the role of hepatobiliary scintigraphy in cystic fibrosis
TRANSCRIPT

The Role of Hepatobiliary Scintigraphy in Cystic Fibrosis
PHIL J. O’CONNOR,1 KEVIN W. SOUTHERN,2 IAN M. BOWLER,2 HENRY C. IRVING,1 PHIL J. ROBINSON,1
AND JAMES M. LITTLEWOOD2
This was a prospective open study that examined the Abnormal liver histology is found with increasing fre-quantitative and qualitative analysis of hepatobiliary quency in older patients with CF,3-5 and clinically overtscintigraphy (DISIDA) in detecting liver involvement in liver disease becomes increasingly prevalent in the sec-cystic fibrosis (CF). Forty-four adult and pediatric pa- ond decade of life.6 The typical hepatic lesions are ini-tients (median age, 12.1 years; range, 1.1-36.3 years) were tially focal in nature but can progress to multilobulardivided into three groups: group 1, no evidence of liver cirrhosis with hepatic failure. Parenchymal liver func-involvement (n Å 8); group 2, biochemical evidence of tion is characteristically preserved until a late stage,liver involvement on two or more occasions (nÅ 26); and
but complications of portal hypertension may occur ear-group 3, clinical evidence of liver disease (n Å 10). Inlier.groups 1 and 2, the most common qualitative scinti-
Recent promising results with ursodeoxycholic acidgraphic finding was focal intrahepatic retention oftracer (26/34 patients, 12 of whom had normal findings (UDCA) in CF liver disease7-9 have led to an increasedon ultrasonography). This finding corresponds to focal interest in early and thorough assessment of the hepa-cholestasis and may warrant treatment with the cholere- tobiliary system. Early detection of liver involvement,tic agent ursodeoxycholic acid (UDCA). In the group 3 however, remains a problem. Clinical, biochemical,patients, the abnormal qualitative scintigraphic appear- pathological, and radiological assessment have, as yet,ances (heterogeneous uptake of tracer and nodular liver not offered early reliable diagnoses using methods suit-outline) added little to the findings on ultrasonography; able for screening the CF population.6however, these patients had a prolonged mean hepatic
Biliary scintigraphy was used by Gaskin et al.10 in aclearance time compared with those in groups 1 and 2study reporting a high incidence of distal common bile(one-way ANOVA; Põ .015). It is proposed that scintigra-duct strictures in patients with CF. Although otherphy with DISIDA has a role in the detection of early liver
involvement in cystic fibrosis. (HEPATOLOGY 1996;23:281- studies have not confirmed these findings, they have287.) all commented on frequent intrahepatic abnormalities
found on scintigraphy.11-14
The aim of the present study was to document theCystic fibrosis (CF) is a recessively inherited multi-range of these scintigraphic abnormalities in CF pa-system disease characterized by recurrent chest infec-tients from both a quantitative and a qualitative view-tions and intestinal malabsorption. Affected individu-point, examining the relationship of these abnormali-als have reduced life expectancy, usually as a result ofties to clinical status and ultrasonographic findings.chronic respiratory failure. More effective treatment of
the chest infection has resulted in a steady improve- PATIENTS AND METHODSment in the median survival rate from 2 years in the
Patients attending the Regional Paediatric and Adult Cys-1950s to more than 30 years in the 1990s.1 Livertic Fibrosis Units were enrolled prospectively. All the pa-involvement in CF has been recognized since the firsttients had clinical features of CF with a positive sweat testreport of the condition2 but is of increasing clinical im-(sweat chloride concentration, ú60 mmol/L) on at least twoportance with improving survival. occasions. Patients with clinical evidence of liver disease orabnormal results of serum liver function tests (LFTs) wereenrolled along with control patients who had some form ofintravenous access (often at the end of a course of intravenousAbbreviations: CF, cystic fibrosis; UDCA, ursodeoxycholic acid; LFT, liverantibiotic therapy).function test; ALT, alanine transaminase; FEV1, forced expiratory volume in 1
Forty-four patients were enrolled, 18 male and 26 female.second; FVC, forced vital capacity; DISIDA, diisopropylphenyl-carboxymethyliminodiacetic acid; CFTR, cystic fibrosis transmembrane conductance regula- Their median age was 12.1 years (range, 1.1-36.3 years).tor. Twenty-nine of the patients had chronic respiratory infection
From the 1Department of Diagnostic Radiology and the 2Regional Paediatric with Pseudomonas aeruginosa (nÅ 25), Burkholderia cepaciaCystic Fibrosis Unit, St. James’ University Hospital, Leeds, England. (n Å 1), or Stenotrophonomas maltophilia (n Å 3).
Received June 12, 1995; accepted September 13, 1995. The patients were examined for hepatomegaly (defined asDrs. Southern and Bowler were supported by the CF Trust (United King- a firm liver edge felt consistently more than 1 cm below thedom).
costal margin) and splenomegaly.Drs. O’Connor and Southern contributed equally to this study.Serum LFTs were performed at the time of radiologicalCopyright q 1996 by the American Association for the Study of Liver
investigation or at the outpatient clinic no earlier than 6Diseases.0270-9139/96/2302-0012$3.00/0 weeks before the scans. Abnormal results of serum LFTs were
281
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology

282 O’CONNOR ET AL. HEPATOLOGY February 1996
TABLE 1. Clinical Groups
Median Age, yr Mean HepaticGroup Description n (range) Sex (M/F) Clearance, min (SEM)
1 No previous evidence of liver involvement 8 14.6 (9.7-29.9) 2:6 21.7 (2.2)2 Abnormal serum LFTs on ú2 occasions 26 12.5 (1.7-36.3) 11:15 28.5 (3.5)3 Clinical evidence of liver disease 10 11.2 (1.1-24.8) 5:5 57.5 (16.1)
alanine transaminase (ALT) concentration of ú35 IU/L or puter acquisition was obtained for 60 minutes (120 30-secondframes with a 64 1 64-W matrix) with spot analogue imagesalkaline phosphatase (ALP) concentration of greater than the
normal range for age15 or bilirubin concentration of ú17 taken at 5-minute intervals.If significant gallbladder activity was found at 60 minutes,mmol/L.
Serum LFTs had been performed annually on all patients a fatty meal (a peanut butter sandwich and a glass of milk)was given to the patient and imaging was continued for aas a routine or more frequently if indicated. The patients’
charts were reviewed for previously abnormal serum LFT further 40 minutes.Computer analysis included calculation of the half-lifelevels.
On the basis of these clinical and biochemical findings, the clearance of the radioisotope from the hepatic parenchymaand the gallbladder emptying fraction following the fattypatients were divided into three groups: group 1, no evidence
of liver involvement (n Å 8); group 2, biochemical evidence meal as described by Brown20 and Newman.21 The qualitativefindings were interpreted by the consensus of opinion be-of liver involvement, abnormal serum LFTs on two or more
occasions (n Å 26); and group 3, clinical evidence of liver tween two observers (P.J.O. and P.J.R.) blinded to the pa-tient’s clinical and ultrasonic findings.involvement (n Å 10) (Table 1).
A number of clinical parameters were noted: Shwachman Normal scintigraphic appearances are shown in Fig. 1.The criteria for abnormal results of hepatobiliary scintigra-Kulczycki clinical score,16 percent weight for height and age,
forced expiratory volume in 1 second (FEV1; percent pre- phy are listed in Table 2.dicted for height and age) and forced vital capacity (FVC;
RESULTSpercent predicted for height and age).Twelve of the patients with evidence of liver involvement The age, sex, and hepatic clearance rate of patients
were started on therapy with UDCA (20 mg/kg/d) and taurine in the three groups are listed in Table 1. The hepatic(30 mg/kg/d). Repeat clinical and radiological assessments clearance time was significantly longer in the group 3were performed after a minimum period of 6 months.patients with clinical evidence of liver involvementLocal ethics committee approval was obtained prior to com-(one-way ANOVA; P õ .015).mencing the study, and informed consent was given by all
There was no significant difference between thepatients and their parents if under 16 years of age.three groups in any of the respiratory, nutritional, or
Imaging clinical parameters measured (one-way ANOVA). Thesize of group 2 reflects the frequent occurrence of ab-
Ultrasonography. The patients underwent upper abdomi- normal serum indicators of liver function in this popu-nal ultrasonography performed by an experienced radiogra-lation.pher using Siemens Quantum (Siemens, Seattle, WA), Acu-
son 128 (Acuson, Mountain View, CA), or Diasonics Ultrasonographic Abnormalities(Diasonics, Milipitas, CA) equipment.The scans were reported by a senior radiologist (H.C.I.). Intrahepatic ultrasonographic abnormalities were
Both the radiographer and radiologist knew the patients had present in only 50% of patients in groups 1 and 2 com-CF but were unaware of their clinical or biochemical status. pared with the abnormal liver parenchyma found in
Abnormalities of liver texture were subjectively recorded17; 80% of patients in group 3 (Fig. 5). Steatosis and livermicrogallbladder was diagnosed if the gallbladder measured nodularity were found in 11 (25%) and 19 patientsless than 3 1 1 cm.18 A spleen of greater than 12 cm in the (43%), respectively. Liver nodularity was more fre-longest axis in adults and extending below the lower pole of
quent in patients with clinical liver disease (P õ .015,the left kidney in children was considered enlarged. The up-Fisher’s Exact Test); steatosis was not associated withper limit of normal for common bile duct caliber was 6 mm.biochemical or clinical liver disease. No patients hadScintigraphy. Hepatobiliary scanning was performed us-intrahepatic duct dilatation. In 2 patients, previouslying the IDA compound diisopropylphenyl-carboxymethyl imi-
nodiacetic acid (DISIDA) labeled with 99mTc. undetected splenomegaly was seen. Gallbladder abnor-Patients fasted overnight. The intravenous dose of DISIDA malities were found in 23 patients (52%), 2 of whom
(Hepatolite, E. I. duPont de Nemours and Co., Stevenage, had gallstones.England) was 120 Mbq for adults; the dose was scaled down There was no age trend in the hepatic ultrasono-for younger patients using recommended guidelines19 with a graphic abnormalities (Mann-Whitney U test).minimum dose of 18.5 Mbq. The whole-body absorbed doseof radiation amounted to 0.4 to 0.6 mGy. Scanning was per- Scintigraphic Intrahepatic Abnormalitiesformed with patients supine for 60 minutes after the injection
Frequent abnormalities were found in all threeusing a large-field-of-view gamma camera (Siemens Orbitergroups including the patients with no clinical or bio-75 Digitrac; Siemens, Oldbury, England) fitted with a low-
energy all-purpose parallel-hole collimator. Continuous com- chemical evidence of liver involvement (group 1) (Fig.
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 O’CONNOR ET AL. 283
FIG. 1. Normal appearances. (A) Fifteen minutes postinjection, there is homogenous hepatic activity. The gallbladder can already beseen clearly (arrow). (B) Forty minutes postinjection, there is good clearance of the hepatic activity with no focal intrahepatic retention.Tracer can be seen within the gallbladder (arrowhead) and small bowel (long arrow).
6). All the patients in group 3 had either heterogeneous Scintigraphic Extrahepatic Abnormalitiesuptake of tracer or a nodular liver outline; these are Extrahepatic scintigraphic abnormalities were foundabnormalities that represent severe liver involvement. in 93% of patients. In half these patients the gallblad-Focal intrahepatic retention was the most frequent der did not fill (nonfunction) and in half the gallbladderqualitative abnormality, occurring in 73%; secondary did not empty following a fatty meal (dysfunction).and tertiary duct visualization occurred in 43%. Intra- These abnormalities were found with equal frequencyhepatic retention was found in 7 of the 8 patients in in the clinical groups (Fig. 6).group 1 with no previous evidence of liver involvement Functional distal common bile duct obstruction wasand in 19 of the 26 patients in group 2. The lower not found in any of the 44 cases.incidence in group 3 can be accounted for by the diffi-culty in evaluating this appearance in the presence of Correlation Between Ultrasonographic anda heterogeneous uptake of tracer. Beading occurred in Scintigraphic Abnormalities36% of patients and was a more frequent finding in
There was a highly significant positive associationgroup 3 patients (P õ .05, Fisher’s Exact Test).between ultrasonographic and scintigraphic nodularityPatients with intrahepatic retention were signifi-(P õ .0001, Fisher’s Exact Test) and a significant posi-cantly older (P õ .05, Mann-Whitney U test); no othertive association between ultrasonically abnormal he-age trends were found in either the intrahepatic orpatic texture and heterogenous scintigraphic activityextrahepatic scintigraphic abnormalities.(P õ .05, Fisher’s Exact Test). No other significant as-sociations were found between the ultrasonographicand scintigraphic abnormalities.TABLE 2. Criteria for Abnormal Results of
Secondary and tertiary bile duct visualization wasHepatobiliary Scintigraphyclosely linked with the presence of intrahepatic reten-
Hepatic tion (P õ .002, Fisher’s Exact Test), suggesting thatNodular liver outline they result from similar pathological processes. ThereHeterogeneous liver activity during the hepatic phase were no other associations between the intrahepatic orFocal intrahepatic retention of tracer 45 min postinjection
extrahepatic scintigraphic abnormalities.(Fig. 2)Visualization of secondary and tertiary bile ducts (Fig. 3)
Follow-up ScansIrregularity (beading) of intrahepatic bile ducts (Fig. 4)Extrahepatic Seven patients from group 2 and 5 from group 3 were
Gallbladder not visualized at 60 min reassessed after treatment with UDCA and taurineGallbladder ejection fraction õ35% following fatty meal (mean treatment period, 13.8 months; range 8-24No activity in the small bowel by 30 min (indicating functional months). There was no progression clinically, and a
distal common bile duct obstruction warranting further significant improvement in serum ALT levels (Põ .01,investigation)Wilcoxon’s matched pairs) was documented. Although
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology

284 O’CONNOR ET AL. HEPATOLOGY February 1996
FIG. 2. (A) Homogenous hepatic activity with an area of focal intrahepatic retention (arrow) 45 minutes postinjection. No gallbladderfilling was observed in this patient. (B) Focal intrahepatic retention (arrow) in a patient with heterogenous hepatic activity 45 minutespostinjection.
the qualitative radiological findings were unchanged monophosphate–stimulated chloride channel situatedin the apical membrane surface of a number of epithe-(ultrasonographic and analogue scintigraphic images)
with no evidence of deterioration, a significant increase lial tissues.23 The absence or malproduction of CFTRis the common link for all individuals with CF.in the rate of hepatic excretion of radioisotope was
found (P õ .05, Wilcoxon’s matched pairs). It is likely that the liver disease in CF is due to acombination of factors. Pathological studies have
DISCUSSION shown evidence of mucus plugging in small intrahe-patic bile ducts.24 There is abundant expression ofThe CF gene is located on the long arm of chromo-
some 7. In 1989, the gene product cystic fibrosis CFTR in normal biliary epithelium,25,26 and its absencein CF may account for the abnormal consistency of bile.transmembrane conductance regulator (CFTR) was
characterized.22 This protein is a cyclic adenosine Another factor is the potential hepatotoxicity of thehydrophobic bile acid pool resulting from excessive fe-cal loss of primary bile acids in patients with cysticfibrosis.27-29
A small but significant percentage of patients withCF develop clinical liver disease, leading in some casesto liver failure, with transplantation being the onlytherapeutic option.30
The identification of liver involvement in CF patientshas, in the past, been made retrospectively. The fre-quent finding of abnormal results of serum LFTs in ourpatients and in other series31 highlights the difficultyin assessing the relevance of abnormal biochemistry ina particular patient.
UDCA, a primary hydrophilic bile acid with cholere-tic properties,32 has been given in high doses to patientswith CF and liver disease. A number of trials havenow shown improvement in results of serum LFTs andhepatic clearance of tracer during scintigraphy.9,14,33
These promising results have emphasized the need forearly identification of patients with liver involvement.
Hepatobiliary scintigraphy in CF represents a rela-tively new application of a technique first described in1977.34 In contrast to other imaging modalities, scintig-raphy gives functional as well as anatomical informa-tion about the liver and biliary tree.
In the 44 patients in the present study, intrahepaticFIG. 3. Secondary and tertiary ducts at 25 minutes. duct irregularity (beading) was found most frequently
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology
HEPATOLOGY Vol. 23, No. 2, 1996 O’CONNOR ET AL. 285
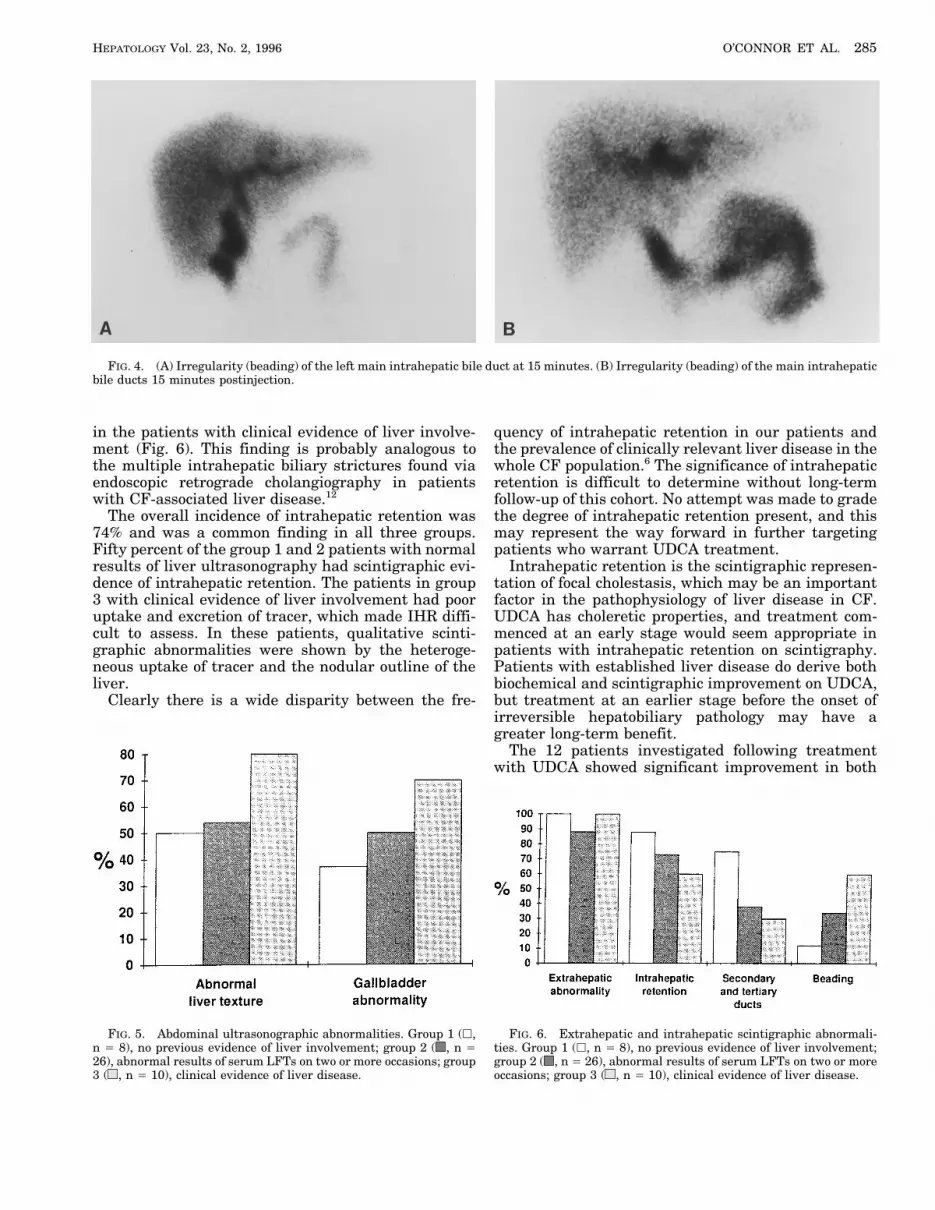
FIG. 4. (A) Irregularity (beading) of the left main intrahepatic bile duct at 15 minutes. (B) Irregularity (beading) of the main intrahepaticbile ducts 15 minutes postinjection.
in the patients with clinical evidence of liver involve- quency of intrahepatic retention in our patients andthe prevalence of clinically relevant liver disease in thement (Fig. 6). This finding is probably analogous to
the multiple intrahepatic biliary strictures found via whole CF population.6 The significance of intrahepaticretention is difficult to determine without long-termendoscopic retrograde cholangiography in patients
with CF-associated liver disease.12 follow-up of this cohort. No attempt was made to gradethe degree of intrahepatic retention present, and thisThe overall incidence of intrahepatic retention was
74% and was a common finding in all three groups. may represent the way forward in further targetingpatients who warrant UDCA treatment.Fifty percent of the group 1 and 2 patients with normal
results of liver ultrasonography had scintigraphic evi- Intrahepatic retention is the scintigraphic represen-tation of focal cholestasis, which may be an importantdence of intrahepatic retention. The patients in group
3 with clinical evidence of liver involvement had poor factor in the pathophysiology of liver disease in CF.UDCA has choleretic properties, and treatment com-uptake and excretion of tracer, which made IHR diffi-
cult to assess. In these patients, qualitative scinti- menced at an early stage would seem appropriate inpatients with intrahepatic retention on scintigraphy.graphic abnormalities were shown by the heteroge-
neous uptake of tracer and the nodular outline of the Patients with established liver disease do derive bothbiochemical and scintigraphic improvement on UDCA,liver.
Clearly there is a wide disparity between the fre- but treatment at an earlier stage before the onset ofirreversible hepatobiliary pathology may have agreater long-term benefit.
The 12 patients investigated following treatmentwith UDCA showed significant improvement in both
FIG. 6. Extrahepatic and intrahepatic scintigraphic abnormali-FIG. 5. Abdominal ultrasonographic abnormalities. Group 1 (h,n Å 8), no previous evidence of liver involvement; group 2 ( , n Å ties. Group 1 (h, n Å 8), no previous evidence of liver involvement;
group 2 ( , n Å 26), abnormal results of serum LFTs on two or more26), abnormal results of serum LFTs on two or more occasions; group3 ( , n Å 10), clinical evidence of liver disease. occasions; group 3 ( , n Å 10), clinical evidence of liver disease.
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology

286 O’CONNOR ET AL. HEPATOLOGY February 1996
6. Scott-Jupp R, Lama M, Tanner MS. Prevalence of liver diseasetheir hepatobiliary clearance of tracer and serum ALTin cystic fibrosis. Arch Dis Child 1991;66:698-701.levels. The qualitative findings on the analogue scinti-
7. Colombo C, Setchell KD, Podda M, Crosignani A, Roda A, Curciographic images remained constant in all 12 patients, L, Ronchi M, et al. Effects of ursodeoxycholic acid therapy forwith no evidence of progression. These patients were liver disease associated with cystic fibrosis. J Pediatr
1990;117:482-489.selected because they had clinical involvement or per-8. Colombo C, Crosignani A, Assaisso M, Battezzati PM, Poddasistently abnormal results of serum LFTs. A recent
M, Giunta A, Zimmer-Nechemias L, et al. Ursodeoxycholic acidstudy35 described follow-up scans on 6 children and therapy in cystic fibrosis-associated liver disease: a dose-re-found quantitative improvement in 3 patients. One of sponse study. HEPATOLOGY 1992;16:924-930.
9. Cotting J, Lentze MJ, Reichen J. Effects of ursodeoxycholic acidthese patients with normal hepatic clearance developedtreatment on nutrition and liver function in patients with cystica qualitative abnormality (dilated intrahepatic ducts)fibrosis and longstanding cholestasis. Gut 1990;31:918-921.on two subsequent scans. These children were not
10. Gaskin KJ, Waters DL, Howman-Giles R, de Silva M, Earl JW,treated with UDCA. Martin HC, Kan AE, et al. Liver disease and common-bile-ductExtrahepatic abnormalities were found frequently in stenosis in cystic fibrosis. N Engl J Med 1988;318:340-346.
11. O’Brien S, Keogan M, Casey M, Duffy G, McErlean D, Fitzgeraldall groups. We found no correlation between the pres-MX, Hegarty JE. Biliary complications of cystic fibrosis. Gutence of liver disease and scintigraphic gallbladder ab-1992;33:387-391.normalities. Previous studies have shown a similar 12. Nagel RA, Westaby D, Javaid A, Kavani J, Meire HB, Lombard
high prevalence of gallbladder abnormality in patients MG, Wise A, et al. Liver disease and bile duct abnormalities inadults with cystic fibrosis. Lancet 1989;2:1422-1425.with CF irrespective of liver involvement.36
13. Dogan AS, Conway JJ, Lloyd-Still JD. Hepatobiliary scintigra-phy in children with cystic fibrosis and liver disease. J Nucl MedCONCLUSION1994;35:432-435.
14. Colombo C, Castellani MR, Balistreri WF, Seregni E, AssaissoHepatobiliary scintigraphy has a role in CF as a com-ML, Giunta A. Scintigraphic documentation of an improvementplementary investigation to ultrasonography. Qualita-in hepatobiliary excretory function after treatment with urso-tive abnormalities not found on ultrasonography were deoxycholic acid in patients with cystic fibrosis and associated
detected, which may represent an early stage of liver liver disease. HEPATOLOGY 1992;15:677-684.involvement in CF. The specificity of these abnormal 15. Clayton BE, Jenkins P, Round JM. Paediatric chemical pathol-
ogy: clinical tests and reference ranges. London, England: Black-findings regarding the development of clinically rele-well, 1980:27-28.vant liver disease is uncertain. Follow-up studies will
16. Shwachman H, Kulczycki LL. Long term study of one hundredbe performed on the patients involved in this study. and five patients with cystic fibrosis. AMA J Dis Child 1958;96:6-In our patients with established liver disease, the 15.
17. Wilson-Sharp RC, Irving HC, Brown RC, Chalmers DM, Lit-qualitative findings offered no additional informationtlewood JM. Ultrasonography of the pancreas, liver and biliaryto the ultrasonographic studies, but because scintigra-system in cystic fibrosis. Arch Dis Child 1984;59:923-926.phy gives functional as well as anatomical information 18. Hubbard VS, Head GL, Shawker TH. Radiological and ultra-
it may prove to be of value in monitoring the progress sound evaluation of the gallbladder in patients with cystic fibro-of these patients. None of the patients had evidence of sis. Pediatr Res 1978;12:437.
19. Alder Hey book of children’s doses. 6th ed. Liverpool, England:distal common bile duct obstruction.Royal Liverpool Children’s NHS Trust, p. 6.Our current practice is to perform ultrasonography
20. Brown PB, Juni JE, Lieberman DA, Krishnamurthy GT. Hepato-and hepatobiliary scintigraphy on all patients with ab- cyte vs. biliary disease: a distinction by deconstitution analysisnormal results of serum LFTs on more than two occa- of Tc99m IDA time-activity curves. J Nucl Med 1988;29:623-630.
21. Newman P, Browne MK, Mowat W. A simple technique for quan-sions. Treatment with UDCA is started on all patientstitative cholescystokinin-HIDA scanning. Br J Radiol 1983;with evidence of hepatic abnormality on imaging.56:500-501.
22. Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzel-Acknowledgment: The authors thank Frances Gar- czak Z, Lok S, et al. Identification of the cystic fibrosis gene:side and the staff of the diagnostic imaging depart- cloning and characterization of complementary DNA. Sciencement, and Drs. R. L. Page and S. P. Conway for 1989;245:1066-1073.
23. Anderson MP, Gregory RJ, Thompson S, Souza DW, Paul S,allowing their patients to take part in the study.Mulligan RC, Welsh MJ. Demonstration that CFTR is a chloridechannel by alteration of its anion selectivity. ScienceREFERENCES1991;253:202-205.
24. Sinaasappel M. Hepatobiliary pathology in patients with cystic1. Dodge JA, Morison S, Lewis PA, Colest EC, Geddes D, Russellfibrosis. Acta Paediatr Suppl 1989;363:45-50.G, Bentley B. Cystic fibrosis in the United Kingdom, 1968-1988:
25. Cohn JA, Strong TV, Picciotto MR, Nairn AC, Collins FS, Fitzincidence, population and survival. Paediatr Perinat EpidemiolJG. Localization of the cystic fibrosis transmembrane conduc-1993;7:157-166.tance regulator in human bile duct epithelial cells. Gastroenter-2. Andersen DH. Cystic fibrosis of the pancreas. Am J Dis Childology 1993;105:1857-1864.1938;56:344-399.
26. Fitz JG, Basavappa S, McGill J, Melhus O, Cohn JA. Regulation3. Roy CC, Weber AM, Morin CL, Lepage G, Brisson G, Yousef I,of membrane chloride currents in rat bile duct epithelial cells.Lasalle R. Hepatobiliary disease in cystic fibrosis: a survey ofJ Clin Invest 1993;91:319-328.current issues and concepts. J Pediatr Gastroenterol Nutr
27. Becker M, Staab D, Leiss O, von Bergmann K. Biliary lipid com-1982;1:469-478.position in patients with cystic fibrosis. J Pediatr Gastroenterol4. Vawter GF, Shwachman H. Cystic fibrosis in adults: an autopsyNutr 1989;8:308-312.study. Pathol Annu 1979;14:357-382.
28. Roy CC, Weber AM, Morin CL, Combes JC, Nussle D, Megevand5. Oppenheimer EH, Esterly JR. Hepatic changes in young infantsA, Lasalle R. Abnormal biliary lipid composition in cystic fibrosis.with CF: possible relationship to focal biliary cirrhosis. J Pediatr
1975;86:683-689. Effect of pancreatic enzymes. N Engl J Med 1977;297:1301-1305.
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 O’CONNOR ET AL. 287
29. Nakagawa M, Colombo C, Setchell KD. Comprehensive study of 33. Galabert C, Lengrand D, Montet JC, Dimier JL, Chazalette JP.Use of ursodeoxycholic acid in the treatment of hepato-biliarythe biliary bile acid composition of patients with cystic fibrosis
and associated liver disease before and after UDCA administra- complications in cystic fibrosis [French]. Pathol Biol1991;39:625-628.tion. HEPATOLOGY 1990;12:322-334.
30. Noble-Jamieson G, Valente J, Barnes ND, Friend PJ, Jamieson 34. Loberg MD, Cooper M, Harvey E, Callery P, Faith W. Develop-ment of a new radiopharmaceutical based on N-substitution ofNV, Rasmussen A, Calne RY. Liver transplantation for hepatic
cirrhosis in cystic fibrosis. Arch Dis Child 1994;71:349-352. iminodiacetic acid. J Nucl Med 1977;17:455-461.35. Semih Dogan A, Conway JJ, Lloyd-Still JD. Hepatobiliary scin-31. Rattenbury JM, Taylor CJ, Heath PK, Howie AF, Beckett GJ.
Serum glutathione S-transferase B1 levels as an index of liver tigraphy in children with cystic fibrosis and liver disease. J NuclMed 1994;35:432-435.function in cystic fibrosis: a three year review (abstr). Paediatr
Pulm 1993;16(Suppl 9):277. 36. Isenberg JN, L’Heureux PR, Warwick WJ, Sharp HL. Clinicalobservations on the biliary system in cystic fibrosis. Am J Gas-32. Hofmann AF, Popper H. Ursodeoxycholic acid for primary biliary
cirrhosis. Lancet 1987;2:398-399. troenterol 1976;65:134-141.
m4730$0025 01-18-96 17:42:15 hepa WBS: Hepatology