student assessment in community settings: a comprehensive approach
TRANSCRIPT

Student assessment in community settings:
a comprehensive approach
Mohi Eldin M. A. Magzoub1, Henk G. Schmidt2, Ahmed A. Abdel-Hameed1,Diana Dolmans2 & Sirag E. Mustafa1
1 University of Gezira, Wad Medani, Sudan, and 2 Maastricht University, The Netherlands
SUMMARY
Student assessment in community settings presents
problems for medical teachers, e.g. dif®culties in as-
sessing the contribution of individual members to
group work, and lack of test standardization due to
varying ®eld conditions. The Faculty of Medicine,
University of Gezira, Sudan is a community-oriented,
community-based medical school which has adopted a
comprehensive approach to student assessment in
community settings using various methods, including
peer assessment, a supervisory checklist, community
feedback, reports from students, short essay questions
(SEQs) and multiple choice questions (MCQs). Each
method focuses on a speci®c aspect of the objectives of
the community-based programme and is weighted in
the ®nal grade according to the extent to which objec-
tives were covered. This assessment programme con-
trasts with the conventional teacher-centred approach,
and is continuously monitored and improved using a
variety of sources of information. A total of 105 stu-
dents participated in a study designed to measure the
reliability and validity of this approach. The reliability
of the methods was tested by computing the alpha co-
ef®cient and was found to range between 0á77 and 0á92.
This was considered acceptable. The validity of the
instruments was examined using con®rmatory factor
analysis, and their content validity was reviewed. The
results show that the comprehensive approach used is
fairly valid. It is suggested that the University's ap-
proach is successful in solving some of the problems of
student assessment in community settings.
Keywords:
Clinical competence; competency-based education;
developing countries; community medicine, *educa-
tion; education, medical, undergraduate, *methods;
Sudan
INTRODUCTION
The aim of community-based education is to produce
graduates who are responsive to the health needs of their
community. Since it is not a conventional form of edu-
cation it requires assessment methods different from
those used in class learning or in the teaching hospital
(Fulop 1976; Kantrowitz et al. 1987). The development
of a valid student assessment system for community-
based education will help innovative medical schools to
support student learning (Hassan et al. 1993).
As more teaching institutions adopt community-
based education to enable graduate health personnel to
respond to community health needs (Schmidt et al.
1991), new problems arise. Of these, the problem of
how to assess students' performance in community
settings is the most urgent, and must be addressed for
three reasons.
First, community-based work competes with other
assessed academic activities, and both students and
staff may consider community-based work as secondary
to the core curriculum. Commitment to community-
based activities may be reduced.
Secondly, assessment is known to stimulate students
to learn and in¯uences what they do and how well they
do it. Many authors have highlighted the close rela-
tionship between assessment and the kind of learning
activities that students actually engage in (Frederickson
& Knox 1984; Newble & Swasan 1988). Irrelevant as-
sessment may reduce motivation and result in irrelevant
activities and negative attitudes.
Thirdly, student assessment and feedback are im-
portant in programme evaluation. If assessment is ir-
relevant to the programme's primary goals, the results
of the assessment will have a direct impact on the way
the programme is operated and further developed.
The Faculty of Medicine, University of Gezira
(FMUG) uses a comprehensive approach to student
assessment in community settings. This article will
discuss this approach following a brief review of the
Correspondence: Dr Mohi Eldin M A Magzoub, Faculty of Medicine, University of Gezira, PO Box 20, Wad Medani, Sudan
50 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd

objectives of the community-based programme at the
FMUG, to indicate which objectives are pursued and
which objectives should therefore be assessed.
The FMUG focuses on community needs and rural
development in its educational, research and services
activities, and has implemented an educational pro-
gramme based on six strategies (Abdel Rahim 1989).
Community-based education plays a signi®cant role
in implementing the educational strategies in Gezira. It
represents 20% of all educational activities as indicated
by the number of credit hours allocated to the different
courses in the curriculum. The students are exposed to
the community from the ®rst semester and throughout
the curriculum.
Community-based education serves two main func-
tions for the faculty, in providing opportunities for
collaboration with the community and the government
and preparing students for a community-oriented ca-
reer. Community-based education provides a chance
for students to work in an environment similar to the
one they are going to face in the future, in particular in
under-served and rural communities.
The speci®c objectives set for the community-based
programme at the FMUG are:
(1) to demonstrate the impact of disease on the family
and the community;
(2) to facilitate student perception of patients as part of
the family and the community;
(3) to clarify how the health system and health team
work;
(4) to enable students to acquire skills in research
methodology, problem-solving, communication,
decision-making, manual clinical skills, leadership,
organization and team work, and
(5) to provide a setting for teaching of the behavioral
sciences, including medical sociology, psychology,
anthropology and economics.
METHODS
Instruments employed for assessment
of community-based courses
By reviewing the fairly limited literature in this area, in
addition to the papers presented at the International
Symposium on Student Assessment in Community
Settings (1993), three main approaches to assessment
may be identi®ed. (1) Knowledge measurement ap-
proaches, essentially pencil and paper methods which
mainly assess the factual recall and, in some cases,
application of knowledge. Tools applied here include
multiple choice questions, essays and reports. This type
of assessment is characteristically conducted at the end
of the community-based education activity (Jinadu &
Davies-Adetugbo 1992; Omatara 1992). (2) Perfor-
mance-based approaches. These are (quasi-) observa-
tional methods mainly assessing the performance of the
students during their ®eld activities. Tools applied
here include logbooks (Des Marchais et al. 1993;
Manalo 1993), supervisory visits (Bollag et al. 1982;
Magzoub et al. 1993), peer assessment (Hassan 1993;
Morales-Sameneigo 1993) and monitoring of atten-
dance (Magzoub & Schmidt 1996). (3) Comprehensive
approaches which combine (1) and (2) using various
tools.
The various methods and instruments employed in
FMUG'S comprehensive approach are described be-
low.
(1) Peer evaluation
It was felt that students were in a better position than
tutors to evaluate each other in four speci®c areas. Each
area required continuous close observation. Conse-
quently, a peer evaluation rating scale was developed,
which included the following. (i) Effort ± eight items
re¯ecting the input of students in the different activities
carried out during the course. (ii) Interaction with the
community ± six items, re¯ecting the students' ability to
communicate with the community, to facilitate data
collection and consent to advice. This skill is consid-
ered to be important for the future work of the doctor
and for developing a doctor±patient±community rela-
tionship. (iii) Leadership ± four items, e.g. leading a
group discussion, decision-making and division of la-
bour. This is a very important skill for doctors in the
Sudan who work as health team leaders in rural hos-
pitals. Objective assessment of this skill is therefore
paramount. (4) Use of knowledge or subject matter
contribution ± four items, re¯ecting the student's ability
to use his or her knowledge to help the group progress
towards the course objectives. The items included in
the rating scale can be found in Table 1. Each student
rates his peers in the group, and the mean of each factor
of all group members' ratings is computed for each
student on a ®ve-point scale.
(2) Community leaders' feedback
Students have close contact with community members
during their posting, particularly with community
leaders, who are responsible for their accommodation
and food, and provide support. Community assessment
is based on a process of feedback, which includes as-
sessment of understanding of the purpose of students'
visits, acceptance of these objectives, level of commu-
nity participation, and impact on the community.
51 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.

Extensive discussion with community leaders and
others is conducted by tutors using a group-discussion
methodology. The tutor summarizes the discussion in a
report, which is analysed at the university using a
checklist consisting of the indicators of student perfor-
mance outlined earlier. Perceived achievement, impact
of the work, and level of participation by the commu-
nity are used to rate the student groups. Based on the
same report, each individual student is evaluated with
respect to community satisfaction, recognition of his or
her achievement, and interaction with the community,
in order to identify differences within each group.
(3) Supervisory checklist
Supervisors assess students posted in villages, primary
health units or rural hospitals, with the aim of assessing
the extent to which progress has been made, identifying
potential problems and helping to solve them. At least
three visits will be made during a student's posting.
FMUG uses these visits to assess students, monitoring
three skills which are essential if students are to survive
in community settings. First, because students are re-
quired to solve real problems, their approach to
identifying problems, and the criteria they use to pri-
oritize them, are assessed. Supervisors rate students'
ability to analyse problems and their approach in re-
solving them. Secondly, students' communication skills
are observed while they interact with individuals or give
a health education presentation to an audience. Items
assessed are whether the student expresses him/herself
in simple and understandable language; whether he or
she communicates ideas by relating them to the local
culture; whether he or she checks to what extent mes-
sages have been understood, and, ®nally, whether his or
her non-verbal behaviour demonstrates an empathic
attitude. Thirdly, organizational ability is assessed, ad-
dressing the extent to which the student has a clear plan
for work in the ®eld; whether the student performs
regular follow-up and daily monitoring, and whether
the student has a time schedule in which to complete a
designated activity. The tutor uses a checklist to allo-
cate scores.
(4) Individual and group report
Following a posting, students are asked to write group
and individual reports documenting all their ®eld ac-
tivities and ®ndings. The report must comply with
standards for scienti®c reporting. It should contain an
introduction, and methods, results and discussion sec-
tions. The reporting ability of students is evaluated by
tutors using criteria such as the organization of ideas in
a logical sequence; the extent to which scienti®c
methods were applied; thoroughness of discussion of
the ®ndings, and the presence of implementable rec-
ommendations. In addition, the general presentation of
the report format is evaluated. One tutor allocates
scores for all reports.
(5) Short essay questions (SEQs)
Short essay questions are given to test knowledge. The
SEQs test a student's ability to summarize ideas in a
clear, logical and condensed fashion in a limited time.
The SEQs test usually includes four questions, three in
the form of short-answer questions such as `Outline the
steps you take to control an epidemic of cholera',a nd
the fourth in the form of a family or a community
problem, for example:
`Ahmed Omer, who is 65 years old, lives in the El-
dibagha area with his family, which has 10 members
including his mother, his eldest divorced daughter and
her son. His house has two rooms, plus a small kitchen
and a pit latrine. He works as a labourer with limited
income. Ahmed and his wife are hypertensive, and his
mother is diabetic. One of his daughters was recently
diagnosed as tuberculous and his 4-year-old nephew has
recurrent attacks of diarrhoea.'
Table 1 Items included in the peer evaluation rating scale
Peer evaluation of effort
1. Contributed well to the design of forms for data collection
2. Contributed well to data collection in the village
3. Participated well in the assigned activities in the village
4. Good problem identi®cation
5. Participated well in report writing
6. Contributed well to the group activities concerning living,
accommodation and housing in the village
7. Participated well in preparation for the group seminar
8. Good physical attendance at announced group activities
Peer evaluation of community interaction
9. The terminology used by the student was understandable
to the community members
10. Always responded to community members' questions in a
clear way
11. A good listener to community problems
12. Advice and suggestions seemed to convince the community
13. Frequently present in the community
14. Able to befriend community members
Peer evaluation of leadership
15. Able to contact community leaders
16. A good leader of group discussion
17. Able to divide labour equally among group members
18. A good decision-maker
Peer evaluation of subject-matter contribution
19. Gave useful information to the group
20. Suggestions and thoughts were helpful to the group's work
21. Formulated good questions
22. Made use of references and other resources
52 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.
Discuss the socio-economic aspects of this family's
problems.
Outline your approach to helping this family.
(6) Multiple choice questions (MCQs)
The MCQs test aims to detect learning outcomes in the
cognitive domain and consists of 30 questions, each
including ®ve true or false statements. Students are
advised to try all questions. They score +1 for a correct
answer, 0 for a blank and )1 for a wrong answer. The
following is an example of an MCQs test.
The egg of Schistosoma manoni:
(a) contains the living miracidium;
( b)has a well-developed terminal spine;
(c) can be found in rectal tissues obtained by a rectal
biopsy;
(d) hatches when exposed to a large volume of water;
(e) is infective to man.
It is important to mention that these methods are not
applied collectively to each community-based course.
The selection of the method depends on the objective
and learning activities in each course. For example, in
the Primary Health Care Centre Practice and Family
Health course, which is mainly conducted in primary
health care units, assessment methods include log-
books, attendance, student reports, the MCQs test and
short essay questions. However, in the interdisciplinary
Field Training Research and Rural Development
course, assessment methods are group report, atten-
dance, community feedback, supervisory checklist and
assessment of oral presentation.
Measures of reliability and validity
To our knowledge, no studies have been conducted to
test the quality of the instruments used in assessing
students in community settings, i.e. measures of reli-
ability and validity. The following section reports on the
reliability and validity of the comprehensive approach
to student assessment in community settings as used at
the FMUG. The performances of 105 students at the
FMUG were measured with a range of instruments
described earlier, which were intended to address all
competencies required in community settings. The data
were analysed using con®rmatory factor analysis and
reliability estimates.
Subjects and procedure
A total of 105 students participated in the interdisci-
plinary Field Training Research and Rural Development
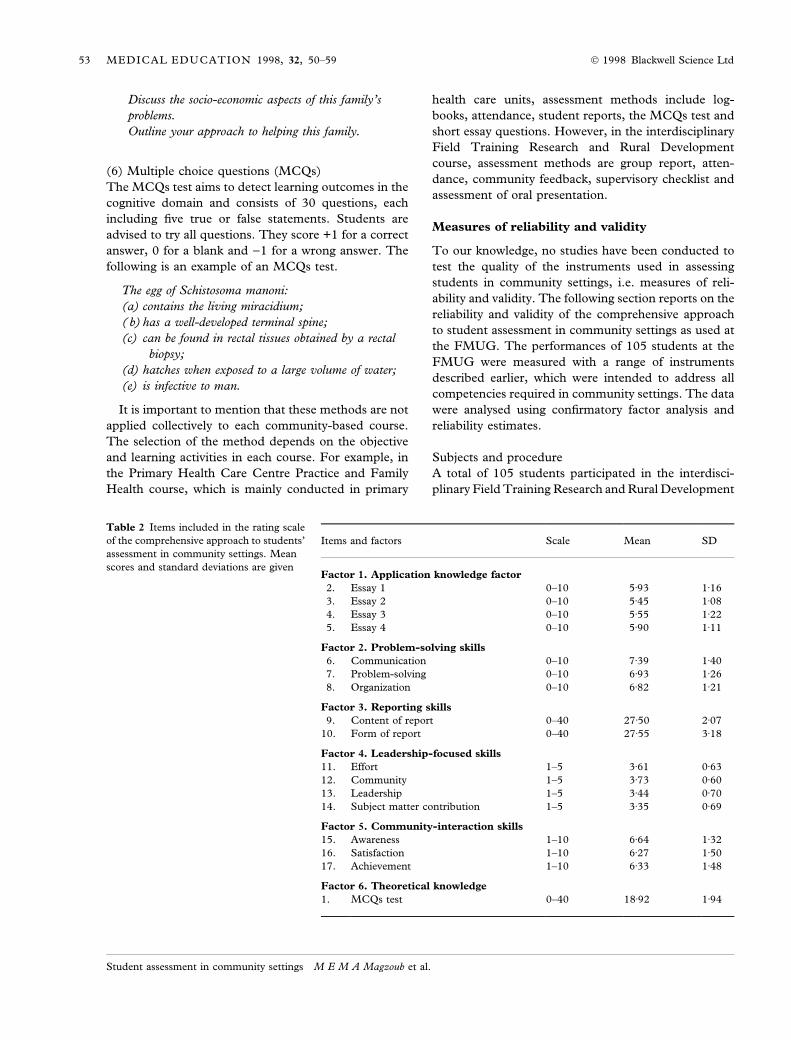
Table 2 Items included in the rating scale
of the comprehensive approach to students'
assessment in community settings. Mean
scores and standard deviations are given
Items and factors Scale Mean SD
Factor 1. Application knowledge factor
2. Essay 1 0±10 5á93 1á16
3. Essay 2 0±10 5á45 1á08
4. Essay 3 0±10 5á55 1á22
5. Essay 4 0±10 5á90 1á11
Factor 2. Problem-solving skills
6. Communication 0±10 7á39 1á40
7. Problem-solving 0±10 6á93 1á26
8. Organization 0±10 6á82 1á21
Factor 3. Reporting skills
9. Content of report 0±40 27á50 2á07
10. Form of report 0±40 27á55 3á18
Factor 4. Leadership-focused skills
11. Effort 1±5 3á61 0á63
12. Community 1±5 3á73 0á60
13. Leadership 1±5 3á44 0á70
14. Subject matter contribution 1±5 3á35 0á69
Factor 5. Community-interaction skills
15. Awareness 1±10 6á64 1á32
16. Satisfaction 1±10 6á27 1á50
17. Achievement 1±10 6á33 1á48
Factor 6. Theoretical knowledge
1. MCQs test 0±40 18á92 1á94
53 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.
course and the Family Health course based in the
community. Groups consisting of 10±11 students were
assigned villages in which to work for three consecu-
tive summers in three phases. During the ®rst phase
(August 1991) students identi®ed problems using var-
ious investigation tools. In the second phase (Septem-
ber 1992), students were engaged in projects which
they set up to solve one of the priority problems
identi®ed in the ®rst phase. In the last phase, students
evaluated projects.
At the end of the second posting, students were as-
sessed using ®ve instruments including community
feedback, supervisory checklists, student reports,
knowledge measures including the MCQs test and
short essay questions, and peer assessment. The dif-
ferent elements of the comprehensive approach can be
found in Table 2.
Analysis
A reliability study was conducted for each instrument
separately and for the total score based on averages of
the scores for each test. The Statistical Package for
Social Sciences program (SPSS) was used to compute
the alpha coef®cient for each instrument. The hypoth-
esis was that all items belonging to a particular instru-
ment measured similar competencies.
A construct validity study was conducted on the
variables involved, using con®rmatory factor analysis.
In the con®rmatory factor model as applied in this
study, the most common factors were correlated. Ob-
served variables 2±5 were affected by the ®rst common
factor, essay score, which is considered to re¯ect ap-
plication knowledge. Observed variables 6±8 were af-
fected by the second common factor, supervisor rating,
which measures mainly problem-solving-related skills.
Variables 9 and 10 were affected by the third common
factor, the reporting skills rating. Variables 11±14 were
affected by the fourth common factor, peer rating,
which focuses on leadership skills, and the last three
variables were affected by the ®fth common factor,
community feedback, which evaluates community
interaction skills. Variable 1, a composite score from
the 30 MCQs-test questions, was considered as the
sixth common factor evaluating theoretical knowledge.
All observed variables were affected by a unique factor
(error), and no pair of unique factors was correlated.
The LISREL VII program (Joreskog & Sorborn 1990) was
used to determine whether the data con®rmed this
theoretical model. Additional analyses were carried out
using EQS, a structural equations program (Bentler
1989). This approach integrates con®rmatory factor
and path analyses.
An attempt was made to check the content validity of
the tests. Content validity describes the extent to which
a test samples, or covers, the area of competencies
under assessment. It answers the question: Have most
of the important things been considered? (Neufeld
1984) In this study, content validity was assessed by
reviewing the coverage of objectives of a community-
based programme described elsewhere (Magzoub et al.
1993), using the different instruments for assessing
students in community settings. The review was con-
ducted by the ®rst author and commented upon by staff
from the FMUG involved in the assessment of students
in community settings. For each instrument, the ob-
jectives covered are indicated by crosses in Table 7,
with three crosses indicating the most coverage and one
cross the least coverage.
RESULTS
Discriminating value
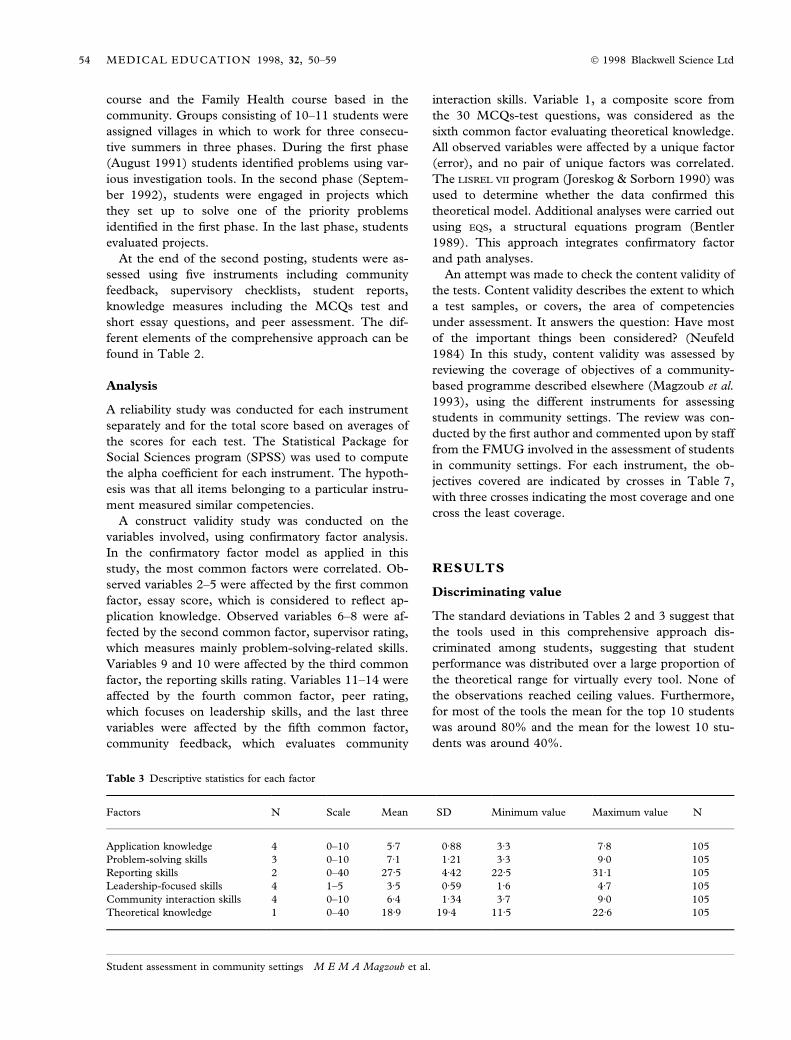
The standard deviations in Tables 2 and 3 suggest that
the tools used in this comprehensive approach dis-
criminated among students, suggesting that student
performance was distributed over a large proportion of
the theoretical range for virtually every tool. None of
the observations reached ceiling values. Furthermore,
for most of the tools the mean for the top 10 students
was around 80% and the mean for the lowest 10 stu-
dents was around 40%.
Table 3 Descriptive statistics for each factor
Factors N Scale Mean SD Minimum value Maximum value N
Application knowledge 4 0±10 5á7 0á88 3á3 7á8 105
Problem-solving skills 3 0±10 7á1 1á21 3á3 9á0 105
Reporting skills 2 0±40 27á5 4á42 22á5 31á1 105
Leadership-focused skills 4 1±5 3á5 0á59 1á6 4á7 105
Community interaction skills 4 0±10 6á4 1á34 3á7 9á0 105
Theoretical knowledge 1 0±40 18á9 19á4 11á5 22á6 105
54 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.
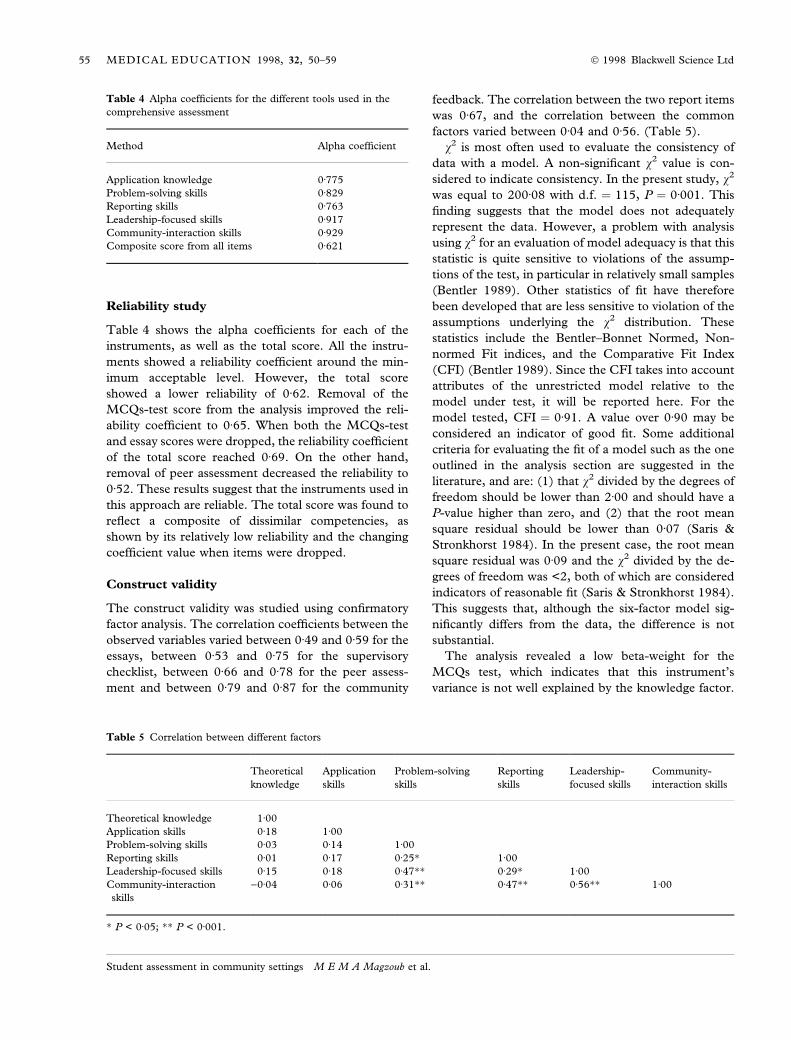
Reliability study
Table 4 shows the alpha coef®cients for each of the
instruments, as well as the total score. All the instru-
ments showed a reliability coef®cient around the min-
imum acceptable level. However, the total score
showed a lower reliability of 0á62. Removal of the
MCQs-test score from the analysis improved the reli-
ability coef®cient to 0á65. When both the MCQs-test
and essay scores were dropped, the reliability coef®cient
of the total score reached 0á69. On the other hand,
removal of peer assessment decreased the reliability to
0á52. These results suggest that the instruments used in
this approach are reliable. The total score was found to
re¯ect a composite of dissimilar competencies, as
shown by its relatively low reliability and the changing
coef®cient value when items were dropped.
Construct validity
The construct validity was studied using con®rmatory
factor analysis. The correlation coef®cients between the
observed variables varied between 0á49 and 0á59 for the
essays, between 0á53 and 0á75 for the supervisory
checklist, between 0á66 and 0á78 for the peer assess-
ment and between 0á79 and 0á87 for the community
feedback. The correlation between the two report items
was 0á67, and the correlation between the common
factors varied between 0á04 and 0á56. (Table 5).
v2 is most often used to evaluate the consistency of
data with a model. A non-signi®cant v2 value is con-
sidered to indicate consistency. In the present study, v2
was equal to 200á08 with d.f. � 115, P � 0á001. This
®nding suggests that the model does not adequately
represent the data. However, a problem with analysis
using v2 for an evaluation of model adequacy is that this
statistic is quite sensitive to violations of the assump-
tions of the test, in particular in relatively small samples
(Bentler 1989). Other statistics of ®t have therefore
been developed that are less sensitive to violation of the
assumptions underlying the v2 distribution. These
statistics include the Bentler±Bonnet Normed, Non-
normed Fit indices, and the Comparative Fit Index
(CFI) (Bentler 1989). Since the CFI takes into account
attributes of the unrestricted model relative to the
model under test, it will be reported here. For the
model tested, CFI � 0á91. A value over 0á90 may be
considered an indicator of good ®t. Some additional
criteria for evaluating the ®t of a model such as the one
outlined in the analysis section are suggested in the
literature, and are: (1) that v2 divided by the degrees of
freedom should be lower than 2á00 and should have a
P-value higher than zero, and (2) that the root mean
square residual should be lower than 0á07 (Saris &
Stronkhorst 1984). In the present case, the root mean
square residual was 0á09 and the v2 divided by the de-
grees of freedom was <2, both of which are considered
indicators of reasonable ®t (Saris & Stronkhorst 1984).
This suggests that, although the six-factor model sig-
ni®cantly differs from the data, the difference is not
substantial.
The analysis revealed a low beta-weight for the
MCQs test, which indicates that this instrument's
variance is not well explained by the knowledge factor.
Table 4 Alpha coef®cients for the different tools used in the
comprehensive assessment
Method Alpha coef®cient
Application knowledge 0á775
Problem-solving skills 0á829
Reporting skills 0á763
Leadership-focused skills 0á917
Community-interaction skills 0á929
Composite score from all items 0á621
Table 5 Correlation between different factors
Theoretical
knowledge
Application
skills
Problem-solving
skills
Reporting
skills
Leadership-
focused skills
Community-
interaction skills
Theoretical knowledge 1á00
Application skills 0á18 1á00
Problem-solving skills 0á03 0á14 1á00
Reporting skills 0á01 0á17 0á25� 1á00
Leadership-focused skills 0á15 0á18 0á47�� 0á29� 1á00
Community-interaction
skills
)0á04 0á06 0á31�� 0á47�� 0á56�� 1á00
� P < 0á05; �� P < 0á001.
55 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.
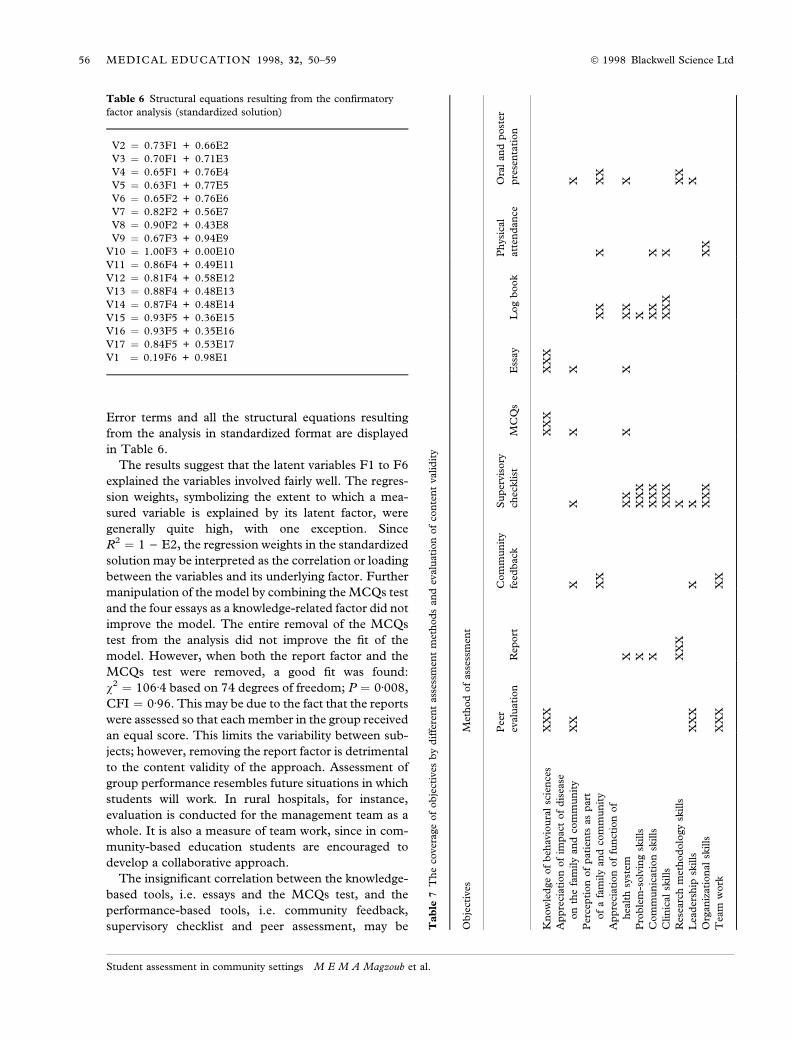
Error terms and all the structural equations resulting
from the analysis in standardized format are displayed
in Table 6.
The results suggest that the latent variables F1 to F6
explained the variables involved fairly well. The regres-
sion weights, symbolizing the extent to which a mea-
sured variable is explained by its latent factor, were
generally quite high, with one exception. Since
R2 � 1 ) E2, the regression weights in the standardized
solution may be interpreted as the correlation or loading
between the variables and its underlying factor. Further
manipulation of the model by combining the MCQs test
and the four essays as a knowledge-related factor did not
improve the model. The entire removal of the MCQs
test from the analysis did not improve the ®t of the
model. However, when both the report factor and the
MCQs test were removed, a good ®t was found:
v2 � 106á4 based on 74 degrees of freedom; P � 0á008,
CFI � 0á96. This may be due to the fact that the reports
were assessed so that each member in the group received
an equal score. This limits the variability between sub-
jects; however, removing the report factor is detrimental
to the content validity of the approach. Assessment of
group performance resembles future situations in which
students will work. In rural hospitals, for instance,
evaluation is conducted for the management team as a
whole. It is also a measure of team work, since in com-
munity-based education students are encouraged to
develop a collaborative approach.
The insigni®cant correlation between the knowledge-
based tools, i.e. essays and the MCQs test, and the
performance-based tools, i.e. community feedback,
supervisory checklist and peer assessment, may be
Table 6 Structural equations resulting from the con®rmatory
factor analysis (standardized solution)
V2 � 0.73F1 + 0.66E2
V3 � 0.70F1 + 0.71E3
V4 � 0.65F1 + 0.76E4
V5 � 0.63F1 + 0.77E5
V6 � 0.65F2 + 0.76E6
V7 � 0.82F2 + 0.56E7
V8 � 0.90F2 + 0.43E8
V9 � 0.67F3 + 0.94E9
V10 � 1.00F3 + 0.00E10
V11 � 0.86F4 + 0.49E11
V12 � 0.81F4 + 0.58E12
V13 � 0.88F4 + 0.48E13
V14 � 0.87F4 + 0.48E14
V15 � 0.93F5 + 0.36E15
V16 � 0.93F5 + 0.35E16
V17 � 0.84F5 + 0.53E17
V1 � 0.19F6 + 0.98E1
Ta
ble
7T
he
cover
age
of
ob
ject
ives
by
dif
fere
nt
ass
essm
ent
met
hod
san
dev
alu
ati
on
of
con
ten
tvalid
ity
Ob
ject
ives
Met
hod
of
ass
essm
ent
Pee
r
evalu
ati
on
Rep
ort
Com
mu
nit
y
feed
back
Su
per
vis
ory
chec
klist
MC
Qs
Ess
ay
Log
book
Ph
ysi
cal
att
end
an
ce
Ora
lan
dp
ost
er
pre
sen
tati
on
Kn
ow
led
ge
of
beh
avio
ura
lsc
ien
ces
XX
XX
XX
XX
X
Ap
pre
ciati
on
of
imp
act
of
dis
ease
on
the
fam
ily
an
dco
mm
un
ity
XX
XX
XX
X
Per
cep
tion
of
pati
ents
as
part
of
afa
mily
an
dco
mm
un
ity
XX
XX
XX
X
Ap
pre
ciati
on
of
fun
ctio
nof
hea
lth
syst
emX
XX
XX
XX
X
Pro
ble
m-s
olv
ing
skills
XX
XX
X
Com
mu
nic
ati
on
skills
XX
XX
XX
X
Clin
ical
skills
XX
XX
XX
X
Res
earc
hm
ethod
olo
gy
skills
XX
XX
XX
Lea
der
ship
skills
XX
XX
XX
Org
an
izati
on
al
skills
XX
XX
X
Tea
mw
ork
XX
XX
X
56 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.

explained by the fact that performance during ®eld
work, with its extensive interpersonal and collaborative
elements, is only drawing in knowledge to a limited
extent. Alternatively, the knowledge gains measured by
the MCQs test and essays may not properly re¯ect the
actual learning taking place in the community settings.
On the other hand, the MCQs test and essays are
comprehensive knowledge-based teats covering a large
spectrum of theoretical community health taken ran-
domly from a bank of examination questions at the end
of the semester, whereas the performance-based in-
struments are applied immediately following commu-
nity-based activities focusing on speci®c skills. An ap-
proach to MCQs test and essay question writing that
better re¯ects the actual learning experiences of stu-
dents in the ®eld may be needed.
It is concluded that the six-factor model does not
adequately represent the data. Removal of the report
factor and the MCQs test improved the ®t, but removal
of the report variables would limit the content validity
of the approach.
Content validity
Table 7 shows that overall the objectives are well cov-
ered by the different methods of assessment. Each
method focuses on a speci®c dimension of the objec-
tives. For example, peer assessment focuses most on
measurement of leadership skills and least on know-
ledge. Essays concentrate on knowledge objectives but
focus less on performance objectives.
DISCUSSION
Since many institutions and health policy makers have
seen the need for health professionals to be trained to
respond more directly to the health needs of the popu-
lation (Schmidt et al. 1991), medical schools have
started to send students to learn in community settings.
Time spent in community settings rather than in other
educational activities may be as high as 50% in some
institutions (Richards et al. 1987). However, the ob-
jective assessment of students in community settings is a
problem that has not yet been solved satisfactorily.
There is a discrepancy between the activities undertaken
by students and the subject of assessment in these
contexts.
Problems with assessment for both staff and students
can be summarized as follows. In community settings,
students usually work in groups, particularly when they
are assigned to villages. When assessing group perfor-
mance, it may be dif®cult to evaluate the students on an
individual basis and to quantify the contribution of each
group member. Secondly, students work in different
community settings, not only for logistic reasons, but
also to share experiences between the different groups.
However, students are asked to ful®l the same objec-
tives and carry out uniform activities. This lack of
standardization of ®eld conditions increases the
subjectivity of student assessment in these courses. In
addition, the fostering of changes in attitude is an
objective that is dif®cult to assess.
The results of the reliability and validity studies
suggested that the comprehensive approach measured
the different competencies developing in community-
based education. The approach seems to give a fair
indication of the whole spectrum of competencies ac-
quired. Thus it is possible to make informed decisions
on issues concerning both students and the pro-
gramme. For instance, some students may display high
achievement on the total score, combined with poor
achievement on one of the competencies, for example
leadership. In this case, a special programme will be
developed for these students to help them overcome
this weakness. On the other hand, it may be possible to
identify average students who are outstanding per-
formers in competencies such as problem-solving,
communication and community interaction. These
students may be able to assist staff in the organization
of community-based education and in tutoring junior
students, and can be targeted as potential future lead-
ers for health services in Sudan. The results of assess-
ments are now used for selecting students to assist in
the organization of CBE activities and even for select-
ing staff to join the Community Medicine Department
responsible for implementing community-based edu-
cation programmes. The validity of the assessments is
supported by the fact that supporting the learning of
students with poor assessment results and involving in
extra activities students with good results has been
found to be bene®cial.
The comprehensive approach described above may
have some disadvantages. First, it requires time and
logistic support. Tutors must be motivated, and con-
tinuous support is provided by the university. Secondly,
participants from the Ministry of Health and the com-
munity might not be as expert in the assessment of
students as academic staff. Most of these participants
collaborate on a voluntary basis and are less committed
to the programme, and their judgements may not be as
reliable. On-going training and orientation sessions for
those collaborating groups is required. Thirdly, as-
sessment is carried out in direct interviews with stu-
dents and in many cases in a face-to-face situation. This
may introduce a leniency error, i.e. students may be
given higher scores than they deserve, resulting in
57 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.

in¯ated grades. In addition, the so-called `halo effect'
may be introduced. Both students and staff may have
their opinions about students in class-based courses,
and their impressions may in¯uence their ratings of the
same students in community-based courses, although
these courses may require different aspects of compe-
tencies to be demonstrated. Fourthly, students may end
up feeling that they are being watched during every
activity undertaken. They might try harder to score
high marks than to achieve the goals of community
medicine.
To overcome these problems, staff participants have
been trained and provided with guidelines. These
describe the purpose of the assessment and how it is
to be conducted, and the criteria to be used for rat-
ings, etc. During their supervisory visits to students in
community settings, supervisors concentrate on ad-
vising students rather than assessing them. Staff
meetings and workshops are therefore opportunities
for them to re¯ect on assessment problems and act
accordingly.
In conclusion, the approach adopted by FMUG has
several advantages. It measures the various competen-
cies needed in the context of community-based work;
considers the impact not only on the student but on the
community as well; appears to be less stressful for
students; provides some measure of the student's atti-
tude, and takes cost-effectiveness into account. The
assessment methods are continuously monitored. The
conventional approach used, for instance, in Depart-
ments of Community Medicine can often be charac-
terized as being teacher-centred, using fewer sources of
information, and concentrating mainly on assessing
knowledge gains at the end of courses.
The high workload and the time needed for applying
this approach constitute the price to be paid for con-
ducting assessment that is sensitive to the objectives of
community-based education and that produces doctors
who are more likely to be responsive to community
health needs.
When tested, the approach was found to be reliable,
to be reasonably valid and to have several advantages
over the conventional approach. It may be a useful al-
ternative to existing methods of assessment of students
and programmes in community-based education.
REFERENCES
Abdel Rahim I M (1989) Six strategies for effective and relevant
medical education as adopted in Gezira Medical School. Saudi
Medical Journal 10, 391±395.
Bentler P M (1989) EQS: Structural Equations Program Manual.
Statistical Software Inc., Los Angeles.
Bollag U, Shmidt HG, Fuges T & Lawari J (1982) Medical
education in action: community-based experience and service
in Nigeria. Medical Education, 16, 282±289.
Des Marchais J E, Dumais B & Allard J (1993) Community
clinical immersion in ®rst year student and programme eval-
uation. In: International Symposium of Student Assessment (With
Special Emphasis on Assessment in Community Settings). Malay-
sia, January 10±15 1993. The Network of Community-Ori-
ented Educational Institutions for Health Sciences,
Maastricht, the Netherlands.
Frederickson K & Knox J D E (1984) The real test item bias.
American Psychologist 39, 193±202.
Fulop T (1976) New approaches to a permanent problem. WHO
Chronicle 30, 443±441.
Hassan F, Ezzat E, Faris R & Fam R (1993) The development of a
valid student assessment system in community-based medical
schools. In: Problem-Based Learning as an Educational Strategy
(ed. by P Bouhuijs, H G Schmidt & H J M Van Berkel),
Network Publications, Maastricht, the Netherlands.
Hassan M H M (1993) Community and Family Study Pro-
gramme at the Universiti Sains Malaysia: an experience in peer
assessment in the fourth and ®nal year. In: International Sym-
posium of Student Assessment (with Special Emphasis on Assess-
ment in Community Settings) Malaysia, January 10±15 1993.
The Network of Community-Oriented Educational Institu-
tions for Health Sciences, Maastricht, the Netherlands.
International Symposium of Student Assessment (with special
emphasis on assessment in community settings) Malaysia,
January 10±15 1993. Organised by the Network of Commu-
nity-oriented Education Institutions for Health Sciences,
Maastricht, the Netherlands.
Jinadu M K & Davies-Adetugbo A (1992) Experience in com-
munity-based education for health professionals. Annals of
Community-Oriented Education 5, 55±60.
Joneskog K G & SoÈrbom D (1990) Liserel VII. User's Guide.
Chicago: National Educational Resources.
Kantrowitz M, Kaufman A, Menin S, Fulop T & Gilbert J J
(1987) Innovative Tracks at Established Institutions for Health
Personnel. An Experimental Approach to Change Relevant to
Health Needs. WHO Offset Publications No. 101. World Health
Organization, Geneva, Switzerland.
Magzoub M M A & Schmidt H G (1996) Community-
based programmes: do they have impact? Education for Health
9, 209±221.
Magzoub M E M A, Abdel-Hameed A A & Ahmed B O (1993)
Assessing group work in community-based learning. In: Inter-
national Symposium of Student Assessment (with Special Emphasis
on Assessment in Community Settings) Malaysia, January 10±15
1993. The Network of Community-Oriented Educational In-
stitutions for Health Sciences, Maastricht, the Netherlands.
Manalo AH (1993) Assessment of second year students doing
community medicine work in a selected community. In: In-
ternational Symposium of Student Assesment (with Special Em-
phasis on Assessment in Community Settings) Malaysia, January
10±15 1993. The Network of Community-Oriented Educa-
58 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.

tional Institutions for Health Sciences, Maastricht, the Neth-
erlands.
Morales-Samaneigo I (1993) Students perception of peer evalu-
ation as an assessment tool in community activities. In: Inter-
national Symposium of Student Assessment (with Special Emphasis
on Assessment in Community Settings) Malaysia, January 10±15
1993. The Network of Community-Oriented Educational In-
stitutions for Health Sciences, Maastricht, the Netherlands.
Neufeld V R (1984) The design and use of assessment methods for
problem-based learning. In: Tutorials in Problem-Based Learning:
A New Direction in Teaching the Health Professions (ed. by H G De
Volder & M L De Volder). Van Gorcum, Assen/Maastricht.
Newble D & Swanson D (1988) Psychometric characteristics of
the objective structured clinical examination. Medical Educa-
tion 22, 325±34.
Norman G R, Smith E K M, Powles A C P, Booney P J, Henry
N L & Dodd P E (1987) Factors underlying performance in
written test of knowledge. Medical Education 21, 297±304.
Omorata B A, Padonu M K O, Passi A P & Amodu M O (1992)
Community-based medical education: The university of Mai-
duguri experience, Annals of Community-oriented Education,
5, 41±6.
Richards R, Fulop T, Bannerman J, Greenholm G, Guilbert J J &
Wunderlich M (1987) Innovative Schools for Health Personnel.
Report of Ten Schools Belonging to the Network of Community-
Oriented Educational Institutions for Health Sciences. WHO Offset
Publication No. 102. World Health Organization, Geneva,
Switzerland.
Saris W E & Stronkhorst L K (1984) Causal Modelling in Nonex-
perimental Research. Sociometric Research Foundation, Am-
sterdam, the Netherlands.
Schmidt H G, Neufeld V R, Nooman Z M & Ogunbode T (1991)
Network of community-oriented educational institutions for
health sciences. Academic Medicine 66, 259±263.
Received 9 June 1994; editorial comments to author 11 October 1994;
accepted for publication 6 May 1997
59 MEDICAL EDUCATION 1998, 32, 50±59 Ó 1998 Blackwell Science Ltd
Student assessment in community settings M E M A Magzoub et al.