the transition to adult health care for youth with special health care needs: do racial and ethnic...
TRANSCRIPT

DOI: 10.1542/peds.2010-1466F 2010;126;S129-S136 Pediatrics
Debra S. Lotstein, Alice A. Kuo, Bonnie Strickland and Fan Tait Do Racial and Ethnic Disparities Exist?
The Transition to Adult Health Care for Youth With Special Health Care Needs:
http://www.pediatrics.org/cgi/content/full/126/Supplement_3/S129located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from
The Transition to Adult Health Care for Youth WithSpecial Health Care Needs: Do Racial and EthnicDisparities Exist?
abstractAlthough the transition to adulthood for youth with special health careneeds (YSHCN) has been gathering attention, the impact of racial andethnic disparities on this process has been relatively unexamined. Inthis review, we explore evidence of disparities in the transition toadulthood for YSHCN, which is important because the problems thatYSHCN face in transitioning to adulthood are, in large part, caused byinterrupted access to high-quality health care and minority YSHCN andadults have many well-described gaps in access to quality care. Under-standing the disparities in the transition process is essential to ensurethat interventions designed to improve this transition will meet theneeds of this high-risk population. We reviewed research on transitionpreparation and outcomes for YSHCN to find evidence of racial andethnic disparities. The results of our review indicate that few YSHCNare receiving adequate transition preparation, and some evidence in-dicates that this situation is worse for racial and ethnic minorities.Furthermore, young adults, including YSHCN, have poorer access tocare than children. Moreover, at some ages, this age-related decline inaccess is worse for Hispanic and black young adults than for others.Finally, low-income YSHCN are at higher risk than other YSHCN of expe-riencing gaps in access to care as they age into adulthood. Possiblecauses of racial and ethnic disparities in health care transitions arerelated to insurance, living in low-income communities, and sociocul-tural factors. Significant efforts in research, policy change, advocacy,and education of providers and families are needed to ensure optimaltransition preparation and adult outcomes for YSHCN from all racialand ethnic backgrounds. Pediatrics 2010;126:S129–S136
AUTHORS: Debra S. Lotstein, MD, MPH,a,b Alice A. Kuo, MD,PhD,a Bonnie Strickland, PhD,c and Fan Tait, MDd
aCenter for Healthier Children, Families and Communities,Department of Pediatrics, David Geffen School of Medicine,University of California, Los Angeles, California; bRand Health,Santa Monica, California; cMaternal and Child Health Bureau,Health Resources and Services Administration, Rockville,Maryland; and dAmerican Academy of Pediatrics, Elk GroveVillage, Illinois
KEY WORDSracial/ethnic disparities, transition of care, adolescents, specialhealth care needs
ABBREVIATIONSYSHCN—youth with special health care needsNS-CSHCN—National Survey of Children With Special Health CareNeedsCSHCN—children with special health care needsPPACA—Patient Protection and Affordable Care Act
www.pediatrics.org/cgi/doi/10.1542/peds.2010-1466F
doi:10.1542/peds.2010-1466F
Accepted for publication Sep 1, 2010
Address correspondence to Debra S. Lotstein, MD, MPH, Divisionof Child Health Policy, UCLA Center for Healthier Children,Families and Communities, David Geffen School of Medicine atUCLA, 10990 Wilshire Boulevard, Suite 900, Los Angeles, CA 90024.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 126, Supplement 3, December 2010 S129. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from
As more children with complex andchronic conditions survive to adult-hood, growing attention is being paidto what happens to this populationas its members leave childhood.1,2
Youth with special health care needs(YSHCN) are at risk of experiencing dif-ficulties as they transfer from pediat-ric to adult health care systems.3,4 Be-cause of their reliance on health careservices to maintain their quality oflife, YSHCN are susceptible to gaps inaccess to high-quality health care ser-vices because of lack of support withthe transition process.
Even before they reach the age atwhich they might need to transfer toadult care, YSHCN from racial and eth-nic minorities face disparities in ac-cess to and quality of care comparedwith white YSHCN.5,6 This subgroup ofYSHCN is also likely to experience diffi-cult transitions to adulthood.
In this article, we review evidence ofdisparities in the transition of YSHCNto adult health care. We present a gen-eral framework for thinking aboutgrowing into adulthood for YSHCN and,using this framework, we review dataon the transition to adult health carefor YSHCN. Because data on racial andethnic disparities in the transition toadult health care are limited, we sum-marize evidence about transitions toadult health care among all youth andhighlight available evidence of dispar-ities. We then explore possible reasonsfor disparities in transitions to adulthealth care and describe actions thatare needed to address these gaps.
CONCEPTUAL TRANSITIONFRAMEWORK
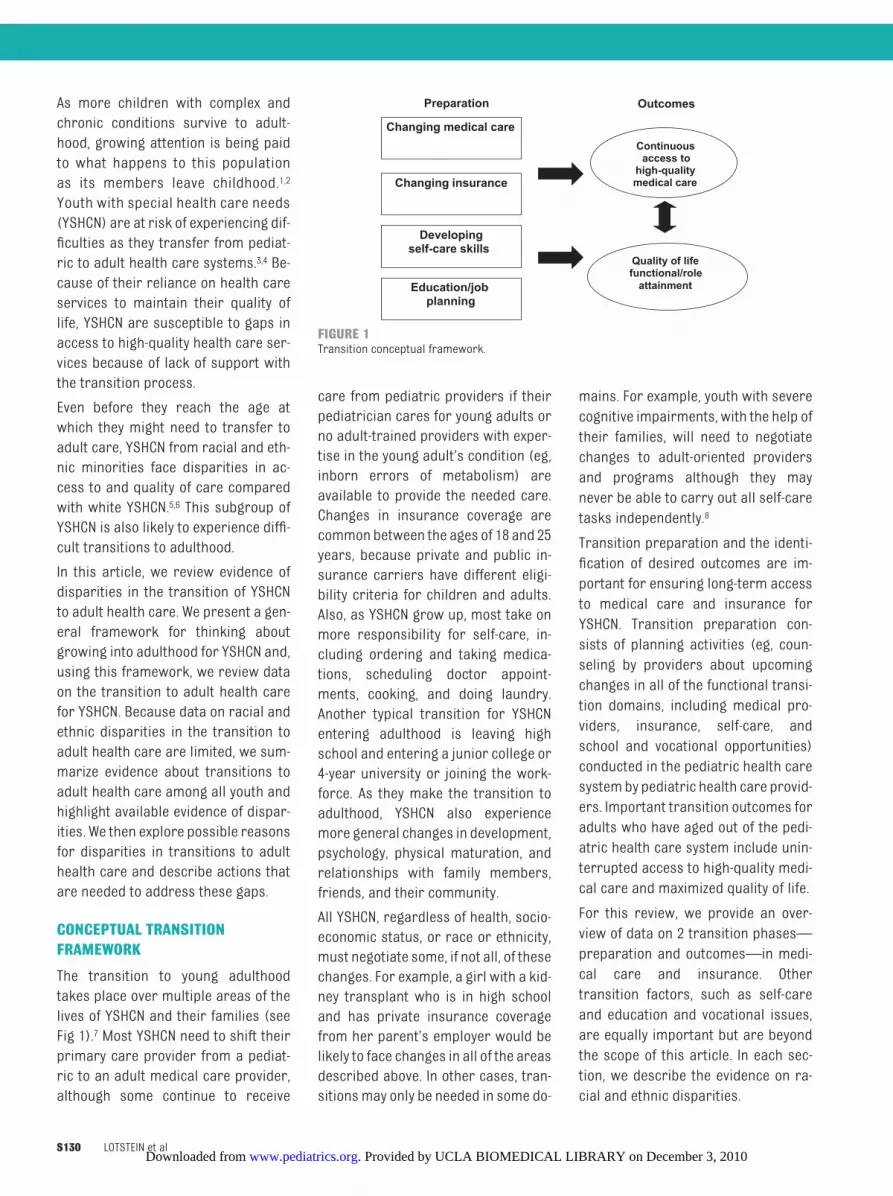
The transition to young adulthoodtakes place over multiple areas of thelives of YSHCN and their families (seeFig 1).7 Most YSHCN need to shift theirprimary care provider from a pediat-ric to an adult medical care provider,although some continue to receive
care from pediatric providers if theirpediatrician cares for young adults orno adult-trained providers with exper-tise in the young adult’s condition (eg,inborn errors of metabolism) areavailable to provide the needed care.Changes in insurance coverage arecommon between the ages of 18 and 25years, because private and public in-surance carriers have different eligi-bility criteria for children and adults.Also, as YSHCN grow up, most take onmore responsibility for self-care, in-cluding ordering and taking medica-tions, scheduling doctor appoint-ments, cooking, and doing laundry.Another typical transition for YSHCNentering adulthood is leaving highschool and entering a junior college or4-year university or joining the work-force. As they make the transition toadulthood, YSHCN also experiencemore general changes in development,psychology, physical maturation, andrelationships with family members,friends, and their community.
All YSHCN, regardless of health, socio-economic status, or race or ethnicity,must negotiate some, if not all, of thesechanges. For example, a girl with a kid-ney transplant who is in high schooland has private insurance coveragefrom her parent’s employer would belikely to face changes in all of the areasdescribed above. In other cases, tran-sitionsmay only be needed in some do-
mains. For example, youth with severecognitive impairments, with the help oftheir families, will need to negotiatechanges to adult-oriented providersand programs although they maynever be able to carry out all self-caretasks independently.8
Transition preparation and the identi-fication of desired outcomes are im-portant for ensuring long-term accessto medical care and insurance forYSHCN. Transition preparation con-sists of planning activities (eg, coun-seling by providers about upcomingchanges in all of the functional transi-tion domains, including medical pro-viders, insurance, self-care, andschool and vocational opportunities)conducted in the pediatric health caresystemby pediatric health care provid-ers. Important transition outcomes foradults who have aged out of the pedi-atric health care system include unin-terrupted access to high-quality medi-cal care and maximized quality of life.
For this review, we provide an over-view of data on 2 transition phases—preparation and outcomes—in medi-cal care and insurance. Othertransition factors, such as self-careand education and vocational issues,are equally important but are beyondthe scope of this article. In each sec-tion, we describe the evidence on ra-cial and ethnic disparities.
Changing insurance
Education/jobplanning
Developingself-care skills
Changing medical care Continuous
access to high-quality medical care
Quality of life functional/role
attainment
Preparation Outcomes
FIGURE 1Transition conceptual framework.
S130 LOTSTEIN et al. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from

PREPARATION
Most studies of transition preparationor planning have been qualitative as-sessments of patient or provider atti-tudes or preferences. Few studieshave compared receipt of transitionpreparation among different racialand ethnic groups.
The only study to examine the fre-quency of transition preparation at thenational level has been the NationalSurvey of Children With Special HealthCare Needs (NS-CSHCN). Fielded in2001 and 2005 by the National Centerfor Health Statistics, the NS-CSHCN is anationally representative telephone-based survey of children and youthfrom birth to the age of 18 years whohave a special health care need.9–11
In 2001, survey personnel asked par-ents and guardians whether their 13-to 17-year-old sons and daughters (1)discussed changing health care needsin adulthood with their health careproviders and, if so, (2) whether theseYSHCN had made plans for the change,and (3) whether these YSHCN had dis-cussed the need to see doctors whotreat adults.12 Overall, only 15.3% of re-spondents reported “yes” to all 3 ques-tions. The investigators found no sig-nificant differences according to raceor ethnicity in a multivariate analysisafter controlling for other socioeco-nomic and health care access factors.Factors associated with achieving thestudy’s transition-performance out-come (an answer of “yes” to all 3 ques-tions) included older age and having amedical home.
In 2005, NS-CSHCN personnel askedparents or guardians of YSHCN aged12 to 17 years whether they or theirchildren had talked to providers aboutthe youth’s changing health careneeds, receipt of care from adult ver-sus pediatric providers, health insur-ance eligibility, and encouragement ofyouth self-responsibility.13 Parents orguardians had to report a need
for transition-related discussions fortheir child’s results to be included inthe study’s performance-outcome cal-culation. Overall, 41.2% of YSHCNachieved the transition-performanceoutcome of having had all 4 of thesediscussions.
Unlike the 2001 survey, the 2005 surveyrevealed significant racial and ethnicdisparities in receipt of transitioncounseling. Although 47.6% of non-Hispanic white youth achieved the2005 transition-performance outcome,only 28.7% of non-Hispanic black youthand 26.3% of Hispanic youth achievedthis outcome. In multivariate analyses,compared with non-Hispanic whiteyouth, non-Hispanic black youth had1.5 times and Hispanic youth had 1.43times the odds of not achieving thetransition outcome (differences signif-icant at P � .05). In the same model,after the investigators controlled forrace and ethnicity, respondents whodid not speak English in the home had2.45 the odds of not achieving the tran-sition outcome compared with Englishspeakers. The 2005 sample had morerespondents overall and more YSHCNof color than did the 2001 survey.These results indicate that fewer thanhalf of YSHCN receive transition prep-aration and that YSHCN of color andfrom non–English-speaking familiesare even less likely to have discussionswith their health care providers thatcould help prepare them to meet theirhealth care and insurance needs asadults.
These disparities in transition prepa-ration are similar to the disparities inpediatric care that racial and ethnicminority populations with specialhealth care needs experience.5 For ex-ample, Strickland et al6 found thatHispanic and non-Hispanic black chil-dren with special health care needs(CSHCN) were significantly less likelyto have a medical home; both groupshad �1.6 the odds of not having ac-
cess to a medical home of non-Hispanic white CSHCN. This finding didnot change when the investigatorstook into consideration other socio-economic factors, disease severity, orinsurance coverage. In these analyses,having a medical home significantlylowered the odds of having delayed orforgone care, having unmet healthcare needs, having an unmet need forfamily support services, or missing 11or more days of school because of ill-ness. Thus, transition-preparation dis-parities must be examined and ad-dressed in the larger context ofpediatric care disparities.
OUTCOMES
In this conceptual framework, goodtransition outcomes for YSHCN includeongoing access to appropriate healthcare providers and comprehensivehealth insurance that meets theirneeds in young adulthood. Althoughthe outcomes of racial and ethnichealth care disparities for older adultshave been well documented,14 fewerstudies have examined the outcomesof disparities in young adults undergo-ing health care transitions. We reviewhere the evidence on transition out-comes for YSHCN and highlight the ra-cial and ethnic disparities described inthe literature.
Studies have revealed that youngadults tend to have high uninsurancerates and those from ethnic and ra-cial minority populations experienceworse access to insurance. An analysisof data from the 2002 and 2003 Na-tional Health Interview Survey re-vealed that full-year insured ratesfollowed a U-shaped curve in adoles-cence and young adulthood, fallingfrom a high of 87% among 13- to 14-year-olds to a low of 61% among 23- to24-year-olds before rising to 75%among 31- to 32-year-olds.15 This studyalso revealed that rates for Hispanicpeople followed the same curve, but
SUPPLEMENT ARTICLES
PEDIATRICS Volume 126, Supplement 3, December 2010 S131. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from

this population had significantly lowerinsured rates than those for white peo-ple of the same age group, even afterthe investigators controlled for con-founding variables. In addition, the gapbetween white and Hispanic youth in-creased from 16 percentage points at13 to 14 years to 32 percentage pointsat 19 to 20 years. After controlling forother socioeconomic factors, the in-vestigators found that white and blackdisparities in insurance coverageacross age groups were only signifi-cantly different at ages 19 to 20 years(74% [white youth] vs 59.8% [blackyouth]) and 21 to 22 years (68.1 [whiteyouth] vs 58.1% [black youth]).
Young adults with chronic health con-ditionsmay not be protected from age-related loss of insurance coverage.Callahan and Cooper,16 who also useddata from the National Health Inter-view Study, found similar uninsurancerates among the 4.7% of individualsaged 19 to 29 years with disablingchronic conditions (on the basis ofself-report) and those without suchconditions: 26% for those with chronicconditions and 28% for those without.However, those with disabling chronicconditions were more likely to haveMedicaid coverage (27.2%) than thosewithout such conditions (5.3%). In ad-dition, young adults without insurancewere more likely to delay medical carebecause of cost, not obtain neededmedical care because of cost, not beable to afford to fill a prescription,have no usual source of care, and havehad no contact with a health profes-sional in the previous year. The au-thors did not report on racial or ethnicdisparities. In another study in whichthe same data set was used, Callahanet al17 found differences in access tohealth care among various Hispanicsubgroups; noncitizens were at thehighest risk of poor access to care.
Two smaller studies examined thetransition to adulthood from a longitu-
dinal perspective. The 2007 Survey ofAdult Transition and Health followed anational sample of YSHCN identified inthe 2001 NS-CSHCN. This sample of10 933 former YSHCN now aged 19 to23 years is not nationally representa-tive (because of the low responserate). The study revealed that 25% ofthese young adults had lost a usualsource of care and 18.8% had lost in-surance coverage since they turned18. Although the study found no racialor ethnic differences in access to care,results of a multivariate analysisshowed that low-income young adultshad poorer health care access thanthose with incomes higher than 400%of the federal poverty level (unpub-lished data).
The second study examined access tocare for young adults who had agedout of a program for children withchronic conditions.7 Among the youthin this group, 65% had at least 1 poortransition outcome; they had no usualsource of care, had forgone or delayedcare in the previous 6 months, had noinsurance, or had experienced a gap ininsurance coverage since leaving theprogram for children. Although mostof those surveyed had insurance, 24%did not have a regular health care pro-vider for their health condition. Thestudy authors could not evaluate racialand ethnic disparities because of thesmall sample size and the fact that52% of the sample was nonwhite.
The results of these studies suggestthat, similar to all young adults, thosewith special health care needs have ahigh risk of having no health care cov-erage and that lack of coverage is as-sociated with poor access to care. Fur-thermore, young adults with specialhealth care needs from traditionallyunderserved communities have aneven greater risk of experiencinghealth care barriers. Preparing for thetransition to adulthood and obtainingcontinuous access to high-quality
health care is a challenge for all YSHCNbut is probably more difficult for mem-bers of racial and ethnic minoritygroups, although data on this issue arelimited. Although the extent of the ra-cial and ethnic health disparities in thetransition to adulthood for YSHCN hasnot been fully defined, this preliminaryevidence indicates that such dispari-ties exist.
POSSIBLE CAUSES
The underlying causes of disparities inhealth care transitions are probablymultifactorial. Some issues that arelikely involved include access to insur-ance, living in low-income communi-ties, and sociocultural factors. Healthcare providers need to be aware ofthese factors to alter their practice tomeet the needs of minority YSHCN.
Health Insurance Factors
Access to health insurance is nearly aprerequisite for access to high-qualityhealth care, and youth from all racialand ethnic backgrounds experiencechallenges in obtaining access to in-surance during the transition fromchildhood to adulthood. Comparedwith CSHCN, young adults with chronicconditions (especially those with a lowincome, which disproportionately af-fects members of minority groups)have more limited private and publicinsurance options. Recent policychanges in access to insurance cover-age enacted with passage of the Pa-tient Protection and Affordable CareAct (PPACA) of 2010 will significantlychange the landscape for both publicand private coverage options for low-income minority YSHCN.18,19 In the sec-tions that follow we describe currentlimitations on access to insurance forminority youth and young adults withspecial health care needs and upcom-ing changes that will be enacted withpassage of the PPACA (either by 2010or in 2014 when full implementation ofthe law goes into effect).
S132 LOTSTEIN et al. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from

Private insurance coverage throughan employer is the most common typeof insurance coverage for both adultsand children (through their parents)in the United States.20 Most CSHCN(60.3% according to the 2005 NS-CSHCN21), similar to their typically de-veloping peers, have private insurancecoverage. Historically, this dependentcoverage typically ends when they turn18, although full-time students may beeligible for longer coverage, depend-ing on state laws.22,23 Because YSHCN,particularly minority youth, are lesslikely than other youth to continue withformal education after high school,24
they are more likely to lose parentalcoverage at an earlier age. Beginningin September 2010, new rules underthe PPACA require insurance plans tocontinue to offer dependent coverageuntil the age of 26 years regardless offinancial, residential, and student sta-tus, thus benefiting minority youthwhose parents have private cover-age.19 Youth who are permanently dis-abled and who continue to be depen-dents of their parents after the age of26 will continue, as in the past, tomain-tain coverage through their parentsinto adulthood.22,23
Young adults can obtain private insur-ance coverage through their own em-ployment, but access to jobs with ben-efits is typically lower for young peoplegenerally and especially for youngadults from low-income minoritybackgrounds.15 During the currenteconomic recession, access to em-ployment in general, and full-timeemployment with benefits especially,has been even more difficult foryoung adults who are newly enteringthe job market.19 Although private in-surance is available for purchase bypeople who do not receive coveragethrough an employer, obtaining suchcoverage has been virtually impossi-ble in the past for young adults withchronic conditions, especially those
with a low income, because of theprohibitive costs of such coverageand the frequent exclusion of benefi-ciaries with a preexisting condi-tion.22,23 Beginning in 2014, the PPACAwill create significant changes inthe nonemployment, self-purchasedinsurance-plan market for all low-income young adults.19 Health planswill be prohibited from limiting cov-erage or charging much higher pre-miums for those with preexistingmedical conditions. Furthermore,health insurance exchanges will cre-ate new options for private coveragewith premium subsidies and caps onout-of-pocket expenses for low-income individuals.18,19
Currently, significant age-related chal-lenges to eligibility for public sourcesof insurance (eg, Medicaid, State ChildHealth Insurance Programs [SCHIPs],and Medicare) also exist. Although it isrelatively generous to poor children,all individuals, regardless of healthstatus, are considered “adults” underMedicaid and SCHIP after the 19thbirthday. Adult Medicaid coverage hasbeen limited to low-income adults whomeet federal disability criteria or arevery low-income parents of young chil-dren. Beginning in 2014, the PPACA ex-pands Medicaid to all adults up to133% of the federal poverty limit (ap-proximately $14 000 per year for an in-dividual, and $30 000 per year for afamily of 4), regardless of disability orparental status.19 As it has been in thepast, young adults are only eligible forMedicare (a program for those olderthan 65) if they have end-stage renaldisease or are dependents of Medi-care beneficiaries.
In the past, this age-related disparity inaccess to public insurance has had adisproportionate impact on young mi-nority adults, who aremore likely to bepublicly insured as children than theirnonminority peers. Specifically, ac-cording to the 2005 NS-CSHCN, 51% of
black YSHCN and 44% of HispanicYSHCN younger than 18 years had pub-lic insurance in 2005, compared with20% of white CSHCN.21 Thus, thePPACA’s Medicaid expansion will likelyhave a significant impact on a largenumber of low-income minority YSHCNwho currently cannot continue theirchildhood Medicaid coverage becausethey are not sick enough to meet dis-ability criteria. These challenges in ac-cess to public insurance are com-pounded for YSHCN who are not UScitizens. Although some (limited)public coverage may be available tononcitizen CSHCN, their eligibilitytypically ends when they becomeadults because, for example, Medic-aid only covers adults who are UScitizens. Furthermore, these YSHCNare less likely than their US citizenpeers to hold jobs that offer privateinsurance coverage.25
Living in Low-Income Communities
The fact that minority YSHCN are morelikely than nonminority YSHCN to live inlow-income communities26 also cre-ates challenges in the transition toadulthood. For example, low-incomecommunities typically have fewer re-sources for youth development,27 suchas schools with resources to meet theneeds of YSHCN who are often absentfrom school because of illness, mighthave mental health service needs (eg,for depression and posttraumaticstress disorders), and often haveother special education needs (suchas cognitive or attention problems be-cause of the disease’s impact onbrain development). Underresourcedschools are also less likely to offer ca-reer and college-preparation services,which are key resources for any youthleaving high school. YSHCN might havedifficulty accessing the services of lo-cal community-based groups becauseof periods of illness and some of thesociocultural factors described below.
SUPPLEMENT ARTICLES
PEDIATRICS Volume 126, Supplement 3, December 2010 S133. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from

Sociocultural Factors
Several sociocultural factors tend tohave a negative impact on the success-ful transition of minority YSHCN toadult health care. Health care provid-ers are often not aware of cultural tra-ditions that are important to this pop-ulation, which can lead to a mismatchbetween patient or family and providerexpectations and needs. Investigatorshave studied these factors in minoritychildren, adolescents, and adults ingeneral, but few empirical studieshave examined the impact of these so-ciocultural factors on transition prep-aration or outcomes.
The most obvious sociocultural factorthat can impose barriers to successfultransitions to adult health care for mi-nority YSHCN is language. Discussionsbetween youth, their parents, andhealth care providers about healthcare transitions can be difficult in En-glish and are even more challengingwhen language barriers exist. Accord-ing to the 2005 NS-CSHCN, 12.5% of par-ents of CSHCN speak a language otherthan English in the home.21 The impactof language barriers in pediatric set-tings generally has been well de-scribed,28 and these findings are prob-ably also relevant to the transitionsetting. Using a child as an interpreteris especially problematic in the contextof conversations about the long-termhealth problems and self-care skills ofyouth. Parents might be uncomfort-able asking difficult questions (eg,about long-term health issues or prob-lems with their child), and childrenmight “selectively interpret” informa-tion from their parents or provider toavoid “getting into trouble” or to pro-tect their parent from bad news.
In navigating between the old, familiarpediatric health care system and thenew, unfamiliar adult system, patientsand families need to interact withmany people in addition to their doc-tors and nurses, including unknown of-
fice staff members, insurance provid-ers, and community service workers.Language barriers make conversa-tions with these individuals challeng-ing and could lead to misunderstand-ings and gaps in the transfer ofservices.
Lower educational attainment (eg, notcompleting high school), which ismore common in minority groups,24
can result in barriers for YSHCN andtheir families in navigating the transi-tion to a complex new adult health caresystem. Interpreting and respondingto information from health insurancecompanies, medical offices, and hospi-tals is particularly challenging for fam-ily members with limited formal edu-cation. Given the complexity of theUS health care system, navigatingchanges for patients with multipleneeds can be challenging even forwell-educated patients and families11; forthose with low education levels, thesechallenges can result in significantgaps in care. Specifically in terms ofracial and ethnic minorities, Ngui andFlores29 found that black and Hispanicparents of CSHCN were more likely toreport problems with ease of use ofhealth care services than whiteparents.
Beliefs and attitudes that can affectthe transition to adulthood and healthcare transitions for YSHCN might alsovary according to socioeconomic sta-tus and culture.3 For example, studieshave revealed that future orientationdiffers according to culture and socio-economic status.30,31 Future orienta-tion is amultidimensional concept thatincludes an individual’s thoughts of hisor her potential future life options andexpectations.32 It includes dimensionssuch as planning abilities, realism, andsense of control. This “model of the fu-ture” provides the grounds for currentgoal-setting and decision-making.Without a future orientation, YSHCNmay be less likely to prioritize activi-
ties that contribute to future well-being, such as continuing their educa-tion or medication adherence.33
Studies in the general adult popula-tions have revealed that patients fromracial and ethnic minority groups areless likely than their nonminoritypeers to have a sense of trust in theirproviders.34 Trust in health care pro-viders plays a large role for YSHCN andtheir families, who often have a specialbond with their pediatric providerwho, in many cases, has helped themaddress life-threatening issues. Leav-ing this protective relationship can bedifficult for all YSHCN.35 Yet, formingnew relationships with adult-orientedprovidersmay take longer for minorityYSHCN and family members who sharethe lack of trust of health care provid-ers found in other racial and ethnicmi-nority groups of patients. Althoughsome skepticism about unknown pro-viders may be appropriate, in extremeit could cause problems such as notfollowing up on a referral to a new phy-sician or resistance to following rec-ommendations for care from that pro-vider. This could result in missingneeded follow-up care. YSHCN andtheir families might delay leaving thepediatric provider until forced to doso by some urgent circumstance (eg,an admission to an adult floor of ahospital) without the benefit of pastrelationship-building or transfer-ence of past records or other keyinformation.
ELIMINATING DISPARITIES INTRANSITIONS TO ADULT HEALTHCARE FOR YSHCN
Significant research, policy change,advocacy, and education efforts involv-ing providers and families are neededto make progress in eliminating racialand ethnic disparities in the transitionto adult health care for YSHCN.
Future research efforts should providea clearer understanding of racial and
S134 LOTSTEIN et al. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from

ethnic differences in the transition-preparation needs of YSHCN. Impor-tant research questions includewhether Hispanic parents have differ-ent expectations from white parentsfor their YSHCN when they becomeadults, how these expectations influ-ence the transition-planning supportthey should receive, and the character-istics of culturally effective transition.Longitudinal studies of transition out-comes in access to care could helpidentify youth at the highest risk ofpoor outcomes. Other research shouldtest the efficacy of tools and interven-tions (such as interventions that con-nect tertiary medical center servicesto community-based services) to im-prove transition preparation andoutcomes.
Policy changes at several levels couldprevent gaps in health care afterYSHCN make the transition to adultcare. Expanding access to public andprivate health insurance for low-income individuals who are not dis-abled but have special health careneeds (as will begin under changes en-
acted by the PPACA) is essential to en-sure that all youth and young adultswith special health care needs receivethe care they need.19,23 Other policychanges to support transition prepa-ration include improved reimburse-ment for care-coordination services,including support for the comprehen-sive medical home model and transi-tion preparation.36 Increased accessto, and utilization of, medical homesfor YSHCN could help eliminate dispar-ities in transitions to adult health care,just as access to medical homes hasreduced racial and ethnic disparitiesin access to, and quality of, care for thegeneral population of adults.37 In addi-tion to its changes in access to healthinsurance coverage, other policychanges in the PPACA could increasethe availability of high-quality medicalhomes for everyone, including those inthis population.38 In addition, changinghealth insurance policies to allow a pe-riod of comanagement by pediatricand adult providers could be helpful tosome YSHCN. Although all of thesechanges would benefit all YSHCN, the
extra support is likely to be most valu-able to YSHCN of color because of theirgreater need for assistance during thetransition period. Advocacy at the fed-eral, state, and local levels will be nec-essary to eliminate disparities in tran-sition. As described above, many of thereforms in the PPACA begin to addressthese policy needs, but careful moni-toring will be required to ensure thatthe PPACA has its intended effects.18,19
Finally, educational efforts are neededin this area. YSHCN and their familiesneed access to professional inter-preter services to permit nuanced dis-cussions among providers, parents,and youth about the transition to adulthealth care. Educational initiatives foradult and pediatrics providers shouldbuild awareness of the cultural as-pects of the transition to adulthoodand add to the growing health careprovider awareness of cultural effec-tiveness.39 Targeted educational ef-forts for parents and YSHCN can helppromote effective transitions toadulthood.
REFERENCES
1. American Academy of Pediatrics, Ameri-can Academy of Family Physicians, Amer-ican College of Physicians. A consensusstatement on health care transitions foryoung adults with special health careneeds. Pediatrics . 2002;110(6 pt 2):1304–1306
2. Rosen DS, Blum RW, Britto M, Sawyer SM,Siegel DM; Society for Adolescent Medicine.Transition to adult health care for adoles-cents and young adults with chronicconditions: position paper of the Society forAdolescent Medicine. J Adolesc Health.2003;33(4):309–311
3. Reiss J, Gibson R. Health care transition:destinations unknown. Pediatrics. 2002;110(6 pt 2):1307–1314
4. McDonagh JE. Growing up and moving on:transition from pediatric to adult care. Pe-diatr Transplant. 2005;9(3):364–372
5. Ngui EM, Flores G. Unmet needs for spe-cialty, dental, mental, and allied health careamong children with special health careneeds: are there racial/ethnic disparities? J
Health Care Poor Underserved. 2007;18(4):931–949
6. Strickland BB, Singh GK, Kogan MD, MannMY, van Dyck PC, Newacheck PW. Access tothe medical home: new findings from the2005–2006 National Survey of Children WithSpecial Health Care Needs. Pediatrics. 2009;123(6). Available at: www.pediatrics.org/cgi/content/full/123/6/e996
7. Lotstein DS, Inkelas M, Hays RD, Halfon N,Brook R. Access to care for youth with spe-cial health care needs in the transition toadulthood. J Adolesc Health. 2008;43(1):23–29
8. Betz CL. Transition of adolescents with spe-cial health care needs: review and analysisof the literature. Issues Compr PediatrNurs. 2004;27(3):179–241
9. McPherson M, Arango P, Fox H, et al. A newdefinition of children with special healthcare needs. Pediatrics. 1998;102(1 pt 1):137–140
10. Blumberg SJ, Welch EM, Chowdhury SR, Up-church HL, Parker EK, Skalland BJ. Design
and operation of the National Survey of Chil-dren With Special Health Care Needs,2005–06. Vital Health Stat 1. 2008;(45):1–188
11. McPherson M, Weissman G, Strickland BB,van Dyck PC, Blumberg SJ, Newacheck PW.Implementing community-based systems ofservices for children and youths with spe-cial health care needs: how well are wedoing? Pediatrics. 2004;113(5 suppl):1538–1544
12. Lotstein DS, McPherson M, Strickland B,Newacheck PW. Transition planning foryouth with special health care needs: re-sults from the National Survey of ChildrenWith Special Health Care Needs. Pediatrics.2005;115(6):1562–1568
13. Lotstein DS, Ghandour R, Cash A, McGuire E,Strickland B, Newacheck P. Planning forhealth care transitions: results from the2005–2006 National Survey of Children WithSpecial Health Care Needs. Pediatrics. 2009;123(1). Available at: www.pediatrics.org/cgi/content/full/123/1/e145
14. Smedley BD, Stith AY, Nelson AR; Institute of
SUPPLEMENT ARTICLES
PEDIATRICS Volume 126, Supplement 3, December 2010 S135. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from
Medicine, Committee on Understanding andEliminating Racial and Ethnic Disparities inHealth Care, Board on Health Sciences Pol-icy. Unequal Treatment: Confronting Racialand Ethnic Disparities in Health Care. Wash-ington DC, National Academies Press; 2002
15. Adams SH, Newacheck PW, Park MJ, BrindisCD, Irwin CE Jr. Health insurance across vul-nerable ages: patterns and disparities fromadolescence to the early 30s. Pediatrics.2007;119(5). Available at: www.pediatrics.org/cgi/content/full/119/5/e1033
16. Callahan ST, Cooper WO. Access to healthcare for young adults with disablingchronic conditions. Arch Pediatr AdolescMed. 2006;160(2):178–182
17. Callahan ST, Hickson GB, Cooper WO. Healthcare access of Hispanic young adults in theUnited States. J Adolesc Health. 2006;39(5):627–633
18. Kaiser Family Foundation. Summary of cov-erage provisions in the Patient Protectionand Affordable Care Act and the Health Careand Education Reconciliation Act of 2010.Available at: www.kff.org/healthreform/8061.cfm. Accessed October 7, 2010
19. Collins S, Nicholson J. Rite of Passage: YoungAdults and the Affordable Care Act of 2010.New York, NY: Commonwealth Fund; 2010.Available at: www.commonwealthfund.org/Content/Publications/Issue-Briefs/2010/May/Rite-of-Passage-Young-Adults-and-the-Affordable-Care-Act-of-2010.aspx. AccessedOctober 7, 2010
20. Kaiser Family Foundation. Chartbook:health insurance coverage in America,2008. Available at: http://facts.kff.org/chartbook.aspx?cb�57. Accessed October7, 2010
21. Child and Adolescent Health MeasurementInitiative. National Survey of Children WithSpecial Health Care Needs, 2005. Availableat : www.cshcndata .org/DataQuery/
DataQueryResults.aspx?q�2285&r1�0&r2�1. Accessed December 10, 2009
22. White PH. Access to health care: health in-surance considerations for young adultswith special health care needs/disabilities.Pediatrics. 2002;110(6 pt 2):1328–1335
23. Nicholson JR, Collins SR, Mahato B, Gould E,Schoen C, Rustgi SD. Rite of Passage? WhyYoung Adults Become Uninsured and HowNew Policies Can Help, 2009 Update. NewYork, NY: Commonwealth Fund; 2009
24. Stoops N. Current population reports: edu-cational attainment in United States2003. Available at: www.census.gov/prod/2004pubs/p20-550.pdf. Accessed March 4,2010
25. Migration Policy Institute. Health insurancecoverage of the foreign born in the UnitedStates: numbers and trends. Available at:www.migrationpolicy.org/pubs/eight_health.pdf. Accessed October 7, 2010
26. DeNavas-Walt C, Proctor BD, Smith JC. Cur-rent Population Reports: Income, Poverty,and Health Insurance Coverage in theUnited States: 2007. Washington, DC: US Gov-ernment Printing Office; 2008. Available at:www.census.gov/prod/2008pubs/p60-235.pdf. Accessed October 7, 2010
27. Kretzmann JP, McKnight JL. Building Com-munities From the Inside Out: A Path TowardFinding and Mobilizing a Community’sAssets. Evanston, IL: Institute for PolicyResearch; 1993
28. Flores G. The impact of medical interpreterservices on the quality of health care: a sys-tematic review. Med Care Res Rev. 2005;62(3):255–299
29. Ngui EM, Flores G. Satisfaction with careand ease of using health care servicesamong parents of children with specialhealth care needs: the roles of race/ethnicity, insurance, language, and ade-quacy of family-centered care. Pediatrics.2006;117(4):1184–1196
30. Greene AL. Great expectations: constructionof the life course during adolescence. JYouth Adolesc. 1990;19(4):289–306
31. Nurmi JE. Age, sex, social class, and qualityof family interaction as determinants of ad-olescent’ future orientation: a developmen-tal task interpretation. Adolescence. 1987;22(88):977–991
32. Nurmi JE. How do adolescents see their fu-ture? A review of the development of futureorientation and planning. Dev Rev. 1991;11(1):1–59
33. Tamaroff MH, Festa RS, Adesman AR, WalcoGA. Therapeutic adherence to oral medica-tion regimens by adolescents with cancer:II. Clinical and psychologic correlates. J Pe-diatr. 1992;120(5):812–817
34. Armstrong K, McMurphy S, Dean LT, et al.Differences in the pattern of health caresystem distrust between blacks and whites.J Gen Intern Med. 2008;23(6):827–833
35. Reiss JG, Gibson RW, Walker LR. Health caretransition: youth, family, and provider per-spectives. Pediatrics. 2005;115(1):112–120
36. Kelly AM, Kratz B, Bielski M, Rinehart PM.Implementing transitions for youth withcomplex chronic conditions using the med-ical home model. Pediatrics. 2002;110(6 pt2):1322–1327
37. Beal AC, Doty MM, Hernandez SE, et al. Clos-ing the Divide: HowMedical Homes PromoteEquitable Care—Results From the Com-monwealth Fund 2006 Health Quality Sur-vey. New York, NY: Commonwealth Fund;2007
38. Williams ED, Redhead CS. Public health,workforce, quality and related provisions inthe Patient Protection and Affordable CareAct (PPACA). Available at: www.aamc.org/reform/summary/ph.pdf. Accessed October7, 2010
39. Beal AC. Policies to reduce racial and ethnicdisparities in child health and health care.Health Aff (Millwood). 2004;23(5):171–179
S136 LOTSTEIN et al. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from
DOI: 10.1542/peds.2010-1466F 2010;126;S129-S136 Pediatrics
Debra S. Lotstein, Alice A. Kuo, Bonnie Strickland and Fan Tait Do Racial and Ethnic Disparities Exist?
The Transition to Adult Health Care for Youth With Special Health Care Needs:
& ServicesUpdated Information
29http://www.pediatrics.org/cgi/content/full/126/Supplement_3/S1including high-resolution figures, can be found at:
References
29#BIBLhttp://www.pediatrics.org/cgi/content/full/126/Supplement_3/S1at: This article cites 23 articles, 12 of which you can access for free
Citations
29#otherarticleshttp://www.pediatrics.org/cgi/content/full/126/Supplement_3/S1This article has been cited by 1 HighWire-hosted articles:
Subspecialty Collections
http://www.pediatrics.org/cgi/collection/developmental:behavior Developmental/Behavior
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by UCLA BIOMEDICAL LIBRARY on December 3, 2010 www.pediatrics.orgDownloaded from