strategies for evaluating the economic value of drugs in alcohol dependence treatment
TRANSCRIPT

R
St
DJa
b
c
d
e
f
a
ARRAA
KAPECCC
C
0d
Drug and Alcohol Dependence 122 (2012) 165– 173
Contents lists available at SciVerse ScienceDirect
Drug and Alcohol Dependence
jo u rn al hom epage: www.elsev ier .com/ locate /drugalcdep
eview
trategies for evaluating the economic value of drugs in alcohol dependencereatment�
avid Schwappacha,b,∗, Svetlana Popovac,d,e, Satya Mohapatrac, Jayadeep Patrac,d, Alexandra Godinhoc,ürgen Rehma,c,d,f
Research Institute for Public Health and Addiction, WHO Collaborating Centre for Substance Abuse, SwitzerlandInstitute of Social and Preventive Medicine (ISPM), University of Bern, SwitzerlandSocial and Epidemiological Research Department, University of Toronto, CanadaDalla Lana School of Public Health, University of Toronto, CanadaFactor-Inwentash Faculty of Social Work, University of Toronto, Ontario M5S 1V4, CanadaEpidemiological Research Unit, Universität Dresden, Germany
r t i c l e i n f o
rticle history:eceived 21 February 2011eceived in revised form 18 August 2011ccepted 20 August 2011vailable online 15 September 2011
eywords:lcohol dependence
a b s t r a c t
Background: To assess existing health economic strategies, which are used to evaluate the economic valueof drugs to treat alcohol dependence (AD) such as acamprosate, naltrexone and any other pharmaceuti-cals.Methods: A systematic literature search on AD treatment economic evaluation studies was performed inmultiple electronic bibliographic and economic databases.Results: A total of seven studies were found that involved economic evaluations of pharmacotherapytreatment of AD. It was seen that all individual pharmacotherapy treatment programs including acam-
harmacotherapyconomic evaluationost minimization analysis (CMA)ost-effectiveness analysis (CEA)ost utility analysis (CUA)
prosate, naltrexone and combined treatments have resulted in a net benefit or cost savings. However,the examined studies used different methods to estimate the costs, cost savings, and cost effectivenessof the treatments.Conclusions: Pharmacotherapy treatment of AD produced marked economic benefits. However, the num-ber of studies on the economic evaluation of pharmacotherapy for AD treatment is limited. The gaps inthese studies have also been identified as necessitating more research.
© 2011 Elsevier Ireland Ltd. All rights reserved.
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1662. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166
2.1. Literature search. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1662.2. Data extraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1662.3. Currency conversions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1662.4. Quality assessment of the examined articles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1663.1. Cost minimization analysis (CMA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1673.2. Cost-effectiveness analysis (CEA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1673.3. Cost–utility analysis (CUA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
4.1. Types of technologies and policies assessed . . . . . . . . . . . . . . . . . . . . . . .4.2. Lack of studies on CUA and CBA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.3. Analytical strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
� Supplementary materials for this article can be found by accessing the online version∗ Corresponding author at: Swiss Patient Safety Foundation, Asylstrasse 77, 8032 Zuric
E-mail address: [email protected] (D. Schwappach).
376-8716/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.drugalcdep.2011.08.026
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
of this paper at http://dx.doi.org. Please see Appendix A for more information.h, Switzerland. Tel.: +41 43 243 7670; fax: +41 43 2437671.

166 D. Schwappach et al. / Drug and Alcohol Dependence 122 (2012) 165– 173
4.4. Measures of health utility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1714.5. Assessment of costs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1724.6. Accuracy of self-report data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1724.7. Substitution between different types of substances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172Role of funding source . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173Appendix A. Supplementary data. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173
. . . . . .
1
aiWcaaeaTa
hayacupooghig2(cq2
edeasCddito
eoeere(
3. Results
In total, 118 abstracts were initially identified. After review-
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
In recent years, several pharmacologic agents have becomevailable for the treatment of alcohol dependence (AD), includ-ng disulfiram, naltrexone (oral and injectable), and acamprosate.
hile several studies have been conducted to assess the clini-al effectiveness of these drugs, the economics of AD treatmentre also important to decision makers when determining whethernd which treatments should become widely available. A healthconomic evaluation is a specific type of analysis that compareslternative courses of action in terms of costs and consequences.his type of analysis aims to support decision makers in resourcellocation decisions.
There are four types of economic analyses used in the study ofealthcare: cost minimization analysis (CMA), cost-effectivenessnalysis (CEA), cost utility analysis (CUA), and cost benefit anal-sis (CBA). In CMA, all health outcomes are assumed to be equalnd only the different costs between alternative treatments areompared. In CEA, the incremental cost of a program from a partic-lar viewpoint is related to the incremental health effects of therogram measured in “natural units” such as a symptom scorer symptom-free days. The results are expressed as cost per unitf effect in these units. In CUA, the incremental cost of a pro-ram from a particular viewpoint is compared to the incrementalealth improvement attributable to that program, where the health
mprovement is measured in quality-adjusted life-years (QALY)ained (Drummond et al., 2005; Rychlik et al., 2003; Zarkin et al.,008). In CBA, all program consequences including health effectse.g., lives saved) are valued in monetary units enabling a directomparison of the costs of the program with its incremental conse-uences in commensurate units of measurement (Drummond et al.,005).
In addition to these four types of analyses, health economicvaluations can also be divided into studies that use patient levelata and those that use decision analytic modelling (Drummondt al., 2005). In the former, data on resource use and effectivenessre collected alongside existing clinical trials (“piggybacked”) or intudies specifically designed to address health economic questions.ontrarily, economic evaluation using decision analytic modellingraws on evidence from multiple sources. It explicitly addressesecision-making under uncertainty. Decision analytic modelling
s particularly useful for the economic evaluation of interven-ions that affect a large variety of outcomes over long periodsf time.
Presently, there are only a few studies that have consid-red economic evaluations of the pharmacotherapy treatmentf AD. The purpose of the present study was to examine
xisting health economic strategies employed in the availableconomic evaluation studies of drugs to treat AD, to map whatesearch has been conducted and identify the major knowl-dge gaps in order to suggest improvements for future studiesAnderson, 2010).. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173
2. Methods
2.1. Literature search
A literature search on pharmacologic AD treatment economic evaluationstudies was performed in multiple electronic bibliographic databases from Jan-uary 1995 to February 2011, including: Ovid MEDLINE, PubMed, EMBASE,Web of Science (Including Science Citation Index, Social Sciences CitationIndex, Arts and Humanities Citation Index), PsycINFO, the Cochrane Databaseof Systematic Reviews and Google Scholar. Health economic databases, suchas CRD NHS EED (http://www.crd.york.ac.uk/crdweb/) and the CEA registry(http://www.tufts-nemc.org/cearegistry/) were also searched. The search was con-ducted using the following keywords: alcohol, addiction, dependence, treatment,pharmacotherapy, cost, cost minimization analysis, cost–benefit analysis, cost–offsetanalysis, cost–effectiveness analysis, cost–utility analysis, return-on-investment anal-ysis, economics, economic strategy, economic evaluation, economic value, disulfiram,acamprosate, naltrexone, and topiramate. As economic technical terms may not beoptimally included into many of the databases, we used wider search strategies tonot miss any study. In addition, we conducted manual reviews of the citations in anyof the relevant articles. The search was not limited to english language publicationsor geography. Studies were included if they were complete economic evaluations,i.e., considered costs and outcomes of treatment of at least two alternatives. Bothpatient level studies and decision analytic modelling studies were included in thisreview.
2.2. Data extraction
Information from the identified studies was independently extracted by twoinvestigators (S.M. and A.G.). Training of coders to achieve sufficient (>0.80) inter-rater reliability (IRR) was conducted. In order to calculate IRR, Fleiss’ kappa statisticsusing attribute agreement analytic method was used. All analyses related to IRR werecomputed using Minitab® statistical software (2007). Discrepancies were reconciledby a third investigator (S.P.), independent of the first process.
Using a standardized spreadsheet (MS-Excel), each study was coded for the fol-lowing variables: reference, country where the study was done, year when studywas conducted, the year of and currency used, perspective of the study, economicevaluation strategy employed and the main results.
2.3. Currency conversions
All monetary findings were reported in original currencies but in addition,converted to a single currency unit for easy comparison between countries andcosting years. We used international monetary fund (IMF) data to adjust for pur-chasing power parities and deflation. All local currencies were adjusted to 2010 US$ (http://eppi.ioe.ac.uk/costconversion/default.aspx) (Shemilt et al., 2008).
2.4. Quality assessment of the examined articles
Checklists, recommended by the British Medical Journal for studies on healtheconomics (Drummond, 1996) were completed for all articles included in thisreview.1 The quality assessments were performed by two independent investigators(A.G. and S.P.) and final scoring was based on consensus (Gerkens et al., 2008).
ing these abstracts, 42 were retained for further consideration that
1 Checklists can be found by accessing the online version of this paper athttp://dx.doi.org. See Appendix A for more information.
D. Schwappach et al. / Drug and Alcohol Dependence 122 (2012) 165– 173 167
Exclud ed du e to violation of bas ic in clu sion cr iteria
(e.g. duplicates, abstracts)
(n=76)
Initial in clusion (n=42)
Fulltext retrieval for critical appraisal
(n=42)
Dropped after critical appra isal (n=33), du e to -No economic evaluation of AD treatment
Identified articles (n= 118)
Includ ed evalu ations (n=9)
CMA (n=2), CEA (n=6), and CUA (n=1)
aluat
iwndCav
aIt
3
htf(ina
dg2lnaetopfctoy
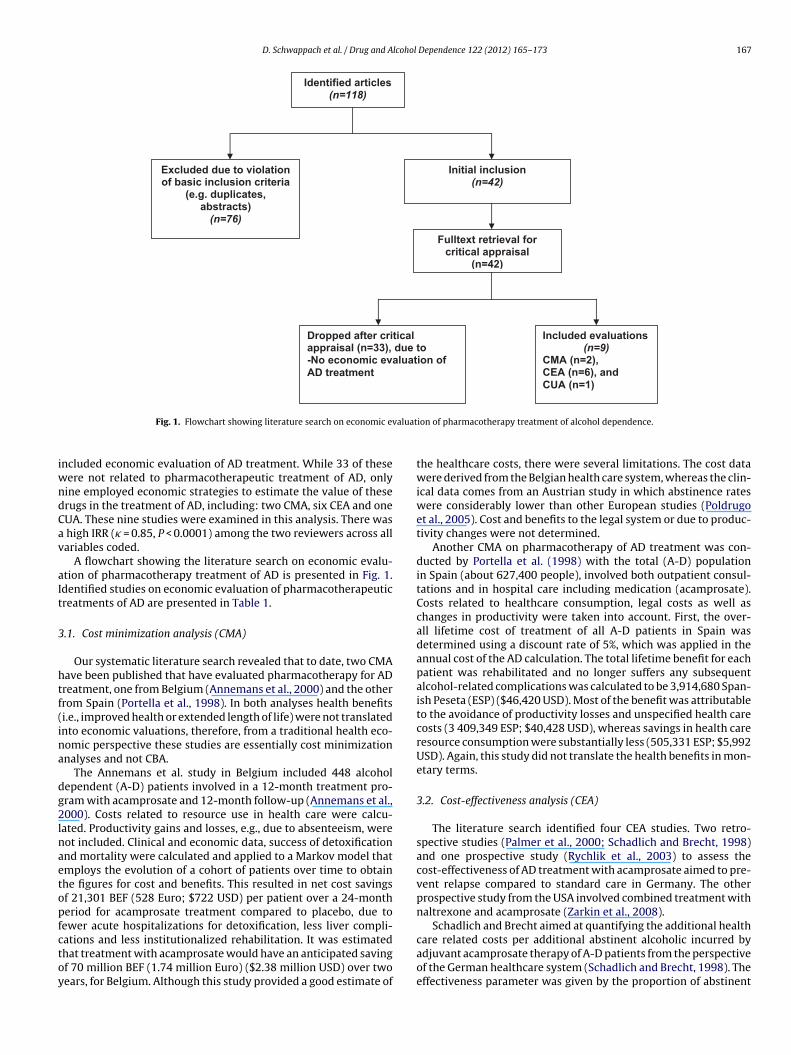
Fig. 1. Flowchart showing literature search on economic ev
ncluded economic evaluation of AD treatment. While 33 of theseere not related to pharmacotherapeutic treatment of AD, onlyine employed economic strategies to estimate the value of theserugs in the treatment of AD, including: two CMA, six CEA and oneUA. These nine studies were examined in this analysis. There was
high IRR (� = 0.85, P < 0.0001) among the two reviewers across allariables coded.
A flowchart showing the literature search on economic evalu-tion of pharmacotherapy treatment of AD is presented in Fig. 1.dentified studies on economic evaluation of pharmacotherapeuticreatments of AD are presented in Table 1.
.1. Cost minimization analysis (CMA)
Our systematic literature search revealed that to date, two CMAave been published that have evaluated pharmacotherapy for ADreatment, one from Belgium (Annemans et al., 2000) and the otherrom Spain (Portella et al., 1998). In both analyses health benefitsi.e., improved health or extended length of life) were not translatednto economic valuations, therefore, from a traditional health eco-omic perspective these studies are essentially cost minimizationnalyses and not CBA.
The Annemans et al. study in Belgium included 448 alcoholependent (A-D) patients involved in a 12-month treatment pro-ram with acamprosate and 12-month follow-up (Annemans et al.,000). Costs related to resource use in health care were calcu-
ated. Productivity gains and losses, e.g., due to absenteeism, wereot included. Clinical and economic data, success of detoxificationnd mortality were calculated and applied to a Markov model thatmploys the evolution of a cohort of patients over time to obtainhe figures for cost and benefits. This resulted in net cost savingsf 21,301 BEF (528 Euro; $722 USD) per patient over a 24-montheriod for acamprosate treatment compared to placebo, due toewer acute hospitalizations for detoxification, less liver compli-
ations and less institutionalized rehabilitation. It was estimatedhat treatment with acamprosate would have an anticipated savingf 70 million BEF (1.74 million Euro) ($2.38 million USD) over twoears, for Belgium. Although this study provided a good estimate ofion of pharmacotherapy treatment of alcohol dependence.
the healthcare costs, there were several limitations. The cost datawere derived from the Belgian health care system, whereas the clin-ical data comes from an Austrian study in which abstinence rateswere considerably lower than other European studies (Poldrugoet al., 2005). Cost and benefits to the legal system or due to produc-tivity changes were not determined.
Another CMA on pharmacotherapy of AD treatment was con-ducted by Portella et al. (1998) with the total (A-D) populationin Spain (about 627,400 people), involved both outpatient consul-tations and in hospital care including medication (acamprosate).Costs related to healthcare consumption, legal costs as well aschanges in productivity were taken into account. First, the over-all lifetime cost of treatment of all A-D patients in Spain wasdetermined using a discount rate of 5%, which was applied in theannual cost of the AD calculation. The total lifetime benefit for eachpatient was rehabilitated and no longer suffers any subsequentalcohol-related complications was calculated to be 3,914,680 Span-ish Peseta (ESP) ($46,420 USD). Most of the benefit was attributableto the avoidance of productivity losses and unspecified health carecosts (3 409,349 ESP; $40,428 USD), whereas savings in health careresource consumption were substantially less (505,331 ESP; $5,992USD). Again, this study did not translate the health benefits in mon-etary terms.
3.2. Cost-effectiveness analysis (CEA)
The literature search identified four CEA studies. Two retro-spective studies (Palmer et al., 2000; Schadlich and Brecht, 1998)and one prospective study (Rychlik et al., 2003) to assess thecost-effectiveness of AD treatment with acamprosate aimed to pre-vent relapse compared to standard care in Germany. The otherprospective study from the USA involved combined treatment withnaltrexone and acamprosate (Zarkin et al., 2008).
Schadlich and Brecht aimed at quantifying the additional health
care related costs per additional abstinent alcoholic incurred byadjuvant acamprosate therapy of A-D patients from the perspectiveof the German healthcare system (Schadlich and Brecht, 1998). Theeffectiveness parameter was given by the proportion of abstinent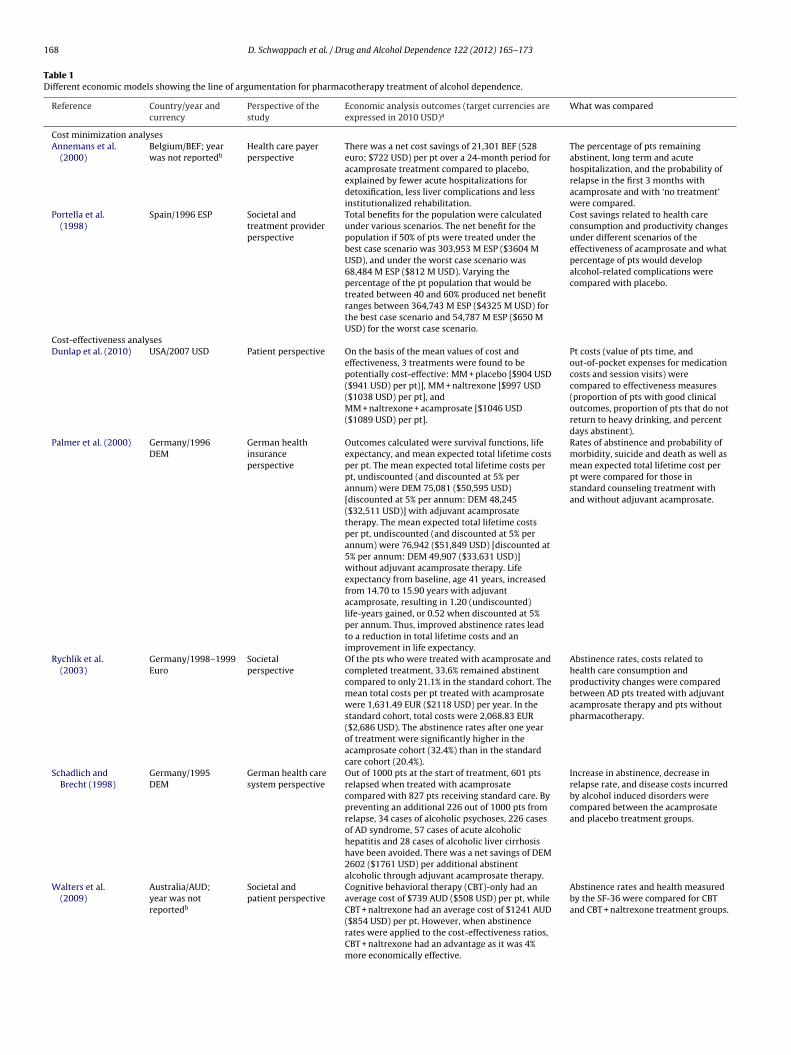
168 D. Schwappach et al. / Drug and Alcohol Dependence 122 (2012) 165– 173
Table 1Different economic models showing the line of argumentation for pharmacotherapy treatment of alcohol dependence.
Reference Country/year andcurrency
Perspective of thestudy
Economic analysis outcomes (target currencies areexpressed in 2010 USD)a
What was compared
Cost minimization analysesAnnemans et al.
(2000)Belgium/BEF; yearwas not reportedb
Health care payerperspective
There was a net cost savings of 21,301 BEF (528euro; $722 USD) per pt over a 24-month period foracamprosate treatment compared to placebo,explained by fewer acute hospitalizations fordetoxification, less liver complications and lessinstitutionalized rehabilitation.
The percentage of pts remainingabstinent, long term and acutehospitalization, and the probability ofrelapse in the first 3 months withacamprosate and with ‘no treatment’were compared.
Portella et al.(1998)
Spain/1996 ESP Societal andtreatment providerperspective
Total benefits for the population were calculatedunder various scenarios. The net benefit for thepopulation if 50% of pts were treated under thebest case scenario was 303,953 M ESP ($3604 MUSD), and under the worst case scenario was68,484 M ESP ($812 M USD). Varying thepercentage of the pt population that would betreated between 40 and 60% produced net benefitranges between 364,743 M ESP ($4325 M USD) forthe best case scenario and 54,787 M ESP ($650 MUSD) for the worst case scenario.
Cost savings related to health careconsumption and productivity changesunder different scenarios of theeffectiveness of acamprosate and whatpercentage of pts would developalcohol-related complications werecompared with placebo.
Cost-effectiveness analysesDunlap et al. (2010) USA/2007 USD Patient perspective On the basis of the mean values of cost and
effectiveness, 3 treatments were found to bepotentially cost-effective: MM + placebo [$904 USD($941 USD) per pt)], MM + naltrexone [$997 USD($1038 USD) per pt], andMM + naltrexone + acamprosate [$1046 USD($1089 USD) per pt].
Pt costs (value of pts time, andout-of-pocket expenses for medicationcosts and session visits) werecompared to effectiveness measures(proportion of pts with good clinicaloutcomes, proportion of pts that do notreturn to heavy drinking, and percentdays abstinent).
Palmer et al. (2000) Germany/1996DEM
German healthinsuranceperspective
Outcomes calculated were survival functions, lifeexpectancy, and mean expected total lifetime costsper pt. The mean expected total lifetime costs perpt, undiscounted (and discounted at 5% perannum) were DEM 75,081 ($50,595 USD)[discounted at 5% per annum: DEM 48,245($32,511 USD)] with adjuvant acamprosatetherapy. The mean expected total lifetime costsper pt, undiscounted (and discounted at 5% perannum) were 76,942 ($51,849 USD) [discounted at5% per annum: DEM 49,907 ($33,631 USD)]without adjuvant acamprosate therapy. Lifeexpectancy from baseline, age 41 years, increasedfrom 14.70 to 15.90 years with adjuvantacamprosate, resulting in 1.20 (undiscounted)life-years gained, or 0.52 when discounted at 5%per annum. Thus, improved abstinence rates leadto a reduction in total lifetime costs and animprovement in life expectancy.
Rates of abstinence and probability ofmorbidity, suicide and death as well asmean expected total lifetime cost perpt were compared for those instandard counseling treatment withand without adjuvant acamprosate.
Rychlik et al.(2003)
Germany/1998–1999Euro
Societalperspective
Of the pts who were treated with acamprosate andcompleted treatment, 33.6% remained abstinentcompared to only 21.1% in the standard cohort. Themean total costs per pt treated with acamprosatewere 1,631.49 EUR ($2118 USD) per year. In thestandard cohort, total costs were 2,068.83 EUR($2,686 USD). The abstinence rates after one yearof treatment were significantly higher in theacamprosate cohort (32.4%) than in the standardcare cohort (20.4%).
Abstinence rates, costs related tohealth care consumption andproductivity changes were comparedbetween AD pts treated with adjuvantacamprosate therapy and pts withoutpharmacotherapy.
Schadlich andBrecht (1998)
Germany/1995DEM
German health caresystem perspective
Out of 1000 pts at the start of treatment, 601 ptsrelapsed when treated with acamprosatecompared with 827 pts receiving standard care. Bypreventing an additional 226 out of 1000 pts fromrelapse, 34 cases of alcoholic psychoses, 226 casesof AD syndrome, 57 cases of acute alcoholichepatitis and 28 cases of alcoholic liver cirrhosishave been avoided. There was a net savings of DEM2602 ($1761 USD) per additional abstinentalcoholic through adjuvant acamprosate therapy.
Increase in abstinence, decrease inrelapse rate, and disease costs incurredby alcohol induced disorders werecompared between the acamprosateand placebo treatment groups.
Walters et al.(2009)
Australia/AUD;year was notreportedb
Societal andpatient perspective
Cognitive behavioral therapy (CBT)-only had anaverage cost of $739 AUD ($508 USD) per pt, whileCBT + naltrexone had an average cost of $1241 AUD($854 USD) per pt. However, when abstinencerates were applied to the cost-effectiveness ratios,CBT + naltrexone had an advantage as it was 4%more economically effective.
Abstinence rates and health measuredby the SF-36 were compared for CBTand CBT + naltrexone treatment groups.

D. Schwappach et al. / Drug and Alcohol Dependence 122 (2012) 165– 173 169
Table 1 (Continued)
Reference Country/year andcurrency
Perspective of thestudy
Economic analysis outcomes (target currencies areexpressed in 2010 USD)a
What was compared
Zarkin et al. (2008) USA/2007 USD Treatment providerperspective
On the basis of the mean values of cost andeffectiveness, 3 interventions are cost-effectiveoptions relative to the other interventions for all 3outcomes: MM + placebo [$409 USD ($426 USD)per pt], MM + naltrexone therapy [$671 USD ($699USD) per pt], and MM + combined naltrexone andacamprosate therapy [$1003 USD ($1044 USD) perpt].
Incremental cost per percentage pointincrease in mean percentage of daysabstinent, incremental cost per pt ofavoiding heavy drinking, andincremental cost per pt of achieving agood clinical outcome were comparedin the COMBINE study.
Cost–utility analysesMortimer and
Segal (2006)Australia/2003AUD
Societalperspective
Naltrexone + counseling was estimated to deliver0.0528 QALYs gained per completer at anincremental cost per completer of $685 AUD ($591USD) as compared to placebo + counseling. The costper QALY gained for the naltrexone + counseling vs.placebo + counseling comparison was estimated at$12,966 AUD ($11,195 USD).
Gain in QALYs was compared betweendifferent interventions for theprevention and treatment of AD.
AD, alcohol dependence; A-D, alcohol-dependent; M, million; MM, medical management; Pt(s), patient(s); QALY, quality-adjusted life-years; AUD, Australian dollar; BEF,Belgian Franc; DEM, Deutsche Mark; ESP, Spanish peseta; USD, United States dollar; EUR, euro.
a International monetary fund (IMF) data were used to adjust for purchasing power parities and deflation. All local currencies were adjusted to 2010 US $(
is use
auM(DteactmpttuaaBia
tawsimbsdolacpewtauDtU
http://eppi.ioe.ac.uk/costconversion/default.aspx) (Shemilt et al., 2008).b A year of currency was not reported, therefore the year of study was published
lcoholics at the end of the 48-week medication-free follow-p period in the prevention of relapse with acamprosate in theanagement of Alcoholism (PRAMA) study, a one-year placebo
standard care), controlled clinical trial and a one-year follow-up.ata on resource consumption and costs were not taken from the
rial but from epidemiological studies and official statistics. Theconomic valuation of the cost parameters was performed usingverage case-related treatment costs of hospital treatment cal-ulated from the average hospitalization periods and costs perreatment day in hospital. This analysis revealed a net savings in
edical costs of about Deutsche Mark (DEM) 2602 ($1761 USD)er additional abstinent alcoholic through adjuvant acamprosateherapy, mainly due to reductions in hospitalization and rehabili-ation costs. This modelling study employed the same time-framesed for the clinical trial allowing precise determination of relativebstinence rates of the acamprosate and placebo groups. The datalso came from the same German Healthcare system [unlike theelgian CMA (Annemans et al., 2000)]. However, the assumption
n this study that abstinent patients would not have any problemfterwards seems unrealistic.
The objective of the Palmer et al. (2000) study was to assesshe lifetime medical and cost outcomes of A-D patients who weredministered acamprosate as adjuvant therapy, in conjunctionith standard counseling therapy, compared with standard coun-
eling therapy alone from the perspective of the German healthnsurance system. The analysis was conducted using a decision
odel based on Markov cycles to assess the long-term costs andenefits. In addition, a set of submodels simulating the progres-ion of important complications of alcoholism (abstinence, liverisease, gastrointestinal disease, alcoholic cardiomyopathy, andther complications) was constructed in parallel. The number ofife-years gained with adjuvant acamprosate over standard ther-py was taken as the measure of effectiveness. The analysis of theosts included the costs for drug acquisition and treating com-lications. Changes in productivity were not included. The lifexpectancy from the baseline of age 41 increased from 14.7 yearsith standard therapy to 15.9 years with adjuvant acamprosate
herapy. The resulting incremental, discounted life-years gained bydjuvant acamprosate over standard therapy was 0.52 (1.20 when
ndiscounted). The cost of 48 weeks of acamprosate therapy wasEM 2177 ($1467 USD). The discounted (and undiscounted) life-ime costs were DEM 48,245 ($32,511 USD) (DEM 75,081; $50,595SD) with adjuvant therapy and DEM 49,907 ($33,631 USD) (DEM
d for conversion rate purposes.
76,942; $51,849 USD) with standard therapy. An incremental CEAwas carried out to combine the costs and health effects. However,adjuvant acamprosate therapy represented the dominant strategyaccording to economic definition, as it was more effective and lesscostly than standard therapy. The major limitation of the study isthat there was no assessment of the patient’s quality of life. Mea-sures of uncertainty (variance) of the cost-effectiveness ratios werenot calculated, although there was wide use of sensitivity analyses.The strength of the study is that the likelihood that successfullytreated subjects would continue to accrue alcohol-related healthcare costs were taken into account, and economic data and clini-cal data were obtained from compatible sources. The weakness ofthe model is that long-term predictions on costs and medical ben-efits are made in the absence of any clinical data on the outcome ofacamprosate-treated subjects beyond 2 years of treatment.
Rychlik et al. (2003) compared the cost-effectiveness of adju-vant acamprosate treatment to any other treatment not usingacamprosate. In this prospective CEA, 814 recently detoxified A-Dpatients in Germany were provided with psychosocial support withadjuvant acamprosate therapy (n = 540) or without pharmacother-apy (n = 274). Real costs of treatment were assessed over a periodof one year. To estimate changes in productivity, time off work wasevaluated by using the human-capital-approach. Travel expensesrelated to treatment were also included. Of the patients whowere treated with acamprosate and completed treatment, 33.6%remained abstinent compared to only 21.1% in the standard cohort.The mean total costs per patient treated with acamprosate were1631.49 EUR ($2118 USD) per year. In the standard cohort, totalcosts were 2068.83 EUR ($2686 USD). Costs relating to healthcareconsumption (including travel expenses) amounted to 77% of thetotal costs, with a 27% difference between the cohorts (p < 0.001).Costs related to productivity changes were 27% higher in the stan-dard cohort. The ratio between costs and abstinence rates werecalculated to evaluate the cost-effectiveness. This patient level datastudy confirmed the favourable cost-effectiveness of acamprosatesuggested by two previous pharmaco-economic modelling studies.
The prospective CEA by Zarkin et al. (2008) in the USA exam-ined the costs and cost-effectiveness of the COMBINE interventions(combined pharmacotherapies involving acamprosate and naltrex-
one along with behavioral therapy) after 16 weeks of treatment.This is the only combined pharmacotherapy study for AD treat-ment to date involving a randomized controlled clinical trial with1383 patients having a diagnosis of primary AD. The study included
1 lcohol
nfbmg
csmmtapswcltppoowf[Uaossti
ttimtgspbtirwMtmettMrmCst
Psbboer
70 D. Schwappach et al. / Drug and A
ine treatment groups. Four groups received medical managementor 16 weeks with naltrexone, 100 mg/d, acamprosate, 3 g/d, oroth, and/or placebo; four groups received the same therapy asentioned above with combined behavioral intervention; and one
roup received combined behavioral intervention only.The investigators used a microcosting approach to estimate the
osts of the COMBINE study therapies from the provider’s per-pective. The costs of all COMBINE study activities (space, labor,edication, and laboratory costs) that would be needed to imple-ent the therapies in clinical practice, rather than in a clinical
rial research protocol, were estimated. The three clinical outcomesssessed in the CEA were the percentage of days abstinent, the pro-ortion of patients who did not return to heavy-drinking days (5tandard drinks per day for men and 4 standard drinks per day foromen), and the proportion of patients who maintained a good
linical outcome (abstinent or moderate drinking without prob-ems). All of these outcomes were measured through the end ofhe 16-week treatment period. Incremental cost per percentageoint increase in percentage of days abstinent, incremental cost peratient of avoiding heavy drinking, and incremental cost per patientf achieving a good clinical outcome were estimated. On the basisf the mean values of cost and effectiveness, three interventionsere found to be cost-effective relative to the other interventions
or all three outcomes: medical management (MM) with placebo$409 USD (426 USD) per patient], MM + naltrexone therapy [$671SD (699 USD) per patient], and MM + combined naltrexone andcamprosate therapy [$1003 USD (1044 USD) per patient]. Focusingnly on effectiveness, MM–naltrexone–acamprosate therapy is notignificantly better than MM–naltrexone therapy. However, con-idering cost and cost-effectiveness, MM–naltrexone–acamprosateherapy may be a better choice, if the cost of the incrementalncrease in effectiveness is justified by the decision maker.
Dunlap et al. (2010) estimated the patient costs for the 9reatments in the COMBINE study (Zarkin et al., 2008) fromhe perspective of the patients. Each patient’s treatment costncluded time costs and out of pocket expenses (copayments for
edications and for session visits). The value of the patient’sime spent participating in treatment, self-help recovery pro-rams, and travel times was calculated by weighting the timepent on relevant activities (treatment, travel) with the unitrice for time. Data on time spent on activities was obtainedy staff and through patient’s self-reports. The unit price forime was obtained by averaging hourly wages across all patientsn all treatments (wages were obtained through patients self-eports). Transportation costs other than travel times, e.g., fares,ere not included. All treatments, except for MM + placebo,M + naltrexone, and MM + naltrexone + acamprosate were found
o be economically dominated, i.e., were less effective butore costly. Effectiveness ratings varied for the three cost-
ffective treatments with MM + placebo being the least effec-ive and MM + naltrexone + acamprosate being the most effec-ive; however, MM + placebo was also the least costly, while
M + naltrexone + acamprosate was the most costly. The studyeveals that patients incur significant costs to participate in treat-ent and devote considerable time and resources to access care.
osts associated with travel times to/from treatment sessions andelf-help meetings accounted for a large portion of total cost ofreatment in all treatment arms (range: 30–40%).
In an Australian study, the Drug Abuse Treatment Cost Analysisrogram was used to estimate treatment costs (costs of per-onnel, supplies and materials, equipment, contracted services,uilding and facilities, and miscellaneous resources) of cognitive
ehavioral therapy (CBT)-only and CBT combined with naltrex-ne (Walters et al., 2009). CBT with naltrexone was 54% morexpensive than CBT-only, however when treatment abstinenceates (36.1% for CBT; 62.6% for CBT + naltrexone) were applied toDependence 122 (2012) 165– 173
the cost-effectiveness ratios, CBT + naltrexone was shown to bemore cost-effective. The cost per 100 completers for CBT-onlywas $206,920 Australian dollars (AUD) ($142,332 USD), whileCBT + naltrexone was $198,650 AUD ($136,644 USD).
3.3. Cost–utility analysis (CUA)
To date, only one CUA has been conducted by Mortimer andSegal in the area of AD (Mortimer and Segal, 2006). This analysiscompared the performance of various competing and complemen-tary interventions for the prevention or treatment of problemdrinking and AD in terms of cost per QALY estimates. Threeinterventions (i) brief interventions for problem drinking, (ii)psychotherapy for mild to moderate dependence, and (iii) drug-therapy adjuvant to counseling for detoxified patients with ahistory of severe physical dependence were selected for evaluation.The study used data from several trials to model a time-dependentstate-transition model with tunnel sequences used to delay thehealth effects of moving from one state to another. Outcomes weremodelled out to full life expectancy. Key health outcomes were typ-ically the fraction of patients drinking on either side of a specifiedthreshold. Incremental program costs have been estimated basedon a description of resource-use in intervention and control groupsobtained from the study reports. Incremental costs and incremen-tal benefits are estimated from a societal perspective, but the rangeof costs and consequences included in the analysis was limiteddue to various practical considerations in estimation. Productivitygains and private costs to access services, e.g., waiting time, werealso excluded. Gains in quality of life were taken from disability-adjusted life year (DALY) – weights from the Netherlands such thatreturning problem- and dependent-drinkers to a ‘safe’ consump-tion pattern is assumed to imply annual QALY-gains of 0.110 and0.330, respectively. Based on the modelled CUA, the brief inter-ventions evaluated were estimated to deliver 0.091 QALYs gainedper treated male and 0.125 QALYs gained per treated female. Thecost per QALY gained is estimated at $671 AUD ($579 USD) inmales and $490 AUD ($423 USD) in females. Moderation-orientedcue exposure was then estimated to deliver 0.116 QALYs gainedper completer at an incremental cost of $249 AUD ($215 USD)per completer as compared to behavioral self-control training.Based on these figures, the cost per QALY gained is estimated at$2145 AUD ($1852 USD) in a predominantly male population withmoderate dependence. The cost per QALY gained for motivationalenhancement therapy was estimated at $3366 AUD ($2906 USD) ascompared to usual care of no further counseling after initial assess-ment and feedback/education. Finally, naltrexone + counseling wasestimated to deliver 0.0528 QALYs gained per completer at an incre-mental cost per completer of $685 AUD ($591 USD) as comparedto placebo + counseling. The cost per QALY gained for the naltrex-one + counseling vs. placebo + counseling comparison is estimatedat $12,966 AUD ($11,195 USD). Under the base-case, interventionsfor problem drinkers appear to offer better value for money thaninterventions targeted at those with a history of severe physicaldependence. The main problem with this modelling study is thatthe DALY – weights that were collected using a specific persontrade-off frame were being used to calculate QALYs. These QALYsare therefore not consistent with standard approaches for estimat-ing gains in QALYs, e.g., standard gamble or time trade-off methods.The results of the study are thus, only to a limited degree compa-rable to other studies.
4. Discussion
Although several medications have been used for treating peo-ple with AD for quite some time, there have been only a fewattempts to economically evaluate such treatments.

lcohol
sopetmhltto
mttof
bko
4
rntaapoiceeT(
4
espmoosinattvaddvaa
rab
D. Schwappach et al. / Drug and A
The studies included in the present analysis have used differenttrategies to estimate the costs and savings due to the treatmentf AD. However, in all cases, it is seen that individual treatmentrograms have resulted in a net savings. The studies used differ-nt methods to estimate the costs and resultant savings due to thereatment programs. The vast majority of included studies esti-
ated only the benefits mainly in the form of cost offsets to theealthcare system, and few assessed the benefits related to the
egal system due to a reduction in the number of crimes or dueo productivity gains. None of the studies used CBA methodologyhat requires valuing both losses and benefits in length and qualityf life – both to the individual and society – in monetary terms.
All economic evaluations including CMA, CEA or CUA have deter-ined economic benefits of pharmaceutical treatments for AD and
hese studies point out a positive economic benefit of addictionreatment with pharmacotherapy. As there are only a few studiesffering an economic evaluation of AD treatment, there is a needor more research on this aspect.
A number of gaps and problems with the current studies haveeen identified, some of which are of a more general nature well-nown from other areas of health economic evaluation, whilethers seem specific to the economics of addiction treatment.
.1. Types of technologies and policies assessed
Evaluations of prevention, health promotion and policies toegulate alcohol consumption are extremely rare. The lack of eco-omic assessments of such broader interventions (as comparedo treatment or clinical prevention) has been observed in otherreas of health care, e.g., cardiovascular disease (Schwappach etl., 2007). Again, as in other areas of health care, there are com-aratively many CEA assessing the outcomes of pharmacotherapy,ften with a very limited focus in terms of time frame and outcomesnvestigated, as compared to other types of treatment, e.g., psy-hotherapy, or combined approaches of care. More recently, healthconomic evaluations have become available that compare differ-nt non-pharmacological treatments, for example, the UK Alcoholreatment Trial (UKATT), and showed favorable cost-effectivenessBarbosa et al., 2010; UKATT Research Team, 2005).
.2. Lack of studies on CUA and CBA
As with other disease areas, more comprehensive types ofconomic evaluations for AD treatment that include a social per-pective are relatively scarce (Schwappach and Boluarte, 2007). Inarticular, “true” CBA and CUA are largely missing for AD treat-ent, while CEA of pharmacotherapy are less rare. The majority
f existing studies simply “omit” effects on quality and quantityf life. Thus, important benefits – both for the individual and forociety – are not being considered. This is a major omission sincet assumes “that drug-misusing individuals have a zero value”, asoted by Godfrey et al. (2004). Cost–benefit approaches evaluatelcohol-attributable mortality and losses in quality of life in mone-ary terms and are necessary to provide a full economic estimate ofhe burden of AD to society. However, methods to assign monetaryalues to quality and life years lost, such as the willingness-to-paypproach, have not yet been extensively applied to AD. The mainisadvantage of the willingness to pay method is that people fromifferent socio-demographic backgrounds may be willing to payastly different dollar amounts for the same health outcomes –s such these differences could drastically bias a study toward orgainst a certain demographic section of the population.
CUA that express health changes in terms of QALYs are war-anted to compare cost/QALY estimates within AD treatment andcross other treatments. Cost/QALY estimates are increasinglyeing used by policy makers to support decision makers in resource
Dependence 122 (2012) 165– 173 171
allocation decisions and though the underlying methodologies arestill being discussed internationally, it can be expected that variouscountries follow the UK National Institute for Health and ClinicalExcellence (NICE) in considering cost/QALY estimates in fundingdecisions (e.g., the German “IQWIG Institute”). It is thus crucial thatvalid and methodologically sound estimates are available for ADtreatment that allow for the comparison of cost/QALY estimateswith the treatment of other diseases.
4.3. Analytical strategy
Both patient-level data and decision analytic modellingapproaches have been applied to evaluate the economics ofAD treatment. Both of these strategies have advantages andlimitations. While trial based studies often follow microcostingapproaches and measure costs and benefits with a high degreeof precision, they are usually limited in scope and time horizon.Decision analytic modelling has the advantage that longer peri-ods of time can be simulated and a variety of outcomes, in andoutside the health care sector, can be incorporated. Data fromdifferent sources can be implemented and the impact of uncer-tainty associated with these data are quantified and made explicit.Indeed, decision analytic modelling, if properly conducted, can beregarded as the meta-analytic approach to economic evaluations(Anderson, 2010). For the evaluation of AD treatments the combi-nation of both approaches seems optimal. A decision analytic modelfed with data from high quality trials wherever possible and supple-mented by observational data or even expert opinion on outcomeshardly accessible through empirical studies could be used to sim-ulate treatments comprehensively. Such a model would also fosterinter-juridical comparisons.
4.4. Measures of health utility
Studies that have tried to model outcomes of treatments asQALYs (i.e., CUA) often use instruments that have not yet beencomprehensively validated for their use in this specific sampleof patients. In the assessment of addiction treatment effects thisaffects two general concerns: (1) how responsive are commoninstruments for utility elicitation to changes in AD, and (2) howvalid are estimates of utility in diseases with considerable externaleffects?
Regarding the responsiveness of utility measurement in A-Dpatients, there is only limited evidence that supports the use ofstandard methodology and instruments, such as the EQ-5D, for theassessment of gains in utility in this patient group. Gunther et al.compared and contrasted the responsiveness of several commu-nity preference-based scores of the EQ-5D in A-D patients withthe responsiveness of composite summary scores of instrumentsmeasuring mental quality of life, psychopathology and social func-tioning (Gunther et al., 2008). In an observational longitudinalcohort study of AD, three different EQ-5D-based utilities (EQ-IndexUnited Kingdom, United States, and Germany) were calculated andcompared with the scores of the WHOQOL-BREF (mental domain),HoNOS (total score), and Global Assessment of Functioning at base-line and at 18 months. The results suggest that the EQ-5D indices areless responsive and require larger patient samples to detect mean-ingful clinical differences compared to the other instruments used.In an earlier study conducted by the same group, the EQ-5D visualanalog scale score (mean 58.0), the British EQ-5D index (mean 0.74)and the German EQ-5D index (mean 0.85) showed poor to moder-ate correlations with other scales (0.28 < r < 0.60) (Gunther et al.,
2007).The second issue relates to the fact that substance abuseis associated with a high degree of external effects and socialconsequences relating to private relationships, social integration,

1 lcohol
esQt(rfiai
scpwuttt
4
2hcdmhsmsibass(e(wcoj
icvnacbHda
4
iosesloc
72 D. Schwappach et al. / Drug and A
ducation and work. Mortimer and Segal showed that the inclu-ion of within-family external effects reduces the cost perALY estimates of interventions for problem drinking and AD,
hereby improving the performance of all evaluated interventionsMortimer and Segal, 2006). They conclude that interventions witheadily quantifiable health benefits (where social costs and bene-ts are predominantly comprised of private costs and benefits) aret a distinct advantage when competing for public funding againstnterventions with quantitatively important external effects.
It remains unclear as to how these effects are captured in mea-ures of health utility, or whether all of the effects can even beaptured within existing economic evaluation methods. For exam-le, it seems plausible that improved family relations or ability toork enter the patient’s utility function to some degree. It is alsonclear whether patients, when answering utility elicitation ques-ions, anticipate improved well-being of their relatives or whetherhese effects have to be modelled separately. Clearly, double or evenhreefold counting has to be avoided.
.5. Assessment of costs
As in other areas of health care costing studies (Stone et al.,000), there is large variability in the assessment of costs in alco-ol studies. Only a few studies include (paid and unpaid) socialosts and productivity losses. The available studies consistentlyemonstrate that these costs are sensitive to the method of esti-ation chosen (whether it is a human capital method, friction or
ybrid approach) and that changes in productivity resulting fromubstance-related morbidity and thus potential gains with treat-ent constitute a substantial portion of total substance-related
ocietal costs. Whether and how to include productivity lossesn economic evaluations conducted from a societal viewpoint haseen subject to substantial methodological and theoretical debatend policies vary (Drummond et al., 2005). For example, NICEupports the inclusion of costs falling outside the NHS budget inubmitted economic evaluations only in exceptional circumstancesClaxton et al., 2010). If productivity changes are considered invaluations of AD treatment, quantities of productivity changese.g., days of work) should be reported separately from prices (e.g.,ages) and expressed separately from costs following from health
are consumption. Following this approach, the appropriatenessf the results can be interpreted by decision makers and inter-urisdictional comparisons can be made.
Another special aspect of costing in AD is that the costs of behav-or associated with AD that fall outside the health care system, e.g.,osts to the law system, economic damage, pain and suffering ofictims involved in crime and motor vehicle crashes, are usuallyot assessed but can be substantial (Fleming et al., 2002). A recentnalysis based on the COMBINE study data show that future socialosts of AD, e.g., costs associated with motor vehicle accidents, cane substantial and outweigh treatment costs (Zarkin et al., 2010).owever, savings were generated three years after treatment ran-omization suggesting that shorter observational periods may biasgainst AD treatment.
.6. Accuracy of self-report data
Studies of AD rely on self-report data from patients relat-ng to health and social care consumption, drinking behaviors,ffences, and other relevant information. The validity of thesetudies thus relies on the accuracy of these self-reports. Whilextensive research has been undertaken to assess the validity of
elf-reports of substance consumption (Del Boca and Noll, 2000)ittle is known about the accuracy of A-D patient’s self-reportsf care consumption. However, research in other areas of healthare suggest that discrepancies in resource utilisation betweenDependence 122 (2012) 165– 173
administrative and patient-supplied data sources can be substan-tial (Bhandari and Wagner, 2006; Pollicino et al., 2002; Marshallet al., 2001). Booth et al. report that agreement between at-riskdrinkers’ self-reports and abstracted provider contacts was mod-erate to good for general medical and specialty mental healthcontacts (kappa = 0.50 and 0.62, respectively) but low for “other”miscellaneous health contacts (0.04) (Booth et al., 2006). Compa-rable figures were obtained in a general patient population studyin the Netherlands (Reijneveld, 2000). As A-D patients consumeresources from a variety of sources and only self-reports may beavailable, future research into their accuracy is warranted so thatthe degree of measurement error associated with self-reports in ADtreatments can be estimated.
4.7. Substitution between different types of substances
Many studies in substance abuse or addiction treatment monitorthe use of specific substances as the primary outcome. For exam-ple, studies in opioid dependent subjects often assess patient’ssubsequent use of illegal substances as measures of effectiveness.Similarly, evaluations of AD treatment typically chose alcohol absti-nence rates or avoided relapses as primary outcomes measures.Most studies fail to include the full spectrum of drugs and alcohol inassessing outcomes. However, this one-dimensional view may notadequately reflect behavior. Subjects may compensate decreasesin one substance with increases in the consumption of other sub-stances. For example, during the “so-called” heroin drought inAustralia, when prices for heroin went up and purity decreased,heroin users increased their consumption of other drugs, in par-ticular methamphetamines and morphine (Longo et al., 2004).Similarly, patients treated for one substance may increase theiruse of other substances. However, such compensation may neveroccur: for instance, higher taxation of cigarettes has been shownto decrease not only smoking but also alcohol consumption (Leeet al., 2010). As compensation or other effects on the use orabuse of other substances could be important, studies in addictiontreatment need to monitor such behavior either by assessing theentire range of used substances, or by modelling consequences ingeneric measures of health and well being (i.e., mortality, qualityof life).
Our study provides an overview about health economic eval-uations of drugs in alcohol dependence treatment. While severalstudies have been conducted in the past years we identified sev-eral knowledge gaps. Currently, evidence seems very fragmentedand most studies have concentrated on short time frames and directaccessible costs and clinical outcomes. This hampers comparisonsbetween different types of treatments and generalisability acrossjurisdictions. A decision-modelling approach that could adopt awide societal perspective, would include a wide range of potentialimpacts of AD (e.g., productivity changes) and would report thesein units of impact. Different models may be necessary for differenttreatment simulations. Units of impact could be synthesized acrossthe available studies and as more trial-based data become availablethese could be included. Such models would allow decision makersto reframe the analysis to their scope of interest (e.g., health caresector, or broader societal perspective) and attach local prices tounits of impact and resources.
Role of funding source
This research was supported by Eli Lilly and Company, Indi-anapolis, USA. The funding source had no other role in study design;
in the collection, analysis and interpretation of the data; in thewriting of the report; or in the decision to submit the paper forpublication.
lcohol
C
Mrovtcccv
C
ti
A
tteO
A
t
R
A
A
B
B
B
C
D
D
D
D
D. Schwappach et al. / Drug and A
ontributors
Authors Rehm and Schwappach designed the study. Authorsohapatra, Popova, Patra, and Godinho conducted a literature
eview and data extraction. Author Mohapatra wrote the first draftf the manuscript, and author Schwappach and Popova super-ised manuscript preparation and revised the second version ofhe manuscript based on the reviewers’ comments. Author Godinhoonducted quality checklists for all examined studies and adjustedosting data for purchasing power parities and deflation. All authorsontributed to interpreting the results and have approved the finalersion of the manuscript.
onflict of interest
All the authors declare that they have no conflicts of interesto report that could inappropriately influence, or be perceived tonfluence this work.
cknowledgements
Support to the Centre for Addiction and Mental Health forhe salaries of scientists and infrastructure has been provided byhe Ontario Ministry of Health and Long-Term Care. The viewsxpressed in this manuscript do not necessarily reflect those of thentario Ministry of Health and Long-Term Care.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at doi:10.1016/j.drugalcdep.2011.08.026.
eferences
nderson, R., 2010. Systematic reviews of economic evaluations: utility or futility.Health Econ. 19, 350–364.
nnemans, L., Vanoverbeke, N., Tecco, J., D’Hooghe, D., 2000. Economic evaluationof campral (acamprosate) compared to placebo in maintaining abstinence inalcohol-dependent patients. Eur. Addict. Res. 6, 71–78.
arbosa, C., Godfrey, C., Parrott, S., 2010. Methodological assessment of economicevaluations of alcohol treatment: what is missing? Alcohol Alcohol. 45, 53–63.
handari, A., Wagner, T., 2006. Self-reported utilization of health care services:improving measurement and accuracy. Med. Care Res. Rev. 63, 217–235.
ooth, B.M., Kirchner, J.E., Fortney, S.M., Han, X., Thrush, C.R., French, M.T., 2006.Measuring use of health services for at-risk drinkers: how brief can you get? J.Behav. Health Serv. Res. 33, 254–264.
laxton, K., Walker, S., Palmer, S., Sculpher, M., 2010. Appropriate perspectives forhealth care decisions. Centre for Health Economics, Research Paper 54. Availablefrom: http://www.york.ac.uk/che/publications/in-house/.
el Boca, F.K., Noll, J.A., 2000. Truth or consequences: the validity of self-report datain health services research on addictions. Addiction 95, S37–S360.
rummond, M., 1996. Guidelines for authors and peer reviewers of eco-nomic submissions to the BMJ. BMJ 313, 275–283, Available from:http://resources.bmj.com/bmj/authors/checklists-forms/health-economics.
rummond, M., O’Brien, B., Stoddart, G.L., Torrance, G.W., 2005. Methods for the Eco-nomic Evaluation of Health Care Programmes, 3rd ed. Oxford University Press,
Oxford.unlap, L.J., Zarkin, G.A., Bray, J.W., Millis, M., Kivlahan, D.R., McKay, J.R., Latham,P., Tonigan, J.S., 2010. Revisiting the cost-effectiveness of the COMBINEstudy for alcohol dependent patients. The patient perspective. Med. Care 48,306–313.
Dependence 122 (2012) 165– 173 173
Fleming, M.F., Mundt, M.P., French, M.T., Manwell, L.B., Stauffacher, E.A., Barry,K.L., 2002. Brief physician advice for problem drinkers: long term efficacy andbenefit–cost analysis. Alcohol. Clin. Exp. Res. 26, 36–43.
Gerkens, S., Crott, R., Cleemput, I., Thissen, J.-P., Closon, M.C., Horsmans, Y., Beguin, C.,2008. Comparison of three instruments assessing the quality of economic eval-uations: a practical exercise on economic evaluations of the surgical treatmentof obesity. Int. J. Technol. Assess. Health Care 24, 318–325.
Godfrey, C., Stewart, D., Gossop, M., 2004. Economic analysis of costs and conse-quences of the treatment of drug misuse: 2-year outcome data from the NationalTreatment Outcome Research Study (NTORS). Addiction 99, 697–707.
Gunther, O., Roick, C., Angermeyer, M.C., Konig, H.H., 2007. The EQ-5D inalcohol dependent patients: relationships among health-related quality oflife, psychopathology and social functioning. Drug Alcohol Depend. 86,253–264.
Gunther, O.H., Roick, C., Angermeyer, M.C., Konig, H.H., 2008. Responsiveness ofEQ-5D utility indices in alcohol-dependent patients. Drug Alcohol Depend. 92,291–295.
Lee, J.M., Chen, M.G., Hwang, T.C., Yeh, C.Y., 2010. Effect of cigarette taxes on theconsumption of cigarettes, alcohol, tea and coffee in Taiwan. Public Health 124,429–436.
Longo, M.C., Henry-Edwards, S.M., Humeniuk, R.E., Christie, P., Ali, R.L., 2004. Impactof the heroin ‘drought’ on patterns of drug use and drug-related harms. DrugAlcohol Rev. 23, 143–150.
Marshall, R., Grayson, D., Jorm, A., O’Toole, B., 2001. Are survey measures of med-ical care utilisation misleading? A comparison of self-reported medical careconsumption with actual medical care utilisation. Aust. Health Rev. 24, 91–99.
Mortimer, D., Segal, L., 2006. Economic evaluation of interventions for problemdrinking and alcohol dependence: do within-family external effects make adifference? Alcohol Alcohol. 41, 92–98.
Palmer, A., Neeser, K., Weiss, C., Brandt, A., Comte, S., Fox, M., 2000. The long-termcost-effectiveness of improving alcohol abstinence with adjuvant acamprosate.Alcohol Alcohol. 35, 478–492.
Poldrugo, F., Haeger, D.A., Comte, S., Walburg, J., Palmer, A., 2005. A criticalreview of pharmacoeconomic studies of acamprosate. Alcohol Alcohol. 40,422–430.
Pollicino, C., Viney, R., Haas, M., 2002. Measuring health system resource usefor economic evaluaton: a comparison of data sources. Aust. Health Rev. 25,171–178.
Portella, E., Ridao, M., Carrillo, E., Ribas, E., Ribó, C., Salvat, M., 1998. Alcohol y suabuso:. Impacto Socio Económico. Editorial Medica Panamericana, Madrid.
Reijneveld, S.A., 2000. The cross-cultural validity of self-reported use of health care:a comparison of survey and registration data. J. Clin. Epidemiol. 53, 267–272.
Rychlik, R., Siedentop, H., Pfeil, T., Daniel, D., 2003. Cost-effectiveness of adjuvanttreatment with acamprosate in maintaining abstinence in alcohol dependentpatients. Eur. Addict. Res. 9, 59–64.
Schadlich, P.K., Brecht, J.G., 1998. The cost effectiveness of acamprosate in the treat-ment of alcoholism in Germany. Pharmacoeconomics 13, 719–730.
Schwappach, D.L., Boluarte, T.A., 2007. HEE-GER: a systematic review of Germaneconomic evaluations of health care published 1990–2004. BMC Health Serv.Res. 7, 7.
Schwappach, D.L., Boluarte, T.A., Suhrcke, M., 2007. The economics of primary pre-vention of cardiovascular disease: a systematic review of economic evaluations.CERA 5, 5.
Shemilt, I., Mugford, M., Byford, S., Drummond, M., Eisenstein, E., Knapp, M., Mallen-der, J., McDaid, D., Vale, L., Walker, D., 2008. Incorporating economics evidence.In: Higgins, J.P.T., Green, S. (Eds.), Cochrane Handbook for Systematic Reviewsof Interventions. The Cochrane Collaboration, Version 5.0.1. , Available fromwww.cohcrane-handbook.org (updated 2008).
Stone, P.W., Chapman, R.H., Sandberg, E.A., Liljas, B., Neumann, P.J., 2000. Measuringcosts in cost–utility analyses. Variations in the literature. Int. J. Technol. Assess.Health Care 16, 111–124.
UKATT Research Team, 2005. Cost effectiveness of treatment for alcohol problems:findings of the randomised UK alcohol treatment trial (UKATT). BMJ 331, 544.
Walters, D., Connor, J.P., Feeney, G.F.X., McD Young, R., 2009. The cost effectivenessof naltrexone added to cognitive-behavioral therapy in the treatment of alcoholdependence. J. Addict. Dis. 28, 137–144.
Zarkin, G.A., Bray, J.W., Aldridge, A., Millis, M., Cisler, R.A., Couper, D., McKay, J.R.,
O’Malley, S., 2010. The effect of alcohol treatment on social costs of alcoholdependence results from the COMBINE study. Med. Care 48, 396–401.Zarkin, G.A., Bray, J.W., Aldridge, A., Mitra, D., Mills, M.J., Couper, D.J., Cisler, R.A.,2008. Cost and cost-effectiveness of the COMBINE study in alcohol dependentpatients. Arch. Gen. Psychiatry 65, 1214–1221.