. B., Emory, W. B., el al. (1981) Efficacy of oophorectomy in lymph- angioleiomyomatosis and benign metastasizing leiomyoma. N Engl J Med 305, 204-209.
460
Cramer, S. F., Meyer, J . S . , Kraner, J . F., Camel, M., Mazur, M. T. & Tenenbaum, M. S. (1980) Meta- stasizing leiomyoma of the uterus, S-phase frac- tion, estrogen receptor, and ultrastructure. Cancer
Ferguson, K. M., Hayes, M. & Jeffcoate, S. L. (1982) A standardised multicentre procedure for plasma gonadotrophin radioimmunoassay. Ann Clin Bio- chem 19, 358-361. ,
Filicori, M., Hall, D. A,, Loughlin, J. S . , Rivier, J . , Vale, W. & Crowley, W. F. (1983) A conservative approach to the management of uterine leiomyoma: pituitary desensitization by a luteiniz- ing hormone-releasing hormone analogue. Am J Obstet Gynecoll47, 726-727.
Graham, M. L., Spelsberg, T. C., Dines, D . E., Payne, W. S. , Bjornsson, J . & Lie, J. T. (1984) Pulmonary lymphangiomyomatosis: with particu- lar reference to steroid-receptor assay studies and pathologic correlation. Mayo Clin Proc 59, 3-11.
Horstmann, J . P., Pietra, G. G., Harman, J . A., Cole, N. G. & Grinspan, S. (1977) Spontaneous regres- sion of pulmonary leiomyomas during pregnancy. Cancer 39,314-321.
Jacobs, H. S. (1979) Hormone replacement therapy (Editorial). J Roy SOC Med 72, 797-798.
King, R. J . B., Hayward, J. L., Kumaoka, S. &
W. M. Hague et al.
45, 932-937.
Yamamoto, H. (1977) Comparison of soluble oestrogen and progestin receptor content of primary breast tumours from Japan and Britain. Eur J Cancer 13, 967-970.
Lipsett, M. B. & Lippman, M. E. (1981) Endocrine responsive cancers of man. In Textbook of Endo- crinology. (Williams, R. H. , ed) w. B. Saunders, Philadelphia, London, Toronto, pp. 1213-1227.
Sandow, J. (1983) Clinical applications of LHRH and its analogues. Clin Endocrinol 18, 571-592.
Soules, M. R. & McCarty, K. S. (1982) Leiomyomas: steroid receptor content. Am J Obstet Gynecoll43, 6-1 1.
Stephenson, C. A., Henley, F. T. & Goldstein, A. R. (1984) Benign metastasizing leiomyoma. Alabama J Med Sci 21,7841.
Sufi, S. B., Donaldson, A. & Jeffcoate, S. L. (1983) Method Manual of the Matched Assay Reagent Pro- gramme (7th Edition). Special programme of research in human reproduction, WHO, Geneva.
Wolff, M., Kaye, G. & Silva, F. (1979) Pulmonary metastases (with admixed epithelial elements) from smooth muscle neoplasms. Am J Surg Pathol 3, 325-342.
Received 10 April 1985 Accepted 26 June 1985