the effect of a periodized resistance training program on
TRANSCRIPT
The Effect of a Periodized Resistance Training Program on Strength and Ambulation in
an Individual with Incomplete Chronic Spinal Cord Injury
An Independent Research Report
Presented to
The Faculty of the College of Health Professions
Florida Gulf Coast University
In Partial Fulfillment
Of the Requirements for the Degree of
Doctor of Physical Therapy
By
Julie Bowditch
2015
APPROVAL SHEET
This Independent Research is submitted in partial fulfillment of
the requirements for the degree of
Doctor of Physical Therapy
____________________________
Julie Bowditch
Approved: April 2015
____________________________
Dennis Hunt, Ed.D., CSCS
Committee Chair / Advisor
____________________________
Mollie Venglar, DSC, MSPT, NCS
Committee Member
The final copy of this Independent Research has been examined by the signatories, and we find that both
the content and the form meet acceptable presentation standards of scholarly work in the above mentioned
discipline.
Acknowledgements
First and foremost, I would like to thank my committee members, Dr. Dennis Hunt and
Dr. Mollie Venglar for their unending support and thoughtful guidance throughout this
process.
Additionally, I would like to thank my parents, classmates, and peers for providing
continuous and uplifting encouragement, companionship, and assistance during this
academic adventure.
Lastly, thank you to Florida Gulf Coast University and the Department of
Rehabilitation Sciences for allowing me to conduct this research as a contribution to my
education and academic career.
Periodized Resistance Training and SCI 1
Table of Contents
Abstract ----------------------------------------------------------------------------------------- 2
Introduction ------------------------------------------------------------------------------------ 3
Spinal Cord Injury -------------------------------------------------------------------- 4
Incomplete Injuries-------------------------------------------------------------------- 5
Effects on Skeletal Muscle --------------------------------------------------------- 6
Muscle Spasticity --------------------------------------------------------------------- 7
Resistance Training & SCI-------------------------------------------------------- 9
Exercise Training Principles ------------------------------------------------------ 14
1-RM Testing -------------------------------------------------------------------------- 15
Periodization Training ---------------------------------------------------------------- 16
Periodization in SCI ----------------------------------------------------------------- 17
Methods ---------------------------------------------------------------------------------------- 20
Participant ----------------------------------------------------------------------------- 20
Study design -------------------------------------------------------------------------- 21
Data collection----------------------------------------------------------------------- 32
Results & Discussion------------------------------------------------------------------------- 34
Discussion Summary ----------------------------------------------------------------------- 56
Conclusion ------------------------------------------------------------------------------------ 60
References ----------------------------------------------------------------------------------- 61
Appendix A-------------------------------------------------------------------------------------- 65
Appendix B--------------------------------------------------------------------------------------- 66
Appendix C---------------------------------------------------------------------------------------- 67
Periodized Resistance Training and SCI 2
Abstract
Muscle atrophy is a primary health concern in individuals suffering from spinal cord
injury (SCI). This change occurs as a result of the injury and subsequent limited mobility.
The population of people with incomplete SCI appears to be increasing. Rehabilitation
and fitness professionals should strive to better understand how an individual’s
capabilities can be improved by focusing on the potential to impact and improve
functional abilities and promote wellness in this population.
PURPOSE: To understand the effect of utilizing a periodized resistance training (RT)
program in addition to a body weight supported aerobic exercise program on improving
strength, endurance, and quality of gait for a community-dwelling ambulatory individual
with a chronic incomplete SCI.
METHODS: The participant was a 38 year old male with a chronic L1 ASIA D SCI. He
completed a 12 week whole body periodized RT and flexibility program involving the
innervated muscle groups of his upper and lower extremities. The intervention included
cardiovascular endurance training once a week on a body weight supported treadmill
along with twice weekly RT sessions. The periodization model included mesocycles
involving one week of an adaptation period followed by three weeks of muscular
endurance training, four weeks of strength training, and four weeks of power training.
Outcomes measures include 1 repetition maximum testing (1RM), the 6-minute walk test
(6MWT), manual muscle testing (MMT), modified Ashworth test for spasticity, body
composition, and joint range of motion (ROM).
RESULTS: The most significant improvements were seen in 1 RM testing and 6MWT.
Upper body strength as measured by 1 RM chest press improved by 30 lbs (22%). Lower
body strength as measured by the 1RM leg press improved by 25 lbs (13%).
Improvement in the 6MWT was 107 feet or 9.7%. No other significant trends were
identified.
CONCLUSION: Strength gains through periodized RT were evident for this individual
with chronic incomplete SCI. Strength gains occurred as seen through the objective 1RM
testing measures looking at the upper and lower body as a whole. Functional
improvements in ambulation distance, endurance, and walking speed are seen in the
results of the 6MWT. Training in a periodized fashion appears to be a viable option for
further study with this population.
Periodized Resistance Training and SCI 3
Introduction
In 2013, the estimated number of people in the United States living with spinal
cord injury (SCI) was approximately 273,000 people (Spinal Cord Injury Facts 2013).
Every year there is estimated to be 40 new cases per million people in the population.
Most injuries are traumatic and happen to young people; with up to 80% of individuals
who have suffered a SCI being males. SCIs lead to a wide variety of functional
disabilities, loss of independence, loss of mobility, loss of sensation, health related
complications, and muscle atrophy below the level of the lesion. The goal of
rehabilitation for individuals with SCI is to address losses in bodily function, minimize
secondary complications, and utilize muscle groups that are still functional in order to
increase independence as much as possible and reintegrate the person back into their
community. The strengthening of muscle groups that are still functional is important in
helping a patient become as independent and functional as he/she can be and in
preventing further injury (Umphred et al 2010 ).
Resistance training (RT) is the voluntary activation of skeletal muscles against
resistance. Resistance can be in the form of using body mass, free weights, and other
modalities such as bands, springs, and manual resistance (McArdle, Katch, & Katch
2010). According to the American College of Sports Medicine (ACSM), RT improves
muscular fitness by increasing strength, endurance, and power. The health-related
benefits of RT include making activities of daily living less physiologically stressful and
managing or preventing chronic diseases. An RT program can provide these desired
benefits from just a few sessions per week (ACSM Guidelines 2010).
Periodized Resistance Training and SCI 4
The purpose of this study was to determine the effect of utilizing a periodized RT
program in addition to a body weight supported treadmill training (BWSTT) program on
strength, endurance, and quality of gait for a participant with a chronic incomplete L1
SCI.
Spinal Cord Injury
SCIs usually occur as traumatic injuries that leave healthy, active, independent
people paralyzed and dependent on others. The mechanism of injury can affect the
severity and type of the spinal cord lesion. The leading causes of SCI are motor vehicle
accidents followed by falls, violent acts, and sports injuries. Birth defects, disease, and
lack of blood flow can also cause spinal cord lesions (Umphred, Lazaro, Roller, & Burton
2013).
Clinical presentations vary depending on the extent of damage to the spinal cord
and the level of the spinal cord that is injured. A detailed physical assessment is needed
to determine which muscles have lost voluntary control and in what areas sensation has
been lost. The American Spinal Injury Association (ASIA) has developed international
standards for the classification of SCI. A SCI can be classified as complete, meaning
there is no sensory or motor function in the lowest sacral segments, or incomplete
meaning there is sensory or motor function in the lowest sacral segments (2011). The
ASIA Impairment Scale classifies injuries as complete or incomplete. The ASIA
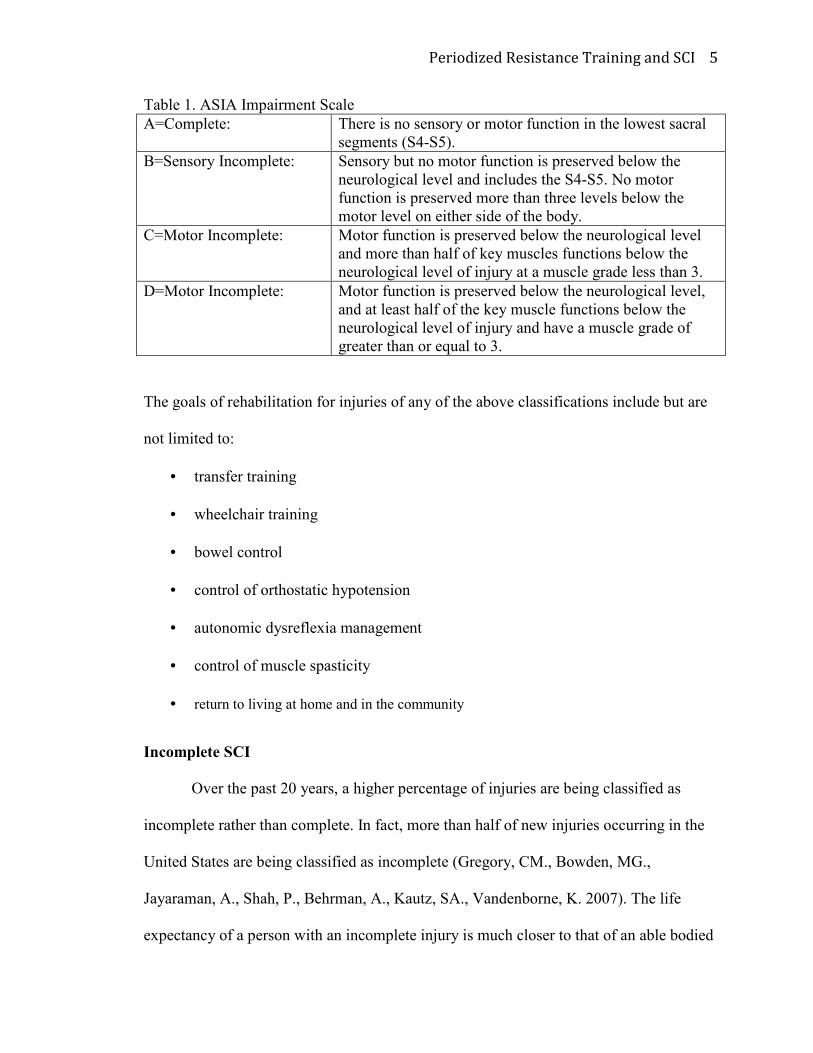
Impairment Scale is provided in Table 1.
Periodized Resistance Training and SCI 5
Table 1. ASIA Impairment Scale
A=Complete: There is no sensory or motor function in the lowest sacral
segments (S4-S5).
B=Sensory Incomplete: Sensory but no motor function is preserved below the
neurological level and includes the S4-S5. No motor
function is preserved more than three levels below the
motor level on either side of the body.
C=Motor Incomplete: Motor function is preserved below the neurological level
and more than half of key muscles functions below the
neurological level of injury at a muscle grade less than 3.
D=Motor Incomplete: Motor function is preserved below the neurological level,
and at least half of the key muscle functions below the
neurological level of injury and have a muscle grade of
greater than or equal to 3.
The goals of rehabilitation for injuries of any of the above classifications include but are
not limited to:
• transfer training
• wheelchair training
• bowel control
• control of orthostatic hypotension
• autonomic dysreflexia management
• control of muscle spasticity
• return to living at home and in the community
Incomplete SCI
Over the past 20 years, a higher percentage of injuries are being classified as
incomplete rather than complete. In fact, more than half of new injuries occurring in the
United States are being classified as incomplete (Gregory, CM., Bowden, MG.,
Jayaraman, A., Shah, P., Behrman, A., Kautz, SA., Vandenborne, K. 2007). The life
expectancy of a person with an incomplete injury is much closer to that of an able bodied
Periodized Resistance Training and SCI 6
person than that of a person with a complete SCI. With incomplete injuries, there is a
strong potential for individuals to be able to walk again. With some muscles rendered not
functioning and others having suffered atrophy, an SCI sufferer must re-learn how to
walk. Through physical therapy with the use of BWSTT, crutches, walkers, and other
devices, many people with paraparesis regain the ability to walk. Limiting factors include
weakness, muscular endurance, fatigue, spasticity, slow gait speed, abnormal gait pattern,
and impractical energy usage. With an increasing population of people with incomplete
injuries, the discipline of physical therapy should strive to better understand how to
improve an individual’s capabilities, focusing on the potential to impact and improve
functional abilities. Evidence-based best practice research is needed to determine an
effective way to return individuals with SCI to walking and to improve the gait pattern to
as near normal as possible.
SCI Effects on Skeletal Muscle
Muscle atrophy is defined as the loss of force generating capacity due to
decreased muscle fiber size and loss of contractile proteins (Kisner& Colby 2007).
Muscles below the level of the SCI will atrophy over time. Two types of atrophy are
present with SCI: denervation and disuse. Denervation atrophy occurs when the nerve
signal to the muscle is absent. Muscles atrophy rapidly because their nerve innervation is
completely cut off. Decreased but not complete denervation of a muscle group can
decrease strength and make initial activation of the muscle difficult. Disuse atrophy is a
result of decreased motor input as well as physical inactivity due to the patient being
hospitalized, immobilized, developing contractures, or being non-weight-bearing.
Muscles that are normally weight bearing prior to the SCI are known to show greater

Periodized Resistance Training and SCI 7
disuse atrophy (Gordon & Mao 1994). For example, the average size of the quadriceps
femoris muscle in patients with SCI is 40% smaller than with able-bodied individuals
(Mahoney, et. al. 2005). Skeletal muscle cross-sectional area can decrease as much as
50% in just a few weeks after injury (Gorgey & Shepherd 2009). Decreased muscle mass
and contractile activity may also contribute to secondary health related complications.
Physical inactivity can contribute to a variety of chronic diseases such as diabetes
mellitus, cardiovascular disease, cancer, obesity, hypertension, bone disease, arthritis, and
osteoporosis (Warburton, Nicol, Bredin, 2006). Chronic SCI sufferers often lead a
sedentary lifestyle which might partially explain a decrease in muscle mass and fitness
for many (Jacobs & Nash 2004). It might also explain why there is a higher risk for
cardiovascular issues, metabolic syndromes, and obesity for those with SCI. These
individuals have much to benefit from reducing the atrophy process and even more if
they increase the mass of muscles that have become small and weak.
Muscle Spasticity in SCI
Muscle spasticity occurs as a result of damage to upper motor neurons. It is
characterized by symptoms of hypertonicity, hyperactive stretch reflexes, and involuntary
movements called clonus below the lesion (O’Sullivan & Schmitz 2007). Causes of
spasticity include decreased motor unit activation, impaired antagonist inhibition, or
impaired presynaptic inhibition of reflex pathways (Pak and Pattern 2008). Prolonged
muscle shortening can lead to contracture, joint damage, muscle damage, and pain which
restrict range of motion (ROM) and voluntary movement (Elbasiouny, S., Moroz, D.,
Bakr, M., Mushahwar, V. 2010). Muscle spasticity is a common issue in individuals with
SCI. It is a stumbling block for those who are trying to increase function and
Periodized Resistance Training and SCI 8
independence. The severity, duration, and frequency of spasticity varies from individual
to individual. It can be triggered by both internal and external stimuli. The symptoms of
spasticity are managed pharmacologically with neurologic antispastic agents. Examples
of common antispastic agents are baclofen, diazepam, and dantrolene (Umphred et al.
2010). To avoid negative side effects of oral baclofen, individuals frequently use an
intrathecal baclofen pump which is surgically inserted under the skin. This pump delivers
the pharmacological effect directly to the spinal cord. The amount of medication
delivered can be adjusted to the individual’s needs by a physician. However, this type of
treatment is not always completely successful at alleviating the symptoms of spasticity
and additionally, a tolerance to the drug can be developed causing the individual to
require adjustments for increased levels of baclofen delivery. Surgical procedures are also
utilized to deliver relief of symptoms including a myotomy (i.e. cutting of the muscle) or
neurectomy (i.e. cutting of the nerve) (O’Sullivan & Schmitz 2007). A drawback to both
of these procedures is that they render the body less able to contract that muscle.
Therapeutic interventions known to benefit and treat muscle spasticity include
prolonged stretching, cryotherapy, weight-bearing exercise, and aquatic therapy
(Umphred et al. 2010). Passive stretching is a mechanism of increasing muscle length,
reducing and preventing contracture, maintaining and increasing ROM, and reducing
muscle tone (Elbasiouny, S., et al 2010). Stretching addresses the biomechanical issues
involved in spasticity that medications do not. Evidence-based duration of stretching
exercises recommended for all individuals is at least 30 seconds (Baechle & Earle 2008).
Periodized Resistance Training and SCI 9
Resistance Training and SCI
It is well established that RT can induce muscle hypertrophy in able-bodied
individuals (Seyness, Boer, Narici 2007). Muscle performance in the areas of strength,
endurance, and power has also been shown to improve with RT (Kisner & Colby 2012).
This type of training maintains or increases strength of musculoskeletal tissues, increases
bone density, decreases stress on joints, decreases risk of injury, and has positive effects
on body composition (Kisner & Colby 2012). The ACSM (2010) guidelines recommend
RT for all individuals, including clinical populations such as those with SCI. Although
special considerations might need to be followed, the benefits of RT can extend to the
SCI’s population.
Researchers have examined various aspects of RT for subjects with chronic SCI.
Gorgey and Shepherd (2009) completed a lower extremity RT program along with
neuromuscular electrical stimulation (NMES). Since the nerve connection between the
brain and the muscles is partially or completely cut off as a result of SCI, NMES was
utilized to induce muscle contraction in order to strengthen the muscle. The use of a
NMES unit allowed for training of muscles that were entirely denervated to participate in
RT. In Gorgey and Shepherd’s (2009) case report, a patient with a complete C5-C6 injury
(ASIA A) underwent RT using NMES to evoke contractions in his knee extensors. The
subject participated in seated RT for his knee extensors, specifically the vastus lateralis,
twice weekly for twelve weeks. Initially the resistance was the weight of the patient’s leg.
Ankle weights were added and intensity increased when the subject was able to perform 4
sets of 10 repetitions. The results of the case study were measured by the patient’s ability
to lift ankle weights as well as T1 weighted magnetic resonance imaging to measure
Periodized Resistance Training and SCI 10
changes in size and cross sectional area of the knee extensors and surrounding
musculature. The researchers concluded that the NMES RT resulted in substantial
increases in muscle hypertrophy (Gorgey& Shepherd 2009).
A similar study examined the increases in skeletal muscle size as evaluated by
MRI after seated knee extension RT was performed twice a week for twelve weeks
(Mahoney et al. 2005). Mahoney et al. (2005), focused more on NMES of the rectus
femoris muscle in five long term SCI sufferers. They concluded that even years after
initial injury, increases in skeletal muscle were remarkable with RT. Increases of up to
37% in muscle cross-sectional area (CSA) were found. These authors performed similar
RT studies on able-bodied and sedentary populations with fewer positive results. In one
of those studies on able-bodied and sedentary populations, subjects performed voluntary
knee extension and reported only 5-10% increases in CSA after 12 weeks. The sedentary
individuals in their study performed knee extension voluntarily and with NMES and
showed gains of only 4%hypertrophy and 10% in CSA. Their conclusions suggest that
the atrophy of muscles in subjects with SCI allowed for greater improvements during RT
program (Mahoney et al 2005).
Improvement in locomotor recovery for individuals with chronic motor
incomplete SCI has also been demonstrated with the use of RT. A study completed in
2010 combined a RT program with a BWSTT program for locomotion to determine the
effects on walking speed, endurance, and balance in an elderly person with a chronic
incomplete SCI (Gorgey, AS., Poarch, H., Miller, J., Castillo, T., & Gaiter, DR. 2010).
The hypothesis for the study was that utilizing a combination of two types of treatment
would stimulate adaptations in both the neuromuscular system and the musculoskeletal
Periodized Resistance Training and SCI 11
system. A drawback of their study was that it involved only one subject who participated
in a program using the treadmill twice a week alternating with twice a week RT program
over a period of 10 weeks. The RT program had a similar design utilized in previous
studies that used a seated knee extension and ankle weights and progressed to 4 sets of 10
repetitions. Outcomes measures for the study included the Berg Balance scale, the
Walking Index for SCI, Functional Independence Measure (FIM), Functional Locomotor
Assessment, and walking speed and duration. Results from the single subject case study
showed that the subject’s body weight and BMI decreased during the training period. The
following increases were also attributed to RT:
• Berg balance score
• FIM level
• Walking speed
• Walking distance (initially increased but decreased when the patient progressed
from using a standard walker to bilateral crutches for ambulation.)
The exercise program also helped the patient to progress to where he was no longer
wheelchair dependent. The author’s concluded that the combination of locomotor training
using BWSTT and RT was effective and efficient at improving walking in a patient over
the age of 60 with chronic SCI. The researchers believed that the combination of the two
interventions was more beneficial because BWSTT alone does not provide the needed
benefits of muscle hypertrophy, diminishing muscle fatigue, and improving bone density
that RT offers (Gorgey et al 2010).
Gregory et al. (2007) examined the effects of RT on locomotor speed and muscle
function in three ambulatory individuals with chronic incomplete SCI. The twelve week
Periodized Resistance Training and SCI 12
study incorporated RT and plyometric training three times weekly. The RT was
performed using selectorized equipment included
• leg press
• knee extension and flexion
• hip extension and flexion
• ankle plantar flexion
Plyometric training included jump exercises in the supine position. The subjects were
tested before and after the twelve week program using MRI to determine muscle CSA of
the knee extensors and plantarflexor groups. These muscle groups were selected based on
their roles in locomotion. These muscle groups were also tested using a Biodex isokinetic
dynamometer to assess strength, peak torque production, time to peak torque, and
average torque development. Gregory et al. (2007) examined and reported voluntary
activation deficits observed in the tested muscle groups before training. The subjects
were also pre and post tested using the GaitRite™ system to determine maximal and self-
selected gait speed changes. GaitRite™ is also able to measure gait pattern. Results of the
study showed that the training program resulted in significant increases in torque and
muscle strength. Increases in strength were considered a result of increased muscle CSA
and an increased ability of the subject to voluntarily initiate contractions in affected
skeletal muscles. Both maximum and self-selected gait speeds demonstrated an increase
by 30%. Increased step lengths as well as improved symmetry during gait cycle were also
reported. Results of this study also suggest that RT can facilitate neuromuscular
improvements as well as strength improvements in those with chronic incomplete SCI.
However, Gregory et al. (2007) stated that few studies have attempted to examine the
Periodized Resistance Training and SCI 13
relationship between lower extremity strength and gait in persons after incomplete SCI.
More research in this very important and expanding area is needed to determine what
interventions are most effective at making improvements in locomotion, increasing
independence and to normalize gait in this population.
A study performed by Jayaraman, Thompson, Rymer, and Hornby (2013) more
recently compared maximal-intensity RT to conventional RT in individuals with an
incomplete SCI to determine and compare the effects. Five individuals with chronic
incomplete SCI were tested before and after a four week program for either maximal-
intensity RT or conventional progressive RT. Effects were measured through the 6-
minute walk test, Berg Balance Scale, and peak isometric torque for strength of lower
extremity muscles. The results of this short 4-week study showed that not only are there
strength increases with short durations of training, but that conventional progressive RT
is not always associated with the greatest functional and strength gains. Maximal-
intensity training for a short duration demonstrated more strength gains as indicated by
greater peak isometric torque. The individuals who participated in this study also had
chronic injuries and had been discharged from therapy many years prior to participation
in this study indicating that strength gains are possible long after a SCI occurs.
Furthermore, this study showed a trend for decreased spasticity of lower extremity
muscles following maximal intensity RT as measured by the modified Ashworth scale.
Muscle weakness is reported to cause pain and dysfunction with aging in persons
with disability due to SCI (Jacobs & Nash 2004). Although more is known about the
effects of endurance and cardiovascular training for people with chronic SCI, current
evidence supports the benefits of increased strength, muscle size, and muscle CSA from

Periodized Resistance Training and SCI 14
RT in this population. Improved torque production and gait speed for locomotor recovery
after incomplete SCI has been shown with the use of RT (Gregory et al 2007). The use of
RT with BWSTT has also been effective in enhancing walking in people with SCI
(Gorgey et al 2010).
Exercise Training Principles
Mcardle, Katch, and Katch (2010) outline general exercise training principles
needed to affect structural and functional adaptations to improve performance. The first
and most important principle greatly applies to the concepts behind RT. This principle,
called the overload principle, says that the load placed on the body must be greater than
what it is accustomed to in order to elicit a training response. The body will adapt and
accommodate to be more efficient at handling that specific load.
The ACSM (2010) provides recommendations for exercise prescription for
muscular fitness for all adults who are untrained or not formally trained. An important
part of any exercise training program should be RT which can produce benefits of
strength, endurance, and power (ACSM 2010). Frequency of RT is suggested to be two
or three days per week per muscle group with at least forty-eight hours of recovery time
between sessions. The overall intensity of each exercise is oftentimes based off
percentages of an individual’s one-repetition maximum (1-RM).
According to the National Strength and Conditioning Association (NSCA),
intensity and volume of exercise are chosen based on the primary training goal (Baechle
& Earl 2008). Better outcomes are achieved when a training program focuses on one
training outcome at a time. Common training goals include hypertrophy, muscle
endurance, strength, and power. The training goal should dictate the number of sets,
Periodized Resistance Training and SCI 15
repetitions, intensity, and amount of recovery time. The amount of recovery time is
directly related to the intensity of training and the goal of training. The greater the
intensity of RT, the longer the recovery period between sets might be. The NSCA
recommends a RT frequency of two to three times a week for a beginner and increased
frequency for intermediate or advanced trainees. In regards to exercise order, the NSCA
recommends that beginning level individuals alternate between upper and lower
extremity exercises if being performed in the same training session. This method reduces
training time and is especially favorable for untrained individuals to decrease stress and
fatigue on muscle groups.
ACSM’s Guidelines for Exercise Testing and Prescription (2010) also outlines
guidelines for exercise testing and prescription for special populations including those
with SCI. They recommend taking into consideration the individual’s capabilities and
effects of the injury, when applying the exercise prescription guidelines for specific
populations. However, at this time there are no specific considerations for the assessment
of muscular strength. The guidelines do advise that a functional assessment is essential in
order to adapt the exercise equipment and program to the individual’s needs. The ACSM
also places an emphasis on stretching and strengthening being performed together to
prevent contracture and promote joint health.
1RM Testing
A 1-repetition maximum (1RM) is the greatest amount of weight that an
individual is able to lift with proper form for one repetition and then is too fatigued to
successfully complete another repetition (Baechle & Earle 2008). A repetition maximum
is the greatest weight able to be lifted for a given number of repetitions with maximal
Periodized Resistance Training and SCI 16
effort. The 1RM is used as a tool to predict appropriate submaximal loads and repetitions
for the purpose of focusing on one specific training goal in RT exercise. The 1RM can be
directly assessed or estimated from the results of a multiple-RM test. Estimating training
intensity from a submaximal multiple-RM test is less accurate than assigning weight
based on percentages of the directly tested 1RM (Baechle & Earle 2008). Furthermore,
utilizing multiple high-repetition tests involved in multiple-RM testing session increases
fatigue which can decrease the accuracy of a test. The 1RM testing protocol outlined by
the NSCA is provided in Appendix C. Exercises used for the 1RM test should involve
multiple joints and larger core muscle groups. These exercises are better equipped to lift
high intensity weight and are less prone to injury. For this reason, the participant in this
study performed 1RM testing with only the chest press and leg press.
Periodization Training
Periodization is an approach to RT that includes planned variations in exercise
over a period of time. This type of training was first developed for athletes who were
looking for a way to maximize training in the off season and to afford peak performance
at a desired point in time (Turner 2011). Most periodized training programs are separated
into periods of time, or phases, with each phase being geared towards a different goal
related to muscular fitness. Phases are also referred to as mesocycles and microcycles and
can range in length by months, weeks, or even days depending on the program.
Appropriate changes in sets, repetitions, exercises, recovery time, or frequency can be
adjusted to meet the specific goal of that phase. Common goals for a particular mesocycle
include increases in overall muscular fitness, endurance, strength, hypertrophy, or power.
The manipulation of variables helps to optimize strength gains, prevent overtraining,
Periodized Resistance Training and SCI 17
prevent joint or muscle damage, and promote psychological interest while challenging the
neuromuscular and musculoskeletal systems to adapt to be efficient at varying capacities
for optimal sport performance (Kraemer & Fleck 2007). Classic periodization RT begins
with high volume, low intensity resistance activities and progresses to low volume, high
intensity activities. Periodization can also begin with generalized strengthening exercises
and progress to more sport specific or competition specific exercises. Studies have
indicated that periodization results in greater strength and power gains than non-
periodized training programs for both men and women of various ages and training
backgrounds (Kell 2011). Rhea and Alderman (2004) conducted a meta-analysis study
comparing periodized and non-periodized training programs. The researchers concluded
that men and women of all ages and training backgrounds would develop greater strength
gains from a periodized training program than from a non-periodized training program
(Rhea & Alderman 2004).
Periodized Training in SCI
There is little research existing using periodization training with diverse
populations, and none found to have been performed with a SCI population. This study
examined whether a whole body periodized RT approach is effective in improving
strength for an individual with chronic incomplete SCI who is ambulatory. By
periodizing the training program, it was hypothesized that optimal muscular fitness (i.e.
strength) gains will be achieved, overtraining will not occur, and participant interest will
be maintained just as in the general population.
In addition, many periodization programs begin with an adaptation phase. An
adaptation phase is a short period of time where the intensity and volume of exercise are
Periodized Resistance Training and SCI 18
intentionally kept at a low to medium level. Referred to as the anatomical adaptation
phase, the goal of this phase is to prevent injury by getting the muscles and connective
tissue accustomed to movements for more intense exercise later in the periodized
program (Bompa & Carrera 2005). Physiologically, tendons, joints, and ligaments begin
to be strengthened, muscles learn the neuromuscular movement patterns needed for
strength training, and muscular fitness begins to be challenged during the anatomical
adaptation phase (Bompa & Carerra 2005). This phase was considered of great
importance in this study because the participant had little prior experience with RT.
This study involved three mesocycles, each with a specific goal, number of sets,
number of repetitions, intensity, and recovery time. This study began in the classical
manner with a focus on muscular fitness and high volume, low intensity resistance
activities. Muscular fitness is defined as the ability to perform many repetitions at a set
weight for longer periods of time (Baechle& Earle 2008). A lower intensity of resistance
will allow for more repetitions to be completed. Four sets of fifteen repetitions at 50% of
the 1RM were completed with short rest periods of 30 seconds.
The next mesocycle focused on increasing muscular strength. Since this phase
was only four weeks long in this program, it was not expected to produce strength gains
due to hypertrophy. Strength gains during this phase were anticipated as a result of neural
adaptations and increased motor unit recruitment (Schoenfeld 2010). Force production is
under neural control which determines the nerves and motor units that will induce muscle
contraction (Baechle & Earle 2008). Force production is higher if more motor units are
recruited and if they are recruited at a faster rate. Therefore, strength increases in the first
few weeks of training are a result of the increasing neurologic control producing better
Periodized Resistance Training and SCI 19
muscle recruitment and force for contractions. The use of the Bod PodTM as an outcomes
measurement in determining body composition was used to assist in determining if any
increases in muscle mass were achieved. For the strength phase, three sets of eight to
twelve repetitions were utilized at an intensity of 80% of 1RM. A two to three minute rest
period between exercises was also used.
The third and final phase of this study was three weeks long and included a
paradigm with the goal of increasing power. Training for power helps an individual to be
better prepared to handle explosive movements. Power is defined as a relationship
between force and velocity (Baechle& Earle 2008). As a result, the two components are
related and cannot function independently of each other in terms of power. Within the
literature, there exists considerable controversy related to how to best achieve adaptations
in power. Studies have shown effectiveness for high intensity (>80 or 90% 1RM) power
training as high intensities are known for their benefit in increasing muscle mass and
cross-sectional area (CSA). The key component for producing high maximum strength
and power is CSA (Hartmann, H., Bob, A., Wirth, K., Schmidtbleicher, D. (2009).
However, other studies have found that to increase power output, individuals should train
at the maximum combination of velocity and intensity in order to produce the maximum
mechanical power. But, according to the “Power = Force x Velocity” equation, as
velocity increases, the amount of force that a muscle is able to generate decreases.
Therefore, maximum mechanical power would only be achieved when an individual lifts
moderate to low intensities (30-45% of 1RM) that allow for greater velocity of movement
(Kawamori, N., Haff, G. 2004). Power increases in this present case were attributed to the
contribution of neuromuscular factors and increased rate of force development (RFD).
Periodized Resistance Training and SCI 20
Since increases in muscle size and CSA are not expected within a study of this short
duration, parameters for the power phase involved low to moderate intensity exercise at a
high velocity of movement. The program variable; exercise for this present study was not
manipulated and the same exercises on selectorized equipment were used for the duration
of each mesocyle.
Methods
Participant
The participant in this study has chronic motor incomplete L1 paraparesis from a
SCI sustained 9 years ago. His injury is classified as ASIA D by the American Spinal
Cord Injury Association. He currently ambulates independently with the assistance of
bilateral canes, bilateral dorsiflexion-assist ankle cuffs, and a Bioness©L300 device on
his right leg designed to electrically assist with ankle dorsiflexion during ambulation. He
was recruited based on his participation in a prior study at Florida Gulf Coast University.
In order to complete the former study, he was deemed medically stable and was
medically cleared for exercise. This study was designed as a continuation and
modification of the previous study and had a primary objective of enhancing muscular
fitness. The prior study involved participation in a BWSTT program twice weekly for
eight weeks, followed by four weeks of no intervention, followed by eight more weeks of
the same BWSTT program twice weekly. The initial study examined elements of
cardiovascular fitness training, effects of training on ambulation, and effects of detraining
after discontinuing exercise. The participant was chosen based on his injury, high level of
physical ability, motivation, and interest in continuing to participate in an associated
study. The participant’s right distal lower extremity was affected most by the SCI. Since
Periodized Resistance Training and SCI 21
active movement in the ankle is almost absent and lacks innervation more than other
muscle groups, strengthening of the ankle complex by itself was not specifically
addressed by this exercise program.
Study Design
This was a quantitative quasi-experimental case study examining the effects of
adding a periodized RT program along with a flexibility program to an existing BWSTT
protocol to an individual’s exercise routine. The participant completed a whole body
periodized RT and flexibility program of the innervated muscle groups of his upper and
lower extremities. The intervention program included a BWSTT routine that was reduced
from twice weekly to once weekly from the previous study and added a twice weekly RT
program.
The periodized program began with a one week adaptation period which included
the participant’s preliminary strength testing. After the adaptation period the participant
performed three weeks of RT focusing on the goal of improving muscular fitness and
endurance, followed by four weeks of RT to increase strength, and then four weeks of RT
with the goal of making power gains. The weekly BWSTT remained consistent
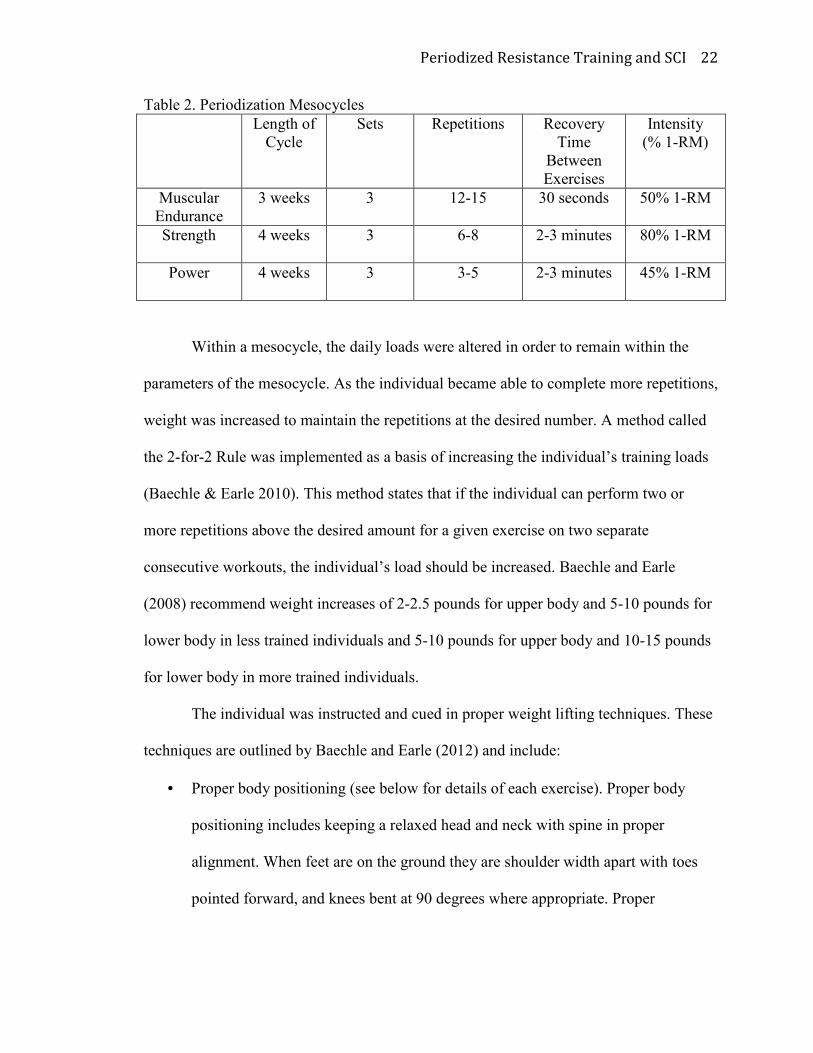
throughout the twelve week exercise program. The variables for the 12 week exercise
program including exercise volume, intensity, duration, and recovery time were
manipulated as depicted in Table 2:
Periodized Resistance Training and SCI 22
Table 2. Periodization Mesocycles
Length of
Cycle
Sets Repetitions Recovery
Time
Between
Exercises
Intensity
(% 1-RM)
Muscular
Endurance
3 weeks 3 12-15 30 seconds 50% 1-RM
Strength 4 weeks 3 6-8 2-3 minutes 80% 1-RM
Power 4 weeks 3 3-5 2-3 minutes 45% 1-RM
Within a mesocycle, the daily loads were altered in order to remain within the
parameters of the mesocycle. As the individual became able to complete more repetitions,
weight was increased to maintain the repetitions at the desired number. A method called
the 2-for-2 Rule was implemented as a basis of increasing the individual’s training loads
(Baechle & Earle 2010). This method states that if the individual can perform two or
more repetitions above the desired amount for a given exercise on two separate
consecutive workouts, the individual’s load should be increased. Baechle and Earle
(2008) recommend weight increases of 2-2.5 pounds for upper body and 5-10 pounds for
lower body in less trained individuals and 5-10 pounds for upper body and 10-15 pounds
for lower body in more trained individuals.
The individual was instructed and cued in proper weight lifting techniques. These
techniques are outlined by Baechle and Earle (2012) and include:
• Proper body positioning (see below for details of each exercise). Proper body
positioning includes keeping a relaxed head and neck with spine in proper
alignment. When feet are on the ground they are shoulder width apart with toes
pointed forward, and knees bent at 90 degrees where appropriate. Proper
Periodized Resistance Training and SCI 23
positioning as a starting point is essential to support the weight being lifted and to
prevent injury.
• Movement pattern: The individual was instructed to move through the full ROM
possible in order to improve strength at all lengths of the muscle.
• Lifting Speed: This refers to the speed of the movement during the exercise. The
individual was instructed to perform slow and controlled motions for the
development of control and to prevent injury. An appropriate verbal cue utilized
in this program was to allow two seconds for the initial push (or pull) during the
concentric phase, and four seconds for the return to original position, or eccentric
phase of the exercise. The exception to this rule occurs during the power phase,
where increased speed of movement is an important component of the mesocycle
and of power.
• Breathing Pattern: The individual was instructed to exhale upon concentric
motion, and to exhale through the sticking point, followed by inhalation during
the eccentric portion of the movement.
Each training session was completed on selectorized equipment. Slight adaptations and
modifications were made to the exercise program as the study progressed to
accommodate the patient’s deficits, promote proper positioning, and to further
individualize the exercise program to the needs of the subject. Modifications were made
based on feedback from the subject, outcomes, and observation. The following exercises
were included in the program in the given order. Changes that were made to the
positioning are noted.
Periodized Resistance Training and SCI 24
• CybexTM Chest Press- The individual assumed a seated position with feet on the
ground. The machine was adjusted so that the individual’s upper chest was just
above the machine handles. Handles were grasped with overhand grip. Handles
were pushed straight forward until arms were extended.
• CybexTM Leg Press- The individual assumed a seated position on the machine
with a padded back. The individual’s legs were elevated in front of him with
knees bent at ninety degrees, hips bent, and feet against a metal plate. The
individual pushed his hips and knees into extension against the metal plate to
complete the exercise. The individual then slowly returned to the original
position.
This exercise was modified after the second week of training. The individual’s
high adductor muscle tone caused by the SCI pulled his knees together for the
duration of the exercise. A soft pool buoy was placed between the individual’s
knees to place his knees the appropriate distance apart and in the optimal position
to exert force for this exercise. As this method was not yet discovered during the
pre test 1RM assessment of lower body strength, it was not implemented in the
post testing 1RM assessment of lower body strength.
• CybexTM Lat Pull-down- The individual assumed a seated position with feet on
the ground. The individual’s knees were held in place with an adjustable pad. The
subject reached overhead to hold onto a weighted overhead bar. The individual
pulled the bar towards his chest while leaning slightly backward. The individual
then slowly returned to the original position.
Periodized Resistance Training and SCI 25
• CybexTM Supine Leg Curls-The individual assumed a seated position with legs off
the ground and knees bent. A weighted pad was placed across the back of the
individual’s ankles and the individual bent his knees as much as possible to
complete the exercise. The individual then slowly returned to the original
position.
The individual was initially unable to complete concentric supine leg curls
independently. He was given assistance with the concentric portion of this
exercise but was able to independently perform the eccentric portion throughout
the duration of the study.
• MagnumTM Shoulder Press- The individual assumed a seated position with feet on
the ground. The machine was adjusted so that the machine handles were at
shoulder level on either side of the subject. Handles were grasped with overhand
grip. Handles were pushed upward until arms were extended.
• CybexTM Leg extension- The individual assumed a seated position slightly
reclined with legs off the ground and knees bent. A weighted pad was placed
across the individual’s ankles and the individual extended his knees till they were
straight out to complete the exercise. The individual then slowly returned to the
original position.
• CybexTM Arm (Bicep) Curls- The individual assumed a seated position with feet
on the ground. The individual’s arms rested on a pad with elbows lined up with
the axis of the machine. The individual held the handles and bent at the elbows
while his arms stayed in contact with the pad.
Periodized Resistance Training and SCI 26
• NautilusTM Hip Abduction- The individual assumed a seated position with back
supported. His legs and feet were elevated off the ground and rested on machine
handles. Weighted pads rested on his outer thigh. The individual pushed the pads
outward as much as possible, and then returned slowly to his original position.
• CybexTM Arm Extension- The individual assumed a seated position with feet on
the ground. The individual’s arms rested on a pad with elbows lined up with the
axis of the machine. The individual held handles and extended the elbows while
arms stayed in contact with the pad. The individual then slowly returned to the
original position.
• CybexTM Back Extension-The individual placed his feet in foot rests while sitting
on a pad. A resisted pad rested against the individual’s back. The individual’s
back was slightly bent forward and he extended his back against the resisted pad
as far as possible. The individual then slowly returned to his original position.
This was another exercise in which the participant’s high adductor muscle tone
posed a problem with proper positioning. At the beginning of the second
mesocycle the pool buoy was also introduced in this exercise as a positioning tool
placed between the individual’s knees to assist in maintaining proper positioning
for the duration of the exercise.
• Supine Abdominal Curls- The individual laid on a mat with hips and knees bent at
90 degree angles. The legs were supported on the seat of a chair. The individual
rested his arms on the mat while flexing his abdominals to lift his upper body
towards the ceiling, and then slowly returned to the original position.
Periodized Resistance Training and SCI 27
Upper and lower extremity exercises were alternated within each individual training
session to hopefully minimize stress and fatigue in muscle groups. In addition to
performing RT the subject performed the following flexibility exercises:
• Thomas Hip Flexor Stretch (Figure 1): The individual sat at the edge of a mat
table and pulled one knee towards his chest as he lied down backwards. The
stretch should be felt in the hip flexor muscles that are on the anterior portion of
the leg hanging off the table.
Image provided by AthleticAdvisor.com (2009)
Figure 1. Thomas Hip Flexor Stretch
• Ober Stretch (for abductors and iliotibial band)(Figure 2): The individual laid on a
mat table on his side with the bottom leg bend upward while the back leg
remained straight and was allowed to drop downwards toward the table. The
stretch affected the abductors that run down the length of the outer thigh.
This stretch was omitted after the endurance phase as the participant reported no
stretch felt and no benefit from the exercise. The individual demonstrated
significant tightness of the adductors throughout the study, it was determined that
the abductors were not in need of lengthening or stretching.

Periodized Resistance Training and SCI 28
Image provided by Stretching-Exercises-Guide (2013)
Figure 2. Ober Stretch
• Standing Calf Stretch (Figure 3): The individual stood with one foot in front of
the other leaning against a wall with both hands. The front leg was bent while the
back leg remained straight with the heel remaining on the ground.
This stretch was modified for the final phase of the program. As time went on, the
individual felt less stretch from this position. It was modified so that he stepped
on a slanted board to place the ankle in a more dorsiflexed position for greater
lengthening of the gastroc/soleus complex.
Image provided by Top End Sports (2015)
Figure 3. Standing Calf Stretch
• Sit and Reach Stretch (Figure 4): The individual sat on a mat with legs extended
and leaned towards one side, then the other while reaching towards his toes as
much as possible. The knees were kept straight.
Periodized Resistance Training and SCI 29
This stretch was modified during the strength phase. A towel was used to wrap
around the foot to allow him to pull himself closer towards the foot and place the
hamstring in a more lengthened position.
Image provided by Edinformatics (1999)
Figure 4. Sit and Reach Stretch
At the beginning of the power phase it was eliminated altogether and a separate
manual hamstring stretch was used in its place (Figure 5). This provided a
progression of the flexibility exercise and was a more comfortable and effective
stretch for the participant.
Image provided by TeachPE.com (2015)
Figure 5. Manual Hamstring Stretch
• Adductor stretch (Butterfly Stretch) (Figure 6): The individual sat on a mat and
pulled his feet towards his body with his arms. The knees were bent, while the
heels touched each other until a stretch was felt in the inner thigh.
Periodized Resistance Training and SCI 30
Image provided by Physiohub (2010)
Figure 6. Adductor Stretch
• Supine Cross-body Gluteal stretch (Figure 7): The individual laid down on a mat
and pulled one knee towards his opposite shoulder with his arms. This was
repeated on both sides.
Image provided by My Physical Therapy Coach (2014)
Figure 7. Supine Cross-body Gluteal Stretch
• Cross body shoulder stretch (Figure 8): The individual extended one arm across
the front of his body and held it in place with the opposite hand until a stretch was
felt across the back of the arm. This was repeated with both sides.
Image provided by Top End Sports (2015)
Figure 8. Cross Body Shoulder Stretch
Periodized Resistance Training and SCI 31
• Overhead Triceps Stretch (Figure 9): The individual bent one elbow behind his
head and pulled posteriorly with the opposite hand until a stretch was felt across
the bottom of the arm. This was repeated on both sides.
Image provided by SuperSets (2013)
Figure 9. Overhead Triceps Stretch
This stretch was modified going into the strength phase of the program. The
individual placed one arm overhead and the other behind the back and was given
a towel to hold within each hand as shown in Figure 10. By pulling the towel with
the lower hand the triceps stretch within the upper hand is increased.
Image provided by All About Tennis (2015)
Figure 10. Modified Overhead Triceps Stretch
• Standing Corner Pectoralis Stretch (Figure 11): The individual stood in a doorway
with arms extended out to both sides. He then leaned in towards the open
doorway until a stretch was felt across the chest.
Periodized Resistance Training and SCI 32
Image provided by Abbott center for Neuromuscular Therapy (2009)
Figure 11. Standing Pectoralis Stretch
Data Collection
Results are quantified by a comparison of preliminary and post testing outcomes
measures including:
• Manual Muscle testing: Manual muscle testing is a basic test for an individual’s
general strength in muscles and muscle groups. It takes into consideration a
muscle groups abilities against the force of gravity and against the force of
manual resistance provided by a clinician. A muscle or muscle group is isolated
and tested for its ability to move through its ROM against gravity, and then for its
ability to hold its position against resistance within the mid-ROM. The standard
grading system of 0-5 for manual muscle testing was used. An outline of the
grading system given by O’Sullivan and Schmitz (2007) is provided in the
Appendix A.
• 1-RM Testing (as described previously)
• Modified Ashworth Scale for muscle spasticity: This is a non-functional measure
of muscle tone based on motions to affect a response to a stretch reflex. The
grading scale measures the severity of muscle tone in response to the stretching
of a muscle. The grading scale for the modified Ashworth scale outlined by
O’Sullivan and Schmitz (2007) is provided Appendix B. It should be noted that
Periodized Resistance Training and SCI 33
the participant in this study received Baclofen through an intrathecal pump for
the duration of the study. The dosage and delivery of this medication was kept
consistent and was not altered in any way at any point during the 12 week study.
• Joint range of motion of the lower extremities via goniometry: This is an
objective measure of an individual’s flexibility and ability to move a single joint
through a ROM.
• 6-minute walk test: The 6-minute walk test is both a speed and endurance test
that measures the distance a person is able to walk for 6 minutes independently.
• Body composition analysis as measured by Bod Pod©: The Bod Pod is a device
that measures an individual’s body composition through the use of air
displacement. The test requires an individual to sit inside a closed vessel for a
few minutes with minimal movement while the device records data.
Periodized Resistance Training and SCI 34
Results & Discussion
Manual Muscle Testing
Manual muscle testing (MMT) has been used in clinical practice since 1912 as a
clinical means to assess and grade muscle strength based on gravity and manually applied
resistance (O’Sullivan 2007). Using this type of assessment, muscles are graded on their
ability to move through a full available ROM, move against gravity, and move against
manual resistance on a scale from zero to five. The ability to move a muscle group
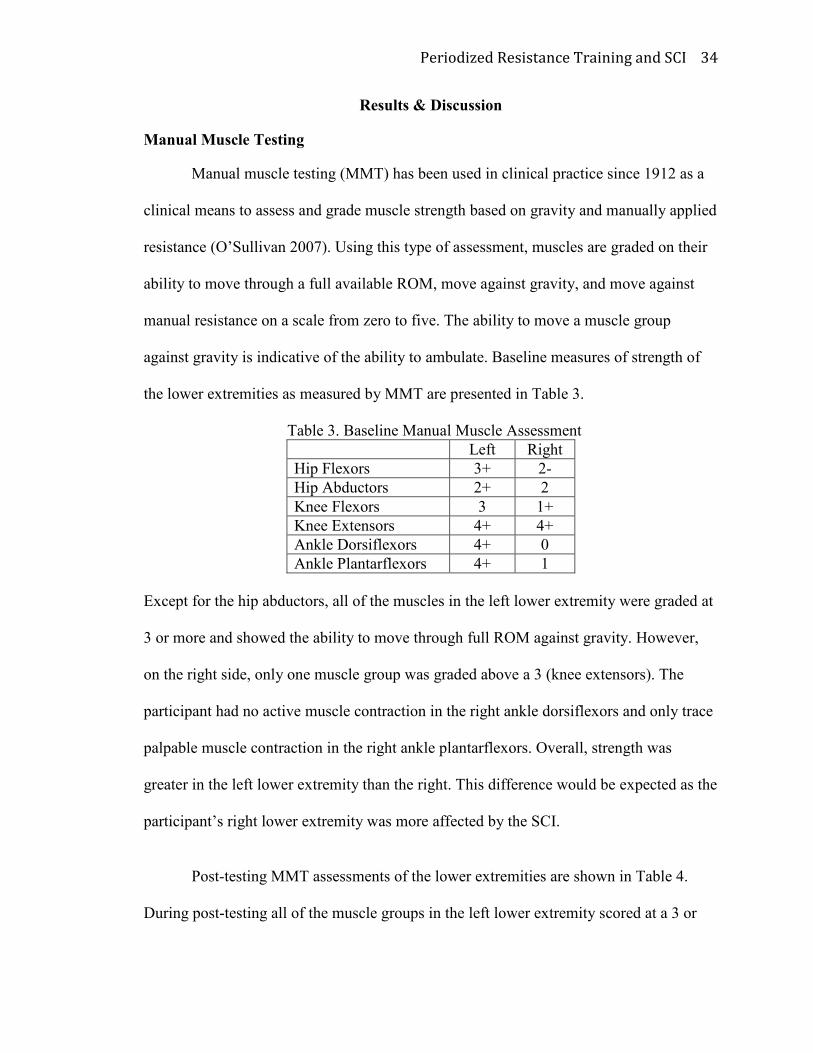
against gravity is indicative of the ability to ambulate. Baseline measures of strength of
the lower extremities as measured by MMT are presented in Table 3.
Table 3. Baseline Manual Muscle Assessment
Left Right
Hip Flexors 3+ 2-
Hip Abductors 2+ 2
Knee Flexors 3 1+
Knee Extensors 4+ 4+
Ankle Dorsiflexors 4+ 0
Ankle Plantarflexors 4+ 1
Except for the hip abductors, all of the muscles in the left lower extremity were graded at
3 or more and showed the ability to move through full ROM against gravity. However,
on the right side, only one muscle group was graded above a 3 (knee extensors). The
participant had no active muscle contraction in the right ankle dorsiflexors and only trace
palpable muscle contraction in the right ankle plantarflexors. Overall, strength was
greater in the left lower extremity than the right. This difference would be expected as the
participant’s right lower extremity was more affected by the SCI.
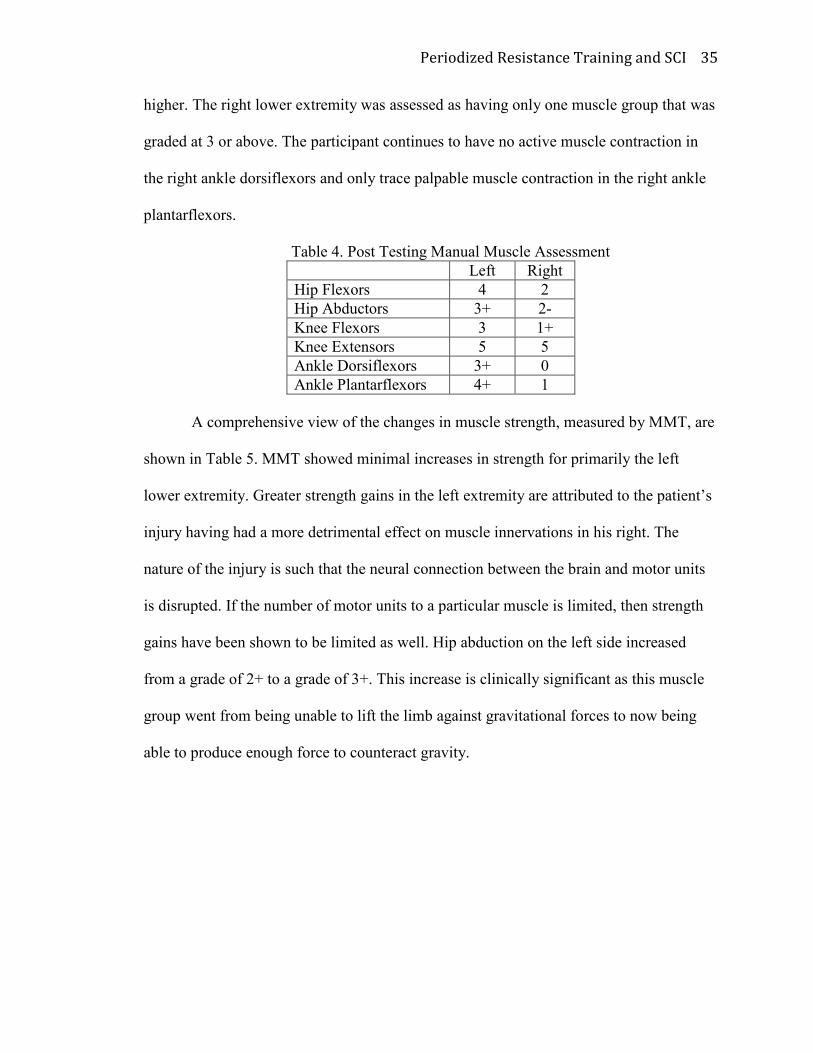
Post-testing MMT assessments of the lower extremities are shown in Table 4.
During post-testing all of the muscle groups in the left lower extremity scored at a 3 or
Periodized Resistance Training and SCI 35
higher. The right lower extremity was assessed as having only one muscle group that was
graded at 3 or above. The participant continues to have no active muscle contraction in
the right ankle dorsiflexors and only trace palpable muscle contraction in the right ankle
plantarflexors.
Table 4. Post Testing Manual Muscle Assessment
Left Right
Hip Flexors 4 2
Hip Abductors 3+ 2-
Knee Flexors 3 1+
Knee Extensors 5 5
Ankle Dorsiflexors 3+ 0
Ankle Plantarflexors 4+ 1
A comprehensive view of the changes in muscle strength, measured by MMT, are
shown in Table 5. MMT showed minimal increases in strength for primarily the left
lower extremity. Greater strength gains in the left extremity are attributed to the patient’s
injury having had a more detrimental effect on muscle innervations in his right. The
nature of the injury is such that the neural connection between the brain and motor units
is disrupted. If the number of motor units to a particular muscle is limited, then strength
gains have been shown to be limited as well. Hip abduction on the left side increased
from a grade of 2+ to a grade of 3+. This increase is clinically significant as this muscle
group went from being unable to lift the limb against gravitational forces to now being
able to produce enough force to counteract gravity.
Periodized Resistance Training and SCI 36
Table 5.Changes in Muscle Strength
∆ ∆
Left Right
Hip Flexors + +
Hip Abductors + -
Knee Flexors 0 0
Knee Extensors + +
Ankle Dorsiflexors - 0
Ankle Plantarflexors 0 0 + : Increase in spasticity after 12 weeks
- : Decrease in spasticity after 12 weeks
0 : No change in spasticity
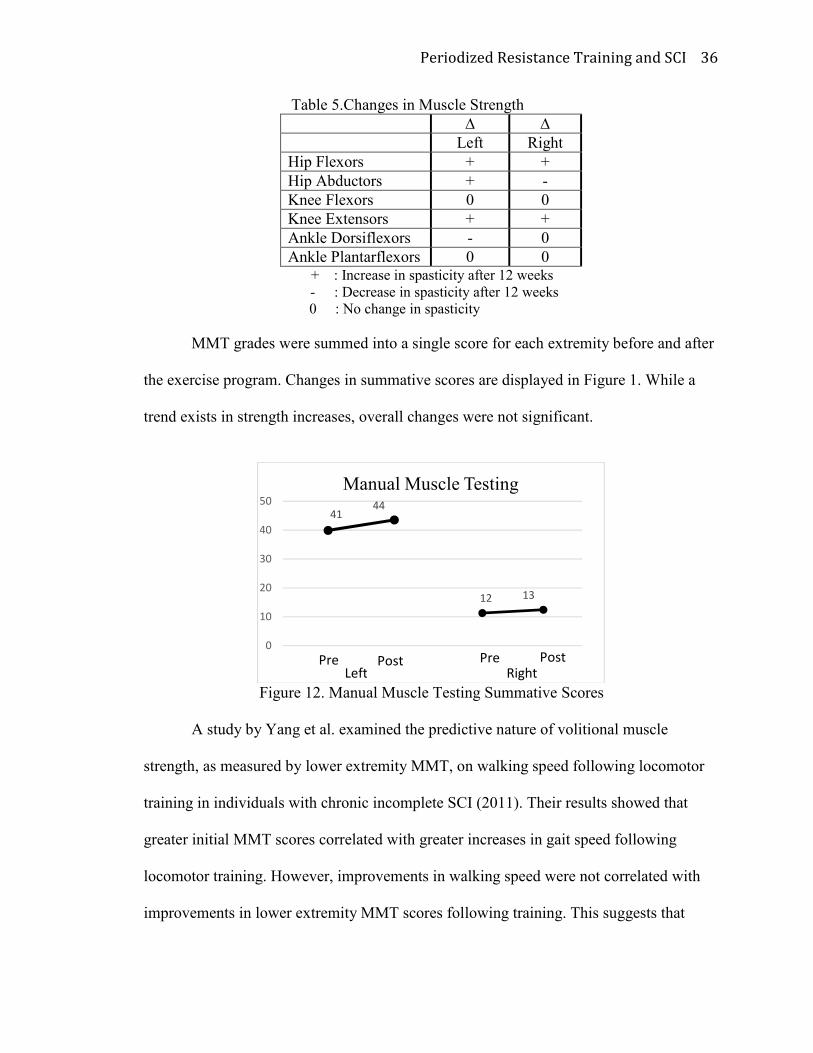
MMT grades were summed into a single score for each extremity before and after
the exercise program. Changes in summative scores are displayed in Figure 1. While a
trend exists in strength increases, overall changes were not significant.
Figure 12. Manual Muscle Testing Summative Scores
A study by Yang et al. examined the predictive nature of volitional muscle
strength, as measured by lower extremity MMT, on walking speed following locomotor
training in individuals with chronic incomplete SCI (2011). Their results showed that
greater initial MMT scores correlated with greater increases in gait speed following
locomotor training. However, improvements in walking speed were not correlated with
improvements in lower extremity MMT scores following training. This suggests that
41
12
44
13
0
10
20
30
40
50
Manual Muscle Testing
Pre Post Pre Post
Left Right
Periodized Resistance Training and SCI 37
improvements in gait speed following locomotor training are related to modified muscle
activation patterns rather than improvements in strength. These findings correlate to the
findings in the current study, where the participant made improvements in gait speed, but
did not show equal improvement in.
1RM Testing
Studies examining strength training in the SCI population are becoming more
prominent but are still sparse compared with other populations. Functional and clinical
outcomes measures are more commonly utilized within studies of the SCI population
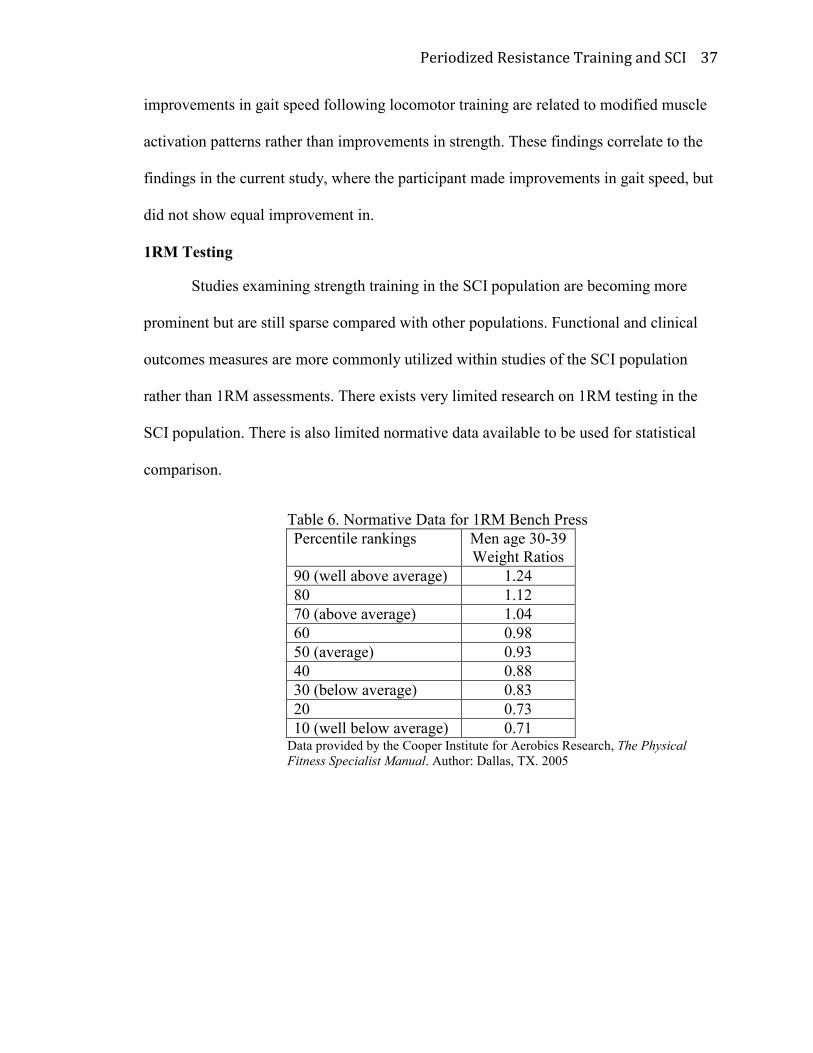
rather than 1RM assessments. There exists very limited research on 1RM testing in the
SCI population. There is also limited normative data available to be used for statistical
comparison.
Table 6. Normative Data for 1RM Bench Press
Data provided by the Cooper Institute for Aerobics Research, The Physical
Fitness Specialist Manual. Author: Dallas, TX. 2005
Percentile rankings Men age 30-39
Weight Ratios
90 (well above average) 1.24
80 1.12
70 (above average) 1.04
60 0.98
50 (average) 0.93
40 0.88
30 (below average) 0.83
20 0.73
10 (well below average) 0.71
Periodized Resistance Training and SCI 38
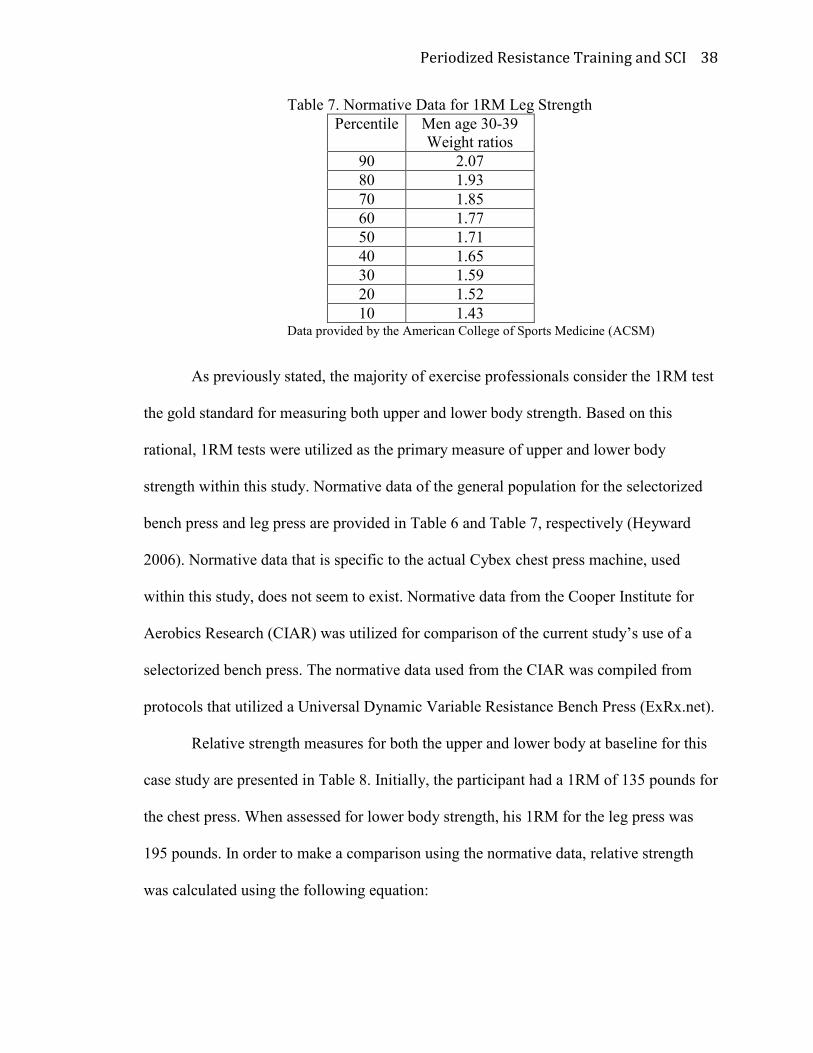
Table 7. Normative Data for 1RM Leg Strength
Percentile Men age 30-39
Weight ratios
90 2.07
80 1.93
70 1.85
60 1.77
50 1.71
40 1.65
30 1.59
20 1.52
10 1.43 Data provided by the American College of Sports Medicine (ACSM)
As previously stated, the majority of exercise professionals consider the 1RM test
the gold standard for measuring both upper and lower body strength. Based on this
rational, 1RM tests were utilized as the primary measure of upper and lower body
strength within this study. Normative data of the general population for the selectorized
bench press and leg press are provided in Table 6 and Table 7, respectively (Heyward
2006). Normative data that is specific to the actual Cybex chest press machine, used
within this study, does not seem to exist. Normative data from the Cooper Institute for
Aerobics Research (CIAR) was utilized for comparison of the current study’s use of a
selectorized bench press. The normative data used from the CIAR was compiled from
protocols that utilized a Universal Dynamic Variable Resistance Bench Press (ExRx.net).
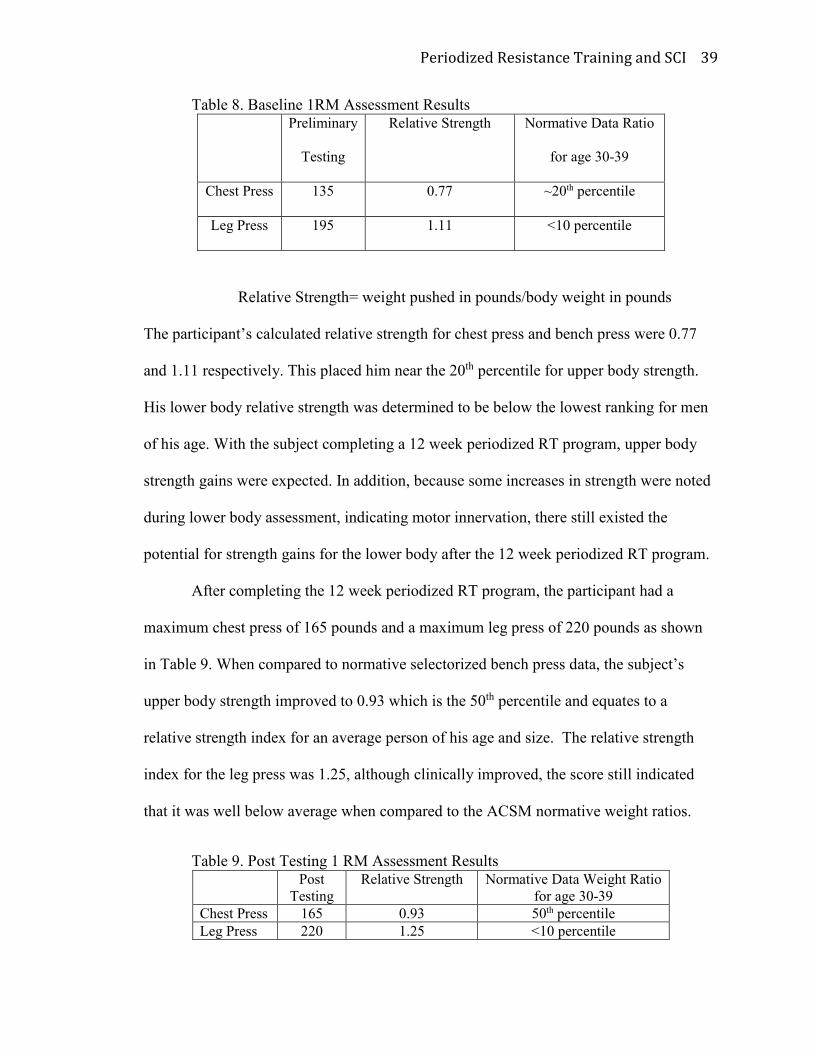
Relative strength measures for both the upper and lower body at baseline for this
case study are presented in Table 8. Initially, the participant had a 1RM of 135 pounds for
the chest press. When assessed for lower body strength, his 1RM for the leg press was
195 pounds. In order to make a comparison using the normative data, relative strength
was calculated using the following equation:
Periodized Resistance Training and SCI 39
Table 8. Baseline 1RM Assessment Results Preliminary
Testing
Relative Strength Normative Data Ratio
for age 30-39
Chest Press 135 0.77 ~20th percentile
Leg Press 195 1.11 <10 percentile
Relative Strength= weight pushed in pounds/body weight in pounds
The participant’s calculated relative strength for chest press and bench press were 0.77
and 1.11 respectively. This placed him near the 20th percentile for upper body strength.
His lower body relative strength was determined to be below the lowest ranking for men
of his age. With the subject completing a 12 week periodized RT program, upper body
strength gains were expected. In addition, because some increases in strength were noted
during lower body assessment, indicating motor innervation, there still existed the
potential for strength gains for the lower body after the 12 week periodized RT program.
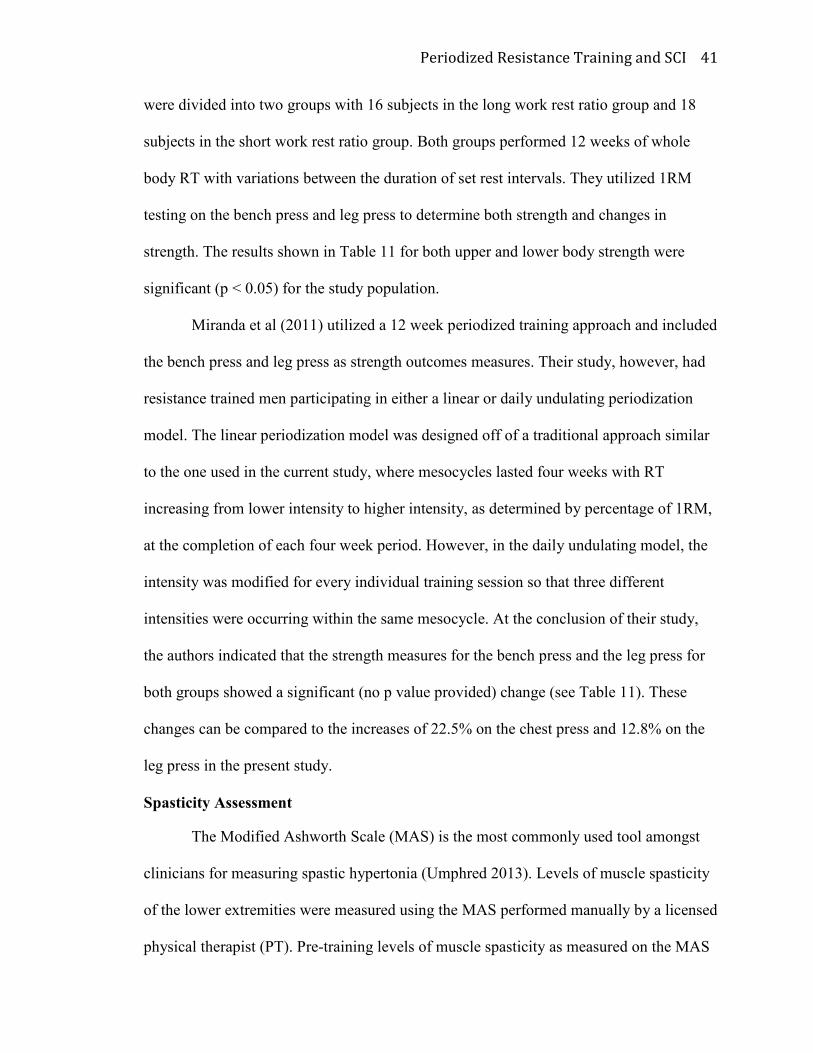
After completing the 12 week periodized RT program, the participant had a
maximum chest press of 165 pounds and a maximum leg press of 220 pounds as shown
in Table 9. When compared to normative selectorized bench press data, the subject’s
upper body strength improved to 0.93 which is the 50th percentile and equates to a
relative strength index for an average person of his age and size. The relative strength
index for the leg press was 1.25, although clinically improved, the score still indicated
that it was well below average when compared to the ACSM normative weight ratios.
Table 9. Post Testing 1 RM Assessment Results Post
Testing
Relative Strength Normative Data Weight Ratio
for age 30-39
Chest Press 165 0.93 50th percentile
Leg Press 220 1.25 <10 percentile

Periodized Resistance Training and SCI 40
Results of both the pre and post assessments for upper and lower body strength,
respectively are depicted in Table 10. As can be observed, strength gains were evidenced
for both upper and lower body strength. The upper body strength test (i.e. chest press)
indicated an increase of 30 pounds, or a 22.2% increase from baseline. The lower body
strength assessment (i.e. leg press) showed an increase of 25 pounds, or a 12.8% increase
in lower body strength from the initial assessment.
Table 10. Changes in 1 RM PreTest Post Testing ∆
(Pounds)
Chest Press 135 165 +30
Leg Press 195 220 +25
Changes in strength are shown in Table 11 and compared to the results from two
other RT studies. These studies were selected because the participants were men, and
each study utilized a 12 week RT intervention. Each study also used 1RM testing as a
measure of upper and lower body strength. Additionally, Gentil et al. was selected
because participants were untrained similar to the participant’s training status in the
current study. The Miranda et al. study was selected because the RT intervention utilized
a periodized paradigm.
Table 11. Comparison to Research Present Study
% change
Miranda et al. (2011)
periodized
trained subjects
Gentil et al. (2010)
not periodized
untrained subjects
Chest Press 22.2% 15% (bench press) 10.5% (bench press)
Leg Press 12.8% 10% 17.5%
Gentil et al. (2010) also manipulated the training variable of rest/recovery
between sets in the study population of young untrained men. The group of participants
Periodized Resistance Training and SCI 41
were divided into two groups with 16 subjects in the long work rest ratio group and 18
subjects in the short work rest ratio group. Both groups performed 12 weeks of whole
body RT with variations between the duration of set rest intervals. They utilized 1RM
testing on the bench press and leg press to determine both strength and changes in
strength. The results shown in Table 11 for both upper and lower body strength were
significant (p < 0.05) for the study population.
Miranda et al (2011) utilized a 12 week periodized training approach and included
the bench press and leg press as strength outcomes measures. Their study, however, had
resistance trained men participating in either a linear or daily undulating periodization
model. The linear periodization model was designed off of a traditional approach similar
to the one used in the current study, where mesocycles lasted four weeks with RT
increasing from lower intensity to higher intensity, as determined by percentage of 1RM,
at the completion of each four week period. However, in the daily undulating model, the
intensity was modified for every individual training session so that three different
intensities were occurring within the same mesocycle. At the conclusion of their study,
the authors indicated that the strength measures for the bench press and the leg press for
both groups showed a significant (no p value provided) change (see Table 11). These
changes can be compared to the increases of 22.5% on the chest press and 12.8% on the
leg press in the present study.
Spasticity Assessment
The Modified Ashworth Scale (MAS) is the most commonly used tool amongst
clinicians for measuring spastic hypertonia (Umphred 2013). Levels of muscle spasticity
of the lower extremities were measured using the MAS performed manually by a licensed
physical therapist (PT). Pre-training levels of muscle spasticity as measured on the MAS
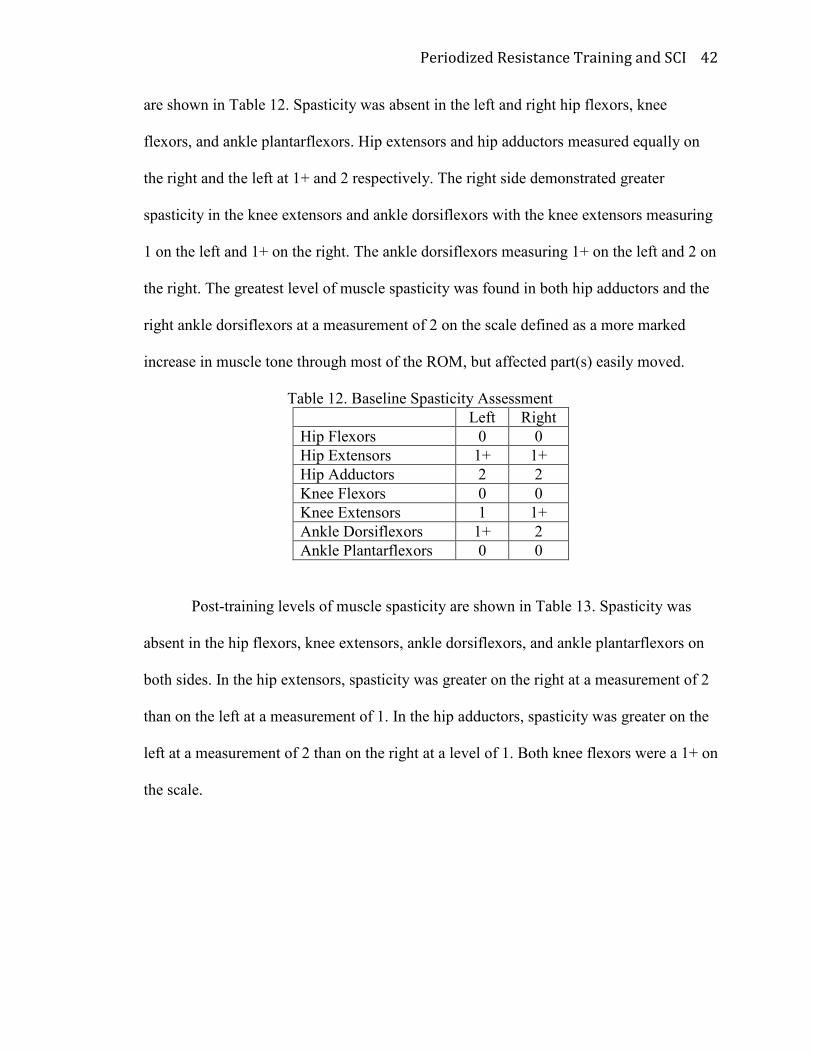
Periodized Resistance Training and SCI 42
are shown in Table 12. Spasticity was absent in the left and right hip flexors, knee
flexors, and ankle plantarflexors. Hip extensors and hip adductors measured equally on
the right and the left at 1+ and 2 respectively. The right side demonstrated greater
spasticity in the knee extensors and ankle dorsiflexors with the knee extensors measuring
1 on the left and 1+ on the right. The ankle dorsiflexors measuring 1+ on the left and 2 on
the right. The greatest level of muscle spasticity was found in both hip adductors and the
right ankle dorsiflexors at a measurement of 2 on the scale defined as a more marked
increase in muscle tone through most of the ROM, but affected part(s) easily moved.
Table 12. Baseline Spasticity Assessment
Left Right
Hip Flexors 0 0
Hip Extensors 1+ 1+
Hip Adductors 2 2
Knee Flexors 0 0
Knee Extensors 1 1+
Ankle Dorsiflexors 1+ 2
Ankle Plantarflexors 0 0
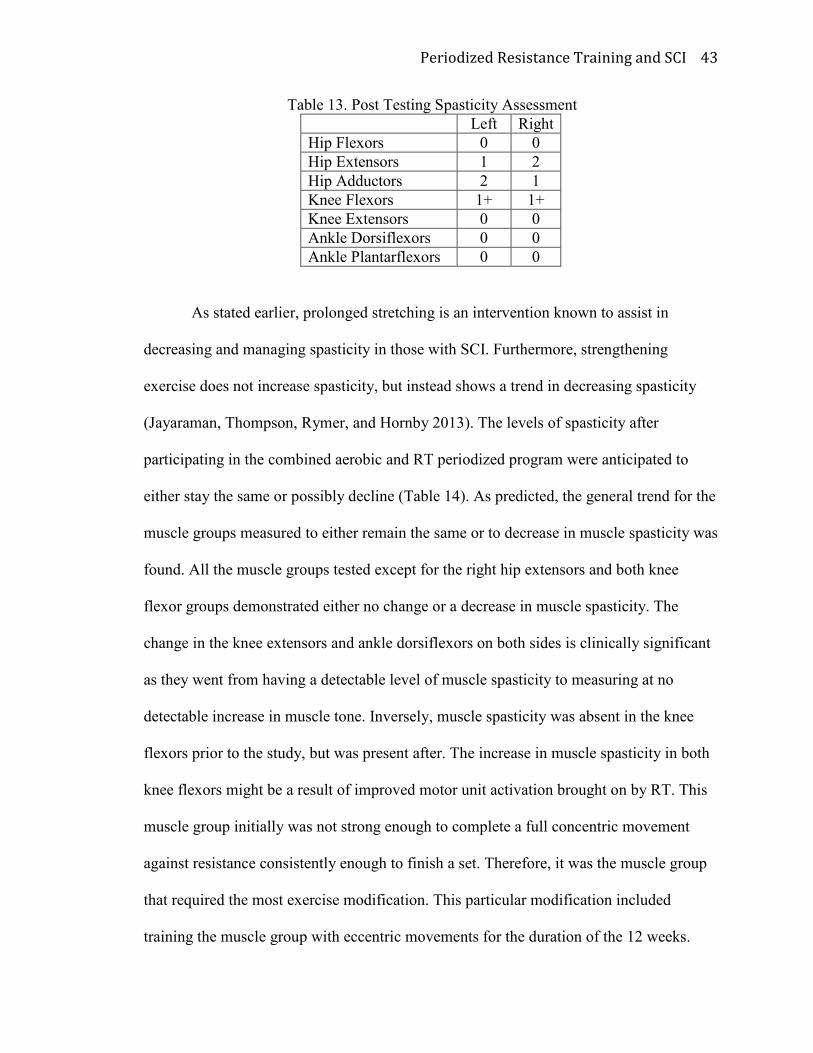
Post-training levels of muscle spasticity are shown in Table 13. Spasticity was
absent in the hip flexors, knee extensors, ankle dorsiflexors, and ankle plantarflexors on
both sides. In the hip extensors, spasticity was greater on the right at a measurement of 2
than on the left at a measurement of 1. In the hip adductors, spasticity was greater on the
left at a measurement of 2 than on the right at a level of 1. Both knee flexors were a 1+ on
the scale.
Periodized Resistance Training and SCI 43
Table 13. Post Testing Spasticity Assessment
Left Right
Hip Flexors 0 0
Hip Extensors 1 2
Hip Adductors 2 1
Knee Flexors 1+ 1+
Knee Extensors 0 0
Ankle Dorsiflexors 0 0
Ankle Plantarflexors 0 0
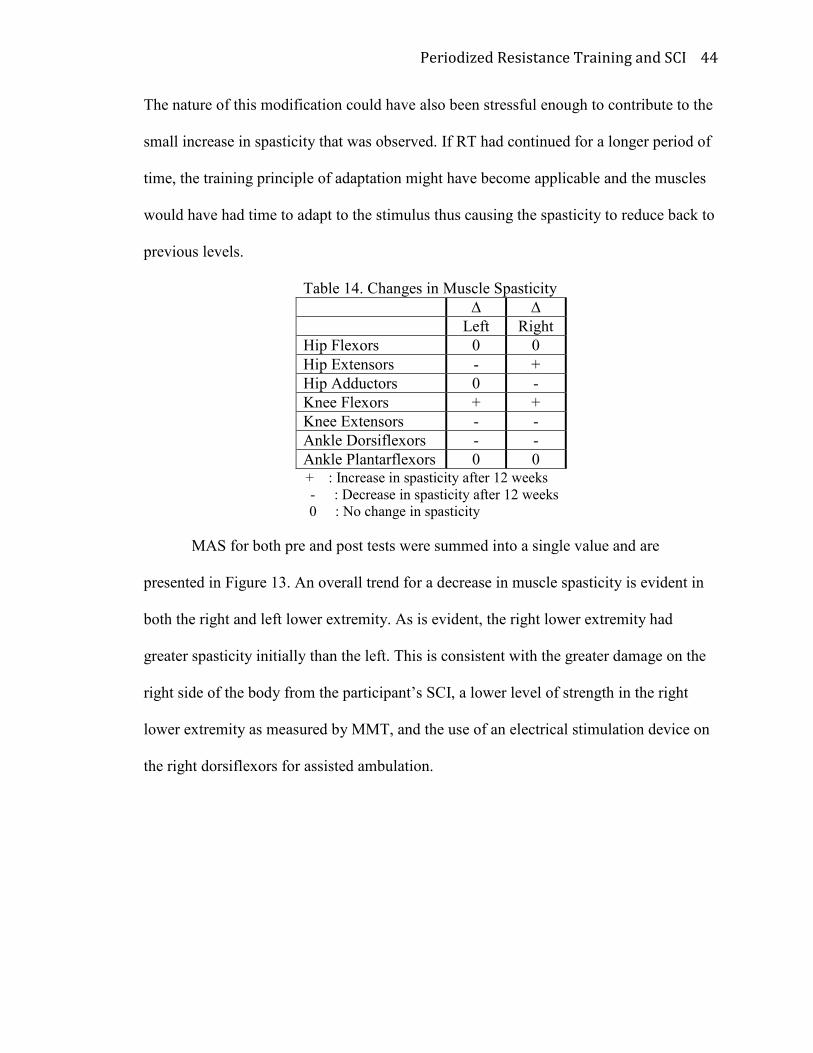
As stated earlier, prolonged stretching is an intervention known to assist in
decreasing and managing spasticity in those with SCI. Furthermore, strengthening
exercise does not increase spasticity, but instead shows a trend in decreasing spasticity
(Jayaraman, Thompson, Rymer, and Hornby 2013). The levels of spasticity after
participating in the combined aerobic and RT periodized program were anticipated to
either stay the same or possibly decline (Table 14). As predicted, the general trend for the
muscle groups measured to either remain the same or to decrease in muscle spasticity was
found. All the muscle groups tested except for the right hip extensors and both knee
flexor groups demonstrated either no change or a decrease in muscle spasticity. The
change in the knee extensors and ankle dorsiflexors on both sides is clinically significant
as they went from having a detectable level of muscle spasticity to measuring at no
detectable increase in muscle tone. Inversely, muscle spasticity was absent in the knee
flexors prior to the study, but was present after. The increase in muscle spasticity in both
knee flexors might be a result of improved motor unit activation brought on by RT. This
muscle group initially was not strong enough to complete a full concentric movement
against resistance consistently enough to finish a set. Therefore, it was the muscle group
that required the most exercise modification. This particular modification included
training the muscle group with eccentric movements for the duration of the 12 weeks.
Periodized Resistance Training and SCI 44
The nature of this modification could have also been stressful enough to contribute to the
small increase in spasticity that was observed. If RT had continued for a longer period of
time, the training principle of adaptation might have become applicable and the muscles
would have had time to adapt to the stimulus thus causing the spasticity to reduce back to
previous levels.
Table 14. Changes in Muscle Spasticity
∆ ∆
Left Right
Hip Flexors 0 0
Hip Extensors - +
Hip Adductors 0 -
Knee Flexors + +
Knee Extensors - -
Ankle Dorsiflexors - -
Ankle Plantarflexors 0 0 + : Increase in spasticity after 12 weeks
- : Decrease in spasticity after 12 weeks
0 : No change in spasticity
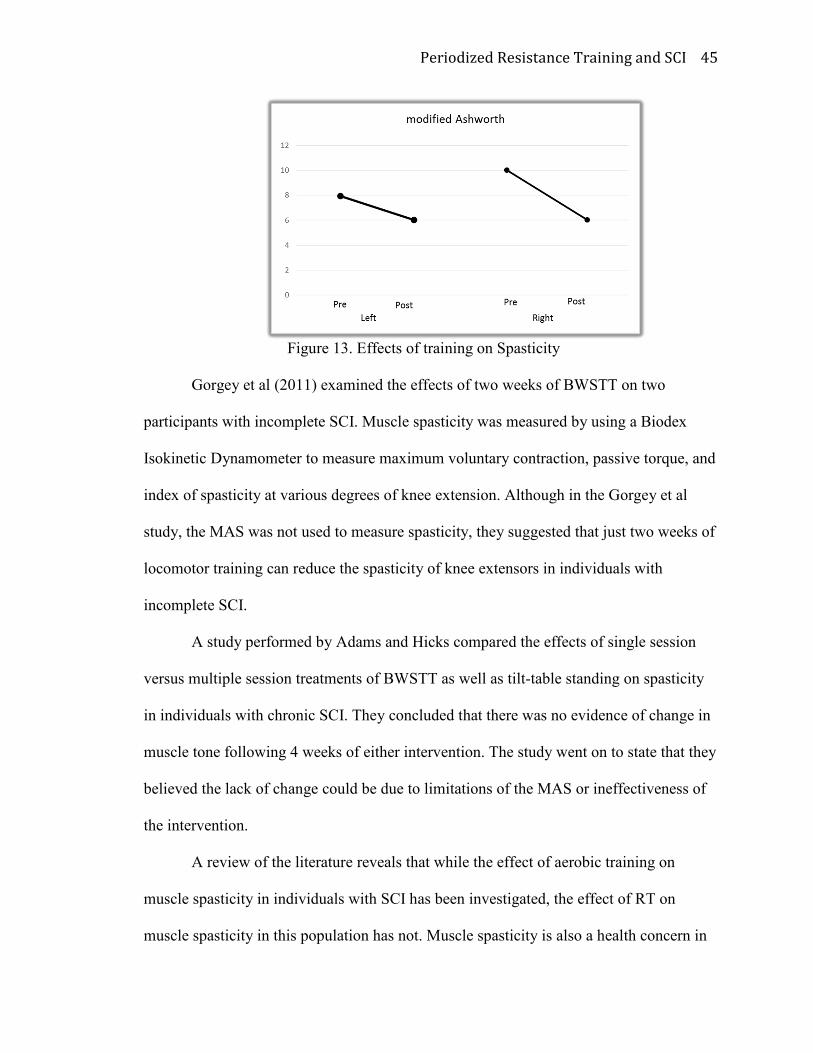
MAS for both pre and post tests were summed into a single value and are
presented in Figure 13. An overall trend for a decrease in muscle spasticity is evident in
both the right and left lower extremity. As is evident, the right lower extremity had
greater spasticity initially than the left. This is consistent with the greater damage on the
right side of the body from the participant’s SCI, a lower level of strength in the right
lower extremity as measured by MMT, and the use of an electrical stimulation device on
the right dorsiflexors for assisted ambulation.
Periodized Resistance Training and SCI 45
Figure 13. Effects of training on Spasticity
Gorgey et al (2011) examined the effects of two weeks of BWSTT on two
participants with incomplete SCI. Muscle spasticity was measured by using a Biodex
Isokinetic Dynamometer to measure maximum voluntary contraction, passive torque, and
index of spasticity at various degrees of knee extension. Although in the Gorgey et al
study, the MAS was not used to measure spasticity, they suggested that just two weeks of
locomotor training can reduce the spasticity of knee extensors in individuals with
incomplete SCI.
A study performed by Adams and Hicks compared the effects of single session
versus multiple session treatments of BWSTT as well as tilt-table standing on spasticity
in individuals with chronic SCI. They concluded that there was no evidence of change in
muscle tone following 4 weeks of either intervention. The study went on to state that they
believed the lack of change could be due to limitations of the MAS or ineffectiveness of
the intervention.
A review of the literature reveals that while the effect of aerobic training on
muscle spasticity in individuals with SCI has been investigated, the effect of RT on
muscle spasticity in this population has not. Muscle spasticity is also a health concern in
Periodized Resistance Training and SCI 46
individuals who suffer from chronic stroke. A review by Pak and Patten examined the
effects of strengthening in individuals following stroke. Their theory is that weakness
contributes to spasticity. Therefore, providing strengthening interventions would not
increase the level of spasticity. They reviewed 11 clinical studies, several of which used
the MAS as an outcomes measure. They concluded that none of the clinical studies they
reviewed reported increased spasticity or hypertonia after a course of strengthening
interventions.
It is important to note that although the test has been shown to have good
intrarater reliability (0.84) and good interrater reliability (0.83), the test itself does not
provide the ability to detect small changes in tone.
Joint Range of Motion
Range of motion was assessed to determine if the exercise program had an effect
on flexibility. Range of motion was assessed via goniometry prior to the exercise
program. Joint ROM can be limited by muscle spasticity, muscle length, connective
tissue extensibility, muscle mass, and improper joint articulation. In addition, active joint
ROM can be limited due to absent or decreased activation or strength of the muscle and
the inability support the movement of the limb. Baseline assessments of passive and
active range of motion in the lower extremities are shown in Table 15 and Table 16
respectively. A box marked with ‘-‘ indicates that there was no active movement of that
muscle group. Due to the nature of his injury, the participant would be expected to have
less active range of motion in his right side rather than his left.
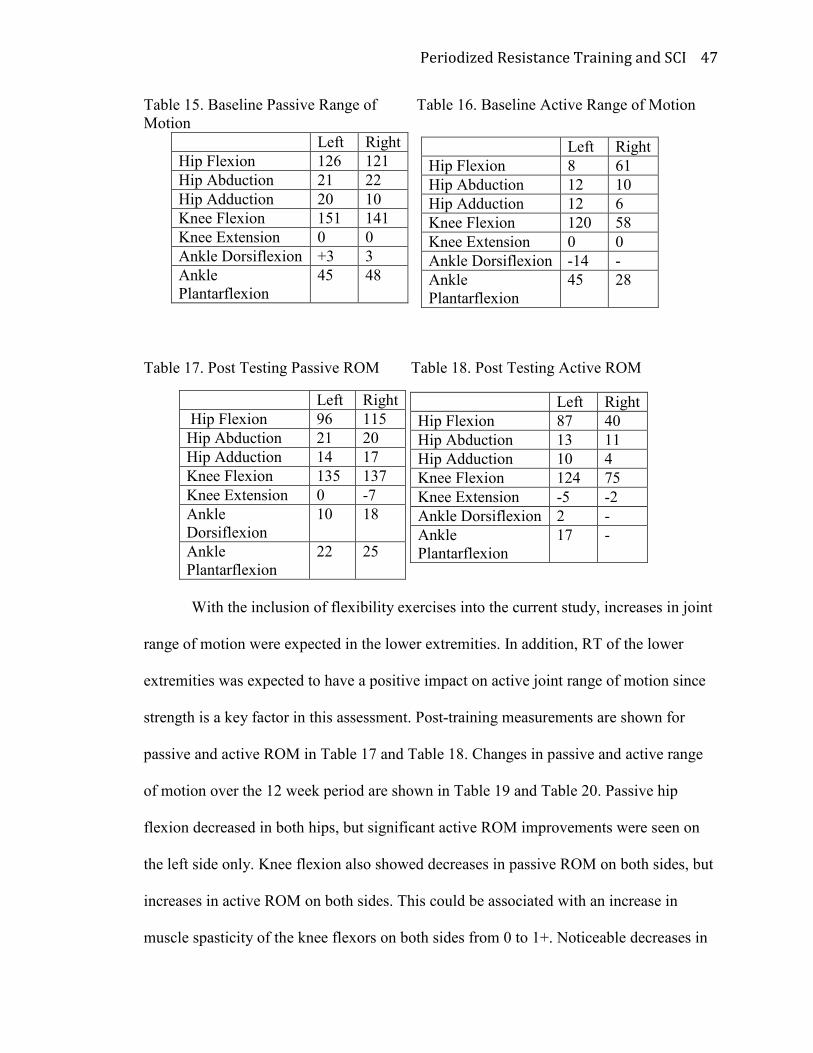
Periodized Resistance Training and SCI 47
Table 15. Baseline Passive Range of Table 16. Baseline Active Range of Motion
Motion
Left Right
Hip Flexion 126 121
Hip Abduction 21 22
Hip Adduction 20 10
Knee Flexion 151 141
Knee Extension 0 0
Ankle Dorsiflexion +3 3
Ankle
Plantarflexion
45 48
Table 17. Post Testing Passive ROM Table 18. Post Testing Active ROM
Left Right
Hip Flexion 96 115
Hip Abduction 21 20
Hip Adduction 14 17
Knee Flexion 135 137
Knee Extension 0 -7
Ankle
Dorsiflexion
10 18
Ankle
Plantarflexion
22 25
With the inclusion of flexibility exercises into the current study, increases in joint
range of motion were expected in the lower extremities. In addition, RT of the lower
extremities was expected to have a positive impact on active joint range of motion since
strength is a key factor in this assessment. Post-training measurements are shown for
passive and active ROM in Table 17 and Table 18. Changes in passive and active range
of motion over the 12 week period are shown in Table 19 and Table 20. Passive hip
flexion decreased in both hips, but significant active ROM improvements were seen on
the left side only. Knee flexion also showed decreases in passive ROM on both sides, but
increases in active ROM on both sides. This could be associated with an increase in
muscle spasticity of the knee flexors on both sides from 0 to 1+. Noticeable decreases in
Left Right
Hip Flexion 8 61
Hip Abduction 12 10
Hip Adduction 12 6
Knee Flexion 120 58
Knee Extension 0 0
Ankle Dorsiflexion -14 -
Ankle
Plantarflexion
45 28
Left Right
Hip Flexion 87 40
Hip Abduction 13 11
Hip Adduction 10 4
Knee Flexion 124 75
Knee Extension -5 -2
Ankle Dorsiflexion 2 -
Ankle
Plantarflexion
17 -
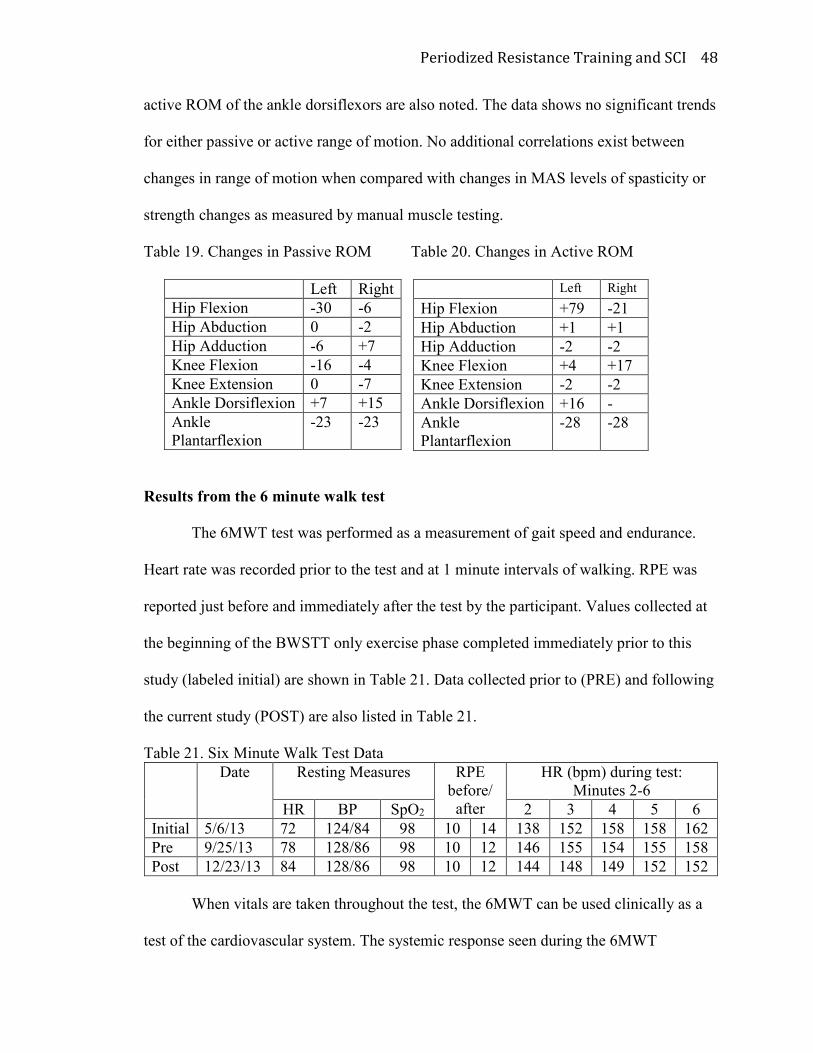
Periodized Resistance Training and SCI 48
active ROM of the ankle dorsiflexors are also noted. The data shows no significant trends
for either passive or active range of motion. No additional correlations exist between
changes in range of motion when compared with changes in MAS levels of spasticity or
strength changes as measured by manual muscle testing.
Table 19. Changes in Passive ROM Table 20. Changes in Active ROM
Left Right
Hip Flexion -30 -6
Hip Abduction 0 -2
Hip Adduction -6 +7
Knee Flexion -16 -4
Knee Extension 0 -7
Ankle Dorsiflexion +7 +15
Ankle
Plantarflexion
-23 -23
Results from the 6 minute walk test
The 6MWT test was performed as a measurement of gait speed and endurance.
Heart rate was recorded prior to the test and at 1 minute intervals of walking. RPE was
reported just before and immediately after the test by the participant. Values collected at
the beginning of the BWSTT only exercise phase completed immediately prior to this
study (labeled initial) are shown in Table 21. Data collected prior to (PRE) and following
the current study (POST) are also listed in Table 21.
Table 21. Six Minute Walk Test Data
Date Resting Measures
RPE
before/
after
HR (bpm) during test:
Minutes 2-6
HR BP SpO2 2 3 4 5 6
Initial 5/6/13 72 124/84 98 10 14 138 152 158 158 162
Pre 9/25/13 78 128/86 98 10 12 146 155 154 155 158
Post 12/23/13 84 128/86 98 10 12 144 148 149 152 152
When vitals are taken throughout the test, the 6MWT can be used clinically as a
test of the cardiovascular system. The systemic response seen during the 6MWT
Left Right
Hip Flexion +79 -21
Hip Abduction +1 +1
Hip Adduction -2 -2
Knee Flexion +4 +17
Knee Extension -2 -2
Ankle Dorsiflexion +16 -
Ankle
Plantarflexion
-28 -28
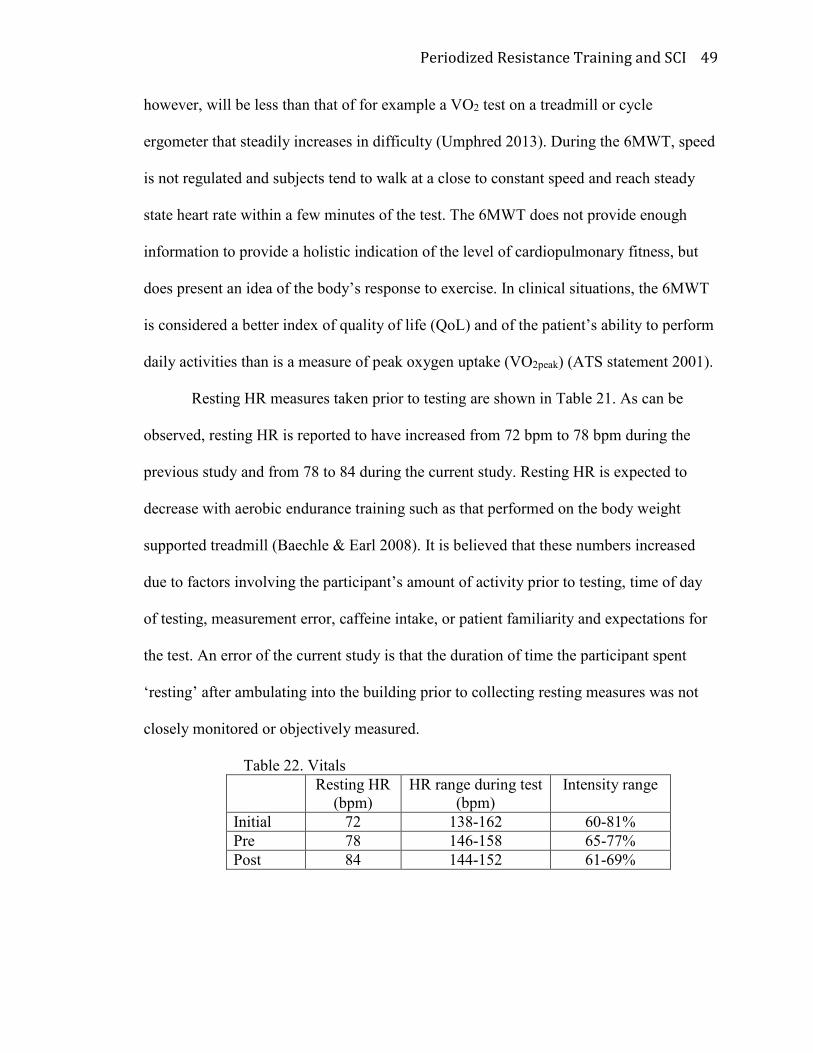
Periodized Resistance Training and SCI 49
however, will be less than that of for example a VO2 test on a treadmill or cycle
ergometer that steadily increases in difficulty (Umphred 2013). During the 6MWT, speed
is not regulated and subjects tend to walk at a close to constant speed and reach steady
state heart rate within a few minutes of the test. The 6MWT does not provide enough
information to provide a holistic indication of the level of cardiopulmonary fitness, but
does present an idea of the body’s response to exercise. In clinical situations, the 6MWT
is considered a better index of quality of life (QoL) and of the patient’s ability to perform
daily activities than is a measure of peak oxygen uptake (VO2peak) (ATS statement 2001).
Resting HR measures taken prior to testing are shown in Table 21. As can be
observed, resting HR is reported to have increased from 72 bpm to 78 bpm during the
previous study and from 78 to 84 during the current study. Resting HR is expected to
decrease with aerobic endurance training such as that performed on the body weight
supported treadmill (Baechle & Earl 2008). It is believed that these numbers increased
due to factors involving the participant’s amount of activity prior to testing, time of day
of testing, measurement error, caffeine intake, or patient familiarity and expectations for
the test. An error of the current study is that the duration of time the participant spent
‘resting’ after ambulating into the building prior to collecting resting measures was not
closely monitored or objectively measured.
Table 22. Vitals
Resting HR
(bpm)
HR range during test
(bpm)
Intensity range
Initial 72 138-162 60-81%
Pre 78 146-158 65-77%
Post 84 144-152 61-69%
Periodized Resistance Training and SCI 50
In order to measure cardiovascular intensity of the participant during the 6-minute
walk test, the HR ranges measured during the test were used to calculate the percent of
heart rate reserve. Heart rate reserve is directly correlated to functional capacity and can
be calculated by subtracting the resting heart rate from the maximum heart rate. The
Karvonen formula is used to determine the percentage of heart rate reserve or functional
capacity. The Karvonen formula is as follows
220 − ��� = max �� ��� �� − ������� �� = ℎ���� ���� ������� ����� ��� � ������������ + ������� �� = ������ ����
The percent ranges of aerobic capacity during the test as calculated by the Karvonen
method are listed in Table 22. The data shows that initially, the participant reached 81%
of heart rate reserve which decreased to only 77% after aerobic BWSTT. After the 12
week RT program, the participant reached a maximum of only 69% of his calculated
functional capacity. This indicates a functional improvement in the cardiovascular
system, as it became more efficient and required fewer heart beats to send oxygen rich
blood to working muscles in order to complete a greater amount of work (increased
distance). Chetta et al (2006) outlines reference values based off a study of 100 healthy
Caucasians ages 20-50 performing the 6MWT. They recorded HR every ten seconds for
the duration of the test to calculate and determine the average percentage of maximal
predicted HR. However, maximal predicted heart rate for their study was calculated
based on a different method and used the following formula:
210 − 0.66 � ��� = max ��
Results suggested that the participants only reached 67±10% of their predicted HRmax.
This has significant implications for the current study. When compared to healthy
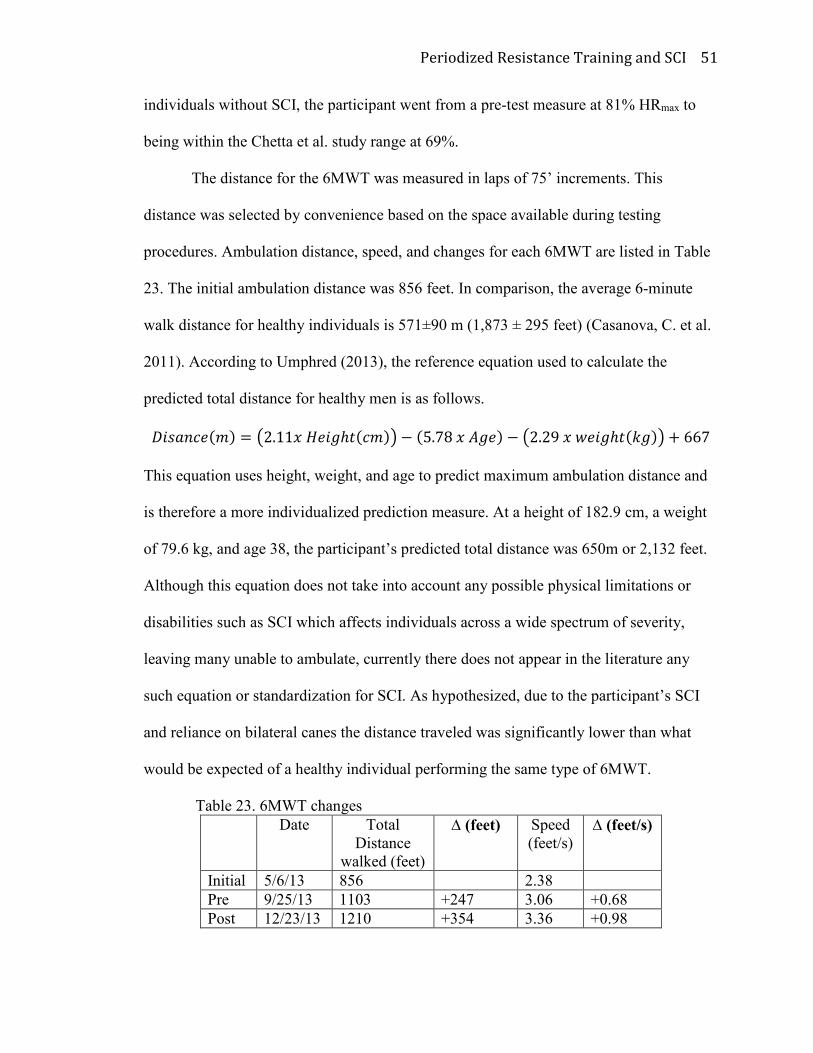
Periodized Resistance Training and SCI 51
individuals without SCI, the participant went from a pre-test measure at 81% HRmax to
being within the Chetta et al. study range at 69%.
The distance for the 6MWT was measured in laps of 75’ increments. This
distance was selected by convenience based on the space available during testing
procedures. Ambulation distance, speed, and changes for each 6MWT are listed in Table
23. The initial ambulation distance was 856 feet. In comparison, the average 6-minute
walk distance for healthy individuals is 571±90 m (1,873 ± 295 feet) (Casanova, C. et al.
2011). According to Umphred (2013), the reference equation used to calculate the
predicted total distance for healthy men is as follows.
"�������#� = $2.11� ����ℎ���#�% − �5.78 � )��� − $2.29 � +���ℎ��,��% + 667
This equation uses height, weight, and age to predict maximum ambulation distance and
is therefore a more individualized prediction measure. At a height of 182.9 cm, a weight
of 79.6 kg, and age 38, the participant’s predicted total distance was 650m or 2,132 feet.
Although this equation does not take into account any possible physical limitations or
disabilities such as SCI which affects individuals across a wide spectrum of severity,
leaving many unable to ambulate, currently there does not appear in the literature any
such equation or standardization for SCI. As hypothesized, due to the participant’s SCI
and reliance on bilateral canes the distance traveled was significantly lower than what
would be expected of a healthy individual performing the same type of 6MWT.
Table 23. 6MWT changes
Date Total
Distance
walked (feet)
∆ (feet)
Speed
(feet/s) ∆ (feet/s)
Initial 5/6/13 856 2.38
Pre 9/25/13 1103 +247 3.06 +0.68
Post 12/23/13 1210 +354 3.36 +0.98
Periodized Resistance Training and SCI 52
With aerobic BWSTT, the participant’s gait speed and endurance were expected
to improve. At the start of the current study, ambulation distance was found to be 1103
ft., demonstrating a change of 247 ft., a 28% increase resulting from the phase of
BWSTT. The participant showed functional gains in ambulation distance and speed after
the addition of the periodized RT program in achieving a distance of 1210 ft at the post
testing. This distance represented a change of 107 feet, or a 9.7% increase after
completing 12 weeks of combined RT and BWSTT. Overall, the subject was able to
demonstrate an increase in distance ambulated by 354 ft (42% increase).
A study by Harkema, Schmidt-Read, Lorenz, Edgerton, and Behrman (2012)
showed that individuals with long term chronic SCIs showed fewer improvements in the
6MWT following intensive locomotor training than those whose injuries occurred more
recently. However, they discovered that significant improvements could be made
regardless of how far removed the individuals were from their SCI. They noted that
individuals whose SCI was greater than three years prior to intervention showed gains of
24±43m (78.7 ± 141.0 ft.) whereas individuals whose SCI had occurred only 1-3 years
before intervention demonstrated improvement of 44±71m (144.3 ±232.9 ft). But,
Harkema et al stated that both resulted in significant gains (p<.001). The results of the
current case study are also similar to the study by Jayaraman et al. (2013) that was
previously mentioned and showed statistically significant changes (p = 0.03) of 12.19 ±
8.29m (or 42 ± 27.2 feet) on the 6MWT with a four week RT program in participants
with chronic SCI.
One major issue that was found in the literature is that there appears to be very
little research utilizing a 12 week period in people with SCI on the 6MWT. A study that
Periodized Resistance Training and SCI 53
combined treadmill and strength training for chronic stroke rehabilitation over a 12 week
period considered a change in 6MWT distance of 35m (114.8 ft) to be statistically
significant, which correlates with the increase of 107 ft in this study (Al-Jarrah, M.,
Shaheen, S., Harries, N., Kissani, N., Molteni, F. 2014).
Musselman (2009) suggests that the minimal clinically important difference for
the 6MWT distance in the SCI population has not been determined and is not known. He
also stated that the clinically relevant difference for the 10-meter walk test is a change in
speed of 0.05 m/s (0.16 ft/s) for community dwelling individuals with SCI. For the
6MWT, a speed increase of 0.30 ft/s was evidenced after RT which would be similar to
what was observed with the present case study. Musselman noted that the results
represented a clinically important improvement. In the current case study, the participant
achieved a speed of 3.36 ft/s which was an improvement from his initial speed of 2.38
ft/s. The increase of 0.98 ft/s over the course of both studies suggests that it was clinically
relevant. A meta-analysis by Bohannan and Andrews determined that normal walking
speed for healthy males age 30-39 is 1.43 m/s (4.69 ft/s) (2011). The studies used to
calculate this speed used distances of 30 meters or less to determine “normal” walking
speed. Therefore these numbers do not take into account any decreases in speed that
would be seen using a longer distance, a test involving turning, or longer duration test
such as the 6MWT.
Body Composition
Body composition data was obtained from the Bod PodTM utilizing the Siri
density-model are found in Table 24. Body composition was measured, to assess the
potential of any increase or decrease in fat free mass or fat mass. As stated previously, it
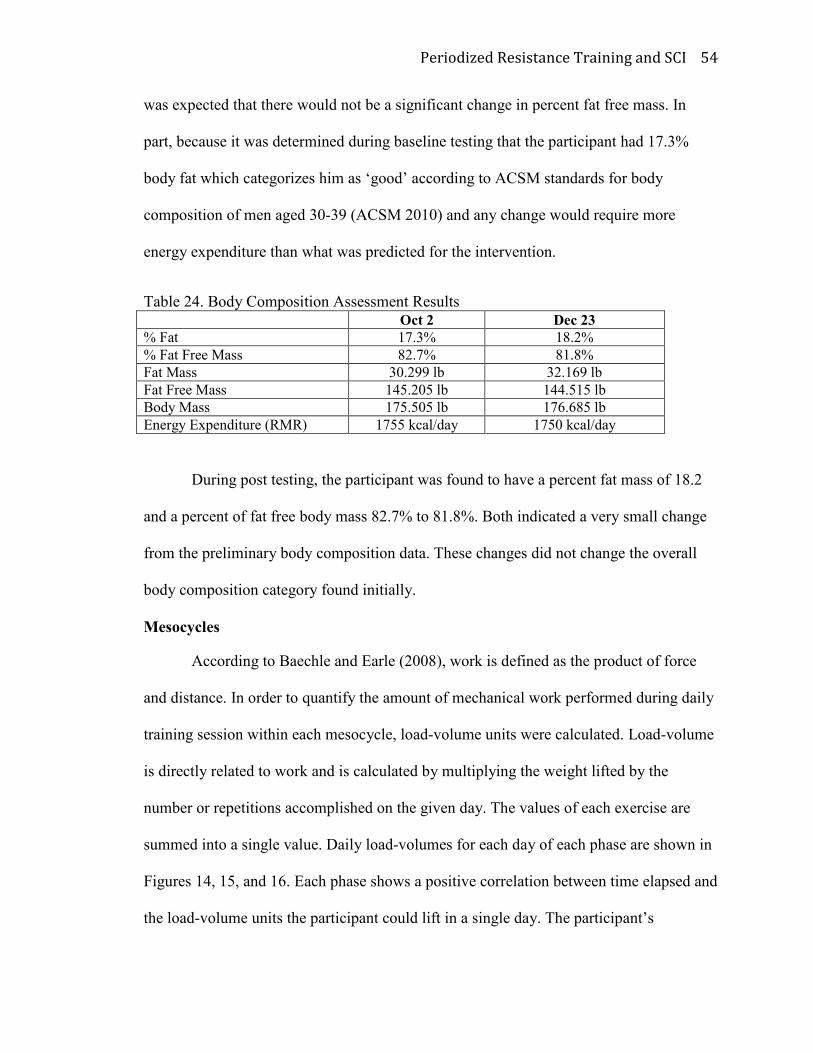
Periodized Resistance Training and SCI 54
was expected that there would not be a significant change in percent fat free mass. In
part, because it was determined during baseline testing that the participant had 17.3%
body fat which categorizes him as ‘good’ according to ACSM standards for body
composition of men aged 30-39 (ACSM 2010) and any change would require more
energy expenditure than what was predicted for the intervention.
Table 24. Body Composition Assessment Results
Oct 2 Dec 23
% Fat 17.3% 18.2%
% Fat Free Mass 82.7% 81.8%
Fat Mass 30.299 lb 32.169 lb
Fat Free Mass 145.205 lb 144.515 lb
Body Mass 175.505 lb 176.685 lb
Energy Expenditure (RMR) 1755 kcal/day 1750 kcal/day
During post testing, the participant was found to have a percent fat mass of 18.2
and a percent of fat free body mass 82.7% to 81.8%. Both indicated a very small change
from the preliminary body composition data. These changes did not change the overall
body composition category found initially.
Mesocycles
According to Baechle and Earle (2008), work is defined as the product of force
and distance. In order to quantify the amount of mechanical work performed during daily
training session within each mesocycle, load-volume units were calculated. Load-volume
is directly related to work and is calculated by multiplying the weight lifted by the
number or repetitions accomplished on the given day. The values of each exercise are
summed into a single value. Daily load-volumes for each day of each phase are shown in
Figures 14, 15, and 16. Each phase shows a positive correlation between time elapsed and
the load-volume units the participant could lift in a single day. The participant’s
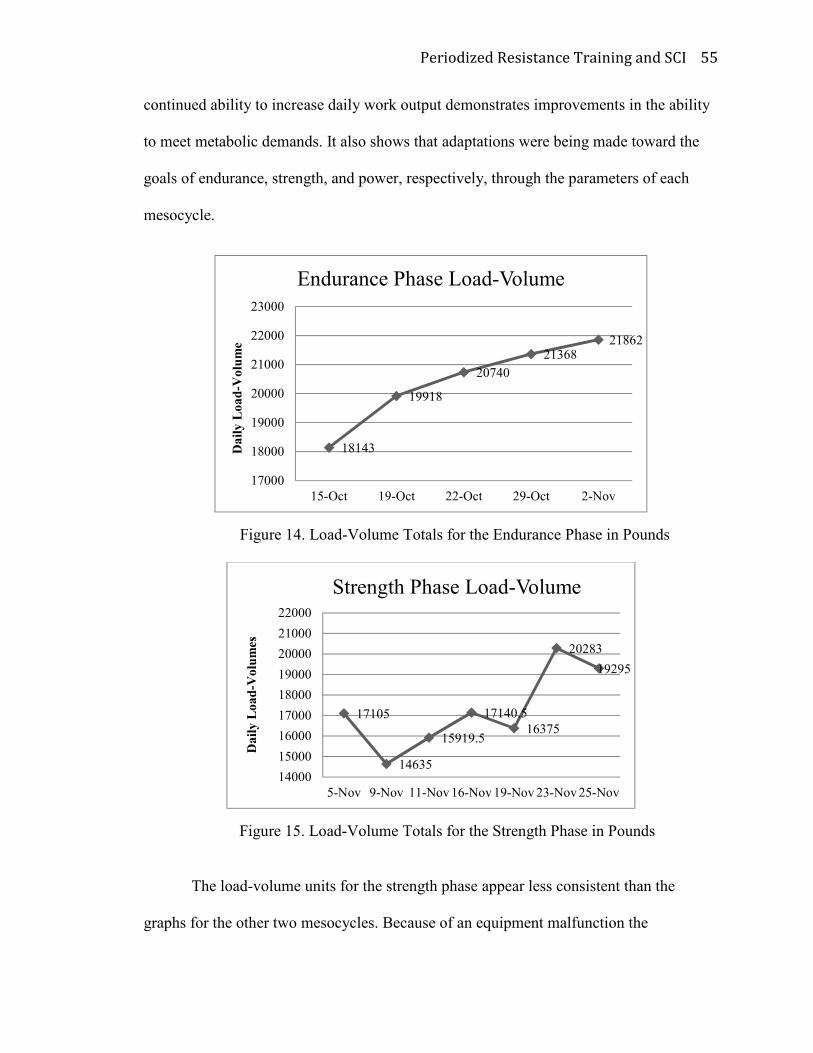
Periodized Resistance Training and SCI 55
continued ability to increase daily work output demonstrates improvements in the ability
to meet metabolic demands. It also shows that adaptations were being made toward the
goals of endurance, strength, and power, respectively, through the parameters of each
mesocycle.
Figure 14. Load-Volume Totals for the Endurance Phase in Pounds
Figure 15. Load-Volume Totals for the Strength Phase in Pounds
The load-volume units for the strength phase appear less consistent than the
graphs for the other two mesocycles. Because of an equipment malfunction the
18143
19918
20740
2136821862
17000
18000
19000
20000
21000
22000
23000
15-Oct 19-Oct 22-Oct 29-Oct 2-Nov
Da
ily
Lo
ad
-Vo
lum
e
Endurance Phase Load-Volume
17105
14635
15919.5
17140.5
16375
20283
19295
14000
15000
16000
17000
18000
19000
20000
21000
22000
5-Nov 9-Nov 11-Nov 16-Nov 19-Nov 23-Nov 25-Nov
Da
ily
Lo
ad
-Vo
lum
es
Strength Phase Load-Volume
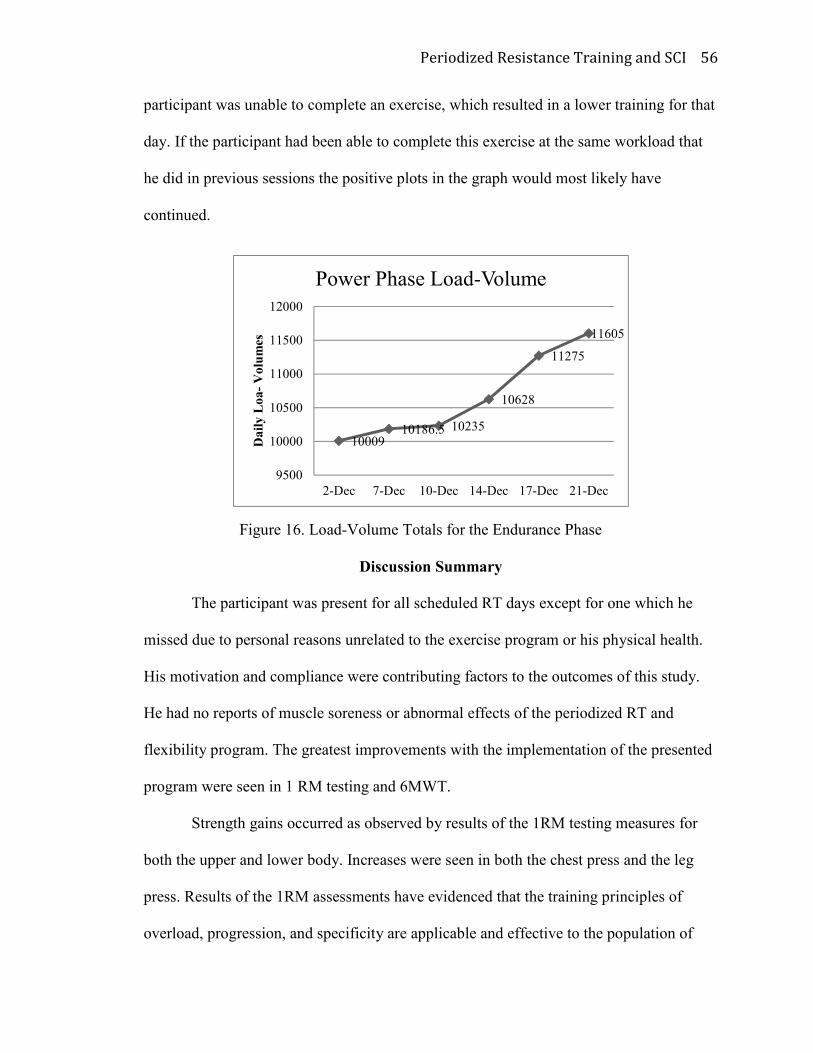
Periodized Resistance Training and SCI 56
participant was unable to complete an exercise, which resulted in a lower training for that
day. If the participant had been able to complete this exercise at the same workload that
he did in previous sessions the positive plots in the graph would most likely have
continued.
Figure 16. Load-Volume Totals for the Endurance Phase
Discussion Summary
The participant was present for all scheduled RT days except for one which he
missed due to personal reasons unrelated to the exercise program or his physical health.
His motivation and compliance were contributing factors to the outcomes of this study.
He had no reports of muscle soreness or abnormal effects of the periodized RT and
flexibility program. The greatest improvements with the implementation of the presented
program were seen in 1 RM testing and 6MWT.
Strength gains occurred as observed by results of the 1RM testing measures for
both the upper and lower body. Increases were seen in both the chest press and the leg
press. Results of the 1RM assessments have evidenced that the training principles of
overload, progression, and specificity are applicable and effective to the population of
1000910186.5 10235
10628
11275
11605
9500
10000
10500
11000
11500
12000
2-Dec 7-Dec 10-Dec 14-Dec 17-Dec 21-Dec
Da
ily
Lo
a-
Vo
lum
es
Power Phase Load-Volume
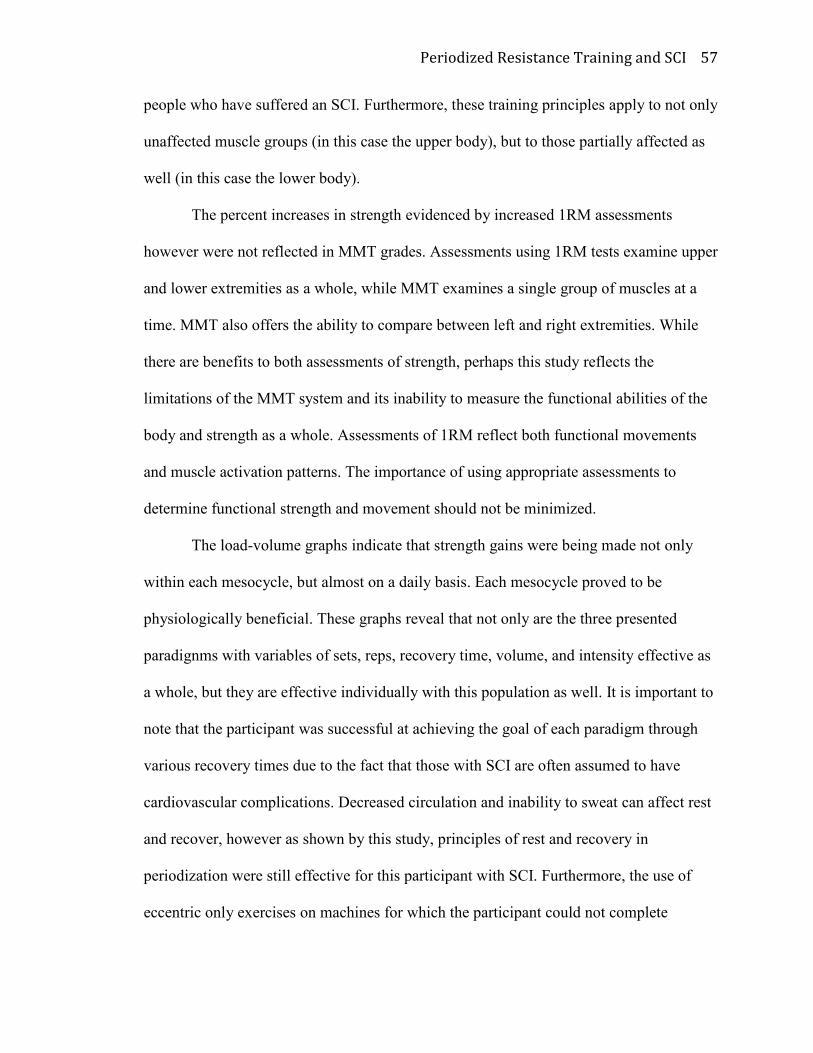
Periodized Resistance Training and SCI 57
people who have suffered an SCI. Furthermore, these training principles apply to not only
unaffected muscle groups (in this case the upper body), but to those partially affected as
well (in this case the lower body).
The percent increases in strength evidenced by increased 1RM assessments
however were not reflected in MMT grades. Assessments using 1RM tests examine upper
and lower extremities as a whole, while MMT examines a single group of muscles at a
time. MMT also offers the ability to compare between left and right extremities. While
there are benefits to both assessments of strength, perhaps this study reflects the
limitations of the MMT system and its inability to measure the functional abilities of the
body and strength as a whole. Assessments of 1RM reflect both functional movements
and muscle activation patterns. The importance of using appropriate assessments to
determine functional strength and movement should not be minimized.
The load-volume graphs indicate that strength gains were being made not only
within each mesocycle, but almost on a daily basis. Each mesocycle proved to be
physiologically beneficial. These graphs reveal that not only are the three presented
paradignms with variables of sets, reps, recovery time, volume, and intensity effective as
a whole, but they are effective individually with this population as well. It is important to
note that the participant was successful at achieving the goal of each paradigm through
various recovery times due to the fact that those with SCI are often assumed to have
cardiovascular complications. Decreased circulation and inability to sweat can affect rest
and recover, however as shown by this study, principles of rest and recovery in
periodization were still effective for this participant with SCI. Furthermore, the use of
eccentric only exercises on machines for which the participant could not complete
Periodized Resistance Training and SCI 58
concentric movements also proved to be successful at improving strength and load-
volume. The use of eccentric strengthening in the population of people with SCI with
weaker, less functional, and more acute injuries for the improvement of strength,
improvement of function, and prevention of secondary complications needs to be
explored further.
Greater strength increases were observed in the participants upper extremities
which were unaffected by the SCI. Anecdotally upper body strength was believed to have
actually increased since the onset of the SCI secondary to use of canes and compensation
for weakness in the lower extremities. As stated earlier, SCIs affect strength and
coordination by damaging motor unit connections. Fewer numbers of functioning motor
units might have prevented the increases in strength one might normally observe in the
lower extremities of a healthy individual that is participating in a periodized RT program.
However, strength increases were still evidenced in the lower extremities despite the
impaired neuromuscular connection.
High levels of muscle spasticity affecting the hip adductors quickly became
obvious as one of the participant’s primary limiting factors in his gait, exercise program,
and daily life. For this reason strengthening of the adductors was not implemented into
the program. Stretching of the hip abductors was also eliminated. To help counteract the
effects of muscle spasticity, the RT and flexibility program focused on strengthening the
hip abductors and stretching the hip adductors.
The participant’s fat free body mass decrease from 145.205lbs to 144.515lbs
suggests that skeletal muscle hypertrophy did not occur. A possible explanation to these
atypical findings might suggest that the length and/or dose of the mesocycles along with
Periodized Resistance Training and SCI 59
the overall duration of the study might not have been sufficient to effect such
morphological changes. In addition, the participant had transitioned from an initial study
that required him to perform aerobic exercise twice a week to the RT program which only
required him to perform aerobic exercise once a week along with the RT. The overall
decrease in aerobic exercise training volume might have also resulted in the small
increase in body fat.
While no significant trends occurred within joint ROM and muscle spasticity
within this study, more research is needed to determine the effects of periodized RT and
flexibility training in individuals with chronic incomplete SCI. Training for specific
aspects of muscle fitness such as endurance, strength, and power have clinical relevance
in the rehabilitation world and coincide with the known benefits of periodization in the
athletic population. In addition, activities of daily living require greater affluence in one
or more of these areas to maintain independence. For example, walking is a muscle
endurance activity and an individual who needs improvement with ambulation would
benefit greatly from training in a fashion that applies the goals of muscular endurance. In
the same fashion, aspects of daily life that include standing and lifting require elements of
strength and power. Individuals who lack these abilities should receive appropriate
exercise training with the appropriate variables adjusted accordingly to achieve the
desired goals of strength and power (muscular fitness).
Inconsistencies could be related to the participant’s diet, amount of sleep, or
amount of physical activity performed prior to training on a given day. This study
recognizes the importance of a participant’s nutrition to his exercise goals and outcomes.
More research is needed that can take advantage of this growing population to determine
Periodized Resistance Training and SCI 60
the potential benefits of this type of training that has largely been used in only training
athletes.
Conclusion
Muscular fitness gains through the use of a periodized RT program were evident
for this individual that exhibited chronic incomplete SCI. Both upper and lower body
strength gains occurred as evidenced by standardized 1RM assessments. Functional
improvements were also found in ambulation distance, endurance, and walking speed as
evidenced by the results of the 6MWT. The case study individual experienced three
different mesocycles or phases of periodized RT. These cycles varied training loads,
repetitions, lifting speeds, and rest periods to focus on the specific goals of muscular
endurance, strength, and power. Training in a periodized fashion appears to be a viable
option for this population and suggests that needed study in this area is warranted.
Periodized Resistance Training and SCI 61
References
Abott, C. (2009). Christina’s Pain Therapy Blog. Abbott Center for Neuromuscular
Therapy. Retrieved from: http://abbottcenter.com/bostonpaintherapy/?p=839
ACSM’s Guidelines for Exercise Testing and Prescription (8th Ed). (2010).Baltimore,
MD: Lippincott Williams & Wilkins.
Activity: Hip adductor stretch: sitting. (2010). Envision Physiotherapy. Physio Hub.
Retrieved from: http://www.physiohub.com/activities/83
Adams, M., Hicks, A. (2011). Comparison of the effects of body-weight-supported
treadmill training and tilt-table standing on spasticity in individuals with chronic
spinal cord injury. The Academy for Spinal Cord Injury Professionals, Inc, 34,
488-494.
Al-Jarrah, M., Shaheen, S., Harries, N., Kissani, N., Molteni, F. (2014). Individualized
Treadmill and Strength Training for Chronic Stroke Rehabilitation: Effects of
Imbalance.
American Thoracic Society. ATS Statement: Guidelines for the Six-Minute Walk Test.
(2002). American Journal of Respiratory and Critical Care Medicine, 166, 111-
117.
Baechle, T.R., Earle, R.W. (4th edition). (2012). Weight Training Steps to Success.
Champaign, IL: Human Kinetics.
Baechle, T.R., Earle, R.W. (3rd edition). (2008). Essentials of Strength Training and
Conditioning: National Strength and Conditioning Association. Champaign, IL:
Human Kinetics.
Bohannan, R., Williams Andrews, A. (2011). Normal Walking Speed: A descriptive
meta-analysis. Physiotherapy, 97, 182-189.
Bompa, T.O., Carrera, M.C. (2nded). (2005). Periodization Training for
Sports.Champaign, IL: Human Kinetics.
Stretching and Flexibility. (2015). Top End Sports. Retrieved from:
http://www.topendsports.com/medicine/stretching.htm
Casanova.C., et al. (2011). The 6-min walk distance in healthy subjects: reference
standards from seven countries. European Respiratory Journal. 37, 150-156.
Chetta, A. et al. (2006). Reference values for the 6-min walk test in healthy subjects 20-
50 years old. Respiratory Medicine, 100, 1573-1578.
Periodized Resistance Training and SCI 62
Dansereau, D. (2014). Physical Therapy Exercise for Low Back Pain. My Physical
Therapy Coach. Retrieved from: http://www.my-physical-therapy-
coach.com/low-back-exercise.html
Edell, D. (2009). Back Stretching. Athletic Advisor.com. Retrieved from:
http://www.athleticadvisor.com/injuries/head_back/back_stretching.htm
Elbasiouny, S., Moroz, D., Bakr, M.,Mushahwar, V. (2010). Management of Spasticity
After Spinal Cord Injury: Current Techniques and Future
Directions.Neurorehabilitaion and Neural Repair, 24, 23-33.
ExRx.net. “Other Fitness Tests”. Retrieved from:
http://www.exrx.net/Testing/OtherTests.html
Gentil, P., et al. (2010). Chronic Effects of Different Between-Set Rest Durations on
Muscle Strength in Nonresistance Trained Young Men. Journal of Strength and
Conditioning Research, 24, 37-42.
Gordon, T. & Mao, J. (1994). Muscle Atrophy and Procedures for Training after Spinal
Cord Injury. Journal of the Amercian Physical Therapy Association, 74, 50-60.
Gorgey, A., et al (2011). Acute Effects of Locomotor training and neuromuscular and
metabolic profile after incomplete spinal cord injury. NeuroRehabilitation,29, 79-
83.
Gorgey, AS., Poarch, H., Miller, J., Castillo, T., Gater, DR. (2010).Locomotor and
resistance training restore walking in an elderly person with a chronic incomplete
spinal cord injury. NeuroRehabilitation, 26, 127-133.
Gorgey, A. S. & Shepherd, C. (2009). Skeletal Muscle Hypertrophy and Decreased
Intramusclular Fat After Unilateral Resistance Training in Spinal Cord Injury: A
Case Report. Journal of Spinal Cord Medicine, 33, 90-95.
Gregory, C. M., Bowden, MG., Jayaraman, A., Shah, P., Behrman, A., Kautz, SA.,
Vandenborne, K. (2007). Resistance Training and Locomotor Recovery after
Incomplete Spinal Cord Injury: A Case Series. Spinal Cord. 45. 522-530.
Harkema, S., Schmidt-Read, M., Lorenz, D., Edgerton, R., Behrman, A. (2012).Balance
and Ambulation in Individuals with Chronic Incomplete Spinal Cord Injury Using
Locomotor Training-Based Rehabilitation. Physical Medicine and Rehabilitation,
93, 1508-1517.
Hartmann, H., Bob, A., Wirth, K., Schmidtbleicher, D. (2009). Effects of Different
Periodization Models on Rate of Development and Power Ability of the Upper
Extremity. Journal of Strength and Conditioning Research, 23, 1921-1932.

Periodized Resistance Training and SCI 63
Warm-Up Exercises and Stretching. (1999). Health and Fitness Education.
Edinformatics. Retrieved from:
http://edinformatics.com/health_fitness/warmup_stretching.htm
Heyward, V. H. (2006). Advanced Fitness Assessment and Exercise Prescription 5th
edition. Champaign, IL: Human Kinetics. 117-140.
Iliotibial Band. (2013). Stretching-Exercises-Guide.com. Retrieved from:
http://www.stretching-exercises-guide.com/iliotibial-band.html
International Standards for Neurological Classification of Spinal Cord Injury. (2011).
American Spinal Injury Association.
Jacobs, P., Nash, M. (2004). Exercise Recommendations for Individuals with Spinal Cord
Injury. Sports Medicine, 34, 727-751.
Jayaraman, A., Thompson, C., Rymer, W., Hornby, G. (2013). Short-term Maximal-
Intensity Resistance Training Increases Volitional Function and Strength in
Chronic Incomplete Spinal Cord Injury: A Pilot Study. Journal of Neurologic
Physical Therapy, 37, 112-117.
Kawamori, N., Haff, G. (2004). The Optimal Training Load for the Development of
Muscular Power. Journal of Strength and Conditioning Research, 18, 675-684.
Kell, RT. (2011). The Influence of Periodized Resistance Training on Strength Changes
in Men and Women. Journal of Strength and Conditioning Research, 25, 735-
744.
Kisner, C., Colby, LA. (6thed). (2012). Therapeutic Exercise: Foundations and
Techniques. Philadelphia, PA: F.A. Davis Company.
Kraemer, W., Fleck, S. (2007). Optimizing Strength Training: Designing Nonlinear
Periodization Workouts. Champaign, IL: Human Kinetics.
Mahoney, ET., Bickel, S., Elder, C., Black, C., Slade, JM., Apple Jr, D., Dudley, GA.
(2005). Changes in Skeletal Muscle Size and Glucose Tolerance with Electrically
Stimulated Resistance Training in Subjects with Chronic Spinal Cord Injury.
Archives of Physical Medicine and Rehabilitation.86. 1502-1504.
McArdle, W., Katch, F., Katch, V. (7thed). (2010). Exercise Physiology: Nutrition,
Energy, and Human Performance. Baltimore, MD: Lippincott Williams &
Wilkins.
Miranda, F., et al. (2011). Effects of Linear vs. Daily Undulatory Periodized Resistance
Training on Maximal and Submaximal Strength Gains. Journal of Strength and
Conditioning Research. 25. 1824-1830.
Periodized Resistance Training and SCI 64
Musselman, K., Fouad, K., Misiaszek, M., Yang, J. (2009). Training of Walking Skills
Overground and on the Treadmill: Case Series on Individuals with Incomplete
Spinal Cord Injury. Physical Therapy, 89, 601-611.
Pak, S., Pattern, C. (2008). Strengthening to Promote Functional Recovery Poststroke:
An Evidence-Based Review. Top Stroke Rehabilitation, 15, 177-199.
Partner Hamstring Stretch (2015). TeachPE. Retrieved from:
http://www.teachpe.com/stretching/hamstring_partner.php
O’Sullivan, S., Schmitz, T. (2007). Physical Rehabilitation 5th edition (497, 945-946).
Philadelphia, PA: F.A. Davis Company.
Rhea, M., Alderman, B. (2004).A Meta-Analysis of Periodized versus Non-periodized
strength and power training programs. Research Quarterly for Exercise and Sport,
75. 413-422.
Schoenfeld, BJ. (2010).The Mechanisms of Muscle Hypertrophy and their Application to
Resistance Training. Journal of Strength & Conditioning Research, 24, 2857-
2872.
Spinal Cord Injury Facts and Figures at a Glance. (2013). National Spinal Cord Injury
Statistical Center. https://www.nscisc.uab.edu/
SuperSets Editorial. (2013). 8 Stretches you Should be Doing. Retrieved from:
http://www.topendsports.com/medicine/stretching.htm
Umphred, D., Lazaro, R., Roller, M., Burton, G.(2013).Traumatic Spinal Cord
Injury.(6thed).Neurological Rehabilitation (pp. 459-520). St. Louis, MO: Elsevier
Mosby.
Turner, Anthony. (2011). The Science and Practice of Periodization: A Brief Review.
Strength and Conditioning Journal, 33, 34-46.
Warburton, D., Nicol, CW., Bredin, S. (2006). Health Benefits of Physical Activity: the
evidence. Canadian Medical Association Journal,174, 801-809.
Warm-Up Exercises. (2015). All About Tennis.com. Retrieved from:
http://www.allabouttabletennis.com/warm-up-exercises.html
Yang, J., et al. (2011). Volitional Muscle Strength in the Legs Predicts Changes in
Walking Speed Following Locomotor Training in People with Chronic Spinal
Cord Injury. Physical Therapy, 91, 931-943.
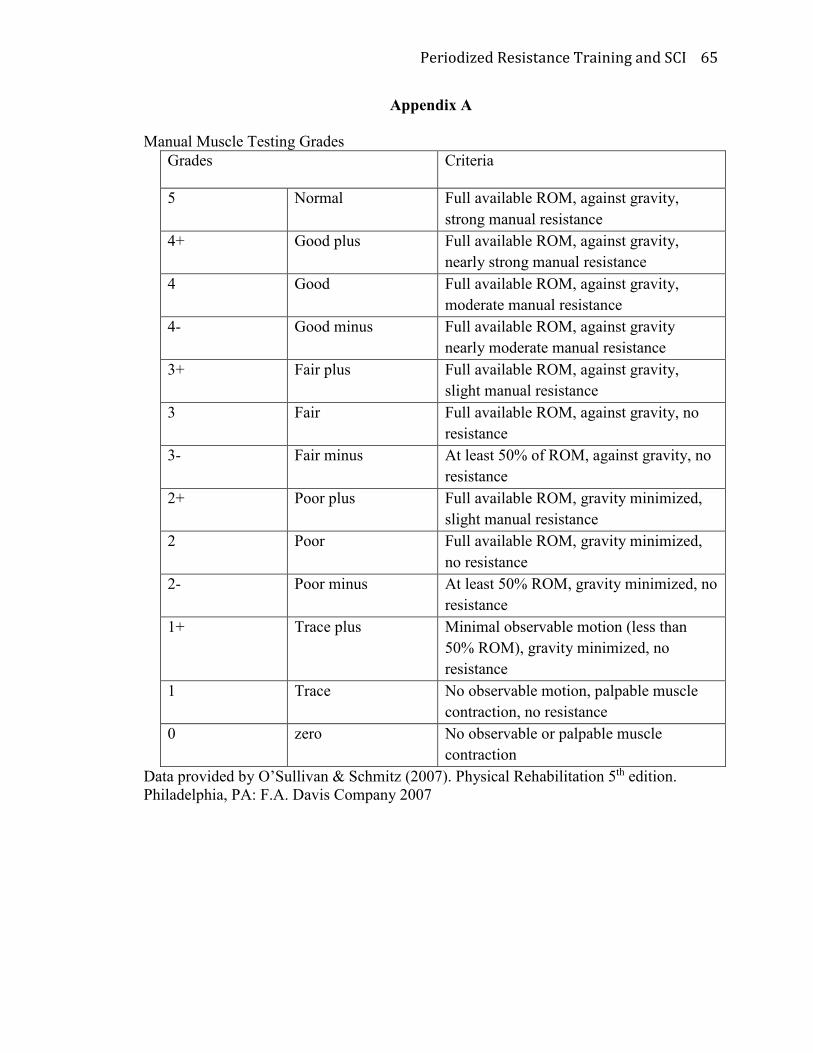
Periodized Resistance Training and SCI 65
Appendix A
Manual Muscle Testing Grades
Grades Criteria
5 Normal Full available ROM, against gravity,
strong manual resistance
4+ Good plus Full available ROM, against gravity,
nearly strong manual resistance
4 Good Full available ROM, against gravity,
moderate manual resistance
4- Good minus Full available ROM, against gravity
nearly moderate manual resistance
3+ Fair plus Full available ROM, against gravity,
slight manual resistance
3 Fair Full available ROM, against gravity, no
resistance
3- Fair minus At least 50% of ROM, against gravity, no
resistance
2+ Poor plus Full available ROM, gravity minimized,
slight manual resistance
2 Poor Full available ROM, gravity minimized,
no resistance
2- Poor minus At least 50% ROM, gravity minimized, no
resistance
1+ Trace plus Minimal observable motion (less than
50% ROM), gravity minimized, no
resistance
1 Trace No observable motion, palpable muscle
contraction, no resistance
0 zero No observable or palpable muscle
contraction
Data provided by O’Sullivan & Schmitz (2007). Physical Rehabilitation 5th edition.
Philadelphia, PA: F.A. Davis Company 2007

Periodized Resistance Training and SCI 66
Appendix B
Modified Ashworth Spasticity Scale
Grade Description
0 No increase in muscle tone
1 Slight increase in muscle tone, manifested by a catch and release or by
minimal resistance at the end of the ROM when the affected part(s) is
moved in flexion or extension
1+ Slight increase in muscle tone, manifested by a catch, followed by
minimal resistance throughout the remainder (less than half) of the
ROM
2 More marked increase in muscle tone through most of the ROM, but
affected part(s) easily moved
3 Considerable increase in muscle tone, passive movement difficult
4 Affected part(s) rigid in flexion or extension
Data provided by O’Sullivan & Schmitz (2007). Physical Rehabilitation 5th edition.
Philadelphia, PA: F.A. Davis Company 2007
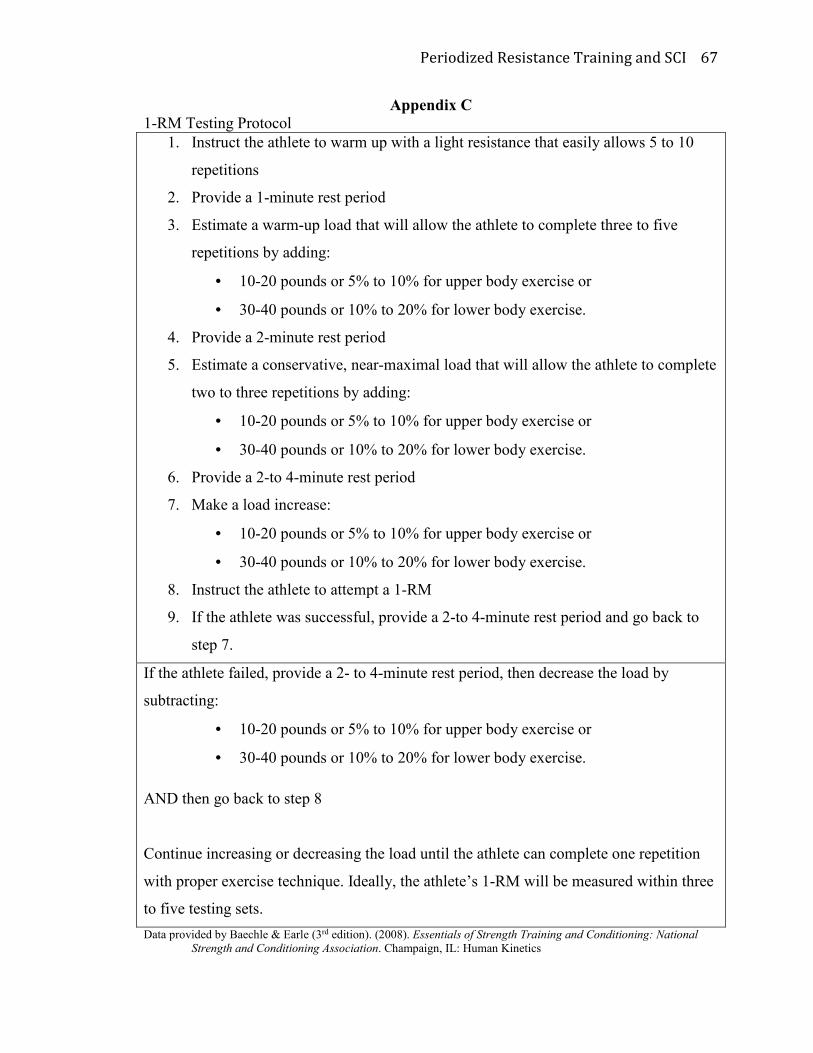
Periodized Resistance Training and SCI 67
Appendix C
1-RM Testing Protocol
1. Instruct the athlete to warm up with a light resistance that easily allows 5 to 10
repetitions
2. Provide a 1-minute rest period
3. Estimate a warm-up load that will allow the athlete to complete three to five
repetitions by adding:
• 10-20 pounds or 5% to 10% for upper body exercise or
• 30-40 pounds or 10% to 20% for lower body exercise.
4. Provide a 2-minute rest period
5. Estimate a conservative, near-maximal load that will allow the athlete to complete
two to three repetitions by adding:
• 10-20 pounds or 5% to 10% for upper body exercise or
• 30-40 pounds or 10% to 20% for lower body exercise.
6. Provide a 2-to 4-minute rest period
7. Make a load increase:
• 10-20 pounds or 5% to 10% for upper body exercise or
• 30-40 pounds or 10% to 20% for lower body exercise.
8. Instruct the athlete to attempt a 1-RM
9. If the athlete was successful, provide a 2-to 4-minute rest period and go back to
step 7.
If the athlete failed, provide a 2- to 4-minute rest period, then decrease the load by
subtracting:
• 10-20 pounds or 5% to 10% for upper body exercise or
• 30-40 pounds or 10% to 20% for lower body exercise.
AND then go back to step 8
Continue increasing or decreasing the load until the athlete can complete one repetition
with proper exercise technique. Ideally, the athlete’s 1-RM will be measured within three
to five testing sets.
Data provided by Baechle & Earle (3rd edition). (2008). Essentials of Strength Training and Conditioning: National
Strength and Conditioning Association. Champaign, IL: Human Kinetics