the health effects of ecstasy: a literature review
TRANSCRIPT
$ “faylor&Francis @ healthsciences
COMJ?REHENSIVE REVIEW
The health effects of ecstasy: a literature review
LINDA R. GOWING’, SUSAN h/f. HENRY-EDWARDS’, RODNEY J. IRVINE2 & ROBERT L. ALI’>
‘Drug and Alcohol Services Council and 2Clinical and Experimental Pharmacology, University of Adelaide, South Australia, Australia
Abstract i Ecstasy (3,4-methy~e~ed~~methamphetam~ne, MDMA,I is the third most used illicit drug, after cannabis and amphetamines. There has been considerable interest in the adverse eflects of use, with particular attention given to a small number of deaths related to ecstasy use, and the neurotoxic effects of MDMA. This paper reviews case reports of adverse efsects attributed to ecstasy use, and the findings of animal and human studies, so as to identify, the health effects of ecstasy use, and factors con~~bu~~ng to their occurrence. The incidence of serious acute adverse events related to ecstasy is low. It t’s the unpred~ctab~li~ of those adverse events and the risk of rno~ali~ and substantial morbidity that makes the health consequences of ecstasy significant, Hyperthermia and hyponatraemia are the most sign$cant acute adverse effects, and can occur even when MDMA is the only drug used. Ecstasy users should be aware of the importance of controlling body temperature and&id intake, early signs of adverse effects, and the need to seek medical assistance promptly. Neurotoxiciy is potential[y the most si~i~ca~t long-term eJjcect of ecstasy. The ~~ini~~ implications of neu~toxiciy are unGerta~n at this time, but short-term memory impairment may be signaficant. [Gowing LR, Henry-Edwards SM, Irvine RJ, Ali RL. The health effects of ecstasy: a literature review. Drug Alcohol Rev 2002;2 1: 53-631
Key words: adverse effects, amphetamine derivatives, ecstasy, 3,4-me~ylenedio~e~amphetamine.
Introduction
In considering the heaith effects of ecstasy, this review defines ecstasy as 3,4-methylenedioxymethampheta- mine or MDMA. However, other drugs are sold as ecstasy, and ecstasy tablets often contain a range of drugs (amphetamine, various amphetamine derivatives, caffeine, aspirin, paracetamol, ketamine) in addition to, or in place of, MDMA [l]. This review gives some consideration to amphetamine derivatives that are chemically related to MDMA (e.g. methylenediox- yamphetamine, or MDA, methylenedioxyethylamphe- tamine or MDEA, and para-methoxyamphetamine or PMA), particularly those that have been substituted for, or combined with, MDMA in ecstasy preparations. In
reviewing the research, we use the term ecstasy to refer to the drug as it is sold on the street, often with the actual composition unknown, and appropriate chemical names (MDMA etc) when a specific, known, substance is being discussed. This review draws together the findings of human and animal studies of the neurotoxic effects of MDMA, together with case reports of adverse events attributed to ecstasy use, to provide an overview of the health effects of ecstasy.
Patterns of use
Data from Australia, Europe indicate that ecstasy has ever
and the United States been tried by between _^.
0.5 and 3% of the general population and from l-S%
Linda R. Gowing PhD, Drug and Alcohol Services Council, Susan M. Henry-Edwards B Ed, Drug and Alcohol Services Council, Rodney J. Irvine PhD, ‘Clinical and Experimental Pharmacology, University of Adelaide, South Australia, Robert L. Ah MBBS, FAFPHM, Grad Dip PI-L, Drug and Alcohol Services Council and 2Clinical and Experimental Pharmacology, University of Adelaide, South Australia, Australia. Correspondence to Dr Linda Gowing, Manager, Evidence-Based Practice Unit, Drug and Alcohol Services Council, 161 Greenhill Road, Parkside SA 5063, Australia.
Received 23 May 2001; accepted for publication 12 December 2001.
ISSN 0959-5235 print/ISSN 1465-3362 online/02/0100S3-11 0 Australian Professional Society on Alcohol and Other Drugs DOI: 10.1080/09595230220119363
of young adults [2,3]. In general, ecstasy is the third most used illicit drug, after cannabis and amphetamines.
In most countries ecstasy is used recreationally as part of a particular youth culture centred on dance parties and “raves” and a preference for specific types of music. The combined stimulant and euphoric proper- ties of MDMA help to explain the association.
Sociability is a major characteristic of ecstasy use. It is taken almost exclusively in a social setting with partners or groups of friends [4,5]. Use of ecstasy by friends is a significant factor in initiation and continuation of ecstasy use [4,6].
Ecstasy is used primarily recreationally, mainly at weekends in association with social events but studies, particularly in the United Kingdom and Australia, have identified regular and intensive use. There may also be a trend of in&easing use by injection [4,7]. Most users appear able to regulate their use of ecstasy but some progress to problematic use [4,6,8,9], Some researchers have suggested that problematic use might constitute dependence, but this is an aspect for further debate [lo-121.
Pharmacology
MDMA has high affinity for serotonin receptors and transport sites in the brain [ 13,141. Serotonin-produc- ing neurones in the brain regulate aggression, mood, sexual activity, sleep and sensitivity to pain. Serotonin is also important in memory and temperature regulation [ 151.
When administered as a single dose, MDMA initially enhances the extracellular brain concentrations of serotonin; this eventually results in depletion of the neurotransmitter and hence a decrease in serotonin levels. In addition, MDMA induces a rapid and subst~tial elevation of another important neurotran- smitter, dopamine, which plays an important role in the control of movement, cognition, motivation and reward [ 161. The release of dopamine in certain areas of the brain is important in mediating ‘the effects of amphetamine and cocaine, and is thought to be the mechanism underlying the stimulant properties of MDMA [17].
In rats, the effect of MDMA is influenced by ambient temperature-between 20 and 22OC, MDMA has a hypothermic effect, but between 28 and 30°C, MDMA has a hyperthermic effect [18], This influence of ambi- ent temperature is significant given that most reports of ecstasy-related hyperthermia in humans are related to use in dance party or nightclub settings where a high ambient temperature is probable. The effect is best characterized as a loss of normal control of body temperature. Hyperthermia has been induced with serotonin [ 191 which suggests that the MDMA-induced
release of this transmitter may be a cause of the temperature control problems [ZO] .
Findings of surveys of users and studies using controlled administration of MDMA are consistent, namely immediate positive psychological effects of euphoria, increased energy and a feeling of closeness xo
others [21--231, and (less commonly) negative psycho- logical effects of paranoia, anxiety and depression. Common short-term physical effects are pupil dilation, increased jaw tension and grinding of teeth, loss of appetite, dry mouth, tachycardia, hot and cold flushes, and sweaty palms. Longer-term effects reported by users include insomnia, depression, headaches and muscle stiffness [2 1,24,25].
Pharmacokinetics and metabolism
MDMA is well absorbed from the gastrointestinal tract 126,271. Following oral administration, effects become apparent in about 20 minutes and last for about 4 hours. Recent evidence indicates that the relationship between MDMA dose and blood concentration may not be linear [28]. Hence, small increases in dose may produce disproportionate increases in effect, possibly contributing to toxicity. Some of the metabolic products of MDMA, e.g. MDA, are themselves bioactive and may also contribute to toxicity [26].
In the liver, MDMA is metabolized by a number of cytochrome P450-mediated pathways. One of the enzymes involved,, CYP2D6, exhibits genetic variability such that some people have low activity of the enzyme and are denoted poor metabolizers [29]. It has been suggested that these people, due to reduced metabo- lism, will be at greater risk of MDMA toxicity However, no evidence has been found to support this hypothesis [30,3%]. It is likely that, in V&G, other enzyme pathways make up for the deficit MDMA is metabolized in the liver and eliminated via the urine [32].
Drug interactions may influence MD&IA toxicity by altering the elimination of MDMA from rhe body, or through an additive effect if the interacting drug has a similar effect to MDMA. Three reported cases of adverse reactions possibly arising from drug interaction involved Buoxetine [33,34] and ritonavir [35].
Neurotoxicity
Animal studies have shown that administration of MDMA produces damage to axons and axon terminal fibres containing serotonin [36]. Decreases in the den- sity of brain serotonin axons have been seen in squirrel monkeys more than 7 years after MDA!&% administra- tion [37]. Some regrowth of axons occurs, but is abnormal and incomplete [38].
55
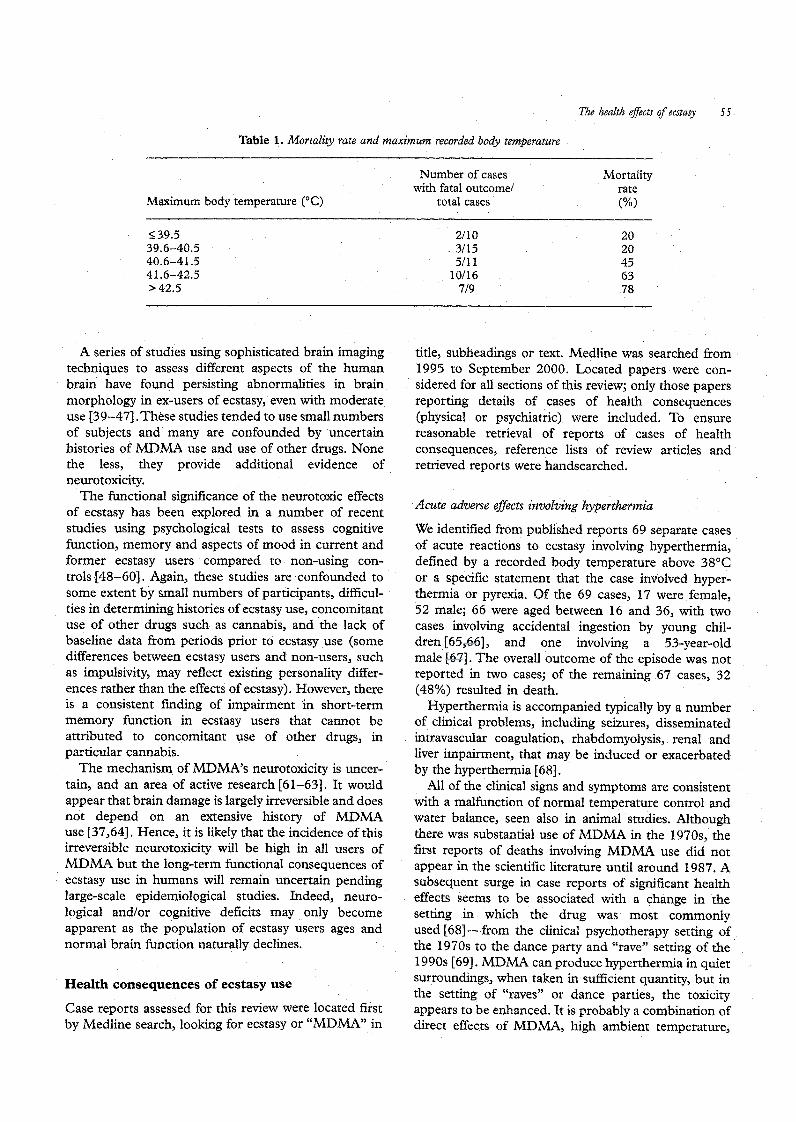
Table 1. Mortality rate and maximum recorded body t~~~~rature
Maximum body temperature (“C)
Number of cases Mortality with fatal outcome/ rate
total cases (%I
$39.5 2flO 20
39.6-40.5 3/15 20
40.6-41.5 5/l 1 45
41.6-42.5 lo/16 63
s42.5 719 78
A series of studies using sophisticated brain imaging techniques to assess different aspects of the human brain have found persisting abnormalities in brain morphology in ex-users of ecstasy, even with moderate use [39-471. These studies tended to use small numbers of subjects and many are confounded by uncertain histories of MDMA use and use of other drugs. None the less, they provide additional evidence of neurotoxicity.
The functional significance of the neurotoxic effects of ecstasy has been explored in a number of recent studies using psychological tests to assess cognitive function, memory and aspects of mood in current and former ecstasy users compared to non-using con- trols [48-601. Again, these studies are confounded to some extent by small numbers of participants, difficul- ties in determining histories of ecstasy use, concomitant use of other drugs such as cannabis, and the lack of baseline data from periods prior to ecstasy use (some differences between ecstasy users and non-users, such as impulsivity, may reflect existing personality differ- ences rather than the effects of ecstasy). However, there is a consistent finding of impairment in short-term memory function in ecstasy users that cannot be attributed to concomitant use of other drugs, in particular cannabis.
The mechanism of MDMA’s neurotoxicity is uncer- tain, and an area of active research [61-631. It would appear that brain damage is largely irreversible and does not depend on an extensive history of MDMA use 137,641. Hence, it is likely that the incidence of this irreversible neurotoxicity will be high in all users of MDMA but the long-term functional consequences of ecstasy use in humans will remain uncertain pending large-scale epidemiological studies. Indeed, neuro- logical and/or cognitive deficits may only become apparent as the population of ecstasy users ages and normal brain function naturally declines.
Health consequences of ecstasy use
Case reports assessed for this review were located first by Medline search, looking for ecstasy or “MDMA” in
title, subheadings or text, Medline was searched from 1995 to September 2000. Located papers were con- sidered for all sections of this review; only those papers reporting details of cases of health consequences (physical or psychiat.ric) were included. To ensure reasonable retrieval of reports of cases of health consequences, reference lists of review articles and retrieved reports were handsearched.
Acute adverse eflects involving hyperthermia
We identified from published reports 69 separate cases of acute reactions to ecstasy involving hyperthermia, defined by a recorded body temperature above 38’C or a specific statement that the case involved hyper- thermia or pyrexia. Qf the 69 cases, 17 were female, 52 male; 66 were aged between 16 and 36, with two cases involving accidental ingestion by young chil- dren [65,66], and one involving a 53-year-old male [67]. The overall outcome of the episode was not reported in two cases; of the remaining 67 cases, 32 (48%) resulted in death.
Hyperthermia is accompanied typically by a number of clinical problems, including seizures, disseminated intravascular coagulation, rhabdomyolysis, renal and liver impairment, that may be induced or exacerbated by the hyperthermia [68].
All of the clinical signs and symptoms are consistent with a malfunction of normal temperature control and water balance, seen also in animal studies. Although there was substantial use of MDMA in the 197Os, the first reports of deaths involving MDMA use did not appear in the scientific literature until around 1987. A subsequent surge in case reports of significant health effects seems to be associated with a change in the setting in which the drug was most commonly used [68] -from the clinical psychotherapy setting of the 1970s to the dance party and “rave” setting of the 1990s [69]. MDMA can produce hyperthermia in quiet surroundings, when taken in sufficient quantity, but in the setting of “raves” or dance parties, the toxicity appears to be enhanced. It is probably a combination of direct effects of MDMA, high ambient temperature,
sustained physical activity and inadequate fluid replace- ment, all impairing temperature regulation, that creates the greatest toxicity [68,70].
It has been suggested that the degree of hyperthermia is predictive of mortality. To investigate this we exam- ined the mortality rate according to the reported maximum body temperature, with cases found dead excluded (Table 1).
These data are clearly suggestive of a correlation between body temperature and the risk of mortality, with around two-thirds of cases where the body temperature exceeded 415°C ending in death. The data support the emphasis placed by others on rapid reduction of temperature as the most important response to hyper- thermia related to ecstasy use. It also indicates the importance of educating users on strategies to avoid hyperthermia, and to seek medical assistance promptly if signs of hyperthermia become apparent.
Acute adverse effects involving disturbances of salt and water balance
We identified 14 cases with features of confusion, reduced consciousness and, in some cases, seizures or convulsions subsequent to ecstasy use and apparently induced by disturbances in salt or water balance. In most cases symptoms resolved as sodium levels were normalized, with full recovery achieved within a few days. However, three of the 14 cases were fatal, due apparently to cerebral oedema associated with excess fluid 7 l-731.
In five of the 14 cases it was reported that copious water had been consumed together with ecstasy. In one case it was reported that consumption of a large amount of water was a deliberate attempt to manage unpleasant alterations of perception caused by the ecstasy [74]. In another case water consumption was estimated at 14 litres in response to thirst induced by MDMA [7 l] . This supports the suggestion that MDMA may result in a sensation of thirst even when there is not a water deficit. Alternatively, behavioural disturbance, including ster- eotyped repetitive actions, may arise from MDMA ingestion [75]. Such an action could include repetitive consumption of water.
The administration of MDMA is associated with inappropriate release of antidiuretic hormone, arginine vasopressin [76,77]. The antidiuretic effect of vasopres- sin, and/or kidney failure associated with hyperthermia, would both reduce urine formation, thereby reducing the body’s capacity to excrete fluid consumed and worsening the effects of excessive fluid consumption. Indeed, the first reports of water intoxication and hyponatraemia occurred after dance club owners encouraged users to take dance breaks in a cool room and drink water [78]. This advice is still sound for prevention of hyperthermia, but clearly the amount of
water consumed needs to be kept within levels able to be handled by the body-an upper limit of 500 ml per hour is appropriate.
Other acute adverse e#ects
Ten cases involved some type of fit or seizure, without hyperthermia or hyponatraemia, suggesting a direct effect on the central nervous system [35,79-831. In five cases the drug involved was confirmed as PMA [79,82]. The presence of MDMA was confirmed for only one case which involved an apparent interaction between MDMA and ritonavir [35]. This suggests that MDMA by itself has minimal direct central nervous system effects.
In six cases (all fatal) aspects of cardiac function appear to have been a primary factor. In three cases there appeared to be pre-existing cardiac dis- ease [34,84,85] suggesting that people with existing cardiovascular conditions may have limited capacity to respond to the stimulatory effects of MDMA.
Twelve cases of haemorrhage or cerebrovascular accident suggest that sudden inappropriate changes in blood pressure or blood flow associated with ecstasy use can result in cerebral ischaemia [86] or blood vessel ruptures, particularly where there are existing weak- nesses such as aneurysms or angioma [87,88). Physical exertion may be a factor, but haemorrhage can also occur in the absence of exercise [87,89]. Intracerebral haemorrhages are also a consequence of abuse of amphetamine and, particularly, cocaine [90,9 11. The stimulatory effect of MDMA may underlie any associa- tion between MDMA use and cerebral haemorrhages, or amphetamines may have been present in the ecstasy preparation consumed, or may have been taken concurrently [88].
In three cases respiratory factors appear to have been central to death, In one case the subject had a history of asthma [92]. In another case death was attributed to inhalation of gastric contents while intoxicated [93], while upper airway obstruction arising from muscle spasms was postulated to have occurred in the third case [94]. These cases indicate that while respiratory difficulties can arise from ecstasy use, MDMA and related amphetamine derivatives do not have a direct effect on respiratory fun&on.
In seven cases use of MDMA or a related amphetamine derivative may have been a factor in behaviour leading to trauma (traffic accidents, falls) [83,85,92,95,96]. In addition, Davies et al. report having treated, over a 3-month period, 16 ecstasy users who had been injured as a result of traffic accidents, all caused by reckless driving. None of the injuries were fatal but ecstasy use was reported to have complicated assessment and treatment [97].
The health effects of ecstasy 57
Six cases of chest pain due to air in tissues in and 6.5 mg/l. (The lowest levels were in cases of hypona- around the thoracic cavity were identified and are traemia where testing occurred around 12 hours after probably attributable to exercise under the influence of drug use.) For those cases with a non-fatal outcome, ecstasy, and not the drug itself [98-1021. In one case serum levels of MDMA ranged from 0.24mg/l to high intra-alveolar pressure resulting from prolonged, 7.0 mg/l. The similarity of these two ranges supports the continuous blowing of a whistle while dancing was conclusion expressed by other commentators, namely considered to have caused the escape of air into the that the dose of MDMA is not predictive of the severity mediastinum [ 10 11. The six cases identified all resolved of outcome [78,107]. without intervention, other than analgesia to manage The lack of correlation between MDMA dose and the pain. Several cases of severe chest pain attributed to mortality rate has caused commentators to look for probable spasm of intercostal muscles as a result of alternative explanations for the occurrence of adverse prolonged dancing under the influence of ecstasy have effects. Suggestions include some form of metabolic also been reported [ 1031. myopathy, as has been suggested in the context of those
Three cases of ophthalmic complications subsequent individuals prone to heat stroke [107] and malignant to ecstasy ingestion were probably also attributable to hyperthermia [ 108,109], or individual variability in the context of use, rather than any direct effects of ecstasy on the eye. It was considered that abnormal
metabolism of MDMA. However, as yet instances of muscle abnormality or impaired MDMA metabolism
exposure of the’ cornea to the air arising from lack of have not been identified in any cases of severe reac- sleep was the likely cause [ 1041. tions [I lo] and there appears to be a mix of first-time
and experienced MDMA users affected, making this explanation unlikely, or at least uncommon.
Other physical consequences It has also been suggested that severe reactions might be due to the presence of contaminants in the urenara-
A significantly greater degree of toothwear has been identified in people reporting ecstasy use in the previous 6 months, compared with a group of 28 people who used other drugs but not ecstasy. The occlusal surfaces were affected more commonly than the incisal, indicat- ing that jaw-clenching rather than tooth-grinding was probably the more significant feature [105].
One limited study has also identified a possible increased risk of birth defects following ecstasy use during pregnancy [ 1061. The study had insufficient statistical power to confirm a causal relation but, given the young age of ecstasy users, the effects of ecstasy on the fetus is an aspect that should be monitored.
- _ tion taken. It is true that acute adverse reactions are not always due to MDMA alone, but the majority of cases we identified primarily involved MDMA. Furthermore, there are reports of the affected person taking from the same supply as others, who did not experience severe reactions. This suggests that contaminants are also an unlikely explanation [ 1071. It seems most likely that it is the combination of dose, setting and individual behav- iour that determines the outcome. Whether this is also true for PMA and other amphetamine derivatives remains unclear.
Liver damage not involving hyperthermia
Effect of MDMA dose Severe liver damage can occur shortly after ingestion of ecstasy, typically in conjunction with hyperthermia.
For 108 of the 158 cases of acute adverse effects identified, drug use was confirmed by analysis of blood and/or urine samples. In 35 of these cases MDMA was the only drug detected, 2 1 involving hyperthermia (10 fatal) and eight cases involving disturbances of salt or water balance (three fatal). These data indicate, first, that MDMA alone can produce adverse effects. Given that hyperthermia and disturbances of salt or water balance generally occur when MDMA is used in nightclub or dance party settings, these data also suggest that the acute adverse effects of MDMA arise primarily from the way it is used.
For 21 of the cases of acute adverse effects where only MDMA was detected, quantitative data from blood toxicology was reported. For cases with a fatal outcome, serum levels of MDMA ranged from O.O4mg/l to
However, liver damage, apparently unrelated to hyper- thermia, can also occur days or weeks after single or multiple episodes of ecstasy use [ 1111. We identified 39 such cases of liver injury, ranging from benign forms mimicking acute viral hepatitis to severe forms such as liver failure due to massive hepatic necrosis [71,112- 1151. The majority of these cases resolved sponta- neously over weeks to months, but 11 cases required some form of transplant and six cases were fatal. It also appears that those who resume ecstasy use after recovery are at risk of a recurrence of their liver damage [ 112,115,116] and the development of chronic hepatitis [ 112,115]. The mechanism of ecstasy-related liver damage is uncertain and, relative to other causes, ecstasy use remains a minor contributor to the inci- dence of liver failure [ 112,113].
58 Lb& R. h&g et al
Psychiatric sequelae hyperthermia theref& comprises rapid cooling with
Depression, or low mood, and concentration and/or intemive monitoring [123]. Sedation to slow down and
memory problems are reported by users as being stop agitated movements may also be appropriate [ 16).
relatively common in the week following ecstasy Rehydration, treatment of metabolic acidosis and sup-
use,[48,117]. The development of psychopa~ologic~ port of failing organ systems are also typical require-
disturbances has also been associated with ecstasy use, ments [ 1071. Alkalin$ation of the urine prevents renal
with the risk of psychopathological disturbances being damage by myoglob&--on this basis, alkalinization is
higher for longer-rerm, larger dosage (acute or cumu- recommended by svme as an early measure [ 1241.
lative) MDMA consumers and those who used MDMA However, alkalinization of the urine reduces renal
in association with other drugs [9,118]. clesrance of amphetsmines and is associated with the
Our search of published literature resulted in the risk of adverse effech in critically ill patients. Conse-
identification of 31 cases of psychiatric sequelae sub- quently the use of alkalinization is controversial. It is
sequent to ecstasy use, generally comprising persistent recommended that urine output is used as the major
episodes of depression, panic disorders, “flashbacks” determinant of adequacy of resuscitation. Rehydration,
and delusions. On the basis of the drug use history while recommended, needs to take into account any
reported, 11 cases appear to have developed subsequent existing htionatraemia [78,125].
to only a short period of ecstasy use (ranging from a There has been considerable discussion in the lit-
single episode of use [ 1191 to four episodes 2-3 weeks erature of the use vf dantrolene. This discussion has
apart [120]). However, 19 cases were related to more tended to rely on comparisons between ecstasy-induced
prolonged, regular use, e.g. several tablets at weekends hyperthermia and heat stroke, malignant hyperthermia
for 6 months or more. In 12 cases a history of cannabis and the serotonin syndrome, Dantrolene is the drug of
use was also reported, and in eight cases a family or choice with malignant hyperthermia, but is not effective
personal history of psychiatric disorders was reported. in heat stroke. Ho&ever, it should be noted that severe
This suggests that the risk of psychiatric sequelae is heat stroke involves an overwhelming of normal ther-
greater when other drugs, particularly cannabis, are moregulatory mechanisms, while MDMA reactions
used in addition to ecstasy, when ecstasy is used appear to involve an abnormality of thermoregula-
repeatedly and at high doses over a period of months, tion [107]. Another argument against dantrolene was
and when there is a family or personal history of that it is’ a peripherally acting muscle relaxant with no
psychiatric disorders. A temporary stress-related state central effects, whereas hyperthermia subsequent to
has also been suggested as a potential source of ecstasy use is attributed to central thermoregulatory
susceptibility [ 12 11. mechanisms. However, Tehan noted that skeletal mus- cle is none the less a major site of increased metabolic activity induced by ecstasy, giving grounds for dan-
Treatment of adverse effects trolene use [126] .’ Another ,aspect raised [Sl] is that each 20 mg vial ok dantrolene contains mannitol (3 g)
Reassurance, observation and monitoring for several zind is reconstituted in solution with pH 9.5. Conse- hours in a subdued environment until symptoms quently the use of dantrolene also results in alkali&a- subside appears to be an appropriate approach to most tion of the urine9 which has associated risks as men-’ cases of adverse effects related to ecstasy tioned above. intoxication [69,122]. As experience of ecstasy-induced h~er~ermia has
The analysis of reported cases of acute adverse effects accumulated, it is becoming apparent that dantrolene related to ecstasy use suggests that hyperthermia and (1 rag/kg i.v. rep.eated up to 10 mg/kg) is of value in hyponatraemia are the most significant complications achieving rapid control of body temperature [ 107). For necessitating intervention. In both conditions the treat- the cases of ecstasy-induced hyperthermia that we ment response needs to be rapid and intense if identified, five of 26 (19%) clearly identified as having significant morbidity and mortality are to be averted. In the case of hyperthermia, the patient may deteriorate
received dantrolene, compared to six of 17 (35%) clearly not administeredl dantrolene, had fatal outcomes, This
rapidly towards multiple organ failure, requiring inten- sive support of cardiovascular, respiratory and renal systems [ 1071. This requires admission to an intensive care unit.
The analysis in Table 1 shows clearly that mortality rate increases with increasing degree of hyperthermia. The duration of hyperthermia is also considered to be an important determinant of mortality [107,109], The recommended medical response to acute reactions with
Isuggests some abvantage, in terms of reduced risk of mortality, arising from the use ofdantrolene.
The use of neuroleptics requires care because of the theoretical risk of producing the neuroleptic malignant syndrome and ‘the possibility of precipitating seiz- ures [68]. Delirium, agitation and seizures should be controlled with increments of diazepam in the first instance, in pre&rence to chlorpromazine [109,127]. In cocaine users it has been found that diazepam is less
The health effects of ecstasy 59
effective if administered after the commencement of potentiate the effects of the released serotonin, worsen- seizures [ 161. ing any adverse effects [68] and limiting their value as a
Many cases of ecstasy-induced liver damage will treatment agent. resolve without intervention, and simply require mon- The non-pharmacological interventions which have itoring. However, patients developing jaundice or with demonstrated the most efficacy) in treating psychosti- evidence of hepatic failure, particularly encephalopathy mulant users are relapse prevention (particularly for and prolongation of the international normalised ratio, heavy users), cue exposure/response prevention, and or both, will require specialist care. Liver transplanta- possibly, multi-faceted behavioural therapy [132]. Con- tion (full or auxiliary) may represent the only chance of tingency management approaches may also be of recovery should they progress to fulminant liver value [ 161. failure [113,114,128]. There remain the issues of attracting users into
treatment and intervening prior to the development of
Treatment for ecstasy use problematic use. An approach that is well suited to these purposes is that of brief intervention [133]. Brief.
In general ecstasy users do not present for treatment. interventions focus on substance use as the target This is likely to largely be a reflection of typical patterns behaviour for change; they aim to investigate a potential of use of ecstasy. It also determines the type of problem and motivate’ an individual to begin to do interventions that can be considered for ecstasy users. something about their substance use. The basic goal of
While the majority of ecstasy users take small doses a brief intervention is to reduce the risk of harm that infrequently, a proportion use more frequently could result from continued substance use. Brief (monthly to weekly) and/or use larger amounts. There interventions on their own can promote behaviour may also be a trend of increasing use by injection rather change, or they can act’as the first stage of more intense than orally [129]. Young, female, polydrug users and treatment [ 1331. those who “binge” on ecstasy are most likely to report These strengths identifjr the potential value of brief, physical, psychological, financial, relationship, and interventions in addressing ecstasy use, but brief occupational problems attributed, at least in part, to interventions need to Ibe structured and much of the their ecstasy use [ 1291, Those, who inject ecstasy are also evidence of their effectiveness relates to alcohol abuse. likely to be at increased risk of harm arising from the It is desirable for there to be development, and more rapid onset of effects and higher peak levels,in the evaluation through structured research, of brief inter- blood following injection, thereby increasing the effect ventions appropriate to ecstasy users and the various on the cardiovascular system and the liver, and the context(s) for delivery of the interventions. There also possibility of physical trauma from loss of control- needs to be developed; approaches to screen for ecstasy during the ?ush” [130]. Those who inject ecstasy are use to aid in the ide~~cation of the target group for also at risk of vein damage and blood-borne viruses due delivery of brief interventions. to their injecting behaviour. These groups of ecstasy Potential settings for opportunistic identification of users therefore constitute targets for preventive ecstasy use include emergency departments of hospi- interventions. tals, subsequent to attendance for acute adverse effects;
In the absende of research into specific interventions support services at major events such as dance parties; for ecstasy users, the closest approximation is inter- and primary health are. Personnel working in these ventions for users of other psychostimulant drugs, i.e. settings need to be i ormed of the range of conditions, 4 cocaine, amphetamine and methamphetamine. Con- that have been assocqated with ecstasy use that might siderable research effort has been directed towards the lead to presentation1 at services, or that might be identification of effective pharmacotherapies for detectable at presentation. There is also potential for cocaine users. To date these efforts have. been largely brief interventions to be administered in law -enforce- unsuccessful and even if an effective pharmacotherapy ment settings, subsewent to being found in possession were found, any transfer to the treatment of ecstasy of an illicit drug, andjthrough computer-based applica- users is questionable because of the differing pharma- tions, given that the target group is likely to be high- cology of the drugs-cocaine acts- primarily through level internet users. dopamine [ 161 whereas MDMA acts primarily through serotonin. Hence pharmacotherapies for ecstasy users, Conclusions should be innovative and specific to the action of MDMA. Selective serotonin reuptake inhibitors Given the prevalenae of ecstasy use, the number of (SSIUs), if taken concurrently with MDM& have been pub;lished cases of adverse effects (we located 160) is shown to block the usual subjective effects of very small, Combined with the findings of the surveys MDMA [ 13 11. However, administration of SSRIs (e.g. of users [8,129,134],~~ this indicates that the incidence of fluoxetine, citalopram) subsequent to MDMA may serious acute adverse events arising from ecstasy use is
low. It is the unpredictability of those adverse events and the risk of mortality and substantial morbidity in’
tives in animals, z’n ptinu, cellular systems and humans..
young people that makes the health consequences of Increased understanding of the mechanisms and tox-
ecstasy significant. icity of these compoimds is critical if we are to respond
Hyperthermia and hyponarraemia are the most sig- to Changes in illicit :$rug markets and predict the likely. adverse effects in any given situation.
nificant, and potentially life-threatening, acute adverse effects associated with ecstasy use. Given that both appear to arise largely as a result of the setting of use Acknowledgements ., ,. and individual behaviour, they are good targets for secondary prevention initiatives. Obvious measures
Dr’Ian Seppelt (St &eorge Hospital, Sydney, Australia),
include the provision of free water and temperature ‘Dr Maristela Mo4tiero and Dr. Jennifer Hillebrand
control at venues, together with education to increase (World Health O@anization) and Dr Linda Chang
the knowledge of users, venue operators and support (Scientist and Chair, Medical Department, Brookhaven
staff, about the importance of controlling body tem- National Laboratqry, Upton, New York, USA) corn- -mented on aspects ‘of the literature review.
peratnre and fluid intake, how to recognize early signs of adverse effects and the importance of seeking medical assistance promptly. A number of countries ’ have developed guidelines for dance parties and nighr-
References ” ;
clubs that support this approach. [l] Wolff K, Hay +W, Sherlock K & ConnekM. Contents of
Testing of ecstasy tablets potentially has some value “ecstasy”. Lark et 1995;346:1100-1.
F in enabling users to avoid more toxic substances, such
: [2] Anonymous. l$stasy. MDA Info&x. National Institute on
as PMA, but most of the available tests simply indicate Drug Abuse, XBQQ. Available from: http:www.nida.nih.gov/
the presence of MDMA, and do not provide informa- Infofax/ecstasirhtml
[3] European M@toring Centre for Drugs and Drug Addic-
tion on the amount of MDMA in the tablet, or the tion. Annual &port on the stare of the drugs problem in the
presence of other substances. It is important thar users European U&a, Luxembourg: Office for Official Publica-
-are aware that use of MDMA by itself can result in adverse effects. Testing of tablets shonld therefore always be accompanied by secondary preventive education.
tions of the &ropean Communities, 1999. [llf Topp L, Haddo J, Degenhardt L, Dillon P; Roche A,
Solowij N. E#stasy use in Australia. NDARC monograph
Medical personnel need to be informed of the nature of adverse effects that may arise subsequent to ecstasy
no. 39. Sy&ey, Australia: National Drug and Alcohol Research Cerpxe, 1997.
[S] M&&in R,.$%rke S, Hayes A, Rmnbold G. Drug Trends 1998. A co&p&son of drug use and trends in three
: use. This would support the opportunistic identification
Australian S*tes; fmdings &om the Illicit Drug Reporting System (ID@). NDARC mouograph no, 41. Sydney,
of ecstasy use, as well as indicating ‘the pattern of Australia: I$tional Drug and Alcohol Research Centre,
monitoring of health status that is appropriate for 1999.
ecstasy users. [6] Sherlock JX, I Conner M. Patterns of ecstasy use amdngst
There remain many gaps and inadequacies in our club-goers qn rhe UK “dance scene”. Int J Drug Policy 1999;10:11’i’-29.
knowledge of the health effects of ecstasy. Systems of [7] Humeniuk @. South Australian Drug Trends 1999. Find- monitoring emergency room attendances should be in@ from *ihe Illicit Drug Repoting System. NDARC
considered as means of monitoring the prevalence of technical rq art no. 88. Sydney, Austiia: National D~xx~
adverse effects. Such systems can also help to ident@ and AicohO:
% Research Centre, 2000.
emerging problems. Controlled epidemiological studies [8] Handy C, ates R, Barrowcliff A. Drug use ‘in South
Wales: whb uses Ecstasy anyway? J Subst Misuse to establish the prevalence of harms, and to quantie the 1998;3:82+8. risks of ecstasy use are highly desirable., Given the [Q] Schifano it. Potential human neurotoxicisy .of MDMA
mounting evidence supporting the concept of Grain c(Ecstasy”$ subjective self-reports, evidence from an
damage associated with ecstasy use, it is also highly ’ btFa&n ,; g addiction centre and clinical case studies.
desirable that further studies are initiated t!o assess the “h Neuropsyc: obiology 2000;42:25-33.
.: [lo] Schuster I$ Lieb R, Lamertz C, Wittchen HU. Is the use of long-term, functional consequences of ecstasy use. At .ecstasy add hallucinogetis increasing? Results from a
this time the clinical implications of this tieurotoxicity communi@ study. Eur Addict Res 1998;4:75-82.
are uncertain, with the most common functional deficit [ 1 I] Topp L, Etfall W, Hando J. Is there a dependence syndrome
revealed so far being in, short-term memory. The for ecstasjri) NDARC ‘technical report no. 51. Sydney, Australia; j National Drug and Alcohol Research Centre,
question of whether ecstasy does produce dependence . : 1997. remains unansw&d. If the .answer is yes; it is then of [12] Jansen K$. Ecstasy (MDMA) dependence. Drug Alcohol
interest to determine whether the assessment of ecstasy Depend A999;53:121-4.
dependence is of diagnostic value.’ A final, important [13] Battaglia G, De Souza EB. Pharmacologic profile of
research direction is that of the pharmacology and’ ampheteine derivatives at various brain recognition sites: selective, j effects on serotonergic systems. NIDA Res
toxicology of MDMA and other amphetamine deriva- Mono&r i989;94:240-58.
T%e h%zM e$ecrs ofecstq 61
[14] Pierce PA, Peroutka SJ. Ring-substituted amphetamine i33] Coore JR. A fatal trip with ecstasy: a case of 3,4-methyle- inreractions with neurotransmitter receptor binding sites in nedioxymethamphetar&ne/3,4-methylenedioxyampheta- human cortex. Neurosci Lett 1988;95:208-12;
(151 Schloss I?, Williams DC. The serotonin transporter: a mine toxicity, J Roy Sot Med 1996;89:51P-52P.
[34] Bingham C, Beaman M, Nicholls AJ, Anthony PP. Necro- primary target for antidepressant drugs. J Psychopharma- tizing renal vasculopathy resulting in chronic renal failure co1 1998;12:115-21.
[ 16) Rawson RA. Treatment for stimulant use disorders. Treat- after ingestion of methamphetamine and 3,4-methylene- ~o~e~~phet~e (“ecstasy”). Nephrol Dial Trans-
ment improvement protocol (TIP) series no, 33. Rockville, plant 1998;13:2654-5. Maryland: US Department of Health and Human Ser- [35] Henry JA, Hill IR. Fatal interaction between ritonavir and vices, 1999. ~~. Lancet 1998!352:1751-2.
[173 Daws L, Irvine RJ, Callaghan PD, Toop PN, White JM, f36] McCann UD, &ulashvili V, Ricaurte GA, Bochner F. Differential behavioural and neurochemical ( + /-)3,4-Methyleneclioxymethamphetamine (“Ecstasy”)- effects of para-methoxyamphetamine and 3,4-methylene- induced serotonin nettrotoxicity: clinical studies. Neuro- dio~e~amphet~ine in the rat. Prog Neuropsycho-’ p~~obioIo~ 2000;4$:11-16. pharmacol Biol Psychiatry 2000;24:955-77, f37] Hatxidimitriou G, McCann UD, Ricaurte GA. Altered
[18] Malberg JP!, Seiden LS. Small changes in ambient tem- serotonin innervation patterns in the forebrain of monkeys peratnre cause large changes in 3,4-methylenedioxyme- treated with ( + I-)3,$-methylenedioxymethamphetamine ~ampheta~ne (MD~)-educed serotonin neurotox-‘ seven years previously: factors i~u~c~g abnormal recov- icity and core body temperature ln the rat. J Neurosci cry. J Neurosci 1999;119:5096-107. 1998;18:5086-94. E381 Boot. BP, McGregor IS, Hall W. MDMA (Rcstasy)
(191 Sternbach H,. The serotonin syndrome. Am J Psychiatry neurotoxicity: asses&g and communicating the risks. .1991;148:705-13. Lancet 2000;355:1818-21.
[20] Loscher W, Witte U, Fredow G, Ganter M, Bickhardt K. [39] McCann UD, Szabo 8, Scheffel U, Dannals RF, Ricaurte Pharmacodynamic effects of serotonin (5-HT) receptor GA. Positron emission tomographic evidence of toxic ligands in pigs: stimulation of 5-HT2 receptors induces effect of MDMA (ecstasy) on brain serotonin neurons in malignant hyperthermia. Naunyn-Schmeideberg’s Arch human beings. Lancet 1998;352:1433-7. Pharmacol 1990;341:483-93, (401 Semple DM, Ebmeier KP, Glabus MF, O’Carroll RE,
[21] Cohen RS. Subjective reports on the effects of the MDMA Johnstone EC. Reduced in &et0 binding to the serotonin (Ecstasy) experience in humans. frog Neuropsychophar- transporter in the cerebral cortex of MDMA (“ecstasy”) macol Biol Psychiatry 1995;19:1137-45. users. Br J Psychiatry 1999;175:63-9.
[22] Peroutka SJ, Newman H, Harris H. Subjective effects of [41] Obrocki J, Buchert I$ Vaterlein 0, Thomasius R, Beyer W, 3,4-me~ylenedio~e~amphetamine in recreational Schiemann T Ecstas
it -long-term effects on the human
users. Neuropsychopharmacology 1988; 1: 273-7. central nervous syst m revealed by positron emission [23] Vollenweider FX, Gamma A, Liechti M, Huber T Psycho- tomography. Br J Psychiatry 1999;175:186-8.
logical and cardiovascular effects and short-term sequelae [42] Chang L, Ernst T, C$rob CS, Poland RR. Cerebral (l)H of MDMA (ecstasy) in ~~-naive healthy volunteers. MRS alterations in recreational 3, 4-me~yl~edio~e- Neuropsychopharmacology 1998;19:241-51. ‘thamphetamine (MAMA, ecstasy) users. J Magn Reson
[24] Peroutka SJ. Recreational use of MDMA. Peroutka SJ, ed. Imaging 1999;10:52# -6. In: Ecstasy: the clinical, pharmacological and neurotoxico- [43] Chang L, Grab, CS,. !E rnst T, et al, Effect of ecstasy [3,4. logical effects of the drug MDh4A. Boston: Kluwer methylenedioxymeth~mphetamine (MDMA)] on cerebral Academic Publishers, 1990:53-62. blood flow: a co-registered SPECT and MRI study.
[25] Siegel RK. MDMA: nonmedical use and intoxication. J Psychiatr Res 2OO@Q@ : 15-28. Psychoact Drugs 1986;18:349-54, 1441 Reneman L, Habraken JB, Majoie CB, Booij J, den Heeten
l26] Mas M, Parre M, de la Torre R, et al, Cardiovascular and GJ. MDMA (ecstasy) and its association with cerebrovas- neuroendocrine effects and pharmacokinetics of cular accidents: preliminary findings. Am J Neuroradiol 3,4-me~yl~edio~e~amphetamine in humans. J Phar- 2~00;21:1001-7. macol Exp Ther 1999;290:136-45. 1451 .Xhfters RI, Duf& F3, O’Donnell PJ, Bouquet C. Levi?1 of
[27] Verebey K. The complications of “ecstasy” (MDMA), use of 3,4-methylenedioxymethamphetamine (MDMA or JAMA 1988;259:1649-50, Ecstasy) in humana correlates with ERG power and
[28] de la Torre R, FarreM, Ortuno J, et al. Non-linear coherence. Psy~o~harmacolo~ (Berlin) 19995145: pharmacokinetics of MDMA (“ecstasy”) in humans. Br J 82-90. Clm l?harmacol2000;49 :104-Q. [46] Gamma A, Frei E, Lehmann D, Pascual-Marqui RD, Hell
[29] Tucker GT, Lennard MS, Ellis SW, &t al. The demethyleni D, Vollenweider FX.I Mood state and brain electric activity ation of me~yl~edio~e~~pheta~e (ecstasy) by in ecstasy users. Neuroreport 2000;11:157-62. debrisoquine hydroxylase (CYP2D6). Biochem Pharma- [47] Kish SJ, Furukawa Y, Ang L, Vorce SP, Kalasinsky KS. co1 1994;47:1151-6. Striatal serotonin is depleted in brain of a human MDMA
[30] G’Donohoe A, O’Flynn K, Shields K, Hawi Z, Gill M. (Ecstasy), user. Neurology 2000;55:294-6. MDMA toxicity: no evidence for a major intluence of [48] Curran HV, Travlll ,RA. Mood and cognitive effects of metabolic genotype at CYP2D6. Addict Biol 1998;3: + l-3,4-methylenedioxymethamphetamine (ML>MA, 309-14. “ecstasy”): week-e@ “high” ‘followed by mid-week low.
[31]. Schwab M, Seyrlnger B, Brauer RR, Heliinger A, Griese Addiction 1997;92:$21-31. EU. Fatal MDMA intoxication. Lancet 1999;353: [49] Parrott AC Lasky J,. Ecstasy (MAMA) effects’upon mood 593-4. and cognition: befoqe, during and after a Saturday night
[32] ,Kreth K, Kovar K, Schwab M, Zanger UM, Ide~ti~cadon dance. Psychophar ,’ acology (Berlin) 1998;139:261-8. of the human cytochromes P450 involved in the oxidative [50] Klugman A, Hardy , BaldewegT, Gruxelier J. Toxic effect 3 metabolism of ecstasy-related designer drugs. Biochem of MDMA on brain serotonin neurons. Lancet Pharmacol,2000;59:1563-71. 1999;353:1269-70.
?
62 LMu R. Gawk. et al
[51] Morgan MJ. Recreational use of ecstasy (MDMA) is VII Henry JA, Jeffreys KJ, Dawling S, Toxicity and deaths from associated with elevated impulsivity. Neuropsychopharma- 3&methylene;~ioxymethamphetamine (“ecstasy”). Lancet cology 1998;19:252-64. 1992;340: 384-7.
[52] Parrott AC, Sisk E, Turner JJ, Psychobiological problems f711 Milroy CM, Clark JC, Forrest AR. Pathology of deaths in heavy “ecstasy” (MDMA) polydrug users, Drug Alcohol associated with ecstasy and “eve” misuse. J Clm Path01 Depend 2000;60:105-10. 1996;49:149-53.
[53] McCann UD, Ridenour A, Shaham Y, Ricaurte GA. 1721 Parr MJ, Low HM, Botterill I?. Hyponatraemia and Serotonin neurotoxicity after ( + /-)3,4-methylenedioxy- death after etstasy ingestion. Med J Aust 1997;166: me~amphetamine (MAMA; “Ectasy”): a controlled study 136-7. in humans. Neuropsychopharmacology 1994;10:129-38. [73] O’Connor A,,‘Cluroe A, Couch R, Galler L, Lawrence J,
[54] Bolla KI, McCann UD, Ricaurte GA. Memory impair- Synek B. Death from hyponatraemia-induced cerebral ment in abstinent MD&%A (ecstasy) users. Neurology oedema assodiated with MDMA (ecstasy) use. NZ Med J 1998;51:1532-37. 1999;112:25$-6.
[55] Morgan MJ. Memory deficits associated with recreational [74] Holden R, Japkson MA. Near-fatal hyponatraemic coma use of ecstasy (MDMA). Psychopharmacology (Berlin) due to 1999;141:30-6.
vasopressin over-secretion after ecstasy (3,4-MAMA). Lancet 1996;347:1052.
[56] McCann UD, MertlM, Eligulashvili V, Ricaurte GA. [75] White JM, B;ochner F, Irvine RJ. The -agony of ecstasy. Cognitive performance in ( +/-) 3,4-methylenedioxyme- Med JAust 1:997;166:117-18. thamphetamine (MDMA, ecstasy) users: a controlled [76] Henry JA, Fallon JK, J&man AT, Hutt AJ, Cowan DA, study, Psy~opharma~olo~ (Berlin) 1999;143:417-25. Forsling M. Low-dose MDMA (ecstasy) induces vasopres-
[57] Renefnan L, Booij J, Schmand B, van den Brink W, sin secretion, Lancet 1998;35 1:1784. Gunning B. Memory disturbances in ecstasy users are [77] Gomez-Balaguer M, Pena H, Morillas C, Hernandez A. correlated with an altered brain serotonin neurotransmis- Syndrome ofiinappropriate antidiuretic hormone secretion sion. Psychopharmacology (Berlin) 2000;148:,322-4. and “design+ drugs” (ecstasy). J Pediatr Bndocrinol
[SS] Wareing M, Fisk JB, Murphy PN. Working memory deficits Metab 2000+3:437-S. in current and previous users of MDMA (“cstasy”). Br J [78] Hegadoren &M-Baker GB, Bourin M. 3,4-Methylene- Psycho1 2000;91:181-8. dioxy analogues of amphetamine: defining the risks to
[59] Gouzoulis-Mayfrank E, Daumann J,?txchtenhagen F, et ai, humans. Neurosci Biobehav Rev 1999;23:539-553. Impaired cognitive performance in drug free users of 1791 Cimbura d: PMA deaths in Ontario. Can Med Assoc J recreational ecstasy (MDMA). J Neurol Neurosurg Psy- 1974;110:1263-7. chiatry 2000;68:719-25. [80] Sawyer J, , Stephens WP. Misuse of ecstasy. BMJ
[60] Rodgers J. Cognitive performance amongst recreational 1992;305:3$0, users of ecstasy. Psychopharmacology (Berlin) 2000; 151: [81] Watson JD, ‘Ferguson C, Hinds CJ, Skinner R, Coakley JH. 19-24. Exertional heat stroke induced by amphetamine analogues.
[61] Colado Ml, O’Shea E, Granados R, Murray TK, Green Does dantrolene have a place? Anaesthesia 1993;48: AR. Is viw evidence for free radical involvement in the 105’7-60. degeneration of rat brain 5-HT following administration of [82] Byard RW,&ilbert J, James R, Lokan RJ. Amphetamine MDMA (“ecstasy”) and p-chloroamphetamine but not the derivative qatalities in South Australia-is ecstasy the degeneration following fenfluramine. Br J Pharmacol culprit? Au&J Forensic Med Path01 1998;19:261-5. 1997;121:889-900. [83] Carter N, Rutty GN, Milroy CM, Forrest AR. Deaths
[62] Aguirre N, BarrionuevoM, Ramirez MJ, De1 Rio J, associated “with MBDB misuse. Int J Legal Med Lasheras B. Alpha-lipoic acid prevents 3,4-methylene- 2000;113:168-70. dio~-me~ampheta~ne (MDMA)-induced neurotoxic- [84] Suarex R\f Riemersma R. Ecstasy and sudden cardiac ity. Neuroreport 1999;10:3675-80. death. Am J Forensic Med Path01 1988;9:339-41.
[63] Sprague JB, Everman SL, Nichols DE. An integrated [85] Lora-Tamayo C, Tena T, Rodriguez A. Amphetamine hypothesis for the serotonergic axonal loss induced by derivative related deaths. Forensic Sci Int 1997;85: 3,4-me~yl~edio~e~ampheta~e. Neurotoxicology 149-57. 1998;19:427-41. [86] Hanyu S, Ikegucbi K, Imai. H, Imai N, Yoshida M,
[64] Gerra G, Zaimovic A, Ferri M, et al. Long-lasting effects of Cerebral ,nfarction associated with 3,4-methylenediox- ( + /-)3,4~me~ylenedio~e~amphetam~e (ecstasy) on ymethamphetamine (“Ecstasy”) abuse. Eur Neural serotonin system function in humans. Biol Psychiatry 1995;35:123. 2000;47: 127-36. [87] Gledhill J+, Moore DF, Bell D, Henry JA. Subarachnoid
1651 Bedford Russell AR, Schwartz RH, Dawling S. Accidental haemorrhage associated with MDMA abuse. J Neurol ingestion of “Ecstasy” (3,4-methylenedioxymethylamphe- Neurosurg Psychiatry 1993;56:1036-7. tarnine), Arch Dis Child 1992;67:1114-15. [88] Hughes J& McCabeM, Evans RJ. Intracranial haemor-
[66] Cooper A, Egleston CV. Accidental ingestion of Ecstasy by, rhage asa#ciated with ingestion of “ecstasy”. Arch Emerg a toddler: unusual cause for convulsion in a febrile child. J Med 199$;10:372-4. Accid Emerg Med 1997;14:183-4. [89] Jacks AS; Hykin PG. Retinal haemorrhage caused by
[67] Walubo A, Seger D, Fatal multi-organ failure after suicidal ecstasy. Br J Ophthalmol 1998;82:842-3. overdose with MDMA, “ecstasy”: case report and review [QO] McEvoy AW, Kitchen ND, Thomas DG. Intracerebral of the literature. Hum Exp Toxic01 1999;18:119-25. haemorrhage caused by drug abuse. Lancet 1998;
[68] Green AR* Cross AJ, Goodwin GM. Review of the 351:1029i. pharmacology and clinical pharmacology of 3,4-methyle- [Ql] Harries ‘bP, de Silva R. “Ecstasy” and intracerebral nedioxymethamphetamine (MDMA or “Ecstasy”). Psy- haemorrhage. Scott Med J 1992;37:150-2. chopharmacology (Berlin) 1995;119:247-60. [92] Dowling GP, McDonough ET, Bost RO. “Bve” and
[69] Henry JA. Ecstasy and the dance of death. BMJ “Bcstasy’~: a report of five deaths associated with the use of 1992;305:5-6. MDEA and MDMA. JAMA 1987;257:1615-17.
The health effects of ecstasy 63
[93] Forrest AR, Galloway JH, Marsh ID, Strachan GA, Clark JC. A fatal overdose with 3,4-methylenedioxyamphetamine derivatives. Forensic Sci Int 1994;64: 57-9.
[94] Weinmann W, Bohnert M. Lethal monointoxication by overdosage of MDEA. Forensic Sci Int 1998;91:91-101.
[95] Dowling GI? Human deaths and toxic reactions attributed to MDMA and MDEA. In: Peroutka SJ, ed. Ecstasy: the clinical, pharmacological and neurotoxicological effects of the drug MDMA. Boston: Kluwer Academic Publishers, 1990:63-75.
[96] Cadier MA, Clarke JA. Ecstasy and Whizz at a rave resulting in a major burn plus complications. Burns 1993;19:239-40.
[97] Davies JP, Evans RO, Newington DP Ecstasy related trauma. J Accid Emerg Med 1998;15:436.
[98] Levine AJ, Drew S, Rees GM. “Ecstasy” induced pneumo- mediastinum. J Roy Sot Med 1993;86:232-3.
[99] Onwudike M. Ecstasy induced retropharyngeal emphy- sema. J Accid Emerg Med 1996;13:359-61.
[loo] Rezvani K, Kurbaan AS, Brenton D. Ecstasy induced pneumomediastinum. Thorax 1996;5 1:960-l.
[loll Pittman JA, Pounsford JC. Spontaneous pneumomediasti- num and Ecstasy abuse. J Accid Emerg Med 1997;14:335-6.
[102] Ahmed JM, Salame MY, Oakley GD. Chest pain in a young girl. Postgrad Med J 1998;74:115-16.
[103] Rittoo D, Rittoo DB. Misuse of ecstasy. BMJ 1992;305:309-10.
[ 1041 O’Neill D, Dart JK. Methylenedioxyamphetamine (“Ecstasy”) associated keratopathy. Eye 1993;7:805-6.
[105] Milosevic A, Agrawal N, Redfearn P, Mair L. The occurrence of toothwear in users of Ecstasy (3,4-methyle- nedioxymethamphetamine). Community Dent Oral Epi- demiol 1999;27:283-7.
[106] McElhatton PR, Bateman DN, Evans C, Pughe KR, Thomas SH. Congenital anomalies after prenatal ecstasy exposure. Lancet 1999;54:1441-2.
[107] Hall Al? Ecstasy and the anaesthetist. Br J Anaesth 1997;79:697-8.
[108] Denborough MA, Hopkinson KC. Dantrolene and ecstasy. Med JAust 1997;166:165-6.
[log] O’Connor B. Hazards associated with the recreational drug Ecstasy. Br J Hosp Med 1994;52):507-14.
[l lo] Tehan B, Hardern R, Bodenham A. Hyperthermia asso- ciated with 3,4-methylenedioxyethamphetamine (“Eve”). Anaesthesia 1993;48:507-10.
[ill] Selim K, Kaplowitz N. Hepatotoxicity of psychotropic drugs. Hepatology 1999;29:1347-51.
[112] Andreu V, Mas A, BrugueraM, et ~2. Ecstasy: a common cause of severe acute hepatotoxicity. J Hepatol 1998;29:394-7.
[113] Jones AL, Simpson KJ. Review article: mechanisms and management of hepatotoxlclty in ecstasy (MDMA) and amphetamine intoxications. Aliment Pharmacol Ther 1999;13:129-33.
[ 1141 Ellis AJ, Wendon JA, Porunann B, Williams R. Acute liver damage and ecstasy ingestion. Gut 1996;38:454-8.
[115] Fidler H, Dhillon A, Gertner D, Burroughs A. Chronic ecstasy (3,4methylenedioxymetamphetamine) abuse: a recurrent and unpredictable cause of severe acute hepatitis.
J Hepatol 1996;25:563-6. [116] Khakoo SI, Coles CJ, Armstrong JS, Barry RE. Hep-
atotoxicity and accelerated fibrosis following 3,4-methyle- nedioxymethamphetamine (ecstasy) usage. J Clin Gastro- enter01 1995;20:244+7.
[117] Curran HV. Is MDM@ (“Ecstasy”) neurotoxic in humans? An overview of evidence and of methodological problems in research. Neuropsychobiology 2000;42:34-41.
[118] Schifano F, Di Furia L, Forza G, Minicuci N, Bricolo R. MDMA (“ecstasy”) consumption in the context of poly- drug abuse: a report on 150 patients. Drug Alcohol Depend 1998;52:85+90.
[119] Cohen RS, Cocores ‘J. Neuropsychiatric manifestations following the use of 3;4-methylenedioxymethamphetamine (MDMA: ecstasy). Prog Neuropsychopharmacol Biol Psychiatry 1997;21:727-34.
[120] Benazzi F, Mazzoli M. Psychiatric illness associated with ecstasy. Lancet 1991;538:1520.
[121] Pallanti S, Mazzi D. MDMA (Ecstasy) precipitation of panic disorder. Biol Psychiatry 1992;32 : 9 l-5,
[ 1221 Williams H, Dratcu L, Taylor R, Roberts M, Oyefeso A. “Saturday night fever”: ecstasy related problems in a London accident and emergency department. J Accid Bmerg Med 1998;15:$22-6.
[ 1231 Hardern R, Tehan B. Ecstasy toxicity. J Accid Emerg Med 1995;12:74.
[124] Murthy BV, Wilkes RG, Roberts NB. Creatine kinase isoform changes following Ecstasy overdose. Anaesth Intensive Care 1997;25:156-9.
[125] Henry JA. Metabolic consequences of drug misuse. Br J Anaesth 2000;85:136-42.
[126] Tehan B. Ecstasy and~,dantrolene. BMJ 1993;306:146. [127] Alciati A, Scaramelli B, Fusi A, Butteri E, Cattaneo ML,
Mellado C. Three cases of delirium after ecstasy ingestion.
[128] J Psychoactive Drugs ~1999;3 1: 167-70. Chenard-Neu MP, Boudjema K, Bernuau J, et al. Auxiliary liver transplantation: regeneration of the native liver and outcome in 30 patients with fulminant hepatic failure-a multicenter Europe$n study. Hepatology 1996;23: 1119-27.
[129] Topp L, Hando J, Dillon P, Roche A, Solowij N. Ecstasy use in Australia: patterns of use and associated harm. Drug Alcohol Depend 1999?55:105-15.
[130] Hum N, Jones K, Shelley H. What happens when ecstasy is injected? Int J Drug Policy 1993;4:161-2.
[131] Stein DJ, Rink J. Effects of ecstasy blocked by serotonin reuptake inhibitors. J Clin Psychiatry 1999;60:485.
[ 1321 Kamieniecki G, Vincent N, Allsop S, tintzeris N. Models of intervention and care for psychostimulant users. National Drug Strategy monograph series no. 32. Can- berra, Australia: Corn onwealth Department of Health
$ and Family Services, 1 98. [133] Barry KL. Brief interventions and brief therapies for
substance abuse. Treatment Improvement Protocol (TIP) series no. 34, Rockville, Maryland: US Department of Health and Human Services, 1999.
[ 1341 Williamson S, Gossop M, Powis B, oriffiths P, Fountain J, Strang J, Adverse effects of stimulant drugs in a commu- nity sample of drug users. Drug Alcohol Depend 1997;44:87-94.