the effect of psychomotor physical therapy on subjective health complaints and psychological...
TRANSCRIPT
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
RESEARCH ARTICLE
The Effect of Psychomotor Physical Therapy on Subjective Health Complaints and Psychological SymptomsMonica H. Breitve1*, Minna J. Hynninen2 & Alice Kvåle3
1Haugesund Hospital, Department of Psychological Health Care, Haugesund, Norway2Faculty of Psychology, University of Bergen, Norway3Section for Physiotherapy Science, Department of Public Health and Primary Health Care, University of Bergen, Norway
Abstract
Background and Purpose. The objective of this study was to examine the effect of Norwegian psychomotor physi-
cal therapy on subjective health complaints and psychological symptoms. Method. A non-randomized waiting list
controlled design was used. Physiotherapists in Norway recruited patients for a treatment group (n = 40) and
waiting list control group (n = 22). Patients on the waiting list could only be included for 6 months, as they then
started treatment. Symptoms registration was obtained from both groups at baseline and 6 months, and only for
the treatment group also at 12 months. The following self-report forms were used; Subjective Health Complaints
Inventory (SCH); Beck Depression Inventory-II (BDI-II); Spielberger State-Trait Anxiety Inventory-Trait (STAI-
T); Bergen Insomnia Scale (BIS); Fatigue Questionnaire (FQ); Quality of Life Inventory (QOLI); The Client Satis-
faction Questionnaire (CSQ). Results. The patients had had widespread and clinically signifi cant health problems
for an average of 9 years upon entrance to the study. After 6 months in psychomotor physical therapy, all the
measured symptoms in the treatment group were signifi cantly reduced, but only quality of life was signifi cantly
reduced when compared to the waiting list control group. After 12 months in therapy, the patients in the treatment
group had continued to improve on all measured variables. The symptoms of anxiety and depression, as well as
quality of life, were improved from clinical to non-clinical level. Conclusions. Norwegian psychomotor physical
therapy seems to have potential for reducing symptoms of subjective health complaints, depression, anxiety, insom-
nia, fatigue and improving quality of life, although the process takes time. Further research is needed to gain more
rigorous data, and randomized controlled studies are highly welcomed. Copyright © 2010 John Wiley & Sons, Ltd.
Received 19 June 2009; Revised 13 October 2009; Accepted 5 January 2010
Keywords
Body awareness; Mental health; Musculoskeletal disorders; Quantitative research; Outcome measurement
*Correspondence
Monica H Breitve, Haugesund Hospital, Department of Psychological Health Care, Pb 2170, Haugesund, Norway, 5504.
Email: [email protected]
Published online in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/pri.462
most frequent reasons for repeated visits to a general
practitioner (Karlsson et al., 1997; Khan et al., 2003).
Medical examination, tests and referrals to specialists
reveal an organic basis for less than 20% of cases
(Kroenke and Mangelsdorff, 1989). Not surprisingly,
Introduction
Vague, diffi cult-to-diagnose complaints, such as
chronic muscular pain, sleep problems, fatigue, head-
ache, and unspecifi c gastrointestinal problems, are the
Effect of psychomotor physical therapy M. H. Breitve et al.
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
health workers tend to think that patients with such
unexplained and long-lasting symptoms are diffi cult to
help (Sharpe et al., 1994). Patients are often dissatisfi ed
with the care (Deyo, 1998) and many have suffered
for several years without adequate treatment. As a
consequence, they may seek assistance from non-
professionals in the fl ourishing health market (Eriksen
and Ursin, 2004).
Eriksen and Ursin (2002) have suggested using the
term ‘subjective health complaints’ (SHC) rather than
‘unexplained symptoms’, as the term is neutral, does
not offer any diagnosis or clues to causality, and avoids
the assumption of disease. Although the complaints are
not accompanied by what is traditionally considered as
objective fi ndings (generally defi ned as radiological
fi ndings or aberrations in laboratory analyses), they are,
however, a real phenomenon and concern for the
patient, with major impacts on both an individual’s
quality of life and health care costs for the society.
Genetics, biological sensitization and psychosocial
factors are likely to play a role in the etiopathogenesis
of SHC, and their degree of impact may differ between
individuals and within groups of people (Wilhelmsen,
2005). Furthermore, aberrations in posture, respira-
tion, movements and muscles, are common. Lack of
fl exibility, increased muscle tension and a restricted
respiration are found in these patients, signifi cantly dif-
ferent from fi ndings in healthy people (Kvåle et al.,
2005). Unexplained somatic symptoms have been
strongly and consistently linked to psychological dis-
tress, in particular anxiety and depression (Simon et al.,
1996). However, viewing such symptoms as ‘psychiat-
ric’ may complicate the interactions between health
workers and patients, as patients may resent ‘all in your
head’ assumptions (Bakal et al., 2006).
Norwegian Psychomotor Physical Therapy (NPPT)
belongs to the realm of so called ‘Body and Mind’ or
‘Body Awareness’ therapies (Kvåle and Ljunggren,
2007). In Norway, the NPPT has been an established
treatment form for almost 50 years, and is commonly
applied for patients with long-lasting pain and psycho-
logical symptoms. General practitioners refer patients
to NPPT for health complaints such as fi bromyalgia,
widespread pain, anxiety or depression, and patients
themselves typically present with more comprehensive
and diffuse complaints (Kamps and Arnesen, 2004).
The majority of patients are women, and their
health problems have often lasted over several years
(Aabakken et al., 1991; Breitve et al., 2008), which
seems to suggest that the approach commonly is uti-
lized as a ‘last resort’, for ‘diffi cult’ patients or when
nothing else seems to work.
In NPPT, as in other body awareness therapies,
patients’ symptom experiences are validated at the
physiological level, even when what is traditionally
defi ned as objective fi ndings are lacking (Kvåle and
Ljunggren, 2007). The body is emphasized as a source
of information and a mediator of previous experiences,
trauma, stress, personality and emotions, and the
patient is invited to a collaborative exploration of what
the bodily symptoms are trying to convey (Øien et al.,
2009). The NPPT is process-oriented and the aim of
treatment is to facilitate change of the affected func-
tions through movement exercises and massage. The
movement exercises generally consist of body aware-
ness through grounding exercises, as well as relaxation
training (Thornquist and Bunkan 1991; Øien et al.
2007). Case descriptions and qualitative studies of
NPPT support the plausibility of the approach for pro-
viding common ground and treatment rational for the
patient and therapist, and describe how creating order
out of chaos also contributes to patients’ ability to self-
soothing and symptom reduction (Ekerholt and
Bergland, 2004; Øien et al., 2009). However, outcome
studies utilizing established measures are lacking.
In the current study, we wanted to examine the effect
of NPPT on subjective health complaints and psycho-
logical symptoms in a heterogenic sample of patients.
In addition to pain, patients with diffuse complaints
also commonly report fatigue and sleep diffi culties
(Malmgren-Olsson and Armelius, 2003), and their
quality of life is likely to suffer (Råheim and Håland,
2006). Therefore, measures of fatigue, sleep and quality
of life were also included as outcome variables.
Method
Design
A non-randomized, non-blinded waiting list controlled
design was used.
Subjects
Participants were recruited by 26 physiotherapists spe-
cialized in NPPT, working in private practice or in a
hospital. To be eligible for inclusion, the participants
were to be 18 years or older, and referred to NPPT by
a general practitioner. For the waiting list group,
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
M. H. Breitve et al. Effect of psychomotor physical therapy
current psychomotor treatment was an exclusion
criterion.
Procedure
For treatment group, patients were recruited during the
fi rst treatment session. Those who agreed to participate
completed baseline assessments during or immediately
after the fi rst session. As long waiting lists for NPPT
are common, physiotherapists contacted waiting list
patients by mail or by telephone and invited them into
the study. These patients completed baseline assess-
ments and returned it by mail. Participants in the
waiting list did not receive any treatment within the
framework of the study. Both groups were followed at
6 months. The treatment group was also followed at 12
months, as NPPT is a process-oriented therapy that
generally is assumed to require longer than 6 months.
However, the waiting lists are seldom more than 6
months, and therefore, in the framework of our natu-
ralistic study, the waiting list patients could not be fol-
lowed as controls for longer. Both follow-up assessments
were conducted by mail.
Norwegian psychomotor physical therapy (NPPT)
The NPPT is based on the assumption that patients
with long-lasting problems, physical and/or psycho-
logical, may react with general aberrations related to
posture, respiration, and movements, as well as with
muscular tension and skin changes (Kvåle and
Ljunggren, 2007). Breathing and feelings are looked
upon as interdependent factors, and the primary differ-
ence between the psychomotor examination and that
of so-called traditional physiotherapy is the emphasis
on respiration and body awareness (Ekerholt and Ber-
gland, 2004). There is no standardized procedure for
the treatment, and thus, the NPPT therapist utilize
various treatment components within the theoretical
framework of the approach, based on their clinical
understanding of the patient. During the treatment,
techniques such as relaxation, massage and active exer-
cises are used for normalizing respiration and muscular
control and helping the patient to become aware of how
the body and mind interact (Bunkan, 2001).
Instruments
Based on fi ndings from previous qualitative studies and
studies using non-validated questionnaires, we chose
established and validated assessment instruments
with sound psychometric properties, covering a wide
spectrum of health complaints. All participants in the
treatment group were asked to fi ll out the self-report
measures at baseline, and at 6- and 12-month follow-
ups. All participants in the waiting list group were asked
to complete the assessment measures at baseline and at
the 6-month follow-up.
Subjective health complaints inventory (SHC) (Eriksen et al., 1999)
SHC measures duration and severity of 29 subjective
somatic and psychological complaints. In addition to a
total score, SHC has fi ve subscales; musculoskeletal
pain, pseudoneurology, gastrointestinal problems,
allergy and fl u.
Beck depression inventory-II (BDI-II) (Beck et al., 1996)
Depression was measured with the BDI-II, which
comprises 21 items. A cut-off score for clinically signifi -
cant depression has been defi ned as 14 or higher (Seggar
et al., 2002).
Spielberger state-trait anxiety inventory-trait (STAI-T) (Spielberger et al., 1983)
The STAI-T was used to measure the tendency for
anxiety. An empirically based cut-off score of 46 has
been defi ned to differentiate between functional and
dysfunctional populations (Fisher and Durham, 1999).
The scale is one of the most frequently used measures
of anxiety in applied clinical research.
Bergen insomnia scale (BIS) (Pallesen et al., 2008)
Sleep disturbances were measured with the BIS,
which contains six items that correspond to the diag-
nostic criteria for insomnia in DSM-IV-TR (American
Psychiatric Association, 2000). BIS provides a total
score on a continuous scale and a categorical score
for the presence of insomnia.
Fatigue questionnaire (FQ) (Chalder et al., 1993)
Fatigue was measured with the FQ. On the basis of
a validation study (Chalder et al., 1993), a categorical
score can be calculated that indicates the presence of

Effect of psychomotor physical therapy M. H. Breitve et al.
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
clinically signifi cant fatigue (sum of dichotomized item
scores >4 and duration >6 months).
Quality of life inventory (QOLI) (Frisch, 1994)
QOLI measures quality of life and satisfaction in 16
domains. Satisfaction in different domains is weighted
by their relative importance for the individual. A score
below 1.6 is estimated to indicate low quality of life.
The client satisfaction questionnaire (CSQ)(Larsen et al., 1979)
Satisfaction with the NPPT treatment was measured
with the CSQ. The scale comprises eight items, and
higher scores indicate more satisfaction.
Statistical analysis
Data were analyzed using SPSS version 14.0 (SPSS Inc,
Chicago, III). Independent samples t-tests and
Pearson’s X2 tests were used to examine demographic
and clinical variables at baseline. A 2 × 2 (time × group)
analysis of covariance was used to investigate differ-
ences between the groups in terms of change from base-
line to 6-month follow-up on the outcome variables,
adjusting for pre-test values. Paired-samples t-tests
were used to compare baseline values with 6-month
follow-up levels, and 6-month values with 12-month
follow-up levels in the treatment group. Within-group
effect sizes were calculated with the Cohen d formula
(Cohen, 1988). An effect size of 0.2 is considered small,
0.5 medium, and 0.8 represent a large effect size.
P-value < 0.05 was regarded as statistically signifi cant.
Ethics
The study was approved by the Regional Committee for
Medical Research Ethics in western Norway (REK
Vest), and by the Norwegian Social Science Data Ser-
vices (NSD). Written informed consent was obtained
from all participants in this study. It was emphasized
that participation is voluntary, and a refusal to partici-
pate or a withdrawal from the study later on would not
have any consequences for treatment. Participation was
not economically rewarded.
Results
Baseline
Sixty-two of the 65 participants originally enrolled in
the study completed baseline assessments (Figure 1
shows participant fl ow in the study). At baseline, there
were no signifi cant differences between the treatment
Figure 1 Participant fl ow in the study
26 physiotherapists recruited patients
Treatment group41 agreed to participate40 completed baseline
assessments
Waiting list 24 agreed to participate22 completed baseline
assessments
Six months35 completed assessments
4 dropped out from treatment
1 could not be contacted
Six months17 completed assessments
4 had started in treatment1 dropped out from the
study due to illness
Twelve months23 completed assessments
8 dropped out from the study- 4 had finished treatment- 4 continued treatment
4 could not be contacted
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
M. H. Breitve et al. Effect of psychomotor physical therapy
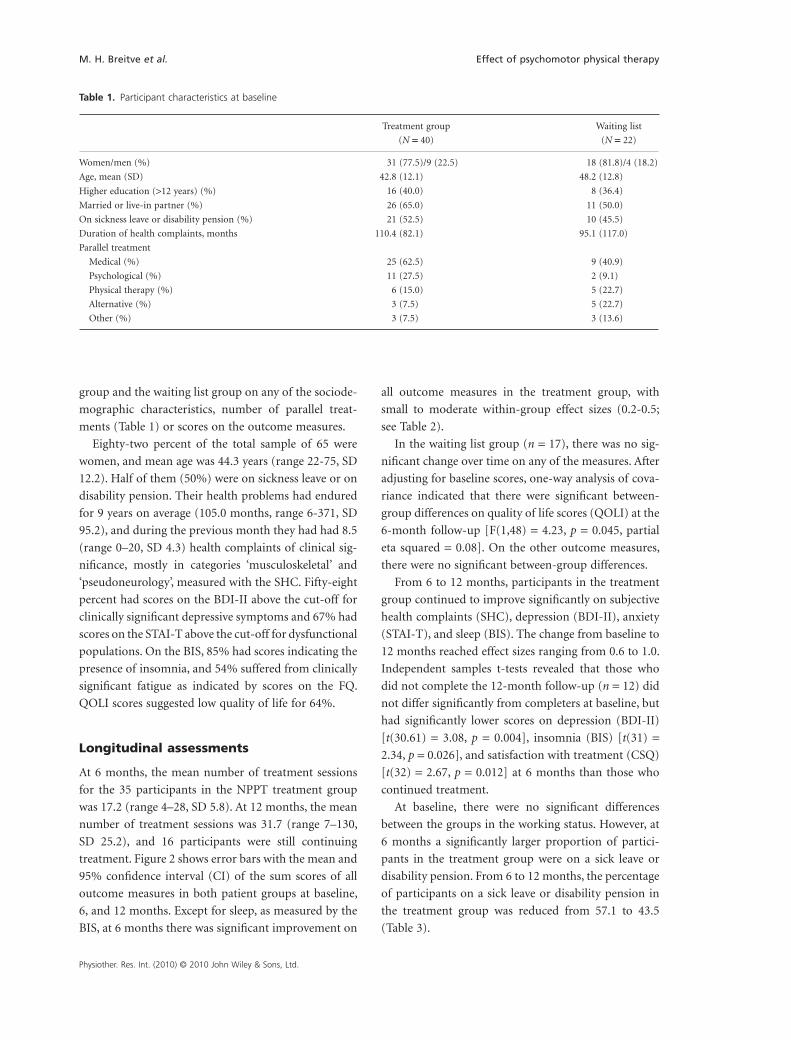
group and the waiting list group on any of the sociode-
mographic characteristics, number of parallel treat-
ments (Table 1) or scores on the outcome measures.
Eighty-two percent of the total sample of 65 were
women, and mean age was 44.3 years (range 22-75, SD
12.2). Half of them (50%) were on sickness leave or on
disability pension. Their health problems had endured
for 9 years on average (105.0 months, range 6-371, SD
95.2), and during the previous month they had had 8.5
(range 0–20, SD 4.3) health complaints of clinical sig-
nifi cance, mostly in categories ‘musculoskeletal’ and
‘pseudoneurology’, measured with the SHC. Fifty-eight
percent had scores on the BDI-II above the cut-off for
clinically signifi cant depressive symptoms and 67% had
scores on the STAI-T above the cut-off for dysfunctional
populations. On the BIS, 85% had scores indicating the
presence of insomnia, and 54% suffered from clinically
signifi cant fatigue as indicated by scores on the FQ.
QOLI scores suggested low quality of life for 64%.
Longitudinal assessments
At 6 months, the mean number of treatment sessions
for the 35 participants in the NPPT treatment group
was 17.2 (range 4–28, SD 5.8). At 12 months, the mean
number of treatment sessions was 31.7 (range 7–130,
SD 25.2), and 16 participants were still continuing
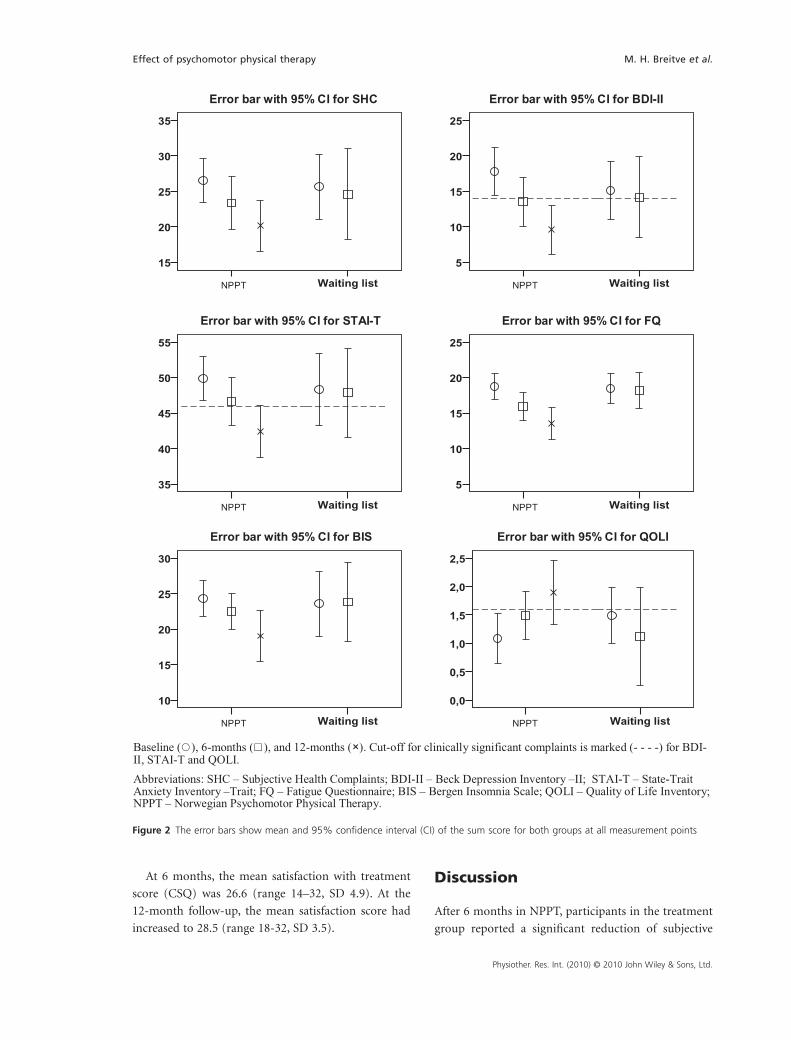
treatment. Figure 2 shows error bars with the mean and
95% confi dence interval (CI) of the sum scores of all
outcome measures in both patient groups at baseline,
6, and 12 months. Except for sleep, as measured by the
BIS, at 6 months there was signifi cant improvement on
all outcome measures in the treatment group, with
small to moderate within-group effect sizes (0.2-0.5;
see Table 2).
In the waiting list group (n = 17), there was no sig-
nifi cant change over time on any of the measures. After
adjusting for baseline scores, one-way analysis of cova-
riance indicated that there were signifi cant between-
group differences on quality of life scores (QOLI) at the
6-month follow-up [F(1,48) = 4.23, p = 0.045, partial
eta squared = 0.08]. On the other outcome measures,
there were no signifi cant between-group differences.
From 6 to 12 months, participants in the treatment
group continued to improve signifi cantly on subjective
health complaints (SHC), depression (BDI-II), anxiety
(STAI-T), and sleep (BIS). The change from baseline to
12 months reached effect sizes ranging from 0.6 to 1.0.
Independent samples t-tests revealed that those who
did not complete the 12-month follow-up (n = 12) did
not differ signifi cantly from completers at baseline, but
had signifi cantly lower scores on depression (BDI-II)
[t(30.61) = 3.08, p = 0.004], insomnia (BIS) [t(31) =
2.34, p = 0.026], and satisfaction with treatment (CSQ)
[t(32) = 2.67, p = 0.012] at 6 months than those who
continued treatment.
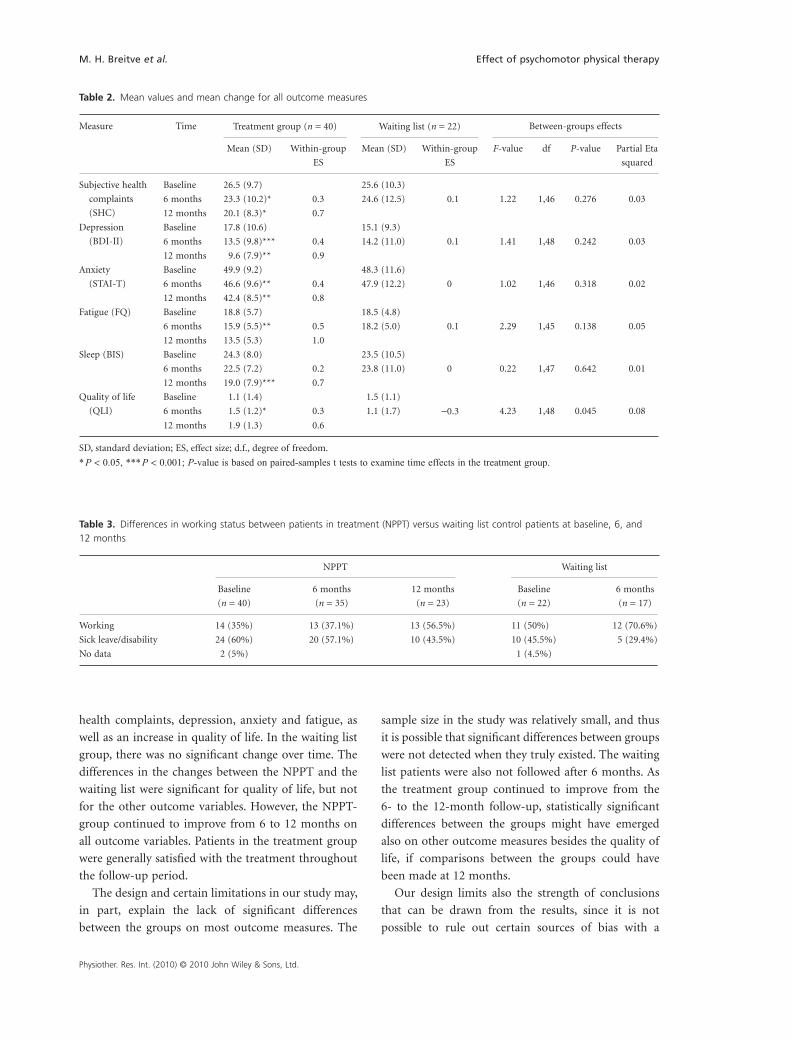
At baseline, there were no signifi cant differences
between the groups in the working status. However, at
6 months a signifi cantly larger proportion of partici-
pants in the treatment group were on a sick leave or
disability pension. From 6 to 12 months, the percentage
of participants on a sick leave or disability pension in
the treatment group was reduced from 57.1 to 43.5
(Table 3).
Table 1. Participant characteristics at baseline
Treatment group
(N = 40)
Waiting list
(N = 22)
Women/men (%) 31 (77.5)/9 (22.5) 18 (81.8)/4 (18.2)
Age, mean (SD) 42.8 (12.1) 48.2 (12.8)
Higher education (>12 years) (%) 16 (40.0) 8 (36.4)
Married or live-in partner (%) 26 (65.0) 11 (50.0)
On sickness leave or disability pension (%) 21 (52.5) 10 (45.5)
Duration of health complaints, months 110.4 (82.1) 95.1 (117.0)
Parallel treatment
Medical (%) 25 (62.5) 9 (40.9)
Psychological (%) 11 (27.5) 2 (9.1)
Physical therapy (%) 6 (15.0) 5 (22.7)
Alternative (%) 3 (7.5) 5 (22.7)
Other (%) 3 (7.5) 3 (13.6)
Effect of psychomotor physical therapy M. H. Breitve et al.
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
At 6 months, the mean satisfaction with treatment
score (CSQ) was 26.6 (range 14–32, SD 4.9). At the
12-month follow-up, the mean satisfaction score had
increased to 28.5 (range 18-32, SD 3.5).
Discussion
After 6 months in NPPT, participants in the treatment
group reported a signifi cant reduction of subjective
II-IDB rof IC %59htiw rabrorrECHS rof IC %59htiw rabrorrE
Error bar with 95% CI for STAI-T Error bar with 95% CI for FQ
Error bar with 95% CI for BIS
Waiting list
35
30
25
20
15
Waiting list
25
20
15
10
5
Waiting list
55
50
45
40
35
Waiting list
25
20
15
10
5
Waiting list
30
25
20
15
10
Waiting list
2,5
2,0
1,5
1,0
0,5
0,0
Error bar with 95% CI for QOLI
Baseline (�), 6-months (�), and 12-months (×). Cut-off for clinically significant complaints is marked (- - - -) for BDI-II, STAI-T and QOLI.
Abbreviations: SHC – Subjective Health Complaints; BDI-II – Beck Depression Inventory –II; STAI-T – State-TraitAnxiety Inventory –Trait; FQ – Fatigue Questionnaire; BIS – Bergen Insomnia Scale; QOLI – Quality of Life Inventory; NPPT – Norwegian Psychomotor Physical Therapy.
_ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _
_ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _
NPPT NPPT
NPPT NPPT
NPPT NPPT
Figure 2 The error bars show mean and 95% confi dence interval (CI) of the sum score for both groups at all measurement points
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
M. H. Breitve et al. Effect of psychomotor physical therapy
health complaints, depression, anxiety and fatigue, as
well as an increase in quality of life. In the waiting list
group, there was no signifi cant change over time. The
differences in the changes between the NPPT and the
waiting list were signifi cant for quality of life, but not
for the other outcome variables. However, the NPPT-
group continued to improve from 6 to 12 months on
all outcome variables. Patients in the treatment group
were generally satisfi ed with the treatment throughout
the follow-up period.
The design and certain limitations in our study may,
in part, explain the lack of signifi cant differences
between the groups on most outcome measures. The
sample size in the study was relatively small, and thus
it is possible that signifi cant differences between groups
were not detected when they truly existed. The waiting
list patients were also not followed after 6 months. As
the treatment group continued to improve from the
6- to the 12-month follow-up, statistically signifi cant
differences between the groups might have emerged
also on other outcome measures besides the quality of
life, if comparisons between the groups could have
been made at 12 months.
Our design limits also the strength of conclusions
that can be drawn from the results, since it is not
possible to rule out certain sources of bias with a
Table 2. Mean values and mean change for all outcome measures
Measure Time Treatment group (n = 40) Waiting list (n = 22) Between-groups effects
Mean (SD) Within-group
ES
Mean (SD) Within-group
ES
F-value df P-value Partial Eta
squared
Subjective health
complaints
(SHC)
Baseline 26.5 (9.7) 25.6 (10.3)
6 months 23.3 (10.2)* 0.3 24.6 (12.5) 0.1 1.22 1,46 0.276 0.03
12 months 20.1 (8.3)* 0.7
Depression
(BDI-II)
Baseline 17.8 (10.6) 15.1 (9.3)
6 months 13.5 (9.8)*** 0.4 14.2 (11.0) 0.1 1.41 1,48 0.242 0.03
12 months 9.6 (7.9)** 0.9
Anxiety
(STAI-T)
Baseline 49.9 (9.2) 48.3 (11.6)
6 months 46.6 (9.6)** 0.4 47.9 (12.2) 0 1.02 1,46 0.318 0.02
12 months 42.4 (8.5)** 0.8
Fatigue (FQ) Baseline 18.8 (5.7) 18.5 (4.8)
6 months 15.9 (5.5)** 0.5 18.2 (5.0) 0.1 2.29 1,45 0.138 0.05
12 months 13.5 (5.3) 1.0
Sleep (BIS) Baseline 24.3 (8.0) 23.5 (10.5)
6 months 22.5 (7.2) 0.2 23.8 (11.0) 0 0.22 1,47 0.642 0.01
12 months 19.0 (7.9)*** 0.7
Quality of life
(QLI)
Baseline 1.1 (1.4) 1.5 (1.1)
6 months 1.5 (1.2)* 0.3 1.1 (1.7) −0.3 4.23 1,48 0.045 0.08
12 months 1.9 (1.3) 0.6
SD, standard deviation; ES, effect size; d.f., degree of freedom.
* P < 0.05, *** P < 0.001; P-value is based on paired-samples t tests to examine time effects in the treatment group.
Table 3. Differences in working status between patients in treatment (NPPT) versus waiting list control patients at baseline, 6, and 12 months
NPPT Waiting list
Baseline
(n = 40)
6 months
(n = 35)
12 months
(n = 23)
Baseline
(n = 22)
6 months
(n = 17)
Working 14 (35%) 13 (37.1%) 13 (56.5%) 11 (50%) 12 (70.6%)
Sick leave/disability 24 (60%) 20 (57.1%) 10 (43.5%) 10 (45.5%) 5 (29.4%)
No data 2 (5%) 1 (4.5%)

Effect of psychomotor physical therapy M. H. Breitve et al.
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
non-randomized, non-blinded study design. As the
physiotherapists who conducted the treatment were
not blind to patients’ study participation, it is possible
that they put a special effort on treating these patients.
This, in turn, may have infl uenced the generalizability
of the treatment effects. Also, as the participants were
not randomized to treatment and waiting list groups,
participant characteristics or factors other than the
NPPT treatment may have caused the observed differ-
ences in change between the groups. However, even
without randomization, the groups did not differ sig-
nifi cantly at baseline on any of the outcome measures
or on the major demographic variables.
Several participants dropped out from the study
during the follow-up period, which may have infl u-
enced the results. The 6-month data suggested that the
participants who did not complete the follow-up period
were less satisfi ed with the treatment, but their depres-
sive symptoms and sleep problems were also reduced
from baseline and, compared to the completers, signifi -
cantly lower (i.e. better) after 6 months in treatment.
The number of participants on sick leave or disability
pension was also reduced from 6 to 12 months but it is
uncertain to what degree this reduction was a conse-
quence of improvement due to treatment or an artifact
caused by the number of drop-outs from the study.
Finally, the choice of outcome measures may not
have been optimal for capturing the benefi cial effects of
NPPT as a holistic and non-symptom focused treat-
ment. Because our intention was to examine the poten-
tial of NPPT as a treatment for diffuse, somatic and
psychological health complaints, we chose instruments
assessing these symptoms as outcome measures.
However, it is uncertain to what degree the change that
can be measured with these instruments corresponds to
the treatment goals as formulated by the therapists, or
to patients’ expectations of treatment outcome.
In spite of these limitations, the fi ndings suggests
that NPPT may have potential as a treatment for
persons with long-lasting and diffuse health com-
plaints: When using the cut-off scores for clinical sig-
nifi cance on depression (BDI-II; Seggar et al., 2002),
anxiety (STAI-T; Fisher and Durham 1999) and quality
of life (QOL; Frisch 1994), NPPT seems to reduce these
symptoms from a clinical to non-clinical level, as shown
in Figure 2. However, as in our study sample, the
patients seeking NPPT have typically suffered from a
heavy symptom burden over long periods of time, and
they may also have failed in different forms of therapies
before. Thus, it can be expected that treatment takes
time.
In the current study, participants who discontinued
treatment after 6 months were characterized by a more
rapid reduction of sleep problems and depressive
symptoms. For some patients, improved sleep might
reduce the need for further treatment and heighten the
tolerance level for pain and discomfort. For those who
completed the 12-month follow-up, the rate of change
appeared to be similar from baseline to 6 months, and
6 to 12 months on all outcome variables, except for
sleep, for which crucial improvement occurred after
6 months. In accordance with literature on NPPT
(Bunkan 2001; Øien et al., 2009), this may indicate that
the treatment will often require a process of up to 1 year
or even longer to reach its full potential.
Within treatment of long-lasting and diffuse pain
and health complaints, a dilemma still exists between
experience-based knowledge and so-called evidence-
based knowledge (Kvåle and Ljunggren, 2007). Psycho-
logical treatments such as CBT have been proven
effi cacious for many patients with long-lasting health
complaints (Sumathipala, 2007). The CBT model aims
at reducing symptoms by helping the patient modify
and change beliefs and behaviours that perpetuate or
maintain the health problems. However, psychological
treatments are not widely available (Sharpe and Carson,
2001) and it has been argued that they may not be
acceptable for all patients (Salmon et al., 1999). Also,
patients with pain and health complaints represent a
heterogeneous group, and a treatment that works for
one subgroup may not have an effect on another.
In contrast to shorter, symptom-focused treatment
forms, psychomotor physiotherapists claim that they
are pursuing a deeper change of the totality of the
person as an indivisible psychosomatic entity, as well as
addressing tension, movements and breathing patterns
(Bunkan 2001; Øien et al., 2009). Unfortunately, this
claim has not been accompanied by any documentation
so far. Previous research has demonstrated changes in
patients’ movement and breathing patterns following
treatment (Kvåle et al., 2005, 2008), and a former mul-
tidisciplinary treatment study including elements of
NPPT also showed that patients who return to work
signifi cantly improve their breathing pattern, more
than those who remained sick-listed (Kvåle et al., 2005).
However, it is yet unclear to what degree a change in
these variables is causative for benefi cial effects such as
symptom relief and increased quality of life.

Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
M. H. Breitve et al. Effect of psychomotor physical therapy
Implications
Currently, most of the evidence for the effect and
mechanisms of NPPT comes from qualitative case
descriptions, interview studies and observational
studies. Even though such qualitative research has its
advantages, effect studies with reliable and validated
outcome measures are also needed. Using established
measures of outcome will facilitate comparisons
between studies as well as with other treatment forms.
Although NPPT may be a process-oriented and holistic
treatment form, it is not enough simply to state the
basic theoretical assumptions of the model; more docu-
mentation on both short- and long-term effects is
needed and the treatment should be compared with
evidence-based treatments, such as CBT. In addition
to examining the effect for patients’ symptom level
and/or quality of life, work-related disability and use of
health care services are important outcomes for such
studies. As different treatment forms may be more suit-
able for some subgroups of patients, investigating the
patient characteristics that moderate treatment effect
would be advantageous.
Although our fi ndings indicate that the NPPT con-
tributes to positive change in patients with long-lasting
and diffuse health complaints, the weaknesses in the
study design limit the strength of the fi ndings. High
quality studies examining the effi cacy of NPPT, as well
as the mechanisms that contribute to benefi cial effects,
are needed in order to document the effects of such
treatments and building a reliable evidence-base. In
order to provide guidelines for best possible care for the
patients, more research is needed to establish what
works and for whom, and what the patients’ want and
fi nd acceptable.
REFERENCES
Aabakken L, Aabakken B, Øfsti L, Schrøder R, Wilhelmsen
T. Psykomotorisk fysioterapi — pasientenes utgangs-
punkt og deres vurdering av behandlingsresultatet.
Tidsskrift for Norsk Lægeforening 1991; 111:
1619–1623.
American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders, 4th ed., text rev.
Washington DC: Author, 2000.
Bakal D, Steiert M, Coll P, Schaefer J. An experiential
mind-body approach to the management of medically
unexplained symptoms. Medical Hypotheses 2006; 67:
1443–1447.
Beck AT, Steer RA, Brown GK. Beck Depression Inven-
tory-II Manual. San Antonio, TX: Hacourt Brace, 1996.
Breitve MH, Hynninen M, Kvåle A. Emosjonelle symp-
tomer og helseplager hos pasienter som oppsøker
psykomotorisk fysioterapi. Fysioterapeuten 2008; 75:
19–26.
Bunkan BH. Psykomotorisk fysioterapi — prinsipper og
retningslinjer. Tidsskrift for Norsk Lægeforening 2001;
121: 2845–2848.
Chalder T, Berelowitz G, Pawlikowska T, Watts L, Wessely
S, Wright D, Wallace EP. Development of a fatigue scale.
Journal of Psychosomatic Research 1993; 37: 147–153.
Cohen J. Statistical Power Analysis for the Behavioral
Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates,
1988.
Deyo R. Low back pain. Scientifi c American 1998; 279:
48–53.
Ekerholt K, Bergland A. The fi rst encounter with Norwe-
gian psychomotor physiotherapy: Patients’ experiences,
a basis for knowledge. Scandinavian Journal of Public
Health 2004; 32: 403–410.
Eriksen HR, Ihlebæk C, Ursin H. A scoring system for
subjective health complaints (SHC). Scandinavian
Journal of Public Health 1999; 1: 63–72.
Eriksen HR, Ursin H. Sensitization and subjective health
complaints. Scandinavian Journal of Psychology 2002;
43: 189–196.
Eriksen HR, Ursin H. Subjective health complaints, sensi-
tization, and sustained cognitive activation (stress).
Journal of Psychosomatic Research 2004; 56: 445–448.
Fisher PL, Durham RC. Recovery rates in generalized
anxiety disorder following psychological therapy: An
analysis of clinically signifi cant change in the STAI-T
across outcome studies since 1990. Psychological
Medicine 1999; 29: 1425–1434.
Frisch MB. Quality of Life Inventory (QOLI). Minneapo-
lis: National Computer Systems, 1994.
Kamps H, Arnesen S. Samhandling mellom allmennlege
og psykomotorisk fysioterapeut. In: Utposten 2004; 33.
http://www.uib.no/isf/utposten/2004nr6/utp04606.htm
[15.08.07].
Karlsson H, Joukamaa M, Lahti I, Lehtinen V, Kokki-
Saarinen T. Frequent attender profi les: Different clinical
subgroups among frequent attender patients in primary
care. Journal of Psychosomatic Research 1997; 42:
157–166.
Khan AA, Khan A, Harezlak J, Tu W, Kroenke K. Somatic
symptoms in primary care: Etiology and outcome.
Psychosomatics 2003; 44: 471–478.
Kroenke K, Mangelsdorff A. Common symptoms in
ambulatory care: Incidence, evaluation, therapy, and
outcome. American Journal of Medicine 1989; 86:
262–266.

Effect of psychomotor physical therapy M. H. Breitve et al.
Physiother. Res. Int. (2010) © 2010 John Wiley & Sons, Ltd.
Kvåle A, Ljunggren AE. Body awareness therapies. In
Schmidt R, Willis W (eds) Encyclopedia of Pain. New
York: Springer, 2007; 1: 167–169.
Kvåle A, Skouen JS, Ljunggren AE. Sensitivity to change
and responsiveness of the Global Physiotherapy
Examination (GPE-52) in patients with long-lasting
musculoskeletal pain. Physical Therapy 2005; 85:
712–726.
Kvåle A, Wilhelmsen K, Fiske HA. Physical fi ndings in
patients with dizziness undergoing a group exercise pro-
gramme. Physiotherapy Research International 2008;
13: 162–175.
Larsen DL, Attkisson CC, Hargreaves WA, Nguyen TD.
Assessment of client/patient satisfaction: Development
of a general scale. Evaluation and Program Planning
1979; 2: 197–207.
Malmgren-Olsson EB, Armelius BÅ. Non-specifi c muscu-
loskeletal disorders in patients in primary care: Sub-
groups with different outcome patterns. Physiotherapy
Theory and Practice 2003; 19: 161–173.
Øien AM, Iversen S, Stensland P. Narratives of embodied
experiences — Therapy processes in Norwegian psycho-
motor physiotherapy. Advances in Physiotherapy 2007;
9: 31–39.
Øien AM, Råheim M, Iversen S, Steihaug S. Self-
perception as embodied knowledge — changing pro-
cesses for patients with chronic pain. Advances in
Physio therapy 2009(3); 121–129. DOI:10.1080/14038
190802315073
Pallesen S, Bjorvatn B, Nordhus IH, Sivertsen B, Hjørnevik
M, Morin CM. A new scale for measuring insomnia: the
Bergen Insomnia Scale. Perceptual & Motor Skills
2008; 107: 691–706.
Råheim M, Håland W. Lived experience of chronic pain
and fi bromyalgia: Women’s stories from daily life.
Qualitative Health Research 2006; 16: 741–761.
Salmon P, Peters S, Stanley I. Patients’ perceptions of
medical explanations for somatisation disorders:
Qualitative analysis. British Medical Journal 1999; 318:
372–376.
Seggar LB, Lambert MJ, Hansen NB. Assessing clinical
signifi cance: Application to the Beck Depression Inven-
tory. Behavior Therapy 2002; 33: 253–269.
Sharpe M, Carson A. ‘Unexplained’ somatic symptoms,
functional syndromes, and somatization: Do we need a
paradigm shift? Annals of Internal Medicine 2001; 134:
926–930.
Sharpe M, Mayou R, Seacroatt V, Surawy C, Warwick H,
Bulstrode C, Dawber R, Lane D. Why do doctors fi nd
some patients diffi cult to help? Quarterly Journal of
Medicine 1994; 87: 187–193.
Simon G, Gater R, Kisely S, Piccinelli M. Somatic symp-
toms of distress: An international primary care study.
Psychosomatic Medicine 1996; 58: 481–488.
Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs
AG. Manual for the State-Trait Anxiety Inventory
(Form Y) (‘Self-Evaluation Questionnaire’). Palo Alto,
CA: Consulting Psychologists Press, 1983.
Sumathipala A. What is the evidence for the effi cacy of
treatments for somatoform disorders? A critical review
of previous intervention studies. Psychosomatic Medi-
cine 2007; 69: 889–900.
Wilhelmsen I. Biological sensitisation and psychological
amplifi cation: Gateways to subjective health complaints
and somatoform disorders. Psychoneuroendocrinology
2005; 30: 990–995.