untitled - 1 file download
TRANSCRIPT
RACE 2003Ramachandra Anaesthesia Continuing Education
February 20 - 23,2003.
Department of Anaesthesiologyand
Critical CareSri Ramachandra Medical College & Research Institute (DU)
Chennai
The R..A..C..E.. is growing
RACE has entered into its 4th successive year. The necessity for the continuing medical education program in the field of Anesthesia, and encouragement and support shown by all of you have made us to continue with the RACE. Our young, still enthusiastic and energetic department has taken up the challenge under the able guidance of Prof. Vijaylakshmi Kamat and we are pleased to be with you this year also.
We constantly made an effort to improve on and make RACE more interesting and more informative. Accordingly we have made some changes in the Scientific Program. We are organizing a hands-on- workshop on the first day and will have three more days of full academic program. We are forced to have limited registration for the workshop, otherwise we cannot make it hands on.
While retaining the Pro & Con Session, PG Symposium and How I Do It?, as demanded by most of the delegates in their feedback, we have included new sessions like “Debate” on few controversial topics and “Group Discussion” which will cover exam going cases and will be handled by the postgraduate examiners from all over India.
To encourage research work, we have included a “Free Paper Session” for the postgraduates in which few selected papers (after peer review) will be allowed to be presented.
Credit for successful publication of this volume goes first to the authors of various articles who in spite of their busy schedule and time constraints made a valuable contribution to the RACE. We gratefully acknowledge their efforts. Efforts have been made to eliminate most of the errors both technical as well as linguistic to the extent possible. We beg the pardon of the readers if there are any. We sincerely apologise to the authors if any errors or distortion have crept into the texts in the editorial process.
We are extremely grateful to our beloved Chancellor Mr.V.R.Venkataachalam and Mrs. Radha Venkataachalam, Chief Executive Director and other members of the management for the encouragement and support extended to us. We are also thankful to Mr.Selvaraj, Proprietor, Archana Group for helping us in providing accommodation.
The team spirit has paid off again. All faculty members have contributed to the successful conduct of RACE. We would like to specially mention the names of few faculty who formed the core group for the RACE like Dr.Arun, Dr.Pradeep, Dr.Aruna and Dr.Pavendhan. Prof.Vijaylakshmi Kamat and Dr.Mahesh Vakamudi played a vital role by providing the guidance and support needed. Ms. Mala has played a good managerial role.
We are extremely thankful to Mr.Arun, who has been man behind the formatting and setting of the articles in this book.
We will be failing in our duty if we do not remember the financial assistance provided by Nicholas Piramal India Limited, in publishing this book. We are also thankful to all the other sponsors who made the RACE 2003 possible.
We look forward to being with you again.
FACULTY OF ANESTHESIA
RACE 2003 Ramachandra Anaesthesia Continuing Education
Lectures
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Gas Laws and the Anaesthetist
New Drugs in Anaesthesia
Management of Acute Pain
Anaesthetic Management of a Pregnant Patient for Non Obstetric Surgery
What’s New in Paediatric Epidural Anaesthesia
Ventilation Perfusion Distribution
Functions of the Diaphragm and Anaesthesia
Management of a Brain Dead Organ Donor
Anaesthetic Management of a Morbidly Obese Patient
Anaesthetic Management of Patients with Haemoglobinopathies
Low Flow Anaesthesia
How to get the most out of your CVP Catheter
Anitha Shenoy
Pankaj Kundra
M.R.Rajagopal
Gopinath
Lakshmi Vas
1
8
22
27
33
RamkumarVenkateswaran 42
Vijayalakshmi Kamat
Joseph Rajesh
Manimala Rao
Chandrasekhar
M.Ravishankar
Jigi Divatia
Anaesthetic Management of a PatientWith ESRD for Renal Transplantation Gita Nath
Sedation and Analgesia in Children for procedures outside the OR Ramesh
49
59
70
76
83
92
100
111
RACE 2003 Ramachandra Anaesthesia Continuing Education
Post Graduate Symposia
15. Cardiovascular Physiology SRMC&RI 119
16. Central Neuraxial Blockade Kurnool Medical College 144
17. Patient Positioning Trivandrum Medical Collegel70
How I Do It
18. A 20 year old primi with severe MS Bharathi. R 186 requires Labour Analgesia
19. A 25 year old otherwise healthy male Manjunath Prabhu 194 with Ludwig’s angina is posted for abscess drainage.
Pros and Cons
20. Induced Hypotension is contraindicated in Children
21. Induced Hypotension is NOT contraindicated in Children
22. Strict preoperative blood sugar control to an FBS of 200mgs% is mandatory before elective surgery
23. Strict preoperative blood sugar control to an FBS of 200mgs% is NOT mandatory before elective surgery
24. Spinal Anaesthesia is contraindicated for day care surgery
25. Spinal Anaesthesia is NOT contraindicated for day care surgery
Raja Manoharan 198
LakshmiVas 201
NaheedAzhar 208
Kalyan Chakravarthy 215
ElsaVarghese 219
Rathna 224
RACE 2003 Ramachandra Anaesthesia Continuing Education
Debate
26. Invasive Monitoring in ASA III and ASA IV patients will influence theoutcome of surgery
27. Invasive Monitoring in ASA III and ASA IV patients will NOT influence the outcome of surgery
28. Preoperative tranfusion threshold is a Hb of 8gms%
29. Preoperative tranfusion threshold is NOT a Hb of 8gms%
Work Shops
30. Airway
31. Cardiopulmonary Resucitation
32. Mechnical Ventilation
33. Nerve Blocks
Ashok Bahde
Rajamanoharan
Manjunath Prabhu
Anitha Shenoy
SrinivasanChandrasekharManjunath
TV. Ramakrishnan
Vijayalakshmi Kamat Gita Nath
Rajamanoharan Azhar Hussain
234
237
242
248
255
260
275
315
RACE 2003 Ramachandra Anaesthesia Continuing Education

Dr. Anitha Shenoy Associate Professor Department of Anaesthesia Kasturba Medical College Manipal.
Dr. Ashok Badhe ProfessorDepartment of Anaesthesia & Critical CareJIPMERPondicherry.
Dr. Azhar Hussain ProfessorDepartment of Anaesthesia Kilpauk Medical College Chennai.
Dr.Bharathi. R.Assistant Professor Department of Anaesthesia SRMC&RI Chennai.
Dr. Chandrasekhar Professor of Anaesthesia Kurnool Medical College Kurnool.
Dr. ElsaVarghese Professor & Head Department of Anaesthesia Kasturba Medical College Manipal.
Dr. Gita NathConsultant Anaesthesiologist Al Jazeria Hospital Abudhabi, UAE.
Dr. Gopinath. R.Professor of AnaesthesiaNizam’s Institute of Medical SciencesHyderabad.
Dr. Hanumantha Rao. JConsultant AnaesthetistPeoples Trauma & Emergency Hospital,Guntur
Dr. Hemalatha Professor of Anaesthesia Trivandrum Medical College Trivandrum
Dr. Jigi Divatia Additional Professor Department of Anaesthesia Tata Memorial Hospital Mumbai.
Dr. Kalyan Chakravathy Consultant Anaesthesiologist Kakinada.
Dr. Lakshmi Vas Consultant Anaesthesiologist Mumbai.
Dr. Manimala Rao. S.Professor & Head Department of Anaesthesia Nizam’s Institute of Medical Sciences Hyderabad.
Dr. Manjunath Prabhu Associate Professor Department of Anaesthesia Kasturba Medical College Manipal.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Dr. Narasimha Reddy Professor of Anaesthesia Kurnool Medical College Kurnool.
Dr. Naheed Azhar Assistant Professor Department of Anaesthesia Stanley Medical College Chennai.
Dr. Pankaj Kundra ProfessorDepartment of Anaesthesia & Critical CareJIPMERPondicherry.
Dr. Rajagopal. M.R Professor of Anaesthesia Amritha Institute of Medical Sciences Cochin.
Dr. Rajamanoharan ProfessorDepartment of Anaesthesia Madurai Medical College Madurai.
Dr. Rajesh Joseph Consultant Anaesthetist Meenakshi Mission Hospital Madurai.
Dr. Ramakrishnan. T.V.Associate Professor and Course Co-ordinatorDepartment of Accident and EmergencyMedicineSRMC&RIChennai.
Dr. Ramesh.S.Consultant Anaesthesiologist Child Trust Hospital Chennai.
Dr. RamkumarVenkateswaran ProfessorDepartment of Anaesthesia Kasturba Medical College Manipal.
Dr. Rathna Professor and Head Department of Anaesthesia M.S. Ramaiah Medical College Bangalore
Dr. Ravishankar. M.Professor & HeadDepartment of Anaesthesia & Critical CareJIPMERPondicherry.
Dr. Srinivasan. R.ProfessorDepartment of Anaesthesia SRMC&RI,Chennai.
Dr. Suresh Rao Associate Professor Department of Anaesthesia SRMC&RI,Chennai.
Dr. Thanikachalam.S.Vice-Chancellor & HOD Cardiology, SRMC&RI,Chennai.
Dr. Vijaylakshmi Kamat Professor and HeadDepartment of Anaesthesiology & Critical CareSRMC & RlChennai
RACE 2003 Ramachandra Anaesthesia Continuing Education
LECTURES
Gases exert pressure, are readily compressed and expanded, fill the spaces available to them by diffusion, dissolve in liquids, are capable of flow and have viscosity. Anaesthesiologists constantly deal with gases and hence it is imperative that he/she has a good knowledge of the behaviour of gases. Several laws define the relationship between gas pressure, volume, mass and temperature. They predict the behaviour of gases under changing conditions.
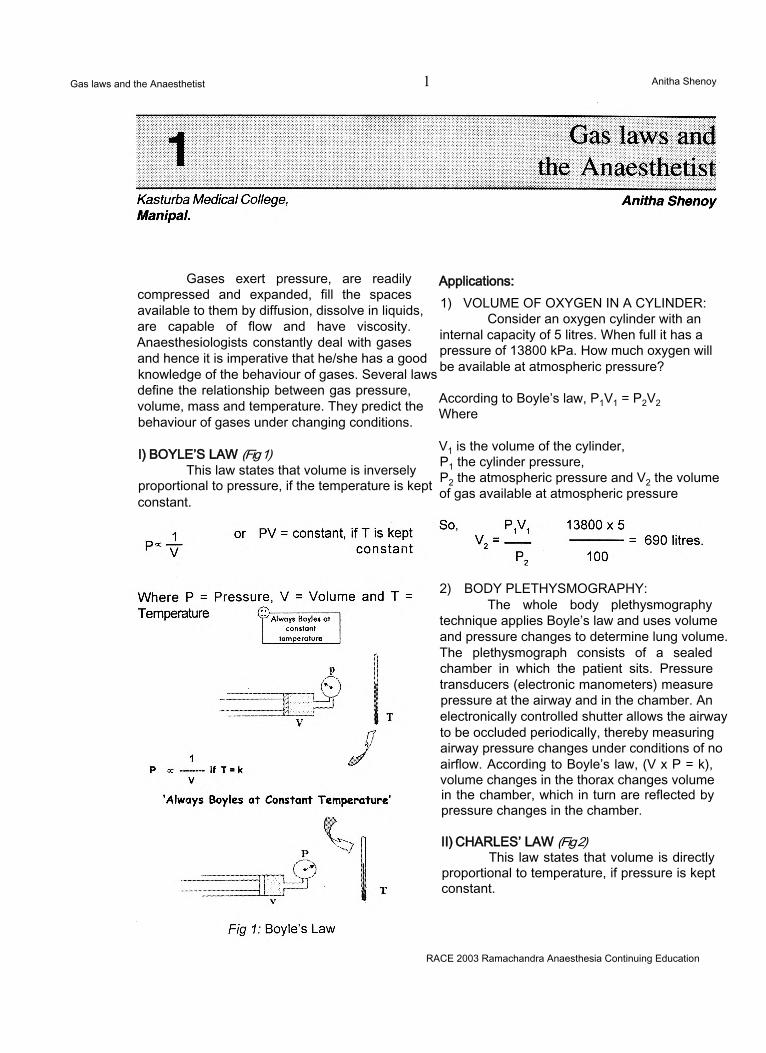
I) BOYLE’S LAW (Fig 1)This law states that volume is inversely
proportional to pressure, if the temperature is kept constant.
Applications:1) VOLUME OF OXYGEN IN A CYLINDER:
Consider an oxygen cylinder with an internal capacity of 5 litres. When full it has a pressure of 13800 kPa. How much oxygen will be available at atmospheric pressure?
According to Boyle’s law, P1V1 = P2V2 Where
V1 is the volume of the cylinder,P1 the cylinder pressure,P2 the atmospheric pressure and V2 the volume of gas available at atmospheric pressure
2) BODY PLETHYSMOGRAPHY:The whole body plethysmography
technique applies Boyle’s law and uses volume and pressure changes to determine lung volume. The plethysmograph consists of a sealed chamber in which the patient sits. Pressure transducers (electronic manometers) measure pressure at the airway and in the chamber. An electronically controlled shutter allows the airway to be occluded periodically, thereby measuring airway pressure changes under conditions of no airflow. According to Boyle’s law, (V x P = k), volume changes in the thorax changes volume in the chamber, which in turn are reflected by pressure changes in the chamber.
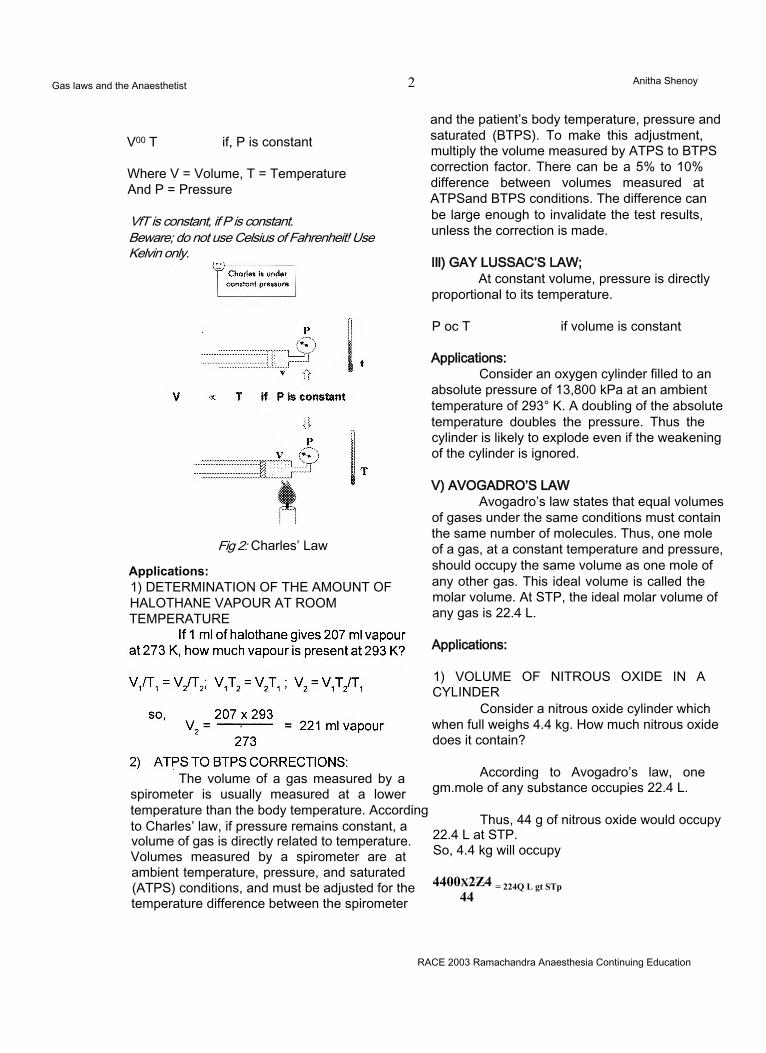
II) CHARLES’ LAW (Fig 2)This law states that volume is directly
proportional to temperature, if pressure is kept constant.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Gas laws and the Anaesthetist 1 Anitha Shenoy
Gas laws and the Anaesthetist 2 Anitha Shenoy
V00 T if, P is constant
Where V = Volume, T = Temperature And P = Pressure
VfT is constant, if P is constant.Beware; do not use Celsius of Fahrenheit! Use Kelvin only.
Fig 2: Charles’ Law
Applications:1) DETERMINATION OF THE AMOUNT OF HALOTHANE VAPOUR AT ROOM TEMPERATURE
and the patient’s body temperature, pressure and saturated (BTPS). To make this adjustment, multiply the volume measured by ATPS to BTPS correction factor. There can be a 5% to 10% difference between volumes measured at ATPSand BTPS conditions. The difference can be large enough to invalidate the test results, unless the correction is made.
Ill) GAY LUSSAC’S LAW;At constant volume, pressure is directly
proportional to its temperature.
P oc T if volume is constant
Applications:Consider an oxygen cylinder filled to an
absolute pressure of 13,800 kPa at an ambient temperature of 293° K. A doubling of the absolute temperature doubles the pressure. Thus the cylinder is likely to explode even if the weakening of the cylinder is ignored.
V) AVOGADRO’S LAWAvogadro’s law states that equal volumes
of gases under the same conditions must contain the same number of molecules. Thus, one mole of a gas, at a constant temperature and pressure, should occupy the same volume as one mole of any other gas. This ideal volume is called the molar volume. At STP, the ideal molar volume of any gas is 22.4 L.
Applications:
1) VOLUME OF NITROUS OXIDE IN A CYLINDER
Consider a nitrous oxide cylinder which when full weighs 4.4 kg. How much nitrous oxide does it contain?
According to Avogadro’s law, one gm.mole of any substance occupies 22.4 L.
Thus, 44 g of nitrous oxide would occupy 22.4 L at STP.So, 4.4 kg will occupy
4400x2Z4 = 224Q L gt STp 44
RACE 2003 Ramachandra Anaesthesia Continuing Education
The volume of a gas measured by a spirometer is usually measured at a lower temperature than the body temperature. According to Charles’ law, if pressure remains constant, a volume of gas is directly related to temperature. Volumes measured by a spirometer are at ambient temperature, pressure, and saturated (ATPS) conditions, and must be adjusted for the temperature difference between the spirometer
Gas laws and the Anaesthetist 3 Anitha Shenoy
V) UNIVERSAL GAS CONSTANT:The concept of gas laws can be combined
with that of Avogadro’s hypothesis and the mole as follows:
PV = K1 V/T = K2 P/T = K3
(Boyle’s law) (Charles’ law)(Gay Lussac’s law)
So, PV/T is constant for a given quantity of any gas. For I mole of any gas PV/T equals a unique constant known as the Universal Gas constant.
So, PV = nRT, where n is the number of
moles of the gas. This is equivalent to 1.987 Joules per degree per mole in SI units
Applications:Consider an oxygen cylinder with a fixed
internal volume V. Therefore V in the equation PV = nRT is a constant. R is a constant value 1.987, and if the cylinder is at a fixed temperature, T is also a constant. Thus, from the formula, P is directly proportional to ‘n’, the number of moles, which is the amount of gas in a cylinder. The pressure gauge then acts as a contents gauge, provided the cylinder contains a gas.
VI) VARIATIONS FROM IDEAL GAS BEHAVIOUR: EXPANSION, COOLING AND ADIABATIC COMPRESSION
Boyle’s law describes the gas behaviour under constant temperature, or isothermal conditions. During isothermal conditions, the temperature of an ideal gas should not change with either expansion or contraction. For example, if an ideal gas were to escape from a high- pressure cylinder into the atmosphere, its temperature should not change. In fact, the rapid expansion of real gases causes substantial cooling. This phenomenon is known as the Joule Thompson effect.
A rapidly expanding gas cools because as it expands, the intermolecular forces are broken down. The energy required for this comes from the gas itself and the temperature must decrease. This drop in temperature can be enough to liquefy the gas. This is the primary method used to liquefy air for the production of oxygen.
Whereas isothermal processes keep gas temperature constant, adiabatic compression and expansion have no such restrictions. During an adiabatic process, the heat energy of the gas is allowed to rise or fall as it undergoes changes in pressure and volume. Adiabatic compression of a gas can cause rapid increases in temperature. This can occur in gas delivery systems where rapid compressions can occur in affixed container. The rise in temperature caused by rapid compression can ignite any combustible material in the system. Hence, care must be taken to clear any combustible material from high-pressure gas delivery systems before pressurization.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Gas laws and the Anaesthetist 4 Anitha Shenoy
VII) CRITICAL TEMPERATURE AND PRESSURE
For every liquid there is a temperature above which the kinetic activity of its molecules is so great that the attractive forces cannot keep them in a liquid state. This temperature is known as the critical temperature. The critical temperature is the highest temperature at which a substance can exist as a liquid. The pressure needed to maintain equilibrium between the liquid and gas phases of a substance at this critical temperature is the critical pressure. Together, the critical temperature and pressure represent the critical point of a substance.
Applications:According to these principles, it is
possible to liquefy any gas with a critical temperature above the ambient, simply by applying pressure. Both C02 and N20 have critical temperatures above ambient. Hence, they can be liquefied by simple compression and stored as liquids at room temperature without cooling. But, liquid oxygen has to be maintained below its boiling point (-183° C) at atmospheric pressure. If higher temperatures are required, higher pressures must be used. If any time, the liquid oxygen exceeds its critical temperature of -118.3° C, it will convert immediately to gas.
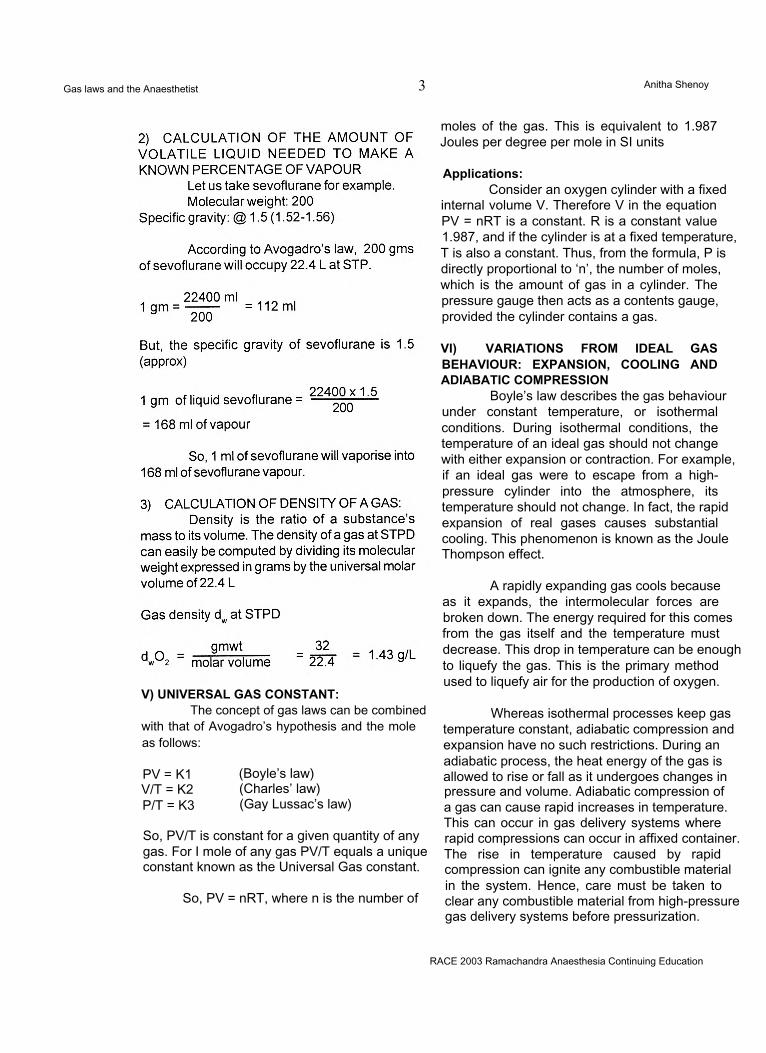
VIII) DALTON’S LAW OF PARTIAL PRESSURE(Fig 3)
This law states that the contribution which each constituent gas makes to the overall pressure, is in proportion to the number of molecules of the constituent. If each gas existed separately in containers of the same size and shape, then the sum of the pressures in the individual containers would equal the combined pressure of all the gases put together in just one of the containers. The pressure exerted by one of the constituent gas is known as the partial pressure of that gas.
Thus, Dalton’s law describes the relationship between the partial pressure and the total pressure in a gas mixture. According to this law, the total pressure of a mixture of gases must equal the sum of the partial pressures of all the component gases. It also states that the partial pressure of a component gas must be proportional
to its percentage in the gas mixture.Partial pressure = Fractional concentration x total pressure
Applications:1) PARTIAL PRESSURE OF GASES AT THE ALVEOLAR LEVEL:
The partial pressure of oxygen at room air is 760 x 0.21 = 159 mmHg. (dry air)
At 25,000 feet (high altitudes), the FI02 is still 0.21 but total atmospheric pressure is only 282 mmHg. The PI02 there would be equal to
282x0.21 =59 mmHg
At a depth of 66 feet under the sea, at about 3 atmospheres, the PI02 will be
3 x 760 x 0.21 = 479 mmHg.
2) ALVEOLAR GASAlveolar gas which is at atmospheric
pressure of 100kPa, is composed of a mixture of gases. Their partial pressures when added will equal the total pressure of one atmosphere.
P02 = 13.3 kPa PC02 = 5.3 kPa PH20 = 6.26 kPa PN2 = 75.2 kPa Total = 100 kPa
Fig 3: Dalton’s law of partial pressure3) FILLING GAS CYLINDERS WITH GAS MIXTURES.
A cylinder is initially filled to 1380 kPa and thereafter 02 is added to make up to a pressure of 13,800 kPa to produce 10% C02in
RACE 2003 Ramachandra Anaesthesia Continuing Education
Gas laws and the Anaesthetist 5 Anitha Shenoy
IX) HENRY’S LAWThis law predicts how much of a given
gas dissolves in a liquid. According to this principle, the volume of gas that dissolves in a liquid is equal to its solubility coefficient times its partial pressure,
V= OC x Pgas
Where
V = volume of the gas dissolved, oc s the solubility coefficient of the gas in the given liquid and Pgas is the partial pressure above the liquid.
Applications:1) THE AMOUNT OF GAS CARRIED IN SOLUTION
The amount of gas carried in solution in blood is governed by Henry’s law. The solubility coefficient of oxygen is 0.003 ml.dL'1. Thus, at 100 mmHg of oxygen tension and in 100 ml, the oxygen that can dissolve in blood would be 0.3 ml.
2) DEEP SEA DIVING:When divers breathe gases under
pressure, nitrogen and other gases pass into solution in the tissues. If they return to atmospheric pressure, the nitrogen comes out of solution as small bubbles in the joints and elsewhere giving rise to decompression sickness or the Caisson’s disease.
X) POISEUILLE’S LAWDuring laminar flow, a fluid moves in
discrete cylindrical layers or streamlines. The difference in pressure required to produce a given flow, under conditions of laminar flow through a smooth tube of fixed size, is defined by Poiseuille’s law.
where A P is the pressure gradient, Ix is the viscosity of the fluid, I is the tube length,
V is the fluid flow, r is the tube radius and n and 8 are constants.
According to this formula, the driving pressure will increase whenever the fluid viscosity, tube length or flow increases. A greater pressure will be required to maintain a given flow if the radius decreases. If the radius reduces by half, the pressure gradient required to maintain the same flow will go up 16 times!
Applications1) INTRAVENOUS INFUSIONS:
The flow rate obtained is governed by the Poiseuille’s law.
Hence, the flow rate obtained is higher when the cannula is large, and short and the pressure head is higher. Doubling the size of the cannula effectively increases the flow 16 times!
2)AIRFLOWTOTHE LUNGS:For air to flow into the lungs, a pressure
gradient must be developed. This depends on the calibre of the airway, rate and pattern of airflow. Laminar flow occurs when the gas passes down parallel-sided tubes at less than a critical velocity. The airflow rate is determined by the Poiseuille’s law.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Variations in the diameter of the smaller bronchi and bronchioles are particularly critical. A decrease in the diameter of the bronchus increases the pressure gradient 16 times and hence an increase in airway pressure is observed. Endotracheal intubation with a smaller tube also has a similar effect.
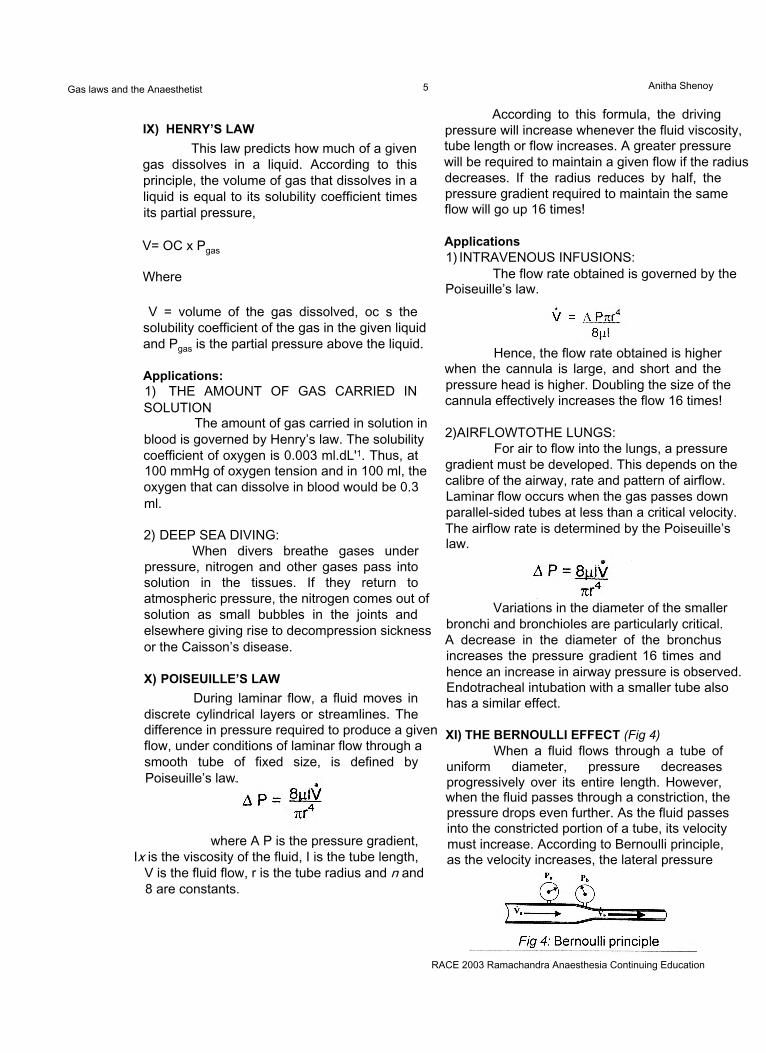
XI) THE BERNOULLI EFFECT (Fig 4)When a fluid flows through a tube of
uniform diameter, pressure decreases progressively over its entire length. However, when the fluid passes through a constriction, the pressure drops even further. As the fluid passes into the constricted portion of a tube, its velocity must increase. According to Bernoulli principle, as the velocity increases, the lateral pressure
Gas laws and the Anaesthetist 6 Anitha Shenoy
exerted by the fluid decreases.
Fluid EntrainmentWhen a flowing fluid encounters a very
narrow passage, its velocity can greatly increase. In some cases, the rise in velocity can be so high as to cause the fluid’s lateral pressure to fall below that exerted by the atmosphere, i.e., negative. If an open tube is placed distal to such a constriction, this negative pressure can actually pull another fluid into the primary flow stream. This effect is called fluid entrainment.
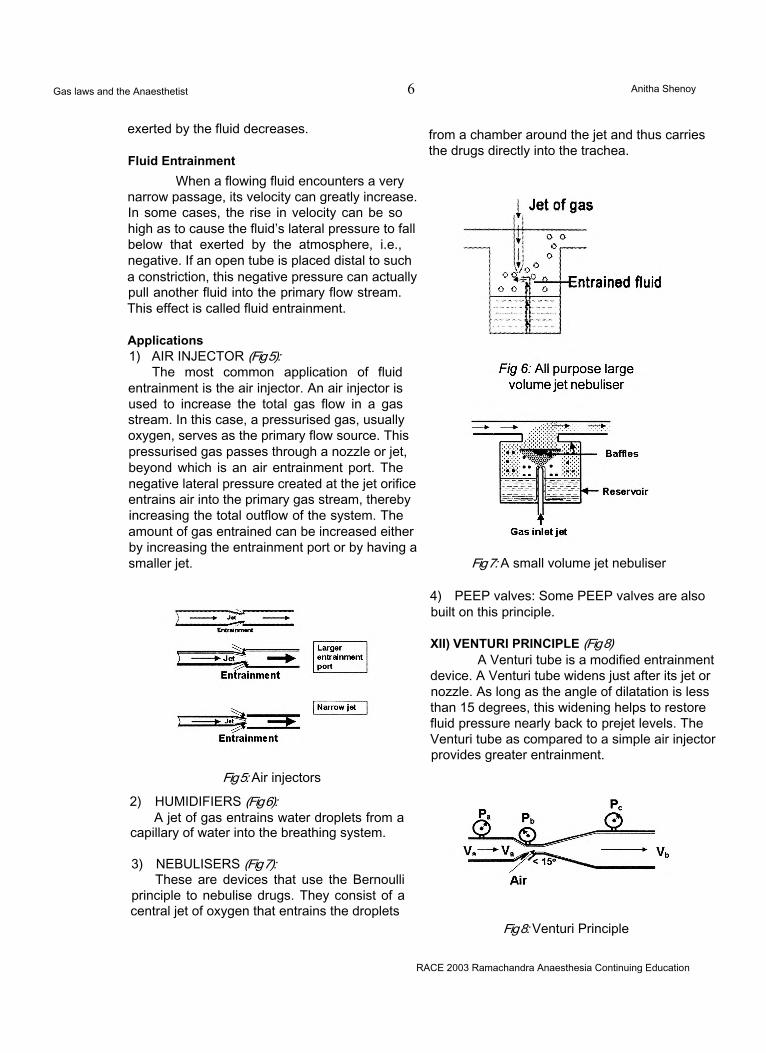
Applications1) AIR INJECTOR (Fig 5):
The most common application of fluid entrainment is the air injector. An air injector is used to increase the total gas flow in a gas stream. In this case, a pressurised gas, usually oxygen, serves as the primary flow source. This pressurised gas passes through a nozzle or jet, beyond which is an air entrainment port. The negative lateral pressure created at the jet orifice entrains air into the primary gas stream, thereby increasing the total outflow of the system. The amount of gas entrained can be increased either by increasing the entrainment port or by having a smaller jet.
from a chamber around the jet and thus carries the drugs directly into the trachea.
Fig 7: A small volume jet nebuliser
Fig 5: Air injectors
2) HUMIDIFIERS (Fig 6):A jet of gas entrains water droplets from a
capillary of water into the breathing system.
3) NEBULISERS (Fig 7):These are devices that use the Bernoulli
principle to nebulise drugs. They consist of a central jet of oxygen that entrains the droplets
4) PEEP valves: Some PEEP valves are also built on this principle.
XII) VENTURI PRINCIPLE (Fig 8)A Venturi tube is a modified entrainment
device. A Venturi tube widens just after its jet or nozzle. As long as the angle of dilatation is less than 15 degrees, this widening helps to restore fluid pressure nearly back to prejet levels. The Venturi tube as compared to a simple air injector provides greater entrainment.
Fig 8: Venturi Principle
RACE 2003 Ramachandra Anaesthesia Continuing Education
Gas laws and the Anaesthetist 7 Anitha Shenoy
ApplicationsVENTURI MASKS:
These have a series of tubes with fixed jet orifice and entrainment. The entrainment of air results in a high total flow to ensure that a fixed FI02can be given.
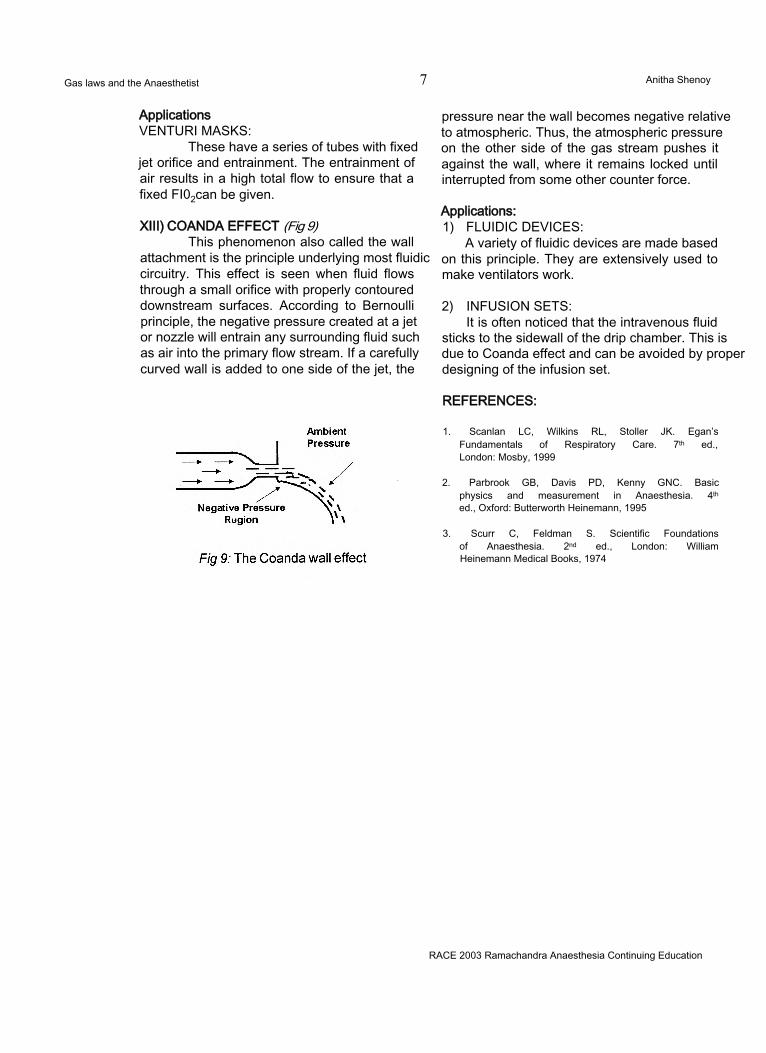
XIII) COANDA EFFECT (Fig 9)This phenomenon also called the wall
attachment is the principle underlying most fluidic circuitry. This effect is seen when fluid flows through a small orifice with properly contoured downstream surfaces. According to Bernoulli principle, the negative pressure created at a jet or nozzle will entrain any surrounding fluid such as air into the primary flow stream. If a carefully curved wall is added to one side of the jet, the
pressure near the wall becomes negative relative to atmospheric. Thus, the atmospheric pressure on the other side of the gas stream pushes it against the wall, where it remains locked until interrupted from some other counter force.
Applications:1) FLUIDIC DEVICES:
A variety of fluidic devices are made based on this principle. They are extensively used to make ventilators work.
2) INFUSION SETS:It is often noticed that the intravenous fluid
sticks to the sidewall of the drip chamber. This is due to Coanda effect and can be avoided by proper designing of the infusion set.
REFERENCES:
1. Scanlan LC, Wilkins RL, Stoller JK. Egan’s Fundamentals of Respiratory Care. 7th ed., London: Mosby, 1999
2. Parbrook GB, Davis PD, Kenny GNC. Basic physics and measurement in Anaesthesia. 4th ed., Oxford: Butterworth Heinemann, 1995
3. Scurr C, Feldman S. Scientific Foundations of Anaesthesia. 2nd ed., London: William Heinemann Medical Books, 1974
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 8 Pankaj Kundra
JIPMER, Pankaj KundraPondicherry.
Promising new anaesthetic agents in the past decadeLocal Anaesthetic Agents: Ropivacaine,LevobupivacaineNarcotics: RemifentanilInhalational Agents: Sevoflurane, DesfluraneIntravenous Induction Agents: PropofolMuscle Relaxants: Rocuronium
Indian Scenario Narcotics: Fentanyl Inhalational: Sevoflurane Intravenous: Propofol, Midazolam Muscle Relaxants: Rocuronium
INTRAVENOUS AGENTS
PROPOFOL
Alkylphenol derivative.(2,6-di-isopropofol)
Physicochemical Properties- pH: 7
Composition10% soyabean Oil
• 2.25% glycerol1.25% purified egg phosphatide
Stable at room temperature
Metabolism1
Liver by conjugation to glucuronide and sulfateMetabolites inactiveClearance of propofol exceeds hepatic blood flow. Thus it is thought to have extrahepatic and extrarenal elimination. Extrahepatic metabolism is confirmed in anhepatic phase of patients receiving liver transplant.
Pharmacokinetics1,2
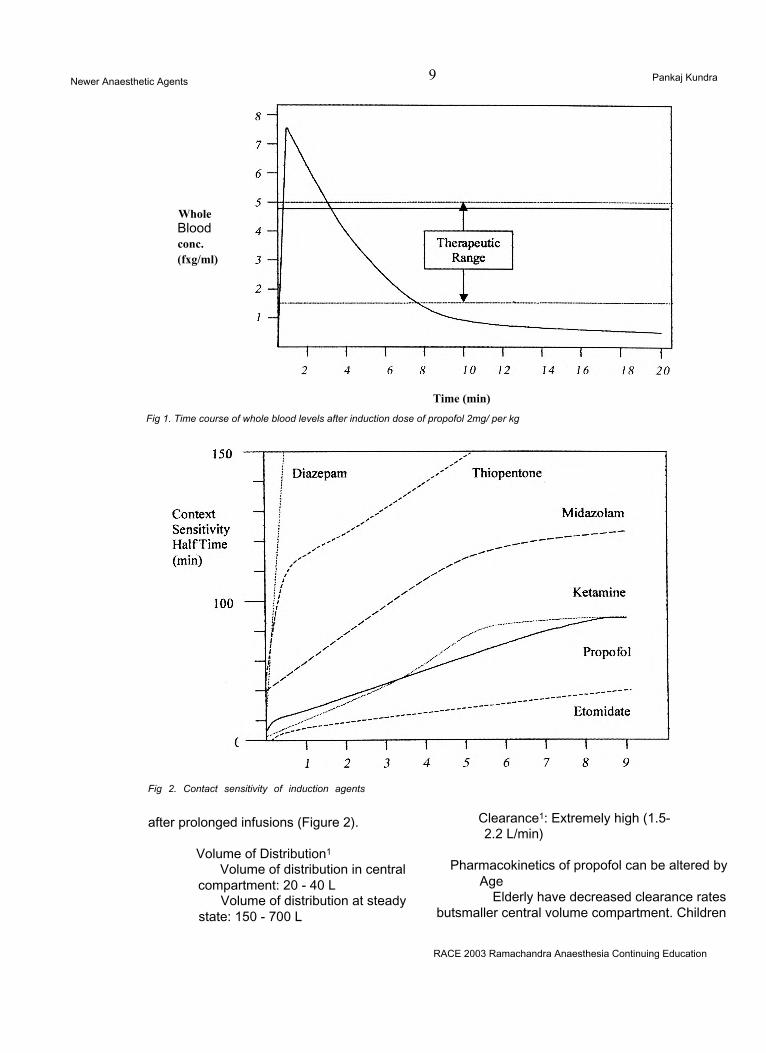
2 and 3 compartment model Following a single bolus injection, whole blood propofol levels decrease very rapidly as a result of both redistribution and elimination (Figure 1)2 compartment model• Initial distribution half life: 2-8
min• Elimination half life: 1-3 hours3 compartment model• Slow distribution half lives: 1 - 8 min and 30 - 70 min
• Elimination half life: 4 - 23.5 hours Owing to very rapid clearance of propofol from
central compartment, the slow return of propofol from deep compartment contributes little to the initial rapid decrease in propofol concentrations
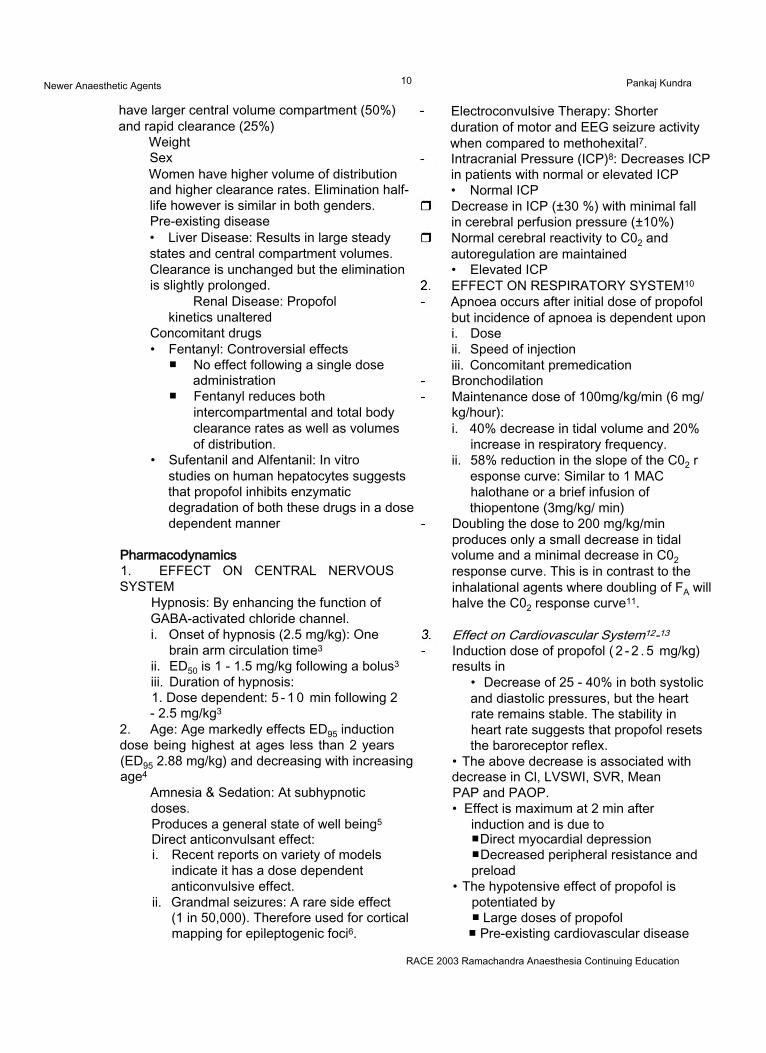
Context Sensitivity2: Defined, as the time required achieving a 50% decrease in drug concentration after termination of a continuous infusidn targeted to maintain a constant concentration. Context sensitivity half time for infusions up to 8 hours is less than 40 min2. As the required decrease in concentration for awakening following anaesthesia or sedation is less than 50%, recovery from propofol will remain rapid even
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 9 Pankaj Kundra
WholeBloodconc.(fxg/ml)
Time (min)Fig 1. Time course of whole blood levels after induction dose of propofol 2mg/ per kg
Fig 2. Contact sensitivity of induction agents
after prolonged infusions (Figure 2).
Volume of Distribution1
Volume of distribution in central compartment: 20 - 40 L
Volume of distribution at steady state: 150 - 700 L
Clearance1: Extremely high (1.5- 2.2 L/min)
Pharmacokinetics of propofol can be altered by Age
Elderly have decreased clearance rates butsmaller central volume compartment. Children
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 10 Pankaj Kundra
have larger central volume compartment (50%) and rapid clearance (25%)
WeightSexWomen have higher volume of distribution and higher clearance rates. Elimination half- life however is similar in both genders. Pre-existing disease• Liver Disease: Results in large steady states and central compartment volumes. Clearance is unchanged but the elimination is slightly prolonged.
Renal Disease: Propofol kinetics unaltered
Concomitant drugs• Fentanyl: Controversial effects
■ No effect following a single dose administration
■ Fentanyl reduces both intercompartmental and total body clearance rates as well as volumes of distribution.
• Sufentanil and Alfentanil: In vitro studies on human hepatocytes suggests that propofol inhibits enzymatic degradation of both these drugs in a dose dependent manner
Pharmacodynamics1. EFFECT ON CENTRAL NERVOUS SYSTEM
Hypnosis: By enhancing the function of GABA-activated chloride channel.i. Onset of hypnosis (2.5 mg/kg): One
brain arm circulation time3
ii. ED50 is 1 - 1.5 mg/kg following a bolus3
iii. Duration of hypnosis:1. Dose dependent: 5 - 1 0 min following 2 - 2.5 mg/kg3
2. Age: Age markedly effects ED95 induction dose being highest at ages less than 2 years (ED95 2.88 mg/kg) and decreasing with increasing age4
Amnesia & Sedation: At subhypnotic doses.Produces a general state of well being5 Direct anticonvulsant effect:i. Recent reports on variety of models
indicate it has a dose dependent anticonvulsive effect.
ii. Grandmal seizures: A rare side effect (1 in 50,000). Therefore used for cortical mapping for epileptogenic foci6.
Electroconvulsive Therapy: Shorter duration of motor and EEG seizure activity when compared to methohexital7. Intracranial Pressure (ICP)8: Decreases ICP in patients with normal or elevated ICP• Normal ICPDecrease in ICP (±30 %) with minimal fall in cerebral perfusion pressure (±10%) Normal cerebral reactivity to C02 and autoregulation are maintained• Elevated ICPEFFECT ON RESPIRATORY SYSTEM10 Apnoea occurs after initial dose of propofol but incidence of apnoea is dependent uponi. Doseii. Speed of injectioniii. Concomitant premedication BronchodilationMaintenance dose of 100mg/kg/min (6 mg/ kg/hour):i. 40% decrease in tidal volume and 20%
increase in respiratory frequency.ii. 58% reduction in the slope of the C02 r
esponse curve: Similar to 1 MAC halothane or a brief infusion of thiopentone (3mg/kg/ min)
Doubling the dose to 200 mg/kg/min produces only a small decrease in tidal volume and a minimal decrease in C02 response curve. This is in contrast to the inhalational agents where doubling of FA will halve the C02 response curve11.
Effect on Cardiovascular System12-13 Induction dose of propofol ( 2 - 2 . 5 mg/kg) results in
• Decrease of 25 - 40% in both systolic and diastolic pressures, but the heart rate remains stable. The stability in heart rate suggests that propofol resets the baroreceptor reflex.
• The above decrease is associated with decrease in Cl, LVSWI, SVR, Mean PAP and PAOP.• Effect is maximum at 2 min after
induction and is due to■ Direct myocardial depression■ Decreased peripheral resistance and preload
• The hypotensive effect of propofol ispotentiated by■ Large doses of propofol■ Pre-existing cardiovascular disease
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 11 Pankaj Kundra
■ Hypovolemia or CVS decompensation■ Advanced age■ Premedication with opioids■ Concomitant use of nitrous oxide
• Both coronary blood flow and myocardial MR02 are reduced, implying the global myocardial supply-demand is maintained.
4. Other EffectsPain on injection, especially in small veinsDuring prolonged infusions consideration must be kept for the effect of volume as well as the energy provided by intralipid (3 mg/ kg/hour provides 555 kcals/24 hours).This is equivalent to 25% of calorie requirements and 50% of lipid requirements per day Preliminary studies indicate it does not
trigger malignant hyperthermia14 It is safe to be used in porphyria.
DOSE REGIMESThe Bristol Model (1988) SirHumphry Davy Dept of Anaesthesia. UK
It is a widely known and quoted model of propofol pharmacokinetics. The study used a computer algorithm based on a 3-compartment model to design a simple infusion scheme for the manual infusion of propofol to achieve a desired target plasma concentration (3 mg/ml) within 2 min and to maintain this level for the duration of surgery.
The study design was as follows:ASA 1 & 2 patients presenting for superficial body surgery
Premedication with temazepam 20 - 30 mg/
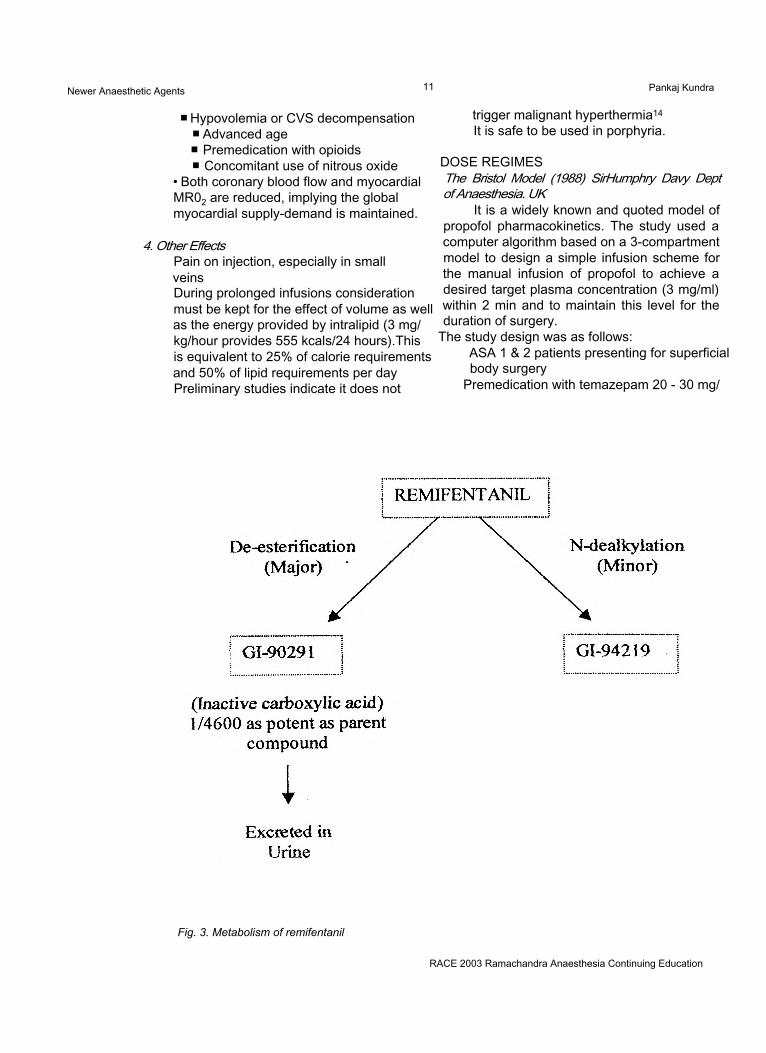
Fig. 3. Metabolism of remifentanil
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 12 Pankaj Kundra
kg, 90 min before surgery.Fentanyl 3 mg/kg 2 min before the injection of propofol.Propofol 1 mg/kg over 20 sec Propofol 10 mg/kg/hr for 10 min Propofol 8 mg/kg/hr for 10 min Propofol 6 mg/kg/kg/hr thereafter. Vecuronium 0.1 mg/kg and tracheal intubationVentilation with 67% nitrous oxide in oxygen. Results in practice showed an overall mean
blood propofol concentration of 3.67 mg/ml, which is maintained over the subsequent 80 - 90 min. It is important to note the figures for the induction dose of propofol used, and that opioid, nitrous oxide and vecuronium provided balanced anaesthesia. If a loading dose of 2 mg/kg of propofol is used, as in common practice, then additional 1 mg/kg is equal to the amount of drug given above a maintenance rate of 6 mg/kg/hr by the higher infusion rates of the first 20 min. If a loading dose 2 mg/kg of propofol is followed by a 10-8-6 regime, the propofol concentration is likely to be higher than predicted, with the attendant cardiovascular effects.
TARGET CONTROL INFUSION (TCI)TCI is an infusion system, which allows the
anaesthesiologist to select the target blood concentration required for a particular effect, considering the patient’s and operation’s needs, then to control depth of anaesthesia by adjusting the requested target concentration during surgery. The pharmacokinetic program of a TCI-device, however, continuously calculates the distribution and elimination of the intravenous anaesthetic agent, and successively adjusts the infusion rate to maintain a predicted blood or plasma drug concentration. One of the main benefits of TCI over manually controlled infusion systems is, therefore, its greater and better control over the drug concentration and the depth of anaesthesia obtained.
OPIOIDS
REMIFENTANIL15
Physicochemical PropertiesUltra-short acting ^-receptor opioid agonist Chemically designated as 3-[4- methoxycarbony l-4-( 1 -
oxopropyl)phenylamino]-1 - poperidine propanoic acid methyl ester.Molecular wt. 413 Structurally similar to fentanyl, sufentanil and alfentanil.Incorporation of methyl ester group onto the N-acyl side chain of the piperidine ring renders remifentanil susceptible to rapid esterhydrolysis.
PharmacokineticsDose dependent pharmacokinetic profile (shape of the blood concentration-time curve is independent of dose).Distribution: 2 or 3 compartment pharmacokinetic model with limited distribution into the 3rd compartment. Clearance: 2.9 L/min. Exceeds normal hepatic blood flow rates. Consistent with widespread extrahepatic metabolism Mean steady state volume of distribution of 31.8 L.Metabolism: Rapid hydrolysis by blood and tissue esterases (Figure 3).Accumulation of GI90291 is demonstrated after prolonged (12 hour) infusions in patients with renal failure. However, there were no obvious effects on minute ventilation in controls and in patients with renal failure as the metabolite is inactive.Hydrolysis of remifentanil is independent of plasma cholinesterase activity. Thus dosage does not require adjustments in pseudocholinestrase deficiency. Remifentanil metabolism is independent of hepatic function. Remifentanil clearance is unchanged during anhepatic phase of liver transplantation.Pharmacokinetics can be influenced by:
Increasing age: Central clearance and distribution volume decreases, whereas potency increases
Obesity: Pharmacokinetics best correlate with lean body weight.
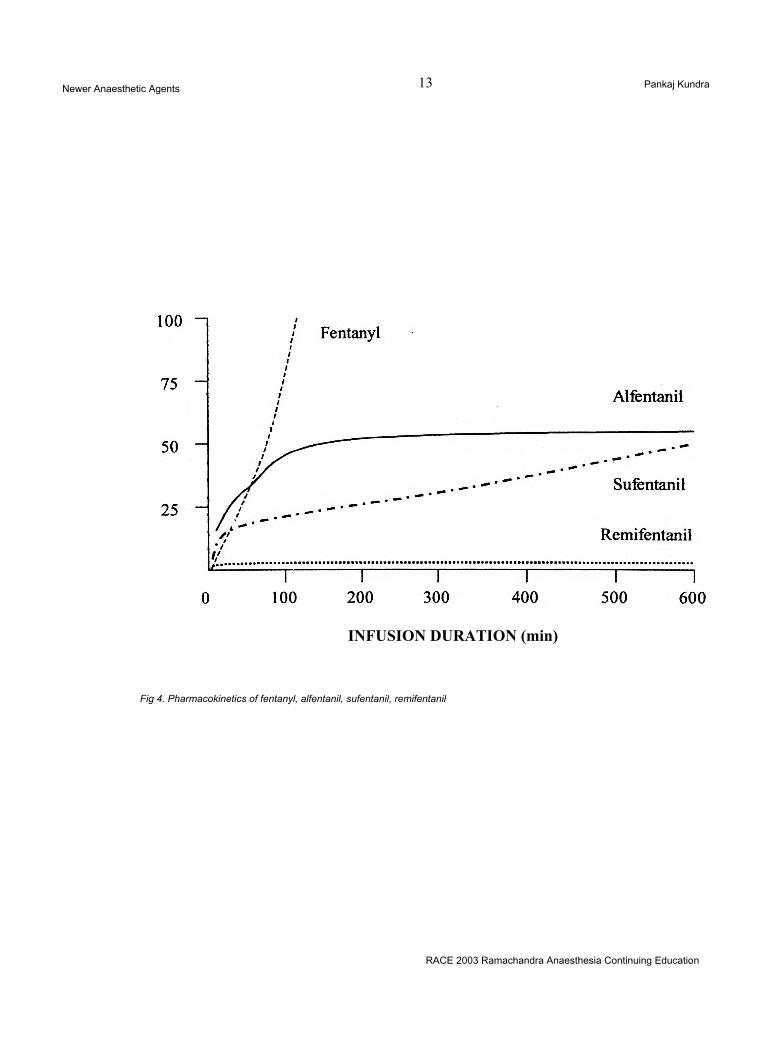
Context sensitive half time: Unique among fentanyl congeners in that its context sensitive half time is short (only 3-4 min) and independent of the duration of infusion. In contrast, context sensitive half time of fentanyl, sufentanil, alfentanil are all dependent on infusion duration and are longer than that of remifentanil (Figure 4).
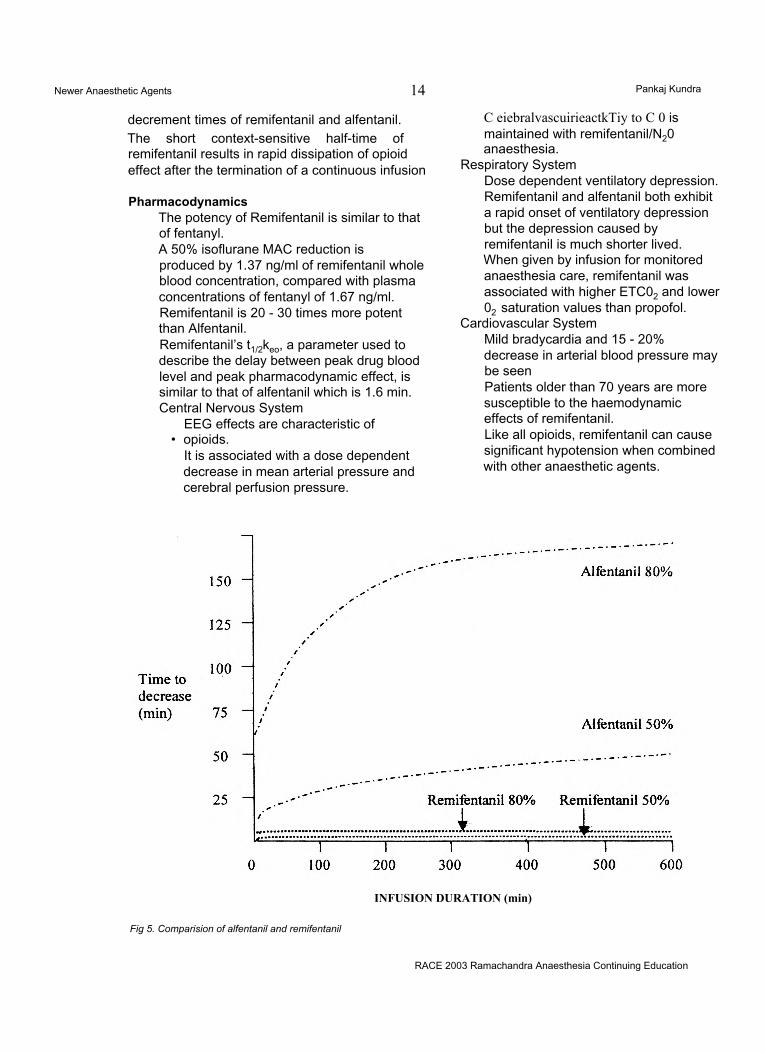
Figure 5 compares the 50% and 80%
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 13 Pankaj Kundra
INFUSION DURATION (min)
Fig 4. Pharmacokinetics of fentanyl, alfentanil, sufentanil, remifentanil
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 14 Pankaj Kundra
decrement times of remifentanil and alfentanil. The short context-sensitive half-time of remifentanil results in rapid dissipation of opioid effect after the termination of a continuous infusion
PharmacodynamicsThe potency of Remifentanil is similar to that of fentanyl.A 50% isoflurane MAC reduction is produced by 1.37 ng/ml of remifentanil whole blood concentration, compared with plasma concentrations of fentanyl of 1.67 ng/ml. Remifentanil is 20 - 30 times more potent than Alfentanil.Remifentanil’s t1/2keo, a parameter used to describe the delay between peak drug blood level and peak pharmacodynamic effect, is similar to that of alfentanil which is 1.6 min. Central Nervous System
EEG effects are characteristic of• opioids.
It is associated with a dose dependent decrease in mean arterial pressure and cerebral perfusion pressure.
C eiebralvascuirieactkTiy to C 0 is maintained with remifentanil/N20 anaesthesia.
Respiratory SystemDose dependent ventilatory depression. Remifentanil and alfentanil both exhibit a rapid onset of ventilatory depression but the depression caused by remifentanil is much shorter lived. When given by infusion for monitored anaesthesia care, remifentanil was associated with higher ETC02 and lower02 saturation values than propofol.
Cardiovascular SystemMild bradycardia and 15 - 20% decrease in arterial blood pressure may be seenPatients older than 70 years are more susceptible to the haemodynamic effects of remifentanil.Like all opioids, remifentanil can cause significant hypotension when combined with other anaesthetic agents.
INFUSION DURATION (min)
Fig 5. Comparision of alfentanil and remifentanil
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 15 Pankaj Kundra
Clinical Uses• MONITORED ANAESTHESIA CARE1. Single Intravenous DoseRemifentanil 0.5 -1.0 mg/kg/over 30 - 60 secs Perform local anaesthetic block 90 secs later Combine with either propofol 0.5 -1.0 mg/kg or midazolam 1 - 2 mg to optimize sedation and decrease side effects.
2. Continuous Intravenous Infusion Remifentanil 0.05-0.1 mg/kg/minPerform local anaesthetic block 5-7 min later Following block titrate remifentanil 0.025 - 0.2 mg/kg/min
When given as continuous infusion, remifentanil may be combined with either midazolam 1 - 2 mg or propofol 10-40 fig/kg/ min to optimize sedation and decrease side effects.
• GENERAL ANAESTHESIA1. Continuous Intravenous Infusion Remifentanil 0.5 - 1.0 mg/kg/min for 2 - 3 min Remifentanil 0.125 - 0.25 mg/kg/min maintenance (range 0.05 - 2.0 mg/kg/min) Remifentanil bolus 0.5 -1.0 mg/kg/min every 3 - 5 min
2. Induction of AnaesthesiaAdminister reduced dose of hypnotic
agent (e.g., propofol 0.75 - 1.0 mg/kg, Thiopentone 1.0 - 1.5 mg/kg) 1 - 2 min after starting remifentanil infusion.Administer neuromuscular blocker following loss of consciousness, as per usual practice.
3. Maintenance of AnaesthesiaIsoflurane 0.4 - 0.8% alone or 0.2 - 0.4% with 66% N20Sevoflurane 0.7 -1.4% alone or 0.4 - 0.8% with 66% N20Desflurane 1.5 - 3.0% alone or 0.75 -1.5% with 66% N20Propofol 75 - 200 mg/kg/min alone or 50-150 mg/kg/min with 66% N20
• SPINAL ADMINISTRATIONPresent formulation contains the
inhibitory neurotransmitter glycine as a vehicle, so continuous intrathecal administration of this formulation produces reversible, naloxone- insensitive motor dysfunction. Hence its
administration is not recommended.
• POSTOPERATIVE ANALGESIABecause of the rapid offset of
opioid effect of remifentanil, it is imperative to address postoperative analgesic needs before the conclusion of surgery. Remifentanil (0.025 - 0.2 mg/kg/min) may be continued into the immediate postoperative period until a longer acting opioid (e.g. morphine) is administered.
INHALATIONAL AGENTS SEVOFLURANE AND DESFLURANE15
Desflurane (CF2H-0-CFH-CF3) and Sevoflurane [CFH2-0-CH-(CF3)2] are
Halogenated ether structures1. Halogenation serves to eliminate
flammability and these drugs are halogenated entirely by fluorine
■ Fluorine significantly changes the solubility of these agents. Solubility is reflected in the blood-gas partition coefficients of 0.45 for desflurane and 0.65 for sevoflurane. The decrease in solubility lends itself to an agent that will provide a faster induction of and emergence from anaesthesia when administered in an equivalent MAC.
■ Fluorine also serves to decrease the MAC of desflurane and sevoflurane.
2. Ether linkage is associated with the drugs’ likelihood to sensitize the myocardium to arrhythmias.
3. Vapour Pressure at 20 degree C■ Desflurane: 669 mm Hg■ Sevoflurane: 170 mm Hg
This pressure allows for the administration of sevoflurane through conventional vaporizers. Desflurane, however, has vapour pressure approaching atmospheric pressure and therefore must be administered through a newly developed vaporizer system.
■ This vaporizer produces a controllable and predictable concentration of desflurane in oxygen regardless of changes in ambient temperature (between 18 - 30°C) and gas flow (between 0.2-10 L/min).
■ The vaporizer works by heating desflurane within an enclosure that is at 1500 mm Hg. The gaseous desflurane then passes from the enclosure through variable resistance transducers as controlled by the set delivery concentration and then mixes with the diluents gas.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 16 Pankaj Kundra
DesfluraneCENTRAL NERVOUS SYSTEM(CNS)
May potentially alter cerebral blood flow (CBF),cerebral metabolic rate for oxygen comsumption (CMR02), CNS activity and cognitive function. Higher MAC concentrations are required for arterial blood pressure support with phenylephrine infusions. A dose dependent decrease in cerebrovascular resistance regardless of arterial blood pressure support. This suggests Desflurane is a cerebral arteriolar dilator.
Dose related depression of EEG activity up to and including burst suppression. No epileptiform activity has been demonstrated.Awakening Time: In ASA I and II patients is about 5.25 min. after discontinuation of 1 MAC during application of dressing.
RESPIRATORY SYSTEMRapid inhalational induction agent (low solubility)High incidence of breath holding, apnoea and coughing.Potential for laryngospasm is high, and these effects. Maintenance of inspired concentration at less than 6% (1 MAC) minimizes the likelihood of airway irritation. Dose dependent decrease in tidal volume and an increase in respiratory rate.Minute ventilation decreases at 1.66 MAC Depresses ventilatory response to C02, which is indistinguishable from the depression reported for isoflurane and enflurane and slightly greater than that reported for halothane.
CARDIOVASCULAR SYSTEMDose dependent increase in right heart filling pressures and a decrease in systemic vascular resistance and mean systemic arterial pressure.Unlike isoflurane, desflurane doesn’t decrease the cardiac index or left ventricular ejection fraction even at deep levels of anaesthesia.Heart Rate: Increase in rate is demonstrated by > 30 beats/min at 1 - 1.5 MAC Unchanged cardiac output in the presence of increased right sided heart filling
pressures, decreased systemic vascular resistance and increased heart rate suggests that desflurane decreases myocardial contractility.Does not sensitize myocardium to catecholamines.Haemodynamic responses get attenuated at 1.66 MAC
PHARMACOKINETICSSingle halogen substitution of a fluorine atom for chlorine in isoflurane makes desflurane a more stable compound. Stability in presence of soda lime maintained at 40°, 60° and 80°C has been compared as the anaesthetic degradation increases as temperature increases:• At 80°C the rate of degradation per hour:
■ Sevoflurane: 92.2 ± 5%■ Halothane: 16 ± 1.6%■ Isoflurane: 13.1 ± 3.7%■ Desflurane: 0.44 ± 0.26%
• This suggests that desflurane strongly resists biodegradation.
Metabolites:• Fluoride ion: Post anaesthesia urinary
excretion of fluoride ion and organic fluoride in volunteers was comparable with pre anaesthesia excretion rates.
• Trifluroacetic acid (TFAA): Increases significantly in both serum and urine of volunteers after desflurane exposure. TFAA increases are 10 fold less than levels seen after isoflurane exposure.
• No evidence towards hepatotoxicity after exposure to 7.35 ± 0.81 MAC hours of desflurane anaesthesia.
• Desflurane does not cause acute renal toxicity.
• Desflurane has the capacity to trigger malignant hyperthermia in susceptible individuals.
SevofluraneCENTRAL NERVOUS SYSTEM
Effects of sevoflurane similar to other halogenated anaesthetics.At 1 MAC both sevoflurane and isoflurane cause• Significant reduction in CMR02 to 50%.• No change in cerebral blood flow occurs
with either of the agent.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 17 Pankaj Kundra
• Significant increase in ICP occurs with both.
• EEG: No evidence of spike or seizure activity.
RESPIRATORY SYSTEMInhalational induction is rapid and pleasant without causing breath holding or coughing. Respiratory depressant Decrease in tidal volume with increasing depth of anaesthesia although respiratory rate is increased.BronchodilationInhibits hypoxic pulmonary vasoconstriction response in a dose dependent manner
CARDIOVASCULAR SYSTEMHalogenated anaesthetic: cardiovascular depressant
• Myocardial depression: More with sevoflurane than isoflurane but less than that with halothane anaesthesia.
• Systemic Vascular Resistance: Decreases SVR but to a lesser degree than isoflurane
• Mean Arterial Pressure: Effect similar to isoflurane.
• Heart Rate: Lesser rise in heart rate as compared to isoflurane
• Does not sensitize myocardial to the arrhythmogenic effects of catecholamines.
METABOLISM AND TOXICITYLacks the stability of halothane or isofluraneRate of degradation at22°C is 6.5% per hour for each degree rise in temperature. Renal effects of prolonged exposure to sevoflurane.• Serum inorganic fluoride levels: 22.1 (± 6.1) mmol/L after 1 hour exposure.• The inorganic fluoride levels associated
with prolonged sevoflurane exposure declined rapidly to less than half the maximal level by 48 hours after cessation of anaesthesia. This is related to a low blood gas partition coefficient, which allows rapid elimination of sevoflurane via the lungs, leaving a little drug to be metabolized after cessation of anaesthesia delivery.
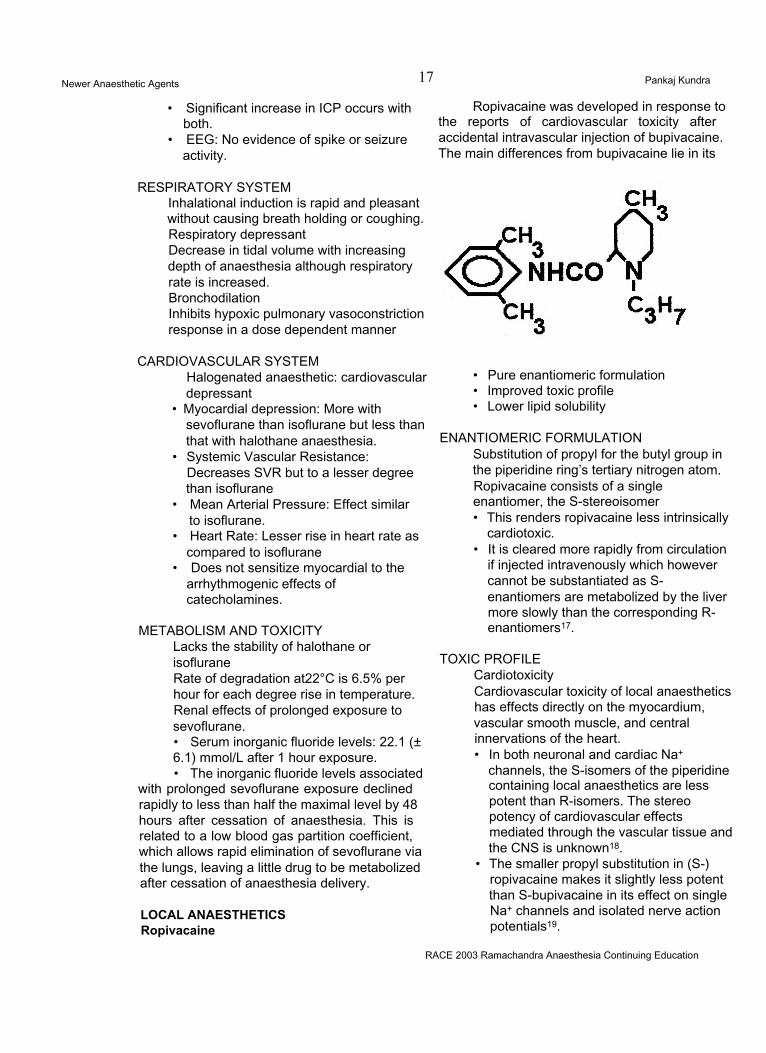
LOCAL ANAESTHETICS Ropivacaine
Ropivacaine was developed in response to the reports of cardiovascular toxicity after accidental intravascular injection of bupivacaine. The main differences from bupivacaine lie in its
• Pure enantiomeric formulation• Improved toxic profile• Lower lipid solubility
ENANTIOMERIC FORMULATIONSubstitution of propyl for the butyl group in the piperidine ring’s tertiary nitrogen atom. Ropivacaine consists of a single enantiomer, the S-stereoisomer• This renders ropivacaine less intrinsically
cardiotoxic.• It is cleared more rapidly from circulation
if injected intravenously which however cannot be substantiated as S- enantiomers are metabolized by the liver more slowly than the corresponding R- enantiomers17.
TOXIC PROFILE CardiotoxicityCardiovascular toxicity of local anaesthetics has effects directly on the myocardium, vascular smooth muscle, and central innervations of the heart.• In both neuronal and cardiac Na+
channels, the S-isomers of the piperidine containing local anaesthetics are less potent than R-isomers. The stereo potency of cardiovascular effects mediated through the vascular tissue and the CNS is unknown18.
• The smaller propyl substitution in (S-) ropivacaine makes it slightly less potent than S-bupivacaine in its effect on single Na+ channels and isolated nerve action potentials19.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 18 Pankaj Kundra
• Very slow reversal of Na+ channel blockade after cardiac action potential is a hallmark of bupivacaine. This reversal is considerably faster with ropivacaine20.
• A greater therapeutic index for ropivacaine than bupivacaine, particularly with regard to cardiotoxicity.
CNS Toxicity• Convulsing doses of ropivacaine are
larger than those of bupivacaine but less than those of lignocaine.
LIPID SOLUBILITY21
• Ropivacaine’s low lipid solubility may result in reduced penetration of the large myelinated A<x motor fibres, so that initially these fibres are relatively spared. However during continuous infusions they get blocked. Therefore, motor block produced with ropivacaine has
• A slower onset with ropivacaine• Less dense• Shorter duration when compared to
bupivacaine.
KINETICSRopivacaine is metabolized in liver by
aromatic hydroxylation, mainly to 3-hydroxy- ropivacaine, but also to 4-hydroxy-ropivacaine, both of which have some local anaesthetic activity21.
LevobupivacaineCLINICAL POTENTIAL:
The S(-)enantiomer of bupivacaine, with less cardiovascular and central nervous toxicity, a slightly longer duration of sensory block, but otherwise similar to its parent.
PHARMACODYNAMICS:Compared to bupivacaine it is as
potent, with a trend towards longer sensory block; with epidural usage it produces less prolonged motor block; Differentiation not seen with peripheral placement; lethal dose 1.3 to 1.6 times higher; less cardiac effect including less depression of contractility and fewer arrhythmias; higher convulsive doses. Has not been compared at equipotent anaesthetic doses with ropivacaine.
PHARMACOKINETICS:
_Elimination t1/21.3 hours VD 67L in adult volunteers Protein binding > 97%Metabolism by CYP1A2 and 3A4 Crosses placenta No racemisation in vivo.
DOSAGE:Minimum effective concentration
0.085%; Recommended maximum dosage 150mg for single dose epidural; 12.5mg/hr (10mls/ hr of 0.125% solution) for labour epidural infusion; 18.75mg/hr (15mls/hr of 0.125% solution) for epidural infusion; and 25mg every 15 or more minutes for epidural bolus doses.
15mg for intrathecal placement. 2.5mg/kg for nerve blocks in paediatric patient.
ADVERSE EFFECTS:Potential for hypotension and
cardiac arrest: observe precautions as for all local anaesthetics. Cardiotoxicity and CNS toxicity as noted.
DRUG INTERACTION: Unknown.Of Note:(1) Don’t use 0.75% in obstetrics;(2) Not for paracervical or Bier’s block;(3) Avoid if hypersensitivity to amides (rare).
EMLA (Eutectic mixture of local anaesthetic)21When two compounds are mixed
to produce a substance that behaves with a single set of physical characteristics, it is said to be eutectic. EMLA (5%) contains mixture of crystalline bases of 2.5% lignocaine and 2.5% prilocaine in a white oil: water emulsion. The mixture has a lower melting point, being oil at room temperature, while the individual components would be crystalline solids.
PRESENTATION AND USESEMLA is presented as an
emulsion in tubes containing 5 or 30 gm. It is used to anaesthetize skin before vascular cannulation or harvesting for skin grafts. It should be applied to intact skin under an occlusive dressing for at least 60 min. to ensure adequate anaesthesia.
CAUTIONSMethaemoglobinaemia is caused
by o-toludine, a metabolite of prilocaine______RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 19 Pankaj Kundra
• Congenital or idiopathic methaemoglobinaemia• Infants less than 12 months receiving treatment with methaemoglobin-inducing drugs• Patients on drugs associated with methaemoglobinaemia (sulfonamides, phenytoin)• Do not use on mucous membranes due to rapid systemic absorption• Patients receiving Class I antiarrhythmic drugs (Tocainide, Mexilitine)
NON DEPOLARIZING MUSCLE RELAXANTS
to limit the duration of the block23.□ Avid liver uptake and elimination into bile
due to increase in the lipophillic nature of the molecule with regard tovecuronium24. At appropriate dose, enables tracheal intubation in 60 - 90 sec and may prove a substitute for succinylcholine in rapid tracheal intubation, other aspects of clinical pharmacology of rocuronium seemssimilar to properties of vecuronium25.
PHARMACODYNAMICS
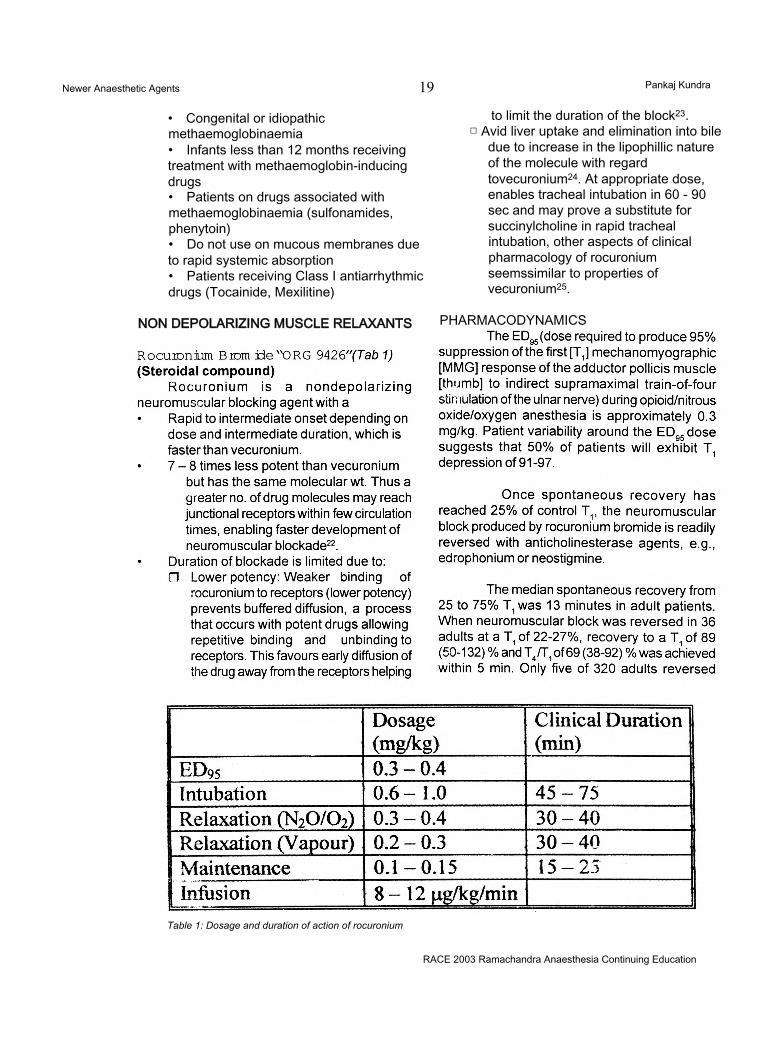
Table 1: Dosage and duration of action of rocuronium
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents Pankaj Kundra
received an additional dose of reversal agent. The median (range) dose of neostigmine was 0.04 (0.01 to 0.09) mg/kg and the median (range) dose of edrophonium was 0.5 (0.3 to 1.0) mg/kg. In geriatric patients (n=51) reversed with neostigmine, the median TA/T: increased from 40 to 88% in 5 min.
METABOLISM & ELIMINATIONNo metabolism of rocuronium has yet been reported. Like vecuronium dual hepatic and renal pathways of elimination exist. Unchanged drug
has been recovered from bile and urine24.
REFERENCES1. Simons PG, Cockshott ID, Douglas EJ. Blood concentrations, metabolism and elimination after subanaesthetic intravenous dose of 14C-propofol to male volunteers. Postgrad Med J 61: 64; 1985.2. Hughes MA, Jacob JR, Glass PSA. Context sensitive half time in multicompartment pharmacokinetic models for intravenous anesthesia. Anesthesiology 76: 334; 1992.3. Major E, Verniquet AJW, Waddell TK et al. A study of 3 doses of ICI 35 868 for induction and maintenance of anaesthesia. Br J Anaesth 53: 267; 1981.4. Aun CST, Short SM, Leung DHY, Oh TE. Induction dose response in unpremedicated children. Br J Anaesth 68: 64; 1992.5. McDonald NJ, Mannion D, Lee P et al. Mood evaluation and out patient anaesthesia. A comparison between propofol and thiopentone. Anaesthesia 43: 68; 1988.6. Anonymus. Convulsions after propofol. Pharm J 249: 745; 1992.7. Dwyer R, McCaughey W, Lavery J et al. Comparison of propofol and methohexitone as anesthetic agents for electroconvulsive therapy. Anaesthesia 43: 459; 1988.8. Stephan H, Sonntag H, Schenk HD, Kohlhausen S.
Effects of disoprivan on cerebral blood flow, cerebral oxygen consumption and cerebral vascular reactivity. Anaesthesiologist 36: 60; 1987.9. Mirakhur RK, Shepherd WFI, Darrah WC. Propofol or thiopentone: effects on intraocular pressure associated with induction of anaesthesia and tracheal intubation (facilitated with suxamethonium) Br J Anaesth 59: 431; 198710. Taylor MB, Grounds RM, Dulrooney PD, Morgan M. Ventilatory effects of propofol during induction of anaesthesia. Comparison with thiopentone. Anaesthesia 41: 816; 1986.11. Goodman NW, Black AMS, Carter JA. Some ventilatory effects of propofol as a sole anaesthetic agent. Br J Anaesth 59: 1497; 1987.12. Coates DP, Monk CR, Prys-Roberts C, Turtle M. Hemodynamic effects of the infusions of the emulsion formulation of propofol during nitrous oxide anesthesia in humans. Anesth Analg 66: 64; 1987.13. Claeys MA, Gepts E, Camu F. Haemodynamic changes during anaesthesia induced and maintained with propofol. Br J Anaesth 60: 3; 1983.14. Hopkinson KC, Denborough M. Propofol and malignant hyperpyrexia (letter). Lancet 1: 191; 1988.15. Johnson SE. Remifentanil: A unique, short acting opioid. Advances in Anesthesia vol. 16, Chapter 4, Mosby Inc. 1999.16. Navarro JR. New Inhalational Anesthetics. Advances in Anesthesia vol. 12, Chapter 4, Mosby - Year Book Inc. 1995.17. Rutten AJ, Mather LE, Mclean CF. Cardiovascular effects and regional clearances of intravenous bupivacaine in sheep: Enantiomeric analysis. Br J Anaesth 67: 247; 1991.18. Lee-Son S, Wang GK, Concus A, et al. Seterioselective inhibition of neuronal sodium channels by local anesthetics. Anesthesiology 77: 324; 1992.19. Wang GK. Binding affinity and stereioselectivity in single batrachotoxin activated Na* channels. J Gen Physiol 96: 1105; 1990.20. Arlock P. Actions of three local anaesthetics: lignocaine, bupivacaine and ropivacaine on guinea pig papillary muscle sodium channels (Vmax). Pharmacol Toxicol 63: 1; 1988.21. Peck TE, Williams MA. Pharmacology for Anaesthesia and intensive care. 1st edition. Chapter 10. Ashford Colour Press, Great Britain.22. Wierda JMKH, Di Wit APM, Kuizenga K et al. Clinical observations of the neuromuscular blocking action of ORG 9426 a new steroidal non-depolarizing agent. Br J Anaesth 64: 521; 1990.23. Min JC, Becavak I, Glavinovic Ml et al. lontophoretic study of speed of action of various muscle relaxants. Anesthesiology 77: 351; 1992.24. Khuenl-Brady K, Castagnoli KP, Canfell PC et al. The neuromuscular blocking effets and pharmacokinetics of ORG 9426 and ORG 9616 in the cat. Anesthesiology 72: 669; 1990.25. Magorian T, Flannery KB, Miller RD. Comparison of rocuronium, succinylcholine and vecuronium for rapid sequence induction of anesthesia in young adults. Anesthesiology 79: 913; 1993.*26. Muir AW, Houston J, Green KL et al. Effects of new neuromuscular blocking agents (ORG 9426) in
RACE 2003 Ramachandra Anaesthesia Continuing Education

Newer Anaesthetic Agents 21 Pankaj Kundra
anesthetized cats and pigs and in isolated nerve muscle preparation. Br J Anaesth 63: 400; 1989.27. Servin FS, Lavaut E, Desmonts JM. Clinical evaluation of ORG 9426 in cirrhotic and control patients.
Anesthesiology 77: A357; 1993.Shanks CA, Fragen RJ, Ling D. Continuous intravenous infusion of rocuronium in patients receiving balanced, enflurane or isoflurane anaesthesia. Anesthesiology 78: 649; 1993.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 22 M R. Rajagopal
INTRODUCTIONIn June 2002, a Californian jury found a
doctor “liable for reckless neglect in under-treating a man’s pain” and ordered him to pay 1.5 million US dollars to the dead man’s children1.
It has started. We cannot get away with it any more. We have always known that a doctor’s duty is to “cure sometimes, relieve often and to comfort always” but we have seldom taken it seriously. But people have started demanding pain relief now, and we better learn to satisfy them.
Unrelieved pain can cause several adverse physiological changes.1. It causes reflex skeletal muscle spasm that,
specially in upper abdominal surgery or chest surgery, can result in regional hypoventilation and result in postoperative chest complications.
2. Pain causes reflex vasoconstriction. It can possibly impair wound healing in any case, but particularly in people with compromised blood flow, this can be very damaging.
3. Pain causes stress response, with adverse circulatory consequences. This can be very detrimental in people with compromised circulation.
4. Pain prevents early mobilization with attendant complications. Pain relief during recovery from acute injury improves survival and speeds rehabilitation by promoting volitional activity2.
For all these reasons, and also because it is simply our duty to relieve suffering, acute pain has to be treated. Lack of resources is certainly not an excuse. Most pain relief
measures are relatively inexpensive. Pain relief is not necessarily something to be done with expensive electronic gadgetry. There are other options.
We will attempt to briefly review the pathophysiology of pain, and use that understanding to describe various means of pain relief. Then wc shall give attention to what could be done even with limited resources.
PATHOPHYSIOLOGY OF PAINLet us start by making some key points
pertaining to pain mechanisms.
Pain is what the patient says hurts.The International Association for Study
of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”3. It is important to remember that people are different, their emotional states could be different and that it would be necessary to take that into consideration while planning treatment.
A simpler definition is, “Pain is what the patient says, hurts”4. The emphasis is on the patient’s experience. He and no one else can assess his pain properly. Once we accept the definition, we shall escape the pit-fall of being judgemental about someone who is 'too sensitive’ or 'too fussy’ and complains 'too much’ about his or her pain.
Hence, the patient is the most appropriate person to assess the severity of his pain. The message is, “Believe the patient about
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 23 M.R. Rajagopal
his pain.”
Pain causes more pain.Unrelieved pain results in steady
worsening of pain. The following description of pathophysiology will make this easier to understand.
Peripheral mechanisms of pain:Any injury causes stimulation of pain
sensing nerve endings, which are called nociceptors. The impulse is transmitted via the C and A-delta sensory nerve fibres to the dorsal horn of the spinai cord. There from, the impulse is transmitted to the thalamus and the sensory cortex.
The initial injury is followed by liberation of chemicals - the nociceptive substances -, which continue to stimulate the nociceptors and perpetuate pain. Of the many such substances (kinins, leukotrienes, substance P, histamine, serotonin, hydrogen and potassium ions and so on), prostaglandins deserve special mention. Prostaglandins sensitize the nociceptor to the other pain producing substances.
It has also been found that silent or sleepy nociceptors are recruited in the face of sustained stimulation. This means that for a particular stimulus, there will be progressively increasing response.
CENTRAL PAIN MECHANISMS AT THE LEVEL OF THE DORSAL HORN
There is some form of sensitization and recruitment at the level the of dorsal horn too. The phenomenon is called “wind-up” - analogous to a wound-up spring. With sustained stimulation from the periphery, the dorsal horn cells seem to get wound up so that with time, there is progressively increasing response to the peripheral stimulus. NMDA receptors are said to play a major role in the development of “windup”.
There is also a process of recruitment at the central level. With time, there is recruitment of adjacent spinal segments so that pain increases not only in intensity, but in extent as well.
In fact with prolonged, unrelieved, acute pain, there can be permanent anatomical changes in the nervous system, so that the pain gets centrally established and becomes chronic pain. It is believed that this is the mechanism of most scar pains.
This entire gamut of changes mean that the earlier pain is treated, the easier it is It also means that in elective trauma (surgery-), pain had better be prevented rather than treated. This is the concept of pre-emptive analgesia.
MANAGEMENT OF ACUTE PAIN:Let us start with some general principles
of pain management.1. All pains are not opioid-sensitive. Roughly
two thirds of acute pain can be treated successfully by opioids. This means that a multi-modal approach works best.
2. Analgesics must be administered round the clock. This may mean the use of continuous infusions or the use of drugs by the clock depending on its duration of action. For example, morphine can be administered either as a continuous subcutaneous or epidural infusion or as 4-hourly bolus doses.
Major pain relief modalities:The following three form the major
modalities of pain relief:1. Prevention of peripheral sensitization by the
use of NSAIDs.2. Application of local anaesthetics, peripherally
or centrally.3. Use of opioids, centrally or peripherally.
By judicious combinations of these, it is possible to achieve adequate analgesia without serious adverse effects. In individual cases, however, there may be other forms of treatment that can be added on. We shall come to them briefly later.
NSAIDs:By preventing sensitisation of
nociceptors and indirectly central sensitisation, NSAIDs contribute to pain relief. However, there are concerns about their safety. The major concerns are:
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 24 M.R. Rajagopal
1. Bleeding tendency because of inhibition of platelet adhesion. There is some controversy; but there does seem to be some evidence at least that it can be a real concern. One study found them to double the bleeding during hip arthroplasty5. But the coxibs appear to be safe. If anything, there seems to be a doubt that coxibs may even have a prothrombotic tendency.
2. Renal dysfunction in those who are predisposed to it. In the surgical context, this can also be a concern in the hypovolaemic. The associated water retention has the potential to worsen hypertension and cardiac failure. It seems doubtful if the chance of this complication is any less with coxibs.
3. Gastritis. But the coxibs appear to be safer than the older generation drugs in this matter.
In spite of these disadvantages, the addition of NSAIDs does seem to improve the quality of analgesia. The combination decreases opioid requirement and decreases the chance of ileus. They are hence recommended particularly in procedures like dental extraction where chance of significant bleeding is negligible.
There is one situation where NSAIDs must be used. In people with chronic arthralgia like in osteoarthritis, rheumatoid arthritis etc, preoperative cessation of NSAIDs causes a flare up of pain (algesic flare). In such cases, it is recommended that coxibs be started and continued through the peri-operative period.
NEWER NSAIDS.Valdecoxib is said to have no effect at
all on platelet function.
Parecoxib is the only Cox-2 selective drug that is recommended for parenteral use.
Etoricoxib is the most potent second generation NSAID yet, three times more selective than rofecoxib.
LOCAL ANAESTHETICSAs used in pain relief, they have a
predominant local effect and some systemic effect (membrane stabilization). The latter,
nevertheless, may be significant when there is a neuropathic component to the pain. Conventionally, they are used most often as epidural injections. Given preoperatively, it can contribute to surgical anaesthesia and confer post-operative analgesia too. Where facilities exist, they had best be given as continuous epidural infusions. An infusion of 0.125- 0.25% bupivacaine would provide adequate analgesia, while permitting ambulation; a dose of 4-8 ml/ hour may be a good starting point. When the pain stimulus is severe, (as in ischaemic pain for example), sometimes it may be necessary to give an anaesthetic concentration of the drug (0.5%) and compromise on mobility. A syringe pump would be the standard equipment for the infusion; a Patient Controlled Analgesia (PCA) device may permit fine-tuning of analgesia.
When a syringe pump is not available, one has to resort to intermittent injections. Too frequent injections are impractical; but on the other hand, at least four hourly injections will be needed if pain relief has to be adequate. And even in that case, the sizeable dose requirement predisposes to hypotension following every bolus injection. Particularly in the context of the unstable circulatory status in many major surgical procedures, this can be quite relevant. Obviously, smaller and more frequent bolus doses are desirable.
Bupivacaine is the local anaesthetic agent used most often. Shorter acting agents like lignocaine have the disadvantage of tachyphylaxis. Ropivacaine seems to have nearly the same duration of action as bupivacaine. It may have an edge over bupivacaine in that it seems to have better selective sensory blockade. With ropivacaine, it is easier to achieve analgesia without motor blockade than with bupivacaine.
Epidural catheters function best for an average of three days. As days go by, blockage, infection, pain on injection and leaks can be problems limiting long term use6.
When epidural infusions of local anaesthetics are not feasible or practical for lack of facilities, even single dose local anaesthetic
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 25 M.R. Rajagopal
blocks can be valuable. By avoiding the maximal pain in the immediate post-operative period, it serves to decrease the sensitization. A single dose epidural block, an interpleural or intercostal block, or a regional block as for herniorrhaphy, can all be very useful, despite the short duration of a single block.
OPIOIDSOpioids can act both centrally and
peripherally. The importance of peripheral opioid receptors is being more and more understood now. Their practical relevance is that the same dose of opioid infiltrated around the incision would be much more effective than a subcutaneous injection elsewhere, because in the former case, we can have the drug acting both on the peripheral receptors as well as systemically.
Addition of opioids to the local anaesthetic agent given epidurally, improves the quality of analgesia. The basic principle is that we are able to achieve rather high neuraxial concentrations compared to systemic drug levels, resulting in excellent analgesia with minimal side effects. Some side effects are possible however, like nausea and vomiting, delayed respiratory depression, urinary hesitancy or retention and itching.
Preservative-free morphine is the agent used most often for this purpose as it has the most opioid-sparing effect compared to IV injection. The dose required is only about one- tenth of the systemic dose. It is about one-third for fentanyl and two-third for buprenorphine. Herein lies the main advantage of morphine over the other opioids for epidural administration - small dose, thus fewer side effects. However, as a practical point, there is the problem of poor availability of preservative-free morphine. (The manufacturers should be able to provide us with this on request.)
However, buprenorphine does have an advantage. It does not have to be given at the required segmental level.
COMBINATION 0!^ DRUGSIn general, we can make the following
recommendations for post-operative analgesia.• NSAIDs, particularly the coxibs would help to
improve the quality of analgesia, but need to be used after weighing the risks and benefits.
• Combination of a local anaesthetic with an opioid would be particularly useful - simple infiltration of these drugs over the site of incision itself may go a long way towards post operative pain relief.
• Preservative free morphine is the best drug for epidural administration, if it can be applied over the segment to be blocked. If the site of administration were distant, buprenorphine would be a better choice.
ANCILLARY MEASURESSeveral other possibilities exist for relief
from acute pain.1. Though not freely available in this country,
Entonox (the compressed mixture of oxygen and nitrous oxide in 50:50 combination) is a good choice for analgesia in the emergency room.
2. It appears that pre-treatment with tricyclic antidepressants decrease opioid requirements presumably by inhibiting reuptake of serotonin and norepinephrine at the inhibitory synapses. While this may have little application as a technique for pain relief in routine practice, this strengthens the case for continuing tricyclics in the peri-operative period in those patients already on it.
3. Sub-cutaneous infusion of lignocaine may supplement analgesia in relatively opioid resistant pains, particularly in patients who have already been in pain for some time, and especially if there is a neuropathic component to the pain (like some patients with burns).
4. Subcutaneous infusion of a sub-anaesthetic dose of ketamine (for example, 5 mg per hour) may help in difficult pains by its action on the NMDA receptors in the dorsal horn of the spina! cord.
5. Transcutaneous electrical nerve stimulation (TENS) is a particularly safe form of pain relief, though it has limited application. The device itself is inexpensive, but they should be used only if sterile conducting pads are available.
RACE 2003 Kamachandra Anaesthesia Continuing Education

Management of Acute Pain 26 M.R. Rajagopal
Organization of an acute pain serviceMore and more is talked now about the
concept of a pain-free hospital. There is a move favouring institutional commitment to pain relief- making pain the 4th vital sign in the patient’s daily hospital record of parameters. Measurement of pain of course mandates adequate control too.
Most acute pain services are anaesthesiologist-led. But it is important to remember that pain service demands teamwork. It would be impossible to achieve assessment and management of pain in a whole hospital, without adequate personnel. Most pain services depend a lot on nurses. It would be essential to have at least one nurse with special training round the clock in the hospital, who will help the staff nurses with evaluation and pain control. Needless to say, this nurse will need expertise in assessment of pain as well as in the mechanical aspects including the use of devices like infusion pumps and PCA devices. Theanaesthesiologist, then, is able to do the consultant’s job. In fact the presence of such a team is much more important than the high tech devices like PCAs. Last but not least, the importance of explanations to the patient and family cannot be overemphasized. If they know what to expect,
anxiety will be less, and that will lessen the pain experience.
REFERENCES
1. Okie.S. Californian jury finds doctor negligent in managing pain. National news', 15 June 2001, Washington.
2. Tuman KJ, Me Carthy RJ, DeLaria GA, Patel RV, Ivankovich AD. Effects of epidural anesthesia and analgesia on coagulation and outcome after major vascular surgery. Anesthesia and Analgesia 1991; 73:696-704.
3. I ASP Sub-committee on Taxonomy. Pain terms: a list with definitions and notes on usage. Pain 1980; 8:249-52.
4. Black RG. The Chronic Pain Syndrome. Surgical Clinics of North America. 1975; 55:999-1011.
5. Robinson CM, Christie J, Malcolm-Smith N. Non-steroidal anti-inflammatory drugs, perioperative blood loss and transfusion requirements in elective hip arthroplasty. J Arthroplasty 1993; 8:607-610.
6. McQuay HJ. Epidural analgesics. In: Wall PD; Melzack R, Eds. Textbook of Pain 3rd ed. Churchill Livingstone, Philadelphia. 1994: 1025-1034.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Qbstetric surgery 27 R. Gopinath
INTRODUCTIONEach year for about 80,000 anaesthetics
administered there are 2 % of parturients who undergo surgery. This is largely due to the increase in the endoscopic procedures undertaken to treat conditions common in the childbearing age group like trauma, ovarian masses, appendicitis, gall bladder disease, breast surgery etc. Major surgical procedures like cardiac surgical, neuro-surgical and liver transplants have been performed during pregnancy with good outcomes for both the foetus and the mother. The known problems of foetal development and drug administration to the mother during pregnancy and the risk of abortions make both the physician and the patient wary of an anaesthetic. To assess the risk one has to understand the physiological changes involved during pregnancy and that two lives are involved during the conduct of anaesthesia raising several unique concerns.
ALTERATIONS IN MATERNAL PHYSIOLOGY.All systems are involved in change but
those important to the anaesthetic management are:Respiratory:
Increased oxygen consumption, reduced functional residual capacity, hypocapnia due to increased minute ventilation, likelihood of difficult intubation and trauma to the airway due to increased vascularity of the mucosa.
Cardiovascular:Increase in both the cardiac output and
the blood volume, dilutional anaemia, decreased vascular responsiveness, increased baroreceptor responsiveness, aortocaval compression in the supine position.
Gastrointestinal:The lower oesophageal sphincter tone is usually reduced though gastric pH, volume and emptying are not much altered.
Central nervous system:Inhalational agent MAC and local
anaesthetic requirements are reduced.
Teratogenicity of anaesthetics is probably minimal and has never been conclusively demonstrated. The use of agents like nitrous oxide, which in animal studies may cause vasoconstriction of the uterine vessels and reduce uterine blood flow are of concern but this, has not been demonstrated in human beings. Benzodiazepines were associated with oro-facial abnormalities but again have not been proven in prospective studies. The inhalational agents, narcotics, intravenous agents and local anaesthetics have long been used safely during pregnancy.
There is a slight increase in miscarriages for OR personnel found during a meta-analysis of anaesthetic exposure in the workplace.
DRUGS AND PREGNANCYDrugs offered for use in pregnancy aregrouped into one of five categories:A. Controlled studies show no riskB. No risk in animal studies or no risk supported
by controlled human studiesC. Animal studies indicate a risk but no human
studies availableD. Evidence of foetal risk but benefits outweigh
risk.X Evidence of high risk to foetus, which
outweighs benefitsNA. Not applicable
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthet/c Management of aPregnant Patient for Non-Obstetric surgery 28 R. Gopinath
Types of drugs taken during pregnancy• Drugs of abuse: Opioids & opiates, marijuana,
cocaine, alcohol and nicotine• Sedatives: Benzodiazepines (class D orX)• Oral contraceptives (low risk, evidence
uncertain), cardiac glycosides (safe)• Antibiotics (most class B, although
aminoglycosides can have foetal toxicity and tetracyclines may give congenital defects)
• Antiparasitics (class C, except quinine, class X)
• Anti-asthmatic drugs (GCs may have latent effects and reduce birth weight, anti-histamines may result in blindness)
• Relaxants/sympathomimetics etc (class C)• Diuretics (most class D)• Anticoagulants (not recommended)• Anti-viral drugs (most category C)
Maternal Pharmacokinetic VariablesDuring pregnancy, a number of
physiological changes occur that affect drug absorption, uptake and metabolism.These changes include:• Changes in body fluid volume• Changes in cardiovascular parameters• Changes in pulmonary function• Alterations in gastric activity• Changes in serum binding protein
concentrations and occupancy• Alterations in kidney function
These maternal variables determine the maternal and foetal therapeutic/toxic responses to drugs! Specifically:• Pregnancy is associated with increased
cardiac output (-30%) and plasma volume (-50%) = increased Vd
• Maternal aqueous and fatty tissue spaces increase dramatically in pregnancy (10-30 weeks mainly); total body water increases by -8 L (mostly extracellular water; 40% maternal, 60% foetal/placental)
• Reduction in motility of stomach and gut - increased intestinal transit time (-30-50%) (P4 effect?) and increased mucus formation = raised gut pH
• Nausea and vomiting may also affect gut
transit time and pH.• Decreased serum albumin concentrations
(-25%), but unchanged alpharacid glycoprotein. Binding sites also taken up by steroid and peptide hormones (= more free drug)
• Glomerular filtration rate increases (-50%) with renal blood flow (-50%), resulting in increased renal excretion & creatinine clearance. Rates of hepatic enzyme activity may also be increased (i.e. phenytoin metabolism) or decreased (theophylline/ caffeine) ?steroid effects
• Hyperventilation and increased pulmonary blood flow = increased alveolar uptake of inhaled drugs (i.e. anaesthetics)
Drug disposition in the maternal-foetal unitDrugs that reach the foetus are (almost)
always administered to the mother!Drug -> Mother-> Placenta -> Foetus -> Placenta-> Mother -> Excretion
Foetal Pharmacokinetic Variables• Blood flow through the placenta (maternal
side) increases during gestation (50 ml/min @ 10 weeks of pregnancy - 600 ml/min @ 38 weeks).
• Foetal plasma binding proteins differ from maternal concentrations: albumin 15% > than maternal, but alpharacid glycoprotein -37% lower (so free fractions of basic drugs such as propranalol and lidocaine are elevated)
• Foetal plasma proteins also appear to bind some drugs with lower affinity than in adults (i.e. ampicillin, benzylpenicillin)
• Ion trapping: Foetal plasma pH > maternal: base drugs (i.e. salicylate) are more ionized on the foetal side, hence lesser drug crosses the placenta back to the maternal plasma = apparent accumulation in foetal plasma. Principle also applies to metabolites (more polar, less mobile)
• Fcetal liver expresses metabolizing enzymes (i.e. CYPs), but metabolizing capacity is less than that of mother (some enzymes are foetal- specific)
• Drugs transferred across the placenta undergo first pass through the foetal liver before reaching systemic circulation (modulated by
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 29 R. Gopinath
ductus venosus shunt, 30-70% by pass)• Foetal kidney immature: GFR is reduced,
increasing with gestational age but only 2-4 ml/min at term (3% of cardiac output vs 25% in adult). Anion (i.e. penicillin) secretion very low, cation (i.e. cimetidine) secretion is efficient.
• Foetal urine enters the amniotic fluid which may be swallowed by the foetus (however, foetal renal blood flow is only 5% of the blood flow)
Placental PharmacokineticsCritical factors that affect drug transfer
across the placenta:• Physicochemical properties i.e. lipid solubility,
ionization, size, protein binding characteristics.
• Transfer of flow-limited drugs affected by placental flow.
• Compounds that alter blood flow alter maternal drug disposition and placental transfer.
• Placental metabolism (dealkylation, hydroxylatior, demethylation) affects drug transfer across the placenta (usually relatively minor effect compared to foetal or maternal liver).
• Foetal metabolism may also be significant, but may change during pregnancy.
Adverse Effects of Drugs on the Foetus DuringPregnancyMECHANISM:1. Effects on maternal tissues primarily, with
only indirect (secondary) effects on the foetus2. Direct effects on developing foetal tissues3. Indirect effects via interference with the
function of the placenta, i.e., placental transferor placental metabolism
TYPE OF EFFECTS:• Teratogenicity (i.e. thalidomide) - readily
detected at, or shortly aftet, birth• Long term latency (i.e. diethylstilbestrol -
increased risk of vaginal adenocarcinoma after puberty, or abnormalities in testicular function and semen production)
• Impaired intellectual or social development (i.e. exposure to phenobarbitone- alters
programming of the brain)• Predisposition to metabolic diseases (i.e.
Barker hypothesis - low birth weight associated with increased risk of diabetes, hypertension, heart disease in adulthood)
DRUGS KNOWN TO EXERT SIGNIFICANT EFFECTS ON THE FOETUS:
Aminopterin, aminoglycosides, barbiturates, chloramphenicol, chlorpropamide, cortisone, diazepam, diethylstilbestrol, ethanol, heroin, iodide, isotretinoin, methadone, methyltestosterone, methylthiouracil, metronidazole, norethindrone, phenytoin, tetracycline, thalidomide, trimethadione, valproic acid, warfarin
Maintenance of uterine perfusion and maternal oxygenation determine and preserve foetal oxygenation. These are of concern and vital for any anaesthetic during pregnancy. Avoid maternal hypoxia and hypotension at all costs and one should be aware of the effects of all agents used on the maternal cardiovascular system and oxygen delivery.
The most difficult perioperative problem is preterm delivery, which is the leading cause of foetal death due to preterm labour. Prevention and management of the same is very important. The anaesthetic management per se is not related as much as the disease process for the surgical intervention and surgery itself.
ANAESTHETIC MANAGEMENTPerioperative management starts with
assessment preoperatively and should include establishment of pregnancy if in doubt, counseling the patient on the risks of anaesthesia (for the foetus on continuation of pregnancy and so considering delaying surgery till the second trimester with explanation of teratogenicity) and the chances of spontaneous miscarriage, the symptoms of preterm labour and the need for uterine displacement to the left if needed. Documentation of the date of the LMP should be recorded.
Preoperative medications to allay anxiety or pain should be given as appropriate and not withheld, since elevated endogenous maternal
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 30 R. Gopinath
catecholamines will reduce uterine blood flow. Prophylaxis against aspiration should be considered and a combination of an antacid (nonparticulate), H2 -receptor blocker or metoclopramide administered. The obstetrician should be involved and perioperative tocolysis discussed. Indomethacin (oral or suppository) and magnesium sulfate as an infusion are commonly used. Indomethacin has few anaesthetic implications but magnesium use should be viewed with caution due to its interactions with neuromuscular blocking agents and the risk and management of hypotension during potential blood loss and volume replacement.
Intraoperative management is not influenced by the anaesthetic technique as long as maternal oxygenation and perfusion is maintained. A review of 49,000 consecutive pregnancies found that 0.14% required surgery during pregnancy. There was no correlation between the type of surgery, type of anaesthetic, trimester in which surgery occurred, length of surgery, estimated surgical blood loss, or the length of anaesthesia and the outcome of the pregnancy.
Monitoring should include blood pressure, oxygenation, ventilation and temperature. Blood glucose should be checked if the procedure is prolonged. If the surgical field is not a hindrance, continuous or intermittent foetal monitoring should be performed after 20-24 wks gestation to ensure the intrauterine environment is optimized. Loss of beat-to-beat variability is normal after anaesthetics are administered, but decelerations are not. They may indicate the need to increase maternal oxygenation, maintain or increase maternal blood pressure, further uterine displacement, reduce surgical retraction, or begin tocolytic drugs. Foetal monitoring can help assess the adequacy of uteroplacental circulation and foetal perfusion during cardiopulmonary bypass, induced hypotension or procedures with major blood loss and volume shifts.
General anaesthesia should include full preoxygenation and denitrogenation, rapid sequence induction with cricoid pressure, high FI02, slow reversal of relaxants to prevent acute rise in acetylcholine that might induce uterine contractions. Inhalational agents should be kept
below 2.0 MAC to prevent cardiovascular compromise. During the first trimester ketamine at doses of > 2.0 mg/kg may cause uterine hypertonus. Nitrous oxide and propofol may be used. Propofol has recently been shown to reduce oxytocin-induced contractions of the uterine smooth muscle. Early pregnancy does not decrease the concentration of propofol required for loss of consciousness. The increase in \nucosal vascularity and potential for difficult airway must be kept in mind during laryngoscopy.
Regional anaesthesia is advantageous in reducing drug administration and reducing the concerns of teratogenicity during the first trimester and minimizing changes in foetal heart rate variability later in gestation. Prevention of hypotension with adequate preload and uterine displacement and aggressive treatment with ephedrine if needed, is mandatory. The dose of local anaesthetic for central neuraxial blocks can be reduced by one-third from that for the nonpregnant patient due to the increased vascularity in the spinal canal with epidural vein engorgement. Regional anaesthesia provides excellent postoperative pain control while reducing maternal sedation needs and maintaining FHR variability.
Postoperatively, monitoring of the foetal heart rate and uterine activity should be continued. Preterm labour must be treated aggressively and at the earliest sign. The patient should be kept in a location like the labour or delivery suite and provision of nursing expertise in the surgical recovery area should be made available. Systemic pain medications will reduce the foetal heart rate variability and this should be borne in mind during monitoring. Regional techniques are thus best suited and should be used wherever feasible. The risk of thromboembolism is very high in these patients and hence they should be mobilized early, which also entails good pain relief postoperatively. In the recovery period also, good maternal oxygenation and left uterine displacement should be maintained. The help of a paediatrician should be enlisted in the management of the patients when the foetus is of a viable gestational age so that preterm labour and delivery can be managed as well as counseling for the parents.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 31 R. Gopinath
SPECIAL SITUATIONSThere are specific anaesthetic
considerations for unusual situations like trauma, neurosurgery, foetal surgery and laparoscopic surgeries.
Emergency surgeryAppendicectomy and adnexal masses
are the most frequent conditions needing surgical treatment. In one study, parturients undergoing appendicectomy had an incidence of 18% of postoperative pulmonary oedema or ARDS. Factors of risk for the same were gestational age> 20 weeks, preoperative respiratory rate of more than 24 breaths/ min, preoperative temperature> 100.4 degrees F, a fluid load ( I/O) greater than 4 liters in the first 48 hrs, and concomitant use of tocolytic agents. Anaesthetists should be conservative in fluid management and have central venous pressure monitoring should there be a fluid overload.
TraumaTrauma is the highest cause of maternal
death. Foetal loss in these situations is due to maternal death or placental abruption. An early ultrasound should be done in the emergency room itself to determine viability of the foetus. The mother should receive all needed diagnostic tests to optimize her management, with lead shielding for the foetus when possible. Exposure to less than 5 rad does not increase the risk to the foetus. Ultrasound or MRI is safer.
There are a few indications for emergency caesarean delivery and would include:1. A stable mother with a viable foetus in distress2. Traumatic uterine rupture.3. Gravid uterus interfering with intra-abdominal
repairs in the mother.4. A mother who is unsalvageable with a viable
foetus.
If the foetus is pre-viable or dead, optimizing the mothers’ condition takes precedence. Vaginal delivery at a later date is better than an emergency caesarean section or a laparotomy.
NeurosurgeryNeurosurgical procedures such as an
aneurysm or AVM repair may be required in this age group. All the usual anaesthetics can be used safely and foetal monitoring will be helpful especially when certain techniques are planned.
Induced hypotension reduces uterine perfusion although most agents like SNP, NTG, hydralazine, esmolol, and inhalational agents have been used safely. Foetal monitoring will determine if uterine perfusion is impaired. The anaesthetist should still provide all necessary care for optimal outcome of the mother while informing the surgeon of any concerns. Hyperventilation reduces maternal cardiac output and shifts the ODC to the left thus decreasing release of oxygen to the foetus. High doses of mannitol have been shown to cause foetal dehydration in animals but should not cause concern in the clinical situation. Endovascular management of acute conditions like ruptured intracranial aneurysms has been successfully undertaken during pregnancy. Foetal shielding should be used at all times.
Foetal SurgeryFoetal surgery is performed in very few
centers and for limited indications. The major problem is postoperative preterm labour. Patients often receive preoperative indomethacin and perioperative magnesium sulfate for tocolysis. A high dose of inhalation agents are used for maternal and foetal anaesthesia and for uterine relaxation during surgery and the possibility of reduced uterine perfusion is to be kept in mind.
Laparoscopic surgeryLaparoscopic procedures have been
employed to avoid laparotomy when abdominal pain presents a diagnostic challenge during pregnancy, as well as for some surgical procedures amenable for such surgery like cholecystectomy. Animal studies have shown that pneumoperitoneum with C02 does not cause significant foetal haemodynamic changes, but does induce foetal respiratory acidosis. Normalizing maternal ETC02 produces late and incomplete correction in the foetus. It is important to maintain intra-abdominal pressure as low as possible and limit operative time to the minimum.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 32 R. Gopinath
Arterial sampling for blood gas analysis is necessary to normalize maternal PC02 if the procedure is'prolonged or difficult. Other technical alterations during pregnancy should include foetal shielding during cholangiograms, pneumatic stockings, left lateral table tilt and an open technique for trocar insertion.
Cardiothoracic surgeryCardiothoracic surgery requiring bypass
has also been successfully performed during pregnancy. The increase in blood volume and cardiac output is maximal at 28-30 weeks and this is the time of high risk for decompensation in patients with cardiac lesions as also immediately post partum. After delivery, the release of aortocaval compression and autotransfusion of uteroplacental blood increases the cardiac output maximally. Those who have severe symptoms and are not responsive to medical management, benefit from surgical interventions, and this should, where possible, be performed in the second trimester when the major risk of teratrogenecity due to drugs, radiation and low flow states of bypass is past and pre term labour is less likely. Combined Caesarean section and bypass too have been successfully performed. Surgery should not be withheld if indicated since mortality is comparable in the mother with non-pregnant states.
After 24 weeks gestation, the foetal status should be monitored and uterine displacement maintained to optimize uterine perfusion. Optimal pressures and flow on bypass are controversial and foetal monitoring is a sensitive measure of perfusion and should be used to optimize flows on bypass. Foetal bradycardia commonly occurs during onset of bypass and slowly returns to baseline with little or no beat-to-beat variability. Hypothermia can oe used although some authors advocate warm
heart surgery. It is essential to avoid high dose vasopressors if possible, to prevent its effect on uterine blood flow, however, optimizing the mothers’ condition is the best way to ensure a good outcome for the foetus.
SUMMARYSurgery during pregnancy may be
necessary and anaesthetists should reassure the mother that anaesthetic agents and techniques do not put the foetus or the pregnancy at risk. Prevention of preterm labour is the greatest concern and may require perioperative use of tocolytics. Good postoperative pain management without sedation will aid in early diagnosis and management of preterm labour and mobilization to prevent thromboembolic complications.
REFERENCES
1. Loebstein, R, Lalkin A, Koren G. Pharmacokinetic changes during pregnancy and their clinical relevance. Clin Pharmacokinet 1997 33(5):328-343
2. organ DJ. Drug disposition in mother and fetus. Clin Exp Pharmacol Physiol 1997 24:869-873.
3. Bailey B, Shinya I. Breast-feeding and maternal drug use. Ped Clin North America 1997 44:41-54.
4. Koren G, Pastuszak A, Ito S. Drugs in pregnancy. New Eng J Med 1998: 338(16): 1128-1137.
5. Garland M. Pharmacology of drug transfer across the placenta. Obstet Gynecol Clin Nth Am. 1998 25(1) 21-42.
6. Boiven JF. Risk of spontaneous abortion in women occupationally exposed to anaesthetic gases: a metaanalysis. Occup Environ Med 1997; 54: 541-8.
7. Friedman JM. Teratogen update: anaesthetic agents, Teratology 1988; 37: 69-77.
8. Hunter JG. Carbon dioxide pneumoperitoneum induces foetal acidosis in a pregnant ewe model. Surg Endosc 1995; 9: 272-9.
9. Rosen MA. Management of anaesthesia for the pregnant surgical patient. Anesthesiology 1999; 91: 1159-63.
10. Weiss BM. Outcome of cardiovascular surgery and pregnancy: a systemic review of the period 1984- 1996. Am J Obstet Gynecol 1998; 179: 1643-53.
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 33 Lakshmi Vas
The single most significant major change in the practice of paediatric anaesthesia in the last two decades has been the introduction of regional anaesthetic techniques. Acceptance of the concept that infants and children feel pain and suffer from its consequences has revolutionized the practice of paediatric anaesthesia in that regional anaesthesia and analgesia have become an integral part of paediatric anaesthesia. In children, light general anaesthesia is required to institute regional blocks. The advantages of this technique are minimal general anaesthesia, preemptive analgesia and attenuation of the stress response to surgery.
Lumbar epidural anaesthesia is very useful in children as an epidural catheter can be positioned and the local anaesthetic drug deposited close to the segment of the cord supplying the dermatomes around the proposed surgical incision. The safety is of a lower volume and dose of local anaesthetic, which by a rough formula is 0.1-0.2 ml/kg/segment to be blocked. The catheter passes quite easily in babies even to levels of the cervical cord. The exact placement can be determined by measuring the distance to be traveled, on the catheter. Recently, connecting a nerve stimulator with a metal needle to the saline filled epidural catheter and passing a current will stimulate the segments of the cord at the tip of the catheter and thus confirms the position of the catheter tip. This produces twitches in the muscles supplied by those segments. Position and spread can also be confirmed by omnipaque (iohexol) injection.
In children, the skin-epidural distance varies with age and weight. A rough guide is 1,5mm/ kg till 1 yr and 1 mm/kg thereafter. Since this is a very short distance, care has to \ be taken not to overshoot this distance and puncture
the dura. The exact technique for introducing an epidural needle in children is different from that of adults. In adults, either a hanging drop or a loss of resistance with incremental advancement of the needle identifies the epidural space. In children, hanging drop technique and incremental advancement of needle is not practicable due to the short skin-epidural distance. The needle is continuously and steadily advanced with a continuous checking for loss of resistance to saline. There is a distinct increase in resistance to the advancement of needle tip and also on the plunger of the syringe, when the needle tip enters the ligamentum flavum. The loss of resistance when the needle leaves this ligament and enters the epidural space is also unequivocally distinct.I prefer saline to elicit this, as it is very easy, obvious and avoids the risks of air embolism, which could be catastrophic considering their size and the volumes of air normally injected.
Many drugs have been used for postoperative analgesia. Various authors have used morphine, fentanyl, pethidine, buprenorphine, pentazocine, tramadol, ketamine clonidine, neostigmine and midazolam. Use of the opioid drugs in neonates and infants has to be done in an ICU setting where an anaesthesiologist is constantly available. This is a luxury many of us do not have. So in this age group we rely solely on bupivacaine in a concentration of 0.05 - 0.1- % solution. In older children, we have used ketamine 0.25-0.5 mg/kg and buprenorphine1-2 microgram/kg. Ketamine has the advantage that there is no fear of any possible respiratory depression, but the problem of unpredictability of duration of action and the possibility of hallucinations remain. Buprenorphine, with its extreme lipophilicity, is very predictable in action, lasts about 24-30 hours, and in the dose mentioned has not given any respiratory depression in any of our patients
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 34 LakshmiVas
who number about 1500. However, older children do complain of severe nausea, which requires prophylactic ondansetron and metoclopramide. We have also used midazolam in a dose of 25 mcg/kg along with the initial dose of local anaesthetic to prolong the analgesia.
Admittedly, the lumbar epidural puncture requires an extreme degree of expertise and delicacy than caudal or lumbar epidural anaesthesia in adults. It can be attempted only after sufficient expertise has been obtained in adults and older children. More importantly, a thorough understanding of the technique is very essential to its scientific practice.
There are many aspects of epidural anaesthesia that are different and sometimes unique to paediatrics. As these differences are being investigated, new and fascinating facts emerge about the epidural space, and the technique itself. Of particular interest is the difficulty in passing the catheter in a small neonate, the calculation of volume, its spread, the back leak of injected solutions and pressure changes in response to epidural injections. The calculation of the volume of injection has been arbitrary, based more on a permissible limit of local anaesthetic dose than as a specific volume to cover a specific number of dermatomes.
The negative epidural pressure described by Janzen in 1926 becomes positive on injection of local anaesthetic solutions as seen by the tracking back of injected solutions around the epidural catheter in children. We undertook studies to investigate the change in epidural pressures in response to local anaesthetic injections at two different rates of injection, as well as the spread of two specific volumes of radio opaque dye injected into the epidural space in a controlled manner in 10 infants. The results of these two studies were published in the journal ‘Paediatric anaesthesia’. The abstracts of these two papers are given below.
Study of epidural pressuresThe pressure changes in the epidural
space of 20 infants due to injection of local anaesthetic solutions were studied. The pressures developed during the passage of the epidural needle through the ligaments of the spine
and in the epidural space, during the injection of 1 ml of the local anaesthetic, at two rates of injection, over 1 and 2 minutes and the residual pressure at 1 and 2 minutes after each injection were studied. The mean pressure while the needle was being advanced through the ligamentum flavum was 69.14+ 36.95 mm of Hg. The epidural pressure, after the needle had just penetrated the ligament, without eliciting the loss of resistance, was 1+.9.759 mms of Hg. A distinct pulsatile waveform identical to the pulse waveform was observed as soon as the epidural space was entered. The pressure rise varied according to the rate of injection. The pressures were 27.79mm of Hg when the rate of injection was 1 ml/1 min, with a residual pressure after 1 minute being 12 + 5.53 mm Hg and it was 10.14+5.53 mm Hg after 2 minutes of injection. When the rate of injection was 1ml/ 2min, the pressures were 15.66+ 9.48 with a residual pressure after 1 minute being 14.79+ 5.15mm Hg and 12.93 + 5.46mm Hg after 2 minutes of injection. The residual pressures seem to vary more with the volume injected than the rate of injection or the pressures developed during the injection. The relationship between the rate of injection and pressures is significant when compared with the adults where the pressures have been measured after an injection rate of 1ml/ sec and 1ml/5secs. This is a very fast rate compared to our rates of injection of 1 ml over 1 and 2 minutes. Based on the findings of this study, we recommend a rate of 1ml/ 2minutes in infants. In neonates, a slower rate of injection would be preferable.
DiscussionBack leak of injected anaesthetic is a
common feature of paediatric epidural injections. It is an indicator that a pressure high enough to create a gradient between the epidural space and the atmosphere is being reached. This leak is not normally seen in young adults, in spite of a much faster injection. But this may be seen in old people, where again the pressures may rise, to cause increased spread because of decreased space around the spinal nerves4.
The main determinant of the backleak would be the pressures developed in the epidural space iri response to the injection of local anaesthetic solutions. The faster rates of injection used in adults produce jets of fluid from the 3
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 35 Lakshmi Vas
holes of the catheter. With our 1 ml/min and 1 ml/ 2min injections, in spite of the pressures 59.09mm of Hg (1 ml/1 min) and 34.93 mm of Hg (1 ml/2min) measured at the proximal end of the 90cm long catheter, the drops formed slowly at the side holes in the distal end.
In an infant, the epidural space is a narrow cylinder, where the pressure on injection can rise to very high levels. The spread inside the annular space will likely be as a surge or a slow rise, depending on the rate of injection. Pressing the dura inwards and compressing the cerebrospinal fluid column around the cord can dissipate this rise in pressure. The CSF is supposed to act as a safety valve2 4 by a cephalad displacement. This is questionable because the area of the CSF column is huge compared to the 1.5 cm area of high pressure around the side holes of the catheter. So, it may act as a buffer to absorb the instantaneous pressure rise, without much disturbance to its own pressure or the intracranial pressures. One study8 has shown a sustained rise in the intracranial pressure in response to the epidural injections. Another stud/ of resin injections in the cadaver9 has shown an intracisternal pressure rise with concomitent lumbar epidural space injection. A concomitant measurement of the fontanelle pressures in infants would probably reflect the rise if any in the CSF pressures, due to a cephalad displacement. Another factor limiting the pressure rise, is the leakage of the local anaesthetic through the intervertebral foramina or through the path of least resistance, the cylindrical tract around the catheter made by the larger epidural needle. A sensation of pain, dizziness and nausea on injection has been reported on injection in adults. An increase in the respiratory and pulse rate in anaesthetized children is also known. The infants in this study showed no specific discernible response to the postoperative injections.
Probably high pressures similar to the peak and residual pressures on injection may develop, when the infant is crying, coughing, breath holding or straining to urinate or defaecate etc, though these have not been studied. The possible deleterious effects if any of the pressure rises on injection are not known. The possibility that complications attributed to regional
techniques may actually be compromises of blood supply already present in the patient due to a congenital vascular malformation or compromised blood supply due to hypotension, which got exacerbated by these pressures, remains to be explored.
Any injection through an epidural catheter, even to air requires an effort. Any increased pressure required for injection when the catheter is in the epidural space may not be appreciated by the operator and be attributed to the long length of the catheter or its small internal diameter. This study showed us that, what would be considered as a slight increase in pressure by the hand, translates into significantly high pressures if they were to be measured. This could lead to a complacence, as most operators would be unaware when excessive pressures are being exerted. After measuring the pressures we taught ourselves to moderate the pressures exerted on the piston on the injecting syringe. Also, making the injections slowly over two minutes confers a safety by reducing the pressures exerted.
The epidural pressures just on entering the space varied mainly on the positive side. Only in 3 patients, negative values were observed. The mean pressure was 1+10. Whether this was because of the narrow potential epidural space with pulsating vessels, or a result of positive pressure ventilation or the pressure on the abdomen in the lateral position with the spine flexed, is uncertain.
In a pilot study of 20 other patients done prior to the present study, using loss of resistance, it was surprising to find pressures of 250 mm of mercury when the tip of the needle was in the ligamentum flavum and the column of saline was being bounced against it. The magnitude of this pressure is determined by two factors. One component is the blocking of the fluid column in the advancing needle by the ligament. The second component is the pressure on the plunger by the operator. However, with awareness of this fact, the pressures in the subsequent cases were lowered to 60-150mms of Hg by consciously exerting less pressure on the plunger. The importance of this pressure is that this is the pressure at which the initial small volume (0.5 - 1 ml) of saline is injected into the epidural space
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 36 Lakshmi Vas
to detect loss of resistance. This leads to a sudden rise of pressure, which decreases rapidly as the injection stops, as soon as the loss of resistance is elicited. This pressure leads to fluid leaking back through the needle, which could be mistaken for CSF, and in our initial practice, this was confirmed by a negative test for glucostix7
The ‘feel’ as the needle passes from the interspinous ligament to the ligamentum flavum was very distinct. When the needle tip was in the former, the feel of bouncing on the plunger of the loss of resistance syringe is less and sometimes, it is even possible to inject a small quantity of saline. This could be misinterpreted as a loss of resistance. This is more likely if air is used for loss of resistance. This is confirmed by the epidurogram, where the spread of the dye in the interspinous ligament is seen. However, once the ligamentum flavum is entered, the bouncing of the piston is distinct and it is impossible to inject anything.
One fairly consistent finding was that the ‘give’ on leaving of ligamentum flavum was so pronounced, that we stopped just short of the epidural space. The catheter, on passing, would encounter a flimsy resistance before passing freely into the space. This felt as if a last thin layer of ligamentum was actually pierced by the catheter. Alternately, a part of the bevel might have been still in the ligamentum giving this impression,The pulsatile waveform seen when the epidural needle tip is in the epidural space was a surprise. It was obviously the pulsations transmitted by the epidural arteries or transmitted from the aorta into the epidural space. This was also registered, even through the fluid filled epidural catheter. Does this mean that the epidural pressure varies with the blood pressure in babies? Does this explain the mildly positive pressure that we found in the epidural space? If there is a pulsatile waveform of pressure in the epidural space, is the loss of resistance elicited a relative one from the high pressures in the ligamentum flavum to that of the lower pressure of the epidural space? We did find subatmospheric pressure in3 cases but in the rest, it was positive. This pulsatile waveform is found so consistently in this study that in other infants it became a test for confirming the epidural placement of needle, especially when a small volume was injected to
transmit these pulsations. Only one study in adults refers to these pulsations. This may be because these pulsations are not very obvious in the capacious adult epidural space but are prominent in the narrow space of infants.
The rates of injection in adults were very fast, with 1 ml/sec or 0.5 ml/sec whereas the recommended rate of injection in children of the whole dose is a few ml over 90-120 seconds11 or 1ml /min 15 Our 1ml over 60 and 120 sec is a very slow rate of injection indeed. However, even at these rates, there was a backleak in many of the babies and epidural pressures were higher than that in adults, 27.79 mm of Hg (37.79 cm of water) against 29 cms of water after 1 ml/minute and 15.09 mms of Hg or 20.52 cm of water after1 ml over 2 minutes. These values were obtained after injection through a 17-gauge needle. In contrast, our pressures were obtained after injection through a 20G catheter, with the solution leaking back along the needle track acting as a relief valve mechanism. This probably reflects the small volume epidural space, which is practically a potential space that gets expanded by the injection of even small volumes of local anaesthetic at very slow rates. We did not record the pressure at which backleak occurs, as it was highly variable. Backleak is important, as it prevents an excessive rise in pressure. However, it causes a loss of effective volume of local anaesthetic remaining in the space to exert an effect. The volume of backleak that correlated with the spread requires to be studied. Interestingly, backleak is not seen commonly when the catheter is introduced from the caudal route, though the injection rate is similar with 1ml/2 min. Probably, the fluid tracking back along the catheter pools in the more capacious caudal epidural space, without steep rises in pressure. Could this mean that there is anaesthesia of the sacral segments in addition to the segmental anaesthesia at the tip of the epidural catheter? Could this also explain the retention of urine associated with central neuraxial blocks instituted from the caudal route? This difference in backleak and its causative pressures with the introduction of catheter between lumbar and caudal routes needs to be studied.
In conclusion, there are many unknown effects associated with epidural injection of local
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 37 Lakshmi Vas
anaesthetic solutions. The resting epidural pressure in infants may not always be negative. It is preferable to make static measurements of pressure, as the pressure drop factor would be eliminated. Measurement of dynamic pressures with steady injections from infusion pumps would eliminate the variations due to the manual injections. The pressure rise in response to lumbar epidural injection in infants is considerably higher than that of adults even with very slow rates of injection. It is safer to use a slow rate of injection like 1ml/2min in infants and may be, even slower rates in neonates. Further studies are required to assess the degree of spread vis- a-vis speed of injection, the effect of residual pressure on the spread and the resultant block height, the effect of backleak on the spread, and the correlation of epidural pressures to fontanelle pressures and the difference in attained pressures with lumbar and caudal routes of introduction of catheters.
STUDY OF THE SPREAD OF RADIOOPAQUE DYE: ABSTRACT AND DISCUSSION.Aim
Prospective study to assess whether the extent of spread of the dye in the epidural space would vary in direct proportion to the volume, by injecting two volumes of the dye.
Patients and methods10 infants aged 2 - 3 6 days, (mean +
SD,13.30+13.68) and weighing 1.8 kg-4.5kg (mean + SD,2.60 + 0.97) undergoing major thoracoabdominal surgery under epidural and general anaesthesia were selected. At the end of surgery, two volumes of radioopaque dye (omnipaque) 0.5ml/kg and 1 ml/kg were injected into the epidural space at a rate of 1 ml/2minutes. The spread of the dye was studied by taking X rays after both injections in the left lateral position.
ResultsThere were ten different patterns of spread
in the 10 cases. Uniformly circumferential and cylindrical spread was seen only in one infant. In others, there were segregated patches of anterior and posterior spread with or without interspersed patches of circumferential spread. There was variation in the extent, location and
the density of spread, filling defects and skipped segments with both volumes. Back leak of dye along the needle track was seen in 3 cases. Statistically Segments were 9.30 + 3.68 for 0.5ml, for 1 ml/kg 11.50 + 3.03, 3.03, S, P=0.014. Circumferential spread for 0.5ml/kg 2.70 + 2.16, for 1 ml/kg 5.90 + 3.14 3.59, S, P=0.006 . Anterior spread for 0.5ml/kg 3.60 + 1.58 and for 1 ml/kg 7.90 + 2.33 5.88, S, P=0.001. Posterior spread for 0.5ml/kg 8.20 + 3.71 and for 1 ml/kg 9.80 + 3.68 3.54, S, P=0.006. Doubling of spread with doubling of the volume occurred in only 1 patient. There was a variable increase in the extent or in the density of spread with reduction of skip segments with 1 ml/kg dose than with 0.5 ml/kg. The probable reasons for this variable spread and the mechanism of epidural anaesthesia in the presence of such spread is discussed.
ConclusionThere is a difference in quantitative as
well as qualitative spread in different patients and in the same patient with different volumes. There were statistically significant increases in the number of segments, circumferential, anterior and posterior locations of the 1.0ml group than the 0.5ml group. Both the extent and the density of spread improve with a higher volume but not in direct proportion to the volume. 1 ml/kg has a better quantitative as well as qualitative spread than 0.5ml and has a better chance of producing adequate anaesthesia.
DiscussionThe extent of spread of the local
anaesthetic solutions injected into the pediatric epidural space depends on many factors like the volume of injection 1'3, speed of injection 4‘5, the backleak of the solution in the needle track around the catheter35' leaks through intervertebral foramina7A the pressures achieved in the epidural space36-8 and the inherent divisions of the epidural space10-17. This study was carried out with the purpose of assessing the extent of spread with two different volumes, but as the study progressed, it became apparent that the quality of spread was as varied as the extent. Logically, the spread of a dose of 1 ml/Kg, should be double that of 0.5 ml/Kg in an ideal predictable situation. However, neither the blind procedure of epidural placement of drugs nor the nature of
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 38 Lakshmi Vas
epidural space seemed to be predictable in this study. There were 10 different patterns of spread in the 10 cases with segregation into anterior and posterior patches instead of a uniform circumferential and cylindrical spread. In the same patient, for the two volumes of injection there were differences in the pattern, the density of spread and the leak (more with the higher volume). There were filling defects and skipped segments in both spreads
Doubling of the number of segments covered by the spread with the doubling of the dose occurred in only one patient, but with a large skip of segments in between. In the other patients, though the spread did not double, the density of the spread was better.
The spread of injections in the closed epidural space determines the number of blocked segments, the upper and lower limits of block and the extent of anaesthesia. The quality of anaesthesia and its patchiness if any, are determined by uneven spread. The factors determining the actual spread of the local anaesthetic solution in the epidural space are as follows.
1) The physical divisions within the epidural space10'17
2) The neuraxial spread versus the physical spread of a solution in the epidural space. It has been suggested that there is a subtle distinction between the physical spread of a solution in the epidural space and its neuraxial spread 16 with the former extending beyond the latter.
3) The pressure rise in the closed epidural space in response to injection of space occupying volumes of local anaesthetic solutions, which determines the pressure head, which in turn will determine the spread. The residual pressure after completion of injection in particular, seems to be important in the extent of spread 1'3 6'7
4) The determinants of this pressure, include speed of injection, volume of the injectate, uniformity of injection pressures, the residual pressure after completion of injection, possible transmission and dissipation of pressure to the body of CSF enclosed within the dura mater3'1819'20
leaks along the nerves, along the needle track around the epidural catheter.
5) Leaks that may mean loss of effective volume of local anaesthetic.
Saitoh et al(8) and Burn et al 16 found from radiographic observations in the elderly that there was no correlation between leak through intervertebral foramina and longitudinal spread.
Backleak around a catheter along the needle track is a unique feature of epidural injections in infants and children, probably due to their small capacity epidural spaces. Whether this adds another dimension to the spread of epidurally injected fluids remains to be explored. In this study, backleak was seen in patients 3,7 and 9, especially with a larger dose. But there was more than doubling in the spread with volume in case 9. Apparently the backleak in this baby did not affect the spread.
In the present study, the variables like speed of injection, volume, age and weight were within a uniform range. However, whether the length, breadth and volume of the epidural space, correlate with the body weight is questionable. Since all the injections were performed by the same person (first author) at the same rate (2ml/ min), the pressures were presumed be in a similar range for all the 10 patients. The only unpredictable variable factors were divisions within the epidural space and other determinants of pressure like leaks, pressure on CSF etc.
The most likely reason for the compartmentalization of the injected fluid , the intriguing skipping of segments could be the physical divisions within the epidural space as described in the previous reports of the anatomy of the epidural space.912
Resin injection studies of Harrison et al9 in autopsies of 20 cadavers found that flow of the resin formed a large posterior bulge with thin antero lateral projections on either side. The anterior spread was seen only in 8 out of 20 cases as very thin and incomplete.
Based on cryomicrotone studies of
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 39 Lakshmi Vas
undisturbed anatomy in a fresh cadaver, Hogan 12 considers the epidural space to have metameric segmentations in the longitudinal axis due to the contact of dura with the ligamentum flavum. These segments start from the middle of the upper lamina to the cephalad edge of the lower lamina. Within each segment also, there is a distinct lateral, anterior and posterior compartments. The posterior compartment has a homogenous pad of fat. In the anterior compartment, the posterior longitudinal ligament (PLL) is closely applied to the dura and blends into the annular ligament at the level of a disc as seen in axial sections. Only caudal to the L4-5, do the dura and PLL part, creating a capacious anterior epidural space.
Savolaine et al described a central midline structure called plica mediana dorsalis 10 with the dorsolateral ligaments issuing from the it 916 of which 4 patterns have been described. Many cases of unilateral spread have been attributed to this 16 21
The findings of Hogan are in contrast to those of Savolair.e and Blomberg.
He proposes that injection of the dye by Savolaine et al and air in the epiduroscopy studies of Blomberg distend the epidural fat pad itself with its lateral attenuations and stretch and suspend it in a posterior epidural compartment to give the artifact called plica and lateral membranes.. Based on pictures in the physiologic state in magnetic resonance imaging22, Savolaine also concedes that plica mediana dorsalis is an artifact due to unnatural transmural dural pressures during distension of epidural space by air or fluid .
The present understanding of epidural space based on these studies is thus :
The homogenous fat in the posterior compartment has no fibrous sections and freely separates from the dura and the ligamenta flava. It is attached by a pedicle to the point where the two left and right portions of the ligamenta flava abut with a vessel entering at this point12. This is the space where the epidural needle and catheter are positioned and the local anaesthetic solution is deposited where it spreads to the other two compartments. This freely separable plane provides a route for the injected fluid or air. The
lateral compartment of the epidural space contains nerve roots, vessels and fat. The fat is lobulated by septae with a plane of septation extending from the exiting nerve root to the PLL. This space is important because this is the area where local anaesthetics come in contact with the nerve roots in their dural cuff. The septae in the lateral and anterior compartments can partially obstruct the flow to cause a pressure rise in response to injections, the decay of the pressure and the residual pressures 36 are independent of the volumes injected123
In our study, the divisions within the epidural space could have confined the dye to the posterior and posterolateral epidural space with less consistent spread to the anterior compartment. Since the volume could not spread in a circumferential manner, it might have spread in a linear manner covering a large number of segments. With the doubling of volume, the pressure head for spread would have been higher, facilitating a denser spread, as well as spread into the less compliant anterior compartment. It is also possible that 0.5ml/kg was an inadequate volume to fill the epidural segments and as a result the higher 1 ml/kg improved the quality rather than the extent of spread . To assess the real effect of volume, the lower dose should probably be 1 ml to study the effects on extent of spread and then double this volume to see if the spread doubles
The spread in patient 1, is interesting in that the lower part spread from T11 to L2 had a helical appearance with alternating anterior and posterior densities. The filling defects in the anterior spread are at the intervertebral discs where the dura is described to merge into the PLL. (12) Thus opposite the bodies, there is a spread with the filling defects opposite the discs. Similarly in the posterior spread, it seems as if there is spread in a metameric segment (12) extending from the upper lamina to the cephalad border of the lower lamina. It was as if the dye flowed from posterior distensible interlaminar areas to the next area that was distensible, the anterior space opposite the vertebral body leaving the non compliant areas in between as filling defects.
Perusal of our epidurograms with their
RACE 2003 Ramachandra Anaesthesia Continuing Education

What’s New in Paediatric Epidural Anaesthesia 40 Lakshmi Vas
predominantly posterior and posterolateral spread raises the question, how exactly does epidural anaesthesia act?24 Is it by blocking of the spinal nerves at the intervertebral foramina as they course through the posterolateral epidural space or by diffusion along the dural sleeves towards the cord or through the dura and CSF towards the spinal cord? Is a lack of spread to the anterior aspect of epidural space likely to matter for the quality of anaesthesia?. Do the vagaries of spread explain the reported failure rate of 4- 50 % of cases with epidural anaesthesia?25 27 In the cord itself, is it the posterior aspect with the sensory tracts that require to be blocked, with the anterior tracts of the cord remaining totally or quasi functional? In which case, could this explain the retention of muscle tone and variable levels of motor activity with epidural anaesthesia which contrasts with the total motor paralysis seen with spinal subarachnoid anaesthesia? In the latter, the quantum of local anaesthetic drug with access to the sensory and motor tracts is such that, dense anesthesia of both sensory and motor tracts ensues with resultant analgesia and motor paralysis.
With epidural anaesthesia, the local anaesthetic drug has comparatively easy access to the spinal nerves, particularly the posterior nerve root encased in the dural arachnoid and pia mater. Only the quantity that diffuses into the cerebrospinal fluid through the dural sleeve has access to the spinal cord. Even here, the physical proximity to the posterior sensory tracts would be more than the anterior motor tracts which are geographically more distal. Whether this explains the difference in the quality of motor block between spinal and epidural remains to be explored. 2428 Do the physical barrier of 3 meningeal layers which have to be crossed by the local anaesthetic drug reduce the efficacy of epidurally deposited drug vis-avis density and totality of blockade? These questions could be addressed probably by injection studies of local anaesthetic coloured with a dye into cadavers and then studying the pattern of spread in both epidural and spinal injections. In our patients there was obvious analgesia as evidenced by absence of tachycardia and a stable blood pressure in response to incision. It is probable that the
posterior spread was enough to provide analgesia. Alternatively, the neuraxial spread of local anaesthetic might have been adequate. Burn et al16 found analgesia of the perineum in patients where the spread had not extended below L3 level, highlighting the disparity between physical and neuraxial spread.
In conclusion, there appears to be considerable individual variations in the extent, quality and uniformity of spread. Doubling of the dose does not necessarily double the extent of spread but improves its density and the extent. As a result, use of 1 ml/kg volume is more likely to ensure a better extent and quality of anaesthesia in this age group. However, epidural anaesthesia remains a blind technique where many aspects of the spread of the local anaesthetic agent and the resultant action are yet to be comprehensively elucidated.
References:
1. R. P. Husemeyer and D. C. White. Lumbar Extradural Injection pressures In Pregnant Women, fir. J. Anaesth 1980; 52: 55-592. D.l. Paul, J.A.W. Wildsmith. Extradural pressures following the injection of two volumes of bupivacaine. fir J. Anaesth 1989; 62: 368-3723.Usubiaga JE, Wikinski JA Usubiaga LE. Epidure pressure and its relation to spread of anesthetic solution in the epidural space. Anesth Analg 1967; 46440-446.4. Y.Hirabayashi, R. Shimizu, I. Matsuda and S. Inoue. Effect of extradural compliance and resistance on spread of extradural analgesia, fir. J. Anaesth 1990; 65: 508-513.5. Cardoso MM, Carvalho JC. Epidural pressure and spread of 2% lidocaine in the epidural space: influence of volume and speed of injection of the local anesthetic solution. Reg Anesth Pain Med 1998 ;23:14-9.6. Janzen E. Der negative Vorschlag bei lumbal Punktion. Dtsch. Z. Nervenheilkd 1926;94: 280.7. Lakshmi Vas Phalguni Naregal Savita Sanzgiri, Anupama Negi, Some vagaries of neonatal lumbar anaesthesia. Paediatric Anaesthesia 1999; 9: 217-2238. Hilt H, Gramm H-J, Link J. Changes intracranial pressure associated withanaesthesia, fir. J. Anaesth 1986; 58: 676-680.9. Harrison GR, Parkin IG, Shah JL. Resin injection studies of the lumbar extra dural space. Br J Anaesth 1985; 57: 333-336.10. Edward Savolaine, Jyoti Pandya, Samuel Greenblattet al. Anatomy of the human lumbar epidural space: new insights using CT epidurography. Anesthesiology; 1088; 68: 217-220.11. Bernard Dalens. Lumbar epidural anaesthesia in Regional anaesthesia in infants, children and adolescents. Edited by Bernard Dalens 1sred. Williams and Wilkins. Baltimore, Maryland. 1993, 207-248,12. Bernard Dalens. Regional anesthesia in children. Anesth
RACE 2003 Ramachandra Anaesthesia Continuing Education

What’s New in Paediatric Epidural Anaesthesia 41 Lakshmi Vas
Analg. 1989;68: 654-7213. Hogan OH. Lumbar epidural anatomy. A new look by cryomicrotome section. Anesthesiology 1991; 75: 765-775.14.Blanco D, Mazo V, Ortiz M, Fernandez - Llamazares J.Vidai F. Spread of local anaesthetic into the epidural caudal space for two rates of injection in children. Reg Anesth 1996 ; 21: 442-515. Claude Ecoffey, Anne-Marie Dubousset, Kamran Samii. Lumbar and Thoracic Epidural Anesthesia for Urologic and upper Abdominal Surgery in infants and Children. Anesthesiology 1986; 65:87-90.
References for study of spread of radioopaque dye:
1. D.l. Paul, J.A.W. Wildsmith. Extradural pressures following the injection of two volumes of bupivacaine. Br. J. Anaesth 1989; 62: 368-3722. Cardoso MM, Carvalho JC. Epidural pressure and spread of 2% lidocaine in the epidural space: influence of volume and speed of injection of the local anesthetic solution. Reg Anesth Pain Med 1998 ;23:14-9.3. Vas L , Raghavendran S, Hosalkar H, et al. A study of epidural pressures in infants Paediatric anaesthesia, in press.4. Blanco D, Mazo V, Ortiz M, et al . Spread of local anaesthetic into the epidural caudal space for two rates of injection in children. Reg Anesth 1996 ; 21: 442-55. Vas L, Naregal N, Sanzgiri S, et al. Some vagaries of neonatal lumbar anaesthesia. Paediatric Anaesthesia 1999; 9: 217-2236. Usubiaga JE, Wikinski JA Usubiaga LE. Epidure pressure and its relation to spread of anesthetic solution the epidural space. Anesth Analg 1967; 46440-446.7. Y.Hirabayashi, R. Shimizu, I. Matsuda and S. Inoue. Effect of extradural compliance and resistance on spread of extradural analgsia. Br. J. Anaesth 1990; 65: 508-513.8. Saitoh K, Hirabayashi Y, Shimuzu R etal. Extensive spread in the elderly may not relate to decresed leakage through intervertebral foramina. BJA 1995, 75: 688-691.9. Harrison GR, Parkin IG, Shah JL. Resin injection studies of the lumbar extra dural space. Br J Anaesth 1985; 57: 333-336.10. Edward Savolaine, Jyoti pandya, Samuel Greenblatt et al. Anatomy of the human lumbar epidural space : new insights using CT epidurography. Anesthesiology; 1088; 68: 217-220.11. Bernard Dalens. Regional anesthesia in children. Anesth Analg. 1989;68: 654-7212. Hogan OH. Lumbar epidural anatomy. A new look by cryomicrotome section. Anesthesiology 1991; 75: 765-775.13. BlombergRG. The lumbar subdural extraarachnoid
space of humans: An anatomical study using spinaloscopy in autopsy cases Anesth Analg 1987 : 66: 177-8014. Blomberg RG.. The dorsomedian connective tissue band in the lumbar epidural space of humans An anatomical study using epiduroscopy in autopsy cases Anesth Analg 1986 : 65: 747-5215. Bromage P.R.Burfoot M.F, Crowell D.E. etal. Quality of epidural blockade: influence of physical factors. Br .J. Anaesth 1964; 36:342-352.16. Burn J.M,GuyerP.B,Langdon L, The spread of solutions injected into the epidural spaceA study using epidurograms in patients with lumbosciatic syndrome. Br.J.Anaesth-1973: 45: 338-34517. Slappendel R, Gielen M.J.M, Hasenbos MAWM. Etal. Spread of radioopaque dye in the thoracic epidural space. Anesthesia 1988; 43: 939-942.18. Van Niekerk J Bax-Vermierre B.M.J, Geurts J.W.M etal . Epidurography in premature infants. Anaesthesia 1990, 45: 722-72519. .StienstraR, DahanA.AIhadi etal. Mechanism of action of an epidural Topup in combined spinal epidural anesthesia Anesth Analg 1996;83:382-6.20. Blumgart C,H. Ryall D, Dennison B. Mechanism of extension of spinal anaesthesia by extradural injections of local anaesthetic. Br. J.Anaesth. 1992;69:457-46021. BoezartA P, Computerized axial tomoepidurographic documentation of unilateral epidural analgesia. Can J anaesth 1989; 36 697-70022. SavolaineER: Reply to a letter. Anesthesiology 69:798, 1988.23. Rocco AG, Scott DA, Boas RA etal The epidural space behaves as a Starling resistor and inflow resistance is elevated in diseased epidural space Reg anesth 1990; 15(suppl):3924. Bromage P.R. Mechanism of action of extradural analgesia Br. J.Anaesth. 1975;47:199-212.25. Curatolo M, Orlando A, Zbinden A.M. et al. A multifactorial analysis to explain inadequate surgical analgesia after extradural block..Br J Anaesth 1995; 75:274-281.26. .Tanaka K .WatanabeR, Harada T etal. Extensive application of epidural anaesthesia and analgesia in a university hospital: Incidence of complications related to technique. Regional anaesthesia 1993; 18 :34-3827. Seeberger M.D Lang M.L.Drewe J et al Comparison of spinal and epidural anesthesia for patients younger than 50 years of age.Anesth Analg1994;78667-73..Huang JS, lYY.TungCC etal Comparison between the effects of epidural and spinal anesthesia for elective cesarian section; Chung Hua Hsueh Tsa Chih (Chin Med J) 1993;51: 40-7
RACE 2003 Ramachandra Anaesthesia Continuing Education
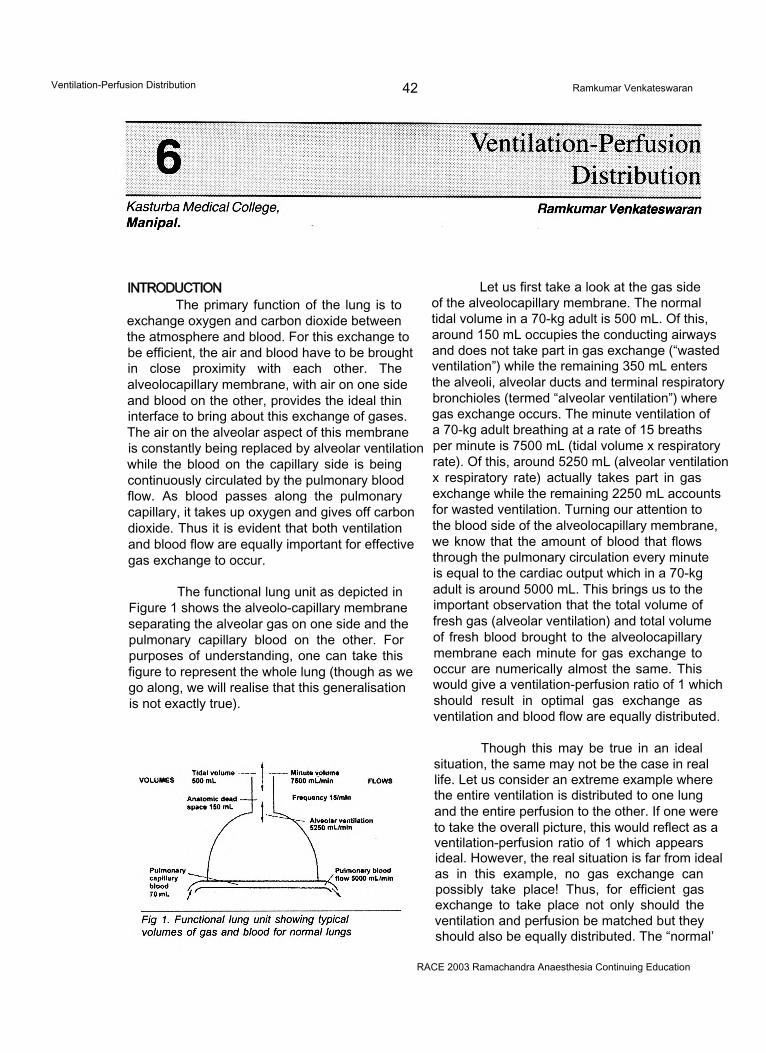
Ventilation-Perfusion Distribution 42 Ramkumar Venkateswaran
INTRODUCTIONThe primary function of the lung is to
exchange oxygen and carbon dioxide between the atmosphere and blood. For this exchange to be efficient, the air and blood have to be brought in close proximity with each other. The alveolocapillary membrane, with air on one side and blood on the other, provides the ideal thin interface to bring about this exchange of gases. The air on the alveolar aspect of this membrane is constantly being replaced by alveolar ventilation while the blood on the capillary side is being continuously circulated by the pulmonary blood flow. As blood passes along the pulmonary capillary, it takes up oxygen and gives off carbon dioxide. Thus it is evident that both ventilation and blood flow are equally important for effective gas exchange to occur.
The functional lung unit as depicted in Figure 1 shows the alveolo-capillary membrane separating the alveolar gas on one side and the pulmonary capillary blood on the other. For purposes of understanding, one can take this figure to represent the whole lung (though as we go along, we will realise that this generalisation is not exactly true).
Let us first take a look at the gas side of the alveolocapillary membrane. The normal tidal volume in a 70-kg adult is 500 mL. Of this, around 150 mL occupies the conducting airways and does not take part in gas exchange (“wasted ventilation”) while the remaining 350 mL enters the alveoli, alveolar ducts and terminal respiratory bronchioles (termed “alveolar ventilation”) where gas exchange occurs. The minute ventilation of a 70-kg adult breathing at a rate of 15 breaths per minute is 7500 mL (tidal volume x respiratory rate). Of this, around 5250 mL (alveolar ventilation x respiratory rate) actually takes part in gas exchange while the remaining 2250 mL accounts for wasted ventilation. Turning our attention to the blood side of the alveolocapillary membrane, we know that the amount of blood that flows through the pulmonary circulation every minute is equal to the cardiac output which in a 70-kg adult is around 5000 mL. This brings us to the important observation that the total volume of fresh gas (alveolar ventilation) and total volume of fresh blood brought to the alveolocapillary membrane each minute for gas exchange to occur are numerically almost the same. This would give a ventilation-perfusion ratio of 1 which should result in optimal gas exchange as ventilation and blood flow are equally distributed.
Though this may be true in an ideal situation, the same may not be the case in real life. Let us consider an extreme example where the entire ventilation is distributed to one lung and the entire perfusion to the other. If one were to take the overall picture, this would reflect as a ventilation-perfusion ratio of 1 which appears ideal. However, the real situation is far from ideal as in this example, no gas exchange can possibly take place! Thus, for efficient gas exchange to take place not only should the ventilation and perfusion be matched but they should also be equally distributed. The “normal’
RACE 2003 Ramachandra Anaesthesia Continuing Education
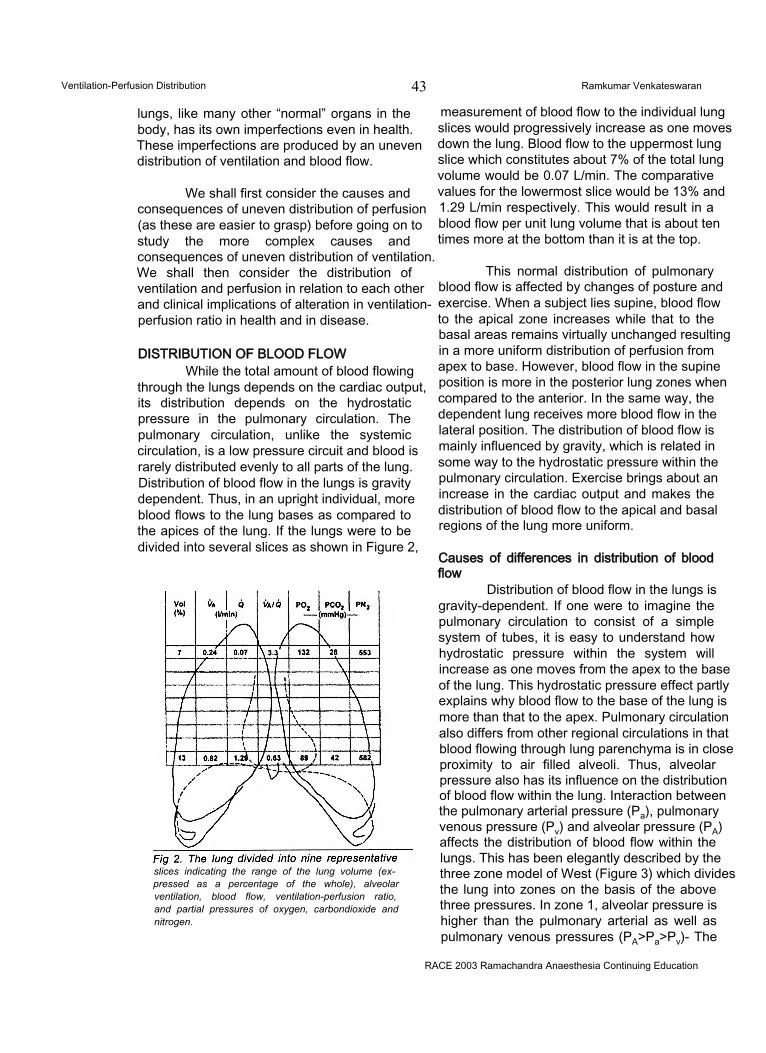
Ventilation-Perfusion Distribution 43 Ramkumar Venkateswaran
lungs, like many other “normal” organs in the body, has its own imperfections even in health. These imperfections are produced by an uneven distribution of ventilation and blood flow.
We shall first consider the causes and consequences of uneven distribution of perfusion (as these are easier to grasp) before going on to study the more complex causes and consequences of uneven distribution of ventilation. We shall then consider the distribution of ventilation and perfusion in relation to each other and clinical implications of alteration in ventilation- perfusion ratio in health and in disease.
DISTRIBUTION OF BLOOD FLOWWhile the total amount of blood flowing
through the lungs depends on the cardiac output, its distribution depends on the hydrostatic pressure in the pulmonary circulation. The pulmonary circulation, unlike the systemic circulation, is a low pressure circuit and blood is rarely distributed evenly to all parts of the lung. Distribution of blood flow in the lungs is gravity dependent. Thus, in an upright individual, more blood flows to the lung bases as compared to the apices of the lung. If the lungs were to be divided into several slices as shown in Figure 2,
slices indicating the range of the lung volume (expressed as a percentage of the whole), alveolar ventilation, blood flow, ventilation-perfusion ratio, and partial pressures of oxygen, carbondioxide and nitrogen.
measurement of blood flow to the individual lung slices would progressively increase as one moves down the lung. Blood flow to the uppermost lung slice which constitutes about 7% of the total lung volume would be 0.07 L/min. The comparative values for the lowermost slice would be 13% and 1.29 L/min respectively. This would result in a blood flow per unit lung volume that is about ten times more at the bottom than it is at the top.
This normal distribution of pulmonary blood flow is affected by changes of posture and exercise. When a subject lies supine, blood flow to the apical zone increases while that to the basal areas remains virtually unchanged resulting in a more uniform distribution of perfusion from apex to base. However, blood flow in the supine position is more in the posterior lung zones when compared to the anterior. In the same way, the dependent lung receives more blood flow in the lateral position. The distribution of blood flow is mainly influenced by gravity, which is related in some way to the hydrostatic pressure within the pulmonary circulation. Exercise brings about an increase in the cardiac output and makes the distribution of blood flow to the apical and basal regions of the lung more uniform.
Causes of differences in distribution of blood flow
Distribution of blood flow in the lungs is gravity-dependent. If one were to imagine the pulmonary circulation to consist of a simple system of tubes, it is easy to understand how hydrostatic pressure within the system will increase as one moves from the apex to the base of the lung. This hydrostatic pressure effect partly explains why blood flow to the base of the lung is more than that to the apex. Pulmonary circulation also differs from other regional circulations in that blood flowing through lung parenchyma is in close proximity to air filled alveoli. Thus, alveolar pressure also has its influence on the distribution of blood flow within the lung. Interaction between the pulmonary arterial pressure (Pa), pulmonary venous pressure (Pv) and alveolar pressure (PA) affects the distribution of blood flow within the lungs. This has been elegantly described by the three zone model of West (Figure 3) which divides the lung into zones on the basis of the above three pressures. In zone 1, alveolar pressure is higher than the pulmonary arterial as well as pulmonary venous pressures (PA>Pa>Pv)- The
RACE 2003 Ramachandra Anaesthesia Continuing Education
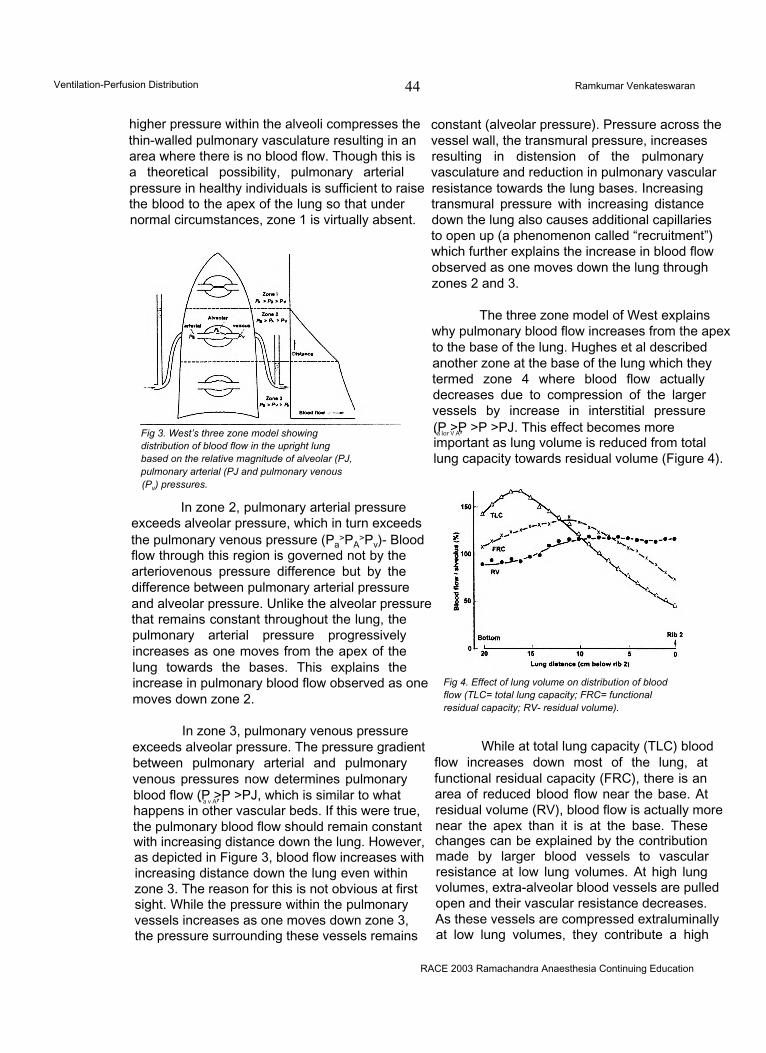
Ventilation-Perfusion Distribution 44 Ramkumar Venkateswaran
higher pressure within the alveoli compresses the thin-walled pulmonary vasculature resulting in an area where there is no blood flow. Though this is a theoretical possibility, pulmonary arterial pressure in healthy individuals is sufficient to raise the blood to the apex of the lung so that under normal circumstances, zone 1 is virtually absent.
Fig 3. West’s three zone model showing distribution of blood flow in the upright lung based on the relative magnitude of alveolar (PJ, pulmonary arterial (PJ and pulmonary venous (Pv) pressures.
In zone 2, pulmonary arterial pressure exceeds alveolar pressure, which in turn exceeds the pulmonary venous pressure (Pa
>PA>Pv)- Blood
flow through this region is governed not by the arteriovenous pressure difference but by the difference between pulmonary arterial pressure and alveolar pressure. Unlike the alveolar pressure that remains constant throughout the lung, the pulmonary arterial pressure progressively increases as one moves from the apex of the lung towards the bases. This explains the increase in pulmonary blood flow observed as one moves down zone 2.
In zone 3, pulmonary venous pressure exceeds alveolar pressure. The pressure gradient between pulmonary arterial and pulmonary venous pressures now determines pulmonary blood flow (P >P >PJ, which is similar to whatx a v A7 1
happens in other vascular beds. If this were true, the pulmonary blood flow should remain constant with increasing distance down the lung. However, as depicted in Figure 3, blood flow increases with increasing distance down the lung even within zone 3. The reason for this is not obvious at first sight. While the pressure within the pulmonary vessels increases as one moves down zone 3, the pressure surrounding these vessels remains
constant (alveolar pressure). Pressure across the vessel wall, the transmural pressure, increases resulting in distension of the pulmonary vasculature and reduction in pulmonary vascular resistance towards the lung bases. Increasing transmural pressure with increasing distance down the lung also causes additional capillaries to open up (a phenomenon called “recruitment”) which further explains the increase in blood flow observed as one moves down the lung through zones 2 and 3.
The three zone model of West explains why pulmonary blood flow increases from the apex to the base of the lung. Hughes et al described another zone at the base of the lung which they termed zone 4 where blood flow actually decreases due to compression of the larger vessels by increase in interstitial pressure (P >P >P >PJ. This effect becomes more' a lor V A7
important as lung volume is reduced from total lung capacity towards residual volume (Figure 4).
Fig 4. Effect of lung volume on distribution of blood flow (TLC= total lung capacity; FRC= functional residual capacity; RV- residual volume).
While at total lung capacity (TLC) blood flow increases down most of the lung, at functional residual capacity (FRC), there is an area of reduced blood flow near the base. At residual volume (RV), blood flow is actually more near the apex than it is at the base. These changes can be explained by the contribution made by larger blood vessels to vascular resistance at low lung volumes. At high lung volumes, extra-alveolar blood vessels are pulled open and their vascular resistance decreases. As these vessels are compressed extraluminally at low lung volumes, they contribute a high
RACE 2003 Ramachandra Anaesthesia Continuing Education
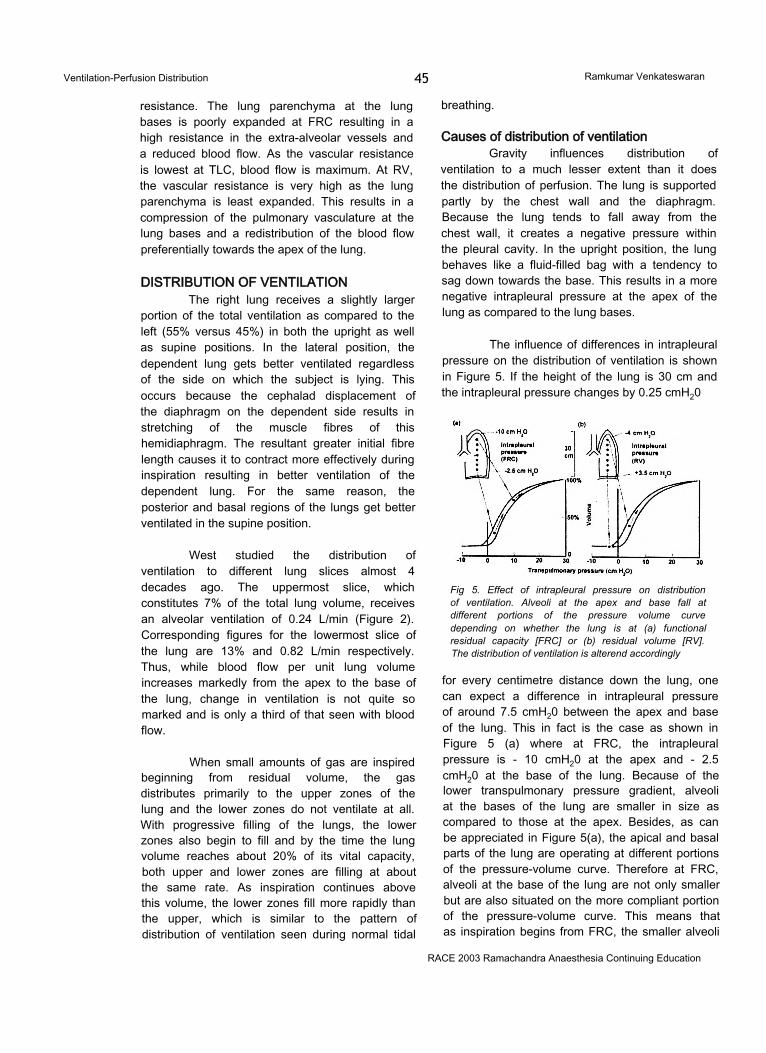
Ventilation-Perfusion Distribution 45 Ramkumar Venkateswaran
resistance. The lung parenchyma at the lung bases is poorly expanded at FRC resulting in a high resistance in the extra-alveolar vessels and a reduced blood flow. As the vascular resistance is lowest at TLC, blood flow is maximum. At RV, the vascular resistance is very high as the lung parenchyma is least expanded. This results in a compression of the pulmonary vasculature at the lung bases and a redistribution of the blood flow preferentially towards the apex of the lung.
DISTRIBUTION OF VENTILATIONThe right lung receives a slightly larger
portion of the total ventilation as compared to the left (55% versus 45%) in both the upright as well as supine positions. In the lateral position, the dependent lung gets better ventilated regardless of the side on which the subject is lying. This occurs because the cephalad displacement of the diaphragm on the dependent side results in stretching of the muscle fibres of this hemidiaphragm. The resultant greater initial fibre length causes it to contract more effectively during inspiration resulting in better ventilation of the dependent lung. For the same reason, the posterior and basal regions of the lungs get better ventilated in the supine position.
West studied the distribution of ventilation to different lung slices almost 4 decades ago. The uppermost slice, which constitutes 7% of the total lung volume, receives an alveolar ventilation of 0.24 L/min (Figure 2). Corresponding figures for the lowermost slice of the lung are 13% and 0.82 L/min respectively. Thus, while blood flow per unit lung volume increases markedly from the apex to the base of the lung, change in ventilation is not quite so marked and is only a third of that seen with blood flow.
When small amounts of gas are inspired beginning from residual volume, the gas distributes primarily to the upper zones of the lung and the lower zones do not ventilate at all. With progressive filling of the lungs, the lower zones also begin to fill and by the time the lung volume reaches about 20% of its vital capacity, both upper and lower zones are filling at about the same rate. As inspiration continues above this volume, the lower zones fill more rapidly than the upper, which is similar to the pattern of distribution of ventilation seen during normal tidal
breathing.
Causes of distribution of ventilationGravity influences distribution of
ventilation to a much lesser extent than it does the distribution of perfusion. The lung is supported partly by the chest wall and the diaphragm. Because the lung tends to fall away from the chest wall, it creates a negative pressure within the pleural cavity. In the upright position, the lung behaves like a fluid-filled bag with a tendency to sag down towards the base. This results in a more negative intrapleural pressure at the apex of the lung as compared to the lung bases.
The influence of differences in intrapleural pressure on the distribution of ventilation is shown in Figure 5. If the height of the lung is 30 cm and the intrapleural pressure changes by 0.25 cmH20
Fig 5. Effect of intrapleural pressure on distribution of ventilation. Alveoli at the apex and base fall at different portions of the pressure volume curve depending on whether the lung is at (a) functional residual capacity [FRC] or (b) residual volume [RV]. The distribution of ventilation is alterend accordingly
for every centimetre distance down the lung, one can expect a difference in intrapleural pressure of around 7.5 cmH20 between the apex and base of the lung. This in fact is the case as shown in Figure 5 (a) where at FRC, the intrapleural pressure is - 10 cmH20 at the apex and - 2.5 cmH20 at the base of the lung. Because of the lower transpulmonary pressure gradient, alveoli at the bases of the lung are smaller in size as compared to those at the apex. Besides, as can be appreciated in Figure 5(a), the apical and basal parts of the lung are operating at different portions of the pressure-volume curve. Therefore at FRC, alveoli at the base of the lung are not only smaller but are also situated on the more compliant portion of the pressure-volume curve. This means that as inspiration begins from FRC, the smaller alveoli
RACE 2003 Ramachandra Anaesthesia Continuing Education
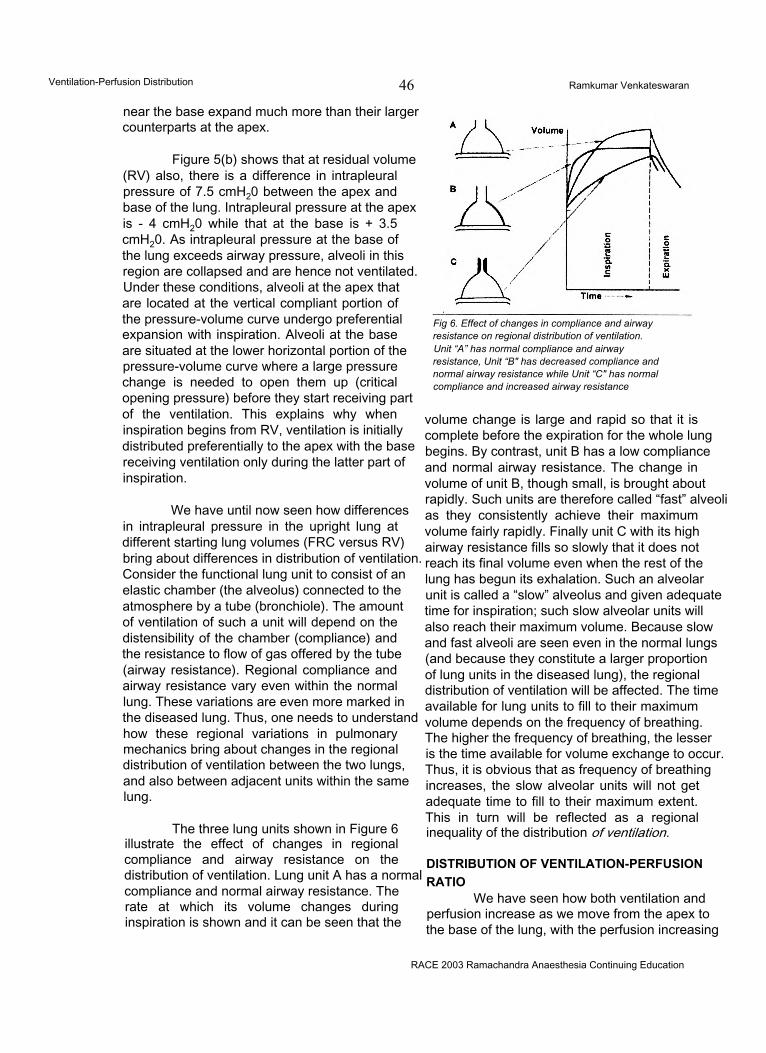
Ventilation-Perfusion Distribution 46 Ramkumar Venkateswaran
near the base expand much more than their larger counterparts at the apex.
Figure 5(b) shows that at residual volume (RV) also, there is a difference in intrapleural pressure of 7.5 cmH20 between the apex and base of the lung. Intrapleural pressure at the apex is - 4 cmH20 while that at the base is + 3.5 cmH20. As intrapleural pressure at the base of the lung exceeds airway pressure, alveoli in this region are collapsed and are hence not ventilated. Under these conditions, alveoli at the apex that are located at the vertical compliant portion of the pressure-volume curve undergo preferential expansion with inspiration. Alveoli at the base are situated at the lower horizontal portion of the pressure-volume curve where a large pressure change is needed to open them up (critical opening pressure) before they start receiving part of the ventilation. This explains why when inspiration begins from RV, ventilation is initially distributed preferentially to the apex with the base receiving ventilation only during the latter part of inspiration.
We have until now seen how differences in intrapleural pressure in the upright lung at different starting lung volumes (FRC versus RV) bring about differences in distribution of ventilation. Consider the functional lung unit to consist of an elastic chamber (the alveolus) connected to the atmosphere by a tube (bronchiole). The amount of ventilation of such a unit will depend on the distensibility of the chamber (compliance) and the resistance to flow of gas offered by the tube (airway resistance). Regional compliance and airway resistance vary even within the normal lung. These variations are even more marked in the diseased lung. Thus, one needs to understand how these regional variations in pulmonary mechanics bring about changes in the regional distribution of ventilation between the two lungs, and also between adjacent units within the same lung.
The three lung units shown in Figure 6 illustrate the effect of changes in regional compliance and airway resistance on the distribution of ventilation. Lung unit A has a normal compliance and normal airway resistance. The rate at which its volume changes during inspiration is shown and it can be seen that the
Fig 6. Effect of changes in compliance and airway resistance on regional distribution of ventilation.Unit “A” has normal compliance and airway resistance, Unit “B" has decreased compliance and normal airway resistance while Unit “C" has normal compliance and increased airway resistance
volume change is large and rapid so that it is complete before the expiration for the whole lung begins. By contrast, unit B has a low compliance and normal airway resistance. The change in volume of unit B, though small, is brought about rapidly. Such units are therefore called “fast” alveoli as they consistently achieve their maximum volume fairly rapidly. Finally unit C with its high airway resistance fills so slowly that it does not reach its final volume even when the rest of the lung has begun its exhalation. Such an alveolar unit is called a “slow” alveolus and given adequate time for inspiration; such slow alveolar units will also reach their maximum volume. Because slow and fast alveoli are seen even in the normal lungs (and because they constitute a larger proportion of lung units in the diseased lung), the regional distribution of ventilation will be affected. The time available for lung units to fill to their maximum volume depends on the frequency of breathing. The higher the frequency of breathing, the lesser is the time available for volume exchange to occur. Thus, it is obvious that as frequency of breathing increases, the slow alveolar units will not get adequate time to fill to their maximum extent. This in turn will be reflected as a regional inequality of the distribution of ventilation.
DISTRIBUTION OF VENTILATION-PERFUSION RATIO
We have seen how both ventilation and perfusion increase as we move from the apex to the base of the lung, with the perfusion increasing
RACE 2003 Ramachandra Anaesthesia Continuing Education
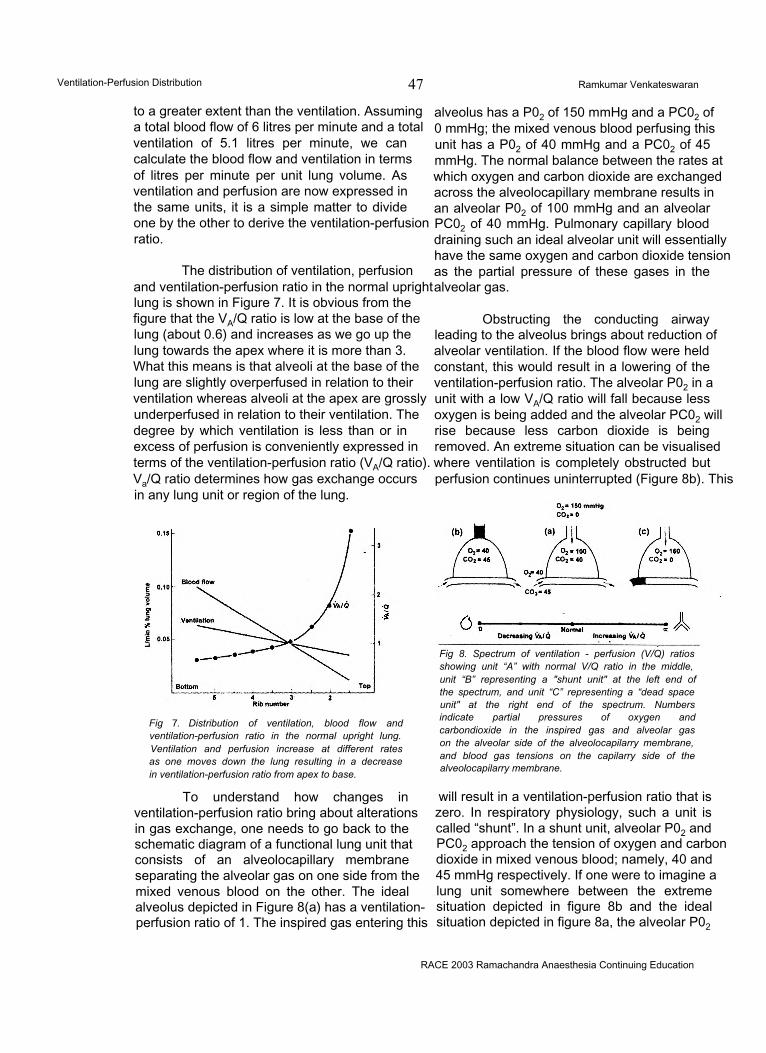
Ventilation-Perfusion Distribution 47 Ramkumar Venkateswaran
to a greater extent than the ventilation. Assuming a total blood flow of 6 litres per minute and a total ventilation of 5.1 litres per minute, we can calculate the blood flow and ventilation in terms of litres per minute per unit lung volume. As ventilation and perfusion are now expressed in the same units, it is a simple matter to divide one by the other to derive the ventilation-perfusion ratio.
The distribution of ventilation, perfusion and ventilation-perfusion ratio in the normal upright lung is shown in Figure 7. It is obvious from the figure that the VA/Q ratio is low at the base of the lung (about 0.6) and increases as we go up the lung towards the apex where it is more than 3. What this means is that alveoli at the base of the lung are slightly overperfused in relation to their ventilation whereas alveoli at the apex are grossly underperfused in relation to their ventilation. The degree by which ventilation is less than or in excess of perfusion is conveniently expressed in terms of the ventilation-perfusion ratio (VA/Q ratio). Va/Q ratio determines how gas exchange occurs in any lung unit or region of the lung.
Fig 7. Distribution of ventilation, blood flow and ventilation-perfusion ratio in the normal upright lung. Ventilation and perfusion increase at different rates as one moves down the lung resulting in a decrease in ventilation-perfusion ratio from apex to base.
To understand how changes in ventilation-perfusion ratio bring about alterations in gas exchange, one needs to go back to the schematic diagram of a functional lung unit that consists of an alveolocapillary membrane separating the alveolar gas on one side from the mixed venous blood on the other. The ideal alveolus depicted in Figure 8(a) has a ventilation- perfusion ratio of 1. The inspired gas entering this
RACE 2003 Ramachandra Anaesthesia Continuing Education
alveolus has a P02 of 150 mmHg and a PC02 of 0 mmHg; the mixed venous blood perfusing this unit has a P02 of 40 mmHg and a PC02 of 45 mmHg. The normal balance between the rates at which oxygen and carbon dioxide are exchanged across the alveolocapillary membrane results in an alveolar P02 of 100 mmHg and an alveolar PC02 of 40 mmHg. Pulmonary capillary blood draining such an ideal alveolar unit will essentially have the same oxygen and carbon dioxide tension as the partial pressure of these gases in the alveolar gas.
Obstructing the conducting airway leading to the alveolus brings about reduction of alveolar ventilation. If the blood flow were held constant, this would result in a lowering of the ventilation-perfusion ratio. The alveolar P02 in a unit with a low VA/Q ratio will fall because less oxygen is being added and the alveolar PC02 will rise because less carbon dioxide is being removed. An extreme situation can be visualised where ventilation is completely obstructed but perfusion continues uninterrupted (Figure 8b). This
Fig 8. Spectrum of ventilation - perfusion (V/Q) ratios showing unit “A” with normal V/Q ratio in the middle, unit “B” representing a "shunt unit" at the left end of the spectrum, and unit “C” representing a “dead space unit" at the right end of the spectrum. Numbers indicate partial pressures of oxygen and carbondioxide in the inspired gas and alveolar gas on the alveolar side of the alveolocapilarry membrane, and blood gas tensions on the capilarry side of the alveolocapilarry membrane.
will result in a ventilation-perfusion ratio that is zero. In respiratory physiology, such a unit is called “shunt”. In a shunt unit, alveolar P02 and PC02 approach the tension of oxygen and carbon dioxide in mixed venous blood; namely, 40 and 45 mmHg respectively. If one were to imagine a lung unit somewhere between the extreme situation depicted in figure 8b and the ideal situation depicted in figure 8a, the alveolar P02

Ventilation-Perfusion Distribution 48 Ramkumar Venkateswaran
would be in between 40 and 100 mmHg (while the alveolar PC02 would lie in between 45 to 40 mmHg). Alveoli at the base of the lung have a VA/ Q ratio of less than 1 and would therefore fall along the spectrum of VA/Q ratios to the left of the normal alveolus as shown at the bottom of figure 8.
What would happen if on the other hand, one gradually obstructs perfusion leaving ventilation undisturbed, thus increasing the VA/Q ratio? The alveolar P02 would rise because less oxygen is being removed, and the alveolar PC02 would fall because less carbon dioxide is being excreted. An extreme situation results when perfusion to a lung unit is completely obstructed with ventilation continuing uninterrupted. This will lead to a VA/Q ratio of infinity. In respiratory physiology, such a unit where ventilation is wasted constitutes “dead space”. In an extreme situation as described above, the composition of the alveolar gas becomes identical with that of inspired gas with a P02 of 150 mmHg and a PC02 of 0 mmHg. Alveoli at the apex of the lung have Va/Q ratios that are typically more than 3. The alveolar P02 and PC02 in alveolar units nearer the apex of the lung will therefore lie somewhere between the ideal alveolar unit shown in figure 8a and the dead space unit shown in figure 8c (with alveolar P02 being between 100 and 150 mmHg and alveolar PC02 being between 40 and 0 mmHg). Apical alveoli will lie along a spectrum of Va/Q ratios to the right of the normal alveolus as shown at the bottom of figure 8.
A reference to figure 2 shows that alveolar units at the apex of the lung with higher VA/Q
ratios have a P02 of 132 mmHg and PC02 of 28 mmHg while those at the base of the lung with lower Va/Q ratios have P02 and PC02 values of 89 mmHg and 42 mmHg respectively.
SUMMARYWe have until now seen how even in the
healthy lung, ventilation and perfusion are not uniformly distributed throughout the lung. We know that though both ventilation and perfusion increase progressively as we move from the apex to the base of the lung, the increase is more significant and rapid with perfusion. The ventilation-perfusion ratio therefore decreases as we move from the apex to the base of the lung. For alveolar units to exchange oxygen and carbon dioxide in a perfect manner, they should have their ventilation and perfusion also perfectly matched. Such an ideal situation does not exist even in the normal lung. Despite variations in ventilation- perfusion ratio, healthy lungs still bring about effective and nearly perfect gas exchange. The situation is different when one considers a diseased lung where gross VA/Q inequalities occur. These VA/Q inequalities have adverse effects on gas exchange that manifest as hypoxaemia and hypercarbia. An understanding of the effects of altered distribution of ventilation and perfusion on gas exchange helps one to appreciate and treat pathological lung conditions. It is hoped that this review has provided the reader with such an insight.
References1. West JB. Ventilation/blood flow and gas exchange. 3rd Edition. Oxford : Blackwell Scientific Publications, 1977.2. Lumb AB. Nunn’s Applied Respiratory Physiology. 5th Edition. Oxford : Butterworth Heinemann, 2000.
RACE 2003 Ramachandra Anaesthesia Continuing Education
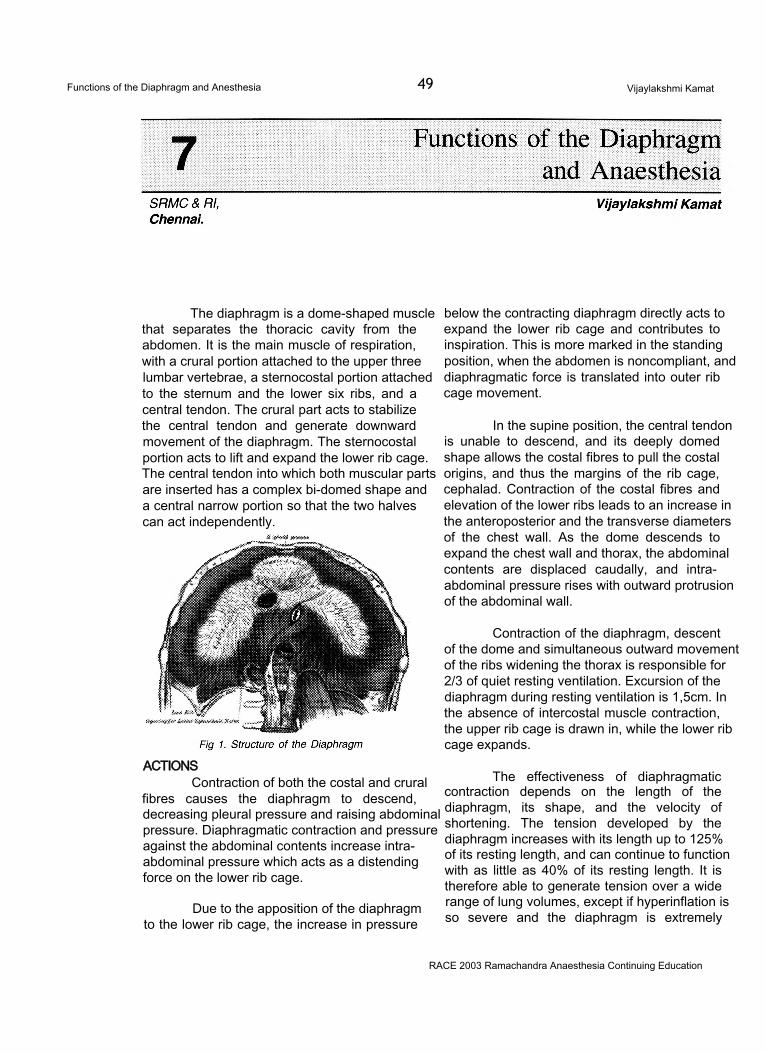
Functions of the Diaphragm and Anesthesia 49 Vijaylakshmi Kamat
The diaphragm is a dome-shaped muscle that separates the thoracic cavity from the abdomen. It is the main muscle of respiration, with a crural portion attached to the upper three lumbar vertebrae, a sternocostal portion attached to the sternum and the lower six ribs, and a central tendon. The crural part acts to stabilize the central tendon and generate downward movement of the diaphragm. The sternocostal portion acts to lift and expand the lower rib cage. The central tendon into which both muscular parts are inserted has a complex bi-domed shape and a central narrow portion so that the two halves can act independently.
ACTIONSContraction of both the costal and crural
fibres causes the diaphragm to descend, decreasing pleural pressure and raising abdominal pressure. Diaphragmatic contraction and pressure against the abdominal contents increase intraabdominal pressure which acts as a distending force on the lower rib cage.
Due to the apposition of the diaphragm to the lower rib cage, the increase in pressure
below the contracting diaphragm directly acts to expand the lower rib cage and contributes to inspiration. This is more marked in the standing position, when the abdomen is noncompliant, and diaphragmatic force is translated into outer rib cage movement.
In the supine position, the central tendon is unable to descend, and its deeply domed shape allows the costal fibres to pull the costal origins, and thus the margins of the rib cage, cephalad. Contraction of the costal fibres and elevation of the lower ribs leads to an increase in the anteroposterior and the transverse diameters of the chest wall. As the dome descends to expand the chest wall and thorax, the abdominal contents are displaced caudally, and intraabdominal pressure rises with outward protrusion of the abdominal wall.
Contraction of the diaphragm, descent of the dome and simultaneous outward movement of the ribs widening the thorax is responsible for 2/3 of quiet resting ventilation. Excursion of the diaphragm during resting ventilation is 1,5cm. In the absence of intercostal muscle contraction, the upper rib cage is drawn in, while the lower rib cage expands.
The effectiveness of diaphragmatic contraction depends on the length of the diaphragm, its shape, and the velocity of shortening. The tension developed by the diaphragm increases with its length up to 125% of its resting length, and can continue to function with as little as 40% of its resting length. It is therefore able to generate tension over a wide range of lung volumes, except if hyperinflation is so severe and the diaphragm is extremely
RACE 2003 Ramachandra Anaesthesia Continuing Education
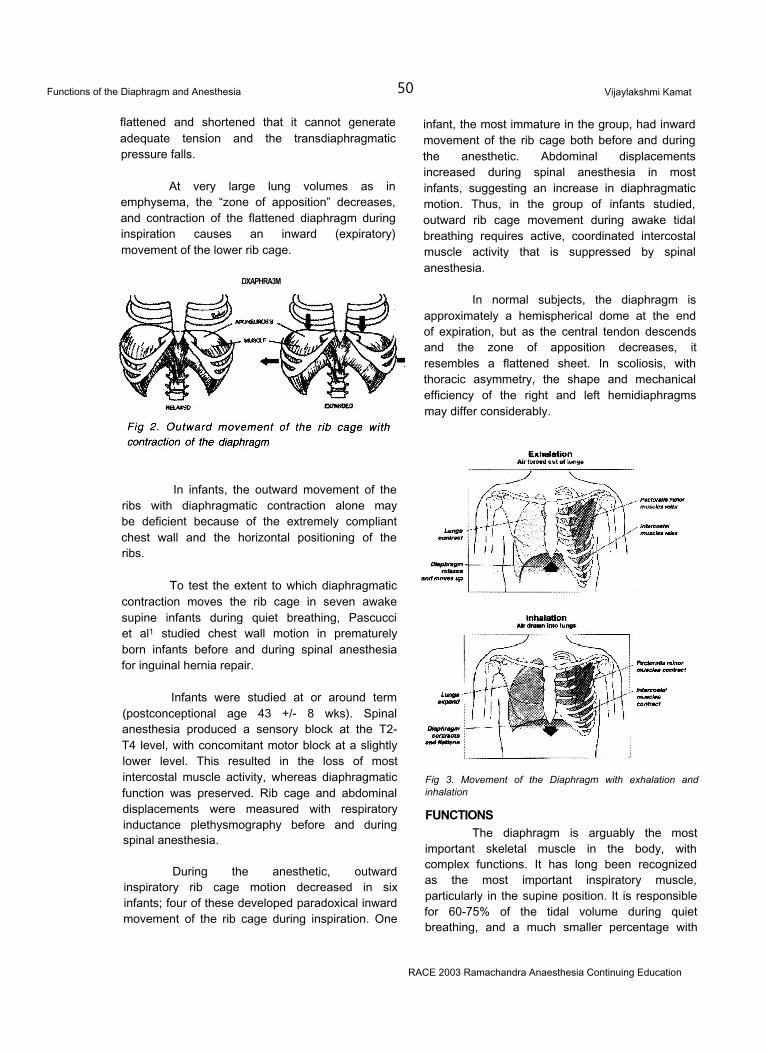
Functions of the Diaphragm and Anesthesia 50 Vijaylakshmi Kamat
flattened and shortened that it cannot generate adequate tension and the transdiaphragmatic pressure falls.
At very large lung volumes as in emphysema, the “zone of apposition” decreases, and contraction of the flattened diaphragm during inspiration causes an inward (expiratory) movement of the lower rib cage.
DXAPHRA3M
In infants, the outward movement of the ribs with diaphragmatic contraction alone may be deficient because of the extremely compliant chest wall and the horizontal positioning of the ribs.
To test the extent to which diaphragmatic contraction moves the rib cage in seven awake supine infants during quiet breathing, Pascucci et al1 studied chest wall motion in prematurely born infants before and during spinal anesthesia for inguinal hernia repair.
Infants were studied at or around term (postconceptional age 43 +/- 8 wks). Spinal anesthesia produced a sensory block at the T2- T4 level, with concomitant motor block at a slightly lower level. This resulted in the loss of most intercostal muscle activity, whereas diaphragmatic function was preserved. Rib cage and abdominal displacements were measured with respiratory inductance plethysmography before and during spinal anesthesia.
During the anesthetic, outward inspiratory rib cage motion decreased in six infants; four of these developed paradoxical inward movement of the rib cage during inspiration. One
infant, the most immature in the group, had inward movement of the rib cage both before and during the anesthetic. Abdominal displacements increased during spinal anesthesia in most infants, suggesting an increase in diaphragmatic motion. Thus, in the group of infants studied, outward rib cage movement during awake tidal breathing requires active, coordinated intercostal muscle activity that is suppressed by spinal anesthesia.
In normal subjects, the diaphragm is approximately a hemispherical dome at the end of expiration, but as the central tendon descends and the zone of apposition decreases, it resembles a flattened sheet. In scoliosis, with thoracic asymmetry, the shape and mechanical efficiency of the right and left hemidiaphragms may differ considerably.
Fig 3. Movement of the Diaphragm with exhalation and inhalation
FUNCTIONSThe diaphragm is arguably the most
important skeletal muscle in the body, with complex functions. It has long been recognized as the most important inspiratory muscle, particularly in the supine position. It is responsible for 60-75% of the tidal volume during quiet breathing, and a much smaller percentage with
RACE 2003 Ramachandra Anaesthesia Continuing Education
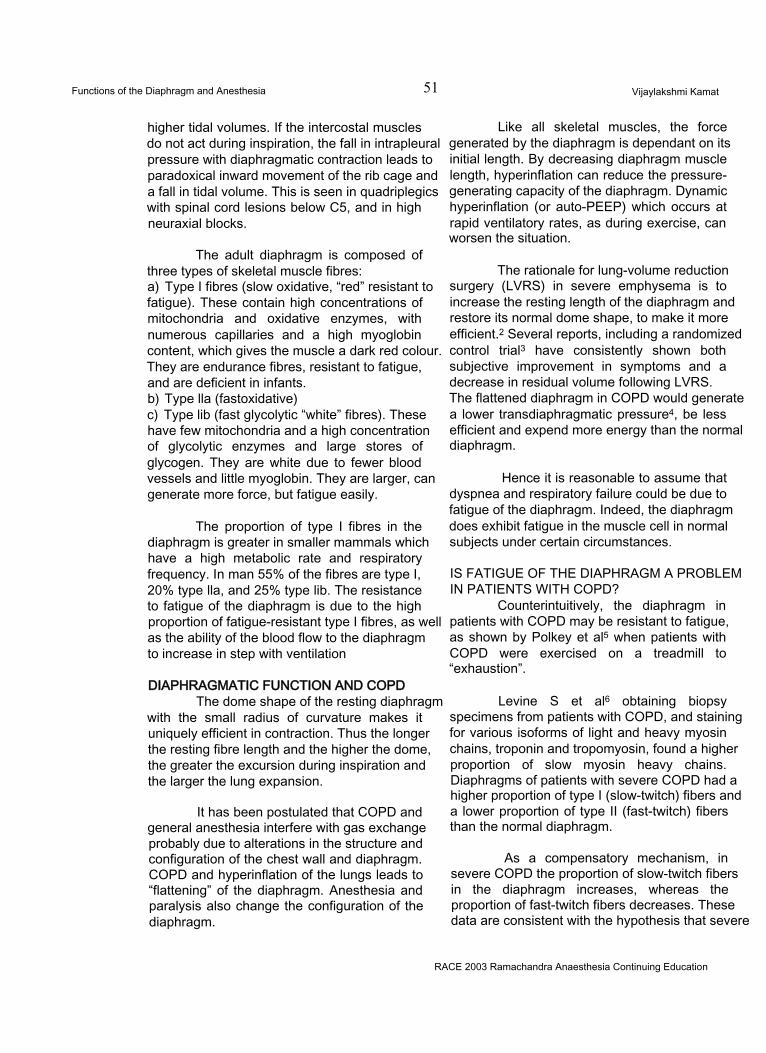
Functions of the Diaphragm and Anesthesia 51 Vijaylakshmi Kamat
higher tidal volumes. If the intercostal muscles do not act during inspiration, the fall in intrapleural pressure with diaphragmatic contraction leads to paradoxical inward movement of the rib cage and a fall in tidal volume. This is seen in quadriplegics with spinal cord lesions below C5, and in high neuraxial blocks.
The adult diaphragm is composed of three types of skeletal muscle fibres:a) Type I fibres (slow oxidative, “red” resistant to fatigue). These contain high concentrations of mitochondria and oxidative enzymes, with numerous capillaries and a high myoglobin content, which gives the muscle a dark red colour. They are endurance fibres, resistant to fatigue, and are deficient in infants.b) Type lla (fastoxidative)c) Type lib (fast glycolytic “white” fibres). These have few mitochondria and a high concentration of glycolytic enzymes and large stores of glycogen. They are white due to fewer blood vessels and little myoglobin. They are larger, can generate more force, but fatigue easily.
The proportion of type I fibres in the diaphragm is greater in smaller mammals which have a high metabolic rate and respiratory frequency. In man 55% of the fibres are type I, 20% type lla, and 25% type lib. The resistance to fatigue of the diaphragm is due to the high proportion of fatigue-resistant type I fibres, as well as the ability of the blood flow to the diaphragm to increase in step with ventilation
DIAPHRAGMATIC FUNCTION AND COPDThe dome shape of the resting diaphragm
with the small radius of curvature makes it uniquely efficient in contraction. Thus the longer the resting fibre length and the higher the dome, the greater the excursion during inspiration and the larger the lung expansion.
It has been postulated that COPD and general anesthesia interfere with gas exchange probably due to alterations in the structure and configuration of the chest wall and diaphragm. COPD and hyperinflation of the lungs leads to “flattening” of the diaphragm. Anesthesia and paralysis also change the configuration of the diaphragm.
Like all skeletal muscles, the force generated by the diaphragm is dependant on its initial length. By decreasing diaphragm muscle length, hyperinflation can reduce the pressure- generating capacity of the diaphragm. Dynamic hyperinflation (or auto-PEEP) which occurs at rapid ventilatory rates, as during exercise, can worsen the situation.
The rationale for lung-volume reduction surgery (LVRS) in severe emphysema is to increase the resting length of the diaphragm and restore its normal dome shape, to make it more efficient.2 Several reports, including a randomized control trial3 have consistently shown both subjective improvement in symptoms and a decrease in residual volume following LVRS. The flattened diaphragm in COPD would generate a lower transdiaphragmatic pressure4, be less efficient and expend more energy than the normal diaphragm.
Hence it is reasonable to assume that dyspnea and respiratory failure could be due to fatigue of the diaphragm. Indeed, the diaphragm does exhibit fatigue in the muscle cell in normal subjects under certain circumstances.
IS FATIGUE OF THE DIAPHRAGM A PROBLEM IN PATIENTS WITH COPD?
Counterintuitively, the diaphragm in patients with COPD may be resistant to fatigue, as shown by Polkey et al5 when patients with COPD were exercised on a treadmill to “exhaustion”.
Levine S et al6 obtaining biopsy specimens from patients with COPD, and staining for various isoforms of light and heavy myosin chains, troponin and tropomyosin, found a higher proportion of slow myosin heavy chains. Diaphragms of patients with severe COPD had a higher proportion of type I (slow-twitch) fibers and a lower proportion of type II (fast-twitch) fibers than the normal diaphragm.
As a compensatory mechanism, in severe COPD the proportion of slow-twitch fibers in the diaphragm increases, whereas the proportion of fast-twitch fibers decreases. These data are consistent with the hypothesis that severe
RACE 2003 Ramachandra Anaesthesia Continuing Education
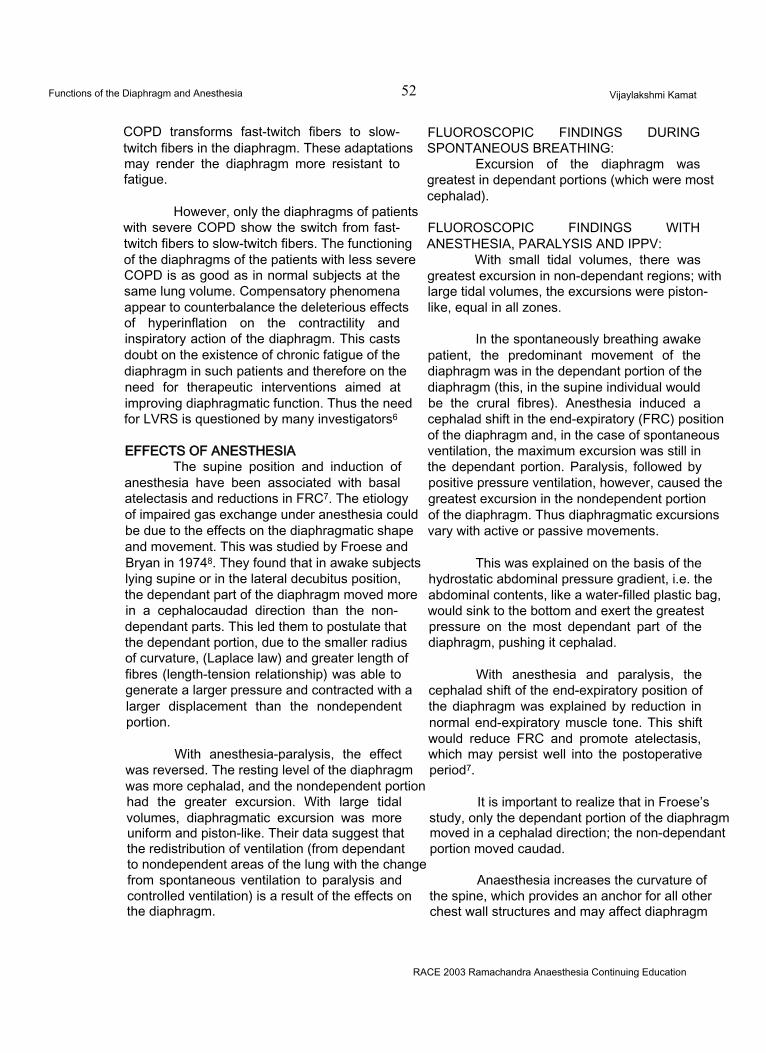
Functions of the Diaphragm and Anesthesia 52 Vijaylakshmi Kamat
COPD transforms fast-twitch fibers to slow- twitch fibers in the diaphragm. These adaptations may render the diaphragm more resistant to fatigue.
However, only the diaphragms of patients with severe COPD show the switch from fast- twitch fibers to slow-twitch fibers. The functioning of the diaphragms of the patients with less severe COPD is as good as in normal subjects at the same lung volume. Compensatory phenomena appear to counterbalance the deleterious effects of hyperinflation on the contractility and inspiratory action of the diaphragm. This casts doubt on the existence of chronic fatigue of the diaphragm in such patients and therefore on the need for therapeutic interventions aimed at improving diaphragmatic function. Thus the need for LVRS is questioned by many investigators6
EFFECTS OF ANESTHESIAThe supine position and induction of
anesthesia have been associated with basal atelectasis and reductions in FRC7. The etiology of impaired gas exchange under anesthesia could be due to the effects on the diaphragmatic shape and movement. This was studied by Froese and Bryan in 19748. They found that in awake subjects lying supine or in the lateral decubitus position, the dependant part of the diaphragm moved more in a cephalocaudad direction than the nondependant parts. This led them to postulate that the dependant portion, due to the smaller radius of curvature, (Laplace law) and greater length of fibres (length-tension relationship) was able to generate a larger pressure and contracted with a larger displacement than the nondependent portion.
With anesthesia-paralysis, the effect was reversed. The resting level of the diaphragm was more cephalad, and the nondependent portion had the greater excursion. With large tidal volumes, diaphragmatic excursion was more uniform and piston-like. Their data suggest that the redistribution of ventilation (from dependant to nondependent areas of the lung with the change from spontaneous ventilation to paralysis and controlled ventilation) is a result of the effects on the diaphragm.
FLUOROSCOPIC FINDINGS DURING SPONTANEOUS BREATHING:
Excursion of the diaphragm was greatest in dependant portions (which were most cephalad).
FLUOROSCOPIC FINDINGS WITH ANESTHESIA, PARALYSIS AND IPPV:
With small tidal volumes, there was greatest excursion in non-dependant regions; with large tidal volumes, the excursions were pistonlike, equal in all zones.
In the spontaneously breathing awake patient, the predominant movement of the diaphragm was in the dependant portion of the diaphragm (this, in the supine individual would be the crural fibres). Anesthesia induced a cephalad shift in the end-expiratory (FRC) position of the diaphragm and, in the case of spontaneous ventilation, the maximum excursion was still in the dependant portion. Paralysis, followed by positive pressure ventilation, however, caused the greatest excursion in the nondependent portion of the diaphragm. Thus diaphragmatic excursions vary with active or passive movements.
This was explained on the basis of the hydrostatic abdominal pressure gradient, i.e. the abdominal contents, like a water-filled plastic bag, would sink to the bottom and exert the greatest pressure on the most dependant part of the diaphragm, pushing it cephalad.
With anesthesia and paralysis, the cephalad shift of the end-expiratory position of the diaphragm was explained by reduction in normal end-expiratory muscle tone. This shift would reduce FRC and promote atelectasis, which may persist well into the postoperative period7.
It is important to realize that in Froese’s study, only the dependant portion of the diaphragm moved in a cephalad direction; the non-dependant portion moved caudad.
Anaesthesia increases the curvature of the spine, which provides an anchor for all other chest wall structures and may affect diaphragm
RACE 2003 Ramachandra Anaesthesia Continuing Education
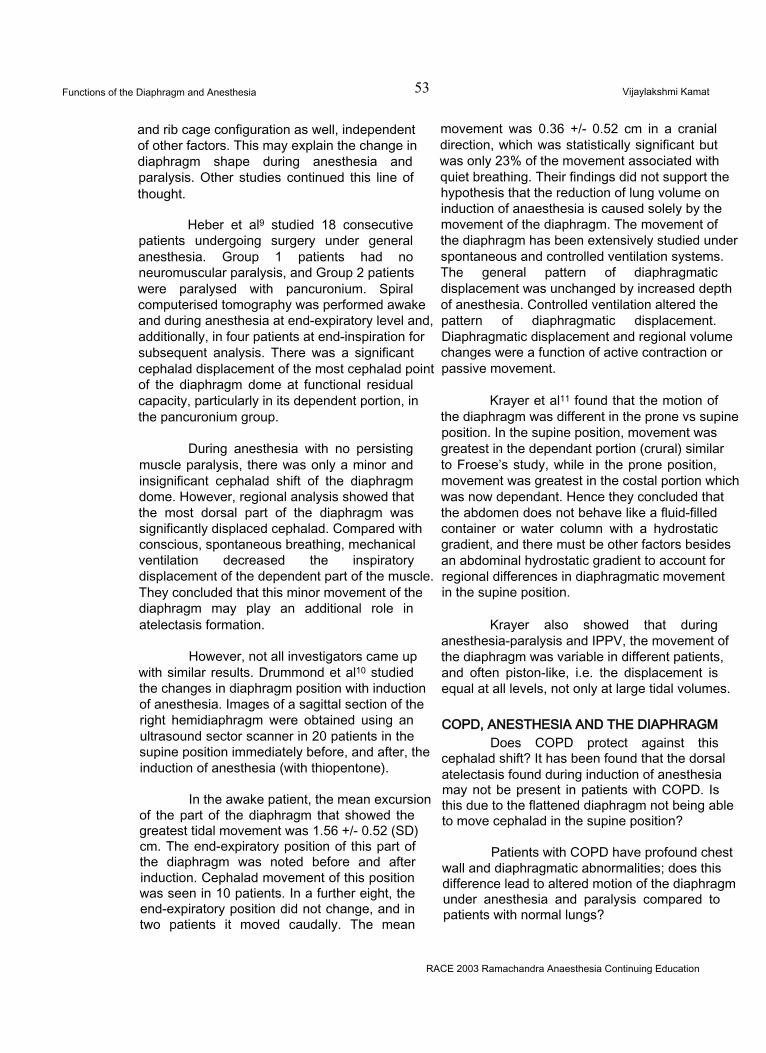
Functions of the Diaphragm and Anesthesia 53 Vijaylakshmi Kamat
and rib cage configuration as well, independent of other factors. This may explain the change in diaphragm shape during anesthesia and paralysis. Other studies continued this line of thought.
Heber et al9 studied 18 consecutive patients undergoing surgery under general anesthesia. Group 1 patients had no neuromuscular paralysis, and Group 2 patients were paralysed with pancuronium. Spiral computerised tomography was performed awake and during anesthesia at end-expiratory level and, additionally, in four patients at end-inspiration for subsequent analysis. There was a significant cephalad displacement of the most cephalad point of the diaphragm dome at functional residual capacity, particularly in its dependent portion, in the pancuronium group.
During anesthesia with no persisting muscle paralysis, there was only a minor and insignificant cephalad shift of the diaphragm dome. However, regional analysis showed that the most dorsal part of the diaphragm was significantly displaced cephalad. Compared with conscious, spontaneous breathing, mechanical ventilation decreased the inspiratory displacement of the dependent part of the muscle. They concluded that this minor movement of the diaphragm may play an additional role in atelectasis formation.
However, not all investigators came up with similar results. Drummond et al10 studied the changes in diaphragm position with induction of anesthesia. Images of a sagittal section of the right hemidiaphragm were obtained using an ultrasound sector scanner in 20 patients in the supine position immediately before, and after, the induction of anesthesia (with thiopentone).
In the awake patient, the mean excursion of the part of the diaphragm that showed the greatest tidal movement was 1.56 +/- 0.52 (SD) cm. The end-expiratory position of this part of the diaphragm was noted before and after induction. Cephalad movement of this position was seen in 10 patients. In a further eight, the end-expiratory position did not change, and in two patients it moved caudally. The mean
movement was 0.36 +/- 0.52 cm in a cranial direction, which was statistically significant but was only 23% of the movement associated with quiet breathing. Their findings did not support the hypothesis that the reduction of lung volume on induction of anaesthesia is caused solely by the movement of the diaphragm. The movement of the diaphragm has been extensively studied under spontaneous and controlled ventilation systems. The general pattern of diaphragmatic displacement was unchanged by increased depth of anesthesia. Controlled ventilation altered the pattern of diaphragmatic displacement. Diaphragmatic displacement and regional volume changes were a function of active contraction or passive movement.
Krayer et al11 found that the motion of the diaphragm was different in the prone vs supine position. In the supine position, movement was greatest in the dependant portion (crural) similar to Froese’s study, while in the prone position, movement was greatest in the costal portion which was now dependant. Hence they concluded that the abdomen does not behave like a fluid-filled container or water column with a hydrostatic gradient, and there must be other factors besides an abdominal hydrostatic gradient to account for regional differences in diaphragmatic movement in the supine position.
Krayer also showed that during anesthesia-paralysis and IPPV, the movement of the diaphragm was variable in different patients, and often piston-like, i.e. the displacement is equal at all levels, not only at large tidal volumes.
COPD, ANESTHESIA AND THE DIAPHRAGMDoes COPD protect against this
cephalad shift? It has been found that the dorsal atelectasis found during induction of anesthesia may not be present in patients with COPD. Is this due to the flattened diaphragm not being able to move cephalad in the supine position?
Patients with COPD have profound chest wall and diaphragmatic abnormalities; does this difference lead to altered motion of the diaphragm under anesthesia and paralysis compared to patients with normal lungs?
RACE 2003 Ramachandra Anaesthesia Continuing Education
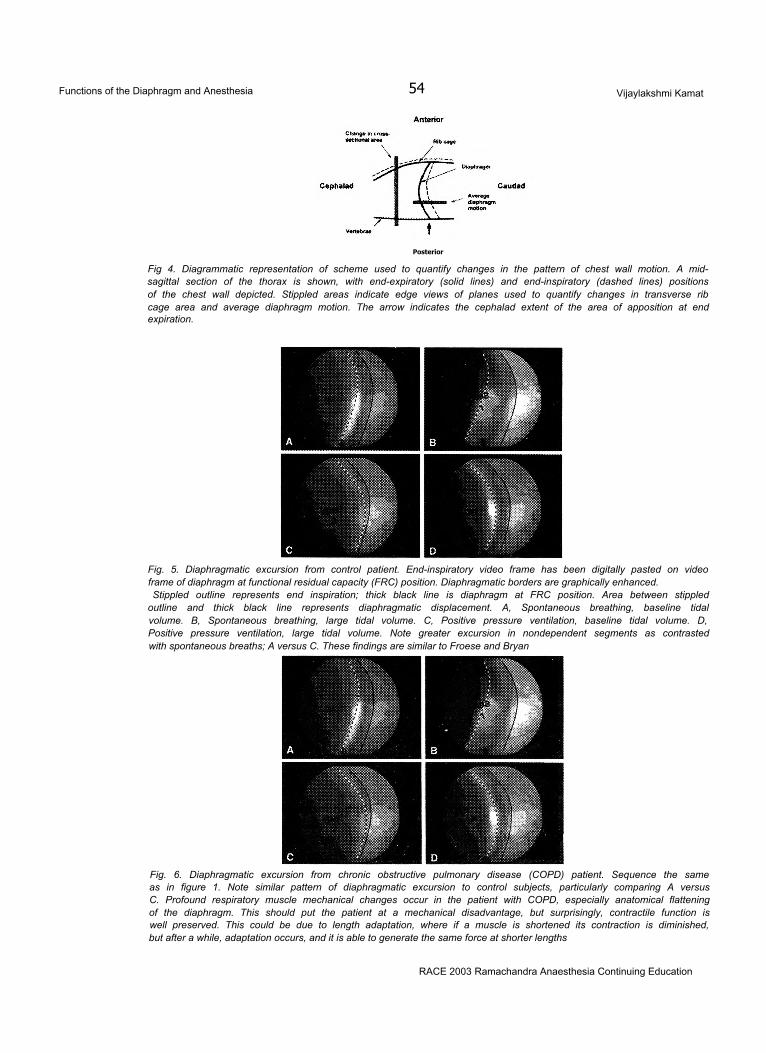
Functions of the Diaphragm and Anesthesia 54 Vijaylakshmi Kamat
Posterior
Fig 4. Diagrammatic representation of scheme used to quantify changes in the pattern of chest wall motion. A mid- sagittal section of the thorax is shown, with end-expiratory (solid lines) and end-inspiratory (dashed lines) positions of the chest wall depicted. Stippled areas indicate edge views of planes used to quantify changes in transverse rib cage area and average diaphragm motion. The arrow indicates the cephalad extent of the area of apposition at end expiration.
Fig. 5. Diaphragmatic excursion from control patient. End-inspiratory video frame has been digitally pasted on video frame of diaphragm at functional residual capacity (FRC) position. Diaphragmatic borders are graphically enhanced.Stippled outline represents end inspiration; thick black line is diaphragm at FRC position. Area between stippled
outline and thick black line represents diaphragmatic displacement. A, Spontaneous breathing, baseline tidal volume. B, Spontaneous breathing, large tidal volume. C, Positive pressure ventilation, baseline tidal volume. D, Positive pressure ventilation, large tidal volume. Note greater excursion in nondependent segments as contrasted with spontaneous breaths; A versus C. These findings are similar to Froese and Bryan
Fig. 6. Diaphragmatic excursion from chronic obstructive pulmonary disease (COPD) patient. Sequence the same as in figure 1. Note similar pattern of diaphragmatic excursion to control subjects, particularly comparing A versus C. Profound respiratory muscle mechanical changes occur in the patient with COPD, especially anatomical flattening of the diaphragm. This should put the patient at a mechanical disadvantage, but surprisingly, contractile function is well preserved. This could be due to length adaptation, where if a muscle is shortened its contraction is diminished, but after a while, adaptation occurs, and it is able to generate the same force at shorter lengths
RACE 2003 Ramachandra Anaesthesia Continuing Education
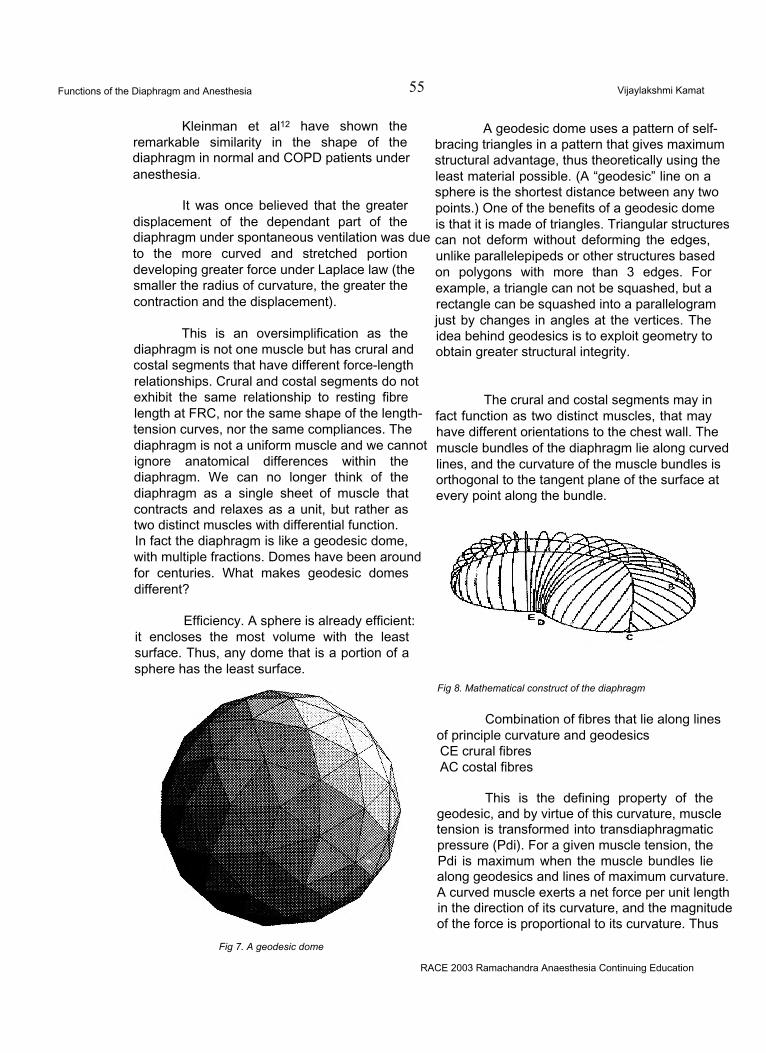
Functions of the Diaphragm and Anesthesia 55 Vijaylakshmi Kamat
Kleinman et al12 have shown the remarkable similarity in the shape of the diaphragm in normal and COPD patients under anesthesia.
It was once believed that the greater displacement of the dependant part of the diaphragm under spontaneous ventilation was due to the more curved and stretched portion developing greater force under Laplace law (the smaller the radius of curvature, the greater the contraction and the displacement).
This is an oversimplification as the diaphragm is not one muscle but has crural and costal segments that have different force-length relationships. Crural and costal segments do not exhibit the same relationship to resting fibre length at FRC, nor the same shape of the length- tension curves, nor the same compliances. The diaphragm is not a uniform muscle and we cannot ignore anatomical differences within the diaphragm. We can no longer think of the diaphragm as a single sheet of muscle that contracts and relaxes as a unit, but rather as two distinct muscles with differential function.In fact the diaphragm is like a geodesic dome, with multiple fractions. Domes have been around for centuries. What makes geodesic domes different?
Efficiency. A sphere is already efficient: it encloses the most volume with the least surface. Thus, any dome that is a portion of a sphere has the least surface.
Fig 7. A geodesic dome
A geodesic dome uses a pattern of selfbracing triangles in a pattern that gives maximum structural advantage, thus theoretically using the least material possible. (A “geodesic” line on a sphere is the shortest distance between any two points.) One of the benefits of a geodesic dome is that it is made of triangles. Triangular structures can not deform without deforming the edges, unlike parallelepipeds or other structures based on polygons with more than 3 edges. For example, a triangle can not be squashed, but a rectangle can be squashed into a parallelogram just by changes in angles at the vertices. The idea behind geodesics is to exploit geometry to obtain greater structural integrity.
The crural and costal segments may in fact function as two distinct muscles, that may have different orientations to the chest wall. The muscle bundles of the diaphragm lie along curved lines, and the curvature of the muscle bundles is orthogonal to the tangent plane of the surface at every point along the bundle.
Fig 8. Mathematical construct of the diaphragm
Combination of fibres that lie along lines of principle curvature and geodesics CE crural fibres AC costal fibres
This is the defining property of the geodesic, and by virtue of this curvature, muscle tension is transformed into transdiaphragmatic pressure (Pdi). For a given muscle tension, the Pdi is maximum when the muscle bundles lie along geodesics and lines of maximum curvature. A curved muscle exerts a net force per unit length in the direction of its curvature, and the magnitude of the force is proportional to its curvature. Thus
RACE 2003 Ramachandra Anaesthesia Continuing Education
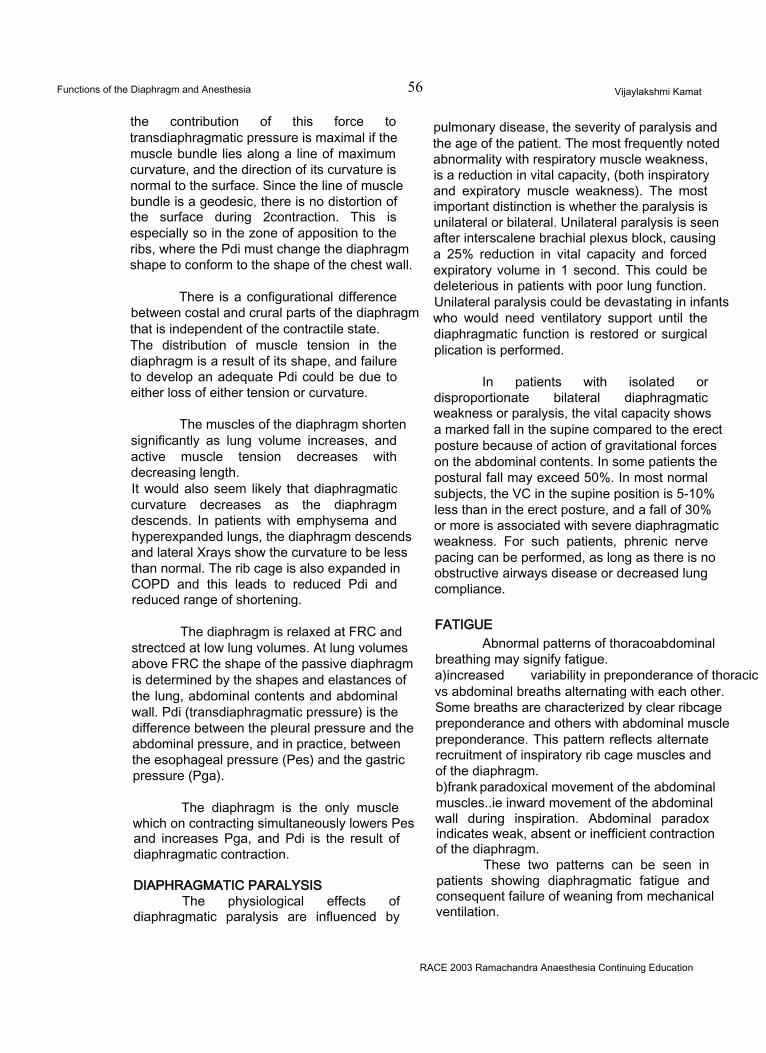
Functions of the Diaphragm and Anesthesia 56 Vijaylakshmi Kamat
the contribution of this force to transdiaphragmatic pressure is maximal if the muscle bundle lies along a line of maximum curvature, and the direction of its curvature is normal to the surface. Since the line of muscle bundle is a geodesic, there is no distortion of the surface during 2contraction. This is especially so in the zone of apposition to the ribs, where the Pdi must change the diaphragm shape to conform to the shape of the chest wall.
There is a configurational difference between costal and crural parts of the diaphragm that is independent of the contractile state. The distribution of muscle tension in the diaphragm is a result of its shape, and failure to develop an adequate Pdi could be due to either loss of either tension or curvature.
The muscles of the diaphragm shorten significantly as lung volume increases, and active muscle tension decreases with decreasing length.It would also seem likely that diaphragmatic curvature decreases as the diaphragm descends. In patients with emphysema and hyperexpanded lungs, the diaphragm descends and lateral Xrays show the curvature to be less than normal. The rib cage is also expanded in COPD and this leads to reduced Pdi and reduced range of shortening.
The diaphragm is relaxed at FRC and strectced at low lung volumes. At lung volumes above FRC the shape of the passive diaphragm is determined by the shapes and elastances of the lung, abdominal contents and abdominal wall. Pdi (transdiaphragmatic pressure) is the difference between the pleural pressure and the abdominal pressure, and in practice, between the esophageal pressure (Pes) and the gastric pressure (Pga).
The diaphragm is the only muscle which on contracting simultaneously lowers Pes and increases Pga, and Pdi is the result of diaphragmatic contraction.
DIAPHRAGMATIC PARALYSISThe physiological effects of
diaphragmatic paralysis are influenced by
pulmonary disease, the severity of paralysis and the age of the patient. The most frequently noted abnormality with respiratory muscle weakness, is a reduction in vital capacity, (both inspiratory and expiratory muscle weakness). The most important distinction is whether the paralysis is unilateral or bilateral. Unilateral paralysis is seen after interscalene brachial plexus block, causing a 25% reduction in vital capacity and forced expiratory volume in 1 second. This could be deleterious in patients with poor lung function. Unilateral paralysis could be devastating in infants who would need ventilatory support until the diaphragmatic function is restored or surgical plication is performed.
In patients with isolated or disproportionate bilateral diaphragmatic weakness or paralysis, the vital capacity shows a marked fall in the supine compared to the erect posture because of action of gravitational forces on the abdominal contents. In some patients the postural fall may exceed 50%. In most normal subjects, the VC in the supine position is 5-10% less than in the erect posture, and a fall of 30% or more is associated with severe diaphragmatic weakness. For such patients, phrenic nerve pacing can be performed, as long as there is no obstructive airways disease or decreased lung compliance.
FATIGUEAbnormal patterns of thoracoabdominal
breathing may signify fatigue.a)increased variability in preponderance of thoracic vs abdominal breaths alternating with each other. Some breaths are characterized by clear ribcage preponderance and others with abdominal muscle preponderance. This pattern reflects alternate recruitment of inspiratory rib cage muscles and of the diaphragm.b)frank paradoxical movement of the abdominal muscles..ie inward movement of the abdominal wall during inspiration. Abdominal paradox indicates weak, absent or inefficient contraction of the diaphragm.
These two patterns can be seen in patients showing diaphragmatic fatigue and consequent failure of weaning from mechanical ventilation.
RACE 2003 Ramachandra Anaesthesia Continuing Education
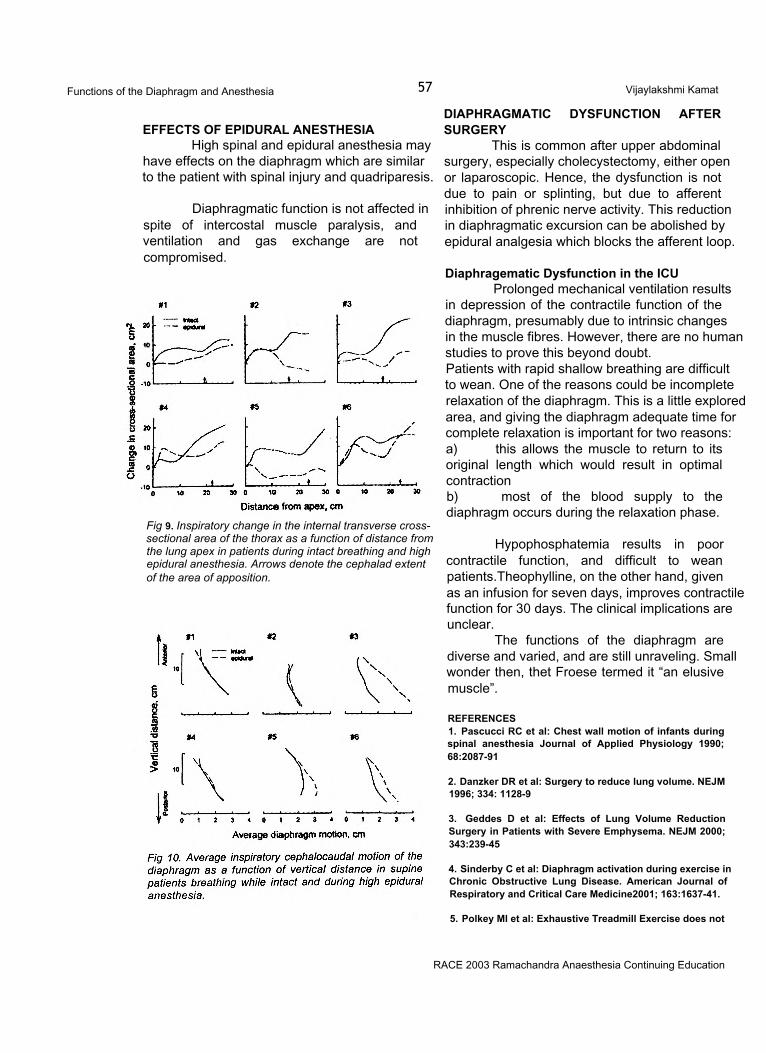
Functions of the Diaphragm and Anesthesia 57 Vijaylakshmi Kamat
EFFECTS OF EPIDURAL ANESTHESIAHigh spinal and epidural anesthesia may
have effects on the diaphragm which are similar to the patient with spinal injury and quadriparesis.
Diaphragmatic function is not affected in spite of intercostal muscle paralysis, and ventilation and gas exchange are not compromised.
Fig 9. Inspiratory change in the internal transverse cross- sectional area of the thorax as a function of distance from the lung apex in patients during intact breathing and high epidural anesthesia. Arrows denote the cephalad extent of the area of apposition.
DIAPHRAGMATIC DYSFUNCTION AFTER SURGERY
This is common after upper abdominal surgery, especially cholecystectomy, either open or laparoscopic. Hence, the dysfunction is not due to pain or splinting, but due to afferent inhibition of phrenic nerve activity. This reduction in diaphragmatic excursion can be abolished by epidural analgesia which blocks the afferent loop.
Diaphragematic Dysfunction in the ICUProlonged mechanical ventilation results
in depression of the contractile function of the diaphragm, presumably due to intrinsic changes in the muscle fibres. However, there are no human studies to prove this beyond doubt.Patients with rapid shallow breathing are difficult to wean. One of the reasons could be incomplete relaxation of the diaphragm. This is a little explored area, and giving the diaphragm adequate time for complete relaxation is important for two reasons:a) this allows the muscle to return to its original length which would result in optimal contractionb) most of the blood supply to the diaphragm occurs during the relaxation phase.
Hypophosphatemia results in poor contractile function, and difficult to wean patients.Theophylline, on the other hand, given as an infusion for seven days, improves contractile function for 30 days. The clinical implications are unclear.
The functions of the diaphragm are diverse and varied, and are still unraveling. Small wonder then, thet Froese termed it “an elusive muscle”.
REFERENCES1. Pascucci RC et al: Chest wall motion of infants during spinal anesthesia Journal of Applied Physiology 1990; 68:2087-91
2. Danzker DR et al: Surgery to reduce lung volume. NEJM 1996; 334: 1128-9
3. Geddes D et al: Effects of Lung Volume Reduction Surgery in Patients with Severe Emphysema. NEJM 2000; 343:239-45
4. Sinderby C et al: Diaphragm activation during exercise in Chronic Obstructive Lung Disease. American Journal of Respiratory and Critical Care Medicine2001; 163:1637-41.
5. Polkey Ml et al: Exhaustive Treadmill Exercise does not
RACE 2003 Ramachandra Anaesthesia Continuing Education

Functions of the Diaphragm and Anesthesia 58 Vijaylakshmi Kamat
reduce twitch transdiaphragmatic pressure in patients with COPD. American Journal of Respiratory and Critical Care Medicine 1995; 152:959-64.
6. Fessler HE et al: Lung volume reduction surgery: is less really more? Am J Respir Crit Care Med 1999; 159:1031- 1035.
7. Hedenstierna G et al : Functional Residual Capacity, thoracoabdominal dimensions, and central blood volume during general anesthesia with muscle paralysis and mechanical ventilation. Anesthesiology 1985; 62:247-54
8. Froese AB, Bryan AC: Effects of anesthesia and paralysis on diaphragmatic mechanics in man. Anesthesiology 1974; 41:242-55
9.. Reber A, Nylund U, Hedenstierna G. Position and shape
of the diaphragm: implications for atelectasis formation. Anaesthesia. 1998 Nov;53(11): 1054-61.
10. Drummond GB et al: Changes in diaphragmatic position in association with the induction of anaesthesia. Br J Anaesth. 1986 Nov;58(11):1246-51.
11. Krayeretal: Position and motion of the human diaphragm during anesthesia-paralysis. Anesthesiology 1989;70:891- 98
12. Kleinman BS, Frey K, VanDrunen M, Sheikh T, DiPinto D, Mason R, Smith T.Motion of the diaphragm in patients with chronic obstructive pulmonary disease while spontaneously breathing versus during positive pressure breathing after anesthesia and neuromuscular blockade.Anesthesiology. 2002 Aug;97(2):298-305.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 59 Joseph Rajesh
INTRODUCTIONIn the past few years, much attention
has been focussed on brain death and artificial support of the organs secondary to catastrophic brain injury. Although brainstem death is irreversible, the ability to recover transplantable organs exists only because the technological advances in intensive care can maintain physiologic homeostasis till the inevitable occurs.
Therapy provided for patients with brain injury is mainly directed towards preservation and restoration of neuronal function. When this becomes unsuccessful the patient may go for brainstem death. The critical care physician thus has the responsibility to offer the patient’s family the opportunity to donate organs and the obligation to unknown recipients to provide the best probable organs.
The recovery of viable organs and successful transplantation are dependent on early and appropriate medical management and timely intervention before and after brain death is declared. This is because, even with intensive support, brain dead donors can be maintained only for a short time, before the pathophysiologic changes induced by brain death overwhelm the resuscitative measures.
The issues related with identification of brain dead donors, criteria for brain death, managing these brain dead donors in the ICU and during the operative period would be discussed here.
THE CONCEPT OF BRAIN DEATHBrain death represents the death of the
organism and not the death or necrosis of the brain in the living body. The organism is an
aggregation of living cells, but it can be said that, the organism exists only when this aggregation is put under the control of some modulating or regulating systems such as the central nervous system, endocrine system, immune system etc. Once any of these fail to function, death is inevitable unless some artificial measures are taken. Without these systems, organized functioning of these cells as a part of the whole organism ceases.
The clinical diagnosis of brain death is equivalent to irreversible loss of all cortical and brainstem function, manifesting as loss of consciousness, lack of motor response to deep painful stimuli, and absence of brainstem reflexes.
THE MECHANISMS OF BRAIN DEATHThe aetiology of brain injury may be
secondary to many things like trauma, cerebrovascular accident or generalized hypoxia, but the ultimate mechanism that produces the change is brain oedema. This oedema can be either vasogenic or cytotoxic in nature.
Vasogenic oedema is caused by an increase in vascular permeability after destruction of the blood brain barrier secondary to release of chemical mediators such as histamine, serotonin, angiotensin and bradykinin. This occurs in hypoxia and ischaemia from the altered cellular osmoregulation, which leads to entry of water into the brain parenchyma.
Brain oedema may be focal initially but later spreads throughout the brain. Since the brain is enclosed in a rigid skull, this is associated with increased intracranial pressure. When the ICP exceeds the arterial pressure, the cerebral circulation ceases and brain death ensues.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 60 Joseph Rajesh
NEURO PHYSIOLOGIC BASIS OF THE BRAINDEATHRespiration:
Since the primary respiratory centre, consisting of both inspiratory and expiratory neurons, is located in the reticular core of the medulla oblongata, there will not be any spontaneous respiration. The C02 drive of respiration is lost even when the PaC02 reaches 55-60 mmHg.
Cardiovascular functions:The central neurons that control the
circulatory system are distributed in the pontine and medullary reticular core. During brainstem death, the outflow of this system is cut off and results in various haemodynamic alterations in the body.
Regulation of body temperature:The heat sensitive centre in the
hypothalamus regulates the body temperature. In brain death, the neural connection between this temperature regulating centre and the peripheral tissues is lost and the patient becomes poikilothermic.
PATHOPHYSIOLOGICAL CHANGES ASSOCIATED WITH BRAIN-STEM DEATH
The sequence of haemodynamic, metabolic and endocrine changes associated with brain death is well documented. Acute ischaemia due to sudden rise in intracranial pressure or alteration in blood flow commonly initiates a series of physiological responses. The earliest phase involves a period of parasympathetic predominance leading to bradycardia, idioventricular rhythms, or even a short period of asystole. The subsequent phase is associated with marked hyperactivity of the sympathetic system leading to a catecholamine storm. The near maximal sympathetic drive causes tachycardia, severe hypertension, ECG signs of myocardial ischaemia and frequent ectopics. Autotransfusion occurring due to constriction of venous capacitance vessels will increase the cardiac filling pressures, which when combined with the massive degree of arterial hypertension, leads to high left ventricular wall tension and therefore high myocardial oxygen consumption. On the other hand, the surge in catecholamines will cause coronary spasm thus reducing the
supply. This imbalance in oxygen supply demand ratio may be so severe as to cause myocardial ischaemia even in normal hearts. During the peak of the catecholamine surge, the vasoconstriction may be sufficiently severe to cause acute left ventricular failure due to sudden increase in afterload.
Once brain death becomes established, many of the changes are reversed. There will be a rapid fall in the level of circulating catecholamines. As a result, the sympathetic tone and SVR will fall and venous capacitance vessels also dilate. Arterial pressures and cardiac filling pressures will thus fall. Heart rate falls to denervated levels.
A few hours following brain stem death, endocrine changes will occur. They are related mainly to the failure of production of hypothalamic release factors and a decline in the production of anterior and posterior pituitary hormones. Failure of production of ADH will cause diabetes insipidus with inappropriate production of large volumes of dilute urine. Circulating levels of cortisol, triiodothyronine and insulin may all fall as release of ACTH, TRH from the pituitary declines.
Thermoregulation is impaired with a progressive fall in the core temperature. This is due to the effects of increased heat loss as a consequence of vasodilatation and in part due to reduced heat production as a result of loss of thyroid and other metabolic hormones.
IDENTIFICATION OF POTENTIAL ORGAN DONORS
The shortage of suitable organs for transplantation is well known to ICU physicians and transplant surgeons, however organs continue to be lost through failure to identify potential donors and tests for brain death. The majority of organ donors will be patients in the ICU who have suffered a catastrophic brain injury that has progressed to brain death. The major causes of severe coma are trauma, CVA, primary intracraniaI tumours and ischaemic brain injury.
CERTIFICATION OF BRAIN DEATHCertification of brain death is an absolute
requirement prior to retrieval of organs for transplantation. Clinical diagnosis of brain stem
RACE 2003 Ramachandra Anaesthesia Continuing Education
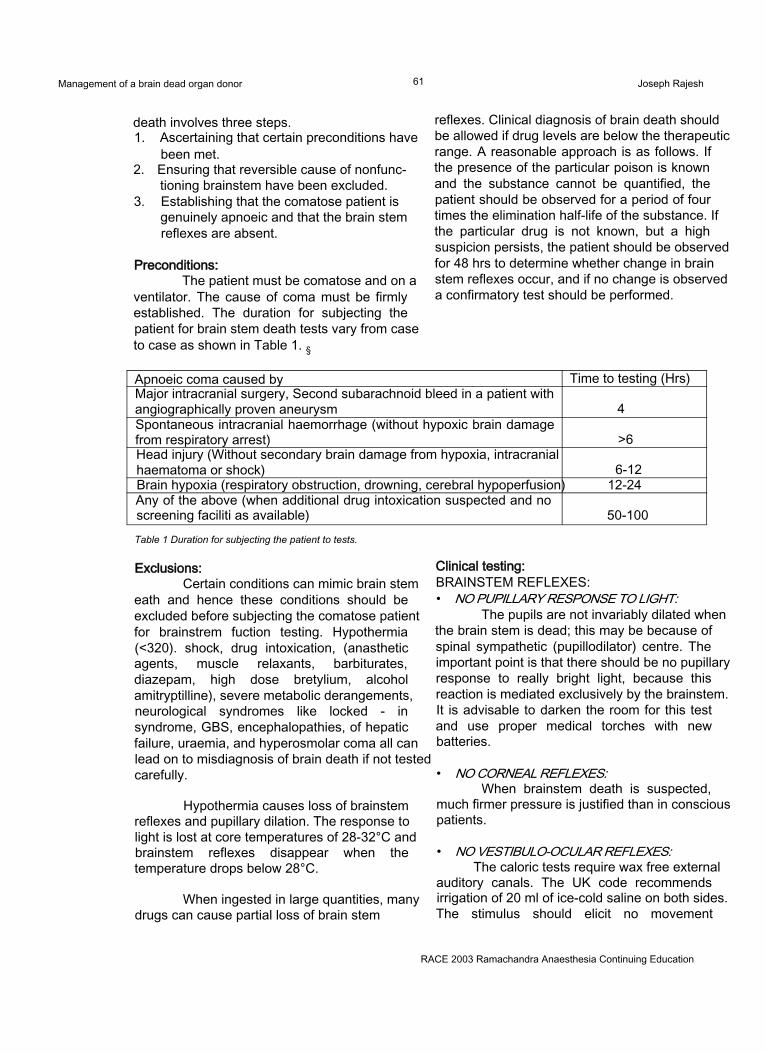
Management of a brain dead organ donor 61 Joseph Rajesh
death involves three steps.1. Ascertaining that certain preconditions have
been met.2. Ensuring that reversible cause of nonfunc
tioning brainstem have been excluded.3. Establishing that the comatose patient is
genuinely apnoeic and that the brain stem reflexes are absent.
Preconditions:The patient must be comatose and on a
ventilator. The cause of coma must be firmly established. The duration for subjecting the patient for brain stem death tests vary from case to case as shown in Table 1. §
Exclusions:Certain conditions can mimic brain stem
eath and hence these conditions should be excluded before subjecting the comatose patient for brainstrem fuction testing. Hypothermia (<320). shock, drug intoxication, (anasthetic agents, muscle relaxants, barbiturates, diazepam, high dose bretylium, alcohol amitryptilline), severe metabolic derangements, neurological syndromes like locked - in syndrome, GBS, encephalopathies, of hepatic failure, uraemia, and hyperosmolar coma all can lead on to misdiagnosis of brain death if not tested carefully.
Hypothermia causes loss of brainstem reflexes and pupillary dilation. The response to light is lost at core temperatures of 28-32°C and brainstem reflexes disappear when the temperature drops below 28°C.
When ingested in large quantities, many drugs can cause partial loss of brain stem
reflexes. Clinical diagnosis of brain death should be allowed if drug levels are below the therapeutic range. A reasonable approach is as follows. If the presence of the particular poison is known and the substance cannot be quantified, the patient should be observed for a period of four times the elimination half-life of the substance. If the particular drug is not known, but a high suspicion persists, the patient should be observed for 48 hrs to determine whether change in brain stem reflexes occur, and if no change is observed a confirmatory test should be performed.
Clinical testing:BRAINSTEM REFLEXES:• NO PUPILLARY RESPONSE TO LIGHT:
The pupils are not invariably dilated when the brain stem is dead; this may be because of spinal sympathetic (pupillodilator) centre. The important point is that there should be no pupillary response to really bright light, because this reaction is mediated exclusively by the brainstem. It is advisable to darken the room for this test and use proper medical torches with new batteries.
• NO CORNEAL REFLEXES:When brainstem death is suspected,
much firmer pressure is justified than in conscious patients.
• NO VESTIBULO-OCULAR REFLEXES:The caloric tests require wax free external
auditory canals. The UK code recommends irrigation of 20 ml of ice-cold saline on both sides. The stimulus should elicit no movement
Apnoeic coma caused by Time to testing (Hrs)Major intracranial surgery, Second subarachnoid bleed in a patient with angiographically proven aneurysm 4Spontaneous intracranial haemorrhage (without hypoxic brain damage from respiratory arrest) >6Head injury (Without secondary brain damage from hypoxia, intracranial haematoma or shock) 6-12Brain hypoxia (respiratory obstruction, drowning, cerebral hypoperfusion) 12-24Any of the above (when additional drug intoxication suspected and no screening faciliti as available) 50-100Table 1 Duration for subjecting the patient to tests.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 62 Joseph Rajesh
whatsoever in either eye within one minute of completion of the test. In deeply unconscious patients with some residual brainstem function, the eye will be deviated towards the irrigated ear.
• NO MOTOR RESPONSE:No motor response should be present
within the cranial nerve distribution, to adequate stimulation of any somatic area.
There should be no grimacing in response to painful stimuli, applied either to the trigeminal fields (firm supraorbital pressure) or to the limbs (the side of a pencil pressed firmly down against the patient’s fingernail or toenail is the most appropriate stimulus). Pinprick should not be used.
•NO GAG REFLEX, OR REFLEX RESPONSE TO BRONCHIAL STIMULATION BY A SUCTION CATHETER.
• THE OCULOCEPHALIC REFLEXThis is best elicited by fast and vigorous
turning of the head from the middle position to 90°on both sides. Normally, the eye deviates to the opposite side. This movement, along with vertical and horizontal eye movements, must be absent in the brain dead.
• NO RESPONSE TO A TROPINEFailure of heart rate to increase > 5 beats
after 1 -2 mg of atropine IV denotes the absent function of vagus nuclei.
• APNOEAApnoea is confirmed by showing no
respiratory movements during disconnection from the ventilator for long enough to ensure that the arterial C02 tension rises to a level of 60mmHg, capable of driving any respiratory centre neurons that may still be alive.
Method of testingHypoxia is prevented by a combination of
preoxygenation and diffuse oxygenation. If the patient is made to breathe 100% oxygen for 10 mts, very high starting levels of arterial oxygen tension are achieved. It is reinforced with the endotracheal delivery of 02 by a catheter (at 61 /mt.) As a result of endogenous metabolism, PaC02will rise by 2 - 3 mmHg/mt. Provided the
starting PaC02 was 30mmHg; the crucial level of 60mmHg will be achieved within 10 mts. This method is simple and free of complications. If events such as hypotension or cardiac arrhythmias occur, they may be due to failure to provide an adequate source of oxygen or lack of preoxygenation. One should look closely for respiratory movements. When in doubt, a spirometer can be attached to confirm the tidal volumes. Apnoea testing by carbondioxide augmentation is less acceptable and potentially dangerous.
ANCILLARY TESTSSome ancillary tests are adopted when
applying the criteria for brain death and should be used in conjunction with proper clinical judgement. These tests are needed for patients in whom specific components of clinical testing cannot be reliably evaluated as in infants.
• TO EVALUATE THE NEURONAL FUNCTION
• Electroencephalography;A flat EEG may indicate irreversible
dysfunction of the cerebrum. In brain death, the recording of isoelectric EEGs should be carried out over 60 mts, and no electrical activity having an amplitude of more than 2 -3 mv should be recorded. However the criteria for brain death clearly indicates that EEG results are not necessary for the diagnosis of brain death.
• TO EVALUATE THE INTRACRANIAL BLOOD FLOW.
• Cerebral angiographyThis selective four-vessel angiography has
some usefulness in distinguishing certain comatose conditions from brainstem death. This is regularly in practice in Scandinavian countries. Here an iodinated contrast medium is injected under high pressure in both the anterior and the posterior circulations. Intracerebral filling is absent in brain death. Since there are no specific guidelines for interpretation, the results can be conflicting.
Isotope AngiographyRapid intravenous injection of serum albumin
labelled with 99mTc is done with imaging by a gamma camera. There will not be any intracranial activity in the brain dead patient.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 63 Joseph Rajesh
Transcranial Doppler Ultrasonography.It is a non-invasive method by which the
velocity of blood flow of intracranial arteries is recorded. Normally blood flows in the same direction during both systole and diastole. After cessation of cerebral blood flow, diastolic flow is initially reversed followed by total loss of perfusion signals. Comparatively, there is huge experience available for this test to other ancillary tests and it can be used in patients who have electroencephalographic activity.
Computed Tomography Simple CT alone does not give any information
regarding the blood flow, but does help in identifying the primary and secondary organic changes. Single photon emission CT, positron emission CT have all been tried with varied success rates in small series of studies.
DECLARATION OF BRAIN DEATHDeclaration of brain death should be done
by a board of medical experts formed by the hospital administration and approved by the government. The UK code now recommends that the tests should be carried out by two medical practitioners who "have expertise in.this field.” One should be the consultant and the other can be either a consultant or a senior resident. When transplantation is planned, neither doctor should be associated with potential recipients. In practice, these doctors can be anaesthetists, neurologists or intensive care physicians.
Practice in various parts of the world differs considerably. Some countries specify the required speciality of the doctors making the diagnosis while others do not.
But all the codes urge that testing should be carried twice. This is to ensure that there has been no error. It ensures that non-functioning of brain stem is not a single finding at one point of time but persisting. The interval period between two testing has been varying in different countries between 3 -6 hrs.
DONOR MAINTENANCEOnce a potential donor is identified and
brain death is certified, medical therapy is directed at maintaining organ function while retrieval is organized. Of primary importance is maintaining adequate tissue oxygenation by the support of
various systems.
Cardiovascular SystemIn brain dead candidates, cardiovascular
instability is inevitable. Hypotension is almost universal and is associated with poor graft function. Other common events encountered are arrhythmias and cardiac arrest, which will become increasingly resistant to therapy with time.
PATHOPHYSIOLOGY:Cause for cardiovascular instability is
multifactorial. It may result from1. The primary (hypoxic) insult leading to brain
death2. Due to the therapy directed at control of
raised ICP3. Physiological changes that result from brain
stem ischaemia and death.4. Direct myocardial contusion resulting in
impaired ventricular function and arrhythmias.
The hypoxic insults severe enough to cause brain death are invariably associated with myocardial damage. The treatment of severe brain injury may include fluid restriction and diuretic therapy, and with the onset of diabetes insipidus, the brain dead patients will become hypovolemic. This will further exacerbate cardiovascular instability. Physiological changes secondary to raised ICP, like hypertension, can cause further structural damage to the heart.
CARDIOVASCULAR SUPPORT:Cardiovascular support is directed at
maintaining tissue perfusion; this requires an adequate cardiac output and tissue perfusion pressure. Immediate therapy is aimed at correcting intravascular fluid depletion with aggressive fluid resuscitation.
Invasive monitoring of arterial and central venous pressure should be instituted if not already in use. In unstable patients, use of a pulmonary artery catheter to monitor cardiac output, PAOP, and SVR is justified. Mean arterial pressure should be maintained at 60 mmHg or greater; CVP up to 15mmHg may be required to achieve this. The choice of resuscitation fluid may be influenced by
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 64 Joseph Rajesh
measurement of haemoglobin, albumin, electrolyte concentrations, coagulation studies and nature of any ongoing blood or fluid losses. Blood, blood products, colloid and crystalloid solution may all be necessary. In the absence of ongoing blood loss, colloid solution may be necessary, as infusion of large volumes of crystalloid solution in patients with increased capillary permeability, may precipitate pulmonary oedema. If Dl is contributing to fluid depletion, an anti diuretic hormone analogue may be used. In many patients, fluid resuscitation may alone restore the cardiovascular instability; but in some, use of vasopressors may be indicated.
As impaired myocardial contractility is associated with vasodilatation, agents with both inotropic and vasopressor properties may be required. Dopamine is the agent most commonly used. At low doses (2-5 ^g/kg/mt), it may preferentially improve the perfusion of transplantable abdominal organs. At higher doses (5 -20ng/kg/mt), (3 and a adrenergic effects will predominate, p stimulation may be necessary if impaired myocardial function is present, but excessive a stimulation may compromise organ perfusion. If hypotension persists despite adequate fluid resuscitation and low dose dopamine, another vasopressor such as dobutamine may be tried. Obviously the lowest dose of least injurious agent is the preferred approach but may not be possible always. In a few cases, prolonged use of vasopressors may be necessary and in these cases, use of a PA catheter may be indicated to monitor cardiac output and SVR and to titrate the use of vasopressor. The ultimate goal is to achieve a normotensive, euvolemic state. The use of hormonal therapy (tri- iodothyronine, cortisol and insulin) has been advocated and is still in experimental use.
Arrhythmias are common and found to be occurring in 27 - 56% cases in any form. Common precipitating causes include myocardial damage and electrolyte abnormalities. Diuretic use, inadequately treated Dl and presence of acidosis may further worsen this. Inotropic agents may initiate or worsen this and dose reduction may be necessary. Once these correctable coexisting conditions are treated, arrhythmias can be managed along the conventional lines.
Respiratory systemRespiratory care has aims of ensuring
adequate gas exchange and maintaining the lungs in a suitable condition for transplantation. The lungs of the potential organ donors may be damaged by a variety of processes namely, bronchopneumonia, pulmonary oedema, pulmonary contusion, atelectasis, pneumothoraces, aspiration pneumonitis etc. Trauma may be accompanied by pulmonary contusion and haemopneumothoraces. In a few, this may progress to ARDS. The sympathetic storm accompanying the coning may damage the pulmonary vasculature. As a result, pulmonary interstitial haemorrhages and increased pulmonary capillary permeability may result. All potential organ donors will be apnoeic and mechanically ventilated; they are therefore at risk of barotrauma, atelectasis and infection. Prolonged intubation will result in colonization of pathogenic bacteria.
RESPIRATORY SUPPORTAny delay in optimising the ventilatory
support should be avoided. In those with injured lungs, use of high-inspired oxygen concentration should be avoided. A Pa02 of 80mmHg and above is necessary. The use of PEEP may allow a reduction in FI02, but PEEP of greater than 15 should be avoided. If hyperventilation is employed to control ICP, it should be discontinued once brain death is confirmed and PaC02 should be maintained in the normal range. If this is not possible, moderate hypercarbia can be allowed.
Endocrine issues:Brain death is accompanied by a
number of endocrine abnormalities. Loss of central sympathetic tone results in subnormal levels of circulating catecholamines. The hypothalamus and pituitary are frequently damaged, resulting in reduced or absent secretion of pituitary hormones.
The most frequent manifestation is the development of diabetes insipidus, which is related to inadequate antidiuretic hormone production by the posterior pituitary gland. Urine output may exceed 15 ml/kg/hr; if not adequately treated, it will contribute to hypovolemia, hypotension, and end organ damage. Treatment is either by replacing the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 65 Joseph Rajesh
excess urine output with an equal volume of electrolyte solution or administration of antidiuretic hormones.
Treatment with fluid replacement may result in the infusion of large volumes of fluid with rapid swings in serum osmolarity and electrolyte concentrations. This may further cause organ damage and predispose to cardiac arrhythmias. Treatment with an antidiuretic hormone analogue is relatively simple and will result in a reduced incidence of hypotension and better function of transplantable organs. Two antidiuretic hormone analogues are available. Vasopressin has a short duration of action and may be given by intravenous infusion at an initial rate of 1 unit /hr, titrated to maintain urine output at 1-2 ml/kg/hr. A potential adverse effect is splanchnic vasoconstriction, which is undesirable in potential liver and kidney donors.
Desmopressin, an analogue, has a long duration of action and causes minimal vasoconstriction. It may be given by subcutaneous, intravascular and intravenous injections or via the endotracheal tube. Intravenous injection of 0.5 to 1 U/hr, is required to control urine output and gives the most predictable response. However, in excess doses it can produce ATN.
Reduction in hepatic blood flow, and increased sensitivity to catecholamines occur and catecholamine doses should be titrated when DDAVP is used. Hyperglycemia is a common complication of Dl and is treated with insulin infusion.
Serum levels of tri-iodothyronine, insulin and cortisol are low in animal models and triiodothyronine administration improves the haemodynamic stability by maintaining myocardial stores of energy and glycogen; however, the beneficial role of this is still unclear in clinical settings.
CoagulopathyDIC may be seen in up to 28% of the
brain dead patients and 80% of head injury donors. This is probably due to the release of thrombolysins from the necrotic or ischaemic tissues. Aggressive treatment with appropriate blood products may stabilize the condition.
HypothermiaHypothermia occurs in up to 54% of the
patients. This is due to the reduction in heat production and increased heat loss due to vasodilatation. Prior hypothermia must be corrected to allow certification of death. It can be treated by warming the intravenous fluids, gases and by using blankets. Correction of hypothermia will also improve the stability of the cardiovascular system.
Infection:Infection is another common problem
encountered in the management of brain dead patients. Common sources of infections are invasive lines and airway instruments. Delay in the certification and organ retrieval will increase the bacterial colonization and cause active infection. Avoiding such delay and following scrupulous aseptic techniques are required to prevent infection that could result in poor graft function.
TREATMENT IMPLICATIONS1. Minimize crystalloid administration except
where mandatory for the administration of drugs (unless serum osmolality exceeds 350 mOsm/Kg).
2. Treat Dl with DDAVP rather than fluid replacement.
3. Maintain circulating volume with colloid solutions as available. A target CVP of 5 - 10 cmH20 is appropriate for most cases.
4. Transfusion of blood may be required to maintain haemoglobin concentration between 9-11 g/dl.
5. Vasoactive drugs should be chosen carefully and used judicially to avoid vasoconstriction and possible ischaemic damage to donor organs.
6. Inotropic support, if already instituted, may be slowly reduced if mean arterial pressures are above 60 -70 mmHg.
7. Lung ventilation should be aimed at maintaining a normal PaC02 and Pa02. PEEP values up to 5 -10 cmH20 can be applied, provided that haemodynamic disturbances are not severe.
8. A FI02of 0.6 is ideal.9. Physiotherapy of the chest including
bronchial toileting should be done aggressively.
10. Complete aseotic techniques should be
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 66 Joseph Rajesh
followed for airway and vascular procedures.11. Chest radiography and blood gas and
biochemical status should be monitored along the lines of any other ventilated patients
12. Antibiotic therapy should be continued if clinical evidence of infection exists
13. All efforts should be made to maintain the core temperature within normal limits like infusing warmed fluids, using HMV filters, blankets etc.
14. Near normal acid base status and electrolytes especially serum potassium and glucose should be maintained within normal limits.
ORGAN SPECIFIC CONSIDERATIONS: • Kidney:
Using Hydroxyethyl starch as a volume expander during resuscitation produces nephrosis like osmosis in the renal tubules, which is associated with greater dialysis requirements in the recipient.
Mean dopamine infusion >7.5 jig/kg/mt seems to be associated with delayed graft functioning.
Low levels of vasopressin are associated with oliguria in the recipient. In some centres, routine vasopressin estimation and prophylactic vasopressin administration is performed.
Donor pre-treatment with IV lignocaine prior to kidney procurement leads to decreased incidence of dialysis and earlier return of kidney function. This is probably secondary to vasodilatory, platelet disaggregating, and Ca channel blocking properties of the drug.
• Liver:A multivariate analysis shows poor initial
graft function seen in donors with1. High levels of alanine transaminase2. ICU stay > 3 days.3. High glucose levels.
PancreasGraft survival rate is inversely
proportionate to the duration of brain death prior to organ procurement.
Pancreas islet cell yield is higher if the donor blood glucose level is at least 120 mg%
without hypotension.
CONTRAINDICATION TO DONOR ACCEPTANCE:
Extracerebral malignancy (except localskin neoplasm, Ca. Cervix in situ)Uncontrolled sepsisActive viral infectionHepatitis A or BCytomegalovirusHerpes simplexAIDS - The presence of HIV antibody is also a contraindication.
When possible hepatitis C - positive donor may be used in a hepatitis C - positive recipient.
CRITERIA FOR INDIVIDUAL ORGANS TO BE ACCEPTABLE FOR TRANSPLANTATION:
Due to the shortage of suitable organs and the increasing success of transplantation, the current trend is to accept the organs that would previously have been considered unsuitable. But the ultimate responsibility for accepting or rejecting a potential donor lies with the transplant surgeon.
Kidneys:• Age<70 years• Adequate renal perfusion• Adequate urine output (Not an
absolute requirement)Liver:
• Age<65 years• Organ size compatible with potential
donor• Haemodynamic stability• No history of alcohol abuse or
hypertensionHeart:
• Age <50 years• Organ size compatible with potential
recipient
• Haemodynamic stability- No prolonged cardiac arrest (not
an absolute requirement)- Cardiac index > 2.5L/m2/mt with- PCWP upto12 cmH20- SVR 500 - 1200 dyne.sec/cm5
- Inotropic support <5mgm/kg/mt.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Management of a brain dead organ donor 67 Joseph Rajesh
- <50% discrepancy between left and right heart filling pressures in the face of abnormal PVR
- No ECG evidence of infarctionLungs:
Age < 50 yearsOrgan size compatible withpotential recipientNo history of chronic lungdiseasesNon smoker (not an absolute requirement)Pa02 >250 mmHg with FI02 0.6 PEEP 10cm H20(max)
ANAESTHETIC MANAGEMENT OF A BRAIN DEAD PATIENT FOR MULTIPLE ORGAN HARVESTING In the operating theatre:
Optimal donor management remains important when the donor is taken to the operating room for organ retrieval. The same principles apply to the intraoperative setting also. Maintaining homeostasis with good haemodynamic stability and good diuresis is the key for successful organ recovery.
GOAL:To avoid ischaemic organ damage by
optimising perfusion and maintaining homeostasis.
PRE ANESTHETIC EVALUATION:It includes review of medical and surgical
histories including the cause of the brain death, haemodynamic stability, ventilatory status, acid base and electrolyte values and other organ functions and various investigations.
INTRAOPERATIVE CARE:It is essentially similar to that of other
critically ill patients undergoing major surgery although management of pathophysiologic changes unique to the donor should be clearly understood.
GENERAL PRECAUTIONS:The OR should be kept warm with the
availability of warming blankets and warmed intravenous fluids. A large volume of crystalloids, colloids, blood and blood products should be made available.
MONITORS:The monitors should include ECG,
Invasive arterial pressure monitoring, Central venous pressure monitoring, oxygen saturation, EtC02, temperature and urinary output.
The donor is positioned on the operating table and ventilation continued with a high tidal volume to achieve a PaC02 that is within the normal range. It is necessary that all infusions and monitors be connected before any surgical incision is placed. General anaesthetic agents are required to blunt sympathetic responses during surgery. Mass reflex is caused by neurogenic vasoconstriction and stimulation of adrenal medulla by the spinal reflex arc and will be manifested as tachycardia, perspiration and involuntary movements, which include arm and hand movements, hence at times muscle relaxants may also be necessary.
Isoflurane is the agent of choice because the degree of myocardial depression is less than other agents, halothane is avoided ,in liver donors, and enflurane is better avoided in kidney donors.
POSITIONING OF VASCULAR LINES:The surgical procedure for thoracotomy
in case of retrieving the thoracic organs may involve early ligation of the left innominate vein and the right subclavian artery. A peripheral arterial line must be started on the left arm either in the radial, ulnar, or brachial artery. Placing the arterial lines in the other areas should be avoided since the ability to measure arterial pressure and sample the blood will be lost at critical times of the procedure.
Venous access and Swan - Ganz is provided by multiple cannulation of the right IJV. The ability to monitor CVP or infusing large volume will be lost, once the left innominate vein is ligated. In the majority of the centres, the Swan - Ganz sheath and triple lumen catheter are inserted separately in the IJV. This approach permits the measurement of CVP, infusion of inotropes, administration of hormone replacement, rapid volume replacement and sampling ability.
MANAGEMENT OF VENTILATION:Ventilation is continued with large tidal
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 68 Joseph Rajesh
volumes, using an FI02 of 0.6, achieved by using either oxygen- air or 02-N20.The use of an FI02 of 0.6 provides the maximum 02 content in the blood, to ensure adequate oxygen saturation, while being unlikely to cause 02 toxicity to the donor lungs. In hypothermic donors, mild respiratory alkalosis is preferred to improve tissue perfusion.
HAEMODYNAMIC MONITORINGHaemodynamic monitoring will include,
monitoring direct arterial pressure through an arterial line, continuous CVP and PA pressures via a Swan - Ganz catheter. Inadvertent wedging should be avoided as it can cause possible lung ischaemia in donors. Baseline values of HR, BP, PAP, CVP, and PCWP are recorded. Baseline acid base status and electrolyte estimations are also done.
MANIPULATION OF CIRCULATING VOLUMEThe goal of the circulatory care is to
preserve perfusion of all organs that are to be procured by maintaining the systolic blood pressure between 100 -120 mmHg, with a CVP of less than 10 cmH20 and minimal inotropic support. Hypotension is associated with increased incidence of ATN and non-functioning of the kidneys as well as poor functioning of the liver. Intravascular volume is adjusted with the guidance of CVP. Colloids or RL can be used to manage the fluid deficit. Hypotonic solutions like 5% dextrose should be used to replace insensible losses. This may decrease the requirement of vasopressin. Excessive urine output (>200 ml/ hr) is replaced by hypotonic solutions with replacement of KCI. If hypotension persists even after volume replacement, inotropic support may be initiated, with dopamine as the first choice. Vasopressors like phenylephrine (Alpha stimulants) should be avoided as they cause reduction in splanchnic and coronary blood flow. Severe cases of tachycardia and hypertension caused by mass reflex may be controlled by general anaesthetics, beta blockers or with calcium channel blockers. Arrhythmias (ventricular and supraventricular) are treated with conventional antiarrhythmic agents. If bradycardia is persisting, it should be treated with isoproterenol or epinephrine, because these patients will not show any response to atropine.
In case of cardiac transplantation,
approximately 10% of the blood volume (500ml) is taken under gravity through Swan Ganz into a blood collection bag. This is subsequently used as the major component of the pulmonary preservation solution and this also reduces the left ventricular filling pressure. It is subsequently replaced by 20% albumin to maintain the colloid oncotic pressure of the plasma. Other crystalloid solutions are inappropriate for volume expansion in these situations. Target values for PCWP are between 5and 8 cmH20 and slightly higher values may be used if lung transplantation is not being considered.
Management During SurgeryASSESSMENT OF THE HEART AND LUNGS:
After median sternotomy, macroscopic examination of thoracic organs is done. In particular, evidence of established coronary artery disease in the donor is sought. The visual impression of ventricular wall motion is also noted. The presence of obvious congenital anomalies of the heart is also excluded.
After the heart is examined, both the pleural cavities are widely opened and examination of the lungs is performed. Areas of lobar collapse may be reinflated using controlled manual ventilation under vision and counter compression of normal lung tissue by the surgeon may allow the reexpansion of such collapsed areas and significantly improve the gas exchange. The application of PEEP of 5 - 10 cm of H20 is essential to maintain the FRC and the haemodynamic consequences will be small as the pleura is opened.
HAEMODYNAMIC MANIPULATION:During the abdominal dissection, adrenal
manipulation, both hypertension with periods of hypotension can occur due to catecholamine excess and impaired venous return respectively. During these events, colloid loading, inotropic support and or vasodilatation are adjusted to maintain homeostasis. Although hypertension is best controlled by vasodilators, the resulting tachycardia carries the risk of inducing ischaemia, which will have a deleterious effect on the heart, if transplantation is planned. Although best avoided, the b adrenergic blockers can be used with caution.
RACE 2003 Ramachandra Anaesthesia Continuing Education
of a brain dead organ donor 69 Joseph Rajesh
HYPOTHERMIAHypothermia is seen among 86% of the
brain dead donors due to the loss of hypothalamic function. As the temperature goes below 32 °C, ECG changes like prolonged PR, QT interval and wide QRS complexes are seen. T wave inversion, ST segment depression and decreased threshold for ventricular fibrillation are seen below 28°C. Hypothermia also produces a left shift of the ODC, increase in blood viscosity, a decrease in splanchnic blood flow and glomerular filtration, hyperglycemia, and metabolic and respiratory acidosis. Hence body temperature must be kept within the normal range by keeping the OR warm, by infusing warmed fluids, and by using blankets, warmer etc.
ANTICOAGULATION:Before cannulating any major vessels,
full anticoagulation doses of heparin are administered .The consequences of unrecognised inadequate anticoagulation and thrombosis within the organs during transport would be disastrous.
PHARMACOLOGICAL INTERVENTIONS:Adequate diuresis is important, because
urine output is c prognostic indicator of graft function. Though low dose dopamine may be effective in maintaining adequate renal perfusion and diuresis, high dose may lead to tubular necrosis and non-functioning of the graft. For persistent oliguria, mannitol (0.25 - 0.5 g/kg) and furosemide 40 mg may be used to induce diuresis before division of the renal pedicle and prevent ischaemia induced ATN.
Alpha-adrenergic receptor blockers such as phenoxybenzamine may be useful to produce renal vasodilatation but have a doubtful effect in multiple organ procurement because of their effects on other organs.Some centres recommend broad-spectrum. antibiotics.
ACID BASE & ELECTROLYTE STATUS:Complete haemodynamic profiles,
including arterial and mixed venous acid-base and02 status are made at regular intervals. Estimations of serum electrolytes, especially potassium and glucose are done and supplemented appropriately. Metabolic acidosis caused by inadequate tissue perfusion can
potentially depress the myocardium and is corrected with sodium bicarbonate or THAM.
Electrolyte imbalances (hypernatremia, hypokalemia, hypocalcemia, hypophosphatemia and hypomagnesemia) due to marked fluid shifts in Dl may cause arrhythmias and myocardial dysfunction, and they are treated along the general guidelines.
Once cardioplegia is induced, no further supportive care is needed. After cross clamping of the aorta, mechanical ventilation and monitoring are disconnected and all cannulas are removed.
The sequence of removal of organs is, heart, lungs, liver, pancreas, intestine and kidneys.
SUMMARY:The ICU and its staff play a major role in
solid organ transplantation. The medical care of the donor may be complex and challenging. Delay in certifying brain death and organizing the organ retrieval will make preservation of organ function more difficult and should be avoided at all costs. Much therapy remains empirical and continued research is required to further define optimum management of the donor.
References:1. David.J. Powner, et al Brain Death
definition, Determination and Physiological effects of donor organs, The Text Book of Critical Care, 1894-1899.
2. Eelco F.M. Wijdicks, The Diagnosis of Brain Death: The New England Journal of Medicine, April 2001, Volume 344: 1215 -1221.
3. Finfer. S. R. Support of the Potential Organ Donor; Principles and Practice of Critical Care; 484 - 493.
4. Johnston. K.R. et al, Optimization of Multiorgan Donors and Selection of Thoracic Organs for Transplantation, Principles and Practice of Critical Care; 431-444.
5. Pallis.C, Brain Stem Death: The evolution of a concept. Text book of transplantation (75-100)
6. Ron Shapiro et al, Management of Potential Cadaveric Donor; up to date 10.1 July 2001.
7. Tarek Razek et al, Issues In Potential Organ Donor Management; Surgical Clinics of North America, June 2000 : Volume 80. No.3.
8. William shoemaker, Ake grenvik : Multiple organ Procurement ; Text book of critical care (fourth edition -1910-1923)
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 70 S. Manimala Rao
Obesity means excessive body fat and the term obese is derived from a Latin word that means fattened by eating. The amount of fat tissue is increased to such an extent that mental and physical health is affected and life expectancy is reduced.
Body mass index (BMI) or Quetelet’s index is calculated from subjects’ height and weight. It is used to indicate obesity. Obesity is indicated by BMI > 30.0 (M), > 28.6 (F). Many clinical parameters depict women as pear shaped, accumulating fat at the bottom and this is regarded as safe, fat being stored between the skin and the body wall. In men, we find the classic beer belly look compared to the rounded apple, here the fat is stored in the internal organs. Morbid obesity is when BMI is more than 40 kg/m2.
PREVALENCE AND EPIDEMIOLOGYThere is a slow but steady increase in
obesity. In UK the statistics showed an increase; in 1980 - 6% males and 8% females and in 1987 - 8% males and 12% females were regarded as obese. Obesity in children is also on the rise. Prevalence varies with the socioeconomic status. In developed countries, poverty is associated with a greater prevalence whereas in developing countries, there is a higher prevalence amongst the affluent. Obesity is complex, wherein the net energy intake exceeds the net energy expenditure over a prolonged period of time.
PATHOPHYSIOLOGYThe brain controls the appetite by means
of signals triggered by dietary breakdown products and also by autonomic signals produced by disturbance of the stomach and intestines.
The multiple signals generated are processed by complex interactions between neuronal networks and neuro transmitters. Most important of them are cholecystokines 8 (CCK 8), which act at the gut and the brain. It induces satiation, is released at the beginning of a meal and promotes pancreatic secretion of insulin, which lowers the sugar and increases the appetite. Insulin crosses the blood brain barrier and triggers the hypothalamus, which juggles many other signals. Therefore, the complexity of weight maintenance is evident. 25-30% of human variations in BMI are genetic and the rest is due to environmental factors. It is a complex picture as to how normal weight is maintained. The pathways regulating weight form a series of redundant regulatory loops. If one is weakened or attenuated, the other can take over. It is this redundancy that regulates calorie storage, but the same redundancy makes it hard to get a handle on how to prevent and treat obesity. It is an imbalance between food intake and energy expenditure. The balancing act involves neural signaling and endocrinal processes. These can be both central and peripheral. Problems can occur any where in this complex system.
GENETIC PREDISPOSITIONObesity tends to be familial. Children of
two obese parents have a 70% chance to become obese. The genetic issues account for 30% and are linked to at least 6 genes. 70% is dependent on environmental factors. Genetic susceptibility may predispose to environmental issues.
ETHNIC INFLUENCESIn USA, the African Americans and
Mexicans have a higher rate of obesity than the Whites. Asian migrates have a more central
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 71 S. Manimala Rao
distribution of fat associated with increased risk of diabetes and coronary artery disease.
MEDICAL DISEASESCushing’s disease, hypothyroidism,
medications like steroids, antidepressants and antihistamines may also lead to obesity.
RISK FACTORSMale gender, middle age, night sedation,
evening alcohol can all compound the problem. Other features which can help identify are BMI > 30 kg/m2, hypertension, observed episodes of apneoea during sleep, hypoxemia, hypercapnia, changes in ECG and ECHO. Definite diagnosis is made by polysomnography in the sleep laboratory. The obese pose great challenges to surgery, anaesthesia, obstetrics, trauma and in the ICU.
Diabetes, hypertension, hyperlipidemia, heart diseases, increased rates of colon and breast cancer, asthma are all linked to rising levels of obesity. A BMI>29 kg/m2 increases the prevalence of pulmonary embolism. The risk of coronary artery disease is doubled if BMI is > 25kg/m2. A BMI of 35kg/m2 leads to a 40-fold increase in developing diabetes, respiratory diseases, sleep apnoea and osteoarthritis. The risk of death increases with body weight. Mortality rises exponentially with increasing body weight.
CHANGES IN VARIOUS SYSTEMS OBESITY AND RESPIRATORY SYSTEM
5% of morbidly obese will have Obstructive Sleep Apnoea (OSA), frequent episodes of apnoea or hypercapnia, snoring and daytime sleepiness. Recurrent apnoea leads to hypoxia, hypercapnia, pulmonary and systemic vascular hypertension, which in turn leads to right ventricle failure. Loss of pharyngeal muscle tone and significant narrowing of airway increases airflow turbulence.
Acid base disturbances of Obstructive Sleep Apnoea (OSA)
Respiratory acidosis is limited to sleep, in the beginning. The longer the problem, alterations occur in breathing patterns with desensitization of the respiratory center to hypercapnia leading to type II respiratory failure.
This leads to increased dependence on the hypoxic drive for ventilation - Pickwickian syndrome, which is characterized by obesity, hypersomnolence, hypoxia, hypercapnia, right ventricular failure and polycythemia.
AirwayPerfect airway, particularly upper is
essential before any anaesthetic management. In obese patients, difficulties are encountered for mask ventilation; tracheal intubations may be difficult. The percentage of difficult intubation is quoted to be 13%. Excessive fat at the upper airway, short neck, high anteriorly placed larynx and restricted cervical spine movements are a few problems.
Obesity and gas exchangeIncreased mass of abdominal and
thoracic contents alters the lung volumes. Decrease in functional residual capacity (FRC) is seen exponentially with increasing BMI. Expiratory reserve volume and total lung capacity are decreased.
FRC may be reduced in the upright position to the extent that it falls within the range of the closing capacity with subsequent small airway closure, ventilation perfusion mismatch, right to left shunting and arterial hypoxemia. The reduction of FRC impairs the capacity of obese patients to tolerate apnoea. They desaturate rapidly after induction of anaesthesia despite preoxygenation due to the smaller 02 reservoir and increased oxygen consumption. Residual volume remains normal or slightly increased due to the increased gas trapping and coexisting obstructive airway disease.
02consumption and C02productionBoth are increased in obese patients as
a result of the metabolic activity of excess fat and increased workload on supportive tissues. With exercise, Oz consumption rises more sharply in the obese than in the non-obese.
Gas exchangeOnly a modest defect in gas exchange
is noted in the obese patients with a reduction in Pa02, increase in Aa02gradient and increase in shunt fraction. This is increased markedly with
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 72 S. Manimala Rao
induction of anaesthesia. PEEP improves the condition, but at the expense of cardiac output and 02 delivery.
Compliance and ResistanceIncreased BMI exponentially decreases
the compliance. As the fat content increases, compliance decreases, but it is also due to a decrease in lung compliance. This is due to the increase in pulmonary blood volume, increased total respiratory resistance and shallow rapid breathing which can limit maximum ventilatory capacity. These are all more marked in the supine position.
Work of breathingThere is a 30% increase observed in the
work of breathing. If hypoventilation occurs in daytime, the work of breathing may approach four times that predicted.
CARDIOVASCULAR SYSTEMA higher incidence of cardiovascular
morbidity is associated with obesity. Mild to moderate hypertension is found in 60-70%, severe in 5-10%. It is the commonest problem followed by ischaemic heart disease. An expansion of extracellular volume resulting in increased blood volume and cardiac output is characteristic of obesity-induced hypertension. The exact mechanism is not known, but an interplay of genetic, hormonal, renal and haemodynamic factors are implicated. Hyperinsulinaemia, activating the sympathetic nervous system and causing sodium retention, increases the pressor norepinephrine and angiotensin II activity. Concentric hypertrophy of the left ventricle leads to cardiac failure. Obesity is an independent risk factor for Ischaemic Heart Disease (IHD) and this is more common in individuals with central obesity. Blood volume is increased, most extra volume being distributed to the fat organ. Splanchnic blood flow is increased by 20%, while renal and cerebral blood flow are normal. A 3- 4mmHg increase in systolic and 2mmHg increase in diastolic pressure is noted for every 10kg increase of weight.
Cardiac arrhythmias can be precipitated in the obese by any number of factors, viz. hypoxia, hypercapnia, electrolyte imbalance,
diuretic therapy or fatty infiltration of the conducting tissue.
Cardiac functionObese patients are at risk of a specific
form of obesity induced cardiac dysfunction. Left ventricular systolic and diastolic functions are affected. Obesity induced cardiomyopathy is well documented. Blood volume is increased and cardiac output increases by 20-30ml/kg of excess body fat. The obese tolerate exercise poorly. Any increase in the cardiac output is by an increase in the heart rate.
OBESITY AND DIABETESType II Diabetes mellitus is an
independent risk factor. The incidence of abnormal glucose tolerance in patients undergoing bariatric surgery is more than 10%.
THROMBOEMBOLIC DISEASEDeep vein thrombosis appears twice as
common in obese patients. It is the commonest complication of bariatric surgery with an incidence of 2.4% - 4.5%. It is due to prolonged immobilization that leads to venous stasis and polycythemia, and increased abdominal pressure with increased pressure on the deep veins. Decreased fibrinolytic activity with increased fibrinogen concentration could also be responsible.
OBESITY AND Gl DISORDERSThe obese have an increased integral
abdominal pressure, a high volume and low pH of gastric contents, delayed gastric emptying and an increased incidence of gastro esophageal reflex. They also have a high risk for aspiration of gastric contents followed by pneumonia. Gastric volume is 75% higher than in normal individuals.
DRUGS, PHARMCODYNAMICS AND KINETICSObesity leads to an alteration in the
distribution, binding and elimination of many drugs. For drugs with narrow therapeutic indices like aminoglycosides and digoxin, toxic reactions can occur if the patients are dosed according to actual body weight. Drug dose should be reduced keeping the lean body mass in view. Absorption of drugs orally remains unchanged in the obese patient.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 73 S. Manimala Rao
Volume Of Distribution (VD)The apparent volume of distribution of a
drug in the obese patient is influenced by a number of factors which include, the size of the fat organ, the increase in lean body mass, the increase in blood volume and cardiac output, reduced total body water, alterations in plasma protein binding and lipophilicity of the drug. Highly lipophilic drugs have an increased volume of distribution (Thiopentone). Increase in the volume of distribution will reduce the elimination half-life unless the clearance is increased. Thiopentone, Benzodiazepines, and potent inhalation agents, may persist for a longer time after discontinuation. Regarding protein binding, alterations may occur due to the high levels of cholesterol, inhibiting protein binding; therefore more free drug is available. In contrast, increased concentrations of a acid glycoprotein may increase the degree of protein binding of other drugs (e.g. local anaesthetics), thus reducing the free plasma fraction.
EliminationClearance is mostly reduced in obese
patients. Cardiac failure and decrease in liver blood flow may slow elimination of midazolam and lignocaine. Renal clearance is increased in obesity because of the increased renal blood flow and GFR. If renal impairment is present, elimination takes a longer time.
Hepatic metabolism is altered in obese patients for volatile agents. Reductive metabolism of halothane is more in obese patients. This may be an important factor in liver injury. Nephrotoxicity can occur due to high fluoride concentrations with halothane and enflurane. Sevoflurane has high hepatic metabolism but does not show adverse effects. Isoflurane does not increase fluoride concentration, and remains the agent of choice in the obese.
ANAESTHETIC IMPLICATIONS Preoperative:
Thorough clinical examination is mandatory with excellent and relevant history taking, checking BP with an appropriate sized cuff to identify hypertension and looking for signs of cardiac failure, viz. increase in jugular pulse, added heart sounds, pulmonary crackles, hepato
jugular reflex and peripheral edema. These signs may be difficult to elicit in the morbidly obese. A thorough assessment of the respiratory system for OSA is very essential.
InvestigationsBesides routine investigations, ECG is
mandatory as tachyarrhythmias are common. Echo may be difficult but will provide valuable information regarding eccentric left ventricular hypertrophy. TEE may provide more insight. Cardiological evaluation is beneficial for further investigation. Optimization of blood pressure, treatment of cardiac failure, or if necessary, coronary angioplasty may be suggested. X-ray chest, lung function tests and baseline arterial blood gases may be useful in the morbidly obese. A thorough history regarding respiratory function and sleep apnoea are a must. Signs of right ventricular failure must be looked for.
Airway assessmentIt is mandatory to plan the type of airway
management. A thorough examination can prevent catastrophes, as it will enable us to select the best technique for the patient. Preoperative evaluation of the airway must include:
1. Assessment of the head and neck; flexion, extension and lateral rotation.
2. Assessment of jaw mobility and mouth opening.
3. Inspection of the oropharynx.4. Checking the patency of the nostrils5. Inspection of previous anaesthetic
charts.
If potential airway obstruction is suspected at direct or indirect laryngoscopy, CT scan of soft tissues would be helpful.
Assessment of veins for placing infusion must be done in the pre- operative visit. Examination of the feet and back for any ulcer or sore is mandatory. Examination of the calf muscles for any redness or tenderness gives a fairly good idea regarding deep vein thrombosis.
Preoperative medicationAvoid narcotics and sedatives. Avoid
intramuscular and subcutaneous injections. If fibre optic intubation is planned, include an
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 74 S. Manimala Rao
antisialogogue. All morbidly obese must have acid aspiration prophylaxis. A combination of the H2 blocker, ranitidine 150mg and prokinetic metaclopramide 10mg orally given 12 hrs and 2hrs before surgery will reduce the risk of aspiration. Some anaesthetists prefer to give 30ml of 0.3 M sodium citrate before induction. Continue the normal medications on the day of surgery. Stop ACE inhibitors the day before surgery. Dextrose- Insulin regimen should follow in all diabetics, unless it is a very short surgical procedure. Insulin requirements may increase in the postoperative period. Prophylactic antibiotics are given as per the hospital protocols, after discussion with the surgeon and the microbiologist.
POSITION AND TRANSFERExtra care, special tables and adequate
padding of pressure areas should be provided. Appropriate manpower to shift is mandatory. Compression of inferior vena cava is avoided by lateral tilt or a wedge. Transfer of obese patients is done in their own bed. Special beds are ordered in other countries.
INTRAVENOUS LINESPeripheral lines may be difficult.
Establish central lines in the beginning to avoid calamities. Even these are difficult in the morbidly obese. Doppler or ultrasound guided placements could reduce complications.
MONITORINGIntraarterial blood pressure measurement
is advocated for all but most minor procedures, ECG, Pulse oximetry, Capnography and neuromuscular monitors are essential. Central venous catheters are essential and PA Catheters should be used where indicated.
REGIONAL ANAESTHESIAWhere it is possible and feasible, regional
anaesthesia should be administered. One can reduce the use of opioids, inhalational agents, reduce postoperative complications, and prevent the loss of airway and aspiration. Excellent postoperative analgesia can be given by placing the epidural catheters in the sitting position, using ultrasound for identification of the space. Local anaesthetic requirements are 50-70% reduced in the morbidly obese. Higher blocks are
common. Blocks extending above T5 can cause cardiorespiratory collapse. All resuscitation equipment should be handy.
SYSTEMIC OPIOIDSThese are hazardous in obese patients;
intramuscular route is not recommended. If intravenous route is preferred, patient controlled analgesia should be the best option. Oral analgesics like paracetamol and cox2 inhibitors may be appropriate. Postoperative analgesia with local anaesthetics and opioids via the epidural catheter will provide ideal pain relief with minimal complications.
OBSTETRICS AND MORBIDLY OBESEAll attending complications are
compounded. Regional anaesthesia is a better choice; avoid general anaesthesia as far as possible. Putting an epidural catheter during labor is a better option. Local anaesthetic requirement may be reduced by up to 25% in the obese pregnant state.
OBESE PATIENTS AND TRAUMAThe out come in obese patients with
trauma is poor. The obese patients have more blunt trauma and chest trauma is more compared to head injury. Investigations are more difficult to handle and interpret. They may require earlier respiratory support and higher oxygen concentration.
OBESE PATIENT IN THE ICUIt is held that the outcome is poor for
these patients. Postoperative pulmonary events are more in obese patients. Morbidly obese may present in the emergency room and intensive care with formidable challenges. A better understanding of the pathophysiology and complications may improve the outcome. Anaesthesiologist has a major role to play as the perioperative physician at every level.
BARIATRIC SURGERY The indications for bariatric surgery are as follows:
BMI >40kg/m2
BMI >35kg/m2 with co morbiditiesShould show that dietary attempts have beenineffective
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 75 S. Manimala Rao
Bariatric surgery (weight reductive surgery) addresses both perioperative care and long-term management. The patients must have a clear understanding of the risks, benefits and complications, and may require life long management strategies.
Types of Bariatric surgeryBariatric surgery comprises two types
namely restrictive and malabsorptive. The common operations include Roux-en-Y grade bypass, vertical banded gastroplasty, bitropancreatic diversion and its variations, various gastric banding procedures, gastric bypass procedures and laparoscopic procedures of the above-mentioned operations.
The preoperative evaluation consists of obesity evaluation, behavioural evaluation, medical evaluation, surgical evaluation, which includes education & potential risk, and anaesthetic evaluation. A team is usually available in other countries for patients with morbid obesity undergoing bariatric surgery.
OBESITY ASSOCIATED -MEDICAL CONDITIONS
The various medical conditions associated with obesity are:
• CAD• Cardiomyopathy• Cerebrovascular disease• Diabetes mellitus and other endocrine
diseases• Infertility
• Hepatobilary disease and gall stones• Malignancies, depression• Degenerative joint disease, chronic back
pain• Respiratory abnormalities• GE reflux• Sudden death
COMPLICATIONSThe complications associated with
bariatric surgery are as follows:• Nutritional deficiencies• Cardiovascular disease and sudden
death
• Pulmonary embolism, which is a leading cause of death
• Bleeding and splenic injury• Gastrointestinal leaks - shown by
tachypnea and tachycardia• Wound infections 1-3%, wound
dehiscence, vomiting and diarrhea• Sternal dilation
The morbidity and mortality has come down for these procedures to <19%.
As we enter the new millennium, severe obesity remains an incurable disease. The consequences and cost to society are significant. Though etiology is becoming more clear, non- surgical treatments are still inadequate for achieving sustained and significant weight loss. Surgical procedures have evolved into safe and effective options. Newer technologies such as laparoscopy should further advance the field. For appropriately selected patients, surgery can achieve the weight loss necessary to prevent the development of significant medical conditions and improve the quality of life. Unfortunately, dietary indiscrimination and malabsorptive eating behaviour can result in weight loss failure despite an excellent surgical result. Therefore, preoperative evaluation and education is a corner stone for long-term success.
CONCLUSIONSMorbidly obese patients can be
encountered more commonly in the West. But with changing lifestyles, a high incidence is now seen in the younger individuals. One may encounter them in the practice of anaesthesia for different types of surgical procedures, bariatric surgeries, trauma and in the ICU setup. They do pose tremendous challenges. Understanding the pathophysiology, anticipating the problem and preventing calamities by a systematic approach will certainly bring down the rate of complications.
REFERENCES
1. J.P.Adams and P.G.Murphy. Obesity in anaesthesia and intensive care. BJA 2000; 85 (1 ):91 -108.
2. Anthony P.Adams, Jereney N Cashnar. Recent Advances in Anaesthesia and Analgesia. Churchill Livingston 2000; Chapter II, Vol 21.
RACE 2003 Ramachandra Anaesthesia Continuing Education
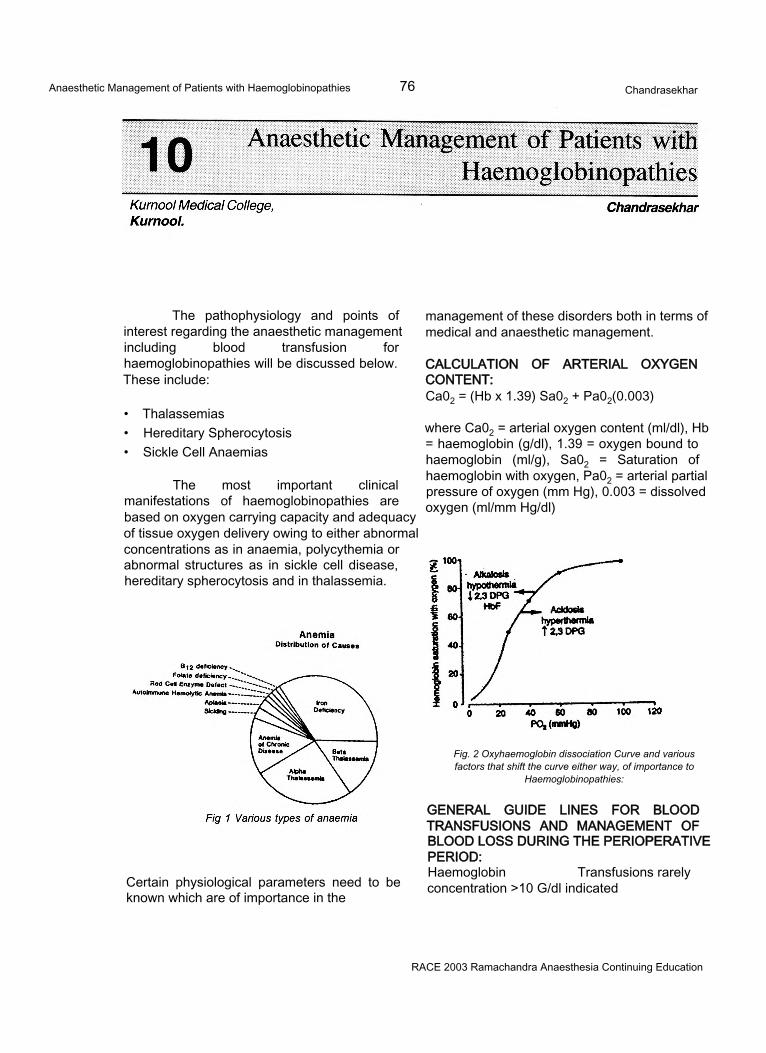
Anaesthetic Management of Patients with Haemoglobinopathies 76 Chandrasekhar
The pathophysiology and points of interest regarding the anaesthetic management including blood transfusion for haemoglobinopathies will be discussed below. These include:
• Thalassemias• Hereditary Spherocytosis• Sickle Cell Anaemias
The most important clinical manifestations of haemoglobinopathies are based on oxygen carrying capacity and adequacy of tissue oxygen delivery owing to either abnormal concentrations as in anaemia, polycythemia or abnormal structures as in sickle cell disease, hereditary spherocytosis and in thalassemia.
management of these disorders both in terms of medical and anaesthetic management.
CALCULATION OF ARTERIAL OXYGEN CONTENT:Ca02 = (Hb x 1.39) Sa02 + Pa02(0.003)
where Ca02 = arterial oxygen content (ml/dl), Hb = haemoglobin (g/dl), 1.39 = oxygen bound to haemoglobin (ml/g), Sa02 = Saturation of haemoglobin with oxygen, Pa02 = arterial partial pressure of oxygen (mm Hg), 0.003 = dissolved oxygen (ml/mm Hg/dl)
Fig. 2 Oxyhaemoglobin dissociation Curve and various factors that shift the curve either way, of importance to
Haemoglobinopathies:
Certain physiological parameters need to be known which are of importance in the
GENERAL GUIDE LINES FOR BLOOD TRANSFUSIONS AND MANAGEMENT OF BLOOD LOSS DURING THE PERIOPERATIVE PERIOD:Haemoglobin Transfusions rarelyconcentration >10 G/dl indicated
RACE 2003 Ramachandra Anaesthesia Continuing Education
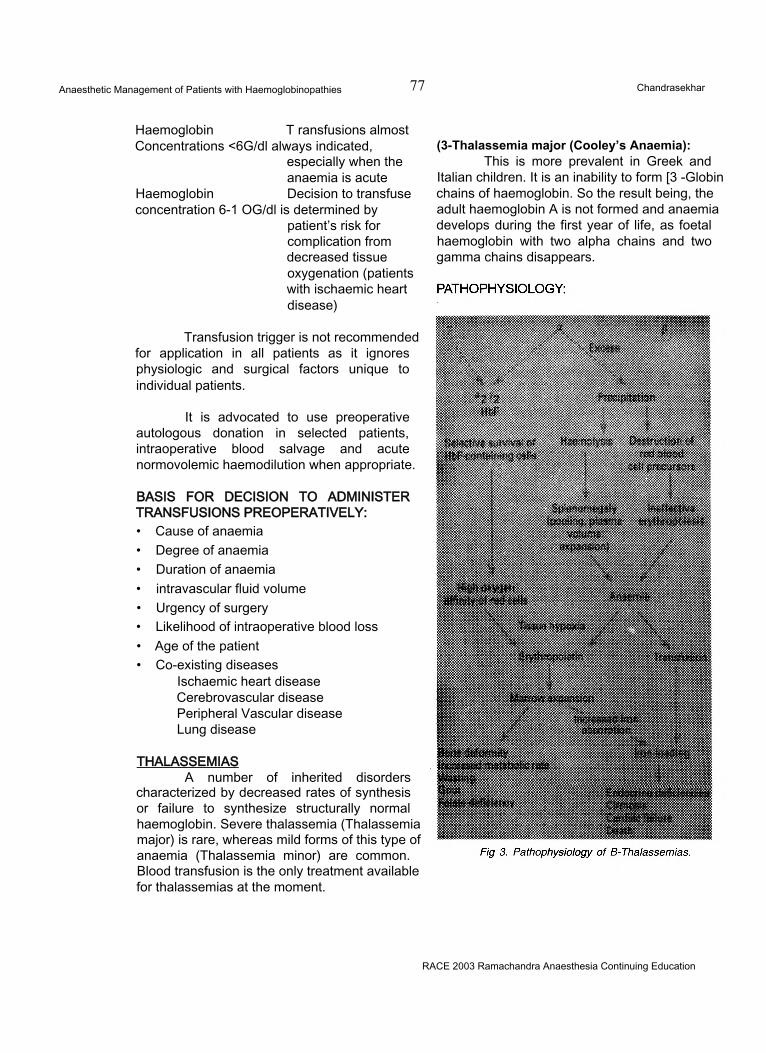
Anaesthetic Management of Patients with Haemoglobinopathies 77 Chandrasekhar
Haemoglobin T ransfusions almostConcentrations <6G/dl always indicated,
especially when the anaemia is acute
Haemoglobin Decision to transfuseconcentration 6-1 OG/dl is determined by
patient’s risk for complication from decreased tissue oxygenation (patients with ischaemic heart disease)
Transfusion trigger is not recommended for application in all patients as it ignores physiologic and surgical factors unique to individual patients.
It is advocated to use preoperative autologous donation in selected patients, intraoperative blood salvage and acute normovolemic haemodilution when appropriate.
(3-Thalassemia major (Cooley’s Anaemia):This is more prevalent in Greek and
Italian children. It is an inability to form [3 -Globin chains of haemoglobin. So the result being, the adult haemoglobin A is not formed and anaemia develops during the first year of life, as foetal haemoglobin with two alpha chains and two gamma chains disappears.
BASIS FOR DECISION TO ADMINISTER TRANSFUSIONS PREOPERATIVELY:• Cause of anaemia• Degree of anaemia• Duration of anaemia• intravascular fluid volume• Urgency of surgery• Likelihood of intraoperative blood loss• Age of the patient• Co-existing diseases
Ischaemic heart disease Cerebrovascular disease Peripheral Vascular disease Lung disease
THALASSEMIASA number of inherited disorders
characterized by decreased rates of synthesis or failure to synthesize structurally normal haemoglobin. Severe thalassemia (Thalassemia major) is rare, whereas mild forms of this type of anaemia (Thalassemia minor) are common. Blood transfusion is the only treatment available for thalassemias at the moment.
RACE 2003 Ramachandra Anaesthesia Continuing Education
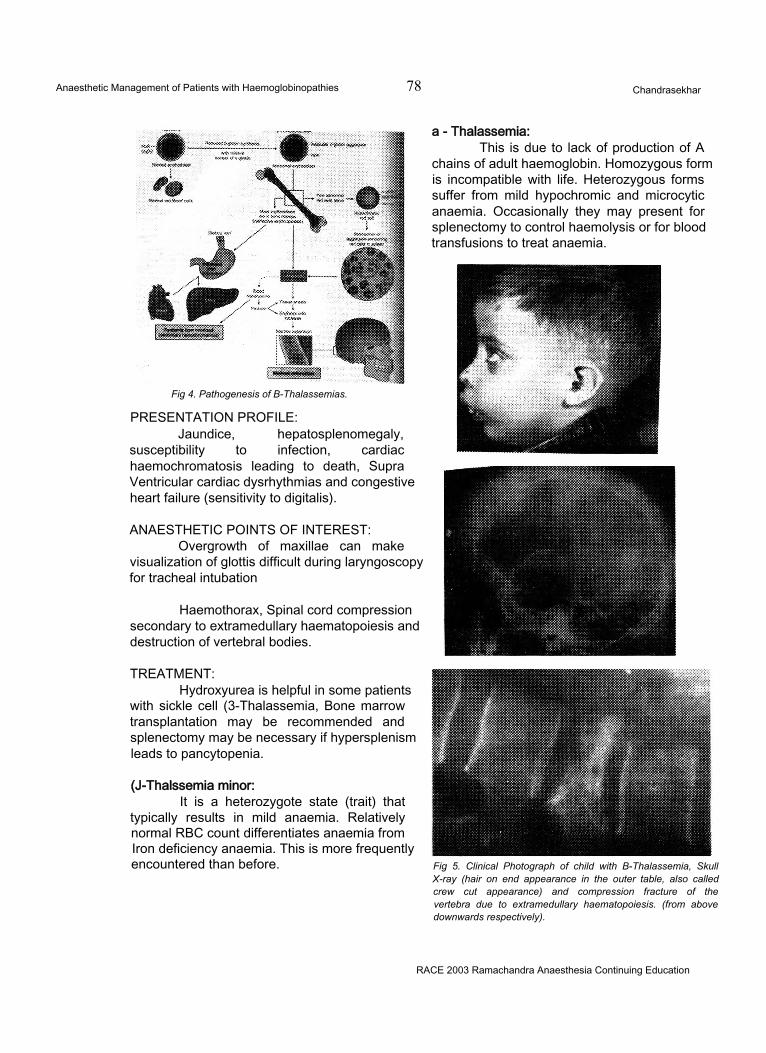
Anaesthetic Management of Patients with Haemoglobinopathies 78 Chandrasekhar
Fig 4. Pathogenesis of B-Thalassemias.
PRESENTATION PROFILE:Jaundice, hepatosplenomegaly,
susceptibility to infection, cardiac haemochromatosis leading to death, Supra Ventricular cardiac dysrhythmias and congestive heart failure (sensitivity to digitalis).
ANAESTHETIC POINTS OF INTEREST:Overgrowth of maxillae can make
visualization of glottis difficult during laryngoscopy for tracheal intubation
Haemothorax, Spinal cord compression secondary to extramedullary haematopoiesis and destruction of vertebral bodies.
TREATMENT:Hydroxyurea is helpful in some patients
with sickle cell (3-Thalassemia, Bone marrow transplantation may be recommended and splenectomy may be necessary if hypersplenism leads to pancytopenia.
(J-Thalssemia minor:It is a heterozygote state (trait) that
typically results in mild anaemia. Relatively normal RBC count differentiates anaemia from Iron deficiency anaemia. This is more frequently encountered than before. Fig 5. Clinical Photograph of child with B-Thalassemia, Skull
X-ray (hair on end appearance in the outer table, also called crew cut appearance) and compression fracture of the vertebra due to extramedullary haematopoiesis. (from above downwards respectively).
a - Thalassemia:This is due to lack of production of A
chains of adult haemoglobin. Homozygous form is incompatible with life. Heterozygous forms suffer from mild hypochromic and microcytic anaemia. Occasionally they may present for splenectomy to control haemolysis or for blood transfusions to treat anaemia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
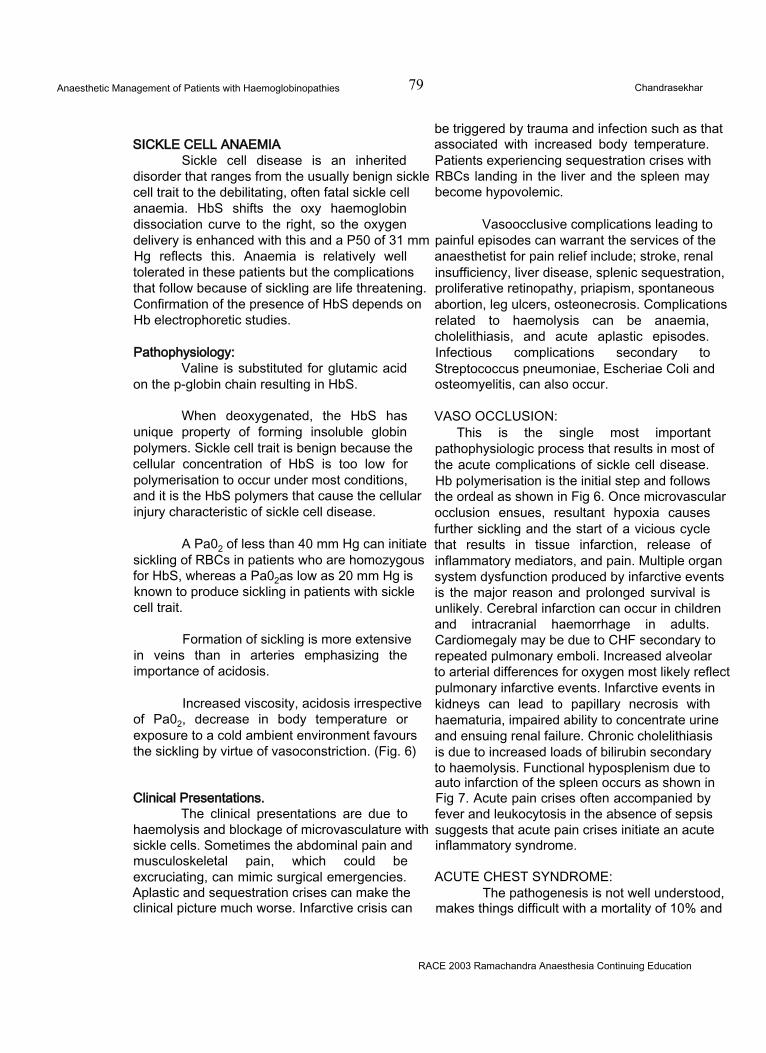
Anaesthetic Management of Patients with Haemoglobinopathies 79 Chandrasekhar
SICKLE CELL ANAEMIASickle cell disease is an inherited
disorder that ranges from the usually benign sickle cell trait to the debilitating, often fatal sickle cell anaemia. HbS shifts the oxy haemoglobin dissociation curve to the right, so the oxygen delivery is enhanced with this and a P50 of 31 mm Hg reflects this. Anaemia is relatively well tolerated in these patients but the complications that follow because of sickling are life threatening. Confirmation of the presence of HbS depends on Hb electrophoretic studies.
Pathophysiology:Valine is substituted for glutamic acid
on the p-globin chain resulting in HbS.
When deoxygenated, the HbS has unique property of forming insoluble globin polymers. Sickle cell trait is benign because the cellular concentration of HbS is too low for polymerisation to occur under most conditions, and it is the HbS polymers that cause the cellular injury characteristic of sickle cell disease.
A Pa02 of less than 40 mm Hg can initiate sickling of RBCs in patients who are homozygous for HbS, whereas a Pa02as low as 20 mm Hg is known to produce sickling in patients with sickle cell trait.
Formation of sickling is more extensive in veins than in arteries emphasizing the importance of acidosis.
Increased viscosity, acidosis irrespective of Pa02, decrease in body temperature or exposure to a cold ambient environment favours the sickling by virtue of vasoconstriction. (Fig. 6)
Clinical Presentations.The clinical presentations are due to
haemolysis and blockage of microvasculature with sickle cells. Sometimes the abdominal pain and musculoskeletal pain, which could be excruciating, can mimic surgical emergencies. Aplastic and sequestration crises can make the clinical picture much worse. Infarctive crisis can
be triggered by trauma and infection such as that associated with increased body temperature. Patients experiencing sequestration crises with RBCs landing in the liver and the spleen may become hypovolemic.
Vasoocclusive complications leading to painful episodes can warrant the services of the anaesthetist for pain relief include; stroke, renal insufficiency, liver disease, splenic sequestration, proliferative retinopathy, priapism, spontaneous abortion, leg ulcers, osteonecrosis. Complications related to haemolysis can be anaemia, cholelithiasis, and acute aplastic episodes. Infectious complications secondary to Streptococcus pneumoniae, Escheriae Coli and osteomyelitis, can also occur.
VASO OCCLUSION:This is the single most important
pathophysiologic process that results in most of the acute complications of sickle cell disease. Hb polymerisation is the initial step and follows the ordeal as shown in Fig 6. Once microvascular occlusion ensues, resultant hypoxia causes further sickling and the start of a vicious cycle that results in tissue infarction, release of inflammatory mediators, and pain. Multiple organ system dysfunction produced by infarctive events is the major reason and prolonged survival is unlikely. Cerebral infarction can occur in children and intracranial haemorrhage in adults. Cardiomegaly may be due to CHF secondary to repeated pulmonary emboli. Increased alveolar to arterial differences for oxygen most likely reflect pulmonary infarctive events. Infarctive events in kidneys can lead to papillary necrosis with haematuria, impaired ability to concentrate urine and ensuing renal failure. Chronic cholelithiasis is due to increased loads of bilirubin secondary to haemolysis. Functional hyposplenism due to auto infarction of the spleen occurs as shown in Fig 7. Acute pain crises often accompanied by fever and leukocytosis in the absence of sepsis suggests that acute pain crises initiate an acute inflammatory syndrome.
ACUTE CHEST SYNDROME:The pathogenesis is not well understood,
makes things difficult with a mortality of 10% and
RACE 2003 Ramachandra Anaesthesia Continuing Education
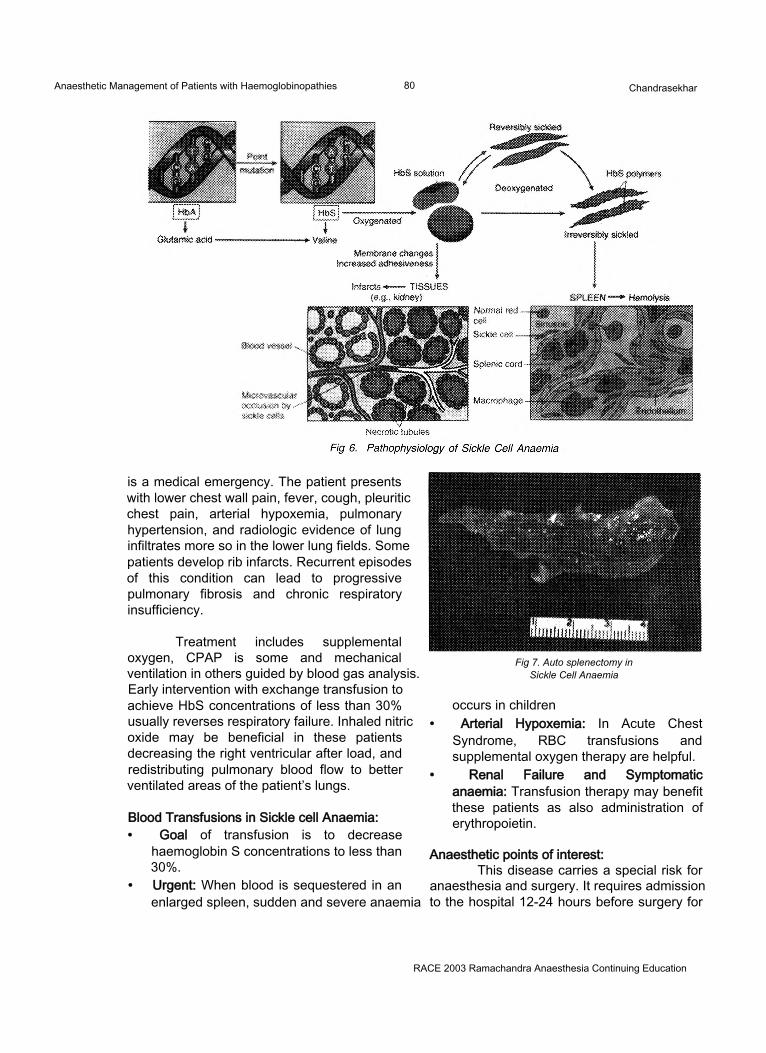
Anaesthetic Management of Patients with Haemoglobinopathies 80 Chandrasekhar
is a medical emergency. The patient presents with lower chest wall pain, fever, cough, pleuritic chest pain, arterial hypoxemia, pulmonary hypertension, and radiologic evidence of lung infiltrates more so in the lower lung fields. Some patients develop rib infarcts. Recurrent episodes of this condition can lead to progressive pulmonary fibrosis and chronic respiratory insufficiency.
Treatment includes supplemental oxygen, CPAP is some and mechanical ventilation in others guided by blood gas analysis. Early intervention with exchange transfusion to achieve HbS concentrations of less than 30% usually reverses respiratory failure. Inhaled nitric oxide may be beneficial in these patients decreasing the right ventricular after load, and redistributing pulmonary blood flow to better ventilated areas of the patient’s lungs.
Blood Transfusions in Sickle cell Anaemia:• Goal of transfusion is to decrease
haemoglobin S concentrations to less than 30%.
• Urgent: When blood is sequestered in an enlarged spleen, sudden and severe anaemia
Fig 7. Auto splenectomy in Sickle Cell Anaemia
occurs in children• Arterial Hypoxemia: In Acute Chest
Syndrome, RBC transfusions and supplemental oxygen therapy are helpful.
• Renal Failure and Symptomatic anaemia: Transfusion therapy may benefit these patients as also administration of erythropoietin.
Anaesthetic points of interest:This disease carries a special risk for
anaesthesia and surgery. It requires admission to the hospital 12-24 hours before surgery for
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of Patients with Haemoglobinopathies 81 Chandrasekhar
optimal hydration with IV fluids. Patients requiring emergency surgery are often at greatest risk for postoperative sickle cell disease related complications (consult haematologist always). Patients with sickle cell trait do not require blood transfusions preoperatively except before open- heart surgery or extensive thoracic surgery. The aim of transfusion is to increase the haematocrit to 30% (only for major surgeries).
Preoperatively, ventilation should not be depressed by aggressive premedication.
Perioperatively, the goal is to maintain near normal arterial oxygenation, hydration, body temperature, proper position, avoiding acidosis that can follow hypoventilation and replacement of blood loss as and when necessary.
Administration of supplemental oxygen is necessary in patients in whom regional techniques are selected.
Avoid overzealous transfusion of RBCs to prevent circulatory stasis. There may be a theoretical hazard in the use of extremity tourniquets as they predispose to localized circulatory stasis, acidosis and hypoxia with subsequent sickling.
There is no evidence that specific anaesthetic drugs are optimal for administration. Regional techniques are preferred over general anaesthesia. In fact there is evidence to show that circulating sickle cells have been reduced during and following general anaesthesia. Epidural and spinal anaesthesia produce compensatory vasoconstriction and decreased Pa02 in the nonblocked areas, making these areas theoretically vulnerable to infarction.
Patients with sickle cell trait tolerate cardiopulmonary bypass with no increased risk whereas attendant low peripheral blood flow, hypothermia and acidosis pose extra risk to patients with sickle cell disease.
The postoperative period is very critical for these patients. Incisional pain, use of analgesics, a high incidence of pulmonary infections and expected decreases in arterial
oxygenation predispose to sickling. So it is necessary to maintain near normal arterial oxygenation, give adequate IVfluids for hydration, consider incentive spirometry for improvement of lung function and oxygenation. The patient should be observed in the hospital overnight as acute chest syndrome may occur as a complication with peak incidence after 48 hours of surgery. PCA or neuraxial opioids are better choices for postoperative analgesia.
Pain Relief in the management of painful episodes.
There is no standard method for pain relief, resulting in institution of all possible measures like:• Fluid Replacement (3-4 litres/day in adults)• Analgesics - Opioids (morphine) in regular
doses and for breakthrough pain as well, PCA with morphine and adjunctive drugs like NSAIDS taking into consideration the standard contraindications forthese drugs. Response is followed up with pain scales and the pain therapy is optimally tailored to the individual patient. Extradural analgesia has been used
Fig 8. Dactylitis in Sickle Cell Anaemia.
in the pain management of sickle cell crises wherever possible.
HEREDITARY SPHEROCYTOSISOwing to the abnormalities in the RBC
cell membrane, water enters the RBCs along with sodium at an increased rate resulting in swollen
RACE 2003 Ramachandra Anaesthesia Continuing Education
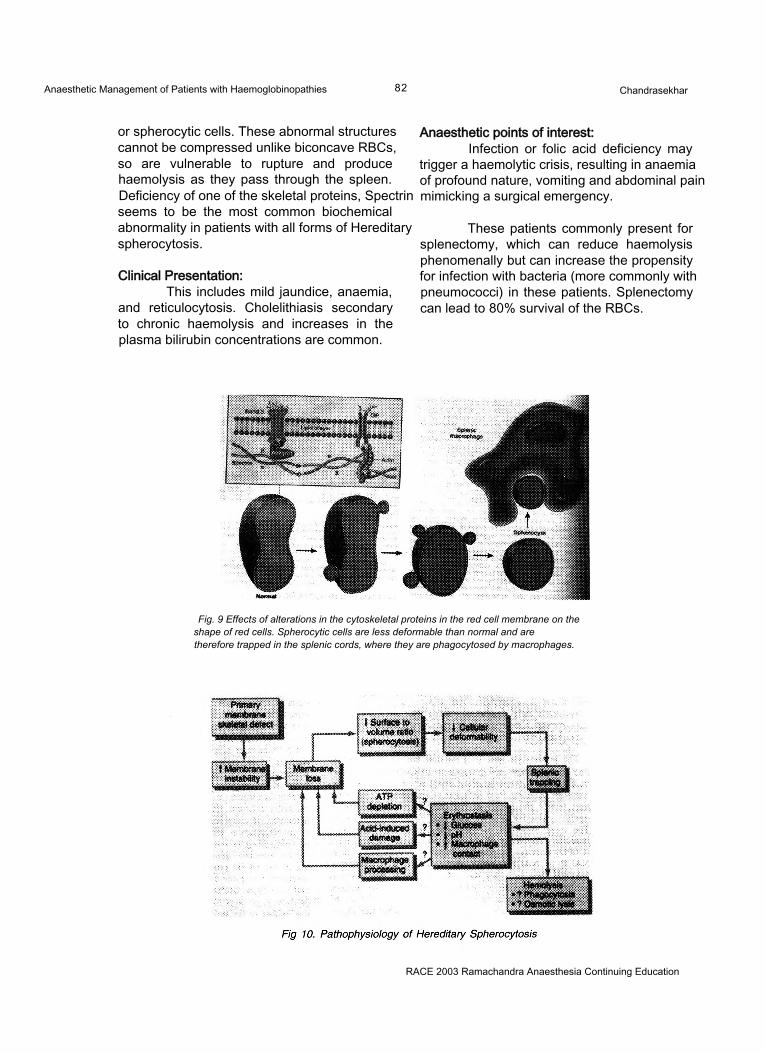
Anaesthetic Management of Patients with Haemoglobinopathies 82 Chandrasekhar
or spherocytic cells. These abnormal structures cannot be compressed unlike biconcave RBCs, so are vulnerable to rupture and produce haemolysis as they pass through the spleen. Deficiency of one of the skeletal proteins, Spectrin seems to be the most common biochemical abnormality in patients with all forms of Hereditary spherocytosis.
Clinical Presentation:This includes mild jaundice, anaemia,
and reticulocytosis. Cholelithiasis secondary to chronic haemolysis and increases in the plasma bilirubin concentrations are common.
Anaesthetic points of interest:Infection or folic acid deficiency may
trigger a haemolytic crisis, resulting in anaemia of profound nature, vomiting and abdominal pain mimicking a surgical emergency.
These patients commonly present for splenectomy, which can reduce haemolysis phenomenally but can increase the propensity for infection with bacteria (more commonly with pneumococci) in these patients. Splenectomy can lead to 80% survival of the RBCs.
Fig. 9 Effects of alterations in the cytoskeletal proteins in the red cell membrane on the shape of red cells. Spherocytic cells are less deformable than normal and are therefore trapped in the splenic cords, where they are phagocytosed by macrophages.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 83 M. Ravishankar
INTRODUCTION:The technique of reusing the expired gas
for alveolar ventilation after absorption of carbon dioxide can be traced to the very beginning of Anaesthesia when Dr. John Snow used caustic potash to absorb C02 from the expired gas. This concept was considerably simplified by the introduction of the “To and Fro” system by Waters and the circle system by Brian Sword, which utilised sodalime for absorption ofC02. It reigned supreme in the early half of this century when expensive and explosive agents like cyclopropane were utilised. The introduction of non-explosive agents like halothane and plenum vaporisers which performed optimally only in the presence of higher flows resulted in low flow anaesthesia becoming less popular. With the added knowledge of the disadvantages of using high percentages of 02 for prolonged periods and the necessity to use a second gas to control the percentage of oxygen, coupled with the complexities involved in the calculation of uptake of anaesthetic agents during the closed circuit anaesthesia made this technique even less popular. However, the awareness of the dangers of theatre pollution with trace amounts of the anaesthetic agents and the prohibitively high cost of the new inhalational agents, have helped in the rediscovery of low flow anaesthesia.
DEFINITIONLow flow anaesthesia has various
definitions. Any technique that utilises a fresh gas flow (FGF) that is less than the alveolar ventilation can be classified as ‘Low flow anaesthesia’. Baum et al1 had defined it as a technique wherein at least 50% of the expired gases had been returned to the lungs after carbon dioxide absorption. This would be satisfied when
the FGF was less than about two litres per minute.
Baker2 in his editorial had classified the FGF used in anaesthetic practice into the following categories:
For most practical considerations, utilisation of a fresh gas flow less than 2 litres/ min may be considered as low flow anaesthesia.
The need for low flow anaesthesia.Completely closed circuit anaesthesia is
based upon the reasoning that anaesthesia can safely be maintained if the gases, which are taken up by the body alone, are replaced into the circuit taking care to remove the expired carbon dioxide with sodalime. No gas escapes out of the circuit and this would provide for maximal efficiency for the utilisation of the fresh gas flow. The very nature of this system requires that the exact amount of anaesthetic agent taken up by the body be known, since that exact amount has to be added into the circuit. Any error in this could lead to a potentially dangerous level of anaesthetic agent being present in the inspired mixture with its attended complications. Hence, there exists a need for a system that provided the advantages of the completely closed circuit and at the same time, reduced the dangers associated with it. Low flow anaesthesia fulfilled these requirements.
Low flow anaesthesia involves utilising a fresh gas flow, which is higher than the metabolic
RACE 2003 Ramachandra Anaesthesia Continuing Education
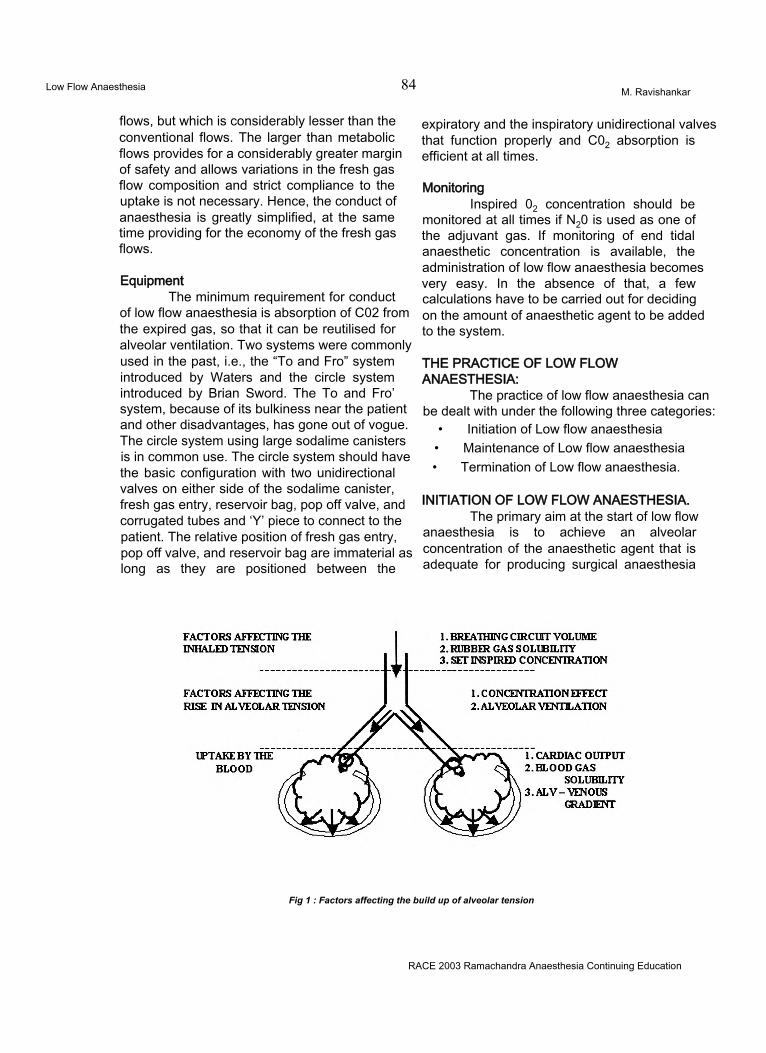
Low Flow Anaesthesia 84 M. Ravishankar
flows, but which is considerably lesser than the conventional flows. The larger than metabolic flows provides for a considerably greater margin of safety and allows variations in the fresh gas flow composition and strict compliance to the uptake is not necessary. Hence, the conduct of anaesthesia is greatly simplified, at the same time providing for the economy of the fresh gas flows.
EquipmentThe minimum requirement for conduct
of low flow anaesthesia is absorption of C02 from the expired gas, so that it can be reutilised for alveolar ventilation. Two systems were commonly used in the past, i.e., the “To and Fro” system introduced by Waters and the circle system introduced by Brian Sword. The To and Fro’ system, because of its bulkiness near the patient and other disadvantages, has gone out of vogue. The circle system using large sodalime canisters is in common use. The circle system should have the basic configuration with two unidirectional valves on either side of the sodalime canister, fresh gas entry, reservoir bag, pop off valve, and corrugated tubes and ‘Y’ piece to connect to the patient. The relative position of fresh gas entry, pop off valve, and reservoir bag are immaterial as long as they are positioned between the
expiratory and the inspiratory unidirectional valves that function properly and C02 absorption is efficient at all times.
MonitoringInspired 02 concentration should be
monitored at all times if N20 is used as one of the adjuvant gas. If monitoring of end tidal anaesthetic concentration is available, the administration of low flow anaesthesia becomes very easy. In the absence of that, a few calculations have to be carried out for deciding on the amount of anaesthetic agent to be added to the system.
THE PRACTICE OF LOW FLOW ANAESTHESIA:
The practice of low flow anaesthesia can be dealt with under the following three categories:
• Initiation of Low flow anaesthesia• Maintenance of Low flow anaesthesia• Termination of Low flow anaesthesia.
INITIATION OF LOW FLOW ANAESTHESIA.The primary aim at the start of low flow
anaesthesia is to achieve an alveolar concentration of the anaesthetic agent that is adequate for producing surgical anaesthesia
Fig 1 : Factors affecting the build up of alveolar tension
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 85 M. Ravishankar
(approximately 1.3 MAC). The factors that can influence the build up of alveolar concentration should all be considered while trying to reach the desired alveolar concentration. These factors can broadly be classified into three groups (fig. 1); 1) Factors governing the inhaled tension of the anaesthetic, 2) Factors responsible for the rise in alveolar tension, 3) Factors responsible for uptake from the lungs thus reducing the alveolar tension.
Factors governing the inhaled tension of the anaesthetic:1 The circle system is often bulky and has a
volume roughly equal to 6-7 litres. Besides this, the FRC of the patient, which is roughly3 litres, together constitutes a reserve volume of 10 litres to which the anaesthetic gases and vapours have to be added. With the addition of FGF, the rate of change of composition of the reserve volume is exponential. The time required for the changes to occur is governed by the time constant, which is equal to this reserve volume divided by the fresh gas flow. This represents the time required for 67% change to occur in the gas concentration. Three time constants are needed for a 95% change in the gas concentration to occur. Hence, if a FGF of 1L/min is used, then 30 minutes will be required for the circuit concentration to reflect the gas concentration of the FGF. If the FGF is still lower, then a correspondingly longer time will be required.
2. The functional residual capacity of the lung and the body as a whole contain nitrogen, which will try to equilibrate with the circuit volume and alter the gas concentration if satisfactory denitrogenation is not achieved at the start of anaesthesia. Hence, as a prelude to the initiation of closed or low flow anaesthesia, thorough denitrogenation must be achieved with either a non-rebreathing circuit or the closed circuit with a large flow of oxygen and a tight fitting facemask.
3. The anaesthetic agent could be lost from the breathing system due to solubility of the agent in rubber, and permeability through the corrugated tubes. Though the amount of loss
will be minimal, it should be considered atthe start if the aimed anaestheticconcentration is low.
Factors responsible for rise in alveolar tension of the anaesthetic agent:1. CONCENTRATION EFFECT:
The concentration effect helps in raising the alveolar tension towards the inspired tension, but hinders it, if an insoluble gas is present in the mixture. The rate of rise of alveolar partial pressure of the anaesthetic agent must bear a direct relationship to the inspired concentration. The higher the inspired concentration, the more rapid is the rise in alveolar concentration. At a low inspired concentration, the alveolar concentration results from a balance between the ventilatory input and the circulatory uptake. If the latter removes half the anaesthetic introduced by ventilation, then the alveolar concentration is half that inspired. The concentration effect modifies this influence of uptake. When appreciable volumes are taken up rapidly, the lungs do not collapse; instead the subatmospheric pressure created in the lung by the anaesthetic uptake causes passive inspiration of an additional volume of gas to replace that lost by uptake, thus increasing the alveolar concentration and offsetting the mathematical calculations. Similarly, if an insoluble gas (e.g., nitrogen) is present in the inspired mixture, as the blood takes up the anaesthetic gas, the concentration of the insoluble gas will go up in the alveoli, reducing the concentration of the anaesthetic agent.
2. ALVEOLAR VENTILATION:The second factor governing the delivery of
anaesthetic agent to the lung is the level of alveolar ventilation. The greater the alveolar ventilation, the more rapid is the rise of alveolar concentration towards the inspired concentration. This effect is limited only by the lung volume; the larger the functional residual capacity, the slower the wash in of the new anaesthetic gas.
Factors responsible for uptake from the lungs thus reducing the alveolar tension:
Uptake from the lung is the product of three factors: solubility of the agent in the blood, the cardiac output and the alveolar to venous partial pressure gradient.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 86 M. Ravishankar
1. BLOOD GAS SOLUBILITY:“Solubility” is the term used to describe
how a gas or vapour is distributed between two media. At equilibrium, that is when the partial pressure of the anaesthetic in the two phases is equal, the concentration of the anaesthetic in the two phases might differ. This is calculated as a coefficient. When it is between blood and gas it is called blood gas solubility coefficient. If other things are equal, the greater the blood/ gas solubility coefficient, the greater the uptake of the anaesthetic, and slower the rate of rise of alveolar concentration.
2. CARDIAC OUTPUT:Because blood carries anaesthetic away
from the lungs, the greater the cardiac output, the greater the uptake, and consequently the slower the rate of rise of alveolar tension. The magnitude of this effect is related to the solubility: the most soluble agents are affected more than the least soluble agents.
3. ALVEOLAR TO VENOUS PARTIAL PRESSURE GRADIENT:
During induction the tissues remove all the anaesthetic brought to them by the blood. This lowers the venous anaesthetic partial pressure far below that of the arterial blood. The result is a large alveolar to venous anaesthetic partial pressure difference, which causes maximum anaesthetic uptake and hence lowers the alveolar partial pressure.
Considering the above mentioned factors at the start of anaesthesia, two facts become apparent:1. Induction if performed using low flows
would take an unacceptably long time.
2. If induction is done with an intravenous agent, unless special precautions are taken, it may take a very long time to achieve the desired alveolar concentration. Once the desired concentration is achieved, it will be difficult to change it. Hence, termination of action would take a long time after the discontinuation of the agents.
Methods to achieve desired gas and agent concentrationUSE OF HIGH FLOWS FOR A SHORT TIME:
This is by and far the commonest and the most effective technique of initiating closed circuit. By using high flows for a short time, the time constant is reduced thereby bringing the circuit concentration to the desired concentration rapidly. Often, a fresh gas flow of 10L of the desired gas concentration and 2 MAC agent concentration is used so that by the end of three minutes (three time constants) the circuit would be brought to the desired concentration. The large flows and high agent concentration also compensate for the large uptake seen at the start of the anaesthesia. Mapleson3 using a spreadsheet model of a circle breathing system has calculated that, by using a FGF equal to minute ventilation and setting the anaesthetic agent partial pressure to 3 MAC, the end expired partial pressure of halothane will reach 1 MAC in4 minutes and that of isoflurane in 1.5 minutes. The major advantages of this method are the rapidity with which the desired concentration is achieved, the ability to prevent unexpected rise in the agent concentration and the ability to use the commonly available plenum vaporisers to achieve the desired concentration. This also has the added advantage of achieving better denitrogenation, so vital to the conduct of low flow anaesthesia. The chief disadvantage would be the high flows required which would compromise on the economy of the gas utilisation and the need for scavenging systems to prevent theatre pollution. This period of using high flows for a short period at initiation goes by the name of “loading”.
PREFILLED CIRCUIT.The second method is utilising a different
circuit like Magills for preoxygenation. Simultaneously, the circle is fitted with a test lung and the entire circuit is filled with the gas mixture of the desired concentration. Following intubation, the patient is connected to the circuit thereby ensuring rapid achievement of the desired concentration in the circuit. But all the factors discussed above will be effective in preventing fast build up of the alveolar concentration to attain surgical anaesthesia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
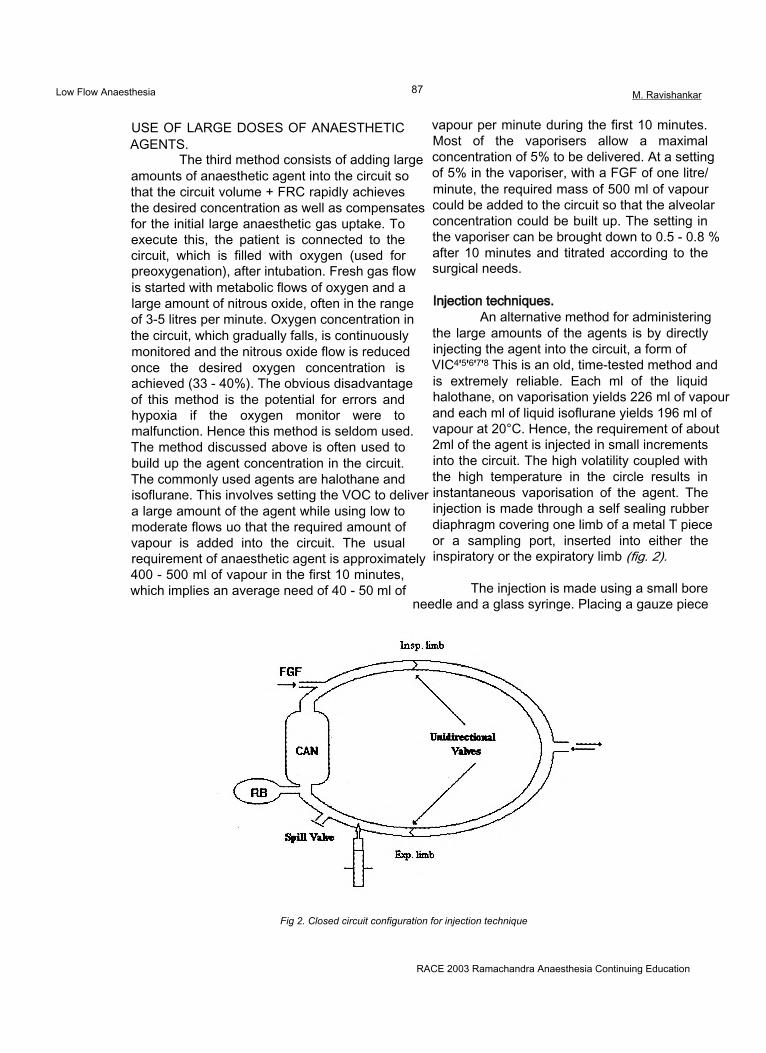
Low Flow Anaesthesia 87 M. Ravishankar
USE OF LARGE DOSES OF ANAESTHETIC AGENTS.
The third method consists of adding large amounts of anaesthetic agent into the circuit so that the circuit volume + FRC rapidly achieves the desired concentration as well as compensates for the initial large anaesthetic gas uptake. To execute this, the patient is connected to the circuit, which is filled with oxygen (used for preoxygenation), after intubation. Fresh gas flow is started with metabolic flows of oxygen and a large amount of nitrous oxide, often in the range of 3-5 litres per minute. Oxygen concentration in the circuit, which gradually falls, is continuously monitored and the nitrous oxide flow is reduced once the desired oxygen concentration is achieved (33 - 40%). The obvious disadvantage of this method is the potential for errors and hypoxia if the oxygen monitor were to malfunction. Hence this method is seldom used. The method discussed above is often used to build up the agent concentration in the circuit. The commonly used agents are halothane and isoflurane. This involves setting the VOC to deliver a large amount of the agent while using low to moderate flows uo that the required amount of vapour is added into the circuit. The usual requirement of anaesthetic agent is approximately 400 - 500 ml of vapour in the first 10 minutes, which implies an average need of 40 - 50 ml of
vapour per minute during the first 10 minutes. Most of the vaporisers allow a maximal concentration of 5% to be delivered. At a setting of 5% in the vaporiser, with a FGF of one litre/ minute, the required mass of 500 ml of vapour could be added to the circuit so that the alveolar concentration could be built up. The setting in the vaporiser can be brought down to 0.5 - 0.8 % after 10 minutes and titrated according to the surgical needs.
Injection techniques.An alternative method for administering
the large amounts of the agents is by directly injecting the agent into the circuit, a form of VIC4'5'6'7'8 This is an old, time-tested method and is extremely reliable. Each ml of the liquid halothane, on vaporisation yields 226 ml of vapour and each ml of liquid isoflurane yields 196 ml of vapour at 20°C. Hence, the requirement of about 2ml of the agent is injected in small increments into the circuit. The high volatility coupled with the high temperature in the circle results in instantaneous vaporisation of the agent. The injection is made through a self sealing rubber diaphragm covering one limb of a metal T piece or a sampling port, inserted into either the inspiratory or the expiratory limb (fig. 2).
The injection is made using a small bore needle and a glass syringe. Placing a gauze piece
Fig 2. Closed circuit configuration for injection technique
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 88 M. Ravishankar
or a wire mesh inside the T piece often helps in the vaporisation of the liquid. The intermittent injections are often made in 0.2-0.5 ml aliquots manually. Doses should never exceed 1 ml at a time. Doses exceeding 2 ml bolus invite disaster. Intermittent injections can often be easily substituted with a continuous infusion with the added advantage of doing away with the peaks and troughs associated with intermittent injections.
The exact dose to be used is calculatedthus:Priming dose (ml vapour) = Desired concentration
x{( FRC + Circuit volume) +(Cardiac output x BG Coeff.)}
The Cardiac output and the FRC can be estimated for the patient based on standard nomograms, minutes of the closed circuit anaesthesia. Besides this, an amount of agent necessary to compensate for the uptake of the body must also be added and this is calculated depending on the uptake model being used (vide infra).
THE MAINTENANCE OF LOW FLOW ANAESTHESIA
This is the most important phase as this is stretched over a period of time and financial savings result directly from this. This phase is characterised by1 Need for a steady state anaesthesia often
meaning a steady alveolar concentration of respiratory gases.
2 Minimal uptake of the anaesthetic agents by the body.
3 Need to prevent hypoxic gas mixtures.
Since the uptake of the anaesthetic agent is small in this phase, the low flow anaesthesia is eminently practical. Adding small amounts of the anaesthetic gases to match the uptake and providing oxygen for the basal metabolism should suffice. If CCA is used, this would be directly equal to the uptake and hence provides for the monitoring of the oxygen consumption and the agent uptake. If low flow anaesthesia is used, then besides the uptake, the amount of gas, which is vented, is also added to the circuit to maintain steady state anaesthesia.
Management of the oxygen and nitrous oxide flow during the maintenance phase:
The need to discuss the flow rates of N20 and 02 arises specifically because of the possible danger of administration of a hypoxic mixture. Let us analyse the following example. 33% oxygen is set using a flow of 500 ml of 02 and 1000 ml of N20. Oxygen is taken up from the lungs at a constant rate of about 4 ml/kg/min. N20 is a relatively insoluble gas and after the initial equilibration with the FRC and vessel rich group of tissues, the uptake is considerably reduced. In this situation, there is a constant removal of02 at a rate of 200 - 250 ml/min, where as the insoluble gas N20 uptake is minimal. Hence the gas returning to the circuit will have more N20 and less of 02. Over a period of time, due to concentration effect, the percentage of N20 will go up and that of 02 will fall, sometimes dangerously to produce hypoxic mixtures.
Various short cuts are available to make low flow anaesthesia easy of which the most popular technique is the ‘Gothenburg technique’9. Most of the other techniques approximate this and hence it deserves a special mention.
THE GOTHENBURG TECHNIQUE:Initially high flows, oxygen at 1.5 l/min
and nitrous oxide at 3.5 l/min had to be used for a period of six minutes after the induction of anaesthesia and this constitutes the loading phase. This is followed by the maintenance phase in which the oxygen flow is reduced to about 4ml/kg and nitrous oxide flow adjusted to maintain a constant oxygen concentration in the circuit. The usual desired oxygen concentration is about 40%. The use of an oxygen analyser is very important since the nitrous oxide added is directly based on its readings and hence any errors would be dangerous.
Other authors have made similar recommendations10'11,12'13'14. Most of the authors opine that the oxygen consumption under anaesthesia is about 200 - 250 ml. However, there is a wide disparity in the amount of nitrous oxide to be added into the circuit. This controversy is consistent with the basic controversy surrounding the uptake of the anaesthetic agents and is dealt with in detail in a later stage. For most practical
RACE 2003 Ramachandra Anaesthesia Continuing Education
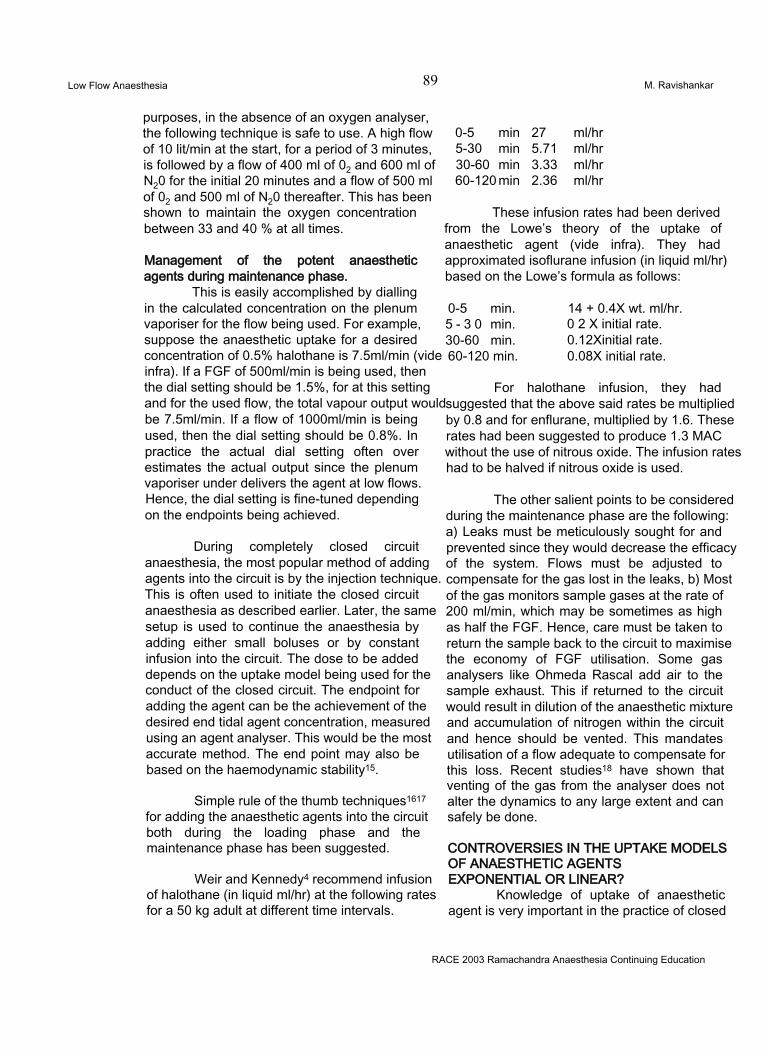
Low Flow Anaesthesia 89 M. Ravishankar
purposes, in the absence of an oxygen analyser, the following technique is safe to use. A high flow of 10 lit/min at the start, for a period of 3 minutes, is followed by a flow of 400 ml of 02 and 600 ml of N20 for the initial 20 minutes and a flow of 500 ml of 02 and 500 ml of N20 thereafter. This has been shown to maintain the oxygen concentration between 33 and 40 % at all times.
Management of the potent anaesthetic agents during maintenance phase.
This is easily accomplished by dialling in the calculated concentration on the plenum vaporiser for the flow being used. For example, suppose the anaesthetic uptake for a desired concentration of 0.5% halothane is 7.5ml/min (vide infra). If a FGF of 500ml/min is being used, then the dial setting should be 1.5%, for at this setting and for the used flow, the total vapour output would be 7.5ml/min. If a flow of 1000ml/min is being used, then the dial setting should be 0.8%. In practice the actual dial setting often over estimates the actual output since the plenum vaporiser under delivers the agent at low flows. Hence, the dial setting is fine-tuned depending on the endpoints being achieved.
During completely closed circuit anaesthesia, the most popular method of adding agents into the circuit is by the injection technique. This is often used to initiate the closed circuit anaesthesia as described earlier. Later, the same setup is used to continue the anaesthesia by adding either small boluses or by constant infusion into the circuit. The dose to be added depends on the uptake model being used for the conduct of the closed circuit. The endpoint for adding the agent can be the achievement of the desired end tidal agent concentration, measured using an agent analyser. This would be the most accurate method. The end point may also be based on the haemodynamic stability15.
Simple rule of the thumb techniques1617 for adding the anaesthetic agents into the circuit both during the loading phase and the maintenance phase has been suggested.
Weir and Kennedy4 recommend infusion of halothane (in liquid ml/hr) at the following rates for a 50 kg adult at different time intervals.
0-5 min 27 ml/hr5-30 min 5.71 ml/hr30-60 min 3.33 ml/hr60-120 min 2.36 ml/hr
These infusion rates had been derived from the Lowe’s theory of the uptake of anaesthetic agent (vide infra). They had approximated isoflurane infusion (in liquid ml/hr) based on the Lowe’s formula as follows:
0-5 min. 5 - 3 0 min. 30-60 min. 60-120 min.
14 + 0.4X wt. ml/hr.0 2 X initial rate. 0.12Xinitial rate.0.08X initial rate.
For halothane infusion, they had suggested that the above said rates be multiplied by 0.8 and for enflurane, multiplied by 1.6. These rates had been suggested to produce 1.3 MAC without the use of nitrous oxide. The infusion rates had to be halved if nitrous oxide is used.
The other salient points to be considered during the maintenance phase are the following: a) Leaks must be meticulously sought for and prevented since they would decrease the efficacy of the system. Flows must be adjusted to compensate for the gas lost in the leaks, b) Most of the gas monitors sample gases at the rate of 200 ml/min, which may be sometimes as high as half the FGF. Hence, care must be taken to return the sample back to the circuit to maximise the economy of FGF utilisation. Some gas analysers like Ohmeda Rascal add air to the sample exhaust. This if returned to the circuit would result in dilution of the anaesthetic mixture and accumulation of nitrogen within the circuit and hence should be vented. This mandates utilisation of a flow adequate to compensate for this loss. Recent studies18 have shown that venting of the gas from the analyser does not alter the dynamics to any large extent and can safely be done.
CONTROVERSIES IN THE UPTAKE MODELS OF ANAESTHETIC AGENTS EXPONENTIAL OR LINEAR?
Knowledge of uptake of anaesthetic agent is very important in the practice of closed
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 90 M. Ravishankar
and low flow anaesthesia since, the very technique calls for the addition of an amount of anaesthetic agent, which is taken up by the body. In fact, mutually contradicting models exist on the uptake of anaesthetic agents. The Lowe’s theory*3'*4, which has wider acceptance, ascribes the anaesthetic uptake to an exponential model. It states that the uptake of agent is inversely proportional to the square root of the time, implying that the uptake decreases exponentially with time. It necessitates calculation of unit dose (Appendix 1). This unit dose is the amount of anaesthetic agent to be added to the closed circuit during the time intervals of 0-1 min, 1-4 min, 4-9 min, 9-16 min, and so on. Besides that, the circuit and the FRC and the circulating blood of the patient had to be brought to the desired concentration with a prime dose.Prime dose = {(circuit volume + FRC) +
(Q xk)} x desired Concentration.
This prime dose had to be added into the circuit during the first 9 minutes of closed circuit anaesthesia.
The practical implication of this is that to maintain closed circuit, one must calculate the agent and gases to be added into the circuit using hair-splitting exponential equations, often frightening the anaesthetist. It has been one of the main causes for the reluctance in the widespread usage of the closed circuit anaesthesia.
In total contrast to this exponential theory is the linear model proposed by CY Lin 1214 He states that the uptake of anaesthetic agents is a near constant over the clinically important concentrations. Hence, he advocated adding the anaesthetic agent as a constant rate infusion into the circuit throughout the anaesthetic procedure. Lin had contended that the FRC constituted an extension of the breathing circuit and the washin into it could not be considered as uptake by the body. He had suggested a simple method of conducting the closed circuit anaesthesia: It had consisted of using a high flow of nitrous oxide and oxygen (6 L/min and 4 L/min respectively) for 3 minutes (three time constants). At the end of 3 minutes, the flows had been reduced to metabolic flows and closed circuit started. Potent agents had
been added either through a VOC (like a copper kettle) or by direct injection into the circuit. The anaesthetic agent required to washin the circuit volume and the FRC of the patient had constituted the prime dose and it should be added to the circuit during the first ten minutes, besides the dose required to compensate for the uptake of the agent. The formula to calculate the amount of agent to be added into the circuit to equal the uptake had been:
Uptake of anaesthetic agent = desired concentration x alveolar ventilation x fractional uptake ( ml of vapour).
The fractional uptake (= 1 - FA/ F,) for halothane had been calculated as 0.5 and that for enflurane, as 0.4. He had concluded that anaesthesia thus conducted produced a nearly constant inspired and expired concentration implying that the uptake of the anaesthetic agents had been a near constant.
Unfortunately very little literature exists on the efficacy of either of these models. The study conducted to compare these two models in our Institute, revealed that predictive performance of both the models were statistically similar, and linear uptake model had scope for improvement where as the exponential model had no such scope. Lin’s linear model however has a distinct superiority in the form of simplicity.
TERMINATION OF LOW FLOW ANAESTHESIA
Unlike the initiation or the maintenance of the closed circuit, termination is less controversial. There are only two recognised methods of termination of the closed circuit. They are as follows:
Towards the end of the anaesthesia, the circuit is opened and a high flow of gas is used to flush out the anaesthetic agents, which accelerates the washout of the anaesthetic agents. This has the obvious advantage of simplicity but would result in wastage of gases.
The second method is the use of activated charcoal8 Activated charcoal when heated to 220°C adsorbs the potent vapours almost completely. Hence, a charcoal-containing
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 91 M. Ravishankar
canister with a bypass is placed in the circuit. Towards the end of the anaesthesia, the gas is directed through the activated charcoal canister. This results in the activated charcoal adsorbing the anaesthetic agent resulting in rapid recovery and at the same time, reducing theatre pollution. Nitrous oxide, due to its low solubility is washed off towards the end by using 100% oxygen.
To conclude, the low flow closed circuit anaesthesia has many advantages to offer. To list a few,1 Enormous financial savings due to use of low
fresh gas flows as well as the agent.2 High humidity in the system leads to fewer
post anaesthetic complications.3 Maintenance of body temperature during
prolonged procedures due to conservation of heat.
4 Reduction in the theatre pollution.
The perceived disadvantages are not real:1 The need to accurately adjust the flows of
gases. The system is inherently stable once a steady state is reached and small errors in the dosage of the agents or the gases would be of no concern.
2 Accumulation of trace gases20. It has, however, been often overestimated21.
3 Need for monitoring equipment. Oxygen monitor is the only one that is necessary and since it is part of the basic monitoring it cannot be considered as a disadvantage.
With a proper understanding of the concepts of practice, the low flow anaesthesia technique can safely be used in all surgical procedures lasting more than an hour.
REFERENCES1 Baum JA, Aithkenhead: Low flow
Anaesthesia. Anaesthesia. 50 (suppl).: 37-44, 1995
2 Baker AB: Editorial. Low flow and Closed Circuits. Anaesthesia and Intensive Care. 22: 341-342, 1994
3 Mapleson W: The theoretical ideal fresh gasflow sequence at the start of low flow anaesthesia Anaesthesia 53(3):264-72, 1998
4 Weir HM, Kennedy RR: Infusing liquid anaesthetic agents into the closed circle anaesthesia. Anaesthesia and Intensive Care. 22: 376-379, 1994
5 Wolfson B: Closed Circuit Anaesthesia by Intermittent Injections of Halothane. British Journal of Anaesthesia. 34: 733 - 737., 1962
6 Thorpe CM, Kennedy RR: Vaporisation of Isoflurane by Liquid Infusion. Anaesthesia and Intensive Care. 22: 380-82, 1994
7 Hampton JL, Flickinger H: Closed Circuit Anesthesia utilising known increments of Halothane.Anesthesiology 22: 413-418, 1961
8 Philip JH: ‘Closed Circuit Anaesthesia’ in ‘Anesthesia Equipment: Principles and Applications’. Edited by Ehrenwerth J, Eisenkraft JB, Mosby Year Book Inc., 1993, Chap 30.
9 Dale O, Stenqvist O: Low flow Anaesthesia : Available today - A routine tomorrow. Survey of Anesthesiology. 36: 334-336, 1992
10 Cullen SC: Who is watching the patient? Anesthesiology 37: 361-362, 1972
11 Baker AB: Back to Basics - A Simplified Non - Mathematical Approach to Low Flow Techniques in Anaesthesia. Anaesthesia and Intensive Care. 22: 394-395., 1994
12 Lin CY, Benson JW, Mostert DW: Closed Circle Systems - A new direction in the practice of Anaesthesia. Acta Anaesthesiologica Scandinavica. 24: 354-361., 1980
13 Lowe HJ: ‘The Anesthetic Continuum’ in the book, ‘Low flow and closed circuit anesthesia’. Edited by Aldrete JA, Lowe HJ, Virtue RW, Grune & Stratton, 1979, pp 11-38
14 Lowe H: ‘Closed- circuit anesthesia’, in the book ‘Clinical Anesthesiology’ Edited byMorgan GE, Mikhail MS, Appleton and Lange, 1992, pp 112 -115.
15 Da Silva CJM, Mapleson WW, Vickers MD: Quantitative study of Lowe’s square root of time method of closed system anaesthesia. British Journal of Anaesthesia. 79: 103-112., 1997
16 El - Attar AM: Guided Isoflurane injection in a totally closed circuit. Anaesthesia. 46.: 1059-1063., 1991.
17 Eger II E: “Uptake and Distribution”, in the book “Anesthesia”, Edited by Miller RD, Ed4, Churchill Livingstone,1994, p118.
18 Bengtson J, Bengtsson J, Bengtsson A, Stenqvist O: Sampled gas need not be returned during low-f!ow anaesthesia. Journal of Clinical Monitoring 9(5): 330-4, 1993
19 Lin CY: Uptake of Anaesthetic Gases and Vapours. Anaesthesia and Intensive Care. 22: 363-373, 1994
20 Morita S, Latta W, Hambro K, Snider MT: Accumilation of methane, acetone and nitrogen in the inspired gas during closed circuit anesthesia. Anesthesia and analgesia. 64: 343-347, 1985
21 Baumgarten R: Much ado about nothing: Trace gaseous metabolites in closed circuit.Anesthesia and Analgesia. 64: 1029-1030, 1985
RACE 2003 Ramachandra Anaesthesia Continuing Education
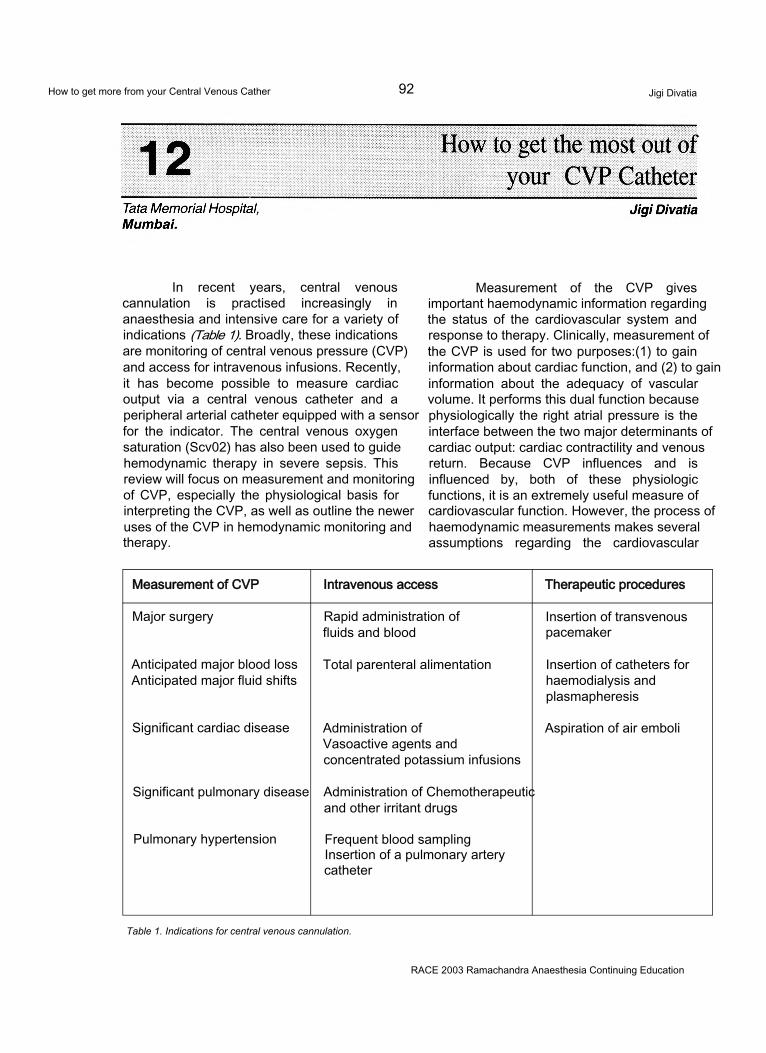
How to get more from your Central Venous Cather 92 Jigi Divatia
In recent years, central venous cannulation is practised increasingly in anaesthesia and intensive care for a variety of indications (Table 1). Broadly, these indications are monitoring of central venous pressure (CVP) and access for intravenous infusions. Recently, it has become possible to measure cardiac output via a central venous catheter and a peripheral arterial catheter equipped with a sensor for the indicator. The central venous oxygen saturation (Scv02) has also been used to guide hemodynamic therapy in severe sepsis. This review will focus on measurement and monitoring of CVP, especially the physiological basis for interpreting the CVP, as well as outline the newer uses of the CVP in hemodynamic monitoring and therapy.
Measurement of the CVP gives important haemodynamic information regarding the status of the cardiovascular system and response to therapy. Clinically, measurement of the CVP is used for two purposes:(1) to gain information about cardiac function, and (2) to gain information about the adequacy of vascular volume. It performs this dual function because physiologically the right atrial pressure is the interface between the two major determinants of cardiac output: cardiac contractility and venous return. Because CVP influences and is influenced by, both of these physiologic functions, it is an extremely useful measure of cardiovascular function. However, the process of haemodynamic measurements makes several assumptions regarding the cardiovascular
Measurement of CVP Intravenous access Therapeutic procedures
Major surgery Rapid administration of fluids and blood
Insertion of transvenous pacemaker
Anticipated major blood loss Anticipated major fluid shifts
Total parenteral alimentation Insertion of catheters for haemodialysis and plasmapheresis
Significant cardiac disease Administration of Vasoactive agents and concentrated potassium infusions
Aspiration of air emboli
Significant pulmonary disease Administration of Chemotherapeutic and other irritant drugs
Pulmonary hypertension Frequent blood sampling Insertion of a pulmonary artery catheter
Table 1. Indications for central venous cannulation.
RACE 2003 Ramachandra Anaesthesia Continuing Education
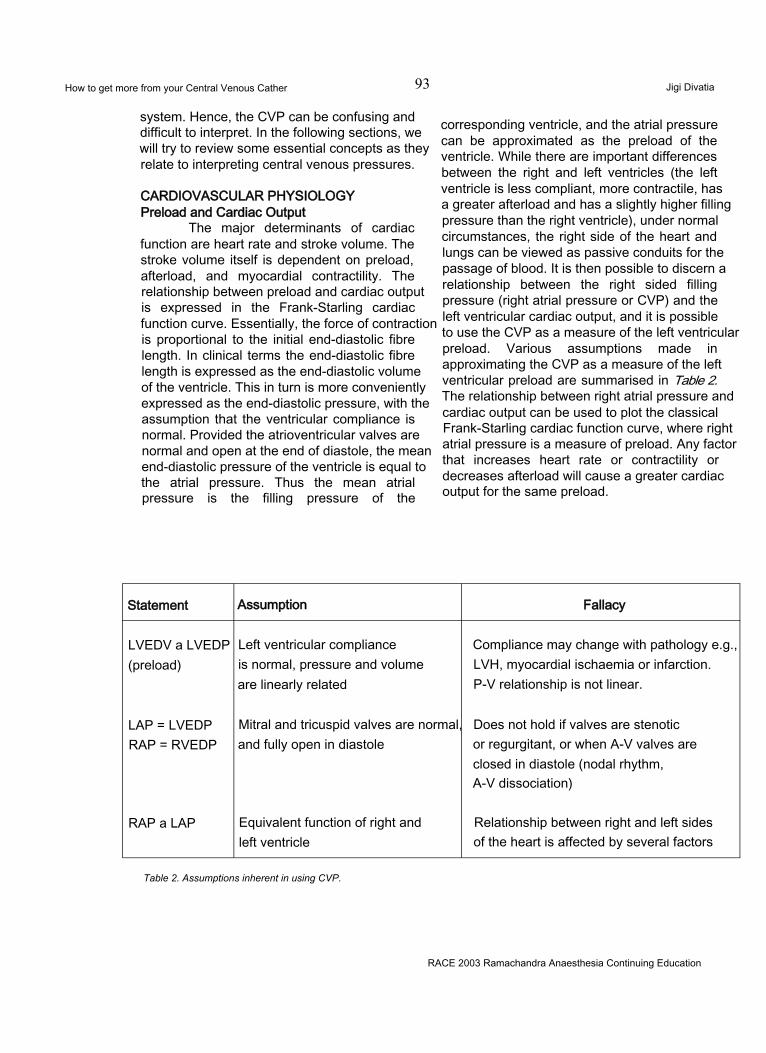
How to get more from your Central Venous Cather 93 Jigi Divatia
system. Hence, the CVP can be confusing and difficult to interpret. In the following sections, we will try to review some essential concepts as they relate to interpreting central venous pressures.
CARDIOVASCULAR PHYSIOLOGY Preload and Cardiac Output
The major determinants of cardiac function are heart rate and stroke volume. The stroke volume itself is dependent on preload, afterload, and myocardial contractility. The relationship between preload and cardiac output is expressed in the Frank-Starling cardiac function curve. Essentially, the force of contraction is proportional to the initial end-diastolic fibre length. In clinical terms the end-diastolic fibre length is expressed as the end-diastolic volume of the ventricle. This in turn is more conveniently expressed as the end-diastolic pressure, with the assumption that the ventricular compliance is normal. Provided the atrioventricular valves are normal and open at the end of diastole, the mean end-diastolic pressure of the ventricle is equal to the atrial pressure. Thus the mean atrial pressure is the filling pressure of the
corresponding ventricle, and the atrial pressure can be approximated as the preload of the ventricle. While there are important differences between the right and left ventricles (the left ventricle is less compliant, more contractile, has a greater afterload and has a slightly higher filling pressure than the right ventricle), under normal circumstances, the right side of the heart and lungs can be viewed as passive conduits for the passage of blood. It is then possible to discern a relationship between the right sided filling pressure (right atrial pressure or CVP) and the left ventricular cardiac output, and it is possible to use the CVP as a measure of the left ventricular preload. Various assumptions made in approximating the CVP as a measure of the left ventricular preload are summarised in Table 2. The relationship between right atrial pressure and cardiac output can be used to plot the classical Frank-Starling cardiac function curve, where right atrial pressure is a measure of preload. Any factor that increases heart rate or contractility or decreases afterload will cause a greater cardiac output for the same preload.
Statement Assumption Fallacy
LVEDV a LVEDP (preload)
Left ventricular compliance is normal, pressure and volume are linearly related
Compliance may change with pathology e.g., LVH, myocardial ischaemia or infarction.P-V relationship is not linear.
LAP = LVEDP RAP = RVEDP
Mitral and tricuspid valves are normal, and fully open in diastole
Does not hold if valves are stenotic or regurgitant, or when A-V valves are closed in diastole (nodal rhythm,A-V dissociation)
RAP a LAP Equivalent function of right and left ventricle
Relationship between right and left sides of the heart is affected by several factors
Table 2. Assumptions inherent in using CVP.
RACE 2003 Ramachandra Anaesthesia Continuing Education

How to get more from your Central Venous Cather 94If it is accepted that the CVP is a
Jigi Divatia
measure of preload, the factors that will affect it are blood volume, venous tone, ventricular compliance, myocardial contractility and afterload. If all the other factors are kept constant, the CVP will give some indication of the contractility, i.e., a failing ventricle is associated with a high CVP. The preload is also affected by changes in afterload. An acute change in the right ventricular afterload by pulmonary embolism causes a rise in CVP, while administration of a peripheral vasoconstrictor like phenylephrine will increase the left ventricular afterload and the CVP. When the acute load is relieved, the CVP will fall. However the commonest causes of variations in CVP during anaesthesia are alterations in blood volume or venous tone, both of wtych are accentuated by posture. For example, during spinal anaesthesia in the supine position, venous tone and venous return are reduced, resulting in a low CVP. Following infusion of fluids, the CVP will return towards normal. However, postoperatively as the anaesthetic-induced vasodilatation recedes, and is replaced by vasoconstriction due to pain, cold, shivering and acidosis, the relative blood volume may be too high, and the CVP will rise.
Ventricular ComplianceThe cardiac function curve uses the right
atrial pressure to represent preload. More accurately, preload is the resting myocardial fiber length or, in the intact heart, end-diastolic ventricular end-diastolic volume. Unfortunately, the relationship between pressure and volume is not linear. The ventricles are able to expand to accept a change in pressure. Cardiac output will increase with little change in the right atrial pressure, until the limits of ventricular expansion are reached. At that point, cardiac output no longer improves but right atrial pressure increases rapidly. Disease states and different physiologic states can change the position & shape of the curve. Consequently, a single measurement of right atrial pressure cannot accurately predict end-diastolic volume. However, determining the compliance (i.e., the change in pressure for a given change in volume) will add valuable information about the system.
Vascular ComplianceJust as the heart demonstrates variable
compliance, the vascular system is able to adjust to changes in volume with minimal changes in
pressure. A rapid increase in vascular volume results in a rapid increase in venous return as well as right atrial & mean systemic pressures. Within seconds, circulatory reflexes begin to adjust these pressures & venous return toward normal. In addition, stress relaxation of the vasculature (not dependent on autonomic reflexes) allows further compensation over the ensuing minutes. Similar compensation occurs for decreases in vascular volume. Consequently, a single measurement of right atrial pressure cannot accurately predict vascular volume. However, determining the compliance of the system can provide valuable clues to the status of the vascular volume.
CLINICAL UTILIZATION OF CVP MEASUREMENT
The most common reasons for CVP measurement are to help determine the state of volume. As can be seen in Table 3, a single measurement of the CVP helps somewhat in defining circulatory status but leaves considerable overlap in possible interpretations.
USING COMPLIANCE TO IMPROVE INTERPRETATION
Rapid changes in vascular volume can help further define the cardiovascular status if the time course of compliance changes is remembered. This is the principle of the “fluid challenge”. A rapid infusion of 300 to 500ml of fluid in a normovolemic adult with good cardiac function will result in a moderate increase in CVP (2 to 4mm Hg) with a return nearly to baseline within 10 to 15 min. A minimal initial rise in CVP implies a reduced vascular volume. A large initial rise in CVP implies a heart that is noncompliant or an elevated vascular volume or both. If the CVP returns to baseline rapidly (within 5min), it implies a reduced vascular volume, which can accommodate additional volume by rapid changes in vasomotor tone. A slower return toward baseline indicates that stress relaxation is occurring & the vascular volume is elevated for the current cardiac status. Table 4 indicates how a fluid challenge can improve the interpretation made on the basis of the CVP alone.
The addition of information about cardiac output can further improve diagnostic accuracy. Actual measurement of cardiac output is best
RACE 2003 Ramachandra Anaesthesia Continuing Education
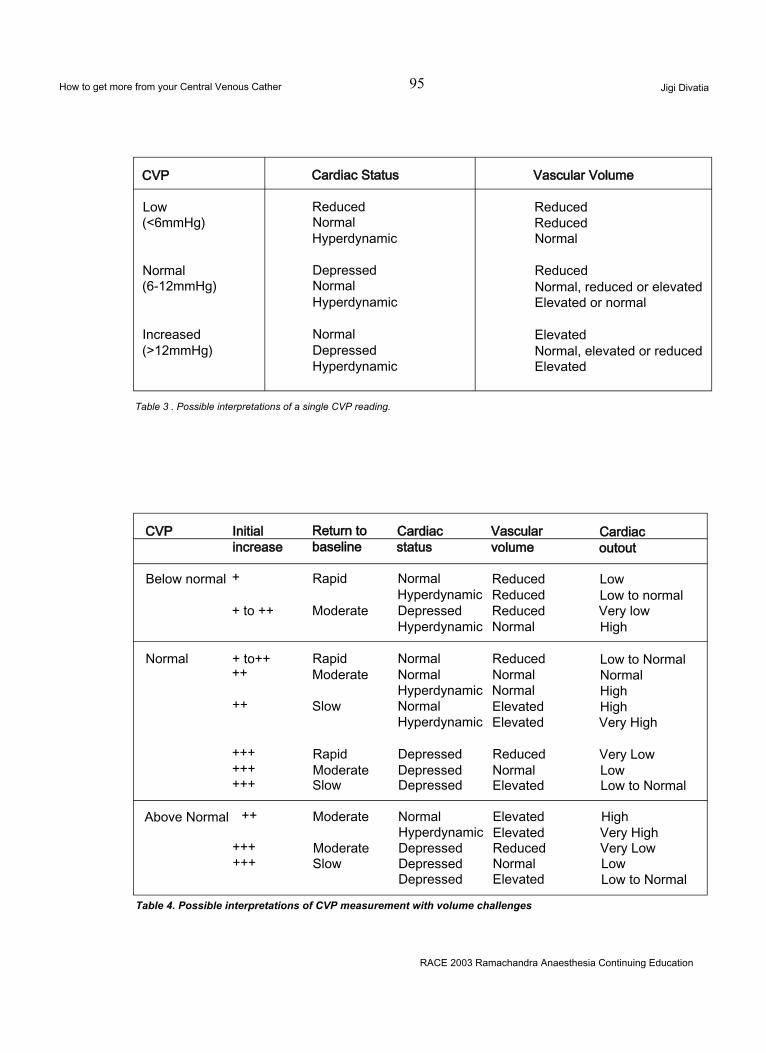
How to get more from your Central Venous Cather 95 Jigi Divatia
CVP Cardiac Status Vascular Volume
Low Reduced Reduced(<6mmHg) Normal Reduced
Hyperdynamic Normal
Normal Depressed Reduced(6-12mmHg) Normal Normal, reduced or elevated
Hyperdynamic Elevated or normal
Increased Normal Elevated(>12mmHg) Depressed Normal, elevated or reduced
Hyperdynamic Elevated
Table 3 . Possible interpretations of a single CVP reading.
CVP Initial Return to Cardiac Vascular Cardiacincrease baseline status volume outout
Below normal + Rapid Normal Reduced LowHyperdynamic Reduced Low to normal
+ to ++ Moderate Depressed Reduced Very lowHyperdynamic Normal High
Normal + to++ Rapid Normal Reduced Low to Normal++ Moderate Normal Normal Normal
Hyperdynamic Normal High++ Slow Normal Elevated High
Hyperdynamic Elevated Very High
+++ Rapid Depressed Reduced Very Low+++ Moderate Depressed Normal Low+++ Slow Depressed Elevated Low to Normal
Above Normal ++ Moderate Normal Elevated HighHyperdynamic Elevated Very High
+++ Moderate Depressed Reduced Very Low+++ Slow Depressed Normal Low
Depressed Elevated Low to Normal
Table 4. Possible interpretations of CVP measurement with volume challenges
RACE 2003 Ramachandra Anaesthesia Continuing Education
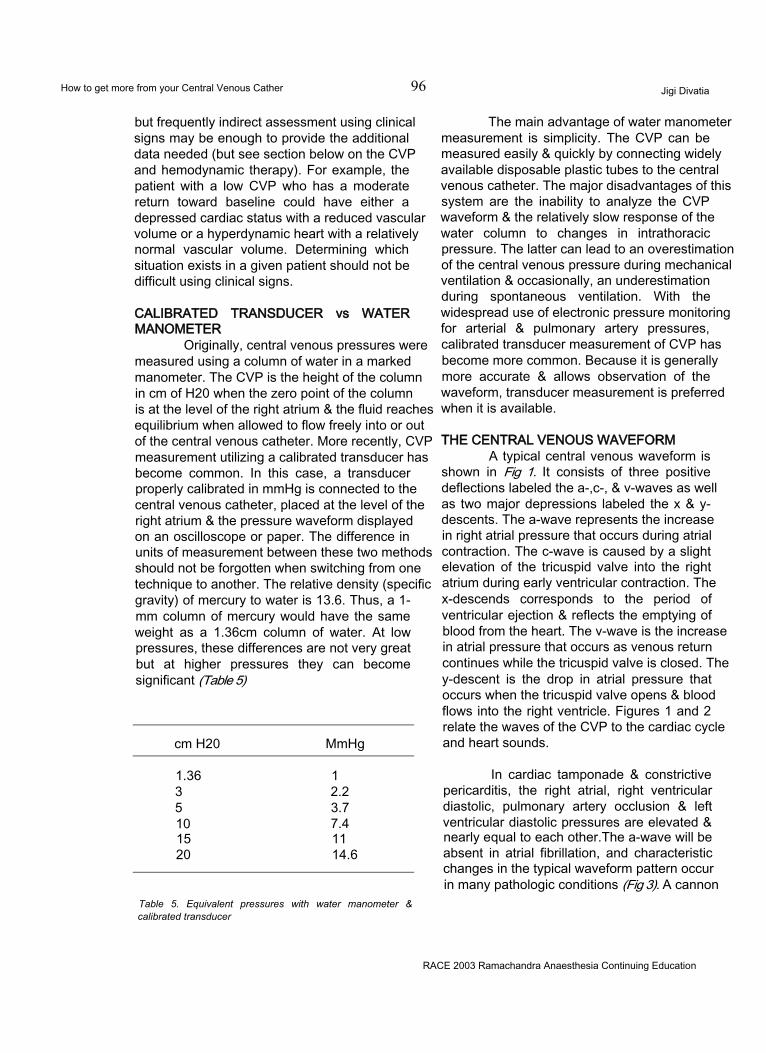
How to get more from your Central Venous Cather 96 Jigi Divatia
but frequently indirect assessment using clinical signs may be enough to provide the additional data needed (but see section below on the CVP and hemodynamic therapy). For example, the patient with a low CVP who has a moderate return toward baseline could have either a depressed cardiac status with a reduced vascular volume or a hyperdynamic heart with a relatively normal vascular volume. Determining which situation exists in a given patient should not be difficult using clinical signs.
CALIBRATED TRANSDUCER vs WATER MANOMETER
Originally, central venous pressures were measured using a column of water in a marked manometer. The CVP is the height of the column in cm of H20 when the zero point of the column is at the level of the right atrium & the fluid reaches equilibrium when allowed to flow freely into or out of the central venous catheter. More recently, CVP measurement utilizing a calibrated transducer has become common. In this case, a transducer properly calibrated in mmHg is connected to the central venous catheter, placed at the level of the right atrium & the pressure waveform displayed on an oscilloscope or paper. The difference in units of measurement between these two methods should not be forgotten when switching from one technique to another. The relative density (specific gravity) of mercury to water is 13.6. Thus, a 1- mm column of mercury would have the same weight as a 1.36cm column of water. At low pressures, these differences are not very great but at higher pressures they can become significant (Table 5)
cm H20 MmHg
1.36 13 2.25 3.710 7.415 1120 14.6
Table 5. Equivalent pressures with water manometer & calibrated transducer
The main advantage of water manometer measurement is simplicity. The CVP can be measured easily & quickly by connecting widely available disposable plastic tubes to the central venous catheter. The major disadvantages of this system are the inability to analyze the CVP waveform & the relatively slow response of the water column to changes in intrathoracic pressure. The latter can lead to an overestimation of the central venous pressure during mechanical ventilation & occasionally, an underestimation during spontaneous ventilation. With the widespread use of electronic pressure monitoring for arterial & pulmonary artery pressures, calibrated transducer measurement of CVP has become more common. Because it is generally more accurate & allows observation of the waveform, transducer measurement is preferred when it is available.
THE CENTRAL VENOUS WAVEFORMA typical central venous waveform is
shown in Fig 1. It consists of three positive deflections labeled the a-,c-, & v-waves as well as two major depressions labeled the x & y- descents. The a-wave represents the increase in right atrial pressure that occurs during atrial contraction. The c-wave is caused by a slight elevation of the tricuspid valve into the right atrium during early ventricular contraction. The x-descends corresponds to the period of ventricular ejection & reflects the emptying of blood from the heart. The v-wave is the increase in atrial pressure that occurs as venous return continues while the tricuspid valve is closed. The y-descent is the drop in atrial pressure that occurs when the tricuspid valve opens & blood flows into the right ventricle. Figures 1 and 2 relate the waves of the CVP to the cardiac cycle and heart sounds.
In cardiac tamponade & constrictive pericarditis, the right atrial, right ventricular diastolic, pulmonary artery occlusion & left ventricular diastolic pressures are elevated & nearly equal to each other.The a-wave will be absent in atrial fibrillation, and characteristic changes in the typical waveform pattern occur in many pathologic conditions (Fig 3). A cannon
RACE 2003 Ramachandra Anaesthesia Continuing Education
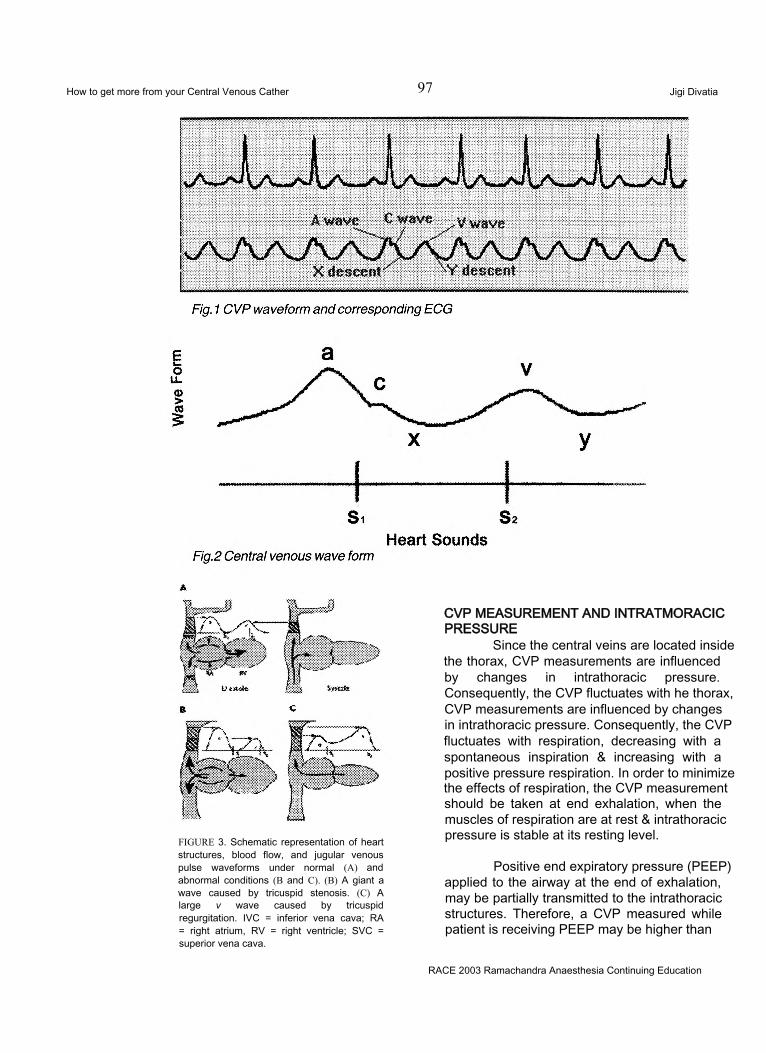
How to get more from your Central Venous Cather 97 Jigi Divatia
FIGURE 3. Schematic representation of heart structures, blood flow, and jugular venous pulse waveforms under normal (A) and abnormal conditions (B and C). (B) A giant a wave caused by tricuspid stenosis. (C) A large v wave caused by tricuspid regurgitation. IVC = inferior vena cava; RA = right atrium, RV = right ventricle; SVC = superior vena cava.
CVP MEASUREMENT AND INTRATMORACIC PRESSURE
Since the central veins are located inside the thorax, CVP measurements are influenced by changes in intrathoracic pressure. Consequently, the CVP fluctuates with he thorax, CVP measurements are influenced by changes in intrathoracic pressure. Consequently, the CVP fluctuates with respiration, decreasing with a spontaneous inspiration & increasing with a positive pressure respiration. In order to minimize the effects of respiration, the CVP measurement should be taken at end exhalation, when the muscles of respiration are at rest & intrathoracic pressure is stable at its resting level.
Positive end expiratory pressure (PEEP) applied to the airway at the end of exhalation, may be partially transmitted to the intrathoracic structures. Therefore, a CVP measured while patient is receiving PEEP may be higher than
RACE 2003 Ramachandra Anaesthesia Continuing Education
How to get more from your Central Venous Cather 98 Jigi Divatia
under the same cardiovascular circumstances if he was not receiving PEER A more accurate measure of right heart filling pressure is the transmural right atrial pressure, that is intravascular right atrial pressure minus intrathoracic pressure. Under most circumstances, measuring CVP referenced to atmosphere is adequate because intrathoracic pressure remains constant. However, when PEEP is applied, pleural pressure increases more than right atrial pressure, so that transmural right atrial pressure(true filling pressure)decreases. This effect is rarely significant if the PEEP is less than 7.5cm H20. The cardiovascular effects of such an increase in CVP are twofold: a decrease in venous return and a decrease in cardiac output. This may be erroneously interpreted as a deterioration in cardiac function. An obvious solution to this problem is to measure the CVP only when the PEEP has been removed. However, the beneficial effect of PEEP on gas exchange is lost very quickly when it is removed and may take a prolonged period to recover when PEEP is reapplied. This subjects the patients to the dangers of hypoxemia. The only accurate method of compensating for the effects of PEEP on central pressure measurements is to measure the transmural pressures. Unfortunately, simple accurate measurement of intrathoracic pressure in the clinical setting is difficult. From a practical standpoint, PEEP does not usually cause a large change in the CVP, especially in patients with stiff lungs. It is best not to remove PEEP for measurements, recognizing that the numbers obtained may be slightly higher than would be found without PEEP, and to assess the change in CVP in response to fluid challenge as a guide to therpy.
Central Venous Catheterisation and Hemodynamic therapy
The pulmonary artery catheter has been considered the gold standard to guide hemodynamic therapy in shock and cardiac failure. The PCWP is considered the most suitable measure of preload (subject to the assumptions outlined in Table 2), and the cardiac output is measured by thermodilution. Modern pulmonary artery catheters allow continuous cardiac output minitoring, continuous mixed venous oxygen saturation (Sv02) monitoring, as well as measurement of right ventricular end-
diastolic volume as the preload, albeit of the right heart. Pulmonary artery catheterization is an invasive procedure, and recent articles have cast doubt on its utility, and there is increasing interest in non-invasive or less invasive methods of measuring cardiac output. The central venous catheter remains central to these measurements in a number of these new technologies.
Use of the Central Venous oxygen saturation (Scv02)
Rivers and colleagues2 studied early goal- directed therapy designed to optimize cardiac preload, afterload, and contractility. Theyrandomly assigned patients to this therapy or to standard (control) therapy at the time of presentation, before admission to the intensive care unit. After arterial and central venous cannulation, the standard- therapy group underwent treatment that included critical care consultation and were transferred to the intensive care unit as soon as possible (on average, after 6.3 hours). The group randomly assigned to early goal-directed therapy was treated in the emergency department for at least 6 hours (average, 8.0 hours) before admission. These patients received, in a sequential fashion, fluid resuscitation, vasopressor or dilator agents, red-cell transfusions, and inotropic medications to achieve target levels of central venous pressure (8 to 12 mm Hg), mean arterial pressure (65 to 90 mm Hg), urine output (at least 0.5 ml per kilogram of body weight per hour), and central venous oxygen saturation (at least 70 percent). Patients who did not have a response to these approaches underwent sedation and mechanical ventilation. In-hospital mortality differed significantly between the two groups: 30.5 percent in the group assigned to early goal-directed therapy and 46.5 percent in the group assigned to standard therapy. During the period from 7 to 72 hours, the patients assigned to early goal-directed therapy had significantly higher mean central venous oxygen saturations and arterial pH values and lower lactate levels, base deficit values, and organ-dysfunotion scores than those assigned to standard therapy.
Thus a hemodynamic therapy based on CVP monitoring and Scv02 measurement, without a pulmonary artery catheter in early sepsis produced dramatic beneficial results. CVCs incorporating a fibreoptic sensor to continuously monitor Scv02 will soon become
RACE 2003 Ramachandra Anaesthesia Continuing Education

How to get more from your Central Venous Cather 99 Jigi Divatia
available. This approach represents a major advance and a simplified method of hemodynamic therapy.
Cardiac OutputThe PiCCO Technology is based on a
hemodynamic monitoring method, which is a combination of transpulmonary thermodilution and arterial pulse contour analysis. The cold bolus traverses the lungs after being injected through a CVP line, and that the thermodilution curve is being measured in a systemic artery. The method provides the user with the following parameters:- Intrathoracic Blood Volume (ITBV) which is a volumetric measure of cardiac preload;- ExtraVascular Lung Water (EVLW) which reflects the level of pulmonary edema, if increased.
The measurement of these and several other parameters requires a single bolus injection of cold saline through any central venous line and a modified (thermistor-tipped) arterial catheter, eliminating the need for a Right Heart Catheter (RHC). The transpulmonary measurement of CO is at least as accurate as the conventional bolus thermodilution using the right heart catheter.3 However, transpulmonary (“arterial”) CO is not affected by respiratory variations meaning that the measurement is not dependent on the moment of bolus injection during the ventilation cycle. ITBV can be regarded as the best bedside measure of static cardiac preload, since it represents total cardiac preload volume.4-6 It may be more representative than conventional filling pressures or right ventricular end-diastolic volume. However ITBV is a calculated parameter based on complex equations, and its routine use requires further validation.
Lithium Dilution cardiac outputThe LiDCO System consists of a
proprietary disposable lithium sensitive sensor which is attached to an existing arterial line, a connector which sends a signal from the sensor to a monitor and a monitor which displays a computation of cardiac output. The LiDCO System provides an indicator dilution method of
measuring cardiac output. A small dose of lithium chloride is injected via a central venous catheter; the resulting arterial lithium concentration-time curve is recorded by withdrawing blood past a lithium sensor. Indicator dilution curves recorded in arterial blood consist of primary and secondary curves due to the initial circulation and then recirculation of the indicator. Clinical trials have been completed that demonstrate that the LiDCO System is at least as accurate as thermodilution.
In conclusion, it is vital to interpret the CVP correctly to make accurate haemodynamic diagnoses and to initiate therapy. The trend of the CVP and responses to fluid challenges and other therapeutic measures are more important than a single value. All information should be ultimately interpreted in the clinical context. Despite its limitations, the CVP remains a vital haemodynamic parameter which can be easily and safety monitored. It may be necessary at some stage to obtain further information, eg, by echocardiography, or by pulmonary artery catheterisation.
REFERENCES
Most of the material including Tables are based on :Otto CW, "Central venous pressure monitoring “ in Monitoring in Anaesthesia and Critical Care Medicine, editor Blitt CD, 1st edition, Churchill Livingstone, New York, 1985.Other references:
1. Karnath B, Thornton W, Beach R. Inspection of Neck veins. Hospital physicians, May 2002. 43-47.
2. Rivers E, Nguyen B, Ressler J, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19): 1368-77.
3. Sakka SG, Reinhart K, Meier-Hellmann A: Comparison of pulmonary artery and arterial thermodilution cardiac output in critically ill patients. Intensive Care Med 25: 843-846, 1999
4. Lichtwarck-Aschoff M, Zeravik J, Pfeiffer U: Intrathoracic blood volume accurately reflects circulatory volume status in critically ill patients with mechanical ventilation. Intensive Care Med 18: 142- 147, 1992;
5. Hedenstierna G: What value does therecording of intrathoracic blood volume have in clinical practice? . Intensive Care Med 187137-138
6. Sakka SG, Meier-Hellmann A, Reinhart K: Assessment of intrathoracic blood volume and extravascular lung water by single transpulmonary thermodilution. Intensive Care Med 26: 180-187, 2000
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 100 Gita Nath
For patients with end-stage renal disease, renal transplantation is the treatment modality which gives the best quality of life and survival.11'21 This patient population includes relatively younger patients with primary renal disease at one end of the spectrum, and older patients with renal failure secondary to diabetes or hypertension, with diffuse atherosclerosis and heart disease at the other end. With improvements in anaesthetic and surgical techniques as well as immunosuppressive drugs, many patients are being accepted for transplantation that would have been considered unsuitable earlier. However, this means we, as anaesthesiologists, have to deal with sicker patients with greater pathophysiological compromise. Hence it is important for us to have a clear understanding of the changes in physiology as well as pharmacology in renal failure.
PATHOPHYSIOLOGIC EFFECTS OF CHRONIC RENAL FAILUREFluid and Electrolyte disturbances
The primary function of the kidneys is to regulate the volume and composition of extracellular fluid. End-stage renal failure is usually associated with hypervolemia due to a greatly reduced glomerular filtration rate and several electrolyte disturbances. 131 Patients presented for renal transplantation are usually well prepared with dialysis and other measures, but even so there is very little margin for error. Overdialysis can lead to hypovolemia and cardiovascular collapse but a positive balance of as little as 500 ml may tip the patient into pulmonary oedema. Most patients produce some urine - 500 to 100 ml/day or even more. But this volume is fixed - it cannot be regulated according to the needs of the body. The few remaining nephrons are, in fact, in a state of maximal osmotic diuresis.
There is a chronic anion gap metabolic acidosis in renal failure due to retention of sulphates and phosphates. Mild acidosis usually persists despite dialysis and is even helpful as it compensates for anaemia. However the decrease is buffer base reduces the margin of safety, and severe acidemia can be caused by relatively mild ventilatory depression. An important point to keep in mind is the relation between H+ and K+. A change in pH of 0.1 results in a 0.5 mEq/L change in serum K+. That is, a decrease in pH from 7.4 to 7.2 may increase the serum K+ from 5.5 to 6.5 mEq/L.
The usual consequence of ESRD on K+ balance is hyperkalemia due to diminished or absent loss through the kidney. The level should be normalized preoperatively by regular dialysis. Hyperkalemia may be worsened or precipitated by conditions such as catabolic stress, acute acidosis - either metabolic or respiratory, and drugs such as ACE inhibitors. Similarly, a patient with borderline low serum K+, maybe due to overzealous dialysis, can be pushed into hypokalemia by hyperventilation. Magnesium is handled by the kidney in a fashion similar to potassium. Hyper-magnesemia is relevant to the anaesthetic assessment, as it causes muscle weakness and potentiates the action of muscle relaxants.
Phosphate elimination depends on the kidneys and hyper-phosphatemia may persist despite dialysis. In addition, renal synthesis of Vitamin D3 (1,25-dihydroxy-chole-calciferol) is deficient in renal failure resulting in reduced calcium absorption from the gut. Both hyperphosphatemia and hypocalcaemia stimulate the parathyroid glands causing parathyroid hyperplasia - this is called secondary hyperparathyroidism. The released parathormone
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 101 Gita Nath
causes bone resorption leading to renal osteodystrophy. In some patients one or more parathyroid glands become autonomous - the so-called tertiary hyperparathyroidism. These patients present with hypercalcaemia and may show metastatic calcification. They may need parathyroidectomy, retaining either a small part of one parathyroid or a forearm autograft of parathyroid tissue. Hypophosphataemia is less common, may be due to excessive dialysis or antacid therapy, and is deleterious as it causes muscle weakness and ventilatory insufficiency.
AnaemiaThis results from decreased
erythropoetin production from the kidney as well as diminished erythrocyte survival.1341 There are also several compensatory mechanisms for this chronic anaemia. The increased level of 2,3 DPG in the erythrocytes and the acidosis present in renal failure result in a rightward shift of the haemoglobin dissociation curve, thus increasing oxygen delivery to the tissues. There is a compensatory increase in the cardiac output and the lowered viscosity helps in better peripheral perfusion. Evalurtion of the effort tolerance of the patient gives one a better idea of his physiological reserve than the Hb value. In fact it has been shown that many haemodialysis patients with hematocrit levels around 25% tolerate treadmill exercise.151 However, in those patients with reduced cardio-respiratory reserve for other reasons, for example coronary artery disease, haematocrit values of around 30% should be aimed for, using recombinant erythropoietin therapy or pre-operative transfusions if necessary.
CoagulopathyPlatelet dysfunction is seen in uremic
patients. It is thought that activation of glycoprotein llb/llla receptors on the platelet membrane is impaired by a dialyzable uremic factor. This results in reduced platelet binding to von Willebrand-Factor VIII complex and fibrinogen, and impaired thrombus generation. Anaemia is an additional contributor to platelet dysfunction as erythrocytes enhance platelet function by releasing ADP and inactivating vascular prostacyclin (PGI2).
The prothrombin time and activated thromboplastin time are usually normal in uremia
unless there is residual heparin in the body after the previous dialysis. Since the platelets counts are normal as well, uremic coagulopathy can be difficult to detect as platelet function tests are not commonly performed. Alternatively, bleeding time can be measured. This is a sensitive indicator of platelet dysfunction but the results are somewhat operator variable.16 71
Platelet function can be improved by effective dialysis. Other measures to treat bleeding diathesis in uremia are desmopressin, which releases von Willebrand-Factor VIII complex from the endothelium, and conjugated oestrogen, whose mechanism of action has not been elucidated. Erythopoetin is helpful by correcting anaemia as well as increasing the number of glycoprotein llb/llla receptors on the platelets. For refractory patients, cryoprecipitate is effective, as it is rich in von Willebrand’s factor and fibrinogen.
HypertensionThis has an intimate relation with renal
failure, as it can be both the cause as well as effect. Expansion of extracellular fluid volume along with disturbances in vascular autoregulation produces hypertension in these patients. There are several mechanisms involved as recently summarized by Mailloux: (1) inappropriately increased angiotensin II in relation to volume and exchangeable sodium, (2) increased vascular sensitivity to endogenous pressors, (3) increased cardiac output in the presence of an inappropriately high peripheral vascular resistance, and (4) failure to fully suppress vasoconstrictor systems[8].
Some patients become normotensive after the initiation of dialysis but many need multiple drugs to bring the blood pressure under control. The exact management of the anti- hypertensive therapy during the peri-operative period needs to be carefully thought out. One concern is to prevent excessive hypertension, especially at critical times such as anaesthetic induction and intubation, so as to avoid adverse effects on the heart and cerebral vasculature. However, after revascularizing the kidney, we need to maintain a good perfusion pressure (at least 130-140 mmHg systolic or 90-100 mmHg mean pressure), as this is one of the most important factors influencing the outcome of the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 102 Gita Nath
transplantation procedure. Overtreatment of the hypertension can make it difficult to achieve this.
Most antihypertensive drugs should be continued till the day of surgery. Sudden cessation of clonidine or beta blockers can result in rebound hypertension. However ACE inhibitors have been found to be associated with intraoperative hypotension, hence it is better to omit this group of drugs on the day of surgery.19101
Post-operatively, many patients become normotensive. Hence it is better to withhold antihypertensives initially and monitor the blood pressure closely. Drugs can be restarted if the patient becomes hypertensive.
Heart and CRFFirst of all we need to consider the effects
of hypertension on the heart, such as left ventricular concentric hypertrophy, decreased LV compliance, diastolic dysfunction and propensity to myocardial ischaemia. Apart from this, the incidence of cardiomyopathy and coronary artery disease is high in these patients, and is a major cause of morbidity and mortality.
LV dysfunction may be caused by ischaemic heart disease, diabetes, hypoalbuminemia, anaemia etc. In addition, uremia itself causes uremic cardiomyopathy which is seen on echocardiography as LV dilatation and ineffective ventricular hypertrophy. This is reversible following renal transplantation, and ejection fractions of less than 30% have been shown to normalize to 69% six months after transplantation.1111 Thus LV dysfunction per se is not a contraindication to transplantation but the presence of congestive heart failure before the patient goes on dialysis is an independent predictor of mortality.1121
Uremic patients show peripheral insulin resistance and decreased lipoprotein lipase activity and are thus prone to hyperglycemia and hypertriglyceridemia. In addition many of them have pre-existing diabetes. For these reasons, coronary artery disease has a high incidence of 17-34 % in uremic patients. Hence all symptomatic or high risk patients (those with diabetes or hyperlipidemia, smokers,) should be screened before surgery. Dipyridamole-thallium
scanning has been found to have a high false negative rate because the myocardial microcirculation has a reduced response to dipyridamole. Dobutamine stress ECG performs better as a screening test in these patients.1131
Uremic pericarditis may cause pericardial effusion which may be haemorrhagic due to the heparin received during dialysis. Pre-operative echocardiography should detect this condition and if cardiac tamponade is present a sub-xiphoid pericardiostomy should be done under monitored anaesthetic care.'141
Miscellaneous Problems.Due to restricted diets and loss of protein
during dialysis, hypoalbuminemia is common, favoring the formation of interstitial and pulmonary oedema. The poor nutrition and anaemia also predispose the patient to infections. Nosocomial infections are especially common at dialysis access sites. The incidence of hepatitis B and C is high in haemodialysis patients due to frequent exposure to blood and blood products. Many of them become asymptomatic carriers.
PHARMACOLOGIC CHANGES IN CRFThe response of patients to many drugs
is different in renal failure, due to pharmacokinetic as well as pharmacodynamic reasons. Clinically, patients seem more sensitive to sedatives and hypnotics. This is because of increased pharmacodynamic effectiveness of the drug as well as increased availability at the effect site. Thiopentone and diazepam are highly protein bound drugs, and the unbound fraction is increased when there is hypoalbuminemia.
In general, to produce the effect of the drug, a therapeutic concentration has to be produced in the volume of distribution. Therefore the initial dose is similar to normal patients, with two exceptions - if the volume of distribution is reduced, as for morphine, alfentanil and remifentanil1151, and secondly if the drug is highly protein bound, as discussed above.
For maintenance dosing, the behaviour of the drug depends on its mode of elimination and whether there are any significant active metabolites. Drugs which totally or predominantly
RACE 2003 Ramachandra Anaesthesia Continuing Education
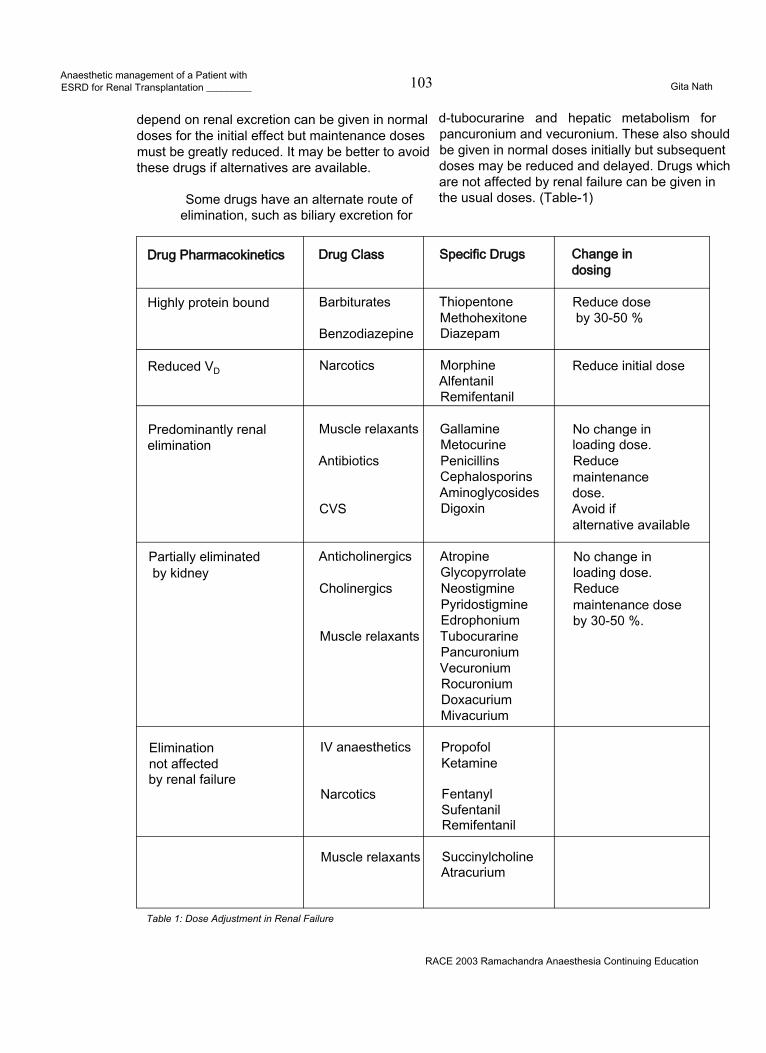
Anaesthetic management of a Patient withESRD for Renal Transplantation _________ 103 Gita Nath
depend on renal excretion can be given in normal doses for the initial effect but maintenance doses must be greatly reduced. It may be better to avoid these drugs if alternatives are available.
Some drugs have an alternate route of elimination, such as biliary excretion for
d-tubocurarine and hepatic metabolism for pancuronium and vecuronium. These also should be given in normal doses initially but subsequent doses may be reduced and delayed. Drugs which are not affected by renal failure can be given in the usual doses. (Table-1)
Drug Pharmacokinetics Drug Class Specific Drugs Change in dosing
Highly protein bound Barbiturates
Benzodiazepine
ThiopentoneMethohexitoneDiazepam
Reduce dose by 30-50 %
Reduced VD Narcotics MorphineAlfentanilRemifentanil
Reduce initial dose
Predominantly renal elimination
Muscle relaxants
Antibiotics
CVS
GallamineMetocurinePenicillinsCephalosporinsAminoglycosidesDigoxin
No change in loading dose. Reduce maintenance dose.Avoid ifalternative available
Partially eliminated by kidney
Anticholinergics
Cholinergics
Muscle relaxants
AtropineGlycopyrrolateNeostigminePyridostigmineEdrophoniumTubocurarinePancuroniumVecuroniumRocuroniumDoxacuriumMivacurium
No change in loading dose. Reducemaintenance dose by 30-50 %.
Elimination not affected by renal failure
IV anaesthetics
Narcotics
PropofolKetamine
FentanylSufentanilRemifentanil
Muscle relaxants SuccinylcholineAtracurium
Table 1: Dose Adjustment in Renal Failure
RACE 2003 Ramachandra Anaesthesia Continuing Education
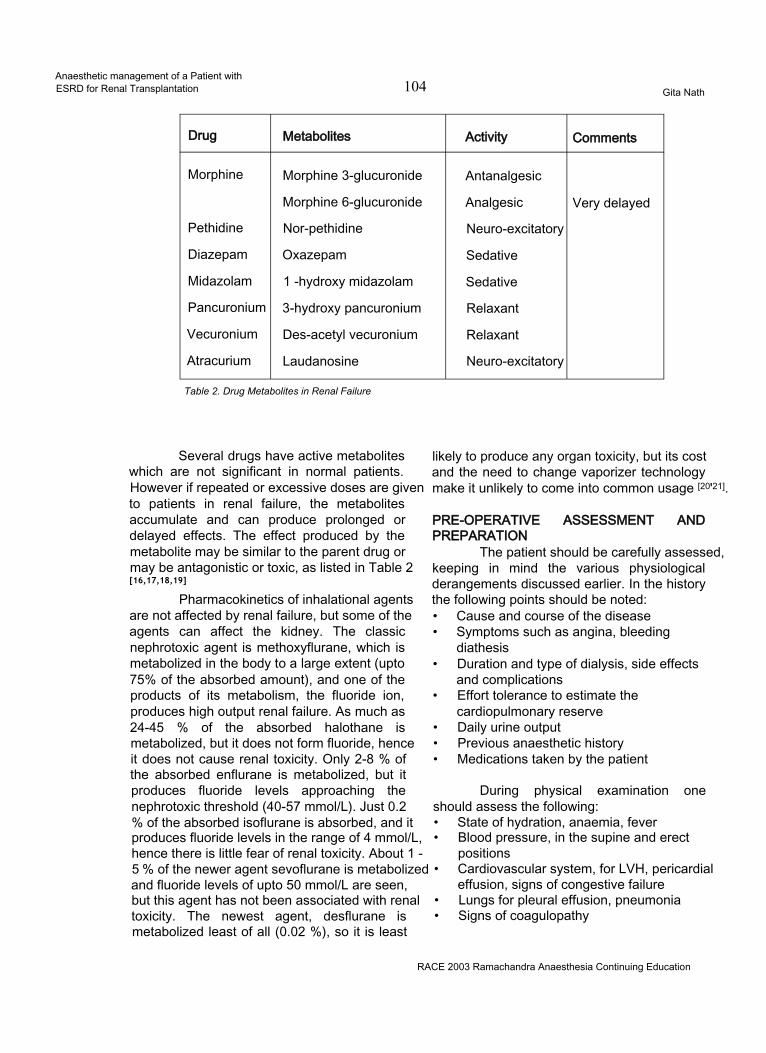
Anaesthetic management of a Patient withESRD for Renal Transplantation 104 Gita Nath
Drug Metabolites Activity Comments
Morphine Morphine 3-glucuronide Antanalgesic
Morphine 6-glucuronide Analgesic Very delayed
Pethidine Nor-pethidine Neuro-excitatory
Diazepam Oxazepam Sedative
Midazolam 1 -hydroxy midazolam Sedative
Pancuronium 3-hydroxy pancuronium Relaxant
Vecuronium Des-acetyl vecuronium Relaxant
Atracurium Laudanosine Neuro-excitatory
Table 2. Drug Metabolites in Renal Failure
Several drugs have active metabolites which are not significant in normal patients. However if repeated or excessive doses are given to patients in renal failure, the metabolites accumulate and can produce prolonged or delayed effects. The effect produced by the metabolite may be similar to the parent drug or may be antagonistic or toxic, as listed in Table 2[16,17,18,19]
Pharmacokinetics of inhalational agents are not affected by renal failure, but some of the agents can affect the kidney. The classic nephrotoxic agent is methoxyflurane, which is metabolized in the body to a large extent (upto 75% of the absorbed amount), and one of the products of its metabolism, the fluoride ion, produces high output renal failure. As much as 24-45 % of the absorbed halothane is metabolized, but it does not form fluoride, hence it does not cause renal toxicity. Only 2-8 % of the absorbed enflurane is metabolized, but it produces fluoride levels approaching the nephrotoxic threshold (40-57 mmol/L). Just 0.2 % of the absorbed isoflurane is absorbed, and it produces fluoride levels in the range of 4 mmol/L, hence there is little fear of renal toxicity. About 1 -5 % of the newer agent sevoflurane is metabolized and fluoride levels of upto 50 mmol/L are seen, but this agent has not been associated with renal toxicity. The newest agent, desflurane is metabolized least of all (0.02 %), so it is least
likely to produce any organ toxicity, but its cost and the need to change vaporizer technology make it unlikely to come into common usage [20'21].
PRE-OPERATIVE ASSESSMENT AND PREPARATION
The patient should be carefully assessed, keeping in mind the various physiological derangements discussed earlier. In the history the following points should be noted:• Cause and course of the disease• Symptoms such as angina, bleeding
diathesis• Duration and type of dialysis, side effects
and complications• Effort tolerance to estimate the
cardiopulmonary reserve• Daily urine output• Previous anaesthetic history• Medications taken by the patient
During physical examination one should assess the following:• State of hydration, anaemia, fever• Blood pressure, in the supine and erect
positions• Cardiovascular system, for LVH, pericardial
effusion, signs of congestive failure• Lungs for pleural effusion, pneumonia• Signs of coagulopathy
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 105 Gita Nath
The following laboratory investigations should be included:• Haematological - Hematocrit, leucocytes,
platelet count, coagulation studies including Ivy bleeding time
• Biochemical - BUN, creatinine, Na+, K+, HCO'3Ca++, Phosphate, Mg++, Albumin, Glucose
• Serological - Hepatitis B and C, HIV status• ECG - for myocardial ischaemia, LVH,
arrhythmias, electrolyte effects• Chest X-ray - Cardiomegaly, pericardial or
pleural effusions, pneumonia• Echocardiography-Assessment of
myocardial function, ventricular hypertrophy, pericardial effusion
If the patient is on haemodialysis, preoperative dialysis should be performed the day before surgery. The amount of fluid removed and the post-dialysis biochemistry should be noted. The effect of residual heparin wears off by 6 hours, and should not interfere with surgery. CAPD may be continued till the time of surgery.
Antihypertensive therapy should be continued till the day of surgery but ACE inhibitors should be omitted. Premedication, if necessary may include a small dose of oral benzodiazepine. For patients at risk of aspiration, a H2 blocker, metoclopramide and sodium bicitrate may be given.
INTRA-OPERATIVE MANAGEMENTRoutine monitoring should include ECG,
oxygen saturation, capnography, neuromuscular monitor and temperature. Care should be taken to protect the arm which has the dialysis access- neither an IV line nor a blood pressure cuff should be placed on that arm. It is better to avoid invasive blood pressure monitoring in case the radial artery is needed for creation of an AV fistula in the future. For the same reason, it is preferable not to use the cephalic vein at the wrist for IV access.
A central venous line is mandatory in all patients, whether under general or regional anaesthesia, to aid in fluid management. Patients with LV dysfunction may need pulmonary artery catheterization.
A urinary catheter is necessary for monitoring the urine output. In should be noted that the bladder is initially filled with saline by the surgical team, and the catheter is clamped, in order to facilitate surgical access to the bladder for re-implantation. This fluid should be excluded, while monitoring urine output after revascularizing the kidney.
Renal transplantation is usually done in the supine position. Great care should be taken to protect the limb with dialysis access. Due to renal osteodystrophy, the bones are very fragile; hence any change in position should be done gently. Attention should be paid to padding the various pressure points - impairment of skin integrity as well as pre-existing peripheral neuropathy should be kept in mind.
Preventive measures should be taken against hypothermia, which may include adjustment of ambient temperature, warming mattress, insulation of all exposed body parts, heater-humidifierfor the inspired air, forced hot air warmers and fluid warming systems. These measures should be continued during the recovery period.
These patients already have impaired immunity because of the primary condition. In addition, immunosuppressive therapy will be instituted to prevent rejection. Hence great attention should be paid towards aseptic technique. On the other hand, they have a higher incidence of blood borne infections such as Hepatitis B and C and HIV. Hence the medical staff should take measures to protect themselves.
Selection of anaesthetic technique:The goals of anaesthetic management
of renal transplantation are:• To tailor the anaesthetic keeping in mind all
the physiological derangements detailed earlier.
• To take measures to optimise functioning of transplanted kidney
• To ensure that there are no residual effects of the anaesthetic drugs or techniques, in case graft functioning is delayed.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic management of a Patient withESRD for Renal Transplantation 106 Gita Nath
• If post-operative dialysis becomesnecessary, to delay it as much as possible so that the interval between surgery and administration of heparin is longer. In essence, this involves avoiding fluid overload and potassium build-up.
As long as the above principles are kept in mind, the actual anaesthetic technique does not make a difference to the outcome. Renal transplantation has been successfully managed using general as well as regional anaesthetic techniques such as spinal and epidural anaesthesia122'. The concern with regional anaesthesia is the risk of hypotension which, if treated with aggressive fluid administration, may lead to pulmonary oedema when the block wears off. Apart from this, expected length of the operation and poor patient cooperation influence the choice of anaesthetic technique. Coagulopathy, which would contraindicate a regional technique, should also be borne in mind, since this may occur even with normal platelet count, prothrombin time and activated thromboplastin time.
Regarding general anaesthesia, both inhalational as well as intravenous techniques can be equally effective. As far as possible drugs whose pharmacokinetics are not affected by renal failure should be used, but this has to be balanced against the availability of resources and the previous experience of the anaesthetist. As with many issues in anaesthesia, it is more important to choose one’s anaesthetist than the anaesthetic technique.
Induction of anaesthesia:Preoxygenation is advisable in these
anaemic patients to improve the oxygen reserve. The intravascular volume is often somewhat depleted after the last dialysis, and carefully titrated fluid increments may be given to avoid hypotension. The goal is to avoid excessive hypotension, but at the same time, prevent excessive hypertensive response to intubation. A bolus dose of a narcotic (e.g. fentanyl 2-3 mic/ kg) helps towards this end.
Thiopentone, etomidate and propofol are the choices available for induction of anaesthesia. Ketamine is not suitable because of its
hypertensive effect. The dose of thiopentone should be reduced because of the reduced protein binding. The usual recommended induction dose of 2 mg/kg propofol causes hypotension even in normal patients, hence carefully titrated doses should be given, checking the blood pressure between doses. Propofol seems to prevent the intubation response much more effectively than thiopentone.
If the risk of aspiration is present, a single dose of succinylcholine may be given as long as the serum potassium is less that 4.5 mEq/L. Rocuronium is the other choice, since it produces satisfactory intubating conditions in 60 to 90 seconds and can be used to maintain relaxation till the end of the procedure. Rapacurium is another steroidal non-depolarizing relaxant, with slightly faster onset than rocuronium, but it has now been withdrawn because of an unacceptably high incidence of adverse events.
If there is no risk of aspiration, the nondepolarising agent can be given directly. Atracurium and cis-atracurium are the relaxants of choice because of their spontaneous breakdown independently of the kidneys or liver. Vecuronium or rocuronium may also be used but the maintenance doses should be reduced and delayed. Pancuronium should be avoided, now that so many alternatives are available. Neuromuscular monitoring is mandatory in these cases t23]. Mivacurium is another agent which doesn’t depend on the kidneys for elimination, but its action is so short-acting that it has to be given by infusion. The large amount required for such a long operation means that it is not cost- effective [24].
After intubation, the patient is ventilated with an oxygen/nitrous oxide or oxygen/air mixture. Excessive hypocapnia or hypercapnia should be avoided, bearing in mind the possible shifts in potassium with changing blood pH. For maintenance of anaesthesia, either a nitrous oxide-oxygen-inhalational agent combination or an intravenous propofol-narcotic infusion can be used with equally good results125 26 271. Isoflurane is probably the best inhalational agent, from the renal point of view Fentanyl, sufentanil or alfentanil can all be used for maintenance of narcotic effect Remifentanil has the advantage of lack of
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation__________ 107 Gita Nath
cumulationt28]. Morphine and pethidine are better avoided, because of accumulation of their metabolites morphine-6-glucuronide and nor- pethidine, with analgesic and neuro-excitatory effects respectively116171.
After induction, minimal fluids are given as long as the blood pressure is adequate. Extra fluid administered at this time redistributes into the extravascular space and is not available for renal perfusion after anastamosis. It is better to fill up more rapidly closer to the time of clamp release. Hartmann’s solution and Ringer Lactate solution should be avoided as they contain potassium.
OPTIMIZING FUNCTION OF THE TRANSPLANTED KIDNEY:
Three aspects of management critically affect the outcome of renal transplantation - the management of the renal donor, how well the graft is preserved and thirdly, perioperative management of the kidney.
1. Management of the donorLiving donors are involved in about 25%
of all renal allografts in the United States, but contribute to the majority of renal transplants in India. All living kidney donors, related or unrelated, should be in excellent health, without any medical problem which increases the risk of anaesthesia. Also they should not have any condition which makes them prone to renal failure in the future, such as hypertension and diabetes.
The operation is performed in the lateral position with the kidney bridge elevated. The key point in managing these patients is to keep the kidneys well oxygenated and perfused, and take measures to reduce their oxygen consumption. Good hydration is mandatory. Some centres make it a practice to give IV fluids overnight. In any case, 1.5 to 2 litres of crystalloids should be infused during the initial part of the operation, and this is followed by 10-12 gm of mannitol. A small dose of lasix may help by blocking the chloride pump in the thick ascending loop of Henle, thus reducing oxygen consumption in a poorly perfused and vulnerable area of the kidney. The urine output should be monitored and a good diuretic response ensured. Maintenance of a good perfusion pressure is important and the colour
and turgidity of the kidney are good indicators of its perfusion. Direct acting vasopressors should be avoided, so that renal artery spasm is not induced. From the surgical side, the kidney and its hilar structures should be handled gently, since spasm of the renal artery can be very troublesome. Some surgeons request 5000 units of heparin before clamping the artery - this can be reversed with protamine 50 mg after the kidney is harvested.
After removal of the kidney, anaesthesia is continued according to one’s normal routine. It is important to ensure that the donor does not come to any harm as the result of his generous action, hence special care should be taken to avoid any anaesthesia or surgery related complications. If the 11th or 12th rib was resected during surgery, a high index of suspicion should be maintained to detect the occurrence of a pneumothorax. Special attention should be directed towards postoperative analgesia, as donor nephrectomy is a very painful operation. Intermittent injections of morphine or pethidine are not really effective. Other methods such as patient controlled analgesia, epidural local anaesthetic or opiate infusions, wound infusion with bupivacaine and other techniques are more effective.
Cadaveric donors contribute to the majority of renal transplants done in the developed world, and cadaveric transplantation is becoming commoner in India as well. The salient points in managing cadaver donors are:
• A protocol for brain death certification should be in place in each institution. This should be followed meticulously so as to afford no chance for anyone to point a finger.
• Haemodynamic stability and good gas exchange criteria give the best results. Contraindications to organ harvesting are prolonged hypotension and hypothermia, systemic sepsis, malignancy, DIC, hepatitis B or C and HIV seropositivity. Relative contraindications are age (above 70), diabetes, vascular diseases, elevated serum creatinine and high requirement for vasopressors.
• A Pa02 of at least 100 should be
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic management of a Patient withESRD for Renal Transplantation 108 Gita Nath
maintained with normocapnia. The arterial pressure should be kept above 100 mmHg, with aggressive fluid treatment. If intravascular volume is adequate but blood pressure is still below 90 mmHg, inotropes can be added, such as dobutamine, low dose dopamine, or low dose adrenaline. High doses of vasopressors, with a vasoconstricting effect such as high dose dopamine, high dose adrenaline and noradrenaline are associated with a worse graft function possibly because of renal vasoconstriction [29], The urine output should be maintained above 100 ml/hr using mannitol, lasix and dopamine, if necessary.
• This treatment is continuedintraoperatively. Muscle relaxants are given to suppress the reflex motor response to surgery. Ventilatory and circulatory support is discontinued after the organs are harvested.
2. Preservation of the harvested organTotal ischaemia time starts when the
donor renal artery is clamped, and ends after the anastamosis when the artery is unclamped in the recipient. Minimizing the ischaemia time is critical in preservation of the kidney. Warm ischaemia is especially deleterious to the kidney as oxygen consumption continues with no oxygen supply. Warm ischaemia starts when the renal artery is clamped and stops when the kidney is cooled by perfusion with a cold solution. Cold ischaemia starts when the core of the kidney becomes cold, as is evidenced by clear perfusion fluid flowing out of the cut end of the renal vein. Cold ischaemia can be maintained for upto 36- 72 hours by storing the kidney at4°C but results are better if the cold ischaemia time is less than 24 hours.
Warm ischaemia time resumes when the kidney is removed from the cold contained and is placed in the recipient and ends when the kidney is perfused again after completion of the vascular anastamosis.
For short ischaemia times, the composition of the perfusate does not matter so much, and perfusion with ice-cold normal saline gives as good results as if a special preservative solution was used. For longer periods of storage, several solutions are available. Euro-Collins solution contains high concentrations of
potassium (110 mM), magnesium sulphate (30 mM), and phosphate (57.5 mM), which mimics intracellular fluid composition; and mannitol which makes the solution hypertonic and prevents cell swelling within the kidney. The UW solution (University of Wisconsin solution) contains lactobionate, raffinose, and hydroxyethyl starch for their osmotic effect, phosphate as a buffer, adenosine for ATP synthesis during reperfusion, glutathione as a free-radical scavenger, allopurinol to inhibit xanthine oxidase and the generation of free radicals, and magnesium and dexamethasone as membrane-stabilizing agents. The UW solution gives better results and can be used for all intra-abdominal organs. Machine perfusion with a cold solution similar to UW solution further extends the cold ischaemia time of the kidney[30).
3. Other measures to optimise graft function• Perfusion Pressure: This is the key factor which influences immediate graft function, and any delay in graft functioning is associated with a worse outcome for the graft in the early posttransplant period as well as long term I31'32). Hence, haemodynamic management is geared towards providing a perfusion pressure of at least 120 mmHg at the time of clamp release. The following measures may be taken towards this goal:• Close haemodynamic monitoring, with frequent checks of blood pressure and CVP• Aggressive intravascular volume expansion. Fluid loading with 1-2 litres of normal saline is done while the vascular anastamosis is being done.• It is important to anticipate and expect hypotension after release of clamps because of reperfusion of the ischaemic vascular bed of the graft and washout of metabolites. Repeated checking of blood pressure is very important. The surgeon’s assessment of the firmness or turgidity of the graft is a useful index of the adequacy of the perfusion pressure.• If verapamil has been added to the renal perfusate, it can cause hypotension on being washed into the circulation when the clamp is released. To cover this, calcium chloride 0.25 gm can be given before and a further 0.25 gm after clamp release.
• Mannitol 10-20 gm before clamp release: This acts by expanding the intravascular volume,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation _________ 109 Gita Nath
reducing cellular swelling, increasing tubular urine flow and reducing the potential for tubular obstruction, scavenging free radicals and increasing the release of intrarenal prostaglandins.
• Albumin has been found to improve the graft outcome at doses of 0.8 to 1.6 gm/Kg [33-34]. Albumin acts by improving the oncotic pressure and thus expanding the intravascular volume, especially in patients with hypoalbuminemia.
• Loop diuretics such as frusemide block the chloride pump in the thick ascending loop of Henle, and increase resistance against ischaemic injury. Despite several theoretical reasons, it is not clear whether they improve transplant outcomel351.
• Verapamil has been shown to improve graft outcome, either when administered to the recipient [36) or added to the renal perfusate.
• Low dose dopamine is said to enhance renal perfusion by selective renal vasodilatation and also promotes natriuresis. However, several studies have not been able to show an improved outcome during cadaver renal transplantation with dopamine 2-3 mic/Kg/min t37 38 39). Hence routine use of dopamine is not recommended.
• The Kidney Cocktail. Some centres infuse a kidney cocktail just before the anastamosis is completed. This consists of 600 ml 1/4 normal saline with albumin 37.5 gm and mannitol 80 gm. For cadaver transplantation, they add 80 mg frusemide[4].
MONITORING OF KIDNEY FUNCTIONThe initial assessment of urine output is
made soon after renal revascularization, by looking out for urine to spurt from the end of the ureter. Once ureteric implantation begins, urine output cannot really be monitored till the bladder is closed. One should be careful to exclude the volume of saline initially used to distend the bladder from the measured urine output.
TROUBLE-SHOOTINGIf there is a delay in urine formation,
prerenal factors should be evaluated first of all, such as perfusion pressure, the anastamosis,
arterial spasm or thrombosis, venous occlusion or thrombosis etc. The consistency of the kidney and thrill at the site of the anastamosis can help confirm good blood flow. Intraoperative Doppler can also evaluate the anastamotic flow.
Post renal factors are outflow tract obstruction due to kinking, clot, oedema; or leakage of urine from the bladder implantation site. The problem may be as simple as a kinked or blocked urinary catheter, or even an air-lock in the catheter drainage bag.
When all these factors are excluded, a biopsy of the transplanted kidney may be necessary to evaluate for acute tubular necrosis or graft rejection.
RECOVERY FROM ANAESTHESIAPotential problems which should be
anticipated at recovery are delayed emergence, respiratory depression, hypo or hypertension, respiratory depression and pulmonary oedema. Adequate recovery of neuromuscular function must be ensured before extubation. Persistent weakness due to hypermagnesaemia may be antagonized by giving calcium. As far as possible it is better to avoid postoperative mechanical ventilation because of the risk of pulmonary infection.
The patient should be transferred to a dedicated transplant unit for postoperative management. Apart from barrier nursing, cardiorespiratory and renal functions are monitored closely for the next few days. Postoperative pain is usually not a problem. Once the kidney has started working, there is no problem with accumulating metabolites, and morphine can be used safely.
CONCLUSIONTransplant anaesthesia is a specialized
field which requires a good understanding of the physiological trespass in patients with renal failure, familiarity with transplant medicine and expertise in the management of these patients. Good anaesthetic management, in liaison with the transplant surgeon and nephrologist, is of paramount importance in avoiding delayed graft function with all its possible sequelae and complications.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic management of a Patient withESRD for Rena( Transplantation 110 Gita Nath
REFERENCES1. Cameron Jl. Differences in quality of life across renal replacement therapies: a meta-analytic comparison. Am J Kidney Dis 2000; 35(4): 629-372. Rabbat CG. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J Am Soc Nephrol 2000; 11(5): 917-223. Sladen RN Anesthetic considerations for the patient with renal failure.- Anesthesiol Clin North America 2000; 18(4): 863-82, x.4. Sprung J, Kapural L, Bourke DL,O’Hara JF. Anesthesia for kidney transplant surgery. Anesthesiol Clin North America2000; 18(4): 919-51.5. Lundin AP, Stein RA, Brown CD, et al: Fatigue, acid-base, and electrolyte changes with exhaustive treadmill exercise in haemodialysis patients. Nephron 1987; 46:57-62.6. Mahesh K. Preoperative Care of Patients with Kidney Disease. American Family Physician 2002; 66: 8.7. Dember LM. Critical care issues in the patient with chronic renal failure. Critical Care Clinics 2002; 18: 2.8. Mailloux LU: Hypertension in chronic renal failure and ESRD: Prevalence, pathophysiology, and outcomes. Semin Nephrol 2001; 21:146-156.9. Powell CG. Severe hypotension associated with angiotensin-converting enzyme inhibition in anaesthesia. Anaesth Intensive Care 1998; 26(1): 107-9.10. Licker M. Cardiovascular responses to anesthetic induction in patients chronically treated with angiotensin- converting enzyme inhibitors. Can J Anaesth 2000; 47(5): 433-40.11. Cho WH, Kim HT, Park CH, et al: Renal transplantation in advanced cardiac failure patients. Transplant Proc 1997; 29:236-238.12. Harnett JD, Foley RN, KentGM, etal: Congestive heart failure in dialysis patients: Prevalence, incidence, prognosis, and risk factors. Kidney Int 1995; 47:884-890.
13. Herzog CA, Marwick TH, Pheley AM: Dobutamine stress echocardiography for the detection of significant coronary artery disease in renal transplant candidates. Am J Kidney Dis 1999; 33:1090.14. Figueroa W, Alankar S, Pai N, et al: Subxiphoid pericardial window for pericardial effusion in end-stage renal disease. Am J Kidney Dis 1996; 27: 664-7.15. Dahaba AA End-stage renal failure reduces central clearance and prolongs the elimination half life of remifentanil- Can J Anaesth 2002; 49(4): 369-74.16. Angst MS, Buhrer M, L6tsch J: Insidious intoxication after morphine treatment in renal failure: Delayed onset of morphine-6-glucuronide action. Anesthesiology 2000; 92: 1473-6.17. Hasselstrfim J, Berg U, Lofgren A, Sawe J: Long lasting respiratory depression induced by morphine-6- glucuronide? Br J Clin Pharmacol 1989; 27: 515-8.18. Sear J: Effect of renal function and failure. In Park GR, Sladen RN (eds): Sedation and Anesthesia in the Critically III. Oxford, Blackwell Science, 1995, pp 108-2919. Hall LG - Analgesic Agents. Pharmacology and Application in Critical Care Crit Care Clin 2001; 17(4): 899- 923, viii.20. Baden JM, Rice SA. Metabolism and Toxicity of Inhaled Anesthetics. In Miller RD (ed): Anesthesia. 5th ed., Copyright © 2000 Churchill Livingstone, Inc, pp 155-167.
21. Conzen PF, Nuscheler M, Melotte A, et al: Renal function and serum fluoride concentrations in patients with stable renal insufficiency after anesthesia with sevoflurane or enflurane. Anesth Analg 1995; 81:569-75.22. Murakami M, Nomiyama S, Ozawa A, et al: Anaesthetic management of pediatric renal transplantation for chronic renal failure. Masui 1993; 42:263-270.23. Murray MJ - Clinical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Crit Care Med 2002; 30(1): 142-56.24. Head-Rapson AG Pharmacokinetics and pharmacodynamics of the three isomers of mivacurium in health, in end-stage renal failure and in patients with impaired renal function. - Br J Anaesth 1995; 75(1): 31-6.25. Ickx B Propofol infusion for induction and maintenance of anaesthesia in patients with end-stage renal disease. - Br J Anaesth 1998; 81(6): 854-60.26. Babacan A Assessment of total intravenous anesthesia in renal transplantation. Transplant Proc 1998; 30(3): 750-3.27. Jirasiritham S Total intravenous anesthesia for general operations in post-renal transplant patients. Transplant Proc 1998; 30(7): 3897-8.28. Hoke JF Pharmacokinetics and pharmacodynamics of remifentanil in persons with renal failure compared with healthy volunteers. Anesthesiology 1997; 87(3): 533-41.29. O’Brien EA, Bour SA, Marshall RL, et al: Effects of use of vasopressors in organ donors on immediate function of renal allografts. Journal of Transplant Coordination 1996; 6:215-216.30. Van der Werf WJ, D’Alessandro AM, Hoffmann RM, Knechtle SJ. Procurement, Preservation, And Transport Of Cadaver Kidneys. Surgical Clinics of North America 1998; 78(1) 41-54.31. Dawidson I, Ar’Rajab A: Perioperative fluid and drug therapy during cadaver kidney transplantation. In Terasaki, Cecka (eds): Clinical Transplants. Los Angeles, 1992, pp 267-27932. Rajamani AR, Kamat VN, Poojara L, Arunkumar AS. Haemodynamic variables affecting kidney allograft function. Intensive Are Medicine 2002; 28: (Suppl 1) S10233. Willms CD, Dawidson IHA, Dickerman R, et al: Intraoperative blood volume expansion induces primary function after renal transplantation: A study of 96 paired cadaver kidneys. Transplant Proc 1991; 23:1338-1339.34. Dawidson IJ Intraoperative albumin administration affects the outcome of cadaver renal transplantation - Transplantation 1992; 53(4): 774-82.35. Shilliday I, Allison ME: Diuretics in acute renal failure. Renal Fail 1994; 16:13-17.36. Dawidson I, Rooth P, Lu C, et al: Verapamil improves the outcome after cadaver renal transplantation. J Am Soc Nephrol 1991; 2:983-990.37. Grundmann R, Kindler J, Meider G, et al: Dopamine treatment of human cadaver kidney graft recipients: A prospectively randomized trial. Klinische Wochenshrift 1982; 60:193-197.38. Kadieva VS, Friedman L, Margoulius LP, et al: The effect of dopamine on graft function in patients undergoing renal transplantation. Anesth Analg 1993; 76:362-365.39. Sandberg J, Tyden G, Groth CG: Low-dose dopamine infusion following cadaveric renal transplantation: No effect on the incidence of ATN. Transplant Proc 1992; 24:357.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Sedation and Analgesia in Children for Procedures outside the OR 111 S. Ramesh
“ 6 year old Master X has been fearful of the repeated lumbar punctures that he must undergo for intrathecal medical administration, as well as his occasional bone marrow aspirations. His previous experiences include being held down while he screamed, with a long period of being silent and withdrawn after each procedure as no sedation or analgesics were given during these procedures. So Master X thereafter refused to come to see any doctor, withdrawn from his friends and needed lot of psychological consults ”
So children who undergo painful medical procedures not only have their physiological function affected, but also face complex psychobiological demands.
Painful diagnostic or therapeutic procedures are often necessary during emergency care of children who have already painful and frightening injuries and illnesses. For example, in a study done by us in 1997, it was found that 90% of lumbar punctures in the paediatric emergency department were performed without sedation or local analgesia. There are many reasons why effective anxiolysis, analgesia and sedation are not in commonplace in the emergency department. The explanations for less use of analgesia or sedation include lack of consensus about optimal safe effective methods, medications, patient monitoring, lack of physician familiarity with local anaesthetic techn^ :?s and dosing, insufficient time to carry outset ■■rd belief that children have only a short tern, of pain.
In India, the past decade has seen what may be considered a revolution in the recognition
and treatment of pain and anxiety in children. Advantages of safe and effective management of pain and anxiety in the emergency department include reduction of psychological trauma and its sequelae, reduction of stress for the paediatricians and parents and a good success for the procedures.
Due to the diversity in population, no ‘cookbook’ is available for the method and medication to be used for a particular procedure. What we must rely on is a broad understanding of the pharmacokinetics and the physiological effects of diverse agents. So this article will review some definitions, pain pathways, various medications available to us, principles of conscious sedation and a few examples of emergency procedures.
NEUROPHYSIOLOGY OF PAIN:‘Pain’
- “ An unpleasant and emotionalexperience associated with actual or potential tissue damage or described in terms of such damage”
_ Pain is ‘suffering’ or ‘distress’_ Pain is what the patient ‘says it is’
The basic mechanism of pain perception has four components, transduction, transmission, perception and modulation. Noxious mechanical, thermal or chemical stimuli excite primary afferent fiores that transmit information about the potential injurious stimuli from the periphery to
dorsal horn of the spinal cord. The pain repulse is transmitted via A delta (large, myelinated) and C (small, unmyelinated) fibres. The tissue injury causes release of inflammatory mediators, (eg.potassium, bradykinin,
RACE 2003 Ramachandra Anaesthesia Continuing Education
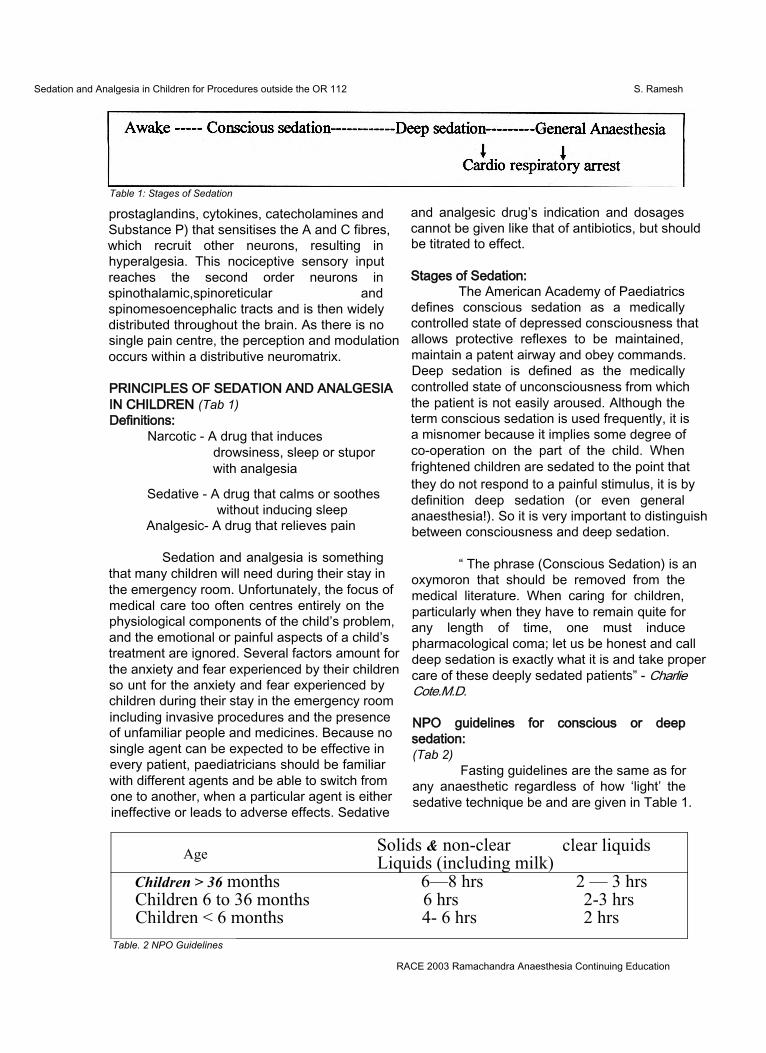
Sedation and Analgesia in Children for Procedures outside the OR 112 S. Ramesh
Table 1: Stages of Sedation
prostaglandins, cytokines, catecholamines and Substance P) that sensitises the A and C fibres, which recruit other neurons, resulting in hyperalgesia. This nociceptive sensory input reaches the second order neurons in spinothalamic,spinoreticular andspinomesoencephalic tracts and is then widely distributed throughout the brain. As there is no single pain centre, the perception and modulation occurs within a distributive neuromatrix.
PRINCIPLES OF SEDATION AND ANALGESIA IN CHILDREN (Tab 1)Definitions:
Narcotic - A drug that inducesdrowsiness, sleep or stupor with analgesia
Sedative - A drug that calms or soothes without inducing sleep
Analgesic- A drug that relieves pain
Sedation and analgesia is something that many children will need during their stay in the emergency room. Unfortunately, the focus of medical care too often centres entirely on the physiological components of the child’s problem, and the emotional or painful aspects of a child’s treatment are ignored. Several factors amount for the anxiety and fear experienced by their children so unt for the anxiety and fear experienced by children during their stay in the emergency room including invasive procedures and the presence of unfamiliar people and medicines. Because no single agent can be expected to be effective in every patient, paediatricians should be familiar with different agents and be able to switch from one to another, when a particular agent is either ineffective or leads to adverse effects. Sedative
and analgesic drug’s indication and dosages cannot be given like that of antibiotics, but should be titrated to effect.
Stages of Sedation:The American Academy of Paediatrics
defines conscious sedation as a medically controlled state of depressed consciousness that allows protective reflexes to be maintained, maintain a patent airway and obey commands. Deep sedation is defined as the medically controlled state of unconsciousness from which the patient is not easily aroused. Although the term conscious sedation is used frequently, it is a misnomer because it implies some degree of co-operation on the part of the child. When frightened children are sedated to the point that they do not respond to a painful stimulus, it is by definition deep sedation (or even general anaesthesia!). So it is very important to distinguish between consciousness and deep sedation.
“ The phrase (Conscious Sedation) is an oxymoron that should be removed from the medical literature. When caring for children, particularly when they have to remain quite for any length of time, one must induce pharmacological coma; let us be honest and call deep sedation is exactly what it is and take proper care of these deeply sedated patients” - Charlie Cote.M.D.
NPO guidelines for conscious or deep sedation:(Tab 2)
Fasting guidelines are the same as for any anaesthetic regardless of how ‘light’ the sedative technique be and are given in Table 1.
Age Solids & non-clear Liquids (including milk)
clear liquids
Children > 36 months 6—8 hrs 2 — 3 hrsChildren 6 to 36 months 6 hrs 2-3 hrsChildren < 6 months 4- 6 hrs 2 hrs
Table. 2 NPO Guidelines
RACE 2003 Ramachandra Anaesthesia Continuing Education
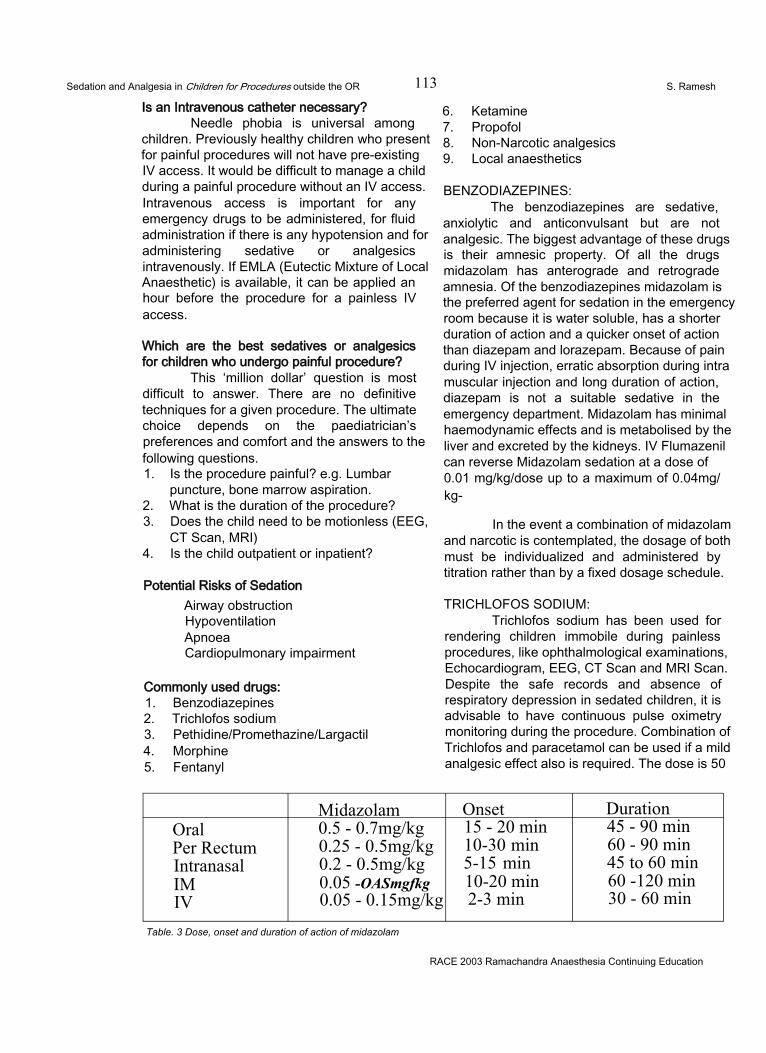
Sedation and Analgesia in Children for Procedures outside the OR 113 S. Ramesh
Is an Intravenous catheter necessary?Needle phobia is universal among
children. Previously healthy children who present for painful procedures will not have pre-existing IV access. It would be difficult to manage a child during a painful procedure without an IV access. Intravenous access is important for any emergency drugs to be administered, for fluid administration if there is any hypotension and for administering sedative or analgesics intravenously. If EMLA (Eutectic Mixture of Local Anaesthetic) is available, it can be applied an hour before the procedure for a painless IV access.
Which are the best sedatives or analgesics for children who undergo painful procedure?
This ‘million dollar’ question is most difficult to answer. There are no definitive techniques for a given procedure. The ultimate choice depends on the paediatrician’s preferences and comfort and the answers to the following questions.1. Is the procedure painful? e.g. Lumbar
puncture, bone marrow aspiration.2. What is the duration of the procedure?3. Does the child need to be motionless (EEG,
CT Scan, MRI)4. Is the child outpatient or inpatient?
Potential Risks of SedationAirway obstructionHypoventilationApnoeaCardiopulmonary impairment
Commonly used drugs:1. Benzodiazepines2. Trichlofos sodium3. Pethidine/Promethazine/Largactil4. Morphine5. Fentanyl
6. Ketamine7. Propofol8. Non-Narcotic analgesics9. Local anaesthetics
BENZODIAZEPINES:The benzodiazepines are sedative,
anxiolytic and anticonvulsant but are not analgesic. The biggest advantage of these drugs is their amnesic property. Of all the drugs midazolam has anterograde and retrograde amnesia. Of the benzodiazepines midazolam is the preferred agent for sedation in the emergency room because it is water soluble, has a shorter duration of action and a quicker onset of action than diazepam and lorazepam. Because of pain during IV injection, erratic absorption during intra muscular injection and long duration of action, diazepam is not a suitable sedative in the emergency department. Midazolam has minimal haemodynamic effects and is metabolised by the liver and excreted by the kidneys. IV Flumazenil can reverse Midazolam sedation at a dose of0.01 mg/kg/dose up to a maximum of 0.04mg/ kg-
In the event a combination of midazolam and narcotic is contemplated, the dosage of both must be individualized and administered by titration rather than by a fixed dosage schedule.
TRICHLOFOS SODIUM:Trichlofos sodium has been used for
rendering children immobile during painless procedures, like ophthalmological examinations, Echocardiogram, EEG, CT Scan and MRI Scan. Despite the safe records and absence of respiratory depression in sedated children, it is advisable to have continuous pulse oximetry monitoring during the procedure. Combination of Trichlofos and paracetamol can be used if a mild analgesic effect also is required. The dose is 50
Midazolam Onset DurationOralPer Rectum Intranasal IM IV
0.5 - 0.7mg/kg 0.25 - 0.5mg/kg 0.2 - 0.5mg/kg 0.05 -OASmgfkg 0.05 - 0.15mg/kg
15 - 20 min 10-30 min 5-15 min 10-20 min 2-3 min
45 - 90 min 60 - 90 min 45 to 60 min 60 -120 min 30 - 60 min
Table. 3 Dose, onset and duration of action of midazolam
RACE 2003 Ramachandra Anaesthesia Continuing Education
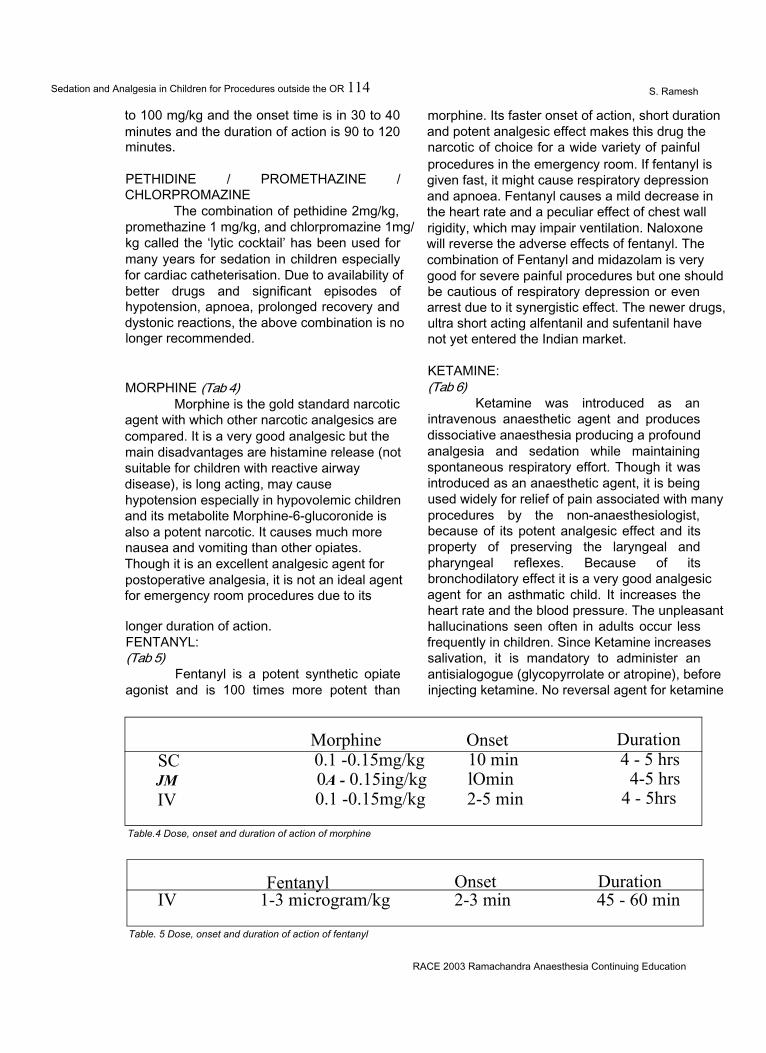
Sedation and Analgesia in Children for Procedures outside the OR 114 S. Ramesh
to 100 mg/kg and the onset time is in 30 to 40 minutes and the duration of action is 90 to 120 minutes.
PETHIDINE / PROMETHAZINE / CHLORPROMAZINE
The combination of pethidine 2mg/kg, promethazine 1 mg/kg, and chlorpromazine 1mg/ kg called the ‘lytic cocktail’ has been used for many years for sedation in children especially for cardiac catheterisation. Due to availability of better drugs and significant episodes of hypotension, apnoea, prolonged recovery and dystonic reactions, the above combination is no longer recommended.
morphine. Its faster onset of action, short duration and potent analgesic effect makes this drug the narcotic of choice for a wide variety of painful procedures in the emergency room. If fentanyl is given fast, it might cause respiratory depression and apnoea. Fentanyl causes a mild decrease in the heart rate and a peculiar effect of chest wall rigidity, which may impair ventilation. Naloxone will reverse the adverse effects of fentanyl. The combination of Fentanyl and midazolam is very good for severe painful procedures but one should be cautious of respiratory depression or even arrest due to it synergistic effect. The newer drugs, ultra short acting alfentanil and sufentanil have not yet entered the Indian market.
MORPHINE (Tab 4)Morphine is the gold standard narcotic
agent with which other narcotic analgesics are compared. It is a very good analgesic but the main disadvantages are histamine release (not suitable for children with reactive airway disease), is long acting, may cause hypotension especially in hypovolemic children and its metabolite Morphine-6-glucoronide is also a potent narcotic. It causes much more nausea and vomiting than other opiates. Though it is an excellent analgesic agent for postoperative analgesia, it is not an ideal agent for emergency room procedures due to its
longer duration of action.FENTANYL:(Tab 5)
Fentanyl is a potent synthetic opiate agonist and is 100 times more potent than
KETAMINE:(Tab 6)
Ketamine was introduced as an intravenous anaesthetic agent and produces dissociative anaesthesia producing a profound analgesia and sedation while maintaining spontaneous respiratory effort. Though it was introduced as an anaesthetic agent, it is being used widely for relief of pain associated with many procedures by the non-anaesthesiologist, because of its potent analgesic effect and its property of preserving the laryngeal and pharyngeal reflexes. Because of its bronchodilatory effect it is a very good analgesic agent for an asthmatic child. It increases the heart rate and the blood pressure. The unpleasant hallucinations seen often in adults occur less frequently in children. Since Ketamine increases salivation, it is mandatory to administer an antisialogogue (glycopyrrolate or atropine), before injecting ketamine. No reversal agent for ketamine
Morphine Onset DurationSC 0.1 -0.15mg/kg 10 min 4 - 5 hrsJM 0A - 0.15ing/kg lOmin 4-5 hrsIV 0.1 -0.15mg/kg 2-5 min 4 - 5hrs
Table.4 Dose, onset and duration of action of morphine
Fentanyl Onset DurationIV 1-3 microgram/kg 2-3 min 45 - 60 min
Table. 5 Dose, onset and duration of action of fentanyl
RACE 2003 Ramachandra Anaesthesia Continuing Education
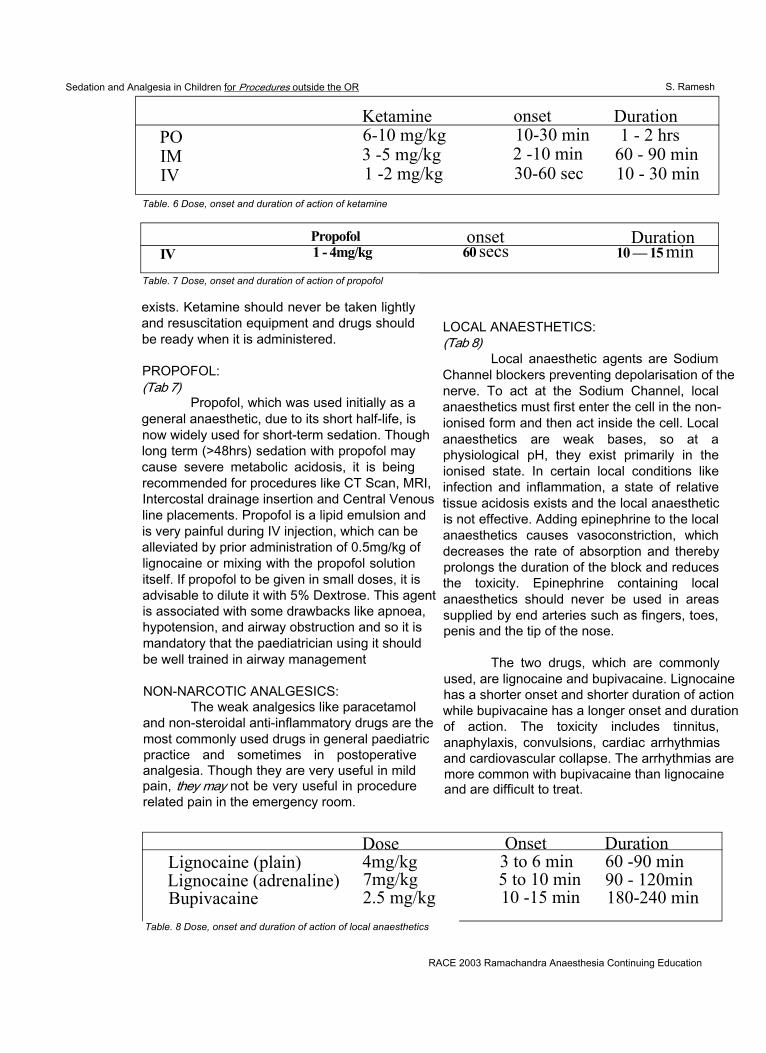
Sedation and Analgesia in Children for Procedures outside the OR S. Ramesh
Ketamine onset DurationPO 6-10 mg/kg 10-30 min 1 - 2 hrsIM 3 -5 mg/kg 2 -10 min 60 - 90 minIV 1 -2 mg/kg 30-60 sec 10 - 30 min
Table. 6 Dose, onset and duration of action of ketamine
Propofol onset DurationIV 1 - 4mg/kg 60 secs 10 — 15 min
Table. 7 Dose, onset and duration of action of propofol
exists. Ketamine should never be taken lightly and resuscitation equipment and drugs should be ready when it is administered.
PROPOFOL:(Tab 7)
Propofol, which was used initially as a general anaesthetic, due to its short half-life, is now widely used for short-term sedation. Though long term (>48hrs) sedation with propofol may cause severe metabolic acidosis, it is being recommended for procedures like CT Scan, MRI, Intercostal drainage insertion and Central Venous line placements. Propofol is a lipid emulsion and is very painful during IV injection, which can be alleviated by prior administration of 0.5mg/kg of lignocaine or mixing with the propofol solution itself. If propofol to be given in small doses, it is advisable to dilute it with 5% Dextrose. This agent is associated with some drawbacks like apnoea, hypotension, and airway obstruction and so it is mandatory that the paediatrician using it should be well trained in airway management
NON-NARCOTIC ANALGESICS:The weak analgesics like paracetamol
and non-steroidal anti-inflammatory drugs are the most commonly used drugs in general paediatric practice and sometimes in postoperative analgesia. Though they are very useful in mild pain, they may not be very useful in procedure related pain in the emergency room.
LOCAL ANAESTHETICS:(Tab 8)
Local anaesthetic agents are Sodium Channel blockers preventing depolarisation of the nerve. To act at the Sodium Channel, local anaesthetics must first enter the cell in the nonionised form and then act inside the cell. Local anaesthetics are weak bases, so at a physiological pH, they exist primarily in the ionised state. In certain local conditions like infection and inflammation, a state of relative tissue acidosis exists and the local anaesthetic is not effective. Adding epinephrine to the local anaesthetics causes vasoconstriction, which decreases the rate of absorption and thereby prolongs the duration of the block and reduces the toxicity. Epinephrine containing local anaesthetics should never be used in areas supplied by end arteries such as fingers, toes, penis and the tip of the nose.
The two drugs, which are commonly used, are lignocaine and bupivacaine. Lignocaine has a shorter onset and shorter duration of action while bupivacaine has a longer onset and duration of action. The toxicity includes tinnitus, anaphylaxis, convulsions, cardiac arrhythmias and cardiovascular collapse. The arrhythmias are more common with bupivacaine than lignocaine and are difficult to treat.
Dose Onset DurationLignocaine (plain) 4mg/kg 3 to 6 min 60 -90 minLignocaine (adrenaline) 7mg/kg 5 to 10 min 90 - 120minBupivacaine 2.5 mg/kg 10 -15 min 180-240 min
Table. 8 Dose, onset and duration of action of local anaesthetics
RACE 2003 Ramachandra Anaesthesia Continuing Education
Sedation and Analgesia in Children for Procedures outside the OR 116 S. Ramesh
EM LAEMLA is a Eutectic mixture of local
anaesthetic cream, which is a mixture of lignocaine, and prilocaine in a water based cream, which provides analgesia even in intact skin. It should be applied at least 60 minutes before. There are some reports of methhaemoglobinaemia in children less than 6 months due to the presence of prilocaine. Its main usage is for IV placement but it can be used for lumbar puncture and circumcision.
General guidelines for using Local anaesthetic agents:1. Use smallest possible needle (24 or 25 g) to
raise the wheal. First inject subcutaneously and then raise the intradermal wheal to prevent pain
2. All resuscitative equipments and drugs should be ready to manage any over dosage or toxicity.
3. It is always safer to have an IV line in place4. To prevent intravascular injection, always
aspirate before injecting the local anaesthetic.
Infiltration local anaesthesia as an adjunct to sedative drugs is very useful in the following situations:1. Lumbar puncture2. Suturing small lacerated wounds3. Central venous line placement4. Arterial line placement5. Intercostal drainage tube insertion6. Bone marrow aspiration and biopsy7. Liver and kidney biopsy
Digital Nerve Block:Of all the other regional nerve blocks,
the most useful block to be learnt is the digital nerve block.
The paired digital nerves enter the digits medially and laterally. Inject 1 to 2 ml of local anaesthetic in the Web space on either sided of the finger or the toe. The usual approach is to enter from the dorsal surface where it is less painful. Epinephrine containing local anaesthetic should never be used. It is very useful for suturing finger injuries, removal of warts and foreign body removal.
Synergism:If you combine two drugs of different
mechanisms of action, one may potentiate the other and reduce the dose requirement of each of them for optimal usage. But at the same time, it may carry the increased risk of respiratory depression.
2 + 2 = 4 Additive effect2 + 2 = 6 Synergistic effect
Example 1- Midazolam and FentanylCombining a sedative and an analgesic
will be very effective for many procedures like lumbar puncture, wound suturing, closed fracture reduction and immobilization. The main advantage of midazolam is amnesia with mild muscle relaxation. Both the drugs should be diluted and injected slowly and titrated to the desired effect without exceeding the upper dose limit of each drug for that particular child. When these combinations are given, it is mandatory to monitor the patient by pulse oximetry. The paediatrician administering these combinations must be skilled in airway management and resuscitation.
Example2 - Atropine or Glycopyrrolate (0.02mg/ kg), Midazolam (0.05mg/kg), Ketamine (0.5 to1 mg/kg)
It is a good combination for painful procedures like wound suturing and fracture reduction. This cocktail effect is not reversible and airway reflexes may not be maintained.
SOME SUGGESTED GUIDELINES FOR THE PROCEDURES:Lumbar puncture:
NPO guide lines ConsentMidazolam 0.1 to 0.2 mg/kg EMLA or local infiltration with 24 Or 25 gauge needleIf airway expert is available, midazolam and fentanyl combination can be tried.
Wound suturingNPO guidelines ConsentMidazolam + Fentanyl combination Local infiltration
RACE 2003 Ramachandra Anaesthesia Continuing Education
Sedation and Analgesia in Children for Procedures outside the OR S. Ramesh
EchocardiographyTrichlofos 50 to 100 mg /kg Intranasal midazolam (0.4mg/kg), onset is in 5 -15 minutes and the duration of action is 25 to 45 minutes.
CT ScanNPO guidelines ConsentTry Midazolam or TrichlofosIf not possible, IV Propofol 2 to 3mg /kgis idealIt is advisable to use IV propofol in the presence of skilled airway personnel.
Haemato- Oncological procedures:NPO guidelines ConsentMidazolam+Fentanyl+Local infiltration Atropine/glycopyrrolate + Midazolam + Ketamine + Local infiltration
RAPID SEQUENCE INTUBATION IN THE EMERGENCY ROOM
The indications and details of the procedure are beyond the purview of this chapter and here, I will be highlighting only the sedatives, induction agents and the muscle relaxants used during the procedure. The main principle here is that the medications are injected fast and theyare preloaded according to the weight of the child.1 Brief history and assessment2. Preperation of equipment and medications3. Preoxygenation4. Premedications5. Sedation and induction of unconsciousness6. Cricoid pressure7. Muscle relaxation8. Intubation9. Verification of ET tube position10. Documentation
Premedication:Atropine or Giycopyrrolate
0.02 mg/kg IV to decrease the secretionsand vagal toneLignocaine 1 mg/kg IV is sometimes is used to provide local airway anaesthesia and blunt ICP response to intubation especially in head trauma.
Sedation and induction of unconsciousness.(Tab 9)
THIOPENTONE:It is an ideal induction agent for this
procedure. It is an ultra short acting barbiturate and has some cerebral protective effect. The major disadvantage is that it causes hypotension. Thiopentone is available in powder form and should be diluted with normal saline and injected as a 2.5% solution and the dose is 4 to 5mg/kg IV.
KETAMINE:There are two clinical situations where
ketamine is considered strongly for induction. One is an asthmatic child because of the bronchodilatory effect and the other is a patient with shock since ketamine is a sympathomimetic agent. The dose is 2mg/kg IV
Midazolam + Fentanyl combination can also be used but higher dosages are needed.
PROPOFOL:Its rapid onset and short duration of
action makes this agent very ideal for rapid induction. Though the manufacturer recommends this agent for children over 3 years, there are many reports of its usage in younger children. It blunts the laryngeal reflexes during intubation. The dose is 2 to 4mg /kg IV.
Muscle relaxants.(Tab 10)
Suxamethonium is the drug of choice for rapid sequence intubation because of its rapid onset and rapid recovery but the disadvantages are bradycardia, fasciculations, and release of potassium.
The alternative to suxamethonium is Rocuronium, which is a non-depolarising muscle relaxant whose onset of action is similar to suxamethonium but the duration of action is longer.
Vecuronium has also been used at a higher dosage of 0.2 to 0.3mg /kg to provide a rapid onset, but the duration is very much prolonged.
RACE 2003 Ramachandra Anaesthesia Continuing Education
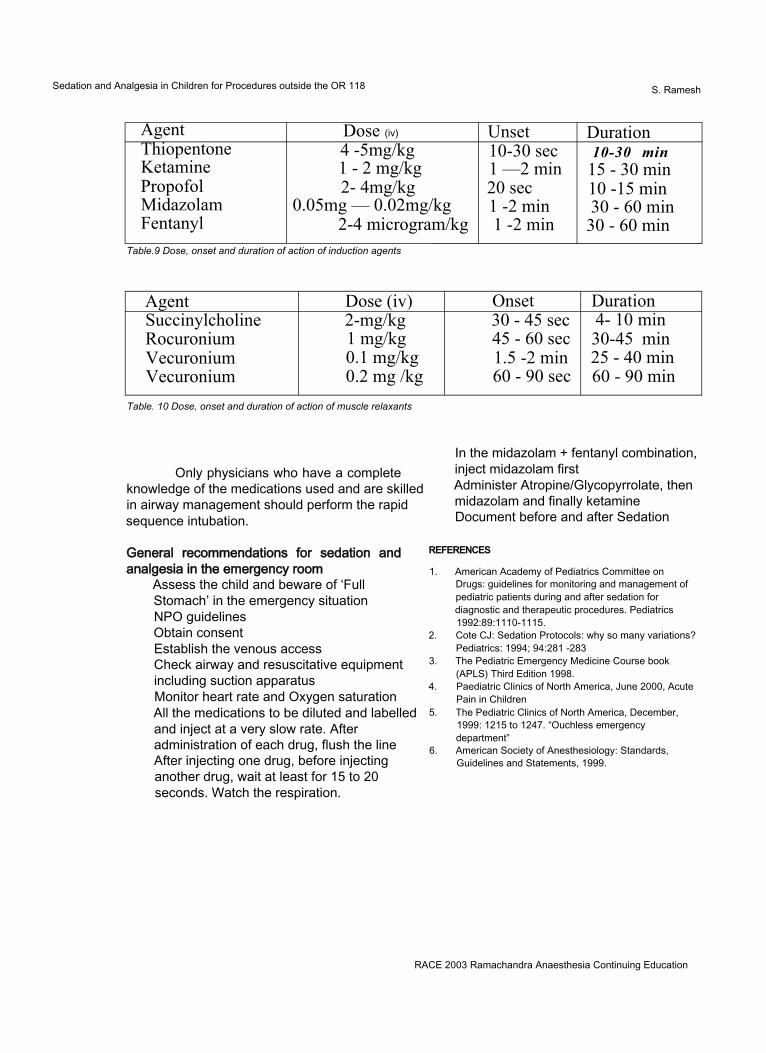
Sedation and Analgesia in Children for Procedures outside the OR 118 S. Ramesh
Agent Dose (iv) Unset DurationThiopentoneKetaminePropofolMidazolamFentanyl
4 -5mg/kg 1 - 2 mg/kg 2- 4mg/kg
0.05mg — 0.02mg/kg2-4 microgram/kg
10-30 sec 1 —2 min 20 sec 1 -2 min 1 -2 min
10-30 min 15 - 30 min 10 -15 min 30 - 60 min
30 - 60 minTable.9 Dose, onset and duration of action of induction agents
Agent Dose (iv) Onset DurationSuccinylcholineRocuroniumVecuroniumVecuronium
2-mg/kg 1 mg/kg 0.1 mg/kg 0.2 mg /kg
30 - 45 sec 45 - 60 sec 1.5 -2 min 60 - 90 sec
4- 10 min 30-45 min 25 - 40 min 60 - 90 min
Table. 10 Dose, onset and duration of action of muscle relaxants
Only physicians who have a complete knowledge of the medications used and are skilled in airway management should perform the rapid sequence intubation.
General recommendations for sedation and analgesia in the emergency room
Assess the child and beware of ‘FullStomach’ in the emergency situationNPO guidelinesObtain consentEstablish the venous accessCheck airway and resuscitative equipmentincluding suction apparatusMonitor heart rate and Oxygen saturationAll the medications to be diluted and labelledand inject at a very slow rate. Afteradministration of each drug, flush the lineAfter injecting one drug, before injectinganother drug, wait at least for 15 to 20seconds. Watch the respiration.
In the midazolam + fentanyl combination, inject midazolam first Administer Atropine/Glycopyrrolate, then midazolam and finally ketamine Document before and after Sedation
REFERENCES
1. American Academy of Pediatrics Committee on Drugs: guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures. Pediatrics 1992:89:1110-1115.
2. Cote CJ: Sedation Protocols: why so many variations? Pediatrics: 1994; 94:281 -283
3. The Pediatric Emergency Medicine Course book (APLS) Third Edition 1998.
4. Paediatric Clinics of North America, June 2000, Acute Pain in Children
5. The Pediatric Clinics of North America, December, 1999: 1215 to 1247. “Ouchless emergency department”
6. American Society of Anesthesiology: Standards, Guidelines and Statements, 1999.
RACE 2003 Ramachandra Anaesthesia Continuing Education

POST GRADUATE SYMPOSIA
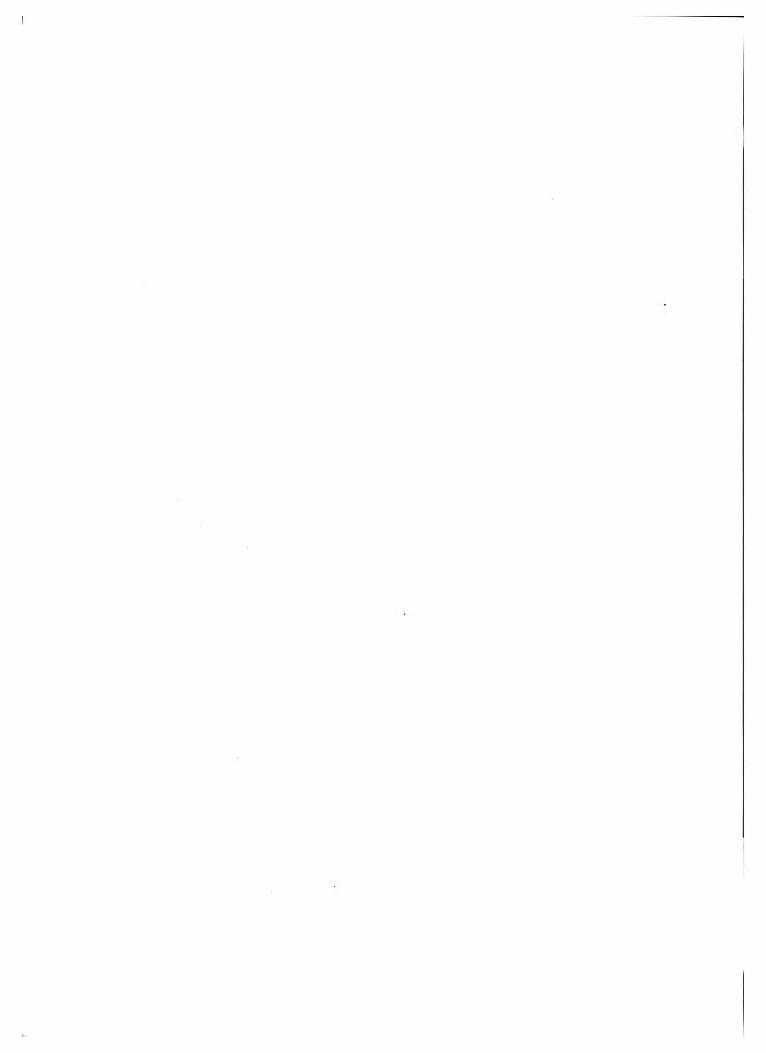
Cardiovascular Physiology 119 Latha, Sathya, Rajkumar
INTRODUCTIONUnderstanding cardiovascular physiology
is mandatory for the treatment of cardiovascular disorders and shock states. This article attempts to deal with CVS physiology from a clinical standpoint, to promote physiology-based treatment of common CVS conditions. It does not intend to be a complete treatise on the subject but merely seeks to kindle interest in the fascinating piece of equipment that is the heart. This article is divided into 3 segments: the first deals with cardiac electrophysiology and the cardiac cycle with an overview of cardiovascular reflexes of relevance to the anaesthesiologist. The second deals with the physiological aspects of ventricular function and its relevance to the anaesthetic management of valvular heart disease. The last part deals with the coronary circulation in health and disease.
THE CARDIAC CYCLEEvents that occur from the beginning of
one heart beat to the next constitute one cardiac cycle. It comprises cardiac filling (diastole) followed by contraction (systole) and is initiated by the spontaneous generation of an action potential in the sinoatrial node. At a heart rate of 72 beats/min, the duration of each cycle is 0.8 sec, of which systole is 0.3 sec and diastole is0.5 sec. At higher heart rates, the shortening of diastole is more than that of systole, a phenomenon that is of significance in many disease states.
Electrophysiology of the HeartWith regard to the electrical activity, the
heart consists of 2 types of fibres: quiescent (those that require an external stimulus for
initiation of electrical activity), and automatic (those that generate electrical activity spontaneously, without any external stimulus). Examples of automatic cells are the SA node and secondary pacemaker cells. Examples of quiescent cells are the atrial and ventricular cells. Before we go into the mechanisms of action potential generation, it is worthwhile discussing the subject of transmembrane potentials.
TRANSMEMBRANE POTENTIAL (TMP)The TMP is recorded by inserting
capillary microelectrodes into single cardiac cells. Depending on the state of cell activation, two types of TMPs may be recorded: the TMP during electrical inactivity (resting membrane potential, or RMP; usually -90 mV), and that during electrical activity (action potential). In the resting state, the inside of the cardiac cell is more negative than the outside, hence the cell is said to be polarized. Stimulation leads to the entry of positive ions causing the cell to lose its polarization, a phenomenon termed depolarization. Finally, the net outward movement of positive charges again restores the TMP to its original state of polarization; this is called repolarization.
FACTORS DETERMINING RMPAt rest, the cardiac cell membrane is
permeable only to K+ and not to any of the other ions. Thus the RMP is mainly determined by the K+concentration inside and outside the cell, given by the formula: RMP= -62 log [K(
+] / [Ko+].
Changes in the ratio between extracellular and intracellular K+ produces a change in the RMP; an acute increase in the K + causes a less
O
negative RMP and vice versa.
RACE 2003 Ramachandra Anaesthesia Continuing Education
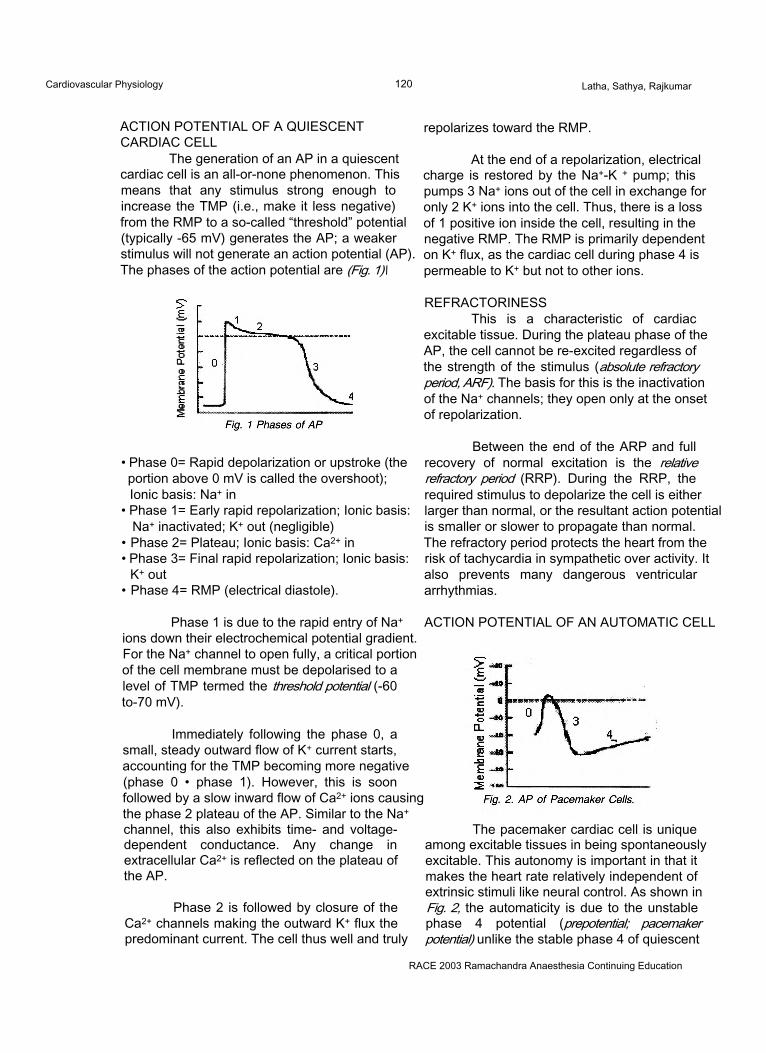
Cardiovascular Physiology 120 Latha, Sathya, Rajkumar
ACTION POTENTIAL OF A QUIESCENT CARDIAC CELL
The generation of an AP in a quiescent cardiac cell is an all-or-none phenomenon. This means that any stimulus strong enough to increase the TMP (i.e., make it less negative) from the RMP to a so-called “threshold” potential (typically -65 mV) generates the AP; a weaker stimulus will not generate an action potential (AP). The phases of the action potential are (Fig. 1)\
repolarizes toward the RMP.
At the end of a repolarization, electrical charge is restored by the Na+-K + pump; this pumps 3 Na+ ions out of the cell in exchange for only 2 K+ ions into the cell. Thus, there is a loss of 1 positive ion inside the cell, resulting in the negative RMP. The RMP is primarily dependent on K+ flux, as the cardiac cell during phase 4 is permeable to K+ but not to other ions.
• Phase 0= Rapid depolarization or upstroke (the portion above 0 mV is called the overshoot); Ionic basis: Na+ in
• Phase 1= Early rapid repolarization; Ionic basis: Na+ inactivated; K+ out (negligible)
• Phase 2= Plateau; Ionic basis: Ca2+ in• Phase 3= Final rapid repolarization; Ionic basis:
K+ out• Phase 4= RMP (electrical diastole).
REFRACTORINESSThis is a characteristic of cardiac
excitable tissue. During the plateau phase of the AP, the cell cannot be re-excited regardless of the strength of the stimulus (absolute refractory period, ARF). The basis for this is the inactivation of the Na+ channels; they open only at the onset of repolarization.
Between the end of the ARP and full recovery of normal excitation is the relative refractory period (RRP). During the RRP, the required stimulus to depolarize the cell is either larger than normal, or the resultant action potential is smaller or slower to propagate than normal. The refractory period protects the heart from the risk of tachycardia in sympathetic over activity. It also prevents many dangerous ventricular arrhythmias.
Phase 1 is due to the rapid entry of Na+ ions down their electrochemical potential gradient. For the Na+ channel to open fully, a critical portion of the cell membrane must be depolarised to a level of TMP termed the threshold potential (-60 to-70 mV).
Immediately following the phase 0, a small, steady outward flow of K+ current starts, accounting for the TMP becoming more negative (phase 0 • phase 1). However, this is soon followed by a slow inward flow of Ca2+ ions causing the phase 2 plateau of the AP. Similar to the Na+ channel, this also exhibits time- and voltage- dependent conductance. Any change in extracellular Ca2+ is reflected on the plateau of the AP.
Phase 2 is followed by closure of the Ca2+ channels making the outward K+ flux the predominant current. The cell thus well and truly
ACTION POTENTIAL OF AN AUTOMATIC CELL
The pacemaker cardiac cell is unique among excitable tissues in being spontaneously excitable. This autonomy is important in that it makes the heart rate relatively independent of extrinsic stimuli like neural control. As shown in Fig. 2, the automaticity is due to the unstable phase 4 potential (prepotential; pacemaker potential) unlike the stable phase 4 of quiescent
RACE 2003 Ramachandra Anaesthesia Continuing Education
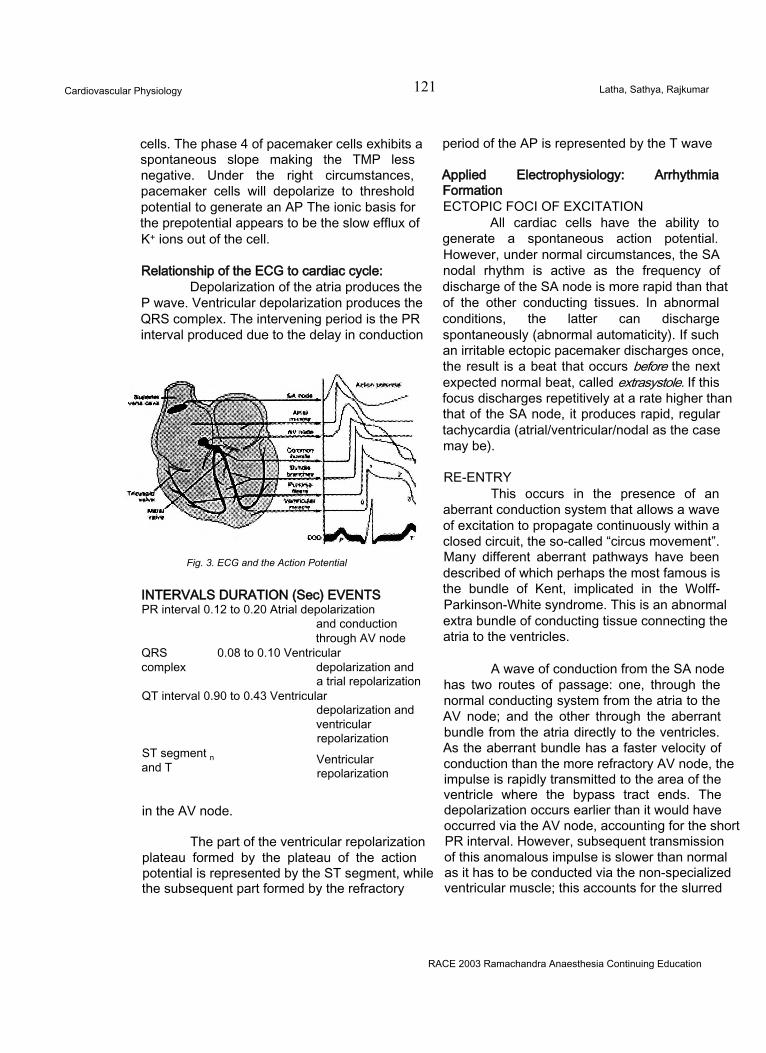
Cardiovascular Physiology 121 Latha, Sathya, Rajkumar
cells. The phase 4 of pacemaker cells exhibits a spontaneous slope making the TMP less negative. Under the right circumstances, pacemaker cells will depolarize to threshold potential to generate an AP The ionic basis for the prepotential appears to be the slow efflux of K+ ions out of the cell.
Relationship of the ECG to cardiac cycle:Depolarization of the atria produces the
P wave. Ventricular depolarization produces the QRS complex. The intervening period is the PR interval produced due to the delay in conduction
Fig. 3. ECG and the Action Potential
INTERVALS DURATION (Sec) EVENTS PR interval 0.12 to 0.20 Atrial depolarization
and conduction through AV node
QRS 0.08 to 0.10 Ventricularcomplex depolarization and
a trial repolarization QT interval 0.90 to 0.43 Ventricular
depolarization andventricularrepolarization
ST segment n and T Ventricular
repolarization
in the AV node.
The part of the ventricular repolarization plateau formed by the plateau of the action potential is represented by the ST segment, while the subsequent part formed by the refractory
period of the AP is represented by the T wave
Applied Electrophysiology: Arrhythmia FormationECTOPIC FOCI OF EXCITATION
All cardiac cells have the ability to generate a spontaneous action potential. However, under normal circumstances, the SA nodal rhythm is active as the frequency of discharge of the SA node is more rapid than that of the other conducting tissues. In abnormal conditions, the latter can discharge spontaneously (abnormal automaticity). If such an irritable ectopic pacemaker discharges once, the result is a beat that occurs before the next expected normal beat, called extrasystole. If this focus discharges repetitively at a rate higher than that of the SA node, it produces rapid, regular tachycardia (atrial/ventricular/nodal as the case may be).
RE-ENTRYThis occurs in the presence of an
aberrant conduction system that allows a wave of excitation to propagate continuously within a closed circuit, the so-called “circus movement”. Many different aberrant pathways have been described of which perhaps the most famous is the bundle of Kent, implicated in the Wolff- Parkinson-White syndrome. This is an abnormal extra bundle of conducting tissue connecting the atria to the ventricles.
A wave of conduction from the SA node has two routes of passage: one, through the normal conducting system from the atria to the AV node; and the other through the aberrant bundle from the atria directly to the ventricles. As the aberrant bundle has a faster velocity of conduction than the more refractory AV node, the impulse is rapidly transmitted to the area of the ventricle where the bypass tract ends. The depolarization occurs earlier than it would have occurred via the AV node, accounting for the short PR interval. However, subsequent transmission of this anomalous impulse is slower than normal as it has to be conducted via the non-specialized ventricular muscle; this accounts for the slurred
RACE 2003 Ramachandra Anaesthesia Continuing Education
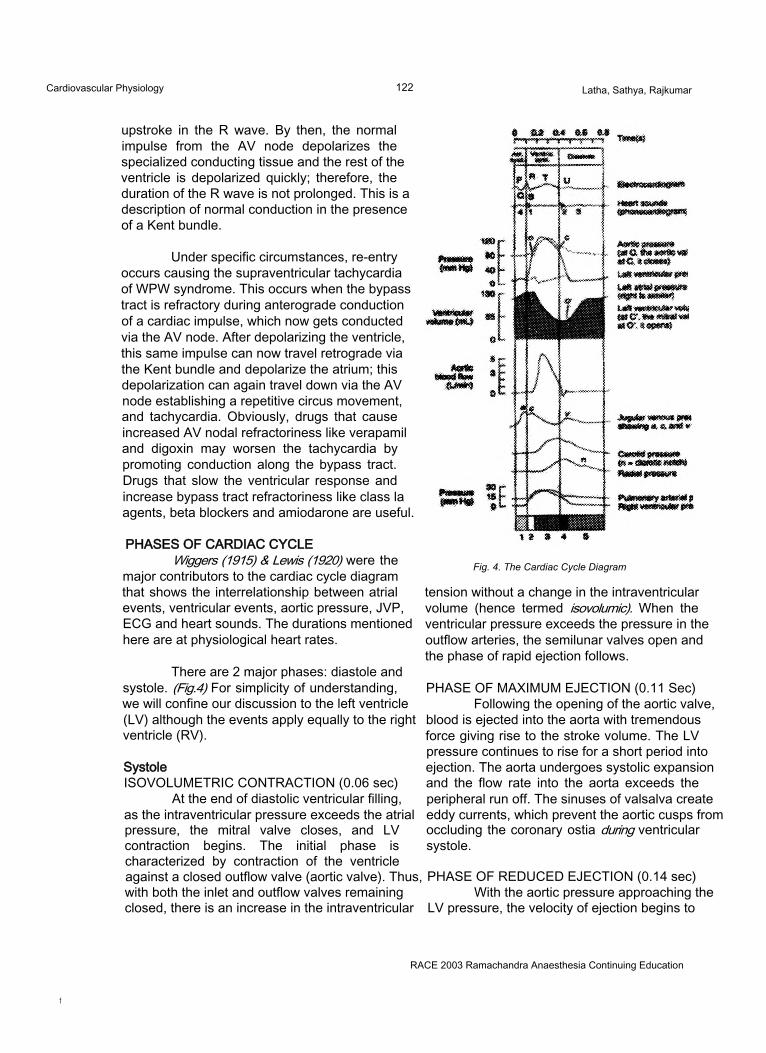
Cardiovascular Physiology 122 Latha, Sathya, Rajkumar
upstroke in the R wave. By then, the normal impulse from the AV node depolarizes the specialized conducting tissue and the rest of the ventricle is depolarized quickly; therefore, the duration of the R wave is not prolonged. This is a description of normal conduction in the presence of a Kent bundle.
Under specific circumstances, re-entry occurs causing the supraventricular tachycardia of WPW syndrome. This occurs when the bypass tract is refractory during anterograde conduction of a cardiac impulse, which now gets conducted via the AV node. After depolarizing the ventricle, this same impulse can now travel retrograde via the Kent bundle and depolarize the atrium; this depolarization can again travel down via the AV node establishing a repetitive circus movement, and tachycardia. Obviously, drugs that cause increased AV nodal refractoriness like verapamil and digoxin may worsen the tachycardia by promoting conduction along the bypass tract. Drugs that slow the ventricular response and increase bypass tract refractoriness like class la agents, beta blockers and amiodarone are useful.
PHASES OF CARDIAC CYCLEWiggers (1915) & Lewis (1920) were the
major contributors to the cardiac cycle diagram that shows the interrelationship between atrial events, ventricular events, aortic pressure, JVP, ECG and heart sounds. The durations mentioned here are at physiological heart rates.
There are 2 major phases: diastole and systole. (Fig.4) For simplicity of understanding, we will confine our discussion to the left ventricle (LV) although the events apply equally to the right ventricle (RV).
SystoleISOVOLUMETRIC CONTRACTION (0.06 sec)
At the end of diastolic ventricular filling, as the intraventricular pressure exceeds the atrial pressure, the mitral valve closes, and LV contraction begins. The initial phase is characterized by contraction of the ventricle against a closed outflow valve (aortic valve). Thus, with both the inlet and outflow valves remaining closed, there is an increase in the intraventricular
Fig. 4. The Cardiac Cycle Diagram
tension without a change in the intraventricular volume (hence termed isovolumic). When the ventricular pressure exceeds the pressure in the outflow arteries, the semilunar valves open and the phase of rapid ejection follows.
PHASE OF MAXIMUM EJECTION (0.11 Sec) Following the opening of the aortic valve,
blood is ejected into the aorta with tremendous force giving rise to the stroke volume. The LV pressure continues to rise for a short period into ejection. The aorta undergoes systolic expansion and the flow rate into the aorta exceeds the peripheral run off. The sinuses of valsalva create eddy currents, which prevent the aortic cusps from occluding the coronary ostia during ventricular systole.
PHASE OF REDUCED EJECTION (0.14 sec) With the aortic pressure approaching the
LV pressure, the velocity of ejection begins to
RACE 2003 Ramachandra Anaesthesia Continuing Education
f
Cardiovascular Physiology 123 Latha, Sathya, Rajkumar
decrease. However, there is still flow of blood from the ventricles to the major vessels due to aortic distensibility (windkessel effect). This phase corresponds to the T wave of ECG. Ejection is terminated when the aortic pressure exceeds the LV pressure leading to closure of the aortic valve. Typically, the end-systolic volume of the LV (LVESV) is 50-60 ml. Ejection fraction is that fraction of end-diastolic volume of LV that is ejected.
DiastoleDiastole marks the phase of relaxation
and filling of the ventricles with blood draining from the atria. It comprises:
PROTODIASTOLE (0.03 sec)The ventricles begin to relax and there is
retrograde flow into the major vessels leading to closure of the semilunar valves (S2 sound).
ISOVOLUMETRIC RELAXATION (0.06 sec)There is a sharp drop in the
intraventricular tension as the ventricular muscle relaxes. With both the AV and semilunar valves being closed, there is no change in the LV volume (isovolumic). The electrical event behind this event is the rapid ATP-dependent uptake of Ca++ from the cytosol into the sarcoplasmic reticulum. This mechanism is impaired in myocardial ischaemia, reperfusion and heart failure.
PHASE OF RAPID FILLING (0.11 sec)When the LV pressure drops below that
in the LA, the mitral valve opens and LV filling starts. Filling is rapid at its onset due to the large pressure gradient, but slows down as the LV pressure approaches the LA pressure.
PHASE OF REDUCED FILLING- DIASTASIS (0.2 sec)
This is the longest phase of diastole as both atrial and ventricular pressures equilibrate and the pressure gradient decreases.
ATRIAL SYSTOLE (0.1 sec)Approximately 25% of the LV filling
results from atrial contraction. It is an important determinant of LV preload in disease states characterized by reduced passive filling like in
mitral stenosis, aortic stenosis, poor LV compliance (hypertensive heart disease, ischaemic heart disease, myocardial fibrosis) and cardiac failure. An effective atrial kick requires coordinated atrial contraction that can only occur in sinus rhythm.
Energy Basis of the Cardiac CycleThe energy requirement for the cardiac
cycle is unequally distributed between systole (85% of the total energy) and diastole (15%). Contrary to popular perception, diastole is also an active process. Energy is required for the Ca++ reuptake that initiates diastole. Ischaemic states impair diastolic relaxation earlier than systolic function. The inequity of energy requirements is utilized by the heart in compensating for altered loading conditions in many disease states (explained in the section on valvular heart disease).
CARDIOVASCULAR REFLEXESNo understanding of the circulatory
reactions of the body is possible unless we start first with the fundamental properties of the heart muscle itself, and then find out how these are modified, protected and controlled under the influence of the mechanisms - nervous, chemical and mechanical - which under normal conditions play on the heart and blood vessels.
-EH Starling, 1920
IntroductionCardiovascular reflexes are integrated
pathways regulating cardiovascular function. They depend on and affect the interplay between the vascular system, the heart and the brain. Understanding cardiac reflexes is important to the anaesthesiologist as they are affected by disease states and anaesthetic techniques alike. Each reflex has a receptor that is stimulated by a specific stimulus, an afferent limb, a centre, an efferent limb and an effector organ (Tabje 1).
Baroreceptor reflex (Fig. 5)Also called the carotid sinus reflex, it is
of primary importance in the maintenance of haemodynamic stability. The primary stimulus for the baroreceptor reflex is a change in blood
RACE 2003 Ramachandra Anaesthesia Continuing Education
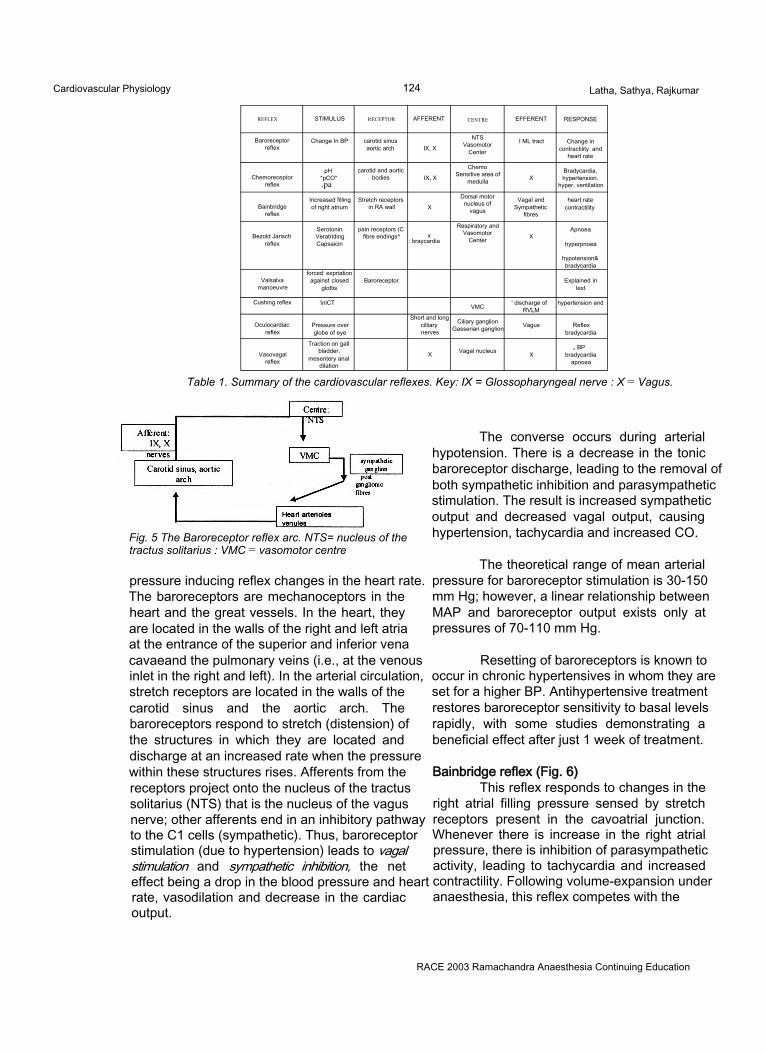
Cardiovascular Physiology 124 Latha, Sathya, Rajkumar
REFLEX STIMULUS RECEPTOR AFFERENT CENTRE EFFERENT RESPONSE
Baroreceptorreflex
Change In BP carotid sinus aortic arch IX, X
NTSVasomotor
Center
I ML tract Change in contractility and
heart rate
Chemoreceptorreflex
.pH*pCO*.pa
carotid and aortic bodies IX, X
Chemo Sensitive area of
medulla XBradycardia, hypertension,
hyper, ventilation
Bainbridgereflex
Increased filling of right atrium
Stretch receptors in RA wall X
Dorsal motor nucleus of
vagus
Vagal and Sympathetic
fibres
heart rate contractility
Bezold Jarisch reflex
SerotoninVeratridingCapsaicin
pain receptors (C fibre endings^ x
: braycardia
Respiratory and Vasomotor
Center XApnoea
hyperpnoea
hypotension&bradycardia
Valsalvamanoeuvre
forced expriation against closed
glottisBaroreceptor Explained in
text
Cushing reflex 'inlCT VMC ' discharge of RVLM
hypertension and
Oculocardiacreflex
Pressure over globe of eye
Short and long cilliary nerves
Ciliary ganglion Gasserian ganglion Vagus Reflex
bradycardia
Vasovagalreflex
Traction on gall bladder,
mesentery anal dilation
X Vagal nucleus X„ BP
bradycardia apnoea
Table 1. Summary of the cardiovascular reflexes. Key: IX = Glossopharyngeal nerve : X = Vagus.
Fig. 5 The Baroreceptor reflex arc. NTS= nucleus of the tractus solitarius : VMC = vasomotor centre
pressure inducing reflex changes in the heart rate. The baroreceptors are mechanoceptors in the heart and the great vessels. In the heart, they are located in the walls of the right and left atria at the entrance of the superior and inferior vena cavaeand the pulmonary veins (i.e., at the venous inlet in the right and left). In the arterial circulation, stretch receptors are located in the walls of the carotid sinus and the aortic arch. The baroreceptors respond to stretch (distension) of the structures in which they are located and discharge at an increased rate when the pressure within these structures rises. Afferents from the receptors project onto the nucleus of the tractus solitarius (NTS) that is the nucleus of the vagus nerve; other afferents end in an inhibitory pathway to the C1 cells (sympathetic). Thus, baroreceptor stimulation (due to hypertension) leads to vagal stimulation and sympathetic inhibition, the net effect being a drop in the blood pressure and heart rate, vasodilation and decrease in the cardiac output.
The converse occurs during arterial hypotension. There is a decrease in the tonic baroreceptor discharge, leading to the removal of both sympathetic inhibition and parasympathetic stimulation. The result is increased sympathetic output and decreased vagal output, causing hypertension, tachycardia and increased CO.
The theoretical range of mean arterial pressure for baroreceptor stimulation is 30-150 mm Hg; however, a linear relationship between MAP and baroreceptor output exists only at pressures of 70-110 mm Hg.
Resetting of baroreceptors is known to occur in chronic hypertensives in whom they are set for a higher BP. Antihypertensive treatment restores baroreceptor sensitivity to basal levels rapidly, with some studies demonstrating a beneficial effect after just 1 week of treatment.
Bainbridge reflex (Fig. 6)This reflex responds to changes in the
right atrial filling pressure sensed by stretch receptors present in the cavoatrial junction. Whenever there is increase in the right atrial pressure, there is inhibition of parasympathetic activity, leading to tachycardia and increased contractility. Following volume-expansion under anaesthesia, this reflex competes with the
RACE 2003 Ramachandra Anaesthesia Continuing Education
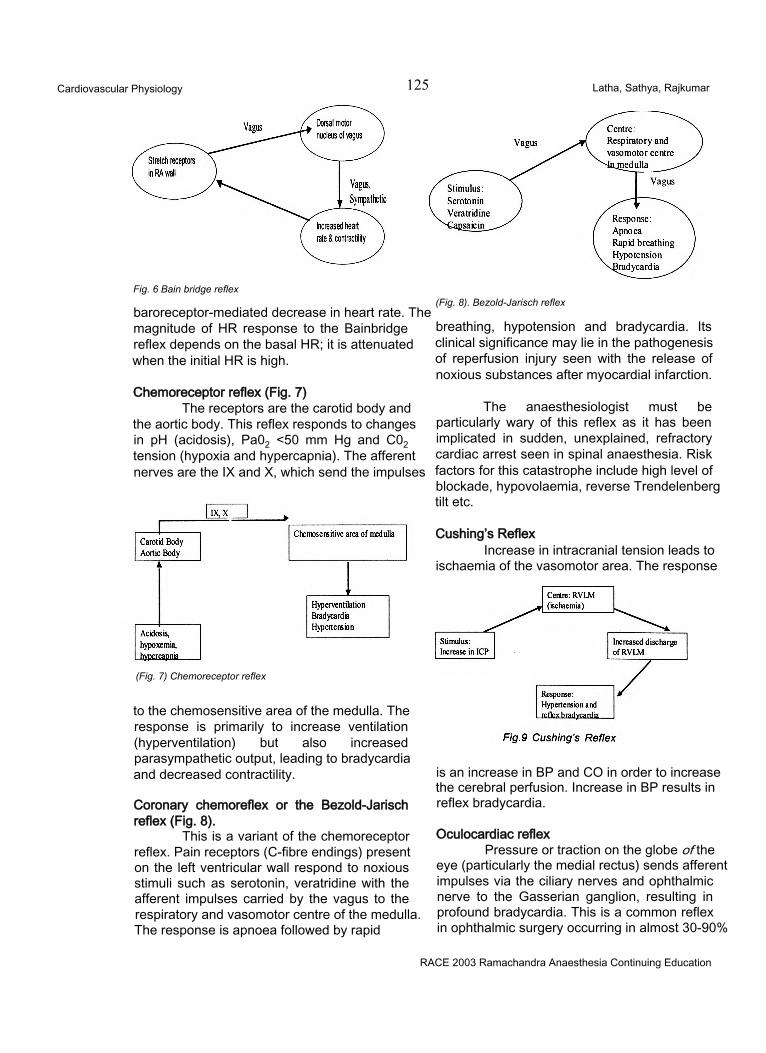
Cardiovascular Physiology 125 Latha, Sathya, Rajkumar
Fig. 6 Bain bridge reflex
baroreceptor-mediated decrease in heart rate. The magnitude of HR response to the Bainbridge reflex depends on the basal HR; it is attenuated when the initial HR is high.
Chemoreceptor reflex (Fig. 7)The receptors are the carotid body and
the aortic body. This reflex responds to changes in pH (acidosis), Pa02 <50 mm Hg and C02 tension (hypoxia and hypercapnia). The afferent nerves are the IX and X, which send the impulses
(Fig. 7) Chemoreceptor reflex
to the chemosensitive area of the medulla. The response is primarily to increase ventilation (hyperventilation) but also increased parasympathetic output, leading to bradycardia and decreased contractility.
Coronary chemoreflex or the Bezold-Jarisch reflex (Fig. 8).
This is a variant of the chemoreceptor reflex. Pain receptors (C-fibre endings) present on the left ventricular wall respond to noxious stimuli such as serotonin, veratridine with the afferent impulses carried by the vagus to the respiratory and vasomotor centre of the medulla. The response is apnoea followed by rapid
(Fig. 8). Bezold-Jarisch reflex
breathing, hypotension and bradycardia. Its clinical significance may lie in the pathogenesis of reperfusion injury seen with the release of noxious substances after myocardial infarction.
The anaesthesiologist must be particularly wary of this reflex as it has been implicated in sudden, unexplained, refractory cardiac arrest seen in spinal anaesthesia. Risk factors for this catastrophe include high level of blockade, hypovolaemia, reverse Trendelenberg tilt etc.
Cushing’s ReflexIncrease in intracranial tension leads to
ischaemia of the vasomotor area. The response
is an increase in BP and CO in order to increase the cerebral perfusion. Increase in BP results in reflex bradycardia.
Oculocardiac reflexPressure or traction on the globe of the
eye (particularly the medial rectus) sends afferent impulses via the ciliary nerves and ophthalmic nerve to the Gasserian ganglion, resulting in profound bradycardia. This is a common reflex in ophthalmic surgery occurring in almost 30-90%
RACE 2003 Ramachandra Anaesthesia Continuing Education
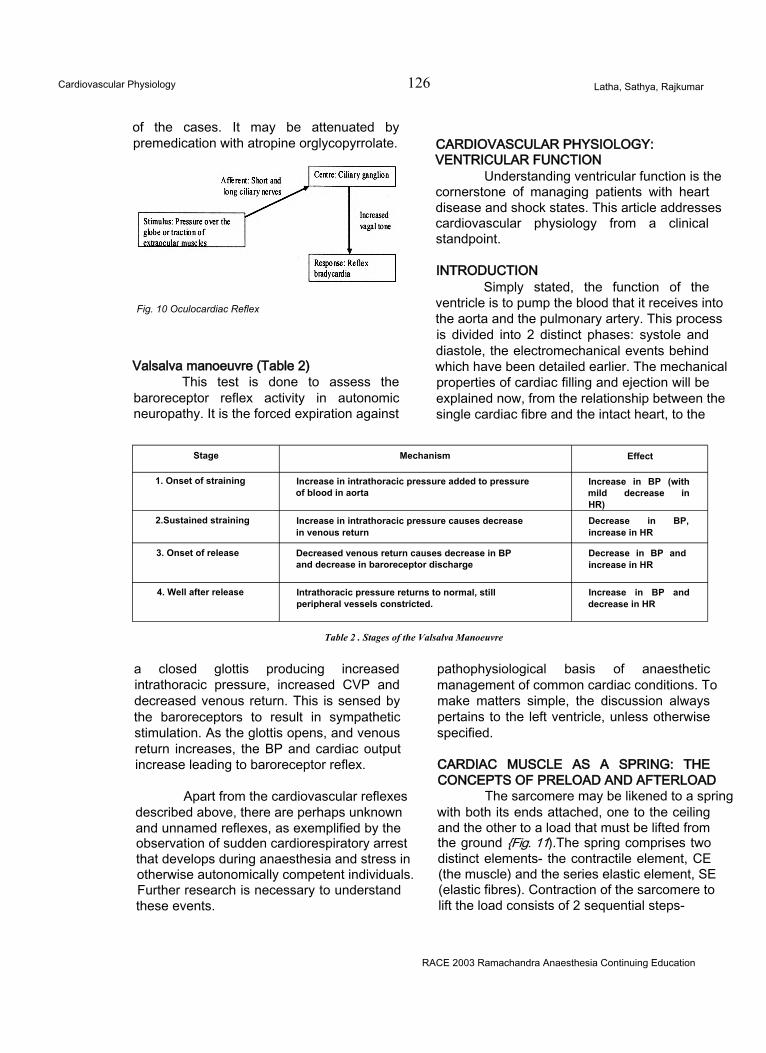
Cardiovascular Physiology 126 Latha, Sathya, Rajkumar
of the cases. It may be attenuated by premedication with atropine orglycopyrrolate.
Fig. 10 Oculocardiac Reflex
Valsalva manoeuvre (Table 2)This test is done to assess the
baroreceptor reflex activity in autonomic neuropathy. It is the forced expiration against
CARDIOVASCULAR PHYSIOLOGY: VENTRICULAR FUNCTION
Understanding ventricular function is the cornerstone of managing patients with heart disease and shock states. This article addresses cardiovascular physiology from a clinical standpoint.
INTRODUCTIONSimply stated, the function of the
ventricle is to pump the blood that it receives into the aorta and the pulmonary artery. This process is divided into 2 distinct phases: systole and diastole, the electromechanical events behind which have been detailed earlier. The mechanical properties of cardiac filling and ejection will be explained now, from the relationship between the single cardiac fibre and the intact heart, to the
Stage Mechanism Effect
1. Onset of straining Increase in intrathoracic pressure added to pressure of blood in aorta
Increase in BP (with mild decrease in HR)
2.Sustained straining Increase in intrathoracic pressure causes decrease in venous return
Decrease in BP, increase in HR
3. Onset of release Decreased venous return causes decrease in BP and decrease in baroreceptor discharge
Decrease in BP and increase in HR
4. Well after release Intrathoracic pressure returns to normal, still peripheral vessels constricted.
Increase in BP and decrease in HR
Table 2 . Stages of the Valsalva Manoeuvre
a closed glottis producing increased intrathoracic pressure, increased CVP and decreased venous return. This is sensed by the baroreceptors to result in sympathetic stimulation. As the glottis opens, and venous return increases, the BP and cardiac output increase leading to baroreceptor reflex.
Apart from the cardiovascular reflexes described above, there are perhaps unknown and unnamed reflexes, as exemplified by the observation of sudden cardiorespiratory arrest that develops during anaesthesia and stress in otherwise autonomically competent individuals. Further research is necessary to understand these events.
pathophysiological basis of anaesthetic management of common cardiac conditions. To make matters simple, the discussion always pertains to the left ventricle, unless otherwise specified.
CARDIAC MUSCLE AS A SPRING: THE CONCEPTS OF PRELOAD AND AFTERLOAD
The sarcomere may be likened to a spring with both its ends attached, one to the ceiling and the other to a load that must be lifted from the ground {Fig. 11).The spring comprises two distinct elements- the contractile element, CE (the muscle) and the series elastic element, SE (elastic fibres). Contraction of the sarcomere to lift the load consists of 2 sequential steps-
RACE 2003 Ramachandra Anaesthesia Continuing Education
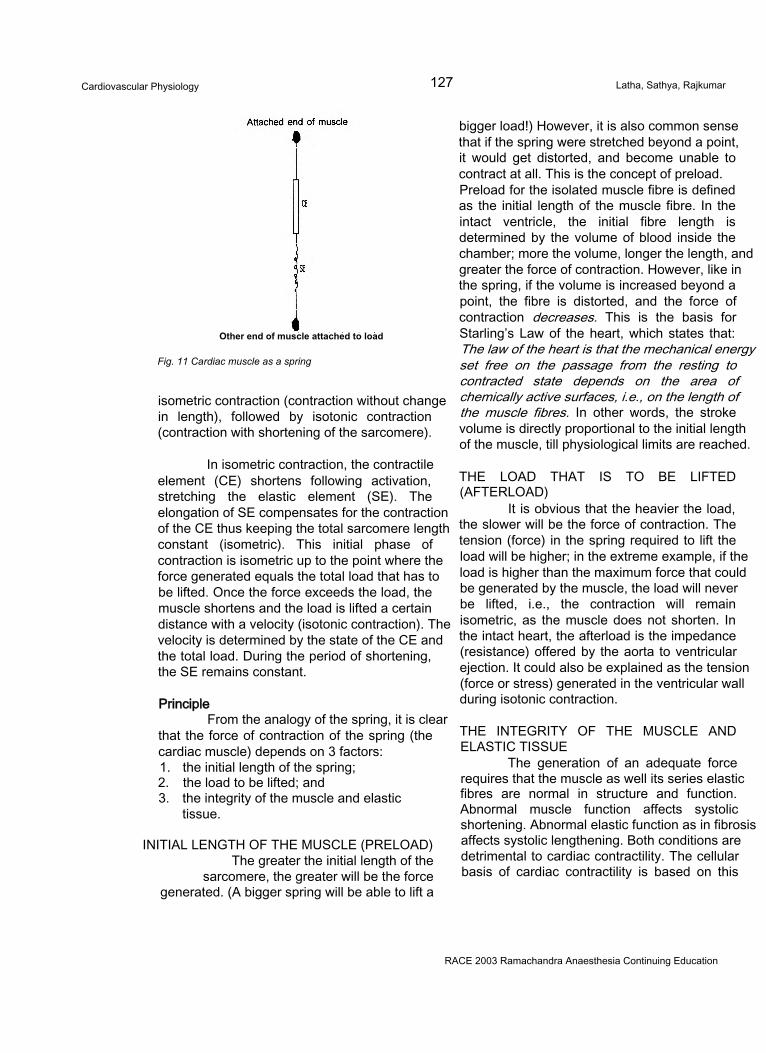
Cardiovascular Physiology 127 Latha, Sathya, Rajkumar
Other end of muscle attached to load
Fig. 11 Cardiac muscle as a spring
isometric contraction (contraction without change in length), followed by isotonic contraction (contraction with shortening of the sarcomere).
In isometric contraction, the contractile element (CE) shortens following activation, stretching the elastic element (SE). The elongation of SE compensates for the contraction of the CE thus keeping the total sarcomere length constant (isometric). This initial phase of contraction is isometric up to the point where the force generated equals the total load that has to be lifted. Once the force exceeds the load, the muscle shortens and the load is lifted a certain distance with a velocity (isotonic contraction). The velocity is determined by the state of the CE and the total load. During the period of shortening, the SE remains constant.
PrincipleFrom the analogy of the spring, it is clear
that the force of contraction of the spring (the cardiac muscle) depends on 3 factors:1. the initial length of the spring;2. the load to be lifted; and3. the integrity of the muscle and elastic
tissue.
INITIAL LENGTH OF THE MUSCLE (PRELOAD) The greater the initial length of the
sarcomere, the greater will be the force generated. (A bigger spring will be able to lift a
bigger load!) However, it is also common sense that if the spring were stretched beyond a point, it would get distorted, and become unable to contract at all. This is the concept of preload. Preload for the isolated muscle fibre is defined as the initial length of the muscle fibre. In the intact ventricle, the initial fibre length is determined by the volume of blood inside the chamber; more the volume, longer the length, and greater the force of contraction. However, like in the spring, if the volume is increased beyond a point, the fibre is distorted, and the force of contraction decreases. This is the basis for Starling’s Law of the heart, which states that: The law of the heart is that the mechanical energy set free on the passage from the resting to contracted state depends on the area of chemically active surfaces, i.e., on the length of the muscle fibres. In other words, the stroke volume is directly proportional to the initial length of the muscle, till physiological limits are reached.
THE LOAD THAT IS TO BE LIFTED (AFTERLOAD)
It is obvious that the heavier the load, the slower will be the force of contraction. The tension (force) in the spring required to lift the load will be higher; in the extreme example, if the load is higher than the maximum force that could be generated by the muscle, the load will never be lifted, i.e., the contraction will remain isometric, as the muscle does not shorten. In the intact heart, the afterload is the impedance (resistance) offered by the aorta to ventricular ejection. It could also be explained as the tension (force or stress) generated in the ventricular wall during isotonic contraction.
THE INTEGRITY OF THE MUSCLE AND ELASTIC TISSUE
The generation of an adequate force requires that the muscle as well its series elastic fibres are normal in structure and function. Abnormal muscle function affects systolic shortening. Abnormal elastic function as in fibrosis affects systolic lengthening. Both conditions are detrimental to cardiac contractility. The cellular basis of cardiac contractility is based on this
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardiovascular Physiology 128 Latha, Sathya, Rajkumar
relationship between the tension (force) and the velocity of shortening.Experimentally, the maximum velocity of shortening has been used in many studies to assess contractility.
CONTRACTILE FUNCTION OF THE INTACT HEART: THE CARDIAC OUTPUT
The cardiac output (CO) is the amount of blood pumped into the peripheral circulation per minute. It is a measurement reflecting the status of the entire circulatory system, not only that of the heart, and is primarily governed by autoregulation in tissues.CO = Stroke Volume (SV) x Heart Rate (HR)
To compare patients with different body sizes, the CO may be corrected in relation to body surface area (BSA). It is then called Cardiac Index (Cl).Cl= CO / BSA Normal 2.5-3.5 L/min/m2.
Stroke VolumeIt is the volume of blood ejected by the
ventricle with each single contraction.SV = End-diastolic volume (EDV) - End-systolic volume(ESV)
DETERMINANTS OF STROKE VOLUME1. Preload2. Afterload3. Contractility4. Heart rate
PRELOADAs explained earlier, preload in the
isolated muscle represents the load imposed on the muscle fibre before contraction, and is the end-diastolic fibre length. In the intact heart, the preload is the ventricular wall stress at end- diastole. However, as the wall-stress is difficult to measure clinically, various approximations have been made substituting for the wall stress. They are:1. Substituting ventricular volume for the wall
stress: LVEDV in an intact heart has been shown to be linearly related to the stroke volume and is thus an excellent estimate of the preload. However, it is difficult to measure clinically. Normal LVEDV = 70- 100 ml /m2.
2. Substituting ventricular pressure for ventricular
volume: These are popular clinical tools owing to their relative simplicity of measurement. However, the relationship between volume and pressure is not linear and may be inaccurate. The various pressures that have been approximated to the LVEDV include:• LVEDP: The most closely related to
LVEDV; difficult to measure, hence clinically not useful. Normal LVEDP = 12 mm Hg.
• Left Atrial Pressure (LAP): Useful in select situations like intra-cardiac surgery, in which a left atrial catheter may be placed by the surgeon.
• Pulmonary artery occlusion pressure (PAOP): Erroneously called the pulmonary capillary wedge pressure (PCWP), this is a less accurate estimate of LVEDV as it is affected by factors such as placement of the pulmonary artery catheter, airway pressure, and positive end-expiratory pressure (PEEP). However, it remains a popular bedside tool due to its simplicity.
• Central venous pressure (CVP): Perhaps the least accurate but the most widely used estimate of preload. In addition to being affected by all the factors affecting PAOP, it is also affected by lung disease, pericardial disease and right ventricular dysfunction. However, despite these limitations, the trend of the CVP and the response to interventions like the fluid challenge may still be used to successfully predict the LV preload.
Determinants of PreloadPreload to the ventricle is determined by:
1. Venous return to the atria, which in turn is determined by:• Total blood volume• Body Position• Venous tone• Pumping action of skeletal muscle
2. Transmural pressure: The pressure gradient for venous filling of the heart is the mean circulatory filling pressure (MCFP) minus the
RACE 2003 Ramachandra Anaesthesia Continuing Education
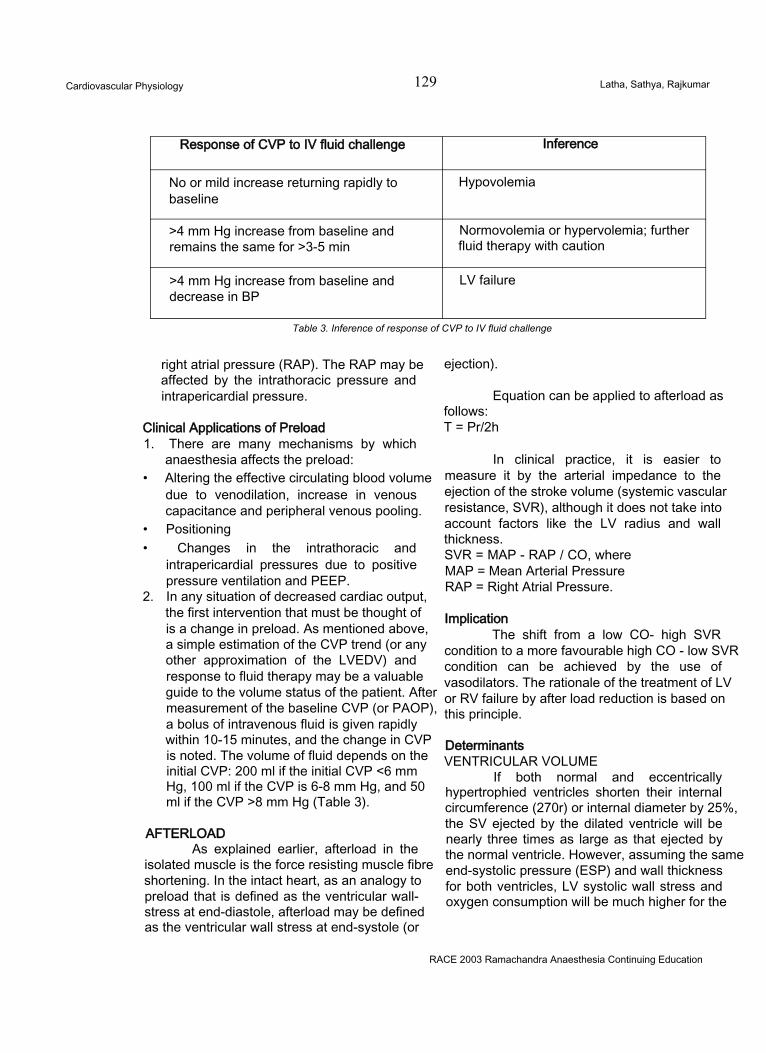
Cardiovascular Physiology 129 Latha, Sathya, Rajkumar
Response of CVP to IV fluid challenge Inference
No or mild increase returning rapidly to baseline
Hypovolemia
>4 mm Hg increase from baseline and remains the same for >3-5 min
Normovolemia or hypervolemia; further fluid therapy with caution
>4 mm Hg increase from baseline and decrease in BP
LV failure
Table 3. Inference of response of CVP to IV fluid challenge
right atrial pressure (RAP). The RAP may be affected by the intrathoracic pressure and intrapericardial pressure.
Clinical Applications of Preload1. There are many mechanisms by which
anaesthesia affects the preload:• Altering the effective circulating blood volume
due to venodilation, increase in venous capacitance and peripheral venous pooling.
• Positioning• Changes in the intrathoracic and
intrapericardial pressures due to positive pressure ventilation and PEEP.
2. In any situation of decreased cardiac output, the first intervention that must be thought of is a change in preload. As mentioned above, a simple estimation of the CVP trend (or any other approximation of the LVEDV) and response to fluid therapy may be a valuable guide to the volume status of the patient. After measurement of the baseline CVP (or PAOP), a bolus of intravenous fluid is given rapidly within 10-15 minutes, and the change in CVP is noted. The volume of fluid depends on the initial CVP: 200 ml if the initial CVP <6 mm Hg, 100 ml if the CVP is 6-8 mm Hg, and 50 ml if the CVP >8 mm Hg (Table 3).
AFTERLOADAs explained earlier, afterload in the
isolated muscle is the force resisting muscle fibre shortening. In the intact heart, as an analogy to preload that is defined as the ventricular wall- stress at end-diastole, afterload may be defined as the ventricular wall stress at end-systole (or
ejection).
Equation can be applied to afterload asfollows:T = Pr/2h
In clinical practice, it is easier to measure it by the arterial impedance to the ejection of the stroke volume (systemic vascular resistance, SVR), although it does not take into account factors like the LV radius and wall thickness.SVR = MAP - RAP / CO, where MAP = Mean Arterial Pressure RAP = Right Atrial Pressure.
ImplicationThe shift from a low CO- high SVR
condition to a more favourable high CO - low SVR condition can be achieved by the use of vasodilators. The rationale of the treatment of LV or RV failure by after load reduction is based on this principle.
DeterminantsVENTRICULAR VOLUME
If both normal and eccentrically hypertrophied ventricles shorten their internal circumference (270r) or internal diameter by 25%, the SV ejected by the dilated ventricle will be nearly three times as large as that ejected by the normal ventricle. However, assuming the same end-systolic pressure (ESP) and wall thickness for both ventricles, LV systolic wall stress and oxygen consumption will be much higher for the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardiovascular Physiology 130 Latha, Sathya, Rajkumar
eccentrically hypertrophied ventricle than for the normal one.
IMPLICATION - Treating cardiac dysfunction with a positive inotrope, such as dobutamine, will decrease the end systolic dimensions of the LV and increase SV, yet leave LV wall stress unchanged or even decreased.
VENTRICULAR WALL THICKNESS (h)Wall thickness is the denominator in the
Laplace formula. Thus when h increases, stress will decrease and vice versa. When comparing concentric with eccentric ventricular hypertrophy, the latter not only has a wider radius (r) but also has a thinner wall (h) compared to the concentrically hypertrophied ventricle. For identical pressures, the systolic ventricular wall stress will be higher in the dilated or “failing" ventricle than in the hypertrophied “hypertensive” left ventricle.
SYSTOLIC INTRAVENTRICULAR PRESSUREIntraventricular pressure is an important
component of afterload, and an inverse relationship exists between SV and LV pressure. When the systolic arterial pressure suddenly increases, as after cross clamping of the thoracic aorta, SV initially decreases, then normalizes through a compensatory increase in LVEDV or heterometric autoregulation. Later, the increase in EDV is followed by an increase in cardiac contractility while LVEDV and LVEDP normalize. This phenomenon is called the Anrep phenomenon and the adaptive mechanism that explains it is called “homeometric autoregulation”. The Anrep phenomenon should be more pronounced under anaesthesia and when cardiac function is already depressed.
CONTRACTILITYAn intrinsic property of cardiac muscle,
it determines the amount of work the heart can perform at a given load. It is primarily determined by the availability of intracellular Ca++. All agents with positive inotropic properties increase intracellular Ca++ while negative inotropes have the opposite effect. In the assessment of ventricular function, the assessment of ventricular contractility is probably the most complex as it is very difficult to devise indices that are
unaffected by loading factors. Some indices that are relatively independent of loading factors are:
Isovolumic indices1. Vmax (maximum velocity of myocardial fibre
shortening)2. Peak pressure development (dp/dt);
Ejection Phase Indices1. Initial ventricular impulse2. Maximum aortic blood acceleration3. Ejection fraction: LVEF is an unreliable index
of LV contractility as it is highly dependent on loading factors. In particular, it is unreliable in patients with VHD.
Pressure Volume LoopAlthough the PV loop allows a more
precise appreciation of LV contractility relatively independent of preload, its technical difficulty makes it unattractive. PV loops are explained in detail in relation to the pathophysiology of valvular heart disease.
Determinants of ContractilityFACTORS INCREASING CONTRACTILITY1. Sympathetic Stimulation: Direct increase of
the force of contraction, as well as indirect increase due to increased heart rate (rate treppe effect or Bowditch phenomenon);• The association between heart rate and
contractility is called the staircase effect. Tachycardia in the range of 60-120 beats/ min leads to a higher availability of Ca++to the contractile proteins and improves contractility (positive staircase effect).
• Further increases in the HR decrease the contractility (negative staircase effect) due to decreased accumulation time for Ca++ in storage sites and diastolic Ca++overload in the cytosol.
2. Administration of positive inotropic drugs.
DECREASING CONTRACTILITY1. Parasympathetic stimulation and bradycardia,2. Sympathetic inhibition via withdrawal of
catecholamines or blockade of adrenergic receptors,
3. Administration of p adrenergic blocking drugs, calcium channel blockers or myocardial
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardiovascular Physiology 131 Latha, Sathya, Rajkumar
depressants,4. Myocardial ischaemia and infarction,5. Intrinsic myocardial diseases such as
cardiomyopathy, and6. Hypoxia and acidosis.
Heart RateThe HR is a major determinant of the
CO. It is primarily governed by the rate of phase 4 depolarisation of the sinoatrial (SA) node. The natural frequency of the SA node is faster (110 times/min) than the other potential pacemakers of the heart, causing an “overdrive suppression” of the latter. Neural and humoral mechanisms are the extrinsic factors controlling the HR. Sympathetic stimulation increases the HR and parasympathetic stimulation decreases it.
The tachycardia induced by sympathetic stimulation and vagal inhibition (atropine) is qualitatively different. In the former instance, there is a shortening of the action potential, systole and diastole. In atropine-mediated tachycardia however, diastole is reduced but there is a prolongation in the duration of the action potential and systole. This impairs coronary filling and increases the myocardial work, both of which are undesirable in ischemic heart disease.
DIASTOLIC FUNCTIONAt physiological heart rates, diastole
oocup:es appmxin ate^2/Srd of the cardiac cycle. Despite this, the study of diastolic function is frequently relegated to the background owing to technical difficulties and lack of awareness of its importance. However, with the realization that diastolic dysfunction and impairment of diastolic ventricular compliance appear earlier than systolic dysfunction in many cardiac conditions, study of diastole is receiving increasing attention.
Phases of Diastole1. Isovolumic relaxation2. Rapid ventricular filling3. Atrial contraction
DeterminantsISOVOLUMIC RELAXATION
This is the period following ventricular ejection, initiated by the rapid re-uptake of Ca++ ions into the sarcoplasmic reticulum. The
decrease in LV pressure can be described by an exponential function and expressed as a time constant (called Trelax). Determinants of relaxation time include:1. Load: The greater the load, the faster the
relaxation.2. Inactivation: This depends on the active
sequestration of Ca++ from the troponin to the sarcoplasmic reticulum (ATP dependent Ca++ pump). Conditions where cytosolic Ca++ may be abnormally high leading to delayed relaxation are:A. Failure of the Ca++ pumpB. Ca++ leaks out of the sarcoplasmic
reticulumC. Myocytes unable to extrude Ca++
D. Increased affinity of troponin for Ca++
3. Coronary blood flow: Adequate blood flow is essential for the supply of ATP.
4. Homogeneity: Segments with regional wall motion abnormalities due to ischaemia will have a prolonged relaxation time
5. Alterations in inotropy affect relaxation.A. Catecholamines increase Ca++ re-uptake
and improve relaxation in normal myocardium. However, by worsening the asynchrony of contraction in compromised myocardium, they decrease Ca++ reuptake and prolong relaxation in ischaemic myocardium.
B. Beta blockade prolongs relaxation in normal myocardium, but improves relaxation in ischaemic myocardium by reducing the asynchrony of contraction.
6. Effect of halogenated agentsA. Halothane and Enflurane prolong Trelax by
decreasing contractility, decreasing load, and decreasing coronary blood flow
B. Isoflurane has no effect on relaxation. The coronary vasodilation produced by isoflurane nullifies the effects of decreased contractility and load.
7. Effect of drugs: Coronary vasodilators like nitrates, inodilators (dobutamine), calcium channel blockers and myocardial revascularization may improve diastolic function or reverse exercise induced ischaemia.
VENTRICULAR FILLINGWhile isovolumic relaxation is caused by
RACE 2003 Ramachandra Anaesthesia Continuing Education
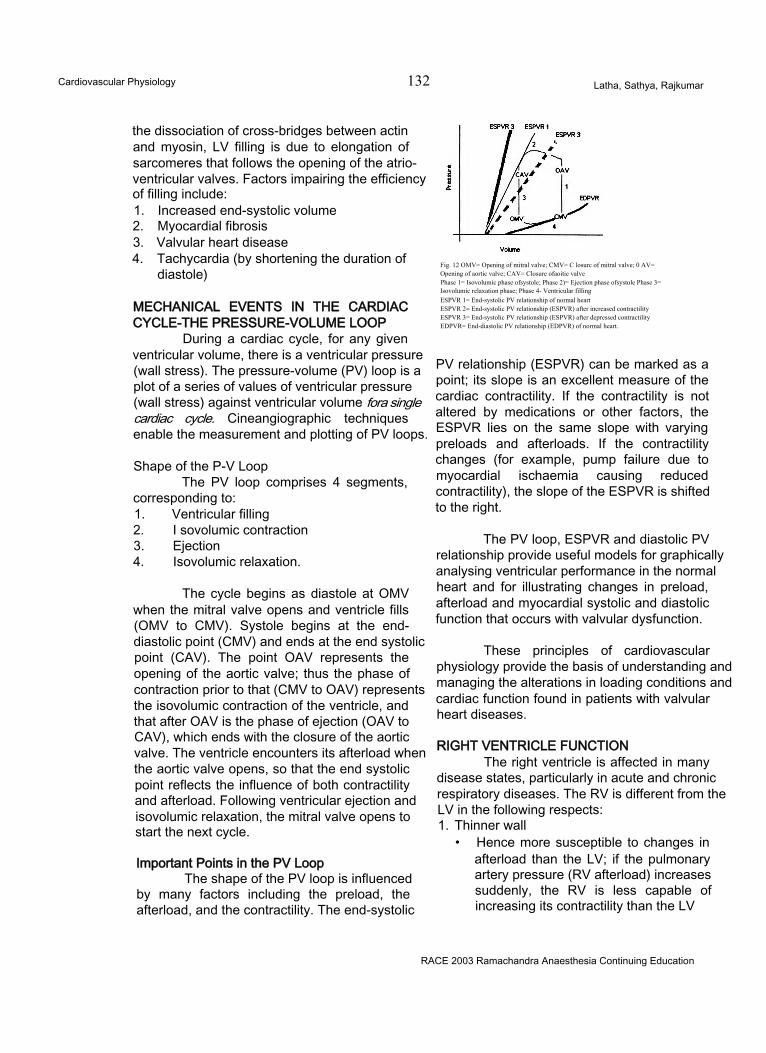
Cardiovascular Physiology 132 Latha, Sathya, Rajkumar
the dissociation of cross-bridges between actin and myosin, LV filling is due to elongation of sarcomeres that follows the opening of the atrioventricular valves. Factors impairing the efficiency of filling include:1. Increased end-systolic volume2. Myocardial fibrosis3. Valvular heart disease4. Tachycardia (by shortening the duration of
diastole)
MECHANICAL EVENTS IN THE CARDIAC CYCLE-THE PRESSURE-VOLUME LOOP
During a cardiac cycle, for any given ventricular volume, there is a ventricular pressure (wall stress). The pressure-volume (PV) loop is a plot of a series of values of ventricular pressure (wall stress) against ventricular volume fora single cardiac cycle. Cineangiographic techniques enable the measurement and plotting of PV loops.
Shape of the P-V LoopThe PV loop comprises 4 segments,
corresponding to:1. Ventricular filling2. I sovolumic contraction3. Ejection4. Isovolumic relaxation.
The cycle begins as diastole at OMV when the mitral valve opens and ventricle fills (OMV to CMV). Systole begins at the end- diastolic point (CMV) and ends at the end systolic point (CAV). The point OAV represents the opening of the aortic valve; thus the phase of contraction prior to that (CMV to OAV) represents the isovolumic contraction of the ventricle, and that after OAV is the phase of ejection (OAV to CAV), which ends with the closure of the aortic valve. The ventricle encounters its afterload when the aortic valve opens, so that the end systolic point reflects the influence of both contractility and afterload. Following ventricular ejection and isovolumic relaxation, the mitral valve opens to start the next cycle.
Important Points in the PV LoopThe shape of the PV loop is influenced
by many factors including the preload, the afterload, and the contractility. The end-systolic
Fig. 12 OMV= Opening of mitral valve; CMV= C losurc of mitral valve; 0 AV= Opening of aortic valve; CAV= Closure ofaoitie valvePhase 1= Isovolumic phase ofsystole; Phase 2)= Ejection phase ofsystole Phase 3=Isovolumic relaxation phase; Phase 4- Ventricular fillingESPVR 1= End-systolic PV relationship of normal heartESPVR 2= End-systolic PV relationship (ESPVR) after increased contractilityESPVR 3= End-systolic PV relationship (ESPVR) after depressed contractilityEDPVR= End-diastolic PV relationship (EDPVR) of normal heart.
PV relationship (ESPVR) can be marked as a point; its slope is an excellent measure of the cardiac contractility. If the contractility is not altered by medications or other factors, the ESPVR lies on the same slope with varying preloads and afterloads. If the contractility changes (for example, pump failure due to myocardial ischaemia causing reduced contractility), the slope of the ESPVR is shifted to the right.
The PV loop, ESPVR and diastolic PV relationship provide useful models for graphically analysing ventricular performance in the normal heart and for illustrating changes in preload, afterload and myocardial systolic and diastolic function that occurs with valvular dysfunction.
These principles of cardiovascular physiology provide the basis of understanding and managing the alterations in loading conditions and cardiac function found in patients with valvular heart diseases.
RIGHT VENTRICLE FUNCTIONThe right ventricle is affected in many
disease states, particularly in acute and chronic respiratory diseases. The RV is different from the LV in the following respects:1. Thinner wall
• Hence more susceptible to changes in afterload than the LV; if the pulmonary artery pressure (RV afterload) increases suddenly, the RV is less capable of increasing its contractility than the LV
RACE 2003 Ramachandra Anaesthesia Continuing Education
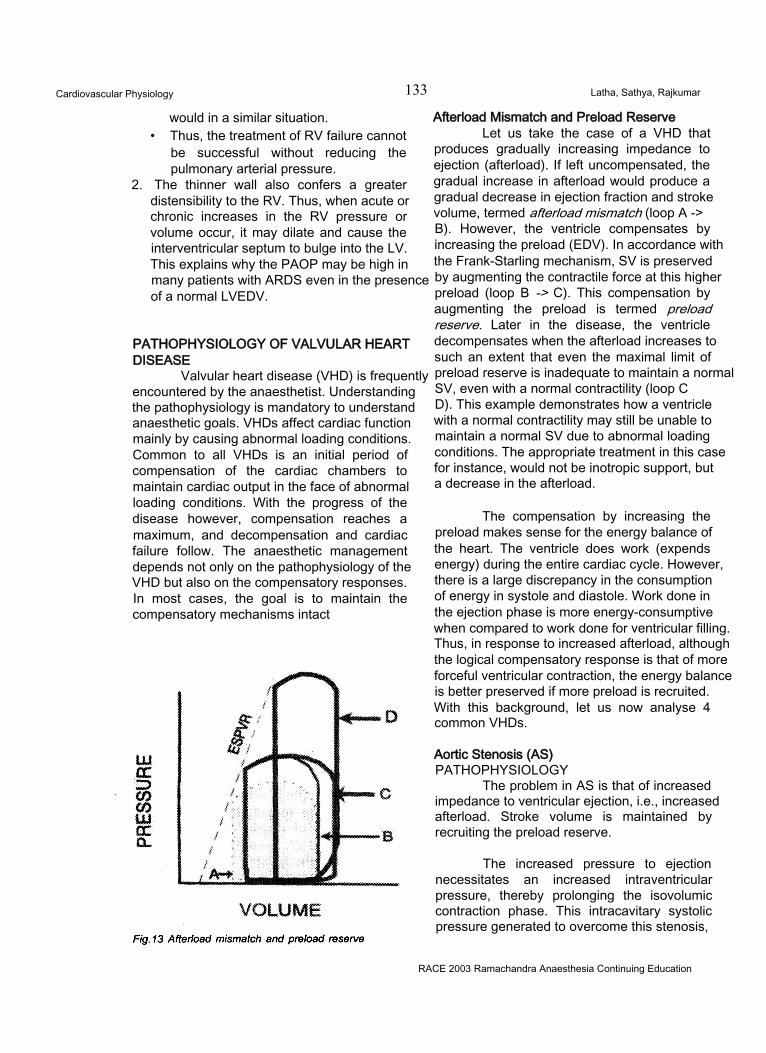
Cardiovascular Physiology 133 Latha, Sathya, Rajkumar
would in a similar situation.• Thus, the treatment of RV failure cannot
be successful without reducing the pulmonary arterial pressure.
2. The thinner wall also confers a greater distensibility to the RV. Thus, when acute or chronic increases in the RV pressure or volume occur, it may dilate and cause the interventricular septum to bulge into the LV. This explains why the PAOP may be high in many patients with ARDS even in the presence of a normal LVEDV.
PATHOPHYSIOLOGY OF VALVULAR HEART DISEASE
Valvular heart disease (VHD) is frequently encountered by the anaesthetist. Understanding the pathophysiology is mandatory to understand anaesthetic goals. VHDs affect cardiac function mainly by causing abnormal loading conditions. Common to all VHDs is an initial period of compensation of the cardiac chambers to maintain cardiac output in the face of abnormal loading conditions. With the progress of the disease however, compensation reaches a maximum, and decompensation and cardiac failure follow. The anaesthetic management depends not only on the pathophysiology of the VHD but also on the compensatory responses. In most cases, the goal is to maintain the compensatory mechanisms intact
Afterload Mismatch and Preload ReserveLet us take the case of a VHD that
produces gradually increasing impedance to ejection (afterload). If left uncompensated, the gradual increase in afterload would produce a gradual decrease in ejection fraction and stroke volume, termed afterload mismatch (loop A ->B). However, the ventricle compensates by increasing the preload (EDV). In accordance with the Frank-Starling mechanism, SV is preserved by augmenting the contractile force at this higher preload (loop B -> C). This compensation by augmenting the preload is termed preload reserve. Later in the disease, the ventricle decompensates when the afterload increases to such an extent that even the maximal limit of preload reserve is inadequate to maintain a normal SV, even with a normal contractility (loop CD). This example demonstrates how a ventricle with a normal contractility may still be unable to maintain a normal SV due to abnormal loading conditions. The appropriate treatment in this case for instance, would not be inotropic support, but a decrease in the afterload.
The compensation by increasing the preload makes sense for the energy balance of the heart. The ventricle does work (expends energy) during the entire cardiac cycle. However, there is a large discrepancy in the consumption of energy in systole and diastole. Work done in the ejection phase is more energy-consumptive when compared to work done for ventricular filling. Thus, in response to increased afterload, although the logical compensatory response is that of more forceful ventricular contraction, the energy balance is better preserved if more preload is recruited. With this background, let us now analyse 4 common VHDs.
Aortic Stenosis (AS)PATHOPHYSIOLOGY
The problem in AS is that of increased impedance to ventricular ejection, i.e., increased afterload. Stroke volume is maintained by recruiting the preload reserve.
The increased pressure to ejection necessitates an increased intraventricular pressure, thereby prolonging the isovolumic contraction phase. This intracavitary systolic pressure generated to overcome this stenosis,
RACE 2003 Ramachandra Anaesthesia Continuing Education
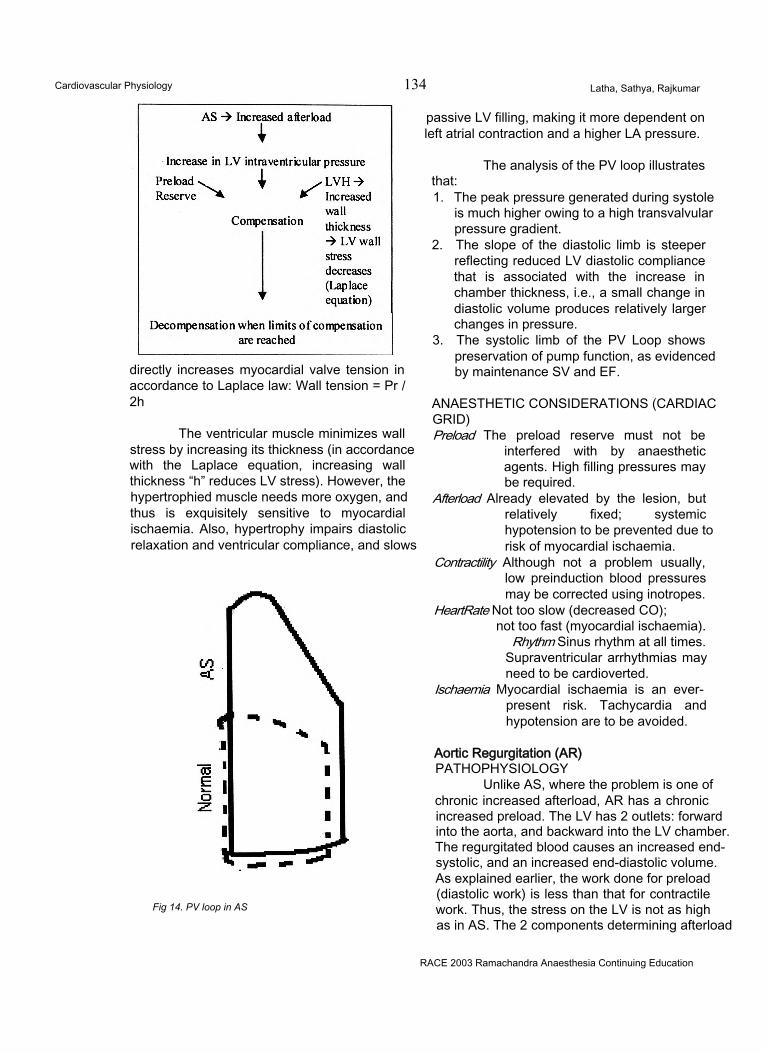
Cardiovascular Physiology 134 Latha, Sathya, Rajkumar
directly increases myocardial valve tension in accordance to Laplace law: Wall tension = Pr / 2h
The ventricular muscle minimizes wall stress by increasing its thickness (in accordance with the Laplace equation, increasing wall thickness “h” reduces LV stress). However, the hypertrophied muscle needs more oxygen, and thus is exquisitely sensitive to myocardial ischaemia. Also, hypertrophy impairs diastolic relaxation and ventricular compliance, and slows
Fig 14. PV loop in AS
passive LV filling, making it more dependent on left atrial contraction and a higher LA pressure.
The analysis of the PV loop illustratesthat:1. The peak pressure generated during systole
is much higher owing to a high transvalvular pressure gradient.
2. The slope of the diastolic limb is steeper reflecting reduced LV diastolic compliance that is associated with the increase in chamber thickness, i.e., a small change in diastolic volume produces relatively larger changes in pressure.
3. The systolic limb of the PV Loop shows preservation of pump function, as evidenced by maintenance SV and EF.
ANAESTHETIC CONSIDERATIONS (CARDIAC GRID)Preload The preload reserve must not be
interfered with by anaesthetic agents. High filling pressures may be required.
Afterload Already elevated by the lesion, but relatively fixed; systemic hypotension to be prevented due to risk of myocardial ischaemia.
Contractility Although not a problem usually, low preinduction blood pressures may be corrected using inotropes.
HeartRate Not too slow (decreased CO);not too fast (myocardial ischaemia).
Rhythm Sinus rhythm at all times.Supraventricular arrhythmias may need to be cardioverted.
Ischaemia Myocardial ischaemia is an everpresent risk. Tachycardia and hypotension are to be avoided.
Aortic Regurgitation (AR)PATHOPHYSIOLOGY
Unlike AS, where the problem is one of chronic increased afterload, AR has a chronic increased preload. The LV has 2 outlets: forward into the aorta, and backward into the LV chamber. The regurgitated blood causes an increased end- systolic, and an increased end-diastolic volume. As explained earlier, the work done for preload (diastolic work) is less than that for contractile work. Thus, the stress on the LV is not as high as in AS. The 2 components determining afterload
RACE 2003 Ramachandra Anaesthesia Continuing Education
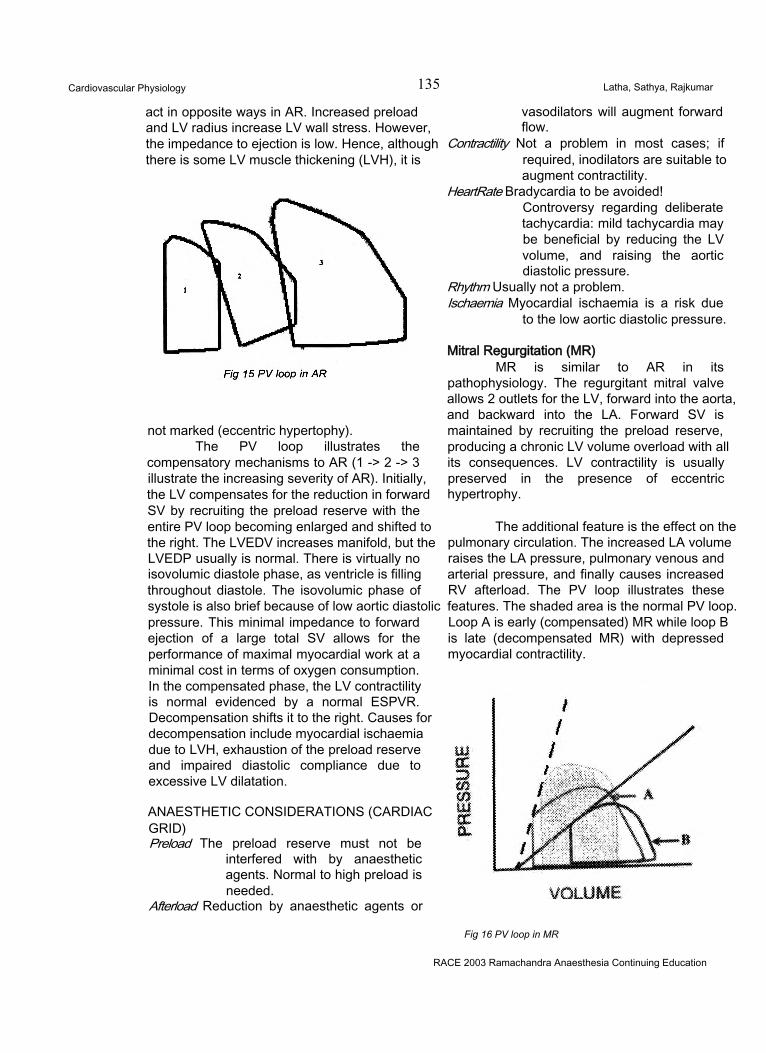
Cardiovascular Physiology 135 Latha, Sathya, Rajkumar
act in opposite ways in AR. Increased preload and LV radius increase LV wall stress. However, the impedance to ejection is low. Hence, although there is some LV muscle thickening (LVH), it is
not marked (eccentric hypertophy).The PV loop illustrates the
compensatory mechanisms to AR (1 -> 2 -> 3 illustrate the increasing severity of AR). Initially, the LV compensates for the reduction in forward SV by recruiting the preload reserve with the entire PV loop becoming enlarged and shifted to the right. The LVEDV increases manifold, but the LVEDP usually is normal. There is virtually no isovolumic diastole phase, as ventricle is filling throughout diastole. The isovolumic phase of systole is also brief because of low aortic diastolic pressure. This minimal impedance to forward ejection of a large total SV allows for the performance of maximal myocardial work at a minimal cost in terms of oxygen consumption. In the compensated phase, the LV contractility is normal evidenced by a normal ESPVR. Decompensation shifts it to the right. Causes for decompensation include myocardial ischaemia due to LVH, exhaustion of the preload reserve and impaired diastolic compliance due to excessive LV dilatation.
ANAESTHETIC CONSIDERATIONS (CARDIAC GRID)Preload The preload reserve must not be
interfered with by anaesthetic agents. Normal to high preload is needed.
Afterload Reduction by anaesthetic agents or
vasodilators will augment forward flow.
Contractility Not a problem in most cases; if required, inodilators are suitable to augment contractility.
HeartRate Bradycardia to be avoided!Controversy regarding deliberate tachycardia: mild tachycardia may be beneficial by reducing the LV volume, and raising the aortic diastolic pressure.
Rhythm Usually not a problem.Ischaemia Myocardial ischaemia is a risk due
to the low aortic diastolic pressure.
Mitral Regurgitation (MR)MR is similar to AR in its
pathophysiology. The regurgitant mitral valve allows 2 outlets for the LV, forward into the aorta, and backward into the LA. Forward SV is maintained by recruiting the preload reserve, producing a chronic LV volume overload with all its consequences. LV contractility is usually preserved in the presence of eccentric hypertrophy.
The additional feature is the effect on the pulmonary circulation. The increased LA volume raises the LA pressure, pulmonary venous and arterial pressure, and finally causes increased RV afterload. The PV loop illustrates these features. The shaded area is the normal PV loop. Loop A is early (compensated) MR while loop B is late (decompensated MR) with depressed myocardial contractility.
Fig 16 PV loop in MR
RACE 2003 Ramachandra Anaesthesia Continuing Education
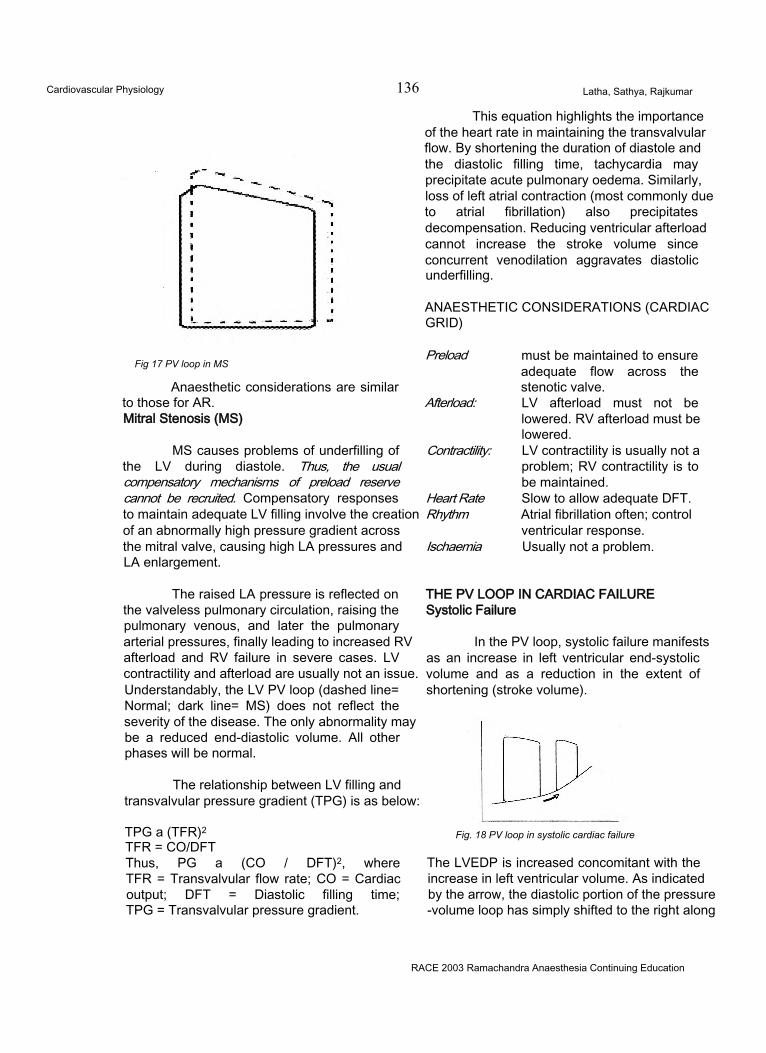
Cardiovascular Physiology 136 Latha, Sathya, Rajkumar
This equation highlights the importance of the heart rate in maintaining the transvalvular flow. By shortening the duration of diastole and the diastolic filling time, tachycardia may precipitate acute pulmonary oedema. Similarly, loss of left atrial contraction (most commonly due to atrial fibrillation) also precipitates decompensation. Reducing ventricular afterload cannot increase the stroke volume since concurrent venodilation aggravates diastolic underfilling.
ANAESTHETIC CONSIDERATIONS (CARDIAC GRID)
Fig 17 PV loop in MS
Anaesthetic considerations are similar to those for AR.Mitral Stenosis (MS)
MS causes problems of underfilling of the LV during diastole. Thus, the usual compensatory mechanisms of preload reserve cannot be recruited. Compensatory responses to maintain adequate LV filling involve the creation of an abnormally high pressure gradient across the mitral valve, causing high LA pressures and LA enlargement.
The raised LA pressure is reflected on the valveless pulmonary circulation, raising the pulmonary venous, and later the pulmonary arterial pressures, finally leading to increased RV afterload and RV failure in severe cases. LV contractility and afterload are usually not an issue. Understandably, the LV PV loop (dashed line= Normal; dark line= MS) does not reflect the severity of the disease. The only abnormality may be a reduced end-diastolic volume. All other phases will be normal.
The relationship between LV filling and transvalvular pressure gradient (TPG) is as below:
TPG a (TFR)2 TFR = CO/DFTThus, PG a (CO / DFT)2, where TFR = Transvalvular flow rate; CO = Cardiac output; DFT = Diastolic filling time; TPG = Transvalvular pressure gradient.
Preload
Afterload:
Contractility:
Heart Rate Rhythm
Ischaemia
must be maintained to ensure adequate flow across the stenotic valve.LV afterload must not be lowered. RV afterload must be lowered.LV contractility is usually not a problem; RV contractility is to be maintained.Slow to allow adequate DFT. Atrial fibrillation often; control ventricular response.Usually not a problem.
THE PV LOOP IN CARDIAC FAILURE Systolic Failure
In the PV loop, systolic failure manifests as an increase in left ventricular end-systolic volume and as a reduction in the extent of shortening (stroke volume).
Fig. 18 PV loop in systolic cardiac failure
The LVEDP is increased concomitant with the increase in left ventricular volume. As indicated by the arrow, the diastolic portion of the pressure -volume loop has simply shifted to the right along
RACE 2003 Ramachandra Anaesthesia Continuing Education
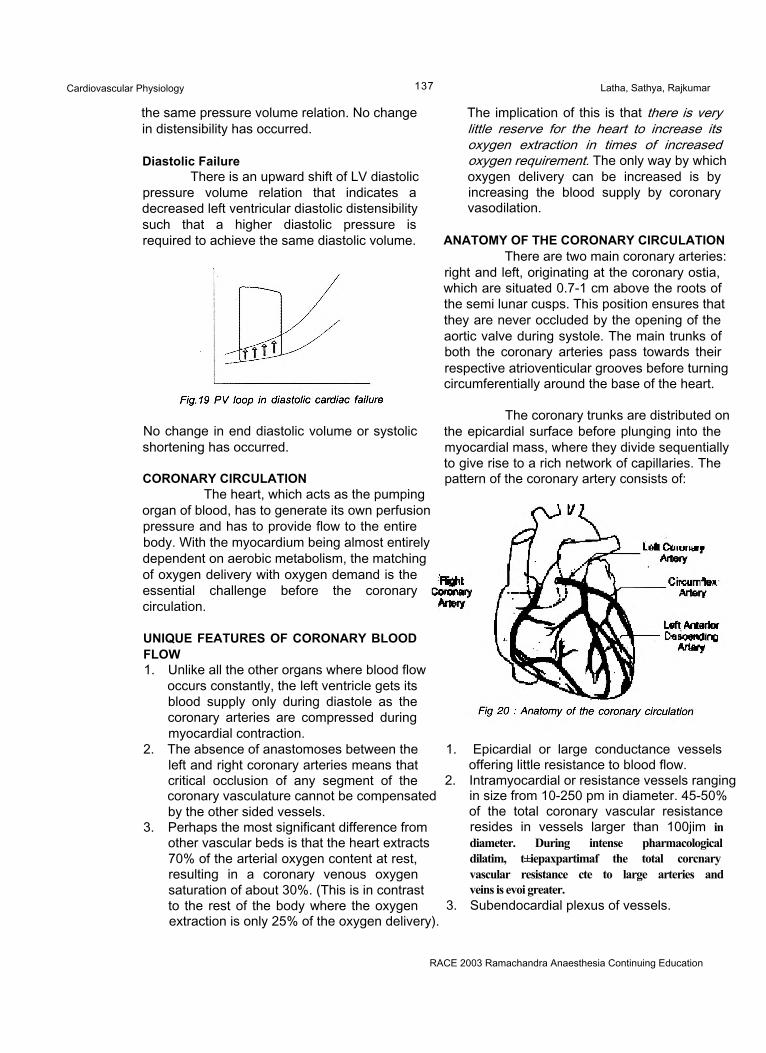
Cardiovascular Physiology 137 Latha, Sathya, Rajkumar
the same pressure volume relation. No change in distensibility has occurred.
Diastolic FailureThere is an upward shift of LV diastolic
pressure volume relation that indicates a decreased left ventricular diastolic distensibility such that a higher diastolic pressure is required to achieve the same diastolic volume.
No change in end diastolic volume or systolic shortening has occurred.
CORONARY CIRCULATIONThe heart, which acts as the pumping
organ of blood, has to generate its own perfusion pressure and has to provide flow to the entire body. With the myocardium being almost entirely dependent on aerobic metabolism, the matching of oxygen delivery with oxygen demand is the essential challenge before the coronary circulation.
UNIQUE FEATURES OF CORONARY BLOOD FLOW1. Unlike all the other organs where blood flow
occurs constantly, the left ventricle gets its blood supply only during diastole as the coronary arteries are compressed during myocardial contraction.
2. The absence of anastomoses between the left and right coronary arteries means that critical occlusion of any segment of the coronary vasculature cannot be compensated by the other sided vessels.
3. Perhaps the most significant difference from other vascular beds is that the heart extracts 70% of the arterial oxygen content at rest, resulting in a coronary venous oxygen saturation of about 30%. (This is in contrast to the rest of the body where the oxygen extraction is only 25% of the oxygen delivery).
The implication of this is that there is very little reserve for the heart to increase its oxygen extraction in times of increased oxygen requirement. The only way by which oxygen delivery can be increased is by increasing the blood supply by coronary vasodilation.
ANATOMY OF THE CORONARY CIRCULATIONThere are two main coronary arteries:
right and left, originating at the coronary ostia, which are situated 0.7-1 cm above the roots of the semi lunar cusps. This position ensures that they are never occluded by the opening of the aortic valve during systole. The main trunks of both the coronary arteries pass towards their respective atrioventicular grooves before turning circumferentially around the base of the heart.
The coronary trunks are distributed on the epicardial surface before plunging into the myocardial mass, where they divide sequentially to give rise to a rich network of capillaries. The pattern of the coronary artery consists of:
1. Epicardial or large conductance vessels offering little resistance to blood flow.
2. Intramyocardial or resistance vessels ranging in size from 10-250 pm in diameter. 45-50% of the total coronary vascular resistance resides in vessels larger than 100jim in diameter. During intense pharmacological dilatim, t±iepaxpartimaf the total corcnary vascular resistance cte to large arteries and veins is evoi greater.
3. Subendocardial plexus of vessels.
RACE 2003 Ramachandra Anaesthesia Continuing Education
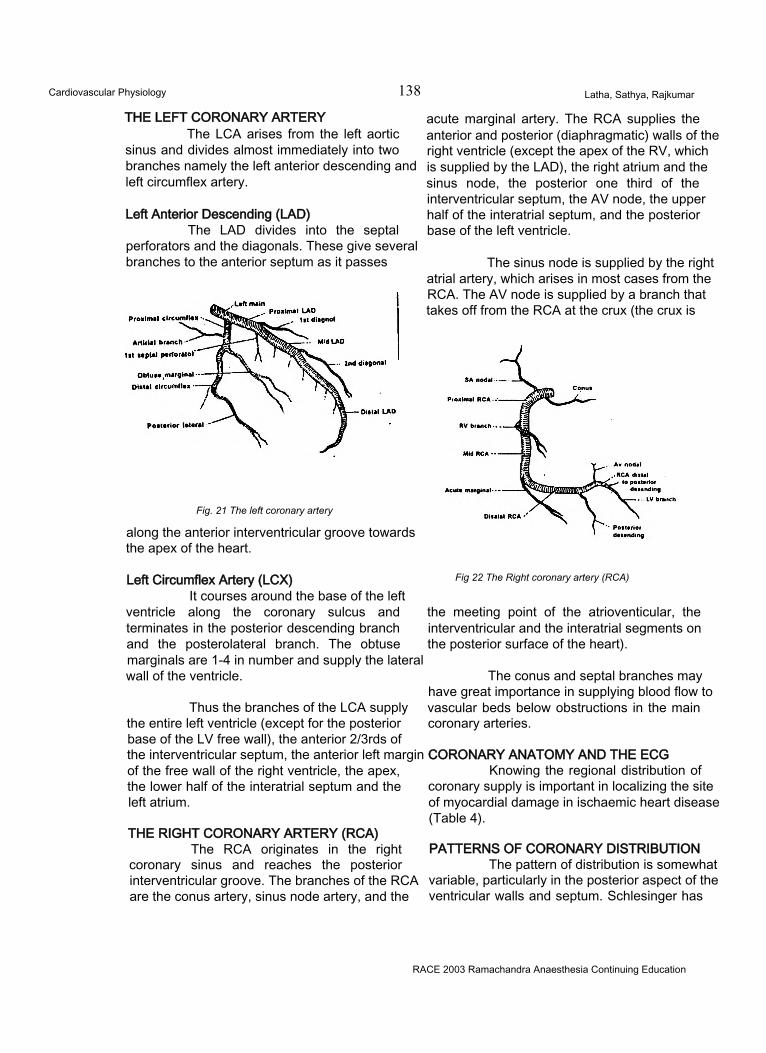
Cardiovascular Physiology 138 Latha, Sathya, Rajkumar
THE LEFT CORONARY ARTERYThe LCA arises from the left aortic
sinus and divides almost immediately into two branches namely the left anterior descending and left circumflex artery.
Left Anterior Descending (LAD)The LAD divides into the septal
perforators and the diagonals. These give several branches to the anterior septum as it passes
Fig. 21 The left coronary artery
along the anterior interventricular groove towards the apex of the heart.
Left Circumflex Artery (LCX)It courses around the base of the left
ventricle along the coronary sulcus and terminates in the posterior descending branch and the posterolateral branch. The obtuse marginals are 1-4 in number and supply the lateral wall of the ventricle.
Thus the branches of the LCA supply the entire left ventricle (except for the posterior base of the LV free wall), the anterior 2/3rds of the interventricular septum, the anterior left margin of the free wall of the right ventricle, the apex, the lower half of the interatrial septum and the left atrium.
THE RIGHT CORONARY ARTERY (RCA)The RCA originates in the right
coronary sinus and reaches the posterior interventricular groove. The branches of the RCA are the conus artery, sinus node artery, and the
acute marginal artery. The RCA supplies the anterior and posterior (diaphragmatic) walls of the right ventricle (except the apex of the RV, which is supplied by the LAD), the right atrium and the sinus node, the posterior one third of the interventricular septum, the AV node, the upper half of the interatrial septum, and the posterior base of the left ventricle.
The sinus node is supplied by the right atrial artery, which arises in most cases from the RCA. The AV node is supplied by a branch that takes off from the RCA at the crux (the crux is
Fig 22 The Right coronary artery (RCA)
the meeting point of the atrioventicular, the interventricular and the interatrial segments on the posterior surface of the heart).
The conus and septal branches may have great importance in supplying blood flow to vascular beds below obstructions in the main coronary arteries.
CORONARY ANATOMY AND THE ECGKnowing the regional distribution of
coronary supply is important in localizing the site of myocardial damage in ischaemic heart disease (Table 4).
PATTERNS OF CORONARY DISTRIBUTIONThe pattern of distribution is somewhat
variable, particularly in the posterior aspect of the ventricular walls and septum. Schlesinger has
RACE 2003 Ramachandra Anaesthesia Continuing Education
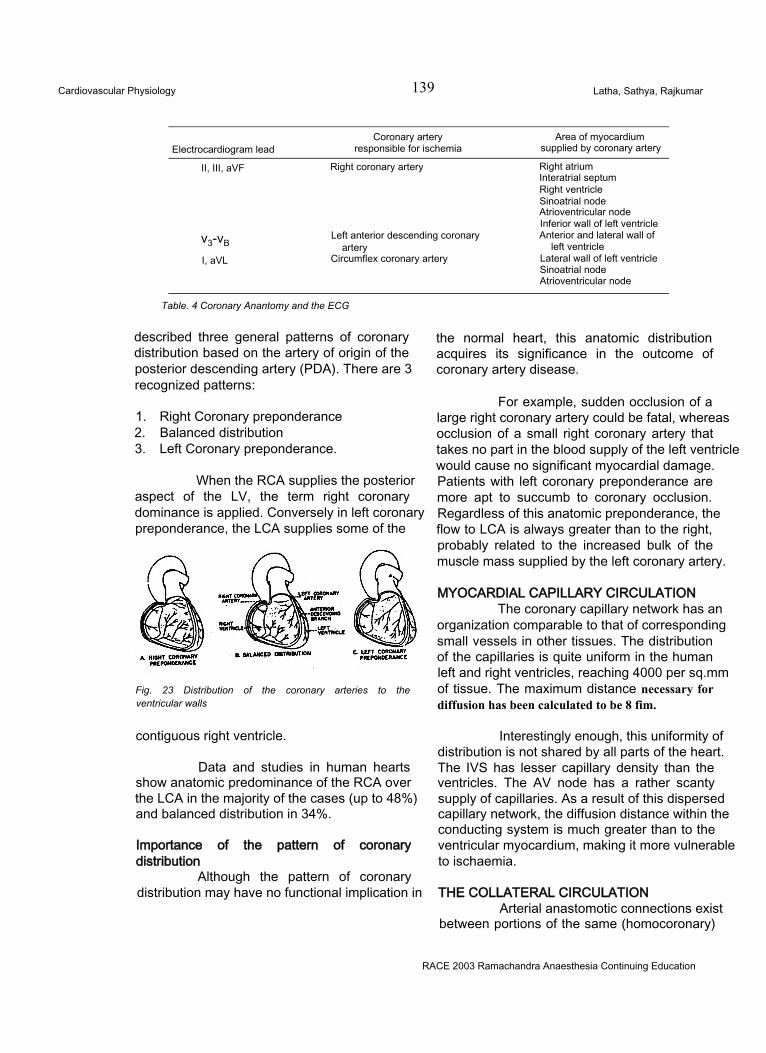
Cardiovascular Physiology 139 Latha, Sathya, Rajkumar
Electrocardiogram leadCoronary artery
responsible for ischemiaArea of myocardium
supplied by coronary artery
II, III, aVF Right coronary artery Right atrium Interatrial septum Right ventricle Sinoatrial node Atrioventricular node Inferior wall of left ventricle
v3-vBLeft anterior descending coronary
arteryAnterior and lateral wall of
left ventricleI, aVL Circumflex coronary artery Lateral wall of left ventricle
Sinoatrial node Atrioventricular node
Table. 4 Coronary Anantomy and the ECG
described three general patterns of coronary distribution based on the artery of origin of the posterior descending artery (PDA). There are 3 recognized patterns:
1. Right Coronary preponderance2. Balanced distribution3. Left Coronary preponderance.
When the RCA supplies the posterior aspect of the LV, the term right coronary dominance is applied. Conversely in left coronary preponderance, the LCA supplies some of the
Fig. 23 Distribution of the coronary arteries to the ventricular walls
contiguous right ventricle.
Data and studies in human hearts show anatomic predominance of the RCA over the LCA in the majority of the cases (up to 48%) and balanced distribution in 34%.
Importance of the pattern of coronary distribution
Although the pattern of coronary distribution may have no functional implication in
the normal heart, this anatomic distribution acquires its significance in the outcome of coronary artery disease.
For example, sudden occlusion of a large right coronary artery could be fatal, whereas occlusion of a small right coronary artery that takes no part in the blood supply of the left ventricle would cause no significant myocardial damage. Patients with left coronary preponderance are more apt to succumb to coronary occlusion. Regardless of this anatomic preponderance, the flow to LCA is always greater than to the right, probably related to the increased bulk of the muscle mass supplied by the left coronary artery.
MYOCARDIAL CAPILLARY CIRCULATIONThe coronary capillary network has an
organization comparable to that of corresponding small vessels in other tissues. The distribution of the capillaries is quite uniform in the human left and right ventricles, reaching 4000 per sq.mm of tissue. The maximum distance necessary for diffusion has been calculated to be 8 fim.
Interestingly enough, this uniformity of distribution is not shared by all parts of the heart. The IVS has lesser capillary density than the ventricles. The AV node has a rather scanty supply of capillaries. As a result of this dispersed capillary network, the diffusion distance within the conducting system is much greater than to the ventricular myocardium, making it more vulnerable to ischaemia.
THE COLLATERAL CIRCULATIONArterial anastomotic connections exist
between portions of the same (homocoronary)
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardiovascular Physiology 140 Latha, Sathya, Rajkumar
coronary artery and between different (intercoronary) coronary arteries. The collaterals have a diameter varying from 40-200 microns. Both types are found throughout the full thickness of the ventricular walls except the layers just under the epicardium. Even repeated brief (2 minute) episodes of ischaemia can serve as stimuli for collateral vessels to open out. The collateral blood supply can prevent the development of infarction and preserve myocardial viability when the obstruction develops gradually over a period of months.
Rest versus exerciseUnlike normal coronary vessels,
collaterals are maximally vasodilated even at rest. They do not have the capability to dilate further in times of increased oxygen requirement, like exertional states. For instance, a patient with 80- 90% obstruction of a major vessel with well- developed collaterals may not complain of anginal pain under basal resting conditions, but may develop ischaemia or even infarction after exertion. It follows that eliciting information about effort tolerance by history or other means may be the best method to unmask the presence of CAD in a patient.
CORONARY VEINSVenous drainage is distinctly different
in the two ventricles. This drainage system forms3 main veins namely:1. The coronary sinus2. The anterior right ventricular veins3. The Thebesian veins.
The main coronary venous drainage tends to retrace the course of the coronary arteries, passing towards the atrioventricular groove and terminating in the coronary sinus, which empties into the right atrium through its posterior wall.
NEURAL CONTROL OF THE HEARTThe atria are abundantly innervated by
the sympathetic and parasympathetic nervous systems, but the ventricles are supplied principally by the sympathetic nervous system. These nerves affect cardiac output by changing the heart rate and strength of myocardial contraction. Maximal sympathetic nervous
system stimulation can increase cardiac output by about 100% above normal. Conversely, maximal parasympathetic nervous system stimulation decreases ventricular contractile strength and subsequent cardiac output only about 30%, emphasizing that parasympathetic nervous system stimulation of the heart is small compared to the effect of sympathetic nervous system stimulation.
Other homeostatic mechanisms forming the cardiovascular reflexes have been dealt with earlier.
CORONARY BLOOD FLOWResting coronary blood flow is 225-250
ml/minute or 4-5% of the cardiac output. Assuming that the normal adult heart weighs about 280 g, this is equivalent to a blood flow of 75 ml/100g/min. The resting myocardial oxygen consumption (Mv02) is 8-10 ml/100g/min, or about 10% of the total body consumption of oxygen. As explained in the section on ventricular function, LV distension is a major determinant of Mv02. For instance, the oxygen consumption of the arrested, non-distended heart is 1 ml/100g/ min compared to 5 ml/100g/min in the arrested but distended heart.
Determinants Of Coronary Blood Flow (CBF)CBF is mainly determined by 4 factors
including:1. Perfusion pressure (coronary perfusion
pressure or CPP)2. Myocardial extravascular compression3. Myocardial metabolism4. Neurohumoral control.
CORONARY PERFUSION PRESSURE (CPP) The CPP is the pressure head that
drives blood into the coronary arteries. The CBF is proportional to the pressure gradient across
the coronary circulation.
The perfusion pressure for any given organ is the pressure difference between the driving pressure in the arterial side minus the pressure in the venous side. In all the other organs the perfusion occurs throughout the cardiac cycle, hence the driving pressure is the mean arterial pressure (MAP). In the LV however, the resistance
RACE 2003 Ramachandra Anaesthesia Continuing Education
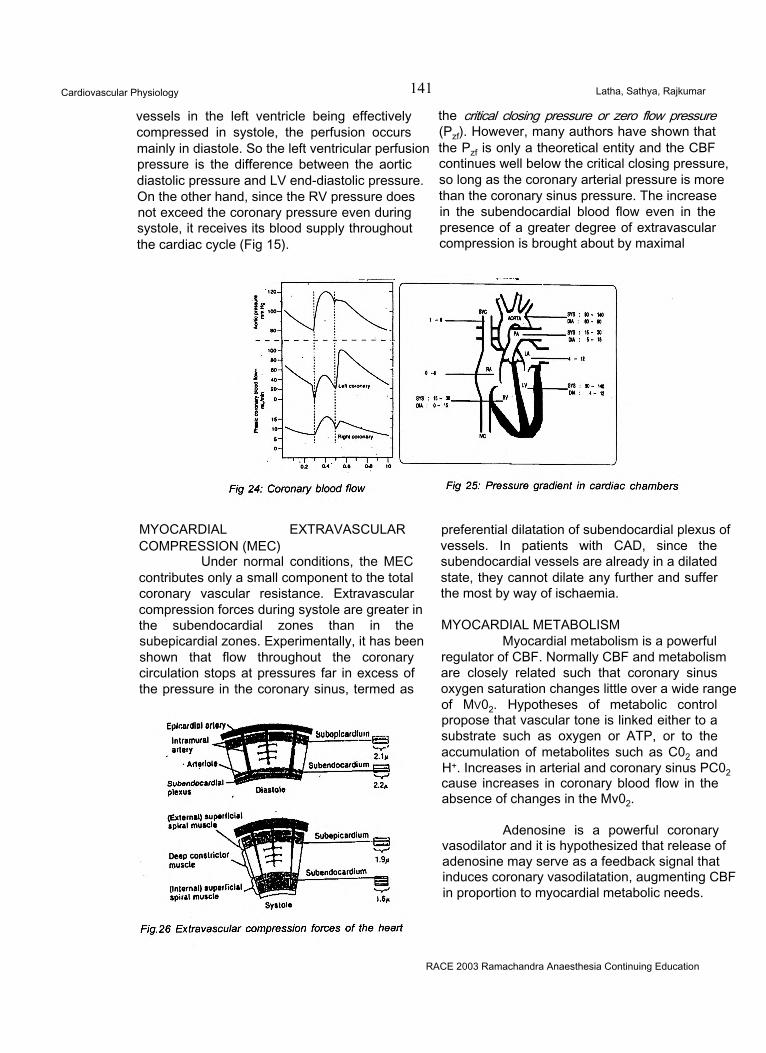
Cardiovascular Physiology 141 Latha, Sathya, Rajkumar
vessels in the left ventricle being effectively compressed in systole, the perfusion occurs mainly in diastole. So the left ventricular perfusion pressure is the difference between the aortic diastolic pressure and LV end-diastolic pressure. On the other hand, since the RV pressure does not exceed the coronary pressure even during systole, it receives its blood supply throughout the cardiac cycle (Fig 15).
the critical closing pressure or zero flow pressure (Pzf). However, many authors have shown that the Pzf is only a theoretical entity and the CBF continues well below the critical closing pressure, so long as the coronary arterial pressure is more than the coronary sinus pressure. The increase in the subendocardial blood flow even in the presence of a greater degree of extravascular compression is brought about by maximal
MYOCARDIAL EXTRAVASCULARCOMPRESSION (MEC)
Under normal conditions, the MEC contributes only a small component to the total coronary vascular resistance. Extravascular compression forces during systole are greater in the subendocardial zones than in the subepicardial zones. Experimentally, it has been shown that flow throughout the coronary circulation stops at pressures far in excess of the pressure in the coronary sinus, termed as
preferential dilatation of subendocardial plexus of vessels. In patients with CAD, since the subendocardial vessels are already in a dilated state, they cannot dilate any further and suffer the most by way of ischaemia.
MYOCARDIAL METABOLISMMyocardial metabolism is a powerful
regulator of CBF. Normally CBF and metabolism are closely related such that coronary sinus oxygen saturation changes little over a wide range of Mv02. Hypotheses of metabolic control propose that vascular tone is linked either to a substrate such as oxygen or ATP, or to the accumulation of metabolites such as C02 and H+. Increases in arterial and coronary sinus PC02 cause increases in coronary blood flow in the absence of changes in the Mv02.
Adenosine is a powerful coronary vasodilator and it is hypothesized that release of adenosine may serve as a feedback signal that induces coronary vasodilatation, augmenting CBF in proportion to myocardial metabolic needs.
RACE 2003 Ramachandra Anaesthesia Continuing Education
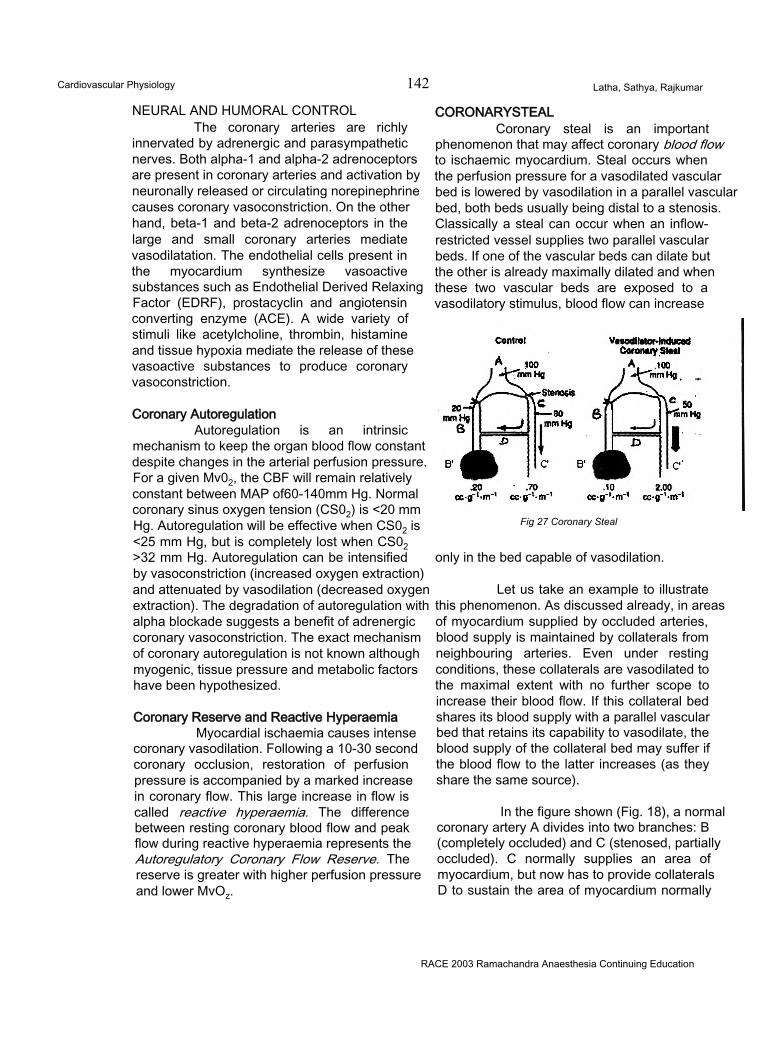
Cardiovascular Physiology 142 Latha, Sathya, Rajkumar
NEURAL AND HUMORAL CONTROLThe coronary arteries are richly
innervated by adrenergic and parasympathetic nerves. Both alpha-1 and alpha-2 adrenoceptors are present in coronary arteries and activation by neuronally released or circulating norepinephrine causes coronary vasoconstriction. On the other hand, beta-1 and beta-2 adrenoceptors in the large and small coronary arteries mediate vasodilatation. The endothelial cells present in the myocardium synthesize vasoactive substances such as Endothelial Derived Relaxing Factor (EDRF), prostacyclin and angiotensin converting enzyme (ACE). A wide variety of stimuli like acetylcholine, thrombin, histamine and tissue hypoxia mediate the release of these vasoactive substances to produce coronary vasoconstriction.
Coronary AutoregulationAutoregulation is an intrinsic
mechanism to keep the organ blood flow constant despite changes in the arterial perfusion pressure. For a given Mv02, the CBF will remain relatively constant between MAP of60-140mm Hg. Normal coronary sinus oxygen tension (CS02) is <20 mm Hg. Autoregulation will be effective when CS02 is <25 mm Hg, but is completely lost when CS02 >32 mm Hg. Autoregulation can be intensified by vasoconstriction (increased oxygen extraction) and attenuated by vasodilation (decreased oxygen extraction). The degradation of autoregulation with alpha blockade suggests a benefit of adrenergic coronary vasoconstriction. The exact mechanism of coronary autoregulation is not known although myogenic, tissue pressure and metabolic factors have been hypothesized.
Coronary Reserve and Reactive HyperaemiaMyocardial ischaemia causes intense
coronary vasodilation. Following a 10-30 second coronary occlusion, restoration of perfusion pressure is accompanied by a marked increase in coronary flow. This large increase in flow is called reactive hyperaemia. The difference between resting coronary blood flow and peak flow during reactive hyperaemia represents the Autoregulatory Coronary Flow Reserve. The reserve is greater with higher perfusion pressure and lower MvOz.
CORONARYSTEALCoronary steal is an important
phenomenon that may affect coronary blood flow to ischaemic myocardium. Steal occurs when the perfusion pressure for a vasodilated vascular bed is lowered by vasodilation in a parallel vascular bed, both beds usually being distal to a stenosis. Classically a steal can occur when an inflow- restricted vessel supplies two parallel vascular beds. If one of the vascular beds can dilate but the other is already maximally dilated and when these two vascular beds are exposed to a vasodilatory stimulus, blood flow can increase
Fig 27 Coronary Steal
only in the bed capable of vasodilation.
Let us take an example to illustrate this phenomenon. As discussed already, in areas of myocardium supplied by occluded arteries, blood supply is maintained by collaterals from neighbouring arteries. Even under resting conditions, these collaterals are vasodilated to the maximal extent with no further scope to increase their blood flow. If this collateral bed shares its blood supply with a parallel vascular bed that retains its capability to vasodilate, the blood supply of the collateral bed may suffer if the blood flow to the latter increases (as they share the same source).
In the figure shown (Fig. 18), a normal coronary artery A divides into two branches: B (completely occluded) and C (stenosed, partially occluded). C normally supplies an area of myocardium, but now has to provide collaterals D to sustain the area of myocardium normally
RACE 2003 Ramachandra Anaesthesia Continuing Education
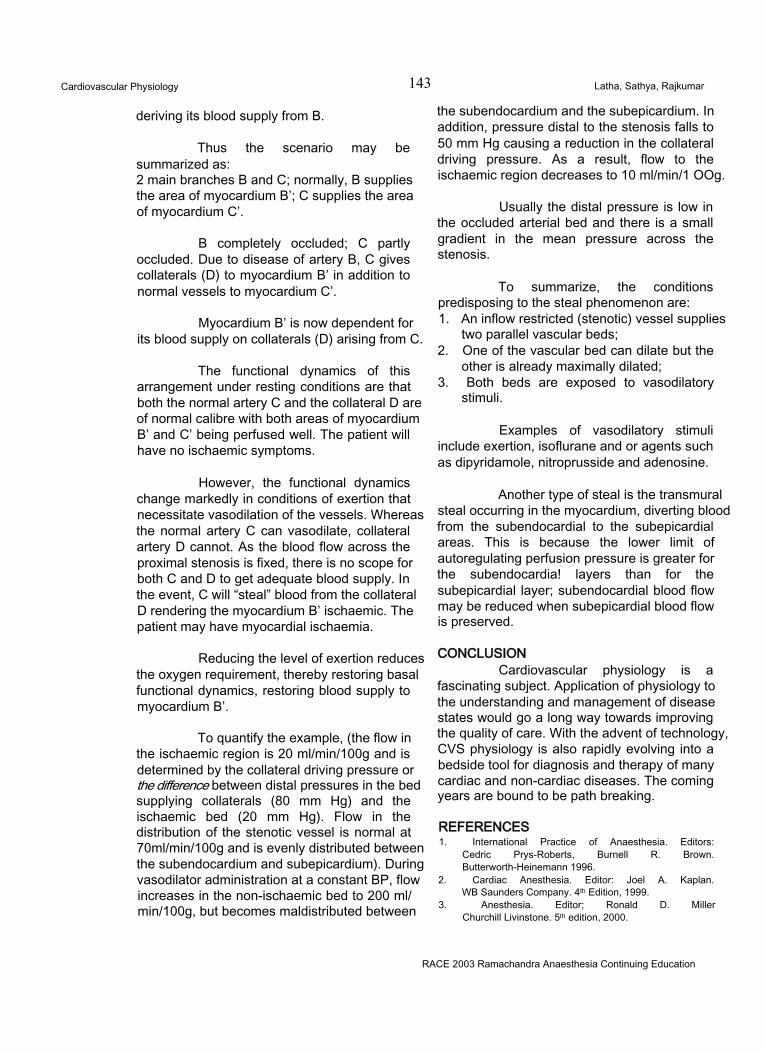
Cardiovascular Physiology 143 Latha, Sathya, Rajkumar
deriving its blood supply from B.
Thus the scenario may be summarized as:2 main branches B and C; normally, B supplies the area of myocardium B’; C supplies the area of myocardium C’.
B completely occluded; C partly occluded. Due to disease of artery B, C gives collaterals (D) to myocardium B’ in addition to normal vessels to myocardium C’.
Myocardium B’ is now dependent for its blood supply on collaterals (D) arising from C.
The functional dynamics of this arrangement under resting conditions are that both the normal artery C and the collateral D are of normal calibre with both areas of myocardium B’ and C’ being perfused well. The patient will have no ischaemic symptoms.
However, the functional dynamics change markedly in conditions of exertion that necessitate vasodilation of the vessels. Whereas the normal artery C can vasodilate, collateral artery D cannot. As the blood flow across the proximal stenosis is fixed, there is no scope for both C and D to get adequate blood supply. In the event, C will “steal” blood from the collateral D rendering the myocardium B’ ischaemic. The patient may have myocardial ischaemia.
Reducing the level of exertion reduces the oxygen requirement, thereby restoring basal functional dynamics, restoring blood supply to myocardium B’.
To quantify the example, (the flow in the ischaemic region is 20 ml/min/100g and is determined by the collateral driving pressure or the difference between distal pressures in the bed supplying collaterals (80 mm Hg) and the ischaemic bed (20 mm Hg). Flow in the distribution of the stenotic vessel is normal at 70ml/min/100g and is evenly distributed between the subendocardium and subepicardium). During vasodilator administration at a constant BP, flow increases in the non-ischaemic bed to 200 ml/ min/100g, but becomes maldistributed between
the subendocardium and the subepicardium. In addition, pressure distal to the stenosis falls to 50 mm Hg causing a reduction in the collateral driving pressure. As a result, flow to the ischaemic region decreases to 10 ml/min/1 OOg.
Usually the distal pressure is low in the occluded arterial bed and there is a small gradient in the mean pressure across the stenosis.
To summarize, the conditions predisposing to the steal phenomenon are:1. An inflow restricted (stenotic) vessel supplies
two parallel vascular beds;2. One of the vascular bed can dilate but the
other is already maximally dilated;3. Both beds are exposed to vasodilatory
stimuli.
Examples of vasodilatory stimuli include exertion, isoflurane and or agents such as dipyridamole, nitroprusside and adenosine.
Another type of steal is the transmural steal occurring in the myocardium, diverting blood from the subendocardial to the subepicardial areas. This is because the lower limit of autoregulating perfusion pressure is greater for the subendocardia! layers than for the subepicardial layer; subendocardial blood flow may be reduced when subepicardial blood flow is preserved.
CONCLUSIONCardiovascular physiology is a
fascinating subject. Application of physiology to the understanding and management of disease states would go a long way towards improving the quality of care. With the advent of technology, CVS physiology is also rapidly evolving into a bedside tool for diagnosis and therapy of many cardiac and non-cardiac diseases. The coming years are bound to be path breaking.
REFERENCES1. International Practice of Anaesthesia. Editors:
Cedric Prys-Roberts, Burnell R. Brown. Butterworth-Heinemann 1996.
2. Cardiac Anesthesia. Editor: Joel A. Kaplan. WB Saunders Company. 4th Edition, 1999.
3. Anesthesia. Editor; Ronald D. Miller Churchill Livinstone. 5th edition, 2000.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 144 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
ANATOMY AND PHYSIOLOGY OF THE SUB ARACHNOID AND THE EPIDURAL SPACE
We anaesthesiologists practice central neuraxial blockade routinely. So it becomes imperative on our part to be well versed with the anatomy and physiology of the subarachnoid and epidural space
VERTEBRAL COLUMN:The vertebral column is composed of 33
vertebrae (7cervical + 12 thoracic + 5 lumbar + 5 fused sacral + 4 coccygeal).
It consists of two curves called the :1) Primary curve and2) Secondary curve
At birth there is only the primary curvature i.e. a single concave curve anteriorly.The secondary curves .namely the cervical and the lumbar curves appear as the neonate starts to support his head and starts to sit and stand respectively.
Noting the directions of the spinous process of these vertebrae is of importance to us at the time of introducing the needle to enter these spaces.
Spinous process of the cervical vertebra:The spinous process of the cervical
vertebra is short and bifid (with the exception of C1 and C7) and is directed almost horizontally to the body of the vertebra.
Spinous process of the thoracic vertebra:The spinous process of the thoracic
vertebra is long and is inclined at an angle of 45 to 60 degrees to the body of the vertebra and the skin.So the needle should be directed at an angle
of 45 to 60 degrees cranially, to follow the upper border of the spine to enter the ligamentum flavum. Spinous Process of the Lumbar Vertebra:
The spinous process of the lumbar vertebra is directed horizontally backwards .virtually 90 degrees to the body of the vertebra and the skin. So the needle is to be directed perpendicular to the skin.
ANATOMY OF THE SPINAL CORD:The spinal cord is the continuation of the
central nervous system from the medulla oblongata.The lower extent of the cord varies with age.• Early fetal life upto 3 months of gestation; it occupies the whole length of the vertebral column• 3 months of gestation to birth: it extends to the 2nd coccygeal vertebra• At birth; it lies at the L3 vertebra and the dural sac ends at S3• At one year: it lies at the lower border of L1 and the dural sac ends at S2• Adult: it lies at the lower border of L1 and the dural sac ends at S2.
Cross section of the spinal cord:It is divided into grey and white matter.
The grey matter is divided in to 9 laminae, namely, LAMINA1 TO LAMINA 9. Lamina 2 and 3 are called the SUBSTANTIA GELATINOSA OF ROLANDO. It acts as a processing center for the information from the somatic receptors and relays it to the brain. It contains ‘C FIBRES’. Lamina 1 and 5 contain ‘ A DELTA FIBRES'.
Receptors of the spinal cord:• Opioid receptors: \i2,kappa,delta• NMDA receptors• GABA receptors• Alpha 2 adrenergic receptors
RACE 2003 Ramachandra Anaesthesia Continuing Education
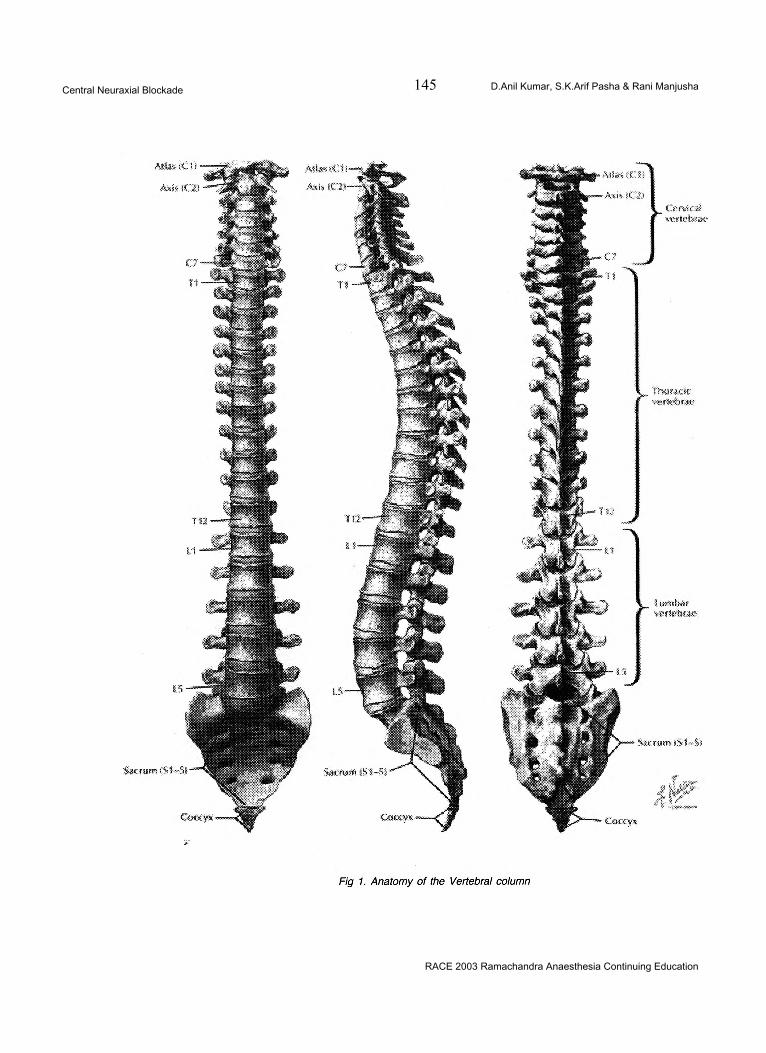
Central Neuraxial Blockade 145 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
RACE 2003 Ramachandra Anaesthesia Continuing Education
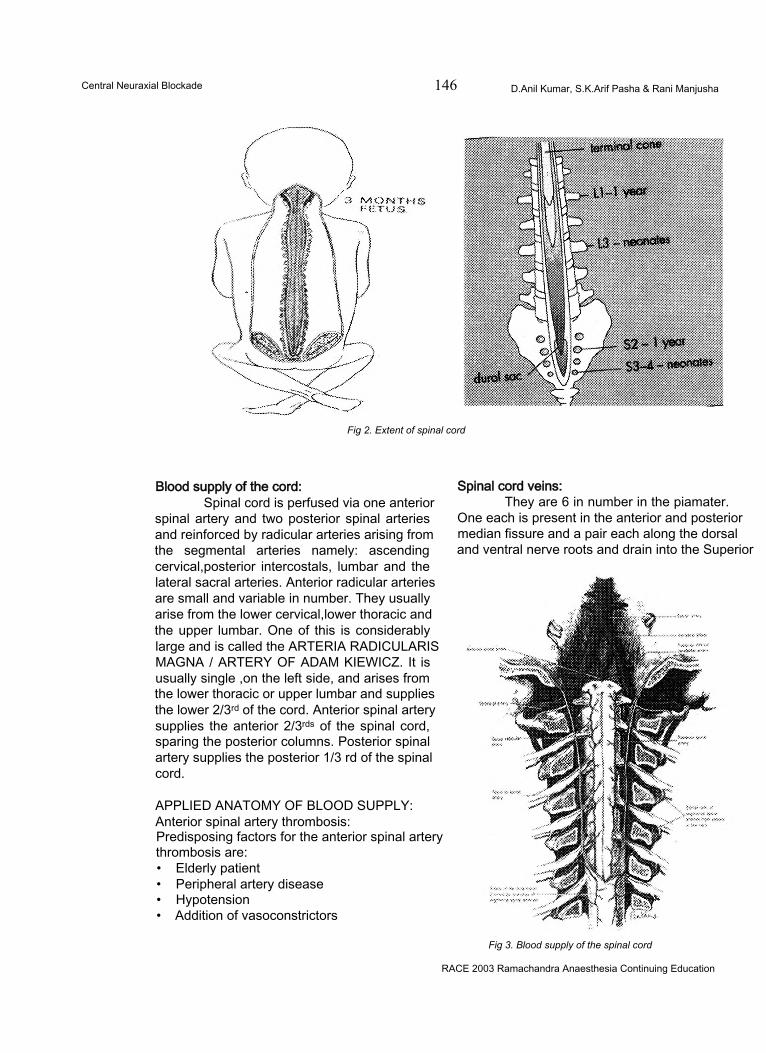
Central Neuraxial Blockade 146 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Fig 2. Extent of spinal cord
Blood supply of the cord:Spinal cord is perfused via one anterior
spinal artery and two posterior spinal arteries and reinforced by radicular arteries arising from the segmental arteries namely: ascending cervical,posterior intercostals, lumbar and the lateral sacral arteries. Anterior radicular arteries are small and variable in number. They usually arise from the lower cervical,lower thoracic and the upper lumbar. One of this is considerably large and is called the ARTERIA RADICULARIS MAGNA / ARTERY OF ADAM KIEWICZ. It is usually single ,on the left side, and arises from the lower thoracic or upper lumbar and supplies the lower 2/3rd of the cord. Anterior spinal artery supplies the anterior 2/3rds of the spinal cord, sparing the posterior columns. Posterior spinal artery supplies the posterior 1/3 rd of the spinal cord.
APPLIED ANATOMY OF BLOOD SUPPLY: Anterior spinal artery thrombosis:Predisposing factors for the anterior spinal artery thrombosis are:• Elderly patient• Peripheral artery disease• Hypotension• Addition of vasoconstrictors
Spinal cord veins:They are 6 in number in the piamater.
One each is present in the anterior and posterior median fissure and a pair each along the dorsal and ventral nerve roots and drain into the Superior
Fig 3. Blood supply of the spinal cord
RACE 2003 Ramachandra Anaesthesia Continuing Education
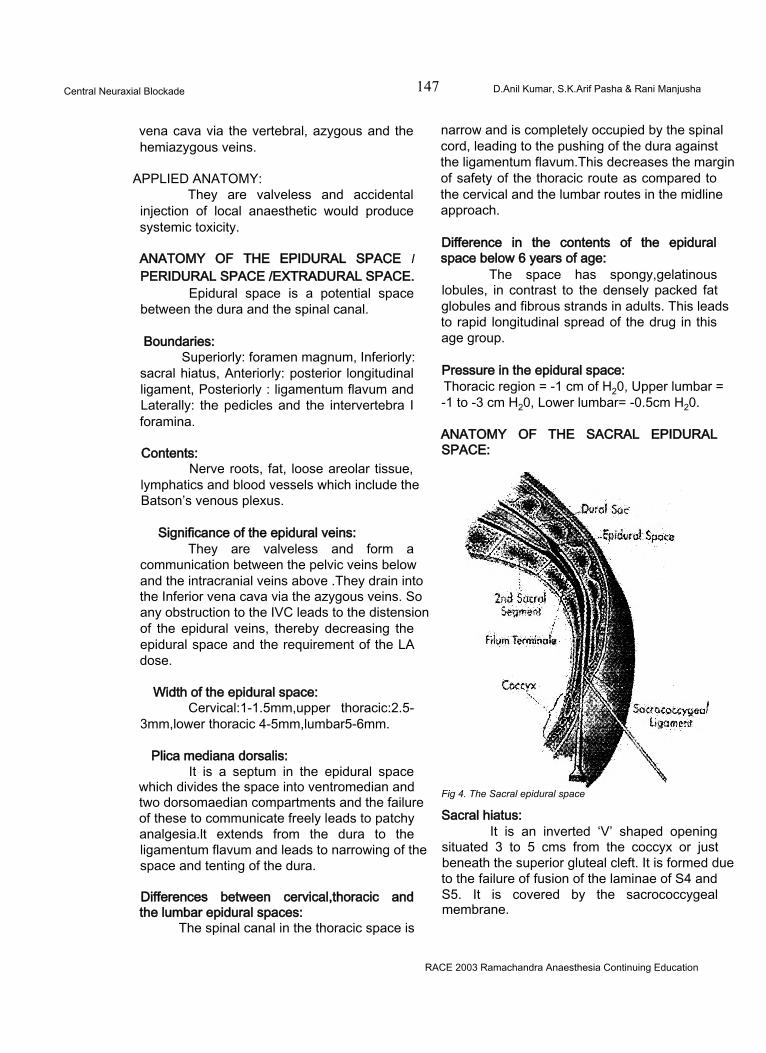
Central Neuraxial Blockade 147 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
vena cava via the vertebral, azygous and the hemiazygous veins.
APPLIED ANATOMY:They are valveless and accidental
injection of local anaesthetic would produce systemic toxicity.
ANATOMY OF THE EPIDURAL SPACE I PERIDURAL SPACE /EXTRADURAL SPACE.
Epidural space is a potential space between the dura and the spinal canal.
Boundaries:Superiorly: foramen magnum, Inferiorly:
sacral hiatus, Anteriorly: posterior longitudinal ligament, Posteriorly : ligamentum flavum and Laterally: the pedicles and the intervertebra I foramina.
Contents:Nerve roots, fat, loose areolar tissue,
lymphatics and blood vessels which include the Batson’s venous plexus.
Significance of the epidural veins:They are valveless and form a
communication between the pelvic veins below and the intracranial veins above .They drain into the Inferior vena cava via the azygous veins. So any obstruction to the IVC leads to the distension of the epidural veins, thereby decreasing the epidural space and the requirement of the LA dose.
Width of the epidural space:Cervical:1-1.5mm,upper thoracic:2.5-
3mm,lower thoracic 4-5mm,lumbar5-6mm.
Plica mediana dorsalis:It is a septum in the epidural space
which divides the space into ventromedian and two dorsomaedian compartments and the failure of these to communicate freely leads to patchy analgesia.lt extends from the dura to the ligamentum flavum and leads to narrowing of the space and tenting of the dura.
Differences between cervical,thoracic and the lumbar epidural spaces:
The spinal canal in the thoracic space is
narrow and is completely occupied by the spinal cord, leading to the pushing of the dura against the ligamentum flavum.This decreases the margin of safety of the thoracic route as compared to the cervical and the lumbar routes in the midline approach.
Difference in the contents of the epidural space below 6 years of age:
The space has spongy,gelatinous lobules, in contrast to the densely packed fat globules and fibrous strands in adults. This leads to rapid longitudinal spread of the drug in this age group.
Pressure in the epidural space:Thoracic region = -1 cm of H20, Upper lumbar = -1 to -3 cm H20, Lower lumbar= -0.5cm H20.
ANATOMY OF THE SACRAL EPIDURAL SPACE:
Fig 4. The Sacral epidural space
Sacral hiatus:It is an inverted ‘V’ shaped opening
situated 3 to 5 cms from the coccyx or just beneath the superior gluteal cleft. It is formed due to the failure of fusion of the laminae of S4 and S5. It is covered by the sacrococcygeal membrane.
RACE 2003 Ramachandra Anaesthesia Continuing Education
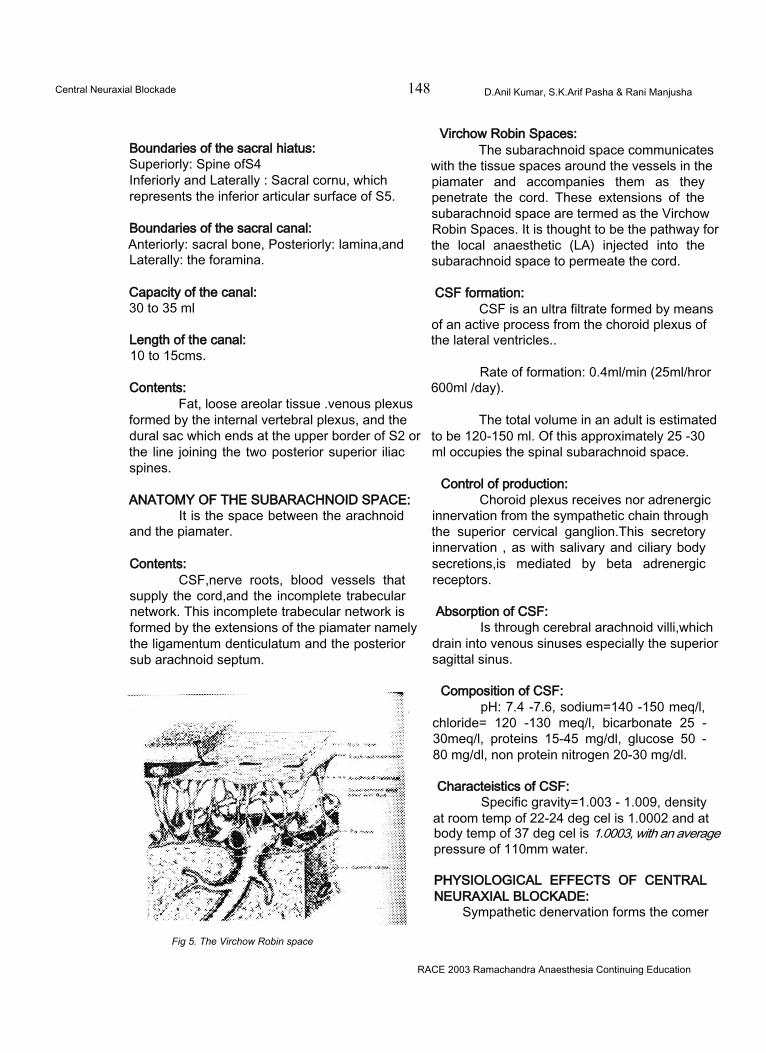
Central Neuraxial Blockade 148 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Boundaries of the sacral hiatus:Superiorly: Spine ofS4Inferiorly and Laterally : Sacral cornu, whichrepresents the inferior articular surface of S5.
Boundaries of the sacral canal:Anteriorly: sacral bone, Posteriorly: lamina,and Laterally: the foramina.
Capacity of the canal:30 to 35 ml
Length of the canal:10 to 15cms.
Contents:Fat, loose areolar tissue .venous plexus
formed by the internal vertebral plexus, and the dural sac which ends at the upper border of S2 or the line joining the two posterior superior iliac spines.
ANATOMY OF THE SUBARACHNOID SPACE:It is the space between the arachnoid
and the piamater.
Contents:CSF,nerve roots, blood vessels that
supply the cord,and the incomplete trabecular network. This incomplete trabecular network is formed by the extensions of the piamater namely the ligamentum denticulatum and the posterior sub arachnoid septum.
Fig 5. The Virchow Robin space
Virchow Robin Spaces:The subarachnoid space communicates
with the tissue spaces around the vessels in the piamater and accompanies them as they penetrate the cord. These extensions of the subarachnoid space are termed as the Virchow Robin Spaces. It is thought to be the pathway for the local anaesthetic (LA) injected into the subarachnoid space to permeate the cord.
CSF formation:CSF is an ultra filtrate formed by means
of an active process from the choroid plexus of the lateral ventricles..
Rate of formation: 0.4ml/min (25ml/hror 600ml /day).
The total volume in an adult is estimated to be 120-150 ml. Of this approximately 25 -30 ml occupies the spinal subarachnoid space.
Control of production:Choroid plexus receives nor adrenergic
innervation from the sympathetic chain through the superior cervical ganglion.This secretory innervation , as with salivary and ciliary body secretions,is mediated by beta adrenergic receptors.
Absorption of CSF:Is through cerebral arachnoid villi,which
drain into venous sinuses especially the superior sagittal sinus.
Composition of CSF:pH: 7.4 -7.6, sodium=140 -150 meq/l,
chloride= 120 -130 meq/l, bicarbonate 25 - 30meq/l, proteins 15-45 mg/dl, glucose 50 - 80 mg/dl, non protein nitrogen 20-30 mg/dl.
Characteistics of CSF:Specific gravity=1.003 - 1.009, density
at room temp of 22-24 deg cel is 1.0002 and at body temp of 37 deg cel is 1.0003, with an average pressure of 110mm water.
PHYSIOLOGICAL EFFECTS OF CENTRAL NEURAXIAL BLOCKADE:
Sympathetic denervation forms the comer
RACE 2003 Ramachandra Anaesthesia Continuing Education
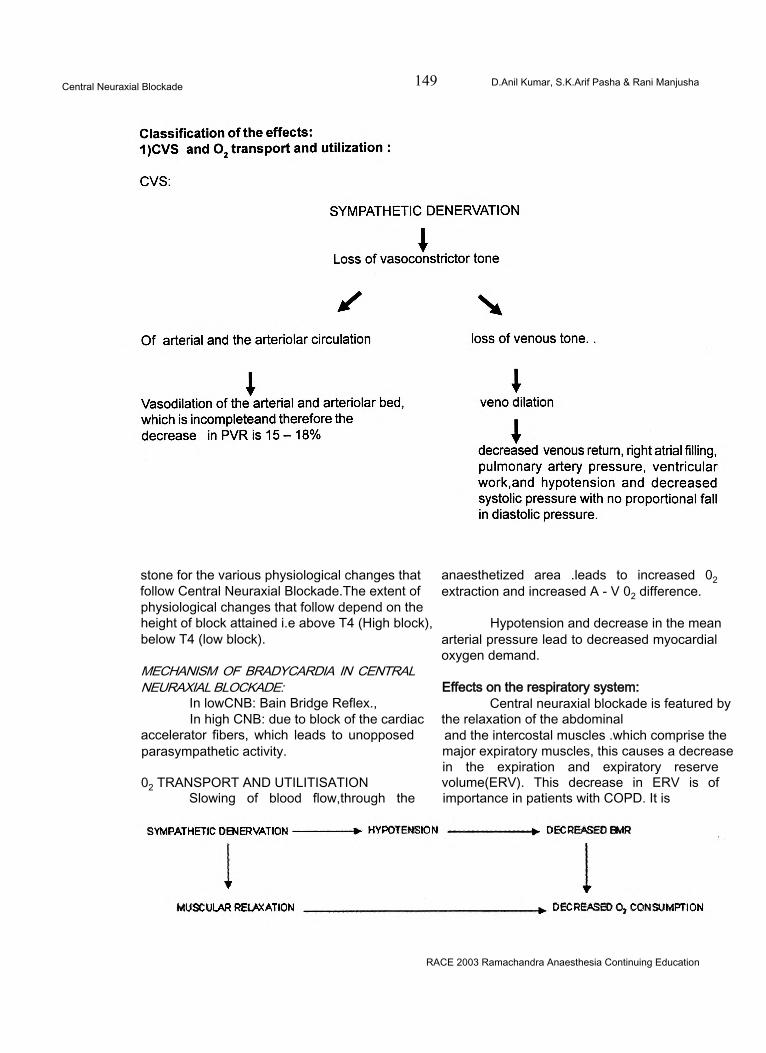
Central Neuraxial Blockade 149 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
stone for the various physiological changes that follow Central Neuraxial Blockade.The extent of physiological changes that follow depend on the height of block attained i.e above T4 (High block), below T4 (low block).
MECHANISM OF BRADYCARDIA IN CENTRAL NEURAXIAL BLOCKADE:
In lowCNB: Bain Bridge Reflex.,In high CNB: due to block of the cardiac
accelerator fibers, which leads to unopposed parasympathetic activity.
02 TRANSPORT AND UTILITISATIONSlowing of blood flow,through the
anaesthetized area .leads to increased 02 extraction and increased A - V 02 difference.
Hypotension and decrease in the mean arterial pressure lead to decreased myocardial oxygen demand.
Effects on the respiratory system:Central neuraxial blockade is featured by
the relaxation of the abdominal and the intercostal muscles .which comprise the major expiratory muscles, this causes a decrease in the expiration and expiratory reserve volume(ERV). This decrease in ERV is of importance in patients with COPD. It is
RACE 2003 Ramachandra Anaesthesia Continuing Education
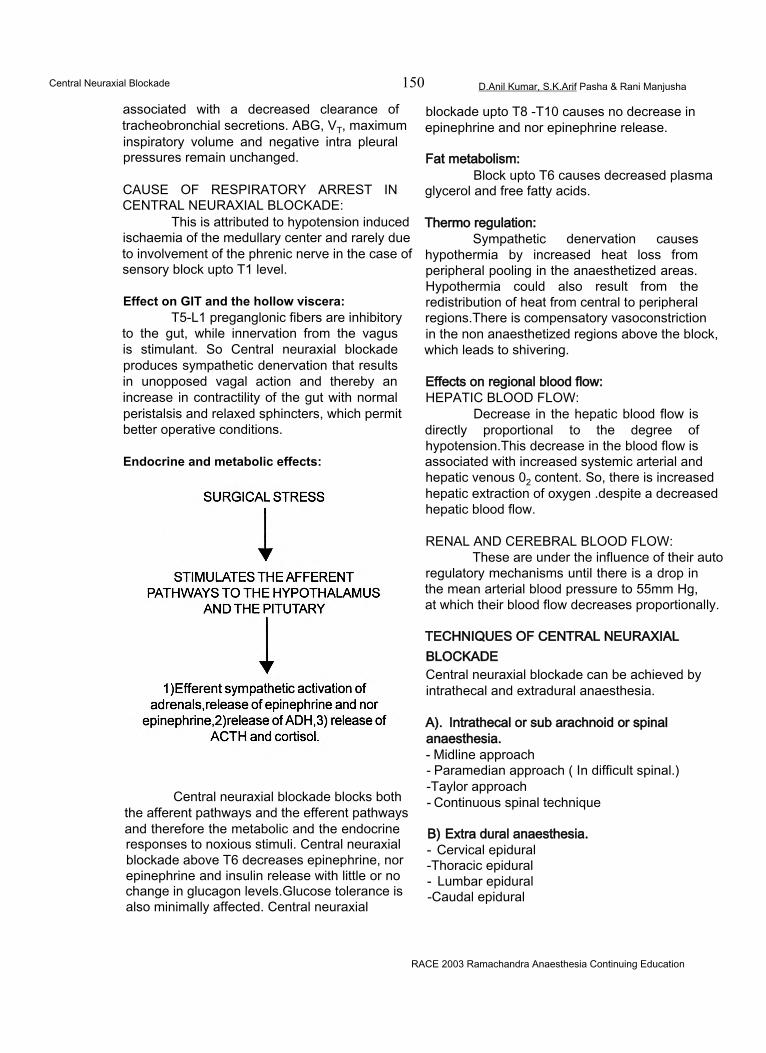
Central Neuraxial Blockade 150 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
associated with a decreased clearance of tracheobronchial secretions. ABG, VT, maximum inspiratory volume and negative intra pleural pressures remain unchanged.
CAUSE OF RESPIRATORY ARREST IN CENTRAL NEURAXIAL BLOCKADE:
This is attributed to hypotension induced ischaemia of the medullary center and rarely due to involvement of the phrenic nerve in the case of sensory block upto T1 level.
Effect on GIT and the hollow viscera:T5-L1 preganglonic fibers are inhibitory
to the gut, while innervation from the vagus is stimulant. So Central neuraxial blockade produces sympathetic denervation that results in unopposed vagal action and thereby an increase in contractility of the gut with normal peristalsis and relaxed sphincters, which permit better operative conditions.
Endocrine and metabolic effects:
Central neuraxial blockade blocks both the afferent pathways and the efferent pathways and therefore the metabolic and the endocrine responses to noxious stimuli. Central neuraxial blockade above T6 decreases epinephrine, nor epinephrine and insulin release with little or no change in glucagon levels.Glucose tolerance is also minimally affected. Central neuraxial
blockade upto T8 -T10 causes no decrease in epinephrine and nor epinephrine release.
Fat metabolism:Block upto T6 causes decreased plasma
glycerol and free fatty acids.
Thermo regulation:Sympathetic denervation causes
hypothermia by increased heat loss from peripheral pooling in the anaesthetized areas. Hypothermia could also result from the redistribution of heat from central to peripheral regions.There is compensatory vasoconstriction in the non anaesthetized regions above the block, which leads to shivering.
Effects on regional blood flow:HEPATIC BLOOD FLOW:
Decrease in the hepatic blood flow is directly proportional to the degree of hypotension.This decrease in the blood flow is associated with increased systemic arterial and hepatic venous 02 content. So, there is increased hepatic extraction of oxygen .despite a decreased hepatic blood flow.
RENAL AND CEREBRAL BLOOD FLOW:These are under the influence of their auto
regulatory mechanisms until there is a drop in the mean arterial blood pressure to 55mm Hg, at which their blood flow decreases proportionally.
TECHNIQUES OF CENTRAL NEURAXIAL BLOCKADECentral neuraxial blockade can be achieved by intrathecal and extradural anaesthesia.
A). Intrathecal or sub arachnoid or spinal anaesthesia.- Midline approach- Paramedian approach ( In difficult spinal.) -Taylor approach- Continuous spinal technique
B) Extra dural anaesthesia.- Cervical epidural -Thoracic epidural- Lumbar epidural -Caudal epidural
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 151 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
C) Combined epidural and spinal anaesthesia.
INDICATIONS:1. Intraoperatively:
• Anaesthesia for lower limb surgeries, perineal procedures and Caesarean section
• ,To provide controlled hypotension
2. For providing analgesia:• Post-operative analgesia• Obstetric analgesia• For relief of intractable pain as in
crush injury chest (Relief from pain reduces paradoxical respiration and allows the patient to clear the lower airways by coughing freely) and lumbar disc lesions (for relief of sciatic pain).
CONTRAINDICATIONS:Absolute:1. Patient refusal.2. Localised infection / Generalised infection.3. Raised ICP / Active CNS disease.4. Coagulation disorders5. Sensitivity to local anaesthetic drugs6. Severe blood loss / shock.
Relative:1. Severe headache / backache2. Medicolegal conditions3. Diseases of the spinal column (arthritis,
metastasis, osteoporosis)4. Blood in CSF - failure to clear after 10 to 15ml
of aspiration.5. Inability to achieve placement of needle after
3 attempts6. Neurological diseases or simulators(residual
paralysis, poliomyelitis).
EQUIPMENT:Spinal needlesThe standard spinal needle consists of 3 parts:1. Hub2. Cannula and3. Stylet with sizes varying from 18 to 29 gauge.
The various needles are/1. Quincke - Babcock needle2. Pitkin needle3. Greene needle
4. Whitacre needle5. Tuohy needle6. Sprotte needle
Epidural needles:1. Tuohy needle with huber point2. Crawford point needle3. Husted needle - modified Tuohy needle with a
rounded tip and bevel opening.
The Spinal, epidural or caudal anaesthesia is preceeded by a preanaesthetic checkup of the patients with examination of the spine, airway and othersystems. On the day of surgery, IV access should be secured. Premedication should be given depending on the patient or circumstances. Preloading is done by adequate volume of fluid infusion if necessary. Patient should be positioned .The area of puncture should be cleaned with antiseptic solution and draped. We can now proceed with our anaesthetic technique.
Drugs:Along with local anaesthetics, other
groups of drugs can also be used for central neuraxial blockade.
TECHNIQUE:Spinal anaesthesia:
Dural puncture can be done in the lateral flexed or sitting position at the widest interspinous space or at the desired space, usually through the midline approach. In difficult cases and in old patients, the paramedian approach can be selected. Needle in the subarachnoid space is confirmed by loss of resistance and aspiration of CSF.
Continuous spinal technique:-In earlier days CSA was achieved by
malleable needle insertion into the dural sac, which is called LEMMON technique.
Tuohy technique:Introduction of wide bore spinal needle
into the dural sac and insertion of micro catheter into the subarachnoid space. This procedure is associated with a lot of complications like :1. Breaking of catheter 2. Kinking of catheter etc.,
Epidural anaesthetic technique:
RACE 2003 Ramachandra Anaesthesia Continuing Education
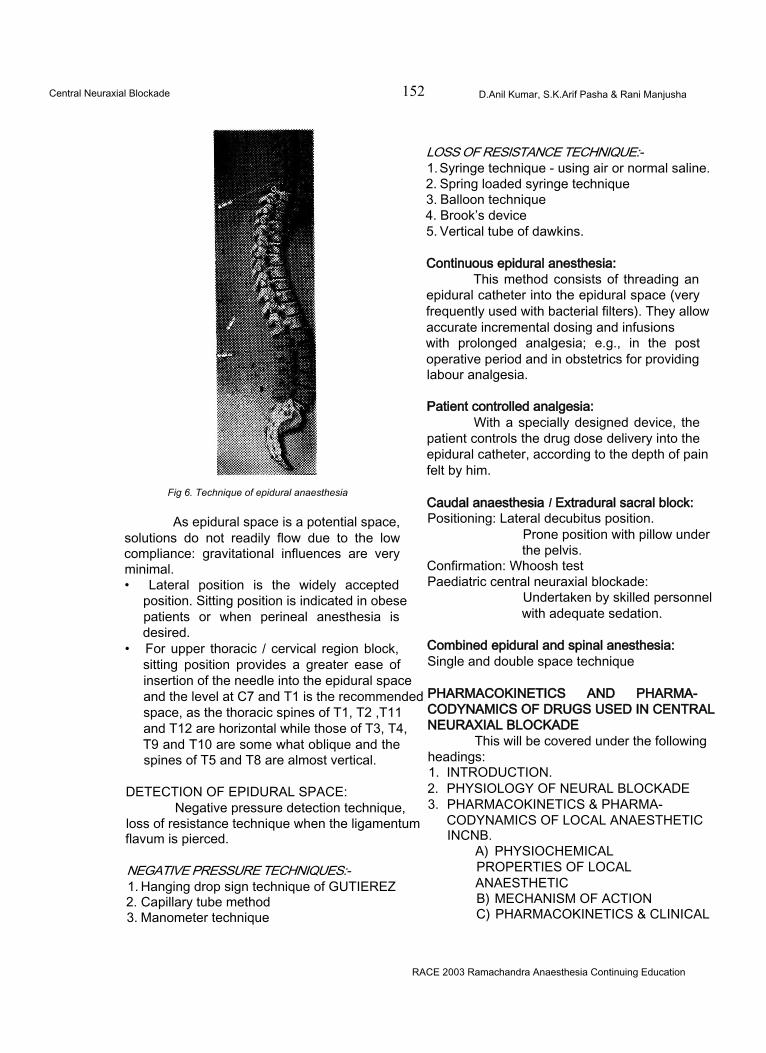
Central Neuraxial Blockade 152 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Fig 6. Technique of epidural anaesthesia
As epidural space is a potential space, solutions do not readily flow due to the low compliance: gravitational influences are very minimal.• Lateral position is the widely accepted
position. Sitting position is indicated in obese patients or when perineal anesthesia is desired.
• For upper thoracic / cervical region block, sitting position provides a greater ease of insertion of the needle into the epidural space and the level at C7 and T1 is the recommended space, as the thoracic spines of T1, T2 ,T11 and T12 are horizontal while those of T3, T4, T9 and T10 are some what oblique and the spines of T5 and T8 are almost vertical.
DETECTION OF EPIDURAL SPACE:Negative pressure detection technique,
loss of resistance technique when the ligamentum flavum is pierced.
NEGATIVE PRESSURE TECHNIQUES:-1. Hanging drop sign technique of GUTIEREZ2. Capillary tube method3. Manometer technique
LOSS OF RESISTANCE TECHNIQUE:-1. Syringe technique - using air or normal saline.2. Spring loaded syringe technique3. Balloon technique4. Brook’s device5. Vertical tube of dawkins.
Continuous epidural anesthesia:This method consists of threading an
epidural catheter into the epidural space (very frequently used with bacterial filters). They allow accurate incremental dosing and infusions with prolonged analgesia; e.g., in the post operative period and in obstetrics for providing labour analgesia.
Patient controlled analgesia:With a specially designed device, the
patient controls the drug dose delivery into the epidural catheter, according to the depth of pain felt by him.
Caudal anaesthesia I Extradural sacral block:Positioning: Lateral decubitus position.
Prone position with pillow under the pelvis.
Confirmation: Whoosh test Paediatric central neuraxial blockade:
Undertaken by skilled personnel with adequate sedation.
Combined epidural and spinal anesthesia:Single and double space technique
PHARMACOKINETICS AND PHARMACODYNAMICS OF DRUGS USED IN CENTRAL NEURAXIAL BLOCKADE
This will be covered under the following headings:1. INTRODUCTION.2. PHYSIOLOGY OF NEURAL BLOCKADE3. PHARMACOKINETICS & PHARMA
CODYNAMICS OF LOCAL ANAESTHETIC INCNB.
A) PHYSIOCHEMICAL PROPERTIES OF LOCAL ANAESTHETICB) MECHANISM OF ACTIONC) PHARMACOKINETICS & CLINICAL
RACE 2003 Ramachandra Anaesthesia Continuing Education
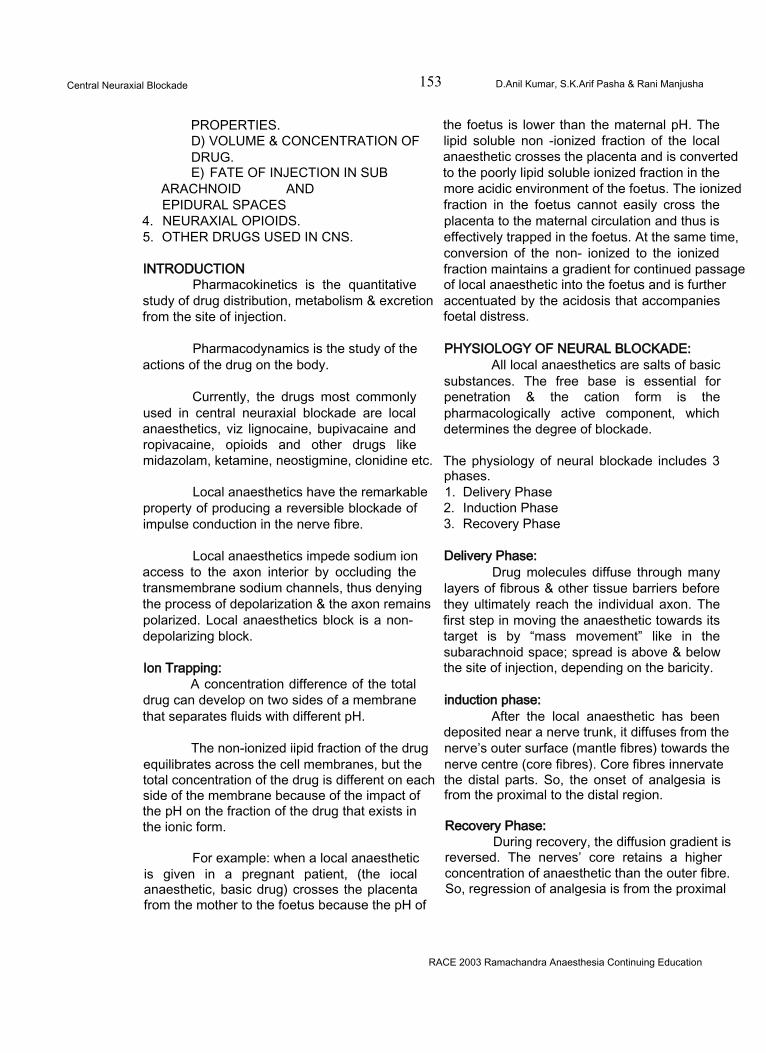
Central Neuraxial Blockade 153 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
PROPERTIES.D) VOLUME & CONCENTRATION OFDRUG.E) FATE OF INJECTION IN SUB
ARACHNOID AND EPIDURAL SPACES
4. NEURAXIAL OPIOIDS.5. OTHER DRUGS USED IN CNS.
INTRODUCTIONPharmacokinetics is the quantitative
study of drug distribution, metabolism & excretion from the site of injection.
Pharmacodynamics is the study of the actions of the drug on the body.
Currently, the drugs most commonly used in central neuraxial blockade are local anaesthetics, viz lignocaine, bupivacaine and ropivacaine, opioids and other drugs like midazolam, ketamine, neostigmine, clonidine etc.
Local anaesthetics have the remarkable property of producing a reversible blockade of impulse conduction in the nerve fibre.
Local anaesthetics impede sodium ion access to the axon interior by occluding the transmembrane sodium channels, thus denying the process of depolarization & the axon remains polarized. Local anaesthetics block is a nondepolarizing block.
Ion Trapping:A concentration difference of the total
drug can develop on two sides of a membrane that separates fluids with different pH.
The non-ionized iipid fraction of the drug equilibrates across the cell membranes, but the total concentration of the drug is different on each side of the membrane because of the impact of the pH on the fraction of the drug that exists in the ionic form.
For example: when a local anaesthetic is given in a pregnant patient, (the iocal anaesthetic, basic drug) crosses the placenta from the mother to the foetus because the pH of
the foetus is lower than the maternal pH. The lipid soluble non -ionized fraction of the local anaesthetic crosses the placenta and is converted to the poorly lipid soluble ionized fraction in the more acidic environment of the foetus. The ionized fraction in the foetus cannot easily cross the placenta to the maternal circulation and thus is effectively trapped in the foetus. At the same time, conversion of the non- ionized to the ionized fraction maintains a gradient for continued passage of local anaesthetic into the foetus and is further accentuated by the acidosis that accompanies foetal distress.
PHYSIOLOGY OF NEURAL BLOCKADE:All local anaesthetics are salts of basic
substances. The free base is essential for penetration & the cation form is the pharmacologically active component, which determines the degree of blockade.
The physiology of neural blockade includes 3 phases.1. Delivery Phase2. Induction Phase3. Recovery Phase
Delivery Phase:Drug molecules diffuse through many
layers of fibrous & other tissue barriers before they ultimately reach the individual axon. The first step in moving the anaesthetic towards its target is by “mass movement” like in the subarachnoid space; spread is above & below the site of injection, depending on the baricity.
induction phase:After the local anaesthetic has been
deposited near a nerve trunk, it diffuses from the nerve’s outer surface (mantle fibres) towards the nerve centre (core fibres). Core fibres innervate the distal parts. So, the onset of analgesia is from the proximal to the distal region.
Recovery Phase:During recovery, the diffusion gradient is
reversed. The nerves’ core retains a higher concentration of anaesthetic than the outer fibre. So, regression of analgesia is from the proximal
RACE 2003 Ramachandra Anaesthesia Continuing Education
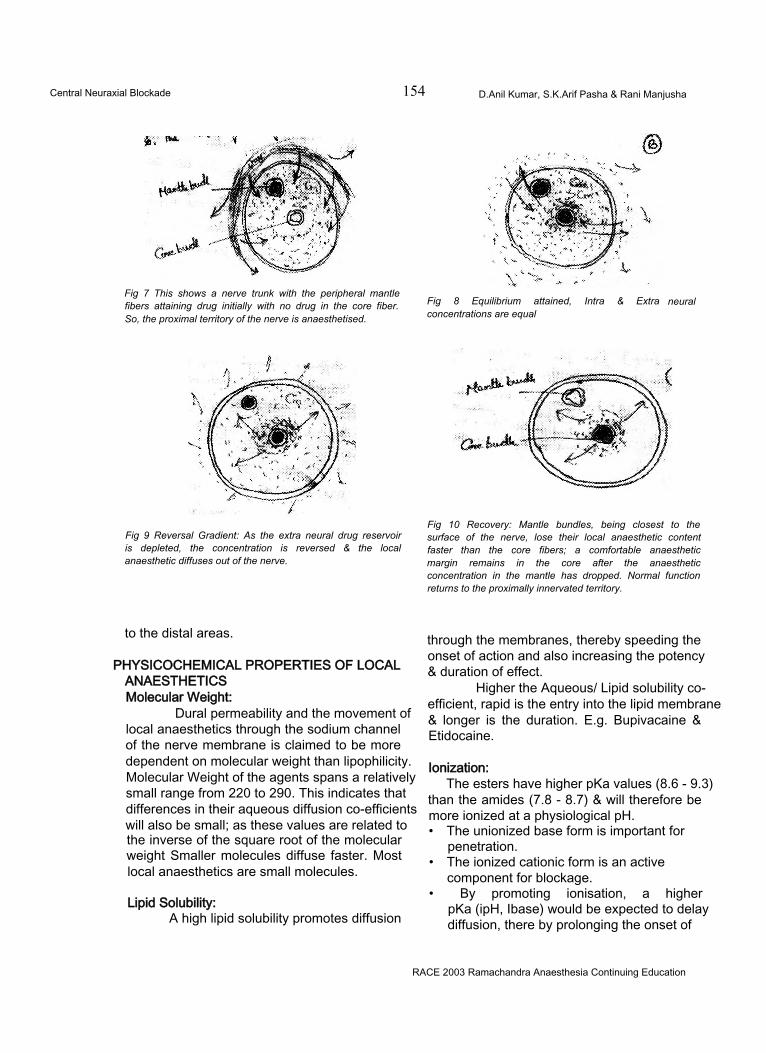
Central Neuraxial Blockade 154 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Fig 7 This shows a nerve trunk with the peripheral mantle fibers attaining drug initially with no drug in the core fiber. So, the proximal territory of the nerve is anaesthetised.
Fig 8 Equilibrium attained, Intra & Extra concentrations are equal
neural
Fig 9 Reversal Gradient: As the extra neural drug reservoir is depleted, the concentration is reversed & the local anaesthetic diffuses out of the nerve.
Fig 10 Recovery: Mantle bundles, being closest to the surface of the nerve, lose their local anaesthetic content faster than the core fibers; a comfortable anaesthetic margin remains in the core after the anaesthetic concentration in the mantle has dropped. Normal function returns to the proximally innervated territory.
to the distal areas.
PHYSICOCHEMICAL PROPERTIES OF LOCALANAESTHETICSMolecular Weight:
Dural permeability and the movement of local anaesthetics through the sodium channel of the nerve membrane is claimed to be more dependent on molecular weight than lipophilicity. Molecular Weight of the agents spans a relatively small range from 220 to 290. This indicates that differences in their aqueous diffusion co-efficients will also be small; as these values are related to the inverse of the square root of the molecular weight Smaller molecules diffuse faster. Most local anaesthetics are small molecules.
Lipid Solubility:A high lipid solubility promotes diffusion
through the membranes, thereby speeding the onset of action and also increasing the potency & duration of effect.
Higher the Aqueous/ Lipid solubility coefficient, rapid is the entry into the lipid membrane & longer is the duration. E.g. Bupivacaine & Etidocaine.
Ionization:The esters have higher pKa values (8.6 - 9.3)
than the amides (7.8 - 8.7) & will therefore be more ionized at a physiological pH.• The unionized base form is important for
penetration.• The ionized cationic form is an active
component for blockage.• By promoting ionisation, a higher
pKa (ipH, Ibase) would be expected to delay diffusion, there by prolonging the onset of
RACE 2003 Ramachandra Anaesthesia Continuing Education
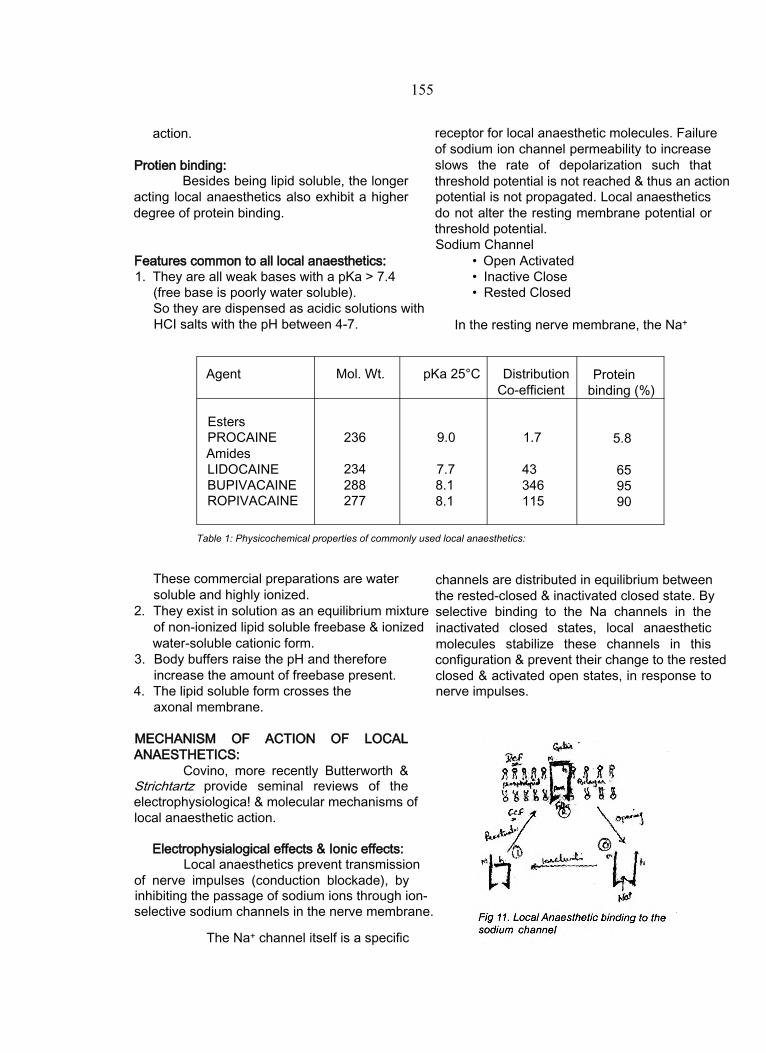
155
action.
Protien binding:Besides being lipid soluble, the longer
acting local anaesthetics also exhibit a higher degree of protein binding.
Features common to all local anaesthetics:1. They are all weak bases with a pKa > 7.4
(free base is poorly water soluble).So they are dispensed as acidic solutions with HCI salts with the pH between 4-7.
receptor for local anaesthetic molecules. Failure of sodium ion channel permeability to increase slows the rate of depolarization such that threshold potential is not reached & thus an action potential is not propagated. Local anaesthetics do not alter the resting membrane potential or threshold potential.Sodium Channel
• Open Activated• Inactive Close• Rested Closed
In the resting nerve membrane, the Na+
Agent Mol. Wt. pKa 25°C DistributionCo-efficient
Protein binding (%)
EstersPROCAINE 236 9.0 1.7 5.8AmidesLIDOCAINE 234 7.7 43 65BUPIVACAINE 288 8.1 346 95ROPIVACAINE 277 8.1 115 90
Table 1: Physicochemical properties of commonly used local anaesthetics:
These commercial preparations are water soluble and highly ionized.
2. They exist in solution as an equilibrium mixture of non-ionized lipid soluble freebase & ionized water-soluble cationic form.
3. Body buffers raise the pH and therefore increase the amount of freebase present.
4. The lipid soluble form crosses the axonal membrane.
channels are distributed in equilibrium between the rested-closed & inactivated closed state. By selective binding to the Na channels in the inactivated closed states, local anaesthetic molecules stabilize these channels in this configuration & prevent their change to the rested closed & activated open states, in response to nerve impulses.
MECHANISM OF ACTION OF LOCAL ANAESTHETICS:
Covino, more recently Butterworth & Strichtartz provide seminal reviews of the electrophysiologica! & molecular mechanisms of local anaesthetic action.
Electrophysialogical effects & Ionic effects:Local anaesthetics prevent transmission
of nerve impulses (conduction blockade), by inhibiting the passage of sodium ions through ion- selective sodium channels in the nerve membrane.
The Na+ channel itself is a specific
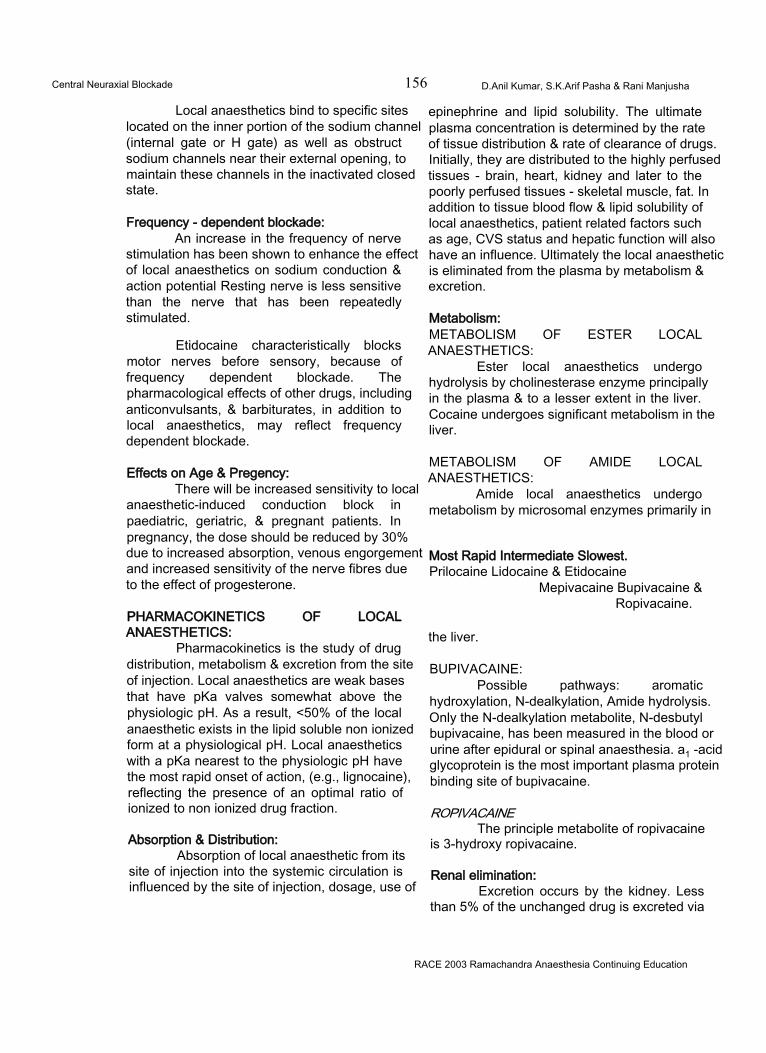
Central Neuraxial Blockade 156 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Local anaesthetics bind to specific sites located on the inner portion of the sodium channel (internal gate or H gate) as well as obstruct sodium channels near their external opening, to maintain these channels in the inactivated closed state.
Frequency - dependent blockade:An increase in the frequency of nerve
stimulation has been shown to enhance the effect of local anaesthetics on sodium conduction & action potential Resting nerve is less sensitive than the nerve that has been repeatedly stimulated.
Etidocaine characteristically blocks motor nerves before sensory, because of frequency dependent blockade. The pharmacological effects of other drugs, including anticonvulsants, & barbiturates, in addition to local anaesthetics, may reflect frequency dependent blockade.
Effects on Age & Pregency:There will be increased sensitivity to local
anaesthetic-induced conduction block in paediatric, geriatric, & pregnant patients. In pregnancy, the dose should be reduced by 30% due to increased absorption, venous engorgement and increased sensitivity of the nerve fibres due to the effect of progesterone.
PHARMACOKINETICS OF LOCAL ANAESTHETICS:
Pharmacokinetics is the study of drug distribution, metabolism & excretion from the site of injection. Local anaesthetics are weak bases that have pKa valves somewhat above the physiologic pH. As a result, <50% of the local anaesthetic exists in the lipid soluble non ionized form at a physiological pH. Local anaesthetics with a pKa nearest to the physiologic pH have the most rapid onset of action, (e.g., lignocaine), reflecting the presence of an optimal ratio of ionized to non ionized drug fraction.
Absorption & Distribution:Absorption of local anaesthetic from its
site of injection into the systemic circulation is influenced by the site of injection, dosage, use of
epinephrine and lipid solubility. The ultimate plasma concentration is determined by the rate of tissue distribution & rate of clearance of drugs. Initially, they are distributed to the highly perfused tissues - brain, heart, kidney and later to the poorly perfused tissues - skeletal muscle, fat. In addition to tissue blood flow & lipid solubility of local anaesthetics, patient related factors such as age, CVS status and hepatic function will also have an influence. Ultimately the local anaesthetic is eliminated from the plasma by metabolism & excretion.
Metabolism:METABOLISM OF ESTER LOCAL ANAESTHETICS:
Ester local anaesthetics undergo hydrolysis by cholinesterase enzyme principally in the plasma & to a lesser extent in the liver. Cocaine undergoes significant metabolism in the liver.
METABOLISM OF AMIDE LOCAL ANAESTHETICS:
Amide local anaesthetics undergo metabolism by microsomal enzymes primarily in
Most Rapid Intermediate Slowest.Prilocaine Lidocaine & Etidocaine
Mepivacaine Bupivacaine & Ropivacaine.
the liver.
BUPIVACAINE:Possible pathways: aromatic
hydroxylation, N-dealkylation, Amide hydrolysis. Only the N-dealkylation metabolite, N-desbutyl bupivacaine, has been measured in the blood or urine after epidural or spinal anaesthesia. a1 -acid glycoprotein is the most important plasma protein binding site of bupivacaine.
ROPIVACAINEThe principle metabolite of ropivacaine
is 3-hydroxy ropivacaine.
Renal elimination:Excretion occurs by the kidney. Less
than 5% of the unchanged drug is excreted via
RACE 2003 Ramachandra Anaesthesia Continuing Education
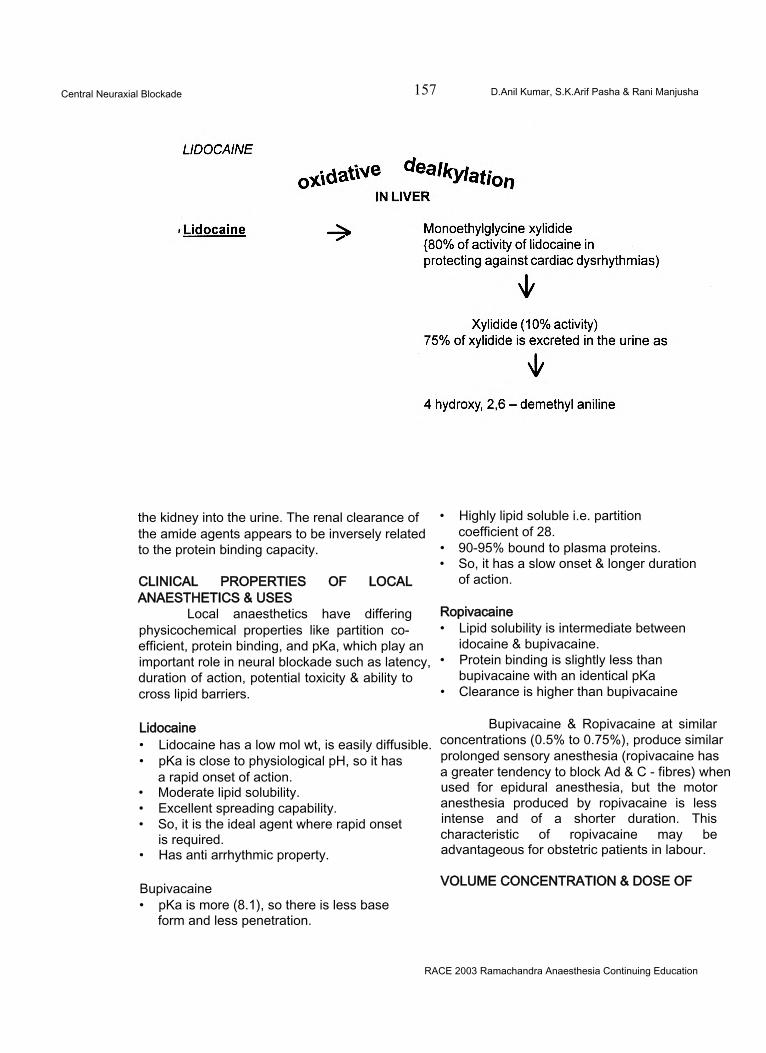
Central Neuraxial Blockade 157 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
the kidney into the urine. The renal clearance of the amide agents appears to be inversely related to the protein binding capacity.
CLINICAL PROPERTIES OF LOCAL ANAESTHETICS & USES
Local anaesthetics have differing physicochemical properties like partition coefficient, protein binding, and pKa, which play an important role in neural blockade such as latency, duration of action, potential toxicity & ability to cross lipid barriers.
Lidocaine• Lidocaine has a low mol wt, is easily diffusible.• pKa is close to physiological pH, so it has
a rapid onset of action.• Moderate lipid solubility.• Excellent spreading capability.• So, it is the ideal agent where rapid onset
is required.• Has anti arrhythmic property.
Bupivacaine• pKa is more (8.1), so there is less base
form and less penetration.
• Highly lipid soluble i.e. partition coefficient of 28.
• 90-95% bound to plasma proteins.• So, it has a slow onset & longer duration
of action.
Ropivacaine• Lipid solubility is intermediate between
idocaine & bupivacaine.• Protein binding is slightly less than
bupivacaine with an identical pKa• Clearance is higher than bupivacaine
Bupivacaine & Ropivacaine at similar concentrations (0.5% to 0.75%), produce similar prolonged sensory anesthesia (ropivacaine has a greater tendency to block Ad & C - fibres) when used for epidural anesthesia, but the motor anesthesia produced by ropivacaine is less intense and of a shorter duration. This characteristic of ropivacaine may be advantageous for obstetric patients in labour.
VOLUME CONCENTRATION & DOSE OF
RACE 2003 Ramachandra Anaesthesia Continuing Education
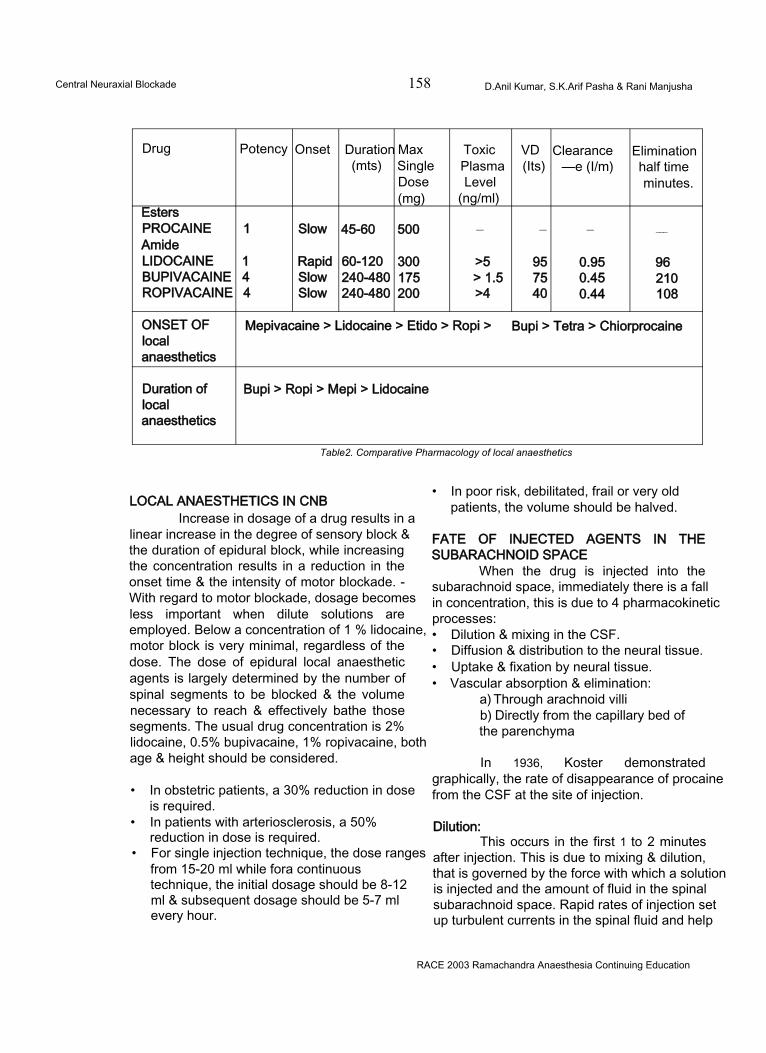
Central Neuraxial Blockade 158 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Drug Potency Onset Duration Max Toxic VD Clearance Elimination(mts) Single Plasma (Its) —e (I/m) half time
Dose Level minutes.(mg) (ng/ml)
EstersPROCAINE 1 Slow 45-60 500 — — — ___
AmideLIDOCAINE 1 Rapid 60-120 300 >5 95 0.95 96BUPIVACAINE 4 Slow 240-480 175 > 1.5 75 0.45 210ROPIVACAINE 4 Slow 240-480 200 >4 40 0.44 108
ONSET OF Mepivacaine > Lidocaine > Etido > Ropi > Bupi > Tetra > Chiorprocainelocalanaesthetics
Duration of Bupi > Ropi > Mepi > Lidocainelocalanaesthetics
Table2. Comparative Pharmacology of local anaesthetics
LOCAL ANAESTHETICS IN CNBIncrease in dosage of a drug results in a
linear increase in the degree of sensory block & the duration of epidural block, while increasing the concentration results in a reduction in the onset time & the intensity of motor blockade. - With regard to motor blockade, dosage becomes less important when dilute solutions are employed. Below a concentration of 1 % lidocaine, motor block is very minimal, regardless of the dose. The dose of epidural local anaesthetic agents is largely determined by the number of spinal segments to be blocked & the volume necessary to reach & effectively bathe those segments. The usual drug concentration is 2% lidocaine, 0.5% bupivacaine, 1% ropivacaine, both age & height should be considered.
• In obstetric patients, a 30% reduction in dose is required.
• In patients with arteriosclerosis, a 50% reduction in dose is required.
• For single injection technique, the dose ranges from 15-20 ml while fora continuous technique, the initial dosage should be 8-12 ml & subsequent dosage should be 5-7 ml every hour.
• In poor risk, debilitated, frail or very old patients, the volume should be halved.
FATE OF INJECTED AGENTS IN THE SUBARACHNOID SPACE
When the drug is injected into the subarachnoid space, immediately there is a fall in concentration, this is due to 4 pharmacokinetic processes:• Dilution & mixing in the CSF.• Diffusion & distribution to the neural tissue.• Uptake & fixation by neural tissue.• Vascular absorption & elimination:
a) Through arachnoid villib) Directly from the capillary bed of the parenchyma
In 1936, Koster demonstrated graphically, the rate of disappearance of procaine from the CSF at the site of injection.
Dilution:This occurs in the first 1 to 2 minutes
after injection. This is due to mixing & dilution, that is governed by the force with which a solution is injected and the amount of fluid in the spinal subarachnoid space. Rapid rates of injection set up turbulent currents in the spinal fluid and help
RACE 2003 Ramachandra Anaesthesia Continuing Education
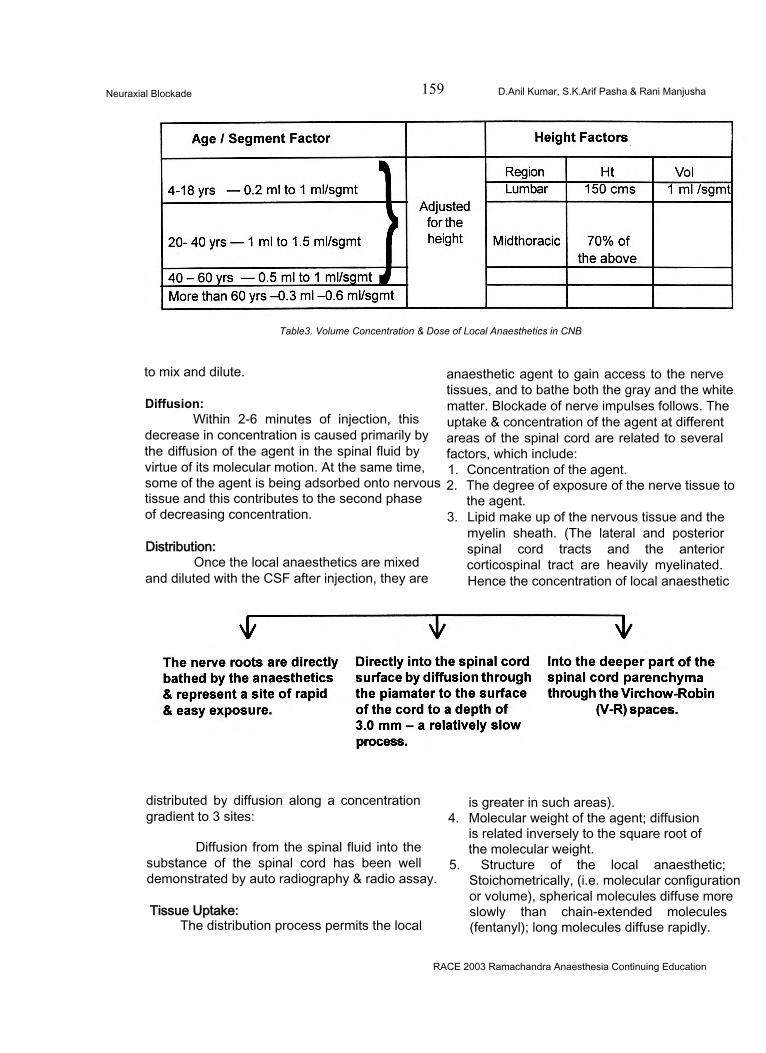
Neuraxial Blockade 159 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Table3. Volume Concentration & Dose of Local Anaesthetics in CNB
to mix and dilute.
Diffusion:Within 2-6 minutes of injection, this
decrease in concentration is caused primarily by the diffusion of the agent in the spinal fluid by virtue of its molecular motion. At the same time, some of the agent is being adsorbed onto nervous tissue and this contributes to the second phase of decreasing concentration.
Distribution:Once the local anaesthetics are mixed
and diluted with the CSF after injection, they are
anaesthetic agent to gain access to the nerve tissues, and to bathe both the gray and the white matter. Blockade of nerve impulses follows. The uptake & concentration of the agent at different areas of the spinal cord are related to several factors, which include:1. Concentration of the agent.2. The degree of exposure of the nerve tissue to
the agent.3. Lipid make up of the nervous tissue and the
myelin sheath. (The lateral and posterior spinal cord tracts and the anterior corticospinal tract are heavily myelinated. Hence the concentration of local anaesthetic
distributed by diffusion along a concentration gradient to 3 sites:
Diffusion from the spinal fluid into the substance of the spinal cord has been well demonstrated by auto radiography & radio assay.
Tissue Uptake:The distribution process permits the local
is greater in such areas).4. Molecular weight of the agent; diffusion
is related inversely to the square root of the molecular weight.
5. Structure of the local anaesthetic; Stoichometrically, (i.e. molecular configuration or volume), spherical molecules diffuse more slowly than chain-extended molecules (fentanyl); long molecules diffuse rapidly.
RACE 2003 Ramachandra Anaesthesia Continuing Education
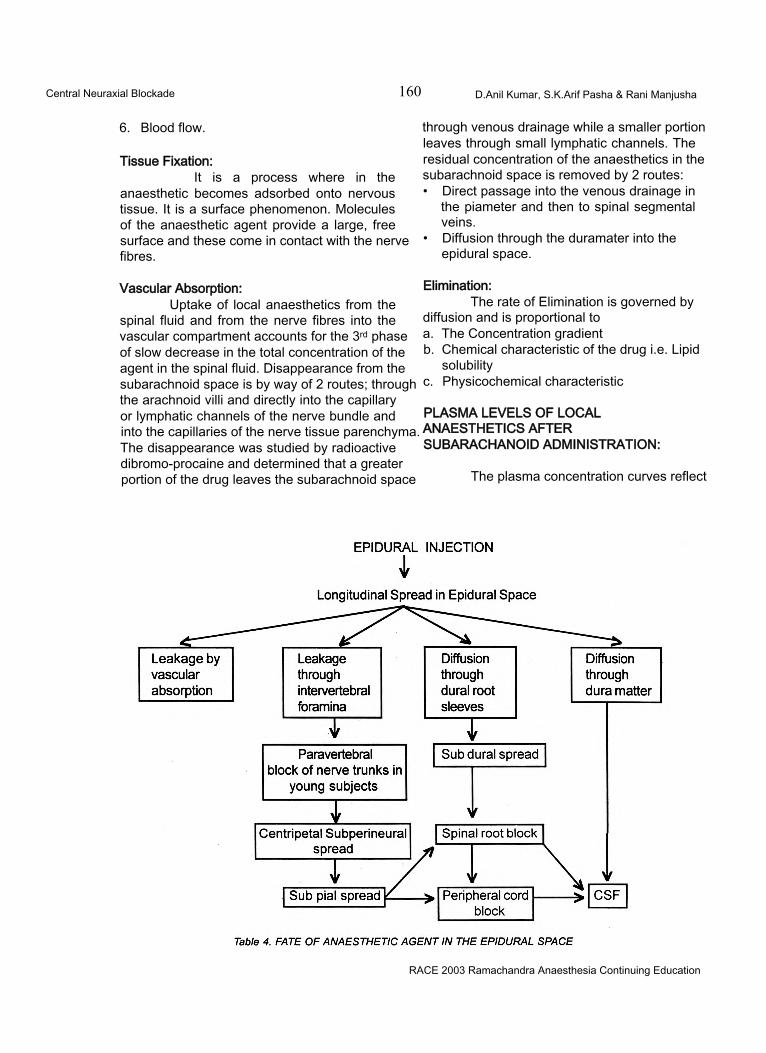
Central Neuraxial Blockade 160 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
6. Blood flow.
Tissue Fixation:It is a process where in the
anaesthetic becomes adsorbed onto nervous tissue. It is a surface phenomenon. Molecules of the anaesthetic agent provide a large, free surface and these come in contact with the nerve fibres.
Vascular Absorption:Uptake of local anaesthetics from the
spinal fluid and from the nerve fibres into the vascular compartment accounts for the 3rd phase of slow decrease in the total concentration of the agent in the spinal fluid. Disappearance from the subarachnoid space is by way of 2 routes; through the arachnoid villi and directly into the capillary or lymphatic channels of the nerve bundle and into the capillaries of the nerve tissue parenchyma. The disappearance was studied by radioactive dibromo-procaine and determined that a greater portion of the drug leaves the subarachnoid space
through venous drainage while a smaller portion leaves through small lymphatic channels. The residual concentration of the anaesthetics in the subarachnoid space is removed by 2 routes:• Direct passage into the venous drainage in
the piameter and then to spinal segmental veins.
• Diffusion through the duramater into the epidural space.
Elimination:The rate of Elimination is governed by
diffusion and is proportional toa. The Concentration gradientb. Chemical characteristic of the drug i.e. Lipid
solubilityc. Physicochemical characteristic
PLASMA LEVELS OF LOCAL ANAESTHETICS AFTER SUBARACHANOID ADMINISTRATION:
The plasma concentration curves reflect
RACE 2003 Ramachandra Anaesthesia Continuing Education
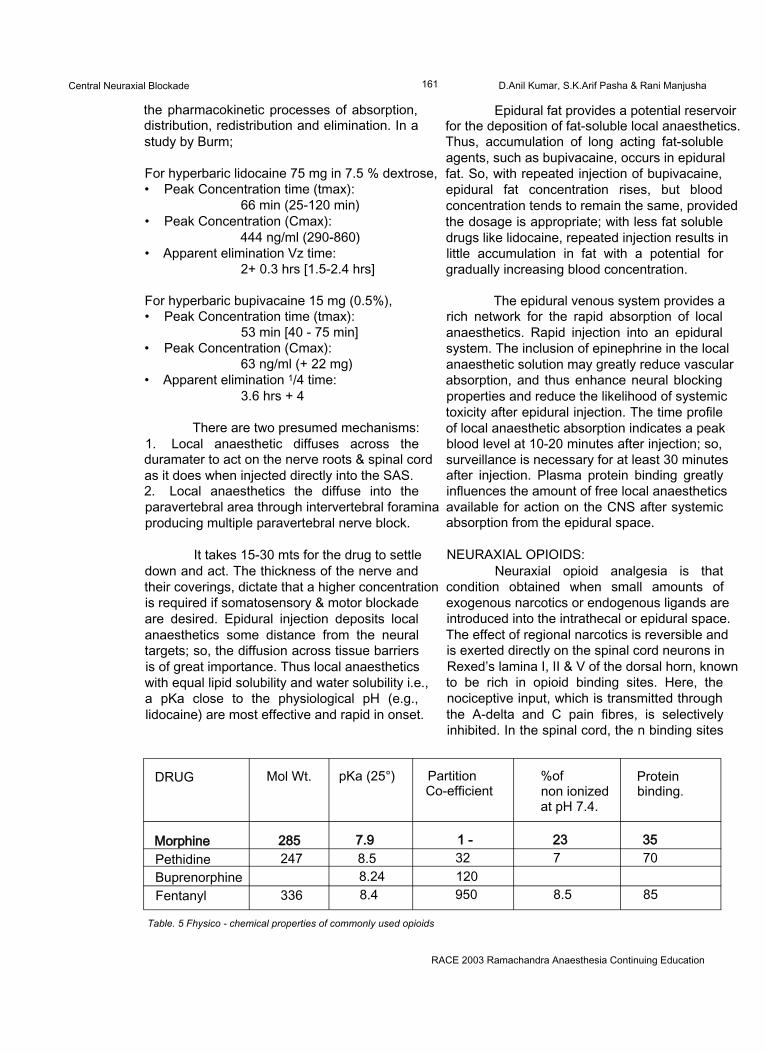
Central Neuraxial Blockade 161 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
the pharmacokinetic processes of absorption, distribution, redistribution and elimination. In a study by Burm;
For hyperbaric lidocaine 75 mg in 7.5 % dextrose,• Peak Concentration time (tmax):
66 min (25-120 min)• Peak Concentration (Cmax):
444 ng/ml (290-860)• Apparent elimination Vz time:
2+ 0.3 hrs [1.5-2.4 hrs]
For hyperbaric bupivacaine 15 mg (0.5%),• Peak Concentration time (tmax):
53 min [40 - 75 min]• Peak Concentration (Cmax):
63 ng/ml (+ 22 mg)• Apparent elimination 1/4 time:
3.6 hrs + 4
There are two presumed mechanisms:1. Local anaesthetic diffuses across the duramater to act on the nerve roots & spinal cord as it does when injected directly into the SAS.2. Local anaesthetics the diffuse into the paravertebral area through intervertebral foramina producing multiple paravertebral nerve block.
It takes 15-30 mts for the drug to settle down and act. The thickness of the nerve and their coverings, dictate that a higher concentration is required if somatosensory & motor blockade are desired. Epidural injection deposits local anaesthetics some distance from the neural targets; so, the diffusion across tissue barriers is of great importance. Thus local anaesthetics with equal lipid solubility and water solubility i.e., a pKa close to the physiological pH (e.g., lidocaine) are most effective and rapid in onset.
Epidural fat provides a potential reservoir for the deposition of fat-soluble local anaesthetics. Thus, accumulation of long acting fat-soluble agents, such as bupivacaine, occurs in epidural fat. So, with repeated injection of bupivacaine, epidural fat concentration rises, but blood concentration tends to remain the same, provided the dosage is appropriate; with less fat soluble drugs like lidocaine, repeated injection results in little accumulation in fat with a potential for gradually increasing blood concentration.
The epidural venous system provides a rich network for the rapid absorption of local anaesthetics. Rapid injection into an epidural system. The inclusion of epinephrine in the local anaesthetic solution may greatly reduce vascular absorption, and thus enhance neural blocking properties and reduce the likelihood of systemic toxicity after epidural injection. The time profile of local anaesthetic absorption indicates a peak blood level at 10-20 minutes after injection; so, surveillance is necessary for at least 30 minutes after injection. Plasma protein binding greatly influences the amount of free local anaesthetics available for action on the CNS after systemic absorption from the epidural space.
NEURAXIAL OPIOIDS:Neuraxial opioid analgesia is that
condition obtained when small amounts of exogenous narcotics or endogenous ligands are introduced into the intrathecal or epidural space. The effect of regional narcotics is reversible and is exerted directly on the spinal cord neurons in Rexed’s lamina I, II & V of the dorsal horn, known to be rich in opioid binding sites. Here, the nociceptive input, which is transmitted through the A-delta and C pain fibres, is selectively inhibited. In the spinal cord, the n binding sites
DRUG Mol Wt. pKa (25°) PartitionCo-efficient
%ofnon ionized at pH 7.4.
Proteinbinding.
Morphine 285 7.9 1 - 23 35Pethidine 247 8.5 32 7 70Buprenorphine 8.24 120Fentanyl 336 8.4 950 8.5 85
Table. 5 Fhysico - chemical properties of commonly used opioids
RACE 2003 Ramachandra Anaesthesia Continuing Education
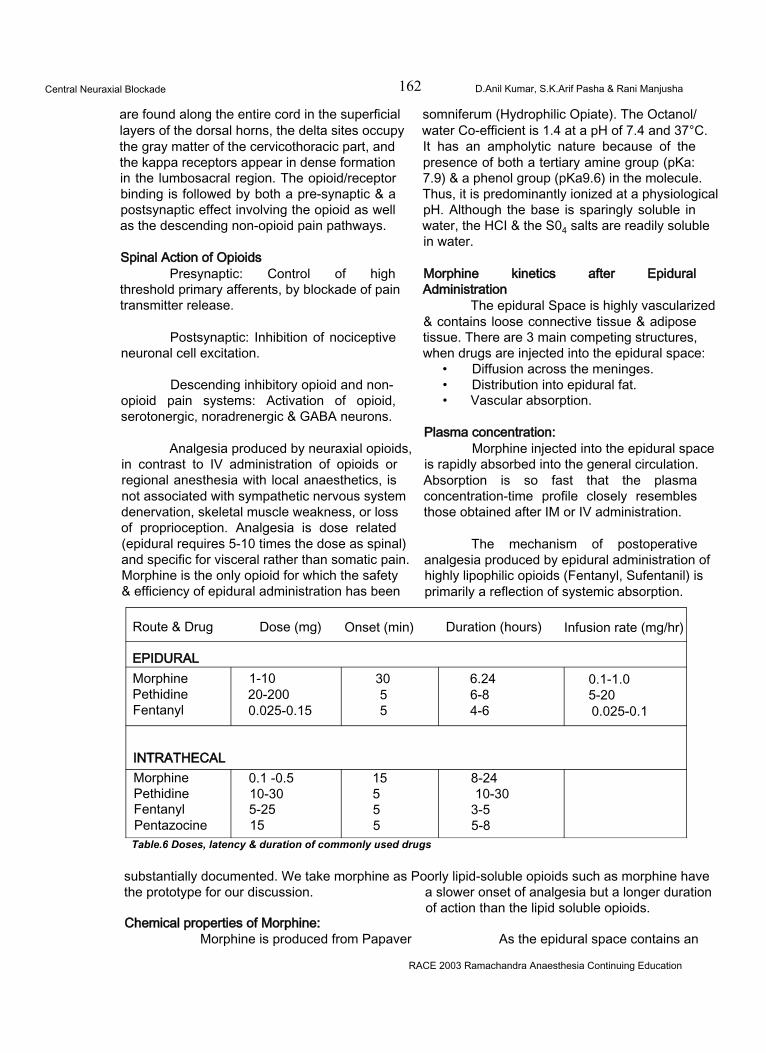
Central Neuraxial Blockade 162 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
are found along the entire cord in the superficial layers of the dorsal horns, the delta sites occupy the gray matter of the cervicothoracic part, and the kappa receptors appear in dense formation in the lumbosacral region. The opioid/receptor binding is followed by both a pre-synaptic & a postsynaptic effect involving the opioid as well as the descending non-opioid pain pathways.
Spinal Action of OpioidsPresynaptic: Control of high
threshold primary afferents, by blockade of pain transmitter release.
Postsynaptic: Inhibition of nociceptive neuronal cell excitation.
Descending inhibitory opioid and nonopioid pain systems: Activation of opioid, serotonergic, noradrenergic & GABA neurons.
Analgesia produced by neuraxial opioids, in contrast to IV administration of opioids or regional anesthesia with local anaesthetics, is not associated with sympathetic nervous system denervation, skeletal muscle weakness, or loss of proprioception. Analgesia is dose related (epidural requires 5-10 times the dose as spinal) and specific for visceral rather than somatic pain. Morphine is the only opioid for which the safety & efficiency of epidural administration has been
somniferum (Hydrophilic Opiate). The Octanol/ water Co-efficient is 1.4 at a pH of 7.4 and 37°C. It has an ampholytic nature because of the presence of both a tertiary amine group (pKa: 7.9) & a phenol group (pKa9.6) in the molecule. Thus, it is predominantly ionized at a physiological pH. Although the base is sparingly soluble in water, the HCI & the S04 salts are readily soluble in water.
Morphine kinetics after Epidural Administration
The epidural Space is highly vascularized & contains loose connective tissue & adipose tissue. There are 3 main competing structures, when drugs are injected into the epidural space:
• Diffusion across the meninges.• Distribution into epidural fat.• Vascular absorption.
Plasma concentration:Morphine injected into the epidural space
is rapidly absorbed into the general circulation. Absorption is so fast that the plasma concentration-time profile closely resembles those obtained after IM or IV administration.
The mechanism of postoperative analgesia produced by epidural administration of highly lipophilic opioids (Fentanyl, Sufentanil) is primarily a reflection of systemic absorption.
Route & Drug Dose (mg) Onset (min) Duration (hours) Infusion rate (mg/hr)
EPIDURALMorphine 1-10 30 6.24 0.1-1.0Pethidine 20-200 5 6-8 5-20Fentanyl 0.025-0.15 5 4-6 0.025-0.1
INTRATHECALMorphine 0.1 -0.5 15 8-24Pethidine 10-30 5 10-30Fentanyl 5-25 5 3-5Pentazocine 15 5 5-8Table.6 Doses, latency & duration of commonly used drugs
substantially documented. We take morphine as Poorly lipid-soluble opioids such as morphine have the prototype for our discussion. a slower onset of analgesia but a longer duration
of action than the lipid soluble opioids.Chemical properties of Morphine:
Morphine is produced from Papaver As the epidural space contains an
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 163 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
extensive venous plexus, vascular absorption is extensive.'After epidural administration, fentanyl blood concentration peaks in 5-10 minutes; in contrast, the blood concentration of morphine peaks after 10-15 minutefe.
Chauvin & colleagues found no significant differences in the areas under the curves after IM, epidural & intrathecal administration of the same dose. This finding suggests that availability is complete, when morphine is administered epidurally or intrathecally.
Bromage & associates reported that simultaneous co-administration of epinephrine, reduced the systemic uptake of morphine in healthy volunteers, whereas Youngstorm & colleagues found that this regimen produced no change in obstetric patients.
CSF Concentration:Epidural administration of opioids
produces considerable CSF concentrations of the drug. To gain access to spinal opioid receptors, the drug must cioss several diffusion barriers, such as the meninges and the neural tissues. Penetration of the dura is considerably influenced by lipid solubility and molecular weight. Fentanyl and Sufentanil are respectively, approximately 800 & 1600 times as lipid soluble as morphine.
After epidural administration, the CSF concentration of fentanyl peaks in about 20 minutes & Sufentanil in 6 minutes. In contract, the CSF concentration of morphine, after epidural administration, peaks after 1-4 hrs. Furthermore, only about 3% of the dose of morphine administered epidurally crosses the dura to enter the CSF.
Morphine kinetics after Intrathecal administration
The intrathecal route of administration circumvents the meningeal diffusion barriers and considerably lower doses of morphine are necessary to produce the same degree of analgesia as that induced by the epidural route.
Cephalad movement of opioids in the
CSF principally depends on lipid solubility.For e.g., lipid soluble opioids such as fentanyl & sufentanil are limited in their cephalad migration by uptake into the spinal cord, whereas the less lipid soluble morphine remains in the CSF for transfer to more cephalad locations.
After lumbar intrathecal morphine administration, appreciable cervical CSF concentration occur 1 to 5 hrs after the injection, whereas cervical CSF concentration of highly lipid-soluble opioids are minimal after their epidural administration.
The underlying cause of ascension of morphine is bulk flow of CSF. CSF ascends in a cephalad direction from the lumbar region reaching the cisterna magna in 1 - 2 hrs, the 4th and lateral ventricle by 3-6 hrs (Chaney, 1995). Coughing or straining, but not body position can affect the movement of CSF.
Relationship between Morphine concentration & analgesic response:
The most outstanding feature of epidural morphine is its ability to produce excellent, long- lasting regional analgesia from doses that are only 20 - 40% of the normal IV dose. I ntrathecal administration of morphine is even more potent, requiring only about 8% of the standard 10 mg IV dose. Clinical experience has shown that analgesic onset of action of epidural morphine is slow (45-60 minutes) compared with that of !V morphine. This delay is due to the physiochemical properties of morphine and the location of the receptors in relation to the site of administration. Being hydrophilic, morphine penetrates the different diffusion barriers much more slowly than the more lipophilic molecules such as fentanyl.
The duration of action of morphine is governed by 2 factors.a) The rate of morphine removal from receptor
sites.b) The magnitude of morphine concentration
surrounding the receptors.
The duration of analgesia varies considerably among patients; due in part to pronounced inter individual differences in pharmacokinetics. Duration is dose dependent,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 164 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
and the usual 4 mg dose is commonly reported to have a duration of 10-17 hrs.
Epidural & Intrathecal Morphine Kinectics in Relation to Adverse Effects
Side effects of neuraxial opioids are caused by the presence of the drug in the CSF or the systemic circulation. The most feared adverse reaction is late respiratory depression, usually due to rostral spread of morphine in the CSF, and is extremely rare. One recent Swedish retrospective study comprising about 10,000 patients, reported an incidence of 0.25 - 0.4%.
The reasons for the rostral spread of morphine may be:a) Bulk flow of CSF.b) Physical activities such as coughing could
cause the CSF pressure wave, capable of moving a substance in a rostral direction.
c) Epidurally injected drugs could be absorbed into the valveless vasculature of the epidural space and subsequently transported to the veins in the brain.
A review of 229 patients in different controlled double-blind studies using 2-5 mg of epidural morphine showed that the three most common side effects were
• Pruritus (14%)• Urinary retention (12)• Nausea & Vomiting (11%)
A most promising study in this context, reported by Rawal & co-workers showed that continuous intravenous infusion of low-dose naloxone could be used to counteract the side effects of epidural morphine, without reducing the analgesia.
OTHER DRUGS USED IN CNBThe other relatively uncommon drugs
used in CNB are1) Benzodiazepines e.g. Midazolam.2) Ketamine3) Clonidine4) Neostigmine5) Steroids.
Spinal GABA System:The spinal GABA system has been used
as a target for newer Benzodiazepines e.g.,
midazolam, and certain neuro active steroids like alphadalone20.
NMDA Receptors and Ketamine:The pain relieving effect of ketamine has
been attributed to blockade of NMDA excitatory neurons; Mccartely, Naguit et al have used ketamine from 30mg to 50mg intrathecally and epidurally with varying results.
Clonidine:Clonidine, an alpha 2 - adrenergic
agonist, is most commonly used centrally to produce relief. It is believed to act on the adrenergic receptors, the opioid receptors and by modulation of G proteins and Substance P. Dose range - 1 to 1.5 (mcg/kg).
Neostigmine:Neostigmine is a familiar drug in the
anaesthesiologist’s armamentarium, which is being used to produce analgesia by inhibiting the breakdown of acetylcholine. The drug has been used epidurally and intrathecally in the dose range of 500 - 750 (meg /kg) and has been found to have dose dependent side effects like nausea and vomiting.
COMPLICATIONS, CLINICAL CONTROVERSIES AND RECENT ADVANCES OF CENTRAL NEURAXIAL BLOCKADE COMPLICATIONS OF CENTRAL NEURAXIAL BLOCKADE:The complications of Central Neuraxial Blockade can be classified as:• Complications due to Spinal anaesthesia.• Complications due to Epidural anaesthesia
COMPLICATIONS OF SPINAL ANAESTHESIAThese can be:During the procedure or immediate complications:A) HYPOTENSION:
Due to the decrease in cardiac output which is due to decreased venous return because of sympathetic block or due to block of sympathetic cardiac fibres.Management: Adequate preloading, head down position, vasopressors and administration of oxygen.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 165 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
B) TOTAL SPINAL ANALGESIA:Characterized by marked hypotension,
apnoea, dilated pupils, loss of consciousness and bradycardia.Management: Intubation and ventilation with 100% oxygen, elevation of the legs, vasopressors and intravenous fluids. The operation can then proceed and spontaneous respiration will probably recommence within an hour, unpleasant sequelae being unlikely.
C) TOXICITY:Due to intravascular injection or by fast
absorption of local anaesthetics. Both CNS and CVS complications occur. Signs are excitement, disorientation, twitching, convulsions, apnoea and severe cardiac depression.Management: Injecting diazepam into the drip, oxygen by IPPV, protection of patient’s teeth and tongue from trauma at the time of convulsions.
D) HYPOVENTILATION:Due to brainstem hypoxia and block of
phrenic nerve roots.Management: Ltngs are ventilated with 100% Oxygen.
E) ALLERGIC RESPONSE TO INJECTED DRUG.Management: Oxygen, I.V. adrenaline,
I.V. Colloid infusion.
F) HYPOTHERMIA:Should be managed by adequately
covering the patient and infusing of warm IV fluids.
G) NAUSEA & VOMITING:As a result of
• Sudden change in position• Hypotension• Parasympathetic mediated traction• Opioid administration.
Management: Exclude hypoxia, take care of hypotension, shift the patient slowly and gently, antiemetic drugs.
H) AFFECTIVE DYSPNOEA:With block of sensory input, patient may
complain of difficulty in breathing. Mechanism is inappropriate response (ventilatory volume) to muscular effort.
Management: Encourage the patient to take deep breaths, provide supplemental oxygen, inhaling of smelling salts like aromatic salts of ammonia and applying pressure over the lower chest helps.
I) APPREHENSION:Attention to premedication is important
in prophylaxis.
J) DIFFICULT SPINAL PUNCTURE.
K) TRAUMATIC SPINAL PUNCTURE:Repeated attempts to achieve a spinal
tap may result in direct trauma to the nerves, the periosteum of the vertebra and to the intervertebral discs. Paraesthesia is noted and may persist. Transient or permanent neurological deficits may ensue.
L) BROKEN NEEDLE OR CATHETERS:Management: Removal of the needle
fragment should be attempted as soon as possible. The proximal part of the stylet should if possible be left in space to serve as a guide to the distal part. If the catheter breaks, it should be noted and the neurosurgeon informed. It is seldom justified to carry out an exploration.
Post operative or late complications of spinal anaesthesia1) POST DURAL PUNCTURE HEADACHE:
It is postural, beginning within 6 to 12 hours after lumbar puncture (but may take 3 days), often occipital and is associated with pain and stiffness of the neck.
Mechanism: It is related to the persistence of dural puncture, with leakage of CSF into surrounding soft tissues leading to lowering of the CSF pressure. This exerts downward traction on the structures of the CNS and on the blood vessels that are attached to the dura and the cranium as well as the brainstem. The result is a headache similar to acute vascular cluster headache Increased incidence is noted
• In young and female patients.• In pregnancy• If needle size is large• With the midline approach• Increased concentration of glucose
Differential diagnosis - Migraine,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 166 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
meningitis, tumour, dehydration, hyponatremia. Management:Avoid in unsuitable patients, with frequent headache.
• Use of fine needles• Prevention of dehydration, strain,
coughing.• Choice of needlepoint: Whitacre, Sprotte
• Epidural blood patch
2) BACKACHE:Due to obliteration of lumbar lordosis and
stretching of ligaments, reflex muscle spasm, positioning and small haematomas. Management: A small pillow under the lumbar region reduces the incidence of backache. Skeletal muscle relaxants and analgesics, reassurance and heat will usually rectify the problem.
3) MAJOR NEUROLOGICAL INJURIES:Cranial nerve disturbances: Paralysis of
every cranial nerve except 1,9 and 10 has been reported.
The primary cause of this is due to CSF dynamics consequent to lumbar puncture. It is basically the same as the cause of headache.
Abducens nerve palsy - it has the longest intracranial course and is more vulnerable to dynamic changes in the CSF.Symptoms: Internal strabismus, blurring, diplopia and difficulty in focussing.Management: 50% cases recover within 1 month, if condition persists, dark glasses may be worn.
Urinary retention: Blockade of S2-S4 is associated with loss of bladder tone and inhibition of voiding reflex leading to overfilling of bladder. Even after resolution of blockade, voiding may be difficult. These problems are more common in male patients and in extreme cases can result in neurogenic bladder requiring intermittent catheterisation.
For prolonged Central Neuraxial Blockade, it is probably wise to avoid this problem by inserting a bladder catheter.
Cauda equina syndrome: - Characterised
by abnormalities of leg reflexes, incontinence of faeces, retention of urine, loss of sexual function, sensory loss in the lumbo sacral plexus distribution and a temporary paralysis of peroneal nerves. Most of them clear spontaneously.
Traction nerve paresis or paralysis; lithotomy position and stirrup pressure may produce peroneal nerve palsies,
4) MENINGITIS OR ARACHNOIDITIS:This may occur even with a seemingly
flawless technique. Aseptic meningitis has been reported.
Contamination with chemical antiseptics, starch powder of gloves, detergents, higher concentration of drugs and variation in pH has been blamed. The need remains for careful adherence to an aseptic technique.
5) ANTERIOR SPINAL ARTERY SYNDROME:Due to spinal cord ischaemia, due to
severe hypotension.
6) VASCULAR INJURY:In patients with coagulation disorders or
on anticoagulants.
COMPLICATIONS OF EPIDURAL ANAESTHESIA: a) Inadvertent dural puncture:
It has been recommended that when this occurs, plan for epidural anaesthesia is stopped and simple spinal / GA is administered. Objective studies indicated that this is unnecessary and we can go for epidural in another inter space or can opt for continuous spinal anaesthesia.
b) Total spinal:Due to accidental sub arachnoid
injection.
c) Neural damage:The incidence is low, but the neurological
deficits are due to trauma, anterior spinal artery syndrome and epidural haematomas.
d) Hypotension:The degree of hypotension is less in EA
than SA, because the onset of action of local
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 167 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
anaesthetic drugs in epidural is delayed and by that time adequate preloading is done so that the incidence and degree of hypotension is reduced.
e) Urinary retention:
f) Toxicity:As relatively large doses of local
anaesthetic drugs are required for EA, and epidural space contains numerous venous plexus, which may be penetrated by epidural needle or catheter, there is more chance of local anaesthetic toxicity with EA.
g) Catheter complications:It may be inserted directly into the blood
vessel or subarachnoid space or breaking of the catheter in the epidural space may occur. No attempt is made to withdraw the catheter through the needle.
h) Failure:
i) Epidural abscess:Following SA or EA, abscess formation
is superficial requiring limited surgical drainage and intravenous antibiotics.
j) Effect of rapid injection:Sensation such as headache, vertigo,
and paraesthesia may be seen when the anaesthetic solution is injected rapidly, as rapid injection increases the CSF pressure. This effect lasts for 3-5 minutes, during which headache is prominent.
RECENT ADVANCES IN REGIONAL ANAESTHESIA
Over the last two decades, there have been considerable innovations in materials, drugs, and techniques of central neuraxial blockade, which have contributed to improving the quality and safety of central neuraxial block. The following are a few of them.
Equipment:1. Use of 25 G epidural needle systems with a modified tip lowers the incidence of post dural puncture headache in the event of an unintentional dural puncture and causes less tissue trauma.
2. The limiting factors for the use of smaller gauge spinal needles are reduced back flow of CSF and decreased tensile strength. But new manufacturing has increased the internal diameter of small gauge needles as well, improving the back flow without a notable decrease in tensile strength. Some needles taper from a 22-gauge shaft to a 24 gauge tip.
3. Another development in neuraxial block technique is the development of effective methods of combining epidural and spinal anaesthesia via a single needle system.
These methods use epidural needle placement followed by insertion of a spinal needle through either a side lumen on the epidural needle, or directly via the epidural needle lumen. This combined technique allows flexibility in a number of clinical settings.
Techniques:1. VERIFICATION OF NEEDLE AND CATHETER INSERTION:
More recently, techniques to aid in location of the epidural space have been reported including the use of1. Auditory amplification of the sound made by the epidural needle as it traverses the interspinous ligament and ligamentum flavum.
• Doppler guidance and• Pressure transducer methods
2. Use of fluoroscopic guidance for epidural needle placement and injection of non-ionic radiopaque contrast solution through the epidural catheter producing the typical epiduralgram appearance. This may also be used to confirm epidural needle (or) catheter placement.
3. Recently low current electrical stimulation resulting in truncal (or) limb motor responses is regarded as a simple, objective and reliable technique for confirmation of epidural catheter placement.
II.EPIDURAL RADIOGRAPHS AND EPIDUROSCOPY: -
Use of epidural radiographic techniques and epiduroscopy have enhanced the knowledge of anatomic characteristics and fluid dynamics within the epidural space & the effect of previous epidural anaesthetic procedures on the cephalad
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 168 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
spread of sensory block during lumbar epidural anaesthesia.
It was noted by epiduroscopy that patients with a history of previous epidural anaesthesia had aseptic inflammatory changes within the epidural space such as, narrowing of epidural space, proliferation of connective tissue and adhesions between the duramater and ligamentum flavum. These changes are responsible for the reduction in cephalad spread of sensory blockade in patients with previous history of epidural anaesthetic producers.
III. METHODS OF DETERMINING THE EXTENT OF EPIDURAL ANAESTHESIA:1. Skin vasomotor reflex testing, using changes in skin blood flow, as measured by laser Doppler, in response to tetanic electrical stimulus.2. Somatosensory evoked potentials in response to electrical and argon laser stimulation have been used to determine the extent of sensory neural blockade during EA & SA.
IV. ANAESTHETIC TECHNIQUES:1. Unilateral epidural analgesic techniques: Insertion of epidural catheters using fluoroscopic guidance has demonstrated the relative ease with which catheters may be directed within the epidural space through changes in location and bevel orientation of the epidural needle and producing unilateral epidural analgesia.
Technique: - Selectively, relatively unilateral distribution of analgesia may be obtained through a technique involving slight angulation (approximately 5 degrees in the horizontal plane) of the epidural needle towards the intended side of location and orientation of the needle bevel between 45 degrees and 135 degrees from the cephalad direction laterally. With this needle location and bevel orientation, the epidural catheter tip is directed to lie in the lateral epidural space.
2. The technique of postoperative epidural administration of 20ml of normal saline hastening the return of motor function from EA has been described. This is related to a dilutional (washout) effect, an ion trapping effect produced by the injection of saline with a relatively low pH and increased uptake of local anaesthetic by greater
area of distribution.
3. Anaesthesia for Ambulatory surgery: Ambulatory surgery demands good surgical anaesthesia with rapid recovery from sensory and motor block & recovery of the ability to void. As lidocaine has been questioned with the possibility of neurotoxicity, hypobaric, hyperbaric and near isobaric bupivacaine solutions are used for ambulatory surgeries.
4. Patient controlled analgesia: Use of microprocessor controlled epidural infusion pumps, with patient activated dosing capability, has become the postoperative pain management technique of choice, as compared with intermittent bolus dose administration method. With this PCEA, it has been noted that there is overall reduced dose requirement and patient satisfaction.
5. Mobile epidurals have already gained popularity in the field of obstetric analgesia as they allow normal mobility with high quality of pain relief.
6. Central neural blockade in children is providing excellent intraoperative and postoperative analgesia. The paediatric regional anaesthetic techniques are greatly reducing the morbidity associated with surgery and anaesthesia in selected groups of patients and can favourably influence the postoperative course.
Drugs: -1. Separation of stereoisomers allowed the development of improved local anaesthetics for safer use, e.g.: Ropivacaine & levobupivacaine which are S.enantiomers of bupivacaine. It has been demonstrated that they have potency almost similar to bupivacaine (less with ropivacaine) while exerting significantly less CNS & CVS toxicity.
2. The most exciting new development in Central Neuraxial Block is the introduction of novel analgesic drugs (nonopioid, nonlocal anaesthetic), analgesic adjuvant medications, and new epidural anaesthetic and analgesic formulations eg.adenosine, midazolam, verapamil, ketorolac and others which are in various stages of clinical (or) preclinical study for
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 169 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
possible spinal analgesic utility.
3. Novel drug formulations and epidural delivery systems may soon include the use of liposome- encapsulated local anaesthetics (or) opioid analgesics capable of, producing an extended duration of analgesic effect from a single epidural dose.
CLINICAL CONTROVERSIESInspite of the many years that neuraxial
blockade techniques have been used, there remain a number of controversies about the appropriate use of these techniques.
1. Related to systemic toxicity of local anaesthetics and premedication.
Inspite of the widely held belief that benzodiazepines should be used with regional anaesthesia to minimize systemic toxicity as they elevate the seizure threshold, it has been shown that benzodiazepines cover up one of the early signs of systemic toxicity (i.e., seizure). Thus resuscitation may be more difficult after cardiovascular collapse, delaying potentially the definitive therapv.
2. Most controversy surrounds the use of epinephrine in obstetric patients in which uterine blood flow may be decreased by intravascular injection there by putting the foetus at risk, but many anaesthesiologists believe epinephrine - containing epidural test doses are useful in obstetric anaesthesia.
3. Some continue to suggest that spinal anaesthesia is inappropriate for out patients because of the occurrence of post dural puncture headache, yet there are data that the occasional headache can be successfully treated even in the out patients and considerable other data are available supporting the use of this technique in out patients.
4. The use of epidural anaesthesia for patients receiving anticoagulants is less clear because epidural anaesthesia is often avoided in these patients but there are studies, which used continuous epidural anaesthesia in vascular operations, in patients receiving preoperative oral anticoagulants without any problem. The acceptable magnitude of preoperative anticoagulation and risk benefit ratio of performing epidural anaesthesia remains undetermined by this time.
The time duration accepted between anti coagulation prophylaxis and Central Neuraxial Block is as follows:
• Low molecular weight heparin-12 hours after the last dose and the same rule applies for the insertion and removal of the catheter.
• Heparin infusion- 4 hours after the cessation of the infusion.
• Warfarin intake- An INR of less than 1.5 is accepted for performing Central Neuraxial Block. Again, it is the element of risk benefit ratio to be kept in mind when such patients are subjected to Central Neuraxial Block
REFERENCES:Anatomy for anaesthetists - Harrold Ellis, Stanely feildman, 6th editionPrinciples of anaesthesiology- Collins, 3rd edition, 1993Indian journal of anaesthesiology Dec 2001 45(6), 414,430Pharmacology and physiology in anaesthetic practice- Stoelting, 3rd edition 1999 Pharmacological basis of therapeutics - Goodman and Gillman Anaesthesia by R.D Miller, 5th edition Lee synopsis of anaesthesia- 13th edition Anaesthesiology clinics of North America - June 2000.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 170 Trivandrum Medical College
INTRODUCTIONThe prone position is also called
‘concorde’ position, ‘face down’ position or the position wherein the ventral surface of the body lies on some surface supporting the body weight. In the Classic prone position the face, chest, abdomen, front of thighs, knees, toes and some surface of hands and arms all touch the supporting surface. People sleep in this posture using crooked arms to hold the face off the bed to prevent pressure on nose.
Patients under GA - Problems :1. Body weight against abdominal wall leads
to decreased diaphragmatic movement and decreased tidal volume
2. Increased intra-abdominal pressure causes decreased venous return
3. Pressure on toes and bony prominences can cause pressure injuries
4. Care must be taken in keeping the head in safe relation with the rest of the body
MODIFICATIONS OF PRONE POSITION :1. Jack knife position :This is used for anorectal surgeries. The patient lies on a flexed operating table with pelvis at the flexion point. Surgical field is clearly visible and the abdominal viscera move cephalad in response to gravity. Arms are beyond the top of the head and face turned to one side.
2. Knee-chest position : This is an exaggeration of jack knife position. Knee and chest are supported, Neck is extended and face turned to one side. Gynaecological examination is facilitated. Uterus and other viscera fall ventrally and cephalad.
3. Buie position : This is a modification of the prone position providing satisfactory exposure
for proctological work. The patient kneels on a wide padded shelf, bends forward over a 90 degree table, placing his chest on the table proper. When the table is tilted into a head down position, gravity moves viscera and venous blood away from the perineum. The operative field exposure is good, blood loss is minimal, proctoscopy greatly simplified and the patient is in a reasonable position for either hypobaric spinal or caudal anaesthesia.
4. Georgia position This is a modification of the knee- chest position. The patient’s weight is supported on his knees and chest. The knees are on a shelf, chest is on a stack of folded sheets. The height of the knee support and the height of stack of sheets are adjusted to leave abdomen free of pressure. Good exposure for perineal and rectal work is obtained, if table is tilted head down.
5. Smith’s recent modification of Georgia position: In this position specially built supports are used to raise the pelvis to a height sufficient to leave abdominal wall completely pressure free. The chest is elevated by stack of folded sheets. The chest and pelvis are elevated, usually to the same height
6. Overholt position : This is used for surgical management of specific thoracic problems to prevent drainage of infected material and blood from the involved lung into the other lung in the course of surgery. Now minimally used since double lumen tubes are available. Exception is a small child whose airway is too small to accommodate the double lumen tube. However, in such a case bronchial blockers can be used rather than Overholt position.
7. Sellor-Brown position : In this position placing the lower part of body, including abdomen
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 171 Trivandrum Medical College
are placed in one plane and the chest, neck and head are on a lower plane. Intent is same as that of the overholt position i.e. to drain blood and infected material from the uninvolved lung.
8. Crouching or ‘carpenter’s rule’ position :In this position knees and hips are flexed
maximally. Patient’s weight rests on the back of the legs. Abdomen on the front of the thighs, back is flexed well to eliminate the lordotic curve. Problems associated in this position are possible knee injury, femoral vein obstruction, free abdominal movement restriction.
INDICATIONS FOR THE PRONE POSITION:1. Spine surgeries like laminectomy, spinal
fusion, scoliosis correction2. Posterior cervical and occipital surgeries3. Adrenal exploration and renal biopsies4. Thoracotomy by posterior approach5. Surgeries on the back of the leg eg.
Varicose vein stripping, tendon repair6. Prone ventilation for ARDS
CONTRAINDICATIONS:1. Patient with contused heart2. Crush injury to the chest3. Full flail chest4. Severe pectus excavatum
TECHNIQUE OF POSITIONING:Turning the anaesthetised patient is
potentially dangerous because1. The autonomic compensatory mechanisms are obtunded by the anaesthetic agents2. There is no muscle tone to protect the joints
Principles:1. The patient should be anaesthetised & turned on the operating table. Trying to control the patient at arms length across the bed is highly inefficient2. The patient is more safely turned if he is very lightly anaesthetised and paralysed. The cardiovascular response to stimulation should be hypertension , not hypotension. This is possible, if he has a functioning vascular control mechanism to oppose the effects of gravity. Heavy premedication with narcotics and deep anaesthesia obtund this mechanism and cause hypotension.3. Before turning -
a. The head end of the table is depressed by 5 -10 degrees. In the head down position, the venous return from lower 2/3rd of the body is maintained even if the upper 1 /3rd of the body is elevated for the turn.b. The anaesthesiologist should manage the head and neck,unless there is a cervical spine fracture . If the neck is unstable, neurosurgeon help should be sought.c. Avoid injury to eyes by the clamps or other objects.d. Avoid damage to intravenous (IV) infusion systems. Use the arm that will be on top of the body as the preferred infusion sitee. BP apparatus should be ready for an immediate measurement after positioningf. The anaesthesiologist directs the turning and must arrange to disconnect the patient from the breathing circuit for the shortest possible period of time4. Skill is more important than strength. Everyone should know what they have to do and how to do it safely.5. The steps involved in positioning the patient are:a. Move the patient towards one side of the table and roll him up onto one side. Two persons should make the lift from back to the side one at his shoulders, one at his hips, both parts to be moved at the same speed. Anaesthesiologist keeps the face in the proper plane. Now the patient is in the lateral decubitus position with one arm under the body and upper arm close to his uppermost side. At least one person should receive the body on the other side of the table.b. Patient now is rolled into 3/-«?h prone position. The underarm is freed of his weight, moved to a position behind him and lowered over the side of the table (without stress on the shoulder). The upper arm is swung forwards to hang free over the other side of the table.c. The hips and the shoulders are lifted back towards the starting edge of the table to return the patient to the middle of the table.d. As the turn is completed, the person controlling the shoulders has an arm under the chest pulling the patient back towards the middle of the table. This person should continue to hold upper part of the patient off the table while anaesthetist gets the head in a safe position, reconnects the breathing circuit, ventilates the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 172 Trivandrum Medical College
patient vigorously for a few breaths and measures blood pressure (BP). After that the supporting arm can be removed from under the chest.e. Now the patient is prone with the head turned to one side, both arms hanging down besides the operating table.f. Any modification of prone position can now be effected.g. After all the movements are completed bring the table back to the horizontal position.
Light plane of anaesthesia, head down tilt etc will decrease the tendency for hypotension. Paraplegics and quadriplegics require IV vasopressor drugs before the turn to avoid severe hypotension. Careful handling during turn decreases the likelihood of injury to the back, neck, shoulders, elbow, wrists and face. Turning requires an anaesthesiologist and at least 3 capable persons !f the patient is very obese additional help may be needed.
PHYSIOLOGICAL EFFECTS: 1. Cardiovascular System (cvs)a. Pressure on the inferior vena cava (IVC) and femoral vein cause decreased venous return and hypotension.The engorged epidural venous plexus cause increased intraoperative blood loss. Avoidance of pressure on the IVC are accomplished by Relton-Hall and Andrews variants of spinal surgery frames.b. Hypotension secondary to spinal, epidural or deep general anaesthesia (GA)c. If the body is properly supported on the chest wall, impairment of cardiac efficiency will not occurd. If the patient is grossly obese it is better to turn the patient into that position during his preoperative visit to see the effect on BP. Those positions which make the patient faint, nauseated or develop headache are to be avoided as these may be the symptoms of hypoxia or hypotension or both.e. Avoid pressure on the carotid sinus when the head is turned to one side as serious arrythmias and hypotension may develop. Pads, rolls can be used to keep the head stablef. The venous return from the head must not be obstructed as engorged (eye vessels, eyelid oedema, post operative headache and even subglottic edema can result.g. Blood supply to the brain must be protected. Severe twisting or extension of neck may impede flow through the vertebral artery.
2. Respiratory system:The abdominal wall should be free to move.
Less airway pressure is required to ventilate obese patients in the prone than supine, as weight of chest and abdomen wall does not have to be lifted. If abdominal wall is not free in prone position, the patient will hypoventilate. Also with every inflation of lung, the entire back will rise. Surgery will be affected on a moving target. Even with perfect positioning upper back will move detectably with artificial ventilation but the upper body weight on the sternum will limit it’s movement. However, back from T 10 down can be kept still, if the patient is properly positioned. Patient’s thorax and pelvis should be raised by supports. In grossly obese patients, lateral decubitus position might be an easier choice.
Now, prone position is utilised to treat ICU patients in acute respiratory failure. Unrestricted abdominal movement is essential. A hand should pass between abdomen & bed.Patient positioned prone with proper support from the supine position, showed market increase in the oxygen tension for the same tidal volume, Fi02and PEEP.
COMPLICATIONS: 1. Neurological Injuries:
Neurological injuries may result from pressure against bones, against hard substances in the operating area, or due to stretching.a. Eyes may be injured during turning or may suffer protracted pressure in the prone position.b. Brachial plexus injury can occur by stretching, during turning or by pressure from an improperly placed support.c. Facial nerve injury can occur by pressure over the infraparotid regiond. Jack knife position may injure the femoral nerve.e. Lateral femoral cutaneous nerve injury can occur while compression against the supporting mechanisms under the pelvis resulting in a symptom complex called meralgia paraesthetica.f. Injury to the nerves and the tendons of the dorsum of foot can occur if the foot rests against the metal edge of the tableg. Ulnar nerve is at risk of injury against sharp edges of supporting devices when the arms are positioned above the head. Flexion of the elbow makes the danger more acute.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 173 Trivandrum Medical College
h. While turning the patient, the hips and shoulders should be on the same plane at all times because improper turning of anaesthetised patient involving relaxation of musculature can result in spine injury.
2. OTHER INJURIESa. Male genitalia should be protected. Precaution are necessary so that electrocautery, grounding plate should not touch them.b. In the female, care must be taken so that the breasts are padded well. Large breasts, can usually be moved laterally, so that the patients weight do not injure themc. Ears must not be folded over and held there by the weight of the head as the elastic cartilage are readily damaged and slow to heal. So pad the ear as well.d. Neck should be turned only after flexion. Turning an extended head leads to protracted neck muscle spasm and headache post operatively (due to pressure on C2 nerve while emerging between the atlas and the axis)e. Skin overlying the bony prominences such as the iliac crest must be protectedf. Toes should be protected from pressure injury using pillows under the anklesg. Air embolism is a risk in any surgical position in which the operating field is higher than the heart, permitting open veins for air entry.h. In moving the patient’s arms from besides the body to beyond the top of the head, the arms are first lowered towards the floor and then swung upwards carefully in a natural arc so as to rest beyond top of the head. Such care prevents shoulder dislocation, brachial plexus injury and tear of ligaments and tendons.i. Nasotracheal tubes must be positioned to avoid pressure on nasal cartilage in the anterior margin.j. Eyes must be protected with no pressure on them. Orbital compression can cause retinal ischaemia leading to blindness. Eyes are to be examined very frequently, and must not be kept open. Head movements may alter the relationship between the eyes and the head support and can cause pressure injury resulting in blindness. To prevent head movements, stabilise it using skull pins in a rigid holder.k. Chest supporting devices must not block the venous return from the neck.lt should be
possible to pass a hand between the base of flexed neck and chest support.I. Injuries to the joints can occur, while turning from supine to prone or, back from prone to supine, m. Varying degrees of pressure necrosis of maxillae and forehead can occur in prolonged spinal procedures.n. In cervical and posterior fossa procedures, flexion of the patient’s neck causes decreased anteroposterior dimension of the hypopharynx that leads to compression ischaemia of base of tongue, macroglossia and unexpected post extubation airway obstruction
3. Accidental extubation:In the prone position there isa. Poor access to the airwayb. Traction from the head movements due to bone drills or saws and also traction from the circuit itself.c. Loosening of the adhesive tapes used to secure the tubes which can be sweated or salivated loose.
SUPINE POSITION
PHYSIOLOGICAL CHANGES IN NORMAL CONCIOUS HUMAN SUBJECT ON CHANGING FROM THE ERECT TO THE SUPINE POSITION
1. Cardiovascular system(CVS) :Human arterial blood pressure remains
within the normal ranges throughout a variety of changes in body position. The principal factors maintaining relatively unaltered systemic blood pressure(BP) on assumption of supine position from erect are,a. Venous and arterial reflexes :As the body shifts from the erect to the supine position, venous return to the heart increases because sympathetic and parasympathetic tone of splanchnic and peripheral arteriolar and venous vessels decrease.This causes increased right atrial filling, increased right ventricular stroke volume, increased pulmonary circulation, increased left ventricle (LV) stroke volume and increased heart rate. This cardioacceleration was attributed to baroreceptors in the great veins and right atrium (Bainbridge 1915). This response is prevented by bilateral vagotomy.b. Pressorecepetor reflexes and autonomic control.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 174 Trivandrum Medical College
The raised cardiac output caused by increased venous return on assuming the supine position, initially tends to increase the arterial BP. Carotid and aortic baroreceptors are stimulated via nerve of Hering to IXth cranial nerve and via vagus respectively to the vasomotor centre and cardiac centre of medulla. From these centre, efferent parasympathetic impulses travel via the vagus to the heart and act on the sinoatrial (SA) node and myocardium. This diminishes the heart rate,stroke volume and decreases the strength of myocardial contraction. Also efferent sympathetic discharge to the heart is decreased and hence decreased heart rate and myocardial contractility.c. Ward and Korner studied the combined reflex effects on changing from the erect to the supine position ,1. MAP, heart rate and peripheral resistance
decreased2. cardiac output and stroke volume increased3. Systolic BP remained the same while
diastolic BP decreased so there was widening of pulse pressure.
2. Respiratory system:a. Pulmonary ventilation: Expansion of the lung during normal quiet inspiration is mainly due to the downward movement of the diaphragm and to a lesser extent by the bucket handle outward movement of the ribs. In the supine position, the abdominal contents limit the diaphragmatic excursion and force the diaphragm cephalad thus decreasing functional residual capacity (FRC) and total lung capacity (TLC). The posterior part of the diaphragm is forced cephalad more than the anterior part owing to the gravitational effect of the abdominal viscera. They are therefore stretched to a greater length and is capable of greater shortening. So, more ventilation of the adjacent posterior segments at the lung base. This has the advantage that dependent lung regions are perfused preferentially, this preferential ventilation makes for more efficient gas exchange.b. Pulmonary circulation: Alveolar capillaries tend to collapse when the external pressure within the alveoli exceeds the internal pressure within the vessels. It occurs more in the apex of the lung in either supine or erect position. The effect is a differential perfusion of the lung at the base than at the apex. This can be explained by dividing the lung into 3 zones.
Zone 1 : At apex pA>pa>pv : no blood flow Zone 2 : pa>pA>pv : flow determined by arterio- alveolar pressure difference Zone 3 : pa>pv>PA: flow dependent on arteriovenous pressure difference Where pA-alveolar pressure
pa-pulmonary arterial pressure pv- pulmonary venous pressure
With the patient in the supine position, the anterior part of the lung lies above the left atrium and the plane from the hilum to the base of the lung lies at the level of the left atrium and these parts function as Zone 2. Posterior part of the entire lung from the apex to the base becomes Zone 3.c. Closing volume increases, FRC decreases.
3. Other systems:a. Blood volume : On changing from erect to supine position, a significant decrease in packed cell volume (PCV) occurs in 5 minutes, maximal decrease of 10 to 20 percent of the erect value at 20 minutes. Also a lowering of serum calcium (7%); total protein (9%) and albumin (6%), PBI (16.3%), cholesterol & triglycerides.b. Renin angiotensin aldosterone axis: There is increase in blood volume and BP decreases. Renin causes decrease in aldosterone secretion and so a 25% increase in sodium excretion.c. Oesophageal sphincter tone decreases.
VARIANTS OF SUPINE POSITION LITHOTOMY POSITION
It is the position in which the patient is on his back with the legs and thighs flexed to right angles.
Indications:Perineal, rectal .vaginal and urological operations
History:William Jones first described the position
in 1839.
Technique of Positioning:First the patient is placed supine with the
gluteal folds at the caudal table break. Anaesthesia is instituted then. The patient’s arms are restrained appropriately by taping the arm
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 175 Trivandrum Medical College
containing the IV needle to an arm board and by wrapping the arm containing the BP cuff in a sheet to the patient’s sides. Now the patient’s legs are elevated together, flexed together and positioned in stirrups. The stirrups can be either of the ankle strapped variety or a part of the total leg support system. Knee supports are rotated medially to facilitate the rotation of the thigh. Thighs are flexed about 90 degrees to the abdomen. Then outward rotation of thigh is accomplished by abducting the knee brace and rotating the thigh by rotating the supporting rods cephalad, flexing the thigh onto the abdomen. Care is taken to cushion the ankle and knee against pressure from metal stirrups.
Disengagement of the Paitent after the procedure:
Stirrup rods with the legs should be brought together to a relatively neutral plane relieving the flexion , abduction and rotation components . Legs lifted and lowered together slowly to avoid a sudden decrease in cardiac output.
Complications1. Venous stasisAny patient placed for more than 15 minutes in lithotomy position should have their legs protected by elastic stockings2. Peripheral nerve injuries:-a. Obturator nerve (L 2,3,4) -Acute flexion of thigh to the groin may result in nerve compression and trauma leading to weakness or paralysis of the adductors of the thigh .b. Saphenous nerve- Sensory to the medial portion of the leg. Legs may get compressed to the medial aspect of the knee brace leading to loss of sensation to the medial aspect of leg.c. Femoral nerve- Injured by acute thigh flexion with angulation against the underlying surface of the pubic ramus. Manifests as abnormal gait and numbness or paraesthesia.d. Common peroneal nerve- L4,5 S1,2 Injured by pressure at the head of fibula. Results in weakness of intrinsic muscles of foot and sensory loss in sole of foot. Foot drop due to palsy of Tibialis Anterior.3. Damage to the hip and knee especially of elder women.4. Injury to the hand and fingers when the caudal portion of the table is lowered .
VARIANTS OF LITHOTOMY POSITION:1. For combined vaginal -abdominal approach to pelvic viscera. Leg elevation is less and flexion of thigh to abduction is less than 90 degrees.2. Walcher position for obstetrics: Thighs pressed firmly onto the trunk and legs kept dangling.3. ForTURP (Blandy’s position): Here the legs are supported in such a way that the thighs create an obtuse rather than an acute angle with the body.
Physiological Changes:1. RESPIRATORY SYSTEM:a. The vital capacity- decreases by 18 % ,the reason being restriction of the movement of diaphragm as well as restriction of volumetric expansion of lungs because of increased pulmonary blood volume.b. Increase in the postoperative respiratory complications due to paralysis of the abdominal wall muscles with resultant inability to cough forcefully during spinal or epidural anaesthesia.c. Tidal volume decreases by 3%d. FEV1 increases by 9% due to the weight of abdominal viscera and flexion of the thighs on abdomen acting as a belt to improve the resting position of diaphragm which increases the inspiratory reserve and added force to maximum expiratory effort.
2. CIRCULATORY SYSTEM:Lower extremities are major
reservoirs of blood. Sudden lowering can cause significant lowering of BP So slow and deliberate lowering of legs should be done in a light plane of anaesthesia.
THE TRENDELENBURG POSITION Introduction:
Historically , the Trendelenburg position describes a supine patient whose head is lower than his heart and whose legs and pelvis are elevated to facilitate surgical access to the lower abdomen and pelvic viscera. Friederich Trendelenburg used this position for urological procedures as early as 1870. The position was originally achieved by placing the patients knees over the shoulders of an orderly while Dr.Trendelenburg operated.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 176 Trivandrum Medical College
Trendelenburg position today implies a head down tilt so that the head is below the horizontal plane. The head down tilt may be anywhere between 1 and 45 degrees, the most common being 10 - 20 degrees tilt.
Advantages:1. Improvement in exposure of the surgical field for pelvic or lower abdominal surgery2. With the surgical field positioned superior to the rest of the body, arterial perfusion pressure at the site of operation is lowered, resulting in less bleeding. Also shed blood falls away from the surgical field enhancing surgeons visualisation. Thus surgical time is decreased.3. Trendelenburg’s position causes engorgement of dependent neck veins thus facilitating the IV placement of needles or catheters.4. Protection of trachea from regurgitated material since they drain by gravity into the more dependent pharynx. So a steep Trendelenburg position might be selected for crash induction to a patient with full stomach.
Disadvantages:1. Displacement of abdominal contents into the surgical field with ventilatory excursions due to rigorous IPPV.2. Tendency of the position to mask unrecognised blood loss through it’s enhancement of central venous return of blood and a preserved cardiac output.3. Cyanosis of the patients face secondary to venous engorgement which makes evaluation of cardiovascular and respiratory status during anaesthesia more difficult.
Anaesthetic Considerations:1. x RESPIRATORY SYSTEM:a. Increase in work of breathing- Abdominal contents are pushed cephalad against the diaphragm so that the diaphragm not only must ventilate the lungs but also lift the abdominal contents .So in obese patients, the added weight of abdominal contents and the weight of the chest wall further decreases compliance and increases the risks of atelectasis and hypoxemia.b. Pulmonary compliance and FRC are decreased - Increase in the pulmonary blood volume and gravitational force on the mediastinal
structures being the causesc. Vital capacity decreasesd. Increase in pulmonary congestion and pulmonary oedema-ln steep Trendelenburg position , most of the lungs becomes zone 3, as most of the lung then lies below the left atrium. In zone 3 , an excessive increase in LAP over the alveolar pressure will enhance fluid transudation into the alveoli increasing pulmonary congestion leading to pulmonary oedema. Hence patients with chronically elevated LAP as in Mitral stenosis tolerate this position poorly.
2. CARDIOVASCULAR SYSTEM:. When the patient is put in the Trendelenburg position, the following things happen .There is autotransfusion of 500-1000 ml of blood from the lower extremities to the central circulation. This increase in volume of blood is pumped from the heart manifesting as an intial increase in cardiac output. There is an increase in the hydrostatic pressure in the arch of aorta and carotid bifurcation. Stimulation of the baroreceptors causes a generalized reflex vasodilatation. This causes decrease in stroke volume,cardiac output and decreased perfusion to vital organ. In a patient with heart disease, this added volume in the central circulation and increased pulmonary blood, flow may cause heart failure.
3. CENTRAL NERVOUS SYSTEM:This position produces an increase in the
intrathoracic pressure thus increasing the central venous pressure leading to an increase in the CSF pressure. At the same time this position decreases cardiac output by sino-aortic reflex thus decreasing cerebral blood flow. Too aggressive use of IPPV to expand the lung will further decrease cerebral blood flow and dangerously increase the CSF pressure while insufficient ventilation will increase the PaC02 which in turn increases CBF and intracranial pressure(ICP).
Technique of positioning:First the patient is placed supine with the
knees placed at the leg section hinge of the table. The operating table mattress must be fixed to the table with adhesive tapes. Ankle straps are secured at the foot of the table with proper
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 177 Trivandrum Medical College
padding of the ankle to protect pressure points .IV cannulae are securely placed and the patients arms are restrained across the chest or placed at the sides taking care to protect the pressure points on the radial and ulnar nerves and that the angle of the arm to the body is less than 90 degrees.
After the patient is anaesthetised, the table is tilted to the desired plane. Concomitantly, the leg piece of the table may be dropped so that the patients knees flex 90 degrees or less. A slight flexion of the hips and small pillows placed under the lumbar and cervical areas may prevent pressure pains and ligament strains. The position of the endotracheal tube should be reconfirmed once the Trendelenburg position has been achieved as the mediastinum may shift cephalad , causing an endobronchial intubation.
If Trendelenburg is combined with lithotomy position, steps are essentially the same except that the feet are placed in stirrups or the legs in leg holders prior to tilting the table. Care should be taken to see that the angle of the thigh with the body is not less than 90 degrees. This position ensures good venous return from the legs.
Disengagement of the Patient:After the procedure, the patient is slowly
returned to the horizontal position, legs slowly straightened allowing for a gradual shunting of central blood volume back into the lower extremities. This will decrease the incidence of sudden hypotension.
Complications:1. Hypotension due to baroreceptor mediated generalized vasodilatation and decrease in cardiac output. These c#n predispose to cardiac arrythmias.2. Venous air embolism by air entrainment into the open pelvic or abdominal veins can occur.3. This position may hide unrecognised blood loss4. Increase in cerebral venous pressure can cause venous thrombosis of cerebral blood vessels, retinal detachment and cerebral oedema.5. Accidental endobronchial intubation.6. Nerve injuries (brachial plexus, superficial peroneal nerve, ulnar and radial) can occur.
Patient in Fracture Table:INDICATION Femur fractures.
This table has a body plate which supports the head and the thorax, a sacral plate for the pelvis, adjustable foot plates and a perineal post. After anaesthetising the patient, the patient is transferred to this table taking care to protect the genitalia against pressure from the perineal post and fibular head protected to avoid pressure on peroneal nerves. Care should be taken to avoid injury to arms, axillary neurovascular bundle and cervical spine.
Lateral Decubitus positionINTRODUCTION
Fron Latin means act of lying on one’s side .The position is conventionally referred to as right or left lateral.INDICATIONS:1. Thoracotomya. Lung surgeries - pneumonectomy, lobectomy, decorticationb. Cardiac surgeries- PDA ligation, CMVc. Mediastinal surgeries- Thymoma, neurogenic tumours2. Laparotomy
In carcinoma of gastrointestinal tract(GIT), strictures, diaphragmatic hernias3. Urological surgeries
Pyeloplasty
HISTORY:Thorek in 1913 described this position for
oesophageal resection for a case of carcinoma oesophagus.
TECHNIQUE OF POSITIONING:
EFFECTING THE LATERAL DECUBITUS POSITION
After induction of anaesthesia and securing all IV and electrical circuits, the patient is turned from supine to the lateral decubitus position . The back should be perpendicular to the end of the table, epigastrium at the level of the kidney rest, the thigh of the dependent lower extremity is flexed upon the trunk to stabilize the pelvis and the knee is flexed. The nondependent lower
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 178 Trivandrum Medical College
extremity is kept straight. Two pillows are placed between the two lower extremities to minimize pressure points. Now the patients trunk is stabilised in the manner that will prevent it’s rolling either forward or backward. Similarly the thighs and buttocks are also stabilised by taping to the sides of the table.
Both forearms are flexed at the elbow and kept out of the operating field and a pillow is kept in between . Another pillow is kept below the dependent axilla to prevent compression of the neurovascular bundle. Excessive abduction on the arms should be avoided to prevent brachial plexus injury. Head is supported on an appropriate sized pillow and the indifferent electrode of the ECG is placed on the upper thigh.
ACHIEVING THE LATERAL DECUBITUS POSITION
Atleast three persons are needed for positioning.a. Patient is supine and intended down arm is abducted.b. Anaesthesiologist is the co-ordinator standing at the head end. He should control turning of head and preservation of airway and the endotracheal tube.c. If the patient is to be turned to the left, anaesthesiologist turns the patients head on its pillow to the left. The two assistants stand on the right at the hip and shoulders of the patient. Assistant 1 at the shoulders places his left hand behind the neck of the patient to grasp the left shoulder and places his right hand on the patients right shoulder. Assistant 2 places his right hand under the patients thighs to grasp the pelvis in the region of the anterior part of left iliac crest
and his left hand on the right iliac crest. On receiving an affirmative reply from both the assistants, anaesthesiologist gives the command “turn”. Then the lateral position is achieved by simultaneously pulling on the patients left hip and left shoulder and pushing on right hip and right shoulder. Once the patient is in the lateral position, a hand on the shoulder of the patient will maintain stability while the limbs are positioned.
PRECAUTIONS1. Care must be taken to control the relaxed head, neck and extremities.2. Possibility of a whiplash injury to the neck should be remembered.3. Avoid pressure on dependent eye and ear.4. Care of the airway, IV lines and monitors.
ADVANTAGES OF LATERAL DECUBITUS POSITION1. Most complete access to one hemithorax2. Best approach for intra pericardial control of hilar vessels.3. Obstetrics -To prevent supine hypotension.
DISADVANTAGES1. Inherently unstable, needs restraints and supports to maintain the desired position which may cause pressure and nerve injuries or interfere with normal blood flow. Overzealously applied restraints across the chest may impair the ventilation of the lungs.2. If IV lines are on dependent limbs interference with free flow may occur.3. If the BP cuff is placed on the dependent limb it can interfere with BP measurement. Also
DO’S DON’TS
Take as many personnel as needed, at least 3 Try to move unconscious patient with
inadequate number of turners
Take care in moving, use smooth movements Use jerky, uncontrolled movements
Have a co-ordinator to call the shots Be satisfied with restraints too tight or
misplaced padding
Pad and restrain adequately Forget that lateral position is unstable
Table 1 Precautions in positioning
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 179 Trivandrum Medical College
can interfere with CVP measurement through a peripherally placed central venous catheter.4. Alteration of the Einthoven triangle between peripherally placed electrodes.5. Atelectasis of lower lung6. Nerve injuries-Brachial plexus
MODIFICATIONS OF LATERAL DECUBITUS POSITION1. Semi supine position for Closed Mitral Valvotomy:
Here the upper leg is straightened; arm is raised by flexing the elbow over the face and the trunk lean back on a small pillow2. Semi prone positionLower leg straightened and trunk rolls forward onto a pillow at the chest.
Physiology of the Lateral Decubitus Position:1. Respira tory system:a. Mechanics of ventilation :
Spontaneously breathing - Dependentlung has better ventilation because with a reduced volume and FRC of the lower lung, the diaphragm on the dependent side lies higher in the chest and is more stretched. This hemidiaphragm has a better mechanical efficiency and produces better ventilation.
Mechanically ventilated patient - The tidal volume is differentially distributed to the non dependent lung because it is more compliant. Reduced FRC in the dependent lung predisposes to alveolar collapse. Also muscle paralysis allows abdominal contents to rise further up against the dependent hemidiaphragm and impede the ventilation of the lower lung. Finally, opening the nondependent side of the chest further accentuates the difference in compliance between the two sides because the upper lung is now less restricted in movement. All these worsen the ventilation perfusion(V/Q) mismatch and predispose to hypoxemia.b. Pulmonary blood flow:
In the lateral position both in spontaneously breathing and mechanically ventilated patients the dependent lung is preferentially perfused to a slightly greater extent because of the effect of gravity. So there is an increase in the zone of nonperfusion of alveoli leading to increase in physiologic dead space on the nondependent side.
2. CVS:In the lateral position, cardiac output is
unchanged unless venous return is obstructed (eg:- use of a kidney rest). Arterial blood pressure may fall as a result of decreased vascular resistance.
COMPLICATIONS:1. Atelectasis : Atelectasis of the dependent lung occurs due to thechanges in the distribution of inspired gas and blood flow more so with controlled ventilation. Prevention is by using large tidal volume >15 ml/Kg and slow rate 10/min with sighs. Postoperative deep breathing exercises, chest physiotherapy and incentive spirometry are recommended.2. Nerve injuries especially of the brachial plexus because of the weight of the body pressing On the lower arm and axilla.
Modifications of the Lateral Position:A. KIDNEY POSITION:
This refers to the posture of a laterally recumbent patient whose spine is flexed laterally to separate the iliac crest of the upper side from the costal margin. This improves the surgical access to the kidney and urinary tract of the exposed flank.
To establish the kidney position, the patient is placed on his side in the middle of the operating table. The break in the table should be at the level of the iliac crest. A pillow is placed between the legs. The lower leg is flexed at the knee and thigh flexed to 90 degrees. Lower thigh and leg are flexed and upper leg remains straight. Table is then flexed or broken so that the muscles of the loin are taut. Final step is the use of a kidney elevator to make the loin muscles extremely taut. Patient is maintained in this position with adhesive tapes. Eyes and arms are well protected.
ANAESTHETIC CONSIDERATIONS:1. Respiratory system:a. Vital capacity decreases by 14.5% due to the restriction of thoracic cage in all the directions. Lateral expansion and diaphragmatic excursion more affected than the anteroposterior expansion.b. Tidal volume decreases by 14%c. Dependent lung prone for atelectasis.d. Surgically induced pneumothorax especially if the surgeon resects the 12th rib
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 180 Trivandrum Medical College
2. Cardiovascular System (CVS) :a. Cardiovascular collapse: This is the most dangerous complication when an anaesthetised patient is turned from supine to either right or left lateral position. So slow and deliberate positioning with constant checking of BP should be done in light planes of anaesthesia.b. Hypotension:1. Morphine frequently given as premedication for renal procedures causes peripheral vasodilatation2. Halothane if used depresses the myocardium and decreases cardiac output.3. G A depresses carotid and aortic sinus reflexes so there is no compensation for cardiovascular instability4. Lateral position especially left lateral, shifts the mediastinum and rotates the heart and interfere with venous return and decreases cardiac output.5. Kidney position produces pooling of blood in both lower extremities. Also there is distortion of upper quadrant of abdomen and obstructs blood flow from lower extremities via inferior vena cava.
COMPLICATIONS OF KIDNEY POSITION.
1. Adhesive tapes - Compression necrosis of the head of femur
2. Injury to the brachial plexus3. Pressure necrosis of the ankle, knees and
feet4. Injury to eyes, ears and cervical spine
B. LATERAL POSITION FOR TOTAL HIP REPLACEMENT:
Anaesthesia is induced in supine position and then turned laterally with the affected hip up. Two pads are kept the first in front of the symphysis pubis to avoid pressure on the genitalia, second is secured posteriorly distal to the iliac crest. Lower leg is flexed at the knee and hip. Additional pads are placed -A. distal to the fibular head to protect the
common peroneal nerveB. under the lateral malleolus of the ankleC. between the kneeD. beneath the dependent axillae
COMPLICATIONS:1. Injury to the dependent hip and leg leading to rhabdomyolysis, myoglobinuria and renal failure.2. Arterial insufficiency of dependent limb and massive swelling of the thigh.
SITTING POSITION INTRODUCTION:
The history of the sitting position for surgical purposes is uncertain, but undeniably lengthy. Barlow, in 1830, reported an episode of air embolism that occurred during the removal of a facial tumor while the patient was in a chair. Dentists seated patients to extract teeth decades before that.The first public demonstration of ether, by W.T.G. Morton in 1846,involved a seated patient undergoing jaw surgery.
The term sitting position describes the posture of the neurosurgical patient whose back is elevated towards the vertical, thighs are flexed on the trunk, legs flexed on the thighs and at the level of his heart.
A much less marked elevation of the head, with the hips and knees only slightly flexed , is used by many surgeons for operations about the jaws, neck and thyroid gland. This is essentially a Lawn chair position with the long axis of the body much more nearly supine than is the classical sitting position.
For pneumoencephalography, the patient is placed in a full sitting position with the spine vertical for a few moments during which air introduced into the lumbar cistern, floats into the skull and initial erect X Ray films of the ventricular system are taken. Surgical procedures, however, are rarely done with the patient in this position.
ANALYSIS:Opinion is divided about the use of sitting
position in Neurosurgery. The sitting and prone positions compete as a means of access to the posterior cranial fossa and cervical spine, whereas the usual choice for approaching the middle cranial fossa is between the sitting and the lateral decubitus positions.
Advantages of the sitting position afe-
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 181 Trivandrum Medical College
1. It allows a better physical access to the operative site from directly behind the wound, rather than from above and to one side, as is the case in prone position.2. Because the head is not weight bearing, this position will permit greater torsion of the head and neck than will prone. This allows the surgeon a more lateral approach to the cerebellopontine angle than could be accomplished with the patient prone.3. Accumulated blood drains out of and away from the operative site, thereby offering more rapid access to the bleeding points, a cleaner surgical field and a technically more favourable operative access.4. The sitting position allows an unobstructed view of the patients face, so that the anaesthesia team may observe motor responses from stimulated cranial nerves.5. Suitable head holders for the sitting position remove the hazard of pressure upon the eyeballs, by the circular or horse shoe shaped face pieces commonly used for prone position.6. Because there is free access to the anterior chest wall in the sitting position than in the prone position, resuscitative measures can be instituted more rapidly if cardiovascular collapse occurs.7. The amount of intrathoracic pressure needed for IPPV is less in the sitting position than in the prone position. A patient who is prone must be lifted off his anterior chest wall by each passive inflation of his lung. This increases venous distension in the wound during expansion of the lung and constitutes a major annoyance to the surgical team if venous bleeding is hard to control.8. Relatively unobstructed access to the chest wall for monitoring purposes or therapeutic needs.9. Arm vessels are more readily available for monitoring, fluid administration or obtaining arterial blood samples.10. Urinary catheter obstructions which upset fluid balance calculations are less likely.11. Sudden dislocation of ETT is unlikely since direct access to the airway by the anaesthesiologist is maintained.
INDICATIONS:1. Posterior cranial fossa surgeries2. Cervical laminectomy3. Suboccipital craniectomy
RELATIVE CONTRAINDICATIONS :1. Ventriculoatrial shunt in position and open2. Cerebral ischemia in the upright awake patient3. LAP<RAP4. Platypnoea-orthodeoxia5. Cervical spine degeneration6. Pre operative demonstration of PFO or right to left shunt7. Cardiac instability8. Extremes of age
PHYSIOLOGICAL EFFECTS OF SITTING POSITION 1. Cardiovascular System (CVS) :
The force of gravity assumes a prominent role in cardiovascular function depending upon the extent to which the long axis of the body becomes vertical in the sitting position, Massaging action of leg muscles useful iri returning dependent venous blood to IVC are absent under anaesthesia and the blood volume in the legs may increase by more than 500 ml as a result. With IPPV there is an additional impedence to the venous return. These forces act to diminish systemic perfusion by decreasing venous return and cardiac output.
Above the level of heart, venous return is aided by gravity. The higher the surgical field is located above the heart, the greater is the pressure differential and the more easily is air entrained in partially severed or patulous vessels. In addition the structure of the dural sinuses is that they do not expand under pressure or collapse when their internal pressure is low. The entrainment capacity of these structures is obvious.
In the arterial tree, gravity antagonises the upward flow of blood into the elevated head and augments it’s accumulation in the dependent lower extremities. With unrestricted arterial pathways cerebral perfusion decreases 2 mm Hg /vertical inch (2.54 cms) of elevation above the heart. 60% of lateral rotation of the head begins to reduce the flow in the contralateral vertebral artery and 80% of rotation obstructs it. Opposing this is a proportional increase in the ipsilateral vertebral artery flow. Another safeguard is the reversal of the normal cephalad flow through the basilar
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 182 Trivandrum Medical College
arteries if the vertebral arteries become ineffective: Brainstem perfusion is then supplied caudal from the circle of Willis.. However any signs of impaired brainstem perfusion (such as unexpected change in BP or appearance of bradyarrhythmias or PVCs) should be recognised early and responded to promptly. Predictable cardiovascular response to tilt includes -1. Increase in heart rate (upto 19%)2. Decrease in stroke volume3. Decrease in cardiac output.(cardiac index <14%)4. Little variation in SBP but an elevation of both DBP and MAP(increase 9-38%)5. Increase in peripheral vascular resistance calculated from the fall in cardiac output and rise in MAP (40%)6. Lengthening of pre ejection period due either to need to open the aortic valve against a higher diastolic pressure or to a reduction in the contractility of the myocardium.
2. Respiratory System(RS):The anaesthetized patient has the benefits
of an almost unimpeded RS when placed in the sitting position. Unlike supine position, in which abdominal viscera tend to restrict the caudad motion of the diaphragm or compress it cephalad at rest, the sitting position permits the downward displacement of the abdominal contents and freer diaphragmatic motion. This should promote better ventilation of the lung bases.
If IPPV is used, the pressures required to expand the lungs of a patient are much less if the patient is in the sitting position than the prone. Since the intrathoracic pressure patterns affect venous return, the pressure of IPPV that is transmitted to the surgical field is less, resulting in less bleeding.
The lung volume at which the small airways begins to close during exhalation has been termed “closing volume”. In healthy adults, Closing Volume(CV) occurs between functional residual capacity (FRC) and residual volume (RV). Both these values are increased in sitting position , but the degree of increase in FRC is more than that of the CV. Hence there is a significant reduction in the volume of trapped gas (VTG) in the sitting position.
A potential detriment of the sitting position was reported by Gurtner & Fowler in 1971. They found a reduction in the diffusing capacity for 02 (A-a D02) in the sitting position because of decreased perfusion of the upper zones of the lung.
3. CNS:The normal CSF pressure in the supine
position is 8-12 mm Hg(100-165 mm H20). With the patient in the sitting position this pressure becomes about 30 mm Hg (400 mm H20) in the lumbar cistern , while at the vertex of the skull it is subatmospheric at -5 mm Hg (-65mmH20). This reduces one force composing the ICP and results in more effective perfusion at lower arterial pressures.
4. Other considerations:a. Pregnancy : Should this position be required in the last trimester of pregnancy, the uterus can impair the two major advantages of this posture - by encroaching upon the downward movement of the diaphragm and compressing the IVC. Careful attention to ventilation and gentle lateral displacement of the uterus should improve the situation.b. Temperature variations : Can be hard to control in the seated patient.
TECHNICAL ASPECTS:The operating table should have a
removable head platform and separate controls for the leg section, for the back and for flexion.
If a thermal mattress or a Gardner-Dohn antigravity suit (G-suit) is used, they should be placed on the table prior to placing the patient on it. 1 or 2 pillows are placed in the thigh section of the table. This serves to elevate the patients seat in the final sitting position, so that when the head platform is removed , the edge of the table corresponds to the 2nd/3rd thoracic vertebra.
Endotracheal intubation in these patients is safest with a non kinkable tube which permits the unusual head position occasionally required for access to the cerebellopontine angle. Tube compression by biting can be prevented by inserting a properly made bite block between the patient’s teeth; a conventional oral airway fails
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 183 Trivandrum Medical College
to separate the teeth widely enough to protect the ETT.
Large calibre IV lines, a right atrial catheter when indicated, an arterial cannula, an esophageal stethoscope, ECG leads, urinary catheter and thermal probes are all put in place with the patient supine. The lower extremities are wrapped with compression stockings or elastic bandages, if needed. Any hypotension associated with induction of anaesthesia is corrected and ventilation is stabilised.
To establish the sitting position, first the table is flexed fully. The foot section is lowered by at least 45 degrees. The thigh straps are loosened temporarily to prevent injuries to the thighs or restricting motion of the table top. The back section is slowly elevated while the chassis is being inclined towards the Trendelenburg position. This combined manoeuvre is coordinated to produce further flexion of the thighs on the trunk. During these manoeuvres BP should be monitored repeatedly.
Continued elevation of the back section will now place the patient in the desired degree of sitting position with the legs at about the level of the heart. The knees should be flexed upon the thighs to prevent stretching of the sciatic nerve or its branches. Slowed elevation of the head and judicious use of a balanced vaspressor, such as ephedrine or mephenteramine, are indicated to ensure BP levels that provide adequate cerebral perfusion.
The traditional method of securing the head was to use a horse shoe shaped head rest placed against the face & to tape the head to it. They, however, seldom fit the face and thereby threaten the eyes, cheeks and the supraorbital nerve with excessive pressure. The strapping can also be sweated loose or ripped off by sustained traction .
The most successful head holder is some form of skull pin & clamp device. There are two versions- the Gardner version and the Mayfield version. Each of these models consists of 3 sterile pins, which firmly penetrate the outer table of the skull & fits into a C shaped skull clamp. The
clamp is then attached to a long supporting arm that is attached to a U shaped brace fastened tightly to the rails of the operating table.
Once the patient’s head is stabilised, the head section of the table is removed. The elbows of the patient are supported by pillows or pads. The patient’s hands are crossed in his laps. Bony prominences are padded and the legs wrapped to mid thigh in elastic bandages to augment venous return.
VARIATIONS:A useful variation was reported by Garcia-
Bengochea & colleagues. They described a position in which the patient was placed in a chair fixed to the operating table in such a way that Durant’s left lateral position can be rapidly established simply by lowering the control end of the table chassis. By arranging the table top in the form of a chair ( back elevated, foot section down), placing a back rest for the patient at 90 degrees to the right edge of the elevated back section, they stabilized the patient in a sitting posture that allowed varied head torsion. Should hypotension or air embolism occur, the usual head end of the table chassis can be lowered rapidly by turning a single crank and the Durant’s position can be attained without losing control of or contaminating the wound.
COMPLICATIONS, PREVENTION AND TREATMENT: 1. Hypotension :
Hypotension in the seated anaesthetised patient is indicative of cerebral hypoperfusion. It is probably the most frequent complication of this position.lt requires rapid detection and prompt correction.a. Fluid volume deficits should be corrected before surgery.b. Vasopressors such as ephedrine or mephenteramine.c. The G suit, though cumbersome, has been shown to be useful in the immediate treatment.d. Alert replacement of intraoperative blood loss.
2. Endotracheal tube migration :An unexpected complication is the
migration of the tip of the ETT into the right
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 184 Trivandrum Medical College
mainstream bronchus. Elevation of the diaphragm produced by the sitting position can easily raise the carina cephalad and cause the tip to migrate. Auscultation of each hemithorax is a must after the positioning and the ETT must be adjusted so that all lung fields are ventilated equally.
Firm tape fixation of the ETT & bite block are mandatory to prevent the ETT from being dislodged by head motion from bone drills or saws or by traction from the breathing circuit itself.
3. Air embolism :Venous air embolism(VAE) is detectable
in the sitting position by precordial Doppler in 40% of patients & in 76% of patients using transesophageal echocardiography.Common sources:The common sources of major VAE are1. Major cerebral venous sinuses
a. transverse sinusb. sigmoid sinusc. posterior half of the sagittal sinus
2. Emissary veinsa. to the suboccipital musculatureb. diploic space of the skull
3. Cervical epidural veins
EFFECTS OF AIR EMBOLISM :Effects depend on the total volume &
perhaps more importantly on the rate of air entry. The air bubbles may pass from the right atrium into the right ventricle, where they may be churned up into froth before being ejected into the pulmonary artery. Pulmonary hypertension with right ventricular strain develops due to mechanical blockage of the pulmonary vessels and neurogenic effect.The cardiac output and BP fall & dysrhythmias including VF, may be precipitated.
Air can then pass into the systemic circulation either through the pulmonary vascular bed or through intracardiac defects like Patent Foramen Ovale. The dangers of systemic air are that it may enter the coronary artery & provoke VF or enter the cerebral vessels & produce permanent neurological damage.
The effect of air embolism is aggravated if the patient is receiving N20 at that time. N20 which is 30 times more soluble than N2, would
diffuse quickly into the bubbles & appreciably increase their size.
MONITORS:1. TEE : This can detect air embolism in 8- 75% of patients in the sitting position. It is a highly sensitive monitor. Emboli as small as 2 microns can be detected. It has the advantage of identifying right to left shunting of air.2. Doppler ultrasound : One of the more sensitive methods to detect air embolism. The receiver is placed over the tricupid valve. The combination of precordial Doppler with ETC02 monitoring is the current standard of care in the sitting position.3. Auscultation : Faintly audible high pitched tinkling sounds can be heard at first. 30 ml of air produces the characteristic mill-wheel murmur. The changes are earlier appreciated with an esophageal stethoscope.4. ECG : Changes are best seen in V1 & comprise of signs of right heart strain(RBBB, T wave depression &tall peaked P waves in the right chest leads)5. ETC02: Sudden falls in ETC02 is produced due to an increase in alveolar dead space secondary to the development of venoarterial shunts in the lung.6. CVS monitoring : There is hypotension secondary to low cardiac output , tachycardia and increase in bothCVPand PAP.7. ETN2: Theoretically attractive, but its use in anything less than catastrophic VAE is small.
MANAGEMENT:1. Prevent further air entrya. Notify the surgeon- compress or ligate the
vessel. If this is not possible flood the wound with saline or pack with saline soaked pads.
b. Apply Jugular compressionc. Change the position of the patient (lower
the patient’s head)2. Support circulation :
External Cardiac Massage (ECM), 100%02, Vasopressors.
3. Removal of air :The classical description is that turning
the patient to the left side head down (Durant’s position) places the right atrium & tricuspid valve above the right ventricle & tends to delay the passage of air into the pulmonary artery. Air can
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 185 Trivandrum Medical College
then be aspirated through a right atrial monitoring catheter. Natural absorption of air is hastened by ventilation with 100% oxygen. Whole body compression of the patient may be valuable to force the gas into solution.
4. Quadriplegia :The sitting position per se has been
implicated as a cause of rare instances of unexplained post operative quadriplegia. It has been hypothesized that neck flexion, which is a common concomitant of the seated position, may result in stretching or compression of the cervical spinal cord. This possibility represents a relative especially when there is evidence of associated cerebral vascular disease.
5. Macroglossia :Swelling of the pharyngeal structures
including the soft palate, post wall, pharynx & base of the tongue have been observed. These have been attributed to trauma/ischemia occurring as a result of foreign body (usually oral airways) causing pressure on these structures in lengthy procedures with sustained neck flexion. It is ideal to maintain at least a finger breadth’s distance between the chin & sternum to prevent excessive reduction of the AP diameter of the oropharynx.
6. Arrythmias :Arrythmias in the seated patients are
classified as perfusing and nonperfusing.
A non perfusing arrythmia is one which causes or accompanies a fall in perfusion pressure & is an emergency. Treatment must be prompt.a. Cessation of the surgical stimulus alone
may be enoughb. Prompt use of vasopressorsc. Restoration of depleted blood volumed. Inflation of the G suit.e. Aspiration of intracardiac air.f. Use of supportive drugs.g- Cardiac massage as needed
A perfusing arrythmmia , that is one notaccompanied by hypotension, may also result from surgical manipulation. If surgical stimulation is not the cause and air embolism can be ruled out, the most frequent cause seems to be C02 excess when blood gases are not being monitored. Other extracardiac causes like electrolyte disturbances should be sought and corrected.
8. Miscellaneous complications :a. Tension pneumocephalusb. Sciatic nerve injury due to prolonged extension of the knees.c. Foot drop due to pressure on the common peroneal nerve.Severe flexion and lateral rotation of the rieck can be traumatic to an arthritic cervical spine.
RACE 2003 Ramachandra Anaesthesia Continuing Education

HOW I DO IT?

A 20 year old Primi with severe MS requires Labour Analgesia 186 R.Bharathi
There is no question that labour and delivery are extremely painful experiences for most women. Unfortunately, many believe that labour pain has an important biological function and should not be relieved and there is a general belief that methods of pain relief are dangerous to the mother and newborn.
IS THERE A NEED TO RELIEVE PAIN?ASOG statement
“Labour results in severe pain for many women. There is no other circumstance, where it is considered acceptable for a person to experience severe pain amenable to safe intervention, while under physician’s care. Maternal request is a sufficient justification for pain relief during labour".
As stated by Hippocrates “Divine is the task to relieve pain”. This is truer than ever when we are considering two lives and we must take every effort to honour the patient’s request for labour analgesia.
When confronted with the patient’s cardiac problem, the anaesthetist must answer the following questions:
1) What are the anatomic abnormalities in mitral stenosis (MS)?2) What changes in preload, afterload, heart rate and contractility will optimise the patient with MS especially with relation to pressure volume loop.3) What are the treatment options for MS?4) What are the important considerations in planning the anaesthetic management of a patient with MS?5) What are the special considerations for anaesthetic management of labour and delivery in MS anticipating haemodynamic swings?6) What are the complications and limitations
of regional anaesthesia in MS?
Although rheumatic heart disease is decreasing worldwide and has become a rare complication of pregnancy in affluent societies, it is still prevalent in poor countries like India and remains an important cause of maternal mortality, MS being the commonest lesion. The overall mortality associated with MS is reported to be 1% but increases to 5% in Class III and IV of the NYHA classification. In the presence of atrial fibrillation, maternal mortality is 14-17%. Similarly, perinatal mortality rates are low in Class I and II, but increase in Class III and IV to 12-31%.
PATHOPHYSIOLOGY:MS causes physiologic abnormalities
both proximal and distal to the abnormal valve. Distally, there is a “protected” or underloaded left ventricle (LV), which may have contractile abnormalities. Proximally, a pressure gradient develops between the left atrium (LA) and LV in order to force blood across the obstruction of the narrowed valve orifices. This elevated LA pressure causes alterations in LA size, compliance and function. In addition, the pressure is reflected back into the pulmonary veins causing changes in pulmonary and right ventricle (RV) function. The area of the valve orifice is the key to the flow, and as the orifice gets smaller, the turbulent flow increases across the valve and total resistance to flow increases.
Diagramatic representation of the transmitral blood flow velocity:
Left ventricular (LV) filling starts with the opening of the mitral valve and continues during the early (rapid) and late (slow) filling phases while atrial blood rushes through the mitral valve into the ventricular cavity. The pressure gradient tends to accelerate the blood flow in the LV cavity.
RACE 2003 Ramachandra Anaesthesia Continuing Education
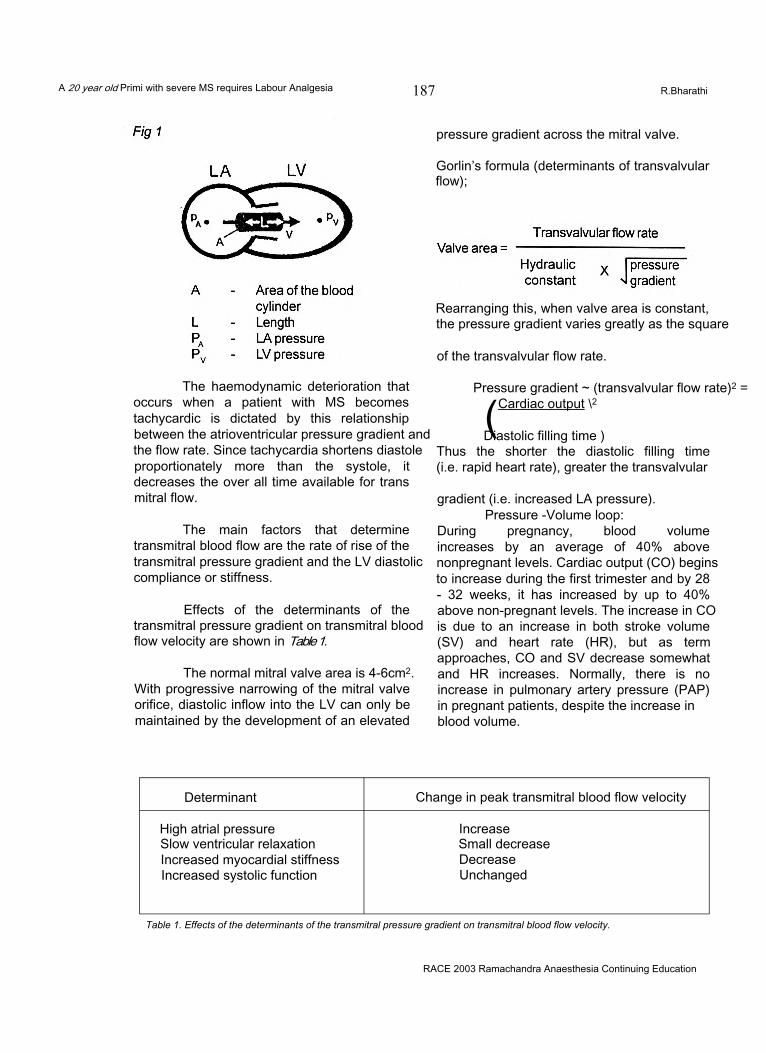
A 20 year old Primi with severe MS requires Labour Analgesia 187 R.Bharathi
The haemodynamic deterioration that occurs when a patient with MS becomes tachycardic is dictated by this relationship between the atrioventricular pressure gradient and the flow rate. Since tachycardia shortens diastole proportionately more than the systole, it decreases the over all time available for trans mitral flow.
The main factors that determine transmitral blood flow are the rate of rise of the transmitral pressure gradient and the LV diastolic compliance or stiffness.
Effects of the determinants of the transmitral pressure gradient on transmitral blood flow velocity are shown in Table 1.
The normal mitral valve area is 4-6cm2. With progressive narrowing of the mitral valve orifice, diastolic inflow into the LV can only be maintained by the development of an elevated
pressure gradient across the mitral valve.
Gorlin’s formula (determinants of transvalvular flow);
Rearranging this, when valve area is constant, the pressure gradient varies greatly as the square
of the transvalvular flow rate.
Pressure gradient ~ (transvalvular flow rate)2 =
(Cardiac output \2
Diastolic filling time )Thus the shorter the diastolic filling time (i.e. rapid heart rate), greater the transvalvular
gradient (i.e. increased LA pressure).Pressure -Volume loop:
During pregnancy, blood volume increases by an average of 40% above nonpregnant levels. Cardiac output (CO) begins to increase during the first trimester and by 28 - 32 weeks, it has increased by up to 40% above non-pregnant levels. The increase in CO is due to an increase in both stroke volume (SV) and heart rate (HR), but as term approaches, CO and SV decrease somewhat and HR increases. Normally, there is no increase in pulmonary artery pressure (PAP) in pregnant patients, despite the increase in blood volume.
Determinant Change in peak transmitral blood flow velocity
High atrial pressure IncreaseSlow ventricular relaxation Small decreaseIncreased myocardial stiffness DecreaseIncreased systolic function Unchanged
Table 1. Effects of the determinants of the transmitral pressure gradient on transmitral blood flow velocity.
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 188 R.Bharathi
In the patient with MS, pregnancy is associated with an increase in CO. There is also an increase in pulmonary artery pressure (PAP), which is probably due to increase in blood volume. If there is pre-existent pulmonary hypertension, the increase in PAP may lead to pulmonary congestion and it may be necessary to initiate diuretic therapy. Symptoms from even mild to moderate MS may become severe as the pregnancy progresses. These haemodynamic changes account for the 25% incidence of pulmonary congestion and 5-17 % mortality rate in the puerperium.
Tachycardia is not well tolerated by patients with MS as it decreases LV diastolic filling time. LA dilatation as a result of increase in central blood volume may lead to atrial fibrillation, which will further impair LV filling. Digoxin is often given prophylactically during pregnancy with MS to prevent tachycardia and atrial fibrillation. Beta- blockers may also be used.
Labour and delivery impose additional stresses on the CVS. In the normal patient, there is a progressive increase in CO during the peripartal period, which is accompanied by an increase in both HR and SV. The increase in CO is due to increased sympathetic stimulation secondary to pain and increased metabolic demand. Uterine contractions cause a further 15- 20% increase in CO, due to blood being transfused from the uterus into the central veins. When the term pregnant patient is turned from the supine to the lateral position aortocaval compression is relieved and CO is increased by 30%
CO and HR are maximal during the immediate postpartum period at which time, CO is approximately 80% above nonpregnant levels (due to disappearance of aortocaval compression and autotransfusion of blood to the central veins by the contracted uterus), This increase in intravascular volume and heart rate makes the MS patient particularly vulnerable to the development of pulmonary oedema at this time.
PAIN PATHWAYS DURING LABOUR:Pain during the first stage of labour is
mainly due to uterine contractions and cervical
dilatation. In the first stage, pain is transmitted via visceral afferents that accompany sympathetic nerve fibres and enter the spinal cord at T10, 11,12 and L1 segments. Visceral pain is severe, dull aching and poorly localized and is easier to block than somatic fibres. Opioids are useful in relieving the pain. In the late first stage and second stage of labour, pain is due to distension of the pelvic floor, vagina and perineum. Opioids are not useful for second stage and local anaesthetic is needed.
WHY PAIN RELIEF?Pain and fear are the main reasons for
maternal hyperventilation during labour, which can lead to respiratory alkalosis, increased oxygen consumption and lactate accumulation. This may not affect a healthy parturient but will affect the parturient with limited cardiac reserve as in mitral stenosis who cannot increase oxygen delivery.
Acid base balance: Inadequate pain relief leads to progressively increasing metabolic acidosis and the foetus becomes more distressed. Failure to relieve labour pain can lead to maternal exhaustion and reduction in the efficacy of uterine work. Maternal pain and stress reduce uterine blood flow secondary to the release of endogenous norepinephrine. There is an increase in cardiac output (25% in the late first stage and 40% during second stage) due to increase in sympathetic activity. This increase in cardiac output is 10-15% less in those who receive labour analgesia, which is beneficial with a narrow mitral valve. Epidural analgesia decreases plasma catecholamine concentrations and attenuates the increase in cardiac output seen in the labouring parturient.
MITRAL STENOSIS:ANAESTHETIC MANAGEMENT IN LABOUR:
Patients with MS often tolerate the haemodynamic changes of pregnancy poorly. Because of the increases in blood volume and cardiac output associated with pregnancy, symptoms from even mild to moderate MS may become severe as the pregnancy progresses. These haemodynamic changes account for the 25% incidence of pulmonary congestion and 5- 17 % mortality rate in the puerperium.
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 189 R.Bharathi
ObjectiveTo minimize left ventricular end diastolic
pressure (LVEDP) and impedance to forward flow and to maximize left ventricular end diastolic volume (LVEDV) and facilitate movement of this relatively fixed CO toward the periphery.
1) Oxygen administration, left lateral position2) Antibiotic prophylaxis - (not necessary for
vaginal delivery as per AHA guidelines)3) Fluid restriction (with monitoring to maintain
preload)4) Slow heart rate: Beta blockade, analgesia,
phenylephrine (not ephedrine?) for hypotension
5) Prevention/Treatment of AF: Digoxin, Verapamil, Beta blockade, DC Cardioversion
MonitoringECG, Pulse oximetry, CVP (use of PA
Catheter is controversial as PCWP does not reflect the left atrial pressure), peripheral arterial line and foetal heart monitoring.
AnaesthesiaREGIONAL ANAESTHESIA FOR LABOUR:
Epidural or CSE the aim is to avoid abrupt decrease in SVR. Suplimental dose will be required during the second stage of labour for elective forceps delivery.
CAESAREAN SECTION:Elective: Epidural probably preferred.
Maintain filling pressures. Emergency: General anaesthesia with
endotracheal intubation. Postpartum high-risk period
First 1-2 hrs critical Possible use of epidural post-op postpartum.
Primi with critical MS for Labour AnalgesiaA 30-year-old primigravida with severe
mitral stenosis (mitral valve area-0.9cm2) requests labour analgesia.
The management begins with a detailed history including prior hospitalisation, drug therapy and decreased exercise tolerance during this pregnancy. I will do a complete physical examination of the cardiovascular and respiratory
systems with particular reference to evidence of cardiac failure (elevated jugular venous pressure, pedal oedema, basal crepitation) and arrhythmias (atrial fibrillation). Airway assessment and spine examination will complete my physical examination.
Investigations that I would like to have will include haemoglobin%, serum electrolytes, blood urea nitrogen, serum creatinine, electrocardiogram and a recent echocardiogram.
I will interact with the obstetrician regarding the progress of labour (cervical dilatation) for the timing of the labour analgesia.
My plan for this patient is combined spinal epidural analgesia.
I will explain to the patient about the benefits of labour analgesia and obtain written consent for the same.
Preparation before the procedure.The patient is given oxygen at 6l/mt and
a wedge kept under the right hip for left uterine displacement. After establishing monitoring including electrocardiogram (ECG), pulseoximetry (Sp02), I will cannulate the left radial artery for invasive pressure measurement and central venous line through the right cubital fossa for central venous pressure monitoring.
Emergency resuscitation trolley, a good working laryngoscope and a working suction are kept ready and the following drugs are loaded before the procedure:1) Thiopentone sodium2) Suxamethonium.3) Atropine.4) Esmolol.5) Phenylepherine.6) Frusemide.7) Fentanyl.
I will explain in detail about the wholeprocedure and allay the patients fear if any.
Combined spinal epidural techniqueNo preloading of intravenous fluid will be
given but ringer lactate will be given at 75 ml/hr
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 190 R.Bharathi
as maintenance fluid. After putting the patient in the left lateral position, the procedure is done as described below. The epidural space is identified with a 16 G tuohy needle in the L3-L4 interspace using loss of resistance to air. Using a needle through needle technique fentanyl 10 meg is given intrathecally with a 26G spinal needle. Alternatively, a separate spinal injection can be given at a lower space. A16 G epidural catheter is inserted 6 cms into the epidural space. All the while, the foetal heart is monitored.
No test dose is givenAn epidural infusion of bupivacaine
0.0625% and fentanyl 2mcg/ml is started at 6 ml/hr. The infusion rate may be increased up to 12 ml/hr so as to achieve a block up to T10 level. Additional doses of fentanyl 25 meg may be given so as to augment analgesia when necessary, as during maximal cervical dilatation. Epidural analgesia facilitates a controlled second stage of labour and can be shortened by the elective use of either vacuum extraction or forceps delivery. During this period, epidural boluses of 0.1% bupivacaine with fentanyl 25 meg can be given in slow incremental doses over a period of 10 to 20 minutes, so as to prevent hypotension. If there is any hypotension during this period, I will manage it with phenylepherine rather than ephedrine, as it will cause tachycardia. There is no evidence that the use of phenylepherine compromises uterine blood flow.
After delivery of the baby, I will give oxytocin 10 units slowly as an infusion over 15 to 20 minutes in order to minimize reflex tachycardia. Since these patients are at risk of developing pulmonary oedema, precipitated by autotransfusion in the postpartum period, I will give frusemide 20 mg in divided doses and as well continue the epidural bupivacaine and fentanyl infusion.
Advantages of combined spinal epidural techniqueINTRATHECAL FENTANYL:
Intrathecal fentanyl alone is effective in early labour (cervical dilatation < 5 cm) conferring the advantage of profound analgesia with complete absence of motor block, greater patient satisfaction and greater reliability. Intrathecal
fentanyl in the range of 5 - 25 meg produces a dose dependent increase in the duration of analgesia (45 -90 mins). Fentanyl doses more than 50mcg do not prolong the analgesic duration. There is a similar analgesic effects, onset, intensity and duration with a smaller dose of fentanyl (15-25mcg) compared to a larger dose (50mcg). There is a modest decrease in maternal blood pressure, likely due to analgesia rather than sympathetic block.
High block, respiratory depression and dysphagia can occur. Ventilatory depression is characterized by reduced tidal volume rather than decreased rate and it can be delayed in onset (30 minutes or more).
Lateral positioning during intrathecal administration may limit the rostral redistribution and limiting the maximum intrathecal dose to 25mcg is likely to reduce these complications.
Appropriate monitoring (Patient observation and pulse oximetry) is strongly recommended when intrathecal techniques are used.
Nausea and pruritis are very common dose dependant side effects. They require treatment infrequently and resolve before the analgesic effect wanes.
There is a low incidence of foetal heart rate (FHR) abnormalities (6-12 %) seen with intrathecal fentanyl 25mcg compared to 30% incidence with 50mcg fentanyl where more of the FHR changes resulted in the need for caesarean delivery. These are transient and resolve spontaneously and are not accompanied by maternal hypotension or emergent interventional delivery.
Foetal bradycardia following the onset of intrathecal analgesia most often is associated with rapid cervical dilatation, or nuchal or prolapsed umbilical cord. Uterine hypertonus can be due to abrupt elimination of beta-adrenergic mediated inhibition of uterine contraction thereby reducing intervillous blood flow.
Epidural testdose1) From the safety point of view, the most
important characteristic of any test to
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 191 R.Bharathi
detect IV or intrathecal catheter malposition is its negative predictive value. This is because the larger therapeutic dose is administered only after the negative test result is obtained. At the same time, a low false positive rate is highly desirable to prevent unnecessary catheter replacement and delay in providing analgesia.
2) Traditional test dose of 45 mg Lignocaine with 15mcg epinephrine is not recommended as there is a risk of high spinal block associated with unrecognised intrathecal catheter malposition, which is hazardous in a labouring cardiac patient as well as tachycardia if it is intravascular, which is detrimental.
3) Unintentional intravascular placement of epidural catheters has been reported to occur with the frequency of 2-9% and is associated with serious outcomes.
Aspiration for blood alone is 98% sensitive in detecting intravascular placement of multiorifice epidural catheters.
Does the air test work for multiport catheter?Inject 1 ml of air through the epidural
catheter and listen for maternal heart sound changes for 15 seconds using a Doppler probe. The test is considered positive if a loud swishing sound lasting atleast 5 seconds is heard in addition to or in place of the normal “lub-dub” heart sounds.
Air test may be less reliable in multiport than in single orifice catheters because gases, to a greater extent than liquids, preferentially exit through the most proximal catheter hole.
Fentanyl test doseAfter 100 meg epidural fentanyl if the
patient has any increased sedation, dizziness or light headedness within the first 5 minutes then it should be interpreted as a positive response for intravascular injection. No adverse foetal outcome has been observed with this method. Yet there may be maternal desaturation, which will require 02 supplementation.
Low dose mixtures of opioid and local anaesthetic are used as a ‘test dose’ combining observation and incremental dosage. At best, intravascular injection results in minimal analgesia
and minimal effects in the mother and the foetus. If the injection is intrathecal, the worst scenario is an increasing degree of slow - onset motor blockade with minimal loss of sympathetic tone.
DisadvantagesEpidural analgesia has potential
disadvantages. A rapid onset of epidural blockade may cause a sudden reduction in SVR. As well as potentially compromising uteroplacental perfusion, marked reduction in SVR can cause a compensatory tachycardia.
Therefore, I chose to use CSA. Intrathecal fentanyl provided rapid initial analgesia without adverse haemodynamic effects. This enabled analgesic maintenance to be established gradually using an infusion of dilute bupivacaine- fentanyl mixture, with the avoidance of large or rapid boluses of local anaesthetic. Epidural infusion has less incidence of hypotension compared to intermittent top ups. Thus sympathetic block and potential haemodynamic changes are likely to be of slow onset and amenable to controlled and titrated management.
If analgesia is insufficient for delivery, pudendal nerve block can be added rather than increase the concentration of local anaesthetic boluses.
In the early postpartum period, the patient is at risk of developing pulmonary oedema, which will be exacerbated by cessation of epidural analgesia and the return of sympathetic tone. Hence, I would like to continue epidural analgesia in the postpartum period.
Patient undergoing Caesarean section for obstetric IndicationFOETAL DISTRESS:-
As there is no time for establishing epidural blockade, general anaesthesia is preferred. Epidural catheter is left for post-op analgesia.
NON-PROGRESSION OF LABOUR: -Incremental injection of boluses of 5ml
of 0.5% bupivacaine are given over 15 minutes interval with careful attention to patient’s mental status (every reinjection is a test dose). CSE is associated with more rapid cervical dilatation
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 192 R.Bharathi
compared to standard epidural analgesia. Obstetric and neonatal outcome are the same with both techniques.
Compared with epidural, the advantages of combined spinal epidural (CSE) are
• Rapid and improved analgesia• Reduced initial and total dose of drugs• An objective procedural end point (CSF)• Nil or minimal motor blockade• Minimal autonomic (sympathetic)
blockade• Selective sensory blockade• Ambulation is possible and safe.
Controversies about CSE:1) Risk of penetration through the dural hole
It is impossible to force a 16G or 18G epidural catheter through a dural hole after a single dural puncture with a 25G spinal needle
2) Perceived increased risk of neurotrauma No evidence that paresthesia on CSE needle
or catheter placement is likely to result in a neurologic deficit.
3) Risk of meningitis is extremely low
4) CSE block and decreased risk of post dural puncture headache (PDPH):
Reasons may bea) The use of a very fine diameter spinal needleb) Tuohy needle as an introducer allows meticulous puncture of the duramaterc) CSF leakage through the dural hole is decreased by the increased pressure from epidural anaesthetic solutions (splints the dura from the arachnoid membrane)d) With the single segment CSE technique, the spinal needle is deflected somewhat, as it exits through the Tuohy needle, approaching the dura at an angle, hence both holes do not overlap.
5) Epidural and intrathecal opioids are prophylactic against PDPH.
ALTERNATIVE METHODSThese include but not limited to
intramuscular opioids, entonox, ketamine and hypnosis’
Regional analgesia is the only effective way of providing complete pain relief, if that is what is desired.
CONCLUSIONPhysiological changes associated with
increased metabolic demand can lead to functional deterioration in women with MS who become pregnant. This is exacerbated in labour when pain, bearing down and autotransfusion can lead to tachycardia, elevations of pulmonary vascular resistance and increases in central blood volume, all of which may be poorly tolerated. Successful management of parturients with MS depends on a multidisciplinary approach and is facilitated by early referral to the cardiology and anaesthesia teams and the use of preoperative echocardiography to delineate the valvular lesion before formulation of the delivery plan.
REFERENCES1) Combined Spinal-Epidural analgesia in the management of labouring parturients with mitral stenosis. W.D Ngankee, J.Shen, A.T.O Chiu, I.Lok, K.S.Khaw. Anaesthesia Intensive Care 1999 27; 523-526.
2) Combined Spinal-Epidural anaesthesia in G.primigravida with valvular heart disease. Tomas VanHelder, Kari G. Smeastad, Can J. Anaesthesia 1998/ 45:5 /488-490.
3) Mitral stenosis in pregnancy: a four-year experience at king Edward VIII hospital, Durban South Africa. British Journal of Obstetrics and Gynaecology. Aug 2000, 107: 953-958.
4) Pain management in the critically ill obstetric patients. Chandra Jayasinghe, Norman H Blass, crit care clinics 1999; Jan 15(1): 201-28
5) Multiport epidural catheter. Barbara et al. Anaesthesiology 2000; 92:1617-20
6) Regional Anaesthesia for the pregnant Cardiac patient Mitterschiffhaler Regional Anaesthesia. Acta anaesthesio scan suppl 1996: 109:180-4
RACE 2003 Ramachandra Anaesthesia Continuing Education

A 20 year old Primi with severe MS requires Labour Analgesia 193 R.Bharathi
7) The incidence of foetal heart changes after intrathecal fentanyl labour analgesia. Craig M Palmer et al. Anaes analg 1999:88:577-81
8) Can Parturients distinguish between intravenous and epidural fentanyl? Morris GF et al. Can J Anaes: 1994:41: 667-72
9) The parturients with cardiac disease. Ridley Smiley Anaesthesiolo Clin? North Ame 1998:16:430-32
10) Labour Epidural Analgesia without an intravascular “Test Dose” Mark C Noris et al. Anaesthesiology
1998:88:1495-501
11) Regional Anaesthesia for obstetrics Anaesthesiolo Clini North Ame 2000:Vol184
12) The Combined Spinal Epidural technique Narinder Rawal, Bjon Holmstrom et al. Anaesthesiology clinics of North America June 2000:V18: 267-288
13) Invasive Monitoring for anaesthetic management of parturient with mitral stenosis. G.T Hemmings et al. Can J Anaest 1987/34:2 182-5
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage
194 Manjunath Prabhu
Ludwig’s angina is a potentially lethal, rapidly spreading cellulitis involving the sublingual and submaxillary spaces. It is manifested by brawny suprahyoid induration, tender swelling in the floor of the mouth, and elevation and posterior displacement of the tongue. This condition is a therapeutic emergency because of inherent life threatening airway obstruction. In 1836, Wilhelm Friedrich von Ludwig described this condition as rapidly spreading cellulitis which produced well defined, woody oedema of the submandibular and sublingual areas with minimal throat inflammation, absence of submandibular lymph node involvement and lack of suppuration. A dental focus of infection can be an initiating factor in the majority of cases. Young adult males are more commonly affected than others. The mortality has come down significantly with the use of early intravenous antibiotics. The most common causative agents are streptococci and staphylococci with anaerobes involving in the mixed infection.
MANAGEMENTAirway obstruction has long been
recognised as the most frequent cause of death in Ludwig’s angina (LA) patients. Airway protection is imperative in the successful treatment plan. Early intravenous antibiotic therapy and exploration of the submandibular spaces in those patients who develop abscesses or fail to respond to initial conservative treatment is important. Continuous observation of the respiratory status is mandatory, as progressive soft tissue oedema compromises the airway insidiously, and total obstruction or laryngospasm secondary to aspiration can be abrupt. In cases of rapidly advancing cellulitis, emergency tracheostomy may be life saving. Nuchal rigidity, trismus and gross distortion of the normal anatomy along with grossly enlarged tongue and pooled secretions
can not only make intubation difficult but also make it traumatic and potentially hazardous.
Prior to detailed examination of the patient a proper planning is a must. Preoperative evaluation of the general condition of the patient and airway examination in particular can give a lot of information that can be of great help in deciding the actual anaesthetic plan. Preinduction intubation may be an ideal way of airway management in these patients. Fibreoptic assisted intubation can be a useful option, but it demands greater skills, a cooperative patient and a Clearfield. These prerequisites are not often encountered in usual clinical settings. Blind nasal intubation can be traumatic causing damage to the inflamed surrounding structures and may precipitate airway obstruction.
Earlier recommendations were for early tracheostomy under local anaesthesia before proceeding with incision and drainage. In recent literature, there are enough evidences suggesting that tracheostomy can be avoided in a large number of patients with careful airway management. In 1982, Patterson etal reported 20 cases of Ludwig’s angina patients and 9 patients underwent surgical exploration.1 Tracheostomy was performed in four patients and in the remaining 5 patients, It was avoided. They reported successful treatment in all 20 patients with the use of antibiotics, surgical drainage and proper airway management. In 1985, Loughnan and colleagues reported successful airway management of nine patients with Ludwig’s angina coming for emergency surgery without tracheostomy.2 Most of their patients had trismus and they were induced with inhalational agents and then intubated under direct vision. Mehrotra et al reported a case report where they have used cervical plexus block and
RACE 2003 Ramachandra Anaesthesia Continuing Education

A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage 195
Manjunath Prabhu
then successfully managed the drainage procedure in a military field hospital in Delhi.3 There are reports of people losing the airway suddenly both while intubating awake as well as under inhalational agents.4 Probably intravenous induction and muscle paralysis before securing the airway may not be a safe technique. After going through the literature it is clear that the airway management is quite tricky in this group of patients and there are more than one way of doing it correctly.
HOW I DO IT:The management of these emergency
cases depends on the actual clinical settings and the available options. The important steps to be remembered are a good skilled assistant, proper planning and option for immediate tracheostomy. In the following part, I have explained the way I would like to manage a young, otherwise healthy Ludwig’s angina patient with no acute airway obstruction coming for abscess drainage.
Starting of intravenous antibiotic will be the first step in the management in these patients. The antibiotics should be active against streptococcus and anaerobes. Minimal blood investigations are needed including haemoglobin and blood grouping. Chest and neck radiographic pictures will be asked for. The neck X- rays will give information regarding the soft tissue swelling and its effect on the upper airway structures. Deviated larynx and trachea or a narrow laryngeal passage would indicate a possible difficulty in airway management.
The preoperative evaluation should include a detailed history and airway examination. Trismus can be a common finding and this may lead to restriction on mouth opening until pain is fully controlled. The space available inside the mouth, with the floor of the mouth pushed upwards and swollen tongue should be assessed. Reassuring the patient and explaining the proposed plan can be very useful since proper airway management and early antibiotic therapy can avoid the mortality in most cases. The preoperative advice include written consent for anaesthesia as well as tracheostomy (elective or emergency), starvation orders and continuation of antibiotic therapy. My premedication includes
intramuscularly administered glycopyrrolate for its antisialogogue effect. I will not administer any sedatives until the patient is under my direct observation in the operating room or in the ICU.
Prior to administration of any anaesthetic to the patient, I would like to keep the difficult airway trolley ready. These include, but not limited to, properly illuminated laryngoscopes, appropriate sized cuffed endotracheal tubes, gum elastic bougie, emergency cricothyrotomy set, emergency tracheostomy set etc. Monitors will include pulseoximeter and capnograph in addition to electrocardiogram and noninvasive blood pressure. Emergency resuscitation drugs and equipments will be kept ready. A good suction apparatus with wide bore suction catheters like Yankauer suckers will be kept ready.
Following establishment of IV fluids and connecting the patient to preinduction monitors,I would like to nebulise lignocaine solution in order to provide topical anaesthesia of the upper airway. Nebulisation of lignocaine should make subsequent airway management less painful and helps in the release of trismus. If the patient is having relatively stable vitals, satisfactory mouth opening and is not in acute airway obstruction, then I would induce the patient with inhalational anaesthetic sevoflurane in oxygen. The rapid induction and rapid emergence property of sevoflurane would be the major advantage over other inhalational anaesthetics. A small dose of a short acting narcotic like fentanyl 100 pgm will be administered slowly before induction. As patient is induced, gentle attempts to assist ventilation will be made. In case of necessity, a soft well lubricated nasal airway will be introduced with minimal force. Once the patient is induced as indicated by regular shallow respiration, trismus is likely to disappear and then laryngoscopy will be tried. Tracheal intubation will be done using Machintosh blade if glottic visualisation is possible. In case of difficulty in passing the tube due to inadequate glottic exposure, a gum elastic bougie will be used as a guide for intubation. I would use a size smaller than the usual cuffed endotracheal tube (6.5 or 7.0 mm ID tube). The important steps to be followed are optimum position of the patient and first laryngoscopy by an experienced person using
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage 196
Manjunath Prabhu
a well illuminated laryngoscope with appropriate size blade. The first attempt at laryngoscopy should be considered as the best attempt and so all the efforts should be made to optimise the first attempt. After confirming proper placement of the endotracheal tube with auscultation and capnography, muscle relaxant will be administered. A close monitoring of oxygen saturation will be done throughout and all attempts will be made to maintain oxygen saturation in the safe range. A skilled surgeon and a assisting nurse should be ready from the beginning of induction so that an emergency tracheostomy will be done immediately if the need arises.
Following successful airway management surgical drainage will be allowed. A proper drainage with proper exploration of the surrounding spaces is encouraged. Pus will be collected and send for culture and sensitivity test. The antibiotic therapy will be continued intraoperatively. Considering the possibility of post operative airway oedema endotracheal tube will be retained for a variable time which will be decided by the further course of the disease.
Postoperatively, the patient will be kept under the direct observation of the anaesthesiologist in a high dependency area. Supplemental oxygen, analgesics (narcotic infusion), antibiotics and adequate intravenous fluids will be administered. Following surgery, the patient will be reassessed on the first postoperative day. The general condition of the patient, airway oedema and other likely complications like pneumonia or spread of infection to the surrounding tissue will be assessed. If the patient is awake, well oriented with improved general condition and decreased airway oedema then extubation is considered. The equipments for intubation along with monitors like capnograph and pulseoximeter will be kept ready. In the presence of a skilled assistant, extubation will be performed over a tube exchanger which will also have option for oxygen therapy. Following extubation, I will closely observe the patient atleast for an hour before removing the tube exchanger. The patient will be kept under observation for a further 24 hours. Postoperative spread of infection to other tissue planes, to the
lungs and mediastinum is assessed. If the recovery is satisfactory and there is no danger of further airway problems then the patient will be sent to the surgical ward.
THE ALTERNATIVE METHODS OF AIRWAY MAINTENANCE INCLUDE:Elective tracheostomy under local anaesthesia:
Even though this was recommended earlier, many clinicians have shown successful airway management without tracheostomy. If we can avoid this in a relatively short lasting crisis, then we can avoid all the morbidity associated with tracheostomy. In more sick patients with significant airway compromise, this can still be a life saving option either as an elective procedure or as an emergency. The technique is difficult considering the distorted anatomy and abnormal feel of the structures. There are enough reports about infection spreading to deeper planes or to the mediastinum.
Awake fibreoptic guided intubation:Awake fibreoptic intubation can be a
useful alternative method of securing the airway in these patients. This requires a skilled operator and the main limiting factors can be an uncooperative patient with partial airway obstruction and possible secretions, pus or blood which may make it impossible to view through the scope.
Awake direct laryngoscopy and intubation:This technique may sound safer but it
has got its own limitations. A compromised difficult airway in a patient with pain and trismus can make direct visualisation impossible. Direct trauma to the inflammed structures in a struggling patient can lead to airway obstruction or laryngospam requiring emergency tracheostomy. Direct trauma and sudden release of pus may precipitate aspiration and related complications.
Blind nasal intubation :Even though experienced persons can
use this technique, it may not be an easy option in a distorted airway anatomy and compromised airway. Possibility of airway trauma and aspiration should be kept in mind.
RACE 2003 Ramachandra Anaesthesia Continuing Education

A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage 197 Manjunath Prabhu
Intubation following intravenous induction and muscle relaxation:
This technique may not be advisable in the majority of patients with Ludwig’s angina. Sudden loss of airway following IV induction can lead to a major crisis. This technique can be applied by experienced people when there is no airway compromise.
Thus a patient coming with Ludwig’s angina for abscess drainage poses several challenges and a management dilemma to the anaesthesiologist. Proper preoperative assessment and adequate preparation can make all the difference. Carefully planned airway management can not only help in avoiding tracheostomy, it can also prevent the possible major complications and help in patient’s recovery.
REFERENCES:
1. Patterson HC, Kelly JH and Strome M. Ludwig’s angina: an update. Laryngoscope 1982; 92: 370 - 7.
2. Loughnan TE, Allen DE. Ludwig’s angina. The anaesthetic management of nine cases. Anaesthesia 1985; 40: 295-7.
3. Allen D, Loughnan TE, Ord RA. A re-evaluation of the role of tracheostomy in Ludwig’s angina. J Oral Maxillofac Surg 1985; 43: 436-9.
4. Mehrotra M and Mehrotra S. Decompression of Ludwig’s angina under cervical block. Anesthesiology 2002; 97: 1625-6.
5. Neff SPW, Merry AF and Anderson B. Airway management in Ludwig’s angina. Anaesth Intensive Care 1999; 27: 659-61.
6. Mostafa SM, Atherton AMJ. Sevoflurane for difficult tracheal intubation. Br J Anaesth 1997; 79: 392-93.
7. Moreland LW, Corey J and McKenzie R. Ludwig’s angina report of a case and review of literature. Arch Intern Med 1988; 148: 461-6.
8. Sparks CJ. Ludwig’s angina causing respiratory arrest in the Solomon Islands. Anaesth Intensive Care 1993; 21: 460-2.
RACE 2003 Ramachandra Anaesthesia Continuing Education

PROS & CONS

Induced hypotension is contraindicated in children 198 A. Rajamanoharan
“The use of deliberate hypotension for paediatric procedures has been more limited because the hazards are relatively high”. At present anaesthesiologists are in a “real dangerous position”. We are "pressurized" from many sides to employ this method in order to save blood or facilitate the work of the surgeon! At the same time we are deeply concerned about our lack of knowledge of the haemodyamics involved and by the unexpected complications.- Robert M.Smith, Anaesthesia for infants and children 4th edition, 268
The mechanism of action of hypotensive drugs differ and produce complex changes in the auto regulatory reflexes, and subsequently blood flow to various organs. Because deliberate hypotension is not without risk, the advantages and disadvantages must be weighed. The “intelligent use" of deliberate hypotension has advantages for "certain” procedures that “may” promote surgical success.- Edward D. Miller Jr- Miller 5th edition, 1470
“As the inappropriate use of induced hypotension can result in irreversible cardiac or brain damage”.- George A. Gregory, Text book on Paediatric anaesthesia,
“Thus a systolic blood pressure of less than 70 mm of Hg is a cause for concern at any age”.- Wylie Churchill Davidson
From the above quotations it is more than clear that induced hypotension in children is to be totally discouraged. Let us see in detail why the text books deliver such “danger signals” on deliberate hypotension.
1. Death rate of induced hypotension of 1 in 1802 as stated by Hugovan Aken (Miller) may be statistically insignificant, but totally avoidable and objectionable, because please remember it is deliberate.
2. The decision to induce hypotension has often been controversial, primarily because of our inability to define the lowest safe MAP with confidence.
3. Most clinical studies do not support the belief that deliberate hypotension decreases operating room time.
4. Patient positioning and attention to ventilation, both of which influence venous return play an important role in minimizing blood loss. Clinical experience suggests that blood loss can be decreased with less or no degree of hypotension and that attention to the surgical field may be a better monitor than the absolute value for MAP.
5. The advantages and contraindications must be weighed carefully when induced hypotension is used, as the inappropriate use of induced hypotension can result in irreversible cardiac or brain damage.
6. Further more, significant deviation from the (routine) management may result in organ damage.
7. Body temperature must be carefully monitored because drug-induced generalized vasoconstriction and vasodilatation may increase heat loss. Normothermia should be maintained, if not, deliberate hypotension is contraindicated.
8. An indwelling arterial cannulation is mandatory as rapid and profound changes in the arterial pressure may require immediate intervention as well as determination of arterial blood gases, electrolytes and glucose level.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced hypotension is contraindicated in children 199 A. Rajamanoharan
9. In Pulseoximetry, the reduced size of the pulse waveform is an indicator of reduced pulse volume.
10. If the patient is positioned in head-up, pressure transducer is placed at the level of the he^d and the CVP at the level of right atrium. Both transducers are to be adjusted.
11. The effects of body position and positive pressure ventilation on blood pressure must be evaluated before induced hypotension is started.
12. Urinary catheter should be inserted after induction of anaesthesia but before induced hypotensaion, and care should be taken to maintain a urine output of 0.5 to 2ml/kg/hr throughout anaesthesia
13. In one study, death from controlled hypotension was mainly due to postoperative complications. So, meticulous care imust be directed to the postoperative period besides the routine monitoring.
14. To minimize the risk of cerebral hypoperfusion, hypocapnia is to be avoided during controlled hypotension.
15. The arterial P02 should be maintained above 300mm of Hg at all times during controlled hypotension which may require
i discontinuation of nitrous oxideL16. Thus a systolic blood pressure of less than
70 mm of Hg is a cause for concern at any age.
17. Parasympathetic control of CVS is well developed at birth and sympathetic control is immature.
18. Decreased sympathetic output may explain the normally low blood pressure in human infants and their INCREASED SUSCEPTIBILITY to bradycardia and hypotension.
19. A low level of baroreceptor activity in infants may reduce their ability to ADAPT to hypotension by an increase in heart rate.
20. Even when a clear indication exists, several relative contraindications abort and out-model the usage of induced hypotension.
21. The usefulness of controlled hypotension during clip ligation of cerebral aneurysm is controversial because wall stress at any given pressure depends on the thinness of the aneurysm sac. Better will be temporary occlusion of the proximal vessel.
22. Farmer et al argue that deliberate hypotension
increases the incidence of vasospasm seriously and compromises border line ischemic brain tissue and impairs cerebral auto regulation. Thus controlled hypotension may place focal areas and the entire brain at a risk of ischaemia.
23. Resistance and development of tachyphylaxis.
24. Rebound haemorrhage in the postoperative period.
CONTRA INDICATIONS TO CONTROLLED HYPOTENSION1. Physicians’ lack of understanding of the
technique; lack of technical expertise or inability to monitor the patient’s condition adequately.
2. Inadequate postoperative care3. Local or generalized, decreased organ blood
flow4. Elevated intracranial pressure.5. Anaemia, haemoglobinopathy and
polycythemia6. Allergy or hypersensitivity to hypotensive
agents7. Hypovolemia8. Cerebrovascular disease9. Ischaemic heart disease10. Peripheral vascular disease11. Severe obstructive lung disease12. Renal impairment or hypertension
COMPLICATIONS OF SODIUM NITROPRUSSIDE
For several years, SNP was believed to be devoid of major toxicity. Side effects were seen infrequently, consisting of nausea, vomiting, twitching, sweating, and apprehension, all of which were believed to be the result of overdosage that could be relieved by decreasing the rate of SNP infusion. Chronic overdosage is reported to have caused hypothyroidism in one patient (Katz and Wolf).
The first abnormal response, thought to be tachyphylaxis, is found in patients whose arterial pressure falls with initial administration of SNP but, on continuation of the drug, rises within 30 to 40 minutes, to be controlled only by increasing dosages. This has been seen several times and is believed to be due to the initial presence of adequate tissue rhodanase and
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced hypotension is contraindicated in children 200 A. Rajamanoharan
sodium thiosulfate, followed by early depletion of one, probably the thiosulfate. When this response develops gradually, Davies and associates have been successful in treating the condition with intravenous administration of 150mg of sodium thiosulfate over a period of 15minutes and subsequently proceeding with SNP.
The second abnormal response is seen in patients whose arterial pressure falls with administration of SNP but who require a high dose from the start (over 3.5fig/kg/min).
The third abnormal response consists of such resistance to SNP that hypotension is unobtainable even with greatly increased dosage. Davies and associates believe that patients who show either of the last two responses are in danger of developing metabolic acidosis and cyanide poisoning, and they recommend discontinuation of the drug.
Special contraindications to the use of SNP• Vitamin B12 deficiency• Leber’s optic atrophy• Tobacco amblyopia
Signs suggesting hypoxia or cyanide poisoning during induced hypotension
• Tachycardia, bradycardia, arrhythmias• Metabolic acidosis• High dose requirement
• Increased mixed venous oxygen content• Decreased arterial - mixed venous
oxygen difference• Dilated pupils• High blood cyanide content• Marked hypothermia
The above said contraindications negate the use of induced hypotension. But more importantly, some of these adverse situations may arise during the intraoperative period, in otherwise normal patients. Such a situation becomes very much complex and complicated.
CONCLUSIONSmooth induction, proper choice of
anaesthetic drugs, maintenance of correct plane of anaesthesia, attention to adequate ventilation, proper posture and unimpeded gravity aided venous return will all benefit the surgeon and even more importantly the paediatric patient from undue surgical bleeding and thereby obviate the relative hazards of deliberate hypotension.Primum non nocere - “first of all do no harm”
REFERENCES
1. Robert M.Smith, Anaesthesia for infants and children 4th edition, 268
2. Edward D.Miller Jr - Miller 5th edition, 1470
3. George A. Gregory, Text book on Paediatric anaesthesia,
4. Text book of Anaesthesia by Wylie Churchill Davidson
5. MacRae, W.R.and Owen, M.: Severe metabolic acidosis following hypotension induced with sodium nitroprusside, Br. J. Anaesth. 46:795.
6. McDowall D. G. Keaney, N.P. Turner, J.M, and others; The toxicity of sodium nitroprusside, Br. J. Anaesth. 46:327
7. McHugh, R.D, Berry, F.A, Jr. and Longnecker, D.E,: Dose requirement of sodium nitroprusside during anaesthesia in children, abstract, annual meeting of the American Society of Anaesthesiologists, Chicago.
8. Ivankovich, A.D, Miletich, D.J, Albrecht, R.F, and Zabed, B: Sodium nitroprusside and cerebral blood flow in the anaesthetized and unanaesthetized goat, Anaesthesiology, 44:21.
RACE 2003 Ramachandra Anaesthesia Continuing Education
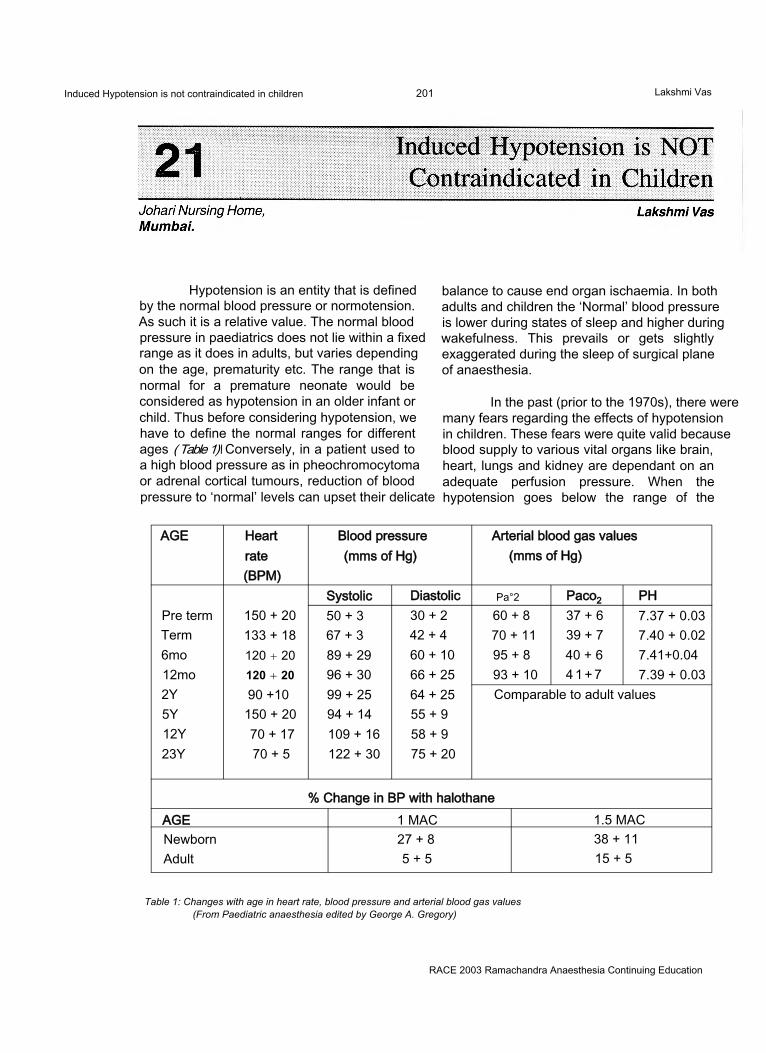
Induced Hypotension is not contraindicated in children 201 Lakshmi Vas
Hypotension is an entity that is defined by the normal blood pressure or normotension. As such it is a relative value. The normal blood pressure in paediatrics does not lie within a fixed range as it does in adults, but varies depending on the age, prematurity etc. The range that is normal for a premature neonate would be considered as hypotension in an older infant or child. Thus before considering hypotension, we have to define the normal ranges for different ages ( Table 1)\ Conversely, in a patient used to a high blood pressure as in pheochromocytoma or adrenal cortical tumours, reduction of blood pressure to ‘normal’ levels can upset their delicate
balance to cause end organ ischaemia. In both adults and children the ‘Normal’ blood pressure is lower during states of sleep and higher during wakefulness. This prevails or gets slightly exaggerated during the sleep of surgical plane of anaesthesia.
In the past (prior to the 1970s), there were many fears regarding the effects of hypotension in children. These fears were quite valid because blood supply to various vital organs like brain, heart, lungs and kidney are dependant on an adequate perfusion pressure. When the hypotension goes below the range of the
AGE Heart Blood pressure Arterial blood gas valuesrate (mms of Hg) (mms of Hg)(BPM)
Systolic Diastolic Pa°2 Paco2 PHPre term 150 + 20 50 + 3 30 + 2 60 + 8 37 + 6 7.37 + 0.03Term 133 + 18 67 + 3 42 + 4 70 + 11 39 + 7 7.40 + 0.026mo 120 + 20 89 + 29 60 + 10 95 + 8 40 + 6 7.41+0.0412mo 120 + 20 96 + 30 66 + 25 93 + 10 4 1 + 7 7.39 + 0.032Y 90 +10 99 + 25 64 + 25 Comparable to adult values5Y 150 + 20 94 + 14 55 + 912Y 70 + 17 109 + 16 58 + 923Y 70 + 5 122 + 30 75 + 20
% Change in BP with halothaneAGE 1 MAC 1.5 MACNewborn 27 + 8 38 + 11Adult 5 + 5 15 + 5
Table 1: Changes with age in heart rate, blood pressure and arterial blood gas values (From Paediatric anaesthesia edited by George A. Gregory)
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 202 Lakshmi Vas
autoregulation for that organ, there can be disastrous consequences of end organ hypoxia. Results of injudicious hypotension could be brain damage and or spinal cord damage in the CNS, renal failure in the kidney, splanchnic ischemia with resultant septicemia in the intestines and so on and so forth.
But all these complications result from an incompetent use of a valuable technique and not as a consequence of its judicious scientific use. It use has to be restricted to specific indications with optimal perioperative monitoring. The general principle is to maintain the highest BP to achieve the desired effect and no lower. The end point is usually a MAP 2/3 the baseline level. The minimum allowable MAP is 55mms of Hg.The onset of hypotension should be gradual over 10-15minutes to allow maximal dilatation of cerebral, coronary and renal vasculature to maintain perfusion pressure and tissue perfusion.
Deliberate or controlled hypotension is a manipulation of the cardiovascular system for:1) Reduction of blood and component loss,
avoiding the risks of blood transfusion and reducing the surgical time.2) Providing a better visibility in the surgical field which is essential for microscopic surgery and procedures inside a narrow or deep cavity that can be flooded by blood (spine) obscuring the whole field including the bleeding vessel.
The common indications are neurosurgery, craniofacial surgery(40% reduction of blood loss), spine surgery , major vascular abnormalities, ENT disorders and burns debridement (1'5)
The contraindications are more discretionary than absolute. Inappropriate use of this good technique can lead to irreversible cardiac and neurological damage. This does not preclude its 3ppropriate scientific use. Obviously the procedure cannot be performed (i) by an inexperienced anaesthesiogist without an understanding of the technique or of paediatric physiology, (ii) when there is lack of technical expertise or (iii) an inability to monitor the patients’ condition adequately ( Table 2) or (iv) an inadequate postoperative care facility.
The relative contraindications applicable to the general patient, both adult and paediatric are focal and generalized reduction of organ blood flow, elevated intracranial pressure, anaemia, haemoglobinopathies (sickle cell anaemia), polycythaemia and allergy or sensitivity to the hypotensive agent.
The mandatory prerequisite for hypotensive anaesthesia is a thorough understanding of the hypotensive agents in a paediatric patient and alteration of physiology by hypotension perse. The hypotensive agents can be subdivided into two types, the volatile agents and the vasodilators.
The anaesthetic agents bring about mild hypotension by maintaing the correct surgical plane of anaesthesia that obtunds any painful stimuli that might cause a haemodynamic response. Their major hypotensive effect is by their effect on the cardiovascular system (negative ionotropy) and/or vasodilatation and depression of central and peripheral sympathetic nerves. Halothane has both effects while isoflurane which has a predominant effect on the peripheral vasculature is preferred. Even nitrous oxide, a weak anaesthetic can cause some hypotension in infants, particularly when their fluid balance is marginal. An initial concentration of 3-4 % and a maintenance level of 2% Isoflurane produces a smooth induction of hypotension, particularly with a reverse Trendelenberg tilt of 20°.
The vasodilators can be subdivided into those that act directly on the vessels (Sodium nitroprusside and nitroglycerin), those that act indirectly, on the sympathetic ganglia (pentolinium) and those that have both direct and indirect actions like Trimethaphan.
THE PHYSIOLOGICAL EFFECTS OF INDUCED HYPOTENSION:Central nervous system:
Most of the data on CBF and metabolism in children have been extrapolated from studies in adults. All volatile agents abolish autoregulation of cerebral blood flow in a dose dependant manner with the effect more pronounced with halothane>enflurane >isoflurane>desflurane. Since we have only halothane and isoflurane in
RACE 2003 Ramachandra Anaesthesia Continuing Education

Induced Hypotension is not contraindicated in children 203 Lakshmi Vas
our country, the obvious choice is isoflurane. It also has the advantage that it reduces the cerebral metabolic rate of oxygen more than it reduces the cerebral blood flow, regardless of hypocapnia.
Hypocapnia reduces the CBF in normotensive subjects by 2% for every 1 mmof Hg reduction of PaC02.6 In hypotensive subjects this effect is attenuated or abolished.8,9 If the reduction in CBF is greater than the reduction in CMR02, cerebral ischaemia may develop. EEG changes occur when CBF is reduced to 40-50% of control values and is isoelectric when it is 60% . Vasodilators like nitroprusside and nitroglycerin dilate cerebral vessels directly without affecting the CMR02. Electrical cortical activity and cortical blood flow are preserved better with nitroprusside than with trimethaphan.(10)
To minimize risks of cerebral ischaemia during controlled hypotension, it has been recommended that MAP should be above 55 mms of Hg and that Isoflurane is the agent of choice with nitroprusside or nitroglycerin as adjuncts. A head up tilt may decrease the cerebral perfusion pressure by2mmHg for every 2.5cm the head is above the arterial transducer.
Respiratory system:Controlled hypotension increases the
alveolar dead space and the intrapulmonary shunt. Head up tilt increases the zone 1 and the VdA/t discrepancy, though to a lesser extent than in adults. This has been attributed to a decrease in pulmonary artery pressure, an increase in zone 3 and a reversal of hypoxic pulmonary vasoconstriction. This reversal is in the order of nitroprusside>nitroglycerin> isoflurane. Nitroprusside directly relaxes the pulmonary vasculature with a reduction of right ventricular afterload. Base line ABG and lactate measurements before and after head up tilt and every 30-60 minutes thereafter are essential to ensure adequate oxygenation and normocapnia.
Cardiovascular system:Hypotensive agents reduce
predominantly the afterload and to a lesser extent
preload. The former improves the left ventricular function so long as there is no exaggerated reduction of preload to compromise the left ventricular filling volume. Fortunately, coronary flow is rarely compromised in children (with the exception of muco polyscharidoses and glycogenoses where IHD is reported). So myocardial ischaemia is not a worry. Reflex tachycardia is a common drawback which can be prevented or treated with (3 blockers, propranolol 60ng/kg in small increments or esmolol infusion 500 fig/kg over 2-3 minutes followed by 300 fig/kg/min are useful.
THE HYPOTENSIVE AGENTS:Can be used in conjunction with volatile
anaesthetics or by themselves in patients where volatile agents have to be withheld for malignant hyperthermia or for SSEP or EEG . In these cases a narcotic , relaxant technique with or without propofol is used with hypotensive agents.
Sodium nitroprusside:This is commonly used in children. Its
action, safe doses, toxicity and its treatment have to be thoroughly understood before embarking on its use in children. It is a direct acting arterial dilator and to a lesser extent venous dilator with a rapid onset of action (1-2mins), a brief duration of action and no myocardial depression. It acts via the release of nitric oxide and cyclic GMP. However, overdose produces cyanide toxicity. It is administered as a 0.01% solution ( 50 mg in 500ml) with an infusion rate starting at 0.1 ng/kg/ min and going up to 8-10 ^g/kg/min. The maximal recommended dose is 2-3 mg/kg/day. As it reduces afterload, preload and myocardial oxygen consumption without reducing contractility, it may increase the cardiac output or decrease it or leave it unchanged. Tachycardia as a common baroreceptor response may reduce its effectiveness and necessitate increasing doses and toxicity. To avoid this, p blockers like IV propranolol 0.015 mg/kg or esmolol 0.2-0.3 mg/ kg/h have been used.
TOXICITY:Cyanide is a toxic metabolite which is
metabolized by the rhodanase enzyme system in the liver(80%) and the methaemoglobin
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 204 Lakshmi Vas
pathway in the RBC(20%). Each molecule of nitroprusside produces 5 ions of cyanide. This combines with thiosulphate or hydroxycobalamin ( both are sulphur atom donors) to form thiocyanate which is excreted by the kidney. However if an overdose is given, the detoxification pathways are overwhelmed and the cyanide binds with the cytochrome oxidases of mitochondria to cause cytotoxic hypoxia. As a result, the cells are unable to utilize the available oxygen and the mixed venous oxygen level rises. As a result of anaerobic metabolism of substrates, the level of lactate rises as the pH decreases.
Immediate treatment comprises stopping the infusion of nitroprusside, administration of 100% oxygen to maximize its cellular availability and sodium nitrite (10mg/kg bolus and 5mg/kg over 30 mins). This drug binds with haemoglobin to form methaemoglobin which has a higher affinity for cyanide than the cytochrome oxidase and so is a temporary measure to release the cytochrome oxidase to relieve the cellular hypoxia. Simultaneously sodium thiosulphate 150mg/kg is also administered to transfer cyanide from cyanmethaemoglobin to form thiocyanate, hydrogen cyanide and methaemoglobin. This methaemoglobin is free to leech some more cyanide from the cytochrome oxidases or is converted to normal haemoglobin by glutathione reductase. Caution has to be exercised to avoid too much nitrite to form excessive methaemoglobin which itself can cause cellular hypoxia. Because the level of haemoglobin is so important in avoiding the toxicity and its treatment, anaemia is a definite contraindication to the use of nitroprusside.
Precautions to be taken with nitroprusside administration are monitoring of oxygenation by oximetry and ABG and lactate levels, direct arterial BP, constant watch for unexplained tachycardia and tachyphylaxis. To avoid tachyphylaxis, hypotension can be augmented by coadministration of isoflurane, captopril, aminophylline and p blockers to reduce the dose of nitroprusside. It should be infused through a central line or a dedicated venous line directly into the hub of the cannula to minimize dead space and delayed response to changes
in infusion rate. Use of an infusion pump ensures accuracy and avoids accidental overdose. The IV Bottle should be shielded, though the IV line need not be shielded as the decomposition takes hours and not minutes that the solution is exposed to light in the tubing.
Nitroglycerin:This is a direct acting venous
capacitance dilator and secondarily an arterial dilator and its action is via nitric oxide. It is a potent coronary vasodilator that decreases cardiac output and pulmonary artery pressure. The onset of hypotension is smooth and gradual without precipitous hypotension. The dose is 1-10 jig/kg/min. All the precautions taken with nitroprusside are applicable to nitroglycerin too, except the shielding of the bottle. A controlled double blind study showed that nitroprusside 6-8 fig/kg/m in produced effective hypotension with a mild increase in A-a Do2 and a mild base deficit. Nitroglycerin was less effective in producing hypotension. The metabolites of nitroglycerin are nitrates and nitrites which have less potent vasodilatory effect and no toxic effect. There is no rebound hypertension either. However, tachyphylaxis, and rarely resistance are common as they are baroreceptor mediated in response to hypotension.
Trimethaphan:This rapidly reduces the systolic BP by
decreasing the systemic vascular resistance. The effect has been attributed to ganglionic blockade, (arterial and venular) direct vasodilatation and in high doses, a adrenergic blockade. All the precautions taken with nitroprusside are applicable.
The dose ranges from 10-200 jig/kg/min. Pressure begins to decrease in 5 minutes and reaches minimal values in 10 minutes. A head up tilt helps the hypotension.
Trimethaphan decreases Cardiac output by either ganglionic blockade or negative inotropic effect. Disadvantages include tachyphylaxis , tachycardia, histamine release, inhibition of pseudocholinesterase activity, mild myoneural blockade, fixed dilated pupils(upto 24 h), urinary
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 205 Lakshmi Vas
retention and gastrointestinal disturbances as an extension of ganglionic blockade.
Pentolinium:This was used in a dose of 0.1 mg/kg
bolus and> repeated to a maximum of 0.3mg/kg. Its onset of action is in 5 minutes reaching a maximum in 30 minutes. The effect is augmented by headhigh tilt, volatile anaesthetics and p blockers, A single dose lasts for 1 -4hrs and can be reversed at the end by change of position to horizontal, stopping the augmenting effect of volatile anaesthetics and p blockers and volume replacement. It has been replaced in paediatric anaesthesia by other better drugs as it has the disadvantages of trimethaphan.
Adenosine:It is an a/a2 agonist. There are a1
receptors in the SA and AV nodes which can cause bradycardia and transient AV block, and those in the kidney that cause renal vasoconstriction. The a2 action causes systemic and pulmonary vasodilation comparable to nitroprusside in the rapidity of and reliability of action but without the disadvantages of tachyphylaxis and rebound hypertension or toxic metabolites. Preload and cardiac output are unchanged or increased. There is no myocardial ischaemia . Both CBF and CMR02 are maintained unlike with nitroprusside. Nor does the hypocapnia cause lowering of CBF to ischaemic levels. However, its a1 action precludes its use. Presently, selective a2 blockers are being developed for clinical use.
Miscellaneous drugs:Likeclonidine, an a2 agonist that is used
for its sedative and hypotensive effects, as an adjunct to isoflurane / metoprolol anaesthesia, magnesium sulphate is being investigated. However, it causes postoperative sedation, coagulation abnormalities and weakness that are a cause for concern, p blockers and calcium channel blockers and propofol have also been used as adjuncts.
ANAESTHETIC MANAGEMENT OF HYPOTENSIVE ANAESTHESIA:
Combined haemodilution (to 30- 20% Hct), hypotension and hypothermia (to 30° C )
have been studied. At lower temperatures, the metabolic demand and oxygen consumption are lower. At 31° C and an FI02of 1, the dissolved oxygen in blood increases to 2ml/100ml representing 30% of Ca02 However these are esoteric techniques to be tried in special centers . In our country, the decision to use controlled hypotension has to be dictated by a favourable risk : benefit ratio and a proper planning of strategies is mandatory. A Hb of 10g/ dl is recommended, though haemodilution with hypotension has been studied.
Premedication can include a venodilator and a ganglion blocker like morphine, droperidol, clonidine (4-8|ig/kg)orchlorpromazine. Vagolytics are avoided.
Intraoperatively, light anaesthesia has to be avoided to prevent hypertension and tachycardia in response to surgical stimulus. Vecuronium is preferred for its slow heart rate. In our country, the best technique to provide analgesia would be an epidural or a regional block if the surgical location permits it. It helps in providing a steady, reliable and total analgesia that is non fluctuant. In addition, the pulse rate goes down as does the blood pressure, to some extent, particularly in children above 6-7 yrs. The vasodilatation associated with epidural also helps in haemodilution . Alternatively, opioids like fentanyl 3 jag/kg stat followed by morphine 0.1 mg/ kg provide a stable level. Positioning with a head up tilt helps with most hypotensive agents.
Intravascular volume should be restored by infusion of colloids (either gelatins or starch) and/or balanced salt solution. A large bore peripheral cannula for replacement of blood loss and a dedicated line for hypotensive infusion is necessary. An arterial line is mandatory for both monitoring and repeated electrolyte, sugar (especially if p blockers like esmolol, metoprolol or labetalol are given), ABG and lactate estimations. An NIBP can both underestimate or overestimate the BP. A dorsalis pedis line may overestimate BP with nitroprusside and underestimate it with isoflurane; so a radial or axillary line is preferred. A central venous line is recommended as right sided filling pressures parallel left sided pressures in children. PA
RACE 2003 Ramachandra Anaesthesia Continuing Education
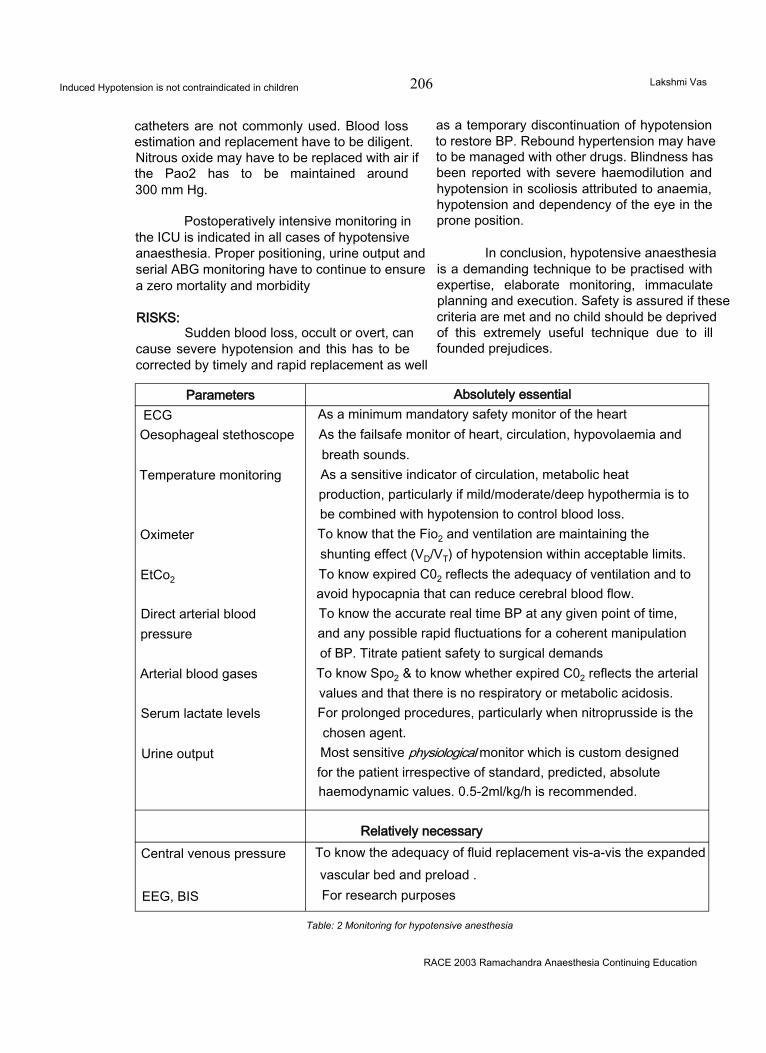
Induced Hypotension is not contraindicated in children 206 Lakshmi Vas
catheters are not commonly used. Blood loss estimation and replacement have to be diligent. Nitrous oxide may have to be replaced with air if the Pao2 has to be maintained around 300 mm Hg.
Postoperatively intensive monitoring in the ICU is indicated in all cases of hypotensive anaesthesia. Proper positioning, urine output and serial ABG monitoring have to continue to ensure a zero mortality and morbidity
RISKS:Sudden blood loss, occult or overt, can
cause severe hypotension and this has to be corrected by timely and rapid replacement as well
as a temporary discontinuation of hypotension to restore BP. Rebound hypertension may have to be managed with other drugs. Blindness has been reported with severe haemodilution and hypotension in scoliosis attributed to anaemia, hypotension and dependency of the eye in the prone position.
In conclusion, hypotensive anaesthesia is a demanding technique to be practised with expertise, elaborate monitoring, immaculate planning and execution. Safety is assured if these criteria are met and no child should be deprived of this extremely useful technique due to ill founded prejudices.
Parameters Absolutely essentialECGOesophageal stethoscope
Temperature monitoring
Oximeter
EtCo2
Direct arterial blood pressure
Arterial blood gases
Serum lactate levels
Urine output
As a minimum mandatory safety monitor of the heart As the failsafe monitor of heart, circulation, hypovolaemia and breath sounds.As a sensitive indicator of circulation, metabolic heat production, particularly if mild/moderate/deep hypothermia is to be combined with hypotension to control blood loss.To know that the Fio2 and ventilation are maintaining the shunting effect (VD/VT) of hypotension within acceptable limits. To know expired C02 reflects the adequacy of ventilation and to avoid hypocapnia that can reduce cerebral blood flow.To know the accurate real time BP at any given point of time, and any possible rapid fluctuations for a coherent manipulation of BP. Titrate patient safety to surgical demands To know Spo2 & to know whether expired C02 reflects the arterial values and that there is no respiratory or metabolic acidosis.For prolonged procedures, particularly when nitroprusside is the chosen agent.Most sensitive physiological monitor which is custom designed for the patient irrespective of standard, predicted, absolute haemodynamic values. 0.5-2ml/kg/h is recommended.
Relatively necessaryCentral venous pressure
EEG, BIS
To know the adequacy of fluid replacement vis-a-vis the expanded vascular bed and preload .For research purposes
Table: 2 Monitoring for hypotensive anesthesia
RACE 2003 Ramachandra Anaesthesia Continuing Education

Induced Hypotension is not contraindicated in children 207 Lakshmi Vas
References
1. Jerrold Lerman In Special techniques ( acute normovolemic haemodilution, controlled hypotension and hypothermia, and ECMO in Paediatric anaesthesia edited by George A . Gregory 4th edition Churchill Livingstone New York, Edinburgh .London, Philadelphia.
2. DiazJH. Lockhart CH: Hypotensive anaesthesia for craniectomy in an infancy. Br.J.Anaesth 51: 233, 1979.
3. Viguera MG., Terry RN., Induced hypotension for an extensive surgery in an infant Anesthesiology 27: 701, 1966.
4. Fairbairn ML., Eltringhamrj, Young PN Robinson JM. Hypotensive anaesthesia for microsurgery of the middle ear A comparison between halothane and isoflurane. Anaesthesia 41: 637 1986
5. Szyfelbein SK Ryan JF Use of controlled hypotension for primary surgical excision in an extensively burned child. Anesthesiology 41:501 1974
6. HarpJR. Wollman H : Cerebral metabolic effects of of
hyperventilation and deliberate hypotension.Br.J.Anaesth 45:256.1973.
7. Artru AA: Partial preservation of cerebral vascular responsiveness to hypocapnia during isoflurane induced hypotension in dogs Anesth Analg 65:660,1986.
8. ArtruAA. Colley PS. Cerebral blood flow response to hypocapnia during hypotension. Strokel 5:878,1984.
9. ArtruAA. . Cerebral vascular response to hypocapnia during nitroglycerin induced hypotension. Neurosurgery 16:468.1985.
10. Thomas WA, Cole PV Etherinton NJ et al.: Electrical activity of the cerebral cortex during induced hypotension in man: a comparison of sodium nitroprusside and trimethaphan Br.J.Anaesth 57:134.1985
11. YasterM., Simmons RS., ToloVT. Etal: A comparison of nitroprusside and nitroglycerin for inducing hypotension in children : a double blind study. Anesthesiology. 65:175, 1986
12. Jean Camboulives in the chapter on Fluid, Transfusion, and blood sparing techniques in PEDIATRIC ANAESTHESIA .Principles and practice edited by Bruno Bisonetteand Bernard Dalens McGraw -Hill.
RACE 2003 Ramachandra Anaesthesia Continuing Education
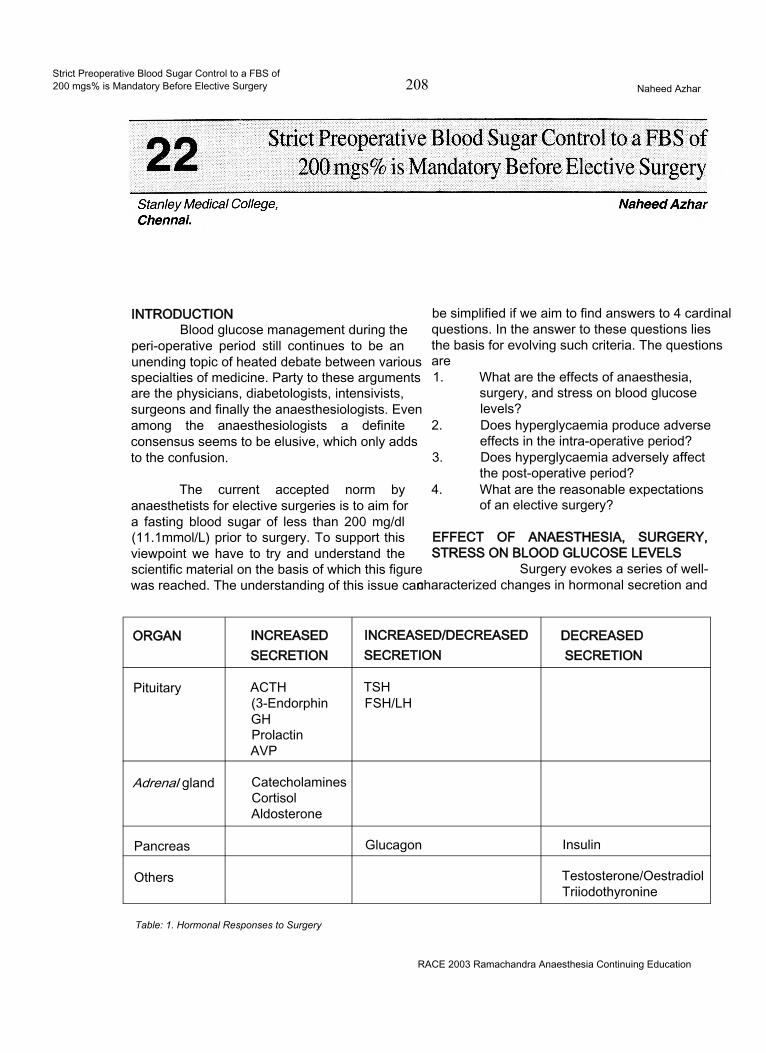
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 208 Naheed Azhar
INTRODUCTIONBlood glucose management during the
peri-operative period still continues to be an unending topic of heated debate between various specialties of medicine. Party to these arguments are the physicians, diabetologists, intensivists, surgeons and finally the anaesthesiologists. Even among the anaesthesiologists a definite consensus seems to be elusive, which only adds to the confusion.
The current accepted norm by anaesthetists for elective surgeries is to aim for a fasting blood sugar of less than 200 mg/dl (11.1mmol/L) prior to surgery. To support this viewpoint we have to try and understand the scientific material on the basis of which this figure was reached. The understanding of this issue can
be simplified if we aim to find answers to 4 cardinal questions. In the answer to these questions lies the basis for evolving such criteria. The questions are1. What are the effects of anaesthesia,
surgery, and stress on blood glucose levels?
2. Does hyperglycaemia produce adverse effects in the intra-operative period?
3. Does hyperglycaemia adversely affect the post-operative period?
4. What are the reasonable expectations of an elective surgery?
EFFECT OF ANAESTHESIA, SURGERY, STRESS ON BLOOD GLUCOSE LEVELS
Surgery evokes a series of well- characterized changes in hormonal secretion and
ORGAN INCREASED INCREASED/DECREASED DECREASEDSECRETION SECRETION SECRETION
Pituitary ACTH(3-EndorphinGHProlactinAVP
TSHFSH/LH
Adrenal gland CatecholaminesCortisolAldosterone
Pancreas Glucagon Insulin
Others Testosterone/OestradiolTriiodothyronine
Table: 1. Hormonal Responses to Surgery
RACE 2003 Ramachandra Anaesthesia Continuing Education
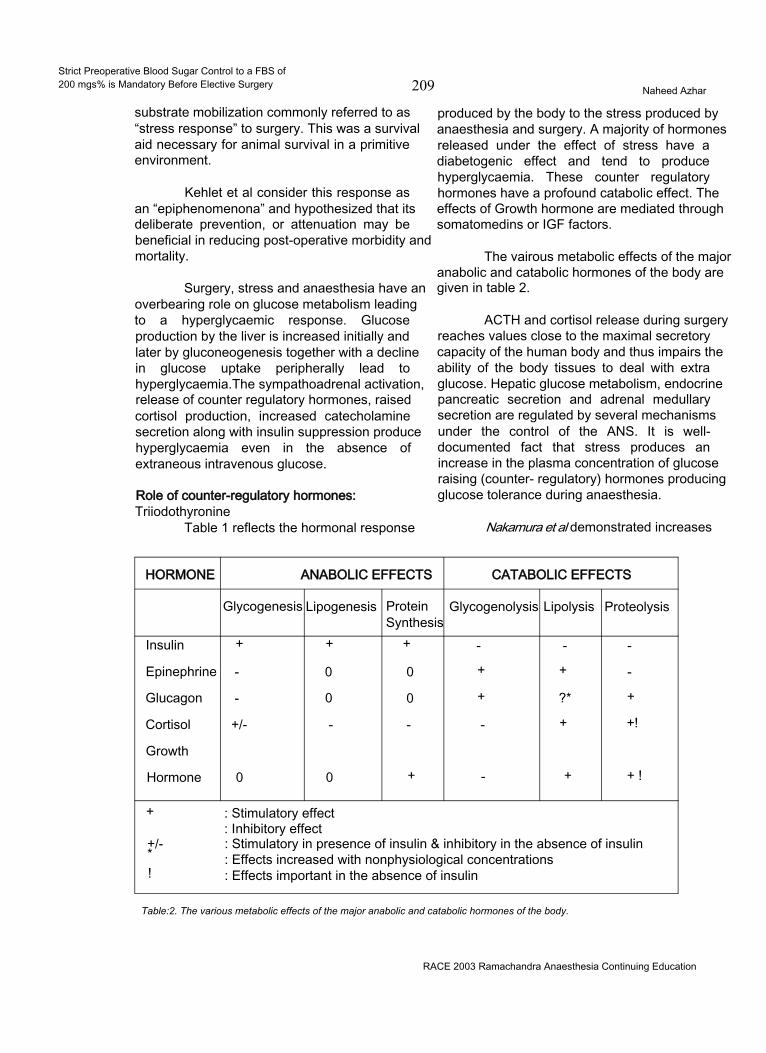
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 209 Naheed Azhar
substrate mobilization commonly referred to as “stress response” to surgery. This was a survival aid necessary for animal survival in a primitive environment.
Kehlet et al consider this response as an “epiphenomenona” and hypothesized that its deliberate prevention, or attenuation may be beneficial in reducing post-operative morbidity and mortality.
Surgery, stress and anaesthesia have an overbearing role on glucose metabolism leading to a hyperglycaemic response. Glucose production by the liver is increased initially and later by gluconeogenesis together with a decline in glucose uptake peripherally lead to hyperglycaemia.The sympathoadrenal activation, release of counter regulatory hormones, raised cortisol production, increased catecholamine secretion along with insulin suppression produce hyperglycaemia even in the absence of extraneous intravenous glucose.
Role of counter-regulatory hormones:Triiodothyronine
Table 1 reflects the hormonal response
produced by the body to the stress produced by anaesthesia and surgery. A majority of hormones released under the effect of stress have a diabetogenic effect and tend to produce hyperglycaemia. These counter regulatory hormones have a profound catabolic effect. The effects of Growth hormone are mediated through somatomedins or IGF factors.
The vairous metabolic effects of the major anabolic and catabolic hormones of the body are given in table 2.
ACTH and cortisol release during surgery reaches values close to the maximal secretory capacity of the human body and thus impairs the ability of the body tissues to deal with extra glucose. Hepatic glucose metabolism, endocrine pancreatic secretion and adrenal medullary secretion are regulated by several mechanisms under the control of the ANS. It is well- documented fact that stress produces an increase in the plasma concentration of glucose raising (counter- regulatory) hormones producing glucose tolerance during anaesthesia.
Nakamura et al demonstrated increases
HORMONE ANABOLIC EFFECTS CATABOLIC EFFECTS
Glycogenesis Lipogenesis ProteinSynthesis
Glycogenolysis Lipolysis Proteolysis
Insulin + + + - - -
Epinephrine - 0 0 + + -
Glucagon - 0 0 + ?* +
Cortisol +/- - - - + +!
Growth
Hormone 0 0 + - + + !
+
+/-*!
: Stimulatory effect : Inhibitory effect: Stimulatory in presence of insulin & inhibitory in the absence of insulin : Effects increased with nonphysiological concentrations : Effects important in the absence of insulin
Table:2. The various metabolic effects of the major anabolic and catabolic hormones of the body.
RACE 2003 Ramachandra Anaesthesia Continuing Education
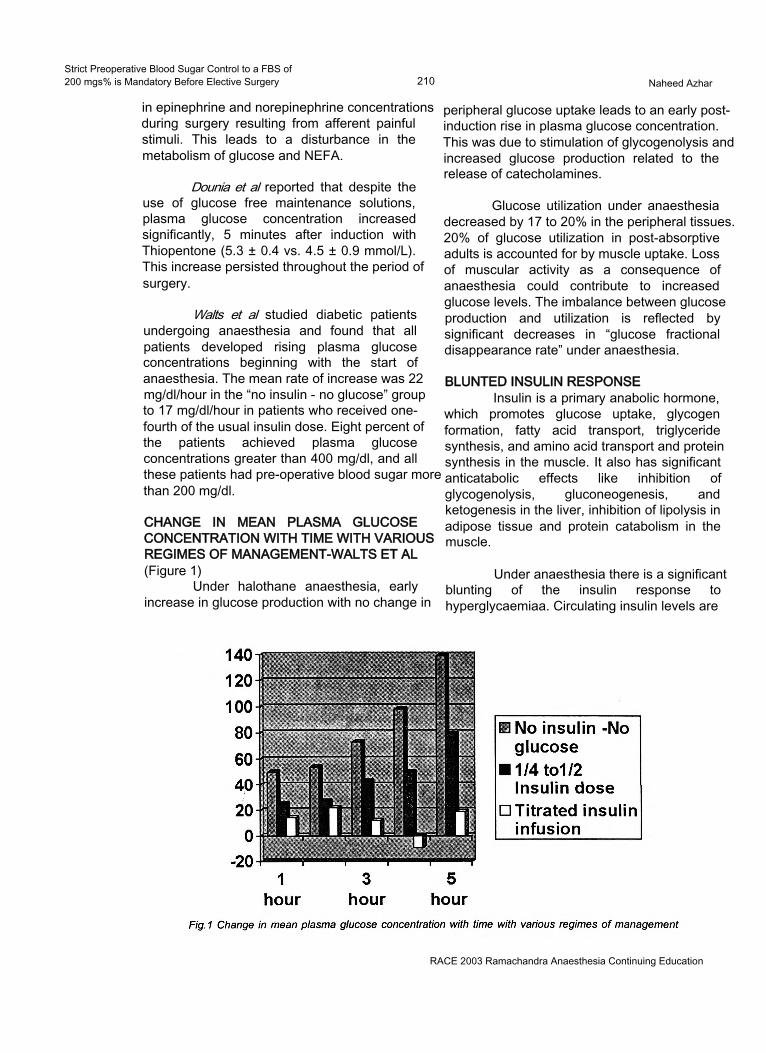
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 210 Naheed Azhar
in epinephrine and norepinephrine concentrations during surgery resulting from afferent painful stimuli. This leads to a disturbance in the metabolism of glucose and NEFA.
Dounia et al reported that despite the use of glucose free maintenance solutions, plasma glucose concentration increased significantly, 5 minutes after induction with Thiopentone (5.3 ± 0.4 vs. 4.5 ± 0.9 mmol/L). This increase persisted throughout the period of surgery.
Walts et al studied diabetic patients undergoing anaesthesia and found that all patients developed rising plasma glucose concentrations beginning with the start of anaesthesia. The mean rate of increase was 22 mg/dl/hour in the “no insulin - no glucose” group to 17 mg/dl/hour in patients who received one- fourth of the usual insulin dose. Eight percent of the patients achieved plasma glucose concentrations greater than 400 mg/dl, and all these patients had pre-operative blood sugar more than 200 mg/dl.
CHANGE IN MEAN PLASMA GLUCOSE CONCENTRATION WITH TIME WITH VARIOUS REGIMES OF MANAGEMENT-WALTS ET AL(Figure 1)
Under halothane anaesthesia, early increase in glucose production with no change in
peripheral glucose uptake leads to an early postinduction rise in plasma glucose concentration. This was due to stimulation of glycogenolysis and increased glucose production related to the release of catecholamines.
Glucose utilization under anaesthesia decreased by 17 to 20% in the peripheral tissues. 20% of glucose utilization in post-absorptive adults is accounted for by muscle uptake. Loss of muscular activity as a consequence of anaesthesia could contribute to increased glucose levels. The imbalance between glucose production and utilization is reflected by significant decreases in “glucose fractional disappearance rate” under anaesthesia.
BLUNTED INSULIN RESPONSEInsulin is a primary anabolic hormone,
which promotes glucose uptake, glycogen formation, fatty acid transport, triglyceride synthesis, and amino acid transport and protein synthesis in the muscle. It also has significant anticatabolic effects like inhibition of glycogenolysis, gluconeogenesis, and ketogenesis in the liver, inhibition of lipolysis in adipose tissue and protein catabolism in the muscle.
Under anaesthesia there is a significant blunting of the insulin response to hyperglycaemiaa. Circulating insulin levels are
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 211 Naheed Azhar
inappropriately low for the prevailing blood glucose values, reflecting a relative lack of circulating insulin during surgery. The factors responsible for this are unclear, but it seems that circulating catecholamines released during surgery have a direct inhibitory effect on the p cells of the pancreas, acting through the a adrenoreceptors.
Desborough et al demonstrated decline in insulin secretion after the induction of anaesthesia, and before the onset of surgery. This inhibition implicated the role of the anaesthetic agents, either directly or indirectly by altering splanchnic blood flow.
Kehlet et al reported increased blood lactate concentrations during surgery under GA.
Desborough et al also demonstrated that inhibition of insulin secretion by halothane, enflurane and isoflurane in clinical concentrations by their inhibitory effect on the stimulus-secretion coupling in the p cells of pancreas and impairment in uptake of glucose in both skeletal and hepatic tissues.
Brandi et al demonstrated that in days after surgery or trauma, circulating insulin values increase above normal values, but the hormone is ineffective metabolically. This period presenting with hyperglycaemia is called the “phase of insulin resistance”. It is related to the effects of catabolic hormones like cortisol and cytokines on insulin receptors along with a post-receptor defect. The moderate resistance to insulin may also be attributable to alteration in the distribution space and serum clearance of insulin.
CONCLUSION NO: 1Anaesthesia and surgery conclusively
produce a hyperglycaemic response due to increased secretion of counter regulatory hormones and relative insulin resistance. This is attributable to decreased glucose tolerance induced by any of the following mechanisms:1. Impaired insulin secretion.2. Decreased biologic response of tissues to
insulin such as diminished peripheral glucose utilization.
3. Impaired gluconeogenesis and /or glycogenolysis.
4. Increased hepatic glucose output and / or
splanchnic release of glucose due to increased anabolic process.
5. Decreased peripheral uptake of glucose.
ADVERSE EFFECTS OF HYPERGLYCAEMIA IN THE INTRA-OPERATIVE PERIOD
Inadequate control of blood glucose and hyperglycaemia in the intra-operative period leads to1. Ketosis.2. Acidemia.3. Electrolyte abnormalities.4. Volume depletion from osmotic diuresis.5. Hyperosmolality.6. Thrombogenesis.7. Lactic Acidosis.8. Disruption of autoregulation.
The renal threshold for glucose is 10 mmol/L. At levels greater than this, the glycosuria causes an osmotic diuresis, with loss of water and electrolytes. High levels of blood glucose can cause severe cellular dehydration due to osmotic transfer of water out of the cells. During renal glycosuria, the osmotic effect on the renal tubules decreases tubular reabsorption of fluids. This leads to massive loss of fluid in the urine causing ECF dehydration, and ultimately compensatory dehydration of the ICF.
Intra-operative hyperglycaemia leads to hyperosmolality. Each mOsmol / L of any substance exerts an osmotic pressure of 19.3 mm Hg. Blood glucose at normal concentrations of 5.6 mmol / L (100 mg / dl) exerts a pressure of 108 mm Hg. The osmotic pressure of plasma is 5443 mm Hg, which is 20 mm Hg more than the pressure of the ECF and ICF, which is 5423 mm Hg. A rise in blood glucose to 20 mmol / L can change the osmotic pressure by as much as 400 mm Hg producing deleterious effects on water and electrolyte homeostasis.
The maximum reabsorptive capacity of renal tubules for glucose averages 320 mg / min. When the tubular load rises above 220 mg / min (plasma glucose = 180 mg / dl), a small amount of glucose begins to appear in the urine, termed as glucose threshold. This glucose excretion keeps rising between plasma levels of 180 to 250 mg / dl. Beyond plasma glucose of 250 mg /dl the absorptive capacity of all nephrons is exceeded showing a steep rise in glycosuria.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 212 Naheed Azhar
Osmotic diuresis is accompanied by a continual loss of electrolytes particularly sodium. Sodium loss is around 150 mmol / L of urine and potassium around 5 mmol / L. Progressive sodium depletion activates the Renin - Angiotensin system and Aldosterone secretion increases, leading to increased sodium resorption from tubules. High aldosterone concentrations reduce potassium resorption and increase urinary potassium excretion. Hyponatremia and Hypokalemia can occur. In rare instances, when oliguria and uremia occur inspite of a substantial osmolar load, potassium starts leaking out of cells into ECF, but can no longer be excreted by diuresis. So although the total potassium stores are depleted the patients may have dangerously high plasma potassium.
Hyperosmolality and dehydration can produce haemodynamic instability and depressed mental state leading to recovery problems. Sodium and potassium derangements may produce arrhythmias and delayed recovery. Hyperglycaemia may increase the viscosity of blood by increasing the osmolal load. Increased viscosity favors slow flow of blood in the blood vessels. Slowflcwing blood causes concentration of pro-coagulants to rise high enough in certain local areas to initiate clotting and thrombogenesis. This is more likely to occur if conditions like dehydration, pre-existing atherosclerosis, high haematocrit, cold induced peripheral vasoconstriction, myocardial depression and hyperglycaemia are present. Controlling peri-operative blood glucose to < 10 mmol / L (200 mg / dl) can eliminate some of the precipitating causes.
Hyperglycaemia increases production of macroglobulins by the liver. They increase the viscosity and promote intracellular swelling by favoring production of non-diffusible molecules like sorbitol.
Hyperglycaemia also disrupts autoregulation. Glucose induced vasodilatation prevents vital target organs from protection against increases in systemic blood pressures. Different degrees of hyperglycaemia may be required before different vascular beds are affected.
Hyperglycaemia promotes lactic acidosis and academia. The increased viscosity and dehydration are major contributory factors
towards it. Acidosis may impair cardiac contractility, provoke arrhythmias, hypotension and interfere with the action and metabolism of drugs. Acidoc s depresses not only the myocardial function but also respiration. Bicarbonate therapy to rapidly correct acidosis is fraught with dangers in alteration of CNS structure and function due to paradoxical CSF and CNS acidosis, decreased CBF, altered CNS oxygenation and development of unfavorable osmotic gradients.
A study of 340 diabetics undergoing open-heart surgery revealed an increases in operative mortality (1.8% vs. 0.6%). During the study a number of cases were reported where inotropic agents were ineffective in maintaining cardiac contractility, although filling pressures, sinus rhythm, serum electrolytes and blood gases were adequate. The blood sugar was high in each of this case. After IV infusion of insulin, effective myocardial contractions returned, allowing easy and rapid bypass weaning.
Intra-operative use of drugs like corticosteroids, p agonists and adrenergic agents all increase the likelihood of intra-operative hyperglycaemia.
CONCLUSION NO: 2Hyperglycaemia is definitely undesirable
during the intra-operative period. The adverse effects of hyperglycaemia are directly or indirectly related to increased blood glucose levels producing1) Ketosis.2) Lactic Acidosis and Acidemia.3) Electrolyte abnormalities.4) Volume depletion from osmotic diuresis.5) Hyperosmolality.6) Thrombogenesis.7) Impaired myocardial contractility.8) Haemodynamic instability.9) Arrythmogenicity.10) Altered drug pharmacodynamics and
pharmacokinetics.11) Disrupted autoregulation of vascular beds.
IMPLICATION OF HYPERGLYCAEMIA IN THE POST/PERI-OPERATIVE PERIOD
Hyperglycaemia during the peri-operative period leads to an increased incidence of infection and delayed wound healing.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 213 Naheed Azhar
Hirsch et al report that impaired wound strength and wound healing occur when plasma glucose levels exceed 11.1 mmol /L (200 mg / dl). Hyperglycaemia interferes with leukocyte chemotaxis, opsonization, phagocytosis, granulocyte adherence and depresses bactericidal activity.
Hyperglycaemia depresses the immune response of the body to infection by producing short-term glycosylation of immunoglobulins thereby inactivating them. Glycosylation of C3 component of complement occurs at its opsonic site, rendering it impotent and unable to bind to the surface of the invading bacteria.
Rassias et al demonstrated that neutrophil phagocytic activity was less depressed when blood sugar was tightly controlled during the peri-operative period (75% vs. 47%). They demonstrated that hyperglycaemia depresses the white cell function and increases the risk of infection after surgery.
Researchers showed that anastomotic healing in both ileum and colon of diabetic animals was better if hyperglycaemia is tightly controlled starting from 4 days before surgery and extending into the entire peri-operative period. Hyperglycaemic animals showed qualitative change in the newly formed collagen causing reduction in wound strength.
Studies reveal that hyperglycaemia results in impaired wound healing due to 1) Accelerated non-enzymatic glycosylation of body proteins due to addition of glucose molecules to the exposed lysine residues on extra cellular proteins. 2) Glycosylation of newly synthesized collagen associated with increased collagenase activity and decreased wound collagen content.
CONCLUSION NO: 3Hyperglycaemia increases the incidence
of infection by interfering with leukocyte function. It also impairs wound healing by altering collagen activity and strength.
GOALS OF ELECTIVE SURGERYAnaesthesia and surgery carry a certain
amount of risk even for the normal patient. The lowest class in ASA classification is Class 1,
with its attendant risks. A class 0 does not exist in anaesthesia. Unanticipated, undesirable events can occur during anaesthesia and these can range from mere hypotension, myocardial depression to the much dreaded arrhythmias, anaphylaxis and failed intubation situations.
During elective surgery, the aim is to plan and to be prepared to minimize these risks to as low as possible. Even if unforeseen complications arise, we should be able to leave the patient undergoing elective surgery with the least possible risk of suffering morbidity or mortality. Uncontrolled hyperglycaemia in the peri-operative period precludes our ability to offer this advantage to the patient undergoing elective surgery.
Hyperglycaemia worsens the neurological outcome in patients who have suffered global CNS ischaemia / hypoxia. Hirsch et al recommend tight control of blood sugar in patients undergoing neurosurgical procedures. Werner et al recommend a plasma glucose of 100 to150 mg / dl for better outcome of patients with stroke or neurotrauma.
Roizen et al recommend blood glucose of less than 200 mg / dl during periods of ischaemia in diabetic patients about to undergo surgery in which hypotension or reduced cerebral blood flow occurs. Hyperglycaemia also worsens neurological outcome after regional CNS blood flow alterations and ischaemia.
In a study of 430 consecutive patients resuscitated after out-of-hospital cardiac arrest, mean blood glucose values were found to be higher in patients who never awakened (341 ± 13 mg / dl) than in those who did (262 ± 7 mg / dl). Among patients who awakened, those with persistent neurological deficits had higher mean glucose levels (286 ± 15 mg / dl) than did those without deficits (251 ± 7 mg / dl). These results are consistent with the findings that hyperglycaemia during stroke is associated with poorer short- and long-term neurological outcomes.
Roizen et al advocate that blood glucose is a major determinant of brain damage following ischaemia. They recommend that until better data is available blood glucose levels should be maintained below 200 mg / dl during periods of likely cerebral ischaemia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 214 Naheed Azhar
Hyperglycaemia in the pregnant diabetic affects her adversely, as well as her offspring. Maternal hyperglycaemia may stimulate insulin secretion in the fetus leading to neonatal hypoglycaemia and delayed release of glucagons. Hypotension in the presence of hypoglycaemia in this sub-sect of patients produced maternal lactic acidosis and consequent fetal acidosis.
Conclusion No: 4During elective surgery enough time is
available to adequately stabilize the patient. This should be utilized to minimize the risk of morbidity and mortality due to anaesthesia and / or surgery. Unanticipated, critical events, if they occur (as they could during anaesthesia) it has been conclusively proven that hyperglycaemia are associated with poor outcome.
CURRENT MOST PRACTISED PROTOCOL FOR DIABETIC MANAGEMENT
Before the advent of bedside glucosimetry, hypoglycaemia being greatly feared, majority of the anaesthetists accepted a moderate hyperglycaemia in the peri-operative period. Since early 1970’s evidence has been accumulating against the harmful effects of even moderate hyperglycaemia.
Dunnet et al in 1985 surveyed the protocols used by anaesthetists in the diabetic management in the peri-operative period. Most of the anaesthetists aimed to maintain the blood glucose in the range of 7 to 10 mmol/L. 35% of respondents chose a value greater than 11 mmol/L.
Eldridge et al restudied the same parameters in 1993. They now found that 26% preferred to maintain blood glucose between 4- to7 mmol/L. 63% preferred a range of 7 to 10 mmol/L. Only 9% selected a range greater than11 mmol/L.
These gross changes amongst the attitude of anaesthesiologists, in their practice of managing blood glucose during the peri-operative period, clearly indicates the emerging trends based on the scientific data that has been made available by recent research. Undoubtedly there is an emerging need to control blood sugar within the normoglycaemic range. The starting point in
this endeavor is to start with pre-operative blood sugar below 200 mg / dl.
CONCLUSIONIn our attempt to seek an answer for
what would be an appropriate pre-operative blood sugar value in a fasting state in an individual posted for elective surgery, we ended up searching the literature to find answers for 4 questions. The search yielded important conclusions, which need to be re-considered at this stage. They are■ Anaesthesia and surgery definitely produce a hyperglycaemic response.• Hyperglycaemia produces undesirable adverse effects in the intra-operative period.■ Hyperglycaemia increases the risk of infection and delays wound healing.■ Unanticipated critical events if they occur in the presence of hyperglycaemia are associated with poor outcome.■ The current approach to blood glucose management in the peri-operative period is to maintain blood glucose within the normoglycaemic range.
The adequate management of blood sugar for the entire peri-operative period should begin with adequate control in the pre-operative period. Fasting blood sugar in elective surgeries, if not all, should strictly be maintained in the normoglycaemic range.
Amongst the majority of workers who have done hall mark studies in peri-operative management of blood glucose, Hirsch, Rassias, Kehletand Roizen all recommend blood glucose to be maintained between 140 to 180 mg/dl. Alberti et al give us the liberty of accepting fasting blood sugar of 180 to 200 mg / dl as an indicator of adequate control.
On the basis of the scientific data available to us at this point of time, it seems reasonable to aim for peri-operative blood sugar in the normoglycaemic range, it would be appropriate to begin this with a fasting blood sugar of less than 200 mg /dl being mandatory for elective surgeries.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Control of Blood Sugar to an FBS of 200mg%is NOT Mandatory Before Elective Surgery 215 Kalyan Chakravarthy
INTRODUCTION:Diabetes Mellitus (DM) with its
devastating consequences has assumed epidemic proportions in many countries of the world. Spectacular increase in the incidence and prevalence of this chronic disease is destined to have enormous impact on mortality, morbidity and health care resources. India would rank first in sharing the global burden of diabetes in the next two decades1. Epidemiological transition including improved socio-economic status, rural to urban migration, adoption to sedentary habit and stress of modern life style is largely responsible for this cataclysmic shift in the burden of diabetes2.
DEFINITION OF DIABETES MELLITUS (DM):Diabetes Mellitus is a syndrome
characterised by chronic hyperglycaemia and disturbances of carbohydrate, fat and protein metabolism associated with absolute or relative deficiencies in insulin secretion and /or insulin action. When fully expressed, diabetes is characterised by fasting hyperglycaemia, but the disease can also be recognised during less overt stages and before fasting hyperglycaemia appears, most usually by the presence of glucose intolerance3.
CURRENT DIAGNOSTIC CRITERIA:The 1997 American Diabetic Association
(ADA) expert committee on the diagnosis and classification of diabetes mellitus and the provisional report of the WHO consultation focus on fasting plasma glucose (FPG) that is 126mg% or greater and confirmed on subsequent day as the preferred criterion for the diagnosis of diabetes mellitus4. This criterion is supported by studies demonstrating that this threshold accurately
differentiates between non-diabetic and diabetic populations and is associated with the development of specific diabetic microvascular complications.
The following points must be remembered while the diagnosis of diabetes mellitus is made.
1. The diagnosis of DM must be based on blood glucose estimations.
2. Urine glucose testing must not be used to diagnose diabetes.
3. True blood glucose should be estimated using enzymatic methods like the glucose oxidase method.
4. Plasma glucose >200mg%, confirmed on repeat testing, in a patient with characteristic signs and symptoms of diabetes is diagnostic.
5. Doing a GTT in a known diabetic patient is not necessary.
6. In all other persons, a GTT must be carried out in order to exclude diabetes.
CLASSIFICATION OF DIABETES MELLITUS5:Diabetes is classified into four major
categories:• Type-1 —IDDM• Type-ll-MODY• Gestational• Secondary
DOES GOOD GLYCAEMIC CONTROL MATTER:
Improved control of blood sugar is protective and this has been confirmed in humans. The Diabetes Control and Complications Trial (DCCT) in the USA compared standard and intensive insulin therapy in a prospective controlled trial of young patients with IDDM6. Even
RACE 2003 Ramachandra Anaeschesia Continuing Education
Strict Preoperative Control of Blood Sugar to an FBS of 2Q0mg%is NOT Mandatory Before Elective Surgery________________________ Kalyan Chakravarthy
in those with intensive therapy, mean blood glucose levels were 40% above the non-diabetic range, but this level of control reduced the risk of progression to retinopathy by 60%, nephropathy by 30% and neuropathy by 20% over seven years of the study.
CELLULAR AND MOLECULAR BASIS OF LONG TERM DIABETIC COMPLICATIONS7:
The complications of DM are attributable to tissue damage due to vascular disease involving micro and macro vasculature. The most common pathology of micro vessels occurs in the retina, kidney, peripheral arteries of the lower limbs, in the coronary vessels and the cerebral arteries.
RELATIONSHIP BETWEEN DIABETIC CONTROL AND COMPLICATIONS:
Patients with type-1 DM have more chance of developing duration dependent complications of disease with better survival. Patients with type-11 DM may have microvascular and macrovascular complications of the disease at the time of detection.
The (UKPDS) UK Prospective Diabetes Study was started in 1977 and included 5702 patients with NIDDM over a period of 20 years6. Summary is:1. Good glycaemic control is necessary for type II diabetes mellitus.2. Early intervention to modify risk factors, and obtain good glycaemic control.3. Control of hypertension in patients with typeII DM needs intensive treatment.4. UKPDS confirms the efficacy of existing treatment for type II DM.
UKPDS and nephropathy - Renal failure and death from renal disease did not differ between the conventional group and the intensive group
UKPDS and neuropathy - No significant difference was seen in the incidence of absent knee and ankle reflexes. Incidence of impotence, abnormal cardiac autonomic functions also did not differ significantly between the groups.
UKPDS and macrovascular complications - The incidence of fatal Ml, heart failure, angina, stroke, amputation and death from
PVD was not lowered significantly.
While a close control of blood glucose is normally mandatory to avoid progressive organ failure, during the peri-operative period, well- standardised insulin protocols appear to be sufficient to manage the diabetic patient7
The peri-operative care of diabetic patients is less dependent on blood glucose control, which needs to be exceptionally tight, and is usually easily obtained thanks to pharmacological improvements, human insulins and analogues, technical progress with blood glucose monitoring at the bedside and infusion with constant flow rates. More important is the influence of end organ pathology, often clinically silent, which must be carefully assessed during the pre-operative evaluation. The organ impairments concern especially the heart, but also all those organs that were modified by abnormal glycosylated proteins. The pre-existing pathology has many consequences on anaesthesia management; the anaesthetic technique depends essentially on their existence. A better long-term control of diabetes both for type I and type II by insulins, and the new oral antidiabetic drugs reduce the incidence of the end organ pathology and the risk linked to organ failure in the peri-operative period8.
Diabetes per se is not a risk factor for post-operative morbidity or mortality, after adjustment for co-morbidities like atherosclerosis. Controlled studies have shown the advantages of tight control of glycaemia, in two acute complications of atherosclerosis, i.e. Ml and CVA. These diseases have a high prevalence rate in diabetic patients, as the probability of macroangiopathy is high. Perioperative tight control of glycaemia is a probable necessity to avoid these complications, which is best achieved by a team.
Reasonable control of blood sugar can best be achieved within a few hours pre-operatively and clinical assessment can be performed on an outpatient basis. Anaesthetic management consists of assessments of control of the disease followed by evaluation of diabetic complications and their severity.
Different views are expressed regarding tight control of blood glucose vs. moderate control
RACE 2003 Ramachandra Anaesthesia Continuing Education
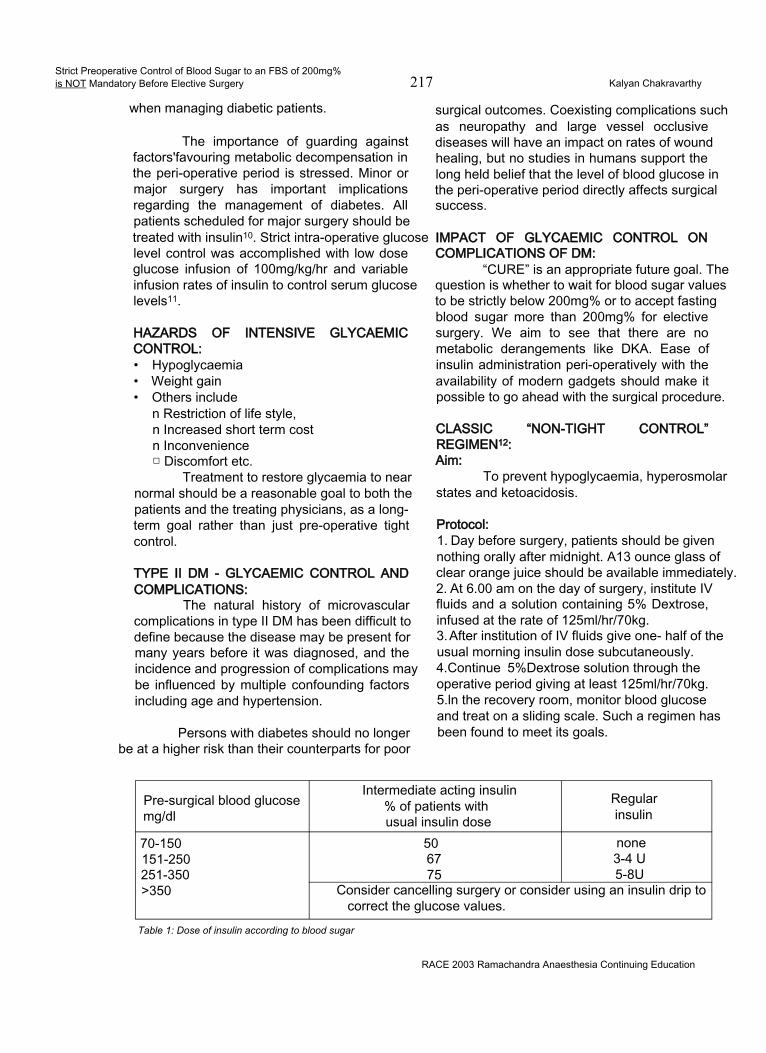
Strict Preoperative Control of Blood Sugar to an FBS of 200mg%is NOT Mandatory Before Elective Surgery 217 Kalyan Chakravarthy
when managing diabetic patients.
The importance of guarding against factors'favouring metabolic decompensation in the peri-operative period is stressed. Minor or major surgery has important implications regarding the management of diabetes. All patients scheduled for major surgery should be treated with insulin10. Strict intra-operative glucose level control was accomplished with low dose glucose infusion of 100mg/kg/hr and variable infusion rates of insulin to control serum glucose levels11.
HAZARDS OF INTENSIVE GLYCAEMIC CONTROL:• Hypoglycaemia• Weight gain• Others include
n Restriction of life style, n Increased short term cost n Inconvenience □ Discomfort etc.
Treatment to restore glycaemia to near normal should be a reasonable goal to both the patients and the treating physicians, as a longterm goal rather than just pre-operative tight control.
TYPE II DM - GLYCAEMIC CONTROL AND COMPLICATIONS:
The natural history of microvascular complications in type II DM has been difficult to define because the disease may be present for many years before it was diagnosed, and the incidence and progression of complications may be influenced by multiple confounding factors including age and hypertension.
Persons with diabetes should no longer be at a higher risk than their counterparts for poor
surgical outcomes. Coexisting complications such as neuropathy and large vessel occlusive diseases will have an impact on rates of wound healing, but no studies in humans support the long held belief that the level of blood glucose in the peri-operative period directly affects surgical success.
IMPACT OF GLYCAEMIC CONTROL ON COMPLICATIONS OF DM:
“CURE” is an appropriate future goal. The question is whether to wait for blood sugar values to be strictly below 200mg% or to accept fasting blood sugar more than 200mg% for elective surgery. We aim to see that there are no metabolic derangements like DKA. Ease of insulin administration peri-operatively with the availability of modern gadgets should make it possible to go ahead with the surgical procedure.
CLASSIC “NON-TIGHT CONTROL” REGIMEN12:Aim:
To prevent hypoglycaemia, hyperosmolar states and ketoacidosis.
Protocol:1. Day before surgery, patients should be given nothing orally after midnight. A13 ounce glass of clear orange juice should be available immediately.2. At 6.00 am on the day of surgery, institute IV fluids and a solution containing 5% Dextrose, infused at the rate of 125ml/hr/70kg.3. After institution of IV fluids give one- half of the usual morning insulin dose subcutaneously.4.Continue 5%Dextrose solution through the operative period giving at least 125ml/hr/70kg. 5.ln the recovery room, monitor blood glucose and treat on a sliding scale. Such a regimen has been found to meet its goals.
Pre-surgical blood glucose mg/dl
Intermediate acting insulin % of patients with usual insulin dose
Regularinsulin
70-150 50 none151-250 67 3-4 U251-350 75 5-8U>350 Consider cancelling surgery or consider using an insulin drip to
correct the glucose values.Table 1: Dose of insulin according to blood sugar
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Control of Blood Sugar to an FBS of 200mg%is NOT Mandatory Before Elective Surgery________________________ Kalyan Chakravarthy
GENERAL GUIDELINES FOR DIABETIC PATIENTS ON THE DAY OF SURGERY13: Tab 1
For type I or type II diabetic patients on insulin therapy: Check blood glucose levels before surgery and use the following guidelines:
In conclusion, an important clinical lesson is that hyperglycaemia is the most important cause of long-term diabetic complications in both types of DM. The available methods of treatment of hyperglycaemia, is effective in achieving near normoglycaemia, which will lessen the morbidity, mortality and cost of management of diabetic complications.
REFERENCES:1. King H et al- Global burden of diabetes 1995-2025, prevalence, numerical estimates and projections. Diabetes Care 1998;21: 1414-31.
2. Ramachandran A, Snehalatha C et al - Diabetes Epidemiology Study Group in India (DESI), High prevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes Survey. Diabetologia 2001 ;44: 1094-101.3. Peter H. Bennett. Chapter 11; Diabetes definition and pathogenesis, Joslin’s Diabetes Mellitus - 13th Edn. Lippincott Williams and Wilkins 193-4, 2000.4. The Expert Committee on Diagnosis and Classification of Diabetes Mellitus.Diabetes Care 1997;20: 1183-97.5. Douglas B. Coursin, et al, Peri-operative care of the diabetic patient. ASA Refresher courses in Anesthesiology 2001 October; 29(1): 1-9.6. Ashok Kumar Das, TS Ashida. Impact of glycaemic control on complications Diabetes Mellitus- Chapter 46. RSSDI-Text book of Diabetes Mellitus, 1st Edn. 2002. 617-22.7. Minerva Anestesiologica. 67(4):258-62, 2001 Apr.8.European Journal of Anaesthesiology. 18(5):277-942001 May.9. Acta Clinica Belgica. 52(5):313-9, 1997.10. South African Journal of Surgery, 30(3);85-9,l!892 Sep.11. JAMA, 244(2): 166-8, 1980 July.12. Ronald D. Miller. Anesthetic implications of concurrent diseases, chapter 25; 5th Edition p-909.s13. Clinical Diabetes vol19, No2, 2001
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia Is Contraindicated for Day Care Surgery 219 Elsa Varghese
The advent of newer short acting general anaesthetic drugs have made day care surgery a reality. Day care surgery involves short duration surgical procedures (not associated with significant alterations in the patient’s normal physiology) on relatively healthy patients. The improvement in surgical technique and the major advancements in anaesthesia drug research has resulted in a large number of medical centres performing the majority of surgical procedures on a day care basis.
In the recent past, the factor of economy has played a major role in increasing the popularity of providing regional anaesthesia for day care surgery. Spinal anaesthesia is being popularised by die-hard fans of this technique as the anaesthetic of choice for surgeries performed below the level of the umbilicus.
To those of us who have performed thousands of spinal anaesthetics and will continue to do so in the future, one may wonder why should there be any contraindication for surgery to be performed on a same day basis, under spinal anaesthesia. There are several reasons why, which this article will address.
COMPLICATIONS AND UNDESIRABLE SIDE EFFECTS OF SPINAL ANAESTHESIA
Complications and undesirable side effects associated with spinal anaesthesia require anaesthesiologists to balance potential risks against potential benefits. Everyday, anaesthesiologists are challenged to make clinical judgements as to the means and methods for ensuring the safety and comfort of their patients. In many cases the administration of spinal anaesthesia may be controversial. The relationship between perceived risk of potential
complications and administration of spinal anaesthesia is a need to be examined.1
Failure to Achieve Anticipated AnaesthesiaSpinal anaesthesia unlike general
anaesthesia is fallible! Even with modern techniques designed to enhance precision, regional anaesthesia may not completely meet the expectations of patients, surgeons or anaesthesiologists. The spectre of unreliability can prejudice its selection.
Informed Consent and Spinal AnaesthesiaWe are obliged to inform our patients of
the potential risks associated with spinal anaesthesia including local anaesthetic toxicity, haematoma, infection, cardiac arrest or death. Shivering, backache, dizziness and urinary retention are unpleasant side effects that may require disclosure.
Controversy of Hyperbaric Spinal LidocaineThe ideal spinal anaesthetic would
combine rapid and adequate surgical anaesthesia with rapid achievement of discharge criteria such as ambulation and urination. The most important determinant of both successful surgical anaesthesia and time until recovery is the dose of local anaesthetic.2
Ideally, local anaesthetics that have an appropriate duration of action with an acceptable side effect profile and the addition of adjuvants which add to the anaesthetic efficacy, without prolonged recovery need to be administered. Hyperbaric spinal lidocaine has long been the gold standard for short acting spinal anaesthesia. Lidocaine has an optimal onset and duration of action of anaesthesia for out-patients but also has the potentially unacceptable side effect of
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia Is Contraindicated for Day Care Surgery 220 Elsa Varghese
transient neurologic symptoms (TNS).3 The incidence of TNS has been found to be highest in out-patients compared with in-patients and in patients undergoing surgery in the lithotomy position (30%) or knee arthroscopies (20%), under spinal anaesthesia.4
Reports of cauda equina neuropathy (CEN), persistent sacral nerve root irritation and unacceptable high incidence of transient neurologic symptoms (TNS) have forced a reappraisal of the safety of hyperbaric spinal lidocaine.
I) CAUDA EQUINA NEUROPATHY (CEN)Auroy et al reported 24 neurologic deficits
following 40,600 spinal anaesthetics.5 Nine of these occurred after lidocaine. CEN has been reported following repeated spinal administration, given to improve the density of a patchy or incomplete subarachnoid block.6
Since CEN can occur after uncomplicated single injections as well, the safety of hyperbaric spinal lidocaine has become controversial. There is mounting laboratory evidence supporting the possibility that a substantial risk exists for prolonged abnormal conduction when 5% Lidocaine is applied to simulated nerve roots.7
The threat of CEN and persistent sacral irritation and transient neurologic symptoms has certainly challenged the clinical decision to persist with providing appropriate spinal anaesthesia for day care surgery.
II) TRANSIENT NEUROLOGIC SYMPTOMS (TNS)
The term TNS is used to describe symptoms of backache with radiation into the buttocks or lower extremities. This syndrome is rarely seen after general anaesthesia and has been demonstrated after spinal anaesthesia. Hyperbaric heavy lidocaine is associated with an increased risk for TNS.8 The aetiology of TNS is unknown. Positioning (lithotomy and knee flexion), sacral stretch, pooling of hyperbaric spinal lidocaine following installation with small-bore pencil point needles have all been implicated as possible risk factors. TNS may occur post
operatively in 4-36% of patients undergoing hyperbaric lidocaine spinals. Alternative approaches for spinal anaesthesia especially for use in outpatients are prompted by the fear of possible neurologic effects of heavy lidocaine.2
ill) CONTROVERSY OF ALTERNATIVES TO HYPERBARIC SPINAL LIDOCAINE
Finding alternatives to hyperbaric spinal lidocaine has challenged clinicians. TNS has been reported with lower concentrations of lidocaine. The addition of epinephrine to isobaric spinal mixtures can increase the incidence of urinary retention.9
Spinal anaesthesia enthusiasts are now ‘dialling down’ the mass of local anaesthetic instilled. But unfortunately dose response data for alternatives such as bupivacaine is scant. There is renewed interest in isobaric and hypobaric alternatives. Laboratory studies suggest a comparative potency of bupivacaine to lidocaine of 9:1. Studies with 2% lidocaine (40mg and lower doses), as well as 0.5% hyperbaric spinal bupivacaine (7.5mg), though providing adequate duration of anaesthesia; have shown a discharge time often exceeding 3 hours for both drugs.1011
IV) MINI DOSE SPINAL ANAESTHESIALow dose lidocaine (20mg) or bupivacaine
6 mg with fentanyl has been advocated for day care spinals of late. Though these combinations may provide satisfactory analgesia and recovery profiles as described by some authors, these concentrations may not provide an immobile extremity during surgery.121314 Moreover, proprioception is preserved with this combination and therefore the patient has the unpleasant awareness of limb manipulation
Post-Dural Puncture Headache (PDPH)Although not a life threatening problem,
PDPH carries substantial morbidity by restricting activities of daily life. A recent survey of 75 consecutive patients suffering from PDPH revealed that approximately 18% had slight restriction of physical activity, 31 % were partially bedridden with restricted physical activity and 51% were entirely bedridden. Furthermore spontaneous resolution of PDPH takes 1 -6 weeks
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia Is Contraindicated for Day Care Surgery 221 Elsa Varghese
after dural puncture thus resulting in frequent and prolonged restriction of daily activities.15
Because no effective non-invasive treatments exist, clinical strategies have focused on prophylactically reducing CSF lost after dural puncture. Traditionally, we have minimised needle size to decrease the size of the CSF leak in the dura, turned cutting needles longitudinally to prevent transverse cutting of longitudinally aligned dural fibres and selected pencil-point needles to maximize the parting and not cutting of dural fibres. Reina et al16 have questioned the concept of less trauma to the dura with pencil-point needles as their study observed similarly sized but more traumatic lesions to the dura with pencil- point needles compared with longitudinally aligned cutting tips.
Evaluation of Closed Claims Data BasesCheny et al17 examined closed claims
database of the American Society of Anaesthesiologists. Of 4183 claims, 16% were for anaesthesia related nerve injury. 84 claims were associated with spinal anaesthesia.
Sudden cardiac arrest during spinal anaesthesia is a significant cause of risk in current medical practice. Interestingly they have been reported in young men undergoing short surgical procedures, where the cardiac arrest occurred almost 30 to 40 minutes following the administration of the spinal anaesthetic. 41 well- documented cases of cardiac arrest have been reported, in which a circulatory mechanism played the primary role in sudden cardiac arrest during spinal or epidural anaesthesia. These arrests were vagal linked or associated with vagal- inducing stimuli like traction, movement, fear and athletic heart syndrome.
Intra-operative cardiac arrest analysis in a prospective study by Biboulet18 suggests that risks and outcomes may be less favourable under conditions of spinal anaesthesia than general anaesthesia. There is persuasive evidence that this phenomenon can occur unexpectedly under conventional conditions of practice and that the associated injury can be very severe.
More so in a situation of day care surgery where there is a rapid turnover and the anaesthetist is under stress to run a schedule in a hurried manner.
BARRIERS TO THE PRACTICE OF SPINAL ANAESTHESIA IN AMBULATORY SURGERY
In ambulatory surgery the use of spinal anaesthesia is subject to the same risk benefit analysis that applies to any anaesthetic technique. There are absolute and relative contraindications.
Patient SelectionSpinal anaesthesia involves very careful
patient selection, the careful positioning and preparation of the patient, introduction of a needle into the subarachnoid space and injection of a local anaesthetic with or without an adjuvant drug and the need to wait for the onset of action of the drug. The possibility of a patchy effect of the block is a reality. The knowledge and expertise in dealing with untoward physiological effects of the block are required. Often, for day care surgery, general anaesthesia has been the preferred anaesthetic of choice mainly for convenience of fast turn overtime and therefore maintaining the hectic OR schedule in a busy day care set up.
Patients are still anxious about being awake during a surgical procedure and more so in the day care setting where premedicant anxiolytic drugs are used minimally. So it is crucial to pick the right patient as inappropriate patients or patients with great anxiety, needle phobia, poorly controlled psychiatric disease or language barriers, are all potentially difficult situations, where though the spinal anaesthetic may provide the analgesia, the patient remains extremely restless and anxious throughout. These patients may require deep sedation, which then defeats the advantages of the technique.
An increasing number of patients are on anti platelet drugs, as the concern for deep vein thrombosis is on the rise. These medications pose an additional risk for spinal anaesthesia and an in-depth information of the medications the patient is on is essential.
>RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia Is Contraindicated for Day Care Surgery 222 Elsa Varghese
Picking the Wrong SurgeonSurgeons must be willing to wait a few
minutes for the onset of action of the block and the choice of spinal anaesthesia may be inappropriate in the outpatient setting when a large number of patients have been scheduled and you have an impatient surgeon on hand.
Picking the Wrong SurgeryPelvic Laparoscopy is a common
procedure performed on a day care basis involving carbon dioxide pneumoperitoneum and steep Trendelenburg. When these procedures are performed under spinal anaesthesia, shoulder tip pain (irritation of the diaphragm) and ascent of spinal level (steep Trendelenburg) are troublesome complications which can occur.
Discharge CriteriaPatients undergoing spinal anaesthesia
need to meet additional discharge criteria before being sent home. As yet there are still no clear- cut guidelines for patient discharge criteria following spinal anaesthesia in ambulatory surgery and they are still being evolved. The ability to void is an important discharge criterion that results in a significant delay in patient discharge after resolution of spinal anaesthesia.19,20
The patient should also be able to stand unaided, walk in a straight line and stand still without swaying. These additional tests would pose an additional strain on recovery room staff especially in a busy day care set-up.
GENERAL ANAESTHESIA FOR DAY CARE SURGERV
Newer anaesthetics have the pharmacokinetic and pharmacodynamic advantages of a shorter duration of action and a more rapid rate of recovery. These factors permit a faster emergence from anaesthesia. Less than 30 years ago, it was unthinkable that patients would be able to return home on the day of surgery. Today, advances in surgery and anaesthesia make it possible to perform surgery safely and effectively on an ambulatory basis.21
With newer agents, propofol, remifentanil, sevoflurane, rapid recovery of patients undergoing anaesthesia permits a patient to be shifted
directly from the operating room to a second stage recovery room and not necessarily the post anaesthesia care unit where nursing care is intensive.
CONCLUSION
Given the uncertainty, along with the time constraints under which day care anaesthesia has to be provided, there has to be a rethink on pushing for the increased use of spinal anaesthesia in the day care setting. There are too many variables out of our control, which does not make it the suitable anaesthetic technique of choice in day care anaesthesia.
REFERENCES
1. Gilbert HC: Complications and controversies in regional anaesthesia. ASA Refresher Course lectures October 2002: No 1232. Liu SS, McDonald SB: Current Issues in Spinal Anaesthesia. Anesthesiology 2001; 94:888-9063. Pollock JE, Neal JM, Stephenson CA et al: Prospective study of the incidence of transient radicular irritation in patients undergoing spinal anaesthesia. Anesthesiology 1996; 84:1361-74. Freedman JM, Li DK, Drasner K, et al: Transient neurologic symptoms after spinal anesthesia. Anesthesiology 1998; 89:1633-415. Auroy Y, Narchi P, Messiah A, et al. Serious complications related to regional anesthesia. Results of a prospective survey in France. Anesthesiology 1997; 87:469-726. Rigler M, Drasur K, Krejue TC et al: Cauda equina syndrome after continuous anesthesia. Anesth Analg 1991; 72:275-817. Lambert L, Lamber D, Strichartz GR: Irreversible conduction block in isolated nerve by high concentrations of local anesthetics. Anesthesiology 1994; 80:10828. Hiller A, Kearjalainen K, Balk M, et al: Transient neurological symptoms after spinal anaesthesia with hyperbaric 5% lidocaine or general anaesthesia. Br J Anaesth 1999; 82:575-99. Chiu A, Liu S, Carpenter RL, et al: The effects of epinephrine on lidocaine spinal anesthesia, a crossover study. Anesth Analg 1995; 80:735-910. Hampi KF, Heinzmann-Wiender S, et al: Transient neurologic symptoms after spinal anesthesia. A lower incidence with prilocaine and bupivacaine than with lidocaine. Anesthesiology 1998; 88:629-3311. Urmey WF, Stanton J, et al: Combined spinal- epidural anesthesia for outpatient surgery. Dose response characteristics of intrathecal isobaric lidocaine using 27 gauge Whitacre spinal needle. Anesthesiology 1995; 83: 528-3412. Ben David B, Mayarsky M, Gurevetch A et al: Comparison of mini dose lidocaine -fentanyl and conventional dose lidocaine spinal anesthesia. Anesth Analg 2000; 91:856-70
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia Is Contraindicated for Day Care Surgery 223 Elsa Varghese
13. Casati A, Fanelli G, Cappelleri G, Berglin B, et al: Low dos£ hyperbaric bupivacaine for unilateral spinal anesthesia. Can J Anesth 1998; 45:850-5414. Ben David B, Solomon E, et al: Intrathecal fentanyl with small dose dilute bupivacaine; better analgesia without prolonged recovery. Anesth Analg 1997; 85: 560-515. Lybecker H, Djernes M, Schmidt JF: Post dural puncture headache (PDPH): onset, duration, severity and associated symptoms: an analysis of 75 consecutive patients with PDPH. Acta Anaesthesiol Scand 1995; 39:605-1216. Reina MA, de Leon-Casasola OA, Lopez A, et al: an in vitro study of dural lesions produces by 25 gauge Quinke and Whitacre needles evaluated by scanning electron microscopy Reg Anesth Pain Med 2001; 25:393- 403
17. Cheny FW et al: Standard of care and anaesthesia liability. JAMA 1989; 261: 1599-160318. Biboulet P: Fatal and non-fatal cardiac arrest related to anesthesia. Can J Anesth 2001; 48:326-3219. Marshall SI, Chung F: Discharge criteria and complications after ambulatory surgery. Anesth Analg 1999; 88:508-1720. Kamphuis ET,lnonescu Tl, Kuipers PW, et al: Recovery of storage and emptying function of urinary bladder after spinal anesthesia with lidocaine and with bupivacaine in men. Anesthesiology 1998; 88:310-621. Lichter JL, Wetchler BV: Outpatient anesthesia, Clinical Anaesthesia, 3rd Edition. Edited by Barash PG, Cullen BF, Stoelting RF, Philadelphia, JP Lippencott Co 1997, pg. 1389-1412
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery Rathna.N.
It is 103 years since the first spinal anaesthetic was administered by Bier in August 1898 in Kiel, Germany. Spinal anaesthesia for a procedure that in many institutions would nowadays be managed on an outpatient basis was reported by Matas in December 1899.1 In spite of the widespread development of ambulatory surgery, there has been relatively little critical evaluation of the role of spinal anaesthesia in outpatients. ‘
Over the past 20 years, the most dramatic change in the delivery of surgical care in the United States has been the shift from inpatient to outpatient and short-stay surgical procedures. Ambulatory surgery in the 1990s, with its demonstrated efforts at cost containment has been enthusiastically accepted by all segments of,health care. Consequently, 65% of all surgical procedures are outpatient based and 35% are in-patients, which in turn has had an impact on the manner in which both surgeons and anaesthesiologists practice.2
“What is an ideal outpatient Anaesthetic”?An ideal outpatient anaesthetic should
provide a safe, simple technique with a quick start (onset of action), rapid stop (offset of effects), minimal postoperative side effects with residual analgesia in the postoperative period. Can spinal anesthesia provide all these? “YES” with selective Spinal anaesthesia.
Why do we think conventional Spinal anaesthesia is contraindicated in ambulatory Surgery?
It is because of the belief and fact that Conventional Dose Spinal Anaesthesia (CDSA)
involves a technique that initiates a block lasting long, with a long time to recovery. Since the time of conventional technique to now, with the better understanding of neurological anatomy, physiology, molecular pharmacology and receptor pharmacology and devices, we have embarked into an era of precision where “selectivity” is the rule with excellent results and benefits, with minimum side effects, which has resulted in a practice of a changed spinal anaesthesia, while exploiting the good aspects of it and succeeding in making it “walk in and walk out” technique for ambulatory surgery.
Professional concernsA survey of 3,651 anaesthetists revealed
that 68 % would choose regional anaesthesia for their own surgery.3 Among the reasons given were ease of administration, fewer complications, pleasant recovery, good operating conditions and less difficulty in the recovery room. More recently, 91 % of anaesthetists who experienced both spinal and epidural anaesthesia expressed a preference for regional anaesthesia.4 Thus, there appears to be a “double standard” within the profession which has lead to pleas that anaesthetists treat their patients as they themselves would like to be treated. Interestingly, 50% of outpatients are afraid of not waking up after anaesthesia. Even though patients’ main preferences are mental clarity and freedom from emesis, pain, dysphoria and myalgias, there is evidence to indicate that administration of general anaesthesia leads to these very problems which may persist for up to 28 days postoperatively.5 Patients’ attitudes towards regional anaesthesia is either favorable(46%) or indifferent (45%), and their main fears are needle pain, backache, seeing and
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia is not Contraindicated for Day Care Surgery 225 Rathna.N.
hearing things, paralysis and the possibility of failure. Thus , a majority of patients would be amenable to regional techniques.
Spinal anaesthesia is not contraindicated for day care surgeries
Regional anaesthesia like spinal and epidural anaesthesia can offer many advantages for the ambulatory patients. In addition to limiting the anaesthetized area, the common side effects of general anaesthesia like nausea, vomiting, dizziness, lethargy etc can be avoided.6 It is said that patients with GA are either “sore, sick or sleepy”. Furthermore, the risks of aspiration, pneumonitis and other side effects of tracheal intubation are avoided. Other advantages include decreased post-operative intensity of care, decreased recovery times, increased mobility, (and) increased post-operative alertness7 and postoperative analgesia. Recently published outcome data have suggested that patients undergoing spinal / epidural anaesthesia alone or combined with general anaesthesia may actually have decreased morbidity and mortality when compared to patients undergoing general anaesthesia alone.8
Minor morbidity, patient satisfaction and costThere are few well-structured
comparisons of regional and general anaesthesia in outpatients. Although general anesthesia continues to be offered as the anaesthetic of choice to most outpatients, its role is being questioned. It is now becoming apparent that minor morbidity is of serious concern. The reported incidence of minor symptoms after outpatient propofol- based general anaesthesia were: hoarse voice (26%), sore throat (24%), headache (10%), backache (20%), emesis (12%), loss of appetite (18%), anxiety (12%), tiredness (28%), delayed recovery of normal function (37%) and postoperative pain (55%).6 A randomised comparison of spinal and general anaesthesia in 433 patients revealed that general anaesthesia was associated with a higher incidence of nausea and vomiting, sore throat, a longer stay in the recovery room with an increased need for opioids, and increased cost.9 Other studies have confirmed a shorter discharge time and decreased cost after spinal anaesthesia. Finally, studies of spinal anaesthesia in outpatients consistently demonstrate that patient satisfaction remains high (>90%).10
Should we abandon conventional dose spinal anaesthesia (CDSA) in outpatients?
A comparison of GA (propofol) and CDSA (15 mg bupivacaine) showed that 180 min after surgery, 15% of GA patients fulfilled home discharge criteria but none of the CDSA patients were able td walk due to residual motor block11. Recently, Vaghadia et al ^demonstrated that small-dose spinal lidocaine was associated with shorter discharge times than CDSA. They have remarked thatthere is a price to be paid for CDSA and the data also revealed what some of us may have suspected - propofol GA may not be the panacea for outpatients. The large standard deviations seen with GA reflect large inter-patient variability depending on whether postoperative complications such as emesis and pain develop, and delay discharge. Interestingly, the short acting spinal anaesthetics have small standard deviations and this suggests that their use will be associated with a more predictable discharge profile, particularly when they are employed with small dose techniques.12
So, conventional dose spinal anaesthesia may not be suitable for routine use in outpatients and anaesthetists need to familiarise themselves with techniques that are associated with a rapid recovery profile.
SELECTIVE SPINAL ANAESTHESIA (SSA)
Definition“ The practice of employing minimal
doses of intrathecal agents so that only the nerve roots supplying a specific area and only the modalities that require to be anaesthetised are affected.”
Drugs used:
LOCAL ANAESTHETICS:
LIDOCAINE:
Investigators have assessed various doses, baricity and concentration. The quality of block, maximum block height and duration are summarised in Table -I. Adjuvants such as fentanyl and sufentanil facilitate reductions in the dose of lidocaine and prolong the sensory block without delaying time to void. In addition, they improve tolerance to visceral sensations such as bladder distension and peritoneal stretch. Addition of
RACE 2003 Ramachandra Anaesthesia Continuing Education
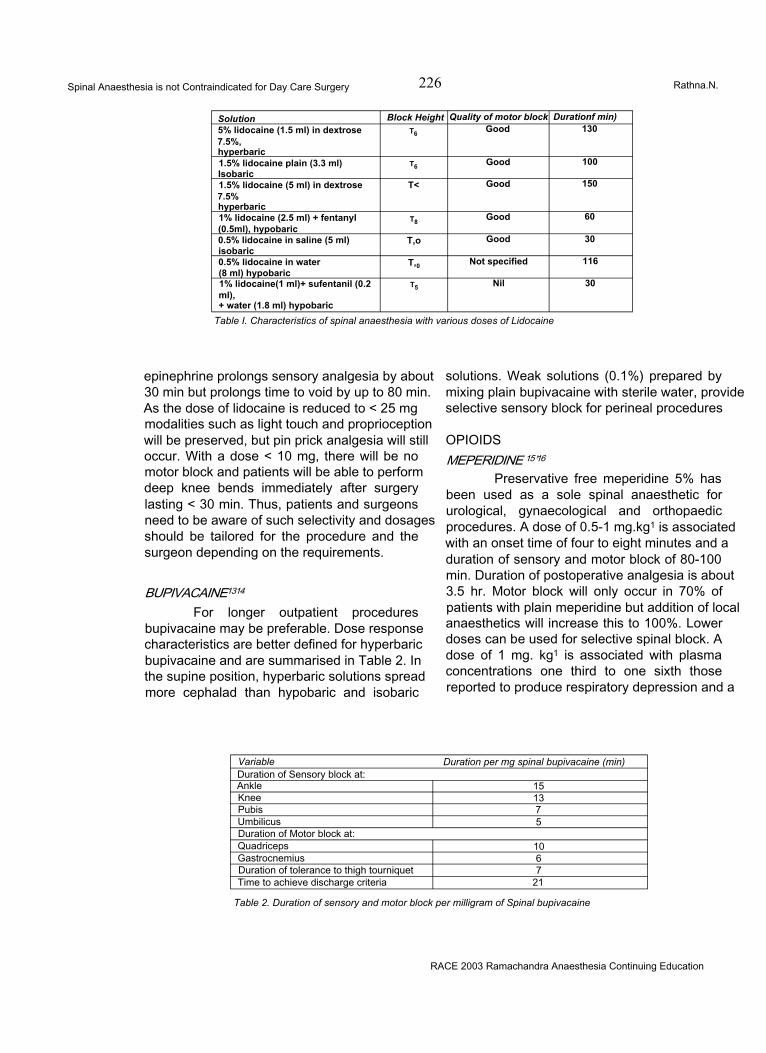
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 226 Rathna.N.
Solution Block Height Quality of motor block Durationf min)5% lidocaine (1.5 ml) in dextrose7.5%,hyperbaric
t6 Good 130
1.5% lidocaine plain (3.3 ml) Isobaric
t6 Good 100
1.5% lidocaine (5 ml) in dextrose7.5%hyperbaric
T< Good 150
1% lidocaine (2.5 ml) + fentanyl (0.5ml), hypobaric
t8 Good 60
0.5% lidocaine in saline (5 ml) isobaric
T,o Good 30
0.5% lidocaine in water (8 ml) hypobaric
T,0 Not specified 116
1% lidocaine(1 ml)+ sufentanil (0.2 ml),+ water (1.8 ml) hypobaric
t5 Nil 30
Table I. Characteristics of spinal anaesthesia with various doses of Lidocaine
epinephrine prolongs sensory analgesia by about 30 min but prolongs time to void by up to 80 min. As the dose of lidocaine is reduced to < 25 mg modalities such as light touch and proprioception will be preserved, but pin prick analgesia will still occur. With a dose < 10 mg, there will be no motor block and patients will be able to perform deep knee bends immediately after surgery lasting < 30 min. Thus, patients and surgeons need to be aware of such selectivity and dosages should be tailored for the procedure and the surgeon depending on the requirements.
BUPIVACAINE1314
For longer outpatient procedures bupivacaine may be preferable. Dose response characteristics are better defined for hyperbaric bupivacaine and are summarised in Table 2. In the supine position, hyperbaric solutions spread more cephalad than hypobaric and isobaric
solutions. Weak solutions (0.1%) prepared by mixing plain bupivacaine with sterile water, provide selective sensory block for perineal procedures
OPIOIDSMEPERIDINE 15’16
Preservative free meperidine 5% has been used as a sole spinal anaesthetic for urological, gynaecological and orthopaedic procedures. A dose of 0.5-1 mg.kg1 is associated with an onset time of four to eight minutes and a duration of sensory and motor block of 80-100 min. Duration of postoperative analgesia is about 3.5 hr. Motor block will only occur in 70% of patients with plain meperidine but addition of local anaesthetics will increase this to 100%. Lower doses can be used for selective spinal block. A dose of 1 mg. kg1 is associated with plasma concentrations one third to one sixth those reported to produce respiratory depression and a
Variable Duration per mg spinal bupivacaine (min)Duration of Sensory block at:Ankle 15Knee 13Pubis 7Umbilicus 5Duration of Motor block at:Quadriceps 10Gastrocnemius 6Duration of tolerance to thigh tourniquet 7Time to achieve discharge criteria 21
Table 2. Duration of sensory and motor block per milligram of Spinal bupivacaine
RACE 2003 Ramachandra Anaesthesia Continuing Education
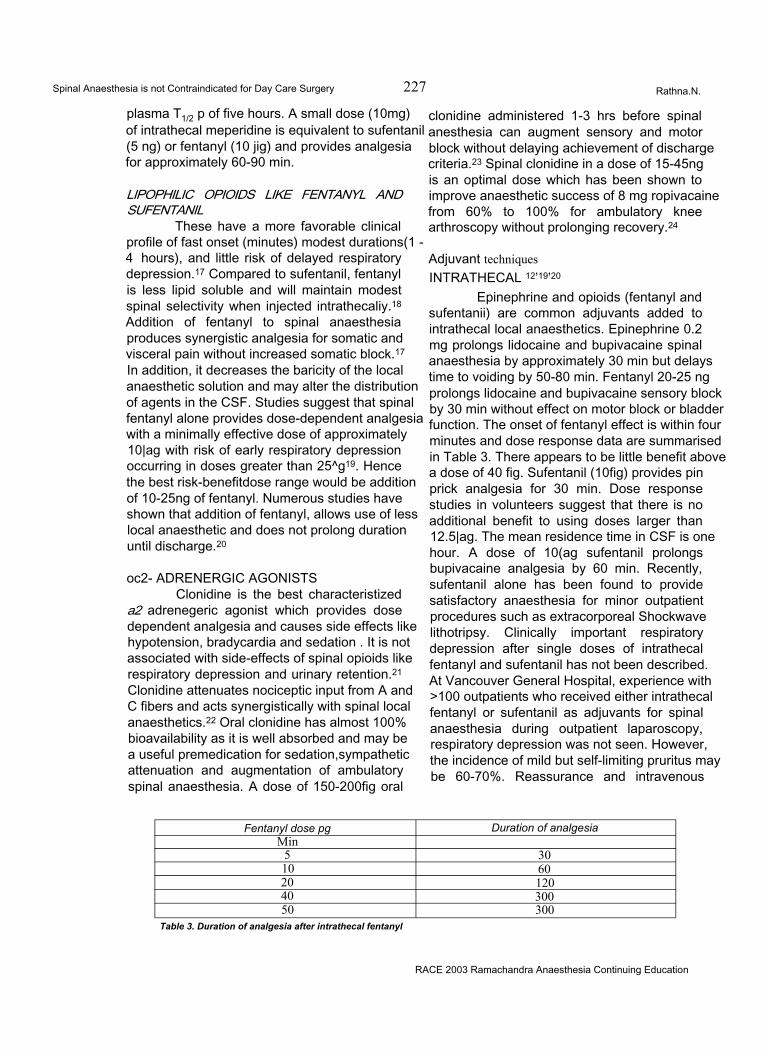
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 227 Rathna.N.
plasma T1/2 p of five hours. A small dose (10mg) of intrathecal meperidine is equivalent to sufentanil (5 ng) or fentanyl (10 jig) and provides analgesia for approximately 60-90 min.
LIPOPHILIC OPIOIDS LIKE FENTANYL AND SUFENTANIL
These have a more favorable clinical profile of fast onset (minutes) modest durations(1 -4 hours), and little risk of delayed respiratory depression.17 Compared to sufentanil, fentanyl is less lipid soluble and will maintain modest spinal selectivity when injected intrathecaliy.18 Addition of fentanyl to spinal anaesthesia produces synergistic analgesia for somatic and visceral pain without increased somatic block.17 In addition, it decreases the baricity of the local anaesthetic solution and may alter the distribution of agents in the CSF. Studies suggest that spinal fentanyl alone provides dose-dependent analgesia with a minimally effective dose of approximately 10|ag with risk of early respiratory depression occurring in doses greater than 25^g19. Hence the best risk-benefitdose range would be addition of 10-25ng of fentanyl. Numerous studies have shown that addition of fentanyl, allows use of less local anaesthetic and does not prolong duration until discharge.20
oc2- ADRENERGIC AGONISTSClonidine is the best characteristized
a2 adrenegeric agonist which provides dose dependent analgesia and causes side effects like hypotension, bradycardia and sedation . It is not associated with side-effects of spinal opioids like respiratory depression and urinary retention.21 Clonidine attenuates nociceptic input from A and C fibers and acts synergistically with spinal local anaesthetics.22 Oral clonidine has almost 100% bioavailability as it is well absorbed and may be a useful premedication for sedation,sympathetic attenuation and augmentation of ambulatory spinal anaesthesia. A dose of 150-200fig oral
clonidine administered 1-3 hrs before spinal anesthesia can augment sensory and motor block without delaying achievement of discharge criteria.23 Spinal clonidine in a dose of 15-45ng is an optimal dose which has been shown to improve anaesthetic success of 8 mg ropivacaine from 60% to 100% for ambulatory knee arthroscopy without prolonging recovery.24
Adjuvant techniquesINTRATHECAL 12’19’20
Epinephrine and opioids (fentanyl and sufentanii) are common adjuvants added to intrathecal local anaesthetics. Epinephrine 0.2 mg prolongs lidocaine and bupivacaine spinal anaesthesia by approximately 30 min but delays time to voiding by 50-80 min. Fentanyl 20-25 ng prolongs lidocaine and bupivacaine sensory block by 30 min without effect on motor block or bladder function. The onset of fentanyl effect is within four minutes and dose response data are summarised in Table 3. There appears to be little benefit above a dose of 40 fig. Sufentanil (10fig) provides pin prick analgesia for 30 min. Dose response studies in volunteers suggest that there is no additional benefit to using doses larger than 12.5|ag. The mean residence time in CSF is one hour. A dose of 10(ag sufentanil prolongs bupivacaine analgesia by 60 min. Recently, sufentanil alone has been found to provide satisfactory anaesthesia for minor outpatient procedures such as extracorporeal Shockwave lithotripsy. Clinically important respiratory depression after single doses of intrathecal fentanyl and sufentanil has not been described. At Vancouver General Hospital, experience with >100 outpatients who received either intrathecal fentanyl or sufentanil as adjuvants for spinal anaesthesia during outpatient laparoscopy, respiratory depression was not seen. However, the incidence of mild but self-limiting pruritus may be 60-70%. Reassurance and intravenous
Fentanyl dose pg Duration of analgesiaMin
5 3010 6020 12040 30050 300
Table 3. Duration of analgesia after intrathecal fentanyl
RACE 2003 Ramachandra Anaesthesia Continuing Education
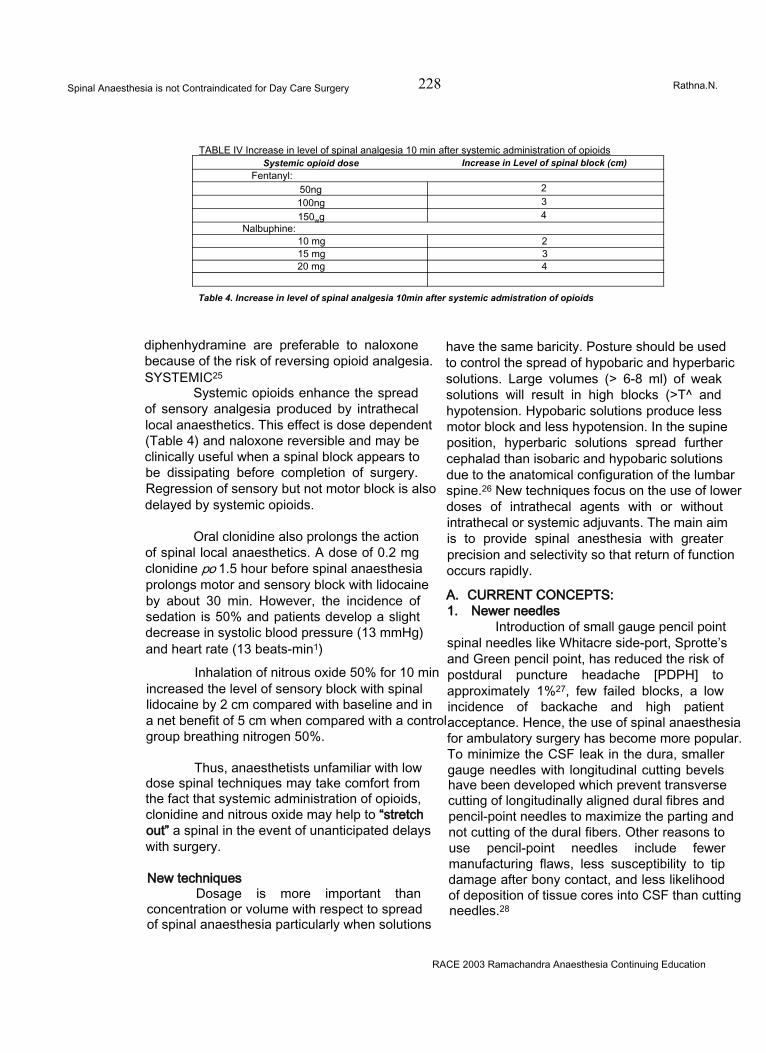
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 228 Rathna.N.
TABLE IV Increase in level of spinal analgesia 10 min after systemic administration of opioidsSystemic opioid dose Increase in Level of spinal block (cm)
Fentanyl:50ng 2100ng 3150wg 4
Nalbuphine:10 mg 215 mg 320 mg 4
Table 4. Increase in level of spinal analgesia 10min after systemic admistration of opioids
diphenhydramine are preferable to naloxone because of the risk of reversing opioid analgesia. SYSTEMIC25
Systemic opioids enhance the spread of sensory analgesia produced by intrathecal local anaesthetics. This effect is dose dependent (Table 4) and naloxone reversible and may be clinically useful when a spinal block appears to be dissipating before completion of surgery. Regression of sensory but not motor block is also delayed by systemic opioids.
Oral clonidine also prolongs the action of spinal local anaesthetics. A dose of 0.2 mg clonidine po 1.5 hour before spinal anaesthesia prolongs motor and sensory block with lidocaine by about 30 min. However, the incidence of sedation is 50% and patients develop a slight decrease in systolic blood pressure (13 mmHg) and heart rate (13 beats-min1)
Inhalation of nitrous oxide 50% for 10 min increased the level of sensory block with spinal lidocaine by 2 cm compared with baseline and in a net benefit of 5 cm when compared with a control group breathing nitrogen 50%.
Thus, anaesthetists unfamiliar with low dose spinal techniques may take comfort from the fact that systemic administration of opioids, clonidine and nitrous oxide may help to “stretch out” a spinal in the event of unanticipated delays with surgery.
New techniquesDosage is more important than
concentration or volume with respect to spread of spinal anaesthesia particularly when solutions
have the same baricity. Posture should be used to control the spread of hypobaric and hyperbaric solutions. Large volumes (> 6-8 ml) of weak solutions will result in high blocks (>T^ and hypotension. Hypobaric solutions produce less motor block and less hypotension. In the supine position, hyperbaric solutions spread further cephalad than isobaric and hypobaric solutions due to the anatomical configuration of the lumbar spine.26 New techniques focus on the use of lower doses of intrathecal agents with or without intrathecal or systemic adjuvants. The main aim is to provide spinal anesthesia with greater precision and selectivity so that return of function occurs rapidly.
A. CURRENT CONCEPTS:1. Newer needles
Introduction of small gauge pencil point spinal needles like Whitacre side-port, Sprotte’s and Green pencil point, has reduced the risk of postdural puncture headache [PDPH] to approximately 1%27, few failed blocks, a low incidence of backache and high patient acceptance. Hence, the use of spinal anaesthesia for ambulatory surgery has become more popular. To minimize the CSF leak in the dura, smaller gauge needles with longitudinal cutting bevels have been developed which prevent transverse cutting of longitudinally aligned dural fibres and pencil-point needles to maximize the parting and not cutting of the dural fibers. Other reasons to use pencil-point needles include fewer manufacturing flaws, less susceptibility to tip damage after bony contact, and less likelihood of deposition of tissue cores into CSF than cutting needles.28
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 229 Rathna.N.
2. Drugs- Local Anaesthetics:A. LIDOCAINE: Spinal lidocaine has long been a popular choice for ambulatory spinal anaesthesia. Although it has enjoyed a long history of safety and popularity since its introduction in 1945, it has come under recent scrutiny because of transient ‘neurologic symptoms [TNS], which has shown to be clearly associated with the spinal lidocaine, with an approximate incidence of 20% in the ambulatory setting.29
B. BUPIVACAINE: TNS is virtually absent in all clinical studies with spinal bupivacaine. Recent studies indicate that small doses [<1 Omg] can be used for ambulatory anaesthesia with time until discharge comparable to lidocaine.30
C. ROPIVACAINE: It is a new local anaesthetic released in the USA in 1996, which is lipid soluble and is approximately 50-60% as potent as spinal bupivacaine with little risk of TNS. Studies have shown that equipotent doses [2:1] of ropivacaine have similar recovery times as bupivacaine.31
D. PRILOCAINE: It is an amide local anaesthetic with pharmacologic properties similar to lidocaine. Recent studies suggest that prilocaine is approximately equipotent to lidocaine with a dose range of 40-70mg and thus may have suitable characteristics for ambulatory spinal anaesthesia with minimal risk of TNS.32
3. Combined Spinal- Epidural Anaesthesia [CSEA]
Has become increasingly popular as its advantages include rapid onset, profound neuraxial block, the ability to titrate or prolong blockade, and lower total drug dosage. Various techniques have been described and technology has provided multiple needle configurations like:
1. Needle through-needle technique
2. Eldor “double barrel” needle
3. Hanaoka “back eye” needle4. Coombs needle.
Availability of the epidural catheter for a rescue anaesthetic allows use of marginal doses of spinal local anaesthetic with resultant rapid recovery and discharge and represents an alternative or complimentary strategy to use of
analgesic additives. However, induction of a CSEA technique probably takes more time than conventional spinal anesthesia, and no current data are available to assess relative cost benefit of increased induction time versus decreased recovery time with CSEA.33
4.. Continuous Spinal Anaesthesia [CSA]The continuous spinal anaesthetic
technique is regaining acceptance in the anaesthesia community. Various needle and catheter designs are available for CSA. Microcatheter (< 24G) and epidural needles and macrocatheters (18-22G) can be used. Newer kits provide an over- the- needle method in which the smaller gauge spinal needle acts as a guide over which the larger gauge catheter ''an be introduced. This needle was designed to reduce the risk of PDPH by not promoting CSF leak. The incidence of PDPH with this technique is 0- 3%.34
One of the advantages of CSA over conventional spinal anaesthesia is the ability to titrate local anaesthetic doses. This slow titration is particularly beneficial in the haemodynamically unstable patient, such as in the elderly or in those with valvular heart disease or trauma.35,36 A number of clinical studies have compared CSA with conventional spinal anaesthesia, demonstrating fewer episodes of hypotension and lesser need for vasopressor with CSA. Another advantage of CSA is the ability to prolong anaesthesia for long surgical cases or even for postoperative analgesia. The ability to use lower anaesthetic doses can lead to faster recovery times, and thus CSA may have applicability to the ambulatory setting, especially in the elderly who are less prone to PDPH.37
TECHNICAL CONSIDERATIONSRecently, it has become apparent that
the pattern of innervation of muscles and deeper structures does not conform strictly to the overlying dermatomes. It has been shown that traditional assumption of a spinal block up to T10 being a prerequisite for urological surgery may not be correct and a mid-lumbar(>L1) level is quite adequate for TURP if bladder pressure is kept <15 mmHg. Systemic adjuvants may also help to improve the adequacy rate of such low block techniques.
The injection rate through a non-cutting
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 230 Rathna.N.
needle (Whitacre) also determines the block height achieved and is important when using low dose techniques. A fast injection rate (0.5 ml.sec-1) results in a greater cephalad spread of spinal anaesthesia (approximately three to four segments) than a slow injection rate (0.02 ml.sec*1).
Continuous spinal anaesthesia with microcatheters would appear a logical method of facilitating selective spinal anaesthesia in outpatients while leaving open the option of further “top ups” as required. An alternative approach is to administer combined spinal-epidural anaesthesia (CSE) with the minimal intrathecal dose required for surgery and utilize the epidural route for back up as necessary. Using a 40 mg initial dose of 2% lidocaine for outpatient arthroscopy, CSE was found to be a reliable technique and was associated with earlier recovery and discharge. Only 10% of patients required intra operative epidural supplementation.
DISCHARGE CRITERIA:Using the newer techniques of spinal
anaesthesia, the patient’s recovery is hastened and the patient can be directly shifted to the step- down recovery by bypassing the Post Anaesthesia Care Unit (PACU). This process is known as “fast tracking” after ambulatory surgery.38lf the patients are awake and oriented in the OR, transfer of these patients directly to the step down unit (Fast tracking) is recommended. The criteria are awake, oriented patients, stable vital signs, minimal pain or bleeding, minimal nausea and vomiting, complete reversal of neuromuscular agents, and oxygen saturation of >94% on room air or resumption to baseline levels. In countries where most or all of the hospital costs are borne by the insurance companies, it results in a significant saving because the major determinant of PACU costs is personnel.39
After spinal anaesthesia, the outpatients must meet the same discharge criteria as patients recovering from general anaesthesia like stable vital signs, ambulation with or without support; no or minimal nausea and vomiting, minimal pain and minimal surgical bleeding.40 In addition, these patients should have prior to ambulation, normal perianal (S4-S5) sensation, the ability to plantar
flex the foot, and proprioception of the big toe as also the ability to void i.e., recovery of sensory, motor and sympathetic nervous functions.40 Patients may be discharged earlier if voiding is not a discharge requirement; however there must be appropriate measures in place if the inability to void persists after discharge.41
POSTOPERATIVE PAIN AND EMESISTwo of the most common problems seen
in the ambulatory surgery patient are pain, and nausea and vomiting. Opioids (e.g., fentanyl, Demerol, morphine) are still the most common and effective method of treating acute, moderate to severe postoperative pain.
Perhaps, as troubling as postoperative pain, is the occurrence of postoperative nausea and vomiting (PONV). For the most susceptible patients (patients with previous history of nausea/ vomiting, motion sickness, women in the luteal phase of the menstrual cycle), prophylactic antiemetic therapy should be considered. The type of surgical procedure also influences PONV; specifically, strabismus repair, laparoscopy, middle ear surgery and orchidopexy are all associated with a relatively high incidence of postoperative vomiting. Despite significant improvement in the pharmacological management of PONV, single drug treatment is not completely effective. However, a multimodal approach has proved successful, including a 92% complete treatment achieved with a combination of droperidol and ondansetron.42 Regional anaesthesia is proven to be associated with a minimal incidence of nausea and vomiting, thereby ameliorating the need for therapeutic interference with drugs.
A LOOK INTO THE FUTURE 43
Experience with new techniques has opened up the possibility of providing “walk-in walk-out” spinal anaesthesia with a real possibility of fast tracking outpatients through the recovery process. Current research is aimed at evaluating the feasibility of bypassing the recovery room after selective spinal anaesthesia (SSA). It has also become apparent that traditional assumptions about the sequence of return of neurological function after spinal anaesthesia (sympathetic, pinprick, motor and finally
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 231 Rathna.N.
propioception) may not apply with SSA. Experience with SSA has demonstrated that pinprick analgesia suitable for surgery can be provided while light touch, proprioception, motor and sympathetic functions are preserved.
CONCLUSIONAmbulatory anaesthesia is continuing to
evolve and has become a recognized anaesthesia subspeciality as more and more surgeries are being performed on an outpatient basis. Ambulatory surgery today represents a new challenge for the anaesthetist as the focus has been shifted and the bottom line is: cost containment and competitive quality care. Spinal anaesthesia with low dose local anaesthetics and analgesic additives provide the double advantage of faster recovery of the central neuraxial blockade and also good postoperative analgesia. New local anaesthetics, analgesic additives, and techniques are being investigated for different applications as the practice of medicine focuses on outpatient care. Safety of spinal agents and complications from spinal anaesthesia continue to be examined and reexamined to improve safety.
With the aforesaid insights into spinal anaesthesia, like• Selective Spinal anesthesia• Modification of techniques - hypobaric and
low dose, adjuvant narcotics• Finer pencil point needles, with an almost
non existent PDPH and• Opportunity for fast tracking the patients• Good post operative analgesia• NoPONV• High acceptance
“ Is Spinal Anaesthesia Contraindicated in Outpatient Surgery”?The answer is a Definite “NO”
REFERENCES:
1 Larson MD. Tait and Caglieri: The first spinal anesthetic in America. Anesthesiology 1996;85: 913-9.
2 White PF, Smith I: Ambulatory anesthesia:PastPresent and future. Int. anesthesia Clin 1994; 32:1.
3 Katz J. A survey of anesthetic choice among anaesthesiologists. Anesth Analg 1973 ; 52: 373-5.
4 Gantt R, Beardsley D,Lindsey J, Setzer V, Stevens RA: Subjective preferences of twelve anesthesiologists undergoing two major neuroaxial blockades : spinal and epidural. Anesthesiology 1994; 81 :A990
5 Watkins S, England AJ, Bolcina A, Yentis SM, Raine G, Feldman SA. Minor morbidity after day -case laparoscopy and the influence of droperidol 0.5 mg: a1 month study. Br J Anaesth 1995; 74: 478P
6 Philip BK: Regional anaesthesia for ambulatory surgery .Can J Anaesth 1992; 39: R3.
7 Neal JM, Dech JJ,Levis MA et al : Hospital discharge after ambulatory knee arthroscopy Reg Anesth 2001; 26: 35-49.
8 Rodgers A, Walker N, Schug SA: Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: Results from an overview of randomized trials, BMJ, 2000; 32:1-12.
9 Standi T, Eckert S, Schulte am Esch J. Postoperative complaints after spinal and thiopentone -isoflurane a n a e s t h e s i a in patients undergoing orthopedics surgery : spinal versus general anaesthesia .Acta Anaesthesiol Scand 1996; 40: 222-6
10 Quaynor H, Corbey M, Berg P. Spinal anaesthesia in day-care surgery with a 26- guage needle.Br J Anaesth 1990; 65: 766-9.
11 Kick O, Megroian B, Lechevalier T, Pinaud M, Souron R, Postoperative comfort and well-being in outpatients: general versus spinal anesthesia. Anesthesiology 1994; 81 :A50
12 Vaghadia H, Me Leod DH, Mitchell GWE, Merrick PM. Small dose hypobaric lidocaine-fentanyl spinal a n a e s t h e s i a
for short duration outpatient laporoscopy.I. A randomized comparison with conventional dose hyperbaric lidocaine. Anesth Analg 1997; 84: 59-64.
13 Liu SS, Ware PD, A//er? HW ,Neal JM, PollockJE. Dose-response haracteristicsof spinal bupivaciane in volunteers. Clinical
implications fora m b u l a t o r y anesthesia. Anaesthesiology 1996; 85: 729-36
14 Maroof M, Khan RM, Siddique M, Tariq M,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery t ____ ___________________________________________________ _—----------------------------- m-----human vokmtees.Rathna.N.
Hypobaric spinal anaesthesia withbupivacaine (0.1%) gives selective sensory block for ano- rectal surgery . Can J Anaesth 1995; 42: 691-4.
15 Tauzin-Fin P, Maurette P, Vincon G, Hecquet D, Houdek M-C, Bonnet F. Clinical and pharmacokinetic aspects of the combination of meperidine and prilocaine for spinal anaesthesia. Can J Anaesth 1992; 39: 655-60.
16 Honet JE, Arkoosh VA, Norris MC, Huffnagle HJ, Silverman NS, Leighton BL. Comparison among intrathecal fentanyl, meperidine, and sufentanil for labor analgesia. Anesth Analg1992; 75: 734-9.
17 Hamber EA, ViscousiCM: Intrathecal lipophilic opioids as adjuvants to surgical
18 spinal anesthetic. Reg Anesth Pain Med 1999; 24:255-63
19 Ummenhofer WC, Arends RH, Shen DD, Bemads CM: Comparative spinal
20 Distribution and clearances kinetics of intrathecally administered morphine,
21 fentanyl, alfentanil and sufentanil. Anaesthesiology 2000; 92:739-53.
22 Ruben SS, Dunn SM, Duprat KM, O’ Sullivan P: An intrathecal fentanyl dose-
23 response study in lower extremity revascularization procedures.
24 Anaesthesiology 1994; 81:1371-5.
25 Liu S, Chin AA, Carpernter RL, Mulrou MF, Allen HW, Neal JM, Pollock JF:
26 Fentanyl prolongs lidocaine spinal anesthesia without prolonging recovery.
27 Anesth Analog 1995; 80:730-4.
28 Eisenach JC, DC kock M, Klimschaw: Alpha (2) adrenergic agonists for
29 regional anesthesia. A clinical review of clonindien (1984-1995)
30 Anaethesiology 1996;85:655-674.
31 Chiari A, Eisenach JC: Spinal Anaesthesia: Mechanism agents, methods, and
32 safety. Reg Anesth Pain Med 1998; 23:357- 362.
33 Liu S, Chig AA, Neal JM, Carpentes RL, Bainton BG, Geerancher JC: O. al
34 clonidine prolongs lidocaine spinal anesthesia
35 Anaesthesiology 1995;82:1353-1359.
36 Dekock M, Gautier PE, Intrathecal ropivacaine and clonindine for 37 ambulatory knee arthroscopy : A dose response study (abstract).
38 Anaesthesiology 2000;93:A6.
39 Sarantipoulos C, Fassoulaki A, Systemic opioids enhance the spread of sensory
40 analgesia produced by intrathecal lidocaine . Anesth Analg 1994;79:94-7.
41 Vaghadia H, Spinal anesthesia for outpatients Controversies and new
42 techniques. Can J Anes.1998;45:R64-R50.
43 Halpan S, Preston R: Post dural puncture headache and spinal needle design:
44 Metganalysis. Anesthesiology 1994; 8:1376- 1383.
45 Greenberg CP, Walit A, Roth JM: Costconscious anesthetic choice for
46 ambulatory surgery (abstract), Anaesthesiology 1994; 81:A1202.
47 Freedman JM,Lid K, Drasner K, Jaskela MC, Larsen B, Wis: Transient
48 neurologic symptoms after spinal anesthesia: An epidemiologic study of 1863
49 patients. Anesthesiology 1998: 89:633-641.
50 Kamphuis ET, Jonscu Tl, Kuipers PW, de Grier J, van vennooij GE, Boon TA:
51 Recovery of storage and ing functions of the urinary bladder after spinal
52 anesthesia with lidocaine and with dupivacaine in men. Anesthesiology 1998;
53 88:310-6.
54 Gautier PF, Dekock M, Vansteenberge A: Intrathecal ropivacine for ambulatory
55 surgery: A comparison between intrathecal dupivaciane and intrathecal
56 ropivacaine for time arthoscopy Anesthesiology 1999; 91:1239-45.
57 Hampl KF, Heinzmann-Weidmen S, Lugmin buch I, Seeberger M, Schneider
58 MC, Drasner K: Transient neurologic sysmptoms after spinal anesthesia: A lower
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 233 Rathna.N.
incidence with prilocaine and bupivacaine than with lidocaine. Anesthesiology 1998; 88:629-33.
59 Liu SS, McDonald SB. Current Issues is spinal Anesthesia. Anesthesiology
60 2001;94:888-906.
61 Muralidhar V, Kaul HL .Mallick P: Over the needle versus microcatheter through needle technique for continuous spinal anesthesia: A prelimnary study.Reg Anesth Pain Med 1999;24:417-21.
62 Collard CD, Eappren S, Lynch EP, conception M: Continuous spinal anaesthesia with invasive hemodynamic monitoring for surgical repair of the hip in 2 patients with severe aortic stenosis Anesth Analy 1995;81:195-198.
63 Wilhelm S, Standi T, Burmeister M, Kessler G, Schulte am Essch J: Comparison of
continuous spinal- epidural anesthesia using plain bupivacaine 0.59% in trauma patients . Anaesth Analg 1997; 85:69-74.
64 Favarel-Garrigues JF, Sztark F, Petitjean MF, Thicoipe M, Larsic P, Dauadic
P:Hemodynamic effects of spinal anesthesia in the elderly: Single dose versus titration through a cather. Anaeth. Analg 196; 82:312-6.
65 Lubarsky DA: Fast track in the post anesthesia care unit:Unlimited possibilities? J Clin Anesth 1996; 8:705.
66 Dexter F, Tinen JH: Analysis of strategies to decrease post anesthesia care unit costs. Anaesthesiology 1995; 82:94.
67 Chung F: Are discharge criteria changing? J Clin Anesth 1993; 5:645.
68 Chung F: Discharge criteria: A new trend. Can J Anaesth 1995; 42:1056.
69 McKenzie R, Lim Uy NT, Riley TJ, Hamilton DL. Droperidol/Ondensetron combination controls nausea and vomiting after tubal ligation. Anesth Analg 1996;83:1081-3.
70 Viskari D.Berril A,Vaghadia H. Walk-in walkout spinal anaesthsia for outpatient laparoscopy: evalution of hreehypobaric solutions. Can J Anaesth 1997; 44: A26-B.
RACE 2003 Ramachandra Anaesthesia Continuing Education
DEBATE

Invasive Monitoring in ASA III and ASA IV patientswill Influence the Outcome of Surgery._______________ 234 Ashok Badhe
The role of Invasive Monitoring in ASA III and ASA IV patients for surgery is quite established by now. Invasive monitoring is quite routinely practsiced in these patients. To single out the influence of invasive monitoring on the outcome of surgery is quite difficult. The outcome of surgery in these groups of patients is influenced by a variety of factors. The factors influencing the outcome of surgery can be broadly categorized as:
1) The patient’s disease2) The Surgery3) Anaesthesia.
The perioperative variables also interact with each other and it is quite difficult to separate the contribution of each to perioperative morbidity and mortality and the postoperative outcome.
To recapitulate (ASA III and IV patients)
ASA classification:1) ASA III - A patient with a severe systemic
disease that limits activity but is not incapacitating.
2) ASA IV - A patient with an incapacitating systemic disease that is a constant threat to life.
The role of monitoring during surgery is not questioned by anybody in the present anaesthesia practice. The basic purpose of monitoring is to help us to know the haemodynamic status and also to guide us about the therapeutic measures to be taken to correct the derangement. Most of the haemodynamic parameters can be monitored by noninvasive techniques, but one must keep in mind the limitations of these techniques in patients of ASAIII and ASA IV. The focus is on this subset of
patients. One must keep in mind that these patients need more intensive and more or less continuous and accurate monitoring which cannot be achieved by noninvasive monitoring techniques. For example, pulse oximetry, one of the most commonly used, and quite useful monitor, can be affected by hypotension, hypothermia and peripheral vasoconstriction which are quite commonly seen in ASA III and ASA IV patients undergoing major surgery.
VARIOUS INVASIVE MONITORING TECHNIQUES : employed during the perioperative period are:
i) Urine output monitoringii) Invasive Arterial Blood Pressure
monitoring.iii) Central Venous Pressure monitoring.iv) Pulmonary Artery Pressure monitoring.
i) Urine Output Monitoring:This is one of the least invasive of all the
monitoring methods. Hourly urine output is quite important in ASA III and ASA IV patients posted for major surgeries. This helps us to know the perfusion of the vital organs and also guides us about the therapeutic modalities. These therapeutic modalities can have an important bearing on the outcome of the surgery.
ii) Invasive Arterial Blood Pressure Monitoring:
Accurate, correct, continuous blood pressure monitoring is mandatory in these groups of patients. Direct Intra-arterial Blood pressure remains the gold standard technique. It provides a beat to beat indication and the waveform. In these patients, wide-swings of arterial pressures may be seen because of surgical manipulations, intravascular volume shifts, effects of anaesthetic agents and arrhythmias. It also helps to obtain
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III and ASA IV patientswill Influence the Outcome of Surgery._______________ 235 Ashok Badhe
repeated blood gas assessment.Indications in these patients:
I. Major surgical procedures involving large fluid shifts, and blood loss.
II. Pulmonary disease patient requiring frequent ABG analysis.
III. Patients with hypovolemic, cardiogenic or septic shock or with multiple organ failure.
IV. Massive TraumaV. Patients requiring Inotropes.VI. Patients with electrolyte and metabolic
disturbances requiring frequent arterial sampling.
VII. Inability to measure arterial pressure non- invasively (morbid obesity).
The indications during cardiovascular, thoracic, and urosurgeries, are not mentioned here.
COMPLICATIONS:1) Infections: This potential common
complication is common to all invasive monitoring techniques. The incidence can be reduced by using a proper aseptic technique and avoiding prolonged catheterization at the same site.
2) Hemorrhage: this is a potential risk because of disconnection. This can be reduced by Luer lock connections and having low pressure alarms.
3) Thrombosis and Distal Ischaemia: Factors that correlate with increased incidence of thrombosis are prolonged cannulation and larger catheters in smaller vessels. This complication is seen in a negligible number of cases and can be reduced by removing arterial catheters with continuous aspiration of catheter by syringe during proximal and distal occlusion of the vessel.
iii) Central venous Pressure Monitoring:Accurate measurements are possible if
the distal end of the catheter lies within one of the large intrathoracic veins or the right atrium. This is quite a useful invasive monitor if the factors affecting it and its limitations are understood. Serial measurements are more useful than a singular measurement and the response of the CVP to a volume infusion is a useful test of right ventricular function. This mainly indicates
intravascular volume.Indications for CVP monitoring include
• Major surgeries involving large fluid shifts and blood loss.
• Intravascular volume assessment when urine output is not reliable or unavailable (Prostate surgery, Renal failure).
• Major trauma• Venous access for vasoactive irritating drugs.• Inadequate peripheral venous access. These
are some of the indications in ASA III and ASAIV patients in the perioperative period.
COMPLICATIONS:A) Arterial Puncture: This is because the veins lie in the close proximity of arteries. This can be minimized by meticulous technique and by using a small gauge (22G) needle initially, to localize the vein.B) PneumothoraxC) Nerve InjuryD) Arrhythmias: Transient atrial and or ventricular arrhythmias commonly occur as the guide wire is passed into the right atrium.
iv) Pulmonary Arterial Pressure Monitoring:The population of patients with multiple
systemic disease is likely to benefit from this “leap” in monitoring. It gives important diagnostic information to decide about the therapeutic management.
INDICATIONS FOR PULMONARY ARTERY CATHETER MONITORING:• Patients with recurrent myocardial infarctions
or unstable angina.• Patients with left ventricular dysfunction
(congestive heart failure).• Patients in hypovolemic, cardiogenic or
septic shock with multiple organ failure.• Patients with massive ascites.• Major procedures involving large fluid shifts
in patients with coronary artery disease.
COMPLICATIONS:1 Unintended arteriotomy2 Pneumothorax3 Arrhythmias4 Sepsis
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III and ASA IV patientswill Influence the Outcome of Surgery._______________ 236 Ashok Badhe
5 Potentially fatal haemorrhage.PAC MONITORING HAS WELL KNOWN POTENTIAL BENEFITS:1. Ability to measure important haemodynamic
indices.2. Additional information regarding fluid
management and drug therapy.3. Also helpful in determining whether it is safe,
for high risk patients to proceed with surgery.
This is one invasive monitoring about which a lot of claims and counter claims appear in the literature by both the technophiles and technophobes. But one must keep in mind that the PAC monitoring is a useful adjunct but it cannot replace the vigilant anaesthetist.
The question most commonly asked is, ‘Does invasive monitoring influence the surgical outcome?’ When one asks a question like this, it is implicit in the question that it does contribute to the surgical outcome atleast in principle. The technology is a discrete, separate feature of our environment; hence we are inclined to think that it can be treated as a single factor and its contribution can be measured or atleast estimated. But in practice it is not so, various prospective and retrospective studies are not able to decide the influence of PAC on the outcome of surgery because most of the studies are not conducted with standard methodology and there are various lacunae in the studies like patient selection, selection of controls etc. ASA established a task force on PAC an 1991 to examine the evidence for benefits and risks from PAC catheters. This report summarizes the task force recommendations based on scientific evidence and experts’ opinions. If you look into statistical analysis, the benefit and the influence
on the outcome of surgery is negative but if you clinically look in to the findings it is quite suggestive that patients do benefit from PAC and it may have influence on the outcome of surgery.
CONCLUSION:To conclude, the principle function of
invasive monitoring technology is to amplify or augment human operator expertise. The benefits of invasive monitoring can be reaped maximum by adequate training, experience and expertise.
REFERENCES:1 Report by ASA Task force on PAC
Anaesthesiology Feb.93, vol.78 No.2
2 Friend and Foe: Why can’t we agree about the effects of new technology in patient safety - Richard I Cook, ASA Refresher course series 2002.
3 Cardiac Anaesthesia - Joel A Kaplan.
4 Bedford RF: Removal of radial artery thrombi following percutaneous cannulation for monitoring. Anaesthesiology 46: 430, 1977.
5 Bedford R.F, Ashfor T.P.: Aspirin pretreatment prevents post cannulation radial
Aspirin pretreatment prevents post cannulation radial artery thrombosis. Anaesthesiology 51: 176, 1979.
6 U. Wolter M.D. et al. - ASA classification and perioperative variables in predictors of post operative outcome. BJA August 1996 Vol.77 No.2.
7 A practice of Anaesthesia - Wylie and Churchil Davidson’s. Edited by Thomas E.J. Healy & Peter Cohen.
8 Anaesthesia Providers, Patient outcome & costs: Anaesth. Analgesia. Jun 1996 Vol.82 No.6 p.1273.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 237 A. Rajamanoharan
Monitoring forms the base or the basis of the conduct and safety of anaesthesia. Measurement is a single observation and monitoring is a serial evaluation. Under anaesthesia the vital parameters must be maintained within the safe limits. The ideal monitoring should be r'mple to apply and observe, cost effective, dynamic, accurate, error free and safe.
The simplicity, safety and the advances in the microprocessor, servo mechanical control technology and photoplethysmography have enabled the non-invasive techniques to be the choice to provide a nearly continuous, correct and accurate assessment of blood flow and pressure.
Invasive monitors without exception carry real dangers and are only used as temporary devices while successful and continued efforts are being made to replace them. Two of the least appreciated disadvantages of extensive monitoring are prolonged immobilisation and the anguish that accompanies it.
Measurement of cardiac output has traditionally been the poor relation to pressure monitoring because of the perceived risks, complexity and expense of pulmonary artery catheterisation. The latest National Confidential Enquiry into Perioperative Deaths highlighted how only a small minority of the reviewed patients had intraoperative pulmonary artery catheter monitoring, yet over three-quarters were classified as being ASA Grade III or higher. No mention was made as to whether cardiac output was actually measured during the operation. The onset of significant haemodynamic deterioration and organ dysfunction is often the cue for its introduction; this belated insertion may partly explain the difficulty in demonstrating any benefit in the critically ill patient. Indeed, a recently
published retrospective analysis has actually suggested possible detriment. This paper has generated considerable debate as to when, how and in whom this invasive approach should be used. It has also given added impetus to the development of alternative flow monitoring techniques that are either non- or minimally invasive and, with advances in technology, increasingly reliable and user-friendly. Many of these techniques also provide additional information on circulatory status, e.g. cardiac preload, ventricular contractility and extravascular lung water, which can further assist therapeutic decision-making. The particular benefits that could arise from non-invasive flow assessment are early identification and either prevention, or faster correction, of circulatory derangements before a significant tissue oxygen debt has been allowed to develop. This proactive philosophy may impact significantly upon postoperative outcome.
Any blinding enthusiasm for non-invasive techniques should be tempered by awareness of the limitations of both the machine and the technology being utilised. Not infrequently, poor equipment design, over-stated abilities and/or inadequate user education have generated unfavourable studies. This may contribute more to an understandable wariness on the part of the clinician rather than to any inherent problem with the technique itself, which is often discredited in the process. It thus behoves prospective users to familiarise themselves fully with both theory and practice underlying a particular device, to develop sufficient expertise to recognise unreliable or erroneous signals, and to be aware of any limitations. All technologies have flaws, and data derived from different methods do not necessarily correlate well. Techniques may often be better at monitoring change rather than delineating absolute output itself. So, let us replace the out-modelled and more harmful
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 238 A. Rajamanoharan
invasive monitoring with non-invasive monitoring equipments and see how they are better, dependable, accurate, totally harmless and user- friendly.
PULSE OXIMETERPulseoximetry (PO) has been arguably
called the most significant technological advance ever made in monitoring the safety of patients during anaesthesia. Prior to the advent of Pulse oximetry, the only monitor for adequate oxygenation of the patient was the “trained” eye of the anaesthesiologist observing skin colour for cyanosis. The pulse oximeter has now become a mandatory intraoperative monitor and in October 1989, the American Society of Anaesthesiologists voted to mandate the use of Pulse oximetry in all anaesthetics after January 1990.
Pulse Oximetry is made possible by the combination of two simple physical principles:1. Every substance has a unique absorbance spectrum2. Of all light absorbing substance in the living tissues, only arterial blood is pulsatile.
Clinical applications1. MONITORING OXYGENATION
- Provides warning of hypoxemia in the operating room (OR), post anaesthesia care unit (PACU), during transport between OR and PACU, and during out-of-hospital transport.
2. MONITORING OXYGEN THERAPY• Helps to titrate supplemental oxygen
in mechanically ventilated patients and patients receiving oxygen therapy by Venturi device. Trends of Sp02 by pulse oximetry should be periodically confirmed by blood gas analysis.
• Pulse oximetry can also be used as a supplement to arterial blood gas analysis to monitor hyperoxia in premature infants
3. ASSESSMENT OF PERFUSIONPresence of pulsatile signal
appropriately tracks the viability of the tissue monitored.
4. MONITORING VASCULAR VOLUME• The amplitude of plethysmographic
waveform provides information about
hypovolaemia during positive pressure ventilation.
Pulse oximeter occupies a unique place among the present day monitors as it provides vital patient information continuously and noninvasively. It also scores over other monitors, as it requires little training for its use and no calibration, making it extremely user-friendly. By helping to detect hypoxemia early, it helps the anaesthesiologist in providing safe patient care in the operating room as well as the intensive care unit.
CAPNOGRAPHYCapnography, the measurement of the
carbon dioxide (C02) content in respired gases, has become part of basic monitoring in anaesthesia and intensive care. Capnographs can provide information regarding the production, transport and excretion of C02. A closed claims study in 1989 has concluded that about 93% of anaesthetic mishaps could have been prevented if capnograph and pulse oximeter had been used as monitors
Indications and uses of capnography• Verification of endotracheal tube placement.• Difficult airway■ Blind nasal intubation• Proper positioning of double lumen tube• Validation of reported end tidal values• Indirect assessment of partial pressure of arterial carbon dioxide tension (normal (a-ET) PC02 varies from 2 to 5mmHg and increases with age, pulmonary disorders like emphysema, pulmonary embolism, decreasing cardiac output, hypovolaemia and general anaesthesia.
■Adequacy of spontaneous ventilation under general endotracheal anaesthesia and also in the awake intubated patient in the recovery room/ICU and in a patient under regional anaesthesia, (apnoea monitor).• Assessment of ventilator, breathing circuit and gas sampling integrity.• Circuit leaks and adjustments of fresh gas flow.■ Instantaneous disconnection, total occlusion and accidental extubation.■ Carbondioxide retention due to faulty circuit (Bains).■ Exhausted carbondioxide absorbent in a semi
RACE 2003 Ramachandra Anaesthesia Continuing Education
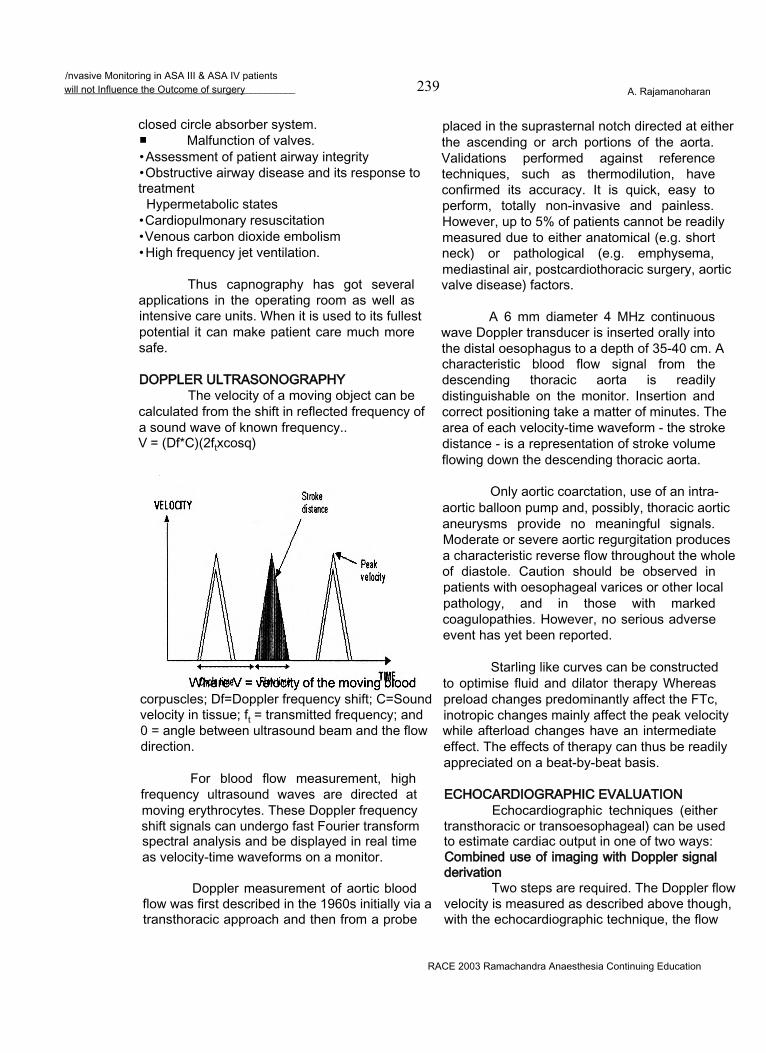
/nvasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 239 A. Rajamanoharan
closed circle absorber system.■ Malfunction of valves.• Assessment of patient airway integrity• Obstructive airway disease and its response to treatment
Hypermetabolic states• Cardiopulmonary resuscitation• Venous carbon dioxide embolism• High frequency jet ventilation.
Thus capnography has got several applications in the operating room as well as intensive care units. When it is used to its fullest potential it can make patient care much more safe.
DOPPLER ULTRASONOGRAPHYThe velocity of a moving object can be
calculated from the shift in reflected frequency of a sound wave of known frequency..V = (Df*C)(2ftxcosq)
corpuscles; Df=Doppler frequency shift; C=Sound velocity in tissue; ft = transmitted frequency; and 0 = angle between ultrasound beam and the flow direction.
For blood flow measurement, high frequency ultrasound waves are directed at moving erythrocytes. These Doppler frequency shift signals can undergo fast Fourier transform spectral analysis and be displayed in real time as velocity-time waveforms on a monitor.
Doppler measurement of aortic blood flow was first described in the 1960s initially via a transthoracic approach and then from a probe
placed in the suprasternal notch directed at either the ascending or arch portions of the aorta. Validations performed against reference techniques, such as thermodilution, have confirmed its accuracy. It is quick, easy to perform, totally non-invasive and painless. However, up to 5% of patients cannot be readily measured due to either anatomical (e.g. short neck) or pathological (e.g. emphysema, mediastinal air, postcardiothoracic surgery, aortic valve disease) factors.
A 6 mm diameter 4 MHz continuous wave Doppler transducer is inserted orally into the distal oesophagus to a depth of 35-40 cm. A characteristic blood flow signal from the descending thoracic aorta is readily distinguishable on the monitor. Insertion and correct positioning take a matter of minutes. The area of each velocity-time waveform - the stroke distance - is a representation of stroke volume flowing down the descending thoracic aorta.
Only aortic coarctation, use of an intra- aortic balloon pump and, possibly, thoracic aortic aneurysms provide no meaningful signals. Moderate or severe aortic regurgitation produces a characteristic reverse flow throughout the whole of diastole. Caution should be observed in patients with oesophageal varices or other local pathology, and in those with marked coagulopathies. However, no serious adverse event has yet been reported.
Starling like curves can be constructed to optimise fluid and dilator therapy Whereas preload changes predominantly affect the FTc, inotropic changes mainly affect the peak velocity while afterload changes have an intermediate effect. The effects of therapy can thus be readily appreciated on a beat-by-beat basis.
ECHOCARDIOGRAPHIC EVALUATIONEchocardiographic techniques (either
transthoracic or transoesophageal) can be used to estimate cardiac output in one of two ways: Combined use of imaging with Doppler signal derivation
Two steps are required. The Doppler flow velocity is measured as described above though, with the echocardiographic technique, the flow
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery 240 A. Rajamanoharan
being interrogated is usually in or close to the heart, e.g. across the mitral valve or, commonly, in the aortic root. Echocardiographic measurement of cross-sectional area at this point will allow calculation of cardiac output as the product of blood velocity averaged over a minute and cross-sectional area. Planimetric measurement, enhanced by recently developed edge-detection technology, may improve the accuracy of calculated cardiac outputs although it may still prove difficult to obtain accurate short- axis views.
The use of combined transoesophageal echocardiographic imaging and Doppler probes allows estimation of cardiac output in the critically ill more readily than transthoracic imaging techniques.
Calculation from ventricular volumesIf ventricular volume at end-systole and
end-diastole are measured, stroke volume can be calculated as the difference between these two values, and cardiac output as the product of this stroke volume and heart rate.
Recently developed technology allows 3- dimensional reconstruction of images of the left ventricle. Routinely, however, ventricular volumes will still be calculated from 2-D and M-Mode images although these often rely upon assumptions about LV shape, namely:
Transthoracic impedanceIn 1966, Kubicek described the thorax
as a cylinder evenly perfused with blood of specific resistivity ‘p’, itself related to the haematocrit. Pulsatile thoracic aortic blood flow caused negative impedance changes (measured from a steady state mean base impedance (Z), with a maximum rate of change [(dZ/dt)m J of Zm during systole between pairs of electrodes placed around the neck and upper abdomen.
SV=p(L2/Z2)ZmWhere SV = stroke volume; p=electrical
resistivity of the blood; L=mean separation of the inner pair of electrodes; Zm = maximum rate of change of impedence (dZ/dt)maxduring systole, and Z = basic impedance between the inner electrodes.
The original Kubicek equation consistently overestimated SV. Furthermore, it
was subsequently shown that the thorax behaves electrically more as a truncated cone rather than as a cylinder. . This, and the application of new technology, renders transthoracic impedance of potential clinical use and the new equations have been incorporated into commercial systems such as the NCCOM-3 (Biomed Medical Manufacturing Ltd, Irvine, CA, USA). Common systems have involved the application of a sensing electrode to either side of the neck root and to opposite sides of the body in a mid-coronal plane at the xiphisternum level. Two pairs of transmitting electrodes are placed 5 cm above the neck sensors and 5 cm below the thoracic sensors, respectively. Accurate electrode placement is crucial using such systems.
Although data derived from this system may, under some circumstances, correlate well with those derived from thermodilution (and even prove more reproducible in individual subjects), the varying impedance technologies and derived equations have yet to be validated in individuals of both sexes and of diverse age and habitus in varied clinical situations. Adoption of the technique in the ICU setting cannot yet be recommended. Its use in the emergency room (to allow rapid and non-invasive monitoring of responses to resuscitation) or on the operating table may prove more readily acceptable.
Pulse Contour AnalysisSince the rate at which blood flows from
arteries to veins is proportional to the rate of fall of arterial pressure, analysis of the contour of the aortic pulse-wave allows determination of cardiac output. The area of the arterial waveform (or pulse contour) was first described as a means of monitoring cardiac output by Frank in 1899. This pulse contour cardiac output technique (PCCO) can be performed non-invasively from a finger pressure waveform using a Finapres device or from an indwelling arterial cannula which is being pressure transduced. However, it cannot be used for quantitation of cardiac output unless a calibration tool such as thermodilution is used. Over the last two decades, various equations have been developed by different researchers for monitoring stroke volume.
The Bradley MethodA clinical means for estimating cardiac
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 241 A. Rajamanoharan
output and peripheral vascular resistance was revised by Bradley. In experienced hands, this has been shown to be a reliable technique, however, a validation study showing good agreement when compared against thermodilution has only been published in abstract form and it has to be shown to be readily transferable to novices.
It relies upon a version of Ohm’s law where the voltage gradient across a circuit equals the product of current and resistance. In the systemic circulation, the pressure gradient across the circuit (mean arterial pressure minus central venous pressure) measured in mmHg equals the product of cardiac output (in 1 /min) and peripheral vascular resistance (in Wood units).
COMPLICATIONS OF INVASIVE MONITORING Complications of arterial puncture
• Infection• Haemorrhage• Thrombosis and distal ischaemia
Skin necrosis EmbolizationHaematoma Neurologic injuryLate complications like pseudoaneurysm and AV fistula
Complications of central venous cannulationsArterial puncturePneumothorax/hydrothoraxChylothoraxPericardial effusion/tamponade
• Venous air embolism Nerve injury Arrhythmias
Complications of pulmonary artery catheterisation
All complications of internal jugular vein cannulation and in addition:
• Complete heart block (in patients with LBBB)Endobronchial haemorrhage Pulmonary infarction Valvular damage Thrombocytopenia
• Thrombus formation Incorrect placement
Balloon rupture
CONCLUSIONKISS the well known acronym for “Keep
it simple, stupid” is often taken to be good advice for life in general. Editorial by C.E. Hahn BJA volume 86-4 April 2001.
Moreover, for the trainee, there is a galaxy of advice, opinion and controversies to be digested. Monitoring has become the sixth sense of the clinician and has contributed in a major way to a safer anaesthetic practice.
Invasive monitoring is time consuming, needs technical expertise, definitely damaging, necessitates immobilization and is vulnerable for disturbances and inaccurate results. Let us eradicate “invasion” anywhere in the universe. To quote Mahatma Gandhi “non-violence”’ (noninvasion) is the strongest but still the most successful method. So let us be non-invasive in monitoring our ASA III & IV patients.
REFERENCES
1. Noninvasive monitoring of cardiac output, Hugh Montgomery, Mervyn Singer, 163, Recent advances in anaesthesia and analgesia 20 by A.P.Adams, J.N.Cashman.
2. Edward D.Miller Jr - Miller 5th edition, 14703. Text book of Anaesthesia by Wylie Churchill Davidson4. Tinker JH, Dull DL, Caplan RA, Ward RJ, Cheney FW.
Monitoring devices in preventing of anaesthetic mishaps: a closed claims analysis. Anaesthesiology 1989; 71:51-46.
5. Shankar KB, Moseley H, Kumar AY, Delph Y, Capnometry and anaesthesia:Can J Anaesth 1992; 39:617-32.
6. Eichhom JH, Prevention of intraoperative Anaesthesia Accidents and Related Severe injury through safety monitoring. Anaesthesiology 1989; 70:572-7.
7. Stock MC, Capnography for Adults. Critical Care Clinics 1995; 11:219-32.
8. Severinghaus JW,, Kelleher JF. Recent developments in pulse oximetry Anaesthesiology 1992; 76:1018-38.
9. Moon RE, Camporesi EM, Respiratory Monitoring. In Miller RD, eds. Anaesthesia. 5th ed.California:Churchill ivingstone; 2000:1:1269-77.
10. Dorsch JA, Dorsch SE Pulseoximetry in: Understanding Anaesthesia Equipment 4th ed. Baltimore:Williams and Wilkins; 1998; 811-48.
11. Wahr JA, Tremper KK.Pulseoximetry. ln:Blitt CD, Hines RL, eds. Monitoring in anaesthesia and critical care medicine.3rd ed. Newyork:Churchill Livingstone; 1995;385-406.
12. RACE 2000 - Postgraduate symposium on Non-invasive monitoring.
RACE 2003 Ramachandra Anaesthesia Continuing Education
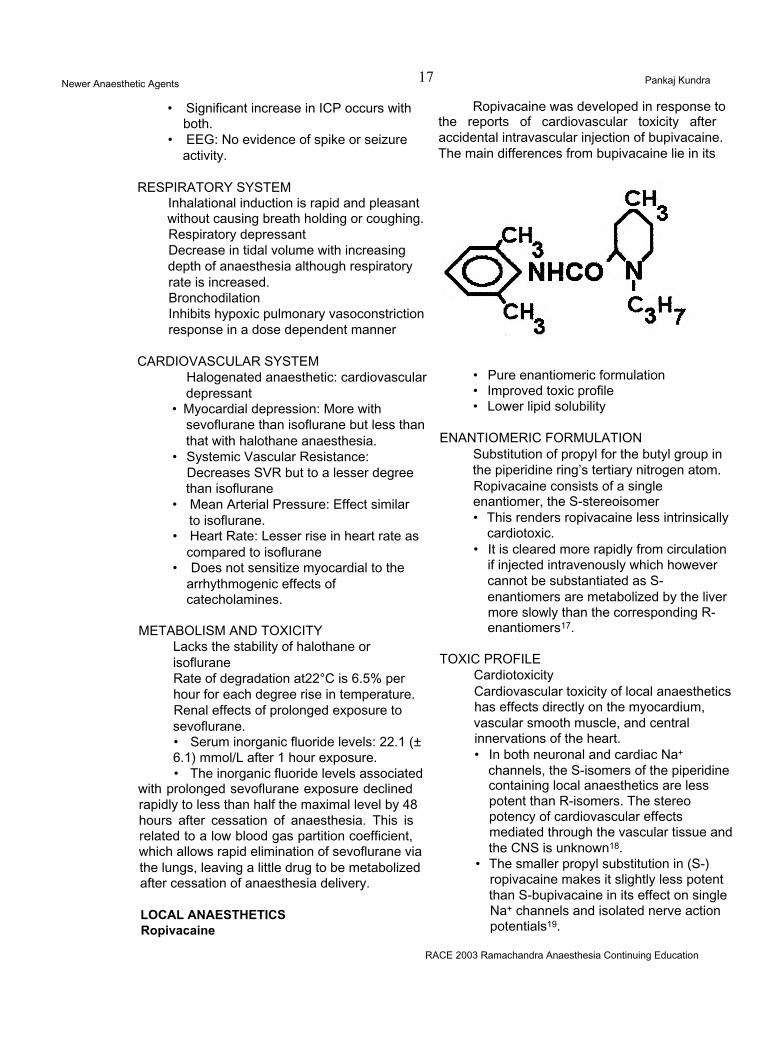
Newer Anaesthetic Agents 17 Pankaj Kundra
• Significant increase in ICP occurs with both.
• EEG: No evidence of spike or seizure activity.
RESPIRATORY SYSTEMInhalational induction is rapid and pleasant without causing breath holding or coughing. Respiratory depressant Decrease in tidal volume with increasing depth of anaesthesia although respiratory rate is increased.BronchodilationInhibits hypoxic pulmonary vasoconstriction response in a dose dependent manner
CARDIOVASCULAR SYSTEMHalogenated anaesthetic: cardiovascular depressant
• Myocardial depression: More with sevoflurane than isoflurane but less than that with halothane anaesthesia.
• Systemic Vascular Resistance: Decreases SVR but to a lesser degree than isoflurane
• Mean Arterial Pressure: Effect similar to isoflurane.
• Heart Rate: Lesser rise in heart rate as compared to isoflurane
• Does not sensitize myocardial to the arrhythmogenic effects of catecholamines.
METABOLISM AND TOXICITYLacks the stability of halothane or isofluraneRate of degradation at22°C is 6.5% per hour for each degree rise in temperature. Renal effects of prolonged exposure to sevoflurane.• Serum inorganic fluoride levels: 22.1 (± 6.1) mmol/L after 1 hour exposure.• The inorganic fluoride levels associated
with prolonged sevoflurane exposure declined rapidly to less than half the maximal level by 48 hours after cessation of anaesthesia. This is related to a low blood gas partition coefficient, which allows rapid elimination of sevoflurane via the lungs, leaving a little drug to be metabolized after cessation of anaesthesia delivery.
LOCAL ANAESTHETICS Ropivacaine
Ropivacaine was developed in response to the reports of cardiovascular toxicity after accidental intravascular injection of bupivacaine. The main differences from bupivacaine lie in its
• Pure enantiomeric formulation• Improved toxic profile• Lower lipid solubility
ENANTIOMERIC FORMULATIONSubstitution of propyl for the butyl group in the piperidine ring’s tertiary nitrogen atom. Ropivacaine consists of a single enantiomer, the S-stereoisomer• This renders ropivacaine less intrinsically
cardiotoxic.• It is cleared more rapidly from circulation
if injected intravenously which however cannot be substantiated as S- enantiomers are metabolized by the liver more slowly than the corresponding R- enantiomers17.
TOXIC PROFILE CardiotoxicityCardiovascular toxicity of local anaesthetics has effects directly on the myocardium, vascular smooth muscle, and central innervations of the heart.• In both neuronal and cardiac Na+
channels, the S-isomers of the piperidine containing local anaesthetics are less potent than R-isomers. The stereo potency of cardiovascular effects mediated through the vascular tissue and the CNS is unknown18.
• The smaller propyl substitution in (S-) ropivacaine makes it slightly less potent than S-bupivacaine in its effect on single Na+ channels and isolated nerve action potentials19.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents 18 Pankaj Kundra
• Very slow reversal of Na+ channel blockade after cardiac action potential is a hallmark of bupivacaine. This reversal is considerably faster with ropivacaine20.
• A greater therapeutic index for ropivacaine than bupivacaine, particularly with regard to cardiotoxicity.
CNS Toxicity• Convulsing doses of ropivacaine are
larger than those of bupivacaine but less than those of lignocaine.
LIPID SOLUBILITY21
• Ropivacaine’s low lipid solubility may result in reduced penetration of the large myelinated A<x motor fibres, so that initially these fibres are relatively spared. However during continuous infusions they get blocked. Therefore, motor block produced with ropivacaine has
• A slower onset with ropivacaine• Less dense• Shorter duration when compared to
bupivacaine.
KINETICSRopivacaine is metabolized in liver by
aromatic hydroxylation, mainly to 3-hydroxy- ropivacaine, but also to 4-hydroxy-ropivacaine, both of which have some local anaesthetic activity21.
LevobupivacaineCLINICAL POTENTIAL:
The S(-)enantiomer of bupivacaine, with less cardiovascular and central nervous toxicity, a slightly longer duration of sensory block, but otherwise similar to its parent.
PHARMACODYNAMICS:Compared to bupivacaine it is as
potent, with a trend towards longer sensory block; with epidural usage it produces less prolonged motor block; Differentiation not seen with peripheral placement; lethal dose 1.3 to 1.6 times higher; less cardiac effect including less depression of contractility and fewer arrhythmias; higher convulsive doses. Has not been compared at equipotent anaesthetic doses with ropivacaine.
PHARMACOKINETICS:
_Elimination t1/21.3 hours VD 67L in adult volunteers Protein binding > 97%Metabolism by CYP1A2 and 3A4 Crosses placenta No racemisation in vivo.
DOSAGE:Minimum effective concentration
0.085%; Recommended maximum dosage 150mg for single dose epidural; 12.5mg/hr (10mls/ hr of 0.125% solution) for labour epidural infusion; 18.75mg/hr (15mls/hr of 0.125% solution) for epidural infusion; and 25mg every 15 or more minutes for epidural bolus doses.
15mg for intrathecal placement. 2.5mg/kg for nerve blocks in paediatric patient.
ADVERSE EFFECTS:Potential for hypotension and
cardiac arrest: observe precautions as for all local anaesthetics. Cardiotoxicity and CNS toxicity as noted.
DRUG INTERACTION: Unknown.Of Note:(1) Don’t use 0.75% in obstetrics;(2) Not for paracervical or Bier’s block;(3) Avoid if hypersensitivity to amides (rare).
EMLA (Eutectic mixture of local anaesthetic)21When two compounds are mixed
to produce a substance that behaves with a single set of physical characteristics, it is said to be eutectic. EMLA (5%) contains mixture of crystalline bases of 2.5% lignocaine and 2.5% prilocaine in a white oil: water emulsion. The mixture has a lower melting point, being oil at room temperature, while the individual components would be crystalline solids.
PRESENTATION AND USESEMLA is presented as an
emulsion in tubes containing 5 or 30 gm. It is used to anaesthetize skin before vascular cannulation or harvesting for skin grafts. It should be applied to intact skin under an occlusive dressing for at least 60 min. to ensure adequate anaesthesia.
CAUTIONSMethaemoglobinaemia is caused
by o-toludine, a metabolite of prilocaine______RACE 2003 Ramachandra Anaesthesia Continuing Education
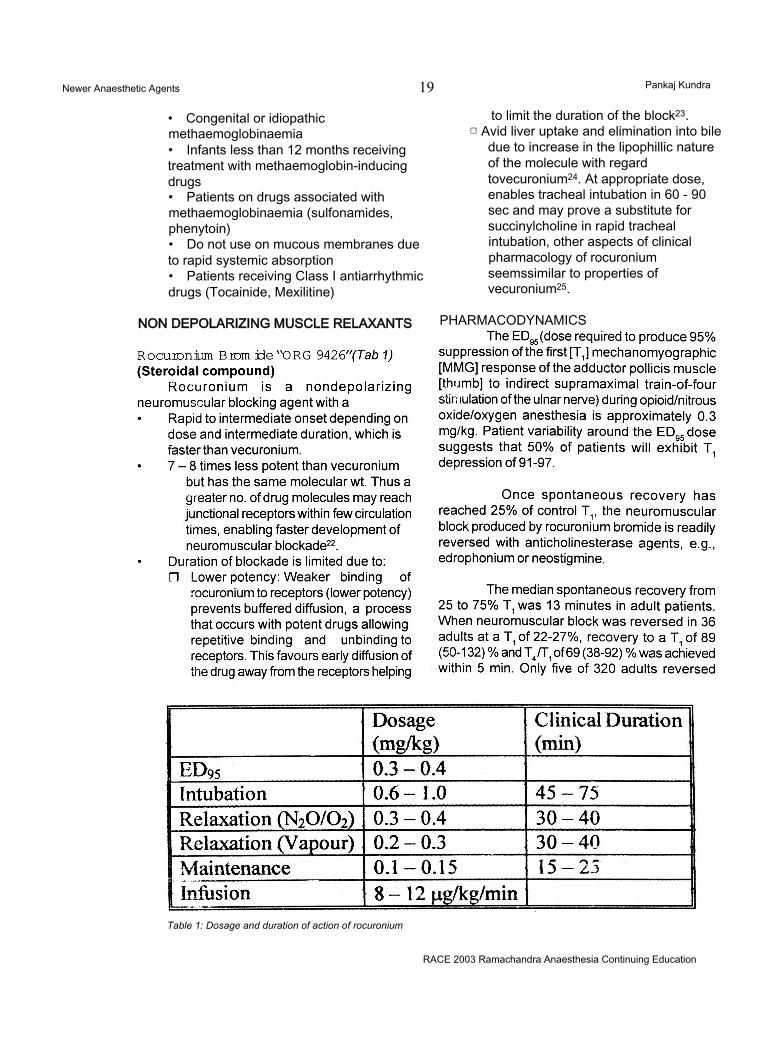
Newer Anaesthetic Agents 19 Pankaj Kundra
• Congenital or idiopathic methaemoglobinaemia• Infants less than 12 months receiving treatment with methaemoglobin-inducing drugs• Patients on drugs associated with methaemoglobinaemia (sulfonamides, phenytoin)• Do not use on mucous membranes due to rapid systemic absorption• Patients receiving Class I antiarrhythmic drugs (Tocainide, Mexilitine)
NON DEPOLARIZING MUSCLE RELAXANTS
to limit the duration of the block23.□ Avid liver uptake and elimination into bile
due to increase in the lipophillic nature of the molecule with regard tovecuronium24. At appropriate dose, enables tracheal intubation in 60 - 90 sec and may prove a substitute for succinylcholine in rapid tracheal intubation, other aspects of clinical pharmacology of rocuronium seemssimilar to properties of vecuronium25.
PHARMACODYNAMICS
Table 1: Dosage and duration of action of rocuronium
RACE 2003 Ramachandra Anaesthesia Continuing Education
Newer Anaesthetic Agents Pankaj Kundra
received an additional dose of reversal agent. The median (range) dose of neostigmine was 0.04 (0.01 to 0.09) mg/kg and the median (range) dose of edrophonium was 0.5 (0.3 to 1.0) mg/kg. In geriatric patients (n=51) reversed with neostigmine, the median TA/T: increased from 40 to 88% in 5 min.
METABOLISM & ELIMINATIONNo metabolism of rocuronium has yet been reported. Like vecuronium dual hepatic and renal pathways of elimination exist. Unchanged drug
has been recovered from bile and urine24.
REFERENCES1. Simons PG, Cockshott ID, Douglas EJ. Blood concentrations, metabolism and elimination after subanaesthetic intravenous dose of 14C-propofol to male volunteers. Postgrad Med J 61: 64; 1985.2. Hughes MA, Jacob JR, Glass PSA. Context sensitive half time in multicompartment pharmacokinetic models for intravenous anesthesia. Anesthesiology 76: 334; 1992.3. Major E, Verniquet AJW, Waddell TK et al. A study of 3 doses of ICI 35 868 for induction and maintenance of anaesthesia. Br J Anaesth 53: 267; 1981.4. Aun CST, Short SM, Leung DHY, Oh TE. Induction dose response in unpremedicated children. Br J Anaesth 68: 64; 1992.5. McDonald NJ, Mannion D, Lee P et al. Mood evaluation and out patient anaesthesia. A comparison between propofol and thiopentone. Anaesthesia 43: 68; 1988.6. Anonymus. Convulsions after propofol. Pharm J 249: 745; 1992.7. Dwyer R, McCaughey W, Lavery J et al. Comparison of propofol and methohexitone as anesthetic agents for electroconvulsive therapy. Anaesthesia 43: 459; 1988.8. Stephan H, Sonntag H, Schenk HD, Kohlhausen S.
Effects of disoprivan on cerebral blood flow, cerebral oxygen consumption and cerebral vascular reactivity. Anaesthesiologist 36: 60; 1987.9. Mirakhur RK, Shepherd WFI, Darrah WC. Propofol or thiopentone: effects on intraocular pressure associated with induction of anaesthesia and tracheal intubation (facilitated with suxamethonium) Br J Anaesth 59: 431; 198710. Taylor MB, Grounds RM, Dulrooney PD, Morgan M. Ventilatory effects of propofol during induction of anaesthesia. Comparison with thiopentone. Anaesthesia 41: 816; 1986.11. Goodman NW, Black AMS, Carter JA. Some ventilatory effects of propofol as a sole anaesthetic agent. Br J Anaesth 59: 1497; 1987.12. Coates DP, Monk CR, Prys-Roberts C, Turtle M. Hemodynamic effects of the infusions of the emulsion formulation of propofol during nitrous oxide anesthesia in humans. Anesth Analg 66: 64; 1987.13. Claeys MA, Gepts E, Camu F. Haemodynamic changes during anaesthesia induced and maintained with propofol. Br J Anaesth 60: 3; 1983.14. Hopkinson KC, Denborough M. Propofol and malignant hyperpyrexia (letter). Lancet 1: 191; 1988.15. Johnson SE. Remifentanil: A unique, short acting opioid. Advances in Anesthesia vol. 16, Chapter 4, Mosby Inc. 1999.16. Navarro JR. New Inhalational Anesthetics. Advances in Anesthesia vol. 12, Chapter 4, Mosby - Year Book Inc. 1995.17. Rutten AJ, Mather LE, Mclean CF. Cardiovascular effects and regional clearances of intravenous bupivacaine in sheep: Enantiomeric analysis. Br J Anaesth 67: 247; 1991.18. Lee-Son S, Wang GK, Concus A, et al. Seterioselective inhibition of neuronal sodium channels by local anesthetics. Anesthesiology 77: 324; 1992.19. Wang GK. Binding affinity and stereioselectivity in single batrachotoxin activated Na* channels. J Gen Physiol 96: 1105; 1990.20. Arlock P. Actions of three local anaesthetics: lignocaine, bupivacaine and ropivacaine on guinea pig papillary muscle sodium channels (Vmax). Pharmacol Toxicol 63: 1; 1988.21. Peck TE, Williams MA. Pharmacology for Anaesthesia and intensive care. 1st edition. Chapter 10. Ashford Colour Press, Great Britain.22. Wierda JMKH, Di Wit APM, Kuizenga K et al. Clinical observations of the neuromuscular blocking action of ORG 9426 a new steroidal non-depolarizing agent. Br J Anaesth 64: 521; 1990.23. Min JC, Becavak I, Glavinovic Ml et al. lontophoretic study of speed of action of various muscle relaxants. Anesthesiology 77: 351; 1992.24. Khuenl-Brady K, Castagnoli KP, Canfell PC et al. The neuromuscular blocking effets and pharmacokinetics of ORG 9426 and ORG 9616 in the cat. Anesthesiology 72: 669; 1990.25. Magorian T, Flannery KB, Miller RD. Comparison of rocuronium, succinylcholine and vecuronium for rapid sequence induction of anesthesia in young adults. Anesthesiology 79: 913; 1993.*26. Muir AW, Houston J, Green KL et al. Effects of new neuromuscular blocking agents (ORG 9426) in
RACE 2003 Ramachandra Anaesthesia Continuing Education

Newer Anaesthetic Agents 21 Pankaj Kundra
anesthetized cats and pigs and in isolated nerve muscle preparation. Br J Anaesth 63: 400; 1989.27. Servin FS, Lavaut E, Desmonts JM. Clinical evaluation of ORG 9426 in cirrhotic and control patients.
Anesthesiology 77: A357; 1993.Shanks CA, Fragen RJ, Ling D. Continuous intravenous infusion of rocuronium in patients receiving balanced, enflurane or isoflurane anaesthesia. Anesthesiology 78: 649; 1993.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 22 M R. Rajagopal
INTRODUCTIONIn June 2002, a Californian jury found a
doctor “liable for reckless neglect in under-treating a man’s pain” and ordered him to pay 1.5 million US dollars to the dead man’s children1.
It has started. We cannot get away with it any more. We have always known that a doctor’s duty is to “cure sometimes, relieve often and to comfort always” but we have seldom taken it seriously. But people have started demanding pain relief now, and we better learn to satisfy them.
Unrelieved pain can cause several adverse physiological changes.1. It causes reflex skeletal muscle spasm that,
specially in upper abdominal surgery or chest surgery, can result in regional hypoventilation and result in postoperative chest complications.
2. Pain causes reflex vasoconstriction. It can possibly impair wound healing in any case, but particularly in people with compromised blood flow, this can be very damaging.
3. Pain causes stress response, with adverse circulatory consequences. This can be very detrimental in people with compromised circulation.
4. Pain prevents early mobilization with attendant complications. Pain relief during recovery from acute injury improves survival and speeds rehabilitation by promoting volitional activity2.
For all these reasons, and also because it is simply our duty to relieve suffering, acute pain has to be treated. Lack of resources is certainly not an excuse. Most pain relief
measures are relatively inexpensive. Pain relief is not necessarily something to be done with expensive electronic gadgetry. There are other options.
We will attempt to briefly review the pathophysiology of pain, and use that understanding to describe various means of pain relief. Then wc shall give attention to what could be done even with limited resources.
PATHOPHYSIOLOGY OF PAINLet us start by making some key points
pertaining to pain mechanisms.
Pain is what the patient says hurts.The International Association for Study
of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”3. It is important to remember that people are different, their emotional states could be different and that it would be necessary to take that into consideration while planning treatment.
A simpler definition is, “Pain is what the patient says, hurts”4. The emphasis is on the patient’s experience. He and no one else can assess his pain properly. Once we accept the definition, we shall escape the pit-fall of being judgemental about someone who is 'too sensitive’ or 'too fussy’ and complains 'too much’ about his or her pain.
Hence, the patient is the most appropriate person to assess the severity of his pain. The message is, “Believe the patient about
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 23 M.R. Rajagopal
his pain.”
Pain causes more pain.Unrelieved pain results in steady
worsening of pain. The following description of pathophysiology will make this easier to understand.
Peripheral mechanisms of pain:Any injury causes stimulation of pain
sensing nerve endings, which are called nociceptors. The impulse is transmitted via the C and A-delta sensory nerve fibres to the dorsal horn of the spinai cord. There from, the impulse is transmitted to the thalamus and the sensory cortex.
The initial injury is followed by liberation of chemicals - the nociceptive substances -, which continue to stimulate the nociceptors and perpetuate pain. Of the many such substances (kinins, leukotrienes, substance P, histamine, serotonin, hydrogen and potassium ions and so on), prostaglandins deserve special mention. Prostaglandins sensitize the nociceptor to the other pain producing substances.
It has also been found that silent or sleepy nociceptors are recruited in the face of sustained stimulation. This means that for a particular stimulus, there will be progressively increasing response.
CENTRAL PAIN MECHANISMS AT THE LEVEL OF THE DORSAL HORN
There is some form of sensitization and recruitment at the level the of dorsal horn too. The phenomenon is called “wind-up” - analogous to a wound-up spring. With sustained stimulation from the periphery, the dorsal horn cells seem to get wound up so that with time, there is progressively increasing response to the peripheral stimulus. NMDA receptors are said to play a major role in the development of “windup”.
There is also a process of recruitment at the central level. With time, there is recruitment of adjacent spinal segments so that pain increases not only in intensity, but in extent as well.
In fact with prolonged, unrelieved, acute pain, there can be permanent anatomical changes in the nervous system, so that the pain gets centrally established and becomes chronic pain. It is believed that this is the mechanism of most scar pains.
This entire gamut of changes mean that the earlier pain is treated, the easier it is It also means that in elective trauma (surgery-), pain had better be prevented rather than treated. This is the concept of pre-emptive analgesia.
MANAGEMENT OF ACUTE PAIN:Let us start with some general principles
of pain management.1. All pains are not opioid-sensitive. Roughly
two thirds of acute pain can be treated successfully by opioids. This means that a multi-modal approach works best.
2. Analgesics must be administered round the clock. This may mean the use of continuous infusions or the use of drugs by the clock depending on its duration of action. For example, morphine can be administered either as a continuous subcutaneous or epidural infusion or as 4-hourly bolus doses.
Major pain relief modalities:The following three form the major
modalities of pain relief:1. Prevention of peripheral sensitization by the
use of NSAIDs.2. Application of local anaesthetics, peripherally
or centrally.3. Use of opioids, centrally or peripherally.
By judicious combinations of these, it is possible to achieve adequate analgesia without serious adverse effects. In individual cases, however, there may be other forms of treatment that can be added on. We shall come to them briefly later.
NSAIDs:By preventing sensitisation of
nociceptors and indirectly central sensitisation, NSAIDs contribute to pain relief. However, there are concerns about their safety. The major concerns are:
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 24 M.R. Rajagopal
1. Bleeding tendency because of inhibition of platelet adhesion. There is some controversy; but there does seem to be some evidence at least that it can be a real concern. One study found them to double the bleeding during hip arthroplasty5. But the coxibs appear to be safe. If anything, there seems to be a doubt that coxibs may even have a prothrombotic tendency.
2. Renal dysfunction in those who are predisposed to it. In the surgical context, this can also be a concern in the hypovolaemic. The associated water retention has the potential to worsen hypertension and cardiac failure. It seems doubtful if the chance of this complication is any less with coxibs.
3. Gastritis. But the coxibs appear to be safer than the older generation drugs in this matter.
In spite of these disadvantages, the addition of NSAIDs does seem to improve the quality of analgesia. The combination decreases opioid requirement and decreases the chance of ileus. They are hence recommended particularly in procedures like dental extraction where chance of significant bleeding is negligible.
There is one situation where NSAIDs must be used. In people with chronic arthralgia like in osteoarthritis, rheumatoid arthritis etc, preoperative cessation of NSAIDs causes a flare up of pain (algesic flare). In such cases, it is recommended that coxibs be started and continued through the peri-operative period.
NEWER NSAIDS.Valdecoxib is said to have no effect at
all on platelet function.
Parecoxib is the only Cox-2 selective drug that is recommended for parenteral use.
Etoricoxib is the most potent second generation NSAID yet, three times more selective than rofecoxib.
LOCAL ANAESTHETICSAs used in pain relief, they have a
predominant local effect and some systemic effect (membrane stabilization). The latter,
nevertheless, may be significant when there is a neuropathic component to the pain. Conventionally, they are used most often as epidural injections. Given preoperatively, it can contribute to surgical anaesthesia and confer post-operative analgesia too. Where facilities exist, they had best be given as continuous epidural infusions. An infusion of 0.125- 0.25% bupivacaine would provide adequate analgesia, while permitting ambulation; a dose of 4-8 ml/ hour may be a good starting point. When the pain stimulus is severe, (as in ischaemic pain for example), sometimes it may be necessary to give an anaesthetic concentration of the drug (0.5%) and compromise on mobility. A syringe pump would be the standard equipment for the infusion; a Patient Controlled Analgesia (PCA) device may permit fine-tuning of analgesia.
When a syringe pump is not available, one has to resort to intermittent injections. Too frequent injections are impractical; but on the other hand, at least four hourly injections will be needed if pain relief has to be adequate. And even in that case, the sizeable dose requirement predisposes to hypotension following every bolus injection. Particularly in the context of the unstable circulatory status in many major surgical procedures, this can be quite relevant. Obviously, smaller and more frequent bolus doses are desirable.
Bupivacaine is the local anaesthetic agent used most often. Shorter acting agents like lignocaine have the disadvantage of tachyphylaxis. Ropivacaine seems to have nearly the same duration of action as bupivacaine. It may have an edge over bupivacaine in that it seems to have better selective sensory blockade. With ropivacaine, it is easier to achieve analgesia without motor blockade than with bupivacaine.
Epidural catheters function best for an average of three days. As days go by, blockage, infection, pain on injection and leaks can be problems limiting long term use6.
When epidural infusions of local anaesthetics are not feasible or practical for lack of facilities, even single dose local anaesthetic
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of Acute Pain 25 M.R. Rajagopal
blocks can be valuable. By avoiding the maximal pain in the immediate post-operative period, it serves to decrease the sensitization. A single dose epidural block, an interpleural or intercostal block, or a regional block as for herniorrhaphy, can all be very useful, despite the short duration of a single block.
OPIOIDSOpioids can act both centrally and
peripherally. The importance of peripheral opioid receptors is being more and more understood now. Their practical relevance is that the same dose of opioid infiltrated around the incision would be much more effective than a subcutaneous injection elsewhere, because in the former case, we can have the drug acting both on the peripheral receptors as well as systemically.
Addition of opioids to the local anaesthetic agent given epidurally, improves the quality of analgesia. The basic principle is that we are able to achieve rather high neuraxial concentrations compared to systemic drug levels, resulting in excellent analgesia with minimal side effects. Some side effects are possible however, like nausea and vomiting, delayed respiratory depression, urinary hesitancy or retention and itching.
Preservative-free morphine is the agent used most often for this purpose as it has the most opioid-sparing effect compared to IV injection. The dose required is only about one- tenth of the systemic dose. It is about one-third for fentanyl and two-third for buprenorphine. Herein lies the main advantage of morphine over the other opioids for epidural administration - small dose, thus fewer side effects. However, as a practical point, there is the problem of poor availability of preservative-free morphine. (The manufacturers should be able to provide us with this on request.)
However, buprenorphine does have an advantage. It does not have to be given at the required segmental level.
COMBINATION 0!^ DRUGSIn general, we can make the following
recommendations for post-operative analgesia.• NSAIDs, particularly the coxibs would help to
improve the quality of analgesia, but need to be used after weighing the risks and benefits.
• Combination of a local anaesthetic with an opioid would be particularly useful - simple infiltration of these drugs over the site of incision itself may go a long way towards post operative pain relief.
• Preservative free morphine is the best drug for epidural administration, if it can be applied over the segment to be blocked. If the site of administration were distant, buprenorphine would be a better choice.
ANCILLARY MEASURESSeveral other possibilities exist for relief
from acute pain.1. Though not freely available in this country,
Entonox (the compressed mixture of oxygen and nitrous oxide in 50:50 combination) is a good choice for analgesia in the emergency room.
2. It appears that pre-treatment with tricyclic antidepressants decrease opioid requirements presumably by inhibiting reuptake of serotonin and norepinephrine at the inhibitory synapses. While this may have little application as a technique for pain relief in routine practice, this strengthens the case for continuing tricyclics in the peri-operative period in those patients already on it.
3. Sub-cutaneous infusion of lignocaine may supplement analgesia in relatively opioid resistant pains, particularly in patients who have already been in pain for some time, and especially if there is a neuropathic component to the pain (like some patients with burns).
4. Subcutaneous infusion of a sub-anaesthetic dose of ketamine (for example, 5 mg per hour) may help in difficult pains by its action on the NMDA receptors in the dorsal horn of the spina! cord.
5. Transcutaneous electrical nerve stimulation (TENS) is a particularly safe form of pain relief, though it has limited application. The device itself is inexpensive, but they should be used only if sterile conducting pads are available.
RACE 2003 Kamachandra Anaesthesia Continuing Education

Management of Acute Pain 26 M.R. Rajagopal
Organization of an acute pain serviceMore and more is talked now about the
concept of a pain-free hospital. There is a move favouring institutional commitment to pain relief- making pain the 4th vital sign in the patient’s daily hospital record of parameters. Measurement of pain of course mandates adequate control too.
Most acute pain services are anaesthesiologist-led. But it is important to remember that pain service demands teamwork. It would be impossible to achieve assessment and management of pain in a whole hospital, without adequate personnel. Most pain services depend a lot on nurses. It would be essential to have at least one nurse with special training round the clock in the hospital, who will help the staff nurses with evaluation and pain control. Needless to say, this nurse will need expertise in assessment of pain as well as in the mechanical aspects including the use of devices like infusion pumps and PCA devices. Theanaesthesiologist, then, is able to do the consultant’s job. In fact the presence of such a team is much more important than the high tech devices like PCAs. Last but not least, the importance of explanations to the patient and family cannot be overemphasized. If they know what to expect,
anxiety will be less, and that will lessen the pain experience.
REFERENCES
1. Okie.S. Californian jury finds doctor negligent in managing pain. National news', 15 June 2001, Washington.
2. Tuman KJ, Me Carthy RJ, DeLaria GA, Patel RV, Ivankovich AD. Effects of epidural anesthesia and analgesia on coagulation and outcome after major vascular surgery. Anesthesia and Analgesia 1991; 73:696-704.
3. I ASP Sub-committee on Taxonomy. Pain terms: a list with definitions and notes on usage. Pain 1980; 8:249-52.
4. Black RG. The Chronic Pain Syndrome. Surgical Clinics of North America. 1975; 55:999-1011.
5. Robinson CM, Christie J, Malcolm-Smith N. Non-steroidal anti-inflammatory drugs, perioperative blood loss and transfusion requirements in elective hip arthroplasty. J Arthroplasty 1993; 8:607-610.
6. McQuay HJ. Epidural analgesics. In: Wall PD; Melzack R, Eds. Textbook of Pain 3rd ed. Churchill Livingstone, Philadelphia. 1994: 1025-1034.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Qbstetric surgery 27 R. Gopinath
INTRODUCTIONEach year for about 80,000 anaesthetics
administered there are 2 % of parturients who undergo surgery. This is largely due to the increase in the endoscopic procedures undertaken to treat conditions common in the childbearing age group like trauma, ovarian masses, appendicitis, gall bladder disease, breast surgery etc. Major surgical procedures like cardiac surgical, neuro-surgical and liver transplants have been performed during pregnancy with good outcomes for both the foetus and the mother. The known problems of foetal development and drug administration to the mother during pregnancy and the risk of abortions make both the physician and the patient wary of an anaesthetic. To assess the risk one has to understand the physiological changes involved during pregnancy and that two lives are involved during the conduct of anaesthesia raising several unique concerns.
ALTERATIONS IN MATERNAL PHYSIOLOGY.All systems are involved in change but
those important to the anaesthetic management are:Respiratory:
Increased oxygen consumption, reduced functional residual capacity, hypocapnia due to increased minute ventilation, likelihood of difficult intubation and trauma to the airway due to increased vascularity of the mucosa.
Cardiovascular:Increase in both the cardiac output and
the blood volume, dilutional anaemia, decreased vascular responsiveness, increased baroreceptor responsiveness, aortocaval compression in the supine position.
Gastrointestinal:The lower oesophageal sphincter tone is usually reduced though gastric pH, volume and emptying are not much altered.
Central nervous system:Inhalational agent MAC and local
anaesthetic requirements are reduced.
Teratogenicity of anaesthetics is probably minimal and has never been conclusively demonstrated. The use of agents like nitrous oxide, which in animal studies may cause vasoconstriction of the uterine vessels and reduce uterine blood flow are of concern but this, has not been demonstrated in human beings. Benzodiazepines were associated with oro-facial abnormalities but again have not been proven in prospective studies. The inhalational agents, narcotics, intravenous agents and local anaesthetics have long been used safely during pregnancy.
There is a slight increase in miscarriages for OR personnel found during a meta-analysis of anaesthetic exposure in the workplace.
DRUGS AND PREGNANCYDrugs offered for use in pregnancy aregrouped into one of five categories:A. Controlled studies show no riskB. No risk in animal studies or no risk supported
by controlled human studiesC. Animal studies indicate a risk but no human
studies availableD. Evidence of foetal risk but benefits outweigh
risk.X Evidence of high risk to foetus, which
outweighs benefitsNA. Not applicable
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthet/c Management of aPregnant Patient for Non-Obstetric surgery 28 R. Gopinath
Types of drugs taken during pregnancy• Drugs of abuse: Opioids & opiates, marijuana,
cocaine, alcohol and nicotine• Sedatives: Benzodiazepines (class D orX)• Oral contraceptives (low risk, evidence
uncertain), cardiac glycosides (safe)• Antibiotics (most class B, although
aminoglycosides can have foetal toxicity and tetracyclines may give congenital defects)
• Antiparasitics (class C, except quinine, class X)
• Anti-asthmatic drugs (GCs may have latent effects and reduce birth weight, anti-histamines may result in blindness)
• Relaxants/sympathomimetics etc (class C)• Diuretics (most class D)• Anticoagulants (not recommended)• Anti-viral drugs (most category C)
Maternal Pharmacokinetic VariablesDuring pregnancy, a number of
physiological changes occur that affect drug absorption, uptake and metabolism.These changes include:• Changes in body fluid volume• Changes in cardiovascular parameters• Changes in pulmonary function• Alterations in gastric activity• Changes in serum binding protein
concentrations and occupancy• Alterations in kidney function
These maternal variables determine the maternal and foetal therapeutic/toxic responses to drugs! Specifically:• Pregnancy is associated with increased
cardiac output (-30%) and plasma volume (-50%) = increased Vd
• Maternal aqueous and fatty tissue spaces increase dramatically in pregnancy (10-30 weeks mainly); total body water increases by -8 L (mostly extracellular water; 40% maternal, 60% foetal/placental)
• Reduction in motility of stomach and gut - increased intestinal transit time (-30-50%) (P4 effect?) and increased mucus formation = raised gut pH
• Nausea and vomiting may also affect gut
transit time and pH.• Decreased serum albumin concentrations
(-25%), but unchanged alpharacid glycoprotein. Binding sites also taken up by steroid and peptide hormones (= more free drug)
• Glomerular filtration rate increases (-50%) with renal blood flow (-50%), resulting in increased renal excretion & creatinine clearance. Rates of hepatic enzyme activity may also be increased (i.e. phenytoin metabolism) or decreased (theophylline/ caffeine) ?steroid effects
• Hyperventilation and increased pulmonary blood flow = increased alveolar uptake of inhaled drugs (i.e. anaesthetics)
Drug disposition in the maternal-foetal unitDrugs that reach the foetus are (almost)
always administered to the mother!Drug -> Mother-> Placenta -> Foetus -> Placenta-> Mother -> Excretion
Foetal Pharmacokinetic Variables• Blood flow through the placenta (maternal
side) increases during gestation (50 ml/min @ 10 weeks of pregnancy - 600 ml/min @ 38 weeks).
• Foetal plasma binding proteins differ from maternal concentrations: albumin 15% > than maternal, but alpharacid glycoprotein -37% lower (so free fractions of basic drugs such as propranalol and lidocaine are elevated)
• Foetal plasma proteins also appear to bind some drugs with lower affinity than in adults (i.e. ampicillin, benzylpenicillin)
• Ion trapping: Foetal plasma pH > maternal: base drugs (i.e. salicylate) are more ionized on the foetal side, hence lesser drug crosses the placenta back to the maternal plasma = apparent accumulation in foetal plasma. Principle also applies to metabolites (more polar, less mobile)
• Fcetal liver expresses metabolizing enzymes (i.e. CYPs), but metabolizing capacity is less than that of mother (some enzymes are foetal- specific)
• Drugs transferred across the placenta undergo first pass through the foetal liver before reaching systemic circulation (modulated by
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 29 R. Gopinath
ductus venosus shunt, 30-70% by pass)• Foetal kidney immature: GFR is reduced,
increasing with gestational age but only 2-4 ml/min at term (3% of cardiac output vs 25% in adult). Anion (i.e. penicillin) secretion very low, cation (i.e. cimetidine) secretion is efficient.
• Foetal urine enters the amniotic fluid which may be swallowed by the foetus (however, foetal renal blood flow is only 5% of the blood flow)
Placental PharmacokineticsCritical factors that affect drug transfer
across the placenta:• Physicochemical properties i.e. lipid solubility,
ionization, size, protein binding characteristics.
• Transfer of flow-limited drugs affected by placental flow.
• Compounds that alter blood flow alter maternal drug disposition and placental transfer.
• Placental metabolism (dealkylation, hydroxylatior, demethylation) affects drug transfer across the placenta (usually relatively minor effect compared to foetal or maternal liver).
• Foetal metabolism may also be significant, but may change during pregnancy.
Adverse Effects of Drugs on the Foetus DuringPregnancyMECHANISM:1. Effects on maternal tissues primarily, with
only indirect (secondary) effects on the foetus2. Direct effects on developing foetal tissues3. Indirect effects via interference with the
function of the placenta, i.e., placental transferor placental metabolism
TYPE OF EFFECTS:• Teratogenicity (i.e. thalidomide) - readily
detected at, or shortly aftet, birth• Long term latency (i.e. diethylstilbestrol -
increased risk of vaginal adenocarcinoma after puberty, or abnormalities in testicular function and semen production)
• Impaired intellectual or social development (i.e. exposure to phenobarbitone- alters
programming of the brain)• Predisposition to metabolic diseases (i.e.
Barker hypothesis - low birth weight associated with increased risk of diabetes, hypertension, heart disease in adulthood)
DRUGS KNOWN TO EXERT SIGNIFICANT EFFECTS ON THE FOETUS:
Aminopterin, aminoglycosides, barbiturates, chloramphenicol, chlorpropamide, cortisone, diazepam, diethylstilbestrol, ethanol, heroin, iodide, isotretinoin, methadone, methyltestosterone, methylthiouracil, metronidazole, norethindrone, phenytoin, tetracycline, thalidomide, trimethadione, valproic acid, warfarin
Maintenance of uterine perfusion and maternal oxygenation determine and preserve foetal oxygenation. These are of concern and vital for any anaesthetic during pregnancy. Avoid maternal hypoxia and hypotension at all costs and one should be aware of the effects of all agents used on the maternal cardiovascular system and oxygen delivery.
The most difficult perioperative problem is preterm delivery, which is the leading cause of foetal death due to preterm labour. Prevention and management of the same is very important. The anaesthetic management per se is not related as much as the disease process for the surgical intervention and surgery itself.
ANAESTHETIC MANAGEMENTPerioperative management starts with
assessment preoperatively and should include establishment of pregnancy if in doubt, counseling the patient on the risks of anaesthesia (for the foetus on continuation of pregnancy and so considering delaying surgery till the second trimester with explanation of teratogenicity) and the chances of spontaneous miscarriage, the symptoms of preterm labour and the need for uterine displacement to the left if needed. Documentation of the date of the LMP should be recorded.
Preoperative medications to allay anxiety or pain should be given as appropriate and not withheld, since elevated endogenous maternal
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 30 R. Gopinath
catecholamines will reduce uterine blood flow. Prophylaxis against aspiration should be considered and a combination of an antacid (nonparticulate), H2 -receptor blocker or metoclopramide administered. The obstetrician should be involved and perioperative tocolysis discussed. Indomethacin (oral or suppository) and magnesium sulfate as an infusion are commonly used. Indomethacin has few anaesthetic implications but magnesium use should be viewed with caution due to its interactions with neuromuscular blocking agents and the risk and management of hypotension during potential blood loss and volume replacement.
Intraoperative management is not influenced by the anaesthetic technique as long as maternal oxygenation and perfusion is maintained. A review of 49,000 consecutive pregnancies found that 0.14% required surgery during pregnancy. There was no correlation between the type of surgery, type of anaesthetic, trimester in which surgery occurred, length of surgery, estimated surgical blood loss, or the length of anaesthesia and the outcome of the pregnancy.
Monitoring should include blood pressure, oxygenation, ventilation and temperature. Blood glucose should be checked if the procedure is prolonged. If the surgical field is not a hindrance, continuous or intermittent foetal monitoring should be performed after 20-24 wks gestation to ensure the intrauterine environment is optimized. Loss of beat-to-beat variability is normal after anaesthetics are administered, but decelerations are not. They may indicate the need to increase maternal oxygenation, maintain or increase maternal blood pressure, further uterine displacement, reduce surgical retraction, or begin tocolytic drugs. Foetal monitoring can help assess the adequacy of uteroplacental circulation and foetal perfusion during cardiopulmonary bypass, induced hypotension or procedures with major blood loss and volume shifts.
General anaesthesia should include full preoxygenation and denitrogenation, rapid sequence induction with cricoid pressure, high FI02, slow reversal of relaxants to prevent acute rise in acetylcholine that might induce uterine contractions. Inhalational agents should be kept
below 2.0 MAC to prevent cardiovascular compromise. During the first trimester ketamine at doses of > 2.0 mg/kg may cause uterine hypertonus. Nitrous oxide and propofol may be used. Propofol has recently been shown to reduce oxytocin-induced contractions of the uterine smooth muscle. Early pregnancy does not decrease the concentration of propofol required for loss of consciousness. The increase in \nucosal vascularity and potential for difficult airway must be kept in mind during laryngoscopy.
Regional anaesthesia is advantageous in reducing drug administration and reducing the concerns of teratogenicity during the first trimester and minimizing changes in foetal heart rate variability later in gestation. Prevention of hypotension with adequate preload and uterine displacement and aggressive treatment with ephedrine if needed, is mandatory. The dose of local anaesthetic for central neuraxial blocks can be reduced by one-third from that for the nonpregnant patient due to the increased vascularity in the spinal canal with epidural vein engorgement. Regional anaesthesia provides excellent postoperative pain control while reducing maternal sedation needs and maintaining FHR variability.
Postoperatively, monitoring of the foetal heart rate and uterine activity should be continued. Preterm labour must be treated aggressively and at the earliest sign. The patient should be kept in a location like the labour or delivery suite and provision of nursing expertise in the surgical recovery area should be made available. Systemic pain medications will reduce the foetal heart rate variability and this should be borne in mind during monitoring. Regional techniques are thus best suited and should be used wherever feasible. The risk of thromboembolism is very high in these patients and hence they should be mobilized early, which also entails good pain relief postoperatively. In the recovery period also, good maternal oxygenation and left uterine displacement should be maintained. The help of a paediatrician should be enlisted in the management of the patients when the foetus is of a viable gestational age so that preterm labour and delivery can be managed as well as counseling for the parents.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 31 R. Gopinath
SPECIAL SITUATIONSThere are specific anaesthetic
considerations for unusual situations like trauma, neurosurgery, foetal surgery and laparoscopic surgeries.
Emergency surgeryAppendicectomy and adnexal masses
are the most frequent conditions needing surgical treatment. In one study, parturients undergoing appendicectomy had an incidence of 18% of postoperative pulmonary oedema or ARDS. Factors of risk for the same were gestational age> 20 weeks, preoperative respiratory rate of more than 24 breaths/ min, preoperative temperature> 100.4 degrees F, a fluid load ( I/O) greater than 4 liters in the first 48 hrs, and concomitant use of tocolytic agents. Anaesthetists should be conservative in fluid management and have central venous pressure monitoring should there be a fluid overload.
TraumaTrauma is the highest cause of maternal
death. Foetal loss in these situations is due to maternal death or placental abruption. An early ultrasound should be done in the emergency room itself to determine viability of the foetus. The mother should receive all needed diagnostic tests to optimize her management, with lead shielding for the foetus when possible. Exposure to less than 5 rad does not increase the risk to the foetus. Ultrasound or MRI is safer.
There are a few indications for emergency caesarean delivery and would include:1. A stable mother with a viable foetus in distress2. Traumatic uterine rupture.3. Gravid uterus interfering with intra-abdominal
repairs in the mother.4. A mother who is unsalvageable with a viable
foetus.
If the foetus is pre-viable or dead, optimizing the mothers’ condition takes precedence. Vaginal delivery at a later date is better than an emergency caesarean section or a laparotomy.
NeurosurgeryNeurosurgical procedures such as an
aneurysm or AVM repair may be required in this age group. All the usual anaesthetics can be used safely and foetal monitoring will be helpful especially when certain techniques are planned.
Induced hypotension reduces uterine perfusion although most agents like SNP, NTG, hydralazine, esmolol, and inhalational agents have been used safely. Foetal monitoring will determine if uterine perfusion is impaired. The anaesthetist should still provide all necessary care for optimal outcome of the mother while informing the surgeon of any concerns. Hyperventilation reduces maternal cardiac output and shifts the ODC to the left thus decreasing release of oxygen to the foetus. High doses of mannitol have been shown to cause foetal dehydration in animals but should not cause concern in the clinical situation. Endovascular management of acute conditions like ruptured intracranial aneurysms has been successfully undertaken during pregnancy. Foetal shielding should be used at all times.
Foetal SurgeryFoetal surgery is performed in very few
centers and for limited indications. The major problem is postoperative preterm labour. Patients often receive preoperative indomethacin and perioperative magnesium sulfate for tocolysis. A high dose of inhalation agents are used for maternal and foetal anaesthesia and for uterine relaxation during surgery and the possibility of reduced uterine perfusion is to be kept in mind.
Laparoscopic surgeryLaparoscopic procedures have been
employed to avoid laparotomy when abdominal pain presents a diagnostic challenge during pregnancy, as well as for some surgical procedures amenable for such surgery like cholecystectomy. Animal studies have shown that pneumoperitoneum with C02 does not cause significant foetal haemodynamic changes, but does induce foetal respiratory acidosis. Normalizing maternal ETC02 produces late and incomplete correction in the foetus. It is important to maintain intra-abdominal pressure as low as possible and limit operative time to the minimum.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic Management of aPregnant Patient for Non-Obstetric surgery 32 R. Gopinath
Arterial sampling for blood gas analysis is necessary to normalize maternal PC02 if the procedure is'prolonged or difficult. Other technical alterations during pregnancy should include foetal shielding during cholangiograms, pneumatic stockings, left lateral table tilt and an open technique for trocar insertion.
Cardiothoracic surgeryCardiothoracic surgery requiring bypass
has also been successfully performed during pregnancy. The increase in blood volume and cardiac output is maximal at 28-30 weeks and this is the time of high risk for decompensation in patients with cardiac lesions as also immediately post partum. After delivery, the release of aortocaval compression and autotransfusion of uteroplacental blood increases the cardiac output maximally. Those who have severe symptoms and are not responsive to medical management, benefit from surgical interventions, and this should, where possible, be performed in the second trimester when the major risk of teratrogenecity due to drugs, radiation and low flow states of bypass is past and pre term labour is less likely. Combined Caesarean section and bypass too have been successfully performed. Surgery should not be withheld if indicated since mortality is comparable in the mother with non-pregnant states.
After 24 weeks gestation, the foetal status should be monitored and uterine displacement maintained to optimize uterine perfusion. Optimal pressures and flow on bypass are controversial and foetal monitoring is a sensitive measure of perfusion and should be used to optimize flows on bypass. Foetal bradycardia commonly occurs during onset of bypass and slowly returns to baseline with little or no beat-to-beat variability. Hypothermia can oe used although some authors advocate warm
heart surgery. It is essential to avoid high dose vasopressors if possible, to prevent its effect on uterine blood flow, however, optimizing the mothers’ condition is the best way to ensure a good outcome for the foetus.
SUMMARYSurgery during pregnancy may be
necessary and anaesthetists should reassure the mother that anaesthetic agents and techniques do not put the foetus or the pregnancy at risk. Prevention of preterm labour is the greatest concern and may require perioperative use of tocolytics. Good postoperative pain management without sedation will aid in early diagnosis and management of preterm labour and mobilization to prevent thromboembolic complications.
REFERENCES
1. Loebstein, R, Lalkin A, Koren G. Pharmacokinetic changes during pregnancy and their clinical relevance. Clin Pharmacokinet 1997 33(5):328-343
2. organ DJ. Drug disposition in mother and fetus. Clin Exp Pharmacol Physiol 1997 24:869-873.
3. Bailey B, Shinya I. Breast-feeding and maternal drug use. Ped Clin North America 1997 44:41-54.
4. Koren G, Pastuszak A, Ito S. Drugs in pregnancy. New Eng J Med 1998: 338(16): 1128-1137.
5. Garland M. Pharmacology of drug transfer across the placenta. Obstet Gynecol Clin Nth Am. 1998 25(1) 21-42.
6. Boiven JF. Risk of spontaneous abortion in women occupationally exposed to anaesthetic gases: a metaanalysis. Occup Environ Med 1997; 54: 541-8.
7. Friedman JM. Teratogen update: anaesthetic agents, Teratology 1988; 37: 69-77.
8. Hunter JG. Carbon dioxide pneumoperitoneum induces foetal acidosis in a pregnant ewe model. Surg Endosc 1995; 9: 272-9.
9. Rosen MA. Management of anaesthesia for the pregnant surgical patient. Anesthesiology 1999; 91: 1159-63.
10. Weiss BM. Outcome of cardiovascular surgery and pregnancy: a systemic review of the period 1984- 1996. Am J Obstet Gynecol 1998; 179: 1643-53.
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 33 Lakshmi Vas
The single most significant major change in the practice of paediatric anaesthesia in the last two decades has been the introduction of regional anaesthetic techniques. Acceptance of the concept that infants and children feel pain and suffer from its consequences has revolutionized the practice of paediatric anaesthesia in that regional anaesthesia and analgesia have become an integral part of paediatric anaesthesia. In children, light general anaesthesia is required to institute regional blocks. The advantages of this technique are minimal general anaesthesia, preemptive analgesia and attenuation of the stress response to surgery.
Lumbar epidural anaesthesia is very useful in children as an epidural catheter can be positioned and the local anaesthetic drug deposited close to the segment of the cord supplying the dermatomes around the proposed surgical incision. The safety is of a lower volume and dose of local anaesthetic, which by a rough formula is 0.1-0.2 ml/kg/segment to be blocked. The catheter passes quite easily in babies even to levels of the cervical cord. The exact placement can be determined by measuring the distance to be traveled, on the catheter. Recently, connecting a nerve stimulator with a metal needle to the saline filled epidural catheter and passing a current will stimulate the segments of the cord at the tip of the catheter and thus confirms the position of the catheter tip. This produces twitches in the muscles supplied by those segments. Position and spread can also be confirmed by omnipaque (iohexol) injection.
In children, the skin-epidural distance varies with age and weight. A rough guide is 1,5mm/ kg till 1 yr and 1 mm/kg thereafter. Since this is a very short distance, care has to \ be taken not to overshoot this distance and puncture
the dura. The exact technique for introducing an epidural needle in children is different from that of adults. In adults, either a hanging drop or a loss of resistance with incremental advancement of the needle identifies the epidural space. In children, hanging drop technique and incremental advancement of needle is not practicable due to the short skin-epidural distance. The needle is continuously and steadily advanced with a continuous checking for loss of resistance to saline. There is a distinct increase in resistance to the advancement of needle tip and also on the plunger of the syringe, when the needle tip enters the ligamentum flavum. The loss of resistance when the needle leaves this ligament and enters the epidural space is also unequivocally distinct.I prefer saline to elicit this, as it is very easy, obvious and avoids the risks of air embolism, which could be catastrophic considering their size and the volumes of air normally injected.
Many drugs have been used for postoperative analgesia. Various authors have used morphine, fentanyl, pethidine, buprenorphine, pentazocine, tramadol, ketamine clonidine, neostigmine and midazolam. Use of the opioid drugs in neonates and infants has to be done in an ICU setting where an anaesthesiologist is constantly available. This is a luxury many of us do not have. So in this age group we rely solely on bupivacaine in a concentration of 0.05 - 0.1- % solution. In older children, we have used ketamine 0.25-0.5 mg/kg and buprenorphine1-2 microgram/kg. Ketamine has the advantage that there is no fear of any possible respiratory depression, but the problem of unpredictability of duration of action and the possibility of hallucinations remain. Buprenorphine, with its extreme lipophilicity, is very predictable in action, lasts about 24-30 hours, and in the dose mentioned has not given any respiratory depression in any of our patients
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 34 LakshmiVas
who number about 1500. However, older children do complain of severe nausea, which requires prophylactic ondansetron and metoclopramide. We have also used midazolam in a dose of 25 mcg/kg along with the initial dose of local anaesthetic to prolong the analgesia.
Admittedly, the lumbar epidural puncture requires an extreme degree of expertise and delicacy than caudal or lumbar epidural anaesthesia in adults. It can be attempted only after sufficient expertise has been obtained in adults and older children. More importantly, a thorough understanding of the technique is very essential to its scientific practice.
There are many aspects of epidural anaesthesia that are different and sometimes unique to paediatrics. As these differences are being investigated, new and fascinating facts emerge about the epidural space, and the technique itself. Of particular interest is the difficulty in passing the catheter in a small neonate, the calculation of volume, its spread, the back leak of injected solutions and pressure changes in response to epidural injections. The calculation of the volume of injection has been arbitrary, based more on a permissible limit of local anaesthetic dose than as a specific volume to cover a specific number of dermatomes.
The negative epidural pressure described by Janzen in 1926 becomes positive on injection of local anaesthetic solutions as seen by the tracking back of injected solutions around the epidural catheter in children. We undertook studies to investigate the change in epidural pressures in response to local anaesthetic injections at two different rates of injection, as well as the spread of two specific volumes of radio opaque dye injected into the epidural space in a controlled manner in 10 infants. The results of these two studies were published in the journal ‘Paediatric anaesthesia’. The abstracts of these two papers are given below.
Study of epidural pressuresThe pressure changes in the epidural
space of 20 infants due to injection of local anaesthetic solutions were studied. The pressures developed during the passage of the epidural needle through the ligaments of the spine
and in the epidural space, during the injection of 1 ml of the local anaesthetic, at two rates of injection, over 1 and 2 minutes and the residual pressure at 1 and 2 minutes after each injection were studied. The mean pressure while the needle was being advanced through the ligamentum flavum was 69.14+ 36.95 mm of Hg. The epidural pressure, after the needle had just penetrated the ligament, without eliciting the loss of resistance, was 1+.9.759 mms of Hg. A distinct pulsatile waveform identical to the pulse waveform was observed as soon as the epidural space was entered. The pressure rise varied according to the rate of injection. The pressures were 27.79mm of Hg when the rate of injection was 1 ml/1 min, with a residual pressure after 1 minute being 12 + 5.53 mm Hg and it was 10.14+5.53 mm Hg after 2 minutes of injection. When the rate of injection was 1ml/ 2min, the pressures were 15.66+ 9.48 with a residual pressure after 1 minute being 14.79+ 5.15mm Hg and 12.93 + 5.46mm Hg after 2 minutes of injection. The residual pressures seem to vary more with the volume injected than the rate of injection or the pressures developed during the injection. The relationship between the rate of injection and pressures is significant when compared with the adults where the pressures have been measured after an injection rate of 1ml/ sec and 1ml/5secs. This is a very fast rate compared to our rates of injection of 1 ml over 1 and 2 minutes. Based on the findings of this study, we recommend a rate of 1ml/ 2minutes in infants. In neonates, a slower rate of injection would be preferable.
DiscussionBack leak of injected anaesthetic is a
common feature of paediatric epidural injections. It is an indicator that a pressure high enough to create a gradient between the epidural space and the atmosphere is being reached. This leak is not normally seen in young adults, in spite of a much faster injection. But this may be seen in old people, where again the pressures may rise, to cause increased spread because of decreased space around the spinal nerves4.
The main determinant of the backleak would be the pressures developed in the epidural space iri response to the injection of local anaesthetic solutions. The faster rates of injection used in adults produce jets of fluid from the 3
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 35 Lakshmi Vas
holes of the catheter. With our 1 ml/min and 1 ml/ 2min injections, in spite of the pressures 59.09mm of Hg (1 ml/1 min) and 34.93 mm of Hg (1 ml/2min) measured at the proximal end of the 90cm long catheter, the drops formed slowly at the side holes in the distal end.
In an infant, the epidural space is a narrow cylinder, where the pressure on injection can rise to very high levels. The spread inside the annular space will likely be as a surge or a slow rise, depending on the rate of injection. Pressing the dura inwards and compressing the cerebrospinal fluid column around the cord can dissipate this rise in pressure. The CSF is supposed to act as a safety valve2 4 by a cephalad displacement. This is questionable because the area of the CSF column is huge compared to the 1.5 cm area of high pressure around the side holes of the catheter. So, it may act as a buffer to absorb the instantaneous pressure rise, without much disturbance to its own pressure or the intracranial pressures. One study8 has shown a sustained rise in the intracranial pressure in response to the epidural injections. Another stud/ of resin injections in the cadaver9 has shown an intracisternal pressure rise with concomitent lumbar epidural space injection. A concomitant measurement of the fontanelle pressures in infants would probably reflect the rise if any in the CSF pressures, due to a cephalad displacement. Another factor limiting the pressure rise, is the leakage of the local anaesthetic through the intervertebral foramina or through the path of least resistance, the cylindrical tract around the catheter made by the larger epidural needle. A sensation of pain, dizziness and nausea on injection has been reported on injection in adults. An increase in the respiratory and pulse rate in anaesthetized children is also known. The infants in this study showed no specific discernible response to the postoperative injections.
Probably high pressures similar to the peak and residual pressures on injection may develop, when the infant is crying, coughing, breath holding or straining to urinate or defaecate etc, though these have not been studied. The possible deleterious effects if any of the pressure rises on injection are not known. The possibility that complications attributed to regional
techniques may actually be compromises of blood supply already present in the patient due to a congenital vascular malformation or compromised blood supply due to hypotension, which got exacerbated by these pressures, remains to be explored.
Any injection through an epidural catheter, even to air requires an effort. Any increased pressure required for injection when the catheter is in the epidural space may not be appreciated by the operator and be attributed to the long length of the catheter or its small internal diameter. This study showed us that, what would be considered as a slight increase in pressure by the hand, translates into significantly high pressures if they were to be measured. This could lead to a complacence, as most operators would be unaware when excessive pressures are being exerted. After measuring the pressures we taught ourselves to moderate the pressures exerted on the piston on the injecting syringe. Also, making the injections slowly over two minutes confers a safety by reducing the pressures exerted.
The epidural pressures just on entering the space varied mainly on the positive side. Only in 3 patients, negative values were observed. The mean pressure was 1+10. Whether this was because of the narrow potential epidural space with pulsating vessels, or a result of positive pressure ventilation or the pressure on the abdomen in the lateral position with the spine flexed, is uncertain.
In a pilot study of 20 other patients done prior to the present study, using loss of resistance, it was surprising to find pressures of 250 mm of mercury when the tip of the needle was in the ligamentum flavum and the column of saline was being bounced against it. The magnitude of this pressure is determined by two factors. One component is the blocking of the fluid column in the advancing needle by the ligament. The second component is the pressure on the plunger by the operator. However, with awareness of this fact, the pressures in the subsequent cases were lowered to 60-150mms of Hg by consciously exerting less pressure on the plunger. The importance of this pressure is that this is the pressure at which the initial small volume (0.5 - 1 ml) of saline is injected into the epidural space
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 36 Lakshmi Vas
to detect loss of resistance. This leads to a sudden rise of pressure, which decreases rapidly as the injection stops, as soon as the loss of resistance is elicited. This pressure leads to fluid leaking back through the needle, which could be mistaken for CSF, and in our initial practice, this was confirmed by a negative test for glucostix7
The ‘feel’ as the needle passes from the interspinous ligament to the ligamentum flavum was very distinct. When the needle tip was in the former, the feel of bouncing on the plunger of the loss of resistance syringe is less and sometimes, it is even possible to inject a small quantity of saline. This could be misinterpreted as a loss of resistance. This is more likely if air is used for loss of resistance. This is confirmed by the epidurogram, where the spread of the dye in the interspinous ligament is seen. However, once the ligamentum flavum is entered, the bouncing of the piston is distinct and it is impossible to inject anything.
One fairly consistent finding was that the ‘give’ on leaving of ligamentum flavum was so pronounced, that we stopped just short of the epidural space. The catheter, on passing, would encounter a flimsy resistance before passing freely into the space. This felt as if a last thin layer of ligamentum was actually pierced by the catheter. Alternately, a part of the bevel might have been still in the ligamentum giving this impression,The pulsatile waveform seen when the epidural needle tip is in the epidural space was a surprise. It was obviously the pulsations transmitted by the epidural arteries or transmitted from the aorta into the epidural space. This was also registered, even through the fluid filled epidural catheter. Does this mean that the epidural pressure varies with the blood pressure in babies? Does this explain the mildly positive pressure that we found in the epidural space? If there is a pulsatile waveform of pressure in the epidural space, is the loss of resistance elicited a relative one from the high pressures in the ligamentum flavum to that of the lower pressure of the epidural space? We did find subatmospheric pressure in3 cases but in the rest, it was positive. This pulsatile waveform is found so consistently in this study that in other infants it became a test for confirming the epidural placement of needle, especially when a small volume was injected to
transmit these pulsations. Only one study in adults refers to these pulsations. This may be because these pulsations are not very obvious in the capacious adult epidural space but are prominent in the narrow space of infants.
The rates of injection in adults were very fast, with 1 ml/sec or 0.5 ml/sec whereas the recommended rate of injection in children of the whole dose is a few ml over 90-120 seconds11 or 1ml /min 15 Our 1ml over 60 and 120 sec is a very slow rate of injection indeed. However, even at these rates, there was a backleak in many of the babies and epidural pressures were higher than that in adults, 27.79 mm of Hg (37.79 cm of water) against 29 cms of water after 1 ml/minute and 15.09 mms of Hg or 20.52 cm of water after1 ml over 2 minutes. These values were obtained after injection through a 17-gauge needle. In contrast, our pressures were obtained after injection through a 20G catheter, with the solution leaking back along the needle track acting as a relief valve mechanism. This probably reflects the small volume epidural space, which is practically a potential space that gets expanded by the injection of even small volumes of local anaesthetic at very slow rates. We did not record the pressure at which backleak occurs, as it was highly variable. Backleak is important, as it prevents an excessive rise in pressure. However, it causes a loss of effective volume of local anaesthetic remaining in the space to exert an effect. The volume of backleak that correlated with the spread requires to be studied. Interestingly, backleak is not seen commonly when the catheter is introduced from the caudal route, though the injection rate is similar with 1ml/2 min. Probably, the fluid tracking back along the catheter pools in the more capacious caudal epidural space, without steep rises in pressure. Could this mean that there is anaesthesia of the sacral segments in addition to the segmental anaesthesia at the tip of the epidural catheter? Could this also explain the retention of urine associated with central neuraxial blocks instituted from the caudal route? This difference in backleak and its causative pressures with the introduction of catheter between lumbar and caudal routes needs to be studied.
In conclusion, there are many unknown effects associated with epidural injection of local
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 37 Lakshmi Vas
anaesthetic solutions. The resting epidural pressure in infants may not always be negative. It is preferable to make static measurements of pressure, as the pressure drop factor would be eliminated. Measurement of dynamic pressures with steady injections from infusion pumps would eliminate the variations due to the manual injections. The pressure rise in response to lumbar epidural injection in infants is considerably higher than that of adults even with very slow rates of injection. It is safer to use a slow rate of injection like 1ml/2min in infants and may be, even slower rates in neonates. Further studies are required to assess the degree of spread vis- a-vis speed of injection, the effect of residual pressure on the spread and the resultant block height, the effect of backleak on the spread, and the correlation of epidural pressures to fontanelle pressures and the difference in attained pressures with lumbar and caudal routes of introduction of catheters.
STUDY OF THE SPREAD OF RADIOOPAQUE DYE: ABSTRACT AND DISCUSSION.Aim
Prospective study to assess whether the extent of spread of the dye in the epidural space would vary in direct proportion to the volume, by injecting two volumes of the dye.
Patients and methods10 infants aged 2 - 3 6 days, (mean +
SD,13.30+13.68) and weighing 1.8 kg-4.5kg (mean + SD,2.60 + 0.97) undergoing major thoracoabdominal surgery under epidural and general anaesthesia were selected. At the end of surgery, two volumes of radioopaque dye (omnipaque) 0.5ml/kg and 1 ml/kg were injected into the epidural space at a rate of 1 ml/2minutes. The spread of the dye was studied by taking X rays after both injections in the left lateral position.
ResultsThere were ten different patterns of spread
in the 10 cases. Uniformly circumferential and cylindrical spread was seen only in one infant. In others, there were segregated patches of anterior and posterior spread with or without interspersed patches of circumferential spread. There was variation in the extent, location and
the density of spread, filling defects and skipped segments with both volumes. Back leak of dye along the needle track was seen in 3 cases. Statistically Segments were 9.30 + 3.68 for 0.5ml, for 1 ml/kg 11.50 + 3.03, 3.03, S, P=0.014. Circumferential spread for 0.5ml/kg 2.70 + 2.16, for 1 ml/kg 5.90 + 3.14 3.59, S, P=0.006 . Anterior spread for 0.5ml/kg 3.60 + 1.58 and for 1 ml/kg 7.90 + 2.33 5.88, S, P=0.001. Posterior spread for 0.5ml/kg 8.20 + 3.71 and for 1 ml/kg 9.80 + 3.68 3.54, S, P=0.006. Doubling of spread with doubling of the volume occurred in only 1 patient. There was a variable increase in the extent or in the density of spread with reduction of skip segments with 1 ml/kg dose than with 0.5 ml/kg. The probable reasons for this variable spread and the mechanism of epidural anaesthesia in the presence of such spread is discussed.
ConclusionThere is a difference in quantitative as
well as qualitative spread in different patients and in the same patient with different volumes. There were statistically significant increases in the number of segments, circumferential, anterior and posterior locations of the 1.0ml group than the 0.5ml group. Both the extent and the density of spread improve with a higher volume but not in direct proportion to the volume. 1 ml/kg has a better quantitative as well as qualitative spread than 0.5ml and has a better chance of producing adequate anaesthesia.
DiscussionThe extent of spread of the local
anaesthetic solutions injected into the pediatric epidural space depends on many factors like the volume of injection 1'3, speed of injection 4‘5, the backleak of the solution in the needle track around the catheter35' leaks through intervertebral foramina7A the pressures achieved in the epidural space36-8 and the inherent divisions of the epidural space10-17. This study was carried out with the purpose of assessing the extent of spread with two different volumes, but as the study progressed, it became apparent that the quality of spread was as varied as the extent. Logically, the spread of a dose of 1 ml/Kg, should be double that of 0.5 ml/Kg in an ideal predictable situation. However, neither the blind procedure of epidural placement of drugs nor the nature of
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 38 Lakshmi Vas
epidural space seemed to be predictable in this study. There were 10 different patterns of spread in the 10 cases with segregation into anterior and posterior patches instead of a uniform circumferential and cylindrical spread. In the same patient, for the two volumes of injection there were differences in the pattern, the density of spread and the leak (more with the higher volume). There were filling defects and skipped segments in both spreads
Doubling of the number of segments covered by the spread with the doubling of the dose occurred in only one patient, but with a large skip of segments in between. In the other patients, though the spread did not double, the density of the spread was better.
The spread of injections in the closed epidural space determines the number of blocked segments, the upper and lower limits of block and the extent of anaesthesia. The quality of anaesthesia and its patchiness if any, are determined by uneven spread. The factors determining the actual spread of the local anaesthetic solution in the epidural space are as follows.
1) The physical divisions within the epidural space10'17
2) The neuraxial spread versus the physical spread of a solution in the epidural space. It has been suggested that there is a subtle distinction between the physical spread of a solution in the epidural space and its neuraxial spread 16 with the former extending beyond the latter.
3) The pressure rise in the closed epidural space in response to injection of space occupying volumes of local anaesthetic solutions, which determines the pressure head, which in turn will determine the spread. The residual pressure after completion of injection in particular, seems to be important in the extent of spread 1'3 6'7
4) The determinants of this pressure, include speed of injection, volume of the injectate, uniformity of injection pressures, the residual pressure after completion of injection, possible transmission and dissipation of pressure to the body of CSF enclosed within the dura mater3'1819'20
leaks along the nerves, along the needle track around the epidural catheter.
5) Leaks that may mean loss of effective volume of local anaesthetic.
Saitoh et al(8) and Burn et al 16 found from radiographic observations in the elderly that there was no correlation between leak through intervertebral foramina and longitudinal spread.
Backleak around a catheter along the needle track is a unique feature of epidural injections in infants and children, probably due to their small capacity epidural spaces. Whether this adds another dimension to the spread of epidurally injected fluids remains to be explored. In this study, backleak was seen in patients 3,7 and 9, especially with a larger dose. But there was more than doubling in the spread with volume in case 9. Apparently the backleak in this baby did not affect the spread.
In the present study, the variables like speed of injection, volume, age and weight were within a uniform range. However, whether the length, breadth and volume of the epidural space, correlate with the body weight is questionable. Since all the injections were performed by the same person (first author) at the same rate (2ml/ min), the pressures were presumed be in a similar range for all the 10 patients. The only unpredictable variable factors were divisions within the epidural space and other determinants of pressure like leaks, pressure on CSF etc.
The most likely reason for the compartmentalization of the injected fluid , the intriguing skipping of segments could be the physical divisions within the epidural space as described in the previous reports of the anatomy of the epidural space.912
Resin injection studies of Harrison et al9 in autopsies of 20 cadavers found that flow of the resin formed a large posterior bulge with thin antero lateral projections on either side. The anterior spread was seen only in 8 out of 20 cases as very thin and incomplete.
Based on cryomicrotone studies of
RACE 2003 Ramachandra Anaesthesia Continuing Education
What’s New in Paediatric Epidural Anaesthesia 39 Lakshmi Vas
undisturbed anatomy in a fresh cadaver, Hogan 12 considers the epidural space to have metameric segmentations in the longitudinal axis due to the contact of dura with the ligamentum flavum. These segments start from the middle of the upper lamina to the cephalad edge of the lower lamina. Within each segment also, there is a distinct lateral, anterior and posterior compartments. The posterior compartment has a homogenous pad of fat. In the anterior compartment, the posterior longitudinal ligament (PLL) is closely applied to the dura and blends into the annular ligament at the level of a disc as seen in axial sections. Only caudal to the L4-5, do the dura and PLL part, creating a capacious anterior epidural space.
Savolaine et al described a central midline structure called plica mediana dorsalis 10 with the dorsolateral ligaments issuing from the it 916 of which 4 patterns have been described. Many cases of unilateral spread have been attributed to this 16 21
The findings of Hogan are in contrast to those of Savolair.e and Blomberg.
He proposes that injection of the dye by Savolaine et al and air in the epiduroscopy studies of Blomberg distend the epidural fat pad itself with its lateral attenuations and stretch and suspend it in a posterior epidural compartment to give the artifact called plica and lateral membranes.. Based on pictures in the physiologic state in magnetic resonance imaging22, Savolaine also concedes that plica mediana dorsalis is an artifact due to unnatural transmural dural pressures during distension of epidural space by air or fluid .
The present understanding of epidural space based on these studies is thus :
The homogenous fat in the posterior compartment has no fibrous sections and freely separates from the dura and the ligamenta flava. It is attached by a pedicle to the point where the two left and right portions of the ligamenta flava abut with a vessel entering at this point12. This is the space where the epidural needle and catheter are positioned and the local anaesthetic solution is deposited where it spreads to the other two compartments. This freely separable plane provides a route for the injected fluid or air. The
lateral compartment of the epidural space contains nerve roots, vessels and fat. The fat is lobulated by septae with a plane of septation extending from the exiting nerve root to the PLL. This space is important because this is the area where local anaesthetics come in contact with the nerve roots in their dural cuff. The septae in the lateral and anterior compartments can partially obstruct the flow to cause a pressure rise in response to injections, the decay of the pressure and the residual pressures 36 are independent of the volumes injected123
In our study, the divisions within the epidural space could have confined the dye to the posterior and posterolateral epidural space with less consistent spread to the anterior compartment. Since the volume could not spread in a circumferential manner, it might have spread in a linear manner covering a large number of segments. With the doubling of volume, the pressure head for spread would have been higher, facilitating a denser spread, as well as spread into the less compliant anterior compartment. It is also possible that 0.5ml/kg was an inadequate volume to fill the epidural segments and as a result the higher 1 ml/kg improved the quality rather than the extent of spread . To assess the real effect of volume, the lower dose should probably be 1 ml to study the effects on extent of spread and then double this volume to see if the spread doubles
The spread in patient 1, is interesting in that the lower part spread from T11 to L2 had a helical appearance with alternating anterior and posterior densities. The filling defects in the anterior spread are at the intervertebral discs where the dura is described to merge into the PLL. (12) Thus opposite the bodies, there is a spread with the filling defects opposite the discs. Similarly in the posterior spread, it seems as if there is spread in a metameric segment (12) extending from the upper lamina to the cephalad border of the lower lamina. It was as if the dye flowed from posterior distensible interlaminar areas to the next area that was distensible, the anterior space opposite the vertebral body leaving the non compliant areas in between as filling defects.
Perusal of our epidurograms with their
RACE 2003 Ramachandra Anaesthesia Continuing Education

What’s New in Paediatric Epidural Anaesthesia 40 Lakshmi Vas
predominantly posterior and posterolateral spread raises the question, how exactly does epidural anaesthesia act?24 Is it by blocking of the spinal nerves at the intervertebral foramina as they course through the posterolateral epidural space or by diffusion along the dural sleeves towards the cord or through the dura and CSF towards the spinal cord? Is a lack of spread to the anterior aspect of epidural space likely to matter for the quality of anaesthesia?. Do the vagaries of spread explain the reported failure rate of 4- 50 % of cases with epidural anaesthesia?25 27 In the cord itself, is it the posterior aspect with the sensory tracts that require to be blocked, with the anterior tracts of the cord remaining totally or quasi functional? In which case, could this explain the retention of muscle tone and variable levels of motor activity with epidural anaesthesia which contrasts with the total motor paralysis seen with spinal subarachnoid anaesthesia? In the latter, the quantum of local anaesthetic drug with access to the sensory and motor tracts is such that, dense anesthesia of both sensory and motor tracts ensues with resultant analgesia and motor paralysis.
With epidural anaesthesia, the local anaesthetic drug has comparatively easy access to the spinal nerves, particularly the posterior nerve root encased in the dural arachnoid and pia mater. Only the quantity that diffuses into the cerebrospinal fluid through the dural sleeve has access to the spinal cord. Even here, the physical proximity to the posterior sensory tracts would be more than the anterior motor tracts which are geographically more distal. Whether this explains the difference in the quality of motor block between spinal and epidural remains to be explored. 2428 Do the physical barrier of 3 meningeal layers which have to be crossed by the local anaesthetic drug reduce the efficacy of epidurally deposited drug vis-avis density and totality of blockade? These questions could be addressed probably by injection studies of local anaesthetic coloured with a dye into cadavers and then studying the pattern of spread in both epidural and spinal injections. In our patients there was obvious analgesia as evidenced by absence of tachycardia and a stable blood pressure in response to incision. It is probable that the
posterior spread was enough to provide analgesia. Alternatively, the neuraxial spread of local anaesthetic might have been adequate. Burn et al16 found analgesia of the perineum in patients where the spread had not extended below L3 level, highlighting the disparity between physical and neuraxial spread.
In conclusion, there appears to be considerable individual variations in the extent, quality and uniformity of spread. Doubling of the dose does not necessarily double the extent of spread but improves its density and the extent. As a result, use of 1 ml/kg volume is more likely to ensure a better extent and quality of anaesthesia in this age group. However, epidural anaesthesia remains a blind technique where many aspects of the spread of the local anaesthetic agent and the resultant action are yet to be comprehensively elucidated.
References:
1. R. P. Husemeyer and D. C. White. Lumbar Extradural Injection pressures In Pregnant Women, fir. J. Anaesth 1980; 52: 55-592. D.l. Paul, J.A.W. Wildsmith. Extradural pressures following the injection of two volumes of bupivacaine. fir J. Anaesth 1989; 62: 368-3723.Usubiaga JE, Wikinski JA Usubiaga LE. Epidure pressure and its relation to spread of anesthetic solution in the epidural space. Anesth Analg 1967; 46440-446.4. Y.Hirabayashi, R. Shimizu, I. Matsuda and S. Inoue. Effect of extradural compliance and resistance on spread of extradural analgesia, fir. J. Anaesth 1990; 65: 508-513.5. Cardoso MM, Carvalho JC. Epidural pressure and spread of 2% lidocaine in the epidural space: influence of volume and speed of injection of the local anesthetic solution. Reg Anesth Pain Med 1998 ;23:14-9.6. Janzen E. Der negative Vorschlag bei lumbal Punktion. Dtsch. Z. Nervenheilkd 1926;94: 280.7. Lakshmi Vas Phalguni Naregal Savita Sanzgiri, Anupama Negi, Some vagaries of neonatal lumbar anaesthesia. Paediatric Anaesthesia 1999; 9: 217-2238. Hilt H, Gramm H-J, Link J. Changes intracranial pressure associated withanaesthesia, fir. J. Anaesth 1986; 58: 676-680.9. Harrison GR, Parkin IG, Shah JL. Resin injection studies of the lumbar extra dural space. Br J Anaesth 1985; 57: 333-336.10. Edward Savolaine, Jyoti Pandya, Samuel Greenblattet al. Anatomy of the human lumbar epidural space: new insights using CT epidurography. Anesthesiology; 1088; 68: 217-220.11. Bernard Dalens. Lumbar epidural anaesthesia in Regional anaesthesia in infants, children and adolescents. Edited by Bernard Dalens 1sred. Williams and Wilkins. Baltimore, Maryland. 1993, 207-248,12. Bernard Dalens. Regional anesthesia in children. Anesth
RACE 2003 Ramachandra Anaesthesia Continuing Education

What’s New in Paediatric Epidural Anaesthesia 41 Lakshmi Vas
Analg. 1989;68: 654-7213. Hogan OH. Lumbar epidural anatomy. A new look by cryomicrotome section. Anesthesiology 1991; 75: 765-775.14.Blanco D, Mazo V, Ortiz M, Fernandez - Llamazares J.Vidai F. Spread of local anaesthetic into the epidural caudal space for two rates of injection in children. Reg Anesth 1996 ; 21: 442-515. Claude Ecoffey, Anne-Marie Dubousset, Kamran Samii. Lumbar and Thoracic Epidural Anesthesia for Urologic and upper Abdominal Surgery in infants and Children. Anesthesiology 1986; 65:87-90.
References for study of spread of radioopaque dye:
1. D.l. Paul, J.A.W. Wildsmith. Extradural pressures following the injection of two volumes of bupivacaine. Br. J. Anaesth 1989; 62: 368-3722. Cardoso MM, Carvalho JC. Epidural pressure and spread of 2% lidocaine in the epidural space: influence of volume and speed of injection of the local anesthetic solution. Reg Anesth Pain Med 1998 ;23:14-9.3. Vas L , Raghavendran S, Hosalkar H, et al. A study of epidural pressures in infants Paediatric anaesthesia, in press.4. Blanco D, Mazo V, Ortiz M, et al . Spread of local anaesthetic into the epidural caudal space for two rates of injection in children. Reg Anesth 1996 ; 21: 442-55. Vas L, Naregal N, Sanzgiri S, et al. Some vagaries of neonatal lumbar anaesthesia. Paediatric Anaesthesia 1999; 9: 217-2236. Usubiaga JE, Wikinski JA Usubiaga LE. Epidure pressure and its relation to spread of anesthetic solution the epidural space. Anesth Analg 1967; 46440-446.7. Y.Hirabayashi, R. Shimizu, I. Matsuda and S. Inoue. Effect of extradural compliance and resistance on spread of extradural analgsia. Br. J. Anaesth 1990; 65: 508-513.8. Saitoh K, Hirabayashi Y, Shimuzu R etal. Extensive spread in the elderly may not relate to decresed leakage through intervertebral foramina. BJA 1995, 75: 688-691.9. Harrison GR, Parkin IG, Shah JL. Resin injection studies of the lumbar extra dural space. Br J Anaesth 1985; 57: 333-336.10. Edward Savolaine, Jyoti pandya, Samuel Greenblatt et al. Anatomy of the human lumbar epidural space : new insights using CT epidurography. Anesthesiology; 1088; 68: 217-220.11. Bernard Dalens. Regional anesthesia in children. Anesth Analg. 1989;68: 654-7212. Hogan OH. Lumbar epidural anatomy. A new look by cryomicrotome section. Anesthesiology 1991; 75: 765-775.13. BlombergRG. The lumbar subdural extraarachnoid
space of humans: An anatomical study using spinaloscopy in autopsy cases Anesth Analg 1987 : 66: 177-8014. Blomberg RG.. The dorsomedian connective tissue band in the lumbar epidural space of humans An anatomical study using epiduroscopy in autopsy cases Anesth Analg 1986 : 65: 747-5215. Bromage P.R.Burfoot M.F, Crowell D.E. etal. Quality of epidural blockade: influence of physical factors. Br .J. Anaesth 1964; 36:342-352.16. Burn J.M,GuyerP.B,Langdon L, The spread of solutions injected into the epidural spaceA study using epidurograms in patients with lumbosciatic syndrome. Br.J.Anaesth-1973: 45: 338-34517. Slappendel R, Gielen M.J.M, Hasenbos MAWM. Etal. Spread of radioopaque dye in the thoracic epidural space. Anesthesia 1988; 43: 939-942.18. Van Niekerk J Bax-Vermierre B.M.J, Geurts J.W.M etal . Epidurography in premature infants. Anaesthesia 1990, 45: 722-72519. .StienstraR, DahanA.AIhadi etal. Mechanism of action of an epidural Topup in combined spinal epidural anesthesia Anesth Analg 1996;83:382-6.20. Blumgart C,H. Ryall D, Dennison B. Mechanism of extension of spinal anaesthesia by extradural injections of local anaesthetic. Br. J.Anaesth. 1992;69:457-46021. BoezartA P, Computerized axial tomoepidurographic documentation of unilateral epidural analgesia. Can J anaesth 1989; 36 697-70022. SavolaineER: Reply to a letter. Anesthesiology 69:798, 1988.23. Rocco AG, Scott DA, Boas RA etal The epidural space behaves as a Starling resistor and inflow resistance is elevated in diseased epidural space Reg anesth 1990; 15(suppl):3924. Bromage P.R. Mechanism of action of extradural analgesia Br. J.Anaesth. 1975;47:199-212.25. Curatolo M, Orlando A, Zbinden A.M. et al. A multifactorial analysis to explain inadequate surgical analgesia after extradural block..Br J Anaesth 1995; 75:274-281.26. .Tanaka K .WatanabeR, Harada T etal. Extensive application of epidural anaesthesia and analgesia in a university hospital: Incidence of complications related to technique. Regional anaesthesia 1993; 18 :34-3827. Seeberger M.D Lang M.L.Drewe J et al Comparison of spinal and epidural anesthesia for patients younger than 50 years of age.Anesth Analg1994;78667-73..Huang JS, lYY.TungCC etal Comparison between the effects of epidural and spinal anesthesia for elective cesarian section; Chung Hua Hsueh Tsa Chih (Chin Med J) 1993;51: 40-7
RACE 2003 Ramachandra Anaesthesia Continuing Education
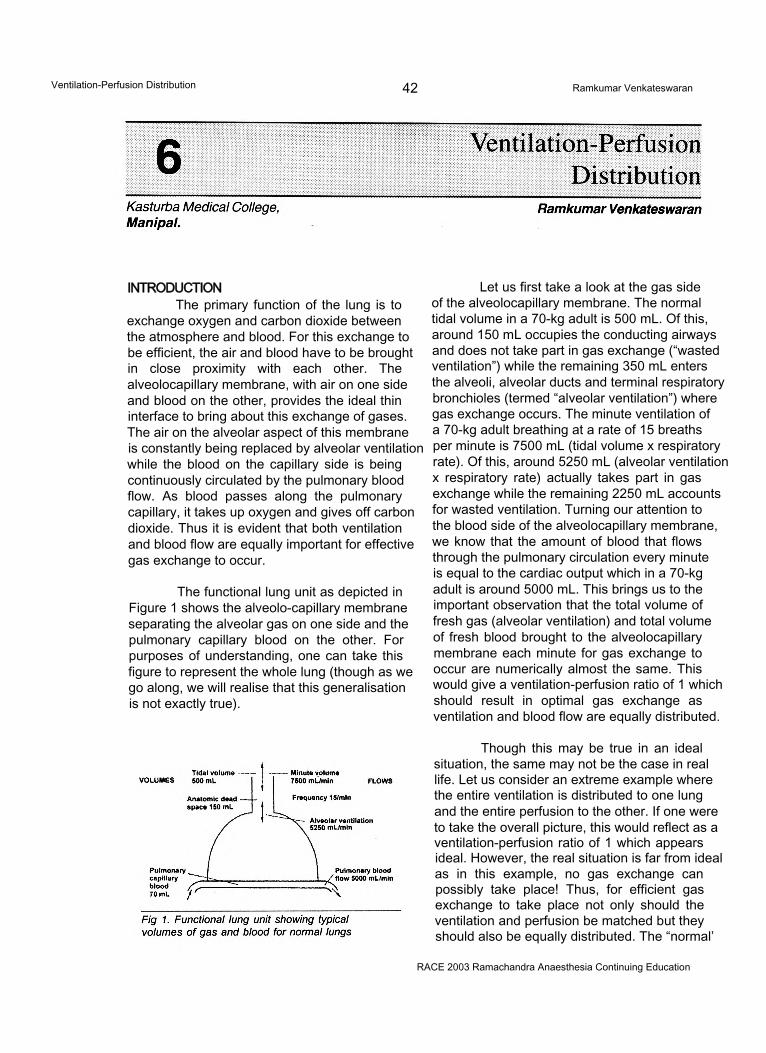
Ventilation-Perfusion Distribution 42 Ramkumar Venkateswaran
INTRODUCTIONThe primary function of the lung is to
exchange oxygen and carbon dioxide between the atmosphere and blood. For this exchange to be efficient, the air and blood have to be brought in close proximity with each other. The alveolocapillary membrane, with air on one side and blood on the other, provides the ideal thin interface to bring about this exchange of gases. The air on the alveolar aspect of this membrane is constantly being replaced by alveolar ventilation while the blood on the capillary side is being continuously circulated by the pulmonary blood flow. As blood passes along the pulmonary capillary, it takes up oxygen and gives off carbon dioxide. Thus it is evident that both ventilation and blood flow are equally important for effective gas exchange to occur.
The functional lung unit as depicted in Figure 1 shows the alveolo-capillary membrane separating the alveolar gas on one side and the pulmonary capillary blood on the other. For purposes of understanding, one can take this figure to represent the whole lung (though as we go along, we will realise that this generalisation is not exactly true).
Let us first take a look at the gas side of the alveolocapillary membrane. The normal tidal volume in a 70-kg adult is 500 mL. Of this, around 150 mL occupies the conducting airways and does not take part in gas exchange (“wasted ventilation”) while the remaining 350 mL enters the alveoli, alveolar ducts and terminal respiratory bronchioles (termed “alveolar ventilation”) where gas exchange occurs. The minute ventilation of a 70-kg adult breathing at a rate of 15 breaths per minute is 7500 mL (tidal volume x respiratory rate). Of this, around 5250 mL (alveolar ventilation x respiratory rate) actually takes part in gas exchange while the remaining 2250 mL accounts for wasted ventilation. Turning our attention to the blood side of the alveolocapillary membrane, we know that the amount of blood that flows through the pulmonary circulation every minute is equal to the cardiac output which in a 70-kg adult is around 5000 mL. This brings us to the important observation that the total volume of fresh gas (alveolar ventilation) and total volume of fresh blood brought to the alveolocapillary membrane each minute for gas exchange to occur are numerically almost the same. This would give a ventilation-perfusion ratio of 1 which should result in optimal gas exchange as ventilation and blood flow are equally distributed.
Though this may be true in an ideal situation, the same may not be the case in real life. Let us consider an extreme example where the entire ventilation is distributed to one lung and the entire perfusion to the other. If one were to take the overall picture, this would reflect as a ventilation-perfusion ratio of 1 which appears ideal. However, the real situation is far from ideal as in this example, no gas exchange can possibly take place! Thus, for efficient gas exchange to take place not only should the ventilation and perfusion be matched but they should also be equally distributed. The “normal’
RACE 2003 Ramachandra Anaesthesia Continuing Education
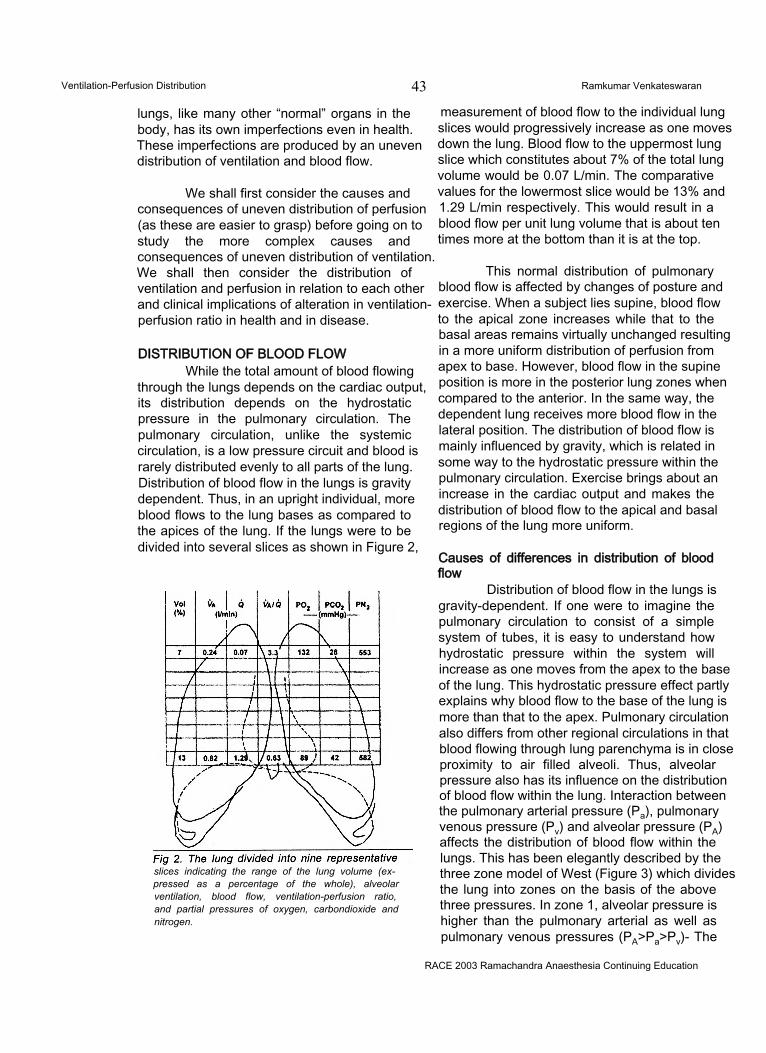
Ventilation-Perfusion Distribution 43 Ramkumar Venkateswaran
lungs, like many other “normal” organs in the body, has its own imperfections even in health. These imperfections are produced by an uneven distribution of ventilation and blood flow.
We shall first consider the causes and consequences of uneven distribution of perfusion (as these are easier to grasp) before going on to study the more complex causes and consequences of uneven distribution of ventilation. We shall then consider the distribution of ventilation and perfusion in relation to each other and clinical implications of alteration in ventilation- perfusion ratio in health and in disease.
DISTRIBUTION OF BLOOD FLOWWhile the total amount of blood flowing
through the lungs depends on the cardiac output, its distribution depends on the hydrostatic pressure in the pulmonary circulation. The pulmonary circulation, unlike the systemic circulation, is a low pressure circuit and blood is rarely distributed evenly to all parts of the lung. Distribution of blood flow in the lungs is gravity dependent. Thus, in an upright individual, more blood flows to the lung bases as compared to the apices of the lung. If the lungs were to be divided into several slices as shown in Figure 2,
slices indicating the range of the lung volume (expressed as a percentage of the whole), alveolar ventilation, blood flow, ventilation-perfusion ratio, and partial pressures of oxygen, carbondioxide and nitrogen.
measurement of blood flow to the individual lung slices would progressively increase as one moves down the lung. Blood flow to the uppermost lung slice which constitutes about 7% of the total lung volume would be 0.07 L/min. The comparative values for the lowermost slice would be 13% and 1.29 L/min respectively. This would result in a blood flow per unit lung volume that is about ten times more at the bottom than it is at the top.
This normal distribution of pulmonary blood flow is affected by changes of posture and exercise. When a subject lies supine, blood flow to the apical zone increases while that to the basal areas remains virtually unchanged resulting in a more uniform distribution of perfusion from apex to base. However, blood flow in the supine position is more in the posterior lung zones when compared to the anterior. In the same way, the dependent lung receives more blood flow in the lateral position. The distribution of blood flow is mainly influenced by gravity, which is related in some way to the hydrostatic pressure within the pulmonary circulation. Exercise brings about an increase in the cardiac output and makes the distribution of blood flow to the apical and basal regions of the lung more uniform.
Causes of differences in distribution of blood flow
Distribution of blood flow in the lungs is gravity-dependent. If one were to imagine the pulmonary circulation to consist of a simple system of tubes, it is easy to understand how hydrostatic pressure within the system will increase as one moves from the apex to the base of the lung. This hydrostatic pressure effect partly explains why blood flow to the base of the lung is more than that to the apex. Pulmonary circulation also differs from other regional circulations in that blood flowing through lung parenchyma is in close proximity to air filled alveoli. Thus, alveolar pressure also has its influence on the distribution of blood flow within the lung. Interaction between the pulmonary arterial pressure (Pa), pulmonary venous pressure (Pv) and alveolar pressure (PA) affects the distribution of blood flow within the lungs. This has been elegantly described by the three zone model of West (Figure 3) which divides the lung into zones on the basis of the above three pressures. In zone 1, alveolar pressure is higher than the pulmonary arterial as well as pulmonary venous pressures (PA>Pa>Pv)- The
RACE 2003 Ramachandra Anaesthesia Continuing Education
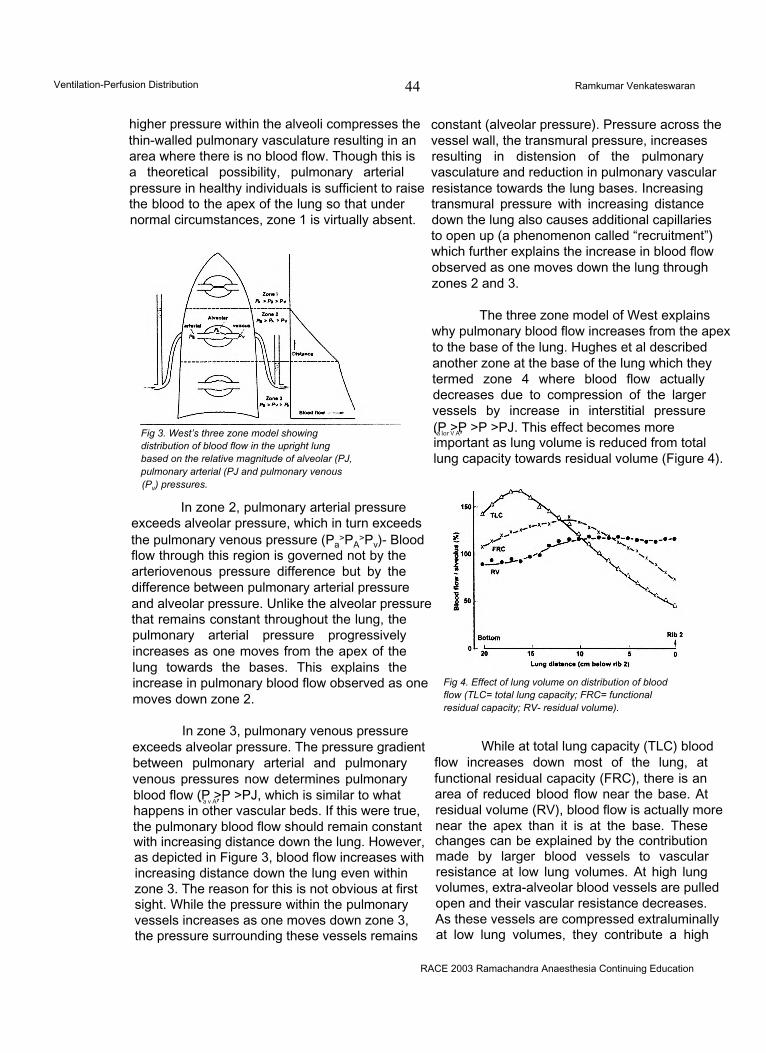
Ventilation-Perfusion Distribution 44 Ramkumar Venkateswaran
higher pressure within the alveoli compresses the thin-walled pulmonary vasculature resulting in an area where there is no blood flow. Though this is a theoretical possibility, pulmonary arterial pressure in healthy individuals is sufficient to raise the blood to the apex of the lung so that under normal circumstances, zone 1 is virtually absent.
Fig 3. West’s three zone model showing distribution of blood flow in the upright lung based on the relative magnitude of alveolar (PJ, pulmonary arterial (PJ and pulmonary venous (Pv) pressures.
In zone 2, pulmonary arterial pressure exceeds alveolar pressure, which in turn exceeds the pulmonary venous pressure (Pa
>PA>Pv)- Blood
flow through this region is governed not by the arteriovenous pressure difference but by the difference between pulmonary arterial pressure and alveolar pressure. Unlike the alveolar pressure that remains constant throughout the lung, the pulmonary arterial pressure progressively increases as one moves from the apex of the lung towards the bases. This explains the increase in pulmonary blood flow observed as one moves down zone 2.
In zone 3, pulmonary venous pressure exceeds alveolar pressure. The pressure gradient between pulmonary arterial and pulmonary venous pressures now determines pulmonary blood flow (P >P >PJ, which is similar to whatx a v A7 1
happens in other vascular beds. If this were true, the pulmonary blood flow should remain constant with increasing distance down the lung. However, as depicted in Figure 3, blood flow increases with increasing distance down the lung even within zone 3. The reason for this is not obvious at first sight. While the pressure within the pulmonary vessels increases as one moves down zone 3, the pressure surrounding these vessels remains
constant (alveolar pressure). Pressure across the vessel wall, the transmural pressure, increases resulting in distension of the pulmonary vasculature and reduction in pulmonary vascular resistance towards the lung bases. Increasing transmural pressure with increasing distance down the lung also causes additional capillaries to open up (a phenomenon called “recruitment”) which further explains the increase in blood flow observed as one moves down the lung through zones 2 and 3.
The three zone model of West explains why pulmonary blood flow increases from the apex to the base of the lung. Hughes et al described another zone at the base of the lung which they termed zone 4 where blood flow actually decreases due to compression of the larger vessels by increase in interstitial pressure (P >P >P >PJ. This effect becomes more' a lor V A7
important as lung volume is reduced from total lung capacity towards residual volume (Figure 4).
Fig 4. Effect of lung volume on distribution of blood flow (TLC= total lung capacity; FRC= functional residual capacity; RV- residual volume).
While at total lung capacity (TLC) blood flow increases down most of the lung, at functional residual capacity (FRC), there is an area of reduced blood flow near the base. At residual volume (RV), blood flow is actually more near the apex than it is at the base. These changes can be explained by the contribution made by larger blood vessels to vascular resistance at low lung volumes. At high lung volumes, extra-alveolar blood vessels are pulled open and their vascular resistance decreases. As these vessels are compressed extraluminally at low lung volumes, they contribute a high
RACE 2003 Ramachandra Anaesthesia Continuing Education
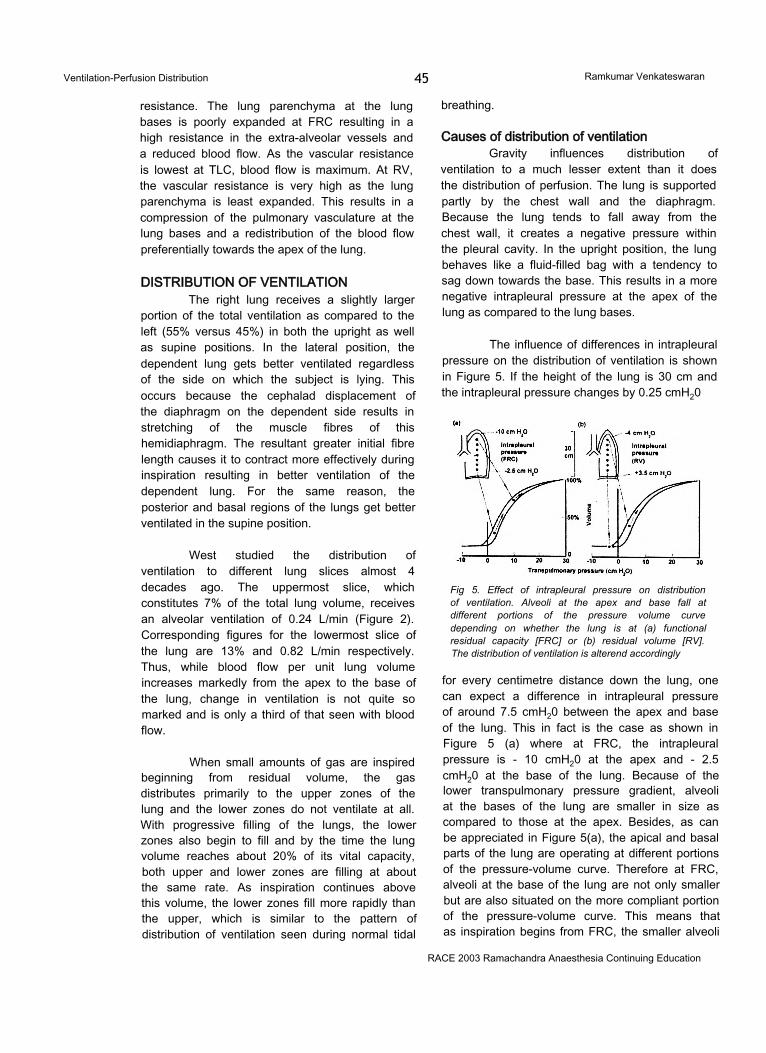
Ventilation-Perfusion Distribution 45 Ramkumar Venkateswaran
resistance. The lung parenchyma at the lung bases is poorly expanded at FRC resulting in a high resistance in the extra-alveolar vessels and a reduced blood flow. As the vascular resistance is lowest at TLC, blood flow is maximum. At RV, the vascular resistance is very high as the lung parenchyma is least expanded. This results in a compression of the pulmonary vasculature at the lung bases and a redistribution of the blood flow preferentially towards the apex of the lung.
DISTRIBUTION OF VENTILATIONThe right lung receives a slightly larger
portion of the total ventilation as compared to the left (55% versus 45%) in both the upright as well as supine positions. In the lateral position, the dependent lung gets better ventilated regardless of the side on which the subject is lying. This occurs because the cephalad displacement of the diaphragm on the dependent side results in stretching of the muscle fibres of this hemidiaphragm. The resultant greater initial fibre length causes it to contract more effectively during inspiration resulting in better ventilation of the dependent lung. For the same reason, the posterior and basal regions of the lungs get better ventilated in the supine position.
West studied the distribution of ventilation to different lung slices almost 4 decades ago. The uppermost slice, which constitutes 7% of the total lung volume, receives an alveolar ventilation of 0.24 L/min (Figure 2). Corresponding figures for the lowermost slice of the lung are 13% and 0.82 L/min respectively. Thus, while blood flow per unit lung volume increases markedly from the apex to the base of the lung, change in ventilation is not quite so marked and is only a third of that seen with blood flow.
When small amounts of gas are inspired beginning from residual volume, the gas distributes primarily to the upper zones of the lung and the lower zones do not ventilate at all. With progressive filling of the lungs, the lower zones also begin to fill and by the time the lung volume reaches about 20% of its vital capacity, both upper and lower zones are filling at about the same rate. As inspiration continues above this volume, the lower zones fill more rapidly than the upper, which is similar to the pattern of distribution of ventilation seen during normal tidal
breathing.
Causes of distribution of ventilationGravity influences distribution of
ventilation to a much lesser extent than it does the distribution of perfusion. The lung is supported partly by the chest wall and the diaphragm. Because the lung tends to fall away from the chest wall, it creates a negative pressure within the pleural cavity. In the upright position, the lung behaves like a fluid-filled bag with a tendency to sag down towards the base. This results in a more negative intrapleural pressure at the apex of the lung as compared to the lung bases.
The influence of differences in intrapleural pressure on the distribution of ventilation is shown in Figure 5. If the height of the lung is 30 cm and the intrapleural pressure changes by 0.25 cmH20
Fig 5. Effect of intrapleural pressure on distribution of ventilation. Alveoli at the apex and base fall at different portions of the pressure volume curve depending on whether the lung is at (a) functional residual capacity [FRC] or (b) residual volume [RV]. The distribution of ventilation is alterend accordingly
for every centimetre distance down the lung, one can expect a difference in intrapleural pressure of around 7.5 cmH20 between the apex and base of the lung. This in fact is the case as shown in Figure 5 (a) where at FRC, the intrapleural pressure is - 10 cmH20 at the apex and - 2.5 cmH20 at the base of the lung. Because of the lower transpulmonary pressure gradient, alveoli at the bases of the lung are smaller in size as compared to those at the apex. Besides, as can be appreciated in Figure 5(a), the apical and basal parts of the lung are operating at different portions of the pressure-volume curve. Therefore at FRC, alveoli at the base of the lung are not only smaller but are also situated on the more compliant portion of the pressure-volume curve. This means that as inspiration begins from FRC, the smaller alveoli
RACE 2003 Ramachandra Anaesthesia Continuing Education
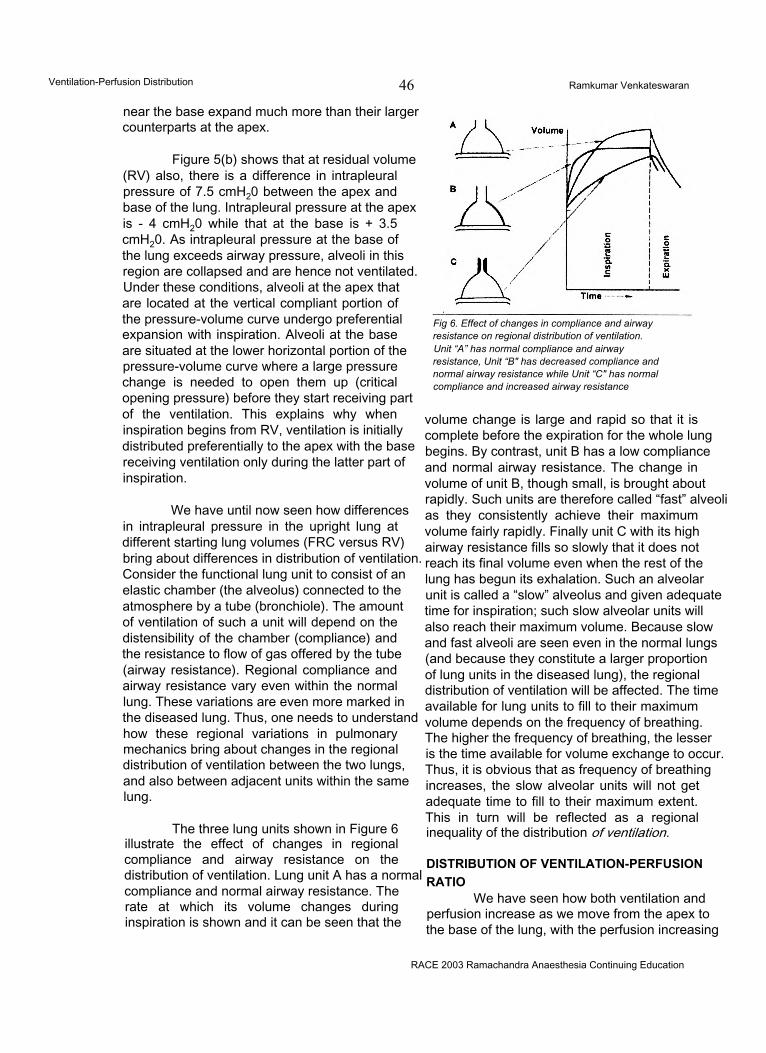
Ventilation-Perfusion Distribution 46 Ramkumar Venkateswaran
near the base expand much more than their larger counterparts at the apex.
Figure 5(b) shows that at residual volume (RV) also, there is a difference in intrapleural pressure of 7.5 cmH20 between the apex and base of the lung. Intrapleural pressure at the apex is - 4 cmH20 while that at the base is + 3.5 cmH20. As intrapleural pressure at the base of the lung exceeds airway pressure, alveoli in this region are collapsed and are hence not ventilated. Under these conditions, alveoli at the apex that are located at the vertical compliant portion of the pressure-volume curve undergo preferential expansion with inspiration. Alveoli at the base are situated at the lower horizontal portion of the pressure-volume curve where a large pressure change is needed to open them up (critical opening pressure) before they start receiving part of the ventilation. This explains why when inspiration begins from RV, ventilation is initially distributed preferentially to the apex with the base receiving ventilation only during the latter part of inspiration.
We have until now seen how differences in intrapleural pressure in the upright lung at different starting lung volumes (FRC versus RV) bring about differences in distribution of ventilation. Consider the functional lung unit to consist of an elastic chamber (the alveolus) connected to the atmosphere by a tube (bronchiole). The amount of ventilation of such a unit will depend on the distensibility of the chamber (compliance) and the resistance to flow of gas offered by the tube (airway resistance). Regional compliance and airway resistance vary even within the normal lung. These variations are even more marked in the diseased lung. Thus, one needs to understand how these regional variations in pulmonary mechanics bring about changes in the regional distribution of ventilation between the two lungs, and also between adjacent units within the same lung.
The three lung units shown in Figure 6 illustrate the effect of changes in regional compliance and airway resistance on the distribution of ventilation. Lung unit A has a normal compliance and normal airway resistance. The rate at which its volume changes during inspiration is shown and it can be seen that the
Fig 6. Effect of changes in compliance and airway resistance on regional distribution of ventilation.Unit “A” has normal compliance and airway resistance, Unit “B" has decreased compliance and normal airway resistance while Unit “C" has normal compliance and increased airway resistance
volume change is large and rapid so that it is complete before the expiration for the whole lung begins. By contrast, unit B has a low compliance and normal airway resistance. The change in volume of unit B, though small, is brought about rapidly. Such units are therefore called “fast” alveoli as they consistently achieve their maximum volume fairly rapidly. Finally unit C with its high airway resistance fills so slowly that it does not reach its final volume even when the rest of the lung has begun its exhalation. Such an alveolar unit is called a “slow” alveolus and given adequate time for inspiration; such slow alveolar units will also reach their maximum volume. Because slow and fast alveoli are seen even in the normal lungs (and because they constitute a larger proportion of lung units in the diseased lung), the regional distribution of ventilation will be affected. The time available for lung units to fill to their maximum volume depends on the frequency of breathing. The higher the frequency of breathing, the lesser is the time available for volume exchange to occur. Thus, it is obvious that as frequency of breathing increases, the slow alveolar units will not get adequate time to fill to their maximum extent. This in turn will be reflected as a regional inequality of the distribution of ventilation.
DISTRIBUTION OF VENTILATION-PERFUSION RATIO
We have seen how both ventilation and perfusion increase as we move from the apex to the base of the lung, with the perfusion increasing
RACE 2003 Ramachandra Anaesthesia Continuing Education
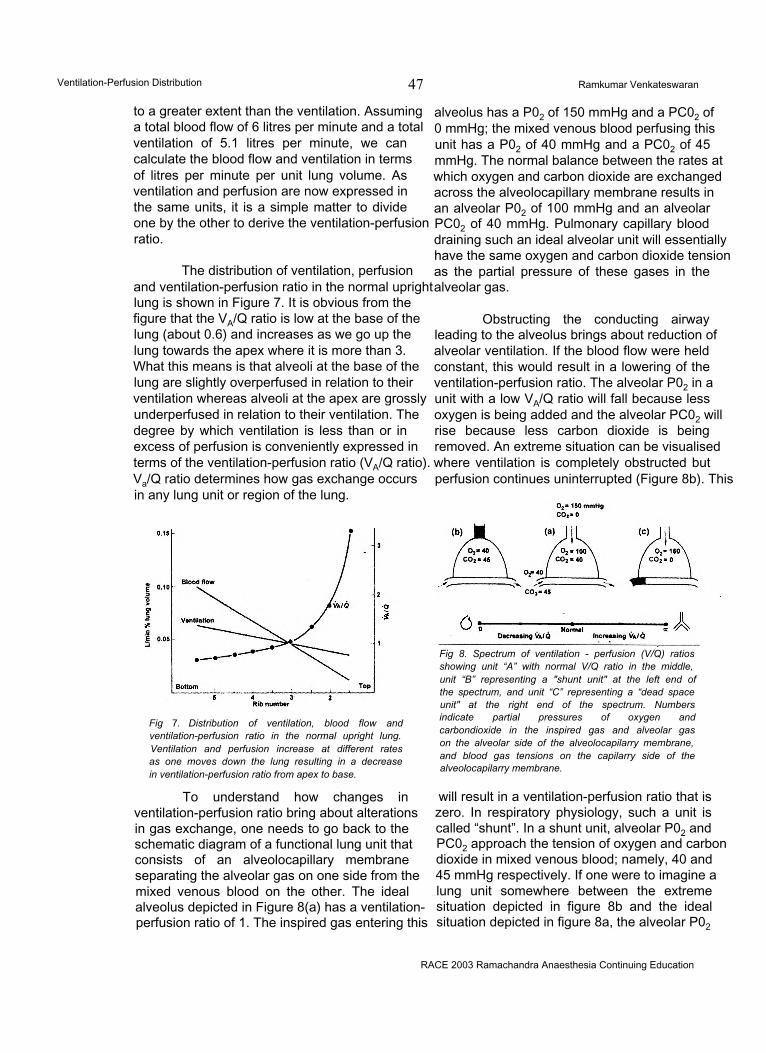
Ventilation-Perfusion Distribution 47 Ramkumar Venkateswaran
to a greater extent than the ventilation. Assuming a total blood flow of 6 litres per minute and a total ventilation of 5.1 litres per minute, we can calculate the blood flow and ventilation in terms of litres per minute per unit lung volume. As ventilation and perfusion are now expressed in the same units, it is a simple matter to divide one by the other to derive the ventilation-perfusion ratio.
The distribution of ventilation, perfusion and ventilation-perfusion ratio in the normal upright lung is shown in Figure 7. It is obvious from the figure that the VA/Q ratio is low at the base of the lung (about 0.6) and increases as we go up the lung towards the apex where it is more than 3. What this means is that alveoli at the base of the lung are slightly overperfused in relation to their ventilation whereas alveoli at the apex are grossly underperfused in relation to their ventilation. The degree by which ventilation is less than or in excess of perfusion is conveniently expressed in terms of the ventilation-perfusion ratio (VA/Q ratio). Va/Q ratio determines how gas exchange occurs in any lung unit or region of the lung.
Fig 7. Distribution of ventilation, blood flow and ventilation-perfusion ratio in the normal upright lung. Ventilation and perfusion increase at different rates as one moves down the lung resulting in a decrease in ventilation-perfusion ratio from apex to base.
To understand how changes in ventilation-perfusion ratio bring about alterations in gas exchange, one needs to go back to the schematic diagram of a functional lung unit that consists of an alveolocapillary membrane separating the alveolar gas on one side from the mixed venous blood on the other. The ideal alveolus depicted in Figure 8(a) has a ventilation- perfusion ratio of 1. The inspired gas entering this
RACE 2003 Ramachandra Anaesthesia Continuing Education
alveolus has a P02 of 150 mmHg and a PC02 of 0 mmHg; the mixed venous blood perfusing this unit has a P02 of 40 mmHg and a PC02 of 45 mmHg. The normal balance between the rates at which oxygen and carbon dioxide are exchanged across the alveolocapillary membrane results in an alveolar P02 of 100 mmHg and an alveolar PC02 of 40 mmHg. Pulmonary capillary blood draining such an ideal alveolar unit will essentially have the same oxygen and carbon dioxide tension as the partial pressure of these gases in the alveolar gas.
Obstructing the conducting airway leading to the alveolus brings about reduction of alveolar ventilation. If the blood flow were held constant, this would result in a lowering of the ventilation-perfusion ratio. The alveolar P02 in a unit with a low VA/Q ratio will fall because less oxygen is being added and the alveolar PC02 will rise because less carbon dioxide is being removed. An extreme situation can be visualised where ventilation is completely obstructed but perfusion continues uninterrupted (Figure 8b). This
Fig 8. Spectrum of ventilation - perfusion (V/Q) ratios showing unit “A” with normal V/Q ratio in the middle, unit “B” representing a "shunt unit" at the left end of the spectrum, and unit “C” representing a “dead space unit" at the right end of the spectrum. Numbers indicate partial pressures of oxygen and carbondioxide in the inspired gas and alveolar gas on the alveolar side of the alveolocapilarry membrane, and blood gas tensions on the capilarry side of the alveolocapilarry membrane.
will result in a ventilation-perfusion ratio that is zero. In respiratory physiology, such a unit is called “shunt”. In a shunt unit, alveolar P02 and PC02 approach the tension of oxygen and carbon dioxide in mixed venous blood; namely, 40 and 45 mmHg respectively. If one were to imagine a lung unit somewhere between the extreme situation depicted in figure 8b and the ideal situation depicted in figure 8a, the alveolar P02

Ventilation-Perfusion Distribution 48 Ramkumar Venkateswaran
would be in between 40 and 100 mmHg (while the alveolar PC02 would lie in between 45 to 40 mmHg). Alveoli at the base of the lung have a VA/ Q ratio of less than 1 and would therefore fall along the spectrum of VA/Q ratios to the left of the normal alveolus as shown at the bottom of figure 8.
What would happen if on the other hand, one gradually obstructs perfusion leaving ventilation undisturbed, thus increasing the VA/Q ratio? The alveolar P02 would rise because less oxygen is being removed, and the alveolar PC02 would fall because less carbon dioxide is being excreted. An extreme situation results when perfusion to a lung unit is completely obstructed with ventilation continuing uninterrupted. This will lead to a VA/Q ratio of infinity. In respiratory physiology, such a unit where ventilation is wasted constitutes “dead space”. In an extreme situation as described above, the composition of the alveolar gas becomes identical with that of inspired gas with a P02 of 150 mmHg and a PC02 of 0 mmHg. Alveoli at the apex of the lung have Va/Q ratios that are typically more than 3. The alveolar P02 and PC02 in alveolar units nearer the apex of the lung will therefore lie somewhere between the ideal alveolar unit shown in figure 8a and the dead space unit shown in figure 8c (with alveolar P02 being between 100 and 150 mmHg and alveolar PC02 being between 40 and 0 mmHg). Apical alveoli will lie along a spectrum of Va/Q ratios to the right of the normal alveolus as shown at the bottom of figure 8.
A reference to figure 2 shows that alveolar units at the apex of the lung with higher VA/Q
ratios have a P02 of 132 mmHg and PC02 of 28 mmHg while those at the base of the lung with lower Va/Q ratios have P02 and PC02 values of 89 mmHg and 42 mmHg respectively.
SUMMARYWe have until now seen how even in the
healthy lung, ventilation and perfusion are not uniformly distributed throughout the lung. We know that though both ventilation and perfusion increase progressively as we move from the apex to the base of the lung, the increase is more significant and rapid with perfusion. The ventilation-perfusion ratio therefore decreases as we move from the apex to the base of the lung. For alveolar units to exchange oxygen and carbon dioxide in a perfect manner, they should have their ventilation and perfusion also perfectly matched. Such an ideal situation does not exist even in the normal lung. Despite variations in ventilation- perfusion ratio, healthy lungs still bring about effective and nearly perfect gas exchange. The situation is different when one considers a diseased lung where gross VA/Q inequalities occur. These VA/Q inequalities have adverse effects on gas exchange that manifest as hypoxaemia and hypercarbia. An understanding of the effects of altered distribution of ventilation and perfusion on gas exchange helps one to appreciate and treat pathological lung conditions. It is hoped that this review has provided the reader with such an insight.
References1. West JB. Ventilation/blood flow and gas exchange. 3rd Edition. Oxford : Blackwell Scientific Publications, 1977.2. Lumb AB. Nunn’s Applied Respiratory Physiology. 5th Edition. Oxford : Butterworth Heinemann, 2000.
RACE 2003 Ramachandra Anaesthesia Continuing Education
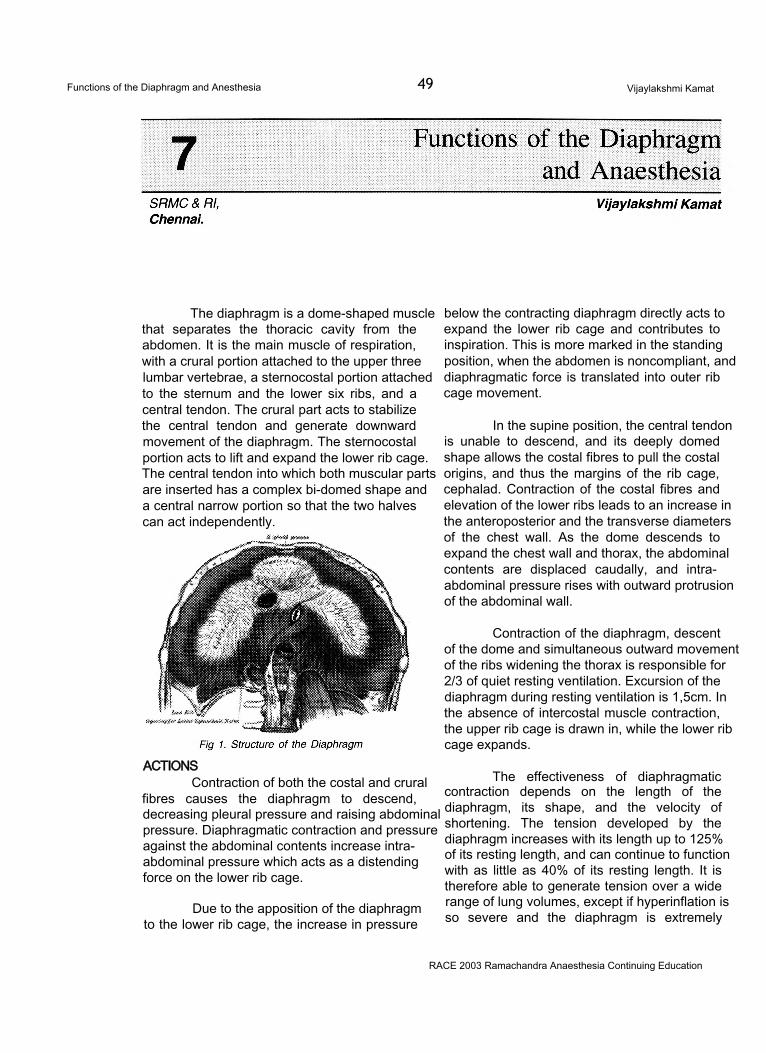
Functions of the Diaphragm and Anesthesia 49 Vijaylakshmi Kamat
The diaphragm is a dome-shaped muscle that separates the thoracic cavity from the abdomen. It is the main muscle of respiration, with a crural portion attached to the upper three lumbar vertebrae, a sternocostal portion attached to the sternum and the lower six ribs, and a central tendon. The crural part acts to stabilize the central tendon and generate downward movement of the diaphragm. The sternocostal portion acts to lift and expand the lower rib cage. The central tendon into which both muscular parts are inserted has a complex bi-domed shape and a central narrow portion so that the two halves can act independently.
ACTIONSContraction of both the costal and crural
fibres causes the diaphragm to descend, decreasing pleural pressure and raising abdominal pressure. Diaphragmatic contraction and pressure against the abdominal contents increase intraabdominal pressure which acts as a distending force on the lower rib cage.
Due to the apposition of the diaphragm to the lower rib cage, the increase in pressure
below the contracting diaphragm directly acts to expand the lower rib cage and contributes to inspiration. This is more marked in the standing position, when the abdomen is noncompliant, and diaphragmatic force is translated into outer rib cage movement.
In the supine position, the central tendon is unable to descend, and its deeply domed shape allows the costal fibres to pull the costal origins, and thus the margins of the rib cage, cephalad. Contraction of the costal fibres and elevation of the lower ribs leads to an increase in the anteroposterior and the transverse diameters of the chest wall. As the dome descends to expand the chest wall and thorax, the abdominal contents are displaced caudally, and intraabdominal pressure rises with outward protrusion of the abdominal wall.
Contraction of the diaphragm, descent of the dome and simultaneous outward movement of the ribs widening the thorax is responsible for 2/3 of quiet resting ventilation. Excursion of the diaphragm during resting ventilation is 1,5cm. In the absence of intercostal muscle contraction, the upper rib cage is drawn in, while the lower rib cage expands.
The effectiveness of diaphragmatic contraction depends on the length of the diaphragm, its shape, and the velocity of shortening. The tension developed by the diaphragm increases with its length up to 125% of its resting length, and can continue to function with as little as 40% of its resting length. It is therefore able to generate tension over a wide range of lung volumes, except if hyperinflation is so severe and the diaphragm is extremely
RACE 2003 Ramachandra Anaesthesia Continuing Education
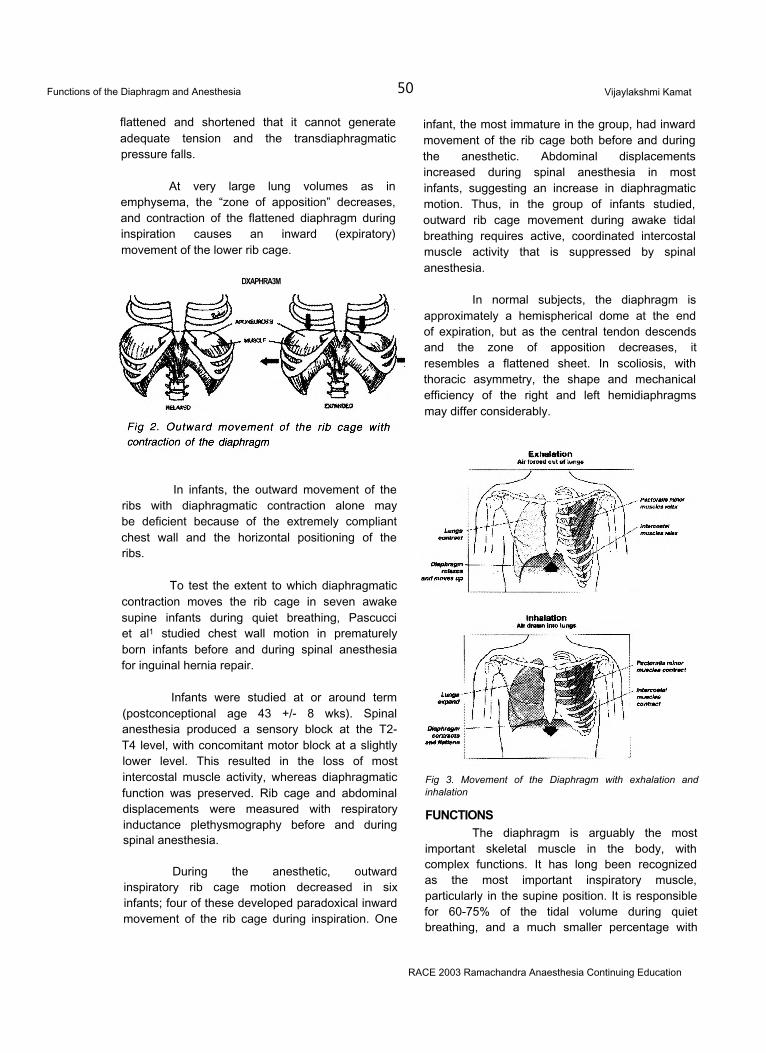
Functions of the Diaphragm and Anesthesia 50 Vijaylakshmi Kamat
flattened and shortened that it cannot generate adequate tension and the transdiaphragmatic pressure falls.
At very large lung volumes as in emphysema, the “zone of apposition” decreases, and contraction of the flattened diaphragm during inspiration causes an inward (expiratory) movement of the lower rib cage.
DXAPHRA3M
In infants, the outward movement of the ribs with diaphragmatic contraction alone may be deficient because of the extremely compliant chest wall and the horizontal positioning of the ribs.
To test the extent to which diaphragmatic contraction moves the rib cage in seven awake supine infants during quiet breathing, Pascucci et al1 studied chest wall motion in prematurely born infants before and during spinal anesthesia for inguinal hernia repair.
Infants were studied at or around term (postconceptional age 43 +/- 8 wks). Spinal anesthesia produced a sensory block at the T2- T4 level, with concomitant motor block at a slightly lower level. This resulted in the loss of most intercostal muscle activity, whereas diaphragmatic function was preserved. Rib cage and abdominal displacements were measured with respiratory inductance plethysmography before and during spinal anesthesia.
During the anesthetic, outward inspiratory rib cage motion decreased in six infants; four of these developed paradoxical inward movement of the rib cage during inspiration. One
infant, the most immature in the group, had inward movement of the rib cage both before and during the anesthetic. Abdominal displacements increased during spinal anesthesia in most infants, suggesting an increase in diaphragmatic motion. Thus, in the group of infants studied, outward rib cage movement during awake tidal breathing requires active, coordinated intercostal muscle activity that is suppressed by spinal anesthesia.
In normal subjects, the diaphragm is approximately a hemispherical dome at the end of expiration, but as the central tendon descends and the zone of apposition decreases, it resembles a flattened sheet. In scoliosis, with thoracic asymmetry, the shape and mechanical efficiency of the right and left hemidiaphragms may differ considerably.
Fig 3. Movement of the Diaphragm with exhalation and inhalation
FUNCTIONSThe diaphragm is arguably the most
important skeletal muscle in the body, with complex functions. It has long been recognized as the most important inspiratory muscle, particularly in the supine position. It is responsible for 60-75% of the tidal volume during quiet breathing, and a much smaller percentage with
RACE 2003 Ramachandra Anaesthesia Continuing Education
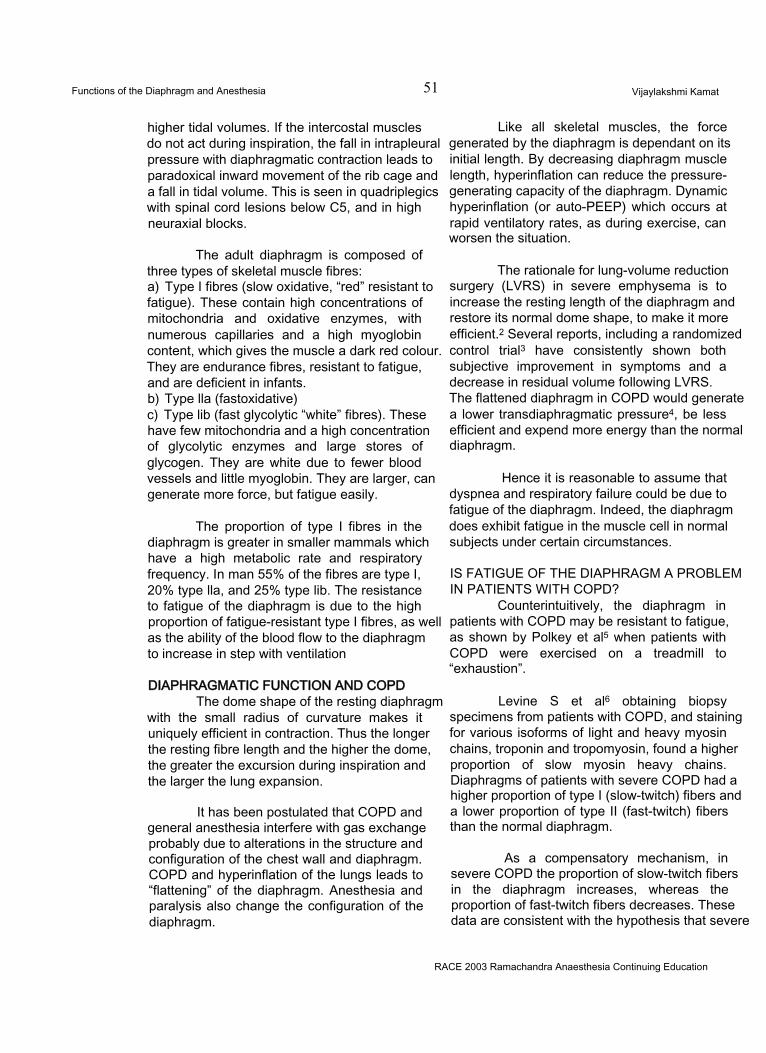
Functions of the Diaphragm and Anesthesia 51 Vijaylakshmi Kamat
higher tidal volumes. If the intercostal muscles do not act during inspiration, the fall in intrapleural pressure with diaphragmatic contraction leads to paradoxical inward movement of the rib cage and a fall in tidal volume. This is seen in quadriplegics with spinal cord lesions below C5, and in high neuraxial blocks.
The adult diaphragm is composed of three types of skeletal muscle fibres:a) Type I fibres (slow oxidative, “red” resistant to fatigue). These contain high concentrations of mitochondria and oxidative enzymes, with numerous capillaries and a high myoglobin content, which gives the muscle a dark red colour. They are endurance fibres, resistant to fatigue, and are deficient in infants.b) Type lla (fastoxidative)c) Type lib (fast glycolytic “white” fibres). These have few mitochondria and a high concentration of glycolytic enzymes and large stores of glycogen. They are white due to fewer blood vessels and little myoglobin. They are larger, can generate more force, but fatigue easily.
The proportion of type I fibres in the diaphragm is greater in smaller mammals which have a high metabolic rate and respiratory frequency. In man 55% of the fibres are type I, 20% type lla, and 25% type lib. The resistance to fatigue of the diaphragm is due to the high proportion of fatigue-resistant type I fibres, as well as the ability of the blood flow to the diaphragm to increase in step with ventilation
DIAPHRAGMATIC FUNCTION AND COPDThe dome shape of the resting diaphragm
with the small radius of curvature makes it uniquely efficient in contraction. Thus the longer the resting fibre length and the higher the dome, the greater the excursion during inspiration and the larger the lung expansion.
It has been postulated that COPD and general anesthesia interfere with gas exchange probably due to alterations in the structure and configuration of the chest wall and diaphragm. COPD and hyperinflation of the lungs leads to “flattening” of the diaphragm. Anesthesia and paralysis also change the configuration of the diaphragm.
Like all skeletal muscles, the force generated by the diaphragm is dependant on its initial length. By decreasing diaphragm muscle length, hyperinflation can reduce the pressure- generating capacity of the diaphragm. Dynamic hyperinflation (or auto-PEEP) which occurs at rapid ventilatory rates, as during exercise, can worsen the situation.
The rationale for lung-volume reduction surgery (LVRS) in severe emphysema is to increase the resting length of the diaphragm and restore its normal dome shape, to make it more efficient.2 Several reports, including a randomized control trial3 have consistently shown both subjective improvement in symptoms and a decrease in residual volume following LVRS. The flattened diaphragm in COPD would generate a lower transdiaphragmatic pressure4, be less efficient and expend more energy than the normal diaphragm.
Hence it is reasonable to assume that dyspnea and respiratory failure could be due to fatigue of the diaphragm. Indeed, the diaphragm does exhibit fatigue in the muscle cell in normal subjects under certain circumstances.
IS FATIGUE OF THE DIAPHRAGM A PROBLEM IN PATIENTS WITH COPD?
Counterintuitively, the diaphragm in patients with COPD may be resistant to fatigue, as shown by Polkey et al5 when patients with COPD were exercised on a treadmill to “exhaustion”.
Levine S et al6 obtaining biopsy specimens from patients with COPD, and staining for various isoforms of light and heavy myosin chains, troponin and tropomyosin, found a higher proportion of slow myosin heavy chains. Diaphragms of patients with severe COPD had a higher proportion of type I (slow-twitch) fibers and a lower proportion of type II (fast-twitch) fibers than the normal diaphragm.
As a compensatory mechanism, in severe COPD the proportion of slow-twitch fibers in the diaphragm increases, whereas the proportion of fast-twitch fibers decreases. These data are consistent with the hypothesis that severe
RACE 2003 Ramachandra Anaesthesia Continuing Education
Functions of the Diaphragm and Anesthesia 52 Vijaylakshmi Kamat
COPD transforms fast-twitch fibers to slow- twitch fibers in the diaphragm. These adaptations may render the diaphragm more resistant to fatigue.
However, only the diaphragms of patients with severe COPD show the switch from fast- twitch fibers to slow-twitch fibers. The functioning of the diaphragms of the patients with less severe COPD is as good as in normal subjects at the same lung volume. Compensatory phenomena appear to counterbalance the deleterious effects of hyperinflation on the contractility and inspiratory action of the diaphragm. This casts doubt on the existence of chronic fatigue of the diaphragm in such patients and therefore on the need for therapeutic interventions aimed at improving diaphragmatic function. Thus the need for LVRS is questioned by many investigators6
EFFECTS OF ANESTHESIAThe supine position and induction of
anesthesia have been associated with basal atelectasis and reductions in FRC7. The etiology of impaired gas exchange under anesthesia could be due to the effects on the diaphragmatic shape and movement. This was studied by Froese and Bryan in 19748. They found that in awake subjects lying supine or in the lateral decubitus position, the dependant part of the diaphragm moved more in a cephalocaudad direction than the nondependant parts. This led them to postulate that the dependant portion, due to the smaller radius of curvature, (Laplace law) and greater length of fibres (length-tension relationship) was able to generate a larger pressure and contracted with a larger displacement than the nondependent portion.
With anesthesia-paralysis, the effect was reversed. The resting level of the diaphragm was more cephalad, and the nondependent portion had the greater excursion. With large tidal volumes, diaphragmatic excursion was more uniform and piston-like. Their data suggest that the redistribution of ventilation (from dependant to nondependent areas of the lung with the change from spontaneous ventilation to paralysis and controlled ventilation) is a result of the effects on the diaphragm.
FLUOROSCOPIC FINDINGS DURING SPONTANEOUS BREATHING:
Excursion of the diaphragm was greatest in dependant portions (which were most cephalad).
FLUOROSCOPIC FINDINGS WITH ANESTHESIA, PARALYSIS AND IPPV:
With small tidal volumes, there was greatest excursion in non-dependant regions; with large tidal volumes, the excursions were pistonlike, equal in all zones.
In the spontaneously breathing awake patient, the predominant movement of the diaphragm was in the dependant portion of the diaphragm (this, in the supine individual would be the crural fibres). Anesthesia induced a cephalad shift in the end-expiratory (FRC) position of the diaphragm and, in the case of spontaneous ventilation, the maximum excursion was still in the dependant portion. Paralysis, followed by positive pressure ventilation, however, caused the greatest excursion in the nondependent portion of the diaphragm. Thus diaphragmatic excursions vary with active or passive movements.
This was explained on the basis of the hydrostatic abdominal pressure gradient, i.e. the abdominal contents, like a water-filled plastic bag, would sink to the bottom and exert the greatest pressure on the most dependant part of the diaphragm, pushing it cephalad.
With anesthesia and paralysis, the cephalad shift of the end-expiratory position of the diaphragm was explained by reduction in normal end-expiratory muscle tone. This shift would reduce FRC and promote atelectasis, which may persist well into the postoperative period7.
It is important to realize that in Froese’s study, only the dependant portion of the diaphragm moved in a cephalad direction; the non-dependant portion moved caudad.
Anaesthesia increases the curvature of the spine, which provides an anchor for all other chest wall structures and may affect diaphragm
RACE 2003 Ramachandra Anaesthesia Continuing Education
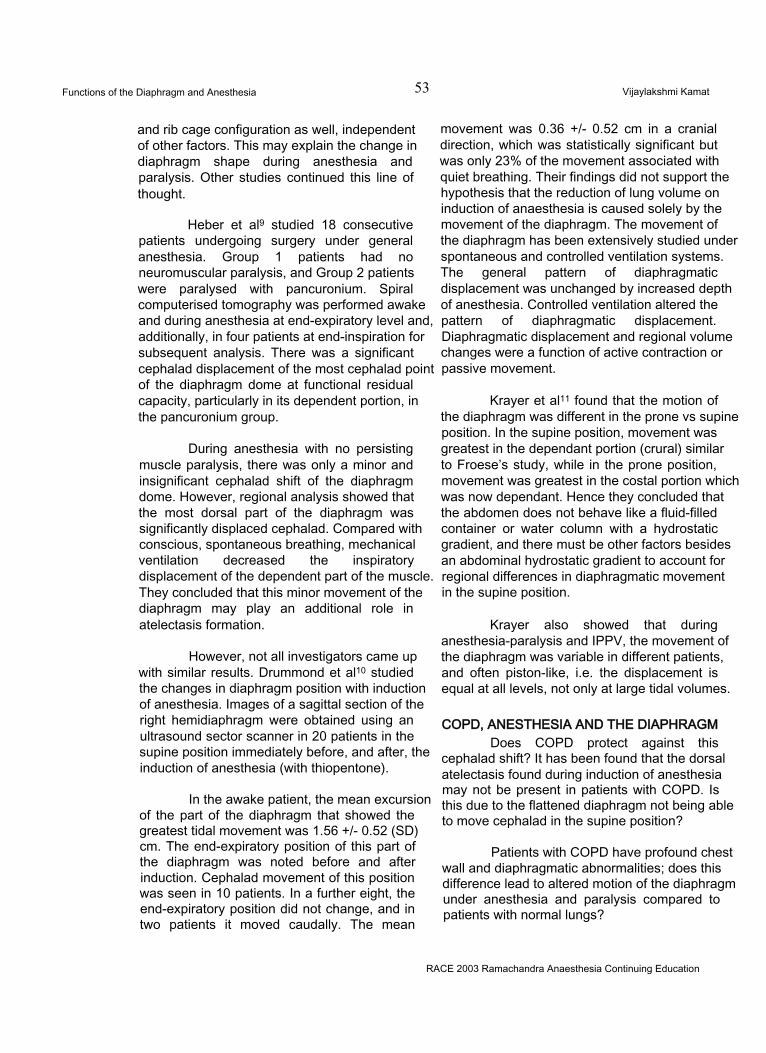
Functions of the Diaphragm and Anesthesia 53 Vijaylakshmi Kamat
and rib cage configuration as well, independent of other factors. This may explain the change in diaphragm shape during anesthesia and paralysis. Other studies continued this line of thought.
Heber et al9 studied 18 consecutive patients undergoing surgery under general anesthesia. Group 1 patients had no neuromuscular paralysis, and Group 2 patients were paralysed with pancuronium. Spiral computerised tomography was performed awake and during anesthesia at end-expiratory level and, additionally, in four patients at end-inspiration for subsequent analysis. There was a significant cephalad displacement of the most cephalad point of the diaphragm dome at functional residual capacity, particularly in its dependent portion, in the pancuronium group.
During anesthesia with no persisting muscle paralysis, there was only a minor and insignificant cephalad shift of the diaphragm dome. However, regional analysis showed that the most dorsal part of the diaphragm was significantly displaced cephalad. Compared with conscious, spontaneous breathing, mechanical ventilation decreased the inspiratory displacement of the dependent part of the muscle. They concluded that this minor movement of the diaphragm may play an additional role in atelectasis formation.
However, not all investigators came up with similar results. Drummond et al10 studied the changes in diaphragm position with induction of anesthesia. Images of a sagittal section of the right hemidiaphragm were obtained using an ultrasound sector scanner in 20 patients in the supine position immediately before, and after, the induction of anesthesia (with thiopentone).
In the awake patient, the mean excursion of the part of the diaphragm that showed the greatest tidal movement was 1.56 +/- 0.52 (SD) cm. The end-expiratory position of this part of the diaphragm was noted before and after induction. Cephalad movement of this position was seen in 10 patients. In a further eight, the end-expiratory position did not change, and in two patients it moved caudally. The mean
movement was 0.36 +/- 0.52 cm in a cranial direction, which was statistically significant but was only 23% of the movement associated with quiet breathing. Their findings did not support the hypothesis that the reduction of lung volume on induction of anaesthesia is caused solely by the movement of the diaphragm. The movement of the diaphragm has been extensively studied under spontaneous and controlled ventilation systems. The general pattern of diaphragmatic displacement was unchanged by increased depth of anesthesia. Controlled ventilation altered the pattern of diaphragmatic displacement. Diaphragmatic displacement and regional volume changes were a function of active contraction or passive movement.
Krayer et al11 found that the motion of the diaphragm was different in the prone vs supine position. In the supine position, movement was greatest in the dependant portion (crural) similar to Froese’s study, while in the prone position, movement was greatest in the costal portion which was now dependant. Hence they concluded that the abdomen does not behave like a fluid-filled container or water column with a hydrostatic gradient, and there must be other factors besides an abdominal hydrostatic gradient to account for regional differences in diaphragmatic movement in the supine position.
Krayer also showed that during anesthesia-paralysis and IPPV, the movement of the diaphragm was variable in different patients, and often piston-like, i.e. the displacement is equal at all levels, not only at large tidal volumes.
COPD, ANESTHESIA AND THE DIAPHRAGMDoes COPD protect against this
cephalad shift? It has been found that the dorsal atelectasis found during induction of anesthesia may not be present in patients with COPD. Is this due to the flattened diaphragm not being able to move cephalad in the supine position?
Patients with COPD have profound chest wall and diaphragmatic abnormalities; does this difference lead to altered motion of the diaphragm under anesthesia and paralysis compared to patients with normal lungs?
RACE 2003 Ramachandra Anaesthesia Continuing Education
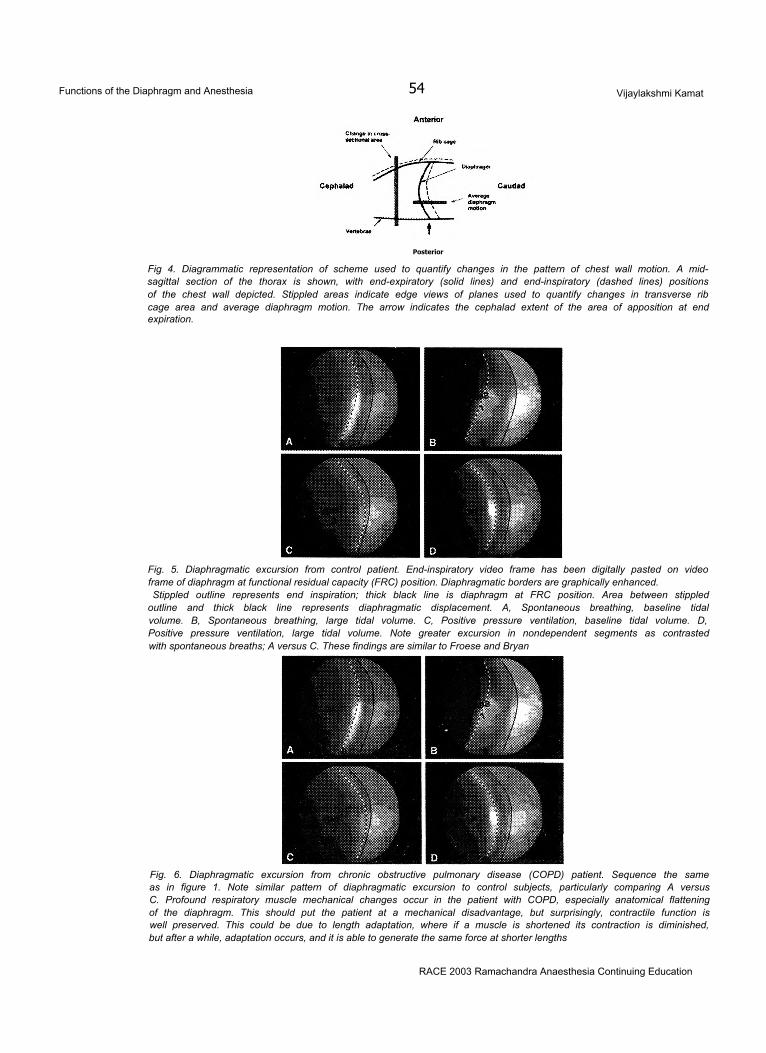
Functions of the Diaphragm and Anesthesia 54 Vijaylakshmi Kamat
Posterior
Fig 4. Diagrammatic representation of scheme used to quantify changes in the pattern of chest wall motion. A mid- sagittal section of the thorax is shown, with end-expiratory (solid lines) and end-inspiratory (dashed lines) positions of the chest wall depicted. Stippled areas indicate edge views of planes used to quantify changes in transverse rib cage area and average diaphragm motion. The arrow indicates the cephalad extent of the area of apposition at end expiration.
Fig. 5. Diaphragmatic excursion from control patient. End-inspiratory video frame has been digitally pasted on video frame of diaphragm at functional residual capacity (FRC) position. Diaphragmatic borders are graphically enhanced.Stippled outline represents end inspiration; thick black line is diaphragm at FRC position. Area between stippled
outline and thick black line represents diaphragmatic displacement. A, Spontaneous breathing, baseline tidal volume. B, Spontaneous breathing, large tidal volume. C, Positive pressure ventilation, baseline tidal volume. D, Positive pressure ventilation, large tidal volume. Note greater excursion in nondependent segments as contrasted with spontaneous breaths; A versus C. These findings are similar to Froese and Bryan
Fig. 6. Diaphragmatic excursion from chronic obstructive pulmonary disease (COPD) patient. Sequence the same as in figure 1. Note similar pattern of diaphragmatic excursion to control subjects, particularly comparing A versus C. Profound respiratory muscle mechanical changes occur in the patient with COPD, especially anatomical flattening of the diaphragm. This should put the patient at a mechanical disadvantage, but surprisingly, contractile function is well preserved. This could be due to length adaptation, where if a muscle is shortened its contraction is diminished, but after a while, adaptation occurs, and it is able to generate the same force at shorter lengths
RACE 2003 Ramachandra Anaesthesia Continuing Education
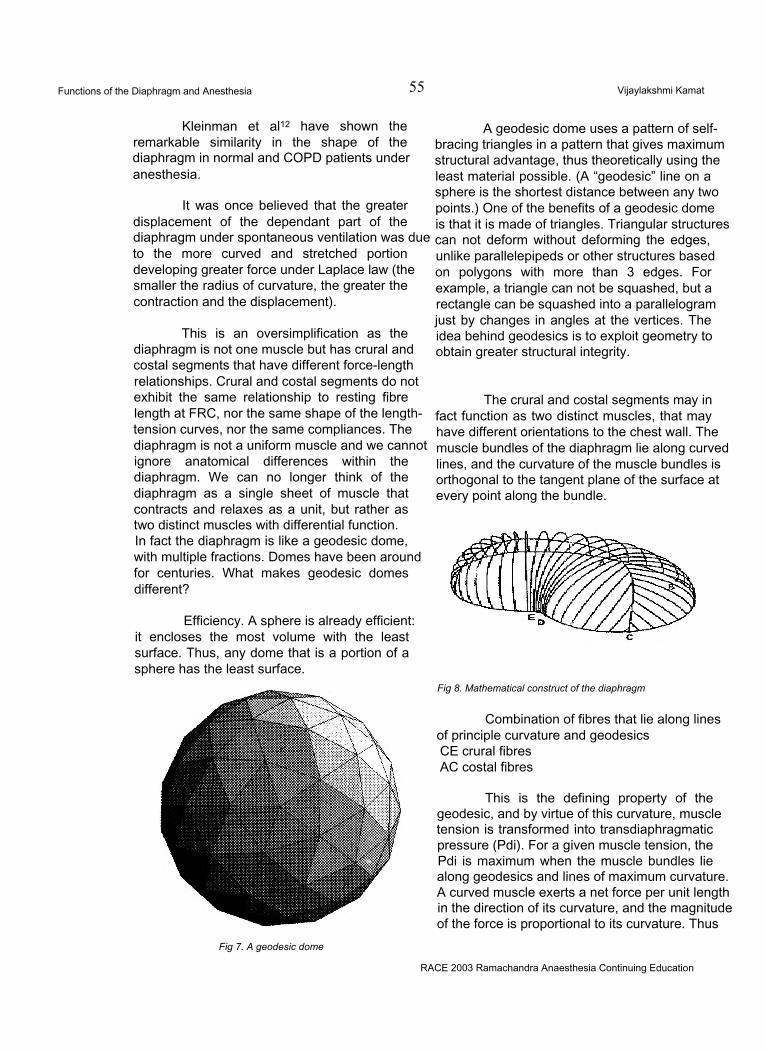
Functions of the Diaphragm and Anesthesia 55 Vijaylakshmi Kamat
Kleinman et al12 have shown the remarkable similarity in the shape of the diaphragm in normal and COPD patients under anesthesia.
It was once believed that the greater displacement of the dependant part of the diaphragm under spontaneous ventilation was due to the more curved and stretched portion developing greater force under Laplace law (the smaller the radius of curvature, the greater the contraction and the displacement).
This is an oversimplification as the diaphragm is not one muscle but has crural and costal segments that have different force-length relationships. Crural and costal segments do not exhibit the same relationship to resting fibre length at FRC, nor the same shape of the length- tension curves, nor the same compliances. The diaphragm is not a uniform muscle and we cannot ignore anatomical differences within the diaphragm. We can no longer think of the diaphragm as a single sheet of muscle that contracts and relaxes as a unit, but rather as two distinct muscles with differential function.In fact the diaphragm is like a geodesic dome, with multiple fractions. Domes have been around for centuries. What makes geodesic domes different?
Efficiency. A sphere is already efficient: it encloses the most volume with the least surface. Thus, any dome that is a portion of a sphere has the least surface.
Fig 7. A geodesic dome
A geodesic dome uses a pattern of selfbracing triangles in a pattern that gives maximum structural advantage, thus theoretically using the least material possible. (A “geodesic” line on a sphere is the shortest distance between any two points.) One of the benefits of a geodesic dome is that it is made of triangles. Triangular structures can not deform without deforming the edges, unlike parallelepipeds or other structures based on polygons with more than 3 edges. For example, a triangle can not be squashed, but a rectangle can be squashed into a parallelogram just by changes in angles at the vertices. The idea behind geodesics is to exploit geometry to obtain greater structural integrity.
The crural and costal segments may in fact function as two distinct muscles, that may have different orientations to the chest wall. The muscle bundles of the diaphragm lie along curved lines, and the curvature of the muscle bundles is orthogonal to the tangent plane of the surface at every point along the bundle.
Fig 8. Mathematical construct of the diaphragm
Combination of fibres that lie along lines of principle curvature and geodesics CE crural fibres AC costal fibres
This is the defining property of the geodesic, and by virtue of this curvature, muscle tension is transformed into transdiaphragmatic pressure (Pdi). For a given muscle tension, the Pdi is maximum when the muscle bundles lie along geodesics and lines of maximum curvature. A curved muscle exerts a net force per unit length in the direction of its curvature, and the magnitude of the force is proportional to its curvature. Thus
RACE 2003 Ramachandra Anaesthesia Continuing Education
Functions of the Diaphragm and Anesthesia 56 Vijaylakshmi Kamat
the contribution of this force to transdiaphragmatic pressure is maximal if the muscle bundle lies along a line of maximum curvature, and the direction of its curvature is normal to the surface. Since the line of muscle bundle is a geodesic, there is no distortion of the surface during 2contraction. This is especially so in the zone of apposition to the ribs, where the Pdi must change the diaphragm shape to conform to the shape of the chest wall.
There is a configurational difference between costal and crural parts of the diaphragm that is independent of the contractile state. The distribution of muscle tension in the diaphragm is a result of its shape, and failure to develop an adequate Pdi could be due to either loss of either tension or curvature.
The muscles of the diaphragm shorten significantly as lung volume increases, and active muscle tension decreases with decreasing length.It would also seem likely that diaphragmatic curvature decreases as the diaphragm descends. In patients with emphysema and hyperexpanded lungs, the diaphragm descends and lateral Xrays show the curvature to be less than normal. The rib cage is also expanded in COPD and this leads to reduced Pdi and reduced range of shortening.
The diaphragm is relaxed at FRC and strectced at low lung volumes. At lung volumes above FRC the shape of the passive diaphragm is determined by the shapes and elastances of the lung, abdominal contents and abdominal wall. Pdi (transdiaphragmatic pressure) is the difference between the pleural pressure and the abdominal pressure, and in practice, between the esophageal pressure (Pes) and the gastric pressure (Pga).
The diaphragm is the only muscle which on contracting simultaneously lowers Pes and increases Pga, and Pdi is the result of diaphragmatic contraction.
DIAPHRAGMATIC PARALYSISThe physiological effects of
diaphragmatic paralysis are influenced by
pulmonary disease, the severity of paralysis and the age of the patient. The most frequently noted abnormality with respiratory muscle weakness, is a reduction in vital capacity, (both inspiratory and expiratory muscle weakness). The most important distinction is whether the paralysis is unilateral or bilateral. Unilateral paralysis is seen after interscalene brachial plexus block, causing a 25% reduction in vital capacity and forced expiratory volume in 1 second. This could be deleterious in patients with poor lung function. Unilateral paralysis could be devastating in infants who would need ventilatory support until the diaphragmatic function is restored or surgical plication is performed.
In patients with isolated or disproportionate bilateral diaphragmatic weakness or paralysis, the vital capacity shows a marked fall in the supine compared to the erect posture because of action of gravitational forces on the abdominal contents. In some patients the postural fall may exceed 50%. In most normal subjects, the VC in the supine position is 5-10% less than in the erect posture, and a fall of 30% or more is associated with severe diaphragmatic weakness. For such patients, phrenic nerve pacing can be performed, as long as there is no obstructive airways disease or decreased lung compliance.
FATIGUEAbnormal patterns of thoracoabdominal
breathing may signify fatigue.a)increased variability in preponderance of thoracic vs abdominal breaths alternating with each other. Some breaths are characterized by clear ribcage preponderance and others with abdominal muscle preponderance. This pattern reflects alternate recruitment of inspiratory rib cage muscles and of the diaphragm.b)frank paradoxical movement of the abdominal muscles..ie inward movement of the abdominal wall during inspiration. Abdominal paradox indicates weak, absent or inefficient contraction of the diaphragm.
These two patterns can be seen in patients showing diaphragmatic fatigue and consequent failure of weaning from mechanical ventilation.
RACE 2003 Ramachandra Anaesthesia Continuing Education
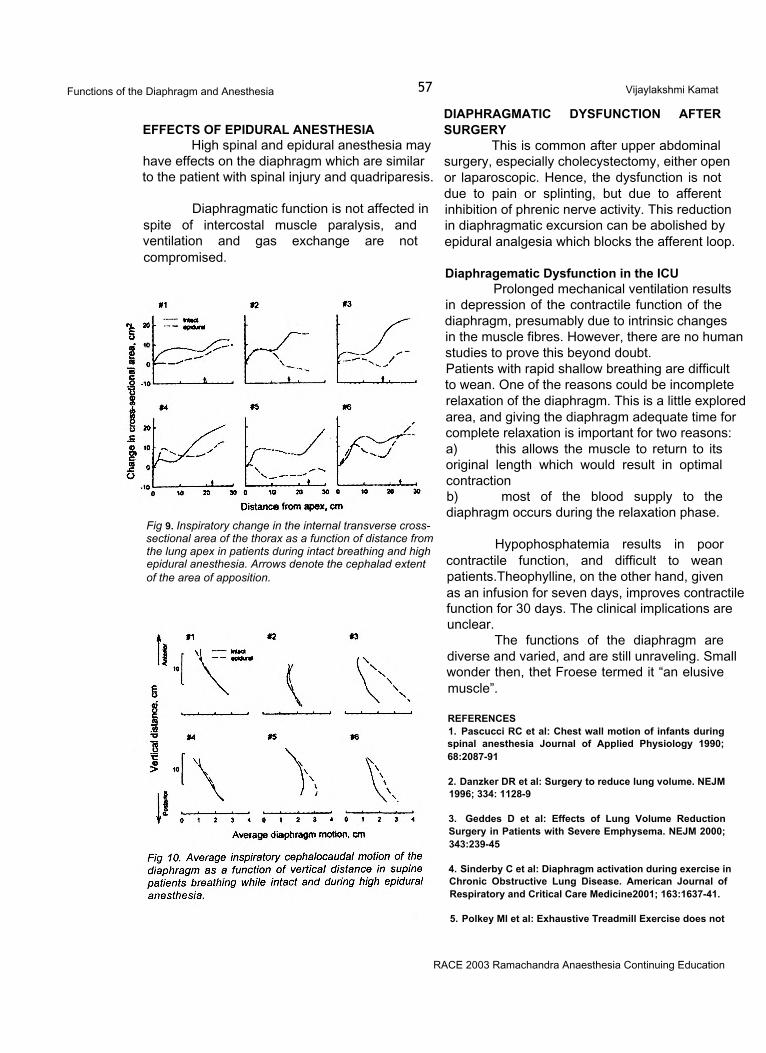
Functions of the Diaphragm and Anesthesia 57 Vijaylakshmi Kamat
EFFECTS OF EPIDURAL ANESTHESIAHigh spinal and epidural anesthesia may
have effects on the diaphragm which are similar to the patient with spinal injury and quadriparesis.
Diaphragmatic function is not affected in spite of intercostal muscle paralysis, and ventilation and gas exchange are not compromised.
Fig 9. Inspiratory change in the internal transverse cross- sectional area of the thorax as a function of distance from the lung apex in patients during intact breathing and high epidural anesthesia. Arrows denote the cephalad extent of the area of apposition.
DIAPHRAGMATIC DYSFUNCTION AFTER SURGERY
This is common after upper abdominal surgery, especially cholecystectomy, either open or laparoscopic. Hence, the dysfunction is not due to pain or splinting, but due to afferent inhibition of phrenic nerve activity. This reduction in diaphragmatic excursion can be abolished by epidural analgesia which blocks the afferent loop.
Diaphragematic Dysfunction in the ICUProlonged mechanical ventilation results
in depression of the contractile function of the diaphragm, presumably due to intrinsic changes in the muscle fibres. However, there are no human studies to prove this beyond doubt.Patients with rapid shallow breathing are difficult to wean. One of the reasons could be incomplete relaxation of the diaphragm. This is a little explored area, and giving the diaphragm adequate time for complete relaxation is important for two reasons:a) this allows the muscle to return to its original length which would result in optimal contractionb) most of the blood supply to the diaphragm occurs during the relaxation phase.
Hypophosphatemia results in poor contractile function, and difficult to wean patients.Theophylline, on the other hand, given as an infusion for seven days, improves contractile function for 30 days. The clinical implications are unclear.
The functions of the diaphragm are diverse and varied, and are still unraveling. Small wonder then, thet Froese termed it “an elusive muscle”.
REFERENCES1. Pascucci RC et al: Chest wall motion of infants during spinal anesthesia Journal of Applied Physiology 1990; 68:2087-91
2. Danzker DR et al: Surgery to reduce lung volume. NEJM 1996; 334: 1128-9
3. Geddes D et al: Effects of Lung Volume Reduction Surgery in Patients with Severe Emphysema. NEJM 2000; 343:239-45
4. Sinderby C et al: Diaphragm activation during exercise in Chronic Obstructive Lung Disease. American Journal of Respiratory and Critical Care Medicine2001; 163:1637-41.
5. Polkey Ml et al: Exhaustive Treadmill Exercise does not
RACE 2003 Ramachandra Anaesthesia Continuing Education

Functions of the Diaphragm and Anesthesia 58 Vijaylakshmi Kamat
reduce twitch transdiaphragmatic pressure in patients with COPD. American Journal of Respiratory and Critical Care Medicine 1995; 152:959-64.
6. Fessler HE et al: Lung volume reduction surgery: is less really more? Am J Respir Crit Care Med 1999; 159:1031- 1035.
7. Hedenstierna G et al : Functional Residual Capacity, thoracoabdominal dimensions, and central blood volume during general anesthesia with muscle paralysis and mechanical ventilation. Anesthesiology 1985; 62:247-54
8. Froese AB, Bryan AC: Effects of anesthesia and paralysis on diaphragmatic mechanics in man. Anesthesiology 1974; 41:242-55
9.. Reber A, Nylund U, Hedenstierna G. Position and shape
of the diaphragm: implications for atelectasis formation. Anaesthesia. 1998 Nov;53(11): 1054-61.
10. Drummond GB et al: Changes in diaphragmatic position in association with the induction of anaesthesia. Br J Anaesth. 1986 Nov;58(11):1246-51.
11. Krayeretal: Position and motion of the human diaphragm during anesthesia-paralysis. Anesthesiology 1989;70:891- 98
12. Kleinman BS, Frey K, VanDrunen M, Sheikh T, DiPinto D, Mason R, Smith T.Motion of the diaphragm in patients with chronic obstructive pulmonary disease while spontaneously breathing versus during positive pressure breathing after anesthesia and neuromuscular blockade.Anesthesiology. 2002 Aug;97(2):298-305.
RACE 2003 Ramachandra Anaesthesia Continuing Education
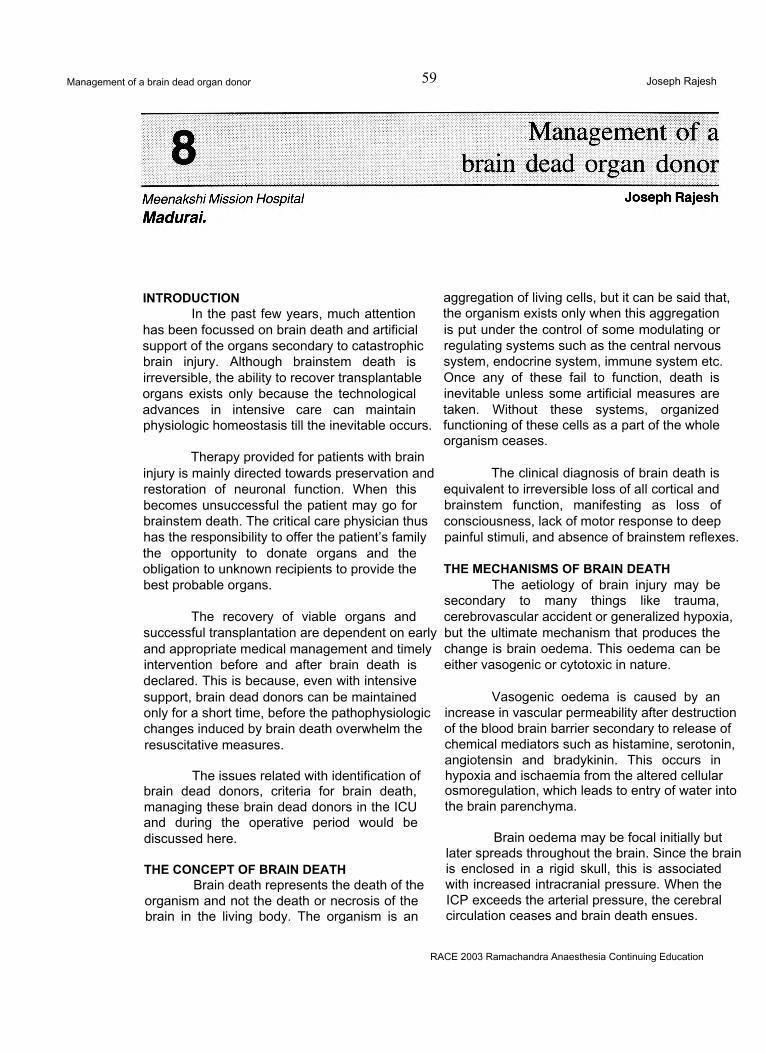
Management of a brain dead organ donor 59 Joseph Rajesh
INTRODUCTIONIn the past few years, much attention
has been focussed on brain death and artificial support of the organs secondary to catastrophic brain injury. Although brainstem death is irreversible, the ability to recover transplantable organs exists only because the technological advances in intensive care can maintain physiologic homeostasis till the inevitable occurs.
Therapy provided for patients with brain injury is mainly directed towards preservation and restoration of neuronal function. When this becomes unsuccessful the patient may go for brainstem death. The critical care physician thus has the responsibility to offer the patient’s family the opportunity to donate organs and the obligation to unknown recipients to provide the best probable organs.
The recovery of viable organs and successful transplantation are dependent on early and appropriate medical management and timely intervention before and after brain death is declared. This is because, even with intensive support, brain dead donors can be maintained only for a short time, before the pathophysiologic changes induced by brain death overwhelm the resuscitative measures.
The issues related with identification of brain dead donors, criteria for brain death, managing these brain dead donors in the ICU and during the operative period would be discussed here.
THE CONCEPT OF BRAIN DEATHBrain death represents the death of the
organism and not the death or necrosis of the brain in the living body. The organism is an
aggregation of living cells, but it can be said that, the organism exists only when this aggregation is put under the control of some modulating or regulating systems such as the central nervous system, endocrine system, immune system etc. Once any of these fail to function, death is inevitable unless some artificial measures are taken. Without these systems, organized functioning of these cells as a part of the whole organism ceases.
The clinical diagnosis of brain death is equivalent to irreversible loss of all cortical and brainstem function, manifesting as loss of consciousness, lack of motor response to deep painful stimuli, and absence of brainstem reflexes.
THE MECHANISMS OF BRAIN DEATHThe aetiology of brain injury may be
secondary to many things like trauma, cerebrovascular accident or generalized hypoxia, but the ultimate mechanism that produces the change is brain oedema. This oedema can be either vasogenic or cytotoxic in nature.
Vasogenic oedema is caused by an increase in vascular permeability after destruction of the blood brain barrier secondary to release of chemical mediators such as histamine, serotonin, angiotensin and bradykinin. This occurs in hypoxia and ischaemia from the altered cellular osmoregulation, which leads to entry of water into the brain parenchyma.
Brain oedema may be focal initially but later spreads throughout the brain. Since the brain is enclosed in a rigid skull, this is associated with increased intracranial pressure. When the ICP exceeds the arterial pressure, the cerebral circulation ceases and brain death ensues.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 60 Joseph Rajesh
NEURO PHYSIOLOGIC BASIS OF THE BRAINDEATHRespiration:
Since the primary respiratory centre, consisting of both inspiratory and expiratory neurons, is located in the reticular core of the medulla oblongata, there will not be any spontaneous respiration. The C02 drive of respiration is lost even when the PaC02 reaches 55-60 mmHg.
Cardiovascular functions:The central neurons that control the
circulatory system are distributed in the pontine and medullary reticular core. During brainstem death, the outflow of this system is cut off and results in various haemodynamic alterations in the body.
Regulation of body temperature:The heat sensitive centre in the
hypothalamus regulates the body temperature. In brain death, the neural connection between this temperature regulating centre and the peripheral tissues is lost and the patient becomes poikilothermic.
PATHOPHYSIOLOGICAL CHANGES ASSOCIATED WITH BRAIN-STEM DEATH
The sequence of haemodynamic, metabolic and endocrine changes associated with brain death is well documented. Acute ischaemia due to sudden rise in intracranial pressure or alteration in blood flow commonly initiates a series of physiological responses. The earliest phase involves a period of parasympathetic predominance leading to bradycardia, idioventricular rhythms, or even a short period of asystole. The subsequent phase is associated with marked hyperactivity of the sympathetic system leading to a catecholamine storm. The near maximal sympathetic drive causes tachycardia, severe hypertension, ECG signs of myocardial ischaemia and frequent ectopics. Autotransfusion occurring due to constriction of venous capacitance vessels will increase the cardiac filling pressures, which when combined with the massive degree of arterial hypertension, leads to high left ventricular wall tension and therefore high myocardial oxygen consumption. On the other hand, the surge in catecholamines will cause coronary spasm thus reducing the
supply. This imbalance in oxygen supply demand ratio may be so severe as to cause myocardial ischaemia even in normal hearts. During the peak of the catecholamine surge, the vasoconstriction may be sufficiently severe to cause acute left ventricular failure due to sudden increase in afterload.
Once brain death becomes established, many of the changes are reversed. There will be a rapid fall in the level of circulating catecholamines. As a result, the sympathetic tone and SVR will fall and venous capacitance vessels also dilate. Arterial pressures and cardiac filling pressures will thus fall. Heart rate falls to denervated levels.
A few hours following brain stem death, endocrine changes will occur. They are related mainly to the failure of production of hypothalamic release factors and a decline in the production of anterior and posterior pituitary hormones. Failure of production of ADH will cause diabetes insipidus with inappropriate production of large volumes of dilute urine. Circulating levels of cortisol, triiodothyronine and insulin may all fall as release of ACTH, TRH from the pituitary declines.
Thermoregulation is impaired with a progressive fall in the core temperature. This is due to the effects of increased heat loss as a consequence of vasodilatation and in part due to reduced heat production as a result of loss of thyroid and other metabolic hormones.
IDENTIFICATION OF POTENTIAL ORGAN DONORS
The shortage of suitable organs for transplantation is well known to ICU physicians and transplant surgeons, however organs continue to be lost through failure to identify potential donors and tests for brain death. The majority of organ donors will be patients in the ICU who have suffered a catastrophic brain injury that has progressed to brain death. The major causes of severe coma are trauma, CVA, primary intracraniaI tumours and ischaemic brain injury.
CERTIFICATION OF BRAIN DEATHCertification of brain death is an absolute
requirement prior to retrieval of organs for transplantation. Clinical diagnosis of brain stem
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 61 Joseph Rajesh
death involves three steps.1. Ascertaining that certain preconditions have
been met.2. Ensuring that reversible cause of nonfunc
tioning brainstem have been excluded.3. Establishing that the comatose patient is
genuinely apnoeic and that the brain stem reflexes are absent.
Preconditions:The patient must be comatose and on a
ventilator. The cause of coma must be firmly established. The duration for subjecting the patient for brain stem death tests vary from case to case as shown in Table 1. §
Exclusions:Certain conditions can mimic brain stem
eath and hence these conditions should be excluded before subjecting the comatose patient for brainstrem fuction testing. Hypothermia (<320). shock, drug intoxication, (anasthetic agents, muscle relaxants, barbiturates, diazepam, high dose bretylium, alcohol amitryptilline), severe metabolic derangements, neurological syndromes like locked - in syndrome, GBS, encephalopathies, of hepatic failure, uraemia, and hyperosmolar coma all can lead on to misdiagnosis of brain death if not tested carefully.
Hypothermia causes loss of brainstem reflexes and pupillary dilation. The response to light is lost at core temperatures of 28-32°C and brainstem reflexes disappear when the temperature drops below 28°C.
When ingested in large quantities, many drugs can cause partial loss of brain stem
reflexes. Clinical diagnosis of brain death should be allowed if drug levels are below the therapeutic range. A reasonable approach is as follows. If the presence of the particular poison is known and the substance cannot be quantified, the patient should be observed for a period of four times the elimination half-life of the substance. If the particular drug is not known, but a high suspicion persists, the patient should be observed for 48 hrs to determine whether change in brain stem reflexes occur, and if no change is observed a confirmatory test should be performed.
Clinical testing:BRAINSTEM REFLEXES:• NO PUPILLARY RESPONSE TO LIGHT:
The pupils are not invariably dilated when the brain stem is dead; this may be because of spinal sympathetic (pupillodilator) centre. The important point is that there should be no pupillary response to really bright light, because this reaction is mediated exclusively by the brainstem. It is advisable to darken the room for this test and use proper medical torches with new batteries.
• NO CORNEAL REFLEXES:When brainstem death is suspected,
much firmer pressure is justified than in conscious patients.
• NO VESTIBULO-OCULAR REFLEXES:The caloric tests require wax free external
auditory canals. The UK code recommends irrigation of 20 ml of ice-cold saline on both sides. The stimulus should elicit no movement
Apnoeic coma caused by Time to testing (Hrs)Major intracranial surgery, Second subarachnoid bleed in a patient with angiographically proven aneurysm 4Spontaneous intracranial haemorrhage (without hypoxic brain damage from respiratory arrest) >6Head injury (Without secondary brain damage from hypoxia, intracranial haematoma or shock) 6-12Brain hypoxia (respiratory obstruction, drowning, cerebral hypoperfusion) 12-24Any of the above (when additional drug intoxication suspected and no screening faciliti as available) 50-100Table 1 Duration for subjecting the patient to tests.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 62 Joseph Rajesh
whatsoever in either eye within one minute of completion of the test. In deeply unconscious patients with some residual brainstem function, the eye will be deviated towards the irrigated ear.
• NO MOTOR RESPONSE:No motor response should be present
within the cranial nerve distribution, to adequate stimulation of any somatic area.
There should be no grimacing in response to painful stimuli, applied either to the trigeminal fields (firm supraorbital pressure) or to the limbs (the side of a pencil pressed firmly down against the patient’s fingernail or toenail is the most appropriate stimulus). Pinprick should not be used.
•NO GAG REFLEX, OR REFLEX RESPONSE TO BRONCHIAL STIMULATION BY A SUCTION CATHETER.
• THE OCULOCEPHALIC REFLEXThis is best elicited by fast and vigorous
turning of the head from the middle position to 90°on both sides. Normally, the eye deviates to the opposite side. This movement, along with vertical and horizontal eye movements, must be absent in the brain dead.
• NO RESPONSE TO A TROPINEFailure of heart rate to increase > 5 beats
after 1 -2 mg of atropine IV denotes the absent function of vagus nuclei.
• APNOEAApnoea is confirmed by showing no
respiratory movements during disconnection from the ventilator for long enough to ensure that the arterial C02 tension rises to a level of 60mmHg, capable of driving any respiratory centre neurons that may still be alive.
Method of testingHypoxia is prevented by a combination of
preoxygenation and diffuse oxygenation. If the patient is made to breathe 100% oxygen for 10 mts, very high starting levels of arterial oxygen tension are achieved. It is reinforced with the endotracheal delivery of 02 by a catheter (at 61 /mt.) As a result of endogenous metabolism, PaC02will rise by 2 - 3 mmHg/mt. Provided the
starting PaC02 was 30mmHg; the crucial level of 60mmHg will be achieved within 10 mts. This method is simple and free of complications. If events such as hypotension or cardiac arrhythmias occur, they may be due to failure to provide an adequate source of oxygen or lack of preoxygenation. One should look closely for respiratory movements. When in doubt, a spirometer can be attached to confirm the tidal volumes. Apnoea testing by carbondioxide augmentation is less acceptable and potentially dangerous.
ANCILLARY TESTSSome ancillary tests are adopted when
applying the criteria for brain death and should be used in conjunction with proper clinical judgement. These tests are needed for patients in whom specific components of clinical testing cannot be reliably evaluated as in infants.
• TO EVALUATE THE NEURONAL FUNCTION
• Electroencephalography;A flat EEG may indicate irreversible
dysfunction of the cerebrum. In brain death, the recording of isoelectric EEGs should be carried out over 60 mts, and no electrical activity having an amplitude of more than 2 -3 mv should be recorded. However the criteria for brain death clearly indicates that EEG results are not necessary for the diagnosis of brain death.
• TO EVALUATE THE INTRACRANIAL BLOOD FLOW.
• Cerebral angiographyThis selective four-vessel angiography has
some usefulness in distinguishing certain comatose conditions from brainstem death. This is regularly in practice in Scandinavian countries. Here an iodinated contrast medium is injected under high pressure in both the anterior and the posterior circulations. Intracerebral filling is absent in brain death. Since there are no specific guidelines for interpretation, the results can be conflicting.
Isotope AngiographyRapid intravenous injection of serum albumin
labelled with 99mTc is done with imaging by a gamma camera. There will not be any intracranial activity in the brain dead patient.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 63 Joseph Rajesh
Transcranial Doppler Ultrasonography.It is a non-invasive method by which the
velocity of blood flow of intracranial arteries is recorded. Normally blood flows in the same direction during both systole and diastole. After cessation of cerebral blood flow, diastolic flow is initially reversed followed by total loss of perfusion signals. Comparatively, there is huge experience available for this test to other ancillary tests and it can be used in patients who have electroencephalographic activity.
Computed Tomography Simple CT alone does not give any information
regarding the blood flow, but does help in identifying the primary and secondary organic changes. Single photon emission CT, positron emission CT have all been tried with varied success rates in small series of studies.
DECLARATION OF BRAIN DEATHDeclaration of brain death should be done
by a board of medical experts formed by the hospital administration and approved by the government. The UK code now recommends that the tests should be carried out by two medical practitioners who "have expertise in.this field.” One should be the consultant and the other can be either a consultant or a senior resident. When transplantation is planned, neither doctor should be associated with potential recipients. In practice, these doctors can be anaesthetists, neurologists or intensive care physicians.
Practice in various parts of the world differs considerably. Some countries specify the required speciality of the doctors making the diagnosis while others do not.
But all the codes urge that testing should be carried twice. This is to ensure that there has been no error. It ensures that non-functioning of brain stem is not a single finding at one point of time but persisting. The interval period between two testing has been varying in different countries between 3 -6 hrs.
DONOR MAINTENANCEOnce a potential donor is identified and
brain death is certified, medical therapy is directed at maintaining organ function while retrieval is organized. Of primary importance is maintaining adequate tissue oxygenation by the support of
various systems.
Cardiovascular SystemIn brain dead candidates, cardiovascular
instability is inevitable. Hypotension is almost universal and is associated with poor graft function. Other common events encountered are arrhythmias and cardiac arrest, which will become increasingly resistant to therapy with time.
PATHOPHYSIOLOGY:Cause for cardiovascular instability is
multifactorial. It may result from1. The primary (hypoxic) insult leading to brain
death2. Due to the therapy directed at control of
raised ICP3. Physiological changes that result from brain
stem ischaemia and death.4. Direct myocardial contusion resulting in
impaired ventricular function and arrhythmias.
The hypoxic insults severe enough to cause brain death are invariably associated with myocardial damage. The treatment of severe brain injury may include fluid restriction and diuretic therapy, and with the onset of diabetes insipidus, the brain dead patients will become hypovolemic. This will further exacerbate cardiovascular instability. Physiological changes secondary to raised ICP, like hypertension, can cause further structural damage to the heart.
CARDIOVASCULAR SUPPORT:Cardiovascular support is directed at
maintaining tissue perfusion; this requires an adequate cardiac output and tissue perfusion pressure. Immediate therapy is aimed at correcting intravascular fluid depletion with aggressive fluid resuscitation.
Invasive monitoring of arterial and central venous pressure should be instituted if not already in use. In unstable patients, use of a pulmonary artery catheter to monitor cardiac output, PAOP, and SVR is justified. Mean arterial pressure should be maintained at 60 mmHg or greater; CVP up to 15mmHg may be required to achieve this. The choice of resuscitation fluid may be influenced by
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 64 Joseph Rajesh
measurement of haemoglobin, albumin, electrolyte concentrations, coagulation studies and nature of any ongoing blood or fluid losses. Blood, blood products, colloid and crystalloid solution may all be necessary. In the absence of ongoing blood loss, colloid solution may be necessary, as infusion of large volumes of crystalloid solution in patients with increased capillary permeability, may precipitate pulmonary oedema. If Dl is contributing to fluid depletion, an anti diuretic hormone analogue may be used. In many patients, fluid resuscitation may alone restore the cardiovascular instability; but in some, use of vasopressors may be indicated.
As impaired myocardial contractility is associated with vasodilatation, agents with both inotropic and vasopressor properties may be required. Dopamine is the agent most commonly used. At low doses (2-5 ^g/kg/mt), it may preferentially improve the perfusion of transplantable abdominal organs. At higher doses (5 -20ng/kg/mt), (3 and a adrenergic effects will predominate, p stimulation may be necessary if impaired myocardial function is present, but excessive a stimulation may compromise organ perfusion. If hypotension persists despite adequate fluid resuscitation and low dose dopamine, another vasopressor such as dobutamine may be tried. Obviously the lowest dose of least injurious agent is the preferred approach but may not be possible always. In a few cases, prolonged use of vasopressors may be necessary and in these cases, use of a PA catheter may be indicated to monitor cardiac output and SVR and to titrate the use of vasopressor. The ultimate goal is to achieve a normotensive, euvolemic state. The use of hormonal therapy (tri- iodothyronine, cortisol and insulin) has been advocated and is still in experimental use.
Arrhythmias are common and found to be occurring in 27 - 56% cases in any form. Common precipitating causes include myocardial damage and electrolyte abnormalities. Diuretic use, inadequately treated Dl and presence of acidosis may further worsen this. Inotropic agents may initiate or worsen this and dose reduction may be necessary. Once these correctable coexisting conditions are treated, arrhythmias can be managed along the conventional lines.
Respiratory systemRespiratory care has aims of ensuring
adequate gas exchange and maintaining the lungs in a suitable condition for transplantation. The lungs of the potential organ donors may be damaged by a variety of processes namely, bronchopneumonia, pulmonary oedema, pulmonary contusion, atelectasis, pneumothoraces, aspiration pneumonitis etc. Trauma may be accompanied by pulmonary contusion and haemopneumothoraces. In a few, this may progress to ARDS. The sympathetic storm accompanying the coning may damage the pulmonary vasculature. As a result, pulmonary interstitial haemorrhages and increased pulmonary capillary permeability may result. All potential organ donors will be apnoeic and mechanically ventilated; they are therefore at risk of barotrauma, atelectasis and infection. Prolonged intubation will result in colonization of pathogenic bacteria.
RESPIRATORY SUPPORTAny delay in optimising the ventilatory
support should be avoided. In those with injured lungs, use of high-inspired oxygen concentration should be avoided. A Pa02 of 80mmHg and above is necessary. The use of PEEP may allow a reduction in FI02, but PEEP of greater than 15 should be avoided. If hyperventilation is employed to control ICP, it should be discontinued once brain death is confirmed and PaC02 should be maintained in the normal range. If this is not possible, moderate hypercarbia can be allowed.
Endocrine issues:Brain death is accompanied by a
number of endocrine abnormalities. Loss of central sympathetic tone results in subnormal levels of circulating catecholamines. The hypothalamus and pituitary are frequently damaged, resulting in reduced or absent secretion of pituitary hormones.
The most frequent manifestation is the development of diabetes insipidus, which is related to inadequate antidiuretic hormone production by the posterior pituitary gland. Urine output may exceed 15 ml/kg/hr; if not adequately treated, it will contribute to hypovolemia, hypotension, and end organ damage. Treatment is either by replacing the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 65 Joseph Rajesh
excess urine output with an equal volume of electrolyte solution or administration of antidiuretic hormones.
Treatment with fluid replacement may result in the infusion of large volumes of fluid with rapid swings in serum osmolarity and electrolyte concentrations. This may further cause organ damage and predispose to cardiac arrhythmias. Treatment with an antidiuretic hormone analogue is relatively simple and will result in a reduced incidence of hypotension and better function of transplantable organs. Two antidiuretic hormone analogues are available. Vasopressin has a short duration of action and may be given by intravenous infusion at an initial rate of 1 unit /hr, titrated to maintain urine output at 1-2 ml/kg/hr. A potential adverse effect is splanchnic vasoconstriction, which is undesirable in potential liver and kidney donors.
Desmopressin, an analogue, has a long duration of action and causes minimal vasoconstriction. It may be given by subcutaneous, intravascular and intravenous injections or via the endotracheal tube. Intravenous injection of 0.5 to 1 U/hr, is required to control urine output and gives the most predictable response. However, in excess doses it can produce ATN.
Reduction in hepatic blood flow, and increased sensitivity to catecholamines occur and catecholamine doses should be titrated when DDAVP is used. Hyperglycemia is a common complication of Dl and is treated with insulin infusion.
Serum levels of tri-iodothyronine, insulin and cortisol are low in animal models and triiodothyronine administration improves the haemodynamic stability by maintaining myocardial stores of energy and glycogen; however, the beneficial role of this is still unclear in clinical settings.
CoagulopathyDIC may be seen in up to 28% of the
brain dead patients and 80% of head injury donors. This is probably due to the release of thrombolysins from the necrotic or ischaemic tissues. Aggressive treatment with appropriate blood products may stabilize the condition.
HypothermiaHypothermia occurs in up to 54% of the
patients. This is due to the reduction in heat production and increased heat loss due to vasodilatation. Prior hypothermia must be corrected to allow certification of death. It can be treated by warming the intravenous fluids, gases and by using blankets. Correction of hypothermia will also improve the stability of the cardiovascular system.
Infection:Infection is another common problem
encountered in the management of brain dead patients. Common sources of infections are invasive lines and airway instruments. Delay in the certification and organ retrieval will increase the bacterial colonization and cause active infection. Avoiding such delay and following scrupulous aseptic techniques are required to prevent infection that could result in poor graft function.
TREATMENT IMPLICATIONS1. Minimize crystalloid administration except
where mandatory for the administration of drugs (unless serum osmolality exceeds 350 mOsm/Kg).
2. Treat Dl with DDAVP rather than fluid replacement.
3. Maintain circulating volume with colloid solutions as available. A target CVP of 5 - 10 cmH20 is appropriate for most cases.
4. Transfusion of blood may be required to maintain haemoglobin concentration between 9-11 g/dl.
5. Vasoactive drugs should be chosen carefully and used judicially to avoid vasoconstriction and possible ischaemic damage to donor organs.
6. Inotropic support, if already instituted, may be slowly reduced if mean arterial pressures are above 60 -70 mmHg.
7. Lung ventilation should be aimed at maintaining a normal PaC02 and Pa02. PEEP values up to 5 -10 cmH20 can be applied, provided that haemodynamic disturbances are not severe.
8. A FI02of 0.6 is ideal.9. Physiotherapy of the chest including
bronchial toileting should be done aggressively.
10. Complete aseotic techniques should be
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 66 Joseph Rajesh
followed for airway and vascular procedures.11. Chest radiography and blood gas and
biochemical status should be monitored along the lines of any other ventilated patients
12. Antibiotic therapy should be continued if clinical evidence of infection exists
13. All efforts should be made to maintain the core temperature within normal limits like infusing warmed fluids, using HMV filters, blankets etc.
14. Near normal acid base status and electrolytes especially serum potassium and glucose should be maintained within normal limits.
ORGAN SPECIFIC CONSIDERATIONS: • Kidney:
Using Hydroxyethyl starch as a volume expander during resuscitation produces nephrosis like osmosis in the renal tubules, which is associated with greater dialysis requirements in the recipient.
Mean dopamine infusion >7.5 jig/kg/mt seems to be associated with delayed graft functioning.
Low levels of vasopressin are associated with oliguria in the recipient. In some centres, routine vasopressin estimation and prophylactic vasopressin administration is performed.
Donor pre-treatment with IV lignocaine prior to kidney procurement leads to decreased incidence of dialysis and earlier return of kidney function. This is probably secondary to vasodilatory, platelet disaggregating, and Ca channel blocking properties of the drug.
• Liver:A multivariate analysis shows poor initial
graft function seen in donors with1. High levels of alanine transaminase2. ICU stay > 3 days.3. High glucose levels.
PancreasGraft survival rate is inversely
proportionate to the duration of brain death prior to organ procurement.
Pancreas islet cell yield is higher if the donor blood glucose level is at least 120 mg%
without hypotension.
CONTRAINDICATION TO DONOR ACCEPTANCE:
Extracerebral malignancy (except localskin neoplasm, Ca. Cervix in situ)Uncontrolled sepsisActive viral infectionHepatitis A or BCytomegalovirusHerpes simplexAIDS - The presence of HIV antibody is also a contraindication.
When possible hepatitis C - positive donor may be used in a hepatitis C - positive recipient.
CRITERIA FOR INDIVIDUAL ORGANS TO BE ACCEPTABLE FOR TRANSPLANTATION:
Due to the shortage of suitable organs and the increasing success of transplantation, the current trend is to accept the organs that would previously have been considered unsuitable. But the ultimate responsibility for accepting or rejecting a potential donor lies with the transplant surgeon.
Kidneys:• Age<70 years• Adequate renal perfusion• Adequate urine output (Not an
absolute requirement)Liver:
• Age<65 years• Organ size compatible with potential
donor• Haemodynamic stability• No history of alcohol abuse or
hypertensionHeart:
• Age <50 years• Organ size compatible with potential
recipient
• Haemodynamic stability- No prolonged cardiac arrest (not
an absolute requirement)- Cardiac index > 2.5L/m2/mt with- PCWP upto12 cmH20- SVR 500 - 1200 dyne.sec/cm5
- Inotropic support <5mgm/kg/mt.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 67 Joseph Rajesh
- <50% discrepancy between left and right heart filling pressures in the face of abnormal PVR
- No ECG evidence of infarctionLungs:
Age < 50 yearsOrgan size compatible withpotential recipientNo history of chronic lungdiseasesNon smoker (not an absolute requirement)Pa02 >250 mmHg with FI02 0.6 PEEP 10cm H20(max)
ANAESTHETIC MANAGEMENT OF A BRAIN DEAD PATIENT FOR MULTIPLE ORGAN HARVESTING In the operating theatre:
Optimal donor management remains important when the donor is taken to the operating room for organ retrieval. The same principles apply to the intraoperative setting also. Maintaining homeostasis with good haemodynamic stability and good diuresis is the key for successful organ recovery.
GOAL:To avoid ischaemic organ damage by
optimising perfusion and maintaining homeostasis.
PRE ANESTHETIC EVALUATION:It includes review of medical and surgical
histories including the cause of the brain death, haemodynamic stability, ventilatory status, acid base and electrolyte values and other organ functions and various investigations.
INTRAOPERATIVE CARE:It is essentially similar to that of other
critically ill patients undergoing major surgery although management of pathophysiologic changes unique to the donor should be clearly understood.
GENERAL PRECAUTIONS:The OR should be kept warm with the
availability of warming blankets and warmed intravenous fluids. A large volume of crystalloids, colloids, blood and blood products should be made available.
MONITORS:The monitors should include ECG,
Invasive arterial pressure monitoring, Central venous pressure monitoring, oxygen saturation, EtC02, temperature and urinary output.
The donor is positioned on the operating table and ventilation continued with a high tidal volume to achieve a PaC02 that is within the normal range. It is necessary that all infusions and monitors be connected before any surgical incision is placed. General anaesthetic agents are required to blunt sympathetic responses during surgery. Mass reflex is caused by neurogenic vasoconstriction and stimulation of adrenal medulla by the spinal reflex arc and will be manifested as tachycardia, perspiration and involuntary movements, which include arm and hand movements, hence at times muscle relaxants may also be necessary.
Isoflurane is the agent of choice because the degree of myocardial depression is less than other agents, halothane is avoided ,in liver donors, and enflurane is better avoided in kidney donors.
POSITIONING OF VASCULAR LINES:The surgical procedure for thoracotomy
in case of retrieving the thoracic organs may involve early ligation of the left innominate vein and the right subclavian artery. A peripheral arterial line must be started on the left arm either in the radial, ulnar, or brachial artery. Placing the arterial lines in the other areas should be avoided since the ability to measure arterial pressure and sample the blood will be lost at critical times of the procedure.
Venous access and Swan - Ganz is provided by multiple cannulation of the right IJV. The ability to monitor CVP or infusing large volume will be lost, once the left innominate vein is ligated. In the majority of the centres, the Swan - Ganz sheath and triple lumen catheter are inserted separately in the IJV. This approach permits the measurement of CVP, infusion of inotropes, administration of hormone replacement, rapid volume replacement and sampling ability.
MANAGEMENT OF VENTILATION:Ventilation is continued with large tidal
RACE 2003 Ramachandra Anaesthesia Continuing Education
Management of a brain dead organ donor 68 Joseph Rajesh
volumes, using an FI02 of 0.6, achieved by using either oxygen- air or 02-N20.The use of an FI02 of 0.6 provides the maximum 02 content in the blood, to ensure adequate oxygen saturation, while being unlikely to cause 02 toxicity to the donor lungs. In hypothermic donors, mild respiratory alkalosis is preferred to improve tissue perfusion.
HAEMODYNAMIC MONITORINGHaemodynamic monitoring will include,
monitoring direct arterial pressure through an arterial line, continuous CVP and PA pressures via a Swan - Ganz catheter. Inadvertent wedging should be avoided as it can cause possible lung ischaemia in donors. Baseline values of HR, BP, PAP, CVP, and PCWP are recorded. Baseline acid base status and electrolyte estimations are also done.
MANIPULATION OF CIRCULATING VOLUMEThe goal of the circulatory care is to
preserve perfusion of all organs that are to be procured by maintaining the systolic blood pressure between 100 -120 mmHg, with a CVP of less than 10 cmH20 and minimal inotropic support. Hypotension is associated with increased incidence of ATN and non-functioning of the kidneys as well as poor functioning of the liver. Intravascular volume is adjusted with the guidance of CVP. Colloids or RL can be used to manage the fluid deficit. Hypotonic solutions like 5% dextrose should be used to replace insensible losses. This may decrease the requirement of vasopressin. Excessive urine output (>200 ml/ hr) is replaced by hypotonic solutions with replacement of KCI. If hypotension persists even after volume replacement, inotropic support may be initiated, with dopamine as the first choice. Vasopressors like phenylephrine (Alpha stimulants) should be avoided as they cause reduction in splanchnic and coronary blood flow. Severe cases of tachycardia and hypertension caused by mass reflex may be controlled by general anaesthetics, beta blockers or with calcium channel blockers. Arrhythmias (ventricular and supraventricular) are treated with conventional antiarrhythmic agents. If bradycardia is persisting, it should be treated with isoproterenol or epinephrine, because these patients will not show any response to atropine.
In case of cardiac transplantation,
approximately 10% of the blood volume (500ml) is taken under gravity through Swan Ganz into a blood collection bag. This is subsequently used as the major component of the pulmonary preservation solution and this also reduces the left ventricular filling pressure. It is subsequently replaced by 20% albumin to maintain the colloid oncotic pressure of the plasma. Other crystalloid solutions are inappropriate for volume expansion in these situations. Target values for PCWP are between 5and 8 cmH20 and slightly higher values may be used if lung transplantation is not being considered.
Management During SurgeryASSESSMENT OF THE HEART AND LUNGS:
After median sternotomy, macroscopic examination of thoracic organs is done. In particular, evidence of established coronary artery disease in the donor is sought. The visual impression of ventricular wall motion is also noted. The presence of obvious congenital anomalies of the heart is also excluded.
After the heart is examined, both the pleural cavities are widely opened and examination of the lungs is performed. Areas of lobar collapse may be reinflated using controlled manual ventilation under vision and counter compression of normal lung tissue by the surgeon may allow the reexpansion of such collapsed areas and significantly improve the gas exchange. The application of PEEP of 5 - 10 cm of H20 is essential to maintain the FRC and the haemodynamic consequences will be small as the pleura is opened.
HAEMODYNAMIC MANIPULATION:During the abdominal dissection, adrenal
manipulation, both hypertension with periods of hypotension can occur due to catecholamine excess and impaired venous return respectively. During these events, colloid loading, inotropic support and or vasodilatation are adjusted to maintain homeostasis. Although hypertension is best controlled by vasodilators, the resulting tachycardia carries the risk of inducing ischaemia, which will have a deleterious effect on the heart, if transplantation is planned. Although best avoided, the b adrenergic blockers can be used with caution.
RACE 2003 Ramachandra Anaesthesia Continuing Education
of a brain dead organ donor 69 Joseph Rajesh
HYPOTHERMIAHypothermia is seen among 86% of the
brain dead donors due to the loss of hypothalamic function. As the temperature goes below 32 °C, ECG changes like prolonged PR, QT interval and wide QRS complexes are seen. T wave inversion, ST segment depression and decreased threshold for ventricular fibrillation are seen below 28°C. Hypothermia also produces a left shift of the ODC, increase in blood viscosity, a decrease in splanchnic blood flow and glomerular filtration, hyperglycemia, and metabolic and respiratory acidosis. Hence body temperature must be kept within the normal range by keeping the OR warm, by infusing warmed fluids, and by using blankets, warmer etc.
ANTICOAGULATION:Before cannulating any major vessels,
full anticoagulation doses of heparin are administered .The consequences of unrecognised inadequate anticoagulation and thrombosis within the organs during transport would be disastrous.
PHARMACOLOGICAL INTERVENTIONS:Adequate diuresis is important, because
urine output is c prognostic indicator of graft function. Though low dose dopamine may be effective in maintaining adequate renal perfusion and diuresis, high dose may lead to tubular necrosis and non-functioning of the graft. For persistent oliguria, mannitol (0.25 - 0.5 g/kg) and furosemide 40 mg may be used to induce diuresis before division of the renal pedicle and prevent ischaemia induced ATN.
Alpha-adrenergic receptor blockers such as phenoxybenzamine may be useful to produce renal vasodilatation but have a doubtful effect in multiple organ procurement because of their effects on other organs.Some centres recommend broad-spectrum. antibiotics.
ACID BASE & ELECTROLYTE STATUS:Complete haemodynamic profiles,
including arterial and mixed venous acid-base and02 status are made at regular intervals. Estimations of serum electrolytes, especially potassium and glucose are done and supplemented appropriately. Metabolic acidosis caused by inadequate tissue perfusion can
potentially depress the myocardium and is corrected with sodium bicarbonate or THAM.
Electrolyte imbalances (hypernatremia, hypokalemia, hypocalcemia, hypophosphatemia and hypomagnesemia) due to marked fluid shifts in Dl may cause arrhythmias and myocardial dysfunction, and they are treated along the general guidelines.
Once cardioplegia is induced, no further supportive care is needed. After cross clamping of the aorta, mechanical ventilation and monitoring are disconnected and all cannulas are removed.
The sequence of removal of organs is, heart, lungs, liver, pancreas, intestine and kidneys.
SUMMARY:The ICU and its staff play a major role in
solid organ transplantation. The medical care of the donor may be complex and challenging. Delay in certifying brain death and organizing the organ retrieval will make preservation of organ function more difficult and should be avoided at all costs. Much therapy remains empirical and continued research is required to further define optimum management of the donor.
References:1. David.J. Powner, et al Brain Death
definition, Determination and Physiological effects of donor organs, The Text Book of Critical Care, 1894-1899.
2. Eelco F.M. Wijdicks, The Diagnosis of Brain Death: The New England Journal of Medicine, April 2001, Volume 344: 1215 -1221.
3. Finfer. S. R. Support of the Potential Organ Donor; Principles and Practice of Critical Care; 484 - 493.
4. Johnston. K.R. et al, Optimization of Multiorgan Donors and Selection of Thoracic Organs for Transplantation, Principles and Practice of Critical Care; 431-444.
5. Pallis.C, Brain Stem Death: The evolution of a concept. Text book of transplantation (75-100)
6. Ron Shapiro et al, Management of Potential Cadaveric Donor; up to date 10.1 July 2001.
7. Tarek Razek et al, Issues In Potential Organ Donor Management; Surgical Clinics of North America, June 2000 : Volume 80. No.3.
8. William shoemaker, Ake grenvik : Multiple organ Procurement ; Text book of critical care (fourth edition -1910-1923)
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 70 S. Manimala Rao
Obesity means excessive body fat and the term obese is derived from a Latin word that means fattened by eating. The amount of fat tissue is increased to such an extent that mental and physical health is affected and life expectancy is reduced.
Body mass index (BMI) or Quetelet’s index is calculated from subjects’ height and weight. It is used to indicate obesity. Obesity is indicated by BMI > 30.0 (M), > 28.6 (F). Many clinical parameters depict women as pear shaped, accumulating fat at the bottom and this is regarded as safe, fat being stored between the skin and the body wall. In men, we find the classic beer belly look compared to the rounded apple, here the fat is stored in the internal organs. Morbid obesity is when BMI is more than 40 kg/m2.
PREVALENCE AND EPIDEMIOLOGYThere is a slow but steady increase in
obesity. In UK the statistics showed an increase; in 1980 - 6% males and 8% females and in 1987 - 8% males and 12% females were regarded as obese. Obesity in children is also on the rise. Prevalence varies with the socioeconomic status. In developed countries, poverty is associated with a greater prevalence whereas in developing countries, there is a higher prevalence amongst the affluent. Obesity is complex, wherein the net energy intake exceeds the net energy expenditure over a prolonged period of time.
PATHOPHYSIOLOGYThe brain controls the appetite by means
of signals triggered by dietary breakdown products and also by autonomic signals produced by disturbance of the stomach and intestines.
The multiple signals generated are processed by complex interactions between neuronal networks and neuro transmitters. Most important of them are cholecystokines 8 (CCK 8), which act at the gut and the brain. It induces satiation, is released at the beginning of a meal and promotes pancreatic secretion of insulin, which lowers the sugar and increases the appetite. Insulin crosses the blood brain barrier and triggers the hypothalamus, which juggles many other signals. Therefore, the complexity of weight maintenance is evident. 25-30% of human variations in BMI are genetic and the rest is due to environmental factors. It is a complex picture as to how normal weight is maintained. The pathways regulating weight form a series of redundant regulatory loops. If one is weakened or attenuated, the other can take over. It is this redundancy that regulates calorie storage, but the same redundancy makes it hard to get a handle on how to prevent and treat obesity. It is an imbalance between food intake and energy expenditure. The balancing act involves neural signaling and endocrinal processes. These can be both central and peripheral. Problems can occur any where in this complex system.
GENETIC PREDISPOSITIONObesity tends to be familial. Children of
two obese parents have a 70% chance to become obese. The genetic issues account for 30% and are linked to at least 6 genes. 70% is dependent on environmental factors. Genetic susceptibility may predispose to environmental issues.
ETHNIC INFLUENCESIn USA, the African Americans and
Mexicans have a higher rate of obesity than the Whites. Asian migrates have a more central
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 71 S. Manimala Rao
distribution of fat associated with increased risk of diabetes and coronary artery disease.
MEDICAL DISEASESCushing’s disease, hypothyroidism,
medications like steroids, antidepressants and antihistamines may also lead to obesity.
RISK FACTORSMale gender, middle age, night sedation,
evening alcohol can all compound the problem. Other features which can help identify are BMI > 30 kg/m2, hypertension, observed episodes of apneoea during sleep, hypoxemia, hypercapnia, changes in ECG and ECHO. Definite diagnosis is made by polysomnography in the sleep laboratory. The obese pose great challenges to surgery, anaesthesia, obstetrics, trauma and in the ICU.
Diabetes, hypertension, hyperlipidemia, heart diseases, increased rates of colon and breast cancer, asthma are all linked to rising levels of obesity. A BMI>29 kg/m2 increases the prevalence of pulmonary embolism. The risk of coronary artery disease is doubled if BMI is > 25kg/m2. A BMI of 35kg/m2 leads to a 40-fold increase in developing diabetes, respiratory diseases, sleep apnoea and osteoarthritis. The risk of death increases with body weight. Mortality rises exponentially with increasing body weight.
CHANGES IN VARIOUS SYSTEMS OBESITY AND RESPIRATORY SYSTEM
5% of morbidly obese will have Obstructive Sleep Apnoea (OSA), frequent episodes of apnoea or hypercapnia, snoring and daytime sleepiness. Recurrent apnoea leads to hypoxia, hypercapnia, pulmonary and systemic vascular hypertension, which in turn leads to right ventricle failure. Loss of pharyngeal muscle tone and significant narrowing of airway increases airflow turbulence.
Acid base disturbances of Obstructive Sleep Apnoea (OSA)
Respiratory acidosis is limited to sleep, in the beginning. The longer the problem, alterations occur in breathing patterns with desensitization of the respiratory center to hypercapnia leading to type II respiratory failure.
This leads to increased dependence on the hypoxic drive for ventilation - Pickwickian syndrome, which is characterized by obesity, hypersomnolence, hypoxia, hypercapnia, right ventricular failure and polycythemia.
AirwayPerfect airway, particularly upper is
essential before any anaesthetic management. In obese patients, difficulties are encountered for mask ventilation; tracheal intubations may be difficult. The percentage of difficult intubation is quoted to be 13%. Excessive fat at the upper airway, short neck, high anteriorly placed larynx and restricted cervical spine movements are a few problems.
Obesity and gas exchangeIncreased mass of abdominal and
thoracic contents alters the lung volumes. Decrease in functional residual capacity (FRC) is seen exponentially with increasing BMI. Expiratory reserve volume and total lung capacity are decreased.
FRC may be reduced in the upright position to the extent that it falls within the range of the closing capacity with subsequent small airway closure, ventilation perfusion mismatch, right to left shunting and arterial hypoxemia. The reduction of FRC impairs the capacity of obese patients to tolerate apnoea. They desaturate rapidly after induction of anaesthesia despite preoxygenation due to the smaller 02 reservoir and increased oxygen consumption. Residual volume remains normal or slightly increased due to the increased gas trapping and coexisting obstructive airway disease.
02consumption and C02productionBoth are increased in obese patients as
a result of the metabolic activity of excess fat and increased workload on supportive tissues. With exercise, Oz consumption rises more sharply in the obese than in the non-obese.
Gas exchangeOnly a modest defect in gas exchange
is noted in the obese patients with a reduction in Pa02, increase in Aa02gradient and increase in shunt fraction. This is increased markedly with
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 72 S. Manimala Rao
induction of anaesthesia. PEEP improves the condition, but at the expense of cardiac output and 02 delivery.
Compliance and ResistanceIncreased BMI exponentially decreases
the compliance. As the fat content increases, compliance decreases, but it is also due to a decrease in lung compliance. This is due to the increase in pulmonary blood volume, increased total respiratory resistance and shallow rapid breathing which can limit maximum ventilatory capacity. These are all more marked in the supine position.
Work of breathingThere is a 30% increase observed in the
work of breathing. If hypoventilation occurs in daytime, the work of breathing may approach four times that predicted.
CARDIOVASCULAR SYSTEMA higher incidence of cardiovascular
morbidity is associated with obesity. Mild to moderate hypertension is found in 60-70%, severe in 5-10%. It is the commonest problem followed by ischaemic heart disease. An expansion of extracellular volume resulting in increased blood volume and cardiac output is characteristic of obesity-induced hypertension. The exact mechanism is not known, but an interplay of genetic, hormonal, renal and haemodynamic factors are implicated. Hyperinsulinaemia, activating the sympathetic nervous system and causing sodium retention, increases the pressor norepinephrine and angiotensin II activity. Concentric hypertrophy of the left ventricle leads to cardiac failure. Obesity is an independent risk factor for Ischaemic Heart Disease (IHD) and this is more common in individuals with central obesity. Blood volume is increased, most extra volume being distributed to the fat organ. Splanchnic blood flow is increased by 20%, while renal and cerebral blood flow are normal. A 3- 4mmHg increase in systolic and 2mmHg increase in diastolic pressure is noted for every 10kg increase of weight.
Cardiac arrhythmias can be precipitated in the obese by any number of factors, viz. hypoxia, hypercapnia, electrolyte imbalance,
diuretic therapy or fatty infiltration of the conducting tissue.
Cardiac functionObese patients are at risk of a specific
form of obesity induced cardiac dysfunction. Left ventricular systolic and diastolic functions are affected. Obesity induced cardiomyopathy is well documented. Blood volume is increased and cardiac output increases by 20-30ml/kg of excess body fat. The obese tolerate exercise poorly. Any increase in the cardiac output is by an increase in the heart rate.
OBESITY AND DIABETESType II Diabetes mellitus is an
independent risk factor. The incidence of abnormal glucose tolerance in patients undergoing bariatric surgery is more than 10%.
THROMBOEMBOLIC DISEASEDeep vein thrombosis appears twice as
common in obese patients. It is the commonest complication of bariatric surgery with an incidence of 2.4% - 4.5%. It is due to prolonged immobilization that leads to venous stasis and polycythemia, and increased abdominal pressure with increased pressure on the deep veins. Decreased fibrinolytic activity with increased fibrinogen concentration could also be responsible.
OBESITY AND Gl DISORDERSThe obese have an increased integral
abdominal pressure, a high volume and low pH of gastric contents, delayed gastric emptying and an increased incidence of gastro esophageal reflex. They also have a high risk for aspiration of gastric contents followed by pneumonia. Gastric volume is 75% higher than in normal individuals.
DRUGS, PHARMCODYNAMICS AND KINETICSObesity leads to an alteration in the
distribution, binding and elimination of many drugs. For drugs with narrow therapeutic indices like aminoglycosides and digoxin, toxic reactions can occur if the patients are dosed according to actual body weight. Drug dose should be reduced keeping the lean body mass in view. Absorption of drugs orally remains unchanged in the obese patient.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 73 S. Manimala Rao
Volume Of Distribution (VD)The apparent volume of distribution of a
drug in the obese patient is influenced by a number of factors which include, the size of the fat organ, the increase in lean body mass, the increase in blood volume and cardiac output, reduced total body water, alterations in plasma protein binding and lipophilicity of the drug. Highly lipophilic drugs have an increased volume of distribution (Thiopentone). Increase in the volume of distribution will reduce the elimination half-life unless the clearance is increased. Thiopentone, Benzodiazepines, and potent inhalation agents, may persist for a longer time after discontinuation. Regarding protein binding, alterations may occur due to the high levels of cholesterol, inhibiting protein binding; therefore more free drug is available. In contrast, increased concentrations of a acid glycoprotein may increase the degree of protein binding of other drugs (e.g. local anaesthetics), thus reducing the free plasma fraction.
EliminationClearance is mostly reduced in obese
patients. Cardiac failure and decrease in liver blood flow may slow elimination of midazolam and lignocaine. Renal clearance is increased in obesity because of the increased renal blood flow and GFR. If renal impairment is present, elimination takes a longer time.
Hepatic metabolism is altered in obese patients for volatile agents. Reductive metabolism of halothane is more in obese patients. This may be an important factor in liver injury. Nephrotoxicity can occur due to high fluoride concentrations with halothane and enflurane. Sevoflurane has high hepatic metabolism but does not show adverse effects. Isoflurane does not increase fluoride concentration, and remains the agent of choice in the obese.
ANAESTHETIC IMPLICATIONS Preoperative:
Thorough clinical examination is mandatory with excellent and relevant history taking, checking BP with an appropriate sized cuff to identify hypertension and looking for signs of cardiac failure, viz. increase in jugular pulse, added heart sounds, pulmonary crackles, hepato
jugular reflex and peripheral edema. These signs may be difficult to elicit in the morbidly obese. A thorough assessment of the respiratory system for OSA is very essential.
InvestigationsBesides routine investigations, ECG is
mandatory as tachyarrhythmias are common. Echo may be difficult but will provide valuable information regarding eccentric left ventricular hypertrophy. TEE may provide more insight. Cardiological evaluation is beneficial for further investigation. Optimization of blood pressure, treatment of cardiac failure, or if necessary, coronary angioplasty may be suggested. X-ray chest, lung function tests and baseline arterial blood gases may be useful in the morbidly obese. A thorough history regarding respiratory function and sleep apnoea are a must. Signs of right ventricular failure must be looked for.
Airway assessmentIt is mandatory to plan the type of airway
management. A thorough examination can prevent catastrophes, as it will enable us to select the best technique for the patient. Preoperative evaluation of the airway must include:
1. Assessment of the head and neck; flexion, extension and lateral rotation.
2. Assessment of jaw mobility and mouth opening.
3. Inspection of the oropharynx.4. Checking the patency of the nostrils5. Inspection of previous anaesthetic
charts.
If potential airway obstruction is suspected at direct or indirect laryngoscopy, CT scan of soft tissues would be helpful.
Assessment of veins for placing infusion must be done in the pre- operative visit. Examination of the feet and back for any ulcer or sore is mandatory. Examination of the calf muscles for any redness or tenderness gives a fairly good idea regarding deep vein thrombosis.
Preoperative medicationAvoid narcotics and sedatives. Avoid
intramuscular and subcutaneous injections. If fibre optic intubation is planned, include an
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 74 S. Manimala Rao
antisialogogue. All morbidly obese must have acid aspiration prophylaxis. A combination of the H2 blocker, ranitidine 150mg and prokinetic metaclopramide 10mg orally given 12 hrs and 2hrs before surgery will reduce the risk of aspiration. Some anaesthetists prefer to give 30ml of 0.3 M sodium citrate before induction. Continue the normal medications on the day of surgery. Stop ACE inhibitors the day before surgery. Dextrose- Insulin regimen should follow in all diabetics, unless it is a very short surgical procedure. Insulin requirements may increase in the postoperative period. Prophylactic antibiotics are given as per the hospital protocols, after discussion with the surgeon and the microbiologist.
POSITION AND TRANSFERExtra care, special tables and adequate
padding of pressure areas should be provided. Appropriate manpower to shift is mandatory. Compression of inferior vena cava is avoided by lateral tilt or a wedge. Transfer of obese patients is done in their own bed. Special beds are ordered in other countries.
INTRAVENOUS LINESPeripheral lines may be difficult.
Establish central lines in the beginning to avoid calamities. Even these are difficult in the morbidly obese. Doppler or ultrasound guided placements could reduce complications.
MONITORINGIntraarterial blood pressure measurement
is advocated for all but most minor procedures, ECG, Pulse oximetry, Capnography and neuromuscular monitors are essential. Central venous catheters are essential and PA Catheters should be used where indicated.
REGIONAL ANAESTHESIAWhere it is possible and feasible, regional
anaesthesia should be administered. One can reduce the use of opioids, inhalational agents, reduce postoperative complications, and prevent the loss of airway and aspiration. Excellent postoperative analgesia can be given by placing the epidural catheters in the sitting position, using ultrasound for identification of the space. Local anaesthetic requirements are 50-70% reduced in the morbidly obese. Higher blocks are
common. Blocks extending above T5 can cause cardiorespiratory collapse. All resuscitation equipment should be handy.
SYSTEMIC OPIOIDSThese are hazardous in obese patients;
intramuscular route is not recommended. If intravenous route is preferred, patient controlled analgesia should be the best option. Oral analgesics like paracetamol and cox2 inhibitors may be appropriate. Postoperative analgesia with local anaesthetics and opioids via the epidural catheter will provide ideal pain relief with minimal complications.
OBSTETRICS AND MORBIDLY OBESEAll attending complications are
compounded. Regional anaesthesia is a better choice; avoid general anaesthesia as far as possible. Putting an epidural catheter during labor is a better option. Local anaesthetic requirement may be reduced by up to 25% in the obese pregnant state.
OBESE PATIENTS AND TRAUMAThe out come in obese patients with
trauma is poor. The obese patients have more blunt trauma and chest trauma is more compared to head injury. Investigations are more difficult to handle and interpret. They may require earlier respiratory support and higher oxygen concentration.
OBESE PATIENT IN THE ICUIt is held that the outcome is poor for
these patients. Postoperative pulmonary events are more in obese patients. Morbidly obese may present in the emergency room and intensive care with formidable challenges. A better understanding of the pathophysiology and complications may improve the outcome. Anaesthesiologist has a major role to play as the perioperative physician at every level.
BARIATRIC SURGERY The indications for bariatric surgery are as follows:
BMI >40kg/m2
BMI >35kg/m2 with co morbiditiesShould show that dietary attempts have beenineffective
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic Management of a Morbidly Obese Patient 75 S. Manimala Rao
Bariatric surgery (weight reductive surgery) addresses both perioperative care and long-term management. The patients must have a clear understanding of the risks, benefits and complications, and may require life long management strategies.
Types of Bariatric surgeryBariatric surgery comprises two types
namely restrictive and malabsorptive. The common operations include Roux-en-Y grade bypass, vertical banded gastroplasty, bitropancreatic diversion and its variations, various gastric banding procedures, gastric bypass procedures and laparoscopic procedures of the above-mentioned operations.
The preoperative evaluation consists of obesity evaluation, behavioural evaluation, medical evaluation, surgical evaluation, which includes education & potential risk, and anaesthetic evaluation. A team is usually available in other countries for patients with morbid obesity undergoing bariatric surgery.
OBESITY ASSOCIATED -MEDICAL CONDITIONS
The various medical conditions associated with obesity are:
• CAD• Cardiomyopathy• Cerebrovascular disease• Diabetes mellitus and other endocrine
diseases• Infertility
• Hepatobilary disease and gall stones• Malignancies, depression• Degenerative joint disease, chronic back
pain• Respiratory abnormalities• GE reflux• Sudden death
COMPLICATIONSThe complications associated with
bariatric surgery are as follows:• Nutritional deficiencies• Cardiovascular disease and sudden
death
• Pulmonary embolism, which is a leading cause of death
• Bleeding and splenic injury• Gastrointestinal leaks - shown by
tachypnea and tachycardia• Wound infections 1-3%, wound
dehiscence, vomiting and diarrhea• Sternal dilation
The morbidity and mortality has come down for these procedures to <19%.
As we enter the new millennium, severe obesity remains an incurable disease. The consequences and cost to society are significant. Though etiology is becoming more clear, non- surgical treatments are still inadequate for achieving sustained and significant weight loss. Surgical procedures have evolved into safe and effective options. Newer technologies such as laparoscopy should further advance the field. For appropriately selected patients, surgery can achieve the weight loss necessary to prevent the development of significant medical conditions and improve the quality of life. Unfortunately, dietary indiscrimination and malabsorptive eating behaviour can result in weight loss failure despite an excellent surgical result. Therefore, preoperative evaluation and education is a corner stone for long-term success.
CONCLUSIONSMorbidly obese patients can be
encountered more commonly in the West. But with changing lifestyles, a high incidence is now seen in the younger individuals. One may encounter them in the practice of anaesthesia for different types of surgical procedures, bariatric surgeries, trauma and in the ICU setup. They do pose tremendous challenges. Understanding the pathophysiology, anticipating the problem and preventing calamities by a systematic approach will certainly bring down the rate of complications.
REFERENCES
1. J.P.Adams and P.G.Murphy. Obesity in anaesthesia and intensive care. BJA 2000; 85 (1 ):91 -108.
2. Anthony P.Adams, Jereney N Cashnar. Recent Advances in Anaesthesia and Analgesia. Churchill Livingston 2000; Chapter II, Vol 21.
RACE 2003 Ramachandra Anaesthesia Continuing Education
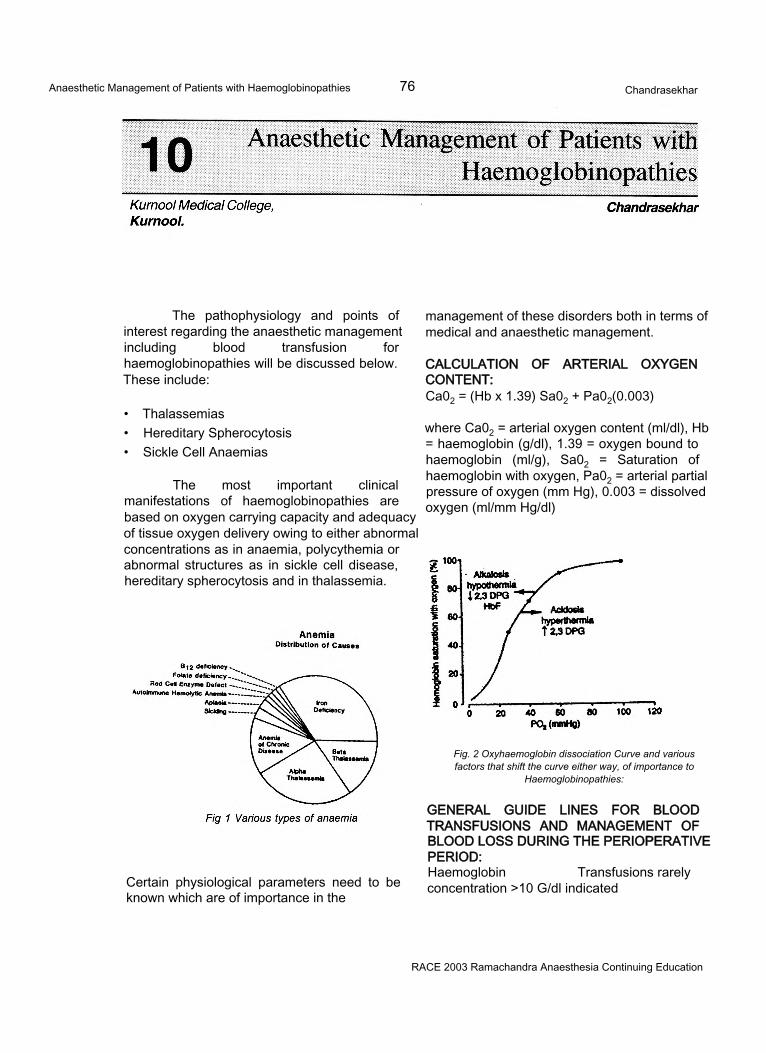
Anaesthetic Management of Patients with Haemoglobinopathies 76 Chandrasekhar
The pathophysiology and points of interest regarding the anaesthetic management including blood transfusion for haemoglobinopathies will be discussed below. These include:
• Thalassemias• Hereditary Spherocytosis• Sickle Cell Anaemias
The most important clinical manifestations of haemoglobinopathies are based on oxygen carrying capacity and adequacy of tissue oxygen delivery owing to either abnormal concentrations as in anaemia, polycythemia or abnormal structures as in sickle cell disease, hereditary spherocytosis and in thalassemia.
management of these disorders both in terms of medical and anaesthetic management.
CALCULATION OF ARTERIAL OXYGEN CONTENT:Ca02 = (Hb x 1.39) Sa02 + Pa02(0.003)
where Ca02 = arterial oxygen content (ml/dl), Hb = haemoglobin (g/dl), 1.39 = oxygen bound to haemoglobin (ml/g), Sa02 = Saturation of haemoglobin with oxygen, Pa02 = arterial partial pressure of oxygen (mm Hg), 0.003 = dissolved oxygen (ml/mm Hg/dl)
Fig. 2 Oxyhaemoglobin dissociation Curve and various factors that shift the curve either way, of importance to
Haemoglobinopathies:
Certain physiological parameters need to be known which are of importance in the
GENERAL GUIDE LINES FOR BLOOD TRANSFUSIONS AND MANAGEMENT OF BLOOD LOSS DURING THE PERIOPERATIVE PERIOD:Haemoglobin Transfusions rarelyconcentration >10 G/dl indicated
RACE 2003 Ramachandra Anaesthesia Continuing Education
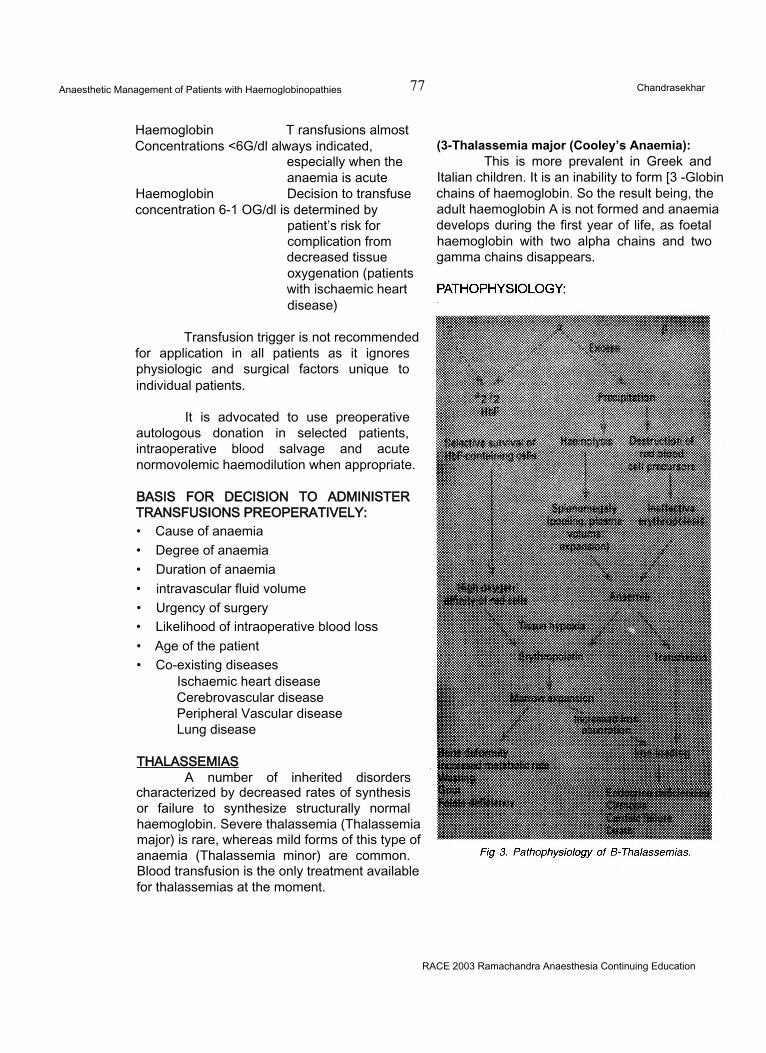
Anaesthetic Management of Patients with Haemoglobinopathies 77 Chandrasekhar
Haemoglobin T ransfusions almostConcentrations <6G/dl always indicated,
especially when the anaemia is acute
Haemoglobin Decision to transfuseconcentration 6-1 OG/dl is determined by
patient’s risk for complication from decreased tissue oxygenation (patients with ischaemic heart disease)
Transfusion trigger is not recommended for application in all patients as it ignores physiologic and surgical factors unique to individual patients.
It is advocated to use preoperative autologous donation in selected patients, intraoperative blood salvage and acute normovolemic haemodilution when appropriate.
(3-Thalassemia major (Cooley’s Anaemia):This is more prevalent in Greek and
Italian children. It is an inability to form [3 -Globin chains of haemoglobin. So the result being, the adult haemoglobin A is not formed and anaemia develops during the first year of life, as foetal haemoglobin with two alpha chains and two gamma chains disappears.
BASIS FOR DECISION TO ADMINISTER TRANSFUSIONS PREOPERATIVELY:• Cause of anaemia• Degree of anaemia• Duration of anaemia• intravascular fluid volume• Urgency of surgery• Likelihood of intraoperative blood loss• Age of the patient• Co-existing diseases
Ischaemic heart disease Cerebrovascular disease Peripheral Vascular disease Lung disease
THALASSEMIASA number of inherited disorders
characterized by decreased rates of synthesis or failure to synthesize structurally normal haemoglobin. Severe thalassemia (Thalassemia major) is rare, whereas mild forms of this type of anaemia (Thalassemia minor) are common. Blood transfusion is the only treatment available for thalassemias at the moment.
RACE 2003 Ramachandra Anaesthesia Continuing Education
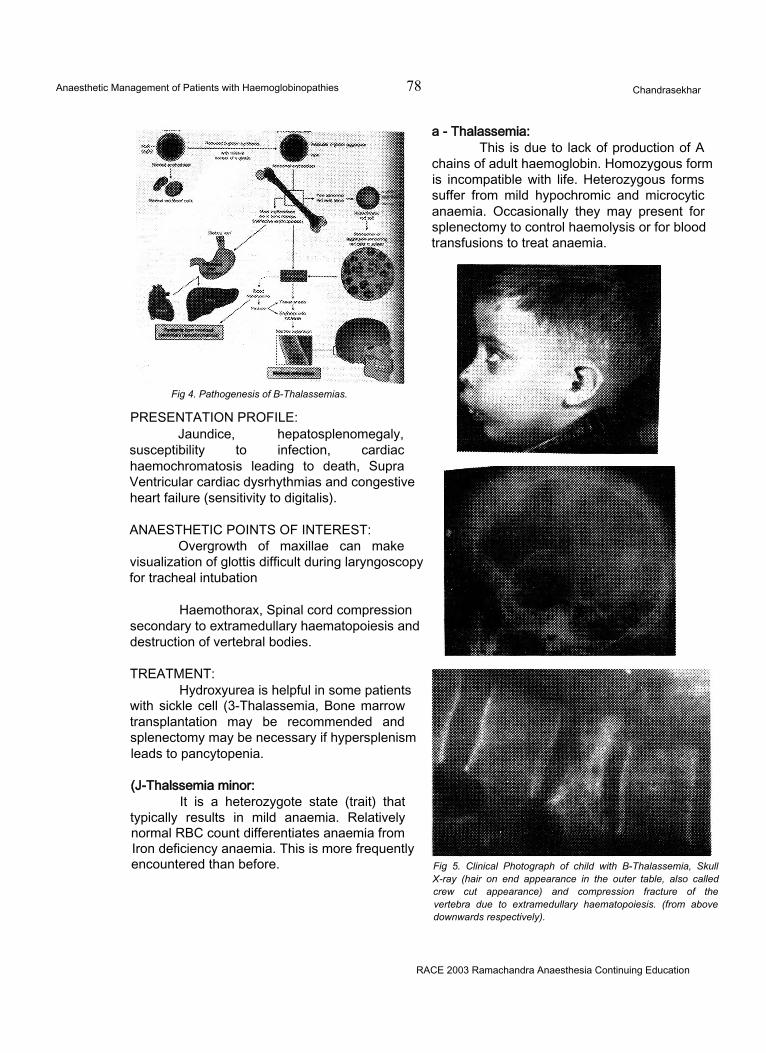
Anaesthetic Management of Patients with Haemoglobinopathies 78 Chandrasekhar
Fig 4. Pathogenesis of B-Thalassemias.
PRESENTATION PROFILE:Jaundice, hepatosplenomegaly,
susceptibility to infection, cardiac haemochromatosis leading to death, Supra Ventricular cardiac dysrhythmias and congestive heart failure (sensitivity to digitalis).
ANAESTHETIC POINTS OF INTEREST:Overgrowth of maxillae can make
visualization of glottis difficult during laryngoscopy for tracheal intubation
Haemothorax, Spinal cord compression secondary to extramedullary haematopoiesis and destruction of vertebral bodies.
TREATMENT:Hydroxyurea is helpful in some patients
with sickle cell (3-Thalassemia, Bone marrow transplantation may be recommended and splenectomy may be necessary if hypersplenism leads to pancytopenia.
(J-Thalssemia minor:It is a heterozygote state (trait) that
typically results in mild anaemia. Relatively normal RBC count differentiates anaemia from Iron deficiency anaemia. This is more frequently encountered than before. Fig 5. Clinical Photograph of child with B-Thalassemia, Skull
X-ray (hair on end appearance in the outer table, also called crew cut appearance) and compression fracture of the vertebra due to extramedullary haematopoiesis. (from above downwards respectively).
a - Thalassemia:This is due to lack of production of A
chains of adult haemoglobin. Homozygous form is incompatible with life. Heterozygous forms suffer from mild hypochromic and microcytic anaemia. Occasionally they may present for splenectomy to control haemolysis or for blood transfusions to treat anaemia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
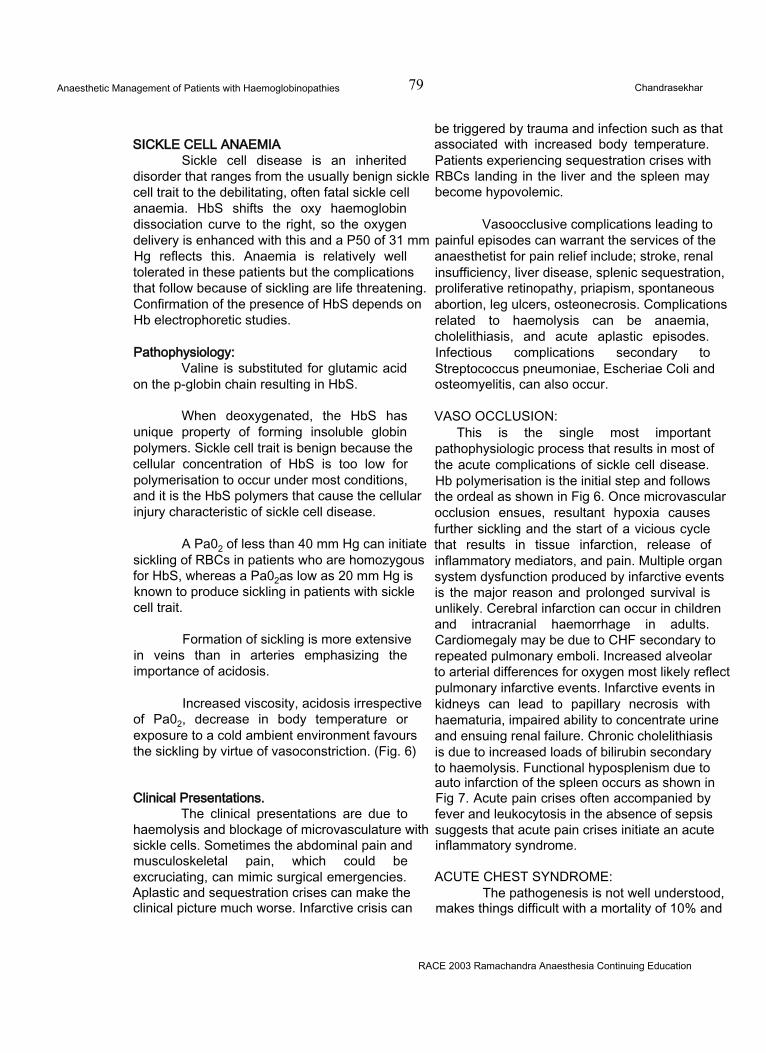
Anaesthetic Management of Patients with Haemoglobinopathies 79 Chandrasekhar
SICKLE CELL ANAEMIASickle cell disease is an inherited
disorder that ranges from the usually benign sickle cell trait to the debilitating, often fatal sickle cell anaemia. HbS shifts the oxy haemoglobin dissociation curve to the right, so the oxygen delivery is enhanced with this and a P50 of 31 mm Hg reflects this. Anaemia is relatively well tolerated in these patients but the complications that follow because of sickling are life threatening. Confirmation of the presence of HbS depends on Hb electrophoretic studies.
Pathophysiology:Valine is substituted for glutamic acid
on the p-globin chain resulting in HbS.
When deoxygenated, the HbS has unique property of forming insoluble globin polymers. Sickle cell trait is benign because the cellular concentration of HbS is too low for polymerisation to occur under most conditions, and it is the HbS polymers that cause the cellular injury characteristic of sickle cell disease.
A Pa02 of less than 40 mm Hg can initiate sickling of RBCs in patients who are homozygous for HbS, whereas a Pa02as low as 20 mm Hg is known to produce sickling in patients with sickle cell trait.
Formation of sickling is more extensive in veins than in arteries emphasizing the importance of acidosis.
Increased viscosity, acidosis irrespective of Pa02, decrease in body temperature or exposure to a cold ambient environment favours the sickling by virtue of vasoconstriction. (Fig. 6)
Clinical Presentations.The clinical presentations are due to
haemolysis and blockage of microvasculature with sickle cells. Sometimes the abdominal pain and musculoskeletal pain, which could be excruciating, can mimic surgical emergencies. Aplastic and sequestration crises can make the clinical picture much worse. Infarctive crisis can
be triggered by trauma and infection such as that associated with increased body temperature. Patients experiencing sequestration crises with RBCs landing in the liver and the spleen may become hypovolemic.
Vasoocclusive complications leading to painful episodes can warrant the services of the anaesthetist for pain relief include; stroke, renal insufficiency, liver disease, splenic sequestration, proliferative retinopathy, priapism, spontaneous abortion, leg ulcers, osteonecrosis. Complications related to haemolysis can be anaemia, cholelithiasis, and acute aplastic episodes. Infectious complications secondary to Streptococcus pneumoniae, Escheriae Coli and osteomyelitis, can also occur.
VASO OCCLUSION:This is the single most important
pathophysiologic process that results in most of the acute complications of sickle cell disease. Hb polymerisation is the initial step and follows the ordeal as shown in Fig 6. Once microvascular occlusion ensues, resultant hypoxia causes further sickling and the start of a vicious cycle that results in tissue infarction, release of inflammatory mediators, and pain. Multiple organ system dysfunction produced by infarctive events is the major reason and prolonged survival is unlikely. Cerebral infarction can occur in children and intracranial haemorrhage in adults. Cardiomegaly may be due to CHF secondary to repeated pulmonary emboli. Increased alveolar to arterial differences for oxygen most likely reflect pulmonary infarctive events. Infarctive events in kidneys can lead to papillary necrosis with haematuria, impaired ability to concentrate urine and ensuing renal failure. Chronic cholelithiasis is due to increased loads of bilirubin secondary to haemolysis. Functional hyposplenism due to auto infarction of the spleen occurs as shown in Fig 7. Acute pain crises often accompanied by fever and leukocytosis in the absence of sepsis suggests that acute pain crises initiate an acute inflammatory syndrome.
ACUTE CHEST SYNDROME:The pathogenesis is not well understood,
makes things difficult with a mortality of 10% and
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic Management of Patients with Haemoglobinopathies 80 Chandrasekhar
is a medical emergency. The patient presents with lower chest wall pain, fever, cough, pleuritic chest pain, arterial hypoxemia, pulmonary hypertension, and radiologic evidence of lung infiltrates more so in the lower lung fields. Some patients develop rib infarcts. Recurrent episodes of this condition can lead to progressive pulmonary fibrosis and chronic respiratory insufficiency.
Treatment includes supplemental oxygen, CPAP is some and mechanical ventilation in others guided by blood gas analysis. Early intervention with exchange transfusion to achieve HbS concentrations of less than 30% usually reverses respiratory failure. Inhaled nitric oxide may be beneficial in these patients decreasing the right ventricular after load, and redistributing pulmonary blood flow to better ventilated areas of the patient’s lungs.
Blood Transfusions in Sickle cell Anaemia:• Goal of transfusion is to decrease
haemoglobin S concentrations to less than 30%.
• Urgent: When blood is sequestered in an enlarged spleen, sudden and severe anaemia
Fig 7. Auto splenectomy in Sickle Cell Anaemia
occurs in children• Arterial Hypoxemia: In Acute Chest
Syndrome, RBC transfusions and supplemental oxygen therapy are helpful.
• Renal Failure and Symptomatic anaemia: Transfusion therapy may benefit these patients as also administration of erythropoietin.
Anaesthetic points of interest:This disease carries a special risk for
anaesthesia and surgery. It requires admission to the hospital 12-24 hours before surgery for
RACE 2003 Ramachandra Anaesthesia Continuing Education
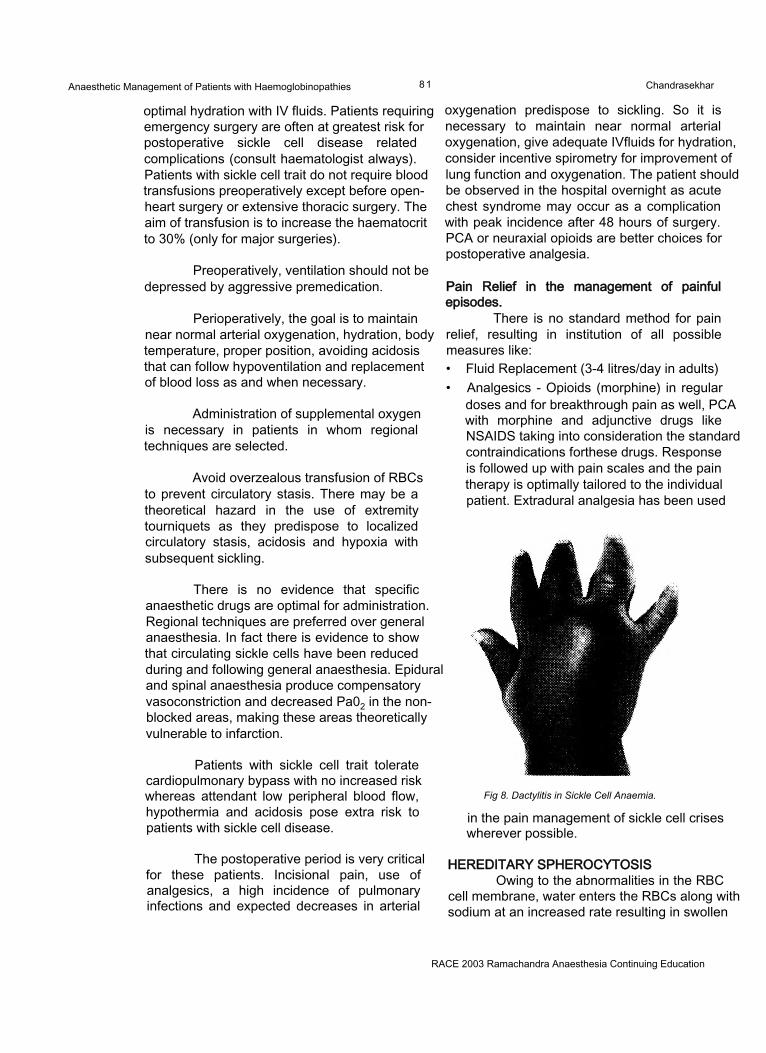
Anaesthetic Management of Patients with Haemoglobinopathies 81 Chandrasekhar
optimal hydration with IV fluids. Patients requiring emergency surgery are often at greatest risk for postoperative sickle cell disease related complications (consult haematologist always). Patients with sickle cell trait do not require blood transfusions preoperatively except before open- heart surgery or extensive thoracic surgery. The aim of transfusion is to increase the haematocrit to 30% (only for major surgeries).
Preoperatively, ventilation should not be depressed by aggressive premedication.
Perioperatively, the goal is to maintain near normal arterial oxygenation, hydration, body temperature, proper position, avoiding acidosis that can follow hypoventilation and replacement of blood loss as and when necessary.
Administration of supplemental oxygen is necessary in patients in whom regional techniques are selected.
Avoid overzealous transfusion of RBCs to prevent circulatory stasis. There may be a theoretical hazard in the use of extremity tourniquets as they predispose to localized circulatory stasis, acidosis and hypoxia with subsequent sickling.
There is no evidence that specific anaesthetic drugs are optimal for administration. Regional techniques are preferred over general anaesthesia. In fact there is evidence to show that circulating sickle cells have been reduced during and following general anaesthesia. Epidural and spinal anaesthesia produce compensatory vasoconstriction and decreased Pa02 in the nonblocked areas, making these areas theoretically vulnerable to infarction.
Patients with sickle cell trait tolerate cardiopulmonary bypass with no increased risk whereas attendant low peripheral blood flow, hypothermia and acidosis pose extra risk to patients with sickle cell disease.
The postoperative period is very critical for these patients. Incisional pain, use of analgesics, a high incidence of pulmonary infections and expected decreases in arterial
oxygenation predispose to sickling. So it is necessary to maintain near normal arterial oxygenation, give adequate IVfluids for hydration, consider incentive spirometry for improvement of lung function and oxygenation. The patient should be observed in the hospital overnight as acute chest syndrome may occur as a complication with peak incidence after 48 hours of surgery. PCA or neuraxial opioids are better choices for postoperative analgesia.
Pain Relief in the management of painful episodes.
There is no standard method for pain relief, resulting in institution of all possible measures like:• Fluid Replacement (3-4 litres/day in adults)• Analgesics - Opioids (morphine) in regular
doses and for breakthrough pain as well, PCA with morphine and adjunctive drugs like NSAIDS taking into consideration the standard contraindications forthese drugs. Response is followed up with pain scales and the pain therapy is optimally tailored to the individual patient. Extradural analgesia has been used
Fig 8. Dactylitis in Sickle Cell Anaemia.
in the pain management of sickle cell crises wherever possible.
HEREDITARY SPHEROCYTOSISOwing to the abnormalities in the RBC
cell membrane, water enters the RBCs along with sodium at an increased rate resulting in swollen
RACE 2003 Ramachandra Anaesthesia Continuing Education
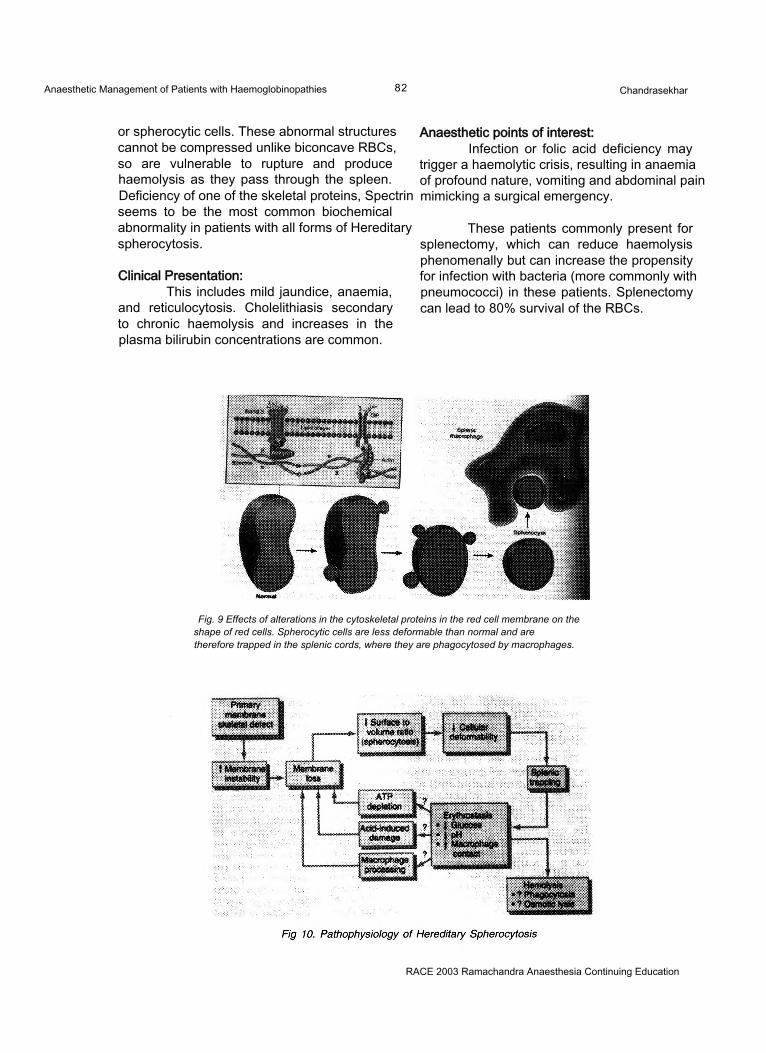
Anaesthetic Management of Patients with Haemoglobinopathies 82 Chandrasekhar
or spherocytic cells. These abnormal structures cannot be compressed unlike biconcave RBCs, so are vulnerable to rupture and produce haemolysis as they pass through the spleen. Deficiency of one of the skeletal proteins, Spectrin seems to be the most common biochemical abnormality in patients with all forms of Hereditary spherocytosis.
Clinical Presentation:This includes mild jaundice, anaemia,
and reticulocytosis. Cholelithiasis secondary to chronic haemolysis and increases in the plasma bilirubin concentrations are common.
Anaesthetic points of interest:Infection or folic acid deficiency may
trigger a haemolytic crisis, resulting in anaemia of profound nature, vomiting and abdominal pain mimicking a surgical emergency.
These patients commonly present for splenectomy, which can reduce haemolysis phenomenally but can increase the propensity for infection with bacteria (more commonly with pneumococci) in these patients. Splenectomy can lead to 80% survival of the RBCs.
Fig. 9 Effects of alterations in the cytoskeletal proteins in the red cell membrane on the shape of red cells. Spherocytic cells are less deformable than normal and are therefore trapped in the splenic cords, where they are phagocytosed by macrophages.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 83 M. Ravishankar
INTRODUCTION:The technique of reusing the expired gas
for alveolar ventilation after absorption of carbon dioxide can be traced to the very beginning of Anaesthesia when Dr. John Snow used caustic potash to absorb C02 from the expired gas. This concept was considerably simplified by the introduction of the “To and Fro” system by Waters and the circle system by Brian Sword, which utilised sodalime for absorption ofC02. It reigned supreme in the early half of this century when expensive and explosive agents like cyclopropane were utilised. The introduction of non-explosive agents like halothane and plenum vaporisers which performed optimally only in the presence of higher flows resulted in low flow anaesthesia becoming less popular. With the added knowledge of the disadvantages of using high percentages of 02 for prolonged periods and the necessity to use a second gas to control the percentage of oxygen, coupled with the complexities involved in the calculation of uptake of anaesthetic agents during the closed circuit anaesthesia made this technique even less popular. However, the awareness of the dangers of theatre pollution with trace amounts of the anaesthetic agents and the prohibitively high cost of the new inhalational agents, have helped in the rediscovery of low flow anaesthesia.
DEFINITIONLow flow anaesthesia has various
definitions. Any technique that utilises a fresh gas flow (FGF) that is less than the alveolar ventilation can be classified as ‘Low flow anaesthesia’. Baum et al1 had defined it as a technique wherein at least 50% of the expired gases had been returned to the lungs after carbon dioxide absorption. This would be satisfied when
the FGF was less than about two litres per minute.
Baker2 in his editorial had classified the FGF used in anaesthetic practice into the following categories:
For most practical considerations, utilisation of a fresh gas flow less than 2 litres/ min may be considered as low flow anaesthesia.
The need for low flow anaesthesia.Completely closed circuit anaesthesia is
based upon the reasoning that anaesthesia can safely be maintained if the gases, which are taken up by the body alone, are replaced into the circuit taking care to remove the expired carbon dioxide with sodalime. No gas escapes out of the circuit and this would provide for maximal efficiency for the utilisation of the fresh gas flow. The very nature of this system requires that the exact amount of anaesthetic agent taken up by the body be known, since that exact amount has to be added into the circuit. Any error in this could lead to a potentially dangerous level of anaesthetic agent being present in the inspired mixture with its attended complications. Hence, there exists a need for a system that provided the advantages of the completely closed circuit and at the same time, reduced the dangers associated with it. Low flow anaesthesia fulfilled these requirements.
Low flow anaesthesia involves utilising a fresh gas flow, which is higher than the metabolic
RACE 2003 Ramachandra Anaesthesia Continuing Education
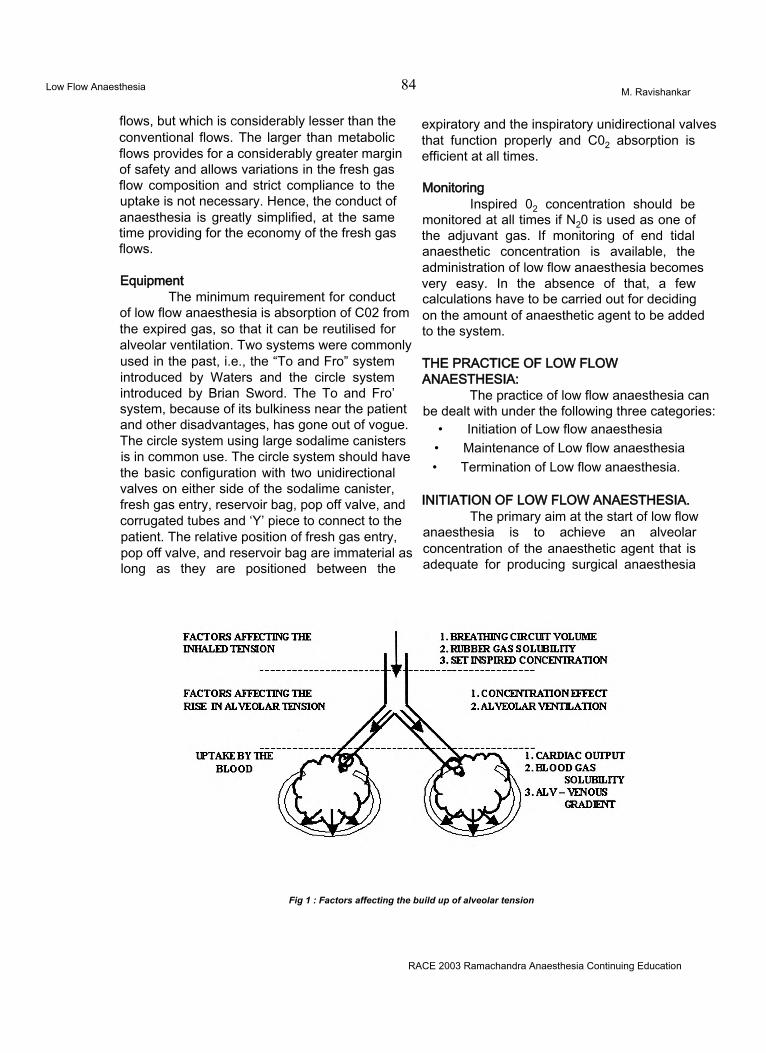
Low Flow Anaesthesia 84 M. Ravishankar
flows, but which is considerably lesser than the conventional flows. The larger than metabolic flows provides for a considerably greater margin of safety and allows variations in the fresh gas flow composition and strict compliance to the uptake is not necessary. Hence, the conduct of anaesthesia is greatly simplified, at the same time providing for the economy of the fresh gas flows.
EquipmentThe minimum requirement for conduct
of low flow anaesthesia is absorption of C02 from the expired gas, so that it can be reutilised for alveolar ventilation. Two systems were commonly used in the past, i.e., the “To and Fro” system introduced by Waters and the circle system introduced by Brian Sword. The To and Fro’ system, because of its bulkiness near the patient and other disadvantages, has gone out of vogue. The circle system using large sodalime canisters is in common use. The circle system should have the basic configuration with two unidirectional valves on either side of the sodalime canister, fresh gas entry, reservoir bag, pop off valve, and corrugated tubes and ‘Y’ piece to connect to the patient. The relative position of fresh gas entry, pop off valve, and reservoir bag are immaterial as long as they are positioned between the
expiratory and the inspiratory unidirectional valves that function properly and C02 absorption is efficient at all times.
MonitoringInspired 02 concentration should be
monitored at all times if N20 is used as one of the adjuvant gas. If monitoring of end tidal anaesthetic concentration is available, the administration of low flow anaesthesia becomes very easy. In the absence of that, a few calculations have to be carried out for deciding on the amount of anaesthetic agent to be added to the system.
THE PRACTICE OF LOW FLOW ANAESTHESIA:
The practice of low flow anaesthesia can be dealt with under the following three categories:
• Initiation of Low flow anaesthesia• Maintenance of Low flow anaesthesia• Termination of Low flow anaesthesia.
INITIATION OF LOW FLOW ANAESTHESIA.The primary aim at the start of low flow
anaesthesia is to achieve an alveolar concentration of the anaesthetic agent that is adequate for producing surgical anaesthesia
Fig 1 : Factors affecting the build up of alveolar tension
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 85 M. Ravishankar
(approximately 1.3 MAC). The factors that can influence the build up of alveolar concentration should all be considered while trying to reach the desired alveolar concentration. These factors can broadly be classified into three groups (fig. 1); 1) Factors governing the inhaled tension of the anaesthetic, 2) Factors responsible for the rise in alveolar tension, 3) Factors responsible for uptake from the lungs thus reducing the alveolar tension.
Factors governing the inhaled tension of the anaesthetic:1 The circle system is often bulky and has a
volume roughly equal to 6-7 litres. Besides this, the FRC of the patient, which is roughly3 litres, together constitutes a reserve volume of 10 litres to which the anaesthetic gases and vapours have to be added. With the addition of FGF, the rate of change of composition of the reserve volume is exponential. The time required for the changes to occur is governed by the time constant, which is equal to this reserve volume divided by the fresh gas flow. This represents the time required for 67% change to occur in the gas concentration. Three time constants are needed for a 95% change in the gas concentration to occur. Hence, if a FGF of 1L/min is used, then 30 minutes will be required for the circuit concentration to reflect the gas concentration of the FGF. If the FGF is still lower, then a correspondingly longer time will be required.
2. The functional residual capacity of the lung and the body as a whole contain nitrogen, which will try to equilibrate with the circuit volume and alter the gas concentration if satisfactory denitrogenation is not achieved at the start of anaesthesia. Hence, as a prelude to the initiation of closed or low flow anaesthesia, thorough denitrogenation must be achieved with either a non-rebreathing circuit or the closed circuit with a large flow of oxygen and a tight fitting facemask.
3. The anaesthetic agent could be lost from the breathing system due to solubility of the agent in rubber, and permeability through the corrugated tubes. Though the amount of loss
will be minimal, it should be considered atthe start if the aimed anaestheticconcentration is low.
Factors responsible for rise in alveolar tension of the anaesthetic agent:1. CONCENTRATION EFFECT:
The concentration effect helps in raising the alveolar tension towards the inspired tension, but hinders it, if an insoluble gas is present in the mixture. The rate of rise of alveolar partial pressure of the anaesthetic agent must bear a direct relationship to the inspired concentration. The higher the inspired concentration, the more rapid is the rise in alveolar concentration. At a low inspired concentration, the alveolar concentration results from a balance between the ventilatory input and the circulatory uptake. If the latter removes half the anaesthetic introduced by ventilation, then the alveolar concentration is half that inspired. The concentration effect modifies this influence of uptake. When appreciable volumes are taken up rapidly, the lungs do not collapse; instead the subatmospheric pressure created in the lung by the anaesthetic uptake causes passive inspiration of an additional volume of gas to replace that lost by uptake, thus increasing the alveolar concentration and offsetting the mathematical calculations. Similarly, if an insoluble gas (e.g., nitrogen) is present in the inspired mixture, as the blood takes up the anaesthetic gas, the concentration of the insoluble gas will go up in the alveoli, reducing the concentration of the anaesthetic agent.
2. ALVEOLAR VENTILATION:The second factor governing the delivery of
anaesthetic agent to the lung is the level of alveolar ventilation. The greater the alveolar ventilation, the more rapid is the rise of alveolar concentration towards the inspired concentration. This effect is limited only by the lung volume; the larger the functional residual capacity, the slower the wash in of the new anaesthetic gas.
Factors responsible for uptake from the lungs thus reducing the alveolar tension:
Uptake from the lung is the product of three factors: solubility of the agent in the blood, the cardiac output and the alveolar to venous partial pressure gradient.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 86 M. Ravishankar
1. BLOOD GAS SOLUBILITY:“Solubility” is the term used to describe
how a gas or vapour is distributed between two media. At equilibrium, that is when the partial pressure of the anaesthetic in the two phases is equal, the concentration of the anaesthetic in the two phases might differ. This is calculated as a coefficient. When it is between blood and gas it is called blood gas solubility coefficient. If other things are equal, the greater the blood/ gas solubility coefficient, the greater the uptake of the anaesthetic, and slower the rate of rise of alveolar concentration.
2. CARDIAC OUTPUT:Because blood carries anaesthetic away
from the lungs, the greater the cardiac output, the greater the uptake, and consequently the slower the rate of rise of alveolar tension. The magnitude of this effect is related to the solubility: the most soluble agents are affected more than the least soluble agents.
3. ALVEOLAR TO VENOUS PARTIAL PRESSURE GRADIENT:
During induction the tissues remove all the anaesthetic brought to them by the blood. This lowers the venous anaesthetic partial pressure far below that of the arterial blood. The result is a large alveolar to venous anaesthetic partial pressure difference, which causes maximum anaesthetic uptake and hence lowers the alveolar partial pressure.
Considering the above mentioned factors at the start of anaesthesia, two facts become apparent:1. Induction if performed using low flows
would take an unacceptably long time.
2. If induction is done with an intravenous agent, unless special precautions are taken, it may take a very long time to achieve the desired alveolar concentration. Once the desired concentration is achieved, it will be difficult to change it. Hence, termination of action would take a long time after the discontinuation of the agents.
Methods to achieve desired gas and agent concentrationUSE OF HIGH FLOWS FOR A SHORT TIME:
This is by and far the commonest and the most effective technique of initiating closed circuit. By using high flows for a short time, the time constant is reduced thereby bringing the circuit concentration to the desired concentration rapidly. Often, a fresh gas flow of 10L of the desired gas concentration and 2 MAC agent concentration is used so that by the end of three minutes (three time constants) the circuit would be brought to the desired concentration. The large flows and high agent concentration also compensate for the large uptake seen at the start of the anaesthesia. Mapleson3 using a spreadsheet model of a circle breathing system has calculated that, by using a FGF equal to minute ventilation and setting the anaesthetic agent partial pressure to 3 MAC, the end expired partial pressure of halothane will reach 1 MAC in4 minutes and that of isoflurane in 1.5 minutes. The major advantages of this method are the rapidity with which the desired concentration is achieved, the ability to prevent unexpected rise in the agent concentration and the ability to use the commonly available plenum vaporisers to achieve the desired concentration. This also has the added advantage of achieving better denitrogenation, so vital to the conduct of low flow anaesthesia. The chief disadvantage would be the high flows required which would compromise on the economy of the gas utilisation and the need for scavenging systems to prevent theatre pollution. This period of using high flows for a short period at initiation goes by the name of “loading”.
PREFILLED CIRCUIT.The second method is utilising a different
circuit like Magills for preoxygenation. Simultaneously, the circle is fitted with a test lung and the entire circuit is filled with the gas mixture of the desired concentration. Following intubation, the patient is connected to the circuit thereby ensuring rapid achievement of the desired concentration in the circuit. But all the factors discussed above will be effective in preventing fast build up of the alveolar concentration to attain surgical anaesthesia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
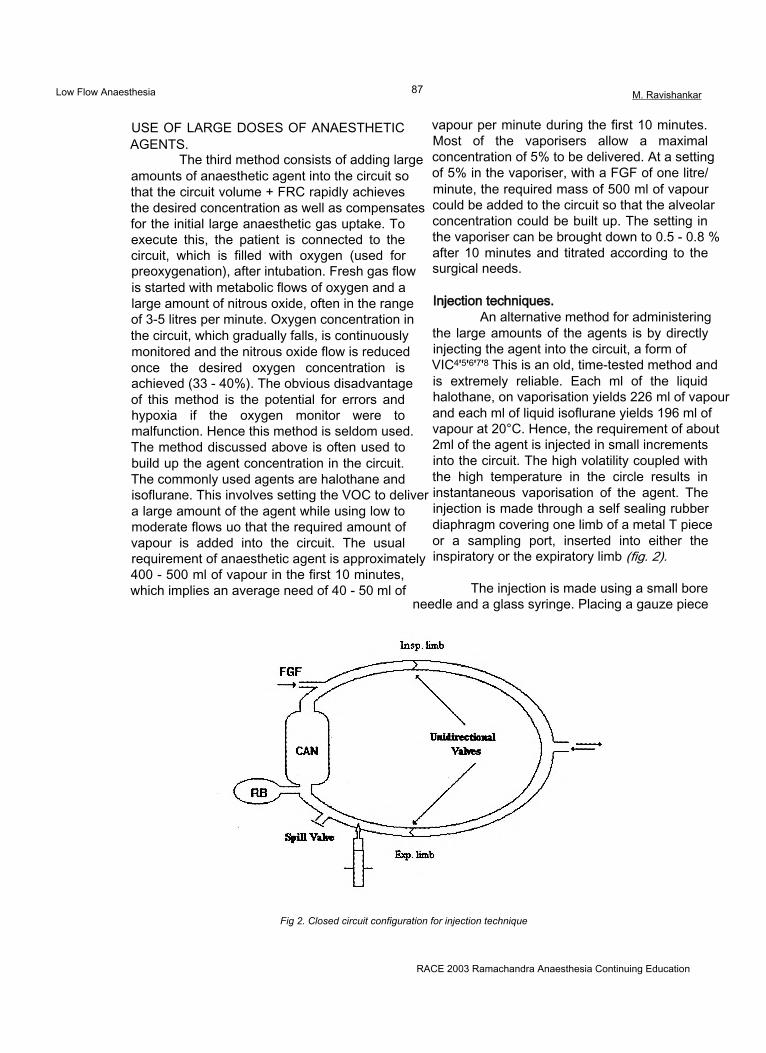
Low Flow Anaesthesia 87 M. Ravishankar
USE OF LARGE DOSES OF ANAESTHETIC AGENTS.
The third method consists of adding large amounts of anaesthetic agent into the circuit so that the circuit volume + FRC rapidly achieves the desired concentration as well as compensates for the initial large anaesthetic gas uptake. To execute this, the patient is connected to the circuit, which is filled with oxygen (used for preoxygenation), after intubation. Fresh gas flow is started with metabolic flows of oxygen and a large amount of nitrous oxide, often in the range of 3-5 litres per minute. Oxygen concentration in the circuit, which gradually falls, is continuously monitored and the nitrous oxide flow is reduced once the desired oxygen concentration is achieved (33 - 40%). The obvious disadvantage of this method is the potential for errors and hypoxia if the oxygen monitor were to malfunction. Hence this method is seldom used. The method discussed above is often used to build up the agent concentration in the circuit. The commonly used agents are halothane and isoflurane. This involves setting the VOC to deliver a large amount of the agent while using low to moderate flows uo that the required amount of vapour is added into the circuit. The usual requirement of anaesthetic agent is approximately 400 - 500 ml of vapour in the first 10 minutes, which implies an average need of 40 - 50 ml of
vapour per minute during the first 10 minutes. Most of the vaporisers allow a maximal concentration of 5% to be delivered. At a setting of 5% in the vaporiser, with a FGF of one litre/ minute, the required mass of 500 ml of vapour could be added to the circuit so that the alveolar concentration could be built up. The setting in the vaporiser can be brought down to 0.5 - 0.8 % after 10 minutes and titrated according to the surgical needs.
Injection techniques.An alternative method for administering
the large amounts of the agents is by directly injecting the agent into the circuit, a form of VIC4'5'6'7'8 This is an old, time-tested method and is extremely reliable. Each ml of the liquid halothane, on vaporisation yields 226 ml of vapour and each ml of liquid isoflurane yields 196 ml of vapour at 20°C. Hence, the requirement of about 2ml of the agent is injected in small increments into the circuit. The high volatility coupled with the high temperature in the circle results in instantaneous vaporisation of the agent. The injection is made through a self sealing rubber diaphragm covering one limb of a metal T piece or a sampling port, inserted into either the inspiratory or the expiratory limb (fig. 2).
The injection is made using a small bore needle and a glass syringe. Placing a gauze piece
Fig 2. Closed circuit configuration for injection technique
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 88 M. Ravishankar
or a wire mesh inside the T piece often helps in the vaporisation of the liquid. The intermittent injections are often made in 0.2-0.5 ml aliquots manually. Doses should never exceed 1 ml at a time. Doses exceeding 2 ml bolus invite disaster. Intermittent injections can often be easily substituted with a continuous infusion with the added advantage of doing away with the peaks and troughs associated with intermittent injections.
The exact dose to be used is calculatedthus:Priming dose (ml vapour) = Desired concentration
x{( FRC + Circuit volume) +(Cardiac output x BG Coeff.)}
The Cardiac output and the FRC can be estimated for the patient based on standard nomograms, minutes of the closed circuit anaesthesia. Besides this, an amount of agent necessary to compensate for the uptake of the body must also be added and this is calculated depending on the uptake model being used (vide infra).
THE MAINTENANCE OF LOW FLOW ANAESTHESIA
This is the most important phase as this is stretched over a period of time and financial savings result directly from this. This phase is characterised by1 Need for a steady state anaesthesia often
meaning a steady alveolar concentration of respiratory gases.
2 Minimal uptake of the anaesthetic agents by the body.
3 Need to prevent hypoxic gas mixtures.
Since the uptake of the anaesthetic agent is small in this phase, the low flow anaesthesia is eminently practical. Adding small amounts of the anaesthetic gases to match the uptake and providing oxygen for the basal metabolism should suffice. If CCA is used, this would be directly equal to the uptake and hence provides for the monitoring of the oxygen consumption and the agent uptake. If low flow anaesthesia is used, then besides the uptake, the amount of gas, which is vented, is also added to the circuit to maintain steady state anaesthesia.
Management of the oxygen and nitrous oxide flow during the maintenance phase:
The need to discuss the flow rates of N20 and 02 arises specifically because of the possible danger of administration of a hypoxic mixture. Let us analyse the following example. 33% oxygen is set using a flow of 500 ml of 02 and 1000 ml of N20. Oxygen is taken up from the lungs at a constant rate of about 4 ml/kg/min. N20 is a relatively insoluble gas and after the initial equilibration with the FRC and vessel rich group of tissues, the uptake is considerably reduced. In this situation, there is a constant removal of02 at a rate of 200 - 250 ml/min, where as the insoluble gas N20 uptake is minimal. Hence the gas returning to the circuit will have more N20 and less of 02. Over a period of time, due to concentration effect, the percentage of N20 will go up and that of 02 will fall, sometimes dangerously to produce hypoxic mixtures.
Various short cuts are available to make low flow anaesthesia easy of which the most popular technique is the ‘Gothenburg technique’9. Most of the other techniques approximate this and hence it deserves a special mention.
THE GOTHENBURG TECHNIQUE:Initially high flows, oxygen at 1.5 l/min
and nitrous oxide at 3.5 l/min had to be used for a period of six minutes after the induction of anaesthesia and this constitutes the loading phase. This is followed by the maintenance phase in which the oxygen flow is reduced to about 4ml/kg and nitrous oxide flow adjusted to maintain a constant oxygen concentration in the circuit. The usual desired oxygen concentration is about 40%. The use of an oxygen analyser is very important since the nitrous oxide added is directly based on its readings and hence any errors would be dangerous.
Other authors have made similar recommendations10'11,12'13'14. Most of the authors opine that the oxygen consumption under anaesthesia is about 200 - 250 ml. However, there is a wide disparity in the amount of nitrous oxide to be added into the circuit. This controversy is consistent with the basic controversy surrounding the uptake of the anaesthetic agents and is dealt with in detail in a later stage. For most practical
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 89 M. Ravishankar
purposes, in the absence of an oxygen analyser, the following technique is safe to use. A high flow of 10 lit/min at the start, for a period of 3 minutes, is followed by a flow of 400 ml of 02 and 600 ml of N20 for the initial 20 minutes and a flow of 500 ml of 02 and 500 ml of N20 thereafter. This has been shown to maintain the oxygen concentration between 33 and 40 % at all times.
Management of the potent anaesthetic agents during maintenance phase.
This is easily accomplished by dialling in the calculated concentration on the plenum vaporiser for the flow being used. For example, suppose the anaesthetic uptake for a desired concentration of 0.5% halothane is 7.5ml/min (vide infra). If a FGF of 500ml/min is being used, then the dial setting should be 1.5%, for at this setting and for the used flow, the total vapour output would be 7.5ml/min. If a flow of 1000ml/min is being used, then the dial setting should be 0.8%. In practice the actual dial setting often over estimates the actual output since the plenum vaporiser under delivers the agent at low flows. Hence, the dial setting is fine-tuned depending on the endpoints being achieved.
During completely closed circuit anaesthesia, the most popular method of adding agents into the circuit is by the injection technique. This is often used to initiate the closed circuit anaesthesia as described earlier. Later, the same setup is used to continue the anaesthesia by adding either small boluses or by constant infusion into the circuit. The dose to be added depends on the uptake model being used for the conduct of the closed circuit. The endpoint for adding the agent can be the achievement of the desired end tidal agent concentration, measured using an agent analyser. This would be the most accurate method. The end point may also be based on the haemodynamic stability15.
Simple rule of the thumb techniques1617 for adding the anaesthetic agents into the circuit both during the loading phase and the maintenance phase has been suggested.
Weir and Kennedy4 recommend infusion of halothane (in liquid ml/hr) at the following rates for a 50 kg adult at different time intervals.
0-5 min 27 ml/hr5-30 min 5.71 ml/hr30-60 min 3.33 ml/hr60-120 min 2.36 ml/hr
These infusion rates had been derived from the Lowe’s theory of the uptake of anaesthetic agent (vide infra). They had approximated isoflurane infusion (in liquid ml/hr) based on the Lowe’s formula as follows:
0-5 min. 5 - 3 0 min. 30-60 min. 60-120 min.
14 + 0.4X wt. ml/hr.0 2 X initial rate. 0.12Xinitial rate.0.08X initial rate.
For halothane infusion, they had suggested that the above said rates be multiplied by 0.8 and for enflurane, multiplied by 1.6. These rates had been suggested to produce 1.3 MAC without the use of nitrous oxide. The infusion rates had to be halved if nitrous oxide is used.
The other salient points to be considered during the maintenance phase are the following: a) Leaks must be meticulously sought for and prevented since they would decrease the efficacy of the system. Flows must be adjusted to compensate for the gas lost in the leaks, b) Most of the gas monitors sample gases at the rate of 200 ml/min, which may be sometimes as high as half the FGF. Hence, care must be taken to return the sample back to the circuit to maximise the economy of FGF utilisation. Some gas analysers like Ohmeda Rascal add air to the sample exhaust. This if returned to the circuit would result in dilution of the anaesthetic mixture and accumulation of nitrogen within the circuit and hence should be vented. This mandates utilisation of a flow adequate to compensate for this loss. Recent studies18 have shown that venting of the gas from the analyser does not alter the dynamics to any large extent and can safely be done.
CONTROVERSIES IN THE UPTAKE MODELS OF ANAESTHETIC AGENTS EXPONENTIAL OR LINEAR?
Knowledge of uptake of anaesthetic agent is very important in the practice of closed
RACE 2003 Ramachandra Anaesthesia Continuing Education
Low Flow Anaesthesia 90 M. Ravishankar
and low flow anaesthesia since, the very technique calls for the addition of an amount of anaesthetic agent, which is taken up by the body. In fact, mutually contradicting models exist on the uptake of anaesthetic agents. The Lowe’s theory*3'*4, which has wider acceptance, ascribes the anaesthetic uptake to an exponential model. It states that the uptake of agent is inversely proportional to the square root of the time, implying that the uptake decreases exponentially with time. It necessitates calculation of unit dose (Appendix 1). This unit dose is the amount of anaesthetic agent to be added to the closed circuit during the time intervals of 0-1 min, 1-4 min, 4-9 min, 9-16 min, and so on. Besides that, the circuit and the FRC and the circulating blood of the patient had to be brought to the desired concentration with a prime dose.Prime dose = {(circuit volume + FRC) +
(Q xk)} x desired Concentration.
This prime dose had to be added into the circuit during the first 9 minutes of closed circuit anaesthesia.
The practical implication of this is that to maintain closed circuit, one must calculate the agent and gases to be added into the circuit using hair-splitting exponential equations, often frightening the anaesthetist. It has been one of the main causes for the reluctance in the widespread usage of the closed circuit anaesthesia.
In total contrast to this exponential theory is the linear model proposed by CY Lin 1214 He states that the uptake of anaesthetic agents is a near constant over the clinically important concentrations. Hence, he advocated adding the anaesthetic agent as a constant rate infusion into the circuit throughout the anaesthetic procedure. Lin had contended that the FRC constituted an extension of the breathing circuit and the washin into it could not be considered as uptake by the body. He had suggested a simple method of conducting the closed circuit anaesthesia: It had consisted of using a high flow of nitrous oxide and oxygen (6 L/min and 4 L/min respectively) for 3 minutes (three time constants). At the end of 3 minutes, the flows had been reduced to metabolic flows and closed circuit started. Potent agents had
been added either through a VOC (like a copper kettle) or by direct injection into the circuit. The anaesthetic agent required to washin the circuit volume and the FRC of the patient had constituted the prime dose and it should be added to the circuit during the first ten minutes, besides the dose required to compensate for the uptake of the agent. The formula to calculate the amount of agent to be added into the circuit to equal the uptake had been:
Uptake of anaesthetic agent = desired concentration x alveolar ventilation x fractional uptake ( ml of vapour).
The fractional uptake (= 1 - FA/ F,) for halothane had been calculated as 0.5 and that for enflurane, as 0.4. He had concluded that anaesthesia thus conducted produced a nearly constant inspired and expired concentration implying that the uptake of the anaesthetic agents had been a near constant.
Unfortunately very little literature exists on the efficacy of either of these models. The study conducted to compare these two models in our Institute, revealed that predictive performance of both the models were statistically similar, and linear uptake model had scope for improvement where as the exponential model had no such scope. Lin’s linear model however has a distinct superiority in the form of simplicity.
TERMINATION OF LOW FLOW ANAESTHESIA
Unlike the initiation or the maintenance of the closed circuit, termination is less controversial. There are only two recognised methods of termination of the closed circuit. They are as follows:
Towards the end of the anaesthesia, the circuit is opened and a high flow of gas is used to flush out the anaesthetic agents, which accelerates the washout of the anaesthetic agents. This has the obvious advantage of simplicity but would result in wastage of gases.
The second method is the use of activated charcoal8 Activated charcoal when heated to 220°C adsorbs the potent vapours almost completely. Hence, a charcoal-containing
RACE 2003 Ramachandra Anaesthesia Continuing Education

Low Flow Anaesthesia 91 M. Ravishankar
canister with a bypass is placed in the circuit. Towards the end of the anaesthesia, the gas is directed through the activated charcoal canister. This results in the activated charcoal adsorbing the anaesthetic agent resulting in rapid recovery and at the same time, reducing theatre pollution. Nitrous oxide, due to its low solubility is washed off towards the end by using 100% oxygen.
To conclude, the low flow closed circuit anaesthesia has many advantages to offer. To list a few,1 Enormous financial savings due to use of low
fresh gas flows as well as the agent.2 High humidity in the system leads to fewer
post anaesthetic complications.3 Maintenance of body temperature during
prolonged procedures due to conservation of heat.
4 Reduction in the theatre pollution.
The perceived disadvantages are not real:1 The need to accurately adjust the flows of
gases. The system is inherently stable once a steady state is reached and small errors in the dosage of the agents or the gases would be of no concern.
2 Accumulation of trace gases20. It has, however, been often overestimated21.
3 Need for monitoring equipment. Oxygen monitor is the only one that is necessary and since it is part of the basic monitoring it cannot be considered as a disadvantage.
With a proper understanding of the concepts of practice, the low flow anaesthesia technique can safely be used in all surgical procedures lasting more than an hour.
REFERENCES1 Baum JA, Aithkenhead: Low flow
Anaesthesia. Anaesthesia. 50 (suppl).: 37-44, 1995
2 Baker AB: Editorial. Low flow and Closed Circuits. Anaesthesia and Intensive Care. 22: 341-342, 1994
3 Mapleson W: The theoretical ideal fresh gasflow sequence at the start of low flow anaesthesia Anaesthesia 53(3):264-72, 1998
4 Weir HM, Kennedy RR: Infusing liquid anaesthetic agents into the closed circle anaesthesia. Anaesthesia and Intensive Care. 22: 376-379, 1994
5 Wolfson B: Closed Circuit Anaesthesia by Intermittent Injections of Halothane. British Journal of Anaesthesia. 34: 733 - 737., 1962
6 Thorpe CM, Kennedy RR: Vaporisation of Isoflurane by Liquid Infusion. Anaesthesia and Intensive Care. 22: 380-82, 1994
7 Hampton JL, Flickinger H: Closed Circuit Anesthesia utilising known increments of Halothane.Anesthesiology 22: 413-418, 1961
8 Philip JH: ‘Closed Circuit Anaesthesia’ in ‘Anesthesia Equipment: Principles and Applications’. Edited by Ehrenwerth J, Eisenkraft JB, Mosby Year Book Inc., 1993, Chap 30.
9 Dale O, Stenqvist O: Low flow Anaesthesia : Available today - A routine tomorrow. Survey of Anesthesiology. 36: 334-336, 1992
10 Cullen SC: Who is watching the patient? Anesthesiology 37: 361-362, 1972
11 Baker AB: Back to Basics - A Simplified Non - Mathematical Approach to Low Flow Techniques in Anaesthesia. Anaesthesia and Intensive Care. 22: 394-395., 1994
12 Lin CY, Benson JW, Mostert DW: Closed Circle Systems - A new direction in the practice of Anaesthesia. Acta Anaesthesiologica Scandinavica. 24: 354-361., 1980
13 Lowe HJ: ‘The Anesthetic Continuum’ in the book, ‘Low flow and closed circuit anesthesia’. Edited by Aldrete JA, Lowe HJ, Virtue RW, Grune & Stratton, 1979, pp 11-38
14 Lowe H: ‘Closed- circuit anesthesia’, in the book ‘Clinical Anesthesiology’ Edited byMorgan GE, Mikhail MS, Appleton and Lange, 1992, pp 112 -115.
15 Da Silva CJM, Mapleson WW, Vickers MD: Quantitative study of Lowe’s square root of time method of closed system anaesthesia. British Journal of Anaesthesia. 79: 103-112., 1997
16 El - Attar AM: Guided Isoflurane injection in a totally closed circuit. Anaesthesia. 46.: 1059-1063., 1991.
17 Eger II E: “Uptake and Distribution”, in the book “Anesthesia”, Edited by Miller RD, Ed4, Churchill Livingstone,1994, p118.
18 Bengtson J, Bengtsson J, Bengtsson A, Stenqvist O: Sampled gas need not be returned during low-f!ow anaesthesia. Journal of Clinical Monitoring 9(5): 330-4, 1993
19 Lin CY: Uptake of Anaesthetic Gases and Vapours. Anaesthesia and Intensive Care. 22: 363-373, 1994
20 Morita S, Latta W, Hambro K, Snider MT: Accumilation of methane, acetone and nitrogen in the inspired gas during closed circuit anesthesia. Anesthesia and analgesia. 64: 343-347, 1985
21 Baumgarten R: Much ado about nothing: Trace gaseous metabolites in closed circuit.Anesthesia and Analgesia. 64: 1029-1030, 1985
RACE 2003 Ramachandra Anaesthesia Continuing Education
How to get more from your Central Venous Cather 92 Jigi Divatia
In recent years, central venous cannulation is practised increasingly in anaesthesia and intensive care for a variety of indications (Table 1). Broadly, these indications are monitoring of central venous pressure (CVP) and access for intravenous infusions. Recently, it has become possible to measure cardiac output via a central venous catheter and a peripheral arterial catheter equipped with a sensor for the indicator. The central venous oxygen saturation (Scv02) has also been used to guide hemodynamic therapy in severe sepsis. This review will focus on measurement and monitoring of CVP, especially the physiological basis for interpreting the CVP, as well as outline the newer uses of the CVP in hemodynamic monitoring and therapy.
Measurement of the CVP gives important haemodynamic information regarding the status of the cardiovascular system and response to therapy. Clinically, measurement of the CVP is used for two purposes:(1) to gain information about cardiac function, and (2) to gain information about the adequacy of vascular volume. It performs this dual function because physiologically the right atrial pressure is the interface between the two major determinants of cardiac output: cardiac contractility and venous return. Because CVP influences and is influenced by, both of these physiologic functions, it is an extremely useful measure of cardiovascular function. However, the process of haemodynamic measurements makes several assumptions regarding the cardiovascular
Measurement of CVP Intravenous access Therapeutic procedures
Major surgery Rapid administration of fluids and blood
Insertion of transvenous pacemaker
Anticipated major blood loss Anticipated major fluid shifts
Total parenteral alimentation Insertion of catheters for haemodialysis and plasmapheresis
Significant cardiac disease Administration of Vasoactive agents and concentrated potassium infusions
Aspiration of air emboli
Significant pulmonary disease Administration of Chemotherapeutic and other irritant drugs
Pulmonary hypertension Frequent blood sampling Insertion of a pulmonary artery catheter
Table 1. Indications for central venous cannulation.
RACE 2003 Ramachandra Anaesthesia Continuing Education
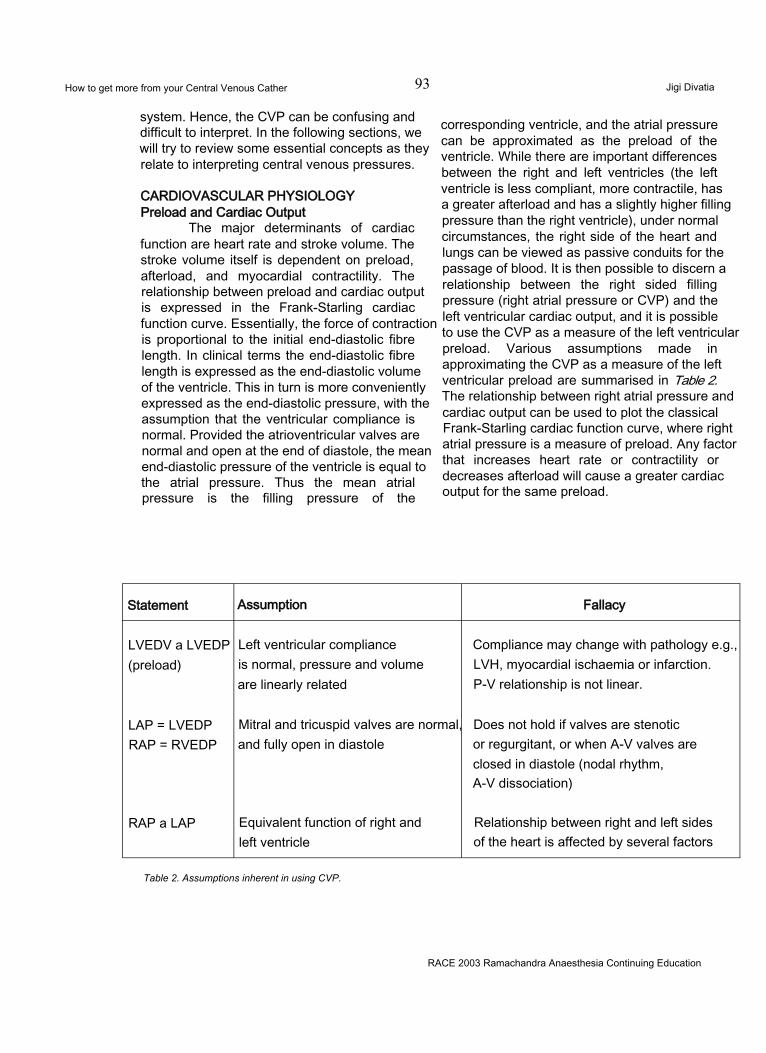
How to get more from your Central Venous Cather 93 Jigi Divatia
system. Hence, the CVP can be confusing and difficult to interpret. In the following sections, we will try to review some essential concepts as they relate to interpreting central venous pressures.
CARDIOVASCULAR PHYSIOLOGY Preload and Cardiac Output
The major determinants of cardiac function are heart rate and stroke volume. The stroke volume itself is dependent on preload, afterload, and myocardial contractility. The relationship between preload and cardiac output is expressed in the Frank-Starling cardiac function curve. Essentially, the force of contraction is proportional to the initial end-diastolic fibre length. In clinical terms the end-diastolic fibre length is expressed as the end-diastolic volume of the ventricle. This in turn is more conveniently expressed as the end-diastolic pressure, with the assumption that the ventricular compliance is normal. Provided the atrioventricular valves are normal and open at the end of diastole, the mean end-diastolic pressure of the ventricle is equal to the atrial pressure. Thus the mean atrial pressure is the filling pressure of the
corresponding ventricle, and the atrial pressure can be approximated as the preload of the ventricle. While there are important differences between the right and left ventricles (the left ventricle is less compliant, more contractile, has a greater afterload and has a slightly higher filling pressure than the right ventricle), under normal circumstances, the right side of the heart and lungs can be viewed as passive conduits for the passage of blood. It is then possible to discern a relationship between the right sided filling pressure (right atrial pressure or CVP) and the left ventricular cardiac output, and it is possible to use the CVP as a measure of the left ventricular preload. Various assumptions made in approximating the CVP as a measure of the left ventricular preload are summarised in Table 2. The relationship between right atrial pressure and cardiac output can be used to plot the classical Frank-Starling cardiac function curve, where right atrial pressure is a measure of preload. Any factor that increases heart rate or contractility or decreases afterload will cause a greater cardiac output for the same preload.
Statement Assumption Fallacy
LVEDV a LVEDP (preload)
Left ventricular compliance is normal, pressure and volume are linearly related
Compliance may change with pathology e.g., LVH, myocardial ischaemia or infarction.P-V relationship is not linear.
LAP = LVEDP RAP = RVEDP
Mitral and tricuspid valves are normal, and fully open in diastole
Does not hold if valves are stenotic or regurgitant, or when A-V valves are closed in diastole (nodal rhythm,A-V dissociation)
RAP a LAP Equivalent function of right and left ventricle
Relationship between right and left sides of the heart is affected by several factors
Table 2. Assumptions inherent in using CVP.
RACE 2003 Ramachandra Anaesthesia Continuing Education

How to get more from your Central Venous Cather 94If it is accepted that the CVP is a
Jigi Divatia
measure of preload, the factors that will affect it are blood volume, venous tone, ventricular compliance, myocardial contractility and afterload. If all the other factors are kept constant, the CVP will give some indication of the contractility, i.e., a failing ventricle is associated with a high CVP. The preload is also affected by changes in afterload. An acute change in the right ventricular afterload by pulmonary embolism causes a rise in CVP, while administration of a peripheral vasoconstrictor like phenylephrine will increase the left ventricular afterload and the CVP. When the acute load is relieved, the CVP will fall. However the commonest causes of variations in CVP during anaesthesia are alterations in blood volume or venous tone, both of wtych are accentuated by posture. For example, during spinal anaesthesia in the supine position, venous tone and venous return are reduced, resulting in a low CVP. Following infusion of fluids, the CVP will return towards normal. However, postoperatively as the anaesthetic-induced vasodilatation recedes, and is replaced by vasoconstriction due to pain, cold, shivering and acidosis, the relative blood volume may be too high, and the CVP will rise.
Ventricular ComplianceThe cardiac function curve uses the right
atrial pressure to represent preload. More accurately, preload is the resting myocardial fiber length or, in the intact heart, end-diastolic ventricular end-diastolic volume. Unfortunately, the relationship between pressure and volume is not linear. The ventricles are able to expand to accept a change in pressure. Cardiac output will increase with little change in the right atrial pressure, until the limits of ventricular expansion are reached. At that point, cardiac output no longer improves but right atrial pressure increases rapidly. Disease states and different physiologic states can change the position & shape of the curve. Consequently, a single measurement of right atrial pressure cannot accurately predict end-diastolic volume. However, determining the compliance (i.e., the change in pressure for a given change in volume) will add valuable information about the system.
Vascular ComplianceJust as the heart demonstrates variable
compliance, the vascular system is able to adjust to changes in volume with minimal changes in
pressure. A rapid increase in vascular volume results in a rapid increase in venous return as well as right atrial & mean systemic pressures. Within seconds, circulatory reflexes begin to adjust these pressures & venous return toward normal. In addition, stress relaxation of the vasculature (not dependent on autonomic reflexes) allows further compensation over the ensuing minutes. Similar compensation occurs for decreases in vascular volume. Consequently, a single measurement of right atrial pressure cannot accurately predict vascular volume. However, determining the compliance of the system can provide valuable clues to the status of the vascular volume.
CLINICAL UTILIZATION OF CVP MEASUREMENT
The most common reasons for CVP measurement are to help determine the state of volume. As can be seen in Table 3, a single measurement of the CVP helps somewhat in defining circulatory status but leaves considerable overlap in possible interpretations.
USING COMPLIANCE TO IMPROVE INTERPRETATION
Rapid changes in vascular volume can help further define the cardiovascular status if the time course of compliance changes is remembered. This is the principle of the “fluid challenge”. A rapid infusion of 300 to 500ml of fluid in a normovolemic adult with good cardiac function will result in a moderate increase in CVP (2 to 4mm Hg) with a return nearly to baseline within 10 to 15 min. A minimal initial rise in CVP implies a reduced vascular volume. A large initial rise in CVP implies a heart that is noncompliant or an elevated vascular volume or both. If the CVP returns to baseline rapidly (within 5min), it implies a reduced vascular volume, which can accommodate additional volume by rapid changes in vasomotor tone. A slower return toward baseline indicates that stress relaxation is occurring & the vascular volume is elevated for the current cardiac status. Table 4 indicates how a fluid challenge can improve the interpretation made on the basis of the CVP alone.
The addition of information about cardiac output can further improve diagnostic accuracy. Actual measurement of cardiac output is best
RACE 2003 Ramachandra Anaesthesia Continuing Education
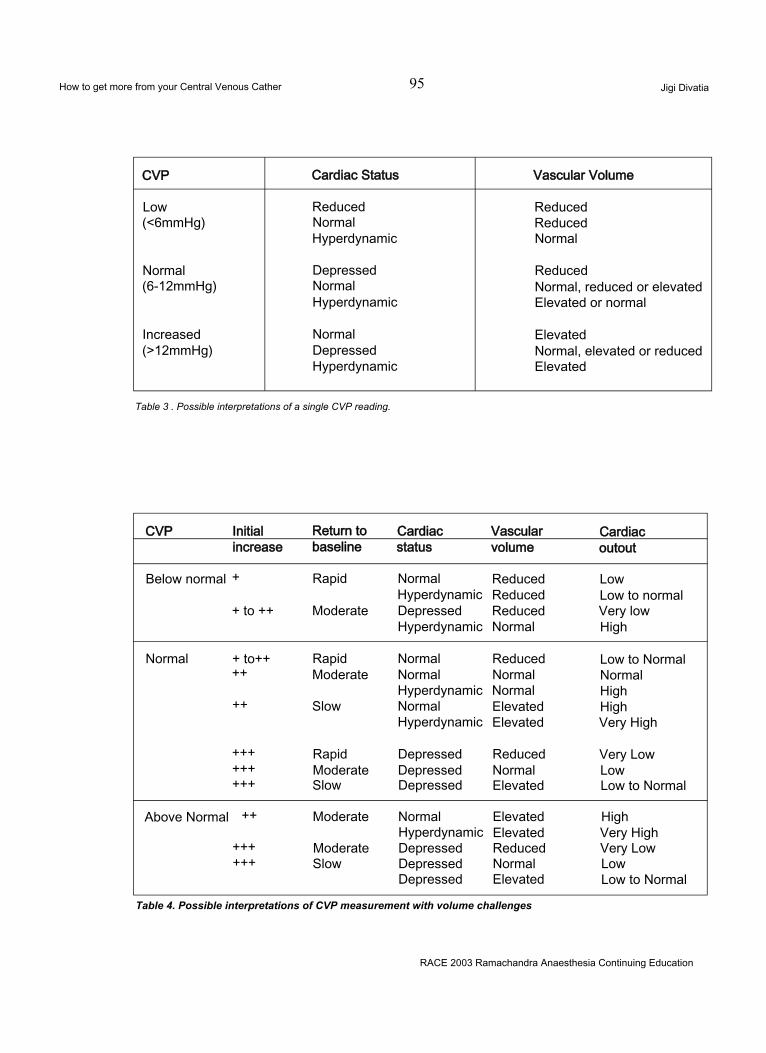
How to get more from your Central Venous Cather 95 Jigi Divatia
CVP Cardiac Status Vascular Volume
Low Reduced Reduced(<6mmHg) Normal Reduced
Hyperdynamic Normal
Normal Depressed Reduced(6-12mmHg) Normal Normal, reduced or elevated
Hyperdynamic Elevated or normal
Increased Normal Elevated(>12mmHg) Depressed Normal, elevated or reduced
Hyperdynamic Elevated
Table 3 . Possible interpretations of a single CVP reading.
CVP Initial Return to Cardiac Vascular Cardiacincrease baseline status volume outout
Below normal + Rapid Normal Reduced LowHyperdynamic Reduced Low to normal
+ to ++ Moderate Depressed Reduced Very lowHyperdynamic Normal High
Normal + to++ Rapid Normal Reduced Low to Normal++ Moderate Normal Normal Normal
Hyperdynamic Normal High++ Slow Normal Elevated High
Hyperdynamic Elevated Very High
+++ Rapid Depressed Reduced Very Low+++ Moderate Depressed Normal Low+++ Slow Depressed Elevated Low to Normal
Above Normal ++ Moderate Normal Elevated HighHyperdynamic Elevated Very High
+++ Moderate Depressed Reduced Very Low+++ Slow Depressed Normal Low
Depressed Elevated Low to Normal
Table 4. Possible interpretations of CVP measurement with volume challenges
RACE 2003 Ramachandra Anaesthesia Continuing Education
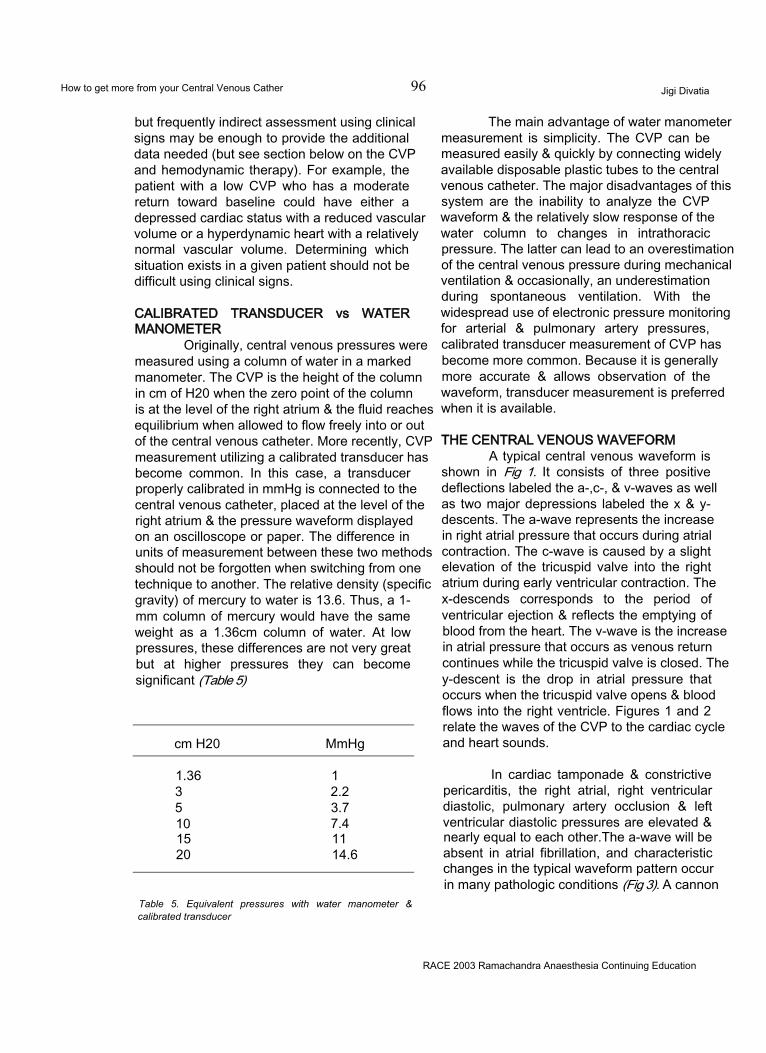
How to get more from your Central Venous Cather 96 Jigi Divatia
but frequently indirect assessment using clinical signs may be enough to provide the additional data needed (but see section below on the CVP and hemodynamic therapy). For example, the patient with a low CVP who has a moderate return toward baseline could have either a depressed cardiac status with a reduced vascular volume or a hyperdynamic heart with a relatively normal vascular volume. Determining which situation exists in a given patient should not be difficult using clinical signs.
CALIBRATED TRANSDUCER vs WATER MANOMETER
Originally, central venous pressures were measured using a column of water in a marked manometer. The CVP is the height of the column in cm of H20 when the zero point of the column is at the level of the right atrium & the fluid reaches equilibrium when allowed to flow freely into or out of the central venous catheter. More recently, CVP measurement utilizing a calibrated transducer has become common. In this case, a transducer properly calibrated in mmHg is connected to the central venous catheter, placed at the level of the right atrium & the pressure waveform displayed on an oscilloscope or paper. The difference in units of measurement between these two methods should not be forgotten when switching from one technique to another. The relative density (specific gravity) of mercury to water is 13.6. Thus, a 1- mm column of mercury would have the same weight as a 1.36cm column of water. At low pressures, these differences are not very great but at higher pressures they can become significant (Table 5)
cm H20 MmHg
1.36 13 2.25 3.710 7.415 1120 14.6
Table 5. Equivalent pressures with water manometer & calibrated transducer
The main advantage of water manometer measurement is simplicity. The CVP can be measured easily & quickly by connecting widely available disposable plastic tubes to the central venous catheter. The major disadvantages of this system are the inability to analyze the CVP waveform & the relatively slow response of the water column to changes in intrathoracic pressure. The latter can lead to an overestimation of the central venous pressure during mechanical ventilation & occasionally, an underestimation during spontaneous ventilation. With the widespread use of electronic pressure monitoring for arterial & pulmonary artery pressures, calibrated transducer measurement of CVP has become more common. Because it is generally more accurate & allows observation of the waveform, transducer measurement is preferred when it is available.
THE CENTRAL VENOUS WAVEFORMA typical central venous waveform is
shown in Fig 1. It consists of three positive deflections labeled the a-,c-, & v-waves as well as two major depressions labeled the x & y- descents. The a-wave represents the increase in right atrial pressure that occurs during atrial contraction. The c-wave is caused by a slight elevation of the tricuspid valve into the right atrium during early ventricular contraction. The x-descends corresponds to the period of ventricular ejection & reflects the emptying of blood from the heart. The v-wave is the increase in atrial pressure that occurs as venous return continues while the tricuspid valve is closed. The y-descent is the drop in atrial pressure that occurs when the tricuspid valve opens & blood flows into the right ventricle. Figures 1 and 2 relate the waves of the CVP to the cardiac cycle and heart sounds.
In cardiac tamponade & constrictive pericarditis, the right atrial, right ventricular diastolic, pulmonary artery occlusion & left ventricular diastolic pressures are elevated & nearly equal to each other.The a-wave will be absent in atrial fibrillation, and characteristic changes in the typical waveform pattern occur in many pathologic conditions (Fig 3). A cannon
RACE 2003 Ramachandra Anaesthesia Continuing Education
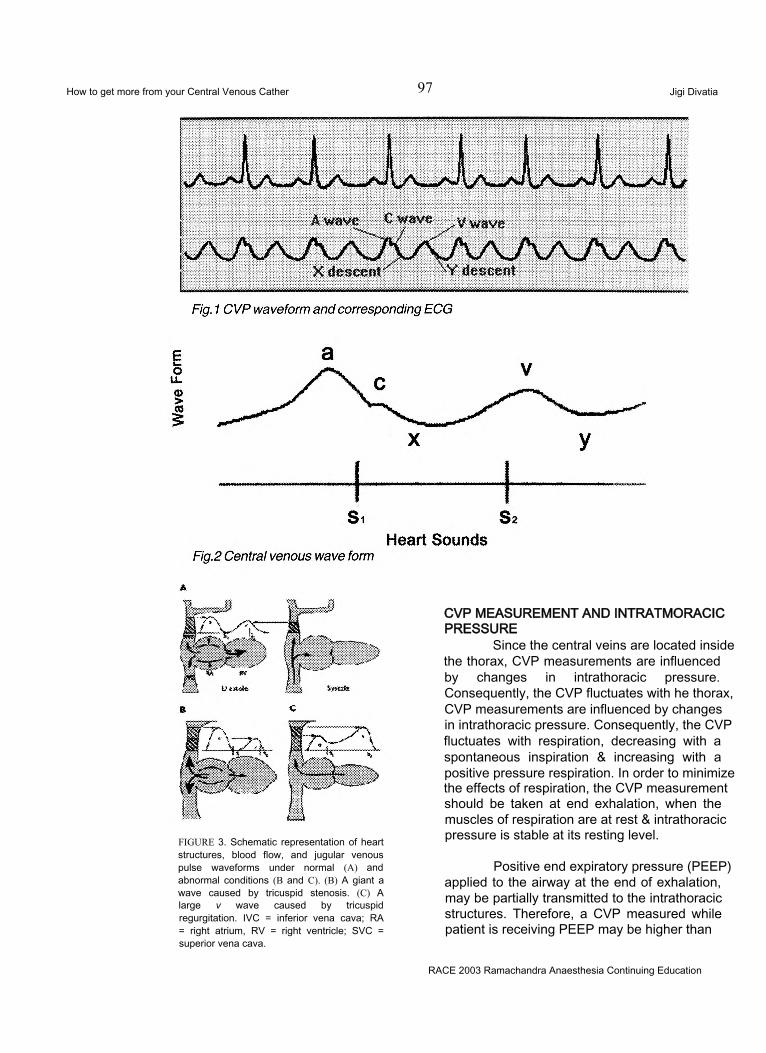
How to get more from your Central Venous Cather 97 Jigi Divatia
FIGURE 3. Schematic representation of heart structures, blood flow, and jugular venous pulse waveforms under normal (A) and abnormal conditions (B and C). (B) A giant a wave caused by tricuspid stenosis. (C) A large v wave caused by tricuspid regurgitation. IVC = inferior vena cava; RA = right atrium, RV = right ventricle; SVC = superior vena cava.
CVP MEASUREMENT AND INTRATMORACIC PRESSURE
Since the central veins are located inside the thorax, CVP measurements are influenced by changes in intrathoracic pressure. Consequently, the CVP fluctuates with he thorax, CVP measurements are influenced by changes in intrathoracic pressure. Consequently, the CVP fluctuates with respiration, decreasing with a spontaneous inspiration & increasing with a positive pressure respiration. In order to minimize the effects of respiration, the CVP measurement should be taken at end exhalation, when the muscles of respiration are at rest & intrathoracic pressure is stable at its resting level.
Positive end expiratory pressure (PEEP) applied to the airway at the end of exhalation, may be partially transmitted to the intrathoracic structures. Therefore, a CVP measured while patient is receiving PEEP may be higher than
RACE 2003 Ramachandra Anaesthesia Continuing Education
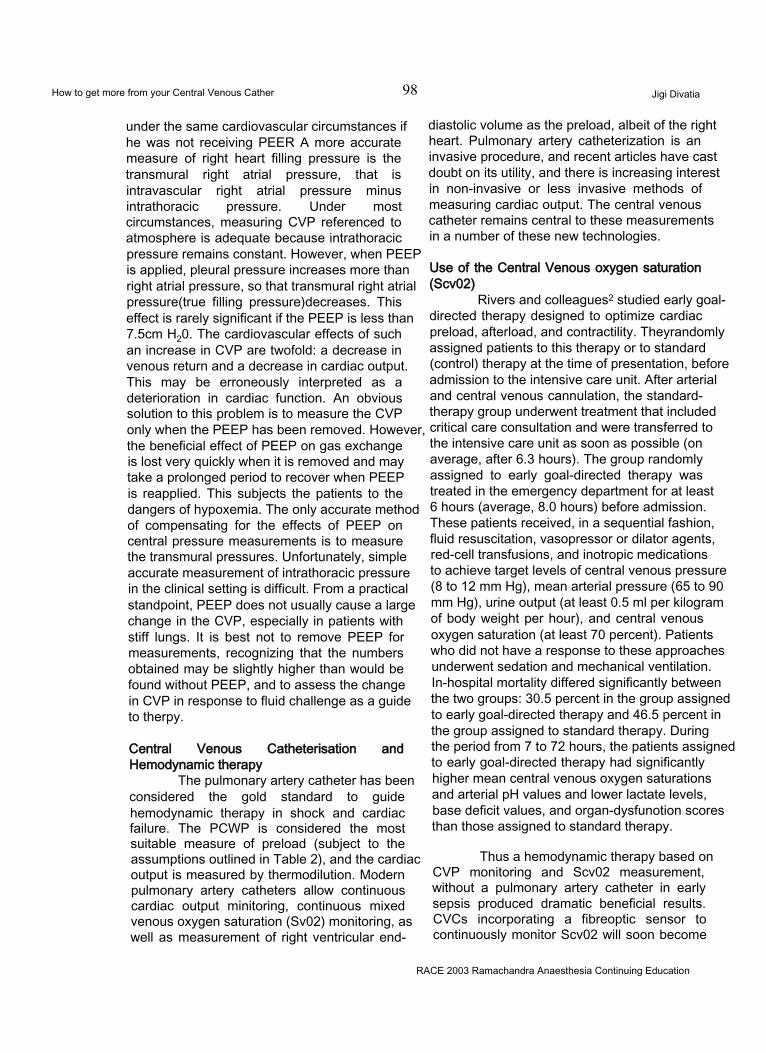
How to get more from your Central Venous Cather 98 Jigi Divatia
under the same cardiovascular circumstances if he was not receiving PEER A more accurate measure of right heart filling pressure is the transmural right atrial pressure, that is intravascular right atrial pressure minus intrathoracic pressure. Under most circumstances, measuring CVP referenced to atmosphere is adequate because intrathoracic pressure remains constant. However, when PEEP is applied, pleural pressure increases more than right atrial pressure, so that transmural right atrial pressure(true filling pressure)decreases. This effect is rarely significant if the PEEP is less than 7.5cm H20. The cardiovascular effects of such an increase in CVP are twofold: a decrease in venous return and a decrease in cardiac output. This may be erroneously interpreted as a deterioration in cardiac function. An obvious solution to this problem is to measure the CVP only when the PEEP has been removed. However, the beneficial effect of PEEP on gas exchange is lost very quickly when it is removed and may take a prolonged period to recover when PEEP is reapplied. This subjects the patients to the dangers of hypoxemia. The only accurate method of compensating for the effects of PEEP on central pressure measurements is to measure the transmural pressures. Unfortunately, simple accurate measurement of intrathoracic pressure in the clinical setting is difficult. From a practical standpoint, PEEP does not usually cause a large change in the CVP, especially in patients with stiff lungs. It is best not to remove PEEP for measurements, recognizing that the numbers obtained may be slightly higher than would be found without PEEP, and to assess the change in CVP in response to fluid challenge as a guide to therpy.
Central Venous Catheterisation and Hemodynamic therapy
The pulmonary artery catheter has been considered the gold standard to guide hemodynamic therapy in shock and cardiac failure. The PCWP is considered the most suitable measure of preload (subject to the assumptions outlined in Table 2), and the cardiac output is measured by thermodilution. Modern pulmonary artery catheters allow continuous cardiac output minitoring, continuous mixed venous oxygen saturation (Sv02) monitoring, as well as measurement of right ventricular end-
diastolic volume as the preload, albeit of the right heart. Pulmonary artery catheterization is an invasive procedure, and recent articles have cast doubt on its utility, and there is increasing interest in non-invasive or less invasive methods of measuring cardiac output. The central venous catheter remains central to these measurements in a number of these new technologies.
Use of the Central Venous oxygen saturation (Scv02)
Rivers and colleagues2 studied early goal- directed therapy designed to optimize cardiac preload, afterload, and contractility. Theyrandomly assigned patients to this therapy or to standard (control) therapy at the time of presentation, before admission to the intensive care unit. After arterial and central venous cannulation, the standard- therapy group underwent treatment that included critical care consultation and were transferred to the intensive care unit as soon as possible (on average, after 6.3 hours). The group randomly assigned to early goal-directed therapy was treated in the emergency department for at least 6 hours (average, 8.0 hours) before admission. These patients received, in a sequential fashion, fluid resuscitation, vasopressor or dilator agents, red-cell transfusions, and inotropic medications to achieve target levels of central venous pressure (8 to 12 mm Hg), mean arterial pressure (65 to 90 mm Hg), urine output (at least 0.5 ml per kilogram of body weight per hour), and central venous oxygen saturation (at least 70 percent). Patients who did not have a response to these approaches underwent sedation and mechanical ventilation. In-hospital mortality differed significantly between the two groups: 30.5 percent in the group assigned to early goal-directed therapy and 46.5 percent in the group assigned to standard therapy. During the period from 7 to 72 hours, the patients assigned to early goal-directed therapy had significantly higher mean central venous oxygen saturations and arterial pH values and lower lactate levels, base deficit values, and organ-dysfunotion scores than those assigned to standard therapy.
Thus a hemodynamic therapy based on CVP monitoring and Scv02 measurement, without a pulmonary artery catheter in early sepsis produced dramatic beneficial results. CVCs incorporating a fibreoptic sensor to continuously monitor Scv02 will soon become
RACE 2003 Ramachandra Anaesthesia Continuing Education

How to get more from your Central Venous Cather 99 Jigi Divatia
available. This approach represents a major advance and a simplified method of hemodynamic therapy.
Cardiac OutputThe PiCCO Technology is based on a
hemodynamic monitoring method, which is a combination of transpulmonary thermodilution and arterial pulse contour analysis. The cold bolus traverses the lungs after being injected through a CVP line, and that the thermodilution curve is being measured in a systemic artery. The method provides the user with the following parameters:- Intrathoracic Blood Volume (ITBV) which is a volumetric measure of cardiac preload;- ExtraVascular Lung Water (EVLW) which reflects the level of pulmonary edema, if increased.
The measurement of these and several other parameters requires a single bolus injection of cold saline through any central venous line and a modified (thermistor-tipped) arterial catheter, eliminating the need for a Right Heart Catheter (RHC). The transpulmonary measurement of CO is at least as accurate as the conventional bolus thermodilution using the right heart catheter.3 However, transpulmonary (“arterial”) CO is not affected by respiratory variations meaning that the measurement is not dependent on the moment of bolus injection during the ventilation cycle. ITBV can be regarded as the best bedside measure of static cardiac preload, since it represents total cardiac preload volume.4-6 It may be more representative than conventional filling pressures or right ventricular end-diastolic volume. However ITBV is a calculated parameter based on complex equations, and its routine use requires further validation.
Lithium Dilution cardiac outputThe LiDCO System consists of a
proprietary disposable lithium sensitive sensor which is attached to an existing arterial line, a connector which sends a signal from the sensor to a monitor and a monitor which displays a computation of cardiac output. The LiDCO System provides an indicator dilution method of
measuring cardiac output. A small dose of lithium chloride is injected via a central venous catheter; the resulting arterial lithium concentration-time curve is recorded by withdrawing blood past a lithium sensor. Indicator dilution curves recorded in arterial blood consist of primary and secondary curves due to the initial circulation and then recirculation of the indicator. Clinical trials have been completed that demonstrate that the LiDCO System is at least as accurate as thermodilution.
In conclusion, it is vital to interpret the CVP correctly to make accurate haemodynamic diagnoses and to initiate therapy. The trend of the CVP and responses to fluid challenges and other therapeutic measures are more important than a single value. All information should be ultimately interpreted in the clinical context. Despite its limitations, the CVP remains a vital haemodynamic parameter which can be easily and safety monitored. It may be necessary at some stage to obtain further information, eg, by echocardiography, or by pulmonary artery catheterisation.
REFERENCES
Most of the material including Tables are based on :Otto CW, "Central venous pressure monitoring “ in Monitoring in Anaesthesia and Critical Care Medicine, editor Blitt CD, 1st edition, Churchill Livingstone, New York, 1985.Other references:
1. Karnath B, Thornton W, Beach R. Inspection of Neck veins. Hospital physicians, May 2002. 43-47.
2. Rivers E, Nguyen B, Ressler J, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19): 1368-77.
3. Sakka SG, Reinhart K, Meier-Hellmann A: Comparison of pulmonary artery and arterial thermodilution cardiac output in critically ill patients. Intensive Care Med 25: 843-846, 1999
4. Lichtwarck-Aschoff M, Zeravik J, Pfeiffer U: Intrathoracic blood volume accurately reflects circulatory volume status in critically ill patients with mechanical ventilation. Intensive Care Med 18: 142- 147, 1992;
5. Hedenstierna G: What value does therecording of intrathoracic blood volume have in clinical practice? . Intensive Care Med 187137-138
6. Sakka SG, Meier-Hellmann A, Reinhart K: Assessment of intrathoracic blood volume and extravascular lung water by single transpulmonary thermodilution. Intensive Care Med 26: 180-187, 2000
RACE 2003 Ramachandra Anaesthesia Continuing Education
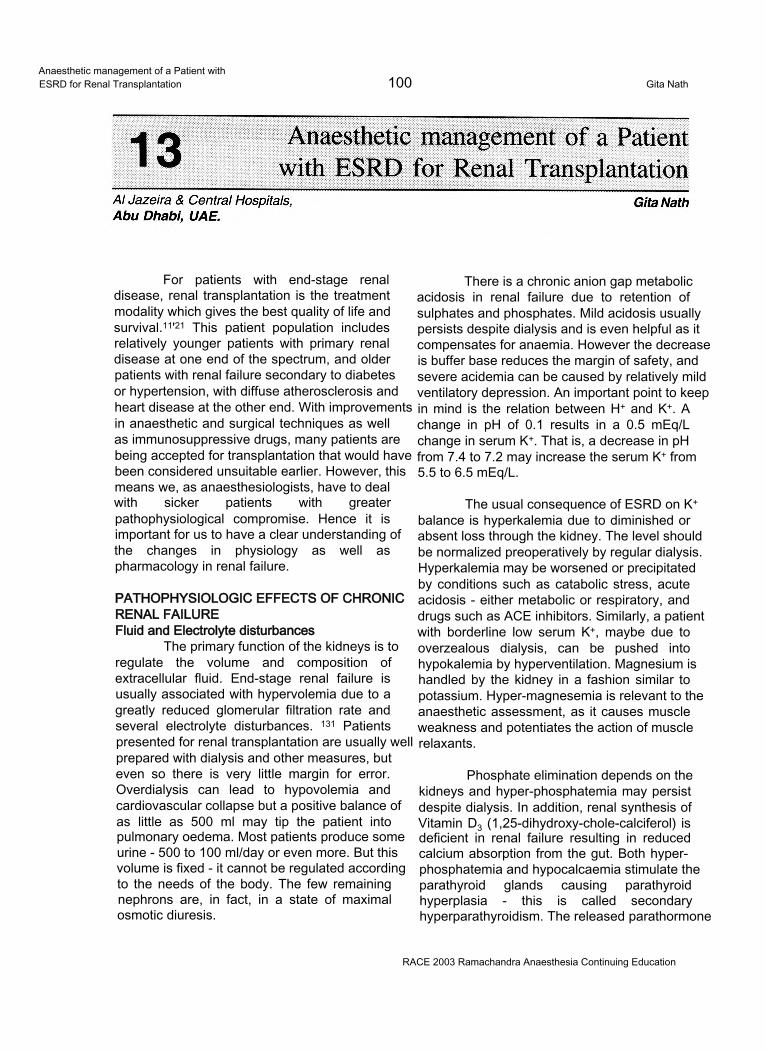
Anaesthetic management of a Patient withESRD for Renal Transplantation 100 Gita Nath
For patients with end-stage renal disease, renal transplantation is the treatment modality which gives the best quality of life and survival.11'21 This patient population includes relatively younger patients with primary renal disease at one end of the spectrum, and older patients with renal failure secondary to diabetes or hypertension, with diffuse atherosclerosis and heart disease at the other end. With improvements in anaesthetic and surgical techniques as well as immunosuppressive drugs, many patients are being accepted for transplantation that would have been considered unsuitable earlier. However, this means we, as anaesthesiologists, have to deal with sicker patients with greater pathophysiological compromise. Hence it is important for us to have a clear understanding of the changes in physiology as well as pharmacology in renal failure.
PATHOPHYSIOLOGIC EFFECTS OF CHRONIC RENAL FAILUREFluid and Electrolyte disturbances
The primary function of the kidneys is to regulate the volume and composition of extracellular fluid. End-stage renal failure is usually associated with hypervolemia due to a greatly reduced glomerular filtration rate and several electrolyte disturbances. 131 Patients presented for renal transplantation are usually well prepared with dialysis and other measures, but even so there is very little margin for error. Overdialysis can lead to hypovolemia and cardiovascular collapse but a positive balance of as little as 500 ml may tip the patient into pulmonary oedema. Most patients produce some urine - 500 to 100 ml/day or even more. But this volume is fixed - it cannot be regulated according to the needs of the body. The few remaining nephrons are, in fact, in a state of maximal osmotic diuresis.
There is a chronic anion gap metabolic acidosis in renal failure due to retention of sulphates and phosphates. Mild acidosis usually persists despite dialysis and is even helpful as it compensates for anaemia. However the decrease is buffer base reduces the margin of safety, and severe acidemia can be caused by relatively mild ventilatory depression. An important point to keep in mind is the relation between H+ and K+. A change in pH of 0.1 results in a 0.5 mEq/L change in serum K+. That is, a decrease in pH from 7.4 to 7.2 may increase the serum K+ from 5.5 to 6.5 mEq/L.
The usual consequence of ESRD on K+ balance is hyperkalemia due to diminished or absent loss through the kidney. The level should be normalized preoperatively by regular dialysis. Hyperkalemia may be worsened or precipitated by conditions such as catabolic stress, acute acidosis - either metabolic or respiratory, and drugs such as ACE inhibitors. Similarly, a patient with borderline low serum K+, maybe due to overzealous dialysis, can be pushed into hypokalemia by hyperventilation. Magnesium is handled by the kidney in a fashion similar to potassium. Hyper-magnesemia is relevant to the anaesthetic assessment, as it causes muscle weakness and potentiates the action of muscle relaxants.
Phosphate elimination depends on the kidneys and hyper-phosphatemia may persist despite dialysis. In addition, renal synthesis of Vitamin D3 (1,25-dihydroxy-chole-calciferol) is deficient in renal failure resulting in reduced calcium absorption from the gut. Both hyperphosphatemia and hypocalcaemia stimulate the parathyroid glands causing parathyroid hyperplasia - this is called secondary hyperparathyroidism. The released parathormone
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 101 Gita Nath
causes bone resorption leading to renal osteodystrophy. In some patients one or more parathyroid glands become autonomous - the so-called tertiary hyperparathyroidism. These patients present with hypercalcaemia and may show metastatic calcification. They may need parathyroidectomy, retaining either a small part of one parathyroid or a forearm autograft of parathyroid tissue. Hypophosphataemia is less common, may be due to excessive dialysis or antacid therapy, and is deleterious as it causes muscle weakness and ventilatory insufficiency.
AnaemiaThis results from decreased
erythropoetin production from the kidney as well as diminished erythrocyte survival.1341 There are also several compensatory mechanisms for this chronic anaemia. The increased level of 2,3 DPG in the erythrocytes and the acidosis present in renal failure result in a rightward shift of the haemoglobin dissociation curve, thus increasing oxygen delivery to the tissues. There is a compensatory increase in the cardiac output and the lowered viscosity helps in better peripheral perfusion. Evalurtion of the effort tolerance of the patient gives one a better idea of his physiological reserve than the Hb value. In fact it has been shown that many haemodialysis patients with hematocrit levels around 25% tolerate treadmill exercise.151 However, in those patients with reduced cardio-respiratory reserve for other reasons, for example coronary artery disease, haematocrit values of around 30% should be aimed for, using recombinant erythropoietin therapy or pre-operative transfusions if necessary.
CoagulopathyPlatelet dysfunction is seen in uremic
patients. It is thought that activation of glycoprotein llb/llla receptors on the platelet membrane is impaired by a dialyzable uremic factor. This results in reduced platelet binding to von Willebrand-Factor VIII complex and fibrinogen, and impaired thrombus generation. Anaemia is an additional contributor to platelet dysfunction as erythrocytes enhance platelet function by releasing ADP and inactivating vascular prostacyclin (PGI2).
The prothrombin time and activated thromboplastin time are usually normal in uremia
unless there is residual heparin in the body after the previous dialysis. Since the platelets counts are normal as well, uremic coagulopathy can be difficult to detect as platelet function tests are not commonly performed. Alternatively, bleeding time can be measured. This is a sensitive indicator of platelet dysfunction but the results are somewhat operator variable.16 71
Platelet function can be improved by effective dialysis. Other measures to treat bleeding diathesis in uremia are desmopressin, which releases von Willebrand-Factor VIII complex from the endothelium, and conjugated oestrogen, whose mechanism of action has not been elucidated. Erythopoetin is helpful by correcting anaemia as well as increasing the number of glycoprotein llb/llla receptors on the platelets. For refractory patients, cryoprecipitate is effective, as it is rich in von Willebrand’s factor and fibrinogen.
HypertensionThis has an intimate relation with renal
failure, as it can be both the cause as well as effect. Expansion of extracellular fluid volume along with disturbances in vascular autoregulation produces hypertension in these patients. There are several mechanisms involved as recently summarized by Mailloux: (1) inappropriately increased angiotensin II in relation to volume and exchangeable sodium, (2) increased vascular sensitivity to endogenous pressors, (3) increased cardiac output in the presence of an inappropriately high peripheral vascular resistance, and (4) failure to fully suppress vasoconstrictor systems[8].
Some patients become normotensive after the initiation of dialysis but many need multiple drugs to bring the blood pressure under control. The exact management of the anti- hypertensive therapy during the peri-operative period needs to be carefully thought out. One concern is to prevent excessive hypertension, especially at critical times such as anaesthetic induction and intubation, so as to avoid adverse effects on the heart and cerebral vasculature. However, after revascularizing the kidney, we need to maintain a good perfusion pressure (at least 130-140 mmHg systolic or 90-100 mmHg mean pressure), as this is one of the most important factors influencing the outcome of the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 102 Gita Nath
transplantation procedure. Overtreatment of the hypertension can make it difficult to achieve this.
Most antihypertensive drugs should be continued till the day of surgery. Sudden cessation of clonidine or beta blockers can result in rebound hypertension. However ACE inhibitors have been found to be associated with intraoperative hypotension, hence it is better to omit this group of drugs on the day of surgery.19101
Post-operatively, many patients become normotensive. Hence it is better to withhold antihypertensives initially and monitor the blood pressure closely. Drugs can be restarted if the patient becomes hypertensive.
Heart and CRFFirst of all we need to consider the effects
of hypertension on the heart, such as left ventricular concentric hypertrophy, decreased LV compliance, diastolic dysfunction and propensity to myocardial ischaemia. Apart from this, the incidence of cardiomyopathy and coronary artery disease is high in these patients, and is a major cause of morbidity and mortality.
LV dysfunction may be caused by ischaemic heart disease, diabetes, hypoalbuminemia, anaemia etc. In addition, uremia itself causes uremic cardiomyopathy which is seen on echocardiography as LV dilatation and ineffective ventricular hypertrophy. This is reversible following renal transplantation, and ejection fractions of less than 30% have been shown to normalize to 69% six months after transplantation.1111 Thus LV dysfunction per se is not a contraindication to transplantation but the presence of congestive heart failure before the patient goes on dialysis is an independent predictor of mortality.1121
Uremic patients show peripheral insulin resistance and decreased lipoprotein lipase activity and are thus prone to hyperglycemia and hypertriglyceridemia. In addition many of them have pre-existing diabetes. For these reasons, coronary artery disease has a high incidence of 17-34 % in uremic patients. Hence all symptomatic or high risk patients (those with diabetes or hyperlipidemia, smokers,) should be screened before surgery. Dipyridamole-thallium
scanning has been found to have a high false negative rate because the myocardial microcirculation has a reduced response to dipyridamole. Dobutamine stress ECG performs better as a screening test in these patients.1131
Uremic pericarditis may cause pericardial effusion which may be haemorrhagic due to the heparin received during dialysis. Pre-operative echocardiography should detect this condition and if cardiac tamponade is present a sub-xiphoid pericardiostomy should be done under monitored anaesthetic care.'141
Miscellaneous Problems.Due to restricted diets and loss of protein
during dialysis, hypoalbuminemia is common, favoring the formation of interstitial and pulmonary oedema. The poor nutrition and anaemia also predispose the patient to infections. Nosocomial infections are especially common at dialysis access sites. The incidence of hepatitis B and C is high in haemodialysis patients due to frequent exposure to blood and blood products. Many of them become asymptomatic carriers.
PHARMACOLOGIC CHANGES IN CRFThe response of patients to many drugs
is different in renal failure, due to pharmacokinetic as well as pharmacodynamic reasons. Clinically, patients seem more sensitive to sedatives and hypnotics. This is because of increased pharmacodynamic effectiveness of the drug as well as increased availability at the effect site. Thiopentone and diazepam are highly protein bound drugs, and the unbound fraction is increased when there is hypoalbuminemia.
In general, to produce the effect of the drug, a therapeutic concentration has to be produced in the volume of distribution. Therefore the initial dose is similar to normal patients, with two exceptions - if the volume of distribution is reduced, as for morphine, alfentanil and remifentanil1151, and secondly if the drug is highly protein bound, as discussed above.
For maintenance dosing, the behaviour of the drug depends on its mode of elimination and whether there are any significant active metabolites. Drugs which totally or predominantly
RACE 2003 Ramachandra Anaesthesia Continuing Education
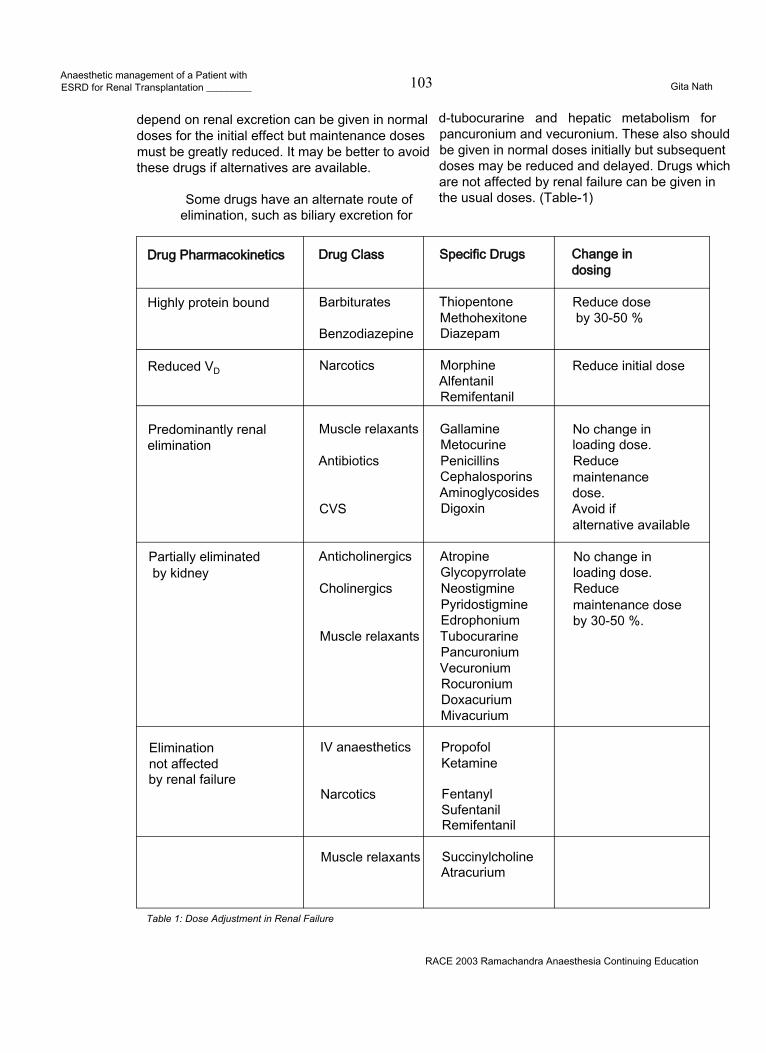
Anaesthetic management of a Patient withESRD for Renal Transplantation _________ 103 Gita Nath
depend on renal excretion can be given in normal doses for the initial effect but maintenance doses must be greatly reduced. It may be better to avoid these drugs if alternatives are available.
Some drugs have an alternate route of elimination, such as biliary excretion for
d-tubocurarine and hepatic metabolism for pancuronium and vecuronium. These also should be given in normal doses initially but subsequent doses may be reduced and delayed. Drugs which are not affected by renal failure can be given in the usual doses. (Table-1)
Drug Pharmacokinetics Drug Class Specific Drugs Change in dosing
Highly protein bound Barbiturates
Benzodiazepine
ThiopentoneMethohexitoneDiazepam
Reduce dose by 30-50 %
Reduced VD Narcotics MorphineAlfentanilRemifentanil
Reduce initial dose
Predominantly renal elimination
Muscle relaxants
Antibiotics
CVS
GallamineMetocurinePenicillinsCephalosporinsAminoglycosidesDigoxin
No change in loading dose. Reduce maintenance dose.Avoid ifalternative available
Partially eliminated by kidney
Anticholinergics
Cholinergics
Muscle relaxants
AtropineGlycopyrrolateNeostigminePyridostigmineEdrophoniumTubocurarinePancuroniumVecuroniumRocuroniumDoxacuriumMivacurium
No change in loading dose. Reducemaintenance dose by 30-50 %.
Elimination not affected by renal failure
IV anaesthetics
Narcotics
PropofolKetamine
FentanylSufentanilRemifentanil
Muscle relaxants SuccinylcholineAtracurium
Table 1: Dose Adjustment in Renal Failure
RACE 2003 Ramachandra Anaesthesia Continuing Education
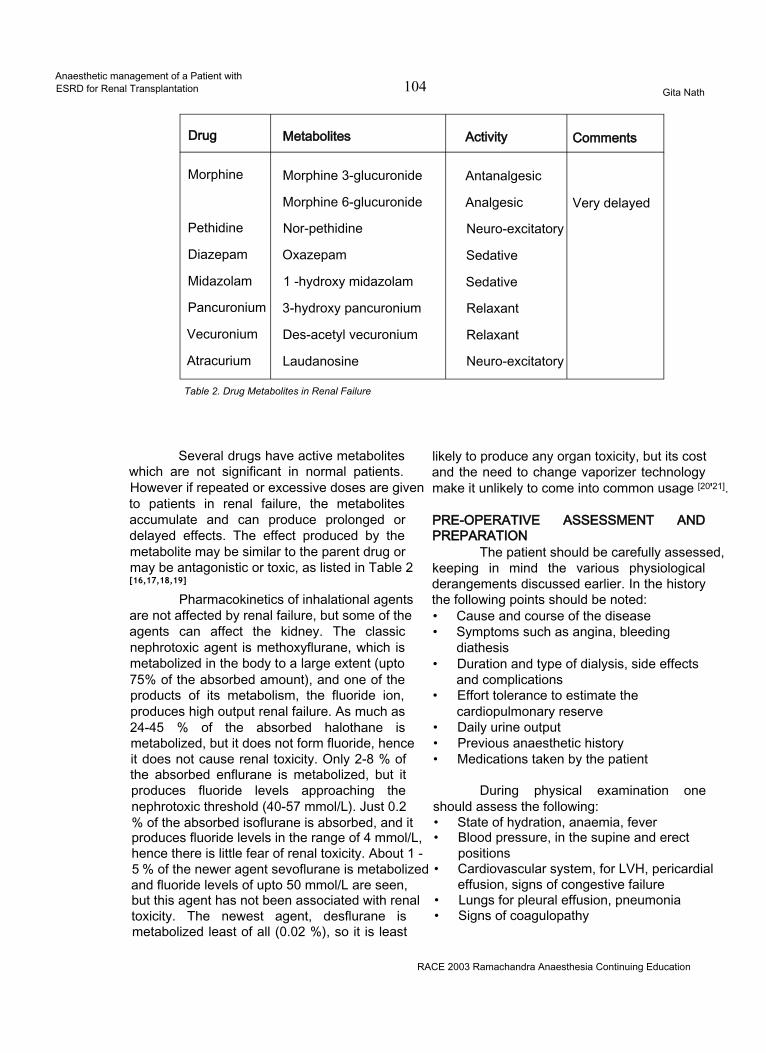
Anaesthetic management of a Patient withESRD for Renal Transplantation 104 Gita Nath
Drug Metabolites Activity Comments
Morphine Morphine 3-glucuronide Antanalgesic
Morphine 6-glucuronide Analgesic Very delayed
Pethidine Nor-pethidine Neuro-excitatory
Diazepam Oxazepam Sedative
Midazolam 1 -hydroxy midazolam Sedative
Pancuronium 3-hydroxy pancuronium Relaxant
Vecuronium Des-acetyl vecuronium Relaxant
Atracurium Laudanosine Neuro-excitatory
Table 2. Drug Metabolites in Renal Failure
Several drugs have active metabolites which are not significant in normal patients. However if repeated or excessive doses are given to patients in renal failure, the metabolites accumulate and can produce prolonged or delayed effects. The effect produced by the metabolite may be similar to the parent drug or may be antagonistic or toxic, as listed in Table 2[16,17,18,19]
Pharmacokinetics of inhalational agents are not affected by renal failure, but some of the agents can affect the kidney. The classic nephrotoxic agent is methoxyflurane, which is metabolized in the body to a large extent (upto 75% of the absorbed amount), and one of the products of its metabolism, the fluoride ion, produces high output renal failure. As much as 24-45 % of the absorbed halothane is metabolized, but it does not form fluoride, hence it does not cause renal toxicity. Only 2-8 % of the absorbed enflurane is metabolized, but it produces fluoride levels approaching the nephrotoxic threshold (40-57 mmol/L). Just 0.2 % of the absorbed isoflurane is absorbed, and it produces fluoride levels in the range of 4 mmol/L, hence there is little fear of renal toxicity. About 1 -5 % of the newer agent sevoflurane is metabolized and fluoride levels of upto 50 mmol/L are seen, but this agent has not been associated with renal toxicity. The newest agent, desflurane is metabolized least of all (0.02 %), so it is least
likely to produce any organ toxicity, but its cost and the need to change vaporizer technology make it unlikely to come into common usage [20'21].
PRE-OPERATIVE ASSESSMENT AND PREPARATION
The patient should be carefully assessed, keeping in mind the various physiological derangements discussed earlier. In the history the following points should be noted:• Cause and course of the disease• Symptoms such as angina, bleeding
diathesis• Duration and type of dialysis, side effects
and complications• Effort tolerance to estimate the
cardiopulmonary reserve• Daily urine output• Previous anaesthetic history• Medications taken by the patient
During physical examination one should assess the following:• State of hydration, anaemia, fever• Blood pressure, in the supine and erect
positions• Cardiovascular system, for LVH, pericardial
effusion, signs of congestive failure• Lungs for pleural effusion, pneumonia• Signs of coagulopathy
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 105 Gita Nath
The following laboratory investigations should be included:• Haematological - Hematocrit, leucocytes,
platelet count, coagulation studies including Ivy bleeding time
• Biochemical - BUN, creatinine, Na+, K+, HCO'3Ca++, Phosphate, Mg++, Albumin, Glucose
• Serological - Hepatitis B and C, HIV status• ECG - for myocardial ischaemia, LVH,
arrhythmias, electrolyte effects• Chest X-ray - Cardiomegaly, pericardial or
pleural effusions, pneumonia• Echocardiography-Assessment of
myocardial function, ventricular hypertrophy, pericardial effusion
If the patient is on haemodialysis, preoperative dialysis should be performed the day before surgery. The amount of fluid removed and the post-dialysis biochemistry should be noted. The effect of residual heparin wears off by 6 hours, and should not interfere with surgery. CAPD may be continued till the time of surgery.
Antihypertensive therapy should be continued till the day of surgery but ACE inhibitors should be omitted. Premedication, if necessary may include a small dose of oral benzodiazepine. For patients at risk of aspiration, a H2 blocker, metoclopramide and sodium bicitrate may be given.
INTRA-OPERATIVE MANAGEMENTRoutine monitoring should include ECG,
oxygen saturation, capnography, neuromuscular monitor and temperature. Care should be taken to protect the arm which has the dialysis access- neither an IV line nor a blood pressure cuff should be placed on that arm. It is better to avoid invasive blood pressure monitoring in case the radial artery is needed for creation of an AV fistula in the future. For the same reason, it is preferable not to use the cephalic vein at the wrist for IV access.
A central venous line is mandatory in all patients, whether under general or regional anaesthesia, to aid in fluid management. Patients with LV dysfunction may need pulmonary artery catheterization.
A urinary catheter is necessary for monitoring the urine output. In should be noted that the bladder is initially filled with saline by the surgical team, and the catheter is clamped, in order to facilitate surgical access to the bladder for re-implantation. This fluid should be excluded, while monitoring urine output after revascularizing the kidney.
Renal transplantation is usually done in the supine position. Great care should be taken to protect the limb with dialysis access. Due to renal osteodystrophy, the bones are very fragile; hence any change in position should be done gently. Attention should be paid to padding the various pressure points - impairment of skin integrity as well as pre-existing peripheral neuropathy should be kept in mind.
Preventive measures should be taken against hypothermia, which may include adjustment of ambient temperature, warming mattress, insulation of all exposed body parts, heater-humidifierfor the inspired air, forced hot air warmers and fluid warming systems. These measures should be continued during the recovery period.
These patients already have impaired immunity because of the primary condition. In addition, immunosuppressive therapy will be instituted to prevent rejection. Hence great attention should be paid towards aseptic technique. On the other hand, they have a higher incidence of blood borne infections such as Hepatitis B and C and HIV. Hence the medical staff should take measures to protect themselves.
Selection of anaesthetic technique:The goals of anaesthetic management
of renal transplantation are:• To tailor the anaesthetic keeping in mind all
the physiological derangements detailed earlier.
• To take measures to optimise functioning of transplanted kidney
• To ensure that there are no residual effects of the anaesthetic drugs or techniques, in case graft functioning is delayed.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic management of a Patient withESRD for Renal Transplantation 106 Gita Nath
• If post-operative dialysis becomesnecessary, to delay it as much as possible so that the interval between surgery and administration of heparin is longer. In essence, this involves avoiding fluid overload and potassium build-up.
As long as the above principles are kept in mind, the actual anaesthetic technique does not make a difference to the outcome. Renal transplantation has been successfully managed using general as well as regional anaesthetic techniques such as spinal and epidural anaesthesia122'. The concern with regional anaesthesia is the risk of hypotension which, if treated with aggressive fluid administration, may lead to pulmonary oedema when the block wears off. Apart from this, expected length of the operation and poor patient cooperation influence the choice of anaesthetic technique. Coagulopathy, which would contraindicate a regional technique, should also be borne in mind, since this may occur even with normal platelet count, prothrombin time and activated thromboplastin time.
Regarding general anaesthesia, both inhalational as well as intravenous techniques can be equally effective. As far as possible drugs whose pharmacokinetics are not affected by renal failure should be used, but this has to be balanced against the availability of resources and the previous experience of the anaesthetist. As with many issues in anaesthesia, it is more important to choose one’s anaesthetist than the anaesthetic technique.
Induction of anaesthesia:Preoxygenation is advisable in these
anaemic patients to improve the oxygen reserve. The intravascular volume is often somewhat depleted after the last dialysis, and carefully titrated fluid increments may be given to avoid hypotension. The goal is to avoid excessive hypotension, but at the same time, prevent excessive hypertensive response to intubation. A bolus dose of a narcotic (e.g. fentanyl 2-3 mic/ kg) helps towards this end.
Thiopentone, etomidate and propofol are the choices available for induction of anaesthesia. Ketamine is not suitable because of its
hypertensive effect. The dose of thiopentone should be reduced because of the reduced protein binding. The usual recommended induction dose of 2 mg/kg propofol causes hypotension even in normal patients, hence carefully titrated doses should be given, checking the blood pressure between doses. Propofol seems to prevent the intubation response much more effectively than thiopentone.
If the risk of aspiration is present, a single dose of succinylcholine may be given as long as the serum potassium is less that 4.5 mEq/L. Rocuronium is the other choice, since it produces satisfactory intubating conditions in 60 to 90 seconds and can be used to maintain relaxation till the end of the procedure. Rapacurium is another steroidal non-depolarizing relaxant, with slightly faster onset than rocuronium, but it has now been withdrawn because of an unacceptably high incidence of adverse events.
If there is no risk of aspiration, the nondepolarising agent can be given directly. Atracurium and cis-atracurium are the relaxants of choice because of their spontaneous breakdown independently of the kidneys or liver. Vecuronium or rocuronium may also be used but the maintenance doses should be reduced and delayed. Pancuronium should be avoided, now that so many alternatives are available. Neuromuscular monitoring is mandatory in these cases t23]. Mivacurium is another agent which doesn’t depend on the kidneys for elimination, but its action is so short-acting that it has to be given by infusion. The large amount required for such a long operation means that it is not cost- effective [24].
After intubation, the patient is ventilated with an oxygen/nitrous oxide or oxygen/air mixture. Excessive hypocapnia or hypercapnia should be avoided, bearing in mind the possible shifts in potassium with changing blood pH. For maintenance of anaesthesia, either a nitrous oxide-oxygen-inhalational agent combination or an intravenous propofol-narcotic infusion can be used with equally good results125 26 271. Isoflurane is probably the best inhalational agent, from the renal point of view Fentanyl, sufentanil or alfentanil can all be used for maintenance of narcotic effect Remifentanil has the advantage of lack of
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation__________ 107 Gita Nath
cumulationt28]. Morphine and pethidine are better avoided, because of accumulation of their metabolites morphine-6-glucuronide and nor- pethidine, with analgesic and neuro-excitatory effects respectively116171.
After induction, minimal fluids are given as long as the blood pressure is adequate. Extra fluid administered at this time redistributes into the extravascular space and is not available for renal perfusion after anastamosis. It is better to fill up more rapidly closer to the time of clamp release. Hartmann’s solution and Ringer Lactate solution should be avoided as they contain potassium.
OPTIMIZING FUNCTION OF THE TRANSPLANTED KIDNEY:
Three aspects of management critically affect the outcome of renal transplantation - the management of the renal donor, how well the graft is preserved and thirdly, perioperative management of the kidney.
1. Management of the donorLiving donors are involved in about 25%
of all renal allografts in the United States, but contribute to the majority of renal transplants in India. All living kidney donors, related or unrelated, should be in excellent health, without any medical problem which increases the risk of anaesthesia. Also they should not have any condition which makes them prone to renal failure in the future, such as hypertension and diabetes.
The operation is performed in the lateral position with the kidney bridge elevated. The key point in managing these patients is to keep the kidneys well oxygenated and perfused, and take measures to reduce their oxygen consumption. Good hydration is mandatory. Some centres make it a practice to give IV fluids overnight. In any case, 1.5 to 2 litres of crystalloids should be infused during the initial part of the operation, and this is followed by 10-12 gm of mannitol. A small dose of lasix may help by blocking the chloride pump in the thick ascending loop of Henle, thus reducing oxygen consumption in a poorly perfused and vulnerable area of the kidney. The urine output should be monitored and a good diuretic response ensured. Maintenance of a good perfusion pressure is important and the colour
and turgidity of the kidney are good indicators of its perfusion. Direct acting vasopressors should be avoided, so that renal artery spasm is not induced. From the surgical side, the kidney and its hilar structures should be handled gently, since spasm of the renal artery can be very troublesome. Some surgeons request 5000 units of heparin before clamping the artery - this can be reversed with protamine 50 mg after the kidney is harvested.
After removal of the kidney, anaesthesia is continued according to one’s normal routine. It is important to ensure that the donor does not come to any harm as the result of his generous action, hence special care should be taken to avoid any anaesthesia or surgery related complications. If the 11th or 12th rib was resected during surgery, a high index of suspicion should be maintained to detect the occurrence of a pneumothorax. Special attention should be directed towards postoperative analgesia, as donor nephrectomy is a very painful operation. Intermittent injections of morphine or pethidine are not really effective. Other methods such as patient controlled analgesia, epidural local anaesthetic or opiate infusions, wound infusion with bupivacaine and other techniques are more effective.
Cadaveric donors contribute to the majority of renal transplants done in the developed world, and cadaveric transplantation is becoming commoner in India as well. The salient points in managing cadaver donors are:
• A protocol for brain death certification should be in place in each institution. This should be followed meticulously so as to afford no chance for anyone to point a finger.
• Haemodynamic stability and good gas exchange criteria give the best results. Contraindications to organ harvesting are prolonged hypotension and hypothermia, systemic sepsis, malignancy, DIC, hepatitis B or C and HIV seropositivity. Relative contraindications are age (above 70), diabetes, vascular diseases, elevated serum creatinine and high requirement for vasopressors.
• A Pa02 of at least 100 should be
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation 108 Gita Nath
maintained with normocapnia. The arterial pressure should be kept above 100 mmHg, with aggressive fluid treatment. If intravascular volume is adequate but blood pressure is still below 90 mmHg, inotropes can be added, such as dobutamine, low dose dopamine, or low dose adrenaline. High doses of vasopressors, with a vasoconstricting effect such as high dose dopamine, high dose adrenaline and noradrenaline are associated with a worse graft function possibly because of renal vasoconstriction [29], The urine output should be maintained above 100 ml/hr using mannitol, lasix and dopamine, if necessary.
• This treatment is continuedintraoperatively. Muscle relaxants are given to suppress the reflex motor response to surgery. Ventilatory and circulatory support is discontinued after the organs are harvested.
2. Preservation of the harvested organTotal ischaemia time starts when the
donor renal artery is clamped, and ends after the anastamosis when the artery is unclamped in the recipient. Minimizing the ischaemia time is critical in preservation of the kidney. Warm ischaemia is especially deleterious to the kidney as oxygen consumption continues with no oxygen supply. Warm ischaemia starts when the renal artery is clamped and stops when the kidney is cooled by perfusion with a cold solution. Cold ischaemia starts when the core of the kidney becomes cold, as is evidenced by clear perfusion fluid flowing out of the cut end of the renal vein. Cold ischaemia can be maintained for upto 36- 72 hours by storing the kidney at4°C but results are better if the cold ischaemia time is less than 24 hours.
Warm ischaemia time resumes when the kidney is removed from the cold contained and is placed in the recipient and ends when the kidney is perfused again after completion of the vascular anastamosis.
For short ischaemia times, the composition of the perfusate does not matter so much, and perfusion with ice-cold normal saline gives as good results as if a special preservative solution was used. For longer periods of storage, several solutions are available. Euro-Collins solution contains high concentrations of
potassium (110 mM), magnesium sulphate (30 mM), and phosphate (57.5 mM), which mimics intracellular fluid composition; and mannitol which makes the solution hypertonic and prevents cell swelling within the kidney. The UW solution (University of Wisconsin solution) contains lactobionate, raffinose, and hydroxyethyl starch for their osmotic effect, phosphate as a buffer, adenosine for ATP synthesis during reperfusion, glutathione as a free-radical scavenger, allopurinol to inhibit xanthine oxidase and the generation of free radicals, and magnesium and dexamethasone as membrane-stabilizing agents. The UW solution gives better results and can be used for all intra-abdominal organs. Machine perfusion with a cold solution similar to UW solution further extends the cold ischaemia time of the kidney[30).
3. Other measures to optimise graft function• Perfusion Pressure: This is the key factor which influences immediate graft function, and any delay in graft functioning is associated with a worse outcome for the graft in the early posttransplant period as well as long term I31'32). Hence, haemodynamic management is geared towards providing a perfusion pressure of at least 120 mmHg at the time of clamp release. The following measures may be taken towards this goal:• Close haemodynamic monitoring, with frequent checks of blood pressure and CVP• Aggressive intravascular volume expansion. Fluid loading with 1-2 litres of normal saline is done while the vascular anastamosis is being done.• It is important to anticipate and expect hypotension after release of clamps because of reperfusion of the ischaemic vascular bed of the graft and washout of metabolites. Repeated checking of blood pressure is very important. The surgeon’s assessment of the firmness or turgidity of the graft is a useful index of the adequacy of the perfusion pressure.• If verapamil has been added to the renal perfusate, it can cause hypotension on being washed into the circulation when the clamp is released. To cover this, calcium chloride 0.25 gm can be given before and a further 0.25 gm after clamp release.
• Mannitol 10-20 gm before clamp release: This acts by expanding the intravascular volume,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Anaesthetic management of a Patient withESRD for Renal Transplantation _________ 109 Gita Nath
reducing cellular swelling, increasing tubular urine flow and reducing the potential for tubular obstruction, scavenging free radicals and increasing the release of intrarenal prostaglandins.
• Albumin has been found to improve the graft outcome at doses of 0.8 to 1.6 gm/Kg [33-34]. Albumin acts by improving the oncotic pressure and thus expanding the intravascular volume, especially in patients with hypoalbuminemia.
• Loop diuretics such as frusemide block the chloride pump in the thick ascending loop of Henle, and increase resistance against ischaemic injury. Despite several theoretical reasons, it is not clear whether they improve transplant outcomel351.
• Verapamil has been shown to improve graft outcome, either when administered to the recipient [36) or added to the renal perfusate.
• Low dose dopamine is said to enhance renal perfusion by selective renal vasodilatation and also promotes natriuresis. However, several studies have not been able to show an improved outcome during cadaver renal transplantation with dopamine 2-3 mic/Kg/min t37 38 39). Hence routine use of dopamine is not recommended.
• The Kidney Cocktail. Some centres infuse a kidney cocktail just before the anastamosis is completed. This consists of 600 ml 1/4 normal saline with albumin 37.5 gm and mannitol 80 gm. For cadaver transplantation, they add 80 mg frusemide[4].
MONITORING OF KIDNEY FUNCTIONThe initial assessment of urine output is
made soon after renal revascularization, by looking out for urine to spurt from the end of the ureter. Once ureteric implantation begins, urine output cannot really be monitored till the bladder is closed. One should be careful to exclude the volume of saline initially used to distend the bladder from the measured urine output.
TROUBLE-SHOOTINGIf there is a delay in urine formation,
prerenal factors should be evaluated first of all, such as perfusion pressure, the anastamosis,
arterial spasm or thrombosis, venous occlusion or thrombosis etc. The consistency of the kidney and thrill at the site of the anastamosis can help confirm good blood flow. Intraoperative Doppler can also evaluate the anastamotic flow.
Post renal factors are outflow tract obstruction due to kinking, clot, oedema; or leakage of urine from the bladder implantation site. The problem may be as simple as a kinked or blocked urinary catheter, or even an air-lock in the catheter drainage bag.
When all these factors are excluded, a biopsy of the transplanted kidney may be necessary to evaluate for acute tubular necrosis or graft rejection.
RECOVERY FROM ANAESTHESIAPotential problems which should be
anticipated at recovery are delayed emergence, respiratory depression, hypo or hypertension, respiratory depression and pulmonary oedema. Adequate recovery of neuromuscular function must be ensured before extubation. Persistent weakness due to hypermagnesaemia may be antagonized by giving calcium. As far as possible it is better to avoid postoperative mechanical ventilation because of the risk of pulmonary infection.
The patient should be transferred to a dedicated transplant unit for postoperative management. Apart from barrier nursing, cardiorespiratory and renal functions are monitored closely for the next few days. Postoperative pain is usually not a problem. Once the kidney has started working, there is no problem with accumulating metabolites, and morphine can be used safely.
CONCLUSIONTransplant anaesthesia is a specialized
field which requires a good understanding of the physiological trespass in patients with renal failure, familiarity with transplant medicine and expertise in the management of these patients. Good anaesthetic management, in liaison with the transplant surgeon and nephrologist, is of paramount importance in avoiding delayed graft function with all its possible sequelae and complications.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Anaesthetic management of a Patient withESRD for Rena( Transplantation 110 Gita Nath
REFERENCES1. Cameron Jl. Differences in quality of life across renal replacement therapies: a meta-analytic comparison. Am J Kidney Dis 2000; 35(4): 629-372. Rabbat CG. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J Am Soc Nephrol 2000; 11(5): 917-223. Sladen RN Anesthetic considerations for the patient with renal failure.- Anesthesiol Clin North America 2000; 18(4): 863-82, x.4. Sprung J, Kapural L, Bourke DL,O’Hara JF. Anesthesia for kidney transplant surgery. Anesthesiol Clin North America2000; 18(4): 919-51.5. Lundin AP, Stein RA, Brown CD, et al: Fatigue, acid-base, and electrolyte changes with exhaustive treadmill exercise in haemodialysis patients. Nephron 1987; 46:57-62.6. Mahesh K. Preoperative Care of Patients with Kidney Disease. American Family Physician 2002; 66: 8.7. Dember LM. Critical care issues in the patient with chronic renal failure. Critical Care Clinics 2002; 18: 2.8. Mailloux LU: Hypertension in chronic renal failure and ESRD: Prevalence, pathophysiology, and outcomes. Semin Nephrol 2001; 21:146-156.9. Powell CG. Severe hypotension associated with angiotensin-converting enzyme inhibition in anaesthesia. Anaesth Intensive Care 1998; 26(1): 107-9.10. Licker M. Cardiovascular responses to anesthetic induction in patients chronically treated with angiotensin- converting enzyme inhibitors. Can J Anaesth 2000; 47(5): 433-40.11. Cho WH, Kim HT, Park CH, et al: Renal transplantation in advanced cardiac failure patients. Transplant Proc 1997; 29:236-238.12. Harnett JD, Foley RN, KentGM, etal: Congestive heart failure in dialysis patients: Prevalence, incidence, prognosis, and risk factors. Kidney Int 1995; 47:884-890.
13. Herzog CA, Marwick TH, Pheley AM: Dobutamine stress echocardiography for the detection of significant coronary artery disease in renal transplant candidates. Am J Kidney Dis 1999; 33:1090.14. Figueroa W, Alankar S, Pai N, et al: Subxiphoid pericardial window for pericardial effusion in end-stage renal disease. Am J Kidney Dis 1996; 27: 664-7.15. Dahaba AA End-stage renal failure reduces central clearance and prolongs the elimination half life of remifentanil- Can J Anaesth 2002; 49(4): 369-74.16. Angst MS, Buhrer M, L6tsch J: Insidious intoxication after morphine treatment in renal failure: Delayed onset of morphine-6-glucuronide action. Anesthesiology 2000; 92: 1473-6.17. Hasselstrfim J, Berg U, Lofgren A, Sawe J: Long lasting respiratory depression induced by morphine-6- glucuronide? Br J Clin Pharmacol 1989; 27: 515-8.18. Sear J: Effect of renal function and failure. In Park GR, Sladen RN (eds): Sedation and Anesthesia in the Critically III. Oxford, Blackwell Science, 1995, pp 108-2919. Hall LG - Analgesic Agents. Pharmacology and Application in Critical Care Crit Care Clin 2001; 17(4): 899- 923, viii.20. Baden JM, Rice SA. Metabolism and Toxicity of Inhaled Anesthetics. In Miller RD (ed): Anesthesia. 5th ed., Copyright © 2000 Churchill Livingstone, Inc, pp 155-167.
21. Conzen PF, Nuscheler M, Melotte A, et al: Renal function and serum fluoride concentrations in patients with stable renal insufficiency after anesthesia with sevoflurane or enflurane. Anesth Analg 1995; 81:569-75.22. Murakami M, Nomiyama S, Ozawa A, et al: Anaesthetic management of pediatric renal transplantation for chronic renal failure. Masui 1993; 42:263-270.23. Murray MJ - Clinical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient. Crit Care Med 2002; 30(1): 142-56.24. Head-Rapson AG Pharmacokinetics and pharmacodynamics of the three isomers of mivacurium in health, in end-stage renal failure and in patients with impaired renal function. - Br J Anaesth 1995; 75(1): 31-6.25. Ickx B Propofol infusion for induction and maintenance of anaesthesia in patients with end-stage renal disease. - Br J Anaesth 1998; 81(6): 854-60.26. Babacan A Assessment of total intravenous anesthesia in renal transplantation. Transplant Proc 1998; 30(3): 750-3.27. Jirasiritham S Total intravenous anesthesia for general operations in post-renal transplant patients. Transplant Proc 1998; 30(7): 3897-8.28. Hoke JF Pharmacokinetics and pharmacodynamics of remifentanil in persons with renal failure compared with healthy volunteers. Anesthesiology 1997; 87(3): 533-41.29. O’Brien EA, Bour SA, Marshall RL, et al: Effects of use of vasopressors in organ donors on immediate function of renal allografts. Journal of Transplant Coordination 1996; 6:215-216.30. Van der Werf WJ, D’Alessandro AM, Hoffmann RM, Knechtle SJ. Procurement, Preservation, And Transport Of Cadaver Kidneys. Surgical Clinics of North America 1998; 78(1) 41-54.31. Dawidson I, Ar’Rajab A: Perioperative fluid and drug therapy during cadaver kidney transplantation. In Terasaki, Cecka (eds): Clinical Transplants. Los Angeles, 1992, pp 267-27932. Rajamani AR, Kamat VN, Poojara L, Arunkumar AS. Haemodynamic variables affecting kidney allograft function. Intensive Are Medicine 2002; 28: (Suppl 1) S10233. Willms CD, Dawidson IHA, Dickerman R, et al: Intraoperative blood volume expansion induces primary function after renal transplantation: A study of 96 paired cadaver kidneys. Transplant Proc 1991; 23:1338-1339.34. Dawidson IJ Intraoperative albumin administration affects the outcome of cadaver renal transplantation - Transplantation 1992; 53(4): 774-82.35. Shilliday I, Allison ME: Diuretics in acute renal failure. Renal Fail 1994; 16:13-17.36. Dawidson I, Rooth P, Lu C, et al: Verapamil improves the outcome after cadaver renal transplantation. J Am Soc Nephrol 1991; 2:983-990.37. Grundmann R, Kindler J, Meider G, et al: Dopamine treatment of human cadaver kidney graft recipients: A prospectively randomized trial. Klinische Wochenshrift 1982; 60:193-197.38. Kadieva VS, Friedman L, Margoulius LP, et al: The effect of dopamine on graft function in patients undergoing renal transplantation. Anesth Analg 1993; 76:362-365.39. Sandberg J, Tyden G, Groth CG: Low-dose dopamine infusion following cadaveric renal transplantation: No effect on the incidence of ATN. Transplant Proc 1992; 24:357.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Sedation and Analgesia in Children for Procedures outside the OR 111 S. Ramesh
“ 6 year old Master X has been fearful of the repeated lumbar punctures that he must undergo for intrathecal medical administration, as well as his occasional bone marrow aspirations. His previous experiences include being held down while he screamed, with a long period of being silent and withdrawn after each procedure as no sedation or analgesics were given during these procedures. So Master X thereafter refused to come to see any doctor, withdrawn from his friends and needed lot of psychological consults ”
So children who undergo painful medical procedures not only have their physiological function affected, but also face complex psychobiological demands.
Painful diagnostic or therapeutic procedures are often necessary during emergency care of children who have already painful and frightening injuries and illnesses. For example, in a study done by us in 1997, it was found that 90% of lumbar punctures in the paediatric emergency department were performed without sedation or local analgesia. There are many reasons why effective anxiolysis, analgesia and sedation are not in commonplace in the emergency department. The explanations for less use of analgesia or sedation include lack of consensus about optimal safe effective methods, medications, patient monitoring, lack of physician familiarity with local anaesthetic techn^ :?s and dosing, insufficient time to carry outset ■■rd belief that children have only a short tern, of pain.
In India, the past decade has seen what may be considered a revolution in the recognition
and treatment of pain and anxiety in children. Advantages of safe and effective management of pain and anxiety in the emergency department include reduction of psychological trauma and its sequelae, reduction of stress for the paediatricians and parents and a good success for the procedures.
Due to the diversity in population, no ‘cookbook’ is available for the method and medication to be used for a particular procedure. What we must rely on is a broad understanding of the pharmacokinetics and the physiological effects of diverse agents. So this article will review some definitions, pain pathways, various medications available to us, principles of conscious sedation and a few examples of emergency procedures.
NEUROPHYSIOLOGY OF PAIN:‘Pain’
- “ An unpleasant and emotionalexperience associated with actual or potential tissue damage or described in terms of such damage”
_ Pain is ‘suffering’ or ‘distress’_ Pain is what the patient ‘says it is’
The basic mechanism of pain perception has four components, transduction, transmission, perception and modulation. Noxious mechanical, thermal or chemical stimuli excite primary afferent fiores that transmit information about the potential injurious stimuli from the periphery to
dorsal horn of the spinal cord. The pain repulse is transmitted via A delta (large, myelinated) and C (small, unmyelinated) fibres. The tissue injury causes release of inflammatory mediators, (eg.potassium, bradykinin,
RACE 2003 Ramachandra Anaesthesia Continuing Education
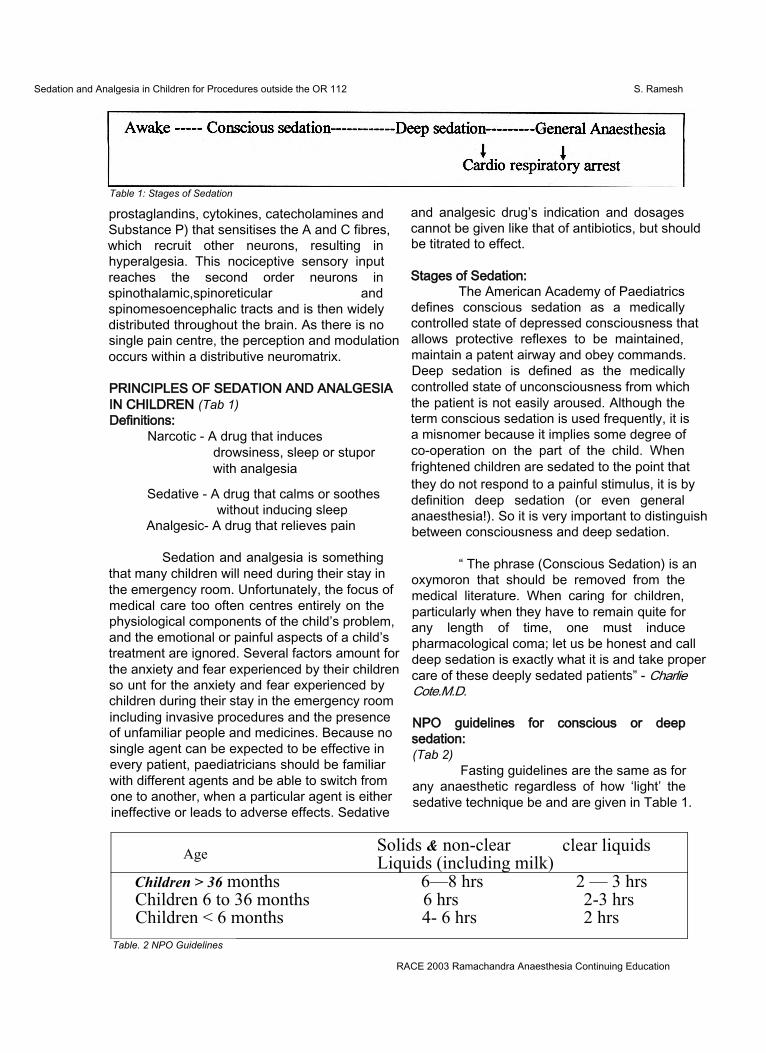
Sedation and Analgesia in Children for Procedures outside the OR 112 S. Ramesh
Table 1: Stages of Sedation
prostaglandins, cytokines, catecholamines and Substance P) that sensitises the A and C fibres, which recruit other neurons, resulting in hyperalgesia. This nociceptive sensory input reaches the second order neurons in spinothalamic,spinoreticular andspinomesoencephalic tracts and is then widely distributed throughout the brain. As there is no single pain centre, the perception and modulation occurs within a distributive neuromatrix.
PRINCIPLES OF SEDATION AND ANALGESIA IN CHILDREN (Tab 1)Definitions:
Narcotic - A drug that inducesdrowsiness, sleep or stupor with analgesia
Sedative - A drug that calms or soothes without inducing sleep
Analgesic- A drug that relieves pain
Sedation and analgesia is something that many children will need during their stay in the emergency room. Unfortunately, the focus of medical care too often centres entirely on the physiological components of the child’s problem, and the emotional or painful aspects of a child’s treatment are ignored. Several factors amount for the anxiety and fear experienced by their children so unt for the anxiety and fear experienced by children during their stay in the emergency room including invasive procedures and the presence of unfamiliar people and medicines. Because no single agent can be expected to be effective in every patient, paediatricians should be familiar with different agents and be able to switch from one to another, when a particular agent is either ineffective or leads to adverse effects. Sedative
and analgesic drug’s indication and dosages cannot be given like that of antibiotics, but should be titrated to effect.
Stages of Sedation:The American Academy of Paediatrics
defines conscious sedation as a medically controlled state of depressed consciousness that allows protective reflexes to be maintained, maintain a patent airway and obey commands. Deep sedation is defined as the medically controlled state of unconsciousness from which the patient is not easily aroused. Although the term conscious sedation is used frequently, it is a misnomer because it implies some degree of co-operation on the part of the child. When frightened children are sedated to the point that they do not respond to a painful stimulus, it is by definition deep sedation (or even general anaesthesia!). So it is very important to distinguish between consciousness and deep sedation.
“ The phrase (Conscious Sedation) is an oxymoron that should be removed from the medical literature. When caring for children, particularly when they have to remain quite for any length of time, one must induce pharmacological coma; let us be honest and call deep sedation is exactly what it is and take proper care of these deeply sedated patients” - Charlie Cote.M.D.
NPO guidelines for conscious or deep sedation:(Tab 2)
Fasting guidelines are the same as for any anaesthetic regardless of how ‘light’ the sedative technique be and are given in Table 1.
Age Solids & non-clear Liquids (including milk)
clear liquids
Children > 36 months 6—8 hrs 2 — 3 hrsChildren 6 to 36 months 6 hrs 2-3 hrsChildren < 6 months 4- 6 hrs 2 hrs
Table. 2 NPO Guidelines
RACE 2003 Ramachandra Anaesthesia Continuing Education
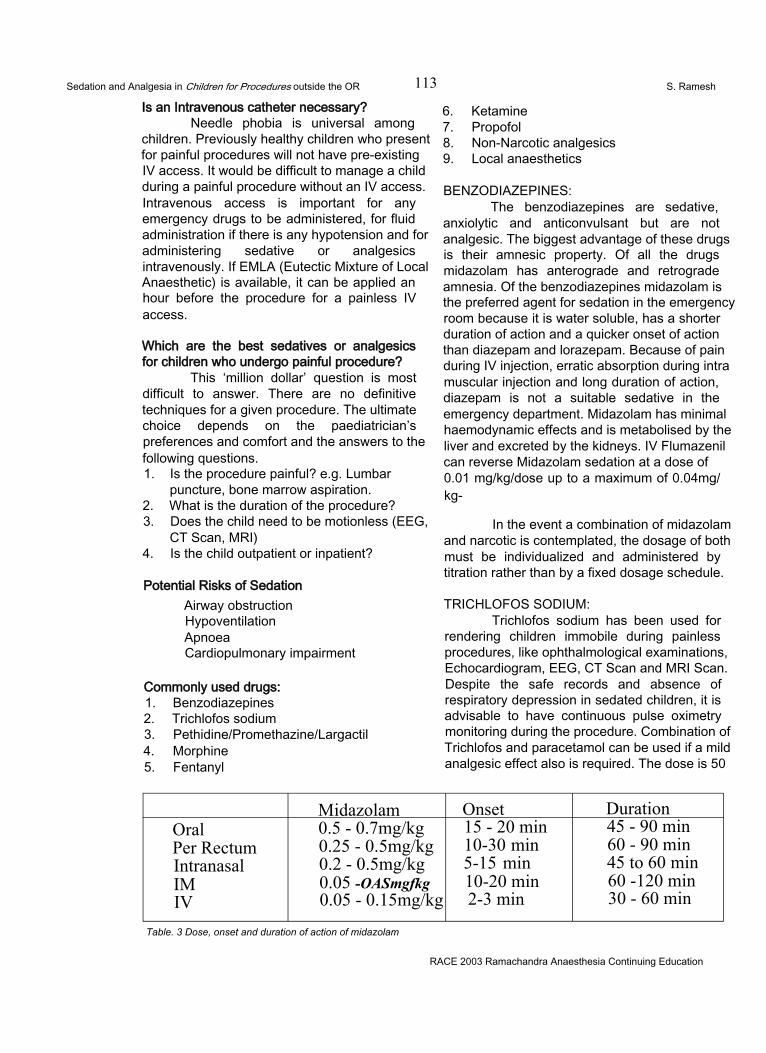
Sedation and Analgesia in Children for Procedures outside the OR 113 S. Ramesh
Is an Intravenous catheter necessary?Needle phobia is universal among
children. Previously healthy children who present for painful procedures will not have pre-existing IV access. It would be difficult to manage a child during a painful procedure without an IV access. Intravenous access is important for any emergency drugs to be administered, for fluid administration if there is any hypotension and for administering sedative or analgesics intravenously. If EMLA (Eutectic Mixture of Local Anaesthetic) is available, it can be applied an hour before the procedure for a painless IV access.
Which are the best sedatives or analgesics for children who undergo painful procedure?
This ‘million dollar’ question is most difficult to answer. There are no definitive techniques for a given procedure. The ultimate choice depends on the paediatrician’s preferences and comfort and the answers to the following questions.1. Is the procedure painful? e.g. Lumbar
puncture, bone marrow aspiration.2. What is the duration of the procedure?3. Does the child need to be motionless (EEG,
CT Scan, MRI)4. Is the child outpatient or inpatient?
Potential Risks of SedationAirway obstructionHypoventilationApnoeaCardiopulmonary impairment
Commonly used drugs:1. Benzodiazepines2. Trichlofos sodium3. Pethidine/Promethazine/Largactil4. Morphine5. Fentanyl
6. Ketamine7. Propofol8. Non-Narcotic analgesics9. Local anaesthetics
BENZODIAZEPINES:The benzodiazepines are sedative,
anxiolytic and anticonvulsant but are not analgesic. The biggest advantage of these drugs is their amnesic property. Of all the drugs midazolam has anterograde and retrograde amnesia. Of the benzodiazepines midazolam is the preferred agent for sedation in the emergency room because it is water soluble, has a shorter duration of action and a quicker onset of action than diazepam and lorazepam. Because of pain during IV injection, erratic absorption during intra muscular injection and long duration of action, diazepam is not a suitable sedative in the emergency department. Midazolam has minimal haemodynamic effects and is metabolised by the liver and excreted by the kidneys. IV Flumazenil can reverse Midazolam sedation at a dose of0.01 mg/kg/dose up to a maximum of 0.04mg/ kg-
In the event a combination of midazolam and narcotic is contemplated, the dosage of both must be individualized and administered by titration rather than by a fixed dosage schedule.
TRICHLOFOS SODIUM:Trichlofos sodium has been used for
rendering children immobile during painless procedures, like ophthalmological examinations, Echocardiogram, EEG, CT Scan and MRI Scan. Despite the safe records and absence of respiratory depression in sedated children, it is advisable to have continuous pulse oximetry monitoring during the procedure. Combination of Trichlofos and paracetamol can be used if a mild analgesic effect also is required. The dose is 50
Midazolam Onset DurationOralPer Rectum Intranasal IM IV
0.5 - 0.7mg/kg 0.25 - 0.5mg/kg 0.2 - 0.5mg/kg 0.05 -OASmgfkg 0.05 - 0.15mg/kg
15 - 20 min 10-30 min 5-15 min 10-20 min 2-3 min
45 - 90 min 60 - 90 min 45 to 60 min 60 -120 min 30 - 60 min
Table. 3 Dose, onset and duration of action of midazolam
RACE 2003 Ramachandra Anaesthesia Continuing Education

Sedation and Analgesia in Children for Procedures outside the OR 114 S. Ramesh
to 100 mg/kg and the onset time is in 30 to 40 minutes and the duration of action is 90 to 120 minutes.
PETHIDINE / PROMETHAZINE / CHLORPROMAZINE
The combination of pethidine 2mg/kg, promethazine 1 mg/kg, and chlorpromazine 1mg/ kg called the ‘lytic cocktail’ has been used for many years for sedation in children especially for cardiac catheterisation. Due to availability of better drugs and significant episodes of hypotension, apnoea, prolonged recovery and dystonic reactions, the above combination is no longer recommended.
morphine. Its faster onset of action, short duration and potent analgesic effect makes this drug the narcotic of choice for a wide variety of painful procedures in the emergency room. If fentanyl is given fast, it might cause respiratory depression and apnoea. Fentanyl causes a mild decrease in the heart rate and a peculiar effect of chest wall rigidity, which may impair ventilation. Naloxone will reverse the adverse effects of fentanyl. The combination of Fentanyl and midazolam is very good for severe painful procedures but one should be cautious of respiratory depression or even arrest due to it synergistic effect. The newer drugs, ultra short acting alfentanil and sufentanil have not yet entered the Indian market.
MORPHINE (Tab 4)Morphine is the gold standard narcotic
agent with which other narcotic analgesics are compared. It is a very good analgesic but the main disadvantages are histamine release (not suitable for children with reactive airway disease), is long acting, may cause hypotension especially in hypovolemic children and its metabolite Morphine-6-glucoronide is also a potent narcotic. It causes much more nausea and vomiting than other opiates. Though it is an excellent analgesic agent for postoperative analgesia, it is not an ideal agent for emergency room procedures due to its
longer duration of action.FENTANYL:(Tab 5)
Fentanyl is a potent synthetic opiate agonist and is 100 times more potent than
KETAMINE:(Tab 6)
Ketamine was introduced as an intravenous anaesthetic agent and produces dissociative anaesthesia producing a profound analgesia and sedation while maintaining spontaneous respiratory effort. Though it was introduced as an anaesthetic agent, it is being used widely for relief of pain associated with many procedures by the non-anaesthesiologist, because of its potent analgesic effect and its property of preserving the laryngeal and pharyngeal reflexes. Because of its bronchodilatory effect it is a very good analgesic agent for an asthmatic child. It increases the heart rate and the blood pressure. The unpleasant hallucinations seen often in adults occur less frequently in children. Since Ketamine increases salivation, it is mandatory to administer an antisialogogue (glycopyrrolate or atropine), before injecting ketamine. No reversal agent for ketamine
Morphine Onset DurationSC 0.1 -0.15mg/kg 10 min 4 - 5 hrsJM 0A - 0.15ing/kg lOmin 4-5 hrsIV 0.1 -0.15mg/kg 2-5 min 4 - 5hrs
Table.4 Dose, onset and duration of action of morphine
Fentanyl Onset DurationIV 1-3 microgram/kg 2-3 min 45 - 60 min
Table. 5 Dose, onset and duration of action of fentanyl
RACE 2003 Ramachandra Anaesthesia Continuing Education
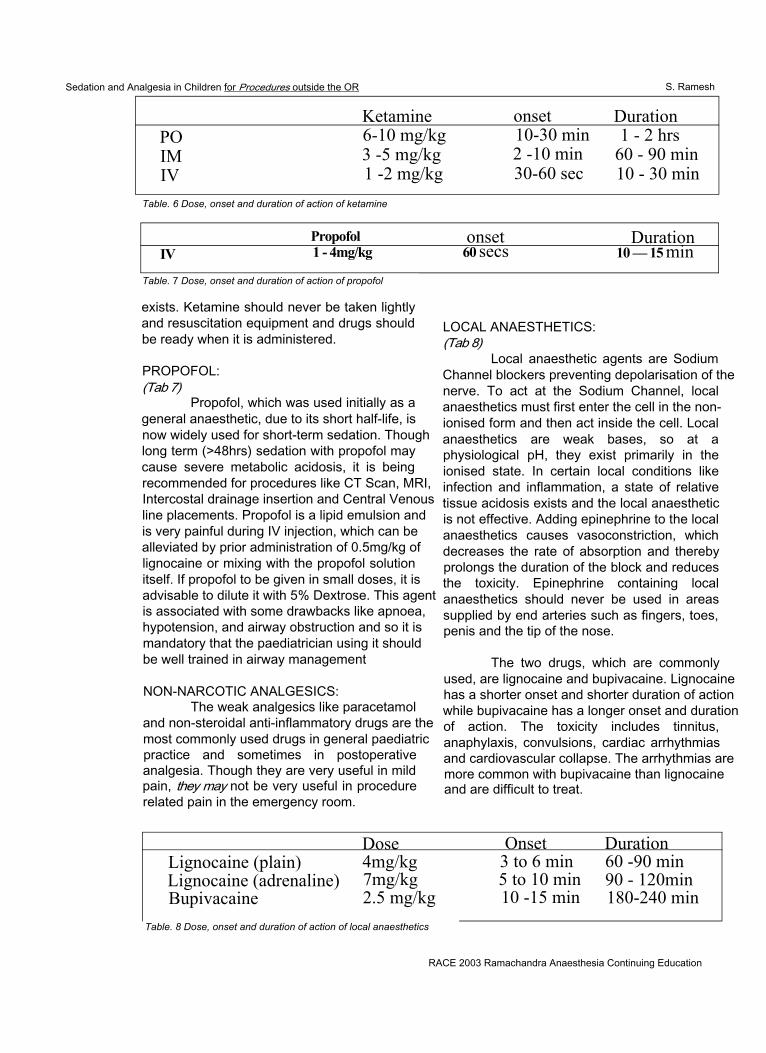
Sedation and Analgesia in Children for Procedures outside the OR S. Ramesh
Ketamine onset DurationPO 6-10 mg/kg 10-30 min 1 - 2 hrsIM 3 -5 mg/kg 2 -10 min 60 - 90 minIV 1 -2 mg/kg 30-60 sec 10 - 30 min
Table. 6 Dose, onset and duration of action of ketamine
Propofol onset DurationIV 1 - 4mg/kg 60 secs 10 — 15 min
Table. 7 Dose, onset and duration of action of propofol
exists. Ketamine should never be taken lightly and resuscitation equipment and drugs should be ready when it is administered.
PROPOFOL:(Tab 7)
Propofol, which was used initially as a general anaesthetic, due to its short half-life, is now widely used for short-term sedation. Though long term (>48hrs) sedation with propofol may cause severe metabolic acidosis, it is being recommended for procedures like CT Scan, MRI, Intercostal drainage insertion and Central Venous line placements. Propofol is a lipid emulsion and is very painful during IV injection, which can be alleviated by prior administration of 0.5mg/kg of lignocaine or mixing with the propofol solution itself. If propofol to be given in small doses, it is advisable to dilute it with 5% Dextrose. This agent is associated with some drawbacks like apnoea, hypotension, and airway obstruction and so it is mandatory that the paediatrician using it should be well trained in airway management
NON-NARCOTIC ANALGESICS:The weak analgesics like paracetamol
and non-steroidal anti-inflammatory drugs are the most commonly used drugs in general paediatric practice and sometimes in postoperative analgesia. Though they are very useful in mild pain, they may not be very useful in procedure related pain in the emergency room.
LOCAL ANAESTHETICS:(Tab 8)
Local anaesthetic agents are Sodium Channel blockers preventing depolarisation of the nerve. To act at the Sodium Channel, local anaesthetics must first enter the cell in the nonionised form and then act inside the cell. Local anaesthetics are weak bases, so at a physiological pH, they exist primarily in the ionised state. In certain local conditions like infection and inflammation, a state of relative tissue acidosis exists and the local anaesthetic is not effective. Adding epinephrine to the local anaesthetics causes vasoconstriction, which decreases the rate of absorption and thereby prolongs the duration of the block and reduces the toxicity. Epinephrine containing local anaesthetics should never be used in areas supplied by end arteries such as fingers, toes, penis and the tip of the nose.
The two drugs, which are commonly used, are lignocaine and bupivacaine. Lignocaine has a shorter onset and shorter duration of action while bupivacaine has a longer onset and duration of action. The toxicity includes tinnitus, anaphylaxis, convulsions, cardiac arrhythmias and cardiovascular collapse. The arrhythmias are more common with bupivacaine than lignocaine and are difficult to treat.
Dose Onset DurationLignocaine (plain) 4mg/kg 3 to 6 min 60 -90 minLignocaine (adrenaline) 7mg/kg 5 to 10 min 90 - 120minBupivacaine 2.5 mg/kg 10 -15 min 180-240 min
Table. 8 Dose, onset and duration of action of local anaesthetics
RACE 2003 Ramachandra Anaesthesia Continuing Education
Sedation and Analgesia in Children for Procedures outside the OR 116 S. Ramesh
EM LAEMLA is a Eutectic mixture of local
anaesthetic cream, which is a mixture of lignocaine, and prilocaine in a water based cream, which provides analgesia even in intact skin. It should be applied at least 60 minutes before. There are some reports of methhaemoglobinaemia in children less than 6 months due to the presence of prilocaine. Its main usage is for IV placement but it can be used for lumbar puncture and circumcision.
General guidelines for using Local anaesthetic agents:1. Use smallest possible needle (24 or 25 g) to
raise the wheal. First inject subcutaneously and then raise the intradermal wheal to prevent pain
2. All resuscitative equipments and drugs should be ready to manage any over dosage or toxicity.
3. It is always safer to have an IV line in place4. To prevent intravascular injection, always
aspirate before injecting the local anaesthetic.
Infiltration local anaesthesia as an adjunct to sedative drugs is very useful in the following situations:1. Lumbar puncture2. Suturing small lacerated wounds3. Central venous line placement4. Arterial line placement5. Intercostal drainage tube insertion6. Bone marrow aspiration and biopsy7. Liver and kidney biopsy
Digital Nerve Block:Of all the other regional nerve blocks,
the most useful block to be learnt is the digital nerve block.
The paired digital nerves enter the digits medially and laterally. Inject 1 to 2 ml of local anaesthetic in the Web space on either sided of the finger or the toe. The usual approach is to enter from the dorsal surface where it is less painful. Epinephrine containing local anaesthetic should never be used. It is very useful for suturing finger injuries, removal of warts and foreign body removal.
Synergism:If you combine two drugs of different
mechanisms of action, one may potentiate the other and reduce the dose requirement of each of them for optimal usage. But at the same time, it may carry the increased risk of respiratory depression.
2 + 2 = 4 Additive effect2 + 2 = 6 Synergistic effect
Example 1- Midazolam and FentanylCombining a sedative and an analgesic
will be very effective for many procedures like lumbar puncture, wound suturing, closed fracture reduction and immobilization. The main advantage of midazolam is amnesia with mild muscle relaxation. Both the drugs should be diluted and injected slowly and titrated to the desired effect without exceeding the upper dose limit of each drug for that particular child. When these combinations are given, it is mandatory to monitor the patient by pulse oximetry. The paediatrician administering these combinations must be skilled in airway management and resuscitation.
Example2 - Atropine or Glycopyrrolate (0.02mg/ kg), Midazolam (0.05mg/kg), Ketamine (0.5 to1 mg/kg)
It is a good combination for painful procedures like wound suturing and fracture reduction. This cocktail effect is not reversible and airway reflexes may not be maintained.
SOME SUGGESTED GUIDELINES FOR THE PROCEDURES:Lumbar puncture:
NPO guide lines ConsentMidazolam 0.1 to 0.2 mg/kg EMLA or local infiltration with 24 Or 25 gauge needleIf airway expert is available, midazolam and fentanyl combination can be tried.
Wound suturingNPO guidelines ConsentMidazolam + Fentanyl combination Local infiltration
RACE 2003 Ramachandra Anaesthesia Continuing Education
Sedation and Analgesia in Children for Procedures outside the OR S. Ramesh
EchocardiographyTrichlofos 50 to 100 mg /kg Intranasal midazolam (0.4mg/kg), onset is in 5 -15 minutes and the duration of action is 25 to 45 minutes.
CT ScanNPO guidelines ConsentTry Midazolam or TrichlofosIf not possible, IV Propofol 2 to 3mg /kgis idealIt is advisable to use IV propofol in the presence of skilled airway personnel.
Haemato- Oncological procedures:NPO guidelines ConsentMidazolam+Fentanyl+Local infiltration Atropine/glycopyrrolate + Midazolam + Ketamine + Local infiltration
RAPID SEQUENCE INTUBATION IN THE EMERGENCY ROOM
The indications and details of the procedure are beyond the purview of this chapter and here, I will be highlighting only the sedatives, induction agents and the muscle relaxants used during the procedure. The main principle here is that the medications are injected fast and theyare preloaded according to the weight of the child.1 Brief history and assessment2. Preperation of equipment and medications3. Preoxygenation4. Premedications5. Sedation and induction of unconsciousness6. Cricoid pressure7. Muscle relaxation8. Intubation9. Verification of ET tube position10. Documentation
Premedication:Atropine or Giycopyrrolate
0.02 mg/kg IV to decrease the secretionsand vagal toneLignocaine 1 mg/kg IV is sometimes is used to provide local airway anaesthesia and blunt ICP response to intubation especially in head trauma.
Sedation and induction of unconsciousness.(Tab 9)
THIOPENTONE:It is an ideal induction agent for this
procedure. It is an ultra short acting barbiturate and has some cerebral protective effect. The major disadvantage is that it causes hypotension. Thiopentone is available in powder form and should be diluted with normal saline and injected as a 2.5% solution and the dose is 4 to 5mg/kg IV.
KETAMINE:There are two clinical situations where
ketamine is considered strongly for induction. One is an asthmatic child because of the bronchodilatory effect and the other is a patient with shock since ketamine is a sympathomimetic agent. The dose is 2mg/kg IV
Midazolam + Fentanyl combination can also be used but higher dosages are needed.
PROPOFOL:Its rapid onset and short duration of
action makes this agent very ideal for rapid induction. Though the manufacturer recommends this agent for children over 3 years, there are many reports of its usage in younger children. It blunts the laryngeal reflexes during intubation. The dose is 2 to 4mg /kg IV.
Muscle relaxants.(Tab 10)
Suxamethonium is the drug of choice for rapid sequence intubation because of its rapid onset and rapid recovery but the disadvantages are bradycardia, fasciculations, and release of potassium.
The alternative to suxamethonium is Rocuronium, which is a non-depolarising muscle relaxant whose onset of action is similar to suxamethonium but the duration of action is longer.
Vecuronium has also been used at a higher dosage of 0.2 to 0.3mg /kg to provide a rapid onset, but the duration is very much prolonged.
RACE 2003 Ramachandra Anaesthesia Continuing Education
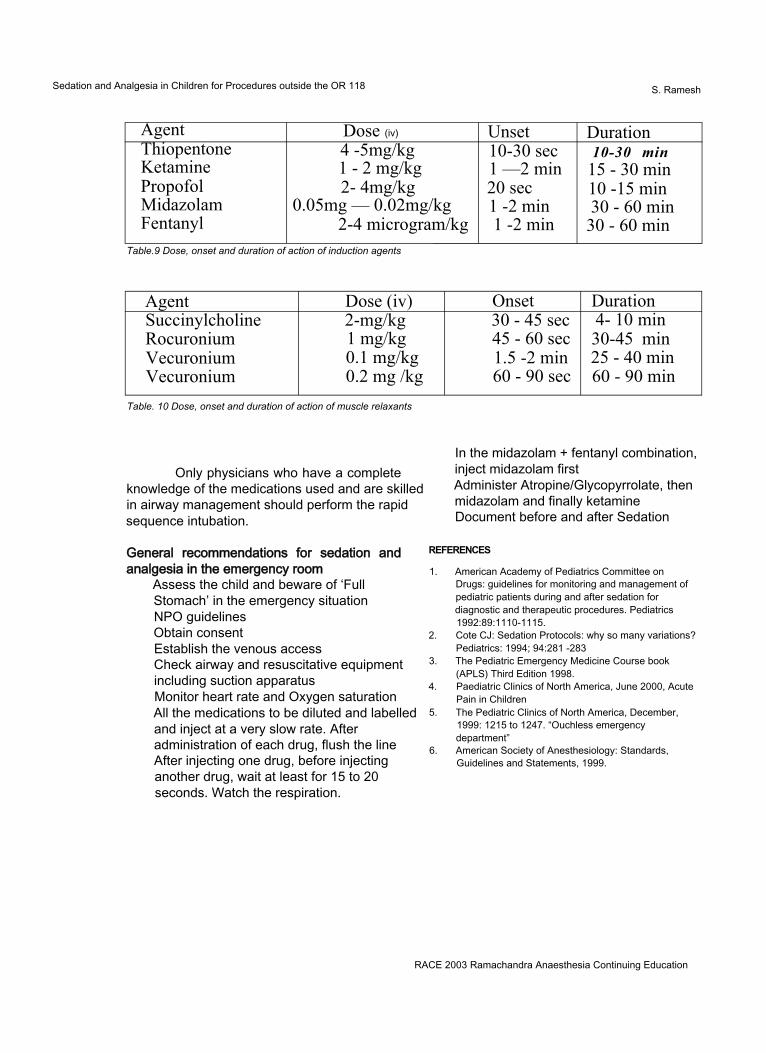
Sedation and Analgesia in Children for Procedures outside the OR 118 S. Ramesh
Agent Dose (iv) Unset DurationThiopentoneKetaminePropofolMidazolamFentanyl
4 -5mg/kg 1 - 2 mg/kg 2- 4mg/kg
0.05mg — 0.02mg/kg2-4 microgram/kg
10-30 sec 1 —2 min 20 sec 1 -2 min 1 -2 min
10-30 min 15 - 30 min 10 -15 min 30 - 60 min
30 - 60 minTable.9 Dose, onset and duration of action of induction agents
Agent Dose (iv) Onset DurationSuccinylcholineRocuroniumVecuroniumVecuronium
2-mg/kg 1 mg/kg 0.1 mg/kg 0.2 mg /kg
30 - 45 sec 45 - 60 sec 1.5 -2 min 60 - 90 sec
4- 10 min 30-45 min 25 - 40 min 60 - 90 min
Table. 10 Dose, onset and duration of action of muscle relaxants
Only physicians who have a complete knowledge of the medications used and are skilled in airway management should perform the rapid sequence intubation.
General recommendations for sedation and analgesia in the emergency room
Assess the child and beware of ‘FullStomach’ in the emergency situationNPO guidelinesObtain consentEstablish the venous accessCheck airway and resuscitative equipmentincluding suction apparatusMonitor heart rate and Oxygen saturationAll the medications to be diluted and labelledand inject at a very slow rate. Afteradministration of each drug, flush the lineAfter injecting one drug, before injectinganother drug, wait at least for 15 to 20seconds. Watch the respiration.
In the midazolam + fentanyl combination, inject midazolam first Administer Atropine/Glycopyrrolate, then midazolam and finally ketamine Document before and after Sedation
REFERENCES
1. American Academy of Pediatrics Committee on Drugs: guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures. Pediatrics 1992:89:1110-1115.
2. Cote CJ: Sedation Protocols: why so many variations? Pediatrics: 1994; 94:281 -283
3. The Pediatric Emergency Medicine Course book (APLS) Third Edition 1998.
4. Paediatric Clinics of North America, June 2000, Acute Pain in Children
5. The Pediatric Clinics of North America, December, 1999: 1215 to 1247. “Ouchless emergency department”
6. American Society of Anesthesiology: Standards, Guidelines and Statements, 1999.
RACE 2003 Ramachandra Anaesthesia Continuing Education

POST GRADUATE SYMPOSIA
Cardiovascular Physiology 119 Latha, Sathya, Rajkumar
INTRODUCTIONUnderstanding cardiovascular physiology
is mandatory for the treatment of cardiovascular disorders and shock states. This article attempts to deal with CVS physiology from a clinical standpoint, to promote physiology-based treatment of common CVS conditions. It does not intend to be a complete treatise on the subject but merely seeks to kindle interest in the fascinating piece of equipment that is the heart. This article is divided into 3 segments: the first deals with cardiac electrophysiology and the cardiac cycle with an overview of cardiovascular reflexes of relevance to the anaesthesiologist. The second deals with the physiological aspects of ventricular function and its relevance to the anaesthetic management of valvular heart disease. The last part deals with the coronary circulation in health and disease.
THE CARDIAC CYCLEEvents that occur from the beginning of
one heart beat to the next constitute one cardiac cycle. It comprises cardiac filling (diastole) followed by contraction (systole) and is initiated by the spontaneous generation of an action potential in the sinoatrial node. At a heart rate of 72 beats/min, the duration of each cycle is 0.8 sec, of which systole is 0.3 sec and diastole is0.5 sec. At higher heart rates, the shortening of diastole is more than that of systole, a phenomenon that is of significance in many disease states.
Electrophysiology of the HeartWith regard to the electrical activity, the
heart consists of 2 types of fibres: quiescent (those that require an external stimulus for
initiation of electrical activity), and automatic (those that generate electrical activity spontaneously, without any external stimulus). Examples of automatic cells are the SA node and secondary pacemaker cells. Examples of quiescent cells are the atrial and ventricular cells. Before we go into the mechanisms of action potential generation, it is worthwhile discussing the subject of transmembrane potentials.
TRANSMEMBRANE POTENTIAL (TMP)The TMP is recorded by inserting
capillary microelectrodes into single cardiac cells. Depending on the state of cell activation, two types of TMPs may be recorded: the TMP during electrical inactivity (resting membrane potential, or RMP; usually -90 mV), and that during electrical activity (action potential). In the resting state, the inside of the cardiac cell is more negative than the outside, hence the cell is said to be polarized. Stimulation leads to the entry of positive ions causing the cell to lose its polarization, a phenomenon termed depolarization. Finally, the net outward movement of positive charges again restores the TMP to its original state of polarization; this is called repolarization.
FACTORS DETERMINING RMPAt rest, the cardiac cell membrane is
permeable only to K+ and not to any of the other ions. Thus the RMP is mainly determined by the K+concentration inside and outside the cell, given by the formula: RMP= -62 log [K(
+] / [Ko+].
Changes in the ratio between extracellular and intracellular K+ produces a change in the RMP; an acute increase in the K + causes a less
O
negative RMP and vice versa.
RACE 2003 Ramachandra Anaesthesia Continuing Education
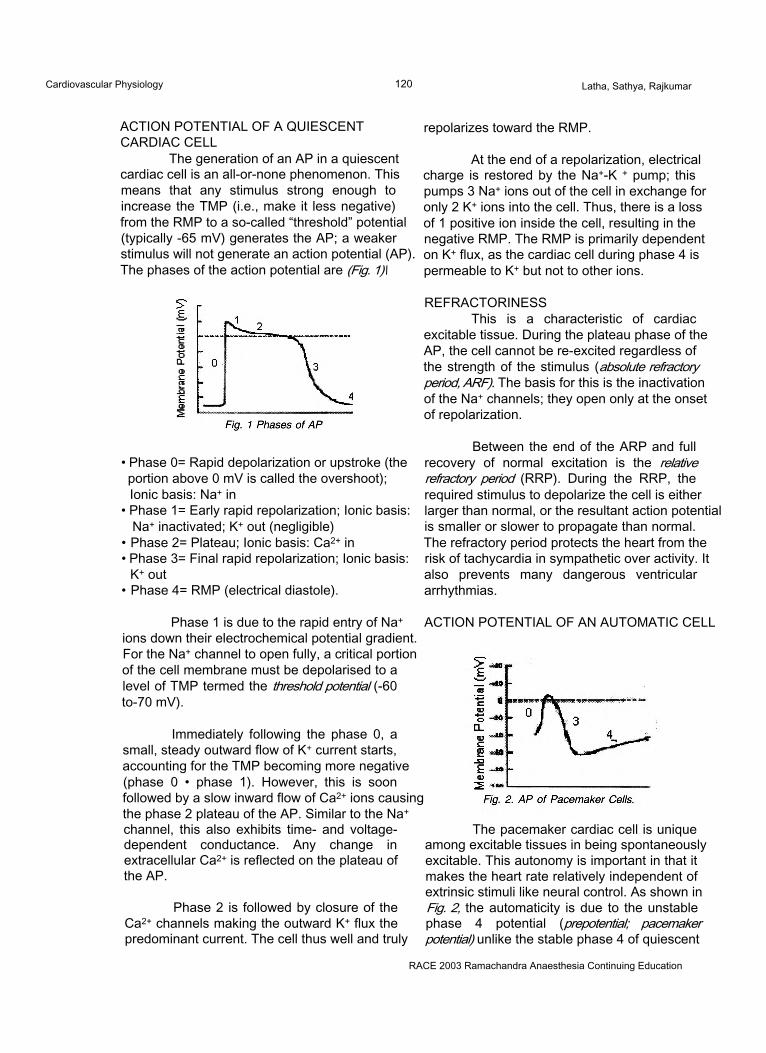
Cardiovascular Physiology 120 Latha, Sathya, Rajkumar
ACTION POTENTIAL OF A QUIESCENT CARDIAC CELL
The generation of an AP in a quiescent cardiac cell is an all-or-none phenomenon. This means that any stimulus strong enough to increase the TMP (i.e., make it less negative) from the RMP to a so-called “threshold” potential (typically -65 mV) generates the AP; a weaker stimulus will not generate an action potential (AP). The phases of the action potential are (Fig. 1)\
repolarizes toward the RMP.
At the end of a repolarization, electrical charge is restored by the Na+-K + pump; this pumps 3 Na+ ions out of the cell in exchange for only 2 K+ ions into the cell. Thus, there is a loss of 1 positive ion inside the cell, resulting in the negative RMP. The RMP is primarily dependent on K+ flux, as the cardiac cell during phase 4 is permeable to K+ but not to other ions.
• Phase 0= Rapid depolarization or upstroke (the portion above 0 mV is called the overshoot); Ionic basis: Na+ in
• Phase 1= Early rapid repolarization; Ionic basis: Na+ inactivated; K+ out (negligible)
• Phase 2= Plateau; Ionic basis: Ca2+ in• Phase 3= Final rapid repolarization; Ionic basis:
K+ out• Phase 4= RMP (electrical diastole).
REFRACTORINESSThis is a characteristic of cardiac
excitable tissue. During the plateau phase of the AP, the cell cannot be re-excited regardless of the strength of the stimulus (absolute refractory period, ARF). The basis for this is the inactivation of the Na+ channels; they open only at the onset of repolarization.
Between the end of the ARP and full recovery of normal excitation is the relative refractory period (RRP). During the RRP, the required stimulus to depolarize the cell is either larger than normal, or the resultant action potential is smaller or slower to propagate than normal. The refractory period protects the heart from the risk of tachycardia in sympathetic over activity. It also prevents many dangerous ventricular arrhythmias.
Phase 1 is due to the rapid entry of Na+ ions down their electrochemical potential gradient. For the Na+ channel to open fully, a critical portion of the cell membrane must be depolarised to a level of TMP termed the threshold potential (-60 to-70 mV).
Immediately following the phase 0, a small, steady outward flow of K+ current starts, accounting for the TMP becoming more negative (phase 0 • phase 1). However, this is soon followed by a slow inward flow of Ca2+ ions causing the phase 2 plateau of the AP. Similar to the Na+ channel, this also exhibits time- and voltage- dependent conductance. Any change in extracellular Ca2+ is reflected on the plateau of the AP.
Phase 2 is followed by closure of the Ca2+ channels making the outward K+ flux the predominant current. The cell thus well and truly
ACTION POTENTIAL OF AN AUTOMATIC CELL
The pacemaker cardiac cell is unique among excitable tissues in being spontaneously excitable. This autonomy is important in that it makes the heart rate relatively independent of extrinsic stimuli like neural control. As shown in Fig. 2, the automaticity is due to the unstable phase 4 potential (prepotential; pacemaker potential) unlike the stable phase 4 of quiescent
RACE 2003 Ramachandra Anaesthesia Continuing Education
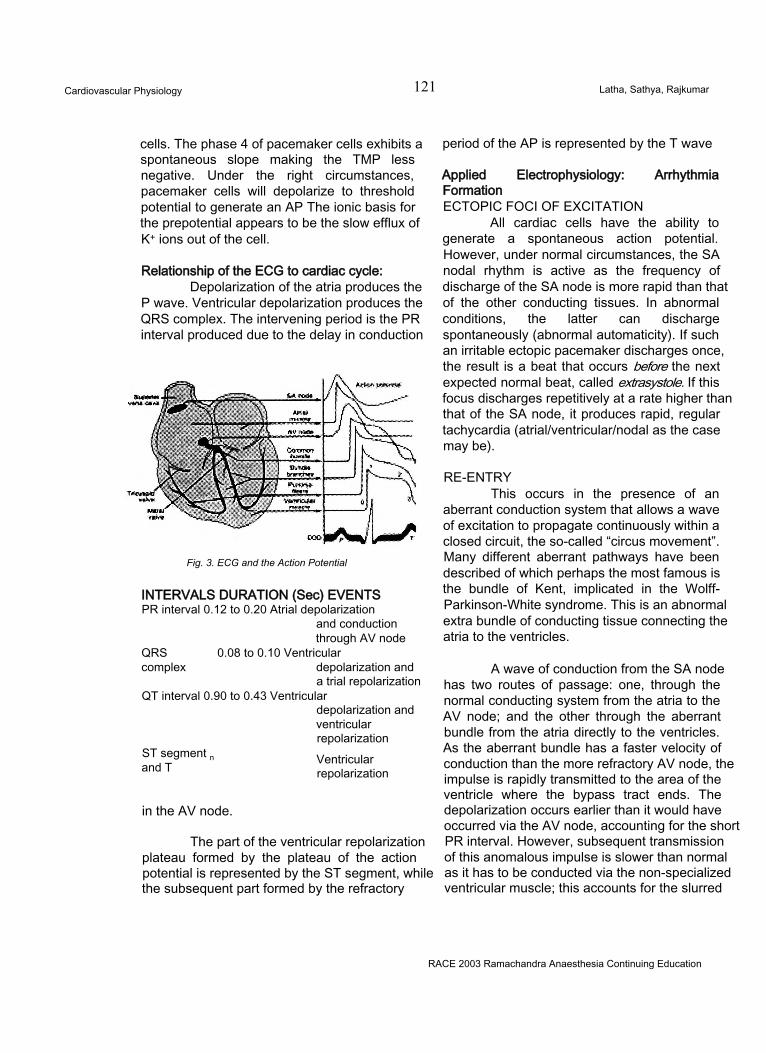
Cardiovascular Physiology 121 Latha, Sathya, Rajkumar
cells. The phase 4 of pacemaker cells exhibits a spontaneous slope making the TMP less negative. Under the right circumstances, pacemaker cells will depolarize to threshold potential to generate an AP The ionic basis for the prepotential appears to be the slow efflux of K+ ions out of the cell.
Relationship of the ECG to cardiac cycle:Depolarization of the atria produces the
P wave. Ventricular depolarization produces the QRS complex. The intervening period is the PR interval produced due to the delay in conduction
Fig. 3. ECG and the Action Potential
INTERVALS DURATION (Sec) EVENTS PR interval 0.12 to 0.20 Atrial depolarization
and conduction through AV node
QRS 0.08 to 0.10 Ventricularcomplex depolarization and
a trial repolarization QT interval 0.90 to 0.43 Ventricular
depolarization andventricularrepolarization
ST segment n and T Ventricular
repolarization
in the AV node.
The part of the ventricular repolarization plateau formed by the plateau of the action potential is represented by the ST segment, while the subsequent part formed by the refractory
period of the AP is represented by the T wave
Applied Electrophysiology: Arrhythmia FormationECTOPIC FOCI OF EXCITATION
All cardiac cells have the ability to generate a spontaneous action potential. However, under normal circumstances, the SA nodal rhythm is active as the frequency of discharge of the SA node is more rapid than that of the other conducting tissues. In abnormal conditions, the latter can discharge spontaneously (abnormal automaticity). If such an irritable ectopic pacemaker discharges once, the result is a beat that occurs before the next expected normal beat, called extrasystole. If this focus discharges repetitively at a rate higher than that of the SA node, it produces rapid, regular tachycardia (atrial/ventricular/nodal as the case may be).
RE-ENTRYThis occurs in the presence of an
aberrant conduction system that allows a wave of excitation to propagate continuously within a closed circuit, the so-called “circus movement”. Many different aberrant pathways have been described of which perhaps the most famous is the bundle of Kent, implicated in the Wolff- Parkinson-White syndrome. This is an abnormal extra bundle of conducting tissue connecting the atria to the ventricles.
A wave of conduction from the SA node has two routes of passage: one, through the normal conducting system from the atria to the AV node; and the other through the aberrant bundle from the atria directly to the ventricles. As the aberrant bundle has a faster velocity of conduction than the more refractory AV node, the impulse is rapidly transmitted to the area of the ventricle where the bypass tract ends. The depolarization occurs earlier than it would have occurred via the AV node, accounting for the short PR interval. However, subsequent transmission of this anomalous impulse is slower than normal as it has to be conducted via the non-specialized ventricular muscle; this accounts for the slurred
RACE 2003 Ramachandra Anaesthesia Continuing Education
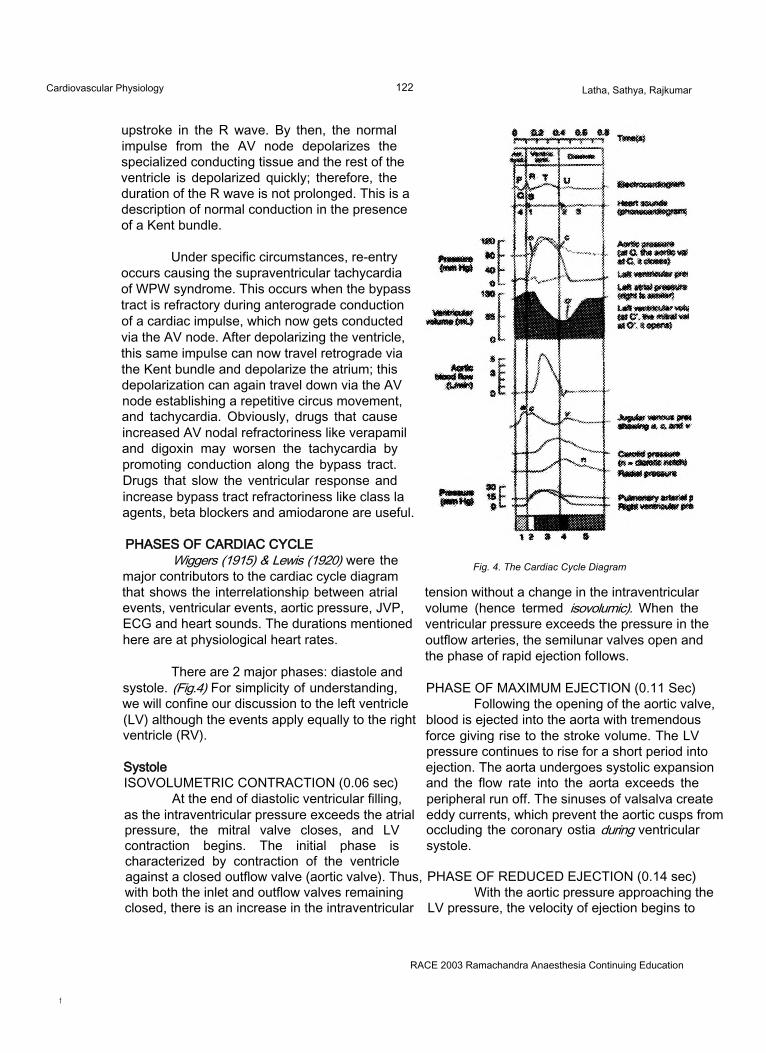
Cardiovascular Physiology 122 Latha, Sathya, Rajkumar
upstroke in the R wave. By then, the normal impulse from the AV node depolarizes the specialized conducting tissue and the rest of the ventricle is depolarized quickly; therefore, the duration of the R wave is not prolonged. This is a description of normal conduction in the presence of a Kent bundle.
Under specific circumstances, re-entry occurs causing the supraventricular tachycardia of WPW syndrome. This occurs when the bypass tract is refractory during anterograde conduction of a cardiac impulse, which now gets conducted via the AV node. After depolarizing the ventricle, this same impulse can now travel retrograde via the Kent bundle and depolarize the atrium; this depolarization can again travel down via the AV node establishing a repetitive circus movement, and tachycardia. Obviously, drugs that cause increased AV nodal refractoriness like verapamil and digoxin may worsen the tachycardia by promoting conduction along the bypass tract. Drugs that slow the ventricular response and increase bypass tract refractoriness like class la agents, beta blockers and amiodarone are useful.
PHASES OF CARDIAC CYCLEWiggers (1915) & Lewis (1920) were the
major contributors to the cardiac cycle diagram that shows the interrelationship between atrial events, ventricular events, aortic pressure, JVP, ECG and heart sounds. The durations mentioned here are at physiological heart rates.
There are 2 major phases: diastole and systole. (Fig.4) For simplicity of understanding, we will confine our discussion to the left ventricle (LV) although the events apply equally to the right ventricle (RV).
SystoleISOVOLUMETRIC CONTRACTION (0.06 sec)
At the end of diastolic ventricular filling, as the intraventricular pressure exceeds the atrial pressure, the mitral valve closes, and LV contraction begins. The initial phase is characterized by contraction of the ventricle against a closed outflow valve (aortic valve). Thus, with both the inlet and outflow valves remaining closed, there is an increase in the intraventricular
Fig. 4. The Cardiac Cycle Diagram
tension without a change in the intraventricular volume (hence termed isovolumic). When the ventricular pressure exceeds the pressure in the outflow arteries, the semilunar valves open and the phase of rapid ejection follows.
PHASE OF MAXIMUM EJECTION (0.11 Sec) Following the opening of the aortic valve,
blood is ejected into the aorta with tremendous force giving rise to the stroke volume. The LV pressure continues to rise for a short period into ejection. The aorta undergoes systolic expansion and the flow rate into the aorta exceeds the peripheral run off. The sinuses of valsalva create eddy currents, which prevent the aortic cusps from occluding the coronary ostia during ventricular systole.
PHASE OF REDUCED EJECTION (0.14 sec) With the aortic pressure approaching the
LV pressure, the velocity of ejection begins to
RACE 2003 Ramachandra Anaesthesia Continuing Education
f
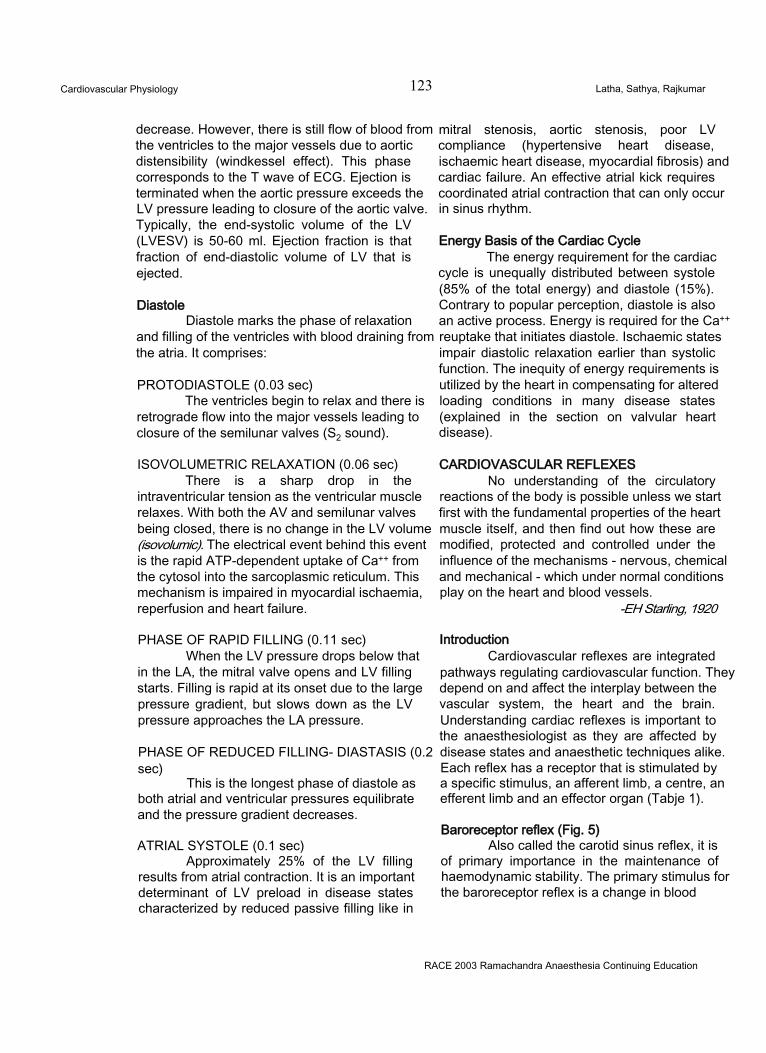
Cardiovascular Physiology 123 Latha, Sathya, Rajkumar
decrease. However, there is still flow of blood from the ventricles to the major vessels due to aortic distensibility (windkessel effect). This phase corresponds to the T wave of ECG. Ejection is terminated when the aortic pressure exceeds the LV pressure leading to closure of the aortic valve. Typically, the end-systolic volume of the LV (LVESV) is 50-60 ml. Ejection fraction is that fraction of end-diastolic volume of LV that is ejected.
DiastoleDiastole marks the phase of relaxation
and filling of the ventricles with blood draining from the atria. It comprises:
PROTODIASTOLE (0.03 sec)The ventricles begin to relax and there is
retrograde flow into the major vessels leading to closure of the semilunar valves (S2 sound).
ISOVOLUMETRIC RELAXATION (0.06 sec)There is a sharp drop in the
intraventricular tension as the ventricular muscle relaxes. With both the AV and semilunar valves being closed, there is no change in the LV volume (isovolumic). The electrical event behind this event is the rapid ATP-dependent uptake of Ca++ from the cytosol into the sarcoplasmic reticulum. This mechanism is impaired in myocardial ischaemia, reperfusion and heart failure.
PHASE OF RAPID FILLING (0.11 sec)When the LV pressure drops below that
in the LA, the mitral valve opens and LV filling starts. Filling is rapid at its onset due to the large pressure gradient, but slows down as the LV pressure approaches the LA pressure.
PHASE OF REDUCED FILLING- DIASTASIS (0.2 sec)
This is the longest phase of diastole as both atrial and ventricular pressures equilibrate and the pressure gradient decreases.
ATRIAL SYSTOLE (0.1 sec)Approximately 25% of the LV filling
results from atrial contraction. It is an important determinant of LV preload in disease states characterized by reduced passive filling like in
mitral stenosis, aortic stenosis, poor LV compliance (hypertensive heart disease, ischaemic heart disease, myocardial fibrosis) and cardiac failure. An effective atrial kick requires coordinated atrial contraction that can only occur in sinus rhythm.
Energy Basis of the Cardiac CycleThe energy requirement for the cardiac
cycle is unequally distributed between systole (85% of the total energy) and diastole (15%). Contrary to popular perception, diastole is also an active process. Energy is required for the Ca++ reuptake that initiates diastole. Ischaemic states impair diastolic relaxation earlier than systolic function. The inequity of energy requirements is utilized by the heart in compensating for altered loading conditions in many disease states (explained in the section on valvular heart disease).
CARDIOVASCULAR REFLEXESNo understanding of the circulatory
reactions of the body is possible unless we start first with the fundamental properties of the heart muscle itself, and then find out how these are modified, protected and controlled under the influence of the mechanisms - nervous, chemical and mechanical - which under normal conditions play on the heart and blood vessels.
-EH Starling, 1920
IntroductionCardiovascular reflexes are integrated
pathways regulating cardiovascular function. They depend on and affect the interplay between the vascular system, the heart and the brain. Understanding cardiac reflexes is important to the anaesthesiologist as they are affected by disease states and anaesthetic techniques alike. Each reflex has a receptor that is stimulated by a specific stimulus, an afferent limb, a centre, an efferent limb and an effector organ (Tabje 1).
Baroreceptor reflex (Fig. 5)Also called the carotid sinus reflex, it is
of primary importance in the maintenance of haemodynamic stability. The primary stimulus for the baroreceptor reflex is a change in blood
RACE 2003 Ramachandra Anaesthesia Continuing Education
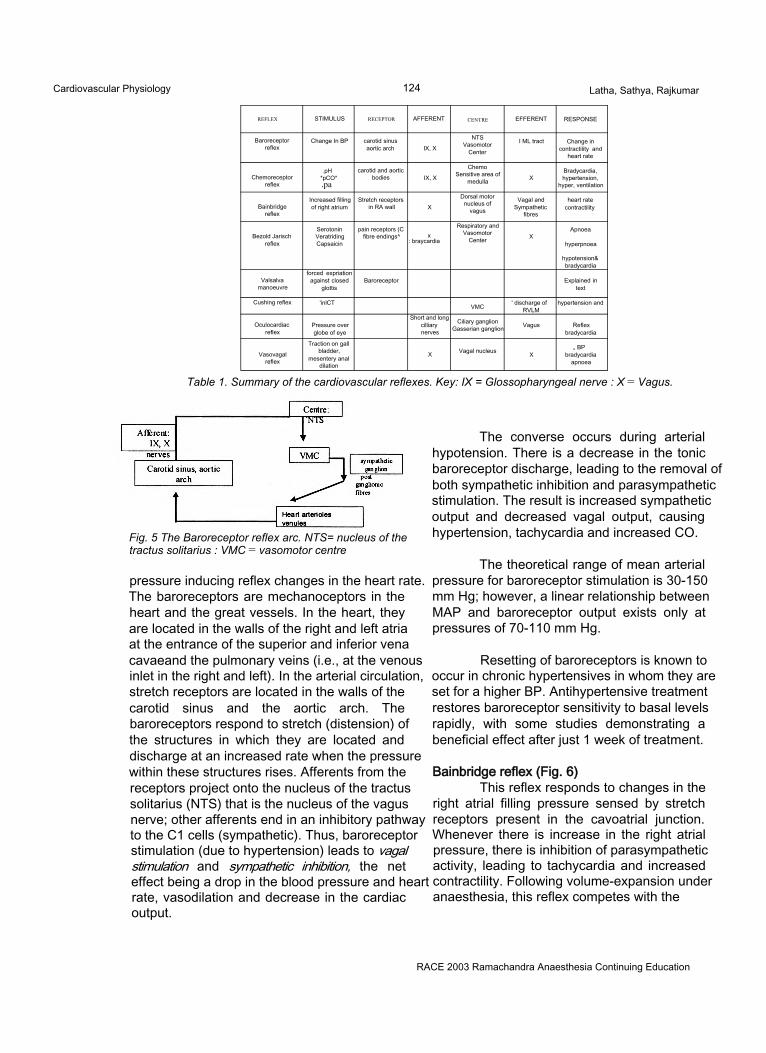
Cardiovascular Physiology 124 Latha, Sathya, Rajkumar
REFLEX STIMULUS RECEPTOR AFFERENT CENTRE EFFERENT RESPONSE
Baroreceptorreflex
Change In BP carotid sinus aortic arch IX, X
NTSVasomotor
Center
I ML tract Change in contractility and
heart rate
Chemoreceptorreflex
.pH*pCO*.pa
carotid and aortic bodies IX, X
Chemo Sensitive area of
medulla XBradycardia, hypertension,
hyper, ventilation
Bainbridgereflex
Increased filling of right atrium
Stretch receptors in RA wall X
Dorsal motor nucleus of
vagus
Vagal and Sympathetic
fibres
heart rate contractility
Bezold Jarisch reflex
SerotoninVeratridingCapsaicin
pain receptors (C fibre endings^ x
: braycardia
Respiratory and Vasomotor
Center XApnoea
hyperpnoea
hypotension&bradycardia
Valsalvamanoeuvre
forced expriation against closed
glottisBaroreceptor Explained in
text
Cushing reflex 'inlCT VMC ' discharge of RVLM
hypertension and
Oculocardiacreflex
Pressure over globe of eye
Short and long cilliary nerves
Ciliary ganglion Gasserian ganglion Vagus Reflex
bradycardia
Vasovagalreflex
Traction on gall bladder,
mesentery anal dilation
X Vagal nucleus X„ BP
bradycardia apnoea
Table 1. Summary of the cardiovascular reflexes. Key: IX = Glossopharyngeal nerve : X = Vagus.
Fig. 5 The Baroreceptor reflex arc. NTS= nucleus of the tractus solitarius : VMC = vasomotor centre
pressure inducing reflex changes in the heart rate. The baroreceptors are mechanoceptors in the heart and the great vessels. In the heart, they are located in the walls of the right and left atria at the entrance of the superior and inferior vena cavaeand the pulmonary veins (i.e., at the venous inlet in the right and left). In the arterial circulation, stretch receptors are located in the walls of the carotid sinus and the aortic arch. The baroreceptors respond to stretch (distension) of the structures in which they are located and discharge at an increased rate when the pressure within these structures rises. Afferents from the receptors project onto the nucleus of the tractus solitarius (NTS) that is the nucleus of the vagus nerve; other afferents end in an inhibitory pathway to the C1 cells (sympathetic). Thus, baroreceptor stimulation (due to hypertension) leads to vagal stimulation and sympathetic inhibition, the net effect being a drop in the blood pressure and heart rate, vasodilation and decrease in the cardiac output.
The converse occurs during arterial hypotension. There is a decrease in the tonic baroreceptor discharge, leading to the removal of both sympathetic inhibition and parasympathetic stimulation. The result is increased sympathetic output and decreased vagal output, causing hypertension, tachycardia and increased CO.
The theoretical range of mean arterial pressure for baroreceptor stimulation is 30-150 mm Hg; however, a linear relationship between MAP and baroreceptor output exists only at pressures of 70-110 mm Hg.
Resetting of baroreceptors is known to occur in chronic hypertensives in whom they are set for a higher BP. Antihypertensive treatment restores baroreceptor sensitivity to basal levels rapidly, with some studies demonstrating a beneficial effect after just 1 week of treatment.
Bainbridge reflex (Fig. 6)This reflex responds to changes in the
right atrial filling pressure sensed by stretch receptors present in the cavoatrial junction. Whenever there is increase in the right atrial pressure, there is inhibition of parasympathetic activity, leading to tachycardia and increased contractility. Following volume-expansion under anaesthesia, this reflex competes with the
RACE 2003 Ramachandra Anaesthesia Continuing Education
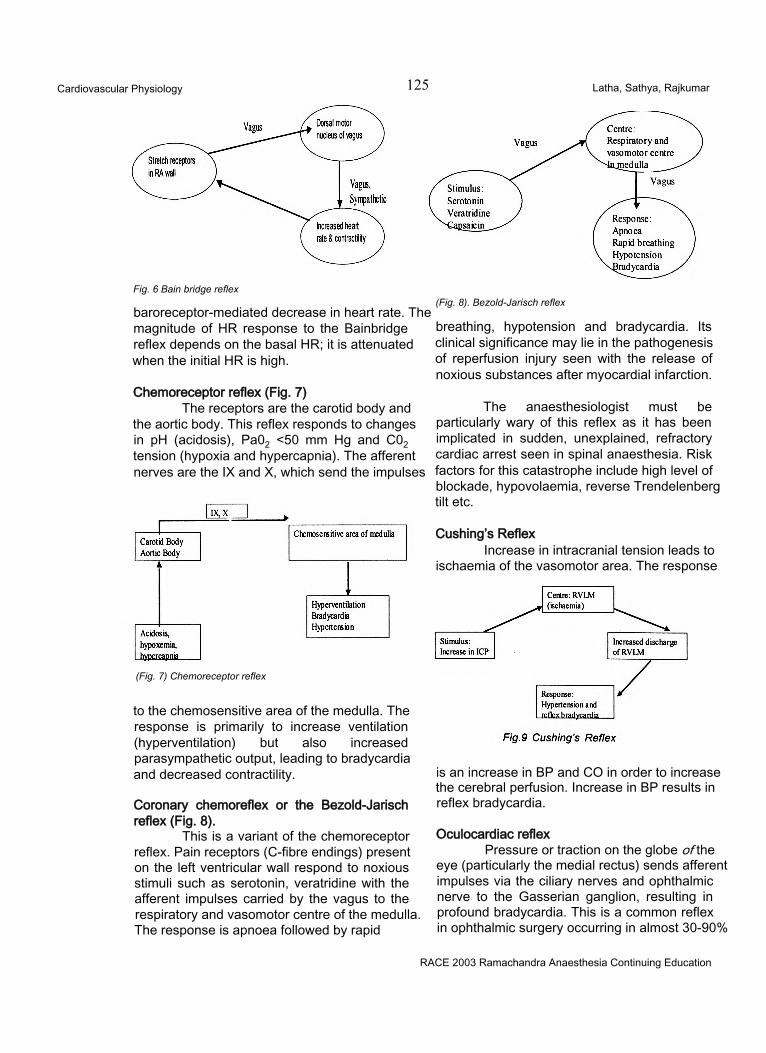
Cardiovascular Physiology 125 Latha, Sathya, Rajkumar
Fig. 6 Bain bridge reflex
baroreceptor-mediated decrease in heart rate. The magnitude of HR response to the Bainbridge reflex depends on the basal HR; it is attenuated when the initial HR is high.
Chemoreceptor reflex (Fig. 7)The receptors are the carotid body and
the aortic body. This reflex responds to changes in pH (acidosis), Pa02 <50 mm Hg and C02 tension (hypoxia and hypercapnia). The afferent nerves are the IX and X, which send the impulses
(Fig. 7) Chemoreceptor reflex
to the chemosensitive area of the medulla. The response is primarily to increase ventilation (hyperventilation) but also increased parasympathetic output, leading to bradycardia and decreased contractility.
Coronary chemoreflex or the Bezold-Jarisch reflex (Fig. 8).
This is a variant of the chemoreceptor reflex. Pain receptors (C-fibre endings) present on the left ventricular wall respond to noxious stimuli such as serotonin, veratridine with the afferent impulses carried by the vagus to the respiratory and vasomotor centre of the medulla. The response is apnoea followed by rapid
(Fig. 8). Bezold-Jarisch reflex
breathing, hypotension and bradycardia. Its clinical significance may lie in the pathogenesis of reperfusion injury seen with the release of noxious substances after myocardial infarction.
The anaesthesiologist must be particularly wary of this reflex as it has been implicated in sudden, unexplained, refractory cardiac arrest seen in spinal anaesthesia. Risk factors for this catastrophe include high level of blockade, hypovolaemia, reverse Trendelenberg tilt etc.
Cushing’s ReflexIncrease in intracranial tension leads to
ischaemia of the vasomotor area. The response
is an increase in BP and CO in order to increase the cerebral perfusion. Increase in BP results in reflex bradycardia.
Oculocardiac reflexPressure or traction on the globe of the
eye (particularly the medial rectus) sends afferent impulses via the ciliary nerves and ophthalmic nerve to the Gasserian ganglion, resulting in profound bradycardia. This is a common reflex in ophthalmic surgery occurring in almost 30-90%
RACE 2003 Ramachandra Anaesthesia Continuing Education
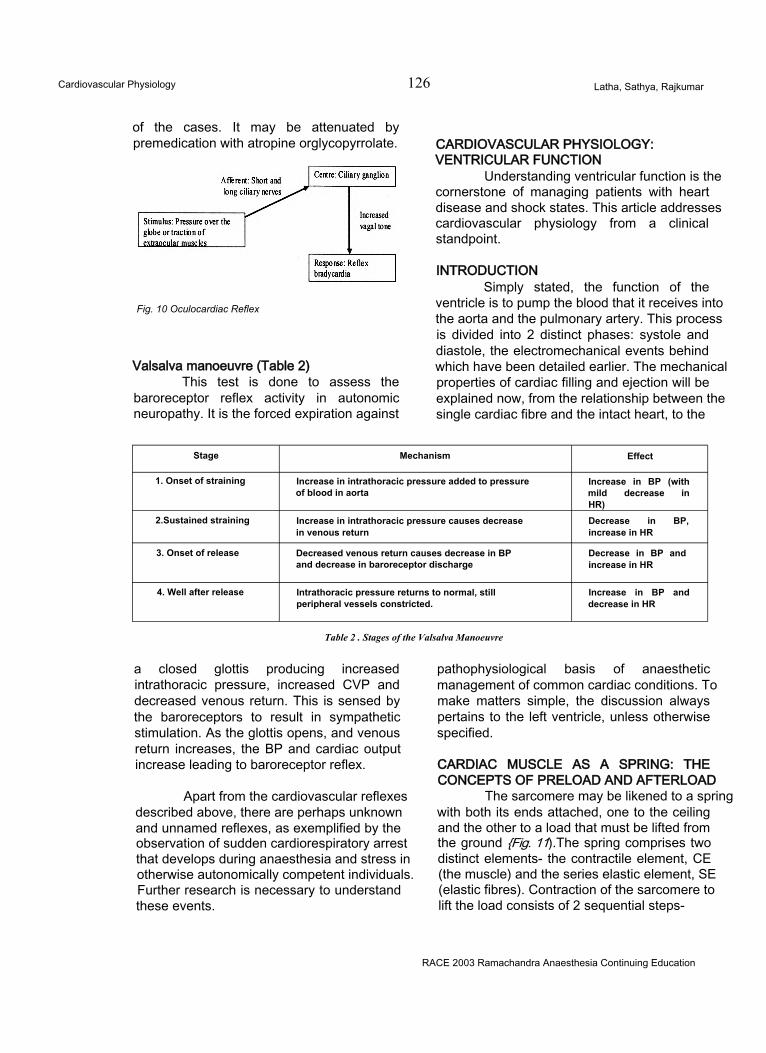
Cardiovascular Physiology 126 Latha, Sathya, Rajkumar
of the cases. It may be attenuated by premedication with atropine orglycopyrrolate.
Fig. 10 Oculocardiac Reflex
Valsalva manoeuvre (Table 2)This test is done to assess the
baroreceptor reflex activity in autonomic neuropathy. It is the forced expiration against
CARDIOVASCULAR PHYSIOLOGY: VENTRICULAR FUNCTION
Understanding ventricular function is the cornerstone of managing patients with heart disease and shock states. This article addresses cardiovascular physiology from a clinical standpoint.
INTRODUCTIONSimply stated, the function of the
ventricle is to pump the blood that it receives into the aorta and the pulmonary artery. This process is divided into 2 distinct phases: systole and diastole, the electromechanical events behind which have been detailed earlier. The mechanical properties of cardiac filling and ejection will be explained now, from the relationship between the single cardiac fibre and the intact heart, to the
Stage Mechanism Effect
1. Onset of straining Increase in intrathoracic pressure added to pressure of blood in aorta
Increase in BP (with mild decrease in HR)
2.Sustained straining Increase in intrathoracic pressure causes decrease in venous return
Decrease in BP, increase in HR
3. Onset of release Decreased venous return causes decrease in BP and decrease in baroreceptor discharge
Decrease in BP and increase in HR
4. Well after release Intrathoracic pressure returns to normal, still peripheral vessels constricted.
Increase in BP and decrease in HR
Table 2 . Stages of the Valsalva Manoeuvre
a closed glottis producing increased intrathoracic pressure, increased CVP and decreased venous return. This is sensed by the baroreceptors to result in sympathetic stimulation. As the glottis opens, and venous return increases, the BP and cardiac output increase leading to baroreceptor reflex.
Apart from the cardiovascular reflexes described above, there are perhaps unknown and unnamed reflexes, as exemplified by the observation of sudden cardiorespiratory arrest that develops during anaesthesia and stress in otherwise autonomically competent individuals. Further research is necessary to understand these events.
pathophysiological basis of anaesthetic management of common cardiac conditions. To make matters simple, the discussion always pertains to the left ventricle, unless otherwise specified.
CARDIAC MUSCLE AS A SPRING: THE CONCEPTS OF PRELOAD AND AFTERLOAD
The sarcomere may be likened to a spring with both its ends attached, one to the ceiling and the other to a load that must be lifted from the ground {Fig. 11).The spring comprises two distinct elements- the contractile element, CE (the muscle) and the series elastic element, SE (elastic fibres). Contraction of the sarcomere to lift the load consists of 2 sequential steps-
RACE 2003 Ramachandra Anaesthesia Continuing Education
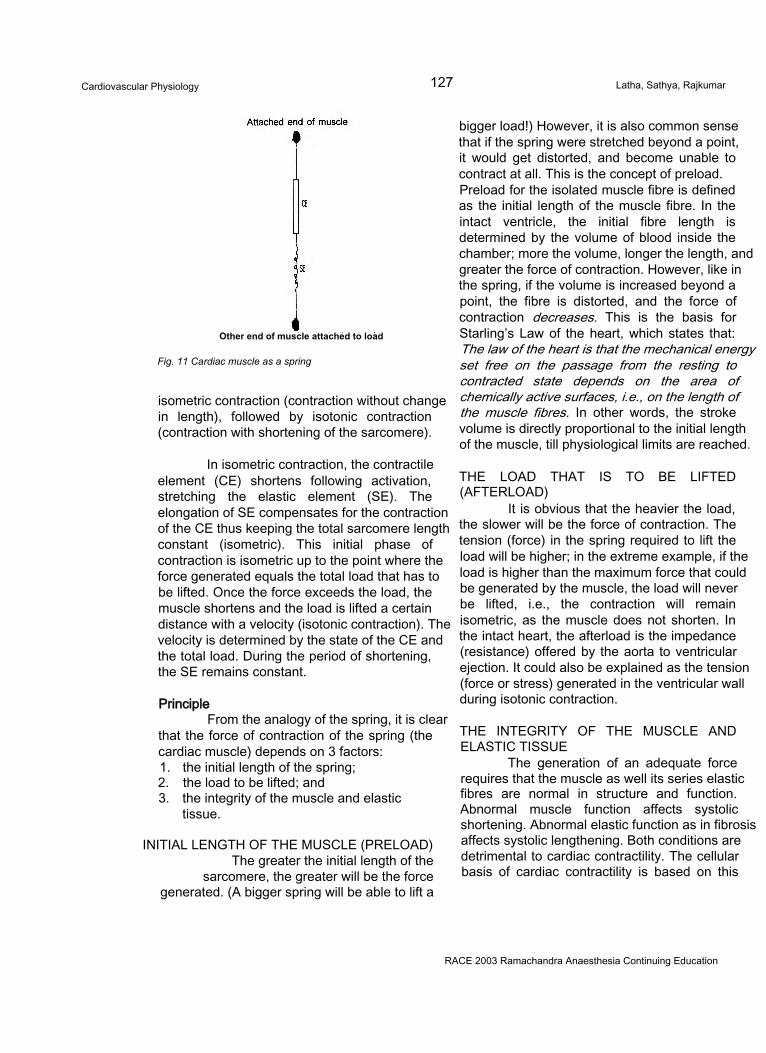
Cardiovascular Physiology 127 Latha, Sathya, Rajkumar
Other end of muscle attached to load
Fig. 11 Cardiac muscle as a spring
isometric contraction (contraction without change in length), followed by isotonic contraction (contraction with shortening of the sarcomere).
In isometric contraction, the contractile element (CE) shortens following activation, stretching the elastic element (SE). The elongation of SE compensates for the contraction of the CE thus keeping the total sarcomere length constant (isometric). This initial phase of contraction is isometric up to the point where the force generated equals the total load that has to be lifted. Once the force exceeds the load, the muscle shortens and the load is lifted a certain distance with a velocity (isotonic contraction). The velocity is determined by the state of the CE and the total load. During the period of shortening, the SE remains constant.
PrincipleFrom the analogy of the spring, it is clear
that the force of contraction of the spring (the cardiac muscle) depends on 3 factors:1. the initial length of the spring;2. the load to be lifted; and3. the integrity of the muscle and elastic
tissue.
INITIAL LENGTH OF THE MUSCLE (PRELOAD) The greater the initial length of the
sarcomere, the greater will be the force generated. (A bigger spring will be able to lift a
bigger load!) However, it is also common sense that if the spring were stretched beyond a point, it would get distorted, and become unable to contract at all. This is the concept of preload. Preload for the isolated muscle fibre is defined as the initial length of the muscle fibre. In the intact ventricle, the initial fibre length is determined by the volume of blood inside the chamber; more the volume, longer the length, and greater the force of contraction. However, like in the spring, if the volume is increased beyond a point, the fibre is distorted, and the force of contraction decreases. This is the basis for Starling’s Law of the heart, which states that: The law of the heart is that the mechanical energy set free on the passage from the resting to contracted state depends on the area of chemically active surfaces, i.e., on the length of the muscle fibres. In other words, the stroke volume is directly proportional to the initial length of the muscle, till physiological limits are reached.
THE LOAD THAT IS TO BE LIFTED (AFTERLOAD)
It is obvious that the heavier the load, the slower will be the force of contraction. The tension (force) in the spring required to lift the load will be higher; in the extreme example, if the load is higher than the maximum force that could be generated by the muscle, the load will never be lifted, i.e., the contraction will remain isometric, as the muscle does not shorten. In the intact heart, the afterload is the impedance (resistance) offered by the aorta to ventricular ejection. It could also be explained as the tension (force or stress) generated in the ventricular wall during isotonic contraction.
THE INTEGRITY OF THE MUSCLE AND ELASTIC TISSUE
The generation of an adequate force requires that the muscle as well its series elastic fibres are normal in structure and function. Abnormal muscle function affects systolic shortening. Abnormal elastic function as in fibrosis affects systolic lengthening. Both conditions are detrimental to cardiac contractility. The cellular basis of cardiac contractility is based on this
RACE 2003 Ramachandra Anaesthesia Continuing Education
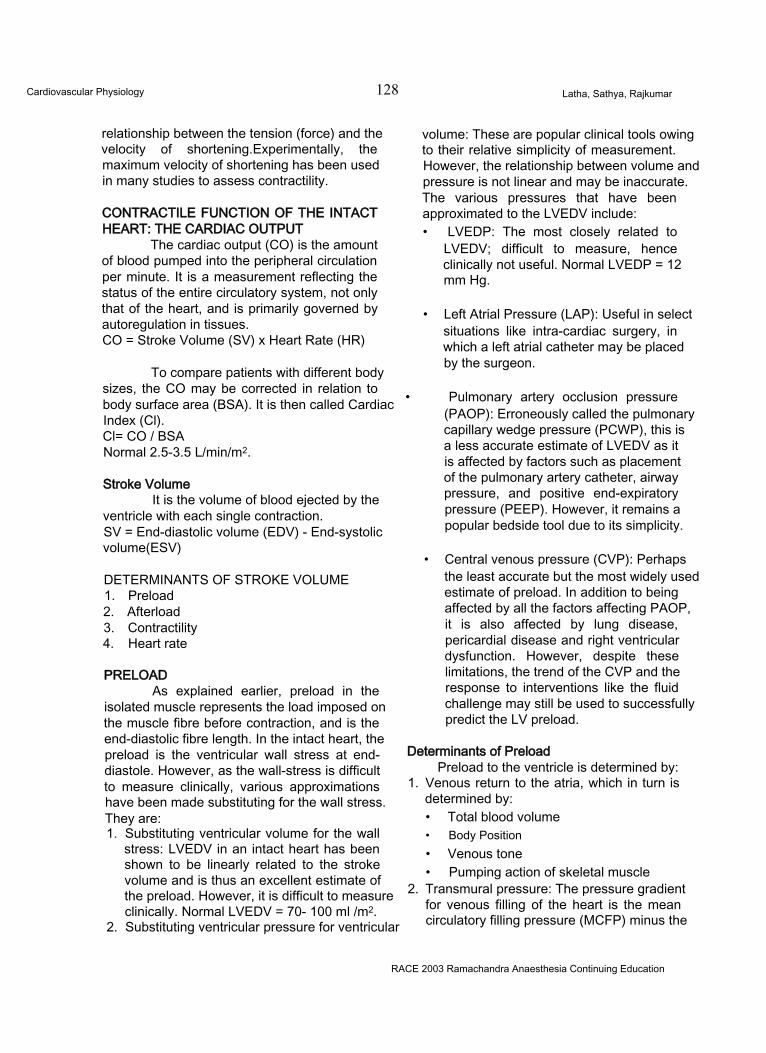
Cardiovascular Physiology 128 Latha, Sathya, Rajkumar
relationship between the tension (force) and the velocity of shortening.Experimentally, the maximum velocity of shortening has been used in many studies to assess contractility.
CONTRACTILE FUNCTION OF THE INTACT HEART: THE CARDIAC OUTPUT
The cardiac output (CO) is the amount of blood pumped into the peripheral circulation per minute. It is a measurement reflecting the status of the entire circulatory system, not only that of the heart, and is primarily governed by autoregulation in tissues.CO = Stroke Volume (SV) x Heart Rate (HR)
To compare patients with different body sizes, the CO may be corrected in relation to body surface area (BSA). It is then called Cardiac Index (Cl).Cl= CO / BSA Normal 2.5-3.5 L/min/m2.
Stroke VolumeIt is the volume of blood ejected by the
ventricle with each single contraction.SV = End-diastolic volume (EDV) - End-systolic volume(ESV)
DETERMINANTS OF STROKE VOLUME1. Preload2. Afterload3. Contractility4. Heart rate
PRELOADAs explained earlier, preload in the
isolated muscle represents the load imposed on the muscle fibre before contraction, and is the end-diastolic fibre length. In the intact heart, the preload is the ventricular wall stress at end- diastole. However, as the wall-stress is difficult to measure clinically, various approximations have been made substituting for the wall stress. They are:1. Substituting ventricular volume for the wall
stress: LVEDV in an intact heart has been shown to be linearly related to the stroke volume and is thus an excellent estimate of the preload. However, it is difficult to measure clinically. Normal LVEDV = 70- 100 ml /m2.
2. Substituting ventricular pressure for ventricular
volume: These are popular clinical tools owing to their relative simplicity of measurement. However, the relationship between volume and pressure is not linear and may be inaccurate. The various pressures that have been approximated to the LVEDV include:• LVEDP: The most closely related to
LVEDV; difficult to measure, hence clinically not useful. Normal LVEDP = 12 mm Hg.
• Left Atrial Pressure (LAP): Useful in select situations like intra-cardiac surgery, in which a left atrial catheter may be placed by the surgeon.
• Pulmonary artery occlusion pressure (PAOP): Erroneously called the pulmonary capillary wedge pressure (PCWP), this is a less accurate estimate of LVEDV as it is affected by factors such as placement of the pulmonary artery catheter, airway pressure, and positive end-expiratory pressure (PEEP). However, it remains a popular bedside tool due to its simplicity.
• Central venous pressure (CVP): Perhaps the least accurate but the most widely used estimate of preload. In addition to being affected by all the factors affecting PAOP, it is also affected by lung disease, pericardial disease and right ventricular dysfunction. However, despite these limitations, the trend of the CVP and the response to interventions like the fluid challenge may still be used to successfully predict the LV preload.
Determinants of PreloadPreload to the ventricle is determined by:
1. Venous return to the atria, which in turn is determined by:• Total blood volume• Body Position• Venous tone• Pumping action of skeletal muscle
2. Transmural pressure: The pressure gradient for venous filling of the heart is the mean circulatory filling pressure (MCFP) minus the
RACE 2003 Ramachandra Anaesthesia Continuing Education
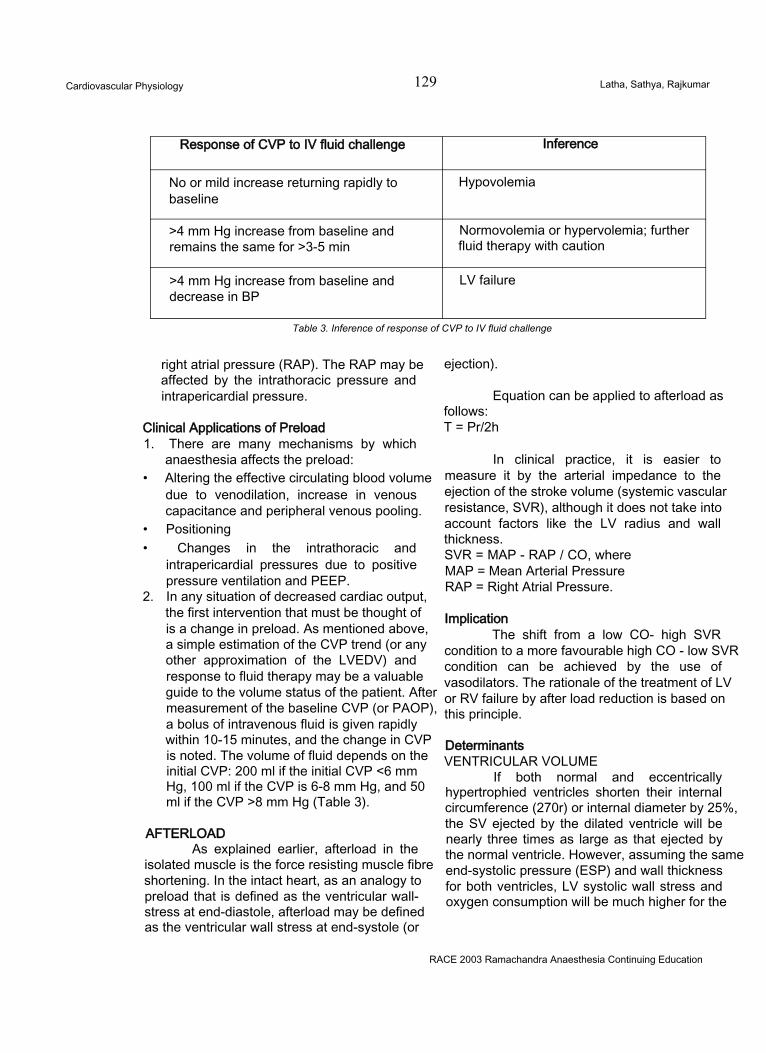
Cardiovascular Physiology 129 Latha, Sathya, Rajkumar
Response of CVP to IV fluid challenge Inference
No or mild increase returning rapidly to baseline
Hypovolemia
>4 mm Hg increase from baseline and remains the same for >3-5 min
Normovolemia or hypervolemia; further fluid therapy with caution
>4 mm Hg increase from baseline and decrease in BP
LV failure
Table 3. Inference of response of CVP to IV fluid challenge
right atrial pressure (RAP). The RAP may be affected by the intrathoracic pressure and intrapericardial pressure.
Clinical Applications of Preload1. There are many mechanisms by which
anaesthesia affects the preload:• Altering the effective circulating blood volume
due to venodilation, increase in venous capacitance and peripheral venous pooling.
• Positioning• Changes in the intrathoracic and
intrapericardial pressures due to positive pressure ventilation and PEEP.
2. In any situation of decreased cardiac output, the first intervention that must be thought of is a change in preload. As mentioned above, a simple estimation of the CVP trend (or any other approximation of the LVEDV) and response to fluid therapy may be a valuable guide to the volume status of the patient. After measurement of the baseline CVP (or PAOP), a bolus of intravenous fluid is given rapidly within 10-15 minutes, and the change in CVP is noted. The volume of fluid depends on the initial CVP: 200 ml if the initial CVP <6 mm Hg, 100 ml if the CVP is 6-8 mm Hg, and 50 ml if the CVP >8 mm Hg (Table 3).
AFTERLOADAs explained earlier, afterload in the
isolated muscle is the force resisting muscle fibre shortening. In the intact heart, as an analogy to preload that is defined as the ventricular wall- stress at end-diastole, afterload may be defined as the ventricular wall stress at end-systole (or
ejection).
Equation can be applied to afterload asfollows:T = Pr/2h
In clinical practice, it is easier to measure it by the arterial impedance to the ejection of the stroke volume (systemic vascular resistance, SVR), although it does not take into account factors like the LV radius and wall thickness.SVR = MAP - RAP / CO, where MAP = Mean Arterial Pressure RAP = Right Atrial Pressure.
ImplicationThe shift from a low CO- high SVR
condition to a more favourable high CO - low SVR condition can be achieved by the use of vasodilators. The rationale of the treatment of LV or RV failure by after load reduction is based on this principle.
DeterminantsVENTRICULAR VOLUME
If both normal and eccentrically hypertrophied ventricles shorten their internal circumference (270r) or internal diameter by 25%, the SV ejected by the dilated ventricle will be nearly three times as large as that ejected by the normal ventricle. However, assuming the same end-systolic pressure (ESP) and wall thickness for both ventricles, LV systolic wall stress and oxygen consumption will be much higher for the
RACE 2003 Ramachandra Anaesthesia Continuing Education
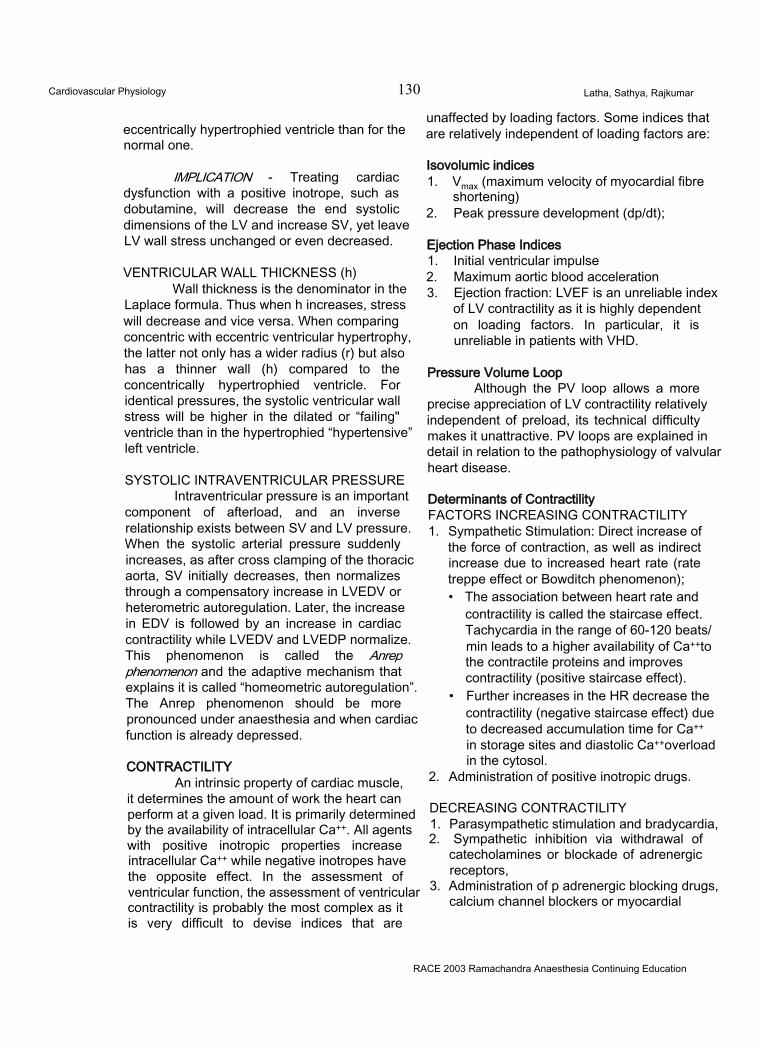
Cardiovascular Physiology 130 Latha, Sathya, Rajkumar
eccentrically hypertrophied ventricle than for the normal one.
IMPLICATION - Treating cardiac dysfunction with a positive inotrope, such as dobutamine, will decrease the end systolic dimensions of the LV and increase SV, yet leave LV wall stress unchanged or even decreased.
VENTRICULAR WALL THICKNESS (h)Wall thickness is the denominator in the
Laplace formula. Thus when h increases, stress will decrease and vice versa. When comparing concentric with eccentric ventricular hypertrophy, the latter not only has a wider radius (r) but also has a thinner wall (h) compared to the concentrically hypertrophied ventricle. For identical pressures, the systolic ventricular wall stress will be higher in the dilated or “failing" ventricle than in the hypertrophied “hypertensive” left ventricle.
SYSTOLIC INTRAVENTRICULAR PRESSUREIntraventricular pressure is an important
component of afterload, and an inverse relationship exists between SV and LV pressure. When the systolic arterial pressure suddenly increases, as after cross clamping of the thoracic aorta, SV initially decreases, then normalizes through a compensatory increase in LVEDV or heterometric autoregulation. Later, the increase in EDV is followed by an increase in cardiac contractility while LVEDV and LVEDP normalize. This phenomenon is called the Anrep phenomenon and the adaptive mechanism that explains it is called “homeometric autoregulation”. The Anrep phenomenon should be more pronounced under anaesthesia and when cardiac function is already depressed.
CONTRACTILITYAn intrinsic property of cardiac muscle,
it determines the amount of work the heart can perform at a given load. It is primarily determined by the availability of intracellular Ca++. All agents with positive inotropic properties increase intracellular Ca++ while negative inotropes have the opposite effect. In the assessment of ventricular function, the assessment of ventricular contractility is probably the most complex as it is very difficult to devise indices that are
unaffected by loading factors. Some indices that are relatively independent of loading factors are:
Isovolumic indices1. Vmax (maximum velocity of myocardial fibre
shortening)2. Peak pressure development (dp/dt);
Ejection Phase Indices1. Initial ventricular impulse2. Maximum aortic blood acceleration3. Ejection fraction: LVEF is an unreliable index
of LV contractility as it is highly dependent on loading factors. In particular, it is unreliable in patients with VHD.
Pressure Volume LoopAlthough the PV loop allows a more
precise appreciation of LV contractility relatively independent of preload, its technical difficulty makes it unattractive. PV loops are explained in detail in relation to the pathophysiology of valvular heart disease.
Determinants of ContractilityFACTORS INCREASING CONTRACTILITY1. Sympathetic Stimulation: Direct increase of
the force of contraction, as well as indirect increase due to increased heart rate (rate treppe effect or Bowditch phenomenon);• The association between heart rate and
contractility is called the staircase effect. Tachycardia in the range of 60-120 beats/ min leads to a higher availability of Ca++to the contractile proteins and improves contractility (positive staircase effect).
• Further increases in the HR decrease the contractility (negative staircase effect) due to decreased accumulation time for Ca++ in storage sites and diastolic Ca++overload in the cytosol.
2. Administration of positive inotropic drugs.
DECREASING CONTRACTILITY1. Parasympathetic stimulation and bradycardia,2. Sympathetic inhibition via withdrawal of
catecholamines or blockade of adrenergic receptors,
3. Administration of p adrenergic blocking drugs, calcium channel blockers or myocardial
RACE 2003 Ramachandra Anaesthesia Continuing Education
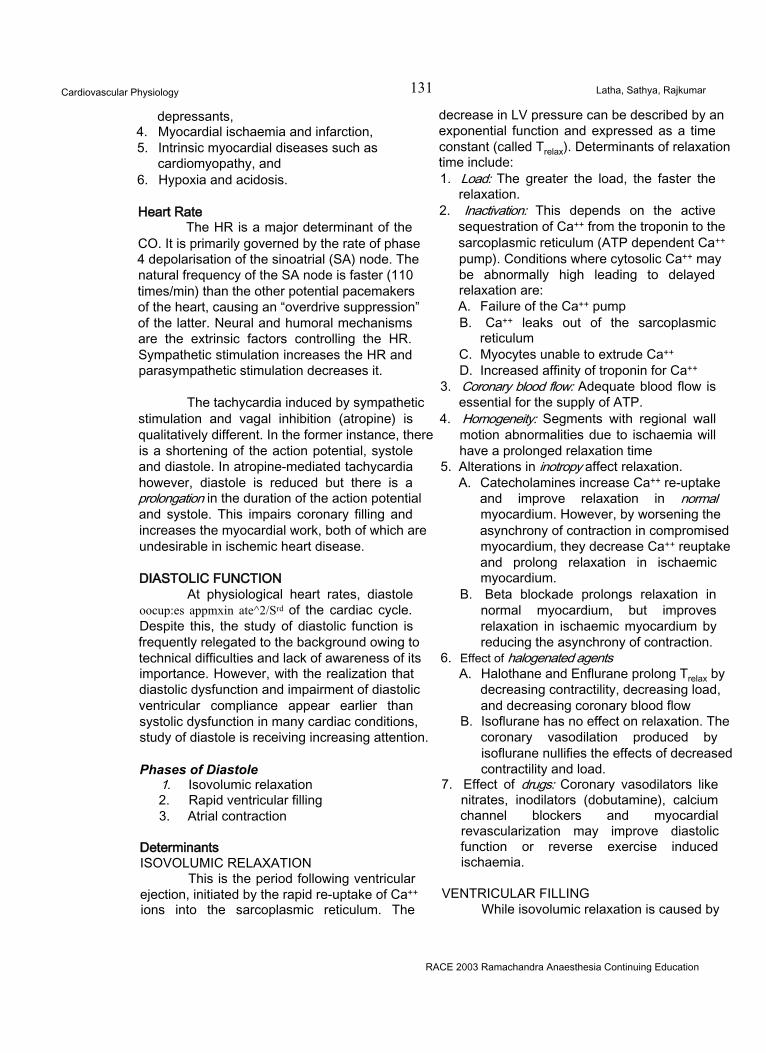
Cardiovascular Physiology 131 Latha, Sathya, Rajkumar
depressants,4. Myocardial ischaemia and infarction,5. Intrinsic myocardial diseases such as
cardiomyopathy, and6. Hypoxia and acidosis.
Heart RateThe HR is a major determinant of the
CO. It is primarily governed by the rate of phase 4 depolarisation of the sinoatrial (SA) node. The natural frequency of the SA node is faster (110 times/min) than the other potential pacemakers of the heart, causing an “overdrive suppression” of the latter. Neural and humoral mechanisms are the extrinsic factors controlling the HR. Sympathetic stimulation increases the HR and parasympathetic stimulation decreases it.
The tachycardia induced by sympathetic stimulation and vagal inhibition (atropine) is qualitatively different. In the former instance, there is a shortening of the action potential, systole and diastole. In atropine-mediated tachycardia however, diastole is reduced but there is a prolongation in the duration of the action potential and systole. This impairs coronary filling and increases the myocardial work, both of which are undesirable in ischemic heart disease.
DIASTOLIC FUNCTIONAt physiological heart rates, diastole
oocup:es appmxin ate^2/Srd of the cardiac cycle. Despite this, the study of diastolic function is frequently relegated to the background owing to technical difficulties and lack of awareness of its importance. However, with the realization that diastolic dysfunction and impairment of diastolic ventricular compliance appear earlier than systolic dysfunction in many cardiac conditions, study of diastole is receiving increasing attention.
Phases of Diastole1. Isovolumic relaxation2. Rapid ventricular filling3. Atrial contraction
DeterminantsISOVOLUMIC RELAXATION
This is the period following ventricular ejection, initiated by the rapid re-uptake of Ca++ ions into the sarcoplasmic reticulum. The
decrease in LV pressure can be described by an exponential function and expressed as a time constant (called Trelax). Determinants of relaxation time include:1. Load: The greater the load, the faster the
relaxation.2. Inactivation: This depends on the active
sequestration of Ca++ from the troponin to the sarcoplasmic reticulum (ATP dependent Ca++ pump). Conditions where cytosolic Ca++ may be abnormally high leading to delayed relaxation are:A. Failure of the Ca++ pumpB. Ca++ leaks out of the sarcoplasmic
reticulumC. Myocytes unable to extrude Ca++
D. Increased affinity of troponin for Ca++
3. Coronary blood flow: Adequate blood flow is essential for the supply of ATP.
4. Homogeneity: Segments with regional wall motion abnormalities due to ischaemia will have a prolonged relaxation time
5. Alterations in inotropy affect relaxation.A. Catecholamines increase Ca++ re-uptake
and improve relaxation in normal myocardium. However, by worsening the asynchrony of contraction in compromised myocardium, they decrease Ca++ reuptake and prolong relaxation in ischaemic myocardium.
B. Beta blockade prolongs relaxation in normal myocardium, but improves relaxation in ischaemic myocardium by reducing the asynchrony of contraction.
6. Effect of halogenated agentsA. Halothane and Enflurane prolong Trelax by
decreasing contractility, decreasing load, and decreasing coronary blood flow
B. Isoflurane has no effect on relaxation. The coronary vasodilation produced by isoflurane nullifies the effects of decreased contractility and load.
7. Effect of drugs: Coronary vasodilators like nitrates, inodilators (dobutamine), calcium channel blockers and myocardial revascularization may improve diastolic function or reverse exercise induced ischaemia.
VENTRICULAR FILLINGWhile isovolumic relaxation is caused by
RACE 2003 Ramachandra Anaesthesia Continuing Education
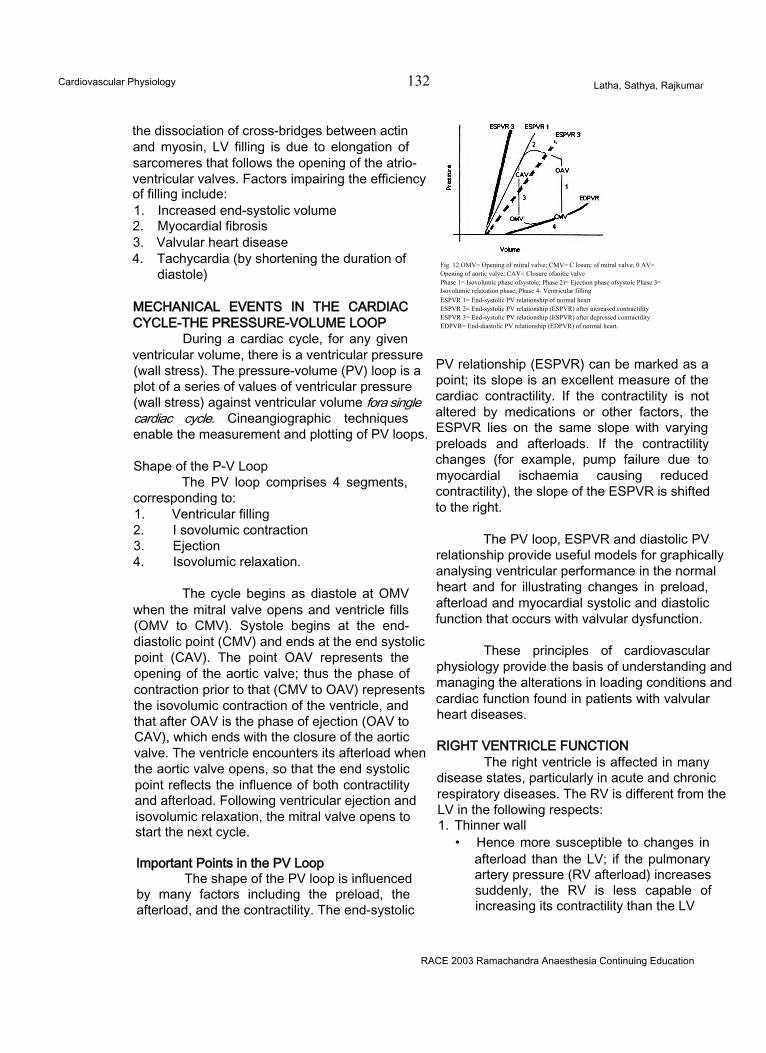
Cardiovascular Physiology 132 Latha, Sathya, Rajkumar
the dissociation of cross-bridges between actin and myosin, LV filling is due to elongation of sarcomeres that follows the opening of the atrioventricular valves. Factors impairing the efficiency of filling include:1. Increased end-systolic volume2. Myocardial fibrosis3. Valvular heart disease4. Tachycardia (by shortening the duration of
diastole)
MECHANICAL EVENTS IN THE CARDIAC CYCLE-THE PRESSURE-VOLUME LOOP
During a cardiac cycle, for any given ventricular volume, there is a ventricular pressure (wall stress). The pressure-volume (PV) loop is a plot of a series of values of ventricular pressure (wall stress) against ventricular volume fora single cardiac cycle. Cineangiographic techniques enable the measurement and plotting of PV loops.
Shape of the P-V LoopThe PV loop comprises 4 segments,
corresponding to:1. Ventricular filling2. I sovolumic contraction3. Ejection4. Isovolumic relaxation.
The cycle begins as diastole at OMV when the mitral valve opens and ventricle fills (OMV to CMV). Systole begins at the end- diastolic point (CMV) and ends at the end systolic point (CAV). The point OAV represents the opening of the aortic valve; thus the phase of contraction prior to that (CMV to OAV) represents the isovolumic contraction of the ventricle, and that after OAV is the phase of ejection (OAV to CAV), which ends with the closure of the aortic valve. The ventricle encounters its afterload when the aortic valve opens, so that the end systolic point reflects the influence of both contractility and afterload. Following ventricular ejection and isovolumic relaxation, the mitral valve opens to start the next cycle.
Important Points in the PV LoopThe shape of the PV loop is influenced
by many factors including the preload, the afterload, and the contractility. The end-systolic
Fig. 12 OMV= Opening of mitral valve; CMV= C losurc of mitral valve; 0 AV= Opening of aortic valve; CAV= Closure ofaoitie valvePhase 1= Isovolumic phase ofsystole; Phase 2)= Ejection phase ofsystole Phase 3=Isovolumic relaxation phase; Phase 4- Ventricular fillingESPVR 1= End-systolic PV relationship of normal heartESPVR 2= End-systolic PV relationship (ESPVR) after increased contractilityESPVR 3= End-systolic PV relationship (ESPVR) after depressed contractilityEDPVR= End-diastolic PV relationship (EDPVR) of normal heart.
PV relationship (ESPVR) can be marked as a point; its slope is an excellent measure of the cardiac contractility. If the contractility is not altered by medications or other factors, the ESPVR lies on the same slope with varying preloads and afterloads. If the contractility changes (for example, pump failure due to myocardial ischaemia causing reduced contractility), the slope of the ESPVR is shifted to the right.
The PV loop, ESPVR and diastolic PV relationship provide useful models for graphically analysing ventricular performance in the normal heart and for illustrating changes in preload, afterload and myocardial systolic and diastolic function that occurs with valvular dysfunction.
These principles of cardiovascular physiology provide the basis of understanding and managing the alterations in loading conditions and cardiac function found in patients with valvular heart diseases.
RIGHT VENTRICLE FUNCTIONThe right ventricle is affected in many
disease states, particularly in acute and chronic respiratory diseases. The RV is different from the LV in the following respects:1. Thinner wall
• Hence more susceptible to changes in afterload than the LV; if the pulmonary artery pressure (RV afterload) increases suddenly, the RV is less capable of increasing its contractility than the LV
RACE 2003 Ramachandra Anaesthesia Continuing Education
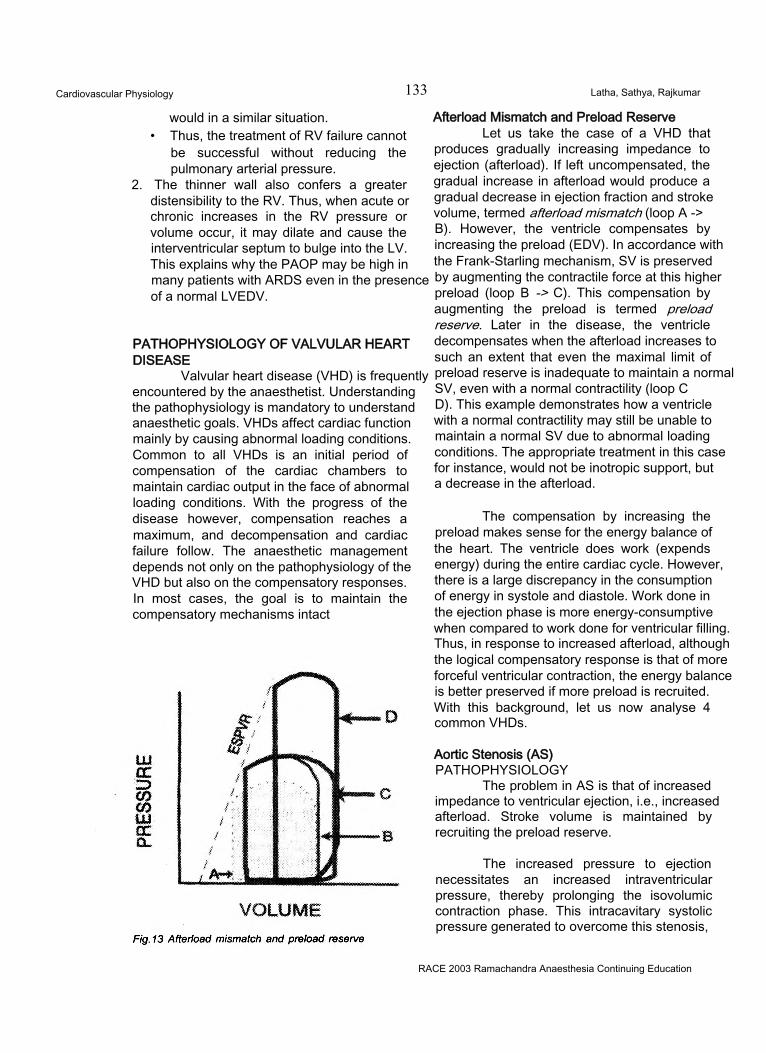
Cardiovascular Physiology 133 Latha, Sathya, Rajkumar
would in a similar situation.• Thus, the treatment of RV failure cannot
be successful without reducing the pulmonary arterial pressure.
2. The thinner wall also confers a greater distensibility to the RV. Thus, when acute or chronic increases in the RV pressure or volume occur, it may dilate and cause the interventricular septum to bulge into the LV. This explains why the PAOP may be high in many patients with ARDS even in the presence of a normal LVEDV.
PATHOPHYSIOLOGY OF VALVULAR HEART DISEASE
Valvular heart disease (VHD) is frequently encountered by the anaesthetist. Understanding the pathophysiology is mandatory to understand anaesthetic goals. VHDs affect cardiac function mainly by causing abnormal loading conditions. Common to all VHDs is an initial period of compensation of the cardiac chambers to maintain cardiac output in the face of abnormal loading conditions. With the progress of the disease however, compensation reaches a maximum, and decompensation and cardiac failure follow. The anaesthetic management depends not only on the pathophysiology of the VHD but also on the compensatory responses. In most cases, the goal is to maintain the compensatory mechanisms intact
Afterload Mismatch and Preload ReserveLet us take the case of a VHD that
produces gradually increasing impedance to ejection (afterload). If left uncompensated, the gradual increase in afterload would produce a gradual decrease in ejection fraction and stroke volume, termed afterload mismatch (loop A ->B). However, the ventricle compensates by increasing the preload (EDV). In accordance with the Frank-Starling mechanism, SV is preserved by augmenting the contractile force at this higher preload (loop B -> C). This compensation by augmenting the preload is termed preload reserve. Later in the disease, the ventricle decompensates when the afterload increases to such an extent that even the maximal limit of preload reserve is inadequate to maintain a normal SV, even with a normal contractility (loop CD). This example demonstrates how a ventricle with a normal contractility may still be unable to maintain a normal SV due to abnormal loading conditions. The appropriate treatment in this case for instance, would not be inotropic support, but a decrease in the afterload.
The compensation by increasing the preload makes sense for the energy balance of the heart. The ventricle does work (expends energy) during the entire cardiac cycle. However, there is a large discrepancy in the consumption of energy in systole and diastole. Work done in the ejection phase is more energy-consumptive when compared to work done for ventricular filling. Thus, in response to increased afterload, although the logical compensatory response is that of more forceful ventricular contraction, the energy balance is better preserved if more preload is recruited. With this background, let us now analyse 4 common VHDs.
Aortic Stenosis (AS)PATHOPHYSIOLOGY
The problem in AS is that of increased impedance to ventricular ejection, i.e., increased afterload. Stroke volume is maintained by recruiting the preload reserve.
The increased pressure to ejection necessitates an increased intraventricular pressure, thereby prolonging the isovolumic contraction phase. This intracavitary systolic pressure generated to overcome this stenosis,
RACE 2003 Ramachandra Anaesthesia Continuing Education
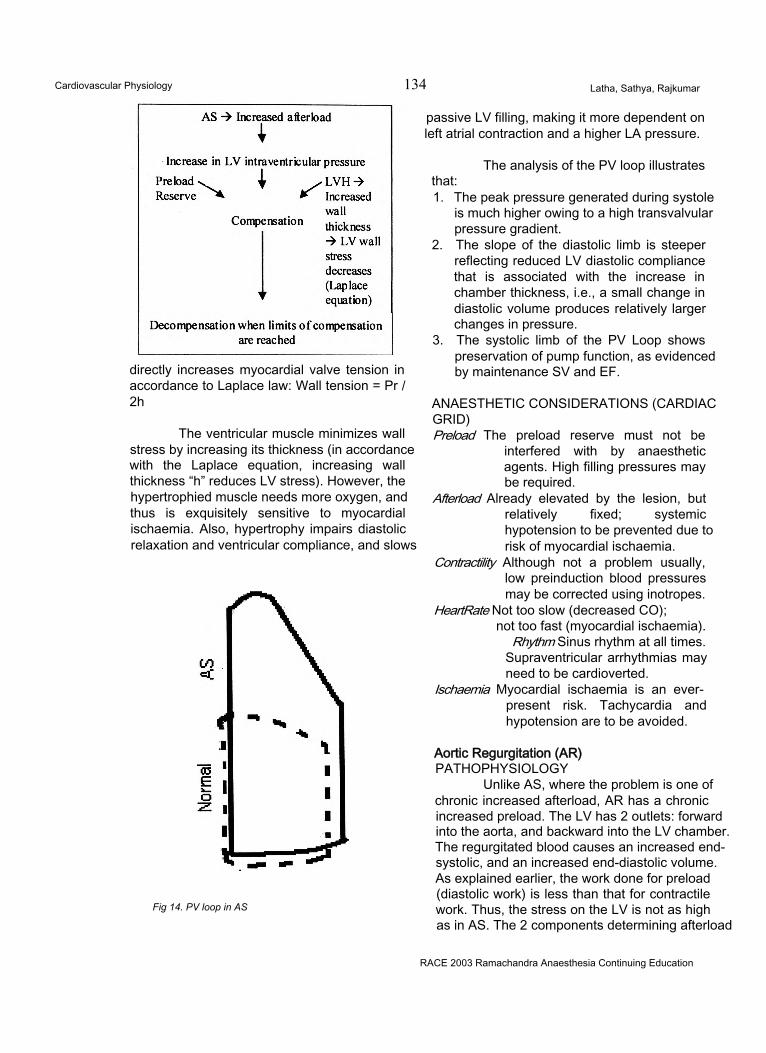
Cardiovascular Physiology 134 Latha, Sathya, Rajkumar
directly increases myocardial valve tension in accordance to Laplace law: Wall tension = Pr / 2h
The ventricular muscle minimizes wall stress by increasing its thickness (in accordance with the Laplace equation, increasing wall thickness “h” reduces LV stress). However, the hypertrophied muscle needs more oxygen, and thus is exquisitely sensitive to myocardial ischaemia. Also, hypertrophy impairs diastolic relaxation and ventricular compliance, and slows
Fig 14. PV loop in AS
passive LV filling, making it more dependent on left atrial contraction and a higher LA pressure.
The analysis of the PV loop illustratesthat:1. The peak pressure generated during systole
is much higher owing to a high transvalvular pressure gradient.
2. The slope of the diastolic limb is steeper reflecting reduced LV diastolic compliance that is associated with the increase in chamber thickness, i.e., a small change in diastolic volume produces relatively larger changes in pressure.
3. The systolic limb of the PV Loop shows preservation of pump function, as evidenced by maintenance SV and EF.
ANAESTHETIC CONSIDERATIONS (CARDIAC GRID)Preload The preload reserve must not be
interfered with by anaesthetic agents. High filling pressures may be required.
Afterload Already elevated by the lesion, but relatively fixed; systemic hypotension to be prevented due to risk of myocardial ischaemia.
Contractility Although not a problem usually, low preinduction blood pressures may be corrected using inotropes.
HeartRate Not too slow (decreased CO);not too fast (myocardial ischaemia).
Rhythm Sinus rhythm at all times.Supraventricular arrhythmias may need to be cardioverted.
Ischaemia Myocardial ischaemia is an everpresent risk. Tachycardia and hypotension are to be avoided.
Aortic Regurgitation (AR)PATHOPHYSIOLOGY
Unlike AS, where the problem is one of chronic increased afterload, AR has a chronic increased preload. The LV has 2 outlets: forward into the aorta, and backward into the LV chamber. The regurgitated blood causes an increased end- systolic, and an increased end-diastolic volume. As explained earlier, the work done for preload (diastolic work) is less than that for contractile work. Thus, the stress on the LV is not as high as in AS. The 2 components determining afterload
RACE 2003 Ramachandra Anaesthesia Continuing Education
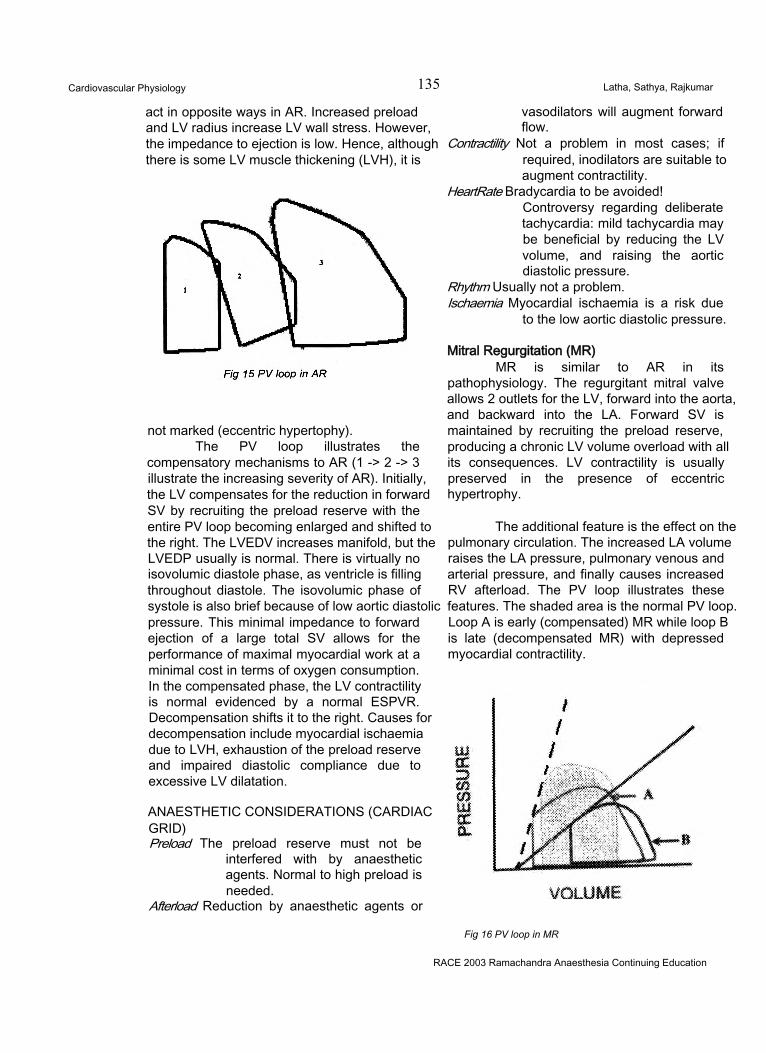
Cardiovascular Physiology 135 Latha, Sathya, Rajkumar
act in opposite ways in AR. Increased preload and LV radius increase LV wall stress. However, the impedance to ejection is low. Hence, although there is some LV muscle thickening (LVH), it is
not marked (eccentric hypertophy).The PV loop illustrates the
compensatory mechanisms to AR (1 -> 2 -> 3 illustrate the increasing severity of AR). Initially, the LV compensates for the reduction in forward SV by recruiting the preload reserve with the entire PV loop becoming enlarged and shifted to the right. The LVEDV increases manifold, but the LVEDP usually is normal. There is virtually no isovolumic diastole phase, as ventricle is filling throughout diastole. The isovolumic phase of systole is also brief because of low aortic diastolic pressure. This minimal impedance to forward ejection of a large total SV allows for the performance of maximal myocardial work at a minimal cost in terms of oxygen consumption. In the compensated phase, the LV contractility is normal evidenced by a normal ESPVR. Decompensation shifts it to the right. Causes for decompensation include myocardial ischaemia due to LVH, exhaustion of the preload reserve and impaired diastolic compliance due to excessive LV dilatation.
ANAESTHETIC CONSIDERATIONS (CARDIAC GRID)Preload The preload reserve must not be
interfered with by anaesthetic agents. Normal to high preload is needed.
Afterload Reduction by anaesthetic agents or
vasodilators will augment forward flow.
Contractility Not a problem in most cases; if required, inodilators are suitable to augment contractility.
HeartRate Bradycardia to be avoided!Controversy regarding deliberate tachycardia: mild tachycardia may be beneficial by reducing the LV volume, and raising the aortic diastolic pressure.
Rhythm Usually not a problem.Ischaemia Myocardial ischaemia is a risk due
to the low aortic diastolic pressure.
Mitral Regurgitation (MR)MR is similar to AR in its
pathophysiology. The regurgitant mitral valve allows 2 outlets for the LV, forward into the aorta, and backward into the LA. Forward SV is maintained by recruiting the preload reserve, producing a chronic LV volume overload with all its consequences. LV contractility is usually preserved in the presence of eccentric hypertrophy.
The additional feature is the effect on the pulmonary circulation. The increased LA volume raises the LA pressure, pulmonary venous and arterial pressure, and finally causes increased RV afterload. The PV loop illustrates these features. The shaded area is the normal PV loop. Loop A is early (compensated) MR while loop B is late (decompensated MR) with depressed myocardial contractility.
Fig 16 PV loop in MR
RACE 2003 Ramachandra Anaesthesia Continuing Education
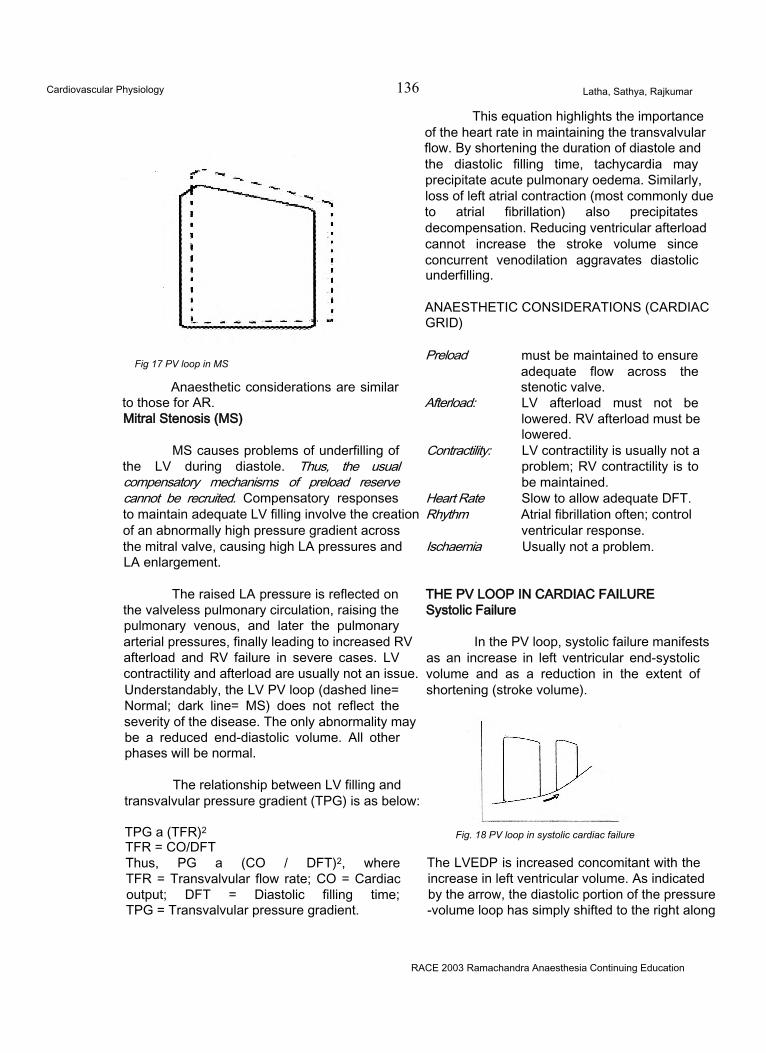
Cardiovascular Physiology 136 Latha, Sathya, Rajkumar
This equation highlights the importance of the heart rate in maintaining the transvalvular flow. By shortening the duration of diastole and the diastolic filling time, tachycardia may precipitate acute pulmonary oedema. Similarly, loss of left atrial contraction (most commonly due to atrial fibrillation) also precipitates decompensation. Reducing ventricular afterload cannot increase the stroke volume since concurrent venodilation aggravates diastolic underfilling.
ANAESTHETIC CONSIDERATIONS (CARDIAC GRID)
Fig 17 PV loop in MS
Anaesthetic considerations are similar to those for AR.Mitral Stenosis (MS)
MS causes problems of underfilling of the LV during diastole. Thus, the usual compensatory mechanisms of preload reserve cannot be recruited. Compensatory responses to maintain adequate LV filling involve the creation of an abnormally high pressure gradient across the mitral valve, causing high LA pressures and LA enlargement.
The raised LA pressure is reflected on the valveless pulmonary circulation, raising the pulmonary venous, and later the pulmonary arterial pressures, finally leading to increased RV afterload and RV failure in severe cases. LV contractility and afterload are usually not an issue. Understandably, the LV PV loop (dashed line= Normal; dark line= MS) does not reflect the severity of the disease. The only abnormality may be a reduced end-diastolic volume. All other phases will be normal.
The relationship between LV filling and transvalvular pressure gradient (TPG) is as below:
TPG a (TFR)2 TFR = CO/DFTThus, PG a (CO / DFT)2, where TFR = Transvalvular flow rate; CO = Cardiac output; DFT = Diastolic filling time; TPG = Transvalvular pressure gradient.
Preload
Afterload:
Contractility:
Heart Rate Rhythm
Ischaemia
must be maintained to ensure adequate flow across the stenotic valve.LV afterload must not be lowered. RV afterload must be lowered.LV contractility is usually not a problem; RV contractility is to be maintained.Slow to allow adequate DFT. Atrial fibrillation often; control ventricular response.Usually not a problem.
THE PV LOOP IN CARDIAC FAILURE Systolic Failure
In the PV loop, systolic failure manifests as an increase in left ventricular end-systolic volume and as a reduction in the extent of shortening (stroke volume).
Fig. 18 PV loop in systolic cardiac failure
The LVEDP is increased concomitant with the increase in left ventricular volume. As indicated by the arrow, the diastolic portion of the pressure -volume loop has simply shifted to the right along
RACE 2003 Ramachandra Anaesthesia Continuing Education
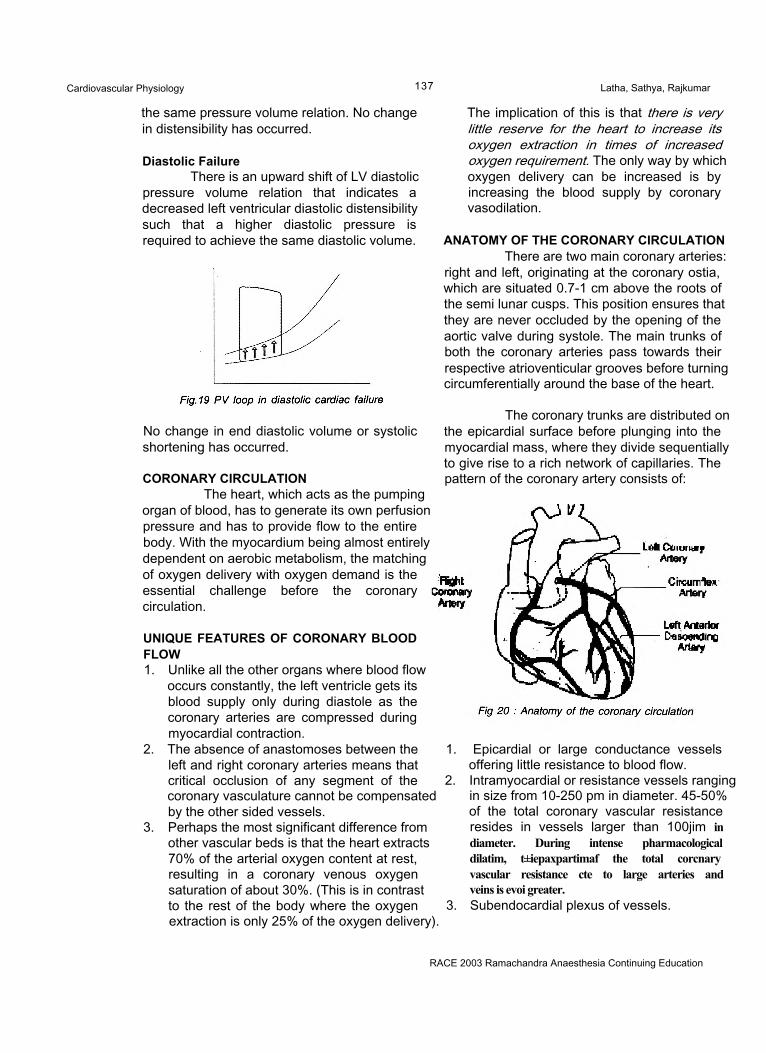
Cardiovascular Physiology 137 Latha, Sathya, Rajkumar
the same pressure volume relation. No change in distensibility has occurred.
Diastolic FailureThere is an upward shift of LV diastolic
pressure volume relation that indicates a decreased left ventricular diastolic distensibility such that a higher diastolic pressure is required to achieve the same diastolic volume.
No change in end diastolic volume or systolic shortening has occurred.
CORONARY CIRCULATIONThe heart, which acts as the pumping
organ of blood, has to generate its own perfusion pressure and has to provide flow to the entire body. With the myocardium being almost entirely dependent on aerobic metabolism, the matching of oxygen delivery with oxygen demand is the essential challenge before the coronary circulation.
UNIQUE FEATURES OF CORONARY BLOOD FLOW1. Unlike all the other organs where blood flow
occurs constantly, the left ventricle gets its blood supply only during diastole as the coronary arteries are compressed during myocardial contraction.
2. The absence of anastomoses between the left and right coronary arteries means that critical occlusion of any segment of the coronary vasculature cannot be compensated by the other sided vessels.
3. Perhaps the most significant difference from other vascular beds is that the heart extracts 70% of the arterial oxygen content at rest, resulting in a coronary venous oxygen saturation of about 30%. (This is in contrast to the rest of the body where the oxygen extraction is only 25% of the oxygen delivery).
The implication of this is that there is very little reserve for the heart to increase its oxygen extraction in times of increased oxygen requirement. The only way by which oxygen delivery can be increased is by increasing the blood supply by coronary vasodilation.
ANATOMY OF THE CORONARY CIRCULATIONThere are two main coronary arteries:
right and left, originating at the coronary ostia, which are situated 0.7-1 cm above the roots of the semi lunar cusps. This position ensures that they are never occluded by the opening of the aortic valve during systole. The main trunks of both the coronary arteries pass towards their respective atrioventicular grooves before turning circumferentially around the base of the heart.
The coronary trunks are distributed on the epicardial surface before plunging into the myocardial mass, where they divide sequentially to give rise to a rich network of capillaries. The pattern of the coronary artery consists of:
1. Epicardial or large conductance vessels offering little resistance to blood flow.
2. Intramyocardial or resistance vessels ranging in size from 10-250 pm in diameter. 45-50% of the total coronary vascular resistance resides in vessels larger than 100jim in diameter. During intense pharmacological dilatim, t±iepaxpartimaf the total corcnary vascular resistance cte to large arteries and veins is evoi greater.
3. Subendocardial plexus of vessels.
RACE 2003 Ramachandra Anaesthesia Continuing Education
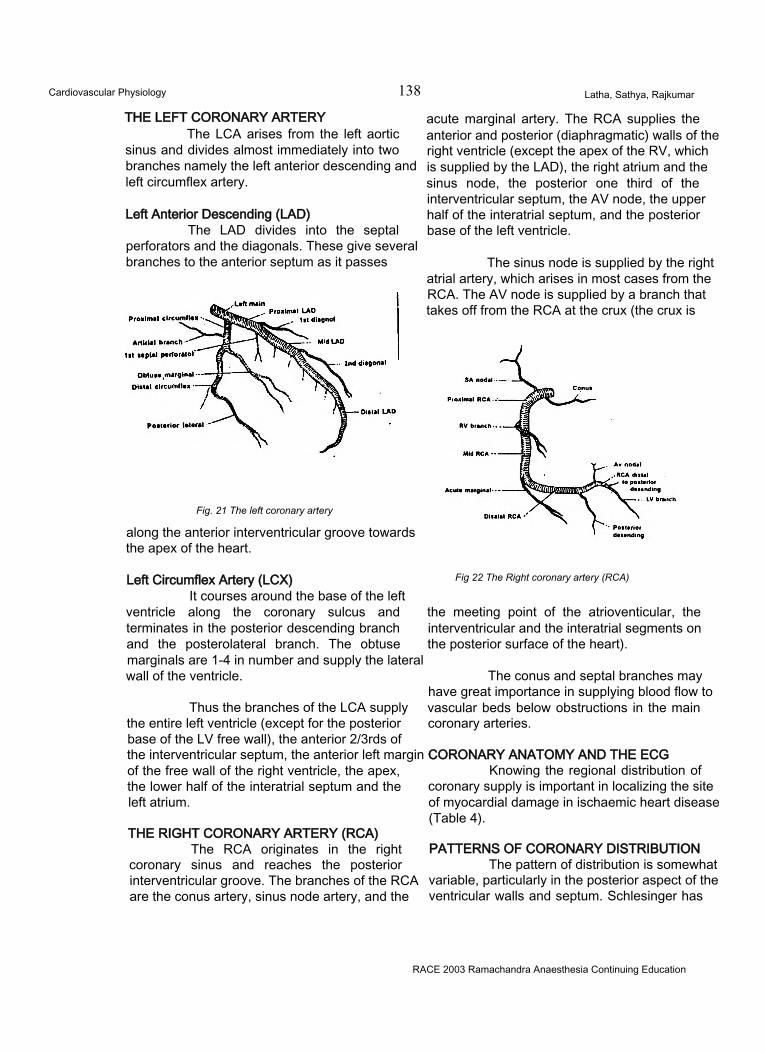
Cardiovascular Physiology 138 Latha, Sathya, Rajkumar
THE LEFT CORONARY ARTERYThe LCA arises from the left aortic
sinus and divides almost immediately into two branches namely the left anterior descending and left circumflex artery.
Left Anterior Descending (LAD)The LAD divides into the septal
perforators and the diagonals. These give several branches to the anterior septum as it passes
Fig. 21 The left coronary artery
along the anterior interventricular groove towards the apex of the heart.
Left Circumflex Artery (LCX)It courses around the base of the left
ventricle along the coronary sulcus and terminates in the posterior descending branch and the posterolateral branch. The obtuse marginals are 1-4 in number and supply the lateral wall of the ventricle.
Thus the branches of the LCA supply the entire left ventricle (except for the posterior base of the LV free wall), the anterior 2/3rds of the interventricular septum, the anterior left margin of the free wall of the right ventricle, the apex, the lower half of the interatrial septum and the left atrium.
THE RIGHT CORONARY ARTERY (RCA)The RCA originates in the right
coronary sinus and reaches the posterior interventricular groove. The branches of the RCA are the conus artery, sinus node artery, and the
acute marginal artery. The RCA supplies the anterior and posterior (diaphragmatic) walls of the right ventricle (except the apex of the RV, which is supplied by the LAD), the right atrium and the sinus node, the posterior one third of the interventricular septum, the AV node, the upper half of the interatrial septum, and the posterior base of the left ventricle.
The sinus node is supplied by the right atrial artery, which arises in most cases from the RCA. The AV node is supplied by a branch that takes off from the RCA at the crux (the crux is
Fig 22 The Right coronary artery (RCA)
the meeting point of the atrioventicular, the interventricular and the interatrial segments on the posterior surface of the heart).
The conus and septal branches may have great importance in supplying blood flow to vascular beds below obstructions in the main coronary arteries.
CORONARY ANATOMY AND THE ECGKnowing the regional distribution of
coronary supply is important in localizing the site of myocardial damage in ischaemic heart disease (Table 4).
PATTERNS OF CORONARY DISTRIBUTIONThe pattern of distribution is somewhat
variable, particularly in the posterior aspect of the ventricular walls and septum. Schlesinger has
RACE 2003 Ramachandra Anaesthesia Continuing Education
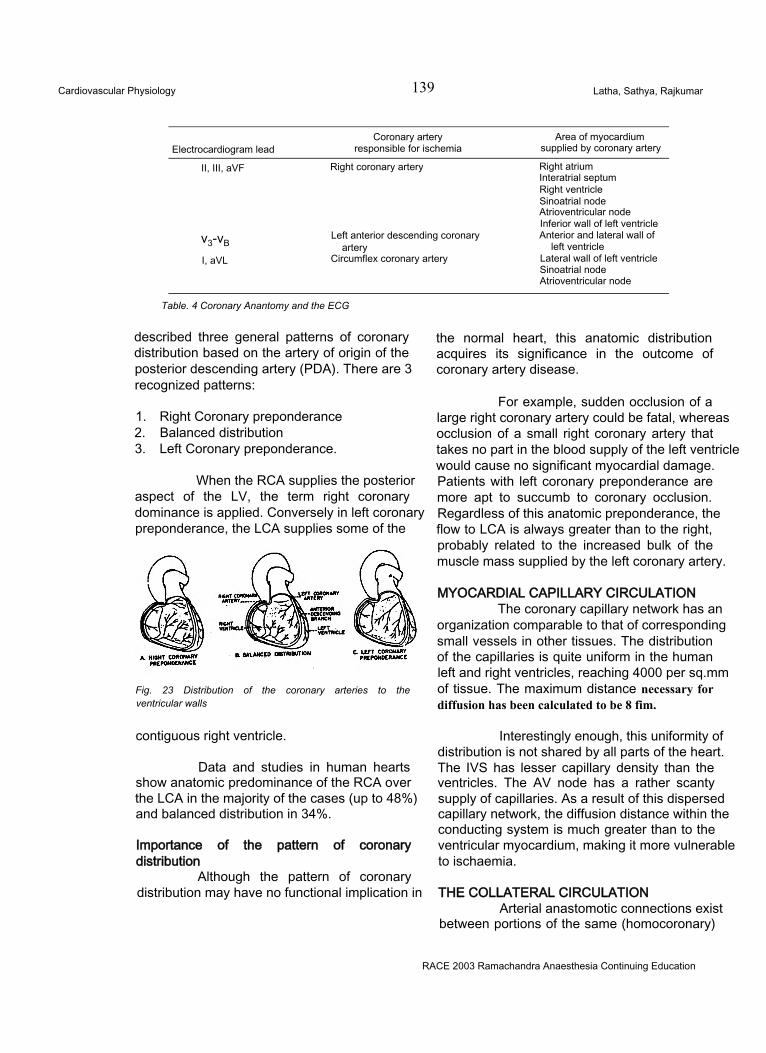
Cardiovascular Physiology 139 Latha, Sathya, Rajkumar
Electrocardiogram leadCoronary artery
responsible for ischemiaArea of myocardium
supplied by coronary artery
II, III, aVF Right coronary artery Right atrium Interatrial septum Right ventricle Sinoatrial node Atrioventricular node Inferior wall of left ventricle
v3-vBLeft anterior descending coronary
arteryAnterior and lateral wall of
left ventricleI, aVL Circumflex coronary artery Lateral wall of left ventricle
Sinoatrial node Atrioventricular node
Table. 4 Coronary Anantomy and the ECG
described three general patterns of coronary distribution based on the artery of origin of the posterior descending artery (PDA). There are 3 recognized patterns:
1. Right Coronary preponderance2. Balanced distribution3. Left Coronary preponderance.
When the RCA supplies the posterior aspect of the LV, the term right coronary dominance is applied. Conversely in left coronary preponderance, the LCA supplies some of the
Fig. 23 Distribution of the coronary arteries to the ventricular walls
contiguous right ventricle.
Data and studies in human hearts show anatomic predominance of the RCA over the LCA in the majority of the cases (up to 48%) and balanced distribution in 34%.
Importance of the pattern of coronary distribution
Although the pattern of coronary distribution may have no functional implication in
the normal heart, this anatomic distribution acquires its significance in the outcome of coronary artery disease.
For example, sudden occlusion of a large right coronary artery could be fatal, whereas occlusion of a small right coronary artery that takes no part in the blood supply of the left ventricle would cause no significant myocardial damage. Patients with left coronary preponderance are more apt to succumb to coronary occlusion. Regardless of this anatomic preponderance, the flow to LCA is always greater than to the right, probably related to the increased bulk of the muscle mass supplied by the left coronary artery.
MYOCARDIAL CAPILLARY CIRCULATIONThe coronary capillary network has an
organization comparable to that of corresponding small vessels in other tissues. The distribution of the capillaries is quite uniform in the human left and right ventricles, reaching 4000 per sq.mm of tissue. The maximum distance necessary for diffusion has been calculated to be 8 fim.
Interestingly enough, this uniformity of distribution is not shared by all parts of the heart. The IVS has lesser capillary density than the ventricles. The AV node has a rather scanty supply of capillaries. As a result of this dispersed capillary network, the diffusion distance within the conducting system is much greater than to the ventricular myocardium, making it more vulnerable to ischaemia.
THE COLLATERAL CIRCULATIONArterial anastomotic connections exist
between portions of the same (homocoronary)
RACE 2003 Ramachandra Anaesthesia Continuing Education
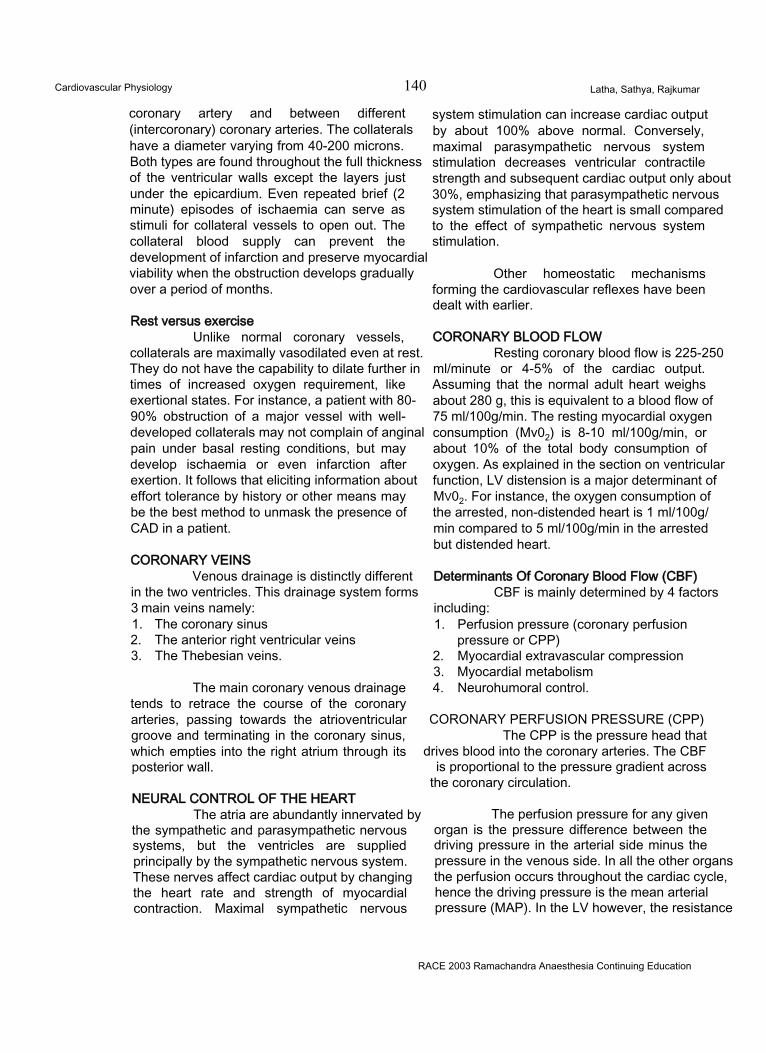
Cardiovascular Physiology 140 Latha, Sathya, Rajkumar
coronary artery and between different (intercoronary) coronary arteries. The collaterals have a diameter varying from 40-200 microns. Both types are found throughout the full thickness of the ventricular walls except the layers just under the epicardium. Even repeated brief (2 minute) episodes of ischaemia can serve as stimuli for collateral vessels to open out. The collateral blood supply can prevent the development of infarction and preserve myocardial viability when the obstruction develops gradually over a period of months.
Rest versus exerciseUnlike normal coronary vessels,
collaterals are maximally vasodilated even at rest. They do not have the capability to dilate further in times of increased oxygen requirement, like exertional states. For instance, a patient with 80- 90% obstruction of a major vessel with well- developed collaterals may not complain of anginal pain under basal resting conditions, but may develop ischaemia or even infarction after exertion. It follows that eliciting information about effort tolerance by history or other means may be the best method to unmask the presence of CAD in a patient.
CORONARY VEINSVenous drainage is distinctly different
in the two ventricles. This drainage system forms3 main veins namely:1. The coronary sinus2. The anterior right ventricular veins3. The Thebesian veins.
The main coronary venous drainage tends to retrace the course of the coronary arteries, passing towards the atrioventricular groove and terminating in the coronary sinus, which empties into the right atrium through its posterior wall.
NEURAL CONTROL OF THE HEARTThe atria are abundantly innervated by
the sympathetic and parasympathetic nervous systems, but the ventricles are supplied principally by the sympathetic nervous system. These nerves affect cardiac output by changing the heart rate and strength of myocardial contraction. Maximal sympathetic nervous
system stimulation can increase cardiac output by about 100% above normal. Conversely, maximal parasympathetic nervous system stimulation decreases ventricular contractile strength and subsequent cardiac output only about 30%, emphasizing that parasympathetic nervous system stimulation of the heart is small compared to the effect of sympathetic nervous system stimulation.
Other homeostatic mechanisms forming the cardiovascular reflexes have been dealt with earlier.
CORONARY BLOOD FLOWResting coronary blood flow is 225-250
ml/minute or 4-5% of the cardiac output. Assuming that the normal adult heart weighs about 280 g, this is equivalent to a blood flow of 75 ml/100g/min. The resting myocardial oxygen consumption (Mv02) is 8-10 ml/100g/min, or about 10% of the total body consumption of oxygen. As explained in the section on ventricular function, LV distension is a major determinant of Mv02. For instance, the oxygen consumption of the arrested, non-distended heart is 1 ml/100g/ min compared to 5 ml/100g/min in the arrested but distended heart.
Determinants Of Coronary Blood Flow (CBF)CBF is mainly determined by 4 factors
including:1. Perfusion pressure (coronary perfusion
pressure or CPP)2. Myocardial extravascular compression3. Myocardial metabolism4. Neurohumoral control.
CORONARY PERFUSION PRESSURE (CPP) The CPP is the pressure head that
drives blood into the coronary arteries. The CBF is proportional to the pressure gradient across
the coronary circulation.
The perfusion pressure for any given organ is the pressure difference between the driving pressure in the arterial side minus the pressure in the venous side. In all the other organs the perfusion occurs throughout the cardiac cycle, hence the driving pressure is the mean arterial pressure (MAP). In the LV however, the resistance
RACE 2003 Ramachandra Anaesthesia Continuing Education
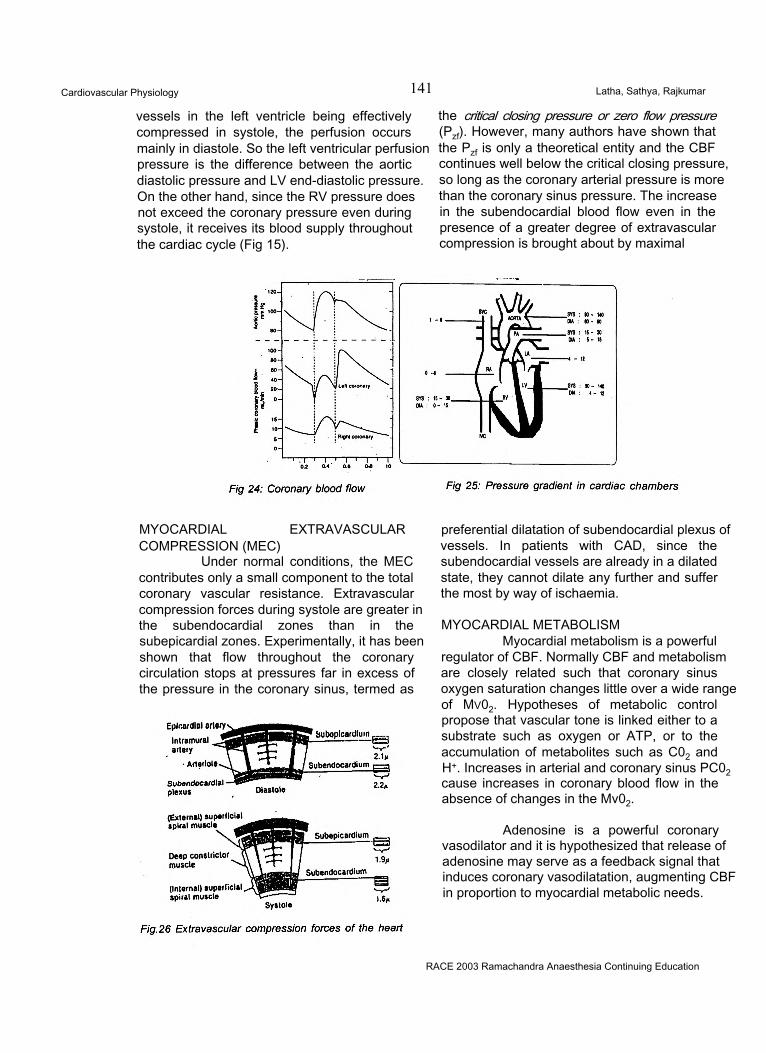
Cardiovascular Physiology 141 Latha, Sathya, Rajkumar
vessels in the left ventricle being effectively compressed in systole, the perfusion occurs mainly in diastole. So the left ventricular perfusion pressure is the difference between the aortic diastolic pressure and LV end-diastolic pressure. On the other hand, since the RV pressure does not exceed the coronary pressure even during systole, it receives its blood supply throughout the cardiac cycle (Fig 15).
the critical closing pressure or zero flow pressure (Pzf). However, many authors have shown that the Pzf is only a theoretical entity and the CBF continues well below the critical closing pressure, so long as the coronary arterial pressure is more than the coronary sinus pressure. The increase in the subendocardial blood flow even in the presence of a greater degree of extravascular compression is brought about by maximal
MYOCARDIAL EXTRAVASCULARCOMPRESSION (MEC)
Under normal conditions, the MEC contributes only a small component to the total coronary vascular resistance. Extravascular compression forces during systole are greater in the subendocardial zones than in the subepicardial zones. Experimentally, it has been shown that flow throughout the coronary circulation stops at pressures far in excess of the pressure in the coronary sinus, termed as
preferential dilatation of subendocardial plexus of vessels. In patients with CAD, since the subendocardial vessels are already in a dilated state, they cannot dilate any further and suffer the most by way of ischaemia.
MYOCARDIAL METABOLISMMyocardial metabolism is a powerful
regulator of CBF. Normally CBF and metabolism are closely related such that coronary sinus oxygen saturation changes little over a wide range of Mv02. Hypotheses of metabolic control propose that vascular tone is linked either to a substrate such as oxygen or ATP, or to the accumulation of metabolites such as C02 and H+. Increases in arterial and coronary sinus PC02 cause increases in coronary blood flow in the absence of changes in the Mv02.
Adenosine is a powerful coronary vasodilator and it is hypothesized that release of adenosine may serve as a feedback signal that induces coronary vasodilatation, augmenting CBF in proportion to myocardial metabolic needs.
RACE 2003 Ramachandra Anaesthesia Continuing Education
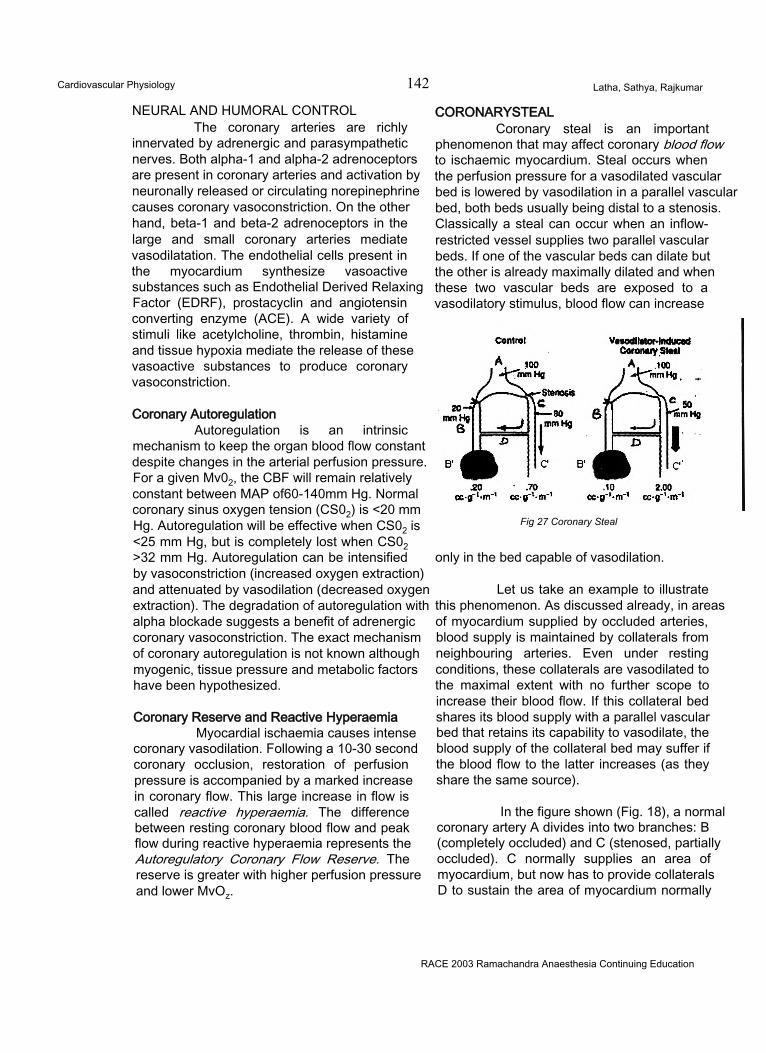
Cardiovascular Physiology 142 Latha, Sathya, Rajkumar
NEURAL AND HUMORAL CONTROLThe coronary arteries are richly
innervated by adrenergic and parasympathetic nerves. Both alpha-1 and alpha-2 adrenoceptors are present in coronary arteries and activation by neuronally released or circulating norepinephrine causes coronary vasoconstriction. On the other hand, beta-1 and beta-2 adrenoceptors in the large and small coronary arteries mediate vasodilatation. The endothelial cells present in the myocardium synthesize vasoactive substances such as Endothelial Derived Relaxing Factor (EDRF), prostacyclin and angiotensin converting enzyme (ACE). A wide variety of stimuli like acetylcholine, thrombin, histamine and tissue hypoxia mediate the release of these vasoactive substances to produce coronary vasoconstriction.
Coronary AutoregulationAutoregulation is an intrinsic
mechanism to keep the organ blood flow constant despite changes in the arterial perfusion pressure. For a given Mv02, the CBF will remain relatively constant between MAP of60-140mm Hg. Normal coronary sinus oxygen tension (CS02) is <20 mm Hg. Autoregulation will be effective when CS02 is <25 mm Hg, but is completely lost when CS02 >32 mm Hg. Autoregulation can be intensified by vasoconstriction (increased oxygen extraction) and attenuated by vasodilation (decreased oxygen extraction). The degradation of autoregulation with alpha blockade suggests a benefit of adrenergic coronary vasoconstriction. The exact mechanism of coronary autoregulation is not known although myogenic, tissue pressure and metabolic factors have been hypothesized.
Coronary Reserve and Reactive HyperaemiaMyocardial ischaemia causes intense
coronary vasodilation. Following a 10-30 second coronary occlusion, restoration of perfusion pressure is accompanied by a marked increase in coronary flow. This large increase in flow is called reactive hyperaemia. The difference between resting coronary blood flow and peak flow during reactive hyperaemia represents the Autoregulatory Coronary Flow Reserve. The reserve is greater with higher perfusion pressure and lower MvOz.
CORONARYSTEALCoronary steal is an important
phenomenon that may affect coronary blood flow to ischaemic myocardium. Steal occurs when the perfusion pressure for a vasodilated vascular bed is lowered by vasodilation in a parallel vascular bed, both beds usually being distal to a stenosis. Classically a steal can occur when an inflow- restricted vessel supplies two parallel vascular beds. If one of the vascular beds can dilate but the other is already maximally dilated and when these two vascular beds are exposed to a vasodilatory stimulus, blood flow can increase
Fig 27 Coronary Steal
only in the bed capable of vasodilation.
Let us take an example to illustrate this phenomenon. As discussed already, in areas of myocardium supplied by occluded arteries, blood supply is maintained by collaterals from neighbouring arteries. Even under resting conditions, these collaterals are vasodilated to the maximal extent with no further scope to increase their blood flow. If this collateral bed shares its blood supply with a parallel vascular bed that retains its capability to vasodilate, the blood supply of the collateral bed may suffer if the blood flow to the latter increases (as they share the same source).
In the figure shown (Fig. 18), a normal coronary artery A divides into two branches: B (completely occluded) and C (stenosed, partially occluded). C normally supplies an area of myocardium, but now has to provide collaterals D to sustain the area of myocardium normally
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardiovascular Physiology 143 Latha, Sathya, Rajkumar
deriving its blood supply from B.
Thus the scenario may be summarized as:2 main branches B and C; normally, B supplies the area of myocardium B’; C supplies the area of myocardium C’.
B completely occluded; C partly occluded. Due to disease of artery B, C gives collaterals (D) to myocardium B’ in addition to normal vessels to myocardium C’.
Myocardium B’ is now dependent for its blood supply on collaterals (D) arising from C.
The functional dynamics of this arrangement under resting conditions are that both the normal artery C and the collateral D are of normal calibre with both areas of myocardium B’ and C’ being perfused well. The patient will have no ischaemic symptoms.
However, the functional dynamics change markedly in conditions of exertion that necessitate vasodilation of the vessels. Whereas the normal artery C can vasodilate, collateral artery D cannot. As the blood flow across the proximal stenosis is fixed, there is no scope for both C and D to get adequate blood supply. In the event, C will “steal” blood from the collateral D rendering the myocardium B’ ischaemic. The patient may have myocardial ischaemia.
Reducing the level of exertion reduces the oxygen requirement, thereby restoring basal functional dynamics, restoring blood supply to myocardium B’.
To quantify the example, (the flow in the ischaemic region is 20 ml/min/100g and is determined by the collateral driving pressure or the difference between distal pressures in the bed supplying collaterals (80 mm Hg) and the ischaemic bed (20 mm Hg). Flow in the distribution of the stenotic vessel is normal at 70ml/min/100g and is evenly distributed between the subendocardium and subepicardium). During vasodilator administration at a constant BP, flow increases in the non-ischaemic bed to 200 ml/ min/100g, but becomes maldistributed between
the subendocardium and the subepicardium. In addition, pressure distal to the stenosis falls to 50 mm Hg causing a reduction in the collateral driving pressure. As a result, flow to the ischaemic region decreases to 10 ml/min/1 OOg.
Usually the distal pressure is low in the occluded arterial bed and there is a small gradient in the mean pressure across the stenosis.
To summarize, the conditions predisposing to the steal phenomenon are:1. An inflow restricted (stenotic) vessel supplies
two parallel vascular beds;2. One of the vascular bed can dilate but the
other is already maximally dilated;3. Both beds are exposed to vasodilatory
stimuli.
Examples of vasodilatory stimuli include exertion, isoflurane and or agents such as dipyridamole, nitroprusside and adenosine.
Another type of steal is the transmural steal occurring in the myocardium, diverting blood from the subendocardial to the subepicardial areas. This is because the lower limit of autoregulating perfusion pressure is greater for the subendocardia! layers than for the subepicardial layer; subendocardial blood flow may be reduced when subepicardial blood flow is preserved.
CONCLUSIONCardiovascular physiology is a
fascinating subject. Application of physiology to the understanding and management of disease states would go a long way towards improving the quality of care. With the advent of technology, CVS physiology is also rapidly evolving into a bedside tool for diagnosis and therapy of many cardiac and non-cardiac diseases. The coming years are bound to be path breaking.
REFERENCES1. International Practice of Anaesthesia. Editors:
Cedric Prys-Roberts, Burnell R. Brown. Butterworth-Heinemann 1996.
2. Cardiac Anesthesia. Editor: Joel A. Kaplan. WB Saunders Company. 4th Edition, 1999.
3. Anesthesia. Editor; Ronald D. Miller Churchill Livinstone. 5th edition, 2000.
RACE 2003 Ramachandra Anaesthesia Continuing Education
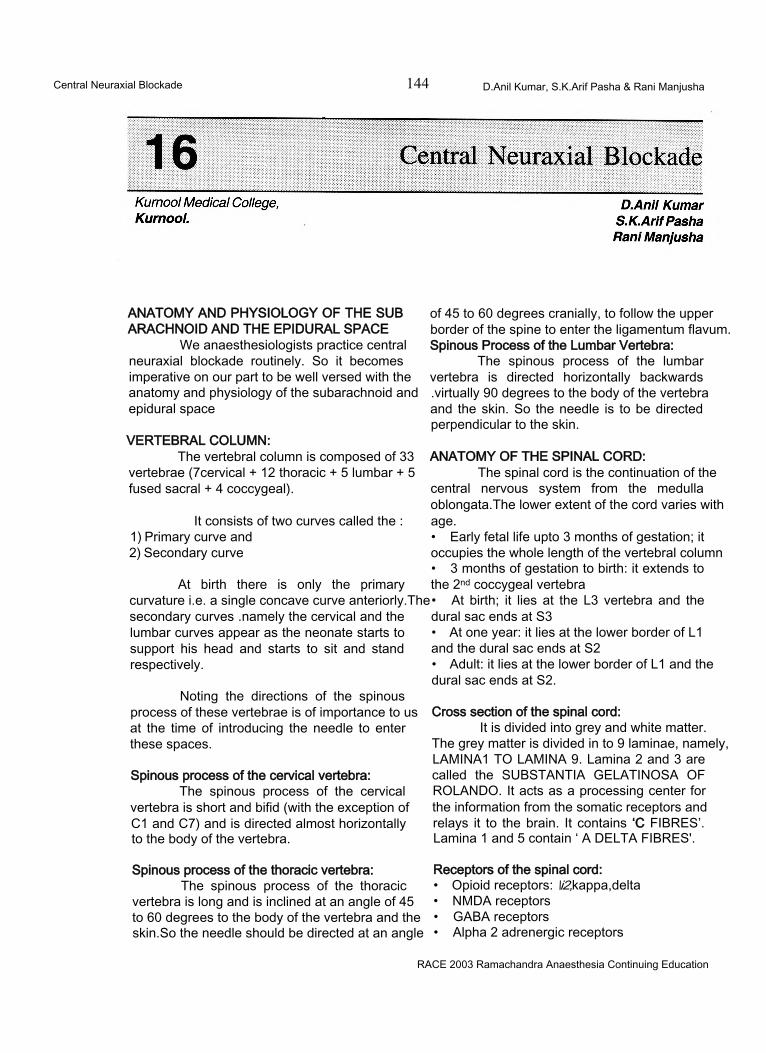
Central Neuraxial Blockade 144 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
ANATOMY AND PHYSIOLOGY OF THE SUB ARACHNOID AND THE EPIDURAL SPACE
We anaesthesiologists practice central neuraxial blockade routinely. So it becomes imperative on our part to be well versed with the anatomy and physiology of the subarachnoid and epidural space
VERTEBRAL COLUMN:The vertebral column is composed of 33
vertebrae (7cervical + 12 thoracic + 5 lumbar + 5 fused sacral + 4 coccygeal).
It consists of two curves called the :1) Primary curve and2) Secondary curve
At birth there is only the primary curvature i.e. a single concave curve anteriorly.The secondary curves .namely the cervical and the lumbar curves appear as the neonate starts to support his head and starts to sit and stand respectively.
Noting the directions of the spinous process of these vertebrae is of importance to us at the time of introducing the needle to enter these spaces.
Spinous process of the cervical vertebra:The spinous process of the cervical
vertebra is short and bifid (with the exception of C1 and C7) and is directed almost horizontally to the body of the vertebra.
Spinous process of the thoracic vertebra:The spinous process of the thoracic
vertebra is long and is inclined at an angle of 45 to 60 degrees to the body of the vertebra and the skin.So the needle should be directed at an angle
of 45 to 60 degrees cranially, to follow the upper border of the spine to enter the ligamentum flavum. Spinous Process of the Lumbar Vertebra:
The spinous process of the lumbar vertebra is directed horizontally backwards .virtually 90 degrees to the body of the vertebra and the skin. So the needle is to be directed perpendicular to the skin.
ANATOMY OF THE SPINAL CORD:The spinal cord is the continuation of the
central nervous system from the medulla oblongata.The lower extent of the cord varies with age.• Early fetal life upto 3 months of gestation; it occupies the whole length of the vertebral column• 3 months of gestation to birth: it extends to the 2nd coccygeal vertebra• At birth; it lies at the L3 vertebra and the dural sac ends at S3• At one year: it lies at the lower border of L1 and the dural sac ends at S2• Adult: it lies at the lower border of L1 and the dural sac ends at S2.
Cross section of the spinal cord:It is divided into grey and white matter.
The grey matter is divided in to 9 laminae, namely, LAMINA1 TO LAMINA 9. Lamina 2 and 3 are called the SUBSTANTIA GELATINOSA OF ROLANDO. It acts as a processing center for the information from the somatic receptors and relays it to the brain. It contains ‘C FIBRES’. Lamina 1 and 5 contain ‘ A DELTA FIBRES'.
Receptors of the spinal cord:• Opioid receptors: \i2,kappa,delta• NMDA receptors• GABA receptors• Alpha 2 adrenergic receptors
RACE 2003 Ramachandra Anaesthesia Continuing Education
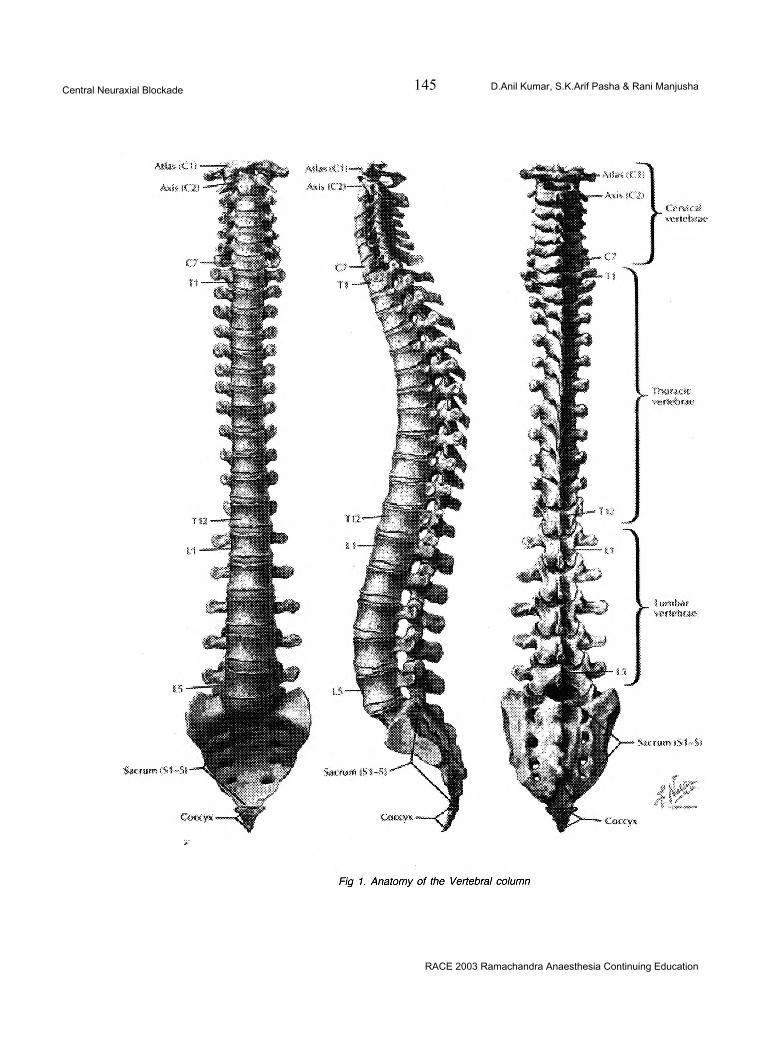
Central Neuraxial Blockade 145 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
RACE 2003 Ramachandra Anaesthesia Continuing Education
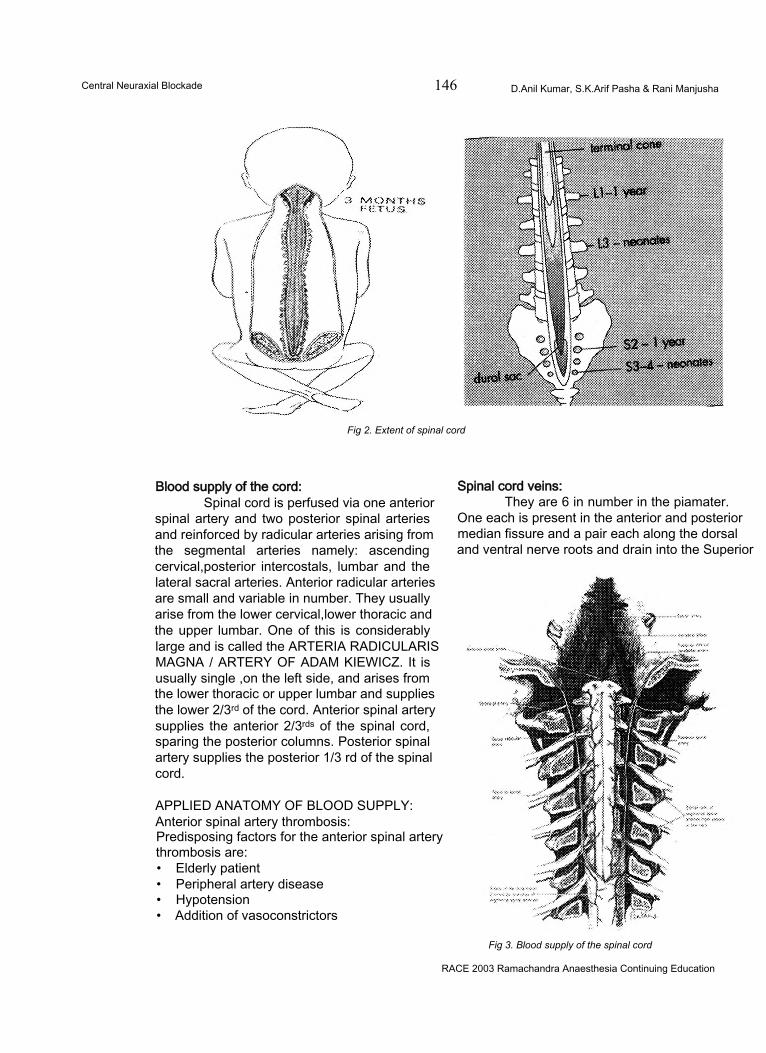
Central Neuraxial Blockade 146 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Fig 2. Extent of spinal cord
Blood supply of the cord:Spinal cord is perfused via one anterior
spinal artery and two posterior spinal arteries and reinforced by radicular arteries arising from the segmental arteries namely: ascending cervical,posterior intercostals, lumbar and the lateral sacral arteries. Anterior radicular arteries are small and variable in number. They usually arise from the lower cervical,lower thoracic and the upper lumbar. One of this is considerably large and is called the ARTERIA RADICULARIS MAGNA / ARTERY OF ADAM KIEWICZ. It is usually single ,on the left side, and arises from the lower thoracic or upper lumbar and supplies the lower 2/3rd of the cord. Anterior spinal artery supplies the anterior 2/3rds of the spinal cord, sparing the posterior columns. Posterior spinal artery supplies the posterior 1/3 rd of the spinal cord.
APPLIED ANATOMY OF BLOOD SUPPLY: Anterior spinal artery thrombosis:Predisposing factors for the anterior spinal artery thrombosis are:• Elderly patient• Peripheral artery disease• Hypotension• Addition of vasoconstrictors
Spinal cord veins:They are 6 in number in the piamater.
One each is present in the anterior and posterior median fissure and a pair each along the dorsal and ventral nerve roots and drain into the Superior
Fig 3. Blood supply of the spinal cord
RACE 2003 Ramachandra Anaesthesia Continuing Education
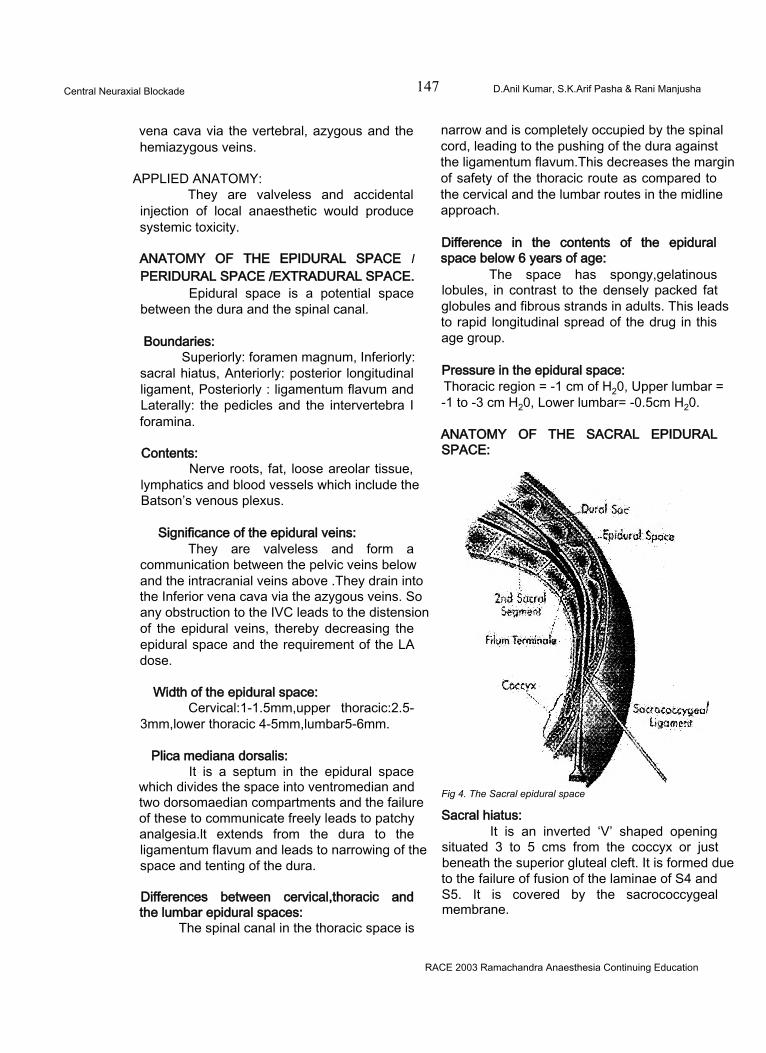
Central Neuraxial Blockade 147 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
vena cava via the vertebral, azygous and the hemiazygous veins.
APPLIED ANATOMY:They are valveless and accidental
injection of local anaesthetic would produce systemic toxicity.
ANATOMY OF THE EPIDURAL SPACE I PERIDURAL SPACE /EXTRADURAL SPACE.
Epidural space is a potential space between the dura and the spinal canal.
Boundaries:Superiorly: foramen magnum, Inferiorly:
sacral hiatus, Anteriorly: posterior longitudinal ligament, Posteriorly : ligamentum flavum and Laterally: the pedicles and the intervertebra I foramina.
Contents:Nerve roots, fat, loose areolar tissue,
lymphatics and blood vessels which include the Batson’s venous plexus.
Significance of the epidural veins:They are valveless and form a
communication between the pelvic veins below and the intracranial veins above .They drain into the Inferior vena cava via the azygous veins. So any obstruction to the IVC leads to the distension of the epidural veins, thereby decreasing the epidural space and the requirement of the LA dose.
Width of the epidural space:Cervical:1-1.5mm,upper thoracic:2.5-
3mm,lower thoracic 4-5mm,lumbar5-6mm.
Plica mediana dorsalis:It is a septum in the epidural space
which divides the space into ventromedian and two dorsomaedian compartments and the failure of these to communicate freely leads to patchy analgesia.lt extends from the dura to the ligamentum flavum and leads to narrowing of the space and tenting of the dura.
Differences between cervical,thoracic and the lumbar epidural spaces:
The spinal canal in the thoracic space is
narrow and is completely occupied by the spinal cord, leading to the pushing of the dura against the ligamentum flavum.This decreases the margin of safety of the thoracic route as compared to the cervical and the lumbar routes in the midline approach.
Difference in the contents of the epidural space below 6 years of age:
The space has spongy,gelatinous lobules, in contrast to the densely packed fat globules and fibrous strands in adults. This leads to rapid longitudinal spread of the drug in this age group.
Pressure in the epidural space:Thoracic region = -1 cm of H20, Upper lumbar = -1 to -3 cm H20, Lower lumbar= -0.5cm H20.
ANATOMY OF THE SACRAL EPIDURAL SPACE:
Fig 4. The Sacral epidural space
Sacral hiatus:It is an inverted ‘V’ shaped opening
situated 3 to 5 cms from the coccyx or just beneath the superior gluteal cleft. It is formed due to the failure of fusion of the laminae of S4 and S5. It is covered by the sacrococcygeal membrane.
RACE 2003 Ramachandra Anaesthesia Continuing Education
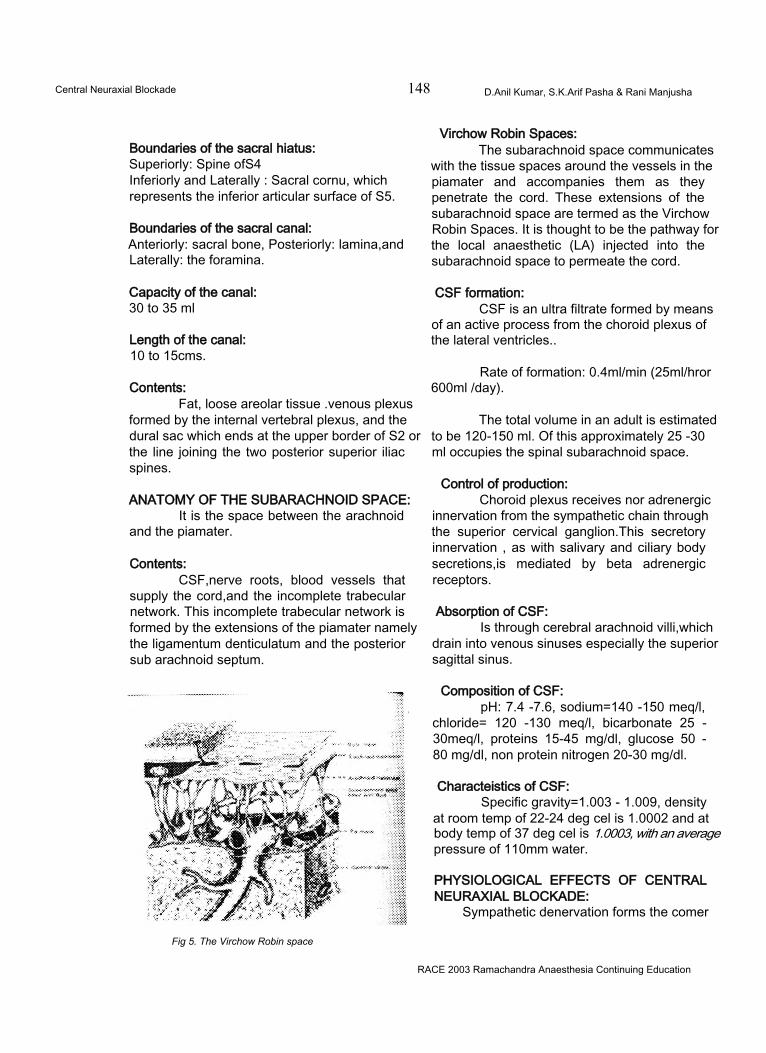
Central Neuraxial Blockade 148 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Boundaries of the sacral hiatus:Superiorly: Spine ofS4Inferiorly and Laterally : Sacral cornu, whichrepresents the inferior articular surface of S5.
Boundaries of the sacral canal:Anteriorly: sacral bone, Posteriorly: lamina,and Laterally: the foramina.
Capacity of the canal:30 to 35 ml
Length of the canal:10 to 15cms.
Contents:Fat, loose areolar tissue .venous plexus
formed by the internal vertebral plexus, and the dural sac which ends at the upper border of S2 or the line joining the two posterior superior iliac spines.
ANATOMY OF THE SUBARACHNOID SPACE:It is the space between the arachnoid
and the piamater.
Contents:CSF,nerve roots, blood vessels that
supply the cord,and the incomplete trabecular network. This incomplete trabecular network is formed by the extensions of the piamater namely the ligamentum denticulatum and the posterior sub arachnoid septum.
Fig 5. The Virchow Robin space
Virchow Robin Spaces:The subarachnoid space communicates
with the tissue spaces around the vessels in the piamater and accompanies them as they penetrate the cord. These extensions of the subarachnoid space are termed as the Virchow Robin Spaces. It is thought to be the pathway for the local anaesthetic (LA) injected into the subarachnoid space to permeate the cord.
CSF formation:CSF is an ultra filtrate formed by means
of an active process from the choroid plexus of the lateral ventricles..
Rate of formation: 0.4ml/min (25ml/hror 600ml /day).
The total volume in an adult is estimated to be 120-150 ml. Of this approximately 25 -30 ml occupies the spinal subarachnoid space.
Control of production:Choroid plexus receives nor adrenergic
innervation from the sympathetic chain through the superior cervical ganglion.This secretory innervation , as with salivary and ciliary body secretions,is mediated by beta adrenergic receptors.
Absorption of CSF:Is through cerebral arachnoid villi,which
drain into venous sinuses especially the superior sagittal sinus.
Composition of CSF:pH: 7.4 -7.6, sodium=140 -150 meq/l,
chloride= 120 -130 meq/l, bicarbonate 25 - 30meq/l, proteins 15-45 mg/dl, glucose 50 - 80 mg/dl, non protein nitrogen 20-30 mg/dl.
Characteistics of CSF:Specific gravity=1.003 - 1.009, density
at room temp of 22-24 deg cel is 1.0002 and at body temp of 37 deg cel is 1.0003, with an average pressure of 110mm water.
PHYSIOLOGICAL EFFECTS OF CENTRAL NEURAXIAL BLOCKADE:
Sympathetic denervation forms the comer
RACE 2003 Ramachandra Anaesthesia Continuing Education
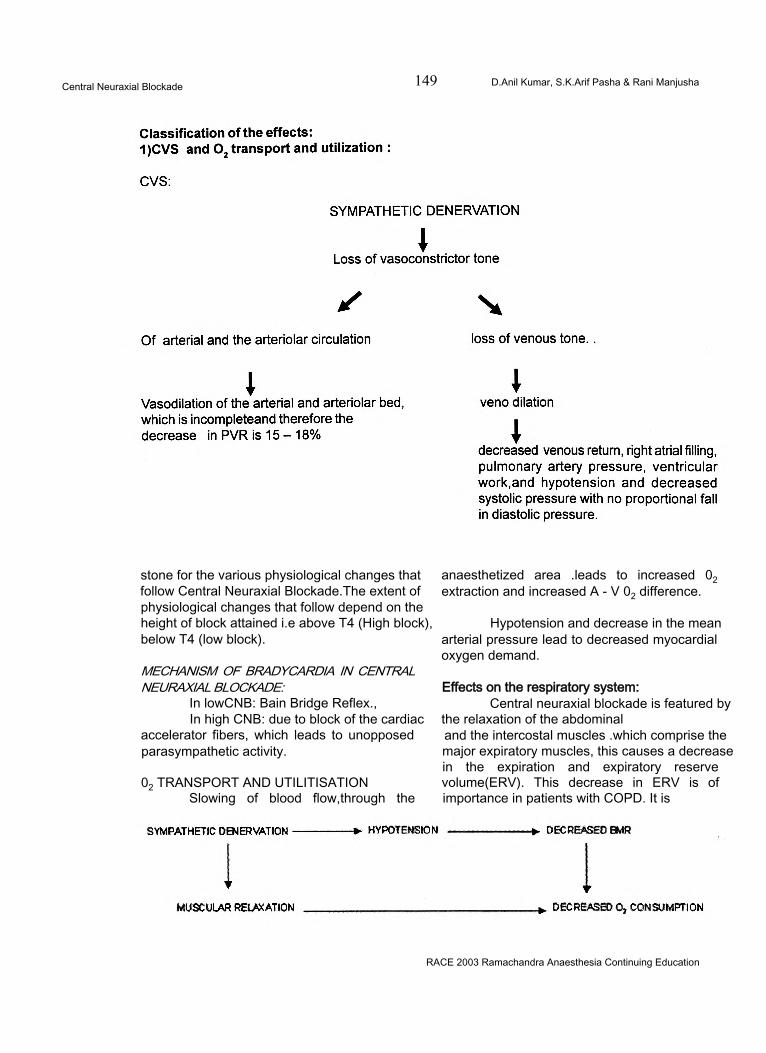
Central Neuraxial Blockade 149 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
stone for the various physiological changes that follow Central Neuraxial Blockade.The extent of physiological changes that follow depend on the height of block attained i.e above T4 (High block), below T4 (low block).
MECHANISM OF BRADYCARDIA IN CENTRAL NEURAXIAL BLOCKADE:
In lowCNB: Bain Bridge Reflex.,In high CNB: due to block of the cardiac
accelerator fibers, which leads to unopposed parasympathetic activity.
02 TRANSPORT AND UTILITISATIONSlowing of blood flow,through the
anaesthetized area .leads to increased 02 extraction and increased A - V 02 difference.
Hypotension and decrease in the mean arterial pressure lead to decreased myocardial oxygen demand.
Effects on the respiratory system:Central neuraxial blockade is featured by
the relaxation of the abdominal and the intercostal muscles .which comprise the major expiratory muscles, this causes a decrease in the expiration and expiratory reserve volume(ERV). This decrease in ERV is of importance in patients with COPD. It is
RACE 2003 Ramachandra Anaesthesia Continuing Education
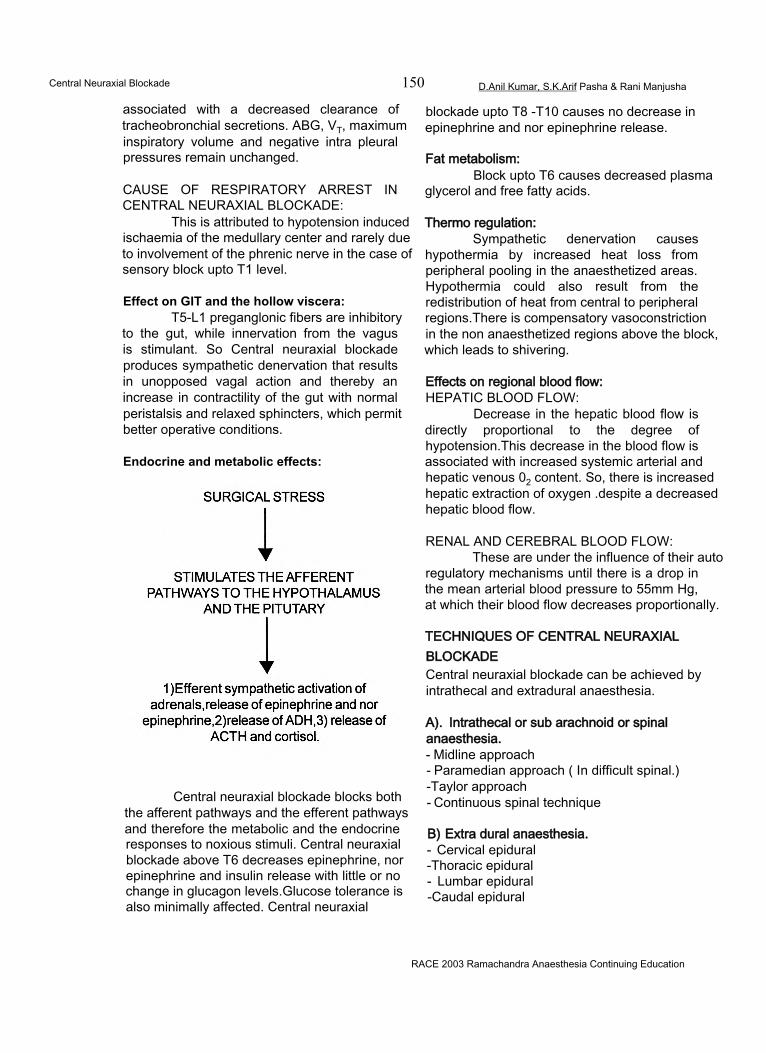
Central Neuraxial Blockade 150 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
associated with a decreased clearance of tracheobronchial secretions. ABG, VT, maximum inspiratory volume and negative intra pleural pressures remain unchanged.
CAUSE OF RESPIRATORY ARREST IN CENTRAL NEURAXIAL BLOCKADE:
This is attributed to hypotension induced ischaemia of the medullary center and rarely due to involvement of the phrenic nerve in the case of sensory block upto T1 level.
Effect on GIT and the hollow viscera:T5-L1 preganglonic fibers are inhibitory
to the gut, while innervation from the vagus is stimulant. So Central neuraxial blockade produces sympathetic denervation that results in unopposed vagal action and thereby an increase in contractility of the gut with normal peristalsis and relaxed sphincters, which permit better operative conditions.
Endocrine and metabolic effects:
Central neuraxial blockade blocks both the afferent pathways and the efferent pathways and therefore the metabolic and the endocrine responses to noxious stimuli. Central neuraxial blockade above T6 decreases epinephrine, nor epinephrine and insulin release with little or no change in glucagon levels.Glucose tolerance is also minimally affected. Central neuraxial
blockade upto T8 -T10 causes no decrease in epinephrine and nor epinephrine release.
Fat metabolism:Block upto T6 causes decreased plasma
glycerol and free fatty acids.
Thermo regulation:Sympathetic denervation causes
hypothermia by increased heat loss from peripheral pooling in the anaesthetized areas. Hypothermia could also result from the redistribution of heat from central to peripheral regions.There is compensatory vasoconstriction in the non anaesthetized regions above the block, which leads to shivering.
Effects on regional blood flow:HEPATIC BLOOD FLOW:
Decrease in the hepatic blood flow is directly proportional to the degree of hypotension.This decrease in the blood flow is associated with increased systemic arterial and hepatic venous 02 content. So, there is increased hepatic extraction of oxygen .despite a decreased hepatic blood flow.
RENAL AND CEREBRAL BLOOD FLOW:These are under the influence of their auto
regulatory mechanisms until there is a drop in the mean arterial blood pressure to 55mm Hg, at which their blood flow decreases proportionally.
TECHNIQUES OF CENTRAL NEURAXIAL BLOCKADECentral neuraxial blockade can be achieved by intrathecal and extradural anaesthesia.
A). Intrathecal or sub arachnoid or spinal anaesthesia.- Midline approach- Paramedian approach ( In difficult spinal.) -Taylor approach- Continuous spinal technique
B) Extra dural anaesthesia.- Cervical epidural -Thoracic epidural- Lumbar epidural -Caudal epidural
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 151 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
C) Combined epidural and spinal anaesthesia.
INDICATIONS:1. Intraoperatively:
• Anaesthesia for lower limb surgeries, perineal procedures and Caesarean section
• ,To provide controlled hypotension
2. For providing analgesia:• Post-operative analgesia• Obstetric analgesia• For relief of intractable pain as in
crush injury chest (Relief from pain reduces paradoxical respiration and allows the patient to clear the lower airways by coughing freely) and lumbar disc lesions (for relief of sciatic pain).
CONTRAINDICATIONS:Absolute:1. Patient refusal.2. Localised infection / Generalised infection.3. Raised ICP / Active CNS disease.4. Coagulation disorders5. Sensitivity to local anaesthetic drugs6. Severe blood loss / shock.
Relative:1. Severe headache / backache2. Medicolegal conditions3. Diseases of the spinal column (arthritis,
metastasis, osteoporosis)4. Blood in CSF - failure to clear after 10 to 15ml
of aspiration.5. Inability to achieve placement of needle after
3 attempts6. Neurological diseases or simulators(residual
paralysis, poliomyelitis).
EQUIPMENT:Spinal needlesThe standard spinal needle consists of 3 parts:1. Hub2. Cannula and3. Stylet with sizes varying from 18 to 29 gauge.
The various needles are/1. Quincke - Babcock needle2. Pitkin needle3. Greene needle
4. Whitacre needle5. Tuohy needle6. Sprotte needle
Epidural needles:1. Tuohy needle with huber point2. Crawford point needle3. Husted needle - modified Tuohy needle with a
rounded tip and bevel opening.
The Spinal, epidural or caudal anaesthesia is preceeded by a preanaesthetic checkup of the patients with examination of the spine, airway and othersystems. On the day of surgery, IV access should be secured. Premedication should be given depending on the patient or circumstances. Preloading is done by adequate volume of fluid infusion if necessary. Patient should be positioned .The area of puncture should be cleaned with antiseptic solution and draped. We can now proceed with our anaesthetic technique.
Drugs:Along with local anaesthetics, other
groups of drugs can also be used for central neuraxial blockade.
TECHNIQUE:Spinal anaesthesia:
Dural puncture can be done in the lateral flexed or sitting position at the widest interspinous space or at the desired space, usually through the midline approach. In difficult cases and in old patients, the paramedian approach can be selected. Needle in the subarachnoid space is confirmed by loss of resistance and aspiration of CSF.
Continuous spinal technique:-In earlier days CSA was achieved by
malleable needle insertion into the dural sac, which is called LEMMON technique.
Tuohy technique:Introduction of wide bore spinal needle
into the dural sac and insertion of micro catheter into the subarachnoid space. This procedure is associated with a lot of complications like :1. Breaking of catheter 2. Kinking of catheter etc.,
Epidural anaesthetic technique:
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 152 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Fig 6. Technique of epidural anaesthesia
As epidural space is a potential space, solutions do not readily flow due to the low compliance: gravitational influences are very minimal.• Lateral position is the widely accepted
position. Sitting position is indicated in obese patients or when perineal anesthesia is desired.
• For upper thoracic / cervical region block, sitting position provides a greater ease of insertion of the needle into the epidural space and the level at C7 and T1 is the recommended space, as the thoracic spines of T1, T2 ,T11 and T12 are horizontal while those of T3, T4, T9 and T10 are some what oblique and the spines of T5 and T8 are almost vertical.
DETECTION OF EPIDURAL SPACE:Negative pressure detection technique,
loss of resistance technique when the ligamentum flavum is pierced.
NEGATIVE PRESSURE TECHNIQUES:-1. Hanging drop sign technique of GUTIEREZ2. Capillary tube method3. Manometer technique
LOSS OF RESISTANCE TECHNIQUE:-1. Syringe technique - using air or normal saline.2. Spring loaded syringe technique3. Balloon technique4. Brook’s device5. Vertical tube of dawkins.
Continuous epidural anesthesia:This method consists of threading an
epidural catheter into the epidural space (very frequently used with bacterial filters). They allow accurate incremental dosing and infusions with prolonged analgesia; e.g., in the post operative period and in obstetrics for providing labour analgesia.
Patient controlled analgesia:With a specially designed device, the
patient controls the drug dose delivery into the epidural catheter, according to the depth of pain felt by him.
Caudal anaesthesia I Extradural sacral block:Positioning: Lateral decubitus position.
Prone position with pillow under the pelvis.
Confirmation: Whoosh test Paediatric central neuraxial blockade:
Undertaken by skilled personnel with adequate sedation.
Combined epidural and spinal anesthesia:Single and double space technique
PHARMACOKINETICS AND PHARMACODYNAMICS OF DRUGS USED IN CENTRAL NEURAXIAL BLOCKADE
This will be covered under the following headings:1. INTRODUCTION.2. PHYSIOLOGY OF NEURAL BLOCKADE3. PHARMACOKINETICS & PHARMA
CODYNAMICS OF LOCAL ANAESTHETIC INCNB.
A) PHYSIOCHEMICAL PROPERTIES OF LOCAL ANAESTHETICB) MECHANISM OF ACTIONC) PHARMACOKINETICS & CLINICAL
RACE 2003 Ramachandra Anaesthesia Continuing Education
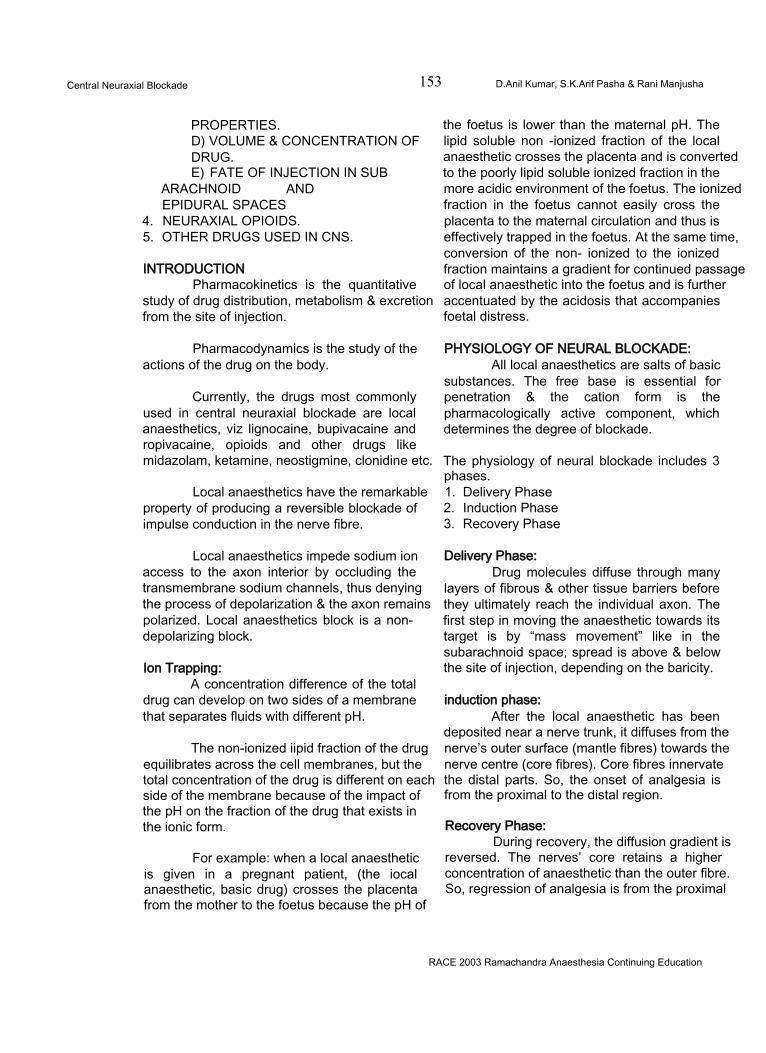
Central Neuraxial Blockade 153 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
PROPERTIES.D) VOLUME & CONCENTRATION OFDRUG.E) FATE OF INJECTION IN SUB
ARACHNOID AND EPIDURAL SPACES
4. NEURAXIAL OPIOIDS.5. OTHER DRUGS USED IN CNS.
INTRODUCTIONPharmacokinetics is the quantitative
study of drug distribution, metabolism & excretion from the site of injection.
Pharmacodynamics is the study of the actions of the drug on the body.
Currently, the drugs most commonly used in central neuraxial blockade are local anaesthetics, viz lignocaine, bupivacaine and ropivacaine, opioids and other drugs like midazolam, ketamine, neostigmine, clonidine etc.
Local anaesthetics have the remarkable property of producing a reversible blockade of impulse conduction in the nerve fibre.
Local anaesthetics impede sodium ion access to the axon interior by occluding the transmembrane sodium channels, thus denying the process of depolarization & the axon remains polarized. Local anaesthetics block is a nondepolarizing block.
Ion Trapping:A concentration difference of the total
drug can develop on two sides of a membrane that separates fluids with different pH.
The non-ionized iipid fraction of the drug equilibrates across the cell membranes, but the total concentration of the drug is different on each side of the membrane because of the impact of the pH on the fraction of the drug that exists in the ionic form.
For example: when a local anaesthetic is given in a pregnant patient, (the iocal anaesthetic, basic drug) crosses the placenta from the mother to the foetus because the pH of
the foetus is lower than the maternal pH. The lipid soluble non -ionized fraction of the local anaesthetic crosses the placenta and is converted to the poorly lipid soluble ionized fraction in the more acidic environment of the foetus. The ionized fraction in the foetus cannot easily cross the placenta to the maternal circulation and thus is effectively trapped in the foetus. At the same time, conversion of the non- ionized to the ionized fraction maintains a gradient for continued passage of local anaesthetic into the foetus and is further accentuated by the acidosis that accompanies foetal distress.
PHYSIOLOGY OF NEURAL BLOCKADE:All local anaesthetics are salts of basic
substances. The free base is essential for penetration & the cation form is the pharmacologically active component, which determines the degree of blockade.
The physiology of neural blockade includes 3 phases.1. Delivery Phase2. Induction Phase3. Recovery Phase
Delivery Phase:Drug molecules diffuse through many
layers of fibrous & other tissue barriers before they ultimately reach the individual axon. The first step in moving the anaesthetic towards its target is by “mass movement” like in the subarachnoid space; spread is above & below the site of injection, depending on the baricity.
induction phase:After the local anaesthetic has been
deposited near a nerve trunk, it diffuses from the nerve’s outer surface (mantle fibres) towards the nerve centre (core fibres). Core fibres innervate the distal parts. So, the onset of analgesia is from the proximal to the distal region.
Recovery Phase:During recovery, the diffusion gradient is
reversed. The nerves’ core retains a higher concentration of anaesthetic than the outer fibre. So, regression of analgesia is from the proximal
RACE 2003 Ramachandra Anaesthesia Continuing Education
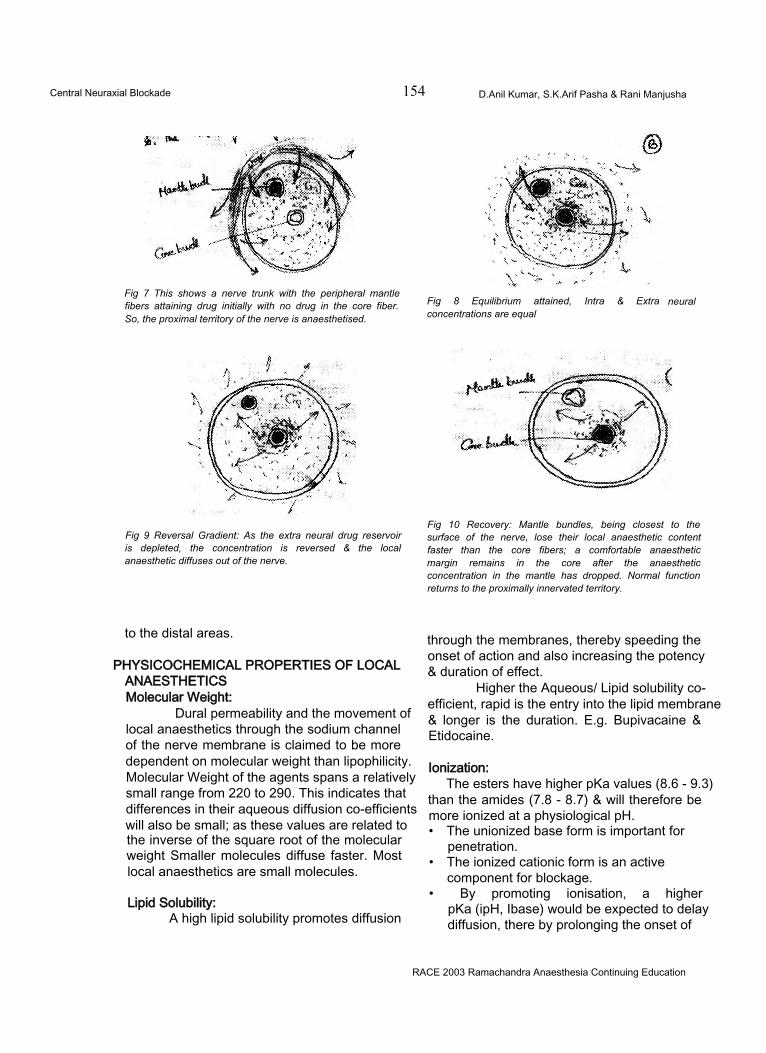
Central Neuraxial Blockade 154 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Fig 7 This shows a nerve trunk with the peripheral mantle fibers attaining drug initially with no drug in the core fiber. So, the proximal territory of the nerve is anaesthetised.
Fig 8 Equilibrium attained, Intra & Extra concentrations are equal
neural
Fig 9 Reversal Gradient: As the extra neural drug reservoir is depleted, the concentration is reversed & the local anaesthetic diffuses out of the nerve.
Fig 10 Recovery: Mantle bundles, being closest to the surface of the nerve, lose their local anaesthetic content faster than the core fibers; a comfortable anaesthetic margin remains in the core after the anaesthetic concentration in the mantle has dropped. Normal function returns to the proximally innervated territory.
to the distal areas.
PHYSICOCHEMICAL PROPERTIES OF LOCALANAESTHETICSMolecular Weight:
Dural permeability and the movement of local anaesthetics through the sodium channel of the nerve membrane is claimed to be more dependent on molecular weight than lipophilicity. Molecular Weight of the agents spans a relatively small range from 220 to 290. This indicates that differences in their aqueous diffusion co-efficients will also be small; as these values are related to the inverse of the square root of the molecular weight Smaller molecules diffuse faster. Most local anaesthetics are small molecules.
Lipid Solubility:A high lipid solubility promotes diffusion
through the membranes, thereby speeding the onset of action and also increasing the potency & duration of effect.
Higher the Aqueous/ Lipid solubility coefficient, rapid is the entry into the lipid membrane & longer is the duration. E.g. Bupivacaine & Etidocaine.
Ionization:The esters have higher pKa values (8.6 - 9.3)
than the amides (7.8 - 8.7) & will therefore be more ionized at a physiological pH.• The unionized base form is important for
penetration.• The ionized cationic form is an active
component for blockage.• By promoting ionisation, a higher
pKa (ipH, Ibase) would be expected to delay diffusion, there by prolonging the onset of
RACE 2003 Ramachandra Anaesthesia Continuing Education
155
action.
Protien binding:Besides being lipid soluble, the longer
acting local anaesthetics also exhibit a higher degree of protein binding.
Features common to all local anaesthetics:1. They are all weak bases with a pKa > 7.4
(free base is poorly water soluble).So they are dispensed as acidic solutions with HCI salts with the pH between 4-7.
receptor for local anaesthetic molecules. Failure of sodium ion channel permeability to increase slows the rate of depolarization such that threshold potential is not reached & thus an action potential is not propagated. Local anaesthetics do not alter the resting membrane potential or threshold potential.Sodium Channel
• Open Activated• Inactive Close• Rested Closed
In the resting nerve membrane, the Na+
Agent Mol. Wt. pKa 25°C DistributionCo-efficient
Protein binding (%)
EstersPROCAINE 236 9.0 1.7 5.8AmidesLIDOCAINE 234 7.7 43 65BUPIVACAINE 288 8.1 346 95ROPIVACAINE 277 8.1 115 90
Table 1: Physicochemical properties of commonly used local anaesthetics:
These commercial preparations are water soluble and highly ionized.
2. They exist in solution as an equilibrium mixture of non-ionized lipid soluble freebase & ionized water-soluble cationic form.
3. Body buffers raise the pH and therefore increase the amount of freebase present.
4. The lipid soluble form crosses the axonal membrane.
channels are distributed in equilibrium between the rested-closed & inactivated closed state. By selective binding to the Na channels in the inactivated closed states, local anaesthetic molecules stabilize these channels in this configuration & prevent their change to the rested closed & activated open states, in response to nerve impulses.
MECHANISM OF ACTION OF LOCAL ANAESTHETICS:
Covino, more recently Butterworth & Strichtartz provide seminal reviews of the electrophysiologica! & molecular mechanisms of local anaesthetic action.
Electrophysialogical effects & Ionic effects:Local anaesthetics prevent transmission
of nerve impulses (conduction blockade), by inhibiting the passage of sodium ions through ion- selective sodium channels in the nerve membrane.
The Na+ channel itself is a specific
Central Neuraxial Blockade 156 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Local anaesthetics bind to specific sites located on the inner portion of the sodium channel (internal gate or H gate) as well as obstruct sodium channels near their external opening, to maintain these channels in the inactivated closed state.
Frequency - dependent blockade:An increase in the frequency of nerve
stimulation has been shown to enhance the effect of local anaesthetics on sodium conduction & action potential Resting nerve is less sensitive than the nerve that has been repeatedly stimulated.
Etidocaine characteristically blocks motor nerves before sensory, because of frequency dependent blockade. The pharmacological effects of other drugs, including anticonvulsants, & barbiturates, in addition to local anaesthetics, may reflect frequency dependent blockade.
Effects on Age & Pregency:There will be increased sensitivity to local
anaesthetic-induced conduction block in paediatric, geriatric, & pregnant patients. In pregnancy, the dose should be reduced by 30% due to increased absorption, venous engorgement and increased sensitivity of the nerve fibres due to the effect of progesterone.
PHARMACOKINETICS OF LOCAL ANAESTHETICS:
Pharmacokinetics is the study of drug distribution, metabolism & excretion from the site of injection. Local anaesthetics are weak bases that have pKa valves somewhat above the physiologic pH. As a result, <50% of the local anaesthetic exists in the lipid soluble non ionized form at a physiological pH. Local anaesthetics with a pKa nearest to the physiologic pH have the most rapid onset of action, (e.g., lignocaine), reflecting the presence of an optimal ratio of ionized to non ionized drug fraction.
Absorption & Distribution:Absorption of local anaesthetic from its
site of injection into the systemic circulation is influenced by the site of injection, dosage, use of
epinephrine and lipid solubility. The ultimate plasma concentration is determined by the rate of tissue distribution & rate of clearance of drugs. Initially, they are distributed to the highly perfused tissues - brain, heart, kidney and later to the poorly perfused tissues - skeletal muscle, fat. In addition to tissue blood flow & lipid solubility of local anaesthetics, patient related factors such as age, CVS status and hepatic function will also have an influence. Ultimately the local anaesthetic is eliminated from the plasma by metabolism & excretion.
Metabolism:METABOLISM OF ESTER LOCAL ANAESTHETICS:
Ester local anaesthetics undergo hydrolysis by cholinesterase enzyme principally in the plasma & to a lesser extent in the liver. Cocaine undergoes significant metabolism in the liver.
METABOLISM OF AMIDE LOCAL ANAESTHETICS:
Amide local anaesthetics undergo metabolism by microsomal enzymes primarily in
Most Rapid Intermediate Slowest.Prilocaine Lidocaine & Etidocaine
Mepivacaine Bupivacaine & Ropivacaine.
the liver.
BUPIVACAINE:Possible pathways: aromatic
hydroxylation, N-dealkylation, Amide hydrolysis. Only the N-dealkylation metabolite, N-desbutyl bupivacaine, has been measured in the blood or urine after epidural or spinal anaesthesia. a1 -acid glycoprotein is the most important plasma protein binding site of bupivacaine.
ROPIVACAINEThe principle metabolite of ropivacaine
is 3-hydroxy ropivacaine.
Renal elimination:Excretion occurs by the kidney. Less
than 5% of the unchanged drug is excreted via
RACE 2003 Ramachandra Anaesthesia Continuing Education
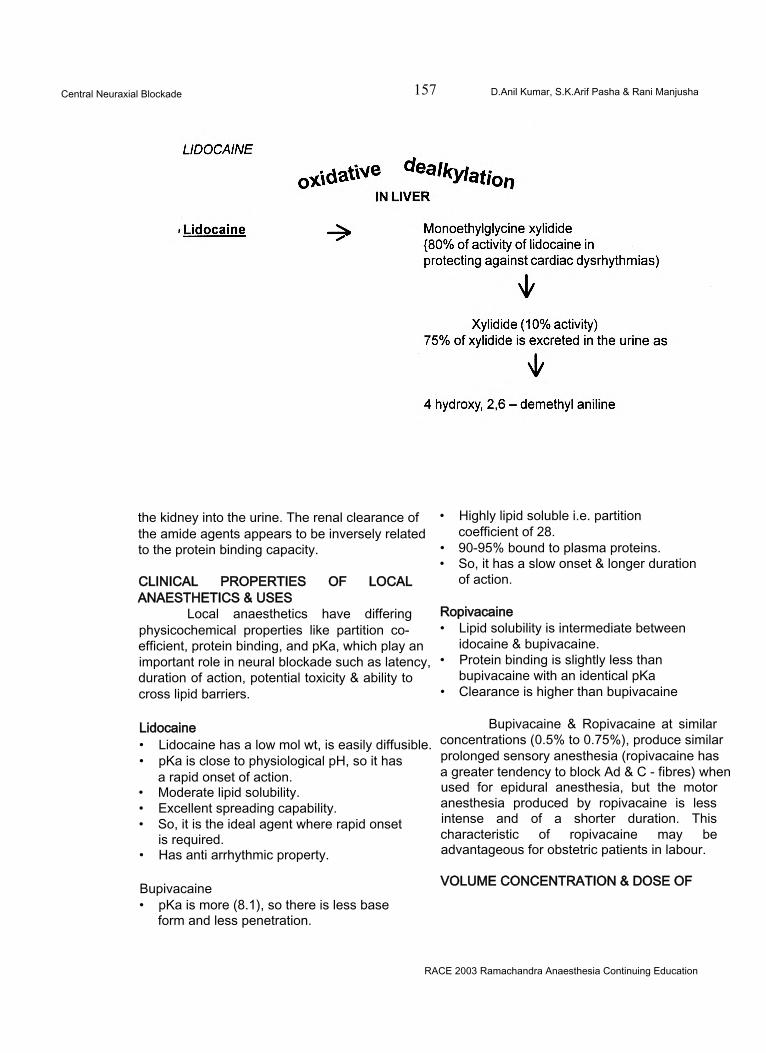
Central Neuraxial Blockade 157 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
the kidney into the urine. The renal clearance of the amide agents appears to be inversely related to the protein binding capacity.
CLINICAL PROPERTIES OF LOCAL ANAESTHETICS & USES
Local anaesthetics have differing physicochemical properties like partition coefficient, protein binding, and pKa, which play an important role in neural blockade such as latency, duration of action, potential toxicity & ability to cross lipid barriers.
Lidocaine• Lidocaine has a low mol wt, is easily diffusible.• pKa is close to physiological pH, so it has
a rapid onset of action.• Moderate lipid solubility.• Excellent spreading capability.• So, it is the ideal agent where rapid onset
is required.• Has anti arrhythmic property.
Bupivacaine• pKa is more (8.1), so there is less base
form and less penetration.
• Highly lipid soluble i.e. partition coefficient of 28.
• 90-95% bound to plasma proteins.• So, it has a slow onset & longer duration
of action.
Ropivacaine• Lipid solubility is intermediate between
idocaine & bupivacaine.• Protein binding is slightly less than
bupivacaine with an identical pKa• Clearance is higher than bupivacaine
Bupivacaine & Ropivacaine at similar concentrations (0.5% to 0.75%), produce similar prolonged sensory anesthesia (ropivacaine has a greater tendency to block Ad & C - fibres) when used for epidural anesthesia, but the motor anesthesia produced by ropivacaine is less intense and of a shorter duration. This characteristic of ropivacaine may be advantageous for obstetric patients in labour.
VOLUME CONCENTRATION & DOSE OF
RACE 2003 Ramachandra Anaesthesia Continuing Education
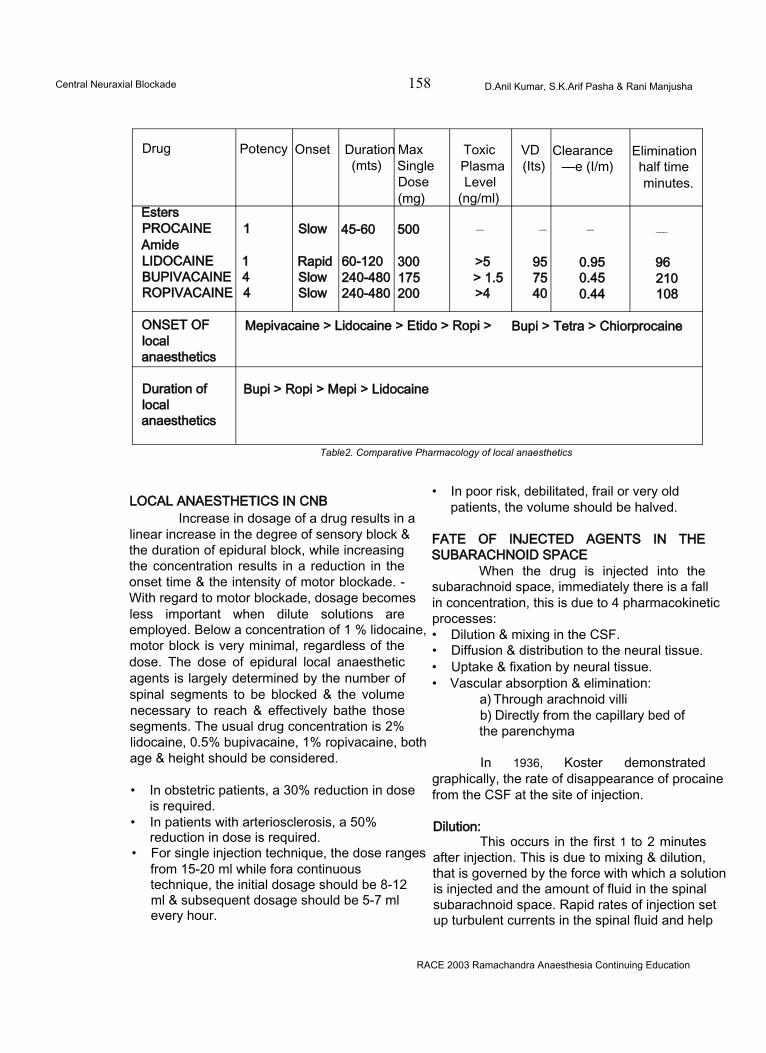
Central Neuraxial Blockade 158 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Drug Potency Onset Duration Max Toxic VD Clearance Elimination(mts) Single Plasma (Its) —e (I/m) half time
Dose Level minutes.(mg) (ng/ml)
EstersPROCAINE 1 Slow 45-60 500 — — — ___
AmideLIDOCAINE 1 Rapid 60-120 300 >5 95 0.95 96BUPIVACAINE 4 Slow 240-480 175 > 1.5 75 0.45 210ROPIVACAINE 4 Slow 240-480 200 >4 40 0.44 108
ONSET OF Mepivacaine > Lidocaine > Etido > Ropi > Bupi > Tetra > Chiorprocainelocalanaesthetics
Duration of Bupi > Ropi > Mepi > Lidocainelocalanaesthetics
Table2. Comparative Pharmacology of local anaesthetics
LOCAL ANAESTHETICS IN CNBIncrease in dosage of a drug results in a
linear increase in the degree of sensory block & the duration of epidural block, while increasing the concentration results in a reduction in the onset time & the intensity of motor blockade. - With regard to motor blockade, dosage becomes less important when dilute solutions are employed. Below a concentration of 1 % lidocaine, motor block is very minimal, regardless of the dose. The dose of epidural local anaesthetic agents is largely determined by the number of spinal segments to be blocked & the volume necessary to reach & effectively bathe those segments. The usual drug concentration is 2% lidocaine, 0.5% bupivacaine, 1% ropivacaine, both age & height should be considered.
• In obstetric patients, a 30% reduction in dose is required.
• In patients with arteriosclerosis, a 50% reduction in dose is required.
• For single injection technique, the dose ranges from 15-20 ml while fora continuous technique, the initial dosage should be 8-12 ml & subsequent dosage should be 5-7 ml every hour.
• In poor risk, debilitated, frail or very old patients, the volume should be halved.
FATE OF INJECTED AGENTS IN THE SUBARACHNOID SPACE
When the drug is injected into the subarachnoid space, immediately there is a fall in concentration, this is due to 4 pharmacokinetic processes:• Dilution & mixing in the CSF.• Diffusion & distribution to the neural tissue.• Uptake & fixation by neural tissue.• Vascular absorption & elimination:
a) Through arachnoid villib) Directly from the capillary bed of the parenchyma
In 1936, Koster demonstrated graphically, the rate of disappearance of procaine from the CSF at the site of injection.
Dilution:This occurs in the first 1 to 2 minutes
after injection. This is due to mixing & dilution, that is governed by the force with which a solution is injected and the amount of fluid in the spinal subarachnoid space. Rapid rates of injection set up turbulent currents in the spinal fluid and help
RACE 2003 Ramachandra Anaesthesia Continuing Education
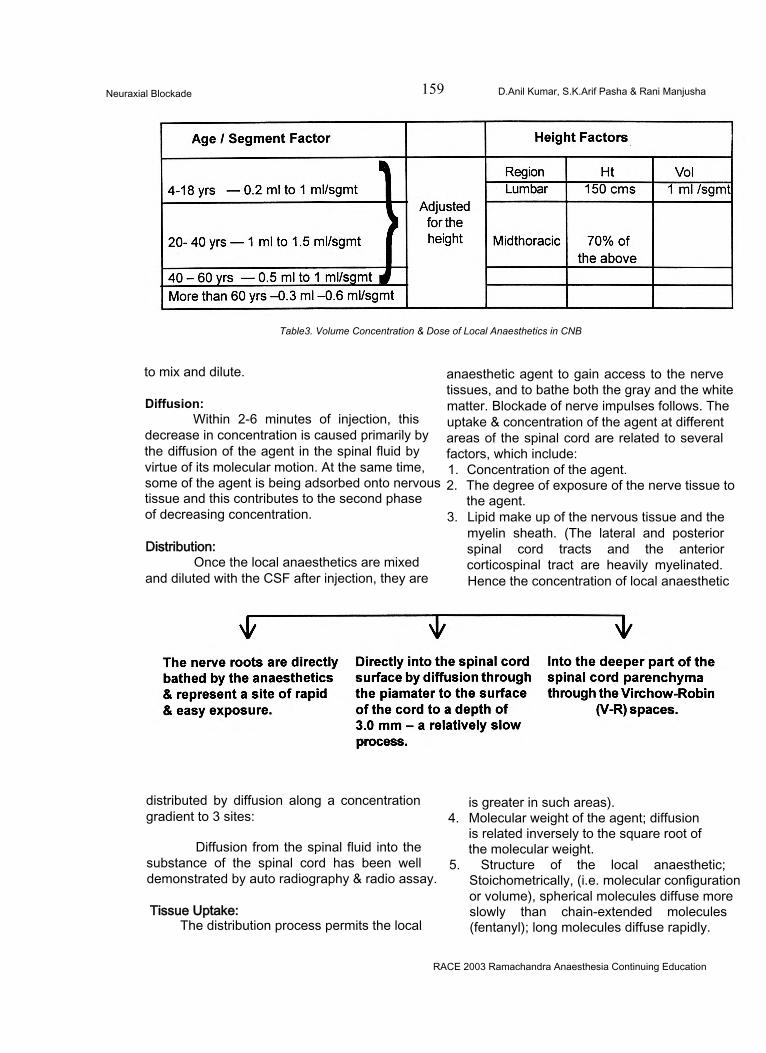
Neuraxial Blockade 159 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
Table3. Volume Concentration & Dose of Local Anaesthetics in CNB
to mix and dilute.
Diffusion:Within 2-6 minutes of injection, this
decrease in concentration is caused primarily by the diffusion of the agent in the spinal fluid by virtue of its molecular motion. At the same time, some of the agent is being adsorbed onto nervous tissue and this contributes to the second phase of decreasing concentration.
Distribution:Once the local anaesthetics are mixed
and diluted with the CSF after injection, they are
anaesthetic agent to gain access to the nerve tissues, and to bathe both the gray and the white matter. Blockade of nerve impulses follows. The uptake & concentration of the agent at different areas of the spinal cord are related to several factors, which include:1. Concentration of the agent.2. The degree of exposure of the nerve tissue to
the agent.3. Lipid make up of the nervous tissue and the
myelin sheath. (The lateral and posterior spinal cord tracts and the anterior corticospinal tract are heavily myelinated. Hence the concentration of local anaesthetic
distributed by diffusion along a concentration gradient to 3 sites:
Diffusion from the spinal fluid into the substance of the spinal cord has been well demonstrated by auto radiography & radio assay.
Tissue Uptake:The distribution process permits the local
is greater in such areas).4. Molecular weight of the agent; diffusion
is related inversely to the square root of the molecular weight.
5. Structure of the local anaesthetic; Stoichometrically, (i.e. molecular configuration or volume), spherical molecules diffuse more slowly than chain-extended molecules (fentanyl); long molecules diffuse rapidly.
RACE 2003 Ramachandra Anaesthesia Continuing Education
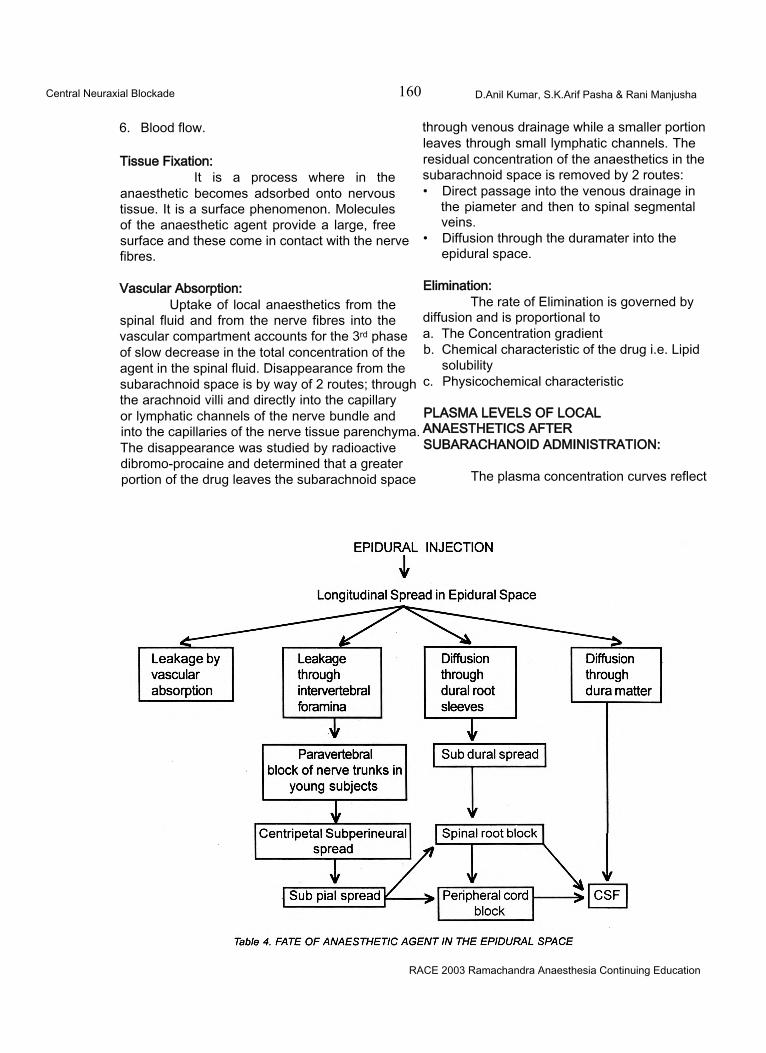
Central Neuraxial Blockade 160 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
6. Blood flow.
Tissue Fixation:It is a process where in the
anaesthetic becomes adsorbed onto nervous tissue. It is a surface phenomenon. Molecules of the anaesthetic agent provide a large, free surface and these come in contact with the nerve fibres.
Vascular Absorption:Uptake of local anaesthetics from the
spinal fluid and from the nerve fibres into the vascular compartment accounts for the 3rd phase of slow decrease in the total concentration of the agent in the spinal fluid. Disappearance from the subarachnoid space is by way of 2 routes; through the arachnoid villi and directly into the capillary or lymphatic channels of the nerve bundle and into the capillaries of the nerve tissue parenchyma. The disappearance was studied by radioactive dibromo-procaine and determined that a greater portion of the drug leaves the subarachnoid space
through venous drainage while a smaller portion leaves through small lymphatic channels. The residual concentration of the anaesthetics in the subarachnoid space is removed by 2 routes:• Direct passage into the venous drainage in
the piameter and then to spinal segmental veins.
• Diffusion through the duramater into the epidural space.
Elimination:The rate of Elimination is governed by
diffusion and is proportional toa. The Concentration gradientb. Chemical characteristic of the drug i.e. Lipid
solubilityc. Physicochemical characteristic
PLASMA LEVELS OF LOCAL ANAESTHETICS AFTER SUBARACHANOID ADMINISTRATION:
The plasma concentration curves reflect
RACE 2003 Ramachandra Anaesthesia Continuing Education
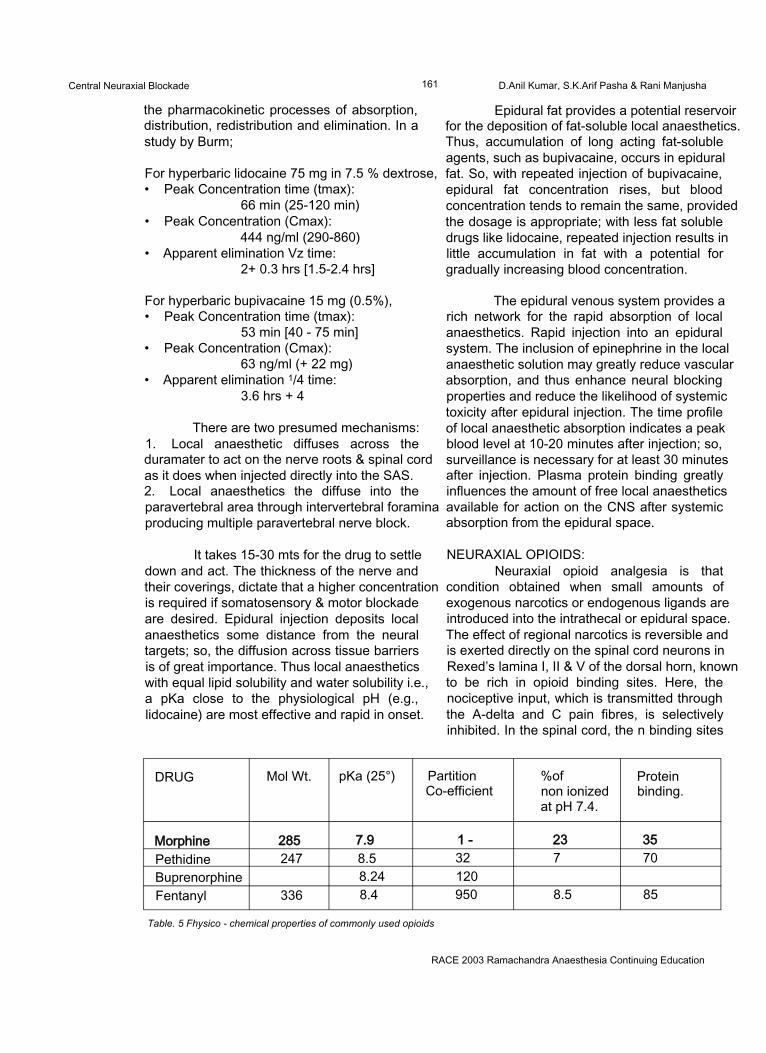
Central Neuraxial Blockade 161 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
the pharmacokinetic processes of absorption, distribution, redistribution and elimination. In a study by Burm;
For hyperbaric lidocaine 75 mg in 7.5 % dextrose,• Peak Concentration time (tmax):
66 min (25-120 min)• Peak Concentration (Cmax):
444 ng/ml (290-860)• Apparent elimination Vz time:
2+ 0.3 hrs [1.5-2.4 hrs]
For hyperbaric bupivacaine 15 mg (0.5%),• Peak Concentration time (tmax):
53 min [40 - 75 min]• Peak Concentration (Cmax):
63 ng/ml (+ 22 mg)• Apparent elimination 1/4 time:
3.6 hrs + 4
There are two presumed mechanisms:1. Local anaesthetic diffuses across the duramater to act on the nerve roots & spinal cord as it does when injected directly into the SAS.2. Local anaesthetics the diffuse into the paravertebral area through intervertebral foramina producing multiple paravertebral nerve block.
It takes 15-30 mts for the drug to settle down and act. The thickness of the nerve and their coverings, dictate that a higher concentration is required if somatosensory & motor blockade are desired. Epidural injection deposits local anaesthetics some distance from the neural targets; so, the diffusion across tissue barriers is of great importance. Thus local anaesthetics with equal lipid solubility and water solubility i.e., a pKa close to the physiological pH (e.g., lidocaine) are most effective and rapid in onset.
Epidural fat provides a potential reservoir for the deposition of fat-soluble local anaesthetics. Thus, accumulation of long acting fat-soluble agents, such as bupivacaine, occurs in epidural fat. So, with repeated injection of bupivacaine, epidural fat concentration rises, but blood concentration tends to remain the same, provided the dosage is appropriate; with less fat soluble drugs like lidocaine, repeated injection results in little accumulation in fat with a potential for gradually increasing blood concentration.
The epidural venous system provides a rich network for the rapid absorption of local anaesthetics. Rapid injection into an epidural system. The inclusion of epinephrine in the local anaesthetic solution may greatly reduce vascular absorption, and thus enhance neural blocking properties and reduce the likelihood of systemic toxicity after epidural injection. The time profile of local anaesthetic absorption indicates a peak blood level at 10-20 minutes after injection; so, surveillance is necessary for at least 30 minutes after injection. Plasma protein binding greatly influences the amount of free local anaesthetics available for action on the CNS after systemic absorption from the epidural space.
NEURAXIAL OPIOIDS:Neuraxial opioid analgesia is that
condition obtained when small amounts of exogenous narcotics or endogenous ligands are introduced into the intrathecal or epidural space. The effect of regional narcotics is reversible and is exerted directly on the spinal cord neurons in Rexed’s lamina I, II & V of the dorsal horn, known to be rich in opioid binding sites. Here, the nociceptive input, which is transmitted through the A-delta and C pain fibres, is selectively inhibited. In the spinal cord, the n binding sites
DRUG Mol Wt. pKa (25°) PartitionCo-efficient
%ofnon ionized at pH 7.4.
Proteinbinding.
Morphine 285 7.9 1 - 23 35Pethidine 247 8.5 32 7 70Buprenorphine 8.24 120Fentanyl 336 8.4 950 8.5 85
Table. 5 Fhysico - chemical properties of commonly used opioids
RACE 2003 Ramachandra Anaesthesia Continuing Education
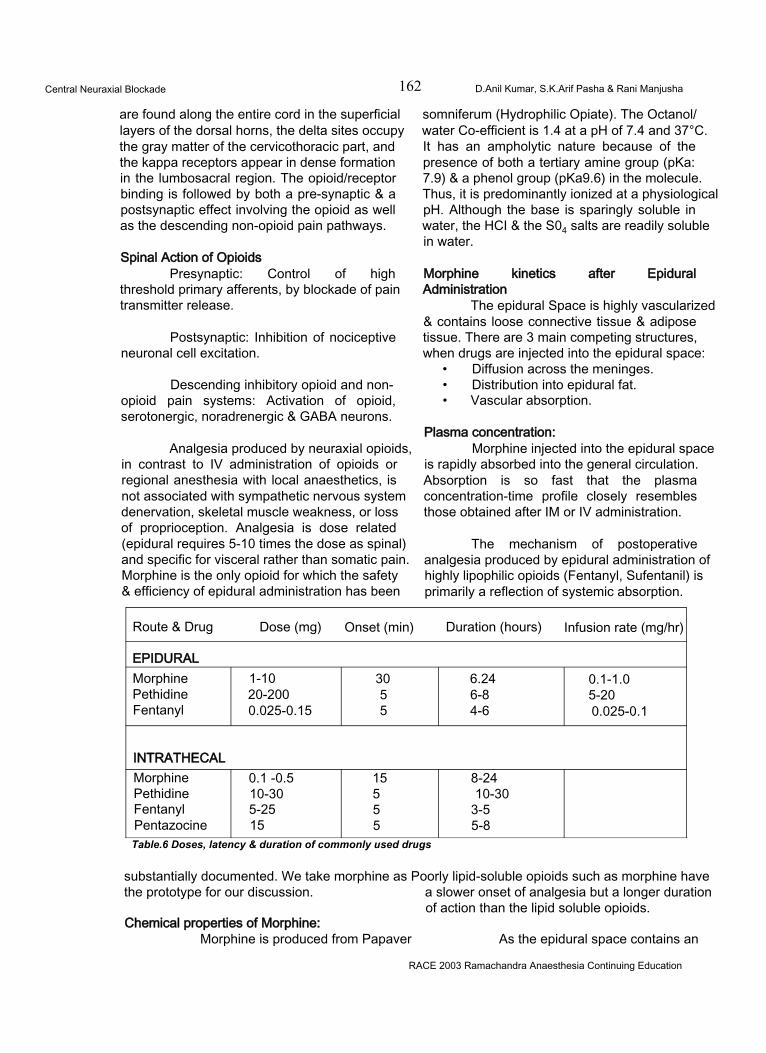
Central Neuraxial Blockade 162 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
are found along the entire cord in the superficial layers of the dorsal horns, the delta sites occupy the gray matter of the cervicothoracic part, and the kappa receptors appear in dense formation in the lumbosacral region. The opioid/receptor binding is followed by both a pre-synaptic & a postsynaptic effect involving the opioid as well as the descending non-opioid pain pathways.
Spinal Action of OpioidsPresynaptic: Control of high
threshold primary afferents, by blockade of pain transmitter release.
Postsynaptic: Inhibition of nociceptive neuronal cell excitation.
Descending inhibitory opioid and nonopioid pain systems: Activation of opioid, serotonergic, noradrenergic & GABA neurons.
Analgesia produced by neuraxial opioids, in contrast to IV administration of opioids or regional anesthesia with local anaesthetics, is not associated with sympathetic nervous system denervation, skeletal muscle weakness, or loss of proprioception. Analgesia is dose related (epidural requires 5-10 times the dose as spinal) and specific for visceral rather than somatic pain. Morphine is the only opioid for which the safety & efficiency of epidural administration has been
somniferum (Hydrophilic Opiate). The Octanol/ water Co-efficient is 1.4 at a pH of 7.4 and 37°C. It has an ampholytic nature because of the presence of both a tertiary amine group (pKa: 7.9) & a phenol group (pKa9.6) in the molecule. Thus, it is predominantly ionized at a physiological pH. Although the base is sparingly soluble in water, the HCI & the S04 salts are readily soluble in water.
Morphine kinetics after Epidural Administration
The epidural Space is highly vascularized & contains loose connective tissue & adipose tissue. There are 3 main competing structures, when drugs are injected into the epidural space:
• Diffusion across the meninges.• Distribution into epidural fat.• Vascular absorption.
Plasma concentration:Morphine injected into the epidural space
is rapidly absorbed into the general circulation. Absorption is so fast that the plasma concentration-time profile closely resembles those obtained after IM or IV administration.
The mechanism of postoperative analgesia produced by epidural administration of highly lipophilic opioids (Fentanyl, Sufentanil) is primarily a reflection of systemic absorption.
Route & Drug Dose (mg) Onset (min) Duration (hours) Infusion rate (mg/hr)
EPIDURALMorphine 1-10 30 6.24 0.1-1.0Pethidine 20-200 5 6-8 5-20Fentanyl 0.025-0.15 5 4-6 0.025-0.1
INTRATHECALMorphine 0.1 -0.5 15 8-24Pethidine 10-30 5 10-30Fentanyl 5-25 5 3-5Pentazocine 15 5 5-8Table.6 Doses, latency & duration of commonly used drugs
substantially documented. We take morphine as Poorly lipid-soluble opioids such as morphine have the prototype for our discussion. a slower onset of analgesia but a longer duration
of action than the lipid soluble opioids.Chemical properties of Morphine:
Morphine is produced from Papaver As the epidural space contains an
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 163 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
extensive venous plexus, vascular absorption is extensive.'After epidural administration, fentanyl blood concentration peaks in 5-10 minutes; in contrast, the blood concentration of morphine peaks after 10-15 minutefe.
Chauvin & colleagues found no significant differences in the areas under the curves after IM, epidural & intrathecal administration of the same dose. This finding suggests that availability is complete, when morphine is administered epidurally or intrathecally.
Bromage & associates reported that simultaneous co-administration of epinephrine, reduced the systemic uptake of morphine in healthy volunteers, whereas Youngstorm & colleagues found that this regimen produced no change in obstetric patients.
CSF Concentration:Epidural administration of opioids
produces considerable CSF concentrations of the drug. To gain access to spinal opioid receptors, the drug must cioss several diffusion barriers, such as the meninges and the neural tissues. Penetration of the dura is considerably influenced by lipid solubility and molecular weight. Fentanyl and Sufentanil are respectively, approximately 800 & 1600 times as lipid soluble as morphine.
After epidural administration, the CSF concentration of fentanyl peaks in about 20 minutes & Sufentanil in 6 minutes. In contract, the CSF concentration of morphine, after epidural administration, peaks after 1-4 hrs. Furthermore, only about 3% of the dose of morphine administered epidurally crosses the dura to enter the CSF.
Morphine kinetics after Intrathecal administration
The intrathecal route of administration circumvents the meningeal diffusion barriers and considerably lower doses of morphine are necessary to produce the same degree of analgesia as that induced by the epidural route.
Cephalad movement of opioids in the
CSF principally depends on lipid solubility.For e.g., lipid soluble opioids such as fentanyl & sufentanil are limited in their cephalad migration by uptake into the spinal cord, whereas the less lipid soluble morphine remains in the CSF for transfer to more cephalad locations.
After lumbar intrathecal morphine administration, appreciable cervical CSF concentration occur 1 to 5 hrs after the injection, whereas cervical CSF concentration of highly lipid-soluble opioids are minimal after their epidural administration.
The underlying cause of ascension of morphine is bulk flow of CSF. CSF ascends in a cephalad direction from the lumbar region reaching the cisterna magna in 1 - 2 hrs, the 4th and lateral ventricle by 3-6 hrs (Chaney, 1995). Coughing or straining, but not body position can affect the movement of CSF.
Relationship between Morphine concentration & analgesic response:
The most outstanding feature of epidural morphine is its ability to produce excellent, long- lasting regional analgesia from doses that are only 20 - 40% of the normal IV dose. I ntrathecal administration of morphine is even more potent, requiring only about 8% of the standard 10 mg IV dose. Clinical experience has shown that analgesic onset of action of epidural morphine is slow (45-60 minutes) compared with that of !V morphine. This delay is due to the physiochemical properties of morphine and the location of the receptors in relation to the site of administration. Being hydrophilic, morphine penetrates the different diffusion barriers much more slowly than the more lipophilic molecules such as fentanyl.
The duration of action of morphine is governed by 2 factors.a) The rate of morphine removal from receptor
sites.b) The magnitude of morphine concentration
surrounding the receptors.
The duration of analgesia varies considerably among patients; due in part to pronounced inter individual differences in pharmacokinetics. Duration is dose dependent,
RACE 2003 Ramachandra Anaesthesia Continuing Education

Central Neuraxial Blockade 164 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
and the usual 4 mg dose is commonly reported to have a duration of 10-17 hrs.
Epidural & Intrathecal Morphine Kinectics in Relation to Adverse Effects
Side effects of neuraxial opioids are caused by the presence of the drug in the CSF or the systemic circulation. The most feared adverse reaction is late respiratory depression, usually due to rostral spread of morphine in the CSF, and is extremely rare. One recent Swedish retrospective study comprising about 10,000 patients, reported an incidence of 0.25 - 0.4%.
The reasons for the rostral spread of morphine may be:a) Bulk flow of CSF.b) Physical activities such as coughing could
cause the CSF pressure wave, capable of moving a substance in a rostral direction.
c) Epidurally injected drugs could be absorbed into the valveless vasculature of the epidural space and subsequently transported to the veins in the brain.
A review of 229 patients in different controlled double-blind studies using 2-5 mg of epidural morphine showed that the three most common side effects were
• Pruritus (14%)• Urinary retention (12)• Nausea & Vomiting (11%)
A most promising study in this context, reported by Rawal & co-workers showed that continuous intravenous infusion of low-dose naloxone could be used to counteract the side effects of epidural morphine, without reducing the analgesia.
OTHER DRUGS USED IN CNBThe other relatively uncommon drugs
used in CNB are1) Benzodiazepines e.g. Midazolam.2) Ketamine3) Clonidine4) Neostigmine5) Steroids.
Spinal GABA System:The spinal GABA system has been used
as a target for newer Benzodiazepines e.g.,
midazolam, and certain neuro active steroids like alphadalone20.
NMDA Receptors and Ketamine:The pain relieving effect of ketamine has
been attributed to blockade of NMDA excitatory neurons; Mccartely, Naguit et al have used ketamine from 30mg to 50mg intrathecally and epidurally with varying results.
Clonidine:Clonidine, an alpha 2 - adrenergic
agonist, is most commonly used centrally to produce relief. It is believed to act on the adrenergic receptors, the opioid receptors and by modulation of G proteins and Substance P. Dose range - 1 to 1.5 (mcg/kg).
Neostigmine:Neostigmine is a familiar drug in the
anaesthesiologist’s armamentarium, which is being used to produce analgesia by inhibiting the breakdown of acetylcholine. The drug has been used epidurally and intrathecally in the dose range of 500 - 750 (meg /kg) and has been found to have dose dependent side effects like nausea and vomiting.
COMPLICATIONS, CLINICAL CONTROVERSIES AND RECENT ADVANCES OF CENTRAL NEURAXIAL BLOCKADE COMPLICATIONS OF CENTRAL NEURAXIAL BLOCKADE:The complications of Central Neuraxial Blockade can be classified as:• Complications due to Spinal anaesthesia.• Complications due to Epidural anaesthesia
COMPLICATIONS OF SPINAL ANAESTHESIAThese can be:During the procedure or immediate complications:A) HYPOTENSION:
Due to the decrease in cardiac output which is due to decreased venous return because of sympathetic block or due to block of sympathetic cardiac fibres.Management: Adequate preloading, head down position, vasopressors and administration of oxygen.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 165 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
B) TOTAL SPINAL ANALGESIA:Characterized by marked hypotension,
apnoea, dilated pupils, loss of consciousness and bradycardia.Management: Intubation and ventilation with 100% oxygen, elevation of the legs, vasopressors and intravenous fluids. The operation can then proceed and spontaneous respiration will probably recommence within an hour, unpleasant sequelae being unlikely.
C) TOXICITY:Due to intravascular injection or by fast
absorption of local anaesthetics. Both CNS and CVS complications occur. Signs are excitement, disorientation, twitching, convulsions, apnoea and severe cardiac depression.Management: Injecting diazepam into the drip, oxygen by IPPV, protection of patient’s teeth and tongue from trauma at the time of convulsions.
D) HYPOVENTILATION:Due to brainstem hypoxia and block of
phrenic nerve roots.Management: Ltngs are ventilated with 100% Oxygen.
E) ALLERGIC RESPONSE TO INJECTED DRUG.Management: Oxygen, I.V. adrenaline,
I.V. Colloid infusion.
F) HYPOTHERMIA:Should be managed by adequately
covering the patient and infusing of warm IV fluids.
G) NAUSEA & VOMITING:As a result of
• Sudden change in position• Hypotension• Parasympathetic mediated traction• Opioid administration.
Management: Exclude hypoxia, take care of hypotension, shift the patient slowly and gently, antiemetic drugs.
H) AFFECTIVE DYSPNOEA:With block of sensory input, patient may
complain of difficulty in breathing. Mechanism is inappropriate response (ventilatory volume) to muscular effort.
Management: Encourage the patient to take deep breaths, provide supplemental oxygen, inhaling of smelling salts like aromatic salts of ammonia and applying pressure over the lower chest helps.
I) APPREHENSION:Attention to premedication is important
in prophylaxis.
J) DIFFICULT SPINAL PUNCTURE.
K) TRAUMATIC SPINAL PUNCTURE:Repeated attempts to achieve a spinal
tap may result in direct trauma to the nerves, the periosteum of the vertebra and to the intervertebral discs. Paraesthesia is noted and may persist. Transient or permanent neurological deficits may ensue.
L) BROKEN NEEDLE OR CATHETERS:Management: Removal of the needle
fragment should be attempted as soon as possible. The proximal part of the stylet should if possible be left in space to serve as a guide to the distal part. If the catheter breaks, it should be noted and the neurosurgeon informed. It is seldom justified to carry out an exploration.
Post operative or late complications of spinal anaesthesia1) POST DURAL PUNCTURE HEADACHE:
It is postural, beginning within 6 to 12 hours after lumbar puncture (but may take 3 days), often occipital and is associated with pain and stiffness of the neck.
Mechanism: It is related to the persistence of dural puncture, with leakage of CSF into surrounding soft tissues leading to lowering of the CSF pressure. This exerts downward traction on the structures of the CNS and on the blood vessels that are attached to the dura and the cranium as well as the brainstem. The result is a headache similar to acute vascular cluster headache Increased incidence is noted
• In young and female patients.• In pregnancy• If needle size is large• With the midline approach• Increased concentration of glucose
Differential diagnosis - Migraine,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 166 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
meningitis, tumour, dehydration, hyponatremia. Management:Avoid in unsuitable patients, with frequent headache.
• Use of fine needles• Prevention of dehydration, strain,
coughing.• Choice of needlepoint: Whitacre, Sprotte
• Epidural blood patch
2) BACKACHE:Due to obliteration of lumbar lordosis and
stretching of ligaments, reflex muscle spasm, positioning and small haematomas. Management: A small pillow under the lumbar region reduces the incidence of backache. Skeletal muscle relaxants and analgesics, reassurance and heat will usually rectify the problem.
3) MAJOR NEUROLOGICAL INJURIES:Cranial nerve disturbances: Paralysis of
every cranial nerve except 1,9 and 10 has been reported.
The primary cause of this is due to CSF dynamics consequent to lumbar puncture. It is basically the same as the cause of headache.
Abducens nerve palsy - it has the longest intracranial course and is more vulnerable to dynamic changes in the CSF.Symptoms: Internal strabismus, blurring, diplopia and difficulty in focussing.Management: 50% cases recover within 1 month, if condition persists, dark glasses may be worn.
Urinary retention: Blockade of S2-S4 is associated with loss of bladder tone and inhibition of voiding reflex leading to overfilling of bladder. Even after resolution of blockade, voiding may be difficult. These problems are more common in male patients and in extreme cases can result in neurogenic bladder requiring intermittent catheterisation.
For prolonged Central Neuraxial Blockade, it is probably wise to avoid this problem by inserting a bladder catheter.
Cauda equina syndrome: - Characterised
by abnormalities of leg reflexes, incontinence of faeces, retention of urine, loss of sexual function, sensory loss in the lumbo sacral plexus distribution and a temporary paralysis of peroneal nerves. Most of them clear spontaneously.
Traction nerve paresis or paralysis; lithotomy position and stirrup pressure may produce peroneal nerve palsies,
4) MENINGITIS OR ARACHNOIDITIS:This may occur even with a seemingly
flawless technique. Aseptic meningitis has been reported.
Contamination with chemical antiseptics, starch powder of gloves, detergents, higher concentration of drugs and variation in pH has been blamed. The need remains for careful adherence to an aseptic technique.
5) ANTERIOR SPINAL ARTERY SYNDROME:Due to spinal cord ischaemia, due to
severe hypotension.
6) VASCULAR INJURY:In patients with coagulation disorders or
on anticoagulants.
COMPLICATIONS OF EPIDURAL ANAESTHESIA: a) Inadvertent dural puncture:
It has been recommended that when this occurs, plan for epidural anaesthesia is stopped and simple spinal / GA is administered. Objective studies indicated that this is unnecessary and we can go for epidural in another inter space or can opt for continuous spinal anaesthesia.
b) Total spinal:Due to accidental sub arachnoid
injection.
c) Neural damage:The incidence is low, but the neurological
deficits are due to trauma, anterior spinal artery syndrome and epidural haematomas.
d) Hypotension:The degree of hypotension is less in EA
than SA, because the onset of action of local
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 167 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
anaesthetic drugs in epidural is delayed and by that time adequate preloading is done so that the incidence and degree of hypotension is reduced.
e) Urinary retention:
f) Toxicity:As relatively large doses of local
anaesthetic drugs are required for EA, and epidural space contains numerous venous plexus, which may be penetrated by epidural needle or catheter, there is more chance of local anaesthetic toxicity with EA.
g) Catheter complications:It may be inserted directly into the blood
vessel or subarachnoid space or breaking of the catheter in the epidural space may occur. No attempt is made to withdraw the catheter through the needle.
h) Failure:
i) Epidural abscess:Following SA or EA, abscess formation
is superficial requiring limited surgical drainage and intravenous antibiotics.
j) Effect of rapid injection:Sensation such as headache, vertigo,
and paraesthesia may be seen when the anaesthetic solution is injected rapidly, as rapid injection increases the CSF pressure. This effect lasts for 3-5 minutes, during which headache is prominent.
RECENT ADVANCES IN REGIONAL ANAESTHESIA
Over the last two decades, there have been considerable innovations in materials, drugs, and techniques of central neuraxial blockade, which have contributed to improving the quality and safety of central neuraxial block. The following are a few of them.
Equipment:1. Use of 25 G epidural needle systems with a modified tip lowers the incidence of post dural puncture headache in the event of an unintentional dural puncture and causes less tissue trauma.
2. The limiting factors for the use of smaller gauge spinal needles are reduced back flow of CSF and decreased tensile strength. But new manufacturing has increased the internal diameter of small gauge needles as well, improving the back flow without a notable decrease in tensile strength. Some needles taper from a 22-gauge shaft to a 24 gauge tip.
3. Another development in neuraxial block technique is the development of effective methods of combining epidural and spinal anaesthesia via a single needle system.
These methods use epidural needle placement followed by insertion of a spinal needle through either a side lumen on the epidural needle, or directly via the epidural needle lumen. This combined technique allows flexibility in a number of clinical settings.
Techniques:1. VERIFICATION OF NEEDLE AND CATHETER INSERTION:
More recently, techniques to aid in location of the epidural space have been reported including the use of1. Auditory amplification of the sound made by the epidural needle as it traverses the interspinous ligament and ligamentum flavum.
• Doppler guidance and• Pressure transducer methods
2. Use of fluoroscopic guidance for epidural needle placement and injection of non-ionic radiopaque contrast solution through the epidural catheter producing the typical epiduralgram appearance. This may also be used to confirm epidural needle (or) catheter placement.
3. Recently low current electrical stimulation resulting in truncal (or) limb motor responses is regarded as a simple, objective and reliable technique for confirmation of epidural catheter placement.
II.EPIDURAL RADIOGRAPHS AND EPIDUROSCOPY: -
Use of epidural radiographic techniques and epiduroscopy have enhanced the knowledge of anatomic characteristics and fluid dynamics within the epidural space & the effect of previous epidural anaesthetic procedures on the cephalad
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 168 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
spread of sensory block during lumbar epidural anaesthesia.
It was noted by epiduroscopy that patients with a history of previous epidural anaesthesia had aseptic inflammatory changes within the epidural space such as, narrowing of epidural space, proliferation of connective tissue and adhesions between the duramater and ligamentum flavum. These changes are responsible for the reduction in cephalad spread of sensory blockade in patients with previous history of epidural anaesthetic producers.
III. METHODS OF DETERMINING THE EXTENT OF EPIDURAL ANAESTHESIA:1. Skin vasomotor reflex testing, using changes in skin blood flow, as measured by laser Doppler, in response to tetanic electrical stimulus.2. Somatosensory evoked potentials in response to electrical and argon laser stimulation have been used to determine the extent of sensory neural blockade during EA & SA.
IV. ANAESTHETIC TECHNIQUES:1. Unilateral epidural analgesic techniques: Insertion of epidural catheters using fluoroscopic guidance has demonstrated the relative ease with which catheters may be directed within the epidural space through changes in location and bevel orientation of the epidural needle and producing unilateral epidural analgesia.
Technique: - Selectively, relatively unilateral distribution of analgesia may be obtained through a technique involving slight angulation (approximately 5 degrees in the horizontal plane) of the epidural needle towards the intended side of location and orientation of the needle bevel between 45 degrees and 135 degrees from the cephalad direction laterally. With this needle location and bevel orientation, the epidural catheter tip is directed to lie in the lateral epidural space.
2. The technique of postoperative epidural administration of 20ml of normal saline hastening the return of motor function from EA has been described. This is related to a dilutional (washout) effect, an ion trapping effect produced by the injection of saline with a relatively low pH and increased uptake of local anaesthetic by greater
area of distribution.
3. Anaesthesia for Ambulatory surgery: Ambulatory surgery demands good surgical anaesthesia with rapid recovery from sensory and motor block & recovery of the ability to void. As lidocaine has been questioned with the possibility of neurotoxicity, hypobaric, hyperbaric and near isobaric bupivacaine solutions are used for ambulatory surgeries.
4. Patient controlled analgesia: Use of microprocessor controlled epidural infusion pumps, with patient activated dosing capability, has become the postoperative pain management technique of choice, as compared with intermittent bolus dose administration method. With this PCEA, it has been noted that there is overall reduced dose requirement and patient satisfaction.
5. Mobile epidurals have already gained popularity in the field of obstetric analgesia as they allow normal mobility with high quality of pain relief.
6. Central neural blockade in children is providing excellent intraoperative and postoperative analgesia. The paediatric regional anaesthetic techniques are greatly reducing the morbidity associated with surgery and anaesthesia in selected groups of patients and can favourably influence the postoperative course.
Drugs: -1. Separation of stereoisomers allowed the development of improved local anaesthetics for safer use, e.g.: Ropivacaine & levobupivacaine which are S.enantiomers of bupivacaine. It has been demonstrated that they have potency almost similar to bupivacaine (less with ropivacaine) while exerting significantly less CNS & CVS toxicity.
2. The most exciting new development in Central Neuraxial Block is the introduction of novel analgesic drugs (nonopioid, nonlocal anaesthetic), analgesic adjuvant medications, and new epidural anaesthetic and analgesic formulations eg.adenosine, midazolam, verapamil, ketorolac and others which are in various stages of clinical (or) preclinical study for
RACE 2003 Ramachandra Anaesthesia Continuing Education
Central Neuraxial Blockade 169 D.Anil Kumar, S.K.Arif Pasha & Rani Manjusha
possible spinal analgesic utility.
3. Novel drug formulations and epidural delivery systems may soon include the use of liposome- encapsulated local anaesthetics (or) opioid analgesics capable of, producing an extended duration of analgesic effect from a single epidural dose.
CLINICAL CONTROVERSIESInspite of the many years that neuraxial
blockade techniques have been used, there remain a number of controversies about the appropriate use of these techniques.
1. Related to systemic toxicity of local anaesthetics and premedication.
Inspite of the widely held belief that benzodiazepines should be used with regional anaesthesia to minimize systemic toxicity as they elevate the seizure threshold, it has been shown that benzodiazepines cover up one of the early signs of systemic toxicity (i.e., seizure). Thus resuscitation may be more difficult after cardiovascular collapse, delaying potentially the definitive therapv.
2. Most controversy surrounds the use of epinephrine in obstetric patients in which uterine blood flow may be decreased by intravascular injection there by putting the foetus at risk, but many anaesthesiologists believe epinephrine - containing epidural test doses are useful in obstetric anaesthesia.
3. Some continue to suggest that spinal anaesthesia is inappropriate for out patients because of the occurrence of post dural puncture headache, yet there are data that the occasional headache can be successfully treated even in the out patients and considerable other data are available supporting the use of this technique in out patients.
4. The use of epidural anaesthesia for patients receiving anticoagulants is less clear because epidural anaesthesia is often avoided in these patients but there are studies, which used continuous epidural anaesthesia in vascular operations, in patients receiving preoperative oral anticoagulants without any problem. The acceptable magnitude of preoperative anticoagulation and risk benefit ratio of performing epidural anaesthesia remains undetermined by this time.
The time duration accepted between anti coagulation prophylaxis and Central Neuraxial Block is as follows:
• Low molecular weight heparin-12 hours after the last dose and the same rule applies for the insertion and removal of the catheter.
• Heparin infusion- 4 hours after the cessation of the infusion.
• Warfarin intake- An INR of less than 1.5 is accepted for performing Central Neuraxial Block. Again, it is the element of risk benefit ratio to be kept in mind when such patients are subjected to Central Neuraxial Block
REFERENCES:Anatomy for anaesthetists - Harrold Ellis, Stanely feildman, 6th editionPrinciples of anaesthesiology- Collins, 3rd edition, 1993Indian journal of anaesthesiology Dec 2001 45(6), 414,430Pharmacology and physiology in anaesthetic practice- Stoelting, 3rd edition 1999 Pharmacological basis of therapeutics - Goodman and Gillman Anaesthesia by R.D Miller, 5th edition Lee synopsis of anaesthesia- 13th edition Anaesthesiology clinics of North America - June 2000.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 170 Trivandrum Medical College
INTRODUCTIONThe prone position is also called
‘concorde’ position, ‘face down’ position or the position wherein the ventral surface of the body lies on some surface supporting the body weight. In the Classic prone position the face, chest, abdomen, front of thighs, knees, toes and some surface of hands and arms all touch the supporting surface. People sleep in this posture using crooked arms to hold the face off the bed to prevent pressure on nose.
Patients under GA - Problems :1. Body weight against abdominal wall leads
to decreased diaphragmatic movement and decreased tidal volume
2. Increased intra-abdominal pressure causes decreased venous return
3. Pressure on toes and bony prominences can cause pressure injuries
4. Care must be taken in keeping the head in safe relation with the rest of the body
MODIFICATIONS OF PRONE POSITION :1. Jack knife position :This is used for anorectal surgeries. The patient lies on a flexed operating table with pelvis at the flexion point. Surgical field is clearly visible and the abdominal viscera move cephalad in response to gravity. Arms are beyond the top of the head and face turned to one side.
2. Knee-chest position : This is an exaggeration of jack knife position. Knee and chest are supported, Neck is extended and face turned to one side. Gynaecological examination is facilitated. Uterus and other viscera fall ventrally and cephalad.
3. Buie position : This is a modification of the prone position providing satisfactory exposure
for proctological work. The patient kneels on a wide padded shelf, bends forward over a 90 degree table, placing his chest on the table proper. When the table is tilted into a head down position, gravity moves viscera and venous blood away from the perineum. The operative field exposure is good, blood loss is minimal, proctoscopy greatly simplified and the patient is in a reasonable position for either hypobaric spinal or caudal anaesthesia.
4. Georgia position This is a modification of the knee- chest position. The patient’s weight is supported on his knees and chest. The knees are on a shelf, chest is on a stack of folded sheets. The height of the knee support and the height of stack of sheets are adjusted to leave abdomen free of pressure. Good exposure for perineal and rectal work is obtained, if table is tilted head down.
5. Smith’s recent modification of Georgia position: In this position specially built supports are used to raise the pelvis to a height sufficient to leave abdominal wall completely pressure free. The chest is elevated by stack of folded sheets. The chest and pelvis are elevated, usually to the same height
6. Overholt position : This is used for surgical management of specific thoracic problems to prevent drainage of infected material and blood from the involved lung into the other lung in the course of surgery. Now minimally used since double lumen tubes are available. Exception is a small child whose airway is too small to accommodate the double lumen tube. However, in such a case bronchial blockers can be used rather than Overholt position.
7. Sellor-Brown position : In this position placing the lower part of body, including abdomen
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 171 Trivandrum Medical College
are placed in one plane and the chest, neck and head are on a lower plane. Intent is same as that of the overholt position i.e. to drain blood and infected material from the uninvolved lung.
8. Crouching or ‘carpenter’s rule’ position :In this position knees and hips are flexed
maximally. Patient’s weight rests on the back of the legs. Abdomen on the front of the thighs, back is flexed well to eliminate the lordotic curve. Problems associated in this position are possible knee injury, femoral vein obstruction, free abdominal movement restriction.
INDICATIONS FOR THE PRONE POSITION:1. Spine surgeries like laminectomy, spinal
fusion, scoliosis correction2. Posterior cervical and occipital surgeries3. Adrenal exploration and renal biopsies4. Thoracotomy by posterior approach5. Surgeries on the back of the leg eg.
Varicose vein stripping, tendon repair6. Prone ventilation for ARDS
CONTRAINDICATIONS:1. Patient with contused heart2. Crush injury to the chest3. Full flail chest4. Severe pectus excavatum
TECHNIQUE OF POSITIONING:Turning the anaesthetised patient is
potentially dangerous because1. The autonomic compensatory mechanisms are obtunded by the anaesthetic agents2. There is no muscle tone to protect the joints
Principles:1. The patient should be anaesthetised & turned on the operating table. Trying to control the patient at arms length across the bed is highly inefficient2. The patient is more safely turned if he is very lightly anaesthetised and paralysed. The cardiovascular response to stimulation should be hypertension , not hypotension. This is possible, if he has a functioning vascular control mechanism to oppose the effects of gravity. Heavy premedication with narcotics and deep anaesthesia obtund this mechanism and cause hypotension.3. Before turning -
a. The head end of the table is depressed by 5 -10 degrees. In the head down position, the venous return from lower 2/3rd of the body is maintained even if the upper 1 /3rd of the body is elevated for the turn.b. The anaesthesiologist should manage the head and neck,unless there is a cervical spine fracture . If the neck is unstable, neurosurgeon help should be sought.c. Avoid injury to eyes by the clamps or other objects.d. Avoid damage to intravenous (IV) infusion systems. Use the arm that will be on top of the body as the preferred infusion sitee. BP apparatus should be ready for an immediate measurement after positioningf. The anaesthesiologist directs the turning and must arrange to disconnect the patient from the breathing circuit for the shortest possible period of time4. Skill is more important than strength. Everyone should know what they have to do and how to do it safely.5. The steps involved in positioning the patient are:a. Move the patient towards one side of the table and roll him up onto one side. Two persons should make the lift from back to the side one at his shoulders, one at his hips, both parts to be moved at the same speed. Anaesthesiologist keeps the face in the proper plane. Now the patient is in the lateral decubitus position with one arm under the body and upper arm close to his uppermost side. At least one person should receive the body on the other side of the table.b. Patient now is rolled into 3/-«?h prone position. The underarm is freed of his weight, moved to a position behind him and lowered over the side of the table (without stress on the shoulder). The upper arm is swung forwards to hang free over the other side of the table.c. The hips and the shoulders are lifted back towards the starting edge of the table to return the patient to the middle of the table.d. As the turn is completed, the person controlling the shoulders has an arm under the chest pulling the patient back towards the middle of the table. This person should continue to hold upper part of the patient off the table while anaesthetist gets the head in a safe position, reconnects the breathing circuit, ventilates the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 172 Trivandrum Medical College
patient vigorously for a few breaths and measures blood pressure (BP). After that the supporting arm can be removed from under the chest.e. Now the patient is prone with the head turned to one side, both arms hanging down besides the operating table.f. Any modification of prone position can now be effected.g. After all the movements are completed bring the table back to the horizontal position.
Light plane of anaesthesia, head down tilt etc will decrease the tendency for hypotension. Paraplegics and quadriplegics require IV vasopressor drugs before the turn to avoid severe hypotension. Careful handling during turn decreases the likelihood of injury to the back, neck, shoulders, elbow, wrists and face. Turning requires an anaesthesiologist and at least 3 capable persons !f the patient is very obese additional help may be needed.
PHYSIOLOGICAL EFFECTS: 1. Cardiovascular System (cvs)a. Pressure on the inferior vena cava (IVC) and femoral vein cause decreased venous return and hypotension.The engorged epidural venous plexus cause increased intraoperative blood loss. Avoidance of pressure on the IVC are accomplished by Relton-Hall and Andrews variants of spinal surgery frames.b. Hypotension secondary to spinal, epidural or deep general anaesthesia (GA)c. If the body is properly supported on the chest wall, impairment of cardiac efficiency will not occurd. If the patient is grossly obese it is better to turn the patient into that position during his preoperative visit to see the effect on BP. Those positions which make the patient faint, nauseated or develop headache are to be avoided as these may be the symptoms of hypoxia or hypotension or both.e. Avoid pressure on the carotid sinus when the head is turned to one side as serious arrythmias and hypotension may develop. Pads, rolls can be used to keep the head stablef. The venous return from the head must not be obstructed as engorged (eye vessels, eyelid oedema, post operative headache and even subglottic edema can result.g. Blood supply to the brain must be protected. Severe twisting or extension of neck may impede flow through the vertebral artery.
2. Respiratory system:The abdominal wall should be free to move.
Less airway pressure is required to ventilate obese patients in the prone than supine, as weight of chest and abdomen wall does not have to be lifted. If abdominal wall is not free in prone position, the patient will hypoventilate. Also with every inflation of lung, the entire back will rise. Surgery will be affected on a moving target. Even with perfect positioning upper back will move detectably with artificial ventilation but the upper body weight on the sternum will limit it’s movement. However, back from T 10 down can be kept still, if the patient is properly positioned. Patient’s thorax and pelvis should be raised by supports. In grossly obese patients, lateral decubitus position might be an easier choice.
Now, prone position is utilised to treat ICU patients in acute respiratory failure. Unrestricted abdominal movement is essential. A hand should pass between abdomen & bed.Patient positioned prone with proper support from the supine position, showed market increase in the oxygen tension for the same tidal volume, Fi02and PEEP.
COMPLICATIONS: 1. Neurological Injuries:
Neurological injuries may result from pressure against bones, against hard substances in the operating area, or due to stretching.a. Eyes may be injured during turning or may suffer protracted pressure in the prone position.b. Brachial plexus injury can occur by stretching, during turning or by pressure from an improperly placed support.c. Facial nerve injury can occur by pressure over the infraparotid regiond. Jack knife position may injure the femoral nerve.e. Lateral femoral cutaneous nerve injury can occur while compression against the supporting mechanisms under the pelvis resulting in a symptom complex called meralgia paraesthetica.f. Injury to the nerves and the tendons of the dorsum of foot can occur if the foot rests against the metal edge of the tableg. Ulnar nerve is at risk of injury against sharp edges of supporting devices when the arms are positioned above the head. Flexion of the elbow makes the danger more acute.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 173 Trivandrum Medical College
h. While turning the patient, the hips and shoulders should be on the same plane at all times because improper turning of anaesthetised patient involving relaxation of musculature can result in spine injury.
2. OTHER INJURIESa. Male genitalia should be protected. Precaution are necessary so that electrocautery, grounding plate should not touch them.b. In the female, care must be taken so that the breasts are padded well. Large breasts, can usually be moved laterally, so that the patients weight do not injure themc. Ears must not be folded over and held there by the weight of the head as the elastic cartilage are readily damaged and slow to heal. So pad the ear as well.d. Neck should be turned only after flexion. Turning an extended head leads to protracted neck muscle spasm and headache post operatively (due to pressure on C2 nerve while emerging between the atlas and the axis)e. Skin overlying the bony prominences such as the iliac crest must be protectedf. Toes should be protected from pressure injury using pillows under the anklesg. Air embolism is a risk in any surgical position in which the operating field is higher than the heart, permitting open veins for air entry.h. In moving the patient’s arms from besides the body to beyond the top of the head, the arms are first lowered towards the floor and then swung upwards carefully in a natural arc so as to rest beyond top of the head. Such care prevents shoulder dislocation, brachial plexus injury and tear of ligaments and tendons.i. Nasotracheal tubes must be positioned to avoid pressure on nasal cartilage in the anterior margin.j. Eyes must be protected with no pressure on them. Orbital compression can cause retinal ischaemia leading to blindness. Eyes are to be examined very frequently, and must not be kept open. Head movements may alter the relationship between the eyes and the head support and can cause pressure injury resulting in blindness. To prevent head movements, stabilise it using skull pins in a rigid holder.k. Chest supporting devices must not block the venous return from the neck.lt should be
possible to pass a hand between the base of flexed neck and chest support.I. Injuries to the joints can occur, while turning from supine to prone or, back from prone to supine, m. Varying degrees of pressure necrosis of maxillae and forehead can occur in prolonged spinal procedures.n. In cervical and posterior fossa procedures, flexion of the patient’s neck causes decreased anteroposterior dimension of the hypopharynx that leads to compression ischaemia of base of tongue, macroglossia and unexpected post extubation airway obstruction
3. Accidental extubation:In the prone position there isa. Poor access to the airwayb. Traction from the head movements due to bone drills or saws and also traction from the circuit itself.c. Loosening of the adhesive tapes used to secure the tubes which can be sweated or salivated loose.
SUPINE POSITION
PHYSIOLOGICAL CHANGES IN NORMAL CONCIOUS HUMAN SUBJECT ON CHANGING FROM THE ERECT TO THE SUPINE POSITION
1. Cardiovascular system(CVS) :Human arterial blood pressure remains
within the normal ranges throughout a variety of changes in body position. The principal factors maintaining relatively unaltered systemic blood pressure(BP) on assumption of supine position from erect are,a. Venous and arterial reflexes :As the body shifts from the erect to the supine position, venous return to the heart increases because sympathetic and parasympathetic tone of splanchnic and peripheral arteriolar and venous vessels decrease.This causes increased right atrial filling, increased right ventricular stroke volume, increased pulmonary circulation, increased left ventricle (LV) stroke volume and increased heart rate. This cardioacceleration was attributed to baroreceptors in the great veins and right atrium (Bainbridge 1915). This response is prevented by bilateral vagotomy.b. Pressorecepetor reflexes and autonomic control.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 174 Trivandrum Medical College
The raised cardiac output caused by increased venous return on assuming the supine position, initially tends to increase the arterial BP. Carotid and aortic baroreceptors are stimulated via nerve of Hering to IXth cranial nerve and via vagus respectively to the vasomotor centre and cardiac centre of medulla. From these centre, efferent parasympathetic impulses travel via the vagus to the heart and act on the sinoatrial (SA) node and myocardium. This diminishes the heart rate,stroke volume and decreases the strength of myocardial contraction. Also efferent sympathetic discharge to the heart is decreased and hence decreased heart rate and myocardial contractility.c. Ward and Korner studied the combined reflex effects on changing from the erect to the supine position ,1. MAP, heart rate and peripheral resistance
decreased2. cardiac output and stroke volume increased3. Systolic BP remained the same while
diastolic BP decreased so there was widening of pulse pressure.
2. Respiratory system:a. Pulmonary ventilation: Expansion of the lung during normal quiet inspiration is mainly due to the downward movement of the diaphragm and to a lesser extent by the bucket handle outward movement of the ribs. In the supine position, the abdominal contents limit the diaphragmatic excursion and force the diaphragm cephalad thus decreasing functional residual capacity (FRC) and total lung capacity (TLC). The posterior part of the diaphragm is forced cephalad more than the anterior part owing to the gravitational effect of the abdominal viscera. They are therefore stretched to a greater length and is capable of greater shortening. So, more ventilation of the adjacent posterior segments at the lung base. This has the advantage that dependent lung regions are perfused preferentially, this preferential ventilation makes for more efficient gas exchange.b. Pulmonary circulation: Alveolar capillaries tend to collapse when the external pressure within the alveoli exceeds the internal pressure within the vessels. It occurs more in the apex of the lung in either supine or erect position. The effect is a differential perfusion of the lung at the base than at the apex. This can be explained by dividing the lung into 3 zones.
Zone 1 : At apex pA>pa>pv : no blood flow Zone 2 : pa>pA>pv : flow determined by arterio- alveolar pressure difference Zone 3 : pa>pv>PA: flow dependent on arteriovenous pressure difference Where pA-alveolar pressure
pa-pulmonary arterial pressure pv- pulmonary venous pressure
With the patient in the supine position, the anterior part of the lung lies above the left atrium and the plane from the hilum to the base of the lung lies at the level of the left atrium and these parts function as Zone 2. Posterior part of the entire lung from the apex to the base becomes Zone 3.c. Closing volume increases, FRC decreases.
3. Other systems:a. Blood volume : On changing from erect to supine position, a significant decrease in packed cell volume (PCV) occurs in 5 minutes, maximal decrease of 10 to 20 percent of the erect value at 20 minutes. Also a lowering of serum calcium (7%); total protein (9%) and albumin (6%), PBI (16.3%), cholesterol & triglycerides.b. Renin angiotensin aldosterone axis: There is increase in blood volume and BP decreases. Renin causes decrease in aldosterone secretion and so a 25% increase in sodium excretion.c. Oesophageal sphincter tone decreases.
VARIANTS OF SUPINE POSITION LITHOTOMY POSITION
It is the position in which the patient is on his back with the legs and thighs flexed to right angles.
Indications:Perineal, rectal .vaginal and urological operations
History:William Jones first described the position
in 1839.
Technique of Positioning:First the patient is placed supine with the
gluteal folds at the caudal table break. Anaesthesia is instituted then. The patient’s arms are restrained appropriately by taping the arm
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 175 Trivandrum Medical College
containing the IV needle to an arm board and by wrapping the arm containing the BP cuff in a sheet to the patient’s sides. Now the patient’s legs are elevated together, flexed together and positioned in stirrups. The stirrups can be either of the ankle strapped variety or a part of the total leg support system. Knee supports are rotated medially to facilitate the rotation of the thigh. Thighs are flexed about 90 degrees to the abdomen. Then outward rotation of thigh is accomplished by abducting the knee brace and rotating the thigh by rotating the supporting rods cephalad, flexing the thigh onto the abdomen. Care is taken to cushion the ankle and knee against pressure from metal stirrups.
Disengagement of the Paitent after the procedure:
Stirrup rods with the legs should be brought together to a relatively neutral plane relieving the flexion , abduction and rotation components . Legs lifted and lowered together slowly to avoid a sudden decrease in cardiac output.
Complications1. Venous stasisAny patient placed for more than 15 minutes in lithotomy position should have their legs protected by elastic stockings2. Peripheral nerve injuries:-a. Obturator nerve (L 2,3,4) -Acute flexion of thigh to the groin may result in nerve compression and trauma leading to weakness or paralysis of the adductors of the thigh .b. Saphenous nerve- Sensory to the medial portion of the leg. Legs may get compressed to the medial aspect of the knee brace leading to loss of sensation to the medial aspect of leg.c. Femoral nerve- Injured by acute thigh flexion with angulation against the underlying surface of the pubic ramus. Manifests as abnormal gait and numbness or paraesthesia.d. Common peroneal nerve- L4,5 S1,2 Injured by pressure at the head of fibula. Results in weakness of intrinsic muscles of foot and sensory loss in sole of foot. Foot drop due to palsy of Tibialis Anterior.3. Damage to the hip and knee especially of elder women.4. Injury to the hand and fingers when the caudal portion of the table is lowered .
VARIANTS OF LITHOTOMY POSITION:1. For combined vaginal -abdominal approach to pelvic viscera. Leg elevation is less and flexion of thigh to abduction is less than 90 degrees.2. Walcher position for obstetrics: Thighs pressed firmly onto the trunk and legs kept dangling.3. ForTURP (Blandy’s position): Here the legs are supported in such a way that the thighs create an obtuse rather than an acute angle with the body.
Physiological Changes:1. RESPIRATORY SYSTEM:a. The vital capacity- decreases by 18 % ,the reason being restriction of the movement of diaphragm as well as restriction of volumetric expansion of lungs because of increased pulmonary blood volume.b. Increase in the postoperative respiratory complications due to paralysis of the abdominal wall muscles with resultant inability to cough forcefully during spinal or epidural anaesthesia.c. Tidal volume decreases by 3%d. FEV1 increases by 9% due to the weight of abdominal viscera and flexion of the thighs on abdomen acting as a belt to improve the resting position of diaphragm which increases the inspiratory reserve and added force to maximum expiratory effort.
2. CIRCULATORY SYSTEM:Lower extremities are major
reservoirs of blood. Sudden lowering can cause significant lowering of BP So slow and deliberate lowering of legs should be done in a light plane of anaesthesia.
THE TRENDELENBURG POSITION Introduction:
Historically , the Trendelenburg position describes a supine patient whose head is lower than his heart and whose legs and pelvis are elevated to facilitate surgical access to the lower abdomen and pelvic viscera. Friederich Trendelenburg used this position for urological procedures as early as 1870. The position was originally achieved by placing the patients knees over the shoulders of an orderly while Dr.Trendelenburg operated.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 176 Trivandrum Medical College
Trendelenburg position today implies a head down tilt so that the head is below the horizontal plane. The head down tilt may be anywhere between 1 and 45 degrees, the most common being 10 - 20 degrees tilt.
Advantages:1. Improvement in exposure of the surgical field for pelvic or lower abdominal surgery2. With the surgical field positioned superior to the rest of the body, arterial perfusion pressure at the site of operation is lowered, resulting in less bleeding. Also shed blood falls away from the surgical field enhancing surgeons visualisation. Thus surgical time is decreased.3. Trendelenburg’s position causes engorgement of dependent neck veins thus facilitating the IV placement of needles or catheters.4. Protection of trachea from regurgitated material since they drain by gravity into the more dependent pharynx. So a steep Trendelenburg position might be selected for crash induction to a patient with full stomach.
Disadvantages:1. Displacement of abdominal contents into the surgical field with ventilatory excursions due to rigorous IPPV.2. Tendency of the position to mask unrecognised blood loss through it’s enhancement of central venous return of blood and a preserved cardiac output.3. Cyanosis of the patients face secondary to venous engorgement which makes evaluation of cardiovascular and respiratory status during anaesthesia more difficult.
Anaesthetic Considerations:1. x RESPIRATORY SYSTEM:a. Increase in work of breathing- Abdominal contents are pushed cephalad against the diaphragm so that the diaphragm not only must ventilate the lungs but also lift the abdominal contents .So in obese patients, the added weight of abdominal contents and the weight of the chest wall further decreases compliance and increases the risks of atelectasis and hypoxemia.b. Pulmonary compliance and FRC are decreased - Increase in the pulmonary blood volume and gravitational force on the mediastinal
structures being the causesc. Vital capacity decreasesd. Increase in pulmonary congestion and pulmonary oedema-ln steep Trendelenburg position , most of the lungs becomes zone 3, as most of the lung then lies below the left atrium. In zone 3 , an excessive increase in LAP over the alveolar pressure will enhance fluid transudation into the alveoli increasing pulmonary congestion leading to pulmonary oedema. Hence patients with chronically elevated LAP as in Mitral stenosis tolerate this position poorly.
2. CARDIOVASCULAR SYSTEM:. When the patient is put in the Trendelenburg position, the following things happen .There is autotransfusion of 500-1000 ml of blood from the lower extremities to the central circulation. This increase in volume of blood is pumped from the heart manifesting as an intial increase in cardiac output. There is an increase in the hydrostatic pressure in the arch of aorta and carotid bifurcation. Stimulation of the baroreceptors causes a generalized reflex vasodilatation. This causes decrease in stroke volume,cardiac output and decreased perfusion to vital organ. In a patient with heart disease, this added volume in the central circulation and increased pulmonary blood, flow may cause heart failure.
3. CENTRAL NERVOUS SYSTEM:This position produces an increase in the
intrathoracic pressure thus increasing the central venous pressure leading to an increase in the CSF pressure. At the same time this position decreases cardiac output by sino-aortic reflex thus decreasing cerebral blood flow. Too aggressive use of IPPV to expand the lung will further decrease cerebral blood flow and dangerously increase the CSF pressure while insufficient ventilation will increase the PaC02 which in turn increases CBF and intracranial pressure(ICP).
Technique of positioning:First the patient is placed supine with the
knees placed at the leg section hinge of the table. The operating table mattress must be fixed to the table with adhesive tapes. Ankle straps are secured at the foot of the table with proper
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 177 Trivandrum Medical College
padding of the ankle to protect pressure points .IV cannulae are securely placed and the patients arms are restrained across the chest or placed at the sides taking care to protect the pressure points on the radial and ulnar nerves and that the angle of the arm to the body is less than 90 degrees.
After the patient is anaesthetised, the table is tilted to the desired plane. Concomitantly, the leg piece of the table may be dropped so that the patients knees flex 90 degrees or less. A slight flexion of the hips and small pillows placed under the lumbar and cervical areas may prevent pressure pains and ligament strains. The position of the endotracheal tube should be reconfirmed once the Trendelenburg position has been achieved as the mediastinum may shift cephalad , causing an endobronchial intubation.
If Trendelenburg is combined with lithotomy position, steps are essentially the same except that the feet are placed in stirrups or the legs in leg holders prior to tilting the table. Care should be taken to see that the angle of the thigh with the body is not less than 90 degrees. This position ensures good venous return from the legs.
Disengagement of the Patient:After the procedure, the patient is slowly
returned to the horizontal position, legs slowly straightened allowing for a gradual shunting of central blood volume back into the lower extremities. This will decrease the incidence of sudden hypotension.
Complications:1. Hypotension due to baroreceptor mediated generalized vasodilatation and decrease in cardiac output. These c#n predispose to cardiac arrythmias.2. Venous air embolism by air entrainment into the open pelvic or abdominal veins can occur.3. This position may hide unrecognised blood loss4. Increase in cerebral venous pressure can cause venous thrombosis of cerebral blood vessels, retinal detachment and cerebral oedema.5. Accidental endobronchial intubation.6. Nerve injuries (brachial plexus, superficial peroneal nerve, ulnar and radial) can occur.
Patient in Fracture Table:INDICATION Femur fractures.
This table has a body plate which supports the head and the thorax, a sacral plate for the pelvis, adjustable foot plates and a perineal post. After anaesthetising the patient, the patient is transferred to this table taking care to protect the genitalia against pressure from the perineal post and fibular head protected to avoid pressure on peroneal nerves. Care should be taken to avoid injury to arms, axillary neurovascular bundle and cervical spine.
Lateral Decubitus positionINTRODUCTION
Fron Latin means act of lying on one’s side .The position is conventionally referred to as right or left lateral.INDICATIONS:1. Thoracotomya. Lung surgeries - pneumonectomy, lobectomy, decorticationb. Cardiac surgeries- PDA ligation, CMVc. Mediastinal surgeries- Thymoma, neurogenic tumours2. Laparotomy
In carcinoma of gastrointestinal tract(GIT), strictures, diaphragmatic hernias3. Urological surgeries
Pyeloplasty
HISTORY:Thorek in 1913 described this position for
oesophageal resection for a case of carcinoma oesophagus.
TECHNIQUE OF POSITIONING:
EFFECTING THE LATERAL DECUBITUS POSITION
After induction of anaesthesia and securing all IV and electrical circuits, the patient is turned from supine to the lateral decubitus position . The back should be perpendicular to the end of the table, epigastrium at the level of the kidney rest, the thigh of the dependent lower extremity is flexed upon the trunk to stabilize the pelvis and the knee is flexed. The nondependent lower
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 178 Trivandrum Medical College
extremity is kept straight. Two pillows are placed between the two lower extremities to minimize pressure points. Now the patients trunk is stabilised in the manner that will prevent it’s rolling either forward or backward. Similarly the thighs and buttocks are also stabilised by taping to the sides of the table.
Both forearms are flexed at the elbow and kept out of the operating field and a pillow is kept in between . Another pillow is kept below the dependent axilla to prevent compression of the neurovascular bundle. Excessive abduction on the arms should be avoided to prevent brachial plexus injury. Head is supported on an appropriate sized pillow and the indifferent electrode of the ECG is placed on the upper thigh.
ACHIEVING THE LATERAL DECUBITUS POSITION
Atleast three persons are needed for positioning.a. Patient is supine and intended down arm is abducted.b. Anaesthesiologist is the co-ordinator standing at the head end. He should control turning of head and preservation of airway and the endotracheal tube.c. If the patient is to be turned to the left, anaesthesiologist turns the patients head on its pillow to the left. The two assistants stand on the right at the hip and shoulders of the patient. Assistant 1 at the shoulders places his left hand behind the neck of the patient to grasp the left shoulder and places his right hand on the patients right shoulder. Assistant 2 places his right hand under the patients thighs to grasp the pelvis in the region of the anterior part of left iliac crest
and his left hand on the right iliac crest. On receiving an affirmative reply from both the assistants, anaesthesiologist gives the command “turn”. Then the lateral position is achieved by simultaneously pulling on the patients left hip and left shoulder and pushing on right hip and right shoulder. Once the patient is in the lateral position, a hand on the shoulder of the patient will maintain stability while the limbs are positioned.
PRECAUTIONS1. Care must be taken to control the relaxed head, neck and extremities.2. Possibility of a whiplash injury to the neck should be remembered.3. Avoid pressure on dependent eye and ear.4. Care of the airway, IV lines and monitors.
ADVANTAGES OF LATERAL DECUBITUS POSITION1. Most complete access to one hemithorax2. Best approach for intra pericardial control of hilar vessels.3. Obstetrics -To prevent supine hypotension.
DISADVANTAGES1. Inherently unstable, needs restraints and supports to maintain the desired position which may cause pressure and nerve injuries or interfere with normal blood flow. Overzealously applied restraints across the chest may impair the ventilation of the lungs.2. If IV lines are on dependent limbs interference with free flow may occur.3. If the BP cuff is placed on the dependent limb it can interfere with BP measurement. Also
DO’S DON’TS
Take as many personnel as needed, at least 3 Try to move unconscious patient with
inadequate number of turners
Take care in moving, use smooth movements Use jerky, uncontrolled movements
Have a co-ordinator to call the shots Be satisfied with restraints too tight or
misplaced padding
Pad and restrain adequately Forget that lateral position is unstable
Table 1 Precautions in positioning
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 179 Trivandrum Medical College
can interfere with CVP measurement through a peripherally placed central venous catheter.4. Alteration of the Einthoven triangle between peripherally placed electrodes.5. Atelectasis of lower lung6. Nerve injuries-Brachial plexus
MODIFICATIONS OF LATERAL DECUBITUS POSITION1. Semi supine position for Closed Mitral Valvotomy:
Here the upper leg is straightened; arm is raised by flexing the elbow over the face and the trunk lean back on a small pillow2. Semi prone positionLower leg straightened and trunk rolls forward onto a pillow at the chest.
Physiology of the Lateral Decubitus Position:1. Respira tory system:a. Mechanics of ventilation :
Spontaneously breathing - Dependentlung has better ventilation because with a reduced volume and FRC of the lower lung, the diaphragm on the dependent side lies higher in the chest and is more stretched. This hemidiaphragm has a better mechanical efficiency and produces better ventilation.
Mechanically ventilated patient - The tidal volume is differentially distributed to the non dependent lung because it is more compliant. Reduced FRC in the dependent lung predisposes to alveolar collapse. Also muscle paralysis allows abdominal contents to rise further up against the dependent hemidiaphragm and impede the ventilation of the lower lung. Finally, opening the nondependent side of the chest further accentuates the difference in compliance between the two sides because the upper lung is now less restricted in movement. All these worsen the ventilation perfusion(V/Q) mismatch and predispose to hypoxemia.b. Pulmonary blood flow:
In the lateral position both in spontaneously breathing and mechanically ventilated patients the dependent lung is preferentially perfused to a slightly greater extent because of the effect of gravity. So there is an increase in the zone of nonperfusion of alveoli leading to increase in physiologic dead space on the nondependent side.
2. CVS:In the lateral position, cardiac output is
unchanged unless venous return is obstructed (eg:- use of a kidney rest). Arterial blood pressure may fall as a result of decreased vascular resistance.
COMPLICATIONS:1. Atelectasis : Atelectasis of the dependent lung occurs due to thechanges in the distribution of inspired gas and blood flow more so with controlled ventilation. Prevention is by using large tidal volume >15 ml/Kg and slow rate 10/min with sighs. Postoperative deep breathing exercises, chest physiotherapy and incentive spirometry are recommended.2. Nerve injuries especially of the brachial plexus because of the weight of the body pressing On the lower arm and axilla.
Modifications of the Lateral Position:A. KIDNEY POSITION:
This refers to the posture of a laterally recumbent patient whose spine is flexed laterally to separate the iliac crest of the upper side from the costal margin. This improves the surgical access to the kidney and urinary tract of the exposed flank.
To establish the kidney position, the patient is placed on his side in the middle of the operating table. The break in the table should be at the level of the iliac crest. A pillow is placed between the legs. The lower leg is flexed at the knee and thigh flexed to 90 degrees. Lower thigh and leg are flexed and upper leg remains straight. Table is then flexed or broken so that the muscles of the loin are taut. Final step is the use of a kidney elevator to make the loin muscles extremely taut. Patient is maintained in this position with adhesive tapes. Eyes and arms are well protected.
ANAESTHETIC CONSIDERATIONS:1. Respiratory system:a. Vital capacity decreases by 14.5% due to the restriction of thoracic cage in all the directions. Lateral expansion and diaphragmatic excursion more affected than the anteroposterior expansion.b. Tidal volume decreases by 14%c. Dependent lung prone for atelectasis.d. Surgically induced pneumothorax especially if the surgeon resects the 12th rib
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 180 Trivandrum Medical College
2. Cardiovascular System (CVS) :a. Cardiovascular collapse: This is the most dangerous complication when an anaesthetised patient is turned from supine to either right or left lateral position. So slow and deliberate positioning with constant checking of BP should be done in light planes of anaesthesia.b. Hypotension:1. Morphine frequently given as premedication for renal procedures causes peripheral vasodilatation2. Halothane if used depresses the myocardium and decreases cardiac output.3. G A depresses carotid and aortic sinus reflexes so there is no compensation for cardiovascular instability4. Lateral position especially left lateral, shifts the mediastinum and rotates the heart and interfere with venous return and decreases cardiac output.5. Kidney position produces pooling of blood in both lower extremities. Also there is distortion of upper quadrant of abdomen and obstructs blood flow from lower extremities via inferior vena cava.
COMPLICATIONS OF KIDNEY POSITION.
1. Adhesive tapes - Compression necrosis of the head of femur
2. Injury to the brachial plexus3. Pressure necrosis of the ankle, knees and
feet4. Injury to eyes, ears and cervical spine
B. LATERAL POSITION FOR TOTAL HIP REPLACEMENT:
Anaesthesia is induced in supine position and then turned laterally with the affected hip up. Two pads are kept the first in front of the symphysis pubis to avoid pressure on the genitalia, second is secured posteriorly distal to the iliac crest. Lower leg is flexed at the knee and hip. Additional pads are placed -A. distal to the fibular head to protect the
common peroneal nerveB. under the lateral malleolus of the ankleC. between the kneeD. beneath the dependent axillae
COMPLICATIONS:1. Injury to the dependent hip and leg leading to rhabdomyolysis, myoglobinuria and renal failure.2. Arterial insufficiency of dependent limb and massive swelling of the thigh.
SITTING POSITION INTRODUCTION:
The history of the sitting position for surgical purposes is uncertain, but undeniably lengthy. Barlow, in 1830, reported an episode of air embolism that occurred during the removal of a facial tumor while the patient was in a chair. Dentists seated patients to extract teeth decades before that.The first public demonstration of ether, by W.T.G. Morton in 1846,involved a seated patient undergoing jaw surgery.
The term sitting position describes the posture of the neurosurgical patient whose back is elevated towards the vertical, thighs are flexed on the trunk, legs flexed on the thighs and at the level of his heart.
A much less marked elevation of the head, with the hips and knees only slightly flexed , is used by many surgeons for operations about the jaws, neck and thyroid gland. This is essentially a Lawn chair position with the long axis of the body much more nearly supine than is the classical sitting position.
For pneumoencephalography, the patient is placed in a full sitting position with the spine vertical for a few moments during which air introduced into the lumbar cistern, floats into the skull and initial erect X Ray films of the ventricular system are taken. Surgical procedures, however, are rarely done with the patient in this position.
ANALYSIS:Opinion is divided about the use of sitting
position in Neurosurgery. The sitting and prone positions compete as a means of access to the posterior cranial fossa and cervical spine, whereas the usual choice for approaching the middle cranial fossa is between the sitting and the lateral decubitus positions.
Advantages of the sitting position afe-
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 181 Trivandrum Medical College
1. It allows a better physical access to the operative site from directly behind the wound, rather than from above and to one side, as is the case in prone position.2. Because the head is not weight bearing, this position will permit greater torsion of the head and neck than will prone. This allows the surgeon a more lateral approach to the cerebellopontine angle than could be accomplished with the patient prone.3. Accumulated blood drains out of and away from the operative site, thereby offering more rapid access to the bleeding points, a cleaner surgical field and a technically more favourable operative access.4. The sitting position allows an unobstructed view of the patients face, so that the anaesthesia team may observe motor responses from stimulated cranial nerves.5. Suitable head holders for the sitting position remove the hazard of pressure upon the eyeballs, by the circular or horse shoe shaped face pieces commonly used for prone position.6. Because there is free access to the anterior chest wall in the sitting position than in the prone position, resuscitative measures can be instituted more rapidly if cardiovascular collapse occurs.7. The amount of intrathoracic pressure needed for IPPV is less in the sitting position than in the prone position. A patient who is prone must be lifted off his anterior chest wall by each passive inflation of his lung. This increases venous distension in the wound during expansion of the lung and constitutes a major annoyance to the surgical team if venous bleeding is hard to control.8. Relatively unobstructed access to the chest wall for monitoring purposes or therapeutic needs.9. Arm vessels are more readily available for monitoring, fluid administration or obtaining arterial blood samples.10. Urinary catheter obstructions which upset fluid balance calculations are less likely.11. Sudden dislocation of ETT is unlikely since direct access to the airway by the anaesthesiologist is maintained.
INDICATIONS:1. Posterior cranial fossa surgeries2. Cervical laminectomy3. Suboccipital craniectomy
RELATIVE CONTRAINDICATIONS :1. Ventriculoatrial shunt in position and open2. Cerebral ischemia in the upright awake patient3. LAP<RAP4. Platypnoea-orthodeoxia5. Cervical spine degeneration6. Pre operative demonstration of PFO or right to left shunt7. Cardiac instability8. Extremes of age
PHYSIOLOGICAL EFFECTS OF SITTING POSITION 1. Cardiovascular System (CVS) :
The force of gravity assumes a prominent role in cardiovascular function depending upon the extent to which the long axis of the body becomes vertical in the sitting position, Massaging action of leg muscles useful iri returning dependent venous blood to IVC are absent under anaesthesia and the blood volume in the legs may increase by more than 500 ml as a result. With IPPV there is an additional impedence to the venous return. These forces act to diminish systemic perfusion by decreasing venous return and cardiac output.
Above the level of heart, venous return is aided by gravity. The higher the surgical field is located above the heart, the greater is the pressure differential and the more easily is air entrained in partially severed or patulous vessels. In addition the structure of the dural sinuses is that they do not expand under pressure or collapse when their internal pressure is low. The entrainment capacity of these structures is obvious.
In the arterial tree, gravity antagonises the upward flow of blood into the elevated head and augments it’s accumulation in the dependent lower extremities. With unrestricted arterial pathways cerebral perfusion decreases 2 mm Hg /vertical inch (2.54 cms) of elevation above the heart. 60% of lateral rotation of the head begins to reduce the flow in the contralateral vertebral artery and 80% of rotation obstructs it. Opposing this is a proportional increase in the ipsilateral vertebral artery flow. Another safeguard is the reversal of the normal cephalad flow through the basilar
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 182 Trivandrum Medical College
arteries if the vertebral arteries become ineffective: Brainstem perfusion is then supplied caudal from the circle of Willis.. However any signs of impaired brainstem perfusion (such as unexpected change in BP or appearance of bradyarrhythmias or PVCs) should be recognised early and responded to promptly. Predictable cardiovascular response to tilt includes -1. Increase in heart rate (upto 19%)2. Decrease in stroke volume3. Decrease in cardiac output.(cardiac index <14%)4. Little variation in SBP but an elevation of both DBP and MAP(increase 9-38%)5. Increase in peripheral vascular resistance calculated from the fall in cardiac output and rise in MAP (40%)6. Lengthening of pre ejection period due either to need to open the aortic valve against a higher diastolic pressure or to a reduction in the contractility of the myocardium.
2. Respiratory System(RS):The anaesthetized patient has the benefits
of an almost unimpeded RS when placed in the sitting position. Unlike supine position, in which abdominal viscera tend to restrict the caudad motion of the diaphragm or compress it cephalad at rest, the sitting position permits the downward displacement of the abdominal contents and freer diaphragmatic motion. This should promote better ventilation of the lung bases.
If IPPV is used, the pressures required to expand the lungs of a patient are much less if the patient is in the sitting position than the prone. Since the intrathoracic pressure patterns affect venous return, the pressure of IPPV that is transmitted to the surgical field is less, resulting in less bleeding.
The lung volume at which the small airways begins to close during exhalation has been termed “closing volume”. In healthy adults, Closing Volume(CV) occurs between functional residual capacity (FRC) and residual volume (RV). Both these values are increased in sitting position , but the degree of increase in FRC is more than that of the CV. Hence there is a significant reduction in the volume of trapped gas (VTG) in the sitting position.
A potential detriment of the sitting position was reported by Gurtner & Fowler in 1971. They found a reduction in the diffusing capacity for 02 (A-a D02) in the sitting position because of decreased perfusion of the upper zones of the lung.
3. CNS:The normal CSF pressure in the supine
position is 8-12 mm Hg(100-165 mm H20). With the patient in the sitting position this pressure becomes about 30 mm Hg (400 mm H20) in the lumbar cistern , while at the vertex of the skull it is subatmospheric at -5 mm Hg (-65mmH20). This reduces one force composing the ICP and results in more effective perfusion at lower arterial pressures.
4. Other considerations:a. Pregnancy : Should this position be required in the last trimester of pregnancy, the uterus can impair the two major advantages of this posture - by encroaching upon the downward movement of the diaphragm and compressing the IVC. Careful attention to ventilation and gentle lateral displacement of the uterus should improve the situation.b. Temperature variations : Can be hard to control in the seated patient.
TECHNICAL ASPECTS:The operating table should have a
removable head platform and separate controls for the leg section, for the back and for flexion.
If a thermal mattress or a Gardner-Dohn antigravity suit (G-suit) is used, they should be placed on the table prior to placing the patient on it. 1 or 2 pillows are placed in the thigh section of the table. This serves to elevate the patients seat in the final sitting position, so that when the head platform is removed , the edge of the table corresponds to the 2nd/3rd thoracic vertebra.
Endotracheal intubation in these patients is safest with a non kinkable tube which permits the unusual head position occasionally required for access to the cerebellopontine angle. Tube compression by biting can be prevented by inserting a properly made bite block between the patient’s teeth; a conventional oral airway fails
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 183 Trivandrum Medical College
to separate the teeth widely enough to protect the ETT.
Large calibre IV lines, a right atrial catheter when indicated, an arterial cannula, an esophageal stethoscope, ECG leads, urinary catheter and thermal probes are all put in place with the patient supine. The lower extremities are wrapped with compression stockings or elastic bandages, if needed. Any hypotension associated with induction of anaesthesia is corrected and ventilation is stabilised.
To establish the sitting position, first the table is flexed fully. The foot section is lowered by at least 45 degrees. The thigh straps are loosened temporarily to prevent injuries to the thighs or restricting motion of the table top. The back section is slowly elevated while the chassis is being inclined towards the Trendelenburg position. This combined manoeuvre is coordinated to produce further flexion of the thighs on the trunk. During these manoeuvres BP should be monitored repeatedly.
Continued elevation of the back section will now place the patient in the desired degree of sitting position with the legs at about the level of the heart. The knees should be flexed upon the thighs to prevent stretching of the sciatic nerve or its branches. Slowed elevation of the head and judicious use of a balanced vaspressor, such as ephedrine or mephenteramine, are indicated to ensure BP levels that provide adequate cerebral perfusion.
The traditional method of securing the head was to use a horse shoe shaped head rest placed against the face & to tape the head to it. They, however, seldom fit the face and thereby threaten the eyes, cheeks and the supraorbital nerve with excessive pressure. The strapping can also be sweated loose or ripped off by sustained traction .
The most successful head holder is some form of skull pin & clamp device. There are two versions- the Gardner version and the Mayfield version. Each of these models consists of 3 sterile pins, which firmly penetrate the outer table of the skull & fits into a C shaped skull clamp. The
clamp is then attached to a long supporting arm that is attached to a U shaped brace fastened tightly to the rails of the operating table.
Once the patient’s head is stabilised, the head section of the table is removed. The elbows of the patient are supported by pillows or pads. The patient’s hands are crossed in his laps. Bony prominences are padded and the legs wrapped to mid thigh in elastic bandages to augment venous return.
VARIATIONS:A useful variation was reported by Garcia-
Bengochea & colleagues. They described a position in which the patient was placed in a chair fixed to the operating table in such a way that Durant’s left lateral position can be rapidly established simply by lowering the control end of the table chassis. By arranging the table top in the form of a chair ( back elevated, foot section down), placing a back rest for the patient at 90 degrees to the right edge of the elevated back section, they stabilized the patient in a sitting posture that allowed varied head torsion. Should hypotension or air embolism occur, the usual head end of the table chassis can be lowered rapidly by turning a single crank and the Durant’s position can be attained without losing control of or contaminating the wound.
COMPLICATIONS, PREVENTION AND TREATMENT: 1. Hypotension :
Hypotension in the seated anaesthetised patient is indicative of cerebral hypoperfusion. It is probably the most frequent complication of this position.lt requires rapid detection and prompt correction.a. Fluid volume deficits should be corrected before surgery.b. Vasopressors such as ephedrine or mephenteramine.c. The G suit, though cumbersome, has been shown to be useful in the immediate treatment.d. Alert replacement of intraoperative blood loss.
2. Endotracheal tube migration :An unexpected complication is the
migration of the tip of the ETT into the right
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 184 Trivandrum Medical College
mainstream bronchus. Elevation of the diaphragm produced by the sitting position can easily raise the carina cephalad and cause the tip to migrate. Auscultation of each hemithorax is a must after the positioning and the ETT must be adjusted so that all lung fields are ventilated equally.
Firm tape fixation of the ETT & bite block are mandatory to prevent the ETT from being dislodged by head motion from bone drills or saws or by traction from the breathing circuit itself.
3. Air embolism :Venous air embolism(VAE) is detectable
in the sitting position by precordial Doppler in 40% of patients & in 76% of patients using transesophageal echocardiography.Common sources:The common sources of major VAE are1. Major cerebral venous sinuses
a. transverse sinusb. sigmoid sinusc. posterior half of the sagittal sinus
2. Emissary veinsa. to the suboccipital musculatureb. diploic space of the skull
3. Cervical epidural veins
EFFECTS OF AIR EMBOLISM :Effects depend on the total volume &
perhaps more importantly on the rate of air entry. The air bubbles may pass from the right atrium into the right ventricle, where they may be churned up into froth before being ejected into the pulmonary artery. Pulmonary hypertension with right ventricular strain develops due to mechanical blockage of the pulmonary vessels and neurogenic effect.The cardiac output and BP fall & dysrhythmias including VF, may be precipitated.
Air can then pass into the systemic circulation either through the pulmonary vascular bed or through intracardiac defects like Patent Foramen Ovale. The dangers of systemic air are that it may enter the coronary artery & provoke VF or enter the cerebral vessels & produce permanent neurological damage.
The effect of air embolism is aggravated if the patient is receiving N20 at that time. N20 which is 30 times more soluble than N2, would
diffuse quickly into the bubbles & appreciably increase their size.
MONITORS:1. TEE : This can detect air embolism in 8- 75% of patients in the sitting position. It is a highly sensitive monitor. Emboli as small as 2 microns can be detected. It has the advantage of identifying right to left shunting of air.2. Doppler ultrasound : One of the more sensitive methods to detect air embolism. The receiver is placed over the tricupid valve. The combination of precordial Doppler with ETC02 monitoring is the current standard of care in the sitting position.3. Auscultation : Faintly audible high pitched tinkling sounds can be heard at first. 30 ml of air produces the characteristic mill-wheel murmur. The changes are earlier appreciated with an esophageal stethoscope.4. ECG : Changes are best seen in V1 & comprise of signs of right heart strain(RBBB, T wave depression &tall peaked P waves in the right chest leads)5. ETC02: Sudden falls in ETC02 is produced due to an increase in alveolar dead space secondary to the development of venoarterial shunts in the lung.6. CVS monitoring : There is hypotension secondary to low cardiac output , tachycardia and increase in bothCVPand PAP.7. ETN2: Theoretically attractive, but its use in anything less than catastrophic VAE is small.
MANAGEMENT:1. Prevent further air entrya. Notify the surgeon- compress or ligate the
vessel. If this is not possible flood the wound with saline or pack with saline soaked pads.
b. Apply Jugular compressionc. Change the position of the patient (lower
the patient’s head)2. Support circulation :
External Cardiac Massage (ECM), 100%02, Vasopressors.
3. Removal of air :The classical description is that turning
the patient to the left side head down (Durant’s position) places the right atrium & tricuspid valve above the right ventricle & tends to delay the passage of air into the pulmonary artery. Air can
RACE 2003 Ramachandra Anaesthesia Continuing Education
Patient Positioning 185 Trivandrum Medical College
then be aspirated through a right atrial monitoring catheter. Natural absorption of air is hastened by ventilation with 100% oxygen. Whole body compression of the patient may be valuable to force the gas into solution.
4. Quadriplegia :The sitting position per se has been
implicated as a cause of rare instances of unexplained post operative quadriplegia. It has been hypothesized that neck flexion, which is a common concomitant of the seated position, may result in stretching or compression of the cervical spinal cord. This possibility represents a relative especially when there is evidence of associated cerebral vascular disease.
5. Macroglossia :Swelling of the pharyngeal structures
including the soft palate, post wall, pharynx & base of the tongue have been observed. These have been attributed to trauma/ischemia occurring as a result of foreign body (usually oral airways) causing pressure on these structures in lengthy procedures with sustained neck flexion. It is ideal to maintain at least a finger breadth’s distance between the chin & sternum to prevent excessive reduction of the AP diameter of the oropharynx.
6. Arrythmias :Arrythmias in the seated patients are
classified as perfusing and nonperfusing.
A non perfusing arrythmia is one which causes or accompanies a fall in perfusion pressure & is an emergency. Treatment must be prompt.a. Cessation of the surgical stimulus alone
may be enoughb. Prompt use of vasopressorsc. Restoration of depleted blood volumed. Inflation of the G suit.e. Aspiration of intracardiac air.f. Use of supportive drugs.g- Cardiac massage as needed
A perfusing arrythmmia , that is one notaccompanied by hypotension, may also result from surgical manipulation. If surgical stimulation is not the cause and air embolism can be ruled out, the most frequent cause seems to be C02 excess when blood gases are not being monitored. Other extracardiac causes like electrolyte disturbances should be sought and corrected.
8. Miscellaneous complications :a. Tension pneumocephalusb. Sciatic nerve injury due to prolonged extension of the knees.c. Foot drop due to pressure on the common peroneal nerve.Severe flexion and lateral rotation of the rieck can be traumatic to an arthritic cervical spine.
RACE 2003 Ramachandra Anaesthesia Continuing Education

HOW I DO IT?

A 20 year old Primi with severe MS requires Labour Analgesia 186 R.Bharathi
There is no question that labour and delivery are extremely painful experiences for most women. Unfortunately, many believe that labour pain has an important biological function and should not be relieved and there is a general belief that methods of pain relief are dangerous to the mother and newborn.
IS THERE A NEED TO RELIEVE PAIN?ASOG statement
“Labour results in severe pain for many women. There is no other circumstance, where it is considered acceptable for a person to experience severe pain amenable to safe intervention, while under physician’s care. Maternal request is a sufficient justification for pain relief during labour".
As stated by Hippocrates “Divine is the task to relieve pain”. This is truer than ever when we are considering two lives and we must take every effort to honour the patient’s request for labour analgesia.
When confronted with the patient’s cardiac problem, the anaesthetist must answer the following questions:
1) What are the anatomic abnormalities in mitral stenosis (MS)?2) What changes in preload, afterload, heart rate and contractility will optimise the patient with MS especially with relation to pressure volume loop.3) What are the treatment options for MS?4) What are the important considerations in planning the anaesthetic management of a patient with MS?5) What are the special considerations for anaesthetic management of labour and delivery in MS anticipating haemodynamic swings?6) What are the complications and limitations
of regional anaesthesia in MS?
Although rheumatic heart disease is decreasing worldwide and has become a rare complication of pregnancy in affluent societies, it is still prevalent in poor countries like India and remains an important cause of maternal mortality, MS being the commonest lesion. The overall mortality associated with MS is reported to be 1% but increases to 5% in Class III and IV of the NYHA classification. In the presence of atrial fibrillation, maternal mortality is 14-17%. Similarly, perinatal mortality rates are low in Class I and II, but increase in Class III and IV to 12-31%.
PATHOPHYSIOLOGY:MS causes physiologic abnormalities
both proximal and distal to the abnormal valve. Distally, there is a “protected” or underloaded left ventricle (LV), which may have contractile abnormalities. Proximally, a pressure gradient develops between the left atrium (LA) and LV in order to force blood across the obstruction of the narrowed valve orifices. This elevated LA pressure causes alterations in LA size, compliance and function. In addition, the pressure is reflected back into the pulmonary veins causing changes in pulmonary and right ventricle (RV) function. The area of the valve orifice is the key to the flow, and as the orifice gets smaller, the turbulent flow increases across the valve and total resistance to flow increases.
Diagramatic representation of the transmitral blood flow velocity:
Left ventricular (LV) filling starts with the opening of the mitral valve and continues during the early (rapid) and late (slow) filling phases while atrial blood rushes through the mitral valve into the ventricular cavity. The pressure gradient tends to accelerate the blood flow in the LV cavity.
RACE 2003 Ramachandra Anaesthesia Continuing Education
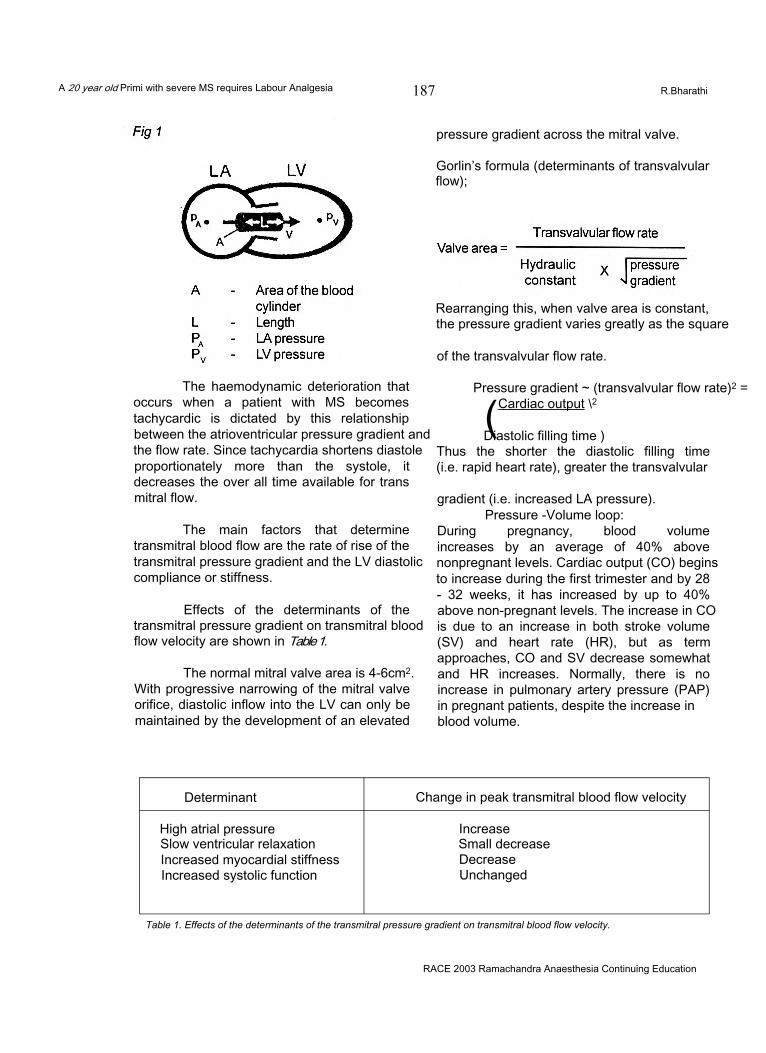
A 20 year old Primi with severe MS requires Labour Analgesia 187 R.Bharathi
The haemodynamic deterioration that occurs when a patient with MS becomes tachycardic is dictated by this relationship between the atrioventricular pressure gradient and the flow rate. Since tachycardia shortens diastole proportionately more than the systole, it decreases the over all time available for trans mitral flow.
The main factors that determine transmitral blood flow are the rate of rise of the transmitral pressure gradient and the LV diastolic compliance or stiffness.
Effects of the determinants of the transmitral pressure gradient on transmitral blood flow velocity are shown in Table 1.
The normal mitral valve area is 4-6cm2. With progressive narrowing of the mitral valve orifice, diastolic inflow into the LV can only be maintained by the development of an elevated
pressure gradient across the mitral valve.
Gorlin’s formula (determinants of transvalvular flow);
Rearranging this, when valve area is constant, the pressure gradient varies greatly as the square
of the transvalvular flow rate.
Pressure gradient ~ (transvalvular flow rate)2 =
(Cardiac output \2
Diastolic filling time )Thus the shorter the diastolic filling time (i.e. rapid heart rate), greater the transvalvular
gradient (i.e. increased LA pressure).Pressure -Volume loop:
During pregnancy, blood volume increases by an average of 40% above nonpregnant levels. Cardiac output (CO) begins to increase during the first trimester and by 28 - 32 weeks, it has increased by up to 40% above non-pregnant levels. The increase in CO is due to an increase in both stroke volume (SV) and heart rate (HR), but as term approaches, CO and SV decrease somewhat and HR increases. Normally, there is no increase in pulmonary artery pressure (PAP) in pregnant patients, despite the increase in blood volume.
Determinant Change in peak transmitral blood flow velocity
High atrial pressure IncreaseSlow ventricular relaxation Small decreaseIncreased myocardial stiffness DecreaseIncreased systolic function Unchanged
Table 1. Effects of the determinants of the transmitral pressure gradient on transmitral blood flow velocity.
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 188 R.Bharathi
In the patient with MS, pregnancy is associated with an increase in CO. There is also an increase in pulmonary artery pressure (PAP), which is probably due to increase in blood volume. If there is pre-existent pulmonary hypertension, the increase in PAP may lead to pulmonary congestion and it may be necessary to initiate diuretic therapy. Symptoms from even mild to moderate MS may become severe as the pregnancy progresses. These haemodynamic changes account for the 25% incidence of pulmonary congestion and 5-17 % mortality rate in the puerperium.
Tachycardia is not well tolerated by patients with MS as it decreases LV diastolic filling time. LA dilatation as a result of increase in central blood volume may lead to atrial fibrillation, which will further impair LV filling. Digoxin is often given prophylactically during pregnancy with MS to prevent tachycardia and atrial fibrillation. Beta- blockers may also be used.
Labour and delivery impose additional stresses on the CVS. In the normal patient, there is a progressive increase in CO during the peripartal period, which is accompanied by an increase in both HR and SV. The increase in CO is due to increased sympathetic stimulation secondary to pain and increased metabolic demand. Uterine contractions cause a further 15- 20% increase in CO, due to blood being transfused from the uterus into the central veins. When the term pregnant patient is turned from the supine to the lateral position aortocaval compression is relieved and CO is increased by 30%
CO and HR are maximal during the immediate postpartum period at which time, CO is approximately 80% above nonpregnant levels (due to disappearance of aortocaval compression and autotransfusion of blood to the central veins by the contracted uterus), This increase in intravascular volume and heart rate makes the MS patient particularly vulnerable to the development of pulmonary oedema at this time.
PAIN PATHWAYS DURING LABOUR:Pain during the first stage of labour is
mainly due to uterine contractions and cervical
dilatation. In the first stage, pain is transmitted via visceral afferents that accompany sympathetic nerve fibres and enter the spinal cord at T10, 11,12 and L1 segments. Visceral pain is severe, dull aching and poorly localized and is easier to block than somatic fibres. Opioids are useful in relieving the pain. In the late first stage and second stage of labour, pain is due to distension of the pelvic floor, vagina and perineum. Opioids are not useful for second stage and local anaesthetic is needed.
WHY PAIN RELIEF?Pain and fear are the main reasons for
maternal hyperventilation during labour, which can lead to respiratory alkalosis, increased oxygen consumption and lactate accumulation. This may not affect a healthy parturient but will affect the parturient with limited cardiac reserve as in mitral stenosis who cannot increase oxygen delivery.
Acid base balance: Inadequate pain relief leads to progressively increasing metabolic acidosis and the foetus becomes more distressed. Failure to relieve labour pain can lead to maternal exhaustion and reduction in the efficacy of uterine work. Maternal pain and stress reduce uterine blood flow secondary to the release of endogenous norepinephrine. There is an increase in cardiac output (25% in the late first stage and 40% during second stage) due to increase in sympathetic activity. This increase in cardiac output is 10-15% less in those who receive labour analgesia, which is beneficial with a narrow mitral valve. Epidural analgesia decreases plasma catecholamine concentrations and attenuates the increase in cardiac output seen in the labouring parturient.
MITRAL STENOSIS:ANAESTHETIC MANAGEMENT IN LABOUR:
Patients with MS often tolerate the haemodynamic changes of pregnancy poorly. Because of the increases in blood volume and cardiac output associated with pregnancy, symptoms from even mild to moderate MS may become severe as the pregnancy progresses. These haemodynamic changes account for the 25% incidence of pulmonary congestion and 5- 17 % mortality rate in the puerperium.
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 189 R.Bharathi
ObjectiveTo minimize left ventricular end diastolic
pressure (LVEDP) and impedance to forward flow and to maximize left ventricular end diastolic volume (LVEDV) and facilitate movement of this relatively fixed CO toward the periphery.
1) Oxygen administration, left lateral position2) Antibiotic prophylaxis - (not necessary for
vaginal delivery as per AHA guidelines)3) Fluid restriction (with monitoring to maintain
preload)4) Slow heart rate: Beta blockade, analgesia,
phenylephrine (not ephedrine?) for hypotension
5) Prevention/Treatment of AF: Digoxin, Verapamil, Beta blockade, DC Cardioversion
MonitoringECG, Pulse oximetry, CVP (use of PA
Catheter is controversial as PCWP does not reflect the left atrial pressure), peripheral arterial line and foetal heart monitoring.
AnaesthesiaREGIONAL ANAESTHESIA FOR LABOUR:
Epidural or CSE the aim is to avoid abrupt decrease in SVR. Suplimental dose will be required during the second stage of labour for elective forceps delivery.
CAESAREAN SECTION:Elective: Epidural probably preferred.
Maintain filling pressures. Emergency: General anaesthesia with
endotracheal intubation. Postpartum high-risk period
First 1-2 hrs critical Possible use of epidural post-op postpartum.
Primi with critical MS for Labour AnalgesiaA 30-year-old primigravida with severe
mitral stenosis (mitral valve area-0.9cm2) requests labour analgesia.
The management begins with a detailed history including prior hospitalisation, drug therapy and decreased exercise tolerance during this pregnancy. I will do a complete physical examination of the cardiovascular and respiratory
systems with particular reference to evidence of cardiac failure (elevated jugular venous pressure, pedal oedema, basal crepitation) and arrhythmias (atrial fibrillation). Airway assessment and spine examination will complete my physical examination.
Investigations that I would like to have will include haemoglobin%, serum electrolytes, blood urea nitrogen, serum creatinine, electrocardiogram and a recent echocardiogram.
I will interact with the obstetrician regarding the progress of labour (cervical dilatation) for the timing of the labour analgesia.
My plan for this patient is combined spinal epidural analgesia.
I will explain to the patient about the benefits of labour analgesia and obtain written consent for the same.
Preparation before the procedure.The patient is given oxygen at 6l/mt and
a wedge kept under the right hip for left uterine displacement. After establishing monitoring including electrocardiogram (ECG), pulseoximetry (Sp02), I will cannulate the left radial artery for invasive pressure measurement and central venous line through the right cubital fossa for central venous pressure monitoring.
Emergency resuscitation trolley, a good working laryngoscope and a working suction are kept ready and the following drugs are loaded before the procedure:1) Thiopentone sodium2) Suxamethonium.3) Atropine.4) Esmolol.5) Phenylepherine.6) Frusemide.7) Fentanyl.
I will explain in detail about the wholeprocedure and allay the patients fear if any.
Combined spinal epidural techniqueNo preloading of intravenous fluid will be
given but ringer lactate will be given at 75 ml/hr
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 190 R.Bharathi
as maintenance fluid. After putting the patient in the left lateral position, the procedure is done as described below. The epidural space is identified with a 16 G tuohy needle in the L3-L4 interspace using loss of resistance to air. Using a needle through needle technique fentanyl 10 meg is given intrathecally with a 26G spinal needle. Alternatively, a separate spinal injection can be given at a lower space. A16 G epidural catheter is inserted 6 cms into the epidural space. All the while, the foetal heart is monitored.
No test dose is givenAn epidural infusion of bupivacaine
0.0625% and fentanyl 2mcg/ml is started at 6 ml/hr. The infusion rate may be increased up to 12 ml/hr so as to achieve a block up to T10 level. Additional doses of fentanyl 25 meg may be given so as to augment analgesia when necessary, as during maximal cervical dilatation. Epidural analgesia facilitates a controlled second stage of labour and can be shortened by the elective use of either vacuum extraction or forceps delivery. During this period, epidural boluses of 0.1% bupivacaine with fentanyl 25 meg can be given in slow incremental doses over a period of 10 to 20 minutes, so as to prevent hypotension. If there is any hypotension during this period, I will manage it with phenylepherine rather than ephedrine, as it will cause tachycardia. There is no evidence that the use of phenylepherine compromises uterine blood flow.
After delivery of the baby, I will give oxytocin 10 units slowly as an infusion over 15 to 20 minutes in order to minimize reflex tachycardia. Since these patients are at risk of developing pulmonary oedema, precipitated by autotransfusion in the postpartum period, I will give frusemide 20 mg in divided doses and as well continue the epidural bupivacaine and fentanyl infusion.
Advantages of combined spinal epidural techniqueINTRATHECAL FENTANYL:
Intrathecal fentanyl alone is effective in early labour (cervical dilatation < 5 cm) conferring the advantage of profound analgesia with complete absence of motor block, greater patient satisfaction and greater reliability. Intrathecal
fentanyl in the range of 5 - 25 meg produces a dose dependent increase in the duration of analgesia (45 -90 mins). Fentanyl doses more than 50mcg do not prolong the analgesic duration. There is a similar analgesic effects, onset, intensity and duration with a smaller dose of fentanyl (15-25mcg) compared to a larger dose (50mcg). There is a modest decrease in maternal blood pressure, likely due to analgesia rather than sympathetic block.
High block, respiratory depression and dysphagia can occur. Ventilatory depression is characterized by reduced tidal volume rather than decreased rate and it can be delayed in onset (30 minutes or more).
Lateral positioning during intrathecal administration may limit the rostral redistribution and limiting the maximum intrathecal dose to 25mcg is likely to reduce these complications.
Appropriate monitoring (Patient observation and pulse oximetry) is strongly recommended when intrathecal techniques are used.
Nausea and pruritis are very common dose dependant side effects. They require treatment infrequently and resolve before the analgesic effect wanes.
There is a low incidence of foetal heart rate (FHR) abnormalities (6-12 %) seen with intrathecal fentanyl 25mcg compared to 30% incidence with 50mcg fentanyl where more of the FHR changes resulted in the need for caesarean delivery. These are transient and resolve spontaneously and are not accompanied by maternal hypotension or emergent interventional delivery.
Foetal bradycardia following the onset of intrathecal analgesia most often is associated with rapid cervical dilatation, or nuchal or prolapsed umbilical cord. Uterine hypertonus can be due to abrupt elimination of beta-adrenergic mediated inhibition of uterine contraction thereby reducing intervillous blood flow.
Epidural testdose1) From the safety point of view, the most
important characteristic of any test to
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 191 R.Bharathi
detect IV or intrathecal catheter malposition is its negative predictive value. This is because the larger therapeutic dose is administered only after the negative test result is obtained. At the same time, a low false positive rate is highly desirable to prevent unnecessary catheter replacement and delay in providing analgesia.
2) Traditional test dose of 45 mg Lignocaine with 15mcg epinephrine is not recommended as there is a risk of high spinal block associated with unrecognised intrathecal catheter malposition, which is hazardous in a labouring cardiac patient as well as tachycardia if it is intravascular, which is detrimental.
3) Unintentional intravascular placement of epidural catheters has been reported to occur with the frequency of 2-9% and is associated with serious outcomes.
Aspiration for blood alone is 98% sensitive in detecting intravascular placement of multiorifice epidural catheters.
Does the air test work for multiport catheter?Inject 1 ml of air through the epidural
catheter and listen for maternal heart sound changes for 15 seconds using a Doppler probe. The test is considered positive if a loud swishing sound lasting atleast 5 seconds is heard in addition to or in place of the normal “lub-dub” heart sounds.
Air test may be less reliable in multiport than in single orifice catheters because gases, to a greater extent than liquids, preferentially exit through the most proximal catheter hole.
Fentanyl test doseAfter 100 meg epidural fentanyl if the
patient has any increased sedation, dizziness or light headedness within the first 5 minutes then it should be interpreted as a positive response for intravascular injection. No adverse foetal outcome has been observed with this method. Yet there may be maternal desaturation, which will require 02 supplementation.
Low dose mixtures of opioid and local anaesthetic are used as a ‘test dose’ combining observation and incremental dosage. At best, intravascular injection results in minimal analgesia
and minimal effects in the mother and the foetus. If the injection is intrathecal, the worst scenario is an increasing degree of slow - onset motor blockade with minimal loss of sympathetic tone.
DisadvantagesEpidural analgesia has potential
disadvantages. A rapid onset of epidural blockade may cause a sudden reduction in SVR. As well as potentially compromising uteroplacental perfusion, marked reduction in SVR can cause a compensatory tachycardia.
Therefore, I chose to use CSA. Intrathecal fentanyl provided rapid initial analgesia without adverse haemodynamic effects. This enabled analgesic maintenance to be established gradually using an infusion of dilute bupivacaine- fentanyl mixture, with the avoidance of large or rapid boluses of local anaesthetic. Epidural infusion has less incidence of hypotension compared to intermittent top ups. Thus sympathetic block and potential haemodynamic changes are likely to be of slow onset and amenable to controlled and titrated management.
If analgesia is insufficient for delivery, pudendal nerve block can be added rather than increase the concentration of local anaesthetic boluses.
In the early postpartum period, the patient is at risk of developing pulmonary oedema, which will be exacerbated by cessation of epidural analgesia and the return of sympathetic tone. Hence, I would like to continue epidural analgesia in the postpartum period.
Patient undergoing Caesarean section for obstetric IndicationFOETAL DISTRESS:-
As there is no time for establishing epidural blockade, general anaesthesia is preferred. Epidural catheter is left for post-op analgesia.
NON-PROGRESSION OF LABOUR: -Incremental injection of boluses of 5ml
of 0.5% bupivacaine are given over 15 minutes interval with careful attention to patient’s mental status (every reinjection is a test dose). CSE is associated with more rapid cervical dilatation
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 20 year old Primi with severe MS requires Labour Analgesia 192 R.Bharathi
compared to standard epidural analgesia. Obstetric and neonatal outcome are the same with both techniques.
Compared with epidural, the advantages of combined spinal epidural (CSE) are
• Rapid and improved analgesia• Reduced initial and total dose of drugs• An objective procedural end point (CSF)• Nil or minimal motor blockade• Minimal autonomic (sympathetic)
blockade• Selective sensory blockade• Ambulation is possible and safe.
Controversies about CSE:1) Risk of penetration through the dural hole
It is impossible to force a 16G or 18G epidural catheter through a dural hole after a single dural puncture with a 25G spinal needle
2) Perceived increased risk of neurotrauma No evidence that paresthesia on CSE needle
or catheter placement is likely to result in a neurologic deficit.
3) Risk of meningitis is extremely low
4) CSE block and decreased risk of post dural puncture headache (PDPH):
Reasons may bea) The use of a very fine diameter spinal needleb) Tuohy needle as an introducer allows meticulous puncture of the duramaterc) CSF leakage through the dural hole is decreased by the increased pressure from epidural anaesthetic solutions (splints the dura from the arachnoid membrane)d) With the single segment CSE technique, the spinal needle is deflected somewhat, as it exits through the Tuohy needle, approaching the dura at an angle, hence both holes do not overlap.
5) Epidural and intrathecal opioids are prophylactic against PDPH.
ALTERNATIVE METHODSThese include but not limited to
intramuscular opioids, entonox, ketamine and hypnosis’
Regional analgesia is the only effective way of providing complete pain relief, if that is what is desired.
CONCLUSIONPhysiological changes associated with
increased metabolic demand can lead to functional deterioration in women with MS who become pregnant. This is exacerbated in labour when pain, bearing down and autotransfusion can lead to tachycardia, elevations of pulmonary vascular resistance and increases in central blood volume, all of which may be poorly tolerated. Successful management of parturients with MS depends on a multidisciplinary approach and is facilitated by early referral to the cardiology and anaesthesia teams and the use of preoperative echocardiography to delineate the valvular lesion before formulation of the delivery plan.
REFERENCES1) Combined Spinal-Epidural analgesia in the management of labouring parturients with mitral stenosis. W.D Ngankee, J.Shen, A.T.O Chiu, I.Lok, K.S.Khaw. Anaesthesia Intensive Care 1999 27; 523-526.
2) Combined Spinal-Epidural anaesthesia in G.primigravida with valvular heart disease. Tomas VanHelder, Kari G. Smeastad, Can J. Anaesthesia 1998/ 45:5 /488-490.
3) Mitral stenosis in pregnancy: a four-year experience at king Edward VIII hospital, Durban South Africa. British Journal of Obstetrics and Gynaecology. Aug 2000, 107: 953-958.
4) Pain management in the critically ill obstetric patients. Chandra Jayasinghe, Norman H Blass, crit care clinics 1999; Jan 15(1): 201-28
5) Multiport epidural catheter. Barbara et al. Anaesthesiology 2000; 92:1617-20
6) Regional Anaesthesia for the pregnant Cardiac patient Mitterschiffhaler Regional Anaesthesia. Acta anaesthesio scan suppl 1996: 109:180-4
RACE 2003 Ramachandra Anaesthesia Continuing Education

A 20 year old Primi with severe MS requires Labour Analgesia 193 R.Bharathi
7) The incidence of foetal heart changes after intrathecal fentanyl labour analgesia. Craig M Palmer et al. Anaes analg 1999:88:577-81
8) Can Parturients distinguish between intravenous and epidural fentanyl? Morris GF et al. Can J Anaes: 1994:41: 667-72
9) The parturients with cardiac disease. Ridley Smiley Anaesthesiolo Clin? North Ame 1998:16:430-32
10) Labour Epidural Analgesia without an intravascular “Test Dose” Mark C Noris et al. Anaesthesiology
1998:88:1495-501
11) Regional Anaesthesia for obstetrics Anaesthesiolo Clini North Ame 2000:Vol184
12) The Combined Spinal Epidural technique Narinder Rawal, Bjon Holmstrom et al. Anaesthesiology clinics of North America June 2000:V18: 267-288
13) Invasive Monitoring for anaesthetic management of parturient with mitral stenosis. G.T Hemmings et al. Can J Anaest 1987/34:2 182-5
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage
194 Manjunath Prabhu
Ludwig’s angina is a potentially lethal, rapidly spreading cellulitis involving the sublingual and submaxillary spaces. It is manifested by brawny suprahyoid induration, tender swelling in the floor of the mouth, and elevation and posterior displacement of the tongue. This condition is a therapeutic emergency because of inherent life threatening airway obstruction. In 1836, Wilhelm Friedrich von Ludwig described this condition as rapidly spreading cellulitis which produced well defined, woody oedema of the submandibular and sublingual areas with minimal throat inflammation, absence of submandibular lymph node involvement and lack of suppuration. A dental focus of infection can be an initiating factor in the majority of cases. Young adult males are more commonly affected than others. The mortality has come down significantly with the use of early intravenous antibiotics. The most common causative agents are streptococci and staphylococci with anaerobes involving in the mixed infection.
MANAGEMENTAirway obstruction has long been
recognised as the most frequent cause of death in Ludwig’s angina (LA) patients. Airway protection is imperative in the successful treatment plan. Early intravenous antibiotic therapy and exploration of the submandibular spaces in those patients who develop abscesses or fail to respond to initial conservative treatment is important. Continuous observation of the respiratory status is mandatory, as progressive soft tissue oedema compromises the airway insidiously, and total obstruction or laryngospasm secondary to aspiration can be abrupt. In cases of rapidly advancing cellulitis, emergency tracheostomy may be life saving. Nuchal rigidity, trismus and gross distortion of the normal anatomy along with grossly enlarged tongue and pooled secretions
can not only make intubation difficult but also make it traumatic and potentially hazardous.
Prior to detailed examination of the patient a proper planning is a must. Preoperative evaluation of the general condition of the patient and airway examination in particular can give a lot of information that can be of great help in deciding the actual anaesthetic plan. Preinduction intubation may be an ideal way of airway management in these patients. Fibreoptic assisted intubation can be a useful option, but it demands greater skills, a cooperative patient and a Clearfield. These prerequisites are not often encountered in usual clinical settings. Blind nasal intubation can be traumatic causing damage to the inflamed surrounding structures and may precipitate airway obstruction.
Earlier recommendations were for early tracheostomy under local anaesthesia before proceeding with incision and drainage. In recent literature, there are enough evidences suggesting that tracheostomy can be avoided in a large number of patients with careful airway management. In 1982, Patterson etal reported 20 cases of Ludwig’s angina patients and 9 patients underwent surgical exploration.1 Tracheostomy was performed in four patients and in the remaining 5 patients, It was avoided. They reported successful treatment in all 20 patients with the use of antibiotics, surgical drainage and proper airway management. In 1985, Loughnan and colleagues reported successful airway management of nine patients with Ludwig’s angina coming for emergency surgery without tracheostomy.2 Most of their patients had trismus and they were induced with inhalational agents and then intubated under direct vision. Mehrotra et al reported a case report where they have used cervical plexus block and
RACE 2003 Ramachandra Anaesthesia Continuing Education

A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage 195
Manjunath Prabhu
then successfully managed the drainage procedure in a military field hospital in Delhi.3 There are reports of people losing the airway suddenly both while intubating awake as well as under inhalational agents.4 Probably intravenous induction and muscle paralysis before securing the airway may not be a safe technique. After going through the literature it is clear that the airway management is quite tricky in this group of patients and there are more than one way of doing it correctly.
HOW I DO IT:The management of these emergency
cases depends on the actual clinical settings and the available options. The important steps to be remembered are a good skilled assistant, proper planning and option for immediate tracheostomy. In the following part, I have explained the way I would like to manage a young, otherwise healthy Ludwig’s angina patient with no acute airway obstruction coming for abscess drainage.
Starting of intravenous antibiotic will be the first step in the management in these patients. The antibiotics should be active against streptococcus and anaerobes. Minimal blood investigations are needed including haemoglobin and blood grouping. Chest and neck radiographic pictures will be asked for. The neck X- rays will give information regarding the soft tissue swelling and its effect on the upper airway structures. Deviated larynx and trachea or a narrow laryngeal passage would indicate a possible difficulty in airway management.
The preoperative evaluation should include a detailed history and airway examination. Trismus can be a common finding and this may lead to restriction on mouth opening until pain is fully controlled. The space available inside the mouth, with the floor of the mouth pushed upwards and swollen tongue should be assessed. Reassuring the patient and explaining the proposed plan can be very useful since proper airway management and early antibiotic therapy can avoid the mortality in most cases. The preoperative advice include written consent for anaesthesia as well as tracheostomy (elective or emergency), starvation orders and continuation of antibiotic therapy. My premedication includes
intramuscularly administered glycopyrrolate for its antisialogogue effect. I will not administer any sedatives until the patient is under my direct observation in the operating room or in the ICU.
Prior to administration of any anaesthetic to the patient, I would like to keep the difficult airway trolley ready. These include, but not limited to, properly illuminated laryngoscopes, appropriate sized cuffed endotracheal tubes, gum elastic bougie, emergency cricothyrotomy set, emergency tracheostomy set etc. Monitors will include pulseoximeter and capnograph in addition to electrocardiogram and noninvasive blood pressure. Emergency resuscitation drugs and equipments will be kept ready. A good suction apparatus with wide bore suction catheters like Yankauer suckers will be kept ready.
Following establishment of IV fluids and connecting the patient to preinduction monitors,I would like to nebulise lignocaine solution in order to provide topical anaesthesia of the upper airway. Nebulisation of lignocaine should make subsequent airway management less painful and helps in the release of trismus. If the patient is having relatively stable vitals, satisfactory mouth opening and is not in acute airway obstruction, then I would induce the patient with inhalational anaesthetic sevoflurane in oxygen. The rapid induction and rapid emergence property of sevoflurane would be the major advantage over other inhalational anaesthetics. A small dose of a short acting narcotic like fentanyl 100 pgm will be administered slowly before induction. As patient is induced, gentle attempts to assist ventilation will be made. In case of necessity, a soft well lubricated nasal airway will be introduced with minimal force. Once the patient is induced as indicated by regular shallow respiration, trismus is likely to disappear and then laryngoscopy will be tried. Tracheal intubation will be done using Machintosh blade if glottic visualisation is possible. In case of difficulty in passing the tube due to inadequate glottic exposure, a gum elastic bougie will be used as a guide for intubation. I would use a size smaller than the usual cuffed endotracheal tube (6.5 or 7.0 mm ID tube). The important steps to be followed are optimum position of the patient and first laryngoscopy by an experienced person using
RACE 2003 Ramachandra Anaesthesia Continuing Education
A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage 196
Manjunath Prabhu
a well illuminated laryngoscope with appropriate size blade. The first attempt at laryngoscopy should be considered as the best attempt and so all the efforts should be made to optimise the first attempt. After confirming proper placement of the endotracheal tube with auscultation and capnography, muscle relaxant will be administered. A close monitoring of oxygen saturation will be done throughout and all attempts will be made to maintain oxygen saturation in the safe range. A skilled surgeon and a assisting nurse should be ready from the beginning of induction so that an emergency tracheostomy will be done immediately if the need arises.
Following successful airway management surgical drainage will be allowed. A proper drainage with proper exploration of the surrounding spaces is encouraged. Pus will be collected and send for culture and sensitivity test. The antibiotic therapy will be continued intraoperatively. Considering the possibility of post operative airway oedema endotracheal tube will be retained for a variable time which will be decided by the further course of the disease.
Postoperatively, the patient will be kept under the direct observation of the anaesthesiologist in a high dependency area. Supplemental oxygen, analgesics (narcotic infusion), antibiotics and adequate intravenous fluids will be administered. Following surgery, the patient will be reassessed on the first postoperative day. The general condition of the patient, airway oedema and other likely complications like pneumonia or spread of infection to the surrounding tissue will be assessed. If the patient is awake, well oriented with improved general condition and decreased airway oedema then extubation is considered. The equipments for intubation along with monitors like capnograph and pulseoximeter will be kept ready. In the presence of a skilled assistant, extubation will be performed over a tube exchanger which will also have option for oxygen therapy. Following extubation, I will closely observe the patient atleast for an hour before removing the tube exchanger. The patient will be kept under observation for a further 24 hours. Postoperative spread of infection to other tissue planes, to the
lungs and mediastinum is assessed. If the recovery is satisfactory and there is no danger of further airway problems then the patient will be sent to the surgical ward.
THE ALTERNATIVE METHODS OF AIRWAY MAINTENANCE INCLUDE:Elective tracheostomy under local anaesthesia:
Even though this was recommended earlier, many clinicians have shown successful airway management without tracheostomy. If we can avoid this in a relatively short lasting crisis, then we can avoid all the morbidity associated with tracheostomy. In more sick patients with significant airway compromise, this can still be a life saving option either as an elective procedure or as an emergency. The technique is difficult considering the distorted anatomy and abnormal feel of the structures. There are enough reports about infection spreading to deeper planes or to the mediastinum.
Awake fibreoptic guided intubation:Awake fibreoptic intubation can be a
useful alternative method of securing the airway in these patients. This requires a skilled operator and the main limiting factors can be an uncooperative patient with partial airway obstruction and possible secretions, pus or blood which may make it impossible to view through the scope.
Awake direct laryngoscopy and intubation:This technique may sound safer but it
has got its own limitations. A compromised difficult airway in a patient with pain and trismus can make direct visualisation impossible. Direct trauma to the inflammed structures in a struggling patient can lead to airway obstruction or laryngospam requiring emergency tracheostomy. Direct trauma and sudden release of pus may precipitate aspiration and related complications.
Blind nasal intubation :Even though experienced persons can
use this technique, it may not be an easy option in a distorted airway anatomy and compromised airway. Possibility of airway trauma and aspiration should be kept in mind.
RACE 2003 Ramachandra Anaesthesia Continuing Education

A 25 year old otherwise healthy male with Ludwig’sangina is posted for abscess drinage 197 Manjunath Prabhu
Intubation following intravenous induction and muscle relaxation:
This technique may not be advisable in the majority of patients with Ludwig’s angina. Sudden loss of airway following IV induction can lead to a major crisis. This technique can be applied by experienced people when there is no airway compromise.
Thus a patient coming with Ludwig’s angina for abscess drainage poses several challenges and a management dilemma to the anaesthesiologist. Proper preoperative assessment and adequate preparation can make all the difference. Carefully planned airway management can not only help in avoiding tracheostomy, it can also prevent the possible major complications and help in patient’s recovery.
REFERENCES:
1. Patterson HC, Kelly JH and Strome M. Ludwig’s angina: an update. Laryngoscope 1982; 92: 370 - 7.
2. Loughnan TE, Allen DE. Ludwig’s angina. The anaesthetic management of nine cases. Anaesthesia 1985; 40: 295-7.
3. Allen D, Loughnan TE, Ord RA. A re-evaluation of the role of tracheostomy in Ludwig’s angina. J Oral Maxillofac Surg 1985; 43: 436-9.
4. Mehrotra M and Mehrotra S. Decompression of Ludwig’s angina under cervical block. Anesthesiology 2002; 97: 1625-6.
5. Neff SPW, Merry AF and Anderson B. Airway management in Ludwig’s angina. Anaesth Intensive Care 1999; 27: 659-61.
6. Mostafa SM, Atherton AMJ. Sevoflurane for difficult tracheal intubation. Br J Anaesth 1997; 79: 392-93.
7. Moreland LW, Corey J and McKenzie R. Ludwig’s angina report of a case and review of literature. Arch Intern Med 1988; 148: 461-6.
8. Sparks CJ. Ludwig’s angina causing respiratory arrest in the Solomon Islands. Anaesth Intensive Care 1993; 21: 460-2.
RACE 2003 Ramachandra Anaesthesia Continuing Education

PROS & CONS

Induced hypotension is contraindicated in children 198 A. Rajamanoharan
“The use of deliberate hypotension for paediatric procedures has been more limited because the hazards are relatively high”. At present anaesthesiologists are in a “real dangerous position”. We are "pressurized" from many sides to employ this method in order to save blood or facilitate the work of the surgeon! At the same time we are deeply concerned about our lack of knowledge of the haemodyamics involved and by the unexpected complications.- Robert M.Smith, Anaesthesia for infants and children 4th edition, 268
The mechanism of action of hypotensive drugs differ and produce complex changes in the auto regulatory reflexes, and subsequently blood flow to various organs. Because deliberate hypotension is not without risk, the advantages and disadvantages must be weighed. The “intelligent use" of deliberate hypotension has advantages for "certain” procedures that “may” promote surgical success.- Edward D. Miller Jr- Miller 5th edition, 1470
“As the inappropriate use of induced hypotension can result in irreversible cardiac or brain damage”.- George A. Gregory, Text book on Paediatric anaesthesia,
“Thus a systolic blood pressure of less than 70 mm of Hg is a cause for concern at any age”.- Wylie Churchill Davidson
From the above quotations it is more than clear that induced hypotension in children is to be totally discouraged. Let us see in detail why the text books deliver such “danger signals” on deliberate hypotension.
1. Death rate of induced hypotension of 1 in 1802 as stated by Hugovan Aken (Miller) may be statistically insignificant, but totally avoidable and objectionable, because please remember it is deliberate.
2. The decision to induce hypotension has often been controversial, primarily because of our inability to define the lowest safe MAP with confidence.
3. Most clinical studies do not support the belief that deliberate hypotension decreases operating room time.
4. Patient positioning and attention to ventilation, both of which influence venous return play an important role in minimizing blood loss. Clinical experience suggests that blood loss can be decreased with less or no degree of hypotension and that attention to the surgical field may be a better monitor than the absolute value for MAP.
5. The advantages and contraindications must be weighed carefully when induced hypotension is used, as the inappropriate use of induced hypotension can result in irreversible cardiac or brain damage.
6. Further more, significant deviation from the (routine) management may result in organ damage.
7. Body temperature must be carefully monitored because drug-induced generalized vasoconstriction and vasodilatation may increase heat loss. Normothermia should be maintained, if not, deliberate hypotension is contraindicated.
8. An indwelling arterial cannulation is mandatory as rapid and profound changes in the arterial pressure may require immediate intervention as well as determination of arterial blood gases, electrolytes and glucose level.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced hypotension is contraindicated in children 199 A. Rajamanoharan
9. In Pulseoximetry, the reduced size of the pulse waveform is an indicator of reduced pulse volume.
10. If the patient is positioned in head-up, pressure transducer is placed at the level of the he^d and the CVP at the level of right atrium. Both transducers are to be adjusted.
11. The effects of body position and positive pressure ventilation on blood pressure must be evaluated before induced hypotension is started.
12. Urinary catheter should be inserted after induction of anaesthesia but before induced hypotensaion, and care should be taken to maintain a urine output of 0.5 to 2ml/kg/hr throughout anaesthesia
13. In one study, death from controlled hypotension was mainly due to postoperative complications. So, meticulous care imust be directed to the postoperative period besides the routine monitoring.
14. To minimize the risk of cerebral hypoperfusion, hypocapnia is to be avoided during controlled hypotension.
15. The arterial P02 should be maintained above 300mm of Hg at all times during controlled hypotension which may require
i discontinuation of nitrous oxideL16. Thus a systolic blood pressure of less than
70 mm of Hg is a cause for concern at any age.
17. Parasympathetic control of CVS is well developed at birth and sympathetic control is immature.
18. Decreased sympathetic output may explain the normally low blood pressure in human infants and their INCREASED SUSCEPTIBILITY to bradycardia and hypotension.
19. A low level of baroreceptor activity in infants may reduce their ability to ADAPT to hypotension by an increase in heart rate.
20. Even when a clear indication exists, several relative contraindications abort and out-model the usage of induced hypotension.
21. The usefulness of controlled hypotension during clip ligation of cerebral aneurysm is controversial because wall stress at any given pressure depends on the thinness of the aneurysm sac. Better will be temporary occlusion of the proximal vessel.
22. Farmer et al argue that deliberate hypotension
increases the incidence of vasospasm seriously and compromises border line ischemic brain tissue and impairs cerebral auto regulation. Thus controlled hypotension may place focal areas and the entire brain at a risk of ischaemia.
23. Resistance and development of tachyphylaxis.
24. Rebound haemorrhage in the postoperative period.
CONTRA INDICATIONS TO CONTROLLED HYPOTENSION1. Physicians’ lack of understanding of the
technique; lack of technical expertise or inability to monitor the patient’s condition adequately.
2. Inadequate postoperative care3. Local or generalized, decreased organ blood
flow4. Elevated intracranial pressure.5. Anaemia, haemoglobinopathy and
polycythemia6. Allergy or hypersensitivity to hypotensive
agents7. Hypovolemia8. Cerebrovascular disease9. Ischaemic heart disease10. Peripheral vascular disease11. Severe obstructive lung disease12. Renal impairment or hypertension
COMPLICATIONS OF SODIUM NITROPRUSSIDE
For several years, SNP was believed to be devoid of major toxicity. Side effects were seen infrequently, consisting of nausea, vomiting, twitching, sweating, and apprehension, all of which were believed to be the result of overdosage that could be relieved by decreasing the rate of SNP infusion. Chronic overdosage is reported to have caused hypothyroidism in one patient (Katz and Wolf).
The first abnormal response, thought to be tachyphylaxis, is found in patients whose arterial pressure falls with initial administration of SNP but, on continuation of the drug, rises within 30 to 40 minutes, to be controlled only by increasing dosages. This has been seen several times and is believed to be due to the initial presence of adequate tissue rhodanase and
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced hypotension is contraindicated in children 200 A. Rajamanoharan
sodium thiosulfate, followed by early depletion of one, probably the thiosulfate. When this response develops gradually, Davies and associates have been successful in treating the condition with intravenous administration of 150mg of sodium thiosulfate over a period of 15minutes and subsequently proceeding with SNP.
The second abnormal response is seen in patients whose arterial pressure falls with administration of SNP but who require a high dose from the start (over 3.5fig/kg/min).
The third abnormal response consists of such resistance to SNP that hypotension is unobtainable even with greatly increased dosage. Davies and associates believe that patients who show either of the last two responses are in danger of developing metabolic acidosis and cyanide poisoning, and they recommend discontinuation of the drug.
Special contraindications to the use of SNP• Vitamin B12 deficiency• Leber’s optic atrophy• Tobacco amblyopia
Signs suggesting hypoxia or cyanide poisoning during induced hypotension
• Tachycardia, bradycardia, arrhythmias• Metabolic acidosis• High dose requirement
• Increased mixed venous oxygen content• Decreased arterial - mixed venous
oxygen difference• Dilated pupils• High blood cyanide content• Marked hypothermia
The above said contraindications negate the use of induced hypotension. But more importantly, some of these adverse situations may arise during the intraoperative period, in otherwise normal patients. Such a situation becomes very much complex and complicated.
CONCLUSIONSmooth induction, proper choice of
anaesthetic drugs, maintenance of correct plane of anaesthesia, attention to adequate ventilation, proper posture and unimpeded gravity aided venous return will all benefit the surgeon and even more importantly the paediatric patient from undue surgical bleeding and thereby obviate the relative hazards of deliberate hypotension.Primum non nocere - “first of all do no harm”
REFERENCES
1. Robert M.Smith, Anaesthesia for infants and children 4th edition, 268
2. Edward D.Miller Jr - Miller 5th edition, 1470
3. George A. Gregory, Text book on Paediatric anaesthesia,
4. Text book of Anaesthesia by Wylie Churchill Davidson
5. MacRae, W.R.and Owen, M.: Severe metabolic acidosis following hypotension induced with sodium nitroprusside, Br. J. Anaesth. 46:795.
6. McDowall D. G. Keaney, N.P. Turner, J.M, and others; The toxicity of sodium nitroprusside, Br. J. Anaesth. 46:327
7. McHugh, R.D, Berry, F.A, Jr. and Longnecker, D.E,: Dose requirement of sodium nitroprusside during anaesthesia in children, abstract, annual meeting of the American Society of Anaesthesiologists, Chicago.
8. Ivankovich, A.D, Miletich, D.J, Albrecht, R.F, and Zabed, B: Sodium nitroprusside and cerebral blood flow in the anaesthetized and unanaesthetized goat, Anaesthesiology, 44:21.
RACE 2003 Ramachandra Anaesthesia Continuing Education
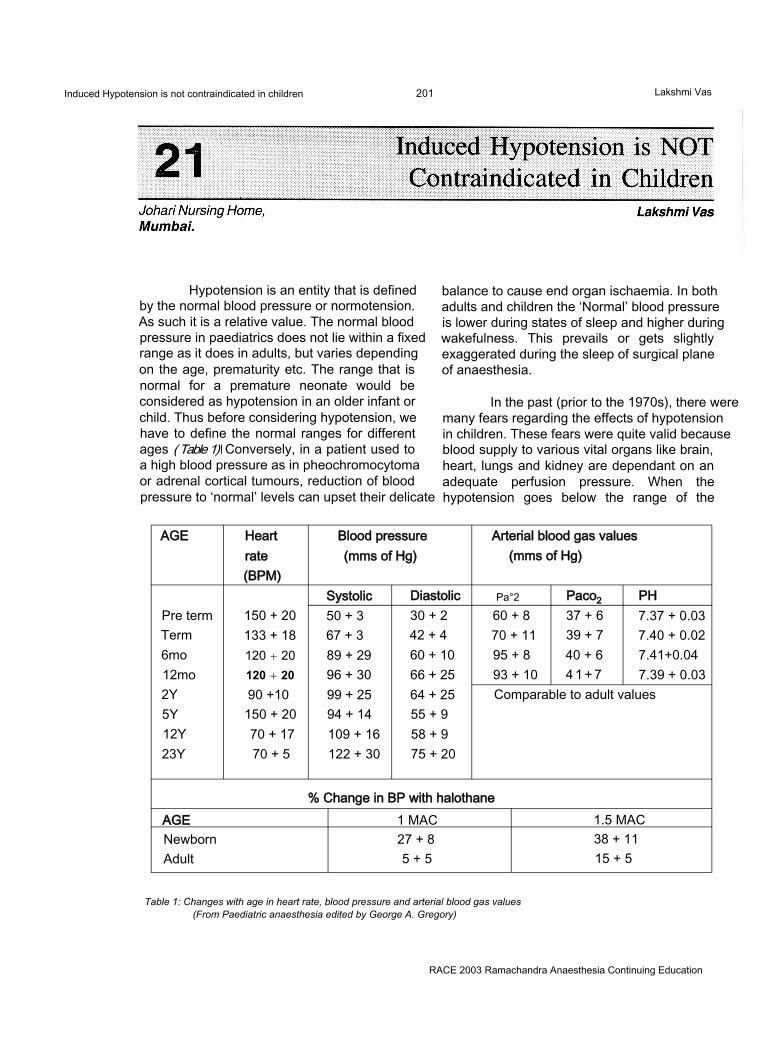
Induced Hypotension is not contraindicated in children 201 Lakshmi Vas
Hypotension is an entity that is defined by the normal blood pressure or normotension. As such it is a relative value. The normal blood pressure in paediatrics does not lie within a fixed range as it does in adults, but varies depending on the age, prematurity etc. The range that is normal for a premature neonate would be considered as hypotension in an older infant or child. Thus before considering hypotension, we have to define the normal ranges for different ages ( Table 1)\ Conversely, in a patient used to a high blood pressure as in pheochromocytoma or adrenal cortical tumours, reduction of blood pressure to ‘normal’ levels can upset their delicate
balance to cause end organ ischaemia. In both adults and children the ‘Normal’ blood pressure is lower during states of sleep and higher during wakefulness. This prevails or gets slightly exaggerated during the sleep of surgical plane of anaesthesia.
In the past (prior to the 1970s), there were many fears regarding the effects of hypotension in children. These fears were quite valid because blood supply to various vital organs like brain, heart, lungs and kidney are dependant on an adequate perfusion pressure. When the hypotension goes below the range of the
AGE Heart Blood pressure Arterial blood gas valuesrate (mms of Hg) (mms of Hg)(BPM)
Systolic Diastolic Pa°2 Paco2 PHPre term 150 + 20 50 + 3 30 + 2 60 + 8 37 + 6 7.37 + 0.03Term 133 + 18 67 + 3 42 + 4 70 + 11 39 + 7 7.40 + 0.026mo 120 + 20 89 + 29 60 + 10 95 + 8 40 + 6 7.41+0.0412mo 120 + 20 96 + 30 66 + 25 93 + 10 4 1 + 7 7.39 + 0.032Y 90 +10 99 + 25 64 + 25 Comparable to adult values5Y 150 + 20 94 + 14 55 + 912Y 70 + 17 109 + 16 58 + 923Y 70 + 5 122 + 30 75 + 20
% Change in BP with halothaneAGE 1 MAC 1.5 MACNewborn 27 + 8 38 + 11Adult 5 + 5 15 + 5
Table 1: Changes with age in heart rate, blood pressure and arterial blood gas values (From Paediatric anaesthesia edited by George A. Gregory)
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 202 Lakshmi Vas
autoregulation for that organ, there can be disastrous consequences of end organ hypoxia. Results of injudicious hypotension could be brain damage and or spinal cord damage in the CNS, renal failure in the kidney, splanchnic ischemia with resultant septicemia in the intestines and so on and so forth.
But all these complications result from an incompetent use of a valuable technique and not as a consequence of its judicious scientific use. It use has to be restricted to specific indications with optimal perioperative monitoring. The general principle is to maintain the highest BP to achieve the desired effect and no lower. The end point is usually a MAP 2/3 the baseline level. The minimum allowable MAP is 55mms of Hg.The onset of hypotension should be gradual over 10-15minutes to allow maximal dilatation of cerebral, coronary and renal vasculature to maintain perfusion pressure and tissue perfusion.
Deliberate or controlled hypotension is a manipulation of the cardiovascular system for:1) Reduction of blood and component loss,
avoiding the risks of blood transfusion and reducing the surgical time.2) Providing a better visibility in the surgical field which is essential for microscopic surgery and procedures inside a narrow or deep cavity that can be flooded by blood (spine) obscuring the whole field including the bleeding vessel.
The common indications are neurosurgery, craniofacial surgery(40% reduction of blood loss), spine surgery , major vascular abnormalities, ENT disorders and burns debridement (1'5)
The contraindications are more discretionary than absolute. Inappropriate use of this good technique can lead to irreversible cardiac and neurological damage. This does not preclude its 3ppropriate scientific use. Obviously the procedure cannot be performed (i) by an inexperienced anaesthesiogist without an understanding of the technique or of paediatric physiology, (ii) when there is lack of technical expertise or (iii) an inability to monitor the patients’ condition adequately ( Table 2) or (iv) an inadequate postoperative care facility.
The relative contraindications applicable to the general patient, both adult and paediatric are focal and generalized reduction of organ blood flow, elevated intracranial pressure, anaemia, haemoglobinopathies (sickle cell anaemia), polycythaemia and allergy or sensitivity to the hypotensive agent.
The mandatory prerequisite for hypotensive anaesthesia is a thorough understanding of the hypotensive agents in a paediatric patient and alteration of physiology by hypotension perse. The hypotensive agents can be subdivided into two types, the volatile agents and the vasodilators.
The anaesthetic agents bring about mild hypotension by maintaing the correct surgical plane of anaesthesia that obtunds any painful stimuli that might cause a haemodynamic response. Their major hypotensive effect is by their effect on the cardiovascular system (negative ionotropy) and/or vasodilatation and depression of central and peripheral sympathetic nerves. Halothane has both effects while isoflurane which has a predominant effect on the peripheral vasculature is preferred. Even nitrous oxide, a weak anaesthetic can cause some hypotension in infants, particularly when their fluid balance is marginal. An initial concentration of 3-4 % and a maintenance level of 2% Isoflurane produces a smooth induction of hypotension, particularly with a reverse Trendelenberg tilt of 20°.
The vasodilators can be subdivided into those that act directly on the vessels (Sodium nitroprusside and nitroglycerin), those that act indirectly, on the sympathetic ganglia (pentolinium) and those that have both direct and indirect actions like Trimethaphan.
THE PHYSIOLOGICAL EFFECTS OF INDUCED HYPOTENSION:Central nervous system:
Most of the data on CBF and metabolism in children have been extrapolated from studies in adults. All volatile agents abolish autoregulation of cerebral blood flow in a dose dependant manner with the effect more pronounced with halothane>enflurane >isoflurane>desflurane. Since we have only halothane and isoflurane in
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 203 Lakshmi Vas
our country, the obvious choice is isoflurane. It also has the advantage that it reduces the cerebral metabolic rate of oxygen more than it reduces the cerebral blood flow, regardless of hypocapnia.
Hypocapnia reduces the CBF in normotensive subjects by 2% for every 1 mmof Hg reduction of PaC02.6 In hypotensive subjects this effect is attenuated or abolished.8,9 If the reduction in CBF is greater than the reduction in CMR02, cerebral ischaemia may develop. EEG changes occur when CBF is reduced to 40-50% of control values and is isoelectric when it is 60% . Vasodilators like nitroprusside and nitroglycerin dilate cerebral vessels directly without affecting the CMR02. Electrical cortical activity and cortical blood flow are preserved better with nitroprusside than with trimethaphan.(10)
To minimize risks of cerebral ischaemia during controlled hypotension, it has been recommended that MAP should be above 55 mms of Hg and that Isoflurane is the agent of choice with nitroprusside or nitroglycerin as adjuncts. A head up tilt may decrease the cerebral perfusion pressure by2mmHg for every 2.5cm the head is above the arterial transducer.
Respiratory system:Controlled hypotension increases the
alveolar dead space and the intrapulmonary shunt. Head up tilt increases the zone 1 and the VdA/t discrepancy, though to a lesser extent than in adults. This has been attributed to a decrease in pulmonary artery pressure, an increase in zone 3 and a reversal of hypoxic pulmonary vasoconstriction. This reversal is in the order of nitroprusside>nitroglycerin> isoflurane. Nitroprusside directly relaxes the pulmonary vasculature with a reduction of right ventricular afterload. Base line ABG and lactate measurements before and after head up tilt and every 30-60 minutes thereafter are essential to ensure adequate oxygenation and normocapnia.
Cardiovascular system:Hypotensive agents reduce
predominantly the afterload and to a lesser extent
preload. The former improves the left ventricular function so long as there is no exaggerated reduction of preload to compromise the left ventricular filling volume. Fortunately, coronary flow is rarely compromised in children (with the exception of muco polyscharidoses and glycogenoses where IHD is reported). So myocardial ischaemia is not a worry. Reflex tachycardia is a common drawback which can be prevented or treated with (3 blockers, propranolol 60ng/kg in small increments or esmolol infusion 500 fig/kg over 2-3 minutes followed by 300 fig/kg/min are useful.
THE HYPOTENSIVE AGENTS:Can be used in conjunction with volatile
anaesthetics or by themselves in patients where volatile agents have to be withheld for malignant hyperthermia or for SSEP or EEG . In these cases a narcotic , relaxant technique with or without propofol is used with hypotensive agents.
Sodium nitroprusside:This is commonly used in children. Its
action, safe doses, toxicity and its treatment have to be thoroughly understood before embarking on its use in children. It is a direct acting arterial dilator and to a lesser extent venous dilator with a rapid onset of action (1-2mins), a brief duration of action and no myocardial depression. It acts via the release of nitric oxide and cyclic GMP. However, overdose produces cyanide toxicity. It is administered as a 0.01% solution ( 50 mg in 500ml) with an infusion rate starting at 0.1 ng/kg/ min and going up to 8-10 ^g/kg/min. The maximal recommended dose is 2-3 mg/kg/day. As it reduces afterload, preload and myocardial oxygen consumption without reducing contractility, it may increase the cardiac output or decrease it or leave it unchanged. Tachycardia as a common baroreceptor response may reduce its effectiveness and necessitate increasing doses and toxicity. To avoid this, p blockers like IV propranolol 0.015 mg/kg or esmolol 0.2-0.3 mg/ kg/h have been used.
TOXICITY:Cyanide is a toxic metabolite which is
metabolized by the rhodanase enzyme system in the liver(80%) and the methaemoglobin
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 204 Lakshmi Vas
pathway in the RBC(20%). Each molecule of nitroprusside produces 5 ions of cyanide. This combines with thiosulphate or hydroxycobalamin ( both are sulphur atom donors) to form thiocyanate which is excreted by the kidney. However if an overdose is given, the detoxification pathways are overwhelmed and the cyanide binds with the cytochrome oxidases of mitochondria to cause cytotoxic hypoxia. As a result, the cells are unable to utilize the available oxygen and the mixed venous oxygen level rises. As a result of anaerobic metabolism of substrates, the level of lactate rises as the pH decreases.
Immediate treatment comprises stopping the infusion of nitroprusside, administration of 100% oxygen to maximize its cellular availability and sodium nitrite (10mg/kg bolus and 5mg/kg over 30 mins). This drug binds with haemoglobin to form methaemoglobin which has a higher affinity for cyanide than the cytochrome oxidase and so is a temporary measure to release the cytochrome oxidase to relieve the cellular hypoxia. Simultaneously sodium thiosulphate 150mg/kg is also administered to transfer cyanide from cyanmethaemoglobin to form thiocyanate, hydrogen cyanide and methaemoglobin. This methaemoglobin is free to leech some more cyanide from the cytochrome oxidases or is converted to normal haemoglobin by glutathione reductase. Caution has to be exercised to avoid too much nitrite to form excessive methaemoglobin which itself can cause cellular hypoxia. Because the level of haemoglobin is so important in avoiding the toxicity and its treatment, anaemia is a definite contraindication to the use of nitroprusside.
Precautions to be taken with nitroprusside administration are monitoring of oxygenation by oximetry and ABG and lactate levels, direct arterial BP, constant watch for unexplained tachycardia and tachyphylaxis. To avoid tachyphylaxis, hypotension can be augmented by coadministration of isoflurane, captopril, aminophylline and p blockers to reduce the dose of nitroprusside. It should be infused through a central line or a dedicated venous line directly into the hub of the cannula to minimize dead space and delayed response to changes
in infusion rate. Use of an infusion pump ensures accuracy and avoids accidental overdose. The IV Bottle should be shielded, though the IV line need not be shielded as the decomposition takes hours and not minutes that the solution is exposed to light in the tubing.
Nitroglycerin:This is a direct acting venous
capacitance dilator and secondarily an arterial dilator and its action is via nitric oxide. It is a potent coronary vasodilator that decreases cardiac output and pulmonary artery pressure. The onset of hypotension is smooth and gradual without precipitous hypotension. The dose is 1-10 jig/kg/min. All the precautions taken with nitroprusside are applicable to nitroglycerin too, except the shielding of the bottle. A controlled double blind study showed that nitroprusside 6-8 fig/kg/m in produced effective hypotension with a mild increase in A-a Do2 and a mild base deficit. Nitroglycerin was less effective in producing hypotension. The metabolites of nitroglycerin are nitrates and nitrites which have less potent vasodilatory effect and no toxic effect. There is no rebound hypertension either. However, tachyphylaxis, and rarely resistance are common as they are baroreceptor mediated in response to hypotension.
Trimethaphan:This rapidly reduces the systolic BP by
decreasing the systemic vascular resistance. The effect has been attributed to ganglionic blockade, (arterial and venular) direct vasodilatation and in high doses, a adrenergic blockade. All the precautions taken with nitroprusside are applicable.
The dose ranges from 10-200 jig/kg/min. Pressure begins to decrease in 5 minutes and reaches minimal values in 10 minutes. A head up tilt helps the hypotension.
Trimethaphan decreases Cardiac output by either ganglionic blockade or negative inotropic effect. Disadvantages include tachyphylaxis , tachycardia, histamine release, inhibition of pseudocholinesterase activity, mild myoneural blockade, fixed dilated pupils(upto 24 h), urinary
RACE 2003 Ramachandra Anaesthesia Continuing Education
Induced Hypotension is not contraindicated in children 205 Lakshmi Vas
retention and gastrointestinal disturbances as an extension of ganglionic blockade.
Pentolinium:This was used in a dose of 0.1 mg/kg
bolus and> repeated to a maximum of 0.3mg/kg. Its onset of action is in 5 minutes reaching a maximum in 30 minutes. The effect is augmented by headhigh tilt, volatile anaesthetics and p blockers, A single dose lasts for 1 -4hrs and can be reversed at the end by change of position to horizontal, stopping the augmenting effect of volatile anaesthetics and p blockers and volume replacement. It has been replaced in paediatric anaesthesia by other better drugs as it has the disadvantages of trimethaphan.
Adenosine:It is an a/a2 agonist. There are a1
receptors in the SA and AV nodes which can cause bradycardia and transient AV block, and those in the kidney that cause renal vasoconstriction. The a2 action causes systemic and pulmonary vasodilation comparable to nitroprusside in the rapidity of and reliability of action but without the disadvantages of tachyphylaxis and rebound hypertension or toxic metabolites. Preload and cardiac output are unchanged or increased. There is no myocardial ischaemia . Both CBF and CMR02 are maintained unlike with nitroprusside. Nor does the hypocapnia cause lowering of CBF to ischaemic levels. However, its a1 action precludes its use. Presently, selective a2 blockers are being developed for clinical use.
Miscellaneous drugs:Likeclonidine, an a2 agonist that is used
for its sedative and hypotensive effects, as an adjunct to isoflurane / metoprolol anaesthesia, magnesium sulphate is being investigated. However, it causes postoperative sedation, coagulation abnormalities and weakness that are a cause for concern, p blockers and calcium channel blockers and propofol have also been used as adjuncts.
ANAESTHETIC MANAGEMENT OF HYPOTENSIVE ANAESTHESIA:
Combined haemodilution (to 30- 20% Hct), hypotension and hypothermia (to 30° C )
have been studied. At lower temperatures, the metabolic demand and oxygen consumption are lower. At 31° C and an FI02of 1, the dissolved oxygen in blood increases to 2ml/100ml representing 30% of Ca02 However these are esoteric techniques to be tried in special centers . In our country, the decision to use controlled hypotension has to be dictated by a favourable risk : benefit ratio and a proper planning of strategies is mandatory. A Hb of 10g/ dl is recommended, though haemodilution with hypotension has been studied.
Premedication can include a venodilator and a ganglion blocker like morphine, droperidol, clonidine (4-8|ig/kg)orchlorpromazine. Vagolytics are avoided.
Intraoperatively, light anaesthesia has to be avoided to prevent hypertension and tachycardia in response to surgical stimulus. Vecuronium is preferred for its slow heart rate. In our country, the best technique to provide analgesia would be an epidural or a regional block if the surgical location permits it. It helps in providing a steady, reliable and total analgesia that is non fluctuant. In addition, the pulse rate goes down as does the blood pressure, to some extent, particularly in children above 6-7 yrs. The vasodilatation associated with epidural also helps in haemodilution . Alternatively, opioids like fentanyl 3 jag/kg stat followed by morphine 0.1 mg/ kg provide a stable level. Positioning with a head up tilt helps with most hypotensive agents.
Intravascular volume should be restored by infusion of colloids (either gelatins or starch) and/or balanced salt solution. A large bore peripheral cannula for replacement of blood loss and a dedicated line for hypotensive infusion is necessary. An arterial line is mandatory for both monitoring and repeated electrolyte, sugar (especially if p blockers like esmolol, metoprolol or labetalol are given), ABG and lactate estimations. An NIBP can both underestimate or overestimate the BP. A dorsalis pedis line may overestimate BP with nitroprusside and underestimate it with isoflurane; so a radial or axillary line is preferred. A central venous line is recommended as right sided filling pressures parallel left sided pressures in children. PA
RACE 2003 Ramachandra Anaesthesia Continuing Education
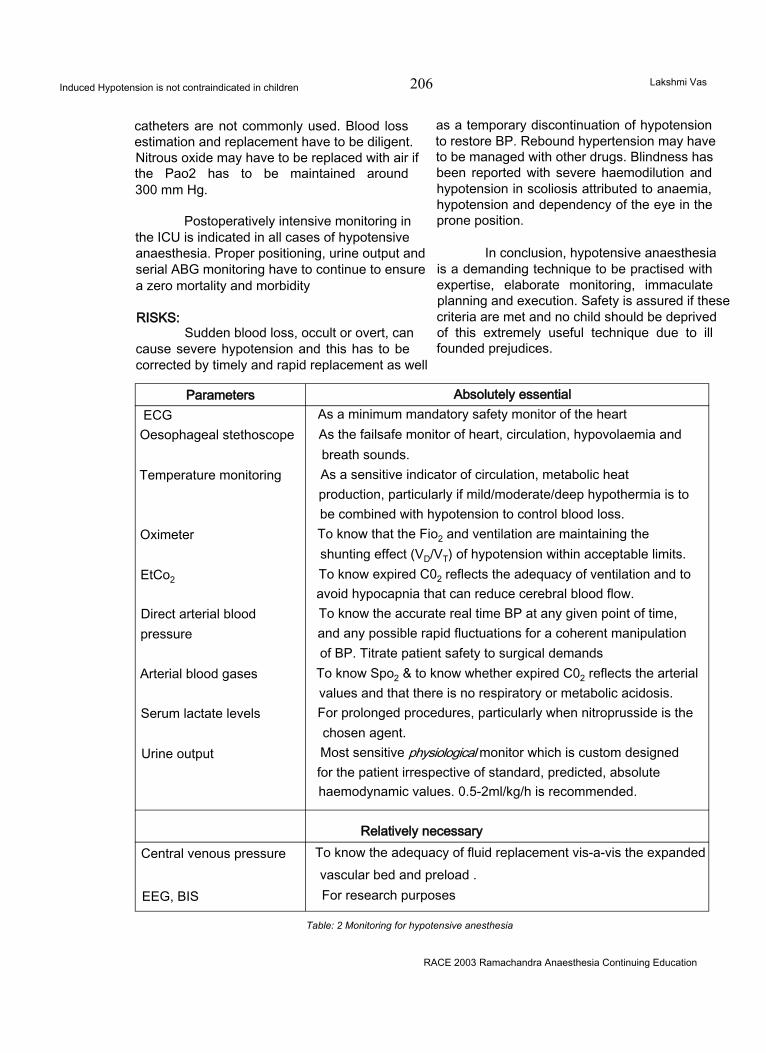
Induced Hypotension is not contraindicated in children 206 Lakshmi Vas
catheters are not commonly used. Blood loss estimation and replacement have to be diligent. Nitrous oxide may have to be replaced with air if the Pao2 has to be maintained around 300 mm Hg.
Postoperatively intensive monitoring in the ICU is indicated in all cases of hypotensive anaesthesia. Proper positioning, urine output and serial ABG monitoring have to continue to ensure a zero mortality and morbidity
RISKS:Sudden blood loss, occult or overt, can
cause severe hypotension and this has to be corrected by timely and rapid replacement as well
as a temporary discontinuation of hypotension to restore BP. Rebound hypertension may have to be managed with other drugs. Blindness has been reported with severe haemodilution and hypotension in scoliosis attributed to anaemia, hypotension and dependency of the eye in the prone position.
In conclusion, hypotensive anaesthesia is a demanding technique to be practised with expertise, elaborate monitoring, immaculate planning and execution. Safety is assured if these criteria are met and no child should be deprived of this extremely useful technique due to ill founded prejudices.
Parameters Absolutely essentialECGOesophageal stethoscope
Temperature monitoring
Oximeter
EtCo2
Direct arterial blood pressure
Arterial blood gases
Serum lactate levels
Urine output
As a minimum mandatory safety monitor of the heart As the failsafe monitor of heart, circulation, hypovolaemia and breath sounds.As a sensitive indicator of circulation, metabolic heat production, particularly if mild/moderate/deep hypothermia is to be combined with hypotension to control blood loss.To know that the Fio2 and ventilation are maintaining the shunting effect (VD/VT) of hypotension within acceptable limits. To know expired C02 reflects the adequacy of ventilation and to avoid hypocapnia that can reduce cerebral blood flow.To know the accurate real time BP at any given point of time, and any possible rapid fluctuations for a coherent manipulation of BP. Titrate patient safety to surgical demands To know Spo2 & to know whether expired C02 reflects the arterial values and that there is no respiratory or metabolic acidosis.For prolonged procedures, particularly when nitroprusside is the chosen agent.Most sensitive physiological monitor which is custom designed for the patient irrespective of standard, predicted, absolute haemodynamic values. 0.5-2ml/kg/h is recommended.
Relatively necessaryCentral venous pressure
EEG, BIS
To know the adequacy of fluid replacement vis-a-vis the expanded vascular bed and preload .For research purposes
Table: 2 Monitoring for hypotensive anesthesia
RACE 2003 Ramachandra Anaesthesia Continuing Education

Induced Hypotension is not contraindicated in children 207 Lakshmi Vas
References
1. Jerrold Lerman In Special techniques ( acute normovolemic haemodilution, controlled hypotension and hypothermia, and ECMO in Paediatric anaesthesia edited by George A . Gregory 4th edition Churchill Livingstone New York, Edinburgh .London, Philadelphia.
2. DiazJH. Lockhart CH: Hypotensive anaesthesia for craniectomy in an infancy. Br.J.Anaesth 51: 233, 1979.
3. Viguera MG., Terry RN., Induced hypotension for an extensive surgery in an infant Anesthesiology 27: 701, 1966.
4. Fairbairn ML., Eltringhamrj, Young PN Robinson JM. Hypotensive anaesthesia for microsurgery of the middle ear A comparison between halothane and isoflurane. Anaesthesia 41: 637 1986
5. Szyfelbein SK Ryan JF Use of controlled hypotension for primary surgical excision in an extensively burned child. Anesthesiology 41:501 1974
6. HarpJR. Wollman H : Cerebral metabolic effects of of
hyperventilation and deliberate hypotension.Br.J.Anaesth 45:256.1973.
7. Artru AA: Partial preservation of cerebral vascular responsiveness to hypocapnia during isoflurane induced hypotension in dogs Anesth Analg 65:660,1986.
8. ArtruAA. Colley PS. Cerebral blood flow response to hypocapnia during hypotension. Strokel 5:878,1984.
9. ArtruAA. . Cerebral vascular response to hypocapnia during nitroglycerin induced hypotension. Neurosurgery 16:468.1985.
10. Thomas WA, Cole PV Etherinton NJ et al.: Electrical activity of the cerebral cortex during induced hypotension in man: a comparison of sodium nitroprusside and trimethaphan Br.J.Anaesth 57:134.1985
11. YasterM., Simmons RS., ToloVT. Etal: A comparison of nitroprusside and nitroglycerin for inducing hypotension in children : a double blind study. Anesthesiology. 65:175, 1986
12. Jean Camboulives in the chapter on Fluid, Transfusion, and blood sparing techniques in PEDIATRIC ANAESTHESIA .Principles and practice edited by Bruno Bisonetteand Bernard Dalens McGraw -Hill.
RACE 2003 Ramachandra Anaesthesia Continuing Education
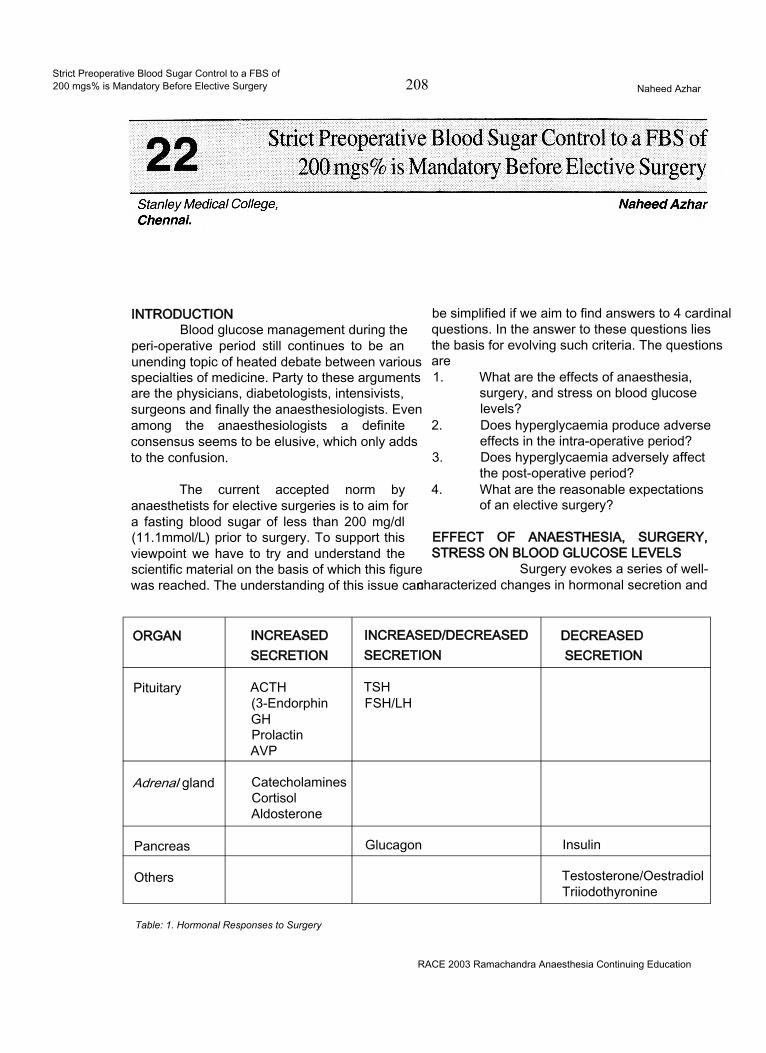
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 208 Naheed Azhar
INTRODUCTIONBlood glucose management during the
peri-operative period still continues to be an unending topic of heated debate between various specialties of medicine. Party to these arguments are the physicians, diabetologists, intensivists, surgeons and finally the anaesthesiologists. Even among the anaesthesiologists a definite consensus seems to be elusive, which only adds to the confusion.
The current accepted norm by anaesthetists for elective surgeries is to aim for a fasting blood sugar of less than 200 mg/dl (11.1mmol/L) prior to surgery. To support this viewpoint we have to try and understand the scientific material on the basis of which this figure was reached. The understanding of this issue can
be simplified if we aim to find answers to 4 cardinal questions. In the answer to these questions lies the basis for evolving such criteria. The questions are1. What are the effects of anaesthesia,
surgery, and stress on blood glucose levels?
2. Does hyperglycaemia produce adverse effects in the intra-operative period?
3. Does hyperglycaemia adversely affect the post-operative period?
4. What are the reasonable expectations of an elective surgery?
EFFECT OF ANAESTHESIA, SURGERY, STRESS ON BLOOD GLUCOSE LEVELS
Surgery evokes a series of well- characterized changes in hormonal secretion and
ORGAN INCREASED INCREASED/DECREASED DECREASEDSECRETION SECRETION SECRETION
Pituitary ACTH(3-EndorphinGHProlactinAVP
TSHFSH/LH
Adrenal gland CatecholaminesCortisolAldosterone
Pancreas Glucagon Insulin
Others Testosterone/OestradiolTriiodothyronine
Table: 1. Hormonal Responses to Surgery
RACE 2003 Ramachandra Anaesthesia Continuing Education
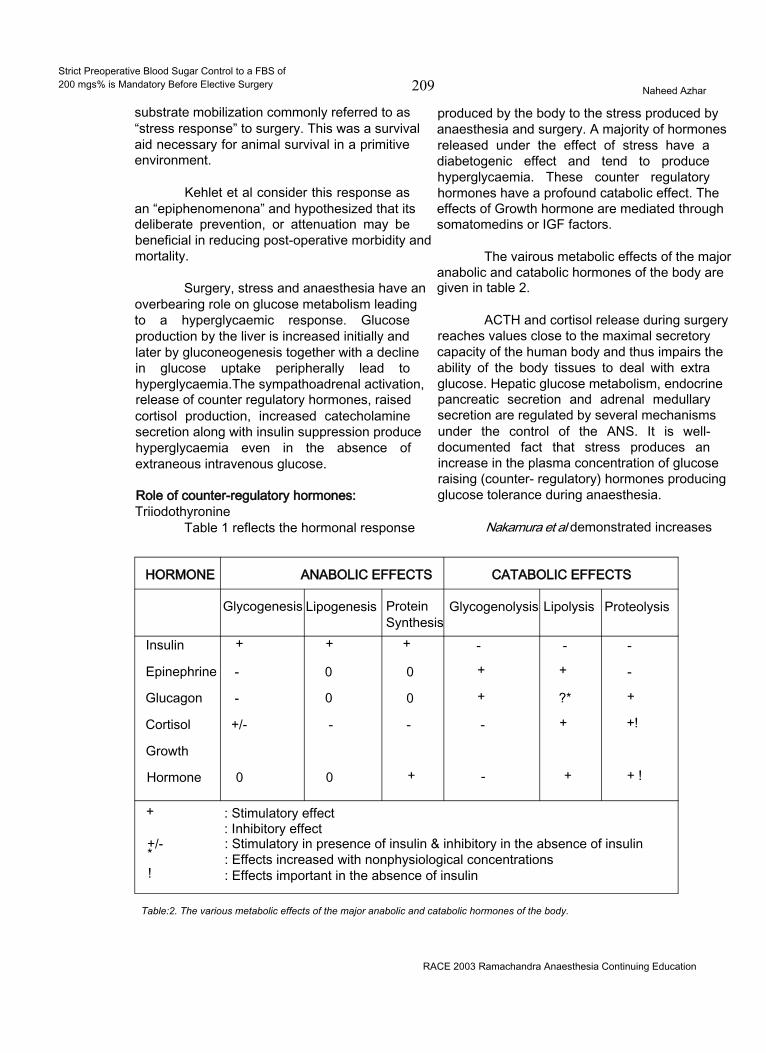
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 209 Naheed Azhar
substrate mobilization commonly referred to as “stress response” to surgery. This was a survival aid necessary for animal survival in a primitive environment.
Kehlet et al consider this response as an “epiphenomenona” and hypothesized that its deliberate prevention, or attenuation may be beneficial in reducing post-operative morbidity and mortality.
Surgery, stress and anaesthesia have an overbearing role on glucose metabolism leading to a hyperglycaemic response. Glucose production by the liver is increased initially and later by gluconeogenesis together with a decline in glucose uptake peripherally lead to hyperglycaemia.The sympathoadrenal activation, release of counter regulatory hormones, raised cortisol production, increased catecholamine secretion along with insulin suppression produce hyperglycaemia even in the absence of extraneous intravenous glucose.
Role of counter-regulatory hormones:Triiodothyronine
Table 1 reflects the hormonal response
produced by the body to the stress produced by anaesthesia and surgery. A majority of hormones released under the effect of stress have a diabetogenic effect and tend to produce hyperglycaemia. These counter regulatory hormones have a profound catabolic effect. The effects of Growth hormone are mediated through somatomedins or IGF factors.
The vairous metabolic effects of the major anabolic and catabolic hormones of the body are given in table 2.
ACTH and cortisol release during surgery reaches values close to the maximal secretory capacity of the human body and thus impairs the ability of the body tissues to deal with extra glucose. Hepatic glucose metabolism, endocrine pancreatic secretion and adrenal medullary secretion are regulated by several mechanisms under the control of the ANS. It is well- documented fact that stress produces an increase in the plasma concentration of glucose raising (counter- regulatory) hormones producing glucose tolerance during anaesthesia.
Nakamura et al demonstrated increases
HORMONE ANABOLIC EFFECTS CATABOLIC EFFECTS
Glycogenesis Lipogenesis ProteinSynthesis
Glycogenolysis Lipolysis Proteolysis
Insulin + + + - - -
Epinephrine - 0 0 + + -
Glucagon - 0 0 + ?* +
Cortisol +/- - - - + +!
Growth
Hormone 0 0 + - + + !
+
+/-*!
: Stimulatory effect : Inhibitory effect: Stimulatory in presence of insulin & inhibitory in the absence of insulin : Effects increased with nonphysiological concentrations : Effects important in the absence of insulin
Table:2. The various metabolic effects of the major anabolic and catabolic hormones of the body.
RACE 2003 Ramachandra Anaesthesia Continuing Education
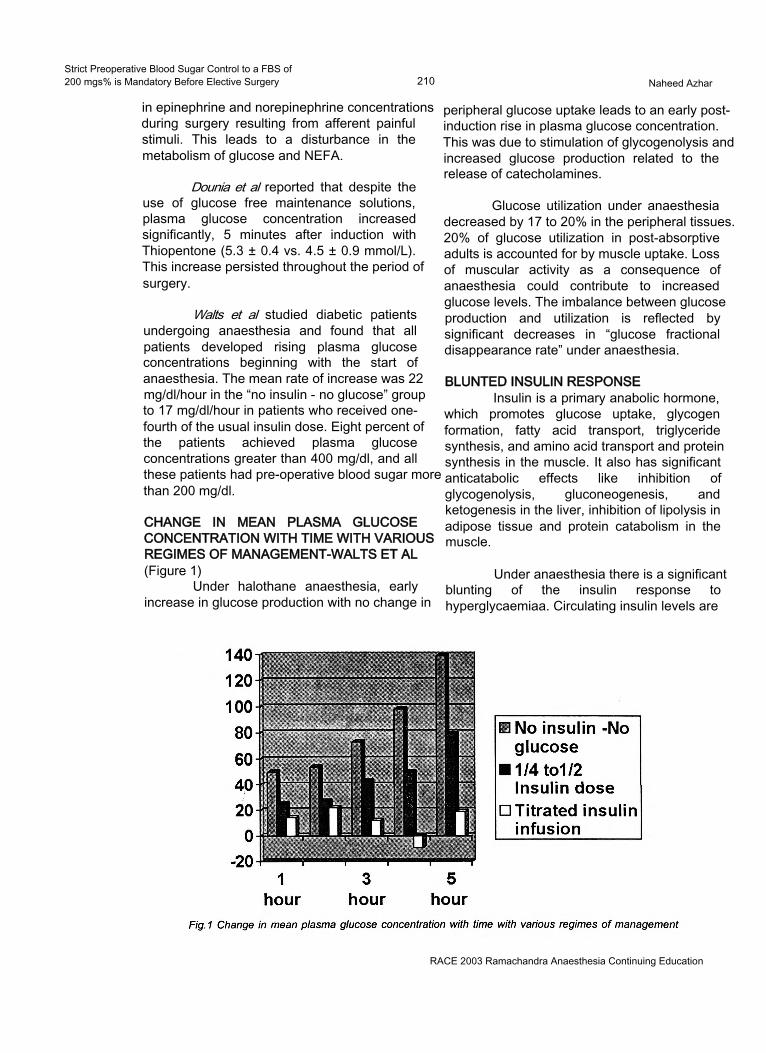
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 210 Naheed Azhar
in epinephrine and norepinephrine concentrations during surgery resulting from afferent painful stimuli. This leads to a disturbance in the metabolism of glucose and NEFA.
Dounia et al reported that despite the use of glucose free maintenance solutions, plasma glucose concentration increased significantly, 5 minutes after induction with Thiopentone (5.3 ± 0.4 vs. 4.5 ± 0.9 mmol/L). This increase persisted throughout the period of surgery.
Walts et al studied diabetic patients undergoing anaesthesia and found that all patients developed rising plasma glucose concentrations beginning with the start of anaesthesia. The mean rate of increase was 22 mg/dl/hour in the “no insulin - no glucose” group to 17 mg/dl/hour in patients who received one- fourth of the usual insulin dose. Eight percent of the patients achieved plasma glucose concentrations greater than 400 mg/dl, and all these patients had pre-operative blood sugar more than 200 mg/dl.
CHANGE IN MEAN PLASMA GLUCOSE CONCENTRATION WITH TIME WITH VARIOUS REGIMES OF MANAGEMENT-WALTS ET AL(Figure 1)
Under halothane anaesthesia, early increase in glucose production with no change in
peripheral glucose uptake leads to an early postinduction rise in plasma glucose concentration. This was due to stimulation of glycogenolysis and increased glucose production related to the release of catecholamines.
Glucose utilization under anaesthesia decreased by 17 to 20% in the peripheral tissues. 20% of glucose utilization in post-absorptive adults is accounted for by muscle uptake. Loss of muscular activity as a consequence of anaesthesia could contribute to increased glucose levels. The imbalance between glucose production and utilization is reflected by significant decreases in “glucose fractional disappearance rate” under anaesthesia.
BLUNTED INSULIN RESPONSEInsulin is a primary anabolic hormone,
which promotes glucose uptake, glycogen formation, fatty acid transport, triglyceride synthesis, and amino acid transport and protein synthesis in the muscle. It also has significant anticatabolic effects like inhibition of glycogenolysis, gluconeogenesis, and ketogenesis in the liver, inhibition of lipolysis in adipose tissue and protein catabolism in the muscle.
Under anaesthesia there is a significant blunting of the insulin response to hyperglycaemiaa. Circulating insulin levels are
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 211 Naheed Azhar
inappropriately low for the prevailing blood glucose values, reflecting a relative lack of circulating insulin during surgery. The factors responsible for this are unclear, but it seems that circulating catecholamines released during surgery have a direct inhibitory effect on the p cells of the pancreas, acting through the a adrenoreceptors.
Desborough et al demonstrated decline in insulin secretion after the induction of anaesthesia, and before the onset of surgery. This inhibition implicated the role of the anaesthetic agents, either directly or indirectly by altering splanchnic blood flow.
Kehlet et al reported increased blood lactate concentrations during surgery under GA.
Desborough et al also demonstrated that inhibition of insulin secretion by halothane, enflurane and isoflurane in clinical concentrations by their inhibitory effect on the stimulus-secretion coupling in the p cells of pancreas and impairment in uptake of glucose in both skeletal and hepatic tissues.
Brandi et al demonstrated that in days after surgery or trauma, circulating insulin values increase above normal values, but the hormone is ineffective metabolically. This period presenting with hyperglycaemia is called the “phase of insulin resistance”. It is related to the effects of catabolic hormones like cortisol and cytokines on insulin receptors along with a post-receptor defect. The moderate resistance to insulin may also be attributable to alteration in the distribution space and serum clearance of insulin.
CONCLUSION NO: 1Anaesthesia and surgery conclusively
produce a hyperglycaemic response due to increased secretion of counter regulatory hormones and relative insulin resistance. This is attributable to decreased glucose tolerance induced by any of the following mechanisms:1. Impaired insulin secretion.2. Decreased biologic response of tissues to
insulin such as diminished peripheral glucose utilization.
3. Impaired gluconeogenesis and /or glycogenolysis.
4. Increased hepatic glucose output and / or
splanchnic release of glucose due to increased anabolic process.
5. Decreased peripheral uptake of glucose.
ADVERSE EFFECTS OF HYPERGLYCAEMIA IN THE INTRA-OPERATIVE PERIOD
Inadequate control of blood glucose and hyperglycaemia in the intra-operative period leads to1. Ketosis.2. Acidemia.3. Electrolyte abnormalities.4. Volume depletion from osmotic diuresis.5. Hyperosmolality.6. Thrombogenesis.7. Lactic Acidosis.8. Disruption of autoregulation.
The renal threshold for glucose is 10 mmol/L. At levels greater than this, the glycosuria causes an osmotic diuresis, with loss of water and electrolytes. High levels of blood glucose can cause severe cellular dehydration due to osmotic transfer of water out of the cells. During renal glycosuria, the osmotic effect on the renal tubules decreases tubular reabsorption of fluids. This leads to massive loss of fluid in the urine causing ECF dehydration, and ultimately compensatory dehydration of the ICF.
Intra-operative hyperglycaemia leads to hyperosmolality. Each mOsmol / L of any substance exerts an osmotic pressure of 19.3 mm Hg. Blood glucose at normal concentrations of 5.6 mmol / L (100 mg / dl) exerts a pressure of 108 mm Hg. The osmotic pressure of plasma is 5443 mm Hg, which is 20 mm Hg more than the pressure of the ECF and ICF, which is 5423 mm Hg. A rise in blood glucose to 20 mmol / L can change the osmotic pressure by as much as 400 mm Hg producing deleterious effects on water and electrolyte homeostasis.
The maximum reabsorptive capacity of renal tubules for glucose averages 320 mg / min. When the tubular load rises above 220 mg / min (plasma glucose = 180 mg / dl), a small amount of glucose begins to appear in the urine, termed as glucose threshold. This glucose excretion keeps rising between plasma levels of 180 to 250 mg / dl. Beyond plasma glucose of 250 mg /dl the absorptive capacity of all nephrons is exceeded showing a steep rise in glycosuria.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 212 Naheed Azhar
Osmotic diuresis is accompanied by a continual loss of electrolytes particularly sodium. Sodium loss is around 150 mmol / L of urine and potassium around 5 mmol / L. Progressive sodium depletion activates the Renin - Angiotensin system and Aldosterone secretion increases, leading to increased sodium resorption from tubules. High aldosterone concentrations reduce potassium resorption and increase urinary potassium excretion. Hyponatremia and Hypokalemia can occur. In rare instances, when oliguria and uremia occur inspite of a substantial osmolar load, potassium starts leaking out of cells into ECF, but can no longer be excreted by diuresis. So although the total potassium stores are depleted the patients may have dangerously high plasma potassium.
Hyperosmolality and dehydration can produce haemodynamic instability and depressed mental state leading to recovery problems. Sodium and potassium derangements may produce arrhythmias and delayed recovery. Hyperglycaemia may increase the viscosity of blood by increasing the osmolal load. Increased viscosity favors slow flow of blood in the blood vessels. Slowflcwing blood causes concentration of pro-coagulants to rise high enough in certain local areas to initiate clotting and thrombogenesis. This is more likely to occur if conditions like dehydration, pre-existing atherosclerosis, high haematocrit, cold induced peripheral vasoconstriction, myocardial depression and hyperglycaemia are present. Controlling peri-operative blood glucose to < 10 mmol / L (200 mg / dl) can eliminate some of the precipitating causes.
Hyperglycaemia increases production of macroglobulins by the liver. They increase the viscosity and promote intracellular swelling by favoring production of non-diffusible molecules like sorbitol.
Hyperglycaemia also disrupts autoregulation. Glucose induced vasodilatation prevents vital target organs from protection against increases in systemic blood pressures. Different degrees of hyperglycaemia may be required before different vascular beds are affected.
Hyperglycaemia promotes lactic acidosis and academia. The increased viscosity and dehydration are major contributory factors
towards it. Acidosis may impair cardiac contractility, provoke arrhythmias, hypotension and interfere with the action and metabolism of drugs. Acidoc s depresses not only the myocardial function but also respiration. Bicarbonate therapy to rapidly correct acidosis is fraught with dangers in alteration of CNS structure and function due to paradoxical CSF and CNS acidosis, decreased CBF, altered CNS oxygenation and development of unfavorable osmotic gradients.
A study of 340 diabetics undergoing open-heart surgery revealed an increases in operative mortality (1.8% vs. 0.6%). During the study a number of cases were reported where inotropic agents were ineffective in maintaining cardiac contractility, although filling pressures, sinus rhythm, serum electrolytes and blood gases were adequate. The blood sugar was high in each of this case. After IV infusion of insulin, effective myocardial contractions returned, allowing easy and rapid bypass weaning.
Intra-operative use of drugs like corticosteroids, p agonists and adrenergic agents all increase the likelihood of intra-operative hyperglycaemia.
CONCLUSION NO: 2Hyperglycaemia is definitely undesirable
during the intra-operative period. The adverse effects of hyperglycaemia are directly or indirectly related to increased blood glucose levels producing1) Ketosis.2) Lactic Acidosis and Acidemia.3) Electrolyte abnormalities.4) Volume depletion from osmotic diuresis.5) Hyperosmolality.6) Thrombogenesis.7) Impaired myocardial contractility.8) Haemodynamic instability.9) Arrythmogenicity.10) Altered drug pharmacodynamics and
pharmacokinetics.11) Disrupted autoregulation of vascular beds.
IMPLICATION OF HYPERGLYCAEMIA IN THE POST/PERI-OPERATIVE PERIOD
Hyperglycaemia during the peri-operative period leads to an increased incidence of infection and delayed wound healing.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 213 Naheed Azhar
Hirsch et al report that impaired wound strength and wound healing occur when plasma glucose levels exceed 11.1 mmol /L (200 mg / dl). Hyperglycaemia interferes with leukocyte chemotaxis, opsonization, phagocytosis, granulocyte adherence and depresses bactericidal activity.
Hyperglycaemia depresses the immune response of the body to infection by producing short-term glycosylation of immunoglobulins thereby inactivating them. Glycosylation of C3 component of complement occurs at its opsonic site, rendering it impotent and unable to bind to the surface of the invading bacteria.
Rassias et al demonstrated that neutrophil phagocytic activity was less depressed when blood sugar was tightly controlled during the peri-operative period (75% vs. 47%). They demonstrated that hyperglycaemia depresses the white cell function and increases the risk of infection after surgery.
Researchers showed that anastomotic healing in both ileum and colon of diabetic animals was better if hyperglycaemia is tightly controlled starting from 4 days before surgery and extending into the entire peri-operative period. Hyperglycaemic animals showed qualitative change in the newly formed collagen causing reduction in wound strength.
Studies reveal that hyperglycaemia results in impaired wound healing due to 1) Accelerated non-enzymatic glycosylation of body proteins due to addition of glucose molecules to the exposed lysine residues on extra cellular proteins. 2) Glycosylation of newly synthesized collagen associated with increased collagenase activity and decreased wound collagen content.
CONCLUSION NO: 3Hyperglycaemia increases the incidence
of infection by interfering with leukocyte function. It also impairs wound healing by altering collagen activity and strength.
GOALS OF ELECTIVE SURGERYAnaesthesia and surgery carry a certain
amount of risk even for the normal patient. The lowest class in ASA classification is Class 1,
with its attendant risks. A class 0 does not exist in anaesthesia. Unanticipated, undesirable events can occur during anaesthesia and these can range from mere hypotension, myocardial depression to the much dreaded arrhythmias, anaphylaxis and failed intubation situations.
During elective surgery, the aim is to plan and to be prepared to minimize these risks to as low as possible. Even if unforeseen complications arise, we should be able to leave the patient undergoing elective surgery with the least possible risk of suffering morbidity or mortality. Uncontrolled hyperglycaemia in the peri-operative period precludes our ability to offer this advantage to the patient undergoing elective surgery.
Hyperglycaemia worsens the neurological outcome in patients who have suffered global CNS ischaemia / hypoxia. Hirsch et al recommend tight control of blood sugar in patients undergoing neurosurgical procedures. Werner et al recommend a plasma glucose of 100 to150 mg / dl for better outcome of patients with stroke or neurotrauma.
Roizen et al recommend blood glucose of less than 200 mg / dl during periods of ischaemia in diabetic patients about to undergo surgery in which hypotension or reduced cerebral blood flow occurs. Hyperglycaemia also worsens neurological outcome after regional CNS blood flow alterations and ischaemia.
In a study of 430 consecutive patients resuscitated after out-of-hospital cardiac arrest, mean blood glucose values were found to be higher in patients who never awakened (341 ± 13 mg / dl) than in those who did (262 ± 7 mg / dl). Among patients who awakened, those with persistent neurological deficits had higher mean glucose levels (286 ± 15 mg / dl) than did those without deficits (251 ± 7 mg / dl). These results are consistent with the findings that hyperglycaemia during stroke is associated with poorer short- and long-term neurological outcomes.
Roizen et al advocate that blood glucose is a major determinant of brain damage following ischaemia. They recommend that until better data is available blood glucose levels should be maintained below 200 mg / dl during periods of likely cerebral ischaemia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Blood Sugar Control to a FBS of200 mgs% is Mandatory Before Elective Surgery 214 Naheed Azhar
Hyperglycaemia in the pregnant diabetic affects her adversely, as well as her offspring. Maternal hyperglycaemia may stimulate insulin secretion in the fetus leading to neonatal hypoglycaemia and delayed release of glucagons. Hypotension in the presence of hypoglycaemia in this sub-sect of patients produced maternal lactic acidosis and consequent fetal acidosis.
Conclusion No: 4During elective surgery enough time is
available to adequately stabilize the patient. This should be utilized to minimize the risk of morbidity and mortality due to anaesthesia and / or surgery. Unanticipated, critical events, if they occur (as they could during anaesthesia) it has been conclusively proven that hyperglycaemia are associated with poor outcome.
CURRENT MOST PRACTISED PROTOCOL FOR DIABETIC MANAGEMENT
Before the advent of bedside glucosimetry, hypoglycaemia being greatly feared, majority of the anaesthetists accepted a moderate hyperglycaemia in the peri-operative period. Since early 1970’s evidence has been accumulating against the harmful effects of even moderate hyperglycaemia.
Dunnet et al in 1985 surveyed the protocols used by anaesthetists in the diabetic management in the peri-operative period. Most of the anaesthetists aimed to maintain the blood glucose in the range of 7 to 10 mmol/L. 35% of respondents chose a value greater than 11 mmol/L.
Eldridge et al restudied the same parameters in 1993. They now found that 26% preferred to maintain blood glucose between 4- to7 mmol/L. 63% preferred a range of 7 to 10 mmol/L. Only 9% selected a range greater than11 mmol/L.
These gross changes amongst the attitude of anaesthesiologists, in their practice of managing blood glucose during the peri-operative period, clearly indicates the emerging trends based on the scientific data that has been made available by recent research. Undoubtedly there is an emerging need to control blood sugar within the normoglycaemic range. The starting point in
this endeavor is to start with pre-operative blood sugar below 200 mg / dl.
CONCLUSIONIn our attempt to seek an answer for
what would be an appropriate pre-operative blood sugar value in a fasting state in an individual posted for elective surgery, we ended up searching the literature to find answers for 4 questions. The search yielded important conclusions, which need to be re-considered at this stage. They are■ Anaesthesia and surgery definitely produce a hyperglycaemic response.• Hyperglycaemia produces undesirable adverse effects in the intra-operative period.■ Hyperglycaemia increases the risk of infection and delays wound healing.■ Unanticipated critical events if they occur in the presence of hyperglycaemia are associated with poor outcome.■ The current approach to blood glucose management in the peri-operative period is to maintain blood glucose within the normoglycaemic range.
The adequate management of blood sugar for the entire peri-operative period should begin with adequate control in the pre-operative period. Fasting blood sugar in elective surgeries, if not all, should strictly be maintained in the normoglycaemic range.
Amongst the majority of workers who have done hall mark studies in peri-operative management of blood glucose, Hirsch, Rassias, Kehletand Roizen all recommend blood glucose to be maintained between 140 to 180 mg/dl. Alberti et al give us the liberty of accepting fasting blood sugar of 180 to 200 mg / dl as an indicator of adequate control.
On the basis of the scientific data available to us at this point of time, it seems reasonable to aim for peri-operative blood sugar in the normoglycaemic range, it would be appropriate to begin this with a fasting blood sugar of less than 200 mg /dl being mandatory for elective surgeries.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Strict Preoperative Control of Blood Sugar to an FBS of 200mg%is NOT Mandatory Before Elective Surgery 215 Kalyan Chakravarthy
INTRODUCTION:Diabetes Mellitus (DM) with its
devastating consequences has assumed epidemic proportions in many countries of the world. Spectacular increase in the incidence and prevalence of this chronic disease is destined to have enormous impact on mortality, morbidity and health care resources. India would rank first in sharing the global burden of diabetes in the next two decades1. Epidemiological transition including improved socio-economic status, rural to urban migration, adoption to sedentary habit and stress of modern life style is largely responsible for this cataclysmic shift in the burden of diabetes2.
DEFINITION OF DIABETES MELLITUS (DM):Diabetes Mellitus is a syndrome
characterised by chronic hyperglycaemia and disturbances of carbohydrate, fat and protein metabolism associated with absolute or relative deficiencies in insulin secretion and /or insulin action. When fully expressed, diabetes is characterised by fasting hyperglycaemia, but the disease can also be recognised during less overt stages and before fasting hyperglycaemia appears, most usually by the presence of glucose intolerance3.
CURRENT DIAGNOSTIC CRITERIA:The 1997 American Diabetic Association
(ADA) expert committee on the diagnosis and classification of diabetes mellitus and the provisional report of the WHO consultation focus on fasting plasma glucose (FPG) that is 126mg% or greater and confirmed on subsequent day as the preferred criterion for the diagnosis of diabetes mellitus4. This criterion is supported by studies demonstrating that this threshold accurately
differentiates between non-diabetic and diabetic populations and is associated with the development of specific diabetic microvascular complications.
The following points must be remembered while the diagnosis of diabetes mellitus is made.
1. The diagnosis of DM must be based on blood glucose estimations.
2. Urine glucose testing must not be used to diagnose diabetes.
3. True blood glucose should be estimated using enzymatic methods like the glucose oxidase method.
4. Plasma glucose >200mg%, confirmed on repeat testing, in a patient with characteristic signs and symptoms of diabetes is diagnostic.
5. Doing a GTT in a known diabetic patient is not necessary.
6. In all other persons, a GTT must be carried out in order to exclude diabetes.
CLASSIFICATION OF DIABETES MELLITUS5:Diabetes is classified into four major
categories:• Type-1 —IDDM• Type-ll-MODY• Gestational• Secondary
DOES GOOD GLYCAEMIC CONTROL MATTER:
Improved control of blood sugar is protective and this has been confirmed in humans. The Diabetes Control and Complications Trial (DCCT) in the USA compared standard and intensive insulin therapy in a prospective controlled trial of young patients with IDDM6. Even
RACE 2003 Ramachandra Anaeschesia Continuing Education
Strict Preoperative Control of Blood Sugar to an FBS of 2Q0mg%is NOT Mandatory Before Elective Surgery________________________ Kalyan Chakravarthy
in those with intensive therapy, mean blood glucose levels were 40% above the non-diabetic range, but this level of control reduced the risk of progression to retinopathy by 60%, nephropathy by 30% and neuropathy by 20% over seven years of the study.
CELLULAR AND MOLECULAR BASIS OF LONG TERM DIABETIC COMPLICATIONS7:
The complications of DM are attributable to tissue damage due to vascular disease involving micro and macro vasculature. The most common pathology of micro vessels occurs in the retina, kidney, peripheral arteries of the lower limbs, in the coronary vessels and the cerebral arteries.
RELATIONSHIP BETWEEN DIABETIC CONTROL AND COMPLICATIONS:
Patients with type-1 DM have more chance of developing duration dependent complications of disease with better survival. Patients with type-11 DM may have microvascular and macrovascular complications of the disease at the time of detection.
The (UKPDS) UK Prospective Diabetes Study was started in 1977 and included 5702 patients with NIDDM over a period of 20 years6. Summary is:1. Good glycaemic control is necessary for type II diabetes mellitus.2. Early intervention to modify risk factors, and obtain good glycaemic control.3. Control of hypertension in patients with typeII DM needs intensive treatment.4. UKPDS confirms the efficacy of existing treatment for type II DM.
UKPDS and nephropathy - Renal failure and death from renal disease did not differ between the conventional group and the intensive group
UKPDS and neuropathy - No significant difference was seen in the incidence of absent knee and ankle reflexes. Incidence of impotence, abnormal cardiac autonomic functions also did not differ significantly between the groups.
UKPDS and macrovascular complications - The incidence of fatal Ml, heart failure, angina, stroke, amputation and death from
PVD was not lowered significantly.
While a close control of blood glucose is normally mandatory to avoid progressive organ failure, during the peri-operative period, well- standardised insulin protocols appear to be sufficient to manage the diabetic patient7
The peri-operative care of diabetic patients is less dependent on blood glucose control, which needs to be exceptionally tight, and is usually easily obtained thanks to pharmacological improvements, human insulins and analogues, technical progress with blood glucose monitoring at the bedside and infusion with constant flow rates. More important is the influence of end organ pathology, often clinically silent, which must be carefully assessed during the pre-operative evaluation. The organ impairments concern especially the heart, but also all those organs that were modified by abnormal glycosylated proteins. The pre-existing pathology has many consequences on anaesthesia management; the anaesthetic technique depends essentially on their existence. A better long-term control of diabetes both for type I and type II by insulins, and the new oral antidiabetic drugs reduce the incidence of the end organ pathology and the risk linked to organ failure in the peri-operative period8.
Diabetes per se is not a risk factor for post-operative morbidity or mortality, after adjustment for co-morbidities like atherosclerosis. Controlled studies have shown the advantages of tight control of glycaemia, in two acute complications of atherosclerosis, i.e. Ml and CVA. These diseases have a high prevalence rate in diabetic patients, as the probability of macroangiopathy is high. Perioperative tight control of glycaemia is a probable necessity to avoid these complications, which is best achieved by a team.
Reasonable control of blood sugar can best be achieved within a few hours pre-operatively and clinical assessment can be performed on an outpatient basis. Anaesthetic management consists of assessments of control of the disease followed by evaluation of diabetic complications and their severity.
Different views are expressed regarding tight control of blood glucose vs. moderate control
RACE 2003 Ramachandra Anaesthesia Continuing Education
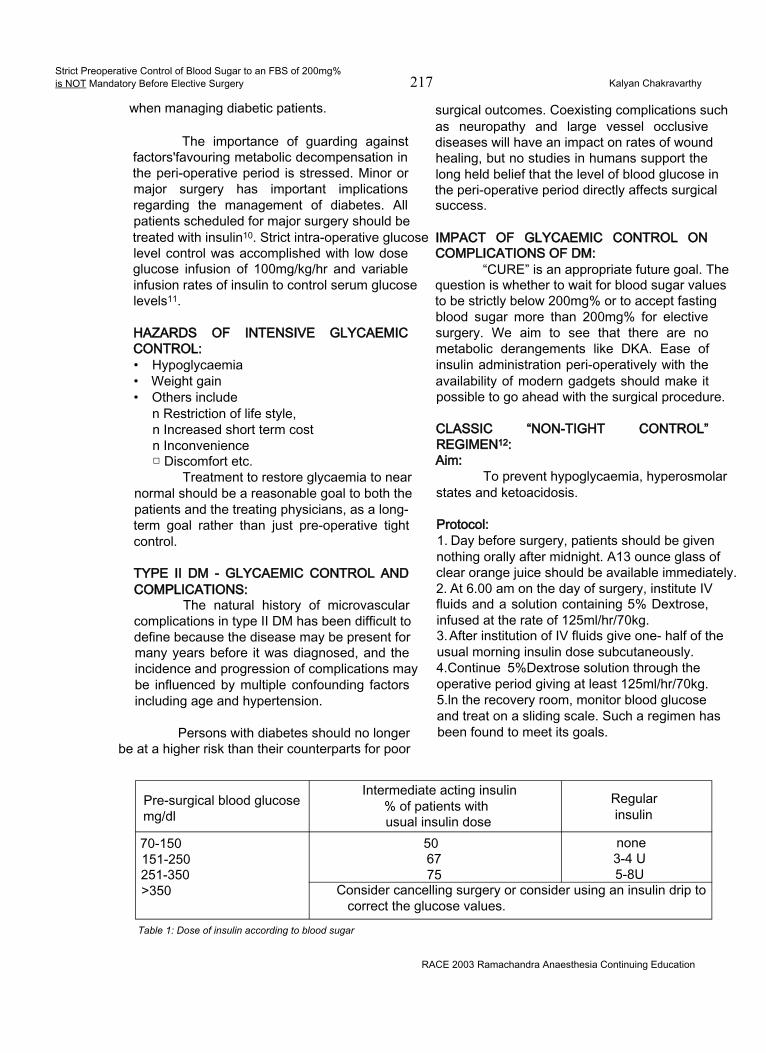
Strict Preoperative Control of Blood Sugar to an FBS of 200mg%is NOT Mandatory Before Elective Surgery 217 Kalyan Chakravarthy
when managing diabetic patients.
The importance of guarding against factors'favouring metabolic decompensation in the peri-operative period is stressed. Minor or major surgery has important implications regarding the management of diabetes. All patients scheduled for major surgery should be treated with insulin10. Strict intra-operative glucose level control was accomplished with low dose glucose infusion of 100mg/kg/hr and variable infusion rates of insulin to control serum glucose levels11.
HAZARDS OF INTENSIVE GLYCAEMIC CONTROL:• Hypoglycaemia• Weight gain• Others include
n Restriction of life style, n Increased short term cost n Inconvenience □ Discomfort etc.
Treatment to restore glycaemia to near normal should be a reasonable goal to both the patients and the treating physicians, as a longterm goal rather than just pre-operative tight control.
TYPE II DM - GLYCAEMIC CONTROL AND COMPLICATIONS:
The natural history of microvascular complications in type II DM has been difficult to define because the disease may be present for many years before it was diagnosed, and the incidence and progression of complications may be influenced by multiple confounding factors including age and hypertension.
Persons with diabetes should no longer be at a higher risk than their counterparts for poor
surgical outcomes. Coexisting complications such as neuropathy and large vessel occlusive diseases will have an impact on rates of wound healing, but no studies in humans support the long held belief that the level of blood glucose in the peri-operative period directly affects surgical success.
IMPACT OF GLYCAEMIC CONTROL ON COMPLICATIONS OF DM:
“CURE” is an appropriate future goal. The question is whether to wait for blood sugar values to be strictly below 200mg% or to accept fasting blood sugar more than 200mg% for elective surgery. We aim to see that there are no metabolic derangements like DKA. Ease of insulin administration peri-operatively with the availability of modern gadgets should make it possible to go ahead with the surgical procedure.
CLASSIC “NON-TIGHT CONTROL” REGIMEN12:Aim:
To prevent hypoglycaemia, hyperosmolar states and ketoacidosis.
Protocol:1. Day before surgery, patients should be given nothing orally after midnight. A13 ounce glass of clear orange juice should be available immediately.2. At 6.00 am on the day of surgery, institute IV fluids and a solution containing 5% Dextrose, infused at the rate of 125ml/hr/70kg.3. After institution of IV fluids give one- half of the usual morning insulin dose subcutaneously.4.Continue 5%Dextrose solution through the operative period giving at least 125ml/hr/70kg. 5.ln the recovery room, monitor blood glucose and treat on a sliding scale. Such a regimen has been found to meet its goals.
Pre-surgical blood glucose mg/dl
Intermediate acting insulin % of patients with usual insulin dose
Regularinsulin
70-150 50 none151-250 67 3-4 U251-350 75 5-8U>350 Consider cancelling surgery or consider using an insulin drip to
correct the glucose values.Table 1: Dose of insulin according to blood sugar
RACE 2003 Ramachandra Anaesthesia Continuing Education

Strict Preoperative Control of Blood Sugar to an FBS of 200mg%is NOT Mandatory Before Elective Surgery________________________ Kalyan Chakravarthy
GENERAL GUIDELINES FOR DIABETIC PATIENTS ON THE DAY OF SURGERY13: Tab 1
For type I or type II diabetic patients on insulin therapy: Check blood glucose levels before surgery and use the following guidelines:
In conclusion, an important clinical lesson is that hyperglycaemia is the most important cause of long-term diabetic complications in both types of DM. The available methods of treatment of hyperglycaemia, is effective in achieving near normoglycaemia, which will lessen the morbidity, mortality and cost of management of diabetic complications.
REFERENCES:1. King H et al- Global burden of diabetes 1995-2025, prevalence, numerical estimates and projections. Diabetes Care 1998;21: 1414-31.
2. Ramachandran A, Snehalatha C et al - Diabetes Epidemiology Study Group in India (DESI), High prevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes Survey. Diabetologia 2001 ;44: 1094-101.3. Peter H. Bennett. Chapter 11; Diabetes definition and pathogenesis, Joslin’s Diabetes Mellitus - 13th Edn. Lippincott Williams and Wilkins 193-4, 2000.4. The Expert Committee on Diagnosis and Classification of Diabetes Mellitus.Diabetes Care 1997;20: 1183-97.5. Douglas B. Coursin, et al, Peri-operative care of the diabetic patient. ASA Refresher courses in Anesthesiology 2001 October; 29(1): 1-9.6. Ashok Kumar Das, TS Ashida. Impact of glycaemic control on complications Diabetes Mellitus- Chapter 46. RSSDI-Text book of Diabetes Mellitus, 1st Edn. 2002. 617-22.7. Minerva Anestesiologica. 67(4):258-62, 2001 Apr.8.European Journal of Anaesthesiology. 18(5):277-942001 May.9. Acta Clinica Belgica. 52(5):313-9, 1997.10. South African Journal of Surgery, 30(3);85-9,l!892 Sep.11. JAMA, 244(2): 166-8, 1980 July.12. Ronald D. Miller. Anesthetic implications of concurrent diseases, chapter 25; 5th Edition p-909.s13. Clinical Diabetes vol19, No2, 2001
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia Is Contraindicated for Day Care Surgery 219 Elsa Varghese
The advent of newer short acting general anaesthetic drugs have made day care surgery a reality. Day care surgery involves short duration surgical procedures (not associated with significant alterations in the patient’s normal physiology) on relatively healthy patients. The improvement in surgical technique and the major advancements in anaesthesia drug research has resulted in a large number of medical centres performing the majority of surgical procedures on a day care basis.
In the recent past, the factor of economy has played a major role in increasing the popularity of providing regional anaesthesia for day care surgery. Spinal anaesthesia is being popularised by die-hard fans of this technique as the anaesthetic of choice for surgeries performed below the level of the umbilicus.
To those of us who have performed thousands of spinal anaesthetics and will continue to do so in the future, one may wonder why should there be any contraindication for surgery to be performed on a same day basis, under spinal anaesthesia. There are several reasons why, which this article will address.
COMPLICATIONS AND UNDESIRABLE SIDE EFFECTS OF SPINAL ANAESTHESIA
Complications and undesirable side effects associated with spinal anaesthesia require anaesthesiologists to balance potential risks against potential benefits. Everyday, anaesthesiologists are challenged to make clinical judgements as to the means and methods for ensuring the safety and comfort of their patients. In many cases the administration of spinal anaesthesia may be controversial. The relationship between perceived risk of potential
complications and administration of spinal anaesthesia is a need to be examined.1
Failure to Achieve Anticipated AnaesthesiaSpinal anaesthesia unlike general
anaesthesia is fallible! Even with modern techniques designed to enhance precision, regional anaesthesia may not completely meet the expectations of patients, surgeons or anaesthesiologists. The spectre of unreliability can prejudice its selection.
Informed Consent and Spinal AnaesthesiaWe are obliged to inform our patients of
the potential risks associated with spinal anaesthesia including local anaesthetic toxicity, haematoma, infection, cardiac arrest or death. Shivering, backache, dizziness and urinary retention are unpleasant side effects that may require disclosure.
Controversy of Hyperbaric Spinal LidocaineThe ideal spinal anaesthetic would
combine rapid and adequate surgical anaesthesia with rapid achievement of discharge criteria such as ambulation and urination. The most important determinant of both successful surgical anaesthesia and time until recovery is the dose of local anaesthetic.2
Ideally, local anaesthetics that have an appropriate duration of action with an acceptable side effect profile and the addition of adjuvants which add to the anaesthetic efficacy, without prolonged recovery need to be administered. Hyperbaric spinal lidocaine has long been the gold standard for short acting spinal anaesthesia. Lidocaine has an optimal onset and duration of action of anaesthesia for out-patients but also has the potentially unacceptable side effect of
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia Is Contraindicated for Day Care Surgery 220 Elsa Varghese
transient neurologic symptoms (TNS).3 The incidence of TNS has been found to be highest in out-patients compared with in-patients and in patients undergoing surgery in the lithotomy position (30%) or knee arthroscopies (20%), under spinal anaesthesia.4
Reports of cauda equina neuropathy (CEN), persistent sacral nerve root irritation and unacceptable high incidence of transient neurologic symptoms (TNS) have forced a reappraisal of the safety of hyperbaric spinal lidocaine.
I) CAUDA EQUINA NEUROPATHY (CEN)Auroy et al reported 24 neurologic deficits
following 40,600 spinal anaesthetics.5 Nine of these occurred after lidocaine. CEN has been reported following repeated spinal administration, given to improve the density of a patchy or incomplete subarachnoid block.6
Since CEN can occur after uncomplicated single injections as well, the safety of hyperbaric spinal lidocaine has become controversial. There is mounting laboratory evidence supporting the possibility that a substantial risk exists for prolonged abnormal conduction when 5% Lidocaine is applied to simulated nerve roots.7
The threat of CEN and persistent sacral irritation and transient neurologic symptoms has certainly challenged the clinical decision to persist with providing appropriate spinal anaesthesia for day care surgery.
II) TRANSIENT NEUROLOGIC SYMPTOMS (TNS)
The term TNS is used to describe symptoms of backache with radiation into the buttocks or lower extremities. This syndrome is rarely seen after general anaesthesia and has been demonstrated after spinal anaesthesia. Hyperbaric heavy lidocaine is associated with an increased risk for TNS.8 The aetiology of TNS is unknown. Positioning (lithotomy and knee flexion), sacral stretch, pooling of hyperbaric spinal lidocaine following installation with small-bore pencil point needles have all been implicated as possible risk factors. TNS may occur post
operatively in 4-36% of patients undergoing hyperbaric lidocaine spinals. Alternative approaches for spinal anaesthesia especially for use in outpatients are prompted by the fear of possible neurologic effects of heavy lidocaine.2
ill) CONTROVERSY OF ALTERNATIVES TO HYPERBARIC SPINAL LIDOCAINE
Finding alternatives to hyperbaric spinal lidocaine has challenged clinicians. TNS has been reported with lower concentrations of lidocaine. The addition of epinephrine to isobaric spinal mixtures can increase the incidence of urinary retention.9
Spinal anaesthesia enthusiasts are now ‘dialling down’ the mass of local anaesthetic instilled. But unfortunately dose response data for alternatives such as bupivacaine is scant. There is renewed interest in isobaric and hypobaric alternatives. Laboratory studies suggest a comparative potency of bupivacaine to lidocaine of 9:1. Studies with 2% lidocaine (40mg and lower doses), as well as 0.5% hyperbaric spinal bupivacaine (7.5mg), though providing adequate duration of anaesthesia; have shown a discharge time often exceeding 3 hours for both drugs.1011
IV) MINI DOSE SPINAL ANAESTHESIALow dose lidocaine (20mg) or bupivacaine
6 mg with fentanyl has been advocated for day care spinals of late. Though these combinations may provide satisfactory analgesia and recovery profiles as described by some authors, these concentrations may not provide an immobile extremity during surgery.121314 Moreover, proprioception is preserved with this combination and therefore the patient has the unpleasant awareness of limb manipulation
Post-Dural Puncture Headache (PDPH)Although not a life threatening problem,
PDPH carries substantial morbidity by restricting activities of daily life. A recent survey of 75 consecutive patients suffering from PDPH revealed that approximately 18% had slight restriction of physical activity, 31 % were partially bedridden with restricted physical activity and 51% were entirely bedridden. Furthermore spontaneous resolution of PDPH takes 1 -6 weeks
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia Is Contraindicated for Day Care Surgery 221 Elsa Varghese
after dural puncture thus resulting in frequent and prolonged restriction of daily activities.15
Because no effective non-invasive treatments exist, clinical strategies have focused on prophylactically reducing CSF lost after dural puncture. Traditionally, we have minimised needle size to decrease the size of the CSF leak in the dura, turned cutting needles longitudinally to prevent transverse cutting of longitudinally aligned dural fibres and selected pencil-point needles to maximize the parting and not cutting of dural fibres. Reina et al16 have questioned the concept of less trauma to the dura with pencil-point needles as their study observed similarly sized but more traumatic lesions to the dura with pencil- point needles compared with longitudinally aligned cutting tips.
Evaluation of Closed Claims Data BasesCheny et al17 examined closed claims
database of the American Society of Anaesthesiologists. Of 4183 claims, 16% were for anaesthesia related nerve injury. 84 claims were associated with spinal anaesthesia.
Sudden cardiac arrest during spinal anaesthesia is a significant cause of risk in current medical practice. Interestingly they have been reported in young men undergoing short surgical procedures, where the cardiac arrest occurred almost 30 to 40 minutes following the administration of the spinal anaesthetic. 41 well- documented cases of cardiac arrest have been reported, in which a circulatory mechanism played the primary role in sudden cardiac arrest during spinal or epidural anaesthesia. These arrests were vagal linked or associated with vagal- inducing stimuli like traction, movement, fear and athletic heart syndrome.
Intra-operative cardiac arrest analysis in a prospective study by Biboulet18 suggests that risks and outcomes may be less favourable under conditions of spinal anaesthesia than general anaesthesia. There is persuasive evidence that this phenomenon can occur unexpectedly under conventional conditions of practice and that the associated injury can be very severe.
More so in a situation of day care surgery where there is a rapid turnover and the anaesthetist is under stress to run a schedule in a hurried manner.
BARRIERS TO THE PRACTICE OF SPINAL ANAESTHESIA IN AMBULATORY SURGERY
In ambulatory surgery the use of spinal anaesthesia is subject to the same risk benefit analysis that applies to any anaesthetic technique. There are absolute and relative contraindications.
Patient SelectionSpinal anaesthesia involves very careful
patient selection, the careful positioning and preparation of the patient, introduction of a needle into the subarachnoid space and injection of a local anaesthetic with or without an adjuvant drug and the need to wait for the onset of action of the drug. The possibility of a patchy effect of the block is a reality. The knowledge and expertise in dealing with untoward physiological effects of the block are required. Often, for day care surgery, general anaesthesia has been the preferred anaesthetic of choice mainly for convenience of fast turn overtime and therefore maintaining the hectic OR schedule in a busy day care set up.
Patients are still anxious about being awake during a surgical procedure and more so in the day care setting where premedicant anxiolytic drugs are used minimally. So it is crucial to pick the right patient as inappropriate patients or patients with great anxiety, needle phobia, poorly controlled psychiatric disease or language barriers, are all potentially difficult situations, where though the spinal anaesthetic may provide the analgesia, the patient remains extremely restless and anxious throughout. These patients may require deep sedation, which then defeats the advantages of the technique.
An increasing number of patients are on anti platelet drugs, as the concern for deep vein thrombosis is on the rise. These medications pose an additional risk for spinal anaesthesia and an in-depth information of the medications the patient is on is essential.
>RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia Is Contraindicated for Day Care Surgery 222 Elsa Varghese
Picking the Wrong SurgeonSurgeons must be willing to wait a few
minutes for the onset of action of the block and the choice of spinal anaesthesia may be inappropriate in the outpatient setting when a large number of patients have been scheduled and you have an impatient surgeon on hand.
Picking the Wrong SurgeryPelvic Laparoscopy is a common
procedure performed on a day care basis involving carbon dioxide pneumoperitoneum and steep Trendelenburg. When these procedures are performed under spinal anaesthesia, shoulder tip pain (irritation of the diaphragm) and ascent of spinal level (steep Trendelenburg) are troublesome complications which can occur.
Discharge CriteriaPatients undergoing spinal anaesthesia
need to meet additional discharge criteria before being sent home. As yet there are still no clear- cut guidelines for patient discharge criteria following spinal anaesthesia in ambulatory surgery and they are still being evolved. The ability to void is an important discharge criterion that results in a significant delay in patient discharge after resolution of spinal anaesthesia.19,20
The patient should also be able to stand unaided, walk in a straight line and stand still without swaying. These additional tests would pose an additional strain on recovery room staff especially in a busy day care set-up.
GENERAL ANAESTHESIA FOR DAY CARE SURGERV
Newer anaesthetics have the pharmacokinetic and pharmacodynamic advantages of a shorter duration of action and a more rapid rate of recovery. These factors permit a faster emergence from anaesthesia. Less than 30 years ago, it was unthinkable that patients would be able to return home on the day of surgery. Today, advances in surgery and anaesthesia make it possible to perform surgery safely and effectively on an ambulatory basis.21
With newer agents, propofol, remifentanil, sevoflurane, rapid recovery of patients undergoing anaesthesia permits a patient to be shifted
directly from the operating room to a second stage recovery room and not necessarily the post anaesthesia care unit where nursing care is intensive.
CONCLUSION
Given the uncertainty, along with the time constraints under which day care anaesthesia has to be provided, there has to be a rethink on pushing for the increased use of spinal anaesthesia in the day care setting. There are too many variables out of our control, which does not make it the suitable anaesthetic technique of choice in day care anaesthesia.
REFERENCES
1. Gilbert HC: Complications and controversies in regional anaesthesia. ASA Refresher Course lectures October 2002: No 1232. Liu SS, McDonald SB: Current Issues in Spinal Anaesthesia. Anesthesiology 2001; 94:888-9063. Pollock JE, Neal JM, Stephenson CA et al: Prospective study of the incidence of transient radicular irritation in patients undergoing spinal anaesthesia. Anesthesiology 1996; 84:1361-74. Freedman JM, Li DK, Drasner K, et al: Transient neurologic symptoms after spinal anesthesia. Anesthesiology 1998; 89:1633-415. Auroy Y, Narchi P, Messiah A, et al. Serious complications related to regional anesthesia. Results of a prospective survey in France. Anesthesiology 1997; 87:469-726. Rigler M, Drasur K, Krejue TC et al: Cauda equina syndrome after continuous anesthesia. Anesth Analg 1991; 72:275-817. Lambert L, Lamber D, Strichartz GR: Irreversible conduction block in isolated nerve by high concentrations of local anesthetics. Anesthesiology 1994; 80:10828. Hiller A, Kearjalainen K, Balk M, et al: Transient neurological symptoms after spinal anaesthesia with hyperbaric 5% lidocaine or general anaesthesia. Br J Anaesth 1999; 82:575-99. Chiu A, Liu S, Carpenter RL, et al: The effects of epinephrine on lidocaine spinal anesthesia, a crossover study. Anesth Analg 1995; 80:735-910. Hampi KF, Heinzmann-Wiender S, et al: Transient neurologic symptoms after spinal anesthesia. A lower incidence with prilocaine and bupivacaine than with lidocaine. Anesthesiology 1998; 88:629-3311. Urmey WF, Stanton J, et al: Combined spinal- epidural anesthesia for outpatient surgery. Dose response characteristics of intrathecal isobaric lidocaine using 27 gauge Whitacre spinal needle. Anesthesiology 1995; 83: 528-3412. Ben David B, Mayarsky M, Gurevetch A et al: Comparison of mini dose lidocaine -fentanyl and conventional dose lidocaine spinal anesthesia. Anesth Analg 2000; 91:856-70
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia Is Contraindicated for Day Care Surgery 223 Elsa Varghese
13. Casati A, Fanelli G, Cappelleri G, Berglin B, et al: Low dos£ hyperbaric bupivacaine for unilateral spinal anesthesia. Can J Anesth 1998; 45:850-5414. Ben David B, Solomon E, et al: Intrathecal fentanyl with small dose dilute bupivacaine; better analgesia without prolonged recovery. Anesth Analg 1997; 85: 560-515. Lybecker H, Djernes M, Schmidt JF: Post dural puncture headache (PDPH): onset, duration, severity and associated symptoms: an analysis of 75 consecutive patients with PDPH. Acta Anaesthesiol Scand 1995; 39:605-1216. Reina MA, de Leon-Casasola OA, Lopez A, et al: an in vitro study of dural lesions produces by 25 gauge Quinke and Whitacre needles evaluated by scanning electron microscopy Reg Anesth Pain Med 2001; 25:393- 403
17. Cheny FW et al: Standard of care and anaesthesia liability. JAMA 1989; 261: 1599-160318. Biboulet P: Fatal and non-fatal cardiac arrest related to anesthesia. Can J Anesth 2001; 48:326-3219. Marshall SI, Chung F: Discharge criteria and complications after ambulatory surgery. Anesth Analg 1999; 88:508-1720. Kamphuis ET,lnonescu Tl, Kuipers PW, et al: Recovery of storage and emptying function of urinary bladder after spinal anesthesia with lidocaine and with bupivacaine in men. Anesthesiology 1998; 88:310-621. Lichter JL, Wetchler BV: Outpatient anesthesia, Clinical Anaesthesia, 3rd Edition. Edited by Barash PG, Cullen BF, Stoelting RF, Philadelphia, JP Lippencott Co 1997, pg. 1389-1412
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery Rathna.N.
It is 103 years since the first spinal anaesthetic was administered by Bier in August 1898 in Kiel, Germany. Spinal anaesthesia for a procedure that in many institutions would nowadays be managed on an outpatient basis was reported by Matas in December 1899.1 In spite of the widespread development of ambulatory surgery, there has been relatively little critical evaluation of the role of spinal anaesthesia in outpatients. ‘
Over the past 20 years, the most dramatic change in the delivery of surgical care in the United States has been the shift from inpatient to outpatient and short-stay surgical procedures. Ambulatory surgery in the 1990s, with its demonstrated efforts at cost containment has been enthusiastically accepted by all segments of,health care. Consequently, 65% of all surgical procedures are outpatient based and 35% are in-patients, which in turn has had an impact on the manner in which both surgeons and anaesthesiologists practice.2
“What is an ideal outpatient Anaesthetic”?An ideal outpatient anaesthetic should
provide a safe, simple technique with a quick start (onset of action), rapid stop (offset of effects), minimal postoperative side effects with residual analgesia in the postoperative period. Can spinal anesthesia provide all these? “YES” with selective Spinal anaesthesia.
Why do we think conventional Spinal anaesthesia is contraindicated in ambulatory Surgery?
It is because of the belief and fact that Conventional Dose Spinal Anaesthesia (CDSA)
involves a technique that initiates a block lasting long, with a long time to recovery. Since the time of conventional technique to now, with the better understanding of neurological anatomy, physiology, molecular pharmacology and receptor pharmacology and devices, we have embarked into an era of precision where “selectivity” is the rule with excellent results and benefits, with minimum side effects, which has resulted in a practice of a changed spinal anaesthesia, while exploiting the good aspects of it and succeeding in making it “walk in and walk out” technique for ambulatory surgery.
Professional concernsA survey of 3,651 anaesthetists revealed
that 68 % would choose regional anaesthesia for their own surgery.3 Among the reasons given were ease of administration, fewer complications, pleasant recovery, good operating conditions and less difficulty in the recovery room. More recently, 91 % of anaesthetists who experienced both spinal and epidural anaesthesia expressed a preference for regional anaesthesia.4 Thus, there appears to be a “double standard” within the profession which has lead to pleas that anaesthetists treat their patients as they themselves would like to be treated. Interestingly, 50% of outpatients are afraid of not waking up after anaesthesia. Even though patients’ main preferences are mental clarity and freedom from emesis, pain, dysphoria and myalgias, there is evidence to indicate that administration of general anaesthesia leads to these very problems which may persist for up to 28 days postoperatively.5 Patients’ attitudes towards regional anaesthesia is either favorable(46%) or indifferent (45%), and their main fears are needle pain, backache, seeing and
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia is not Contraindicated for Day Care Surgery 225 Rathna.N.
hearing things, paralysis and the possibility of failure. Thus , a majority of patients would be amenable to regional techniques.
Spinal anaesthesia is not contraindicated for day care surgeries
Regional anaesthesia like spinal and epidural anaesthesia can offer many advantages for the ambulatory patients. In addition to limiting the anaesthetized area, the common side effects of general anaesthesia like nausea, vomiting, dizziness, lethargy etc can be avoided.6 It is said that patients with GA are either “sore, sick or sleepy”. Furthermore, the risks of aspiration, pneumonitis and other side effects of tracheal intubation are avoided. Other advantages include decreased post-operative intensity of care, decreased recovery times, increased mobility, (and) increased post-operative alertness7 and postoperative analgesia. Recently published outcome data have suggested that patients undergoing spinal / epidural anaesthesia alone or combined with general anaesthesia may actually have decreased morbidity and mortality when compared to patients undergoing general anaesthesia alone.8
Minor morbidity, patient satisfaction and costThere are few well-structured
comparisons of regional and general anaesthesia in outpatients. Although general anesthesia continues to be offered as the anaesthetic of choice to most outpatients, its role is being questioned. It is now becoming apparent that minor morbidity is of serious concern. The reported incidence of minor symptoms after outpatient propofol- based general anaesthesia were: hoarse voice (26%), sore throat (24%), headache (10%), backache (20%), emesis (12%), loss of appetite (18%), anxiety (12%), tiredness (28%), delayed recovery of normal function (37%) and postoperative pain (55%).6 A randomised comparison of spinal and general anaesthesia in 433 patients revealed that general anaesthesia was associated with a higher incidence of nausea and vomiting, sore throat, a longer stay in the recovery room with an increased need for opioids, and increased cost.9 Other studies have confirmed a shorter discharge time and decreased cost after spinal anaesthesia. Finally, studies of spinal anaesthesia in outpatients consistently demonstrate that patient satisfaction remains high (>90%).10
Should we abandon conventional dose spinal anaesthesia (CDSA) in outpatients?
A comparison of GA (propofol) and CDSA (15 mg bupivacaine) showed that 180 min after surgery, 15% of GA patients fulfilled home discharge criteria but none of the CDSA patients were able td walk due to residual motor block11. Recently, Vaghadia et al ^demonstrated that small-dose spinal lidocaine was associated with shorter discharge times than CDSA. They have remarked thatthere is a price to be paid for CDSA and the data also revealed what some of us may have suspected - propofol GA may not be the panacea for outpatients. The large standard deviations seen with GA reflect large inter-patient variability depending on whether postoperative complications such as emesis and pain develop, and delay discharge. Interestingly, the short acting spinal anaesthetics have small standard deviations and this suggests that their use will be associated with a more predictable discharge profile, particularly when they are employed with small dose techniques.12
So, conventional dose spinal anaesthesia may not be suitable for routine use in outpatients and anaesthetists need to familiarise themselves with techniques that are associated with a rapid recovery profile.
SELECTIVE SPINAL ANAESTHESIA (SSA)
Definition“ The practice of employing minimal
doses of intrathecal agents so that only the nerve roots supplying a specific area and only the modalities that require to be anaesthetised are affected.”
Drugs used:
LOCAL ANAESTHETICS:
LIDOCAINE:
Investigators have assessed various doses, baricity and concentration. The quality of block, maximum block height and duration are summarised in Table -I. Adjuvants such as fentanyl and sufentanil facilitate reductions in the dose of lidocaine and prolong the sensory block without delaying time to void. In addition, they improve tolerance to visceral sensations such as bladder distension and peritoneal stretch. Addition of
RACE 2003 Ramachandra Anaesthesia Continuing Education
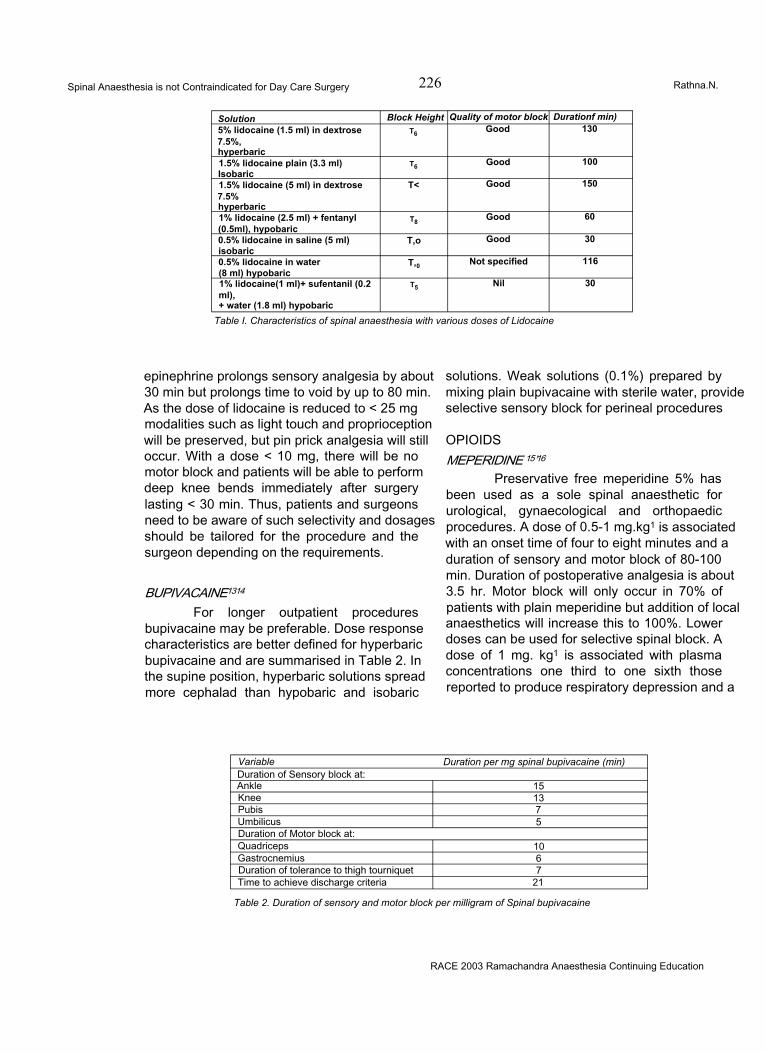
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 226 Rathna.N.
Solution Block Height Quality of motor block Durationf min)5% lidocaine (1.5 ml) in dextrose7.5%,hyperbaric
t6 Good 130
1.5% lidocaine plain (3.3 ml) Isobaric
t6 Good 100
1.5% lidocaine (5 ml) in dextrose7.5%hyperbaric
T< Good 150
1% lidocaine (2.5 ml) + fentanyl (0.5ml), hypobaric
t8 Good 60
0.5% lidocaine in saline (5 ml) isobaric
T,o Good 30
0.5% lidocaine in water (8 ml) hypobaric
T,0 Not specified 116
1% lidocaine(1 ml)+ sufentanil (0.2 ml),+ water (1.8 ml) hypobaric
t5 Nil 30
Table I. Characteristics of spinal anaesthesia with various doses of Lidocaine
epinephrine prolongs sensory analgesia by about 30 min but prolongs time to void by up to 80 min. As the dose of lidocaine is reduced to < 25 mg modalities such as light touch and proprioception will be preserved, but pin prick analgesia will still occur. With a dose < 10 mg, there will be no motor block and patients will be able to perform deep knee bends immediately after surgery lasting < 30 min. Thus, patients and surgeons need to be aware of such selectivity and dosages should be tailored for the procedure and the surgeon depending on the requirements.
BUPIVACAINE1314
For longer outpatient procedures bupivacaine may be preferable. Dose response characteristics are better defined for hyperbaric bupivacaine and are summarised in Table 2. In the supine position, hyperbaric solutions spread more cephalad than hypobaric and isobaric
solutions. Weak solutions (0.1%) prepared by mixing plain bupivacaine with sterile water, provide selective sensory block for perineal procedures
OPIOIDSMEPERIDINE 15’16
Preservative free meperidine 5% has been used as a sole spinal anaesthetic for urological, gynaecological and orthopaedic procedures. A dose of 0.5-1 mg.kg1 is associated with an onset time of four to eight minutes and a duration of sensory and motor block of 80-100 min. Duration of postoperative analgesia is about 3.5 hr. Motor block will only occur in 70% of patients with plain meperidine but addition of local anaesthetics will increase this to 100%. Lower doses can be used for selective spinal block. A dose of 1 mg. kg1 is associated with plasma concentrations one third to one sixth those reported to produce respiratory depression and a
Variable Duration per mg spinal bupivacaine (min)Duration of Sensory block at:Ankle 15Knee 13Pubis 7Umbilicus 5Duration of Motor block at:Quadriceps 10Gastrocnemius 6Duration of tolerance to thigh tourniquet 7Time to achieve discharge criteria 21
Table 2. Duration of sensory and motor block per milligram of Spinal bupivacaine
RACE 2003 Ramachandra Anaesthesia Continuing Education

Spinal Anaesthesia is not Contraindicated for Day Care Surgery 227 Rathna.N.
plasma T1/2 p of five hours. A small dose (10mg) of intrathecal meperidine is equivalent to sufentanil (5 ng) or fentanyl (10 jig) and provides analgesia for approximately 60-90 min.
LIPOPHILIC OPIOIDS LIKE FENTANYL AND SUFENTANIL
These have a more favorable clinical profile of fast onset (minutes) modest durations(1 -4 hours), and little risk of delayed respiratory depression.17 Compared to sufentanil, fentanyl is less lipid soluble and will maintain modest spinal selectivity when injected intrathecaliy.18 Addition of fentanyl to spinal anaesthesia produces synergistic analgesia for somatic and visceral pain without increased somatic block.17 In addition, it decreases the baricity of the local anaesthetic solution and may alter the distribution of agents in the CSF. Studies suggest that spinal fentanyl alone provides dose-dependent analgesia with a minimally effective dose of approximately 10|ag with risk of early respiratory depression occurring in doses greater than 25^g19. Hence the best risk-benefitdose range would be addition of 10-25ng of fentanyl. Numerous studies have shown that addition of fentanyl, allows use of less local anaesthetic and does not prolong duration until discharge.20
oc2- ADRENERGIC AGONISTSClonidine is the best characteristized
a2 adrenegeric agonist which provides dose dependent analgesia and causes side effects like hypotension, bradycardia and sedation . It is not associated with side-effects of spinal opioids like respiratory depression and urinary retention.21 Clonidine attenuates nociceptic input from A and C fibers and acts synergistically with spinal local anaesthetics.22 Oral clonidine has almost 100% bioavailability as it is well absorbed and may be a useful premedication for sedation,sympathetic attenuation and augmentation of ambulatory spinal anaesthesia. A dose of 150-200fig oral
clonidine administered 1-3 hrs before spinal anesthesia can augment sensory and motor block without delaying achievement of discharge criteria.23 Spinal clonidine in a dose of 15-45ng is an optimal dose which has been shown to improve anaesthetic success of 8 mg ropivacaine from 60% to 100% for ambulatory knee arthroscopy without prolonging recovery.24
Adjuvant techniquesINTRATHECAL 12’19’20
Epinephrine and opioids (fentanyl and sufentanii) are common adjuvants added to intrathecal local anaesthetics. Epinephrine 0.2 mg prolongs lidocaine and bupivacaine spinal anaesthesia by approximately 30 min but delays time to voiding by 50-80 min. Fentanyl 20-25 ng prolongs lidocaine and bupivacaine sensory block by 30 min without effect on motor block or bladder function. The onset of fentanyl effect is within four minutes and dose response data are summarised in Table 3. There appears to be little benefit above a dose of 40 fig. Sufentanil (10fig) provides pin prick analgesia for 30 min. Dose response studies in volunteers suggest that there is no additional benefit to using doses larger than 12.5|ag. The mean residence time in CSF is one hour. A dose of 10(ag sufentanil prolongs bupivacaine analgesia by 60 min. Recently, sufentanil alone has been found to provide satisfactory anaesthesia for minor outpatient procedures such as extracorporeal Shockwave lithotripsy. Clinically important respiratory depression after single doses of intrathecal fentanyl and sufentanil has not been described. At Vancouver General Hospital, experience with >100 outpatients who received either intrathecal fentanyl or sufentanil as adjuvants for spinal anaesthesia during outpatient laparoscopy, respiratory depression was not seen. However, the incidence of mild but self-limiting pruritus may be 60-70%. Reassurance and intravenous
Fentanyl dose pg Duration of analgesiaMin
5 3010 6020 12040 30050 300
Table 3. Duration of analgesia after intrathecal fentanyl
RACE 2003 Ramachandra Anaesthesia Continuing Education
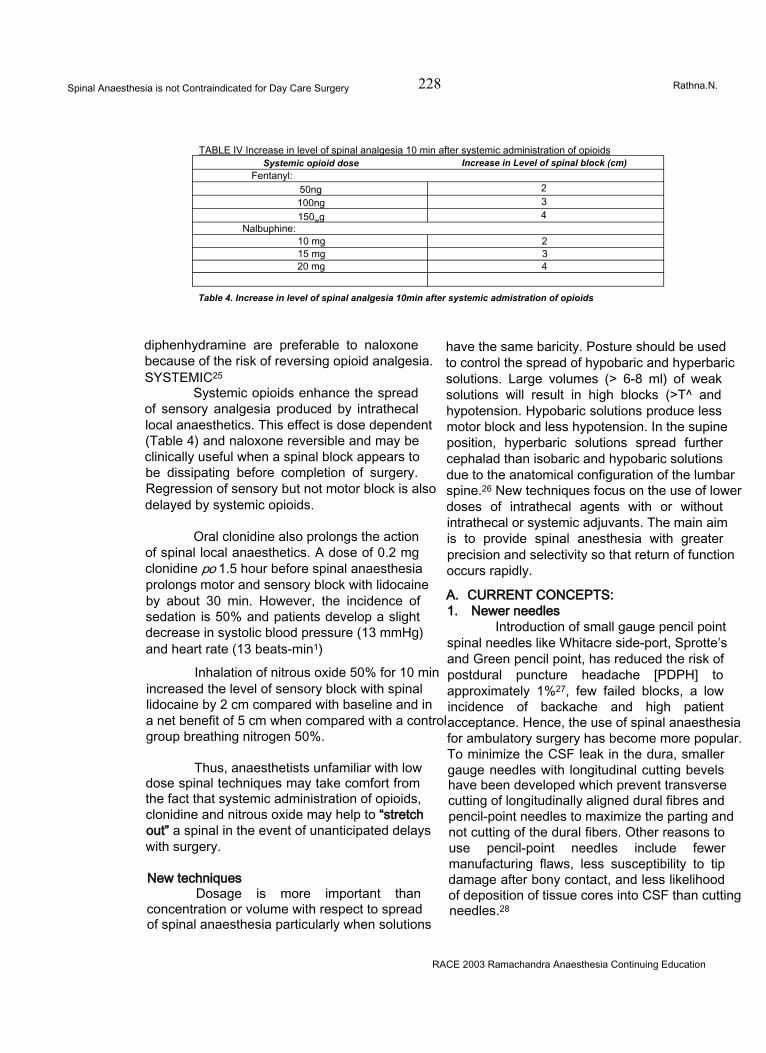
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 228 Rathna.N.
TABLE IV Increase in level of spinal analgesia 10 min after systemic administration of opioidsSystemic opioid dose Increase in Level of spinal block (cm)
Fentanyl:50ng 2100ng 3150wg 4
Nalbuphine:10 mg 215 mg 320 mg 4
Table 4. Increase in level of spinal analgesia 10min after systemic admistration of opioids
diphenhydramine are preferable to naloxone because of the risk of reversing opioid analgesia. SYSTEMIC25
Systemic opioids enhance the spread of sensory analgesia produced by intrathecal local anaesthetics. This effect is dose dependent (Table 4) and naloxone reversible and may be clinically useful when a spinal block appears to be dissipating before completion of surgery. Regression of sensory but not motor block is also delayed by systemic opioids.
Oral clonidine also prolongs the action of spinal local anaesthetics. A dose of 0.2 mg clonidine po 1.5 hour before spinal anaesthesia prolongs motor and sensory block with lidocaine by about 30 min. However, the incidence of sedation is 50% and patients develop a slight decrease in systolic blood pressure (13 mmHg) and heart rate (13 beats-min1)
Inhalation of nitrous oxide 50% for 10 min increased the level of sensory block with spinal lidocaine by 2 cm compared with baseline and in a net benefit of 5 cm when compared with a control group breathing nitrogen 50%.
Thus, anaesthetists unfamiliar with low dose spinal techniques may take comfort from the fact that systemic administration of opioids, clonidine and nitrous oxide may help to “stretch out” a spinal in the event of unanticipated delays with surgery.
New techniquesDosage is more important than
concentration or volume with respect to spread of spinal anaesthesia particularly when solutions
have the same baricity. Posture should be used to control the spread of hypobaric and hyperbaric solutions. Large volumes (> 6-8 ml) of weak solutions will result in high blocks (>T^ and hypotension. Hypobaric solutions produce less motor block and less hypotension. In the supine position, hyperbaric solutions spread further cephalad than isobaric and hypobaric solutions due to the anatomical configuration of the lumbar spine.26 New techniques focus on the use of lower doses of intrathecal agents with or without intrathecal or systemic adjuvants. The main aim is to provide spinal anesthesia with greater precision and selectivity so that return of function occurs rapidly.
A. CURRENT CONCEPTS:1. Newer needles
Introduction of small gauge pencil point spinal needles like Whitacre side-port, Sprotte’s and Green pencil point, has reduced the risk of postdural puncture headache [PDPH] to approximately 1%27, few failed blocks, a low incidence of backache and high patient acceptance. Hence, the use of spinal anaesthesia for ambulatory surgery has become more popular. To minimize the CSF leak in the dura, smaller gauge needles with longitudinal cutting bevels have been developed which prevent transverse cutting of longitudinally aligned dural fibres and pencil-point needles to maximize the parting and not cutting of the dural fibers. Other reasons to use pencil-point needles include fewer manufacturing flaws, less susceptibility to tip damage after bony contact, and less likelihood of deposition of tissue cores into CSF than cutting needles.28
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 229 Rathna.N.
2. Drugs- Local Anaesthetics:A. LIDOCAINE: Spinal lidocaine has long been a popular choice for ambulatory spinal anaesthesia. Although it has enjoyed a long history of safety and popularity since its introduction in 1945, it has come under recent scrutiny because of transient ‘neurologic symptoms [TNS], which has shown to be clearly associated with the spinal lidocaine, with an approximate incidence of 20% in the ambulatory setting.29
B. BUPIVACAINE: TNS is virtually absent in all clinical studies with spinal bupivacaine. Recent studies indicate that small doses [<1 Omg] can be used for ambulatory anaesthesia with time until discharge comparable to lidocaine.30
C. ROPIVACAINE: It is a new local anaesthetic released in the USA in 1996, which is lipid soluble and is approximately 50-60% as potent as spinal bupivacaine with little risk of TNS. Studies have shown that equipotent doses [2:1] of ropivacaine have similar recovery times as bupivacaine.31
D. PRILOCAINE: It is an amide local anaesthetic with pharmacologic properties similar to lidocaine. Recent studies suggest that prilocaine is approximately equipotent to lidocaine with a dose range of 40-70mg and thus may have suitable characteristics for ambulatory spinal anaesthesia with minimal risk of TNS.32
3. Combined Spinal- Epidural Anaesthesia [CSEA]
Has become increasingly popular as its advantages include rapid onset, profound neuraxial block, the ability to titrate or prolong blockade, and lower total drug dosage. Various techniques have been described and technology has provided multiple needle configurations like:
1. Needle through-needle technique
2. Eldor “double barrel” needle
3. Hanaoka “back eye” needle4. Coombs needle.
Availability of the epidural catheter for a rescue anaesthetic allows use of marginal doses of spinal local anaesthetic with resultant rapid recovery and discharge and represents an alternative or complimentary strategy to use of
analgesic additives. However, induction of a CSEA technique probably takes more time than conventional spinal anesthesia, and no current data are available to assess relative cost benefit of increased induction time versus decreased recovery time with CSEA.33
4.. Continuous Spinal Anaesthesia [CSA]The continuous spinal anaesthetic
technique is regaining acceptance in the anaesthesia community. Various needle and catheter designs are available for CSA. Microcatheter (< 24G) and epidural needles and macrocatheters (18-22G) can be used. Newer kits provide an over- the- needle method in which the smaller gauge spinal needle acts as a guide over which the larger gauge catheter ''an be introduced. This needle was designed to reduce the risk of PDPH by not promoting CSF leak. The incidence of PDPH with this technique is 0- 3%.34
One of the advantages of CSA over conventional spinal anaesthesia is the ability to titrate local anaesthetic doses. This slow titration is particularly beneficial in the haemodynamically unstable patient, such as in the elderly or in those with valvular heart disease or trauma.35,36 A number of clinical studies have compared CSA with conventional spinal anaesthesia, demonstrating fewer episodes of hypotension and lesser need for vasopressor with CSA. Another advantage of CSA is the ability to prolong anaesthesia for long surgical cases or even for postoperative analgesia. The ability to use lower anaesthetic doses can lead to faster recovery times, and thus CSA may have applicability to the ambulatory setting, especially in the elderly who are less prone to PDPH.37
TECHNICAL CONSIDERATIONSRecently, it has become apparent that
the pattern of innervation of muscles and deeper structures does not conform strictly to the overlying dermatomes. It has been shown that traditional assumption of a spinal block up to T10 being a prerequisite for urological surgery may not be correct and a mid-lumbar(>L1) level is quite adequate for TURP if bladder pressure is kept <15 mmHg. Systemic adjuvants may also help to improve the adequacy rate of such low block techniques.
The injection rate through a non-cutting
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 230 Rathna.N.
needle (Whitacre) also determines the block height achieved and is important when using low dose techniques. A fast injection rate (0.5 ml.sec-1) results in a greater cephalad spread of spinal anaesthesia (approximately three to four segments) than a slow injection rate (0.02 ml.sec*1).
Continuous spinal anaesthesia with microcatheters would appear a logical method of facilitating selective spinal anaesthesia in outpatients while leaving open the option of further “top ups” as required. An alternative approach is to administer combined spinal-epidural anaesthesia (CSE) with the minimal intrathecal dose required for surgery and utilize the epidural route for back up as necessary. Using a 40 mg initial dose of 2% lidocaine for outpatient arthroscopy, CSE was found to be a reliable technique and was associated with earlier recovery and discharge. Only 10% of patients required intra operative epidural supplementation.
DISCHARGE CRITERIA:Using the newer techniques of spinal
anaesthesia, the patient’s recovery is hastened and the patient can be directly shifted to the step- down recovery by bypassing the Post Anaesthesia Care Unit (PACU). This process is known as “fast tracking” after ambulatory surgery.38lf the patients are awake and oriented in the OR, transfer of these patients directly to the step down unit (Fast tracking) is recommended. The criteria are awake, oriented patients, stable vital signs, minimal pain or bleeding, minimal nausea and vomiting, complete reversal of neuromuscular agents, and oxygen saturation of >94% on room air or resumption to baseline levels. In countries where most or all of the hospital costs are borne by the insurance companies, it results in a significant saving because the major determinant of PACU costs is personnel.39
After spinal anaesthesia, the outpatients must meet the same discharge criteria as patients recovering from general anaesthesia like stable vital signs, ambulation with or without support; no or minimal nausea and vomiting, minimal pain and minimal surgical bleeding.40 In addition, these patients should have prior to ambulation, normal perianal (S4-S5) sensation, the ability to plantar
flex the foot, and proprioception of the big toe as also the ability to void i.e., recovery of sensory, motor and sympathetic nervous functions.40 Patients may be discharged earlier if voiding is not a discharge requirement; however there must be appropriate measures in place if the inability to void persists after discharge.41
POSTOPERATIVE PAIN AND EMESISTwo of the most common problems seen
in the ambulatory surgery patient are pain, and nausea and vomiting. Opioids (e.g., fentanyl, Demerol, morphine) are still the most common and effective method of treating acute, moderate to severe postoperative pain.
Perhaps, as troubling as postoperative pain, is the occurrence of postoperative nausea and vomiting (PONV). For the most susceptible patients (patients with previous history of nausea/ vomiting, motion sickness, women in the luteal phase of the menstrual cycle), prophylactic antiemetic therapy should be considered. The type of surgical procedure also influences PONV; specifically, strabismus repair, laparoscopy, middle ear surgery and orchidopexy are all associated with a relatively high incidence of postoperative vomiting. Despite significant improvement in the pharmacological management of PONV, single drug treatment is not completely effective. However, a multimodal approach has proved successful, including a 92% complete treatment achieved with a combination of droperidol and ondansetron.42 Regional anaesthesia is proven to be associated with a minimal incidence of nausea and vomiting, thereby ameliorating the need for therapeutic interference with drugs.
A LOOK INTO THE FUTURE 43
Experience with new techniques has opened up the possibility of providing “walk-in walk-out” spinal anaesthesia with a real possibility of fast tracking outpatients through the recovery process. Current research is aimed at evaluating the feasibility of bypassing the recovery room after selective spinal anaesthesia (SSA). It has also become apparent that traditional assumptions about the sequence of return of neurological function after spinal anaesthesia (sympathetic, pinprick, motor and finally
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 231 Rathna.N.
propioception) may not apply with SSA. Experience with SSA has demonstrated that pinprick analgesia suitable for surgery can be provided while light touch, proprioception, motor and sympathetic functions are preserved.
CONCLUSIONAmbulatory anaesthesia is continuing to
evolve and has become a recognized anaesthesia subspeciality as more and more surgeries are being performed on an outpatient basis. Ambulatory surgery today represents a new challenge for the anaesthetist as the focus has been shifted and the bottom line is: cost containment and competitive quality care. Spinal anaesthesia with low dose local anaesthetics and analgesic additives provide the double advantage of faster recovery of the central neuraxial blockade and also good postoperative analgesia. New local anaesthetics, analgesic additives, and techniques are being investigated for different applications as the practice of medicine focuses on outpatient care. Safety of spinal agents and complications from spinal anaesthesia continue to be examined and reexamined to improve safety.
With the aforesaid insights into spinal anaesthesia, like• Selective Spinal anesthesia• Modification of techniques - hypobaric and
low dose, adjuvant narcotics• Finer pencil point needles, with an almost
non existent PDPH and• Opportunity for fast tracking the patients• Good post operative analgesia• NoPONV• High acceptance
“ Is Spinal Anaesthesia Contraindicated in Outpatient Surgery”?The answer is a Definite “NO”
REFERENCES:
1 Larson MD. Tait and Caglieri: The first spinal anesthetic in America. Anesthesiology 1996;85: 913-9.
2 White PF, Smith I: Ambulatory anesthesia:PastPresent and future. Int. anesthesia Clin 1994; 32:1.
3 Katz J. A survey of anesthetic choice among anaesthesiologists. Anesth Analg 1973 ; 52: 373-5.
4 Gantt R, Beardsley D,Lindsey J, Setzer V, Stevens RA: Subjective preferences of twelve anesthesiologists undergoing two major neuroaxial blockades : spinal and epidural. Anesthesiology 1994; 81 :A990
5 Watkins S, England AJ, Bolcina A, Yentis SM, Raine G, Feldman SA. Minor morbidity after day -case laparoscopy and the influence of droperidol 0.5 mg: a1 month study. Br J Anaesth 1995; 74: 478P
6 Philip BK: Regional anaesthesia for ambulatory surgery .Can J Anaesth 1992; 39: R3.
7 Neal JM, Dech JJ,Levis MA et al : Hospital discharge after ambulatory knee arthroscopy Reg Anesth 2001; 26: 35-49.
8 Rodgers A, Walker N, Schug SA: Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: Results from an overview of randomized trials, BMJ, 2000; 32:1-12.
9 Standi T, Eckert S, Schulte am Esch J. Postoperative complaints after spinal and thiopentone -isoflurane a n a e s t h e s i a in patients undergoing orthopedics surgery : spinal versus general anaesthesia .Acta Anaesthesiol Scand 1996; 40: 222-6
10 Quaynor H, Corbey M, Berg P. Spinal anaesthesia in day-care surgery with a 26- guage needle.Br J Anaesth 1990; 65: 766-9.
11 Kick O, Megroian B, Lechevalier T, Pinaud M, Souron R, Postoperative comfort and well-being in outpatients: general versus spinal anesthesia. Anesthesiology 1994; 81 :A50
12 Vaghadia H, Me Leod DH, Mitchell GWE, Merrick PM. Small dose hypobaric lidocaine-fentanyl spinal a n a e s t h e s i a
for short duration outpatient laporoscopy.I. A randomized comparison with conventional dose hyperbaric lidocaine. Anesth Analg 1997; 84: 59-64.
13 Liu SS, Ware PD, A//er? HW ,Neal JM, PollockJE. Dose-response haracteristicsof spinal bupivaciane in volunteers. Clinical
implications fora m b u l a t o r y anesthesia. Anaesthesiology 1996; 85: 729-36
14 Maroof M, Khan RM, Siddique M, Tariq M,
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery t ____ ___________________________________________________ _—----------------------------- m-----human vokmtees.Rathna.N.
Hypobaric spinal anaesthesia withbupivacaine (0.1%) gives selective sensory block for ano- rectal surgery . Can J Anaesth 1995; 42: 691-4.
15 Tauzin-Fin P, Maurette P, Vincon G, Hecquet D, Houdek M-C, Bonnet F. Clinical and pharmacokinetic aspects of the combination of meperidine and prilocaine for spinal anaesthesia. Can J Anaesth 1992; 39: 655-60.
16 Honet JE, Arkoosh VA, Norris MC, Huffnagle HJ, Silverman NS, Leighton BL. Comparison among intrathecal fentanyl, meperidine, and sufentanil for labor analgesia. Anesth Analg1992; 75: 734-9.
17 Hamber EA, ViscousiCM: Intrathecal lipophilic opioids as adjuvants to surgical
18 spinal anesthetic. Reg Anesth Pain Med 1999; 24:255-63
19 Ummenhofer WC, Arends RH, Shen DD, Bemads CM: Comparative spinal
20 Distribution and clearances kinetics of intrathecally administered morphine,
21 fentanyl, alfentanil and sufentanil. Anaesthesiology 2000; 92:739-53.
22 Ruben SS, Dunn SM, Duprat KM, O’ Sullivan P: An intrathecal fentanyl dose-
23 response study in lower extremity revascularization procedures.
24 Anaesthesiology 1994; 81:1371-5.
25 Liu S, Chin AA, Carpernter RL, Mulrou MF, Allen HW, Neal JM, Pollock JF:
26 Fentanyl prolongs lidocaine spinal anesthesia without prolonging recovery.
27 Anesth Analog 1995; 80:730-4.
28 Eisenach JC, DC kock M, Klimschaw: Alpha (2) adrenergic agonists for
29 regional anesthesia. A clinical review of clonindien (1984-1995)
30 Anaethesiology 1996;85:655-674.
31 Chiari A, Eisenach JC: Spinal Anaesthesia: Mechanism agents, methods, and
32 safety. Reg Anesth Pain Med 1998; 23:357- 362.
33 Liu S, Chig AA, Neal JM, Carpentes RL, Bainton BG, Geerancher JC: O. al
34 clonidine prolongs lidocaine spinal anesthesia
35 Anaesthesiology 1995;82:1353-1359.
36 Dekock M, Gautier PE, Intrathecal ropivacaine and clonindine for 37 ambulatory knee arthroscopy : A dose response study (abstract).
38 Anaesthesiology 2000;93:A6.
39 Sarantipoulos C, Fassoulaki A, Systemic opioids enhance the spread of sensory
40 analgesia produced by intrathecal lidocaine . Anesth Analg 1994;79:94-7.
41 Vaghadia H, Spinal anesthesia for outpatients Controversies and new
42 techniques. Can J Anes.1998;45:R64-R50.
43 Halpan S, Preston R: Post dural puncture headache and spinal needle design:
44 Metganalysis. Anesthesiology 1994; 8:1376- 1383.
45 Greenberg CP, Walit A, Roth JM: Costconscious anesthetic choice for
46 ambulatory surgery (abstract), Anaesthesiology 1994; 81:A1202.
47 Freedman JM,Lid K, Drasner K, Jaskela MC, Larsen B, Wis: Transient
48 neurologic symptoms after spinal anesthesia: An epidemiologic study of 1863
49 patients. Anesthesiology 1998: 89:633-641.
50 Kamphuis ET, Jonscu Tl, Kuipers PW, de Grier J, van vennooij GE, Boon TA:
51 Recovery of storage and ing functions of the urinary bladder after spinal
52 anesthesia with lidocaine and with dupivacaine in men. Anesthesiology 1998;
53 88:310-6.
54 Gautier PF, Dekock M, Vansteenberge A: Intrathecal ropivacine for ambulatory
55 surgery: A comparison between intrathecal dupivaciane and intrathecal
56 ropivacaine for time arthoscopy Anesthesiology 1999; 91:1239-45.
57 Hampl KF, Heinzmann-Weidmen S, Lugmin buch I, Seeberger M, Schneider
58 MC, Drasner K: Transient neurologic sysmptoms after spinal anesthesia: A lower
RACE 2003 Ramachandra Anaesthesia Continuing Education
Spinal Anaesthesia is not Contraindicated for Day Care Surgery 233 Rathna.N.
incidence with prilocaine and bupivacaine than with lidocaine. Anesthesiology 1998; 88:629-33.
59 Liu SS, McDonald SB. Current Issues is spinal Anesthesia. Anesthesiology
60 2001;94:888-906.
61 Muralidhar V, Kaul HL .Mallick P: Over the needle versus microcatheter through needle technique for continuous spinal anesthesia: A prelimnary study.Reg Anesth Pain Med 1999;24:417-21.
62 Collard CD, Eappren S, Lynch EP, conception M: Continuous spinal anaesthesia with invasive hemodynamic monitoring for surgical repair of the hip in 2 patients with severe aortic stenosis Anesth Analy 1995;81:195-198.
63 Wilhelm S, Standi T, Burmeister M, Kessler G, Schulte am Essch J: Comparison of
continuous spinal- epidural anesthesia using plain bupivacaine 0.59% in trauma patients . Anaesth Analg 1997; 85:69-74.
64 Favarel-Garrigues JF, Sztark F, Petitjean MF, Thicoipe M, Larsic P, Dauadic
P:Hemodynamic effects of spinal anesthesia in the elderly: Single dose versus titration through a cather. Anaeth. Analg 196; 82:312-6.
65 Lubarsky DA: Fast track in the post anesthesia care unit:Unlimited possibilities? J Clin Anesth 1996; 8:705.
66 Dexter F, Tinen JH: Analysis of strategies to decrease post anesthesia care unit costs. Anaesthesiology 1995; 82:94.
67 Chung F: Are discharge criteria changing? J Clin Anesth 1993; 5:645.
68 Chung F: Discharge criteria: A new trend. Can J Anaesth 1995; 42:1056.
69 McKenzie R, Lim Uy NT, Riley TJ, Hamilton DL. Droperidol/Ondensetron combination controls nausea and vomiting after tubal ligation. Anesth Analg 1996;83:1081-3.
70 Viskari D.Berril A,Vaghadia H. Walk-in walkout spinal anaesthsia for outpatient laparoscopy: evalution of hreehypobaric solutions. Can J Anaesth 1997; 44: A26-B.
RACE 2003 Ramachandra Anaesthesia Continuing Education
DEBATE

Invasive Monitoring in ASA III and ASA IV patientswill Influence the Outcome of Surgery._______________ 234 Ashok Badhe
The role of Invasive Monitoring in ASA III and ASA IV patients for surgery is quite established by now. Invasive monitoring is quite routinely practsiced in these patients. To single out the influence of invasive monitoring on the outcome of surgery is quite difficult. The outcome of surgery in these groups of patients is influenced by a variety of factors. The factors influencing the outcome of surgery can be broadly categorized as:
1) The patient’s disease2) The Surgery3) Anaesthesia.
The perioperative variables also interact with each other and it is quite difficult to separate the contribution of each to perioperative morbidity and mortality and the postoperative outcome.
To recapitulate (ASA III and IV patients)
ASA classification:1) ASA III - A patient with a severe systemic
disease that limits activity but is not incapacitating.
2) ASA IV - A patient with an incapacitating systemic disease that is a constant threat to life.
The role of monitoring during surgery is not questioned by anybody in the present anaesthesia practice. The basic purpose of monitoring is to help us to know the haemodynamic status and also to guide us about the therapeutic measures to be taken to correct the derangement. Most of the haemodynamic parameters can be monitored by noninvasive techniques, but one must keep in mind the limitations of these techniques in patients of ASAIII and ASA IV. The focus is on this subset of
patients. One must keep in mind that these patients need more intensive and more or less continuous and accurate monitoring which cannot be achieved by noninvasive monitoring techniques. For example, pulse oximetry, one of the most commonly used, and quite useful monitor, can be affected by hypotension, hypothermia and peripheral vasoconstriction which are quite commonly seen in ASA III and ASA IV patients undergoing major surgery.
VARIOUS INVASIVE MONITORING TECHNIQUES : employed during the perioperative period are:
i) Urine output monitoringii) Invasive Arterial Blood Pressure
monitoring.iii) Central Venous Pressure monitoring.iv) Pulmonary Artery Pressure monitoring.
i) Urine Output Monitoring:This is one of the least invasive of all the
monitoring methods. Hourly urine output is quite important in ASA III and ASA IV patients posted for major surgeries. This helps us to know the perfusion of the vital organs and also guides us about the therapeutic modalities. These therapeutic modalities can have an important bearing on the outcome of the surgery.
ii) Invasive Arterial Blood Pressure Monitoring:
Accurate, correct, continuous blood pressure monitoring is mandatory in these groups of patients. Direct Intra-arterial Blood pressure remains the gold standard technique. It provides a beat to beat indication and the waveform. In these patients, wide-swings of arterial pressures may be seen because of surgical manipulations, intravascular volume shifts, effects of anaesthetic agents and arrhythmias. It also helps to obtain
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III and ASA IV patientswill Influence the Outcome of Surgery._______________ 235 Ashok Badhe
repeated blood gas assessment.Indications in these patients:
I. Major surgical procedures involving large fluid shifts, and blood loss.
II. Pulmonary disease patient requiring frequent ABG analysis.
III. Patients with hypovolemic, cardiogenic or septic shock or with multiple organ failure.
IV. Massive TraumaV. Patients requiring Inotropes.VI. Patients with electrolyte and metabolic
disturbances requiring frequent arterial sampling.
VII. Inability to measure arterial pressure non- invasively (morbid obesity).
The indications during cardiovascular, thoracic, and urosurgeries, are not mentioned here.
COMPLICATIONS:1) Infections: This potential common
complication is common to all invasive monitoring techniques. The incidence can be reduced by using a proper aseptic technique and avoiding prolonged catheterization at the same site.
2) Hemorrhage: this is a potential risk because of disconnection. This can be reduced by Luer lock connections and having low pressure alarms.
3) Thrombosis and Distal Ischaemia: Factors that correlate with increased incidence of thrombosis are prolonged cannulation and larger catheters in smaller vessels. This complication is seen in a negligible number of cases and can be reduced by removing arterial catheters with continuous aspiration of catheter by syringe during proximal and distal occlusion of the vessel.
iii) Central venous Pressure Monitoring:Accurate measurements are possible if
the distal end of the catheter lies within one of the large intrathoracic veins or the right atrium. This is quite a useful invasive monitor if the factors affecting it and its limitations are understood. Serial measurements are more useful than a singular measurement and the response of the CVP to a volume infusion is a useful test of right ventricular function. This mainly indicates
intravascular volume.Indications for CVP monitoring include
• Major surgeries involving large fluid shifts and blood loss.
• Intravascular volume assessment when urine output is not reliable or unavailable (Prostate surgery, Renal failure).
• Major trauma• Venous access for vasoactive irritating drugs.• Inadequate peripheral venous access. These
are some of the indications in ASA III and ASAIV patients in the perioperative period.
COMPLICATIONS:A) Arterial Puncture: This is because the veins lie in the close proximity of arteries. This can be minimized by meticulous technique and by using a small gauge (22G) needle initially, to localize the vein.B) PneumothoraxC) Nerve InjuryD) Arrhythmias: Transient atrial and or ventricular arrhythmias commonly occur as the guide wire is passed into the right atrium.
iv) Pulmonary Arterial Pressure Monitoring:The population of patients with multiple
systemic disease is likely to benefit from this “leap” in monitoring. It gives important diagnostic information to decide about the therapeutic management.
INDICATIONS FOR PULMONARY ARTERY CATHETER MONITORING:• Patients with recurrent myocardial infarctions
or unstable angina.• Patients with left ventricular dysfunction
(congestive heart failure).• Patients in hypovolemic, cardiogenic or
septic shock with multiple organ failure.• Patients with massive ascites.• Major procedures involving large fluid shifts
in patients with coronary artery disease.
COMPLICATIONS:1 Unintended arteriotomy2 Pneumothorax3 Arrhythmias4 Sepsis
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III and ASA IV patientswill Influence the Outcome of Surgery._______________ 236 Ashok Badhe
5 Potentially fatal haemorrhage.PAC MONITORING HAS WELL KNOWN POTENTIAL BENEFITS:1. Ability to measure important haemodynamic
indices.2. Additional information regarding fluid
management and drug therapy.3. Also helpful in determining whether it is safe,
for high risk patients to proceed with surgery.
This is one invasive monitoring about which a lot of claims and counter claims appear in the literature by both the technophiles and technophobes. But one must keep in mind that the PAC monitoring is a useful adjunct but it cannot replace the vigilant anaesthetist.
The question most commonly asked is, ‘Does invasive monitoring influence the surgical outcome?’ When one asks a question like this, it is implicit in the question that it does contribute to the surgical outcome atleast in principle. The technology is a discrete, separate feature of our environment; hence we are inclined to think that it can be treated as a single factor and its contribution can be measured or atleast estimated. But in practice it is not so, various prospective and retrospective studies are not able to decide the influence of PAC on the outcome of surgery because most of the studies are not conducted with standard methodology and there are various lacunae in the studies like patient selection, selection of controls etc. ASA established a task force on PAC an 1991 to examine the evidence for benefits and risks from PAC catheters. This report summarizes the task force recommendations based on scientific evidence and experts’ opinions. If you look into statistical analysis, the benefit and the influence
on the outcome of surgery is negative but if you clinically look in to the findings it is quite suggestive that patients do benefit from PAC and it may have influence on the outcome of surgery.
CONCLUSION:To conclude, the principle function of
invasive monitoring technology is to amplify or augment human operator expertise. The benefits of invasive monitoring can be reaped maximum by adequate training, experience and expertise.
REFERENCES:1 Report by ASA Task force on PAC
Anaesthesiology Feb.93, vol.78 No.2
2 Friend and Foe: Why can’t we agree about the effects of new technology in patient safety - Richard I Cook, ASA Refresher course series 2002.
3 Cardiac Anaesthesia - Joel A Kaplan.
4 Bedford RF: Removal of radial artery thrombi following percutaneous cannulation for monitoring. Anaesthesiology 46: 430, 1977.
5 Bedford R.F, Ashfor T.P.: Aspirin pretreatment prevents post cannulation radial
Aspirin pretreatment prevents post cannulation radial artery thrombosis. Anaesthesiology 51: 176, 1979.
6 U. Wolter M.D. et al. - ASA classification and perioperative variables in predictors of post operative outcome. BJA August 1996 Vol.77 No.2.
7 A practice of Anaesthesia - Wylie and Churchil Davidson’s. Edited by Thomas E.J. Healy & Peter Cohen.
8 Anaesthesia Providers, Patient outcome & costs: Anaesth. Analgesia. Jun 1996 Vol.82 No.6 p.1273.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 237 A. Rajamanoharan
Monitoring forms the base or the basis of the conduct and safety of anaesthesia. Measurement is a single observation and monitoring is a serial evaluation. Under anaesthesia the vital parameters must be maintained within the safe limits. The ideal monitoring should be r'mple to apply and observe, cost effective, dynamic, accurate, error free and safe.
The simplicity, safety and the advances in the microprocessor, servo mechanical control technology and photoplethysmography have enabled the non-invasive techniques to be the choice to provide a nearly continuous, correct and accurate assessment of blood flow and pressure.
Invasive monitors without exception carry real dangers and are only used as temporary devices while successful and continued efforts are being made to replace them. Two of the least appreciated disadvantages of extensive monitoring are prolonged immobilisation and the anguish that accompanies it.
Measurement of cardiac output has traditionally been the poor relation to pressure monitoring because of the perceived risks, complexity and expense of pulmonary artery catheterisation. The latest National Confidential Enquiry into Perioperative Deaths highlighted how only a small minority of the reviewed patients had intraoperative pulmonary artery catheter monitoring, yet over three-quarters were classified as being ASA Grade III or higher. No mention was made as to whether cardiac output was actually measured during the operation. The onset of significant haemodynamic deterioration and organ dysfunction is often the cue for its introduction; this belated insertion may partly explain the difficulty in demonstrating any benefit in the critically ill patient. Indeed, a recently
published retrospective analysis has actually suggested possible detriment. This paper has generated considerable debate as to when, how and in whom this invasive approach should be used. It has also given added impetus to the development of alternative flow monitoring techniques that are either non- or minimally invasive and, with advances in technology, increasingly reliable and user-friendly. Many of these techniques also provide additional information on circulatory status, e.g. cardiac preload, ventricular contractility and extravascular lung water, which can further assist therapeutic decision-making. The particular benefits that could arise from non-invasive flow assessment are early identification and either prevention, or faster correction, of circulatory derangements before a significant tissue oxygen debt has been allowed to develop. This proactive philosophy may impact significantly upon postoperative outcome.
Any blinding enthusiasm for non-invasive techniques should be tempered by awareness of the limitations of both the machine and the technology being utilised. Not infrequently, poor equipment design, over-stated abilities and/or inadequate user education have generated unfavourable studies. This may contribute more to an understandable wariness on the part of the clinician rather than to any inherent problem with the technique itself, which is often discredited in the process. It thus behoves prospective users to familiarise themselves fully with both theory and practice underlying a particular device, to develop sufficient expertise to recognise unreliable or erroneous signals, and to be aware of any limitations. All technologies have flaws, and data derived from different methods do not necessarily correlate well. Techniques may often be better at monitoring change rather than delineating absolute output itself. So, let us replace the out-modelled and more harmful
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 238 A. Rajamanoharan
invasive monitoring with non-invasive monitoring equipments and see how they are better, dependable, accurate, totally harmless and user- friendly.
PULSE OXIMETERPulseoximetry (PO) has been arguably
called the most significant technological advance ever made in monitoring the safety of patients during anaesthesia. Prior to the advent of Pulse oximetry, the only monitor for adequate oxygenation of the patient was the “trained” eye of the anaesthesiologist observing skin colour for cyanosis. The pulse oximeter has now become a mandatory intraoperative monitor and in October 1989, the American Society of Anaesthesiologists voted to mandate the use of Pulse oximetry in all anaesthetics after January 1990.
Pulse Oximetry is made possible by the combination of two simple physical principles:1. Every substance has a unique absorbance spectrum2. Of all light absorbing substance in the living tissues, only arterial blood is pulsatile.
Clinical applications1. MONITORING OXYGENATION
- Provides warning of hypoxemia in the operating room (OR), post anaesthesia care unit (PACU), during transport between OR and PACU, and during out-of-hospital transport.
2. MONITORING OXYGEN THERAPY• Helps to titrate supplemental oxygen
in mechanically ventilated patients and patients receiving oxygen therapy by Venturi device. Trends of Sp02 by pulse oximetry should be periodically confirmed by blood gas analysis.
• Pulse oximetry can also be used as a supplement to arterial blood gas analysis to monitor hyperoxia in premature infants
3. ASSESSMENT OF PERFUSIONPresence of pulsatile signal
appropriately tracks the viability of the tissue monitored.
4. MONITORING VASCULAR VOLUME• The amplitude of plethysmographic
waveform provides information about
hypovolaemia during positive pressure ventilation.
Pulse oximeter occupies a unique place among the present day monitors as it provides vital patient information continuously and noninvasively. It also scores over other monitors, as it requires little training for its use and no calibration, making it extremely user-friendly. By helping to detect hypoxemia early, it helps the anaesthesiologist in providing safe patient care in the operating room as well as the intensive care unit.
CAPNOGRAPHYCapnography, the measurement of the
carbon dioxide (C02) content in respired gases, has become part of basic monitoring in anaesthesia and intensive care. Capnographs can provide information regarding the production, transport and excretion of C02. A closed claims study in 1989 has concluded that about 93% of anaesthetic mishaps could have been prevented if capnograph and pulse oximeter had been used as monitors
Indications and uses of capnography• Verification of endotracheal tube placement.• Difficult airway■ Blind nasal intubation• Proper positioning of double lumen tube• Validation of reported end tidal values• Indirect assessment of partial pressure of arterial carbon dioxide tension (normal (a-ET) PC02 varies from 2 to 5mmHg and increases with age, pulmonary disorders like emphysema, pulmonary embolism, decreasing cardiac output, hypovolaemia and general anaesthesia.
■Adequacy of spontaneous ventilation under general endotracheal anaesthesia and also in the awake intubated patient in the recovery room/ICU and in a patient under regional anaesthesia, (apnoea monitor).• Assessment of ventilator, breathing circuit and gas sampling integrity.• Circuit leaks and adjustments of fresh gas flow.■ Instantaneous disconnection, total occlusion and accidental extubation.■ Carbondioxide retention due to faulty circuit (Bains).■ Exhausted carbondioxide absorbent in a semi
RACE 2003 Ramachandra Anaesthesia Continuing Education
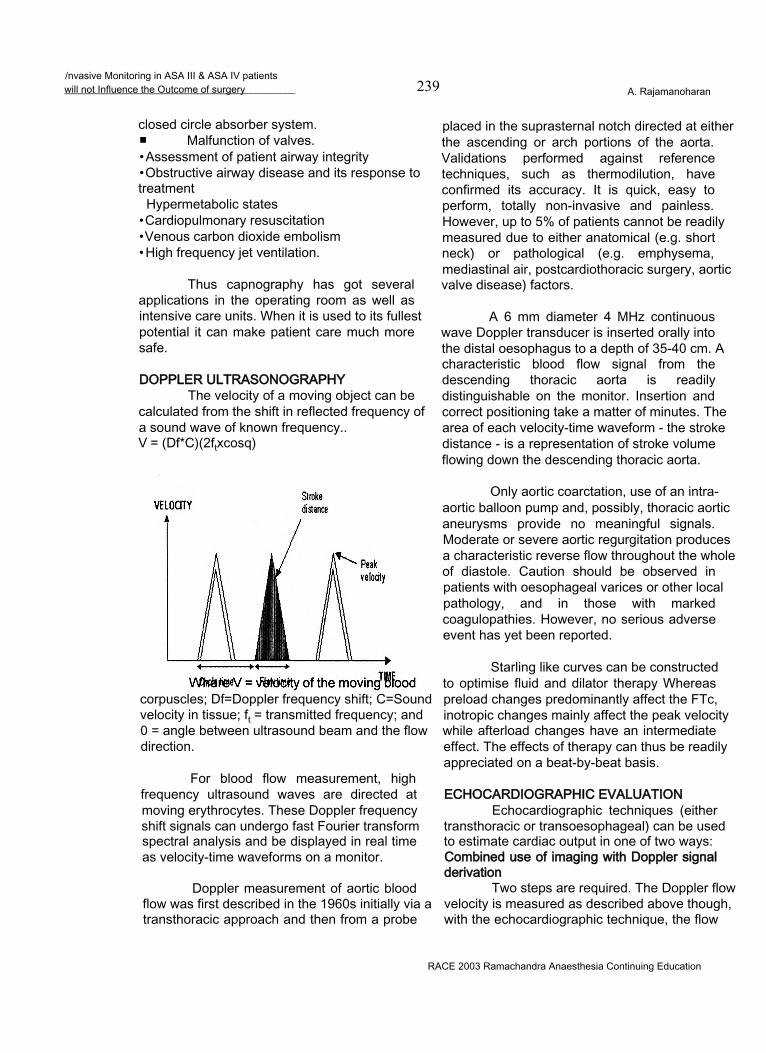
/nvasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 239 A. Rajamanoharan
closed circle absorber system.■ Malfunction of valves.• Assessment of patient airway integrity• Obstructive airway disease and its response to treatment
Hypermetabolic states• Cardiopulmonary resuscitation• Venous carbon dioxide embolism• High frequency jet ventilation.
Thus capnography has got several applications in the operating room as well as intensive care units. When it is used to its fullest potential it can make patient care much more safe.
DOPPLER ULTRASONOGRAPHYThe velocity of a moving object can be
calculated from the shift in reflected frequency of a sound wave of known frequency..V = (Df*C)(2ftxcosq)
corpuscles; Df=Doppler frequency shift; C=Sound velocity in tissue; ft = transmitted frequency; and 0 = angle between ultrasound beam and the flow direction.
For blood flow measurement, high frequency ultrasound waves are directed at moving erythrocytes. These Doppler frequency shift signals can undergo fast Fourier transform spectral analysis and be displayed in real time as velocity-time waveforms on a monitor.
Doppler measurement of aortic blood flow was first described in the 1960s initially via a transthoracic approach and then from a probe
placed in the suprasternal notch directed at either the ascending or arch portions of the aorta. Validations performed against reference techniques, such as thermodilution, have confirmed its accuracy. It is quick, easy to perform, totally non-invasive and painless. However, up to 5% of patients cannot be readily measured due to either anatomical (e.g. short neck) or pathological (e.g. emphysema, mediastinal air, postcardiothoracic surgery, aortic valve disease) factors.
A 6 mm diameter 4 MHz continuous wave Doppler transducer is inserted orally into the distal oesophagus to a depth of 35-40 cm. A characteristic blood flow signal from the descending thoracic aorta is readily distinguishable on the monitor. Insertion and correct positioning take a matter of minutes. The area of each velocity-time waveform - the stroke distance - is a representation of stroke volume flowing down the descending thoracic aorta.
Only aortic coarctation, use of an intra- aortic balloon pump and, possibly, thoracic aortic aneurysms provide no meaningful signals. Moderate or severe aortic regurgitation produces a characteristic reverse flow throughout the whole of diastole. Caution should be observed in patients with oesophageal varices or other local pathology, and in those with marked coagulopathies. However, no serious adverse event has yet been reported.
Starling like curves can be constructed to optimise fluid and dilator therapy Whereas preload changes predominantly affect the FTc, inotropic changes mainly affect the peak velocity while afterload changes have an intermediate effect. The effects of therapy can thus be readily appreciated on a beat-by-beat basis.
ECHOCARDIOGRAPHIC EVALUATIONEchocardiographic techniques (either
transthoracic or transoesophageal) can be used to estimate cardiac output in one of two ways: Combined use of imaging with Doppler signal derivation
Two steps are required. The Doppler flow velocity is measured as described above though, with the echocardiographic technique, the flow
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery 240 A. Rajamanoharan
being interrogated is usually in or close to the heart, e.g. across the mitral valve or, commonly, in the aortic root. Echocardiographic measurement of cross-sectional area at this point will allow calculation of cardiac output as the product of blood velocity averaged over a minute and cross-sectional area. Planimetric measurement, enhanced by recently developed edge-detection technology, may improve the accuracy of calculated cardiac outputs although it may still prove difficult to obtain accurate short- axis views.
The use of combined transoesophageal echocardiographic imaging and Doppler probes allows estimation of cardiac output in the critically ill more readily than transthoracic imaging techniques.
Calculation from ventricular volumesIf ventricular volume at end-systole and
end-diastole are measured, stroke volume can be calculated as the difference between these two values, and cardiac output as the product of this stroke volume and heart rate.
Recently developed technology allows 3- dimensional reconstruction of images of the left ventricle. Routinely, however, ventricular volumes will still be calculated from 2-D and M-Mode images although these often rely upon assumptions about LV shape, namely:
Transthoracic impedanceIn 1966, Kubicek described the thorax
as a cylinder evenly perfused with blood of specific resistivity ‘p’, itself related to the haematocrit. Pulsatile thoracic aortic blood flow caused negative impedance changes (measured from a steady state mean base impedance (Z), with a maximum rate of change [(dZ/dt)m J of Zm during systole between pairs of electrodes placed around the neck and upper abdomen.
SV=p(L2/Z2)ZmWhere SV = stroke volume; p=electrical
resistivity of the blood; L=mean separation of the inner pair of electrodes; Zm = maximum rate of change of impedence (dZ/dt)maxduring systole, and Z = basic impedance between the inner electrodes.
The original Kubicek equation consistently overestimated SV. Furthermore, it
was subsequently shown that the thorax behaves electrically more as a truncated cone rather than as a cylinder. . This, and the application of new technology, renders transthoracic impedance of potential clinical use and the new equations have been incorporated into commercial systems such as the NCCOM-3 (Biomed Medical Manufacturing Ltd, Irvine, CA, USA). Common systems have involved the application of a sensing electrode to either side of the neck root and to opposite sides of the body in a mid-coronal plane at the xiphisternum level. Two pairs of transmitting electrodes are placed 5 cm above the neck sensors and 5 cm below the thoracic sensors, respectively. Accurate electrode placement is crucial using such systems.
Although data derived from this system may, under some circumstances, correlate well with those derived from thermodilution (and even prove more reproducible in individual subjects), the varying impedance technologies and derived equations have yet to be validated in individuals of both sexes and of diverse age and habitus in varied clinical situations. Adoption of the technique in the ICU setting cannot yet be recommended. Its use in the emergency room (to allow rapid and non-invasive monitoring of responses to resuscitation) or on the operating table may prove more readily acceptable.
Pulse Contour AnalysisSince the rate at which blood flows from
arteries to veins is proportional to the rate of fall of arterial pressure, analysis of the contour of the aortic pulse-wave allows determination of cardiac output. The area of the arterial waveform (or pulse contour) was first described as a means of monitoring cardiac output by Frank in 1899. This pulse contour cardiac output technique (PCCO) can be performed non-invasively from a finger pressure waveform using a Finapres device or from an indwelling arterial cannula which is being pressure transduced. However, it cannot be used for quantitation of cardiac output unless a calibration tool such as thermodilution is used. Over the last two decades, various equations have been developed by different researchers for monitoring stroke volume.
The Bradley MethodA clinical means for estimating cardiac
RACE 2003 Ramachandra Anaesthesia Continuing Education
Invasive Monitoring in ASA III & ASA IV patientswill not Influence the Outcome of surgery__________ 241 A. Rajamanoharan
output and peripheral vascular resistance was revised by Bradley. In experienced hands, this has been shown to be a reliable technique, however, a validation study showing good agreement when compared against thermodilution has only been published in abstract form and it has to be shown to be readily transferable to novices.
It relies upon a version of Ohm’s law where the voltage gradient across a circuit equals the product of current and resistance. In the systemic circulation, the pressure gradient across the circuit (mean arterial pressure minus central venous pressure) measured in mmHg equals the product of cardiac output (in 1 /min) and peripheral vascular resistance (in Wood units).
COMPLICATIONS OF INVASIVE MONITORING Complications of arterial puncture
• Infection• Haemorrhage• Thrombosis and distal ischaemia
Skin necrosis EmbolizationHaematoma Neurologic injuryLate complications like pseudoaneurysm and AV fistula
Complications of central venous cannulationsArterial puncturePneumothorax/hydrothoraxChylothoraxPericardial effusion/tamponade
• Venous air embolism Nerve injury Arrhythmias
Complications of pulmonary artery catheterisation
All complications of internal jugular vein cannulation and in addition:
• Complete heart block (in patients with LBBB)Endobronchial haemorrhage Pulmonary infarction Valvular damage Thrombocytopenia
• Thrombus formation Incorrect placement
Balloon rupture
CONCLUSIONKISS the well known acronym for “Keep
it simple, stupid” is often taken to be good advice for life in general. Editorial by C.E. Hahn BJA volume 86-4 April 2001.
Moreover, for the trainee, there is a galaxy of advice, opinion and controversies to be digested. Monitoring has become the sixth sense of the clinician and has contributed in a major way to a safer anaesthetic practice.
Invasive monitoring is time consuming, needs technical expertise, definitely damaging, necessitates immobilization and is vulnerable for disturbances and inaccurate results. Let us eradicate “invasion” anywhere in the universe. To quote Mahatma Gandhi “non-violence”’ (noninvasion) is the strongest but still the most successful method. So let us be non-invasive in monitoring our ASA III & IV patients.
REFERENCES
1. Noninvasive monitoring of cardiac output, Hugh Montgomery, Mervyn Singer, 163, Recent advances in anaesthesia and analgesia 20 by A.P.Adams, J.N.Cashman.
2. Edward D.Miller Jr - Miller 5th edition, 14703. Text book of Anaesthesia by Wylie Churchill Davidson4. Tinker JH, Dull DL, Caplan RA, Ward RJ, Cheney FW.
Monitoring devices in preventing of anaesthetic mishaps: a closed claims analysis. Anaesthesiology 1989; 71:51-46.
5. Shankar KB, Moseley H, Kumar AY, Delph Y, Capnometry and anaesthesia:Can J Anaesth 1992; 39:617-32.
6. Eichhom JH, Prevention of intraoperative Anaesthesia Accidents and Related Severe injury through safety monitoring. Anaesthesiology 1989; 70:572-7.
7. Stock MC, Capnography for Adults. Critical Care Clinics 1995; 11:219-32.
8. Severinghaus JW,, Kelleher JF. Recent developments in pulse oximetry Anaesthesiology 1992; 76:1018-38.
9. Moon RE, Camporesi EM, Respiratory Monitoring. In Miller RD, eds. Anaesthesia. 5th ed.California:Churchill ivingstone; 2000:1:1269-77.
10. Dorsch JA, Dorsch SE Pulseoximetry in: Understanding Anaesthesia Equipment 4th ed. Baltimore:Williams and Wilkins; 1998; 811-48.
11. Wahr JA, Tremper KK.Pulseoximetry. ln:Blitt CD, Hines RL, eds. Monitoring in anaesthesia and critical care medicine.3rd ed. Newyork:Churchill Livingstone; 1995;385-406.
12. RACE 2000 - Postgraduate symposium on Non-invasive monitoring.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Preoperative transfusion threshold is a haemoglobin of 8 g% 242 Manjunath Prabhu
Transfusion of blood in general and the red blood cells in particular can be a life saving measure in the management of variety of medical and surgical conditions but inadvertent administration of blood cannot be justifiable, more so considering its limited availability. A time- honoured method to assist physicians decision making regarding any intervention is the risk benefit ratio. Minimising the risk and maximising efficacy improves the likelihood of a good response. Physicians as well as their patients are quiet familiar with the ever growing list of complications of homologous blood transfusion, little information is available regarding the benefits of administering blood.
Following the screening for antibodies to HIV in March 1985, the transmission of HIV infection has decreased significantly but still there are about 5 cases of transfusion related HIV being reported every year in the United States. This is inspite of strict screening and public awareness programs there. Considering the less than optimal screening in general, and poor public awareness, the danger is likely to be much more in our country.
Hepatitis A, B and C are the other type of viral disease, transmitted by blood transfusions. The incidence and frequency per transfusion has been given below (table-1).
PROBLEMS ASSOCIATED WITH BLOOD TRANSFUSION
The risks of red blood cell transfusion are many. Some of them can be immediate whereas many other may manifest later. Many of them are known but many more are being added regularly. Any infectious agent that is present in the donor at the time of donation is potentially transmissible to a susceptible recipient. The consequence may be seen as clinical morbidity and mortality after an incubation period characteristic of that agent. Considering the screening tests before accepting blood, it is unlikely that bacterial infection can be transmitted through blood often. The viral infection transmission can be significantly reduced by proper screening but the fact is that disease transmission can still occur during the "window period' (the period soon after infection during which a blood donor is infectious but screening tests will be negative).
Transmission of HIV:The first description of transmission
associated HIV infection was reported in 1983.1
Blood and blood products can be contaminated with bacteria and can be dangerous when stored incorrectly.2 A report from New Zealand says that the rate of contamination by Yersinia enterocolitica, the most commonly implicated bacterial contamination, was 1 per 65,000 red cell units transfused, with a fatality rate of 1 per 104,000.3
Transfusion associated acute lung injury (TRALI)
TRALI is usually caused by donor plasma that contains antibodies against patient’s leucocytes. This is characterised by a rapid detoriation of pulmonary function within 1 to 4 hours of starting transfusion, with diffuse opacity on the chest X- ray. The estimated frequency of this problem is 200 per million units.4 5
Acute and delayed haemolytic transfusion reaction:
Despite advances in the understanding of red-cell antigens, haemolytic reactions both acute and chronic continue to occur. Fatal acute haemolytic reactions, to transfusion occur in the
RACE 2003 Ramachandra Anaesthesia Continuing Education
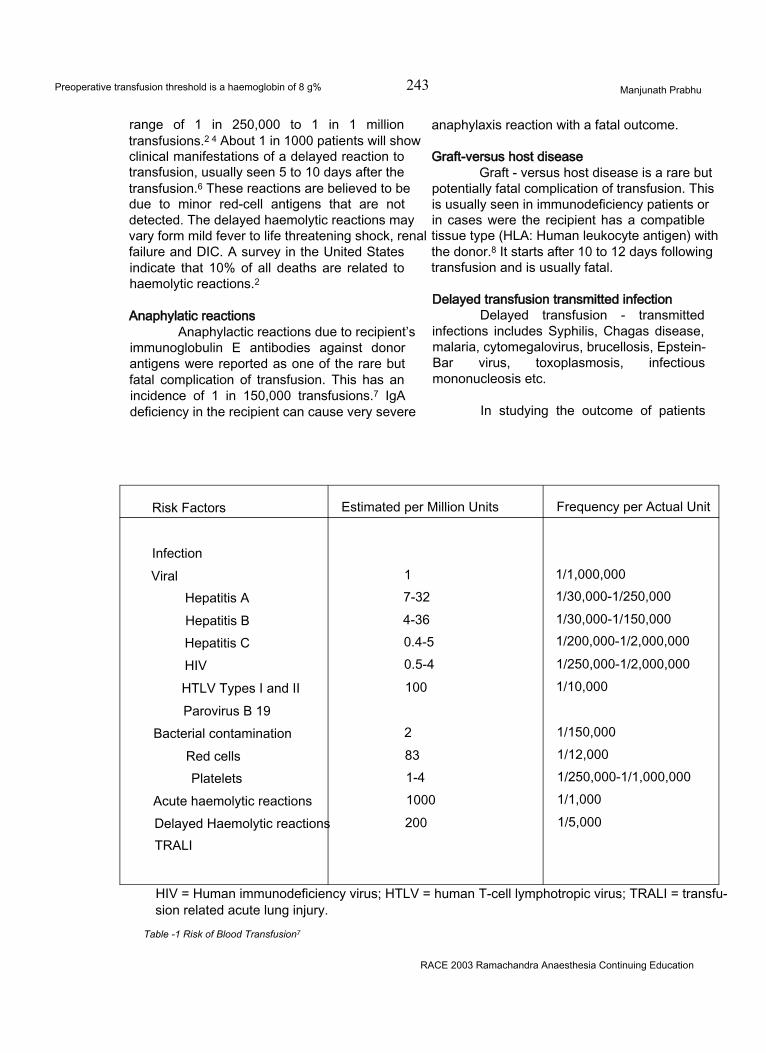
Preoperative transfusion threshold is a haemoglobin of 8 g% 243 Manjunath Prabhu
range of 1 in 250,000 to 1 in 1 million transfusions.2 4 About 1 in 1000 patients will show clinical manifestations of a delayed reaction to transfusion, usually seen 5 to 10 days after the transfusion.6 These reactions are believed to be due to minor red-cell antigens that are not detected. The delayed haemolytic reactions may vary form mild fever to life threatening shock, renal failure and DIC. A survey in the United States indicate that 10% of all deaths are related to haemolytic reactions.2
Anaphylatic reactionsAnaphylactic reactions due to recipient’s
immunoglobulin E antibodies against donor antigens were reported as one of the rare but fatal complication of transfusion. This has an incidence of 1 in 150,000 transfusions.7 IgA deficiency in the recipient can cause very severe
anaphylaxis reaction with a fatal outcome.
Graft-versus host diseaseGraft - versus host disease is a rare but
potentially fatal complication of transfusion. This is usually seen in immunodeficiency patients or in cases were the recipient has a compatible tissue type (HLA: Human leukocyte antigen) with the donor.8 It starts after 10 to 12 days following transfusion and is usually fatal.
Delayed transfusion transmitted infectionDelayed transfusion - transmitted
infections includes Syphilis, Chagas disease, malaria, cytomegalovirus, brucellosis, Epstein- Bar virus, toxoplasmosis, infectious mononucleosis etc.
In studying the outcome of patients
Risk Factors Estimated per Million Units Frequency per Actual Unit
InfectionViral 1 1/1,000,000
Hepatitis A 7-32 1/30,000-1/250,000
Hepatitis B 4-36 1/30,000-1/150,000
Hepatitis C 0.4-5 1/200,000-1/2,000,000
HIV 0.5-4 1/250,000-1/2,000,000
HTLV Types I and II 100 1/10,000
Parovirus B 19Bacterial contamination 2 1/150,000
Red cells 83 1/12,000
Platelets 1-4 1/250,000-1/1,000,000
Acute haemolytic reactions 1000 1/1,000
Delayed Haemolytic reactions 200 1/5,000
TRALI
HIV = Human immunodeficiency virus; HTLV = human T-cell lymphotropic virus; TRALI = transfusion related acute lung injury.
Table -1 Risk of Blood Transfusion7
RACE 2003 Ramachandra Anaesthesia Continuing Education

Preoperative transfusion threshold is a haemoglobin of S g% 244 Manjunath Prabhu
undergoing major abdominal surgery, Maetani et al found that the highest risk factor for developing organ system failure was blood transfusion.9 Postoperative septicaemia has been found to be highly linked to transfusion practice in a large study by Wobbes and colleagues.10 Those who received 3 or more units of red blood cells were at a much higher risk (P = 0.003) to develop septic complications than those not receiving transfusions.
There is evidence that blood transfusions received in the perioperative period for cancer surgery have adverse effects on disease-free survival and overall survival. In a study done by Blumberg et al, tumour recurrence and death rates in patients following colorectal cancer surgery was the single most important predictor for poor outcome.11 In an editorial, Kitchens C writes “If transfusion has an aggregate potential risk of 20% per transfusion, then what guarantee is there that transfusions are of such benefit that these risks are justifiable and acceptable?”12 In a survey on transfusion decision making, the risks of transfusion were recognised.13 Most unnecessary transfusions appear to result from excessive and unfound fear of the risk from not transfusing. These same researchers pointed out that a physician’s confidence in his or her decisions regarding transfusion ordering was inversely related to the practitioner’s actual knowledge of transfusion medicine. They suggested that changing a physician’s transfusion ordering habits would probably be better affected by information on the limited benefit of transfusion rather than by further knowledge of the risk of transfusion.
PREOPERATIVE TRANSFUSION - ANY BENEFITS?
Two concepts form the basis for the use of Hb as a transfusion trigger, the optimal Hb and the minimally acceptable Hb. For many years, these two were considered to be the same. In 1941, Lundy recommended that all patients with preoperative Hb levels below 10 g% be transfused before surgery, basing this decision on his clinical experience and understanding of oxygen transport dynamics.14 A few years later, Clark et al. also recommended 10 g% of Hb or a haematocrit value of 30%.15 The 10 g% Hb level, or 10/ 30 rule, for
transfusion, soon became a doctrine that has persisted for many years. It is important to separate the effects of hypovolemia and decreased perfusion from that of anaemia. If there is normal intravascular volume and normal tissue perfusion, then there is no adverse effect on cardiovascular function until anaemia is profound. Healing of surgical wound depends on angiogenesis and collagen deposition, and epithelialisation. Healing is not compromised with normovolemic haemodilution unless it is extreme. The oxygen extraction ratio of the healing tissue is 3%. The critical Hb at which anaemia may influence tissue repair is about 5 g%.
The clinical experience with Jehovah’s Witness patients, who refuse transfusion due to religious reasons, has given a lot of scope for rethinking about transfusion practice. Clinicians started reconsidering the minimum Hb level needed before surgery. Several studies designed to establish an optimal Hb concentration noted that levels lower than 10 g% were well tolerated by most of the patients. Several clinical studies provided further information regarding the minimally acceptable Hb level in the form of mortality and morbidity data in anaemic surgical patients. Rawstron et al. noted similar postop complications in 145 patients with Hb less than 10g% and in 412 patients with Hb levels 10 g% or above.16 Alexiu et al. compared the post operative mortality rates in patients with gastrointestinal bleeding.17 Sixty-nine transfused patients were compared with 72 who were resuscitated with large volumes of dextrose and normal saline. In patients not given blood the postoperative haematocrit ranged from 10 to 37% with a mean of 23.3% on the second postoperative day. There were no deaths in the nontransfused group and the complication rate was lower than that in the transfused group. Their study indicates that keeping a normal volume in an anaemic patient is important and the absolute Hb value is less important unless it is very low.
Spence and colleagues reported their findings of postoperative morbidity and death in Jehovah’s Witnesses.18 In 125 patients, mortality rate was higher when Hb level was less than 8 g%. There was comparable mortality with patients having Hb between 8 g% and 10g% and with Hb
RACE 2003 Ramachandra Anaesthesia Continuing Education
Preoperative transfusion threshold is a haemoglobin of 8 g% 245 Manjunath Prabhu
more than 10g% (0 % and 7.1% respectively). They also observed that when the Hb level was more than 8 g% and blood loss was less than 500 ml, there was no mortality. In a study done by Nelson et al comparing 100 operations for total hip replacement in Jehovah’s Witness with 100 patients who were not Jehovah’s Witness having same age, sex and health status operated by the same surgeon,19 the overall morbidity and mortality of the both groups were same. The elderly Jehovah’s Witness patients did not experience any increase in the incidence of stroke, myocardial infarction or renal failure despite blood loss of 5 units. Nelson and colleagues implied that by not transfusing the 100 Jehovah’s Witness undergoing total hip replacement, at least 200 units of blood was saved. This conservative method had not only represent a sizeable expense spared, it also unknowingly avoided an estimated 20% of complications associated with transfusions. Two more studies raise concerns regarding blood transfusion in the ICU patients. In 23 medical and surgical patients with sepsis, the measured V02 did not improve after transfusion from 9.0g% to11.9g% regardless of the lactate level. However, when the blood was more than 15 days old gastric intramucosal pH fell, indicating possible splanchnic ischaemia.20 Purdy and colleagues showed a clear correlation of mortality from severe sepsis and age of transfused RBC units.21
WHAT COULD BE THE MINIMUM HAEMOGLOBIN REQUIRED FOR A RESTING INDIVIDUAL?
Lieberman and colleagues studied the effect of isovolumic haemodilution in 8 healthy young adult human volunteers.22 They reduced the Hb level from 12.5 g% to 4.8 g% with isovolumic haemodilution using 5% albumin and autologos plasma. They monitored the haemodynamics of these volunteers and studied the oxygen delivery (D02) and oxygen consumption (V02) along with plasma lactate levels. The D02 decreased to 9.9 ± 2.0 ml02 .kg1.min'1 from 14.0 ± 2.9 ml02 .kg1.min1. V02and plasma lactate level was slightly raised and further reducing the D02 to 7.3 ± 1.4 ml02 .kg-1.min1 did not increase the plasma lactate levels. They concluded that the a decrease in
D02 to 7.3 ± 1.4 ml02.kg-1.min'1 in resting, healthy, conscious humans does not produce evidence of inadequate systemic oxygenation. The critical D02 in healthy, conscious humans appears to be less than 7.3 ml02.kg‘1.min'1. This study confirms that healthy individuals can tolerate very low Hb levels without showing any evidence of inadequate tissue oxygenation provided normal intravascular volume is maintained.
Clinical evidence with acute normovolemic haemodilution indicates that Hb levels of approximately 7 g% are well tolerated, even in elderly patients. 23 Cardiac output is usually increased approximately 35%, but tachycardia is not prominent if normovolemia is maintained. In healthy teenagers, Hb levels of 5 g% were well tolerated during acute normovolemic haemodilution.24 There are case reports of patients having an introperative Hb of 2 g% and how were still able to recover fully.
The lower limit of Hb tolerated in humans is not known. If the goal is to provide adequate global oxygen supply to meet normal oxygen consumption in an otherwise healthy person, the lowest level of Hb can be calculated mathematically.
V02 is the difference between arterial oxygen delivery (D02) and venous oxygen return t V02 = Do2 - 02 return
= CO L.min-1x ( Ca02 mL.dL-1- Cv02 mL.dL’1) x 10 dL.L'1
= CO x [ 1.38 (Hb) (Sa02- SvO2)/ 100]x 10
= CO x 13.8 x Hb x (Sa02 - Sv02) /100 where CO is cardiac output, Ca02 is arterial oxygen content, Sa02 is saturation of arterial blood with oxygen, Cv02 is venous oxygen content, and Sv02 is saturation of venous blood with oxygen.
When the normal values are substitutedV02 = 5x 13.8 x 15 x (100-75)/100
= 259 mL.min-1.
In healthy adults there are a number of compensatory mechanisms by which oxygen delivery (D02) can be maintained in the presence of anaemia. These are, by increased oxygen
RACE 2003 Ramachandra Anaesthesia Continuing Education
Preoperative transfusion threshold is a haemoglobin of 8 g% 246 Manjunath Prabhu
extraction by tissues, a rightward shift of oxyhaemoglobin dissociation curve (ODC) and increased cardiac output. Cardiac output (CO) can be increased by increases in contractility, heart rate, stroke volume or preload. In healthy adults CO can be increased to 15L.min'1 and Sv02 can fall to 31%. Even if we take a minimum Sv02 of 50%, the Hb required to provide a normal V02 can be as low as:
Hb = VO2/ CO L.min1x 13.8 x (100-50)/100 Hb = 259/15 x 13.8 x ( 100-50) /100 Hb = 2.5g%
This is an extreme condition assuming a normal V02, extraordinary cardiopulmonary reserve and instantaneous ability to increase oxygen extraction. These assumptions may not hold good in elderly, critically ill patients or reduced cardiopulmonary reserve. This also does not take into consideration the specific organs like heart and brain. This may give some indication about how some patients reported in the literature where able to compensate extremes of anaemia. In the real clinical situation we should always provide enough reserve so that unexpected sudden change in supply or demand can be met with. We should also see that our unsuspected patients are not exposed to unwanted transfusion related complications.
The 1992 clinical guideline by American College of Physicians for practice strategies for elective red blood cell transfusion recommends:25
PATIENT UNDER ANESTHESIA Patients with stable vital signs:• Assess the patients risk for myocardial or
cerebral ischemia• In the absence of risks, transfusion is not
indicated, independent of hemoglobin level.• Intravascular volume of patients at risk should
be adequately restored with crystalloids. Normovolemic anaemia has been shown to be well tolerated.
Patients with unstable vital signs:• Assess the patients risk for myocardial or
cerebral ischemia• In the absence of risks, intravascular volume
should be adequately restored with crystalloids.
• Patients at risk should receive autologous blood transfusion. If autologous blood is not available, homologous blood should be used on a unit by unit basis to stabilise vital signs. Remember: One unit may be sufficient.
There are many known and several more unknown complications associated with blood transfusion. Unnecessary blood transfusion not only exposes patients to these risks but also puts a strain on the limited resources. There is no evidence to show that Hb more than 8 g% is associated with a better outcome. All the newer recommendations condemn unnecessary blood transfusion and recommend transfusions only when the patient is symptomatic. Considering the fact that in developing countries such as ours complications of blood transfusion are likely to be higher when compared to Western data, we should refrain from administering unwanted blood transfusions. Whenever one considers blood transfusion, one must weigh the risk: benefit ratio before taking the final decision to transfuse.
References :
1. Ammann AJ, Cowan MJ, Wara DW, et al. Acquired immunodeficiency in an infant: possible transmission by means of blood products. Lancet 1983; 1: 956-8.2. Sazama K. Reports of 355 transfusion-associated deaths:1976 through 1985. Transfusion 1990; 30: 583-90.3. Theakston EP, Moriss AJ, Streat SJ, et al. Transfusion transmitted Yersinia enterocolitica infection in New Zealand. Aust NZJ Med 1997; 27: 62-7.4. Linden JV, Tourault MA, Scribner CL. Decrease in frequency of transfusion fatalities. Transfusion 1997; 37:243-4.5. Popovsky MA, Moore SB. Diagnostic and pathogenetic considerations in transfusion-related acute lung injury. Transfusion 1997; 37: 719-26.6. Ness PM, Shirley RS, Thoman SK, et al. The differentiation of delayed serologic and delayed haemolytic transfusion reactions; incidence, long term serologic findings, and clinical significance. Transfusion 1990; 30: 688-93.7. Goodnough LT, Brecher ME, Kanter MH, et al. Transfusion medicine. First of two parts-blood transfusion. N Eng J Med 1999; 340: 438-47.8. Greenbaum BH. Transfusion-associated graft- versus-host disease: historical prospectives, incidence,and current use of irradiated blood products. J Clin Oncol 1991; 9: 1889-1902.9. Maetani S, Nishikawa T, Hirakawa A et al. Role of blood transfusion in organ system failure following major abdominal surgery. Ann Surg 1986; 203: 275-81.10. Wobbes T, Bemelmans BLH, Kuypers JHC, et al. Risk of postoperative septic complications after abdominal surgical treatment in relation to perioperative blood transfusion. Surg Gynecol Obstet 1990; 171:59-62.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Preoperative transfusion threshold is a haemoglobin of 8 g% 247 Manjunath Prabhu
11. Blumberg N, Agarwal MM, Chaung C. Relation between recurrence of cancer of the colon and blood transfusion. BMJ1985; 290: 1037-9.12. Kitchens CS. Are transfusions overrated? Surgical outcome of Jehovah’s Witness. Am J Med 1993; 94: 117-9.13. Salem-Schatz SR, Avorn J, Soumerai SB. Influence of clinical knowledge, organizational context, and practice style on transfusion decision making. Implications for practice change strategies. JAMA 1990; 264: 476-83.14. Ad^ms RC, Lundy JS. Anesthesia in cases of poor surgical risk. Some suggestions for decreasing the risk. Surg Gynecol Obstet 1942; 74: 1011.15. Clark JH, Nelson W, Lysons C et al. Chronic shock: the problem of reduced blood volume in the chronically ill patient. Ann Surg 1947; 125: 618.16. Rawstron ER. Anemia and surgery. A retrospective clinical study. Aust N Z J Surg 1970; 39 : 425.17. Alexiu O, Mircea N, Balaban M et al. Gastrointestinal haemorrhage from peptic ulcer. An evaluation of bloodless transfusion and early surgery. Anaesthesia 1975; 30: 609.18. Spence RK, Carson JA, Poses R et al. Elective surgery without transfusion: influence of preoperative hemoglobin level and blood loss on mortality. Am J Surg 1990; 59 : 320.
19. Nelson CL, Bowen WS. Total hip arthroplasty in Jehovah’s Witness without blood transfusion. J Bone Joint Surg (Am) 1986; 68: 350-3.20. Mark PE, Sibbald WJ. Effect of stored-blood transfusion on oxygen delivery in patients with sepsis. JAMA 1993; 269: 3024-9.21. Purdy FR, Tweeddale MG, Merrick PM> Association of mortality with age of blood transfused in septic ICU patients. Can J Anaesth 1997; 44: 1256-61.22. Lieberman JA, Weiskopf RB, Kelley SD, et al. Critical oxygen delivery in conscious human is less than 7.3 ml 02 . kg-’ . min-1. Anesthesiology 2000; 92 : 407.23. Stehling L, Zauder HL. Acute normovolemic hemodilution. Transfusion 1991; 31: 857.24. Haberkern M, Dangel P. Normovolaemic haemodilution and intraoperative auto transfusion in children: experience with 30 cases of spinal fusion. Eur J Paediatr Surg. 1991; 1 : 30.25. American College of Physicians. Practice strategies for elective red blood cell transfusion. Ann Int Med 1992; 116: 403.26. Anderson KC, Weinstein HS. Transfusion associated graft-versus host disease. N Engl J Med 1990; 323: 315-21.
RACE 2003 Ramachandra Anaesthesia Continuing Education
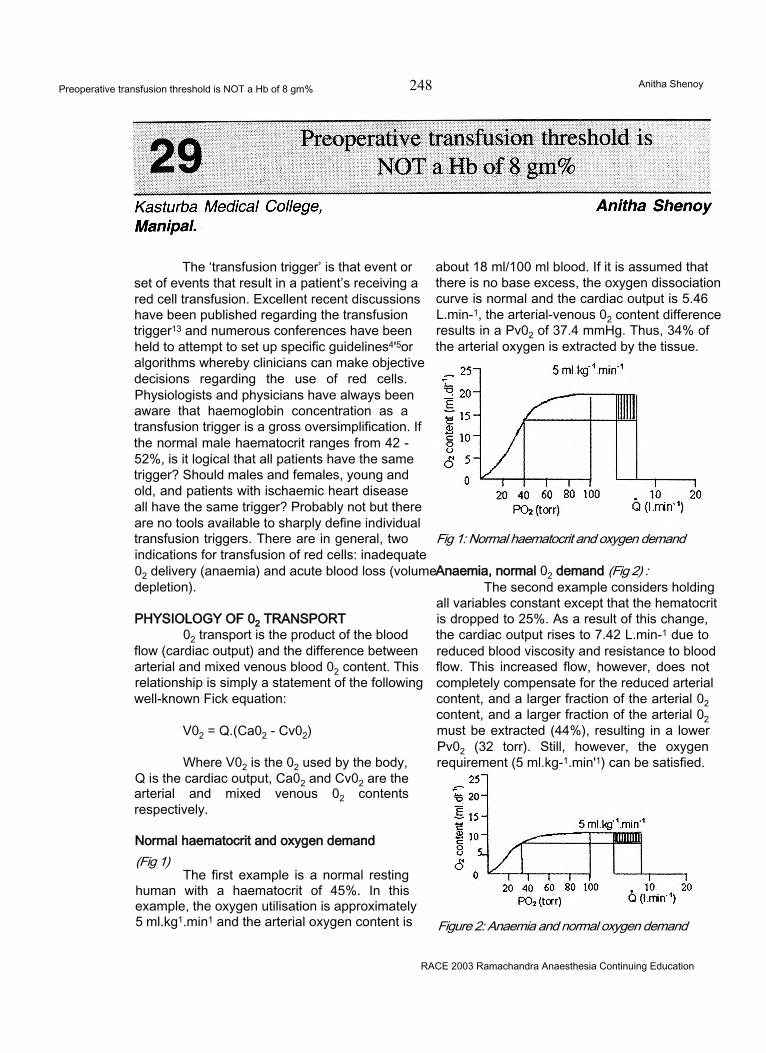
Preoperative transfusion threshold is NOT a Hb of 8 gm% 248 Anitha Shenoy
The ‘transfusion trigger’ is that event or set of events that result in a patient’s receiving a red cell transfusion. Excellent recent discussions have been published regarding the transfusion trigger13 and numerous conferences have been held to attempt to set up specific guidelines4'5or algorithms whereby clinicians can make objective decisions regarding the use of red cells. Physiologists and physicians have always been aware that haemoglobin concentration as a transfusion trigger is a gross oversimplification. If the normal male haematocrit ranges from 42 - 52%, is it logical that all patients have the same trigger? Should males and females, young and old, and patients with ischaemic heart disease all have the same trigger? Probably not but there are no tools available to sharply define individual transfusion triggers. There are in general, two indications for transfusion of red cells: inadequate 02 delivery (anaemia) and acute blood loss (volume depletion).
PHYSIOLOGY OF 02 TRANSPORT02 transport is the product of the blood
flow (cardiac output) and the difference between arterial and mixed venous blood 02 content. This relationship is simply a statement of the following well-known Fick equation:
V02 = Q.(Ca02 - Cv02)
Where V02 is the 02 used by the body, Q is the cardiac output, Ca02 and Cv02 are the arterial and mixed venous 02 contents respectively.
Normal haematocrit and oxygen demand(Fig 1)
The first example is a normal resting human with a haematocrit of 45%. In this example, the oxygen utilisation is approximately5 ml.kg1.min1 and the arterial oxygen content is
about 18 ml/100 ml blood. If it is assumed that there is no base excess, the oxygen dissociation curve is normal and the cardiac output is 5.46 L.min-1, the arterial-venous 02 content difference results in a Pv02 of 37.4 mmHg. Thus, 34% of the arterial oxygen is extracted by the tissue.
Fig 1: Normal haematocrit and oxygen demand
Anaemia, normal 02 demand (Fig 2) :The second example considers holding
all variables constant except that the hematocrit is dropped to 25%. As a result of this change, the cardiac output rises to 7.42 L.min-1 due to reduced blood viscosity and resistance to blood flow. This increased flow, however, does not completely compensate for the reduced arterial content, and a larger fraction of the arterial 02 content, and a larger fraction of the arterial 02 must be extracted (44%), resulting in a lower Pv02 (32 torr). Still, however, the oxygen requirement (5 ml.kg-1.min'1) can be satisfied.
Figure 2: Anaemia and normal oxygen demand
RACE 2003 Ramachandra Anaesthesia Continuing Education
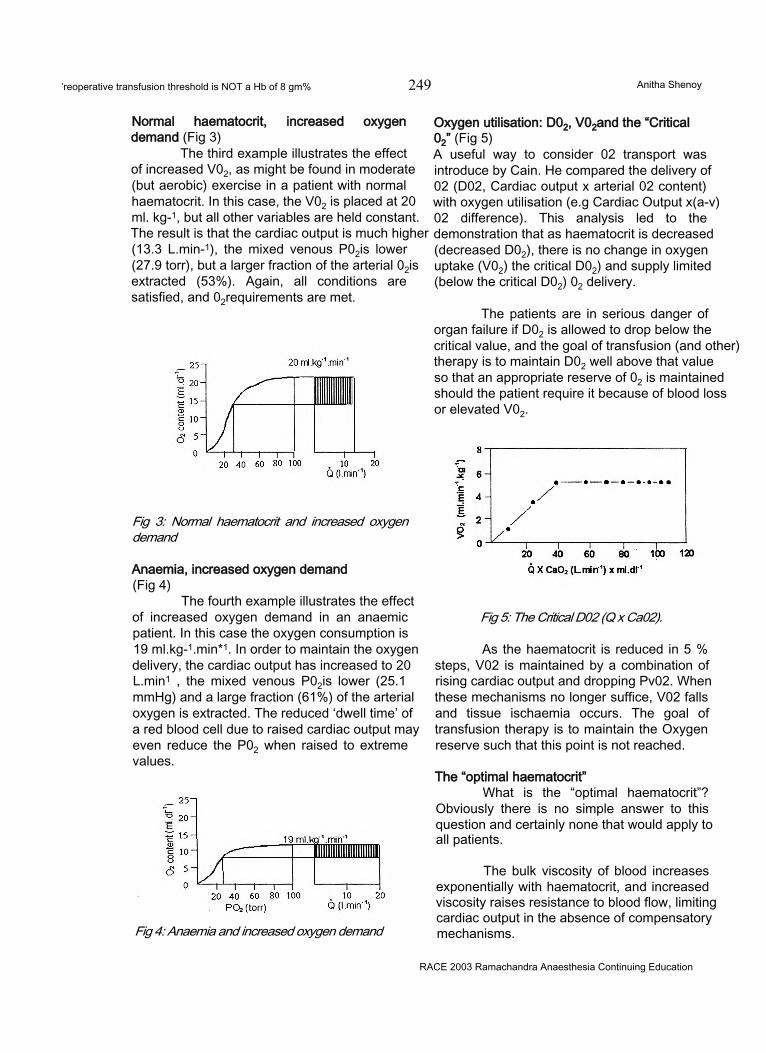
’reoperative transfusion threshold is NOT a Hb of 8 gm% 249 Anitha Shenoy
Normal haematocrit, increased oxygen demand (Fig 3)
The third example illustrates the effect of increased V02, as might be found in moderate (but aerobic) exercise in a patient with normal haematocrit. In this case, the V02 is placed at 20 ml. kg-1, but all other variables are held constant. The result is that the cardiac output is much higher (13.3 L.min-1), the mixed venous P02is lower (27.9 torr), but a larger fraction of the arterial 02is extracted (53%). Again, all conditions are satisfied, and 02requirements are met.
Fig 3: Normal haematocrit and increased oxygen demand
Anaemia, increased oxygen demand(Fig 4)
The fourth example illustrates the effect of increased oxygen demand in an anaemic patient. In this case the oxygen consumption is 19 ml.kg-1.min*1. In order to maintain the oxygen delivery, the cardiac output has increased to 20 L.min1 , the mixed venous P02is lower (25.1 mmHg) and a large fraction (61%) of the arterial oxygen is extracted. The reduced ‘dwell time’ of a red blood cell due to raised cardiac output may even reduce the P02 when raised to extreme values.
Oxygen utilisation: D02, V02and the “Critical02” (Fig 5)A useful way to consider 02 transport was introduce by Cain. He compared the delivery of 02 (D02, Cardiac output x arterial 02 content) with oxygen utilisation (e.g Cardiac Output x(a-v) 02 difference). This analysis led to the demonstration that as haematocrit is decreased (decreased D02), there is no change in oxygen uptake (V02) the critical D02) and supply limited (below the critical D02) 02 delivery.
The patients are in serious danger of organ failure if D02 is allowed to drop below the critical value, and the goal of transfusion (and other) therapy is to maintain D02 well above that value so that an appropriate reserve of 02 is maintained should the patient require it because of blood loss or elevated V02.
Fig 4: Anaemia and increased oxygen demand
Fig 5: The Critical D02 (Q x Ca02).
As the haematocrit is reduced in 5 % steps, V02 is maintained by a combination of rising cardiac output and dropping Pv02. When these mechanisms no longer suffice, V02 falls and tissue ischaemia occurs. The goal of transfusion therapy is to maintain the Oxygen reserve such that this point is not reached.
The “optimal haematocrit”What is the “optimal haematocrit”?
Obviously there is no simple answer to this question and certainly none that would apply to all patients.
The bulk viscosity of blood increases exponentially with haematocrit, and increased viscosity raises resistance to blood flow, limiting cardiac output in the absence of compensatory mechanisms.
RACE 2003 Ramachandra Anaesthesia Continuing Education
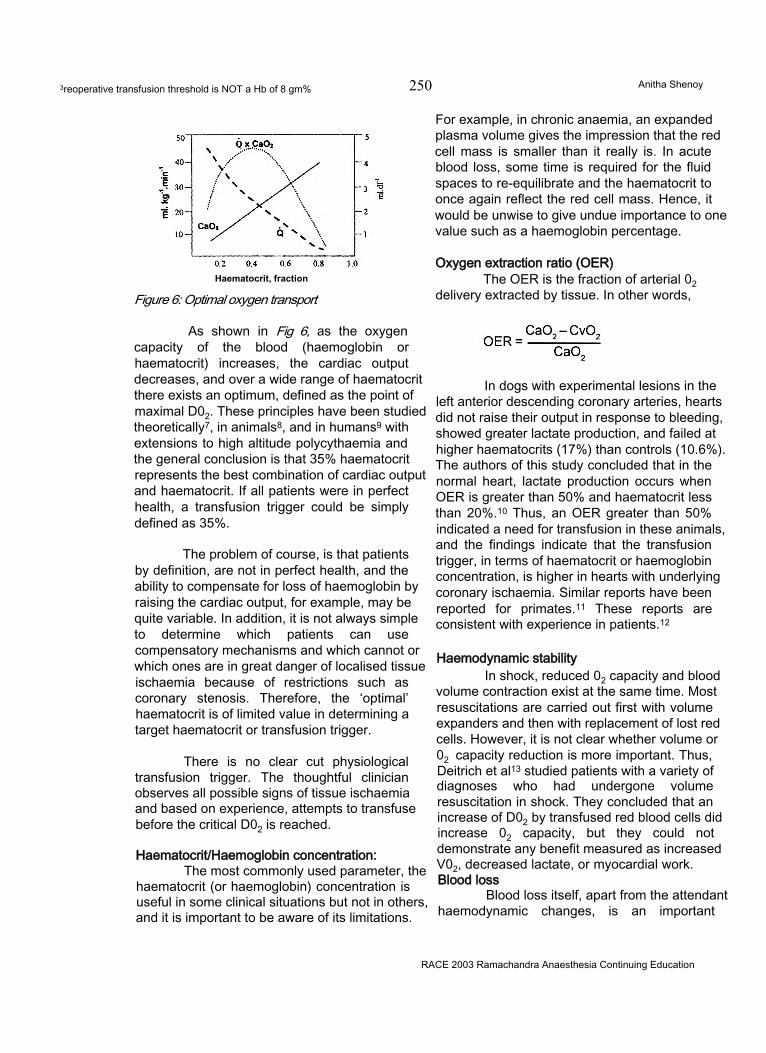
3reoperative transfusion threshold is NOT a Hb of 8 gm% 250 Anitha Shenoy
Haematocrit, fraction
Figure 6: Optimal oxygen transport
As shown in Fig 6, as the oxygen capacity of the blood (haemoglobin or haematocrit) increases, the cardiac output decreases, and over a wide range of haematocrit there exists an optimum, defined as the point of maximal D02. These principles have been studied theoretically7, in animals8, and in humans9 with extensions to high altitude polycythaemia and the general conclusion is that 35% haematocrit represents the best combination of cardiac output and haematocrit. If all patients were in perfect health, a transfusion trigger could be simply defined as 35%.
The problem of course, is that patients by definition, are not in perfect health, and the ability to compensate for loss of haemoglobin by raising the cardiac output, for example, may be quite variable. In addition, it is not always simple to determine which patients can use compensatory mechanisms and which cannot or which ones are in great danger of localised tissue ischaemia because of restrictions such as coronary stenosis. Therefore, the ‘optimal’ haematocrit is of limited value in determining a target haematocrit or transfusion trigger.
There is no clear cut physiological transfusion trigger. The thoughtful clinician observes all possible signs of tissue ischaemia and based on experience, attempts to transfuse before the critical D02 is reached.
Haematocrit/Haemoglobin concentration:The most commonly used parameter, the
haematocrit (or haemoglobin) concentration is useful in some clinical situations but not in others, and it is important to be aware of its limitations.
For example, in chronic anaemia, an expanded plasma volume gives the impression that the red cell mass is smaller than it really is. In acute blood loss, some time is required for the fluid spaces to re-equilibrate and the haematocrit to once again reflect the red cell mass. Hence, it would be unwise to give undue importance to one value such as a haemoglobin percentage.
Oxygen extraction ratio (OER)The OER is the fraction of arterial 02
delivery extracted by tissue. In other words,
In dogs with experimental lesions in the left anterior descending coronary arteries, hearts did not raise their output in response to bleeding, showed greater lactate production, and failed at higher haematocrits (17%) than controls (10.6%). The authors of this study concluded that in the normal heart, lactate production occurs when OER is greater than 50% and haematocrit less than 20%.10 Thus, an OER greater than 50% indicated a need for transfusion in these animals, and the findings indicate that the transfusion trigger, in terms of haematocrit or haemoglobin concentration, is higher in hearts with underlying coronary ischaemia. Similar reports have been reported for primates.11 These reports are consistent with experience in patients.12
Haemodynamic stabilityIn shock, reduced 02 capacity and blood
volume contraction exist at the same time. Most resuscitations are carried out first with volume expanders and then with replacement of lost red cells. However, it is not clear whether volume or02 capacity reduction is more important. Thus, Deitrich et al13 studied patients with a variety of diagnoses who had undergone volume resuscitation in shock. They concluded that an increase of D02 by transfused red blood cells did increase 02 capacity, but they could not demonstrate any benefit measured as increased V02, decreased lactate, or myocardial work. Blood loss
Blood loss itself, apart from the attendant haemodynamic changes, is an important
RACE 2003 Ramachandra Anaesthesia Continuing Education

Preoperative transfusion threshold is NOT a Hb of 8 gm% 251 Anitha Shenoy
indicator of the need for transfusion. Carson et al14 carried out a careful study of 125 surgical patients who declined to be transfused on religious grounds and found that mortality was inversely related to haemoglobin concentration. Mortality rose from 7.1% for patients with haemoglobin concentrations over 10 g.dM. Mortality was 8% for patients in whom 500 ml or less blood was lost but rose to 42.9% for those in whom loss was greater than 2000 ml.
Most healthy patients can tolerate blood loss upto 40% of their blood vloume. However, many surgical patients who are not healthy may be much less tolerant of blood loss. For example, elderly patients with ischaemic heart disease may suffer tissue infarction as a result of decreased organ blood flow. Patients with borderline or inadequate pulmonary function may not be able to maintain arterial oxygenation when red cell capillary transit time decreases with increased cardiac output. Patients with liver disease may not be able to increase albumin synthesis to increase plasma oncotic pressure and so on. These factors must be kept in mind when considering the clinical indications for transfusion in an individual patient.
The risk of undertransfusionIn our enthusiasm to spare patients the
risks of blood transfusions, there is a risk of undertransfusion. Although a National Institutes of Health consensus conference recommended that the lower safe limit of haemoglobin concentration could be below 10g.dl \ no definite lower limit guideline was provided.5
Animal studies underscore the risks of undertransfusion. Spahn et al15 haemodiluted dogs in whom experimental stenoses had been placed on the left anterior descending coronary artery. They then measured regional function of the myocardium by sonomicrometry and found that the lowest haemoglobin concentration tolerated without compromised function was 7.5 g.dl1 and an increase of as little as 1.9 g.dl1 by transfusion restored function and 02 consumption in the affected region.
Similar observations have been made in patients. A haematocrit lower than 29% was
associated with significant cardiac ischaemia in a group of surgical patients with peripheral vasaikrcLi5ease .16 Significantly more coronary ischaemia occurred in peripheral vasular reconstructive surgery in whom the haematocrit was less than 28%.17 A haematocrit value of 28% appears to be the lower limit that can be safely reached in patients with clear evidence of coronary ischaemia.18
In patients in whom the haematocrit must fall below approximately 28%, the astute clinician must assess the patient’s ability to compensate for the reduced 02 capacity, and if there is evidence of ischaemia, careful monitoring of ECG, blood pressure, oxygen saturation and ST segment analysis is indispensable.19
Ciinicai transfusion triggerAlthough a physiological transfusion
trigger is elusive, actual clinical situations are far more complicated. For example, not all patients can raise cardiac output in response to the challenge of anaemia. In others, tissue ischaemia, such as in coronary artery disease, can raise the local D02 requirement, reducing the Oz reserve for that area. In other patients, pulmonary disease may impose a diffusion barrier (increased DM02) or restrict ventilation, which can restrict pulmonary 02 uptake.
In some ways, focusing attention on this issue has resulted in physician’s atttitudes drifting away from using ‘clinical judgement’ toward the search for hard quantitative triggers that relieve the clinician from the responsibility of making a decision.20 In reality, the decision to transfuse (or not to transfuse) is a clinical judgement, and the astute clinician distils many different data, objective and subjective, in coming to a final decision.
LITERATURE SUPPORTING A HIGHERHAEMATOCRITIschaemic heart disease
Carson et al21 conducted a retrospective study in 1958 patients, 18 years and older, who underwent surgery and declined blood transfusion for religious reasons. The primary outcome was 30-day mortality and the secondary outcome was 30-day mortality or in-hospital 30-day morbidity.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Preoperative transfusion threshold is NOT a Hb of 8 gm% 252 Anitha Shenoy
Cardiovascular disease was defined as a history of angina, myocardial infarction, congestive heart failure, or peripheral vascular disease. The 30- day mortality was 3.2% (95% Cl 2.4-4.0). The mortality was 1.3% (0.8 - 2.0) in patients with preoperative haemoglobin 12g.dl1 or greater and 33.1% (18.6-51.0) in patients with preoperative haemoglobin less than 6 g.dl1. The increase in death associated with low preoperative haemoglobin was more pronounced in patients with cardiovascular disease than in patients without.(interaction p < 0.03).
Wu et al22 conducted a retrospective study of data on 78,974 Medicare beneficiaries 65 years old or older who were hosptalised with acute Ml. Patients were categorised according to haematocrit on admission (5.0 to 24%, 24.1 to 27%, 27.1 to 30%, 30.1 to 33.0%, 33.1 to 36.0% , 36.1 to 39% or 39.1 to 48.0% and data were evaluated to determine whether there was an association between the use of transfusion and 30-day mortality. Patients with lower haematocrit had a higher 30-day mortality rates. Blood transfusion was associated with a reduction in 30 day mortality among patients whose haematocrit fell into the categories ranging from 5.0 to 24% (adjusted odds ratio, 0.22; 95% confidence interval, 0.11 to 0.45) to 30.1 to 33.0 percent (adjusted odds ratio, 0.69; 95% confidence interval, 0.53 to 0.89). It was not associated with decrease in mortality with haematocrit values of 30.1% or higher. Their conclusion was that blood transfusion was associated with a lower short term mortality rate among elderly patients with acute Ml if the haematocrit on admission is 30.0% or lower and may be effective in patients with a haematocrit as high as 33% on admission.
Spine SurgeryPostoperative vision loss is a rare
complication of spine surgery that has been reported with increasing frequency over the last decade, occurring in 0 - 1 % of cases2327. Postoperative vision loss is most often due to anterior or posterior ischaemic optic neuropathy (AION, PION) and rarely due to other less common perioperative complications such as, central retinal artery or vein occlusion and occipital lobe infarcts. Causes of ION include 1.
decreased perfusion pressure due to systemic hypotension, increased venous pressure, or large vessel occlusive disease, 2. increased resistance to blood flow due to increased viscosity of blood, local artery disease, or increased external pressure and 3. decreased oxygen carrying capacity. While postoperative ION appears to occur more commonly in patients over age 40 to 50, it does develop in young patients also.28
Reported risk factors for postoperative AION and PION include patient factors such as risk factors for atherosclerotic disease and intraoperative factors such as hypotension, anaemia, excessive blood loss, massive fluid resuscitation, prone position, long operative duration and head dependent positioning. Intraoperative hypotension and anaemia are the most consistent observations in patients developing postoperative ION. Long operative duration, high intraoperative blood loss, and large volume resuscitation have been reported to be associated with increased risk for ION.25 Because most patients undergoing even long prone spine surgery with large intraoperative blood loss do not develop ION, other as yet unidentified factors are felt to exist.27 It has been suggested that changes in transfusion practice over the last decade to lower haematocrit values as triggers for transfusion may lead to an increased incidence of postoperative ION.23
One of the suggestions include choosing minimum haematocrit and blood pressure levels in those patients that may be higher than for patients not felt to be at particular risk for ION.
Critically ill patientsHebert et al29 examined the impact of
transfusion practice on mortality rates in 4,470 critically ill patients. As compa.ed with survivors, patients who died in intensive care units (ICU) had lower haemoglobin values (95 ± 26 versus 104 ± 23 g.l1, p < 0.0001) and were transfused red cells more frequently (42.6% versus 28%, p < 0.0001). In patients with cardiac disease, there was a trend toward an increased mortality when haemoglobin values were <9.5 gm% (55% versus 42%, p = 0.09) as compared with anaemic patients with other diagnoses. They concluded that anaemia increases the risk of death in
RACE 2003 Ramachandra Anaesthesia Continuing Education
Preoperative transfusion threshold is NOT a Hb of 8 gm% 253 Anitha Shenoy
critically ill patients with cardiac disease. Blood transfusions appear to decrease this risk. This finding is reinforced by a subsequent study (multicentred, randomised, controlled clinical trial of transfusion requirements) by the same group.30 They concluded that younger patients and those who are not so severely ill may tolerate a haemoglobin level of 7 gm%. However, some groups of patients who may benefit from transfusion and require further study include those with cardiac disease, emphysema, more severe illness, cerebrovascular disease, and trauma, as well as older patients. The last group may require a liberal strategy of transfusion.
Acute gastrointestinal bleedIt is recommended that patients
presenting with moderate or severe acute gastrointestinal bleeding should have blood transfused to a Hb level of > 9 gm% until one is fairly confident that the patient is unlikely to have a further large bleed.31
Many practitioners will accept a threshold Hb level of approximately 7-8 gm% in a well compensated and otherwise healthy patient presenting for minor surgery. However, a higher preoperative haemoglobin level will be needed before elective surgery in the following situations32
1) Inadequate compensation for anaemia2) Significant co-existing cardiopulmonary disease3) Major surgery or significant blood loss is expected.
The decision to transfuse should be supported by the need to relieve clinical signs and symptoms and prevent significant morbidity or mortality. A blanket treatment meted out to every patient cannot be acceptable. Thus, the patient’s haemoglobin value, although important, should not be the sole deciding factor in starting or avoiding transfusion.
REFERENCES
1) Stehling L, Simon Tl. The red cell transfusion trigger. Physiological and clinical studies. Arch Pathol Lab Med 1994;118:429-34
2) Goodnough LT, Vertbrugge D, Vizmeg K, Riddell J IV.
Identifying elective orthopaedic surgical patients transfused with amounts of blood in excess of need: the transfusion trigger revisit [published erratum appears in Transfusion 1992;32:838]. Transfusion 1992;32:648-53
3) Levine E, Rosen A, Sehgal L, Gould S, Sehgal H, Moss G. Physiological effects of acute anaemia:implications for a reduced transfusion trigger.Transfusion 1990;30:11-4
4) Robertie PG, Gravlee GP,. Safe limits of isovolaemic haemodilution and recommendations for erythrocyte transfusion. Int Anesth Clin 1990;28:197-204
5) NIH consensus conference. Perioperative Red Cell Transfusion. JAMA 1988;260:2700-3
6) Cain SM. Oxygen delivery and uptake in dogs during anaemic and hypoxic hypoxia. J Appl Physiol 1977;42:228-34
7) Crowell JW, Smith EE. Determination of the optimal haematocrit. J Appl Physiol 1967;22:501-4
8) Guyton AC, Jones CE, Coleman TG. Cardiac output and its regulation. 2nd ed. Philadelphia: WB Saunders, 1973
9) Winslow RM, Monge CC. Hypoxia, polycythaemia,and chronic mountain sickness. Baltimore: Johns
Hopkins University Press, 1987
10) Levy Ps, Chavez RP, Crystal GJ, et al. Oxygen extraction ratio : a valid indicator of transfusion need in I coronary vascular reserve? J Trauma 1992;32:769-74
11) Wilkerson DK, Rosen AL, Gould SA, Sehgal LR, Sehgal HL, Moss GS. Whole body oxygen extraction ratio as an indicator of cardiac status in anaemia. Curr Surg 1988;45:214-7
12) Mathru M, Kleinman B, Blakeman B, Sullivan H, Kumar P, Dries DJ. Myocardial metabolism and adaptation during extreme hemodilution in humans after coronary revascularisation. Crit Care Med 1992;20:1420-5
13) Dietrich KA, Conrad SA, Hebert CA, Levy GL, Romero MD. Cardiovascular and metabolic response to red cell transfusion in critically ill volume resuscitated nonsurgical patients. Crit Care Med 1990;18:940-4
14) Carson JL, Spence RK, Poses RM, Bonavita G. Severity of anaemia and operative mortality and morbidity. Lancet 1988;1:727-9
15) Spahn DR, Smith LR, Veronee CD, et al. Acute isovolaemic hemodilution and blood transfusion. Effects on regional function and metabloism in myocardium with compromised coronary blood flow. J Thorac Cardiovasc Surg 1993;105:694-704
RACE 2003 Ramachandra Anaesthesia Continuing Education
Preoperative transfusion threshold is NOT a Hb of 8 gm% 254 Anitha Shenoy
16) Christopherson R, Frank S, Norris E, Rock P, GottliebS, Beattie C. Low postoperative hematocrit is asscoiated with cardiac ischaemia in high risk patients. Anesthesiology 1991;75:A99
17) Nelson AH, Fleisher LA, Rosenbaum SH. Relationship between postoperative anemia and cardiac morbidity in high risk vascular patients in the intensive care unit. Crit Care Med 1993;21:860-6
18) Johnson RG, Thurer RL, Kruskall MS, et al. Comparison of two tranfusion strategies after elective operations for myocardial revascularisation. J Thorac Cardiovasc Surg 1992;104:307-14
19) Dick W, Baur C, Reiff K. Which factors determine the critical haematocrit as an indication of transfusion? (published erratum appears in Anaesthetist 1992;41:113). Anaesthetist 1992;41:1-14
20) Faust RJ. Perioperative indications for red blood cell transfusion: has the pendulum swung too far? Mayo Clin Proc 1993;68:512-4
21) Carson JL, Duff A, Poses RM, Berlin JA, Spence RK, Trout R et al. Effects of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996;348:1055-60
22) Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med 2001; 345:1230-6
23) Williams EL, Hart WM, Tempelhoff R: Postoperative ischaemic optic neuropathy. Anesth Analg 1995;80:1018-29
24) Stevens WR, Glazer PA, Kelley SD, Lietman TM, Bradford DS: Ophthalmic complications after spine surgery. Spine 1997;22:1319-24
25) Myers MA, Hamilton SR, Bogosian AJ, Smith CH, Wagner TA: Visual loss as a complication of spine surgery. A review of 37 cases. Spine 1997(22): 1329
26) Cheng MA, Sigurdson W, Tempelhoff R, Lauryssen C: Visual loss after spine surgery: a survey. Neurosurgery 2000;46(3):625-31
27) Warner ME, Warner MA, Garrity JA, Mackenzie RA, Warner DO: The frequency of perioperative vision loss. Anesth Analg 2001; 93:1417-21
28) Roth S, Barash P: Postoperative vision loss. Anesthesiology 2001;95:575-7
29) Hebert PC, Wells G, Tweeddale M, Martin C, et al. Does transfusion Practice Affect Mortality In CriticallyIII Patients? Am J Respir Crit Care Med 1997;155:1618-23
30) Hebert PC, Wells G, Blajchman MA et al. A multicentre, randomised, controlled clinical trial of transfusion requirements in critical care. N Engl J Med 1999;340:409-17
31) WHO. The current use of blood. Handbook. Blood transfusion safety. Geneva 2001
32) Winslow RM. A physiological basis for the transfusion trigger. In Perioperative transfusion medicine. Spiess BDed., Baltimore: William & Wilkins, 1998
RACE 2003 Ramachandra Anaesthesia Continuing Education

WORKSHOPS
Airway 255 Srinivasan, Chandrasekhar, Majunath Prabhu
Over the last three decades, anaesthesia related mortality has probably declined, but airway catastrophes continue to be well represented in all large series of anaesthesia deaths. Perhaps, this is not surprising since airway management is central to the practice of anaesthesia. Although the incidence of difficult or failed tracheal intubations is comparatively low, unexpected difficulties and poorly managed situations may produce a life threatening condition or even death.
The normal anatomy of the airway, its assessment including clinical and radiological, the techniques to anaesthetise the upper airway, various adjuncts in securing the airway, fibreoptic guided airway control and retrograde intubation have all been dealt with in RACE 2000. Hence difficult and failed tracheal intubation will be discussed in this session under the following headings:
• RECOGNITION OF DIFFICULT INTUBATION• CLINICAL TESTS OF CORRECT
PLACEMENT• ADVANCES IN MANAGEMENT OF
DIFFICULT INTUBATION• ADVANCES IN MANAGEMENT OF FAILED
INTUBATION
RECOGNITION OF DIFFICULT INTUBATIONAnatomical factors in failed intubation
It is the unexpected difficult intubation that leads to disaster. Predicting a problem at intubation should not be difficult when there is obvious pathology involving the neck, maxillofacial, pharyngeal and laryngeal structures, whether or not this is associated with certain medical conditions or congenital syndromes. However, several patients of apparently normal appearance unexpectedly
present great difficulty at intubation. A study of anatomical factors in these patients should improve the ability to predict and manage a potential failed intubation.
The importance must be stressed of correct positioning of the head and neck during laryngoscopy in order to achieve alignment of the axes of the mouth, pharynx and larynx to permit tracheal intubation. The position of flexion of the lower portion of the cervical spine combined with extension of the head at the atlanto-occipital joint is defined as the standard intubating position. Inability to extend the head at the atlanto-occipital joint is an important cause of difficult intubation. The amount of extension that can be achieved at this joint is limited by the abutment of the occiput against the posterior tubercle of the atlas. The greater the distance in the neutral position, the greater the degree of extension that is possible. When the posterior tubercle of the atlas is already in contact with the occiput in the neutral position, attempts to extend the head result in anterior bowing of the cervical spine and forward displacement of the larynx. Consequently, laryngoscopy is difficult.
It is necessary to raise the occiput above the shoulders by means of a pillow before testing for head extension. This manoeuvre helps to eliminate the error in assessment from anterior bowing of the cervical spine.
Despite correct positioning of the head and neck, other anatomic factors may interfere with the line of vision from the mouth to the vocal cords. Cormack and Lehane have categorized these as:
FORWARD DISPLACEMENT OF THE LARYNX OR UPPER TEETH
There is a marked descent of the larynx
RACE 2003 Ramachandra Anaesthesia Continuing Education
Airway 256 Srinivasan, Chandrasekhar. Majunath Prabhu
relative to the cervical spine during the first two years of life. This position remains static until puberty when further descent of laryngeal structures occurs. There is no advantage in visualisation of the larynx by flexion of the neck in children less than 2 yrs of age, as there are no intervertebral joints above the level of the larynx. A more effective procedure is to apply external pressure to the larynx, thus increasing the intubation angle and improving the view. Similarly, a high anterior larynx in an adult may be brought to view by external laryngeal manipulation. Marked anterior convexity of the cervical spine is associated with an anterior larynx. Furthermore, if there is marked convexity of the cervical spine, there is no atlanto-occipital gap.
UPPER TEETH AS A CAUSE OF DIFFICULT INTUBATION
Buckteeth is an important risk factor in predicting difficult intubation. Relative overgrowth of the premaxilla resulting in protruding upper incisors is a predictor of difficult intubation. Edentulous patients do no usually present an intubation problem, although this is not always the case. Mandibular configuration, tongue mass and mobility of these structures are important determinants of laryngeal visibility.
BACKWARD DISPLACEMENT OF THE TONGUE
Using radiological techniques, the ratio of the mandibular space to the total length of the tongue is a good predictor of difficult intubation thus introducing the important concept that bony structures should be considered in conjunction with soft tissues with which they are closely associated. Mass of the tongue with the mandibular space is the Mallampati classification. Limited movement of the mandible is a recognized cause of difficult intubation. This may be related to TM joint dysfunction or trismus, but in addition, a short thick neck, a relatively large mandible with short descending rami may contribute to the problems. Interdental gap and subluxation of the jaw are significant in assessment as risk factors for difficult intubation. While mouth opening permits adequate insertion of the laryngoscope, good forward movement of the mandible provides additional space for forward displacement of the tongue.
CLINICAL TESTS OF CORRECT PLACEMENT:
Clinical aidsDetection of oesophageal intubation is
significant because it contributes to 15% of major anaesthetic catastrophes. Hence the need for clinical aids for correct placement. These are:
Direct visualisation of the tube passing through the larynx Observation of chest movement
• Auscultation of breath sounds• Auscultation of the epigastrium
Observation for abdominal movements Observation for moisture condensation in the tubeMovement of reservoir bag in unparalyzed patients
Diagnostic aidsClinical methods of detecting
oesophageal intubation cannot be relied upon solely but every piece of available information should be utilized. Various diagnostic aids are available which include:1.FIBREOPTIC SCOPE
The best method of confirming tracheal intubation is visualization of the carina and tracheal rings by fibreoptic scope, probably impractical for routine use, but mandatory in case of doubt and certainly in the case of difficult intubation.
2. EXHALED CARB0NDI0XIDE(C02)Inadvertent ventilation of the stomach by
a misplaced endotracheal tube will not be accompanied by the presence of exhaled C02 and C02 monitoring should offer a reliable means of detecting oesophageal intubation. But if alveolar gas is forced into the stomach during mask ventilation, the C02 concentration in the stomach may be similar to that in the alveoli and this will produce a normal capnograph. However C02 waveform rapidly falls due to dilution of C02 in the stomach. Ingestion of a carbonated soft drink preoperatively also results in the simulation of a normal capnograph for the first few breaths following oesophageal intubation. Hence exhaled C02 waveform must be observed for a minimum of 6 cycles post intubation.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Airway 257 Srinivasan, Chandrasekhar, Majunath Prabhu
ASA Closed Claims analysis review suggests that a combination of both Sp02 and EtC02 prevented adverse respiratory events. Both were recommended for preventing oesophageal intubation but Sp02 alone was favoured for prevention of adverse outcomes associated with difficult intubations.
3.OESOPHAGEAL DETECTOR DEVICE (ODD):An oesophageal detector device is a 60
ml catheter tip syringe fitted to one end of a standard catheter mount with an international 15mm tracheal tube fitting at the distal end. It works because the oesophagus is a fibromuscular tube with no intrinsic structure to maintain its patency whereas the trachea is kept patent by C shaped cartilages. If the endotracheal tube is in the trachea and the ODD is attached to it, withdrawal of the plunger will aspirate gases from the patient’s lungs without any resistance apart from that inherent to the device. However, if the tube is in the non-rigid oesophagus, withdrawal of the plunger of the syringe will cause apposition of the wall of the oesophagus around the tube, which will occlude the lumen and cause negative pressure or resistance when the plunger is pulled back. The same disadvantage as of EtC02 is possible here since an inflated stomach behaves like lungs. Hence, ODD must be applied before starting ventilation through the tube. Ellick’s evacuator bulb is a modified version of this device.
4.TRANSTRACHEAL ILLUMINATION:The use of an illuminated introducer for
the tracheal tube is an aid to blind intubation and for difficult intubations using a standard technique under direct vision. A lighted stylet placed inside an endotracheal tube just proximal to the cuff, with cricoid pressure applied and overhead lights dimmed, facilitates tracheal intubation. When the lighted stylet was introduced into the oesophagus, no trans-oesophageal illumination was demonstrated. The method would not work with midline neck masses or red rubber tubes.
ADVANCES IN MANAGEMENT OF DIFFICULT INTUBATIONS:Adjuncts to difficult intubation
There are several devices, which are useful in managing difficult intubations. These are:
1.GUM ELASTIC BOUGIE:This is useful where the vocal cords
cannot be seen. There are 3 ways of identification of tracheal placement of a bougie:
a) Tracheal rings may be felt as clicks as the bougie slides in
b) The bougie may be held up as the small bronchi are reached whereas the whole length may be inserted into the oesophagus
c) The patient may cough
2.FIBREOPTIC SCOPE:Fibreoptic intubation may be oral or
nasal and can be performed under local or general anaesthesia. Fibreoptic nasal intubation is technically easier than oral intubation. Fibreoptic scope is invaluable in anticipated difficult intubation but requires expertise.
ADVANCES IN MANAGEMENT OF FAILED INTUBATION:
The essence of all failed intubation drill isa) Maintenance of oxygenationb) Prevention of aspiration
The risk to the patient is greatly increased if the anaesthetist is inexperienced or if the stomach is full.
Adjuncts to failed intubation include1. LMA
The LMA is invaluable in the management of failed intubation because of the high rate of successful insertion even in inexperienced hands. The l-LMA has the LMA, which serves as a guide to blind placement of the endotracheal tube. The currently available version has a fenestration so that a 6 mm tube can be passed through. A bougie can be inserted through the LMA, the mask removed and then an 8 or 9mm endotracheal tube can be threaded over the bougie.
The LMA has a place in every failed intubation routine to allow the patient to be oxygenated while the effect of the anaesthetic wears off. Risk of aspiration is not eliminated by insertion of laryngeal mask although it may provide some protection. Also in distorted upper airway anatomy, LMA would make proper placement difficult.
2.THE OESOPHAGEAL OBTURATOR AIRWAY AND OESOPHAGEAL GASTRIC TUBE AIRWAY:
These are intended to be emergency
RACE 2003 Ramachandra Anaesthesia Continuing Education
Airway 258 Srinivasan, Chandrasekhar, Majunath Prabhu
methods of maintaining the airway but the complications outweigh the safety these offer (like oesophageal rupture and tracheal placement, inadequate oxygenation and ventilation).
3. TRANSTRACHEAL VENTILATION:In the event of inability to ventilate a
patient by facemask or laryngeal mask following failed intubation, TTV is the only resort. There are 3 methods:
Needle cricothyrotomy MinitrachSurgical cricothyrotomy
MANAGEMENT OF FAILED INTUBATIONPatients with risk of vomiting/regurgitation
(as in obstetrics where hypoxia and aspiration are likely):STEPS TO PREVENT ASPIRATION
Early implementation of Turnstall’s drill before complication occurs Call for senior help Maintain cricoid pressure Left lateral with head down position Suction of pharynx as necessary If adoption of left lateral position not
possible, insert an EGTA, ventilate the lungs with 100% 02 using bag and facemask
STEPS TO ENSURE OXYGENATIONMethods to improve patient’s airway
includeExtend the head on neck Open the mouth Push the mandible forward Insertion of an Oropharyngeal airway Release cricoid pressure only if lateral head down position is possible Use of EGTA device
PARTIAL AIRWAY OBSTRUCTIONIf there is partial airway obstruction, but
sufficient oxygenation is taking place with return to spontaneous ventilation, persist with IPPV until patient recovers and consider alternative techniques. These include GA with facemask with spontaneous ventilation, awake intubation and subsequent GA, regional anaesthesia, local infiltration of LA and TTV with IV anaesthesia. Etomidate is suggested with IV opioids after delivery of the child.
NO AIRWAY OBSTRUCTIONIf the patient has a clear airway, there is
an option at this stage to establish spontaneous inhalation anaesthesia. If necessary, a wide bore stomach tube may be passed through, with the patient in the head down lateral position .The stomach is emptied, antacid instilled (20 ml of0.3.molar sodium citrate), after which the tube is withdrawn and the pharynx cleared. When spontaneous respiration resumes, the patient may be repositioned supine with a wedge.
OXYGENATION IMPOSSIBLEIf oxygenation is impossible consider
transtracheal ventilation. An LMA may be introduced through which a 6mm cuffed tube may be passed into the trachea. IPPV with LMA predisposes to regurgitation and aspiration, hence spontaneous ventilation is preferred.
Awake fibreoptic intubation in a patient at risk from vomiting or regurgitation with a difficult airway as indicated by a previous failed intubation has some advantages.They are:1. Spontaneous ventilation and pharyngeal
muscle tone are preserved2. The co-operation of the patient is
maintained3. Lower oesophageal sphincter tone is
maintained if no sedation is given. Patients may be aware of impending vomiting and can assist in turning themselves to the lateral position.Some simple precautions can be taken to minimise aspiration. No topical anaesthesia should be administered below the vocal cords until the tube is passed to maintain cough reflex. No sedation is to be given. Cricoid pressure may still be applied in the awake patient if it is acceptable and does not itself induce vomiting. Patients may be intubated in the sitting position but this approach is less familiar to many.
Patients not at risk for vomiting/regurgitationIn this group of patients, there is more
time for careful planning of airway management. The poorly maintained airway in a patient with impending hypoxia obviously requires a different and urgent approach.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Airway 259 Srinivasan, Chandrasekhar, Majunath Prabhu
IF THE AIRWAY IS MAINTAINED EASILYThe anaesthetist must consider if
tracheal intubation is necessary because general anaesthesia with mask may be preferable to risking further traumatic attempts at intubation. LMA is an important advance in the airway management. Fibreopticscope can also be used in the failed intubation in an awake patient. Another option i6 the use of the Bullard intubating laryngoscope. It is designed to facilitate rapid visualisation of the larynx without requiring alignment of the pharyngeal, laryngeal and oral axes. Guided blind tracheal intubation like retrograde is an alternative technique where intubation has failed. TTV has been used where intubation is likely to be extremely difficult or impossible. Tracheostomy under general anaesthesia is the final option.
IF THE AIRWAY IS DIFFICULT TO MAINTAIN:There is always the danger of progressive
hypoxia developing when the airway is difficult to maintain and the priority is to awaken the patient. TTV may be necessary when complete inspiratory obstruction occurs. In the majority of patients, anaesthesia may be aborted successfully with conventional oxygenation techniques after which an elective awake intubation may be performed.
CONCLUSIONThe key points for clinical practice are:
1. Formal assessment of the airway should form part of every pre-operative evaluation.
2. Minimum monitoring standards apply equally to the anaesthetic induction and operating room.
3. Auscultation of breath sounds cannot be relied upon to detect oesophageal intubation.
4. The exhaled C02 waveform must be observed for a minimum of 6 cycles post intubation to confirm tracheal intubation.
5. All practising anaesthesiologists should be thoroughly versed in a failed intubation drill.
6. The LMA has an important role in the case of failed intubation.
7. In the event of inability to ventilate the patient by facemask or LMA following failed intubation, TTV is the only resort.
REFERENCES.1. M.Cobleyand R.S.Vaughan. Recognition
and Management of Difficult Airway Problems. British Journal of Anaesthesia; 1992;68:90-97.
2. E.M.Wright, E.Major. Airway catastrophes and solutions. Recent Advances in Anaesthesia and Analgesia.
3. T. A. King, P. Adams. Failed tracheal intubation. British Journal Anaesthesia 1990;65:400-414.
RECOMMENDED READINGRACE 2000. Difficult Airway.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardio Pulmonary Resuscitation 260 T.V. Ramakrishnan
Cardio Pulmonary Resuscitation (CPR) will be discussed under the following topics.
TOPICSBasic Life Support
Airway Management
Arrythmias Recognition
Defibrillation
• AED
Drugs
Special Situations in Cardiac Arrest
T reatment Algorithms
BASIC LIFE SUPPORT Introduction
The purpose of basic life support is to maintain circulation and ventilation until the underlying cause of the carc^o-respiratory arrest is reversed. Failure of circulation for 3-4 minutes will lead to irreversible brain damage. Basic Life Support guidelines imply that no equipment is employed.
Mechanism for forward blood flow(i) Cardiac pump - Direct compression of the heart(ii) Thoracic pump-Generalized increase in intrathoracic pressure. Venous collapse at the thoracic inlet prevents backflow of blood.
Even when performed optimally chest
compressions achieve less than 30% of the normal cardiac output.
Risks to the RescuerENVIRONMENT: Before approaching any unconscious person out-of-hospital, make sure there are no immediate dangers from the environment like traffic, electricity, gas and particularly if you are rescuing the victim from the water.
POISONING:If the victim is exposed to poisonous gas
e.g., hydrogen cyanide or hydrogen sulphide or corrosive chemicals e.g., strong acids, alkalis avoid direct contact with the victim and use nonreturn system for ventilation. Organophosphates are easily absorbed through the skin or respiratory tract. Adequate protective clothing including gloves should be worn.
INFECTION:The possibility of transmission of infection
like HIV and other viruses is a real concern. There are only 15 documented cases of CPR related infection have been reported. Most of them are Neisseria meningitidis. No cases of hepatitis B, C or Cytomegalovirus viruses. All three cases of HIV transmission during resuscitation were due to deep needle stick injuries and contamination of excoriated hands. There is at least one case of tuberculosis transmission during resuscitation.
PRECAUTIONS:Use of protective gloves, eye protection
and sharp bins for prompt disposal of sharps is important. Face-masks with one-way valves prevent the transmission bacteria to the rescuer side of the mask.
RACE 2003 Ramachandra Anaesthesia Continuing Education
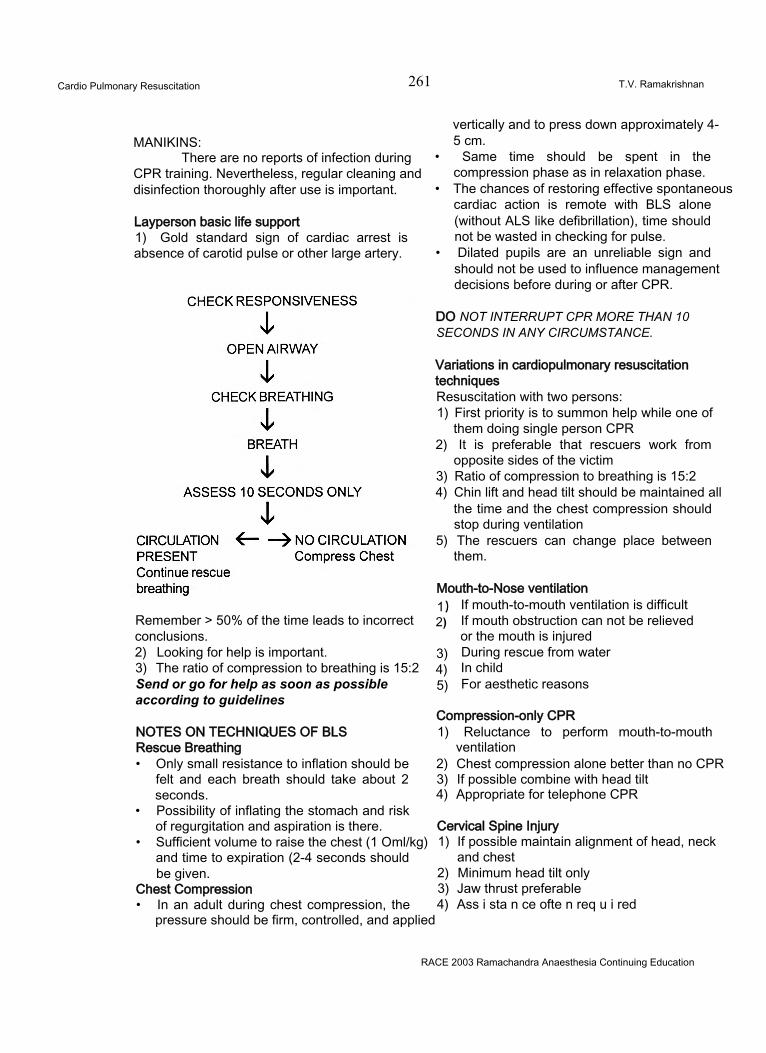
Cardio Pulmonary Resuscitation 261 T.V. Ramakrishnan
MANIKINS:There are no reports of infection during
CPR training. Nevertheless, regular cleaning and disinfection thoroughly after use is important.
Layperson basic life support1) Gold standard sign of cardiac arrest is absence of carotid pulse or other large artery.
Remember > 50% of the time leads to incorrectconclusions.2) Looking for help is important.3) The ratio of compression to breathing is 15:2Send or go for help as soon as possibleaccording to guidelines
NOTES ON TECHNIQUES OF BLSRescue Breathing• Only small resistance to inflation should be
felt and each breath should take about 2 seconds.
• Possibility of inflating the stomach and risk of regurgitation and aspiration is there.
• Sufficient volume to raise the chest (1 Oml/kg) and time to expiration (2-4 seconds should be given.
Chest Compression• In an adult during chest compression, the
pressure should be firm, controlled, and applied
vertically and to press down approximately 4-5 cm.
• Same time should be spent in the compression phase as in relaxation phase.
• The chances of restoring effective spontaneous cardiac action is remote with BLS alone (without ALS like defibrillation), time should not be wasted in checking for pulse.
• Dilated pupils are an unreliable sign and should not be used to influence management decisions before during or after CPR.
DO NOT INTERRUPT CPR MORE THAN 10 SECONDS IN ANY CIRCUMSTANCE.
Variations in cardiopulmonary resuscitationtechniquesResuscitation with two persons:1) First priority is to summon help while one of
them doing single person CPR2) It is preferable that rescuers work from
opposite sides of the victim3) Ratio of compression to breathing is 15:24) Chin lift and head tilt should be maintained all
the time and the chest compression should stop during ventilation
5) The rescuers can change place between them.
Mouth-to-Nose ventilation1) If mouth-to-mouth ventilation is difficult2) If mouth obstruction can not be relieved
or the mouth is injured3) During rescue from water4) In child5) For aesthetic reasons
Compression-only CPR1) Reluctance to perform mouth-to-mouth
ventilation2) Chest compression alone better than no CPR3) If possible combine with head tilt4) Appropriate for telephone CPR
Cervical Spine Injury1) If possible maintain alignment of head, neck
and chest2) Minimum head tilt only3) Jaw thrust preferable4) Ass i sta n ce ofte n req u i red
RACE 2003 Ramachandra Anaesthesia Continuing Education
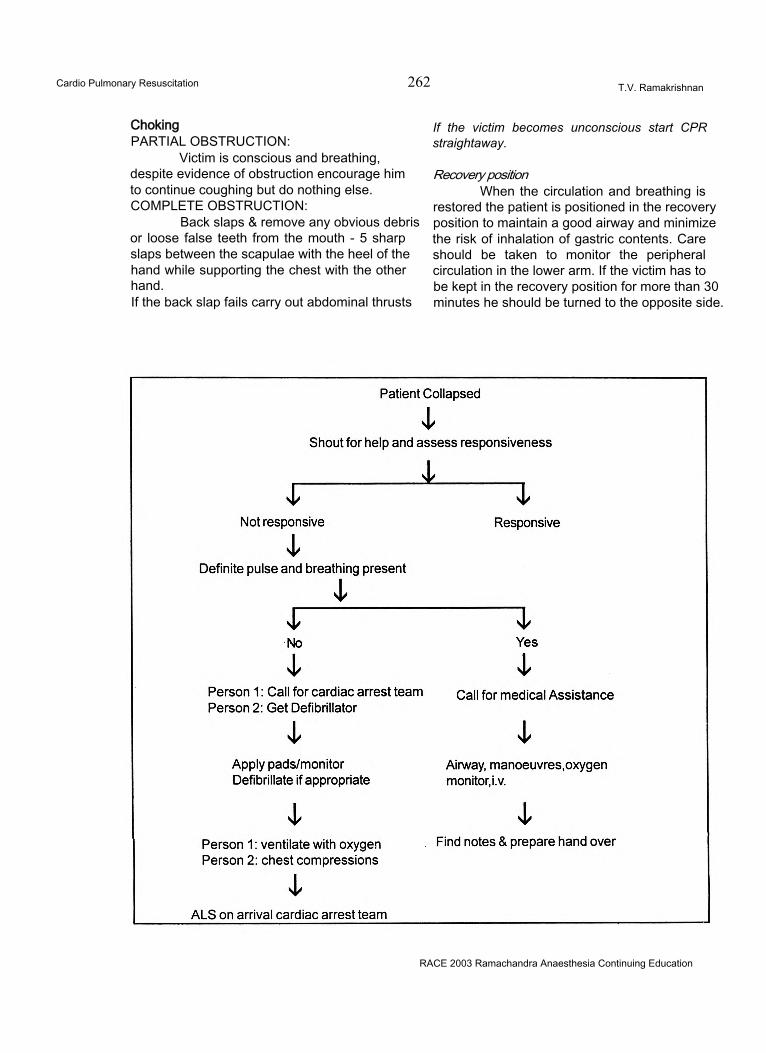
Cardio Pulmonary Resuscitation 262 T.V. Ramakrishnan
ChokingPARTIAL OBSTRUCTION:
Victim is conscious and breathing, despite evidence of obstruction encourage him to continue coughing but do nothing else. COMPLETE OBSTRUCTION:
Back slaps & remove any obvious debris or loose false teeth from the mouth - 5 sharp slaps between the scapulae with the heel of the hand while supporting the chest with the other hand.If the back slap fails carry out abdominal thrusts
If the victim becomes unconscious start CPR straightaway.
Recovery positionWhen the circulation and breathing is
restored the patient is positioned in the recovery position to maintain a good airway and minimize the risk of inhalation of gastric contents. Care should be taken to monitor the peripheral circulation in the lower arm. If the victim has to be kept in the recovery position for more than 30 minutes he should be turned to the opposite side.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardio Pulmonary Resuscitation 263 T.V. Ramakrishnan
AIRWAY MANAGEMENT Introduction:
Patients requiring resuscitation often have an obstructed airway, usually due to loss of consciousness, or less commonly due to cardio respiratory arrest. Assessment must be prompt with airway control and provision of ventilation. This helps to present hypoxic damage to brain and other vital organs and more importantly it may be impossible to restart an arrested myocardium without adequate reoxygenation.
Causes of airway obstruction:Obstruction may be partial or complete.
The commonest site of obstruction is at the level of the pharynx, which may become occluded by the tongue falling backwards as a result of loss of consciousness. Vomitus or blood can also contribute to obstruction. Obstruction at the larynx may be due to bums, inflammation or anaphylaxis. Obstruction below the larynx can arise from bronchospasm, pulmonary edema, aspiration and pneumothorax.
Recognition of airway obstruction:Best achieved by the look, listen and feel
approach. Look for movement of chest and abdomen. Listen for breath sounds, gurgling, snoring and crowing. Feel for the expired air.
Opening the airway:Once any obstruction is recognized,
immediate measures must be taken to maintain airway patency. The three maneuvers used are
• Head tilt• Chin lift• Jaw thrust
Jaw thrust is the technique of choice in patients with suspected injury to the cervical spine. It is essential, however, to open the airway as death from hypoxic airway obstruction is more common than cervical cord damage arising as a result of airway manipulation.
Adjuncts to basic airway techniques:Simple airway adjuncts are often helpful,
but sometimes essential to maintain an open airway particularly when resuscitation is prolonged.
Oropharyngeal airways are introduced into the oral cavity in the ‘upside-down’ position and then rotated through 180° as it passes below the hard palate and into the oropharynx. This minimizes the chance of pushing the tongue backwards and downwards. An estimate of the size required may be done by selecting a airway with a length corresponding to the distance between the corner of the patients mouth and the angle of the jaw.
The nasopharyngeal airway can be life saving in patients with clenched jaws, trismus or maxillofacial injuries.
It is better tolerated than oral airways in patients who are not deeply unconscious. It is inserted with the bevel end first, vertically along the floor of the nose with a slight twisting action. The tip should eventually lie in the pharynx.
Ventilation:It is prudent to start artificial ventilation
as soon as possible. Expired air ventilation is effective, but the inspired oxygen concentration is only 16% so it should be substituted by ventilation with oxygen enriched air at the earliest. The pocket mask is a simple adjunct, which avoids direct person-to-person contact. This decreases the potential for cross infection and allows oxygen enrichment. However it is difficult to maintain a airtight seal and the possibility of gastric inflation exists.
The most common device used to ventilate patients who are apneic or breathing inadequately, is the self inflating bag with a one way valve. It avoids direct person-to-person contact, allows oxygen supplementation (upto 85%), and can be used with a face mask, LMA, combitube and a tracheal tube. When used with a facemask there is a risk of inadequate ventilation and gastric inflation. Two persons are needed for optimal use.
LARYNGEAL MASK AIRWAY:The LMA can be inserted rapidly and
easily. It comes in a variety of sizes.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardio Pulmonary Resuscitation 264 T.V. Ramakrishnan
LMA size chartSize Cuff inflation (ml air)3 Small adult 20\ Normal adult 305 Large adult 40
Ventilation using the LMA is more efficient and easier than with a bag-valve-mask assembly. It avoids the need for laryngoscopy. The LMA has certain limitations. There is no absolute guarantee against aspiration. It is not suitable when very high inflation pressures are needed. If the patient is not deeply unconscious, they may cough, strain or develop laryngospasm during insertion.
The LMA is held like a pen and introduced into the mouth with the distal aperture facing towards the patients feet. The tip is advanced with the upper surface applied to the palate until it reaches the posterior pharyngeal wall. The mask is then pressed backwards and downwards around the corner of the pharynx until a resistance is felt as it locates in the back of the hypopharynx. The cuff is inflated with the predetermined amount of air. The tube lifts 1- 2cm out of the mouth as the cuff is inflated indicating proper placement.
COMBITUBE:It is a double lumen tube introduced
blindly over the tongue and is designed to achieve ventilation whether the tube has passed into the trachea or esophagus. The tracheal channel has open distal end, whereas the esophageal tube is without an opening at the end, but has several small side holes some centimeters proximal to the tip. There are two cuffs: a small distal cuff and a large (100ml) cuff designed to inflate within the hypopharynx.
The rationale of its use is that when introduced blindly, if the tube enters the esophagus (which is usual), the patient can be ventilated through the esophageal channel via the side openings which are hopefully situated at or above the larynx.
The inflating gas cannot pass down the esophagus because of the blind end of the
esophageal channel, and the cuff, just proximal to the blind end. The cuff in the hypopharynx is designed to prevent air leak from the mouth. If on the other hand, the tube enters the trachea, ventilation is achieved via the tracheal port through its open end. Because it is double channel tube, each channel is necessarily narrow and the resistance to ventilation is therefore high. This device has developed from the original esophageal obturator airway, but many advantages are claimed for it and it is currently being evaluated for use by high dependency nurses and paramedics.
Technique for introduction ofCombitube:• Place the patient in a supine position with the
head and neck aligned in the normal position.• The mouth is opened and the chin supported
(this is best done by an assistant).• The Combitube is weH lubricated and passed
blindly over the tongue until the proximal black marking line on the tube is at the level of the teeth. Some resistance may be encountered as the tube passes around the corner of the oropharynx, and then passes the laryngeal opening.
• The large proximal cuff (clear) is inflated with approximately 100ml of air. The distal cuff is inflated with 15 - 20ml of air.
• Ventilation is first applied to the esophageal tube and chest movement or abdominal distension observed and chest sounds sought by auscultation.
• If no breath sounds are heard on auscultation, then the tracheal port is next used to ventilate and again by observation and auscultation, evidence of inflation of the lungs is sought.
• If ventilation of the lungs cannot be achieved via either port, then the tube is removed. Alternative forms of ventilation must then be utilized.
It can be inserted rapidly and easily. There is no need for laryngoscopy. It can be used even with high inflation pressures. There are a few disadvantages. It is suitable only for adults. There is always the danger of ventilation through the wrong lumen, damage to cuffs on insertion.
TRACHEAL INTUBATION:This is the best method of providing and
maintaining a clear and secure airway. It allows
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardio Pulmonary Resuscitation 265 T.V. Ramakrishnan
ventilation with 100% oxygen. It isolates the airway, thereby preventing aspiration. It provides a route for both tracheal suctioning as well as for drug administration. It has a few limitations. Training and experience is essential, failed intubation is a possibility and an undetected oesophageal intubation is fatal. Attempts at intubation1 can worsen a cervical cord or head injury.
It is important to get all the essential equipment available before attempting intubation. Always pre-oxygenate the patient and never attempt for more than 30 seconds. Make it a point to insert the tube only under direct vision. If in doubt or difficulty, re-oxygenate before further attempts. It is important to remember that patients are harmed by failure of oxygenation and not failure of intubation.
Confirmation of correct placement of the tracheal tube is done by:• Direct visualization at laryngoscopy• Auscultation - Bilaterally, midaxillary line, over
the epigastrium• Symmetrical movement of chest during
ventilation.• Esophageal detector device.• Capnometry.
Potential problems during tracheal intubation are:• Anatomical variations which can make
intubation difficult short neck, trismus, receding lower jaw, stiff neck.
• Loose teeth or dental prosthesis• Vomiting or regurgitation• Clenching of teeth• Facial burns and trauma• Unrecognized esophageal intubation.• Cervical spine injury - Manual in line traction
should be given to immobilize the neck during intubation.
Cricoid pressure:A trained assistant carries out this
maneuver during intubation with the aim of preventing regurgitation and consequent pulmonary aspiration. Anteroposterior pressure on the cricoid cartilage occludes the esophagus against the cervical vertebra. It is useful during
intubation, ventilation with facemask or LMA. It has a few limitations. It may make intubation more difficult, may impair ventilation via facemask and LMA. It should not be used in cases of active vomiting as it can result in damage to the esophagus.
NEEDLE CRICOTHYROIDOTOMY:Indications for a needle
cricothyroidotomy are failure to provide an airway by any other means.
Occasionally it will be impossible to ventilate an apneic patient with a bag-valve-mask, or to pass a tracheal tube or another advanced airway device. Examples are in patients suffering extensive facial trauma, or when there is mechanical laryngeal obstruction. In these circumstances, it will be necessary to create a surgical airway below the level of the obstruction. An emergency tracheotomy is not appropriate as it is time consuming, hazardous and requires considerable surgical skill and equipment. Needle cricothyroidotomy is the immediate technique of choice as it is less hazardous, more rapid, and requires only simple equipment. However, it can only be a temporary measure until a definitive surgical airway can be created.
Procedure:• Place the patient supine with the head slightly extended.• Identify the cricothyroid membrane as the recess between the thyroid cartilage (Adam’s apple) and the horizontal cricoid cartilage.■ The membrane is punctured vertically using a large bore (14 gauge or larger) intravenous cannula attached to a syringe. Aspiration of air confirms the correct position. The trachea is situated just deep to the subcutaneous tissue and should be encountered at a very shallow depth.• The cannula is advanced towards the feet at 45° into the trachea in a similar manner to its insertion into the vein. The needle should be removed and the cannula attached to a high- pressure oxygen supply at 12 - 15 l/min via a Y connector, or purpose designed Sanders injector.■ It is essential that the chest be observed for both inspiratory and expiratory movement. Failure to allow air to escape from the chest between
RACE 2003 Ramachandra Anaesthesia Continuing Education
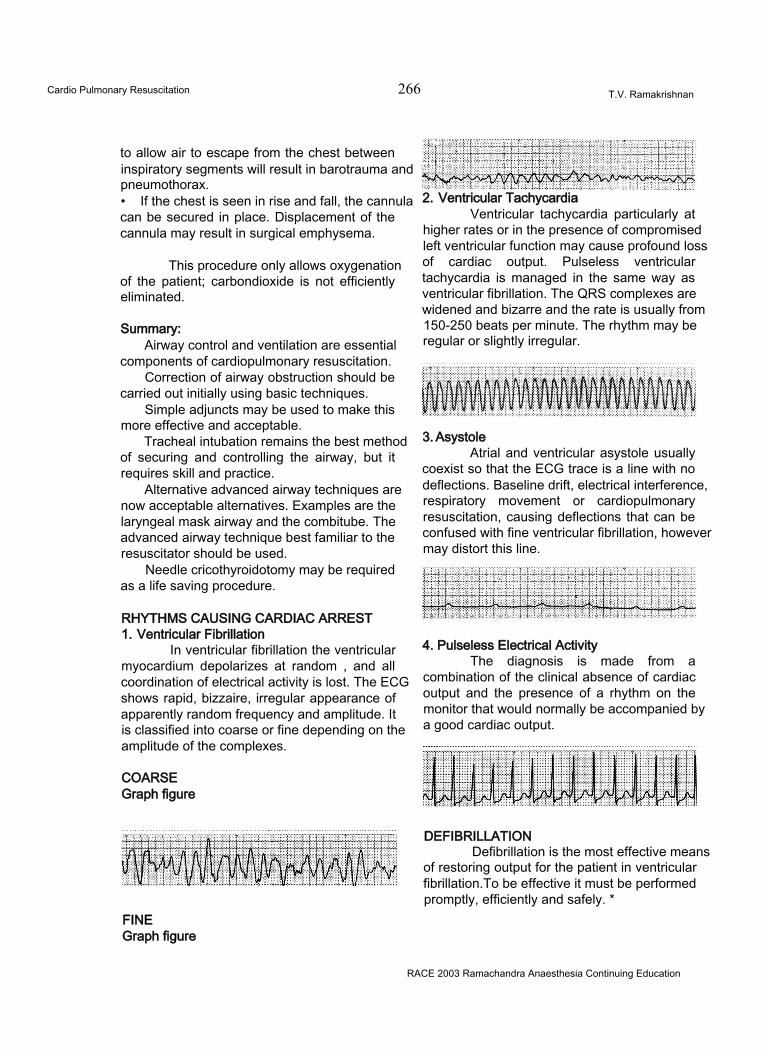
Cardio Pulmonary Resuscitation 266 T.V. Ramakrishnan
to allow air to escape from the chest between inspiratory segments will result in barotrauma and pneumothorax.• If the chest is seen in rise and fall, the cannula can be secured in place. Displacement of the cannula may result in surgical emphysema.
This procedure only allows oxygenation of the patient; carbondioxide is not efficiently eliminated.
Summary:Airway control and ventilation are essential
components of cardiopulmonary resuscitation.Correction of airway obstruction should be
carried out initially using basic techniques.Simple adjuncts may be used to make this
more effective and acceptable.Tracheal intubation remains the best method
of securing and controlling the airway, but it requires skill and practice.
Alternative advanced airway techniques are now acceptable alternatives. Examples are the laryngeal mask airway and the combitube. The advanced airway technique best familiar to the resuscitator should be used.
Needle cricothyroidotomy may be required as a life saving procedure.
RHYTHMS CAUSING CARDIAC ARREST1. Ventricular Fibrillation
In ventricular fibrillation the ventricular myocardium depolarizes at random , and all coordination of electrical activity is lost. The ECG shows rapid, bizzaire, irregular appearance of apparently random frequency and amplitude. It is classified into coarse or fine depending on the amplitude of the complexes.
COARSE Graph figure
3. AsystoleAtrial and ventricular asystole usually
coexist so that the ECG trace is a line with no deflections. Baseline drift, electrical interference, respiratory movement or cardiopulmonary resuscitation, causing deflections that can be confused with fine ventricular fibrillation, however may distort this line.
4. Pulseless Electrical ActivityThe diagnosis is made from a
combination of the clinical absence of cardiac output and the presence of a rhythm on the monitor that would normally be accompanied by a good cardiac output.
DEFIBRILLATIONDefibrillation is the most effective means
of restoring output for the patient in ventricular fibrillation.To be effective it must be performed promptly, efficiently and safely. *
FINEGraph figure
2. Ventricular TachycardiaVentricular tachycardia particularly at
higher rates or in the presence of compromised left ventricular function may cause profound loss of cardiac output. Pulseless ventricular tachycardia is managed in the same way as ventricular fibrillation. The QRS complexes are widened and bizarre and the rate is usually from 150-250 beats per minute. The rhythm may be regular or slightly irregular.
RACE 2003 Ramachandra Anaesthesia Continuing Education
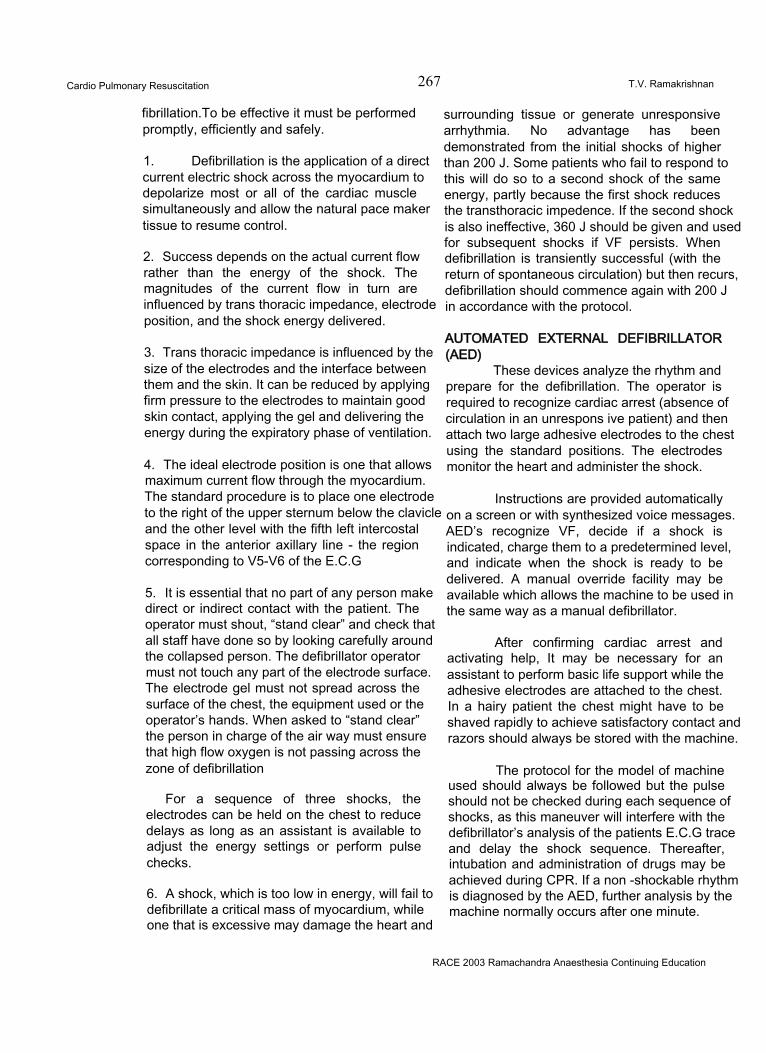
Cardio Pulmonary Resuscitation 267 T.V. Ramakrishnan
fibrillation.To be effective it must be performed promptly, efficiently and safely.
1. Defibrillation is the application of a direct current electric shock across the myocardium to depolarize most or all of the cardiac muscle simultaneously and allow the natural pace maker tissue to resume control.
2. Success depends on the actual current flow rather than the energy of the shock. The magnitudes of the current flow in turn are influenced by trans thoracic impedance, electrode position, and the shock energy delivered.
3. Trans thoracic impedance is influenced by the size of the electrodes and the interface between them and the skin. It can be reduced by applying firm pressure to the electrodes to maintain good skin contact, applying the gel and delivering the energy during the expiratory phase of ventilation.
4. The ideal electrode position is one that allows maximum current flow through the myocardium. The standard procedure is to place one electrode to the right of the upper sternum below the clavicle and the other level with the fifth left intercostal space in the anterior axillary line - the region corresponding to V5-V6 of the E.C.G
5. It is essential that no part of any person make direct or indirect contact with the patient. The operator must shout, “stand clear” and check that all staff have done so by looking carefully around the collapsed person. The defibrillator operator must not touch any part of the electrode surface. The electrode gel must not spread across the surface of the chest, the equipment used or the operator’s hands. When asked to “stand clear” the person in charge of the air way must ensure that high flow oxygen is not passing across the zone of defibrillation
For a sequence of three shocks, the electrodes can be held on the chest to reduce delays as long as an assistant is available to adjust the energy settings or perform pulse checks.
6. A shock, which is too low in energy, will fail to defibrillate a critical mass of myocardium, while one that is excessive may damage the heart and
surrounding tissue or generate unresponsive arrhythmia. No advantage has been demonstrated from the initial shocks of higher than 200 J. Some patients who fail to respond to this will do so to a second shock of the same energy, partly because the first shock reduces the transthoracic impedence. If the second shock is also ineffective, 360 J should be given and used for subsequent shocks if VF persists. When defibrillation is transiently successful (with the return of spontaneous circulation) but then recurs, defibrillation should commence again with 200 J in accordance with the protocol.
AUTOMATED EXTERNAL DEFIBRILLATOR (AED)
These devices analyze the rhythm and prepare for the defibrillation. The operator is required to recognize cardiac arrest (absence of circulation in an unrespons ive patient) and then attach two large adhesive electrodes to the chest using the standard positions. The electrodes monitor the heart and administer the shock.
Instructions are provided automatically on a screen or with synthesized voice messages. AED’s recognize VF, decide if a shock is indicated, charge them to a predetermined level, and indicate when the shock is ready to be delivered. A manual override facility may be available which allows the machine to be used in the same way as a manual defibrillator.
After confirming cardiac arrest and activating help, It may be necessary for an assistant to perform basic life support while the adhesive electrodes are attached to the chest. In a hairy patient the chest might have to be shaved rapidly to achieve satisfactory contact and razors should always be stored with the machine.
The protocol for the model of machine used should always be followed but the pulse should not be checked during each sequence of shocks, as this maneuver will interfere with the defibrillator’s analysis of the patients E.C.G trace and delay the shock sequence. Thereafter, intubation and administration of drugs may be achieved during CPR. If a non -shockable rhythm is diagnosed by the AED, further analysis by the machine normally occurs after one minute.
RACE 2003 Ramachandra Anaesthesia Continuing Education
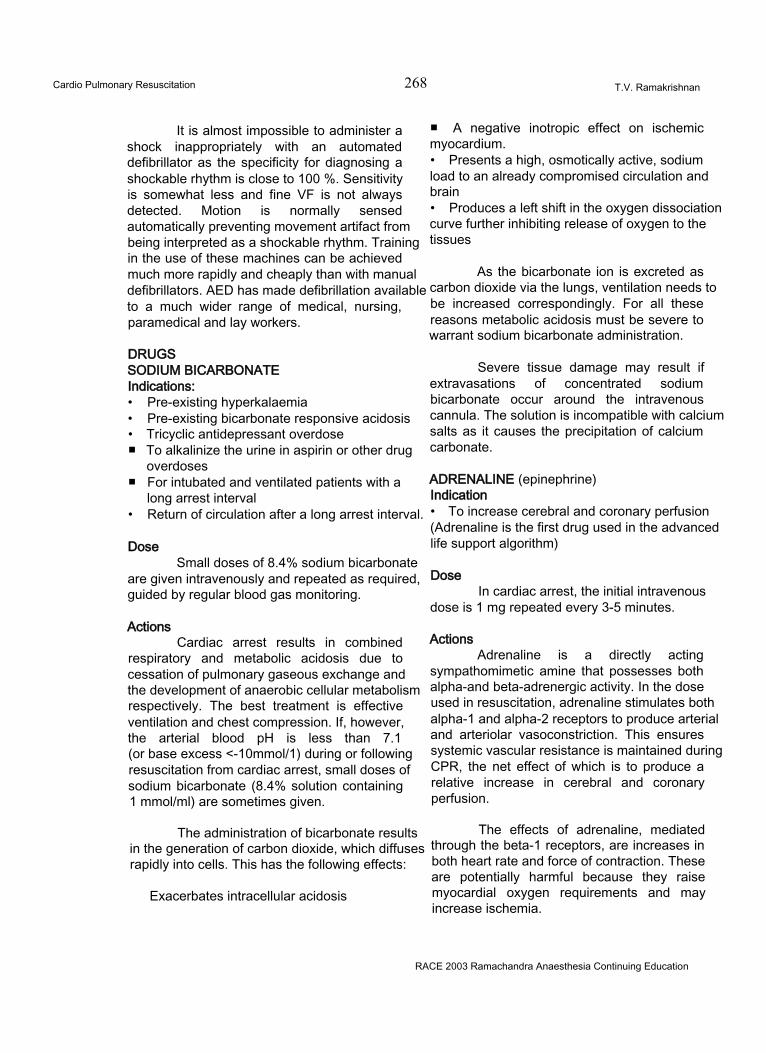
Cardio Pulmonary Resuscitation 268 T.V. Ramakrishnan
It is almost impossible to administer a shock inappropriately with an automated defibrillator as the specificity for diagnosing a shockable rhythm is close to 100 %. Sensitivity is somewhat less and fine VF is not always detected. Motion is normally sensed automatically preventing movement artifact from being interpreted as a shockable rhythm. Training in the use of these machines can be achieved much more rapidly and cheaply than with manual defibrillators. AED has made defibrillation available to a much wider range of medical, nursing, paramedical and lay workers.
DRUGSSODIUM BICARBONATE Indications:• Pre-existing hyperkalaemia• Pre-existing bicarbonate responsive acidosis• Tricyclic antidepressant overdose■ To alkalinize the urine in aspirin or other drug
overdoses■ For intubated and ventilated patients with a
long arrest interval• Return of circulation after a long arrest interval.
DoseSmall doses of 8.4% sodium bicarbonate
are given intravenously and repeated as required, guided by regular blood gas monitoring.
ActionsCardiac arrest results in combined
respiratory and metabolic acidosis due to cessation of pulmonary gaseous exchange and the development of anaerobic cellular metabolism respectively. The best treatment is effective ventilation and chest compression. If, however, the arterial blood pH is less than 7.1 (or base excess <-10mmol/1) during or following resuscitation from cardiac arrest, small doses of sodium bicarbonate (8.4% solution containing 1 mmol/ml) are sometimes given.
The administration of bicarbonate results in the generation of carbon dioxide, which diffuses rapidly into cells. This has the following effects:
Exacerbates intracellular acidosis
■ A negative inotropic effect on ischemic myocardium.• Presents a high, osmotically active, sodium load to an already compromised circulation and brain• Produces a left shift in the oxygen dissociation curve further inhibiting release of oxygen to the tissues
As the bicarbonate ion is excreted as carbon dioxide via the lungs, ventilation needs to be increased correspondingly. For all these reasons metabolic acidosis must be severe to warrant sodium bicarbonate administration.
Severe tissue damage may result if extravasations of concentrated sodium bicarbonate occur around the intravenous cannula. The solution is incompatible with calcium salts as it causes the precipitation of calcium carbonate.
ADRENALINE (epinephrine)Indication• To increase cerebral and coronary perfusion (Adrenaline is the first drug used in the advanced life support algorithm)
DoseIn cardiac arrest, the initial intravenous
dose is 1 mg repeated every 3-5 minutes.
ActionsAdrenaline is a directly acting
sympathomimetic amine that possesses both alpha-and beta-adrenergic activity. In the dose used in resuscitation, adrenaline stimulates both alpha-1 and alpha-2 receptors to produce arterial and arteriolar vasoconstriction. This ensures systemic vascular resistance is maintained during CPR, the net effect of which is to produce a relative increase in cerebral and coronary perfusion.
The effects of adrenaline, mediated through the beta-1 receptors, are increases in both heart rate and force of contraction. These are potentially harmful because they raise myocardial oxygen requirements and may increase ischemia.
RACE 2003 Ramachandra Anaesthesia Continuing Education
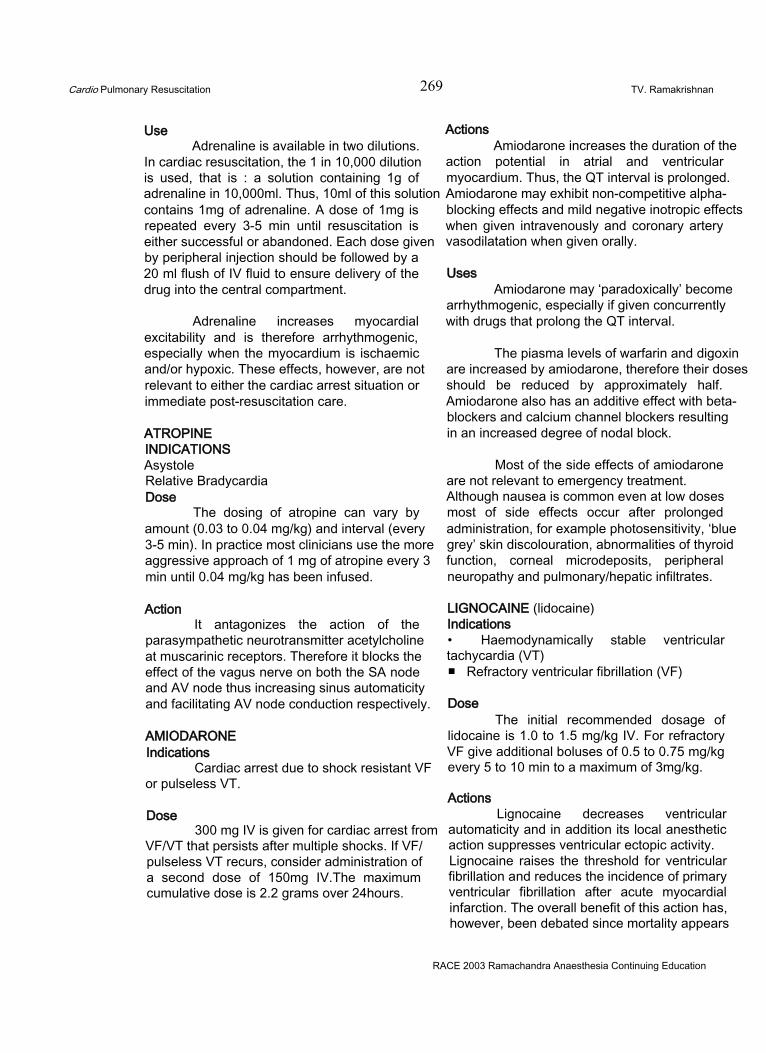
Cardio Pulmonary Resuscitation 269 TV. Ramakrishnan
UseAdrenaline is available in two dilutions.
In cardiac resuscitation, the 1 in 10,000 dilution is used, that is : a solution containing 1g of adrenaline in 10,000ml. Thus, 10ml of this solution contains 1mg of adrenaline. A dose of 1mg is repeated every 3-5 min until resuscitation is either successful or abandoned. Each dose given by peripheral injection should be followed by a 20 ml flush of IV fluid to ensure delivery of the drug into the central compartment.
Adrenaline increases myocardial excitability and is therefore arrhythmogenic, especially when the myocardium is ischaemic and/or hypoxic. These effects, however, are not relevant to either the cardiac arrest situation or immediate post-resuscitation care.
ATROPINEINDICATIONSAsystoleRelative Bradycardia Dose
The dosing of atropine can vary by amount (0.03 to 0.04 mg/kg) and interval (every 3-5 min). In practice most clinicians use the more aggressive approach of 1 mg of atropine every 3 min until 0.04 mg/kg has been infused.
ActionIt antagonizes the action of the
parasympathetic neurotransmitter acetylcholine at muscarinic receptors. Therefore it blocks the effect of the vagus nerve on both the SA node and AV node thus increasing sinus automaticity and facilitating AV node conduction respectively.
AMIODARONEIndications
Cardiac arrest due to shock resistant VF or pulseless VT.
Dose300 mg IV is given for cardiac arrest from
VF/VT that persists after multiple shocks. If VF/ pulseless VT recurs, consider administration of a second dose of 150mg IV.The maximum cumulative dose is 2.2 grams over 24hours.
ActionsAmiodarone increases the duration of the
action potential in atrial and ventricular myocardium. Thus, the QT interval is prolonged. Amiodarone may exhibit non-competitive alpha- blocking effects and mild negative inotropic effects when given intravenously and coronary artery vasodilatation when given orally.
UsesAmiodarone may ‘paradoxically’ become
arrhythmogenic, especially if given concurrently with drugs that prolong the QT interval.
The piasma levels of warfarin and digoxin are increased by amiodarone, therefore their doses should be reduced by approximately half. Amiodarone also has an additive effect with beta- blockers and calcium channel blockers resulting in an increased degree of nodal block.
Most of the side effects of amiodarone are not relevant to emergency treatment. Although nausea is common even at low doses most of side effects occur after prolonged administration, for example photosensitivity, ‘blue grey’ skin discolouration, abnormalities of thyroid function, corneal microdeposits, peripheral neuropathy and pulmonary/hepatic infiltrates.
LIGNOCAINE (lidocaine)Indications• Haemodynamically stable ventricular tachycardia (VT)■ Refractory ventricular fibrillation (VF)
DoseThe initial recommended dosage of
lidocaine is 1.0 to 1.5 mg/kg IV. For refractory VF give additional boluses of 0.5 to 0.75 mg/kg every 5 to 10 min to a maximum of 3mg/kg.
ActionsLignocaine decreases ventricular
automaticity and in addition its local anesthetic action suppresses ventricular ectopic activity. Lignocaine raises the threshold for ventricular fibrillation and reduces the incidence of primary ventricular fibrillation after acute myocardial infarction. The overall benefit of this action has, however, been debated since mortality appears
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardio Pulmonary Resuscitation 270 T.V. Ramakrishnan
unchanged by its routine use. Lignocaine has no clinically important effects on atrial arrhythmias.
VASOPRESSINVasopressin, the naturally occurring anti-
diuretic hormone, becomes a powerful vasoconstrictor when used at much higher doses than those normally observed in the body.Vasopressin produces the same positive effects as epinephrine in terms of vasoconstriction and increasing the blood flow to the brain and heart during CPR. Moreover, vasopressin does not have the negative, adverse effects of epinephrine on the heart, such as increased ischemia and irritability.
DoseVasopressin is given as a single one-time
dose (40 U IV), a regimen based on the much longer half-life of vasopressin (10-20 min) compared with epinephrine (3-5 min). After the single dose of vasopressin, if there is no clinical response in 10 to 20 min, it is acceptable to return to 1 mg epinephrine every 3-5 min. The possibility of giving a second dose of vasopressin at the 10 to 20 min mark seems rational but is not supported by human data.
CARDIAC ARREST IN SPECIALCIRCUSTANCESHypothermia1. Hypothermia exists when the body core temperature falls below 35°c
2. All the principles of basic and advanced life support apply to the hypothermic patient
3. Open, clear and maintain the airway, and if there is no spontaneous respiration ventilate with high concentration of oxygen, preferably warmed and humidified.
4. As the pulse can be very slow and difficult to find, palpate a major artery for a minimum of one minute before concluding that there is no cardiac output.
5. Consider hypothermia as a cause of bradycardia.
6. Hypothermia may cause stiffness of the chest wall, so that more resistance is met. This may result in both ventilation and compression having to be performed more slowly. The aims should be to inflate with a volume of air sufficient to cause the chest to rise visibly, and to compress the chest to a depth of 4 to 5cms.
7. Cannulate a central or a large peripheral vein. All drugs should be given by this route with doses being kept at the lower end of the therapeutic range during rewarming to reduce drug pooling at the periphery.
8. Monitor for arrhythmias. As the body temperature falls, sinus bradycardia tends to give way to atrial fibrillation followed by ventricular fibrillation and finally asystole. If the core temperature is less than 30°c ventricular fibrillation may not respond to cardioversion. In that event rapid core rewarming is needed, with cardio pulmonary resuscitation being continued until defibrillation becomes effective.
9. Lignocaine has no significant effect on VF in hypothermic patients.
10. Arrhythmias other than VF tend to revert spontaneously as the core temperature rises, and usually do not require immediate treatment.
11. Hypothermic patients should be handled carefully as mechanical disturbances can precipitate VF.
12. Elderly patients with insidious onset hypothermia should not be rewarmed actively because of the risk of pulmonary and cerebral edema.
13. If the patient is profoundly hypothermic and unconscious, the following methods of rewarming can be used.
• Ventilating with warm humidified oxygen.• Administration of warm fluids through a central
venous line.• Gastric, peritoneal, pleural lavage.• Heated blankets• Blood rewarming by hemodialysis or CPB
RACE 2003 Ramachandra Anaesthesia Continuing Education
Cardio Pulmonary Resuscitation 271 T.V. Ramakrishnan
Near drowningThe primary effect of submersion is
respiratory arrest; cardiac arrest is a secondary event. The initial care of the patient is the same whether the water is salt or fresh.
1. To reduce the chances of aspiration the patient should be removed from the water in a horizontal or head- down posture; this also reduces postural hypotension.
2. If there is a suspicion of head or neck injury, associated with water sport or diving, the airway should be opened by using chin lift or jaw thrust rather than head tilt.
3. BLS is very difficult to perform unsupported in deep water, but rescue breathing may be attempted once the rescuer can stand or has reached a point of support.
4. The air way should be inspected and cleared manually.
5. Ventilate with 100 % oxygen and early intubate early as regurgitation or vomiting are common.02
6. Hypothermia and bradycardia are common in near drowning, so additional time should be allowed to detect a major pulse.
7. During prolonged immersion, the hydrostatic pressure of the surrounding water exerts a ‘squeeze’ effect that reduces the body volume and results in a compensatory reduction in the body fluid. On removal from the water, loss of this ‘squeeze’ and loss of blood pressure regulatory reflexes due to hypothermia may result in severe and life- threatening hypovolaemia, that must be corrected with IV fluids.
8. Stomach should be decompressed with a nasogastric tube.
Pregnancy1. During pregnancy there are two lives to resuscitate, but to optimize foetal outcome effective life support must be given to the mother.
2. Early tracheal intubation with cricoid pressure, to prevent aspiration as the gastric emptying is poor.
3. To improve venous return and cardiac output it is vital that pressure on the inferior vena cava from the pregnant uterus be relieved by:
I Placing sand bags, pillows or a wedge under the right side of the patient
I Moving the uterus to the left by manual displacement
I Raising the mothers right hip
4. Difficult chest compression may be anticipated because of breast hypertrophy and splinting of the diaphragm.
5. After 5mins of unsuccessful in-hospital resuscitation, emergency caesarean section is indicated to save the foetus, and improve the mother’s chances of survival by decompressing the inferior vena cava. ACLS must be continued during and after surgery.
Electrocution1. The severity of injury depends on the magnitude, area of contact and path of the current.2. The. rescuer must ensure that any power source is switched off and not approach the victim unless it is safe. It should always be remembered that high voltage electricity could conduct through the ground up to several feet around the victim.3. Standard basic and advanced life support should be started immediately, as muscular paralysis may persist for up to 30mins during which time respiratory support will be required.4. VF is the commonest initial arrhythmia; particularly after high voltage AC current shock and this should be treated promptly by defibrillation. Asystole is more common after DC shock.5. In the case of mass electrocution, attend to the unconscious victims first.6. Those who have survived an electric shock should be monitored in hospital if they have suffered:
I Loss of consciousness I Cardiac arrest I E.C.G abnormalities I Contact injuryI History of cardiac problems
RACE 2003 Ramachandra Anaesthesia Continuing Education
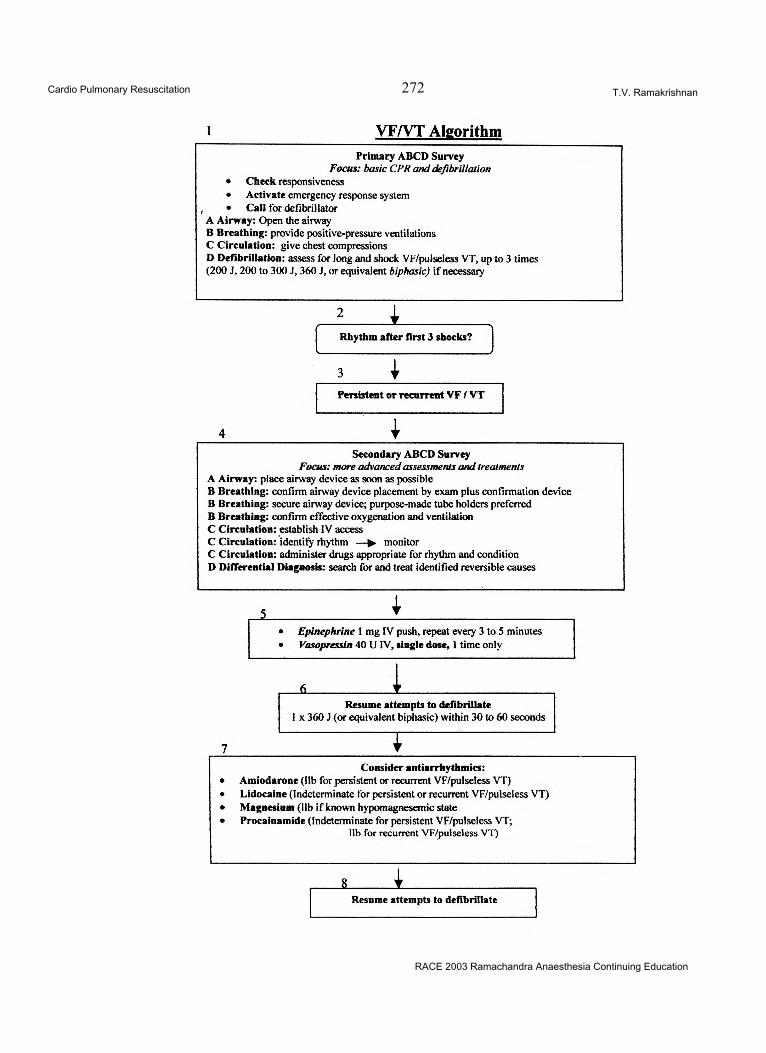
Cardio Pulmonary Resuscitation 272 T.V. Ramakrishnan
RACE 2003 Ramachandra Anaesthesia Continuing Education
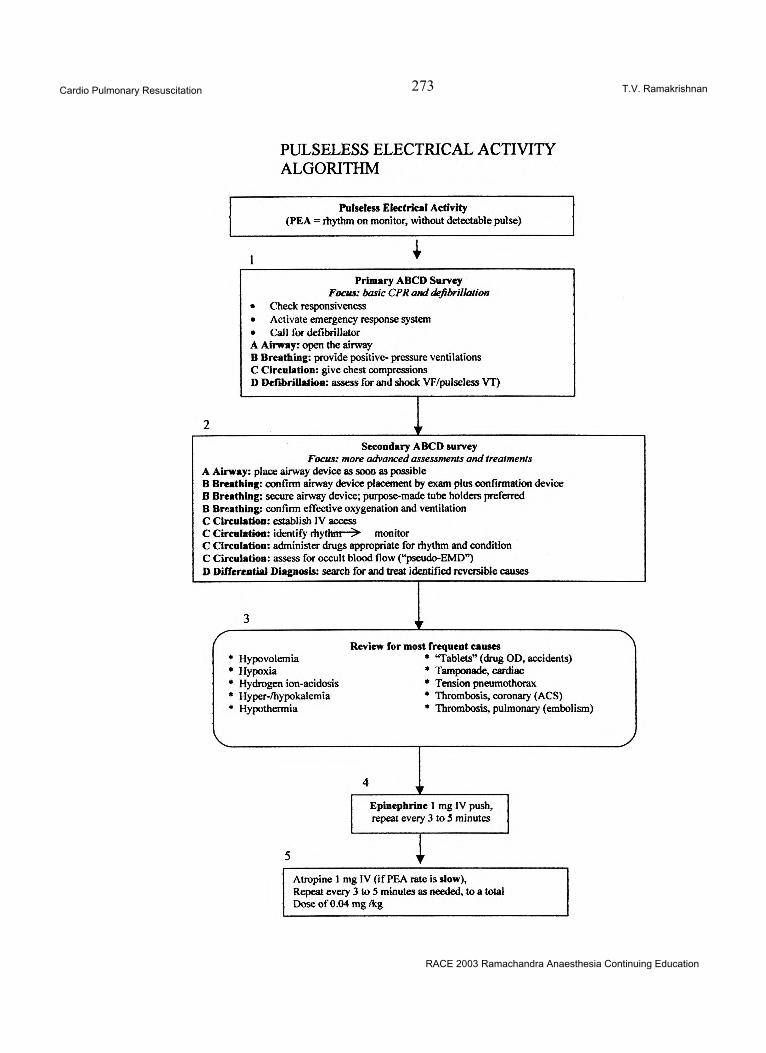
Cardio Pulmonary Resuscitation 273 T.V. Ramakrishnan
RACE 2003 Ramachandra Anaesthesia Continuing Education
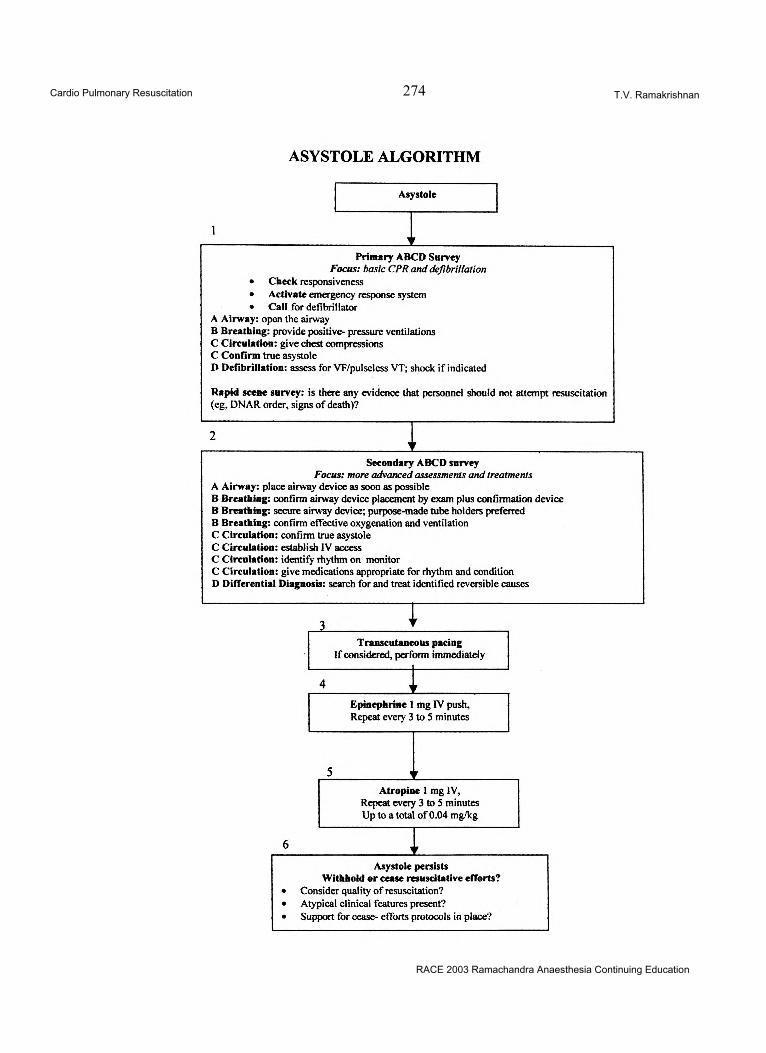
Cardio Pulmonary Resuscitation 274 T.V. Ramakrishnan
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 275 Vijaylakshmi Kamat & Gita Nath
OVERVIEWMechanical Ventilation: When?1. Routine Anaesthesia and post-operative
management of major surgery2. Respiratory impairment (parenchymal,
airways or chest wall)3. Central nervous system or neuromuscular
impairment4. Circulatory failure
BASIC CHARACTERISTICS OF MECHANICAL VENTILATORS:1. Power source or input power: Can be
electrical or pneumatic or a combination of both.
2. Internal control system - which in turn has 5 components
Power source or input powerELECTRICALLY POWERED ventilators
are those in which electricity operates fans, bellows, solenoids and transducers, all of which help to achieve a controlled gas flow to patients. It has an on/off switch for control of motors, electro-magnets, potentiometers or rheostats, which control the mechanism for inspiration/ expiration, flow of gas and alarm systems eg. MA-1, Emerson 3-PV. Internally, electricity powered circuits can also control electronic devices such as resistors, capacitors, diodes and transistors. A combination of these components form the basis for the integrated circuits and circuit board which in turn form microprocessors.
PNEUMATICALLY POWERED Ventilators can be pneumatic or fluidic. Pneumatic eg. Bird mark 7; these ventilators use needle valves, venturi entrainers (injectors), flexible diaphragms and spring loaded bulbs to control
flow, volume delivery and inspiratory/expiratory function.
Fluidic ventilators use the principles of fluidics ie., the Coanda effect for control of operation eg. Monaghan 225/SIMV. In the Siemens servo 900, gas power provides the driving force or flow to the patient. Electricity controls a special stepper motor that regulates the opening or closing of scissor like valves for inspiration/ expiration. Electronic logic controls the function of the scissor valves. These ventilators are therefore pneumatically powered and electronically controlled.
The Internal Control system has 5 componentsa) THE CONTROL SYSTEM: This might be an open loop "unintelligent” system or a closed loop “intelligent” system. An example is the servo feed back control system where the flow, pressure and timing of the respiratory gases are regulated electronically by two servo valves which receive information 500 times per second from the flow meters and pressure meters via the electronic unit.
b) MECHANICAL DRIVE MECHANISM: A variety of devices are used in various ventilators including spring loaded bellows, needle valves, linear drive pistons, rotary wheel driven pistons, venturi injectors and weighted bellows. The Siemens servo 900 series uses spring-loaded bellows as the mechanical drive mechanism.
c) CONTROL PANEL: Has a variety of available knobs or settings which include tidal volume, rate, inspiratory time, FI02 etc. These controls are set by the operator and basically they control 4 parameters: flow, volume, pressure and time.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 276 Vijaylakshmi Kamat & Gita Nath
These valves can be varied over a wide range.
d) OUTPUT CONTROL VALVES: Different output valves interact with the drive mechanism in determining the pattern of flow delivery in a ventilator.e) PNEUMATIC CIRCUIT: refers to the series of tubes that allows gas to flow inside the ventilator and between the ventilator and the patient.
Additional Items in the ventilator include:1. Device to warm and humidify inspired air2. Thermometer to measure inspired air
temperature3. Apnoea or low pressure alarm4. Nebulizer line5. Volume measuring devices for patient’s
exhaled volumes6. Bacterial filters7. Pressure Gauge: (Usually built into the
ventilator)
THE INSPIRATORY PHASEThe internal delivery of gas is the
important single characteristic of a ventilator. Inspiration is generated by the drive mechanism of the ventilator. The ability of a ventilator to maintain flow, volume and pressure pattern during inspiration depends on the drive mechanism and the output control valve. Volume delivery to the lungs depends on the compliance of the lungs and resistance to gas flow. A simplified equation; “equation of motion of the respiratory system”, derived by Chatburn is expressed as follows: Muscle pressure + ventilatory pressure = elastic recoil pressure + flow resistance pressure
Chatburn’s guide to ventilators classification:To determine whether the ventilator is a
pressure, time or flow controller, use the following guide:From the operator’s manual, experiments and previous knowledge, answer the following questions:1. Does the pressure wave form at the upper
airway change when the patient’s resistance or compliance changes?If not, the ventilator is a pressure controller (stop here)If yes, go to number 2
2. Does the volume waveform stay constant when
the patient’s resistance or compliance changes?If not, the ventilator is a time controller (stop here)If yes, go to number 3
3. Is the volume measured directly by either a volume displacement device or a flow transducer?If not, the ventilator is a flow controller (stop here)If yes, the ventilator is a volume controller.
CONSTANT FLOW GENERATORS1. Most commonly encountered2. Delivers constant flow (squares or rectangular
waves)3. Flow stays constant regardless of changes
in the patient’s lung condition4. Pressure measured during gas delivery varies
with lung condition.5. Pressure due to flow resistance is constant6. Volume is not measured although flow may
be measured and displayed as volume7. Pressures at the manometer and in the alveoli
rise linearly throughout inspiration
Ventilators that have a high internal or working pressure have flow generation capabilities. Such a ventilator uses a 50-psig-gas source (i.e. 3500 cm H20 pressure). Flow = 3500 cm H20 cf 10-100 cm H20 generated at the mouth. Therefore, changes in lung compliance and airway resistance will not affect the flow rate. If a ventilator can produce 5 times or more of the amount of pressure seen at peak inspiration, it is considered as a constant flow generator. The volume increases with time owing to the constant flow rate and inspiration is either time or volume cycled. Volume delivered by the ventilator during inspiration is constant.
Most currently used commeicial ventilators have the capability of being constant flow controllers and can be time or volume eye led ie., inspiration ends after a predetermined ti.ne or volume have been reached. These ventilak\ s have a pressure-limiting feature, which prevents upper airway pressure exceeding a preset value. If the preset pressure limit is reached before the machine either time cycles or volume cycles out of inspiration, then the volume will not be delivered
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 277 Vijaylakshmi Kamat & Gita Nath
as described. Reaching a preset pressure limit will prevent a constant volume delivery. This can occur if the patient’s lungs are much stiffer and if the airways resistance is increased significantly.
CONSTANT PRESSURE GENERATORSWhen a ventilator provides a constant
pressure at the upper airway, it is called a constant pressure generator. This type of machine has 4 important characteristics.1. It provides a rectangular or constant waveform.2. The wave-form and pressure are not affected
by changes in the patient’s lung characteristics (compliance and resistance)
3. The flow waveform starts at a high rate and decreases during inspiration (descending ramp flow pattern)
Microprocessor ventilators that use the modes called pressure support and pressure control also act as constant pressure ventilators. They use devices such as solenoids to achieve this. A constant pressure ventilator is usually one in which the drive mechanism or output control valve produces a pressure that is less than 5 times the pressure at the upper airway at the end of inspiration. During pressure support, inspiration usually ends at predetermined flow rates of gas, during pressure control, inspiration usually ends at a preset inspiratory time.
Beginning of inspiration: The triggering mechanism
The mechanism, which begins inspiration and marks the end of expiration, is the triggering mechanism. The ventilator may be triggered by pressure, flow, time and volume. The volume variable is seldom used.
TIME TRIGGERING:Controlled ventilation is time triggered.
The control knob is the rate control knob.
PRESSURE TRIGGERING:Assisted ventilation is pressure triggered.
The operator must set the sensitivity setting, which is also called the patient effort or patient- triggering device. This sensitivity determines how much of pressure change must be detected before the ventilator is triggered. Less pressure means that the machine is more sensitive. The assist
and SIMV modes of ventilation are pressure triggered into inspiration.
PRESSURE OR TIME TRIGGEREDThe assist control ventilation mode is one
in which a minimum rate is determined by the ventilator control knob but the patient has the option of initiating inspiration at a faster time. For the mode to work correctly, the ventilator operator must always be sure that the ventilator is sensitive to the patient’s efforts.
FLOW TRIGGERINGIf a ventilator is capable of measuring the
inspiratory flow effort from the patient and of then triggering flow delivery, it is said to be flow triggered. At the present time, only a few ventilators use flow-triggering - the Puritan Bennett 7200 a, originally in the Flow-by-Mode only and the servo 300 when set for flow sensitivity. When a stimulator detects a certain drop in the gas flow due to patient inspiration, it will increase the gas flow through the circuit. Whether it augments flow or actually provides a pressure limited breath depends on the ventilator and modes in use.
Limiting Inspiration:During the inspiratory phase, the operator
can set on the ventilator, a limit on the value of one of the pressure, volume or flow. A limiting characteristic on a parameter is the maximum value a variable (pressure, volume or flow) can attain. This limits the variable during inspriation, but does not end the inspiratory phase.
PRESSURE LIMITING:Examples of pressure limiting are the
modes called pressure support and pressure control; when a value is present in either of these two modes, the pressure that can go to the airway is limited.
VOLUME LIMITINGVolume limiting ventilators have a
prefixed volume contained in a bag, bellows device, or piston cylinder. Volume is limited to what is contained in the piston cylinder.
FLOW LIMITINGIf the flow reaches a constant value before
the end of inspiration, then a ventilator is
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 278 Vijaylakshmi Kamat & Gita Nath
considered to be flow limited. Volume delivery is determined by the rate of gas flow (L/min or \J sec) and the length of inspiration.
Termination of Inspiratory phase: Cycling mechanism:
The way in which a ventilator marks the end of inspiratory gas flow and begins expiratory flow is called the cycling method or cycling mechanism.There are 4 parameters the ventilator can control to cycle out of inspiration; pressure, flow, volume and time. For any single breath, only one of the four can be operating. Most ventilators have more than one mode in which they can be cycled.
PRESSURE CYCLED VENTILATION:When a preset pressure threshold (limit)
is reached at the mouth or the upper airway, a ventilator in the pressure-cycled mode will terminate inspiration. The volume delivered to the patient depends on the flow pattern delivered, the length of inspiration, and the patient’s lung characteristics.
Pressure cycled ventilators have the disadvantage of delivering a lower tidal volume when decreases in compliance and increases in resistance occur. They have the advantage of limiting peak pressure, which may be damaging to the lungs. For a short term, ventilation of patients with fairly stable lung conditions, such as the post operative patient, these ventilators are adequate. One possible advantage with most pressure cycled ventilators using low generating pressure and decelerating flow pattern is the distribution of ventilation. Theoretically, as the flow decreases, the amount of turbulence in the airway is reduced. This helps contribute to better distribution of air into airways with varying resistance levels.
VOLUME CYCLED VENTILATION:When a ventilator terminates the
inspiratory phase after the desired volume has been delivered from the ventilator, then it is referred to as a volume cycled ventilator.The volume delivered from the ventilator is not the volume that enters the patient’s lungs.The best way to evaluate the actual volume delivered to the patient is to measure the exhaled volume at the
endotracheal or tracheostomy tube. If the patient were to develop an increased airway resistance and a decreased compliance, the flow rate would drop off slightly. In flow controllers, the preset inspiratory time and flow rate do not change with alterations in patient’s lungs’ characteristics. These ventilators are useful in delivering a fixed minute volume since the rate and volume coming out of the ventilator remain the same. Some microprocessor ventilators, like the 7200a, have computers, which can correct for volumes lost to the tubing. The volume displayed on these ventilators indicates what is intended for the patient’s lungs, having corrected for tubing compliance loss.
TIME CYCLED VENTILATORSA ventilator can be considered time
cycled if the inspiratory phase ends when a predetermined time has elapsed. This is controlled by a timing mechanism within the ventilator, which is not affected by conditions in the patient’s lungs. This time remains fixed e.g. Schrist IV -100, servo 900 C. If a flow controller (either constant or nonconstant) is being time cycled, any increase in airway resistance or decrease in compliance will not affect the flow rate. As a result, the volume delivery in a fixed time frame will be the same while the pressure changes. Pressure support also has a safety backup maximum inspiratory time on most ventilators. Usually a lapsed time of about 5 sec will end inspiration if it is not ended normally by flow.
FLOW CYCLED VENTILATIONFlow can be used to determine the end
of the inspiratory phase. Once a pre-determined flow has been achieved, the ventilator cycles in to the expiratory phase. Volume and time vary according to changes in patient’s lung characteristics. Microprocessor ventilators that provide pressure support normally flow cycle out of inspiration. Volume and flow delivery vary with patient efforts and lung characteristics.
Inflation HoldInflation hold is designed to maintain air
in the lungs at the end of inspiration. This helps to increase the peripheral distribution of gas and improve oxygenation. The pressure reading during the phase is called the plateau pressure. This
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 279 Vijaylakshmi Kamat & Gita Nath
technique of breath holding is referred to as inspiratory pause, inspiratory hold or inflation hold. This manoeuvre increases inspiratory time and mean airway pressure (Paw). Use of inflation hold is primarily for measuring plateau pressure and calculation of static compliance. It has been replaced by PEEP or CPAP for improving oxygenation.
EXPIRATORY PHASEWith the use of IPPV, expiration is
passive and depends upon the recoil of the elastic tissues in the lungs to remove air out of the alveoli and in to the ambient air.
Expiratory holdExpiratory hold or expiratory pause is
accomplished by allowing the patient to exhale and then having the ventilator pause prior to delivering the next machine breath. The purpose of this manoeuvre is to see if there is any pressure from the trapped air still in the lungs before the next positive pressure breath.
Expiratory RetardThis adds a certain amount of resistance
to expiration, which theoretically prevents early airway closure and improves ventilation. While popular in the early 1970, the method has lost its popularity and low levels of PEEP can be used for the same purpose.
PEEP/CPAPCPAP is continuous spontaneous
breathing at pressures above ambient to improve oxygenation. PEEP is pressure at the airway above ambient, at the end of expiration. CPAP and PEEP theoretically help to prevent early airway closure or airway collapse or both at the end of expiration by increasing the FRC of the lungs. This allows for better 02 exchange at the alveolocapillary membranes. PEEP also increases mean airway pressure.
Auto PEEPAuto PEEP is defined as an unintentional
PEEP that occurs with mechanically ventilated patients, when a new inspiratory breath is delivered before expiration has ended. It is a complication that may escape detection unless looked for. Auto PEEP differs from PEEP, which
is a pre-selected value at the end expiratory gas flow.AUTO PEEP = OCCULT PEEP = INADVERTENT PEEP = INTRINSIC PEEP = GASTRAPPING = BREATH STACKING.
PHYSIOLOGIC FACTORSThere are 3 distinct forms of AUTO PEEP1. Auto PEEP without lung distension; which occurs because the expiratory muscles are actively contracting during exhalation. This raises the alveolar pressure at end exhalation without increasing the volume at end exhalation2. Auto PEEP which occurs in patients with normal airway resistance, in whom air trapping occurs in the presence of high minute volume, long inspiratory times and factors that increase resistance to exhalation such as small ET tubes and exhalation lines (normally less than 4 cm H20/L/sec).3. Auto PEEP also occurs in patients with airflow obstruction who tend to have airway collapse during exhalation and flow limitation during normal tidal breathing. In these patients, an increased expiratory effort only increases the alveolar pressure and does not improve the expiratory flow rate.
FACTORS THAT INCREASE THE RISK OF AUTO PEEP1. COPD2. Minute ventilation of > 10L/min (39%
incidence; with minute ventilation > 20L/min, the incidence is 100%)
3. Increased age, particularly patients aged > 60 years (the minute ventilation requirement for auto PEEP decreases with age)
4. Decreases in ET tube size5. Increases in compliance6. As respiratory frequency increases, the risk
of gas trapping increases, particularly as inspiratory time approaches expiratory time in value (in adult volume cycled ventilation and infant pressure limited, time cycled ventilation)
7. Reduced inspiratory flow leading to a shorter expiratory time, even though peak pressure decreases
8. Increase in tidal volume particularly in patients with airway obstruction.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 280 Vijaylakshmi Kamat & Gita Nath
DETECTION OF AUTO PEEPAir trapping can be detected with volume
ventilation by observing an increase in peak and plateau pressures, a transient reduction in exhaled volumes, a reduction in breath sounds, a decrease in compliance and an increase in resonance on percussion of the chest wall. It can also be detected by measuring the auto PEEP level. Some ventilators have end expiratory pause buttons. These are usually microprocessor ventilators that can time the closing of the exhalation valve. They close the valve just prior to the next positive pressure breath. They then delay the next breath and measure the pressure in the circuit.
Auto PEEP can also be measured during mechanical ventilation by occluding the expiratory limb of the patient circuit just prior to the next positive pressure breath. Detecting auto PEEP by measuring end-expiratory pressure requires a quiet patient and controlled ventilation. Auto PEEP will actually slow the beginning of the gas flow during inspiration.
Auto PEEP when present, may increase the patient’s work of breathing, as the patient’s inspiratory effort must equal the set end expiratory level plus the auto PEEP level in order to trigger the ventilator. Auto PEEP can be reduced by providing a longer exhalation time, which can be achieved by using higher inspiratory flow rates, smaller tidal volume settings, lower respiratory rates, less compliant circuits, low resistance exhalation valves, larger ET tubes and bronchodilators for reactive airways.
Alternative strategies that can be chosen when auto PEEP is inevitable are1. Mild hypoventilation (permissive hypercapnia)2. Partial support modes such as SIMV/IMV, PS
and CPAP are thought to benefit patients in clinical situations of acute hypoxaemic respiratory failure as it improves oxygenation.
CHANGING AND MAINTENANCE OF VENTILATORS
In general, the external circuit requires dismantling and the tubings, patient Y, humidifier, bacterial filters and the components of the expiratory channel should be cleaned and
sterilized between every patient use. The flow transducer should be cleaned in 70% ethyl solution for about one hour. All the other parts should be cleaned in a disinfectant solution and then rinsed in water. After cleaning and rinsing, all the parts including the flow transducer can be autoclaved at a temperature of up to 150 degree centigrade. Individual operating manuals should be consulted for the entire cleaning routine and a check of function should be made after every cleaning. After every 1000 hours of operation or after every six months at the least, a 1000 hours overhaul with complete cleaning should be carried out and this should be followed by a calibration of the ventilator and the oxygen cells.
MODELS OF VENTILATION Goals of mechanical ventilation:1. To improve arterial blood oxygenation by
applying optimal FI02, improving V/Q mismatch or recruiting previously non-ventilated alveoli.
2. Decrease/eliminate the energy consumed by the respiratory muscles by having the ventilators provide some or all of the power required to breathe.
3. Control the rate of alveolar ventilation.
Choosing an appropriate ventilatorConstant flow generators, which are
volume or time cycled can maintain ventilation, oxygenation and compliance better than pressure cycled ventilators. They are recommended for use in all types of patient situations. These ventilators require an electrical source and at least one compressed gas source, if not two. The most recent generations of microprocessor ventilators can operate as flow or pressure generators and can provide volume preset, pressure preset and weaning modes. Many also provide a variety of flow patterns including constant flow, sine wave and descending and ascending ramps.
Constant pressure, pressure cycled machines use the descending flow pattern, which results in a better distribution of air throughout the lungs. In addition, these ventilators are small, portable, require no electricity, operate from compressed gas and have leak compensating mechanisms. They are of value in patient transport, use during emergency situations and for short-term ventilation in the post-operative
RACE 2003 Ramachandra Anaesthesia Continuing Education
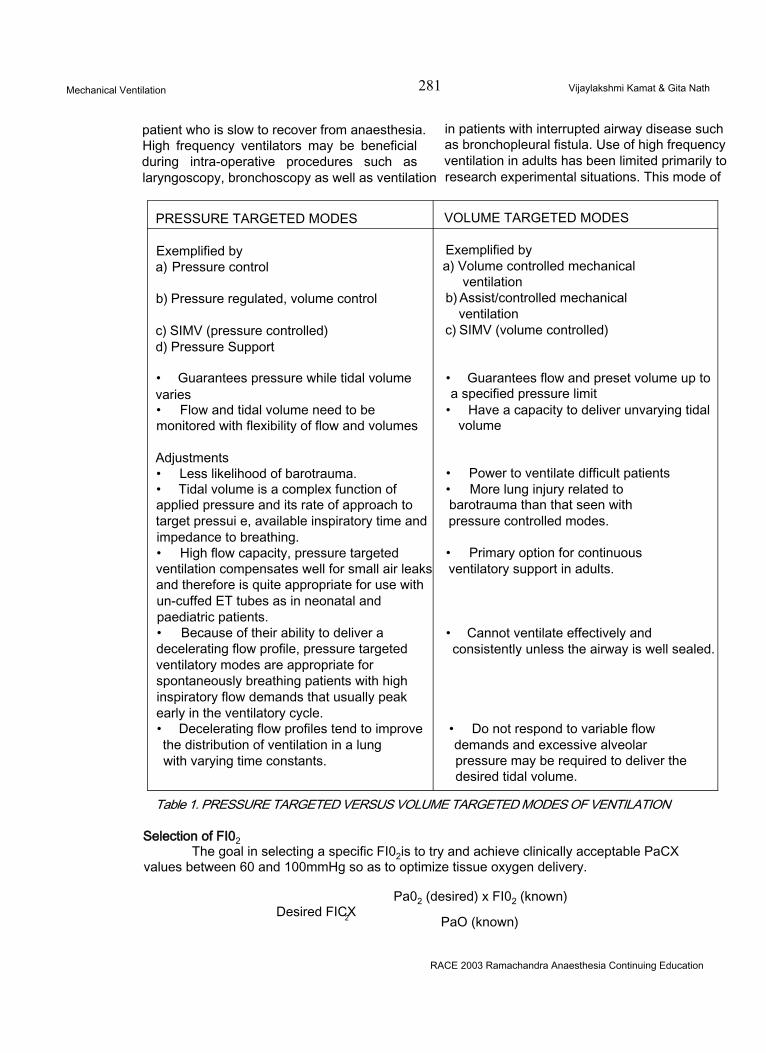
Mechanical Ventilation 281 Vijaylakshmi Kamat & Gita Nath
patient who is slow to recover from anaesthesia. High frequency ventilators may be beneficial during intra-operative procedures such as laryngoscopy, bronchoscopy as well as ventilation
in patients with interrupted airway disease such as bronchopleural fistula. Use of high frequency ventilation in adults has been limited primarily to research experimental situations. This mode of
PRESSURE TARGETED MODES VOLUME TARGETED MODES
Exemplified bya) Pressure control
b) Pressure regulated, volume control
c) SIMV (pressure controlled)d) Pressure Support
• Guarantees pressure while tidal volume varies• Flow and tidal volume need to be monitored with flexibility of flow and volumes
Adjustments• Less likelihood of barotrauma.• Tidal volume is a complex function of applied pressure and its rate of approach to target pressui e, available inspiratory time and impedance to breathing.• High flow capacity, pressure targeted ventilation compensates well for small air leaks and therefore is quite appropriate for use with un-cuffed ET tubes as in neonatal and paediatric patients.• Because of their ability to deliver a decelerating flow profile, pressure targeted ventilatory modes are appropriate for spontaneously breathing patients with high inspiratory flow demands that usually peak early in the ventilatory cycle.• Decelerating flow profiles tend to improve the distribution of ventilation in a lungwith varying time constants.
Exemplified bya) Volume controlled mechanical
ventilationb) Assist/controlled mechanical
ventilationc) SIMV (volume controlled)
• Guarantees flow and preset volume up to a specified pressure limit
• Have a capacity to deliver unvarying tidal volume
• Power to ventilate difficult patients• More lung injury related to barotrauma than that seen with pressure controlled modes.
• Primary option for continuous ventilatory support in adults.
• Cannot ventilate effectively and consistently unless the airway is well sealed.
• Do not respond to variable flow demands and excessive alveolar pressure may be required to deliver the desired tidal volume.
Table 1. PRESSURE TARGETED VERSUS VOLUME TARGETED MODES OF VENTILATION
Selection of FI02The goal in selecting a specific FI02is to try and achieve clinically acceptable PaCX
values between 60 and 100mmHg so as to optimize tissue oxygen delivery.
Pa02 (desired) x FI02 (known)Desired FICX2 PaO (known)
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 282 Vijaylakshmi Kamat & Gita Nath
ventilation is most often used in infants.
Rational Settings of Ventilator controls:Full ventilatory support (FVS) implies
that the ventilation provides all the energy necessary to maintain effective alveolar ventilation and can be defined as mechanical rates of 12 or more breaths/min and tidal volume 6-8ml/kg; this can be provided by the use of control modes like IMV or SIMV or pressure control.
Partial ventilatory support (PVS) is that in which the patient actively participates in ventilation to maintain safe levels of PaC02 and can be provided by using any mode of ventilation. In acute respiratory failure, the initial goal is to provide full ventilatory support and after reasonable recovery and stabilization, partial ventilatory support is advocated.
A mode may be defined as a particular set of control and phase variables and can be described by the pressure, flow and volume patterns that occur over time when the method of ventilation is used.
Tidal VolumeThe initial tidal volume to satisfy minute
ventilation requirements and to arrest progressive atelectasis that can occur in supine patients is 6-8ml/kg, up to a maximum of 1 litre. A lower tidal volume may be selected in patients with sever airway obstruction, where there is a concern about air trapping and in patients with only one lung. Initial respiratory rate of 12/min is selected.
Inspiratory flow rateDuring constant flow, the average flow
rate is almost equal to the peak inspiratory flow rate. During decelerating or sinusoidal flow patterns, the inspiratory flow rate set on the ventilator is again equal to PI FR, but the average flow rate is lower and the respiratory time is therefore longer for the same settings of peak flow and tidal volume.
Considerations Guiding Flow Rate
Selection1. Faster flows require greater airway pressures
to deliver the same tidal volume.2. Higher flow rates increase shear forces
risking further airway and parenchymal damage.
3. Low inspiratory flow rates can lead to dangerous air trapping.
4. If machine flow rate is less than the patient’s inspiratory flow demand, then the patient will struggle, fight the ventilator and increase his WOB and oxygen consumption.
Flow rate settings:1. Peak flow in the constant flow rates should
be 4 times the minute ventilation.2. For patients who are spontaneously
breathing, flow demands are highest in the beginning of inspiration and therefore, a decelerating flow profile is helpful. For the same inspiratory tidal volume and time, peak flow should be set to 20-25% higher than in the constant flow mode.
3. Relatively higher flow rates should be used for patients with air flow obstruction.
4. In pressure cycled ventilation, the flow rate has a decelerating pattern but cannot be adjusted independent of other variables. In this situation, the inspiratory time can be adjusted by a timing mechanism. In most circumstances, the l/E ratio can be set at 1:3
Inspiratory PauseInspiratory pause shortens the expiratory
phase of the respiratory cycle, increasing the l:E ratio. This feature is useful to estimate alveolar pressure at end inspiration and thereby derive static compliance. It can be used as an alternative to PCIRV. It guarantees tidal volume and is readily accessible in patients already on volume-cycled ventilations.
Mean Airway Pressure and its ImplicationsMany complications can be associated
with positive pressure ventilation. Of these, the two most important are interference with cardiovascular function and interference with gas exchange. In order to minimize the cardiovascular side effects, the term mean airway pressure (Paw), its determinations and implications have to be understood.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 283 Vijaylakshmi Kamat & Gita Nath
THE UPPER AIRWAY PRESSURES DURING A POSITIVE PRESSURE BREATH:
Pressure rises during inspiration to peak inspiratory pressure (PIP). With the breath held, the plateau pressure can be measured. Pressure falls back to baseline during expiration. Normally base line pressure is zero. Baseline pressure takes on a higher value than zero if PEEP is set.
PEAK PRESSUREThis is the highest pressure recorded at
the end of inspiration. It is called peak inspiratory pressure (PIP). This is equal to the sum of trans airway (PTA) and alveolar pressure(PA).
PLATEAU PRESSUREPlateau pressure is actually a pressure
measurement that is taken after a breath has been delivered to the patient and before exhalation has begun. Plateau pressure reflects the effect of the elastic recoil of the lungs and chest wall on the gas volume inside the alveoli and any pressure (P ) exerted by the volume in the ventilator circuit. Plateau pressure reflects alveolar pressure.
MEAN AIRWAY PRESSURE (Paw):This is the area enclosed between the
curve and the baseline for one respiratory cycle, divided by the duration of the cycle. Paw can be monitored using a variety of devices that use various algorithms to calculate and display the average value of Paw during mechanical ventilation of the subject. In a constant flow, volume cycled ventilator, the pressure rise is nearly linear with time and produces essentially a triangular pressure waveform.
Paw can be estimated by the following equation: Paw = 1/4 (Ppeak x(insp time/total Resp cycle) with PEEP addedPAW = V2 (Ppeak - PEEP) x (Insp time/total cycle time) + PEEP
The Paw generated during IPPV undergoes variations and may produce different wave forms (pressure curves) depending upon the types of ventilator employed, the mode of ventilation used and the patient’s pulmonary characteristics. Modes such as inflation hold, expiratory retard, pressure control, and PEEP
have high Paw values compared to normal IPPV and ZEEP.
It is essential to avoid large values of Paw in order to minimize the harmful cardiovascular effects of IPPV. Lower Paw can be achieved by changing inspiratory flow rates, l/E ratio, inflation hold, PEEP and expiratory retard. IMV or SIMV, and possible modes such as pressure support may also reduce Paw.
Inspiratory flow ratesRaised inspiratory flows may increase
PIP but with normal conductive airways they can deliver the desired VTin a shorter time and have a lower Paw However, with high PIP, more pressure is lost to the patient circuit and airway resistance and uneven ventilation might occur. In general terms, the goal is to use the highest possible flow rates and carefully monitor the effects of the flow changes oh volume delivery, VD/VT, V/Q and
l/E RatioA range of l/E ratios of 1:1.5 to 1:4 or
smaller in the adult is considered acceptable for mechanical ventilation. Values of 1:1, 2:1 and higher may result in significant increases in Paw, air trapping and significant haemodynamic complications unless the lung tissue is very stiff. Values of 1:2,1:3,1:4 and smaller have a lower Paw and fewer associated hazards. In patients with poor airway conductance (increased resistance), a longer expiratory time also has the benefit of allowing alveolar emptying. Short l/E ratios that is, 1:6 or smaller in a non- spontaneously breathing patient may increase the physiological dead space. This is due to rapid inspiratory flow rates with inspiratory times of less than 0.5 sec.
FEATURES OF INDIVIDUAL VENTILATORY MODESControl mode ventilation (CMV)
Can provide only mandatory breaths, which are triggered by the ventilator, are flow limited and are time/volume cycled. This mode is usually indicated in patients who are first intubated prior to full evaluation, those who require high minute volumes, those with unstable respiratory drive, those with respiratory muscle
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 284 Vijaylakshmi Kamat & Gita Nath
fatigue and those with a poor cardiac output. CMV has the advantages of guaranteeing minute ventilation and reducing the oxygen and energy consumption of the respiratory muscles. The disadvantages of this mode are that it requires a quiet sedated paralyzed patient and the ventilator’s disconnection will result in an apnoiec patient. This mode is unresponsive to the changing minute volume requirements and might result in alkalosis and high mean airway and intrathoracic pressures. It may also lead to atrophy of the respiratory muscles if used for prolonged periods. The initial settings on this mode include a respiratory rate of 10-12/min and a tidal volume of 10-12ml/kg ideal body weight with an I: E ratio of 1:2 or less. Settings may be re-adjusted in accordance with the blood gases.
Assist/control mode of ventilationA/CMV is an adaptation of CMV that
allows the patient to initiate a volume cycled breath at a rate greater than the set backup respiratory rate. The backup rate on A/CMV is a safety feature. It is usually set to provide about 80% of the baseline minute ventilation. Situations in which the back up rate is set above the patient’s respiratory rate are the following:a) A dyspnoeic patient with unstable angina or a
low Cardiac output.b) Patient with an unstable respiratory drive who
requires a tight control of pH and PaC02c) Patient with a flail chest.
To actuate an assisted breath, the patient must generate negative pressure in the airway. Therefore trigger sensitivity must be adjusted for using this mode.
The intermittent mandatory ventilation mode (IMV)
IMV was developed and incorporated from 1975 into most ventilators designed for neonatal and infant applications. It was simple, relatively fool proof, easy to convert to CMV or to lower level applications like CPAP. Modification of the Ayre’s “T” piece is the basis of intermittent mandatory ventilation. Continuous gas flow allows spontaneous breathing whereas occlusion of the end of the “T” tube diverts the flow into the infant’s lungs. A positive pressure inflation results, the volume of which is controlled by gas flow rates
and the duration of ventilation.
In this, two types of breaths, mandatory and spontaneous, are possible. Inspiration can be triggered by the ventilator or the patient, limited by flow and cycled either by volume (if it is a ventilator breath) or by the patient.
IMV can be used as a full ventilatory support mode or as a weaning mode. Reputed advantages include:a) Avoidance of respiratory alkalosisb) Decreased requirement for sedation/muscle
relaxation.c) Lower mean airway pressuresd) Better ventilation to perfusion matchinge) Expedited weaningf) Prevention of respiratory muscle atrophy or
disco-ordination.g) Reduced likelihood of cardiac decompensation.
DISADVANTAGES INCLUDE1. Increased risk of carbon dioxide retention.2. Increased work of breathing and respiratory
muscle fatigue.
SETTINGS FOR THIS MODE INCLUDE1. Mandatory rate2. Mandatory tidal volume/minute ventilation3. I: E ratio4. Trigger sensitivity5. High/low pressure alarms6. Apnoea alarms7. Respiratory rate/tidal volume display
Synchronized intermittent mandatory ventilation (SIMV)
SIMV differs from IMV in adults in that the mandated breath is synchronized with the patient’s inspiratory effort, thereby preventing the possibility of the ventilator stacking a mechanical tidal volume on top of a spontaneous one. This makes SIMV an interactive mode of ventilation. From the mid 1980s, the primary modification to the traditional IMV/SIMV (and indeed to all ventilator modes) was the introduction of microprocessor technology that allowed more precise applications and expanded capabilities.
Therefore 2 options are possible on the
RACE 2003 Ramachandra Anaesthesia Continuing Education
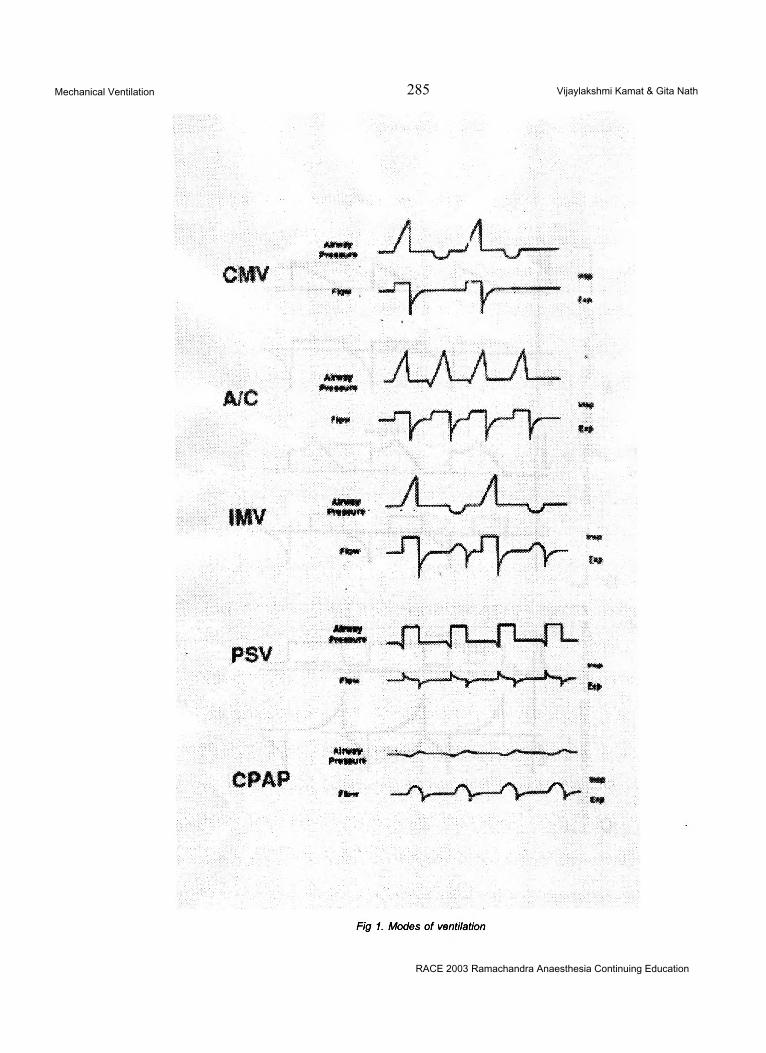
Mechanical Ventilation 285 Vijaylakshmi Kamat & Gita Nath
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 286 Vijaylakshmi Kamat & Gita Nath
SIMV mode,1. Volume controlled SIMV mandatory breaths
(SIMV-VC)2. Pressure controlled SIMV mandatory breaths
(SIMV-PC)
The SIMV mode is capable of providing 2 types of breaths, mandatory and spontaneous, and inspiration can be triggered either by the ventilator or the patient. Mandatory breaths are flow limited and volume cycled in the SIMV (VC) mode, or pressure limited and time cycled in the SIMV (PC) mode.
SIMV modes can be used as full ventilatory support modes or as weaning nodes. All the advantages and disadvantages of IMV listed above also apply to SIMV. All SIMV machines are not equally effective. The time taken for the inspiratory valve to open after the pressure sensor has been triggered varies between machines. If the time taken is longer, the work of breathing is increased. Although subjectively patients usually appear more comfortable on SIMV than IMV, there is no evidence that it reduces morbidity or mortality.
Mandatory minute ventilation (MMV)This mode was developed to fill the
lacunae in the SIMV mode. Ideally in this mode, the ventilator should monitor exhaled volumes and “top up” the patients’ respiratory efforts, if needed. This is the basis of the mandatory minute ventilation. In this mode of ventilation, a preset volume is selected. If the patient’s own respiratory efforts produce a minute ventilation in excess of the preset value, the ventilator does not activate. If the preset minute volume is not achieved, the ventilator gives some assistance to the patient, to bring the minute ventilation back to the target value. The method used to provide ventilatory assistance depends on the design of the ventilator. The Ohmeda CPU 1 and Engstrom Erica provide synchronized mandatory breaths of a preset tidal volume at an increasing frequency as the patient’s own respiratory efforts diminish.The Hamilton Veolar uses a different approach and provides increasing inspiratory pressure support, as the patient’s own efforts decrease. Whichever method is used, the machines ensure that the patient always receives
a predetermined minute volume. While theoretically attractive, the technique has not been widely adopted. The system works well if the patient’s respiratory rate is relatively normal, but if the patient develops rapid shallow breathing, the ventilator will measure an adequate minute ventilation even though the bulk of the ventilation will be delivered to the anatomical dead space and so will not contribute to carbondioxide elimination.
Pressure control mode (PCV)PCV mode is used as a control mode
with a normal l:E ratio or with an increased l:E ratio. It could be used as an assist mode or in combination with PSV. At present, the primary indication for pressure control is for the ventilatory support of patients with ARDS, in whom conventional IPPV with PEEP is not effective i.e specifically those patients who are on a FI02 of 1.0, have a PIP of 50cm H20 or higher, PEEP levels of 15 cm H20 or higher, assist control rates of > 16 breaths/min, have a low Pa02 value and low lung compliance. Traditional pressure control mode is capable of delivering only mandatory breaths which can be triggered by the ventilator or the patient, are limited by pressure and are time cycled.
Advantages with this mode include:1. Less barotrauma than CMV2. Better distribution of ventilation in the lungs in regions of varying time constants.
The main disadvantage is that paralysis and sedation are necessary, especially if the mode is used with inverse ratio ventilation, as it is uncomfortable for patients.
SETTINGS ON THE PRESSURE CONTROL MODE1. A preset pressure about half the PIP on IPPV2. PEEP setting to half the PEEP level on CMV (only if the PEEP level on CMV was greater than 8 cm H20)3. I:E ratio of 1:2 or less4. Measurements of intrinsic PEEP are mandatory for correct calculation of compliance, for reading haemodynamic data and for carrying out cardiovascular pharmacological interventions. The pressure regulated volume control mode is
RACE 2003 Ramachandra Anaesthesia Continuing Education
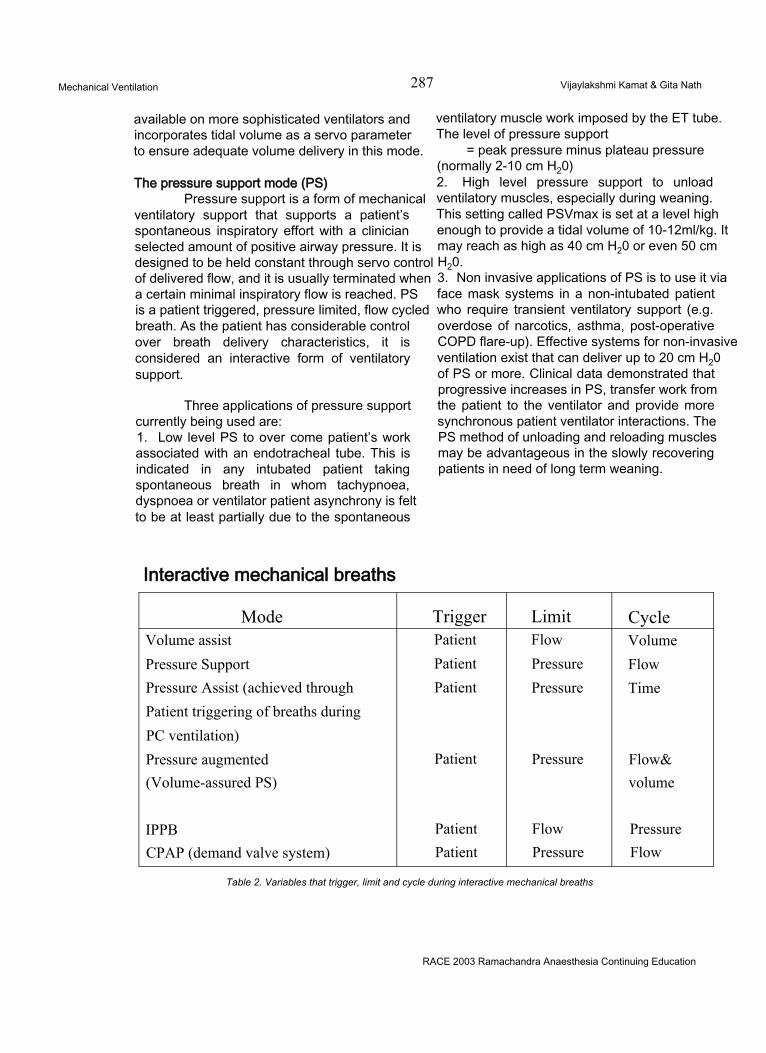
Mechanical Ventilation 287 Vijaylakshmi Kamat & Gita Nath
available on more sophisticated ventilators and incorporates tidal volume as a servo parameter to ensure adequate volume delivery in this mode.
The pressure support mode (PS)Pressure support is a form of mechanical
ventilatory support that supports a patient’s spontaneous inspiratory effort with a clinician selected amount of positive airway pressure. It is designed to be held constant through servo control of delivered flow, and it is usually terminated when a certain minimal inspiratory flow is reached. PS is a patient triggered, pressure limited, flow cycled breath. As the patient has considerable control over breath delivery characteristics, it is considered an interactive form of ventilatory support.
Three applications of pressure support currently being used are:1. Low level PS to over come patient’s work associated with an endotracheal tube. This is indicated in any intubated patient taking spontaneous breath in whom tachypnoea, dyspnoea or ventilator patient asynchrony is felt to be at least partially due to the spontaneous
ventilatory muscle work imposed by the ET tube. The level of pressure support
= peak pressure minus plateau pressure (normally 2-10 cm H20)2. High level pressure support to unload ventilatory muscles, especially during weaning. This setting called PSVmax is set at a level high enough to provide a tidal volume of 10-12ml/kg. It may reach as high as 40 cm H20 or even 50 cm H20.3. Non invasive applications of PS is to use it via face mask systems in a non-intubated patient who require transient ventilatory support (e.g. overdose of narcotics, asthma, post-operative COPD flare-up). Effective systems for non-invasive ventilation exist that can deliver up to 20 cm H20 of PS or more. Clinical data demonstrated that progressive increases in PS, transfer work from the patient to the ventilator and provide more synchronous patient ventilator interactions. The PS method of unloading and reloading muscles may be advantageous in the slowly recovering patients in need of long term weaning.
Interactive mechanical breaths
Mode Trigger Limit CycleVolume assist Patient Flow VolumePressure Support Patient Pressure FlowPressure Assist (achieved through Patient Pressure TimePatient triggering of breaths duringPC ventilation)Pressure augmented Patient Pressure Flow&(Volume-assured PS) volume
IPPB Patient Flow PressureCPAP (demand valve system) Patient Pressure Flow
Table 2. Variables that trigger, limit and cycle during interactive mechanical breaths
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 288 Vijaylakshmi Kamat & Gita Nath
PEEP/CPAPEnd-expiratory pressure may be applied
during continuous mechanical ventilation (PEEP) : or spontaneous breathing with or without partial < ventilatory support (CPAP). PEEP and CPAP i typically are: I1. Used to reduce or prevent expiratory atelectasis in patients with acute lung injury. ;2. To reduce LV afterload in patients with congestive heart failure. i3. To reduce inspiratory load in patients with COPD.
Various valves are used to produce end expiratory pressure1. Hydrostatic tension valves2. Spring tension valves3. Pneumatic valves4. Electromagnetic valves5. Weighted ball valves
Ideally, an end expiratory pressure mechanism should permit unrestricted expiration, until the pressure in the breathing circuit reaches the level of PEEP selected.
TITRATING PEEP/CPAP THERAPY TO A DESIRABLE END POINT
Respiratory system mechanics and gas exchange are evaluated as PEEP/CPAP is titrated.a) Conservative ApproachPEEP to achieve an adequate Pa02 (usually >60 to 65 torr or Sa02>90%) with a FI02=0.5 without a significant reduction in cardiac output.b) Best PEEPPEEP titrated to achieve optimal respiratory system compliance.c) Optimal PEEPTitration of PEEP until Qs/Qt is < 15%If the cardiac output deteriorates before achieving optimal PEEP, intravenous fluids and inotropes can be administered depending on the measured PCWP.
Airway pressure release ventilation (APRV)APRV is a CPAP system that allows
augmentation of alveolar ventilation by briefly interrupting CPAP. APRV is designed to deliver CPAP, to simultaneously augment alveolar ventilation and to allow unrestricted spontaneous ventilation.
The APRV circuit is a high flow CPAP system with a release valve in the expiratory limb. Opening this release valve for 1-2 seconds allows circuit and airway pressure to drop from the CPAP level to near ambient pressure (or to a lower CPAP level). This brief interruption of CPAP causes airway pressure to fall and thereby allows the lung volume to decrease. When the release valve closes, airway pressure increases to higher CPAP levels and the lung volume is restored to the augmented FRC. Thus each mechanical breath is created by the brief interruption and restoration of CPAP. As each breath is delivered by releasing (decreasing) pressure rather than increasing airway pressure, the peak airway pressure cannot exceed the CPAP level.
APRV can be delivered successfully only with the equipments that meet stringents which include:a) Flow capability of 90-100 Lit/min and demand
valves with low inertia.b) Humidifier, circuit, tubings and connections,
which offer minimal flow resistance of 1-2 cmH20/100L/min.
c) Expiratory valve which can attain the fully opened or closed position in 10 m.secs.
The APRV mode is a flexible alternative to conventional ventilation, to augment alveolar ventilation in patients with acute lung injury of mild to moderate severity. The detrimental haemodynamic effects of conventional ventilatory support do not occur with APRV .The APRV’s haemodynamic pattern was indistinguishable from that during spontaneous ventilation with CPAP.
RACE 2003 Ramachandra Anaesthesia Continuing Education
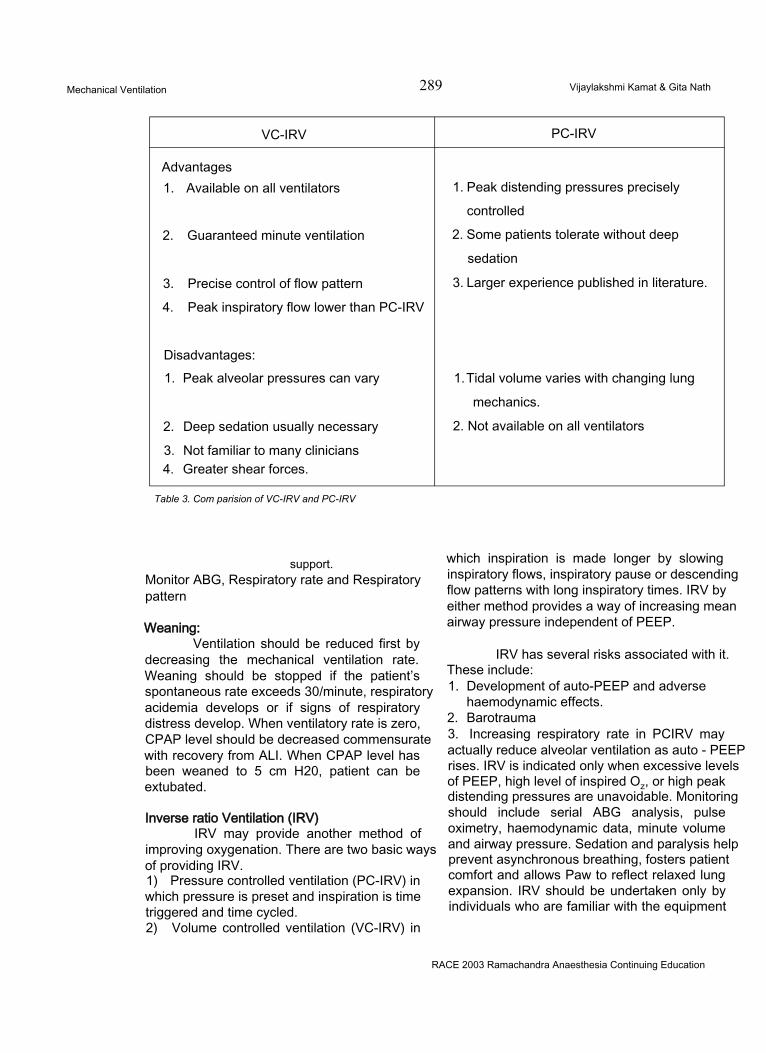
Mechanical Ventilation 289 Vijaylakshmi Kamat & Gita Nath
VC-IRV PC-IRV
Advantages1. Available on all ventilators
2. Guaranteed minute ventilation
3. Precise control of flow pattern
4. Peak inspiratory flow lower than PC-IRV
Disadvantages:1. Peak alveolar pressures can vary
2. Deep sedation usually necessary
3. Not familiar to many clinicians4. Greater shear forces.
1. Peak distending pressures precisely
controlled
2. Some patients tolerate without deep
sedation
3. Larger experience published in literature.
1. Tidal volume varies with changing lung
mechanics.
2. Not available on all ventilators
Table 3. Com parision of VC-IRV and PC-IRV
support.Monitor ABG, Respiratory rate and Respiratory pattern
Weaning:Ventilation should be reduced first by
decreasing the mechanical ventilation rate. Weaning should be stopped if the patient’s spontaneous rate exceeds 30/minute, respiratory acidemia develops or if signs of respiratory distress develop. When ventilatory rate is zero, CPAP level should be decreased commensurate with recovery from ALI. When CPAP level has been weaned to 5 cm H20, patient can be extubated.
Inverse ratio Ventilation (IRV)IRV may provide another method of
improving oxygenation. There are two basic ways of providing IRV.1) Pressure controlled ventilation (PC-IRV) in which pressure is preset and inspiration is time triggered and time cycled.2) Volume controlled ventilation (VC-IRV) in
which inspiration is made longer by slowing inspiratory flows, inspiratory pause or descending flow patterns with long inspiratory times. IRV by either method provides a way of increasing mean airway pressure independent of PEEP.
IRV has several risks associated with it. These include:1. Development of auto-PEEP and adverse
haemodynamic effects.2. Barotrauma3. Increasing respiratory rate in PCIRV may actually reduce alveolar ventilation as auto - PEEP rises. IRV is indicated only when excessive levels of PEEP, high level of inspired Oz, or high peak distending pressures are unavoidable. Monitoring should include serial ABG analysis, pulse oximetry, haemodynamic data, minute volume and airway pressure. Sedation and paralysis help prevent asynchronous breathing, fosters patient comfort and allows Paw to reflect relaxed lung expansion. IRV should be undertaken only by individuals who are familiar with the equipment
RACE 2003 Ramachandra Anaesthesia Continuing Education
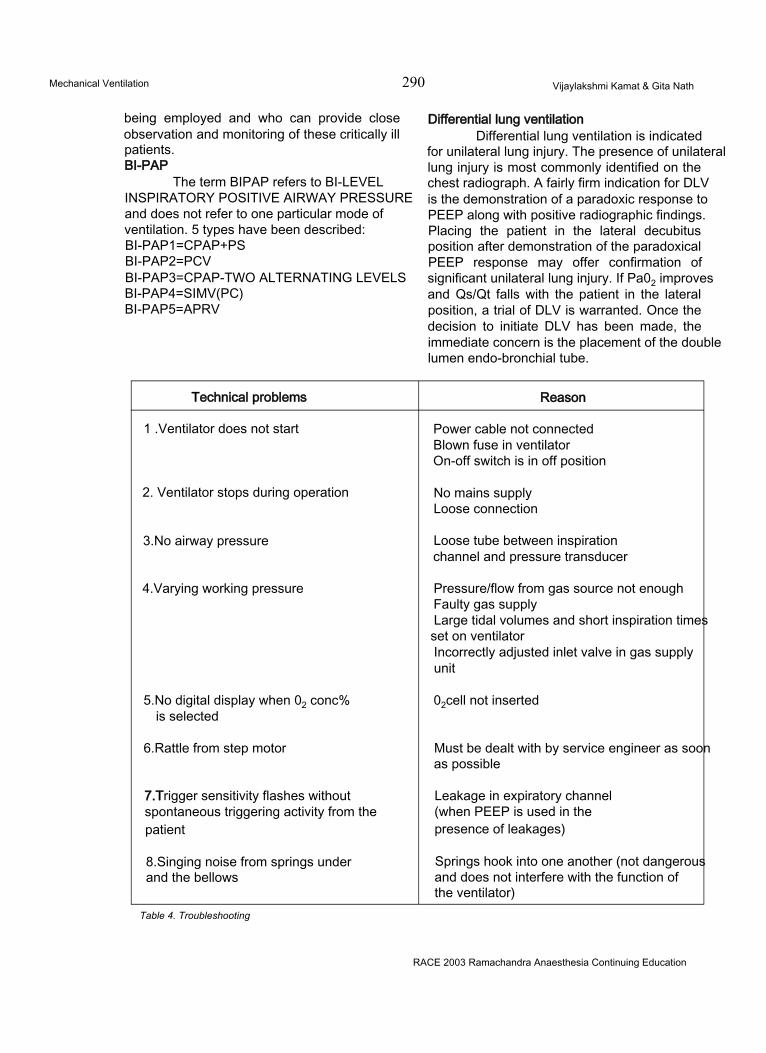
Mechanical Ventilation 290 Vijaylakshmi Kamat & Gita Nath
being employed and who can provide close observation and monitoring of these critically ill patients.BI-PAP
The term BIPAP refers to BI-LEVEL INSPIRATORY POSITIVE AIRWAY PRESSURE and does not refer to one particular mode of ventilation. 5 types have been described: BI-PAP1=CPAP+PS BI-PAP2=PCVBI-PAP3=CPAP-TWO ALTERNATING LEVELS BI-PAP4=SIMV(PC)BI-PAP5=APRV
Differential lung ventilationDifferential lung ventilation is indicated
for unilateral lung injury. The presence of unilateral lung injury is most commonly identified on the chest radiograph. A fairly firm indication for DLV is the demonstration of a paradoxic response to PEEP along with positive radiographic findings. Placing the patient in the lateral decubitus position after demonstration of the paradoxical PEEP response may offer confirmation of significant unilateral lung injury. If Pa02 improves and Qs/Qt falls with the patient in the lateral position, a trial of DLV is warranted. Once the decision to initiate DLV has been made, the immediate concern is the placement of the double lumen endo-bronchial tube.
Technical problems Reason
1 .Ventilator does not start Power cable not connected Blown fuse in ventilator On-off switch is in off position
2. Ventilator stops during operation No mains supply Loose connection
3.No airway pressure Loose tube between inspiration channel and pressure transducer
4.Varying working pressure Pressure/flow from gas source not enough Faulty gas supplyLarge tidal volumes and short inspiration times set on ventilatorIncorrectly adjusted inlet valve in gas supply unit
5.No digital display when 02 conc% is selected
02cell not inserted
6.Rattle from step motor Must be dealt with by service engineer as soon as possible
7.Trigger sensitivity flashes without spontaneous triggering activity from the patient
Leakage in expiratory channel (when PEEP is used in the presence of leakages)
8.Singing noise from springs under and the bellows
Springs hook into one another (not dangerous and does not interfere with the function of the ventilator)
Table 4. Troubleshooting
RACE 2003 Ramachandra Anaesthesia Continuing Education
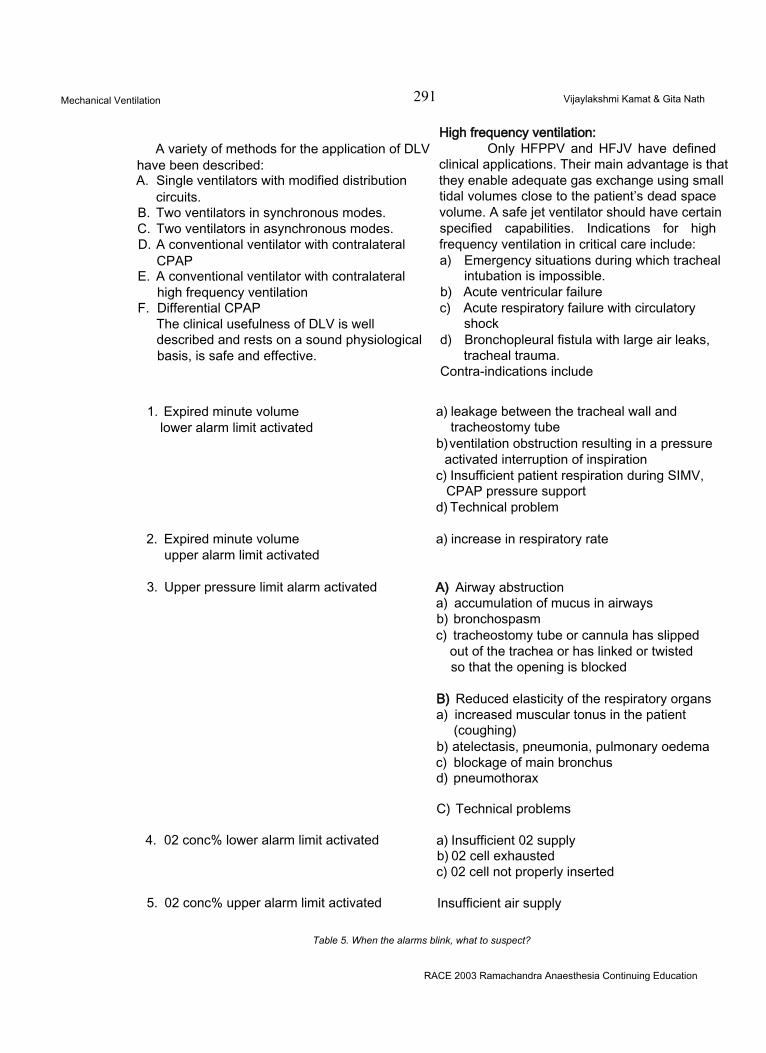
Mechanical Ventilation 291 Vijaylakshmi Kamat & Gita Nath
A variety of methods for the application of DLV have been described:A. Single ventilators with modified distribution
circuits.B. Two ventilators in synchronous modes.C. Two ventilators in asynchronous modes.D. A conventional ventilator with contralateral
CPAPE. A conventional ventilator with contralateral
high frequency ventilationF. Differential CPAP
The clinical usefulness of DLV is well described and rests on a sound physiological basis, is safe and effective.
High frequency ventilation:Only HFPPV and HFJV have defined
clinical applications. Their main advantage is that they enable adequate gas exchange using small tidal volumes close to the patient’s dead space volume. A safe jet ventilator should have certain specified capabilities. Indications for high frequency ventilation in critical care include:a) Emergency situations during which tracheal
intubation is impossible.b) Acute ventricular failurec) Acute respiratory failure with circulatory
shockd) Bronchopleural fistula with large air leaks,
tracheal trauma.Contra-indications include
1. Expired minute volume lower alarm limit activated
2. Expired minute volume upper alarm limit activated
3. Upper pressure limit alarm activated
4. 02 conc% lower alarm limit activated
5. 02 conc% upper alarm limit activated
a) leakage between the tracheal wall and tracheostomy tube
b) ventilation obstruction resulting in a pressure activated interruption of inspiration
c) Insufficient patient respiration during SIMV, CPAP pressure support
d) Technical problem
a) increase in respiratory rate
A) Airway abstructiona) accumulation of mucus in airwaysb) bronchospasmc) tracheostomy tube or cannula has slipped
out of the trachea or has linked or twisted so that the opening is blocked
B) Reduced elasticity of the respiratory organsa) increased muscular tonus in the patient
(coughing)b) atelectasis, pneumonia, pulmonary oedemac) blockage of main bronchusd) pneumothorax
C) Technical problems
a) Insufficient 02 supplyb) 02 cell exhaustedc) 02 cell not properly inserted
Insufficient air supply
Table 5. When the alarms blink, what to suspect?
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 292 Vijaylakshmi Kamat & Gita Nath
a) COPDb) Status asthmaticus
MONITORING WITH THE VENTILATORThis includes various alarm settings for
pressure, volume, timing, etc and also monitoring airway pressures, compliance, airway resistance, volumes, temperatures etc.Monitoring airway pressures
Airway pressure is continually monitored to be sure that very high pressure limits are not exceeded but that a minimal pressure (low pressure limit) is maintained. The various pressures that give information about the patient condition are peak pressure(PIP), plateau pressure (Pplateau), transairway pressure (PIP- Plateau), mean airway pressure (Paw) and expiratory pressure (EEP). A pressure exceeding a limit indicates a change in the patient’s condition that may signal that the airway needs to be suctioned, the Raw is increased, that lung compliance is decreased etc.
Monitoring Cuff pressure:It is monitored 8th hrly and it should not
exceed 25mm of Hg as the tracheal wall arterial end-capillary pressure is about 30 mm Hg. There are devices that provide gauge or digital readings of cuff pressures. The use of MLT “minimum leak technique”, can provide adequate cuff inflation to allow for ventilation and reduce the intracuff pressure. To perform MLT, the cuff is inflated until no air leak is heard around the airway during a positive pressure inspiration. Then a small volume of air is removed from the cuff until a small leak is heard at the end of inspiration when listening over the trachea.
Monitoring compliance:Compliance is a change in volume per
unit of pressure change. The respiratory system has a dynamic compliance and a static compliance. The measurement of lung and chest wall compliance is static compliance.lt is normally 70-160 ml/cm H20 Cs=Vt/(Pplateau - EEP)
Reduced Cs implies that ventilation is less effective and can result in decreased Pa02 and increased PaC02.
DYNAMIC COMPLIANCE (CDYN):
It is a measurement of both the recoil of the lungs and the chest wall plus the pressure caused by Raw.Cdyn=Vt/(PIP - EEP)
From these values of Cs and Cdyn, we can interpret a clinical situation. If Cdyn is constant or decreasing and Cs is decreasing, then most likely the lung compliance is decreasing. If Cdyn is decreasing and Cs is constant, the airway resistance is increasing.
Monitoring airway resistance:It is one more important parameter to
be monitored as it increases with increased secretions, mucosal edema, bronchospasm and aspiration. Normal Raw ranges from 0.6-2.4 cm H20/L/sec. With the placement of an ET tube, this can increase to 6cm H20/L/sec or more. Raw=PTA/flow (L/sec).
WEANING FROM VENTILATORMechanical ventilation is an effective form
of therapy for respiratory failure. The clinician taking care of the ventilated patient should be able to determine the optimal time and method of discontinuing ventilatory support. There are two ways of removing the patient form artificial ventilation.1) Discontinuation (abrupt withdrawal from
ventilator)2) Weaning (gradual withdrawal from ventilator)
Before weaning is considered, a series of conditions should be fulfilled:• Underlying disease process should have been improved.• Patient must be
haemodynamically stable In good clinical condition without sepsis and overt CNS depression Psychologically stable and mentally prepared for the weaning process.
• Patient must have optimal internal milieu i.e. Pa02>60 mm of Hg with FI02<0.4 and PEEP<5cm of H20.
Therapeutic Strategies for Weaning:Counter balance of intrinsic PEEP: The
use of PEEP or CPAP provides a means of counterbalancing and reducing the inspiratory
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 293 Vijaylakshmi Kamat & Gita Nath
threshold load imposed by intrinsic PEEP.
Therefore, patient’s inspiratory effort and energy demands of the respiratory muscles can be decreased. The optimal level of PEEP or CPAP is the value just below the level of intrinsic PEEP. The useful way of monitoring intrinsic PEEP and the response to PEEP and CPAP is measurement of end expiratory pressure (expiratory hold). This pressure should not rise after the application of PEEP or CPAP.
Ventilatory Techniques:There are generally two ventilatory
weaning techniques1) T-Piece weaning2) Partial support weaning
• IMV• SIMV• PS• SIMV+PS
Before either technique is applied, some ventilatory adjustments regarding the PaC02 level and the machine delivered tidal volume are important. The PaC02achieved with the ventilator should be in accordance with the PaC02 the patient is anticipated to maintain once breathing spontaneously again. In order to minimize changes in the breathing pattern that occur during transition from full machine support to either T- piece or partial support, the tidal volume delivered by the ventilator should be gradually reduced to the approximate level expected to be maintained spontaneously during the weaning trial.
T-PIECE WEANING:T-piece weaning can be accomplished
by alternating periods of full ventialtory support with increasing periods of independent breathing through the T-piece circuit. The T-piece trial is terminated if any of the following develops:• Increase in the respiratory rate by greater than
10 breaths/mt or to more than 40 breaths/mt• Increase or decrease in BP by 20mm of Hg• Increase or decrease in HR by 20 beats/mt• 02 desaturation to 90% or Pa02 less than
60mm of Hg• Increase in PaC02 by greater than 5mm of
Hg or a decrease in pH to less than 7.3• Development of cardiac dysrhythmias
• Signs of increased work of breathing signaling impending respiratory muscle fatigue
• Diaphoresis, complaints of dyspnoea and fatigue not relieved by reassurance.
Following each T-piece trial, the patient is rested on the ventilator. Patients are best weaned while sitting in bed or in the semi- recumbent position. Weaning trial should begin early in the morning and end by late evening so that the patient will rest at night. Initially 3 to 4 T- piece trials are performed daily. Gradually the rest periods are shortened and finally eliminated. Once the patient is able to breathe spontaneously for 24 hrs, weaning is considered complete and the patient is extubated. The tracheal gas insufflations technique using an intra-tracheal catheter reduces dead space ventilation and improves the efficiency of C02 elimination, thereby augmenting T-piece weaning by diminishing minute volume and ventilatory demands.
PARTIAL SUPPORT WEANING:IMV AND SIMV:
Ventilator delivered breaths are interspersed with spontaneous breaths so as to achieve an adequate PaC02 without the development of any sign of respiratory difficulty. The IMV rate is then reduced in a stepwise pattern as tolerated by the patient. The IMV rate is again increased if the patient develops signs of deterioration. The cause for weaning difficulty is searched for and treated before reduction in IMV rate is restored. IMV rate is reduced gradually. It is useful to allow the patient’s respiratory muscles to rest at night by increasing the IMV rate. When the IMV rate is reduced to zero and the patient can breathe spontaneously for 24 hrs, weaning is complete.
PRESSURE SUPPORT:Pressure support provides a preset level
of airway pressure throughout spontaneous inspiratory efforts. During weaning, the pressure support is gradually refused. If the patient develops tachypnoea, the support level is again increased. Etiology of deterioration is searched and reversed. Weaning is complete when the patient is able to breathe spontaneously at a PS level of 3-5 cm of H20 (to maintain the endotracheal tube and ventilator circuit
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 294 Vijaylakshmi Kamat & Gita Nath
resistance). Because the frequency and tidal volume are dependent on the patient, pressure support does not guarantee a specific level of back-up ventilation. To solve this problem, a combination of SIMV + PS is available on many ventilators.
SIMV+PS :Initially, the stepwise reduction of SIMV
rate allows the patient to gradually take an increasing number of spontaneous breaths. At the same time, each breath is supported, so that adequate ventilation is achieved. When this amount of ventilation has been stabilized, there is no need of back-up ventilation and the SIMV mode is turned off. Now the pressure support is gradually reduced as the patient becomes able to generate a greater amount of pressure and finally can take up the whole ventilatory task. This gradual reduction of the ventilator support is beneficial not only for the failing ventilatory pump but also for the failing cardiac pump. The positive intra-thoracic pressure decreases venous return at the same time as it assists the cardiac system by decreasing the left ventricular afterload. The stepwise reduction in ventilatory support withdraws this cardiac assistance, gradually allowing enough time for the compensatory mechanisms and the pharmacological interventions to prevent heart failure. Restoring full mechanical ventilatory support, by increasing the SIMV rate during the evening, ideally with normal periods of sleep, is considered important.
Irrespective of which method of mechanical ventilation is used, potential criteria of extubation would be the ability to breathe spontaneously without any form of assistance for a prescribed period of time (24 hrs). The patient can be made to breathe spontaneously through the simple T-piece or through the ventilator circuit, the latter offering the potential advantages of convenience, ease of application, access to ventilatory monitoring systems and alarms. However, spontaneous breathing through the ventilatory circuit may further add to the ventilatory load owing to factors such as circuit dead space, inspiratory & expiratory circuit resistance and demand valve operation.
During spontaneous breathing trials using
either system, it should be recognized that endotracheal tube resistance is significant and it often greatly exceeds that of the native upper airway. In fact, patients may do better without an ET Tube in place owing to an improved ability to cough and spontaneously clear secretions. Conversely, upper airway dysfunction post extubation may contribute to weaning failure in a patient who otherwise could breathe spontaneously without positive pressure assistance from the ventilator. Options other than reintubation exist for the patient who has a failed extubation, namely non-invasive ventilation.
Criteria predicting weaning out come:There is a lack of precise definition of
weaning outcome. Weaning success is defined as successful spontaneous ventilation for 24 hrs. Weaning failure however is not defined by clear cut endpoints. Strict objective criteria are used by some authors while many use subjective clinical criteria. Absence of standardized objective criteria of weaning failure has resulted in the evolution of a large number of weaning indices. No single index is highly predictive of weanability.
From a physiological point of view, these indices can be divided into:I. Those that assess simple ventilatory parameters• Vital capacity• Minute ventilation• Tidal volume
II. Those that assess oxygenation• PaOz• pao2• Pa02/FI02• P*VPA• P(A-a)02 on corresponding FI02 values
III. Those that assess respiratory muscle strength (Plmax) or(MIP)
IV. Those that assess central respiratory drive (P0.1)
V. Those that measure respiratory muscle reserve Such as Maximal voluntary ventilation
Minute ventilation and Mean transdiaphraqmatic pressure per breath
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 295 Vijaylakshmi Kamat & Gita Nath
Maximal transdiaphragmatic pressure |
VI. Those that record and analyze the pattern of spontaneous breathing in terms of respiratory rate (f), tidal volume (Vt),Total compartmental displacement (TCP)
Tidal volume(which is a measure of ribcage-abdominal wall , asynchrony) respiratory alternans or f/Vt (the measure of rapid shallow breathing)
VII. Those that alter the work of breathing
VIII. Composite indices such as CROP, P 0.1 X f/Vt or weaning index.
The indices may not accurately reflect patho-physiological determinants of weaning outcome because weaning success or failure is multi-factorial in origin and an index usually assesses only a single physiological function. Moreover, the indices do not assess the function of other organ systems important for successful weaning such as the cardiovascular system.
Physiological basis of weaning indicesI. THOSE THAT ASSESS SIMPLE VENTILATORY PARAMETERSa) VITAL CAPACITY: Preferably the vital capacity should be greater than 15-20 ml per Kg of ideal body weight. 20ml/kg or 3 x Vt (predicted) is needed for the patient to be able to cough or deep breathe on their own. If less than 13ml/kg or2xVt (predicted), weaning may be a problem.
b) MINUTE VENTILATION: Less than 10 Lits/mt is usually acceptable. If greater than 20 Lits/mt, the patient cannot support this spontaneously for longer periods.
c) TIDAL VOLUME: 6-10ml/kg body weight or greater than 300ml. In adults, if tidal volume is less than 300ml or greater than 700ml, there may be difficulty in weaning the patient.
II. THOSE THAT ASSESS OXYGENATIONa) Pa02>60mm of Hg on FI02<0.4b) Pa02/FI02>200mm of Hgc) P(A-a)02<350 mm of Hg with FI02=1.0
III. ASSESSING RESPIRATORY MUSCLE STRENGTH (PI MAX) OR (MIP)
If the patient is able to generate a MIP > -20 cm of H20 within 20 seconds, then the patient probably has a vital capacity > 15ml/kg. “Preferably greater than -30cm of H20” is necessary for weaning (normal MIP is greater than or equal to -80cm of H20 within 10 seconds)
IV. ASSESSING THE CENTRAL RESPIRATORY DRIVE (P 0.1)
It is difficult to measure drive at the bedside, and the conventional method is an indirect index which is difficult to interpret. This is P 0.1 which refers to the pressure generated after 100m sec of an occluded inspiration and has a threshold value of 6cm of H20.
V. THOSE THAT MEASURE RESPIRATORY MUSCLE RESERVEa) MW: MW should be at least greater than twice the minute ventilation. If the patient is able to double spontaneous minute ventilation on command, it is a good sign.b) Those indices which determine load vs. capacity balance.(i) PDi
PDI maxi.e., the ratio of mean Trans diaphragmatic pressure per breath to the maximal Trans diaphragmatic pressure.
If this is higher than 40%, it implies that ventilation cannot be sustained i.e. patient cannot be weaned.
(ii) T.T.I = PDI x TiPDI max Ttot
The T.T.I. relates inspiratory resistive loading and inspiratory time as a fraction of the total respiratory cycle. During resting ventilation, T.T.I. is about 0.05. When it exceeds 0.15 through an increase either in the duration of inspiration or the inspiratory pressure, ventilation cannot be sustained. The inspiratory effort co-efficient relates load, capacity and fatigue in patients in the ICU.
I. E co-efficient = KxVt/CdvnPI maxXTi/Ttot
I EC is low in patients who wean from
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 296 Vijaylakshmi Kamat & Gita Nath
mechanical ventilation. When the co-efficient exceeds 0.23, weaning is unlikely.
VI (I) RR preferably <25/mt (normal 12-18/mt)(II) f/Vt<105. The f/Vt is recommended as
the best single index available.A combination of P 01 x fA/t less than or equal to 450 is a predicator of weaning success
VII. NORMAL WORK OF BREATHING should not exceed 15% of total
VIII. COMPOSITE INDICESCROP is an index that indicates
compliance, rate, oxygenation and P max. A value greater than or equal to 13ml/breath/mt is considered a predictor of weaning success.
NONINVASIVE VENTILATION IN ACUTE RESPIRATORY FAILURE INTRODUCTION
Interest in noninvasive ventilation originated from concern for patients with hypoventilatory syndromes. Recently, however, randomized controlled trials established noninvasive ventilation as an alternative to endotracheal intubation in patients with acute respiratoryfailure.
During acute respiratoryfailure, the main objectives are to avoid complications of endotracheal intubation and to deliver ventilatory support to patients for whom endotracheal intubation is not desirable. Although mechanical ventilation is a lifesaving procedure, its use is complicated by serious morbidity and mortality. For instance, endotracheal intubation can precipitate cardiac arrest, cause aspiration of foreign materials into the lungs, laryngeal or tracheal injury, and it can result in long-term adverse sequelae.
Tracheal tubes are implicated in the genesis of nosocomial pneumonia, which is frequently accompanied by bacterial colonization of the pharynx and the upper gastrointestinal tract that results in repeated micro aspiration of contaminated secretions around the tracheal tube. Nosocomial pneumonia is responsible for prolonged hospital stays and it significantly increases mortality. Tracheal tubes also are
associated with a high incidence of nosocomial sinusitis because of abnormal (or no) sinus drainage, especially when the tube resides in the nose. Indirectly, the need for heavy sedation and some of the difficulties in weaning from ventilatory support may be related to the presence of an endotracheal tube.
In other cases, withholding endotracheal intubation and mechanical ventilation may be justified by poor short-term prognosis due to the physiology or severity of the underlying disease. In addition, some patients with late-stage disease refuse to be intubated. The decision not to intubate a patient is formed by the patient and/or family and the primary physician. For such patients, noninvasive ventilation may allow adequate support for respiratory distress with a lower risk of complications. In the same way, because the decision whether or not to intubate may be difficult at an early phase of acute respiratoryfailure, noninvasive ventilation may be used to postpone endotracheal intubation.
TECHNIQUES AND THEIR PHYSIOLOGIC EFFECTSPerithoracic Ventilation
Several devices generating a perithoracic negative pressure have been proposed for neuromuscular disorders, including iron lung, cuirass, or poncho-wrap ventilators. Most of these devices use conventional respiratory frequency. Recently developed devices synchronize spontaneous respiratory effort and the negative pressure breath. In a tank ventilator (iron-lung), the whole body, except the head and the neck, is submitted to intermittent negative pressure, whereas with the two other techniques only the thorax and the abdomen (poncho) or the thorax alone (cuirass) is exposed to the changes in pressure. The cuirass ventilator also has been used to deliver negative pressure high-frequency oscillations. Lastly, inflatable vests have been used in chronic obstructive pulmonary disease (COPD) patients to deliver positive-pressure high- frequency oscillations.
Several studies suggested beneficial effects after 6 to 8 hour periods of negative pressure ventilation in COPD patients with mild or moderate decompensation. Most studies
RACE 2003 Ramachandra Anaesthesia Continuing Education

Mechanical Ventilation 297 Vijaylakshmi Kamat & Gita Nath
concerning negative pressure ventilation during acute respiratory failure describe only short-term effects, have no or questionable control groups, and suggest only a mild efficacy.
Reported side effects noted, mainly during chronic use of these techniques, include obstructive sleep apnoea and back pain. Negative pressure ventilator use is also limited by the scarcity of the equipment and because the apparatus may restrict routine intensive care unit (ICU) procedures.
Positive Pressure VentilationVENTILATORY MODESCONTINUOUS POSITIVE AIRWAY PRESSURE
Continuous positive airway pressure (CPAP) has been used for many years in patients with hypoxemic respiratory failure. Improvement in respiratory system compliance has led to a decrease in the work of breathing and to an increase in comfort. There also has been an improvement in oxygenation. Delivered via a facemask, this type of therapy may be poorly tolerated by some patients. CPAP has also been used in patient* with left ventricular failure to improve both haemodynamics and respiratory mechanics. In fact, acute hypercapnic cardiogenic pulmonary edema is the only situation in which a clear benefit of CPAP has been demonstrated in a randomized controlled trial. In a study by Bersten et al., CPAP significantly improved several cardiac and pulmonary physiologic parameters and reduced the number of patients requiring intubation.
Classically, CPAP and positive end- expiratory pressure (PEEP) were considered to be contraindicated for patients with COPD for fear of enhancing hyperinflation and thereby worsening abnormal pulmonary mechanics. The notion of dynamic hyperinflation, which might be responsible for the respiratory system’s positive elastic recoil at end-expiration in such patients, suggests that perhaps CPAP or PEEP might be beneficial. Appendini etal. demonstrated that the combination of CPAP and pressure support ventilation with a mask in COPD patients had greater efficacy than use of each one alone to reduce inspiratory muscle effort.
INTERMITTENT POSITIVE-PRESSURE VENTILATION
Volume-limited and pressure-limited modes have been used for noninvasive ventilation. Assist-control ventilation can be used with conventional settings for breathing frequency and inspiratory flow rate. If ventilation is volume- limited, any leakage around the mask will decrease the volume delivered to the patient. Therefore, some authors have recommended using larger tidal volumes than usually chosen for intubated patients.
Pressure support ventilation also has been used widely for noninvasive ventilation. This ventilatory mode usually decreases the inspiratory work of breathing, increases tidal volume, and reduces spontaneous breathing frequency. During noninvasive ventilation, the presence of leaks is roughly compensated by the ventilator because the inspiratory pressure is maintained constant; it may, however, cause problems in the cycling mechanism from inspiration to expiration based on the flow decay. Thus, some authors prefer to use pressure-control ventilation, in which the inspiratory time is preset, or they add conventional positive pressure volume-limited breaths using synchronized intermittent mandatory ventilation to pressure support. Using an adjustable flow threshold for cycling may also solve this problem. Thus, the problem of how to make the ventilator compensate for leaks around the mask requires sophisticated knowledge of ventilators and may limit use of noninvasive ventilation if sophisticated problem-solvers are not available.
PHYSIOLOGIC EFFECTSIn initial reports on noninvasive ventilation,
blood gas abnormalities were corrected partially and failures (i.e., patients who eventually required endotracheal intubation) were most often not related to ventilation failure by itself. In an open study, Meduri et al. described the treatment of hypercapnic respiratory distress in 18 patients using essentially pressure support ventilation. In 13 of 18 patients, intubation was avoided and the authors noted that an improvement in PaC02 and pH during the first 2 hours was a good predictor of technique success (absence of intubation).
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 298 Vijaylakshmi Kamat & Gita Nath
Physiologic studies of the effects of noninvasive pressure support or pressure-limited ventilation on breathing pattern and respiratory muscle activity have been reported in patients with chronic respiratory insufficiency Comparable results were obtained in severe, but stable COPD patients, and in patients admitted for acute exacerbation of their disease. Delivered noninvasively, pressure support assists each spontaneous breath and can reduce the transdiaphragmatic pressure, respiratory muscle pressure-time index, or the diaphragmatic electromyographic activity. This reduction in muscle effort is accompanied by alterations in the breathing pattern with increase in tidal volume, reduction in breathing frequency, and, frequently, an increase in minute ventilation. Oxygenation parameters are improved with a concomitant increase in alveolar ventilation.
MECHANISMS OF ACTIONThe first mechanism of action is simply
to oxygenate the patient. In patients with COPD, however, oxygen may worsen hypercapnia and respiratory acidosis, which may constitute a major limitation for oxygen therapy alone. By increasing alveolar ventilation, noninvasive ventilation may allow sufficient oxygenation without raising PaC02. Fernandez etal. reported that pressure support ventilation via a full face mask suppressed oxygen-induced hypercapnia in COPD patients. In patients successfully treated noninvasively, the rate at which PaC02 decreased was much slower than the increase in oxygenation.
As mentioned, noninvasive pressure support ventilation results in partial unloading of the respiratory muscles. The mechanism by which beneficial effects are observed, therefore, may be a combination of adequate oxygenation and partial unloading of the respiratory muscles, which allow the patient to put his or her muscles partially at rest while keeping alveolar ventilation initially constant.
INFLUENCE OF THE TECHNIQUE Ventilatory Mode
The effects of intermittent positive pressure breathing (IPPB) were markedly different from those of pressure support when delivered in
nonintubated subjects in a high ventilatory demand situation. Breathing with IPPB may induce extra work owing to the superimposed impedance to the respiratory circuit and the poor response of the ventilatory device. This problem emphasizes the importance of the ventilatory mode and the equipment used when treating patients with ventilatory failure or high ventilatory demand.
Pressure support ventilation and assist- control ventilation have been the two most frequently used ventilatory modes, with or without PEEP. Vitacca et al. compared the clinical efficacy of the two ventilation modes in a randomized study in 29 COPD patients. The efficacy of the technique was similar in the two groups with regard to the need for endotracheal intubation. Interestingly, treatment compliance was better and the side effects were fewer with pressure support ventilation. This observation may be explained by the higher peak mask pressure generated with assist-control ventilation and the lower level of comfort in the presence of high peak airway pressure.
Patient-Ventilator InterfaceIn patients with chronic respiratory
failure, noninvasive ventilation usually has been delivered through a nasal mask. Commercially available models can be used and high-quality masks of multiple sizes are now available. Customized silicone masks can be individually moulded to the patient’s nose. Masks are secured to the head with straps.
In the acute care settings, many clinicians use full-face masks on their patients. Nasal masks, however, present many advantages compared with full-face masks, including better patient comfort, ease of use, and lower internal dead space. During nasal ventilation, however, inadvertent loss of volume through the mouth may cause serious problems. Patients can experience marked patient-ventilator asynchrony during air leakage through the mouth. Because gas insufflated through the nose may escape through the mouth, mouth closure is mandatory. Many patients with acute respiratory failure do not choose to breathe solely via the nose and are often not cooperative enough to do so on request. Disadvantages of the full face mask are the high
RACE 2003 Ramachandra Anaesthesia Continuing Education
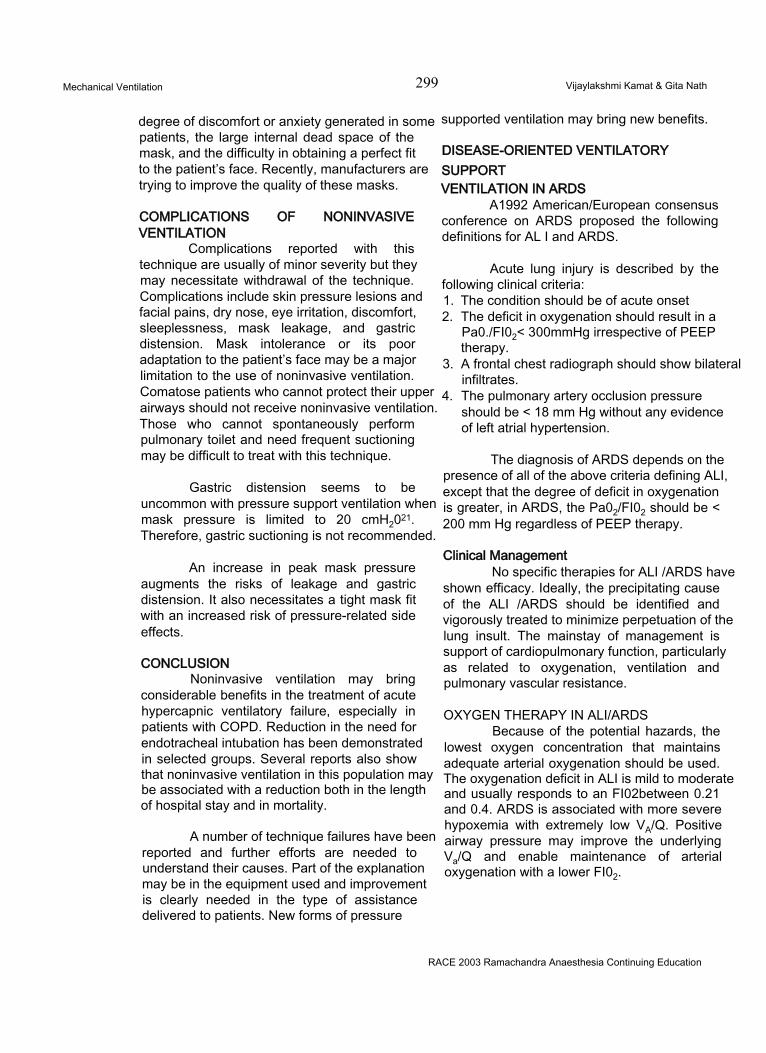
Mechanical Ventilation 299 Vijaylakshmi Kamat & Gita Nath
degree of discomfort or anxiety generated in some patients, the large internal dead space of the mask, and the difficulty in obtaining a perfect fit to the patient’s face. Recently, manufacturers are trying to improve the quality of these masks.
COMPLICATIONS OF NONINVASIVE VENTILATION
Complications reported with this technique are usually of minor severity but they may necessitate withdrawal of the technique. Complications include skin pressure lesions and facial pains, dry nose, eye irritation, discomfort, sleeplessness, mask leakage, and gastric distension. Mask intolerance or its poor adaptation to the patient’s face may be a major limitation to the use of noninvasive ventilation. Comatose patients who cannot protect their upper airways should not receive noninvasive ventilation. Those who cannot spontaneously perform pulmonary toilet and need frequent suctioning may be difficult to treat with this technique.
Gastric distension seems to be uncommon with pressure support ventilation when mask pressure is limited to 20 cmH2021. Therefore, gastric suctioning is not recommended.
An increase in peak mask pressure augments the risks of leakage and gastric distension. It also necessitates a tight mask fit with an increased risk of pressure-related side effects.
CONCLUSIONNoninvasive ventilation may bring
considerable benefits in the treatment of acute hypercapnic ventilatory failure, especially in patients with COPD. Reduction in the need for endotracheal intubation has been demonstrated in selected groups. Several reports also show that noninvasive ventilation in this population may be associated with a reduction both in the length of hospital stay and in mortality.
A number of technique failures have been reported and further efforts are needed to understand their causes. Part of the explanation may be in the equipment used and improvement is clearly needed in the type of assistance delivered to patients. New forms of pressure
supported ventilation may bring new benefits.
DISEASE-ORIENTED VENTILATORY SUPPORTVENTILATION IN ARDS
A1992 American/European consensus conference on ARDS proposed the following definitions for AL I and ARDS.
Acute lung injury is described by the following clinical criteria:1. The condition should be of acute onset2. The deficit in oxygenation should result in a
Pa0./FI02< 300mmHg irrespective of PEEP therapy.
3. A frontal chest radiograph should show bilateral infiltrates.
4. The pulmonary artery occlusion pressure should be < 18 mm Hg without any evidence of left atrial hypertension.
The diagnosis of ARDS depends on the presence of all of the above criteria defining ALI, except that the degree of deficit in oxygenation is greater, in ARDS, the Pa02/FI02 should be < 200 mm Hg regardless of PEEP therapy.
Clinical ManagementNo specific therapies for ALI /ARDS have
shown efficacy. Ideally, the precipitating cause of the ALI /ARDS should be identified and vigorously treated to minimize perpetuation of the lung insult. The mainstay of management is support of cardiopulmonary function, particularly as related to oxygenation, ventilation and pulmonary vascular resistance.
OXYGEN THERAPY IN ALI/ARDSBecause of the potential hazards, the
lowest oxygen concentration that maintains adequate arterial oxygenation should be used. The oxygenation deficit in ALI is mild to moderate and usually responds to an FI02between 0.21 and 0.4. ARDS is associated with more severe hypoxemia with extremely low VA/Q. Positive airway pressure may improve the underlying Va/Q and enable maintenance of arterial oxygenation with a lower FI02.
RACE 2003 Ramachandra Anaesthesia Continuing Education
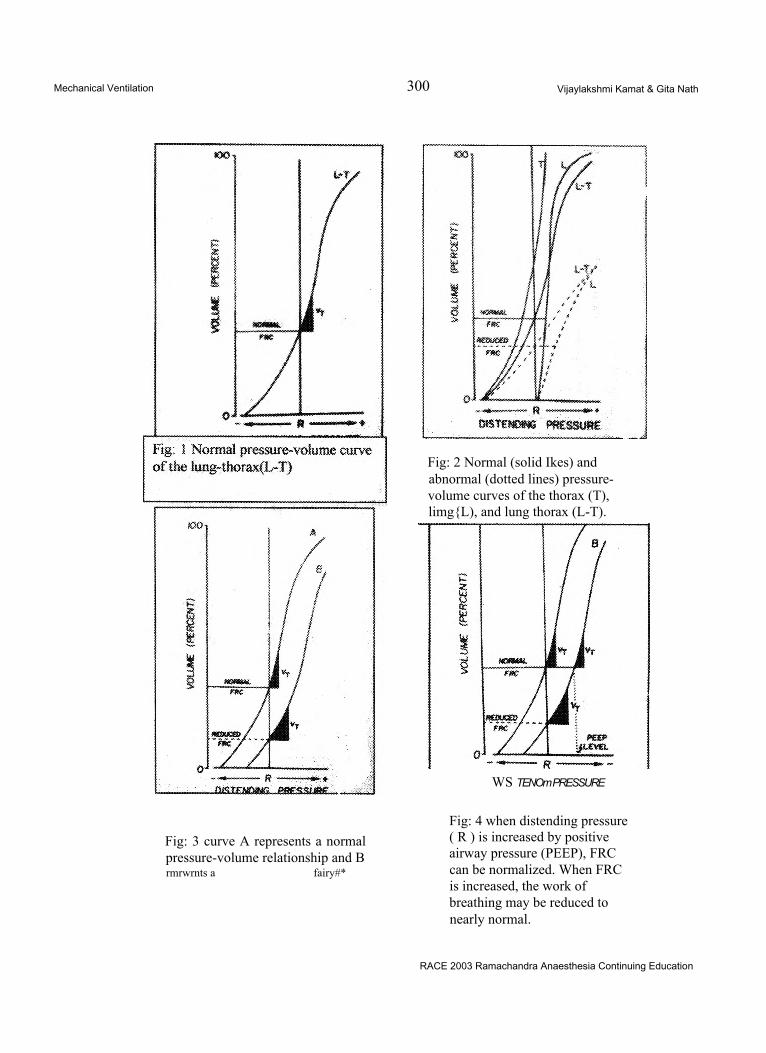
Mechanical Ventilation 300 Vijaylakshmi Kamat & Gita Nath
Fig: 2 Normal (solid Ikes) and abnormal (dotted lines) pressure- volume curves of the thorax (T), limg{L), and lung thorax (L-T).
WS TENOm PRESSURE
Fig: 3 curve A represents a normal pressure-volume relationship and Brmrwrnts a fairy#*
Fig: 4 when distending pressure ( R ) is increased by positive airway pressure (PEEP), FRC can be normalized. When FRC is increased, the work of breathing may be reduced to nearly normal.
RACE 2003 Ramachandra Anaesthesia Continuing Education
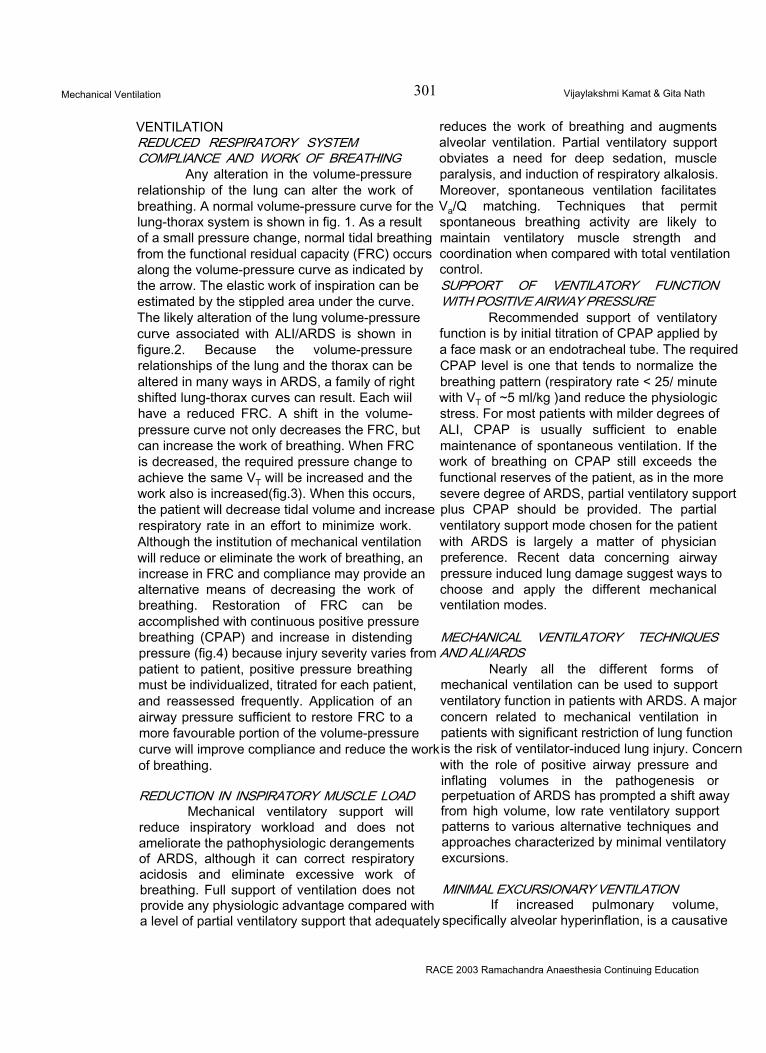
Mechanical Ventilation 301 Vijaylakshmi Kamat & Gita Nath
VENTILATIONREDUCED RESPIRATORY SYSTEM COMPLIANCE AND WORK OF BREATHING
Any alteration in the volume-pressure relationship of the lung can alter the work of breathing. A normal volume-pressure curve for the lung-thorax system is shown in fig. 1. As a result of a small pressure change, normal tidal breathing from the functional residual capacity (FRC) occurs along the volume-pressure curve as indicated by the arrow. The elastic work of inspiration can be estimated by the stippled area under the curve. The likely alteration of the lung volume-pressure curve associated with ALI/ARDS is shown in figure.2. Because the volume-pressure relationships of the lung and the thorax can be altered in many ways in ARDS, a family of right shifted lung-thorax curves can result. Each wiil have a reduced FRC. A shift in the volume- pressure curve not only decreases the FRC, but can increase the work of breathing. When FRC is decreased, the required pressure change to achieve the same VT will be increased and the work also is increased(fig.3). When this occurs, the patient will decrease tidal volume and increase respiratory rate in an effort to minimize work. Although the institution of mechanical ventilation will reduce or eliminate the work of breathing, an increase in FRC and compliance may provide an alternative means of decreasing the work of breathing. Restoration of FRC can be accomplished with continuous positive pressure breathing (CPAP) and increase in distending pressure (fig.4) because injury severity varies from patient to patient, positive pressure breathing must be individualized, titrated for each patient, and reassessed frequently. Application of an airway pressure sufficient to restore FRC to a more favourable portion of the volume-pressure curve will improve compliance and reduce the work of breathing.
REDUCTION IN INSPIRATORY MUSCLE LOAD Mechanical ventilatory support will
reduce inspiratory workload and does not ameliorate the pathophysiologic derangements of ARDS, although it can correct respiratory acidosis and eliminate excessive work of breathing. Full support of ventilation does not provide any physiologic advantage compared with a level of partial ventilatory support that adequately
reduces the work of breathing and augments alveolar ventilation. Partial ventilatory support obviates a need for deep sedation, muscle paralysis, and induction of respiratory alkalosis. Moreover, spontaneous ventilation facilitates Va/Q matching. Techniques that permit spontaneous breathing activity are likely to maintain ventilatory muscle strength and coordination when compared with total ventilation control.SUPPORT OF VENTILATORY FUNCTION WITH POSITIVE AIRWAY PRESSURE
Recommended support of ventilatory function is by initial titration of CPAP applied by a face mask or an endotracheal tube. The required CPAP level is one that tends to normalize the breathing pattern (respiratory rate < 25/ minute with VT of ~5 ml/kg )and reduce the physiologic stress. For most patients with milder degrees of ALI, CPAP is usually sufficient to enable maintenance of spontaneous ventilation. If the work of breathing on CPAP still exceeds the functional reserves of the patient, as in the more severe degree of ARDS, partial ventilatory support plus CPAP should be provided. The partial ventilatory support mode chosen for the patient with ARDS is largely a matter of physician preference. Recent data concerning airway pressure induced lung damage suggest ways to choose and apply the different mechanical ventilation modes.
MECHANICAL VENTILATORY TECHNIQUES AND ALI/ARDS
Nearly all the different forms of mechanical ventilation can be used to support ventilatory function in patients with ARDS. A major concern related to mechanical ventilation in patients with significant restriction of lung function is the risk of ventilator-induced lung injury. Concern with the role of positive airway pressure and inflating volumes in the pathogenesis or perpetuation of ARDS has prompted a shift away from high volume, low rate ventilatory support patterns to various alternative techniques and approaches characterized by minimal ventilatory excursions.
MINIMAL EXCURSIONARY VENTILATIONIf increased pulmonary volume,
specifically alveolar hyperinflation, is a causative
RACE 2003 Ramachandra Anaesthesia Continuing Education
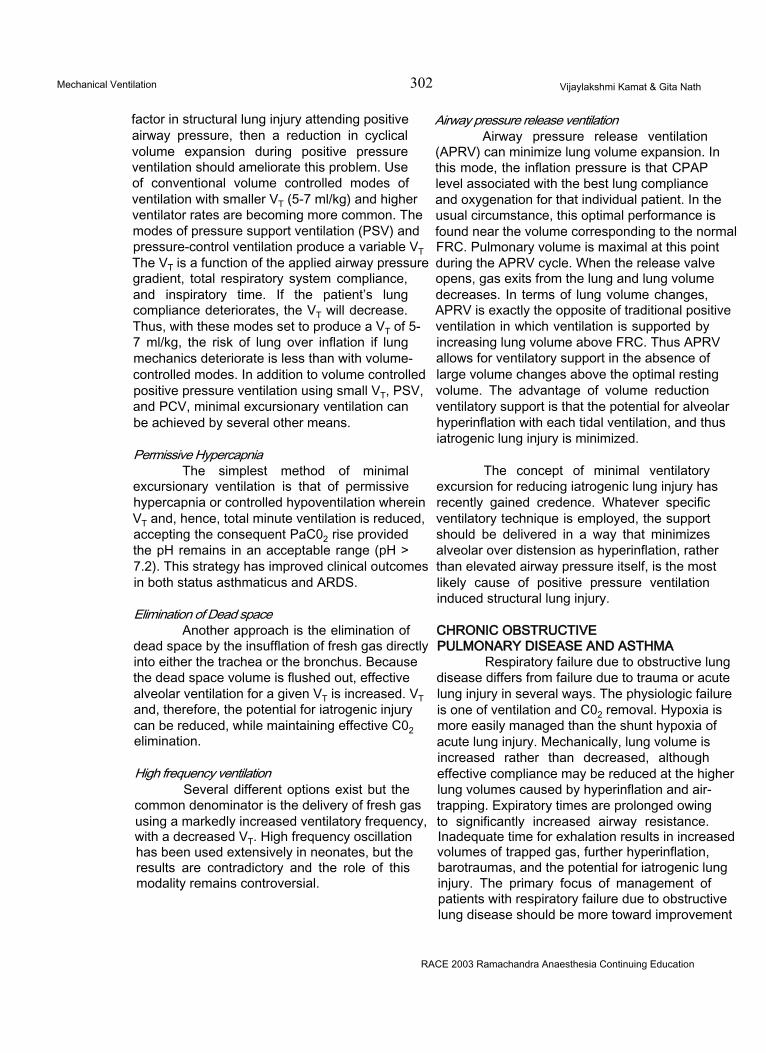
Mechanical Ventilation 302 Vijaylakshmi Kamat & Gita Nath
factor in structural lung injury attending positive airway pressure, then a reduction in cyclical volume expansion during positive pressure ventilation should ameliorate this problem. Use of conventional volume controlled modes of ventilation with smaller VT (5-7 ml/kg) and higher ventilator rates are becoming more common. The modes of pressure support ventilation (PSV) and pressure-control ventilation produce a variable VT The VT is a function of the applied airway pressure gradient, total respiratory system compliance, and inspiratory time. If the patient’s lung compliance deteriorates, the VT will decrease. Thus, with these modes set to produce a VT of 5- 7 ml/kg, the risk of lung over inflation if lung mechanics deteriorate is less than with volume- controlled modes. In addition to volume controlled positive pressure ventilation using small VT, PSV, and PCV, minimal excursionary ventilation can be achieved by several other means.
Permissive HypercapniaThe simplest method of minimal
excursionary ventilation is that of permissive hypercapnia or controlled hypoventilation wherein VT and, hence, total minute ventilation is reduced, accepting the consequent PaC02 rise provided the pH remains in an acceptable range (pH > 7.2). This strategy has improved clinical outcomes in both status asthmaticus and ARDS.
Elimination of Dead spaceAnother approach is the elimination of
dead space by the insufflation of fresh gas directly into either the trachea or the bronchus. Because the dead space volume is flushed out, effective alveolar ventilation for a given VT is increased. VT and, therefore, the potential for iatrogenic injury can be reduced, while maintaining effective C02 elimination.
High frequency ventilationSeveral different options exist but the
common denominator is the delivery of fresh gas using a markedly increased ventilatory frequency, with a decreased VT. High frequency oscillation has been used extensively in neonates, but the results are contradictory and the role of this modality remains controversial.
Airway pressure release ventilationAirway pressure release ventilation
(APRV) can minimize lung volume expansion. In this mode, the inflation pressure is that CPAP level associated with the best lung compliance and oxygenation for that individual patient. In the usual circumstance, this optimal performance is found near the volume corresponding to the normal FRC. Pulmonary volume is maximal at this point during the APRV cycle. When the release valve opens, gas exits from the lung and lung volume decreases. In terms of lung volume changes, APRV is exactly the opposite of traditional positive ventilation in which ventilation is supported by increasing lung volume above FRC. Thus APRV allows for ventilatory support in the absence of large volume changes above the optimal resting volume. The advantage of volume reduction ventilatory support is that the potential for alveolar hyperinflation with each tidal ventilation, and thus iatrogenic lung injury is minimized.
The concept of minimal ventilatory excursion for reducing iatrogenic lung injury has recently gained credence. Whatever specific ventilatory technique is employed, the support should be delivered in a way that minimizes alveolar over distension as hyperinflation, rather than elevated airway pressure itself, is the most likely cause of positive pressure ventilation induced structural lung injury.
CHRONIC OBSTRUCTIVE PULMONARY DISEASE AND ASTHMA
Respiratory failure due to obstructive lung disease differs from failure due to trauma or acute lung injury in several ways. The physiologic failure is one of ventilation and C02 removal. Hypoxia is more easily managed than the shunt hypoxia of acute lung injury. Mechanically, lung volume is increased rather than decreased, although effective compliance may be reduced at the higher lung volumes caused by hyperinflation and air- trapping. Expiratory times are prolonged owing to significantly increased airway resistance. Inadequate time for exhalation results in increased volumes of trapped gas, further hyperinflation, barotraumas, and the potential for iatrogenic lung injury. The primary focus of management of patients with respiratory failure due to obstructive lung disease should be more toward improvement
RACE 2003 Ramachandra Anaesthesia Continuing Education

Mechanical Ventilation 303 Vijaylakshmi Kamat & Gita Nath
of deranged mechanics than to defense of gas exchange.
ACUTE SEVERE ASTHMA Indications for Ventilation
Only about 5% of patients with acute severe asthma will require intubation and mechanical ventilation. The decision to ventilate a patient is a clinical one. It should be based on deteriorating status, impending or actual cardiac or respiratory arrest, decreasing level of consciousness, cyanosis, a silent chest, worsening paradox, or diaphoresis. Orthopneic patients often require intubation as do patients with a respiratory rate > 30 breaths/minute, a heart rate > 120 beats/minute, or a pulsus paradoxus >12 mmHg. Response in the first 2 hours to the medical regimen outlined above may have predictive utility. The clinical trend is probably more important than the initial findings. Objective measurements of airflow may be helpful, but spirometric efforts may paradoxically worsen bronchospasm or precipitate respiratory arrest. This reaction can be blocked with intravenous atropine. Arterial blood gases should be checked initially; serial blood gases are usually not needed. An increasing PaC02 correlates with severe obstruction with FEV, < 25% predicted, but does not absolutely predict the need for intubation. Metabolic acidosis is seen in 28% of patients. This is most often due to lactic acidemia, due either to respiratory muscle activity or to beta- adrenergic agonists.
Management of VentilationIn the acute asthmatic state, airway
resistance is markedly increased and time constants for expiration are significantly prolonged. When a patient breathes at high respiratory rates and minute volumes, there may be insufficient time for complete exhalation before the next inspired breath. This leads to progressive hyperinflation. Dynamic functional residual capacity (FRC) will be established at a lung volume above the static FRC of the respiratory system, often on a flatter portion of the lung’s pressure-volume curve. The degree of dynamic hyperinflation is proportional to tidal volume, and inversely related to the ratio of expiratory time (Te) to the time constant for expiration. The recoil pressure associated with the increased FRC is auto-PEEP, which constitutes an added
mechanical load against which the patient must work to initiate inspiratory airflow. The reduction in effective compliance at these higher lung volumes adds a further elastic load to the patient’s work of breathing. Elevated alveolar pressure at end-inspiration poses a significant risk for barotrauma.
GOALThe goal of mechanical ventilation in
acute severe asthma is to provide a physiologically adequate minute volume, while minimizing the risk of dynamic hyperinflation, auto-PEEP and barotrauma. Mechanical considerations, especially the optimization of expiratory time, should take precedence over the normalization of blood gases. Ventilation to eucapnia often leads to dynamic hyperinflation and should not be regarded as an appropriate objective.
VENTILATOR SETTINGSMechanically ventilated asthmatics
should initially be placed in the controlled ventilation mode (CMV). Initial settings should provide a tidal volume of 8-10 ml/kg, a rate of 8- 14 breaths/minute, with an inspiratory flow rate of 80-100 L/minute. Minute volume should be kept <115 ml/kg/minute. These settings generally result in a moderate respiratory acidosis with a pH ~ 7.2, and they usually avoid an unacceptable degree of hyperinflation, defined as an end- inspiratory volume > 20 ml/kg. Further adjustments should be made to minute volume and Te based on arterial blood gases and examination of the patient. Prolongation of TE may be accomplished by reduction of frequency or tidal volume, or by increases in inspiratory flow rate or the inspiratory-to-expiratory (l/E) ratio. Closer examination of the relationships among volume, flow, and TE demonstrates that increase in the I/ E ratio or reductions in tidal volume are relatively inefficient in prolonging TE. Increases in inspiratory flow can be some what helpful at higher minute volumes, but the most efficient manoeuvre to prolong TE is to decrease the respiratory rate or minute volume (VE). Use of a square waveform will shorten inspiratory pressure but it does not affect alveolar pressure. Low compliance tubing permits a lower set tidal volume to produce a given delivered tidal volume. Increases in inspiratory flow rates will produce higher peak inflation
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 304 Vijaylakshmi Kamat & Gita Nath
pressures, but these are not reflected in significantly increased alveolar pressure or in increased risk of barotrauma.
Extrinsic PEEP is an option that should be used with caution. Applied PEEP at levels up to 85% of the auto-PEEP level may reduce the work of breathing, relieving airflow obstruction by strutting open narrowed airways, and by counteracting the inspiratory threshold load imposed by auto-PEEP. If too much external PEEP is applied, however, alveolar volume may increase, worsening hyperinflation. Auto-PEEP and applied PEEP are additive in terms of effects on cardiac preload.
DELIVERY OF BRONCHODILATORSIntensive bronchodilator therapy should
continue even after the asthmatic patient is placed on mechanical ventilation. The best site for delivering bronchodilators is above the Y- connection into the inspiratory limb. A longer inspiratory time gives better delivery but at the cost of decreased TE and increased dynamic hyperinflation. Deposition is improved by low tidal and minute volumes and by a longer inspiratory pause. Humidifiers in the ventilator circuit decrease deposition'and should be bypassed during bronchodilator delivery.
CONTROLLED HYPOVENTILATIONIn mechanical ventilation for asthma and
acute respiratory failure in chronic obstructive pulmonary disease (COPD), avoidance of ventilator-associated injury should take precedence over normalization of blood gases. The level of ventilatory support should be titrated to a tolerable level of respiratory acidosis. It has been demonstrated that hypercapnia is usually well tolerated up to a PaC02 of 90 mm Hg, particularly when evolution is slow. If the patient cannot be safely ventilated to normocapnia because of high minute volumes, auto-PEEP, dynamic hyperinflation, or excessive alveolar pressure, minute volume may be reduced, allowing the PaC02 to rise by 10 mmHg/hour to a maximum of 80-90 mm Hg. Pa02 should be kept > 50 mmHg. Heavy sedation and paralysis may be needed because of increased drive. Elevated intracranial pressure represents an absolute contraindication to controlled hypoventilation. Although papilledema due to
hypercapnia is relatively uncommon, funduscopic examinations should be followed.
Deliberate acidosis should be reversed slowly to avoid post-hypercapnic alkalosis. The common practice is to attempt to correct pH when pH falls below 7.15-7.20. The goal is partial, rather than complete correction of pH. When controlled hypoventilation leads to significant respiratory acidosis, choice for correction are sodium bicarbonate, TRIS (THAM, tromethamine), and carbicarb.
Adjunctive MeasuresSEDATION AND PARALYSIS
Sedation and muscular relaxation are recommended during the initial stages of mechanical ventilation, allowing the patient to sleep and to rest the respiratory muscles. Sedatives should not be used to correct dyssynchrony with the ventilator unless attempts at ventilator adjustment have failed to produce better patient-ventilator interaction. Sedatives should be titrated to drowsiness and response to voice or light touch.
Neuromuscular blocking agents should be employed for paralysis only when necessary and then as briefly as possible. Indications for paralysis include asynchrony with the ventilator or excessively high inflation pressures. Neuromuscular blockers should never be administered until adequate sedation has been obtained. The paralysis level should be monitored with a nerve stimulator set to train-of-four. Abolition of three of four twitches is considered an appropriate level of paralysis.
MonitoringThe safe ventilatory management of the
acute asthmatic calls for the balancing of gas exchange considerations against the risk of hyperinflation and barotrauma. The important determinants of dynamic hyperinflation, tidal volume, and expiratory time should be optimized and followed carefully. Changes in frequency, tidal volume, wave from, and inspiratory flow rates will be reflected in changes in measured < <rway pressures. Barotrauma, however, has been snown to correlate most closely with trapped gas volume, and with alveolar, rather than airway
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 305 Vijaylakshmi Kamat & Gita Nath
pressure.
Although high peak pressures are commonly encountered in ventilated asthmatics, most of the measured pressure is related to airway resistance rather than to elevated alveolar pressure. PIP correlates poorly with barotrauma in obstructive pulmonary diseases and no reliable threshold value can be identified. Likewise, the presence or level of auto-PEEP has not been shown to predict the development of barotrauma. Plateau pressure (Pplat) measures airway pressure at the end of inspiration and better reflects alveolar pressure. Peak pressure falls to a plateau exponentially and this process may be prolonged in the presence of airflow obstruction. When measuring Pplat, sufficient time should be allowed to permit a true plateau to be reached. Airway pressure traces on ventilators equipped with graphics mode can be especially helpful for judging plateau adequacy. Pplat somewhat overestimates alveolar pressure. It is advisable to keep Pplat < 35 cmH20 to maintain alveolar pressure > 30 cmH20. Pplat, like PIP, may not correlate well with the incidence of barotrauma. Pplat may also vary in reliability because of variations in lung compliance. End-inspiratory lung volume (VEI) has been shown to correlate well with complications of mechanical ventilation. VEI is determined by measuring the amount of air exhaled during a 60-second apnoea added to the delivered tidal volume. VEI should be kept > 20 ml/kg. This is best accomplished by prolonging Te as much as possible, which is most efficiently achieved by reducing minute ventilation, especially at low breathing frequencies 22 (Fig.20.2).
Both VEI and auto-PEEP may underestimate the actual degree of hyperinflation and air trapping if airway closure prevents the free communication of alveoli with the airway opening. Measurement of lung volumes by impedance pneumography or examination of pressure-volume traces may provide alternative evidence of the presence of hyperinflation, the pressure-volume trace will show an end- inspiratory flattening manifesting as a “beak” in the curve.
WeaningAsthma patients should be supported on
mechanical ventilation until the bronchospastic
process begins to remit. Characteristically, improvement is slow for most of the course, followed by a precipitous improvement in airflow and dyspnea, and a reduction in audible wheezing. As bronchospasm remits, the patient may be switched from CMV to partial support ventilatory modes, such as assist-control (A/CMV), intermittent mandatory ventilation (IMV), synchronized intermittent mandatory ventilation (SIMV), or pressure support ventilation (PSV). IMV and PSV are preferable to A/CMV because of a lower risk for hyperinflation, auto-PEEP, and barotrauma.
With further improvement, patients may be evaluated for weaning, the progressive withdrawal of ventilatory support. Forty percent can be extubated after 24 hours, 70% by 48 hours, and 85% by 5 days. The remainder may take up to 3 weeks to resolve to the point at which extubation is possible. Although clinical judgment usually suffices, a combination of objective measures has been approximately 75% accurate in predicting weanability, including maximal inspiratory pressure < - 25 cmH20, breathing frequency < 35 breaths/minute, vital capacity > 10 ml/kg body weight, and arterial oxygen saturation > 90% on an FI 02 of < 40%2324
Once asthmatics “break,” they can usually be quickly weaned. Because of this, the method used, whether T-piece, IMV, pressure support, or a combination thereof, is relatively unimportant. The respiratory muscles should be reloaded as rapidly as the patient tolerates.
ComplicationsThe major complications associated with
mechanical ventilation for acute severe asthma relate to the mechanical consequences of airflow obstruction and are manifested as auto-PEEP and other forms of barotrauma. Acute myopathy associated with corticosteroids and neuromuscular blocking agents is a newly recognized complication of the management of asthmatic respiratory failure.
AUTO-PEEPBecause bronchospasm increases
airway resistance several times above normal, time constants for exhalation are significantly prolonged in acute severe asthma. If the asthma
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 306 Vijaylakshmi Kamat & Gita Nath
patient is breathing spontaneously at high rates or is ventilated at high rates, insufficient time is available for the lung to empty before the next mechanical breath is delivered. This leads to an end-expiratory volume above the mechanical functional residual capacity (FRC) of the respiratory system and is termed dynamic hyperinflation. The elastic recoil pressure associated with the elevated volume at end- expiration is manifested as auto-PEEP (intrinsic PEEP, PEEPi, occult PEEP). Virtually 100% of patients ventilated for acute severe asthma for exacerbations of chronic obstructive lung disease have measurable levels of auto-PEEP that may be as high as 15-20 cmH20.
Auto-PEEP is associated with dynamic hyperinflation and an increased risk of barotrauma. Auto-PEEP acts in the same way as externally applied PEEP to increase intrathoracic pressure and interferes with venous return to the heart. The consequence is hypotension and a fall in cardiac output. Hypotension due to auto-PEEP may develop within 1 -2 minutes of assumption of a rapid breathing pattern and may be reversed as quickly by stopping or slowing the ventilator. Auto- PEEP markedly increases the work of breathing by placing the lung higher on its pressure-volume curve in a region of lower compliance, and by posing an inspiratory threshold load on the respiratory muscles. Airflow cannot be triggered by the patient until a negative pressure equal to set trigger sensitivity plus auto-PEEP is generated. This accounts for the observation of patients expending considerable muscular effort without triggering the ventilator, and may contribute significantly to prolonged ventilator dependence.
Auto-PEEP can be measured by (a) imposing an end-expiratory hold on the ventilator and measuring airway pressure at end-expiration, (b) the change in oesophageal pressure necessary to produce inspiratory airflow, (c) comparing Pplat before and after a prolonged apnoea, {d) by determining the level of applied PEEP that begins to produce an increase in lung volume. Auto-PEEP can be detected by examination of flow-volume curves on graphics- capable ventilators. Expiratory flow fails to return to zero before the next inspiration begins. Newer
generations of microprocessor-driven ventilators are beginning to offer measurements of auto- PEEP as part of their monitoring option packages.
COPDMany of the management principles
discussed above for acute severe asthma are applicable to the care of patients with acute on chronic respiratoryfailure (ACRF) associated with chronic obstructive pulmonary disease. The two conditions differ largely in the time course and the degree of clearing that may be expected as a result of treatment.
Medical ManagementAs in the acute asthmatic episode,
aggressive inhaled bronchodilator therapy combined with corticosteroids is used to forestall the need for intubation and mechanical ventilation. The COPD patient, however, may present additional challenges in clinical judgement. The basic principles of management are to correct life-threatening hypoxemia, correct life- threatening acidosis, treat underlying precipitants, and treat and prevent complications.
OXYGENTo correct life-threatening hypoxemia in
ACRF, only small increases in FI02 are generally necessary. If FI02 requirements are > 40%, superimposed disease such as congestive heart failure or pneumonia should be suspected. The chest roentgenogram should be used to determine if another process is present that may call for higher doses of 02. In response to oxygen administration, most COPD patients will increase their PaC02 by 10-15 mm Hg but then stabilize. The elevation of PaC02 may result from hypoventilation due to blunted hypercapnic and hypoxic drives, increased C02 production, and an increased dead space. Correction of hypoxemia may further exacerbate hypercapnia via the Haldane effect, which shits the carbon dioxide dissociation curve to the right in the presence of increased oxygen. Patients presenting with a pH<7.35 and a Pa02<50 mmHg are at highest risk for C02 retention. Establishing a Pa02 of 55-65 mmHg should avoid excessive hypercapnia in most instances. Initial FI02 levels should range between 24% and 30% by mask or
RACE 2003 Ramachandra Anaesthesia Continuing Education

Mechanical Ventilation 307 Vijaylakshmi Kamat & Gita Nath
3-5 L/minute by nasal cannula and patients should be observed closely for progressive C02 retention. Because masks are sometimes uncomfortable and poorly tolerated by patients, nasal cannulas should be provided at mealtimes.
Indications for VentilationIntubation and ventilation for ACRF is
indicated for failure of response to medical management and for PaC02>50 mmHg with evidence of obtundation. Before committing to a course of intubation and ventilation, issues such as the patient’s quality of life, prognosis, wishes, and values should be explored as thoroughly as time permits. When doubt exists, however, intubation should proceed. If the intervention is subsequently inappropriate or against the patient’s wishes, ventilatory support may be withdrawn. Noninvasive ventilation offers an alternative approach to the support of the ACRF patient.
Management of VentilationBASIC CONSIDERATIONS
The prolonged time constants associated with ACRF call for the same balance of dynamic hyperinflation wit.i gas exchange as with the acute asthmatic. Hyperinflation poses more of a problem in liberation from ventilation than it does in safely ventilating the ACRF patient, and weaning may be a much more prolonged process than for the acute asthmatic. Unlike asthma, high PIP levels are unusual. If PIP is high or C02 removal is difficult, coexisting problems (e.g., pneumothorax, pulmonary oedema, or mucus plugging) need to be considered.
ALTERNATIVE TECHNIQUES NONINVASIVE VENTILATION
Tracheobronchial toilet is more efficient through an intact glottis than through an endotracheal tube. Complications increase with the duration of mechanical ventilation and weaning is often a difficult proposition in ACRF. For these reasons, alternative approaches to intubation should be considered whenever possible. Accumulating experience indicates that most ACRF patients, 56%-92%, can be successfully supported through an acute episode by noninvasive ventilation. Where successful, noninvasive ventilation is associated with shorter
intensive care unit (ICU) stays and fewer complications. Mask ventilation requires close cooperation between the patient and the respiratory therapist, especially in the first 30-60 minutes. Failure is more likely in anxious, uncooperative, pursed lip breathing patients. Mask ventilation should be avoided in patients with high aspiration risk, impaired swallowing, haemodynamic instability, severe hypoxia, or acute abdominal problems. Nasogastric tubes, which increase the risk of gastric distention, should be avoided. Aspiration of gastric contents is a rare complication. Full face masks should be carefully fitted for each patient and they give better results than nasal masks. Duoderm patches and benzoin improve the seal of the mask and minimize skin necrosis, while allowing small air leaks. Patients selected for noninvasive ventilation should be placed in a semi-Fowler position with a 45% tilt. Ventilation can be delivered with a bi-level positive airway pressure (BiPAP) device with inspiratory positive airway pressure (IPAP) set to 15 cmH20 and expiratory positive airway pressure (EPAP) to 8-10 cmH20. Volume-cycled ventilators may also be used with initial settings of pressure support 10-20 cmH20 (usually 12-15), with CPAP 3-5 cmH20, and F102 0.4-1.0 as needed. Pressure support should be titrated to produce a tidal volume > 7 ml/kg and a breathing frequency <25/minute with Sa02> 90%. Small air leaks can be tolerated and are of concern only when tidal volume is compromised. Leaks can be minimized by reducing CPAP or pressure support levels. If leaks are severe, flow triggering should be used, adjusting base flow to maintain desired PEEP levels. Alternatively, pressure control or volume control modes (IMV, A/CMV) can be tried. The success or failure of mask ventilation is usually readily apparent within 2 hours of initiation. Successfully treated patients will show a significant decrease in PaC02 and increase in pH. Patients may be allowed 15 minutes holiday for comfort and for eating. Weaning is accomplished by gradually withdrawing the level of support.
TRACHEAL GAS INSUFFLATIONTracheal gas insufflation (TGI) has been
described as an adjunct to C02 clearance in the setting of hypercapnia. Oxygen is delivered by continuous flow at 10 L/minute through a 2.2 mm outer diameter catheter threaded through the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 308 Vijaylakshmi Kamat & Gita Nath
endotracheal tube to 1 cm above the carina. Ventilator tidal volume is titrated against catheter flow to produce a constant total volume. TGI produces-; on an average, a 15% reduction in PaC02 with best results when the PaC02 is high. TGI causes slight increases in PIP, but no increase in mean airway pressure.
WeaningWeaning patients with ACRF from
mechanical ventilation is a more prolonged and difficult proposition than weaning the acute asthmatic. Patients with COPD are often malnourished and weaker compared to asthmatics, coexisting pathology is often present, and their underlying disease is less completely reversible. These individuals are iess able to deal with any residual hyperinflation that may put their diaphragms at a mechanical disadvantage. Particular attention needs to be paid to nutritional repletion and to minimizing hyperinflation. The principles of determining readiness for weaning are the same as for the acute asthmatic but the weaning progress may be slow. Few data exist to suggest the best available weaning modality for ACRF patients, but it would be expedient to avoid any method likely to produce high respiratory rates predisposing to dynamic hyperinflation and further prolonging the weaning process. One study suggested that a combination of IMV and pressure support is better than IMV alone in weaning patients with ACRF
ComplicationsProblems of varying severity are
commonly encountered such as right mainstem intubation, and alveolar hypoventilation. Several other concerns are particularly germane to ventilation in obstructive diseases.
Auto-PEEP is a major risk in ACRF of COPD. Because lung compliance tends to be high, most airway pressure is transmitted to the pleural space, causing more interference with venous return and hypotension. A sudden onset of hypotension in a ventilated patient with obstructive lung disease is often due to auto- PEEP, but it may also raise the question of tension pneumothorax. Auto-PEEP can be quickly identified as the cause of the problem by giving 100% 02 and disconnecting the ventilator
for 30-45 seconds or reducing the rate to 2-3 breaths/minute for a similar time. Blood pressure will rapidly return to baseline if hyperinflation is relieved. Problems with auto-PEEP are typically associated with high minute volumes, high tidal volumes, and high respiratory rates. All of these conditions should be avoided where possible.
Tube trauma, nosocomial pneumonias, upper gastrointestinal bleeding, venous thromboembolism, right-sided heart failure and ventricular and supraventricular tachyarrhythmias are major complications associated with mechanical ventilation for COPD.
AN APPROACH TO ARTERIAL BLOOD GASANALYSIS
Arterial blood gas (ABG) analysis gives us valuable information about ventilation, oxygenation and acid-base status of the patient. This coupled with Venous Blood Gases (VBG) and haemodynamic data gives oxygen transport of the patient.
VENTILATIONTidai Volume (VT) is the amount of air
that goes in and out of the respiratory passages during each respiratory cycle.
VT x Respiratory Rate (RR) = Minute Ventilation
The air we breathe goes through the trachea and the bronchial tree to the alveoli. The bronchial tree up to the 18th division acts as a conducting zone, i.e., down to but not including the respiratory bronchioles. This is called the Anatomical Dead Space (VD) because it does not take part in gas exchange. The air that enters beyond the 18th division of the bronchial tree participates in gas exchange across the capillary membrane. This is called the Alveolar Dead Space (VA)
VT - VD + VA
in healthy lungs, physiological dead space is equal to anatomical dead space.
Normal Values (ABG) pH 7.36 to 7.44
RACE 2003 Ramachandra Anaesthesia Continuing Education

Mechanical Ventilation 309 Vijaylakshmi Kamat & Gita Nath
pC02 36 to 44 mm Hg HC03 22 to 26 mEq/L
Calculating Alveolar Partial Pressure of Oxygen (PA02):
P aPDP O = FIO (P - P ) - Z
A 2 2 ' B H20' R
_ Respiratory _ C02 production _ q 8 Quotient o2 consumption
Normal barometric pressure is 760 mm of Hg at sea level. The air comprises of nitrogen and oxygen in the ratio of 79% and 21%. At atmospheric temperature, they do not react with each other. So, the partial pressure of 02 in air can be calculated as follows:
P02 = 0.21/100 x 760 = 159.6 mm of Hg.
As we breathe air in, it passes through the nose, nasopharynx and the airways and in the process, gets humidified. At the end of inspiration the pressure in the airways is equal to that of the atmosphere. But air in the airways has nitrogen, oxygen and water vapor. Water vapor pressure at body temperature is 47 mm of Hg. So pressure exerted by N2 and 02 is 713 mm of Hg. So, the partial pressure of 02 in the airways can be calculated by
P02in airways =0.21/100 x 713 = 159.6 mm of Hg.
By the time air moves into the alveoli, C02 is added. At the end of inspiration the pressure in the alveoli is 760 mm of Hg. It is now comprised of C02, N2,02 and H20.
The partial Pressure in the alveoli (PA02) can be calculated by the modified alveolar gas equation (at sea level, breathing room air):
Pa02=FI02x (PBP-PH20) - PaC02/ .8 PA02=0.21x (760-47) - 40/ .8 PA02=100 mm of Hg
The difference between alveolar 02 and arterial 02 is known as the A-aOz gradient. Normal Aa02 gradient is 0-10. A-a02 indicates the severity
of hypoxia and also helps to know whether the cause of hypoxia is hypoventilation or not.
Example 1. A patient with morphine overdose comes with a PA02 of 40mmHg and a PAC02 of 80mmHg.The A-a02 gradient on room air can be calculated as:
PA02=FI02x(PBP-PH20)-PaC02/0.8 0.21 x (760-47) - 80/0.8 0.21 x (713)-100 150-100 = 50 mm of Hg Arterial 02 = 40 mm of Hg
A-a02 gradient is 10, which is within the normal range. In this patient hypoxia is due to hypoventilation.
Example 2. A patient with pneumonia comes with a Pa02 of 40mmHg, a PaC02 of 40mmHg on room air. A-a02 can be calculated as:
PA02=FI02x(PBP-PH20)-PaC02/0.8 0.21 x (760-47)-40/0.8 0.21 x 713-50 150-50= 100 Arterial 02 is = 40 mm of Hg A-a02 = 60 mm of Hg
The cause of hypoxia is other than hypoventilation.
Diffusion: Once air reaches the alveoli 02 moves into the pulmonary capillary and C02 moves into the alveoli by a simple process of diffusion. The factors that determine diffusion are the pressure gradient between the alveoli and the capillary, thickness of the membrane which includes alveolar membrane interstitium and capillary membrane, K - which is the diffusability of individual gases and surface area (300 million alveoli). Higher the pressure gradient, more gas will diffuse across a membrane. That is why a patient gets supplemental oxygen in hypoxia to improve the gradient. For an amount of ventilation, there is an amount of perfusion (Blood Flow). Ventilation in the upright lung can be divided into three zones - upper, middle and lower zones. Upper zone has more ventilation and lower zone has less ventilation. Likewise, the lower lung field has more perfusion and the upper part has less perfusion. Best V/Q matching occurs in the
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 310 Vijaylakshmi Kamat & Gita Nath
dependent part of the lung and the best ratio is0.8.
PULMONARY SHUNT: (QS/QT)If there is alveolar collapse or alveolar
oedema - there is no oxygen diffusing through that capillary blood. This is called pulmonary shunt or venous admixture. Normal pulmonary shunt is 0 - 5%. Pulmonary shunt refers to that amount of blood flow that goes through the lungs from the right side of the heart to the left side of the heart without getting oxygenated adequately.
HIGH ALTITUDE:At high altitude the barometric pressure
is low so that the partial pressure of oxygen in atmosphere is low. That is why people living in high altitudes have chronic hypoxia.
Pa02 = 104.2-(0.27 x age)
Hypoxia refers to reduced oxygen pressure in the alveolus. Hypoxemia refers to low arterial Pa02.CAUSES OF ACID BASE DISTURBANCE Metabolic acidosisA. NORMAL ANION GAP - METABOLIC ACIDOSIS
1. NORMAL OR HYPERKALEMIAa. Early renal failureb. Tubulointerstitial diseasec. Adrenal deficiencyd. Type IV renal tubular acidosise. Addition of acid (e.g., HCI, Arg HCI, TPN)
2. HYPOKALEMIAa. Diarrhoeab. Enterocutaneous fistulac. Pancreatic drainaged. Biliary drainagee. Ureteral diversionsf. Renal tubular acidosis, types I & IIg. Carbonic anhydrase inhibitorsh. Post-hypocapniai. Dilutional acidosis (normal saline) j. Villous adenomak. Some cases of DKA
INCREASED ANION GAP - METABOLIC ACIDOSIS (MUD PILES)1. Methanol poisoning
2. Uremia3. Diabetic ketoacidosis4. Paraldehyde5. Lactic acidosis6. Ethylene glycol poisoning7. Salicylate intoxication
Metabolic alkalosisA. CHLORIDE RESPONSIVE1. GASTROINTESTINAL CAUSESa. Vomitingb. Nasogastric suctionc. Villous adenoma
2. RENAL CAUSESa. Diuretic inducedb. Carbenicillin, penicillinc. Sulphates, phosphatesd. Post-hypercapnia
3. CONTRACTION ALKALOSIS
4. EXOGENOUS ALKALOSISa. Bicarbonate therapyb. Acid salts, e.g., acetatec. Blood transfusionsd. Antacid therapy
■ Absorbable antacids■ Nonabsorbables + ion resins
CHLORIDE RESISTANT1.NORMOTENSIVE VARIANTSa. Bartter’s syndromeb. Profound potassium depletionc. Refeeding alkalosisd. Hypercalcemiae. Hyperparathyroidism
2. HYPERTENSIVE VARIANTSa. Endogenous mineralocorticoid
■ Primary aldosteronism■ Cushing’s syndrome■ Hyperreninism■ 11 or 17 - hydroxylase deficiency■ Liddle’s syndrome
b. Exogenous mineralocorticoid■ Steroid therapy■ Carbenoxolone
STEPWISE APPROACH TO DIAGNOSING
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 311 Vijaylakshmi Kamat & Gita Nath
ACID-BASE DISORDERSThe following is a seven-step logical
approach to analyzing acid-base disorders utilizing the ABG and serum electrolyte data. It was originally proposed by Narins and Emmet and furthur refined by Morganroth.
Step 1: Acidemic or Alkalemic?The pH of the arterial blood gas
measurement identifies the disorder as alkalemic or acidemic. Normal arterial blood pH = 7.40 +0.05Acidemic: pH<7.35 Alkalemic: pH>7.45
Step2: Is the primary disturbance respiratory or metabolic?
This step requires one to determine whether the disturbance affects-primarily the arterial PaC02orthe serum HC03'
A respiratory disturbance alters the arterial PaC02(normal value 40mmHg, range 35- 45mmHg).Go to step 3.
A metabolic disturbance alters the serum HC03‘(normal value 24meq/L, range 20-28meq/L).If HC03' <20meq/L, metabolic acidosis is present. Go to step 4.
If HC03' >28meq/L, metabolic alkalosis is present, is respiratory compensatic n adequate?Go to step 6.
The Henderson - Hasselbach equation provides the basis for the relationship between the blood pH, PaC02 and HC03-, and is shown below. The calculation however has no practical value.
Thco;! „PH = PK + log [p^JxKor
Step 3: For a respiratory disturbance, determine whether it is acute or chronic.
A respiratory acidosis results from
accumulation of PaC02 and a respiratory alkalosis results from hyperventilation and a low PaC02. For acute disturbances, a PaC02 variation from normal by 10 mm Hg is accompanied by a pH shift of approximately 0.08 units. A chronic disturbance reflects renal mediated HC03* shifts. Renal compensation requires several hours to develop and is maximal after days. Therefore, during chronic disturbances, a PaC02 variation from normal by 10mmHg is accompanied by a smaller pH shift of only 0.03 units. Also the renal correction brings the pH back towards normal but not completely. These relationships are spelled out in the following equations:
Acute respiratory acidosis:pH decrease=0.08 x (PaC02 - 40)/10
Chronic respiratory acidosis:pH decrease=0.03 x (PaC02 - 40)/10
Acute respiratory alkalosis:pH increase=0.08 x (40 - PaC02)/10
Chronic respiratory alkalosis.pH increase=0.03 x (40 - PaC02)/10
Step 4: For a respiratory disorder, is the compensation OK?
A knowledge of the empirical limits of com" ^nsation is essential to evaluate if the change in HC03' is appropriate for the change in PaC02. The limits of compensation are dictated not only by the nature of the disorder (respiratory acidosis vs alkalosis), but also by the duration of the disorder (acute vs chronic). Thus the upper limits for compensation are:
Respiratory acidosis:<24 hrs: D [HC03] = 1/10 D PC02 >24 hrs: D HC03] = 3/10 D PC02
Respiratory alkalosis:1-2 hrs: D [HC03 ] = 2/10 D PC02 >2 days: D [HC03 ] = 6/10 D PC02
Step 5: Assess the normal compensation by the respiratory system for a metabolic disturbance.
Thj respiratory system responds quickly to a metabolic disturbance and most predictably to a metabolic acidosis. The change in PaCOz exhibits a linear correlation with the change in HC03-. The equation that predicts the respiratory response to a metabolic acidosis is called
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 312 Vijaylakshmi Kamat & Gita Nath
Unmeasured Anions vs Unmeasured Cations
Proteins, mostly albumin Calcium 5 mEq/L15 mEq/LOrganic acids 5 mEq/L Potassium 4.5mEq/L
Phosphates 2mEq/L Magnesium 1.5 mEq/LSulphates 1 mEq/LTotals: 23 mEq/L 11 mEq/L
Table. 6 Unmeasured Cations and Anions
Winter’s formula:
Expected PaC02 = (1.5* HC03) + 8 + 2
In the setting of a simple metabolic acidosis, the measured PaC02 will fall within the range predicted by Winter’s formula. If a respiratory disturbance is occurring concurrently with a metabolic acidosis, it would be defined by the direction the PaC02 varies outside the range predicted by the Winter’s formula, not from the normal value of 40mmHg.
Working through the following example illustrates how to utilize Winter’s formula to assess the respiratory compensation to a metabolic acidosis. If the serum HC03' is 10 m eq/L, the PaC02 should be between 21 and 25 according to Winter’s formula. If the measured PaC02 falls outside this range, then an additional respiratory disturbance must be occurring concurrently. If the measured PaC02 is less than 21, then the additional disturbance is a respiratory alkalosis. If the measured PaC02 is greater than 25, then the additional disturbance is a respiratory acidosis. Winter’s formula does not predict the respiratory response to a metabolic alkalosis. The magnitude of the respiratory response to a metabolic alkalosis is not easily predictable. When present, the respiratory response to metabolic alkalosis is hypoventilation, but the degree of PaC02 increase does not exhibit a linear relationship with the HC03\
Two general rules hold up for the respiratory response to a metabolic alkalosis:1) a patient will be alkalemic (pH >7.42) if the PaC02 is elevated to compensate for a metabolic alkalosis, 2)if the patient is academic,(pH <7.38), then an additional respiratory acidosis is present).
Step 6. For a metabolic acidosis, determine whether an anion gap is present.
The anion gap calculation simplifies the diagnosis of the cause for a metabolic acidosis. The normal anion gap is the calculated difference between negatively charged (anion) and positively charged (cation) electrolytes, which are measured in routine serum assays. The total of measured cations represented by sodium (Na+), is greater then the total measured anions, HC03‘ and chloride (Cl ). Turned around, that difference or gap also can be viewed as the unmeasured anion concentration. The unmeasured anion concentration dominates the balance between the unmeasured serum anions and cations. Anion Gap reflects the unmeasured anions and cations.
Thus the balance favours the unmeasured anions by 12 mEq/L, which is the normal anion gap. The unmeasured anions rarely change enough to affect anion gap interpretation. Knowledge of the unmeasured anions is not essential to the calculation of the anion gap. However, one needs to understand the concept in order to recognize the rare instances when the anion gap is not 12 for reasons other than a metabolic acidosis.
The causes of an anion gap acidosis differ from those of a normal or non-anion gap acidosis. The anion gap determination is an excellent tool for narrowing the list of potential causes of a metabolic acidosis. The simple calculation requires values for the serum Na+ Cl" and HC03'
Anion gap = Na+ - (Cl* + HC03 )
Anion gap metabolic acidosis, if anion gap >12 Normal or non-anion gap acidosis, if anion gap
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 313 Vijaylakshmi Kamat & Gita Nath
<12
The calculation of the anion gap provides reliable data with the following rare exceptions. Patients with a low serum albumin (e.g. cirrhosis, nephrotic syndrome, malnutrition) have an anion gap acidosis, but the measured anion gap is normal or < 12. The reason is that albumin has many negative charges on its surface and accounts for a significant proportion of the unmeasured anions. Severe hypoalbuminemia may exhibit a normal anion gap as low as 4. Therefore in severe hypoalbuminemia, if the anion gap increases and approaches 12, one must suspect an additional metabolic cause for the increased anion gap. In alkalemic patients with a pH >7.5, the anion gap may be elevated due to metabolic alkalosis and not because of additional metabolic acidosis. This is probably due to unmeasured anion accumulation. Specifically, the negative charges on the surface of albumin become more negative in alkalemic conditions, which would increase the unmeasured anions and the anion gap.
The distinction between whether an anion gap is due to alkalemia or an underlying acidosis in an alkalemic patient needs to be considered in some clinical situations.
Step 7: Determine whether other metabolic disturbances co-exist with an anion gap acidosis.
A non-anion gap acidosis or a metabolic alkalosis may exist concurrently with an anion gap acidosis. This determination requires one to account for the increase in the anion gap and determine whether additional variation in HC03' exists. If no other metabolic disturbance exists, then the following calculation would result in 24meq/L.Corrected HCO ' = measured HCO ' + (anion gap-12)
If the corrected HC03' varies significantly above or below 24, then a mixed or more complex metabolic disturbance exists. To be more specific, if the corrected HC03' is greater than 24, a metabolic alkalosis co - exists. If the corrected HCQ3- is less than 24,
then a non-anion gap acidosis co-exists.
The following examples help one understand how this step works. A patient with an anion gap has a HC03‘ of 10 mEq/L and an anion gap of 26. By calculating the corrected HC03- one finds the result to be 24 and we can conclude that no other metabolic disturbance co-exists. If this patient had a HC03 of 15 and an anion gap of 26, then the corrected HC03‘ would be 29, a value significantly greater than 24. One would then conclude that metabolic alkalosis co-exists with the anion gap acidosis.
IV. SPECIFIC ACID-BASE DISORDERS AND DIAGNOSES 1 .Respiratory Acidosis:
Respiratory acidosis results from hypoventilation, which is manifested by the accumulation of C02 in the blood and a drop in blood pH. Examples of specific causes can be categorized as follows:• Central Nervous System Depression
(Sedatives, CNS disease, Obesity Hypoventilation syndrome)
• Pleural Disease (Pneumothorax)• Lung Disease (COPD, pneumonia)• Musculoskeletal disorders (Kyphoscoliosis,
Guillain-Barre, Myasthenia Gravis, Polio)
2.Respiratory Alkalosis:Respiratory alkalosis results from
hyperventilation, which is manifested by excess elimination of C02 from the blood and a rise in the blood pH. Examples of specific causes are listed below:• Catastrophic CNS event (CNS Haemorrhage)• Drugs (salicylates, progesterone)• Pregnancy (especially the 3rd trimester)• Decreased lung compliance (interstitial lung
disease)• Liver cirrhosis• Anxiety
3.Anion Gap Metabolic AcidosisAnion gap acidosis results from the
accumulation of acidic metabolites and is manifested by a low HC03' and an anion gap > 12 (anion gap calculation discussed in step 3). Examples of specific causes:■ Uremia
RACE 2003 Ramachandra Anaesthesia Continuing Education
Mechanical Ventilation 314 Vijaylakshmi Kamat & Gita Nath
■ Ketoacidosis (diabetic hyperglycemia, EtOH withdrawal).
■ Alcohol poisons or drug intoxication (methanol, ethylene glycol, paraldehyde, salicylates)
■ Lactic acidosi? (sepsis, left ventricular failure)
One may use a mnemonic to remember these items. MULEPAK is a mnemonic commonly used (Methanol, Uremia, Lactic acidosis, Ethylene glycol intoxication, Paraldehyde intoxication, Aspirin, Ketoacidosis).(Also KUSMAL & MUDPILES)
4.Non-Anion Gap AcidosisNon-Anion gap acidosis results from the
loss of bicarbonate or external acid infusion and is manifested by a low HC03', but the anion gap is < 12.Examples of specific causes:■ Gl loss of HC03' (diarrhoea)■ Renal loss of HC03‘■ Compensation for respiratory alkalosis■ Carbonic anhydrase inhibitor (Diamox)■ Renal tubular acidosis■ Ureteral diversion■ Other causes: HCI or NH4CI infusion, Cl gas
inhalation, Hyperalimentation.
The commonly used mnemonic is ACCURED (acid infusion, compensation for respiratory alkalosis, Carbonic anhydrase inhibitor, renal tubular acidosis, Ureteral diversion, “Extra" alimentation or hyperalimentation, Diarrhoea).
5.Metabolic AlkalosisMetabolic alkalosis results from
elevation of serum bicarbonate. Examples of specific causes:■ Volume contraction (vomiting, overdiuresis,
ascites)■ Hypokalemia■ Alkali ingestion (bicarbonate)■ Excess gluco- or mineralo corticoids■ Bartter’s syndrome
Urinary Anion GapA. A rough index of appropriate NH3 generation Urinary anion gap
AG = Na+ + K+ - Clin acidotic patients,AG < 23 meq/d - appropriate NH3 AG > 0 < 75 meq/d - inappropriate NH3 AG > 75 meq/d - look for organic
ammonuriaB. Gl anion gap
AG = Na+ + K+ - Cra. StoolIf AG positive - acidosis likely outcome If AG negative - alkalosis likely outcome
b. GastricQualification can estimate quantity of H+ lost.
CONCLUSIONA new era has emerged with the
anaesthesiologists becoming intensivists as well, running multidisciplinary ICUs. So it is mandatory that the anaesthesiologist is well versed with the fundamentals of acid base balance and mechanical ventilation.
RACE 2003 Ramachandra Anaesthesia Continuing Education
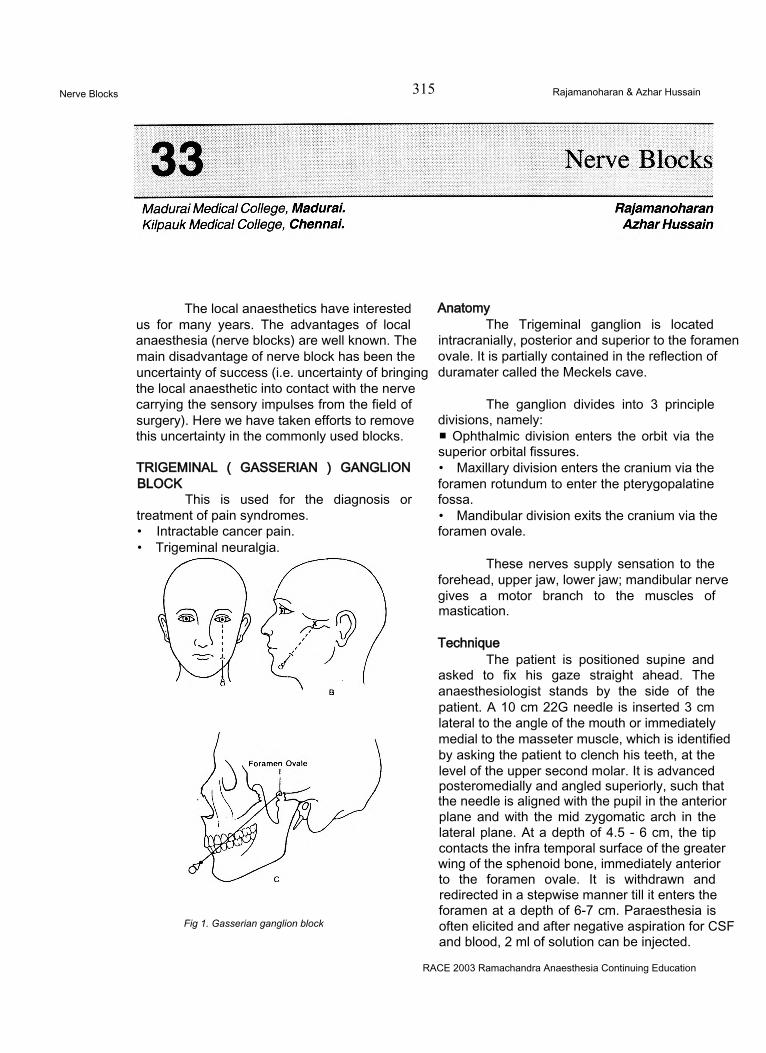
Nerve Blocks 315 Rajamanoharan & Azhar Hussain
The local anaesthetics have interested us for many years. The advantages of local anaesthesia (nerve blocks) are well known. The main disadvantage of nerve block has been the uncertainty of success (i.e. uncertainty of bringing the local anaesthetic into contact with the nerve carrying the sensory impulses from the field of surgery). Here we have taken efforts to remove this uncertainty in the commonly used blocks.
TRIGEMINAL ( GASSERIAN ) GANGLION BLOCK
This is used for the diagnosis or treatment of pain syndromes.• Intractable cancer pain.• Trigeminal neuralgia.
Fig 1. Gasserian ganglion block
AnatomyThe Trigeminal ganglion is located
intracranially, posterior and superior to the foramen ovale. It is partially contained in the reflection of duramater called the Meckels cave.
The ganglion divides into 3 principle divisions, namely:■ Ophthalmic division enters the orbit via the superior orbital fissures.• Maxillary division enters the cranium via the foramen rotundum to enter the pterygopalatine fossa.• Mandibular division exits the cranium via the foramen ovale.
These nerves supply sensation to the forehead, upper jaw, lower jaw; mandibular nerve gives a motor branch to the muscles of mastication.
TechniqueThe patient is positioned supine and
asked to fix his gaze straight ahead. The anaesthesiologist stands by the side of the patient. A 10 cm 22G needle is inserted 3 cm lateral to the angle of the mouth or immediately medial to the masseter muscle, which is identified by asking the patient to clench his teeth, at the level of the upper second molar. It is advanced posteromedially and angled superiorly, such that the needle is aligned with the pupil in the anterior plane and with the mid zygomatic arch in the lateral plane. At a depth of 4.5 - 6 cm, the tip contacts the infra temporal surface of the greater wing of the sphenoid bone, immediately anterior to the foramen ovale. It is withdrawn and redirected in a stepwise manner till it enters the foramen at a depth of 6-7 cm. Paraesthesia is often elicited and after negative aspiration for CSF and blood, 2 ml of solution can be injected.
RACE 2003 Ramachandra Anaesthesia Continuing Education
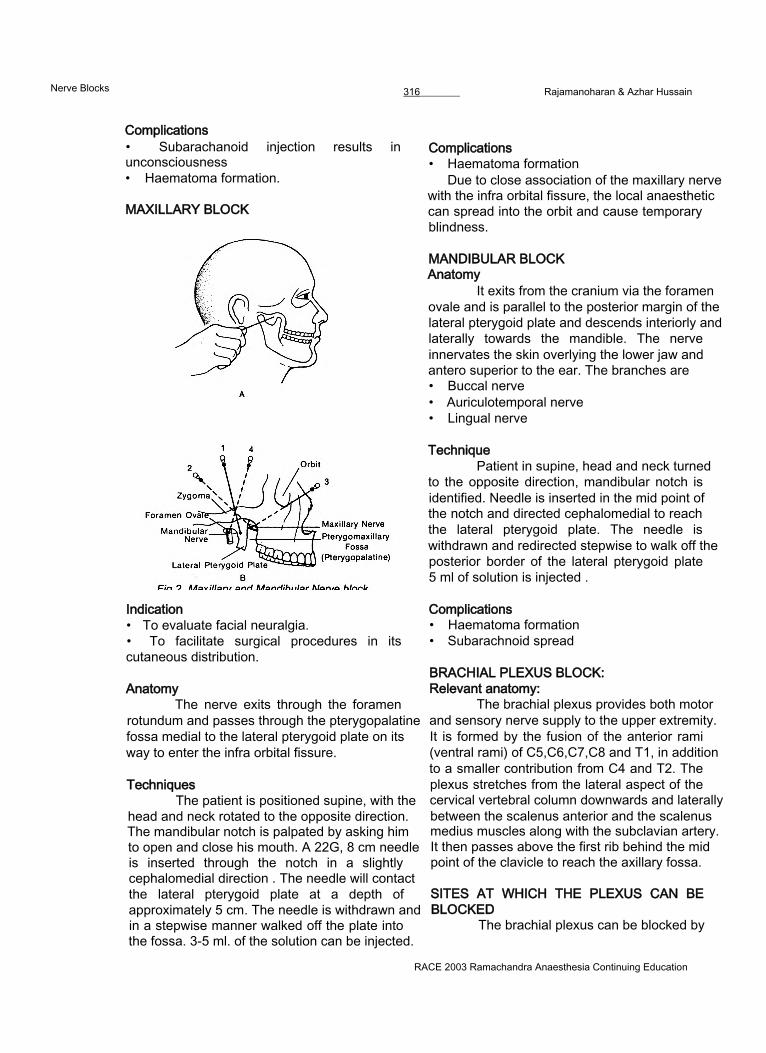
Nerve Blocks 316________ Rajamanoharan & Azhar Hussain
Complications• Subarachanoid injection results in unconsciousness• Haematoma formation.
MAXILLARY BLOCK
Complications• Haematoma formation
Due to close association of the maxillary nerve with the infra orbital fissure, the local anaesthetic can spread into the orbit and cause temporary blindness.
MANDIBULAR BLOCK Anatomy
It exits from the cranium via the foramen ovale and is parallel to the posterior margin of the lateral pterygoid plate and descends interiorly and laterally towards the mandible. The nerve innervates the skin overlying the lower jaw and antero superior to the ear. The branches are• Buccal nerve• Auriculotemporal nerve• Lingual nerve
Indication• To evaluate facial neuralgia.• To facilitate surgical procedures in its cutaneous distribution.
AnatomyThe nerve exits through the foramen
rotundum and passes through the pterygopalatine fossa medial to the lateral pterygoid plate on its way to enter the infra orbital fissure.
TechniquesThe patient is positioned supine, with the
head and neck rotated to the opposite direction. The mandibular notch is palpated by asking him to open and close his mouth. A 22G, 8 cm needle is inserted through the notch in a slightly cephalomedial direction . The needle will contact the lateral pterygoid plate at a depth of approximately 5 cm. The needle is withdrawn and in a stepwise manner walked off the plate into the fossa. 3-5 ml. of the solution can be injected.
TechniquePatient in supine, head and neck turned
to the opposite direction, mandibular notch is identified. Needle is inserted in the mid point of the notch and directed cephalomedial to reach the lateral pterygoid plate. The needle is withdrawn and redirected stepwise to walk off the posterior border of the lateral pterygoid plate 5 ml of solution is injected .
Complications• Haematoma formation• Subarachnoid spread
BRACHIAL PLEXUS BLOCK:Relevant anatomy:
The brachial plexus provides both motor and sensory nerve supply to the upper extremity. It is formed by the fusion of the anterior rami (ventral rami) of C5,C6,C7,C8 and T1, in addition to a smaller contribution from C4 and T2. The plexus stretches from the lateral aspect of the cervical vertebral column downwards and laterally between the scalenus anterior and the scalenus medius muscles along with the subclavian artery. It then passes above the first rib behind the mid point of the clavicle to reach the axillary fossa.
SITES AT WHICH THE PLEXUS CAN BE BLOCKED
The brachial plexus can be blocked by
RACE 2003 Ramachandra Anaesthesia Continuing Education
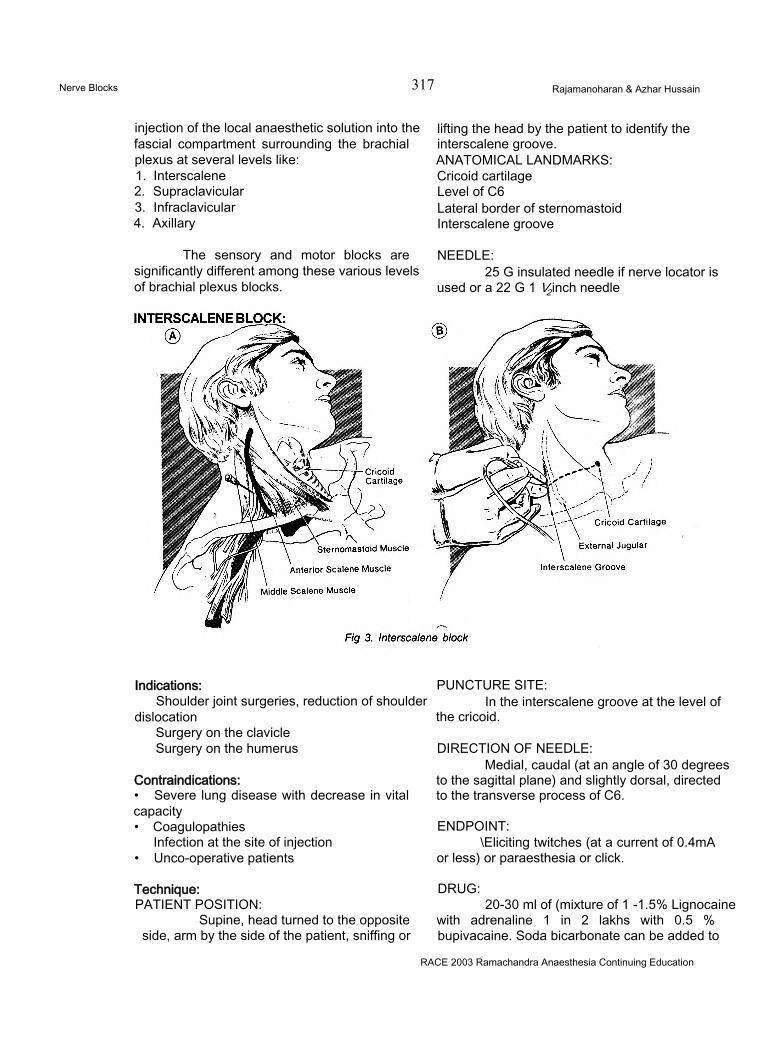
Nerve Blocks 317 Rajamanoharan & Azhar Hussain
injection of the local anaesthetic solution into the fascial compartment surrounding the brachial plexus at several levels like:1. Interscalene2. Supraclavicular3. Infraclavicular4. Axillary
lifting the head by the patient to identify the interscalene groove.ANATOMICAL LANDMARKS:Cricoid cartilage Level of C6Lateral border of sternomastoid Interscalene groove
The sensory and motor blocks are significantly different among these various levels of brachial plexus blocks.
NEEDLE:25 G insulated needle if nerve locator is
used or a 22 G 1 V2 inch needle
Indications:Shoulder joint surgeries, reduction of shoulder
dislocationSurgery on the clavicle Surgery on the humerus
Contraindications:• Severe lung disease with decrease in vital capacity• Coagulopathies
Infection at the site of injection• Unco-operative patients
Technique:PATIENT POSITION:
Supine, head turned to the opposite side, arm by the side of the patient, sniffing or
PUNCTURE SITE:In the interscalene groove at the level of
the cricoid.
DIRECTION OF NEEDLE:Medial, caudal (at an angle of 30 degrees
to the sagittal plane) and slightly dorsal, directed to the transverse process of C6.
ENDPOINT:\Eliciting twitches (at a current of 0.4mA
or less) or paraesthesia or click.
DRUG:20-30 ml of (mixture of 1 -1.5% Lignocaine
with adrenaline 1 in 2 lakhs with 0.5 % bupivacaine. Soda bicarbonate can be added to
RACE 2003 Ramachandra Anaesthesia Continuing Education
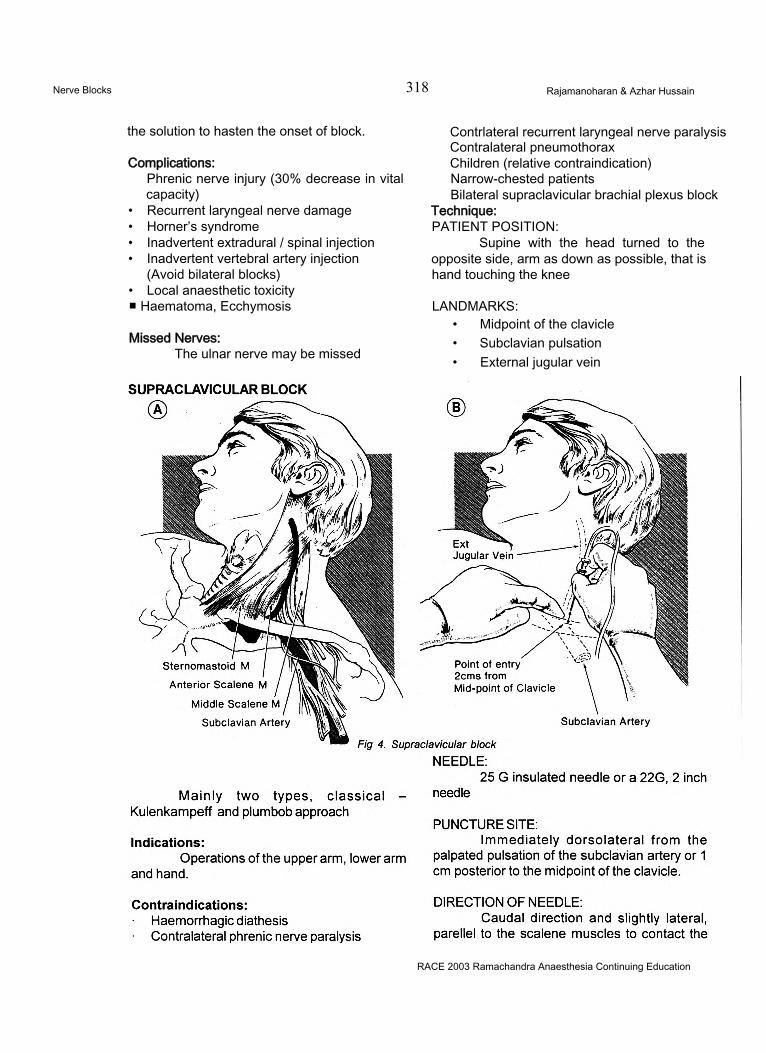
Nerve Blocks 318 Rajamanoharan & Azhar Hussain
the solution to hasten the onset of block.
Complications:Phrenic nerve injury (30% decrease in vital capacity)
• Recurrent laryngeal nerve damage• Horner’s syndrome• Inadvertent extradural / spinal injection• Inadvertent vertebral artery injection
(Avoid bilateral blocks)• Local anaesthetic toxicity ■ Haematoma, Ecchymosis
Missed Nerves:The ulnar nerve may be missed
Contrlateral recurrent laryngeal nerve paralysis Contralateral pneumothorax Children (relative contraindication) Narrow-chested patients Bilateral supraclavicular brachial plexus block
Technique:PATIENT POSITION:
Supine with the head turned to the opposite side, arm as down as possible, that is hand touching the knee
LANDMARKS:• Midpoint of the clavicle• Subclavian pulsation• External jugular vein
RACE 2003 Ramachandra Anaesthesia Continuing Education
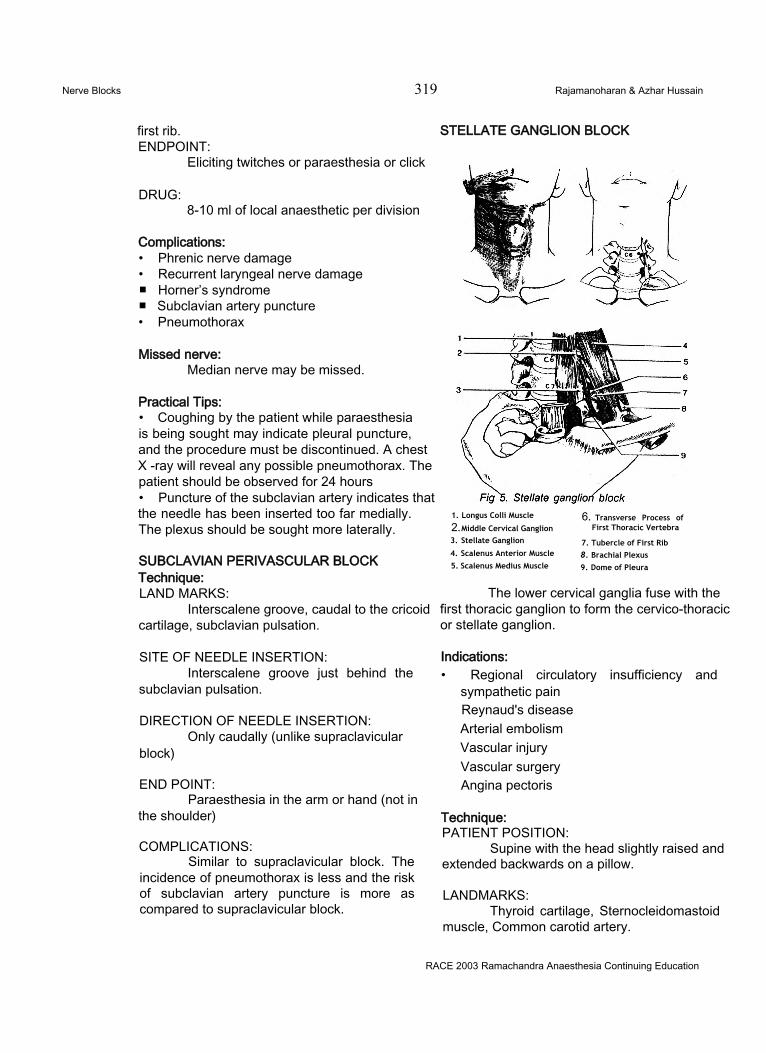
Nerve Blocks 319 Rajamanoharan & Azhar Hussain
first rib.ENDPOINT:
Eliciting twitches or paraesthesia or click
STELLATE GANGLION BLOCK
DRUG:8-10 ml of local anaesthetic per division
Complications:• Phrenic nerve damage• Recurrent laryngeal nerve damage■ Horner’s syndrome■ Subclavian artery puncture• Pneumothorax
Missed nerve:Median nerve may be missed.
Practical Tips:• Coughing by the patient while paraesthesia is being sought may indicate pleural puncture, and the procedure must be discontinued. A chest X -ray will reveal any possible pneumothorax. The patient should be observed for 24 hours• Puncture of the subclavian artery indicates that the needle has been inserted too far medially. The plexus should be sought more laterally.
SUBCLAVIAN PERIVASCULAR BLOCK Technique:LAND MARKS:
Interscalene groove, caudal to the cricoid cartilage, subclavian pulsation.
SITE OF NEEDLE INSERTION:Interscalene groove just behind the
subclavian pulsation.
DIRECTION OF NEEDLE INSERTION:Only caudally (unlike supraclavicular
block)
END POINT:Paraesthesia in the arm or hand (not in
the shoulder)
COMPLICATIONS:Similar to supraclavicular block. The
incidence of pneumothorax is less and the risk of subclavian artery puncture is more as compared to supraclavicular block.
1. Longus Colli Muscle
2. Middle Cervical Ganglion3. Stellate Ganglion
4. Scalenus Anterior Muscle
5. Scalenus Medius Muscle
6. Transverse Process of First Thoracic Vertebra
7. Tubercle of First Rib8. Brachial Plexus9. Dome of Pleura
The lower cervical ganglia fuse with the first thoracic ganglion to form the cervico-thoracic or stellate ganglion.
Indications:• Regional circulatory insufficiency and
sympathetic pain Reynaud's disease Arterial embolism Vascular injury Vascular surgery Angina pectoris
Technique:PATIENT POSITION:
Supine with the head slightly raised and extended backwards on a pillow.
LANDMARKS:Thyroid cartilage, Sternocleidomastoid
muscle, Common carotid artery.
RACE 2003 Ramachandra Anaesthesia Continuing Education
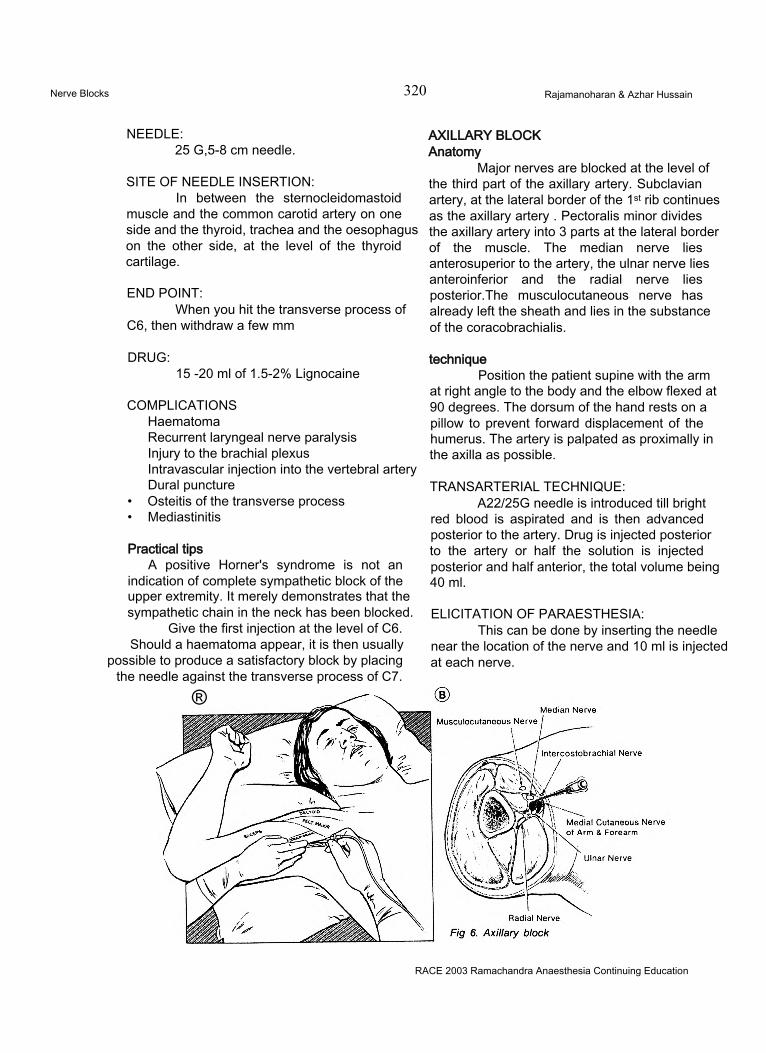
Nerve Blocks 320 Rajamanoharan & Azhar Hussain
NEEDLE:25 G,5-8 cm needle.
SITE OF NEEDLE INSERTION:In between the sternocleidomastoid
muscle and the common carotid artery on one side and the thyroid, trachea and the oesophagus on the other side, at the level of the thyroid cartilage.
END POINT:When you hit the transverse process of
C6, then withdraw a few mm
AXILLARY BLOCK Anatomy
Major nerves are blocked at the level of the third part of the axillary artery. Subclavian artery, at the lateral border of the 1st rib continues as the axillary artery . Pectoralis minor divides the axillary artery into 3 parts at the lateral border of the muscle. The median nerve lies anterosuperior to the artery, the ulnar nerve lies anteroinferior and the radial nerve lies posterior.The musculocutaneous nerve has already left the sheath and lies in the substance of the coracobrachialis.
DRUG:15 -20 ml of 1.5-2% Lignocaine
COMPLICATIONSHaematomaRecurrent laryngeal nerve paralysis Injury to the brachial plexus Intravascular injection into the vertebral artery Dural puncture
• Osteitis of the transverse process• Mediastinitis
Practical tipsA positive Horner's syndrome is not an
indication of complete sympathetic block of the upper extremity. It merely demonstrates that the sympathetic chain in the neck has been blocked.
Give the first injection at the level of C6. Should a haematoma appear, it is then usually
possible to produce a satisfactory block by placing the needle against the transverse process of C7.
®
techniquePosition the patient supine with the arm
at right angle to the body and the elbow flexed at 90 degrees. The dorsum of the hand rests on a pillow to prevent forward displacement of the humerus. The artery is palpated as proximally in the axilla as possible.
TRANSARTERIAL TECHNIQUE:A22/25G needle is introduced till bright
red blood is aspirated and is then advanced posterior to the artery. Drug is injected posterior to the artery or half the solution is injected posterior and half anterior, the total volume being 40 ml.
ELICITATION OF PARAESTHESIA:This can be done by inserting the needle
near the location of the nerve and 10 ml is injected at each nerve.
RACE 2003 Ramachandra Anaesthesia Continuing Education
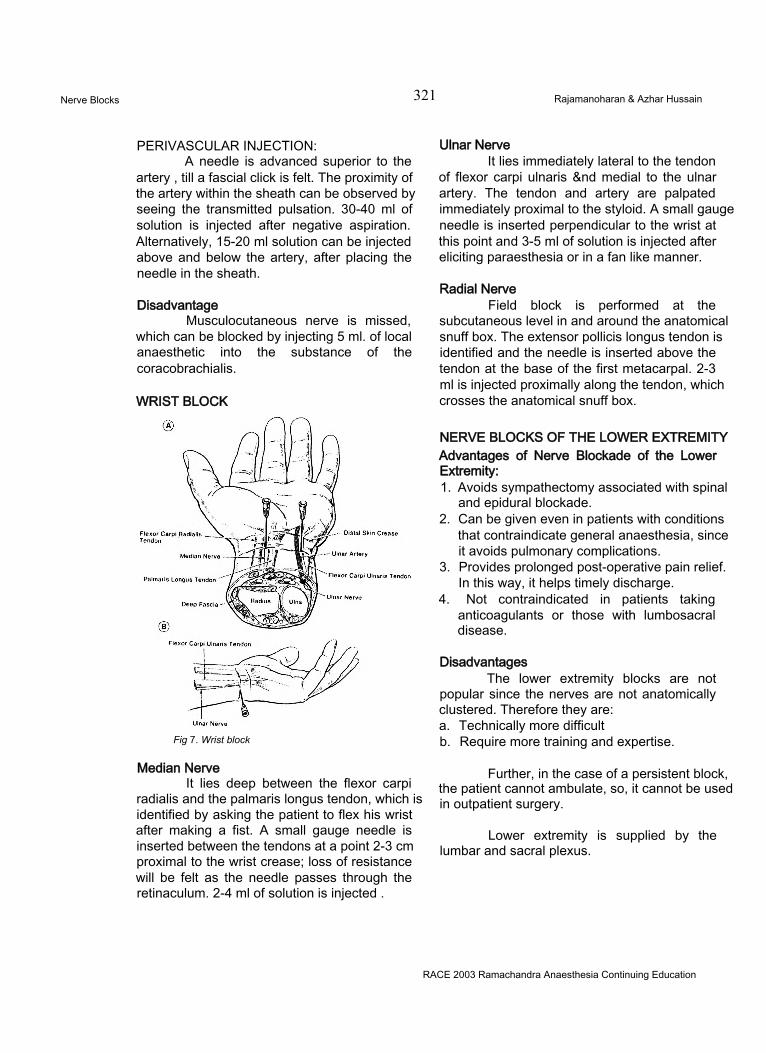
Nerve Blocks 321 Rajamanoharan & Azhar Hussain
PERIVASCULAR INJECTION:A needle is advanced superior to the
artery , till a fascial click is felt. The proximity of the artery within the sheath can be observed by seeing the transmitted pulsation. 30-40 ml of solution is injected after negative aspiration. Alternatively, 15-20 ml solution can be injected above and below the artery, after placing the needle in the sheath.
DisadvantageMusculocutaneous nerve is missed,
which can be blocked by injecting 5 ml. of local anaesthetic into the substance of the coracobrachialis.
WRIST BLOCK
Fig 7. Wrist block
Median NerveIt lies deep between the flexor carpi
radialis and the palmaris longus tendon, which is identified by asking the patient to flex his wrist after making a fist. A small gauge needle is inserted between the tendons at a point 2-3 cm proximal to the wrist crease; loss of resistance will be felt as the needle passes through the retinaculum. 2-4 ml of solution is injected .
Ulnar NerveIt lies immediately lateral to the tendon
of flexor carpi ulnaris &nd medial to the ulnar artery. The tendon and artery are palpated immediately proximal to the styloid. A small gauge needle is inserted perpendicular to the wrist at this point and 3-5 ml of solution is injected after eliciting paraesthesia or in a fan like manner.
Radial NerveField block is performed at the
subcutaneous level in and around the anatomical snuff box. The extensor pollicis longus tendon is identified and the needle is inserted above the tendon at the base of the first metacarpal. 2-3 ml is injected proximally along the tendon, which crosses the anatomical snuff box.
NERVE BLOCKS OF THE LOWER EXTREMITY Advantages of Nerve Blockade of the Lower Extremity:1. Avoids sympathectomy associated with spinal
and epidural blockade.2. Can be given even in patients with conditions
that contraindicate general anaesthesia, since it avoids pulmonary complications.
3. Provides prolonged post-operative pain relief. In this way, it helps timely discharge.
4. Not contraindicated in patients taking anticoagulants or those with lumbosacral disease.
DisadvantagesThe lower extremity blocks are not
popular since the nerves are not anatomically clustered. Therefore they are:a. Technically more difficultb. Require more training and expertise.
Further, in the case of a persistent block, the patient cannot ambulate, so, it cannot be used in outpatient surgery.
Lower extremity is supplied by the lumbar and sacral plexus.
RACE 2003 Ramachandra Anaesthesia Continuing Education
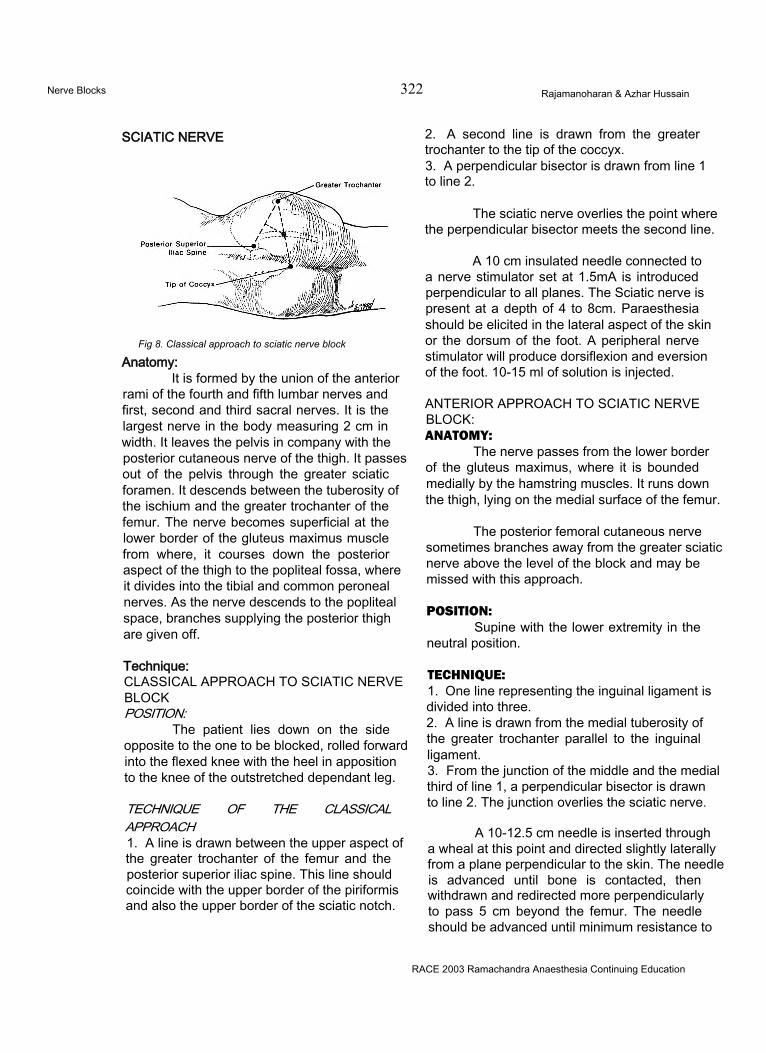
Nerve Blocks 322 Rajamanoharan & Azhar Hussain
SCIATIC NERVE
Fig 8. Classical approach to sciatic nerve block
Anatomy:It is formed by the union of the anterior
rami of the fourth and fifth lumbar nerves and first, second and third sacral nerves. It is the largest nerve in the body measuring 2 cm in width. It leaves the pelvis in company with the posterior cutaneous nerve of the thigh. It passes out of the pelvis through the greater sciatic foramen. It descends between the tuberosity of the ischium and the greater trochanter of the femur. The nerve becomes superficial at the lower border of the gluteus maximus muscle from where, it courses down the posterior aspect of the thigh to the popliteal fossa, where it divides into the tibial and common peroneal nerves. As the nerve descends to the popliteal space, branches supplying the posterior thigh are given off.
Technique:CLASSICAL APPROACH TO SCIATIC NERVEBLOCKPOSITION:
The patient lies down on the side opposite to the one to be blocked, rolled forward into the flexed knee with the heel in apposition to the knee of the outstretched dependant leg.
TECHNIQUE OF THE CLASSICAL APPROACH1. A line is drawn between the upper aspect of the greater trochanter of the femur and the posterior superior iliac spine. This line should coincide with the upper border of the piriformis and also the upper border of the sciatic notch.
2. A second line is drawn from the greater trochanter to the tip of the coccyx.3. A perpendicular bisector is drawn from line 1 to line 2.
The sciatic nerve overlies the point where the perpendicular bisector meets the second line.
A 10 cm insulated needle connected to a nerve stimulator set at 1.5mA is introduced perpendicular to all planes. The Sciatic nerve is present at a depth of 4 to 8cm. Paraesthesia should be elicited in the lateral aspect of the skin or the dorsum of the foot. A peripheral nerve stimulator will produce dorsiflexion and eversion of the foot. 10-15 ml of solution is injected.
ANTERIOR APPROACH TO SCIATIC NERVE BLOCK:ANATOMY:
The nerve passes from the lower border of the gluteus maximus, where it is bounded medially by the hamstring muscles. It runs down the thigh, lying on the medial surface of the femur.
The posterior femoral cutaneous nerve sometimes branches away from the greater sciatic nerve above the level of the block and may be missed with this approach.
POSITION:Supine with the lower extremity in the
neutral position.
TECHNIQUE:1. One line representing the inguinal ligament is divided into three.2. A line is drawn from the medial tuberosity of the greater trochanter parallel to the inguinal ligament.3. From the junction of the middle and the medial third of line 1, a perpendicular bisector is drawn to line 2. The junction overlies the sciatic nerve.
A 10-12.5 cm needle is inserted through a wheal at this point and directed slightly laterally from a plane perpendicular to the skin. The needle is advanced until bone is contacted, then withdrawn and redirected more perpendicularly to pass 5 cm beyond the femur. The needle should be advanced until minimum resistance to
RACE 2003 Ramachandra Anaesthesia Continuing Education
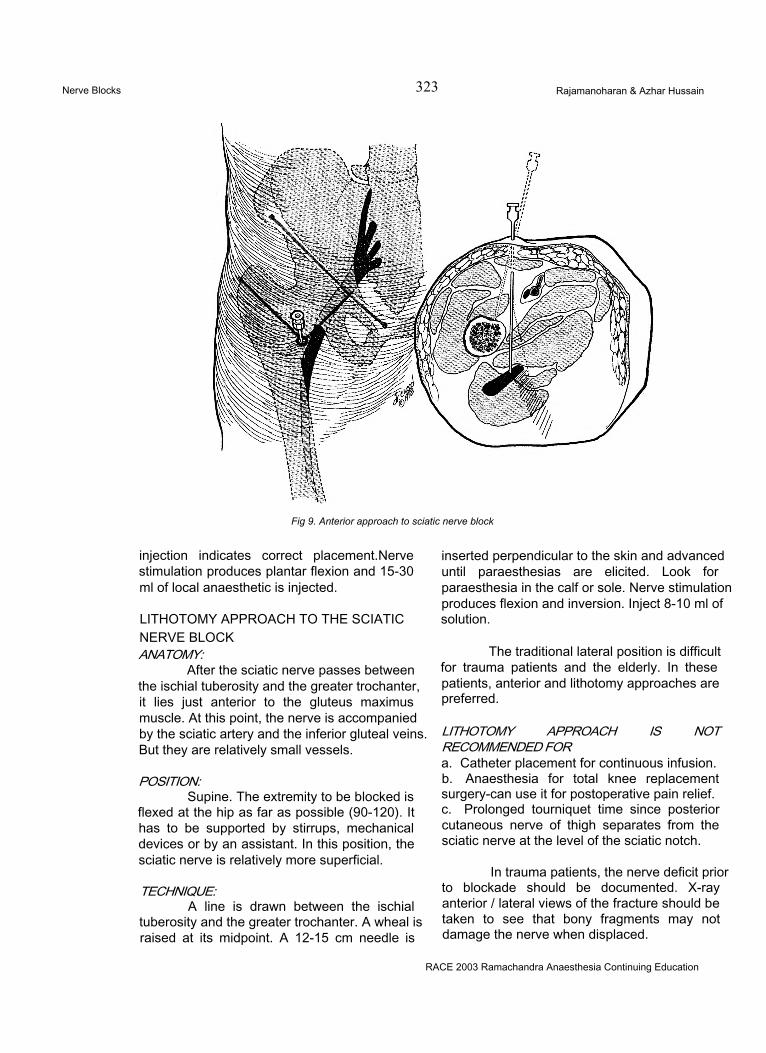
Nerve Blocks 323 Rajamanoharan & Azhar Hussain
Fig 9. Anterior approach to sciatic nerve block
injection indicates correct placement.Nerve stimulation produces plantar flexion and 15-30 ml of local anaesthetic is injected.
LITHOTOMY APPROACH TO THE SCIATICNERVE BLOCKANATOMY:
After the sciatic nerve passes between the ischial tuberosity and the greater trochanter, it lies just anterior to the gluteus maximus muscle. At this point, the nerve is accompanied by the sciatic artery and the inferior gluteal veins. But they are relatively small vessels.
POSITION:Supine. The extremity to be blocked is
flexed at the hip as far as possible (90-120). It has to be supported by stirrups, mechanical devices or by an assistant. In this position, the sciatic nerve is relatively more superficial.
TECHNIQUE:A line is drawn between the ischial
tuberosity and the greater trochanter. A wheal is raised at its midpoint. A 12-15 cm needle is
inserted perpendicular to the skin and advanced until paraesthesias are elicited. Look for paraesthesia in the calf or sole. Nerve stimulation produces flexion and inversion. Inject 8-10 ml of solution.
The traditional lateral position is difficult for trauma patients and the elderly. In these patients, anterior and lithotomy approaches are preferred.
LITHOTOMY APPROACH IS NOT RECOMMENDED FORa. Catheter placement for continuous infusion.b. Anaesthesia for total knee replacement surgery-can use it for postoperative pain relief.c. Prolonged tourniquet time since posterior cutaneous nerve of thigh separates from the sciatic nerve at the level of the sciatic notch.
In trauma patients, the nerve deficit prior to blockade should be documented. X-ray anterior / lateral views of the fracture should be taken to see that bony fragments may not damage the nerve when displaced.
RACE 2003 Ramachandra Anaesthesia Continuing Education

Nerve Blocks 324 Rajamanoharan & Azhar Hussain
Test of sciatic nerve blockade:Toes cannot be moved.
Distribution of anaesthesia:Muscles: Back of the thigh
Leg Foot
Skin: Back of the thighBack and lateral aspect of the leg Lateral side, bottom and all the toes of the foot with the occasional exception of the dorsal surface of the big toe.
Articular branches to the hip joint, knee joint and ankle joint.
Complications:a. Primarily a somatic nerve, but it does carry some sympathetic fibers to the extremity, does not usually cause significant hypotension.b. Residual dysesthesias for 1 -3 days - usually self-limiting.
AnatomyThe femoral nerve (L2-L4) proceeds from
the lumbar plexus in the groove between the psoas major and the iliac muscles, where it enters the thigh by passing deep to the inguinal ligament. At the level of the inguinal ligament, the femoral nerve lies anterior to the ilio-psoas muscle and slightly lateral to the femoral artery. The femoral nerve divides into an anterior and posterior bundle at or even above the level of the inguinal ligament.
TechniqueThe patient is in the supine position. The
femoral artery is palpated immediately below the inguinal ligament and a wheal is raised immediately lateral to the artery. The wheal lies 1 -2 cm below the line joining the anterior superior iliac spine to the pubic symphysis. A 3-4 cm needle without syringe is advanced perpendicular to the skin until a paraesthesia is elicited or the needle undergoes maximum lateral pulsation from its position adjacent to and at the level of the artery. If paresthesias occur, 7-10 ml of local anaesthetic solution should be injected after careful aspiration. If no paresthesias occur, 20 ml of local anaesthetic is deposited fanwise lateral to the artery. A wall of anaesthetic solution should extend from the skin to a depth of 3.2 cm and from the artery laterally for at least 2.5 cm.
Complications and Side effects1. Some sympathetic fibres are blocked. It does
not produce systemic hypotension. The advantage is that blood flow is increased.
2. Intravascular injection3. Haematoma formation4. Presence of vascular grafts of the femoral
artery is a relative contraindication for elective femoral nerve block
Distribution of anaesthesia
ANTERIOR BRANCHES• Skin of the thigh from the inguinal ligament to
the knee.• Sartorius muscle.
POSTERIOR BRANCHES• Quadriceps muscles.• Hip joint, knee joint.
RACE 2003 Ramachandra Anaesthesia Continuing Education
Nerve Blocks 325 Rajamanoharan & Azhar Hussain
• Medial ligament of the knee joint• Saphenous nerve
It descends over the medial side of the calf to supply the skin down to the medial malleolus.
Test of Femoral Nerve blockadeWhen the femoral block is successful,
the patient cannot extend the knee
Indications of femoral block1. Analgesia in patients with a fractured shaft of
the femur.2. Muscle biopsy of quadriceps.3. Surgery limited to anterior thigh.4. Knee arthroscopy
WINNIE’S THREE IN ONE BLOCKThree in one - By using 20-30 ml of
solution, we can block the femoral, obturator and the lateral cutaneous nerve of thigh.
LATERAL FEMORAL CUTANEOUS NERVE BLOCK (L2-L3)Anatomy
It emerges at the lateral border of the psoas muscle at a level lower than the ilioinguinal nerve. It passes obliquely under the iliac fascia and across the iliac muscle to enter the thigh deep to the inguinal ligament at a point approximately 1-2 cm medial to the anterior superior iliac spine. It courses beneath the fascia lata. It emerges from the fascia lata at a point 7- 10cm below the anterior superior iliac spine. Here it divides into anterior and posterior branches. Lateral femoral cutaneous nerve is in close relation to the iliac bone.
TechniqueWith the patient in the supine position,
a skin wheal is raised 2.5 cm below and medial to the anterior superior iliac spine. A 2-4 cm needle with syringe attached is inserted through the wheal perpendicular to the skin. A pop is felt as the needle penetrates the fascia lata. 10 ml of solution is deposited fanwise as the needle is moved upward and downward both above and below the fascia.
To ensure complete blockage, the needle is redirected to contact the iliac bone just below
the anterior superior iliac spine. The needle is withdrawn, directed medially and reinserted 2.5 cm immediately adjacent to the medial side of the shelving edge of the iliac bone.
Distribution of anaesthesia
ANTERIOR BRANCHSkin over the antero-lateral aspect of the
thigh as low as the knee
POSTERIOR BRANCHSkin on the lateral side of the thigh from
just below the greater trochanter to about the middle of the thigh.
Complications:No known risks except remotely possible
dysesthesias or hypoaesthesias.
Indications:1. Anaesthetizing donor site prior to the removal of small skin grafts.2. Supplement to femoral & sciatic nerve blocks to provide analgesia for tourniquet pain.3. Should be blocked for operation on the knee, with or without tourniquet, since it forms a part of the patellar plexus.
POPLITEAL BLOCK:The sciatic nerve is composed of two
separate nerves travelling side by side in a common epidural sheath.
Anatomy:a) The saphenous nerve is the terminal extension
of the femoral nerve.b) Common peroneal nerve & tibial nerve are
extensions from the sciatic nerve.
They bifurcate at the upper end of the popliteal space.
TechniqueCLASSICAL APPROACH1. The patient is placed in the prone position. The patient is made to flex the leg. The triangular popliteal fossa is bounded by the biceps femoris and the semitendinosus muscles. The base of the triangle is the skin crease behind the knee.2. A perpendicular is drawn from the midpoint of
RACE 2003 Ramachandra Anaesthesia Continuing Education
Nerve Blocks 326 Rajamanoharan & Azhar Hussain
the base to the apex of the triangle. Six centimeters from the base, an X is drawn 1cm lateral to this line.3. A 7.5 or 10cm needle is introduced through this “X” and directed 45 degrees cephalad. A fanwise search is conducted perpendicular to this line till the nerve is contacted. The nerve lies midway between the skin and the femur.4. If paraesthesia or muscle response is obtained, 30-40ml of local anaesthetic is injected.
The femoral branches are blocked by a subcutaneous wheal of 5-10ml of local anaesthetic solution along the medial tibial head just below the knee.
LATERAL APPROACH:The patient is in the supine position
1. The groove between the biceps femoris tendon and the vastus lateralis is identified. An "X” is placed 7cm cephalad to the lateral femoral epicondyle.2. A 22-gauge 10cm needle is inserted at this mark in a horizontal plane. The femur is usually contacted within 5cm. The needle is directed 30 c^grees posteriorly. The tibial and common peroneal nerves are looked for by identifying paraesthesia or muscle movement. 10-15ml of anaesthetic injected around each nerve provides adequate anaesthesia.
Distribution of AnaesthesiaSAPHENOUS NERVE:
Skin over the medial, anteromedial and posteromedial aspects of the leg from the knee to the ball of the great toe.
TIBIAL NERVE:Muscular branch to the back of the leg,
cutaneous branches in the popliteal fossa and down the back of the legs to the ankle.
COMMON PERONEAL NERVE:It is one half the size of the tibial nerve. It gives- Articular branches to the knee joint.- Cutaneous nerves to the lateral side of the
leg, heel and ankle.
Complications:• Minor residual dysesthesias■ Haematoma
Indications:Below knee surgery:
Popliteal block + subcutaneous infiltration to branches of the saphenous nerve.
Advantages:The function of the thigh extensors and
flexors are preserved which can help in early ambulation.
The trunk and the most proximal part of the lower extremity are supplied by the iliohypogastric and ilio-ingiunal nerves. So we may need to block these also along with the genitofemoral nerve.
OBTURATOR NERVE BLOCK( L2 - L4) Anatomy:
It appears at the medial border of the psoas muscle, covered anteriorly by the external iliac vessels and passes downward in the pelvis. It passes with the obturator vessels along the obturator foramen into the thigh. In the obturator canal, it divides into anterior and posterior branches.
Technique:POSITION:
The patient is in the supine position with the leg in slight abduction.
Caution: To protect genitalia from irritant antiseptic solution used for skin preparation.
The pubic tubercle is palpated. A skin wheal is raised 1-2cm below and 1-2cm,lateral to it. A 7-8cm needle without syringe attached is introduced through the wheal medially to strike the horizontal pubic ramus. It is then withdrawn and redirected 45 degree cephalad to identify the superior bony portion of the obturator canal. The depth of the bone in each direction is noted. The needle is withdrawn again & directed laterally and inferiorly to pass into the obturator canal. It should be advanced 2-3cm beyond the previously noted depth of the bone. After aspiration to ensure that the obturator vessels have not been entered, 10- 15ml of local anaesthetic solution is injected.
Indication of successful blockade:The patient is unable to adduct his legs
strongly.
RACE 2003 Ramachandra Anaesthesia Continuing Education
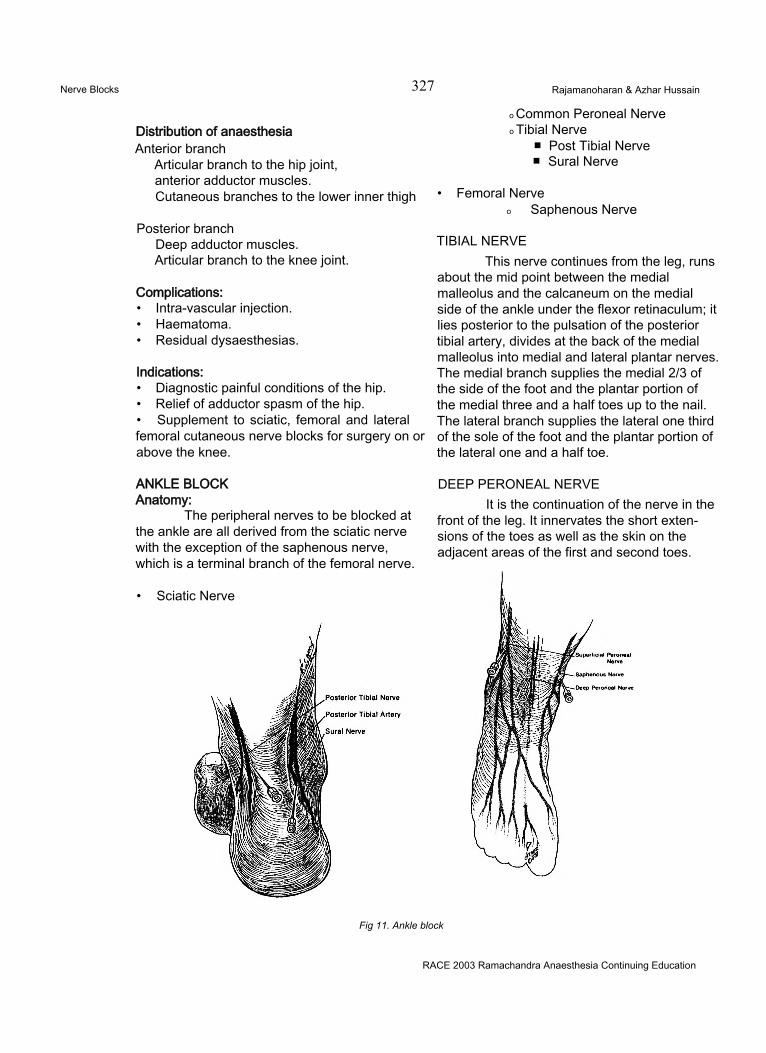
Nerve Blocks 327 Rajamanoharan & Azhar Hussain
Distribution of anaesthesiaAnterior branch
Articular branch to the hip joint, anterior adductor muscles.Cutaneous branches to the lower inner thigh
Posterior branchDeep adductor muscles.Articular branch to the knee joint.
Complications:• Intra-vascular injection.• Haematoma.• Residual dysaesthesias.
Indications:• Diagnostic painful conditions of the hip.• Relief of adductor spasm of the hip.• Supplement to sciatic, femoral and lateral femoral cutaneous nerve blocks for surgery on or above the knee.
o Common Peroneal Nerve o Tibial Nerve
■ Post Tibial Nerve■ Sural Nerve
• Femoral Nerveo Saphenous Nerve
TIBIAL NERVEThis nerve continues from the leg, runs
about the mid point between the medial malleolus and the calcaneum on the medial side of the ankle under the flexor retinaculum; it lies posterior to the pulsation of the posterior tibial artery, divides at the back of the medial malleolus into medial and lateral plantar nerves. The medial branch supplies the medial 2/3 of the side of the foot and the plantar portion of the medial three and a half toes up to the nail. The lateral branch supplies the lateral one third of the sole of the foot and the plantar portion of the lateral one and a half toe.
ANKLE BLOCK Anatomy:
The peripheral nerves to be blocked at the ankle are all derived from the sciatic nerve with the exception of the saphenous nerve, which is a terminal branch of the femoral nerve.
• Sciatic Nerve
DEEP PERONEAL NERVEIt is the continuation of the nerve in the
front of the leg. It innervates the short extensions of the toes as well as the skin on the adjacent areas of the first and second toes.
Fig 11. Ankle block
RACE 2003 Ramachandra Anaesthesia Continuing Education
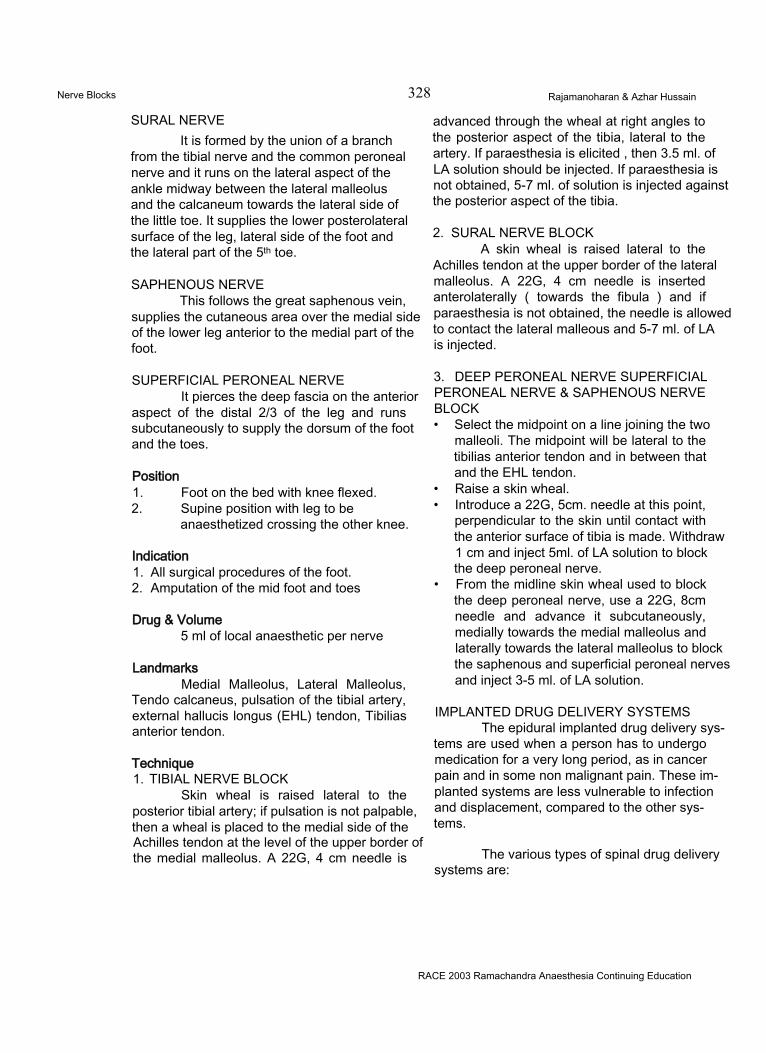
Nerve Blocks 328 Rajamanoharan & Azhar Hussain
SURAL NERVEIt is formed by the union of a branch
from the tibial nerve and the common peroneal nerve and it runs on the lateral aspect of the ankle midway between the lateral malleolus and the calcaneum towards the lateral side of the little toe. It supplies the lower posterolateral surface of the leg, lateral side of the foot and the lateral part of the 5th toe.
SAPHENOUS NERVEThis follows the great saphenous vein,
supplies the cutaneous area over the medial side of the lower leg anterior to the medial part of the foot.
SUPERFICIAL PERONEAL NERVEIt pierces the deep fascia on the anterior
aspect of the distal 2/3 of the leg and runs subcutaneously to supply the dorsum of the foot and the toes.
Position1. Foot on the bed with knee flexed.2. Supine position with leg to be
anaesthetized crossing the other knee.
Indication1. All surgical procedures of the foot.2. Amputation of the mid foot and toes
Drug & Volume5 ml of local anaesthetic per nerve
LandmarksMedial Malleolus, Lateral Malleolus,
Tendo calcaneus, pulsation of the tibial artery, external hallucis longus (EHL) tendon, Tibilias anterior tendon.
Technique1. TIBIAL NERVE BLOCK
Skin wheal is raised lateral to the posterior tibial artery; if pulsation is not palpable, then a wheal is placed to the medial side of the Achilles tendon at the level of the upper border of the medial malleolus. A 22G, 4 cm needle is
advanced through the wheal at right angles to the posterior aspect of the tibia, lateral to the artery. If paraesthesia is elicited , then 3.5 ml. of LA solution should be injected. If paraesthesia is not obtained, 5-7 ml. of solution is injected against the posterior aspect of the tibia.
2. SURAL NERVE BLOCKA skin wheal is raised lateral to the
Achilles tendon at the upper border of the lateral malleolus. A 22G, 4 cm needle is inserted anterolaterally ( towards the fibula ) and if paraesthesia is not obtained, the needle is allowed to contact the lateral malleous and 5-7 ml. of LA is injected.
3. DEEP PERONEAL NERVE SUPERFICIAL PERONEAL NERVE & SAPHENOUS NERVE BLOCK• Select the midpoint on a line joining the two
malleoli. The midpoint will be lateral to the tibilias anterior tendon and in between that and the EHL tendon.
• Raise a skin wheal.• Introduce a 22G, 5cm. needle at this point,
perpendicular to the skin until contact with the anterior surface of tibia is made. Withdraw1 cm and inject 5ml. of LA solution to block the deep peroneal nerve.
• From the midline skin wheal used to block the deep peroneal nerve, use a 22G, 8cm needle and advance it subcutaneously, medially towards the medial malleolus and laterally towards the lateral malleolus to block the saphenous and superficial peroneal nerves and inject 3-5 ml. of LA solution.
IMPLANTED DRUG DELIVERY SYSTEMSThe epidural implanted drug delivery sys
tems are used when a person has to undergo medication for a very long period, as in cancer pain and in some non malignant pain. These implanted systems are less vulnerable to infection and displacement, compared to the other systems.
The various types of spinal drug delivery systems are:
RACE 2003 Ramachandra Anaesthesia Continuing Education
Nerve Blocks 329 Rajamanoharan & Azhar Hussain
Type I Percutaneous epidural or subarachnoid catheterType II Percutaneous epidural or subarachnoid catheter with
subcutaneous tunnelingType III Totally implanted epidural or subarachnoid catheter with subcutaneous
injection portType IV Totally implanted epidural or subarachnoid catheter with implanted manually
activated pumpType V Totally implanted epidural or subarachnoid catheter with implanted
infusioin pumpType VI Totally implanted epidural or subarachnoid catheter with implanted
programmable infusion pump
Table 1. Spinal drug delivery systems
The methods of implantation of the epidural catheter will be demonstrated at the workshop.
RACE 2003 Ramachandra Anaesthesia Continuing Education

R x
isoflurane U
uquid for Inh100 mlContains : ls°flurane USP ” non-flammable, ^halation anaesth!'0 avoid leakage, container tiqhtlv a
ISORANEIsoflurane
An ideal Inhalational Anaesthetic for High Risk Patients