trigger points and classical acupuncture points
TRANSCRIPT

AkupunkturD e u t s c h e Z e i t s c h r i f t f ü r
DZ
AOriginalia | original articles
DOI : 10. 10 16/ j .dza .2008.10.001 6 Dt Z tschr f Akup. 5 1 , 4 / 2008
P. T. Dorsher1, J. Fleckenstein2
Trigger Points and Classical Acupuncture PointsPart 2: Clinical Correspondences in Treating Pain and Somatovisceral Disorders
Trigger-Punkte und klassische AkupunkturpunkteTeil 2: Klinische Korrespondenzen in der Behandlung von Schmerzen und
somatoviszeralen Störungen
AbstractBackground: Anatomic comparisons of the locations of myofascial trigger points (mTrPs) to those of classical acu-puncture points in the fi rst part of this study showed that at least 238 (93.3 %) of 255 “common” mTrPs described by the Trigger Point Manual have proximate, anatomically corresponding classical acupoints that anatomy references document enter the same muscle regions of those mTrPs.Objectives: To determine whether these correlated com-mon mTrP–classical acupoint pairs have similar indica-tions for treating pain and somatovisceral disorders.Methods: The clinical indications of the 238 anatomically corresponding classical acupoints were examined in acu-puncture references to determine whether they include in-dications for treating pain and/or somatovisceral disorders that are comparable to those described for their correlated common mTrPs by the Trigger Point Manual.Results: 93 % (221/238) of the correlated common mTrPs have pain indications described by the Trigger Point Ma-nual. Of their anatomically corresponding classical acu-points, 208/221 (94 %) have similar regional pain indi-cations described, and another 6 (3 %) of these acupoints have indications for painful conditions in the distributions of their correlated mTrPs’ described referred-pain. Only 7 classical acupoints that anatomically corresponded to common mTrPs had no comparable pain indications. The Trigger Point Manual describes somatovisceral eff ects for 60 (24 %) of its common mTrPs. Of their anatomically corresponding classical acupoints, 82 % (49/60) have “de-fi nite” and another 11 % (7/60) have “probable” clinical correspondences of their somatovisceral eff ects.Conclusions: The marked correspondences of the pain in-dications (up to 97 %) and somatovisceral indications (up to 93 %) of anatomically corresponding common mTrP-classical acupoint pairs provide a second, clinical line of evidence that trigger points and acupuncture points likely describe the same physiologic phenomena.
Peter T. Dorsher, MDDepartment of Physical Medicine and RehabilitationMayo Clinic
4500 San Pablo RoadJacksonville, FL 32224
1 From the Department of Physical Medicine and Rehabilitation, Mayo Clinic, Jacksonville, Flo2 and the Interdisciplinary Pain Center, Department of Anesthesiology, University of Munich
KeywordsAcupuncture, acupuncture point, myofascial pain, trigger point therapy
ZusammenfassungHintergrund: Der Vergleich der Lokalisationen myofaszialer Triggerpunkte (mTrPs) mit der von klassischen Akupunktur-punkten im ersten Teil dieser Studie zeigte, das mindestens 238 (93,3 %) der 255 „allgemeinen“ mTrPs, die im Trigger Point Manual beschrieben werden, mit in ihrer Nähe gelegenen Akupunkturpunkten dieselben Muskelregionen versorgen.Zielsetzung: Festzustellen, ob diese Korrelations-Paare aus mTrP und klasssischen Akupunkturpunkten ähnliche Indikationen zur Behandlung von Schmerzen und somato-viszeralen Störungen besitzen.Methoden: Die klinischen Indikationen der 238 anatomisch korrespondierenden klassischen Akupunkturpunkte wurden daraufhin untersucht, ob ihre Indiaktionen für die Therapie von Schmerzen und/oder somatoviszeralen mit den Indika-tionen für die mTrP des Trigger Point Manual korrelieren.Ergebnisse: 93 % (221/238) der korrelierenden allgemei-nen mTrPs des Trigger Point Manual besitzen Schmerz-Indikationen. Für 208/221 (94 %) der mit ihnen korrelie-renden klassischen Akupunktupunkte werden ähnliche regionale Schmerz-Indikationen angegeben. Weitere sechs (3 %) dieser Akupunkturpunkte besitzen Schmerz-Indika-tionen für die Regionen des übertragenen Schmerzes der korrelierenden mTrPs. Nur 7 klassische Akupunkturpunkte, die mit mTrPs korrelieren, haben keine vergleichbare Schmerz-Indikation. Das Trigger Point Manual beschreibt somatoviszerale Eff ekte für 60 (24 %) der allgemeinen mTrPs. 82 % (49/60) der mit ihnen anatomisch korrelie-renden klassischen Akupunkturpunkte haben sichere, wei-tere 11 % (7/60) wahrscheinliche korrespondierende soma-toviszerale Eff ekte.Schlussfolgerungen: Die deutliche Übereinstimmung der Schmerz-Indikationen (bis zu 97%) und somatoviszeralen Indikationen (bis zu 93 %) der Paare der anatomisch korre-spondierenden allgemeinen mTrPs mit klassischen Akupunk-turpunkten liefern einen zweiten klinischen Beweis, dass Trig-gerpunkte und Akupunkturpunkte mit hoher Wahrscheinlich-keit dieselben physiologischen Phänomene beschreiben.
rida
SchlüsselwörterAkupunktur, Akupunkturpunkt, myofaszialer Schmerz, Triggerpunkttherapie

Originalia | original articles
P. T. Dorsher, J . F leckenste in Trigger Points and Classical Acupuncture Points
Introduction
Less than 30 % of the acupuncture literature is devoted
and allopathic physicians. All but 2 of the 361 classical
17 (the latter point has no clinical indications). Thus, though their pain uses are often not their primary cli-nical indications, virtually every classical acupuncture point has at least one indication for treating pain disor-ders that derives from thousands of years of accumulated clinical experience. Trigger point therapy is primarily used to treat myofascial pain and dysfunction, and continues to be a widely used pain treatment method in contemporary medical practice both by primary care physicians and pain management
The qualitative and quantitative comparisons of the ana-tomic locations of common mTrPs and classical acupoints
that at least 93.3 % (238/255) of common mTrP regions
tomic correspondence with classical acupoints. Anatomic correspondence was defi ned as being present when a classical acupoint was proximate to a common mTrP and demonstrated by anatomic references to enter the same muscle region of that trigger point. Another 6 common mTrPs demonstrated anatomic and physiologic (referred-pain) relationships to the acupuncture meridians coursing over them, though there were no proximate classical acu-points. If these mTrPs were considered as corresponding, then the anatomic correspondence of common mTrPs and classical acupoints rises to nearly 96 %. The quantitative analysis of the anatomic proximity of correlated common mTrP- classical acupoint pairs produced estimates that 82 % of these point pairs are located within 2 cm of each other, and 95 % within 3 cm of each other. Though this high degree of anatomic correspondence found between common mTrPs and classical acupoints is unlikely to oc-cur by chance, skeptics might still raise this possibility to challenge the correspondences of the myofascial pain and acupuncture traditions in treating pain. If it can be de-monstrated that these anatomically corresponding trigger points and acupuncture points also have marked similari-ty of their clinical uses and/or physiologic properties (re-ferred-pain and meridian distributions), then this would provide corroborating clinical and physiologic evidence that trigger points and acupoints likely describe the same clinical phenomena. This in turn would suggest that the myofascial pain tradition likely represents an indepen-dent discovery of the acupuncture tradition’s fi ndings in the treatment of pain disorders.The purpose of the second part of this study is to compare the acupuncture and myofascial pain traditions’ clinical indications both in the treatment of pain and somatovis-ceral disorders.
this is likely its most familiar indication to the public
acupuncture points do have pain indications described [2–4], with the exceptions being points BL-8 and ST-
specialists [7, 8].
in the fi rst part of the present study [9] demonstrated
delineated in the Trigger Point Manual [5, 6] have ana-
to its use in the treatment of pain conditions [1], yet
Methods
The clinical indications described in three authoritative acu-
correlated classical acupuncture points from the fi rst part of
disorders. Since the main purpose of this study is specifi cally to compare the acupuncture and myofascial pain traditions in the treatment of pain disorders, pain was not required to be the primary indication of a given classical acupuncture point as long as that acupoint had a pain indication descri-bed by one or more of those acupuncture references.For the analysis of the somatovisceral correspondences of the acupuncture and myofascial pain traditions, the somatovis-ceral eff ects of common mTrPs described in the Trigger Point
acupoints that anatomically corresponded to those mTrPs were examined for similarities in their clinical eff ects.
Results
Of the 238 common mTrPs that anatomically corresponded
221 (93 %) have pain indications described in the Trigger
that have no pain indications described- only somatovis-ceral eff ects. These include the pectoralis major “cardiac arrythmia”, the abdominal external oblique “belch but-ton”, and 15 lower abdominal wall musculature “causes
Another 43 common mTrP regions also have somatovisce-
Thus, a total of 60 common mTrP regions have somatovis-ceral eff ects described.
Pain Correspondences
Comparable regional musculoskeletal or neurologic (“inter-costal neuralgia”, for example) pain indications are descri-bed for 208 (94 %) of the 221 anatomically corresponding
classical acupoints have clinical indications for other pain-ful conditions in the distributions of their anatomically cor-
to 214/221 (~97 %) of classical acupoints have clinical pain indications that are comparable to those described for their anatomically corresponding common trigger point regions.Only 3 % (7/221) of mTrPs had clinical pain indications that diff ered from those of their anatomically corresponding clas-sical acupuncture points. This represented 6 distinct classical acupoints (LI-17, LR-3, LR-9, MH-4, SP-8, and SP-11).
Somatovisceral Correlations
fects for 60 common mTrP regions, which represents nearly 25 % of all trigger points outlined in that text. 17/60 (28 %) of
responding mTrPs’ referred pain (Table 2). Overall, then, up
are distinct from their regional pain indications (Table 1).
this study [9] were examined for their uses in treating pain
puncture references [2–4] for each of the 238 anatomically
Manual [5, 6] were compiled. The somatovisceral indications described by acupuncture references [2–4] for the classical
to a classical acupoint in the fi rst part of this study [ 9],
Point Manual [5, 6]. There are 17 common mTrP regions
diarrhea” mTrP regions [5, 6].
ral eff ects described by the Trigger Point Manual [5, 6] that
classical acupuncture points [2–4]. Another 6 (3 %) of the
The Trigger Point Manual [5, 6] describes somatovisceral ef-
Dt Z tschr f Akup. 5 1 , 4 / 2008 7 DZA

AkupunkturD e u t s c h e Z e i t s c h r i f t f ü r
DZ
AOriginalia | original articles
those common mTrP regions have only non-painful, soma-
“causes diarrhea” trigger point regions represent 15 of those regions; and as demonstrated in Figure 1, those common mTrP regions are located in the distribution of the Spleen and Stomach meridians over the lower anterior abdominal wall musculature. These common mTrPs are proximate to classical acupoints SP-13 and SP-14 laterally and ST-27,
intestinal disorder indications of these classical acupoints
Trigger Point Muscle Region Somatovisceral Eff ect
trapezius, mid-point upper portion
dizziness and “vertigo”
sternocleidomastoid, ster-nal head, middle portion, inferior
“sore throat”
sternocleidomastoid, sternal head, lower portion
paroxysmal dry cough
sternocleidomastoid, clavicu-lar head, lower portion
postural dizziness & less often vertigo
sternocleidomastoid, sternal head, middle portion, su-perior
“sore throat”
sternocleidomastoid, clavicu-lar head, middle portion
postural dizziness & less often vertigo
sternocleidomastoid, clavicu-lar head, upper portion
postural dizziness & lessoften vertigo
sternocleidomastoid, sternal head, upper portion
“sore throat”
masseter, superfi cial layer, upper portion, anterior
posterior upper teeth pain
masseter, superfi cial layer, upper portion, posterior
posterior upper teeth pain
masseter, superfi cial layer, middle portion, anterior
posterior lower teeth pain
masseter, superfi cial layer, middle portion, posterior
posterior lower teeth pain
masseter, deep layer tinnitus
temporalis, anterior portion maxillary incisor pain
temporalis, middle portion, anterior
pain in maxillary teethjust behind incisor (“intermediate teeth“)
temporalis, middle portion, posterior
posterior maxillary teeth pain
lateral pterygoid, superior portion
“sinusitis”
lateral pterygoid, inferior portion
“sinusitis”
Table 1 Somatovisceral Eff ects of Myofascial Trigger Points That Also Have Pain Indications
ST-28, and ST-29 medially. Table 3 delineates the gastro-
tovisceral indications described [5, 6], as outlined above. The
[2–4]. Note that some of these acupoints have indications for
DZA 8 Dt Z tschr f Akup. 5 1 , 4 / 2008
digastric, posterior belly diffi culty swallowing
splenius capitis “ache inside the skull”, vertex headache
splenius cervicis, upper portion
“ache inside the skull“, blurred near vision, diff use pain inside head focusing behind the eye
rectus capitis posterior major “headache ghosts”
obliquus capitis inferior “headache ghosts”
pectoralis major, intermedi-ate sternal section, upper
“heart attack”
pectoralis major, intermedi-ate sternal section, middle
“heart attack”
pectoralis major, intermedi-ate sternal section, lower
“heart attack”
pectoralis major, lateral free margin, medial
breast pain
pectoralis major, lateral free margin, lateral
breast pain
pectoralis major, parasternal section, upper
“heart attack”
pectoralis major, parasternal section, lower
“heart attack”
pectoralis minor, upper mimics cardiac ischemia
pectoralis minor, lower mimics cardiac ischemia
sternalis mimics cardiac ischemia
serratus anterior “short of breath”
iliocostalis thoracis, mid-thoracic level
mimics cardiac ischemia or pleurisy
external oblique, anterior upper portion
“heartburn”
external oblique, anterior middle portion
“inguinal and testicular pain, lower quadrant abdominal pain”
external oblique, anterior lower portion
“inguinal and testicular pain, lower quadrant abdominal pain”
rectus abdominus, upper portion
“abdominal fullness, nausea, and vomitting”
both constipation and enteritis. A clinician can theoretically produce opposite clinical eff ects at a given acupoint depen-ding on how the needle is manipulated there. Overall, the somatovisceral indications of 49/60 (82 %) of common mTrP regions were defi nitely comparable to those of their anatomically corresponding classical acu-points, and another 7 (11 %) of anatomically correspon-ding common mTrP- classical acupoint pairs had probab-
(7 %) point pairs had no correlation of their somatovisceral le corresponding somatovisceral eff ects (Table 4). Only 4
eff ects (Table 5).

Originalia | original articles
P. T. Dorsher, J . F leckenste in Trigger Points and Classical Acupuncture Points
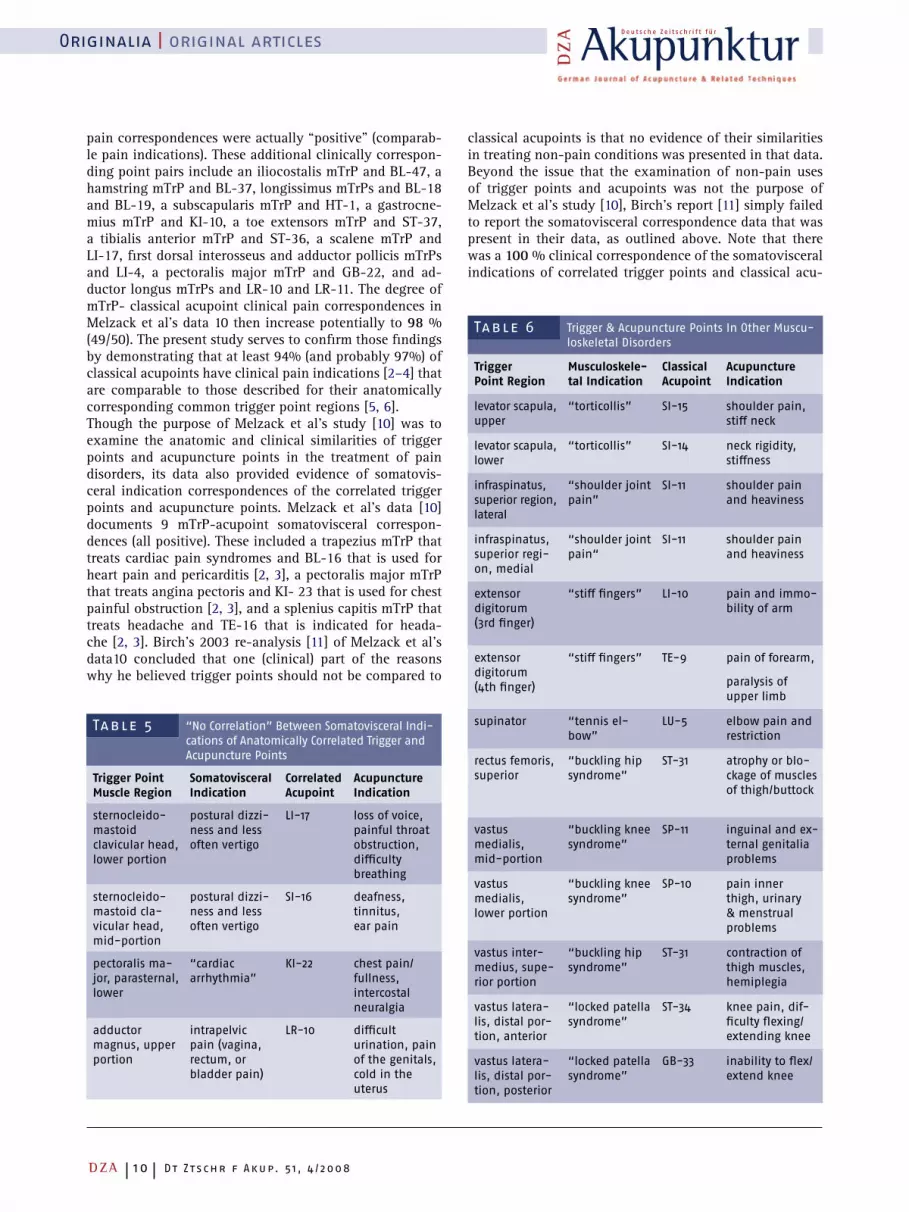
Other musculoskeletal eff ects of trigger point regions were described for 15 regions which are generally non-painful
sponding classical acupoints demonstrated defi nite or pro-bable agreement for 11/13 (85 %) of these point pairs.
Discussion
dence of 48 trigger points with 50 acupuncture points tradi-tionally used to treat pain disorders but found their clinical correspondence in treating pain disorders was somewhat lower (71 %). In reality, however, if the data of Melzack et
probably 14 of their 15 “negative” mTrP-acu point clinical
Trigger Point Muscle
Region
Corres-
ponding
Acupoint
Acupuncture Point
Pain Indication(s)
sphincter ani, superior region (perianal referred pain)
GV-1 hemorrhoid pain, heaviness of sacrum
sphincter ani, lateral region (perianal referred pain)
GV-1 hemorrhoid pain, heaviness of sacrum
levator ani (perianal referred pain)
GV-1 hemorrhoids, anal prolapse, lumbar pain
gluteus medius, medial region (referred pain to ipsilateral low lumbar region & medial buttock)
BL-27 testicular pain radia-ting to lumbar region
adductor magnus, upper region (referred pain into pelvis)
BL-36 diffi cult urination or defecation, hemor-rhoids, cold in uterus
soleus, exceptional point (referred pain to ipsilateral face & jaw)
GB-35 facial swelling, leg pain
Table 2 Acupoints With Clinical Pain Indications in the Distribution of Their Anatomically Correspon-ding Trigger Points’ Referred-Pain
(Table 6), and the indications of their anatomically corre-
Melzack et al. [10] reported a 100 % anatomic correspon-
al’s study [10] is carefully examined, then at least 9 and
Figure 1. The “Causes Diarrhea” Trigger Point Regions & Their Relationships to the Principal Meridians with their Classical Acupuncture Points(adapted from Primal Pictures images, with permission)
Trigger Point
Muscle Region
Myofascial
Indication
Classical
Acupoint
Acupoint
Indication
temporalis, middle portion, posterior
posterior uppertooth pain
GB-7 used to treat tooth decay with ST-42
lateral pterygoid, upper
“sinusitis” ST-7 pain/swelling of cheek
lateral pterygoid, lower
“sinusitis” ST-7 pain/swelling of cheek
lower abdominal obliques, right
“causesdiarrhea”
ST-28 distension abdo-men, retention feces
lower abdominal obliques, left
“causesdiarrhea”
ST-28 distension abdomen, retenti-on feces
soleus “exceptio-nal” lower portion, lateral
pain to jaw and cheek
GB-35 swelling of face/eyes, throat pain-ful obstruction
Table 4 “Probable” Agreement Between Somatovisce-ral Indications of Trigger Points and Classical Acupuncture Points
Dt Z tschr f Akup. 5 1 , 4 / 2008 9 DZA
Table 3 “Causes Diarrhea” Trigger Points and Gastrointestinal Indications of their Anatomically Corresponding Classical Acupoints (D = Deadman, S = Shanghai, and C = Chen)
Trigger Point Region Myofascial Indication Classical Acupoint Acupoint Indication(s)
abdominal obliques (3 regions) “causes diarrhea” SP-13 constipation (D) enteritis (C)
abdominal obliques (4 regions) “causes diarrhea” SP-14 diarrhea and dysentery (D)enteritis (C)
abdominal obliques (4 regions) “causes diarrhea” ST-27 abdominal distension (D)constipation, enteritis (C)
abdominal obliques (2 regions) “causes diarrhea” ST-28 retention of feces (D)lower abdomen distension (C)
abdominal obliques (2 regions) “causes diarrhea” ST-29 colic (S)
AkupunkturD e u t s c h e Z e i t s c h r i f t f ü r
DZ
AOriginalia | original articles
pain correspondences were actually “positive” (comparab-le pain indications). These additional clinically correspon-ding point pairs include an iliocostalis mTrP and BL-47, a hamstring mTrP and BL-37, longissimus mTrPs and BL-18 and BL-19, a subscapularis mTrP and HT-1, a gastrocne-mius mTrP and KI-10, a toe extensors mTrP and ST-37, a tibialis anterior mTrP and ST-36, a scalene mTrP and LI-17, fi rst dorsal interosseus and adductor pollicis mTrPs and LI-4, a pectoralis major mTrP and GB-22, and ad-ductor longus mTrPs and LR-10 and LR-11. The degree of mTrP- classical acupoint clinical pain correspondences in Melzack et al’s data 10 then increase potentially to 98 % (49/50). The present study serves to confi rm those fi ndings by demonstrating that at least 94% (and probably 97%) of
are comparable to those described for their anatomically
examine the anatomic and clinical similarities of trigger points and acupuncture points in the treatment of pain disorders, its data also provided evidence of somatovis-ceral indication correspondences of the correlated trigger
documents 9 mTrP-acupoint somatovisceral correspon-dences (all positive). These included a trapezius mTrP that treats cardiac pain syndromes and BL-16 that is used for
that treats angina pectoris and KI- 23 that is used for chest
treats headache and TE-16 that is indicated for heada-
data10 concluded that one (clinical) part of the reasons why he believed trigger points should not be compared to
Table 5 “No Correlation” Between Somatovisceral Indi-cations of Anatomically Correlated Trigger and Acupuncture Points
Trigger Point
Muscle Region
Somatovisceral
Indication
Correlated
Acupoint
Acupuncture
Indication
sternocleido-mastoid clavicular head, lower portion
postural dizzi-ness and less often vertigo
LI-17 loss of voice, painful throat obstruction, diffi culty breathing
sternocleido-mastoid cla-vicular head, mid-portion
postural dizzi-ness and less often vertigo
SI-16 deafness, tinnitus, ear pain
pectoralis ma-jor, parasternal, lower
“cardiac arrhythmia”
KI-22 chest pain/ fullness, intercostal neuralgia
adductor magnus, upper portion
intrapelvic pain (vagina, rectum, or bladder pain)
LR-10 diffi cult urination, pain of the genitals, cold in the uterus
classical acupoints have clinical pain indications [2–4] that
corresponding common trigger point regions [5, 6].Though the purpose of Melzack et al’s study [10] was to
points and acupuncture points. Melzack et al’s data [10]
heart pain and pericarditis [2, 3], a pectoralis major mTrP
painful obstruction [2, 3], and a splenius capitis mTrP that
che [2, 3]. Birch’s 2003 re-analysis [11] of Melzack et al’s
DZA 10 Dt Z tschr f Akup. 5 1 , 4 / 2008
classical acupoints is that no evidence of their similarities in treating non-pain conditions was presented in that data. Beyond the issue that the examination of non-pain uses of trigger points and acupoints was not the purpose of
to report the somatovisceral correspondence data that was present in their data, as outlined above. Note that there was a 100 % clinical correspondence of the somatovisceral indications of correlated trigger points and classical acu-
Table 6 Trigger & Acupuncture Points In Other Muscu-loskeletal Disorders
Trigger
Point Region
Musculoskele-
tal Indication
Classical
Acupoint
Acupuncture
Indication
levator scapula, upper
“torticollis” SI-15 shoulder pain, stiff neck
levator scapula, lower
“torticollis” SI-14 neck rigidity, stiff ness
infraspinatus, superior region, lateral
“shoulder joint pain”
SI-11 shoulder pain and heaviness
infraspinatus, superior regi-on, medial
“shoulder joint pain“
SI-11 shoulder pain and heaviness
extensor digitorum (3rd fi nger)
“stiff fi ngers” LI-10 pain and immo-bility of arm
extensor digitorum (4th fi nger)
“stiff fi ngers” TE-9 pain of forearm,
paralysis of upper limb
supinator “tennis el-bow”
LU-5 elbow pain and restriction
rectus femoris, superior
“buckling hipsyndrome”
ST-31 atrophy or blo-ckage of muscles of thigh/buttock
vastus medialis, mid-portion
“buckling kneesyndrome”
SP-11 inguinal and ex-ternal genitalia problems
vastus medialis, lower portion
“buckling kneesyndrome”
SP-10 pain inner thigh, urinary & menstrual problems
vastus inter-medius, supe-rior portion
“buckling hipsyndrome”
ST-31 contraction of thigh muscles, hemiplegia
vastus latera-lis, distal por-tion, anterior
“locked patellasyndrome”
ST-34 knee pain, dif-fi culty fl exing/extending knee
vastus latera-lis, distal por-tion, posterior
“locked patellasyndrome”
GB-33 inability to fl ex/extend knee
Melzack et al’s study [10], Birch’s report [11] simply failed

Originalia | original articles
P. T. Dorsher, J . F leckenste in Trigger Points and Classical Acupuncture Points
Summary
93 % (221/238) of anatomically corresponding • mTrPs have pain indications described by the Trig-ger Point Manual. 94 % (208/221) of anatomically corresponding • classical acupoints have comparable regional pain indications described. Another 6 classical acupoints (3• %) have indica-tions for painful conditions in the distributions of their correlated mTrPs’ described referred-pain. 60 (24• %) of common mTrPs described by the Trig-ger Point Manual have somatovisceral eff ects At least 93 % (56/60) of their anatomically corre-• sponding classical acupoints have somatovisceral indications described that are defi nitely or proba-bly comparable.
ted to generalize his demonstrably incorrect conclusion about the lack of reported somatovisceral eff ects of trigger
ted in the present study to document somatovisceral eff ects for nearly 25 % of the 255 trigger point regions reported. More over, the somatovisceral eff ects described for those
in over 93 % of comparisons!This near-complete clinical correspondence of common mTrPs and classical acupuncture points in the treatment of pain disorders (at least 94 %) as well as somatovisceral disorders (at least 93 %) documented in the present study provides clinical evidence that complements the evidence of their anatomic correspondences (at least 93.3 %) presented
and classical acupoints likely are describing the same phy-siologic phenomena. Even if skeptics were to argue that the 93.3 % anatomic correspondence found between common mTrP regions and classical acupuncture points found in this study could occur by chance (however unlikely), it would be even more improbable that these anatomically correlated point pairs would, by chance, also demonstrate nearly 97 % correlation in their pain indications and a 94 % correlation in their somatovisceral eff ects.
to Birch for over a decade before his report) is demonstra-
points in Melzack et al’s data [10] to all trigger points, even
their anatomically corresponding classical acupoints [2–4]
points in that data [10]! Birch’s 2003 report [11] attemp-
though the Trigger Point Manual [5, 6] (that was available
common mTrPs [5, 6] are similar to those described for
in the fi rst part of this study [9] to suggest that trigger points
The third (fi nal) part of this study will provide yet an-other line of evidence of the similarities of the myofascial pain and acupuncture traditions by demonstrating the strong correspondences of the distributions of the myo-fascial referred-pain patterns and acupuncture meridians of anatomically corresponding common mTrP-classical acupoint pairs.
Conclusions
to 97 %) and somatovisceral indications (> 93 %) of ana-tomically corresponding common trigger point-classical acupuncture point pairs (classical acupoints that are pro-ximate to and enter the muscle region of their correlated common mTrPs). This provides a second, clinical line of evidence that trigger points and acupuncture points likely are describing the same physiologic phenomena.
ReferencesHelms JM. Acupuncture energetics: a clinical approach for physicians. Ber- 1. keley: Medical Acupuncture Publishers; 1995Deadman P, Al-Khafaji M, Baker K. A manual of acupuncture. Hove, East 2. Sussex (UK): Journal of Chinese Medicine Publications; 1998O’Connor J, Bensky D. Acupuncture: a comprehensive text. Chicago: 3. Eastland Press; 1981Chen E. Cross-sectional anatomy of acupoints. Edinburgh: Churchill 4. Livingstone; 1995Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point 5. manual. Vol 1. Baltimore: Williams and Wilkins; 1983Travell JG, Simons DG. Myofascial pain and dysfunction: the trigger point 6. manual. Vol 2. Baltimore: Williams and Wilkins; 1992Manchikanti, L. Medicare in interventional pain management: a critical 7. analysis. Pain Physician. 2006;9(3):171–197Peng PW, Castano ED. Survey of chronic pain practice by anesthesiologists 8. in Canada. Canadian J Anesth. 2005;52(4):383–389Dorsher PT, Fleckenstein J. Trigger points and classical acupuncture 9. points: part 1: qualitative and quantitative anatomic correspondences. Dt Ztschr f Akup. 2008;51,3:15–24Melzack R, Stillwell DM, Fox EJ. Trigger points and acupuncture points for 10. pain: correlations and implications. Pain. 1977;3:3–2Birch S. Trigger point: acupuncture point correlations revisited. J Altern 11. Complement Med. 2003;9:91-103Wiseman N, Ellis A. Fundamentals of chinese medicine. Brookline, Para-12. digm Publishers, 1996
The Trigger Point Manual [5, 6] and authoritative acu-
clinical correspondences of both the pain indications (up puncture references [2–4] document that there are marked
Dt Z tschr f Akup. 5 1 , 4 / 2008 1 1 DZA