tobacco awareness in three u.s. medical schools
TRANSCRIPT

This article was downloaded by: [Columbia University]On: 30 September 2014, At: 18:04Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Journal of Addictive DiseasesPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/wjad20
Tobacco Awareness in Three U.S. Medical SchoolsJoshua G. Schkrohowsky MD a , Bindu Kalesan MSc, MPH b & Anthony J. Alberg PhD, MPH ba Johns Hopkins University School of Medicine , Baltimore, MD, USAb Department of Epidemiology , Johns Hopkins University Bloomberg School of PublicHealth , Baltimore, MD, USAPublished online: 04 Oct 2008.
To cite this article: Joshua G. Schkrohowsky MD , Bindu Kalesan MSc, MPH & Anthony J. Alberg PhD, MPH (2007) TobaccoAwareness in Three U.S. Medical Schools, Journal of Addictive Diseases, 26:3, 101-106, DOI: 10.1300/J069v26n03_11
To link to this article: http://dx.doi.org/10.1300/J069v26n03_11
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Tobacco Awareness in Three U.S. Medical Schools
Joshua G. Schkrohowsky, MDBindu Kalesan, MSc, MPH
Anthony J. Alberg, PhD, MPH
ABSTRACT. Purpose: To evaluate the attitudes, knowledge, and beliefs of future physicians re-garding smoking cessation and tobacco-related issues and the development of these attributes dur-ing the course of medical education.
Methods: In a cross-sectional survey, questionnaires were completed by 298 first- and fourth-yearmedical students at three medical schools from 2003 through 2004. The primary outcomes wereknowledge of the health effects of tobacco and smoking cessation strategies, attitudes towardsmoking cessation, and anticipated clinical behavior with respect to addressing smoking behaviorand cessation with future patients.
Results: Fourth-year medical students had knowledge scores that were 13% higher thanfirst-year students for smoking-caused morbidity and mortality and understanding the physician’srole in smoking cessation. The average proportion of correct responses for specific knowledge ofsmoking cessation was only 64% and did not differ significantly between fourth- and first-yearmedical students. Three-quarters of fourth-year students felt they needed further training in coun-seling patients to stop smoking.
Conclusion: In this study, medical students had not received adequate education to provide ef-fective and appropriate smoking cessation counseling to their patients. In general, this indicates aneed for medical schools to place greater emphasis on developing the knowledge-base and skillsrequired for future physicians to effectively guide their nicotine-dependent patients to stop smok-ing. doi:10.1300/J069v26n03_11 [Article copies available for a fee from The Haworth Document DeliveryService: 1-800-HAWORTH. E-mail address: <[email protected]> Website: <http://www.HaworthPress.com> © 2007 by The Haworth Press, Inc. All rights reserved.]
KEYWORDS. Smoking cessation, medical education, nicotine-dependent patients
INTRODUCTION
Cigarette smoking is the single largest causeof preventable morbidity and premature deathin the United States.1 Primary care physiciansplay a major role in tobacco control efforts.2-4
However, high percentages of primary carephysicians feel inadequately trained to counselpatients regardingsmokingcessation.2,3,5 Inad-equate medical school education regardingsmoking cessation contributes to physician’slack of confidence in their ability to effectively
Joshua G. Schkrohowsky was affiliated with The Johns Hopkins University School of Medicine, Baltimore, MD,at the time of study.
Bindu Kalesan and Anthony J. Alberg were affiliated with the Department of Epidemiology, Johns Hopkins Uni-versity Bloomberg School of Public Health, Baltimore, MD at the time of the study.
Address correspondence to: Anthony J. Alberg, Hollings Cancer Center, Medical University of South Carolina,86 Jonathan Lucas Street, P.O. Box 250955, Charleston, SC 29425 (E-mail: [email protected]).
The authors thank Sally Santon, MD, and David McDowell, MD, for assistance with IRB approvals and data col-lection; Anne Roche, MD, for assistance with survey instrument; Gordon Lindsay, PhD, for constructive comments;and Cynthia Lochhead for assistance in preparation of the manuscript.
Journal of Addictive Diseases, Vol. 26(3) 2007Available online at http://jad.haworthpress.com
© 2007 by The Haworth Press, Inc. All rights reserved.doi:10.1300/J069v26n03_11 101
Dow
nloa
ded
by [
Col
umbi
a U
nive
rsity
] at
18:
04 3
0 Se
ptem
ber
2014

counsel their patients who smoke cigarettes.6,7
Proper training of medical students will posi-tively impact the tobacco cessation counselingthey will provide their future patients.7 Physi-cians who feel sufficiently prepared in inter-vention techniques are more likely to incorpo-rate smoking cessation into their practice andachieve higher success rates.8,9
Medical school is the most effective point ina physician’s career to incorporate smokingcessation education. To provide data to addresswhether tobacco cessation was incorporatedinto medical school curricula, the present studywascarriedout in threemedicalschools toeval-uate the attitudes, knowledge, and beliefs of fu-ture physicians regarding smoking cessationand thedevelopmentof tobaccocessationskillsduring medical school.
MATERIALS AND METHODS
This study took place at three universitymedical schools: Vanderbilt, Columbia, andJohns Hopkins. All first-year medical students(class of 2007) and fourth-year medical stu-dents (classes of 2003 and 2004) of theseschools were asked to completean anonymous,self-administered questionnaire. The fourth-year students at each school were contacted inthe spring of 2003 and both first- and fourth-year students were contacted during the2003-2004 school year. During the 2003 re-search year, the survey instrument and consentform were distributed, along with an intra-de-partmental return envelope, to the on-campusmailbox of all fourth-year students at eachschool. The students were informed of the sur-vey via a class email. Due to a low initial re-sponse rate, the data collection methods wererevised at Columbia and Johns Hopkins duringthe 2004 academic year. At Columbia, thequestionnaires were handed out during class-room lectures. Students placed completedquestionnaires in a box outside the classroom.At Johns Hopkins, the first-year class wasgiven access to the questionnaire on the studentcourse website and the fourth-year class re-ceived it in their campus mailboxand via email.Questionnaires were given to a total of 920medical students (83% of enrolled students); ofthese, 298 (32.3%) completed the question-
naire. The response rates were22%atVanderbilt(n = 65, 33 first-years student, 32 fourth-yearstudents), 29% at Columbia (n = 105, 34first-year students, 71 fourth-year students), and39% at Johns Hopkins (n = 128, 69 first-yearstudents, 59 fourth-year students). InstitutionalReview Board approval was obtained at eachmedical school and the Johns Hopkins Univer-sity Bloomberg School of Public Health.
Thestudyquestionnairewasderivedfromanexisting instrument.10 The questionnaire wascomprised of 8 questions concerning demo-graphic characteristics (e.g., age, gender, yearin medical school), 31 knowledge-based ques-tions,6 items toassess studentattitudes relatingto smoking cessation, 3 items regarding barri-ers to cessation success, and 2 questions onanticipated clinical behavior.
In the data analyses, the knowledge itemswere grouped into the following categories:(1) smoking-related morbidity/mortality, (2) smo-king cessation modalities and effectiveness,(3) the role of the physician in smoking cessa-tion, and (4) tobacco pharmacology. Meanscores were calculated for all the knowledgeitems combined and within each of these cate-gories. As a measure of progress achieved dur-ing medical school, the results of fourth-yearmedical students were compared to those offirst-year medical students. For these analyses,the differences were compared using thechi-square test. A two-sided p-value of 0.05 orless was considered to be statistically signifi-cant.ThedatawereanalyzedusingSTATA8.2.
RESULTS
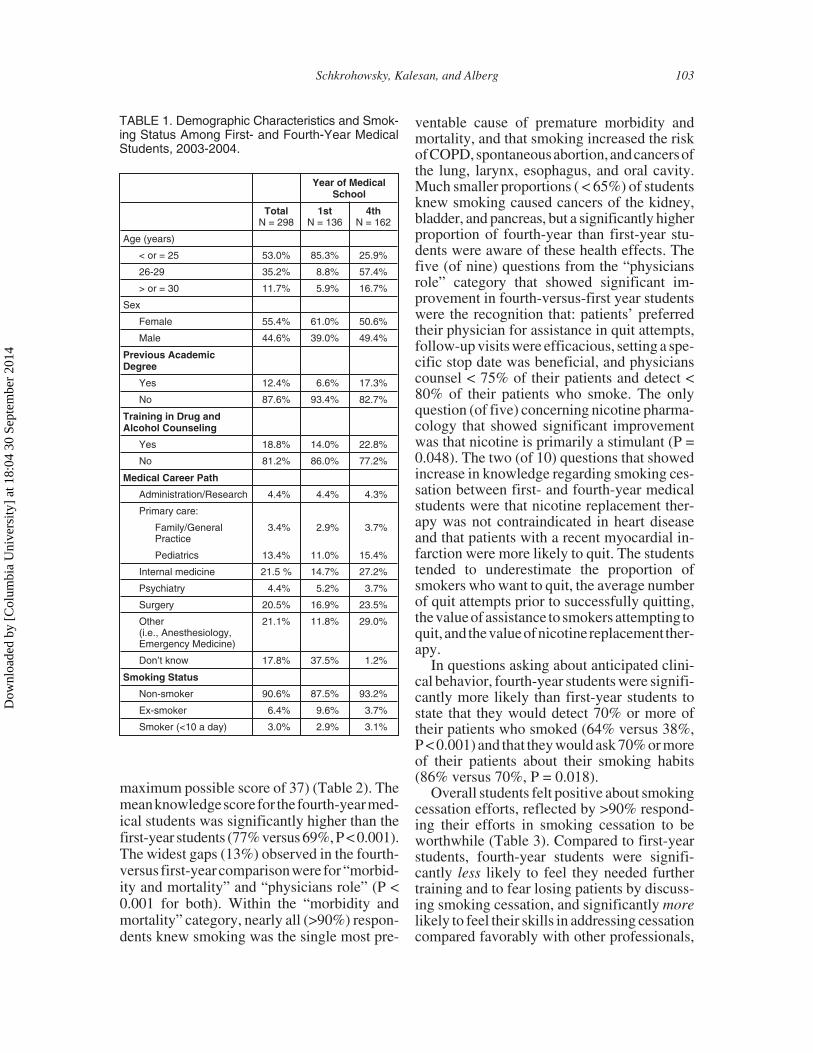
Participants were comprised of 136 first-year (average age 23.3 years) and 162 fourth-year (average age 26.7 years) students. Moststudents (>80%) did not have previous profes-sional qualifications or specific training rele-vant to counseling patients on smoking cessa-tion (Table 1). Of those who indicated a careerpath, the most common specialties were inter-nalmedicine(21.5%),surgery(20.5%),andpe-diatrics (13.4%) (Table 1). The prevalence ofcurrent (3%)andformer(6%)smokingwas low(Table 1).
On average, the respondents answered 74%of the knowledge items correctly (27.2 out of a
102 JOURNAL OF ADDICTIVE DISEASES
Dow
nloa
ded
by [
Col
umbi
a U
nive
rsity
] at
18:
04 3
0 Se
ptem
ber
2014
maximum possible score of 37) (Table 2). Themeanknowledgescorefor thefourth-yearmed-ical students was significantly higher than thefirst-year students (77% versus 69%, P < 0.001).The widest gaps (13%) observed in the fourth-versus first-yearcomparisonwere for“morbid-ity and mortality” and “physicians role” (P <0.001 for both). Within the “morbidity andmortality” category, nearly all (>90%) respon-dents knew smoking was the single most pre-
ventable cause of premature morbidity andmortality, and that smoking increased the riskofCOPD,spontaneousabortion,andcancersofthe lung, larynx, esophagus, and oral cavity.Much smaller proportions ( < 65%) of studentsknew smoking caused cancers of the kidney,bladder, and pancreas, but a significantly higherproportion of fourth-year than first-year stu-dents were aware of these health effects. Thefive (of nine) questions from the “physiciansrole” category that showed significant im-provement in fourth-versus-first year studentswere the recognition that: patients’ preferredtheir physician for assistance in quit attempts,follow-up visits were efficacious, setting a spe-cific stop date was beneficial, and physicianscounsel < 75% of their patients and detect <80% of their patients who smoke. The onlyquestion (of five) concerning nicotine pharma-cology that showed significant improvementwas that nicotine is primarily a stimulant (P =0.048). The two (of 10) questions that showedincrease in knowledge regarding smoking ces-sation between first- and fourth-year medicalstudents were that nicotine replacement ther-apy was not contraindicated in heart diseaseand that patients with a recent myocardial in-farction were more likely to quit. The studentstended to underestimate the proportion ofsmokers who want to quit, the average numberof quit attempts prior to successfully quitting,the valueof assistance to smokers attempting toquit, and thevalueofnicotinereplacement ther-apy.
In questions asking about anticipated clini-cal behavior, fourth-year students were signifi-cantly more likely than first-year students tostate that they would detect 70% or more oftheir patients who smoked (64% versus 38%,P < 0.001) and that they would ask 70% or moreof their patients about their smoking habits(86% versus 70%, P = 0.018).
Overall students felt positive about smokingcessation efforts, reflected by >90% respond-ing their efforts in smoking cessation to beworthwhile (Table 3). Compared to first-yearstudents, fourth-year students were signifi-cantly less likely to feel they needed furthertraining and to fear losing patients by discuss-ing smoking cessation, and significantly morelikely to feel their skills in addressing cessationcompared favorably with other professionals,
Schkrohowsky, Kalesan, and Alberg 103
TABLE 1. Demographic Characteristics and Smok-ing Status Among First- and Fourth-Year MedicalStudents, 2003-2004.
Year of MedicalSchool
TotalN = 298
1stN = 136
4thN = 162
Age (years)
< or = 25 53.0% 85.3% 25.9%
26-29 35.2% 8.8% 57.4%
> or = 30 11.7% 5.9% 16.7%
Sex
Female 55.4% 61.0% 50.6%
Male 44.6% 39.0% 49.4%
Previous AcademicDegree
Yes 12.4% 6.6% 17.3%
No 87.6% 93.4% 82.7%
Training in Drug andAlcohol Counseling
Yes 18.8% 14.0% 22.8%
No 81.2% 86.0% 77.2%
Medical Career Path
Administration/Research 4.4% 4.4% 4.3%
Primary care:
Family/GeneralPractice
3.4% 2.9% 3.7%
Pediatrics 13.4% 11.0% 15.4%
Internal medicine 21.5 % 14.7% 27.2%
Psychiatry 4.4% 5.2% 3.7%
Surgery 20.5% 16.9% 23.5%
Other(i.e., Anesthesiology,Emergency Medicine)
21.1% 11.8% 29.0%
Don’t know 17.8% 37.5% 1.2%
Smoking Status
Non-smoker 90.6% 87.5% 93.2%
Ex-smoker 6.4% 9.6% 3.7%
Smoker (<10 a day) 3.0% 2.9% 3.1%
Dow
nloa
ded
by [
Col
umbi
a U
nive
rsity
] at
18:
04 3
0 Se
ptem
ber
2014
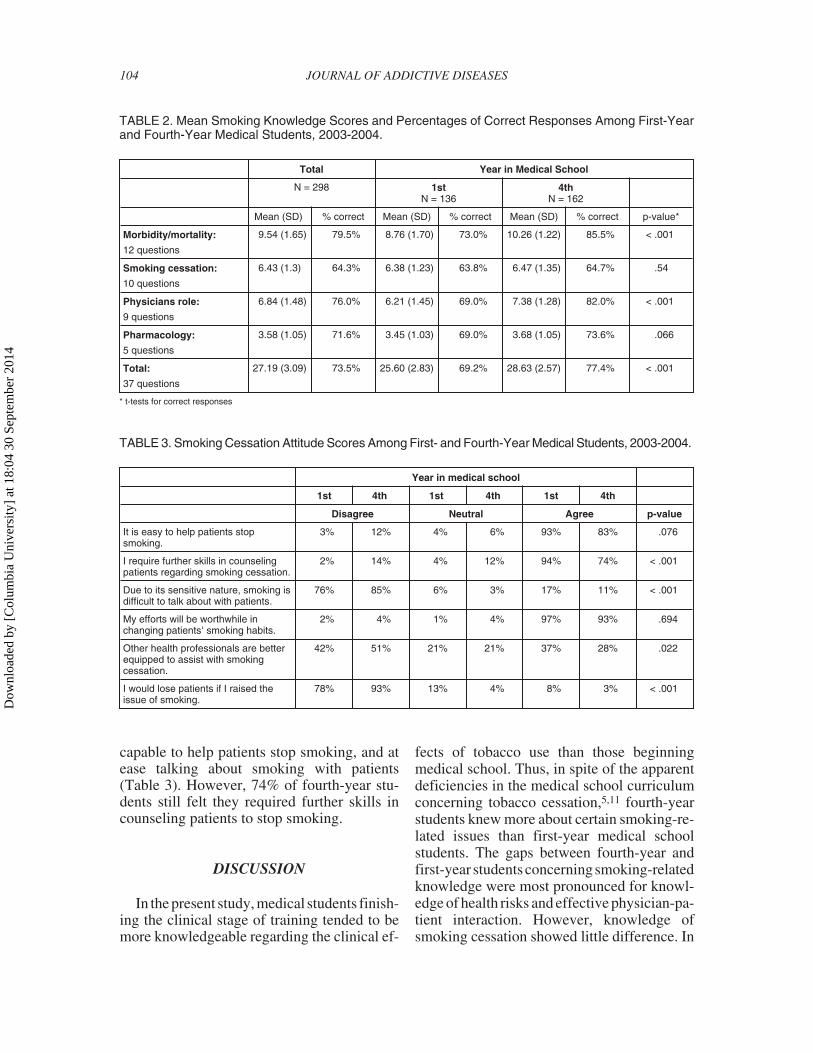
capable to help patients stop smoking, and atease talking about smoking with patients(Table 3). However, 74% of fourth-year stu-dents still felt they required further skills incounseling patients to stop smoking.
DISCUSSION
In the present study, medical students finish-ing the clinical stage of training tended to bemore knowledgeable regarding the clinical ef-
fects of tobacco use than those beginningmedical school. Thus, in spite of the apparentdeficiencies in the medical school curriculumconcerning tobacco cessation,5,11 fourth-yearstudents knew more about certain smoking-re-lated issues than first-year medical schoolstudents. The gaps between fourth-year andfirst-year studentsconcerningsmoking-relatedknowledge were most pronounced for knowl-edge of health risks and effective physician-pa-tient interaction. However, knowledge ofsmoking cessation showed little difference. In
104 JOURNAL OF ADDICTIVE DISEASES
TABLE 2. Mean Smoking Knowledge Scores and Percentages of Correct Responses Among First-Yearand Fourth-Year Medical Students, 2003-2004.
Total Year in Medical School
N = 298 1stN = 136
4thN = 162
Mean (SD) % correct Mean (SD) % correct Mean (SD) % correct p-value*
Morbidity/mortality:
12 questions
9.54 (1.65) 79.5% 8.76 (1.70) 73.0% 10.26 (1.22) 85.5% < .001
Smoking cessation:
10 questions
6.43 (1.3) 64.3% 6.38 (1.23) 63.8% 6.47 (1.35) 64.7% .54
Physicians role:
9 questions
6.84 (1.48) 76.0% 6.21 (1.45) 69.0% 7.38 (1.28) 82.0% < .001
Pharmacology:
5 questions
3.58 (1.05) 71.6% 3.45 (1.03) 69.0% 3.68 (1.05) 73.6% .066
Total:
37 questions
27.19 (3.09) 73.5% 25.60 (2.83) 69.2% 28.63 (2.57) 77.4% < .001
* t-tests for correct responses
TABLE 3. Smoking Cessation Attitude Scores Among First- and Fourth-Year Medical Students, 2003-2004.
Year in medical school
1st 4th 1st 4th 1st 4th
Disagree Neutral Agree p-value
It is easy to help patients stopsmoking.
3% 12% 4% 6% 93% 83% .076
I require further skills in counselingpatients regarding smoking cessation.
2% 14% 4% 12% 94% 74% < .001
Due to its sensitive nature, smoking isdifficult to talk about with patients.
76% 85% 6% 3% 17% 11% < .001
My efforts will be worthwhile inchanging patients' smoking habits.
2% 4% 1% 4% 97% 93% .694
Other health professionals are betterequipped to assist with smokingcessation.
42% 51% 21% 21% 37% 28% .022
I would lose patients if I raised theissue of smoking.
78% 93% 13% 4% 8% 3% < .001
Dow
nloa
ded
by [
Col
umbi
a U
nive
rsity
] at
18:
04 3
0 Se
ptem
ber
2014

an evaluation of 12 U.S. medical schools, 8schools devoted less time to tobacco awarenessteaching during the third and fourth years (clin-icalyears) thanduringthefirstandsecondyears(basic science years).11
Our results indicate deficiencies in knowl-edge of smoking cessation. For example, themajority of medical students held mispercep-tions about nicotine replacement therapy. Theavailability of nicotine replacement therapiesadd to the likelihood of a successful quit at-tempt12,13 but our results suggest this topic isnot being adequately incorporated into themedical school education. This finding corrob-orates previous findings among osteopathicmedical schools.14 Without a better under-standing of the full menu of effective smokingcessation modalities,15 physicians will remainless effective in counseling patients in smokingcessation.2,3,5,10
Approximately one-half of medical studentsdid not know that physicians are the patient’sfirst choice for a smoking cessation advocateand underestimated the percentage of smokerswho want to quit smoking. The majority ofmedical students felt that patients continuesmoking due to a lack of willingness to quit,when in fact the percentage of smokers who de-sire toquit reaches70%.16 Theseprevalentmis-conceptions about patients’ desire to quitsmoking and their needs could impact futurephysicians’ practices and their effectiveness inpatient counseling.17
Consistent with the findings of others,10
medical students overestimated the actualsmoking quit rate and the ease with which pa-tients can stop smoking. High proportions ofmedical students believed that helping a patientstop smoking was not difficult and most smok-ers do not need specialized cessation assis-tance, and underestimated the average numberof attempts it takes a patient to quit smoking.These optimistic views may lead newly trainedphysicians to takeanactiverole insmokingces-sation early in their careers, but may eventuallylead to frustration as their careers advance, pro-viding a disincentive to engage in smoking ces-sation counseling in the long term.10,18
Furthermore, there was a large discrepancybetween what medical students believed physi-cians could do and what they thought physi-cians actually do to promote smoking cessa-
tion.Moststudentsbelievedthatphysicianscanhave a significant impact on quit rates, yet onlya few believed that physicians counseled morethan 75% of their patients. Scott et al. describedsimilar attitudes among medical students 20years ago.7
When comparing medical students percep-tion of physician interaction to theirown antici-patedbehavior, first-yearstudentsbelievedthatphysicians were more capable of detecting themajorityof theirpatientswhosmoked than theyfelt themselves capable of doing. In contrast,only a small percentage of fourth-year medicalstudents felt that physicians could detect a ma-jority of their patients who smoked while twiceas many students felt that they could detect thisamount. Students seemed to lose confidenceduring medical school in the ability and will-ingness of practicing physicians to providesmoking cessation counseling to their patients.This is disconcerting, as the role models prac-ticing physicians’ provide will greatly affectthe future practice of students.7
Most students felt that their efforts in smok-ing intervention would be worthwhile and be-lieved they would routinely ask the majority oftheir patients about tobacco use. Yet eventhree-fourths of fourth-year students felt theydid not receive adequate training to counsel pa-tients to stop smoking.19
A notable strength of this study is that it wasmulti-institutional, including students enrolledin three medical schools. However, we wereunable to contact 17% of students and of thosecontacted only approximately 1 in 3 actuallyparticipated. The low response rate is a sourceof concern, but in this situation it seems likelythat themedical studentswith thegreatest inter-est in the subject would respond. To the extentthis is true, our results present an overly opti-mistic picture when compared to results if theparticipationratehad been higher. Thus, our re-sults seem likely to portray the best case sce-nario of medical students’ knowledge, atti-tudes, and behaviors toward tobacco control.Nevertheless, our final sample size makes thisone of the larger studies and, to our knowledge,there are no other published studies of U.S.medical students that compare first-year tofourth-year medical students with respect toknowledge and attitudes towards smoking ces-sation during medical school. We have used the
Schkrohowsky, Kalesan, and Alberg 105
Dow
nloa
ded
by [
Col
umbi
a U
nive
rsity
] at
18:
04 3
0 Se
ptem
ber
2014

comparison of the fourth-year to first-year stu-dents to infer that the differences representchanges due to additional medical school train-ing. However, this was a cross-sectional study,providing a comparison of fourth-year andfirst-year medical students at a point in time.Future studies that follow cohorts of medicalstudents longitudinally over time will providestronger inferences concerning increases in to-bacco cessation awareness during medicalschool. Despite these limitations, this studyprovides a useful initial assessment and thesehypothesis-generating results emphasize theneed for more intensive future investigation.
Theresultsof thepresentstudyingeneralsup-port previously reported findings.5,7,11,14,18,19
For example, Ferry et al.5 and Powers et al.11
stated that less time is devoted to tobacco edu-cation during clinical years than basic scienceyears. This supports our findings that medicalstudents’ knowledge of smoking-associatedhealth risks improved, whereas little changewas evident in theirknowledgeof smokingces-sation counseling. Also, Geller et al. reportedthat greater than fifty percent of fourth-yearmedical students felt they had too little expo-sure to cancer control education and we foundseventy-four percent of fourth-year studentsfelt they needed further training in smokingcessation.19
Effectively training medical school studentsin tobacco cessation interventions will instillfuture physicians with the requisite skills andconfidence to help their future patients effec-tively quit smoking. Reemphasis is needed onthe National Cancer Institute’s recommenda-tion to introducetobaccoeducationinto thecur-ricula of all U.S. medical schools. Our resultsindicate that when such programs are imple-mented they should seek to develop the specificskills and knowledge required to provideappropriate smoking cessation guidance topatients.
REFERENCES
1. Centers for Disease Control and Prevention. An-nual smoking-attributable mortality, years of potentiallife lost, and economic costs: United States, 1995-1999.MMWR Morb Mortal Wkly Rep. 2002;51:300-303.
2. Spangler JG, George G, Foley KL, Crandall SJ.Tobacco intervention training: current efforts and gapsin U.S. medical schools. JAMA. 2002;288:1102-1109.
3. Richmond R. Teaching medical students abouttobacco. Thorax. 1999;54:70-78.
4. Raw M, McNeill A. The prevention of tobacco-related disease. Addiction. 1994;89:1505-1509.
5. Ferry LH, Grissino LM, Runfola PS. Tobaccodependence curricula in US undergraduate medical edu-cation. JAMA. 1999;282:825-829.
6. Patkar AA, Hill K, Batra V, Vergare MJ, LeoneFT. A comparison of smoking habits among medicaland nursing students. Chest. 2003;124:1415-1420.
7. Scott CS, Neighbor WE. Preventative care atti-tudes of medical students. Soc Sci Med. 1985;21:299-305.
8. Wilson DM, Taylor DW, Gilbert JR, et al. A ran-domized trial of a family physician intervention forsmoking cessation. JAMA. 1988;260:1570-1574.
9. Fried JL, Reid BC, DeVore LE. A comparison ofhealth professions student attitudes regarding tobaccocurricula and interventionist roles. J Dent Educ. 2004;68:370-377.
10. Roche AM, Eccleston P, Jordan D. Smoking-re-lated knowledge and attitudes of senior Australian med-ical students. Tob Control. 1996;5:271-279.
11. Powers CA, Zapka JG, Bognar B, et al. Evalua-tion of current tobacco curriculum at 12 US medicalschools. J Cancer Educ. 2004;19:212-219.
12. Shiffman S, Di Marino ME, Pillitteri JL. The ef-fectiveness of nicotine patch and nicotine lozenge invery heavy smokers. J Subt Abuse Treat. 2005;28:49-55.
13. Silagy C, Lancaster T, Stead L, Mant D, FowlerG. Nicotine replacement therapy for smoking cessation.Cochrane Database Syst Rev. 2004;(3):CD000146.
14. Montalto NJ, Ferry LH, Stanhiser T. Tobacco de-pendence curricula in undergraduate osteopathic medi-cal education. J Am Osteopath Assoc. 2004;104:317-323.
15. Ellerbeck EF, Choi WS, McCarter K, JolicoeurDG, Greiner A, Ahluwalia JS. Impact of patient charac-teristics on physician’s smoking cessation strategies.Prev Med. 2003;36:464-470.
16. Centers for Disease Control and Prevention. Cig-arette smoking among adults: United States, 2000.MMWR Morb Mortal Wkly Rep. 2002;51:642-645.
17. Roche AM, Eccleston P, Sanson-Fisher R. Teach-ing smoking cessation skills to senior medical students:a block-randomized controlled trial of four different ap-proaches. Prev Med. 1996;25:251-258.
18. Nieman LZ, Velasquez MM, Groff JY, Cheng L,Foxhall LE. Implementation of a smoking cessationcounseling module in a preceptorship program. FamMed. 2005;37:105-111.
19. Geller AC, Prout M, Sun T, Lew RA, CulbertAL, Koh HK. Medical students’ knowledge, attitudes,skills, and practices of cancer prevention and detection.J Cancer Educ. 1999;14:72-77.
doi:10.1300/J069v26n03_11
106 JOURNAL OF ADDICTIVE DISEASES
Dow
nloa
ded
by [
Col
umbi
a U
nive
rsity
] at
18:
04 3
0 Se
ptem
ber
2014