ultrasound characteristics of the deep abdominal muscles during the active straight leg raise test
TRANSCRIPT

O
UDDSS
SJd2
autb
tt
iut1l
nd
2fw(eiti
pd
SCo
NG
sw
AMa
ao
761
RIGINAL ARTICLE
ltrasound Characteristics of the Deep Abdominal Musclesuring the Active Straight Leg Raise Test
eydre S. Teyhen, PT, PhD, Jared N. Williamson, PT, DPT, Nathan H. Carlson, PT, DPT,ean T. Suttles, PT, DPT, Shaun J. O’Laughlin, PT, DPT, Jackie L. Whittaker, BScPT,
tephen L. Goffar, PT, PhD, John D. Childs, PT, PhDswupds
M
AcpmtbT
tdhtpketaclw(inaKcausp
m
ABSTRACT. Teyhen DS, Williamson JN, Carlson NH,uttles ST, O’Laughlin SJ, Whittaker JL, Goffar SL, ChildsD. Ultrasound characteristics of the deep abdominal musclesuring the active straight leg raise test. Arch Phys Med Rehabil009;90:761-7.
Objective: To determine whether changes in the transversusbdominis (TrA) and internal oblique (IO) muscles, as seen onltrasound imaging, during the active straight leg raise (ASLR)est differ between subjects with and without unilateral lum-opelvic pain.Design: Cross-sectional, case-control study.Setting: Clinical laboratory.Participants: Subjects (n�15) with unilateral symptoms in
he lumbopelvic region and age-matched and sex-matched con-rol subjects (n�15).
Interventions: Bilateral measurements of the deep abdom-nal muscles (TrA and IO) were obtained simultaneously usingltrasound imaging to compare the percent change in musclehickness from rest with (1) immediately on raising, (2) after a0-second hold, and (3) within 5 seconds after returning theower extremity to the plinth.
Main Outcome Measure: Percent change in muscle thick-ess of both muscles from rest to the other 3 time intervalsuring the ASLR test.Results: The 3-way group � side measured � time and
-way side measured � time interactions were not significantor either the TrA (P�.34) or the IO (P�.14) muscles. The 2-ay interaction group � time was significant for both the TrA
P�.003) and the IO (P�.02) muscles. On lifting the lowerxtremity, the control group demonstrated a 23.7% and 11.2%ncrease in TrA and IO muscle thickness, respectively, whilehose with lumbopelvic pain demonstrated a 6.4% and 5.7%ncrease in TrA and IO muscle thickness, respectively.
Conclusions: Although subjects with unilateral lumbopelvicain demonstrated a smaller increase in muscle thickness,uring the ASLR test there appears to be a symmetrical re-
From the US Army-Baylor University Doctoral Program in Physical Therapy, Ft.am Houston, TX (Teyhen, Williamson, Carlson, Suttles, O’Laughlin, Goffar,hilds); and the School of Health Professions and Rehabilitation Sciences, Universityf Southampton, Highfield Campus, Southampton, UK (Whittaker).Presented to the American Physical Therapy Association, February 6–9, 2008,
ashville, TN; and to the Texas Physical Therapy Association, October 18–21, 2007,alveston, TX.We certify that no party having a direct interest in the results of the research
upporting this article has or will confer a benefit on us or on any organization withhich we are associated.Reprint requests to Deydre S. Teyhen, PT, PhD, Dept of Physical Therapy, US
rmy Medical Department Center and School, 3150 Stanley Rd, Room 1303, ATTN:CCS-HMT, Fort Sam Houston, TX 78234, e-mail: deydre.teyhen@amedd.
rmy.mil.The opinions or assertions contained herein are the private views of the Authors
nd are not to be construed as official or as reflecting the views of the Departmentsf the Army, Air Force, or Defense.
0003-9993/09/9005-00775$36.00/0doi:10.1016/j.apmr.2008.11.011
ponse in both of the deep abdominal muscles regardless ofhich lower extremity is lifted during the ASLR test or thenilateral nature of the symptoms. This study attests to theotential construct validity of using the ASLR test to assessifferent motor control strategies of the TrA and IO muscles inubjects with unilateral lumbopelvic pain.
Key Words: Low back pain; Rehabilitation.© 2009 by the American Congress of Rehabilitationedicine
LTERED NEUROMUSCULAR control and muscularfunction are thought to contribute to the development of
hronic lumbopelvic pain, one of the most common reasonseople seek medical attention in the United States.1 One com-on presentation of lumbopelvic pain is unilateral pain over
he sacroiliac joint region. Patients with lumbopelvic pain haveeen shown to have altered muscle recruitment patterns of therA and IO muscles.2-4
The ASLR test has been used to assess the functional abilityo transfer loads through the pelvis,5-8 and has been used toiscriminate between patients with lumbopelvic pain andealthy subjects.5,6 The ASLR test is performed with the pa-ient lying supine. The test is judged to be positive when theatient flexes the hip by lifting the lower extremity with thenee fully extended off the table 5cm and experiences unilat-ral pain, discomfort, or a feeling of heaviness relative to whenhe opposite leg is lifted.4,7 The ASLR test has been validatedgainst radiographic mobility of the pelvic joints7 and has beenorrelated with other disease severity scales in patients withumbopelvic pain.6 O’Sullivan et al4 demonstrated that subjectsith a positive ASLR test used different load transfer strategies
ie, increased pelvic floor descent and changes in intra-abdom-nal pressure) during the test than those in whom the test wasegative. However, they did not assess the role of the deepbdominal muscles (TrA and IO) during the ASLR test.nowledge of muscle performance (ie, a change in mus-
le thickness) of deep abdominal muscles during the ASLR testnd comparing differences between those with and withoutnilateral lumbopelvic dysfunction may provide valuable in-ights into underlying motor control deficits in this patientopulation.Despite the purported usefulness of the ASLR test, onlyinimal evidence has been reported regarding the muscular
List of Abbreviations
ASLR active straight leg raiseCI confidence intervalICC intraclass correlation coefficientIO internal obliqueMDC minimal detectable changeTrA transversus abdominis
USI ultrasound imagingArch Phys Med Rehabil Vol 90, May 2009

raasrnntHbpdItTitswtuctc
S
oanmsAplosiSIaC
P
wpatpAtv
A
wrplDj“
csperme
tlooaa
U
aopasepcawd
ntnpsatmwt(smb
762 DEEP ABDOMINALS ACTIVE STRAIGHT LEG RAISE, Teyhen
A
esponse of the pelvic floor muscles during this test.4 Recentdvancements in the field of rehabilitative USI9 have allowedssessments of the deep abdominal muscles’ behavior duringpecific tasks.10-12 USI is a noninvasive tool that has proven aeliable and valid measurement of muscle activity and thick-ess based on comparisons with electromyography and mag-etic resonance imaging, respectively,13-20 including differen-iating changes in thickness of the TrA and IO muscles.owever, limited information exists regarding the muscularehavior of the deep abdominal muscles in subjects with aositive ASLR test. The primary purpose of this study was toetermine whether changes in muscle thickness of the TrA andO muscles during performance of the ASLR test differ be-ween subjects with and without unilateral lumbopelvic pain.he secondary purpose was to determine whether differences
n percent change in muscle thickness exist based on whetherhe lower extremity lifted was ipsilateral or contralateral to theide of symptoms. Understanding the answer to these questionsill help provide additional evidence of construct validity for
he ASLR test in patients with lumbopelvic pain. A betternderstanding of the performance of the deep abdominal mus-les during limb movement may ultimately prove beneficial inerms of prescribing specific therapeutic exercises to help de-rease the severity and recurrence of lumbopelvic pain.
METHODS
ubjectsWe recruited a sample of 30 adults between 18 to 50 years
f age, 15 subjects with lumbopelvic pain and 15 healthyge-matched (�2y) and sex-matched control subjects who didot meet any of the exclusion criteria (appendix 1). The deter-ination of lumbopelvic pain was based on at least 1 positive
acroiliac provocation test (see appendix 1)21-24 and a positiveSLR test.4,7 These tests were selected based on their use inrevious research to identify a subgroup of patients with uni-ateral lumbopelvic pain and to facilitate our ability to compareur findings with previous research on the ASLR test.4,21-24 Allubjects were Department of Defense health care beneficiaries,ncluding active duty military, family members, and retirees.ubjects provided written informed consent and signed Healthnsurance Portability and Accountability Act privacy formspproved by the Brooke Army and Wilford Hall Medicalenters’ Institutional Review Board prior to participation.
roceduresThis study used a cross-sectional, case-control design in
hich all data were collected in a single session. We screenedotential subjects with lumbopelvic pain with a physical ex-mination including the ASLR and sacroiliac joint provocationests. Eligible consenting subjects completed an additionalhysical examination, history, and demographic questionnaire.dditionally, we provided subjects with educational informa-
ion about the abdominal musculature and a standardized over-iew of the testing procedures.
ctive Straight Leg Raise TestThe ASLR test was performed with the subject lying supine
ith lower extremities straight on a standard plinth, handsesting on the chest, and elbows on the plinth. The feet wereositioned 20cm apart prior to the subject being asked to raise theower extremity 5cm off the plinth without bending the knee.4
uring the initial instructions, the investigator lifted the sub-ect’s lower extremity to the correct position (5cm) and stated,
This is the position we are going to use for the ASLR test.” ToFi
rch Phys Med Rehabil Vol 90, May 2009
oordinate the timing of the ASLR test and the USI assessment,ubjects were told which lower extremity to lift, then given thereparatory command, “prepare to lift,” and the command ofxecution, “lift.” After holding the lower extremity in theaised position for 10 seconds, subjects were given the com-ands “prepare to lower,” and “lower,” to return the lower
xtremity to the resting position.All subjects performed the ASLR test with both lower ex-
remities. An average of 3 repetitions of the ASLR test perower extremity was used to assess changes in muscle thicknessf the deep abdominal muscles during the ASLR test. Testrder was counter-balanced to protect against the potential forn order effect to occur. To minimize the influence of fatigue,30-second rest period was provided between each condition.
ltrasound ImagingChanges in muscle thickness during the ASLR test were
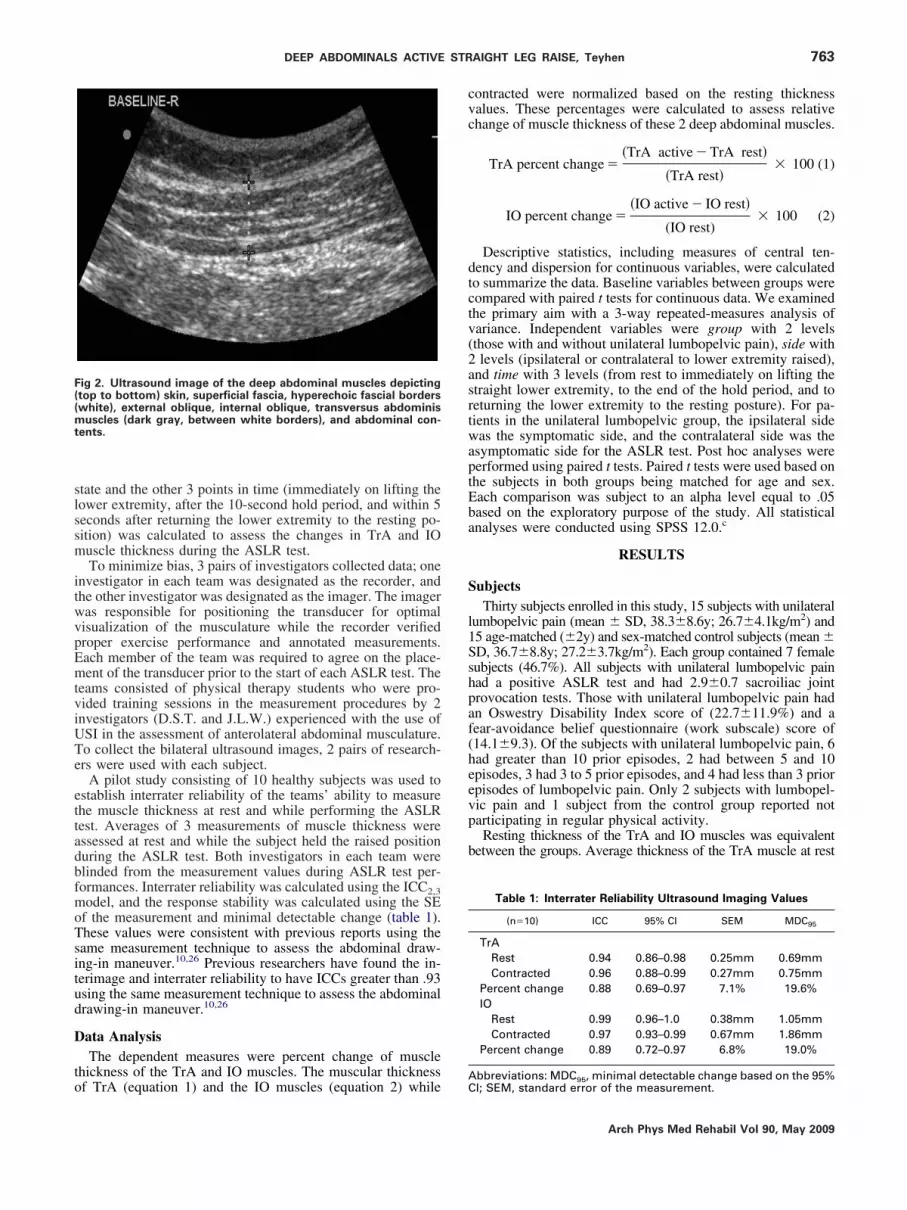
ssessed with USI. Bilateral ultrasound measurements werebtained simultaneously by 2 pairs of researchers using 2ortable ultrasound unitsa with 5-MHz, 60-mm curvilinearrrays (fig 1). USI was obtained as outlined by previous re-earchers.10,25,26 The transducers were placed on the anterolat-ral aspect of the abdominal wall just superior to the iliac crest,erpendicular to the body’s axillary line,10,25,26 and oriented toapture the anterior insertion of the TrA. During quantitativessessment, the interface of the thoracolumbar fascia and TrAas visualized in the upper right margin of the onscreenisplay.Resting thickness values were obtained at the end of a
ormal expiration as determined based on visual observation ofhe ultrasound image.10,25,26 To assess change in muscle thick-ess, resting thickness values were compared with 3 differentoints during the ASLR test: (1) immediately on lifting thetraight lower extremity, (2) after the 10-second hold period,nd (3) within 5 seconds after returning the lower extremity tohe final (resting) phase of the ASLR test. Measurements ofuscle thickness were performed using Image-Pro Plus Soft-are version 4.5.b Electronic onscreen calipers were aligned at
he superficial border of each muscle’s hyperechoic fascial linefig 2). A vertical straight line through the center of the ultra-ound image was used to ensure standardized placement of theeasurement line in relation to the center of the TrA muscle
elly. Percent change in thickness between the initial resting
ig 1. Experimental set-up depicting 2 rater groups, 2 ultrasoundmaging units, and subject positioning.
slssm
itwvpEmtviUTe
ettadbfmoTsitud
D
to
cvc
dtctv(2asrtwaptEba
S
l1Sshpaf(heevp
b
F((mt
763DEEP ABDOMINALS ACTIVE STRAIGHT LEG RAISE, Teyhen
tate and the other 3 points in time (immediately on lifting theower extremity, after the 10-second hold period, and within 5econds after returning the lower extremity to the resting po-ition) was calculated to assess the changes in TrA and IOuscle thickness during the ASLR test.To minimize bias, 3 pairs of investigators collected data; one
nvestigator in each team was designated as the recorder, andhe other investigator was designated as the imager. The imageras responsible for positioning the transducer for optimalisualization of the musculature while the recorder verifiedroper exercise performance and annotated measurements.ach member of the team was required to agree on the place-ent of the transducer prior to the start of each ASLR test. The
eams consisted of physical therapy students who were pro-ided training sessions in the measurement procedures by 2nvestigators (D.S.T. and J.L.W.) experienced with the use ofSI in the assessment of anterolateral abdominal musculature.o collect the bilateral ultrasound images, 2 pairs of research-rs were used with each subject.
A pilot study consisting of 10 healthy subjects was used tostablish interrater reliability of the teams’ ability to measurehe muscle thickness at rest and while performing the ASLRest. Averages of 3 measurements of muscle thickness weressessed at rest and while the subject held the raised positionuring the ASLR test. Both investigators in each team werelinded from the measurement values during ASLR test per-ormances. Interrater reliability was calculated using the ICC2,3odel, and the response stability was calculated using the SE
f the measurement and minimal detectable change (table 1).hese values were consistent with previous reports using theame measurement technique to assess the abdominal draw-ng-in maneuver.10,26 Previous researchers have found the in-erimage and interrater reliability to have ICCs greater than .93sing the same measurement technique to assess the abdominalrawing-in maneuver.10,26
ata AnalysisThe dependent measures were percent change of muscle
hickness of the TrA and IO muscles. The muscular thickness
ig 2. Ultrasound image of the deep abdominal muscles depictingtop to bottom) skin, superficial fascia, hyperechoic fascial borderswhite), external oblique, internal oblique, transversus abdominis
uscles (dark gray, between white borders), and abdominal con-ents.
f TrA (equation 1) and the IO muscles (equation 2) whileAC
ontracted were normalized based on the resting thicknessalues. These percentages were calculated to assess relativehange of muscle thickness of these 2 deep abdominal muscles.
TrA percent change ��TrA active � TrA rest�
�TrA rest�� 100 (1)
IO percent change ��IO active � IO rest�
(IO rest)� 100 (2)
Descriptive statistics, including measures of central ten-ency and dispersion for continuous variables, were calculatedo summarize the data. Baseline variables between groups wereompared with paired t tests for continuous data. We examinedhe primary aim with a 3-way repeated-measures analysis ofariance. Independent variables were group with 2 levelsthose with and without unilateral lumbopelvic pain), side withlevels (ipsilateral or contralateral to lower extremity raised),
nd time with 3 levels (from rest to immediately on lifting thetraight lower extremity, to the end of the hold period, and toeturning the lower extremity to the resting posture). For pa-ients in the unilateral lumbopelvic group, the ipsilateral sideas the symptomatic side, and the contralateral side was the
symptomatic side for the ASLR test. Post hoc analyses wereerformed using paired t tests. Paired t tests were used based onhe subjects in both groups being matched for age and sex.ach comparison was subject to an alpha level equal to .05ased on the exploratory purpose of the study. All statisticalnalyses were conducted using SPSS 12.0.c
RESULTS
ubjectsThirty subjects enrolled in this study, 15 subjects with unilateral
umbopelvic pain (mean � SD, 38.3�8.6y; 26.7�4.1kg/m2) and5 age-matched (�2y) and sex-matched control subjects (mean �D, 36.7�8.8y; 27.2�3.7kg/m2). Each group contained 7 femaleubjects (46.7%). All subjects with unilateral lumbopelvic painad a positive ASLR test and had 2.9�0.7 sacroiliac jointrovocation tests. Those with unilateral lumbopelvic pain hadn Oswestry Disability Index score of (22.7�11.9%) and aear-avoidance belief questionnaire (work subscale) score of14.1�9.3). Of the subjects with unilateral lumbopelvic pain, 6ad greater than 10 prior episodes, 2 had between 5 and 10pisodes, 3 had 3 to 5 prior episodes, and 4 had less than 3 priorpisodes of lumbopelvic pain. Only 2 subjects with lumbopel-ic pain and 1 subject from the control group reported notarticipating in regular physical activity.Resting thickness of the TrA and IO muscles was equivalent
etween the groups. Average thickness of the TrA muscle at rest
Table 1: Interrater Reliability Ultrasound Imaging Values
(n�10) ICC 95% CI SEM MDC95
TrARest 0.94 0.86–0.98 0.25mm 0.69mmContracted 0.96 0.88–0.99 0.27mm 0.75mm
Percent change 0.88 0.69–0.97 7.1% 19.6%IO
Rest 0.99 0.96–1.0 0.38mm 1.05mmContracted 0.97 0.93–0.99 0.67mm 1.86mm
Percent change 0.89 0.72–0.97 6.8% 19.0%
bbreviations: MDC95, minimal detectable change based on the 95%I; SEM, standard error of the measurement.
Arch Phys Med Rehabil Vol 90, May 2009

wltw
CAG
nma(tsT(
lcdea(
CW
tCdttppwusfmtmpwtd(tC
CA
mitpOt(t
Fcseg
*tp† e wat
764 DEEP ABDOMINALS ACTIVE STRAIGHT LEG RAISE, Teyhen
A
as 4.4�0.1mm and 3.8�0.7mm for those without and withumbopelvic pain, respectively (P�.07). Average thicknesses ofhe IO muscle at rest were 8.7�3.0mm and 7.9�2.4mm for thoseithout and with lumbopelvic pain, respectively (P�.45).
hanges in Muscle Thickness During the Phases of thective Straight Leg Raise Test Based onroup and Side MeasuredThe 3-way group � side measured � time interaction was
ot significant for either the TrA (P�.34) or the IO (P�.20)uscles. Additionally, the 2-way side measured � time inter-
ction was not significant for either the TrA (P�.37) or the IOP�.14) muscles. The bilateral ultrasound measurements ob-ained during the ASLR test demonstrated a symmetrical re-ponse (table 2, fig 3) in changes in muscle thickness of therA muscle from rest to when the lower extremity was lifted
P�.91), during the hold phase (P�.46), and on lowering the
ig 3. Percent changes in muscle thickness of the TrA and IO mus-les were not statistically significant based on whether the ultra-ound measurements were obtained on the ipsilateral or contralat-
Table 2: Percent Change in Muscle Thickness During the Active StSympto
N�30 Ipsilateral
MuscleMeasured
Stage ofASLR Mean � SD 95% CI
TrA (%) To lift 15.3�2.9 9.4 to 21.2To hold 11.9�3.0 5.9 to 17.8To return 2.7�1.3 0.1 to 5.4
IO (%) To lift 5.5�2.1 1.2 to 9.8To hold 6.8�2.7 1.4 to 12.2To return 0.7�1.1 –1.4 to 2.9
The 3-way group � side measured � time interaction was not signhe 2-way side measured � time interaction was not significant foresented represent all 30 subjects.For patients in the unilateral lumbopelvic group, the ipsilateral sidomatic side for the ASLR test.
mral side (symptomatic or asymptomatic side for the lumbopelvicroup), or based on group membership.
rch Phys Med Rehabil Vol 90, May 2009
ower extremity (P�.65). A bilateral response of the IO mus-les from rest to when the lower extremity was lifted (P�.06),uring the hold phase (P�.13), and on lowering the lowerxtremity (P�.38) was also noted. However, a post hoc an-lysis showed that the power was low for both musclesTrA�.20; IO�.35) for the 2-way interaction.
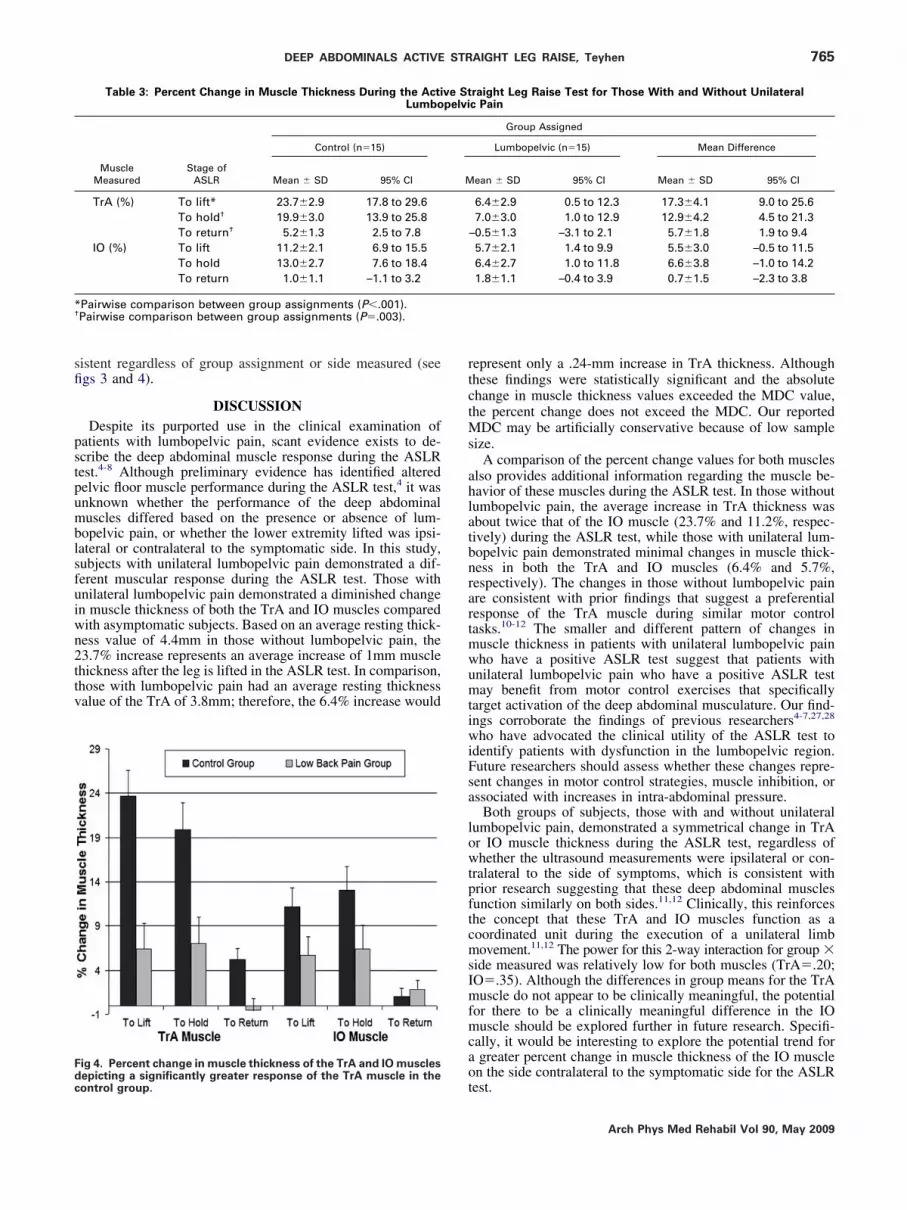
hanges in Muscle Thickness in Subjects With andithout Lumbopelvic PainThe 2-way interaction group � time was significant for both
he TrA (P�.003) and the IO (P�.02) muscles (table 3, fig 4).omparison of measurements between groups demonstrated aecreased percent change in muscle thickness during the ASLRest in subjects with unilateral lumbopelvic pain compared withhe age-matched and sex-matched control subjects. The meanercent change in TrA muscle thickness during the liftedhases of the ASLR test ranged from 20% to 24% in thoseithout lumbopelvic pain and was only 6% to 7% in those withnilateral lumbopelvic pain, and this response was statisticallyignificant (P�.003). The mean difference between the groupsrom rest to leg lift was 17.3% (95% CI, 9.0%–25.6%), and theean difference between the groups from rest to the end of
he 10-second hold time was 12.9% (95% CI, 4.5%–21.3%). Theean percent change in IO muscle thickness during the lifted
hases of the ASLR test ranged from 11% to 13% in thoseithout unilateral lumbopelvic pain and was only 5% to 6% in
hose with unilateral lumbopelvic pain (P�.07). The meanifference between the groups from rest to leg lift was 5.5%95% CI, –0.5% to 11.5%), and the mean difference betweenhe groups from rest to the 10-second hold time was 6.6% (95%I, –1.0% to 14.2%).
hanges in Muscle Thickness During the Phases of thective Straight Leg Raise TestThere was a main effect of time for both the TrA and IOuscles (P�.001). In general, the muscle thickness values
ncreased on lifting the leg, and these changes in musclehickness were maintained throughout the 10-second holdhase for both the TrA (P�.56) and the IO (P�.29) muscles.n lowering the lower extremity to the plinth, the muscle
hickness values decreased for both the TrA and the IOP�.001) muscles. Although the percent change in musclehickness for those with unilateral lumbopelvic pain was di-
t Leg Raise Test Based on Measurement of the Asymptomatic orSide*
Side Measured†
Contralateral Mean Difference
ean � SD 95% CI Mean � SD 95% CI
4.8�2.9 8.9 to 20.7 0.5�4.1 –7.9 to 8.85.0�3.0 9.1 to 20.9 –3.1�4.2 –11.5 to 5.31.9�1.3 –0.7 to 4.5 0.8�1.8 –2.9 to 4.51.4�2.1 7.1 to 15.6 –5.9�3.0 –11.9 to 0.22.6�2.7 7.2 to 18.0 –5.8�3.8 –13.4 to 1.82.1�1.1 –0.1 to 4.2 –1.3�1.5 –4.4 to 1.7
t for either the TrA (P�.34) or the IO (P�.20) muscles. Additionally,er the TrA (P�.37) or the IO (P�.14) muscles. Therefore, the data
s the symptomatic side and the contralateral side was the asymp-
raighmatic
M
11
11
ificanr eith
inished, the pattern of change in muscle thickness was con-
sfi
pstpumblsfuiwn2ttv
rtctMs
ahlatbnrartmwumtiwiFsa
lowtpftcmsImfmcao
*†
Fdc
765DEEP ABDOMINALS ACTIVE STRAIGHT LEG RAISE, Teyhen
istent regardless of group assignment or side measured (seegs 3 and 4).
DISCUSSIONDespite its purported use in the clinical examination of
atients with lumbopelvic pain, scant evidence exists to de-cribe the deep abdominal muscle response during the ASLRest.4-8 Although preliminary evidence has identified alteredelvic floor muscle performance during the ASLR test,4 it wasnknown whether the performance of the deep abdominaluscles differed based on the presence or absence of lum-
opelvic pain, or whether the lower extremity lifted was ipsi-ateral or contralateral to the symptomatic side. In this study,ubjects with unilateral lumbopelvic pain demonstrated a dif-erent muscular response during the ASLR test. Those withnilateral lumbopelvic pain demonstrated a diminished changen muscle thickness of both the TrA and IO muscles comparedith asymptomatic subjects. Based on an average resting thick-ess value of 4.4mm in those without lumbopelvic pain, the3.7% increase represents an average increase of 1mm musclehickness after the leg is lifted in the ASLR test. In comparison,hose with lumbopelvic pain had an average resting thicknessalue of the TrA of 3.8mm; therefore, the 6.4% increase would
Table 3: Percent Change in Muscle Thickness During the ActiLumbo
Control (n�15)
MuscleMeasured
Stage ofASLR Mean � SD 95% CI
TrA (%) To lift* 23.7�2.9 17.8 to 29.6To hold† 19.9�3.0 13.9 to 25.8To return† 5.2�1.3 2.5 to 7.8
IO (%) To lift 11.2�2.1 6.9 to 15.5To hold 13.0�2.7 7.6 to 18.4To return 1.0�1.1 –1.1 to 3.2
Pairwise comparison between group assignments (P�.001).Pairwise comparison between group assignments (P�.003).
ig 4. Percent change in muscle thickness of the TrA and IO muscles
tepicting a significantly greater response of the TrA muscle in theontrol group.
epresent only a .24-mm increase in TrA thickness. Althoughhese findings were statistically significant and the absolutehange in muscle thickness values exceeded the MDC value,he percent change does not exceed the MDC. Our reported
DC may be artificially conservative because of low sampleize.
A comparison of the percent change values for both muscleslso provides additional information regarding the muscle be-avior of these muscles during the ASLR test. In those withoutumbopelvic pain, the average increase in TrA thickness wasbout twice that of the IO muscle (23.7% and 11.2%, respec-ively) during the ASLR test, while those with unilateral lum-opelvic pain demonstrated minimal changes in muscle thick-ess in both the TrA and IO muscles (6.4% and 5.7%,espectively). The changes in those without lumbopelvic painre consistent with prior findings that suggest a preferentialesponse of the TrA muscle during similar motor controlasks.10-12 The smaller and different pattern of changes inuscle thickness in patients with unilateral lumbopelvic painho have a positive ASLR test suggest that patients withnilateral lumbopelvic pain who have a positive ASLR testay benefit from motor control exercises that specifically
arget activation of the deep abdominal musculature. Our find-ngs corroborate the findings of previous researchers4-7,27,28
ho have advocated the clinical utility of the ASLR test todentify patients with dysfunction in the lumbopelvic region.uture researchers should assess whether these changes repre-ent changes in motor control strategies, muscle inhibition, orssociated with increases in intra-abdominal pressure.
Both groups of subjects, those with and without unilateralumbopelvic pain, demonstrated a symmetrical change in TrAr IO muscle thickness during the ASLR test, regardless ofhether the ultrasound measurements were ipsilateral or con-
ralateral to the side of symptoms, which is consistent withrior research suggesting that these deep abdominal musclesunction similarly on both sides.11,12 Clinically, this reinforceshe concept that these TrA and IO muscles function as aoordinated unit during the execution of a unilateral limbovement.11,12 The power for this 2-way interaction for group �
ide measured was relatively low for both muscles (TrA�.20;O�.35). Although the differences in group means for the TrAuscle do not appear to be clinically meaningful, the potential
or there to be a clinically meaningful difference in the IOuscle should be explored further in future research. Specifi-
ally, it would be interesting to explore the potential trend forgreater percent change in muscle thickness of the IO musclen the side contralateral to the symptomatic side for the ASLR
raight Leg Raise Test for Those With and Without Unilateralc Pain
Group Assigned
Lumbopelvic (n�15) Mean Difference
ean � SD 95% CI Mean � SD 95% CI
6.4�2.9 0.5 to 12.3 17.3�4.1 9.0 to 25.67.0�3.0 1.0 to 12.9 12.9�4.2 4.5 to 21.3
–0.5�1.3 –3.1 to 2.1 5.7�1.8 1.9 to 9.45.7�2.1 1.4 to 9.9 5.5�3.0 –0.5 to 11.56.4�2.7 1.0 to 11.8 6.6�3.8 –1.0 to 14.21.8�1.1 –0.4 to 3.9 0.7�1.5 –2.3 to 3.8
ve Stpelvi
M
est.
Arch Phys Med Rehabil Vol 90, May 2009
timsptenTdt
S
cobhgp
srp
sjalsdptua
Aa
A
766 DEEP ABDOMINALS ACTIVE STRAIGHT LEG RAISE, Teyhen
A
Results from this study may also assist future researchers inhe assessment of the deep abdominal muscles using ultrasoundmaging during the ASLR test. In the absence of a difference inuscular response bilaterally, it may make intuitive sense to
elect the symptomatic side for future assessment of muscularerformance. Additionally, the percent changes in musclehickness on lifting the lower extremity and after the lowerxtremity was held for 10 seconds were not statistically sig-ificant for either those with or without lumbopelvic pain.herefore, measurements to represent the activated state of theeep abdominal muscles could be assessed at any time duringhe lifted phase of the ASLR test.
tudy LimitationsThere are several limitations to this study that should be
onsidered. Our sample size was relatively low. Additionally,ur sample included only those subjects with unilateral lum-opelvic pain with symptoms over the sacroiliac region whoad a positive ASLR test; therefore, our results may not beeneralizable to a wide spectrum of patients with low back
fbbreviations: Sn, Sensitivity; Sp, Specificity.
since pregnancy. Spine 2001;26:1167-71.
1
rch Phys Med Rehabil Vol 90, May 2009
tabilization exercise regimen on the clinical and muscularesponse of the ASLR test in those with unilateral lumbopelvicain.
CONCLUSIONSAlthough subjects with unilateral lumbopelvic pain demon-
trated a different muscular response than asymptomatic sub-ects, there appears to be a symmetrical response in the deepbdominal muscles regardless of which lower extremity isifted during the ASLR test or the unilateral nature of theymptoms. Subjects with unilateral lumbopelvic pain did notisplay a preferential change in TrA muscle thickness com-ared with those without lumbopelvic pain during the ASLRest. This study provides an element of construct validity forsing the ASLR test to assess muscular response of the TrAnd IO muscles in subjects with unilateral lumbopelvic pain.
Acknowledgments: In memoriam, we acknowledge Captainnna Kelly, USAF, who assisted in the development of the methods
nd data collection during this study. Additionally, we thank the
ollowing personnel for assistance in data collection: Nichole Bluemle,ain. Future researchers should assess the influence of a lumbar PT, DPT, Jeff Dolbeer, PT, DPT, and Sarah Baker, PT, DPT.
APPENDIX 1: INCLUSION AND EXCLUSION CRITERIA
Inclusion criteria for the lumbopelvic paingroup
1. Unilateral pain over the sacroiliac joint. Defined as not proximal to the iliaccrests3-5,29,30 and not distal to the popliteal fossa.
2. A positive ASLR test.4,7
3. Pain lasting over 3mo without signs of abating.4
4. A positive result on 1 of 6 sacroiliac joint provocation tests (Sn�1.00; Sp�0.44).4,21,22
A. Distraction.B. Compression.C. Posterior shear test (thigh-thrust test).D. Gaenslen provocation test (right).E. Gaenslen provocation test (left).F. Sacral thrust test.
General exclusion criteria for both groups 1. Known pregnancy, or pregnancy less than 6mo postpartum.4,5
2. A history of fracture, neoplasm, or previous surgery of the lumbar spine, the pelvicgirdle, the hip joint, or the femur.5
3. Signs of radiculopathy, as defined by 2 of the 4 neurologic signs: diminishedsensation to touch in a dermatomal region, a positive neural tension test, motorweakness not secondary to pain, or diminished reflexes.5
4. Bilateral sacroiliac pain or a bilaterally positive ASLR test.Exclusion criteria for the control group 1. A history of low back, sacroiliac, pelvic, hip, or thigh pain in the last year resulting in
lost work days, inability to perform recreational activities, or symptoms that requiredmedical attention.31
2. A history of congenital lumbar or pelvic anomalies.29
3. An inability to perform or a positive ASLR test.4,29
References1. Crisco JJ 3rd, Panjabi MM. The intersegmental and multisegmen-
tal muscles of the lumbar spine: a biomechanical model compar-ing lateral stabilizing potential. Spine 1991;16:793-9.
2. Ferreira PH, Ferreira ML, Hodges PW. Changes in recruitment ofthe abdominal muscles in people with low back pain: ultrasoundmeasurement of muscle activity. Spine 2004;29:2560-6.
3. Hungerford B, Gilleard W, Hodges P. Evidence of altered lum-bopelvic muscle recruitment in the presence of sacroiliac jointpain. Spine 2003;28:1593-600.
4. O’Sullivan PB, Beales DJ, Beetham JA, et al. Altered motor controlstrategies in subjects with sacroiliac joint pain during the activestraight-leg-raise test. Spine 2002;27:E1-8.
5. Mens JM, Vleeming A, Snijders CJ, Koes BW, Stam HJ. Reliabilityand validity of the active straight leg raise test in posterior pelvic pain
6. Mens JM, Vleeming A, Snijders CJ, Koes BW, Stam HJ. Validityof the active straight leg raise test for measuring disease severityin patients with posterior pelvic pain after pregnancy. Spine 2002;27:196-200.
7. Mens JM, Vleeming A, Snijders CJ, Stam HJ, Ginai AZ. Theactive straight leg raising test and mobility of the pelvic joints. EurSpine J 1999;8:468-73.
8. O’Sullivan PB, Twomey L, Allison GT. Altered abdominal musclerecruitment in patients with chronic back pain following a specificexercise intervention. J Orthop Sports Phys Ther 1998;27:114-24.
9. Teyhen D. Rehabilitative ultrasound imaging symposium SanAntonio, TX, May 8-10, 2006. J Orthop Sports Phys Ther 2006;36:A1-3.
0. Teyhen D, Miltenberger C, Deiters H, et al. The use of ultrasoundimaging of the abdominal drawing-in maneuver in subjects with
low back pain. J Orthop Sports Phys Ther 2005;35:346-55.
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
a
b
767DEEP ABDOMINALS ACTIVE STRAIGHT LEG RAISE, Teyhen
1. Hides JA, Wong I, Wilson SJ, Belavy DL, Richardson CA.Assessment of abdominal muscle function during a simulatedunilateral weight-bearing task using ultrasound imaging. J OrthopSports Phys Ther 2007;37:467-71.
2. Hides J, Wilson S, Stanton W, et al. An MRI investigation into thefunction of the transversus abdominis muscle during “drawing-in”of the abdominal wall. Spine 2006;31:E175-8.
3. Dietz HP, Jarvis SK, Vancaillie TG. The assessment of levatormuscle strength: a validation of three ultrasound techniques. IntUrogynecol J Pelvic Floor Dysfunct 2002;13:156-9; discussion 9.
4. Dietz HP, Steensma AB, Hastings R. Three-dimensional ultra-sound imaging of the pelvic floor: the effect of parturition onparavaginal support structures. Ultrasound Obstet Gynecol 2003;21:589-95.
5. Dietz HP, Clarke B. The influence of posture on perineal ultra-sound imaging parameters. Int Urogynecol J Pelvic Floor Dys-funct 2001;12:104-6.
6. Heit M. Intraurethral sonography and the test-retest reliability ofurethral sphincter measurements in women. J Clin Ultrasound2002;30:349-55.
7. Juul-Kristensen B, Bojsen-Moller F, Holst E, Ekdahl C. Compar-ison of muscle sizes and moment arms of two rotator cuff musclesmeasured by ultrasonography and magnetic resonance imaging.Eur J Ultrasound 2000;11:161-73.
8. Peschers UM, Gingelmaier A, Jundt K, Leib B, Dimpfl T. Eval-uation of pelvic floor muscle strength using four different tech-niques. Int Urogynecol J Pelvic Floor Dysfunct 2001;12:27-30.
9. McMeeken JM, Beith ID, Newham DJ, Milligan P, Critchley DJ.The relationship between EMG and change in thickness of trans-versus abdominis. Clin Biomech (Bristol, Avon) 2004;19:337-42.
0. Hodges PW, Pengel LH, Herbert RD, Gandevia SC. Measurementof muscle contraction with ultrasound imaging. Muscle Nerve2003;27:682-92.
1. Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis ofsacroiliac joint pain: validity of individual provocation tests andcomposites of tests. Man Ther 2005;10:207-18.
2. Laslett M, Williams M. The reliability of selected pain provoca-
tion tests for sacroiliac joint pathology. Spine 1994;19:1243-9. c3. Ronchetti I, Vleeming A, van Wingerden JP. Physical character-istics of women with severe pelvic girdle pain after pregnancy: adescriptive cohort study. Spine 2008;33:E145-51.
4. Vleeming A, Albert HB, Ostgaard HC, Sturesson B, Stuge B.European guidelines for the diagnosis and treatment of pelvicgirdle pain. Eur Spine J 2008;17:794-819.
5. Painter EE, Ogle MD, Teyhen DS. Lumbopelvic dysfunctionand stress urinary incontinence: a case report applying rehabil-itative ultrasound imaging. J Orthop Sports Phys Ther 2007;37:499-504.
6. Springer B, Mielcarek B, Nesfield T, Teyhen D. Relationshipsamong lateral abdominal muscles, gender, body mass index,and hand dominance. J Orthop Sports Phys Ther 2006;36:289-97.
7. Mens JM, Vleeming A, Snijders CJ, Ronchetti I, Ginai AZ, StamHJ. Responsiveness of outcome measurements in rehabilitation ofpatients with posterior pelvic pain since pregnancy. Spine 2002;27:1110-5.
8. Roussel NA, Nijs J, Truijen S, Smeuninx L, Stassijns G. Low backpain: clinimetric properties of the Trendelenburg test, activestraight leg raise test, and breathing pattern during active straightleg raising. J Manipulative Physiol Ther 2007;30:270-8.
9. Hungerford B, Gilleard W, Lee D. Altered patterns of pelvic bonemotion determined in subjects with posterior pelvic pain usingskin markers. Clin Biomech 2004;19:456-64.
0. Maigne JY, Aivaliklis A, Pfefer F. Results of sacroiliac jointdouble block and value of sacroiliac pain provocation tests in 54patients with low back pain. Spine 1996;21:1889-92.
1. Hayes MA, Howard TC, Gruel CR, Kopta JA. Roentgenographicevaluation of lumbar spine flexion-extension in asymptomaticindividuals. Spine 1989;14:327-31.
Suppliers. Ultrasound imaging device, Sonosite TITAN; Sonosite Inc, 21919
30th Dr SE, Bothell, WA 98021.. Image Processing Solutions Inc, 761 Silver Spring Ave, Ste B,
Silver Spring, MD 20910.
. SPSS Inc, 233 S. Wacker Dr., 11th Fl, Chicago, IL 60606.Arch Phys Med Rehabil Vol 90, May 2009