treatment of superior limbic keratoconjunctivitis with a unilateral bandage contact lens
TRANSCRIPT

PostScript..............................................................................................
LETTERS
Treacher Collins syndrome withnovel ophthalmic findings andvisceral anomaliesTreacher Collins syndrome (TCS) (mandibu-lofacial dysostosis (MFD) or zygoauroman-dibular dysplasia) is one of a group ofcongenital malformation syndromes thathave in common maldevelopment of the firstand second branchial arches.1 Clinical featurestypically include hypoplasia of the mandibleand zygoma; a complex variety of ear abnor-malities including malformed pinnae, atresiaof the external auditory canals and anomaliesof the middle ear ossicles; cleft palate;receding chin; and sinus and choanal atresia.2
We present a pair of twins that possessed notonly classic features of TCS but also unusualvisceral and previously unreported ophthal-mic pathology.
Case reportsA 32 year old, gravida 3 para 2-0-0-2 womanunderwent elective abortion after fetal deathand major fetal malformations were diag-nosed during pregnancy. Ultrasound exam-ination at 20 weeks of gestation displayedmonozygotic, diamniotic twins. Fetus A, notedalive at 16 weeks, was dead and surrounded
by minimal amniotic fluid. Fetus B was alivewith several anomalies including bilateralinfraorbital cystic masses, protruding tongue,and large median facial cleft. Amniocentesisrevealed a 46XY karyotype without numericalor structural chromosomal abnormalities. Theparents denied any significant medical his-tory, family history, of congenital anomalies,or use of drugs or alcohol. Their two otherchildren, ages 17 and 33 months, werenormal. No family members exhibited fea-tures of TCS on visual examination.
Necropsy measurements were consistentwith 16 weeks of gestational age for twin Aand 21 weeks for twin B. Both twins hadbilaterally hypoplastic zygomas, maxillae, andrelated muscles; severely hypoplastic andmisplaced pinnae; bilaterally agenic externalauditory canals; bilateral lateral facial clefts,and severe micognathia (Fig 1). Twin Aexhibited left sided choanal atresia, agenesisof the hard and soft palate, and multiplevisceral anomalies, including dual superiorvena cava, bilobed right and unilobed leftlungs, bilateral renal and ureteral agenesis,rudimentary urinary bladder, and absentepididymides. Twin B was noted to have rightsided choanal atresia, soft palate aplasia, hardpalate hypoplasia, and a left sided cleft; twin Bhad no visceral anomalies. Ocular pathologi-cal dissection of twin A illustrated bilateralmicrophthalmia; corneal scleralisation; andmaldevelopment of the uvea, lens, and retina.Ocular dissection of twin B revealed microph-thalmia, aniridia, congenital cataracts, andbilateral vascularisation of the corneas.
CommentThese twins had multiple features character-istic of TCS, most notably hypoplastic zygo-mas, maxillae, and related muscles—perhapsthe most characteristic features of TCS. Incontrast, visceral anomalies, such as those oftwin A, are rare. Only two cases have beenpreviously reported: one with tracheoesopha-geal fistula, rectovaginal fistula, and analatresia; another with achalasia.3 Renal agen-esis, found in twin A, has not been previouslydescribed in association with TCS. While oph-thalmological features in TCS are often exten-sive, they seldom involve the intraocularstructures. Common findings include a defec-tive inferior lateral angle of the orbit, caudaldisplacement of the superolateral orbit, true
and pseudocolobomas of the lids, lateral can-thal dystopia, orbital lipodermoids, corneo-scleral dermoids, and microphthalmos.4 Cata-racts, lacrimal duct atresia, pupillary ectopia,distichiasis, and uveal colobomas have beenreported less commonly. The extensive in-traocular involvement in these twins is rare inTCS. Furthermore, aniridia, corneal scleralisa-tion, and uveal, lens, and retinal maldevelop-ment are previously unreported.
TCS is an autosomal dominant disorderaffecting one in 50 000 live births. Thedisorder appears to have arisen in these twinswith no relevant family history, as occurs in60% of cases.5 Expressivity is highly variable,ranging from clinically undetectable to peri-natal death secondary to airway compromise6;the disease severity that resulted in the fetaldeath of twin A is highly unusual. Theresponsible gene, TCOF1, has been mapped to5q32–33.2 7 and the structure of its proteinproduct, treacle, elucidated.8 To date, 51disease causing mutations have beenidentified,9 nearly all resulting in a prematuretermination codon.10 Significantly, no relationhas been found between any single mutationand phenotype severity. The ophthalmicpathology observed in these twins may haveresulted from a focal TCOF1 mutation and ayet to be defined role treacle may have in eye(and renal) development. Considering thenumber and severity of abnormalities, thefailure to identify a single “genetic hot spot,”and the novel ophthalmic features, an alter-native and perhaps more likely explanation isthat a second gene, itself involved in ophthal-mic embryology, was affected along withTCOF1. This unidentified gene may have beendisrupted from a translocation involving5q32–33.2 or from a deletion large enough toresult in a contiguous gene syndrome. A finalconsideration is that these twins may not havehad TCS but rather a new though closelyrelated syndrome. Further genetic investiga-tion may shed light upon these speculations.
AcknowledgementsJLP and GB contributed equally to this work.
J L Prenner, G Binenbaum,D F Carpentieri, S M Goldstein,
R S Douglas, E Ruchelli, J A KatowitzScheie Eye Institute, Department of Ophthalmology,University of Pennsylvania; Departments of PediatricOphthalmology and Pathology, Children’s Hospital
of Philadelphia; Philadelphia, Pennsylvania, USA
R W HertleThe Laboratory of Sensorimotor Research, The
National Eye Institute, The National Institutes ofHealth; Bethesda, Maryland, USA
Correspondence to: J L Prenner, MD, Department ofOphathalmology, Scheie Eye Institute, University ofPennsylvania, 51 North 39th Street, Philadelphia,
PA 19106, USA; [email protected]
Accepted for publication 7 September 2001
References1 Van der Meulen J, Mazzola R, Stricker M, et
al. Classification of craniofacialmalformations. In: Stricker M, Van der MeulenJ, Raphael B, Mazzola R, eds. Craniofacialmalformations. New York: ChurchillLivingstone, 1989:149–309.
2 Phelps PD, Poswillo D, Lloyd GAS. The eardeformities in mandibulofacial dysostosis. ClinOtolaryngol 1981;61:15–28.
If you have a burning desire to respond toa paper published in the BJO, why notmake use of our “rapid response” option?
Log on to our website(www.bjophthalmol.com), find the paperthat interests you, and send your responsevia email by clicking on the “eLetters”option in the box at the top right handcorner.
Providing it isn’t libellous or obscene, itwill be posted within seven days. You canretrieve it by clicking on “read eLetters”on our homepage.
The editors will decide as beforewhether to also publish it in a futurepaper issue.
Figure 1 Gross photographs of fetal twins with features of Treacher Collins syndrome: (A)and (B) are twin B (21 weeks of gestational age); (C) is twin A (16 weeks of gestational age).
Br J Ophthalmol 2002;86:472–488472
www.bjophthalmol.com

3 Robb LJ. Treacher Collins-Franceschettisyndrome with tracheoesophageal fistula,rectovaginal fistula, and anal atresia: variantor new syndrome? Am J Med Genet1991;39:119–20.
4 Hertle RW, Ziylan S, Katowitz JA.Ophthalmic features and visual prognosis inthe Treacher-Collins syndrome. Br JOphthalmol 1993;77:642–5.
5 Jones KL, Smith DW, Harvey MA, et al.Older paternal age and fresh gene mutation:data on additional disorders. J Pediatr1975;86:84–8.
6 Edwards SJ, Fowlie A, Cust MP, et al.Prenatal diagnosis in Treacher Collinssyndrome using combined linkage analysisand ultrasound imaging. J Med Genet1996;33:603–6.
7 Treacher Collins Syndrome CollaborativeGroup. Positional cloning of a gene involvedin the pathogenesis of Treacher Collinssyndrome. Nat Genet 1996;12:130–6.
8 Wise CA, Chiang LC, Paznekas WA, et al.TCOF1 gene encodes a putative nucleolarphosphoprotein that exhibits mutations inTreacher Collins syndrome throughout itscoding region. Proc Nat Acad Sci1997;94:3110–5.
9 Splendore A, Silva EO, Alonso LG, et al.High mutation detection rate in TCOF1 amongTreacher Collins syndrome patients revealsclustering of mutations and 16 novelpathogenic changes. Hum Mutat2000;16:315–22.
10 Edwards SJ, Gladwin AJ, Dixon MJ. Themutational spectrum in Treacher Collinssyndrome reveals a predominance ofmutations that create a premature-terminationcodon. Am J Hum Genet 1997;60:515–24.
Acute postural drop in opticnerve perfusion after vitrectomyand gas in a patient withdiabetic autonomic neuropathyWe report the case of an insulin dependentdiabetic who suffered transient blindness as aresult of a change of posture following vitrec-tomy surgery with injection of gas.
This 34 year old woman with longstandingdiabetic disease, postural hypotension, andproliferative retinopathy had undergoneargon laser panretinal photocoagulation(PRP) to both eyes. Her right eye was ambly-opic and had visual acuity of counting fingers(CF), whereas the left eye, at best, had visionof 6/12 that was frequently impaired by recur-rent vitreous haemorrhage. She underwentleft vitrectomy and required 30% sulphurhexafluoride (SF6) gas to support an inciden-tal small, inferior detachment related to around hole. The patient postured supine over-night and remained under the care of thephysicians.
The following day her vision droppedsuddenly and severely on her way to the eyeclinic. Visual acuity was no perception of light(NPL) in the operated eye and CF in the righteye. The left pupil was already dilated andanterior segment examination was satisfac-tory. The view of the fundus was limitedowing to the presence of gas and residualhaemorrhage but the retina was flat. Theintraocular pressure (IOP) was 42 mm Hg andher blood pressure (BP) was 70/40. A decisionto withdraw 0.5 ml of gas from the eye wasmade. While the patient was lying down forthis procedure she immediately noted animprovement in vision to light perception. Herblood pressure improved in the supine posi-tion to 150/80. Following removal of gas theIOP fell to 20 mm Hg and the vision improvedto counting fingers. Four weeks later, withdisappearance of the gas her best correctedvision had improved to 6/18 and the retinaremained flat.
CommentJudging by the severity of the visual loss webelieve that it was due to obstruction of boththe central retinal artery and optic nerve per-fusion. The precipitating factor in this casewould appear to have been the change in pos-ture from supine to erect. The presence of gasin the operated eye had raised the intraocularpressure to a level such that the perfusionpressure to the eye was effectively eliminatedresulting in a period of no light perception.Restoring the patient to the supine positionwas sufficient alone to reverse the conditionand improve the perfusion of the eye. Whenthe IOP was reduced to normal she was out ofthis critical situation and was able to maintainthe ocular perfusion, even when sitting.
Collapse of the central retinal artery isknown to occur in conditions of high IOP1 butvision does not fluctuate with posture. How-ever, it is known that raised IOP also reducesorthograde axonal transport and compro-mises nerve head perfusion.2
Postural hypotension in diabetics is second-ary to autonomic neuropathy. The patho-physiology is not clear but it seems the mainfactor is blunted catecholamine response tostanding and failure of the lower limb vascu-lar resistance to increase adequately.3 Sys-temic hypotension can reduce optic nerveblood flow as illustrated by numerous reportsin the literature of non-arteritic anteriorischaemic optic neuropathy (NA-AION) oc-curring following acute blood loss.4–6 Patientswith NA-AION have a significantly greaterpostural pressure change in IOP comparedwith healthy subjects as shown by James andSmith.7 In the same study they demonstrateda higher pulsatile ocular blood flow (POBF) onstanding compared with supine. In thispatient with autonomic neuropathy it is likelythat the normal increase in POBF on standingwas inadequate.
We advise particular caution in diabeticsundergoing ocular surgery in which theremay be a significant postoperative pressurerise. Similar problems can occur duringsurgery if hypotensive anaesthesia is eitherdeliberately or inadvertently employed in dia-betics. Beware of assuming poor postoperativevision to be purely the result of the presence ofhaemorrhage or gas; patients may have quitepoor vision immediately after vitreoretinalsurgery but will rarely have NPL unless thereis also optic nerve compromise. We alsosuggest one should to aim for a lower postop-erative IOP in diabetics.
A Al Khaier, J C Khan, R L BurtonDepartment of Ophthalmology, The West NorwichHospital, Bowthorpe Road, Norwich NR2 3TQ, UK
Correspondence to: Mr Burton;[email protected]
Accepted for publication 12 September 2001
References1 Abrams GW, Swanson DE, Sabates WI, et al.
The result of sulfur hexoflurride gas in vitreoussurgery. Am J Ophthalmol 1982;94:165.
2 Hayreh SS, March W, Anderson DR.Pathogenesis of block of rapid orthogradeaxonal transport by elevated intraocularpressure. Exp Eye Res 1979;28:515–23.
3 Purewal TS, Goss DE, Zanone MM, et al. Thesplanchnic circulation and posturalhypotension in diabetic autonomicneuropathy. Diabet Med 1995;12:513–22.
4 Sharma R, Desai S. Postpartum haemorrhageproducing acute ischaemic optic neuropathy.Asia Oceania J Obstet Gynaecol1993;19:249–51.
5 Connolly SE, Gordon KB, Horton JC. Salvageof vision after hypotension induced ischaemic
optic neuropathy. Am J Ophthalmol1994;117:235–42.
6 Chopra KB, Banka NH, Chandalia HB.Bilateral optic nerve infarction following acutesystemic hypotension and anaemia, a casereport. Indian J Ophthalmol 1992;40:66–9.
7 James CB, Smith SE. The effect of posture onthe intraocular pressure and pulsatile ocularblood flow in patients with non-arteriticanterior ischaemic optic neuropathy. Eye1991;5 (Pt 3):309–14.
Optical coherence tomographyimaging of severe commotioretinae and associated macularholeCommotio retinae results in retinal opacifica-tion following blunt trauma. Mild commotioretinae usually settles spontaneously withminimal sequelae but more severe cases areassociated with visual loss. We are not awareof any previous reports describing opticalcoherence tomography (OCT) imaging ofsevere commotio retinae with an associatedfull thickness macular hole (FTMH).
Case reportA 15 year old boy presented 24 hours afterblunt trauma from a football striking his righteye. On examination his best corrected visualacuity was counting fingers right eye and 6/6left. Biomicroscopic examination revealedextensive commotio retinae over the posteriorpole, no posterior vitreous detachment (PVD),and a FTMH. Colour photography and OCTimaging (OCT 2000 scanner, Zeiss-Humphrey) were performed (Fig 1). OCTconfirms a FTMH and demonstrates extensivedisruption of photoreceptor outer segmentsand retinal pigment epithelium (RPE).
Figure 1 (A) Right macula of 15 year oldboy with extensive commotio retinae overposterior pole and an associated macularhole at 1 day after blunt injury. (B)Horizontal OCT scan through centre ofmacula confirms a full thickness macular holeand demonstrates extensive disruption ofphotoreceptor outer segment/retinal pigmentepithelium layer. The optic disc is seen at thenasal edge of the scan.
PostScript 473
www.bjophthalmol.com

He was treated conservatively with a shortcourse of topical steroids. The colour fundusand OCT appearance at 1 month are shown inFigure 2. Despite spontaneous macular holeclosure, visual acuity remained at countingfingers at 1 year follow up.
CommentThe major site of retinal trauma appeared onOCT to be at the level of the photoreceptorouter segment/RPE interface. The OCT imagesare consistent with fragmentation of photore-ceptor outer segments and damaged cell bod-ies, as suggested by Sipperley et al1 in theirstudy of the histological changes in commotioretinae in primates.
The exact pathogenesis of macular holesremains uncertain. Ho et al2 outlined the threebasic historical theories regarding aetiology—the traumatic theory, the cystic degenerationand vascular theory, and the vitreous theory.Of these, the latter has gathered the most sup-port in the context of idiopathic macular holes.
In our case, the OCT imaging reveals thatthe edges of the macular hole are ellipticaland irregular with no associated PVD, corticalvitreous condensation, or overlying prefovealopacity. The characteristics suggest a differentmechanism of hole formation from thatproposed in idiopathic senile macular holes.We believe that mechanical distortion of theretina, relative to the vitreous and underlyingsclera, created disruption of the photoreceptorouter segments and creation of a FTMH in thiscase. It is at the fovea and photoreceptor outersegment level that the retina has the leastsupport from Müller cells and is thereforelikely to undergo greatest deformation.
In the only previous report of OCT imagingin traumatic macular hole, a case with mildcommotio retinae was described in which
extensive outer retinal disruption was notobserved.3 There have been some encouragingreports suggesting that vitrectomy can suc-cessfully close traumatic macular holes as wellas improve visual function in many cases.4 5
However, it seems unlikely that cases withsevere commotio retinae, and associatedphotoreceptor/RPE damage, as demonstratedin our cases, would gain any benefit from sur-gical as opposed to spontaneous closure of atraumatic FTMH. The final visual prognosis isseverely limited by the extent of initialphotoreceptor damage, and the excessive pig-ment atrophy and clumping that follows.
We believe OCT imaging provides additionalinformation both on the pathogenesis ofcommotio retinae and in the assessment ofouter retina disruption following oculartrauma. This information may help in theselection of patients likely to benefit fromsurgical intervention.
R Ismail, V TannerRoyal Berkshire Hospital, London Road, Reading,
RG1 5AN, UK
T H WilliamsonSt Thomas’s Hospital, Lambeth Palace Road,
London SE1 7EH, UK
Correspondence to: Mr V Tanner;[email protected]
Accepted for publication 26 September 2001
References1 Sipperley JO, Quigley HA, Gass DM.
Traumatic retinopathy in primates. Theexplanation of commotio retinae. ArchOphthalmol 1978;96:2267–73.
2 Ho AC, Guyer DR, Fine SL. Macular hole.Surv Ophthalmol 1998;42:393–416.
3 Parmar DN, Stanga PE, Reck AC, et al.Imaging of a traumatic macular hole withspontaneous closure. Retina 1999;19:470–2.
4 Amari F, Ogino N, Matsumura M, et al.Vitreous surgery for traumatic macular holes.Retina 1999;19:410–3.
5 Johnson RN, McDonald R, Lewis H, et al.Traumatic macular hole. Observations,pathogenesis, and results of vitrectomysurgery. Ophthalmology 2001;108:853–7.
Acute ocular ischaemia andorbital inflammation associatedwith systemic lupuserythematosusWe report a patient with systemic lupuserythematosus (SLE) who developed bilateralocular ischaemic syndrome in associationwith orbital inflammation leading to devas-tating visual loss.
Case reportA 73 year old white woman presented withunilateral acute anterior uveitis and polyar-thropathy of the hands, knees, and neck. Overthe next 4 years she suffered recurrentanterior uveitis, marginal keratitis, and epis-cleritis, which were treated with topicalsteroids. She had bilateral age related cataractand underwent left cataract surgery. Postop-eratively, her visual acuities were 6/60 righteye and 6/9 left eye.
She was admitted 7 months later withextensive erythematous, scaly plaques on sunexposed areas and a purpuric eruption overthe abdomen, buttocks, and legs. Biopsy of aplaque showed changes consistent with SLEincluding follicular keratin plugging, epider-mal atrophy, degeneration of the basal layerwith colloid body formation, basement mem-brane thickening, myxoid change in the
dermis, and periappendageal lymphocyte in-filtrates. Biopsy of the purpuric eruption wasconsistent with a leucocytoclastic vasculitis.Further investigations revealed positive rheu-matoid factor (1/100), ANA (1/25), pANCA(1/100), and anti-EN antibodies (1/100).There was reduced C3 and C4, polyclonalincrease in IgA and IgM, lymphopenia,thrombocytopenia, and reduced creatinineclearance but no proteinuria. Anticardiolipinantibodies were negative. A diagnosis of SLEwas made and oral prednisolone (0.8 mg/kg)was commenced.
Three weeks later she developed a rapidonset of marked bilateral conjunctival and lidoedema, subconjunctival haemorrhage, andproptosis. Visual acuity deteriorated to per-ception of light in each eye. There was grossrestriction of ocular movements. Signs of ocu-lar ischaemia developed in both eyes withcorneal oedema, iris neovascularisation, fibri-nous anterior uveitis, hyphaema, and raisedintraocular pressure (Fig 1). Computed tom-ography and B-scan ultrasonography of theorbits showed posterior scleritis, choroidaldetachment, vitreous haemorrhage, andthickening of the extraocular muscles (Fig 2).
She was treated with topical dexametha-sone 0.1% and carteolol 1%, oral acetazola-mide 500 mg daily, intravenous cyclophospha-mide (10 mg/kg), and subsequentlyintravenous immunoglobulin (0.5 g/kg/dayfor 3 days). Over the following month therewas regression of the proptosis, conjunctivaland lid oedema, corneal oedema, and fibri-nous uveitis. The intraocular pressure wascontrolled and the visual acuity remainedperception of light in each eye. Subsequently,the patient developed pneumonia, VIIth nervepalsy, left sided hemiparesis, and died 7 weeksafter admission. Postmortem examinationrevealed bronchopneumonia, lung abscess,pleural effusions,fibrinous pericarditis,cardio-megaly, and jejunal mucosal haemorrhages.
Figure 2 (A) Right macula 1 month afterinjury with extensive retinal pigmentepithelium disruption, marked epiretinalmembrane, and spontaneous closure of themacular hole. (B) Horizontal OCT scanthrough centre of right macular confirmsresolution of commotio retinae, spontaneousclosure of macular hole, and disruption of thephotoreceptor/retinal pigment epitheliumreflex.
Figure 1 Anterior segment of right eyeshowing conjunctival injection, cornealoedema, hyphaema, rubeosis iridis, andcataract
Figure 2 B-scan ultrasound of left eyeshowing marked posterior scleritis (crosses)and choroidal detachment (arrow).
474 PostScript
www.bjophthalmol.com

The family did not consent to histopathologi-cal examination of the eyes.
CommentAcute orbital inflammation and orbital myosi-tis leading to proptosis are rare manifestationsof SLE.1–7 To our knowledge acute ocularischaemic syndrome with orbital inflamma-tion is a novel complication of SLE. Theophthalmic manifestations may have resultedfrom a vasculitis involving the vessels supply-ing the globe and extraocular muscles. Thelimitation of ocular movements was mostprobably the result of mechanical restriction.Although the proptosis, lid and conjunctivaloedema improved with immunosuppression,the visual acuity did not recover. This mayhave been because of irreversible visual lossfrom optic nerve dysfunction due to ischae-mia, compression from the acute orbitalinflammation, or secondary to raised in-traocular pressure. Close cooperation betweenophthalmologist and rheumatologist is essen-tial in the management of these patients, inorder to try and prevent blindness.
P Stavrou, P I MurrayBirmingham and Midland Eye Centre,
City Hospital NHS Trust, Birmingham, UK
K BattaBirmingham Skin Centre,
City Hospital NHS Trust, Birmingham, UK
C GordonDepartment of Rheumatology,
City Hospital NHS Trust, Birmingham, UK
Correspondence to: Professor P I Murray, AcademicUnit of Ophthalmology, Division of Immunity andInfection, Birmingham and Midland Eye Centre,City Hospital NHS Trust, Birmingham B18 7QU,
Accepted for publication 10 October 2001
References1 Brenner EH, Shock JP. Proptosis secondary to
systemic lupus erythematosus. ArchOphthalmol 1974;91:81–2.
2 Wildinson LS, Panush RS. Exophthalmosassociated with systemic lupus erythematosus.Arthritis Rheum 1975;18:188–9.
3 Grimson BS, Simons KB. Obitalinflammation, myositis and systemic lupuserythematosus. Arch Ophthalmol1983;101:736–8.
4 Bankhurst AD, Carlow TJ, Reidy RW.Exophthalmos in systemic lupus erythematosus.Ann Ophthalmol 1984;16:669–71.
5 Fossaluzza V, Dal Mas P. Proptosis andsystemic lupus erythematosus. Clin ExpRheumatol 1987;5:192–3.
6 Gray RE, Jenkins EA, Hall MA, et al.Recurrent acute proptosis in atypical systemiclupus erythematosus. Clin Rheumatol1989;8:528–32.
7 Serop S, Vianna RN, Claeys M, et al. Orbitalmyositis secondary to systemic lupuserythematosus. Acta Ophthalmol1994;72:520–3.
Chickenpox neuroretinitis in a 9year old childChickenpox in children is usually thought ofas a benign infectious disease with few ocularcomplications. Posterior segment involvementfrom primary varicella zoster infection hasrarely been reported in children. We describethe clinical features and visual outcome of anunusual case of neuroretinitis presenting in a9 year old child.
Case reportAn immunocompetent 9 year old boy acquiredprimary varicella zoster virus (VZV) infection
from his sibling and developed the character-istic exanthematous vesicular rash. Four daysafter the onset of the rash he woke withdiscomfort in his right eye and described hisvision as being “all grey” on that side. He pre-sented to the emergency department thesame day and was found to have a visual acu-ity of 3/6 on the right and 3/3 on the left (log-MAR). A relative afferent pupillary defect(RAPD) was present on the right. His anteriorsegment was quiet with no vitritis; however,he had slight macular thickening and a subtlecherry red spot on funduscopy, along withsome mild peripapillary swelling and dischaemorrhage.
On review in the ophthalmology clinic 2days later his vision had reduced to 1/60(Sheridan Gardiner singles) on the right. Hehad no new skin lesions and all those presenthad crusted. No lid lesions were present. Hehad a marked RAPD, red desaturation, andmild conjunctival injection. His anterior seg-ment and vitreous remained clear. The rightdisc was hyperaemic with peripapillary swell-ing and haemorrhage. The macular area waspale and oedematous (Fig 1). Examination ofthe left eye was completely normal.
Considering the onset of ocular symptomsand signs following the appearance of thetypical VZV skin lesions, a presumptivediagnosis of chickenpox neuroretinitis wasmade. He was admitted and commenced onintravenous aciclovir (250 mg × 3 per day).Confirmatory IgM titres for VZV were unfor-tunately not performed. No change in hisacuity was observed over the next few days;however, his right disc was noted to becomeslightly pale after 2 days of treatment. At thispoint intravenous methyl prednisolone wasinstituted at a dose of 5 mg/kg per day. Despitea gradual resolution of the macular and peri-papillary oedema over the next 5 days, his discremained pale (Fig 2) and his acuitymeasured as 3/30 (logMAR) after 7 days ofintravenous aciclovir and 5 days of methyl
prednisolone. Systemically he remained com-pletely well and afebrile on treatment. He wasdischarged with a further 3 day course of oralaciclovir and a 6 day reducing course of oralprednisolone.
Over 5 months of follow up his acuity hasnot improved beyond 3/30 (logMAR). Theright optic disc is pale and a yellow lipiddeposit is present at the macula with somereticular macular pigmentation. The left eyehas been normal throughout.
CommentPosterior segment involvement as part of pri-mary VZV infection in children has only beenreported twice to our knowledge.Copenhaver1 reported a 3 year old withbilateral papillitis and a unilateral macularlesion associated with encephalitis followingVZV infection. In this case there was completerecovery of vision and resolution of the macu-lar lesion within 3 weeks of presentation.Capone and Meredith2 describe a case of uni-lateral central visual loss in a 2 year old childcaused by chickenpox retinitis with opticneuritis resulting in a poor visual outcome.Their patient presented with an acute exo-tropia 24–48 hours before the onset ofcutaneous VZV. Funduscopy revealed papilli-tis, phlebitis, and a macular lipid star; retinalopacification just outside the arcades andscattered intraretinal haemorrhages were alsodescribed. In these two cases sequential acuitymeasurement or photography were not possi-ble because of the young age of the subjects.
Our case is particularly interesting, not onlybecause these are the first published fundalphotographs of VZV neuroretinitis in a child,but also because of the relatively mild ocularfindings which have resulted in severe visualloss. The young age of the patient is atypical ofocular VZV infection.3 Adults who contractprimary VZV infection tend to run a moresevere course than children.4 Ocular complica-tions in children are extremely rare.5
The typical posterior segment involvementof VZV is acute retinal necrosis (ARN).4 Theyoungest case of ARN in association withchickenpox has been reported in a 4 yearold.5 In adults, ARN is described as being lesssevere when presenting at the time of primaryzoster infection than as a result of secondaryreactivation of latent, previously acquiredVZV.6 The changes typical of ARN were absentin this case. Unilateral papillitis and retinitisconfined to the macular area were the mainfeatures. Optic neuritis has been reported byseveral authors in association with primaryVZV.7–9 Many of these cases are bilateral andcoincident with encephalitis7 or occurring inthose who are immunocompromised.8 Unilat-eral optic neuritis has been described in an 18year old several weeks following a varicellarash which remitted without sequelae follow-ing the administration of corticosteroid.9
The mainstay of treatment of VZV retinitisis with intravenous aciclovir. Whether anyadvantage is gained in administering systemicsteroid with the aciclovir is controversial.4 Wedo not know if a more positive visual outcomemay have been achieved if intravenoustherapy had been commenced on presenta-tion. It is therefore suggested that prompttreatment of VZV retinitis with intravenousaciclovir be started in patients, particularly ina child, presenting with any posterior seg-ment signs.
J R MacKinnon, T Lim Joon,J E Elder
Department of Ophthalmology, Royal Children’sHospital, Melbourne, Australia
Figure 1 Right fundus: neuroretinitis withloss of vision to 1/60.
Figure 2 Right fundus: following treatmentwith intravenous aciclovir and methylprednisolone.
PostScript 475
www.bjophthalmol.com

Correspondence to: Jane R MacKinnon, Departmentof Ophthalmology, Aberdeen Royal Infirmary,
Foresterhill, Aberdeen AB25 2ZD, UK;[email protected]
Accepted for publication 17 October 2001
References1 Copenhaver RM. Chickenpox with retinopathy.
Arch Ophthalmol 1966; 75:199–200.2 Capone A, Meredith TA. Central visual loss
caused by chickenpox retinitis in a 2-year-oldchild. Am J Ophthalmol 1992;113:592–3.
3 Van Gelder RN, Willig JL, Holland GN, etal. Herpes simplex virus type 2 as a cause ofacute retinal necrosis syndrome in youngpatients. Ophthalmology 2001;108:869–76.
4 Yoser SL, Forster DJ, Rao NA. Systemic viralinfections and their retinal and choroidalmanifestations. Surv Ophthalmol 1993;37:313–52.
5 Lee WH, Charles SJ. Acute retinal necrosisfollowing chickenpox in a healthy 4 year oldpatient. Br J Ophthalmol 2000;84:667–8.
6 Culbertson WW, Brod RD, Flynn HW, et al.Chickenpox-associated acute retinal necrosissyndrome. Ophthalmology 1991;98:1641–5.
7 Selbst RG, Selhorst JB, Harbison JW, et al.Parainfectious optic neuritis. Report andreview following varicella. Arch Neurol1983;40:347–50.
8 Lee MS, Cooney EL, Stoessel KM, et al.Varicella zoster virus retrobulbar optic neuritispreceding retinitis in patients with acquiredimmune deficiency syndrome. Ophthalmology1998;105:467–71.
9 Pina MA, Ara JR, Capablo JL, et al. Myelitisand optic neuritis caused by varicella. RevNeurol 1997;25:1575–6.
Bilateral central retinal arteryocclusion in Wegener’sgranulomatosis and α1
antitrypsin deficiencyVisual loss occurs in up to 8% of patients withWegener’s granulomatosis (WG) during thedisease lifetime,1 although only a smallproportion of these cases are the result ofcentral retinal artery occlusion (CRAO). Wedescribe an unusual case of a patient withbilateral CRAO as a presenting feature of WGand α1 antitrypsin (AAT) deficiency.
Case reportA 58 year old white man presented with sud-den painless loss of vision to the right eye.Vision was hand movements in the right eyeand 6/6 in the left. Funduscopy revealed anacute right CRAO with macular oedema.There were no signs of uveitis or retinalvasculitis. Management consisted of intra-venous acetazolamide (500 mg), ocular mas-sage, and anterior chamber paracentesis. Hewas subsequently sent home with aspirintreatment, and referred to his family doctorfor routine risk factors assessment.
The following morning, he returned to theeye casualty department with a left CRAO,which was treated in the same way. Visionwas 6/60 in the right eye and hand move-ments in the left. Systemic inquiry revealed a2 month history of general malaise, arthral-gia, and myalgia. General examination re-vealed evidence of vasculitic rash (Fig 1)affecting the right elbow and nailfold infarcts(Fig 2). He was admitted for further investiga-tion. His erythrocyte sedimentation rate in thefirst hour was 128 mm and C reactive protein(171 mg/l) were markedly raised. Liver en-zymes were slightly abnormal (γGT, 165 IU/l,ALT, 85, alkaline phosphatase, 153). Therewere traces of blood and protein in the urine,with a normal creatinine clearance (86 mmol/l). He was commenced on oral prednisolone
(60 mg/day) for presumed systemic vasculitis.Normal echocardiography and blood culturesexcluded endocarditis. Ultrasound of hiscarotid arteries was normal. His vision gradu-ally improved, and was recorded 6 days lateras 6/12 in the right eye and 6/6 in the left.Patchy peripheral field defects remained.
Subsequently, his serum was positive forcytoplasmic antineutrophil cytoplasmic anti-body (cANCA) at a titre of 1/160, confirmingthe diagnosis of WG. Monthly pulses of intra-venous cyclophosphamide were employed,with gradual tapering of oral prednisolonedose. There was also an incidental finding ofhomozygous AAT deficiency (Z allele) fromserum protein electrophoresis.
CommentWG is a rare disease with a reported annualincidence of 8.5 per million population2 in theUK, of which up to 16% present initially withocular disease.3 CRAO in patients with WG israre, with only several reported cases3 4 since1960. Ocular and ocular adnexal involvementis the result of parenchymal necrosis, smallvessel vasculitis, and granulomatous inflam-mation. The orbit may be the site of primaryinflammation or become secondarily involvedfrom disease of the paranasal sinuses andnasopharynx. Mechanisms by which visualloss occurs in WG include vascular occlusion,macular oedema, inflammatory destruction ofretina, optic nerve, or corneoscleral tissue.3
Systemically, the most commonly affected tis-sues are the lungs and kidneys. The currenttherapy for WG is cyclophosphamide (daily orpulse) and corticosteroids. Multicentre trialsare in progress to assess the optimumtreatment duration for induction, and subse-quent maintenance of remission.5
This is the first reported case of bilateralCRAO in WG and AAT deficiency. AAT is nor-mally present in serum and inhibits uncon-trolled enzymic destruction of connective tis-sue during inflammation. Deficiency of AATresults in progressive emphysema and liverinjury.6 Research suggests an increased inci-dence of WG in patients with AAT deficiency.7
The incidence of AAT deficiency has beenreported as being significantly increased in
patients with anterior uveitis.8 We are notaware of any reports implicating AAT defi-ciency in CRAO, although it is possible thatthis is contributing to the ongoing inflamma-tory process underlying his vasculitis.
S C Wong, R L Boyce, T C DowdDepartment of Ophthalmology, North Riding
Infirmary, Middlesbrough, UK
J N FordhamDepartment of Rheumatology, James Cook
University Hospital, Middlesbrough, UK
Correspondence to: Dr Sui Chien Wong,Department of Ophthalmology, North Riding
Infirmary, Newport Road,Middlesbrough, TS1 5JE, UK
Accepted for publication 19 October 2001
References1 Hoffman GS, Kerr GS, Leavitt RY. Wegener
granulomatosis: an analysis of 158 patients.Ann Intern Med 1992;116:488–98.
2 Carruthers DM, Watts RA, Symmons DP, etal. Wegener’s granulomatosis—increasedincidence or increased recognition? Br JRheumatol 1996;35:142–5.
3 Harman LE, Margo CE. Wegener’sgranulomatosis. Surv Ophthalmol1998;42:458–80.
4 Lamprecht P, Lerin-Lozano C, Reinhold-KellerE, et al. Retinal artery occlusion in Wegener’sgranulomatosis. Rheumatology2000;39:928–9.
5 Savage CO, Harper L, Cockwell P, et al. ABCof arterial and vascular disease: vasculitis[Review]. BMJ 2000;320:1325–8.
6 Perlmutter DH. Alpha-1-antitrypsin deficiencybiochemistry and clinical manifestations.[Review]. Ann Med 1996;28:385–94.
7 Borgmann S, Endisch G, Urban S, et al. Alinkage disequilibrium between genes at theserine protease inhibitor gene cluster onchromosome 14q32.1 is associated withWegener’s granulomatosis. Clin Immunol2001;98:244–8.
8 Breit SN, Wakefield D, Robinson JP. The roleof α1-antitrypsin deficiency in thepathogenesis of immune disorders. ClinImmunol Immunopathol 1985;35:363–80.
Complication of acupuncture ina patient with Behçet’s diseaseWe would like to bring to your attention acomplication resulting from acupuncture in apatient with Behçet’s disease.
Case reportA 35 year old white man, who fulfilled theInternational Study Group criteria1 for Be-hçet’s disease, attended the Behçet’s clinic atthe Birmingham and Midland Eye Centre. Hecomplained of four red areas on his left arm(Fig 1). Two days earlier he had undergoneacupuncture for what he described as “tenniselbow.” These red areas corresponded towhere the acupuncture needles had beeninserted. Examination revealed these areas tobe pustules (inset) that were characteristic ofa positive pathergy test.
Figure 1 Photograph of right elbowshowing vasculitic rash.
Figure 2 Retroillumination photograph ofright and left index fingers showing nailfoldinfarcts.
Figure 1 Arrows indicating pustulescorresponding to a positive pathergy test.Inset: magnified image of one pustule.
476 PostScript
www.bjophthalmol.com

CommentA positive pathergy test is an important diag-nostic sign of Behçet’s disease.1 Its prevalencevaries by geographic region, being less com-mon in patients from Northern Europe.Nevertheless, patients with Behçet’s diseaseshould be made aware of this potentialcomplication if they intend to undergo acu-puncture.
P I Murray, N AboteenBirmingham and Midland Eye Centre, Birmingham
B18 7QU, UK
Correspondence to: Professor P I Murray, AcademicUnit of Ophthalmology, Division of Immunity andInfection, Birmingham and Midland Eye Centre,
City Hospital NHS Trust, Dudley Road, BirminghamB18 7QU, UK; [email protected]
Accepted for publication 22 October 2001
Reference1 International Study Group For Behçet’s
Disease. Criteria for diagnosis of Behçet’sdisease. Lancet 1990;335:1078–80.
Corneoscleral fibroushistiocytomaFibrous histiocytomas of the corneosclerallimbus are rare tumours. We present a casereport and a review of the clinical andhistopathological findings from cases pre-sented in the literature.
Case reportA 19 year old white male presented with a 6month history of a painless growth on theinferior corneoscleral limbus of the left eye(Fig 1A and B). There were no other ocularsymptoms. He had no medical history of note.His vision was 6/5 unaided in the right eye,and 6/6 unaided in the left eye. The growthwas approximately 5 mm in diameter, vascu-larised, and yellowish in appearance. Therewere no other ocular abnormalities. The lesionwas excised by conjunctival excision andsuperficial keratectomy under a general an-aesthetic and sent for histopathological opin-ion.
Histological sections of the lesion showed astromal hypercellular nodule consisting ofspindle cells, small lymphocytes, multinucle-ated giant cells, and histiocytes. (Fig 1C–F).Some histiocytes had foamy cytoplasm. Manycapillary sized blood vessels were present. Inareas, the spindle cells were arranged in astoriform pattern. A fine collagenous mesh-work extended throughout the lesion. Immu-nohistochemistry confirmed the cellular com-position of the lesion (Fig 1G, H) as rich inmacrophages (CD68), lymphoid cells (CD45),capillary sized blood vessels (CD34), andvimentin positive spindle cells. Mitotic figureswere not evident after a careful search. Thelesion was diagnosed as a benign fibrous his-tiocytoma. The tumour was incompletelyexcised and extended into the deep aspect ofthe lamella in the conjunctiva. However, 16months after excision there has been norecurrence of the tumour.
CommentFibrous histiocytomas are soft tissue tumoursand may be benign or malignant, the benignvariety being the most common.1 They areusually found on the extremities, but canoccur in any part of the body, including orbitaltissues. Fibrous histiocytomas account for 1%of all orbital tumours, and are the most com-mon primary mesenchymal tumour of theorbit.2 Benign fibrous histiocytomas havebeen reported in the orbit,3 eyelid,4 and
episclera.5 Symptoms and signs depend on thesite, but may include decreased vision, pain,restricted eye movements, diplopia, and discswelling. To date, there are only 18 cases offibrous histiocytoma arising from the corneo-scleral limbus reported in the literature1 6; 11of these were classified as benign. Theyusually present as painless masses and candevelop at any age, but most commonlybetween the ages of 20–40 years. Their grossappearance is of a circumscribed yellow orwhite mass, and they may have focal areas ofhaemorrhage, which can make them appearbrown or black in colour.
The histopathological appearance of a be-nign fibrous histiocytoma includes a mixture offibroblastic and histiocytic cells that are oftenarranged in a cartwheel or storiform pattern,and accompanied by varying numbers ofinflammatory cells, including foam cells and
siderophages. No atypical nuclei or mitotic fig-ures are present. Although some authorsregard these tumours as reactive proliferationsof fibroblasts, others do not accept this viewbecause the lesions tend not to regress sponta-neously. Recurrence is rare, with less than 5%of cutaneous benign fibrous histiocytomasrecurring after local excision.7
In contrast, malignant fibrous histiocytomasof the corneoscleral limbus characteristicallyappear in later life, between the ages of 50–70years, with an equal distribution of males tofemales.1 They are highly aggressive tumours,and have been reported to have a localrecurrence rate of 100% if a limited excision isperformed.8 Recurrence can occur within a fewmonths of excision. There are seven reportedcases of corneoscleral malignant fibrous histio-cytoma. Two of the cases had an enucleationand two cases underwent orbital exenteration.
Figure 1 Fibrous histiocytoma arising from the corneoscleral limbus, showing the tumourextending into the cornea. It is moderately vascular and has a similar appearance to adermoid. (B) Fibrous histiocytoma showing the inferior margin of the tumour. (C) Haematoxylinand eosin (H&E) stain, original magnification ×20. (D) H&E stain, original magnification×100. (E) H&E stain, original magnification ×400. (F) H&E stain, original magnification×400. (G) Immunoperoxidase CD68. Original magnification ×200. (H) ImmunoperoxidaseCD45. Original magnification ×200.
PostScript 477
www.bjophthalmol.com

Follow up of these patients ranged from 18months to 5 years and all were free from recur-rence. The other three patients had a local exci-sion. One patient developed local scleral recur-rence 2 months later. (It is not evident from theliterature if the borders of excision were clear oftumour.) He was found to have a metastasis inthe “parotid gland” 4 months later, and evenafter a parotidectomy and radical neck dissec-tion, the patient developed multiple pulmonarymetastases and died within 1 year.9 One of thepatients was lost to follow up. The third patientwho had a local excision went on to developtwo recurrences, which subsequently neededexcision and cryotherapy.6 However, after 1 yearhe was free of any recurrence. Malignantfibrous histiocytomas have a broad range ofhistological appearances; storiform-pleomorphic, myxoid, giant cell, and inflam-matory.10 The storiform-pleomorphic type isthe most common. The cells are predominantlyplump pleomorphic spindle-shaped with occa-sional large, ovoid histiocyte-like cells. Modestamounts of inflammatory cells, such as lym-phocytes and plasma cells may be present. Thedifferential diagnosis of a malignant fibroushistiocytoma includes pleomorphic carcinoma,malignant melanoma, and other sarcomas.
For those limbal fibrous histiocytomas witha benign histopathological appearance, themanagement should be local surgical exci-sion. Malignant fibrous histiocytomas need tobe managed cautiously, preferably by widelocal excision and cryotherapy at the earliestopportunity. If necessary, enucleation shouldbe considered to fully excise a limbal malig-nant fibrous histiocytoma.
C S Daniel, B J Clark, S J TuftMoorfields Eye Hospital, 162 City Road, London,
EC1V 2PD, UK
Correspondence to: Miss Daniel, Department ofPathology, Institute of Ophthalmology, University
College London, Bath Street, London EC1V 9EL, UK
Accepted for publication 22 October 2001
References1 Mietz H, Severin M, Arnold G, et al.
Management of fibrous histiocytoma of thecorneoscleral limbus: report of a case andreview of the literature. Graefes Arch Clin ExpOphthalmol 1997;235:87–91.
2 Ulloa TK, Anderson SF. Orbital fibroushistiocytoma: case report and literaturereview. J Am Optom Assoc 1999;70:253–60.
3 Font RL, Hidayat AA. Fibrous histiocytoma ofthe orbit. Hum Pathol 1982;13:199–209.
4 Font RL. Eyelids and lacrimal drainagesystem. In: Spencer WH, ed. Ophthalmicpathology: an atlas and textbook. 4th ed.Philadelphia: WB Saunders,1996:2218–437.
5 Iwamoto T, Jakobiec FA, Darrel RW. Fibroushistiocytoma of the corneoscleral limbus.Ophthalmology 1981;88:1260–8.
6 Allaire GS, Corriveau C, Teboul N.Malignant fibrous histiocytoma of theconjunctiva. Arch Ophthalmol1999;117:685–7.
7 Niemi KM. The benign fibrohistiocytictumours of the skin. Acta Dermatovener1970;50(suppl 63):1.
8 Weiss SW. Malignant fibrous histiocytoma. Areaffirmation. Am J Surg Pathol1982;6:773–84.
9 Margo CE, Horton MB. Malignant fibroushistiocytoma of the conjunctiva with metasasis.Am J Ophthalmol 1989;107:433–4.
10 Enzinger FM, Weiss SW. Soft tissue tumours.3rd ed. St Louis: CV Mosby, 1995:351–466.
Haemophilus influenzae cornealulcer associated with atopickeratoconjunctivitis and herpessimplex keratitisHaemophilus influenzae is a rare cause ofcorneal ulceration, usually associated withprevious corneal damage. To ensure appropri-ate treatment, the organism must first beidentified by cultures in enriched media. Wedescribe a case of keratitis caused by Hinfluenzae associated with two risk factors—herpetic keratitis and atopic keratoconjuncti-vitis.
Case reportA 43 year old Hispanic male presented with 1week of redness, blurred vision, pain, burning,and itching in the left eye. Past ocular historywas remarkable for bilateral epithelial andinterstitial herpetic keratitis and atopic kera-toconjunctivitis with a previous shield ulcer inthe left cornea. The patient was not using anymedications at the onset of the currentepisode. He had a history of anhidroticectodermal dysplasia and atopic dermatitissince birth. On examination, uncorrectedvisual acuity was 20/100 in the left eye. Theskin of the eyelids was wrinkled, thickened,and hyperpigmented bilaterally with madaro-sis of the lashes. The conjunctiva had a mildpapillary reaction on the right and a severereaction on the left, with giant papillae in thesuperior tarsal area. In the left eye, cornealsensation was markedly decreased and a cen-tral corneal epithelial defect of 1.0 × 0.5 mmwas present with an underlying anterior stro-mal infiltrate measuring 2.5 × 1.5 mm (Fig 1).Scant keratic precipitates and a small hy-popyon were also present.
Scrapings of the corneal ulcer were takenand inoculated on blood and chocolate agar aswell as in thioglycollate broth. Viral culturesand polymerase chain reaction (PCR) werealso performed to rule out the possibility of arecurrent herpes simplex infection. They weresubsequently negative. The patient wasstarted on ofloxacin and fortified cefazolin(50 mg/ml) drops every hour. He was alsostarted on oral aciclovir 800 mg five times aday. On the fourth day, corneal cultures werepositive with a heavy growth of H influenzaesensitive to ofloxacin (Fig 2). On the sixth dayof treatment, uncorrected visual acuity im-proved to 20/30, the stromal infiltrate de-creased to 1 × 1 mm, with a small epithelialdefect, and there was no hypopyon. Asupratarsal injection of dexamethasone wasgiven and topical prednisolone acetate 1%three times a day was added. The papillaeregressed and the corneal lesion healed com-pletely, leaving a central scar with a deep stro-mal vessel.
CommentH influenzae is a tiny Gram negative coccoba-cillus that is an uncommon cause of cornealulceration. In most series it accounts for lessthan 2% of all corneal ulcers.2 3 5 7 8 10 It is acommon cause of acute bacterial conjunctivi-tis, especially in children.9 Unlike Staphylococ-cus aureus, Streptococcus pneumoniae, and otherbacterial causes of conjunctivitis, H influenzaeseldom produces corneal ulceration. This is inmarked contrast with H egyptus ocular infec-tions where peripheral ulcers, infiltrates, andphlyctenules are commonly seen as complica-tions of conjunctivitis. For H influenzae toinfect the cornea, there must be an epithelialdefect. Most of the reported cases of H influen-zae keratitis have been associated with specificrisk factors such as contact lens wear, applica-tion of cyanoacrylate glue, or systemic debili-tating diseases.1 4 6 In this case, the patient hadtwo significant risk factors—severe atopickeratoconjunctivitis and herpetic keratitis.Despite the negative results of the viralcultures and HSV-DNA PCR, we cannot ruleout the possibility that a viral aetiology playeda part in this case. Also, it seems likely thatcomplications from the patient’s atopic dis-ease, delayed the healing of the ulcer.
H influenzae is a fastidious organism thatneeds media enriched with nicotinamideadenine dinucleotide (NAD), such as choco-late agar for growth. It will not grow in bloodagar, unless there are also colonies of Staphylo-coccus aureus, which provide NAD. In that situ-ation, H influenzae will then grow as satellitecolonies around the Staphylococcus aureus. Thiscase illustrates the importance of utilisingchocolate agar as well as blood agar to makean aetiological diagnosis.
In conclusion, H influenzae is a rare cause ofcorneal ulceration, which can occur in pa-tients with previous corneal damage from
Figure 1 Haemophilus influenzae cornealulcer.
Figure 2 Corneal cultures: (A) no bacterialgrowth on blood agar; (B) heavy growth of Hinfluenzae on chocolate agar.
478 PostScript
www.bjophthalmol.com

diseases such as herpetic keratitis and atopickeratoconjunctivitis. To ensure appropriatetreatment the organism must first be identi-fied by cultures in enriched media.
C D Siverio Jr, J P WhitcherThe Francis I Proctor Foundation-UCSF, San
Francisco, CA 94143-0944, USA
Correspondence to: Dr John P Whitcher;[email protected]
Accepted for publication 31 October 2001
References1 Armstrong JR, Cohen KL, McCarthy LR.
Haemophilus influenzae corneal ulcer in atherapeutic contact lens wearer. Br JOphthalmol 1984;68:188–91.
2 Asbell P, Stenson S. Ulcerative keratitis:survey of 30 years’ laboratory experience.Arch Ophthalmol 1982;100:77–80.
3 Carmichael TR, Wolpert M, Koornhof HJ.Corneal ulceration at an urban Africanhospital. Br J Ophthalmol 1985;69:920–6.
4 Cavanaugh TB, Gottsch JD. Infectiouskeratitis and cyanoacrylate adhesive. Am JOphthalmol 1991;111:466–72.
5 Coster DJ, Wilhelmus K, Peacock J, et al.Suppurative keratitis in London. In:Trevor-Roper PD, ed. VIth Congress of TheEuropean Society of Ophthalmology. Thecornea in health and disease. InternationalCongress and Symposium Series 1981, No40. The Royal Society of Medicine, AcademicPress, Grune and Stratton.
6 Leahey AB, Jones D. Haemophilus influenzaecentral corneal ulcer associated with cosmeticlens wear. CLAO J 1996;22:213–14.
7 Liesegang TK, Forster RK. Spectrum ofmicrobial keratitis in south Florida. Am JOphthalmol 1980;90:38–47.
8 Seal DV, Barrett SP, McGill JI. Aetiology andtreatment of acute bacterial infection of theexternal eye. Br J Ophthalmol1982;66:357–60.
9 Soukiasian SH, Baum J. Bacterialconjunctivitis. In: Krachmer JH, Mannis MJ,Holland EJ, eds. Cornea. St Louis: Mosby-YearBook, 1997:759–71.
10 Upadhyay MP, Karmacharya PCD, KoiralaS, et al. Epidemiologic characteristics,predisposing factors and etiologic diagnosisof corneal ulceration in Nepal. Am JOphthalmol 1991;111:92–9.
Blinking and operating:cognition versus visionThe difference in the refractive indices be-tween the air and the tear film results in thetear film having the greatest optical power ofany part of the eye. Eyelid blinks areimportant for maintenance of the tear film.Between blinks there is progressive thinningof the tear film, which becomes non-uniformon the ocular surface and may break up. Thisproduces an irregular air/tear interface, with areduction in image quality.1 The longer theperiod between blinks the greater the effecton the tear film and reduction in vision.Restoration of the tear film occurs immedi-ately following a blink so that the ability tomaintain a regular tear film is dependent on
the blink rate. A reduction in the blink ratesuch as, for example, a pause between blinksof 15 seconds has been associated with achange in the shape of the profile of thecorneal tear film and up to a 6% reduction invisual acuity.2 More importantly, however, areduction in blink rate leads to a reduction incontrast visual acuity.1
The ability to distinguish between differentlayers during surgery, such as the posteriorcapsule of the lens and anterior vitreous face,or peeling a layer off the retinal surface in vit-reoretinal surgery, is dependent on the sur-geon having and maintaining good contrastacuity. Blink rates and blink amplitude varyaccording to vision related behaviour and areduction in the blink rate occurs with tasksof increasing visual difficulty.3 For example,visual tasks requiring concentration, such asvideo display terminal use, result in a decreasein average blink rate from 18.4/mm to 3.6blinks/min.4
In order to determine whether the blinkrate of ophthalmic surgeons alters duringintraocular surgery, the blink rate patterns ofnine ophthalmic surgeons were recorded. Twoobservers recorded the blink rate duringcasual conversation and when the surgeonswere using the operating microscope. None ofthe surgeons were aware that their blink rateswere being recorded, which was done by twomedical students during their ophthalmicattachment—that is, their presence in thetheatre was accepted as part of their ophthal-mic training. The blink rate for each surgeonwas recorded in each condition between fourand 10 times. The mean blink rate for eachsurgeon during casual conversation and whileoperating are presented in Table 1. There was asignificant reduction in the average blink ratebetween both conditions (16.69/min and4.75/min, p= 0.0002 paired t test), on averagea three and a half fold decrease occurred whileoperating. It was also noted that the onset ofconversation such as the request for aninstrument or demonstration of an intraocu-lar structure, was associated with the onset ofa blink response.
The reduction in blink rates observed in thisstudy—that is, 16.69 to 4.75, are similar tothat found by Patel et al for visual tasks suchas video display terminal use. A reduction inblink rate to 4.75 translates to a reduction incontrast acuity of approximately 10% withfour surgeons having an expected reductionof more than 60%.1 Such a reduction incontrast acuity is likely to have an effect onthe ability to differentiate between differentintraocular surgical layers. Blinking occursbetween visual fixations and may be timed soas not to interfere with significant visualinput.5 Blink rate is low when informationmemory is operating, and cognitive processesutilising display areas accessible to visualinput are disrupted during the blackoutperiod of a blink.5 Blinking is thus suspendedduring certain cognitive activities to avoiddisrupting these processes.5
Tear evaporation is dependent on the widthof the palpebral fissure and the surrounding
humidity. Evaporation increases with widen-ing of the palpebral aperture leading to a lowertear film stability. This has led to a recommen-dation that video display unit screens be keptbelow eye level. During ophthalmic surgerythe eye pieces are roughly perpendicular to theface, so that it might be reasonable to lower theheight of the eye pieces to reduce the width ofthe palpebral aperture. Frequent instillation ofartificial tears during surgery is not practicableand might also create an abnormal tear filmand image contrast. Likewise, increasing thehumidity of the theatre may not be feasible. Itmight be reasonable to make surgeons, andanyone who uses the microscope, aware of thispotential problem so that they can train them-selves to blink during parts of the operation orinvestigation where good contrast acuity is notessential and where disruption of the cognitiveprocesses is likely to have a minimal effect.
K K W Wong, W Y Wan,S B Kaye
St Paul’s Eye Unit, 8z Link, Royal LiverpoolUniversity Hospital, Prescot Street,
Liverpool L7 8XP, UK
Correspondence to: Mr Kaye;[email protected]
Accepted for publication 21 November 2001
References1 Tutt R, Bradey A, Begley C, et al. Optical
and visual impact of tear break-up in humaneyes. Invest Ophthalmol Vis Sci 2000;41:4117–23.
2 Nemeth J, Erdelyi B, Csakany B. Cornealtopography changes after a 15 second pausein blinking. J Cataract Refract Surg 2001;27:589–92.
3 Cho P, Sheng C, Chan C, et al. Baseline blinkrates and the effect of visual task difficulty andposition of gaze. Curr Eye Res2000;20:64–70.
4 Patel S, Henderson R, Bradley L, et al. Effectof visual display unit use on blink rate andtear stability. Optom Vis Sci 1991;68:888–92.
5 Holland MK, Tarlow G. Blinking andthinking. Percept Mot Skills 1975;41:505–6.
Should we vaccinate forglaucoma surgery?Trabeculectomy is the most common non-laser surgical procedure performed for treat-ment of all forms of glaucoma. It involves thefashioning of a fistula from the anteriorchamber of the eye to the subconjunctivalspace. This allows for extra drainage of aque-ous humour to the subconjunctival space. Thisproduces a localised elevation of the conjunc-tiva in the area of the trabeculectomy called a“filtering bleb.” Antimetabolites may be usedintraoperatively and perioperatively to in-crease the success of glaucoma filteringsurgery by their action on wound healing. 5-Fluorouracil or mitomycin C is administeredto the scleral flap during the procedure. Post-operatively; subconjunctival injections of
Table 1 Average blink rates (No/min) for ophthalmic surgeons during periods of casual conversation and whileoperating using the microscope
Surgeon 1 2 3 4 5 6 7 8 9 Mean (SD)
Casual 17.29 17.75 7.75 17.60 27.44 24.67 11.50 13.86 12.33 16.69Operating 9.71 9.00 0.29 7.40 1.68 8.67 1.59 3.86 0.54 4.75p Value 0.000002 0.002 0.002 0.002 0.0001 0.0001 0.00003 0.0004 0.0002 0.0003
PostScript 479
www.bjophthalmol.com

5-fluorouracil may be given. This is known asan augmented trabeculectomy.
Infective endophthalmitis is a recognisedcomplication of glaucoma filtering surgery. Itmay occur in the early postoperative period orit may happen years after surgery. Anotherentity, possibly a precursor to endophthalmi-tis has been described as blebitis.1 Blebitis isan infection of the trabeculectomy bleb with-out vitreous involvement.
Clinical features of blebitis include pain,photophobia, conjunctival discharge, andsevere conjunctival injection centred on anopalescent filtering bleb. A Siedel test may bepositive (this indicates aqueous leakage fromthe bleb) and there may be an anterior cham-ber reaction. There is no vitritis.2
As many as one per 100 patients/year maydevelop infection of the bleb.3 Factors associ-ated with increased risk of bleb related endo-phthalmitis include increased axial length,thin leaky bleb, conjunctivitis, upper respira-tory tract infection, hibernal occurrence,trauma, and vitreous wicks.4 5 With theincreased use of antimetabolites in glaucomasurgery, the incidence of thin walled cysticblebs seems to be increasing.6 These blebs aremore prone to leakage.7 Some studies con-clude the incidence of bleb related endoph-thalmitis is higher when antimetabolites areused.8 This is more common with inferior lim-bal trabeculectomy.7 8 However, some studiesshow equal incidence in augmented trab-eculectomy and trabeculectomy withoutantimetabolite augmentation.5
There are few data available for theincidence of blebitis. In most reported casesconjunctival swabs were performed for cul-ture and sensitivity, but organisms causingendophthalmitis may only be present tran-siently on the ocular surface. In many reports,ocular surface cultures came back positive forStaphylococcus epidermidis and S aureus, whichmay both be found on healthy normal eyes.
The microbiology of bleb associated endo-phthalmitis is different from other causes ofendophthalmitis. Clinicians should not ex-trapolate the results of the EndophthalmitisVitrectomy study to the post-filtration surgeryendophthalmitis given the differing patho-genesis and unique spectrum of organisms.2
The most common organisms are Streptococcusspecies.6 The second most common is Haemo-philus influenzae type b at over 23%.8 Of thestreptococci, S pneumoniae may account forapproximately 12%.9 Between them H influen-zae type b and S pneumoniae probably causemore than 35% of blebitis and bleb associatedendophthalmitis.
The treatment of endophthalmitis is expen-sive. It usually involves admission of thepatient and frequent use of expensive drops aswell as surgical intervention. Inpatient treat-ment for blebitis has been priced at US$892(approximately £540) per 24 hours.10 This canwork out to more than £5000 for a 10 day stayin hospital. Furthermore, the cost of follow upvisits and the morbidity that is involved needto be taken into account. Frequently thesepatients have pre-existing visual compromiseand an episode of endophthalmitis may resultin partially sighted or blind registration, anindividual disaster with wider social implica-tions.
H influenzae type b vaccine is licensed for usein infants. However, its use is allowed in thosepatients considered to be at risk for invasive Hinfluenzae type b disease such as sickle cell dis-ease and those receiving treatment formalignancy.11 After the age of 13 months thevaccine is effective after a single dose. Thisvaccine has already shown benefit in ophthal-
mology by the dramatic decrease in theincidence of orbital cellulitis in immunisedchildren.12 It consists of a capsular polysaccha-ride of H influenzae type b conjugated to a pro-tein carrier. Side effects of the vaccine includefever, headache, malaise, irritability, loss ofappetite, vomiting, diarrhoea, rash, urticaria,convulsions, erythema multiforme, and tran-sient cyanosis of the lower limbs.11 Its cost tothe NHS is as low as £8.83 for a single dose of0.5 ml.11
Pneumococcal vaccine is available. It is apolyvalent pneumococcal polysaccharide fromeach of 23 capsular types of S pneumoniae. Thevaccine is recommended from the age of 2 forpeople with the following conditions: homo-zygous sickle cell disease, asplenia or dysfunc-tion of the spleen, chronic renal disease,nephrotic syndrome, immunodeficiency, im-munosuppression, chronic heart disease,chronic lung disease, chronic liver disease, anddiabetes mellitus. It is effective after a singledose if the strains of S pneumoniae prevalent inthe community are reflected in the poly-saccharides contained in the vaccine. Its costto the NHS is £9.49 for a 0.5 ml vial.11
There have been no reports of epidemics ofinfective blebitis. If it were contagious, therewould have been epidemics or clustering inour glaucoma clinics. We can find no evidenceof case to case transmission. In fact, allreported cases and series appear sporadic. Theassociation with upper respiratory tract infec-tions and hibernal occurrence are stronglysuggestive of respiratory infection with conse-quent spread to the predisposed eye.4 5 We areuncertain whether this is systemic or dropletspread. However, the need for topical antibodyprotection is negated by the presence ofsystemic antibodies against the specific bacte-ria. We believe that by minimising thepossibility of systemic infections with theseagents we diminish the likelihood of blebitis.
It is possible that these vaccines could begiven to patients who are destined fortrabeculectomy. The cost for both vaccineswould be less than £20.00.
Two hundred and fifty vaccinations couldbe paid for by the price of a single episode ofbleb associated endophthalmitis. Assuming along term infection rate of 2%, these vaccinescould possibly prevent two cases of bleb asso-ciated endophthalmitis, representing a savingof £5000 to the NHS.
Apart from the cost, vaccination has thepotential to prevent significant ocular morbid-ity. At the very least, these vaccines should beconsidered in high risk patients undergoingaugmented trabeculectomy. We plan to con-duct a prospective study of the effect of thesevaccinations upon the incidence of blebitisand bleb related endophthalmitis.
R R Seemongal-Dass, T E JamesDepartment of Ophthalmology, Calderdale Royal
Hospital, Salterhebble, Halifax HX3 0PW,West Yorkshire, UK
Correspondence to: R R Seemongal-Dass
Accepted for publication 21 November 2001
References1 Brown RH, Yang LH, Walker SD, et al.
Treatment of bleb infection after glaucomasurgery. Arch Ophthalmol 1994;112:57–61.
2 Ciulla TA, Beck AD, Topping TM, et al.Blebitis, early endophthalmitis, and lateendophthalmitis after glaucoma filteringsurgery. Ophthalmology 1997;104:986–95.
3 Doyle JW, Smith M F. Complications ofglaucoma surgery and their management. In:Yanoff M, Duker JS, eds. Ophthalmology.Mosby International, 1999:12.33.1–6.
4 Ashkenazi I, Melamed S, Avni I, et al. Riskfactors associated with late infection offiltering blebs and endophthalmitis.Ophthalmic Surg 1991;22:570–4.
5 Mochizuki K, Jikihara S, Ando Y, et al.Incidence of delayed onset infection aftertrabeculectomy with adjunctive mitomycin Cor 5-fluorouracil treatment. Br J Ophthalmol1997;81:877–83.
6 Ayyala RS, Bellows AR, Thomas JV, et al.Bleb infections: clinically different courses of“blebitis” and endophthalmitis. OphthalmicSurg Lasers 1997;28:452–60.
7 Higginbotham EJ, Stevens RK, Musch DC, etal. Bleb-related endophthalmitis aftertrabeculectomy with mitomycin C.Ophthalmology 1996;103:650–6.
8 Greenfield DS, Suner IJ, Miller MP, et al.Endophthalmitis after filtering surgery withmitomycin. Arch Ophthalmol1996;114:943–9.
9 Mandelbaum S, Forster RK, Gelender H, etal. Late onset endophthalmitis associated withfiltering blebs. Ophthalmology1985l;92:964–72.
10 Chen PP, Gedde SJ, Budenz DL, et al.Outpatient treatment of bleb infection. ArchOphthalmol 1997;115:1124–8.
11 British National Formulary 39. London: BritishMedical Association and RoyalPharmaceutical Society of Great Britain,March 2000.
12 Donahue SP, Schwartz G. Preseptal andorbital cellulitis in childhood. A changingmicrobiologic spectrum. Ophthalmology1998;105:1902–5; discussion 1905–6.
The wide field multifocalelectroretinogram reveals retinaldysfunction in early retinitispigmentosaThe diagnosis of retinitis pigmentosa (RP) ismade on the basis of characteristic retinalpigmentation changes, visual field defects,and reduction in amplitude or loss of rod sco-topic standard electroretinography (ERG)responses, with a possible history of nightblindness and a positive family history of RP.1
Multifocal electrophysiology (mfERG), is anew technique that constructs a topographi-cal map reflecting retinal function.2 Reportshave suggested that the spatial resolution ofmfERG is sufficient to detect focal changes inretinal function as RP progresses.3–5
We describe a case of early RP in which theamplitude and implicit times of the patient’sstandard ERG rod and maximal responseswere normal in the right eye and equivocal inthe left eye. However, the peripheral retinalmfERG amplitude and implicit times werereduced and delayed. These abnormalitieswere obtained using a custom built wide fieldmfERG,6 which facilitates assessment of a 90degree retinal field.
Case reportA 29 year old woman was referred to the eyeclinic by her optometrist. Abnormal retinalpigmentation was found in both fundi onroutine examination. She had no visual prob-lems and was otherwise systemically well. Her51 year old mother is known to have RP.
On examination, she had 0.50 dioptres ofhypermetropia in both eyes. Her best cor-rected logMAR visual acuities were −0.075 inthe right eye and −0.025 in the left. Her colourvision, anterior segment examination, andintraocular pressures were normal in botheyes. Fundal examination revealed semicircu-lar arcs of intraretinal “bone spicule” pigmen-tation in the inferior mid-periphery of eachretina. Her optic discs appeared normal andthere was no evidence of attenuation of theretinal vasculature.
480 PostScript
www.bjophthalmol.com
A Humphrey 120 point threshold relatedperimetry test was performed and the patientmaintained fixation throughout the test.There was an arc of absolute visual field defectin the superior field, symmetrical in both eyes,40 degrees from fixation, which was moreextensive superotemporally than superona-sally.
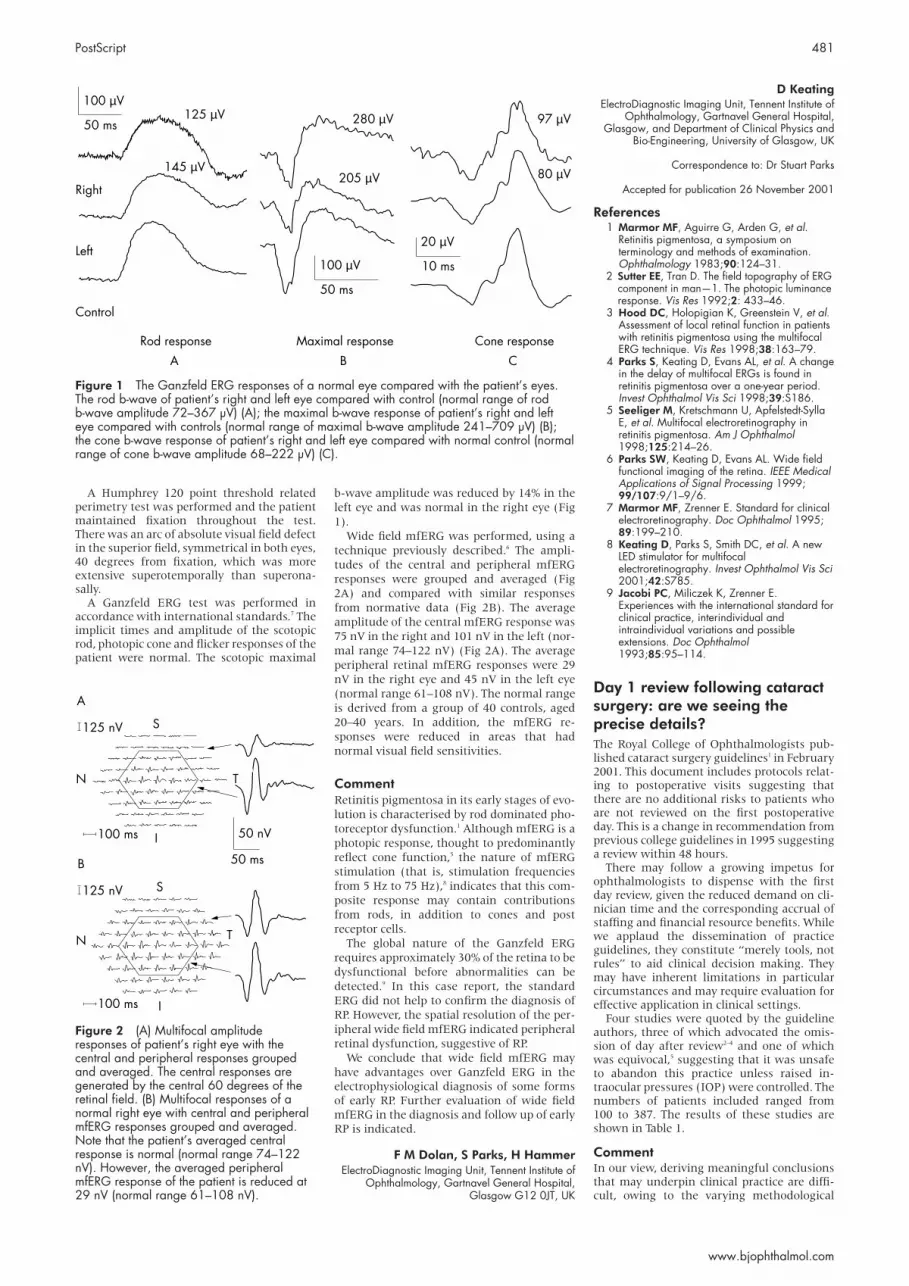
A Ganzfeld ERG test was performed inaccordance with international standards.7 Theimplicit times and amplitude of the scotopicrod, photopic cone and flicker responses of thepatient were normal. The scotopic maximal
b-wave amplitude was reduced by 14% in theleft eye and was normal in the right eye (Fig1).
Wide field mfERG was performed, using atechnique previously described.6 The ampli-tudes of the central and peripheral mfERGresponses were grouped and averaged (Fig2A) and compared with similar responsesfrom normative data (Fig 2B). The averageamplitude of the central mfERG response was75 nV in the right and 101 nV in the left (nor-mal range 74–122 nV) (Fig 2A). The averageperipheral retinal mfERG responses were 29nV in the right eye and 45 nV in the left eye(normal range 61–108 nV). The normal rangeis derived from a group of 40 controls, aged20–40 years. In addition, the mfERG re-sponses were reduced in areas that hadnormal visual field sensitivities.
CommentRetinitis pigmentosa in its early stages of evo-lution is characterised by rod dominated pho-toreceptor dysfunction.1 Although mfERG is aphotopic response, thought to predominantlyreflect cone function,5 the nature of mfERGstimulation (that is, stimulation frequenciesfrom 5 Hz to 75 Hz),8 indicates that this com-posite response may contain contributionsfrom rods, in addition to cones and postreceptor cells.
The global nature of the Ganzfeld ERGrequires approximately 30% of the retina to bedysfunctional before abnormalities can bedetected.9 In this case report, the standardERG did not help to confirm the diagnosis ofRP. However, the spatial resolution of the per-ipheral wide field mfERG indicated peripheralretinal dysfunction, suggestive of RP.
We conclude that wide field mfERG mayhave advantages over Ganzfeld ERG in theelectrophysiological diagnosis of some formsof early RP. Further evaluation of wide fieldmfERG in the diagnosis and follow up of earlyRP is indicated.
F M Dolan, S Parks, H HammerElectroDiagnostic Imaging Unit, Tennent Institute of
Ophthalmology, Gartnavel General Hospital,Glasgow G12 0JT, UK
D KeatingElectroDiagnostic Imaging Unit, Tennent Institute of
Ophthalmology, Gartnavel General Hospital,Glasgow, and Department of Clinical Physics and
Bio-Engineering, University of Glasgow, UK
Correspondence to: Dr Stuart Parks
Accepted for publication 26 November 2001
References1 Marmor MF, Aguirre G, Arden G, et al.
Retinitis pigmentosa, a symposium onterminology and methods of examination.Ophthalmology 1983;90:124–31.
2 Sutter EE, Tran D. The field topography of ERGcomponent in man—1. The photopic luminanceresponse. Vis Res 1992;2: 433–46.
3 Hood DC, Holopigian K, Greenstein V, et al.Assessment of local retinal function in patientswith retinitis pigmentosa using the multifocalERG technique. Vis Res 1998;38:163–79.
4 Parks S, Keating D, Evans AL, et al. A changein the delay of multifocal ERGs is found inretinitis pigmentosa over a one-year period.Invest Ophthalmol Vis Sci 1998;39:S186.
5 Seeliger M, Kretschmann U, Apfelstedt-SyllaE, et al. Multifocal electroretinography inretinitis pigmentosa. Am J Ophthalmol1998;125:214–26.
6 Parks SW, Keating D, Evans AL. Wide fieldfunctional imaging of the retina. IEEE MedicalApplications of Signal Processing 1999;99/107:9/1–9/6.
7 Marmor MF, Zrenner E. Standard for clinicalelectroretinography. Doc Ophthalmol 1995;89:199–210.
8 Keating D, Parks S, Smith DC, et al. A newLED stimulator for multifocalelectroretinography. Invest Ophthalmol Vis Sci2001;42:S785.
9 Jacobi PC, Miliczek K, Zrenner E.Experiences with the international standard forclinical practice, interindividual andintraindividual variations and possibleextensions. Doc Ophthalmol1993;85:95–114.
Day 1 review following cataractsurgery: are we seeing theprecise details?The Royal College of Ophthalmologists pub-lished cataract surgery guidelines1 in February2001. This document includes protocols relat-ing to postoperative visits suggesting thatthere are no additional risks to patients whoare not reviewed on the first postoperativeday. This is a change in recommendation fromprevious college guidelines in 1995 suggestinga review within 48 hours.
There may follow a growing impetus forophthalmologists to dispense with the firstday review, given the reduced demand on cli-nician time and the corresponding accrual ofstaffing and financial resource benefits. Whilewe applaud the dissemination of practiceguidelines, they constitute “merely tools, notrules” to aid clinical decision making. Theymay have inherent limitations in particularcircumstances and may require evaluation foreffective application in clinical settings.
Four studies were quoted by the guidelineauthors, three of which advocated the omis-sion of day after review2–4 and one of whichwas equivocal,5 suggesting that it was unsafeto abandon this practice unless raised in-traocular pressures (IOP) were controlled. Thenumbers of patients included ranged from100 to 387. The results of these studies areshown in Table 1.
CommentIn our view, deriving meaningful conclusionsthat may underpin clinical practice are diffi-cult, owing to the varying methodological
Figure 1 The Ganzfeld ERG responses of a normal eye compared with the patient’s eyes.The rod b-wave of patient’s right and left eye compared with control (normal range of rodb-wave amplitude 72–367 µV) (A); the maximal b-wave response of patient’s right and lefteye compared with controls (normal range of maximal b-wave amplitude 241–709 µV) (B);the cone b-wave response of patient’s right and left eye compared with normal control (normalrange of cone b-wave amplitude 68–222 µV) (C).
50 ms
100 µV125 µV
145 µV
Rod response
A
Maximal response
B
Cone response
C
205 µV
280 µV 97 µV
80 µVRight
Left
Control
50 ms
100 µV 10 ms
20 µV
Figure 2 (A) Multifocal amplituderesponses of patient’s right eye with thecentral and peripheral responses groupedand averaged. The central responses aregenerated by the central 60 degrees of theretinal field. (B) Multifocal responses of anormal right eye with central and peripheralmfERG responses grouped and averaged.Note that the patient’s averaged centralresponse is normal (normal range 74–122nV). However, the averaged peripheralmfERG response of the patient is reduced at29 nV (normal range 61–108 nV).
50 ms
125 nV
N
A
100 ms
T
S
I 50 nV
125 nV
N
B
100 ms
T
S
I
PostScript 481
www.bjophthalmol.com

approaches used in these studies. In Tufail’sstudy,2 extracapsular cataract extraction wasthe predominant surgical technique used.Cohen et al5 excluded more than 50% ofpatients with complicated ocular histories orcomplicated surgery and Whitefield et al3 hadsimilar extensive exclusion criteria, althoughthe number excluded was not mentioned.
We would draw attention to a recently pub-lished study by McKellar and Elder,6 which toour knowledge is one of the largest cohortstudies, aside from national cataract surveys,reporting on first and seventh day complica-tions of cataract surgery. Of 1000 patients, thestudy found that on the first postoperativeday, complications were observed in 10% ofeyes, of which 88% was raised IOP. Unlikemost of the previous studies, all patients withavailable records were eligible, includingthose with preoperative risk factors and thosewith surgical complications. These figuresalign more closely with our “gold standard” ofthe National Cataract Surgery Survey7 thanthe previous mentioned studies. The eventsmost frequently occurring within 48 hoursafter surgery in the national survey were cor-neal oedema (9.5%), raised IOP (7.9%), anduveitis (5.6%). Overall, 23.3% of patients hadearly postoperative complications rangingfrom minor to sight threatening conditions.The survey also found that several risk indica-tors were associated with poorer visual out-comes and complications related to cataractsurgery: age, ocular co-morbidity (glaucoma,macular disease, amblyopia, and previousocular surgery), diabetes mellitus, stroke, typeof surgical procedure, and grade of surgeon.
In summary, up to 20 000 patients a year inthe United Kingdom (10%) may have anundetected early postoperative complicationsuch as corneal oedema or raised IOP, if firstday review was abandoned. And if McKellar’sstudy is representative, then 5% of patientswould have raised pressure without anyprevious history or surgical complication and0.9% of patients could have other potentiallyserious early complications. Nationally, thatequates to almost 12 000 patients annually. Itis worth noting that the American Academyof Ophthalmology in its white paper,8 con-cludes that there are enough significant earlypostoperative complications to warrant firstday review. Are we sufficiently confident inour own practices to diverge?
Credit should be apportioned to the dis-tinguished authors of the cataract surgeryguidelines suggesting 24 hour follow up ofpatients who had undergone complicatedsurgery, had coexisting eye disease, or hadlarge incision cataract surgery. We would liketo reiterate the importance of explicit criteriaas part of any review policy and suggest thatclinical interpretation of individual circum-stances is paramount.
To reconcile the need for an efficient, costeffective review protocol together with anecessity to give due consideration to theentirety of detrimental post-cataract compli-cations, especially given the NHS resource
constraints, is difficult. A pragmatic approachmay be for clinicians to be discriminatelyaware of those patients most at risk of devel-oping early complications and institutingreview policies accordingly, together with anopen door policy for patients who need orwant reassurance on the first day followinguncomplicated surgery. Furthermore, a multi-professional management approach involvingthe extended role of trained ophthalmicnurses in postoperative care may reducedemands on physician time.
At the moment, there is a paucity of a goodprospective literature on the subject and aneed for future studies to address whetherthose identified complications would result ina change of management at the first postop-erative day visit and whether patients wouldhave a poorer outcome if the changes were notinstituted.
D GohRoyal Surrey County Hospital,
Guildford GU2 5XX, UK
N LimThe Western Eye Hospital, Marylebone Road,
London NW1 5YE, UK
Correspondence to: Dr Goh; [email protected]
Accepted for publication 29 November 2001
References1 Royal College of Ophthalmologists. Cataract
surgery guidelines. London: RCO, 2001.2 Tufail A, Forse AJE, Hamilton AMP. Is the first
day postoperative review necessary aftercataract extraction? Br J Ophthalmol1995;79:646–8.
3 Whitefield L, Crowston J, Little BC. First dayfollow-up for routine phacoemulsification? Br JOphthalmol 1996;80:148–50.
4 Tan JHY, Newman DK, Klunker C, et al.Phacoemulsification cataract surgery: isroutine review necessary on the firstpostoperative day. Eye 2000;14:53–5.
5 Cohen VM, Demetria H, Jordan K, et al. Firstday post-operative review followinguncomplicated phacoemulsification. Eye1998;12:634–6.
6 McKellar MJ, Elder MJ. The earlycomplications of cataract surgery: is routinereview of patients 1 week after cataractextraction necessary. Ophthalmology2001;108:930–5.
7 Desai P, Minassian DC, Reidy A. Nationalcataract surgery survey 1997–1998: a reportof the results of the clinical outcomes. Br JOphthalmol 1999;83:1336–40.
8 American Academy of Ophthalmology,American Society of Cataract and RefractiveSurgery. White paper on cataract surgery.Ophthalmology 1996;103:1152–6.
Choroidal abnormalities inneurofibromatosis type 1 withnon-invasive infrared imagingRetinal abnormalities have been reportedworldwide in patients with neurofibromatosistype 1.1–3 However, there have been few reportsof choroidal abnormalities.4 We report apatient with choroidal abnormalities, associ-ated with neurofibromatosis type 1, using ascanning laser ophthalmoscope (SLO).
Case reportA 37 year old woman presented for an exam-ination with hard contact lenses. Her best cor-rected visual acuity was 20/20 in both eyes. Adiagnosis of neurofibromatosis type 1 wasmade on the basis of multiple cafe au laitspots, plexiform neurofibroma, and Sakurai-Lisch nodules in the iris in both eyes. The con-ventional ophthalmoscopic and biomicro-scopic fundus examinations wereunremarkable. A general medical examina-tion showed no abnormalities except signs ofneurofibromatosis type 1. SLO examinationshowed no abnormalities with a helium-neonlaser (633 nm) and regions of multiple, brightpatches with infrared imaging (780 nm)using the direct confocal mode4 (Fig 1) anddark patches with the indirect mode5 (Fig 2)at the corresponding regions in the posteriorpole in both eyes. There were no scotomas inthose regions using SLO microperimetry.
CommentIn this case, we observed choroidal abnor-malities in a patient with neurofibromatosistype 1. The conventional fundus examination,including biomicroscopic examination andfundus colour photography, did not showremarkable changes. However, the SLO exam-ination showed regions of bright patches withinfrared imaging using the direct confocalmode and dark patches using the indirectmode at both posterior poles. Infrared lightpenetrates the retina into the choroid morethan visible light.6 Therefore, the brightpatchy regions seen with confocal infraredimaging and the absence of such regionsunder helium-neon light examination indi-cates that the patchy regions are of choroidalorigin, as reported by Yasunari andcolleagues.4 In addition, we observed darkpatchy regions in the corresponding areausing the indirect mode of infrared imaging(which also can obtain images of the deeperretinal layers non-invasively) instead of usingindocyanine green fundus angiography. Yasu-nari and colleagues reported that choroidalabnormalities (100%) occurred more fre-quently than plexiform neurofibroma (29%)and Sakurai-Lisch nodules in the iris (76%).4
Table 1 Day 1 postoperative complications noted in clinical studies
Study/(n) patients Cornea oedema Raised IOP Uveitis Others
Tufail et al2 (387) 4 (1%) 8 (2%) – 12 (3.1%)Whitefield et al3 (100) 10 (10%) 3 (3%) – –Cohen et al5 (201) 26 (13%) 12 (6%) – –Tan et al4 (227) 5 (4.4%) 3 (1.3%) 1 (0.4%) 3 (1.3%)
Figure 1 SLO image of the right eye usingthe infrared direct confocal mode.
Figure 2 SLO image of the right eye usingthe infrared indirect mode.
482 PostScript
www.bjophthalmol.com

They also reported that bright patchy choroi-dal regions should be a new diagnosticcriterion for neurofibromatosis type 1. Thenon-invasive SLO examination with confocaland indirect infrared imaging may be usefulin the diagnosis of patients with neurofi-bromatosis type 1.
F Mori, N Kitaya, T Hikichi, A YoshidaDepartment of Ophthalmology, Asahikawa Medical
College, Asahikawa, Japan
Correspondence to: Fumihiko Mori, MD, PhD,Department of Ophthalmology, Asahikawa MedicalCollege, Midorigaoka Higashi 2-1-1-1, Asahikawa
078-8510, Japan; [email protected]
The authors have no proprietary interest in anyaspect of this report.
Accepted for publication 5 October 2001
References1 Destro M, D’Amico DJ, Gragoudas ES, et al.
Retinal manifestations of neurofibromatosis.Arch Ophthalmol 1991;109:662–6.
2 Mori F, Nozu K, Kado M, et al. A case of vonRecklinghausen’s disease with retinal tumor.Folia Ophthalmol Jpn 1994;45:883–5.
3 Mori F, Kawai M, Sato E, et al. Branch retinalvein occlusion in a Japanese patient withneurofibromatosis 1. Jpn J Ophthalmol2001;45:634–5.
4 Yasunari T, Shiraki K, Hattori H, et al.Frequency of choroidal abnormalities inneurofibromatosis type 1. Lancet2000;356:988–92.
5 Haynes RJ, Manivannan A, Walker S, et al.Imaging of optic nerve head drusen with thescanning laser ophthalmoscope. Br JOphthalmol 1997;81:654–7.
6 Shiraki K. Fundus examination using ascanning laser ophthalmoscope. FoliaOphthalmol Jpn 1996;47:629–36.
Corneal melt and perforationsecondary to floppy eyelidsyndrome in the presence ofrheumatoid arthritisFloppy eyelid syndrome (FES) is an uncom-mon condition that it is often underdiagnosedor misdiagnosed owing to the somewhattrivial and non-specific symptoms with whichit often presents.1 2 In association with the dryeye of rheumatoid arthritis it can, however,have devastating effects.
Case reportA 60 year old moderately obese man with wellcontrolled rheumatoid arthritis (RA) presentedto the eye clinic with recurrent red and grittyeyes. A diagnosis of dry eye syndrome withblepharitis was made. He was also found tohave a mucocoele of the left lacrimal sac. Lidhygiene and ocular lubricants yielded an initialencouraging response and he was discharged.
He re-presented 5 years later with similarsymptoms and reduced visual acuity (VA) of6/36 in the left eye. A diagnosis of dry eyesyndrome with secondary corneal epithelialchanges was made. Topical lubricants failed torelieve the condition satisfactorily and he wastherefore scheduled for punctal occlusion.However, upon admission for this 8 weekslater, he was found to have an asymptomaticperforation of the left cornea, with a VA of6/60. The perforation was treated with glueand a bandage contact lens, topical antibiotic,steroids, and lubricants. Systemic immuno-suppression was considered in view of thehistory of RA, but was withheld as a heavygrowth of staphylococcus had been culturedfrom the cornea. The right eye demonstratedsigns of dryness but was otherwise healthywith VA of 6/9.
Bilateral punctal occlusion was undertakenas planned, and in addition a left dacro-cystorhinostomy (DCR) to eliminate the muco-coele as a potential reservoir of infection. Theeye, however, continued to slowly deteriorate,with persisting mucopurulent discharge, de-spite the DCR. Eventually uncontrolled endo-phthalmitis developed requiring evisceration.
He re-presented 8 months later with re-duced VA of 6/60 in the right eye secondary toa corneal melt (Fig 1A). A chronic mucopuru-lent discharge had also developed in the righteye, but no lacrimal sac mucocoele was identi-fiable. On this occasion, however, it was notedon examination that while everting the eye-lids, all four lids exhibited excessive laxity (Fig1B). This, together with a florid papillary tarsalconjunctival reaction and the chronic mucusdischarge, led to a diagnosis of RA associateddry eye syndrome exacerbated by FES.
All four eyelids were immediately subjectedto considerable shortening by pentagonalexcision; the corneal melt was treated with abandage contact lens, with topical antibiotic,steroids and lubricants. The response tosurgery was dramatic with complete resolu-tion of discharge and gradual spontaneousrepair of the corneal melt (Fig 2). The VAeventually recovered to 6/9.
CommentFES occurs most frequently in middle agedobese males,1 although it has been described
in young, slim males, females, and one child.2
Typically, the upper tarsus is rubbery and theupper eyelid everts easily with gentle upwardpressure. A florid papillary conjunctivitis andchronic mucus discharge are common. Severecorneal involvement is rare, with only fourreports in the literature of ulceration inassociation with FES and only two cases ofperforation.2–4
Although the exact pathophysiology of FESis uncertain, a sequence of events that maylead to its development and to the secondarycorneal changes has been proposed.1 4 Un-known predisposing factors, possibly congeni-tal, create a floppy upper tarsus. Whereasexamination of post-excisional specimens hasrevealed normal tarsal collagen, elastin fibresare nearly absent.5 It is unclear whether thisfinding is causative or secondary. Duringsleep, a local pressure induced ischaemia maydevelop in the tarsus that, when relieved,results in a reperfusion injury which couldinjure tarsal elastin. In addition, there is ahigh incidence of obstructive sleep apnoea inFES patients and nocturnal dips in PaO2 couldfurther contribute to the local ischaemia andsubsequent elastin damage.2
Corneal involvement may occur throughone or more mechanisms. Spontaneous noc-turnal lid eversion resulting from pressure ofthe pillow on the lax upper lid may lead torepeated trauma of the corneal epithelium.Lash ptosis may contribute to this directtrauma. The cornea, however, may be dam-aged from a more subtle but important mech-anism. Affected lid specimens demonstrate amarked polymorphonuclear infiltrate, whichmay be the sequelae of the reperfusion injurydescribed above; this tarsal infiltrate and theassociated papillary response may have directtoxic effects on corneal epithelium andstroma.4 It is perhaps intuitive that thecorneal complications found in FES may bemore severe when, as in our case, co-existingpathologies are present. Blepharitis and RAassociated dry eye may both independentlycause significant corneal pathology.
This case serves as a reminder that multiplepathologies may contribute to the clinical pic-ture. If FES is not to be missed, ocular exam-ination must include lid eversion and inspec-tion of the tarsus.
J D RossiterSouthampton Eye Unit, Southampton General
Hospital, Tremona Road,Southampton SO16 6YD, UK
R EllinghamBristol Eye Hospital, Lower Maudlin Street,
Bristol BS1 2LX, UK
K N Hakin, J M TwomeyDepartment of Ophthalmology, Taunton and
Somerset Hospital, Taunton TA1 5DA, UK
Correspondence to: Mr RossiterAccepted for publication 10 October 2001
References1 Culbertson WW, Ostler HB. The floppy
eyelid syndrome. Am J Ophthalmol1981;92:568–75.
2 McNab AA. Floppy eyelid syndrome andobstructive sleep apnea. Ophthalmic PlastReconstr Surg 1997;13:98–114.
3 Moore MB, Harrington J, McCulley JP. Floppyeyelid syndrome: management includingsurgery. Ophthalmology 1986;93:184–8.
4 Culbertson WW, Tseng SCG. Cornealdisorders in floppy eyelid syndrome. Cornea1994;13:33–42.
5 Netland PA, Sugrue SP, Albert DM, et al.Histopathologic features of the floppy eyelidsyndrome. Ophthalmology1994;101:174–81.
Figure 1 Right eye before eyelid shorteningshowing (A) the corneal melt and (B) markedlaxity of the upper and lower lids with achronic mucus discharge.
Figure 2 Postoperative photograph of righteye demonstrating the marked improvement.
PostScript 483
www.bjophthalmol.com

Ocular trauma with smallframed spectaclesPenetrating injuries are widely reported withspectacle related eye trauma, particularly incar accidents.1–4 The use of high grade plasticsand secure frames have been shown to reducethe incidence of spectacle related eyetrauma.5 Spectacle safety may be compro-mised in the trend for small frames andframeless spectacles and may place patients atrisk of serious ocular injury.3
We present the case of an aphakic patientwho sustained a blunt injury following ocularcompression by her spectacles. Her injuriescould have been avoided if larger framedspectacles had been worn.
Case reportA 79 year old aphakic woman sustained anon-penetrating injury to her left globe bywalking into a door. She noted a sharp painand sudden loss of vision. The globe was com-pressed by her spectacles, which were smallerthan her orbital rim. Her glasses were notdamaged and there was minimal periocularsoft tissue injury.
She was aphakic, following bilateral cata-ract extraction for congenital cataracts. Thespectacle refraction was +9.00 with a shortback vertex distance of 5 mm (Fig 1).
The pinhole acuity was 6/36, a quiet, deepanterior chamber was noted with no aqueousleak, the intraocular pressure was 0 mm Hg.Funduscopy revealed a light vitreous haemor-rhage, peripapillary choroidal ruptures, and a360 degree suprachoroidal haemorrhage(Fig 2).
Hypotony following traumatic ciliary arteryspasm was diagnosed and the patient wastreated conservatively, with topical atropinetwice daily and dexamethasone four timesdaily. After 4 days the hypotony resolved andthe intraocular pressure returned to 14 mm Hg.The suprachoroidal haemorrhages resolvedover 2 weeks and the visual acuity improved to6/24.
CommentThe potential ocular damage from framed andframeless spectacles has been highlighted in a
number of reports.1–4 These often result fromminor road traffic accidents or inflation of airbags that damage the spectacles. The traumais usually sufficient to break the lenses in thespectacles and the resultant globe laceration isthe main cause of morbidity.
The recent trends towards smaller framedspectacles has not been reported as a potentialrisk to the patient; however, in this case, withsmall framed spectacles (with a short backvertex distance), minor trauma was sufficientto cause serious eye injury. The patient’sprevious larger framed spectacles would haveprevented such an injury as the lenses wouldhave been supported by the orbital marginand not the globe.
This case demonstrates the previouslyunconsidered risk of small framed spectaclesin aphakic patients. The back vertex distancemay be short, increasing the risk of bluntinjury.
J Clarke, R Newsom, C CanningSouthampton Eye Unit, Southampton, UK
Correspondence to: Mr J C K Clarke, SouthamptonEye Unit, Southampton General Hospital, Tremona
Road, Southampton SO16 6YD, UK
Accepted for publication 10 October 2001
References1 Christianson MD, Parker JA, Arndt J.
Material and thickness: the important factorsin the impact resistance of spectacles. Canad JOphthalmol 1977;12:300–3.
2 Gault JA, Vichnin MC, Jaeger EA, et al.Ocular injuries associated with eyeglass wearand airbag inflation. J Trauma Injury InfectCrit Care 1995;38:494–7.
3 Newsom RSB, Williamson TH. Globeperforation with frameless spectacles. Br JOphthalmol 2000;84:668–9.
4 Vichnin MC, Jaeger EA, Gault JA, et al.Ocular injuries related to air bag inflation.Ophthalmic Surg Lasers 1995;26:542–8.
5 Keeney AH, Renaldo D. Newly defined lensand frame factors in the reduction of eyeinjuries. Eye Ear Nose Throat Monthly1973;52:19–24.
Late opacification of SC60B-OUVacrylic intraocular lensesOptical clarity of the intraocular lens (IOL) isparamount in maintaining visual improve-ment after cataract extraction. While theadvent of newer foldable IOLs have revolu-tionised cataract surgery by the smallerincisions required, their long term safety willbe established only with time. There havebeen recent reports of two separate groupsof hydrophilic IOLs that have shownvarious degrees of opacification, 6 monthsto 2 years after implantation.1 These includethe Hydroview lens (Bausch & Lomb
Surgical, Claremont, CA, USA) and themodel SC60B-OUV (Medical DevelopmentalResearch, Clearwater, FL, USA).1 2 We reportour experiences with two patients who hadpermanent reduction in visual acuity 1–2years after implantation of the SC60B-OUVIOL.
Case reportsCase 1An 82 year old man with visual acuities of6/60 in both eyes because of a right macularhole and left posterior subcapsular cataractunderwent routine left phacoemulsificationand intraocular lens implantation in March1998. A foldable hydrophilic acrylic IOL(Model SC60B-OUV, MDR, Inc) was im-planted in the capsular bag. Postoperativerecovery was uneventful, with left visual acu-ity improving to 6/4 with correction, 6 weeksafter the surgery.
He was referred back to the clinic in March2000 with symptoms of intermittent binocu-lar diplopia, which was relieved with fresnelprisms. His left visual acuity was 6/6, but theintraocular lens was found to be uniformlycloudy (Fig 1A). As the patient was not expe-riencing any symptoms from his cloudy IOL,no intervention was advised. Over the next 6months the brownish discoloration of the IOLincreased in intensity and the patient com-plained of “foggy vision.” His visual acuitydropped to 6/12 and he was disturbed by thedistorted, but clear images from his right eyeand hazy images from his left eye. Fundusexamination of the left eye has also becomeprogressively difficult. IOL exchange is beingconsidered, bearing in mind the presence ofthe macular hole in the fellow eye and therisks of removing a posterior chamber IOL 3years after implantation.
Case 2A 78 year old woman with bilateral Fuchs’corneal endothelial dystrophy and long stand-ing central retinal vein occlusion in the lefteye, underwent uneventful right phacoemul-sification with intraocular lens implantation(Model SC60B-OUV, MDR, Inc) in August1998. Her right visual acuity improved to 6/9,
Figure 1 Note the short back vertexdistance in this aphakic correction.
Figure 2 The choroidal rupture followingblunt injury to the globe.
Figure 1 (A) Diffuse opacification of theIOL 2 years after implantation in case 1. (B)The explanted opacified IOL optic from case2 is compared to a normal acrylic IOL.
484 PostScript
www.bjophthalmol.com

but approximately 1 year after the surgerythere was gradual deterioration of vision to6/24 in August 2000. At this stage the IOL wasnoted to be cloudy; there was also progressionof her endothelial dystrophy. She underwentuneventful right penetrating keratoplastywith exchange of posterior chamber IOL inNovember 2000 and has a current right visualacuity of 6/12. The explanted opacified IOL iscompared to a normal clear acrylic IOL in Fig-ure 1B.
CommentThe safety and efficacy of AcrySof polyacrylicIOLs has been reported to be equal to or betterthan poly(methylmethacrylate) IOLs.3 Theunexpected late opacification of the acrylicIOL (SC60B-OUV), implanted in the only“good” eye of both our patients, resulted insignificant visual disability and clinical di-lemma. This model of IOL was first producedin June 1997 by Medical Development Re-search (MDR, Inc). More than 60 000 of theselenses have been implanted worldwide, butonly outside the United States.1 Reports ofopacification of the IOL started comingthrough to the manufacturer in May 1999.(Summary of SC60B-OUV lens opacificationinvestigation, personal communication fromMDR, Inc, 20 July 2001.)
Several theories have been put forward toexplain the late clouding of the IOL optic.2 4 5
Analysis of 23 explanted IOLs of the samemodel has shown that degeneration of theultraviolet filtration material and calciumdeposits within the optic biomaterial areresponsible for the opacification of the IOL.1
Werner et al analysed nine explanted IOLs ofthe same model and demonstrated the pres-ence of calcium phosphate salts in the depos-its within the optics of the IOL.6 Investigationsby the manufacturers identified four lots ofpolymer biomaterial formulated and preparedby Vista Optics (London) and used by MDR,Inc in the IOL manufacture, that correlatedwith opacification complaints (Summary ofSC60B-OUV lens opacification investigation,personal communication from MDR, Inc, 20July 2001).
Ninety two of the estimated 60 0000SC60B-OUV IOLs implanted were explantedand returned to the company. MDR, Incceased exporting SC60B-OUV lenses in June2000 and claims that the opacification repre-sents only 0.15% of total SC60B-OUV IOLsimplanted. (Summary of SC60B-OUV lensopacification investigation, personal commu-nication from MDR, Inc, 20 July 2001). How-ever, this does not account for those patientswho have not yet had their opaque IOLs iden-tified or explanted. The lateness of the onsetof opacification and resulting visual disabilitymay mean that we are seeing only the tip ofthe iceberg.
A Joseph, H S DuaDivision of Ophthalmology and Visual Sciences,
University of Nottingham
Correspondence to: Professor H S Dua, Division ofOphthalmology and Visual Sciences, B Floor, Eye
Ear Nose and Throat Block, University Hospital,Queen’s Medical Centre, Nottingham NG7 2UH,
Accepted for publication 3 December 2001
References1 Apple DJ, Werner L, Pandey SK. Newly
recognized complications of posteriorchamber intraocular lenses. Arch Ophthalmol2001;119:581–2
2 Chang BYP, Davey KG, Gupta M, et al. Lateclouding of an acrylic intraocular lens
following routine phacoemulsification. Eye1999;13:807–8.
3 Kobayashi H, Ikeda H, Imamura S, et al.Clinical assessment of long-term safety andefficacy of a widely implanted polyacrylicintraocular lens material. Am J Ophthalmol2000;130:310–21.
4 Woodruff SA, Khan J, Dhingra N, et al. Letterto the editor. Eye 2001;15:361–2.
5 Sharma A, Ram J, Gupta A. Letter to theeditor. Eye 2001;15:362.
6 Werner L, Apple J, Kaskaloglu M, et al.Dense opacification of the optical componentof a hydrophiphilic acrylic intraocular lens: aclinicopathological analysis of 9 explantedlenses. J Cataract Refract Surg2001;27:1485–92.
Treatment of superior limbickeratoconjunctivitis with aunilateral bandage contact lensThe typical patient with superior limbic kera-toconjunctivitis (SLK) is a woman agedbetween 20 and 60 years of age with chronicred and irritable eyes.1 Although both eyes areusually affected, the condition maybeasymmetrical.1 After episodes of exacerbationand remission it usually resolves. The patientmay also have abnormal thyroid function.2
SLK has been treated with silver nitrate orthermal cauterisation of the superior bulbarconjunctiva, pressure patching, and largediameter bandage contact lenses (BCL), topi-cal trans-retinoic acid 0.1%, and recessionor resection of the superior bulbarconjunctiva.1 3 Over 50% of patients with SLKare said to have keratoconjunctivitis sicca4 andrecently upper punctal plugs have been usedto treat SLK.5
We report two cases in which a unilateralBCL wear ameliorated the symptoms of bilat-eral SLK and a possible explanation isdiscussed.
Case reportsCase 1A 38 year old woman presented with a 3month history of irritable photophobic eyesthat were unresponsive to preserved lubri-cants. Her right eye was amblyopic. Onsystemic review she reported weight loss, heatintolerance, and insomnia.
Slit lamp examination revealed bilateralsuperior conjunctival hyperaemia, superiorpunctate epithelial erosions, and four to fivefilaments and micropannus on the superiorcornea of each eye. Both superior tarsalconjunctivae had moderate papillary reac-tions. Schirmer’s test without anaesthesia was14 mm on the right and 15 mm on the left at5 minutes. Non-preserved lubricants every1–2 hours and Lacrilube ointment at nightwere prescribed. Thyroid function tests re-vealed hyperthyroidism and she was referredto an endocrinologist who commenced carbi-mazole.
Three months later she returned stillcomplaining of persistent severe discomfort,photophobia, and a burning sensation in botheyes. The ocular examination was unchanged.A silicone hydrogel BCL (Pure Vision, Bauschand Lomb, 36% water content) was insertedinto the right eye and within an hour she hadsymptomatic relief in both eyes. Non-preserved lubricants were continued for theleft eye.
On review 2 months after insertion of theBCL she remained asymptomatic. Mild supe-rior limbal hyperaemia on the right andpunctate staining of the superior conjunctivaand adjacent cornea on the left were found onexamination.
Case 2A 54 year old woman was referred with a 3year history of sore, gritty eyes, worse on theleft. The tear break up time was <10 secondsand Schirmer test without anaesthesia wasright 0 mm and left 1 mm after 3 minutes.There was some relief from lubricants, thoughon occasion the pain was so severe that sherequired oral analgesia.
On examination punctate epithelial ero-sions were found on the superior bulbar con-junctiva of both eyes, but were more markedon the left (Fig 1). A silicone hydrogel BCL(Pure Vision, Bausch and Lomb) was insertedinto the left eye, which rapidly amelioratedthe symptoms in both eyes. Lubricants werecontinued for the right eye.
Three months later she remained asympto-matic and no fluorescein staining was seen.The BCL was removed. Within a month herbilateral ocular discomfort returned and theleft BCL was refitted with immediate sympto-matic relief in both eyes. Two months later theBCL was lost and her bilateral ocular discom-fort recurred within 2 days. Since then herBCL has been replaced every 3 months. Occa-sionally she has used lubricants for the righteye.
One year following her presentation shebecame tachycardic and hyperthyroidism wasdiagnosed. Her endocrinologist commencedcarbimazole and β blockers. Her treatmentwas later changed to propylthiouracil aftershe suffered from carbimazole induced ar-thralgia. Thyroid function tests were normal 6months later and the propylthiouracil wasstopped.
CommentThe pathogenesis of SLK is unclear. It may bethe result of mechanical irritation fromincreased pressure of the upper eyelid againstthe globe and/or increased motility of theupper bulbar conjunctiva from hypothyroid-ism or ageing.2 6 Increased upper eyelid tight-ness may be the result of thyroid eye diseaseor chronic inflammation and, in addition, may
Figure 1 Case 2, left eye. (A) The superiorbulbar conjunctiva, at presentation, showinghyperaemia and rose bengal staining. (B)After 3 months of bandage contact lens wearthe superior conjunctival hyperaemia hadresolved and the patient was asymptomatic.
PostScript 485
www.bjophthalmol.com

impair the normal turnover of bulbar con-junctival epithelial cells.2 6 This may be aggra-vated, in some patients, by blepharospasm,which increases the force on the globe.1 3
Therapeutic lenses can produce rapid symp-tom relief in SLK.2 3 They may be helpful in thetreatment of SLK as they relieve pain,facilitate healing of punctate epithelial ero-sions by protecting the ocular surface fromthe eyelids, reduce upper lid pressure on theglobe, and alter tear dynamics.7 During blink-ing as the upper lid moves downwards to meetthe lower lid significant forces are exerted onthe globe.8 The lens can reduce the force onthe superior limbus from blinking as it has alower mechanical stiffness and elasticmodulus.3 9
In the first week of contact lens wear tearproduction increases dramatically and teartonicity decreases.8 Tear production then nor-malises and tear tonicity rises as evaporationincreases.8 A lens may then aid aqueous teardeficiency, which can accompany SLK,4 byensuring a continuous precorneal tear film.7
It is difficult to be certain of the mechanismof bilateral symptom relief from unilateralBCL wear in SLK. One possible explanation isthat BCL wear reduces the tactile cornealreflex, measurable 1–2 hours after lens inser-tion, and this reduction, which increases withthe duration of lens wear, would thendecrease bilateral reflex blinking.8 10 Thiswould protect the superior limbus in both eyesfrom the mechanical friction associated withblinking and may also break the cycle thatleads to blepharospasm in SLK.3
It should not be forgotten that continuousBCL wear carries risks including microbialkeratitis and corneal vascularisation.6 11 Newextended wear silicone BCL, as used in ourpatients, increase oxygen transfer and havebeen shown to reduce such risks.11
S Watson, A B Tullo, F CarleyCorneal Unit, Manchester Royal Eye Hospital,
Oxford Road, Manchester M13 9WH, UK
Correspondence to: Mr Tullo;[email protected]
Accepted for publication 17 December 2001
References1 Theodore FH. Further observations on
superior limbic keratoconjunctivitis. Trans AmAcad Ophthalmol Otolaryngol 1967;71:341–51.
2 Wright P. Superior limbic keratoconjunctivitis.Trans Ophthalmol Soc UK 1972;92:555–60.
3 Mondino BJ, Zaidman GW, Salamon SW.Use of pressure patching and soft contact lensin superior limbic keratoconjunctivitis. ArchOphthalmol 1982;100:1932–4.
4 Udell IJ, Kenyon KR, Sawa M, et al.Treatment of superior limbickeratoconjunctivitis by thermocauterisation ofthe superior bulbar conjunctiva.Ophthalmology 1986;93:162–6.
5 Yang H-Y, Fujishima H, Toda I, et al.Lacrimal punctal occlusion for the treatment ofsuperior limbic keratoconjunctivitis. Am JOphthalmol 1997;124:87.
6 Cher I. Superior limbic keratoconjunctivitis:multifactorial mechanical pathogenesis. ClinExp Ophthalmol 2000;28:181–4.
7 John T, Mobilia EF, Kenyon KR. Therapeuticsoft contact lens. In: Ruben M, Guillon M, eds.Contact lens practice. 1st ed. London:Chapman and Hall, 1994:889–890, 906–7,910.
8 Larke JR. The eye in contact lens wear. 2nded. Oxford: Butterworth-Heinemann, 1997:9,43, 141.
9 Guillon M, Sammons WA. Contact lensdesign. In: Ruben M, Guillon M, eds. Contactlens practice. 1st ed. London: Chapman andHall, 1994:108.
10 Burton H. Somatic sensations from the eye.In: Hart WM, ed. Adler’s physiology of theeye. 9th ed. St Louis: Mosby-Year Book,1992:90.
11 Sankaridurg PR, Sweeney DF, Sharma S, etal. Adverse events with extended wear ofdisposable hydrogels: results for the first 13months of lens wear. Ophthalmology1999;106:1671–80.
MAILBOX
Keratectasia after PTKTakahashi and colleagues have elegantlydescribed an interesting and rare complica-tion of phototherapeutic keratectomy (PTK)in their recent report of an unusual case ofkeratectasia after PTK.1 The hypothesis thatrisk of ectasia is proportional to residual stro-mal base, or depth of ablation, fits with theassumed biomechanical aetiology of thisrecently reported complication of laser refrac-tive surgery. The generally accepted empiricalminimum thickness of 250–300 µm of cornealstroma, excluding flap thickness, remainsspeculative, as we do not understand theunderlying pathophysiology. Indeed, althoughHolland et al highlighted the association ofthin residual stromal thicknesses, post-PRKand LASIK, with keratectasia, they alsodescribed this complication after surfacebased hypermetropic PRK ablation, where thecentre was minimally ablated and residualstromal thickness was greater than 360 µm.2
The authors suggest, in the reported case,that band-shaped keratopathy (BSK) mayhave compromised the tensile strength of thecornea. This seems unlikely as this conditiongenerally affects the superficial anterior cor-nea, and usually does not penetrate deeperthan Bowman’s layer, hence its suitability fortreatment by PTK. However, further clinicaldetail which the authors have not providedmight reveal underlying corneal pathologywith secondary “rough” BSK rather than“smooth” BSK.
However, there are a number of reasons,other than simple biomechanical compro-mise, for keratectasia following PTK in thiscase: (1) forme fruste keratoconus—as nopreoperative topography or surface asymme-try values are presented to enable the readerto rule this out; (2) clinical keratoconus,which seems less likely in respect of patient’sage and a preoperative cylindrical error ofonly −1.5D; (3) idiopathic keratectasia, possi-bly secondary to widespread deregulatedkeratocyte apoptosis. The latter has beendemonstrated after LASIK, with a consider-able and longstanding decrease in keratocytesin the peri-ablation area.3 Also, Helena et al4
demonstrated apoptosis to a depth of at least50 µm after all of the following procedures:epithelial scrape, corneal scrape PRK, tran-sepithelial PRK, and LASIK. Epithelial scrapeand LASIK demonstrated keratocyte apopto-sis to depths of up to 75 µm and 100 µm,respectively. The authors have recently identi-fied a keratocyte free zone 160 µm into thestroma following LASIK, and theoreticallymore widespread apoptosis as a response toexcimer laser photorefractive surgery, maycontribute to keratectasia.
While it is difficult to ascertain why kerate-ctasia occurs, in this case with a residual stro-mal thickness of over 500 µm, from the dataprovided the most likely aetiologies wouldseem to be either undiagnosed forme frustekeratoconus or idiopathic keratectasia.Currently,5 recent reviews illustrate the dearth
of substantial information available regardingidiopathic keratectasia (iatrogenic kerato-conus), with a little over 60 cases published.At this point, although some are likely to bedue to over-ablation, for many cases such asthis the exact aetiology remains unknownand is likely to be multifactorial, and one ofthese factors is residual corneal thickness. Thefact that keratectasia can occur, after whatwould be considered minimal ablation, high-lights the unpredictability of occurrence, butwith over a million cases of LASIK or PRKoccurring each year, the stimulus to identifycontributing factors is significant.
Simon J Dean, Charles N J McGheeDiscipline of Ophthalmology, Faculty of Medicine
and Health Sciences, University of Auckland,Private Bag 92019, Auckland, New Zealand
Correspondence to: Professor C N J McGhee;[email protected]
References1 Miyata K, Takahashi T, Tomidokoro A, et al.
Iatrogenic keratectasia after phototherapeutickeratectomy. Br J Ophthalmol2001;85:247–8.
2 Holland SP, Srivannaboon S, Reinstein DZ.Avoiding serious corneal complications of laserassisted in situ keratomileusis andphotorefractive keratectomy. Ophthalmology2000;107:640–52.
3 Vesaluoma M, Perez-Santonja J, Petroll WM,et al. Corneal stromal changes induced bymyopic LASIK. Invest Ophthalmol Vis Sci2000;41:369–76.
4 Helena MC, Baerveldt F, Kim WJ, et al.Keratocyte apoptosis after corneal surgery.Invest Ophthalmol Vis Sci 1998;39:276–83.
5 Edwards M, Kent D, McGhee CNJ.Keratectasia (iatrogenic keratoconus)following laser refractive surgery. J CMEOphthalmol 2001;50:70–3.
BOOK REVIEWS
Age Related MacularDegeneration—CurrentTreatment Concepts.
Eds WE Alberti, G Richard, RH Sagerman. Pp150; £51.50. Berlin: Springer, 2000. ISBN3-540-66643-5.
This book is one in a large series of medicalradiology textbooks concentrating on diag-nostic imaging and radiation oncology. Thereare 71 authors in all, the majority of whomwork either in the eastern United States orGermany, and the book contains 24 chapters.
The text is aimed at specialists in radio-therapy rather than ophthalmology. The ma-jority of the chapters are concerned withradiotherapy of age related macular degenera-tion (ARMD) with contributions from expertsin this field. Some of the chapters containresults of controlled studies and are of goodvalue, whereas others have less scientificmerit in that they are long term follow upstudies without controls. For ophthalmolo-gists wishing to look into the subject of
486 PostScript
www.bjophthalmol.com

radiotherapy for ARMD this would be a goodsource of material and is well referenced.
There are a few chapters on the clinicalmanifestations, diagnosis, and surgery ofARMD but there is no real mention of lasertreatment. Many of these chapters are of lim-ited scope and do not provide a comprehen-sive overview of the ophthalmic assessmentand management of ARMD.
Although not stated in the book it reads asif it is the proceedings of a clinical meeting.The chapters do not read in a coordinated wayand essentially present the results of indi-vidual units describing their methods andresults of radiotherapy. As such it is a usefulsource of information for those with an inter-est in this topic but it is of limited value forophthalmologists wishing to obtain a bal-anced view of current treatment of ARMD.
R H B GreyBristol Eye Hospital, Lower Maudlin Street, Bristol
BS1 2LX, UK
Clinical Ophthalmic Pathology.John Harry, Gary Misson. Pp 376; £125.Oxford: Butterworth-Heinemann, 2001 ISBN0 7506 2171 0.
This is an excellent, easy to read, wellillustrated book. It is one of the first of its kindto bring pathology alive by describing diseasesvia pathogenesis as opposed to anatomy. Forthe trainee in ophthalmology, optometry, andvisual science it, therefore, provides a morelogical approach to the understanding of ocu-lar diseases. As the book attempts to covermany subjects it sometimes does not dojustice to the basic science. It would have beenbetter to have had the reading lists at the endof each chapter. However, as it stands the bookis an excellent introduction to pathologycomplementing clinical textbooks. If readtogether with clinical texts it certainly willbroaden the knowledge base of all traineeophthalmologists. As a result of its logical andsimple approach I was left frustrated at timeswith the lack of background knowledge.However, going through pathologically basedchapters including injury and repair, immu-nity, genetics, growth, degeneration, vasculardisorders, and disorders of the nerve andmuscle, I was left entertained, as a clinician,with a greater understanding of pathologicalprocesses.
The final chapter for the clinician in thelaboratory I felt could have been expanded,delivering more detail, particularly, on thecurrent molecular methods used in pathologi-cal practice today.
A Dick
NOTICES
Childhood blindnessThe latest issue of Community Eye Health (No40) discusses new issues in childhood blind-ness, with an editorial by Clare Gilbert, seniorlecturer at the International Centre for EyeHealth. For further information please con-tact: Journal of Community Eye Health,
International Centre for Eye Health, Instituteof Ophthalmology, 11–43 Bath Street, LondonEC1V 9EL, UK (tel: +44 (0)20 7608 6910; fax:+44 (0)20 7250 3207; email: [email protected]; website: www.jceh.co.uk). Annualsubscription (4 issues) UK£25/US$40. Free toworkers in developing countries.
International Centre for EyeHealth
The International Centre for Eye Health haspublished a new edition of the Standard List ofMedicines, Equipment, Instruments and OpticalSupplies (2001) for eye care services indeveloping countries. It is compiled bythe Task Force of the International Agengy forthe Prevention of Blindness. Further details:Sue Stevens, International Centre for EyeHealth, 11–43 Bath Street, London EC1V 9EL,UK (tel: +44 (0)20 7608 6910; email:[email protected]).
Second Sight
Second Sight, a UK based charity whose aimsare to eliminate the backlog of cataract blindin India by the year 2020 and to establishstrong links between Indian and British oph-thalmologists, is regularly sending volunteersurgeons to India. Details can be found at thecharity website (www.secondsight.org.uk) orby contacting Dr Lucy Mathen ([email protected]).
SPecific Eye ConditionS (SPECS)
Secific Eye ConditionS (SPECS) is a not forprofit organisation which acts as an umbrellaorganisation for support groups of any condi-tions or syndrome with an integral eye disor-der. SPECS represents over fifty differentorganisations related to eye disorders rangingfrom conditions that are relatively commonto very rare syndromes. We also includegroups who offer support of a more generalnature to visually impaired and blind people.Support groups meet regularly in the Board-room at Moorfields Eye Hospital to offer sup-port to each other, share experiences andexplore new ways of working together. Theweb site www.eyeconditions.org.uk acts as aportal giving direct access to support groupsown sites. The SPECS web page is a valuableresource for professionals and may also be ofinterest to people with a visual impairmentor who are blind. For further detailsabout SPECS contact: Kay Parkinson, SPECSDevelopment Officer (tel: +44 (0)1803524238; email: [email protected];www.eyeconditions.org.uk).
XXIXth International Congress ofOphthalmology
The XXIXth International Congress of Oph-thalmology will be held on 21–25 April 2002in Sydney, Australia. Further details: CongressSecretariat, C/- ICMS Australia Pty Ltd, GPOBox 2609, Sydney, NSW 2001, Australia (tel:+61 2 9241 1478; fax: +61 2 9251 3552;email: [email protected]; website:www.ophthalmology.aust.com).
12th Meeting of the EuropeanAssociation for the Study ofDiabetic Eye Complications(EASDEC)The 12th meeting of the EASDEC will be heldon 24–26 May 2002 in Udine, Italy. The dead-line for abstracts is 15 February 2002. Threetravel grants for young members (less than35 years of age at the time of the meeting) areavailable. For information on the travelgrants, please contact Pr CD Agardh, Presi-dent of EASDEC, Malmö University Hospital,SE-205 02 Malmö, Sweden (tel +46 40 33 1016; fax: +46 40 33 73 66; email: [email protected]). Further de-tails: NORD EST CONGRESSI, Via Aquilea,21.–33100 Undine, Italy (tel: +30 043221391; fax: +39 0432 50687; email:nordest.congressi@ ud.nettuno.it)
3rd Interdisciplinary Symposiumon the Treatment ofAutoimmune DisordersThe 3rd Interdisciplinary Symposium on theTreatment of Autoimmune Disorders will beheld in Leipzig, Germany on the 6–8 June2002. Topics to be covered include: basicaspects of autoimmune diseases, experimen-tal therapeutic concepts, and clinical studiesproviding novel concepts or novel focus onestablished therapies. There will also be thepresentation of the Nils-Ilja-Richter Award(application deadline is April 2002, furtherdetails on the web site). Further details: Prof.Dr. med. Michael Sticherline, Department ofDermatology, University of Leipzig (email:[email protected]; website: ww-w.autoimmun.org); Fördergesellschaft zurTherapie von Autoimmunerkrankugen e.V.(email: [email protected])
International Society for Behçet’sDiseaseThe 10th International Congress on Behçet’sDisease will be held in Berlin 27–29 June2002. Further details: Professor Ch Zouboulis(email: [email protected]).
Singapore National Eye Centre5th International MeetingThe Singapore National Eye Centre 5th Inter-national Meeting will be held on 3–5 August2002 in Singapore. Further details: Ms AmyLim, Organising Secretariat, Singapore Na-tional Eye Centre, 11 Third Hospital Avenue,Singapore 168751 (tel: (65) 322 8374;fax: (65)227 7290; email: [email protected]).
BEAVRS MeetingThe next BEAVRS meeting will be held in theDalmahoy Hotel near Edinburgh on 31 Octoberto 1 November 2002. Further details: SusanCampbell, Medical Secretary, Gartnavel Gen-eral Hospital (email: [email protected]).
CORRECTION
The authors of the letter “Recurrent cornealulceration as late complication of toxic kerati-tis”, appearing in the February issue of BJO(2002;86:245–6), would like to add an author,SH Santander.
PostScript 487
www.bjophthalmol.com