toxicity of volatile poisons (alcohols, ethylene glycol, kerosene)
TRANSCRIPT
VOLATILE POISONS
الطاهر عبدالعزيز .د
ETHANOL TOXICITY
ETHANOL
Uses 1- Ingredient for many tinctures, elixirs, spirits
2- Cosmetic industry: perfumes, aftershaves, colognes
3- Solvent
4- Antidote
5- Wide recreational (prohibited in Libya) use
- Beers 3-6%
- Wines 10-12%
- Distilled beverages (Whisky, Vodka..) 20-60%
Absorption: 20% stomach & 80% upper small intestine.
GASTRIC EMPTYING
• INCREASED – Tolerance to the alcohol.
– Gastrectomy.
– Type of beverage.
• DECEASED
• Presence of food in the stomach (milk & carbohydrates). – Drugs (e.g. atropine).
– Emotional state.
– Solutions with concentrations above 20% are absorbed slowly , inhibit gastric peristalsis and cause pylorospasm.
Blood
Concentration
Alcohol in blood can be detected after 5 min
Maximum concentration within 30-90 min.
One unit alcohol increases blood level in females more
than that in males because of:
– Smaller body mass in women
– Higher fats & lesser fluids in the body.
– Diminished “first-pass” metabolism of alcohol in the
gastric mucosa because of lesser alcohol
dehydrogenase
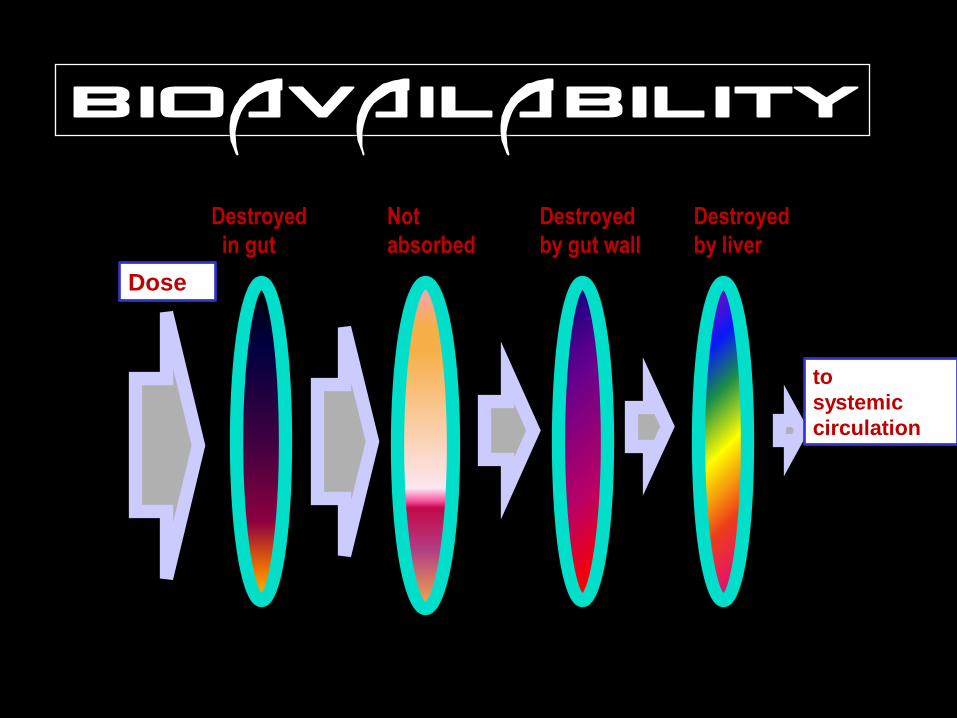
Dose
Destroyed
in gut
Not
absorbed
Destroyed
by gut wall
Destroyed
by liver
to
systemic
circulation
• Peak blood ethanol concentrations
develop more slowly after rapid ingestion
due to the irritant properties of ethanol.
• Little difference in rate of absorption of the
same dose of ethanol administered in the
form of different alcoholic beverages.
– This is important for forensic considerations,
i.e., blood ethanol concentration is not
significantly influenced by the type of
alcoholic beverage consumed.
Distribution & Equilibrium • Alcohol enters various organs of the body as
well as spinal fluid, urine, and pulmonary
alveolar air, etc.
• Alcohol is distributed in body water. Tissues rich in
water take up more alcohol than those rich in fat do.
• Equilibrium between tissues and blood takes place
within 1-2 hours.
Elimination
• About 10% of alcohol are excreted as such mainly
through urine and breath and only negligible amount in
sweat and faeces.
Metabolism in the liver
First Step 1- About 90% of the ingested alcohol are oxidized in
the cytoplasm by alcohol dehydrogenase. 2- Catalase system: peroxisomes & mitochondria. 3- Microsomal ethanol-oxidizing system: smaller
amount of alcohol is converted to acetaldehyde. Second step metabolism of acetaldehyde, which is converted to
acetate by the effect of aldehyde dehydrogenase and the presence of NAD as cofactor.
Ethanol Acetaldehyde acetate H2O + CO2
Acetaldehyde might be responsible for alcohol intoxication and addiction:
• Flushers (Chinese & some other Asians) differ from other non-flushers in that addiction is lesser among them but this not a fact as American Indians are more alcoholic than other ethnic groups.
• Acetaldehyde combines with norepinephrine, epinephrine, and serotonin to make substances similar in structures to plant alkaloids that cause addiction such as morphine.
Metabolic adaptation (Tolerance)
• Besides CNS adaptation, alcoholics (in
the absence of liver disease) often have
an increased rate of blood alcohol
clearance.
• This is called metabolic tolerance
Suggested mechanisms include:
1. Induction of ADH.
2. Increased reoxidation of NADH
3. Induction of CYP2E1 (the most active cytochrome P450 for oxidizing ethanol).
Clearance: rate of chemical elimination from the body per unit
of time.
Blood Alcohol Curve
• Alcohol concentration rises steeply to a distinct maximum (absorption phase). Peak concentration is reached after 30-90 minutes (average 60 minutes).
• Irregularly curved fall due to a period of diffusion within the tissues to equilibrium (15-30 minutes).
• The BAC then falls progressively in linear fasion (elimination phase).
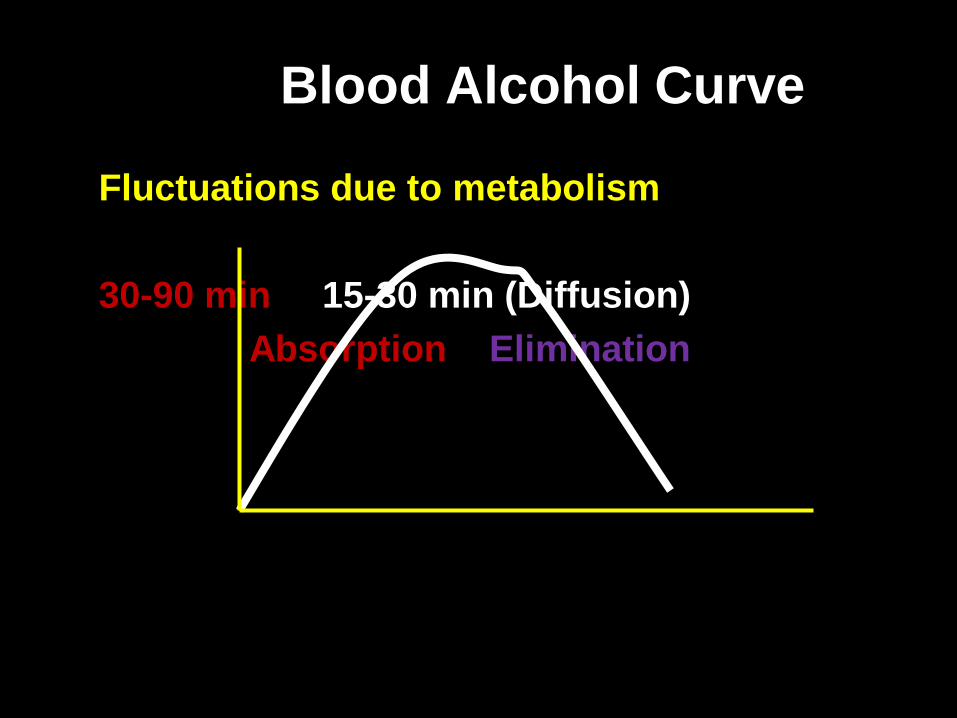
Blood Alcohol Curve
Fluctuations due to metabolism
30-90 min 15-30 min (Diffusion)
Absorption Elimination
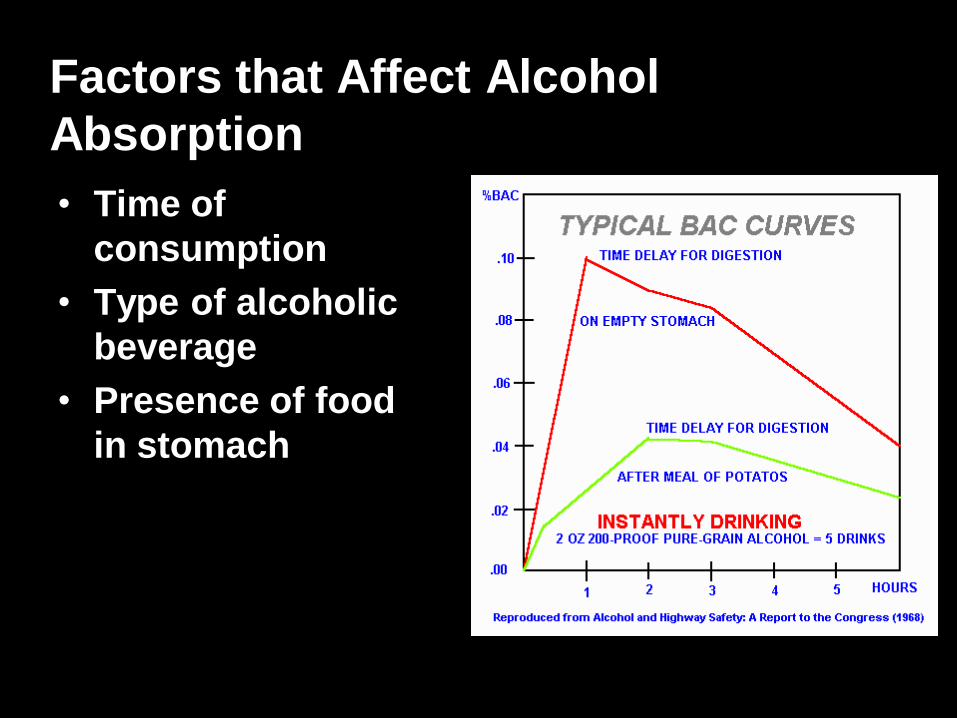
Factors that Affect Alcohol
Absorption
• Time of
consumption
• Type of alcoholic
beverage
• Presence of food
in stomach
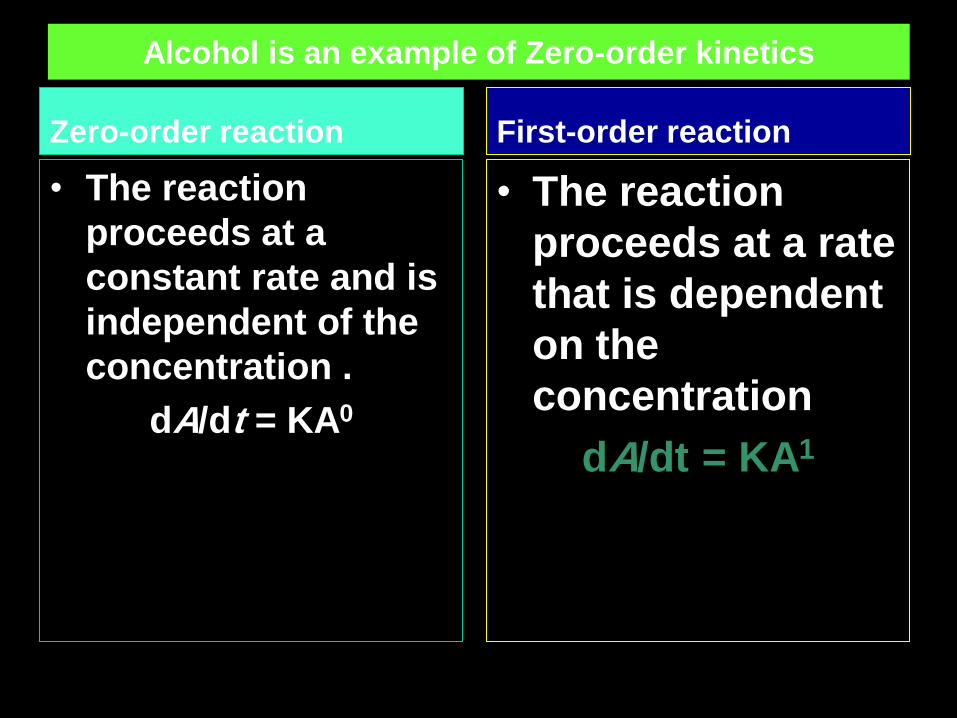
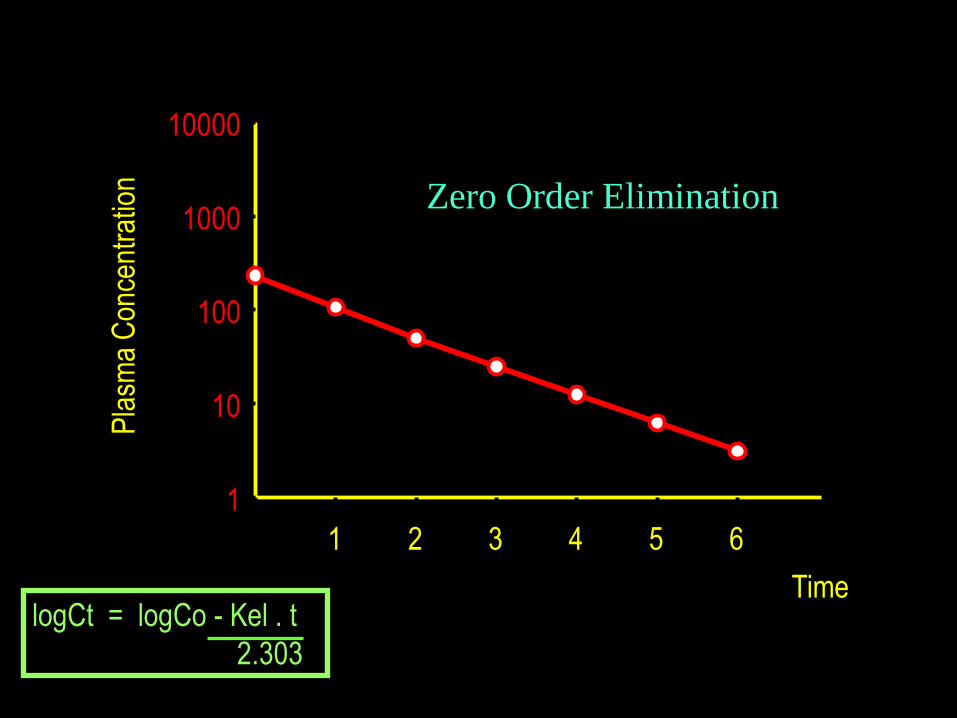
Alcohol is an example of Zero-order kinetics
Zero-order reaction
• The reaction
proceeds at a
constant rate and is
independent of the
concentration .
dA/dt = KA0
First-order reaction
• The reaction
proceeds at a rate
that is dependent
on the
concentration
dA/dt = KA1
Time
Pla
sma
Con
cent
ratio
n
0 1 2 3 4 5 6
1
10
100
1000
10000
Zero Order Elimination
logCt = logCo - Kel . t
2.303
Forensic Significance of Zero-order kinetics
• The rate of elimination of ethanol is 15-20
mg/dl/hour
• At very high concentrations >200mg% over 12
hours are required to eliminate 200mg%.
Limits of blood alcohol content (BAC)
In Libya, alcohol is prohibited.
The alcohol level at which a person is
considered to be legally impaired varies
by country.
The list below gives limits by country.
These are typically BAC limits for the
operation of a vehicle.
Criminal Code of Canada reports legal limit for
ethanol as 80 milligrams per 100 millilitres of
blood (80 mg%).
Also expressed as 0.08 g/100 ml blood.
Serum/Plasma versus Whole Blood
Serum contains more alcohol than whole blood by a
factor of 1.12:1.
Serum level 112 mg% = 100 mg% in whole blood.

Blood Alcohol legal lmits (g/dl) ZERO 0.02 0.03 0.04 0.05 0.08
LIBYA China India lituania Australia Canada
Islamic
countries?
?
Estonia Japan Others Malaysia
Slovakia Poland Russia Malta
Romania Norway Urguay Mexico
Brazil Sweden USA
Chech Rep Puorto Rico United
kingdom
Hungary
Mode of Action
• Direct effect by its lipid solubility, interacts with
membrane lipoproteins.
1- Depression of CNS.
– Releasing inhibition: euphoric effect.
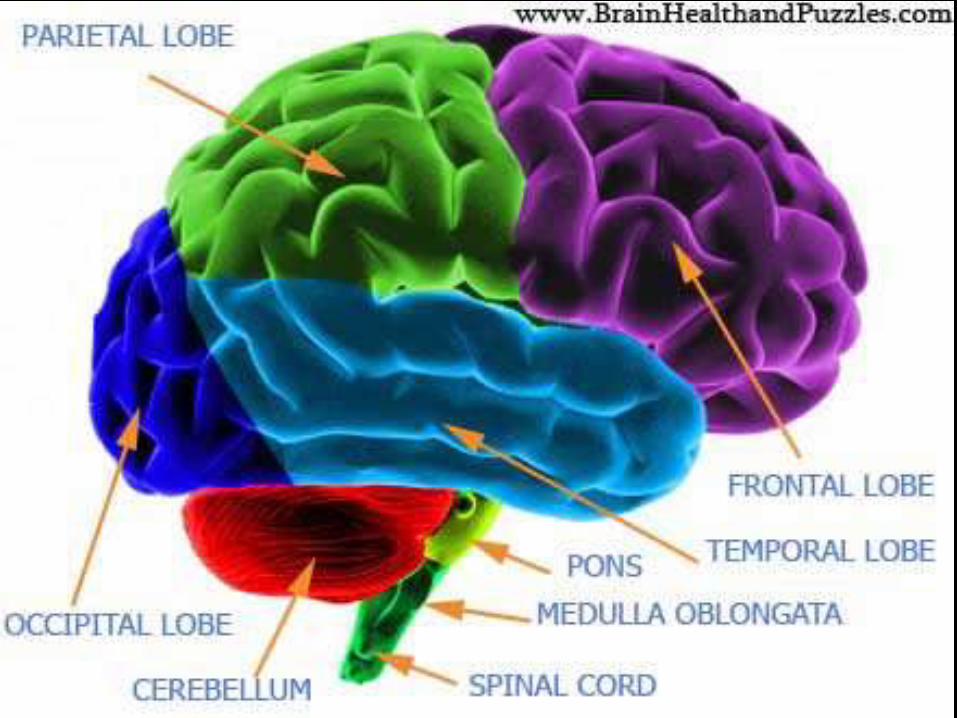
– Acts on the frontal lobe, psychic area,
cerebellum, spinal cord, and finally the medulla.
– Inhibits (1) higher nervous centers (control
conduct & judgment), (2) motor centers (3) the
vital organs.
• The effect on the spinal cord leads to initial
increase in deep tendon reflexes.
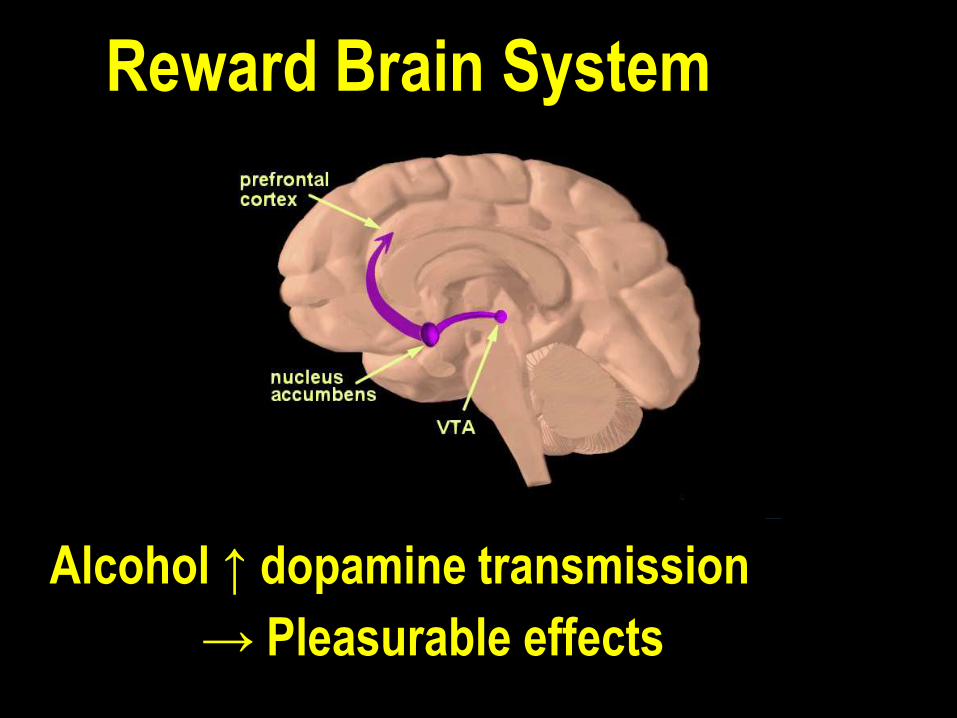
Alcohol ↑ dopamine transmission
Reward Brain System
→ Pleasurable effects
Movement: Slower, Inaccurate, Random
Impairment of mental function:
– interfering with the speed of perception
– Interfering with the mental processing
slower learning, decreased focusing,
concentration, judgment, discrimination, and
thinking.
2- Acid-base disturbances: HIGH ANION GAP
METABOLIC ACIDOSIS
3- Hypoglycemia (or hyperglycemia).
Hypoglycemia most common.
4- Hypothermia
CLINICAL MANIFESTATIONS
Phase I: Excitation (50-150 mg/100ml)
• Excitement, euphoria, and increased confidence
• Talkative and argues on every point
• Inhibition of self-control.
• Face is flushed and the conjunctiva is injected
• Pupils are dilated with sluggish light and accommodation reactions.
• Judgment is impaired while mental alertness can be retained.
Phase II: Incoordination (Confusion) BAC up to 300mg/100ml.
• Important for medicolegal purposes
• Incoordination of thought, speech, and action
• Pupils are dilated and react sluggishly to light and accommodation
• Sense of perceptions and skilled movements are affected
• Ataxia.
• There may be hangover due to brain edema, toxic effects of alcohol on the brain, GIT, and liver.
Phase III: Coma (Narcosis) BAC is more than 300mg/100ml.
• Motor and sensory cells are deeply affected.
• Speech becomes thick and slurring
• Incoordination is more marked the person
staggers and falls
• Gradually, he enters into coma and cannot be
awakened by deep stimuli and reflexes are
abolished.
• Pupils may be constricted.
Clinical Diagnosis
Serum level (mg/100ml)
=
Osmolar gap x 4.6
Analysis of BAC
• Breath Tests
• Field Sobriety Tests
• Blood Tests
The Breathalyzer
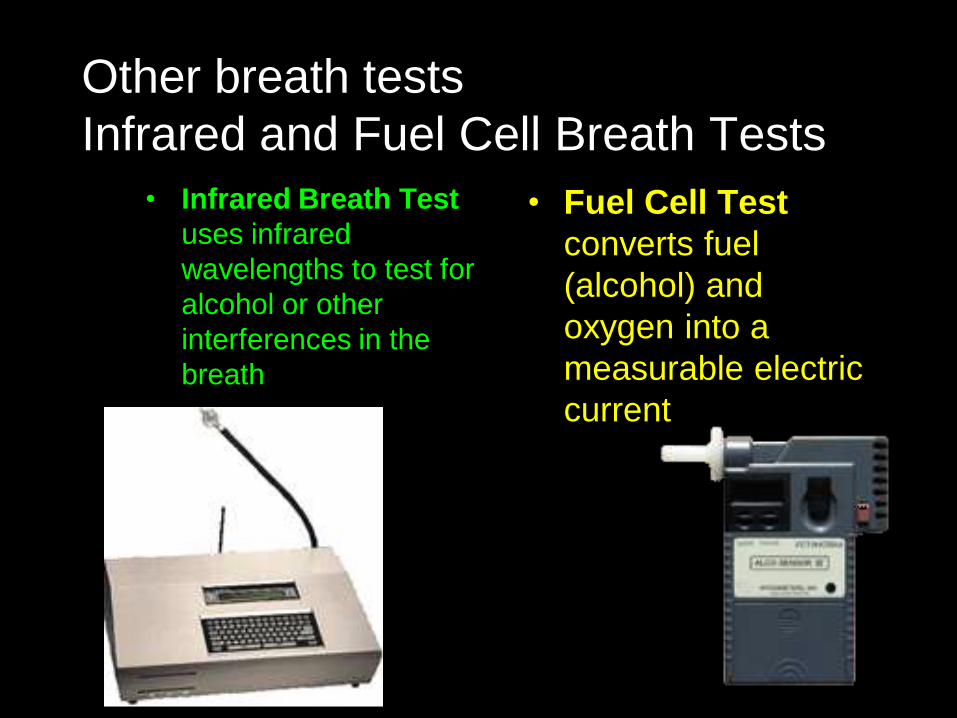
Other breath tests
Infrared and Fuel Cell Breath Tests
• Infrared Breath Test
uses infrared
wavelengths to test for
alcohol or other
interferences in the
breath
• Fuel Cell Test
converts fuel
(alcohol) and
oxygen into a
measurable electric
current
Field Sobriety Tests
• Horizontal Gaze Nystagmus – Involuntary eye jerk as eye moves horizontally
• Walk and Turn (divided attention tasks)
• One-Leg Stand
Collection and preservation of blood
• Use nonalcoholic disinfectant like
– Povidone-iodine (Betadine)
– Benzalkonium chloride (Zepiran)
– Mercuric chloride
• Stored in airtight container with
anticoagulant and preservative under
refrigeration
Pathological Alcohol intoxication
(mania a potu)
• Rare
• Extraordinary severe response
• Marked by apparently senseless violent
behavior, usually followed by exhaustion, sleep
and amnesia for the episode.
• It is used by criminals to form
legal defense against their criminal activities.
TREATMENT • ABC: IV dextrose & 100 mg of thiamine.
• Gastric lavage in noncomatose patients, if the patient comes early after the ingestion. The lavage should be done, at the beginning, with plain water, from which a sample should be sent for chemical analysis. The next wash will be done by NaHCO3. This will prevent further absorption and help for acidosis.
• Maintain body temperature, especially in cold
weather.
• Others causes of coma should be excluded.
• Treat acidosis if ABG results show low pH.
• Hemodialysis or hemoperfusion may be
considered in severe cases.
ALCOHOLISM Alcoholism is a term used to mean compulsive & uncontrolled consumption of alcohol.
Several other terms are used, specifically "alcohol abuse" and "alcohol dependence" which have more specific definitions.
Alcohol dependence : an individual uses alcohol despite significant areas of dysfunction, evidence of physical dependence, and/or related hardship, and also may cause stress and bipolar disorder.
In 1979 an expert WHO committee discouraged the use of "alcoholism" in medicine, preferring the category of "alcohol dependence syndrome“.
The WHO estimates that there are 140 million people with alcoholism worldwide.2001-2003
In USA, It costs annually 40-50 billion dollars
In LIBYA, NO DATA
CHRONIC ALCOHOLISM
• Daily use of large amounts of alcohol
for adequate functioning.
• Regular heavy drinking limited to
weekends.
• Long periods of sobriety interspersed
with binges of heavy alcohol intake
lasting for weeks or months.
CHRONIC ALCOHOLISM
• Associated behaviors as:
Inability to stop drinking: Repeated efforts to control or
reduce excessive drinking or restricting drinking to
certain times
Binges (remaining intoxicated for at least 2 days).
The continuation of drinking despite a Binges.
Amnestic periods for events while intoxicated (blackouts).
The continuation of drinking despite a serious physical
disorder that the person knows is exacerbated by alcohol
use.
The drinking of nonbeverage alcohol such as fuel.
Impaired social and occupational functioning
Complications of Alcohol Withdrawal 1- Withdrawal Seizures
2- Impendin g delirium Tremens: common alcohol withdrawal syndrome. Mild to moderate agitation, tremor, insomnia, loss of blood pressure control. Acute alcoholic hallucinations, with auditory hallucinations.
Generalized tremor the most is the most obvious feature of the illness.
3- Delirium Tremens – Most severe form of withdrawal syndrome.
– A medical emergency.
– Due to severe cortical and brainstem hyperexcitability, cerebral edema, and increased pressure of CSF.
– Onset follows 3-5 days after cessation of drinking.
– Mortality is 20% if untreated, usually as a result of an intercurrent medical illness such as pneumonia, renal disease, hepatic insufficiency, pancreatitis, or heart failure.
Forensic Considerations
1. Time lag from consumption to peak level
determined by factors affecting absorption.
2. Ethanol elimination rates; genetic, sex, age, Wt.
3. Partition ratio: differences between blood, breath,
and urine ratios.
4. Fluctuations and anomalies: factors that change in
blood levels of alcohol due to changes in
absorption and elimination.
Postmortem appearance
• External: congestion of conjunctiva, odor of
alcohol around mouth and nose.
• Internal: congestion of GIT, pulmonary and
cerebral edema, congestion of other
viscera.
• In chronic alcoholism there may be
additional features:
– Fatty or cirrhotic liver
– Degenerative changes in the brain.
METHANOL
TOXICITY
Also called wood alcohol obtained
by destructive distillation of wood.
Widely used as solvent and found
in paint, varnish
Used as Antifreeze
Surgical spirit: Ethanol & Methanol.
Methanol Uses
• Gas Line Antifreeze 100%
• Windshield washer fluid 30%
• Varnish removers
• Fuel for food warming 3-70%
• Industrial uses
Mechanism of toxicity
• Methanol is slowly metabolized by ADH to formaldehyde and subsequently by aldehyde dehydrogenase to formic acid (formate).
• Systemic acidosis is caused by the formic acid as well as by lactic acid, while blindness is caused primarily by formate.
• Both ethanol and methanol compete for the enzyme alcohol dehydrogenase; the preference of this enzyme for metabolizing ethanol forms the basis for ethanol therapy in methanol poisonings
Toxicokinetics
Methanol is readily absorbed and quickly distributed to the body water . It is not protein bound.
It is metabolized slowly by alcohol dehydrogenase at a rate about one-tenth that of ethanol.
The reported “half-life” ranges from 2–24 hours.
Only about 3% is excreted unchanged by the kidneys and less than 10% through the breath.
METHANOL FORMALDEHYDE FORMATE
Formate is responsible for:
1- Ocular Toxicity
2- Acidosis
Mortality & Morbidity is related more to formate concentration (time between ingestion & initiation of therapy) rather than to initial methanol concentration).
Clinical Features
Initially similar to ethanol toxicity
After a latent period (8-36 hours): nausea, vomiting, abdominal pain, severe metabolic acidosis, visual disturbances, cerebral edema, seizures, coma, & death.
• Optic neuritis leads to blindness. The pupils are dilated and fixed.
In over dose, death is caused by respiratory paralysis.
Fatal Dose: approximately 60-300 ml. Even as little as 10 ml may cause serious illness. Blindness has occurred even after a dose of 4 ml.
Toxicity, also, occur by inhalation and through skin.
Fatal Period: (6 – 30 hours).
Methanol Toxicity
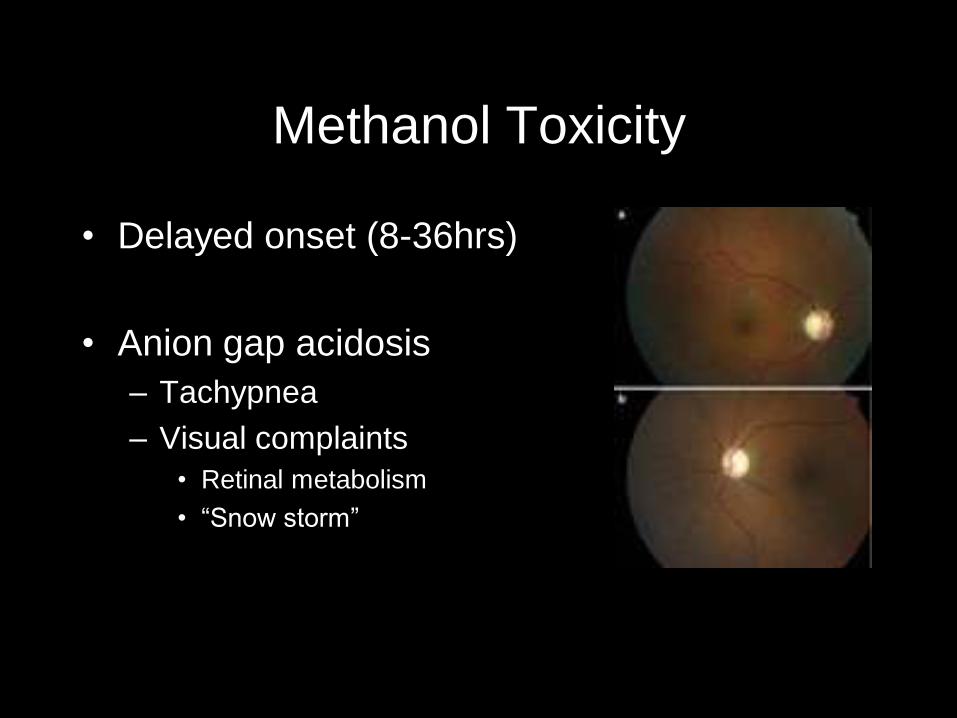
• Delayed onset (8-36hrs)
• Anion gap acidosis
– Tachypnea
– Visual complaints
• Retinal metabolism
• “Snow storm”
Yang CS et al Eye 2005;19:806-809
Methanol Toxicity
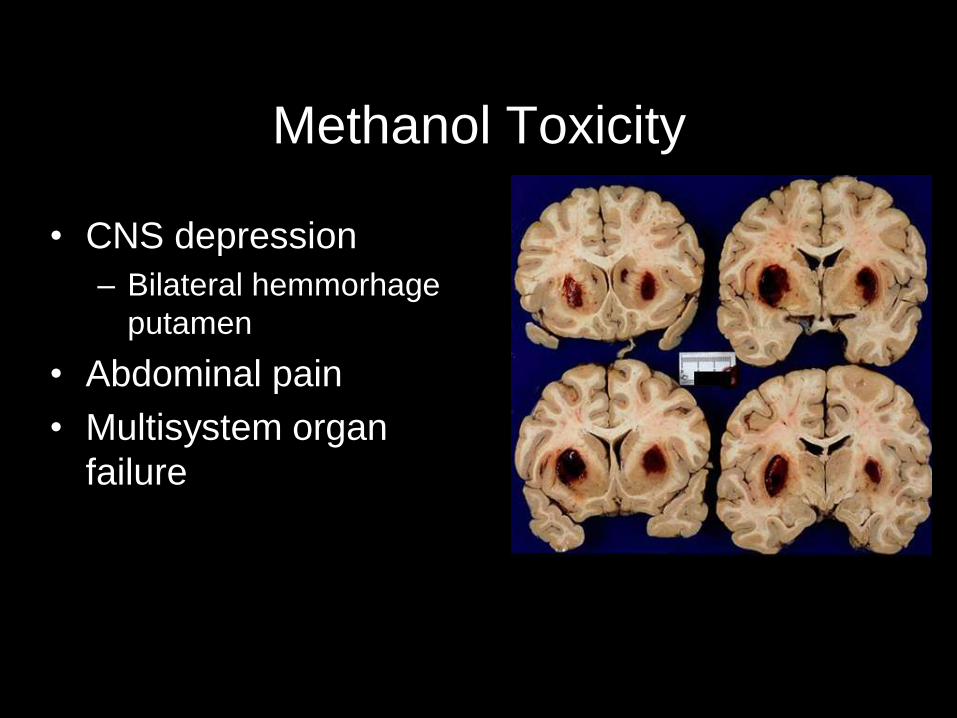
• CNS depression
– Bilateral hemmorhage
putamen
• Abdominal pain
• Multisystem organ
failure
University of Western Ontario:
Neurology Collection
Diagnosis Diagnosis is usually based on the history,
symptoms, and laboratory findings because
methanol levels are rarely available.
Methanol level = osmolal gap x 3.2
A large anion gap (not due to elevated lactate)
suggests possible methanol (or ethylene
glycol) poisoning.
Diagnosis Specific levels
1. Serum methanol levels higher than 20 mg/dL should
be considered toxic, and levels higher than 40 mg/dL
should be considered very serious. After the latent
period, a low or nondetectable methanol level does
not rule out serious intoxication in a symptomatic
patient because all the methanol may already have
been metabolized to formate.
2. Elevated serum formate concentrations may confirm
the diagnosis and are a better measure of toxicity,
but formate levels are not yet widely available.
Treatment • Stabilization of the patient
• Correction of metabolic acidosis by IV NaHCO3
• Elimination – Induction of emesis or gastric lavage may be done.
– Hemodialysis • Methanol level > 25 mg/dl
• Formate level > 50mg/dl
• Severe metabolic acidosis
• Antidotes – Ethyl alcohol as the antidote.
– The new antidote Fomepizole.
– Folinic Acid it accelerates the conversion of formic acid to carbon dioxide and water
Postmortem appearance
• Similar to ethanol
• Toxic damage in liver and kidney
• Lungs may reveal edema
ETHYLENE
GLYCOL
TOXICITY
Ethylene Glycol
• Ethylene glycol is the primary
ingredient (up to 95%) in antifreeze.
• It is sometimes intentionally
consumed as an alcohol substitute
by alcoholics and is tempting to
children because of its sweet taste.
Intoxication
Mechanism of toxicity. • Metabolized by alcohol dehydrogenase to
glycoaldehyde, which is then metabolized to glycolic, glyoxylic, and oxalic acids. These acids, along with excess lactic acid, are responsible for the anion gap metabolic acidosis.
• Oxalate readily precipitates with calcium to form insoluble calcium oxalate crystals. Tissue injury is caused by widespread deposition of oxalate crystals and the toxic effects of glycolic and glyoxylic acids
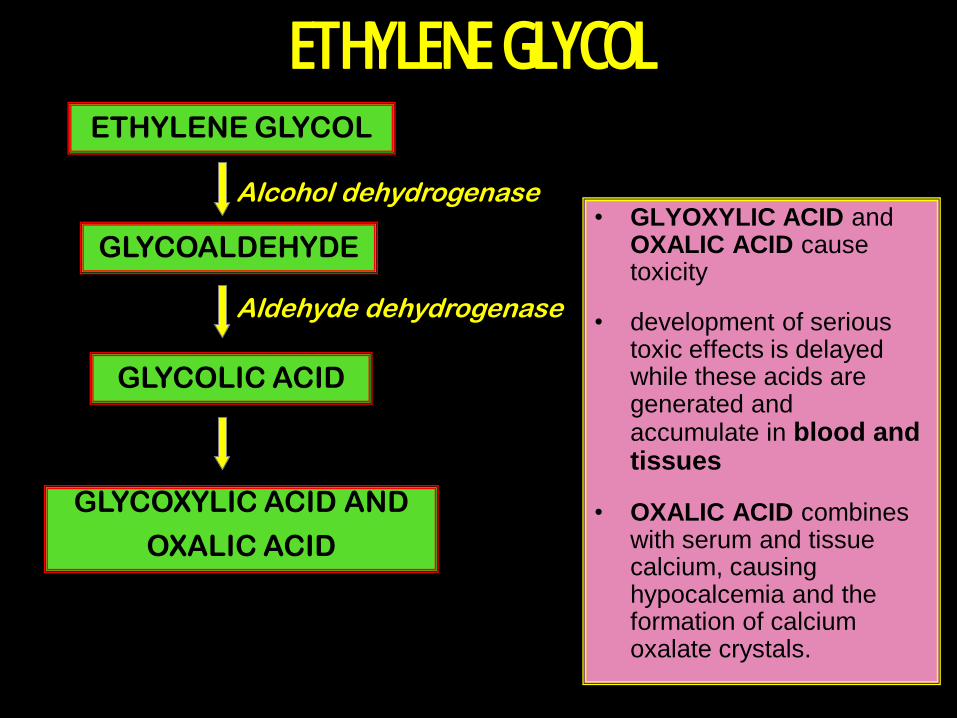
ETHYLENE GLYCOL
• GLYOXYLIC ACID and OXALIC ACID cause toxicity
• development of serious toxic effects is delayed while these acids are generated and accumulate in blood and tissues
• OXALIC ACID combines with serum and tissue calcium, causing hypocalcemia and the formation of calcium oxalate crystals.
ETHYLENE GLYCOL
GLYCOALDEHYDE
GLYCOLIC ACID
GLYCOXYLIC ACID AND
OXALIC ACID
Alcohol dehydrogenase
Aldehyde dehydrogenase
Clinical Manifestations • Stage 1: Neurological (30 minutes to 12 hours after ingestion)
– Within minutes to several hours, similar to ethanol symptoms
of may be observed. Nausea and vomiting can also occur.
– As metabolism progresses, metabolic acidosis and CNS
depression can replace earlier symptoms.
– Approximately 4-12 hours after ingestion, symptoms
associated with toxic metabolites of EG predominate.
– In severe cases, these symptoms can include coma
associated with hypotonia, hyporeflexia, occasional seizures,
and meningismus.
– Cytotoxicity and the deposition of calcium oxalate can lead
to cerebral damage and contribute to CNS depression.
– Other neurological symptoms may include nystagmus, ataxia,
opthalmoplegia, and myoclonic jerks. In most cases of ethylene glycol
poisoning, the optic fundus is normal; however, in some situations, the
presence of papilledema may confuse the clinical presentation with that of
methanol poisoning.
• Stage 2: Cardiopulmonary (12-24
hours after ingestion)
tachycardia and mild hypertension
frequently occur.
In serious cases, severe metabolic
acidosis with compensatory
hyperventilation can develop
accompanied by multiple organ failure.
Most deaths occur in this stage.
• Stage 3: Renal (24-72 hours after ingestion)
• The symptoms of the third stage can include
oliguria, flank pain, acute tubular necrosis,
renal failure and, in rare instances, bone
marrow suppression.
• In severe cases of ethylene glycol poisoning,
renal failure may appear early and progress
to anuria.
• Recovery of renal function is often complete
but may require several months of
hemodialysis.
• Serious damage to the liver is rare.
Diagnosis • History of antifreeze ingestion, typical
symptoms, and elevation of the osmolar and
anion gaps.
• Oxalate or hippurate crystals may be present in
the urine (crystals may be cuboidal or elongate in
form).
• Because many antifreeze products contain
fluorescein, the urine may fluoresce under
Wood’s lamp, depending on the amount
ingested, the time since ingestion, and the urine
concentration.
Estimation of serum level (mg/dl)= Osmolar gap x 6.2
Calcium oxalate crystals
Serum Level
• Serum levels higher than 50 mg/dL are usually associated with serious intoxication, although lower levels do not rule out poisoning if the parent compound has already been metabolized (in such a case, the anion gap should be markedly elevated).
• Calculation of the osmolar gap may be used to estimate the ethylene glycol level.
• False-positive ethylene glycol levels can be caused by elevated triglycerides
• In the absence of a serum ethylene glycol level, if the osmolar and anion gaps are both normal and the patient is asymptomatic, then serious ingestion is not likely to have occurred.
Treatment
• Stomach lavage with calcium salts.
• Forced diuresis to eliminate the nonmetabolized part.
• In the IV infusion 10% calcium gluconate will be added as an antidote to oxalic acid.
• Ethyl alcohol to prevent further oxidation
• Fomepizole is the newer antidote.
• Pyridoxine, folate, and thiamine cofactors required for the metabolism of ethylene glycol that may decreasetoxicity by enhancing metabolism of glyoxylic acid to nontoxic metabolites.
• Correction of metabolic acidosis.
• Treatment of complications; pulmonary edema, shock, etc.
Fomepizole
• 4-methylpyrazole (4MP)
• Potent inhibitor of ADH
• Has an affinity for ADH x 500-1000 of ethanol
• Limited toxicity
• Safely used in France since 1981(1)
• 2 US multi centre prospective trials confirmed
efficacy(2,3)
1. Megarbane B, Borron SW, Trout H et al. treatment of acute methanol poisoning with fomepizole. Intensive
Care Med. 2001. 27:1370-1378
2. Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of ethylene glycol poisoning. NEJM. 1999.
340:832-838
3. Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of methanol poisoning. NEJM. 2001.
344:424-429
Current recommendations for treatment of severe toxic alcohol
poisonings. Intensive care med. 2005
• Fomepizole
• Due to efficacy & safety profile
• Recommended as 1st line antidote in confirmed ethylene glycol / methanol poisoning
• Also recommend initial fomepizole dose – Suspicion of toxic alcohol ingestion
– In presence of metabolic acidosis with elevated anion gap unexplained by equivalent increase in serum lactate
• Peritoneal dialysis, hemodialysis or hemoperfusion.
• Fatal Dose: 20-120 ml. In children 3-4 ml/kg.
Postmortem appearance
• cerebral edema
• Toxic damage of liver and
kidneys
• Oxalate crystals in brain,
spinal cord and kidneys
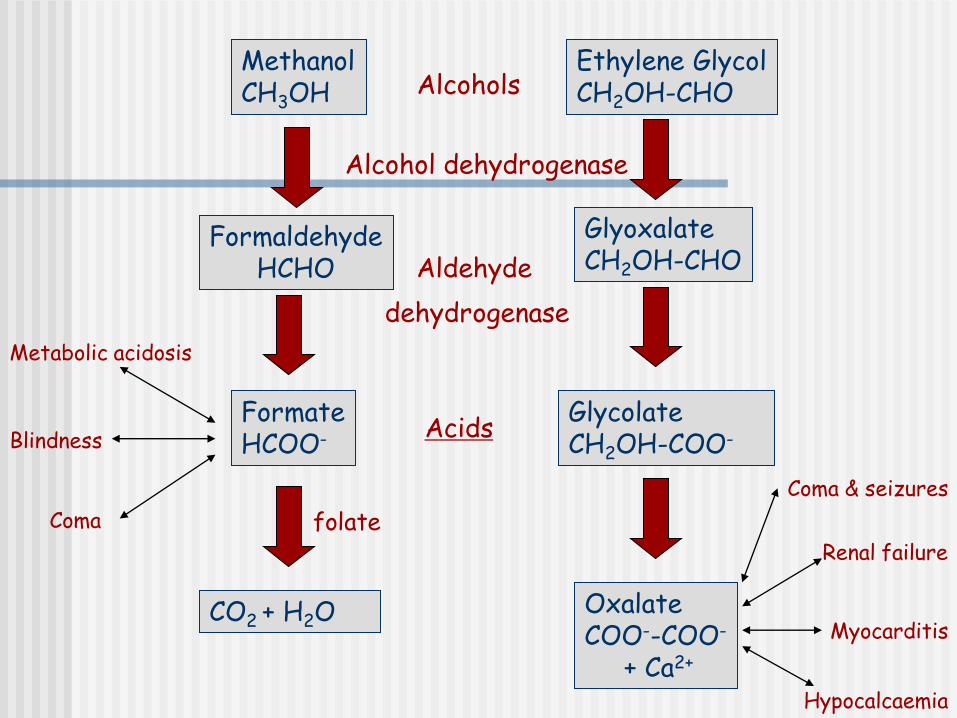
Methanol CH3OH
Ethylene Glycol CH2OH-CHO
Formaldehyde HCHO
Glyoxalate CH2OH-CHO
Formate HCOO-
Glycolate CH2OH-COO-
CO2 + H2O Oxalate COO--COO-
+ Ca2+
Alcohols
Metabolic acidosis
Blindness
Coma
Coma & seizures
Renal failure
Myocarditis
Hypocalcaemia
Alcohol dehydrogenase
Aldehyde
dehydrogenase
folate
Acids
HYDROCARBONS
Petrolium Distillates
• Widely used in the petroleum, plastic, agricultural, and chemical industries as solvents, degreasers, fuels, and pesticides.
• A hydrocarbon is any chemical containing hydrogen and carbon (essentially, any organic compound).
• There are many subcategories of hydrocarbons, including aliphatic (saturated carbon structure), alicyclic (ring compounds), aromatic (containing one or more benzene ring structures), halogenated (containing chlorine, bromine, or fluoride atoms), alcohols and glycols, ethers, ketones, carboxylic acids, and many others.
• Aliphatic form: includes kerosene, gasoline, furniture polish, petroleum ether, petroleum naphtha, lubricating oils
• Aromatic hydrocarbons: benzene, xylenes,
etc.
• The toxicity of hydrocarbons is generally indirectly proportional to the agent’s viscosity. Products with high viscosity (150 – 250), such as heavy greases and oils, considered to have limited toxicity.
Mechanism of Toxicity
Pulmonary Aspiration: Chemical peumonitis.
Ingestion:
1- Aliphatic (kerosene) poorly absorbed by GIT giving less systemic toxicity.
2- Aromatic (benzene) are capable of causing systemic toxicity after ingestion such as convulsion, coma, cardiac arrhythmias.
Inhalation: vapors in an enclosed space may cause systemic intoxication.

Clinical Manifestations
After Inhalation:
Gasoline and kerosene produce symptoms resembling alcoholic intoxication.
The early effects of exposure are: headache, nausea, vomiting, dyspnea, and variety degrees of cyanosis and confusion.
Within few hours may progress to tachypnea, wheezing, chemical pneumonitis.
Muscular incoordination, convulsions, coma.
With more severe injury, pulmonary edema, hemoptysis.
Cardiorespiratory arrest.
After Ingestion • Often causes- abrupt nausea, vomiting.
• Irritation of upper GIT.
• Occasionally hemorrhagic gastroenteritis.
• Diarrhea (may be bloody), less common.
• Some compounds may be absorbed and produce systemic toxicity:
There may be confusion, ataxia, lethargy, headache.
With severe exposure; syncope, coma, and respiratory arrest
Postmortem Appearance
• 1- characteristic odor
• Froth at mouth and nostrils
• Cyanosis of extremities
• Congestion of GIT
• Pulmonary edema, lung changes
• Fatty change in liver
• Cardiomyopathic changes