treatment of inflammatory diseases by selective eicosanoid inhibition: a double-edged sword?
TRANSCRIPT
Treatment of inflammatory diseases byselective eicosanoid inhibition:a double-edged sword?Saul Yedgar1, Miron Krimsky1, Yuval Cohen2 and Roderick J. Flower3
1 Department of Biochemistry, Hebrew University-Hadassah Medical School, Jerusalem, 91120, Israel2 Morria Biopharmaceuticals Plc, 53 Davies Street, London W1K 5JH, UK3 Biochemical Pharmacology Centre, The William Harvey Research Institute, Queen Mary University of London, Charterhouse
Square, London EC1M 6BQ, UK
Review TRENDS in Pharmacological Sciences Vol.28 No.9
Eicosanoids are generally considered to be potent pro-inflammatory mediators, and their suppression has,therefore, been a desirable therapeutic goal. However,analysis of the literature reveals that inhibition ofspecific eicosanoids per se is a simplistic approachbecause it overlooks the fact that net pathophysiologicaleffects of these lipid mediators arise from a complexbalance between eicosanoids derived from differentpathways, which might exhibit both pro-and anti-inflam-matory activities (depending on organs and diseasestage), or which might have essential physiologicalroles. An alternative strategy, discussed in this review,might be to control inflammatory lipid mediators in sucha way as to avoid disrupting this intricate inter-eicosa-noid balance and its physiological sequelae.
Inflammation is mediated by a plethora of bioactivelipidsThe production of eicosanoids is initiated by the release ofarachidonic acid (AA) after the hydrolysis of membranephospholipids by phospholipase A2 (PLA2) and otherenzymes. AA is further metabolized into different eicosa-noid families by several enzyme systems. The two mainpathways are the cyclooxygenases COX-1 and COX-2 (andpossibly COX-3 in some species), producing the prostaglan-dins (PGs) and thromboxanes (TXs), and the lipoxygenasepathways (5-LOX, 12-LOX, 15-LOX), producing the leuko-trienes (LTs), hydroperoxy fatty acids and derivativesthereof (Figure 1). The products of both pathways areinvolved in the induction and facilitation of numerouspathologies, particularly inflammatory diseases, and theirsuppression has, therefore, been a major therapeutic goalfor anti-inflammatory drug development. Largely forhistorical reasons, the prevalent strategy has been to blockselectively the enzymatic pathways leading to the pro-duction of inflammatory PGs or LTs (COX or LOX, respect-ively), or to suppress the production or action of a specificPG or LT, believed to be a key player in a specific disease.However, despite the attraction of this notion and theconsiderable resources invested, this approach has yieldedmixed results, and high-profile drugs (e.g. some COX-2
Corresponding author: Flower, R.J. ([email protected]).Available online 10 August 2007.
www.sciencedirect.com 0165-6147/$ – see front matter � 2007 Elsevier Ltd. All rights reserve
inhibitors) have been withdrawn from the market becauseof safety concerns.
A review of the field and analysis of the intricate path-ways of eicosanoid production and action point to severalpotential reasons for the unsatisfactory experience withsuch inhibitors. These can be mainly grouped under fourheadings:
� Ed. d
icosanoids mediating particular functions might beproduced by alternative pathways of AA metabolism.
� E
icosanoids producing opposing effects on particularfunctions might be produced by the same pathway.� T
he same eicosanoids might exert opposing effects indifferent organs and tissues and might switch roles,from pro- to anti-inflammatory, during the course ofdisease.� S
ome ‘pro-inflammatory’ eicosanoids and AA-metabo-lizing enzymes also have essential physiological func-tions.should be taken into account when considering the inhi-
The present review aims to highlight the factors thatbition of eicosanoid production/action for the treatment ofinflammatory diseases. Because of the enormous body ofliterature on this subject, the arguments discussed in thisreview are supported by illustrative examples and thecoverage of the area is not exhaustive.
Eicosanoids mediating particular functions might beproduced by alternative pathways of AA metabolismIt is well known that both COX and LOX pathways produceeicosanoids that mediate the inflammatory response. Forexample, the COX-derived TXA2 and PGD2, and the LOX-produced cysteinyl leukotrienes (cys-LTs) and LTB4 arepotent inducers of smooth muscle contraction and/or con-striction of airways and blood vessels [1–4]. These eicosa-noids, as well as PGE2, also induce intestinal inflammation[5,6], as well as other inflammatory conditions, as illus-trated in Table 1. By blocking only one pathway, AA mightbe diverted into the other pathway; this would clearly notmitigate, and might even exacerbate, the pathologicalcondition [7–9]. A well-known example is Aspirin1, themost widely used non-steroidal anti-inflammatory drug(NSAID), which by inhibiting COX can shift the AAmetabolism to increased production of LTs, which might
oi:10.1016/j.tips.2007.07.005
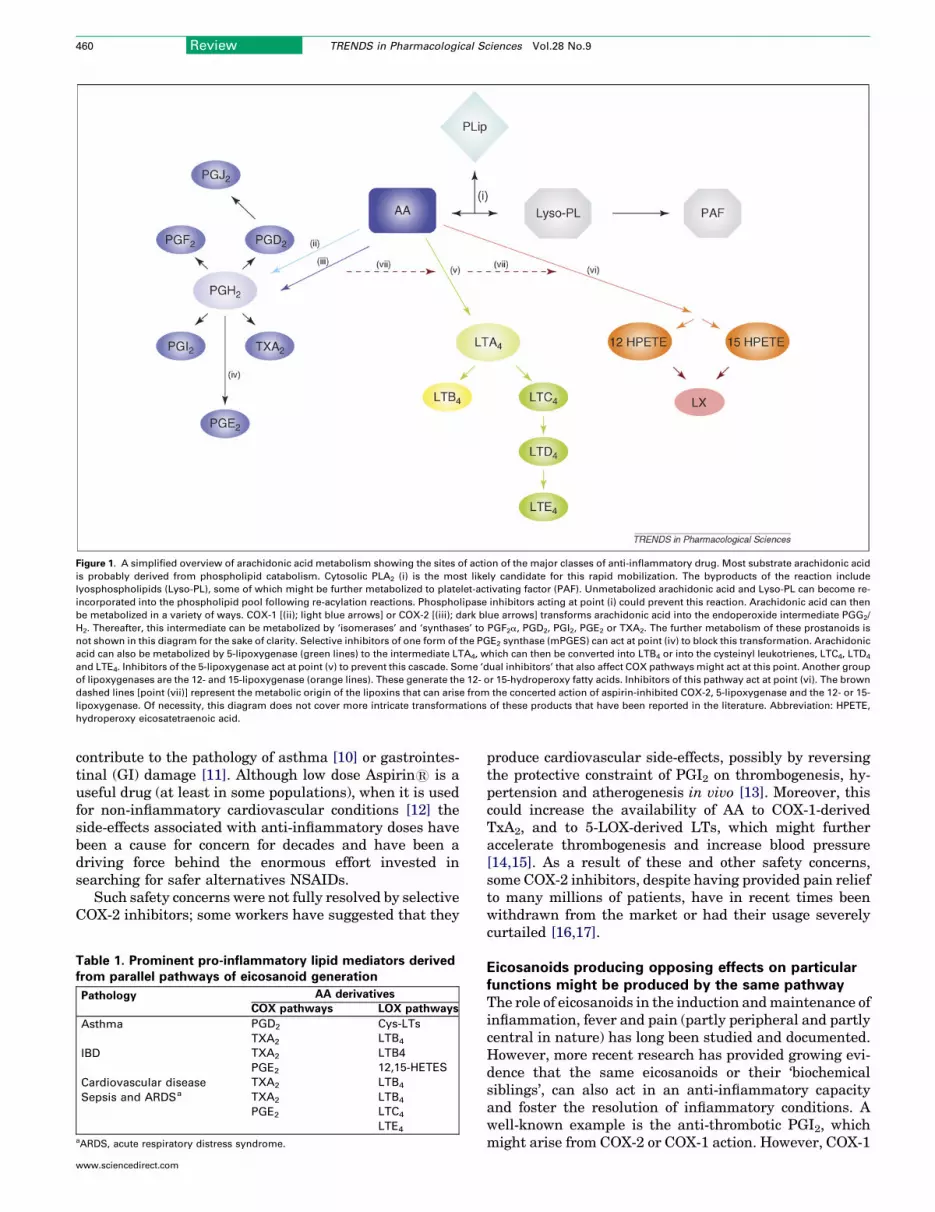
Figure 1. A simplified overview of arachidonic acid metabolism showing the sites of action of the major classes of anti-inflammatory drug. Most substrate arachidonic acid
is probably derived from phospholipid catabolism. Cytosolic PLA2 (i) is the most likely candidate for this rapid mobilization. The byproducts of the reaction include
lyosphospholipids (Lyso-PL), some of which might be further metabolized to platelet-activating factor (PAF). Unmetabolized arachidonic acid and Lyso-PL can become re-
incorporated into the phospholipid pool following re-acylation reactions. Phospholipase inhibitors acting at point (i) could prevent this reaction. Arachidonic acid can then
be metabolized in a variety of ways. COX-1 [(ii); light blue arrows] or COX-2 [(iii); dark blue arrows] transforms arachidonic acid into the endoperoxide intermediate PGG2/
H2. Thereafter, this intermediate can be metabolized by ‘isomerases’ and ‘synthases’ to PGF2a, PGD2, PGI2, PGE2 or TXA2. The further metabolism of these prostanoids is
not shown in this diagram for the sake of clarity. Selective inhibitors of one form of the PGE2 synthase (mPGES) can act at point (iv) to block this transformation. Arachidonic
acid can also be metabolized by 5-lipoxygenase (green lines) to the intermediate LTA4, which can then be converted into LTB4 or into the cysteinyl leukotrienes, LTC4, LTD4
and LTE4. Inhibitors of the 5-lipoxygenase act at point (v) to prevent this cascade. Some ‘dual inhibitors’ that also affect COX pathways might act at this point. Another group
of lipoxygenases are the 12- and 15-lipoxygenase (orange lines). These generate the 12- or 15-hydroperoxy fatty acids. Inhibitors of this pathway act at point (vi). The brown
dashed lines [point (vii)] represent the metabolic origin of the lipoxins that can arise from the concerted action of aspirin-inhibited COX-2, 5-lipoxygenase and the 12- or 15-
lipoxygenase. Of necessity, this diagram does not cover more intricate transformations of these products that have been reported in the literature. Abbreviation: HPETE,
hydroperoxy eicosatetraenoic acid.
460 Review TRENDS in Pharmacological Sciences Vol.28 No.9
contribute to the pathology of asthma [10] or gastrointes-tinal (GI) damage [11]. Although low dose Aspirin1 is auseful drug (at least in some populations), when it is usedfor non-inflammatory cardiovascular conditions [12] theside-effects associated with anti-inflammatory doses havebeen a cause for concern for decades and have been adriving force behind the enormous effort invested insearching for safer alternatives NSAIDs.
Such safety concerns were not fully resolved by selectiveCOX-2 inhibitors; some workers have suggested that they
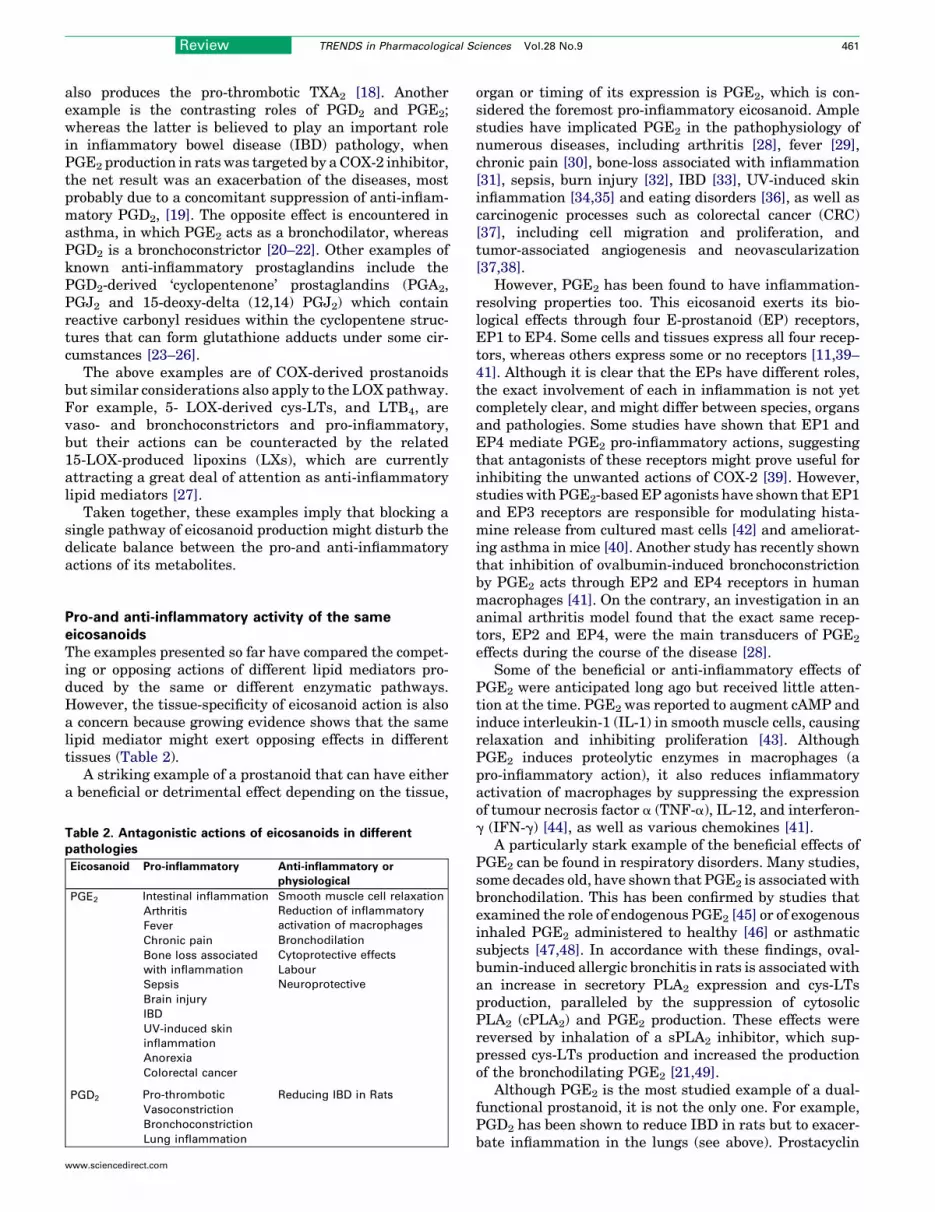
Table 1. Prominent pro-inflammatory lipid mediators derivedfrom parallel pathways of eicosanoid generation
Pathology AA derivatives
COX pathways LOX pathways
Asthma PGD2 Cys-LTs
TXA2 LTB4
IBD TXA2 LTB4
PGE2 12,15-HETES
Cardiovascular disease TXA2 LTB4
Sepsis and ARDSa TXA2 LTB4
PGE2 LTC4
LTE4
aARDS, acute respiratory distress syndrome.
www.sciencedirect.com
produce cardiovascular side-effects, possibly by reversingthe protective constraint of PGI2 on thrombogenesis, hy-pertension and atherogenesis in vivo [13]. Moreover, thiscould increase the availability of AA to COX-1-derivedTxA2, and to 5-LOX-derived LTs, which might furtheraccelerate thrombogenesis and increase blood pressure[14,15]. As a result of these and other safety concerns,some COX-2 inhibitors, despite having provided pain reliefto many millions of patients, have in recent times beenwithdrawn from the market or had their usage severelycurtailed [16,17].
Eicosanoids producing opposing effects on particularfunctions might be produced by the same pathwayThe role of eicosanoids in the induction andmaintenance ofinflammation, fever and pain (partly peripheral and partlycentral in nature) has long been studied and documented.However, more recent research has provided growing evi-dence that the same eicosanoids or their ‘biochemicalsiblings’, can also act in an anti-inflammatory capacityand foster the resolution of inflammatory conditions. Awell-known example is the anti-thrombotic PGI2, whichmight arise from COX-2 or COX-1 action. However, COX-1
Review TRENDS in Pharmacological Sciences Vol.28 No.9 461
also produces the pro-thrombotic TXA2 [18]. Anotherexample is the contrasting roles of PGD2 and PGE2;whereas the latter is believed to play an important rolein inflammatory bowel disease (IBD) pathology, whenPGE2 production in rats was targeted by aCOX-2 inhibitor,the net result was an exacerbation of the diseases, mostprobably due to a concomitant suppression of anti-inflam-matory PGD2, [19]. The opposite effect is encountered inasthma, in which PGE2 acts as a bronchodilator, whereasPGD2 is a bronchoconstrictor [20–22]. Other examples ofknown anti-inflammatory prostaglandins include thePGD2-derived ‘cyclopentenone’ prostaglandins (PGA2,PGJ2 and 15-deoxy-delta (12,14) PGJ2) which containreactive carbonyl residues within the cyclopentene struc-tures that can form glutathione adducts under some cir-cumstances [23–26].
The above examples are of COX-derived prostanoidsbut similar considerations also apply to the LOX pathway.For example, 5- LOX-derived cys-LTs, and LTB4, arevaso- and bronchoconstrictors and pro-inflammatory,but their actions can be counteracted by the related15-LOX-produced lipoxins (LXs), which are currentlyattracting a great deal of attention as anti-inflammatorylipid mediators [27].
Taken together, these examples imply that blocking asingle pathway of eicosanoid production might disturb thedelicate balance between the pro-and anti-inflammatoryactions of its metabolites.
Pro-and anti-inflammatory activity of the sameeicosanoidsThe examples presented so far have compared the compet-ing or opposing actions of different lipid mediators pro-duced by the same or different enzymatic pathways.However, the tissue-specificity of eicosanoid action is alsoa concern because growing evidence shows that the samelipid mediator might exert opposing effects in differenttissues (Table 2).
A striking example of a prostanoid that can have eithera beneficial or detrimental effect depending on the tissue,
Table 2. Antagonistic actions of eicosanoids in differentpathologies
Eicosanoid Pro-inflammatory Anti-inflammatory or
physiological
PGE2 Intestinal inflammation Smooth muscle cell relaxation
Arthritis Reduction of inflammatory
activation of macrophagesFever
Chronic pain Bronchodilation
Bone loss associated
with inflammation
Cytoprotective effects
Labour
Sepsis Neuroprotective
Brain injury
IBD
UV-induced skin
inflammation
Anorexia
Colorectal cancer
PGD2 Pro-thrombotic Reducing IBD in Rats
Vasoconstriction
Bronchoconstriction
Lung inflammation
www.sciencedirect.com
organ or timing of its expression is PGE2, which is con-sidered the foremost pro-inflammatory eicosanoid. Amplestudies have implicated PGE2 in the pathophysiology ofnumerous diseases, including arthritis [28], fever [29],chronic pain [30], bone-loss associated with inflammation[31], sepsis, burn injury [32], IBD [33], UV-induced skininflammation [34,35] and eating disorders [36], as well ascarcinogenic processes such as colorectal cancer (CRC)[37], including cell migration and proliferation, andtumor-associated angiogenesis and neovascularization[37,38].
However, PGE2 has been found to have inflammation-resolving properties too. This eicosanoid exerts its bio-logical effects through four E-prostanoid (EP) receptors,EP1 to EP4. Some cells and tissues express all four recep-tors, whereas others express some or no receptors [11,39–41]. Although it is clear that the EPs have different roles,the exact involvement of each in inflammation is not yetcompletely clear, and might differ between species, organsand pathologies. Some studies have shown that EP1 andEP4 mediate PGE2 pro-inflammatory actions, suggestingthat antagonists of these receptors might prove useful forinhibiting the unwanted actions of COX-2 [39]. However,studies with PGE2-basedEP agonists have shown that EP1and EP3 receptors are responsible for modulating hista-mine release from cultured mast cells [42] and ameliorat-ing asthma in mice [40]. Another study has recently shownthat inhibition of ovalbumin-induced bronchoconstrictionby PGE2 acts through EP2 and EP4 receptors in humanmacrophages [41]. On the contrary, an investigation in ananimal arthritis model found that the exact same recep-tors, EP2 and EP4, were the main transducers of PGE2
effects during the course of the disease [28].Some of the beneficial or anti-inflammatory effects of
PGE2 were anticipated long ago but received little atten-tion at the time. PGE2 was reported to augment cAMP andinduce interleukin-1 (IL-1) in smooth muscle cells, causingrelaxation and inhibiting proliferation [43]. AlthoughPGE2 induces proteolytic enzymes in macrophages (apro-inflammatory action), it also reduces inflammatoryactivation of macrophages by suppressing the expressionof tumour necrosis factor a (TNF-a), IL-12, and interferon-g (IFN-g) [44], as well as various chemokines [41].
A particularly stark example of the beneficial effects ofPGE2 can be found in respiratory disorders. Many studies,some decades old, have shown that PGE2 is associatedwithbronchodilation. This has been confirmed by studies thatexamined the role of endogenous PGE2 [45] or of exogenousinhaled PGE2 administered to healthy [46] or asthmaticsubjects [47,48]. In accordance with these findings, oval-bumin-induced allergic bronchitis in rats is associatedwithan increase in secretory PLA2 expression and cys-LTsproduction, paralleled by the suppression of cytosolicPLA2 (cPLA2) and PGE2 production. These effects werereversed by inhalation of a sPLA2 inhibitor, which sup-pressed cys-LTs production and increased the productionof the bronchodilating PGE2 [21,49].
Although PGE2 is the most studied example of a dual-functional prostanoid, it is not the only one. For example,PGD2 has been shown to reduce IBD in rats but to exacer-bate inflammation in the lungs (see above). Prostacyclin
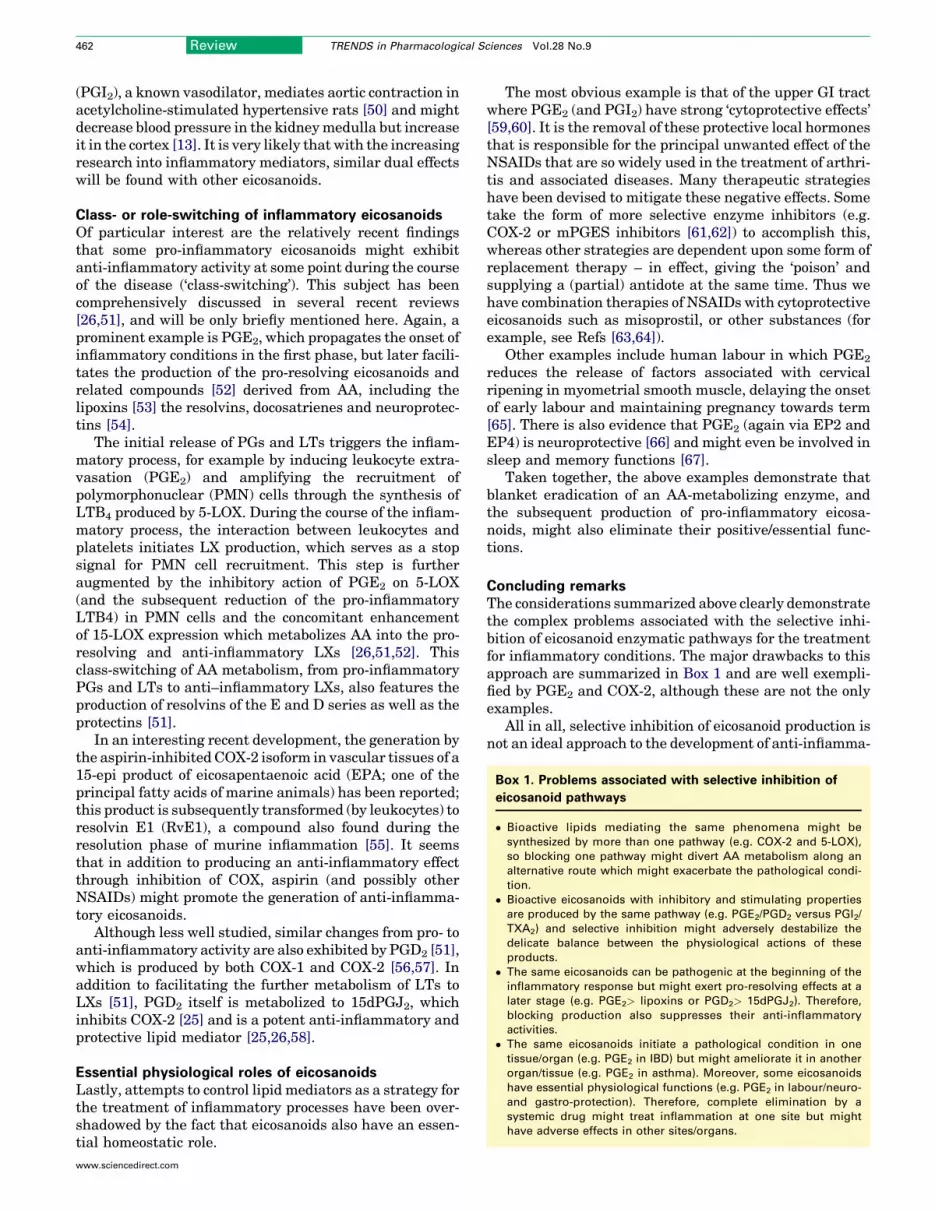
Box 1. Problems associated with selective inhibition of
eicosanoid pathways
� Bioactive lipids mediating the same phenomena might be
synthesized by more than one pathway (e.g. COX-2 and 5-LOX),
so blocking one pathway might divert AA metabolism along an
alternative route which might exacerbate the pathological condi-
tion.
� Bioactive eicosanoids with inhibitory and stimulating properties
are produced by the same pathway (e.g. PGE2/PGD2 versus PGI2/
TXA2) and selective inhibition might adversely destabilize the
delicate balance between the physiological actions of these
products.
� The same eicosanoids can be pathogenic at the beginning of the
inflammatory response but might exert pro-resolving effects at a
later stage (e.g. PGE2> lipoxins or PGD2> 15dPGJ2). Therefore,
blocking production also suppresses their anti-inflammatory
activities.
� The same eicosanoids initiate a pathological condition in one
tissue/organ (e.g. PGE2 in IBD) but might ameliorate it in another
organ/tissue (e.g. PGE2 in asthma). Moreover, some eicosanoids
have essential physiological functions (e.g. PGE2 in labour/neuro-
and gastro-protection). Therefore, complete elimination by a
systemic drug might treat inflammation at one site but might
have adverse effects in other sites/organs.
462 Review TRENDS in Pharmacological Sciences Vol.28 No.9
(PGI2), a known vasodilator, mediates aortic contraction inacetylcholine-stimulated hypertensive rats [50] and mightdecrease blood pressure in the kidneymedulla but increaseit in the cortex [13]. It is very likely that with the increasingresearch into inflammatory mediators, similar dual effectswill be found with other eicosanoids.
Class- or role-switching of inflammatory eicosanoidsOf particular interest are the relatively recent findingsthat some pro-inflammatory eicosanoids might exhibitanti-inflammatory activity at some point during the courseof the disease (‘class-switching’). This subject has beencomprehensively discussed in several recent reviews[26,51], and will be only briefly mentioned here. Again, aprominent example is PGE2, which propagates the onset ofinflammatory conditions in the first phase, but later facili-tates the production of the pro-resolving eicosanoids andrelated compounds [52] derived from AA, including thelipoxins [53] the resolvins, docosatrienes and neuroprotec-tins [54].
The initial release of PGs and LTs triggers the inflam-matory process, for example by inducing leukocyte extra-vasation (PGE2) and amplifying the recruitment ofpolymorphonuclear (PMN) cells through the synthesis ofLTB4 produced by 5-LOX. During the course of the inflam-matory process, the interaction between leukocytes andplatelets initiates LX production, which serves as a stopsignal for PMN cell recruitment. This step is furtheraugmented by the inhibitory action of PGE2 on 5-LOX(and the subsequent reduction of the pro-inflammatoryLTB4) in PMN cells and the concomitant enhancementof 15-LOX expression which metabolizes AA into the pro-resolving and anti-inflammatory LXs [26,51,52]. Thisclass-switching of AA metabolism, from pro-inflammatoryPGs and LTs to anti–inflammatory LXs, also features theproduction of resolvins of the E and D series as well as theprotectins [51].
In an interesting recent development, the generation bythe aspirin-inhibited COX-2 isoform in vascular tissues of a15-epi product of eicosapentaenoic acid (EPA; one of theprincipal fatty acids of marine animals) has been reported;this product is subsequently transformed (by leukocytes) toresolvin E1 (RvE1), a compound also found during theresolution phase of murine inflammation [55]. It seemsthat in addition to producing an anti-inflammatory effectthrough inhibition of COX, aspirin (and possibly otherNSAIDs) might promote the generation of anti-inflamma-tory eicosanoids.
Although less well studied, similar changes from pro- toanti-inflammatory activity are also exhibited by PGD2 [51],which is produced by both COX-1 and COX-2 [56,57]. Inaddition to facilitating the further metabolism of LTs toLXs [51], PGD2 itself is metabolized to 15dPGJ2, whichinhibits COX-2 [25] and is a potent anti-inflammatory andprotective lipid mediator [25,26,58].
Essential physiological roles of eicosanoidsLastly, attempts to control lipid mediators as a strategy forthe treatment of inflammatory processes have been over-shadowed by the fact that eicosanoids also have an essen-tial homeostatic role.
www.sciencedirect.com
The most obvious example is that of the upper GI tractwhere PGE2 (and PGI2) have strong ‘cytoprotective effects’[59,60]. It is the removal of these protective local hormonesthat is responsible for the principal unwanted effect of theNSAIDs that are so widely used in the treatment of arthri-tis and associated diseases. Many therapeutic strategieshave been devised to mitigate these negative effects. Sometake the form of more selective enzyme inhibitors (e.g.COX-2 or mPGES inhibitors [61,62]) to accomplish this,whereas other strategies are dependent upon some form ofreplacement therapy – in effect, giving the ‘poison’ andsupplying a (partial) antidote at the same time. Thus wehave combination therapies of NSAIDs with cytoprotectiveeicosanoids such as misoprostil, or other substances (forexample, see Refs [63,64]).
Other examples include human labour in which PGE2
reduces the release of factors associated with cervicalripening in myometrial smooth muscle, delaying the onsetof early labour and maintaining pregnancy towards term[65]. There is also evidence that PGE2 (again via EP2 andEP4) is neuroprotective [66] and might even be involved insleep and memory functions [67].
Taken together, the above examples demonstrate thatblanket eradication of an AA-metabolizing enzyme, andthe subsequent production of pro-inflammatory eicosa-noids, might also eliminate their positive/essential func-tions.
Concluding remarksThe considerations summarized above clearly demonstratethe complex problems associated with the selective inhi-bition of eicosanoid enzymatic pathways for the treatmentfor inflammatory conditions. The major drawbacks to thisapproach are summarized in Box 1 and are well exempli-fied by PGE2 and COX-2, although these are not the onlyexamples.
All in all, selective inhibition of eicosanoid production isnot an ideal approach to the development of anti-inflamma-

Review TRENDS in Pharmacological Sciences Vol.28 No.9 463
tory drugs. Instead, the desired treatment should providemore inclusive control of lipid mediator production, takinginto account the disparate/opposing functions of differentmediators in different organs/tissues under varying con-ditions, and their possible role-switching during the courseof the disease. On these grounds, combined inhibition ofCOX and LOX activities has been proposed for treatment ofinflammatory conditions (e.g. Licofelone1). This approachmight be unsatisfactory too. First, because these enzymesand their products subserve essential physiological roles,their systemic obliteration would also deprive the organismof their desirable positive functions. Second, in addition tobeing metabolized into eicosanoids by these pathways, AAitself can induce cell activation and inflammation. Finally, amajor disadvantage of current approaches to controlling AAmetabolism is that they ignore the role of LysoPL (the co-product of PL hydrolysis along with AA) which is a potentinducer of diverse inflammatory processes, from leukocyteactivation to atherosclerosis or proliferation of cancer andsmooth muscle cells. Possibly because AAmetabolites havedominated our attention, the control of LysoPL productionand action has been generally ignored as a target for anti-inflammatory treatment.
Upstream control of both AA and LysoPL production byinhibition of PLA2 could represent a superior strategy andattempts to develop suitable PLA2 inhibitors have longbeen explored but so far with no clinical success. This lackof success might be because some of the drawbacks dis-cussed above might also apply to PLA2 inhibition as wellbecause these enzymes (mainly cPLA2 and iPLA2) alsohave homeostatic/house-keeping functions. Total suppres-sion of lipid mediator production would therefore alsoeliminate their vital/beneficiary functions. Here again,any strategy aimed at inhibiting PLA2 activity should takeinto account the diverse activities of the downstreammediators and the need to control their activation whilemaintaining their basal activities. This subject is beyondthe scope of this review, and has been addressed in recentarticles [68,69].
In conclusion, selective manipulation of eicosanoid pro-duction for the control of inflammatory processes appearsto be a simplistic approach. An alternative approach wouldbe a more comprehensive and inclusive control of lipidmediator production, which will take into considerationtheir multiple intricate and opposing activities.
AcknowledgementsRJF is supported by the Wellcome Trust. S.Y.’s research is mainlysupported by a Grant from the Israel Ministry of Health.
Disclosure of interestYuval Cohen is an employee of Morria Biopharmaceuticals Plc, acompany which is sponsoring research in the laboratory of Prof. SaulYedgar. Roderick J Flower consults for Antibe Therapeutics, PalauPharma and Sosei RD Ltd, and has undertaken legal work for Pfizer Inc.
References1 Devillier, P. and Bessard, G. (1997) Thromboxane A2 and related
prostaglandins in airways. Fundam. Clin. Pharmacol. 11, 2–182 Shoseyov, D. et al. (2005) Treatment of ovalbumin-induced
experimental allergic bronchitis in rats by inhaled inhibitor ofsecretory phospholipase A(2). Thorax 60, 747–753
www.sciencedirect.com
3 Sakata, K. et al. (2004) The contractile action of leukotriene B4 in theguinea-pig lung involves a vascular component. Br. J. Pharmacol. 141,449–456
4 Trandafir, C.C. et al. (2005) Cysteinyl leukotrienes and leukotriene Bmediate vasoconstriction to arginine vasopressin in rat basilar artery.Clin. Exp. Pharmacol. Physiol. 32, 1027–1033
5 Abir, F. et al. (2005) The role of arachidonic acid regulatory enzymes incolorectal disease. Dis. Colon Rectum 48, 1471–1483
6 Zamuner, S.R. et al. (2005) Predisposition to colorectal cancer in ratswith resolved colitis: role of cyclooxygenase-2-derived prostaglandinD2. Am. J. Pathol. 167, 1293–1300
7 Yeomans, N.D. et al. (1998) Selective COX-2 inhibitors: are they safe forthe stomach? Gastroenterology 115, 227–229
8 Lauritsen, K. et al. (1994) Inhibition of eicosanoid synthesis andpotential therapeutic benefits of ‘dual pathway inhibition’.Pharmacol. Toxicol. 75 (Suppl 2), 9–13
9 Brune, K. and Hinz, B. (2004) Selective cyclooxygenase-2 inhibitors:similarities and differences. Scand. J. Rheumatol. 33, 1–6
10 Bovill, J.G. (1997) Mechanisms of actions of opioids and non-steroidalanti-inflammatory drugs. Eur. J. Anaesthesiol. Suppl. 15, 9–15
11 Wilson, D.E. (1991) Role of prostaglandins in gastroduodenal mucosalprotection. J. Clin. Gastroenterol. 13 (Suppl 1), S65–S71
12 Patrono, C. et al. (2005) Low-dose aspirin for the prevention ofatherothrombosis. N. Engl. J. Med. 353, 2373–2383
13 Grosser, T. et al. (2006) Biological basis for the cardiovascularconsequences of COX-2 inhibition: therapeutic challenges andopportunities. J. Clin. Invest. 116, 4–15
14 Khanapure, S.P. et al. (2007) Eicosanoids in inflammation:biosynthesis, pharmacology, and therapeutic frontiers. Curr. Top.Med. Chem. 7, 311–340
15 Lotzer, K. et al. (2005) The 5-lipoxygenase pathway in arterial wallbiology and atherosclerosis. Biochim. Biophys. Acta 1736, 30–37
16 Dogne, J.M. et al. (2006) Coxibs and cardiovascular side-effects: fromlight to shadow. Curr. Pharm. Des. 12, 971–975
17 Mukherjee, D. et al. (2001) Risk of cardiovascular events associatedwith selective COX-2 inhibitors. JAMA. 286, 954–959
18 Bezugla, Y. et al. (2006) COX-1 and COX-2 contribute differentially tothe LPS-induced release of PGE2 and TxA2 in liver macrophages.Prostaglandins Other Lipid Mediat. 79, 93–100
19 Ajuebor, M.N. et al. (2000) Cyclooxygenase-2-derived prostaglandinD(2) is an early anti-inflammatory signal in experimental colitis. Am.J. Physiol. Gastrointest. Liver Physiol. 279, G238–G244
20 Hart, P.H. (2001) Regulation of the inflammatory response in asthmaby mast cell products. Immunol. Cell Biol. 79, 149–153
21 Offer, S. et al. (2005) Negative feedback between secretory and cytosolicphospholipase A2 and their opposing roles in ovalbumin-inducedbronchoconstriction in rats. Am. J. Physiol. Lung Cell. Mol. Physiol.288, L523–L529
22 Vancheri, C. et al. (2004) The lung as a privileged site for the beneficialactions of PGE2. Trends Immunol. 25, 40–46
23 Cuzzocrea, S. et al. (2003) The cyclopentenone prostaglandin 15-deoxy-delta(12,14)- PGJ2 attenuates the development of colon injury caused bydinitrobenzene sulphonic acid in the rat.Br. J. Pharmacol. 138, 678–688
24 Kawahito, Y. et al. (2000) 15-deoxy-delta(12,14)-PGJ(2) inducessynoviocyte apoptosis and suppresses adjuvant-induced arthritis inrats. J. Clin. Invest. 106, 189–197
25 Tsubouchi, Y. et al. (2001) Feedback control of the arachidonatecascade in rheumatoid synoviocytes by 15-deoxy-Delta(12,14)-prostaglandin J2. Biochem. Biophys. Res. Commun. 283, 750–755
26 Lawrence, T. et al. (2002) Anti-inflammatory lipid mediators andinsights into the resolution of inflammation. Nat. Rev. Immunol. 2,787–795
27 Goh, J. et al. (2003) Lipoxins: pro-resolution lipid mediators inintestinal inflammation. Gastroenterology 124, 1043–1054
28 Honda, T. et al. (2006) Prostacyclin-IP signaling and prostaglandin E2-EP2/EP4 signaling bothmediate joint inflammation inmouse collagen-induced arthritis. J. Exp. Med. 203, 325–335
29 Ivanov, A.I. and Romanovsky, A.A. (2004) Prostaglandin E2 as amediator of fever: synthesis and catabolism. Front. Biosci. 9, 1977–1993
30 Mabuchi, T. et al. (2004) Membrane-associated prostaglandin Esynthase-1 is required for neuropathic pain. Neuroreport 15, 1395–1398
464 Review TRENDS in Pharmacological Sciences Vol.28 No.9
31 Ha, H. et al. (2006) alpha-Lipoic acid inhibits inflammatory boneresorption by suppressing prostaglandin E2 synthesis. J. Immunol.176, 111–117
32 Hahn, E.L. and Gamelli, R.L. (2000) Prostaglandin E2 synthesis andmetabolism in burn injury and trauma. J. Trauma 49, 1147–1154
33 Subbaramaiah,K. etal. (2004)MicrosomalprostaglandinEsynthase-1 isoverexpressed in inflammatory bowel disease. Evidence for involvementof the transcription factor Egr-1. J. Biol. Chem. 279, 12647–12658
34 Goulet, J.L. et al. (2004) E-prostanoid-3 receptors mediate theproinflammatory actions of prostaglandin E2 in acute cutaneousinflammation. J. Immunol. 173, 1321–1326
35 Tober, K.L. et al. (2006) Importance of the EP(1) receptor in cutaneousUVB-induced inflammation and tumor development. J. Invest.Dermatol. 126, 205–211
36 Pecchi, E. et al. (2006) Involvement of central microsomalprostaglandin E synthase-1 in IL-1beta-induced anorexia. Physiol.Genomics 25, 485–492
37 Backlund, M.G. et al. (2005) Mechanisms for the prevention ofgastrointestinal cancer: the role of prostaglandin E2. Oncology 69(Suppl 1), 28–32
38 Namkoong, S. et al. (2005) Prostaglandin E2 stimulates angiogenesisby activating the nitric oxide/cGMP pathway in human umbilical veinendothelial cells. Exp. Mol. Med. 37, 588–600
39 Brochhausen, C. et al. (2006) Cyclooxygenases and prostaglandin E2receptors in growth plate chondrocytes in vitro and in situ -prostaglandin E2 dependent proliferation of growth platechondrocytes. Arthritis Res. Ther. 8, R78
40 Chung, K.F. (2005) Evaluation of selective prostaglandin E2 (PGE2)receptor agonists as therapeutic agents for the treatment of asthma.Sci. STKE 2005, pe47
41 Takayama, K. et al. (2002) Prostaglandin E2 suppresses chemokineproduction in human macrophages through the EP4 receptor. J. Biol.Chem. 277, 44147–44154
42 Wang, X.S. and Lau, H.Y. (2006) Prostaglandin E potentiates theimmunologically stimulated histamine release from humanperipheral blood-derived mast cells through EP1/EP3 receptors.Allergy 61, 503–506
43 Libby, P. et al. (1988) Interleukin 1: a mitogen for human vascularsmooth muscle cells that induces the release of growth-inhibitoryprostanoids. J. Clin. Invest. 81, 487–498
44 van der Pouw Kraan, T.C. et al. (1996) Regulation of IL-12 productionby human monocytes and the influence of prostaglandin E2. Ann. N. Y.Acad. Sci. 795, 147–157
45 Pavord, I.D. and Tattersfield, A.E. (1995) Bronchoprotective role forendogenous prostaglandin E2. Lancet 345, 436–438
46 Mathe, A.A. and Hedqvist, P. (1975) Effect of prostaglandins F2 alphaand E2 on airway conductance in healthy subjects and asthmaticpatients. Am. Rev. Respir. Dis. 111, 313–320
47 Gauvreau, G.M. et al. (1999) Protective effects of inhaled PGE2 onallergen-induced airway responses and airway inflammation. Am. J.Respir. Crit. Care Med. 159, 31–36
48 Pasargiklian, M. et al. (1976) Clinical, functional and pathogeneticaspects of bronchial reactivity to prostaglandins F2alpha, E1, and E2.Adv. Prostaglandin Thromboxane Res. 1, 461–475
49 Escoubet-Lozach, L. et al. (2001) Increased expression of cytosolicphospholipase A2, 5-lipoxygenase and 5-lipoxygenase-activatingprotein in rat peritoneal macrophages during ovalbumin-inducedsensitisation. Clin. Exp. Allergy 31, 1094–1104
www.sciencedirect.com
50 Gluais, P. et al. (2005) Acetylcholine-induced endothelium-dependentcontractions in the SHR aorta: the Janus face of prostacyclin. Br. J.Pharmacol. 146, 834–845
51 Serhan, C.N. and Savill, J. (2005) Resolution of inflammation: thebeginning programs the end. Nat. Immunol. 6, 1191–1197
52 Levy, B.D. et al. (2001) Lipid mediator class switching during acuteinflammation: signals in resolution. Nat. Immunol. 2, 612–619
53 Paul-Clark, M.J. et al. (2004) 15-epi-lipoxin A4-mediated induction ofnitric oxide explains how aspirin inhibits acute inflammation. J. Exp.Med. 200, 69–78
54 Serhan, C.N. et al. (2004) Resolvins, docosatrienes, andneuroprotectins, novel omega-3-derived mediators, and theiraspirin-triggered endogenous epimers: an overview of theirprotective roles in catabasis. Prostaglandins Other Lipid Mediat. 73,155–172
55 Serhan, C.N. et al. (2000) Novel functional sets of lipid-derivedmediators with antiinflammatory actions generated from omega-3fatty acids via cyclooxygenase 2-nonsteroidal antiinflammatorydrugs and transcellular processing. J. Exp. Med. 192, 1197–1204
56 Gilroy, D.W. et al. (1999) Inducible cyclooxygenase may have anti-inflammatory properties. Nat. Med. 5, 698–701
57 Yoshikawa, K. et al. (2006) Profiling of eicosanoid production in the rathippocampus during kainic acid-induced seizure: dual phaseregulation and differential involvement of COX-1 and COX-2. J.Biol. Chem. 281, 14663–14669
58 Lin, T.N. et al. (2006) 15d-prostaglandin J2 protects brain fromischemia-reperfusion injury. Arterioscler. Thromb. Vasc. Biol. 26,481–487
59 Main, I.H. and Whittle, B.J. (1973) The effects E and A prostaglandinson gastric mucosal blood flow and acid secretion in the rat. Br. J.Pharmacol. 49, 428–436
60 Nezamis, J.E. et al. (1971) Inhibition by prostaglandin E 1 of gastricsecretion in the dog. J. Physiol. 218, 369–383
61 Gudis, K. et al. (2005) Microsomal prostaglandin E synthase (mPGES)-1, mPGES-2 and cytosolic PGES expression in human gastritis andgastric ulcer tissue. Lab. Invest. 85, 225–236
62 Trebino, C.E. et al. (2005) Redirection of eicosanoid metabolism inmPGES-1-deficient macrophages. J. Biol. Chem. 280, 16579–16585
63 Wallace, J.L. and Cirino, G. (1994) The development ofgastrointestinal-sparing nonsteroidal anti-inflammatory drugs.Trends Pharmacol. Sci. 15, 405–406
64 Wallace, J.L. et al. (1995) Nitric oxide-releasingNSAIDs: a novel class ofGI-sparing anti-inflammatory drugs.Agents Actions Suppl. 46, 121–129
65 Slater, D.M. et al. (2006) Anti-inflammatory and relaxatory effects ofprostaglandin E2 inmyometrial smoothmuscle.Mol. Hum. Reprod. 12,89–97
66 Echeverria, V. et al. (2005) Stimulation of PGE receptors EP2 and EP4protects cultured neurons against oxidative stress and cell deathfollowing beta-amyloid exposure. Eur. J. Neurosci. 22, 2199–2206
67 Chen, C. and Bazan, N.G. (2005) Lipid signaling: sleep, synapticplasticity, and neuroprotection. Prostaglandins Other Lipid Mediat.77, 65–76
68 Menschikowski, M. et al. (2006) Secretory phospholipase A2 of groupIIA: is it an offensive or a defensive player during atherosclerosis andother inflammatory diseases? Prostaglandins Other Lipid Mediat. 79,1–33
69 Murakami,M. (2004) Hot topics in phospholipase A2 field.Biol. Pharm.Bull. 27, 1179–1182